Session 6 PD, Mitigating the Cost Impact of Trends in Hospital Billing Practices. Moderator/Presenter: Sabrina H.
|
|
|
- Egbert Owens
- 5 years ago
- Views:
Transcription

1 Session 6 PD, Mitigating the Cost Impact of Trends in Hospital Billing Practices Moderator/Presenter: Sabrina H. Gibson, FSA, MAAA Presenters: Dawna Nibert Lawrence R. Smart, FSA, MAAA


2 Society of Actuaries Health Meeting June 2016
3 Moderator: Sabrina Gibson, FSA, MAAA Speakers: Larry Smart, FSA, MAAA Dawna Nibert, MS
4 Larry Smart is a Vice President and the Chief Actuary for WellCare Health Plans located in Tampa, Florida. He is a Fellow of the Society of Actuaries and a Member of the American Academy of Actuaries and has worked as a health care actuary for almost 20 years and in Medicaid and Medicare for 10 years. He has led teams for reserving, medical economics, PDP program design and rate development as well as his current Chief Actuary role. Larry is a graduate of George Mason University with a major in Mathematics.
5 Dawna is a Senior Director of Medical Economics for WellCare Health Plans based in Tampa Florida. She brings over 20 years of extensive knowledge around all facets of health care analytics including health plan provider contracting analytics, value based and alternative payment models, actuarial rate setting and modeling, health plan financial and operational management, health care information systems, and predictive modeling and outcomes. Her health plan and consulting experience span both government sponsored and commercial health plans, but she has primarily worked with Managed Medicaid and Medicare Advantage plans over the last 10 years. Dawn received her graduate degree in Information Systems from Marshall University in WV. Her undergraduate degrees in Computer Science and Mathematics are from the West Virginia Institute of Technology.
6 Hospital cost control is the number one goal of every health plan. Hospital billing practices have become more complex. The health plan s job of controlling these costs becomes more difficult.
7 This session will discuss some of the most common ways hospitals increase revenue through billing practices and how the health plan can implement strategies to manage these practices. What are the practices. How to identify them in the claim data. How to address the practice to reduce the cost impact
8 Managing Inpatient Authorizations
9 Hospital will request an inpatient authorization for a service that should be classified as observation stay (generally<48 hours Two-Midnight rule) Example of the difference in cost for a 2 day inpatient versus an observation. Program IP Cost Observation Cost Medicaid $5,000 $800 Medicare $8,000 $1,100 Commercial $12,000 $1,700
10 What to look for when reviewing IP authorizations data: Average requested lengths of stay and admits per 1000 How do they compare to benchmarks? Focus on short stays two days or less Has there been recent decreases in the average length of stay? Recent changes in the authorization process? Recent staffing changes? Recent regulatory changes?
11 What to look for when reviewing IP authorizations data: Percentage of authorizations reviewed by a Medical Director (MD) Nurses review authorizations and can approve them, but an MD is the only one that can deny for an IP stay (would be billed at OP rate) Get external benchmarks for appropriate levels of MD review Percentage of authorizations auto-approved Required turnaround times Staffing levels will impact What evidence based medical criteria is being used Is it being applied consistently?
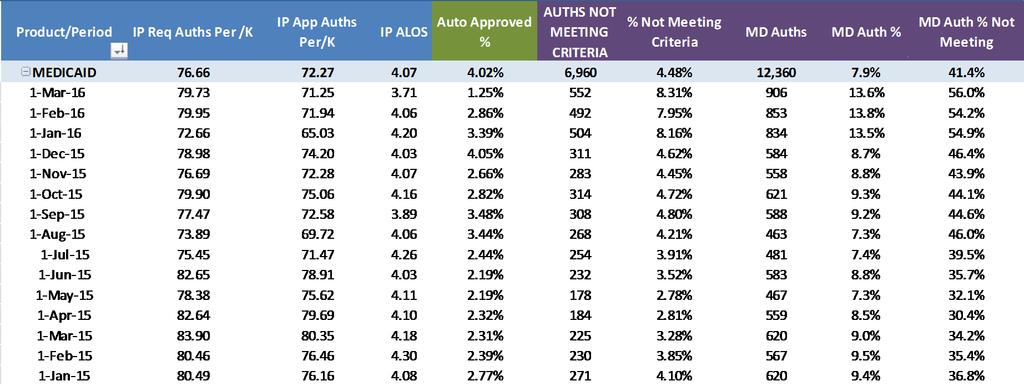
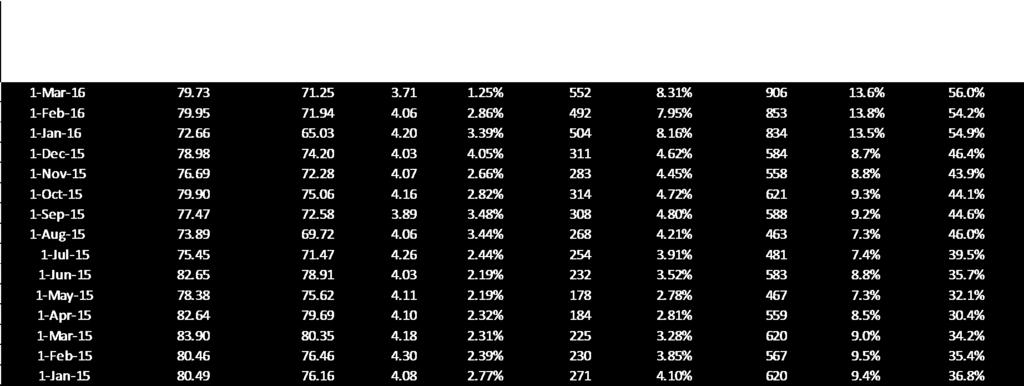
12 Create a operational chart to monitor
13 Action plan Staff appropriately to reduce auto approvals Under staffing causes increases in auto approvals Clearly define medical evidence based criteria Make sure staff is trained appropriately Use external vendor to help set internal benchmarks Periodic audits of nurses and medical directors
14 Action plan Use early indicators to identify process gaps Identify changes in top IP diagnosis Headaches Respiratory Abdominal Pain Chest pain Etc. Monitor unexplained changes in: Auto approvals Medical director review Does not meet criteria percentage Staff properly for increased appeals
15 Hospital Billing and Pricing Practices
16 What is Upcoding? Generally upcoding refers to a situation when the level of service billed is higher than the intensity of service rendered or required at the time of service The National Uniform Billing Committee has established objective standards/thresholds for the billing codes that are used to bill daily room and board charges. Level of care standards are outlined for ICU, CCU, Nursery, and Sub Acute For example, Revenue Code 174 (the highest acuity revenue code for Neonatal Intensive Care) is defined as being appropriate for newborns who need constant nursing and continuous cardiopulmonary and other support [over 12 hours per day] for severely ill infants (considered to be intensive care).
