Reducing Mortality and Harm in ABMU Local Health Board
|
|
|
- Beverly Fleming
- 6 years ago
- Views:
Transcription

1 10 th June 2011 Reducing Mortality and Harm in ABMU Local Health Board Insert name of presentation on Master Slide
2 Programme Driver Diagram Aims/Outcome Measure Reduce Mortality Reduce RAMI to <100 by Harm Reduce Secondary Care GTT Indicator by 50% by Key Interventions/Domains Infection Control Pathways Communication Mortality Reviews Key Areas for Action Cleaning Standards Antimicrobial Governance Hand Hygiene Dress Code Single Room provision Urinary Catheter Bundle SSI Surveillance Inpatient Falls Intermediate Care Falls Stroke Care Fractured Neck of Femur Thrombo prophylaxis SBAR Discharge Interface WHO Surgical Checklist Initial Review Investigation Data Quality Errors Timeliness
3 Patient Safety & Quality Walkrounds A total of 86 patient safety and quality walkround visits were undertaken during January to March 2011, increasing the total to 173 visits since April Performance against an ABMU target set in September for each ward, unscheduled care area and theatre suite to have been visited at least once within a 12 month cycle was achieved in March 2011.
4 Patient Safety & Quality Walkrounds - Themes Estates and environmental issues, particularly ability to treat patients with dignity and respect, the building fabric on some wards, storage space, security access within sites, access to car parking, dining rooms not fit for purpose Effective communication and engagement with staff when implementing changes to practice, avoiding rumours and poor service reputation with public Replacement equipment issues Development of strong multidisciplinary team working restricted by availability of psychology and therapy services, together with staff continuity within the team Challenges regarding access to medical records Staffing issues, particularly within Swansea Hospitals Frustration at not being able to enact change. These key themes are not new to the Health Board and Executive Members through existing groups and committees are driving improvement in all of these areas.
5 MORTALITY AND HARM Risk Adjusted Mortality Index * * * Coding completeness <95%
6 MORTALITY AND HARM Risk Adjusted Mortality Index
7 MORTALITY AND HARM Global Trigger Tool Sample size increased to 20 per acute site (Total of 80) per month from June 2010 discharges onwards
8 MORTALITY AND HARM Global Trigger Tool
9 MORTALITY AND HARM Global Trigger Tool
10 MORTALITY AND HARM Mortality Reviews Mortality Review Team: Bruce Ferguson; Anne Biffin Aims/Outcome Measures Improve Key Interventions Initial Screening Key Areas for Action Develop Screening Tool Establish Weekly Screening Cause of death established (100%) RCA recommendations implemented (100%) Unexpected Death Review Mortality Review Tool Establish Weekly Review RCA Training Lessons Learned Mortality Review Report
11 % MORTALITY AND HARM Mortality Reviews Total number of screening forms completed for HB % of total deaths with a completed screening form NPTH Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 0 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 NPTH % Screening Forms completed
12 MORTALITY AND HARM Mortality Reviews Reviews being undertaken consistently at NPTH Between 20 65% of deaths screened at NPTH were identified as needing more in depth review Limited spread to PoWH, Morriston & Singleton Further spread constrained by availability of Consultant medical staff to undertake full reviews Process to be revised and implementation across the Health Board restarted July 2011 Key themes Consultant review not always undertaken promptly Times of entries are not always recorded Suitable patients are not being put on the Care of the Dying Pathway Appropriateness of investigations (imaging) needs to be evaluated against patients suitability for aggressive treatment such as surgery
13 Infection Control Infection Control Committee: Victoria Franklin; Nicola Williams AIM INTERVENTION OVERARCHING MEASURE/DATA SOURCE MEASURE Reduce Hospital Acquired Infections C.Difficile 20% (AOF) C.Section Wound Infection (AOF) Joint Replacement Surgery (AOF) MRSA Urinary Catheter Infections Fully implement Bare Below Elbows Full compliance with appropriate hand hygiene Achieve compliance with NSOC (meet minimum standards of cleanliness) Achieve full compliance with Health Board Antimicrobial Policy Health Board wide Infection Surveillance data and WHAIP surveillance data C.Difficile acquired rates (HCAI) MRSA bacteraemia New: Spot audits New: Provide graphs audit quarterly Current: Ward level overall compliance Nursing Metrics New: Monthly C4C compliance Current: Monthly environmental audits Nurse Metrics New: Quarterly Directorate audits Current: Antimicrobial Pharmacist targeted reviews Increase single room provision/develop surge capacity and isolation ward Full roll out Short Term Urinary Catheter Bundle Achieve full compliance with SSI Mandatory Surveillance Programmes MSSA bacteraemia Beds closed due to norovirus New: Quarterly review New: Monthly compliance Current: Urinary tract infections rates Ward Metrics Current: Quarterly WHAIP SSI reports
14 INFECTION CONTROL Infection Reduction Activities undertaken in the last year Targeted hand hygiene actions Bed Cleaning video Commode cleaning bundle fully rolled out Monthly infection control environmental audits Antimicrobial / Microbiology ward rounds Revised antimicrobial prescribing policy reduction in prescribing C. diff high risk antibiotics Implementation of antibiotic stickers within drug charts Norovirus toolkit 50% reduction in bed days lost this year Increased Incidences of C.difficile meetings implemented > 2 cases in 28 days Suite of ward infection prevention & control metrics implemented keeping infection a high priority Infection control data visible on every ward Urinary Catheter Bundle fully rolled out Peripheral Venflon bundle pilot commenced
15 Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb March No.of dosage units Feb Mar Apr May jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar NO.OF UNITS INFECTION CONTROL Trends in Antibiotic TAZOCIN USAGE IN DOSAGE UNITS MORRISTON HOSPITAL FEBRUARY 2008 TO MARCH 2011 Prescribing Total Issues of Ciprofloxacin and Cefuroxime Morriston Hospital August 2007 to March 2011 TAZOCIN MONTH Linear (TAZOCIN) 13, , , R 2 = , , Month/Year Total Poly. (Total)
16 INFECTION CONTROL 21.5% Reduction in C.difficile Infection rates
17 INFECTION CONTROL ABMU Health Board
18 INFECTION CONTROL MRSA MSSA ABMU Health Board
19 INFECTION CONTROL Hand Hygiene Monthly Observational Audit undertaken in all areas Hand Hygiene video on intranet Zero Tolerance to non compliance with WHO 5 moments implemented 569 staff trained as Hand Hygiene Trainers 1,510 staff trained between April and September
20 INFECTION CONTROL Hand Hygiene
21 INFECTION CONTROL Hand Hygiene Audit
22 % compliance % compliance INFECTION CONTROL Peripheral Venflon Bundle Peripheral venflon bundle being piloted within a medical ward 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% % compliance with maintenance bundle by week Ward E 02/05/11 09/05/11 % compliance w ith maintenance bundle 16/05/11 % compliance with insertion bundle by week Ward E 100% 98% 96% 94% 92% 90% 88% 86% 84% 02/05/11 09/05/11 % compliance w ith insertion bundle 16/05/11
23 INFECTION CONTROL Bacteraemia in Intensive Care Incidence of CVC related infection 01/01/10 to 31/12/2010 HELICS defined CVC infections/1000 catheter days WHAIP defined CVC infections/1000 catheter days Neath Port Talbot Princess of Wales Swansea All Wales Rate
24 INFECTION CONTROL Bacteraemia in Intensive Care Incidence of Critical Care Ventilator Associated Pneumonia 01/01/10 to 31/12/2010 HELICS defined VAP rate/1000 ICU ventilator days Neath Port Talbot 0.0 Princess of Wales 0.0 Swansea 1.5 All Wales Rate 1.0
25 FALLS IC Falls Pathway Intermediate Care Falls Reduction Implementation Group: Victoria Franklin: Nicola Williams Aims/Outcome Measures Reduce The mortality associated with falls in the community The harm associated with falls in the community Key Interventions Trigger Bundle Assessment Bundle Intervention Bundle Key Areas for Action Complete the initial screening using an agreed tool Log the fall on central Falls Register Notification of the fall as per locally agreed pathway, copy to GP Take falls history Complete falls risk assessment Provide falls prevention information Refer as appropriate for specialist assessment Initiate bespoke plan Agree plan with patient and carers Agree timescale and review date Copy plan to GP Monitoring Bundle Review Plan compliance Evaluate efficacy Update or close plan as appropriate
26 FALLS IP Falls Pathway Inpatient Falls Reduction Implementation Group: Victoria Franklin: Nicola Williams Aims/Outcome Measures Key Interventions Initial Falls Risk Assessment Key Areas for Action Compliance Improvement Reduce The number of inpatient falls (50%) Bed Rails Assessment Risk Reassessment Compliance Improvement Compliance Improvement Falls Bundle Develop and Implement Safe Rounds Roll Out to all Wards
27 FALLS Falls Reduction An inpatient Falls Reduction Bundle is being established and will be rolled out across the organisation Falls reduction aids introduced sensor pads SAFE Rounds significantly reduced incidence of in-patient falls A Community Falls Reduction Collaborative is being established Integrated falls group established and Integrated falls strategy under development
28 FALLS Inpatient falls Ward Metrics data
29 PATIENT ID Improving Patient Identification Health Board wide focus to reduce the incidence of patient identification errors Electronic bar coded wrist bands (bed side) that contain the NHS number as unique identifier rolled out across the whole Health Board

30 PATIENT ID Wristband Audit
31 RRAILS Rapid Response to Acute Illness
32 RRAILS RRAILS
33 RRAILS RRAILS
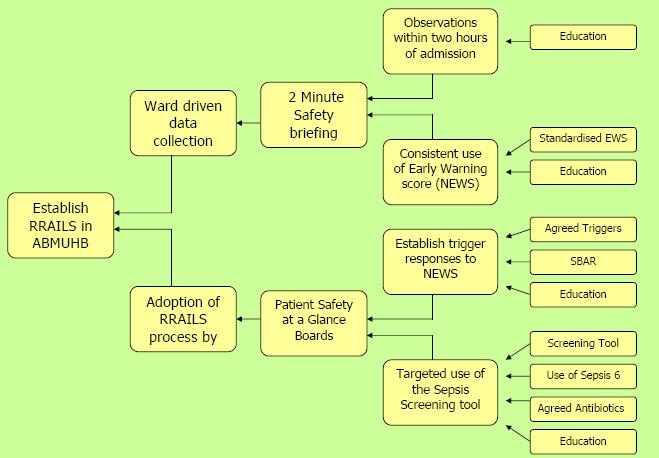
34 RRAILS

35 RRAILS RRAILS Implementation plan
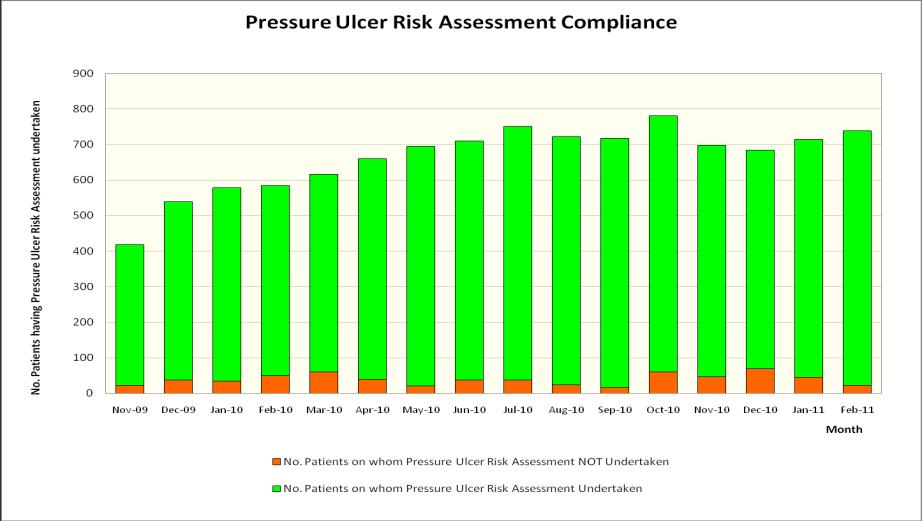
36 PRESSURE ULCERS Zero Tolerance to hospital acquired pressure ulcers Nutritional & Pressure Ulcer risk assessments audited monthly SKIN bundle rolled out across all inpatient areas SKIN Bundle pilot within a District Nurse Team Commenced Successful Care Home SKIN Bundle Pilot
37 Preventing Pressure Ulcers
38 Pressure Ulcer Incidence Swansea Hospitals Feb 2011 No of patients Patients with acquired pressure ulcers Percentage % 10% 6.59% 6.08% 1.99% 1% Zero Tolerance to any hospital acquired pressure ulcer Significant organisational cultural change
39
40 HOSPITAL ACQUIRED THROMBOSIS Thromboprophylaxis Thromboprophylaxis and Anticoagulation Committee: Bruce Ferguson: Andrea Croft:Anne Biffin Aims/Outcome Measures Reduce Mortality Deaths related to HAT Harm % of patients diagnosed with DT or PE who ve been in hospital in last 3 months Key Interventions Risk Assessment Prophylactic Treatment Patient involvement Key Areas for Action Documented Risk Assessment on admission Reassessment of risk every 24 hours / When there is a change in the patient s condition Mechanical Methods Pharmacological methods Patient awareness of risk factors and symptoms
41 HOSPITAL ACQUIRED THROMBOSIS HAT Collaborative Team Executive Lead Medical Director Project Board - Thromboprophylaxis & Anticoagulation Committee (Chaired by Medical Director) Local HAT Collaborative Team: Anticoagulation CNS, Orthopaedic Surgical Practitioner, 3 Clinical Pharmacists, CE & Governance Manager
42 HOSPITAL ACQUIRED THROMBOSIS Adoption of HAT Risk Assessment Tools Three HAT Risk Assessment & Treatment Tools have been developed through repeated PDSA cycles and wide consultation with clinicians: Combined Acute Admissions Elective General Surgery Elective Orthopaedic Surgery Acute Admissions Tool embedded as part of the admission process in the Clinical Decision Unit at POWH, in use for acute admissions at Singleton and soon to be piloted in Morriston CDU Elective General and Elective Orthopaedic Tools fully embedded into the HB s Pre Assessment Process at POWH and NPTH. Cardiac at Morriston will be adopting the Acute and Elective General Surgery Tools from end May 2011
43 % HOSPITAL ACQUIRED THROMBOSIS Elective Orthopaedic Surgery HAT Risk Assessment All patients attending for pre-assessment at POW & NPT have a documented risk assessment All patients admitted to POW & NPT for elective orthopaedic surgery who have no contraindications receive thromboprophylaxis Risk assessment is being undertaken at Morriston but data collection needs to be formalised Elective Orthopaedics HAT Risk Assessment Compliance POWH & NPTH Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 % risk assessed at preassessment % risk assessed on admission % prescribed of eligible
44 % HOSPITAL ACQUIRED THROMBOSIS Combined Acute Admissions HAT Risk Assessment CDU POWH Consultants in CDU at POWH and Morriston identified as Clinical Champions Training provided for trainee doctors by the Anticoagulation CNS Combined Acute Admissions HAT Risk Assessment Compliance 0 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 % completed RA % prescribed of eligible
45 % HOSPITAL ACQUIRED THROMBOSIS Elective General Surgery HAT Risk Assessment POWH & NPTH All patients attending for preassessment at POW & NPT have a documented risk assessment This includes Adult General Surgery, Gynaecology majors and Ophthalmology patients Now needs to be embedded into pre-assessment at Morriston and Singleton Data collection to establish % of eligible, at risk, patients prescribed thromboprophylaxis required % Risk Assessed at pre-assessment Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 NPTH % risk assessed at preassessment POWH % risk assessed at preassessment
46 STROKE Stroke Pathway Acute Stroke Care Pathway Group: Bruce Ferguson: Andrew Phillips: Hilary Dover Aims/Outcome Measures Reduce Mortality within 30 days of emergency admission Readmission within 28 days Improve Percentage of people discharged to usual address Average Functional outcome (Barthel) score on discharge Key Interventions First Hours Bundle First Day Bundle First 3 Days Bundle 7 Days Bundle Key Areas for Action Compliance Improvement Compliance Improvement Compliance Improvement Compliance Improvement
47 STROKE Stroke First Hours Bundle Princess of Wales Hospital Morriston Hospital % compliance with First Hours bundle Stroke patients from Feb 2009 to May FebM araprm ayjun Jul AugSepOctNovDec JanFebM araprm ayjun Jul AugSepOctNovDecJanFebM araprm ay Months % compliance with First Hours bundle Stroke patients from Jan 2010 to May 2011 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Months
48 STROKE Stroke First Day Bundle Princess of Wales Hospital Morriston Hospital % compliance with First Days bundle Stroke patients from Feb 2009 to May FebM araprm ayjun Jul AugSepOctNovDec JanFebM araprm ayjun Jul AugSepOctNovDecJanFebM araprm ay Months % compliance with First Days bundle Stroke patients from Jan 2010 to May 2011 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Months
49 STROKE Stroke 3 Day Bundle Princess of Wales Hospital Morriston Hospital % compliance with First 3 Days bundle Stroke patients from Feb 2009 to May 2011 % compliance with First 3 Days bundle Stroke patients from Jan 2010 to May FebM araprm ayjun Jul AugSepOctNovDec JanFebM araprm ayjun Jul AugSepOctNovDecJanFebM araprm ay Months Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Months
50 STROKE Stroke 7 Day Bundle Princess of Wales Hospital Morriston Hospital % compliance with First 7 Days bundle Stroke patients from Feb 2009 to May 2011 % compliance with First 7 Days bundle Stroke patients from Jan 2010 to May FebM araprm ayjun Jul AugSepOctNovDec JanFebM araprm ayjun Jul AugSepOctNovDecJanFebM araprm ay Months Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Months
51 STROKE Stroke Length of Stay POWH Morriston
52 FRACTURED NOF PATHWAY # NOF Pathway MSK Directorate: Dougie Russell: Mike Bond Aims/Outcome Measures Reduce Key Interventions Diagnosis Key Areas for Action Diagnostic Protocols Mortality Number of missed diagnoses Improve The number of patients having surgery within 24 hours of admission (90%) Peer Review Guidance Peer Review of all Cases Pathway Development Performance Feedback Theatre availability Prioritise on Theatre Lists
53 FRACTURED NOF PATHWAY # NoF Pathway
54 #NoF Pathway
55 THEATRE COMMUNICATION Theatre Communication ACCT Directorate: Push Mangat; Ceri Mathews Aims/Outcome Measures Key Interventions Completion of Time Out Key Areas for Action Time Out Compliance Reduce Wrong site surgery cases Incidence of theatre related incidents Completion of Sign Out Sign Out Compliance Awareness Incident Investigation Performance Feedback
56 WHO Surgical Checklist Compliance with WHO / NPSA Surgical Checklist Abertawe Bro Morgannwg University Health Board 100% 80% 60% 40% 20% 0% Jul 2010 Aug 2010 Sep 2010 Oct 2010 Nov 2010 Dec 2010 Jan 2011 Feb 2011 Mar 2011
57 DATA QUALITY Data Quality Clinical Outcomes Steering Group: Bruce Ferguson Aims/Outcome Measures Improve Timeliness of clinical coding (95% within 6 weeks) Coding Completeness (Coding depth in peer group upper quartile) Key Interventions Coding Timeliness Coding Depth Coding Accuracy Key Areas for Action Ward based coding Access to closed libraries Workforce reorganisation Use of electronic resources Coding Bookmark Co Morbidities Coding awareness sessions Qualified staff Coder training Coding Clinics Feedback Feedback reports Coder Liaison
58 DATA QUALITY Data Quality Clinical coding performance has improved over the past year with the Health Board achieving the national target of 95% completeness within 3 months of discharge for the past 7 months. Coding completeness for April 2010 to January 2011 is currently 96%. Clinical Coding Completeness Jan 2010 to end of Dec 2010 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct- 10 Nov- 10 Dec-10 98% 98% 98% 98% 98% 98% 98% 98% 97% 97% 96% 93% Percentage of Deaths Z515 code Jan 2010 to end of Dec 2010 (CHKS Figs) Jan- 10 Feb- 10 Mar- 10 Apr- 10 May- 10 Jun- 10 Jul- 10 Aug- 10 Sep- 10 Oct- 10 Nov Dec- 10
59 ENHANCED RECOVERY AFTER SURGERY ERAS in Colorectal Surgery MDT with the patient at the centre- Patient education provided preoperatively, Patients collect their own data for each ERAS Goal Compliance with data collection
60 ENHANCED RECOVERY AFTER SURGERY ERAS in Colorectal Surgery The median length of stay for major colorectal resections within the ERAS programme is just 4 days compared to 11 days previous to ERAS, with 86% being performed laparoscopically. This reduced length of stay is not associated with an increase in readmission rate
61 MEDICINES MANAGEMENT Clydach Anticoagulation Pilot The new model of care involves monitoring of Anticoagulation therapy through point of care testing (POCT) together with dosing and prescribing being undertaken by Independent Pharmacist/Nurse Prescribers, in a one-stop, network-based clinic. Clydach Pilot: Initial Comparative Data March May 2011 Clydach Acute Sites - Swansea % INR in range % INR below range % INR above range %INR >1 below target %INR > %INR >
62 ENHANCED RECOVERY AFTER SURGERY Benefits of monitoring INR in Primary Care Improves patient convenience by providing INR testing nearer to patients which is easily accessible. This should encourage attendance and decrease DNA rates Combining monitoring and dosing improves patient safety by - reducing potential dosing errors - establishing high INRs immediately, whilst the patient is present Improves anticoagulation control could reduce number of INR tests required to maintain in-range control as patient reviewed by Independent Prescriber at each visit Ensures that maintenance of patients is properly controlled, the need for continuation of therapy is reviewed regularly and therapy is discontinued where appropriate
Andrea Croft RGN Lead Advanced Nurse Practitioner Anticoagulation. Welsh Nurse Director Thrombosis UK
 Andrea Croft RGN Lead Advanced Nurse Practitioner Anticoagulation Welsh Nurse Director Thrombosis UK Background Venous Thromboembolism (VTE), the collective term for deep vein thrombosis (DVT) and pulmonary
Andrea Croft RGN Lead Advanced Nurse Practitioner Anticoagulation Welsh Nurse Director Thrombosis UK Background Venous Thromboembolism (VTE), the collective term for deep vein thrombosis (DVT) and pulmonary
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
MRSA: National developments, Progress, Challenges and Targets
 MRSA: National developments, Progress, Challenges and Targets Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London The MRSA challenge - 2007 Bacteraemia
MRSA: National developments, Progress, Challenges and Targets Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London The MRSA challenge - 2007 Bacteraemia
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Bwrdd Iechyd Prifysgol Betsi Cadwaladr University Health Board
 Thursday 25 th November 2010 Liberty Stadium / Optic Technium Bwrdd Iechyd Prifysgol Betsi Cadwaladr University Health Board Betsi Cadwaladr University Health Board Ysbyty Glan Clwyd Ysbyty Gwynedd Ysbyty
Thursday 25 th November 2010 Liberty Stadium / Optic Technium Bwrdd Iechyd Prifysgol Betsi Cadwaladr University Health Board Betsi Cadwaladr University Health Board Ysbyty Glan Clwyd Ysbyty Gwynedd Ysbyty
NHS Highland Infection Prevention & Control Annual Work Plan End of Year
 NHS Highland Board 5 April Item 5.7 NHS Highland & Control Annual Work Plan End of Year Update for COIC Prepared by Catherine Stokoe and Jonty Mills (as of 01/03/) Objective Activity Time Scale Lead Officer
NHS Highland Board 5 April Item 5.7 NHS Highland & Control Annual Work Plan End of Year Update for COIC Prepared by Catherine Stokoe and Jonty Mills (as of 01/03/) Objective Activity Time Scale Lead Officer
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Radiology CPG Annual Report for Quality, Safety and Experience Sub-Committee- April 2015
 Radiology CPG Annual Report for Quality, Safety and Experience Sub-Committee- April 2015 1. Purpose of report To provide assurance to the QSE sub-committee of the Radiology CPG s commitment to quality,
Radiology CPG Annual Report for Quality, Safety and Experience Sub-Committee- April 2015 1. Purpose of report To provide assurance to the QSE sub-committee of the Radiology CPG s commitment to quality,
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
REPORT SUMMARY SHEET
 Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 27 th October 2016 Infection Prevention and Control
Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 27 th October 2016 Infection Prevention and Control
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Quality and Safety Committee. Prevention and Control of Healthcare Acquired Infections performance to February 2012
 Betsi Cadwaladr University Health Board Committee Paper 05.04.12 Item QS12/37.5 Name of Committee: Subject: Summary or Issues of Significance National / Local Objectives Addressed: Legislation or Healthcare
Betsi Cadwaladr University Health Board Committee Paper 05.04.12 Item QS12/37.5 Name of Committee: Subject: Summary or Issues of Significance National / Local Objectives Addressed: Legislation or Healthcare
REPORT SUMMARY SHEET
 Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 29 th September 2016 Infection Prevention and Control
Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 29 th September 2016 Infection Prevention and Control
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36
 Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Ensuring quality outcomes
 Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
This paper provides an update on the the recent national SPSP conference the programme of work for Tissue Viability Acute Adult Care SPSP
 Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Sheffield Teaching Hospitals NHS Foundation Trust
 Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST REDUCING HARM TISSUE VIABILITY PROGRESS REPORT
 Agenda item A5(iv) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST REDUCING HARM TISSUE VIABILITY PROGRESS REPORT EXECUTIVE SUMMARY The Tissue Viability Team assists wards and departments to reduce
Agenda item A5(iv) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST REDUCING HARM TISSUE VIABILITY PROGRESS REPORT EXECUTIVE SUMMARY The Tissue Viability Team assists wards and departments to reduce
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Paper 8 DECISION NOTE. Recommendation
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
Sign up to Safety Drivers and Measurement
 Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
Mission Statement: 1) Patient safety and clinical quality. 2) Patient and staff experience. 3) Productivity and efficiency.
 Patient safety and clinical quality. 2) Patient and staff experience. 3) Productivity and efficiency.") Quality Accounts Mission Statement: The Trust aims to become the leading integrated health, teaching, research and innovation campus in the NHS and to position itself on an international basis alongside
Quality Accounts Mission Statement: The Trust aims to become the leading integrated health, teaching, research and innovation campus in the NHS and to position itself on an international basis alongside
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Board of Directors Infection Prevention and Control Report. Dr Claire Thomas, DIPC
 Board of Directors 25 November Report to: Title: Author: Sponsoring Director Purpose: Decision Sought: Board of Directors Infection Prevention and Control Report Dr Claire Thomas, DIPC Donna Green 6 monthly
Board of Directors 25 November Report to: Title: Author: Sponsoring Director Purpose: Decision Sought: Board of Directors Infection Prevention and Control Report Dr Claire Thomas, DIPC Donna Green 6 monthly
To Dip or Not To Dip
 To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
Infection Prevention and Control Annual Report 2012/13
 Infection Prevention and Control Annual Report 2012/13 Infection Prevention and Control Annual Report 2012/13 1 Contents 1. Executive Overview 2. Key Achievements 3. Infection Prevention and Control Team
Infection Prevention and Control Annual Report 2012/13 Infection Prevention and Control Annual Report 2012/13 1 Contents 1. Executive Overview 2. Key Achievements 3. Infection Prevention and Control Team
Elaine Andrews, Assistant Director of Nursing & Safety and Caroline Booton Quality Analyst Jill Asbury, Acting Director of Nursing
 Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT
 WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT 2006-2007 Author(s) Gill Harris, Director of Infection Prevention and Control EXECUTIVE
WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT 2006-2007 Author(s) Gill Harris, Director of Infection Prevention and Control EXECUTIVE
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Quality Improvement Strategy
 / Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
/ Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Mortality and harm reduction in Welsh Ambulance Services NHS Trust
 25 th November 2010 Mortality and harm reduction in Welsh Ambulance Services NHS Trust Insert name of presentation on Master Slide Introduction First ambulance service in the world to take part in 1000
25 th November 2010 Mortality and harm reduction in Welsh Ambulance Services NHS Trust Insert name of presentation on Master Slide Introduction First ambulance service in the world to take part in 1000
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
abc INFECTION CONTROL STRATEGY
 abc INFECTION CONTROL STRATEGY 1. INTRODUCTION East and North Hertfordshire NHS Trust (ENHT) considers the reduction of Healthcare Associated infections (HCAI) a key component of patient safety systems
abc INFECTION CONTROL STRATEGY 1. INTRODUCTION East and North Hertfordshire NHS Trust (ENHT) considers the reduction of Healthcare Associated infections (HCAI) a key component of patient safety systems
Integrated Quality Report
 Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Connolly Hospital Infection Prevention and Control Quality Improvement Plan 14 th March 2013
 Connolly Hospital Infection Prevention and Control Quality Improvement Plan 14 th March 2013 1. Summary The Infection Prevention and Control Quality Improvement Plan clearly defines the priorities for
Connolly Hospital Infection Prevention and Control Quality Improvement Plan 14 th March 2013 1. Summary The Infection Prevention and Control Quality Improvement Plan clearly defines the priorities for
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Two years to make a difference in Welsh Healthcare
 Two years to make a difference in Welsh Healthcare 2008-2010 1000 Lives Campaign reaches aim of saving 1,000 lives The Campaign is estimating that 1,199 additional lives have been saved by NHS staff in
Two years to make a difference in Welsh Healthcare 2008-2010 1000 Lives Campaign reaches aim of saving 1,000 lives The Campaign is estimating that 1,199 additional lives have been saved by NHS staff in
Cluster Network Action Plan Neath Cluster. Abertawe Bro Morgannwg University Health Board Neath Cluster Action Plan
 Cluster Network Action Plan 2016-17 Neath Cluster 1 Introduction The Neath Cluster Network includes a cluster of 8 GP practices, seven of the practices are engaged in GP training. The cluster network estate
Cluster Network Action Plan 2016-17 Neath Cluster 1 Introduction The Neath Cluster Network includes a cluster of 8 GP practices, seven of the practices are engaged in GP training. The cluster network estate
Chief Executive s Statement. I am pleased to welcome you to our Quality Accounts 2015.
 Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2015. Now in their sixth year, Quality Accounts continue to provide a truly objective metric for us, and others, to gauge
Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2015. Now in their sixth year, Quality Accounts continue to provide a truly objective metric for us, and others, to gauge
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Infection Prevention and Control (IPC) Annual Programme 20010/11
 Annual Programme 20010/11") Infection Prevention and Control (IPC) Annual Programme 20010/11 1. Introduction The Code of Practice for the Prevention and Control of Healthcare Associated Infections (DH, 2009) otherwise known as the
Infection Prevention and Control (IPC) Annual Programme 20010/11 1. Introduction The Code of Practice for the Prevention and Control of Healthcare Associated Infections (DH, 2009) otherwise known as the
IR(ME)R Inspection (Announced) Abertawe Bro Morgannwg University Health Board Princess of Wales Hospital Radiology Department
R Inspection (Announced) Abertawe Bro Morgannwg University Health Board Princess of Wales Hospital Radiology Department") DRIVING IMPROVEMENT THROUGH INDEPENDENT AND OBJECTIVE REVIEW IR(ME)R Inspection (Announced) Abertawe Bro Morgannwg University Health Board Princess of Wales Hospital Radiology Department 18 and 19 August
DRIVING IMPROVEMENT THROUGH INDEPENDENT AND OBJECTIVE REVIEW IR(ME)R Inspection (Announced) Abertawe Bro Morgannwg University Health Board Princess of Wales Hospital Radiology Department 18 and 19 August
NHS Awards 2013 Endoscopy Unit
 NHS Awards 201 Endoscopy Unit 1. Storyboard Title Improving the quality of the patients experience of the endoscopy service: achieving full JAG accreditation in Bronglais District General Hospital utilising
NHS Awards 201 Endoscopy Unit 1. Storyboard Title Improving the quality of the patients experience of the endoscopy service: achieving full JAG accreditation in Bronglais District General Hospital utilising
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH The aim of this report is to provide NHS Borders Board with a thematic review of:-
 Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS 22 FEBRUARY 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
Infection Prevention. & Control. Report
 Infection Prevention & Control Report April 2012 March 2013 Author Joanne Raper, Infection Prevention & Control Nurse Manager Page 1 of 10 1.0 Purpose of the Paper The purpose of this report is to provide
Infection Prevention & Control Report April 2012 March 2013 Author Joanne Raper, Infection Prevention & Control Nurse Manager Page 1 of 10 1.0 Purpose of the Paper The purpose of this report is to provide
Quality Accounts April 2015 to March 2016
 Quality Accounts April 2015 to March 2016 Group Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2016. Our 2016 Quality Accounts provide a transparent picture of BMI Healthcare
Quality Accounts April 2015 to March 2016 Group Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2016. Our 2016 Quality Accounts provide a transparent picture of BMI Healthcare
Specialised Services Service Specification. Adult Congenital Heart Disease
 Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Infection Prevention and Control Strategy (NHSCT/11/379)
") Infection Prevention and Control Strategy (NHSCT/11/379) September 2010 September 2010 Contents Page No. 1. Foreword 1 2. Introduction 2-3 3. Key Principles 4-5 4. Objectives 6-13 5. Organisational Arrangements
Infection Prevention and Control Strategy (NHSCT/11/379) September 2010 September 2010 Contents Page No. 1. Foreword 1 2. Introduction 2-3 3. Key Principles 4-5 4. Objectives 6-13 5. Organisational Arrangements
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Harm Across the Board Reporting: How your Hospital Can Get There
 Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Antimicrobial stewardship in Scotland: quality improvement agenda
 Antimicrobial stewardship in Scotland: quality improvement agenda Dr Jacqueline Sneddon Project Lead Scottish Antimicrobial Prescribing Group Background Scottish Antimicrobial Prescribing Group (SAPG)
Antimicrobial stewardship in Scotland: quality improvement agenda Dr Jacqueline Sneddon Project Lead Scottish Antimicrobial Prescribing Group Background Scottish Antimicrobial Prescribing Group (SAPG)
National Programme to Prevent Central-Line Associated Bacteraemia. Project Charter October 2011 to April 2013
 National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
Policy for Venous Thromboembolism Prevention and Treatment
 Policy for Venous Thromboembolism Prevention and Treatment Start date: May 2013 Next Review: May 2015 Committee approval: Endorsed by: Distribution: Location Thrombosis and Thromboprophylaxis Steering
Policy for Venous Thromboembolism Prevention and Treatment Start date: May 2013 Next Review: May 2015 Committee approval: Endorsed by: Distribution: Location Thrombosis and Thromboprophylaxis Steering
After reading this learning module, the nurse should be able to:
 After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Performance Improvement Bulletin
 SPECIAL DELIVERY UNIT/ NATIONAL TREATMENT PURCHASE FUND Issue No.1 08/12 Performance Improvement Bulletin Featured Work underway - Maximum Waiting Time Targets 2 Case Study No. 1 Galway & Roscommon University
SPECIAL DELIVERY UNIT/ NATIONAL TREATMENT PURCHASE FUND Issue No.1 08/12 Performance Improvement Bulletin Featured Work underway - Maximum Waiting Time Targets 2 Case Study No. 1 Galway & Roscommon University
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
On behalf of COMMIT Team
 Dr Rashmi Sharma & Dr Achyut Guleri On behalf of COMMIT Team Quality Safety People Delivery Environment Cost Consultant Microbiologist Clinical Director- Laboratory Medicine, Blackpool Teaching Hospitals
Dr Rashmi Sharma & Dr Achyut Guleri On behalf of COMMIT Team Quality Safety People Delivery Environment Cost Consultant Microbiologist Clinical Director- Laboratory Medicine, Blackpool Teaching Hospitals
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study
 Case Study") Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Storyboard Submission NHS Wales Awards Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated INRs
 Storyboard Submission 1. Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated 2. Brief Outline of Context As part of the 1000 Lives Plus initiative, ward pharmacists throughout ABHB
Storyboard Submission 1. Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated 2. Brief Outline of Context As part of the 1000 Lives Plus initiative, ward pharmacists throughout ABHB
NHS Greater Glasgow and Clyde Alison Noonan
 NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
West Hertfordshire Hospitals NHS Trust Reducing Clostridium difficile infection Action Plan [Updated 19/3/13] Item 37/13
![West Hertfordshire Hospitals NHS Trust Reducing Clostridium difficile infection Action Plan [Updated 19/3/13] Item 37/13](/thumbs/78/78298479.jpg "West Hertfordshire Hospitals NHS Trust Reducing Clostridium difficile infection Action Plan [Updated 19/3/13] Item 37/13") Introduction purpose: West Hertfordshire Hospitals NHS Trust Reducing Clostridium difficile infection Action Plan 2012-2013 [Updated 19/3/13] Item 37/13 This action plan has been developed by West Hertfordshire
Introduction purpose: West Hertfordshire Hospitals NHS Trust Reducing Clostridium difficile infection Action Plan 2012-2013 [Updated 19/3/13] Item 37/13 This action plan has been developed by West Hertfordshire
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Appendix 10a SBAR REPORT MARCH 2010 FREE TO LEAD FREE TO CARE, EMPOWERING WARD SISTER / CHARGE NURSE SITUATION
 SBAR REPORT MARCH 2010 FREE TO LEAD FREE TO CARE, EMPOWERING WARD SISTER / CHARGE NURSE SITUATION The purpose of this report is to inform the Board members of the current position and progress of Cwm Taf
SBAR REPORT MARCH 2010 FREE TO LEAD FREE TO CARE, EMPOWERING WARD SISTER / CHARGE NURSE SITUATION The purpose of this report is to inform the Board members of the current position and progress of Cwm Taf
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
System enablers practical aspects Chair Lesley Anne Smith
 System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users