Time No. Item Lead Action OPENING ADMINISTRATION Declarations of Interest Chair, Dr Debbie Frost Note 5-8
|
|
|
- Imogene Lillian Henry
- 6 years ago
- Views:
Transcription
1 Barnet Clinical Commissioning Group Governing Body Meeting in Public Thursday 11 January to Committee Room 1 Hendon Town Hall, The Borroughs, Hendon, London NW4 4BG Time No. Item Lead Action OPENING ADMINISTRATION Page number Introductions and apologies for absence Chair, Dr Debbie Frost Note Verbal Declarations of Interest Chair, Dr Debbie Frost Note Gifts and Hospitality Chair, Dr Debbie Frost Note Verbal Minutes of meeting, 02 November 2017 and amended minute extract 06 July 2017 Chair, Dr Debbie Frost Approve Action Log and Matters Arising Chair, Dr Debbie Frost Note CHAIR, ACCOUNTABLE OFFICER, PATIENT STORY AND QUALITY Chair s Report Chair, Dr Debbie Frost Note Accountable Officer s Report Accountable Officer, NCL CCGs, Helen Pettersen Note Patient Story Interim Director of Quality and Clinical Services, Vicky Aldred Note Verbal 09: Performance and Quality Report Deputy Director, POD, NELCSU, Richard Pearson/Chair of Clinical Quality and Risk Committee, Dr Murtaza Khanbhai Note CORPORATE BUSINESS and BUSINESS CASES Ophthalmology Business Case Director of Care Closer to Home, Colette Wood Approve Care Closer to Home progress report Director of Care Closer to Home, Colette Wood Note
2 Proposal to take in-house a range of Commissioning Support Unit Services Director of Performance and Acute Commissioning, Paul Sinden Note / approve FINANCE, PERFORMANCE AND GOVERNANCE Finance Report Month 8 Chief Finance Officer NCL CCGs, Simon Goodwin Note Health and Wellbeing Strategy (includes Progress on Strategy at appendix 2 (unnumbered) Chair, Dr Debbie Frost Note Safeguarding Annual Report Children s Safeguarding Annual Report Adults Associate Director of Safety of Safeguarding, Siobhan McGovern Associate Director of Safety of Safeguarding, Siobhan McGovern Approve Approve SUMMARY REPORTS and MINUTES OF COMMITTEES OF THE GOVERNING BODY Finance, Performance and QIPP, summaries of meetings held 28 September and 26 October 2017 Committee Chair, Dr Barry Subel Note Audit Committee 24 August 2017 meeting and summary of 23 November 2017 meeting Committee Chair, Robin Somerville Note Primary Care Procurement Committee, summaries of 5 October 2017 and 2 November 2017 meetings Committee Chair, Bernadette Conroy Note Clinical Quality and Risk Committee meeting 12 October 2017 Committee Chair, Dr Murtaza Khanbhai Note NCL Joint Commissioning Committee meetings, 3 August 2017 and 5 October 2017 Accountable Officer, NCL CCGs, Helen Pettersen Note
3 16.50 NCL Primary Care Committee in Common meeting, 22 September 2017 Accountable Officer, NCL CCGs, Helen Pettersen Note Health and Well Being Board meeting, 14 September 2017 Chair, Dr Debbie Frost Note CLOSING ADMINISTRATION Any Other Business Chair, Dr Debbie Frost Verbal 17.1 Glossary of Acronyms Chair, Dr Debbie Frost QUESTIONS FROM THE PUBLIC RELATING TO ITEMS ON THE AGENDA 3
4 4
5 Item 2 Name Position (s) held in the CCG i.e. Governing Body member; Committee member; Member practice; CCG employee or other Declared Interest (Name of the organisation and nature of business) Type of Interest Is the interest direct or indirect? Nature of Interest Date of Interest Financial Interest Non-Financial Professional Interest Elected Voting Members Dr Debbie Frost Elected GP Representative Millway Medical Practice yes yes no Direct GP Partner - Personal Medical Services (PMS) Practice. 01/03/ /10/2017 Non-Financial Personal Interest From To Updated Barndoc Healthcare no no yes indirect One of the Partners in Millway Medical Practice is the Chair of Barndoc Healthcare Ltd. 01/03/ /10/2017 Pan Barnet Federated GPs Network Board. no no no indirect GP Partner is a member 01/03/ /10/2017 KPMG Banking Sector no no no indirect Son is a graduate trainee 01/03/ /10/2017 Helen Pettersen Simon Goodwin Dr Aashish Bansal Accountable Officer and NCL STP Convenor Chief Finance Officer Elected GP Representative Health and Well Being Boards for the LGA no no yes indirect Facilitator of a Leadership Essentials Course 30/11/2017 NCL CCGs no no no n/a nil return 01/05/ /09/2017 NCL CCGs no no no 01/06/ /09/2017 East London NHS FT no no yes indirect wife is a senior manager 01/06/ /09/2017 Everglade Medical Practice yes yes no Direct GP Partner 30/05/ /09/2017 Tavistock and Portman NHS Trust no no yes indirect wife is a consultant pyschiatrist for CAMHS 30/05/ /10/2017 Watling Medical Centre, Burnt Oak Barnet GP Federation yes yes no Direct GP Partner 01/05/ /10/2017 no no yes indirect member 01/05/ /10/2017 Colindale BurntOak Healthcare Network the company name of the network no no yes indirect Director 01/05/ /10/2017 Dr Murtaza Khanbhai Elected GP Representative Thornhill Clinic Ltd Yes Yes No indirect 25% shareholder, a primary care clinic in Luton, there is no connection to Barnet CCG or patients and no NHS activity 01/05/ /10/2017 Ravenscroft Medical Centre Yes Yes no Direct GP Principal 01/03/ /09/2017 Dr Barry Subel Dr Charlotte Benjamin Elected GP Representative Elected GP Representative South Locality Barnet Practices Network Ltd no no Yes indirect Member 01/05/ /09/2017 St George's Medical Centre Yes Yes Yes Direct GP Partner 01/03/ /10/2017 JFS Brent No No No indirect school Governor 01/03/ /10/2017 Chelsea and Westminster NHS FT no no yes indirect husband is clinical lead for ENT 01/03/ /10/2017 Speedwell Practice. Yes Yes No direct GP Partner 01/03/ /11/2017 Speedwellness Health Ltd Yes Yes No direct Director, this is a wholly owned subsidiary company and is dormant 01/03/ /11/2017 Barnet GP Federation no no yes indirect member 01/03/ /11/2017 NHS England s Medical Directorate, and its Transforming Cancer Services Team No No Yes indirect member 01/03/ /11/2017 North Central London Cancer Commissioning Board. no no Yes indirect Chair 01/03/ /11/2017 Pan-London Cancer Commissioning Board No No Yes indirect Representative for NCL CCGs 01/03/ /11/2017 National Clinical Review Group for Bowel Can no no yes indirect GP Member 01/03/ /11/2017 Clinical advisory group to the pan cancer LondNo no yes indirect member 01/11/ /11/2017 All-party Parliamentary Groups for cancer. No no Yes indirect By invitation she makes ad-hoc contributions 01/03/ /11/2017 International Council for Standardisation in Haematology in association with the World Health Organisation No No Yes indirect Her father is a Board member 01/03/ /11/2017 Beating Bowel Cancer UK no no yes indirect Member of the Clinical Advisory Board 01/03/ /03/2017 Item 2 5
6 Item 2 Dr Clare Stephens Dr Tal Helbitz Dr Jonathan Lubin Bernadette Conroy Elected GP Representative Elected GP Representative Elected GP Representative Lay member (Strategy and Organisational Development St Michael s Grammar School, Finchley no no yes indirect Foundation Governor 01/03/ /11/2017 Air Cadets 393 Squadron local group charity no no yes indirect civilian committee member 01/03/ /11/2017 East Barnet Health Centre Yes Yes No direct GP Partner 01/03/ /09/2017 Barnet GP Federation no no yes indirect Practice is a member 01/03/ /09/2017 Barnet Healthcare Ltd Yes Yes No Direct Practice is a member 01/03/ /09/2017 Social Finance No No Yes indirect Spouse is a director. Social Finance, engages with various Barnet stakeholders on health and social care matters. 01/03/ /09/2017 Derwent Crescent Medical Centre Yes Yes No direct GP Principal 01/03/ /10/2017 Barnet GP Federation Yes Yes no Direct Practice is a member 01/03/ /10/2017 Barndoc Healthcare No No Yes indirect shareholder - 50 shares 01/03/ /10/2017 Cherry Tree Bereavement Charity no no Yes indirect partner is trustee 01/03/ /10/2017 Stroke Service in Islington No No Yes indirect daughter works in this service 01/03/ /10/2017 Lady Sarah Cohen House and Nursing Home yes yes no Direct Derwent Crescent Medical Centre Contract 01/03/ /10/2017 Rosetrees Residential Home yes yes no Direct Derwent Crescent Medical Centre Contract 01/03/ /10/2017 Occupational Health Services for School in Barnet Occupational Health Services for Barnet Homes Occupational Health Services for School in Haringey and Enfield yes yes yes yes no Direct Derwent Crescent Medical Centre Contract 01/03/ /10/2017 yes no Direct Derwent Crescent Medical Centre Contract 01/03/ /10/2017 yes no Direct Derwent Crescent Medical Centre Contract 01/03/ /10/2017 Joint Jewish Burial Society no no no indirect wife, Clare Lubin is Treasurer to JJBS 22/12/2017 Occupational Health Services for Middlesex yes University yes no Direct Derwent Crescent Medical Centre Contract 01/03/ /10/2017 University of Cambridge no no yes indirect Independent Chair of Building and Estates Committee 01/03/ /10/2017 North London NHS Estates Partnership. no no yes indirect Non-executive Director 01/03/ /10/2017 Community Health Partnership. no no yes indirect Non-executive Director 01/03/ /10/2017 Bancrofts school no no yes indirect Governor 01/03/ /10/2017 St Paul s Way Trust School. no no yes indirect Trustee 01/03/ /10/2017 Network Hones no no yes indirect Chair 01/03/ /10/2017 Royal Free Hospitals no no yes indirect spouse is a consultant anaethetist 01/03/ /10/2017 Ian Bretman Citizens Advice Bureau, Barnet no no yes indirect Chair 01/04/ /09/2017 The company is a potential supplier to the no Son is a senior technical manager in a company offering an NHS no yes indirect App for people to manage prescription requests and longterm medication programmes 01/04/ /09/2017 Dominic Tkaczyk Associate Lay Member (Finance) no no no no interests declared 04/04/ /09/2017 Robin Somerville Helen Donovan Lay Member (Governance and Conflicts of Interest Guardian) Registered Nurse Nursing and Midwifery Council no no yes indirect Panel Chair 01/06/2017 Medical Practitioners Tribunal Service no no yes indirect Member 01/06/2017 Barnet CEPN and via the University of Hertfordshire Provide immunisation training, and on self-employed basis immunisation training and consultancy 01/03/ /10/2017 Self-Care Forum no no yes indirect Board member 01/03/ /10/2017 Sanofi Pasteur / Sanofi MSD no no yes indirect Have provided training 01/03/ /10/2017 Royal College of Nursing, no no yes indirect Professional Lead for Public Health nursing at the RCN 01/03/ /10/2017 University of Hertfordshire no no yes indirect Senior Lecturer (Honorary Contract). 01/03/ /10/2017 Dr Jon Baker Secondary Care Doctor GP Surgery in Hendon no no yes indirect spouse is a GP in Barnet 27/09/2017 Non-Voting Members Lay Member (Patient and Public Involvement) Rev Dr Jeff Lake Consultant in Public Health at LBB Consultant in Public Health no no no n/a nil return 01/12/2017 Item 2 6
7 Item 2 Selina Rodrigues Dawn Wakeling Head of Healthwatch, Barnet Strategic Director for Adults, Communities and Health, LBB Head of Healthwatch Barnet Yes yes no Direct Staff member of Community Barnet (lead charity which is the contracting organisation for the Healthwatch Barnet contract) 01/12/2017 Community Barnet no no yes indirect Staff member of Community Barnet which has the following CCG contracts: Health and Wellbeing Hub (to Sept 2019). Wellbeing seminars(to Oct 2019) PPE Project (1year to February 2018) 01/12/2017 Andrew Howe Director of Public Health, LBB Director of Public Health no no no n/a nil return 01/12/2017 Attendees Kay Matthews Chief Operating Officer No interests declared no no no n/a nil return 11/10/2017 Matt Backler Deputy Chief Finance Officer No interests declared no no no n/a nil return 29/09/2017 Colette Wood Director, Care Closer to Home No interests declared no no no n/a nil return 27/10/2017 Ruth Donaldson Sarah d'souza Vicky Aldred Jenny Goodridge Joint Director of Commissioning Joint Director of Commissioning Interim Director of Quality and Clinical Services Director of Quality and Clinical Services No interests declared no no no Regional Lead for Patient Safety / Head of Quality North East Central London NHSE 16/11/2017 Richard Pearson Deputy Director (Barnet, Enfield and Haringey MDTs) NEL Commissioning Support Unit Item 2 7
8 8
9 Item 4 NHS BARNET CLINICAL COMMISSIONING GROUP Minutes of the Governing Body held on Thursday 2 November 2017, 09:00 to 12:00hrs Finchley Memorial Hospital, Greenlands Road, London, N12 0JE Members: Dr Debbie Frost Ms Helen Pettersen Dr Aashish Bansal Dr Jon Baker Dr Charlotte Benjamin Ms Bernadette Conroy Mr Ian Bretman Ms Helen Donovan Mr Simon Goodwin Dr Tal Helbitz Dr Murtaza Khanbhai Mr Robin Somerville Dr Clare Stephens Dr Barry Subel Mr Dominic Tkaczyk Non-Voting Members: Mr Matt Backler Mr Andrew Howe Mr Jeff Lake Ms Kay Matthews Ms Maria DaSilva Ms Selina Rodrigues Mr Paul Sinden Ms Colette Wood Ms Dawn Wakeling Chair, GP and Governing Body Member, West Locality, BCCG Accountable Officer, NCL CCGs GP and Governing Body Member, West Locality, BCCG Secondary Care Doctor, BCCG GP and Governing Body Member, South Locality, BCCG Lay Member (Strategy and OD), BCCG Lay Member (PPI), BCCG Registered Nurse, Governing Body Member, BCCG Chief Finance Officer, NCL CCGs GP and Governing Body Member, North Locality, BCCG GP and Governing Body Member, West Locality, BCCG Lay Member, (Governance), BCCG GP and Governing Body Member, North Locality, BCCG GP and Governing Body Member, South Locality, BCCG Associate Lay Member (Finance), BCCG Deputy Director of Finance, BCCG Director of Public Health, LBB Consultant in Public Health at LBB Chief Operating Officer, BCCG Interim Director of Commissioning, BCCG Head of Healthwatch, Barnet Director of Performance and Acute Commissioning, NCL CCGs Director Care Closer to Home, BCCG Strategic Director for Adults, Communities and Health, LBB In Attendance Ms Ursula Madine Head of Clinical Quality, BCCG (Item 7) Mr Richard Pearson Deputy Director, POD, NELCSU Minutes: Andrew Tillbrook Apologies: Ms Jenny Goodridge Dr Jonathan Lubin Mr Will Huxter Board Secretary (interim), CCCG Director, Quality and Clinical Services, BCCG GP and Governing Body Member, North Locality, BCC Director of Strategy, NCL CCGs Page 1 of 12 9
10 Introduction 1.1 Introductions, Welcome and Apologies for Absence Dr Frost opened the meeting, introductions were made and apologies noted and recorded as above. Ms Colette Wood was welcomed as the CCG s recently appointed Director of Care Closer to Home and Mr Matt Backler, has recently been appointed Deputy Director of Finance. 2.0 Declaration of Interests 2.1 Members were invited to proffer any new declarations of interest, for which none were given. It was noted that the Register should be updated to take account of the recent guidance issued by NHSE. Dr Subel advised that there was reference to his own practice (Ravenscroft) in the minutes of the Primary Care Committee in Common meeting. 3.0 Minutes of the previous meeting, 7 th September The minutes of the meeting held on the 7 th September 2017 were considered and approved after the following amendments were made at Mr Somerville s request: to rephrase paragraph 12.4 by removing the word materially in the penultimate sentence and remove the last sentence, so that the paragraph now reads as: Members discussed the financial position at length, particular regard was given to the increasing risk that plan would not be achieved and whether it would be appropriate to continue to forecast this at month five. A number of members expressed concern with doing so unless there was assurance provided that a realistic set of actions would be feasible to bring the plan into balance given the current likely risks to the position. It was acknowledged that the position could improve through actions such as year-end settlements, release of additional central funds or risk share across NCL CCGs. AGREED: to approve the minutes of the 7 th September Matters Arising and Action Log and updates 4.1 The Chair sought progress on clarifying the approval of the NCL Joint Commissioning Terms of Reference paragraph 8.1 et seq - noting there remained some matters for clarification, especially with respect to budgetary authority it was agreed that Paul Sinden would progress this matter. (Action 101) 4.2 The Action Log was considered and noted, the following updates were provided and accompanying recommendations: GB/073 - Care Closer to Home a report is scheduled for the January 2018 Governing Body Meeting - Action open GB/078 Finance Month 11 and use of contingency money to improve patient care noting that RFL had attended the NCL Joint Commissioning Committee in September 2017 their slide presentation which explains this matter would be circulated to all GB members Action closed GB/090 Young people and mental health information had been provided - Action closed GB/093 Children and Young Persons Plan (STP) information to Dr Helbitz sent - Action closed GB/092 - NCL Joint Commissioning Committee financial modelling re Transformation Programme - agenda item for November report provided - Action closed GB/095 Better Care Fund - - agenda item for November - Action closed GB/096 - Declaration of Interests clarification sought and agreed no new declarations required - Action closed. Page 2 of 12 10
11 GB/097 - Declaration of Interest Register Update all GB members updated Action closed GB/098 - Patient Story - Review content, purpose agenda item - Action closed GB/099 - Update the GBAF to include the relevant NCL risks which need to be brought to the attention of the GB - Action open GB/100 - Children s services and safeguarding and issues to be considered as an informal GB meeting - Action open AGREED: the Committee agreed to note the Action Log updates Chair, Accountable Officer, Patient Story and Quality 5.0 Chair s Report Dr Frost introduced the above report which was taken as read; particular highlights included: the AGM was well attended by members and the public alike the Strategic Partnership Committee which is represented by the CCG, Local Authority and community / business partners. The view, endorsed by the Governing Body, was that this Forum should be used to support the CCG with some of its strategic work the outcome of the OFSTED Review - the Improvement Plan in response to the review, had been praised by Ms Frankie Sulke, CBE, a Commissioner with the Department for Education. It was agreed to circulate the Action Plan to the Governing Body in January via the CQRC (Action KM: GB/ 102) the approval of the opening of the Adams Ward at Finchley Memorial Hospital to support the Discharge to Assess initiative. The meeting noted that this had been agreed by the Governing Body on the 12th October 2017 in order to meet the deadline to enable the ward to open by early December. The meeting noted and supported the resolution to commission seventeen Discharge to Assess beds on Adams Ward at Finchley Memorial Hospital from 4th December 2017 managed by Central London Community Health Care Services (CLCH), including additional investment requirement of 123k in 2017/18 and 202k in 2018/19 the Children s Therapies Business Case, which had been reviewed by FP&Q Committee in March 2017, which was broadly endorsed subject to some issues of clarification. Following the August FP&Q meeting at which a request for additional expenditure was approved ( 54,000), it came to light that as the total contract value exceeded 1.5million, Governing Body consideration and decision was required for approval. The Governing Body considered the business case on the 12th October 2017 at which it agreed to support the total aligned budget of 3,217,518 available across the LBB and Barnet CCG and to go out to procure an integrated therapies service. The Governing Body also agreed that: o the length of contract to be 5 years plus 2. o the current Section 75 agreement is amended to include all three services and with the new financial amounts as agreed in the Business Case and covering report Members discussed the AGM part of the report with particular reference to the resolutions regarding GP representation across the three localities that constitute the CCG. Although there was a range of opinions, the resolution presented does provide flexibility for the Governing Body. Whilst some concern was expressed as to the time frame given for the membership to consider the resolution at the AGM, calls for members to come forward to be considered for Governing Body membership had been made on several occasions as well as promoting the resolution proposal via the GP newsletter. AGREED: to note the report Page 3 of 12 11
12 6.0 Accountable Officer s Report 6.1. Ms Pettersen referred the meeting to the above report which was taken as read, from which attention was drawn to: the CCG now had a fully appointed directorate team, which would provide stability and direction for the organisation good progress was being made with the plans for Finchley Memorial Hospital NHSE London provided positive feedback to the CCG senior team following a meeting at which its financial recovery plans were discussed recently the financial recovery plan, submitted to NHSE London, had been accepted; Ms Matthews, Mr Backler, Mr Goodwin and Mr Eaton were thanked for their work building confidence with NHSE. AGREED: to note the report 7.0 Review of Patient Stories in Ms Madine presented the report which was taken as read. The meeting was reminded of the recommendation to review the value and purpose of collecting and relaying patient stories to the Governing Body. In considering the report, members provided a range of views and comments: providing context of the patient story with regard to their condition as well as the service(s) they receive and / or seek, noting that this would require research, interviewing patients as well linking the story / topic with the CCG s Commissioning Team the patient story could be helpful as a way to review patient pathways, linking their experience to CCG initiatives the potential opportunity for the CCG s Public and Patient Involvement (PPI) Committee to provide an oversight function identifying ways to help improve communications to augment the patient voice Healthwatch could provide potential patient case studies via its Outreach service the granularity of the patient story was appreciated and whether the exercise could focus more on the quality perspective and if there might be common themes encourage members of the CCG s Commissioning Team to visit services that they have commissioned to gain first-hand knowledge and experience of the clinician providing treatment and the patient receiving treatment providing patients with feedback as to how effective the commissioned service is, as well as any shortcomings in the service and identify changes in quality of the service (which would require live ongoing patient engagement) linking the patient story with service design (and redesign) as a way of assessing the quality of care and benchmarking improvements to provide greater focus on themes where possible rather than individual patients to avoid the perception that the Governing Body assumed a role of sorting out a particular problem for a patient. 7.2 Members were reminded that the provision of the Patient Story as a standing item at Governing Body was to centre its membership on their role, that of patient care and quality of service. Ms Matthews endorsed the view that patients should be interviewed to help develop the story and context. 7.3 In considering a way forward, the following suggestions were made: the PPI Committee to consider and identify themes for patient stories by April 2018 for the Governing Body to receive an annual review of patient stories to act as a reflective tool and a mechanism for development for the year ahead publishing patient stories on the CCG website (subject to the appropriate consents). 7.4 Following further discussion, the Governing Body: Page 4 of 12 12
13 AGREED: to note the report for a progress report from the PPI Committee to be received at the March 2018 Governing Body meeting for a patient story to be developed and presented at the January 2018 meeting an Annual Review of patient stories to be presented at the November 2018 Governing Body and annually thereafter. 8.0 Quality and Performance Report 8.1 Mr Pearson referred the meeting to the above report which was taken as read. Particular note was made of: the worsening Referral To Treatment (RTT) waiting times at Royal Free London, which was being supported via the Intensive Support Team and NHS Improvements and NELCSU a remedial action plan was being developed and should be in place by mid-november UCLH had also missed its RTT targets and it was expected that this would have a knock on effect at the Royal Free London Cancer waiting times remained a concern with five of the eight waiting time targets met in August 2017, though some of the targets were missed because of the small numbers of patients causing significant swings in percentage performance. Concern was also highlighted that there was an increase in referrals in dermatology and lower gastric intestinal conditions and the potential issue of capacity following capability problems at the North Middlesex University Hospital (NMUH). In the short term, RFL was employing greater use of tele-dermatology clinics and hiring an additional consultant though this was not regarded as a long term solution. It was noted that although there was intention to meet the 62-day urgent GP target by September 2017, the target had been missed and it was now not expected that it would be met by November 2017 Dr Stephens expressed concern about funding being withdrawn for early intervention and early diagnosis for cancer patients as the 62 cancer referral target had not been met. This was expected to have a detrimental effect on quality of care and patient support. The STP had contacted the national cancer team to express concern but it was unlikely that this funding would be reinstated. However, a second tranche of funding would be made available to help fund the ITT tracker. It was noted that this matter had been escalated to NHSE via the provider trusts as well as the relevant CCGs in north central London Accident and Emergency Waits - there had been recent improvements to meeting targets, Barnet Hospital was conducting its Perfect Week (a national initiative designed by the Emergency Care Intensive Support Team (ECIST) to help improve acute and emergency care performance). It was hoped that the improved performance could be sustained. Community Services performance had continued to improve and targets against the Remedial Action Plan set in August had been met. As a result of this improvement, the contract performance notice had been withdrawn. However, there remained concern that some patients were exceeding their twelve week stay and leading to delayed transfers of care; the Barnet Integrated Care Team was investigating the reasons for the delays Mental Health, Improved Access to Psychological Services (IAPT) workloads were increasing, which was leading to an increased risk on the service to meet performance targets. 8.2 Dr Khanbhai highlighted some of the issues raised in the quality section, particularly with regard to serious incidents and never events: the delayed report on the serious incident at RFL in June 2017 had recently been published and significant learning had been gained Page 5 of 12 13
14 reports for one of the three never events in August 2017 had been published, with the other two to follow shortly. The findings were and would be scrutinised at the providers Clinical Quality Reference Group (CQRG) feedback from the Royal National Orthopaedic Hospital had proved more challenging as Barnet CCG was now represented at their CQRG meetings indirectly. Dr Khanbhai advised he would follow up how to ensure improved oversight. Following further discussion, it was agreed that Mr Sinden would progress this matter Action: GB/ The meeting noted that there were some 52 week wait (re RTT) breaches at RFL as well as 62 day cancer wait breaches which may have resulted in significant harm to patients. Assurance was given that NHSE was reviewing, individually, those patients who exceeded the 52 week wait and an action plan was being developed. Concern remained that RTT waits had been a long running issue with RFL and there were effects on patient care and potential harm. Whilst there was intensive work addressing and manage the RTT breaches, there was general agreement that a Contract Performance Notice (CPN) should be issued in order to trigger a contractual process to provide a Remedial Action Plan and data sharing within a prescribed time period. Members were reminded that RTT waits was of such concern three years ago, with NHSE, that the CCG was placed into special directions. It was noted that the issue of RTT breaches remained the responsibility of the provider to ensure that patients were referred to other providers if the RFL did not have the capacity. Dr Helbitz sought assurance that patient care and quality would not be compromised if RFL referred patients to other providers. 8.4 Following further discussion, Mr Sinden recommended that an intention to serve notice of a CPN should be expressed first to provide forewarning to the provider before issuing the CPN. 8.5 Ms Da Silva advised that it was the CCG s intention to discuss the Remedial Action Plan with RFL and NHSE so that all key stakeholders were engaged, week commencing 20 November. 8.6 Dr Khanbhai advise that the CCG s Clinical Quality and Risk Committee (CQRC) was reviewing its role and some of its reporting lines. Noting, for example, that care homes came under the aegis of the Local Authority, the Committee was considering that it should have local authority representation to strengthen its oversight of the quality aspects of care. 8.7 Clarity was sought as to how the smaller contracts with a range of providers under the CCG s domain was being managed from a quality perspective. Ms Matthews confirmed that an initial piece of work had been conducted, and when the results were available, a prioritisation process was planned. It was noted that some contracts were directly related to the Care Closer to Home initiative. Following further discussion the Governing Body noted that report on smaller contracts would be brought to the Governing Body meeting in March 2018 (preceded by review by the Quality Committee, GB/104 action MDS) AGREED: to note the report to give notice of an intention to serve a CPN to RFL to receive a progress report on RTT at the next Finance, Performance and QIPP Committee Corporate Business and Business Cases 9.0 Better Care Fund 2017/ Ms Da Silva presented the above report. Members were advised that the BCF plan to NHSE was submitted on the 11th September and subsequently approved as a pan-london plan. Four national conditions had been set by NHSE: Plans to be jointly agreed NHS contribution to adult social care is maintained in line with inflation Page 6 of 12 14
15 Agreement to invest a specific proportion of the fund in NHS commissioned out-ofhospital services; (or retain it as part of local risk-sharing) Managing Transfers of Care (to ensure people s care transfers smoothly between services and settings). 9.2 Whilst there would be some flexibility as to how the budget was spent, the CCG needed to remain mindful of four performance metrics with a view to help improve performance: Delayed transfers of care (DTOCs) Non-elective admissions (General and Acute) Admissions to residential and nursing homes Effectiveness of reablement. 9.3 In terms of planning, members noted that some of the money would be allocated directly to the Local Authority (known as the IBCF) which would amount to 21m over three years, details of which were set out in section 3 of the report. 9.4 There would be a focus on DTOC; meetings had already started between the CCG and the provider, Central London Community Healthcare Trust (CLCH) and a drive to integrate the various but related services for planned care including Care Closer to Home, and unplanned care including admissions avoidance, rapids response and enablement services. 9.5 Ms Wakeling provided a verbal update on the 18/19 performance against the approved plan, Currently Barnet are not meeting the DTOC metric; which has been further compounded by the fact that the data submitted by CLCH now needed to be refreshed. It was noted that NHSE had been made aware of the inconsistencies and are working with the provider to refresh the data. 9.6 Members, in deliberating on the report, gave rise to the following comments / clarifications: references to pooled budget should be rephrased as an aligned budget the logistics of discharging patients from hospital to care homes on a Friday to help improve transfers of care was countered by risk that some patients may not always have access to their regular medication and receive the appropriate clinical care until the Monday. it was noted that the level of support would need to be assessed in each care home as their capacity to provide adequate care over the weekend between discharge and assessment by a doctor varied. it was noted that a new service funded by the RFL charity to help cover this aspect was being commissioned. Nevertheless, some patients presented a range of complex needs and there would be occasion when staying in hospital over the weekend gave the best provision of care. The GB sought assurance that the CCG would not be funding the void space for Ruby ward at Edgware Hospital once it was decommissioned GB/105 action MB to clarify if the CCG was liable for the Ruby Ward void space costs post decommissioning. AGREED: to note the report to note the approval of the submission of the plan and budget submitted to NHSE in September 2017 for the Finance, Performance and Quality Committee to progress and monitor the Better Care Fund with updates to the Governing Body when appropriate 10.0 NCL Winter Planning 10.1 Ms DaSilva presented the above report. The meeting noted that: Barnet CCG had just appointed a dedicated Resilience Manager to cover winter planning An Urgent and Emergency Care Transformation Board has been set up at the Royal Free site to mirror the approach being taken at Barnet Hospital Page 7 of 12 15
16 Patient flow worked reasonably well at Royal Free Hampstead Royal Free Hampstead s accident and emergency centre had been redesigned; and it was expected that patient flow would be improved Barnet Hospital patient flow was less assured; the CCG and NHS Improvement had met with the provider to assess the challenges and help support and develop an improvement plan which had led to more collaborative working between the stakeholders, represented by senior level staff. This motivation had led to better availability of beds in A&E and better ambulance handovers and reduced mixed sex breaches and fewer Delayed Transfers of Care (DTOCs) Whilst assurance was given to improvements across the RFL, concern remained on the potential fallout if a neighbouring provider hospital was unable to meets its targets with increased demand on providers in Barnet. Members noted that the North Middlesex University Hospital (NMUH) was making significant progress in meeting its A&E targets; complemented with a robust management team with a view to improve and sustain performance Nevertheless, concerns remained across providers across the outer London boroughs that border Essex, Middlesex and Hertfordshire as there had been an increased demand on A&E services with patients being brought in from these counties via the East of England Ambulance Service Trust (EEAST). Ms Pettersen s team were due to meet with representatives from NHSE, the London Ambulance Service (LAS) and EEAST to review this position and devise a plan to address this issue Assurance on ensuring appropriately senior clinical staff deployed at key points in the A&E system was provided as RFL and the Whittington hospitals had embraced these recommendations and were now able to demonstrate the benefits. AGREED: to note the report Finance, Performance and Governance 11.0 Finance and QIPP Report, month Mr Goodwin introduced the above report by reminding members of the developments made since the last Governing Body meeting on the 7th September 2017: in September, discussion focussed on the level of risk and whether it realistic to continue to forecast achievement of budget by month 5, it was apparent that the forecast would be a deficit of 4.6m which was an adverse variance to plan of 8.3m, which was subsequently declared to NHSE NHSE s response to this declaration asked the CCG to devise and submit a recovery plan, from which would trigger an external financial review which was due to start by December the Recovery Plan, submitted in October 2017, indicated mitigations against the forecast deficit of 2.3m. The forecast deficit at month 6 was therefore 2.3m (reduced from 4.6m) the Recovery Plan appeared to generally accepted by NHSE, partly due to the plan demonstrating that the run-rate would be recovered in year compared to plan. The recovery plan represents a stretching but achievable position and there is material risk to delivery which will need to be actively managed 11.2 Mr Backler advised the Governing Body that QIPP savings for 2018/19 of 21.8m would be required to deliver financial balance based on current forecasts. Of the 21.8m, 7m would be delivered through full year effect savings (to be achieved) for 2017/18. Page 8 of 12 16
17 11.3 In discussion, it was noted that Barnet CCG had accumulated surpluses of 5.2m and would be used to offset the in-year forecasted deficit of 2.3m, meaning the CCG would not be required to recover the 2017/18 deficit in 2018/ The Chair thanked the senior team responsible for devising the Recovery Plan and its submission to NHSE which had instilled a sense of confidence that the Plan was realistic and achievable. AGREED: to note the report /19 Barnet CCG Commissioning Intentions 12.1 Ms Da Silva introduced the above report. Members noted that the submission of the Commissioning Intentions had been made to NHSE on the 29 September 2017; these were in two parts - at NCL level to address a wider strategic level of interfacing with main providers and via the CCG to address more locally focussed services. It was noted that strategic challenge at NCL level focused on prevention based services Mr Sinden advised that the planning round for 2018/19 had started and that there was provision for negotiating and resetting base lines (support for which had been provided by the Commissioning Support Unit) on year two contracts agreed and set for It was noted that baselines would be set on a consistent basis across the CCGs. Agreement was expected to be reached by the 20 December Ms Rodrigues suggested that the commissioning intentions should be presented to the (shortly to be inaugurated) CCG s Public and Patient Involvement Committee to enable comment and provide a patient s perspective, when this process was undertaken next year. AGREED: to note the report 13.0 Transforming Care Update (Learning Disabilities) 13.1 Mr Sinden presented a progress report on the transforming care programme that had been presented to the NCL Joint Commissioning Committee (JCC) in October In October 2017 the JCC agreed that monies released from CCG funded inpatient placements would be used to cover the costs for CCGs and Social Care of transferring packages of care into the community A second cohort of patients were in inpatient placements funded by NHS England (Specialist Commissioning), and a funding transfer agreement was not in place for any transfer of care for this cohort into locally funded community packages. For Barnet CCG and Social Care this represented a potential cost pressure of 0.7m if funds did not follow the patient At the October 2017 meeting the JCC agreed that a letter be sent to NHS England on its behalf seeking clarity on the transfer of funds to match transfers of care. Following this a meeting with NHS England was held on 2 nd November to discuss funding mechanisms Nevertheless, concern remained that there would be additional cost pressures on the local authority, primary and secondary care services and it was therefore paramount that adequate funding was received via NHSE to support this group of patients. AGREED: to note the report 14.0 Sustainability and Transformation Partnerships (STP Half yearly update) 14.1 Ms Pettersen presented the above update on behalf of Mr Huxter; an overview of which was provided. Members noted the progress which had been made: Page 9 of 12 17
18 from planning to implementation of plans, including recalibration of plans the increasing improvement of joint working between commissioners and providers streamlining and joining up of processes across the five CCGs at STP level, focussing on improving working relationships with the Health Overview and Scrutiny Committees, Health and Wellbeing Boards reviewing and scoping what part of the services could be managed at NCL level (and so reviewed once) whilst ensuring that more locally based services, e.g. primary care, remained with each CCG the NCL Director of Strategy s team was now established which now enabled greater opportunity to develop NCL wide projects, such as determining a Health Information Exchange financially, the STP and NCL CCGs remained challenged due to the capped expenditure process, but this was a common issue across London In response, the progress of the STP was welcomed, supporting in particular, the importance of building on the communication and engagement with stakeholders and the public to help develop a better understanding of how the health and care system was working. It was noted that there should be an opportunity for lay members to be engaged and help shape and promote the emerging health and care structures The meeting noted that Communications and Engagement Leads across NCL were due to attend a Workstream meeting on 22 November with the aim of gaining a better understanding of the various components that constituted NCL as well as the related stakeholders It was noted that there was a potential resource and expertise that could be called upon with lay members and clinical leads identified in slide 14 of the report, noting that there should be more clinical input, especially from Barnet CCG. AGREED: to note the presentation 15.0 NCL Primary Care Co-Commissioning Terms of Reference 15.1 Mr Sinden provided an update to a report previously presented to the Governing Body outlining some amendments to the Terms of Reference. The changes outlined in the Terms of Reference were noted: the Committee could approve non contentious, low level decisions between meetings that decision making would be by the relevant CCG lay member, rather than any lay member Following further deliberation, clarification was sought on clause 5.1 geographical coverage - to be amended as persons registered in Barnet clause 11.7 as to whether all three persons needed to approve or any one of the three was sufficient - it was noted that it should be ALL three persons clause 12.1 quoracy it was not the intention that if one CCG was not present, that the committee would be rendered inquorate regarding clauses 12.2 and to clarify that the co-opted person should be from the relevant CCG rather than any CCG the detail in schedule 1 should be job titles only and not names. AGREED: to note the recommended amendments to enable Ms Conroy and Mr Sinden to further review the Terms of Reference to ensure they are fit for purpose to approve the revised Terms of Reference based on the proviso of the aforementioned review Page 10 of 12 18
19 16.0 Terms of Reference, Public and Patient Involvement (PPI) Committee 16.1 Mr Bretman introduced the above report and proposed Terms of Reference. Members noted that the PPI Committee was due to meet on the 16th November The ToR had been considered with a range of stakeholders, and, whilst there some final appointments to be identified to the Committee, it was practicable to form and start its work in the interim, to maintain momentum. The purpose of the Committee was to promote engagement and oversight of the services commissioned by the CCG In discussion it was noted that the PPI Committee needed adequate resourcing, which would and was being addressed indirectly by way of a Corporate Services Review across NCL. It was recommended that the ToR should make provision for substitution of members and creation of a vice Chair if the Chair was unable to attend. Ms Wakeling confirmed that the Local Authority could provide support by sharing relevant policies about volunteering Dr Frost welcomed the progress made with the creation of this Committee and thanked Mr Bretman for his work. AGREED: to approve the Terms of Reference, subject to inclusion of the recommendations set out in para Annual General Meeting Minutes 7th September The minutes were considered were noted, with clarification that Ms Conroy left the meeting at para 3.6 AGREED: to approve the minutes and recommend their adoption at the next Annual General Meeting Reports and Minutes of Committees of the Governing Body 18.1 Finance Performance and QIPP Committee, 27th June 2017 and 31st August 2017 AGREED: to note the minutes of the meetings 18.2 Primary Care Procurement Committee, 6th July 2017 AGREED: to note the minutes of the meeting 18.3 Clinical Quality and Risk Committee 27th July 2017 AGREED: to note the minutes of the meeting and recommend a deep dive with a future set of minutes at a forthcoming meeting 18.4 NCL Primary Care Committee in Common 19th July 2017 AGREED: to note the minutes of the meeting 18.5 Health and Well Being Board Minutes 20th July 2017 AGREED: to note the minutes of the meeting Consideration was given whether to provide summaries of minutes of CCG Committees in future, noting, however, the resourcing required to achieve this made this unviable except for the Primary Care Procurement Committee. Page 11 of 12 19
20 Closing Administration 19.0 Any Other Business 19.1 Health Information Exchange the Chair advised that a review of the HIE was being undertaken and whether there may be occasion for a decision to be made between meetings. It was noted that NCL would be eligible to receive funding from the Estates and Technology Transformation Fund. Where a decision was required before the next Governing Body meeting, the members agreed that this should be delegated to Ms Conroy and Mr Goodwin Diabetes Freestyle Libre - the CCG had received numerous enquiries from patients as to whether this device would be funded by the CCG. The matter has been discussed across NCL and primary care leads who had concluded that for now Barnet CCG, as well as the other CCGs in NCL were unable to fund the device on the grounds of cost, in both primary and secondary care settings. This holding position had been agreed by the NCL Joint Formulary Committee. It was agreed to circulate the decision via the GP Bulletin and provide the evidence to GPs to support their dialogue with relevant patients. It is anticipated that North Central London Formulary Committee liaising with other NHS Medicines groups in London will provide further guidance in the future Review of meeting effectiveness and items for next Governing Body meeting, 11th January 2018 The breadth of reports and discussion was noted as balanced and robust The date of the next meeting was scheduled to take place on 11th January 2018 between 09:00 to 12:00 at Hendon Town Hall. There was no further business. The meeting closed at Page 12 of 12 20
21 Barnet CCG Item 4.1 Governing Body minutes, 6 July 2017 A question was raised by a member of the public at the July 2017 Governing Body meeting. Following publication of these minutes after the September Governing Body Meeting, the member of the public sought clarification as to how the minute was recorded. After consideration with the Governing Body Chair, Dr Frost and Governing Body Member, Dr Talbitz, it was agreed to revise the minute to read: Questions from members of the public Mr D R Hurley put forward some questions concerning the role of the Referral Management System in Barnet (RMS), with particular respect to: What is the mission statement for the RMS and are there performance measures for monitoring the service and if so what are they? Whether these measures of the RMS performance were reviewed by the CCG s Governing Body? Dr Farooqi provided an overview of the RMS and explained that it was set up with the aim that patients received the right appropriate care in a timely and efficient way. It was noted that there were delays occurring in the system, these may be influenced by patient choice, or where a series of tests were required for a patient prior to diagnosis and treatment. Dr Helbitz explained how patient records were held and indicated that all GP Practices in Barnet had adopted a web-based system called EMIS (an electronic patient record system managed by EMIS Health). The system enabled the transfer of electronic patient records between surgeries when a patient moved address. Although an overview of the RMS was explained, greater clarity was sought as to the level of oversight the Governing Body had of referral service. Mr. Hurley also expressed the view, from his experience of performance management, that one of the reasons Bernadette Conroy raised questions on 62 day cancer performance was because that measure does not give good visibility of actual hospital performance, and process measures would be more appropriate for that. Dr Frost suggested that Mr Hurley should discuss this with Mr. David Willmott (who had left the meeting) as he would be more familiar with this area of process measures. Mr Hurley agreed to provide his contact details. The Governing Body is asked to confirm the above text. For completeness the original extract from the July meeting is copied below: There were a number of questions put forward by Mr Hurley a patient in Barnet. He had encountered significant delays and problems with the Referral Management Service (RMS). He asked the Governing Body if GPs were actively managed and what kind of systems GP practices used, as from his experience they appeared to be inefficient. He specifically asked if patient records were stored electronically. 21
22 Ahmer Farooqi responded that he was the CCG s clinical lead for the RMS. He was sorry to hear about Mr Hurley s difficulties with the service. He confirmed that patient records are held electronically by GPs, the RMS was setup with the aim to ensure that patients received the right treatment in the most appropriate setting, by the right person at the right time. There were many reasons why a referral may be delayed, sometimes it could be as a result of patient choice, other times due to a GP requiring a particular pathway, and there may also be a need to complete a range of investigations before the referral proceeded. The RMS was intended to improve efficiency and therefore be more cost effective. Tal Helbitz commented that all practices used EMIS web-based system and this had improved how general practices managed patient records. It was noted that Barndoc operated the RMS and that there were regular meetings between the CCG and Barndoc to performance monitor the service. Debbie Frost suggested that Mr Hurley discussed his particular case with David Willmott, Associate Director of Quality so that he could look into his particular case with the practice. 22
23 Paper 5.0 Decision and action log for meeting held in Public Minute Reference Date Agreed Action Lead / Owner Due Date Action Status Item for future Governing Body Status GB/ Care Closer to Home The Strategic Plan including resources for Care Closer to Home will be produced and submitted to FP&Q in July / August. Leigh Griffin/ Tal Helbitz Colette Wood Work is progressing on the production of a joint Health and Care Closer to Home resourcing and delivery plan with Barnet Borough Council. This plan is being produced under the auspices of the Joint Commissioning Executive, recast as a Care Closer to Home Programme Board, reporting to Barnet s Health and Wellbeing Board as well as to constituent organisational partners. An update will be given at the September GB. Colette Wood to be appointed as Director of Care Closer to Home from 9 October. Kay Matthews to retain oversight. Work with Local Authority continued. Agreed to give a progress report at Jan GB meeting. Yes Recommend close Agenda item Jan 2018 meeting Report on decision taken action points arising from Governing Body Meeting held in Public ITEM 5 Page 1 of 3 23
24 Paper 5.0 Decision and action log for meeting held in Public GB/ GB/ GB/ GB/ GB/ Update the GBAF to include the relevant NCL risks which need to be brought to the attention of the GB Children s services and safeguarding and issues to be considered at an Informal GB Meeting NCL Joint Commissioning ToR clarification sought re budgetary authority Ofsted Action Plan circulate plan to next meeting via the Dec CQRC Quality and performance report Get appropriate representation at the RNOH CQRG because of concerns Paul Sinden Andrew Tillbrook Paul Sinden Kay Matthews Paul Sinden Update the GBAF to include relevant NCL risks to be brought to the attention of the GB This work is in progress and an updated GBAF will be presented to the Audit Committee in January and will include any NCL relevant risks which require inclusion onto the GBAF To be arranged suggest January / February 2018 Terms of reference for JCC signed off Barnet CCG Children s Improvement Action Plan has been circulated to GB 18/12/2017 CCGG Director of Quality is now attending the RNOH CQRG Yes No No No No Open Recommend close Recommend close Open Report on decision taken action points arising from Governing Body Meeting held in Public ITEM 5 Page 2 of 3 24
25 Paper 5.0 Decision and action log for meeting held in Public GB/ GB/ Quality and performance report Management of the smaller contracts with a range of providers under the CCG s domain was being managed from a quality perspective. Noted that a report on smaller contracts would be brought to the Governing Body meeting in March 2018 (preceded by review by the Quality Committee in February 2018) Better Care Fund 2017/19 Check if Barnet CCG is liable for paying for Ruby Ward at Edgware Hospital void costs post decommissioning Maria DaSilva No Open Matt Backler It has been confirmed that Barnet CCG is not liable for void costs No Recommend close Report on decision taken action points arising from Governing Body Meeting held in Public ITEM 5 Page 3 of 3 25
26 26
27 Item 6 MEETING NHS Barnet CCG Governing Body Meeting DATE 11 January 2018 REPORT LEAD DIRECTOR / GOVERNING BODY MEMBER AUTHOR CONTACT DETAILS Report of the Chair Dr Debbie Frost, Chair of Barnet CCG Dr Debbie Frost, Chair of Barnet CCG Debbiefrost@nhs.net EXECUTIVE SUMMARY The purpose of this report is to provide the Governing Body members with an update on relevant chair s actions and key strategic work streams that are currently taking place within the CCG since the last meeting on 2 November RECOMMENDED ACTION The Governing Body members are asked to: Note the update provided in this report. Objective(s) / Plans supported by this paper: This paper supports the following strategic objectives of the CCG as highlighted within the Constitution. This paper supports the Chair of the CCG in fulfilling their responsibilities in accordance with the CCG s constitution and also to ensure that the CCG works collaboratively with the North Central London CCGs on external governance arrangements to support NCL wide strategy. Outcomes Expected: Ensure that the Governing Body members and the member practices are kept informed of key changes. 1 P a g e 27
28 Audit Trail: N/A Patient & Public Involvement (PPI): N/A Equality Impact Assessment: N/A Risks : None 2 P a g e 28
29 Key themes and events 1.0 Finchley Memorial Hospital 1.1 I am pleased to report that there has been real progress on services going into Finchley Memorial Hospital (FMH). Adams ward a 17 bedded ward for Discharge to Assess provided by CLCH opened on 04 December and took 5 patients in the first week. The CCG continues to progress the other key work streams to maximise the usage of FMH. This includes: Opening the CT scanner suite to support the lung cancer research project. This work is on track and is expected to open in June Exploring the possibility of opening a Breast Screening facility. Developing a service specification for a General Practice to be provided from FMH. 1.2 I met with the Right Honourable Mr Jeremy Hunt MP, Secretary of State for Health, on 03 November with Kay Matthews, local MP Mike Freer and Sir David Sloman, Chief Executive of the RFL, to discuss Finchley Memorial Hospital and the opportunity this facility presents for the residents for Barnet. 1.3 On the 08 November I met with local Councillors from the Barnet Health and Overview Scrutiny Committee, who have taken a close interest in Finchley Memorial Hospital. This meeting was with Kay Matthews and Councillor Alison Cornelius (Totteridge Ward) and Councillor Grahame Old (Finchley Church End) to discuss progress on Finchley Memorial Hospital, and an update on the Procedures of Limited Clinical Effectiveness. 1.4 I also attended the Health Overview Scrutiny Committee (HOSC) on 04 December with Kay Matthews and Alan Gavurin, Finchley Memorial project lead, to give a formal update on the progress being made to maximise the usage of Finchley Memorial Hospital. The HOSC warmly welcomed the progress being made. They will continue to scrutinise progress at their bi-monthly meetings for the coming future. 2.0 Management and Strategy 2.1 On 03 November, I attended a summit to discuss the Emergency Department workforce in North Central London together with Dr Aash Bansal and Maria DaSilva, Director of Commissioning. The summit focused on the workforce across North Central London looking at both the short term and long term strategies needed to manage winter and beyond. 2.2 NHS Improvement (NHSI) and the other arms-length bodies have announced plans for enhancing the staffing of emergency and urgent care. Locally there is workforce development funding available to support the system and we need to determine collectively how best to use this resource. 2.3 On November, I attended the London CCG Chairs and Trust Medical Directors workshop at Cumberland Lodge in Windsor. We had an opportunity on the 14 November to discuss CCG issues with Professor Jane Cummings, Chief Nurse for England and NHSE Regional Director for London. The following day we met with Medical Directors from Trusts across London, as well as the Medical Directors for NHS England and NHS Improvement in London. As well as discussing strategy and working 3 P a g e 29
30 together, we also heard a very interesting presentation from Nottingham about their approach to forming an Accountable Care System (ACS) and their progress so far. 2.4 On 05 December I attended a fascinating breakfast meeting at the Kings Fund. Speakers included a Kings Fund analyst, an ex-ccg Chair (who is the clinical lead for an STP) and the former Chief Executive of NHS Improvement - who all gave their views of the recent budget. 3 Working with our partners in Barnet 3.1 Health and Wellbeing Board (HWBB) I attended the Health and Wellbeing Board as Vice Chair. Of particular interest was the report on the London Borough of Barnet s Ofsted Improvement plan as well as two interesting papers from Barnet Mencap following their work with Healthwatch Barnet. One report focused on care for patients with learning disabilities, with very telling feedback about some of the carers; the other report was on experiences of having blood tests. Following the Board meeting, I circulated a copy of, and advice on, easy read materials to all the GPs in Barnet via the GP bulletin. 3.2 Healthy Barnet Week I held the first meeting to start planning for an event where we will hope to increase our prevalence of diabetes and atrial fibrillation by finding the undiagnosed patients as well as promoting the Mayor s Golden Kilometre. This was together with Councillor Caroline Stock as well as Louise Pavli, a public health strategist, Luke Robertshaw from Public Health and Dr Lesley Isenberg, retired GP and Chair of the Barnet branch of Diabetes UK. Especially exciting was using the Diabetes UK tool Know your Risk During, the last two months, Kay Matthews and I have also met with the Medical Director, Director of Strategy and Director of Finance of CLCH, John Hooton, Chief Executive of the London Borough of Barnet and Matthew Offord MP the latter meeting at Portcullis House in Westminster. 3.3 Improving Patient Discharge from Acute Care Both Dr Barry Subel and I participated in the Barnet Hospital MADE (Multi Agency Discharge Event). This brings together the local health system to support improved patient flow across the system, identifies patients appropriate to discharge and unblocks delays to discharge and challenges, helping to improve and simplify complex discharge processes. The outcome of this is to ensure the hospital learns from these events how to improve their discharge processes to ensure patients do not stay in hospital longer than clinically necessary. This also resets the hospitals in preparation for the seasonal pressure expected over the holiday period. 4 Joint Commissioning Committee 4 P a g e 30
31 4.1 I attended the NCL Joint Commissioning Committee, where we discussed the performance of the trusts within NCL as well as Procedures of Limited Clinical effectiveness (PoLCE), dermatology services and planning for winter. 5.0 Better Health 5.1 I attended the North Central London Primary Care Strategy Development Workshop on 14 December, along with Dr Tal Helbitz who is the Governing Body Clinical lead for Care Closer to Home. Helen Pettersen, Will Huxter, Paul Sinden as well as the other Chairs, COOs, Primary care clinical and managerial leads from all the NCL CCGs. This was the first workshop to start the process of developing a Primary Care Strategy across North Central London and will be followed by a series of further workshops and wider engagement to shape and test the strategy during its development phase. I used this workshop as an opportunity to highlight the work we are doing on Care Closer to Home Integrated Networks (CHINs) in Barnet. 6.0 Governing Body Vacancies 6.1 Following the recent advertisement in the GP Bulletin, a candidate for the appointment of GP representative for all three localities in Barnet CCG was interviewed on the 13 December Nick Dattani was the only applicant who applied for this post. He was interviewed and assessed as successfully meeting the required criteria to go forward for election by the GP members. This election will take place in January 2018, in line with the CCG s constitution. 7.0 Welcome to Maria Kane at North Middlesex University Hospital NHS Trust 7.1 I would like to extend a warm welcome to Maria Kane, who has been appointed as the chief executive of North Middlesex University Hospital NHS Trust. I m delighted with Maria s appointment and look forward to working with her across NCL. Dr Debbie Frost Chair of Barnet Clinical Commissioning Group 18 December P a g e 31
32 32
33 Item 7 MEETING: NHS Barnet CCG Governing Body Meeting DATE: Thursday, 11 January 2017 TITLE: LEAD DIRECTOR/ MANAGER: AUTHOR: CONTACT DETAILS: Accountable Officer Report Helen Pettersen Accountable Officer, and STP Convenor for North Central London Kay Matthews, Chief Operating Officer kay.matthew5@nhs.net SUMMARY: This report updates the Governing Body on developments in the local NHS and wider policy issues. SUPPORTING PAPERS: There are no supporting papers. RECOMMENDED ACTION: The Governing Body is asked to: NOTE the Accountable Officer s Report Objective(s) / Plans supported by this paper: This report is for information only. Audit Trail: This report is for information only. Patient & Public Involvement (PPI): This report is for information only. Equality Impact Assessment: This report is for information only. Risks: This report is for information only. Resource Implications: This report is for information only. Page 1 of 4 33
34 Accountable Officers Report 1 INTRODUCTION 1.1 This report focuses on the key activities that the senior team and I have been involved in and work that has progressed since the last Governing Body meeting. 2 The CCG s Director s Team 2.1 The CCG will welcome Ruth Donaldson and Sarah D Souza to the Director s team on the 2 nd January 2018 as the substantive Director of Commissioning on a substantive, job share basis. I would like to express my thanks to Maria da Silva who has been covering this role on an interim basis since June 2017 and who has, in partnership with her clinical colleagues, successfully progressed the commissioning agenda locally. 2.2 Other director level changes include: o Mark Eaton, Interim Director of QIPP completing his technical assignment to develop the 2018/19 QIPP programme and returning to Enfield CCG to support their programme going forward. o Recruitment of an Interim Director of QIPP delivery whose assignment will focus on strengthening the mobilisation of the workforce to deliver the 2018/19 QIPP programme. This is Mark Easton, who will join the organisation from the 8 th January 2018 and will work for the CCG on a part-time basis, shared with Camden CCG. We look forward to working with Mark who will bring a wealth of experience to the CCG. 3 Corporate services in the CCG 3.1 The Consultation on corporate services completed in December. The initial proposal was strengthened through staff feedback, amendments were made to the proposals and an agreed North Central London wide structure will be implemented from the 8 th January This new arrangement will greatly strengthen the management of governance, risk, communications and engagement for Barnet CCG. The benefits for the CCG includes moving to a substantive staffing arrangement with the appropriate level of skills and expertise, which is affordable because it is provided at scale using the do it once and share philosophy, where appropriate. We look forward to welcoming new colleagues to the CCG. 4 Winter 4.1 The RFL system Winter Funding bid of 2,201,000 has been approved by NHSE. This funding must be spent by 31 March 2018 and deliver 90% A and E performance over Quarter 4 of 2017/18. The funding will be used for additional beds at both Barnet Hospital and Royal Free Hospital sites. The winter allocation also includes funding to increase Health Care Assistants, Occupational Therapists and Social Work capacity to support the Discharge to Assess model and enable more patients to be discharged home with enablement support. It will also fund the piloting of GP streaming within the Urgent Care Centres and provide enhanced support to Barnet Nursing homes through additional nurses and pharmacists. These schemes will start in early January In addition to this the urgent care commissioners have developed an Urgent and Emergency Care (UEC) Transformation Plan with the Royal Free London Hospital and established a refocused A&E Delivery Board to oversee the delivery of progress being Page 2 of 4 34
35 made to achieve the 95% of patients being seen at A&E within 4 hours across the Royal Free London Hospitals Group. 4.3 Both Barnet Hospital and the Royal Free Hospital sites have held Perfect Week and Multi- Agency Discharge Events (MADE) supported by Emergency Care Improvement Programme (ECIP) support consultants. 4.4 There has also been intensive work with Barnet Council and the Central London Community Healthcare NHS Trust (CLCH) regarding delayed transfers (DTOCs) of care in CLCH beds. As a result, DTOCs have reduced from 25% on average to 6%. 4.5 We have also started the redesign of community nursing and intermediate care services with CLCH. This will streamline services through integration and alignment to CHINs, as well as further supporting admissions avoidance and rapid discharge from hospital. 5 Finchley Memorial Hospital (FMH) 5.1 The CCG has been working to improve the usage and occupation levels at FMH and has a work programme specifically focused on this objective. 5.2 The first key output from this work programme was delivered on December 4th when Adams Ward opened. Adams ward is a 17 bed non-acute community care bed service that supports Discharge to Assess in Barnet. This has opened in a phased fashion and is now up to its full 17 bed capacity. 5.3 The mobilisation of this service so quickly demonstrates the excellent level of collaboration between the CCG and CLCH, who are providing the service. Our gratitude is expressed to CLCH for their commitment to open this service so quickly. 5.4 Adams Ward is a key part of the CCG s strategy to support the health care system, particularly over winter. This facility provides beds for patients who are medically fit but need some additional support before they can go home or to their ongoing place of care. 6 Care Closer to Home 6.1 We are pleased to confirm that the CCG has now fully recruited to a substantive primary care team which will enhance the primary care support to the CCG and its member practices. Dan Glasgow formally took up his role as Deputy Director of Care Closer to Home on the 8th December and Conan Cowley, Lisa Savage and Sandra Grinze will commence their roles as Senior Locality Managers together with Shahreen Shurmni as Project Support Officer in the New Year. 6.2 In support of Care Closer to Home and the development of CHINs, Barnet CCG has been successful in a bid to the Diabetes Transformation programme for money to support diabetes management in primary care. This has seen investment in the first Diabetes- Quality Improvement Support Team (D-QIST). The Barnet GP Federation has been commissioned by the CCG to deliver the D-QIST working in partnership with Central London Community Healthcare NHS Trust and this will be operational to support the Burnt Oak Care Closer to Home Integrated Network (CHIN) in January Information Advice and Signposting and Communication and Engagement are key workstreams in Barnet s Care Closer to Home programme. Scoping workshops were held in December 2017 and were attended by representatives from the CCG, Barnet Council, community and voluntary sector stakeholders. Page 3 of 4 35
36 7 Financial Recovery 7.1 A financial forecasting exercise was undertaken in October as part of the 2017/18 recovery plan. This identified a 21.8m target for QIPP savings in 2018/19. During October and November a centralised North Central London process was undertaken to identify, develop and align QIPP schemes across all CCGs. 7.2 Project initiation documents for the QIPP programme have been developed locally and, where appropriate, on a North Central London basis, which has put the QIPP programme on firm foundations for 2018/ Clinical Services and Quality 8.1 The first meeting of the CCG Safeguarding Forum occurred in November. This is a successor to the Safeguarding Children s Health Advisory Group which was reconfigured in order to incorporate children s and adult safeguarding and to strengthen governance and oversight of the effectiveness of safeguarding policy and procedures. 8.2 The CCG Adult Safeguarding Lead has supported Barnet, Enfield & Haringey Mental Health NHS Trust with a project funded by NHS England (the first of its kind in the country) where an Independent Domestic Violence Advocate is embedded within the trust. This project was shortlisted for an HSJ award this November. 8.3 A refreshed Patient and Public Involvement Committee was established in November to oversee engagement work on behalf of the Governing Body and to identify ways of improving clinical commissioning through a strengthened patient voice shaping services. This has served to strengthen relations with key stakeholders (Healthwatch Barnet, local authority, voluntary and community sectors) to support greater collaboration in engagement work. Helen Pettersen Accountable Officer, 20 th December 2017 Page 4 of 4 36
37 Item 9 MEETING NHS Barnet CCG Governing Body DATE 11 January 2017 REPORT Performance and Quality Report LEAD DIRECTOR Kay Matthews, Chief Operating Officer, Barnet CCG AUTHOR Ashi Naveed, Performance Manager & Richard Pearson, Deputy Director, NEL CSU CONTACT DETAILS EXECUTIVE SUMMARY This report (attached) sets out pertinent issues relating to the performance of key commissioned provider organisations, in addition to various corporate performance measures. The report details performance to date and actions that are in place to address any identified issues Key exceptions are: Referral To Treatment Waiting Times The Providers commissioned by Barnet CCG have been non-compliant on the Referral to Treatment (RTT) standard for three consecutive months. Overall performance in October 2017 was 88.17%, against the national RTT standard of 92%. Both Royal Free London (RFL) and University College London Hospitals (UCLH) RTT performance continue to be challenging each achieved 86.9% and 90.6% respectively in October. North Middlesex University Hospital (NMUH) has achieved RTT compliance at 94.4% in October The number of Barnet CCG patients waiting over 52 weeks has slightly increased to 16 in October 2017 from 13 in September Of the 16 Barnet patients waiting over 52 weeks, 11 are at RFL, 4 at Imperial College HealthCare and 1 at Royal National Orthopaedic hospital. RFL has submitted an RTT recovery action plan (RAP) to NHSE, NHSI and Commissioners. Whilst the plan addresses various speciality-related issues, it still requires improvement in order to provide the necessary detail and assurance to Commissioners. The Trust have also been asked to re-consider the recovery trajectory which suggested a return to compliance by August Table 1 (below) sets out the latest position at speciality level. 37


 and the 62 day Screening target).")
38 Table 1: RFL RTT waiting times by specialty (Barnet CCG only) UCLH is expected to deliver RTT compliance by January A number of waiting list initiatives is being organised to meet the demand and to reduce the backlog. The lead commissioner (Camden CCG) is scrutinising the performance through the monthly contractual meetings. Table 2, below sets out the latest position at speciality level. Table 2: UCLH RTT waiting times by speciality (Barnet CCG only) Cancer Waiting Times Barnet CCG achieved 6 out of 8 of the cancer waiting times targets in October 2017 (the noncompliant targets were the 62 day urgent (GP referral) and the 62 day Screening target). Table 3, below shows a summary of all the Cancer waiting time targets for Barnet CCG. North Middlesex University hospital (NMUH) achieved all the Cancer waiting times target in October


39 Table 3: Barnet CCG Cancer waiting time targets summary RFL has achieved the 62-day performance trajectory two months in a row achieving 83.1% in October 2017 against the trajectory target of 81.7%. The overall waiting list has reduced to circa1800 per week to-date. (this is a reduction of 400 pathways) At RFL, Urology, Lower GI and Dermatology continue to contribute to majority of the 62-day breaches. Waiting list initiative are planned to continue in November 2017 and January 2018 for these specialties. Regarding capacity, the Trust have, or are about to increase capacity in key specialities, with: Renal theatre capacity has been increased since October 2017 An additional surgical Fellow for skin has also been in post since November Two additional Lower GI consultants are expected to be in post in January RFL is working NHS Improvement and is progressing with the recovery plans for cancer services and these are shared with Barnet CCG regularly. Camden CCG continue to monitor UCLH recovery action plans and Commissioning Managers are closely monitoring performance issue in the contractual meetings. Diagnostic target Barnet CCG have not achieved the diagnostic waiting times target for two months in a row - the target was narrowly missed at 98.7% against the national standard of 99% in October The main contributor to this under-performance was RFL. However, both UCLH and NMUH were compliant on the diagnostic target in the same period. RFL has an ongoing capacity issue in Echo-Cardiography and Computer Tomography (CT). In addition to the above modalities, the waiting list has also increased in other areas, such as Cystoscopy, Gastroscopy and Colonoscopy. RFL are continuing to outsource capacity for Echo- Cardiography and an additional new CT scanner has been operational since November Accident and Emergency Waits In October 2017, Barnet CCG underperformed against the A&E target overall. The main contributors to position were the RFL, NMUH and UCLH, which did not achieve their planned performance trajectories in this period. The 17 bedded Adams Ward at Finchley Memorial Hospital has been operational since 4 December This facility is designed to support complex patients on the discharge to assess (DTA) pathway 2 and 3 and thereby improve patient flow within both the Barnet and Hampstead sites. A multi-agency discharge event (MADE) was held at RFL between the 11 th and 14 th December The purpose of this event was for system wide stakeholders to focus on early discharge for medically fit patients. The event was well attended and it expected that recommendations for further improvement will feed into A&E recovery action plans. 39
40 Community Services (CLCH) Central London Community Hospital (CLCH) have concluded a deep dive review into Musculoskeletal Services (MSK), demonstrating new ways of working - including telephone assessments, triage stratification, group education and promotion of self-management are having a positive impact on waiting times. Overall, within Barnet 6 week wait performance has improved and Commissioners currently expect that the March 2018 trajectory to be delivered. The specialist Voice Service is provided by a single clinician and is therefore not able to respond to variances in demand. As a result of this, Commissioners and the Trust have agreed to review the current service model. The Parkinson s Service is still suffering from capacity problems within Speech and Language Therapy due to recruitment problems. The Provider has cited a national staff shortage as the main issue and are currently considering what can be done to improve this situation. In October 2017, the 18 week 92% standard was narrowly missed. Mental Health The new Barnet Instant Access to Psychological Therapy (IAPT) service, provided by Barnet Enfield and Haringey Mental Health Trust (BEH MHT) began in October Initial, unvalidated data shows that the IAPT recovery rate was 43.08% against national target of 50% in and the IAPT access target was 0.33% against the monthly target of 1.25%. Commissioners understand that a contributory factor to this non-compliance the transition to the new Providers which resulted in some rescheduling of patient appointments to a later date. The Provider is committed to achieve required performance within November 2017 it is expected that the shortfall from October 2017 will be made up in Quarter four. All other mental health standards were achieved for Barnet CCG. Quality Seven (un-validated) cases of Clostridium Difficile were for reported in October Six of these occurrences were at the Royal Free Hospital and one was at Barnet Hospital. Overall, there have been 47 cases year to date (YTD) which means that RFL have breached the YTD plan of 39. In October 2017, Royal Free London (RFL) reported eight Serious Incidents (SIs). These were in relation to, two diagnostic incidents, one sub-optimal care of the patient and two treatment delays. There were also two overdue SI Reports (SIRs) at the end of the month and 13 open further information requests (FIRs). There was two Sis reported for University College London Hospital (UCLH), one was related to abused/alleged abuse of adult patient by staff and the other one was pending a category to be selected. Four Sis were not submitted within the deadline are overdue as at the end of October 2017 by UCLH. There were 10 Sis reported at North Middlesex University Hospital, of those two were diagnostic incidents, two treatment delays, two surgical invasive procedures, two slip/falls, one maternity/baby and one pending a view for a category. RFL reported one never event (NE) in October This NE was a result of wrong site surgery. There were 41 mixed sex accommodation breaches reported in October 2017 at RFL. The majority of the breaches were at the Barnet site in recovery or in ITU. There were no breaches of the mixed sex accommodation standard at the Hampstead site l in October RFL has commenced harm reviews for the increasing number of patients waiting over 52 weeks for treatment. The criteria for the harm reviews will be shared with the RFL Clinical Quality Review Group (CQRG) and the CQRG will oversee the process. 40
41 RECOMMENDED ACTION The Committee is asked to note this report Objective(s) / Plans supported by this paper: High quality, high performing services Approval Route: The report has been considered by the CCG s Finance Performance and QIPP Committee on the 21 December 2017 Patient & Public Involvement (PPI): n/a Stakeholder Engagement: n/a Key Risks To Note: Resource Implications: see each scheme within the report n/a Next Steps n/a 41
42 42





43 Barnet Clinical Commissioning Group Quality and Performance Report to Governing Body December 2017 working together with the Barnet population to improve health and well-being 43
44 IAF Ref. Indicator Target Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 YTD Trend AS01 Percentage of incomplete pathways within 18 weeks for patients on incomplete pathways * 92% 92.2% 93.1% 92.7% 92.5% 92.6% 92.1% 88.7% 88.8% 88.2% 90.8% AS03 AS04 AS05 Percentage of patients treated within 18 weeks of referrals - admitted patients Percentage of patients treated within 18 weeks of referrals - non-admitted patients Number of patients waiting more than a year for treatment (Incomplete pathways) % 81.1% 83.2% 80.2% 80.7% 81.0% 81.6% 81.8% 81.3% 81.4% % 92.8% 92.3% 92.4% 90.9% 89.3% 90.4% 92.4% 92.5% 91.4% AS06 Percentage of patients waiting 6 weeks or more for a diagnostic test* 1% 1.3% 0.4% 0.6% 0.7% 0.8% 1.0% 0.9% 1.2% 1.3% 0.9% AS07 Percentage of patients waiting 6 weeks or Percentage of patients admitted, discharged or 1.0% 1.0% 1.0% 1.0% AS08 transferred out within 4 hours of arrival in the 95% 87.3% 86.2% 88.0% 90.4% 88.0% 87.4% 89.0% 85.3% 87.8% 88.0% AS09 dept.* Percentage of patients admitted, discharged or 89.6% 89.8% 90.1% IAF Ref. Indicator Target Royal Free London NHS Foundation Trust University College Hospital London North Middlesex University Hospital NHS Trust Oct-17 YTD Trend Oct-17 YTD Trend Oct-17 YTD Trend AS01 Percentage of incomplete pathways within 18 weeks for patients on incomplete pathways * 92% AS01R 86.9% 90.1% AS01U 90.6% 91.7% AS01N 94.4% 95.6% AS03 AS04 AS05 AS06 AS08 Percentage of patients treated within 18 weeks of referrals - admitted patients Percentage of patients treated within 18 weeks of referrals - non-admitted patients Number of patients waiting more than a year for treatment (Incomplete pathways) Percentage of patients waiting 6 weeks or more for a diagnostic test* Percentage of patients admitted, discharged or transferred out within 4 hours of arrival in the dept.* * NHS Constitutional Standard - AS03R 81.6% 81.2% AS03U 85.3% 84.9% AS03N 73.6% 80.4% - AS04R 91.5% 91.4% AS04U 91.9% 93.3% AS04N 94.4% 95.7% 0 AS05R AS05U 5 17 AS05N 0 0.0% 1% AS06R 1.52% 0.94% AS06U 0.83% 0.72% AS06N 0.61% 0.7% 95% AS08R 87.0% 87.3% AS08U 88.2% 89.5% AS08N 87.2% 83.2% - Page 2-44
45 Cancer Access standards IAF Ref Target Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 CA01 All Cancers - two week wait 93% 93.0% 93.4% 91.3% 94.0% 94.3% 93.7% 91.5% 91.7% 93.1% 92.8% CA02 CA03 CA04 CA05 CA06 CA07 CA08 CA09 CA10 IAF Ref. Two week wait for breast symptoms (where cancer not initially suspected) Percentage of patients receiving first definitive treatment within 31 days of a cancer diagnosis. 31 Day standard for subsequent cancer treatments - anti cancer drug regimens 31 Day standard for subsequent cancer treatments - radiotherapy 31 Day standard for subsequent cancer treatments - surgery All cancer 62 day urgent referral to first treatment wait (Actual)* All cancer 62 day urgent referral to first treatment wait (Planned trajectory) 62 day wait for first treatment following referral from an NHS cancer screening service 62 day wait for first treatment for cancer following a consultant's decision to upgrade the patients priority 93% 96.5% 94.6% 89.2% 93.0% 90.7% 93.1% 96.3% 94.5% 96.4% 93.3% 96% 98.9% 100.0% 99% 97.0% 96.3% 97.2% 98.2% 97.7% 100.0% 97.9% 98% 98% 100% 100% 100% 97% 100% 100% 100% 100% 99.2% 94% 97.3% 97% 93% 100.0% 97% 97% 97% 100% 100% 99.6% 94% 93.8% 100% 94% 100% 100% 100.0% 100.0% 100% 100% 97.8% 85% 80.8% 76.9% 84.8% 78.0% 81.9% 78.5% 77.6% 77.2% 83.1% 80.1% 85.5% 85.7% 86.4% 86.4% 85.5% 86.1% 85.5% 85.5% 85.5% 90% 43% 90.9% 85% 100% 88% 90.0% 100.0% 100.0% 86% 92.5% % 100% 93% 100% 92% 77% 92% 100% 88% 91.9% Royal Free London NHS University College Hospital North Middlesex University Foundation Trust London Hospital NHS Trust Oct-17 YTD Trend Oct-17 YTD Trend Oct-17 YTD Trend CA01 All Cancers - two week wait 93% CA01R 93.8% 93.8% CA01U 93.9% 94.2% CA01N 94.5% 95.0% CA02 CA03 CA04 CA05 CA06 CA07 CA09 CA10 Indicator Indicator Two week wait for breast symptoms (where cancer not initially suspected) Percentage of patients receiving first definitive treatment within 31 days of a cancer diagnosis. 31 Day standard for subsequent cancer treatments - anti cancer drug regimens 31 Day standard for subsequent cancer treatments - radiotherapy 31 Day standard for subsequent cancer treatments - surgery All cancer 62 day urgent referral to first treatment wait (Actual)* 62 day wait for first treatment following referral from an NHS cancer screening service 62 day wait for first treatment for cancer following a consultant's decision to upgrade the patients priority Target 93% CA02R 95.8% 93.5% CA02U 99.0% 93.6% CA02N 98.7% 96.1% 96% CA03R 99.2% 97.4% CA03U 96.9% 93.4% CA03N 100% 98.8% 98% CA04R 100% 97.1% CA04U 100% 100% CA04N 100% 100.0% 94% CA05R 100% 100% CA05U 100.0% 99.6% CA05N 100% 99.6% 94% CA06R 97.8% 100% CA06U 94.9% 93.4% CA06N 100% 98.0% 85% CA07R 83.2% 82.1% CA07U 71.4% 66.8% CA07N 88.2% 84.9% 90% CA09R 86% 92.7% CA09U 84.6% 72.1% CA09N 100% 94.0% - CA10R 87.5% 86.4% CA10U 79.5% 81.2% CA10N 91.1% 89.8% CA01U YTD Trend - Page 3-45
 * 1.25% 1.03% 1.13% 1.04% 1.")

46 Mental Health standards IAF Ref. Indicator Target Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Trend MH01 IAPT Access Roll-out (NHS Digital published data) * 1.25% 1.03% 1.13% 1.04% 1.26% 1.26% 1.00% 1.11% 1.0% 0.33% MH02 IAPT Recovery rate (NHS Digital published data) 50% 43.2% 42.0% 37.5% 37.0% 43.0% 38.0% 45.0% 41.1% 43.06% MH03 MH04 MH05 The proportion of people that wait 6 weeks or less from referral to entering a course of IAPT treatment against the number of people who finish a course of treatment in the reporting period. The proportion of people that wait 18 weeks or less from referral to entering a course of IAPT treatment against the number of people who finish a course of treatment in the reporting period. Estimated diagnosis rate for people with dementia (65 years+) 75% 94.0% 98.0% 96.0% 95.0% 92.0% 90.0% 86.00% 87.1% 82.72% 95% 98% 100.0% 99.0% 99% 99.0% 100% 100% 98% % 66.7% 75.1% 75.1% 74.6% 73.8% 73.5% 74.1% 74.11% 74.4% 73.78% MH06 Proportion of patients on a CPA who were followed up within seven days after discharge from psychiatric 95.0% 0.0% 100.0% 0.0% 0.0% 98.3% 0.0% 0.0% 100.0% 0.00% inpatient care (quarterly) MH08 Outpatient Did Not Attend rate - Adult ** 10% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.00% 0.0% 0.00% Early intervention Psychosis (2 week Referral To MH10 Treatment) ** 50% 50% 80.0% 66.7% 100.0% 83% 100.0% 75% 50.0% % * IAPT access targets is 15% annualised or equivalent to 3.75% Quarterly and 1.25% monthly ** Barnet CCG only *** Sept & Oct data are not published - Page 4-46
47 Quality and Responsiveness Measures and Standards IAF Ref Indicator YTD Trend Target Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 ##### Sep-17 Oct-17 QU01 Number of never events (Royal Free) QU02 New SIRIs reported in the month (Royal Free) QU03 Overdue SIRIs (Royal Free) QU04 Patient Falls - Royal Free (Safety Thermometer) - 2.0% 2.5% 2.8% 1.3% 1.9% 2.1% 2.4% 1.3% 0.62% QU05 New CAUTIs - Royal Free (Safety Thermometer) - 0.9% 0.3% 0.5% 0.5% 0.9% 0.2% 0.4% 0.3% 0.00% QU06 New Pressure Ulcers - Royal Free (Safety Thermometer) - 0.1% 0.1% 0.6% 0.2% 0.9% 0.6% 1.3% 0.4% 0.62% QU07 New VTEs - Royal Free (Safety Thermometer) - 0.1% 0.4% 0.6% 0.4% 0.4% 0.1% 0.4% 0.5% 0.31% QU08 Friends and Family Test Score - Recommend A&E (Royal Free) 89.7% 84.1% 82.3% 83.5% 84.6% 82.7% 81.1% 84.6% 83.3% 84.2% QU09 Friends and Family Test Score - Recommend Inpatients (Royal Free) 95.1% 87.7% 91.1% 87.3% 89.0% 89.6% 89.2% 89.8% 90.4% 90.8% QU10 VTE Assessments undertaken upon admission - Royal Free 95.0% 87.0% 94.3% 96.2% 95.7% 91.0% 90.9% 89.2% 91.9% 89.8% QU11 Mixed Sex Accommodation breaches - Royal Free QU12A Cumulative cases of Clostridium difficile - actual (CCG-wide) QU12P Cumulative cases of Clostridium difficile monthly ceiling plan (CCG-wide) QU13 Cases of MRSA bacteraemia (CCG-wide) AM01 AM02 Ambulance Handover - 15 minutes (Royal Free London Hampstead site) Ambulance Handover - 30 minutes (Royal Free London Hampstead site) 100% 33.6% 30.6% 17.4% 16.3% 25.7% 23.7% 33.5% 27.8% 25.0% 24.2% 100% 75.8% 71.6% 76.6% 65.7% 74.9% 71.8% 84.2% 77.7% 71.7% 74.7% AM03 Category A 8 minute response time (LAS) - Red 1 75% 70.0% 74.9% 79.2% 73.7% 73.3% 72.3% 74.5% 70.7% 73.9% AM04 Category A 8 minute response time (LAS) - Red 2 75% 67.7% 73.6% 73.6% 71.9% 69.7% 68.5% 72.0% 68.5% 70.7% DC01 Delayed transfers of Care - All reasons (Royal Free only) 3.0% 4.1% 2.9% 3.4% 2.4% 2.85% 2.05% 1.90% 2.30% 1.60% DC02 Delayed transfers of Care - All reasons (Barnet Hospital only) 3.0% 4.4% 5.4% 6.5% 6.4% 2.2% 2.2% 0 DC03 Delayed transfers of Care - All reasons (Chase Farm Hospital only) 3.0% 7.1% 6.3% 1.8% 12.5% 2.8% 2.5% 5.5% DC04 Delayed transfers of Care (RF Trust) 3.0% 3.5% 4.3% 3.5% 4.0% 2.3% 1.9% - Page 5-47
48 * Annual C.Difficile ceiling (all providers aggregated to Barnet CCG) of 84 cases - Page 6-48
49 Internal Key Performance Indicators IAF Indicator Target Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Ref. Risk Management Number of risks on the Operational Risk Register RM01 (ORR) RM02 Number of ORR risks rated as 'Extreme' - 12 Trend RM03 Number of ORR risks rated as 'High' Number of risks where the rating (composite score) RM04 has increased from last month Number of risks where the rating (composite score) RM05 has decreased from last month IF01 IF02 Individual Funding Requests (data published quarterly) Number of new applications received for IFR in the quarter Turnaround time - Percentage of cases closed within four weeks % 96.0% 97.0% 95.0% IF03 CCG Triage: Approved - Percentage of cases closed % 83.0% 82.0% IF04 CCG Triage: Declined - Percentage of cases closed % 15.0% 12.0% IF05 Closed for other reasons (inappropriate referrals) - 0.0% 3.0% 6.0% IF06 Number of appeals received per quarter CH01 CH02 CH03 CH04 CH05 CH06 Continuing Health Care Percentage of patients who passed away in preferred place of death Percentage of patients in receipt of scheduled reviews completed within 3 months Percentage of patients in receipt of scheduled reviews completed within 12 months Percentage of appeals upheld both Local Appeal and Independent Review Panels (NA - No Appeals made in the month) Percentage of completed MDT referrals carried out jointly by health and social care professionals Number of formal DToCs in a hospital setting attributed to Continuing Healthcare 74.0% 77.4% 81.0% 73.0% 76.0% 83.8% 79.0% 74.0% 76.0% 80% 100.0% 100.0% 83.0% 100.0% 91% 100.0% 88% 96% 100% 80% 100.0% 100.0% 83.0% 96.0% 100.0% 80.0% 68% 97.0% 89% 0.0% 100% 100% 0% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% Page 7-49
50 Internal Key Performance Indicators IAF Ref. Indicator Programme Management Office Target Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 12m rolling YTD Trend PM01 Number of schemes signed off per month (FBC to Live Template) PM02 Number of schemes commenced in the month PM03 PM04 Percentage of schemes on track as per project plan (Green on monthly 'Highlight Report') Number of projects formally closed in the month 61.0% 58.0% 64.0% 67.0% 67.0% 61.0% 57.0% 55.0% 49.0% PM05 Project/scheme abandonment Workforce WF01 Staff sickness - short term 2.0% 2.37% 0.17% 2.76% 2.35% 0.51% 3.35% 0.73% 1.01% 0.23% WF02 Staff sickness - long term 0.5% 2.70% 2.95% 1.76% 1.74% 1.78% 1.76% 1.68% 3.04% 4.65% WF03 Staff turnover 10% 0.00% 0.93% 0.93% 3.23% 3.33% 1.64% 0.00% 3.08% 0.00% WF05 Mandatory training compliance 90% 0.00% 0.00% 99.00% 99.00% 95.00% 75.00% 77.00% 65.00% 70.00% IAF Ref Finance to month 7 (October 2017) Year to Date (YTD) Forecast Outturn (FOT) Plan Actual Var. Plan Actual Var. FI02 Surplus/(Deficit) - Year to Date ( '000s) 0-2,680-2,680 R YTD Rating FOT Rating FI03 Surplus - Full Year Forecast ( '000s) 0-6,023-6,023 R FI04 1% Non Recurrent Funds ( '000s) ,700 2,350 2,350 G FI05 QIPP - Year to Date ( '000s) 7,150 3,540-3,610 R Overall rating: FI06 QIPP - Full Year Forecast ( '000s) 18,149 8,510-9,639 R R FI07 Running Costs ( '000s) 4,969 4, ,732 8,732 0 G G FI10 Percentage expenditure on interim, temporary and agency staff 0.0% 38.0% 0.0% 31.0% R R - Page 8-50
 MAR, August 2017 94,777 55,507 53,065-4.40% CO03 E.M.7b Total Other Referrals (General and Acute) MAR, August 2017 61,190 35,835 34,556-3.")
51 Operational Planning 2017/18 - activity status IAF Ref. EM. Code Point of Delivery (acute care) Source & Period Annual activity plan 2016/17 Year To Date Plan Year To Date Actual Variance CO01 E.M.7 Total Referrals (General and Acute) MAR, August ,967 91,342 87, % CO02 E.M.7a Total GP Referrals (General and Acute) MAR, August ,777 55,507 53, % CO03 E.M.7b Total Other Referrals (General and Acute) MAR, August ,190 35,835 34, % CO04 E.M.8 Consultant Led First Outpatient Attendances SUS, August ,403 91,010 89, % CO05 E.M.9 Consultant Led Follow-Up Outpatient Attendances SUS, August , , , % CO06 E.M.10 Total Elective Admissions SUS, August ,293 23,597 21, % CO07 E.M.11 Total Non-Elective Admissions SUS, August ,015 17,601 17, % CO08 E.M.12 Total A&E Attendances excluding Planned Follow Ups SUS, August , , , % CO09 E.M.18 Number of Completed Admitted RTT Pathways Unify, August ,522 18,461 15, % CO10 E.M.19 Number of Completed Non-Admitted RTT Pathways Unify, August ,914 60,858 55, % CO11 E.M.20 Number of New RTT Pathways (Clockstarts) Unify, August , ,250 89, % CO12 E.J.3 Number of specific acute bed days relating to hospital provider spells SUS, August ,600 94,160 98, % * Key to sources of data MAR Monthly Activity Returns SUS Secondary Use Service DM01 Monthly Diagnostic return Unify2 Department of Health portal - Page 9-51
52 - Page 10-52
53 NHSE Improvement and Assessment Framework Indicators The table below details those indicators in the IAF which are currently available. Further background information on the IAF is provided on the following page. IAF Ref. Measure Source / Period of measurement Barnet CCG (most recent data) Change since last reported data Last reported data Peer group CCGs London CCGs England CCGs DOMAIN: BETTER HEALTH 101a Maternal Smoking At Delivery Q3 2016/ % q 3.40% 6.65% 5.11% 10.64% 102a Percentage of children aged classified as overweight or obese National Child Measurement Programme (2011/12 to 2014/15) 33.2% q 33.4% 32.6% 37.0% 33.4% 103a Diabetes patients that have achieved all the NICE recommended treatment targets: Three (HbA1c, cholesterol and blood pressure) for adults and one (HbA1c) for children National Diabetes Audit 2015/ % q 42.2% 40.9% 39.1% 39.0% 103b Newly Diagnosed Diabetics On A Structued Education Course % p 1.5% 4.9% 6.5% 7.4% 104a Injuries from falls per 100,000 population (65 years and over) Rolling Annual. Latest October 2016 to December ,694.0 p 1, , , , a Utilisation of the NHS e-referral service to enable choice at first routine elective referral HSCIC March % p 31.7% 36.4% 37.3% 52.1% 105b Number of personal health budgets in place per 100,000 CCG population (based on the population the CCG is responsible for) Voluntary collection from CCGs, collected by NHS England (not RAG rated ) Q4 2016/ u c Percentage of deaths which take place in hospital ONS, National EoL Care Intelligence Network Q2 2016/ % p 50.0% 49.1% 53.3% 47.1% 105d People with a long-term condition feeling supported to manage their condition(s) HSCIC Indicator Portal (July 2015 to March 2016) 60.1% p 57.1% 61.8% 59.4% 64.1% 107a Anti-microbial resistance: Appropriate prescribing of antibiotics in primary care. The number of antibiotics prescribed in primary care per Item based Specific Therapeutic group Age-Sex related Prescribing Unit STAR-PU Antibiotic QP dashboard published on the NHS England website - 12 Months rolling data to February q b Anti-microbial resistance: Appropriate prescribing of antibiotics in primary care. The number of co-amoxiclav, cephalosporins and quinolones as a percentage of the total number of selected antibiotics prescribed in primary care. Antibiotic QP dashboard published on the NHS England website - 12 Months rolling data to February % q 13.2% 9.7% 10.0% 8.9% 108a The directly standardised average health status (EQ-5D ) for individuals reporting that they are carers, measured based on responses to a question from the GP Patient Survey General Practice Patient Survey (July 2015 to March 2016) DOMAIN: BETTER CARE 121a Provision of high quality care - hospitals (Score from 0 to 100) My NHS (Q4 16/17) 59.0 q a Cancer diagnosed at an early stage: New cases of cancer diagnosed at stage 1 and 2 as a proportion of all new cases of cancer diagnosed Cancer Analysis System, National Cancer Registry, PHE: 2015 data 51.5% q 52.2% 51.2% 50.2% 52.4% 122b People with urgent GP referral having first definitive treatment for cancer within 62 days of referral NHS England Statistics (derived from cancer waiting times database) Q4 16/ % q 75.0% 84.6% 81.1% 81.1% 122c Percentage of adults diagnosed with any type of cancer in a year who are still alive one year after diagnosis Adults diagnosed in 2014 (ONS data) 73.8% p 73.1% 71.1% 70.3% 70.4% 122d Cancer patient experience - Percentage of responses to the question "Overall, how would you rate your care?" which were positive (score of 1 worst, score of 10 best) National Cancer Patient Experience Survey average score given by patients asked to rate their care on a scale from 1 to a Improving Access to Psychological Therapies recovery rate HSCIC Rolling Quarterly data to January % q 46.5% 49.2% 48.5% 49.2% 123b The percentage of people referred to the service experiencing a first episode psychosis or at risk mental state that start NICE-recommended care package in the reporting period. Unify2 Early Intervention in Psychosis Waiting Times collection - rolling quarter to March % p 61.5% 71.4% 71.5% 74.4% 124a Reliance on specialist inpatient care for people with a learning disability and/or autism NHS Digital assuring transformation collection, plus GP registered population Quarter /17 59 q b Proportion of people with a learning disability on the GP register receiving an annual health check NHS Digital 2015/ % p 44.5% 45.6% 41.4% 37.1% Above one or more peers or on target Worse than one peer Worse than at least two peers or off target - Page 11-53
54 NHSE Improvement and Assessment Framework Indicators IAF Ref. Measure Source / Period of measurement Barnet CCG (most recent data) Change since last reported data Last reported data Peer group CCGs London CCGs England CCGs DOMAIN: BETTER CARE 125a Neonatal Mortality and Stillbirths - deaths per 1,000 births HSCIC p b Women's experience in Maternity Services - score out of 100 based on six survey questions CQC Maternity Services Survey. Annual c Choices in Maternity Services - score out of 100 based on six survey questions CQC Maternity Services Survey. Annual a Estimated diagnosis rate for people with dementia Estimated prevalence rate from the CFAS II study and ONS population figures (March 2017) 75.1% u 75.1% 67.3% 73.8% 67.6% 126b The percentage of patients diagnosed with dementia whose care plan has been reviewed in a face-to-face review in the preceding 12 months HSCIC, published Quality and Outcomes Framework (QoF) / % q 85.1% 78.9% 79.3% 84.0% 127a Assessment of progress in implementation of delivering functionally integrated, 24/7, Urgent Care service accessed via NHS 111 (positive responses against eight key elements of Integrated Urgent Care) NHS England quarterly data collection - January 2017) 7.0 p b Delivery of an Integrated Urgent Care service: Rate of unplanned hospital admissions for urgent care sensitive conditions, per 100,000 registered patients (age-sex standardised) Hospital Episodes Statistics (NHS DIGITAL) and population figures (NHAIS) - rolling 12 months up to Q3 2016/17 1,599 q 1,615 1, , , c Percentage of patients admitted, transferred or discharged from A&E within 4 hours (rating against peers, not 95% target) A&E attendances and emergency admissions monthly return (MSitAE via UNIFY2) - March % q 92.1% 90.4% 88.6% 90.0% 127e Delayed transfers of care attributable to the NHS per 100,000 population Monthly Delayed Transfers of Care Return (MSitDT via UNIFY2) - February p f Population use of hospital beds following emergency admission (occupied bed days per 1,000 population) Quarterly. Latest Quarter / p a Management of long term conditions - number of emergency admissions per 100,000 population NHS Digital HES data: 12 month rolling data to Q3 2016/ p b Patient experience of GP services - percentage of people who rated their experience as 'Good' GP Patient Survey (GPPS) - data published in July % p 80.2% 82.2% 80.9% 85.1% 128c Percentage of practices within a CCG that registered patients have access to pre-bookable appointments on Saturdays, and on Sundays, and on each weekday for at least 1.5 hours, either in the early-morning before 8 am, or in the evening after 6.30pm or both morning and evening through the practice or a group of which the practice is a member GP practices bi-annual survey (March 2017) Peer, London and England figures exclude nil returns 35.5% p 26.7% 46.1% 48.5% 22.5% 128d Number of GPs and practice nurses (full-time equivalent) per 1,000 weighted patients by CCG 0.81 q a The percentage of patients waiting to start non-emergency consultant-led treatment who were waiting less than 18 weeks at the end of the reporting period NHS England UNIFY2 system (March 2017) 0.93 p 92.2% 89.9% 90.4% 90.3% 131a People eligible per 50,000 population for standard NHS Continuing Healthcare NHS England Continuing Healthcare Report (Q3 2016/17) 34.3 q Above one or more peers or on target Worse than one peer Worse than at least two peers or off target - Page 12-54
55 NHSE Improvement and Assessment Framework Indicators IAF Ref. Measure Source / Period of measurement Barnet CCG (most recent data) Change since last reported data Last reported data Peer group CCGs London CCGs England CCGs DOMAIN: SUSTAINABILITY 141a The indicator assesses compliance of financial plans with business rules NHS England Green b Assessment of whether CCG is likely to meet its financial plan NHS England Green a 142b 143a 144a Improvement score based on a CCG s performance for three baskets of outcomes metrics for three programmes selected in advance by each CCG Improvement score for expenditure on primary care, prescribing, elective and non-elective admissions (experimental data collection and not all CCGs currently participating in 'Wave One' phase ) - not RAG rated Indicator to determine if the CCG is leading the development of a population health vanguard (Multispecialty Community Provider, Primary and Acute Care System, or Enhanced Health in Care Homes). Indicator to determine if the CCG is a member of a footprint that has an approved Local Digital Roadmap, based on completed Digital Maturity assessments from primary and key secondary care providers. NHS England (Q3 2016/17) u NHS England (Q4 2016/17) u NHS England (Q4 2016/17) No u No NHS England Technology Strategy Team (Q4 2016/17) Yes u Yes 144b Digital interactions between primary and secondary care - the unweighted average of four key measures of use of digital systems between primary and secondary care. NHS Digital report for EPS2, ers and SCR/local system usage; DMA for electronic discharge summaries. Q4 2016/ a As local system leaders, CCGs can facilitate the national agenda through the creation of a strategic estates plan (SEP) covering their area of responsibility. The indicator reports whether a plan is in place (Yes/No statement). NHS England Yes DOMAIN: LEADERSHIP 161a The indicator is designed to make a one-off assessment of each CCG s participation in / contribution to ensuring a successful STP, during the first year of STP development. Assessment rated as Red/Amber/Green. This is not an assessment of the overall STP. NHS England 162a This indicator assesses CCGs compliance with a number of requirements of the revised statutory guidance on managing conflicts of interest for CCGs. NHS England u 163a Staff engagement index - engagement index on a 1 to 5 scale (5 good) NHS England - NHS Staff Survey u b Race equality progress indicator created as a composite score, looking at the difference between the BME and White response to four questions on the NHS staff survey (Higher scores indicate higher average inequality) NHS England - NHS Staff Survey a Effectiveness of working relationships in the local system - indicator is based on the responses given to two questions asked of all stakeholders in the CCG Stakeholder 360 survey - Percentage score achieved NHS England annual CCG stakeholder 360 survey (2016/17) 65.42% p 59.29% 68.71% 69.48% 68.53% 165a Quality of CCG Leadership - An assessment based on four key lines of enquiry to determine how robustly the leaders of a CCG are performing their role (Robust culture/leadership sustainability, Quality, Governance and Engagement) NHS England (Q4 2016/17) p Above one or more peers or on target Worse than one peer Worse than at least two peers or off target - Page 13-55
56 CLCH Community Waits 6 Weeks Compliance % 6 Weeks Direction from Previous 18 Weeks Compliance % 18 Weeks Direction from Previous 6 Weeks Compliance % 18 Weeks Compliance % Oct-17 Services Service Line Diabetes - Barnet 58.94% 14.77% 98.68% 0.34% 96.80% Heart Function 88.89% % % 0.00% % ICMSK 94.02% -4.98% % 0.00% % Falls 96.34% 20.64% % 0.00% % Respiratory/COPD 51.69% 5.84% 99.44% -0.56% 91.58% Parkinson's Service 72.38% 21.03% 87.62% 3.84% 97.87% Adult Services Children Services 6 Weeks and 18 Weeks monitoring Waiting Podiatric Surgery 38.26% 2.42% 97.32% -0.95% 80.65% Podiatry 55.71% 1.33% 35.48% ICUD 98.47% -1.53% 94.69% ICMD 98.31% -1.69% 95.31% ICSLT 29.19% 29.19% 15.63% MSK Physio 46.80% 5.17% 34.63% Nutrition and Dietetics 90.74% 1.27% 77.08% Continence Service % 0.00% % Stoma Care % Tissue Viability 93.88% -3.80% 94.00% Orthotics 51.30% 10.75% 36.11% Orthoptics 47.78% 5.28% 81.97% Complex Care % 0.00% % Occupational Therapy 47.06% 20.14% 21.05% Physiotherapy 63.79% 1.67% 23.53% Alternative waiting times( Seen) Service Line Target 01/04/ /05/ /06/ /07/ /08/ /09/ /10/2017 Trend Response Time 24hr Nursing (excluding Phlebotomy) 90.00% 95.00% 95.00% 95.00% 96.00% 95.00% 92.00% 91.00% Urgent 48 Hrs 24hr Nursing (excluding Phlebotomy) 90.00% 83.00% 80.00% % 97.00% % 85.00% Urgent to OOH Nursing 2 Hrs Early Supported Discharge 95.00% % 97.00% % % % % 96.00% 24 hours from referral/discharge Rapid Response 85.00% 98.00% 87.00% 93.00% 93.00% 97.00% 97.00% 92.00% 2 hours from Referral Continence Service 95.00% 99.00% % 99.00% 99.00% 99.00% 99.00% 97.00% Respond to within 1 day Diabetes Urgent 14 days COPD days to first patient contact Paediatric HEFT 95.00% % % % % % % % Urgent 48 Hrs Heart Function Improvement Service (1) 95.00% % % 4 hours of referral Heart Function Improvement Service (2) 95.00% % % Complex - 14 days from referral Heart Function Improvement Post Acute - 14 days from 95.00% % % Service (3) referral Heart Function Improvement Service (4) 95.00% % % Urgent 14 days WIC - FMH 95.00% % % % % % % 98.00% Percent wait more than 4 hours (National Target for A&E / Urgent Care) WIC - EGH 95.00% % % % % % % 98.00% The table above captures performance measures that are less than six weeks; Hours and Days Seen 56
57 Oct-17 Adult Services Children Services Service Performance breakdown - Waiting within 6 Weeks Service Line 01/04/ /05/ /06/ /07/ /08/ /09/ /10/2017 Trendline ICUD 48.46% 78.52% 86.67% % 95.06% % 98.47% ICMD 51.59% 72.73% % % % % 98.31% ICSLT 29.90% 52.63% 52.63% 0.00% 0.00% 0.00% 29.19% MSK Physio 66.19% 60.31% 50.17% 47.94% 42.29% 41.63% 46.80% Nutrition and Dietetics 66.67% 79.49% 79.41% 84.75% 86.21% 89.47% 90.74% Podiatry 40.75% 47.63% 50.97% 46.20% 49.81% 54.37% 55.71% Continence Service % % % % % % % Stoma Care Tissue Viability 94.44% 84.62% 88.89% 87.18% 91.67% 97.67% 95.92% Orthotics 31.71% 40.56% 51.30% Orthoptics 58.75% 96.84% 79.10% 74.44% 42.50% 47.78% Complex Care % % % % Occupational Therapy 48.98% 37.93% 60.00% 41.30% 26.92% 47.06% Physiotherapy 48.98% 50.00% 82.69% 48.89% 62.12% 63.79% Adult Services Service Performance breakdown - Waiting within 18 Weeks Service Line 01/04/ /05/ /06/ /07/ /08/ /09/ /10/2017 Trendline Diabetes - Barnet 98.45% 97.54% 95.95% 98.26% 96.86% 98.33% 98.68% Heart Function % % % % % % % Falls % 99.30% % % % % % ICMSK % % 99.82% 98.27% % % % Parkinson's Service 84.54% 81.05% 90.76% 94.29% 89.16% 83.78% 87.62% Podiatric Surgery 99.19% % 99.17% 97.35% % 98.27% 97.32% Respiratory/COPD 99.41% 99.63% % % 98.88% % % 57
58 58
59 Item 10 MEETING NHS Barnet CCG Governing Body DATE 11 January 2018 REPORT Ophthalmology Business Case LEAD Colette Wood DIRECTOR/GOVERNING BODY MEMBER AUTHOR Yasmeen Farooqi/ Teresa Callum CONTACT DETAILS EXECUTIVE SUMMARY: The proposal outlined in the business case is to develop and procure a new commissioning model for the Community Ophthalmology service. The service aims to enhance the patient treatment pathway, allowing access to a high quality, cost effective service that meets the patient s clinical needs and supports the right care, right time and right place objective. The overall aim is to provide: An innovative and improved service Seamless, timely and co-ordinated pathways across primary and secondary care A holistic patient centred service A one stop service where appropriate Outline business case to Directors March 2017 PODG - business case sign off April 2017 Public/Stakeholder engagement June 2017 Executive team 27 th November 2017 FPQ committee (spec, business case sign off) 30 th November 2017 Governing Body (spec, business case sign off) 11 th January 2018 Run procurement process (Tender submission, interviews, Alcatel, award report, contract) January March 2018 Tender open to bidders Evaluation Interview Award contract Alcatel Mobilisation **Progress of the procurement will be managed through QDG** 22 nd January 13 th February 1 st March 5 th March 19 th March April - July Governing Body - sign off award report (virtual sign off) April 2018 New service commences September P a g e 59
60 RECOMMENDED ACTION The Governing Body is asked to note and approve the decision of the FPQ to proceed with this procurement. Objective(s) / Plans supported by this paper: The proposal aims to provide right care first time, value for money, care closer to home and a better patient experience, which in turn, supports Barnet CCG s strategic goals. Audit Trail: The project has been through: PRG March 2017 PODG 26 th April 2017 FPQ Committee 30 th November 2017 Will be going to: Governing Body 11 th January 2018 Patient & Public Involvement (PPI): We have two patient representatives on the panel who have provided input into the development of the service specification and will be part of the procurement process. Equality Impact Assessment: Impact neutral Risks: Identified in Business Case Procurement process challenged, reduced tariff doesn t interest any provider, new service model failing to deliver any QIPP savings. Resource Implications: The development of this business case, service specification and management of this procurement will be met through the Planned Care Team existing budgeted staffing resources. The additional resources required to deliver this work programme equates to 6,230 for clinical expertise. Next Steps: Decommission service letters to existing providers stipulating the new service commence date and arrangements To start the procurement process and award the contract to the new service provider(s) Inform Barnet Referral Management Service, GP and service users of the change. 2 P a g e 60
61 61
62 62
63 63
64 64
65 65

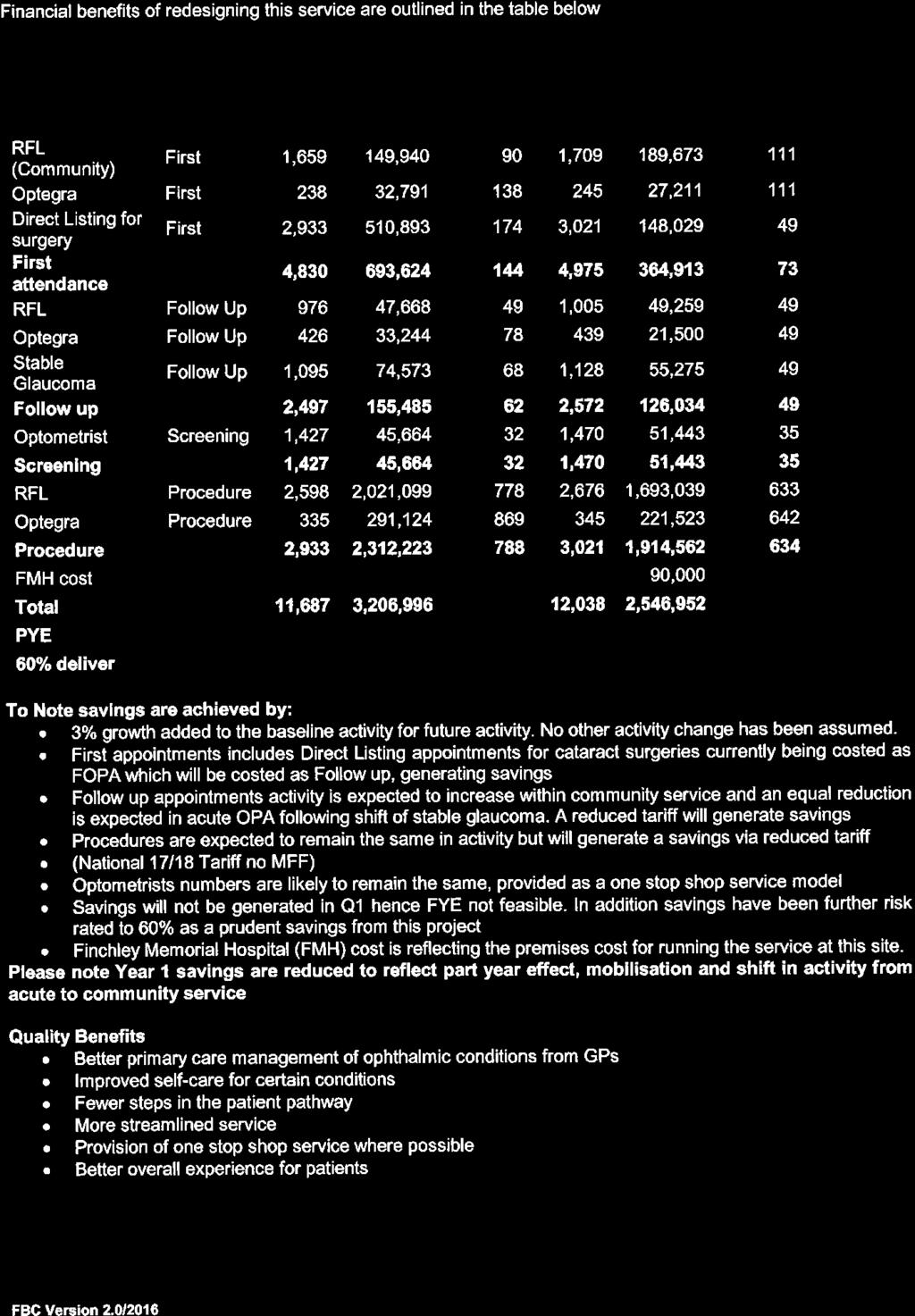

66 66

67 a total cost of 6,230 67
68 68
69 69
70 70
71 71
72 72
73 Item 11 MEETING NHS Barnet CCG Governing Body DATE 11 th January 2018 REPORT Care Closer to Home LEAD Colette Wood DIRECTOR/GOVERNING BODY MEMBER AUTHOR Colette Wood CONTACT DETAILS EXECUTIVE SUMMARY: The report provides further details on component elements of a local Care Closer to Home approach, highlighting the importance attached to a partnership approach with Barnet Borough Council and the Barnet GP Federation. The report gives an update on progress on the key components of Care Closer to Home: Extended access Care Closer to Home Integrated Networks (CHINs) Quality Improvement Support Teams (QISTs) Prevention and self-management It gives a commitment to produce an investment and delivery plan which will be presented to the March 2018 meeting of the CCG s Governing Body for approval. RECOMMENDED ACTION Governing Body members are asked to note this progress report on plans and developments with regard to Care Closer to Home. Governing Body members are asked to note that an investment and delivery plan will be developed and presented to the March 2018 meeting of the CCG s Governing Body for approval. Objective(s) / Plans supported by this paper: NCL Care Closer to Home Strategy Audit Trail: The project has been through: Governing Body March 2017 North Central London Care Closer to Home Board October/November/December 2017 Care Closer to Home Programme Board October/November 2017 Will be going to: Governing Body 11 th January 2018 Patient & Public Involvement (PPI): We have patient representatives on the North Central London Care Closer to Home Board. Patient representatives will also be on each Care Closer to Home Integrated Network (CHIN). 1 P a g e 73
74 Equality Impact Assessment: A full equality impact assessment will be undertaken as the Care Closer to Home Programme is rolled out Risks: Risk of a failure to effectively deliver the Care Closer to Home programme, as contextualised by the North Central London Sustainability and Transformation Plan Resource Implications: Investment plan presented to March 2018 Governing Body meeting for approval Next Steps: An investment and delivery plan will be developed and presented to the March 2018 meeting of the CCG s Governing Body for approval. 2 P a g e 74
75 BARNET CARE CLOSER TO HOME PROGRAMME 1. Introduction 1.1 Barnet CCG has previously signalled its commitment to the spirit and principles of Care Closer to Home, which at its heart is a place based population health system of care delivery supporting a programme of work to deliver more care and treatment in local community settings. The benefits of this model are that it will reduce dependence on avoidable and unnecessary hospital attendances and admissions, enable earlier interventions, promote individual and community health and wellbeing and provide more integrated, coordinated support to those most in need, including the frail elderly, children and those with long term conditions. 1.2 In Barnet the Care Closer to Home programme of work has been co-designed with the London Borough of Barnet, in full recognition of the imperative of a coordinated and integrated approach to promote local health and social care delivery in ways which best meet the needs of the residents and registered population of Barnet. Design and delivery work is being taken forward under the direction of the local Joint Commissioning Executive Group, itself overseen by the Barnet Health and Wellbeing Board and CCG Governing Body. This ensures that action to promote the delivery of care closer to home is consistent with our broader commitment to improvements in local health and wellbeing. 1.3 The Care Closer to Home work stream within North Central London is over seen by the Health and Care Closer to Home Board. This is chaired by Andrew Ridley, Chief Executive of Central London Community Healthcare Trust. The Senior Responsible Officer for the Programme is Tony Hoolaghan, Haringey and Islington Chief Operating Officer. Barnet s Primary Care team are delivering this work within existing resource with support from a Programme Director covering North Central London. 1.4 This report provides further detail on the component elements of a Care Closer to Home and progress to date in Barnet: 2. Context: The North Central London Sustainability and Transformation Plan (STP) 2.1 The strengthening of health and care closer to home is one of the fundamental platforms for change in the North Central London STP. The STP identifies a number of delivery/enabling mechanisms for the enhancement of care closer to home. Collectively, these require an integrated approach across health and social care and strengthened federated working by providers, including primary care. This should include the more flexible deployment of workforce skills across organisations. 2.2 The three main drivers of change are: Improved Access Patients will be able to access consultations with GPs or other Primary Care professionals in their local area for pre-bookable and unscheduled care appointments between 8am and 8pm seven days a week. Planned outcomes are improved patient satisfaction with access to primary care and a reduced number of patients seen in A&E/Urgent Care with a primary care appropriate problem. 1 P a g e 75
76 2.2.2 Care Closer to Home Integrated Networks (CHINs) CHINS may be virtual or physical. Typically covering populations of c50-80,000, they will be home to a number of services, providing an integrated, holistic, person-centred model of health and social care and support. At the heart of this will be integrated health and social care multi-disciplinary teams, care planning, risk stratification and care coordination. Support from specialist consultants should be accessible to enable GPs and their teams to manage more care closer to home. Planned outcomes are a reduction in clinical variation, a reduction in secondary (hospital) care activity and cost, a reduction in the number of residents dying prematurely, an enhancement of the quality of life for people with long-term conditions and an increase in the number of patients having a positive experience of care Quality Improvement Support Teams (QISTs) These GP-led teams will be tasked with improving quality in primary care and reducing unwarranted variation. They will play a central role in supporting CHINs, providing hands-on practical help for individual GP practices to ensure a consistent quality standard and offer of service. They will help to identify, promote and roll out best practice, clinical innovation and proven technologies in a systematic and consistent way. This will include support to maximise early identification and support and the proactive management of high blood pressure, atrial fibrillation, chronic kidney disease and diabetes. Planned outcomes are a reduction in clinical variation, a reduction in secondary (hospital) care activity and cost, a reduction in the number of residents dying prematurely, an enhancement of the quality of life for people with long-term conditions and an increase in the number of patients having a positive experience of care. 3. Progress in 2017/ Extended access Following a procurement exercise, a contract award for extended access was made to the Barnet GP Federation. Extended access is now provided from 3 community hubs with 6 satellite sites, the service has been operational since April 2017 and will provide an additional 38,000 appointment slots per annum for local patients Investment to enable the above comes from a mix of pre-existing CCG investment and further dedicated resources received from NHS England The CCG has monthly contract meetings with the GP Federation to assure progress. 3.2 Care Closer to Home Integrated Networks (CHINs) Working closely with the Barnet GP Federation, expressions of interest from local practices to become CHINs were invited. Five expressions of interest from local clusters of practices were received and evaluated and three were approved. The first Barnet CHIN is centred on a group of five practices located in Edgware/Burnt Oak/Watling Way. Together these practices have a registered population of c50, 000, equating to c12.5% of the Borough s total GP registered population and will focus on diabetes and paediatric access. 2 P a g e 76
77 3.2.2 The second CHIN will be centred across a group of practices in the North Locality and will focus on frailty based on prevalence and demography The aim was to launch the Burnt Oak CHIN in September 2017, and the second CHIN through the second half of 2017/18. However this timeline has slipped and it is now envisaged that the first CHIN will become operational in January 2018 with the second CHIN coming online in March The Barnet GP Federation has indicated a desire to progress this first phase of CHIN development and it has been agreed that they will work in partnership with the CCG to take this forward. Discussions are now progressing with the Barnet GP Federation to agree a programme of mobilisation and a deployment of resources and to agree the future footprint for CHIN development to achieve universal coverage in Barnet Over time the aspiration is to shape all community commissioning and delivery around the delivery vehicle of CHINs, aligning resource and giving permission to front line staff to work differently. CHINs will be used as a vehicle for testing new ways of working such as the sharing of diabetic registers and practice resources. 3.3 Quality Improvement Support Teams Barnet CCG were successful in a bid to the Diabetes Transformation programme for money to support diabetes management in primary care and received 249k to be invested in a D-QIST. The aim of the D-QIST is to work collaboratively with the CHINs to deliver three treatment targets. Barnet have now commissioned the Barnet GP Federation to deliver the D-QIST working in partnership with CLCH and this will be operational to support the Burnt Oak CHIN in January The D-QIST will be used as a prototype for QIST development in Barnet and pending review of its outcomes discussion will extend to consider how the concept and intended outcomes of a QIST can be rolled out across Barnet and developed for the CHIN footprint. 4. Resources 4.1 No dedicated funding has been received by the CCG to support the development of CHINs and QISTs however it is clear that to support their development investment will be required to support their infrastructure and operational costs. Their impact, in terms of reducing avoidable demand and costs in other sectors is therefore of particular importance in developing a return on investment plan. In addition, the CCG and Barnet Borough Council will actively consider how existing resources can be re-purposed in support of a more integrated and federated approach which is central to the development of CHINs and QISTs. 5. Prevention and supported self-management 5.1 Supported self-management is key to developing a clear social prescribing offer across North Central London. Barnet will continue to build on a strong foundation of work to support self-management. Our supported self-management programmes and recovery model component of re-imaginings in mental health are all geared to a more empowering model of health care. 3 P a g e 77
78 6. Communications and Engagement 6.1 Communication and Engagement is a key work-stream in Barnet s Care Closer to Home Programme. A public engagement event was held in June 2017 which was attended by 85 delegates, including 29 members of the public and 33 representatives from community and voluntary sector stakeholders. The event was organised by Barnet CCG in conjunction with Healthwatch Barnet and CommUNITY Barnet. It focused on Care Closer to Home, particularly in relation extended access, new models of provider working and GP online services. 6.2 A further engagement event Reimagining Care Closer to Home was held on 7 th December with local people, voluntary organisations, the NHS and local government representatives from Enfield, Haringey, Camden, Islington and Barnet. to agree key messages to be communicated. 6.3 The communication strategy for the programme will be further developed over coming months. 7. Conclusion 7.1 The Care Closer to Home work stream of the North Central London STP has brought a renewed focus on the need to build a sustainable and robust primary care system that has the capacity and capability to support out of hospital care and is an opportunity to transfer services over time. There remain challenges, however, with workforce and estates continuing to undermine efforts to meet demand which must be addressed as a key enabler for this programme of work. In addition a transformational change programme at this scale will require resourcing and investment. 7.2 With the establishment of CHINs and QISTs there is a unique opportunity to consider how they can potentially be used as a platform for broader working between providers and commissioners to deliver good patient outcomes, create resilience in primary care and transfer services from acute to primary and community care over time. 8. Recommendation and next steps 8.1 Governing Body members are invited to note the progress report on plans and developments with regard to Care Closer to Home. 8.2 An investment and delivery plan will be developed and presented to the March 2018 meeting of the CCG s Governing Body for approval. 4 P a g e 78
79 Item 12 MEETING NHS Barnet CCG Governing Body DATE 11 January 2018 REPORT Proposal to take in-house a range of Commissioning Support Unit Services DATE OF REPORT 18 December 2017 LEAD DIRECTOR / Paul Sinden, NCL Director of Performance and Acute GOVERNING BODY Commissioning MEMBER AUTHOR David Stout, Senior Programme Director CONTACT DETAILS David.stout3@nhs.net DIRECTOR SIGN OFF Helen Pettersen, 18 December 2017 EXECUTIVE SUMMARY This report sets out a proposal to take in-house a range of services from North East London Commissioning Support Unit (NELCSU) to the five CCGs across North Central London. RECOMMENDED ACTION The Governing Body is asked to: Note the report; Support the proposed approach; and Agree to give notice to NELCSU of the CCG s intention to bring services in-house Objective(s) / Plans supported by this paper: The in-housing of the provision of a range of NELCSU services will contribute to the successful delivery of all of the CCG s objectives Audit Trail: N/A Patient & Public Involvement (PPI): N/A Equality Impact Assessment: N/A Risks: There are a number of risks which will be managed through the transfer process. A full risk register will be developed as part of the change programme to ensure risks are considered and mitigated. Resource Implications: Section 6.4 of the report sets out the financial work to be undertaken in relation to the proposal. Next Steps: Section 4 of the report sets out the proposed timetable for next steps 1 P a g e 79
80 Proposal to take in-house a range of Commissioning Support Unit Services 1. Introduction This paper sets out a proposals to take in-house a range of services currently provided by North East London Commissioning Support Unit (NELCSU) to the five CCGs across North Central London (NCL). The paper sets out the key issues which will need to be considered and an outline timetable, together with a proposed project approach. 2. Background NELCSU provides a range of services to NCL CCGs under a service level agreement (SLA) with a total value of 16.0m in 2017/18, which reduces to 15.4m in 2018/19 see Appendix One for details. Over the last few weeks the CCG management team has reviewed the current service provision from NELCSU in light of the new management arrangements for the five NCL CCGs and the development of the NCL Sustainability & Transformation Partnership (STP). The review concluded that it would be beneficial to bring in-house NELCSU s Point of Delivery Multi-Disciplinary Team (POD MDT) services for the NCL CCGs. This conclusion was not driven by concerns about the quality of the services provided, but that this change would support work to reduce duplication across the five boroughs, provide improved value for money and better support the CCGs. It would also deliver a more effective alignment of these services with the new CCG management structures across the 5 CCGs and with the NCL STP footprint. There have been informal discussions with senior managers within NELCSU who have confirmed that they understand the logic of these proposed changes and that they will work with NCL CCGs to ensure the proposed changes are managed effectively. The next step is for the five NCL CCGs to give formal notice to NELCSU. This paper seeks approval from the Governing Body to proceed to give notice. 3. Proposed approach We recognise that changes of this sort bring risks. Therefore we want to approach these proposed changes collaboratively between the CCGs and the CSU so that this is a shared change programme. We believe that this will maximise the likelihood of a successful transfer and minimise the risk of loss of confidence of staff and of unintended consequences on remaining CSU services so that services are effectively maintained during the transition period. We want to implement these changes as quickly as is reasonable without compromising due process. This will enable us to minimise the period of uncertainty for staff. As such we will need to discuss whether it would be appropriate to transfer services more quickly than the formal 6 month notice period as specified in the SLA. 4. High level deliverables and timetable At a high level, the proposed deliverables and timetable are as follows: CCG Governing Body agreement of intention to take a range of CSU services in house January 2018 Confirmation of services to transfer January P a g e 80
81 CCGs to issue formal notice to CSU end January 2018 Agreement of structure for CSU staff to transfer into within the CCGs February 2018 Sign off NHS England business case February 2018 Formal consultation with CSU staff up to three months from beginning of March 2018 Sign-off of decisions following consultation early June 2018 Agreement of asset transfer details June 2018 Agreement of revised SLA value for services remaining with CSU by June 2018 Transfer of staff to be completed 1 July 2018 (preferred date but subject to agreement with CSU regarding notice period) The issues which will need to be addressed to achieve this timetable are set out in the next section of this paper. 5. Implementation There are two phases to the implementation: Phase 1 Mobilisation, Due Diligence & Decision Making Develop an overarching HR work stream plan ensuring that all parties are working to an agreed timetable and within agreed governance arrangements. Identify and develop a risks and issues log and escalate/propose mitigation as appropriate to NCL SMT. Oversee the joint consultation and engagement with NELCSU, and staff side for both sender and receiver organisations. Work with NELCSU to manage staff communications and responses to questions from staff, key stakeholders and staff side within an agreed communications protocol. Develop a score card of key metrics as part of the reporting process for the NCL CCG Senior Management Team (SMT). Working closely together with NELCSU to consider what staff well-being interventions need developing as part of the support offer to staff Develop a dependencies log as appropriate e.g. estates, finance, communications. Phase 2 Transition Implementation Oversee the implementation of the work stream plan, ensuring that all staff are appropriately jointly consulted on the HR transition process and are treated in a fair and consistent manner. Monitor progress, and continue to mitigate/escalate risks and issues, and provide regular reports to NCL CCG SMT Oversee the TUPE/COSOP transfer to receiver organisations under management of change policy 6. Issues 6.1 Confirmation of services to transfer We have agreed that we intend to transfer the POD MDT services back in-house. These currently comprise approximately 84 staff. There may however be some further central CSU services which it would make sense to also transfer where they are integral to the work of the POD MDT and so to dislocate them would not make operational sense. There may also be other changes instigated by other 3 P a g e 81
82 STP areas in London or the London-wide work on business intelligence which may have a knock-on effect which will need to be taken into account. We will confirm the full scope of services to transfer during January. We will also agree what degree of redesign of these services we wish to achieve during the transfer. 6.2 HR issues We will ensure that any HR issues associated with the transfer are addressed. Michelle Chadwick, Director of HR/OD, NCL CCGs will provide expert HR advice. This will include agreement of which CCG will employ the staff transferring from NELCSU. 6.3 Estates/assets We will need to ensure that we have adequate office accommodation for any staff who transfer. CSU POD MDT staff already spend significant portions of their time in CCG accommodation, but also spend an amount of time back in CSU HQ at Clifton House. We need to consider whether we still need a central location to bring them together and if so whether we continue to use Clifton House in the short term or find an alternative location within the NCL CCG footprint. We also need to ensure planning for relocation from Stephenson House for Camden CCG takes the accommodation needs of transferred staff into account. In principle we would expect transferring staff to bring associated assets with them (most notably IT kit). However we need to consider compatibility of IT kit with local CCG systems. 6.4 Finance We have already agreed financial savings as part of the existing SLA for CSU services (see Appendix One). The POD MDT services which transfer will incorporate these cost reductions. If we wish to achieve further savings on services which transfer then this will need to be included as part of any service redesign. We will need to agree a revised SLA value for the CSU services which will continue to be provided to NCL CCGs from the date of transfer. We recognise that the transfer of services may leave the CSU with some stranded costs as a result of for example vacated office space or management overheads. The expectation is that these will be short-term as they can be anticipated and planned for. However we will need to agree the value of any stranded costs and timescale which they will remain alongside the pricing of the remaining services. Matt Backler, Deputy Director of Finance, Barnet CCG will lead finance input into the process. We will ensure that CCG audit committees are briefed on the transfer process. 6.5 Communications/stakeholder engagement Excellent communications will be key to success. Communications with CSU staff and CCG staff need to be regular and consistent throughout the process. The approach will need to be agreed, but is likely to be in the form of a regular newsletter/ , backed up by line management briefings and periodic open staff meetings throughout the process. During the staff consultation period, these will be particularly critical. Initial communications have been sent to staff affected within NELCSU and to CCG staff. There will also be a need for wider stakeholder management. In particular there will be a need to engage NHS England and the other CCGs/STPs in London to ensure that we have a mutual understanding of plans in relation to the CSU. 4 P a g e 82
83 7. Project Management and oversight Clearly this change programme is complex. David Stout has been asked to act as Programme Director to oversee the work, reporting to Paul Sinden (Director of Performance & Acute Commissioning, NCL CCGs) and liaising directly with Steve Rubery (CSU sector director North London) We will establish a project team to oversee the work from January The Project Team will report to the CCG SMT and to the CSU executive management team. We propose to establish a CCG Governing Body subgroup with membership from each of the five CCG bodies to provide oversight of the transfer process. 8. Conclusion The Governing Body is asked to: Note the report; Support the proposed approach; and Agree to give notice to NELCSU of the CCG s intention to bring services in-house 5 P a g e 83
84 NCL SLA Values Closing 16/17 Appendix One NCL Barnet CCG Camden CCG Enfield CCG Haringey CCG Islington CCG NCL Total Business Support Services 296, , , , ,870 1,376,525 Comms 38,204 36,952 36,042 23,380 23, ,958 Continuing Health Care Contracting 1,820,871 1,388,570 1,486,996 1,338,516 1,122,019 7,156,972 Finance Services 306, , , , ,136 1,402,767 FOI 0 6,929 7, ,137 HR 137, , , ,676 80, ,420 IFR Process Management 117,715 79,403 53,709 43, , ,948 Medicines Management (Primary and Secondary Care) 41,254 41,992 39,684 39,860 43, ,710 Quality 70,581 54,039 61,901 56,695 50, ,129 Reporting & BI 1,111, , , , ,199 4,697,305 3,940,825 3,205,820 3,474,153 2,984,402 2,755,671 16,360, /18 Percentage Reduction 2.5% NCL Barnet CCG Camden CCG Enfield CCG Haringey CCG Islington CCG NCL Total Business Support Services 288, , , , ,423 1,342,112 Comms 37,249 36,028 35,141 22,796 22, ,009 Continuing Health Care Contracting 1,775,349 1,353,856 1,449,821 1,305,053 1,093,969 6,978,048 Finance Services 299, , , , ,108 1,367,698 FOI 0 6,756 7, ,784 HR 134, , , ,984 78, ,260 IFR Process Management 114,772 77,418 52,366 41, , ,749 Medicines Management (Primary and Secondary Care) 40,223 40,942 38,692 38,864 42, ,542 Quality 68,816 52,688 60,353 55,278 49, ,776 Reporting & BI 1,083, , , , ,644 4,579,872 3,842,304 3,125,675 3,387,299 2,909,792 2,686,779 15,951, /19 Percentage Reduction 3.5% NCL Barnet CCG Camden CCG Enfield CCG Haringey CCG Islington CCG NCL Total Business Support Services 278, , , , ,718 1,295,138 Comms 35,945 34,767 33,911 21,998 21, ,619 Continuing Health Care Contracting 1,713,212 1,306,471 1,399,077 1,259,376 1,055,680 6,733,816 Finance Services 288, , , , ,514 1,319,828 FOI 0 6,519 6, ,301 HR 129, , , ,310 75, ,565 IFR Process Management 110,755 74,708 50,533 40, , ,463 Medicines Management (Primary and Secondary Care) 38,815 39,509 37,338 37,503 41, ,488 Quality 66,408 50,844 58,241 53,343 47, ,739 Reporting & BI 1,045, , , , ,221 4,419,577 3,707,824 3,016,276 3,268,744 2,807,949 2,592,742 15,393,535 6 P a g e 84
85 Item 13 MEETING NHS Barnet CCG Governing Body DATE 11 January 2018 REPORT Finance Report Month 8 (November 2017) LEAD DIRECTOR Simon Goodwin, Chief Finance Officer, NCL CCGs AUTHOR Matt Backler, Deputy CFO CONTACT DETAILS Matt.backler@nhs.net EXECUTIVE SUMMARY Forecast outturn (FOT) is a deficit of 2.3m, which is an adverse variance to plan of 6.0m. This is mainly driven by: under-delivery of the QIPP plan by 9.6m; acute over-performance of 1.5m; under-accrual of prior year invoices of 1.3m; cost pressures in continuing healthcare of 1.5m; partially offset by release of mandatory reserves and contingencies of 5.5m, deferral of investment of 1.3m and marginal rate of 1.1m The delivery of the FOT looks challenging primarily due to uncertainty around the impact of any agreements at the Royal Free Hospital on a number of disputed items which have a material impact on the likely financial performance. The position agreed for Q1 has been extrapolated over the full year and has added pressure of around 1.1m compared to forecast in M6 (last finance report viewed by the governing body) and M7. However the overall risk profile has reduced materially to 10.1m (compared to over 15m before items were agreed) with a worst case scenario of 4.8m deficit. There is scope to improve the FOT based on further delivery of the recovery plan and improvement in forecast QIPP delivery which has been limited to a modest value in the forecast. As at month 8 YTD the CCG is 4.2m worse than plan, this is in line with the forecast year end position (of 6.0m worse than plan). Conclusion The committee, executive and wider governing body will need to consider what further corrective actions can be taken whilst actively managing further risks and mitigations. RECOMMENDED ACTION The Committee is asked to note the financial position and forecast. Objective(s) / Plans supported by this paper: Close management of the financial position supports the CCG s on-going delivery of its financial requirements and ensures that any corrective action is taken at the earliest opportunity. Outcomes Expected: Discussion of financial report by the Committee. Audit Trail: This paper has been prepared from information provided by North and East London Commissioning Support Unit and CCG internal management and budgetary control processes. Next Steps Any actions noted and revisions incorporated into future financial reports to the FPQ Committee and CCG Governing Body. 85
86 86
87 17/18 bridge Barnet CCG 2017/18 Month 6 The forecast outturn (FOT) is a deficit of ( 2.3m) this is 6.0m adverse to plan and is driven mainly by QIPP slippage. Plan to FOT bridge ( m) Driven by: Numerous small over-performances totalling 2.4m; partially offset by Underperformance at UCLH of 0.9m 5.0m of Mandatory Reserves, 0.5m of Local Reserves and 1.3m of Investment has been deferred compared to plan. A further 1.8m of mitigations are included as part of the recovery plan submitted in mid October. - (2.0) 8.7 (2.3) (4.0) (6.0) (9.7) (1.5) (1.3) (3.4) (8.0) 1.1 (10.0) (12.0) 17/18 Plan QIPP slippage Acute performance Forecast QIPP slippage of ( 9.7m) against plan of 18.1m. Full year effect of schemes is 15.6m. Marginal rate All in sector acutes have agreed a marginal rate around contract baseline Prior year items Other Mitigations FOT Driven by: Continuing Healthcare 1.5m; Winter resilience overspend of 0.6m;and Prescribing 0.4m 870
88 Overview Barnet CCG 2017/18 Month 8 The FOT of a 2.3m looks increasing stretched although not unfeasible, against this total risk exposure has decreased Summary financial position ( m) Bud Actual Var Bud FOT Var Revenue Resource Limit Acute Non-Acute Corporate & running costs (0.0) (0.3) Centrally held QIPP (3.2) (1.9) 1.3 (5.3) (4.5) 0.8 Total Recurrent Total Non-Recurrent (2.0) (3.7) Total Expenditure Surplus / (Deficit) 2.5 (1.7) (4.2) 3.7 (2.3) (6.0) Acute bridge ( m) Trust / Service Plan QIPP sliggage Over perfor mance Marginal rate FOT Var Royal Free (0.8) UCLH (0.9) (0.0) 25.2 (0.8) Other (0.3) In sector (1.1) Other Acute Total Acute (1.1) QIPP ( m) Area YTD YTD Full Year Full Year Bud Act Var Del Bud FOT Var Del Planned care (0.4) 70% (1.6) 58% Care Closer to home % (0.1) 93% UEC (0.4) 55% (0.9) 53% Other (1.2) 61% (1.9) 63% Discontinued (2.3) 0% (5.1) 0% Total QIPP (4.3) 52% (9.7) 47% Summary position Due to a number of pressures - in particular likely impact of Q1 RF settlement - hitting the FOT of 2.3m is challenging although not unfeasible, we have for this month held the FOT constant but will review this carefully each month. Year to date (YTD) shows a deficit to plan of ( 4.2m), this is in line with the FOT variance Material issues to note including changes since the governing body last considered the finance report: a (1.1)m impact ( (0.7)m YTD) as a result of the Q1 Royal Free agreement this has however materially reduced the risk outside of QIPP slippage acute performance is on plan for in-sector acutes, however out of sector acutes are over-performing by 1.4m cost pressures in CHC continue to be an issue and are worsening every month, prescribing has improved in the last month or so There is scope to improve the FOT based on further delivery of the recovery plan and improvement in forecast QIPP delivery which has been limited to a modest value in the forecast The main driver of the acute variance is a slippage of 7.4m for Acute Focused QIPP (out of the total 9.7m slippage including Non-Acute) and out of sector over performance of 1.4m; partially offset by the marginal rate benefit of 1.1m. Underlying in-sector acute performance is in-line with plan with underperformance in planned care, critical care and diagnostics offset by overperformance in A&E and outpatients. Forecast QIPP delivery is 8.5m against a plan of 18.1m. Of the slippage against acute schemes ( 7.4m) effectively 50% of this is mitigated by the impact of marginal rate The run rate used in the FOT has been adjusted down for expected QIPP delivery in the final four months by 1.2m. 881
89 Risks Barnet CCG 2017/18 Month 8 There is gross emergent risk of 10.1m over and above that recognised in the FOT worst case analysis is a 4.8m deficit Risk analysis has identified emergent risk over above that recognised in the FOT of 10.1m, this is mainly driven by acute (over-performance, RTT pressures & contractual disputes) and risk of delivering the recovery plan. Given the stretch included in the recovery plan it is not considered reasonable to present a best case over and above this. The worst case is a deficit of 4.8m which represents deterioration against the FOT of 2.5m. This has been derived by applying a 10%, 25% and 40% to the emergent risk rated low, medium and high respectively Risks & worst case analysis Emergent '000 Emergent Risk Description Prescribing (650) High Various items - driven by rises in individual prices where substitution is limited or unavailable Acute over-performance (1,216) Med Acute performance continues to be volatile and present both a risk and opportunity to the position with a high degree of uncertainty. We have made assumptions around seasonality, claims, challenges and CQUIN performance as well as QIPP delivery (which is back loaded) and over performance. These assumptions in totality are reasonably aggressive will have the potential to materially impact the positon one way or another. Performance issues (500) Med The Winter Resilience budget is already over committed to support A&E performance at our main providers is becoming strained. However, we understand that RTT will not be hit for August and there may be some costs recovered to mitigate Contractual issues (1,814) Med There remains a number of items of a contractual dispute nature being negotiated with a number of providers Emergent % Worst case ( '000) FOT (2,311) 40% (260) 25% (304) 25% (125) 25% (453) CHC (500) Med CHC continues to increase as a cost pressure each month 25% (125) Provider sustainability (800) Low External reviews of some of the providers suggest financial pressure 10% (80) Prior year invoices/balances (2,300) Low over and above the contract value. We are working with the providers in question Subsequent to agree to year an end approach a number of invoices which had not been 10% (230) accrued for appear likely to be payable. We are currently in negotiations with providers around a settlement Total (7,780) (1,577) Recovery plan non-delivery (2,300) High 40% (920) Total (10,080) (2,497) Worst case (4,808) 892
90 90
91 Item 14.0 MEETING NHS Barnet CCG Governing Body DATE 11 January 2018 REPORT Joint Health and Wellbeing Strategy Implementation plan ( ) annual progress report DATE OF REPORT November 2017 LEAD DIRECTOR / GOVERNING BODY Dr Debbie Frost, Chair of Barnet Clinical Commissioning Group (Barnet CCG) MEMBER AUTHOR Catherine Searle, Interim Assistant Director of Joint Commissioning CONTACT DETAILS catherine.searle1@nhs.net DIRECTOR SIGN OFF Kay Matthews, Chief Operating Officer, Barnet CCG EXECUTIVE SUMMARY In November 2015 the Health and Wellbeing Board (HWBB) approved the Joint Health and Wellbeing (JHWB) Strategy The HWBB has received regular updates on progress to deliver the JHWB Strategy at each meeting. The Board agreed to receive a full annual report each November on progress in delivering the strategy, including performance targets, indicators and activity which allows the Board to review progress and refine priorities for the coming year. This report: Sets out the progress made in delivering the JHWB Strategy over the past year Reviews Barnet s Health Profile (as produced by Public Health England) for 2016 and 2017 Recommends the priority areas of focus for November RECOMMENDED ACTION The Governing Body is asked to note the attached report. Objective(s) / Plans supported by this paper: The JHWB Strategy is the Barnet s overarching strategy to improve health outcomes for local people, keep our residents well and promote independence. The JHWB Strategy focuses on health and social care related factors that influence people s health and wellbeing, with clear recognition of the importance of prevention, early intervention and supporting individuals to take responsibility for themselves and their families. Actions in the JHWB Strategy may also be included in other key strategies and action plans such as the Primary Care Strategy, Better Care Fund plans and the Children s and Young People s Plan to ensure delivery across the health and social care system in Barnet. 1 P a g e 91
92 The JHWB Strategy supports evidence-based decision making across the Health and Wellbeing Board and its partners. The JHWB Strategy has been developed to align and bring together national and local strategies and priorities including Barnet Clinical Commissioning Group s strategic plans and Barnet Council s Corporate Plan Audit Trail: This paper has been discussed at the Health and Wellbeing Board meeting on 9 th November Patient & Public Involvement (PPI): A number of partners have been involved in the development of the JHWB Strategy including a public consultation. Equality Impact Assessment: The JHWB Strategy has used evidence presented in the JSNA to produce an evidence based resource. The JSNA has equalities embedded, explicitly covering the current and future needs of people in Barnet from each equalities group. Risks: There is a risk that, if the JSNA and JHWB Strategy are not used to inform decision making in Barnet, that work to reduce demand for services, prevent ill health, and improve the health and wellbeing of residents be sub optimal, resulting in poorly targeted services and an increase in avoidable demand pressures across the health and social care system in the years ahead. Risk is managed through progress updates at the Joint Commissioning Executive Group (JCEG) and escalated to the HWBB as necessary. Barnet CCG, the LBB and selected partners discuss local priorities for commissioning and delivery across health and care in Barnet within the context of the local STP at the JCEG. Barnet CCG and the LBB recognise that the delivery and implementation of STP plans and of services delivered through Better Care Fund and Section 75 agreements are strategically linked. Resource Implications: The JHWB Strategy sets the priorities of the Health and Wellbeing Board for the period , building on current strategies and focusing on areas of joint impact within current resources. The priorities highlighted in the JWHB Strategy will be considered by all the relevant organisations when developing activities. The JHWB Strategy will support the work of all partners to improve the health and wellbeing of the population. Each project will be individually funded however, using the existing resources of the participating organisations. Appendices Health profile for the Borough Appendix 1 Strategy Progress report Appendix 2 (pages 1 to 16) Next Steps: Barnet CCG will continue to monitor the implementation of the work streams within the Implementation Plan. 2 P a g e 92
93 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Item 14 England Barnet Clinical Commissioning Group 93
94 2 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Contents 1. Foreword 3 2. What we are trying to achieve 4 Aims 5 Themes and priorities 5 3. Where we are now 7 Barnet at a glance 7 Policy context 9 4. Preparing for a healthy life 11 Highlights 11 What does Barnet s JSNA tell us? 11 What we plan to do 12 How will we know we have made a difference? Wellbeing in the community 15 Highlights 15 What does Barnet s JSNA tell us? 17 What we plan to do 18 How will we know we have made a difference? How we live 23 Highlights 23 What does Barnet s JSNA tell us? 24 What we plan to do 25 How will we know we have made a difference? Care when needed 29 Highlights 29 What we plan to do 31 Primary care 34 How will we know we have made a difference? Target setting, monitoring and governance Appendix: Barnet s Health and Wellbeing Board 37 94
, our Joint Health and Wellbeing Strategy (JHWB) provides the framework and direction for local")

95 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Foreword As one of the most important responsibilities of the Health and Wellbeing Board (HWBB), our Joint Health and Wellbeing Strategy (JHWB) provides the framework and direction for local commissioning and service planning. Our new Joint Strategic Needs Assessment (JNSA) on which our JHWB Strategy is based tells us that thankfully on average people in Barnet are living much longer. However, it is the health and wellbeing quality of that longer life which our Joint Health and Wellbeing Strategy seeks to improve adding life to years not just years to life. We would like to thank the wide range of partners who have contributed to the development of the JHWB Strategy especially all those residents who took the time to feed into the consultation; your opinions are much valued and we have reflected many of these in the final JHWB Strategy. Using our recently updated and renewed JSNA as an evidence base, we outline our priority areas for action to meet our ambition to keep our residents well and to promote independence; we are particularly concerned with improving the health and wellbeing of people with mental health problems and those increasingly affected by dementia. As Chairman and Vice Chairman of the Health and Wellbeing Board and reflecting the truly joint nature of the JHWB Strategy, we are absolutely committed to its implementation. With help and support from pregnancy and throughout the life course and recognising the vital role that carers play, we hope to inspire residents and partners with our plans and look forward to working together to achieve the most positive impact possible for our residents over the next few years. Of paramount importance is our emphasis on prevention, self-management, early intervention to prevent disease and secondary intervention so vital to slowing the progression of disease. Councillor Helena Hart Chairman, Barnet HWBB Dr Debbie Frost Vice Chairman, Barnet HWBB and Chair of Barnet Clinical Commissioning Group 95
96 4 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy What we are trying to achieve Barnet is a great place to live and is now the largest borough in London by population. People in Barnet can expect to live longer and in better health than in many parts of London and England as a whole. This is not by chance but is linked to a range of factors including levels of family support, lifestyle, wealth, access to healthcare and green spaces, as well as the ability to access the right support when needed. While the overall picture is positive, the current Barnet Joint Strategic Needs Assessment (JSNA) has shown that there are marked differences in health and wellbeing outcomes, between places and different demographic groups, within Barnet. With less and less public money available, the JHWB Strategy aims to align and combine our efforts on a focused list of priorities where together we can make the largest impact to reduce health inequalities. The JHWB Strategy focuses on health and social care related factors that influence people s health and wellbeing, with clear recognition of the importance of addressing wider factors such as education, employment, income and welfare. These wider factors can both impact on and be impacted by the health and wellbeing of an individual or population, and need to be considered in order to make sustainable improvements to health and wellbeing. We hope to inspire and encourage both individuals and partners with the JHWB Strategy and our vision for health and wellbeing in Barnet; we will do this through the following approach: providing a shared vision and strategic direction across partners continuing the emphasis on prevention and early intervention including secondary prevention (slowing the progression of disease) making health and wellbeing a personal agenda as well as increasing individual responsibility and building resilience whilst ensuring provision for people with complex needs and/or special access needs joining up services so residents have a better experience developing greater community capacity; increasing community responsibility and opportunities for residents to design services with us strengthening partnerships to effect change and improvement putting emphasis on working holistically to reduce health inequalities in order to enhance each individual s health and wellbeing. It is our vision for Barnet residents, where appropriate, to be able to far better manage their own health and wellbeing. Barnet has a strong foundation for using resources within local communities with 88% of residents satisfied with their local area and 90% of residents saying that they help their neighbours out when needed (Resident Perception Survey, autumn 2014). 28% of residents volunteer regularly (weekly or monthly) and over 1,400 voluntary and community sector organisations are active in the borough. The JHWB Strategy reflects Barnet s Strategic Equalities Objective that: Citizens will be treated equally, with understanding and respect, and will have equal access to quality services which provide value to the taxpayer. 96
97 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy In September 2015 Barnet became the first London Borough to sign a faith covenant. The All Parliamentary Party Covenant for Engagement between Faith Communities and Local Authorities sets out how Barnet council and faith groups can work together in the borough. The Covenant will be upheld in the design and delivery of the activities described in the JHWB Strategy as faith communities are a valuable partner for improving health and wellbeing in the borough. The Health and Wellbeing Board and its partners are well placed to seek to improve wellbeing and tackle inequalities locally. Organisations, partners and residents tell us that they all want the same thing to keep well and promote independence. This strategy is a guide as to how, together, we can have the biggest impact. We have consulted widely on the JHWB Strategy not only to ensure that people feel it is appropriate but also to embed our vision across the public sector and to develop joint services to make the biggest difference. Aims The Joint Health and Wellbeing Strategy has two overarching aims consistent with the aims of the previous strategy: 1. Keeping Well Based upon a strong belief that prevention is better than cure, the JHWB Strategy aims to begin at the very earliest opportunity by giving every child in Barnet the best possible start to live a healthy life. It aims to create more opportunities to develop healthy and flourishing neighbourhoods and communities as well as to support people to adopt healthy lifestyles in order to prevent avoidable disease and illness. 2. Promoting Independence The JHWB Strategy aims to support residents and communities to become equal partners, with public services, to improve health and wellbeing. It also aims to ensure that when extra care is needed, this is delivered in a way which enables everyone (children, young people, adults and older people) to regain as much independence as possible, as soon as possible, and as ever supported by health and social care services working together. possible, and as ever supported by health and social care services working together. It is our aim that the JHWB Strategy should be used to inform service planning and service development across the public, private and voluntary and community sectors in the borough. Barnet s Health and Wellbeing Board is responsible for the development of the JHWB Strategy and for overseeing its implementation. Further information about the Barnet Health and Wellbeing Board, its membership, subgroups and associated groups can be found at the Appendix. Themes and priorities Annually the Health and Wellbeing Board has reviewed the progress made against the previous Health and Wellbeing Strategy ( ) and, based on the progress made, has identified a number of priorities. Using the updated JSNA we are now able to review the progress made and redefine our approach for the lifetime of this refreshed JHWB Strategy ( ). Our current Health and Wellbeing Strategy focuses on priorities across four theme areas and these priorities have been retained for the refreshed strategy. The table below gives an overview of the theme areas and the priorities we will focus on within each theme area: 97
98 6 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Vision Theme Objective What we will do to achieve our objective Preparing for a healthy life Improving outcomes for babies, young children and their families Focus on early years settings and providing additional support for parents who need it To help everyone to keep well and to promote independence Wellbeing in the Community How we live Creating circumstances that enable people to have greater life opportunities Encouraging healthier lifestyles Focus on improving mental health and wellbeing for all Support people to gain and retain employment and promote healthy workplaces Focus on reducing obesity and preventing long term conditions through promoting physical activity Assure promotion and uptake of all screening including cancer screening and the early identification of disease Care when needed Providing care and support to facilitate good outcomes and improve user experience Focus on identifying unknown carers and improving the health of carers (especially young carers) Work to integrate health and social care services Our efforts across the priorities will have a cumulative positive impact. Our aspirations for all children, young people, adults and older people are embedded across the theme areas. 98
99 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Where we are now Barnet at a glance The latest Barnet JSNA, formulated in 2015, is an impartial and up-to-date evidence base to be used as an effective means for joined up decision making across all sectors. The JSNA provides the data and information from which we can determine our priorities. The key headlines from the JSNA are: Barnet is now the largest borough in London by population (projected to be 367,265 by the end of 2015) and is continuing to grow. The highest rates of population growth are forecast to occur around the planned development works in the west of the borough, with over 113% growth in Golders Green and 56% in Colindale by ,265 Barnet population projected to be by the end of 2015 the west of the borough has generally the highest levels of deprivation in the wards of Colindale, West Hendon and Burnt Oak. There are pockets of deprivation across the borough such as the Strawberry Vale estate in East Finchley and the Dollis Valley estate in Underhill Barnet s population is becoming more diverse, driven predominantly by natural change in the established population. The highest proportion of the population from white ethnic backgrounds are found in the 90 years and over age group (93.3%) whereas the highest proportion of people from Black, Asian and minority ethnic (BAME) groups are found in the 0 4 age group (55.4%). The wards of Colindale, Burnt Oak and West Hendon have populations of whom more than 50% are from BAME backgrounds in Barnet, as in the rest of the country, women have a higher average life expectancy (85 years) than men (81.9 years). The life expectancy of men has increased at a higher rate than that of women, reducing the life expectancy gap between genders from 5.1 years (1991/93) to 3.1 years Life expectancy gap reducing 3.1 years between genders the life expectancy of individuals living in the most deprived areas of the borough are on average 7.6 years less for men and 4.7 years less for women than those in the most affluent areas. By ward, Burnt Oak has the lowest average life expectancy from birth of 78.8 years, 4.2 years behind the Barnet average and 8.3 years behind Garden Suburb, which has the highest life expectancy of 87.1 from birth gains in life expectancy have outstripped gains in healthy life expectancy. 99
100 8 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy This indicates that although women are living (on average) longer than men, a larger proportion of women s lives is spent in poor health; 19.1% (16.2 years) for women and 17.0% (13.9 years) for men Coronary Heart Disease is the number one cause of death amongst men and women, followed by Cancer due to the projected population increase in those 65 and over, the number of people aged over 65 living with moderate or severe learning disabilities is estimated to rise from 143 in 2015 to 187 in 2030 in 2015, it is predicted that 56,333 people aged have a mental health problem it is estimated that over 4,000 people in Barnet are living with dementia and even greater numbers of families and friends are adversely impacted by the condition. By 2021 the number of people with dementia in Barnet is expected to increase by 24% compared with a London-wide figure of 19% during 2013/14, 4,957 people were diagnosed as having had a stroke. The rate of emergency hospital admissions for stroke in Barnet (235.4 / 100,000) was higher than the national rate (174.3 / 100,000) in , breastfeeding initiation in Barnet was the 11th highest among all 326 English local authorities and 9th highest among the 33 London boroughs Barnet has a relatively low level of smoking prevalence compared with other areas (15% of adults over 18 years, compared to 18.4% nationally) Barnet has a relatively high percentage of the adult population with a healthy weight (42.1%). Although the percentage of adults with excess weight (55.7%) (combined overweight 35.2%, plus obese 20.5%) is low compared to the national average it nonetheless covers a large proportion of the adult population. Barnet also has a high percentage of underweight adults (2.3%) compared to the national level (1.2%) for children aged 4 5 years, the percentage of excess weight (overweight and obese) was 21% in 2013/14 was lower than London (23.1%) and England (22.5%) averages and has declined over the past five years. However, the proportion of excess weight for children aged years has increased to 34.4% in 2013/14 compared to 33.6% in 2012/13 this is similar to the national rate but still lower than the London region (37.59%) Barnet is ranked 16th and 14th out of all London boroughs in relation to lifesatisfaction and worthwhileness wellbeing scores out of the 33 London boroughs. Both of these indicators have experienced a decline in Barnet since Resident satisfaction levels vary throughout the borough peaking in Finchley Church End, Garden Suburb and Totteridge with satisfaction being lowest in Burnt Oak. The full JSNA can be accessed here: 100

101 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Policy context Although it has only been three years since the last JHWB Strategy the policy context has moved on greatly with a number of major legislative changes and policy developments. Locally, the council approved its Corporate Plan 1 ( ) in April 2015 which strives to ensure that Barnet is the place of opportunity, where people are helped to help themselves, where responsibility is shared and where high quality services are delivered effectively and at low cost to the taxpayer. The council s Corporate Plan sets the framework for each of the commissioning Committees five year commissioning plans. Whether the plans are covering social care services or concern universal services such as the environment and waste, there are a number of core and shared principles which underpin the commissioning outcomes the principles of fairness, responsibility and opportunity. With the Corporate Plan, the JHWB Strategy will provide strategic direction to council strategies and action plans, including those on housing, regeneration, transport, employment and business. 1 Barnet Council s Corporate Plan ( ) The Barnet Clinical Commissioning Group s (BCCG) Five Year Strategic Plan ( ) outlines its strategic vision to work with local people to develop seamless, accessible care for a healthier Barnet. BCCG goals are to promote health and wellbeing; transform primary care; ensure the right care, first time and develop joined up care. Nationally it is proposed that GPs provide services on a seven-day a week, 8am 8pm basis by BCCG had submitted a collaborative bid with Enfield CCG in partnership with Barnet constituent GP federated networks regarding the Prime Minister s Fund Wave Two. Although the bid was unsuccessful the proposals explored networks delivering extended access (8am to 8pm, seven days a week) and digital primary care. 8 to 8 The continuing financial pressures across the health and social care economy underlies the importance of changing the way in which we work for example crossing organisational boundaries and providing services in a more collaborative and effective way. NHS England approved the council and BCCG joint Better Care Fund bid in January 2015 which laid out how we plan to better care for people with complex needs. Barnet s Better Care Fund represented a single pooled budget of 23,312,00 for 2015/16, to support health and social care services to work more closely together. The council and BCCG are working together, within the Health and Social Care Integration model, to deliver a robust programme of work including Healthy Living Pharmacies and Barnet s Integrated Locality Team (BILT). The Five Year Forward View, published in October 2014 by NHS England, set out a radical increase in emphasis on prevention and public health focusing on greater individual and community control and responsibility through a new relationship with patients and communities. Four new models of care are identified in the NHS England planning guidance for the Five Year Forward View including multispecialty community providers, integrated primary and acute care 101
102 10 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy system, additional approaches to creating smaller viable hospital and models of enhanced health in care homes. Relevant here is the shift to local determination of how resources are most effectively deployed, one example is the Great Manchester devolution deal with NHS England, this would enable decisions to be made closer to the population being served. In 2014, NHS England asked for CCGs to put forward their bids for co-commissioning (with NHS England) of primary care. The North Central London (NCL) CCGs Co Commissioning application to be involved at Level 2 decision making only has been approved. Following changes to their constitutions, the CCGs in NCL (Barnet, Enfield, Haringey, Camden, Islington) will be able to collaborate to decisionmaking within the Joint Co-Committee arrangements set out by NHS England. The Care Act 2014, the most comprehensive overhaul of social care since 1948, provided an opportunity to build on and improve the care and support that we deliver. The Care Act called for care to be focused on the individual, their needs and their wellbeing, including increasing the importance of individuals choosing who they buy their care from. The Care Act has also put carers on an equal platform as their cared for in terms of eligibility for support. The Care Act came into force on 1 April 2015 and is therefore a key driver in refreshing the JHWB Strategy alongside challenges of increased demand for adult social care support. Increased demand for adult social care support The Children and Families Act, another major piece of legislation, was implemented in September In particular, the Act introduced a single assessment process, Special Educational Needs (SEN) reforms (including Education, Health and Care plans replacing statements) and a comprehensive local offer of services available to children, young people and their families. The council and BCCG have been working together to implement changes including cross-over with the Care Act. In December 2012, the Department of Health published the Winterbourne View Concordat. This has developed into the Transforming Care programme of action designed to transform services for people with learning disabilities, autism and mental health conditions. There is ongoing work in Barnet to improve and adapt current services, such as a new model for community learning disability services, embedding new care and treatment review processes to include people at risk of admission and a new Learning Disability Skills and Competency Framework for staff. The JHWB Strategy also considers wider influences on health and wellbeing such as changes to the welfare and benefits system, housing policy and developments in the built environment. We are aware that the policy context is likely to change in the lifetime of the JHWB Strategy and while we will be as flexible as possible in order to meet these demands, our ambition and priorities are unlikely to change. 102
103 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Preparing for a healthy life Highlights The council, BCCG and voluntary and community sector have been working hard to implement the reforms from the Children and Families Act (2014) in order to be compliant to deliver a system designed around the needs of children and able to support them until they are 25. We have developed our commitment to improving the life experiences of children and young people with complex disabilities into a vision for a new and improved 0 25 disability service which aims to foster resilience and independence. The new service intends to reduce the cliff edge of care our young people and their families often report during the transition from children s services to adults. The council is working to align with BCCG as the same service challenges are experienced by young people and their families accessing health services. New models of health visiting and school nursing have been completed in time for the transfer of the responsibility of services from NHS England to the local authority in October The Healthy Children s Centre Project supports Children s Centre staff and health professionals to work together to provide high quality services to support young children and families health and wellbeing. Taking a whole family approach the project has focused on a range of health and wellbeing outcomes such as involving families in healthy eating, reducing obesity through healthy lifestyles, promoting successful breastfeeding and children s oral health. An Oral Health Co-ordinator, started in 2014 and has trained staff to deliver the Brushing for Life Programme (promoting effective tooth brushing and fluoride s indisputable role in preventing tooth decay). Oral Health Champions in Children s Centres have also been identified. Schools in areas of high deprivation or with a high number of overweight children have been prioritised. At centres for children, baby clinics (or self service weighing services at centres without baby clinics) are providing a valuable opportunity for centre staff to engage with new families about services and support available. Engaging with new families at children s centres What does Barnet s JSNA tell us? Population growth the 0 15 age group shows growth at a greater rate than the age group until 2026, after which the child population is expected to decline slightly. This pattern of growth suggests that families are moving to Barnet with children. The high rates of population growth for children and young people (CYP) is expected to largely occur in wards with planned regeneration works and are predominantly in the west of the borough. 103
104 12 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Deprivation overall, in comparison with the national picture, children in Barnet have above average good health, educational attainment and life chances. However, this is not uniform for all children across the borough although the number of children living in poverty 2 has reduced slightly from the last Health and Wellbeing Strategy, from 18,000 to 17,330, this remains a significant proportion of children in the borough (21.2%), located notably in the western areas of Barnet. The poor outcomes for children in poverty are well documented especially poor educational attainment and ill health. Health childhood immunisation rates seem to remain a problem in Barnet with rates worse than the national rates, we will continue to work with NHS England to ensure accurate data is collected. Barnet s Public Health team is looking at immunisation uptake with partners, overseen 2 According to the 2010 Child Poverty Act, a child is defined as being in poverty when he/she lives in a household with an income below 60% of the UK s average. Throughout the refreshed JSNA and JHWB Strategy child poverty will be defined based upon the definition put forward by the 2010 Child Poverty Act. by the Health Overview and Scrutiny Committee poor dental health is associated with poor health outcomes in later life. Child dental decay is the top cause for non-emergency hospital admissions in Barnet for children Poor dental health the number of post-16 pupils remaining in special schools is placing pressure on the availability of places for admission of younger pupils. Safety keeping people safe is a key component of health and wellbeing. The safety of children in Barnet is overseen by a partnership of colleagues on the Safeguarding Children Board and the Children, Education, Libraries and Safeguarding Committee over half of children and young people with a child protection plan have suffered neglect. 65% of known cases of child sexual exploitation (CSE) in Barnet are females in their teenage years. The pattern of CSE in Barnet is wide and varied. Key characteristics have been youth violence or gang related activity and male adults talking to young females and males through the internet. What we plan to do Improve oral health for children We will seek to improve access to dental services for children and young people. In June 2015, Healthwatch reported problems with NHS dentists accepting new patients (including children) and have commissioned Homestart Barnet to explore the dentistry experiences of families with young (pre-school children). This study will look at the impact of accessibility to dental services for young children, availability of NHS dental services, family attitudes and opinions to dental care and the availability of clear information on how to access dental services. For Oral Health Champions, we will increase stakeholder networking and increase community 104
105 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy activity, outside of the classroom and centres for children to ensure that good oral health practices are embedded. Provide effective services for children, young people and their families Poor oral health is an indicator of wider difficulties including neglect; we are committed to supporting parents and families to create positive and supportive environments for children. The best chance for intervention with lasting positive impact is during the first 1001 critical days 3 of a child s life which is a critical period for brain development as well as attachment. We aim to improve outcomes for our children and young people through developing a supportive environment so children can thrive in their early years. We will provide a variety of support for parents especially older and first time mothers. All of our centres for children are working towards Healthy Children s Centre Status anticipating five centres will be awarded this status in late We will continue to support our centres for children to become registered as Healthy Children s Centres by late An Early Years review has been undertaken and will be continually reviewed in light of Critical Days UserFiles/files/1001_days_jan28_15_final.pdf emerging legislation. A locality model for centres for children has been developed which supports integrated working with partners with an early years offer being led jointly by BCCG and the council. The model will deliver a broader offer of services which incorporates external provision and builds on community capacity; it will also consider co-location and integration of health services. The offer will aim to improve outcomes and reduce inequalities for children. The locality model focuses on three areas (east/central, south and west) of the borough aiming to improve flexibility, effectiveness and also join up services to create a clear, identifiable Early Years offer which is trusted by residents and facilitates strong support networks. Our partners are key to ensuring centres for children are able to make a positive impact on the health and wellbeing of children and their families. Pregnancy and the birth of a baby are a critical window of opportunity when parents are especially receptive to offers of advice and support. Promotion of support and linking new parents with early years provision is vital and effective. The Early Years Service provides brokerage and outreach across the borough to seek to ensure all parents of targeted two year olds and universal three and four year olds access their free entitlement offer. Currently 42% of eligible two year olds and 86% of eligible three and four year olds access their offer. There is a targeted approach to increase uptake as well as to link with employment opportunities. Increasing the uptake of the free early years education offer The JSNA identifies Burnt Oak and Colindale as areas of particular need given the levels of deprivation. Just over one third of the children in Burnt Oak and in Colindale are living in low-income families. Burnt Oak is the only ward where the average household income in 2015 at 25,000 per year was lower than in Targeted, multi-agency, place based commissioning programmes have been developed including a GP-led well-being pilot, Love Burnt Oak s Health Coaches funded by the Area Forums, a town centre regeneration project and a multi-agency employment service (Burnt Oak Opportunity Support Team, BOOST). 105
106 14 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy We will seek to support more of our looked after children locally, especially those with a range of complex needs, enabling them to benefit from the quality of local schools and other local services. We are committed to increasing the number of Barnet children fostered by Barnet foster carers. From mapping of voluntary and community sector services documented in the JSNA, local voluntary and community sector provision for children is relatively low in the areas where the population of children and young people is forecast to be highest (Colindale and Burnt Oak). Targeted social action, volunteering and employment projects, delivered by our local infrastructure partners, aim to rectify this. Our local infrastructure partners, with the council, will support voluntary and community organisations to deliver services and offer solutions to help sustainability. The Health and Wellbeing Board recognises and supports the priorities of the Safeguarding Children Board including CSE and Female Genital Mutilation (FGM). The Health and Wellbeing Board has a role to ensure CSE issues are championed across partners. How will we know we have made a difference? Our performance measures for the theme Preparing for a healthy life are: five of centres for children to be Healthy Children s Centres by 2016 with all centres being accredited by 2020 have 85% (65% from vulnerable groups) of families with child/ren under 5 registered and accessing services at centres for children by 2015/16 and 96% (65% vulnerable groups) by 2019/20 increase the percentage of children in care in Barnet foster care as a percentage of all children in care from 35% (2014/15) to 39% (2015/16) and 53% (2019/20) enhance our corporate parenting approach across Barnet by, for example, increasing the percentage of free entitlement early years places taken up by parents/carers (where eligible) from 41% (2014/15) to 50% (2015/16) and 85% (2019/20) reduce the prevalence of early childhood dental caries from 6.1% (2013) to the national average (3.8%) by 2020 remain above the school readiness national average (60.4%) for the percentage of children achieving a good level of development at the end of reception 65.4% for Barnet s children in 2013/14 increase satisfaction of children and parents with services for children and young people (aged 0 25 years old) through the development of our 0 25 disability service increase uptake of childhood immunisations (six vaccinations) to be at or above the England average increase the frequency of occurrences whereby children and young people are engaged and involved in the design, planning and review of services and commissioning processes increase social action and voluntary and community sector activity through the work of our Local Infrastructure Partners. 106
107 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Wellbeing in the community Highlights The previous Health and Wellbeing Strategy identified excess cold hazards (such as cold homes, the cost of energy bills, social isolation, access to services and risk of falls) as a priority. The Winter Well scheme, led by Regional Enterprise Ltd. (Re), working in partnership with the council, BCCG and voluntary and community sector partners, was successfully delivered in The scheme aims to reduce negative health outcomes and excess winter deaths by providing practical assistance to the most vulnerable and eligible residents. To date the scheme has included training and advice to over 110 professionals and 210 residents on energy matters to prevent and reduce fuel poverty. The scheme includes a Winter Well helpline and has provided emergency supplies and services such as heaters, damp proofing and boiler repairs. To date energy switches have saved borough residents a total of 24,004 (total for 97 residents). Warm places have been set up across the borough for people who had difficulty heating their homes and/ or found themselves isolated over the colder months. Seventy new Community Friends (part of Altogether Better) were recruited during the scheme showing the community s response to help others in the event of cold weather. Warm places have been set up for people who found themselves isolated over the colder months Altogether Better officers work in small geographical localities, have an open door, access to information and small amounts of funding, but most importantly a remit to nurture local solutions and keep people independent. The projects aim to build and unlock community resources and bring people together. Currently there are four Altogether Better sites covering the following the areas: Burnt Oak East Finchley Edgware and Stonegrove High Barnet, Arkley and Underhill. Activities include Talkie Walkies (walking groups), Wellbeing Cafés and Men in Shed projects. Also, restaurants offer discounted meals for older people as part of the Silver Service initiative (in two localities). We will seek to promote the expansion of these opportunities where the Council engage with providers in relation to Healthy Catering Commitments. As part of the wider Ageing Well programme, Barnet has borough wide projects. The Barnet Timebank is in its second year; 121 exchanges have included CV help, gardening, befriending, fitness advice and language lessons. There are also a number of volunteer led intergenerational reading groups including for people with dementia and their carers. 107
108 16 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy The condition of and access to local housing has an important role in the quality of life and health of both individuals and communities. The council has developed a new Housing Strategy ( ) which sets out how the council and partners will deliver the additional housing that is required in the borough due to the growing population. The Housing Strategy details how more affordable housing will be provided as well as promoting independence through the provision of wheelchair accessible housing. In Barnet, there are also a number of plans in place to improve housing such as removing health and safety hazards in homes (particularly in the private rented sector), re-locating and improving the quality of an in-house children s home, and work to better understand the causes of homelessness and how to prevent it as part of the Housing Strategy. We are also working with private landlords to ensure good quality private sector housing. Improving mental health and wellbeing is a key priority. In 2014, BCCG and Barnet Council signed up to the Crisis Care Concordat and the Government emphasised the importance of achieving parity of esteem between physical and mental health; valuing mental health equally with physical health. Action already taking place includes: Barnet Council s Network Enablement Service BCCG and the council working with Barnet, Enfield and Haringey Mental Health Trust to improve and modernise the current secondary care services towards a community based model of care delivery within the community BCCG South Locality Primary Care Liaison Pilot which is reporting a reduction in secondary care referrals the Burnt Oak and Colindale Wellness Service Pilot involving a navigator role to support people through their health and wellbeing journey BCCG implementing a locally enhanced service to improve access to primary care for people with mental health problems who are homeless reducing the waiting list for IAPT as well as encouraging self-referrals to IAPT Public Health has developed a Suicide Prevention Strategy, Working Group and action plan. Self-harm and suicide prevention workshops have been held for professionals and volunteers who work with vulnerable groups two public health commissioned employment support services Motivational and Psychological Support based in local Job Centres and an Individual Placement and Support (IPS) scheme for people with severe and enduring mental health needs and based in community mental health teams Barnet is leading a West London Alliance (WLA) programme looking at developing IPS for people with common mental health conditions. Learning from other similar schemes suggests that we should expect to see between a third and a half of people supported gain and retain employment a number of befriending schemes running such as Alzheimer s Society supporting people with dementia and their carers and Homestart supporting families. Befriending schemes supporting individuals and families 108
109 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy A Barnet Schools Health and Wellbeing programme has been in place since 2013, and is both established and performing well. The emotional health and wellbeing element of this programme offers support to develop programmes, a directory for signposting as well as training to build capacity within schools. We seek to build on existing work in schools which will promote early identification of Tier Two (child adolescent mental health specialists working in community and primary care settings) needs and offer appropriate interventions. A project is underway to pilot an evidence based manualised treatment group for managing severe anxiety which impacts on school attendance. Barnet s Community Education Provider Network (CEPN) has commissioned a programme for primary care staff to consider how patients with medically unexplained symptoms (MUS) can be empowered and how primary care can aid recovery. Service users were included in the delivery of these sessions. The work is yet to be evaluated but it lays the foundation for further work in Barnet to address the needs of patients with MUS and help to redress the balance of supporting mental health with equal importance as physical health. What does Barnet s JSNA tell us? Mental health, mental wellbeing and social isolation Barnet has a lower prevalence of depression (4.3%) in adults than the national average (5.8%) across all ages, the prevalence of schizophrenic, bipolar affective disorder and other psychoses (0.95%) is lower than the London average (1.03%) emergency admissions for self-harm (109.9 / 100,000) are lower than the average for England (191 / 100,000) and the suicide rate (6.9 / 100,000) is lower than the national rate (8.5 / 100,000) the hospital admissions rate for poor mental health in children (aged less than 18 years) in Barnet is higher (167.6 / 100,000) than the average national rate (87.6 / 100,000) prevalence varies by age and gender, with males more likely (11.4%) to have experienced or be experiencing a mental health problem than girls (7.8%). Children aged 11 to 16 years olds are also more likely (11.5%) than 5 to 10 year olds (7.7%) to experience mental health problems. Domestic violence and violence against women and girls domestic violence along with parental mental ill health and substance abuse are the most common causes for referrals into social care and result in the poorest outcomes for children and young people the number of Multi Agency Risk Assessment Conference (MARAC) cases of domestic abuse associated with drug and alcohol use in Barnet nearly doubled between 2011 and Employment Barnet has a lower than average percentage of people with mental health conditions and learning disabilities in work than other areas there are significant differences in the proportion of working-age people receiving Job Seekers Allowance in different wards, the areas with the highest proportions being in Burnt Oak, Childs Hill and Underhill. 109
110 18 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy What we plan to do Mental health and wellbeing The number of people with mental health conditions is predicted to increase as the population grows. In November 2014, the Health and Wellbeing Board identified prevention of and early intervention in mental health problems as a priority. Mental health is our key priority in year one 4 of the JHWB Strategy with partners coming together to make a positive impact for all of our residents. We will continue to implement national guidance including the recommendations that will come from the NHS England established taskforce to develop a five year forward view for mental health. We are hoping, through the JHWB Strategy, to build prevention and early identification into all we can to prevent and reduce mental health problems for our borough s residents. Many Public Health and community initiatives contribute to mental wellbeing across the lifespan such as pregnancy and parenting support, physical activity and self care. 4 From agreement of the JHWB Strategy in November April 2017 Barnet will run a wellbeing campaign focusing on taking responsibility for and improving mental wellbeing as well as tackling stigma. The campaign will embed wellbeing into current activity, share success stories and celebrate World Mental Health Day. We will also: develop a health champion programme in primary care focused on improving mental health and wellbeing review local pathways for antenatal and postnatal depression including promoting peer support be part of the pan London digital mental health support service maximise the potential of improvements to and changes in the management of open spaces, where this could support improved mental wellbeing. Health champion programme focused on improving mental health All services and activities working with residents have a responsibility to identify where someone could benefit from support. Healthwatch Barnet Youth has been undertaking a survey into the awareness, training and confidence of schools staff regarding mental health, following a series of workshops and focus groups with young people to determine their priorities and concerns on health. Early mortality for people with severe mental health problems is widely documented. Treatment services are required to make changes at scale to re-focus on recovery, social inclusion and enablement. The Reimagining Mental Health project, facilitated by BCCG, is putting residents at the centre of mental health service delivery. 110
111 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy The co-designed and co-produced model aims to deliver better, more targeted health services through a community based approach. BCCG has committed to the following commissioning intentions to: work with Enfield and Haringey CCGs to review Psychiatric Liaison Service provision review each 2015/16 contract for services for older people relating to multidisciplinary care in people s own homes that link with primary, secondary, social and voluntary and community sectors, and including access to Rapid Care, Triage Rapid Elderly Assessment Team, Post-Acute Care Enablement Service, Integrated Care Team and the Barnet Integrated Locality Team undertake, collaboratively across North Central London, an end-to-end pathway redesign of existing Child and Adolescent Mental Health Services (CAMHS) as our response to the national CAMHS Transformation agenda including a focus on the most vulnerable (including those with complex needs and/or special access needs) produce CAMHS out of hour s service, working with North Central London partners. Alongside this, a new specification for mental health social work has been developed by the council to re-focus social work. Work is now underway to embed the model which includes Consultant Social Workers and integrated pathways as well as improving employment and accommodation. Social isolation Feelings of social isolation and loneliness can be detrimental to a person s health and wellbeing. We will seek to improve the identification of people (children, young people, adults and older people) at risk of or experiencing social isolation (across the borough) through our Healthy Living Pharmacies, hospital discharge teams and substance misuse treatment services. In Barnet, social isolation is especially prevalent in older women who live alone (more likely to be in areas of higher affluence and lower population density). We will develop targeted initiatives, building on current good practice and working with the voluntary and community sector, to encourage greater social contact. We will engage volunteers through befriending schemes (particularly as a respite offer for carers) and promote ways for people to get involved locally such as in the borough s parks and green spaces and libraries. 111
112 20 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Preventing loneliness and isolation The Barnet Provider Group has expanded its programme of activities which includes lunch clubs and befriending activities, tea dances and games afternoons. Activities have reached over 2,500 new people over the last 12 months. Many of these activities are delivered by volunteers (over 500 are involved). The benefits of volunteering are well documented and the majority of volunteers are older people themselves. The Barnet Provider Group plans to expand its befriending services during 2015/16 so that it can continue its work to prevent loneliness and isolation. Employment and healthy workplaces There has been growing recognition that the relationship between health and work has a significant effect on the lives of individuals and on wider society. 5 When out of work, an individual s health is more likely to deteriorate and they risk falling into poverty. Nationally, for too long it was assumed that people with health conditions should be protected from work but in recent years evidence has shown how detrimental this approach can be to individuals and their families. Barnet has been responding to the Welfare Reform agenda with a Welfare Reform Task Force. The Task Force brought together the council s housing officers, Jobcentre staff and health advisers into a single team to work with those impacted by Welfare Reform. This integrated team has engaged with 96% of residents affected by the Benefit Cap and helped over a third of them into work. 96 % of residents affected by the Benefit Cap Engaged with 5 Fitness for Work, Department for Work and Pensions (2013) system/uploads/attachment_data/file/181072/healthat-work-gov-response.pdf In the past, local authorities, Jobcentre Plus, Work Programme providers, and the local voluntary and community sector have generally operated in silos to help people into work. While this has produced some positive results, there remain pockets of disadvantage where communities are missing out on the opportunities that growth brings. Burnt Oak Opportunity Support Team (BOOST), launched in April 2015 and based in the library, helps people find work through holistic support in their local area. The project is part of a West London Alliance approach called Working People, Working Places and puts all relevant services together under one roof so all residents (whether they claim benefits or not) can access the targeted support they need to help them develop new skills and overcome any obstacles to employment that stand in their way. Key to the success of the model is the involvement of the local community facilitated by Love Burnt Oak who will help the service engage with more isolated residents. 112
113 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy The service is also supported by a commissioned service called Future Path that supports people with their mental health, physical health and employability side by side. The aim of the two year project is to boost incomes in the area, supporting people into work as well as supporting a measurable increase in the wellbeing of those supported. The BOOST team have already supported 63 people into work. We will continue to take a personalised approach to support individuals to pursue their interest within their capabilities. There are opportunities for more partners to get involved in the BOOST project and work together to increase incomes and improve wellbeing. When residents gain employment (including a return to employment following a period of ill health) we want them to be healthy and we need to create healthy workplaces that support this. Around 300,000 people across the country fall out of work a year and into the welfare system because of health-related issues. The state spends 13 billion a year on health-related benefits, with employers facing an annual bill of around 9 billion for sick pay and associated costs. Costs to individuals are around 4 billion in lost income. A healthy and happy workforce also improves the experience of our customers. As we ask residents to take more responsibility for their own health, employers also need to take responsibility for the health and wellbeing of their staff, creating healthy environments and modelling healthy behaviours. The council and BCCG are two of the largest employers in the borough. The council is looking to achieve an excellence level for the London Healthy Workplace Charter and BCCG is implementing its Health and Wellbeing Policy. HWBB member organisations are committed to supporting their staff to be healthy at work and will promote and champion this agenda to partners such as Re and our health and social care providers as well as via Entrepreneurial Barnet which is Barnet s public sector approach to making the best place in London to be a small business. As not all of our residents will actually work in the borough, the HWBB will share its learning and experience across London, through the London Healthy Workplace Charter, to promote to other boroughs and partners. The London Healthy Workplace Charter, a Greater London Authority programme, asks employers to review the support they offer their employees in a number of areas including stress prevention, the promotion of mental wellbeing, smoke free spaces, active travel, healthy eating, a reduction of excess alcohol consumption and the prevention of substance misuse. London Healthy Workplace Charter asks employers to review the support they offer their employees 113
114 22 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy How will we know we have made a difference? Our performance measures for the theme Wellbeing in the community are: recruit 50 Health Champions in 2015/16 with further roll out to 2020 increase the proportion of adults in contact with secondary mental health services in paid employment from 5.7% (2013/14) to 7% (2015/16) and continue to increase (2019/20) increase the proportion of adults with mental health needs who live in stable accommodation from 70.90% (2014/15) to 75% (2015/16) with the aim of being in the top 25% of comparable boroughs by 2019/20 through improved CAMHS we will reduce the waiting time for eating disorder services, reduce self-harm admissions and A&E presentations, every young person presenting with self-harm or crisis to be seen within two hours regardless of setting and improve parent and teacher reported Strength and Difficulties Questionnaire (SDQ) to below threshold for referral support 240 people into work via BOOST in 2015/16 and 2016/17 Barnet Council to achieve (by 2016) and maintain London Healthy Workplace Charter maintain or reduce the percentage of employees who have had at least one day off in the previous week (1.3% in ) increase the percentage of adult social care users who have as much social contact as they would like from 41.4% in 2014/15 to being in the top 25% in England. More stable accommodation for adults with mental health needs 114
115 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy How we live Highlights Barnet has embraced the transition of public health from the NHS to the Local Authority using this as a key way to address the wider aspects critical to health and wellbeing. Some successes include the commission of substance misuse services which will address fragmentation of services, school nursing, health visitors transfer preparation and increase in NHS Health Checks. Public Health has also developed a Substance Misuse Strategy which coordinates activities to prevent and protect residents from harmful substance misuse as well as promote and sustain recovery through collaboration, training, social marketing and reviewing local licensing. An Implementation Group, led by Public Health, has been established to take forward key areas of action overseen by the HWBB as well as the Community Safety Partnership. Further to this, enhanced training of Barnet GPs in health promotion for patients with mental illness is part of the Reimagining Mental Health plan. Barnet and Harrow joint Public Health service is working in collaboration with the West London Alliance (WLA) and the majority of boroughs across London as part of collaborative sexual health (genitourinary medicine, GUM) service commissioning arrangements. The major new service tendering, expected in 2017, will reduce service fragmentation, improve access and early intervention which in turn will reduce unwanted pregnancies and onward transmission of sexually transmitted infections (STIs) as well as aiming to tackle escalating costs. Taking action locally, we have organised a number of pop up screening events to increase the early identification of disease. The pop up shops and health promotion events have provided information on healthy lifestyles and their contribution to cancer prevention, symptoms and the importance of early presentation and diagnosis and screening. The Obesity Pathway group, with a membership of BCCG, schools, leisure and providers, has been exploring improvements to the child weight management pathway. Healthy Weight Nurses were appointed in 2015 and after being in place for six months, the nurses had engaged with 25 children on a 1:1 basis, reporting that almost all had shown positive behaviour change and, as a consequence, six had already lost weight. The team has also noticed behaviour changes in the families of the children they have engaged with. Another aspect of our Child Weight Management programme is Alive and Kicking which, through information on nutrition and physical activities, is successfully supporting weight loss. Alive and Kicking is also engaging with schools and parents to embed healthy weight principles. Embedding healthy weight principles For adults, the Obesity Strategy Group has expanded following a commitment to develop a Healthy Weight (Obesity) Strategy and action plan. An adult Weight Management Service development is underway. 115
116 24 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Barnet Council is committed to working with its contracted leisure provider to enhance and develop varied opportunities. This has been highlighted by the total number of GLL Better Inclusive members, a membership aimed at encouraging participation of people with disabilities which peaked at 733 in What does Barnet s JSNA tell us? Healthy Lifestyles smoking, bad diet, and a lack of exercise are the main causes of premature death in Barnet rates of sexually transmitted infections are lower than London rates. However, there are lower detection rates of chlamydia (16%) than England (24.9%) in Barnet, only 1% of all trips between 2007/ /10 (baseline figures) were made by bike pollution levels are higher along arterial routes, particularly the North Circular, M1, A1 and A5. Long term conditions the rate of emergency hospital admissions due to stroke is significantly higher in Barnet than London or England the prevalence rate of diabetes is forecast to rise at both national and local levels and this increase could be even higher if diabetes risk factors such as obesity are not addressed. Screening screening rates for cervical cancer (68.8%) and breast cancer (71.2%) are significantly lower in Barnet than the England average (74.2%; 75.9% respectively). Sport England Active People Survey Data (APS) The number of people playing sport is tracked continuously through Active People the largest survey of sport and active recreation ever carried out in Europe. Active People provides information on the national and local picture of who is taking part in sport and how are they participating. APS 9 Quarter 2 (April 14/2015) evidences significant levels of inactivity within Barnet: 37.9% of the population currently participate in activity at least once a week (moderate intensity for 30m or more) 17.1% total number of population participating in activity 3 or more times per week (moderate intensity for 30m or more) 51.9% of the population do not currently take part in any sport inequalities are apparent as current research demonstrates 46.1% of men currently participate in activity once or more per week (30m more) 30.2% of women currently participate in activity once or more per week (30m more). physical activity rates are below the national average 116
117 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy What we plan to do Sport and physical activity Barnet Sport and Physical Activity Needs Assessment (2012) highlighted that whilst health behaviours and outcomes are more favourable in Barnet than in England as a whole, sport and physical activity rates and the use of outdoor spaces are below the national average. A breadth of evidence demonstrates that a more active lifestyle is essential for physical and mental wellbeing. Regular physical activity helps to reduce the risk of stroke, type II diabetes, development of dementia, incidences of heart disease, cancers and high blood pressure. Physical activity supports the prevention and management of long term conditions as well as being a component of achieving and maintaining a healthy weight. Physical inactivity currently costs the UK economy 7.2 billion. Additional costs are incurred via the wider economy; through sickness absence, premature death of productive individuals and increased costs for individuals and their carers. Within Barnet, the health costs of physical inactivity currently cost 6.7 million. This is approximately 1.9 million per 100,000 of the Borough population. However as measured by the Sport England Active People Survey Data (APS9 Quarter 2) 43.8% of the Borough are currently inactive and would like to do more. We aspire to ensure our residents lead an active and healthy lifestyle. Our ambition is underpinned by a commitment to: improve and enhance Barnet leisure facilities, ensuring that opportunities are accessible for all residents: reflect public health outcomes within a new leisure management contract (from 2018) refurbish and redevelop of leisure facilities. advocate investment and innovative policies to support the delivery of high quality, accessible facilities and delivery of services: facilitate mutually beneficial partnerships that connect and align services to deliver a more cost effective physical activity pathway develop the Fit & Active Barnet network that encourages engagement and collaboration. facilitate partnerships and develop opportunities that demonstrate a commitment to embed an active habit. We will: work with local, regional and national partners ensure opportunities are concentrated in a range of settings to sustain future activity; schools/colleges, workplace, community, leisure, travel and open environment assess the supply, demand and quality of playing pitches. Leading to the adoption of a Barnet Playing Pitch Strategy develop and improve the accessibility and quality of open spaces across the borough to support healthy outcomes, underpinned by the Barnet Open Spaces Strategy (including allotments and safety) utilise open space to coordinate and support recreational and competitive activity, inclusive of Outdoor Gyms promote and support of clubs, initiatives and activities within Barnet 117
118 26 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy through local infrastructure organisations, we will support individuals and communities to take ownership and responsibility for sustainable sports and physical activity options facilitate a Community Sport and Health Activation project in Burnt Oak and Colindale. A project targeting young people 11 19yrs, supported by Sport England and additional partners work with our Volunteer Centre to develop volunteering opportunities and recruit and retain volunteers, increasing and tailoring workforce development provide the structures required for individuals to recognise their sporting potential make healthy choices the easiest and first in the built environment such as consideration of the placement of stairs in new buildings. target those who do not traditionally engage. To increase participation amongst under-represented groups such as women and girls, people with disabilities, people from BAME communities, children and young people and older adults we will: widen access to ensure that facilities and open spaces are better used by the communities they serve work in partnership with providers to develop sustainable activities targeted at those people at risk of developing long term health conditions support early intervention and health promotion pathways such as the children and young people s obesity pathway and cardiovascular disease, highlighting the benefits of leading an active lifestyle. We will improve the post Health Check service offer to ensure that people engage in services and lifestyle changes where necessary support and promote activities provided by local organisations such as Love to Move for people over 50 delivered by Age UK Barnet and Saracens Sport Foundation create and support stronger and safer communities ensuring that activity venues are welcoming, secure and experiences are positive tackle the barriers facing the most disadvantaged and enabling them to reach individual potential ensure there is a commitment to provide affordable participation opportunities for those who experience cost as a barrier for example concessionary based schemes within leisure centres engage community and faith leaders retain English Federation of Disability Sport (EFDS) Inclusive Fitness Initiative Accreditation at Burnt Oak Sports Centre, exploring expansion and commitment within the leisure facility portfolio support Barnet Centre for Independent Living (BCIL) to deliver The Into Sport project which is a Sport England funded initiative assembled through 118
119 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy a partnership between Inclusion London, Interactive and five London DPOs (disabled people s user led organisations). The project takes a creative approach to tackling barriers faced by disabled people in accessing sport and physical activity. Wider public health workforce The definition of the Public Health workforce is changing to highlight how public health is everyone s business. To make the biggest impact we need to utilise the wider public health workforce which consists of individuals who are not specialists in Public Health but who have the opportunity to improve the public s health and to create inclusive communities and places. A training resource will be developed to upskill staff (from all sectors) who interact with residents to maximise the opportunities for face-to-face contact to promote good health, social care and wellbeing information, messages and signposting. The training will also support the identification of hidden carers. Specific training is also available such as Raising the Issue of Weight training to support professionals to discuss weight issues with residents. We will also promote and improve signposting resources. Regeneration The borough s ambitious regeneration and growth programme provides an opportunity to develop new lifetime neighbourhoods that promote independence and wellbeing. Being aware that the environment in which people live impacts their health, we will build public health into all our regeneration and transport projects including the provision of new health facilities and plans to encourage active travel. The high street, at the heart of local community, offers an ideal platform for health promotion. Where possible, we will create healthy high streets including health champions and stores making healthy options easier. We will also consider the proximity of fast food outlets to schools, colleges, leisure centres and other places children gather. We will also link regeneration programmes with child friendly and dementia friendly community developments. We will drive this through our Entrepreneurial Barnet Board supported by national programmes such as NHS England s Healthy New Towns. We will also look at the role Health Impact Assessments play in planning. Where comprehensive development and regeneration is taking place across the borough (particularly at Colindale and Brent Cross), a wide range of investment programmes are planned to secure improvements to health outcomes for those populations already living in and new residents moving to those areas. These include: expanded or new integrated use local primary care facilities new high quality and energy efficient housing to replace existing non-decent housing stock travel planning, public transport, parking measures and highways improvements to enable travel choices new schools that can help improve educational and family lifestyle outcomes new community and youth facilities to promote social engagement and support positive local community activities. 119
120 28 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Screening Increasing screening uptake remains a priority. NHS England has lead responsibility for screening performance. Public Health will work with NHS England to explore appropriate service delivery in line with best practice to improve the uptake of all screening including cancer screening programmes. How will we know we have made a difference? Our performance measures for the theme How we live are: increase by 1%, the percentage of active adults 14 years and over (as measured by Sport England Active People Survey) by 2020 (currently 37.9%) increase the total number of leisure centre members (all categories) from 26,400 to 30,000 in 2020 increase total leisure centre attendances (1,149,290) by 2% by 2020 older adults (55 and over), currently 27% people with disabilities, currently 733. reduce excess weight in adults (55.7% in 2014/15) cumulative percentage of the eligible population aged who are offered (33.4%) and take up (8%) a NHS Health Checks to become more targeted reduce the prevalence of children classified as overweight and obese by 0.5% for each group (4 5 year olds overweight, 4 5 year olds obese, year olds overweight, year olds obese) by 2020 increase the uptake of screening. We will also monitor the following: an increase in life expectancy and healthy life expectancy including decreasing inequalities (between wards and genders) reducing the prevalence of CHD and cancers. increase participation (as measured by Sport England active people survey) by 1% for the following groups by 2020: females 16 years and over, currently 30% 120
121 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Care when needed Highlights Barnet has improved access to care and support by: launching a new universal deferred payments scheme providing prevention services, promoting wellbeing and focusing on delaying or preventing the need for social care services improving information and advice services, enabling people, carers and families to take control of, and make well-informed choices about, their care and support and how to fund it implementing a service to support self-funders to arrange and manage their community care (users pay a fee to cover costs) promoting Information and Advice providers including Social Care Direct changes to support services for carers as well as establishing an assessment for carers own needs and implementing changes of eligibility for carers continuing to meet Equalities Duties and provide a person centred approach, for those with specific access needs we provide interpreters and information in a variety of formats. We are currently reviewing our telecare and sensory equipment offer. Carers can access mainstream and prevention services to promote their health and wellbeing for example they can receive health checks for themselves and obtain information and advice about benefits. Following a carers assessment and development of a personalised Support Plan, the council offers further support options including obtaining a direct payment to meet their identified and eligible needs and outcomes; and respite given to the person they look after. There are specialist support services for carers delivered through a lead provider who work with voluntary and community sector partners to provide short breaks so carers can have time off from caring; peer and group support; training in manual handling and help with emergency planning. With support from the council, a Parent Carer Forum has been established in Barnet with a membership of over 100 parent carers. The forum will be a resource for consultation, vital at a time of service development alongside the wider Carer s Forum. Integrated care and encouraging self-care were identified as priority areas by the Health and Wellbeing Board in November 2014 and since then a key focus of the board has been to deliver better care for people with complex health care needs. The council, BCCG, voluntary and community sector as well as providers are working together to create ways for people to remain in their own homes for longer. In line with our prevention aims and to reduce the pressure on accident and emergency departments, we have been developing community models of care. The borough has established a Healthy Living Pharmacy (HLP) model with 28 pharmacies (of the 78 in Barnet) signed up to providing a health and wellbeing support service to patients. 28/78 pharmacies have signed up to providing support services 121
122 30 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Our commitment to support people to live meaningful, fulfilling lives whatever their ability or disability is also evident in our Winterbourne View Concordat progress. There are active discharge plans in place for many of the remaining patients. Commissioners and care co-ordinators are working closely with existing and new providers to develop solutions which are in the patients best interests % Dementia diagnosis rate Barnet achieved the 67% dementia diagnosis national target for 2014/15 with a 67.7% result and, as of August 2015, we have achieved a 77.1% diagnosis rate. This means that three quarters of the people estimated to be living with dementia in Barnet have a diagnosis. The re-configured Memory Assessment Service, provided by Barnet, Enfield and Haringey Mental Health Trust, became fully operational in July The service provides a holistic assessment for people with memory problems and has the capacity to meet the needs of a growing population of older people with dementia. Located with this service, is Barnet s Dementia Advisor service which provides specialist information and advice at the point of diagnosis and a point of contact on an ongoing basis. Four Dementia café s provide opportunities for people with dementia and their carers to gain information and advice and take part in a range of activities. The Early Stroke Discharge team provides specialist stroke rehabilitation care and a seamless transfer from hospital to home for stroke survivors. Barnet s post-acute services such as stroke review and specialist information and advice ensure that the recovery potential for people following a stroke is maximised. The stroke review service re-assesses an individual s health, social care and therapy needs at six months post stroke, improving their recovery potential. The review can pick up the need for further prevention services so reducing the likelihood of a second stroke. What does Barnet s JSNA tell us? Our older population Barnet has a higher proportion of people aged 85 and over (3.1%) compared to Outer London (1.8%) and the UK (2.3%) currently, Garden Suburb and High Barnet have the largest proportion of people who are over 65, both at 18.1% of the population within the ward. Over this period, Brunswick Park and Hale are projected to experience relatively higher levels of growth in the proportion of the population aged 65 and over, increasing by 5.8% and 5.5% respectively the over-65 population is forecast to grow three times faster than the overall population between 2015 and 2030, and the rate goes higher in successive age bands; over-65 population will grow by 34.5% by 2030, whereas the 85 and over population will increase by 66.6%. Health and social care despite continued growth in the adult population, the number of people in receipt of residential care and nursing care has decreased from 1,441 in 2011/12 to 1,367 in 2013/14 (a decrease of 5.1%) overall the percentage of diabetic people having all 8 health checks in Barnet is below the national rate increasing demand on urgent and emergency care with Barnet Accident 122
 in")
123 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy and Emergency activity recording an increase in 14/15 compared to 2013/14 Barnet has a higher population of people with dementia than many London boroughs and the highest number of care home places registered for dementia per 100 population aged 65 and over in London the incidence of tuberculosis (TB) in Barnet (25.9 per 100,000, three year average) is lower than the London regional rate (39.6 per 100,000) but higher than the rate in England (14.8 per 100,000). Barnet has a higher number of drug resistant TB cases than the average number of these cases in London. Carers in 2011 there were 32,256 residents who classified themselves as a carer in Barnet. The year old age group had the largest number of carers (12,746) in relation to the total population, Brunswick Park and Underhill have the highest rate of carers (10.5% of the population), whereas Colindale has the lowest (6.90% of the population) young carers are at particular risk of remaining hidden from services, in Barnet we have identified 2% of under 18s to be carers but there is a large gap in identification of year olds with a caring responsibility 2 % of under 18s have been identified as carers on average carers are more likely to report having poor health (5.2%) than non-carers (4.2%), especially among carers who deliver in excess of 50 hours of care per week. One in 5 young carers describe their health as being only fairly good or even poor young carers are also 1.5 times more likely to have a disability, long term condition and special educational needs than non-young carers young carers are twice as likely not to speak English as their first language the Carer s Survey shows that whilst carers reporting satisfaction with the services they received has decreased from 74.7% 2012/13 to 68.1% in 2014/15, satisfaction has remained stable for people who are cared for (88.3% of service users in 2013/14 and 88.2% of service users in 2014/15). What we plan to do Carers Carers are being recognised nationally for their contribution. Carers are being prioritised in the JHWB Strategy due to their crucial role and their own health and wellbeing needs which will increase as more people choose and are supported to remain at home for longer. According to Carers UK, there are 6.4 million carers in the UK reducing the national care bill by an estimated 119bn per year, equivalent to 18,594 per carer. Each caring situation is unique and every carer has different needs and priorities. It is important to identify carers, and where needed, support them to carry out their caring role whilst protecting their own health and wellbeing. A caring role can develop and change gradually overtime or an individual (parent, partner and sibling) may not regard what they do as caring which means that identifying carers is difficult. Awareness needs to be raised with residents to understand what caring is and that it is ok to ask for help. To increase the identification of unknown carers we will: develop campaigns for the following: 123
124 32 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy areas with a high population of older people such as Garden Suburb work with schools and colleges to develop effective outreach to identify carers who are aged people from BAME communities to ensure literature and information is accessible. work with businesses (including pharmacies), through Entrepreneurial Barnet, to ensure that businesses understand their responsibility, as employers and in interactions with residents, to identity and provide carers with the flexibility they require to work and care ensure services working with adults identify children and young people (and where they have caring responsibility) at an early stage and make referrals as necessary such as drug and alcohol services and enablement services as well as voluntary and community sector providers. To support carers to have a life of their own, positive health and wellbeing as well as supporting our most vulnerable carers, we will embed the needs of carers across the priorities of the JHWB Strategy as well as: making sure carers have access to high quality support when they need it including advice about their entitlements and services available providing specific training for young carers in the areas of learning disability, physical disability and mental health (including dementia) so they are better equipped in their caring role developing the respite offer for carers, through our local volunteering service and through the council s contracted lead provider ensuring that services are developed with carers and their cared for in mind particularly prevention provision and services for people with long term conditions such as dementia and stroke actively involving carers in at all stages of strategic and service commissioning. The council and BCCG are committed to making sure that the voice of carers shapes the services available to them, and monitor the effectiveness and standards of what is available. Dementia Our aim has been to focus on early and timely diagnosis, improving information and supporting people with dementia and their carers in the early stages. Our Barnet Dementia Manifesto sets out what we aim to do next, for example, increase public and professional awareness and understanding of dementia. Recognising particular housing needs, the council will increase the supported housing options for people with dementia and their carers, linked to health and care support and other community facilities by Increasing the supported housing options 124
125 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Palliative and End of Life Care Two thirds of people that die every year are 75 years of age or older. However deaths in England and Wales are expected to rise by 17% from 2012 to Traditionally palliative care services have been oriented towards cancer care; however people with a whole range of other conditions including cardiovascular, respiratory, neurological disorders and dementia should also be accommodated. To date the proportion of people with non-cancer diagnoses accessing specialist palliative care services has remained low. With both the palliative and end of life care being a priority for Barnet, a review of the current pathway is underway in order to ensure that patients are supported to die in their preferred place of choice. We will: work with the voluntary and community sector to: improve the availability of relevant information to individuals and their carer raise awareness of the importance of talking about dying and death as well as getting your affairs in order. continue to ensure timely identification of the end of life phase, this will involve linking the palliative care register with other long-term condition registers further develop our local processes for access to rapid response end of life care in the community. Health and social care integration The Health and Wellbeing Board has a clear vision for the integration of health and social care for frail elderly people and people with long-term conditions in Barnet (to deliver our Better Care Fund objectives) and has set up an ongoing programme of work to deliver it which includes: encouraging residents to be involved in and take responsibility for their health and wellbeing in order to support independence. Programmes which develop social capital are achieving great outcomes such as the neighbourhood services and voluntary and community sector initiatives: building teams across primary and community health and social care to support people with complex long term conditions Barnet Integrated Locality Team to improve the coordination and quality of care develop the Health Living Pharmacy model to improve the public health service offer across the borough looking at where integration of commissioning can be explored with neighbouring boroughs. encouraging friends and families to refer to social care services, earlier as currently a large majority of referrals to social care are from either primary or secondary care settings embedding prevention through system transformation including changing the patient-professional conversation which our Heath Champion pilot in 2016 aims to achieve with roll out from We will design and develop services with voluntary and community sector groups and residents to ensure that needs are considered, for example we will work with Barnet Senior Assembly to improve the quality of and access to information and advice for older people. 125
126 34 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy In terms of the Winterbourne View Concordat (Assuring Transformation), there have been no new in or out of borough hospital admissions since September The BCCG s Continuing Health Care team continues to work closely with the Integrated Community Learning Disabilities service to identify and plan appropriate support for those at risk of admission. A whole system approach is required to achieve better outcomes for our residents. When someone needs care and support, they need services that are joined up around individual needs, including those of carers. Personal Budgets and Personal Health Budgets (PHBs) are central to this approach. NHS England guidance requires CCGs to include people with learning disabilities in long stay hospitals for PHBs. Gearing Up is a partnership programme led by Barnet Mencap alongside Barnet BCCG (Continuing Healthcare Staff), the council and parent carers piloting Personal Health Budgets for people with learning disabilities. PHBs aim to develop innovative, personalised accommodation, care and wellbeing solutions for individuals and presents a huge opportunity for the health and social care market to diversify and personalise their service offer to creatively meet the needs of residents. There are also opportunities to explore this with neighbouring boroughs. At the present time, there are 10 individuals who have a PHB in Barnet. With local stakeholders we will develop a local offer during 2016 where PHBs become the default offer for people receiving Continuing Healthcare and other individuals. Primary care The success of the Health and Social Care Integration model relies on significant changes in primary care delivery. Improving access, quality and outcomes in primary care will reduce hospital admissions. Improving primary care is a key strategic goal of BCCG and across North Central London to: jointly co-commission primary care with NHS England coordinate care around the needs of the patient building on existing Primary Care Networks, support the continued development of Networks, across the borough, to deliver a wider range of enhanced services, delivered at scale, within a primary or community setting, that allows for improved access to seven days a week promote health and wellbeing (improve uptake of Health Checks for people aged 40 74) recruit and retain the best staff provide high quality and safe premise and practice. Locally, building on the work of Healthwatch Barnet, we will encourage service user feedback and improve the collection of patient experience information. Primary care services are keen to work with partners to improve service quality such as Barnet Mencap detailing the experiences of people with learning disabilities and autism. Tuberculosis (TB) is a disease that is preventable and treatable yet it remains a major public health problem in London. In January 2015, Public Health England and Department of Health released the Collaborative TB Strategy for England, In July 2015, the Health and Wellbeing discussed a new approach to control TB in the borough which includes developing a Latent TB Infection screening programme for new registrants targeted a people aged and from countries of high prevalence. This will require a local programme network to develop and an application for available funding. 126
127 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy How will we know we have made a difference? Our performance measures for the theme Care when needed are: in 2014/15 Adult Social Care assessed 1364 carers and there were 5950 registered carers at the Carers Centre. We aim to increase the identification of unknown carers by 10% by 2015/16 and continue to increase this to 2019/20 increase the number of carer assessments resulting in information, advice and services being provided from 1160 who received direct support following an Adult Social Care assessment in 2014/15 to being in the top 25% of comparable boroughs by 2019/20 increase the percentage of adult carers who have as much social contact as they would like from 35.8% (2013/14) to being in the top 25% of comparable boroughs by 2019/20 increase the proportion of carers satisfied with social services from 34.6% (2013/14) to 35.7% (2015/16) aiming for the top 25% of comparable boroughs by 2019/20 increase the proportion of people who feel in control of their own lives from 73.3% (2014/15) to the top 25% in England by 2019/20 increasing choice and control through Personal Health Budget, moving from we do this for some people to we do this for most people in 2016 (Makers of Progress scorecard) reduce permanent admissions to residential and nursing care homes of 13.5 per 100,000 population (of year olds) in 2014/15 to be in the upper quartile in our comparator group by 2019/20 increase the proportion of older people still at home 91 days after discharge from 73.8% (2014/15) to 81.5% (2015/16) with the aim of being in the top 10% in the country by 2019/20 increase the detection of TB, targets for the latent screening programme to be confirmed working with NHS England and partner organisations to reduce the proportion of people reporting a very poor GP experience. maintain the diagnosis rate of 77.1% and continue to meet the 12 week referral to diagnosis target 127
128 36 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Target setting, monitoring and governance The targets chosen in the JHWB Strategy are considered most relevant to the strategic priorities. Most of the data which will be used to monitor achievement against targets is already being collected and monitored by one of more of the agencies on the Health and Wellbeing Board, which avoids duplication. The targets will be regularly monitored and reported to the Health and Wellbeing Board to assess progress. While this is a four year strategy, the targets will be reviewed annually, taking on board the latest intelligence and recommendations. The results will be published so that the public are easily able to track our progress in achieving our priorities set out in our Joint Health and Wellbeing Strategy. Regular monitoring of targets 128
129 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Appendix: Barnet s Health and Wellbeing Board The Health and Social Care Act 2012 established Health and Wellbeing Boards as forums where key leaders from the health and care system work together to improve the health and wellbeing of local communities. The Health and Wellbeing Board plays a key role in the local commissioning of health care, social care and public health through development and implementation of Barnet s Joint Strategic Needs Assessment (JSNA) and Joint Health and Wellbeing Strategy. The membership of the HWBB (November 2015) Chairman: Vice-Chairman: Councillor Helena Hart Dr Debbie Frost (Barnet Clinical Commissioning Group Chair) London Borough of Barnet Barnet Clinical Commissioning Two Councillors: group (BCCG) Chairman of Adults Safeguarding Committee Two BCCG Board Members Chairman of Children, Chief Operating Officer Education, Libraries and Safeguarding Committee NHS England Director of Adults Social Services Director of Children s Services Director of Public Health One representative Observer member (Speaking, non-voting rights) Independent Chair of the Safeguarding Adults and Children Boards Healthwatch Barnet working together to improve health and wellbeing Head of Healthwatch Barnet 129
130 38 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy Barnet s Health and Wellbeing Board has been functioning in shadow form since 2012 and functioning a statutory body in April 2013 and has achieved the following: agreed the final plans for Barnet s Better Care Fund supported Barnet CCG s proposal to joint co-commission (with NHS England) primary care alongside the North Central London CCGs approved Public Health 5-year Commissioning Plan agreed for Public Health to commission the Fit and Active Partnership Board to be set up supported the commissioning of a Tier 2 adult weight management service reviewed our progress against the Disability Charter identified the need for a local Dementia Manifesto received Healthwatch Barnet reports highlighting issues on: meals in hospitals the hospital discharge process improving awareness of local services. took responsibility for health and wellbeing issues in the Children and Young People Plan. Barnet s Health and Wellbeing Board has three subgroups: Early Years Subgroup, Finance Group and the Health and Social Care Integration Board. The Health and Wellbeing Board works closely with Barnet s five Partnership Boards (Older People s Partnership Board; Mental Health Partnership Board; Learning Disabilities Partnership Board; Carers Strategy Partnership Board; Physical and Sensory Impairments Partnership Board). Members of the Health and Wellbeing Board and the Partnership Boards are bought together at twice yearly summits which are a forum for collaborative working. To access more information about the Board including the Board s work programme, agenda and papers visit: co.uk/ielistmeetings.aspx?cid=177&year=0 130
131 Keeping Well, Promoting Independence A Joint Health and Wellbeing Strategy
132 Ref: _HWB Strategy A4 Booklet 09/12/2015 For more information visit: 132
133 Item 14 Appendix 1 Barnet Unitary authority This profile was published on 4th July 2017 Health Profile 2017 Health in summary The health of people in Barnet is generally better than the England average. About 17% (12,600) of children live in low income families. Life expectancy for both men and women is higher than the England average. N Barnet Health inequalities Life expectancy is 7.3 years lower for men and 5.0 years lower for women in the most deprived areas of Barnet than in the least deprived areas. Edgware East Barnet Friern Barnet Child health In Year 6, 19.6% (714) of children are classified as obese. The rate of alcohol-specific hospital stays among those under 18 is 22*, better than the average for England. This represents 20 stays per year. Levels of teenage pregnancy, GCSE attainment, breastfeeding initiation and smoking at time of delivery are better than the England average. Hendon Finchley Adult health The rate of alcohol-related harm hospital stays is 488*, better than the average for England. This represents 1,598 stays per year. The rate of self-harm hospital stays is 103*, better than the average for England. This represents 399 stays per year. The rate of smoking related deaths is 205*, better than the average for England. This represents 353 deaths per year. Estimated levels of adult excess weight are better than the England average. Rates of sexually transmitted infections and TB are worse than average. Rates of hip fractures and people killed and seriously injured on roads are better than average. Rates of violent crime, long term unemployment, early deaths from cardiovascular diseases and early deaths from cancer are better than average. Local priorities Priorities in Barnet include environmental planning, early years, mental health and wellbeing, encouraging healthy lifestyles and self care, empowering the community and voluntary sector and care closer to home. For more information see 2 miles Contains National Statistics data Crown copyright and database right 2017 Contains OS data Crown copyright and database right 2017 This profile gives a picture of people s health in Barnet. It is designed to help local government and health services understand their community s needs, so that they can work together to improve people s health and reduce health inequalities. Visit for more profiles, more information and interactive maps and tools. on Twitter * rate per 100,000 population Crown Copyright Barnet - 4 July
134 Population: summary characteristics Age profile Males Age Females % of total population Barnet (population in thousands) Barnet 2015 (Male) Barnet 2015 (Female) England 2015 Males Females Persons Population (2015): Projected population (2020): % people from an ethnic minority group: 31.6% 34.3% 33.0% Dependency ratio (dependants / working population) x % England (population in thousands) Population (2015): 27,029 27,757 54,786 Projected population (2020): 28,157 28,706 56,862 % people from an ethnic minority group: 13.1% 13.4% 13.2% Dependency ratio (dependants / working population) x % The age profile and table present demographic information for the residents of the area and England. They include a 2014-based population projection (to 2020), the percentage of people from an ethnic minority group (Annual Population Survey, October 2014 to September 2015) and the dependency ratio. The dependency ratio estimates the number of dependants in an area by comparing the number of people considered less likely to be working (children aged under 16 and those of state pension age or above) with the working age population. A high ratio suggests the area might want to commission a greater level of services for older or younger people than those areas with a low ratio. Barnet 2020 estimate Deprivation: a national view The map shows differences in deprivation in this area based on national comparisons, using national quintiles (fifths) of the Index of Multiple Deprivation 2015 (IMD 2015), shown by lower super output area. The darkest coloured areas are some of the most deprived neighbourhoods in England. This chart shows the percentage of the population who live in areas at each level of deprivation. 100 Contains OS data Crown copyright and database rights 2017 N Lines represent electoral wards (2016) % Residents England Barnet Most deprived quintile Least deprived quintile Crown Copyright Barnet - 4 July
135 Life expectancy: inequalities in this local authority The charts show life expectancy for men and women in this local authority for The local authority is divided into local deciles (tenths) by deprivation (IMD 2015), from the most deprived decile on the left of the chart to the least deprived decile on the right. The steepness of the slope represents the inequality in life expectancy that is related to deprivation in this local area. If there was no inequality in life expectancy the line would be horizontal. Life expectancy gap for men: 7.3 years 95 Life expectancy gap for women: 5.0 years 95 Life expectancy at birth (years) Life expectancy at birth (years) Most deprived Inequality slope for men Least deprived Life expectancy for men 65 Most deprived Inequality slope for women Least deprived Life expectancy for women Health inequalities: changes over time These charts provide a comparison of the changes in death rates in people under 75 (early deaths) between this area and England. Early deaths from all causes also show the differences between the most and least deprived local quintile in this area. Data from onwards have been revised to use IMD 2015 to define local deprivation quintiles (fifths), all prior time points use IMD In doing this, areas are grouped into deprivation quintiles using the Index of Multiple Deprivation which most closely aligns with time period of the data. This provides a more accurate way of discriminating changes between similarly deprived areas over time Early deaths from all causes: men IMD 2010 IMD Early deaths from all causes: women IMD 2010 IMD Age-standardised rate per 100,000 population Age-standardised rate per 100,000 population Years 250 Early deaths from heart disease and stroke Years Early deaths from cancer Age-standardised rate per 100,000 population Age-standardised rate per 100,000 population Years Years Data points are the midpoints of three year averages of annual rates, for example 2005 represents the period 2004 to Where data are missing for local least or most deprived, the value could not be calculated as the number of cases is too small. England average Local average Local least deprived Local most deprived Local inequality Crown Copyright Barnet - 4 July
136 E Health summary for Barnet The chart below shows how the health of people in this area compares with the rest of England. This area s result for each indicator is shown as a circle. The average rate for England is shown by the black line, which is always at the centre of the chart. The range of results for all local areas in England is shown as a grey bar. A red circle means that this area is significantly worse than England for that indicator; however, a green circle may still indicate an important public health problem. Significantly worse than England average Not significantly different from England average Significantly better than England average Not compared Domain Indicator Period England worst Local count Regional average Local value 25th percentile Eng value Eng worst England average 75th percentile England range England best Eng best 1 Deprivation score (IMD 2015) 2015 n/a Our communities 2 Children in low income families (under 16s) , Statutory homelessness 2015/ GCSEs achieved 2015/16 2, Violent crime (violence offences) 2015/16 5, Long term unemployment ^ ^ Children's and young people's health Adults' health and lifestyle Disease and poor health Life expectancy and causes of death 7 Smoking status at time of delivery 2015/ $ Breastfeeding initiation 2014/15 4, Obese children (Year 6) 2015/ Admission episodes for alcohol-specific conditions (under 18s) 2013/14-15/ Under 18 conceptions Smoking prevalence in adults 2016 n/a Percentage of physically active adults 2015 n/a Excess weight in adults n/a Cancer diagnosed at early stage Hospital stays for self-harm 2015/ Hospital stays for alcohol-related harm 2015/16 1, , Recorded diabetes 2014/15 18, Incidence of TB New sexually transmitted infections (STI) , , Hip fractures in people aged 65 and over 2015/ Life expectancy at birth (Male) n/a Life expectancy at birth (Female) n/a Infant mortality Killed and seriously injured on roads Suicide rate Smoking related deaths , Under 75 mortality rate: cardiovascular Under 75 mortality rate: cancer Excess winter deaths Aug Jul Indicator notes 1 Index of Multiple Deprivation (IMD) % children (under 16) in low income families 3 Eligible homeless people not in priority need, crude rate per 1,000 households 4 5 A*-C including English & Maths, % pupils at end of key stage 4 resident in local authority 5 Recorded violence against the person crimes, crude rate per 1,000 population 6 Crude rate per 1,000 population aged % of women who smoke at time of delivery 8 % of all mothers who breastfeed their babies in the first 48hrs after delivery 9 % school children in Year 6 (age 10-11) 10 Persons under 18 admitted to hospital due to alcohol-specific conditions, crude rate per 100,000 population 11 Under-18 conception rate per 1,000 females aged 15 to 17 (crude rate) 12 Current smokers (aged 18 and over), Annual Population Survey 13 % adults (aged 16 and over) achieving at least 150 mins physical activity per week, Active People Survey 14 % adults (aged 16 and over) classified as overweight or obese, Active People Survey 15 Experimental statistics - % of cancers diagnosed at stage 1 or 2 16 Directly age sex standardised rate per 100,000 population 17 Admissions involving an alcohol-related primary diagnosis or an alcohol-related external cause (narrow definition), directly age standardised rate per 100,000 population 18 % people (aged 17 and over) on GP registers with a recorded diagnosis of diabetes 19 Crude rate per 100,000 population 20 All new diagnoses (excluding chlamydia under age 25), crude rate per 100,000 population aged 15 to Directly age-sex standardised rate of emergency admissions, per 100,000 population aged 65 and over 22, 23 The average number of years a person would expect to live based on contemporary mortality rates 24 Rate of deaths in infants aged under 1 year per 1,000 live births 25 Rate per 100,000 population 26 Directly age standardised mortality rate from suicide and injury of undetermined intent per 100,000 population (aged 10 and over) 27 Directly age standardised rate per 100,000 population aged 35 and over 28 Directly age standardised rate per 100,000 population aged under Directly age standardised rate per 100,000 population aged under Ratio of excess winter deaths (observed winter deaths minus expected deaths based on non-winter deaths) to average non-winter deaths (three years) Indicator has had methodological changes so is not directly comparable with previously released values. "Regional" refers to the former government regions. ^20 Value based on an average of monthly counts $ 1 There is a data quality issue with this value If 25% or more of areas have no data then the England range is not displayed. Please send any enquiries to healthprofiles@phe.gov.uk You may re-use this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit Crown Copyright Barnet - 4 July
137 Appendix 3: 2 Joint Health and Wellbeing Strategy progress report, November 2016 November 2017 This progress report provides an overview of areas where we achieved and did not achieve our targets as set out in the Joint Health and Wellbeing Strategy ( ) as well as providing a narrative for the Barnet Health Profile for Based on our progress, recommendations are made for areas of focus for the next year (to November 2018). Theme Preparing for a healthy life Objectives Improving outcomes for babies, young children and their families Areas of focus 1. Improving the health & wellbeing of Looked After Children Target a) All initial health assessments completed within time frame (20 days) b) Review Health assessments for children looked after for a year or more Increase the proportion of locally placed looked after children to at least 46% (2017/18) to 53% (2019/20) Continue to closely monitor the provider including staff vacancies. 2. Increasing the uptake of childhood immunisations Target Increase uptake of childhood immunisations to be above the England average HWBB to receive regular reports from NHSE, scrutinising performance against targets and NHSE and local remedial action plans. 3. Early years review Target - The council (including Public Health) will work with Barnet CCG to further integrate the service offer of health-related services in early years settings, improving service delivery for families. 3 What did we achieve? 1. Improving the health & wellbeing of Looked After Children It is a statutory requirement that all children have an Initial Health Assessment (IHA) within 20 working days (28 calendar days) of coming into care; the target is for over 95% to be completed within the timescales. Data from 2015/16 and the beginning of 2016/17 showed that this was only the case for 30% of children coming into care. a) Significant improvements have been seen on IHA performance in 2017(being within statutory timeframes): AGENDA ITEM 6 1
138 o o o o o o o o 50% in January 19% in February 92% in March 100% in April 93% in May 79% in June 86% in July 100% in August b) All review health assessments (RHAs) have been completed within the timescales. All health assessments are young person-led and focus on the child. Improvements can be attributed to: o Clearly documented process, with timescales, communicated to all professionals involved to avoid performance slipping o Commissioners increased monitoring and implemented an improvement plan which included regularly meeting with GP practices o The nursing team increasing the number of reminders that young people and foster carers receive prior to the appointment which includes calls and s the day before the appointment o Improved communication and working between CLCH and children s social care o Previously key workers were reporting that no-one was able to attend appointments with the young people, this issue has now been resolved o Independent Reviewing Officers are now involved in any key issues, this has been particularly helpful for out of borough placements c) The CCG Executive, in August 2017, agreed an increase in resource for the LAC Health team for an additional Band 7 nurse, likely to start November/December. This will enable the Designated Nurse to focus on more strategic work for example overseeing the paediatric model for IHAs, following up on the most vulnerable CYP (including children and young people with SEND) and improving the offer for care leavers. o Paediatric model for IHAs for LAC aged In March 2017, the CCG Executive approved the move to a paediatric model for IHAs for children aged 0 9. Currently IHAs are completed by GPs. It is best practice for these to be 4 2
139 o completed by paediatricians, particularly for young children due to the identification of developmental delay, working with cases of neglect and providing a continued point of contact From September 2017, 0-2s coming into care have been seen by a paediatrician; initial feedback is positive from all stakeholders and the service will continue to be monitored. 2. Increasing the uptake of childhood immunisations Supporting the national immunisation campaign and promotion of childhood immunisations throughout the year to GP s, children centres, front line staff and volunteers. Includes sharing information and campaign resources with children centres through quarterly news letters Improving and increasing awareness amongst GP s and practice managers (using the GP bulletin and Practice Manager bulletin) of the MMR 2 coverage to improve uptake and achieve 95% coverage target Delivery of childhood immunisations training to all children centres Utilised MECC (making every contact count) training to engage and train front line staff and volunteers for brief interventions on childhood immunisations Awareness raising with Barnet residents by updating the Barnet PH children s webpage to include information on immunisations and immunisations schedule 3. Early years review Development of Integrated Hubs for Children, Families and Young People Also kept continued good registration and access of targeted families at children s centres Successful delivery of the peri-natal health coaches programme Launched in September the 30 hour offer for 3 and 4 year olds as per DfE requirements Where are the gaps? 1. Improving the health & wellbeing of Looked After Children Improve the quality of Initial Health Assessments To improve the quality of IHAs the Designated Doctor and Designated Nurse for LAC will be: o Working with social workers to improve the information provided to GPs and 5 3
140 paediatricians completing IHAs regarding the child s history o Completing an audit of IHAs and feeding back to GPs (by December 2017) o Providing training to GPs (November December 2017) What remains a priority? (suggested areas of focus up to November 2018) 2. Increasing the uptake of childhood immunisations o Uptake and data quality require further improvement 3. Early years review The take up of free two year old places achieved is 60% for the 2016/17 academic year. There is a clear strategy to improve the upward trajectory and it is anticipated that take up will increase. 1. Improving the health & wellbeing of Looked After Children to continue as a priority for 2018 Working with social workers to improve the information provided to GPs and Paediatrician completing the Initial health assessments regarding the child s history Completing an audit if Initial health assessments and feeding back to GPs (by December 2017) Providing training to GPs (November December 2017) Special educational needs and disability SEND embedding the SEND reforms 2. Increasing the uptake of childhood immunisations Working to increase the uptake of all pre-school boosters amongst the under 5s To increase the uptake of flu immunisation amongst 2 and 3 year olds and pregnant women during autumn and winter seasons To maintain messaging to health professionals including GPs, children s centre staff, midwives, in order to increase uptake and keep them up to date on latest policy and guidance Support national immunisation campaign at local level To take part and support NCL immunisation assurance programme 3. Early years review Continue roll out of Early Years hubs in Barnet. 6 4
141 Theme Objectives Areas of focus Wellbeing in the community Creating circumstances that enable people to have greater life opportunities 4a. Child and Adolescent Mental Health Services (CAMHS) In order to improve CAMHS provision, Barnet CCG and Barnet Council agreed to jointly recommission CAMHS at the HWBB in September 2016 Public health supported the redesign of CAMHS; developing a programme of work based on the Thrive Model. The approach aimed to improve access to services by improving sign posting, self-management and enabling one off contact in order to improve coping mechanisms in children and young people. 4b. Adult mental health services o The priority area was to develop new service models that provided earlier intervention, recovery and different ways of working. What did we achieve? 5. Employment Increase the proportion of adults in contact with secondary mental health services in paid employment. Increase the proportion of adults with learning disabilities in paid employment Planned actions: o Developing the market and engaging with providers not yet operating in the borough and procuring an approved list in 2017 o Embed employment in care plans develop the role for brokerage in securing employment pathways, embedding strengths based practice and continue to develop the Mental Health Enablement model o Raising quality of provision within existing day-care including the Your Choice Barnet transformation and hold Job Coaching and Brokerage Skills training(delivered by British Association for Supported Employment) The Council as a public sector leader - leverage to create job opportunities through contracting and becoming a disability confident employer 4a. Child and Adolescent Mental Health Services - (CAMHS) Procurement has been delayed due to negotiations in regard to BEH NHST Trust. Transformation of services supported by the Barnet allocation for CAMHS Transformation Fund (NHS England) has continued outside of the procurement programme. Through targeted resourcing and a waiting times reduction programme, 7 5
142 Barnet has reduced the number of young people waiting for treatment for over 12 weeks from 119 to 65 and average waiting times reduced from 131 days to 90 days (30 th September 2016 to 30 th September 2017). In addition Barnet has developed new Early Help services and programmes including: o Resilient Schools Programme-jointly led between BCCG and Barnet Public Health o Kooth Online Counselling and Support which has been used by 120 young people in the first month (June 2017) o Emotional Wellbeing Team (part of Resilient Families Service-Barnet Council) o CVS Partnership Space2Grow fund with Young Barnet Foundation o Raphael House (a local CVS) Counselling Project o o Specialist Education Psychology provision for Youth Offending Service The above programmes combined will provide emotional wellbeing and mental health support to an additional 500+ young people by June 2018, primarily for those children and young people who would not have met the CAMHS clinical threshold Planned activity: o The CAMHS Transformation Plan is being refreshed and will be presented to JHWB in January 2018 o Two new posts have been created with the Youth Offending Service 1. Clinical Psychologist (starts 6 th November 2017) and Mental Health Liaison and Diversion Worker (interview November 2017) o Space2Grow funded projects to begin November b. Adult mental health services - Different ways of working with secondary and primary care for adults mental health services: o o o The Barnet Wellbeing Hub was established and its impact monitored Work was carried out to improve talking therapies, with the aim that IAPT services will become part of the Wellbeing Hub The Council remodelled its mental health workforce to focus on recovery and expanded the Network mental health enablement service to offer mental health enablement and recovery support to more people. The Reimagining Mental Health Programme is continuing, organisations are continuing to 8 6
143 work collaboratively, with minimal investment in transformation, to deliver improvements for individuals via primary care with dedicated BEH Mental Health Trust Primary Care MH Linkworkers and from community providers following a social prescribing model. The Linkworker team comprises Psychiatrists, Psychologist, Social Worker, Occupational Therapists, Mental Health Nurses, Graduate Mental Health Workers There have been fewer referrals to secondary care, especially to crisis care and mental health liaison Linkworkers are embedded in the new Wellbeing Collaborative delivering wellbeing services to people across Barnet. Organisations are working closely with commissioners to ensure that social prescribing sits alongside clinical and social care support o Coverage has been rolled out across all Barnet localities and referrals have been received from all 62 practices o Lead GPs in each locality promote the direct benefits of the Linkworker and integrated service to their colleagues o o Linkworkers attend locality and community meetings to promote the service Patient feedback continues to be positive It was really good that you came to the doctor s surgery and It was very good. I now know what is available and how I can progress Most significant and measurable results: Achieved 40% reduction in referrals to secondary care from South Barnet since commencement of linkworker service (first quarter) Average of 94% of a total 225 referrals to linkworkers were acknowledged within 24 hours and were contacted within 5 working days in the first quarter of operation There has been a reduction to average length of stay with the Crisis Resolution Home Treatment Team since the introduction of Linkworkers, suggesting that people are able to be discharged sooner back to the care of their GP and can be stepped up as required Presentations to Psychiatric liaison in A&E remained high in January and February from the North Locality. Despite this increase at the beginning of the year, the overall picture has since been lower across all areas since prior to the Link Working service starting. This has reduced the incidence of breaches in the 1 hour target at Barnet Hospital and reduced presentations at the Royal Free, Hampstead 9 7
144 The Network has developed stronger links with the Wellbeing Hub and has established a weekly joint referral meeting and a drop-in session for the Wellbeing centre at the Network building. The service is recruiting a Peer Support worker to work with the wider wellbeing services. Emotional health checks are being delivered by Wellbeing Practitioners across Barnet following staff training and referrals have increased at a pace since February. More than 40 organisations are lead and delivery members of the Wellbeing Hub, which is currently based at the Meritage Centre in Hendon. Staff in all voluntary sector organisations has been trained in Emotional Health Checks which only need to be delivered once before individuals are supported with their individual social prescribing plan to access the support they need. People are supported to access a range of options based on the issues they themselves want to address. Individuals are still reporting high satisfaction with the service and further development of 3 rd Sector High volume web-based IAPT services have been in test phase throughout September and October from digital provider Mind Time Therapies working with CommUNITY Barnet and results are proving positive. The new IAPT provision, Let s Talk IAPT began operating from 1 st October 2017 and is working closely with GPs, Linkworkers and the Wellbeing Hub to receive referrals. They also have partners the Multi-lingual Wellbeing Service (own-language IAPT service) and Twining Enterprise IPS (Employment Support) working with them to deliver integrated support to people with common mental illness Barnet is part of the London Digital Mental Wellbeing is a two year programme to develop, test and evaluate a 24/7 digital mental wellbeing service. The service is began its pilot phase in May 2017 and is expected to be available more widely before the end of the year. Community Centred practice aims to improve community wellbeing through community champions in General Practice The programme is now taking place in five surgeries - due to a surgery closure - and one in a care home. We now have over 60 champions providing a wide range of activities across five surgeries including walking 10 8
145 groups, story time for children, diabetes self-help and gardening. Where are the gaps? What remains a priority? (suggested areas of focus up to November 2018) 5. Employment - Increase the proportion of adults in paid employment Proportion of adults in contact with secondary mental health services in paid employment was 7.6 % at quarter 4 (2016/17) against a target of 7.2% for 2015/16 The council have commissioned new employment support and employment retention services, for working age adults with social care needs. The services will be available from November 2017 The council have commissioned new day opportunity provision for people with learning disabilities and autism, which will support people to develop their life skills, increase their confidence and progress them on their pathway to employment BOOST- The council continues to work with partners to promote employment and skills. In the first quarter of 2017/18 BOOST Childs Hill launched- this takes the multiagency approach to the south of the borough. BOOST Burnt Oak continues to develop and is now working side by side with around 14 other organisations on a sessional basis at the library. Together the teams have engaged over 400 residents and supported over 100 into work. In this period the Council has brought two additional employment to the borough: the Skills Escalator which aims to help people who are in work to find a better job and the Mental Health and Employment Trailblazer which supports people with common mental Illness to find work. The borough s largest learning disability provider, Your Choice Barnet, transformed its services to focus on access to employment and increasing independence in the community. New employment support and retention teams were established, working with 22 service users initially of which 10 users gained employment and 8 started volunteering to date. 4a. Further work is needed on the development and quality improvement of Child and Adolescent Mental Health Services (CAMHS) 4b. Performance improvement of IAPT services 5. Employment ensuring as many people as possible are support to access new services and employment opportunities. 4a. Child and Adolescent Mental Health Services (CAMHS) 4b. Focus on mental health and wellbeing by Undertaking formal post-implementation evaluation of the Reimagining Mental 11 9
146 Health programme Closely monitoring transferred Improving access to psychological therapies services and work towards improving access targets Working on wider wellbeing as part of the ThriveLDN initiative 5. support disabled people to gain and retain employment by Implementing new employment support and retention services for adults with mental health needs and learning disabilities Ensuring the mental Health Network provides mental health recovery and enablement to all eligible residents who would benefit The BOOST team to continue working with partners to promote employment and skills The Employment Trailblazer to continue support people with common mental health illness to find work and to support Improving access to psychological therapies Your Choice Barnet rolling out new employment support and retention support for people with learning disabilities (PWLD) Recommissioning universal access employment support for people with autistic spectrum conditions and PWLD Theme How we live Objectives Encouraging healthier lifestyles Areas of focus 6. Reduce excess weight in children (10-11 years old) & in Adults (overweight and obese) Target: reduce excess weight in adults and children Develop and agree an Obesity Strategy and Action plan Establish the Fit and Active Barnet Partnership Through a multi-agency approach (Saracens Sport Foundation, England Athletics, LBB, Barnet Partnership for School Sport and MDX University) primary schools were encouraged to increase physical activity levels by participating in the Mayor s Golden KM Challenge, encouraging 15 minutes of physical activity every day. Seven schools engaged with the pilot phase and the initiative is currently recruiting more primary schools, focusing on recruiting PH 'priority schools' (schools with the highest prevalence of overweight and obese children according to the National Child Measurements Programme) 12 10
147 What did we achieve? Focus on the built environment and how we can maximise the built environments role in encouraging healthy lifestyles for all residents A new leisure management contract to be developed with an increased focus on public health outcomes. A formal procurement process commenced in October 2016, a successful bidder will be appointed in October 2017 and the new contract will commence on 1 January Increase screening uptake To increase screening uptake PH to work with PC colleagues in CCG and NHSE to explore local actions to improve uptake 6. Reduce excess weight in children (10-11 years old) Barnet has developed a successful & cost-effective weight management programme The Healthy Weight Nurse (HWN) service: 31% lost weight and 69% who were known to reduce or maintain their BMI in 16/17 Alive n Kicking (ANK): 80% either reduced or maintained BMI z-score. This includes ANK afterschool Programmes, 1:1 and SEN Programmes Successful behaviour change in parents: o 81% of parents accessing the ANK service increased their confidence in reading and understanding labels and changed their behaviour o 100% made positive improvements to their eating behaviours o 100% reduced their consumption of junk food o 80% increased fruit consumption o 60% increase physical activity the most popular being walking and swimming o 60% reduced screen time (including TV and computer time) Supported vulnerable children: The HWN service had 13 (21%) of children on the caseload who presented with Autistic spectrum conditions. 5 (8%) of children presented with Learning disabilities and 43 (71%) were vulnerable with a safeguarding plan. Reduce excess weight in adults (overweight and obese) Year Target Reported 2016/ % Current (2016/17 quarter 2) 56.75% 13 11
148 The development of the Healthier catering Commitment continues to develop successfully with a focus on takeaways and food suppliers. There has also been successful liaison with Kocher providers to tackle healthier supply issues. Tier 1 and tier 2 weight management services have been integrated into the new leisure contract to start in January Increase screening uptake PH continues to work with PC colleagues in CCG to explore local actions to improve uptake In partnership with Jo s Trust, Public Health put together a series of events and activities to promote awareness uptake of cervical cancer screening A diabetes awareness campaign was conducted the week of 12 th June This included a partnership event at Brent Cross co-ordinated by Cllr Stock where approximately 100 people completed a risk assessment questionnaire and 8 people were identified with diabetes A Diabetes UK information stall was set up outside Edgware Broadwalk shopping Centre and Millway Medical practice offered diabetes testing and advice to Barnet residents. Approximately 20 people had blood tests. Instructors were placed at 11 outdoor gyms across the borough and councillors joined residents in an Oakhill Park Run to raise Diabetic Awareness Prevention and Wellbeing Training based on the Making Every Contact Count (MECC) principles has been delivered Where are the gaps? 6. Continue to work to reduce excess weight in children (10-11 years old) & in Adults (overweight and obese, a refreshed action plan will be presented to the HWB in early Continue to work to increase screening uptake. This requires continued focus and improvement. What remains a priority? (suggested areas of focus up to November 2018) 6. Reduce excess weight in children (10-11 years old) & in Adults (overweight and obese) Improving current services based on children s Tier 2 service evaluation recommendations Improving the current 0-19 Healthy Weight Care pathway to ensure that it reflects all services available within Barnet Re-commissioning Tier 2 weight management services (as contacts are due to expire 14 12
149 on 31st March 2018) Developing and implementing healthy weight action plans for children & young people (CYP) and adults Implementing a new range of opportunities for Barnet residents to be physically active through the new leisure service (from January 2018) Implementing a new range of health promotion and prevention activities through the new leisure service (from January 2018) 7. Increase screening uptake Sending GP endorsed text reminders to encourage uptake of screening Learning from NHS England funded Imperial University survey to identify the barriers to attendance of cervical screening in London and funded opportunistic cervical screening in sexual health clinics for women who were overdue screening Replacing in 2018/19, faecal occult blood testing with faecal immunochemical testing within the bowel screening programme across England. Pilot studies have shown that uptake will increase by up to 7% Carrying out promotion of bowel cancer screening Theme Care when needed Objectives Providing care and support to facilitate good outcomes and improve user experience Areas of focus 8. Care closer to home The CCG and Council have establishing executive support to a programme of work designed to radically enhance the delivery of appropriate Care Closer to Home. In order to develop a new Care Closer to Home approach a key requirement is to create a major shift of balance from avoidable hospital admissions to integrated health, social care and third sector models delivered in community and primary care settings. The implementation of the care closer to home vision will be overseen by the JCEG, reporting into the HWB, CCG governing body and the STP programme board. 9. Carers - delivering the Carer and Young Carer Strategy 15 13
150 Focus on identifying unknown carers Improving the health of carers (especially young carers) What did we achieve? 8. Care closer to home Barnet CCG and LB Barnet are working closely with the Barnet GP Federation and provider organisations to deliver the Care Closer to Home programme in Barnet. The programme has four key elements: Developed and improved access to core general practice from 8am to 8pm. This service is now operational. Care delivered across clinically-led partnerships known as Care Closer to Home Integrated Networks (CHINs). The first pilot area (Burnt Oak) has been selected and has identified its priority areas as Diabetes and paediatric urgent access. This CHIN should commence work in early T he Care Closer to Home Programme Board has agreed a vision, development approach, development process and programme delivery plan for the rollout of CHINs across Barnet, including wider health and social care services. Quality Improvement Support Teams (QISTs) will work with general practice to improve quality, reduce variation and build resilience through tailored information and analytics. The Barnet GP Federation and CLCH have been engaged to provide this service to the Burnt Oak CHIN. In close collaboration with the local community and voluntary sector, deliver prevention and supported self-management services that help people stay healthy, strong, safe and connected as contributing citizens. The Programme Board has agreed that it is a priority for CHINs to draw effectively upon the many preventative services for children and adults that are available in Barnet. Building on the community centred practice initiative and the extension of Ageing Well into a full Local Area Coordination model, a social prescribing offer is planned for incorporation into the developing CHINs 9. Carers Good progress has been made on the Carers and Young Carers Strategy Action Plan The contract for integrated support services for carers and young carers continues to be delivered and is performing well
151 LBB continues to be a member of the Employers for Carers Scheme (membership no ~EFC 1588) which allows all LBB employees and all SMEs in the borough (businesses which employee less than 250 staff) to access resources such as: o Supporting working carers- a carers guide o Supporting carers in your workforce- an employer s guide o Supporting carers in your workforce- a manager s guide The council established a Specialist Dementia Support Service for adults with dementia and their carers, focused on helping to improve their health and wellbeing, maximise their independence and help sustain carers in their caring role. The council supported Carers Week 2017 with our Lead Provider for Carers and Young Carers Support Services to help support raising awareness of and championing carers, highlighting the challenges that they face and the contribution they make to families and communities and promoting local support available to carers The Council introduced dementia friendly swimming in the borough The council provides monthly training to staff to identification of carers and young carers, carers assessments, support planning and understanding the carers support offer Family Services commissioned specialist training for their staff on supporting young carers The council s carers web pages have been refreshed to improve how carers can access information, advice and support Where are the gaps? 8. Care closer to home continued implementation of the programme, at pace. 9. Carers Further work needs to occur in health settings to promote identification of unknown carers (and young carers) Further work needs to occur in health settings to promote health support available to carers in the borough (e.g. Free health checks and flu vaccinations) What remains a priority? (suggested 8. Care closer to home areas of focus up to November 2018) Mobilisation of CHIN and QIST teams across Barnet Establishing an overarching partnership between commissioners and providers to support the roll-out of CHINs 17 15
152 Broadening the range of services that are available through CHINs beyond the initial scope of Primary Care and Community Services. Implementing prevention, social prescribing and information and signposting services linked to each CHIN Developing an emergency care attendance prevention pathway for CYP within CHINs 9. Carers Continuing to focus on identifying unknown carers and young carers Continuing to improve the health of carers (especially young carers) Continuing to promote Employers for carers so that more Barnet carers can access and retain employment Providing advice and information to carers through the dedicated carers service Providing specialist support for carers of people with dementia 18 16
153 Item 15 MEETING NHS Barnet CCG Governing Body Meeting DATE 11 January 2018 REPORT Annual Safeguarding Children s Report LEAD DIRECTOR Vicky Aldred, Interim Director Quality and Clinical Services AUTHOR Siobhan McGovern Associate Director Safeguarding/ Designated Nurse NHS Barnet CCG Dr Paul de Keyser Designated Doctor Safeguarding Children NHS Barnet CCG Dr Prashant Desai Named General Practitioner NHS Barnet CCG CONTACT DETAILS siobhan.mcgovern@nhs.net EXECUTIVE SUMMARY 1. Introduction This report provides the annual Safeguarding Children update to Barnet CCG s Governing Body. The report provides information regarding assurance and identified gaps and risks regarding the CCG and its providers' compliance with safeguarding children arrangements and duties as per Section 11 of the Children Act 2004 across health services commissioned for Barnet children. The report will outline any recent developments in the following areas: Governance arrangements National and Local Context Participation in Local Safeguarding Board and Partnership arrangements Progress with Serious Case Reviews, including embedding of learning Provider performance and assurances Risks and Challenges Conclusion and Recommendations An Ofsted Inspection of Children s Services and the Barnet Safeguarding Children s Board was carried out in May Barnet s rating overall was Inadequate. An improvement plan has been developed by the Local Authority in conjunction with statutory partners which has been reviewed by Ofsted in a follow-up visit in November 2017 and the outcome of this is Ofsted have noted the required steps to take the service forward are being taken. NHS Barnet CCG have developed a Children s Services Improvement Plan to support the overarching Ofsted Improvement Plan. Progress against this plan is overseen by a CCG Children s Services Task and Finish Group which is a sub group of the Quality Committee. This is Chaired by the Chief Operating Officer. This plan has also been reviewed by the Quality Committee and will also be reviewed at the NHS Barnet CCG Bi-monthly Safeguarding Children s Committee
154 2. Risks and Challenges Requirements of the Ofsted improvement plan require significant time resources from the CCG Safeguarding Team which may have a potential impact on their ability to fulfil other aspects of their role. The delivery of Primary Care Safeguarding training remains a challenge for the CCG safeguarding team, as does the collection of information regarding the impact of the training on the working practices of the General Practitioners following attendance at the sessions. Ensuring that provider organisations are compliant with the required safeguarding competencies at the appropriate levels for each professional. Working with Children s commissioning to ensure that plans for CAMHS Out of Hours Services at Barnet Hospital address the needs of the vulnerable children requiring their service. Further discussion is required regarding access to Child Protection Information System (CP-IS) for Locum staff in Out of Hours Hubs. 3. Conclusion The Ofsted report into Barnet Children s Services and the Barnet Children s Safeguarding Board arrangements highlights significant improvement requirements to ensure that Barnet children are protected from harm, and that there is appropriate support in place when there are difficulties within the family. However, all statutory partners are ensuring that the Improvement Plan is prioritised in organisational business. 4. Recommendations The CCG safeguarding team will continue to work with BCCG Chief Operating Officer, the BCCG Chair, and the Associate Director Quality and Clinical Services to ensure that London Borough of Barnet s Improvement Plan is implemented from a health perspective. NHS Barnet CCG Chief Operating Officer and Chair will be statutory partners at the BSCB Leadership group. The Associate Director NHS Barnet CCG/ Designated Nurse, Designated Doctor Children's Safeguarding and Named General Practitioner will attend the BSCB Executive Board to ensure that with our provider colleagues the voice of health is heard across the partnership. Actions and learning from the Ofsted Report, Serious Case Reviews and other serious incidents pertaining to children and young people will be embedded and highlighted in training and future learning across the health partnership. Provider organisations not meeting or maintaining required Safeguarding training levels are to provide action plans to Barnet CCG demonstrating how they will address this issue. CCG safeguarding training figures to be monitored on a monthly basis. Actions from Barnet Serious Case Reviews to be monitored within the BCCG Safeguarding Forum and reported to the CQRC on a quarterly basis. The Safeguarding team in partnership with Barnet CCG Children s Commissioners to monitor continued arrangements for CAMHS out of hours services, to ensure that the service provided is safe and does not place Barnet children at risk. NHS Barnet will work with Barnet Safeguarding Children s Board to embed the priorities for 2017/18 in healthcare practice. 2 RECOMMENDED ACTION: For Assurance 138
155 Objective(s) / Plans supported by this paper: Promote health and wellbeing Ensure right care, right time Approval Route: Director Quality and Clinical Services NHS Barnet CCG Clinical Quality and Risk Committee 14/12/2017 Patient & Public Involvement (PPI): N/A Stakeholder Engagement: Named General Practitioner Safeguarding Children has been involved in the content of the paper. Key Risks To Note: Ofsted rating of Children s Services and Barnet Safeguarding Board as Inadequate. Resource Implications: No current additional CCG resources envisaged. However, it is to be noted that the CCG has committed further funding to the Safeguarding Board. Next Steps: Quarterly Update Report to NHS Barnet Clinical Quality and Risk Committee April Appendices N/A 3 139
156 Annual Safeguarding Children s Report 1. Introduction This report provides the annual update to NHS Barnet CCG s Governing Body. The report provides information regarding assurance and identified gaps and risks regarding the CCG and its provider s compliance with safeguarding children arrangements and duties as per Section 11 of the Children Act 2004 across health services commissioned for Barnet children. The report will outline any recent developments in the following areas: Demographic Changes Governance arrangements National and Local Context Participation in Local Safeguarding Board and Partnership arrangements Progress with Serious Case Reviews, including embedding of learning Provider performance and assurances Risks and Challenges Conclusion and Recommendations Barnet Demographic Changes Barnet is home to a diverse and changing population; the Borough is forecast to have the largest child population in London by The majority of children and young people in Barnet achieve good outcomes, however, there is a small percentage (2%) of children and young people who require targeted or specialist support to achieve better outcomes. There are approximately 93,590 children and young people under the age of 19 years living in Barnet representing 25% of the borough's total population. Barnet s population is estimated to reach 98,914 by 2020, representing a growth of 6%. 2. Governance Arrangements 2.1 NHS Barnet CCG Children s safeguarding team Since the last report to Barnet CCG Governing Body, the NHS Barnet CCG Safeguarding Children s team remains unchanged and comprises of: Associate Director of Safeguarding (the role incorporates that of the Designated Nurse Safeguarding Children). Designated Doctor for Children's Safeguarding. Named GP Safeguarding Children. Senior Safeguarding Administrator (commencing 27/11/2017, following a short gap). 2.2 Resources for Role of Designated Doctor for Children s Safeguarding 4 140
157 The business case to support additional resources for the role of the Designated Doctor for Children s Safeguarding in Barnet CCG has been approved and additional resources have been in place since June This ensures that resources provided are in line with the Intercollegiate document: Safeguarding Children and Young People: Roles and Competencies for Health Care Safeguarding Forum (Formerly Safeguarding Children s Health Advisory Group (SCHAG) The Safeguarding Forum meets on a bi-monthly basis and is chaired by a member of the CCG Safeguarding Team. The Terms of Reference for the group have been reviewed to strengthen governance and oversight 1. The forum, as part of its agenda, will however, continue to provide the opportunity for case discussion and supervision for complex cases crossing health providers. 3 National and Local Context 3.1 Children and Social Work Act 2017 Findings in a review of safeguarding arrangements for children by Alan Wood in 2015 were that fundamental reforms should take place to the current Local Safeguarding Children s Board (LSCB) framework, as service delivery arrangements have become more complex for the function of the LSCB's and accountability for them has become less clear. Legislation was brought forward in the Children and Social Work Bill, now enacted, which allowed for the disbanding of the requirement for Local Safeguarding Children s Boards. Instead it is proposed that there will be a requirement for local safeguarding partners, in particular health, police and the local authority, to work together in exercising their functions in safeguarding and promoting the welfare of children in the area. The aim of these changes is to introduce a stronger and more flexible statutory framework which will engender greater accountability on the three key agencies involved in safeguarding children, namely local authorities, the police and the health service. This also enables local areas to determine the best way to organise themselves. There is ongoing dialogue as to how best to include senior education leaders at the highest levels of this framework. The review stated the need to consider the context of each of the partners governance and transformation arrangements and future plans, such as the CCG s Sustainability and Transformation Plans and the Metropolitan Police Service s move to a super borough structure. These will have implications on the safeguarding arrangements for the future. 3.2 Inspections Ofsted Inspection In July 2017 the Local Authority and Barnet Safeguarding Children s Board (BSCB), were both judged as Inadequate by Ofsted. From a Safeguarding Board perspective the key reason for this judgement was that the Board had not been effective in discharging all of its statutory functions. In particular it had not assessed the effectiveness of the help being provided to children and their families, 5 141
158 quality assured practice or comprehensively monitored and evaluated the quality and impact of safeguarding training for multi-agency practitioners. The BSCB have in conjunction with Statutory Partners, developed an improvement plan to ensure that the Barnet Safeguarding Board is able to demonstrate how it is effectively delivering its statutory duties as a safeguarding partnership and how it is supporting the Local Authority to improve safeguarding services to children and young people. The framework for improvement will ensure that: The Safeguarding partnership arrangements deliver strong, strategic local leadership that measurably improves outcomes for vulnerable children, There is an embedded accountability mechanism which will result in confident, regular evaluation and improvement in the quality of help, care and protection that is provided by the partnership. There is improved professional practice across the partnership which is based on effective and continuous learning. The views and experiences of children, young people and their families are at the centre of service design and will influence development and strategic thinking. The CCG has developed an action plan which is incorporated in the overall BSCB action plan, which was discussed in detail with our health statutory partners at the Safeguarding Children s Forum in November The review identified a requirement for improvement in respect to workforce training across the health partnership and NHSB CCG will continue to monitor both structural and training issues within the services they commission. 3.3 Child Sexual Abuse Hubs The Child Sexual Abuse (CSA) Transformation Programme for London has received additional funding from NHS England Safeguarding until September The CSA Hub for North Central London is already operational, and the sector is scheduled to have London s pilot Child House, with an anticipated launch date of July Child Protection Information System The national implementation of the Child Protection Information System (CP-IS) is now live in Barnet and accessible to all unscheduled care facilities. This includes The Integrated Urgent Care Centres which have taken over Barndoc and 111 provision. However, further discussion is required regarding access to CP-IS for Locum staff in Out of Hours Hubs. Information is shared on Children Subject to a Child Protection plan, and on Looked after Children. 3.5 CAMHS Out of Hours Service As highlighted within this paper the support of young people who are at risk of suicide and self-harm is considered a priority by both the Children s Safeguarding Board and also Barnet CCG. Barnet Children s Commissioning team have been working with the community CAMHS provider (BEHMHT) to develop a service which will include expanded community based crisis support and outreach. North Central London (NCL) STP are also developing specialist services including Out of Hours CAMHS Crisis Service and a Perinatal Mental Health pathway
159 3.6 Children in Need and Children Subject to a Child Protection Plan At 30 October 2017, 2060 Barnet children had been identified as children in need of statutory social work intervention. This is an increase from 1876 on 31st October At 30 October 2017, 163 Barnet children were subject to a Child Protection Plan. This is a reduction from 281 at 31 October Participation in Local Safeguarding Board and Partnership arrangements 4.1 Barnet Safeguarding Children Board Multi-agency working with the Barnet Safeguarding Children s Board Barnet is developing a new safeguarding strategic framework as allowed by the Children and Social Work Act. The Chief Officer and Chair NHS Barnet CCG sit on the Leadership Board for Children s Safeguarding in conjunction with the Director of Children s Social Care and the Police Commander. Sitting beneath this senior Leadership Board is an Executive Group, which from Health comprises the CCG Director of Quality and Clinical Services, Designated Nurse and Doctor and Named General Practitioner, with health providers represented by their Heads of Safeguarding. There are various subgroups including: BSCB Serious Case Review Committee Barnet Child Death Overview Panel Each of the local provider Trusts and Barnet CCG provide a financial contribution to the work of the BSCB on an annual basis. NHS Barnet CCG have substantially increased funding to the BSCB in recognition of the necessity of an appropriately resourced partnership to achieve the improvements necessary to ensure that children and young people achieve best outcomes and are protected from harm BSCB Safeguarding Board Priorities NHS Barnet CCG Safeguarding Children s team have worked both within the Board itself and with provider organisations to embed the board s priorities for 2016/2017 within partner organisations. These include Priority 1: Child and Adolescent Mental Health / Self-Harm Priority 2: Neglect Priority 3: Domestic Abuse Priority 4: E-Safety Priority 5: Information Sharing Priority 6: Resilience Based Practice In addition to these six priorities the BSCB has maintained oversight on the coordination and effectiveness of services for children at risk or victims of child sexual exploitation, missing from home or care, and vulnerability within gangs
160 In response to recognition of the impact of these issues on children and young people, Barnet CCG included within the Safeguarding update for General Practitioners at the Annual General Meeting in September 2017 a session by Consultants from Barnet Enfield and Haringey Mental Health Trust to discuss how General Practitioners can work to support children and young people at risk of suicide and self-harm. The CCG Safeguarding Team also delivered a presentation based on a National Serious Case Review in respect to children who Do not Attend health appointments. In response to the Neglect priority, the CCG safeguarding team have highlighted the need for General Practitioners to understand the inappropriateness of the DNA acronym sometimes used within records and to consider that any child requiring medical treatment and not attending as not being brought to appointments. This point has also been highlighted to General Practitioners in CCG bulletins and will continue to be reiterated in training sessions carried out by the safeguarding team throughout the year Multi-Agency Hubs As part of the Ofsted Improvement Plan, work is underway to further improve service integration across the partnership, to ensure that families receive seamless support. In September 2017 a pilot of the first of three integrated locality hubs began. This will join up referral and decision making pathways for all children aged 0-19 who need early help. It will also promote seamless delivery and joined up assessment and intervention. The other two localities will begin operations in The intention is to have an integrated model of delivery Thresholds for Intervention The multi-agency partnership of the Safeguarding Children Board agreed a threshold document in March 2017 which professionals within the MASH use as a tool to aid decision making which will be revised to ensure it addresses thresholds across Social Care as well as Early Help. A full evaluation of the thresholds will be undertaken in 2017/18 as part of the overall review of policies and procedures operating across the Barnet safeguarding partnership Multi-Agency Audits As part of the Ofsted improvement plan, Barnet Local Authority are taking the lead on audits of a child s journey across the partnerships. To date there have been audits of: Children who have experienced or are at risk of Child Sexual Exploitation. Children who have experienced neglect Plans are in place to audit cases where children have lived in environments in which domestic violence is part of their lives Female Genital Mutilation 8 Since it is thought that health practitioners are often best placed to identify Female Genital Mutilation, Barnet CCG Designated Nurse and Doctor and Named GP have taken the lead in ensuring that health professionals are following DOH guidance to support women who have experienced FGM. The identification of FGM remains a high profile concern, and is part of level 3 training for health practitioners and is highlighted within GP training sessions. 144
161 4.1.7 Looked After Children Arrangements CCGs have a responsibility to ensure that the health needs of Looked after Children are met in accordance with statutory guidance (Statutory Guidance on Promoting the Health and Well-being of Looked after Children, 2009.) CCGs are also required to employ the services of a Designated Doctor Looked after Children and a Designated Nurse Looked after children. Resources have been identified to seek to ensure that the Designated Doctor is able to provide front line Initial Medicals for the younger children who come into care. The role also focuses on the training of General Practitioners who have also been commissioned to provide the services and on quality assuring of their reports. The Designated Nurse Looked after Children Barnet is based within a provider organisation. However, as part of her designated role she works closely with Barnet CCG Children s commissioning team to advise the CCG of commissioning requirements for Looked after Children. In Barnet there are currently 343 Looked After children within the borough, all of whom required initial assessment by a medical practitioner when they first came into the care of the Local Authority. The children are then reviewed on an annual basis by a member of the Health Looked after Children s team. It is anticipated that these additional investments will prevent backlogs of children who have not in the past been seen within statutory timescales (This was a situation which arose in 2016 but has now been resolved). In response to findings from the Serious Case Review into the death of Child E, the CCG have also funded an additional post for a Band 7 Specialist Nurse to work within the team. This will enable the Designated Nurse for Looked after Children to develop her role strategically and ensure that the health needs of Looked after Children are being met. 5. Progress with Serious Case Reviews The CCG Safeguarding team continue to work closely with the multi-agency partnership regarding the embedding of learning points into healthcare practice, from reviews that have been completed or are in progress. 6. Provider Performance and Assurances 6.1 Arrangements for monitoring Compliance by Provider Trusts and Independent Contractors The CCG Associate Director/ Children s Designated Nurse receives assurances regarding provider organisations compliance with safeguarding requirements through attendance at Provider Quarterly Integrated safeguarding committees and submission to the CCG of Quarterly Safeguarding provider safeguarding performance information. Provider Trust Safeguarding reports are presented on a quarterly basis to the Clinical Quality and Review Group meetings. Safeguarding Serious Incidents reported through the Strategic Executive Information System (STEIS) are reviewed by the Associate Director Safeguarding in collaboration 9 145
162 with the CCG Quality leads and the Commissioning Support Unit s Patient Safety Team. The Associate Director/ Children s Designated Nurse is also informed of safeguarding referrals to the Local Authority Designated Officer (LADO) if safeguarding allegations are made against health professionals. The Safeguarding Children s Forum(formerly known as the Safeguarding Children s Health Group), is a where Senior Professionals from across the health economy can gain assurance regarding safeguarding practice, demonstrate areas of good practice and identify issues that may impact on the wider group. 6.2 Training Compliance Health providers continue to be represented at the London Borough of Barnet Safeguarding Partnership Executive Board and also at the Barnet CCG Safeguarding Committee (Formerly Safeguarding Children s Advisory Group) where action plans for improvement are monitored. The outcomes of provider safeguarding audits are reviewed within their internal safeguarding committees (attended by relevant designated professionals and also within CQRG process) Q4 Training data for Provider trusts Central London Community Healthcare Trust (CLCH) L1 L2 L3 97% 95% 83% Barnet, Enfield and Haringey Mental Health Trust (BEH MHT) L1/2 L3 92% 79% Royal Free London NHS Foundation Trust (RFL NHS FT) L1 L2 L3 88% 81% 74% East London NHS Foundation Trust (ELFT) L1 L3 100% 66% East London NHS Foundation Trust is the provider of Speech and Language services to Barnet child residents, having been commissioned by NHS Barnet CCG since October They employ 33 staff all of whom are mapped at Level 3. The Trust s L3 percentages are low due to lack of provision for Level 3 training to date within multiagency training slots. However, the issue is being addressed by Barnet Safeguarding team in conjunction with the Local Authority and Royal Free London NHS Foundation Trust
163 6.2.2 NHS Barnet CCG L1 73% CCG staff have been alerted as to the need to ensure their statutory training is up to date and monthly reviews of the statistics will be maintained General Practice GPs access safeguarding training in a variety of ways including through local providers, national study days etc. GPs are required to provide evidence of compliance with safeguarding training for their annual appraisal. The CCG Safeguarding team provide several safeguarding update sessions for General Practice throughout the year. In addition to these sessions, GP Safeguarding Leads are offered additional input to ensure that they are aware of changes in legislation or practice requirements. Safeguarding teaching was a key element of The CCG Annual General Meeting in September 2017 and Dr Cathy Wainhouse and Dr Jonathon Bindman presented on Suicide and Self harm strategies (This was the CCG response to ensure that General Practitioners are skilled in supporting children and young people who are at risk of this type of harm). The Safeguarding team also delivered a presentation on the impact of neglect at the Annual General Meeting. 7. Risks and Challenges Requirements of the Ofsted improvement plan require significant time resources from the CCG Safeguarding Team which may have a potential impact on their ability to fulfil other aspects of their role. The delivery of Primary Care Safeguarding training remains a challenge for the CCG safeguarding team, as does the collection of information regarding the impact of the training on the working practices of the General Practitioners following attendance at the sessions. Ensuring that provider organisations are compliant with the required safeguarding competencies at the appropriate levels for each professional. Working with Children s commissioning to ensure that plans for CAMHS out of Hours Services at Barnet Hospital address the needs of the vulnerable children requiring their service. Further discussion is required regarding access to CP-IS for Locum staff in Out of Hours Hubs. 8. Conclusion The Ofsted report into Barnet Children s Services and the Barnet Children s Safeguarding Board arrangements highlights significant improvement requirements to ensure that Barnet children are both protected from harm, and have the appropriate support in place, when there are difficulties within the family. However, all statutory partners are ensuring that the Improvement Plan is prioritised in organisational business
164 9. Recommendations The CCG safeguarding team will continue to work with BCCG Chief Operating Officer, the BCCG Chair, and the Associate Director Quality and Clinical Services to ensure that London Borough of Barnet s Improvement Plan is implemented from a health perspective. NHS Barnet CCG Chief Operating Officer and Chair will be statutory partners at the BSCB Leadership group. The Associate Director NHS Barnet CCG/ Designated Nurse, Designated Doctor Children's Safeguarding and Named General Practitioner will attend the BSCB Executive Board to ensure that with our provider colleagues the voice of health is heard across the partnership. Actions and learning from the Ofsted Report, Serious Case Reviews and other serious incidents pertaining to children and young people will be embedded and highlighted in training and future learning across the health partnership. Provider organisations not meeting or maintaining required Safeguarding training levels are to provide action plans to Barnet CCG demonstrating how they will address this issue. CCG safeguarding training figures to be monitored on a monthly basis. Actions from Barnet Serious Case Reviews to be monitored within the BCCG Safeguarding Forum and reported to the CQRC on a quarterly basis. The Safeguarding team in partnership with Barnet CCG Children s Commissioners to monitor continued arrangements for CAMHS out of hour s services, to ensure that the service provided is safe and does not place Barnet children at risk. NHS Barnet will work with Barnet Safeguarding Children s Board to embed the priorities for 2017/18 in healthcare practice. 10. Next Steps CCG Safeguarding team will provide an update to NHS Barnet Clinical Quality and Review Committee in April Authors: Siobhan McGovern Associate Director Safeguarding /Designated Nurse Safeguarding Children Dr Paul de Keyser Designated Doctor for Children's Safeguarding Dr Prashant Desai Named Doctor for Children's Safeguarding Date: 30 th November
165 Item 15.1 MEETING NHS Barnet CCG Governing Body DATE 11 January 2018 REPORT Annual Safeguarding Adult s Report LEAD DIRECTOR Vicky Aldred, Interim Director Quality and Clinical Services AUTHOR Heather Wilson, Adult Safeguarding Lead NHS Barnet CCG Siobhan McGovern, Associate Director Safeguarding/ Designated Nurse NHS Barnet CCG Dr Raju Raithatha, Named General Practitioner Safeguarding Adults CONTACT DETAILS heatherwilson3@nhs.net EXECUTIVE SUMMARY 1. Introduction This report provides the annual Safeguarding Adults update to Barnet CCG s Governing Body. The report provides information regarding assurance and identified gaps and risks regarding the CCG and its provider s compliance with safeguarding adult arrangements and duties as required within the Care Act 2014 across health services commissioned for Barnet Adults. The report will outline any recent developments in the following areas: Governance arrangements National and Local Context Participation in Local Safeguarding Board and Partnership arrangements Progress with Serious Adult and Domestic Homicide Reviews, including embedding of learning Provider performance and assurances Risks and Challenges Conclusion/ Recommendations 2. Risks and Challenges Working with the CCG Quality team, Continuing Healthcare Team and the local authority to ensure that residents placed in Care Homes/ Nursing Homes which have enforcement action by the Care Quality Commission are Safeguarded from harm whilst improvements are being monitored and placements suspended, or alternative care provision is being arranged. In conjunction with the Quality team, Monitoring improvement plans for those homes rated as inadequate by the CQC. Ensuring that the proposed Adult Multi-Agency Safeguarding Hub (MASH) has the required health input resourced to facilitate full health information sharing and input. This should not impact on staff currently providing day to day community care for patients. Assessing the risk of poor legal literacy across the health economy and working to improve the understanding of the Mental Capacity Act
166 3. Conclusion/ Recommendations Safeguarding reviews continue to find themes of poor legal literacy regarding the Mental Capacity Act and the Mental Health Act. The CCG Safeguarding team will consider how this can be approved across the health economy and monitor and implement action plans from the reviews. The CCG Safeguarding team will promote and support the use of the new Hoarding and Self Neglect policy by General Practitioners and other health providers in Barnet. The CCG Safeguarding team to work with the Local Authority to ensure that the proposed Adult MASH is resourced to enable full health input. RECOMMENDED ACTION: For assurance Objective(s) / Plans supported by this paper: Promote health and wellbeing Ensure right care right time Approval Route: (delete as applicable) Director Quality and Clinical Services 22/11/2017 Clinical Quality and Risk Committee 14/12/2017 Patient & Public Involvement (PPI): N/A Stakeholder Engagement: Named General Practitioner Safeguarding Adults has been involved in the development of the content of this paper Key Risks To Note: There are currently 3 nursing homes in Barnet with inadequate CQC inspections and placements suspended. The CCG Adult Safeguarding Lead, CHC nurses and Quality lead are working with the local authority to support and monitor these homes. Ensuring that the proposed Adult MASH has the required health input resourced to facilitate full health information sharing and input. This should not impact on staff currently providing day to day community care for patients. Resource Implications: Health input to the Adult MASH will need to be resourced. Next Steps: Quarterly update to NHS Barnet CCG Clinical Quality and Risk Committee April 2018 Appendices N/A 2 150
167 Annual Safeguarding Adults Report 1 Introduction 1.1 This report provides the annual update to the CCG Governing Body. The report provides information regarding assurance and identified gaps and risks regarding the CCG and its provider s compliance with safeguarding adult arrangements and duties as required within the Care Act 2014 across health services commissioned for Barnet children. 1.2 The report will outline any recent developments in the following areas: Governance arrangements National and Local Context Participation in Local Safeguarding Board and Partnership arrangements Progress with Serious Adult and Domestic Homicide Reviews, including embedding of learning Provider performance and assurances Risks and Challenges Conclusion Recommendations 2 Governance Arrangements The CCG Adult safeguarding team includes: Associate Director for Safeguarding: The post holder manages the Adult Safeguarding Lead and provides advice and leadership support to the role. Lead for Adult Safeguarding: The post holder provides advice and safeguarding knowledge within the CCG, across commissioned services and across local partnerships. The Adult Safeguarding Lead is also lead for Mental Capacity Act (MCA), Prevent and Domestic Abuse. They lead on the implementation of the CCG Adult Safeguarding Policy. The post holder since March 2014 is Heather Wilson. Named GP for Adult Safeguarding: The post holder provides specialist advice and knowledge to the CCG board, and to GP colleagues. The post holder since July 2013 is Dr Raju Raithatha. Senior Safeguarding Administrator: The post holder provides administrative support for adults and children s safeguarding and arranges safeguarding training. 3. National and Local Context 3.1 Care Act Guidance The Care Act 2014 came into force in April The CCG Adults at Risk Policy was developed to ensure the CCG was compliant with the Act and was ratified by the CCG board in November The Care Act Guidance was refreshed on March 10 th 2016 by the Department of Health. 151
168 3.2 Intercollegiate document for Safeguarding Adults The Intercollegiate document for Safeguarding Adults was made available in final draft form by NHS England in January Health providers were asked to prepare training and competencies according to this draft. Barnet Health Providers have been developing and delivering level 3 training for their staff according to the competencies specified. However, the final document has not been published as a decision has been made to align it with the Children s guidance, which is due to be published in early Whilst this guidance is awaited, providers are delivering training at the required levels and including level 3 training where appropriate. 3.3 National learning from Safeguarding Adults Reviews Safeguarding Adults Boards (SABS) must arrange a Safeguarding Adult Review (SAR) when: An adult dies as a result of abuse or neglect, or experiences serious abuse or neglect and There is concern about how agencies worked together to safeguard them. The purpose To identify lessons to be learnt from the case and apply those lessons to future cases. To improve how agencies work, singly and together, to safeguard adults. A report into reviews across London was commissioned in 2017 by the Association of Directors of Adult Social Services (ADASS). This review found: More cases involved men, of all age groups Most involved group living such as care homes or supported living schemes Organisational abuse and self-neglect were most common Common themes were: Lack of legal literacy Poor information sharing Silo working Lack of safeguarding literacy Absence of challenge to poor standards Absence of leadership and coordination Missing the obvious Barnet Safeguarding Adults Board (SAB) has developed an action plan based on these recommendations, which will be implanted and monitored by its subgroups. 3.4 Making Safeguarding Personal A national review of Making Safeguarding Personal (MSP) has been completed in Areas for development were identified as: Working with and managing risk A focus on MCA and making safeguarding personal for those who lack capacity Focus on Core Safeguarding Principles Focus on Prevention and including MSP in prevention strategies Development of a Multi-Agency Safeguarding Hub (MASH) to help with interagency working, especially in mental health There is an action plan based on this review which will be monitored by the Personalisation sub group of the Barnet SAB
169 3.5 Safeguarding Adults in Barnet In 2016/ safeguarding concerns were raised to the local authority. Of these, 298 were referred for further enquiry due to suspected abuse. The other concerns were addressed with actions such as reviews of care and support, or further assessments for the adult and their carers. Neglect and Acts of Omission are the main category of abuse, making up 34% of cases. Care homes are the main area where abuse occurs. The largest category for the person who caused the harm are friends and family, with paid carers being the second largest group. The abuse was fully or partially substantiated in 47% of cases. Actions taken as part of a safeguarding plan include: increased monitoring of services (by local authority with CQC informed), reviews and or changes in care packages, moving the individual, police action and disciplinary action. 3.6 The Mental Capacity Act 2005 (MCA) and Deprivation of Liberty Safeguards 2009 (DoLS) Lack of literacy in the Mental Capacity Act continues to be a theme emerging from Safeguarding reviews and enquiries. Barnet Providers complete yearly MCA audits for the CCG, and MCA training is mandatory across all providers. Actions from SARs related to the MCA will be monitored by the CCG, these include: Specialist training for primary care staff in managing complex patients where Mental Capacity is a concern, and provision of Court of Protection updates for clinical staff. The CCG Safeguarding team is considering the best way of providing these updates. To support Primary Care, NHS England has developed EMIS tools for the MCA. These are very simple forms that are specific for GPs and practice nurses to use, for example there is a form for use in flu vaccine clinics. These were piloted by Hillingdon CCG and are being rolled out across London Deprivation of Liberty Safeguards (DoLS) Legislation proposed by the Law Commission to streamline the current DoLS system has not been scheduled for the next two years of parliamentary business. Therefore, the Department of Health is consulting with MCA Leads across local authorities, CCGs and Health Providers in order to determine what changes are possible to implement in the interim. 4 Safeguarding Adults Reviews and Domestic Homicide Reviews 4.1 Safeguarding Adult Reviews (SAR) (AB) A learning event was held in May 2017 following a review into a Barnet resident who had life changing medical complications and concerns were identified as to how agencies had worked together to manage risk. The final Safeguarding Adults Review report and recommendations are being completed. The action plan will be monitored by the Safeguarding Adults Board, and the learning from the review has been incorporated into training by providers and the CCG. The recommendations include: The need for legal literacy regarding the Mental Capacity Act and the Mental Health Act, including access to expert advice for Primary Care when working with complex patients Multi-Agency training on complex capacity assessments focussing on the time specific nature of capacity, and the difficulty of assessing how individuals use and weigh information A second Safeguarding Adults Review has been commissioned after the death of a vulnerable adult in a fire. The initial concerns after the fire have been picked up by the CCG with information sent to all GPs about the use of emollient creams and associated fire risks
170 4.1.3 (YY) Camden local authority have published a Safeguarding Adult Review (YY) into a person who died after serious self-neglect and an eating disorder. The person previously lived in Barnet. The review recommendations for health include: All staff should be working to the NICE guidelines on eating disorders GP involvement in multi-agency safeguarding arrangements are strengthened 4.2 Domestic Homicide Reviews (DHR) A Domestic Homicide Review is required by the Home Office when a person is killed by a partner or close family member. This year the Home Office updated the guidance on reviews, and emphasised the involvement of families. Previous reviews have identified where services missed opportunities to intervene and improve the safety of domestic abuse victims. The CCG Adult Safeguarding Lead and Local Authority colleagues delivered multi-agency learning events for a previous DHR to GPs, CCG senior colleagues, Safeguarding Boards and Mental Health Staff. The CCG safeguarding team monitor the action plans via provider reporting and internal committees. CCG actions from this review included commissioning Identification and Referral to Improve (IRIS) for Barnet GPs, this has now been commissioned in Barnet There is one current Domestic Homicide Review in process in Barnet. 5. Participation in Local Safeguarding Board and Local Partnership Arrangements 5.1 Safeguarding Adults Board (SAB) The CCG is one of three statutory partners on the SAB (representation from Associate Director Safeguarding, Adult Safeguarding Lead and Named General Practitioner Safeguarding Adults), along with the Local Authority and Police, and contributes to the operational work of its subgroups. 6 The SAB priorities for are as below: Personalisation: The SAB is required to ensure multi-agency partners adopt Making Safeguarding Personal (MSP). Barnet CCG has incorporated MSP in its Adults at Risk policy and is committed to involving adults in safeguarding processes. Personalisation also covers Self Neglect, which is a new category of abuse since the Care Act A hoarding and self-neglect policy has been developed and adopted by the Safeguarding Adults Board, all partners are requested to adopt this policy. It includes an assessment tool that professionals can use to assess the risk of hoarding behaviours. The multi-agency risk panel, of which the CCG is a core member, was extended in 2017 to formally include hoarding and self-neglect. The Barnet Fire Brigade has taken a lead on this area of work. The policy and updated procedures for working with self-neglect will be launched in Barnet early next year Pressure Ulcers: The Pressure Ulcer Safeguarding Protocol that was adopted by Barnet SAB has now been embedded across community health services in Barnet. This has led to a significant reduction in inappropriate referrals to adult social care. This protocol is now being extended to nursing homes. This SAB priority is being led by the CCG and CLCH and the adult safeguarding leads will be auditing the use of the protocol in the fourth quarter Domestic Abuse: The SAB has decided to focus on domestic abuse in situations where there is an adult in need of care or support, and those who are carers for them. Disabled women are twice as likely to be victims of abuse. 154
171 5.1.4 Access to Justice: There has been significant under reporting of hate crimes in Barnet. The SAB sub group has implemented on a new process for reporting hate crimes. There are now 19 hate crime reporting sites (third party sites) in Barnet, to make reporting easier for victims. This has led to a small increase in reports up from 1 to Adult Multi Agency Safeguarding Hub (MASH): The SAB has employed a project officer to deliver an Adult MASH. The CCG is on the project board. The proposal is for the Adult MASH to be co-located with the Children s MASH at the Local Authority. Health involvement in the MASH will support GPs and health providers with referrals for adult safeguarding, and allow for timely information gathering from health systems. 7 The format for the Adult MASH is being scoped currently. 5.2 Domestic Violence and Violence against Women and Girls (DV and VAWG) The CCG is a partner on the Domestic Violence and Violence against women and girls Delivery Board Identification and Referral to Improve Safety (IRIS) IRIS has now been commissioned for Barnet and is a jointly funded project by the London Borough of Barnet, Barnet Clinical Commissioning Group and NHS England. The provider is Solace Advocacy and Support, who provide Domestic Violence and Abuse (DVA) support services in Barnet, and have been providing IRIS services in neighboring boroughs. An advocate educator will work with 25 selected GP Practices to deliver DVA training to GP practice teams and act as an ongoing consultant and support the team, working with patients who are at medium risk of domestic abuse, and ensuring referral for those who are high risk. The advocate educator will work with a local clinical lead to implement the project Mental Health Domestic Abuse project. (LINKS project) NHS England have funded a pilot for the first Mental Health Independent Domestic Violence Advocate in England, who is placed in Barnet and works at the Springwell Unit in Barnet Hospital and the Dennis Scott Unit at Edgware hospital. The CCG is a partner on the project board. The IDVA is providing DVA training for staff, which is mandatory, and is doing case work with mental health patients. The project has so far achieved a 150% increase in referrals to DVA services and to the MARAC in Barnet. An unexpected finding has been the identification of perpetrators who have been referred for support and interventions outside the criminal justice system. This project has been shortlisted for a HSJ award under Innovations in Mental Health Barnet Multi Agency Risk Assessment Conference (MARAC) The Barnet MARAC is chaired by the police, and the CCG is a partner. The MARAC is a problem solving meeting to discuss high risk cases of domestic abuse, victims/survivors of abuse are referred with their consent to the meeting. The CCG Adult Safeguarding Lead is a member of the MARAC and supports GP referrals, and liaison with GPs for those referred by other agencies, as well as supporting health providers. Health Referrals are still low to the MARAC, but have improved since the provision of IDVA services within the acute hospitals and the Mental Health Trust. The roll out of IRIS is expected to increase referrals from primary care. 5.3 The Community Safety Multi-agency Risk Assessment Case Conference (CS MARAC) The CS MARAC is a panel which meets every six weeks to consider the most persistent and complex Anti-Social Behaviour cases in Barnet. The CCG adult safeguarding Lead supports the CS MARAC with those referrals where Primary Care or other health provider liaison is 155
172 needed to reduce risk, and facilitate support and services for the individual, both victims and perpetrator. 5.4 Prevent Prevent is a part of the governments Counter Terrorism Strategy which focuses on those at risk of being radicalised into terrorist activities. Prevent is a safeguarding intervention that is voluntary for the person at risk to choose to participate in. The Prevent Duty requires all NHS Trusts to train healthcare staff to recognise vulnerability to radicalisation. The Barnet Lead for Prevent is within the local authority. Counter Terrorism police lead on managing Prevent referrals. The CCG Prevent lead is a core member of the Barnet Channel Panel, and the Prevent Delivery Board, as required by NHS England. 6. Provider performance and assurances 6.1 NHS Providers: Royal Free London NHS Foundation Trust, Central London Community Healthcare NHS Trust (CLCH), Barnet, Enfield and Haringey Mental Health NHS Trust (BEHMHT) The Trusts have integrated safeguarding committees which meet quarterly and are attended by CCG safeguarding leads for assurance. The committee receives reports on patients and families who have the opportunity to ask questions or request changes. Provider Trusts safeguarding reports are presented to the Clinical Quality and Risk Group meetings every quarter. Duty of Candour and Making Safeguarding Personal requirements ensure that all Safeguarding Enquiries involve patients and their families. NHS Reports are always shared with patients and families who have the opportunity to ask questions or request changes The committee also receives reports on Adult Safeguarding activity, including training compliance, alerts raised against the Trust and their outcomes, Mental Capacity Act assessments, and Deprivation of Liberty Safeguard applications and outcomes. The CCG Adult Safeguarding Lead attends the committees as one way of assuring that the Trust is providing high quality safeguarding for its patients. All NHS providers are responsible for ensuring that all Serious Incidents, including those with safeguarding elements, are reported to the Strategic Executive Information System (STEIS), which reports to the Department of Health via NHS England. The CCG Adult Safeguarding Lead reviews all Safeguarding Serious Incidents, in collaboration with the CCG Quality Leads and the Commissioning Support Unit s Patient Safety Team. Training compliance Quarter 2 Royal Free Hospitals: Adult Safeguarding L1 80% L2 91% Mental Capacity Act 80% CLCH: Adult Safeguarding L1 92% L2 92.5% Mental Capacity Act 92% BEHMHET Adult Safeguarding L1 & 2 90% Mental Capacity Act 90% 8 156
173 Primary Care: GPs access safeguarding training in a variety of ways including through local providers, national study days, and private study and practice reviews of cases. GPs are required to provide evidence of compliance with safeguarding training for CQC inspection. This includes demonstrating compliance with the MCA The CCG Safeguarding team provide several safeguarding update sessions for General Practice throughout the year. In addition to these sessions, safeguarding leads are offered additional input to ensure that they are aware of changes in legislation or practice requirements to embed in their practices Bespoke MCA and DoLS training was commissioned for GPs across Barnet in Safeguarding was a key element of The CCG Annual General Meeting in September 2017 The Fire Brigade presented in response to a death in Barnet that has led to a Safeguarding Review Royal Free London NHS Foundation Trust also offers training places for GPs CCG staff CCG staff training compliance is monitored and reported to us by the commissioning support unit. Adult safeguarding training is part of induction and also available online for staff. Training compliance Quarter 2: Adult Safeguarding L1 75% The CCG safeguarding team are supporting and promoting improvement in compliance of safeguarding training and monitoring of the statistics in ongoing. 6.2 Third Sector Providers As the Lead Commissioner for the North London Hospice, Barnet CCG provides support and monitors safeguarding performance at the Hospice. The Hospice provides quarterly metrics to the CCG, including training compliance, safeguarding referrals and Deprivation of Liberty Safeguard applications. The CCG has supported the hospice to improve their training levels, and to commission training sessions, including Prevent training. Bespoke training to improve confidence with complex safeguarding cases has also been developed. Adult Safeguarding training: L1 89% L2 76% 6.3 Independent Providers: Nursing/Residential Care Homes, Private Hospitals and Domiciliary Care. Oversight of independent provider safeguarding performance is via a multi-agency partnership approach in Barnet, consisting of: Provider concerns: a bi monthly meeting between the Local Authority, CCG and CQC which examines all safeguarding concerns reported relating to Care Homes or Domiciliary Care Agencies Continuing Healthcare (CHC) patient reviews: Any patient subject to a safeguarding concern will be reviewed by the CHC team review nurse. Allegations against the provider are monitored by the CCG and Local authority Contract monitoring visits by the local authority contract team and Quality in Care Homes team 9 157
174 Establishment concerns processes, triggered when there are significant concerns about a provider. This is a multi-agency meeting, which includes the provider. Suspension of placements to a provider can be decided on by the local authority from this meeting 7. Risks and Challenges 7.1 CQC Inspections and Outcomes The CCG Quality Lead, CHC team and Adult Safeguarding Lead has worked closely with the local authority to support a local nursing home that was found inadequate by the CQC with enforcement notices and a suspension of placements in early Regular meetings with the home and CQC inspector, monitoring of action plans, and safeguarding enquiries have resulted in the home being able to turn itself around and receive a good CQC result. Placements have now been reinstated There are currently three nursing homes in Barnet with inadequate CQC inspections and placements suspended. The CCG Adult Safeguarding Lead, CHC nurses and Quality lead are working with the local authority to support and monitor these homes Ensuring that the proposed Adult MASH has the required health input resourced to facilitate full health information sharing and input. This should not impact on staff currently providing day to day community care for patients. 8. Conclusion/ Recommendations Safeguarding reviews continue to find themes of poor legal literacy regarding the Mental Capacity Act and the Mental Health Act. The CCG Safeguarding team will consider how this can be approved across the health economy and monitor and implement action plans from the reviews. The CCG Safeguarding team will promote and support the use of the new Hoarding and Self Neglect policy by General Practitioners and other health providers in Barnet. The CCG Safeguarding team to work with the Local Authority to ensure that the proposed Adult MASH is resourced to enable full health input
175 Item Barnet Clinical Commissioning Group Finance Performance and QIPP Committee Meeting 28 September2017 Report title Finance Performance and QIPP Committee Chair Report author Dr Barry Subel Mr Andrew Tillbrook. Board Secretary, interim Report summary This paper presents a summary of the meeting of the Finance Performance and QIPP Committee which took place on the 28 September Recommendation The Governing Body is asked to Note the summary report. Strategic objectives links The strategic objectives are: Improve health and wellbeing and reduce inequalities Provide value and live within our means Enhance Quality Be excellent Clinically Well Led 159
176 Report of the Finance Performance and QIPP Committee meeting Summary of the Meeting Held on 28 September 2017 Items of Business Monthly Finance Report Month 5 (incorporating QIPP status for 2017/18), from which the committee considered: the forecast outturn is an adverse variance to plan of 8.3m (made up of slippage in QIPP ( 7m), acute over performance (5.2m) and offset by mitigating actions of 6.4m overall QIPP slippage The CCG would be reviewing its Budget and commitments for 2017/18 to identify where additional savings could be made and report to NHSE London. Members discussed the budgetary implications at length which covered: the level and spend in acute over performance with the providers the level of QIPP that related to acute over performance a new management team was being established in the CCG which was beginning to make a positive impact by reviewing practice and systems which was leading to greater clarity of the CCG s financial position Consideration was also given to longer term planning, focussing on savings and increased efficiencies with a view to having greater control over the CCG s budget. Accuracy and coherency of data from providers was considered as a major issue, noting that there should be greater contractual oversight to prescribe providers to give accurate data in a timely way. It was recommended that: there should be CCG clinical input to help shape services CCG clinical input should be integral to QIPP management and review. 2018/19 QIPP Planning, which was considered by the Committee, noting the CCG s resolve to deliver the savings identified in the QIPP plans. Early modelling suggested that the QIPP target for 18/19 would be at least 15.5m. Of this 3.3m is expected to be delivered by the full year effect of the 2017/18 QIPP, which left a gap of 12.2m. It was agreed that clinical leadership should be integral to QIPP planning. Quality and Performance Report was reviewed at length from which the following issues were reviewed: the Referral to Treatment Target (RTT) compliance of 18 weeks was achieved in July 2017 by the Royal Free Hospital. However, the RTT waiting list was increasing and the issue of capacity was being monitored by the CCG and Trust managers. the number of patients waiting over 52 weeks had increased from 3 to 7 in July 2017; whilst not significant at this stage, any further increase in waiting time would require additional remedial plans delays in developing a robust patient reporting system which was leading to delays in providing accurate reports to the CCG. accident and emergency care waits were not achieved, but it was expected that the implementation of a Discharge to Assess Home model would bring waiting times into target. The CCG s senior management team was focussing its attention with the provider to reduce waiting times. Work was ongoing with regard to improving social care to help delayed transfer of care patients, working with the local authority 160
177 the gradual improvement in achieving recovery and access rate for IAPT services. Barnet Enfield Haringey Mental Health Trust (BEHMHT) Pricing Review considered a report which reviewed of the financial position of BEHMHT. It was noted that BEHMHT was subject to a programme review, supported by NHS Improvements (NHSI), as well as the continuing issue about the level of contribution CCGs in north central London provided. Members considered this aspect, noting that the CCGs were due to commit any additional contributions, and, coupled with the uncertainty of whether the funding for special commissioning would be given to the CCGs from NHSE there remained a concern on the level of service. 2018/19 CCG Commissioning Intentions were considered, particularly with regard to the development of the commissioning intentions in Barnet and across the other four CCGs in NCL. As part of the appraisal, intentions that were potentially similar, were identified in order to avoid duplication of work as well as ensuring that all they are material. The review has led to streamlining the list of intentions. Members agreed and recommended that IT systems should be an embedded part of each commissioning intention and that the effectiveness should be monitored by using KPIs each proposal should state that a single secure point of access to communicate between commissioner Business Cases Care Homes QIPP Scheme was considered. This related to an enhanced care home healthcare support service (CHESS), - a pilot scheme which was due to end in October A new service model had been was agreed at this Committee s sub group (PODG) in September from which is projected to deliver 27k savings this financial year against a QIPP target of 24.5k, plus 971k savings in 2018/19. The initiative was proposed to be of a longer term strategy, with the effect to reduce the number of patient admissions to A&E department. Early indications suggested that this initiative was having a beneficial effect on reducing admissions and that there was a collaborative approach with the Local Authority. Members agreed to approve the proposed service budget of 163,500 for the remainder of 2017/18 (additional to the CHESS spend due to end in October), and 195,500 for 2018/19, on an invest to save basis, to achieve the 2017/18 QIPP target, with a much larger savings potential for 2018/
178 162
179 Item Barnet Clinical Commissioning Group Finance Performance and QIPP Committee Meeting 26 October 2017 Report title Finance Performance and QIPP Committee Chair Report author Dr Barry Subel Mr Andrew Tillbrook. Board Secretary, interim Report summary This paper presents a summary of the meeting of the Finance Performance and QIPP Committee which took place on the 26 October Recommendation The Governing Body is asked to Note the summary report. Strategic objectives links The strategic objectives are: Improve health and wellbeing and reduce inequalities Provide value and live within our means Enhance Quality Be excellent Clinically Well Led 163
180 Report of the Finance Performance and QIPP Committee meeting Summary of the Meeting Held on 26 October 2017 Items of Business Monthly Finance Report Month 6 (September 2017) was considered in depth, noting draw up year-end surplus target (indicating 3.7m) whilst still continuing to show the forecast outturn deficit of 4.5m; an adverse variance of 8.2m year to date. A recovery plan had been developed by the CCG and submitted to NHSE. The plan included an additional savings plan of 2.3m. Attention was drawn to the level of acute over-performance, which was being assessed and subject to continuing negotiation with the Royal Free London (RFL) Collectively, across NCL, the forecast outturn still indicated an overall deficit. There remained ongoing concerns with the costs of patient transport and clarification work of the productivity metrics. The management of reducing patient referral to treatment times (RTT) was debated from which it was noted that the provider was in the process of implementing a new reporting system. There was also an increase in demand, which coincided with a decrease in capacity, which had resulted in a worsening position of 5%. RFL was scheduled to publish a recovery plan by the end of October; from which the CCG would then be in a position to assess further. Monitoring of this issue was also being provided by NHSE. Assurance was given that the NHSE and the Commissioners were engaged with the provider. Members noted that work was starting on the 2018/19 QIPP schemes; a draft plan had been drawn up with which to base the CCG s negotiation with providers over the coming weeks. For 2017/18, consideration was given to the challenge of achieving the 7.0m FYE. However, it was noted that there is a significant overlap of services and schemes between Barnet and Enfield. Part of the drive for efficiency was to stop duplication of managing similar schemes, their prioritisation and identifying where the biggest impact could be made. Quality and Performance Report the Committee focussed on: Cancer Waiting Times Accident and Emergency waiting times this continues to be challenging. However, the level of delayed transfers of care (DTOC) had been better than target and it was suggested that this achievement was the result of effective management in the prior months, at the RFL and Finchley Memorial Hospital Community Services (CLCH) - an improvement in Muscular Skeletal Services had been evidenced and the Commissioners had now lifted the Contract Performance Notice. Mental Health a gradual improvement of referral waiting time had been shown since August 2017 to IAPT services. In considering the report, the following issues and comments were raised; The demand for dermatology services (and already significant waiting times for patients), It was noted that there was a national shortage of dermatologists (and so a strategic issue). Additional capacity to help manage demand was being addressed by introducing a tele-dermatology service in the short term. Some of the care homes referenced in the report (particularly those that had been suspended) were outside of the borough. 164
181 to consider whether there were more opportunities to assess and identify ways to act more strategically across Barnet and NCL. QIPP Schemes and Plans - the Committee noted that contract negotiations for the 2018/19 contracts would be underway soon.. Business Cases Lead Provider Update (MSK / Urology Service) A proposal to develop an integrated service as well as for commissioners (Barnet and Enfield) to forge systems together, becoming more efficient and cost effective was presented. Note was made of the budgetary implications of between 200m and 250m (for Barnet) over a five year period and, given the size of the project, the project should form a standing item at this committee to ensure regular and formal oversight of the project. It was noted that the proposal was at a high level stage and agreed that the committee would require a more detailed plan to include, resourcing, contractual arrangements so that the CCG could determine the commitment required by the CCG to support and manage the project. It was agreed to provide an update to the next meeting for consideration. Ophthalmology Business Case - the Committee noted that an outline business case had already been presented to this Committee earlier in the year and minimal changes were being presented at this meeting. Key points to note included: a more streamlined patient referral process a shift in activity from the acute sector to the community sector an expected saving per annum of around 400,000. Some points of clarification were raised, including; where surgery would be conducted, the percentage of time that an ophthalmic consultant should be available for, the degree of how much the proposed service would improve patient experience and whether the service could be conducted directly from their specialist surgery (which could decrease the need for patients to attend the main hospital. Consideration was given to the service model which had been adopted by Enfield CCG and whether Barnet should follow this approach. With further scrutiny it was agreed to place a moratorium on this business case, and that it should be reconsidered by the Barnet CCG Executive Team, and in turn to provide an update and recommendations to the November meeting of this Committee 165
182 166
183 Item Members: Mr Robin Somerville Dr Aashish Bansal Mr Ian Bretman Mr Dominic Tkaczyk In Attendance Mr Matt Backler Mr Simon Goodwin Mr Charlie Medley Ms Erin Sims Mr Clive Makombera Minutes: Andrew Tillbrook Apologies: Ms Joanna Lees Ms Kay Matthews NHS BARNET CLINICAL COMMISSIONING GROUP Minutes of the Audit Committee held on Thursday 24 August 2017, Meeting room G2, 09:00 to 10:10am North London Business Park, London, N11 1NP Lay Member Governing Body, BCCG GP and Governing Body Member, West Locality, BCCG Lay Member (PPI), BCCG Associate Lay Member (Finance), BCCG Deputy Chief Finance Officer, BCCG Chief Finance Officer, NCL CCGs Audit Manager, External Audit, KPMG Local Counter Fraud Specialist, Internal Audit, RSM Director, Internal Audit, RSM Deputy Board Secretary, CCCG Director, KPMG Chief Operating Officer, BCCG 1. Introduction 1.1 Welcome and Apologies for Absence Mr Somerville opened the meeting, introductions were made and apologies noted and recorded above. 2.0 Declaration of Interests 2.1 Members were invited to proffer any new declarations of interest, for which none were given. 3.0 Minutes of the previous meetings, 18 and 25 May The Minutes of the meetings held on 18 and 25 May 2017 were considered and agreed as an accurate record. It was noted and agreed that summaries of minutes would be provided to future Governing Body meetings in the interests of succinctness. Agreed: To approve the minutes of the meetings held on 18 and 25 May 2017 Minutes of meetings would be summarised for future Governing Body meetings 4.0 Action Log and updates 4.1 The Action Log was considered and noted, confirming to remove actions agreed as Closed and retain items agreed as Open for reporting on at the next meeting. Page 1 of 6 167
184 Noting that the change in commissioning arrangements will not change how counter fraud matters would be conducted with regard to general medical services; clarifying that the investigations that pre date transfer still remain with NHSE It was agreed to clarify if the agreement was an understanding or a more formal agreement; noting that a report on this matter had been brought to Islington CCG Audit Committee in July Action: to circulate this report to Barnet CCG (SG) The Committee agreed to note the Action Log updates. Governance and Audit 5.0 Internal Audit management Actions Follow Up Report Clive Makombera introduced the above report, from which the Committee noted the following points: Of the twenty two management actions had been identified, of which 85% were now implemented. Of the remaining four, one was rated as a high risk and the other, a medium risk and two low rated, all of which were being managed Clarification on completion dates were sought regarding: o Contract monitoring by the CSU (high risk), noting that KPIs were to be developed with the aim to have a greater awareness across all CCGs in the NCL group. A draft report was with Paul Sinden, Director of Acute Commissioning, NCL, for review. Noting the timescales and progress to date, RSM was invited to provide a substantive report in time for the November meeting of this Committee. (Action AC/17/01: CM) o Continuing Health Care an update should be brought to the November meeting of this Committee (Action AC/17/01: CM) o Board Assurance Framework (BAF) for which a joined up systems approach across the five CCGs was being progressed (noting that the current Risk Manager it was agreed that he should brief his successor and provide an update to the November meeting of this Committee o The NCL Governance Review was being managed by Andrew Spicer, NCL Governance Lead. Following a brief discussed, it was agreed that Simon Goodwin would check progress with Andrew Spicer and confirm that Robin Somerville would be included in future correspondence. (Action AC/17/01: SG) o Risk Management Strategy, noting the Committee s wish to conclude this management action, from which it was agreed that Clive Makombera would progress this matter with Kevin Street, the CCG s Risk Manager (Action AC/17/01:CM). AGREED: to note the report and progress 6.0 Internal Audit 6.1 CCG Progress Report, includes benchmarking Report Clive Makombera reminded the Committee of the plan to harmonise the Internal Audit Plan across all five CCGs. The Plan remained work in progress to take account of the variations in maturity across the NCL group, which required a flexible approach on areas such as governance framework and board assurance. Nevertheless, there was A draft report for initial evaluation with Paul Sinden on CSU contract monitoring A report would shortly be available on delegated commissioning The governance framework was likely take longer than expected due to the complexities across the five CCG Provider performance was in progress, completion of which would be influenced by when the governance framework would reach a coordinated conclusion. Page 2 of 6 168
185 6.1.2 In considering the overall, it was hoped that this Committee would receive the report on contract monitoring at the November meeting (Action CM to progress this with Paul Sinden with the aim it is completed in time). The Committee noted no undue concerns with regards to the other elements of the Internal Audit Plan. AGREED: to note the report 6.2 CSU Quality Assurance Plan 2017/ Clive Makombera summarised the arrangements to the committee of how Barnet CCG, as one of twelve CCGs across London procured services (including IT, HR, Contracts) from the Commissioning Support Unit, who themselves were audited by Deloittes. Deloittes provided RSM with their Service Auditor Report which focussed on the financial systems and payroll. However, there remained a gap in audit overview, hence the existence of a Quality Assurance Group (composed of representatives from the CSU and CCGs to review the Quality Assurance Programme, which provided a forum to hold the CSU to account on the delivery of services The Committee noted that this report had been presented to the Audit Committee in the other CCGs across NCL and the issues raised the report generally applied to all five CCGs. AGREED: to note the report 6.3 CSU Quality Assurance Plan Progress Report Clive Makombera introduced the above report. Members noted: Concerns in some areas of services provided by the CSU, which were currently being reviewed as to how improvements could be made, in terms of efficiency, effectiveness and cost for the benefit of all CCGs and STP level Assurance was provided that the merging of the two CSUs would not impact as to the data quality issues arising from provider management Members noted the progress to date with particular respect to: Provider quality management Procurement Cyber security Recruitment Which would be reviewed initially by the Quality Assurance Group and then to the respective CCG Audit Committees for consideration. 6.4 Health Matters It was confirmed that all management actions were being implemented Clarity was sought whether it was the CCG s or the CSU s responsibility to have a defined and agreed procurement strategy; noting that this ambiguity was likely to be due to inadequate KPIs. However, CM agreed to confirm the position and advise SG in the interim, prior to waiting for the final report (Action AC/17/02) CM). It was further noted that the key concern related to how contracts were reviewed in adequate time to enable considered decision making (i.e. whether to re-procure, re-tender, and / or cease a service); (Action AC/17/02) SG to update the position at the November meeting) The Committee noted the above report which RSM published for its clients as a way of keeping them informed of developments. AGREED: to note the report Page 3 of 6 169
186 7.0 External Audit 7.1 Audit letter from BDO The Committee noted the above letter which had been prepared and issued by the erstwhile auditors, BDO. In consideration to the preparation of the CCG s Annual Report and Accounts, members agreed that improvements were required as to their preparation and entirety prior to committee review, given the extensive comments required of the draft files and their eleventh-hour presentation. It was agreed that earlier and better presentation was required for the 2017/18 Annual Report and Accounts so that the first draft was ready at the end of April, and final draft ready by the end of May so that the deadlines for submission to NHSE could be met more comfortably It was recommended that the external auditors should be brought in earlier in the process so that any concerns can be raised prior to the formal audit. This was seen as particularly pertinent as KPMG were newly appointed to Barnet CCG. Members noted that Simon Goodwin and Matt Backler were due to meet Charlie Medley and Joanne Lees shortly which would include discussions of the auditing timetable. It was agreed that Charlie Medley would provide a plan of work to the November meeting (Action AC/17/03) CMe) The Committee considered the wording of the BDO Audit Letter, agreeing that the CCG s 2017/18 QIPP Programme was a function of the national efficiency requirement. It was further confirmed that the overall representation of Barnet s state of affairs provided by BDO remained unchanged Introduction from KPMG Charlie Medley was welcomed to the meeting, from which members noted the meetings that had been established for the KPMG Audit Team to meet key staff and committee members from Barnet CCG in order to prepare for the 2017/18 audit and beyond. AGREED: To note the report To note the audit letter, which would be published on the CCG s website 8.1 Counter Fraud Report Update Progress Report Erin Sims advised that the Local Counter Fraud Work Plan had been agreed across all CCGs in the NCL area. Members noted The progress being made against the proactive plan, which included relevant policy reviews, working with Andrew Spicer, the NCL Governance Lead. Raising awareness of counter fraud work across the CCGs, liaising with Simon Goodwin to agree the scope from which a bespoke fraud risk register would be developed The reactive work which highlighted two low level risk cases which included o the fraudulent use of an NHS number by a patient. (loss was incurred by the Provider) o an ongoing case that was being managed by NHS Protect to which information was still sought by RSM. It remained unclear when the information would be available, influenced by the reorganisation that was taking place in NHS Protect Discussion ensued as to the scale of the fraud and time taken to investigate the fraud / potential fraud. It was agreed that more detail would be provided in future to help make a judgement as to time spent on working on cases. However, it was agreed that a balance needed to be struck as to how investigations should be managed, akin to a triage system to Page 4 of 6 170
187 determine if the fraud was wider or a systems issue. It was important that the CCG should not be exposed to undue and / or fraud. It was agreed that the triage criteria should be developed further (Action SG to provide to ES and include RS, Chair, on progress) Later note, with regard to the above action: Across each of the five CCGs, it is important that staff / others have an opportunity to report suspected fraud issues to the LCFS/NHS Protect. A triage point is however needed to ensure that the CCG does not embark on expensive investigations unless there is potential for the gain (whether financial - e.g. a potential recovery, or an improvement in systems and processes to prevent a recurrence / something similar happening or non-financial e.g. reputational or patient safety / quality) to be worth the cost. It is therefore proposed that no LCFS investigation is embarked on without approval by the CFO of NCL; whose judgement will be based on the balance of cost, potential recovery, likelihood of recovery, potential system improvements and potential non-financial benefits. It is impossible to be prescriptive or have a set of metrics to apply each case needs to be reviewed on its merits. This is how I have operated in my previous NHS DoF roles, over 16 years as an NHS DoF. Where a potential case is difficult to judge I would propose to discuss with the Audit Committee Chair prior to deciding whether to proceed. In previous roles I have ensured that the LCFS update to the Audit Committee to also document cases where I have decided not to proceed, so that the Committee has oversight on this and can question any such decisions, and I would propose that we do this across NCL Consideration was given with the apparent low incidents that occurred. However, it was suspected that with delegated commissioning now being part of the CCG s remit, the number of incidents may increase. Nevertheless, consideration was given as to the robustness of the current systems. It was noted that RSM relied on individuals raising concerns as well as their pro-active work. In discussion it was suggested: ES to provide a benchmarking report across all CCGs in RSM s client base to see how Barnet compared ES to check if there were adequate, clear routes for staff, member and public to know how to raise concerns (AC/17/04) With a view to provide assurance the Committee. It was noted however that some referrals may approach NHS Protect rather than RSM, However there was an internal on line system called FIRST which enabled internal audit firms across England and Wales to relay information relevant to the particular organisation Part of RSM s work would include assessing the areas of where fraud might occur and associated risks. A scoping plan was being developed for review and approval and the timescale for the work would be clarified (Action AC/17/05: ES / SG) It was noted that the proactive deep dive element of the counter fraud work had been agreed earlier in the year across the 5 CCGs that a fraud risk assessment exercise would be conducted In conclusion, whilst there was a perception of systemic under reporting of fraud, members were assured that there was a project in progress to address this issue and due to report to this Committee by spring AGREED: to note the report 8.2 Notice Fraud Newsletter AGREED: to note the report 8.3 RSM Benchmarking NHS Reactive Cases 2016 Summary and Report Page 5 of 6 171
188 AGREED: to note the report 8.4 NHS Fraud Facts AGREED: to note the report CLOSING ADMINISTRATION 9.0 Any Other Business 9.1 Following discussion, it was agreed that there not a need to hold the scheduled meeting on 21 September. It was also agreed to set an annual meeting frequency of four times a year plus one meeting specifically to agree and sign off the annual report and accounts prior to submission to NHSE at the end of May. It was agreed that the timings of the meetings needed adequate timing to consider the draft annual report. There was no further business Review of the meeting and Clinical Effectiveness 10.1 This item was not discussed The dates of future meetings were scheduled to take place on Thursday 23 November 2017 between 08:30 to 10:30 at Barnet CCG Thursday 25 January 2018 between 08:30 to 10:30 at Barnet CCG The meeting closed at 10.10am. Page 6 of 6 172
189 Item Barnet Clinical Commissioning Group Audit Committee Meeting 23 November 2017 Report title Audit Committee Chair Report author Mr Robin Somerville Mr Andrew Tillbrook. Board Secretary, interim Report summary This paper presents a summary of the meeting of the Audit Committee which took place on the 23 November Recommendation The Governing Body is asked to Note the summary report, and in particular, the Committee s approval of two policies: Anti-Fraud and Anti-Bribery policies Strategic objectives links The strategic objectives are: Improve health and wellbeing and reduce inequalities Provide value and live within our means Enhance Quality Be excellent Clinically Well Led 173
190 Report of the Audit Committee meeting Summary of the Meeting Held on 23 November 2017 Items of Business Internal Audit Management Actions follow up report As per the agreed work plan, the Committee received reports on Primary Care Delegated Commissioning Part One; and CSU Contract Monitoring, both of which had received partial assurance as well as draft reports on Conflicts of Interest and Provider Performance Management. Nearly all of the management actions had been completed and closed. The Committee considered and commented on the proposal for the creation of an NCL wide Audit Committee, noting that this was subject to further discussion between the Audit Chairs across the 5 CCGs with senior management. Progress on the CSU Quality Assurance Plan was considered, with particular reference to cyber security and recruitment. Cyber security was a follow up review which had initially been conducted in November 2016 and note was made of the progress on improving systems to protect the IT system. Looking ahead, there are four further reviews in progress: Procurement (all 12 CCGs) draft report stage NHS Continuing Healthcare WELC POD only Provider Quality Management (NCL CCGs for provider Quality and all twelve for Patient Experience/Complaints) Acute and Non-Acute Contracting (All twelve CCGs). A Conflicts of Interest Benchmarking exercise (London and south east England CCGs) was noted, from which is was agreed to draw on and learn from the good practice. External Audit -the Committee was apprised of the preliminary work in preparing for the audit of the CCG s Annual Report and Accounts, noting that written plan would be presented at the next meeting. Counter Fraud Report Update note was made: of the organisational change that NHS Protect had been superseded by the NHS Counter Fraud Authority Fraud Awareness month was ongoing which included CCG staff training Clarification of the routes for reporting potential and actual fraud The Anti-Fraud and Anti Bribery Policies were presented and considered, noting that the revised version had taken account of legislative changes and correct reporting lines. The policy would be presented across all five CCGs in NCL for consideration. The Committee supported and approved the updated policies, in accordance with Schedule E of the CCG s Constitution. It was agreed to delegate responsibility to the Committee Chair if the policy required amendment following its review at other CCGs, providing they were minor and not material. The Conflicts of Interest Policy was presented for consideration. Noting that the Internal Auditors were in the midst of reviewing conflicts of interest as part of the Internal Audit Plan, it was recommended the policy presented should be deferred to wait for the outcome of the their work in case there are recommendations for changing the policy. It was agreed to let the current policy stand and reconsider the policy at the next meeting. 174
191 Item Barnet Clinical Commissioning Group Primary Care Procurement Committee Meetings 05 October and 02 November 2017 Report title Primary Care Procurement Committee Chair Report author Ms Bernadette Conroy Mr Andrew Tillbrook. Board Secretary, interim Report summary This paper presents a summary of the meetings of the primary Care Procurement Committee which took place on the 05 October and 02 November Recommendation The Governing Body is asked to Note the summary report. Strategic objectives links The strategic objectives are: Improve health and wellbeing and reduce inequalities Provide value and live within our means Enhance Quality Be excellent Clinically Well Led 175
192 Report of the Primary Care Procurement Committee meeting Summary of the Meeting Held on 05 October 2017 Items of Business 2017/18 General Practice Resilience Programme The Resilience Funding scheme, provided by NHSE, was for the CCG to support how best allocate the money to practices to their benefit and ultimately, to improve patient care. Consideration was given to establishing reporting mechanisms to enable this Committee to have oversight to how the money was spent with the aim of demonstrating material change. It was agreed that this principle should apply to all Practices listed in the report. The general view was that a prioritisation exercise against the ten criteria listed in the report would have provided greater clarity when allocating funding to practices. Following further discussion, it was confirmed that: The allocations for each of the GP Practices stated in the report had already agreed which meant that the funds could not be for other purposes though, It was within the CCG s gift to identity and recommended GP Practices that it felt may also need support to increase their resilience In practical terms, the CCG was not in a position to authorise the funding could be spent in any other way as this aspect had been determined by an STP Panel (which included Barnet representation) with London Medical Committee representatives. The Committee recommended that the GP Practices who would be awarded this funding should be monitored and be asked to demonstrate how it would improve the quality of their service. Looking ahead, on the assumption that this exercise may be repeated next year, it was recommended that the CCG should take a system wide approach Local Incentive Schemes Improved Access Service Specification The Committee discussed the allocations presented, noting that there had also been a view to use some of the funding towards the CHINs (Care Closer to Home Integrated Networks) and QISTs, (Quality Improvement. Support Teams. The option presented a more flexible approach to how the allocation could be used. NHSE had just issued guidance which included: to stimulate development of providers for improved in hours access to stimulate implementation of the ten high impact actions to free up GP time and to secure sustainability of general practice. It was noted that the funding requested for the CHINs and QIST elements was about 100,000. Discussion focussed on the degree of impact of the additional funding across the Borough and whether there was an opportunity to adopt a more coordinated approach. It was agreed that the work in developing a system of opening up a limited number of appointment slots at GP Practices so that patients could be referred to their GP via A&E and Urgent Care Centres using an on line booking system was regarded a very positive to reduce demand on A&E. It was expected that the system could be rolled out by January 2018, subject to costing (and agreement). The Committee supported the approval of stage 1 of the LCS to commence 1 October 2017 as a whole system (and not piecemeal), subject to the 176
193 functionality costs of developing and establishing an online appointment system for the provider to make to refer patients seeking admittance to A&E and / or urgent care centres to their GP practice for an appointment where appropriate to do so, by January. Summary of the Meeting Held on 02 November 2017 Item of Business Personal Medical Services (PMS) Commissioning Intentions (CIs) The Committee noted the NCL wide approach was being adopted, noting that each of the CCGs in the group had different ratios of practices holding GMS and PMS contracts. Barnet had recently undertaken an engagement process with GP Practices, noting that Barnet had a relatively high proportion of PMS GP Practices The intention of this exercise was to equalise the funding for both GP Practice types The timescale for working up the commissioning intentions was tight, with a report due to be submitted w/c 6 November to NCL setting out the budget lines for years 1 and 2 (i.e. 2018/19 and 2019/20) Account of other activities such as Care Close to Home and Joint Strategic Needs Assessment was being taken into account Note was made that practice funding in isolation showed part of the whole picture with regards to investment into primary care services, Consideration was given as to ensure the processes used to devise the commissioning intentions were conducted robustly. Note was made of the fair and transparent approach with the membership: The Committee considered the next steps, from which members noted: A fully developed set of Commissioning Intentions needed to be ready to submit to Enfield CCG (who is leading on this project) by the 6 November Enfield CCG, as coordinator for this project across NCL was due submit its final proposal to the Director of Performance, NCL, on the 8 November for review and submission to the Primary Care Committee in Common (NCL), in time for the NHSE Assurance meeting. Subject to approval of these commissioning intentions, offer letters would be sent to all GPs on the 4 December and providing them with a three month period for GP to review and sign up to the revised contract. 177
194 178
 Dr Jon Baker Mr Ian Bretman Ms Helen Donovan Dr Rachel Mellins Ms Lisa Robbins NHS BARNET CLINICAL COMMISSIONING GROUP Minutes of the Clinical Quality and Risk")
195 Item Members: Dr Murtaza Khanbhai Chair) Dr Jon Baker Mr Ian Bretman Ms Helen Donovan Dr Rachel Mellins Ms Lisa Robbins NHS BARNET CLINICAL COMMISSIONING GROUP Minutes of the Clinical Quality and Risk Committee held on Thursday 12 October 2017, Shannon Room Building 4, to North London Business Park, London, N11 1NP GP and Governing Body Member, West Locality, BCCG Secondary Care Doctor and Governing Body Member, BCCG Lay Member (PPI), Governing Body Member, BCCG Registered Nurse, Governing Body Member BCCG External GP, Heathfields Medical Centre, Barnet Healthwatch Representative, Barnet In Attendance Mr Eamann Devlin CAMHS Officer, BCCG Ms Valerie Hanson Head of Quality Assurance, BCCG Ms Lisa Savage Commissioning Manager, Planned Care, BCCG (Item 10) Ms Swetlana Wolf Head of Quality Assurance, NELCSU Minutes: Andrew Tillbrook Apologies: Ms Jenny Goodridge Ms Ursula Madine Board Secretary, Interim, BCCG Director of Quality and Clinical Services, BCCG Head of Clinical Quality, BCCG 1. Introduction 1.1 Welcome and Apologies for Absence Dr Murtaza Khanbhai opened the meeting, introductions were made and apologies noted and recorded above. In particular, Ms Swetlana Wolf was welcomed in her capacity to provide support to this Committee during Ms Goodridge s absence, noting that her role was to: maintain quoracy of the Committee by having a member representing the executive lead (ie Ms Goodridge) provide guidance and suggestions to the Committee where appropriate. 2.0 Declaration of Interests 2.1 Members were invited to proffer any new declarations of interest, Dr Khanbhai advised there could be a potential conflict of interest with regard to the Urology service report as it could have a bearing on primary care services. 3.0 Minutes of the previous meeting, 27 July The Minutes of the meeting held on the 27 July 2017 were considered and agreed as an accurate record. Agreed: to approve the minutes of the 27 July 2017 Page 1 of 6 179
NORTH CENTRAL LONDON ( NCL ) JOINT COMMISSIONING COMMITEE
 JOINT COMMISSIONING COMMITEE") NORTH CENTRAL LONDON ( NCL ) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 3 rd August 2017 from 3pm - 4.20pm Seminar Room 2, Resource for London, 356 Holloway Road, London
NORTH CENTRAL LONDON ( NCL ) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 3 rd August 2017 from 3pm - 4.20pm Seminar Room 2, Resource for London, 356 Holloway Road, London
Governing Body Vice Chair and Lay Member, Camden CCG. Governing Body Lay Member, Barnet CCG
 Present: NORTH CENTRAL LONDON (NCL) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 5 October 2017, 15:00-17:00 Conference Hall Cypriot Community Centre Earlham Grove London
Present: NORTH CENTRAL LONDON (NCL) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 5 October 2017, 15:00-17:00 Conference Hall Cypriot Community Centre Earlham Grove London
Commissioning Arrangements in North Central London
 Commissioning Arrangements in North Central London 1 Summary The NHS 5 Year Forward View sets out the direction for the NHS In response, 44 areas across England have been developing Sustainability and
Commissioning Arrangements in North Central London 1 Summary The NHS 5 Year Forward View sets out the direction for the NHS In response, 44 areas across England have been developing Sustainability and
As Chair, DW welcomed attendees to the meeting and apologies were noted. DW also welcomed AL, CWo, LM and NM to their first Programme Board meeting.
 Appendix 1 Joint Commissioning Executive, Care Closer to Home Programme Board Thursday 19 October 2017, 13:30 15:00 Chapman Room, Building 2, North London Business Park Part 1 Commissioners and Providers
Appendix 1 Joint Commissioning Executive, Care Closer to Home Programme Board Thursday 19 October 2017, 13:30 15:00 Chapman Room, Building 2, North London Business Park Part 1 Commissioners and Providers
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April The Broadway, Wimbledon, SW19 1RH
 MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
APPROVED MINUTES OF THE NCL STP PROGRAMME DELIVERY BOARD
 P a g e 1 APPROVED MINUTES OF THE NCL STP PROGRAMME DELIVERY BOARD 15:00-17:00 on Tuesday 10 July 2018 Room 11.10-11.12, 5 Pancras Square, London, N1C 4AG Members PDB role / job title Attended Deputy Apologies
P a g e 1 APPROVED MINUTES OF THE NCL STP PROGRAMME DELIVERY BOARD 15:00-17:00 on Tuesday 10 July 2018 Room 11.10-11.12, 5 Pancras Square, London, N1C 4AG Members PDB role / job title Attended Deputy Apologies
Professional Interests Non-Financial. Personal Interests Is the interest direct or indirect? X Direct Practice Partner
 Haringey CCG Declarations 7.3.18 Name Current position (s) held- i.e. Governing, Member practice, Employee or other Declared Interest- (Name of the organisation and nature of business) Financial Interests
Haringey CCG Declarations 7.3.18 Name Current position (s) held- i.e. Governing, Member practice, Employee or other Declared Interest- (Name of the organisation and nature of business) Financial Interests
AGENDA. Appendix: 0. Action required 1. Introduction 1.1 Apologies for Absence Declarations of Interest Declarations of Gifts and Hospitality
 Appendix: 0 Islington Clinical Commissioning Group Governing Body Business Meeting Wednesday, 9 May 2018 9.30-11.30 Laycock PDC, Laycock Street London N1 1TH AGENDA PART 1 Please look over the agenda and
Appendix: 0 Islington Clinical Commissioning Group Governing Body Business Meeting Wednesday, 9 May 2018 9.30-11.30 Laycock PDC, Laycock Street London N1 1TH AGENDA PART 1 Please look over the agenda and
North Central London Medicines Optimisation Network. Terms of Reference. North Central London Medicines Optimisation Network 1 of 8
 North Central London Medicines Optimisation Network Medicines Optimisation Committee Terms of Reference North Central London Medicines Optimisation Network 1 of 8 Document control Date Version Amendments
North Central London Medicines Optimisation Network Medicines Optimisation Committee Terms of Reference North Central London Medicines Optimisation Network 1 of 8 Document control Date Version Amendments
Governing Body Vice Chair and Lay Member, Camden. Governing Body Chair, Camden CCG
 NCL Joint Commissioning Committee Thursday 5 th October 2017 3-5pm Main Conference Hall Cypriot Community Centre Earlham Grove London N22 5HJ Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel
NCL Joint Commissioning Committee Thursday 5 th October 2017 3-5pm Main Conference Hall Cypriot Community Centre Earlham Grove London N22 5HJ Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel
PRESENT ACTION OPENING ADMINISTRATION
 PRESENT NHS Barnet Clinical Commissioning Group Governing Body Meeting held in Public Thursday 26 January 2017 09:30 to 12:00 Committee Room One, Hendon Town Hall Debbie Frost DF NHS Barnet CCG Chair (West
PRESENT NHS Barnet Clinical Commissioning Group Governing Body Meeting held in Public Thursday 26 January 2017 09:30 to 12:00 Committee Room One, Hendon Town Hall Debbie Frost DF NHS Barnet CCG Chair (West
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years
 Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Haringey CCG Governing Body 9 November STP 6 month progress report
 Haringey CCG Governing Body 9 November 2017 STP 6 month progress report Helen Pettersen Accountable Officer & STP Convenor Will Huxter Director of Strategy North Central London CCGs Ambition of the STP
Haringey CCG Governing Body 9 November 2017 STP 6 month progress report Helen Pettersen Accountable Officer & STP Convenor Will Huxter Director of Strategy North Central London CCGs Ambition of the STP
Appendix 5.2 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Thursday, 15 March 2018 TITLE: LEAD DIRECTOR:
 Appendix 5.2 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Thursday, 15 March 2018 TITLE: LEAD DIRECTOR: AUTHOR: CONTACT DETAILS: Performance & Quality Summary (P&Q) Alex
Appendix 5.2 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Thursday, 15 March 2018 TITLE: LEAD DIRECTOR: AUTHOR: CONTACT DETAILS: Performance & Quality Summary (P&Q) Alex
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
1.1.1 Apologies were received from Dr Dina Dhorajiwala, David Graham, Tony Hoolaghan, and Rachel Lissauer.
 Minutes Meeting of the Haringey Clinical Commissioning Group Finance and Performance Committee 14 December 2017 at 1.00pm Room 7, Level 4, River Park House Present: Dr John Rohan JR GP Governing Body Member,
Minutes Meeting of the Haringey Clinical Commissioning Group Finance and Performance Committee 14 December 2017 at 1.00pm Room 7, Level 4, River Park House Present: Dr John Rohan JR GP Governing Body Member,
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
The North Central London Sustainability and Transformation Plan. and. Camden Local Care Strategy. Caz Sayer Chair, Camden CCG
 The North Central London Sustainability and Transformation Plan and Camden Local Care Strategy Caz Sayer Chair, Camden CCG About the Sustainability & Transformation Plan (STP) N C L North Central London
The North Central London Sustainability and Transformation Plan and Camden Local Care Strategy Caz Sayer Chair, Camden CCG About the Sustainability & Transformation Plan (STP) N C L North Central London
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING A&E DELIVERY AND URGENT CARE BOARD UPDATE
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING A&E DELIVERY AND URGENT CARE BOARD UPDATE Date of the meeting 17/05/2017 Author Sponsoring GB member Purpose of Report Recommendation Stakeholder
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING A&E DELIVERY AND URGENT CARE BOARD UPDATE Date of the meeting 17/05/2017 Author Sponsoring GB member Purpose of Report Recommendation Stakeholder
Governing Body Vice Chair and Lay Member, Enfield CCG. Governing Body Lay Member, Camden CCG
 NCL Joint Commissioning Committee Thursday 5 th April 2018 3-5pm Hendon Town Hall Committee Room 1 The Burroughs London NW4 4BG Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel Brookes Dr Peter
NCL Joint Commissioning Committee Thursday 5 th April 2018 3-5pm Hendon Town Hall Committee Room 1 The Burroughs London NW4 4BG Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel Brookes Dr Peter
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
NWL STP plans for the last phase of life
 NWL STP plans for the last phase of life Dr Tim Spicer, GP & Chair of Hammersmith & Fulham CCG & Toby Hyde, Head of Strategy Hammersmith & Fulham CCG NW London Sustainability & Transformation Plan Improving
NWL STP plans for the last phase of life Dr Tim Spicer, GP & Chair of Hammersmith & Fulham CCG & Toby Hyde, Head of Strategy Hammersmith & Fulham CCG NW London Sustainability & Transformation Plan Improving
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Therefore to accommodate these conflicting issues, the following contracting arrangements are proposed:
 Appendix: 3.3b North Central London CCGs Collaboration Arrangements for Contracting 22-1-13 Introduction Across the 5 CCGs in North Central London, the total value of all contracts excluding non clinical
Appendix: 3.3b North Central London CCGs Collaboration Arrangements for Contracting 22-1-13 Introduction Across the 5 CCGs in North Central London, the total value of all contracts excluding non clinical
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016
 Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Appendix 5.5. AUTHOR & POSITION: Jill Shattock, Director of Commissioning CONTACT DETAILS:
 Appendix 5.5 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE Wednesday, 30 July 2014 TITLE: North Central London (NCL) NHS 111 and GP Out of Hours LEAD GOVERNING Jill Shattock,
Appendix 5.5 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE Wednesday, 30 July 2014 TITLE: North Central London (NCL) NHS 111 and GP Out of Hours LEAD GOVERNING Jill Shattock,
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 26 th January 2106 Agenda No: 5 Attachment: 04 Title of Document: Clinical Chair and Chief Officer Report Report Author: Adam
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 26 th January 2106 Agenda No: 5 Attachment: 04 Title of Document: Clinical Chair and Chief Officer Report Report Author: Adam
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Developing primary care in Barnet
 Developing primary care in Barnet Introduction In January 2012, the Joint Boards of NHS North Central London (NCL) approved a NCL Primary Care Strategy, which describes development of the primary care
Developing primary care in Barnet Introduction In January 2012, the Joint Boards of NHS North Central London (NCL) approved a NCL Primary Care Strategy, which describes development of the primary care
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
A meeting of Bromley CCG Primary Care Commissioning Committee 22 March 2018
 A meeting of Bromley CCG Primary Care Commissioning Committee 22 March 2018 ENCLOSURE 7 PROPOSAL FOR ENHANCED MEDICAL SUPPORT TO BROMLEY CARE HOMES SUMMARY: Bromley CCG gained agreement at the CCG Clinical
A meeting of Bromley CCG Primary Care Commissioning Committee 22 March 2018 ENCLOSURE 7 PROPOSAL FOR ENHANCED MEDICAL SUPPORT TO BROMLEY CARE HOMES SUMMARY: Bromley CCG gained agreement at the CCG Clinical
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY. TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10. Chair Dr Tony Martin
 - 13:00-13:10. Chair Dr Tony Martin") NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY HELD IN THE HARBOUR SANDS MEETING ROOM, 3 RD FLOOR, THANET DISTRICT COUNCIL TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10 Chair
NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY HELD IN THE HARBOUR SANDS MEETING ROOM, 3 RD FLOOR, THANET DISTRICT COUNCIL TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10 Chair
Reviewing and Assessing Service Redesign and/or Change Proposals
 Reviewing and Assessing Service Redesign and/or Change Proposals RCN guidance CLINICAL PROFESSIONAL RESOURCE Acknowledgements Helen Donovan, RCN Professional Lead for Public Health Nursing David Dipple,
Reviewing and Assessing Service Redesign and/or Change Proposals RCN guidance CLINICAL PROFESSIONAL RESOURCE Acknowledgements Helen Donovan, RCN Professional Lead for Public Health Nursing David Dipple,
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Update Report to Clinical Members. Quarter 3; what have we done so far
 Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
North West London Accident and Emergency Performance Report for the winter of 2016/17. North West London Joint Health Overview and Scrutiny Committee
 North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
Minutes: Quality and Safety Committee (QSC) Date Wednesday 20 May 2015 Time 10:00-13:00 Venue. 5.3, 15 Marylebone Road, London, NW1 5JD
 Date Wednesday 20 May 2015 Time 10:00-13:00 Venue. 5.3, 15 Marylebone Road, London, NW1 5JD") Minutes: Quality and Safety Committee (QSC) Date Wednesday 20 May 2015 Time 10:00-13:00 Venue 5.3, 15 Marylebone Road, London, NW1 5JD Present Dr Neville Purssell NP GP, CLCCG and Governing Body Member
Minutes: Quality and Safety Committee (QSC) Date Wednesday 20 May 2015 Time 10:00-13:00 Venue 5.3, 15 Marylebone Road, London, NW1 5JD Present Dr Neville Purssell NP GP, CLCCG and Governing Body Member
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
WOLVERHAMPTON CCG. Governing Body Meeting 9 th September 2014
 WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Contract Award Recommendation for NCL Direct Access Diagnostics Service Tim Deeprose/Leo Minnion
 Appendix 5.4 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Wednesday, 26 March 2014 TITLE: LEAD DIRECTOR/ MANAGER: CLINICAL LEADS AUTHORS: CONTACT DETAILS: Contract Award
Appendix 5.4 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Wednesday, 26 March 2014 TITLE: LEAD DIRECTOR/ MANAGER: CLINICAL LEADS AUTHORS: CONTACT DETAILS: Contract Award
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
MEMORANDUM OF UNDERSTANDING
 MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
Quarterly Reporting Template - Guidance
 Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Cabinet Member for Education, Children and Families
 Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
CCG Annual General Meeting (AGM) AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs
 AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs") CCG Annual General Meeting (AGM) AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs Riverside Centre, The Quay, Newport, Isle of Wight, PO30 2QR Item Item Title/Heading Initial Paper No /Attachment 1.
CCG Annual General Meeting (AGM) AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs Riverside Centre, The Quay, Newport, Isle of Wight, PO30 2QR Item Item Title/Heading Initial Paper No /Attachment 1.
AGENDA Lead Action required Appendices
 Meeting in Public of the Enfield Clinical Commissioning Group Governing Body 11 May 2016 2.30pm to 5pm Millfield House Silver Street Edmonton N18 1PJ AGENDA Lead Action required Appendices 1. Welcome and
Meeting in Public of the Enfield Clinical Commissioning Group Governing Body 11 May 2016 2.30pm to 5pm Millfield House Silver Street Edmonton N18 1PJ AGENDA Lead Action required Appendices 1. Welcome and
Integrated Care in North Central London
 Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Kingston Clinical Commissioning Group Report Summary
 Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 7 th November 2017 Report Title Health & Well Being Board Minutes 14 th September 2017 Agenda Item 15 Attachment
Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 7 th November 2017 Report Title Health & Well Being Board Minutes 14 th September 2017 Agenda Item 15 Attachment
Paper 5.0 SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE.
 SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE December 2015 Version 2.2 Paper 5.0 1 Purpose This document sets out the proposed new
SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE December 2015 Version 2.2 Paper 5.0 1 Purpose This document sets out the proposed new
Lincolnshire County Council: Councillors Mrs W Bowkett, R L Foulkes, C R Oxby and N H Pepper
 1 PRESENT: COUNCILLOR MRS S WOOLLEY (CHAIRMAN) LINCOLNSHIRE HEALTH AND WELLBEING BOARD Lincolnshire County Council: Councillors Mrs W Bowkett, R L Foulkes, C R Oxby and N H Pepper Lincolnshire County Council
1 PRESENT: COUNCILLOR MRS S WOOLLEY (CHAIRMAN) LINCOLNSHIRE HEALTH AND WELLBEING BOARD Lincolnshire County Council: Councillors Mrs W Bowkett, R L Foulkes, C R Oxby and N H Pepper Lincolnshire County Council
TERMS OF REFERENCE. Transformation and Sustainability Committee. One per month (Second Thursday) GP Board Member (Quality) Director of Commissioning
 GP Board Member (Quality) Director of Commissioning") TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
In Attendance: Arlene Sheppard (AMS) Note Taker WNCCG Sarah Haverson (SHv) Commissioning Support Officer WNCCG
 Note Taker WNCCG Sarah Haverson (SHv) Commissioning Support Officer WNCCG") Agenda Item: 17.62 DRAFT Minutes of West Norfolk Primary Care Commissioning Committee Part One (Quorate) Held on 26th May 2017 2pm Education Room, Town Hall, Saturday Market Place, Kings Lynn PE30 5DQ
Agenda Item: 17.62 DRAFT Minutes of West Norfolk Primary Care Commissioning Committee Part One (Quorate) Held on 26th May 2017 2pm Education Room, Town Hall, Saturday Market Place, Kings Lynn PE30 5DQ
Engagement Summary. North London Partners Urgent and Emergency Care Programme. Camden Barnet Enfield Haringey Islington
 Engagement Summary North London Partners Urgent and Emergency Care Programme Camden Barnet Enfield Haringey Islington Introduction This report summarises a year-long programme of engagement undertaken
Engagement Summary North London Partners Urgent and Emergency Care Programme Camden Barnet Enfield Haringey Islington Introduction This report summarises a year-long programme of engagement undertaken
MINUTES. Name of meeting. Quality and Clinical Governance Committee. Date and time Tuesday 2 May :30-17:00. Venue. Board Room, Dominion House
 MINUTES Name of meeting Quality and Clinical Governance Committee Date and time Tuesday 2 May 2017 14:30-17:00 Venue Board Room, Dominion House Name Title Chair Dr Sue Tresman (ST) Lay Vice Chair (Lay
MINUTES Name of meeting Quality and Clinical Governance Committee Date and time Tuesday 2 May 2017 14:30-17:00 Venue Board Room, Dominion House Name Title Chair Dr Sue Tresman (ST) Lay Vice Chair (Lay
Adults and Safeguarding Committee 19 March Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy.
 Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
CONTINUING HEALTHCARE POLICY
 BEFORE USING THIS POLICY ALWAYS ENSURE YOU ARE USING THE MOST UP TO DATE VERSION CONTINUING HEALTHCARE POLICY 1 SUMMARY This policy describes the way in which the five Primary Care Trusts in NHS North
BEFORE USING THIS POLICY ALWAYS ENSURE YOU ARE USING THE MOST UP TO DATE VERSION CONTINUING HEALTHCARE POLICY 1 SUMMARY This policy describes the way in which the five Primary Care Trusts in NHS North
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
City Integrated Commissioning Board
 Meeting-in-common of the City & Hackney Clinical Commissioning Group and City of London Corporation City Integrated Commissioning Board Meeting on Tuesday 23 May, 09:30-11:30 Tomlinson Centre, Queensbridge
Meeting-in-common of the City & Hackney Clinical Commissioning Group and City of London Corporation City Integrated Commissioning Board Meeting on Tuesday 23 May, 09:30-11:30 Tomlinson Centre, Queensbridge
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality and Safety
 Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow
 CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow Present In Attendance Prash Gupta (PG) HCCG (Chair) Natasha Malhotra (NM)
CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow Present In Attendance Prash Gupta (PG) HCCG (Chair) Natasha Malhotra (NM)
UCLH CANCER COLLABORATIVE VANGUARD BOARD TERMS OF REFERENCE
 UCLH CANCER COLLABORATIVE VANGUARD BOARD TERMS OF REFERENCE 1. PURPOSE & SCOPE Picking up the challenge and aspirations of the five year forward view and the Taskforce, the UCLH Collaborative provides
UCLH CANCER COLLABORATIVE VANGUARD BOARD TERMS OF REFERENCE 1. PURPOSE & SCOPE Picking up the challenge and aspirations of the five year forward view and the Taskforce, the UCLH Collaborative provides
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Apologies Lay Member Financial Management & Audit
 Primary Care Commissioning Committee Unratified Minutes of the Public Meeting held on Thursday 2 August 2018, 09:30 10:45 Committee Room, Gedling Civic Centre, Arnot Hill Park Members Mike Wilkins (MW)
Primary Care Commissioning Committee Unratified Minutes of the Public Meeting held on Thursday 2 August 2018, 09:30 10:45 Committee Room, Gedling Civic Centre, Arnot Hill Park Members Mike Wilkins (MW)
Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper
 1. Purpose of this paper Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper This paper sets out the rationale for investment in new more effective urgent care pathways for people
1. Purpose of this paper Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper This paper sets out the rationale for investment in new more effective urgent care pathways for people
FINAL MINUTES. Associate Director of Quality and Improvement. Senior Quality and Performance Analyst. Deputy Director of Clinical Commissioning
 Item No: 5.3 Paper No: 24 Name of meeting FINAL MINUTES Quality and Clinical Governance Committee Date and time Tuesday 6 September 2016; 14:30-16:30 Venue Board Room, Dominion House Name Title Chair Dr
Item No: 5.3 Paper No: 24 Name of meeting FINAL MINUTES Quality and Clinical Governance Committee Date and time Tuesday 6 September 2016; 14:30-16:30 Venue Board Room, Dominion House Name Title Chair Dr
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Co-Commissioning Arrangements in Primary Care (GP practices) - Principles and Process for managing Quality and Contracting
 - Principles and Process for managing Quality and Contracting") Co-Commissioning Arrangements in Primary Care (GP practices) - Principles and Process for managing and Contracting 1. Purpose The CCG will have delegated authority to commission primary care (For clarity,
Co-Commissioning Arrangements in Primary Care (GP practices) - Principles and Process for managing and Contracting 1. Purpose The CCG will have delegated authority to commission primary care (For clarity,
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT
 9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...