17 Potential upcoding situations include: Billing a high acuity room on the date the patient was discharged to a home setting. Facilities will bill Revenue Code 174 (frequently at over $7,000 per day) on the date of service prior to discharge to a home care environment. How can a patient require constant nursing and continuous cardiopulmonary and other support on a Thursday, but be stable enough to not require any nursing care on a Friday? Continuing to bill a high acuity Revenue Code after resource consumption falls below that Revenue Code s thresholds. Similarly, although Revenue Code 174 is only appropriate for patients that require continuous cardiopulmonary support, facilities will continue to bill Revenue Code 174 after all forms of respiratory therapy have been discontinued and the patient no longer requires any cardiopulmonary support. Overlap of levels/services on transition days involving a step down Moving from ventilator to CPAP machine 24 hrs of both billed on transition day
18 Hospital per diem contracts need to be monitored to ensure proper level gets reimbursed Per Diem contracts require complex concurrent review monitoring Authorization systems have limitations; often authorize length of stay and not levels Even if the authorization is captured at the level of care claims systems can t match the claim to the authorization day by day Hospital contracts paying on DRG can also be impacted by the upcoding issue Increased billed charges associated with the higher room and board levels will pay out more in outlier costs
19 Strategies to mitigate the impact of room and board upcoding Identification and retro-review to identify outliers for recovery Analyze claims by looking at DRGs and progression of level of R&B billed through discharge Review itemized bills to find overlap of services billed for transitions Contractual approaches Build per diem levels based on DRG groupings not individual Room and Board codes MS DRG 795 Level 1 per diem MS DRGs 789, 792, Level 2 per diem MS DRGs 791, 793 Level 3 per diem MS DRG 790 Level 4 per diem
20 What is Unbundling? Unbundling refers to a billing practice where services that should be packaged together are broken out and billed separately. CMS payment guidelines state that daily room and board charges includes basic nursing services and minor medical supplies and it is inappropriate for facilities to unbundle these charges from the underlying room and board charge. It is appropriate for a facility to bill these services/supplies in an outpatient setting and/or in other settings where such services/supplies are not already elements of the underlying standard of care. Since the UB claim form used to bill payers rolls routine and nonroutine service supply charges into the same revenue codes, it s very difficult to identify instances of potential unbundling without obtaining and reviewing the itemized bill that lists each charge billed by the facility.
21 Separately billed regular nursing services include: routine venipunctures (frequently billed at over $100 per blood draw) bedside glucose testing (performed with the same reusable glucometer used by diabetics and frequently billed at over $50 per test) medication administration (frequently billed at over $50 per medication) Separately billed minor medical/surgical supplies include such basic supplies as: 4 x4 gauze (frequently billed at over $20 each) sponges, (frequently billed at over $30 each) and sterile water for irrigation (frequently billed at over $100 per 100ml)
22 Hospital costs for contracts paying on both DRG and per diem can be impacted by unbundling Additional services billed will accumulate more charges toward triggering DRG outlier payments and stop loss outlier thresholds Strategies to mitigate the impact of unbundling Reviewing itemized billed charges to determine payments excluding any items not allowable. Such reviews routinely disclose that many facilities inpatient claims continue to include separate charges for the very regular nursing services and minor supply items that were already included in the underlying daily room charges, resulting in double billing. Potential Savings of 10% - 20% of large claims
23 Hospital Chargemaster - a comprehensive list of every itemized price for every service, procedure, and supply item that can be billed by a hospital. Chargemasters are proprietary to every hospital and can contain anywhere from thousands to tens of thousands of codes. Hospitals update chargemasters at least yearly and often more frequently; CMS regulation states that hospitals can only have one chargemaster across all payers. As payer payment has become more complex hospitals tend to push up charges overall to ensure they are covering costs across all payers.
