20.0 Date and time of next meeting: 9.30 a.m. on 24 January 2013, The Board Room, RJAH Orthopaedic Hospital NHS Foundation Trust, Oswestry
|
|
|
- Stephany Garrison
- 5 years ago
- Views:
Transcription
1 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 AT 9.30 A.M. THE BOARD ROOM Russell Hardy 4358 Chairman AGENDA PART ONE - PUBLIC MEETING 1.0 Apologies: James Turner 2.0 Minutes of the previous meeting held on 25 th October 2012 Paper Matters Arising 4.0 Declarations of Interest STRATEGY 5.0 Patient DVD Presentation: Day Surgery at the Menzies Unit Presentation 6.0 NHS National Commissioning Board Mandate Paper 02/ Presentation 7.0 Marketing Update Presentation PERFORMANCE 8.0 Month 7 Integrated Performance Report Paper 03 GOVERNANCE, QUALITY AND SAFETY 9.0 RJAH Safeguarding Children Annual Report Paper RJAH Safeguarding Adult Annual Report Paper Shropshire's Safeguarding Children Board Annual Report Paper Revised SFIs and Detailed Scheme of Delegation Paper Board Governance Arrangements Paper Update on Revalidation Paper Sub Committee Dates Paper Chairman s Report from Board Sub Committee: Paper 11 Business Risk and Investment Committee 3 rd October Foundation Trust Bulletin: October Any Other Business: None notified 19.0 Questions from the Public 20.0 Date and time of next meeting: 9.30 a.m. on 24 January 2013, The Board Room, RJAH Orthopaedic Hospital NHS Foundation Trust, Oswestry Paper 12 Questions from the Public on Agenda items time limit of 15 minutes There will be an opportunity for the public to ask questions on agenda items. These should be limited to two questions per person and the time in total for each person should be limited to five minutes. If topics are likely to exceed this, they should be the subject of discussions between the hospital management and the individual concerned or there should be a formal request agreed by the Trust Board or the item to be included on the next agenda. If questions are detailed and require information that is not instantly available, the hospital will respond to the question within ten working days. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Agenda - 30 November 2012.doc
2 To resolve, in accordance with Trust Standing Orders, that representatives of the press and other members of the public be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest. (Section 1(2) Public Bodies (Admission to Meeting) Act 1960) AGENDA PART TWO PRIVATE CLOSED SESSION 21.0 Minutes of the previous meeting held on 25 October 2012 Paper Matters Arising 23.0 Chief Executive s Report Paper 14/ Presentation 24.0 Our Hospital Values Paper 15/ Discussion Weeks Referral to Treatment Target Position Update Presentation Paper 16 Outcome from Monitor Escalation Meeting 26.0 Award of Internal Audit Tenders Paper Minutes from Board Sub Committees: Business Risk and Investment Committee 3 rd October 2012 Paper Any Other Business 29.0 Date and Time of Next Meeting: 24 January 2013 following the Public Board of Directors meeting U:\Trust Board & Committees\Public Trust Board\ \November 2012\Agenda - 30 November 2012.doc
3 Paper 1 BOARD OF DIRECTORS 25 TH OCTOBER 2012 MINUTES OF MEETING Russell Hardy 4358 Chairman PRESENT: IN ATTENDANCE: Russell Hardy, Chairman Wendy Farrington Chadd, Chief Executive Val Doyle, Director of Operations John Grinnell, Director of Finance Jayne Downey, Director of Nursing Steve White, Medical Director James Turner, Non Executive Director Glen Lawes, Non Executive Director Peter Jones, Non Executive Director Richard Clarke, Non Executive Director Ruth Tyrrell, Associate Director of HR Margaret Surrage, Head of Board Governance (Trust Secretary) Janet Cox, Minutes Secretary MEMBERS OF THE PUBLIC: June Jones, Shropshire Patient Group PART ONE PUBLIC MEETING MINUTE NO TITLE ACTION 25/10/1.0 APOLOGIES There were no apologies. 25/10/2.0 MINUTES OF THE PREVIOUS MEETING The minutes of the previous meeting were agreed as an accurate record. 25/10/3.0 MATTERS ARISING The Chairman went through the actions which had been completed. 25/10/4.0 DECLARATIONS OF INTEREST There were no new declarations of interest recorded. STRATEGY 25/10/5.0 MANAGEMENT OF PRESSURE SORES PRESENTATION The Director of Nursing gave a presentation which explained the differences between the grading of pressure sores and how these are managed and treated by the Trust. She confirmed that there had been no RJAH hospital acquired Grade 3 or 4 pressure ulcers for the past six years and for the period April to September 2012 there had been eight Grade 2 hospital acquired pressure ulcers. Pressure sores is one of the four harms included within the harm free care initiative which aims for Trusts to be 95% harm free by December U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 1
4 Paper Currently the Trust is meeting this target. Richard Clarke, Non Executive Director clarified whether the 95% was all harms or related just to the pressure sores. The Director of Nursing confirmed that this related to all four harms pressure sores, VTE, Falls and Catheter Associated Urinary Tract Infection. Richard Clarke, Non Executive Director congratulated the hospital on the excellent achievement of no hospital acquired Grade 3 or 4 pressure sores at the hospital for six years. He queried whether the low instance of Grade 2 pressure sores were avoidable. The Director of Nursing explained that a recent initiative of intentional rounding had been introduced whereby all patients are spoken to in a planned way every couple of hours to ensure that their pain is being managed; whether they need assistance to visit the toilet and to check pressure areas. A booklet which had been written by and for staff on the spinal injuries unit is being further developed to be shared throughout the Cluster on the good management of patients with pressure sores. Glen Lawes, Non Executive Director queried whether the patient in the presentation with the Grade 3 pressure sore had been referred to the hospital to cure this condition. The Director of Nursing explained that the spinal injuries patient had been referred to the hospital with the pressure sore and it had taken three years for the pressure sore to heal. James Turner, Non Executive Director asked whether it was typical for a pressure sore to take so long to heal. The Director of Nursing explained that this had been a severe case but that the use of VAK therapy helps. Glen Lawes, Non Executive Director asked for more detail around the impact on the Cluster of achieving harm free care. The Director of Nursing explained that all the Trusts within the Cluster are working together to share best practice and learning from the treatment of patients. Peter Jones, Non Executive Director commented that the Quality and Safety Committee had discussed this at their meeting and he congratulated the team on their fantastic performance achieving the 95% harm free care. He said that it was difficult to compare patients from RJAH against patients from a district general hospital as patients are more likely to stay in bed longer at RJAH. The Chairman asked how long it would take for a patient to deteriorate to a Grade 3 pressure sore. The Director of Nursing responded that it could be hours depending on the patient, what medication they are taking, their skin condition to a few days. The Chairman then asked a supplementary question regarding the development of pressure sores whilst people are sleeping. The Director of Nursing said that generally people move about in their sleep so pressure sores do not then develop. She confirmed that there is a regular turning programme for patients together with specialist bed U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 2
5 Paper 1 tilts which are used, as spinal injury patients are not able to move naturally. The Chairman then asked what was happening with regards to drug therapy or wound management. The Director of Nursing explained that VAK therapy forms a clean area which allows the skin to heal. The Chairman queried who was best in class that RJAH could learn from and improve performance even further. The Director of Nursing said that this is an area of national focus and that RJAH are leading in this regard although we continue to look to other hospitals for improvements from which to learn. The Chief Executive reminded the Board of Directors that the 95% harm free care initiative was an SHA ambition as no other region was attempting this and that we are ahead in this regard. The Chairman asked whether the Trust could benchmark with its Specialist Orthopaedic Alliance colleagues. The Director of Nursing said that performance is very similar but that the Cluster Nurse Directors would review this as a collaborative. The Director of Operations commented that other specialist organisations do not have spinal injuries units so RJAH may well be best in class. The Director of Nursing said that Stoke Mandeville hospital would be one similar organisation with which to benchmark. The Medical Director commented that he had recently operated on a patient with a pressure sore and he had been impressed with the way that the nurses knew what to do in treating this patient. The Director of Nursing said that nursing staff would be going out to the trauma network to support other hospital staff on early management of pressure sores. Richard Clarke, Non Executive Director asked that the performance report include narrative about Grade 2 pressure sores in future. This was agreed. DIRECTOR OF NURSING The Board of Directors noted the presentation. PERFORMANCE 25/10/6.0 MONTH 6 INTEGRATED PERFORMANCE REPORT The Chief Executive introduced the Month 6 integrated performance report and reported that the position was showing improvement around overall activity and 18 Week RTT performance. She reminded the Board of Directors that the need to treat more patients has had an impact financially although this has not affected the quality indicators. She added that focus remains on cost control around the use of bank and agency staff and sickness management and said it was encouraging that sickness absence had fallen to below 3%. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 3
6 Paper 1 Domain 1 Patient Safety The Medical Director reported that the underlying performance for the domain remains strong with continued focus on monitoring and assessing patient falls. He highlighted that: There were no cases of hospital acquired MRSA bacterium or Clostridium Difficile in month. There were no never events. There had been an outbreak of infection on one ward which was treated as a serious incident although this had since been downgraded by the SHA as there had been no impact on capacity. There had been no unexpected deaths. There had been 17 medication incidents, none of which led to serious harm. Patient falls had reduced slightly. The Director of Nursing commented that nurses were now proactively asking patients if they needed to get up rather than patients pressing the call bell for assistance. There had been no hospital acquired Grade 3 or 4 pressure ulcers in month. Performance against the CQUIN targets remains strong with detailed progress tracked by the Quality and Safety Committee. James Turner, Non Executive Director asked whether there had been any deaths, not just unexpected. The Director of Nursing responded that there had been one which was a patient on an end of life pathway. It was agreed that in future the narrative would include any deaths, not just unexpected. James Turner, Non Executive Director asked if there was any benchmarking data available regarding medicines management and patient falls that could give the Board of Directors further assurance. The Medical Director agreed that he would circulate the national data for information. MEDICAL DIRECTOR MEDICAL DIRECTOR Peter Jones, Non Executive Director said that he believed that the level of detail regarding patient falls was sufficient. He also assured the Board of Directors that the Quality and Safety Committee discuss these issues in great detail at each meeting. Glen Lawes, Non Executive Director welcomed the intentional rounding initiative and asked whether this was sustainable with the current level of staff. The Director of Nursing said that this would be reviewed in the coming months and suggested that when the Non Executive Directors carry out their ward visits, they ask the staff for their view. James Turner, Non Executive Director queried whether the 2 hour frequency was enough and whether this ought to be more. The Director of Nursing confirmed that it was hourly on Sheldon Ward and if patients are more severely ill, this is done more often. She added that when the round has been completed, this is documented in patient notes. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 4
7 Paper 1 Domain 2 Patient experience The Director of Nursing reported that focus remains high on the delivery of the access time recovery plan and active management of delayed discharges. She highlighted that: The Trust remains in the top quartile for the net promoter question for patient satisfaction at 85% against the SHA target of 71% Patient Satisfaction surveys were undertaken in Physiotherapy and Rheumatology and 99% of the respondents rated their experience as excellent or good. There had been 7 complaints in month. One complaint had been referred to the Ombudsman. There had been 68 compliments in month. Delayed Discharges were slightly above target at 3.79% with all delayed patients awaiting external care packages. The Chief Executive informed the Board of Directors that the Trust had produced a graph showing the net promoter question performance for the past 6 months which showed that the Trust was well above the average. It was agreed that this would be circulated via . She added that it was likely to become an increasing feature of hospital performance as this is rolled out nationally. James Turner, Non Executive Director queried the methodology which was being applied to this measure. The Director of Nursing confirmed that the prescribed methodology was being used. CHIEF EXECUTIVE The Director of Operations reported that: All key Cancer wait times were achieved in month. The English 6-week diagnostic target was maintained in month. Work continues on reducing the backlog. Work continues on achieving the agreed trajectories for admitted and non-admitted 18 Week RTT. The number of patients on an incomplete pathway reduced in month and is at 75% against the 92% target. To assist with achievement of the 36-week RTT for North Wales patients by December, Powys UHB has relaxed their waiting times. The Inpatient waiting list remains within tolerance levels. The Outpatient waiting list has increased although this is likely to reduce in the coming months as a result of additional outpatient clinics being arranged. Reportable cancellations remain in line with the Trust and national KPIs. James Turner, Non Executive Director asked if reportable cancellations are as a result of patients not attending for treatment. The Director of Operations confirmed that reportable cancellations are Trust cancellations, for example if there was not enough Theatre time to carry out a procedure. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 5
8 Paper 1 Domain 3 Efficiency The Director of Operations reported that performance in month has improved. She highlighted that: Surgical activity had been lower than planned. Medicine activity remains ahead of plan. New to follow up ratio is within target. BADS Activity continues to increase. The Day Case Working Group has been reinstated and is led by the Clinical Director, Mr Karlakki. Admission on Day of Surgery was above the 82% target at 87%. Theatre utilisation increased in month. Average length of stay was below target at 1.97 days. Work continues on the Enhanced Recovery programme. The Director of Nursing added that the Joint School for patients recommenced in mid- October. James Turner, Non Executive Director commented that the progress which had been reported was very encouraging and demonstrates good management. Peter Jones, Non Executive Director queried whether the decision to treat a patient as a day case was dependent on the fitness of the patient and/or the procedure involved. The Medical Director confirmed that it is mainly down to the procedure. The Chairman thanked the Team for the work which has been done to restore the metrics into balance. The Chief Executive commented that it was pleasing that almost 50% of patients having a primary hip or knee replacement were being discharged within 3 days. She added that the Medical and Clinical Director were carrying out some in-depth work on patients who were staying for longer which will be discussed in more detail over the coming months. Domain 4 Resources The Director of Finance reported that there had been a high percentage of premium costs incurred to reduce the waiting list backlog but this should return to more sustainable levels from October. He added that the CIP delivery remains key to delivering the planned 1.5m surplus. He highlighted that: A 380k surplus was achieved in month. Cumulatively the Trust is at 800k which is broadly on plan. The Financial Risk Rating of 3 has been maintained. A new delivery framework has been agreed to achieve the planned 1.5m surplus. Confirmation from the PCT on additional support for the premium rate activity is awaited. Income overachieved in month and cumulatively is 450k ahead of plan. The cost base showed pressures around the private sector and use of Out of Job Plan activity which has impacted negatively on the CIP performance which is U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 6
9 Paper 1 200k behind plan. The cash balance reduced to 3.5m but this is expected to improve over the latter part of the year. Capital expenditure was slightly behind plan. The Chief Executive asked for further information regarding the Commissioner support. The Director of Finance explained that negotiations continue with the PCT for them to re-invest the penalty they had levied relating to last year s performance. He added that confirmation was expected from the PCT in November that they had agreed to this support of 300k. James Turner, Non Executive Director commented that the area of tactical/miscellaneous appeared to be making the most contribution as opposed to workforce productivity and operational efficiency. He asked whether these were recurring benefits or one-offs as he was concerned that these may assist in the short term but then any underlying issues will come to a head. The Director of Finance said that more detail would be given in the private session of the meeting but acknowledged that the description of tactical/miscellaneous was misleading as it covered areas such as procurement and back office efficiencies. Richard Clarke, Non Executive Director queried whether the Commissioner support should be included as it had not yet been approved. The Director of Finance said that given the level of assurance around this from the discussions with the PCT, he was comfortable including this in the figures. The Chairman commented that the Director of Finance was best placed to assess the overall likelihood of this being approved. The Director of Finance said that he would be very disappointed if this was not forthcoming. Richard Clarke, Non Executive Director asked what headroom the Trust has on the financial risk rating of 3 on the income projected and if the Commissioner support is not forthcoming. The Director of Finance confirmed that the full year position of a financial risk rating of 3 is not at risk. The Associate Director of Human Resources reported that: Sickness absence reduced in month although as this is above target, work continues to reduce this. Over 200 staff have had the flu jab. The health and wellbeing day had been very well attended and over 200 staff attended received mini health checks. Staff appraisals have improved following a reminder campaign. The Chairman commented that it was good that the Trust was promoting health and wellbeing for staff. Domain 5 External Perception The Quality Governance forecast on the balanced scorecard is amber-red which correlates to the rating applied using the U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 7
10 Paper 1 Monitor methodology. The Board of Directors noted the Month 6 (September) performance. GOVERNANCE, QUALITY AND SAFETY 25/10/7.0 CARE QUALITY COMMISSION COMPLIANCE REPORT The Chief Executive presented the report prepared by the Care Quality Commission (CQC) following their unannounced inspection on 12 th September She explained that the CQC had visited three wards and concluded that the organisation met the required standards on the following areas which were reviewed: Respecting and involving people who use services Care and welfare of people who use services Safeguarding people who use services from abuse Staffing Complaints She added that some issues were highlighted around staffing and sickness which the Trust was aware of and work will continue to progress improvements in these areas. James Turner, Non Executive Director commented that he felt that it was a very small sample size on which to assess the organisation and questioned whether this was realistic. Peter Jones, Non Executive Director said that it depended on what they were looking for but that this was enough to allow triangulation. The Chairman commented that the visit was not unexpected and the inspection had reviewed the Trust s performance against the essential standards of quality and safety. He added that this was a good example of what to expect from the monitoring system. Richard Clarke, Non Executive Director said that the comments regarding patients waiting for staff to respond to the call bell did not correlate with his experience when he has visited wards. Glen Lawes, Non Executive Director queried whether there were regular views on each ward to ensure that the balance of staff was correct. The Director of Nursing confirmed that each ward has a staffing template and that a trial was currently being undertaken using the safer nursing tool which looks at the acuity of patients. She added that discussion is ongoing on a daily basis between the nursing staff and Matrons to ensure that wards are adequately staffed. The Board of Directors noted the report. 25/10/8.0 QUARTER 2 BOARD ASSURANCE FRAMEWORK The Head of Board Governance (Trust Secretary) introduced the Quarter 2 Board Assurance Framework and reminded the Board that the document is a live document. She explained that the ratings of four risks had been changed since the last U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 8
11 Paper 1 Board discussion in July 2012 and had been discussed in detail at the Business Risk and Investment Committee at its meeting on 3 rd October. The risks which had changed were detailed as follows: Risk Delivery of Open Pathways RTT has increased. Risk 1217 Delivery of RTT performance has reduced. Risk 1230 In year Cost pressures has increased. Risk 1004 Management of Sickness Absence has increased. The Director of Operations explained that risk 1229 delivery of open pathways RTT was at risk as this would not be achieved from October 2012 and a new trajectory has been agreed with the PCT. The Business Risk and Investment Committee discussed and agreed the increased rating on this risk. The Director of Operations explained that risk 1217 delivery of RTT performance had decreased because of the assurance that this target would be achieved from October. The Director of Finance explained that risk 1230 in year cost pressures has been increased as a result of the pressures faced in Months 1-6 around the delivery of the RTT action plan. He added that a mitigation for this is the new delivery framework for the remaining 6 months of the year which has been agreed. He confirmed the forecast Financial Risk Rating of 3 was achievable. The Associate Director of Human Resources explained that risk 1004 management of sickness absence had been increased in acknowledgement of the challenging target to achieve 2% by She added that further work to meet this challenge will continue. The Chief Executive reiterated that support from the Commissioners is a key mitigating factor for the risks around cost pressures and RTT delivery. The Chairman commented that he was encouraged by the live nature of this important document and the fact that this is ingrained in the work that the Trust undertakes. The Board of Directors approved the Quarter 2 Board Assurance Framework. 25/10/9.0 QUARTER 2 INFECTION CONTROL REPORT The Director of Nursing presented the Quarter 2 Infection Prevention and Control and Cleanliness report which outlined the Trust s performance against the registration requirements. She highlighted that: Performance remains strong across the organisation. There had been no instances of hospital acquired MRSA Bacteraemia or Clostridium Difficile during the quarter. Peer reviews between wards along with spot checks U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 9
12 Paper 1 means that the Trust continues to maintain its high standards on cleaning. Infection control remains a high priority. Focus continues on the rolling programme of monthly infection control audits and mandatory training for staff. Excellent performance continues around Surgical Site Infections. The outbreak of Diarrhoea and Vomiting had been reported to the SHA as a serious incident but as this had not impacted on capacity, this had been downgraded. This was not attributed specifically to either Clostridium Difficile or Norovirus. The Medical Director commented that he had displayed the hand hygiene graph in Theatres to remind staff of the importance of this. It was noted that the scores for medics had improved. Richard Clarke, Non Executive Director said that he was surprised that no comment had been made regarding the excellent performance around surgical site infections of one out of 549 procedures. The Medical Director responded that the organisation would expect this to be low. Richard Clarke, Non Executive Director said that he would like to congratulate everyone for this excellent result but that the pressure would need to continue to ensure that this high standard did not slip. The Chairman reiterated this comment and reminded all of the need to not become complacent. The Board of Directors noted the progress outlined in the Quarter 2 report approved the report. 25/10/10.0 QUARTER 2 MONITOR SUBMISSION The Chief Executive presented the Quarter 2 performance return which provides assurance to the Board of Directors in relation to the key targets and declarations required by Monitor which is to be submitted on 31 st October She explained that the Trust had declared compliance to all targets and indicators with the exception of the three 18- Week Referral to Treatment measures. She added that this was consistent with the previous Monitor return and overall gives the Trust an amber-red Governance rating and a Finance Risk Rating of Level 3. She concluded that it is expected that the 90%/95% targets would be achieved from Quarter 3. The Board of Directors approved the Quarter 2 Monitor Return. 25/10/ BOARD OF DIRECTOR MEETING DATES The Chairman presented the proposed dates for the Board of Director meetings in 2013 and the Board Development Sessions for discussion and approval. James Turner, Non Executive Director stated that he was U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 10
13 Paper 1 unable to attend any of the Board Development Sessions arranged for the last Friday of the month, as had been the case in The Chief Executive noted this and said that the Board Development Session dates were to be confirmed. A discussion then took place on the date for the January Board of Directors meeting and it was noted that this had been brought forward to accommodate the Board of Directors discussing the Quarter 3 Monitor submission in advance of the deadline of 31 st January. It was also noted that the May Board of Directors meeting was to be confirmed to meet the deadline for submitting the Trust s annual accounts. A discussion then took place on the proposed Sub Committee meeting dates and it was agreed that the individual Sub Committee Chairs would liaise with the Head of Board Governance (Trust Secretary) to finalise these for approval at the next meeting. The Board of Directors noted the proposed Board of Directors meeting dates for 2013 and agreed to discuss the Sub Committee meeting dates at the next Board of Directors meeting on 30 November SUB COMMITTEE CHAIRS MINUTES SECRETARY 25/10/12.0 FOUNDATION TRUST BULLETIN : SEPTEMBER 2012 The Chief Executive presented the September Foundation Trust Bulletin from Monitor which the Head of Board Governance (Trust Secretary) had reviewed to ensure that required actions were being progressed. James Turner, Non Executive Director brought the Board s attention to an event on the 15 th November 2012 which had been arranged by the Kings Fund for Non Executive Directors. Richard Clarke, Non Executive Director commented that he had recently attended the CASS Non Executive Director Development Course which he had found very worthwhile. He suggested that any new Non Executive Directors to the Trust should attend this in the first 12 months of their tenure. The Board of Directors noted the September Foundation Trust Bulletin. 25/10/13.0 ANY OTHER BUSINESS There was no additional business to discuss. 25/10/14.0 QUESTIONS FROM THE PUBLIC There were no questions from the public. 25/10/15.0 DATE OF NEXT MEETING: Friday 30 th November 2012 at 9.30 a.m. in the Board Room. CHAIRMAN S CLOSING REMARKS The Chairman thanked everyone for their contribution and closed the public session of the meeting. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 11
14 Paper 1 BOARD OF DIRECTORS MEETING 25 TH OCTOBER 2012 SUMMARY OF KEY ACTIONS Action Lead Responsibility Progress 25/10/5.0 MANAGEMENT OF PRESSURE SORES PRESENTATION Performance report narrative to include details of Grade 2 pressure sores. Director of Nursing Completed. 25/10/6.0 MONTH 6 INTEGRATED PERFORMANCE REPORT Performance report narrative to include details of all deaths. National data around patient falls and medication incidents to be circulated. Net promoter question graph to be circulated. Medical Director Medical Director Chief Executive Completed. Completed. Completed. 25/10/ BOARD OF DIRECTOR MEETING DATES Sub Committee Chairs to liaise with the Head of Board Governance (Trust Secretary) re dates for Item to be included on the Board of Directors agenda in November. Sub Committee Chairs Minutes Secretary Completed. Completed. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 01 Minutes of the previous meeting held on 25th October 2012.doc 12
15 Paper 02 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title NHS Commissioning Board Mandate Executive Responsible Paper prepared by (if different from above) Nature of Report Category of Item Context Wendy Farrington Chadd, Chief Executive Sir David Nicholson, NHS Chief Executive For Information For Discussion For Approval Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary The Secretary of State published the first mandate to the NHS Commissioning Board on 13 November 2012 which sets out the Government s ambitions for the NHS, which it is asking the NHS Commissioning Board to achieve from April 2013 to the end of Received or approved by Legal Implications Recommendation The Board of Directors are asked to note the mandate. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 02 NHS Commissioning Board Mandate.doc
16 Date: 13 November 2012 To: All Chairs and Chief Executives in NHS trusts in England All Chairs and Chief Executives in NHS foundation trusts in England All Chairs and Chief Executives in primary care trusts in England All Chairs and Chief Executives in strategic health authorities in England Regional Directors, NHS Commissioning Board Richmond House 79 Whitehall London SW1A 2NS Cc: All Chief Executives of Local Authorities in England Monitor Gateway reference: Dear colleagues PUBLICATION OF THE NHS MANDATE The Secretary of State for Health has today published the first mandate to the NHS Commissioning Board (NHS CB). The NHS mandate sets out the Government s ambitions for the NHS, which it is asking the NHS CB to achieve from April 2013 to the end of The mandate has been informed by a wide range of organisations and stakeholders across the health and care system. It sets a number of objectives for the Commissioning Board, based on the five domains identified in the NHS Outcomes Framework, an updated version of which is also published today. As leaders of the health and care system, it is important that you understand exactly what the NHS is being asked to do over the next few years. This applies both to those of you supporting organisations in their transition to the new system, and to those of you who will be helping deliver these objectives. You can read the NHS mandate at In the coming weeks I will be writing out to many of you in my role as Chief Executive of the NHS CB to set out details of the Board s approach to the 2013/14 planning round.
17 I look forward to continue to working with you all as we continue our transition to the new health and care system. Kind regards Sir David Nicholson KCB CBE NHS Chief Executive
18 The Mandate A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 November 2012
19 The Mandate A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 Presented to Parliament pursuant to Section 13A(1) of the National Health Service Act 2006
20 Crown copyright 2012 You may re-use this information (excluding logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit or Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned. Any enquiries regarding this publication should be sent to us by filling in the web form at: or calling This publication is available for download from our website at:
21 Contents Foreword 3 Introduction 4 1. Preventing people from dying prematurely 7 2. Enhancing quality of life for people with long-term conditions 9 3. Helping people to recover from episodes of ill health or following injury Ensuring that people have a positive experience of care Treating and caring for people in a safe environment and protecting them from avoidable harm Freeing the NHS to innovate The broader role of the NHS in society Finance Assessing progress and providing stability 27 1
22 Foreword Now in its sixty-fifth year, the NHS remains as vital and as respected as ever. Millions of us depend upon it every week, and through the dedication of thousands of professionals, we do so in confidence that it will be there for us, whatever our background or needs. I am immensely proud of what the NHS has achieved, not only for the extraordinary things it does for us as individuals, but also for what it says about us as a nation. This mandate the first of its kind in the world underlines my responsibility as Health Secretary to preserve and defend those principles to which we all remain indebted. The most important of these is that the NHS remains comprehensive and universal, free at the point of delivery, and available to all based on clinical need. Under this Government, that will never change. Yet the Mandate reflects a second responsibility to ensure the NHS stays relevant and trusted in a rapidly changing world. Never in its history has the NHS had to face such a profound shift in our needs and expectations. An ageing population, rising costs of treatments, and a huge increase in the number of us with long term, often multiple conditions are rewriting our relationship with health and care, all at a time of acute pressure on public finances. These challenges go to the heart of the objectives I am setting the NHS Commissioning Board. By offering health professionals more power and space, and by focusing on the things that people tell us matter most, we will make sure the NHS responds decisively and stays ahead of the game. Similarly, whilst most people experience excellent care, nobody claims the NHS today is perfect. I therefore want us to open every possible window into performance, so that we expose and prevent poor care, inspire the whole NHS to aim higher, and give everyone more confidence in the services they use. Last century, the NHS set itself the highest ideals of compassion and dignity, carried by a commitment to the very best standards of treatment and support. This mandate shows how we will honour that promise for the 21st century and ensure our proudest creation continues to be our finest. JEREMY HUNT Secretary of State for Health 3
23 Introduction The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill, and when we cannot fully recover, to stay as well as we can to the end of our lives. It works at the limits of science bringing the highest levels of human knowledge and skill to save lives and improve health. It touches our lives at times of most basic human need, when care and compassion matter most. The NHS is founded on a set of common principles and values that bind together the communities and people it serves patients and the public and the staff who work for it. The NHS Constitution 1. As a nation, we are proud of what the NHS has achieved and the values it stands for. But public expectations of good healthcare do not stand still. So on behalf of the people of England, patients and those who care for them, this first mandate to the NHS Commissioning Board sets out our ambitions for how the NHS needs to improve. It covers the period from April 2013 to the end of March It is the Government s privilege to serve as guardian of the NHS and its founding values. We will safeguard, uphold and promote the NHS Constitution; and this is also required of the NHS Commissioning Board. 3. The NHS is there for everyone, irrespective of background. The Government will continue to promote the NHS as a comprehensive and universal service, free at the point of delivery and available to all based on clinical need, not ability to pay. We will increase health spending in real terms in each year of this Parliament. We will not introduce new patient charges. 4. The creation of an independent NHS Commissioning Board, and this mandate to the Board from the Government, mark a new model of leadership for the NHS in England, in which Ministers are more transparent about their objectives while giving local healthcare professionals independence over how to meet them. 5. The NHS budget is entrusted to the Board, which shares with the Secretary of State for Health the legal duty to promote a comprehensive health service. The Board oversees the delivery of NHS services, including continuous improvement of the quality of treatment and care, through healthcare professionals making decisions about services based on the needs of their communities. The Board is subject to a wide range of statutory duties, and is accountable to the Secretary of State and the public for how well it performs these. 4
24 Introduction 6. This mandate plays a vital role in setting out the strategic direction for the Board and ensuring it is democratically accountable. It is the main basis of Ministerial instruction to the NHS, which must be operationally independent and clinically-led. Other than in exceptional circumstances, including a general election, it cannot be changed in the course of the year without the agreement of the Board. The Mandate is therefore intended to provide the NHS with much greater stability to plan ahead. 7. The Board is legally required to pursue the objectives in this document 1. However it will only succeed through releasing the energy, ideas and enthusiasm of frontline staff and organisations. The importance of this principle is reflected in the legal duties on the Secretary of State and the NHS Commissioning Board as to promoting the autonomy of local clinical commissioners and others. 8. The scale of what we ask will take many years to achieve, but if the Board is successful, by March 2015 improvement across the NHS will be clear. By then, patients will see real and positive change in how they use health services, and how different organisations work together to support them. 9. The Government s ambition for excellent care is not just for those services or groups of patients mentioned in this document, but for everyone regardless of income, location, age, gender, ethnicity or any other characteristic. Yet across these groups there are still too many longstanding and unjustifiable inequalities in access to services, in the quality of care, and in health outcomes for patients. The NHS is a universal service for the people of England, and the NHS Commissioning Board is under specific legal duties in relation to tackling health inequalities and advancing equality. The Government will hold the Board to account for how well it discharges these duties. 10. The objectives in this mandate focus on those areas identified as being of greatest importance to people. They include transforming how well the NHS performs by: preventing ill-health, and providing better early diagnosis and treatment of conditions such as cancer and heart disease, so that more of us can enjoy the prospect of a long and healthy old age (see section 1); managing ongoing physical and mental health conditions such as dementia, diabetes and depression so that we, our families and our carers can experience a better quality of life; and so that care feels much more joined up, right across GP surgeries, district nurses and midwives, care homes and hospitals (see section 2); helping us recover from episodes of ill health such as stroke or following injury (see section 3); 1 See section 13A(2) of the National Health Service Act 2006, as inserted by the Health and Social Care Act
25 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 making sure we experience better care, not just better treatment, so that we can expect to be treated with compassion, dignity and respect (see section 4); providing safe care so that we are treated in a clean and safe environment and have a lower risk of the NHS giving us infections, blood clots or bed sores (see section 5). 11. These areas correspond to the five parts of the NHS Outcomes Framework, which are listed in this document and will be used to measure progress. The framework will be kept up to date to reflect changing public and professional priorities, and balanced to reduce distortion or perverse incentives from focusing inappropriately on some areas at the expense of others. In order to allow space for local innovation at the front line, both the Government and the NHS Commissioning Board will seek to ensure that local NHS organisations are held to account through outcome rather than process objectives. As one of its objectives, the Board will need to demonstrate progress against the five parts and all of the outcome indicators in the framework including, where possible, by comparing our services and outcomes with the best in the world. 12. As part of this, the Government has identified the following priority areas where it is expecting particular progress to be made: (i) improving standards of care and not just treatment, especially for older people and at the end of people s lives; (ii) the diagnosis, treatment and care of people with dementia; (iii) supporting people with multiple long-term physical and mental health conditions, particularly by embracing opportunities created by technology, and delivering a service that values mental and physical health equally; (iv) preventing premature deaths from the biggest killers; (v) furthering economic growth, including supporting people with health conditions to remain in or find work. The Board is also expected to play a full role in supporting public service reform. 13. These priorities reflect the Government s absolute commitment to high quality healthcare for all, while highlighting the important additional role the NHS can play in supporting economic recovery. 14. The Mandate is not exhaustive. As part of the changes in the relationship between the Government and the NHS, the Board has agreed to play its full part in fulfilling pre-existing government commitments not specifically mentioned in the Mandate. For its part, the Government will exercise discipline by not seeking to introduce new objectives for the Board between one mandate and the next. 15. In all it does, whether in the Mandate or not, whether supporting local commissioners or commissioning services itself, the Commissioning Board is legally bound to pursue the goal of continuous improvement in the quality of health services. 6
26 1. Preventing people from dying prematurely 1.1 We want people to live longer, and with a better quality of life. Too many people die too soon from illnesses that can be prevented or treated. From cancer, liver and lung disease and for babies and young children, England s rates of premature mortality are worse than those in many other European countries. There are also persistent inequalities in life expectancy and healthy life expectancy between communities and groups, which need to be urgently addressed by the NHS Commissioning Board. 1.2 About 20,000 lives a year would be saved if our mortality rates were reduced to the level of the best in Europe. We are under a moral imperative to act, so that more of us, our families, friends and neighbours, may enjoy the prospect of an independent and active old age. Our ambition is for England to become one of the most successful countries in Europe at preventing premature deaths, and our objective for the NHS Commissioning Board is to make measurable progress towards this outcome by National and local government, the NHS Commissioning Board, Public Health England and others will all need to take action, with each organisation having the same goal. All will need to invest time now in developing strong partnerships, so that rapid progress can be made from April Only after many years of sustained effort and innovation will this ambition be realised. Along the way, the NHS Commissioning Board s objective is to make significant progress: in supporting the earlier diagnosis of illness, particularly through appropriate use of primary care, and tackling risk factors such as high blood pressure and cholesterol. This includes working with Public Health England to support local government in the roll out of NHS Health Checks; in ensuring people have access to the right treatment when they need it, including drugs and treatments recommended by the National Institute for Health and Care Excellence (NICE), and services for children and adults with mental health problems; in reducing unjustified variation between hospitals in avoidable deaths, so that standards in all hospitals are closer to those of the best. The NHS should measure and publish outcome data for all major services by 2015, broken down by local clinical commissioning groups (CCGs) where patient numbers are adequate, as well as by those teams and organisations providing care. To support this, the Government will strengthen quality accounts, which all providers are legally required to publish to account for the quality of their services; 7
27 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 in focusing the NHS on preventing illness, with staff using every contact they have with people as an opportunity to help people stay in good health by not smoking, eating healthily, drinking less alcohol, and exercising more. As the country s largest employer, the NHS should also make an important contribution by promoting the mental and physical health and wellbeing of its own workforce. Preventing people from dying prematurely: Key areas where progress will be expected (Part one of the NHS Outcomes Framework) Overarching indicators 1a Potential Years of Life Lost (PYLL) from causes considered amenable to health care (This is a measure of premature deaths that can be avoided through timely and effective healthcare.) i Adults ii Children and young people 1b Life expectancy at 75, i males ii females Improvement areas: Reducing premature mortality from the major causes of death 1.1 Under 75 mortality rate from cardiovascular disease 1.2 Under 75 mortality rate from respiratory disease 1.3 Under 75 mortality rate from liver disease 1.4 Under 75 mortality from cancer i One- and ii Five-year survival from all cancers iii One- and iv Five-year survival from breast, lung and colorectal cancer Reducing premature death in people with serious mental illness 1.5 Excess under 75 mortality rate in adults with serious mental illness Reducing deaths in babies and young children 1.6.i Infant mortality 1.6.ii Neonatal mortality and stillbirths 1.6.iii Five-year survival from all cancers in children Reducing premature death in people with learning disabilities 1.7 Excess under 60 mortality in adults with learning disabilities 8
28 2. Enhancing quality of life for people with long-term conditions 2.1 We want to empower and support the increasing number of people living with long term conditions. One in three people are living with at least one chronic condition, such as hypertension, diabetes or depression. By 2018 nearly three million people, mainly older people, will have three or more conditions all at once. 2.2 Too many people with ongoing health problems are treated as a collection of symptoms not a person. Simple things like getting a repeat prescription or making an appointment need to be much easier. People should expect the right support to help them manage their long term conditions so that they do not end up in hospital needlessly or find that they can no longer work because of mental or physical illness. We need the NHS to do much better for people with long term conditions or disabilities in the future. To stay relevant to our changing needs, different parts of the NHS have to work more effectively with each other and with other organisations, such as social services, to drive joined-up care. 2.3 To address these challenges, the NHS Commissioning Board s objective is to make measurable progress towards making the NHS among the best in Europe at supporting people with ongoing health problems to live healthily and independently, with much better control over the care they receive. 2.4 By 2013, the new 111 phoneline will be up and running for non-emergency care. By March 2015, we expect the Board to have made particular progress in four key areas: (i) involving people in their own care; (ii) the use of technology; (iii) better integration of services; and (iv) the diagnosis, treatment and care of those with dementia. 2.5 The NHS Commissioning Board s objective is to ensure the NHS becomes dramatically better at involving patients and their carers, and empowering them to manage and make decisions about their own care and treatment. For all the hours that most people spend with a doctor or nurse, they spend thousands more looking after themselves or a loved one. Achieving this objective would mean that by 2015: far more people will have developed the knowledge, skills and confidence to manage their own health, so they can live their lives to the full; everyone with long-term conditions, including people with mental health problems, will be offered a personalised care plan that reflects their preferences and agreed decisions; 9
29 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 patients who could benefit will have the option to hold their own personal health budget, subject to the evaluation of the pilot programme, as a way to have even more control over their care; the five million carers looking after friends and family members will routinely have access to information and advice about the support available including respite care. 2.6 In a digital age, it is crucial that the NHS not only operates at the limits of medical science, but also increasingly at the forefront of new technologies. The Board s objective is to achieve a significant increase in the use of technology to help people manage their health and care. In particular, the Government expects that by March 2015: everyone who wishes will be able to get online access to their own health records held by their GP. The Board should promote the implementation of electronic records in all health and care settings and should work with relevant organisations to set national information standards to support integration; clear plans will be in place to enable secure linking of these electronic health and care records wherever they are held, so there is as complete a record as possible of the care someone receives; clear plans will be in place for those records to be able to follow individuals, with their consent, to any part of the NHS or social care system; everyone will be able to book GP appointments and order repeat prescriptions online; everyone will be able to have secure electronic communication with their GP practice, with the option of e-consultations becoming much more widely available; significant progress will be made towards three million people with long term conditions being able to benefit from telehealth and telecare by 2017; supporting them to manage and monitor their condition at home, and reducing the need for avoidable visits to their GP practice and hospital. 2.7 As a leader of the health system, the NHS Commissioning Board is uniquely placed to coordinate a major drive for better integration of care across different services, to enable local implementation at scale and with pace from April The focus should be on what we are achieving for individuals rather than for organisations in other words care which feels more joined-up to the users of services, with the aim of maintaining their health and wellbeing and preventing their 10
30 Enhancing quality of life for people with long-term conditions condition deteriorating, so far as is possible. We want to see improvements in the way that care: is coordinated around the needs, convenience and choices of patients, their carers and families rather than the interests of organisations that provide care; centres on the person as a whole, rather than on specific conditions; ensures people experience smooth transitions between care settings and organisations, including between primary and secondary care, mental and physical health services, children s and adult services, and health and social care thereby helping to reduce health inequalities; empowers service users so that they are better equipped to manage their own care, as far as they want and are able to. 2.9 In taking forward this objective, we are asking the Board to drive and coordinate engagement with local councils, CCGs and providers; and at national level, to work with the Department of Health, Monitor, Health Education England, Public Health England, and the Local Government Association, as well as other organisations that want to contribute. The challenge is to tackle practical barriers that stop services working together effectively, and for national organisations to provide help and expertise where this will be needed, rather than to design and impose a blueprint. Local commissioners have the vital role of stimulating the development of innovative integrated provision for example, across primary, secondary and social care, or for frail elderly patients. In responding to the barriers revealed by their work, further national action will be needed in a number of areas, including: better measurement of user experience of seamless care; better use of technology to share information; open and fair procurement practice; and new models of contracting and pricing which reward value-based, integrated care that keeps people as healthy and independent as possible Dementia is the illness most feared by people in England over the age of 55, yet in the past it has not received the attention it needs. This has inspired the Prime Minister s Challenge on Dementia, which was launched in March The Government s goal is that the diagnosis, treatment and care of people with dementia in England should be among the best in Europe The objective for the NHS Commissioning Board is to make measurable progress towards achieving this by March 2015, in particular ensuring timely diagnosis and the best available treatment for everyone who needs it, including support for their carers. We want the Board to work with CCGs, driving significant improvements in diagnosis of dementia, and capturing this in a national ambition for diagnosis rates built up from local plans. 11
31 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March The NHS Commissioning Board will publish the expected level of diagnosis across the country through to March And because people with dementia, their carers and professionals rightly need to feel confident that a diagnosis of dementia will improve the lives of people with the disease, the Board should work with CCGs to support local proposals for making the best treatment available across the country. Enhancing quality of life for people with long-term conditions: Key areas where progress will be expected (Part two of the NHS Outcomes Framework) Overarching indicator 2 Health related quality of life for people with long-term conditions Improvement areas Ensuring people feel supported to manage their condition 2.1 Proportion of people feeling supported to manage their condition Improving functional ability in people with long-term conditions 2.2 Employment of people with long-term conditions Reducing time spent hospital by people with long-term conditions 2.3.i Unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) (Chronic ambulatory care sensitive conditions are those where the right treatment and support in the community can help prevent people needing to be admitted to hospital.) 2.3.ii Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s Enhancing quality of life for carers 2.4 Health-related quality of life for carers Enhancing quality of life for people with mental illness 2.5 Employment of people with mental illness Enhancing quality of life for people with dementia 2.6.i Estimated diagnosis rate for people with dementia 2.6.ii A measure of the effectiveness of post-diagnosis care in sustaining independence and improving quality of life 12
32 3. Helping people to recover from episodes of ill health or following injury 3.1 Every year, millions of people rely on the NHS to help them recover after an illness or rehabilitate after injury. It does so not only through effective treatment but also through ongoing help in recovering quickly and regaining independence whether from a planned operation such as a hip or knee replacement, an injury from a fall or other accident, a respiratory infection in a young child, or a major emergency like a stroke. Helping people get back as quickly or as much as possible to their everyday lives is not something the NHS can achieve alone, but requires better partnership with patients, families and carers, social services and other agencies. 3.2 Many parts of the NHS are world-leading in helping people to recover from ill health or injury. Because standards are high overall, most people assume all NHS services are equally good. Yet there are huge and unwarranted differences in quality and results between services across the country even between different teams in the same hospital, or GP practices in the same vicinity. 3.3 An objective for the NHS Commissioning Board is to shine a light on variation and unacceptable practice, to inspire and help people to learn from the best. We want a revolution in transparency so that the NHS leads the world in the availability of information about the quality of services. This means: reporting results at the level of local councils, clinical commissioning groups, providers of care and consultant-led teams; the systematic development of clinical audit and patient-reported outcome and experience measures; real consideration of how to make it easy for patients and carers to give feedback on their care and see reviews by other people, so that timely, easy-to-review feedback on NHS services becomes the norm. 3.4 Better information may expose the need for change. For example, stroke services in London have recently been brought together to provide rapid access to highly specialised emergency treatment, significantly reducing mortality rates. Priority should be given to changes to services which improve outcomes whilst also maintaining access. Where local clinicians are proposing significant change to services, we want to see better informed local decision-making about services, in which the public are fully 13
