Appendix 3. Option Appraisal The Provision of Intermediate Care Services in the North Down and Ards Areas
|
|
|
- Milo Wood
- 6 years ago
- Views:
Transcription
1 Appendix 3 Option Appraisal The Provision of Intermediate Care Services in the North Down and Ards Areas January 2015
2 Contents Section 1.0 Introduction 3 Page number 2.0 Background Future Service Model Strategic Context Existing Service Profile Objectives and constraints Formulation and Evaluation of Options Non-Financial Benefits Appraisal Quantitative Analysis Conclusion 73 2
3 1.0 Introduction This document presents the strategic context and options appraisal process for the future provision of intermediate care services for the North Down and Ards localities in the South Eastern Health and Social Care Trust (SET). The current service profile section describes the existing service provision; and the strategic context section identifies the case for change through analysis of regional, national and local policy context and the requirement for future service provision. This paper details the appraisal process undertaken by the Trust including the establishment of project objectives, an explanation of constraints, the generation of options to meet objectives and an evaluation of costs and benefits of shortlisted options, financial evaluation and the identification of the preferred option. 2.0 Background On 1 April 2007, the South Eastern Health & Social Care Trust (SET) was established amalgamating the former Down &Lisburn and Ulster Community & Hospitals HSS Trusts. The SET is a community and acute hospitals Trust that provides integrated health and social services to the population of North Down, Lisburn, Down and Ards Council areas and acute services to a wider catchment, which takes in parts of east Belfast. The Trust provides acute and community services to a resident population of 349,618 in the above local government districts (source: Northern Ireland Statistics and Research Agency (NISRA) Mid-Year Population Estimates). 3

4 The South Eastern Health and Social Care Trust vision is to be a leading provider of high quality health and social care for our patients, clients and carers. We will achieve this, in partnership with others, by making sure that our services are safe and effective, improving and providing a positive outcome and experience. 2.1 Financial Context All Trusts have a statutory breakeven duty (contained in circular HSS (F) 25/2000) by the end of each financial year (1 April to 31 March). During this financial year 2014/15, the South Eastern Trust recognised a shortfall in the funding to meet all the costs of delivering services due to increasing financial pressures and the lateness of the budgetary settlement for the NI Executive. A number of factors, including an ageing population, complexity of conditions and an increase in demand for our services have contributed to these pressures. The entire health and social care sector is facing unprecedented financial challenges in the current year with a deficit forecast at around 200m. A significant element of this, approximately ( 160m) has been resolved regionally in year; however, the remaining 30m - 40m rests with the health and social care trusts to deliver. The South Eastern Trust was required to implement a series of contingency measures to 4
5 deliver 5m of savings in order to achieve financial breakeven for the 2014/15 financial year. In its contingency plan, the Trust identified a number of proposals that would contribute to achieving the required savings by the end of the year. When developing the proposals, the Trust s top priority was ensuring patient and client safety. The Trust had to focus both on areas that could result in reduced spend quickly and, where possible, on areas in line with strategic direction of travel. Meeting the savings targets outlined in contingency plans is extremely challenging. One of the contingency measures proposed by the Trust was the temporary closure of 20 inpatient beds in Bangor Hospital, which was introduced to assist the Trust to achieve financial breakeven. This was approved by the HSCB / PHA / and the Minister of the Department of Health, Social Services and Public Safety on 30 October 2014 and the temporary closure took effect on 1 December Whilst it was not feasible to carry out a consultation on the temporary closure, the Trust is committed to consulting on a permanent arrangement for intermediate care provision in North Down and Ards. The Temporary closure will remain in place until the public consultation and associated decision making processes are concluded. For the 2015/16 financial year the current estimated deficit identified for the South Eastern Trust is 17.5m. The Trust is therefore required to implement a range of savings plans to ensure financial break even. One of the proposals the Trust is considering and which this document addresses, is the review of intermediate care services for the North Down and Ards area. 2.2 Service Context Intermediate care is an in-patient stay in one of the Trusts Intermediate Care beds. These beds provide a period of recovery and rehabilitation for a patient after a spell of acute illness or trauma. The beds are mainly used by patients after they have had a stay in an acute hospital and no longer need acute medical input but are not quite ready to go home. The Health and Social Care Board in 2013 issued guidance on Principles for Medical Cover for Intermediate Care Beds this guidance outlines the King s Fund definition of Intermediate Care as follows 5
6 A short-term intervention to promote and preserve the independence of people who might otherwise face unnecessarily prolonged hospital stays, or inappropriate admission to hospital or residential care. The care is person centred, focused on rehabilitation and delivered by a combination of professional groups with either a therapeutic or specialist medical lead where required. The current service model for Intermediate Care services is provided at section 5 of this report. The Trust is in the process of implementing new service initiatives, supported through Integrated Care Partnerships (ICP) to deliver the recommendations of Transforming Your Care, in that patients will have rapid access to diagnosis and treatment and receive enhanced care services in their own homes. Coupled with unscheduled care reform and an internal review of the beds purchased in the Independent Sector, the Trust believes that this review of Intermediate Care is timely. This is in-line with the future service model for intermediate care services which is described in full at section 3 of this report. 6
7 3.0 Future Service Model This section outlines the proposed model of care for the future development of health and social care delivery for the South Eastern Trust. The service model is patient centred and based on a five level approach: Level 0 Patient Home; Level 1 Local Health and Care Centres ( Spoke ); Level 2 Primary and Community Care Centres ( Hub ); Level 3 Local Hospitals; and Level 4 Acute Hospitals. Figure 1 South Eastern Trust Model of Care Patient Level 1 - Health Centres (spokes) Local GP Practices. District Nursing Specialist Nursing. Treatment Room Nursing. Health Visiting. Level 2 - PCCCs (hubs). Community Mental Health. Family Planning (including Sexual Health). Shared Services - Diagnostics. Imaging. Cancer-supportive and chemotherapies. AHP. ICATS. Social Services. Psychology. Rehabilitation. Marie Curie. One Stop Assessment. Patient experience Level 3 - Local/Sub Acute Hospitals ED/Enhanced GP Out of Hours. Day Surgery. Endoscopy. Specialist Investigations testing. Level 4 - Acute Hospital General Surgery. General Medicine. Gynaecology. Cardiology. Trauma and Orthopaedic Surgery. Plastic Surgery. Maxillofacial Surgery. Healthcare for Elderly. ED. Critical Care services. Paediatric Medicine (including infectious diseases). Paediatric Surgery Renal Services. Haematology. Chemotherapy. Comprehensive range of outpatient services The development of a new integrated model of care for community and hospital services reflects the recommendations within Transforming Your Care 2011(TYC). 7
8 The focus is on placing the individual at the centre of the model with services becoming increasingly accessible in the local community which will promote a better outcome for the user, carer and their family. By redesign of primary, community services, links to the local hospital network and the Acute Hospital the Trust intends to develop integrated care which fosters positive working relationships. This model will be a significant shift from the provision of services in hospitals to the provision of services within the community, in the GP surgery and closer to home, where it is safe and effective to do this. This will result in the delivery of a quality service which provides safe and effective care outcomes for the patient/client. Throughout the review that informed Transforming Your Care, people expressed their preference for care at home or as close to home as possible. In response to this, any new model should provide more support to help people who are sick or frail to maintain their independence and stay in their own homes for as long as possible. This applies whether that home is the family home, supported housing, nursing home or residential home. Since its formation in 2007, the Trust has developed a strategic vision for a Single Acute Hospital at the Ulster Hospital site, and a local hospital model for Downe and Lagan Valley Hospitals supported by a Primary and Community Care Centre in each of the four Trust localities. The Trust is committed to develop specialist centres of chronicity, through the provision of a Primary and Community Care Centre or Hub in each locality. This is in keeping with the Bamford Review, Older People s Strategy and Regional Dementia Strategy. 8

9 Figure 2 South Eastern Trust Hubs The new model focuses on providing opportunities to integrate care which crosses professional boundaries to benefit patients, clients and families. The emphasis has been placed on creating an environment to maximise multi-disciplinary and multiprofessional team working and encourage shared opportunities for developing links within Health and Social Care and with external health care partners. The success of this model will be dependent on the ability to maximise the use of appropriate technology to promote service integration thereby improving patient outcomes. This model will be integral to the Trust s four significant change areas as outlined in the Trust s Population Plan in response to Transforming Your Care: Early Intervention and the promotion of disease prevention models to improve health and wellbeing. Acute reconfiguration to deliver hospital services in the South Eastern Locality that improve quality and optimise the use of resources. Greater service integration and a shift of services from secondary to primary care settings to promote patient centred care. Supporting our older population to help them live independently in their own homes for as long as possible. 9
10 Model of Care for Level 3 Local Hospital Services Down Hospital Lagan Valley Hospital Emergency Department / Enhanced GP Out of Hours; Day Surgery; Endoscopy; Specialists Investigations e.g. Cardiology, Imaging, Pulmonary Function testing; Inpatient Medical Beds including Endocrine, Respiratory, GI, Cardiology, Care of Elderly and Stroke; Midwife Led Unit; Mental Health (Adult); Dementia Inpatient Beds; Rehabilitation; Ambulatory Care; and Specialist Outpatients. Model of Care for Level 2 PCCC Hub Bangor PCCC GP Practices; District Nursing/Specialist Nurses; Treatment Room Nursing; Health Visiting; Community Mental Health; Psychology Services; Family Planning (including Sexual Health); Social Care for Older People; Children s Centre (including CAMHS); Cancer Health and Wellbeing Centre; Voluntary Groups; 10
11 Complementary therapies; Bookable space for use by e.g. Maternity services, Integrated Clinical Assessment and Treatment Services (ICATS), Outpatient clinics; Dentistry; Allied Health Professionals including Physiotherapy, Occupational Therapy, Podiatry, Speech and Language Therapy; ICATS; and Health Development. Model of Care for Level 2 PCCC Hub including Urgent Care Centre Lisburn PCCC Downe PCCC Ards PCCC The following services will be included within three of the four Trust PCCC Hubs: Reference: HSCB Commissioning Plan 2014/15 Section 8.2 and These services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. Minor Injuries Intermediate Care Beds GP Out of Hours (GPOOHs) It is the Trust s view that intermediate care beds should be consolidated and collocated with both Minor Injuries and GP OOHs services, in order to maximise clinical adjacencies. Shared / Integrated Services The opportunity for integrated care for the patient will be considered through the access to and use of the following: Diagnostics; Imaging; Cancer- supportive and chemotherapy treatments; 11
12 Allied Health Professions (Dietetics, Dental, Physiotherapy, Occupational Therapy, and Speech and Language Therapy); ICATS; Social Services; Psychology; Rehabilitation; Voluntary sector; One Stop Assessment; and Patient Experience. Ultimately, it is anticipated that this service model will: Ensure that the professionals providing health and social care services will be required to work together in a much more integrated way to plan and deliver consistently high quality care for patients; Ensure that most services will be provided locally, for example, diagnostics, outpatients and urgent care, and local services will be better joined up with specialist hospital services; Reduce inpatient surgical beds and reconfigure medical inpatient beds; Increase day surgery/endoscopy; Increase screening/ prevention therapies; Increase ambulatory care to include Outpatients/Diagnostic services; Develop Emergency /GP Out of Hours Urgent Care Model integration; 3.1 North Down & Ards Supporting Information The 2013 South Eastern Local Commissioning Group s Strategic Commissioning Statements in regards to Primary and Community Care Infrastructure Service Requirements notes that: Bangor also has a community hospital which includes 20 step-up/step-down beds as well as a range of clinic and diagnostic facilities. There is no capacity within this site 12
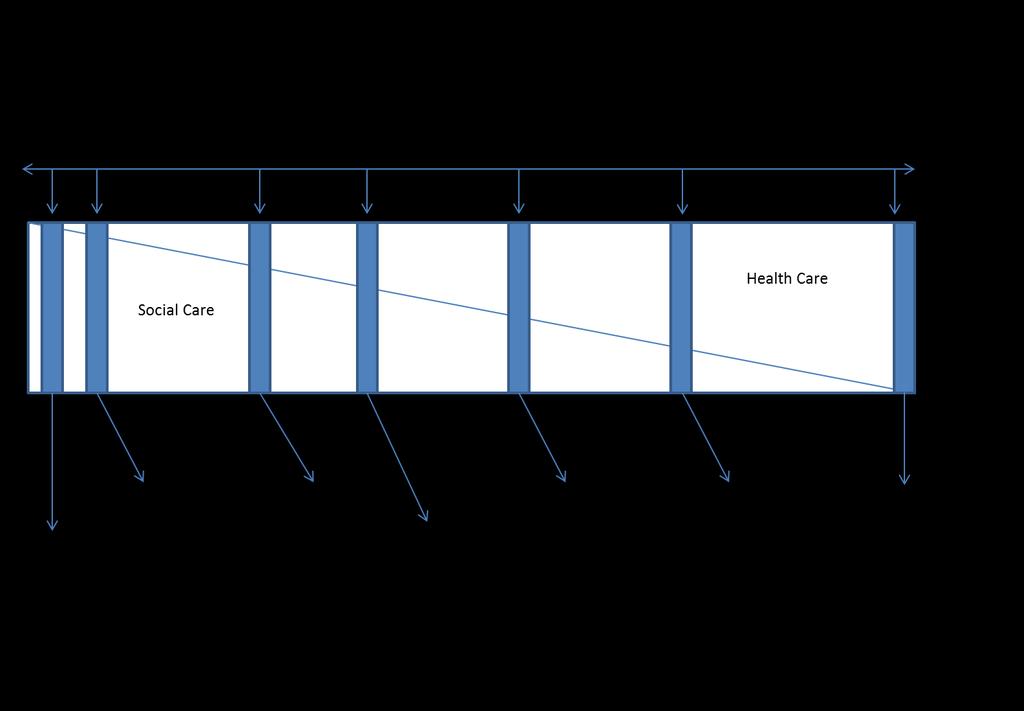
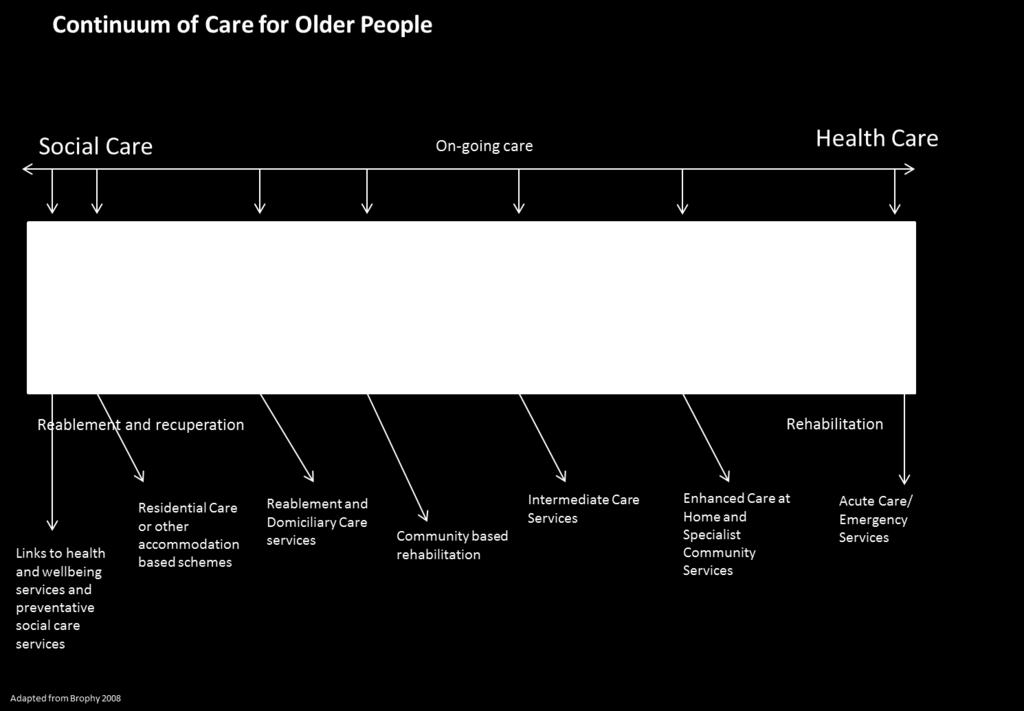