24 Hospital costs for contracts paying on both DRG and per diem can be impacted by chargemaster increases Increased chargemasters accumulate more charges toward triggering DRG outlier payments and stop loss outlier thresholds Strategies to mitigate the impact of chargemaster increases Contract language that allows for offset of chargemaster increases to contracted rates. However, limitations for vertical increases can lead to horizontal increases (such as upcoding and unbundling) Hospitals often report chargemaster increases aggregated across all payers but methodology can be developed to measure chargemaster impact based on the health plan s experience with the hospital
25 Methodology to measure Chargemaster Increase specific to health plan Period 1 Period 2 Normalized Charges using Period 1 units Charge Master change Normalized Charges using Period 2 units Revenue Code Revenue Code Description Units Charges Unit Charge Units Charges Unit Charge Period 1 Charges Period 2 Charges Period 1 Charges Period 2 Charges 0110 Room & Board (Private) 42 77,154 1, ,975 1,932 77,154 81,136 5% 189, ,975 5% 0113 Pediatric 22 40,414 1, ,941 1,929 40,414 42,438 5% 53,273 55,941 5% 0114 Psychiatric 31 56,947 1, ,432 1,929 56,947 59,799 5% 14,696 15,432 5% 0120 Room & Board (Semi-Private 2 beds) 565 1,037,905 1,837 1,134 2,190,654 1,932 1,037,905 1,091,461 5% 2,083,158 2,190,650 5% 0121 Medical/Surgical/Gyn 3 5,511 1, ,858 1,929 5,511 5,787 5% 3,674 3,858 5% 0123 Pediatric 47 86,339 1, ,604 1,929 86,339 90,663 5% 139, ,604 5% 0124 Psychiatric 39 71,643 1, ,373 1,929 71,643 75,231 5% 67,969 71,373 5% 0128 Rehab 20 36,740 1, ,296 1,929 36,740 38,580 5% 44,088 46,296 5% 0130 Room&Board (Semi private 3-4 beds) ,625 1, ,439 1, , ,125 5% 350, ,439 5% 0170 Nursery 18 28,387 1, ,612 1,307 28,387 23,534-17% 23,656 19,612-17% 0172 Newborn-Level II ,330 3, ,403 3, , ,329 3% 436, ,403 3% 0173 Newborn-Level III 397 1,344,432 3, ,696 3,703 1,344,433 1,469,960 9% 629, ,697 9% 0174 Newborn-Level IV ,625 3, ,442 3, , ,485 2% 318, ,442 2% 0200 Intensive care ,849 4, ,177 4, , ,695 5% 230, ,177 5% 0202 Medical 1 4,043 4, ,847 4,254 4,043 4,254 5% 92,989 97,847 5% 0203 Pediatric 28 82,162 2, ,404 3,791 82, ,162 29% 205, ,404 29% 0206 Intermediate ICU 22 54,626 2, ,054 2,607 54,626 57,354 5% 302, ,054 5% Plan Derived Increase 4,570,733 4,843, % 5,187,244 5,505, % Adult R&B 1,757,228 1,846, % 3,330,430 3,500, % Nursery/NICU/Pediatric 2,695,937 2,873, % 1,614,330 1,749, % Charge Master change
26 CMS regulation also states that charges need to reasonably and consistently relate back to underlying cost of a service Certain higher cost services should be reviewed High cost drugs can be compared to Medicare AWP ( Implants can be compared to the amount that facilities have reported to a central database as their cost for these supplies. Since this database is used by facilities to create a level playing field when contracting with implant suppliers, it provides an accurate benchmark for facilities presumptive costs for these supplies.
27 Scenario #1: Hospital cherry picked the higher of their contracted rate or the old physician rate when billing Hospital contract was silent on acquired groups Solution: Add specific language in the hospital contracts around acquired physician groups: acquired physician groups will be reimbursed at 100% of the Medicaid fee schedule until such time as the parties have negotiated a mutually agreed upon rate OR all physicians will be paid at the prevailing contract fee
28 Scenario #2: Physicians brought on as staff physicians of hospital, so bills using outpatient place of service Also leads to physicians billing lab, diagnostics, etc as outpatient such as ultrasounds if it is OB/GYN Solution: Add very specific language in the hospital contracts around the definition of staff physician or add language specifying how physician groups can bill.