33 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 consulted and involved. The NHS Commissioning Board s objective is to ensure that proposed changes meet four tests: (i) strong public and patient engagement; ii) consistency with current and prospective need for patient choice; iii) a clear clinical evidence base; and iv) support for proposals from clinical commissioners. 3.5 Treating mental and physical health conditions in a coordinated way, and with equal priority, is essential to supporting recovery. Yet people with mental health problems have worse outcomes for their physical healthcare, and those with physical conditions often have mental health needs that go unrecognised. The NHS Commissioning Board s objective is to put mental health on a par with physical health, and close the health gap between people with mental health problems and the population as a whole. 3.6 By March 2015, we expect measurable progress towards achieving true parity of esteem, where everyone who needs it has timely access to evidence-based services. This will involve extending and ensuring more open access to the Improving Access to Psychological Therapies (IAPT) programme, in particular for children and young people, and for those out of work. The Board has agreed to play its full part in delivering the commitments that at least 15% of adults with relevant disorders will have timely access to services, with a recovery rate of 50%. The Board will work with stakeholders to ensure implementation is at all times in line with the best available evidence. Helping people to recover from episodes of ill health or following injury: Key areas where progress will be expected (Part three of the NHS Outcomes Framework) Overarching indicators 3a Emergency admissions for acute conditions that should not usually require hospital admission 3b Emergency readmissions within 30 days of discharge from hospital Improvement areas Improving outcomes from planned treatments 3.1 Total health gain as assessed by patients for elective procedures 3.1.i Hip ii Knee replacement iii Groin Hernia iv Varicose veins v Psychological therapies (These indicators will measure the number of people accessing particular treatments and whether patients report that they are effective.) Preventing lower respiratory tract infections (LRTI) in children from becoming serious 3.2 Emergency admissions for children with lower respiratory tract infections (LRTI) 14
34 Helping people to recover from episodes of ill health or following injury Helping people to recover from episodes of ill health or following injury: Key areas where progress will be expected (Part three of the NHS Outcomes Framework) Improving recovery from injuries and trauma 3.3 Proportion of people who recover from major trauma Improving recovery from stroke 3.4 Proportion of stroke patients reporting an improvement in activity/lifestyle on the Modified Rankin Scale at 6 months (The Modified Rankin Scale is commonly used to measure the degree of disability or dependence following a stroke.) Improving recovery from fragility fractures 3.5 The proportion of patients with fragility fractures recovering to their previous levels of mobility/walking ability at i 30 days and ii 120 days Helping older people to recover their independence after illness or injury 3.6.i Proportion of Older People (65 and over) who were still at home 91 days after discharge from hospital into reablement/rehabilitation services 3.6.ii Proportion offered rehabilitation following discharge from acute or community hospital. 15
35 4. Ensuring that people have a positive experience of care 4.1 The NHS is not there just to offer excellent treatment and support. It is there to care for us. Quality of care is as important as quality of treatment, but the public are less confident about consistency in care provision than they are about treatment. 4.2 No one going in to hospital should have to worry about being left in pain, unable to eat or drink, or go to the toilet. And those who have relatives or friends who need support should have peace of mind that they will be treated with compassion, respect and dignity whether at home or in residential care. 4.3 While most people receive excellent care, we have all been shocked by incidents of major failings in care. It is frequently those who are very old or vulnerable who bear the brunt those with complex conditions, who are unlikely or unable to complain, and who in some instances no longer have friends or family members who can fight for them. As a society, as a health and care system, and as a Government, we all find such failings abhorrent and intolerable. The Government is clear that, where serious failures of care and treatment have occurred, managers in both the NHS and social care sector will be better held to account. 4.4 In the early months of 2013, Robert Francis QC will publish the report of his independent Public Inquiry into the lessons from Mid-Staffordshire NHS Foundation Trust. Working in partnership with national agencies, including the Care Quality Commission and Healthwatch England, Monitor, the professional regulators and Royal Colleges, the NHS Commissioning Board and Health Education England, the Government will bring about a response that is comprehensive, effective and lasting. It will be important to ensure there is a credible, robust and independent inspection regime across the entire health and care system. 4.5 Later in the autumn of 2012, the Government will issue a full and detailed response to the appalling abuse that was witnessed at Winterbourne View private hospital. The NHS Commissioning Board s objective is to ensure that CCGs work with local authorities to ensure that vulnerable people, particularly those with learning disabilities and autism, receive safe, appropriate, high quality care. The presumption should always be that services are local and that people remain in their communities; we expect to see a substantial reduction in reliance on inpatient care for these groups of people. 16
36 Ensuring that people have a positive experience of care 4.6 Our ambition stretches beyond ensuring that all parts of the health and care system will satisfy minimum standards of care. The NHS Commissioning Board s objective is to pursue the long-term aim of the NHS being recognised globally as having the highest standards of caring, particularly for older people and at the end of people s lives. 4.7 The quality of care is closely related to how well organisations engage, manage and support their own staff. The NHS Constitution includes important pledges to staff who provide NHS care, and the NHS Commissioning Board is required to promote the NHS Constitution in carrying out its functions. The Board also has a statutory duty as to promoting education and training, to support an effective system for its planning and delivery. The Board should support Health Education England in ensuring that the health workforce has the right values, skills and training to enable excellent care. 4.8 The Government also expects to see the Board make significant progress by March 2015 in two principal areas. The first objective is to make rapid progress in measuring and understanding how people really feel about the care they receive and taking action to address poor performance. The NHS staff survey provides important information about organisations health, and it already asks whether staff would recommend their place of work to a family member or friend as a high-quality place to receive treatment and care (the friends and family test ). However, staff are only asked this question annually, and the Board should ensure that much more regular feedback on the friends and family test becomes the norm. 4.9 Part of this objective is for the NHS Commissioning Board to introduce the friends and family test for patients across the country: for all acute hospital inpatients and Accident and Emergency patients from April 2013; for women who have used maternity services from October 2013; and as rapidly as possible thereafter for all those using NHS services. Hospitals with good scores on the friends and family test will be financially rewarded We want to boost professional and public pride in all the caring professions, and to empower patients to demand improvements where care is not as good as it could be. By 2015, a further part of this objective is to increase the proportion of people, across all areas of care, who rate their experience as excellent or very good The second objective for the Board, which will require joined-up care between the NHS and local authorities across health, education and social services, is to improve the standards of care and experience for women and families during pregnancy and in the early years for their children. As part of this, we want the Board to work with partner organisations to ensure that the NHS: offers women the greatest possible choice of providers; 17
37 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 ensures every woman has a named midwife who is responsible for ensuring she has personalised, one-to-one care throughout pregnancy, childbirth and during the postnatal period, including additional support for those who have a maternal health concern; reduces the incidence and impact of postnatal depression through earlier diagnosis, and better intervention and support Our ambition is to help give children the best start in life, and promote their health and resilience as they grow up; and the Government s commitment to an additional 4,200 health visitors by 2015 will help to ensure this vital support for new families. We expect to see the NHS, working together with schools and children s social services, supporting and safeguarding vulnerable, looked-after and adopted children, through a more joined-up approach to addressing their needs. We welcome the Board s commitment to its full participation in local safeguarding arrangements for vulnerable children and adults. We will work with the NHS Commissioning Board, and Healthwatch England, to consider how best to ensure that the views of children, especially those with specific healthcare needs, are listened to One area where there is a particular need for improvement, working in partnership across different services, is in supporting children and young people with special educational needs or disabilities. The Board s objective is to ensure that they have access to the services identified in their agreed care plan, and that parents of children who could benefit have the option of a personal budget based on a single assessment across health, social care and education Timely access to services is a critical part of our experience of care. The NHS should be there for people when they need it; this means providing equally good care seven days of the week, not just Monday to Friday. More generally, over the last decade, the NHS has made enormous improvements in reducing waiting times for services. The people of England expect all parts of the NHS to comply with the rights, and fulfil the commitments set down in the NHS Constitution, including to maintain high levels of performance in access to care. The Board s objective is to uphold these rights and commitments, and where possible to improve the levels of performance in access to care Too often, access to services for people with mental health problems is more restricted and waiting times are longer than for other services, with no robust system of measurement in place even to quantify the scale of the problem. As part of its objective to put mental health on a par with physical health, we expect the Board to be able to comprehensively identify levels of access to, and waiting times for, mental health services. We want the Board to work with CCGs to address unacceptable delays and significantly improve access and waiting times for all mental health 18
38 Ensuring that people have a positive experience of care services, including IAPT. We will also work with the Board to consider new access standards, including waiting times, for mental health services, including the financial implications of any such standards. Ensuring that people have a positive experience of care: Key areas where progress will be expected (Part four of the NHS Outcomes Framework) Overarching indicators 4a Patient experience of primary care i GP services ii GP out-of-hours services iii NHS Dental Services 4b Patient experience of hospital care 4c Friends and Family test Improvement areas Improving people s experience of outpatient care 4.1 Patient experience of outpatient services Improving hospitals responsiveness to personal needs 4.2 Responsiveness to in-patients personal needs Improving people s experience of accident and emergency services 4.3 Patient experience of A&E services Improving access to primary care services 4.4 Access to i GP services and ii NHS dental services Improving women and their families experience of maternity services 4.5 Women s experience of maternity services Improving the experience of care for people at the end of their lives 4.6 Bereaved carers views on the quality of care in the last 3 months of life Improving the experience of healthcare for people with mental illness 4.7 Patient experience of community mental health services Improving children and young people s experience of healthcare 4.8 An indicator is under development Improving people s experience of integrated care 4.9 An indicator is under development 19
39 5. Treating and caring for people in a safe environment and protecting them from avoidable harm 5.1 As indicated in the NHS Constitution, patients should be able to expect to be treated in a safe and clean environment and to be protected from avoidable harm. In recent years the NHS has made progress in developing a culture of patient safety in the NHS, through the introduction of stronger clinical governance within organisations. But much remains to be done. 5.2 Improving patient safety involves many things: treating patients with dignity and respect; high quality nursing care; creating systems that prevent both error and harm; and creating a culture of learning from patient safety incidents, particularly events that should never happen, such as wrong site surgery, to prevent them from happening again. 5.3 The NHS Commissioning Board s objective is to continue to reduce avoidable harm and make measurable progress by 2015 to embed a culture of patient safety in the NHS including through improved reporting of incidents. 5.4 It is also important for the NHS to take action to identify those groups known to be at higher risk of suicide than the general population, such as people in the care of mental health services and criminal justice services. The Board will need to work with clinical commissioning groups to ensure that providers of mental health services take all reasonable steps to reduce the number of suicides and incidents of serious selfharm or harm to others, including effective crisis response. 20
40 Treating and caring for people in a safe environment and protecting them from avoidable harm Treating and caring for people in a safe environment and protecting them from avoidable harm: Key areas where progress will be expected (Part five of the NHS Outcomes Framework) Overarching indicators 5a Patient safety incident reporting 5b Safety incidents resulting in severe harm or death 5c Hospital deaths attributable to problems in care Improvement areas Reducing the incidence of avoidable harm 5.1 Incidence of hospital-related venous thromboembolism (VTE) 5.2 Incidence of healthcare assosiated infection (HCAI) i Incidence of MRSA ii Incidence of C. difficile 5.3 Incidence of newly-acquired category 2, 3 and 4 pressure ulcers 5.4 Incidence of medication errors causing serious harm Improving the safety of maternity services 5.5 Admission of full-term babies to neonatal care Delivering safe care to children in acute settings 5.6 Incidence of harm to children due to failure to monitor 21
41 6. Freeing the NHS to innovate 6.1 The Government and the NHS Commissioning Board are of one mind in recognising that the scale of the ambitions in this mandate cannot be achieved through a culture of command and control. Only by freeing up local organisations and professionals, and engaging the commitment of all staff to improve and innovate, can the NHS achieve the best health outcomes in the world. This mandate, together with new legal duties that relate to promoting autonomy, demands a new style of leadership from Ministers and from the Board which is about empowering individuals and organisations at the front line of the NHS. We welcome the Board s commitment to support improved outcomes, including by understanding and responding to the needs and preferences of patients and communities locally. 6.2 The Board s objective is to get the best health outcomes for patients by strengthening the local autonomy of clinical commissioning groups, health and wellbeing boards, and local providers of services. The Government will hold the Board to account for achieving this; and it will be supported by a process of comprehensive feedback for assessing the Board s performance. 6.3 The establishment of CCGs and health and wellbeing boards is a critical part of the process of decentralising power, as is the progression of NHS trusts through the pipeline to Foundation Trust status under the leadership of the NHS Trust Development Authority. The Board has a vital role in completing the safe transition to a system of fully authorised CCGs. By engaging and supporting emerging CCGs, the Board can ensure that as many CCGs as are willing and able can be authorised fully, without conditions, by April For each of those authorised with conditions, the Board intends to set out a clear timetable and path to full authorisation. CCGs will be in full control over where they source their commissioning support. A sign of the Board s success will be that it sets out and operates a transparent system for intervention in CCGs where this is needed. 6.4 The objectives in this mandate can only be realised through local empowerment. The Board s role in the new system will require it to consider how best to balance different ways of enabling local and national delivery. These may include: the power of its expertise and its professional leadership, working with partners such as the Royal Colleges; its ability to bring NHS organisations together across larger geographical areas, not as the manager of the system, but as its convener; 22
42 Freeing the NHS to innovate its ability to work in partnership with local authorities and commissioners, particularly through health and wellbeing boards; its duties and capabilities for engaging and mobilising patients, professionals and communities in shaping local health services; its duties to promote research and innovation the invention, diffusion and adoption of good practice; the transformative effect of information and transparency, enabling patients to make fully informed decisions, and encouraging competition between peers for better quality; its control over incentives such as improving the basis of payment by results, introducing the quality premium for CCGs, and the quality and outcomes framework in the GP contract; leading the continued drive for efficiency savings, while maintaining quality, through the Quality Innovation Productivity and Prevention (QIPP) programme; and by spreading better commissioning practice, including redesigning services, open procurement and contracting for outcomes, to ensure consistently high standards across all areas of commissioning. 6.5 To support the NHS to become more responsive and innovative, the NHS Commissioning Board s objective by 2015 is to have: fully embedded all patients legal rights to make choices about their care, and extended choice in areas where no legal right yet exists. This includes offering the choice of any qualified provider in community and mental health services, in line with local circumstances. The Government will shortly publish a Choice Framework, following consultation, which will help patients understand the choices they can expect to have, and the Board is working further with Monitor on how choice can best be used to improve outcomes for patients; supported the creation of a fair playing field, so that care can be given by the best providers, whether from the public, independent or voluntary sector. This calls for the Board to lead major improvements in how the NHS undertakes procurement, so that it is more open and fair, and allows providers of all sizes and from all sectors to contribute, supporting innovation and the interests of patients; made significant improvements in extending and improving the system of prices paid to providers, so that it is transparent, and rewards people for doing the right thing. 6.6 The previous administration commissioned an independent evaluation of the impact of many of its policies on the NHS, and during 2013 the Department of Health will commission a similar evaluation programme. 23
43 7. The broader role of the NHS in society 7.1 The NHS is the biggest public service in the country, accounting for eight per cent of national income. It contributes to the growth of the economy: not only by addressing the health needs of the population, thereby enabling more people to be economically active; but also through supporting the life sciences industry, by adopting and spreading new technologies; and through exporting innovation and expertise internationally. 7.2 The NHS Commissioning Board s objective is to ensure that the new commissioning system promotes and supports participation by NHS organisations and NHS patients in research funded by both commercial and non-commercial organisations, most importantly to improve patient outcomes, but also to contribute to economic growth. This includes ensuring payment of treatment costs for NHS patients taking part in research funded by Government and Research Charity partner organisations. 7.3 The NHS and its public sector partners need to work together to help one another to achieve their objectives. This is a core part of what the NHS does and not an optional extra, whether it is working with local councils, schools, job centres, housing associations, universities, prisons, the police or criminal justice agencies such as Police and Crime Commissioners and Community Safety Partnerships. The NHS Commissioning Board s objective is to make partnership a success. This includes, in particular, demonstrating progress against the Government s priorities of: continuing to improve services for both disabled children and adults; continuing to improve safeguarding practice in the NHS; contributing to multi-agency family support services for vulnerable and troubled families; upholding the Government s obligations under the Armed Forces Covenant; contributing to reducing violence, in particular by improving the way the NHS shares information about violent assaults with partners, and supports victims of crime; improving services through the translation of scientific developments into benefits for patients; helping people experiencing ill health, whether mental or physical, to remain in or return to work, and avoid homelessness; 24
44 The broader role of the NHS in society developing better healthcare services for offenders and people in the criminal justice system which are integrated between custody and the community, including through development of liaison and diversion services; championing the Time to Change campaign to raise awareness of mental health issues and reduce stigma, including in the NHS workforce. 25
45 8. Finance 8.1 The NHS Commissioning Board s revenue budget for is 95,623 million (of which 1,843 million is for delivery of the section 7A agreement 2 with the Secretary of State) and its capital budget is 200 million 3. At a time of great pressure on the public finances, it is vital to deliver this mandate within available resources, both in the current spending review period and beyond. Therefore, the Board s objective is to ensure good financial management and unprecedented improvements in value for money across the NHS, including ensuring the delivery of its contribution, and that of CCGs, to the QIPP programme. The Board will also need to comply with the financial directions made under the NHS Act 2006 and published alongside this mandate, which set out further technical limits, including spending on administration. Like any other public body it will be covered by all relevant government guidance on the management of public finances, which are summarised in the Framework Agreement between the Department of Health and the NHS Commissioning Board. 8.2 The Board will be responsible for allocating the budgets for commissioning NHS services. This will prevent any perception of political interference in the way that money is distributed between different parts of the country. The Government expects the principle of ensuring equal access for equal need to be at the heart of the Board s approach to allocating budgets. This process will also need to be transparent, and to ensure that changes in allocations do not result in the destabilising of local health economies. 2 The NHS Commissioning Board will be responsible for carrying out some specific public health functions on behalf of the Secretary of State for Health. These functions, and further details of the funding granted to support them, will be set out in an agreement made under section 7A of the NHS Act See section 223D of the NHS Act 2006 (financial duties of the Board); the revenue and capital budgets are the amounts specified as the limits on total resource use under subsections (2) and (3). 26
46 9. Assessing progress and providing stability 9.1 The Government is formally setting the NHS Commissioning Board the objectives in this document under section 13A of the National Health Service Act 2006, as amended by the Health and Social Care Act We will assess annually the success of the Board against the progress it makes against this mandate, and in carrying out other legal duties and functions. 9.2 The NHS Commissioning Board will be directly commissioning NHS services provided by GPs, dentists, community pharmacists and community opticians; specialised care; health services for people in custody; and military health. This offers a great opportunity to improve standards and national consistency, for example in services for people with rare conditions. The Board has an important responsibility to drive improvements in the quality of primary care, reflecting the vital role that stronger primary care will play in supporting delivery of objectives across this mandate. 9.3 The Department will hold the Board to account for the quality of its direct commissioning, and how well it is working with clinical commissioners, health and wellbeing boards, and local healthcare professionals. An objective is to ensure that, whether NHS care is commissioned nationally by the Board or locally by clinical commissioning groups, the results the quality and value of the services should be measured and published in a similar way, including against the relevant areas of the NHS Outcomes Framework. Success will be measured not only by the average level of improvement but also by progress in reducing health inequalities and unjustified variation. 9.4 Every year, the Board must report on its progress, and the Government will publish an annual assessment of the Board s performance. To ensure that our assessment is fair, the Government will invite feedback from CCGs, local councils, patients and any other people and organisations that have a view. This will mean successes can be recognised, and areas for improvement can be acted on. 4 The Secretary of State also has power to use the Mandate to set any requirements that he thinks are necessary for the purpose of achieving the objectives; these must be backed up by regulations. This mandate does not include any requirements. 27
47 The Mandate: A mandate from the Government to the NHS Commissioning Board: April 2013 to March This mandate provides democratic legitimacy for the work of the Board. It will be updated annually and laid before Parliament. The Government will maintain constancy of purpose, and strive to keep changes between mandates to the minimum necessary. In this way the Mandate will help provide greater stability for the NHS to plan ahead, innovate and excel to bring the greatest benefit to all those who use it. 28
48 Crown copyright Nov 2012 Produced by Williams Lea for the Department of Health
49 Paper 03 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title October (Month 7) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Esyllt Edwards, Information Analyst Craig Macbeth, Deputy Director of Finance Nature of Report Category of Item Context For Information For Discussion For Approval Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary The Trust s month 7 Performance Report is detailed in the attached paper. Received or approved by Legal Implications None Recommendation It is recommended that the Board note: The performance at October 2012 (Month 7). U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 1
50 Paper 03 BOARD OF DIRECTORS INTEGRATED PERFORMANCE REPORT OCTOBER Introduction 1.1 This paper presents the Trust s performance at the end of October 2012, the seventh month of the 2012/13 financial year. 1.2 The 2012/13 performance report details performance against the core standards set nationally by Monitor, the Department of Health and Care Quality Commission, locally agreed CQUIN quality improvement targets and internally driven improvement targets. 1.3 The scorecard and performance report format and metrics have been developed using the Trust s electronic planning and performance system (interplan) and reflect the format agreed by the Board in the May 2012 Trust Board paper 2012/13 Trust Balanced Scorecard. 1.4 Domain 5, of this report looks at the external perception of the Trust and includes further details of performance against Monitor s compliance framework which supports the Trust s self declarations to Monitor at the end of each quarter. 2. Chief Executive s Overview 2.1 The position for October shows a much improved position in terms of overall activity delivery and performance on RTT measures. Performance on quality remains strong. In terms of resources, although we are achieving to date this requires continued focus for the remainder of the year. We have been successful in securing additional support from the PCT to manage the cost of delivery on 18 weeks and it is really encouraging to note our return to performance on the 90%/95% measures. 2.2 Focus continues on the 92% achievement and we are tracking progress against our delivery plan to March Monitor have informed us that we will be rated as red until we achieve compliance on this measure. 2.3 In terms of overall productivity, our treatment of patients on a day case basis continues to grow and our stays for the main procedures reduces we have made huge improvements in these areas and are focussing on the longer stays which will support overall further improvements in these metrics. 3. October Performance Overview 3.1 Domain 1 Patient Safety Patient Safety: Directors Assessment Underlying performance for this domain remains strong with focus continuing on monitoring and assessing patient falls Infection Control and Screening There were no cases of hospital acquired MRSA bacterium or C. difficile in October. We continue to forecast delivery of the C. Difficile target however recognising the risk of delivery given a low in year target of 2 cases for the year. It should be noted that within the 2012/13 Compliance Framework a de-minimis of 12 cases per year has been applied providing a level of buffer for the Trust should the C. difficile target be breached Never Events There were no never events in October. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 2
51 Paper Serious Incidents A fracture as a result of a patient fall was reported as a serious incident in October. The incident has been investigated and recommendations introduced regarding mobility of patients post treatment. The infection outbreak incident in September has now been downgraded from a Serious Incident by the Local Cluster with the graph updated accordingly Mortality Rates There were three patient deaths during the month. All three patients had been placed on the Liverpool Care Pathway and the deaths were not unexpected Medicines Management There were 18 medication incidents relating to patient care during October. There were 10 administration errors, 3 dispensing error, 3 regarding storage, 1 relating to risk of procedure having to be cancelled and 1 relating to medication a patient received on transfer from another hospital. All incidents have been or are under investigation by the area manager with the hospital involved in the last incident being informed of the error to enable their own investigation. The 18 incidents represented 1.25% of the total Trust inpatient activity for the month and is reported as amber in the scorecard Patient Falls As a result of a data audit, the year to date falls figures have been updated. There were 20 patient falls in October a slight reduction from last month, which relates to 2.61% of the inpatient activity. This remains above the target ceiling of 1.6% and is reported as red in the scorecard. In addition to the serious incident reported in section above, another two patients required treatment as a result of their falls. The Falls Protocol was followed in all incidents and a route cause analysis completed for each incident. Although work continues to reduce patient falls with targeted training through the senior nurse forum and at ward level, the year-end forecast is currently amber in reflection of the trend in the level of falls over the last few months. Since the introduction of regular rounding on one of the Orthopaedic Wards in August, there has been a reduction in the number of falls on that ward. The practice of ward rounding will be extended to the other wards over the coming months Pressure Ulcer Assessments - The Trust continues to maintain its performance with regards to pressure ulcer assessments undertaking 99.82% of pressure ulcer assessments against a target of 99%. There were two hospital acquired grade 2 pressure ulcers during October which relates to 0.15% of the inpatient contract activity in month. There were no hospital acquired Grade 3 or 4 pressure ulcers CQUINs The Trust has ten CQUIN goals in 2012/2013 which are made up of 16 separate indicators. The VTE Risk Assessment target continues to be achieved with 100% of the relevant patients having an assessment completed during October. Detailed progress on all of the indicators is tracked by the Quality and Safety Committee with work continuing to deliver the goals during the year. 3.2 Domain 2 - Patient Experience Patient Experience: Directors Commentary The key area of focus for this domain remains the delivery of the access time targets and the continued active management of delayed discharges Patient Satisfaction Net Promoter Question In October, the Trust achieved a score of 87.50, which maintains our excellent position across the Local Cluster Complaints and Compliments A total of 71 compliments were received in October following episodes of care in various departments within the Trust. The feedback provided included comments regarding the overall quality of care, support and information provided by staff and friendly care environment within the hospital. 5 complaints were received which represents 0.05% of the contract activity. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 3
52 Paper 03 Four complaints were regarding the quality of care and were related to length of time it took to be admitted to a ward from the admission on day of surgery unit, lack of support and information when requesting post-operative advice, content of clinic note following consultation and the length of time to process referral for an MRI scan The remaining complaint was an operational issue regarding the handling of booking an ultrasound appointment Access to Bone Tumour Services - The Trust achieved all of the key cancer waiting times targets in month Access to Services (Waiting Times) The English 6 week diagnostic target was maintained in month with 99.55% of patients seen in 6 weeks. The Trust is now delivering performance on two of the 18 week RTT targets in line with the original plan and trajectories agreed by Monitor and the PCT. In month, 91.33% of admitted patients were treated within 18 weeks against of target of 90% whilst 95.15% of non-admitted patients were seen within 18 week against a target of 95%. We have now agreed new trajectories with the Local Health Economy for delivery of the 92% incomplete pathway target by the end of March % of patients on an incomplete pathway at the end of October were waiting less than 18 weeks against the target of 92%. As part of the on-going work with Welsh Commissioners to improve the performance back to within tolerance levels, in October 89.11% of Welsh patients completed their RTT pathways within the 26 weeks against a target of 95%. As the end of the month 90.34% of patients on an incomplete pathway were waiting under 26 weeks against a target of 95% with a reduction in the number of patients waiting over 36 weeks. It should be noted that Powys LHB have written to the Trust formally to ask us, for all future patients bookings, to extend the time patients wait to be treated to 36 weeks (from 26 weeks). This is as a result of financial pressures. Powys LHB has written to all their GPs to inform them of this instruction. The Inpatient Waiting List remains within tolerance levels. There continues to be a decrease in the number of patients on the outpatient waiting list as part of the work to reduce the waiting time for the first milestone in the referral to treatment pathway. The number waiting is expected to continue to decrease as additional clinics are arranged in order to support the plans for recovery of delivery of all RTT targets Reportable Cancellations This is a cumulative metric which compares on the day cancellations to the number of elective discharges in month. The metric remains in line with the target at the end of October with a cumulative performance of 0.66% against a target of less than 0.8%. All patients cancelled have been re-dated within the 28 day standard cancellation guarantee period with the work of the pre-surgical contact team having a positive effect in reducing avoidable on the day cancellations Delayed Discharges As a result of the specialist care packages required by some patients post discharge, the percentage of delayed discharges against occupied beds on the last Thursday of the month was above the SHA target of 3.5% at the end of October at 5.43%. This represented seven patients being delayed at the month end. The Nursing Team have regular meetings with community partners to try and ensure that these care packages are arranged but the majority of delays are beyond the control of the Trust Day Readmission Rates to RJAH for all Specialties Four patients were readmitted as an emergency within 30 days of initial discharge in August, which represents 0.64% of the patients discharged against a target of less than 1.10%. All U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 4
53 Paper 03 readmissions are monitored by the Infection Control Team who complete a full analysis regarding the reasons for readmission. 3.3 Domain 3 Efficiency Efficiency: Directors Commentary Although October has been a challenging month in efficiency as the focus has been on improving the Trust s RTT performance, a number of the metrics have improved in month and are expected to return in line with targets going forward in Quarter Referrals Received for Consultant Led Services This metric monitors the number of referrals received from all sources into Consultant led clinics. The main increase over the last few months have been as a result of GP referrals to the orthopaedic sub-specialties which include additional referrals from Betsi Cadwaladr University Health Board as part of a two year agreement for delivery of additional activity. The year to date data has been refreshed at the end of October; this has not resulted in a significant change to previously reported data Activity - Surgery The arrangement of additional clinic and theatre sessions and the continuation of agreements to deliver certain procedures externally during October resulted in increased throughput in-month in line with monthly plans. Work will continue to ensure utilisation of clinic and theatre sessions over the coming months to support the delivery of the waiting time targets and recover the shortfall in activity from earlier in the year Activity Medicine The year to date performance against plan for the medicine division remains ahead of plan New to Follow Up Ratio The new to follow up ratio in month was 1:1.86 which is within the target level of 1: BADS Activity 75.40% of patients whose procedure met the British Association of Day Surgery (BADS) recommendations were treated as daycases in October against a target of 84%. Work continues to assess the clinical pathways of patients admitted for a BADS procedure with the aim to continue to increase the number treated as daycase. The daycase percentage continues to increase for the procedures of autograft anterior cruciate ligament reconstruction, bunion and subacromial decompression procedures where in the past the majority of patients would have had a one night hospital stay Admission on the Day of Surgery 87.76% of the inpatients discharged during October had been admitted on the day of their surgery against a target of 84%. Work continues to ensure that patients are admitted on the day of surgery where appropriate with performance over the last four months ahead of the year-end target of 85% Theatre Efficiency (Utilisation of Available Staffed Sessions) With an average of 2.33 cases per session, the theatre utilisation rate was slightly below the target of 95% during October at 93.33%. Work is continuing to ensure that theatre sessions are being utilised where possible in order to support the delivery of the annual activity plans and delivery of the RTT targets Average Length of Stay For patients discharged during October, the overall average length of stay (including daycases) was 2.27 days. This was slightly above the target of 2.10 and was linked to a richer casemix in month and a small number of long stay patients due to medical co-morbidities Enhanced Recovery (Hips and Knees) Over 250 patients were discharged following primary hip or knee replacements during October. Of these 42.74% were discharged within 3 days of admission as part of the enhanced recovery protocol. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 5
54 Paper 03 The average length of stay for primary hips (4.63 days) and knees (4.42 days) was slightly above the target of 4.25 days and continues to be distorted by a number of patients whose stay was over 10 days due to complexity, co-morbidities and other medical reasons. The Medical Director has instigated a working group to look into the issues causing the longer stays Bed Occupancy Linked with the increase in activity during the month, the average percentage bed occupancy on the adult orthopaedic wards during October was 84.14%. Variation in occupancy levels is being monitored at ward level to ensure the continued availability of beds for admission and provision of high level clinical care. 3.4 Domain 4 Resources Resources: Directors Commentary October was the first month of operating under a new delivery framework that has been introduced to ensure the achievement of waiting list reductions required to sustain RTT targets within the additional financial resources secured from Commissioners. This has been largely successful although there needs to be continued focus to ensure we maintain delivery. Sickness levels increased in month which given the increased volumes of work has placed further pressure on our workforce budgets. The Department of Health Reference Cost Index (RCI) for 2011/12 has been published and this once again places the Trust in a favourable position compared to our peer organisations in the Orthopaedic Alliance our published RCI is 106 compared to 105 the previous year. This underlines the significant sustainable improvements we have made as an organisation to our operating model and looking forward it is essential that we maintain this to allow us to continue to progress our collective aims Finance Overall A surplus of 0.24m was made during October which fell marginally short of the 0.28m that had been planned under the new delivery framework. Cumulatively we have now hit just over 1m surplus for the year which equates to two thirds of our overall target after seven months of the year. Our financial risk rating remains at a level three which is essential for our external perception by Monitor. Income We have agreed a revised contract value with SCPCT that incorporates the RTT delivery plan and which also secures a re-investment of the contract penalty levied earlier in the year in respect of old year breaches. This positive outcome had been factored into our September financial position. The overall income position for October was an over achievement against the new delivery framework of 0.6m driven by increased outpatients and private patient billing Expenditure The overall cost position was 0.65m overspent against the new delivery plan in month. The main drivers for this were: 0.25m of additional implant costs driven by both the volume and mix of work undertaken. An audit of the new Theatre stock management system has been requested to ensure the integrity of the new reports. 0.17m of additional spend with the private sector ( 0.27m in total). This is expected to cease from December although specific long wait patients may cause additional pressures in this area. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 6
55 Paper 03 Out of Job Plan (OJP) Expenditure increased in outpatients however this was covered by additional income. A residual area of focus is OJP usage in Anaesthetics Cost Improvements We are reporting the delivery of an additional 0.29m of efficiencies in month which was in line with plan. This position was driven by a number of substitute schemes coming on line during the month, many of which focused on improvements in productivity of our support services. As activity continues to increase and exceed last year levels there will be scope for further efficiencies to be realised provided that the cost base is tightly managed. This will be essential in delivering the full programme Cash Balances increased from 3.5m to 4m in month but remain 0.4m behind the original plan. This is largely as a result of the additional income earned from our Commissioner performance not yet being cash backed although this position will be rectified over the coming months Capital Expenditure in month amounted to 0.19m which was 0.06m ahead of plan in month and 0.3m behind plan cumulatively. Expenditure is expected to increase in the remainder of the year as per our revised capital programme linked to the new Tumour development Sickness Rates Sickness absence increased in October to 3.78%, which was due to increased short term absences caused by colds, diarrhoea/vomiting, infections and long term absences related to pregnancy and cardiac/coronary causes. As this is still above the target of 2.5%, work continues to reduce absence, and a revised sickness absence management policy is currently under review with staff side representatives. The Trust s 2012 flu vaccine campaign continues with 480 (37%) staff having received a vaccine up to mid November Staff Turnover Staff turnover remained similar to the previous month at 4.23% in October, and remains well below the 10% ceiling Staff Appraisal Appraisal data continues to improve and is reported to the end of October at 85.28%. 3.5 Domain 5 External Perception The balanced scorecard reflects the Trust s position at the end of October 2012 the seventh month of 2012/ The Quality Governance in-month position is reported as amber-green on the Balanced Scorecard front sheet. Two of the referral to treatment waiting times indicators returned in line with targets in October as described in section which has resulted in an improved rating at the end of the month. Using Monitor s own methodology this results in a risk rating of 1 amber-green (as per appendix 1). Monitor have an override position on the rating they report when we fail a core target for 3 quarters in succession. On this basis whilst our underlying governance rating is amber-green Monitor have overridden this to a Red rating which is discussed in more detail under a separate agenda item The Trust remains compliant with all other remaining Monitor s targets and indicators including MRSA, Cancer waiting times, and Learning Difficulties. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 7
56 Paper Recommendation 4.1 It is recommended that the Board: Note the performance for October (Month 7) John Grinnell Director of Finance, Contracting and Performance U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 8
57 Paper 03 Balanced Scorecard Trust Board 2012 / 2013 Month - 7 Patient Safety Overall Performance Period Key Metric Actual Year to date Change Forecast Oct-12 Infection Control g g same g Oct-12 Serious Incidents g g same g Oct-12 Never Events g g same g Oct-12 Medicine Management a a same g Oct-12 Unexpected Deaths g g same g Oct-12 Patient Falls r r same g Oct-12 Pressure Ulcer Assessments g g same g Oct-12 CQUIN g g same g Patient Experience Overall Performance Period Key Metric Actual Year to date Change Forecast Oct-12 Patient Satisfaction - Net Promoter Question g g same g Oct-12 Number of Complaints g a same g Oct-12 Access to Bone Tumour Services g g same g Oct-12 Access to Services a r better g Oct-12 Reportable Cancellations g g same g Oct-12 Delayed Discharges r r worse g Sep day Readmission Rates to RJAH for all specialties g g same g VISION To be the leading centre for high quality, sustainable Orthopaedic and related care, achieving excellence in both experience and outcomes for our patients Resources Overall Performance Oct-12 Key Metric Actual Year to date Change Forecast Oct-12 EBITDA g g same g Oct-12 Net Surplus a a worse g Oct-12 CIP Delivery g r better g Oct-12 Capital Expenditure g a better g Oct-12 PSPP g g same g Oct-12 Cash Balance a a better g Oct-12 Sickness Absence a a same g Oct-12 Staff Turnover g g same g Oct-12 Staff Appraisal a a same g Efficiency Overall Performance Period Key Metric Actual Year to date Change Forecast Sep-12 Demand for Services g g same g Oct-12 Activity - Surgery g a same g Oct-12 Activity - Medicine g g better g Oct-12 New to Follow Up Ratio (Consultant Led Activity) g g same g Oct-12 BADS Activity a a same g Oct-12 Admission on Day of Surgery g g same g Oct-12 Theatre Efficiency a r worse g Oct-12 Average Length of Stay a r worse g Oct-12 Enhanced Recovery a a better g Oct-12 Bed Occupancy - Adult Orthopaedic Wards a r better g External Perception Overall Performance Period Key Metric Actual Year to date Change Forecast Oct-12 Monitor Risk Rating - Finance g g same g Oct-12 Monitor Risk Rating - Quality Governance a/g a/g better g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 9
58 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Patient Safety Infection Control Hospital Acquired MRSA Patient Safety Infection Control Hospital Acquired C. Difficile Patient Safety Serious Incidents Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g a g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 10
59 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Patient Safety Never Events Patient Safety Medicine Management Medication Errors - Total Numbers Patient Safety Medicine Management Medication Errors as % of activity Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a g r g a a % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a a a g a a U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 11
60 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Patient Safety Patient Safety Patient Safety Unexpected Deaths Patient Falls Pressure Ulcer Assessments Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r g r g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a r r r r r % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 12
61 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Patient Safety CQUIN VTE Risk Assessments % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 13
62 Balanced Scorecard - Trust Board 2012/13 Month - 07 Patient Experience Patient Satisfaction - Net Promoter Question Patient Experience Number of Complaints Patient Experience Access to Bone Tumour Services 2 week cancer referral target Paper % Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Period Target Actual Performance Apr g Oct-12 Nov- 12 Dec- 12 May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Jan- 13 Feb-13 g g g g g g Mar-13 Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a a g g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 14
63 Balanced Scorecard - Trust Board 2012/13 Month - 07 Patient Experience Access to Bone Tumour Services Cancer 1 month wait Patient Experience Access to Bone Tumour Services Cancer 2 month wait Patient Experience Access to Services Paper weeks RTT (Completed Pathways) % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r r r r r r U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 15
64 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Patient Experience Access to Services 26 week RTT (Incomplete Pathways) Patient Experience Access to Services Patients waiting over 36 weeks Patient Experience Access to Services 18 weeks RTT Admitted % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a a a a a a Number Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Period Target Actual Performance Apr r Oct-12 Nov- 12 Dec- 12 May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Jan- 13 Feb-13 r r r r r r Mar-13 % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r r r r r g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 16
65 Patient Experience Access to Services Balanced Scorecard - Trust Board 2012/13 Month weeks RTT Non-Admitted Patient Experience Access to Services 18 weeks RTT Incomplete Patient Experience Access to Services Paper 03 6 week wait for diagnostics - English Patients % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r r r r r g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r r r r r r % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 17
66 Patient Experience Access to Services Balanced Scorecard - Trust Board 2012/13 Month - 07 Inpatient Waiting List Total Patient Experience Access to Services Outpatient Waiting List (Consultant Led Activity Only) Patient Experience Reportable Cancellations Paper 03 Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr-12 3, , a May-12 3, , Jun-12 3, , Jul-12 3, , Aug-12 3, , Sep-12 3, , Oct-12 3, , Nov-12 3, Dec-12 3, Jan-13 3, Feb-13 3, Mar-13 3, a g g g g g Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr-12 4, , r May-12 4, , Jun-12 4, , Jul-12 3, , Aug-12 3, , Sep-12 3, , Oct-12 3, , Nov-12 3, Dec-12 3, Jan-13 3, Feb-13 3, Mar-13 3, r r r r r r % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g a a g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 18
67 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Patient Experience Delayed Discharges % delayed discharges against occupied beds on last Thursday of month 7 Patient Experience 30 Days Readmission Rates to RJAH for all specialties 2.0 % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g a g g a r % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct no data Nov Dec Jan Feb Mar a r g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 19
68 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Resources Resources Resources Sickness Absence Staff Turnover Staff Appraisal % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a a r r a a % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a a a a a a U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 20
69 Efficiency Demand For Services Balanced Scorecard - Trust Board 2012/13 Month - 07 Referrals Received for Consultant Led Services Efficiency Activity - Surgery Surgical Division Activity - Inpatient Contract Efficiency Activity - Surgery Paper 03 Surgical Division Activity - Outpatient Contract Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr-12 2, , g May-12 2, , Jun-12 2, , Jul-12 2, , Aug-12 2, , Sep-12 2, , Oct-12 2, no data Nov-12 2, Dec-12 2, Jan-13 2, Feb-13 2, Mar-13 2, g g g g g Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May-12 1, Jun-12 1, Jul-12 1, , Aug-12 1, , Sep-12 1, , Oct-12 1, , Nov-12 1, Dec Jan-13 1, Feb-13 1, Mar-13 1, a r r r r r Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr-12 4, , g May-12 6, , Jun-12 6, , Jul-12 6, , Aug-12 6, , Sep-12 6, , Oct-12 6, , Nov-12 7, Dec-12 6, Jan-13 6, Feb-13 6, Mar-13 6, g a r r g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 21
70 Efficiency Activity - Medicine Balanced Scorecard - Trust Board 2012/13 Month - 07 Medicine Division Activity - Inpatient Contract Efficiency Activity - Medicine Medicine Division Activity - Outpatient Contract Efficiency Paper 03 New to Follow Up Ratio (Consultant Led Activity) Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a r g a g a Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr-12 1, a May-12 1, , Jun-12 1, , Jul-12 1, , Aug-12 1, Sep-12 1, , Oct-12 1, , Nov-12 1, Dec Jan-13 1, Feb-13 1, Mar-13 1, g g a r g g Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g a g g g g U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 22
71 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Efficiency BADS Activity Efficiency Admission on Day of Surgery Efficiency Theatre Efficiency % Staffed Theatre Lists Utilised % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a a a a a a % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g a g g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a r a r g a U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 23
72 Balanced Scorecard - Trust Board 2012/13 Month - 07 Efficiency Average Length Of Stay - Elective Including Daycase Efficiency Enhanced Recovery Average Length of Stay Primary Hips Efficiency Enhanced Recovery Paper 03 Average Length of Stay Primary Knees Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr a May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a r r r g a Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar a g r g a r Number Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r r r r r r U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 24

73 Balanced Scorecard - Trust Board 2012/13 Month - 07 Paper 03 Efficiency Enhanced Recovery % of hip and knee patients discharged in 3 days or less Efficiency Bed Occupancy - Adult Orthopaedic Wards % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr g May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar g g g g g g % Apr-11 May- 11 Jun- 11 Jul-11 Aug- 11 Sep- 11 Oct-11 Nov- 11 Dec- 11 Jan- 12 Feb-12 Mar-12 Apr-12 May- 12 Jun- 12 Jul-12 Aug- 12 Sep- 12 Oct-12 Nov- 12 Dec- 12 Jan- 13 Feb-13 Mar-13 Period Target Actual Performance Apr r May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar r r a r r a U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 25
74 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 A) Income and Expenditure Account m C) Cashflow Statement '000 Clinical Income from activity Private Patient income Other income Original Annual Plan Original Plan In Month Revised Plan Actual Variance Original Plan Pay (46.17) (48.27) (3.83) (4.05) (4.24) (0.19) (27.09) (27.86) Non-pay EBITDA (31.78) 6.02 Finance Costs (4.52) (4.52) (0.38) (0.38) (0.39) (0.00) (2.61) (2.61) Surplus/ Loss Before Impairment Impairment Revised Plan (33.03) (2.80) (2.90) (3.36) (0.46) (18.29) (18.75) 0.62 (0.05) Year to Date Annual In Month Year To Date Revised Plan Actual Variance Forecast Risk Plan Actual Plan Actual (28.05) (19.21) 0.03 (0.19) (0.46) (0.05) (0.09) 0.00 (2.59) (0.11) (48.27) (33.03) 6.02 (4.52) EBITDA Impairments Working Capital Movement Operating Cash Flow Capital Expenditure Proceeds from sale of assets Operating Cash Flow after Capital Net Interest Paid / Received Provisions Movement Loans Received Loan Repayment Lease Payment PDC Received PDC Dividend Paid Cash Flow for Period Opening Cash Balance ,588 3, (288) (1,457) ,300 2,160 (143) (159) (2,869) (2,431) (271) 0 (8) (5) 5 (4) (164) (28) (382) (25) (25) (2) (6) (14) (16) (573) (573) (214) (1,263) 4,171 3,543 5,273 5,273 Net Surplus (0.05) (0.09) 1.50 Closing Cash Balance 5,059 4,010 5,059 4,010 B) Statement of Financial Position '000 D) Predicted Monitor Risk Assessment/Ratio's Sep-12 Oct-12 Movement Annual Plan YTD Actual YTD Risk Rating Annual Forecast Forecast Risk Rating Fixed Assets Non current receivables Total Non Current Assets Inventories (Stocks) Receivables Cash at Bank and in hand Total Current Assets Payables (Creditors) Borrowings Current Provisions Total Current Liabilities 51,077 50,998 (79) Depreciation in excess of capital expenditure (64) Reduction in new RTA notifications 51,886 51,742 (144) 1,427 1,375 (52) Adjustments from Theatre and Pharmacy reports 5,953 6, Increased accrued income 3,543 4, ,924 12,050 1,126 (8,876) (9,793) (916) Increased system creditors (73) (79) (6) (305) (155) 150 Reduction in pay provisions (9,254) (10,026) (772) EBITDA Margin 6.2% EBITDA Achieved 101.0% Return on Assets (ROA) I&E Surplus Margin 1.7% 2.0% Liquidity Ratio (Days) 32 Overall risk rating 3 5.7% 96.3% 1.6% 0.8% % 1.7% % 5 1.6% Total Assets less Current Liabilities Non Current Borrowings Non Current Provisions Creditors due after more than one year Total Assets Employed 53,555 53, (295) (284) 11 (333) (319) 14 Executive Commentary (628) (603) 25 52,927 53, Public Dividend Capital 31,220 31,220 0 Revenue Position 791 1, In month surplus / (loss) Retained Earnings 7,916 7,916 0 Revaluation Reserve 13,001 13,001 0 Total Taxpayers Equity U:\Trust Board & Committees\Public Trust Board\ \November 52,927 53, \Month 7 Integrated Performance Report 26 A surplus of 0.24m was made during October which fell marginally short of the 0.28m that had been planned under the new delivery framework. Budgets for both income and expenditure have been rebased in line with the new framework and all variances referred to in this report have been measured against the revised targets. Income was stronger than anticipated in the month as a result of additional outpatient activity and private patient billing. This was however offset by higher than expected premium costs for OJP and Private sector.