13 for further development. As part of TYC, ICPs will be bringing forward a range of plans to manage many of the conditions for which patients use the Bangor Hospital. The document also reflects the Trust s future vision for the North Down and Ards area. Locality meetings with GPs confirmed their support for the suggested development of four South Eastern Trust Hubs in Lisburn, Downpatrick, Newtownards and Bangor. There was, however, some initial discussion around the potential of a single hub that might serve the populations of Newtownards, Bangor and Comber together with the more dispersed population of the Ards peninsula. However, after further consideration and engagement on this option, there was general consensus that these localities merited separate hubs based on the geographical spread and demographic profile of the population - though given their close proximity the service model should be carefully considered to avoid unnecessary duplication of services. (Source: SELCG Strategic Commissioning Statement re Primary and Community Care Infrastructure Service Requirements July 2013). The Trust s vision clearly articulates a model of four Primary and Community Care Centre Hubs, two of which will be located in North Down and Ards localities. As noted above, the Bangor facility will be a PCCC Hub whist the Ards facility will encompass a PCCC including Urgent Care Centre. The ongoing Primary Care Infrastructure Development programme has been established to facilitate the required investment in community facilities to enable the shift of services outlined in TYC. Both new build facilities required by the Trust have been included in its Strategic Capital Priorities Review to the DHSSPSNI, outlining the key projects / capital investments required for the Trust to deliver its strategic objectives, based on the recommendations of Transforming Your Care. 3.2 Future Service Model for Older People In line with the recommendations from Transforming Your Care 2011 for the Future Model for Integrated Health and Social Care, the Trust s vision for services for older people in the future has been developed. The Trust model of care for older people, aims to encapsulate the wide range of statutory and community based services, as a continuum of care, spanning health and wellbeing, social care, rehabilitation and reablement linking through to long term care and acute care. This model will be 13

14 better at preventing ill health, will provide patient-centred care, will help manage demand for services, will tackle health inequalities, deliver high-quality evidence based services, and ensure sustainability and value for money. The model has four key pillars:- The model builds on the care already being provided focusing on Improving the health and wellbeing of older people through the development of a targeted range of health and wellbeing services that will address the specific locality based needs of the older population. This will be via a coordinated local network model with a single access point for all services including, falls prevention, social isolation, physical activity, nutrition, information and medication. Better and more responsive care at home to manage those with complex health and social care needs in the most appropriate place. This will be through multi-disciplinary community based services, such as Enhanced Care at Home, working with Integrated Care Partnerships and General Practitioners aiming to avoid hospital admission and ensure direct access for General Practitioners to the appropriate diagnostic services. An ethos of reablement and rehabilitation so that older people regain the maximum level of independence possible and are able to remain in their own home safely. 14
15 Sustaining the continuum of care (of which intermediate care is a function) that incorporates a wide range of services, to support the local population to receive acute care when necessary, to receive on-going care as appropriate and to access specialist care at the right time and in the right place. The provision of rapid access to assessment and treatment for older people and bridge the gap between Primary and Secondary Care services by creating the opportunity for same day discussion and support on patient management and treatment options between General Practitioners and Senior Hospital Doctors. This also will link with initiatives to develop one stop assessment centres for older people and with the development of a frailty unit, which would ensure the comprehensive assessment of older people seeking emergency care. Increased focus on the role of technology to support our services and service users to manage and support their health and wellbeing. This would be through maximising the use of Telehealth and Telecare services that support a range of long term conditions and help ensure a person s safety at home. Innovation and service development, will be enabled through working in partnership with local industry and through research and development to seek out new and innovative ways to support older people to live independent lives, while remaining safe and confident to manage their health and wellbeing. This model will enhance and maintain the health and wellbeing and independence of older people and provide a range of integrated services that will promote faster recovery from illness, prevent unnecessary acute hospital admission and premature admission to long-term residential care, support timely discharge from hospital and maximise independent living. 15
16 16
17 3.3 Intermediate Care The Trust has agreed a number of general principles in its approach to reviewing Intermediate Care services. These include: Services will be safe, sustainable, person-centred. They will be planned, implemented and evaluated in partnership with users and carers. Services will promote independence, recovery and rehabilitation, supporting people to live at home. Everyone has the right to experience the same level of service regardless of location. To ensure appropriate access to Intermediate Care services based on assessed need. Services will be provided in an environment which is fit for purpose with the appropriate level of medical intervention The services we deliver will be evidence-based, of high quality, and provide improved outcomes for patients and clients. Staff will be supported in their professional and personal development. Services will be delivered in an efficient and effective manner. Services will promote positive health, wellbeing and early intervention. As described above, TYC has outlined a shift from the provision of services in hospitals to the provision of services within the community, in the GP surgery and closer to home. It is anticipated that Intermediate Care beds should be provided as close to the patient home as possible, with enhanced Community Stroke Rehabilitation, Reablement and Intermediate Care services provided within the patient home or within a PCCC Hub. The Reablement programme will assist the Trust in driving the transformation outlined in the population plan by promoting greater independence for older people at home using short-term support services following a hospital admission or health or social care crisis at home and reduce referrals for long term domiciliary care support. This approach will ensure that older people receive the level of support required to maximise independence. 17
18 4.0 Strategic Context This section sets out the strategic context which underpins the review of Intermediate Care Services, which is significant in determining how services will be delivered in the future. The Trust s strategic direction has largely been influenced by a number of drivers for change. These include the Transforming Your Care, December 2011 and the commissioning intentions as indicated by the Health and Social Care Board through Commissioning Plan and Commissioning Specifications 2013/14 and the Commissioning plan and Commissioning Specifications of 2014/ Transforming Your Care (2011) The Review of the Provision of Health and Social Care Services in Northern Ireland announced by the Minister for Health, Social Services and Public Safety in June 2011, has produced a report which offers an assessment of all aspects of health and social care, and includes 99 recommendations. Overall, the Review is positive in tone, identifies and addresses the challenges that lie ahead and sets in place a framework for future changes in Health and Social Care. The Review has presented a methodology to implement change over the next five years. It outlines a clear direction of travel as follows: starting with the individual. looking to a greater focus on prevention. maintaining care close to home. re-designing primary care. re-shaping hospitals. 4.2 Commissioning Plan 2013/14 The 2013/14 South Eastern LCG Commissioning Plan outlined a commitment to four Primary and Community Care Centre Hubs for the South Eastern Trust within 18
19 Lisburn, Newtownards, Bangor and Downpatrick. This was further clarified within the 2014/15 document. 4.3 Commissioning Plan 2014/15 (January 2015) The 2014/15 Health and Social Care Board and Public Health Agency Commissioning Plan highlights the Commissioner s intention for further reform of the urgent care model in the South Eastern Trust. The document states, at section 8.2, that The South Eastern LCG views our service hubs (referred to as PCCC Hubs with Urgent Care Centres within Trust Model of Care in section 3) in the Downe Hospital, the Ards Hospital site and the Lagan Valley Hospital site as key enablers to ensuring good community access to future local services. Note: This document does not reference commissioner support for the inclusion of an Urgent Care Centre within the Bangor PCCC Hub. Section 8.4.1, of the plan indicates that the Ulster Hospital should continue as the main provider of consultant-led 24/7 emergency care services, whilst new care arrangements in Downpatrick, Lisburn and North Down and Ards should now begin to evolve. Specifically the South Eastern Trust is expected to develop intermediate care services in line with the delivery of appropriate clinical care for patients in order to meet the shift left objective of Transforming Your Care that is to provide care at home. 4.3 South Eastern LCG, Strategic Commissioning Statements in regards to Primary and Community Care Infrastructure Service Requirements This paper outlines a service model that illustrates the integrated nature and interdependent relationships between Hubs and Spokes and their interface with secondary care (Hubs being centres with a mix of primary, community and secondary care providers and Spokes being more community based primary care centres i.e. GP practices). The document confirms commitment to the development of four proposed Hubs for the South Eastern Trust area within Downpatrick, Lisburn, Newtownards and Bangor, with new build facilities proposed for both Bangor and Newtownards. 19
20 4.5 South Eastern LCG, Frail Elderly Commissioning Specification, July 2013 For Frail Elderly, ICPs will remodel their intermediate bed provision and support to carers through reinvestment in the independent sector and provision of alternative community based models of care. 4.6 Improving the Patient & Client Experience Standards Patients and clients have a right to experience respectful and professional care, in a considerate and supportive environment, where their privacy is protected and dignity maintained. This principle should be promoted and supported by all health and social care organisations and professional bodies, enabling staff to provide a quality service. There are many complex factors relevant to the quality of patient and client experience. The following five areas have been identified as important towards ensuring a positive patient or client experience. Respect Attitude Behaviour Communication Privacy and dignity All of these standards should involve the patient and client or their representatives, organisational leaders charged with the quality of patient and client experience as well as members of staff and teams charged with ensuring a positive patient and client experience in the delivery of health and social care. 4.7 DHSSPS Guidance for HSC Organisations on Arrangements for Implementing Effective Personal Public Involvement Policy in the HSC 2012 Personal and Public Involvement (PPI) describes the process of including those who use health and social care services, their carers, relatives, friends, neighbours, 20
21 voluntary workers, members of community groups and employees of voluntary organisations in the decision-making of those services. It builds on the values and principles which were set out in the 2007 Departmental guidance on PPI and incorporates the requirements set out in the Health and Social Care Reform Act 2009, which formally requires health and social care bodies to provide information about the services it provides, to receive information from users about how well they receive those services and to encourage service users to take up care in the best way possible. 4.8 Section 75 of the Northern Ireland Act, 1998 This Act requires Trusts to have due regard to the need to promoting equality of opportunity, in respect of a number of defined groups, including people of different ages. 4.9 Trust Strategic Direction In response to the Commissioning plan the South Eastern Trust has developed a draft Trust Delivery Plan 2014/15. The document outlines how the Trust plans to deliver services in line with the Commissioning priorities and identifies pressures in relation to the Trust s ability to deliver on key Departmental and Executive financial commitments/requirements: To set out the Trust s Strategic Direction the Trust has developed a Strategic Hospital Network Reform Board and associated Action Group which has identified the need to review the provision of services of services in response to this reform agenda and with a strategic emphasis on the provision of appropriate care South Eastern Health & Social Care Trust Corporate Plan ( ) The following key objectives and priorities are included in the Trust s Corporate Plan for and are relevant to this appraisal: Key Theme To ensure that services are safe, of a high quality and Priority Flexible use and development of facilities across both the hospital and community setting to support the 21
22 Key Theme contribute towards improving the experience and outcomes for patients, clients and carers. To ensure that patients and clients receive services in a timely and accessible manner. To develop partnerships to promote and maintain health and wellbeing. To focus on the efficiency and effectiveness of services, improve organisational capability within available finances. To build a stable, highly motivated workforce that is Priority delivery of safe and effective care. Reduce admissions to hospital and enhance patient experience through the development of new care pathways and more outpatient services where appropriate. Reduce admissions and unnecessary stays in hospital through better links and communication between hospital and community services and better use of community based services. Further development of clinical networks to ensure best use of resources across the Trust area. Continue to improve the provision of high quality, innovative and inclusive community services. Enable people to live as independently as possible through the development of community and home based services. To ensure that methods of engagement are tailored to meet the specific needs of service users, including children and young people. Continue to develop services in response to changing demand. Ensure fair access to services across the Trust area. Provide support and services to help people to remain well and live in their own communities. Develop early intervention and prevention approaches. Further develop integrated working across professions to provide a more seamless service and an improved experience for service users, families and carers. Ensure that follow-up services for patients are easily understood and readily available to help them to live to their full potential. Deliver local services where possible and centralise services where required. Provide hospital care for those who need it and appropriate community care for those who can live in their own homes and communities. Exploit opportunities for efficiencies in the way equipment and other services are purchased. Engage with service users, interested parties and local communities regarding decisions required to achieve service reform. Continue to develop appropriate multidisciplinary teams to ensure that patient and clients receive a seamless, truly integrated service. 22