29 Scenario #3: Group begins billing injectables through outpatient instead of at the historic AWP they used when billing as a physician office Solution: Add specific language in the hospital contracts around acquired injectables supplied by physician groups:
30 One goal of the Affordable Care Act (ACA) is to reduce costs to hospitals for unwanted outcomes and to provide quality care more efficiently. The following provisions from the ACA directly impact the reimbursements to hospitals: Hospital Acquired Conditions, Never Events, and other Provider-Preventable Conditions (PPCs) Day Hospital Readmission Rates for select conditions 2015 Hospital Acquired Infections top quartile Health Plan s Provider Manual should indicate that CMS guidelines are followed for claims payment procedure Follow CMS s lead and draft specific policy and procedures for your Health Plan
31 Section 3025 of the Affordable Care Act added section 1886(q) to the Social Security Act establishing the Hospital Readmissions Reduction Program. CMS defines readmission as an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital; Medicare allows for a 30 day lookback with any similar diagnosis Exclusions for certain facilities, major diagnostic categories, patient status, interim bills Pre pay edit looks for two categories of potential readmission Category 1 Same DRG and similar primary diagnosis Category 2 Same DRG and any similar diagnosis Retrospective review also done for Category 1 and 2 Hospital can appeal and submit medical records
32 California Hospital Chargemasters aspx High cost drugs can be compared to Medicare AWP at CMS Provider Reimbursement Manuals Guidance/Guidance/Manuals/Paper-Based- Manuals-Items/CMS html
33 Questions
Clinical. Financial. Integrated.
 Clinical. Financial. Integrated. April 2015 Table of Contents When are the rule changes effective? What is changing? What requirements must be met to avoid payment at the site neutral rate? How is the
Clinical. Financial. Integrated. April 2015 Table of Contents When are the rule changes effective? What is changing? What requirements must be met to avoid payment at the site neutral rate? How is the
Medi-Cal APR-DRG Updates. Medi-Cal Updates. Agenda. Medi-Cal APR-DRG Updates Quality Assurance Fee (QAF) Program
 Program") Medi-Cal Updates Amber Ott California Hospital Association Agenda Medi-Cal APR-DRG Updates Quality Assurance Fee (QAF) Program Current QAF Law (SB239) Prop 52 Medicaid Managed Care Final Rules QAF 5 Development
Medi-Cal Updates Amber Ott California Hospital Association Agenda Medi-Cal APR-DRG Updates Quality Assurance Fee (QAF) Program Current QAF Law (SB239) Prop 52 Medicaid Managed Care Final Rules QAF 5 Development
June 18, 2009 Page 1
 Base Year Current LOC base rates calculated using: Wyoming Medicaid inpatient hospital claims data from July 1, 1994 through December 31, 1996 Most recently audited Medicare cost report with provider fiscal
Base Year Current LOC base rates calculated using: Wyoming Medicaid inpatient hospital claims data from July 1, 1994 through December 31, 1996 Most recently audited Medicare cost report with provider fiscal
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
Critical Care Services Benefits to Change for the CSHCN Services Program
 Critical Care Services Benefits to Change for the CSHCN Services Program Information posted July 14, 2008 Effective for dates of service on or after September 1, 2008, the benefit criteria for critical
Critical Care Services Benefits to Change for the CSHCN Services Program Information posted July 14, 2008 Effective for dates of service on or after September 1, 2008, the benefit criteria for critical
BCBSTX Admission Type Definitions Grouper Version 33
 Shared NPI between Acute Care and Specialty Provider numbers NPI is not shared between Acute Care and Specialty Provider numbers Residential Treatment Center, Eating Disorder Inpatient DRG 876, 880-887
Shared NPI between Acute Care and Specialty Provider numbers NPI is not shared between Acute Care and Specialty Provider numbers Residential Treatment Center, Eating Disorder Inpatient DRG 876, 880-887
Facility-Based Behavioral Health Program Professional Fees Reimbursement Policy Annual Approval Date. Approved By
 Policy Number 2016RP505A Facility-Based Behavioral Health Program Professional Fees Reimbursement Policy Annual Approval Date 09/30/2016 Approved By Optum Behavioral Reimbursement Committee IMPORTANT NOTE
Policy Number 2016RP505A Facility-Based Behavioral Health Program Professional Fees Reimbursement Policy Annual Approval Date 09/30/2016 Approved By Optum Behavioral Reimbursement Committee IMPORTANT NOTE
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Ralph Wuebker, MD, MBA Chief Medical Officer Executive Health Resources