75 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 E) Income and activity analysis In-patient Spells In-patient Income m In-patient income per spell Inpatients Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb 1213 Spells Plan 1112 Spells Actual 1213 Spells Actual Mar #REF! #REF! 1213 Income m #REF! Plan 1112 Income m Income m Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 3,250 3,200 3,150 3,100 3,050 3,000 2,950 2,900 2,850 2,800 2,750 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb 1213 Income per Spell Plan 1112 Income per Spell Mar During October, we delivered the highest number of inpatient spells of the year so far. This was in line with the new delivery framework which has set increased levels of activity for the second half of the year to recover the shortfalls from quarter 1 and ensure both Commissioner contracts and waiting time targets are maintained. Out-patient Attendances Out-patient Income m Other Income Out-patients Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Monthly Attendances Plan 1213 Attendances 1112 Attendances 1213 Income m Plan 1112 Income m 1213 Income m Private Patients Income m Other Income m Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Outpatient activity showed a sharp increase in month as operational attention switched to patients waiting less than 18 weeks. This pattern is expected to continue throughout quarter 3 as outpatient wait times are brought down to a level that will allow ongoing achievement of waiting time targets. This strong performance further bolstered our income. Private Patient income exceeded plan in month driven by the first tranche of retrospective bills sent out to fully recover all chargeable activities undertaken by the Trust historically. This follows a review undertaken by an independent consultant employed by the Trust to maximise income recoverable from insurance companies Plan m 1112 Actual m 1213 Actual m 1213 Plan m 1112 Actual m 1213 Actual m U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 27
76 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 F) Cost Improvement Programme In Month CIP Achievement 000's In Month CIP Achievement 000's Trust YTD Achievement Against YTD Plan 000's Workforce productivity Staffing 1, , Tactical/miscellaneous Realising the benefits of technology Improving operational efficiency Improved contributions Estates rationalisation Back office functions Diagnostics Corporate Medicine Surgery 1, , , CIP by Theme Oct Plan Oct Actual Year To Date CIP Achievement 000's Workforce productivity Tactical/miscellaneous Realising the benefits of technology Improving operational efficiency Improved contributions Estates rationalisation Back office functions CIP by Division Oct Plan Oct Actual Year To Date CIP Achievement 000's Staffing Diagnostics Corporate Medicine Surgery YTD Plan Total YTD Actual We recognised the delivery of an additional 0.29m of efficiencies in month which was in line with plan. This brings the total ytd to 1.45m which is 0.26m behind plan. The in month position was driven by a number of substitute schemes coming on line during the month, many of which focused on improvements in productivity of our support services. As activity continues to increase and exceed last year levels there will be scope for further efficiencies to be realised provided that the cost base is tightly managed. This will be essential in delivering the full programme. YTD Plan YTD Actual YTD Plan YTD Actual G) Commissioner Performance Year To Date Commissioner Income against Plan m YTD Total Income Against Plan m Clinical Income Shropshire County Telford & Wrekin Other England Contracted Specialised Commissioners Betsi Cadwaladr Powys Other Wales Contracted Non Contracted Activity Exclusions and other Grand Total We have agreed a revised contract value with SCPCT that incorporates the RTT delivery plan and which also secures a reinvestment of the contract penalty levied earlier in the year in respect of old year breaches. This positive outcome had been factored into our September financial position. In delivering our contractual obligations to the end of the year there needs to be a continuation of the push on Shropshire and Telford patients as well as a recovery of the BCU performance. All of these requirements are captured in the delivery framework. YTD Plan m Actual m YTD Plan m Actual m U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 28
77 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 H) Pay Expenditure related Key Drivers/Financial Assumptions Total Pay Expenditure ( m) Trust Pay Cost Per In-patient Spell ( ) Total Pay Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 5,000 4,500 4,000 3,500 3,000 2,500 2,000 1,500 1, Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Pay costs were 0.19m higher than had been budgeted for under the new delivery framework as a result of additional Out of Job plan payments. The overall pay cost per in patient spell did however fall in month. Reserves allocated to divisions in month amounted to 0.12m relating entirely to planned developments Plan 1112 Actual 1213 Actual 1213 Plan 1112 Actual 1213 Actual Out of Job Plan Expenditure ( m) Average OJP Cost Per In-patient Spell ( ) Out of Job Plan Expenditu ure Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar An additional 0.16m of OJP costs were incurred in month above the levels planned in the new delivery framework. Of this an additional 0.08m was undertaken in Outpatients and was funded by a corresponding increase in outpatient income and 0.03m was worked in Radiology as a consequence of the increased outpatient activity. The remaining 0.05m related to anaesthetics. Controls on OJP bookings are still to be fully implemented and this area will continue to be focused upon to ensure it does not compromise our financial plan Plan 1112 Actual 1213 Actual 1213 Plan 1112 Actual 1213 Actual Clinical Bank & Agency Expenditure (,000) Non-Clinical Bank & Agency Expenditure (,000) Bank & Agency Expenditure Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Overall Bank and Agency spend held steady in month. Given the increased outpatient activity that has necessitated the need for both outpatients and diagnostics to flex up capacity, in real terms this marks an improvement upon earlier months Actual 1213 Actual 1112 Actual 1213 Actual U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 29
78 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 I) Non-Pay Expenditure related Key Drivers/Financial Assumptions Total Non-pay Expenditure ( m) Trust Average Non-pay Cost Per In-patient Spell ( ) Total Non-pay Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 1213 Plan 1112 Actual 1213 Actual 3,000 2,500 2,000 1,500 1,000 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 1213 Plan 1112 Actual 1213 Actual Non Pay costs were 0.46m higher than had been budgeted for under the new delivery framework. There have been two main drivers for this adverse position as follows: Increased implant expenditure of 0.28m discussed further below. An additional 0.17m cost of using the private sector (the framework had allowed for 0.1m only). This has been driven by a particularly heavy case mix as we have been reliant upon the private sector to assist with the clearance of some of our longest waiters. A detailed review of each patient episode undertaken in the private sector has been undertaken and further restrictions are to be applied from December onwards to minimise usage of this high premium cost area. Non-pay reserves allocated in month amounted to 0.14m and related to authorised developments only. Implant Expenditure ( m) Average Implant Cost Per Surgical In-patient Spell ( ) Implants Expenditure Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Implant costs exceeded planned values by 0.28 in month. This has been driven by both the volume and mix of work undertaken during the period. An audit of the new Theatre stock management system has been requested to ensure the integrity of the new reports Plan 1112 Actual 1213 Actual 1213 Plan 1112 Actual 1213 Actual Drugs Expenditure ( m) Average Drugs Cost Per In-patient Spell ( ) Drugs Expenditure Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Drugs expenditureremains reasonably steady with a slight increase in line with activity, expenditure above plan continues to relate to specific high cost drugs which are income backed Plan 1112 Actual 1213 Actual 1213 Plan 1112 Actual 1213 Actual U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 30
79 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 J) Balance Sheet Items Analysis Receivables over 90 Days Invoices over 90 days old and over 5K 18.00% Debtor Detail Amount Status 16.00% Insurance Company Private Patient 25,326 Payment pending Debtors 14.00% 12.00% 10.00% 8.00% 6.00% 4.00% 2.00% 0.00% Receivables over 90 Days excl CRU Sep Oct Rugby Club Former employee London PCT W Mids PCTs North West Trust Partner Organisation Private Outpatients Equipment Non contracted activity Old year over performance Salary Recharge Recharge 47,507 11,901 Total invoices over 90 days > 5K 135,748 18,779 Discussions ongoing 20,985 5,913 5,337 With debt recovery agent Discussions ongoing Awaiting final reconciliation Discussions ongoing Payment made in October The percentage of invoices outstanding over 90 days has decreased by a further 1.61% compared to last month but remains in excess of Monitor's 5% target. A detailed review of the aged debt is currently ongoing. Creditors over 90 Days Public Sector Payments Policy Cash Creditors 5.00% 2.50% 0.00% 7, , , , , , , Current Invoices over 90 days % Sep Oct Cash Plan v Actual % 99.00% Date Invested Date of Maturity 23/08/12 23/11/12 Barclays Cash Placed on Investment Accounts Investment Organisation Invested Amount 2,000, Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar TOTAL 2,000,000 Cash Plan Cash Actual U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report % 97.00% 96.00% 95.00% 94.00% 93.00% 92.00% 91.00% 90.00% Sep PSPP Oct Interest rate secured Additional Interest earned 0.56% 1,563 1,563 Creditors over 90 days remain within the Monitor threshold of 5%. The in month performance improved again at 3.5% down from 4.9% last month. Our PSPP metric for invoices paid within 30 days reduced slightly to 96.01% of all invoices paid but remains ahead of the 95% target. Our cash balances increased from 3.5m to 4m in month but remain 0.4m behind the original plan. This is largely as a result of the additional income earned from our Commissioner performance not yet being cash backed although this position will be rectified over the coming months The table to the left is an extract from our investment register showing our investment activity for the year to date and the additional interest that this has secured.
80 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 K) Capital Programme In Month Capital Expenditure '000s Cumulative Capital Expenditure '000s Capital Projects Listing Capital In Month Capital Plan Oct In Month Capital Expenditure Capital Expenditure in month amounted to 0.19m which is 0.06m ahead of plan Cumulative Capital Plan Oct Cumulative Capital Expenditure Cumulatively the programme is behind plan by 0.3m, however the shortfall is expected to be recovered and exceeded in the second half of The full revised capital programme which was approved by the Capital Planning Group during September can now been seen in theforecast outturn on the table to the right. The 0.5m increase being directly linked to the construction of the new Tumour Unit which has beenbrought forward from the programme. Project Estates Backlog Main Entrance Main Entrance - LOF Medical Equipment Diagnostics Equip't X-Ray Refurbishment IT Investment Orthotics Redesign Site Redevelopment Denbighs Stores Sheldon Ward Alice Ward Tumour Unit Other Capital NHS Capital Expenditure Annual Plan In Month Capital Projects 2012/13 In Month 000s Plan Actual Variance ed 000s 000s 000s (35) (30) (37) (76) (9) (40) 40 0 (40) (241) (50) (25) (116) 240 3, In Month 64 YTD Plan 000s YTD Complet 2,728 2,424 YTD Variance (304) Forecast Outturn 4,387 L) Service Line Performance M) Key Financial Risks Service Level Reporting Service Level Reporting Q2 Contribution Analysis Q3 Q4 Q1 Q2 Joint Surgery 23% 22% 20% 16% Medicine 6% 17% 13% 17% Paediatric Services 33% 37% 30% 28% Spinal Services 19% 21% 15% 23% Commentary Use of private sector and increased OJP has impacted margins across Surgery. Continued strong performance from Metabolic Medicine & Rheumatology, Care of the Elderly still operates at a loss despite non recurrent support from the PCT. Reduction in outpatient activity for Paediatric Medicine has reduced the margin. Use of private sector is beneficial for certain spinal surgery procedures compared to in house delivery, RTA income also driving fluctuations. Key Risk Description Delivery of 4% Efficiency programme incorporated into annual plan Emerging cost pressures not captured in plan including inflation Failure to deliver full C-QUIN programme leading to lost income Delivery of additional activity to achieve RTT waiting times at cost in excess of tariff Economic squeeze on public spending leading to Commissioner unaffordability of current contract values Risk Rating Mitigating Action Monthly Divisional Performance reviews to monitor progress. Over identification of schemes to protect from slippage Plan has built in cost pressure reserve Each C-QUIN has a nominated operational and exec lead. Contingency for delivery built into plan Capacity working group in place to consider value for money of all capacity proposals Close working relationships with Commissioners in introducing mutually beneficial demand management schemes Resulting Risk Rating Trading Directorate 24% 21% 25% 28% Physiotherapy now profitable due to new local tariffs and implementation of new staffing structure. The top five financial risks to the delivery of our financial plan have been captured in the table above. Also included are the mitigating actions in place from which a residual risk position has been assessed. All risks and the effectiveness of mitigations are re-assessed each month. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 32
81 Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust Finance Report for period ending 31st October 2012 Paper 03 N) Rolling Cashflow Forecast INCOME Actual Forecast Apr May June July August Sept Oct Nov Dec Jan Feb Mar Apr May June July August Sept Oct Actual Actual Actual Actual Actual Actual Actual Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan Clinical SLA Income 5,964 5,625 6,113 5,970 5,918 5,905 5,909 7,274 6,060 6,060 6,060 6,059 5,914 5,914 5,914 5,914 5,914 5,914 5,914 Clinical SLA Overperformance Clinical SLA Underperformance refunds Other NHS Income 1, , Non NHS Income Recharges Donated Capital Total Cash receipts 7,689 6,810 7,207 7,806 7,164 6,898 7,671 8,402 7,033 7,635 7,335 7,334 7,489 7,189 7,189 7,489 7,189 7,189 7,489 Cashflow EXPENDITURE Payroll 2,315 2,237 2,221 2,243 2,266 2,305 2,295 2,300 2,300 2,300 2,300 2,300 2,300 2,300 2,300 2,300 2,300 2,300 2,300 Tax,NI,SPN 1,575 1,631 1,567 1,522 1,544 1,590 1,613 1,603 1,600 1,600 1,600 1,600 1,600 1,600 1,600 1,600 1,600 1,600 1,600 Theatre rental 839 Non-Pay via Accs Payable (Trade) 2,620 1,930 2,539 2,277 3,490 2,437 2,573 3,697 2,100 2,000 2,000 2,000 2,250 2,250 2,250 2,250 2,250 2,250 2,250 Non-Pay via Accs Payable (NHS) Capital (NHS) Capital (Donated) Investments 4,000-1,000 1,000-1,000-1,000-2,000 Loan Repayment Loan Interest PDC Dividend Total Cash Payments 11,526 5,827 7,185 6,834 9,374 7,562 6,197 6,435 6,939 6,628 6,728 8,037 7,000 7,000 7,000 7,000 7,000 7,605 7,000 CASH BALANCE Opening Balance 5,271 1,434 2,417 2,439 3,411 1, ,011 3,978 4,072 5,079 5,686 4,983 5,472 5,661 5,850 6,339 6,528 6,112 Cash Movement -3, , ,474 1, , Closing Balance 1,434 2,417 2,439 3,411 1, ,011 3,978 4,072 5,079 5,686 4,983 5,472 5,661 5,850 6,339 6,528 6,112 6,601 Total cash including investments Add short term investments 4,000 3,000 3,000 3,000 4,000 3,000 2,000 Total Cash Holding 5,434 5,417 5,439 6,411 5,201 3,537 4,011 3,978 4,072 5,079 5,686 4,983 5,472 5,661 5,850 6,339 6,528 6,112 6,601 Previous month forecast cash holding 5,006 4,534 5,453 5,782 6,188 3,921 3,718 4,133 4,431 4,746 5,038 4,421 4,710 4,999 5,288 5,577 5,866 6,155 Variance U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 33
82 Paper 03 Appendix 1 - Declaration of performance against healthcare targets and indicators These targets and indicators are set out in the 2012/13 Compliance Framework Definitions can be found in the "2012/13 Compliance Framework" Target or Indicator (per 2012/13 Compliance Framework) Threshold/ agreed target YTD Weighting Month 7 Achieved / Not Met Clostridium Difficile -meeting the C.Diff objective Achieved explanation MRSA - meeting the MRSA objective Achieved Cancer 62 Day Waits for first treatment (from urgent GP referral) >85% 1.0 Achieved Referral to treatment time, 18 weeks in aggregate, admitted patients >90% Achieved Referral to treatment time, 18 weeks in aggregate, non-admitted patients >95% 3.0 Achieved Referral to treatment time, 18 weeks in aggregate, incomplete pathways >92% Failed to Meet Cancer 31 day wait from diagnosis to first treatment >96% 0.5 Achieved Cancer 2 week (all cancers) >93% 0.5 Achieved Compliance with requirements regarding access to healthcare for people with a learning disability N/A 0.5 Achieved Risk of, or actual, failure to deliver mandatory services N/A 4.0 No CQC compliance action outstanding (as at 30 Sep 2012) N/A special No CQC enforcement action within last 12 months (up to 30 Sep 2012) N/A special No CQC enforcement notice currently in effect (as at 30 Sep 2012) N/A 4.0 No Moderate CQC concerns or impacts regarding the safety of healthcare provision (as at 30 Sep 20 N/A special No Major CQC concerns or impacts regarding the safety of healthcare provision (as at 30 Sep 2012) N/A 2.0 No Unable to maintain, or certify, a minimum published CNST level of 1.0 or have in place appropriate alternative arrangements N/A 2.0 No Score of 7 or less in standard 1 assessment at last NHSLA CNST inspection (maternity or all N/A special No services) Trust unable to declare ongoing compliance with minimum standards of CQC registration N/A special No Results left to complete 0 Total Score 1 Overall rating Overide Rating RED U:\Trust Board & Committees\Public Trust Board\ \November 2012\Month 7 Integrated Performance Report 34
83 Paper 04 Russell Hardy 4358 Chairman BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Subject/Title Safeguarding Children s Annual Report 2011/12 Executive Responsible Paper prepared by (if different from above) Jayne Downey, Director of Nursing Suzanne Marsden, Designated Nurse, Safeguarding Nature of Report For Information For Discussion For Approval Category of Item Context Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary Received or approved by The Annual Report provides information on the work undertaken in relation to Safeguarding Children across the organisation. This includes information regarding designated leads, incident over the past 12 months, local and external meetings. Approved by the Quality and Safety Committee Legal Implications Recommendation The Board of Directors are asked to note the contents of the Annual Report. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 04 RJAH Safeguarding Children Annual Report.doc 1

84 Annual Report for Safeguarding Children and Young People 1 st April st March
85 1 Introduction This is the statutory Annual Report for Safeguarding Children and Young People for 2012 as prepared by Suzanne Marsden, Named Nurse for Safeguarding Children and Young people. This report covers the time period from April 2011 until March The purpose of this report is to provide an update to The Robert Jones and Agnes Hunt (RJAH) Orthopaedic Hospital NHS Foundation Trust Board in relation to Safeguarding Children and to provide assurance to the Board that the Trust is fulfilling its statutory responsibilities. The RJAH Trust Board has adopted the Shropshire Safeguarding Boards (SSCB) policy and incorporates this into the Trusts own Safeguarding Children and Young Peoples policy. This report should be read in conjunction with the Shropshire Safeguarding Children Board Annual Report on arrangements for Safeguarding Children and Young People county wide. Safeguarding children and young people remains high on the national agenda and for all departments within the Trust that come into contact with children. We define children and young people as those who have not yet reached their 18 th Birthday. 2 Child Protection RJAH takes the safeguarding of children very seriously. It recognizes the need to maintain vigilance and to ensure that there are robust systems in place to monitor this work throughout the Trust. There has been a continued focus during the past three years to ensure that lessons have been learnt from previous child protection reviews. For example from the death of Baby Peter in Haringey and the subsequent Eileen Munro Independent Review of Child Protection in England The final report focused on a child-centred system looking at the child s journey with recommendations based on four key themes: a system that values professional expertise; sharing responsibility for the provision of early help; developing social work expertise; and finally clarifying accountabilities and improving learning. In addition, key recommendations from Lord Laming s review included learning from Serious Case Reviews (SCRs) and these are now shared in the SSCB subgroup and County wide Named Nurse meetings. Children in Need Safeguarding is not just child protection. Early intervention is a key theme in the Allen Report Early Intervention, the next steps and the Health Visitor Intervention Plan which is reinforced in Munro s recommendations. Health providers are expected to respond to families at three levels: Universal: Working to keep all children and young people safe and create safe environments for children. Targeted: Some groups of children are more at risk than others, and it is important to target policies and services to these groups, to help keep them safe from harm. Responsive: There will always be some children and young people who suffer harm. Services need to respond quickly and appropriately when this happens to 3
86 support these children and deal with those who harm them. 3 SAFEGUARDING CHILDREN ACCOUNTABILITY STRUCTURE ACROSS THE TRUST Chief Executive RJAH Board Lead for Safeguarding Children Named Nurse (supported by the Designated Nurse) Named Doctor (supported by the Designated Doctor) The lead roles for safeguarding children remain the same within the Trust. The Named Doctor who is a Paediatric Orthopaedic Consultant continues to undertake this post on a temporary basis, and he is hopeful that the Trust will be able to recruit a paediatrician to undertake this role as per national guidance. He is currently allocated ½ PA per week protected time, to undertake this role. The Named Doctor provides all staff groups across the Trust with expert advice and support regarding safeguarding children issues. He is supported and supervised as necessary from the County wide Designated Doctor The Named Nurse for safeguarding children is the ward manager on Alice ward and has 7.5 hrs per week allocated time, to undertake this role. However this time is frequently overridden by the need to work on the ward and maintain safe staffing levels. We are monitoring the situation closely to ensure adequate time is available to undertake this role. The Named Nurse works closely with the Named Doctor to ensure that the Trust meets its statutory responsibilities in safeguarding children as defined in Working Together to Safeguard Children document, (2010) and the Children Act (2004). In May 2011, the Named Nurse and Doctor both attended level 4 Safeguarding children training in London. The Named Nurse represents the Trust at the Shropshire County and Telford and Wrekin Health governance Safeguarding Committee in Shropshire on a quarterly basis, as well as the County Named Nurse meetings bimonthly. The Designated nurse in Shropshire, Telford and Wrekin provides supervision for the Named nurse and meetings routinely take place bimonthly to ensure effective support. During July, August & September 2011 due to a high ratio of complex safeguarding cases in the Trust, supervision was increased to monthly. The Named nurse coordinates and delivers level one and two training for staff working in the Trust and provides all staff groups across the Trust with expert advice and support regarding safeguarding children issues. The Trust has an interim executive lead for safeguarding (interim Director of Nursing) and she is supported by the Deputy Director of Nursing. The Executive Lead provides support for the named professionals and champions Safeguarding Children at a Board level. These staff maintain strong safeguarding links with the county wide Safeguarding meetings and are key links within the organisation. The Trust now needs to consider appointing a non executive lead for safeguarding children and Young people. 4
87 4 Safeguarding Activity Over the last two years, child protection activity has steadily increased within the Trust and during the early part of 2011; fifteen children were highlighted as requiring Safeguarding support during the period April Sept This is more than the whole of the previous year and at times has been extremely difficult to manage. Several of these cases have been complex cases and have involved attendance at case conferences and Team around the Child meetings in Telford and Wolverhampton. During the second half of the year the increasing trend seems to have turned and the numbers appear to have stabilized with four cases, one of which was reported as a Serious Untoward incident (SUI):- Changes in practice as a result of the incident included parents being given a leaflet highlighting the risks associated with the use of a PCA. There have been no reported allegations made against any members of staff in 2011/12. Group Supervision was provided for staff on the Midlands Centre for Spinal Injuries in October 2011 and January 2012 due to concerns raised over a delay in responding to a 16 year old suffering both emotional and physical abuse from a family member. These sessions where held by the Named nurse and Designated Nurse for Safeguarding children. The sessions included debrief, lessons learnt and training on Dealing with hostile parents and children living with domestic violence in the household. These sessions were well received by staff. During this year the Trust saw the second suicide of a family member whose relative had recently suffered a serious spinal cord injury. The first case occurred in 2008 This is a concern to the Trust and an increase in psychological support for vulnerable parents has been identified on the Spinal Injuries Unit. As a direct result of the issues raised on the Spinal Injuries unit, the Trust was visited by the West Mercia Cluster team who reviewed the safeguarding arrangements in the Trust. A list of recommendations was proposed and an action plan was developed to meet these objectives, most of which have now been completed (appendix 1). It is clearly evident that safeguarding children is everyone s responsibility and as a Trust it is crucial that the appropriate procedures are put in place to improve outcomes for children. These include the following: senior managements commitment to the importance of safeguarding and promoting children s welfare; a clear line of accountability within the organisation for work on safeguarding and promoting the welfare of children; service development that takes account of the need to safeguard and promote children s welfare. This should be informed, where appropriate, by the views of children and families; staff training on safeguarding and promoting the welfare of children for all staff working with or in contact with children and families; safe recruitment procedures in place; 5
88 effective inter-agency working to safeguard and promote the welfare of children; and effective information sharing Review of statutory compliance of section 11 (Children s Act 2004) through an audit at least 4 times per year. Performance Monitoring Safeguarding Children is reviewed four times per year in the form of a report which is shared with the Shropshire Telford and Wrekin Health Governance Safeguarding Children Committee. These reports highlight any safeguarding concerns and these arrangements have been formalised with all other county providers to monitor and assess how effective safeguarding arrangements are throughout the county. The indicators which are monitored include: Training uptake Safe recruitment and staffing issues Section 11 compliance under the Children Act 2004 (appendix 2) Completion of Safeguarding documentation audits - once per year Serious Case Reviews Comment on trends or unresolved issues in relation to reported incidents (if applicable Serious Untoward Incidents Supervision During the early part of the Year the Trust held Bimonthly Safeguarding Children and Adult meetings. The remit of these meetings was to monitor compliance, discuss any safe guarding incidents and to learn from them. Documentation Audit The annual documentation audit was completed in August Priorities for 2012 / 2013 Review of safeguarding service within the Trust in relation to children s safeguarding. To review both Named Professional roles within the Trust in line with Intercollegiate and Working together (2010), and ensure protected time is supported. The appointment of a Non Executive Lead for safeguarding children To reintroduce the Trust Safeguarding Children and adult meetings To monitor the training database and compliance in levels 1,2,3 and 4 training. To increase Paediatric Medical staff compliance with level 3 child protection training To continue to work on improving Section 11 compliance within the Trust To continue to work through quality assurance subgroup to monitor outcome 6
89 from child protection cases and serious case reviews. To ensure that the local LADO (Local Authority Designated Officer) is involved with all allegations made against members of staff. To work with partner agencies in achieving the Shropshire Safeguarding Children Board Key targets for 2012/13: 1. Compromised parenting including children living in households with mental ill health, Substance misuse & Domestic violence 2. Children who go missing, including sexual exploitation 3. Communication RJAH will continue to focus on both local and national priorities for children s safeguarding in 2012/13. The revised Working Together to Safeguard Children s document (2012) and subsequent changes to the West Mercia Consortium Child Protection Procedures together with additional key performance indicators for safeguarding will guide this work. In conclusion, the Named Nurse, Named Doctor and Executive Lead strive to maintain high standards of practice within the Trust. This will be achieved by continually reviewing safeguarding procedures and practices, ensuring that training requirements are fulfilled and auditing child protection practices. This will ensure that the safeguarding needs of children and young people in this Trust remain of paramount importance and that any safeguarding needs are met with competent and skilled staff. Update April 2012 October 2013 Appointment of New Director of Nursing / Executive Lead for Safeguarding - April 2012 The Trust Safeguard Children and Adults Committee, was reconvened by Executive Lead in July 2012 and Designated Nurse has joined the group. Named Nurse protected time. Due to a high number of vacant hours on the ward throughout the summer, protected time has been difficult to achieve and we have agreed to continue to monitor the situation through the Trust safeguarding committee to ensure compliance. Sept The current Named Doctor has now resigned from his position and a Locum Paediatrician has now taken up this post. Reviews - Shropshire Peer Review May 2012 and an Internal Safeguarding Adult and Children review by Assistant Director of Nursing safeguarding adults and children Salford Royal Foundation Trust May Action plan in progress. 7
90 Trust Quality Review October 2011 Appendix 1 Name of person completing baseline assessment - Suzanne Marsden May 2012 updated Sept 12 Recommendations Is it met? Y/N/Partially/ Planned Comments (Examples of good practice or deficiencies identified) Action required Timescale Person responsible Leadership & Governance A Trust Board Executive Director Lead should be identified and developed to new national Child Protection training standards. Monthly and/or as required meetings should be held with Named Safeguarding Professionals to discuss future and present complex cases. The Named Safeguarding Nurse is only allocated 1 day a week for safeguarding activities. This is now insufficient due to the dramatic increase in workload both strategically and operationally. The Executive Nurse for Safeguarding should report this deficit to Trust Board/HR in order to achieve further investment in line with national statutory guidance. This must include a review of the Named Nurse s allocated grade, time and development (minimal 2-3 days a week is more appropriate as current training commitments are not factored into the Named Nurse s protected time. The Executive/ Named Professionals should be members LSCB/ LSCB sub groups. RJAH SSCB training sub group representation essential to ensure that RJAH CP training is maintained to multi-agency standard (Elearning incorporated to raise Level 1 training to all RJAH staff). Audit/ policy and procedures/ performance partnership sub group representation would be a future area Yes Partial Director of Nursing Monthly 1:1 commenced SM is allocated 1 day per week for Safeguarding duties. These hours depend greatly on ward dependency. Issue raised with DON Bimonthly supervision with Designated Nurse Named Nurse and Doctor have specific Job descriptions relating to their role. E mail sent to all post office accounts to update on named professionals for safeguarding children DON to attend the safeguarding board for formal introductions. SM attends County Health governance Safeguarding Committee. NB Deputy Director of Nursing attends Board and Health Governance meetings. SM is on the training pool for the SSCB. Corporate induction training level 1. Trust booklet - To appoint a non exec lead -To consider taking Child Protection days away from ward environment -SM to consider joining Audit sub group Dec 12 DON Designated Nurse Designated Nurse 8
91 Recommendations for further development if safeguarding capacity. The Executive/ Named Nurse should report via quarterly template to Health Governance Safeguarding Children Committee all SUIs, Safeguarding Case/ Supervision Activity, Training Levels, IMR/ SCR recommendations feedback/ policy and procedures update with review dates in header and footers. SUIs should also be reported to SHA. The Executive/ Named professionals for safeguarding should have a safeguarding reporting mechanism with pathway flowchart safeguarding reporting from Executive Board Level to front-line staff level. All safeguarding contact information and policy and procedures should be on RJAH intranet site including links to SSCB West Mercia CP procedures and child exploitation, domestic abuse policy (MARAC representation as required), suicide prevention and neglect strategy/ toolkits to assist front-line staff. Staff should be informed about strategies in training. A Caldicott guardian, Information Governance should be aware of RJAH Safeguarding Professionals to provide support in Information Sharing Arrangement in and out of county. Legal advice/ guidance should be sought if required especially in complex cases. Is it met? Y/N/Partially/ Planned Yes Yes Yes Comments (Examples of good practice or deficiencies identified) Level 1 & 2 training provided internally Level 3 &4 provided externally Board training completed in Oct 11 Doctors complete E-learning West Midlands deanery package. Safeguarding Nurse reports quarterly to the Health governance Safeguarding children group. Recent SUI was reported as per policy. An Annual report is submitted to board SSCB tool kits available for staff Neglect, Suicide prevention and Child exploitation strategies. The Trust has a safeguarding children page on the Alice Ward Intranet page. This includes Link to county safeguarding children policies, Trust policies, SSCB Strategies and tool kits, contact numbers and named professional information. Trust poster, Library leaflet and Safeguarding children Booklet Safeguarding file developed for spinal injuries The Caldicott Guardian the Director of Nursing. Trust solicitor involved in sharing of information re complex cases. Action required Timescale Person responsible Designated Nurse Designated Nurse DON 9
92 Recommendations The Executive / Named Nurse/Dr should have safeguarding supervision via other Executives/ Designated Professionals and then they provide safeguarding supervision to staff within RJAH. RJAH IT department need to develop and procure an in house IT flagging system for children subjected to CP plan. At present staff have to phone Social Services/ SaTH Action and Emergency department to determine if a child or young person subjected to a plan. RJAH need to develop a safeguarding protocol for pre admission and discharge planning of children and young people admitted to hospital with extra consideration to out of area complex cases in spinal injuries and/or children s wards The Named Nurse/ Doctor will conduct any future Individual Management Reviews (IMR) on behalf of their organisations. The Executive/ Named Nurse should be advocating that all staff follow Working Together to Safeguarding Children (2010) statutory guidance in respect of safeguarding case management and information sharing. Record Keeping Audits should be yearly with development of multi-agency case tracking audits if further RJAH invested capacity to identify lessons learned, improving safeguarding clinical practice and staff Is it met? Y/N/Partially/ Planned Yes Yes Comments (Examples of good practice or deficiencies identified) The named nurse has regular safeguarding supervision from the Designate nurse for safeguarding children. Session is documented. Named doctor contacts Designated Doctor as required. Currently not available, process in place to address through IT Action required Timescale Person responsible DON to discuss funding costs with SaTH. Nov 12 No Protocol currently being developed Dec 12 Designated Nurse Yes Designated Nurse of would undertake as necessary Designated Nurse attended SCIE training 30 th May 2012 Yes Awaiting new updated guidance. Yes Annual record keeping audits are undertaken. Last completed in Aug 2011 DON Re audit Oct 12 Oct 12 Designated Nurse 10
93 Recommendations competence An out of area safeguarding admissions should have a list of professional contacts for Shropshire and out of area address this should be included in notes, admission and discharge plans with best practice record keeping. Management of Allegations made against Persons in Positions of Trust RJAH is accountable for ensuring that the policy in relation to allegations made against persons in positions of trust is implemented via liaison with the Local Authority Designated Officer who leads the process and provision of advice and ongoing support throughout RJAH, including- Provision of advice and support to Human Resources department/ Confident Board as appropriate. Supporting managers and staff according to procedures Attendance at strategy meetings as appropriate Is it met? Y/N/Partially/ Planned Yes Yes Comments (Examples of good practice or deficiencies identified) Prior to last high risk admission. All necessary telephone numbers where documented on Safeguarding sheet for all staff to access. Information sharing DOH document shared with staff. Trust information sharing policy in place Managing allegations policy in place Clinical holding guideline in place for children Clinical Holding Training provided Designated Nurse attended safe recruitment training 2011 The local LADO information shared with HR July 12. Action required Timescale Person responsible Domestic Violence policy to be developed. Information shared. Jan 13 Complete HR 11
94 Safeguarding Children s Work plan Monthly level one training Induction 2 nd Mon Supervision with Audrey bimonthly to be arranged. Safeguarding leaflet to be sent out with wages. To check with Jo Bayliss Dec 2012 Safeguarding children policy to be update to include x-ray document. Managing allegations policy to be updated HR to introduce a policy for dealing with staff who are suffering from domestic violence. Annual documentation audit to be started Oct 2012 DV training to be introduced for clinical staff via E learning April 2013 RJAH need to develop a safeguarding protocol for pre admission and discharge planning of children and young people admitted to hospital with extra consideration to out of area complex cases in spinal injuries and/or children s wards Trust flagging system to be implements for children at Risk. JD working with IT re access to SEMA system in RSH Quarterly report Health Gov meeting Dec, Feb Attend Trust, Named Nurse, training Pool and Health Gov meetings Section 11 review Quarterly SM to consider joining one of the SSCB sub groups if work capacity allows Training programme sourced and to be discussed with roll out April 13 JD liaising with IT Section 11 audit Work to improve No Aim - Exceeds requirements Current evidence 1.2 Corporate Plans include appropriate reference to the need to safeguard and promote children s welfare and are communicated effectively to staff, who have a clear understanding of their role in relation to safeguarding and promoting the welfare of children. All staff are involved in the development of Corporate Plans and have a sense of ownership of the Plans and team and individual plans contain clear objectives in relation to safeguarding and relate to the overall plan The Named Nurse undertakes this role as a band 7. Plans in place for re banding of this role to a band 8. Protected time needs further consideration 1.3 A named person at senior management level is identified and responsible for championing the importance of safeguarding and promoting the welfare of children and the championing role is clearly contained within the job description, with identified actions in relation to this role as part of the individual work plan/ performance management plan Effective systems in place for children, staff and other people to make a complaint about non- The divisional, annual and IBP all reference the issues surrounding safeguarding and promote a culture of safety and openness within the Trust. 12
95 No Aim - Exceeds requirements Current evidence adherence to the agency s procedures. Childfriendly complaints information is available to all children and families. The organisation can clearly demonstrate the effectiveness of recommendations/outcomes on practice and these are reported to staff e.g. through the annual report. 2.2 Effective systems in place for children, staff and other people to make a complaint about nonadherence to the agency s procedures. Childfriendly complaints information is available to all children and families. The organisation can clearly demonstrate the effectiveness of recommendations/outcomes on practice and these are reported to staff e.g. through the annual report. 2.4 Children, young people and families are involved in the writing and reviewing of the equal opportunities policy. 4.2 Children, young people and families are actively involved in the design, development and delivery of services. The organisation can demonstrate how, at various levels, they enable children, young people and families to engage in service development. There is a responsive process in place which acts upon identified unmet need. 6.4 The organisation can demonstrate via audit activity that they have policy and procedures compliant with LSCB defined safer recruitment and selection policy 6.5 The organisation can demonstrate via audit activity that they have policy and procedures compliant with LSCB defined safer recruitment and selection policy 6.7 The organisation s policy and guidance on whistleblowing promotes a positive and open culture within organisations that enables staff to report unsuitable behaviour with confidence. The organisation includes confidential reporting/ whistle blowing within interagency training 6.11 The organisation has a defined business plan that ensures effective procedures for dealing with allegations against people who work with children are in operation and are monitored and reported on. Procedures are disseminated to all employees working with children and young people and guidance is available to those employees facing allegations of abuse. 8.2 The organisation can demonstrate that they have a clear policy which encourages appropriate information sharing and can evidence how this impacts on outcomes for children and families. 8.3 The organisation can demonstrate that they have a clear policy which encourages appropriate The Trust has a clear complaints process in place; however we recognise the need to develop a child friendly document which is in progress. The Trust has an equal opportunities policy in place; however children and young people are not currently involved in the review process. The children's ward holds a bimonthly parent and children focus group. This group assists with the development of service. E.g. Developing a child friend patient experience document. Involved in the development of the ward garden. All Trust policies are reviewed at regular intervals The Trust has a Safe recruitment policy in place which is regularly reviewed The Trust has a "Managing Allegations policy and this incorporates the inclusion of the County LADO in all cases. The Trust has a "Managing Allegations policy and this incorporates the inclusion of the County LADO in all cases. The Trust has an Information Governance policy which is audited to monitor staff knowledge. We are currently unable to evidence how this impacts on the outcomes for children The Trust has an Information Governance policy which is audited to monitor staff 13
96 No Aim - Exceeds requirements Current evidence information sharing and can evidence how this impacts on outcomes for children and families. knowledge. We are currently unable to evidence how this impacts on the outcomes for children 8.4 The organisation can demonstrate that they have a clear policy which encourages appropriate information sharing and can evidence how this impacts on outcomes for children and families. The Trust has an Information Governance policy which is audited to monitor staff knowledge. We are currently unable to evidence how this impacts on the outcomes for children 14
97 Paper 05 Russell Hardy 4358 Chairman BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Subject/Title Safeguarding Adults Annual Report 2011/12 Executive Responsible Paper prepared by (if different from above) Jayne Downey, Director of Nursing Anne Worrall, Matron Nature of Report For Information For Discussion For Approval Category of Item Context Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary Received or approved by The Annual Report provides information on the work undertaken in relation to Safeguarding Adults across the organisation. This includes information regarding designated leads, incident over the past 12 months, local and external meetings. Approved by the Quality and Safety Committee Legal Implications Recommendation The Board of Directors are asked to note the contents of the Annual Report. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 05 RJAH Safeguarding Adults Annual Report.doc
98 Annual Report for Adult Safeguarding 1.0 Introduction In March 2000 the Department of Health issued the No Secrets document which provided the framework for interagency collaboration on the development and implementation of procedures for the protection of adults vulnerable from abuse Vulnerable adults are defined by government guidance NO Secrets Act 2000 as people Who are or may be in need of community care services because of mental or other disability, age, or illness. Who are unable to care for themselves or unable to protect themselves from significant harm or exploitation The guidance refers to harm in terms of abuse. This might be physical, sexual, psychological, financial or material, neglect and acts of omission, discriminatory or institutional. The lead organisation is the local social services authority who act as the coordinating agency for safeguarding adults. However other organisations with responsibilities include the National Health Service (NHS), independent (private and voluntary) social and healthcare providers, housing providers, the police, the crown prosecution services (CPS), the probation services and benefits agency. Joint working between all the above agencies is seen as essential in safeguarding activity including the sharing of information. To ensure effective multiagency and multidisciplinary joint working there are policies and procedures in place to represent commitment of organisations to: Work together to prevent and protect adults at risk from abuse Empower and support people to make their own choices Investigate actual or suspected abuse or neglect Support adults and provide a service to those at risk who are experiencing abuse, neglect and exploitation 2.0 Adult Safeguarding at the Robert Jones & Agnes Hunt NHS Foundation Trust The Robert Jones and Agnes Hunt Orthopaedic NHS Foundation Trust continue to be fully committed to encompassing the six key concepts in adult safeguarding; empowerment, protection, prevention, proportionate responses, partnership and accountability into our working practices at the organisation.
99 As an organisation we have continued to work with Shropshire and Telford and Wrekin Safeguarding Adults Board contributing to effective interagency working, and joint working partnerships to provide the most effective means of safeguarding vulnerable adults. As an organisation we aim to ensure that the dignity, safety and wellbeing of the individual is our priority. To be the provider of choice for patients through the provision of safe, effective, high quality orthopaedic and related care has been identified as one of the main trust strategic aims. To deliver this objective, the Trust has continued to: provide safeguarding vulnerable adults training for all staff, and provides specific Mental Capacity training and Deprivation of Liberty safeguards (DOLs) training. These two training topics are provided as facilitated training sessions (face to face) which have proven to be extremely informative, enhancing staff learning and awareness. Additionally, staff undertakes an e- learning mandatory training package for adult protection which is completed on 3 yearly basis. raise staff awareness (through training provision) which has enabled them to understand their role and responsibilities in regard to policy and procedure. This enables staff to promote good practice for responding to concerns on a multiagency basis strengthen links with outside agencies, and work in collaboration, to ensure service users are safe from harm, and maintain independence, well-being and choice. hold quarterly meetings of the Safeguarding Committee meet to provide a forum to discuss children and adult safeguarding issues, and has the appropriate accountability for safeguarding across the trust. The committee report to the Trusts Quality and Effectiveness committee. support compliance with the Care Quality Commission Standards Outcome 7 through the actions listed above adopt the Shropshire and Telford & Wrekin Multiagency Adult Protection Policy which is accessible through the Trust intranet. Additionally, the Clinical Psychologist has been part of the local DOLS Safeguarding Board and has completed the Best interest assessor training. Having undertaken this additional training it has enabled staff to share best practice, and enhance their knowledge and skills within this specific area. 3.0 Review Adult safeguarding is recognised as everyone s business, and it is the responsibility of all organisations including the NHS to have a continued commitment to ensure safeguarding becomes fully integrated into NHS systems. Openness and transparency is key for effective working between agencies and effective clinical incident reporting and RJAH continues to embed these principles which support achieving our strategic aims.
100 In August 2011, a review was undertaken by the West Midlands Quality Review Service who looked at Trust-wide guidelines and policies within the organisation and tested their implementation in some of the clinical areas within the organisation. The aim of the West Midlands Quality Review Service (WMQRS) is a collaborative venture by NHS organisations in the West Midlands to help improve the quality of health services by developing evidence-based quality standards, and carrying out developmental and supportive quality reviews. This is undertaken through peer review visits, producing comparative information on the quality of services and providing development and learning for all involved. The expected outcomes by having these reviews is for better quality, safety and clinical outcomes, better patient and carer experience, organisations with better information about quality of clinical services, and organisations with more confidence and competence in reviewing the quality of clinical services The general comments and achievements from the review were: Staff at Robert Jones and Agnes Hunt NHS Foundation Trust had made significant efforts to improve the care of vulnerable people. Staff were welcoming and clinical areas appeared well-organised. Pathways for major and minor surgery were in place. There were good working relationships across the Trust and the Nursing Director and Deputy Director undertook regular clinical work. Standards of recordkeeping were good and an IPAD information tracker was planned which would give real time patient experience feedback. The reviewers identified good practice, and the following points were made: The Deprivation of Liberty Poster on the wards was very clear and easy to read. In collaboration with service users the Trust had produced an easy read information booklet for people with learning disabilities who attended the Trust. The Falls Assessment Intervention Tool was very good and had been extended to cover two hourly interactions with the patients and intentional rounds. Since implementation there had been a 12% reduction in falls. Following the review there were further considerations made by the reviewers to assist the Trust to continue improving the care of vulnerable adults, listed below are some of the recommendations Several staff commented that the Trust was a low risk organisation for safeguarding and improving the care of vulnerable adults because the organisation undertook mainly elective and rehabilitation work. Raising awareness of the orthopaedic and rehabilitation aspects of safeguarding and the contribution of the Trust to the care of vulnerable adults may be helpful.
101 A medical lead with responsibility for safeguarding and improving the care of vulnerable adults within the Trust may help to support the Safeguarding Lead and raise awareness and training among medical staff. The Violence and Aggression Policy may benefit from review to include the management of behaviours that challenge. Staff were clear about access to interpretation services for Welsh speakers but some staff were not clear about interpretation services for people speaking other languages and access to sign language interpreters for people with hearing problems. Criteria for access to rehabilitation may benefit from review. It appeared that, due to the current screening process for surgery, people with dementia may be deemed ineligible for rehabilitation when, in practice, they may benefit. Telephone advice was available from the Mytton Oak Learning Disabilities Team, but this team was not able to visit patients within the Trust to advise on their care. Further consideration of the support needed by Trust patients with learning disabilities may be helpful. Following the review, the Trust has reviewed these comments and included pertinent actions points within their Adult Safeguarding action plan for 2012/ Referrals The Robert Jones & Agnes Hunt Orthopaedic NHS Trust has had two adult protection referrals to the local social services from April 2011 March 2012 The first referral was about a patient who attended the outpatient clinic and reported to a member of staff that her husband had hit her around the head when they had a disagreement the previous week. The patient did inform the member of staff that there was a course of action underway in which she had reported the incident direct to the police. The member of staff reported the incident through the Trust s reporting datix system as per policy, and the patients local safeguarding services were contacted who actioned the referral. The second referral involved a patient s daughter witnessed shouting at her father, who abruptly pulled her fathers dentures out of his mouth, and then slapped her father across his shoulder when he refused to have his dentures put back in his mouth after she had cleaned them. Action was immediately taken when the daughter was questioned by the Ward Manager, witness statements taken, and senior nurse management informed. This was also reported through the datix reporting system. A formal referral was made to the local adult protection service who actioned accordingly. A formal meeting through the adult protection service was undertaken. 5.0 Training The Trust currently provides the following mandatory training for clinical staff with direct patient contact which needs to be completed every 3 years by staff identified within the Trust Training Needs Analysis:
102 Mental Capacity Act 2005 Awareness This is provided as a facilitated session delivered by an external training company. Deprivation of Liberty Safeguarding Awareness (DOLS) Training This is provided as a facilitated session delivered by an external training company. Safeguarding Vulnerable Adults Staff complete this training via an internally produced e-learning module. For the period 1 st March st March 2012 the following number of staff have completed the training listed above: Name of training No of staff completing training in % of staff completed training No of staff completing training in % of staff completed training Total number of staff required to complete training as identified organisation TNA DOLS Training % % 751 Mental Capacity Act 2005 Awareness Safeguarding Vulnerable Adults % % * *New training package only available since 1 st April 2011 Training in these subject areas continues to be delivered in 2012/13. 9% % 751 in Additionally in April 2012, the Trust also launched Learning Disabilities Awareness training. This training can be completed either as an e-learning module or via a facilitated session in collaboration with Shropshire County Training. Since 1 st April st August 2012, 277 staff (37%) have completed this training. We continue to work with Shropshire County Training and are currently co-producing another e-learning package to provide Autism Awareness training for staff. We have also launched Dementia Awareness training workshops which have been delivered by Staffordshire University in this financial year and to date 135 clinical staff have attended these sessions. 6.0 Conclusion The Trust is actively making progress towards ensuring the Safeguarding Adults is embedded into everyday working practices at the Trust and be able to demonstrate best practice. The Trust works in collaboration with the local Safeguarding Board and disseminates appropriate information to prevent and protect adults at risk from abuse and if necessary investigate actual or suspected abuse or neglect. Training staff enables the Trust to empower and support adults at risk and provide a comprehensive service to them. Reviews of practice have enabled the Trust to develop a robust action plan for which will further enhance Safeguarding Adults practices at the Trust.