23 Key Theme committed to a culture of continuous development and ultimately service improvement. To ensure that consideration is given to the views of patients, clients, carers and other interested parties in the planning and delivery of services Efficency & Service Reform. The Trust will continue to focus on the efficiency and effectiveness of services, improve organisational capability within available finances. The national and local financial environment will present both challenges and opportunities for the organisation. Delivery of services within available finances each year will continue to be a key responsibility for the Trust. Priority Benchmark services against others as we strive to achieve excellence in all that we do. Further develop partnerships with independent, voluntary, community groups and volunteers to enhance choice. Ensure clear and meaningful engagement processes are in place with regard to all service modernisation proposals. Involve users and carers in planning and delivery through service specific or special interest groups. To improve productivity across all areas of the Trust, thereby delivering the best we can with what we have available to us. Deliver local services where possible and centralise services where required. This will involve reviewing how and where we deliver a range of services across the Trust The South Eastern Trust s Corporate Plan highlights the priorities for the Primary Care & Older People Directorate: To provide a person centred service that is readily accessible and responsive to the needs of users; 23
24 To provide a co-ordinated, integrated service focusing on prevention, health education and effective self-care; To plan for investment to respond to demographic changes. 24
25 5.0 Existing Service Profile 5.1 Demography Northern Ireland (NI) has the fastest growing population in the United Kingdom. Table 1 below demonstrates the 2013 mid-year population estimates with table 2 highlighting the estimated population by Table 1: Resident Populations: Northern Ireland and SEHSCT LGDs Mid Year Population Estimate 2013 Age Northern Ireland Ards Down North Down Lisburn SEHSCT ,155 14,073 13,978 13,822 24,877 66, ,212 9,101 9,516 8,710 15,811 43, ,870 19,070 17,943 19,899 32,525 89, ,354 21,795 18,205 21,540 30,845 92, ,850 12,878 9,796 13,429 15,922 52, ,284 1,632 1,387 2,024 2,010 7,053 Total 1,829,725 78,549 70,825 79, , ,788 25
26 Table 2 Population Projected Change Age Regional Population Profile NI Projection 2023 NI % Change 2013 to 2023 Trust Sector Population Projections 2023 Ards North Down Down Lisburn Trust Projection 2023 Change in Trust Population Profile Trust % change 2013 to , % 4,208 4,426 4,850 8,723 22, % , % 4,532 4,654 4,878 8,801 22, % , % 4,798 4,860 4,933 8,962 23, % , % 4,673 4,388 4,462 8,071 21, % , % 3,719 3,515 3,823 6,909 17, % , % 4,074 4,215 4,496 8,096 20, % , % 4,468 4,793 4,732 8,970 22, % , % 4,607 5,025 4,607 8,907 23, % , % 4,754 5,061 4,400 8,600 22, % , % 4,753 4,842 4,249 7,843 21, % , % 5,576 5,606 4,841 8,660 24, % , % 6,083 5,777 5,211 9,177 26, % , % 5,707 5,531 4,725 8,283 24, % , % 5,053 4,892 4,072 6,697 20, % , % 4,505 4,549 3,536 5,583 18, % , % 4,142 4,280 2,982 4,860 16, % , % 2,621 2,716 2,013 3,429 10, % , % 1,506 1,671 1,329 2,027 6, % , % 929 1, ,193 4, % Total 1,926, % 80,708 81,888 75, , , % These tables demonstrate that the NI population will increase by 5.17% by The demographical statistics (as per NISRA reports) for NI population over 65 years old show an anticipated growth rate of 26.4% between 2013 and For the population over 85 years old the growth rate over the same time period is 41.7%. Current Intermediate Care Service Provision within the North Down and Ards Area Intermediate care is a short term in-patient stay in one of the Trusts funded Intermediate Care beds. These beds provide a period of recovery and rehabilitation for a patient after a spell of acute illness or trauma. The beds are mainly used by patients after they have had a stay in an acute hospital and no longer need acute 26
27 medical input but are not quite ready to go home, needing some more therapy or rehabilitation. For the most part, the medical care provided is outside General Medical Services (General Practitioner Services) and would be provided by a Trust appointed medical officer or Consultant. Where a patient s need is solely for social or nursing care they would be admitted to a normal nursing or residential care bed and the medical cover in this case would be provided by a General Practitioner (GP) through General Medical Services in the same way as if living at home. 27
28 Table 3 Existing Bed Profile in North Down and Ards Facility Location Number of Beds Bangor Hospital Bangor 20 designated as 10 GP led beds and 10 that may be used for Stroke Rehabilitation Ards Hospital Newtownards 20 (10 Consultant led beds and 10 GP led Beds) Independent Sector Various locations, 65* Average use currently - (29 Consultant led fracture rehabilitation) Dundonald, Holywood, Comber, (22 Independent Provider Beds) (14 Statutory Residential beds currently Newtownards and Northfield) Donaghadee Total 105 * The Trust can also spot purchase up to 20 Nursing Beds across the Trust area to meet demand when required and these can be anywhere across the locality to suit an individual s needs As at 1 December 2014, 20 beds in Bangor Hospital have been closed temporarily as a result of contingency measures imposed to enable the Trust to achieve financial breakeven. 28
29 Table 4 Existing Bed Profile in the Down and Lisburn Area Facility Location Number of Beds Lisburn Lisburn 10 Consultant led beds Intermediate Care Centre (LICC) Drumlough House Lisburn 10 Statutory residential beds Ardview House Downpatrick 10 Statutory residential beds Independent Sector Various locations 15* Average use throughout the locality dependent on capacity Total 45 * The Trust can also spot purchase up to 20 Nursing Beds across the Trust area to meet demand when required and these can be anywhere across the locality to suit an individual s needs. There is greater demand for Intermediate Care in the North Down and Ards sector due to an increased number of complex patients requiring discharges for fracture rehabilitation. 29
30 5.2 Bed Usage The following tables show the bed usage across the North Down and Ards Areas for the full years for 2012/13 and 2013/ North Down and Ards Bed Supply and Use Year 2012/13 Bed Supply Bangor Ards Independent Fracture Residential Totals / Usage Hospital Hospital Sector Rehab Care Number of overall beds Number of available bed days Number of admissions ,624 Occupied Bed Days , ,190 Bed Occupancy 92% 90% 99% 86% 59% Levels (%) Average Length of stay 1 Owing to demand the equivalent of up to 32 beds were purchased at any one time 2 20 beds were in place in 2012/13 For the year 2012/13 this table highlights that there were 106 beds available to the Trust in the North Down and Ards area at any given point in time. This was with a total of 38,690 bed days available for utilisation. Throughout the year there were a total of 1,624 admissions with 34,190 bed days used. 30
31 5.2.2 North Down and Ards 2013/14 Bed Supply and Use Year 2013/14 Bed Supply Bangor Ards Independent Fracture Residential Totals / Usage Hospital Hospital Sector Rehab Care Number of overall beds Number of available bed days Number of admissions Occupied Bed Days Bed Occupancy 86% 91% 97% 96% 46% Levels (%) Average Length of stay 1 Owing to demand the equivalent of up to 25 beds were purchased at any one time 2 21 beds were in place in 2013/14 For the year 2013/14 this table highlights that there were 100 beds in the North Down and Ards area, available to the Trust at any given point in time. This was with a total of 36,500 bed days available for utilisation. Throughout the year there were a total of 1,627 admissions with 31,496 bed days used. Comparing the two years there has been a trend in the reduction of the length of stay overall, but in particular in the independent sector beds and residential care. This means that the Trust was able to cope with additional admissions but used 2694 fewer bed days. 31
32 5.2.3 Down and Lisburn Area Bed Supply and Use 2012/13 Year 2012/13 Independent Totals Lisburn Independent Bed Supply Drumloug Ardview Sector Intermediate Sector Spot / Usage h House House floating Care Centre purchased purchased Number of overall beds Number of available bed days Number of admissions Occupied Bed Days Bed Occupancy 54% 73% 75% 100% 100% Levels (%) Average Length of stay 1 Lisburn Intermediate Care Centre closed 5 beds in September which then reopened in October Drumlough closed 5 beds for the whole of September 2012 For the year 2012/13 this table shows that there were 54 beds available to the Trust in the Down and Lisburn area at any given point in time. This was with a total of 16,009 bed days available for utilisation. Throughout the year there were a total of 467 admissions with 12,409 bed days used. 32
33 5.2.4 Down and Lisburn Area Bed Supply and Use 2013/14 Bed Supply / Usage Number of overall beds Number of available bed days Number of admissions Occupied Bed Days Bed Occupancy Levels (%) Average Length of stay Year 2013/14 Independent Totals Lisburn Independent Drumloug Ardview Sector Intermediate Sector Spot h House House floating Care Centre purchased purchased % 73% 75% 100% 100% For the year 2013/14 this table shows that there were 54 beds available to the Trust in the Down and Lisburn area at any given point in time. This was with a total of 16,009 bed days available for utilisation. Throughout the year there were a total of 449 admissions with 13,030 bed days used. Comparing the two years there has been a slight increase in the length of stay overall, however, the number of admissions has decreased. 33
34 5.3 Community Based Services The Trust has a wide range of Community based Services that it currently provides which can offer an alternative to Intermediate Care beds and support individuals to remain in their own homes. It is important to note that where appropriate all patients that require acute hospital admission will continue to be admitted to an acute hospital bed when required. The main objective of community care services are: To help people remain in their own homes, or in as near domestic environment as possible, for as long as they wish and it is safe and appropriate to do so. To provide practical support to carers to support them in their caring role. To ensure that residential care, nursing home care and hospital is reserved for those whose needs cannot be met in any other way. The following are examples of the range of services that are available to patients across the Trust area Supported Living The Trust is committed to maintaining the lifestyles of older people by promoting their independence whilst at the same time receiving support from staff on site, who assist with daily tasks and are able to respond to emergency situations as they arise. The direction of the Trust has been to develop the model of Supported Living and develop one Supported Housing scheme in each of the Trust localities, in North Down, Ards, Lisburn and Downpatrick. Across the Trust there are 66 supported living schemes providing 1,667 units of accommodation. The Trust is currently in development of a new scheme in Bangor on the site of the former Ravara House Residential Home. 34
35 5.3.2 Community Care The Trust provides a range of Community Care packages which include placement in a Nursing Home or Residential Home and Domiciliary Care services. At the end of October 2014 the Trust was providing 6046 Community Care Packages, Trust wide, for older people, which includes 2805 Community Care Packages in the North Down and Ards area. These packages are based on an individual s assessment of need and personal choice. The Trust has invested significantly in Community Care each year as demonstrated in the table below: 2012/ / /15* Community Care Packages *Up to December Case Management Case Management is a planned, coordinated, process to manage and review the care of an individual. It delivers health care to the most vulnerable people with chronic long term conditions who are admitted frequently to hospital. A range of services are coordinated and clients are admitted to a Virtual Ward. This is achieved through enhanced community nursing services, integrated primary care working and a case finding model delivered by a case coordinator. The virtual ward in place in the Trust currently supports up to 18 patients across the Trust, with 12 in the North Down and Ards area. The Trust is currently working as part of an Integrated Care Partnership and has plans to implement an Enhanced Care at Home model in The aim of this service will be to provide tailored medical, nursing and social care, to suit the circumstances of patients presenting with acute needs, to ensure the best care in the most appropriate environment, either in the patient s own home or other community setting. The model is intended for patients who do not need the full range of services provided in an acute hospital, but do require a more intensive care package than that typically provided by existing GP and district nursing services. The service will be operated 24 hours a day
36 days a year and will include access to Specialist Nursing, Allied Health Professions, such as Physiotherapy, Occupational Therapy, Heart Failure, Palliative Care and enable access to clinical advice and support through General Practitioners and Consultants when appropriate Rapid Response Service The Community Nursing Rapid Response Service is the 24 hour provision and delivery of intensive levels of nursing care for people in their own homes or as close to their own homes as possible across the Trust. Patients are cared for by the Team and their medical care is the responsibility of the General Practitioner and in some cases their Hospital Consultant. The Community Nursing Rapid Response Service is suitable for a range of conditions/illnesses which would normally be treated as an inpatient in hospital or require attendance at an emergency department, outpatient facility or day procedure unit. The service works in partnership with the District Nursing Services and other professionals to deliver patient-centred care services and enable the Trust to deliver patient-centred care in the Community. The following table shows the caseload, referrals and contacts for the service comparing the first quarter of each year. 1 st Quarter April-June Total Quarterly New Referrals Total Quarterly Caseload contacts / Telecare Telecare is used to help people to be as safe as possible within their own homes so that families and carers can be given the peace of mind that their loved ones are safe, secure and remain as independent as possible for as long as possible. The system can be used for a wide spectrum of people in need of added safety and monitoring at home. The technology assists in the maximisation of independence 36