 The Invisible Denial: A Closer Look at Commercial Denials and Appeals Strategies Ralph Wuebker, MD, MBA Chief Medical Officer Executive Health Resources AHA Solutions, Inc., a subsidiary of the American
The Invisible Denial: A Closer Look at Commercial Denials and Appeals Strategies Ralph Wuebker, MD, MBA Chief Medical Officer Executive Health Resources AHA Solutions, Inc., a subsidiary of the American
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions Version Date: September 22, 2014 UPDATE: The District of Columbia Department of Health Care Finance (DHCF) is submitting
District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions Version Date: September 22, 2014 UPDATE: The District of Columbia Department of Health Care Finance (DHCF) is submitting
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Florida Medicaid. Outpatient Hospital Services Coverage Policy. Agency for Health Care Administration. Draft Rule
 Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid
 Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
PROPOSED POLICY AND PAYMENT CHANGES FOR INPATIENT STAYS IN ACUTE-CARE HOSPITALS AND LONG-TERM CARE HOSPITALS IN FY 2014
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
Ohio Hospital Association Finance Committee 2018 Hospital Inpatient Reimbursement Recommendations
 Ohio Hospital Association Finance Committee 2018 Hospital Inpatient Reimbursement Recommendations Freddie L. Johnson, JD, MPA Chief Medical Services & Compliance Officer August 10, 2017 2018 Inpatient
Ohio Hospital Association Finance Committee 2018 Hospital Inpatient Reimbursement Recommendations Freddie L. Johnson, JD, MPA Chief Medical Services & Compliance Officer August 10, 2017 2018 Inpatient
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
ICD-10/APR-DRG. HP Provider Relations/September 2015
 ICD-10/APR-DRG HP Provider Relations/September 2015 Agenda ICD-10 ICD-10 General Overview Who is affected Preparation Testing Prior Authorization APR-DRG Inpatient hospital rates Crosswalks Questions 2
ICD-10/APR-DRG HP Provider Relations/September 2015 Agenda ICD-10 ICD-10 General Overview Who is affected Preparation Testing Prior Authorization APR-DRG Inpatient hospital rates Crosswalks Questions 2
Executive Summary, December 2015
 CMS Revises Two-Midnight Rule to Allow An Exception for Part A Payment for Hospital Services Provided to Patients Requiring Inpatient Care for Less Than Two Midnights Executive Summary, December 2015 Sponsored
CMS Revises Two-Midnight Rule to Allow An Exception for Part A Payment for Hospital Services Provided to Patients Requiring Inpatient Care for Less Than Two Midnights Executive Summary, December 2015 Sponsored
THE INVISIBLE DENIAL: A Closer Look at Commercial Denials and Appeals Strategies
 THE INVISIBLE DENIAL: A Closer Look at Commercial Denials and Appeals Strategies Marc Tucker, DO, FACOS, MBA Sr. Medical Director ACE AHA Solutions, Inc., a subsidiary of the American Hospital Association,
THE INVISIBLE DENIAL: A Closer Look at Commercial Denials and Appeals Strategies Marc Tucker, DO, FACOS, MBA Sr. Medical Director ACE AHA Solutions, Inc., a subsidiary of the American Hospital Association,
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL
 Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
Indiana Hospital Assessment Fee -- DRAFT
 Indiana Hospital Assessment Fee -- DRAFT September 27, 2011 Inpatient Fee The initial Indiana Inpatient Hospital Fee applies to inpatient days from each hospital's most recent FYE as taken from the cost
Indiana Hospital Assessment Fee -- DRAFT September 27, 2011 Inpatient Fee The initial Indiana Inpatient Hospital Fee applies to inpatient days from each hospital's most recent FYE as taken from the cost
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Learning Objectives. It Starts With an Order and an Expectation
 1 Under What Condition: Understanding Condition Codes 44 and W2 Debbie Mackaman, RHIA, CPCO, CCDS Regulatory Specialist HCPro, an H3.Group Brand Middleton, MA Learning Objectives At the completion of this
1 Under What Condition: Understanding Condition Codes 44 and W2 Debbie Mackaman, RHIA, CPCO, CCDS Regulatory Specialist HCPro, an H3.Group Brand Middleton, MA Learning Objectives At the completion of this
LTCH Payment Reform & Patient Criteria
 LTCH Payment Reform & Patient Criteria Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Overview Objectives What happened? Describe new LTACH payment system
LTCH Payment Reform & Patient Criteria Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Overview Objectives What happened? Describe new LTACH payment system
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015)
") 7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
AMENDATORY SECTION (Amending WSR , filed 8/27/15, effective. WAC Inpatient psychiatric services. Purpose.