103 Adult Safeguarding Action Plan 2012/13 Objective Action Lead Date to be achieved Review of Named Professional is undertaken, to assess their knowledge and expertise and understanding of their role and responsibilities for Adult Safeguarding. Ensuring that Named Roles have been developed in line with Working Together Director of Nursing to identify the named professionals i.e. Named Nurse, and Named doctor for the organisation. Development of clear outlined roles and responsibilities to provide assurance for CQC Outcome 7.which need to be reflected in job descriptions and job plans Director of Nursing To ensure compliance with Outcome 7 CQC Essential standards, and provide board assurance that these standards are being met Development of strong links in relation to safeguarding and capability/performance management Compliance of Quality Standards : Care of Vulnerable Adults in Acute Hospitals (WMQRS) Provision of evidence to ensure compliance through policies and procedures, datix reporting and root cause analysis. Training records, risk management Evidence through the Trust s safeguarding board who meets quarterly. Report to Trust board giving updates annually, and through risk management. Development of risk register for safeguarding committee. Development of evidence portfolio Evidence links with the local health economy Attend the adult safeguarding network group for the Shropshire area. Director of Nursing /Adult Safeguarding lead Director of Nursing Director Of Nursing Adult Safeguarding lead Adult Safeguarding lead Adult Safeguarding work plan/aw Sept
104 Adult Safeguarding Action Plan 2012/13 Objective Action Lead Date to be achieved Trust to undertake a training need analysis for Adult safeguarding outlining the different levels of training Implementation of the training through the training department within the Trust. Ensure clear reporting systems are in place for the review of targets on a regular basis. Report training figures to the Trust s Safeguarding board on a quarterly basis Training Manager Dissemination of clear adult safeguarding policies so that processes are embedded within the organisation. Policies need to be accessible for all staff within clinical areas. Development of Adult safeguarding resource file for each ward area. Identify safeguarding link professional within ward areas Adult Safeguarding lead Supervision for the designated nurse/ Doctor needs to be reviewed and expanded A supervision policy needs to be in place. Evidence supervision with documentation to support this. Set up regular meetings with the lead for Adult safeguarding and the Adult Safeguarding Lead Nurse Shropshire County PCT/NHS Telford and Wrekin Director Of Nursing Adult Safeguarding lead Clear CRB processes, and monitoring Process for identification of people with learning difficulties/disabilities The implementation of the ISA framework is currently ongoing. Inform staff of the changes so they can be prepared for the impact it may have on them Create strong links within the local health economy re: leaning disabilities Human Resources Manager Adult Safeguarding lead Adult Safeguarding work plan/aw Sept
105 Implementation for the Patient Passport within the organisation, and provide staff awareness. Provide staff with the necessary information within the Adult Safeguarding Resource File Adult Safeguarding work plan/aw Sept
106 Paper 06 Russell Hardy 4358 Chairman BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Subject/Title Shropshire Safeguarding Children Board Annual Report Executive Responsible Paper prepared by (if different from above) Jayne Downey, Director of Nursing - Nature of Report For Information For Discussion For Approval Category of Item Context Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary The Annual Report for the Shropshire Safeguarding Children Board provides an assessment of the effectiveness of local safeguarding arrangements during the last twelve months, identifies challenges to be addressed and sets out priorities for the coming year. Received or approved by Legal Implications Recommendation The Board of Directors are asked to note the contents of the Annual Report. Acronyms and Abbreviations SSCB Shropshire Safeguarding Children Board U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 06 Shropshire Safeguarding Children Board Annual Report.doc



107 Annual Report Keeping our children safe from harm draft
108 SSCB Annual report Foreword I am pleased to present the Shropshire Safeguarding Children Board annual report , which provides an assessment of the effectiveness of local safeguarding arrangements during the last twelve months, identifies challenges to be addressed and sets out priorities for the coming year. The report covers a period that has been characterised as ever - by significant change both nationally and locally. Professor Eileen Munro s Review of Child Protection was published during the year. She argues that the child protection system has lost its focus on the things that matter most: the views and experiences of children themselves; and recommends a move towards a child protection system with less central prescription and interference, where greater trust and responsibility is placed on skilled professionals at the front line. The government accepted her analysis, stating that there is now a significant opportunity to build a child-centred system that values professional expertise; shares responsibility for the provision of early help; develops social work expertise and supports effective social work practice; and strengthens accountabilities and promotes learning. This has resulted in a revision to Working Together (awaited later this year), and indications that LSCBs will play a significantly enhanced role in acting as the regulator of the local safeguarding system. Within Shropshire, much work has already been undertaken to develop early help services to children and families. Safeguarding is everyone s responsibility. Locally, safeguarding and looked after children services were inspected by Ofsted, which judged the overall effectiveness of safeguarding, and the capacity of the council and its partners to improve as adequate. A number of strengths were noted, including the well-established nature of partnership working. Nevertheless, a number of challenges were identified, and a series of recommendations made for the local authority and its partners, some of which were directed at the SSCB. The resulting action plan led, amongst other things, to developments in the governance, structure, membership, and operation of the SSCB, including the welcome appointment of two community members. There is now an independent chair, appointed specifically to strengthen the ability of the SSCB to challenge and hold its partners to account. For many of the board s partner agencies, there is considerable organisational change. National government has introduced new policies and structures for education and for health services; the local authority has merged its services for children and adults, with the former Director of Children s Services having significantly enlarged responsibilities; forthcoming changes to policing will have an impact locally. SSCB is responding by adapting and strengthening its arrangements as needed to ensure an unwavering focus is maintained on the safety and well-being of children. The continuing reports of the harm and exploitation of children and young people in the media are a stark and sad reminder of why we are here: to learn and apply lessons in order to safeguard children as effectively as we can. They are also a reminder of the challenges facing front-line workers and managers, who deserve our thanks as they undertake each day the challenging, difficult and often distressing work of safeguarding Shropshire s children. Sally Halls Independent 2 Chair
109 Contents 1. Summary page 4 2. Governance and accountability arrangements page Role, function and structure of the Board page Membership and attendance page Subgroups page Financial arrangements page 9 3. Quality assurance page The Audit and Quality Assurance framework page The approach to auditing in Shropshire page The scorecard page Exit Interviews Feedback from children and parents/carers page Children subject to Child Protection Plans page Performance page Progress on 2009/12 priorities page Training and development page Serious case review page Looking to the future page Key priorities page Business Plan page 21 Appendices page Appendix 1: Sub Group report Appendix 2: Scorecard Appendix 3: Business Plan Appendix 4: Business Plan Appendix 5: Training delivery
110 1. Summary Shropshire is one of England s most rural and sparsely populated counties with a large geographic area of 1,235 square miles. Situated in the West Midlands, bordering Wales to the west and Cheshire to the north, the area has a population of just under 291,000. Shropshire s population is largely of White British ethnic origin. The numbers of residents from minority ethnic groups is low, at 1.2% of the population, an increase of 0.5% since the 1991 census. Fifty-five per cent of Shropshire s population live in Shrewsbury or in the other main market towns of Oswestry, Whitchurch, Market Drayton, Ludlow, Bridgnorth and Church Stretton. Children and young people aged 0 19 make up 23.4% of Shropshire s population, a proportion that is line with England averages. However, the number of people living in the county aged fell by 16.2% between 1991 and 2007, a figure significantly higher that the England average figure of 6.4%. There are currently 35,751 children and young people of school age (4 16). Between mid-1981 and mid 2007 the population of Shropshire increased by 13.9%, largely due to people moving into the county, which is a more rapid growth rate than nationally (8.9%). According to the Indices of Deprivation Affecting Children Index, Shropshire ranks as seventeenth least deprived local authority in England. However, this statistic masks pockets of deprivation in the more rural areas, where five areas, each covering up to 1500 people, are amongst the 20% most deprived nationally in terms of their income, and a further 11 are among the 30% most deprived cohort. The most recent data shows that 13.3% of children are living in income deprived households. At the time of the Ofsted inspection (February 2011) there were 201 children subject to child protection plans, 225 looked after children, including one unaccompanied asylum-seeking child, and 181 care leavers. Shropshire had 110 foster carer households and 18 children in independent fostering agency placements. Fifty children were currently placed in residential care, 42 of which are in external provision, the remainder being placed in the council s own provision. In the previous two years, 15 looked after children were adopted or secured permanence through special guardianship orders. By the end of 2011/12, there were: 180 children subject of a child protection plan 7 fewer than at the end of the previous year 3.3% of child protection plans lasted for 2 years or more, a reduction from 11.8% the previous year 9.7% of children subject to a child protection plan for the second or subsequent time a small rise 205 Looked After Children per 10,000 offences against children reported a rise from per 10,000 the previous year 764 CAFs completed 40 children who had been missing from home for more than 24 hours, of whom 4 were looked after by Shropshire Council, compared with a total of 55 (6 LAC) the previous year 4
111 Further details are given in the report, and in Appendix 2. Ofsted inspected Shropshire s safeguarding and looked after children s services in February 2011 and judged the overall effectiveness of safeguarding to be adequate. The Children s Trust and the SSCB were judged as fulfilling their statutory functions. Across the partnership, Ofsted noted a strong commitment to safeguarding and evidence of thorough planning to protect front line services as much as is possible in an acutely challenging financial climate. The capacity of the council and its partners to improve was also judged to be adequate. Partnership working was found to be well established with a long history of sound professional relationships at all levels, with significant and successful work being undertaken to modernise and refocus strategic partnerships so that they were well placed to tackle emerging demands and opportunities. Ofsted noted that similar modernisation plans were in place to improve the effectiveness of the SSCB, but progress was not able to proceed as quickly as some members would wish due to organisational uncertainty in some key agencies such as health services. Nevertheless, the core business was being undertaken adequately. Ofsted (February 2011) found that.. modernisation plans are in place to improve the effectiveness of the LSCB, but progress cannot proceed as quickly as some members would wish due to organisational uncertainty in some key agencies such as health services. Nevertheless, the core business is being undertaken adequately. The Ofsted inspection provides a baseline for performance and a backdrop to this report, which sets out progress made since then, together with future priorities for SSCB. 2. Governance and accountability arrangements 2.1 Role, function and structure of the Board Shropshire Safeguarding Children Board (SSCB) was established in April 2006 and is the key statutory mechanism for co-ordinating local work to safeguard and promote the welfare of children and ensuring the effectiveness of that work. Its core functions are: Developing policies, procedures and protocols for safeguarding and promoting the welfare of children and young people in the area, including: Action to be taken where there are concerns about a child s safety or welfare (including thresholds for intervention); Training for people working with children or in services affecting their safety and welfare; Recruitment and supervision of persons working with children; Investigation of allegations concerning persons working with children; Safety and welfare of children who are privately fostered; Communicating and raising awareness; 5
112 Monitoring and evaluation; Participating in planning and commissioning; Actions relating to child deaths; Undertaking Serious Case Reviews. SSCB board members are accountable for delivering the objectives and actions agreed by the Board and for ensuring that their agency delivers on safeguarding children responsibilities. However, the SSCB is not accountable for the operational work of partners nor does it have the power to direct them. The SSCB is comprised of senior members from a range of Shropshire agencies that work with and/or have contact with children and who are able to: Speak for their agency; Hold their agency to account and challenge its practices; Make decisions about safeguarding as required and allocate resources; Ensure that safeguarding is given strategic priority within their own agency. Partners work: Collaboratively to ensure that good outcomes for the most vulnerable children are achieved through quality services, which place children and young people at the centre; To safeguard children and promote their wellbeing with a particular focus on children who are in need of protection. 2.2 Membership and attendance The following agencies are represented on the Board itself, with many more contributing to the work of its sub-groups: Shropshire Council Shropshire PCT, Hospitals, Community and Foundation Trusts West Mercia Probation West Mercia Police CAFCASS Youth Offending Service Lead (Elected) Member for Safeguarding Dedicated SSCB Officers also attend. Following the inspection, a review of SSCB structure and membership was carried out which resulted in significant changes, including the appointment of an Independent Chair and two lay members representing the local community. The 6
113 chair has a crucial role in making certain that the Board operates effectively and secures an independent voice for the SSCB. The role of the community members is to support stronger public engagement in local child safety issues, bring a grass roots perspective, to contribute to an improved understanding of the LSCB s child protection work in the wider community and to challenge the LSCB on the accessibility by the public and children and young people of its plans and procedures. The Board itself has also evolved within the context of significant public services restructures. Whilst significant challenges remain present for the public sector, the streamlining and consolidation of the SSCB has been successfully implemented. These steps have reduced the numbers on the main board to 21. The Chair of the Board now attends the Children s Trust on a regular basis, including presenting the Annual Report, to ensure a strong relationship between the two bodies, and will also be attending the newly established Health and Wellbeing Board. Arrangements for ensuring scrutiny within the local authority are under discussion and will be in place during 2012/13. The independent Chair also has regular meetings with the Director of Children s Services, who is held to account for the effective working of the LSCB by the Chief Executive of Shropshire Council, and challenged where appropriate by the Lead Member. The Lead Member is a participating observer of the SSCB, routinely attending meetings as an observer and receiving all its written reports. Diagram 1 below shows the structure and strategic links of SSCB. The Board also has explicit links with other strategic groups with safeguarding responsibilities, including: MAPPA (Multi Agency Public Protection Arrangements) MARAC (Multi Agency Risk Assessment Conference via Criminal Justice Sub Group) Domestic Abuse Forum 7
114 Diagram 1: Structure of SSCB Association of Directors of Children s Services West Midlands LADO Network West Midlands Runaways, Sexually Exploited & Trafficked Children Network West Midlands IRO Network Shropshire Children s Trust Executive Regional Networks: West Midlands Regional Safeguarding Network Association of Chief Police Officers MAPPA Education Executive Sub-Group Chair: Kath Edwards, Group Manager Safeguarding (SC) Partnerships Sub-Group Chair: Janet Graham, Group Manager Health and Wellbeing (SC) Chair: Sally Halls Child Death Overview Panel Chair: Audrey Scott-Ryan, Designated Nurse - Safeguarding Healthcare Governance - Safeguarding Children Committee Chair: Prof. Rod Thomson, Director Public Health Communications Sub-Group Chair: Lisa Charles, SSCB Development Officer Training Sub-Group - Chair: Donna Chapman, SSCB Training Coordinator Audit & Evaluation Sub-Group Chair: Steve Ladd, Service Specialist Safeguarding (SC) e-safety Sub-Group Chair: Lisa Charles, SSCB Development Officer Suicide Prevention Sub-Group Chair: Kath Edwards, Group Manager Safeguarding (SC) Criminal Justice Sub-Group Chair: Steve Hoskings/Sue Horne, YOS Serious Case Review Sub-Group Chair: Claire Porter, Corporate Head of Legal & Democratic Services (SC) Child Sexual Exploitation Sub- Group Chair: Steve Ladd, Service Specialist Safeguarding (SC) SCR Panel Tri-X West Mercia Consortium Child Protection Procedures Policy & Procedures Sub-Group Chair: Steve Ladd, Service Specialist Safeguarding (SC) Culture, Leisure & Learning Sub- Group Chair: Erica Garner soon to be subsumed by Area Strategic Fora 8
115 2.3 Sub Groups The SSCB carries out much of its work through a number of subgroups (Diagram 1) and task and finish groups. These groups support the work of the Board through progressing actions and fulfilling the functions of the SSCB, including specified activity as directed by the Board and the business plan, and are well supported by a wide range of agencies, including schools, colleges, voluntary sector organisations as well as the larger statutory organisations who also contribute to the main Board. The work plans of the sub-groups are included in the Board s business plan. Further details of the focus, membership and activity of the sub-groups are included in Appendix Financial arrangements To function effectively, LSCBs have to be supported by their member organisations with adequate and reliable resources. In Shropshire, the core financial contributions are provided by the local authority, the NHS organisations in Shropshire, and the police. Other organisations contribution both in cash and in kind according to their resources and local circumstances, for example through making staff and premises available to deliver SSCB training,. The budget for 2011/12 was as follows: LSCB CAFCASS Health Local Authority Probation Police Other SSCB 11/ (0.36%) 44,570 (29.15%) 58,000 (37.94%) 4,500 (2.94%) 26,910 (17.6%) Colleges 6,250 (4.09%) Schools 10,540 (6.90%) YOS 1,560 (1.02%) The SSCB budget has been used to support key SSCB officers posts including the appointment of an Independent Chair, progress of the business plan (Appendix 3) and significant safeguarding training across agencies. A contingency budget has also been set aside for Serious Case Reviews. 9
116 3. Quality Assurance LSCBs are required to monitor the quality of professional practice within their area. This role has been reinforced following the death of Peter Connelly in Haringey, and the revision of Working Together, with a clear expectation that LSCBs consider the quality of front-line practice and challenge any deficits. Robust assessment and decision-making in safeguarding services, in respect of individual families and children, depends on good internal and cross-agency practice that draws appropriately on the most up-to-date knowledge base. This good practice depends in turn on adequate organisational engagement, processes and structures. Assuring the quality of both professional practice and organisational processes and structures depends on robust internal and crossagency audit systems. Ofsted inspected Shropshire s safeguarding and looked after children services in February 2011 and found that. Revised quality assurance and performance management processes are established and increasingly effective, although the use of data in parts of front line services is more variable and audit processes are not sufficiently outcome focussed. They concluded that performance management and quality assurance were adequate overall. Recommendations specified improvements to be made regarding the reporting of allegations against adults who work with children, and complaints in relation to child protection processes and decisions. Ofsted also commented that the quality assurance role of child protection conference chairs was underdeveloped, and that auditing arrangements needed to be more outcome focused and evaluative. 3.1 The quality assurance framework Shropshire s Safeguarding Children Board in June 2011 requested that the Audit and Evaluation sub-group prepare proposals for strengthening quality assurance arrangements. A new framework for audit and quality assurance was developed to build a cumulative picture of practice, share good practice and plan for further improvement where needed. The final framework was presented to, and agreed by, SSCB in September The framework is explicitly designed to build a cumulative picture focussed on practice, outcomes and compliance rather than just one-off snapshots. The framework sets out tiers of activity relating to oversight, practice, and compliance. Most of the activity described in the framework is essentially what we collectively do already and the associated tools enable a better capture of this information. 10
117 Diagram 2: Audit and Quality Assurance Model Oversight \ Analysis 3 Multi agency file audits per term (3.5) months 1 st Report December 2011 Practice - 10 files per term (3.5 months) summary to A/E group at end of each Term Audit and Evaluation Sub Group Practice Agencies Police, Health, Education, Social Care Compliance All Agencies SSCB Compliance Audit - all agencies annual June 2012 responses back to SSCB business manager Section 11 Winter / Spring 2011 / 12 (Joint with Telford and Wrekin) 11
118 The SSCB approach to quality assurance includes: looking systematically and objectively at samples of practice, using the audit and quality assurance framework and its associated tools; the child protection conference chairs quality assuring each child protection conference, including seeking the views of service users through exit interviews ; collating and analysing the findings, taking a wide view; sharing the issues which emerge with staff, managers and others as relevant; deciding the actions needed both to promote the good practice identified and to make improvements where needed; providing support for staff to achieve required changes; re-auditing to measure that improvements have been achieved and maintained. The audit and quality assurance model is illustrated in diagram The approach to auditing in Shropshire The overall aim of the audit programme is to ensure SSCB s work is effective and high quality, demonstrate continuous improvement and meet national requirements for self-assessment and quality assurance. Audits in Shropshire are undertaken in a range of circumstances. The following audit activity in relation to active child protection cases has taken place or is underway Oversight tier There have been 3 multi-agency audits undertaken and outcomes presented to SSCB by the audit and evaluation subgroup since September The audit focussed on children subject to Child Protection Plans where domestic abuse had featured. Practice tier Over 70 case files in total were audited by agencies between September and December These audits involved direct operational managers and front line practitioners from education, police, children s social care health services. 12
119 Compliance A joint Section 11 (of the Children Act 2004) audit was undertaken between November and December 2011 by Shropshire and Telford and Wrekin Safeguarding Children Boards, in order to examine the degree to which member agencies were carrying out their statutory duty to safeguard and promote children s welfare, in all aspects of their delivery of services and functions. Results were based on a self-assessment by each agency, and identified a number of areas which are in need of improvement or development, and also highlighted areas of good practice. Overall, the audit has given a baseline of information against which each LSCB will be able to assess progress. Quality Assurance Child protection conferences have continued to be quality assured by the Child Protection Conference Chairs 120 Conferences as at end December In general the outcomes of the above activities were positive, although the process itself posed some challenges for service areas that were not routinely involved in audits. There is evidence that the child protection process works well and is understood by statutory agencies, with cases being progressed appropriately once in the formal child protection arena. However, there remain a number of agencies whose contribution to core child protection activity needs improving. Notably, West Mercia Police has taken immediate steps to address this through appointment of a child protection conference coordinator. The audits also indicated that the TAC and CAF process started well but lost momentum, showing high levels of professional activity and repetition of intervention strategies with limited outcomes; and of poor record keeping across agencies. These findings, along with the outcomes of Eileen Munro s review of child protection system, led to a review of our early offers of help to families and this review will affect the way in which we respond to the need for early intervention. A number of recommendations were made as a result of the audits. These relate to improved participation by key agencies, and availability of accessible information for parents regarding child protection processes. An additional action relates to the development of guidance to assist partner agencies with completing audits, particularly practice audits. 3.3 The scorecard An additional tool has recently been developed by the SSCB which seeks to take the integration of performance, quality assurance and demographic data a step further in the form of a combined scorecard. The scorecard is presented to the SSCB, on a quarterly basis, giving quantitative and qualitative information around 13
120 selected outcomes, multi-agency service quality measures, threshold indicators and staffing information. In some instances, measures have been suggested where data is not yet readily available, e.g. referral sources and average time of assessments. These work towards the direction indicated by the Munro Review final report of May While none of these measures are intended for use individually as absolute indicators of success or failure, together they are intended to give a picture of overall performance. The most recent scorecard is included as appendix Exit Interviews feedback from children and parents/carers Independent Child Protection Conference Chairs are a key part of the SSCB quality assurance framework. They monitor the quality of the child protection process in relation to a range of measures. An increasingly important element of their work involves gaining feedback from parents and young people on their experience of the child protection process. Feedback to date includes the following comments: A young person said: A lot of things have changed, my health is better I have no worries about my older brother s behaviour and I am happy now. Young people generally did not feel the child protection conference process was explained to them but, by contrast, in one case the youngest and the eldest child participated in the conferences; each came prepared with what they wished to say. Some parents say that being part of the child protection process was helpful and recognised the changes that they themselves made with multi-agency support. A consistent message is that more information needs to be made available to parents about the child protection process, including the conference. 3.5 Children subject of child protection plans Following the death of Peter Connolly ( Baby P ) in Haringey and other factors, Shropshire, like many authorities nationally, experienced a significant rise in the numbers of children referred under the auspices of child protection, and an increase of the numbers of children subject to child protection plans through /11. This picture has now stabilised. 14


121 When Ofsted visited Shropshire in February 2011 for its announced 2 week long inspection of safeguarding arrangements, it commented that the number of children who were the subject of child protection plans for 2 or more years was higher than would or should be expected. Work had already begun to attend to this area in 2010 and efforts were reinforced through strong performance management in SSCB has been kept informed of the progress via the newly-introduced scorecard system. The two charts below demonstrate the progress made over the last 12 months in addressing lengthy episodes of children remaining subject of a child protection plan. The latest data suggests that over 85% of child protection plans are fewer than 12 months old. This data, when coupled with the low rate of re-registrations, indicates that child protection plans are achieving suitable safeguarding outcomes for children in a timely fashion. 15
122 st March Children 2 years + Less than 2 years less than 1 year 6 Total 16
123 4. Performance Progress on 2009/2012 priorities In addition to objectives relating to strengthening governance and improving overall performance described above, SSCB agreed four core practice priorities in its business plan : Suicide Prevention, Neglect, Child Sexual Exploitation and Information Sharing. (i) Suicide Prevention SSCB aimed to establish a multi-agency collaborative approach to suicide prevention in Shropshire. A Suicide Prevention Strategy and Care Pathway has been developed which sets out a common understanding and approach to suicide prevention, including a practitioner s toolkit to assist front line workers with identifying risk of suicide. The strategy and care pathway was formally launched in the spring of (ii) Neglect SSCB aimed to assist practitioners with identifying childhood neglect at the earliest opportunity in order to plan early intervention. A strategy, practitioner s toolkit and guidance has been developed which together set out a common understanding and approach to identification of and interventions in relation to childhood neglect. These were formally launched with key managers across agencies including schools. Staff who attended the launch events were provided with session plans and resources to disseminate the briefings to their teams. An evaluation of the impact that this work has had on the early identification of neglect cases and the management of the escalation/de-escalation of cases will be carried out over the summer of 2012 and reported to SSCB in the autumn. (iii) Child Sexual Exploitation (CSE) SSCB aimed to examine areas of good practice across the country including Derbyshire, Dudley and our immediate neighbour, Telford and Wrekin in order to develop our approach to CSE and trafficking. A strategy, guidance and toolkit to assist with the identification, prevention and intervention in relation to CSE and trafficking has been developed. In addition, a CSE panel has been established as the key mechanism for agreeing how relevant organisations will co-operate and work together to safeguard and promote the welfare of individual children and young people who are identified as experiencing or at risk of experiencing CSE in Shropshire, and for monitoring their effectiveness. The activities described above are in their first 12 months of implementation and their effectiveness will become clearer over time. What is already known is that the dozen children who have been identified as either experiencing or at 17
124 risk of experiencing CSE have received a co-ordinated response, including the police using strategies of disruption such as issuing of harbouring notices; one case is subject to a criminal investigation; and effective care planning is in place for a looked after child. (iv) Information sharing SSCB aimed to improve information sharing within and between agencies. An Information Sharing Themed conference was held in May 2011 which focussed on exploring the barriers to information sharing and how these could be overcome to improve the safeguarding of children and young people in Shropshire. It was a presenter led event with a range of keynote speakers focusing on topics such as the research review Safeguarding in 21 st Century (by the report s author Jane Barlow), Hearing from the Voices of our Children in Care (Shropshire s Care Council Crew), Sex Offender Disclosure Scheme & Domestic Abuse Protection Orders ( Martin Lakeman West Mercia Police HQ) and A Legal and practical Tool Kit for Sharing Information (Tim Collard, Head of Legal Services and Roy Morris, Information Governance Officer - Shropshire Council). In Addition SSCB reviewed, renewed and re-launched the Missing from Home and Care Protocol in collaboration with Herefordshire, Worcestershire, Telford and Wrekin LSCBs and West Mercia Police. This protocol also links to child sexual exploitation. The SSCB Child Protection procedures were updated to reflect the changes in Working Together 2010, and systems put in place to ensure that these remain updated and compliant with statutory changes. 4.2 Training and development The training sub-group oversees and manages multi-agency training on behalf of SSCB informed by the requirements set out in Working Together to Safeguard Children 2010, and the priorities set within the business plan. In the past 12 months the SSCB training project has planned, commissioned and delivered a varied range of training opportunities for Shropshire for a large number of agencies and practitioners. In addition, a series of one-off events and manager briefings were delivered through the year to meet additional training needs identified. Details are set out in Appendix 5. The training pool has continued to be sustained and there have been three development sessions provided for trainers throughout the year, attended by an 18
125 average of 40 trainers, which has continued to develop their skills and knowledge to deliver training for the SSCB. The training sub-group and the training co-ordinator have developed good links with the Fire Service, Independent Schools and the Education Advisory team, who deliver child protection training in schools and to designated school safeguarding leads. The training sub-group has also introduced a new charging policy, agreed by the SSCB, to ensure consistency in charging, and is exploring new income generation developments. As the new financial year progresses, the training sub-group plans to make stronger links to the audit and evaluation sub-group and develop good quality assurance mechanisms for single agency and multi-agency child protection training. 4.3 Serious case review There were no serious cases in Shropshire during 2011/12 which met the criteria for a serious case review, which are set out in chapter 8 of Working Together However, there were two instances where SSCB wished to review the effectiveness of work and derive learning, so decided to undertake a review of multi-agency safeguarding practice in respect of each. There were points of learning in relation to improving the support of young people who are Looked After or Children in Need. As a result, there were a number of changes in practice that were identified and addressed. These changes were attended to through training events and team briefings in the majority of agencies to address a number of compliance issues, and to further raise awareness of key strategies and tools developed by SSCB including the Suicide Prevention Care Pathway. In addition, an Information Sharing conference was delivered by the SSCB, which underlined the importance of swift and comprehensive information sharing on an inter and intra agency basis. Action plans were developed by agencies and collated into a multi-agency action plan, against which progress will be monitored by the Serious Case Review Subgroup of the LSCB. It is hoped that the actions taken prior to, and during the process of these reviews, will help to protect other children and young people from experiencing further harm, whilst being provided with a multi-agency safeguarding plan. 5. Looking to the future Members of SSCB attended a development day in December 2011 to review progress of their work, and to agree the priorities for the 2012 \15 period. A range of information and evidence was considered, including relevant data, the outcomes of local audit activity including prevalent factors in Shropshire s child protection population, government reviews, initiatives and research, including analysis of serious case reviews. 5.1 Key Priorities
126 The following three priorities will be a particular focus of activity during the next three years and are reflected in the Board s Business Plan for : 1) Compromised Parenting To include: Domestic abuse Substance misuse Parental mental health This priority has been chosen because evidence from serious case reviews and elsewhere demonstrates that children living in households where there is domestic abuse, and/ or parents/carers who suffer from poor mental health, or misuse drugs or alcohol, are more likely to suffer significant harm. This is also the case in Shropshire, with one or more of these factors being a feature in the lives of children on child protection plans or entering the care system. This work is being taken forward as part of the work of the Partnership Subgroup, with the aims of: Establishing a common understanding, commitment and approach to identifying children and young people who are experiencing, or are risk of experiencing, harm due to domestic abuse, substance misuse or adult mental ill health; Ensuring that children living in such circumstances are recognised as being at risk of harm/being harmed not hidden; Delivering a co-ordinated response to these children and young people that reduces the risk of harm and ensures that they receive a joined up service; Ensuring that children and young people feel safe and supported. 2) Missing To include: Trafficking Child Sexual Exploitation This priority has been chosen for a number of reasons. Examination of data in Shropshire has revealed that, in addition to its own children in care population of around 205 children, there are around 350 children placed within Shropshire who are looked after by another local authority. Of these, a small but significant number go missing regularly. An increasing body of evidence is indicating that this population of young people is particularly vulnerable to exploitation of various kinds. A task and finish group has been established to take this forward. We will be aiming to keep children safe through: Developing and embedding policies & procedures that are effective in reducing missing children in each 20
127 organisation, agency, school and children s home; Achieving a reduction in the number of children reported as having been harmed when missing; Achieving a reduction in the number of missing episodes; Developing greater knowledge of where missing children have been; Ensuring that there is a named person responsible for missing in each relevant agency. In relation to child sexual exploitation & trafficking, our measures of success are: A reduction in young people s vulnerability to child sexual exploitation and trafficking; An improvement in young people s resilience; Disruption and prevention of the activities of perpetrators; Reducing tolerance of exploitative behaviour; Successful identification and prosecution of abusers. 3) Communication To include: Promotion Community engagement Inter-agency communication Voice of children and young people Information Sharing This priority has been chosen to reflect the importance we place as a board on promoting awareness and understanding of the need to safeguard and promote the welfare of children and young people, and that we regard this as a collective responsibility. This will include listening to and consulting children and young people and ensuring that their views and opinions are taken into account in planning and delivering safeguarding and promoting welfare services. The following strap-line for SSCB has been adopted to reflect the Board s childcentred approach: Keeping our children safe from harm Through improved communication and awareness, we aim to achieve the following: Earlier and more effective identification of vulnerable young people; Workforce awareness of their responsibilities, board priorities and the contribution they can make; The public having an understanding of safeguarding issues and the role of the LSCB; Active community involvement in safeguarding children; All members of council to understand safeguarding issues; Different methods of communication being used for different audiences; SSCB to be regularly informed by children and young people s views. 5.2 Business Plan
128 In addition to the above priorities, the Board will be continuing to deliver on its statutory responsibilities, as well as monitoring and responding to the extensive public sector change which has already taken place in relation to public sector finance, human resources and statutory guidance, with more to come in the next 12 months. A safeguarding peer review has been commissioned in order to provide an independent look at SSCB progress and development following the Ofsted inspection and assist us with our improvement journey. This will take place in May There are also developments both locally and nationally to which the SSCB will be responding in the next year. These include: The Back to basics review, which is developing the approach in Shropshire to early intervention in the light of the Munro Review and the government response, will be completed in the late summer of The outcome and any proposals will be presented to SSCB in Autumn The partnerships sub-group will be leading this work; The revised Working Together to Safeguard Children guidance, which is in the process of being consulted on nationally, and will doubtless have implications will need to be considered and implemented; including revision of the SSCB policies and/or procedures; The Protection of Freedoms Bill, which has brought changes to the disclosure scheme. This will be a particular focus of work by the policy and procedures sub-group. In this context of significant change, maintaining the momentum of multiagency collaboration has its challenges. However, the continuing effort and commitment of our partner agencies will enable the good work of the Board to progress next year and beyond. The SSCB business plan is attached at Appendix 4. 22

129 Appendix 1 Current working arrangements by sub-group 2.1 Executive Sub-group Membership: Chair: Safeguarding Group Manager, Shropshire Council SSCB Independent Chair Safeguarding Group Service Specialist & SSCB Business Manager Corporate Head of Legal & Democratic Services, Shropshire Council Designated Nurse for Shropshire, Telford & Wrekin Assistant Chief Officer, West Mercia Probation SSCB Training Officer Area Commander, West Mercia Police SSCB Development Officer Designated Doctor for Shropshire and Telford & Wrekin Quarterly Frequency of meetings: Focus: Developing the SSCB agenda Activity: The Executive Sub-group debates and clarifies the issues that are scheduled for the SSCB, receives all performance management reports and reports from sub-groups and determines the matters to be considered by the full SSCB. Future work: Communications Sub-group Membership: Chair: SSCB Development Officer PCT Communications Officer Shropshire Councils Communications Officer Regional Safe Network Officer Family Information Service West Mercia Police Communications Officer Community Member Hoping to recruit: Education, CVS, Equalities and Diversity rep Frequency of meetings: Focus: Activity: Future work: 2.2 Training Sub-group Membership: Bi-monthly Communications Strategy and SSCB website development The Communications Sub-Group has led the development of a SSCB Communications Strategy. This group will lead on the SSCB s Communications priority, and ensure that the message about safeguarding children being everybody s responsibility is disseminated amongst the widest numbers of the population as possible. They will also undertake tasks on behalf of the Board which are related to the publicising of safeguarding work in Shropshire, and the engagement of children and young people in the work of the Board. Chair: Inter-agency Training Officer, SSCB Shropshire Council (SSCB) Shropshire Council (LETS) West Mercia Police SSSFT (South Staffordshire & Shropshire Healthcare NHS Foundation Trust), 23
130 Frequency of meetings: Focus: Activity: Future work: 2.3 Audit & Evaluation Sub-group Membership: Frequency of meetings: Focus: Activity: Lead Nurse for Child Protection Shropshire Council (IRU) Walford & North Shropshire College Shropshire Council (Prevention & Inclusion) Shropshire Early Years & Child Care NSPCC Shropshire Community NHS Trust & SATH, Named Nurse for Child Protection Shropshire Council, Joint Training for Adult Community & Health Services Shropshire Council Shrewsbury Children s Centre Shropshire Council Raising Achievement & Inclusion Shropshire Council Social Care & Safeguards Bi Monthly Co-ordinating the delivery and quality assurance of Safeguarding training in Shropshire for all those working with children, safeguarding or child protection. The group is developing a quality assurance model to achieve this consistently. The group has reviewed developing practice modules, and has agreed training priorities for 2012 in line with Board Priorities. It ensures that learning from Serious Case Reviews and other developments is embedded into the Safeguarding Training packages. The group has commissioned suitable e-learning packages for Group 1 as defined in Working Together to Safeguard Children It is currently working on reviewing developing practice modules, and agreeing priorities for 2012 in line with Board Priorities. Developing and co-ordinating a Safeguarding training Audit Tool. Developing ways of communicating Learning from SCR s. Chair: Safeguarding Group Service Specialist SSCB Development Officer West Mercia Police Education Welfare PCT Army Welfare Shropshire Council Performance Manager NHS Bi-monthly Scrutinising and evaluating practice to ensure this is effective and complies with standards. The Audit and Evaluation sub group developed and launched the Audit and Quality Assurance Framework (tiered audits) throughout last year and is currently implementing this Framework. Section 11 audits feed into this framework. These were completed in January 2012, in conjunction with Telford and Wrekin LSCB. Proposals for quality assuring returns will be presented at the April SSCB meeting. Future work: Further embedding and improvement of the Audit Framework (Oversight, Practice, Compliance) Development of the SSCB scorecard based on audit, quality assurance activities (such as agencies attendance at child protection conferences 24
131 2.4 e-safety Sub-group Membership: and views of children and families) Considering proposed Munro performance information and incorporating it into SSCB processes. Chair: SSCB Development Officer Education Harnessing Technology Officer Youth Association Independent Schools Connexions Broadplaces West Mercia Police School Nurse Manager SSCB Training Officer Secondary School Deputy Head Primary School Head Library Service Frequency of Quarterly meetings: Focus: Delivery of e-safety strategy Activity: An e-safety training audit identified that schools require help with resources and training for parents, would welcome CPD opportunities and the chance to network and share good practice with others. An e-safety Conference for schools was organised by the sub-group in January 2012 to address some of the issues arising from the audit and follow-up work to organise training events and develop resources for parents is underway. The group has signed up to a West Mercia wide e-safety website for young people, parents and carers. It was launched to young people in Shropshire during Anti-Bullying week. It is hoped that as many young people as possible will complete the online questionnaire on an annual basis, which will identify the e-safety issues they face and further inform the groups work. Future work: The recently developed e-safety Policy Guidance for non-school settings will be launched along with the Online Compass self-assessment tool in May Suicide Prevention Sub-group Membership: Chair: Group Manager Safeguarding SSCB Development Officer SSCB Training Co-ordinator Education Welfare Head of Multi-Agency Teams TAMHS Co-ordinator Education Psych Samaritans PCT Assistant Director MAP CAMHS Frequency of Currently bi-monthly meetings: Focus: This group was developed in late 2009 to determine the nature and level of self-harming and risk of suicidal attempts by children and young people in Shropshire, to outline the support services available and how these are 25
132 Activity: coordinated, and to agree a strategy for service development. The Suicide Prevention Strategy was launched by SSCB in Spring The sub-group continues to monitor the implementation of the Suicide Prevention Care Pathway (part of the strategy) which was launched in March 2011 and disseminates learning taken from recent cases. The Pathway provides: A systematic approach to identifying and addressing the needs of children and young people at risk of suicide; Risk assessment guidance, early intervention questions and baseline risk assessment questions; A care pathway flowchart for workers to follow; Additional supporting information and guidance. Suicide Prevention Training is being delivered to practitioners across Shropshire in the form of STORM Training (Skills Training on Risk Management) continues to be delivered to multi-agency audiences by a pool of six qualified trainers. The training has been well received and has equipped practitioners with the confidence and skills that they need when working with young people at risk of suicide. Future work: A mini-storm raising awareness training package has been developed and will be delivered to foster carers in May Criminal Justice Sub-group Membership: Chair: Service Manager, YOS West Mercia Probation West Mercia Police Independent Reviewing Officer Stoke Heath Army Welfare Assessment & Support Service Independent Domestic Violence Advocate Frequency of Quarterly meetings: Focus: Monitors criminal justice agencies activity in relation to safeguarding children, for example the management of offenders in the community, including reviewing, monitoring and ensuring implementation of PPRC. Activity: The group, in conjunction with the Community Safety Partnership has: carried out a scoping exercise in relation to provision of domestic abuse services in relation to the SSCB priority of Compromised Parenting ; completed a 2 year workplan, which has included overseeing implementation of the West Midlands revised procedures for criminal justice agencies Persons Posing a Risk to Children. The group was represented at a regional level during the revision and has subsequently reviewed local compliance levels and issues with practice. Monitored the safeguarding of children at Stoke Heath YOI until the YJB s decision to decommission places for under 18 years old at this institution. The county now has no secure custodial facilities for under 18 year olds. Future work: This group is being discontinued. 2.7 Serious Case Review Sub-group Membership: Chair: Head of Legal and Democratic Services Group Manager Safeguarding Service Manager Safeguarding & Review 26
133 Frequency of meetings: Focus: Activity: Future work: Service Specialist Safeguarding SSCB Development Officer West Mercia Probation West Mercia Police Designated Nurse/Doctor Bi-monthly 2.8 Policy & Procedures Sub-group Membership: Frequency of meetings: Activity: Future work: This group is responsible for considering whether or not cases meet the Serious Case Review criteria or require Management Reviews to be undertaken. Other work-streams involve monitoring agencies compliance with SCR recommendations/action plans, analysing cases for key themes, learning and identifying trends. Two Management Reviews have been completed in the last twelve months and work is ongoing on a review of teenage suicides. This group is also considering the implementation of a systems model for undertaking SCRs and is exploring training opportunities. Chair: Service Specialist Safeguarding Service Manager Safeguarding & Review SSCB Development Officer Human Resources Designated Nurse Education Welfare West Mercia Police Hope House Bi Monthly 2.9 Child Sexual Exploitation Sub-group Membership: Since West Mercia consortia has been established, updates to procedures have been subsumed by this group which consists of the 4 LSCB business managers and Tri X as well as priority groups such as Sexual Exploitation and Suicide Prevention. Changes to Safer Recruitment procedures will be a priority area of work for this group following the introduction of the Protection of Freedoms Bill. This renewed group will be looking at arrangements for ensuring a safe workforce, including recruitment and developments with the Protection of Freedoms Bill (vetting \ barring) and LADO activity. Chair: Service Manager Safeguarding & Review Service Specialist Safeguarding SSCB Development Officer SSCB Training Co-ordinator Education Welfare PCT West Mercia Police Assessment & Support Service YOS Residential Independent Reviewing Officer LAC Nurse Connexions 27
134 Frequency of Quarterly meetings: Focus: Development and delivery of CSE strategy Activity: The group has recently developed and launched the CSE Strategy and Practitioner s Toolkit to aid front line practitioners to take a common approach based on shared understanding in the identification of CSE. Over 100 managers from different agencies have attended the briefings to launch the strategy and referrals are now being received. The group has also initiated the development of a CSE Multi-Agency Panel that considers cases on a monthly basis, and ensures adequate resources are available to attend to them and enable progress to be maintained. This panel has been meeting on a monthly basis since December 2011 and has already considered 12 cases of child sexual exploitation and have agreed safeguarding plans for the young people affected. Future work: The group will develop an action plan in response to the Government s Action Plan for tackling CSE. A Task and Finish group is to be formed to review the missing children arrangements currently in place and ensure they fit with the recently revised Joint Protocol For Reporting Missing Children and Young People. The CSE sub group will report on the number of cases heard and the overall effect it has had on Child Sexual Exploitation in Shropshire in the 2012/13 annual report Partnerships Sub-group Membership: Chair: Group Manager Care & Wellbeing Group Manager Safeguarding SSCB Training Officer West Mercia Police Designated Nurse Service Manager Assessment & LAC Service Specialist, Safeguarding Group Headteacher, Oldbury Wells Headteacher, Weston Ryn CVS Representative Education Welfare Named Nurse Inclusion Officer Service Manager, Family Care & Wellbeing Health Development Manager, Family Care & Wellbeing Programme Lead for Childhood Obesity Service Manager, Support Services CAMHS Children & Specialist Services, NHS Frequency of Monthly meetings: Focus: Review thresholds and work on early intervention strategies: Developing interagency collaboration across all tiers, with a particular eye on early intervention and support; including review of thresholds; also leading the response to the Munro Review. Activity: This group is a recent addition (October 2011). The group has commissioned a Back to Basics Review to consider the arrangements regarding early intervention and prevention including the 28
135 systems, support, resources, tools and training involved. It is consulting all agencies including schools. This review is due to be completed in the summer 2012 and outcomes and proposals will be presented to SSCB in the autumn Future work: Co-ordinate work on the priority theme of Compromised Parenting, with other sub-groups contributing. The following groups have been asked to carry out a scoping exercise on the provision of the adult services, to begin this piece of work; Group Scoping exercise Hidden Harm Group Adult Substance Misuse Services Health Governance Group Adult Mental Health Services Criminal Justice Sub-group Domestic Abuse Services Consider the use of the CWDC funding in providing Early Intervention services Establish task and finish group to develop programmes and resources for parenting support 2.11 Health Governance Safeguarding Children Committee Membership: Chair: Director of Public Health for Shropshire Group Manager Safeguarding Designated Nurse Director of Nursing & Quality Nurse Director (Shropshire Doctors Ltd) Designated Nurse LAC Named Nurse SSSFT Service Delivery Manager Safeguarding (T&W) Services Manager Safeguarding (T&W) Director of Nursing (RJ&AH) Head of Safeguarding (Powys) Deputy Director of Child & Family Support Services (T&W) Named Nurse (RJ&AH) Named Nurse for Safeguarding (SATH) Named Midwife (SATH) Lead Nurse (CDOP) Joint Lead Commissioner (T&W) Consultant Paediatrician/Designated Doctor Designated Nurse for Children in Care (T&W) Managing Director for Community Health Services (T&W) Deputy Director for Children & Specialist Services West Midlands Ambulance Service Service Specialist for Safeguarding, Shropshire Council Named Nurse (T&W) Director of Quality & Safety/Chief Nurse (SATH) Frequency of Quarterly meetings: Focus: Providing assurance to the SSCB and Care Quality Commission (CQC) that safeguarding children remains a key agenda item for the Shropshire, Telford and Wrekin health economy and that: all statutory requirements are met, healthcare standards relating to safeguarding children are performance monitored,and appropriate action taken to ensure compliance. 29
136 Activity: This group was formally requested to become a sub group of SSCB in January An extraordinary meeting of this group was convened in February 2012 and the Terms of Reference are currently being re drafted to positively reflect the SSCBs proposal. Future work: To oversee the safe transition of the heath organisations to new arrangements, ensuring continued priority is given to safeguarding children Child Death Overview Panel Sub Group Membership: SSCB and Telford & Wrekin LSCB share the Child Death Overview Panel (CDOP) Frequency of Monthly meetings: Focus: Monitor and review child deaths during the year on behalf of both LSCBs. Reviewing child deaths includes collecting information about the circumstances of the child s death, with the overall purpose of understanding how and why children die, making recommendations to protect other children and preventing future deaths. The group is responsible for the submission of CDOP national data. Activity: There were 25 deaths during the year 2010/11, 17 fewer than the 42 which occurred in 2009/10 and 30 fewer than the 55 that occurred in 2008/09. Of the 25 deaths, a Rapid Response was carried out for 9 deaths. The total number of child deaths notified to CDOP since commencing in April 2008 is 122. There were no child deaths due to deliberately inflicted harm, trauma or acute or chronic medical conditions over the last 12 months. Key achievements include securing agreement to the appointment of a CDOP Lead Nurse, and developing effective partnership working with the coroner. Future work: To continue to monitor and review child deaths during the year on behalf of both LSCBs, as required. 30

137 31 Appendix 2
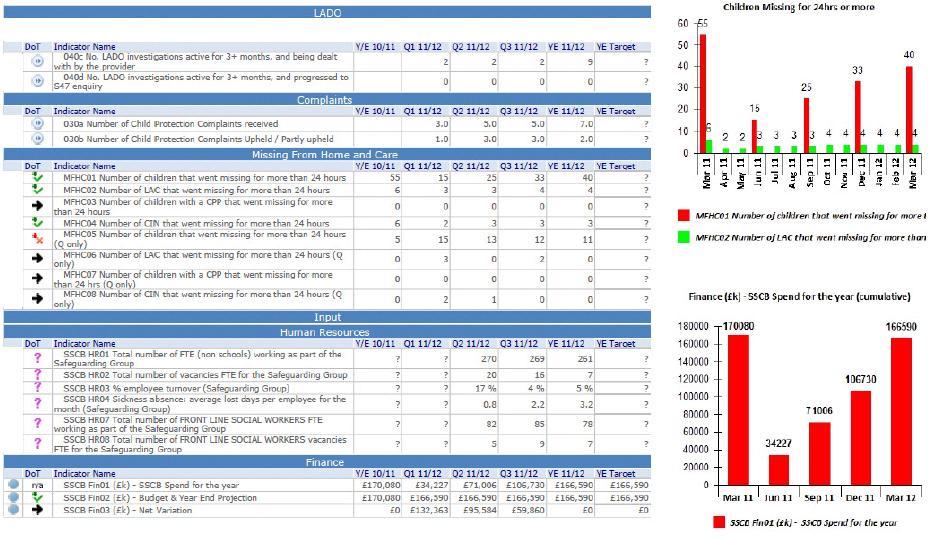
138 32
139 Shropshire Safeguarding Children Board Business Plan Progress Appendix 3 The overall aim of this business plan is to enable the Shropshire Safeguarding Children Board to fulfil its objectives, which are: 1. to support local work to safeguard and promote the welfare of children and 2. to ensure the effectiveness of that work. Business Priorities for Activity Area Objectives When RAG Rating Notes Governance Following revision of Working Together to Safeguard Children 2006, review current relationship with Shropshire s Children Trust to ensure compliance with new statutory guidance. Sept 2010 A report was presented to the SSCB meeting in June 2010 on the relationship between the Board and The Children s Trust and the roles and responsibilities of both. Review the arrangements for the Chair of SSCB. June 2010 A new Independent Chair was appointed in September 2011 on a 2 year fixed term contract. Ensure Lead Member for Children s Services is able participate fully in the work of SSCB. Agree reporting arrangement between SSCB and Shropshire Council Scrutiny Committee. Review SSCB Subgroups Terms Of Reference and reporting process. Dec 2009 Mar 2010 Mar 2010 Cllr Anne Hartley involved in the work of SSCB and attends Board meetings. Completed Completed and reported to SSCB in March Revise SSCB Member Agreements. Mar 2010 Member roles and responsibilities revised and agreed at the Development Day in December
140 Performance Ensure new SSCB members complete Section 11 Audits, when necessary. Undertake annual interagency case file audit, reporting findings to SSCB. Report detailed data on Missing Children to SSCB from 2010 onwards. Dec 2010 Section 11 Audits completed by all Board member agencies and findings reported to Board in January Annual Three inter-agency case file audits will now be completed every term in line with the new Audit Framework. Annual Report to SSCB April Undertake SSCB Self Audit exercise every two years to ensure effectiveness maintained. Establish CDOP Action Planning process for SSCB to ensure issues relating to preventable child deaths are addressed. Audit the implementation by SSCB members of new guidance. Report on outcome of annual Compliance Audit process. June 2012 June 2010 On-going Annual Timing to be decided by the Board in April 2012 (to be completed during a Board meeting?) CDOP Annual Reports are presented at Board This is done on a project specific basis and also measured using the Audit Framework and scorecard. To be discussed at Exec (to be completed June 2012) Report annually on outcomes of SSCB Performance Data Set. Annual Activity Area Objectives When Performance Data for the last quarter is critically analysed and presented at each Board meeting. Practice Revise SSCB Tri X Child Protection Guidance once Working Together to Safeguard Children 2006 is revised and published. Sep 2010 Completed Explore with SSCB members how information sharing between agencies can be improved. Dec 2010 Inter-agency Information Sharing Conference took place in May
141 SSCB to agree specific strategies regarding: Accident Prevention 2011 Strategy has been presented to Board. Child Sexual Exploitation 2010 The CSE Sub-group has re-convened, developed and launched a strategy and has set-up a Multi-Agency Panel to consider CSE cases on a monthly basis. Suicide Prevention 2010 A Suicide Prevention Care Pathway and toolkit has been developed and launched. The Suicide Prevention sub-group continues to meet to monitor progress and work together to prevent the suicides of children and young people. Neglect 2010 A Neglect Strategy and Practitioner s Toolkit has been developed and launched. A review of progress since the launch of the strategy will take place in Spring 2012 Communication, including Young People, their Carers and the Children s Workforce Annual Conference to address Information Sharing The Media Sub-group to consider this areas of work in the development of a Communication Strategy in 2012 Dec 2010 Completed Provide briefings on the Safeguarding Agenda to elected members, trustees and governors to ensure a strategic understanding of the issues. Dec 2010 Consideration is being given to developing a briefing on CSE for elected members early in Re-launch People Posing A Risk To Children protocol. Feb 2010 The PPRC protocol was re-launched in 2010, however its implementation is currently under review through the Criminal Justice Sub-group. Ensure all SSCB members are prepared for the implementation of the Vetting and Barring Scheme. Nov Awaiting the outcome of the Freedoms Bill in order to consider the implications for
142 Assist Shropshire Children s Trust in its work addressing Domestic Abuse within the county. Receive annual report on children missing from education and those educated at home. agencies of the changes to the disclosure scheme. Ongoing SSCB has representation on the County DV Forum. Inter-agency training on Domestic Abuse was developed and piloted in 2010 and is now being delivered as part of the SSCB training programme. Annual Report due in April 2012 Review e-safety Strategy and Training content to reflect evolving understanding of Cyber-bullying and the wider e-safety area. Dec 2010 e-safety Annual Action Plan ( ) has been developed and progress is monitored at each e-safety sub-group meeting. Last updated April
143 Governance SSCB Business Plan Appendix 4 Priority Key Activities Measure of success Lead Role Timescale RAG & progress Strengthen the governance of the Board Develop a Board Constitution to include Terms of Reference and Board Structure diagram Board Constitution in place and adhered to by all members SSCB Business Manager Apr-12 Share in the development and delivery of the new Area Strategic Forum meetings Re-convene Law & Procedures Subgroup, re-name as Policy & Procedures Sub-Group and revise terms of reference. Sub-group to initially focus on Safe Recruitment. Review the arrangements for the Independent Chair and Community Members SSCB priorities are shared with and owned by the Area Fora Safe Recruitment messages communicated to partner agencies prior to launch of Protection of Freedom's Bill Successful reappointment/appointment of Independent Chair and Community Members SSCB Business Manager & Group Manager for Safeguarding SSCB Business Manager SSCB Development Officer & SSCB Members During 2012 Apr Sept 2012 Spring
144 Performance Further develop links with scrutiny/children's Trust with reporting across partnerships Governance arrangements in place. SCT commitment to SSCB recommendations about the service improvements. DCS & SSCB Chair Sep-12 Ensure each sub-group has terms of reference and an action plan Documents in place for each subgroup SSCB Development Officer Jul-12 Respond to and implement Government legislation, strategies and guidance Audit and evaluate practice objectively to ensure compliance with standards and highlight areas for improvement Ensure all SSCB members are prepared for the implementation of the Disclosure and Barring Scheme. Undertake Back to Basics Review of early intervention. Revise SSCB Tri X Child Protection Guidance following the revision of Working Together to Safeguard Children 2010 and the outcome of the Back to Basics Review Undertake SSCB Self Audit exercise every two years to ensure effectiveness maintained. SSCB member agencies effectively implementing the DBS Update report to July SSCB Agencies acknowledging and agreeing to early intervention \ prevention approach. New procedures online and updates announced to be decided at Exec Meeting in June 2012 Policy & Procedures Sub- Group Partnership Sub- Group Policy & Procedures Sub- Group Audit & Evaluation Sub- Group Dec-12 Oct-12 Sep Dec 2012 to be decided at Exec Meeting in June
145 Practice Maintain the S11 Audit as a 'live' document to be updated every 6 months by agencies and carry out sample audits for quality assurance on an annual basis Agencies produce and implement safeguarding action plans and demonstrate continuous improvement Audit & Evaluation Sub- Group Update June & Dec 2012 QA Sep Jan 2013 Further embed and improve the Audit Framework (Oversight, Practice, Compliance). Review the Audit Framework Develop the SSCB scorecard on a flexible basis to reflect audit and quality assurance activities Consider the proposed Munro performance information and comparative data Reports to SSCB collate findings and highlight areas for development and improvement Identifying areas for improvement and measuring the effectiveness off SSCBs work Audit & Evaluation Sub- Group Audit & Evaluation Sub- Group & Performance Team Sep-12 Quarterly Priority 1 - Missing Children, CSE & Trafficking Keeping our children safe from harm by coordinating our response to the issues of Missing, CSE & Trafficking Implement the Missing Joint Protocol in Shropshire through the creation of a Task/Finish Group Monitor and evaluate the implementation of the Missing From Home and Care Protocol. Reduction in the number of children reported as having been harmed when missing Reduction in the number of missing episodes Greater knowledge of where missing children have been Missing Task/Finish Group Missing Task/Finish Group May - Dec 2012 Report to Board in April 2013 Improve SSCBs awareness of LAC children placed in Shropshire from other local authorities and improve notification systems LAC Census to be reported to Board in July 2012 to better establish a baseline population count of this cohort of young people. LAC Strategy Group July
146 Establish data collection processes for Missing, CSE and Trafficking Added to SSCB scorecard and reported on at the end of each quarter SSCB Business Manager & Performance Team Quarterly Reduce incidences of CSE, Missing and Trafficking through the disruption of perpetrators, including those targeting private care homes. Evidence of disrupted activity West Mercia Police via CSE sub-group On-going Develop training and education for schools and colleges to include case studies Raised awareness of the issues, increased young people's resilience and created a culture of zero tolerance - measured through number of referrals Training Subgroup & CSE Subgroup Sep-12 Number of young people receiving training Priority 2 - Communication Keeping our children safe from harm by communicating safeguarding messages effectively Revise Terms of Reference for Media Sub Group and re-name as Communications Sub-Group. Develop draft Communications Strategy to include areas of work agreed at the SSCB Development Day and begin implementation. Community actively involved in safeguarding children Workforce aware of their responsibilities, Board priorities and the contribution they can make Communications sub-group May Dec
147 Develop the SSCB website for Professionals, Parents and Children and Young People Number of hits to be monitored and feedback to be collected Public having a realistic understanding of the role of the LSCB and safeguarding issues SSCB Development Officer & Communications sub-group Sep-12 Engage with children and young people and seek their views to help shape the work of the Board Children and young people's views are presented to the Board and are used to inform service developments SSCB advocates children's views to partner agencies SSCB Development Officer & Communications sub-group On-going Priority 3 - Compromised Parenting Keeping our children safe from harm by creating a common understanding, commitment and approach to identifying children and young people who are experiencing, or are at risk of Undertake a scoping exercise/mapping of existing groups, personnel, protocols and services in respect of domestic abuse, substance misuse and adult mental health. To have a better understanding of the range of services available and to have identified gaps in provision to inform the development of protocols to enable agencies to work together more effectively Each steering group to have identified outcomes they would like to see achieved SSCB Development Officer & Domestic Abuse Forum, Hidden Harm Group, Health Governance Group & Area Strategic Fora March 2012 for consideration by Exec Sub- Group to decide how work is progressed. 41
148 experiencing, harm due to domestic abuse, substance misuse or adult mental health. Deliver a co-ordinated response to children and young people to reduce the risk of harm from compromised parenting Young person s confirmation that they feel supported/safer Better identification of young people at risk of harm Joined up approach to working with the young person Partnership Subgroup April 2012 for consideration by Partnership Sub-group as to how work is progressed On-going work streams Understand how and why children die, make recommendations to protect other children and to prevent future deaths. Embed CDOP Action Planning process for SSCB to ensure issues relating to preventable child deaths are addressed Multi-Agency Panel review child deaths across Shropshire. Contribute to the review and revision West Mercia SUDIC Protocol. Promote the reduction in child deaths due to accidents Lessons learnt incorporated in Child Death Overview Panel Achieve consistency of response across the West Mercia area for Sudden and Unexpected Death in Childhood. CDOP On-going Annual report to SSCB April 2012 Delivering the core functions required of the LSCB as detailed in Working Together through the operational sub- Develop a quality assurance model for SSCB training modules that measures the impact that training has on practice Positive changes in working practice as a result of training SSCB Training Officer & Training Sub- Group Dec-12 42
149 groups. Continue to monitor the effectiveness of the PPRC process Referrals are sent to the appropriate contact; Criminal Justice Sub-Group Jul 2012 Consider the implications of the Domestic Homicide Review process Staff are aware of the PPRC process Work with the Community Safety Partnership to ensure that children are appropriately safeguarded from domestic abuse and MARAC processes are working effectively Reduction in number of children affected by domestic abuse On-going Raise awareness of the risks associated with online technologies and provide resources/support networks for professionals, parents and young people Consider the implementation of systems approach model for undertaking SCR s and explore training opportunities Continue to monitor the implementation of the Suicide Prevention Care Pathway Pilot raising awareness training for crisis fosters carers Young people are effectively safeguarded Professionals and parents feel supported Appropriate managers to have attended SCIE training event Implementing a systems model for SCRs Reduction in number of suicides of young people Practitioner's feel more confident when dealing with suicidal young people Raised awareness amongst foster carers e-safety Sub- Group On-going SCR Sub-Group Jun 2012 Suicide Prevention Sub- Group Dec 2012 On-going June
150 Developing collaborative Health contribution to SSCB Improved NHS reporting to LADO. Improved NHS \ PCT engagement within Child Protection Conferences Health Governance Sub- Group On- going Monitor the effectiveness and productivity of the sub-groups through producing a report of progress against work plans. Sub-groups review their work plans and terms of reference in light of Board developments and/or recommendations. All Sub-group Chairs Oct 2012 & April
151 Appendix 5 Multi-Agency Core Training delivered in 2011 \ 12 Modules No. delivered No. delegates Multi-agency / single Raising Awareness in CP Multi-agency Raising Awareness 4 51 Single agency (commissioned) CDOP briefing 3 62 Multi-agency Case conference & core group 2 39 Multi-agency Neglect DP Module Multi-agency Physical Abuse Multi-agency Sexual Abuse 6 80 Multi-agency MAPPA Briefing 3 64 Multi-agency STORM 6 63 Multi-agency Totals Multi-agency Additional Training delivered in 2011 \ 12 Fabricated and induced illness Information Sharing Conference 1 92 Multi-agency Multi-agency Train the trainers in Raising Awareness in CP Managers Briefing CSE Strategy Managers Briefing Neglect Strategy Managers Briefing Suicide Prevention strategy 2 25 Multi-agency 3 87 Multi-agency Multi-agency Multi-agency Totals Multi-agency 45
152 46
153 Paper 07 TRUST BOARD 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title Standing Financial Instructions (SFI s) and the Detailed Scheme of Delegation Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Margaret Surrage, Head of Board Governance (Trust Secretary) Monitor Nature of Report Category of Item Context For Information For Discussion For Approval Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary The SFI s and Detailed scheme of delegation have been reviewed and some minor updates have been proposed. The revised documents are attached with the proposed changes shown as tracked changes. The revised documents have been reviewed by the Audit Committee, which has recommended their approval. Received or approved by Legal Implications Recommendation The Trust Board are asked to approve the updated Standing Financial Instructions and Detailed Scheme of Delegation. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
154 Paper 07 TRUST BOARD 30 TH NOVEMBER 2012 REVIEW OF SFI S AND DETAILED SCHEME OF DELEGATION The SFI s and detailed scheme of delegation were subject to thorough scrutiny to ensure that they were fit for purpose for a Foundation Trust prior to their adoption in September The current SFI s and detailed scheme of delegation have been reviewed to ensure that they are still appropriate and that no issues have occurred during the first year of operation as an foundation Trust which have prompted a change. SFI s Following feedback from colleagues two changes are proposed to provide clarification The references to Standing Orders have been replaced by the Constitution, as the standing orders now form part of the constitution and staff were unclear as how to access them. Also some issue which are pertinent to the SFI s are found in sections of the constitution other than the Board of Directors Standing orders, so the generic term Constitution is preferred. An additional paragraph has been included at paragraph to direct readers to the detailed scheme of delegation to confirm the levels of delegation to budget managers Further minor changes have been made to reflect changes in terminology, eg in paragraph 2.11 the Statement of Internal Control becomes the Annual Governance Statement and the reference to the Secretary of States direction on counter fraud has been replaced by the instructions contained in the NHS Standard Contract. A copy of the SFIs is attached at appendix 1, with the proposed changes shown as tracked changes. Detailed Scheme of Delegation Three minor changes have been proposed: The limits for tendering have been updated to reflect the latest EU procurement regulations The Director of Finance has replaced the Director of Operations as the person responsible for reviewing compliance with environmental legislation The maximum maturity date for investment has been reduce from 95 to 90 days, to reflect the agreed changes in the Treasury management policy. A copy of the Detailed Scheme of Delegation is attached at appendix 2, with the proposed changes shown as tracked changes. Recommendation That the Board approve the revised Standing Orders and Detailed Scheme of Delegation. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
155 Paper 07 Appendix 1 STANDING FINANCIAL INSTRUCTIONS The Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust DRAFT NOVEMBER 2012 Approved by the Board of Directors September 2011 Review date September 2012 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
156 Paper 07 STANDING FINANCIAL INSTRUCTIONS STANDING FINANCIAL INSTRUCTIONS CONTENTS 1. INTRODUCTION 2. AUDIT 3. BUSINESS PLANNING, BUDGETS, BUDGETARY CONTROL AND MONITORING 4. ANNUAL ACCOUNTS AND REPORTS 5. BANK AND GOVERNMENT BANKING SERVICE 6. INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS 7. TENDERING AND CONTRACTING PROCEEDURE 8. CONTRACTS FOR THE PROVISION OF HEALTHCARE SERVICES 9. TERMS OF SERVICE AND PAYMENT OF DIRECTORS AND EMPLOYEES 10. NON-PAY EXPENDITURE 11. FINANCIAL FRAMEWORK 12. CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS AND SECURITY OF ASSETS 13 STORES AND RECEIPT OF GOODS 14. DISPOSALS AND CONDEMNATIONS, LOSSES AND SPECIAL PAYMENTS 15. INFORMATION TECHNOLOGY 16. PATIENTS' PROPERTY 17. FUNDS HELD ON TRUST 18. ACCEPTANCE OF GIFTS BY STAFF 19. RETENTION OF DOCUMENTS 20. RISK MANAGEMENT 2 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
157 STANDING FINANCIAL INSTRUCTIONS Paper INTRODUCTION 1.1 General The Trust s Standing Financial Instructions (SFI s) have been compiled in accordance with the requirements and provisions of The NHS Act They shall have effect as if incorporated in the Board of Directors Standing Orders (SOs).Trust Constitution These Standing Financial Instructions detail the financial responsibilities, policies and procedures adopted by the Trust. They are designed to ensure that the Trust's financial transactions are carried out in accordance with the law and with Government policy in order to achieve probity, accuracy, economy, efficiency and effectiveness. They should be used in conjunction with the Schedule of Decisions Reserved to the Board and the Scheme of Delegation adopted by the Trust These Standing Financial Instructions identify the financial responsibilities which apply to everyone working for the Trust and its constituent organisations including Trading Units. They do not provide detailed procedural advice and should be read in conjunction with the detailed departmental and financial procedure notes. All financial procedures must be approved by the Finance Director Should any difficulties arise regarding the interpretation or application of any of the Standing Financial Instructions then the advice of the Finance Director must be sought before acting. The user of these Standing Financial Instructions should also be familiar with and comply with the provisions of the Trust Constitution Board of Directors Standing Orders (SOs) The failure to comply with Standing Financial Instructions and Standing Orders as included in the Constitution, can in certain circumstances be regarded as a disciplinary matter that could result in dismissal Overriding Standing Financial Instructions If for any reason these Standing Financial Instructions are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around the noncompliance shall be reported to the next formal meeting of the Audit Committee for referring action or ratification. All members of the Board and staff have a duty to disclose any non-compliance with these Standing Financial Instructions to the Finance Director as soon as possible. 3 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
158 STANDING FINANCIAL INSTRUCTIONS Paper TERMINOLOGY Any expression to which a meaning is given in Health Service Acts, or in Directions made under the Acts, shall have the same meaning in these instructions; and "ACCOUNTING OFFICER" means the person who from time to time discharges the functions specified in paragraph 25 (5) in Schedule 7 to the 2006 Act. "BOARD" means the Board of Directors of the Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust, as constituted in accordance with the Trust s Constitution; "BUDGET" means a resource, expressed in financial terms, proposed by the Board of Directors for the purpose of carrying out, for a specific period, any or all of the functions of the Trust; "BUDGET HOLDER" means the director or employee with delegated authority to manage finances (Income and Expenditure) for a specific area of the organisation; "CHIEF EXECUTIVE" means the chief executive (and accounting officer) of the Trust; "CONSTITUTION" means the constitution, including the annexes, which was approved on authoristion as a Foundation Trustattached to the Authorisation with any subsequent variationsammendments from time to time approved by the Regulatorin accordance with current legislation.. "DIRECTOR" means a person appointed as a Director in accordance with the Constitution. The Directors of the Trust will be either: Executive Director means a Member of the Board of Directors who holds an executive office of the Trust and who was appointed in accordance with the Constitution. or Non Executive Director means a Member of the Board of Directors who does not hold an executive office of the Trust and who was appointed by the Council of Governors in accordance with the Constitution. FINANCE DIRECTOR" means the chief financial officer of the Trust; FUNDS HELD ON TRUST means those funds which the Trust holds on date of incorporation, receives on distribution by statutory instrument or chooses subsequently to accept under powers derived under the 2006 Act. Such funds may or may not be charitable. INDEPENDENT REGULATOR means the independent corporate body established under the National Health Service 2006 Act, responsible for authorising, monitoring and regulating NHS Foundation Trusts. "LEGAL ADVISER" means the properly qualified person appointed by the Trust to provide legal advice. "OFFICER" means employee of the Trust or any other person holding a paid appointment or office with the Trust. SIRO means Senior Information Risk Officer. This role is undertaken by the Finance Director TRUST, means the Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust. 4 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
159 STANDING FINANCIAL INSTRUCTIONS Paper All references in these instructions to the masculine gender shall be read as equally applicable to the feminine gender Wherever the title Chief Executive, Finance Director, or other nominated officer is used in these instructions, it shall be deemed to include such other director or employees who have been duly authorised to represent them Wherever the term "employee" is used and where the context permits it shall be deemed to include employees of third parties contracted to the Trust when acting on behalf of the Trust. 1.3 Responsibilities and delegation The Trust Board exercises financial supervision and control by: (a) (b) (c) (d) (e) Formulating the financial strategy; Requiring the submission and approval of budgets within approved allocations/overall income; Defining and approving essential features in respect of important procedures and financial systems (including the need to obtain value for money); Defining specific responsibilities placed on members of the Board and employees as indicated in the Scheme of Delegation document. Receiving regular reports on financial performance The Board has resolved that certain powers and decisions may only be exercised by the Board in formal session. These are set out in the Reservation of Matters Reserved to the Board document. All other powers have been delegated to such other committees as the Trust has established or to the Chief Executive or Finance Director The Chief Executive and Finance Director will, as far as possible, delegate their detailed responsibilities, but they remain accountable for financial control. The Chief Executive is ultimately accountable to the Board, and as Accounting Officer, to parliament, for ensuring that the Board meets its obligation to perform its functions within the available financial resources. The duties as Accounting Officer are set out in the NHS Foundation Trust Accounting Officer Memorandum. The Chief Executive has overall executive responsibility for the Trust s activities; is responsible to the Chairman and the Board for ensuring that its financial obligations and targets are met and has overall responsibility for the Trust s system of internal control It is a duty of the Chief Executive to ensure that Members of the Board and, employees and all new appointees are notified of, and put in a position to understand their responsibilities under these Instructions The Finance Director is responsible for: (a) Implementing the Trust s financial policies and for coordinating any corrective action necessary to further these policies; 5 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
160 STANDING FINANCIAL INSTRUCTIONS Paper 07 (b) (c) Maintaining an effective system of internal financial control including ensuring that detailed financial procedures and systems incorporating the principles of separation of duties and internal checks are prepared, documented and maintained to supplement these instructions; Ensuring that sufficient records are maintained to show and explain the Trust s transactions, in order to disclose, with reasonable accuracy, the financial position of the Trust at any time; and, without prejudice to any other functions of the Trust, and employees of the Trust, the duties of the Finance Director include: (d) (e) (f) The provision of financial advice to other members of the Board and employees; The design, implementation and supervision of systems of internal financial control; The preparation and maintenance of such accounts, certificates, estimates, records and reports as the Trust may require for the purpose of carrying out its statutory duties All members of the Board and employees, severally and collectively, are responsible for: (a) (b) (c) (d) (e) The security of the property of the Trust; Avoiding loss; Achieving economy, effectiveness and efficiency in the use of resources; Conforming with the requirements of the Trust Constitution, Standing Orders, Standing Financial Instructions, Financial Procedures and the Scheme of Delegation; Maintaining effective risk management arrangements Any contractor or employee of a contractor who is empowered by the Trust to commit the Trust to expenditure or who is authorised to obtain income shall be covered by these instructions. It is the responsibility of the Chief Executive to ensure that such persons are made aware of this For all members of the Board and any employees who carry out a financial function, the form in which financial records are kept and the manner in which members of the Board and employees discharge their duties must be to the satisfaction of the Director of Finance. 6 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
161 STANDING FINANCIAL INSTRUCTIONS Paper AUDIT 2.1 Audit Committee In accordance with the constitution and with reference to the Audit Code for NHS Foundation Trusts and the Code of Governance, issued by the Independent Regulator, the Board of Directors shall formally establish an Audit Committee, with clearly defined terms of reference. The Committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the organisation s activities (both clinical and non clinical) that supports the achievement of the organisation s objectives. In particular, the Committee will review the adequacy of: (a) (b) (c) (d) (e) (f) All risk and control related disclosure statements (in particular the Statement on Internal Control/ Annual Governance Statement), together with any accompanying Head of Internal Audit statement or other appropriate independent assurances; The underlying assurance processes that indicates the degree of the Achievement of corporate objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements; The policies for ensuring compliance with relevant regulatory, legal and code of conduct requirements and related reporting and self-certification; The policies and procedures for all work related to fraud and corruptions as set out in NHS Standard contractsecretary of State Directions and as required by NHS Protect and review and confirm the level of resources assigned for countering fraud; The Internal Audit Service ensuring that it meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Chief Executive and Board; The work of the External Auditor and consider the findings, implications and management s responses to their work; Agree the Accounting Policies to be adopted for the preparation of the financial statements and receive the External Auditor s annual governance report prepared in accordance with the relevant International Accounting Standards. The Audit Committee shall review the Annual Report and Financial Statements before submission to the Board The Audit Committee must assess the work and the fees of external audit on an annual basis to ensure that the work is of a sufficiently high standard and that the fees are reasonable. The Audit Committee shall make a recommendation to the Council of Governors with respect to the re-appointment of the external auditors. The Trust will undertake market-testing for the appointment of external auditors at least once every five years. 7 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
162 STANDING FINANCIAL INSTRUCTIONS Paper Where the Audit Committee considers there is evidence of ultra vires transactions, evidence of improper acts, or if there are other important matters that the committee wish to raise, the Chairman of the Audit Committee should raise the matter at a full meeting of the Board of Directors. Exceptionally, the matter may need to be referred to the Independent Regulator via the Finance Director It is the responsibility of the Finance Director to ensure an adequate internal audit service is provided and the Audit Committee shall be involved in the selection process when/if an internal audit service provider is changed Further detail on the role, responsibility and powers of the Audit Committee are contained it its Terms of Reference. 2.2 Finance Director The Finance Director is responsible for: (a) (b) Ensuring there are arrangements to review, evaluate and report on the effectiveness of internal financial control including the establishment of an effective Internal Audit function; Ensuring that the Internal Audit is adequate and meets the NHS mandatory audit standards; (c) (d) Deciding at what stage to involve the police in cases of misappropriation and other irregularities not involving fraud or corruption; Ensuring that an annual internal audit report is prepared for the consideration of the Audit Committee and the Board. The report must cover: (i) A clear opinion on the effectiveness of internal control; (ii) Major internal financial control weaknesses discovered; (iii) Progress on the implementation of internal audit recommendations; (iv) Progress against plan over the previous year; (v) Strategic audit plan covering the coming three years; (vi) A detailed plan for the coming year The Finance Director and designated internal and external auditors are entitled without necessarily giving prior notice to require and receive: (a) Access to all records, documents and correspondence relating to any financial or other relevant transactions, including documents of a confidential nature; (b) Access at all reasonable times to any land, premises or members of the Board or employee of the Trust; (c) The production of any cash, stores or other property of the Trust under a member of the Board or an employee's control; and (d) Explanations concerning any matter under investigation. 8 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
163 STANDING FINANCIAL INSTRUCTIONS Paper Role of Internal Audit Internal Audit will review, appraise and report upon: (a) (b) (c) (d) The extent of compliance with, and the financial effect of, relevant established policies, plans and procedures; The adequacy and application of financial and other related management controls; The suitability and reliability of financial and other related management data; The extent to which the Trust s assets and interests are accounted for and safeguarded from loss of any kind, arising from: (i) (ii) (iii) Fraud and other offences; Waste, extravagance, inefficient administration; Poor value for money or other causes. (e) Internal Audit shall also independently verify the Assurance Statements in accordance with guidance from the Independent Regulator Whenever any matter arises which involves, or is thought to involve, irregularities concerning cash, stores, or other property or any suspected irregularity in the exercise of any function of a pecuniary nature, the Director of Finance must be notified immediately The Head of Internal Audit will normally attend Audit Committee meetings and has a right of access to all Audit Committee members, the Chairman and Chief Executive of the Trust The Head of Internal Audit shall be accountable to the Finance Director. The reporting system for internal audit shall be agreed between the Finance Director, the Audit Committee and the Chief Internal Auditor. The agreement shall be in writing and shall comply with the guidance on reporting contained in the NHS Internal Audit Standards. The reporting system shall be reviewed at least every three years The designated officers must carry out agreed audit recommendations within the timescale for action agreed with the Head of Internal Audit. Failure to do so shall be reported to the Audit Committee and to the Chief Executive who shall take necessary action to ensure compliance with such recommendations. 2.4 External Audit The external auditor is appointed by the Council of Governors and paid for by the Trust. The Audit Committee must ensure a cost-efficient service The Trust must ensure that the external auditor appointed by the Council of Governors meets the criteria of Monitor set out in the Audit Code for NHS 9 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
164 STANDING FINANCIAL INSTRUCTIONS Paper 07 Foundation Trust s at the date of appointment and on an on-going basis throughout the term of their appointment External audit must comply with the responsibilities and functions set out in Monitor s Audit Code for NHS Foundation Trusts and under Part 1 of the Health and Social Care Act Fraud and Corruption In line with their responsibilities, the Trust Chief Executive and Finance Director shall monitor and ensure compliance with Directions issued by the Secretary of State for Health on fraud and corruption, and the requirements of the Bribery Act 2010 and other relevant legislation the has been or may be enacted The Trust shall nominate a suitable person to carry out the duties of the Local Counter Fraud Specialist as specified by the Department of Health Fraud and Corruption Manual and guidance The Local Counter Fraud Specialist shall report to the Trust Director of Finance and shall work with staff in NHS Protect in accordance with the Department of Health Fraud and Corruption Manual The Local Counter Fraud Specialist will provide regular reports to the Audit Committee, including a written Annual Report. 2.6 Security Management In line with their responsibilities, the Trust Chief Executive will monitor and ensure compliance with Directions issued by the Secretary of State for Health on NHS security management The Trust shall nominate a suitable person to carry out the duties of the Local Security Management Specialist (LSMS) as specified by the Secretary of State for HealthNHS Protect guidance on NHS security management The Trust shall nominate a Non-Executive Director to be responsible to the Board for NHS security management The Chief Executive has overall responsibility for controlling and coordinating security. However, key tasks are delegated to the Security Management Director (SMD) and the appointed Local Security Management Specialist (LSMS). 10 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
165 STANDING FINANCIAL INSTRUCTIONS Paper BUSINESS PLANNING, BUDGETS, BUDGETARY CONTROL, AND MONITORING 3.1 Preparation and Approval of Plans and Budgets The Chief Executive will compile and submit to the Board an Annual Plan which complies with the requirements of the Independent Regulator The plan will be approved by the Board of Directors and have regard to the views of the Council of Governors The plan will be submitted to the Independent Regulator in accordance with their timetable Prior to the start of the financial year the Finance Director will, on behalf of the Chief Executive, prepare and submit budgets for approval by the Board. Such budgets will: (a) (b) (c) (d) (e) be in accordance with the aims and objectives set out in the Annual Plan; accord with workload and manpower plans; be produced following discussion with appropriate budget holders; be prepared within the limits of available funds; identify potential risks The Finance Director shall monitor financial performance against budget and plan, periodically review them, and report to the Board All budget holders must provide information as required by the Finance Director to enable budgets to be compiled All budget holders will sign to agree their allocated budgets at the commencement of each financial year The Finance Director is responsible for ensuring that adequate training is delivered on an on-going basis to budget holders to help them manage their budgets successfully. 3.2 Budgetary Delegation The Chief Executive may delegate the management of a budget to permit the performance of a defined range of activities. This delegation must be in writing and be accompanied by a clear definition of: (a) (b) (c) The amount of the budget; The purpose(s) of each budget heading; Individual and group responsibilities; 11 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
166 STANDING FINANCIAL INSTRUCTIONS Paper 07 (d) (e) Achievement of planned levels of service; The provision of regular reports The Chief Executive and delegated budget holders must not exceed the budgetary total Any budgeted funds not required for their designated purpose(s) revert to the immediate control of the Chief Executive Non-recurring budgets should not be used to finance recurring expenditure without the authority in writing of the Chief Executive, as advised by the Director of Finance. 3.3 Budgetary Control and Reporting The Director of Finance will devise and maintain systems of budgetary control. These will include: (a) Monthly financial reports to the Board in a form approved by the Board containing: (i) (ii) (iii) Income and expenditure to date showing trends and forecast year-end position; Movements in working capital; Movements in cash and capital; (iv) Capital project spend and projected outturn against plan; (v) Explanations of any material variances from plan; (vi) Details of any corrective action where necessary and the Chief Executive's and/or Finance Director s view of whether such actions are sufficient to correct the situation; (b) (c) (d) (e) The issue of timely, accurate and comprehensible advice and financial reports to each budget holder, covering the areas for which they are responsible; Investigation and reporting of variances from financial, workload and manpower budgets; Monitoring of management action to correct variances; and Arrangements for the authorisation of budget transfers Each Budget Holder is responsible for ensuring that: (a) (b) Any likely overspending or reduction of income is not incurred without the prior consent of the Board; The amount provided in the approved budget is not used in whole or in part for any purpose other than that specifically authorised. 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
167 STANDING FINANCIAL INSTRUCTIONS Paper 07 (c) No permanent employees are appointed without the approval of the Chief Executive other than those provided for within the available resources and manpower establishment as approved by the Board The Chief Executive is responsible for identifying and implementing cost improvements and income generation initiatives in accordance with the requirements of the Annual Plan and a balanced budget. 3.4 Capital Expenditure The general rules applying to delegation and reporting shall also apply to capital expenditure. (The particular applications relating to capital are contained in SFI Section 12.) The Capital Programme and any amendments will be approved in advance by the Board of Directors. 3.5 Monitoring Returns The Chief Executive is responsible for ensuring that the appropriate monitoring forms are submitted to the requisite monitoring organisation. 4. ANNUAL ACCOUNTS AND REPORTS 4.1 The Chief Executive, as the Accounting officer, will sign the Annual accounts 4.2 The Chief Executive will direct the Finance Director, to: (a) (b) (c) Prepare financial returns in accordance with the accounting policies and guidance given by the Independent Regulator, the Trust's accounting policies, and generally accepted accounting practice; Prepare and submit annual financial reports to the Independent Regulator and Parliament in accordance with current guidelines; and Submit financial returns to the Independent Regulator and Parliament for each financial year in accordance with the prescribed timetable. 4.3 The Trust's audited annual accounts must be presented to the Board of Directors for approval and received at a public meeting of the Council of Governors. A copy should be forwarded to the Independent Regulator and made available to the public. 4.4 The Trust will publish an annual report, in accordance with the Constitution and present it at the Council of Governors general meeting. The document will comply with the Independent Regulator s Financial Reporting Manual. 13 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
168 STANDING FINANCIAL INSTRUCTIONS Paper BANK AND GOVERNMENT BANKING SERVICES ACCOUNTS 5.1 General The Finance Director is responsible for managing the Trust s banking arrangements and for advising the Trust on the provision of banking services and operation of accounts. This advice will take into account guidance and directions issued from time to time by the Independent Regulator, Only the Director of Finance shall open or close bank accounts in the name of the Trust. The Board shall approve the banking arrangements. 5.2 Bank and Government Banking Services Accounts The Director of Finance is responsible for all bank accounts and the Government Banking Services (GBS) accounts including: (a) (b) (c) Establishing separate bank accounts for the Trust s non-exchequer funds; Ensuring payments made from bank accounts do not exceed the amount credited to the account except where arrangements have been made; and Reporting to the Board all arrangements made with the Trust s bankers for accounts to be overdrawn. 5.3 Banking Arrangements The Finance Director will prepare detailed instructions on the operation of bank and GBS accounts which must include: (a) (b) (c) (d) The conditions under which each bank and GBS account is to be operated; The limit to be applied to any overdraft; and Those authorised to sign cheques or other orders drawn on the Trust s accounts; Arrange a working capital and capital loan facility if required and in accordance with the recommendations of Monitor and within the Trust Prudential Borrowing Limit (PBL) The Director of Finance must advise the Trust s bankers in writing of the conditions under which each account will be operated. 5.4 Tendering and Review The Finance Director will review the banking arrangements of the Trust at regular intervals, and at least every five years, to ensure they reflect best practice and represent value for money. Following such reviews the Finance Director shall 14 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
169 STANDING FINANCIAL INSTRUCTIONS Paper 07 determine whether or not retendering for services is necessary and seek the approval of the Business Risk & Investment Committee to pursue his proposed course of action. 15 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
170 STANDING FINANCIAL INSTRUCTIONS Paper INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS 6.1 Income Systems The Finance Director is responsible for designing, maintaining and ensuring compliance with systems for the proper recording, invoicing, collection and coding of all monies due The Finance Director is also responsible for the prompt banking of all monies received The Finance Director will issue instructions that the Trust will not accept cash payments of amounts greater than 10, Fees and Charges The Trust shall follow the Department of Health guidance in the Operating Framework in setting prices for NHS service agreements The Finance Director is responsible for approving and regularly reviewing the level of all fees and charges other than those determined by the Department of Health or by statute. Independent professional advice on matters of valuation shall be taken as necessary. Where sponsorship income (including items in kind such as subsidised goods or loans of equipment) is considered the guidance in the Department of Health s Commercial Sponsorship Ethical standards in the NHS shall be followed All employees must inform the Finance Director promptly of money due arising from transactions which they initiate/deal with, including all contracts, leases, tenancy agreements, private patient undertakings and other transactions. 6.3 Debt Recovery The Finance Director is responsible for the appropriate recovery action on all outstanding debts Income not received and deemed to be irrecoverable should be dealt with in accordance with losses procedures Overpayments should be detected (or preferably prevented) and recovery initiated promptly. 6.4 Security of Cash, Cheques and other Negotiable Instruments The Finance Director is responsible for: (a) Approving the form of all receipt books, agreement forms, or other means of officially acknowledging or recording monies received or receivable; 16 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
171 STANDING FINANCIAL INSTRUCTIONS Paper 07 (b) (c) (d) Ordering and securely controlling any such stationery; The provision of adequate facilities and systems for employees whose duties include collecting and holding cash, including the provision of safes or lockable cash boxes, the procedures for keys, and for coin operated machines; Prescribing systems and procedures for handling cash and negotiable securities on behalf of the Trust Official money shall not under any circumstances be used for the encashment of private cheques or IOUs All cheques, postal orders, cash etc., shall be banked intact. Disbursements shall not be made from cash received, except under arrangements approved by the Finance Director The holders of safe keys shall not accept unofficial funds for depositing in their safes unless such deposits are in special sealed envelopes or locked containers. It shall be made clear to the depositors that the Trust is not to be held liable for any loss, and written indemnities must be obtained from the organisation or individuals absolving the Trust from responsibility for any loss, before the deposit is accepted. 17 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
172 STANDING FINANCIAL INSTRUCTIONS Paper TENDERING AND CONTRACTING PROCEDURE The procedure for making all contracts by or on behalf of the Trust shall comply with these Standing Financial Instructions Directives by the Council of the European Union promulgated by the Department of Health (DH) prescribing procedures for awarding all forms of contracts shall have effect as if incorporated in these Standing Financial Instructions The Trust shall comply as far as is practicable with the requirements of Monitor guidance, the Government Financial Reporting Manual and Estatecode in respect of capital investment and estate and property transactions Orders must not be placed for goods or services which have been split or otherwise placed in a manner to avoid the financial thresholds for tendering. 7.2 Formal Competitive Tendering General Applicability The Trust shall ensure that competitive tenders are invited for: (a) the supply of goods, materials and manufactured articles; (b) the rendering of services including all forms of management consultancy services (other than specialised services sought from or provided by the DH); (c) the design, construction and maintenance of building and engineering works (including construction and maintenance of grounds and gardens); for disposals Exceptions and instances where formal tendering need not be applied Formal tendering procedures need not be applied where: (a) (b) (c) The estimated expenditure or income does not, or is not reasonably expected to, exceed 49,999; Where the supply is proposed under special arrangements negotiated by the DH or other NHS procurement agency in which event the said special arrangements must be complied with; Regarding disposals as set out in Standing Financial Instructions No. 25; Formal tendering procedures may be waived in the following circumstances: (d) Where the Chief Executive decides that formal tendering procedures would not be practicable or the estimated expenditure or income would not warrant formal tendering procedures, and the circumstances are detailed in an appropriate Trust record; (e ) Where the requirement is covered by an existing contract; (f) Where NHS Supply Chain, Office of Government Commerce or other NHS agreements can be utilised; or 18 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
173 STANDING FINANCIAL INSTRUCTIONS Paper 07 (g) (h) (i) (j) (k) (l) Where a consortium arrangement is in place and a lead organisation has been appointed to carry out tendering activity on behalf of the consortium members; Where the timescale genuinely precludes competitive tendering but failure to plan the work properly would not be regarded as a justification for a single tender; Where specialist expertise is required and is available from only one source; When the task is essential to complete the project, and arises as a consequence of a recently completed assignment and engaging different consultants for the new task would be inappropriate; There is a clear benefit to be gained from maintaining continuity with an earlier project. However in such cases the benefits of such continuity must outweigh any potential financial advantage to be gained by competitive tendering; For the provision of legal advice and services providing that any legal firm or partnership commissioned by the Trust is regulated by the Law Society for England and Wales for the conduct of their business (or by the Bar Council for England and Wales in relation to the obtaining of Counsel s opinion) and are generally recognised as having sufficient expertise in the area of work for which they are commissioned. The Finance Director will ensure that any fees paid are reasonable and within commonly accepted rates for the value of such work; (m) The waiving of competitive tendering procedures should not be used to avoid competition or for administrative convenience or to award further work to a consultant originally appointed through a competitive procedure. Where it is decided that competitive tendering is not applicable and should be waived, the fact of the waiver and the reasons should be documented and recorded in an appropriate Trust record and reported to the Audit Committee at each meeting Where the exceptions set out in paragraph apply, the Trust shall ensure that invitations to tender are sent to a sufficient number of firms/individuals to provide fair and adequate competition as appropriate, and in no case less than two firms/individuals, having regard to their capacity to supply the goods or materials or to undertake the services or works required Items estimated to be below the limits set in this Standing Financial Instruction for which formal tendering procedures are not used which subsequently prove to have a value above such limits shall be reported to the Chief Executive, and be recorded in an appropriate Trust record. 19 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
174 STANDING FINANCIAL INSTRUCTIONS Paper Contracting/Tendering Procedure Invitation to tender (a) (b) All invitations to tender shall state the date and time as being the latest time for the receipt of tenders. All invitations to tender shall state that no tender will be accepted unless: (i) (ii) Submitted in a plain sealed package or envelope bearing a pre-printed label supplied by the Trust (or the word "tender" followed by the subject to which it relates) and the latest date and time for the receipt of such tender addressed to the Chief Executive or nominated Manager; tender envelopes/ packages do not bear any names or marks indicating the sender. The use of courier/postal services must not identify the sender on the envelope or on any receipt so required by the deliverer. (c) (d) Every tender for goods, materials, services or disposals shall embody such of the NHS Standard Contract Conditions as are applicable; Every tender for building or engineering works (except for maintenance work, when Estmancode guidance shall be followed) shall embody or be in the terms of the current edition of one of the Joint Contracts Tribunal Standard Forms of Building Contract or Department of the Environment (GC/Wks) standard forms of contract amended to comply with concode; or, when the content of the work is primarily engineering, the General Conditions of Contract recommended by the Institution of Mechanical and Electrical Engineers and the Association of Consulting Engineers (Form A), or (in the case of civil engineering work) the General Conditions of Contract recommended by the Institute of Civil Engineers, the Association of Consulting Engineers and the Federation of Civil Engineering Contractors. These documents shall be modified and/or amplified to accord with Department of Health guidance and, in minor respects, to cover special features of individual projects. Any other significant amendments must be notified to the Business Risk and Investment Committee Receipt and safe custody of tenders The Chief Executive or his nominated representative will be responsible for the receipt, endorsement and safe custody of tenders received until the time appointed for their opening. The date and time of receipt of each tender shall be endorsed on the tender envelope/package Opening tenders and Register of tenders (a) (c) As soon as practicable after the date and time stated as being the latest time for the receipt of tenders, they shall be opened by two Executive Directors or Associate Directors, who will not be from the originating department; The originating Department will be taken to mean the Department sponsoring or commissioning the tender; 20 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
175 STANDING FINANCIAL INSTRUCTIONS Paper 07 (d) (e) Every tender received shall be marked with the date of opening and initialled, alongside the tender total, by those present at the opening; A register shall be maintained by the Chief Executive, or a person authorised by him, to show for each set of competitive tender invitations despatched; (i) (ii) (iii) (iv) (v) (vi) The name of all firms individuals invited; The names of firms individuals from which tenders have been received; The date the tenders were opened; The persons present at the opening; The price shown on each tender; A note where price alterations have been made on the tender. Each entry to this register shall be signed by those present. (f) A note shall be made in the register if any one tender price has had so many alterations that it cannot be readily read or understood; (g) Incomplete tenders, i.e. those from which information necessary for the adjudication of the tender is missing, and amended tenders i.e., those amended by the tenderer upon his own initiative either orally or in writing after the due time for receipt, but prior to the opening of other tenders, should be dealt with in the same way as late tenders. (paragraph below) Admissibility (a) (b) If for any reason the designated officers are of the opinion that the tenders received are not strictly competitive (for example, because their numbers are insufficient or any are amended, incomplete or qualified) no contract shall be awarded without the approval of the Chief Executive; Where only one tender is sought and/or received, the Chief Executive and Director of Finance shall, as far practicable, ensure that the price to be paid is fair and reasonable and will ensure value for money for the Trust Late tenders (a) (b) Tenders received after the due time and date, but prior to the opening of the other tenders, may be considered only if the Chief Executive or his nominated officer decides that there are exceptional circumstances i.e. despatched in good time but delayed through no fault of the tenderer; Only in the most exceptional circumstances will a tender be considered which is received after the opening of the other tenders and only then if the tenders that have been duly opened have not left the custody of the Chief Executive or his nominated officer or if the process of evaluation and adjudication has not started and the provisional results of the tender exercise have not been communicated to the originating department. 21 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
176 STANDING FINANCIAL INSTRUCTIONS Paper 07 (c) While decisions as to the admissibility of late, incomplete or amended tenders are under consideration, the tender documents shall be kept strictly confidential, recorded, and held in safe custody by the Chief Executive or his nominated officer; Acceptance of formal tenders (a) (b) Any discussions with a tenderer which are deemed necessary to clarify technical aspects of his tender before the award of a contract will not disqualify the tender; The lowest tender, if payment is to be made by the Trust, or the highest, if payment is to be received by the Trust, shall be accepted unless there are good and sufficient reasons to the contrary. Such reasons shall be set out in either the contract file, or other appropriate record. It is accepted that for professional services such as management consultancy, the lowest price does not always represent the best value for money. Other factors affecting the success of a project include: (i) (ii) (iii) (iv) Experience and qualifications of team members; Understanding of client s needs; Feasibility and credibility of proposed approach; Ability to complete the project on time. Where other factors are taken into account in selecting a tenderer, these must be clearly recorded and documented in the contract file prior to requesting tenders, and the reason(s) for not accepting the lowest tender clearly stated. (c) (d) No tender shall be accepted which will commit expenditure in excess of that which has been allocated by the Trust and which is not in accordance with these Instructions except with the authorisation of the Chief Executive. The use of these procedures must demonstrate that the award of the contract was: (i) Not in excess of the going market rate / price current at the time the contract was awarded; (ii) That best value for money was achieved. (iii) All tenders should be treated as confidential and should be retained for inspection Tender reports to the Trust Board Reports to the Trust Board will be made on an exceptional circumstance basis only Approved firms (a) Firms invited to tender shall ensure that when engaging, training, promoting or dismissing employees or in any conditions of employment, they do not 22 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
177 STANDING FINANCIAL INSTRUCTIONS Paper 07 discriminate against any person because of colour, race, ethnic or national origins, religion, gender or sexual orientation and that they comply with the provisions of the Equal Pay Act 1970, Equality legislation, the Bribery Act 2010 or related legislation. (b) (c) Firms shall conform at least with the requirements of the Health and Safety at Work Act and any amending and/or other related legislation concerned with the health, safety and welfare of workers and other persons, and to any relevant British Standard Code of Practice issued by the British Standard Institution. Firms must provide to the appropriate manager a copy of its safety policy and evidence of the safety of plant and equipment, when requested. The Finance Director may make or institute any enquiries he deems appropriate concerning the financial standing and financial suitability of approved contractors. The Director with lead responsibility for clinical governance will similarly make such enquiries as is felt appropriate to be satisfied as to their technical / medical competence. 7.4 Quotations: Competitive and non-competitive Quotations are required where formal tendering procedures are not adopted and where the intended expenditure or income exceeds, or is reasonably expected to exceed 10,000 but not exceed 49, Competitive Quotation (a) (b) (c) (d) Quotations should be obtained from at least 3 firms/individuals, unless the intended income or expenditure is less than 19,999 when 2 quotations will be acceptable. The quotations will be based on specifications or terms of reference prepared by, or on behalf of, the Trust; Quotations should be in writing unless the Chief Executive or his nominated officer determines that it is impractical to do so in which case quotations may be obtained by telephone. Confirmation of telephone quotations should be obtained as soon as possible and the reasons why the telephone quotation was obtained should be set out in a permanent record; All quotations should be treated as confidential and should be retained for inspection; The Chief Executive or his nominated officer should evaluate the quotation and select the quote which gives the best value for money. If this is not the lowest quotation if payment is to be made by the Trust, or the highest if payment is to be received by the Trust, then the choice made and the reasons why must be recorded in a permanent record Non-Competitive Quotations Non-competitive quotations in writing may be obtained in the following circumstances: (a) The supply of proprietary or other goods of a special character and the rendering of services of a special character, for which it is not, in the opinion 23 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
178 STANDING FINANCIAL INSTRUCTIONS Paper 07 of the responsible officer, possible or desirable to obtain competitive quotations; (b) The supply of goods or manufactured articles of any kind which are required quickly and are not obtainable under existing contracts; (c) Where the goods or services are for building and engineering maintenance the responsible works manager must certify that the first two conditions of this paragraph apply Quotations to be within Financial Limits No quotation shall be accepted which will commit expenditure in excess of that which has been allocated by the Trust and which is not in accordance with Standing Financial Instructions except with the authorisation of either the Chief Executive or Finance Director. 7.5 Authorisation of Tenders and Competitive Quotations Providing all the conditions and circumstances set out in these Standing Financial Instructions have been fully complied with, formal authorisation and awarding of a contract may be decided by the following staff to the value of the contract as follows: Designated budget holders up to 999 Divisional Managers up to 4,999 Directors up to 19,999 Finance Director up to 49,999 Chief Executive up to 74,999 Chief Executive and Finance Director up to 249,999 Trust Board over 250,000 These levels of authorisation may be varied or changed and need to be read in conjunction with the Trust Board s Scheme of Delegation. Formal authorisation must be put in writing. In the case of authorisation by the Trust Board this shall be recorded in their minutes. 7.6 Instances where formal competitive tendering or competitive quotation is not required Where competitive tendering or a competitive quotation is not required the Trust should adopt one of the following alternatives: (a) (b) The Trust shall use the local procurement service for procurement of all goods and services unless the Chief Executive or nominated officers deem it inappropriate. The decision to use alternative sources must be documented. If the Trust does not use the local procurement service - where tenders or quotations are not required, because expenditure is below 10,000, the Trust shall procure goods and services in accordance with procurement procedures approved by the Director of Finance. 24 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
179 STANDING FINANCIAL INSTRUCTIONS Paper Significant and Material Transactions All significant and material transactions, as defined in the Compliance Framework, must comply with the requirements of the Compliance Framework and the Trust Constitution. Formal notification must be received from the Independent Regulator to confirm compliance before entering into a legally binding agreement, All major transactions whether or not they comply with the definitions of Significant or Material transactions will be risk assessed in line with best practice and in line with the Risk Evaluation for Investment Decisions by NHS Foundation Trusts (REID) manual All major transactions must be explicitly approved by the Board. 7.8 Compliance requirements for all contracts The Board may only enter into contracts on behalf of the Trust within the statutory powers delegated to it by the Secretary of State and shall comply with: (a) (b) (c) (d) (e) (f) (g) The Trust s Trust ConstitutionStanding Orders and Standing Financial Instructions; EU Directives and other statutory provisions; Any relevant directions including the Capital Investment Manual, Estatecode and guidance on the Procurement and Management of Consultants; Such of the NHS Standard Contract Conditions as are applicable; Contracts with Foundation Trusts must be in a form compliant with appropriate NHS guidance; contracts shall be in or embody the same terms and conditions of contract as was the basis on which tenders or quotations were invited. If a departure becomes necessary the reasons for the departure must be recorded in a permanent record and in the project file; In all contracts made by the Trust, the Board shall endeavour to obtain best value for money by use of all systems in place. The Chief Executive shall nominate an officer who shall oversee and manage each contract on behalf of the Trust. 7.9 Agency or Temporary Staff Contracts The Chief Executive shall nominate officers with delegated authority to enter into contracts of employment, regarding staff, agency staff or temporary staff service contracts. 25 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
180 STANDING FINANCIAL INSTRUCTIONS Paper Healthcare Services Agreements (see overlap with SFI No. 8) Service agreements with NHS providers for the supply of clinical and non clinical support services shall be drawn up in accordance with guidance issued by the independent regulator, or subsequent responsible NHS body Disposals (See overlap with SFI No. 14) Competitive Tendering or Quotation procedures shall not apply to the disposal of: (a) (b) (c) (d) (e) Any matter in respect of which a fair price can be obtained only by negotiation or sale by auction as determined (or pre-determined in a reserve) by the Chief Executive or his nominated officer; Obsolete or condemned articles and stores, which may be disposed of in accordance with the supplies policy of the Trust; Items to be disposed of with an estimated sale value of less than 10,000, this figure to be reviewed on a periodic basis; Items arising from works of construction, demolition or site clearance, which should be dealt with in accordance with the relevant contract; Land or buildings concerning which Secretary of State guidance has been issued but subject to compliance with such guidance In-house Services The Chief Executive shall be responsible for ensuring that best value for money can be demonstrated for all services provided on an in-house basis. The Trust may also determine from time to time that in-house services should be market tested by competitive tendering In all cases where the Board determines that in-house services should be subject to competitive tendering the following groups shall be set up: (a) (b) (c) Specification group, comprising the Chief Executive or nominated officers and specialist. In-house tender group, comprising a nominee of the Chief Executive and technical support. Evaluation team, comprising normally a specialist officer, a supplies officer and a Director of Finance representative All groups should work independently of each other and individual officers may be a member of more than one group but no member of the in-house tender group may participate in the evaluation of tenders. 26 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
181 STANDING FINANCIAL INSTRUCTIONS Paper The evaluation team shall make recommendations to the Board The Chief Executive shall nominate an officer to oversee and manage the contract on behalf of the Trust Applicability of SFIs on Tendering and Contracting to funds held in trust. These Instructions shall not only apply to expenditure from Exchequer funds but also to works, services and goods purchased from the Trust s trust funds and private resources. 27 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
182 STANDING FINANCIAL INSTRUCTIONS Paper CONTRACTS FOR THE PROVISION OF HEALTHCARE SERVICES 8.1 The Chief Executive is responsible for signing the annual legally binding contract, with Commissioners, using the standard NHS contract terms and conditions where appropriate, detailing the basis on which the Trust will provide healthcare services. Any variations to the standard terms and conditions will be approved in accordance with the Scheme of Delegation. 8.2 The Chief Executive is responsible for negotiating contracts for the provision of services to patients in accordance with the annual Business Plan. In carrying out these functions, the Chief Executive should take into account the advice of the Finance Director regarding costing and pricing of services, payment terms and conditions and amendments to service agreements. 8.3 Contracts should be so devised as to achieve activity and performance targets, minimise risk, and maximise the Trust s opportunity to generate income. The Trust will produce a local tariff in accordance with NHS guidelines, for services outside the scope of the national tariff. 8.4 The Finance Director will report any negotiated contract which uses terms other than those laid down in the NHS Contract or the Operating Framework to the Trust Board. 8.5 The Finance Director shall ensure that a summary of the Trust s agreed contracts is reported annually to the Board, prior to the start of the financial year. The Director Finance shall also produce regular reports to the Board detailing actual and forecast contract income with a detailed assessment of the variable elements of income. 28 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
183 STANDING FINANCIAL INSTRUCTIONS Paper TERMS OF SERVICE, ALLOWANCES AND PAYMENT OF MEMBERS OF THE TRUST BOARD AND EXECUTIVE COMMITTEE AND EMPLOYEES 9.1. Remuneration and Terms of Service (see overlap with SO No. 6) In accordance with the Constitution the Board shall establish a Remuneration Committee, with clearly defined terms of reference, specifying which posts fall within its area of responsibility, its composition, and the arrangements for reporting. The Committee will advise the Board about appropriate remuneration and terms of service for the Chief Executive, and other senior employees not on Agenda for Change terms and conditions, including: (a) (b) (c) All aspects of salary (including any performance-related Elements/bonuses); Provisions for other benefits, including pensions and cars; Arrangements for termination of employment and other contractual terms; having proper regard to the Trust s circumstances and performance and to the provisions of any national arrangements for such members and staff where appropriate The Council of Governors will agree the remuneration for the Chairman and non executive members of the Board. 9.2 Funded Establishment The manpower plans incorporated within the annual plan will form the funded establishment The funded establishment of any department may not be varied without the approval of the Director of Finance The total funded establishment of the Trust may not be varied without the approval of the Chief Executive. 9.3 Staff Appointments No officer or Member of the Trust Board or employee may engage, re-engage, or regrade employees, either on a permanent or temporary nature, or hire agency staff, or agree to changes in any aspect of remuneration unless the following conditions are met: (a) (b) They have delegated authority, in accordance with the Scheme of Delegation. The appointment is within the limit of their approved budget and funded establishment. 29 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
184 STANDING FINANCIAL INSTRUCTIONS Paper 07 (c) The appointment has been made in accordance with procedures agreed by the Chief Executive The Board will approve procedures presented by the Chief Executive for the determination of commencing pay rates, condition of service, etc, for employees. 9.4 Processing Payroll The Finance Director is responsible for: (a) (b) (c) (d) Specifying timetables for submission of properly authorised time records and other notifications; The final determination of pay and allowances; Making payment on agreed dates; Agreeing method of payment The Finance Director will issue instructions regarding: (a) (b) (c) (d) (e) (f) (g) (h) (i) (j) (k) (l) Verification and documentation of data; The timetable for receipt and preparation of payroll data and the payment of employees and allowances; Maintenance of subsidiary records for superannuation, income tax, social security and other authorised deductions from pay; Security and confidentiality of payroll information; Checks to be applied to completed payroll before and after payment; Authority to release payroll data under the provisions of the Data Protection Act; Methods of payment available to various categories of employee and officers; Procedures for payment by cheque, bank credit, or cash to employees and officers; Procedures for the recall of cheques and bank credits; Pay advances and their recovery; Maintenance of regular and independent reconciliation of pay control accounts; Separation of duties of preparing records and handling cash; (m) A system to ensure the recovery from those leaving the employment of the Trust of sums of money and property due by them to the Trust. 30 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
185 STANDING FINANCIAL INSTRUCTIONS Paper Appropriately nominated managers have delegated responsibility for: (a) (b) (c) Submitting time records and other notifications in accordance with agreed timetables; Completing time records and other notifications in accordance with the Director of Finance's instructions and in the form prescribed by the Director of Finance; Submitting termination forms in the prescribed form immediately upon knowing the effective date of an employee's or officer s resignation, termination or retirement. Where an employee fails to report for duty or to fulfil obligations in circumstances that suggest they have left without notice, the Finance Director must be informed immediately Regardless of the arrangements for providing the payroll service, the Finance Director shall ensure that the chosen method is supported by appropriate (contracted) terms and conditions, adequate internal controls and audit review procedures and that suitable arrangements are made for the collection of payroll deductions and payment of these to appropriate bodies. 9.5 Contracts of Employment The Board shall delegate responsibility to an officer for: (a) (b) Ensuring that all employees are issued with a Contract of Employment in a form approved by the Board and which complies with employment legislation. Dealing with variations to, or termination of, contracts of employment. 31 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
186 STANDING FINANCIAL INSTRUCTIONS Paper NON-PAY EXPENDITURE 10.1 Delegation of Authority The Board will approve the level of non-pay expenditure on an annual basis and the Chief Executive will determine the level of delegation to budget managers The levels to be delegated are set out in the Detailed Scheme of Delegation, which should be referred to for further detail The Chief Executive will set out: (a) (b) The list of managers who are authorised to place requisitions for the supply of goods and services; The maximum level of each requisition and the system for authorisation above that level The Chief Executive shall set out procedures on the seeking of professional advice regarding the supply of goods and services Ordering, Receipt and Payment for Goods and Services Requisitioning The requisitioner, in choosing the item to be supplied (or the service to be performed) shall always obtain the best value for money for the Trust. In so doing, the advice of the Trust s adviser on supply shall be sought. Where this advice is not acceptable to the requisitioner, the Finance Director (and/or the Chief Executive) shall be consulted System of Payment and Payment Verification The Director of Finance shall be responsible for the prompt payment of accounts and claims. Payment of contract invoices shall be in accordance with contract terms, or otherwise, in accordance with national guidance. The Finance Director will: (a) (b) (c) (d) Advise the Board regarding the setting of thresholds above which quotations (competitive or otherwise) or formal tenders must be obtained; and, once approved, the thresholds should be incorporated in Standing Orders and Standing Financial Instructions and regularly reviewed; Prepare procedural instructions or guidance within the Scheme of Delegation on the obtaining of goods, works and services incorporating the thresholds; Be responsible for the prompt payment of all properly authorised accounts and claims; Be responsible for designing and maintaining a system of verification, recording and payment of all amounts payable. The system shall provide for: (i) A list of employees (including specimens of their signatures) authorised to certify invoicesapprove payments; 32 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
187 STANDING FINANCIAL INSTRUCTIONS Paper 07 (ii) Certification that: - Goods have been duly received, examined and are in accordance with specification and the prices are correct; - Work done or services rendered have been satisfactorily carried out in accordance with the order, and, where applicable, the materials used are of the requisite standard and the charges are correct; - In the case of contracts based on the measurement of time, materials or expenses, the time charged is in accordance with the time sheets, the rates of labour are in accordance with the appropriate rates, the materials have been checked as regards quantity, quality, and price and the charges for the use of vehicles, plant and machinery have been examined; - Where appropriate, the expenditure is in accordance with regulations and all necessary authorisations have been obtained; - The account is arithmetically correct; - The account is in order for payment. (iii) (iv) A timetable and system for submission to the Finance Director of accounts for payment; provision shall be made for the early submission of accounts subject to cash discounts or otherwise requiring early payment. Instructions to employees regarding the handling and payment of accounts within the Finance Department. (e) Be responsible for ensuring that payment for goods and services is only made once the goods and services are received. The only exceptions are set out in paragraph below Prepayments Prepayments are only permitted where exceptional circumstances apply. In such instances: (a) (b) (c) Prepayments are only permitted where the financial advantages outweigh the disadvantages (i.e. where material, cash flows must be discounted to net present value at the prevailing discount rate); The appropriate officer must provide, in the form of a written report, a case setting out all relevant circumstances of the purchase. The report must set out the effects on the Trust if the supplier is at some time during the course of the prepayment agreement unable to meet his commitments; The Director of Finance will need to be satisfied with the proposed arrangements before contractual arrangements proceed (taking into account the EU public procurement rules where the contract is above a stipulated financial threshold); 33 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
188 STANDING FINANCIAL INSTRUCTIONS Paper 07 (d) The budget holder is responsible for ensuring that all items due under a prepayment contract are received and they must immediately inform the appropriate Director or Chief Executive if problems are encountered Official orders Official Orders must: (a) (b) (c) (d) (e) (f) Be uniquely identified by use of an internally approved process; Be in a form approved by the Finance Director; State the Trust s terms and conditions of trade, including the need for suppliers to quote a valid order number when submitting invoices for payment; Only be issued to, and used by, those duly authorised by the Chief Executive. Lists of authorised officers shall be maintained and a copy of each list supplied to the Finance Director; May be transmitted by a system of Electronic Data Interchange (EDI) approved by the Finance Director; Be authorised, prior to being issued, according to the values detailed in the Scheme of Reservation and Delegation Duties of Managers and Officers Managers and officers must ensure that they comply fully with the guidance and limits specified by the Finance Director and that: (a) (b) (c) (d) All contracts (except as otherwise provided for in the Scheme of Delegation), leases, tenancy agreements and other commitments which may result in a liability are notified to the Finance Director in advance of any commitment being made; Contracts above specified thresholds are advertised and awarded in accordance with EU rules on public procurement; Where consultancy advice is being obtained, the procurement of such advice must be in accordance with best practice; No order shall be issued for any item or items to any firm which has made an offer of gifts, reward or benefit to directors or employees. As laid out in the Standards of Business Conduct policy. This excludes; (i) (ii) Isolated gifts of a trivial character or inexpensive seasonal gifts, such as calendars; conventional hospitality, such as reasonable lunches in the course of working visits; (e) No requisition/order is placed for any item or items for which there is no budget provision unless authorised by the Finance Director on behalf of the Chief Executive; 34 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
189 STANDING FINANCIAL INSTRUCTIONS Paper 07 (f) (g) (h) (i) (j) (k) (l) All goods, services, or works are ordered on an official order except works and services executed in accordance with a contract and purchases from petty cash or purchasing card; Verbal orders must only be issued very exceptionally - by an employee designated by the Chief Executive and only in cases of emergency or urgent necessity. These must be confirmed by an official order and clearly marked "Confirmation Order"; Orders are not split or otherwise placed in a manner devised so as to avoid the financial thresholds; Goods are not taken on trial or loan in circumstances that could commit the Trust to a future uncompetitive purchase; Changes to the list of employees and officers authorised to certify invoices are notified to the Director of Finance; Purchases from petty cash or purchasing card are restricted in value and by type of purchase in accordance with instructions issued by the Director of Finance; Petty cash and purchasing card records are maintained in a form as determined by the Director of Finance; (m) Drugs shall only be ordered via the Pharmacy Department The Chief Executive and Director of Finance shall ensure that the arrangements for financial control and financial audit of building and engineering contracts and property transactions comply with the guidance contained within ESTATECODE or CONCODE. The technical audit of these contracts shall be the responsibility of the relevant Director All staff have a responsibility for the maintenance of confidentiality of all information. No member of staff shall reveal information that could: a) Prejudice fair competition; b) Result in the Trust failing to achieve the most advantageous price in respect of purchases or income in respect of sales. Any breach of confidentiality, whether or not for personal gain, may render an individual open to disciplinary action in accordance with the Trust s Disciplinary Procedures and which may ultimately result in dismissal Payments to local authorities and voluntary organisations made under the powers of section 256 of the NHS Act 2006 (previously known as Section 28a payments) shall comply with procedures laid down by the Director of Finance which shall be in accordance with this Act. 35 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
190 STANDING FINANCIAL INSTRUCTIONS Paper FINANCIAL FRAMEWORK 11.1 External Borrowing The Finance Director will advise the Board concerning the ability of the Foundation Trust to pay interest and make repayments on any proposed new borrowing, within the limits set by the Prudential Borrowing Limit guidance from the Office of the Independent Regulator. The Finance Director is also responsible for reporting periodically to the Board concerning the Public Dividend Capital (PDC) and overdrafts Any application for additional PDC or overdraft facilities will only be made by the Finance Director and the Chief Executive or by an employee so delegated The Finance Director must prepare detailed procedural instructions concerning applications for additional PDC and overdrafts All short term borrowing should be kept to a minimum period of time possible, consistent with the cash flow position. Any short term borrowing requirement in excess of one month must be authorised by the Finance Director and Chief Executive or an employee so delegated All long term borrowing must be consistent with the plans outlined in the Annual Plan and in accordance with the Investment Decision Making Policy Investments Temporary cash surpluses must be held only in such public or private sector investments as authorised by the Board of Directors and in line with the Treasury Management Policy and the Independent Regulator s guidance, Managing Operating Cash in NHS foundation trusts as outlined in the Trust s Treasury Management Policy The Finance Director is responsible for advising the Board of Directors on investments and shall therefore report annually to the Board of Directors concerning the performance of investments held The Finance Director will prepare detailed procedural instructions on the operation of investment accounts and on the records to be maintained The Trust must comply with all relevant guidance published on investments from time to time in force Working Capital Facility The Board will ensure that funds are available for short-term cash flow management by negotiating an irrevocable working capital facility with a commercial bank. The value of this facility shall not exceed the limit set in the Trust s authorisation. 36 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
191 STANDING FINANCIAL INSTRUCTIONS Paper CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS AND SECURITY OF ASSETS 12.1 Capital Investment The Chief Executive: (a) (b) (c) Shall ensure that there is an adequate appraisal and approval process in place for determining capital expenditure priorities and the effect of each proposal upon business plans; Is responsible for the management of all stages of capital schemes and for ensuring that schemes are delivered on time and to budget; Shall ensure that the capital investment is not undertaken without confirmation of commissioners support and the availability of resources to finance all revenue consequences, including capital charges For every capital expenditure proposal greater than 75,000, the Chief Executive shall ensure: (a) That a business case in line with best practice as set out in such guidance as the Capital Investment Manual and Risk Evaluation for Decision Making issued by the Independent Regulator. This should include (i) (ii) (iii) An option appraisal of potential benefits compared with known costs to determine the option with the highest ratio of benefits to costs; The involvement of appropriate Trust personnel and external agencies; Appropriate project management and control arrangements. (b) That the Finance Director has reviewed and confirmed the costs and revenue consequences detailed in the business case For capital schemes where the contracts stipulate stage payments, the Chief Executive will issue procedures for their management, incorporating the recommendations of Estatecode The Finance Director shall issue procedures for the regular reporting of expenditure and commitment against authorised budgets The approval of a capital programme shall not constitute approval for expenditure on any scheme. The Chief Executive shall issue to the manager responsible for any scheme: (a) Specific authority to commit expenditure; (b) Authority to proceed to tender (see overlap with SFI No. 7); (c) Approval to accept a successful tender (see overlap with SFI No. 7). 37 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
192 STANDING FINANCIAL INSTRUCTIONS Paper 07 The Chief Executive will issue a scheme of delegation for capital investment management in accordance with "Estatecode" guidance and the Trust s Standing Orders The Finance Director shall issue procedures governing the financial management, including variations to contract, of capital investment projects and valuation for accounting purposes Private Finance (including Leasing) When the Trust proposes to use private finance or leasing either a finance lease or an operating lease the following procedures shall apply: (a) (b) (c) The proposal must obtain approval commensurate with that which is required were the assets, goods or services are to be obtained by outright purchase, i.e. employees must follow annual planning guidance. The Director of Finance shall demonstrate that the financing represents value for money and genuinely transfers risk to the private sector in accordance with relevant guidance. Any finance or operating leases must be agreed and signed by the Director of Finance Asset Registers The Chief Executive is responsible for the maintenance of registers of assets, taking account of the advice of the Finance Director concerning the form of any register and the method of updating, and arranging for a physical check of assets against the asset register to be conducted once a year The Trust shall maintain an asset register recording fixed assets Additions to the fixed asset register must be clearly identified to an appropriate budget holder and be validated by reference to: (a) (b) (c) Properly authorised and approved agreements, architect's certificates, supplier's invoices and other documentary evidence in respect of purchases from third parties; Stores, requisitions and wages records for own materials and labour including appropriate overheads; Lease agreements in respect of assets held under a finance lease and capitalised Where capital assets are sold, scrapped, lost or otherwise disposed of, their value must be removed from the accounting records and each disposal must be validated by reference to authorisation documents and invoices (where appropriate) The Finance Director shall approve procedures for reconciling balances on fixed assets accounts in ledgers against balances on fixed asset registers. 38 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
193 STANDING FINANCIAL INSTRUCTIONS Paper The value of each asset shall be indexed to current values in accordance the Trust s accounting policies The value of each asset shall be depreciated using methods and rates as specified in the Trust s accounting policies The Finance Director of the Trust shall calculate and pay capital charges as specified in the guidance issued by the Independent regulator The Trust shall maintain a property register recording protected property, in accordance with guidance issued by the independent regulator Security of Assets The overall control of fixed assets is the responsibility of the Chief Executive Asset control procedures (including fixed assets, cash, cheques and negotiable instruments, and also including donated assets) must be approved by the Finance Director. This procedure shall make provision for: (a) (b) (c) (d) (e) (f) (g) Recording managerial responsibility for each asset; Identification of additions and disposals; Identification of all repairs and maintenance expenses; Physical security of assets; Periodic verification of the existence of, condition of, and title to, assets recorded; Identification and reporting of all costs associated with the retention of an asset; Reporting, recording and safekeeping of cash, cheques, and negotiable instruments All discrepancies revealed by verification of physical assets to fixed asset register shall be notified to the Finance Director Whilst each employee and officer has a responsibility for the security of property of the Trust, it is the responsibility of Board members and senior employees in all disciplines to apply such appropriate routine security practices in relation to NHS property as may be determined by the Board. Any breach of agreed security practices must be reported in accordance with agreed procedures. (see SFI 2) Any damage to the Trust s premises, vehicles and equipment, or any loss of equipment, stores or supplies must be reported by Board members and employees in accordance with the procedure for reporting losses. (see SFI 2) Where practical, assets should be marked as Trust property. 39 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
194 STANDING FINANCIAL INSTRUCTIONS Paper STORES AND RECEIPT OF GOODS 13.1 General position Stores, defined in terms of controlled stores and departmental stores (for immediate use) should be: (a) (b) (c) Kept to a minimum; Subjected to annual stock take; Valued in accordance with the Trusts accounting policies Control of Stores, Stocktaking, condemnations and disposal Subject to the responsibility of the Finance Director for the systems of control, overall responsibility for the control of stores shall be delegated to an employee by the Chief Executive. The day-to-day responsibility may be delegated by him to departmental employees and stores managers/keepers, subject to such delegation being entered in a record available to the Finance Director. The control of any Pharmaceutical stocks shall be the responsibility of a designated Pharmaceutical Officer; the control of any fuel oil and coal of a designated estates manager The responsibility for security arrangements and the custody of keys for any stores and locations shall be clearly defined in writing by the designated manager/pharmaceutical Officer. Wherever practicable, stocks should be marked as health service property The Finance Director shall set out procedures and systems to regulate the stores including records for receipt of goods, issues, and returns to stores, and losses Stocktaking arrangements shall be agreed with the Finance Director and there shall be a physical check covering all items in store at least once a year Where a complete system of stores control is not justified, alternative arrangements shall require the approval of the Finance Director The designated Manager/Pharmaceutical Officer shall be responsible for a system approved by the Finance Director for a review of slow moving and obsolete items and for condemnation, disposal, and replacement of all unserviceable articles. The designated Officer shall report to the Finance Director any evidence of significant overstocking and of any negligence or malpractice (see also overlap with SFI No. 25 Disposals and Condemnations, Losses and Special Payments). Procedures for the disposal of obsolete stock shall follow the procedures set out for disposal of all surplus and obsolete goods Receipt of Goods 40 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
195 STANDING FINANCIAL INSTRUCTIONS Paper A delivery note shall be obtained from the supplier at the time of delivery and shall be signed by the person receiving the goods. All goods received shall be checked, by the appropriate department, as regards quantity and/or weight and inspected as to quality and specification. Instructions shall be issued to staff covering the procedures to be adopted in those cases where a delivery note is not available All goods received shall be entered onto an appropriate goods received/stock record (whether a computer or manual system) on the day of receipt. If goods received are unsatisfactory, the records shall be marked accordingly. Further, where the goods received are found to be unsatisfactory or short on delivery, they shall only be accepted on the authority of the designated officer and the supplier shall be notified immediately Goods supplied by NHS Supply Chain For goods supplied via the NHS Logistics central warehouses, the Chief Executive shall identify those authorised to requisition and accept goods from the store. The authorised person shall check receipt against the delivery note before forwarding this to the Finance Director who shall satisfy himself that the goods have been received before accepting the recharge. 41 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
196 STANDING FINANCIAL INSTRUCTIONS Paper DISPOSALS AND CONDEMNATIONS, LOSSES AND SPECIAL PAYMENTS 14.1 Disposals and Condemnations Procedures The Finance Director must prepare detailed procedures for the disposal of assets including condemnations, and ensure that these are notified to managers When it is decided to dispose of a Trust asset, the Head of Department or authorised deputy will determine and advise the Finance Director of the estimated market value of the item, taking account of professional advice where appropriate All unserviceable articles shall be: (a) (b) Condemned or otherwise disposed of by an employee authorised for that purpose by the Finance Director; Recorded by the Condemning Officer in a form approved by the Finance Director which will indicate whether the articles are to be converted, destroyed or otherwise disposed of. All entries shall be confirmed by the countersignature of a second employee authorised for the purpose by the Finance Director The Condemning Officer shall satisfy himself as to whether or not there is evidence of negligence in use and shall report any such evidence to the Finance Director who will take the appropriate action Any disposal of IT equipment must also comply with the IT Security Policy Losses and Special Payments Procedures The Finance Director must prepare procedural instructions on the recording of and accounting for condemnations, losses, and special payments Any employee or officer discovering or suspecting a loss of any kind must either immediately inform their head of department, who must immediately inform the Chief Executive and the Director of Finance or inform an officer charged with responsibility for responding to concerns involving loss. This officer will then appropriately inform the Finance Director and/or Chief Executive. Where a criminal offence is suspected, the Finance Director must immediately inform the police if theft or arson is involved. In cases of fraud and corruption or of anomalies which may indicate fraud or corruption, the Finance Director must inform the relevant LCFS and NHS Protect in accordance with Secretary of State for Health s Directions For losses apparently caused by theft, arson, neglect of duty or gross carelessness, except if trivial, the Finance Director must immediately notify: (a) The Board, 42 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
197 STANDING FINANCIAL INSTRUCTIONS Paper 07 (b) (c) The External Auditor. NHS Protect The Trust Board shall approve the delegation of the writing-off of losses, on an annual basis The Finance Director shall take any necessary steps to safeguard the Trust s interests in bankruptcies and company liquidations For any loss, the Finance Director should consider whether any insurance claim can be made The Finance Director shall maintain a Losses and Special Payments Register in which write-off action is recorded All losses and special payments must be reported to the Audit Committee at every meeting. 43 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
198 STANDING FINANCIAL INSTRUCTIONS Paper INFORMATION TECHNOLOGY 15.1 Responsibilities and duties of the Senior Information Risk Officer (SIRO) The Trust s nominated Senior Information Risk Officer (SIRO), who is responsible for the accuracy and security of the computerised data of the Trust, shall: a) Devise and implement any necessary procedures to ensure adequate protection of the Trust s data, programs and computer hardware for which the Director is responsible from accidental or intentional disclosure to unauthorised persons, deletion or modification, theft or damage, having due regard for the Data Protection Act 1998 (updated 2000); b) Ensure that adequate controls exist over data entry, processing, storage, transmission and output to ensure security, privacy, accuracy, completeness, and timeliness of the data, as well as the efficient and effective operation of the system; c) Ensure that adequate controls exist such that the routine computer operation is separated from system controls including development, maintenance and amendment; d) Ensure that an adequate management (audit) trail exists through the computerised system and that such computer audit reviews as the Director may consider necessary are being carried out; e) Ensure that adequate controls exist to maintain the security, privacy, accuracy and completeness of financial data sent via transmission networks. f) Shall ensure that risks to the Trust arising from the use of IT are effectively identified and considered and appropriate action taken to mitigate or control these risks. This shall include the preparation and testing of appropriate disaster recovery plans Responsibilities and duties of other Directors and Officers in relation to computer systems of a general application The Foundation Trust Secretary shall publish and maintain a Freedom of Information (FOI) Publication Scheme, or adopt a model Publication Scheme approved by the information Commissioner In the case of computer systems which are procured jointly with other NHS organisations, the responsible officer will send to the Finance Director (a) (b) Details of the outline design of the system; In the case of packages acquired either from a commercial organisation, from the NHS, or from another public sector organisation, the operational requirement. 44 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
199 STANDING FINANCIAL INSTRUCTIONS Paper Contracts for Computer Services with other health bodies or outside agencies The Finance Director shall ensure that contracts for computer services for financial applications with another health organisation or any other agency shall clearly define the responsibility of all parties for the security, privacy, accuracy, completeness, and timeliness of data during processing, transmission and storage. The contract should also ensure rights of access for audit purposes. Where another health organisation or any other agency provides a computer service for financial applications, the Finance Director shall periodically seek assurances that adequate controls are in operation Requirements for Computer Systems which have an impact on corporate financial systems Where computer systems have an impact on corporate financial systems the Finance Director shall need to be satisfied that: (a) (b) (c) (d) Systems acquisition, development and maintenance are in line with corporate policies such as, but not limited to, an Information Technology Strategy; Data produced for use with financial systems is adequate, accurate, complete and timely, and that a management (audit) trail exists; Finance Director s staff and the Trust s auditors have access to such data; Such computer audit reviews as are considered necessary are being carried out. 45 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
200 STANDING FINANCIAL INSTRUCTIONS Paper PATIENTS' PROPERTY 16.1 The Trust has a responsibility to provide safe custody for money and other personal property (hereafter referred to as "property") handed in by patients, in the possession of unconscious or confused patients, or found in the possession of patients dying in hospital or dead on arrival The Chief Executive is responsible for ensuring that patients or their guardians, as appropriate, are informed before or at admission by: - Notices and information booklets; (notices are subject to sensitivity guidance) - Hospital admission documentation and property records; - The oral advice of administrative and nursing staff responsible for admissions, that the Trust will not accept responsibility or liability for patients' property brought into Health Service premises, unless it is handed in for safe custody and a copy of an official patients' property record is obtained as a receipt The Finance Director must provide detailed written instructions on the collection, custody, investment, recording, safekeeping, and disposal of patients' property (including instructions on the disposal of the property of deceased patients and of patients transferred to other premises) for all staff whose duty is to administer, in any way, the property of patients. Due care should be exercised in the management of a patient's money in order to maximise the benefits to the patient Where Department of Health instructions require the opening of separate accounts for patients' moneys, these shall be opened and operated under arrangements agreed by the Finance Director In all cases where property of a deceased patient is of a total value in excess of 5,000 (or such other amount as may be prescribed by any amendment to the Administration of Estates, Small Payments, Act 1965), the production of Probate or Letters of Administration shall be required before any of the property is released. Where the total value of property is 5,000 or less, forms of indemnity shall be obtained Staff should be informed, on appointment, by the appropriate departmental or senior manager of their responsibilities and duties for the administration of the property of patients Where patients' property or income is received for specific purposes and held for safekeeping the property or income shall be used only for that purpose, unless any variation is approved by the donor or patient in writing. 46 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
201 STANDING FINANCIAL INSTRUCTIONS Paper FUNDS HELD ON TRUST 17.1 Corporate Trustee The Trust Board is responsible, as a corporate trustee, for the management of funds it holds on trust. The Trust Board is responsible for ensuring compliance with Charities Commission latest guidance and best practice. The discharge of the Trust s corporate trustee responsibilities are distinct from its responsibilities for exchequer funds and may not necessarily be discharged in the same manner, but there must still be adherence to the overriding general principles of financial regularity, prudence and propriety. Trustee responsibilities cover both charitable and non-charitable purposes. The Director of Finance shall ensure that each trust fund which the Trust is responsible for managing is managed appropriately with regard to its purpose and to its requirements Accountability to Charity Commission and Secretary of State for Health The trustee responsibilities must be discharged separately and full recognition given to the Trust s dual accountabilities to the Charity Commission for charitable funds held on trust and to the Secretary of State for all funds held on trust The Schedule of Matters Reserved to the Board and the Scheme of Delegation make clear where decisions regarding the exercise of discretion regarding the disposal and use of the funds are to be taken and by whom. All Trust Board members and Trust officers must take account of that guidance before taking action Applicability of Standing Financial Instructions to funds held on Trust In so far as it is possible to do so, most of the sections of these Standing Financial Instructions will apply to the management of funds held on trust The over-riding principle is that the integrity of each Trust must be maintained and statutory and Trust obligations met. Materiality must be assessed separately from Exchequer activities and funds 47 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
202 STANDING FINANCIAL INSTRUCTIONS Paper ACCEPTANCE OF GIFTS BY STAFF AND LINK TO STANDARDS OF BUSINESS CONDUCT The Foundation Trust Secretary shall ensure that all staff are made aware of the Trust Code of Business Conduct, which gives guidance on the acceptance of gifts and other benefits in kind by staff. 19. RETENTION OF RECORDS 19.1 The Chief Executive shall be responsible for maintaining archives for all records required to be retained in accordance with Department of Health guidelines The records held in archives shall be capable of retrieval by authorised persons Records held in accordance with latest Department of Health guidance shall only be destroyed at the express instigation of the Chief Executive. Detail shall be maintained of records so destroyed. 20. RISK MANAGEMENT AND INSURANCE 20.1 Programme of Risk Management The Chief Executive shall ensure that the Trust has a programme of risk management, in accordance with current guidance from the Independent Regulator, which must be approved and monitored by the Board. The programme of risk management shall include: (a) (b) (c) (d) (e) (f) (g) A process for identifying and quantifying risks and potential liabilities; Engendering among all levels of staff a positive attitude towards the control of risk; Management processes to ensure all significant risks and potential liabilities are identified and addressed including effective systems of internal control, cost effective insurance cover, and decisions on the acceptable level of retained risk; Contingency plans to offset the impact of adverse events; Audit arrangements including; Internal Audit, clinical audit, health and safety review; A clear indication of which risks shall be insured; Arrangements to review the Risk Management programme. The existence, integration and evaluation of the above elements will assist in providing a basis to make an Annual Governance Statement within the Annual Report and Accounts as required by current guidance from the Independent regulator. 48 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
203 STANDING FINANCIAL INSTRUCTIONS Paper Insurance: Risk Pooling Schemes administered by NHSLA The Board shall decide if the Trust will insure through the risk pooling schemes administered by the NHS Litigation Authority or self insure for some or all of the risks covered by the risk pooling schemes. If the Board decides not to use the risk pooling schemes for any of the risk areas (clinical, property and employers/third party liability) covered by the scheme this decision shall be reviewed annually Insurance arrangements with commercial insurers Any decision to enter insurance arrangements with commercial insurers must be taken by the Trust Board the one exception being (a) The Trust may enter commercial arrangements for insuring motor vehicles owned by the Trust including insuring third party liability arising from their use without board approval Arrangements to be followed by the Board in agreeing Insurance cover (a) (b) (c) Where the Board decides to use the risk pooling schemes administered by the NHS Litigation Authority the Finance Director shall ensure that the arrangements entered into are appropriate and complementary to the risk management programme. The Finance Director shall ensure that documented procedures cover these arrangements. Where the Board decides not to use the risk pooling schemes administered by the NHS Litigation Authority for one or other of the risks covered by the schemes, the Finance Director shall ensure that the Board is informed of the nature and extent of the risks that are self insured as a result of this decision. The Finance Director will draw up formal documented procedures for the management of any claims arising from third parties and payments in respect of losses which will not be reimbursed. All the risk pooling schemes require Scheme members to make some contribution to the settlement of claims (the deductible ). The Finance Director should ensure documented procedures also cover the management of claims and payments below the deductible in each case. 49 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
204 Paper 07 Appendix 2 Detailed Scheme of Delegation DRAFT 2012 The delegation shown below is the lowest level to which authority is delegated, this delegation may be suspended in order to increase control response to special circumstances. Delegation to lower levels is only permitted with written approval of the Chief Executive who will, before authorising such delegation, consult with other Senior Officers as appropriate. In the absence of the officer with delegated authority; if arrangements in place for a deputy to act up, which have been formally recorded, the deputy may exercise that delegated authority, if no such arrangement in place the matter should be referred to the next highest senior officer. All items concerning Finance must be carried out in accordance with Standing Financial Instructions. DELEGATED MATTER AUTHORITY DELEGATED TO REFERENCE DOCUMENTS 1. Management of Budgets SFIs Section Responsibility of keeping revenue expenditure within budgets (a) Designation of Budget Holder (b) At Individual Budget level (Pay and Non Pay) (c) At Divisional Level (d) Other areas (eg reserves) Chief Executive Budget Holders Nominated Executive Director Finance Director 1.2 Responsibility of keeping Capital expenditure within budgets (a) Designation of Budget Holder (b) At Individual Budget level Chief Executive Finance Director 1.3 Responsibility for Activity Income (a) Designation of Budget Holder (b) At Divisional level Chief Executive Nominated Executive Director Page 1 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
205 Paper 07 Appendix 2 2 Investment & Banking SFIs Section 5 & 11 Opening & Closure of Bank accounts Finance Director Investment of surplus cash Up to 1m Up to 28 days Deputy FD Up to days Finance Director Over days Finance Director with BRIC approval. Up to 5m Up to 7 days Deputy FD Up to days FD Over days Finance Director with BRIC approval. Over 5m Up to days Finance Director Over days Finance Director with Board approval. External Borrowing Establishment of Working Capital Facility Finance Director Chief Executive and Finance Director 3. Non Pay Revenue and Capital Expenditure Authorising Non Pay Requisitions, Orders and Payments, (excluding locums & agency staff), where there is sufficient budget available. This is includes requisitions and payments made using the Oracle on line system. SFIs Section Routine Goods & Services (a) Approve requisitions/payments up to 999 (b) Approve requisitions/payments up to 4,999 (c) Approve requisitions/payments up to 19,999 Budget Holder Divisional Manager Director and Finance Director or Nominated Deputy (d) Approve requisitions/payments up to 49,999 (e) Approve requisitions/payments up to 74,999 (f) Approve requisitions/payments over 75,000 Finance Director Chief Executive or Finance Director & one other Executive Director Chief Executive & Finance Director Page 2 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
206 Paper Specialist Goods & Services and exceptional items Appendix 2 (a) Approve pharmacy orders/payments up to 74,999 (b) Approve pharmacy orders/payments over 75,000 (c) Approve works /Capital requisitions/payments up to 9,999 (d) Approve works/capital requisitions/payments, where scheme has been approved by the Board, up the approved budget (e) Approve theatre requisitions/ payments up to 9,999 For amounts greater than 9,999 section 3.1 will apply (see above) (f) Orders exceeding 12 month period (g) All contracts for goods & services for a period greater than one year and subsequent variations to those contracts. Head of Pharmacy Head of Pharmacy & Finance Director or Chief Executive Deputy Director of Estates Chief Executive Theatre Manager Finance Director or Chief Executive Finance Director or Chief Executive 4. Capital Schemes SFIs Section 12 a) Selection of architects, quantity surveyors, consultant engineer and other professional advisors within EU regulations. b) Financial monitoring and reporting on all capital scheme expenditure. c) Granting and termination of leases with annual rent < 100k d) Granting and termination of leases of > 100k Deputy Director of Estates Finance Director or Nominated Deputy Finance Director Chief Executive and Finance Director 5. Quotations, Tendering & Contract Procedures SFIs Section Quotations and Tendering Limits a) Obtaining 2 written quotations for goods/services expected to be from 10,000 to 19,999 b) Obtaining 3 written quotations for goods/services expected to be from 20,000 to 49,000 Budget Holder in conjunction with SHPS Budget Holder in conjunction with SHPS Page 3 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
207 Paper 07 Appendix 2 c) Obtaining 3 written competitive tenders for goods/services expected to be from 50,000 to ,999 d) Obtaining competitive tenders in accordance with European legislation for goods/services expected to be over ,000 Executive Director/Divisional manager in conjunction with SHPS Executive Director and Director of Finance in conjunction with SHPS 5.2 Wavering of Quotations & Tenders subject to SFIs. a) Waiving of Quotations up to 49,000 Director of Finance b) Waiving of Tenders over 50,000 up Chief Executive to 112,999101,000 c) Waiving of Tenders over N/A ,000. No waiver or single tender action is allowed which would exceed the EU procurement limit. 5.3 Tender Opening /Evaluation and Acceptance / Recording a) Opening Tenders Two Executive Directors or Associate Directors. b) Evaluation of Tenders Panel including Divisional lead, Finance manager and appropriate specialist advisor(s) c) Acceptance of Tenders up to the Two Executive Board Directors value of 249,999 d) Acceptance of Tenders over 250,000 Trust Board Decision e) Approving expenditure over the Finance Director agreed tender/quotation budget where the tender/quotation price is greater than 10% up to the value of 15,000. f) Approving expenditure over the Chief Executive agreed tender/quotation budget where the tender/quotation price is greater than 10% and over 15,000. g) Maintenance of Tender Register Foundation Trust Secretary 6. Healthcare Contracts SFIs Section 8 a) Signing of Contracts over 5m Chief Executive b) Signing of Contracts up to the value Finance Director of 5m c) Price of NHS Contracts Charges for all Finance Director Activity not covered by PBR Tariff. d) Private Patient, Overseas Visitors, Income Generation and other patient related services. Finance Director e) Reporting to the Trust Board where a Finance Director negotiated contract does not comply with the terms of the NHS Contract or the Operating Framework 7. Personnel & Pay SFIs Section 9 & Page 4 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
208 Paper 07 Trust Policies Appendix 2 a) Authority to fill funded post on the establishment with permanent staff b) Authority to appoint staff to post not on the formal establishment with permanent staff c) Authority to appoint Additional staff to the agreed establishment with specifically allocated finance. d) The granting of additional increments to staff within budget and in accordance with Trust policy e) All requests for upgrading/regrading shall be dealt with in accordance with Trust Procedure 7.1 Pay a) Authority to complete standing data forms affecting pay, new starters, variations and leavers b) Authority to complete and authorise positive reporting forms. Associate Director of Human Resources (in line with post approval procedures) Associate Director of Human Resources (in line with post approval procedures) Associate Director of Human Resources (in line with post approval procedures) Associate Director of Human Resources Associate Director of Human Resources Budget Holder Budget Holder c) Authority to authorise overtime Appropriate Manager/Director d) Authority to authorise travel and Appropriate Manager/Director subsistence claims e) Approval of Performance related pay. Chief Executive or Nomination and Remuneration Committee 7.2 Leave a) Approval of annual leave Line/Departmental Manager b) Annual leave approval of carry Line/Departmental Manager forward up to a maximum of 5 days c) Annual leave approval of carry over Associate Director of Human in excess of 5 days but less than 10 Resources days. d) Special leave up to 5 days. Line/Departmental Manager. In line with Trust policy. e) vii) Special leave in addition to 5 days Associate Director of Human Resources In line with Trust policy. f) Unpaid leave - up to 5 days Line/Departmental Manager In line with Trust policy. g) Unpaid leave - over 5 days Associate Director of Human Resources In line with Trust policy. h) Medical Staff Leave of Absence paid Medical Director and Associate Page 5 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
209 Paper 07 and unpaid (over and above normal annual leave entitlement) Director of Human Resources. Appendix 2 i) Time off in lieu. Automatic approval of Line manager within the requirements of the organisation. j) Maternity leave paid and unpaid. Automatic approval within guidance. 7.3 Absence due to Sickness a) Any extension of Sick Leave over employee conditions of service b) Return to work part-time on full pay to assist recovery. 7.4 Study Leave a) All study leave outside of the UK, excluding CME/professional leave b) Medical staff CME/professional leave (UK and overseas) except any associated with the receipt of Divisional Manager or Director in conjunction with The Associate Director of Human Resources. Associate Director of Human Resources in conjunction with the Divisional Manager or Director. Chief Executive Clinical Divisional Director or Medical Director (plus Associate Director of Human Resources if hospitality is involved). hospitality. c) All other study leave Divisional manager/director with support from line manger 7.5 Relocation Expenses a) Authorisation of payment of removal expenses incurred by officers taking up new appointments (in accordance with local policy) Up to 5,000 Associate Director of Human Resources Over 5,000 Chief Executive 7.6 Grievance Procedure All grievance cases must be dealt with strictly in accordance with the Grievance Procedure and the advice of a Human Resources Officer must be sought. Associate Director of Human Resources in accordance with Trust policy. 7.7 Authorised Car & Mobile Phone Users a) Requests for new posts to be authorised as car users. b) Requests for existing posts to be authorised as car users. c) Requests for posts to be authorised as mobile telephone users 7.8 Renewal of Fixed Term and Temporary Contracts Associate Director of Human Resources/ Finance Director in liaison with Divisional Manager/Director Associate Director of Human Resources/ Finance Director in liaison with Divisional Manager/Director Associate Director of Human Resources/ Finance Director in liaison with Divisional Manager/Director Page 6 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
210 Paper 07 a) Renewal of Fixed Term and Temporary Contracts 7.9 Staff Retirement Policy Authorisation of extensions of contract beyond agreed retirement age Associate Director of Human Resources (in line with post approval procedures) Associate Director of Human Resources in liaison with Divisional Manager/Director Appendix Redundancy Chief Executive and Associate Director of Human Resources 7.11 Ill Health Retirement Decision to pursue retirement on the grounds of ill-health The Associate Director of Human Resources in conjunction with Divisional Manager or Director Dismissal The Associate Director of Human Resources and authorised directors or Nomination and Remuneration Committee as appropriate 8. Engagement of Staff other than employees SFIs Section 7 a) Non Medical Consultancy Staff Chief Executive or Finance Director b) Engagement of Trust s Solicitors Chief Executive or Finance Director and one other Director c) Booking of Bank or Agency Staff - Medical Locums - Nursing - Clerical Associate Director of Human Resources (in line with Bank, Agency Procedure). 9. Expenditure on Charitable and Endowment Funds SFIs Section Approval to fundraising/appeal Launching a) Projected Fundraising up to 5000 Executive Director b) Projected Fundraising between 5001 Charitable Funds Committee. and 250,000 c) Projected Fundraising between over 250, Expenditure a) Up to 500 Fund Manager Trust Board Approval subject to Charitable Funds Committee and following Divisional Manager / Director support b) Up to 10,000 per request Chief Executive or Finance Director c) Up to 20,000 per request Chief Executive & Finance Director d) Over 20,000 per request Charitable Funds Committee, or between meetings Director of Finance Director and Chief Executive in consultation with other Trustees. Page 7 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
211 Paper 07 e) Over 50,000 Charitable Funds Committee. Appendix Agreement/Licences a) Preparation and signature of all tenancy agreements/licences for all staff, subject to Trust Policy on accommodation for staff. Finance Director/ Associate Director of Human Resources / Deputy Director of Estates b) Extensions to existing leases Finance Director/ Associate Director of Human Resources / Deputy Director of Estates c) Letting of premises to outside organisations d) Approval of rent based on professional assessment Finance Director & Chief Executive Finance Director 11. Condemning & Disposal of Assets SFIs Section 14 a) Items obsolete, obsolescent, redundant, and irreparable or cannot be repaired cost effectively.(including x-ray films, mechanical & engineering plant) With a current estimated value of less than 2,500 With a current estimated value over than 2, Write off of Losses and Special Payments Divisional Manager/ Director / Associate Director/Deputy Director of Estates Finance Director All Losses, Write-Offs & Special Payments must be reported to the Audit Committee 12.1 Losses a) Losses resulting from loss of cash, fruitless payments, bad debts and damage to buildings or loss of equipment Less than 50,000 Finance Director Between 50,000 and 100,000 Finance Director and Chief Executive Over 100,000 Finance Director and Chief Executive and a member of the Audit Committee Special Payments a) Special Payments (excluding severance payments), including Compensation made under legal obligation, Personal Injury claim following legal advice, maladministration and loss of Page 8 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
212 Paper 07 personal effects. Less than 50,000 Finance Director Appendix 2 Between 50,000 and 100,000 Finance Director and Chief Executive Over 100,000 Finance Director and Chief Executive and a member of the Audit Committee Severance Payments Nomination & Remuneration Committee following Treasury 12.4 Novel, contentious or repercussive special payments- to be notified to the Department of Health approval. Director of Finance 13. Reporting of Incidents to the Police SFIs Section 2 a) Where a criminal offence is suspected. The Duty Manager in conjunction with Local Security Management Specialist b) Where a fraud is involved Finance Director in conjunction with the Local Counter Fraud Specialist. 14. Petty Cash Disbursements a) Expenditure up to 25 per item Petty Cash Holder b) Reimbursement of patients monies up to 100 c) Reimbursement of patients monies in excess of 100 Finance Director or nominated deputy Finance Director 15. Receiving Hospitality SFIs Section 18, Applies to both individual and collective hospitality. (Small items such as pens, diaries or chocolates need not be declared). 16. Implementation of Internal and External Audit Recommendations 17. Maintenance & update of Trust Financial Procedures All staff are required to make a declaration in Trust s Hospitality Register and follow the Trusts Standards of Business Conduct Appropriate Director SFIs Section 2 Finance Director SFIs Section Investment of Funds (including Charitable & Endowment Funds) Finance Director in conjunction with the Business Risk and Investment Committee. SFIs Sections 11/17 Page 9 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
213 Paper 07 Appendix Authorisation of New Drugs Estimated total yearly cost up to 25,000 Estimated total yearly cost above 25, Authorisation of Clinical Sponsorship deals Medical Director and Finance Director following advise from the Drugs & Therapeutics Committee Medical Director and Chief Executive in conjunction with the Executive team, following advise from the Drugs & Therapeutics Committee Medical Director SFIs Section Authorisation of Research Projects Medical Director 22. Authorisation of Clinical Trials Medial Director and Director of Nursing and Governance 23. Insurance Policies Finance Director 24. Risk Management Chief Executive SFIs Section Patients & Relatives Complaints a) Overall responsibility for ensuring that all complaints are dealt with effectively b) Responsibility for ensuring complaints relating to a directorate are investigated thoroughly c) Medico-Legal complaints Co ordination of their management Director of Nursing and Governance Director of Nursing and Governance Director of Nursing and Governance 26. Relationships with Press a) Non Emergency Enquiries - within hours - outside b) Emergency - within hours - outside hours 27. Infectious Diseases & Notifiable Outbreaks Chief Executive Duty Officer or Senior Manager On Call Chief Executive Duty Officer or Senior Manager on call Director of Infection Prevention and Control 28. Extended Role Activities Page 10 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
214 Paper 07 Approval of Nurses to undertake duties/ procedures which can properly be described as beyond the normal scope of Nursing Practice. 29. Patient Services a) Variation of operating and clinic sessions within existing numbers - Outpatients - Theatres - Other Director of Nursing and Governance Director of Operations Director of Operations Director of Operations Nurse/Midwives/H ealth Visitors Act Midwives Rules/Code of Practice UKCC Code of Professional Conduct. Appendix 2 b) All proposed changes in bed allocation and use - Temporary Change - Permanent Change 30. Facilities for staff not employed by the Trust to gain practical experience. a) Professional Recognition, Honorary Contracts, and Insurance of Medical Staff Director of Nursing & Governance Chief Executive Associate Director of Human Resources in accordance with Trust Policy b) Work experience students Associate Director of Human Resources in accordance with Trust Policy 31. Review of Fire Precautions Director of Operations 32. Review of all statutory compliance with legislation and Health and Safety requirements including control of Substances Hazardous to Health Regulations 33. Review of Medicines Inspectorate Regulations 34. Review of compliance with environmental regulations, for example those relating to clean air and waste disposal 35. Review of Trust s compliance with the Data Protection Act 36. Monitor proposals for contractual arrangements between the Trust and outside bodies Director of Operations Medical Director in conjunction with the Head of Pharmacy Director of Operations Finance in conjunction with the Deputy Director of Estates Director of Nursing and Governance SFIs Section 15 Finance Director SFIs Section 8 Page 11 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
215 Paper 07 Appendix Review of the Trust s compliance with the Code of Practice for Handling Confidential Information in the Contracting Environment and compliance with safe haven per EL 92/ The keeping of a Declaration of Interests Register 39. Attestation of Sealings in accordance with Standing Orders 40. The keeping of a register of Sealings Finance Director SFIs Section 15 Foundation Trust Secretary SFIs Section 19, Chairman/Chief Executive or nominated deputy Foundation Trust Secretary 41. The keeping of the Hospitality Foundation Trust Secretary SFIs Section 18, Register 42. Retention of Records Chief Executive SFIs Section Clinical Audit Medical Director Page 12 of 12 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 07 revised SFIs and Detailed Scheme of Delegation
216 Paper 08 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title Board Governance Arrangements Executive Responsible Paper prepared by (if different from above) Wendy Farrington Chadd, Chief Executive Margaret Surrage, Head of Board Governance (Trust Secretary) Nature of Report Category of Item For Information For Discussion For Approval Strategic Direction and Development Performance and Governance Context Previous Board discussion Reviewed at Board Development session May 2009 Revised document approved October 2010 Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary The Board Governance Arrangements have been reviewed and updated. The Standards for NHS Board Members, produced by the Professional Standards Authority, has been added to the suite of documents. Received or approved by Legal Implications Recommendations That the Board approve the adoption of the Standards for NHS Board members. That the Board approves the proposed changes to the Board Governance Arrangements document. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 1
217 Paper 08 Board Governance Arrangements Introduction The attached suite of documents describes the overarching arrangements for Board Governance within the Trust. They were developed in preparation for the Trust becoming a Foundation Trust and were approved by the Board in October As well as giving a high level assurance on board governance these documents also fulfil some of the detailed requirements from the NHS Foundation Trust Code of Governance. There should be a formal schedule of matters specifically reserved for decision by the board of directors (A.1.1) The division of responsibilities between the chairman and chief executive should be clearly established, set out in writing and agreed by the board of directors. (A.2.1) Given this it is appropriate that the board reviews and affirms this suite of documents. Standards for NHS Board Members The Professional Standards Authority issued a set off standards for the members of NHS Boards in November These were commissioned in the wake of the Francis inquiry and are intended to complement rather replace the existing managements standards. The standards cover three domains Personal behaviour Technical Competence Business Practices and are intended to put compassion and respect at the heart of NHS leadership These standards have been added to the suite of Governance documents, see appendix A. For completeness, the Code of Conduct for NHS Managers, which all of the Trust s managers are required to adhere to, has been attached at Appendix B. Updates to the Board Governance Arrangements A number of changes have been proposed to update the documents, many of them to reflect the changes brought about by the Health and Social care Act. The Collective role of the Board has been updated to include the duties set out in the Health and Social care Act (page 2) The composition of the Board has been updated to include the Deputy Chair and the Senior Independent director (page 2) The adoption of the Standards for NHS Board members has been added(page 4) Executive Roles have been amended to reflect: o the transfer of duties from the Director of Operations to the Director of Finance. (pages 9&10) o that the Director of Operations is also the Deputy Chief Executive (page 10) U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 2
218 Paper 08 The role of the Council of Governors has been updated to include the duties set out in the Health and Social Care Act (page 11) The composition of the Council of Governors has been updated to reflect the current constitution, this will require a further update once any changes have been made in response to the Health and Social Care Act. (page 11). The matters reserved to the Board o Inclusion of decision to increase Non NHS activity by more than 5% of total income (page 17) o Approval of the Trust Constitution (page 19) Membership and responsibility of key committees. The current Terms of Reference (TOR) have been amended to include: o Audit committee TOR amended to include clarification of its role in the oversight of Information Governance. (page 23) o The paper previously approved by the Board setting out the risk management duties of the Audit Committee and its interaction with the other committees has been included (page 26) o The TORs for Audit, Quality & Safety, Business Risk and Investment Committees have been amended to include the authority to approve policies. (pages 25, 32, 29) o The Nominations and Remunerations Committee has been changed to the Remuneration Committee as this more accurately reflects its duties. Recommendations That the Board approve the adoption of the Standards for NHS Board members. That the Board approves the proposed changes to the Board Governance Arrangements Document, as shown above. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 3
219 Paper 08 BOARD GOVERNANCE FOR RJAH THE ROBERT JONES AND AGNES HUNT ORTHOPAEDIC HOSPITAL NHS FOUNDATION TRUST The Board of Directors Contents 1. The collective role of the Board 2. The composition of the Board 3. The operation of the Board 4 The Standards for NHS Board Members Individual roles within the Board of Directors Non-executive roles 1. All non-executive directors 2. Trust Chairman 3. Deputy Chairman 4. Senior Independent Director Executive roles 5. Chief Executive and Accounting Officer 6. Finance Director 7. Medical Director 8. Director of Nursing 9. Director of Operations Board support 10. Foundation Trust Secretary Reservation and delegation of responsibilities 1. Matters reserved to the Board of Directors 2. Delegation to officers 3. Delegation to committees of the Board: The Council of Governors 1. The role of the Council of Governors 2. The composition of the Council of Governors 3. The operation of the Council of Governors Appendices: A: NHS Board Standards B: Code of Conduct for NHS Managers C: A: Statement on the division of responsibilities between the Trust Chairman and the Chief Executive D:B: Schedule of matters reserved to the Board E:C: Membership and key responsibilities of Board committees C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 1 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 4
220 Paper 08 DF: Job Descriptions : Board Directors 1. The collective role of the Board THE BOARD OF DIRECTORS The collective role of the Board of Directors is to: The general duty of the Board of Directors and of each director individually, is to act with a view to promoting the success of the trust so as to maximise the benefits for the members of the trust as a whole and for the public.( Health and Social Care Act 2012) - Formulate Strategy - Ensuring accountability by holding the organisation to account for the delivery of the strategy and through seeking assurance that systems of control are robust provide active leadership of the Trust within a framework of prudent and effective controls which enables risk to be assessed and managed Formatted: Normal, Space After: 0 pt, Bulleted + Level: 1 + Aligned at: 0 cm + Tab after: 0.6 cm + Indent at: 0.6 cm, Don't adjust space between Latin and Asian text, Don't adjust space between Asian text and numbers Formatted: Bullets and Numbering Formatted: Normal, Indent: Left: 0 cm, Space After: 0 pt, Don't adjust space between Latin and Asian text, Don't adjust space between Asian text and numbers Formatted: Indent: Left: 0 cm, Hanging: 0.63 cm ensure compliance by the Trust with its terms of authorisation, its Constitution, mandatory guidance issued by Monitor, relevant statutory requirements and contractual obligations set the Trust's strategic aims, taking into consideration the views of the Council of Governors and ensuring that the necessary financial and human resources are in place for the Trust to meet its objectives, and to review management performance ensure the quality and safety of healthcare services, education, training and research delivered by the Trust and apply the principles and standards of clinical governance set out by the Department of Health, the Care Quality Commission and other relevant NHS bodies ensure that the Trust exercises its functions effectively, efficiently and economically set the Trust s values and standards of conduct and ensure that its obligations to its members, patients and other stakeholders are understood and met 2. The composition of the Board The Board of Directors will comprises: a non-executive Chairman no fewer than four and no more than six other non-executive directors one of the non-executive directors will act as the vice chair one of the non-executive directors will act as the senior independent director Formatted: Bullets and Numbering Formatted: Bullets and Numbering C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 2 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 5
221 Paper 08 no fewer than four and no more than six executive directors, including a Chief Executive, a Finance Director, a registered medical practitioner or registered dentist and a registered nurse or registered midwife At any time, at least half the Board (excluding the Chairman) will be made up of nonexecutive directors. RJAH Trust Board is constituted as follows: Board Structure Non Executive Directors Chairman Non Executive Director Non Executive Director (Chair of Audit Committee) Non Executive Director (Chair of Quality and Safety Committee) Non Executive Director (Chair of Business Risk And Investment Committee) Non Executive Director The position of Vice Chairman is currently held by the Chair of the Business Risk and Investment Committee. Board Structure Executive Directors Chief Executive Director of Finance and Performance Director of Operations Director of Nursing Medical Director The Trust has a Foundation Trust Secretary to support the work of the Board. This role will also support the Council of Governors. 3. The operation of the board The Board of Directors operates as a unitary body which is collectively responsible for the performance of the Trust and the exercise of its statutory powers. Accordingly all directors, whether executive or non-executive: have joint responsibility for every decision of the Board and are required to take decisions objectively in the interests of the Trust C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 3 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 6
222 Paper 08 are responsible for leading and directing the Trust's activities and for helping to develop proposals on strategy are responsible for monitoring the conduct and performance of management and for constructively challenging the decisions of the Board are responsible for adding value and promoting the success of the Trust 4. Standards for NHS Board members Formatted: Bullets and Numbering The Board has adopted the Standards for members of NHS Boards and Clinical Commissioning Group governing bodies in England, which has been developed by the Professional Standards Authority (November 2012) All members of the Board are expected to adhere to these standards. The Standards are attached at Appendix A In addition to this all managers in the Trust are required to comply with the Code of Conduct for NHS Mangers Formatted: Left A copy of the code is attached at Appendix B C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 4 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 7
223 Paper 08 INDIVIDUAL ROLES WITHIN THE BOARD OF DIRECTORS 1. All non-executive directors Non-executive roles The Board of Directors is a unitary body which is collectively responsible for the performance of the Trust and the exercise of its statutory powers. Within the unitary Board, all directors, whether executive or non-executive, have joint responsibility for every decision of the Board and are required to take decisions objectively in the interests of the Trust. Non-executive as well as executive directors are responsible for leading and directing the Trust's activities and for helping to develop proposals on strategy. Conversely, executive as well as non-executive directors are responsible for monitoring the conduct and performance of management and for constructively challenging the decisions of the Board As part of their role as members of the unitary Board, non-executive directors have a particular duty to ensure that the decisions of the Board are subject to constructive challenge and to scrutinise management performance in meeting agreed goals and objectives. In addition, non-executive directors who are determined by the Board to be independent in character and judgement and free from any business or other relationship which could materially interfere with the exercise of their judgement will be responsible, as the members of key committees of the Board, for: monitoring the integrity of financial, clinical and other information ensuring that financial and clinical quality controls and systems of risk management are robust determining appropriate levels of remuneration of executive directors playing a prime supporting role in appointing and, where necessary, removing executive directors, and in succession planning 2. Trust Chairman The Trust Chairman provides leadership for the Board of Directors and the Council of Governors and ensure their effectiveness in all aspects of their role and agenda. Key responsibilities include: ensuring the provision of accurate, timely and clear information to directors and governors facilitating the effective contribution of non-executive directors, executive directors and governors and ensuring constructive relations between them ensuring that the Board establishes clear objectives for the delivery of agreed plans and meeting the Trust's terms of authorisation and regularly reviews performance against these objectives C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 5 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 8
224 Paper 08 A statement on the division of responsibilities between the Trust Chairman and the Chief Executive, as agreed by the Board of Directors, is attached as Appendix A to this document. 3. Deputy Chairman The Deputy Chairman will beis appointed from amongst the Trust's non-executive directors by the Council of Governors. Where the Trust Chairman has died or has ceased to hold office, or where he or she is unable to perform his or her duties as Chairman owing to illness, conflict of interest or any other cause, the Deputy Chairman will: preside at meetings of the Board of Directors and the Council of Governors exercise all the authorities vested in the Trust Chairman by the Standing Orders of those bodies, including the right to a casting vote where necessary. 4. Senior Independent Director The Senior Independent Director is to be appointed from amongst the Trust's independent non-executive directors by the Board of Directors, in consultation with the Council of Governors. In addition to his or her responsibilities as a non-executive director, the Senior Independent Director will: lead the non-executive directors in the evaluation of the Trust Chairman's performance as part of a process agreed with the Council of Governors convene a meeting of the non-executive directors, without the Trust Chairman, at least annually and on such other occasions as are deemed appropriate be available to members and governors if they have concerns which contact through the normal channels of Trust Chairman, Chief Executive or Finance Director has failed to resolve or for which such contact is inappropriate maintain sufficient contact with, and attend sufficient meetings of, the governors to listen to their views in order to help develop a balanced understanding of their issues and concerns. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 6 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 9
225 Paper 08 INDIVIDUAL ROLES WITHIN THE BOARD OF DIRECTORS Executive roles 5. Chief Executive and Accounting Officer The Chief Executive will manage the Trust in accordance with the values, objectives, policies and specific decisions of the Board of directors and ensure that all activities are directed towards their achievement. Key responsibilities include: evaluating present and future opportunities, threats and risks in the external environment and current and future strengths, weaknesses and risks to the Trust producing the annual business plan and ensuring that it is geared to achieving he Trust's vision and strategy managing executive directors and senior managers and developing effective working relationships and communications with other staff ensuring that the Board of Directors is given the advice and information it needs to perform its duties and that the business of the Board is properly conducted establishing systems of control and limits of delegation and providing the Board of Directors with regular assurance on their effectiveness establishing strong systems for performance management, focused on continuous improvement in the delivery of services, and maintaining close relationships with relevant regulatory bodies promoting effective joint working with external stakeholders and other key partners In his or her capacity as the Accounting Officer, the Chief Executive has personal responsibility for: the propriety and regularity of public finances, the keeping of proper accounts, prudent and economical administration, the avoidance of waste and extravagance and the efficient and effective use of the Trust's resources ensuring that appropriate advice is tendered to the Board of Directors and the Council of Governors on all matters of financial propriety and regularity, prudent and economical administration, efficiency and effectiveness if necessary, informing Monitor of any proposed course of action which might infringe the requirements of financial propriety and regularity, prudent and economical administration, efficiency and effectiveness appearing before the Public Accounts Committee as required to give evidence on any report by the Comptroller & Auditor General on the economy, efficiency and effectiveness with which the Trust has used its resources A statement on the division of responsibilities between the Trust Chairman and the Chief Executive, as agreed by the Board of Directors, is attached as Appendix A to this document. 6. Finance Director The Finance Director will advise the Chief Executive, the Board of Directors and the Council of Governors on all aspects of financial strategy and financial management. Key responsibilities include: C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 7 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 10
226 Paper 08 providing strategic leadership for finance across the organisation and helping to strengthen its contribution to the Trust s activities providing comprehensive financial services to the Trust including the production of budget proposals, the development of effective budgetary control systems, the provision of accurate and timely information and advice and the compilation of monthly management returns and year-end accounts for statutory and regulatory purposes managing financial agreements between the Trust and its stakeholders effectively in order to ensure appropriate recovery of costs overseeing all financial systems and internal controls, including the development and modification of accounting systems when required managing relationships with the Trust's internal and external auditors Providing strategic leadership for the development of the Trust s Estate, ensuring its contribution to the Trust s activities. ensure the Trust has a robust IM&T strategy in place to support the objectives of the organisation. Ensure that there ae robust systems in place to provide the Board with high quality data to support performance management and decision making Formatted: Bullets and Numbering Formatted: Bullets and Numbering Formatted: Font: (Default) Arial, 11 pt Formatted: Bullets and Numbering 7. Medical Director The Medical Director will advise the Chief Executive, the Board of Directors and the Council of Governors on medical and clinical matters, including compliance with national policy, and will provide professional leadership to all medical staff within the Trust. Key responsibilities, carried out in collaboration with other executive directors, include: developing a culture within the Trust which promotes clinical governance and ensures its effectiveness planning and implementing the clinical services strategy for the Trust leading the Trust s relationships with bodies representing general practitioners and with the medical schools associated with the Trust leading on medical workforce planning and developing plans for the Trust and the wider health economy taking the lead on research on behalf of the Trust and developing relationships with universities and the wider research community 8. Director of Nursing The Director of Nursing will advise the Chief Executive, the Board of Directors and the Council of Governors on nursing matters, including compliance with national C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 8 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 11
227 Paper 08 policy, and will provide professional leadership to all nursing staff and Allied Health Professionals within the Trust. Key responsibilities include: developing and implementing nursing policies that achieve the Trust s strategic direction fostering a culture that values continuing professional development and strives for excellence in the delivery of patient care in collaboration with the Medical Director, developing the clinical governance culture of the Trust and monitoring its effectiveness leading patient and public involvement in the Trust and managing the Patient Advice and Liaison Service (PALS) and complaints service 9. Director of Operations The Director of Operations will advise the Chief Executive, the Board of Directors and the Council of Governors regarding the delivery of operational performance within the Trust. The post carries Board level responsibility for Risk including compliance with Health and Safety legislation The Director of Nursing will advise the Chief Executive, the Board of Directors and the Council of Governors on nursing matters, including compliance with national policy, and will provide professional leadership to all nursing staff and Allied Health Professionals within the Trust. Key responsibilities include: - Deputy Chief Executive - Providing strategic leadership for the development of the Trust s Estate, ensuring its contribution to the Trust s activities. - Ensuring the delivery of operational activity in accordance with agreements between the Trust and its stakeholders and national targets. - Meet agreed targets and objectives, and deliver within defined costs, timescales and resources. - Board responsibility for Health and Safety. 10. Foundation Trust Secretary Board and Council Support All directors and governors have access to the advice and services of the Trust Secretary, who has the following primary responsibilities: ensuring good information flows within the Board of Directors, the Council of Governors and their committees and between senior management, non-executive directors and governors ensuring that the procedures and Standing Orders of the Board of Directors and the Council of Governors are complied with C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 9 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 12
228 Paper 08 advising the Board of Directors and the Council of Governors (through the chairman) on all governance matters supporting the induction of new directors and governors and assisting with their professional development C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 10 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 13
229 Paper 08 RESERVATION AND DELEGATION OF RESPONSIBILITIES 1. Matters reserved to the Board As recommended by the NHS Foundation Trust Code of Governance, the Board of Directors has expressly reserved certain key matters for its collective consideration and decision. The schedule of matters reserved to the Board of Directors is set out in Appendix B to this document. 2. Delegation to officers Matters which the Board of Directors considers suitable for delegation to individual directors and officers of the Trust are contained in the Scheme of Delegation and Standing Financial Instructions (SFIs), which are regularly reviewed and revised by the Board. 3. Delegation to committees of the Board The Board of Directors has established the following committees, all of which are chaired by non-executive directors, to exercise delegated responsibilities on behalf of the Board: Audit Committee Quality & Safety Committee Business Risk & Investment Committee Nomination & Remuneration Committee The membership and key responsibilities of these committees of the Board are summarised in Appendix C to this document. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 11 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 14
230 Paper 08 THE COUNCIL OF GOVERNORS 1. The role of the Council of Governors The specific statutory powers and duties of the Council of Governors are to:-the general duties of the Council of Governors are to hold the non-executive directors individually and collectively to account for the performance of the Board of Directors, and Formatted: Indent: Left: 1.27 cm to represent the interests of the members of the trust as a whole and the interests of the public. (Health & Social care act 2012) The specific statutory powers and duties of the Council of Governors are to: appoint and, if appropriate, remove the Trust Chairman appoint and, if appropriate, remove the other non-executive directors decide the remuneration and allowances, and the other terms and conditions of office, of the Chair and the other non-executive directors approve the appointment of the Chief Executive appoint and, if appropriate, remove the External Auditor receive the Trust s annual accounts, any report of the External Auditor on them and the annual report. approve significant transactions, including plans to increase the proportion of income received from activities other than the health service in England by 5% Formatted: Bullets and Numbering In addition, in preparing the Trust s forward plan, the Board of Directors must have regard to the views of the Council of Governors. In exercising its powers and duties, governors are required by the NHS Foundation Trust Code of Governance to: represent the interests of Trust members and Partnership Organisations in the governance of the Trust act in the best interests of the Trust and adhere to its values and code of conduct hold the Board of Directors collectively to account for the Trust's performance and ensure that the Board of Directors acts in such a way that the Trust does not breach the terms of its Authorisation feed back information about the Trust, its vision and its performance to the constituencies and stakeholder organisations that elected or appointed them. 2. The composition of the Council of Governors In accordance with the Trust's Constitution, the Council of Governors will consist of governors, to be composed as follows: eleven ten governors elected by the Public Constituency three governors elected by the Staff Constituency seven six governors elected by Partnership Organisations, appointed by Shropshire County PCT and including one governor appointed by Shropshire Council. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 12 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 15
231 Paper The operation of the Council of Governors Meetings of the Council of Governors will be held at least four times a year, one of which will be an AGM. The Council of Governors is not permitted to delegate any of its powers or responsibilities to any committee or individual governor, but is able to appoint committees to assist it in the proper performance of its functions. The Trust's Constitution provides for the appointment by the Council of Governors of an ad hoc Nomination Committee for the purpose of making recommendations to it on each exercise of its powers to appoint and re-appoint the Trust Chairman and other non-executive directors and to remove another non-executive director (including the Trust Chairman). C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 13 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 16

232 Paper 08 Appendix A Standards for members of NHS boards and Clinical Commissioning Group governing bodies in England All members of NHS boards and CCG governing bodies should understand and be committed to the practice of good governance and to the legal and regulatory frameworks in which they operate. As individuals they must understand both the extent and limitations of their personal responsibilities. To justify the trust placed in me by patients, service users, and the public, I will abide by these Standards at all times when at the service of the NHS. I understand that care, compassion and respect for others are central to quality in healthcare; and that the purpose of the NHS is to improve the health and well-being of patients and service users, supporting them to keep mentally and physically well, to get better when they are ill and, when they cannot fully recover, to stay as well as they can to the end of their lives. I understand that I must act in the interests of patients, service users and the community I serve, and that I must uphold the law and be fair and honest in all my dealings. Professional Standards Authority Buckingham Palace Road, London SW1W 9SP Telephone: info@professionalstandards.org.uk Web: Professional Standards Authority, November 2012 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 17
233 Paper 08 Appendix A Personal behaviour 1. As a Member 1 I commit to: The values of the NHS Constitution Promoting equality Promoting human rights in the treatment of patients and service users, their families and carers, the community, colleagues and staff, and in the design and delivery of services for which I am responsible. 2. I will apply the following values in my work and relationships with others: Responsibility: I will be fully accountable for my work and the decisions that I make, for the work and decisions of the board 2, including delegated responsibilities, and for the staff and services for which I am responsible Honesty: I will act with honesty in all my actions, transactions, communications, behaviours and decision-making, and will resolve any conflicts arising from personal, professional or financial interests that could influence or be thought to influence my decisions as a board member Openness: I will be open about the reasoning, reasons and processes underpinning my actions, transactions, communications, behaviours and decision-making and about any conflicts of interest Respect: I will treat patients and service users, their families and carers, the community, colleagues and staff with dignity and respect at all times Professionalism: I will take responsibility for ensuring that I have the relevant knowledge and skills to perform as a board member and that I reflect on and identify any gaps in my knowledge and skills, and will participate constructively in appraisal of myself and others. I will adhere to any professional or other codes by which I am bound Leadership: I will lead by example in upholding and promoting these Standards, and use them to create a culture in which their values can be adopted by all Integrity: I will act consistently and fairly by applying these values in all my actions, transactions, communications, behaviours and decision-making, and always raise concerns if I see harmful behaviour or misconduct by others. 1 The term Member is used throughout this document to refer to members of NHS boards and CCG governing bodies in England. 2 The term board is used throughout this document to refer collectively to NHS boards and CCG governing bodies in England. Standards for members of NHS boards and CCG governing bodies in England U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 18
234 Paper 08 Appendix A Technical competence 3. As a Member, for myself, my organisation, and the NHS, I will seek: Excellence in clinical care, patient safety, patient experience, and the accessibility of services To make sound decisions individually and collectively Long term financial stability and the best value for the benefit of patients, service users and the community. 4. I will do this by: Always putting the safety of patients and service users, the quality of care and patient experience first, and enabling colleagues to do the same Demonstrating the skills, competencies, and judgement necessary to fulfil my role, and engaging in training, learning and continuing professional development Having a clear understanding of the business and financial aspects of my organisation s work and of the business, financial and legal contexts in which it operates Making the best use of my expertise and that of my colleagues while working within the limits of my competence and knowledge Understanding my role and powers, the legal, regulatory, and accountability frameworks and guidance within which I operate, and the boundaries between the executive and the non-executive Working collaboratively and constructively with others, contributing to discussions, challenging decisions, and raising concerns effectively Publicly upholding all decisions taken by the board under due process for as long as I am a member of the board Thinking strategically and developmentally Seeking and using evidence as the basis for decisions and actions Understanding the health needs of the population I serve Reflecting on personal, board, and organisational performance, and on how my behaviour affects those around me; and supporting colleagues to do the same Looking for the impact of decisions on the services we and others provide, on the people who use them, and on staff Listening to patients and service users, their families and carers, the community, colleagues, and staff, and making sure people are involved in decisions that affect them Communicating clearly, consistently and honestly with patients and service users, their families and carers, the community, colleagues, and staff, and ensuring that messages have been understood Respecting patients rights to consent, privacy and confidentiality, and access to information, as enshrined in data protection and freedom of information law and guidance. Standards for members of NHS boards and CCG governing bodies in England U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 19
235 Paper 08 Appendix A Business practices 5. As a Member, for myself and my organisation, I will seek: To ensure my organisation is fit to serve its patients and service users, and the community To be fair, transparent, measured, and thorough in decision-making and in the management of public money To be ready to be held publicly to account for my organisation s decisions and for its use of public money. 6. I will do this by: Declaring any personal, professional or financial interests and ensuring that they do not interfere with my actions, transactions, communications, behaviours or decision-making, and removing myself from decision-making when they might be perceived to do so Taking responsibility for ensuring that any harmful behaviour, misconduct, or systems weaknesses are addressed and learnt from, and taking action to raise any such concerns that I identify Ensuring that effective complaints and whistleblowing procedures are in place and in use Condemning any practices that could inhibit or prohibit the reporting of concerns by members of the public, staff, or board members about standards of care or conduct Ensuring that patients and service users and their families have clear and accessible information about the choices available to them so that they can make their own decisions Being open about the evidence, reasoning and reasons behind decisions about budget, resource, and contract allocation Seeking assurance that my organisation s financial, operational, and risk management frameworks are sound, effective and properly used, and that the values in these Standards are put into action in the design and delivery of services Ensuring that my organisation s contractual and commercial relationships are honest, legal, regularly monitored, and compliant with best practice in the management of public money Working in partnership and co-operating with local and national bodies to support the delivery of safe, high quality care Ensuring that my organisation s dealings are made public, unless there is a justifiable and properly documented reason for not doing so. Standards for members of NHS boards and CCG governing bodies in England U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 20
236 Paper 08 Appendix B Code of Conduct for NHS Managers October 2002 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 21
237 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 22 Paper 08 Appendix B
238 Paper 08 Appendix B Code of Conduct for NHS Managers U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 23
239 Paper 08 Appendix B Crown Copyright 2002 Produced by Department of Health p 1k Oct 02 (CWP) CHLORINE FREE PAPER The text of this document may be reproduced without formal permission or charge for personal or in-house use. First published October /Code of Conduct for NHS Managers can also be made available on request in braille, on audio cassette tape, on disk, in large print, and in other languages on request. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 24
240 Paper 08 Appendix B Introduction 1. As part of the response to the Kennedy Report, the attached Code of Conduct for NHS Managers has been produced by a Working Group chaired by Ken Jarrold CBE. 2. The Code sets out the core standards of conduct expected of NHS managers. It will serve two purposes: to guide NHS managers and employing health bodies in the work they do and the decisions and choices they have to make. to reassure the public that these important decisions are being made against a background of professional standards and accountability. 3. The environment in which the Code will operate is a complex one. NHS managers have very important jobs to do and work in a very public and demanding environment. The management of the NHS calls for difficult decisions and complicated choices. The interests of individual patients have to be balanced with the interests of groups of patients and of the community as a whole. The interests of patients and staff do not always coincide. Managerial and clinical imperatives do not always suggest the same priorities. A balance has to be maintained between national and local priorities. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements Introduction 1 25
241 4. The Code should apply to all managers and should be incorporated in the contracts of senior managers at the earliest possible opportunity. A document on implementation is attached. Paper 08 Appendix B NIGEL CRISP 9 October 2002 NHS Chief Executive U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 2 Code of Conduct for NHS Managers 26
242 Paper 08 Appendix B Code of Conduct for NHS Managers As an NHS manager, I will observe the following principles: make the care and safety of patients my first concern and act to protect them from risk; respect the public, patients, relatives, carers, NHS staff and partners in other agencies; be honest and act with integrity; accept responsibility for my own work and the proper performance of the people I manage; show my commitment to working as a team member by working with all my colleagues in the NHS and the wider community; take responsibility for my own learning and development. This means in particular that: 1 I will: respect patient confidentiality; use the resources available to me in an effective, efficient and timely manner having proper regard to the best interests of the public and patients; U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements Code of Conduct for NHS Managers 3 27
243 be guided by the interests of the patients while ensuring a safe working environment; act to protect patients from risk by putting into practice appropriate support and disciplinary procedures for staff; and seek to ensure that anyone with a genuine concern is treated reasonably and fairly. 2 I will respect and treat with dignity and fairness, the public, patients, relatives, carers, NHS staff and partners in other agencies. In my capacity as a senior manager within the NHS I will seek to ensure that no one is unlawfully discriminated against because of their religion, belief, race, colour, gender, marital status, disability, sexual orientation, age, social and economic status or national origin. I will also seek to ensure that: the public are properly informed and are able to influence services; patients are involved in and informed about their own care, their experience is valued, and they are involved in decisions; relatives and carers are, with the informed consent of patients, involved in the care of patients; partners in other agencies are invited to make their contribution to improving health and health services; and NHS staff are: valued as colleagues; properly informed about the management of the NHS; given appropriate opportunities to take part in decisionmaking. given all reasonable protection from harassment and bullying; provided with a safe working environment; helped to maintain and improve their knowledge and skills and achieve their potential; and helped to achieve a reasonable balance between their working and personal lives. 3 I will be honest and will act with integrity and probity at all times. I will not make, permit or knowingly allow to be made, any untrue or misleading statement relating to my own duties or the functions of my employer. Paper 08 Appendix B U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 4 Code of Conduct for NHS Managers 28
244 Paper 08 Appendix B I will seek to ensure that: the best interests of the public and patients/clients are upheld in decision-making and that decisions are not improperly influenced by gifts or inducements; NHS resources are protected from fraud and corruption and that any incident of this kind is reported to the NHS Counter Fraud Services; judgements about colleagues (including appraisals and references) are consistent, fair and unbiased and are properly founded; and open and learning organisations are created in which concerns about people breaking the Code can be raised without fear. 4 I will accept responsibility for my own work and the proper performance of the people I manage. I will seek to ensure that those I manage accept that they are responsible for their actions to: the public and their representatives by providing a reasonable and reasoned explanation of the use of resources and performance; patients, relatives and carers by answering questions and complaints in an open, honest and well researched way and in a manner which provides a full explanation of what has happened, and of what will be done to deal with any poor performance and, where appropriate giving an apology; and NHS staff and partners in other agencies by explaining and justifying decisions on the use of resources and give due and proper consideration to suggestions for improving performance, the use of resources and service delivery. I will support and assist the Accountable Officer of my organisation in his or her responsibility to answer to Parliament, Ministers and the Department of Health in terms of fully and faithfully declaring and explaining the use of resources and the performance of the local NHS in putting national policy into practice and delivering targets. For the avoidance of doubt, nothing in paragraphs two to four of this Code requires or authorises an NHS manager to whom this Code applies to: make, commit or knowingly allow to be made any unlawful disclosure; make, permit or knowingly allow to be made any disclosure in breach of his or her duties and obligations to his or her employer, save as permitted by law. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements Code of Conduct for NHS Managers 5 29
245 If there is any conflict between the above duties and obligations and this Code, the former shall prevail. 5 I will show my commitment to working as a team by working to create an environment in which: teams of frontline staff are able to work together in the best interests of patients; leadership is encouraged and developed at all levels and in all staff groups; and the NHS plays its full part in community development. 6 I will take responsibility for my own learning and development. I will seek to: take full advantage of the opportunities provided; keep up to date with best practice; and share my learning and development with others. Paper 08 Appendix B Department of Health October 2002 U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 6 Code of Conduct for NHS Managers 30
246 Paper 08 APPENDIX AC DIVISION OF RESPONSIBILITIES BETWEEN THE TRUST CHAIRMAN AND THE CHIEF EXECUTIVE The following division of responsibilities between the Chairman and the Chief Executive has been agreed by the Board of Directors. Key responsibilities Chairman: managing the business of the Board of Directors and the Council of Governors so as to ensure their effective performance promoting the highest levels of integrity, probity and corporate governance and ensuring that these standards are embodied in the conduct of the Board of Directors and the Council of Governors ensuring that the Board as a whole is able to play a full and constructive role in the development of the Trust's strategy and business aims ensuring that the Board pays sufficient attention to the development of the Trust's business and the protection of its reputation Chief Executive: executive management of the Trust's business consistent with the strategic and business objectives agreed by the Board as a whole ensuring that the affairs of the Trust are carried out in accordance with the highest standards of integrity, probity and corporate governance and that these standards are embedded at all levels ensuring that the strategy and business aims set by the Board are aligned with statutory, regulatory and contractual requirements formulating annual objectives, budgets and operational plans to deliver the strategy and business objectives set by the Board Detailed responsibilities a) Board of Directors Chairman: setting the Board's agenda and managing the conduct of its business ensuring that all directors receive accurate, timely and clear information on performance, the issues, challenges and opportunities facing the Trust and matters which are reserved to the Board for decision Chief Executive: leading, motivating and directing the other executive directors and senior managers ensuring that the Board is given the advice and information it needs to carry out its duties effectively and (in consultation with the Chairman) that the business of the Board is properly conducted C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 14 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 31
247 Paper 08 facilitating the effective contribution of all directors and ensuring constructive relationships between executive directors and NEDs ensuring that NEDs receive full, formal and tailored induction and participate in the Board development programme ensuring that the Board undertakes and acts on formal and rigorous evaluation of its own performance and that of its committees appraising the performance of NEDs and acting on the outcomes of performance evaluation where necessary promoting the effective contribution of executive directors and senior managers to the proceedings of the Board and its committees contributing to induction programmes for new directors and ensuring that management time is made available for this purpose. providing input to the evaluation of the performance of the Board and its committees appraising the performance of executive directors in their corporate and functional roles. b) Council of Governors Chairman: leading the Council of Governors and setting its agendas ensuring that governors receive accurate, timely and clear information that is appropriate for their duties ensuring that governors receive full, formal and tailored induction and are enabled to update their skills, knowledge and familiarity with the Trust leading the Council of Governors in periodically assessing its collective performance ensuring constructive relationships between the Board of Directors and the Council of Governors and that the views of governors and members are Chief Executive: facilitating the work of the Council of Governors and its committees, ensuring that they have sufficient resources and are able to meet sufficiently regularly to discharge their duties ensuring that the Council of Governors is given the advice and information it needs to carry out its duties effectively and (in consultation with the Chairman) that the business of the Council of Governors is properly conducted contributing to induction and development programmes for governors and ensuring that management time is available for this purpose. providing input to the assessment of the performance of the Council of Governors ensuring that the views of governors and members are taken into account in the conduct of the Trust's business and the C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 15 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 32
248 Paper 08 communicated to the Board development of its strategic aims c) Stakeholders Formatted Table Chairman being a visible and accessible figurehead for the Trust's staff and the leading champion of its vision, values and objectives taking the lead at ceremonial events and other corporate formalities promoting mutual understanding with external partners and stakeholder bodies through dialogue with their non-executive or elected leads supporting the Chief Executive in contacts with MPs and other political figures taking the lead at public meetings and events and with voluntary groups, as the public face of the Trust, with the participation of the Chief Executive as appropriate acting as a confidential sounding board for the Chief Executive on key issues and decisions and providing advice, support or challenge as appropriate Chief Executive performing the role of senior line manager and employer taking the lead on employee relations and internal communications on operational matters fostering good working relationships with external partners and stakeholders through the conduct of business with their executive officer leads taking the lead on contact with MPs and other political figures, with the participation of the Chairman as appropriate taking the lead on communications with the media, with the participation of the Chairman as appropriate informing and consulting the Chairman on key issues and decisions and ensuring that the Chairman is aware of emerging opportunities and threats to the achievement of objectives d) Accountability Chairman accountable to the Board of Directors and the Council of Governors for the effective conduct of their activities Chief Executive accountable to the Chairman (acting on behalf of the Board) and to the Board direct C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 16 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 33
249 Paper 08 e) Reporting lines Chairman The Chairman is not responsible for the executive management of the Trust. Other than the Chief Executive and (in respect of matters relating directly to the Board of Directors or the Council of Governors) the Trust Secretary, no executive director, senior manager or other member of staff reports to the Chairman other than through the Board Chief Executive The Chief Executive is responsible for all executive management matters relating to the Trust. All members of executive management report, directly or indirectly, to the Chief Executive. The appointment and removal of the Trust Secretary is a matter for the Chairman and the Chief Executive jointly C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 17 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 34
250 Paper 08 APPENDIX BD SCHEDULE OF MATTERS RESERVED TO THE BOARD OF DIRECTORS The matters set out in the schedule below are specifically reserved for the collective decision of the Board of Directors. 1. STRATEGY AND MANAGEMENT 1.1 Responsibility for the overall management of the Trust 1.2 Approval of the Trust's long-term objectives and business strategy 1.3 Approval of the annual operating and capital expenditure budgets and any material changes to them 1.4 Oversight of the Trust's operations ensuring: competent and prudent management sound planning an adequate system of internal control adequate accounting and other records compliance with its terms of authorisation, constitution, mandatory guidance issued by the independent regulator, relevant statutory requirements and contractual obligations the quality and safety of healthcare services, education, training and research delivered by the Trust the application of the principles and standards of clinical governance set out by the Department of Health, the Care Quality Commission and other relevant NHS bodies 1.5 Review of performance in the light of the Trust's strategy, objectives, business plans and budgets and ensuring that any necessary corrective action is taken 1.6 Extension of the Trust's activities into new business areas 1.7 Any decision to cease to operate all or a material part of the Trust's business 1.8 Ratify decisions made under emergency powers 1.9 Any decision to increase by 5% or more the proportion of its total income attributable to activities other than the provision of goods and services for the purposes of health service, subject to approval by the Council of Governors C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 18 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 35
251 Paper CORPORATE STRUCTURE AND STATUS 2.1 Major changes to the Trust's corporate structure 2.2 Major changes to the Trust's management and control structure 2.3 Any changes to the Trust's status as an NHS Foundation Trust 2.4 Any proposal to establish a subsidiary company, joint venture or other corporate vehicle for the purpose of carrying out any current or proposed activity of the Trust 2.5 Any proposal involving a merger of the Trust with or takeover of the Trust by another organisation 2.6 Any acquisition or disposal of land 2.7 Any application to a planning authority for planning permission 2.7 Any proposal involving the Trust operating in another organisation (whether within the NHS or not) in the provision of services 2.9 Any use of the RJAH name or brand by another organisation for any purpose. 3. FINANCIAL REPORTING AND CONTROLS 3.1 Approval of the quarterly financial report to the Independent Regulator. 3.2 Approval of the annual report and accounts, including the corporate governance statement and the remuneration report 3.3 Approval of any significant changes in accounting policies or practices 3.4 Approval of treasury policies, including foreign currency exposure and the use of financial derivatives 3.5 Receive Annual Audit Letter 4. INTERNAL CONTROLS 4.1 Ensuring the maintenance of a sound system of internal control and risk management including: receiving reports on, and reviewing the effectiveness of, the group's risk and control processes to support its strategy and objectives undertaking an annual assessment of these processes approving an appropriate statement for inclusion in the annual report Approving Standing Financial Instructions. 5. CONTRACTS 5.1 Major capital projects and Business Cases 5.2 Contracts which are material, strategically or by reason of size, or length of commitment entered into by the Trust in the ordinary course of business. Contracts, other than NHS, over 250k or three years in duration. 5.3 Contracts entered into by the Trust which are not in the ordinary course of C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 19 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 36
252 Paper 08 its business. 6. COMMUNICATION 6.4 Approval of formal submissions to the Department of Health, the Independent Regulator, the Care Quality Commission and other relevant NHS bodies concerning the Trust's compliance with applicable targets and standards 7. BOARD MEMBERSHIP AND OTHER APPOINTMENTS 7.1 Nomination of a Deputy Chairman for formal appointment by the Council of Governors 7.2 Appointment of the Senior Independent Director in consultation with the Council of Governors 7.3 Establishment, Membership and chairmanship of Board committees 7.4 Nomination of Board representatives to any joint committee of the Board of Directors and the Council of Governors that may be established from time to time for any purpose 7.5 Continuation of any director in office at any time, including the suspension or termination of service of an executive director as an employee of the Trust, subject to the law and their service contract 7.6 Appointments to the boards of any subsidiary company, joint venture or other corporate vehicle established by the Trust for the purpose of carrying out any current or proposed activity 8. DELEGATION OF AUTHORITY 8.1 Approval of the statement on the division of responsibilities between the Chairman and the Chief Executive, which should be in writing 8.2 Approval and review of the terms of reference of Board committees 8.3 Receiving reports from Board committees on their activities 9. CORPORATE GOVERNANCE MATTERS 9.1 Approval of the Trust Constitution, in conjunction with the Council of Governors 9.2 Undertaking at least annually a formal and rigorous review of the Board's own performance and that of its committees and individual directors 9.3 Determining the independence of non-executive directors 9.4 Review of the Trust's overall corporate governance arrangements 9.5 Receiving reports on the views of the Trust's members, patients, carers and members of the public 10. POLICIES 10.1 Approval and revision of Trust-wide Policy Management guidance 10.2 Approval of key policies of general application throughout the Trust, including: C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 20 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 37
253 Paper OTHER codes of conduct health and safety policy whistle blowing business continuity risk management 11.1 Approval of the appointment of the Trust's principal professional advisers, with the exception of the external auditor 11.2 Decisions relating to overall levels of insurance for the Trust, including proposals for the purchase of commercial directors' and officers' liability insurance and indemnification of directors Approve the arrangements relating to the discharge of the Trusts responsibilities as a corporate trustee for funds held on trust 11.4 This schedule of matters reserved for board decisions Matters which the Board considers suitable for delegation are contained in the terms of reference of its committees and in the scheme of delegation. In addition, the Board will receive reports and recommendations from time to time on any matter which it considers significant to the Trust. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 21 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 38
254 Paper 08 APPENDIX CE MEMBERSHIP AND KEY RESPONSIBILITIES OF BOARD COMMITTEES 1. Constitution Audit Committee Terms of Reference The Board hereby resolves to establish a Committee of the Board to be known as the Audit Committee. The Committee is a non-executive Committee of the Board and has no executive powers other than those specifically delegated in these Terms of Reference. 2. Membership The Committee shall be appointed by the Board from amongst the Non-Executive Directors of the Trust and shall consist of not less than 3 members. At least one of the members should have recent relevant financial experience. A quorum shall be 2 members. One of the members will be appointed Chair of the Committee by the Board. The Chairman of the Trust Board shall not be a member of the committee. 3. Attendance The Director of Finance, & the Foundation Trust Secretary, as well as appropriate Internal and External audit representatives will be expected to attend each Audit Committee meeting. At least once a year the Committee will meet privately with the Internal and External Auditors. The Chairs of the Quality and Safety Committee and the Business Risk and Investment Committee will be invited to attend at least on an annual basis to report on how the work of their committee has enabled them to gain assurance that risks are being appropriately monitored and managed in their areas of responsibility. The Chief Executive and other Executive Directors may be invited to attend, particularly when the Committee is discussing areas of risk or operations that is the responsibility of that director. The Chief Executive shall be invited to attend the meeting at which the draft Statement on Internal Control/Annual Governance Statement is discussed with the Audit Committee and the process for assurance which supports it. The Chair of the Board is not a member of the Audit Committee and will not attend unless invited by the Chair of the Audit Committee to attend certain meetings or for specific agenda items either to form a view and understanding of the Committees operations or to provide assurances and explanation to the Committee on certain issues. The Foundation Trust Secretary shall agree the agenda with the Chair of the Audit Committee and other attendees, organise the collation and distribution of the papers and keep a record of matters arising and issues to be carried forward. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 22 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 39
255 Paper Frequency Not less than quarterly, including at least one meeting a year with both the internal and external auditors but without Executive Board members. The external auditors or internal auditors may request a meeting if they consider that one is necessary. 5. Authority The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. 6. Reporting The Chair of the Committee will report to the Board in as soon as practically possible following the Committee meeting, this will be no later than Board meeting in the following month. A summary of the main issues of the discussion, drawing attention to any issues that require full Board or Executive action, will be presented. In addition to this the approved minutes of the meeting will also be submitted to the private session of the Board. This is in line with the sub-committee reporting process agreed by the Board. The Committee will report to the Board annually on its work in support of the Statement on Internal Control, specifically commenting on the fitness for purpose of the Assurance Framework, the completeness and embeddedness of risk management in the Trust, the integration of governance arrangements and the appropriateness of the self-assessment against the Care Quality Commission (CQC) regulations. The Committee will undertake an annual self assessment, which will be presented to the Trust board, along with the Annual Report of the Committee s activities. The Duties of the Committee can be categorised as: 1 Governance, Risk Management and Internal Control The Committee shall review the establishment and maintenance of an effective system of integrated governance, internal control and risk management, across the whole of the Trust activities (both clinical and non-clinical) that supports the achievement of the Trust objectives. In particular, the Committee will review the adequacy of: All risk and control related disclosure statements (in particular the Statement on Internal Control and declarations of compliance with the CQC regulations), together with any accompanying Head of Internal Audit statement, external audit opinion or other appropriate independent assurances, prior to endorsement by the Board. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 23 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 40
256 Paper 08 The underlying assurance processes that indicate the degree of the achievement of corporate objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements. The policies for ensuring that there is compliance with relevant regulatory, legal and code of conduct requirements. The policies and procedures for all work related to fraud and corruption as set out in Secretary of State Directions and as required by NHS Protect and best practice. The policies and procedures promoting an anti-bribery and corruption culture. This will include the Whistle blowing and Standards of Business Conduct policies and the Declaration of Interests and Hospitality registers The Committee will also rely, as far as possible, on assurance provided by the Quality and Safety and Business Risk and Investment Committees. In carrying out this work the Committee will primarily utilise the work of Internal Audit, External Audit and other assurance functions, but will not be limited to these audit functions. It will also seek reports and assurances from directors and managers as appropriate, concentrating on the over-arching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness. This will be evidenced through the Committee s use of an effective Assurance Framework to guide its work and that of the audit and assurance functions that report to it. 2 Information Governance The Audit Committee are responsible for maintaining an oversight of Information Governance principally by monitoring the progress against the Information Governance toolkit. The Audit Committee has a specific role with regard to data quality The Quality & Safety Committee has a specific role to review data governance issues relating to patient information, in particular in investigating any Patient Identifiable Data SI s The BRIC has a specific role to review data governance issues relating to IM&T infrastructure and the management of the IM&T function. The Audit Committee has a duty to ensure that these specific matters have been referred to the appropriate sub committee and dealt with appropriately. 32 Internal Audit The Committee shall ensure that there is an effective internal audit function established by management, which meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Chief Executive and Board. This will be achieved by: Considering the appointment of the internal audit service, the audit fee and any questions of resignation and dismissal. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 24 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 41
257 Paper 08 Reviewing and approving the internal audit strategy, operational plan and more detailed programme of work, ensuring that this is consistent with the audit needs of the Trust as identified in the Assurance Framework. Considering the major findings of internal audit investigations (and management s response), and ensure co-ordination between the Internal and External Auditors. Ensuring that the Internal Audit function is adequately resourced and has appropriate standing within the Trust. Conducting an annual review of the effectiveness of Internal Audit and providing feedback to the Board and the Internal Auditors. 34 External Audit The Committee shall review the work and findings of the External Auditor and consider the implications and management s responses to their work. This will be achieved by: Considering the appointment of the external audit service, the audit fee and any questions of resignation and dismissal, in accordance with the procedures governing NHS Foundation Trusts as appropriate Discuss and agree with the External Auditor, before the audit commences, the nature and scope of the audit as set out in the Annual Plan, and ensure coordination, as appropriate, with other External Auditors in the local health economy. Discussion with the External Auditors of their local evaluation of audit risks and assessment of the Trust and associated impact on the audit fee. Review all External Audit reports, including agreement of the annual audit letter before submission to the Board and any work carried outside the annual audit plan, together with appropriateness of management responses. Conduct an annual review of the effectiveness of External Audit and provide feedback to the Board and the External Auditors. 45 Other Assurances Functions The Audit Committee shall be made aware of the findings of other significant assurance functions, both internal and external to the Trust, and consider the implications to the governance of the Trust. These will include, but will not be limited to, any reviews by Department of Health Arms Length Bodies or Regulators/Inspectors (e.g. CQC, NHS Litigation Authority, Monitor etc.), professional bodies with responsibility for the performance of staff or functions (e.g. Royal Colleges, accreditation bodies, etc.) In addition, the Committee will review the work of other Committees within the Trust, whose work can provide relevant assurance to the Audit Committee s own scope of work. This will particularly include the Quality and Safety Committee, the Business Risk and Investment Committee and any Risk Management committees that are established. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 25 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 42
258 Paper 08 In reviewing the work of the Quality and Safety Committee, and issues around clinical risk management, the Audit Committee will wish to satisfy themselves on the assurance that can be gained from the clinical audit function. 56 Management The Committee shall request and review, as appropriate, reports and positive assurances from directors and managers on the overall arrangements for governance, risk management and internal control. They may also request specific reports from individual functions within the Trust (e.g. clinical audit) as they may be appropriate to the overall arrangements. 7 Policies The Committee shall approve such policies as the Board has not reserved to itself and as required by the Trust s Policy Control Policy. These will include Counter Fraud Policy 68 Other Matters Financial Reporting: The Audit Committee shall review the Annual Report and Financial Statements before submission to the Board, focusing particularly on: The wording of the Statement on Internal ControlAnnual Governance Statement and other disclosures relevant to the Terms of Reference of the Committee; Changes in, and compliance with, accounting policies and practices; Unadjusted mis-statements in the financial statements; Major judgmental areas; and Significant adjustments resulting from the audit. The Committee should also ensure that the systems for financial reporting to the Board, including those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the Board. Date prepared: 21 st May 2009 Amended 4 th June Approved Trust Board 22 July 2010 Amended 8 th September 2011 Approved by the Board 29 th September 2011 Review Date: by 20 th May 2012 C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 26 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 43
259 Paper 08 MEMBERSHIP AND KEY RESPONSIBILITIES OF BOARD COMMITTEES Membership and Operation of the Audit Committee The Terms of Reference for the Audit Committee give it responsibility for Governance, Risk Management and Internal Control as described below: The committee shall review the establishment and maintenance of an effective system of integrated governance, internal control and risk management, across the whole of the Trust activities (both clinical and non-clinical) that supports the achievement of the Trust objectives. The Quality and Safety Committee and the Business Risk and Investment Committee both have responsibility for reviewing risk arrangements over certain designated areas. This paper sets out recommendations for the relationships between the committees so that the Business Risk and Investment Committee and the Quality and Safety Committee are able to oversee matters within their areas of responsibility whilst providing a framework for the Audit Committee to maintain a comprehensive overview of integrated governance, internal control and risk management within the Trust. In order to fulfil this function the Audit Committee needs to gain assurance from the other committees, whilst remaining independent from them. It is proposed that this will be achieved by: The Chairs of the other two committees will not be regular members of the Audit Committee and the Chair of the Audit Committee will not be a regular member of either of the other two Committees; The Chairs of the Business Risk and Investment Committee and the Quality and Safety Committee will attend the Audit Committee on an annual basis to report on their work and how that work has enabled them to gain assurance that risks are being appropriately monitored and managed in their areas of responsibility; the Non-Executive Directors being made aware of issues being handled by other Committees, by receiving all the papers which are issued to all Committees. All Non- Executive Directors should be able to raise issues with the Chairs of any of the Committees and may attend any committee meeting if they wish and should be able to fully participate in the meeting; The Chair of the Audit Committee will attend a meeting of each of the other two committees on an annual basis. Formatted: Bullets and Numbering C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 27 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 44
260 Paper 08 MEMBERSHIP AND KEY RESPONSIBILITIES OF BOARD COMMITTEES 1. Constitution Quality & Safety Committee Terms of Reference The Board hereby resolves to establish a Committee of the Board to be known as the Quality and Safety Committee. The Committee is a non-executive Committee of the Board and has no executive powers other than those specifically delegated in these Terms of Reference. 2. Membership The membership of the Committee shall consist of three Non Executive Directors plus; Medical Director; Director of Nursing and Governance; Chief Executive; Director of Operations and others as appropriate. A quorum will be two Non Executive members and one Executive member. 3. Attendance The Chief Executive, Medical Director, Director of Nursing and Director of Operations would be expected to attend each meeting. The Chair of the Trust can attend at the invitation of the Chair of the Committee. The Foundation Trust Secretary shall agree the agenda with the Chair of the Committee and other attendees, organise the collation and distribution of the papers and keep a record of matters arising and issues to be carried forward. 4. Frequency of meetings Not less than four times a year. 5. Authority The Committee is authorised by the Board to investigate any activity and is expected to make recommendations to the full board, within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the board to obtain outside legal or other independent professional advice and to secure the attendance of others from outside the Trust with relevant experience and expertise if it considers this necessary. 6. Reporting The Chair of the Committee will report to the Board in as soon as practically possible following the Committee meeting, this will be no later than the Board meeting in the following month. A summary of the main issues of the discussion, drawing attention to any issues that require full Board or Executive C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 28 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 45
261 Paper 08 action, will be presented. In addition to this the approved minutes of the meeting will also be submitted. This is in line with the sub-committee reporting process agreed by the Board. The Committee will undertake an Annual self assessment, which will be presented to the Trust board, along with an Annual Report. The Chair of the Committee will also attend the Audit Committee on an annual basis to provide assurance on the Committee s processes. Where attendance is not possible a written report will be prepared and submitted to the Audit Committee. 7. Key responsibilities Promote excellence in patient care in all aspects of quality and safety, and monitor and review the Clinical Quality Improvement Strategy. To ensure the Trust is meeting core standards and is compliant with national guidelines to include (but not be limited to) prevention and control of infection and effective and efficient use of resources through evidence based clinical practice. To receive an agreed level of clinical data and trend analysis from clinical forums and working groups, which provides adequate clinical matrix to inform and analyse the clinical services provided at the Trust. To ensure that the Committee has adequate information on which to advise and assure the Board on standards of care provision. To receive reports from appropriate specialist committees. Clinical outcomes Monitoring the effectiveness of the Trust's arrangements for the systematic monitoring of mortality and other patient outcomes. Receiving and commenting on action plans and progress reports proposed by management in response to monitoring data on patient outcomes. Incident reporting and investigation Monitoring the effectiveness of the Trust's systems for reporting and investigating Serious Incidents (SIs), near misses and other incidents. Reviewing the outcomes of investigations, ensuring that the information is presented in sufficient detail to enable systemic failings in patient care to be identified; receiving and commenting on action plans and progress reports proposed by management in response to SIs, near misses and other incidents. Patient experience Monitoring the effectiveness of the Trust's systems for complaints handling and reviewing complaints for trends and themes. Monitoring the effectiveness of the Trusts systems for advocacy and the encouragement of feedback from patients and relatives. Clinical risk / Quality risk C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 29 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 46
262 Paper 08 Reviewing the Trust's strategy for management of clinical risk and monitoring the overall level of clinical risk within the Trust, taking account of NHSLA and CQC requirements and applicable regulatory guidance. Supporting the Audit Committee in assessing the overall scope and effectiveness of the Trust's risk management systems. Reviewing the entries of the Trust s risk register which are relevant to the Committee and in line with the terms of reference. Clinical audit Monitoring the effectiveness of clinical audit. Reviewing clinical audit findings and the action plans proposed by management in response to these. Patient Information Governance Monitoring the arrangements to ensure the security of personally identifiable data. Policies The Committee shall approve such policies as the Board has not reserved to itself and as required by the Trust s Policy Control Policy. These will include Formatted: Indent: Left: 1.27 cm Formatted: Bullets and Numbering Formatted: Indent: Left: 1.21 cm Complaints Consent Being Open Clinical audit Falls Date prepared: 28th May 2009 Review date: by 20 th May 2012 Amended 12 th August 2011 Review date August 2012 C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 30 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 47
263 Paper 08 MEMBERSHIP AND KEY RESPONSIBILITIES OF BOARD COMMITTEES Business Risk and Investment Committee Terms of Reference 1. Constitution The Board hereby resolves to establish a Committee of the Board to be known as the Business Risk and Investment Committee. The Committee is a nonexecutive Committee of the Board and has no executive powers other than those specifically delegated in these Terms of Reference. 2. Membership The membership of the Committee shall consist of three Non Executive Directors plus the Chief Executive, Director of Finance,Director of Operations and the Associate Director of Human Resources. A quorum will be two Non Executive members and one Executive member. 3. Attendance The Chief Executive, Director of Finance and Director of Operations would be expected to attend each meeting. Other Executive directors to attend as appropriate. The Chair of the Trust may attend at the invitation of the Chair of the Committee. The Foundation Trust Secretary shall agree the agenda with the Chair of the Committee and other attendees, organise the collation and distribution of the papers and keep a record of matters arising and issues to be carried forward.. 4. Frequency of meetings Not less than four times a year 5. Authority The Committee is authorised by the board to investigate any activity and expected to make recommendations to the full board, within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The committee is authorised by the board to obtain outside legal or other independent professional advice and to secure the attendance of others from outside the Trust with relevant experience and expertise if it considers this necessary. 6. Reporting C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 31 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 48
264 Paper 08 The Chair of the Committee will report to the Board by the month following the Committee meeting at the latest. A summary of the main issues of the discussion, drawing attention to any issues that require full Board or Executive action, will be presented. In addition to this the approved minutes of the meeting will also be submitted. This is in line with the sub-committee reporting process agreed by the Board. The Committee will undertake an Annual self assessment, which will be presented to the Trust board, along with an Annual Report. The Chair of the Committee will also attend the Audit Committee on an annual basis to provide assurance on the Committee s processes, or provide a written report where attendance is not possible. 7. Key responsibilities Business Risk To support the Audit Committee in:- Assessing the overall scope and effectiveness of the Trust s non clinical risk management systems; Reviewing the Trust s strategies for the management of business risk Reviewing the business risks included on the Trusts Corporate and Strategic register. Monitoring the overall level of business risk within the Trust, taking account of Monitor, CQC and other applicable regulatory guidance. Business Investment Establish the overall methodology, processes and controls which govern investments, and to evaluate and monitor investments against these arrangements. In particular, the Committee will: Oversee the continued development the Trust s Investment Policy and ensure this is maintained to fit with best practice and in line with Monitor guidance; Review in advance of Board submission significant investment proposals. The definition of a significant investment proposal being one where the capex exceeds the Chief Executive's sign off limit (ie in excess of 250,000) or where a proposed investment meets the Monitor definition of a significant investment Appraising the potential financial, commercial, service and other investment opportunities offered by FT status; Identifying and evaluating specific investment opportunities; Reviewing capital investment proposals within the capital investment programme and monitoring its implementation; Ensure appropriate independent professional advice is sought in line with SHA/Monitor s guidance relating to significant investments; Consider post project evaluation reports on significant capital investments (i.e. those over 250,000); Develop the Trust s Operating Cash Policy and Monitor compliance. Oversight and Scrutiny C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 32 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 49
265 Paper 08 Receiving reports from appropriate specialist sub committees. Receiving relevant Internal Audit reports. Review progress made in delivering key enabling strategies such as (but not limited to) Workforce, Estates, Marketing, Sustainability and IT raising any significant risks regarding their delivery to the Trust Board Review the Trust s investment register Promoting sustainability and receiving sustainability KPI s Policies The Committee shall approve such policies as the Board has not reserved to itself and as required by the Trust s Policy Control Policy. Formatted: Indent: Left: 0.95 cm Formatted: Bullets and Numbering Formatted: Indent: Left: 1.27 cm Date prepared: 28 th May 2009 Review date: by 20 th May 2012 Amended 3 rd September 2009 Amended 28 th June 2010 Amended 27 th October 2011 Review date by October 2012 C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 33 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 50
266 Paper 08 MEMBERSHIP AND KEY RESPONSIBILITIES OF BOARD COMMITTEES 1. Constitution Nomination & Remuneration Committee Terms of Reference The Board hereby resolves to establish a Committee of the Board to be known as the Nomination and Remuneration Committee. The Committee is a nonexecutive Committee of the Board and has no executive powers other than those specifically delegated in these Terms of Reference. 2. Membership The membership of the Committee will vary according to the nature of the business to be discharged at a particular meeting, as follows. 1. Where a meeting or part-meeting of the Committee is convened for the purpose of considering any question relating to: the structure, size and composition of the Board of Directors; succession planning the appointment of executive directors (other than Chief Executive) advising the Governors prior to the recruitment of nonexecutives directors the Committee shall consist of the Trust Chairman, the Chief Executive and all non-executive directors. Quorum at least three members of the committee 2. Where a meeting or part-meeting of the Committee is convened for the purpose of considering any question relating to the appointment of a Chief Executive, the Committee shall consist of the Trust Chairman and all non-executive directors Quorum at least three members of the committee 3. Where a meeting or part-meeting of the Committee is convened for the purpose of considering any question relating to the remuneration of the executive directors, the Committee shall consist of the Trust Chairman, the Chief Executive and all non-executive directors. Quorum at least three independent non-executive directors 4. Where a meeting or part-meeting of the Committee is convened for the purpose of considering any question relating to the remuneration of the Chief Executive, the Committee shall consist of the Trust Chairman and all non-executive directors. Quorum at least three independent non-executive directors 5. The Chairman of the Trust Board of Directors will Chair the meeting. C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 34 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 51
267 Paper Attendance Other officers of the Trust may attend the meetings at the express invitation of the remuneration committee. 4. Frequency of meetings Not less than twice a year. 5. Authority The Committee is authorised by the board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The committee is authorised by the board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. 6. Reporting The Chair of the Committee will report to the next meeting of the Board following the Committee, summarising the main issues of the discussion and drawing the Board s attention to any issues the require disclosure to the full Board or require Executive action. The approved or draft minutes will also be submitted to that meeting. 7. Key responsibilities Board structure, size and composition reviewing the structure, size and composition (including the skills, knowledge and experience) required of the Board as a whole compared to its current position; making recommendations to the Board on any changes and development needs. Succession planning considering succession planning for executive directors and other senior managers, taking into account the challenges and opportunities facing the Trust and the skills and expertise needed on the Board in the future. Appointment of executive directors (other than Chief Executive) where a new executive director (other than a new Chief Executive) is to be appointed, being responsible for the selection and appointment process on behalf of the Board. Appointment of Chief Executive where a new Chief Executive is to be appointed, being responsible for the selection and appointment process on behalf of the Board. Appointment of non-executive directors: interface with Council of Governors C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 35 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 52
268 Paper 08 where a new Trust Chairman or non-executive director is to be appointed by the Council of Governors, communicating views on the balance of skills, knowledge and experience required on the Board and its description of the role and capabilities required for the particular appointment to the Nomination Committee of the Council of Governors. Executive remuneration setting the remuneration of all executive directors, including salary, any performance-related elements/bonuses or allowances and provision for other benefits including cars; ensuring the contractual terms of Executive Directors are in accordance with national policy and guidance, particularly in relation to the termination of employment, notice periods and pension benefits; determining whether a proportion of executive directors' remuneration should be linked to corporate and individual performance and, if so, approving an appropriate scheme of performance-related remuneration. Date prepared: 28 th May 2009 Review date: by 27 th May 2012 C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 36 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 53
269 Paper 08 APPENDIX CF JOB DESCRIPTIONS : BOARD DIRECTORS Job Descriptions and Person Specifications for the following roles which constitute the Board of Directors. 1. Chairman U:drive : Trust Board and Committees : Job Descriptions Board Directors : Chairman 2. Non Executive Directors (which also identify the following Non Executive responsibilities: Deputy Trust Chairman Chair of Audit Committee Chair of Business Risk and Investment Committee Chair of Quality and Safety Committee Senior Independent Director 3. Chief Executive and Accountable Accounting Officer U:drive : Trust Board and Committees : Job Descriptions Board Directors : Non Executive Directors U:drive : Trust Board and Committees : Job Descriptions Board Directors : Chief Executive 4. Director of Finance U:drive : Trust Board and Committees : Job Descriptions Board Directors : Director of Finance 5. Medical Director U:drive : Trust Board and Committees : Job Descriptions Board Directors : Medical Director 6. Director of Nursing U:drive : Trust Board and Committees : Job Descriptions Board Directors : Director of Nursing 7. Director of Operations U:drive : Trust Board and Committees : Job Descriptions Board Directors : Director of Operations Board Support 8. Foundation Trust Secretary U:drive : Trust Board and Committees : Job Descriptions Board Directors : Foundation Trust Secretary C:\Documents and Settings\owenja.RJAH\My Documents\Margaret Surrage\Trust Board Papers\Board Governance for NHS FT ammended Nov docU:\FINANCE\group\Margaret 37 Surrage\new company secretary role\governance Documents\November Board\Board Governance for NHS FT ammended Nov 2012.docU:\FINANCE\group\Margaret Surrage\new company secretary role\governance Documents\Board Governance for NHS FT.doc U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 08 Board Governance Arrangements 54
270 Paper 09 Russell Hardy 4358 Chairman BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Subject/Title Medical Revalidation Executive Responsible Paper prepared by (if different from above) Mr Stephen White, Medical Director - Nature of Report For Information For Discussion For Approval Category of Item Context Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary Received or approved by The Board of Directors are asked to take note of the letter received from Sir David Nicholson, NHS Chief Executive and Sir Bruce Keogh, NHS Medical Director in relation to Revalidation. Our ORSA submissions are green rated, and submitted on a regular basis to the Department of Health. We have identified the first 20% of doctors to go through revalidation in the first cycle. Revalidation starts in December Legal Implications Recommendation The Board of Directors are asked to note the contents of the letter. Acronyms and Abbreviations ORSA Organisational Readiness Self Assessment GMC General Medical Council RJAH Robert Jones and Agnes Hunt Orthopaedic Hospital GMC General Medical Council U:\Trust Board & Committees\Public Trust Board\ \November\Paper 09 Update on Revalidation
271 Paper 09 Russell Hardy 4358 Chairman BOARD OF DIRECTORS 30 TH NOVEMBER 2012 BOARD SUMMARY OF REVALIDATION A summary of medical revalidation is provided in the letter received from Sir David Nicholson, NHS Chief Executive and Sir Bruce Keogh, NHS Medical Director in relation to Revalidation. The implications for doctors working at the Robert Jones and Agnes Hunt (RJAH) Orthopaedic Hospital are as follows;- Revalidation is a process by which the General Medical Council (GMC) assures the public that doctors are up to date and fit to practice The GMC will receive recommendations by Responsible Officers Each Trust has a Responsible Officer and doctors at RJAH Orthopaedic Hospital whose contracts are held here will be allocated to this Trust as their designated body Doctors whose contracts are held by other trusts will report to that designated body Members of the armed forces will report to the armed forces Responsible Officer Trainees will report to the Deanery The system is based upon strengthened appraisal. Appraisals have been carried out here for 10 years. This annual process has been largely based on information provided by the doctor. Strengthened appraisal requires specified information according to Royal College guidelines per speciality and a systematic review of quality information gathered by the hospital. The process is also more complex as it requires our doctors, who also work elsewhere, to bring quality assurance data from those other hospitals. Similarly doctors based elsewhere will require RJAH Orthopaedic Hospital to supply quality assurance data to support the appraisals at those other hospitals. Feedback from patients and colleagues often known as 360 degree appraisal is required on a five yearly cycle. At appraisal the following information is considered; Continuous professional development Quality improvement activity Significant events Feedback from colleagues and patients (where applicable) Review of complaints and compliments. Appraisers need training to carry out strengthened appraisal and many consultants have in 2012 been on strengthened appraisal top up training. At RJAH Orthopaedic Hospital we have an electronic spreadsheet / dashboard containing the outcomes of the appraisals. These outcomes will be used to make a decision by the Responsible Officer of whether a doctor can be: Recommended to the General Medical Council (GMC) for revalidation Alternatively, whether the revalidation should be deferred Whether the doctor should be referred to the GMC. U:\Trust Board & Committees\Public Trust Board\ \November\Paper 09 Update on Revalidation
272 Paper 09 To avoid any misunderstandings please note: Are appraisals the time to deal with concerns about a doctor? o No, don t wait for appraisals, concerns about a doctor should be dealt with when they arise. Patient safety is paramount. The benefit of dealing with problems when they arise is that by the time the appraisal occurs these concerns will have been addressed and hopefully will no longer be a concern. Even at appraisal if there is a concern this is not necessarily a bar to satisfactory appraisal. If it is being satisfactorily corrected, the most important thing is the dealing with concerns appropriately. Usually this will avoid escalation Remediation the varying standards required of doctors is noticeable between hospitals. There is an intense process of responsible officer networking currently to provide greater consistency of application of standards expected of doctors My intention as Responsible Officer is to encourage reflection by doctors annually to continuously strive to improve, and for appraisers to signpost appraisee s to facilitate learning and improvement. My philosophy is to try and identify problems at an early stage so that mild concerns can be dealt with and prevent escalation through amber and then through to red. This approach is surely better for patients and doctors the reputation of the hospital, the profession and healthcare in the UK generally. Mr Stephen White Medical Director U:\Trust Board & Committees\Public Trust Board\ \November\Paper 09 Update on Revalidation
273 U:\Trust Board & Committees\Public Trust Board\ \November\Paper 09 Update on Revalidation Paper 09
274 U:\Trust Board & Committees\Public Trust Board\ \November\Paper 09 Update on Revalidation Paper 09
275 Paper 10 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title Proposed Sub Committee dates 2013 Executive Responsible Paper prepared by (if different from above) Russell Hardy, Chairman Margaret Surrage, Head of Board Governance (Trust Secretary) Nature of Report For Information For Discussion For Approval Category of Item Strategic Direction and Development Performance and Governance Context Previous Board discussion Draft timetable discussed at the October Board meeting. Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary Following discussions with the Chairs of the Sub Committees the dates for their meetings have been confirmed. One late change to note is that the February Charitable Funds Committee meeting has been moved to Monday February 25th Risk if No Action is Taken Received or Approved by Legal Implications Recommendation The Board is asked to note the dates for the Sub Committee meetings Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper Sub Committee Dates.doc 1
276 Paper 10 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan FORMAL TRUST BOARD (monthly) 24th 28th 27th 25th Weds 29th 27th 25th - 26th 24th 28th - 30th ANNUAL GENERAL MEETING (annual) 25th Council of Governors meeting dates (quarterly) TBC 28th 29th 25th 28th BOARD DEVELOPMENT SESSIONS TBC 25th pm 28th 27th 29th 31st Board Strategy Day 28th Sub Committees Audit Committee - Regular (Tuesday) 15th 16th 16th 15th 14th Audit Committee - Extraordinary (draft & final accounts) 19th? 28/29th? Quality & Safety - Regular (Thursday) 17th 4th 11th 17th 16th Quality & Safety - Extraordinary (quality accounts ) BRIC (Wednesday) 5th 9th 10th 16th 15th Charitable Funds 25th 27th 26th 29th Nomination & Remuneration committee as & when required 28/29th? U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper Sub Committee Dates.doc 2
277 Paper 11 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title Executive Responsible Paper prepared by (if different from above) Report from the Chair of the Business Risk & Investment Committee (BRIC) James Turner, Non Executive Director Nature of Report For Information For Discussion For Approval Category of Item Context Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary This report highlights the key business undertaken by the BRIC at its meeting on 3 rd October Received or approved by Legal Implications Recommendation The Trust Board are asked to note the Chairman s Report. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 11 BRIC Chairs Report.doc 1
278 Paper 11 James Turner Non-Executive Director BOARD OF DIRECTORS 30 TH NOVEMBER 2012 BUSINESS RISK & INVESTMENT COMMITTEE CHAIRMAN S REPORT OF THE MEETING OF 3 RD OCTOBER 2012 Risk The Committee reviewed all of the Corporate and Strategic risks which had been allocated to the BRIC, paying particular attention to the risks which had increased and the new risk. Increased cost pressures as a result of the RTT recovery programme increased risk Reduction in staff sickness increased risk Repatriation of Welsh patients new risk Governance - RTT Action Plan The Committee noted that all of the actions had now been implemented. They noted the progress which had been made against the targets for patients on admitted and nonadmitted pathways. They discussed the obstacles to achieving the open pathway target of 92%. They were reassured by the PCT s engagement in these issues and noted that Monitor would be engaged on this. - Sickness Absence Review The committee received a detailed report on the progress made in reducing sickness absence and considered options for further action. The committee agreed that the target should remain 2% whilst acknowledging the challenge this involved. Business Cases - APCS The Committee noted that the due diligence exercise was now complete were given an overview of the issues involved prior to the full business case being developed. - MRI Scanner PPE The Committee noted the technological benefits brought by the scanner, but that further work was required to fully realise the potential benefits and agreed that the Chair should write to the Clinical Lead to request further assurance. Strategies The Committee approved the minor changes which had been proposed for the Treasury Management Policy. The Committee considered the revised Capital Programme, they noted that the changes had been made in order to facilitate the early completion of the new tumour unit and that the programme remained within the original cost envelope. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 11 BRIC Chairs Report.doc 2
279 Paper 11 Regular Reports The Committee noted the following reports: Health & Safety report IM&T Report SMS Annual report Human Resources, this included an ad hoc report on the management of temporary contracts which were nearing their end date Treasury Management (Investment Register) The Work Plan was revised to include an in depth report on CIPs James Turner Non Executive Director U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 11 BRIC Chairs Report.doc 3
280 Paper 12 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 Russell Hardy 4358 Chairman Subject/Title FT Bulletin October 22nd Executive Responsible Paper prepared by (if different from above) Wendy Farrington Chadd, Chief Executive Margaret Surrage, Head of Board Governance (Trust Secretary) Monitor Nature of Report For Information For Discussion For Approval Category of Item Context Strategic Direction and Development Performance and Governance Previous Board discussion Link to National Policy Link to Trust s Strategic Objectives Risk if no action taken Executive Summary The October edition of the FT Bulletin published by Monitor is attached and a summary of progress of the key actions required by the Trust is included in this report. Received or approved by Legal Implications Recommendation The Trust Board are asked to note the actions taken in response to the FT Bulletin. Acronyms and Abbreviations U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 12 Foundation Trust Bulletin.doc 1
281 Paper 12 BOARD OF DIRECTORS 30 TH NOVEMBER 2012 FT BULLETIN (22ND OCTOBER 2012) SUMMARY OF KEY ACTIONS ARISING Action Lead Responsibility Progress Cost Improvement Plans Boards must ensure that they have effective processes in place for ensuring quality whilst introducing cost saving measures that procedures are subject to regular, robust audit. that cost improvement plans have clinical signoff where appropriate. Chief Executive This issue has been flagged as part of the BAF and as such is regularly reviewed by the Board. Update on private patient income cap for NHS foundation trusts The Board should note the changes to the provisions governing private patient income Trust Board Complete. These changes were covered in the Revised Constitution which was approved at the September Board. Schedule 6 has been updated Note that this schedule, which lists the information that FT s have a legal obligation to provide, has been updated Head of Board Governance (Trust Secretary) Complete, these have been noted. U:\Trust Board & Committees\Public Trust Board\ \November 2012\Paper 12 Foundation Trust Bulletin.doc 2

282 FT Bulletin 22 October 2012 Issue 62 Welcome to the October edition of Monitor s FT Bulletin. This bulletin is sent to foundation trust chief executives, chairs, finance, medical and nursing directors and the Foundation Trust Network. Click on the links below to jump straight to the relevant sections of the bulletin. For information Gaming to meet targets Regulatory Assessment Framework and Enforcement Guidance - consultations out soon Monitor's new executive team Mid Staffordshire contract award Monitor s recruitment website goes live Webinar on Cost Improvement Programmes Consultation & Engagement Consultation on the new NHS provider licence - closes 23 October For action Cost Improvement Plans Update on private patient income cap for NHS foundation trusts Schedule 6 has been updated Events & development programmes Monitor at the first Foundation Trust Network National Conference Monitor publications NHS foundation trusts: review of three months to 30 June 2012 Getting in touch Queries or feedback News alerts Consultation on guidance for commissioners on ensuring continuity of health services - closes 8 November Foundation Trust ARM consultation Department of Health Consultations Medical engagement and leadership seminar The FT NED role: meeting the challenges conference How to engage clinicians in cost improvement Strategic Financial Leadership Programme Publications 3
283 For information For action Monitor publications Consultation & Engagement Events & development programmes Getting in touch Jump straight to a section using the quick links above For information Gaming to meet health care targets Monitor would like to stress the importance of trusts ensuring that patient care is not being compromised by inappropriate practices designed to achieve health care targets. In particular, there have been reports in the press recently of trusts allegedly keeping patients in ambulances for extended periods before admitting them into hospital, in order to delay the start of the four hour A&E waiting time target. In fact, the clock starts for the A&E target either when the ambulance crew hands the patient over to an A&E clinician OR 15 minutes after the time the ambulance arrives at the A&E department (whichever is sooner). If a patient is kept in an ambulance for an extended period, it therefore does not delay the start of the clock for the purposes of the A&E Total Time target (or indeed any of the other A&E Clinical Indicators). Keeping any patient who requires hospital care in an ambulance for an extended period of time, is clearly poor patient care and could have serious clinical implications for patients with certain medical conditions. Delaying ambulances at hospitals also restricts the capacity of ambulance services to reach other patients who may be in need of urgent medical attention. We would encourage all trusts to ensure that such practices are not taking place at your hospitals. Evidence of foundation trusts carrying out these practices would be taken very seriously by Monitor. Please also refer to a letter on this matter from David Flory, Chief Executive of the NHS Trust Development Authority, which went to all trusts including foundation trusts earlier this year. Regulatory Assessment Framework and Enforcement Guidance - consultations out soon Next month, Monitor will publish for consultation its Regulatory Assessment Framework (RAF) and Enforcement Guidance. The Regulatory Assessment Framework will play a similar role to the Compliance Framework for Foundation Trusts. Both documents will be key regulatory tools for the future. It is important that trusts feed into these consultations to inform the future regulatory framework. Please look out for these documents next month when they will be ed to trusts and published on the Monitor website. Back Return to main menu Forward 4

284 For information For action Monitor publications Consultation & Engagement Events & development programmes Getting in touch Jump straight to a section using the quick links above For information Monitor's new executive team Monitor's new role as sector regulator for health means the organisation needs to adapt and take on a range of new responsibilities from April As part of this transition process, Monitor has re-structured its executive team and made a range of senior appointments. You can read more about this here. Mid Staffordshire contract award In September 2012, Monitor announced a competitive tender for experts to draw up a rescue plan to protect health services for patients at Mid Staffordshire NHS Foundation Trust. The contract for this project has now been awarded to a consortium headed by Ernst & Young and supported by McKinsey. Further details on this are included on our website here. You can also read about the engagement exercise that is now underway with the local population, the trust, local commissioners and clinicians to find a sustainable long term solution at Mid Staffs. Monitor s recruitment website goes live Monitor has launched a new recruitment website Joinmonitor.com The website enables applicants to view and apply for the new roles we are recruiting to. Visitors to joinmonitor.com can register their details to receive the latest job alerts tailored to their skills. Back Return to main menu Forward 5
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
July (Month 4) Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval
 Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval") BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
A consultation on the Government's mandate to NHS England to 2020
 A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
National Clinical Audit programme
 National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
Commissioning for Value insight pack
 Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators April Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Indicators April 2011 Report to: Trust Board 24 May 2011 Report from: Sponsoring Executive: Aim of Report / Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Indicators April 2011 Report to: Trust Board 24 May 2011 Report from: Sponsoring Executive: Aim of Report / Principle Topic: Review History to date:
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Open and Honest Care in your local Trust
 Agenda Item: 3 Encl. 3.3 Open and Honest Care in your local Trust Open and Honest Report for Black Country Partnership NHS Foundation Trust February 2017 NHS England INFORMATION READER BOX Directorate
Agenda Item: 3 Encl. 3.3 Open and Honest Care in your local Trust Open and Honest Report for Black Country Partnership NHS Foundation Trust February 2017 NHS England INFORMATION READER BOX Directorate
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Implementation of the right to access services within maximum waiting times
 Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
NHS Rotherham. The Board is recommended to note the proposal to adopt the NHS EDS and to approve the development and implementation of the EDS
 NHS Rotherham Management Executive 31 May 2011 NHS Rotherham Board 6 June 2011 Equality Delivery System This report has been informed by a briefing note from the SHA Contact Details: Lead Director: Sarah
NHS Rotherham Management Executive 31 May 2011 NHS Rotherham Board 6 June 2011 Equality Delivery System This report has been informed by a briefing note from the SHA Contact Details: Lead Director: Sarah
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Draft Minutes. Agenda Item: 16
 Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Technical Guidance Refreshing NHS plans for 2018/19. Published by NHS England and NHS Improvement
 Technical Guidance Refreshing NHS plans for 2018/19 Published by NHS England and NHS Improvement Technical Guidance for Refreshing NHS plans for 2018/19 Version number: 1.1 First published: 23 February
Technical Guidance Refreshing NHS plans for 2018/19 Published by NHS England and NHS Improvement Technical Guidance for Refreshing NHS plans for 2018/19 Version number: 1.1 First published: 23 February
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Our Achievements. CQC Inspection 2016
 Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Quality Account 2016/17 & 2017/18 Quality Priorities
 Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 25 th February 2009 at 2.00 pm in Rooms 2 and 3 at Hertford County Hospital DRAFT Present:
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 25 th February 2009 at 2.00 pm in Rooms 2 and 3 at Hertford County Hospital DRAFT Present:
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Overall rating for this service Good
 Dr Rajesh Sarafaf Quality Report Moorside Medical Centre 681 Ripponden Road Oldham OL1 4JU Tel: 0161 909 8388 Website: www.doctorsatmoorside.co.uk/saraf Date of inspection visit: 09/06/2016 Date of publication:
Dr Rajesh Sarafaf Quality Report Moorside Medical Centre 681 Ripponden Road Oldham OL1 4JU Tel: 0161 909 8388 Website: www.doctorsatmoorside.co.uk/saraf Date of inspection visit: 09/06/2016 Date of publication:
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Outcomes benchmarking support packs: CCG level
 Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Staff Health and Wellbeing Strategy
 Staff Health and Wellbeing Strategy 1. Background Dr Steve Boorman undertook a review of NHS health and wellbeing during 2009 (The NHS Health and Wellbeing Review). He gathered a wealth of evidence of
Staff Health and Wellbeing Strategy 1. Background Dr Steve Boorman undertook a review of NHS health and wellbeing during 2009 (The NHS Health and Wellbeing Review). He gathered a wealth of evidence of
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
CARERS POLICY. All Associate Director of Patient Experience. Patient & Carers Experience Committee & Trust Management Committee
 CARERS POLICY Department / Service: Originator: All Associate Director of Patient Experience Accountable Director: Chief Nursing Officer Approved by: Patient & Carers Experience Committee & Trust Management
CARERS POLICY Department / Service: Originator: All Associate Director of Patient Experience Accountable Director: Chief Nursing Officer Approved by: Patient & Carers Experience Committee & Trust Management
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Quality, Safety and Patient Experience Strategy
 Quality, Safety and Patient Experience Strategy November 2015 www.castlepointandrochfordccg.nhs.uk Document Name Quality, Safety & Patient Experience Strategy Version V7 Author/s Name Job Title/s Jenny
Quality, Safety and Patient Experience Strategy November 2015 www.castlepointandrochfordccg.nhs.uk Document Name Quality, Safety & Patient Experience Strategy Version V7 Author/s Name Job Title/s Jenny
Quality Assurance Committee Annual Report April 2017 March 2018
 Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
REQUIREMENT. Identify a minimum of 4 theme areas which are considered to have caused concern for patients during 2012/13
 2012/13 SSOTP CQUIN INDICATOR TARGETS INDICATOR REQUIREMENT 1. Patient Experience Milestone 1 (15th working day of April 2012) Identify a minimum of 4 theme areas which are considered to have caused concern
2012/13 SSOTP CQUIN INDICATOR TARGETS INDICATOR REQUIREMENT 1. Patient Experience Milestone 1 (15th working day of April 2012) Identify a minimum of 4 theme areas which are considered to have caused concern
THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST QUALITY ACCOUNTS 2011/12
 THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST Quality Narrative QUALITY ACCOUNTS 2011/12 (WORKING DRAFT OF CONTENT) 1. Statement from the Chief Executive, and summary of the quality of NHS services
THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST Quality Narrative QUALITY ACCOUNTS 2011/12 (WORKING DRAFT OF CONTENT) 1. Statement from the Chief Executive, and summary of the quality of NHS services
Our NHS, our future. This Briefing outlines the main points of the report. Introduction
 the voice of NHS leadership briefing OCTOBER 2007 ISSUE 150 Our NHS, our future Lord Darzi s NHS next stage review, interim report Key points The interim report sets out a vision of an NHS that is fair,
the voice of NHS leadership briefing OCTOBER 2007 ISSUE 150 Our NHS, our future Lord Darzi s NHS next stage review, interim report Key points The interim report sets out a vision of an NHS that is fair,
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Why do we need this project? What is Mouth Care Matters? Why Does it Matter? Mary. Oral Health Champion Volunteers. August 2018
 This month, I am pleased to inform you about this important project, Mouth Care Matters, and am proud to support the Dental Service within the MaxilloFacial Department as the Executive Lead on this. 1
This month, I am pleased to inform you about this important project, Mouth Care Matters, and am proud to support the Dental Service within the MaxilloFacial Department as the Executive Lead on this. 1
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
is asked to NOTE the update provided on fragile services.
 Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement
 Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Your Guide to the proposed NHS Constitution
 Your Guide to the proposed NHS Constitution I like to feel that I am making a difference We want to start looking after our own health Everybody should be treated as an individual It s your NHS. Know your
Your Guide to the proposed NHS Constitution I like to feel that I am making a difference We want to start looking after our own health Everybody should be treated as an individual It s your NHS. Know your
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Marie Curie Hospice Liverpool Speke Road, Woolton, Liverpool,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Marie Curie Hospice Liverpool Speke Road, Woolton, Liverpool,
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Public Services Reform (Scotland) Bill. Scottish Independent Hospitals Association
 Bill. Scottish Independent Hospitals Association") Public Services Reform (Scotland) Bill Scottish Independent Hospitals Association The following submission is presented to the Health and Sport Committee of the Scottish Government as an outline of the
Public Services Reform (Scotland) Bill Scottish Independent Hospitals Association The following submission is presented to the Health and Sport Committee of the Scottish Government as an outline of the
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
National Cancer Peer Review Programme Evidence Guide for: Gynaecology Specialist MDT
 Intelligence National Cancer Action Team Part of the National Cancer Programme National Cancer Peer Review Programme Evidence Guide for: Gynaecology Specialist MDT Foreword This evidence guide has been
Intelligence National Cancer Action Team Part of the National Cancer Programme National Cancer Peer Review Programme Evidence Guide for: Gynaecology Specialist MDT Foreword This evidence guide has been
REVIEW AND UPDATE OF THE COMMITTEE WORK PROGRAMME
 AGENDA ITEM 3.1 14 June 2013 REVIEW AND UPDATE OF THE COMMITTEE WORK PROGRAMME Executive Lead: Committee Chair Author: Assistant Director of Patient Safety & Quality Contact Details for further information:
AGENDA ITEM 3.1 14 June 2013 REVIEW AND UPDATE OF THE COMMITTEE WORK PROGRAMME Executive Lead: Committee Chair Author: Assistant Director of Patient Safety & Quality Contact Details for further information:
QUALITY STRATEGY
 QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Section 1 - Key Performance Indicators
 Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within