37 and safety by sensing activity, learning patterns of behaviour, establishing normal patterns and taking action if pre-agreed triggers are activated. If appropriate a signal will be sent through the telephone system to the Safety/ Triage Centre and an alert raised. Dementia patients could have fitted into their homes a range of sensors which would be monitored over 24-hours/7-days a week. Currently the Trust has 173 clients being supported with a Telecare package at home. Some examples of these are: Bed or chair occupancy Falls Movement Smoke/Flooding Temperature extremes Open doors and windows Resident calls for assistance Vital Signs e.g. Blood pressure monitoring or weight linked to the case management programme Wandering alerts utilising GPS technology Remote Telemonitoring (Telehealth) Remote Telemonitoring is a means of monitoring patients using technology in a community based setting. It allows patients with heart and respiratory conditions, diabetes and those who have suffered a stroke who are suitable to have their vital signs such as pulse, blood pressure, body weight and oxygen saturation monitored at home on a daily basis. The Trust currently has 254 patients using remote Telemonitoring. How it works All Trust Specialist Nurses, Registered Community Nurses, appropriate Allied Health Professional staff and hospital Consultants can identify potential patients from their caseloads or clinics, patients who have attended the Emergency Department and/or 37
38 GP out of hours service can also be identified. General Practice (i.e. GP and Practice Nurses) can identify patients through local knowledge of their patients, Long Term Conditions registers and the Quality and Outcomes Framework. Hospital ward staff can also identify patients with a diagnosis of Chronic obstructive pulmonary disease, Chromic Heart Failure, Diabetes, Gestational Diabetes, Stroke/ transient ischaemic attack or Hypertension, who have been admitted to Hospital. Equipment is installed in a patient s own home and readings and measurements outlined in the patient plan are completed, are monitored and triaged centrally by nursing staff who, if necessary escalate patients to the Trust response teams Self Directed Support Self Directed Support (SDS) transforms Social Care Services from a service led system to one that promotes individuals' autonomy and independence. SDS allows individuals to develop support plans to meet their assessed need and the provision of a personalised budget results in individuals having greater choice, independence and control over how their support needs are met. SDS can take the form of Direct Payments which are cash payments made to individuals or their representatives in lieu of the Trust providing a social care service. Personal Budgets can be used more flexibly by individuals to spend in ways that makes sense to them. A person must be able to consent to have a direct payment and have the capacity to manage one, although they can have assistance to manage their payment on a dayto-day basis. At the end of October 2014 Trust is supporting 449 people with direct payments, having grown from 377 at the end of March Reablement Reablement is a person-centred approach which is about promoting and maximising independence to allow people to remain in their own home as long as possible. It is designed to enable people to gain or regain their confidence, ability, and necessary 38
39 skills to live independently, especially after having experienced a health or social care crisis, such as illness, deterioration in health or injury. The aim of Reablement is to help people perform their necessary daily living skills such as personal care, walking, and preparing meals, so that they can remain independent within their own home. The reablement service is available across the entire Trust area, It is different from conventional domiciliary home care as it adopts a more hands off approach to supporting people, encouraging and enabling people to carry out activities of daily living for themselves instead of doing things for people. The table overview provides a breakdown of the number of clients who started reablement by month during the financial year 2013/14. 39
40 Table 5. Number of Clients Starting Reablement (April 13 March 14) Month Number of clients starting reablement April May June July August September October November December January February March Total 1277 Over the 12 month period April 13 to March 14, 1277 people were started on the reablement Service Enhanced Care At Home The implementation of new Enhanced Care At Home services will assist in reducing acute admissions of frail elderly patients to, for example, acute medical wards, elderly assessment beds and acute psychiatric wards and also reduce length of hospital stay. In particular being able to maintain a frail older person in their own home should reduce the potential for the rapid onset of confusion, reduce the possibility of hospital acquired infections and reduce the potential of a fall occurring in unfamiliar surroundings such as wards in a hospital. As noted earlier, in response to TYC, the general public responded and advised that their preference would be to remain in their own home if possible. 40
41 6.0 Objectives and constraints This section outlines the main objectives and constraints relevant to the provision of Intermediate Care Service in the North Down and Ards area. 6.1 Project Objectives: The aim of the project is to identify the most effective and efficient way to provide Intermediate Care Services in the North Down and Ards areas in line with available resources and Regional Principles of Medical Cover. In order to achieve this, the project objectives were identified as follows- Objective 1 Strategic Direction To facilitate a structure that will result in a high quality of service with improved outcomes and improved service efficiency in terms of use of resources. Measures: Compliance with the Trust strategic direction i.e. The future overarching service model and the future service model for older people as outlined in Section 3 of this report Compliance with the Commissioner direction for reform of Urgent Care Services as outlined in Section 4 Compliance with Commissioner Specifications for clinical priority areas. No increase in intermediate care length of stay in line with regional average and best practice across the different levels of Intermediate Care No increase in readmission rates to intermediate and acute care on current baseline Improved service user satisfaction from improved clinical outcomes for patients No increase in patient incidents Increase the number of patients receiving care closer to home and enable patients to remain in their own homes Increase in number of patients enabled to stay in their own homes Maximise efficiencies through consolidation of services Admission criteria for each facility Multi-disciplinary management plans developed for each patient 41
42 Objective 2 Medical Cover To ensure that the Trust has adequate Intermediate Care Provision in the locality with the appropriate level of medical cover which complies with the Regional principles for Medical Cover. Measure Adequate staff capacity within the locality to manage the current number of admissions to intermediate care beds as outlined in section 5. The appointment and sustainability of the most appropriate medical cover to ensure that patients receive care that is safe and effective Staff employed are appropriately skilled and trained to provide the level of medical input needed Outcome focused multi-disciplinary management plans in place for all patients Appropriate lengths of stay in line with regional average and best practice Appropriate medical care (routine and emergency) available to patients at all times. Adherence with Regulation and Quality Improvement Authority (RQIA) regulations Objective 3 Flexibility / Sustainability To provide a service which is sufficiently flexible to respond to future changes in service delivery and volumes. Measure Flexibility to increase or reduce the number of beds as demand requires and in line with emerging service reform, such as Enhanced Care at Home Objective 4 Speed and Ease of Implementation To minimise disruption and disturbance to on-going patient care. Measure Speed of implementation of changes changes should not take more than 6 months to implement Numbers of patients that are enabled to receive care in their own homes. 42
43 Intermediate care that is part of a seamless continuum of services linking health and wellbeing, preventative services, primary care, community based services, social care, carers support services and acute hospital care. 43
44 6.2 Project Constraints: The project could be constrained by the following factors- Constraint 1: Staffing models Any model of care must be supported by suitably qualified, competent professional staff with the assurance of sustainability through workload/ patterns and activity. Constraint 2: Demand & Capacity Any service model must manage the demand and have adequate capacity to ensure sustainable delivery. Constraint 3: Affordability That any option must be affordable within the current and predicted future financial climate. Constraint 4: Site Limitations/ Accessibility Availability and suitability of facilities. 44
45 7.0 Formulation and Evaluation of Options 7.1 Option Identification A key component of any formal option appraisal is the assessment of the nonfinancial benefits that are likely to accrue from the options under consideration. The following sections provide a description of the process used to assess the potential benefits of the short-listed options together with the outcomes of the exercise. In considering the proposed service model for the future provision of Intermediate Care Services the Trust has considered a number of options as outlined in the long list below. 45
46 7.2 Long list of Options Option 1 Status Quo - Do Nothing. 2 Do minimum Description This option is to continue to provide all 125 intermediate care beds, with the current medical model in place in the North Down and Ards area as follows- 29 Consultant led fracture rehabilitation beds Currently Domnall 22 Independent Provider block purchased Beds with GP GMS Medical support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 20 Beds in Bangor Hospital with GP Medical Support 14 Beds in Northfield House with GP GMS Medical Support. Up to 20 spot purchased beds on a temporary basis when demand requires This option is to provide up to 95 beds, the same number of beds provided following the temporary closure in Bangor Hospital. 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP GMS Medical support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 14 Beds in Northfield House with GP GMS Medical Support. Up to 10 spot purchased beds on a temporary basis when demand requires. Please note that there would be no intermediate care beds at Bangor Hospital within this option and would therefore result in a permanent closure of the 20 beds at Bangor Hospital. This option would also include a reduction in the spot purchase beds from 20 to 10 3 This option is to provide up to 95 beds, the same number of beds provided following the temporary closure in Bangor Hospital. 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP GMS Medical support 20 beds in Bangor Hospital 10 with GP Medical Support and 10 with Consultant support 14 Beds in Northfield House with GP GMS Medical Support. Up to 10 spot purchased beds on a temporary basis when demand requires Please note that there would be no intermediate care beds at Ards Hospital within this option and would therefore result in a permanent closure of the 20 beds at Ards Hospital. This option would also include a reduction in the spot purchase beds from 20 to 10 4 This option is to provide up to 95 intermediate care beds in the North Down and Ards area as follows 29 Consultant led fracture rehabilitation beds Currently Domnall 2 Independent Provider Beds with GP Medical support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 20 Beds in Bangor Hospital with GP Medical Support 14 Beds in Northfield House with GP GMS Medical Support. Up to 10 spot purchased beds on a temporary basis when demand requires Please note that the option would result in a reduction in the Trust block purchase of beds from the independent sector. This option would also include a reduction in the spot purchase beds from 20 to 10 5a This option is to provide up to 105 intermediate care beds in the North Down and Ards area as follows 29 Consultant led fracture rehabilitation beds Currently Domnall 46
47 Option Description 22 Independent Provider Beds with GP Medical support 20 Consultant led Beds in Bangor Hospital 14 Beds in Northfield House with GP GMS Medical Support. Up to 20 additional spot purchased beds on a temporary basis when demand requires. Please note that there would be no intermediate care beds at Ards Hospital within this option and would therefore result in a permanent closure of the 20 beds at Ards Hospital. 5b This option is to provide up to 105 intermediate care beds in the North Down and Ards area as follows 29 Consultant led fracture rehabilitation beds Currently Domnall 22 Independent Provider Beds with GP Medical support 20 beds in Bangor Hospital with GP Medical Support 14 Beds in Northfield House with GP GMS Medical Support. Up to 20 additional spot purchased beds on a temporary basis when demand requires. Please note that there would be no intermediate care beds at Ards Hospital within this Option and would therefore result in a permanent closure of the 20 beds at Ards Hospital. 6a This option is to provide up to 105 intermediate care beds in the North Down and Ards area as follows 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP Medical support 20 Consultant led beds in Ards Hospital 14 Beds in Northfield House with GP GMS Medical Support. Up to 20 additional spot purchased beds on a temporary basis when demand requires. Please note that there would be no intermediate care beds at Bangor Hospital within this Option and would therefore result in a permanent closure of the 20 beds at Bangor Hospital. 6b This option is to provide up to 105 intermediate care beds in the North Down and Ards area as follows 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP Medical support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 14 Beds in Northfield House with GP GMS Medical Support. Up to 20 additional spot purchased beds on a temporary basis when demand requires. Please note that there would be no intermediate care beds at Bangor Hospital within this Option and would therefore result in a permanent closure of the 20 beds at Bangor Hospital. 7 This option is to provide up to 105 intermediate care beds in the North Down and Ards area as follows 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP Medical support 10 Consultant led beds in Ards Hospital 10 Consultant led Beds in Bangor Hospital 14 Beds in Northfield House with GP GMS Medical Support. Up to 20 additional spot purchased beds on a temporary basis when demand requires. Please note that this option would result in the permanent closure of 10 beds at Ards Hospital and 10 beds at Bangor Hospital 47
48 7.3 Preliminary Sift of Options The long list of options described in Section 4.1 was reviewed by the Trust to ensure compliance with all of the objectives and constraints of the project. The preliminary sift eliminated all options which were clearly not feasible so that a reduced number of options can be considered in greater detail. The outcome of this sift is shown in the table below with the following symbols: - complies with objective / constraint. X - fails to meet the objective / constraint.? - might / might not meet the objective / constraint and should therefore be evaluated further. 48