 AMENDATORY SECTION (Amending WSR 15-18-065, filed 8/27/15, effective 9/27/15) WAC 182-550-2600 Inpatient psychiatric services. Purpose. (1) The medicaid agency, on behalf of the mental health division
AMENDATORY SECTION (Amending WSR 15-18-065, filed 8/27/15, effective 9/27/15) WAC 182-550-2600 Inpatient psychiatric services. Purpose. (1) The medicaid agency, on behalf of the mental health division
CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS
 10 th Annual HCCA Compliance Institute Session Las Vegas, NV April 25, 2006 CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS MARK HARDIMAN HOOPER, LUNDY & BOOKMAN, INC. 1875
10 th Annual HCCA Compliance Institute Session Las Vegas, NV April 25, 2006 CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS MARK HARDIMAN HOOPER, LUNDY & BOOKMAN, INC. 1875
3M Health Information Systems. The standard for yesterday, today and tomorrow: 3M All Patient Refined DRGs
 3M Health Information Systems The standard for yesterday, today and tomorrow: 3M All Patient Refined DRGs From one patient to one population The 3M APR DRG Classification System set the standard from the
3M Health Information Systems The standard for yesterday, today and tomorrow: 3M All Patient Refined DRGs From one patient to one population The 3M APR DRG Classification System set the standard from the
INPATIENT/COMPREHENSIVE REHAB AUDIT DICTIONARY
 Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients
 Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
I. Cost Finding and Cost Reporting
 FLORIDA TITLE XIX INPATIENT HOSPITAL REIMBURSEMENT PLAN VERSION XLIV EFFECTIVE DATE July 1, 2017 I. Cost Finding and Cost Reporting A. Each hospital participating in the Florida Medicaid program shall
FLORIDA TITLE XIX INPATIENT HOSPITAL REIMBURSEMENT PLAN VERSION XLIV EFFECTIVE DATE July 1, 2017 I. Cost Finding and Cost Reporting A. Each hospital participating in the Florida Medicaid program shall
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule
 CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor. NJHFMA Finance for Clinicians Session March 24, 2016
 1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
INPATIENT HOSPITAL REIMBURSEMENT
 HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
State FY2013 Hospital Pay-for-Performance (P4P) Guide
 Guide") State FY2013 Hospital Pay-for-Performance (P4P) Guide Table of Contents 1. Overview...2 2. Measures...2 3. SFY 2013 Timeline...2 4. Methodology...2 5. Data submission and validation...2 6. Communication,
State FY2013 Hospital Pay-for-Performance (P4P) Guide Table of Contents 1. Overview...2 2. Measures...2 3. SFY 2013 Timeline...2 4. Methodology...2 5. Data submission and validation...2 6. Communication,
Minnesota health care price transparency laws and rules
 Minnesota health care price transparency laws and rules Minnesota Statutes 2013 62J.81 DISCLOSURE OF PAYMENTS FOR HEALTH CARE SERVICES. Subdivision 1.Required disclosure of estimated payment. (a) A health
Minnesota health care price transparency laws and rules Minnesota Statutes 2013 62J.81 DISCLOSURE OF PAYMENTS FOR HEALTH CARE SERVICES. Subdivision 1.Required disclosure of estimated payment. (a) A health
Hospital Strength INDEX Methodology
 2017 Hospital Strength INDEX 2017 The Chartis Group, LLC. Table of Contents Research and Analytic Team... 2 Hospital Strength INDEX Summary... 3 Figure 1. Summary... 3 Summary... 4 Hospitals in the Study
2017 Hospital Strength INDEX 2017 The Chartis Group, LLC. Table of Contents Research and Analytic Team... 2 Hospital Strength INDEX Summary... 3 Figure 1. Summary... 3 Summary... 4 Hospitals in the Study
Place of Service Code Description Conversion
 Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
Abbreviated Client Stay means an Inpatient stay ending in client death or in which the client leaves against medical advice.
 DEPARTMENT OF HEALTH CARE POLICY AND FINANCING Medical Services Board MEDICAL ASSISTANCE - SECTION 8.300 10 CCR 2505-10 8.300 [Editor s Notes follow the text of the rules at the end of this CCR Document.]
DEPARTMENT OF HEALTH CARE POLICY AND FINANCING Medical Services Board MEDICAL ASSISTANCE - SECTION 8.300 10 CCR 2505-10 8.300 [Editor s Notes follow the text of the rules at the end of this CCR Document.]
Payment Methodology. Acute Care Hospital - Inpatient Services
 Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
UTILIZATION MANAGEMENT Section 4. Overview The Plan s Utilization Management (UM)
") Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
HCA APR-DRG and EAPG Rebasing Revised February 2017
 HCA APR-DRG and EAPG Rebasing Revised February 2017 Inpatient and Outpatient Pricing Effective 11/01/2014 to Current Inpatient pricing From AP DRG to APR DRG HCA is using 3M Standard Weights Pricing goes
HCA APR-DRG and EAPG Rebasing Revised February 2017 Inpatient and Outpatient Pricing Effective 11/01/2014 to Current Inpatient pricing From AP DRG to APR DRG HCA is using 3M Standard Weights Pricing goes
Outpatient Observation Services
 Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
3M Health Information Systems. 3M Clinical Risk Groups: Measuring risk, managing care
 3M Health Information Systems 3M Clinical Risk Groups: Measuring risk, managing care 3M Clinical Risk Groups: Measuring risk, managing care Overview The 3M Clinical Risk Groups (CRGs) are a population
3M Health Information Systems 3M Clinical Risk Groups: Measuring risk, managing care 3M Clinical Risk Groups: Measuring risk, managing care Overview The 3M Clinical Risk Groups (CRGs) are a population
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
INFORMATION ABOUT YOUR OXFORD COVERAGE REIMBURSEMENT PART I OXFORD HEALTH PLANS OXFORD HEALTH PLANS (NJ), INC.
, INC.") OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
PATIENT STATUS DEFINITIONS, 2 MIDNIGHT RULE AND 96 HOUR RULE
 PURPOSE It is the policy of Mason General Hospital and Family of Clinics (MGH&FC) that based on the Patient Status Definitions, all placements concerning the use of observation beds, or placements made
PURPOSE It is the policy of Mason General Hospital and Family of Clinics (MGH&FC) that based on the Patient Status Definitions, all placements concerning the use of observation beds, or placements made
The In and Out of the Medicare Two Midnight Rule. Disclaimer. Objectives 3/31/2014
 The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
FY2018 Proposed Rule: Payment and Quality Reporting
 FY2018 Proposed Rule: Payment and Quality Reporting Mary Dalrymple Managing Director, LTRAX Objectives Describe effects of reimbursement updates Look at new short stay payment system Touch on miscellaneous
FY2018 Proposed Rule: Payment and Quality Reporting Mary Dalrymple Managing Director, LTRAX Objectives Describe effects of reimbursement updates Look at new short stay payment system Touch on miscellaneous
Hospital Payments and Quality Initiatives
 Hospital Payments and Quality Initiatives December 2014 John McCarthy Ohio Medicaid Director Today s Overview How Ohio Medicaid pays hospitals - Prospective Payment Methods - Inpatient Hospital Payment
Hospital Payments and Quality Initiatives December 2014 John McCarthy Ohio Medicaid Director Today s Overview How Ohio Medicaid pays hospitals - Prospective Payment Methods - Inpatient Hospital Payment
Chapter 13 Section 2. Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups
 Groups") Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics
 Hot Reimbursement Topics Rural Area Hospitals May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics RICHARD S. REID, MPA, FHFMA, CPA, Director,
Hot Reimbursement Topics Rural Area Hospitals May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics RICHARD S. REID, MPA, FHFMA, CPA, Director,
CARING & CODING FOR MALNUTRITION
 CARING & CODING FOR MAL Sandy Routhier RHIA, CCS, CDIP, AHIMA Approved ICD-10CM/PCS Trainer CloudMed Solutions Michelle Mathura, RDN, LRD, CDE Director, Nutrition Division DM&A Our Presenters Sandra Routhier,
CARING & CODING FOR MAL Sandy Routhier RHIA, CCS, CDIP, AHIMA Approved ICD-10CM/PCS Trainer CloudMed Solutions Michelle Mathura, RDN, LRD, CDE Director, Nutrition Division DM&A Our Presenters Sandra Routhier,
Inpatient Hospital Rates Rebasing Report
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Inpatient Hospital
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Inpatient Hospital
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
EMERGENCY DEPARTMENT CASE MANAGEMENT
 EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
DC Inpatient APR-DRG Payment for Acute Care Hospitals
 DC Inpatient APR-DRG Payment for Acute Care Hospitals Provider Training 2014 Xerox Corporation. All rights reserved. Xerox and Xerox Design are trademarks of Xerox Corporation in the United States and/or
DC Inpatient APR-DRG Payment for Acute Care Hospitals Provider Training 2014 Xerox Corporation. All rights reserved. Xerox and Xerox Design are trademarks of Xerox Corporation in the United States and/or
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CMS -1599F. The 2 Midnight Rule Effective October 1, 2013
 Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
Connecting the Revenue and Reimbursement Cycles
 Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
Session 74 PD, Innovative Uses of Risk Adjustment. Moderator: Joan C. Barrett, FSA, MAAA
 Session 74 PD, Innovative Uses of Risk Adjustment Moderator: Joan C. Barrett, FSA, MAAA Presenters: Jill S. Herbold, FSA, MAAA Robert Anders Larson, FSA, MAAA Erica Rode, ASA, MAAA SOA Antitrust Disclaimer
Session 74 PD, Innovative Uses of Risk Adjustment Moderator: Joan C. Barrett, FSA, MAAA Presenters: Jill S. Herbold, FSA, MAAA Robert Anders Larson, FSA, MAAA Erica Rode, ASA, MAAA SOA Antitrust Disclaimer
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Clinical Episode-Based Payment (CEBP) Measures Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach
Clinical Episode-Based Payment (CEBP) Measures Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach
Inpatient orders and Physician Certification MUST BE authenticated PRIOR to discharge No EXCEPTIONS.
 2 Midnight Rule for InPatient Admission On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule (CMS- 1599-F) updating Medicare payment policies which modifies and clarifies
2 Midnight Rule for InPatient Admission On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule (CMS- 1599-F) updating Medicare payment policies which modifies and clarifies
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Facilities and Ancillaries This supplement of the Optima Health Provider Manual provides information of specific interest to Optima Health contracted
Optima Health Provider Manual Supplemental Information For Facilities and Ancillaries This supplement of the Optima Health Provider Manual provides information of specific interest to Optima Health contracted
Observation Care Evaluation and Management Codes Policy
 Policy Number Observation Care Evaluation and Management Codes Policy 2017R0115A Annual Approval Date 3/8/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible
Policy Number Observation Care Evaluation and Management Codes Policy 2017R0115A Annual Approval Date 3/8/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
Wisconsin Medicaid Hospital Update
 Rural Hospital Finance Workshop Division of Health Care Access and Accountability Bureau of Fiscal Management August 26, 2016 1 Agenda 1. SFY 2016 Hospital Medicaid Expenditures 2. 3. APR DRG Training
Rural Hospital Finance Workshop Division of Health Care Access and Accountability Bureau of Fiscal Management August 26, 2016 1 Agenda 1. SFY 2016 Hospital Medicaid Expenditures 2. 3. APR DRG Training
Reimbursement Policy. Subject: Inpatient Readmissions Committee Approval Obtained: Effective Date: 10/01/13
 Reimbursement Policy Subject: Inpatient Readmissions Committee Approval Obtained: Effective Date: 10/01/13 Section: Facilities 04/03/17 *****The most current version of the Reimbursement Policies can be
Reimbursement Policy Subject: Inpatient Readmissions Committee Approval Obtained: Effective Date: 10/01/13 Section: Facilities 04/03/17 *****The most current version of the Reimbursement Policies can be
PATIENT ADMISSIONS 2.0
 PATIENT ADMISSIONS 2.0 HOSPITAL DIVISION FINANCIAL POLICIES and PROCEDURES MANUAL SECTION 2.0 PATIENT ADMISSIONS 2.4 Admissions General Information Patient Classification Inpatient An inpatient is a person
PATIENT ADMISSIONS 2.0 HOSPITAL DIVISION FINANCIAL POLICIES and PROCEDURES MANUAL SECTION 2.0 PATIENT ADMISSIONS 2.4 Admissions General Information Patient Classification Inpatient An inpatient is a person
LOUISIANA MEDICAID PROGRAM ISSUED: 11/30/12 REPLACED: 07/01/11 CHAPTER 25: HOSPITAL SERVICES SECTION 25.7: REIMBURSEMENT PAGE(S) 17 REIMBURSEMENT
 17 REIMBURSEMENT") REIMBURSEMENT This chapter is an overview of inpatient reimbursement methodology and does not address all issues or questions that a hospital may have regarding reimbursement. If a provider has a question
REIMBURSEMENT This chapter is an overview of inpatient reimbursement methodology and does not address all issues or questions that a hospital may have regarding reimbursement. If a provider has a question
AAPC Webinar 3/28/2016
 Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Table 8.2 FORM CMS County Hospital - Fiscal Year One Worksheet A
 Table 8.2 Worksheet A A-6 Reclassified A-8 Net Expenses Salaries Other Total Reclassifications Trial Balance Adjustments For Allocation Cost Center Descriptions 1 2 3 4 5 6 7 General Service Cost Centers
Table 8.2 Worksheet A A-6 Reclassified A-8 Net Expenses Salaries Other Total Reclassifications Trial Balance Adjustments For Allocation Cost Center Descriptions 1 2 3 4 5 6 7 General Service Cost Centers
Hospital-Based Ambulatory Care
 C H A P T E R 2 Hospital-Based Ambulatory Care ANSWERS TO KNOWLEDGE-BASED QUESTIONS 1. What has been the trend in the utilization of hospital-based services? What factors help to account for this trend?
C H A P T E R 2 Hospital-Based Ambulatory Care ANSWERS TO KNOWLEDGE-BASED QUESTIONS 1. What has been the trend in the utilization of hospital-based services? What factors help to account for this trend?
Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape
 Presenting a live 90-minute webinar with interactive Q&A Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape Navigating the Interplay of Inpatient and
Presenting a live 90-minute webinar with interactive Q&A Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape Navigating the Interplay of Inpatient and
Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014, the Centers
Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014, the Centers
Basis of Payment and Appeal Procedure; Out-of-State Hospital Services. Authorized By: Jennifer Velez, Commissioner, Department of Human Services.
 HUMAN SERVICES 45 NJR 2(2) February 19, 2013 Filed January 17, 2013 DIVISION OF MEDICAL ASSISTANCE AND HEALTH SERVICES Hospital Services Manual Basis of Payment and Appeal Procedure; Out-of-State Hospital
HUMAN SERVICES 45 NJR 2(2) February 19, 2013 Filed January 17, 2013 DIVISION OF MEDICAL ASSISTANCE AND HEALTH SERVICES Hospital Services Manual Basis of Payment and Appeal Procedure; Out-of-State Hospital
2013 Health Care Regulatory Update. January 8, 2013
 2013 Health Care Regulatory Update January 8, 2013 Quality-Based Payment Reform, ACOs and Clinical Integration Bruce Johnson and Tom Donohoe Overview Quality-based payment reform programs Major programs
2013 Health Care Regulatory Update January 8, 2013 Quality-Based Payment Reform, ACOs and Clinical Integration Bruce Johnson and Tom Donohoe Overview Quality-based payment reform programs Major programs
MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes. UB-04 Revenue Codes
 Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
Same Day/Same Service Policy, Professional
 Same Day/Same Service Policy, Professional Policy Number 2018R0002D Annual Approval Date 7/11/2018 Approved By REIMBURSEMENT POLICY CMS-1500 Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT
Same Day/Same Service Policy, Professional Policy Number 2018R0002D Annual Approval Date 7/11/2018 Approved By REIMBURSEMENT POLICY CMS-1500 Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER