The Use of Non-Invasive Ventilation in Patients with Acute Type 2 Respiratory Failure
|
|
|
- Maurice Carpenter
- 6 years ago
- Views:
Transcription
1 POLICY UNDER REVIEW Please note that this policy is under review. It does, however, remain current Trust policy subject to any recent legislative changes, national policy instruction (NHS or Department of Health), or Trust Board decision. For guidance, please contact the Author/Owner. The Use of Non-Invasive Ventilation in Patients with Acute Type 2 Respiratory Failure V1.0 May 2014 Page 1 of 17
2 Table of Contents 1. Introduction Purpose of this Policy/Procedure Scope Definitions / Glossary Ownership and Responsibilities Role of the Managers Role of Individual Staff Standards and Practice Selection criteria Set Up Monitoring Escalation Treatment Duration and Weaning from Ventilation Palliation Trouble Shooting Dissemination and Implementation Monitoring compliance and effectiveness Updating and Review Equality and Diversity Equality Impact Assessment References... 9 Appendix 1. Governance Information Appendix 2. Initial Equality Impact Assessment Form Appendix 3. RCHT care plan and pathway Page 2 of 17
3 1. Introduction 1.1. Non-invasive ventilation (NIV) in the management of acute type II respiratory failure represents one of the major technical advances in respiratory care over the last decade. It has been shown to improve survival, reduce need for invasive ventilation and ICU, reduce length of hospital stay, reduce complication rates and reduce hospital costs This version supersedes any previous versions of this document. 2. Purpose of this Policy/Procedure 2.1. The aim of this policy is to provide guidance for all healthcare professionals involved in the delivery of acute NIV and to ensure that this is done both safely and effectively. This policy has been written in keeping with national evidence-based guidelines 2,3 This policy is not intended for patients on long-term domicillary NIV. 3. Scope 3.1. This policy is intended for healthcare professionals involved in the decision to implement NIV (clinicians) and those delivering NIV (clinicians, trained staff). 4. Definitions / Glossary 4.1. The following abbreviations will be used throughout this document ABG Arterial blood gas NIV Non-invasive ventilation IPPV Invasive positive pressure ventilation BiPAP Bilevel positive pressure ventilation CPAP Continuous positive pressure ventilation CCU Coronary Care Unit ph ph PaO2 Arterial oxygen tension PaCO2 Arterial carbon dioxide tension PtCO2 Transcutaneous carbon dioxide HR Heart rate RR Respiratory rate 4.2. The following terms will be used throughout this document 4.3. BiPAP Focus, BiPAP Vision and BiPAP V60 are the three types of ventilator used outside of critical care. It is mandatory for all staff delivering NIV to undergo training. Appendix 3, provides details on each separate ventilator which can be used as a reference. 5. Ownership and Responsibilities 5.1. This guideline has been developed by Dr Meme Wijesinghe, consultant chest physician, RCHT with input from the other four RCHT chest physicians (Jon Myers, Ian Coutts, Stephen Iles, Lisa Hosking). It has been based on standards set by the British Thoracic Society and Royal College of Physicians2,3 Page 3 of 17
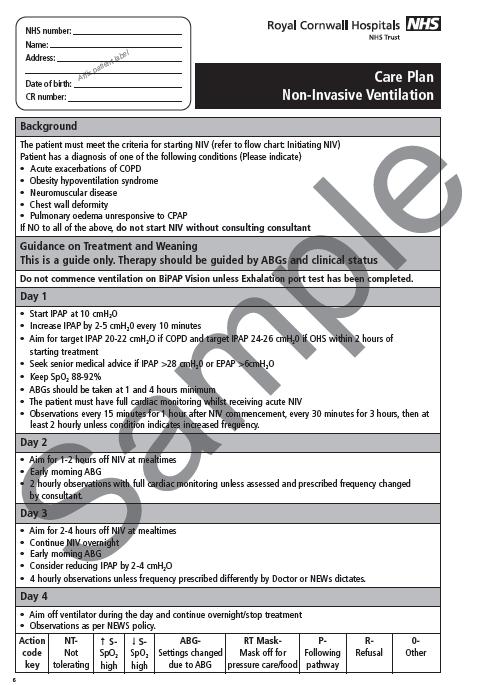
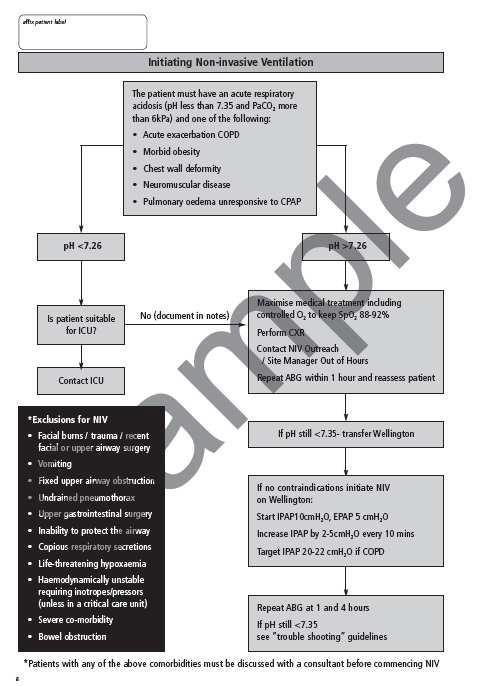
4 5.2. It has been endorsed by Critical Care and the Emergency Medicine Department Role of the Managers Line managers are responsible for: Ensuring the policy is adhered to Provisions are made to deliver the service 5.4. Role of Individual Staff All staff members are responsible for: Delivering safe and effective NIV as stated in the policy Ensuring they are up-to-date with training and competencies 6. Standards and Practice 6.1. Selection criteria 6.2. The RCHT NIV care plan and pathway (appendix 4) must be followed and completed from selection of patients for NIV, initiation of treatment and monitoring whilst on NIV. This must be signed by the clinician and nursing staff delivering NIV Prior to starting NIV, patients must receive immediate maximum standard medical treatment which should include controlled oxygen therapy in all patients to keep SpO % (refer to Emergency Oxygen Policy) for no more than one hour If a respiratory acidosis (PaCO2>6kPa, ph < ) persists in the following patients, NIV should be considered: Acute exacerbations of COPD Obesity hypoventilation syndrome Neuromuscular disease Chest wall deformity Cardiogenic pulmonary oedema unresponsive to CPAP 6.5. They must also meet the following inclusion and exclusion criteria 6.6. Inclusion Criteria for NIV Sick but not moribund *Able to protect airway *Conscious and cooperative No excessive respiratory secretions Potential for recovery to quality of life acceptable to the patient Patient s wishes considered Page 4 of 17
5 6.7. *Consider NIV if unconscious and endo-tracheal intubation deemed inappropriate or NIV is to be provided in a critical care setting. There are data to support the use of NIV in patients who are in a state of coma secondary to hypercapnoea and who respond rapidly to this treatment 6.8. Exclusion criteria for NIV facial burns/trauma/recent facial or upper airway surgery vomiting fixed upper airway obstruction undrained pneumothorax upper gastrointestinal surgery inability to protect the airway copious respiratory secretions life-threatening hypoxaemia haemodynamically unstable requiring inotropes/pressors (unless in a critical care unit) severe co-morbidity confusion/agitation bowel obstruction Patients with any of the above comorbidities should be discussed with the consultant responsible for the patient (critical care, cardiology, respiratory, medicine) before commencing NIV. NIV may be commenced if deemed to be appropriate in individual situations Patients with a ph <7.26 should be discussed with Critical Care if deemed appropriate by the admitting clinician Set Up Location Acute NIV should only be delivered in the following areas: Emergency Department, Critical Care, Wellington Ward and Coronary Care Unit. For those patients in the ED who require NIV, a bed should be identified on Wellington, Critical or CCU and the patient must be transferred as soon as possible. During office hours (Monday to Friday 0830 to 1630) the NIV outreach physio should be contacted on bleep All patients should be on a cardiac monitor for the first 24 hours of treatment Patients on CCU who are in pulmonary oedema and do not respond to standard medical treatment should be commenced on CPAP first and only put on BiPAP if they fail to respond. Where possible, only patient with pulmonary oedema should be managed on CCU, all other patients should be managed on Critical Care or Wellington. If there are no beds available on Critical Care or Wellington, non-cardiac patients on NIV should be under the care of a nominated respiratory consultant If NIV is initiated elsewhere in the hospital, the NIV outreach team, critical care outreach or other appropriately trained staff (site coordinator, hospital at night) will need to remain with the patient until a bed is identified on Wellington, Critical Care or CCU. If patients develop acute hypercapnic respiratory failure at any site outside Page 5 of 17
6 Treliske their medical management should be optimised and if NIV is deemed appropriate they should be transferred to Treliske Continuous positive pressure airway ventilation (CPAP), is outside the scope of this policy, but should only be delivered on the coronary care unit or Critical Care Decision to start treatment The decision to commence NIV should only be made by a doctor of ST level 2 or above. The initiation of NIV should only be performed by a health care professional trained and competent in the set-up of NIV. All patients initiated on NIV should be reviewed by a respiratory physician as soon as is practicable. The patient s consent should be sought wherever possible. Written information about NIV should be provided to patients and/or the relatives (See patient information leaflet: NIV The Treatment Explained) All patients must have a CXR to exclude a pneumothorax or other comorbidity excluding them from NIV. If a pneumothorax is identified it must be drained prior to starting treatment Mask fit and positioning The patient should be in a sitting leaning forward, or semi-recumbent position when started on NIV. Mask size should be assessed using the templates provided with the masks. A full-face mask should be used for most patients for the first 24 hours followed by switch to a nasal mask for patient comfort when requested. Only Respironics masks and disposables should be used Ventilators and starting pressures Only Respironics Vision, Focus and V60 machines are to be used in the trust. All machines used outside of Critical Care must be fitted with a red plug. Plugs should be only removed by a member of staff who has been fully trained in the use of NIV Patients should be commenced on an initial inspiratory positive airway pressure (IPAP) of 10cms H2O and expiratory positive airway pressure (EPAP) of 5cms H2O. These pressures may not significantly improve gas exchange but allow acclimatization of the patient to the machine. The IPAP should be gradually increased by 2-5cm increments at a rate of approximately 5 cms H2O each 10 minutes until a therapeutic response is achieved or patient tolerability has been reached. An IPAP of 20cmH2O should be therapeutic in most patients, but should be assessed with ABGs. Patients who are morbidly obese are likely to need a higher target IPAP Other treatments Oxygen should be entrained to achieve a saturation of 88-92%. The BiPAP Vision and BiPAP V60 allows a precise fraction of inspired oxygen to be delivered, whereas the BiPAP Focus provides a variable oxygen concentration. Oxygen should not be directly entrained into the mask as lower oxygen concentrations are delivered to the patient. Page 6 of 17
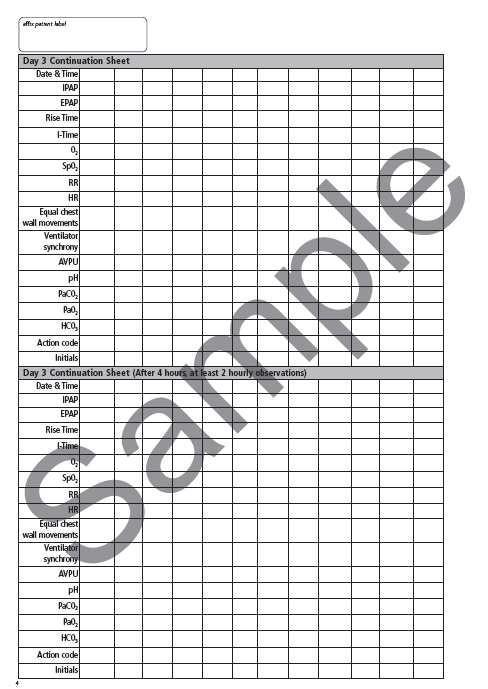
7 6.26. Bronchodilators should preferably be administered off NIV but may be administered on NIV and when so should be entrained between the expiration port and the face mask. Delivery of both oxygen and nebulised solutions is affected by NIV pressure settings Non-invasive ventilation can be used with a naso-gastric tube in place, in which case this should be a fine bore tube to minimise mask leakage Infection Control Equipment should be cleaned according to manufacturer and Infection Control guidelines. A bacterial filter must be attached to the ventilator outlet port. This should be changed between patients and at 24 hour intervals. The filters in the machine s air entrainment mechanism should be changed when visibly dirty and between patients. Single patient use items should not be reused and should be disposed of appropriately. A system should be in place to enable traceability of equipment e.g. in the event of product failure to enable recall of equipment Monitoring All patients receiving NIV require continuous cardiac monitoring for the first 24 hours of treatment. Thereafter the need for cardiac monitoring should be risk assessed RR, HR, level of consciousness, chest wall movement, ventilator synchrony, accessory muscle use, patient comfort, and SpO2 must be monitored and recorded at the following intervals: First hour: every 15 minutes 1-4 hours: every 30 minutes 4-12 hours: every 1 hour After 12 hours of treatment patients should have hourly observations whilst on NIV but this can be reduced in accordance with the NEWS policy whilst off NIV Observations must be recorded on the NIV Care Plan in addition to the NEWS chart A clinical assessment of mask fit to include skin condition and degree of leak (particularly onto the corneas) should be performed at the same time As a standard ABG should be taken and used to assist in the management plan at 4 hours or earlier if judged clinically necessary and again at 12 hours unless the clinical improvement in the patient obviates the need for further ABG analysis Escalation At the initiation of treatment there must be a written plan if NIV fails. This should include whether escalation of care is indicated or whether NIV is the ceiling of treatment and whether the patient is for resuscitation or specific palliative care measures. If the patient is deemed not for resuscitation, an Allow Natural Death Order needs to be completed and communicated to all relevant staffing members in keeping with the AND policy. Page 7 of 17
8 6.38. Treatment Duration and Weaning from Ventilation Treatment duration Patients who appear to benefit from NIV during the first few hours of treatment should receive NIV for as long as possible (minimum of 6 hours) with appropriate breaks for oral intake, nebulisers etc, during the first 24 hours. Attention should be paid to skin care on the bridge of the nose during this period. In patients in whom NIV is successful (ph 7.35 achieved, resolution of underlying cause and symptoms, respiratory rate normalised) following an appropriate duration of treatment, it is appropriate to start a weaning plan. Gradual reduction of the duration of NIV should be determined by clinical improvement Weaning Initially weaning should be during the day with extended periods off the ventilator for meals, physiotherapy, nebulised therapy etc. Patients may require continued ventilation overnight if stable during the day. Early morning ABGs are required to monitor gas exchange. Most patients should be weaned within 2-3 days Palliation Palliation of symptoms is appropriate in patients in whom standard medical treatment and NIV fails or where patients have chosen not to receive this treatment and where a decision has been made and documented not to escalate to intubation and mechanical ventilation. In exceptional circumstances NIV may be continued to palliate breathlessness, but should not be initiated for this reason. Opioids and benzodiazepines can be used to treat breathlessness in this situation. Initiation of palliative care pathways should where possible include appropriate discussion with the patient and family Trouble Shooting See appendix Dissemination and Implementation 7.1. This policy will be disseminated throughout all relevant areas in the trust through lead clinicians, ward managers/sisters and managers 7.2. Provision of training is provided by consultant respiratory physicians and the Learning and Development department. Training is mandatory for all staff delivering NIV. 8. Monitoring compliance and effectiveness Element to be monitored Lead Tool Frequency All aspects of the NIV service in keeping with standards set by the British Thoracic Society (see website) Dr Meme Wijesinghe British Thoracic Society (see website) Annually Page 8 of 17
9 Reporting arrangements Acting on recommendations and Lead(s) Change in practice and lessons to be shared A report is generated annually. This will allow us to benchmark our practice with the rest of the country. Dr Meme Wijesinghe will disseminate audit results If deficiencies are identified, Dr Wijesinghe will identify how changes can be actioned and improvements to the service implemented 9. Updating and Review 9.1. This policy will be reviewed every three years 10. Equality and Diversity This document complies with the Royal Cornwall Hospitals NHS Trust service Equality and Diversity statement which can be found in the 'Equality, Diversity & Human Rights Policy' or the Equality and Diversity website Equality Impact Assessment The Initial Equality Impact Assessment Screening Form is at Appendix References 1. Ram FS, Picot J, Lightowler J, et al. Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2004;3:CD British Thoracic Society Standards of Care Committee. Non-invasive ventilation in acute respiratory failure. Thorax. 2002;57: Roberts, C.M.; Brown, J.L.; Reinhardt, A.K.; Kaul, S.; Scales, K.; Mikelsons, C.; Reid, K.; Winter, R.; Young, K.; Restrick, L.; Plant, P.K. Non-invasive ventilation in chronic obstructive pulmonary disease: management of acute type 2 respiratory failure. Clinical Medicine, Journal of the Royal College of Physicians, Volume 8, Number 5, October 2008, pp (5) Page 9 of 17
10 Appendix 1. Governance Information Document Title Date Issued/Approved: 13 Jun 14 Date Valid From: 13 Jun 14 Date Valid To: 13 Jun 17 The Use of Non-Invasive Ventilation in Patients with Acute Type 2 Respiratory Failure Directorate / Department responsible (author/owner): Meme Wijesinghe, Respiratory Medicine Consultant Contact details: Brief summary of contents The aim of this policy is to provide guidance for all healthcare professionals involved in the delivery of NIV and to ensure that this is done both safely and effectively. Suggested Keywords: Ventilation, Respiratory Failure,. Target Audience Executive Director responsible for Policy: RCHT PCH CFT KCCG Medical Director Date revised: 13 Jun 14 This document replaces (exact title of previous version): Approval route (names of committees)/consultation: Divisional Manager confirming approval processes The Use of Non-Invasive Ventilation in Patients with Acute Type 2 Respiratory Failure Robert Taylor, Consultant in Emergency Medicine Jonathan Paddle, Consultant in Critical Care Audrius Simiatis, Consultant Cardiologist Bruce Daniels Name and Post Title of additional signatories Signature of Executive Director giving approval Publication Location (refer to Policy on Policies Approvals and Ratification): Document Library Folder/Sub Folder Links to key external standards Related Documents: Training Need Identified? Not Required {Original Copy Signed} Internet & Intranet Intranet Only Clinical / Respiratory None None No Page 10 of 17
11 Version Control Table Date Version No 30 Oct 12 V1.0 Initial Issue 13 Jun 14 V2.0 Complete rewrite. Summary of Changes Changes Made by (Name and Job Title) Meme Wijesinghe, Respiratory Medicine Consultant Meme Wijesinghe, Respiratory Medicine Consultant All or part of this document can be released under the Freedom of Information Act 2000 This document is to be retained for 10 years from the date of expiry. This document is only valid on the day of printing Controlled Document This document has been created following the Royal Cornwall Hospitals NHS Trust Policy on Document Production. It should not be altered in any way without the express permission of the author or their Line Manager. Page 11 of 17
12 Appendix 2. Initial Equality Impact Assessment Form Name of the strategy / policy /proposal / service function to be assessed (hereafter referred to as policy) (Provide brief description): The Use of Non-Invasive Ventilation in Patients with Acute Type 2 Respiratory Failure Directorate and service area: Clinical / Is this a new or existing Policy? New Respiratory Name of individual completing Telephone: assessment: Meme Wijesinghe 1. Policy Aim* Who is the strategy / policy / proposal / service function aimed at? 2. Policy Objectives* See section 2. The aim of this policy is to provide guidance for all healthcare professionals involved in the delivery of NIV and to ensure that this is done both safely and effectively. 3. Policy intended Outcomes* 4. *How will you measure the outcome? 5. Who is intended to benefit from the policy? 6a) Is consultation required with the workforce, equality groups, local interest groups etc. around this policy? See section 6. See section 8. All NIV patients. No b) If yes, have these *groups been consulted? C). Please list any groups who have been consulted about this procedure. 7. The Impact Please complete the following table. Are there concerns that the policy could have differential impact on: Equality Strands: Yes No Rationale for Assessment / Existing Evidence Age Page 12 of 17
13 Sex (male, female, transgender / gender reassignment) Race / Ethnic communities /groups Disability - Learning disability, physical disability, sensory impairment and mental health problems Religion / other beliefs Marriage and civil partnership Pregnancy and maternity Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian You will need to continue to a full Equality Impact Assessment if the following have been highlighted: You have ticked Yes in any column above and No consultation or evidence of there being consultation- this excludes any policies which have been identified as not requiring consultation. or Major service redesign or development 8. Please indicate if a full equality analysis is recommended. Yes No 9. If you are not recommending a Full Impact assessment please explain why. Signature of policy developer / lead manager / director Date of completion and submission Names and signatures of members carrying out the Screening Assessment 1. Meme Wijesinghe 2. Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead, c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa, Truro, Cornwall, TR1 3HD A summary of the results will be published on the Trust s web site. Signed Date Page 13 of 17


14 Appendix 3. RCHT care plan and pathway Page 14 of 17

15 Page 15 of 17

16 Page 16 of 17

17 Page 17 of 17
Clinical Guideline for Post-Operative Nausea and Vomiting 1. Aim/Purpose of this Guideline
 Clinical Guideline for Post-Operative Nausea and Vomiting 1. Aim/Purpose of this Guideline 1.1. The purpose of this guideline is to provide anaesthetists with an algorithm to work with when dealing with
Clinical Guideline for Post-Operative Nausea and Vomiting 1. Aim/Purpose of this Guideline 1.1. The purpose of this guideline is to provide anaesthetists with an algorithm to work with when dealing with
CLINICAL GUIDELINE FOR THE MANAGEMENT OF SEPSIS IN ADULT PATIENTS 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR THE MANAGEMENT OF SEPSIS IN ADULT PATIENTS 1. Aim/Purpose of this Guideline 1.1. This guideline aims to improve outcomes for patients presenting with sepsis or developing sepsis
CLINICAL GUIDELINE FOR THE MANAGEMENT OF SEPSIS IN ADULT PATIENTS 1. Aim/Purpose of this Guideline 1.1. This guideline aims to improve outcomes for patients presenting with sepsis or developing sepsis
CLINICAL GUIDELINE FOR REFERRAL TO PAIN SERVICE 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR REFERRAL TO PAIN SERVICE 1. Aim/Purpose of this Guideline To provide guidance for appropriate referral to the acute pain service for in-patient review. 2. The Guidance PAIN SERVICES
CLINICAL GUIDELINE FOR REFERRAL TO PAIN SERVICE 1. Aim/Purpose of this Guideline To provide guidance for appropriate referral to the acute pain service for in-patient review. 2. The Guidance PAIN SERVICES
Loading Dose Worksheet for Oral Amiodarone
 This applies to adult patients only Key: General Notes ED/MAU/SRU/Acute GP/Amb-Care GP/SWASFT In-patient wards Start Prescribe as per loading dose worksheet below End 1. Aim/Purpose of this Guideline 1.1.
This applies to adult patients only Key: General Notes ED/MAU/SRU/Acute GP/Amb-Care GP/SWASFT In-patient wards Start Prescribe as per loading dose worksheet below End 1. Aim/Purpose of this Guideline 1.1.
CLINICAL GUIDELINE FOR THE ADMISSION OF PATIENTS TO PAEDIATRIC HIGH DEPENDANCY UNIT V4.0
 CLINICAL GUIDELINE FOR THE ADMISSION OF PATIENTS TO PAEDIATRIC HIGH DEPENDANCY UNIT V4.0 Page 1 of 13 Abbreviation (P/A)HDU (P/A)ICU GCS IPPV CPAP BiPAP DKA Reg Meaning (Paediatric/Adult) High Dependency
CLINICAL GUIDELINE FOR THE ADMISSION OF PATIENTS TO PAEDIATRIC HIGH DEPENDANCY UNIT V4.0 Page 1 of 13 Abbreviation (P/A)HDU (P/A)ICU GCS IPPV CPAP BiPAP DKA Reg Meaning (Paediatric/Adult) High Dependency
Diagnostic Testing Procedures in Urodynamics V3.0
 V3.0 09 01 18 Table of Contents Summary.... 1. Introduction... 3 1.1. Diagnostic testing information... 3 2. Purpose of this Policy/Procedure... 3 2.1. Approved Document Process... 3 3. Scope... 3 3.1.
V3.0 09 01 18 Table of Contents Summary.... 1. Introduction... 3 1.1. Diagnostic testing information... 3 2. Purpose of this Policy/Procedure... 3 2.1. Approved Document Process... 3 3. Scope... 3 3.1.
Policy for the authorising of blood components by the Haematology Clinical Nurse Specialist V1.0
 Policy for the authorising of blood components by the Haematology Clinical Nurse Specialist V1.0 January 2016 Summary. This policy applies only to selected staff within the Haematology Department at the
Policy for the authorising of blood components by the Haematology Clinical Nurse Specialist V1.0 January 2016 Summary. This policy applies only to selected staff within the Haematology Department at the
CLINICAL GUIDELINE FOR THE ASSESSMENT AND DOCUMENTATION OF PAIN (ADULTS)
") CLINICAL GUIDELINE FOR THE ASSESSMENT AND DOCUMENTATION OF PAIN (ADULTS) 1. Aim/Purpose of this Guideline 1.1. Pain is whatever the experiencing person says it is, existing whenever the experiencing person
CLINICAL GUIDELINE FOR THE ASSESSMENT AND DOCUMENTATION OF PAIN (ADULTS) 1. Aim/Purpose of this Guideline 1.1. Pain is whatever the experiencing person says it is, existing whenever the experiencing person
Diagnostic Test Reporting & Acknowledgement Procedures. - Pathology & Clinical Imaging
 Diagnostic Test Reporting & Acknowledgement Procedures V2.0 November 2014 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5.
Diagnostic Test Reporting & Acknowledgement Procedures V2.0 November 2014 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5.
Policy on Governance Arrangements Relating to Medicines V2.0
 V2.0 August 2015 Summary. The policy outlines the governance arrangements for medicines within the Trust, specifically; 1. The committee structure in the Trust and the county for medicine related matters
V2.0 August 2015 Summary. The policy outlines the governance arrangements for medicines within the Trust, specifically; 1. The committee structure in the Trust and the county for medicine related matters
The initial care and management of patients admitted to RCHT with a Ventricular Assist Device (VAD). V2.0
. V2.0") The initial care and management of patients admitted to RCHT with a Ventricular Assist Device (VAD). V2.0 October 2016 Summary. Start See section 6.2 of this document for important information regarding
The initial care and management of patients admitted to RCHT with a Ventricular Assist Device (VAD). V2.0 October 2016 Summary. Start See section 6.2 of this document for important information regarding
CLINICAL GUIDELINE FOR: Management of low-risk upper GI haemorrhage. Page 1 of 10. Management of low-risk upper GI haemorrhage
 CLINICAL GUIDELINE FOR: Page 1 of 10 Summary AGE
CLINICAL GUIDELINE FOR: Page 1 of 10 Summary AGE
OXYGEN THERAPY AND SATURATION MONITORING OF THE NEONATE - CLINICAL GUIDELINE V3.0
 OYGEN THERAPY AND SATURATION MONITORING OF THE NEONATE - CLINICAL GUIDELINE V3.0 1. Aim/Purpose of this Guideline 1.1 To provide guidance on the assessment and management of infants requiring oxygen therapy
OYGEN THERAPY AND SATURATION MONITORING OF THE NEONATE - CLINICAL GUIDELINE V3.0 1. Aim/Purpose of this Guideline 1.1 To provide guidance on the assessment and management of infants requiring oxygen therapy
CLINICAL GUIDELINE FOR USE OF BED AND CHAIR SENSOR ALARM MATS FOR PREVENTING FALLS IN ADULT PATIENTS
 CLINICAL GUIDELINE FOR USE OF BED AND CHAIR SENSOR ALARM MATS FOR PREVENTING FALLS IN ADULT PATIENTS 1. Aim/Purpose of this Guideline This guideline is to support the use of bed and chair sensor alarm
CLINICAL GUIDELINE FOR USE OF BED AND CHAIR SENSOR ALARM MATS FOR PREVENTING FALLS IN ADULT PATIENTS 1. Aim/Purpose of this Guideline This guideline is to support the use of bed and chair sensor alarm
CLINICAL GUIDELINE FOR THE USE OF INTRAVENOUS SLIDING SCALE REGIMEN FOR ADULTS 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR THE USE OF INTRAVENOUS SLIDING SCALE REGIMEN FOR ADULTS 1. Aim/Purpose of this Guideline This guideline is for the management of for the management of Adult patients with Mellitus
CLINICAL GUIDELINE FOR THE USE OF INTRAVENOUS SLIDING SCALE REGIMEN FOR ADULTS 1. Aim/Purpose of this Guideline This guideline is for the management of for the management of Adult patients with Mellitus
A list of authorised referrers will be retained by the Colposcopy team and the Clinical Imaging Department.
 Clinical Guideline for Clinical Imaging Referral Protocol for Nurse Colposcopist within Colposcopy Dept. Royal Cornwall Hospital 1. Aim/Purpose of this Guideline 1.1 This protocol applies to Nurse Colposcopist
Clinical Guideline for Clinical Imaging Referral Protocol for Nurse Colposcopist within Colposcopy Dept. Royal Cornwall Hospital 1. Aim/Purpose of this Guideline 1.1 This protocol applies to Nurse Colposcopist
Clinical Guideline for Nurse-Led Indocyanine Green Angiography Summary.
 Clinical Guideline for Nurse-Led Indocyanine Green Angiography Summary. Obtain brief medical history including allergies & renal function. Informed verbal consent gained and documented and procedure and
Clinical Guideline for Nurse-Led Indocyanine Green Angiography Summary. Obtain brief medical history including allergies & renal function. Informed verbal consent gained and documented and procedure and
CLINICAL GUIDELINE FOR THE USE OF RECTUS SHEATH CATHETERS IN CHILDREN. 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR THE USE OF RECTUS SHEATH CATHETERS IN CHILDREN. 1. Aim/Purpose of this Guideline 1.1. Guidelines for the use of rectus sheath catheters for the management of pain following laparotomy
CLINICAL GUIDELINE FOR THE USE OF RECTUS SHEATH CATHETERS IN CHILDREN. 1. Aim/Purpose of this Guideline 1.1. Guidelines for the use of rectus sheath catheters for the management of pain following laparotomy
CLINICAL GUIDELINE FOR IPRATROPIUM BROMIDE NEBULISER INHALER PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR IPRATROPIUM BROMIDE NEBULISER INHALER PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline 1.1. This Patient Group Direction (PGD) applies to all nursing and clinical
CLINICAL GUIDELINE FOR IPRATROPIUM BROMIDE NEBULISER INHALER PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline 1.1. This Patient Group Direction (PGD) applies to all nursing and clinical
Clinical Guideline for Clinical Imaging Referral Protocol for Upper & Lower GI Non medical Endoscopist within RCHT. 1. Aim/Purpose of this Guideline
 Clinical Guideline for Clinical Imaging Referral Protocol for Upper & Lower GI Non medical Endoscopist. 1. Aim/Purpose of this Guideline 1.1 This protocol applies to upper & lower GI Non medical Endoscopist
Clinical Guideline for Clinical Imaging Referral Protocol for Upper & Lower GI Non medical Endoscopist. 1. Aim/Purpose of this Guideline 1.1 This protocol applies to upper & lower GI Non medical Endoscopist
CLINICAL GUIDELINE FOR CLINICAL IMAGING REFERRAL PROTOCOL FOR NURSE SPECIALISTS IN HEART FUNCTION WITHIN RCHT Summary. Start
 CLINICAL GUIDELINE FOR CLINICAL IMAGING REFERRAL PROTOCOL FOR NURSE SPECIALISTS IN HEART FUNCTION WITHIN RCHT Summary. Start The non-medical practitioner has received sufficient training to make clinical
CLINICAL GUIDELINE FOR CLINICAL IMAGING REFERRAL PROTOCOL FOR NURSE SPECIALISTS IN HEART FUNCTION WITHIN RCHT Summary. Start The non-medical practitioner has received sufficient training to make clinical
1.3 Referrer: in the context of this protocol the term referrer refers to a health care worker who is authorised to refer individuals for X-rays.
 Clinical Guideline for Clinical Imaging Referral Protocol for Nurse Endoscopist (Lower GI) within the Royal Cornwall Hospitals Trust 1. Aim/Purpose of this Guideline 1.1 This protocol applies to Nurse
Clinical Guideline for Clinical Imaging Referral Protocol for Nurse Endoscopist (Lower GI) within the Royal Cornwall Hospitals Trust 1. Aim/Purpose of this Guideline 1.1 This protocol applies to Nurse
PARACETAMOL PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline
 PARACETAMOL PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline 1.1. This Patient Group Direction (PGD) applies to all nursing and clinical staff in the Child Health Department and its
PARACETAMOL PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline 1.1. This Patient Group Direction (PGD) applies to all nursing and clinical staff in the Child Health Department and its
School Vision Screening Policy V2.0
 School Vision Screening Policy V2.0 05 April 2016 Summary. Vision screening test in school PASS Visual acuity LogMAR 0.2 both eyes Kays 0.1 both eyes Outcome letter sent home Test result information put
School Vision Screening Policy V2.0 05 April 2016 Summary. Vision screening test in school PASS Visual acuity LogMAR 0.2 both eyes Kays 0.1 both eyes Outcome letter sent home Test result information put
Tissue Viability Referral Pathway. April 2017
 Tissue Viability Referral Pathway V4 April 2017 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities...
Tissue Viability Referral Pathway V4 April 2017 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities...
WARD CLOSURE POLICY V
 WARD CLOSURE POLICY V3.0 29.07.15 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 4 5.1.
WARD CLOSURE POLICY V3.0 29.07.15 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 4 5.1.
IBUPROFEN PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline
 IBUPROFEN PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline 1.1. This Patient Group Direction (PGD) applies to all nursing and clinical staff in the Child Health Department and its
IBUPROFEN PATIENT GROUP DIRECTION CHILD HEALTH 1. Aim/Purpose of this Guideline 1.1. This Patient Group Direction (PGD) applies to all nursing and clinical staff in the Child Health Department and its
CLINICAL IMAGING REFERRAL PROTOCOL FOR REGISTERED NURSE PRACTITIONERS IN THE EMERGENCY DEPARTMENT, URGENT CARE CENTRE AND AMBULATORY CARE
 CLINICAL IMAGING REFERRAL PROTOCOL FOR REGISTERED NURSE PRACTITIONERS IN THE EMERGENCY DEPARTMENT, URGENT CARE CENTRE AND AMBULATORY CARE CLINICAL GUIDELINE V4. Summary. Start The non-medical practitioner
CLINICAL IMAGING REFERRAL PROTOCOL FOR REGISTERED NURSE PRACTITIONERS IN THE EMERGENCY DEPARTMENT, URGENT CARE CENTRE AND AMBULATORY CARE CLINICAL GUIDELINE V4. Summary. Start The non-medical practitioner
Safe Bathing Policy V1.3
 V1.3 April 2018 Summary Safe hot water temperatures The hot water distribution temperatures, which are required for the control and prevention of Legionella, can lead to discharge temperatures in excess
V1.3 April 2018 Summary Safe hot water temperatures The hot water distribution temperatures, which are required for the control and prevention of Legionella, can lead to discharge temperatures in excess
This guideline is for nursing staff within the Pain Services assisting with the administration of botulinum toxin.
 CLINICAL GUIDELINE FOR THE SAFE ADMINISTRATION OF BOTULINUM NEURO TOIN FOR INJECTION within the PAIN SERVICE. Botox and eomin (trade names) 1. Aim/Purpose of this Guideline This guideline is for nursing
CLINICAL GUIDELINE FOR THE SAFE ADMINISTRATION OF BOTULINUM NEURO TOIN FOR INJECTION within the PAIN SERVICE. Botox and eomin (trade names) 1. Aim/Purpose of this Guideline This guideline is for nursing
CLINICAL GUIDELINE FOR THE EMERGENCY DEFILL OF AN ADJUSTABLE GASTRIC BAND
 CLINICAL GUIDELINE FOR THE EMERGENCY DEFILL OF AN ADJUSTABLE GASTRIC BAND 1. Aim/Purpose of this Guideline The aim of this guideline to enable the effective care of patients needing emergency defill of
CLINICAL GUIDELINE FOR THE EMERGENCY DEFILL OF AN ADJUSTABLE GASTRIC BAND 1. Aim/Purpose of this Guideline The aim of this guideline to enable the effective care of patients needing emergency defill of
2.1. Applicable areas: Royal Cornwall Hospitals Trust; Neonatal Unit and Delivery Suite
 ADVANCED NEONATAL NURSE PRACTITIONERS (ANNPs) BLOOD COMPONENT AND BLOOD PRODUCT REQUESTING PROTOCOL NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1 The purpose of this protocol is to guide
ADVANCED NEONATAL NURSE PRACTITIONERS (ANNPs) BLOOD COMPONENT AND BLOOD PRODUCT REQUESTING PROTOCOL NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1 The purpose of this protocol is to guide
2.1. It is essential that promoting and safeguarding the welfare of children and young people is integral to all NHS Trust policies and procedures.
 Was Not Brought, Cancellation and Refusal of Appointments Policy for Children and Young People up to the Age of 18 Years (up to the age of 25 years for people with a Learning Disability) 1. Aim/Purpose
Was Not Brought, Cancellation and Refusal of Appointments Policy for Children and Young People up to the Age of 18 Years (up to the age of 25 years for people with a Learning Disability) 1. Aim/Purpose
Newborn Hearing Screening Programme Policy
 Newborn Hearing Screening Programme Policy V3.0 December 2015 Page 1 of 16 Summary - Screening Pathway for Newborn Hearing Screening Newborn hearing screening Check eligibility Eligible for screening Not
Newborn Hearing Screening Programme Policy V3.0 December 2015 Page 1 of 16 Summary - Screening Pathway for Newborn Hearing Screening Newborn hearing screening Check eligibility Eligible for screening Not
Procedure for the Application of a Cast and its subsequent care V1.3
 Procedure for the Application of a Cast and its subsequent care V1.3 May 2015 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary...
Procedure for the Application of a Cast and its subsequent care V1.3 May 2015 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary...
Diagnostic Testing Procedures in Neurophysiology V1.0
 V1.0 10 September 2012 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the
V1.0 10 September 2012 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the
Diagnostic Testing Procedures for Ophthalmic Science
 V4.0 01/08/17 Table of Contents 1. Introduction... 3 2. Purpose of this Policy... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the Managers... 3 5.3.
V4.0 01/08/17 Table of Contents 1. Introduction... 3 2. Purpose of this Policy... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the Managers... 3 5.3.
ESCALATION PLAN PAEDIATRICS AND NEONATAL UNIT 1. Aim/Purpose of this Guideline
 ESCALATION PLAN PAEDIATRICS AND NEONATAL UNIT 1. Aim/Purpose of this Guideline 1.1. This guidance is designed to aid staff to monitor capacity and staffing in Child Health. 2. The Guidance 2.1. The majority
ESCALATION PLAN PAEDIATRICS AND NEONATAL UNIT 1. Aim/Purpose of this Guideline 1.1. This guidance is designed to aid staff to monitor capacity and staffing in Child Health. 2. The Guidance 2.1. The majority
Safeguarding Children Supervision Policy V4.0. November 2016
 Safeguarding Children Supervision Policy V4.0 November 2016 Page 1 of 20 Summary Part 1 Part 2 Safeguarding supervision for Nursing and Midwifery staff, Paediatricians, Medical Staff and other Allied Health
Safeguarding Children Supervision Policy V4.0 November 2016 Page 1 of 20 Summary Part 1 Part 2 Safeguarding supervision for Nursing and Midwifery staff, Paediatricians, Medical Staff and other Allied Health
MANAGEMENT OF HEREDITARY SPHEROCYTOSIS IN THE NEONATAL PERIOD CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline
 MANAGEMENT OF HEREDITARY SPHEROCYTOSIS IN THE NEONATAL PERIOD CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1 This guideline aimed at all clinical staff responsible for the management of infants
MANAGEMENT OF HEREDITARY SPHEROCYTOSIS IN THE NEONATAL PERIOD CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1 This guideline aimed at all clinical staff responsible for the management of infants
Health and Safety Policy and Guidance for Staff Working During Night Time Hours V2.0
 Health and Safety Policy and Guidance for Staff Working During Night Time Hours V2.0 January 2016 Summary Purpose of the document: The purpose of this policy is to provide an outline of the requirements
Health and Safety Policy and Guidance for Staff Working During Night Time Hours V2.0 January 2016 Summary Purpose of the document: The purpose of this policy is to provide an outline of the requirements
CEREBRAL FUNCTION MONITORING (aeeg). NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline
. NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline") CEREBRAL FUNCTION MONITORING (aeeg). NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1. To provide guidance on the operation and interpretation of Cerebral Function Monitoring (CFM) in neonates.
CEREBRAL FUNCTION MONITORING (aeeg). NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1. To provide guidance on the operation and interpretation of Cerebral Function Monitoring (CFM) in neonates.
Patient Experience Strategy
 POLICY UNDER REVIEW Please note that this policy is under review. It does, however, remain current Trust policy subject to any recent legislative changes, national policy instruction (NHS or Department
POLICY UNDER REVIEW Please note that this policy is under review. It does, however, remain current Trust policy subject to any recent legislative changes, national policy instruction (NHS or Department
Occupational Health Surveillance Policy V2.1
 Occupational Health Surveillance Policy V2.1 May 2016 Table of Contents 1. Introduction... 2 2. Purpose of this Policy... 2 3. Scope... 2 4. Definitions/Glossary... 3 5. Ownership and Responsibilities...
Occupational Health Surveillance Policy V2.1 May 2016 Table of Contents 1. Introduction... 2 2. Purpose of this Policy... 2 3. Scope... 2 4. Definitions/Glossary... 3 5. Ownership and Responsibilities...
PRESCRIBING, DISPENSING AND ADMINISTRATION OF CHEMOTHERAPY TO CHILDREN AND YOUNG PEOPLE - CLINICAL GUIDELINE V4.0
 PRESCRIBING, DISPENSING AND ADMINISTRATION OF CHEMOTHERAPY TO CHILDREN AND YOUNG PEOPLE - CLINICAL GUIDELINE V4.0 Clinical Guideline Template Page 1 of 14 1. Aim/Purpose of this Guideline 1.1. This guideline
PRESCRIBING, DISPENSING AND ADMINISTRATION OF CHEMOTHERAPY TO CHILDREN AND YOUNG PEOPLE - CLINICAL GUIDELINE V4.0 Clinical Guideline Template Page 1 of 14 1. Aim/Purpose of this Guideline 1.1. This guideline
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Questions. Background to the ICNARC Case Mix Programme
 Number of admissions, unit length of stay and days of mechanical ventilation for admissions with blunt chest trauma to critical care in England, Wales and Northern Ireland Questions What were the number,
Number of admissions, unit length of stay and days of mechanical ventilation for admissions with blunt chest trauma to critical care in England, Wales and Northern Ireland Questions What were the number,
A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs.
 6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
RCHT Non-Ionising Radiation Safety Policy
 V3.0 June 2015 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 4 4. Definitions / Glossary... 5 5. Ownership and Responsibilities... 5 6. Standards and Practice...
V3.0 June 2015 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 4 4. Definitions / Glossary... 5 5. Ownership and Responsibilities... 5 6. Standards and Practice...
Unit length of stay and APACHE II scores for ventilated admissions to critical care in England, Wales and Northern Ireland
 Unit length of stay and APACHE II scores for ventilated admissions to critical care in England, Wales and Northern Ireland Questions What was the unit length of stay and APACHE II scores for ventilated
Unit length of stay and APACHE II scores for ventilated admissions to critical care in England, Wales and Northern Ireland Questions What was the unit length of stay and APACHE II scores for ventilated
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
Safe Staffing Levels for. Midwifery, Nursing and Support Staff. For Maternity Service - Approved. Document V1.5. June 2017
 Safe Staffing Levels for Midwifery, Nursing and Support Staff For Maternity Service - Approved V1.5 June 2017 Jan Walters Head of Midwifery Women, Children and Sexual Health Division CONTENTS Section Page
Safe Staffing Levels for Midwifery, Nursing and Support Staff For Maternity Service - Approved V1.5 June 2017 Jan Walters Head of Midwifery Women, Children and Sexual Health Division CONTENTS Section Page
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services
 Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Severe Weather Plan V5.5 March 2018
 V5.5 March 2018 Table of Contents 1. Introduction 3 2. Purpose of this Plan. 3 3. Scope. 3 4. Ownership and Responsibilities. 3 5. Escalation Levels and Actions 5 6. Staffing Contingency and Guidance.
V5.5 March 2018 Table of Contents 1. Introduction 3 2. Purpose of this Plan. 3 3. Scope. 3 4. Ownership and Responsibilities. 3 5. Escalation Levels and Actions 5 6. Staffing Contingency and Guidance.
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
NCEPOD and BTS Acute NIV
 NCEPOD and BTS Acute NIV Key points by Dr Lisa Vincent-Smith and Iain Wheatley Nurse Consultant BTS NIV Quality Standards (draft consultations Sept 17) Case study 1 An elderly patient was admitted with
NCEPOD and BTS Acute NIV Key points by Dr Lisa Vincent-Smith and Iain Wheatley Nurse Consultant BTS NIV Quality Standards (draft consultations Sept 17) Case study 1 An elderly patient was admitted with
Hand Hygiene Policy V2.1
 V2.1 October 2017 Summary. Effective hand hygiene is shown to significantly reduce the carriage of potential pathogens and decrease the risk and occurrence of healthcare associated infections. Each individual
V2.1 October 2017 Summary. Effective hand hygiene is shown to significantly reduce the carriage of potential pathogens and decrease the risk and occurrence of healthcare associated infections. Each individual
COPD Management in the community
 COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS
 GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
It is essential that patients are aware of, and in agreement with, their referral to palliative care.
 Title: Directorate: Responsible for review: Ratified by: CHRONIC HEART FAILURE REFERRAL TO PALLIATIVE CARE SERVCES Palliative Care Consultant in Palliative Care Care and Clinical Policies Group Ref No:
Title: Directorate: Responsible for review: Ratified by: CHRONIC HEART FAILURE REFERRAL TO PALLIATIVE CARE SERVCES Palliative Care Consultant in Palliative Care Care and Clinical Policies Group Ref No:
CLINICAL GUIDELINE FOR Management of NON-VARICEAL Upper GI haemorrhage
 CLINICAL GUIDELINE FOR Management of NON-VARICEAL Upper GI haemorrhage Suspected Non Variceal upper GI haemorrhage If any features suggest liver disease consult the variceal haemorrhage guideline http://www.rcht.nhs.uk/documentslibrary/royalcornw
CLINICAL GUIDELINE FOR Management of NON-VARICEAL Upper GI haemorrhage Suspected Non Variceal upper GI haemorrhage If any features suggest liver disease consult the variceal haemorrhage guideline http://www.rcht.nhs.uk/documentslibrary/royalcornw
SCHEDULE 2 THE SERVICES. A. Service Specifications. E07/S/c Paediatric Long Term Ventilation
 Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
CLINICAL GUIDELINE FOR TRANSFERS AND DISCHARGES IN THE LAST FEW WEEKS OF LIFE 1. Aim/Purpose of this Guideline
 POLICY UNDER REVIEW Please note that this policy is under review. It does, however, remain current Trust policy subject to any recent legislative changes, national policy instruction (NHS or Department
POLICY UNDER REVIEW Please note that this policy is under review. It does, however, remain current Trust policy subject to any recent legislative changes, national policy instruction (NHS or Department
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Implementation Policy for NICE Guidelines
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Implementation Policy for NICE Guidelines Version No.: 5.3 Effective From: 08 May 2017 Expiry Date: 02 March 2019 Date Ratified: 23 February 2017
The Newcastle upon Tyne Hospitals NHS Foundation Trust Implementation Policy for NICE Guidelines Version No.: 5.3 Effective From: 08 May 2017 Expiry Date: 02 March 2019 Date Ratified: 23 February 2017
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
PROCESS FOR INITIATING A SYRINGE DRIVER FOR COMMUNITY NURSE PATIENTS OUT OF HOURS
 STANDARD OPERATING PROCEDURE PROCESS FOR INITIATING A SYRINGE DRIVER FOR COMMUNITY NURSE PATIENTS OUT OF HOURS Issue History Issue Version one Purpose of Issue/Description of Change To facilitate patients
STANDARD OPERATING PROCEDURE PROCESS FOR INITIATING A SYRINGE DRIVER FOR COMMUNITY NURSE PATIENTS OUT OF HOURS Issue History Issue Version one Purpose of Issue/Description of Change To facilitate patients
NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY
 PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
Prone Ventilation of the Critically Ill Patient
 Prone Ventilation of the Critically Ill Patient Statement of Best Practice Patients who require prone ventilation will be clinically assessed by the appropriate medical team, taking into account indications/contraindications,
Prone Ventilation of the Critically Ill Patient Statement of Best Practice Patients who require prone ventilation will be clinically assessed by the appropriate medical team, taking into account indications/contraindications,
Domiciliary non-invasive ventilation for recurrent acidotic exacerbations of COPD: an economic analysis Tuggey J M, Plant P K, Elliott M W
 Domiciliary non-invasive ventilation for recurrent acidotic exacerbations of COPD: an economic analysis Tuggey J M, Plant P K, Elliott M W Record Status This is a critical abstract of an economic evaluation
Domiciliary non-invasive ventilation for recurrent acidotic exacerbations of COPD: an economic analysis Tuggey J M, Plant P K, Elliott M W Record Status This is a critical abstract of an economic evaluation
Guidelines on Postanaesthetic Recovery Care
 Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Pediatric Private Duty Nursing Qualification Assessment Background. Section 1. Section 2
 Background The Pediatric Private Duty Nursing Qualification Assessment tool is designed to accurately determine a client s need for private duty nursing hours, while considering all conditions which require
Background The Pediatric Private Duty Nursing Qualification Assessment tool is designed to accurately determine a client s need for private duty nursing hours, while considering all conditions which require
WHY. Regional Acute Non-invasive Ventilation Training and Competencies? Joint Project. Dr Lisa Vincent-Smith. Eva Lazar
 WHY Regional Acute Non-invasive Ventilation Training and Competencies? Joint Project Dr Lisa Vincent-Smith Clinical Lead, KSS AHSN Respiratory Progranme Eva Lazar Improvement Co-ordinator NPSA Alert Non-invasive
WHY Regional Acute Non-invasive Ventilation Training and Competencies? Joint Project Dr Lisa Vincent-Smith Clinical Lead, KSS AHSN Respiratory Progranme Eva Lazar Improvement Co-ordinator NPSA Alert Non-invasive
Early detection, management and control of carbapenemase-producing Enterobacteriaceae Policy V3.0
 Early detection, management and control of carbapenemase-producing Enterobacteriaceae Policy V3.0 01.05.2018 Summary - Patient admission flow chart for the infection prevention and control of carbapenemase-producing
Early detection, management and control of carbapenemase-producing Enterobacteriaceae Policy V3.0 01.05.2018 Summary - Patient admission flow chart for the infection prevention and control of carbapenemase-producing
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
PHARMACEUTICAL REPRESENTATIVE POLICY NOVEMBER This policy supersedes all previous policies for Medical Representatives
 PHARMACEUTICAL REPRESENTATIVE POLICY VEMBER 2017 This policy supersedes all previous policies for Medical Representatives Policy title Pharmaceutical Representative Policy Policy PHA39 reference Policy
PHARMACEUTICAL REPRESENTATIVE POLICY VEMBER 2017 This policy supersedes all previous policies for Medical Representatives Policy title Pharmaceutical Representative Policy Policy PHA39 reference Policy
NCEPOD On the Right Trach?
 NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
Northern Ireland COPD Audit
 Northern Ireland COPD Audit A regional audit of chronic obstructive pulmonary disease (COPD) care September 2017 www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care Contents
Northern Ireland COPD Audit A regional audit of chronic obstructive pulmonary disease (COPD) care September 2017 www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care Contents
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Patients Wills Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Version No: 5.0 Effective From: 7 September 2017 Expiry Date: 31 August 2018 Date Ratified: 30 August 2017 Ratified By: Executive Team 1 Introduction
The Newcastle upon Tyne Hospitals NHS Foundation Trust Version No: 5.0 Effective From: 7 September 2017 Expiry Date: 31 August 2018 Date Ratified: 30 August 2017 Ratified By: Executive Team 1 Introduction
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Procedure for Monitoring of Delayed Transfers of Care
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Procedure for Monitoring of Delayed Transfers of Care Version No.: 2.2 Effective From: 17 March 2015 Expiry Date: 17 March 2018 Date Ratified: 25
The Newcastle upon Tyne Hospitals NHS Foundation Trust Procedure for Monitoring of Delayed Transfers of Care Version No.: 2.2 Effective From: 17 March 2015 Expiry Date: 17 March 2018 Date Ratified: 25
Respiratory Nursing 2015
 QRC: 2208 Price One Day : $363 inc. GST Two Days: $490 inc. GST Date 25-26 May 2015 Venue Hotel IBIS - Therry Street 15-21 Therry Street, Melbourne, VI, 3000 CPD Hours 12 Hours 0 Mins Respiratory Nursing
QRC: 2208 Price One Day : $363 inc. GST Two Days: $490 inc. GST Date 25-26 May 2015 Venue Hotel IBIS - Therry Street 15-21 Therry Street, Melbourne, VI, 3000 CPD Hours 12 Hours 0 Mins Respiratory Nursing
Inspiring Change. summary. A review of the quality of care provided to patients receiving acute non-invasive ventilation
 Inspiring Change A review of the quality of care provided to patients receiving acute non-invasive ventilation summary Improving the quality of healthcare Inspiring Change A review of the quality of care
Inspiring Change A review of the quality of care provided to patients receiving acute non-invasive ventilation summary Improving the quality of healthcare Inspiring Change A review of the quality of care
RESPIRATORY MASK FIT TESTING POLICY
 RESPIRATORY MASK FIT TESTING POLICY Printed copies must not be considered the definitive version DOCUMENT CONTROL Policy Group: Author: Reviewer: POLICY NO. IC - 130 Occupational Health & Safety/Infection
RESPIRATORY MASK FIT TESTING POLICY Printed copies must not be considered the definitive version DOCUMENT CONTROL Policy Group: Author: Reviewer: POLICY NO. IC - 130 Occupational Health & Safety/Infection
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Strong Potassium Solutions Safe Handling and Storage
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Strong Potassium Solutions Safe Handling and Storage Version : 5.3 Effective From: 19 January 2016 Expiry Date: 19 January 2019 Date Ratified: 14
The Newcastle upon Tyne Hospitals NHS Foundation Trust Strong Potassium Solutions Safe Handling and Storage Version : 5.3 Effective From: 19 January 2016 Expiry Date: 19 January 2019 Date Ratified: 14
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Guidelines for the appointment of. General Practitioners with Special Interests in the Delivery of Clinical Services. Respiratory Medicine
 Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Access to Drugs Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Access to Drugs Policy Version No.: 3.0 Effective From: 25 January 2016 Expiry Date: 25 January 2019 Date Ratified: 4 November 2015 Ratified By: Medicines
The Newcastle upon Tyne Hospitals NHS Foundation Trust Access to Drugs Policy Version No.: 3.0 Effective From: 25 January 2016 Expiry Date: 25 January 2019 Date Ratified: 4 November 2015 Ratified By: Medicines
Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy
 Policy") Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy 1 Policy Title: Executive Summary: Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy Cardiopulmonary resuscitation (CPR) can be attempted
Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy 1 Policy Title: Executive Summary: Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy Cardiopulmonary resuscitation (CPR) can be attempted
National Early Warning Scoring System
 National Early Warning Scoring System A common language for health care The deteriorating patient Professor Derek Bell January 2013 Adult National Early Warning Score Background Overview of NEWS Next Steps
National Early Warning Scoring System A common language for health care The deteriorating patient Professor Derek Bell January 2013 Adult National Early Warning Score Background Overview of NEWS Next Steps
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease
 Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
does staff intervene; used? If not, describe.
 Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
HAWAII HEALTH SYSTEMS CORPORATION
 All Positions HE-13 6.822 Function and Location This position works in the respiratory therapy unit of a hospital and is responsible for supervising several respiratory therapy technicians in providing
All Positions HE-13 6.822 Function and Location This position works in the respiratory therapy unit of a hospital and is responsible for supervising several respiratory therapy technicians in providing
Other (please specify): Note: This policy has been assessed for any equality, diversity or human rights implications
: Note: This policy has been assessed for any equality, diversity or human rights implications") Post holder responsible for Procedural Document Author of Policy Division/ Department responsible for Procedural Document Contact details Judy Potter, Lead Nurse, Infection Prevention & Control Judy Potter,
Post holder responsible for Procedural Document Author of Policy Division/ Department responsible for Procedural Document Contact details Judy Potter, Lead Nurse, Infection Prevention & Control Judy Potter,
CLINICAL GUIDELINE FOR MAXIMUM SURGICAL BLOOD ORDER SCHEDULE (MSBOS) Summary.
 Summary.") CLINICAL GUIDELINE FOR MAXIMUM SURGICAL BLOOD ORDER SCHEDULE (MSBOS) Summary. Start Elective procedure identified, blood requirement listed in guideline Patient attends PAC and has a group and screen (G&S)
CLINICAL GUIDELINE FOR MAXIMUM SURGICAL BLOOD ORDER SCHEDULE (MSBOS) Summary. Start Elective procedure identified, blood requirement listed in guideline Patient attends PAC and has a group and screen (G&S)
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation
 Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
AICU/CICU guidelines for Prone Ventilation in Severe Hypoxic ARDS
 AICU/CICU guidelines for Prone Ventilation in Severe Hypoxic ARDS Issue:- Version2 Issue Date:- March2014 Review Date:- March 2017 Issued To:- All staff AICU Consultant Jonathan Chantler, Senior Sister
AICU/CICU guidelines for Prone Ventilation in Severe Hypoxic ARDS Issue:- Version2 Issue Date:- March2014 Review Date:- March 2017 Issued To:- All staff AICU Consultant Jonathan Chantler, Senior Sister
The Newcastle upon Tyne NHS Hospitals Foundation Trust. Latex Operational Policy
 The Newcastle upon Tyne NHS Hospitals Foundation Trust Version No.: 4.2 Effective From: 27 October 2015 Expiry Date: 27 October 2018 Date Ratified: 1 July 2015 Ratified By: Clinical Risk Group 1 Introduction
The Newcastle upon Tyne NHS Hospitals Foundation Trust Version No.: 4.2 Effective From: 27 October 2015 Expiry Date: 27 October 2018 Date Ratified: 1 July 2015 Ratified By: Clinical Risk Group 1 Introduction