49 Table 6: Preliminary Sift of Options Objectives Constraints Shortlist? Option Strategic Medical Flexibility Speed & Staffing Demand & Affordability Site Direction Cover Sustainability Ease Models Capacity Limitation 1 X X Y 2 X Y 3 X X X N 4 X X X N 5a X N 5b X N 6a Y 6b Y 7 X X N 49
50 The table below sets out the long-list of options that has been identified along with details of the options that have been shortlisted for detailed consideration and the rationale for not short listing the remaining options: Option Description 1 Status Quo Provide 125 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed Consultant and GP Medical Cover, 20 in Bangor Hospital with GP Medical Cover and 14 residential care beds and up to 20 spot purchase beds in the independent sector. 2 Do Minimum Provide up to 95 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed Consultant and GP Medical Cover and 14 residential care beds. Up to 10 spot purchased beds on a temporary basis when demand requires Shortlisted for further consideration Yes Yes Rationale for shortlisting / not shortlisting Did not meet Objective 1 as The option is not in line with the Commissioning Plan 2014/15. Minor Injuries, Intermediate Care beds and GP OOHs services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. The Plan confirms that the Urgent Care Centre for North Down and Ards will be based at Newtownards, therefore this option, which provides beds at Bangor Hospital is not in-line with the commissioner s intentions. Constraints The option did not successfully address the Constraints of the project in that- This option is unaffordable as intermediate care beds across two sites would not offer any financial savings The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation Shortlisted as a requirement for baseline purposes. Constraints The option was limited in terms of capacity for the future. The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation Shortlisted to enable comparison between all of the do something options 50
51 Option Description 3 Provide up to 95 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Bangor Hospital with mixed Consultant and GP Medical Cover and 14 Residential Care beds. Up to 10 spot purchased beds on a temporary basis when demand requires Shortlisted for further consideration No Rationale for shortlisting / not shortlisting Did not meet Objective 1 as- The option is not in line with the Commissioning Plan 2014/15. Minor Injuries, Intermediate Care beds and GP OOHs services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. The Plan confirms that the Urgent Care Centre for North Down and Ards will be based at Newtownards, therefore this option, which provides beds at Bangor Hospital is not in-line with the commissioner s intentions. Did not meet Objective 3 as- The option does not offer suitable flexibility when demand dictates as the independent sector beds to spot purchase are more limited at 10. Constraints The option did not successfully address the Constraints of the project in that- The option was limited in terms of capacity for the future as the option only provides 95 beds. Although Bangor is accessible, and meets the constraints outlined in the sift, the group noted that it does not provide as good access to the whole of the North Down and Ards locality. The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation 4 Provide up to 95 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 2 Independent Sector, 20 in Ards Hospital with mixed Consultant and GP Medical Cover, 20 in Bangor Hospital with GP medical cover and 14 Residential Care beds. Up to 10 spot purchased beds on a temporary basis when demand requires No Did not meet Objective 1 as- The option is not in line with the Commissioning Plan 2014/15. Minor Injuries, Intermediate Care beds and GP OOHs services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. The Plan confirms that the Urgent Care Centre for North Down and Ards will be based at Newtownards. Did not meet Objective 3 as- The option does not offer suitable flexibility when demand dictates as the independent sector beds to spot purchase are more limited at 10. Constraints The option did not successfully address the Constraints of the project in that- The option was limited in terms of capacity for the future as the option only provides 95 beds. Although Bangor is accessible, and meets the constraints outlined in the sift, the group noted that it does not provide as good access to the whole of the North Down and Ards locality. The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation 5a Provide up to 105 No Did not meet Objective 1 as- 51
52 Option Description beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Bangor Hospital with Consultant Medical Cover, 14 Residential Care beds and up to 20 additional spot purchased beds. Shortlisted for further consideration Rationale for shortlisting / not shortlisting The option is not in line with the Commissioning Plan 2014/15. Minor Injuries, Intermediate Care beds and GP OOHs services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. The Plan confirms that the Urgent Care Centre for North Down and Ards will be based at Newtownards, therefore this option, which provides beds at Bangor Hospital is not in-line with the commissioner s intentions. Constraints The option did not successfully address the Constraints of the project in that- Although Bangor is accessible, and meets the constraints outlined in the sift, the group noted that it does not provide as good access to the whole of the North Down and Ards locality The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation 5b Provide up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Bangor Hospital with GP Medical Cover, 14 Residential Care beds and up to 20 additional spot purchased beds No Did not meet Objective 1 as- The option is not in line with the Commissioning Plan 2014/15. Minor Injuries, Intermediate Care beds and GP OOHs services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. The Plan confirms that the Urgent Care Centre for North Down and Ards will be based at Newtownards, therefore this option, which provides beds at Bangor Hospital is not in-line with the commissioner s intentions. Constraints The option did not successfully address the Constraints of the project in that- Although Bangor is accessible, and meets the constraints outlined in the sift, the group noted that it does not provide as good access to the whole of the North Down and Ards locality. The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation 6a Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with Consultant Medical Cover, 14 residential care beds and up to 20 Yes Meets all objectives Addresses all constraints 52
53 Option Description additional spot purchased beds 6b Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed GP and Consultant Medical Cover, 14 residential care beds and up to 20 additional spot purchased beds 7 Provide up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 10 in Ards with Consultant Medical Cover, 10 in Bangor Hospital with Consultant Medical Cover, 14 Residential Care beds and up to 20 additional spot purchased beds. Shortlisted for further consideration Yes No Rationale for shortlisting / not shortlisting Meets all objectives Addresses all constraints Did not meet Objective 1 as- The option is not in line with the Commissioning Plan 2014/15. Minor Injuries, Intermediate Care beds and GP OOHs services should be co-located to maximise clinical integration and efficiencies and together will form an urgent care centre within the PCCC Hub. The Plan confirms that the Urgent Care Centre for North Down and Ards will be based at Newtownards, therefore this option, which provides beds at Bangor Hospital is not in-line with the commissioner s intentions. Constraints The option did not successfully address the Constraints of the project in that- In terms of constraints it was considered that having a consultant provide cover on each of both Ards and Bangor sites would be unsustainable and impractical considering working patterns. Nurse staffing for two 10-bedded wards on two separate sites would also be financially inefficient. This option is unaffordable as 10 intermediate care beds in both Ards and Bangor Hospitals would not offer the required financial savings The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation As such, the short list consists of four options to be taken forward for detailed evaluation. The detailed evaluation of these options has been set out in the following sections. 53
54 8.0 Non-Financial Benefits Appraisal 8.1 Overview The appraisal underpinning the proposal for the provision of intermediate care services for North Down and Ards must include a Qualitative (Non-Financial) Assessment of shortlisted options, in line with DFP guidance within the Northern Ireland Guide to Expenditure Appraisal and Evaluation (NIGEAE). The Qualitative Assessment aims to capture the impact of non-monetary aspects of the project, such as health and social effects impacts which could not otherwise be expressed in a monetary form. As noted in the NIGEAE, non-monetary costs and benefits of a project should not be regarded as any less important than the monetary value. Generally, the Qualitative Assessment should relate closely to the objectives of the project, with an analysis of how well each shortlisted option meets the objectives and the Qualitative Assessment can be used as a means of ranking the shortlisted options on a non-monetary basis and/or assisting in the selection of a preferred option. 8.2 Methodology The Weighted Scoring Method has been used for the purposes of scoring the qualitative risks and benefits relating to the provision of intermediate care services for North Down and Ards appraisal. The Weighted Scoring Method involves attributing weights to each non-monetary element (reflecting its relative importance); scoring each option based on its performance against each objective or assessment criterion; and calculating a weighted score for each option. The following table sets out the steps undertaken in the Weighted Scoring Method: 54
55 Step 1) Identify the relevant nonmonetary attributes 2) Decide the weights for each attribute 3) Score each option 4) Calculate the weighted scores 5) Test the robustness of the results 6) Interpret the results Description This step involves selecting the qualitative aspects of the project which are to be considered these may be health, social, etc. These attributes should be closely linked to the objectives of the project and define the non-monetary benefits which are sought to be achieved by the project. There should be no overlap between any of the non-monetary attributes and/or any issue with a cost already attached. These non-monetary attributes were agreed with the Project Team prior to their inclusion within the appraisal. In this step, each attribute is given a weighting (as a percentage), based on the perceived relative importance of the attribute. Clear justification will be required in the appraisal as to the reasoning behind the relative weightings applied to each selected non-monetary attribute included. In this step, each shortlisted option is given a score against each nonmonetary attribute selected in Step One. The scores may range from, for example, zero to 10. This score reflects how well it is expected that each shortlisted option would deliver the benefits associated with each non-monetary attribute of the project. It is important to try and distinguish between the benefits derived from each option and the benefits which would be derived anyway. Following the agreement of the scorings in Step Three, each of these is multiplied by the relevant weightings attributed to each non-monetary aspect and decided in Step Two. These weighted scores are then summated to give an overall nonmonetary score for each of the shortlisted economic options. In this step, the results reached following the first four steps previously are tested for robustness through altering assumptions, as a means of sensitivity analysis. This can be achieved by potentially reconsidering the weightings and/or scorings identified in Steps Two and Three. As indicated previously, justification should be documented in the appraisal as to the reasoning behind the weightings and scorings applied throughout the analysis. Furthermore, the results of the process should be interpreted in the context of the overall project and its objectives. These results will then be incorporated, along with results from the monetary assessment, into the final decision on the selection of the preferred option. 8.3 Non Financial Benefits Workshop A benefits appraisal scoring workshop was held on 5 th January 2015 to assess the relative level of benefits delivered by the short-listed options. The aim of the workshop was to:- 55
56 Establish a common understanding and agreed approach to the benefits appraisal process; Review and describe the list of options to be evaluated, Ratify the sift including the shortlisting of the option long list; Develop the list of criteria against which each of the options would be evaluated; Rank and weight the criteria; Score the options against the agreed criteria using the assigned weightings. Identify and agree a qualitative preferred option To ensure that the views of stakeholders were at the forefront of the process; and that the benefits appraisal process was conducted in an open and transparent manner, a broadly representative group of individuals were invited to attend the workshop. The group was made up from a wide range of key stakeholders. This included: Director of Planning Performance and Informatics, Director of Nursing, Older People and Primary Care, Assistant Director of Primary Care, Assistant Director Older People s Services, Assistant Director Allied Health Professions, Representatives from: Trust Finance, Strategic and Capital Development Human Resources Planning and Service Improvement Estates Community and Voluntary Groups Northern Ireland Ambulance Service Health and Social Care Board Clinical Director of Primary Care (GP) Union representatives (observer status for scoring) Apologies were received from the ICP GP lead for North Down, ICP GP lead for Ards and the Chair of the GP Executive for North Down. 56
57 The workshop was independently facilitated by a member of the Performance Improvement and Commissioning team who has extensive experience in carrying out non-financial benefits appraisals. Following the workshop the preferred option was acceptable to all members of the group and all members of the group confirmed that they were content with the process and that their views were appropriately reflected in decision making. 8.4 Benefits Criteria The role of the benefit criteria in the non-financial appraisal is to provide a basis against which each of the options can be evaluated in terms of their potential for meeting the objectives of the proposed capital investment. The criteria have been specifically developed in a manner which minimises the extent to which there may be double counting arising from overlap in the attributes or features. In addition due care has been taken of the need to ensure that the full range of attributes are covered even if they are likely to be common to all of the short listed options. On considering the unique requirements for this scheme, the following criteria have been produced for evaluating the relative merits of each option and to ensure that they meet the specific project objectives. Taking into account the objectives and constraints of the proposed project, a list of salient benefits has been devised which could accrue from the project if implemented successfully. The Criteria listed below are non financial benefit criteria and will provide the basis of a non-financial evaluation. 57
58 The criteria to select and evaluate the options are: Criteria Accessibility and Experience Clinical Quality and Integration Speed of Implementation Strategic Alignment Description of Key Features The Trust's ability to deliver more effective model of care to the local population. Access to locally based appropriate services Travel time for patients and relatives Access to public transport Access to different levels of care Choice for service users Enabling and maximising safety and quality of care Appropriate medical and pharmacy cover Appropriate diagnostic services Improved outcomes for patients. Improved Model of Care Minimised time to implementation Access and availability of medical cover Impact on staff and patients In line with draft Commissioners priorities and stated intention In line with Trust strategic vision and avoidance of service duplication Regional priorities Sustainability Trust can provide appropriate medical cover Recruitment, retention and training Capacity Affordable within existing budget Demographic trends/ growth Medium to long term sustainability 58
59 The appropriate linkages between project objectives and benefit criteria are set out below. PROJECT OBJECTIVES To facilitate a structure that will result in a high quality of service with improved outcomes and improved efficiency in terms of use of resources. To ensure that the Trust has adequate Intermediate Care Provision in the locality with the appropriate level of medical cover which complies with the Regional principles for Medical Cover. To provide a service which is sufficiently flexible to respond to future changes in service delivery and volumes. To minimise of disruption and disturbance to on-going patient care. BENEFITS CRITERIA Clinical Quality and Integration Compatibility with strategic vision. Clinical Quality and Integration Accessibility and Experience Quality of the Physical Environment; Compatibility with strategic vision. Accessibility and Experience Sustainability Compatibility with strategic vision. Speed of Implementation Accessibility and Experience Compatibility with strategic vision Clinical Quality and Integration Accessibility and Experience Weighting the Criteria The Project Team allocated weighting factors to each of the criteria as a means of reflecting their relative effect in the success of each option in the scoring. i. ii. iii. iv. v. Benefit Criteria % Accessibility and Experience 25 Clinical Quality and Integration 30 Speed of Implementation 5 Strategic Alignment 15 Sustainability 25 Total
60 Accessibility and Experience The team considered that accessibility for the public to services was important. Consideration was given to Trust area demographics and geographic situation, in conjunction with access to car parking, public transport and the ability to co-locate services. This criterion attracted a weighting of Clinical Quality and Integration The team considered that the ability to enable and maximise clinical safety and support an improved model of care resulted in this being the most important criterion. This reflected the fact that the success of the preferred option will be primarily judged on how far it goes in providing a safe and effective service that meets professional recommendations (both national and local) in terms of the provision of Intermediate Care Services. This criteria therefore attracted a weighting of Speed of Implementation Although this may be seen to be a short-term criterion, it is nevertheless an important one as the Trust wishes to ensure that a sustainable option is implemented as soon as possible to avoid a situation where unplanned short-term measures would have to be put into effect. As a result, this criterion attracted a weighting of Strategic Alignment The team considered that any option must reflect current strategic priorities, including the Commissioner s intentions as outlined in the Commissioning Plan, and the Trust s strategic priorities. This criterion attracted a weighting of Sustainability This criterion, which encompasses the ability to recruit and retain staff as an essential component in maintaining a service, must also reflect the need for any changes to future proof the service so far as is possible to ensure that envisaged demands for the service can be met. Therefore this criterion was ranked quite highly and thus attracted the same weighting Accessibility and Experience of
61 8.4.2 Scoring the Options The scoring of the options against the benefits criteria is designed to assess the extent to which the potential solutions meet the objectives of the proposed service. Scoring provides a means to assess how each of the options compares both in relation to the optimal position (i.e. meeting all the criteria in their totality) as well as with other options. The capability of each of the options to meet the objectives was assessed using scores ranging from 0 (extremely poor- many reservations) to 10 (fully meets criterion no reservations) as outlined in the table below. Scoring was undertaken as a single group involving all attendees using a consensus approach. The group was tasked with assessing the extent to which each of the options met the criteria using the scoring scale detailed below: Scoring Scale Score Definition 10 Fully meets criterion - no reservations 9 Excellent - some very minor reservations 8 Very Good 7 Good 6 Quite Good 5 Satisfactory 4 Somewhat unsatisfactory 3 Poor 2 Very Poor - some reservations 1 Extremely poor - many reservations The table below will be used to summarise the agreed scores for each criterion against each option, which will be multiplied by the respective weighting to give the overall weighted score. 61
62 Benefit Criteria Accessibility and Experience Clinical Quality and Integration Speed of Implementation Strategic Alignment Weight Option 1 Maintain Status Quo Score Weighted Score Option 2 Do Minimum Score Weighted Score Option 6a Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with Consultant Medical Cover, 14 residential care beds and up to 20 spot Score purchased beds. Weighted Score Option 6b Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed GP and Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. Score Weighted Score Sustainability Total
63 8.5 Option Ranking Table - Scoring Rationale At the start of the Workshop the Assistant Director for Older Peoples Services requested an amendment the option descriptions for options 2, 3 and 4, from 85 beds to 95 beds. It was also noted that whilst the long term future of Northfield House is not confirmed, the Trust s long term plan is to continue to provide 14 beds either at this facility or an alternative. Option no 1. Status Quo Provide 125 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed Consultant and GP Medical Cover, 20 in Bangor Hospital with GP Medical Cover,14 residential care beds and up to 20 spot purchase beds in the independent sector. Criterion Score Rationale Accessibility and Experience Clinical Quality and Integration 8 Whilst generally good this option would not deliver a more effective or improved model of care / patient experience. The option scored highly as it maintains the current two wards therefore making it accessible for patients from both the Ards and Bangor Areas; therefore the group agreed that it should score one point higher than option 2. There was no issue regarding access via public transport for the entire locality Facilitated good access to the entire population of North Down and Ards. However the group noted that the provision of spot purchase beds in a patient s area would offer enhanced accessibility and therefore this option scored very good. 7 This option scored well as maintaining both Ards and Bangor Hospital beds would enable a safe and quality service including diagnostic services. Whilst the group noted that this option offered very good benefits in terms of clinical quality, the provision of beds across two sites would not maximise integration of services and therefore the option was scored as good. Speed Implementation Strategic Alignment Sustainability of 4 This option was deemed as somewhat unsatisfactory and therefore the group agreed should be awarded a score of 4 as the group noted that the speed of implementation would be in the region of 12 months. The option also scored low because the Human Resources representative advised that the timescale for implementation could take up to 12 months 2 The group agreed that this score should score 2 as this option is very poor in terms of strategic alignment as the inclusion of beds at both Ards and Bangor is not in line with the Commissioning plan, which states that the intention is to commission urgent care centres within PCCCs at Downpatrick, Lisburn and Newtownards. 3 Although it was noted that this option would provide the required up to 105 beds, the group agreed that the overall sustainability should be marked as poor. 63
64 The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation The option was viewed as not being affordable within the permissible budget as the bed complement offered limited flex in terms of rationalisation if demand reduced. The group therefore awarded this option a score of 3. Total score Weighted 535 Option no 2. Do Minimum This option is to provide up to 95 beds, the same number of beds provided following the temporary closure in Bangor Hospital. Ability to spot purchase up to 10 beds in the independent sector 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP GMS Medical support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 14 Beds in Northfield House with GP GMS Medical Support. Up to 10 spot purchased beds on a temporary basis when demand requires. Criterion Score Rationale Accessibility Experience and 7 This option provides 20 beds in Ards and spot purchase beds via the Independent sector across the entire locality and therefore was deemed a good option in terms of scoring level Accessibility to the Bangor population would be slightly reduced, however facilitated through other independent sector beds available and allowing adequate access to services for those living further away in the Peninsula, eg Portaferry. The group agreed therefore that this option should score one point lower than option 1. Public transport from the Ards peninsula is optimised in this option as there are more direct services to Ards than Bangor. Choice for service users would still be good. Clinical Quality and Integration Speed of Implementation Strategic Alignment 7 The option enabled a safe and quality service which was good. The option provided good access to the appropriate diagnostic services. Whilst there was some reservations regarding medical cover in Ards hospital, in the main, as consultant cover was already in place it was agreed that this was still a good option. The group agreed that this option should therefore score 7 10 This option scored the maximum because the option is currently in place following the temporary closure of Bangor Hospital beds, therefore no changes need to be made and the model could be implemented with immediate effect. 6 The group requested that this option should score higher than Option 1 as it is inline with the Commissioning Plan direction, which states that the intention is to commission urgent care centres within PCCCs in Downpatrick, Lisburn and Newtownards. The Trust strategic model of care for North Down and Ards is dependent on an appropriate level of inpatient intermediate care beds, the group felt this would be challenging to achieve within a bed complement of 95 when compared to other options. Sustainability 4 This option would provide up to 95 beds and therefore is not as 64
65 sustainable as other options which provide up to 105 beds. The group agreed that this option offered more long term flexibility that option 1 and should therefore score 1 point higher. The group did note that in terms of medical and staffing cover, there would be challenges in relation to implementation Total score Weighted
66 Option no 6a. Option to provide 105 intermediate care beds in North Down and Ards area as follows: 29 Consultant led fracture rehabilitation beds 22 Independent provider beds with GP Medical Support 20 Consultant led beds in Ards Hospital 14 beds in Northfield House with GP GMS Medical Support Up to 20 additional spot purchased beds on a temporary basis when demand requires Criterion Score Rationale Accessibility Experience and Clinical Quality and Integration Speed of Implementation Strategic Alignment Sustainability Total score Weighted 9 The group agreed this option was better than option 2 in that services could be delivered more effectively right across the locality The option was viewed as excellent as it promoted local access to different levels of care with the additional ability to purchase independent sector beds in the patient s home area. The option was therefore viewed as providing excellent choice for service users and their families The group therefore agreed that this option should score 9. 8 It was deemed very good because there was a range of different levels of care available. The centralisation of beds on one Hospital site would provide good integration. The option was scored as very good because it provided access to the appropriate levels of diagnostic services. 7 The group agreed this option could be in place quite quickly as in the main it was already in place and there was a consultant presence for medical cover for some of the beds in Ards hospital already. Therefore it was agreed that this option should score less than option 2 as it is not currently in operation and would take some time to implement in full. This option was also viewed as good as the Trust already have approved funding in place to facilitate the spot purchase beds. 7 The group felt that this option should be viewed as good in terms of meeting with strategic direction of the Trust and the Commissioners stated intentions. It was agreed that this option should score one point more than option 2 as it has a greater ability to purchase spot beds within a patient s own area which is more in line with TYC and Trust strategic direction. 7 This option scored well in terms of sustainability as it was viewed as being affordable and in line with available resources. This option provides flexibility with ability to spot purchase up to 20 beds The option would enable the Trust to cope with demand through the availability of spot purchased beds There would be minimal issues with the recruitment and retention of staff The group therefore agreed that an overall score of 7 should be awarded
67 Option no 6b. Option to provide 105 intermediate care beds in North Down and Ards area as follows: 29 Consultant led fracture rehabilitation beds 22 Independent provider beds with GP Medical Support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 14 beds in Northfield House with GP GMS Medical Support Up to 20 additional spot purchased beds on a temporary basis when demand requires Criterion Score Rationale Accessibility and Experience Clinical Quality and Integration 9 The group agreed this option was better than option 2 in that services could be delivered more effectively right across the locality The option was viewed as excellent as it promoted local access to different levels of care with the additional ability to spot purchase independent sector beds in the patient s home area. The option was viewed as providing excellent choice for service users and their families The group therefore agreed that this option should score 9. 7 It was deemed very good because there was a range of different levels of care available with the option to access additional beds when demand dictates. The group agreed that this option should score one less point than option 6a as some of the beds would be staffed by GPs and therefore the integration of the beds would not be as good as option 6a, where all beds would be managed by the same staff cohort. The option was scored as very good because it provided access to the appropriate levels of diagnostic services. Speed Implementation Strategic Alignment of 4 Option scored lower that Option 6a because the group felt implementation could be difficult specifically with regards to GP Medical Cover. It was agreed that this cover may take longer to secure and therefore the option should score 4. 6 This option was viewed as quite good in terms of meeting with strategic direction The group agreed that this option should score one point less than option 6a due as it is not as compliant with the regional principles of medical cover. Sustainability Total Weighted score 6 While the option was considered to be affordable within the available budget it was considered quite good with regards to sustainability in the long term The group agreed that this option should score one point less than option 6a as there is concern over current and future availability of appropriate medical cover. This option was agreed as quite good in that it would provide flexibility with the 20 additional spot purchase beds thus addressing demography and demand issues
68 8.6 Option Ranking Analysis of results Rank Option Option 6a Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. Option 6b Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed GP and Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. Option 2 Do Minimum This option is to provide up to 95 beds, the same number of beds provided following the temporary closure in Bangor Hospital. Ability to spot purchase up to 10 beds in the independent sector 29 Consultant led fracture rehabilitation beds - Currently Domnall 22 Independent Provider Beds with GP GMS Medical support 20 beds in Ards Hospital 10 with GP Medical Support and 10 with Consultant support 14 Beds in Northfield House with GP GMS Medical Support. Up to 10 spot purchased beds on a temporary basis when demand requires. 4 Option 1 Status Quo Provide 125 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed Consultant and GP Medical Cover, 20 in Bangor Hospital with GP Medical Cover, 14 residential care beds and up to 20 spot purchase beds in the independent sector 8.7 Sensitivity Testing To test the robustness of the results of the benefits appraisal it is necessary to assess the sensitivity of the ranking of the scores to changes in key variables and assumptions. Accordingly an equal weighting was applied to all criteria and the results are outlined overleaf. 68
69 Benefit Criteria Accessibility and Experience Clinical Quality and Integration Speed of Implementation Strategic Alignment Weight Option 1 Maintain Status Quo Score Weighted Score Option 2 Do Minimum Score Weighted Score Option 6a Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. Score Weighted Score Option 6b Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed GP and Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. Score Weighted Score Sustainability Total
70 8.8 Qualitative statement of the preferred option In overall terms the results of the benefits scoring exercise were conclusive. Based on the composite scores, Option 6a (780) clearly delivers the highest level of benefits when measured against the criteria. The robustness of the results is confirmed in sensitivity testing whereby the outcome is the same when the criteria are given equal weighting. The Trust is seeking to provide a solution, which will provide a sustainable and affordable Intermediate Care provision to the population of North Down and Ards. Following the option appraisal, Option 6a has been identified as the preferred option in qualitative terms as it best meets the objectives set out above and scores the highest in terms of the benefit criteria. The Trust is confident that this proposal will ensure that the Service can be sustained over the long term, will improve quality of care, patient experience, enhance clinical networks and is in line with the Trust s strategic direction and the Commissioning Plan direction. However, the Trust will continue to monitor and review arrangements for Intermediate Care Provision for North Down and Ards on a regular basis. 70

71 9.0 Quantitative Analysis 9.1 Methodology This section examines the monetary costs associated with each of the shortlisted options. Quantitative Analysis of Shortlisted Options Option 1 Option 2 Option 6a Option 6b Maintain Do Up to 105 beds, Status Quo Minimum configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. 29 Consultant Led Fracture Rehabilitation Beds Independent Sector 20 Ards Hospital Bangor Hospital Residential care Beds Spot Purchase TOTAL Savings against Status Quo Up to 105 beds, configured as follows, 29 Consultant led Fracture Rehabilitation, 22 Independent Sector, 20 in Ards Hospital with mixed GP and Consultant Medical Cover, 14 residential care beds and up to 20 spot purchased beds. 71
Intermediate Care Provision in North Down and Ards. Consultation Document. January 2015
 Intermediate Care Provision in North Down and Ards Consultation Document January 2015 Contents Page number 1.0 INTRODUCTION AND BACKGROUND 6 2.0 ABOUT THE TRUST 7 3.0 CONTEXT 8 4.0 OVERVIEW OF PROCESS
Intermediate Care Provision in North Down and Ards Consultation Document January 2015 Contents Page number 1.0 INTRODUCTION AND BACKGROUND 6 2.0 ABOUT THE TRUST 7 3.0 CONTEXT 8 4.0 OVERVIEW OF PROCESS
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality care for you, with you Southern Health & Social Care Trust Three Year Strategic Plan Improving Through Change
 Quality care for you, with you Southern Health & Social Care Trust Three Year Strategic Plan 2015-2018 Improving Through Change Trust Board 22 nd October 2015 1 Contents Section 1: Why have we produced
Quality care for you, with you Southern Health & Social Care Trust Three Year Strategic Plan 2015-2018 Improving Through Change Trust Board 22 nd October 2015 1 Contents Section 1: Why have we produced
corporate management plan
 corporate management plan 2012-2013 2 Contents 1. Introduction 2. Overview of the Trust 3. Our purpose, values and core objectives 4. Safety & Quality Corporate Objectives 5. Modernisation Corporate Objectives
corporate management plan 2012-2013 2 Contents 1. Introduction 2. Overview of the Trust 3. Our purpose, values and core objectives 4. Safety & Quality Corporate Objectives 5. Modernisation Corporate Objectives
Living With Long Term Conditions A Policy Framework
 April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Northern Local Commissioning Group Locality Population Plan
 Northern Local Commissioning Group Locality Population Plan Foreword The Northern Local Commissioning Group and the Northern Health and Social Care Trust have collaborated to produce this Population Plan
Northern Local Commissioning Group Locality Population Plan Foreword The Northern Local Commissioning Group and the Northern Health and Social Care Trust have collaborated to produce this Population Plan
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
A Managed Change Briefing Paper : An Agenda for Creating a. Sustainable Basis for Domiciliary Care in Northern Ireland
 A Managed Change Briefing Paper : An Agenda for Creating a Sustainable Basis for Domiciliary Care in Northern Ireland November 2015 Contact You can contact us in the following ways: Telephone: 0300 555
A Managed Change Briefing Paper : An Agenda for Creating a Sustainable Basis for Domiciliary Care in Northern Ireland November 2015 Contact You can contact us in the following ways: Telephone: 0300 555
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74
 Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Corporate Plan
 Corporate Plan 2016-2017 FINAL Contents Page number Foreword... 3 Section 1: About the Trust ------------------------------------------- 5 Section 2: Vision, Values and Strategic Direction -------------
Corporate Plan 2016-2017 FINAL Contents Page number Foreword... 3 Section 1: About the Trust ------------------------------------------- 5 Section 2: Vision, Values and Strategic Direction -------------
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY. (for use by Health and Social Care Trusts)
") REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Briefing paper on Systems, Not Structures: Changing health and social care, and Health and Wellbeing 2026: Delivering together
 Briefing paper on Systems, Not Structures: Changing health and social care, and Health and Wellbeing 2026: Delivering together Judith Cross Head of policy and committee services November 2016 Briefing
Briefing paper on Systems, Not Structures: Changing health and social care, and Health and Wellbeing 2026: Delivering together Judith Cross Head of policy and committee services November 2016 Briefing
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Review by RQIA of Northern Ireland Single Assessment Tool Stage One
 Review by RQIA of Northern Ireland Single Assessment Tool Stage One Overview Report October 2011 Section 1 Contents Page 1.0 The Regulation and Quality Improvement Authority 1 2.0 Context for the Review
Review by RQIA of Northern Ireland Single Assessment Tool Stage One Overview Report October 2011 Section 1 Contents Page 1.0 The Regulation and Quality Improvement Authority 1 2.0 Context for the Review
REPORT SUMMARY SHEET
 Meeting: Date: Title: REPORT SUMMARY SHEET Trust Board 11th June 2015 Executive Director of Nursing s presentation on the Nursing Quality Indicator (NQI) Framework Providing assurance on the quality of
Meeting: Date: Title: REPORT SUMMARY SHEET Trust Board 11th June 2015 Executive Director of Nursing s presentation on the Nursing Quality Indicator (NQI) Framework Providing assurance on the quality of
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Transforming Clinical Services. Our developing clinical strategy
 Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Modernising Learning Disabilities Nursing Review Strengthening the Commitment. Northern Ireland Action Plan
 Modernising Learning Disabilities Nursing Review Strengthening the Commitment Northern Ireland Action Plan March 2014 INDEX Page A MESSAGE FROM THE MINISTER 2 FOREWORD FROM CHIEF NURSING OFFICER 3 INTRODUCTION
Modernising Learning Disabilities Nursing Review Strengthening the Commitment Northern Ireland Action Plan March 2014 INDEX Page A MESSAGE FROM THE MINISTER 2 FOREWORD FROM CHIEF NURSING OFFICER 3 INTRODUCTION
Southern Local Commissioning Group Locality -Population Plan. Changing For A Better Future
 Southern Local Commissioning Group Locality -Population Plan Changing For A Better Future 1 Foreword Foreword The Southern LCG and the Southern Health and Social Care Trust have together developed this
Southern Local Commissioning Group Locality -Population Plan Changing For A Better Future 1 Foreword Foreword The Southern LCG and the Southern Health and Social Care Trust have together developed this
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Future of Respite (Short Breaks) Services for Children with Disabilities
 Services for Children with Disabilities") Future of Respite (Short Breaks) Services for Children with Disabilities Consultation Feedback Report 2014 Foreword from the Director of Children s Services Within the Northern Trust area we know that
Future of Respite (Short Breaks) Services for Children with Disabilities Consultation Feedback Report 2014 Foreword from the Director of Children s Services Within the Northern Trust area we know that
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Trust Strategy
 Trust Strategy 2012 2022 Approved November 2012 Contents Introduction 3 Overview of St George s Healthcare NHS Trust 4 The drivers for change 6 Our mission, vision and values 7 Our guiding principles (values
Trust Strategy 2012 2022 Approved November 2012 Contents Introduction 3 Overview of St George s Healthcare NHS Trust 4 The drivers for change 6 Our mission, vision and values 7 Our guiding principles (values
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
grampian clinical strategy
 healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
ASPIRE. Allied Health Professions Supporting and Promoting Improvement, Rehabilitation and Enabling Others ADVANCED PRACTICE SPECIALIST GENERALIST
 ASPIRE Allied Health Professions Supporting and Promoting Improvement, Rehabilitation and Enabling Others ADVANCED PRACTICE SPECIALIST GENERALIST ENABLING OTHERS AHP Strategy 2017 2021 CONTENTS Introduction
ASPIRE Allied Health Professions Supporting and Promoting Improvement, Rehabilitation and Enabling Others ADVANCED PRACTICE SPECIALIST GENERALIST ENABLING OTHERS AHP Strategy 2017 2021 CONTENTS Introduction
JOB DESCRIPTION. Acute Services Patient Flow Coordinator. Band of Post: Band 7. Acute Community Services Manager
 JOB DESCRIPTION Title of Post: Acute Services Patient Flow Coordinator Band of Post: Band 7 Directorate: Reports to: Accountable to: Initial Location: Type of Contract: Hours: Adult Services Acute Community
JOB DESCRIPTION Title of Post: Acute Services Patient Flow Coordinator Band of Post: Band 7 Directorate: Reports to: Accountable to: Initial Location: Type of Contract: Hours: Adult Services Acute Community
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Our community nursing roles
 Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Hazel Winning AHP Lead Officer DHSSPS
 Hazel Winning AHP Lead Officer DHSSPS Promoting service and role redesign to AHPs to increase capacity and add value to service delivery. Ensuring robust governance arrangements, including supervision,
Hazel Winning AHP Lead Officer DHSSPS Promoting service and role redesign to AHPs to increase capacity and add value to service delivery. Ensuring robust governance arrangements, including supervision,
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Daisy Hill Hospital Profile
 Daisy Hill Hospital Profile 2012 Daisy Hill Hospital Profile Mairead McAlinden, Southern Trust Chief Executive, and Chair Roberta Brownlee welcome Health Minister Edwin Poots on a recent visit to Daisy
Daisy Hill Hospital Profile 2012 Daisy Hill Hospital Profile Mairead McAlinden, Southern Trust Chief Executive, and Chair Roberta Brownlee welcome Health Minister Edwin Poots on a recent visit to Daisy
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Agenda Item 3.3 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE
 FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Delivering excellent care and support to patients at home, in the community and in hospital - first time, every time.
 The Integrated County Durham & Darlington NHS Foundation Trust: Delivering excellent care and support to patients at home, in the community and in hospital - first time, every time. 1.0 Introduction The
The Integrated County Durham & Darlington NHS Foundation Trust: Delivering excellent care and support to patients at home, in the community and in hospital - first time, every time. 1.0 Introduction The
Annual Review and Evaluation of Performance 2012/2013. Torfaen County Borough Council
 Annual Review and Evaluation of Performance 2012/2013 Local Authority Name: Torfaen County Borough Council This report sets out the key areas of progress in Torfaen Social Services Department for the year
Annual Review and Evaluation of Performance 2012/2013 Local Authority Name: Torfaen County Borough Council This report sets out the key areas of progress in Torfaen Social Services Department for the year
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
TYC POST PROJECT EVALUATION
 TYC POST PROJECT EVALUATION Provider: SEHSCT Project/Enabler Title: TYC Telecare Prepared By: Position Held: Robert Moore (in lieu of J-A Augusto) Lead Nurse Primary Care Specialist Nursing Approved By:
TYC POST PROJECT EVALUATION Provider: SEHSCT Project/Enabler Title: TYC Telecare Prepared By: Position Held: Robert Moore (in lieu of J-A Augusto) Lead Nurse Primary Care Specialist Nursing Approved By:
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
A review of people s views on Health and Social Care as expressed to the Patient and Client Council since April 2009
 The People s Priorities for Transforming Your Care A review of people s views on Health and Social Care as expressed to the Patient and Client Council since April 2009 The Initial Draft People s Report
The People s Priorities for Transforming Your Care A review of people s views on Health and Social Care as expressed to the Patient and Client Council since April 2009 The Initial Draft People s Report
AHP Services Data Definitions Guidance. Guidance for monitoring the Ministerial AHP 13 Week Access Target
 AHP Services Data Definitions Guidance Guidance for monitoring the Ministerial AHP 13 Week Access Target 2015/16 Status Live from July 1 st 2014 Version Control Number of this Version: Date of this Version:
AHP Services Data Definitions Guidance Guidance for monitoring the Ministerial AHP 13 Week Access Target 2015/16 Status Live from July 1 st 2014 Version Control Number of this Version: Date of this Version:
Statement of Purpose Kerry General Hospital 2013
 Statement of Purpose Kerry General Hospital 2013 Table of Contents Introduction...3 Description of Services Provided...3 Kerry General Hospital Services...4 Models of service delivery and aligned resources
Statement of Purpose Kerry General Hospital 2013 Table of Contents Introduction...3 Description of Services Provided...3 Kerry General Hospital Services...4 Models of service delivery and aligned resources
Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay. Statement of Intent
 Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay Statement of Intent March 2014 1 1. Introduction This document sets out our commitment to deliver integrated
Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay Statement of Intent March 2014 1 1. Introduction This document sets out our commitment to deliver integrated
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
Performance Evaluation Report Gwynedd Council Social Services
 Performance Evaluation Report 2013 14 Gwynedd Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Gwynedd Council Social Services for the year
Performance Evaluation Report 2013 14 Gwynedd Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Gwynedd Council Social Services for the year
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
STATEMENT OF PURPOSE August Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008)
") 1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
IMProVE Outline Business Case, Community Transformation across South Tees
 IMProVE Outline Business Case, Community Transformation across South Tees 1 Acknowledgements The assistance with and contributions to this business case from departments throughout NHS South Tees Clinical
IMProVE Outline Business Case, Community Transformation across South Tees 1 Acknowledgements The assistance with and contributions to this business case from departments throughout NHS South Tees Clinical
NHS BORDERS CLINICAL STRATEGY. 'A plan for person-centred, innovative healthcare to help the Borders flourish'
 NHS BORDERS CLINICAL STRATEGY 'A plan for person-centred, innovative healthcare to help the Borders flourish' CONTENTS NHS BORDERS CLINICAL STRATEGY FOREWORD 3 EXECUTIVE SUMMARY 4 THE CASE FOR CHANGE 5
NHS BORDERS CLINICAL STRATEGY 'A plan for person-centred, innovative healthcare to help the Borders flourish' CONTENTS NHS BORDERS CLINICAL STRATEGY FOREWORD 3 EXECUTIVE SUMMARY 4 THE CASE FOR CHANGE 5
A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services
 A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services Clinical Strategy and Programmes Division Vision for Paediatric Health Services Introduction
A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services Clinical Strategy and Programmes Division Vision for Paediatric Health Services Introduction
Discharge to Assess Standards for Greater Manchester
 Discharge to Assess Standards for Greater Manchester 1 Contents 1. Introduction... 3 2. Definition of Discharge to Assess... 3 3. Discharge to Assess Pathways... 4 4. Greater Manchester Standards for Discharge
Discharge to Assess Standards for Greater Manchester 1 Contents 1. Introduction... 3 2. Definition of Discharge to Assess... 3 3. Discharge to Assess Pathways... 4 4. Greater Manchester Standards for Discharge
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
OUTLINE BUSINESS CASE FOR THE DEVELOPMENT OF A&E SERVICES AT ANTRIM AREA HOSPITAL
 OUTLINE BUSINESS CASE FOR THE DEVELOPMENT OF A&E SERVICES AT ANTRIM AREA HOSPITAL Executive Summary August 2009 0.0 EXECUTIVE SUMMARY 0.1 Introduction and background There are two strands to the case for
OUTLINE BUSINESS CASE FOR THE DEVELOPMENT OF A&E SERVICES AT ANTRIM AREA HOSPITAL Executive Summary August 2009 0.0 EXECUTIVE SUMMARY 0.1 Introduction and background There are two strands to the case for
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Agenda Item: REPORT TO PUBLIC BOARD MEETING 31 May 2012
 Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Better Care, Closer to Home
 Better Care, Closer to Home Our three-year strategy for coordinated, high quality care out of hospital 2012 2015 V0.3 17.05.2012 Ealing Clinical Commissioning Group Foreword Ealing Clinical Commissioning
Better Care, Closer to Home Our three-year strategy for coordinated, high quality care out of hospital 2012 2015 V0.3 17.05.2012 Ealing Clinical Commissioning Group Foreword Ealing Clinical Commissioning
Introduction. Context
 Introduction Delivering Care aims to support the provision of high quality care which is safe and effective in hospital and community settings, through the development of a framework to determine staffing
Introduction Delivering Care aims to support the provision of high quality care which is safe and effective in hospital and community settings, through the development of a framework to determine staffing
Midlothian Health and Social Care Partnership
 Midlothian Health and Social Care Partnership the right care the right support the right time This document is a draft, work in progress version. It includes current thinking on priorities / direction
Midlothian Health and Social Care Partnership the right care the right support the right time This document is a draft, work in progress version. It includes current thinking on priorities / direction
Belfast Local Commissioning Plan 2013/14 14 March 2013
 Belfast Local Commissioning Plan 2013/14 14 March 2013 Belfast LCG Commissioning Plan 2013/14 Page 1 Contents 1. Belfast LCG Population & Need... 3 2. Key successes in 2012/13... 17 3. Key challenges for
Belfast Local Commissioning Plan 2013/14 14 March 2013 Belfast LCG Commissioning Plan 2013/14 Page 1 Contents 1. Belfast LCG Population & Need... 3 2. Key successes in 2012/13... 17 3. Key challenges for
Quality Improvement Strategy 2017/ /21
 Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
New Directions. The Teams. Chart showing New Directions Project Structure. What s next for New Directions?
 May 2016 Volume 1, Issue 1 New Directions A blueprint for future health and social care delivery in Belfast Trust The purpose of New Directions is to determine, with Trust Teams, the future shape of services
May 2016 Volume 1, Issue 1 New Directions A blueprint for future health and social care delivery in Belfast Trust The purpose of New Directions is to determine, with Trust Teams, the future shape of services
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
HEALTH AND SOCIAL CARE BOARD PUBLIC HEALTH AGENCY COMMISSIONING PLAN 2010/2011
 HEALTH AND SOCIAL CARE BOARD PUBLIC HEALTH AGENCY COMMISSIONING PLAN 2010/2011 Contents Foreword Page Numbers SECTION ONE SUMMARIES AND OVERVIEWS 1. Strategic Context 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9
HEALTH AND SOCIAL CARE BOARD PUBLIC HEALTH AGENCY COMMISSIONING PLAN 2010/2011 Contents Foreword Page Numbers SECTION ONE SUMMARIES AND OVERVIEWS 1. Strategic Context 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Nurse Recruitment in South Eastern HSC Trust
 Nurse Recruitment in South Eastern HSC Trust Why choose South Eastern H&SC Trust? In the South Eastern H&SC Trust person centredness is at the centre of all that we do. We encourage our staff to look after
Nurse Recruitment in South Eastern HSC Trust Why choose South Eastern H&SC Trust? In the South Eastern H&SC Trust person centredness is at the centre of all that we do. We encourage our staff to look after
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
GOULBURN VALLEY HEALTH Strategic Plan
 GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
Devon Pre-Consultation Business Case
 Devon Pre-Consultation Business Case 21 September 2016 Contents 1 Executive summary... 5 1.1 Introduction... 5 1.2 Stakeholder engagement... 5 1.3 Context... 6 1.4 Case for change... 6 1.5 Responding to
Devon Pre-Consultation Business Case 21 September 2016 Contents 1 Executive summary... 5 1.1 Introduction... 5 1.2 Stakeholder engagement... 5 1.3 Context... 6 1.4 Case for change... 6 1.5 Responding to
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service
 Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Craigavon Area Hospital Profile
 Craigavon Area Hospital Profile 2012 Craigavon Area Hospital Profile Craigavon Area Hospital is located in Craigavon, County Armagh and is an essential part of the hospital network provided by the Southern
Craigavon Area Hospital Profile 2012 Craigavon Area Hospital Profile Craigavon Area Hospital is located in Craigavon, County Armagh and is an essential part of the hospital network provided by the Southern
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts