AGENDA. Appendix: 0. Action required 1. Introduction 1.1 Apologies for Absence Declarations of Interest Declarations of Gifts and Hospitality
|
|
|
- Bryce McBride
- 6 years ago
- Views:
Transcription
1 Appendix: 0 Islington Clinical Commissioning Group Governing Body Business Meeting Wednesday, 9 May Laycock PDC, Laycock Street London N1 1TH AGENDA PART 1 Please look over the agenda and think about which of these topics might present an area of conflict for you. This means an item where a decision or recommendation made may advantage you, your family, and your workplace or business interests. These advantages might be financial or in another form, perhaps the ability to exert unseen influence. Where anything on the agenda has the potential to put you in such a position, or is raised during the meeting, you should tell us all about it. This means we can ensure that our decisions, recommendations or actions can be protected from the impact of any possible conflict you or others could have. If you are unsure, it is always best to raise the possibility with the Chair before the meeting, or at any point during the meeting. This openness is important as we can all discuss how to manage decision making in a complex environment that involves public money. Item Lead Action required Papers Page No 1. Introduction 1.1 Apologies for Absence Chair Note Declarations of Interest Declarations of Gifts and Hospitality In addition to being published with this agenda, the Register of Interests is available on the CCG s website ( or from the Business Support Team, 2 nd Floor Laycock PDC, Laycock Street, London, N1 1TH 1.2 Chair s Introduction and Chair Note Opening Remarks 1.3 Minutes and Actions of the Meeting held on 14th March 2018 Chair For approval Matters Arising Chair Questions from the Public Chair --
2 Appendix: 0 Item Lead Action required Papers NB: Members of the public will be given the opportunity to ask questions. These must relate to items that are on the agenda for this meeting and should not take longer than three minutes per person. 2. Overview Reports 2.1 Accountable Officer s Report Accountable Officer Page No For approval Quality, Performance and Finance 3.1 Finance Report Chief Finance Officer 3.2 Performance Report Director of Planning, Performance and Delivery 3.3 Pre-Consultation Business Case for the Redevelopment of the St Pancras Hospital site and Mental Health Community Hubs Chief Operating Officer For discussion For discussion For approval Request to Delegate Authority for Approval of the Annual Report and Accounts to the Islington CCG Audit Committee 4. Governance and Assurance 4.1 Governing Body Risk Assurance Framework (With NCL Section of Risk Reports) 4.2 Audit Committee In Common Terms of Reference (TOR) 5. For Information 5.1 Minutes of the Quality & Performance Committee available here 5.2 Minutes of the Patient and Public Participation Committee available here Chief Operating Officer Director of Planning, Performance and Delivery NCL Chief Finance Officer Chair, Quality & Performance Committee Chair, Patient and Public Participation Committee For approval For discussion For approval To note 5.1 To note
3 Appendix: 0 Item 5.3 Minutes of the Strategy & Finance Committee - available here 5.4 NCL Primary Care Joint Committee minutes - available here 5.5 NCL Joint Committee minutes available here 6. Any Other Business Lead Chair, Strategy & Finance Committee Action required Papers To note 5.3 To note 5.4 To note 5.5 Date of Next Meeting Wednesday 11 th July 2018, Page No
4 Item: 1.3 Part One Minutes Meeting of the Islington Clinical Commissioning Group Governing Body 14th March 2018 Laycock PDC, Laycock Street, London, N1 1TH Members Present: Dr Jo Sauvage Sorrel Brookes Lucy de Groot Dr Rue Roy Dr Rathini Ratnavel Jennie Hurley Dr Karen Sennett Helen Pettersen Simon Goodwin Deborah Snook Non-Voting Members: Clare Henderson Rachel Lissauer Alex Smith Anthony Browne Will Huxter Tony Hoolaghan Chair, Islington Clinical Commissioning Group Lay Vice Chair Lay Member North Locality GP Representative South West Locality GP Representative Practice Nurse Representative South East Locality GP Representative NCL Accountable Officer NCL Chief Finance Officer Practice Manager Representative Director of Commissioning Director of Wellbeing Partnership Director of Planning, Performance and Delivery Deputy Chief Finance Officer Director of Strategy Chief Operating Officer In attendance: Dr Imogen Bloor Julie Billett Rose McDonald Dr Katie Coleman Rosie Peregrine-Jones Jess Macgregor Apologies: Shelagh Prosser Jennie Williams Sara Lightowlers Paul Sinden Sarah Mcilwaine Not expected: Ian Huckle Minutes: Karl Thompson Primary Care Lead Director of Public Health for Camden and Islington Healthwatch Observer GP Representative Assistant Director of Quality & Safety (Haringey CCG) Service Director Adult Social Care Strategy & Commissioning Healthwatch Observer Director of Quality & Executive Nurse Secondary Care Consultant representative NCL Director of Acute Commissioning and Performance Director of Care Closer to Home Practice Manager Representative (job share) Head of NCL Corporate Services 4 of 402
5 1 Introduction 1.1 Apologies for Absence and Declarations of Interest Jo Sauvage noted apologies from Sorrel Brookes, Shelagh Prosser, Jennie Williams, Sarah Lightowlers, Paul Sinden, Sarah Mcilwaine and that the practice manager role as being covered this month by Deborah Snook. Jo Sauvage reiterated the importance of managing conflicts and noted the statement included in the agenda, regarding the ongoing importance and the responsibilities everyone has in this respect. Jo Sauvage declared that she is a GP provider and that her practice was a member of the local GP Federation. Jo Sauvage clarified that all GP and practice members of the Governing Body are linked to GP practices who also form part of the membership of the Islington GP Federation. Jo Sauvage also reiterated the importance of completing the gifts and hospitality register as appropriate. 1.2 Chair s Introduction and opening Remarks Jo Sauvage welcomed everyone to the meeting and reiterated the hard work continuing across teams in support of the ongoing winter pressures. 1.3 Minutes and Actions of the Meeting held on 10th January Minutes Part 1 Amendments as follows: Katie Coleman asked for her new positon with the Islington GP Federation, to be recorded as GP Director for the GP Federation. Katie Coleman asked that the ihub audit date be captured, noting when this would be available for review. Deborah Snook asked if reference to patient representatives should be amend to community members as she understood this was the correct title. Simon Goodwin also noted that Barnet Governing Body had now supported the recommendation for NCL CCG audit Committees to meet in common with some minor amendments to the terms of reference The minutes for Part 1 of the meeting on 10 th January 2018 were APPROVED as an accurate record subject to the above changes. Part 2 JS Amendments as follows: 2.0 Replace the word not in the last sentence with the word into The minutes for Part 2 of the meeting on 10th January 2018 were APPROVED as an accurate record subject to the above change. 5 of 402
6 Action Log The following updates were provided: Jennie Hurley reiterated her request that when the CCG refer to the 'GP Five Year Forward View' that we also include the '10 Point Plan for general Practice Nursing' Karen Sennett amended the action relating to LAS. It was clarified that this was a request for information regarding the percentage of calls made to 111 that subsequently result in an ambulance conveyance that are assessed by a clinician. Alex Smith agreed to find out from Enfield CCG, if this information could be provided, as lead commissioner. Deborah Snook asked on behalf of Ian Huckle if the action related to RTT could be updated to request if some regular data could be added to the performance report. In respect to the ihub performance review and audit, Lucy de Groot asked that this be noted as an action. Clare Henderson confirmed the review preparation was underway and that the Strategy and Finance committee would receive a report in June 2018 ACTION: 14/03 01 Jennie Hurley reiterated her request that when the CCG refer to the 'GP Five Year Forward View' that we also include the '10 Point Plan for general Practice Nursing' ACTION: 14/03 02 In respect to the ihub performance review and audit, Lucy de Groot asked that this be noted as an action. Clare Henderson confirmed the review preparation was underway and that the Strategy and Finance committee would receive a report in June 2018 ACTION: 14/03 03 Alex Smith to find out from Enfield CCG, if they can provide information on the percentage of calls made to 111, as lead commissioner. 1.4 Matters Arising None 1.5 Questions from the Public A representative from Islington ADHD Champions provided the following statement We would like to thank the CCG efforts especially Jill Britton for her help in addressing the shortfall in care. Sadly, instead of having a care driven health care system, a target driven culture has developed. Our efforts will now be directed on a national level. We do hope that Islington CCG will continue with the actions it has set out with in improving services for ADHD service users. Jo Sauvage thanked Islington ADHD Champions for their comments and expressed her thanks for their input and wished them good luck with their future national role. Tony Hoolaghan confirmed he would pass on the thanks to Jill Britton for her good work. 2 Overview Reports 2.1 Accountable Officers Report All referred to the Accountable Officers Report that was circulated ahead of the meeting. Helen Pettersen referred members to the following highlights in her report: 6 of 402
7 St Pancras Hospital redevelopment Tony Hoolaghan continues to develop the public consultation documentation which is likely to be available for public consultation during late Spring or early Summer Moorfields eye hospital early discussions with the hospital continue regarding a potential move to the re-developed St Pancras Hospital site with a further update due at the Governing Body meeting in May 2018 Staff Survey results Tony Hoolaghan is leading a cross section of staff from both Haringey and Islington CCGs to review the feedback. Overall there were very positive remarks, although there remains room for improvement which will be worked on by the staff representatives and the executive team Internal audit and counter fraud services the procurement process has now completed and the contract for NCL CCGs has been awarded to RSM Risk Assurance Services who are the current provider. The contract is for three years with an option to extend for a further two. Chairs action was sought in February to approve the re-appointment and the Governing Body were asked to ratify this decision NEL Commissioning Support Unit a notice letter was issued to take in-house contract management services and acute medicines management services. A project group met on 22 nd February 2018 to commence review of the project plan and associated risks and additionally confirmed that the five NCL CCGs would be asked to approve the final business case. Given the timescales it was requested that this be delegated to the sub group to make the decision. Ian Huckle is keen for the Governing Body to make the decision and so the Chair indicated that a sensible compromise would be to review any business case outside of a formal Governing Body meeting, adopting the urgent decisions process and that this would then be ratified at a future Governing Body meeting Haringey and Islington CCG Committees work is underway to streamline decision making and reduce duplication through committees initially meeting in common, with the potential for joint committees to be established, in the future, where appropriate A Remuneration Committee in common took place on 1 st March 2018 and supported the recommendation for the creation of the following two new posts: o Director of Acute Commissioning and Director of Performance, Planning and Primary Care o These posts have been created by splitting the existing NCL Director of Acute Commissioning and Performance role o Paul Sinden was confirmed as moving into the Director of Performance, Planning and Primary Care role o The Governing Body were asked to NOTE the decision taken as delegated authority had been given to the remuneration committee Helen Pettersen concluded her update and asked if there were any questions in relation to the report. Katie Coleman supported the change to the NCL Director roles and asked for assurance that primary care would receive sufficient attention given the complexity of the area. Helen Pettersen explained that with the additional resource and with the proposed changes to move contracts management into the CCGs, that there should be an increased focus Simon Goodwin explained that the funding for the additional post would be met from reducing the existing costs attributed to the Healthy London Partnership programme Lucy de Groot asked for a summary of the source of funding in relation to the new NCL post for Director of Acute Commissioning Deborah Snook asked in relation to the Staff Survey results, what arrangements were in place regarding supporting staff to speak up. Tony Hoolaghan explained that under guidance for Freedom To Speak Up that there are mechanisms in place and that the reference regarding concerns over bullying and harassment was made by a very small number of respondents 7 of 402
8 although it was recognised that this issue would be taken seriously in order to ensure that all staff felt supported in the work place In addition, Helen Pettersen noted that Whittington Health and Camden & Islington Foundation Trust (CIFT) had both done very well in achieving a rating of good at their recent Care Quality Commission (CQC) inspections. Rathini Ratnaval noted that within the CIFT report, there were two services that received outstanding ratings The Community Aging Service and Substance Misuse Service. The Substance Misuse Service is currently only a Camden service although from the 1 st April 2018, this is being extended to Islington residents. ACTION: 14/03-04 Lucy de Groot asked for a summary of the source of funding in relation to the new NCL post for Director of Acute Commissioning The Governing Body; 1) NOTED the report and 2) NOTED that an urgent decision regarding the NELCSU contract would be taken outside of the formal Governing Body meeting 3) RATIFIED the decision taken by the Remuneration Committee taken under Chairs Action 3 Quality, Performance and Finance 3.1 Finance Report All referred to the Finance Report that was circulated ahead of the meeting. Anthony Browne highlighted a number of key points in the report: An improved in-year surplus of 2.5M was reported, noting this was mainly the result of non-recurrent items off setting underlying pressure Acute contracting forecast an overall pressure of 3.6M at year end UCLH continue to pose the greatest risk to CCG financial performance with a 2.4M year end forecast variance Non acute services are forecasting a year end 1.6M overspend. The overall non acute position moved adversely from month 9 due to increases within the continuing healthcare and prescribing costs Reference was made to table 3.11 in which underspends in diagnostics and maternity were noted. Diagnostic underspend relates to a drop in MRI scans Non elective outpatient pressure was also noted with the mitigation that this would be the focus of the developing care closer to home integrated networks (CHINs) and quality improvement support team (QIST) activity during Whittington Health have experienced a spike in general A&E attendance although a reduction in mental health concerns Royal Free are recognised to have a plan artificially high and as such significant variance remain which will be rectified for contracting round QIPP full year performance is reporting a slippage of 3.9M against the target of 11.7M. This relates mainly to delays in planned care QIPP risks were noted and it was reported that pressure can be offset by nonrecurrent mitigating items allowing the year end forecast surplus of 2.5M to still be achieved Simon Goodwin provided the following update: For it was reiterated that the surplus being declared for Islington is supported by 7.5M of non-recurrent contingency funding For month 10 there has been greater scrutiny of the accounts in order to give an accurate year end forecast The 0.5% reserve of 1.7M is also likely to be returned from NHSE which will increase the overall year end surplus 8 of 402
9 The Islington position remains the strongest for the NCL CCGs with Camden forecasting breakeven and Barnet, Enfield and Haringey all forecasting a year end deficit For table 7.7 summarises changes in funding and the required QIPP targets based and three different models Contracts deadline is scheduled for the end of March and as it stands it is likely that a greater than 3.28% QIPP target will be required Anthony Browne and Simon Goodwin concluded their update asking if there were any question relating to the report. Whilst it was noted that the Islington CCG financial performance was forecast to move into a year-end surplus positon, Lucy de Groot asked for transparency across NCL CCGs and requested the detail for the other forecast positons be shared with members. Simon Goodwin agreed to include this in future reporting Karen Sennett indicated that the NICE guidance requiring changes in the process for GPs requesting diagnostics has yet to be implemented and may have had some impact on the level of diagnostic underspend Karen Sennett asked when the CCG budget would be finalised. Simon Goodwin explained that values relied upon final contract sign off and agreement of QIPP targets and explained that from a governance perspective, the operating plan and agreed budgets need to be submitted by the end of April and so the intention is to use the 26 th April Strategy & Finance committee meeting to review and finalise the operating plan Karen Sennett asked how prevention should be included in QIPP plans. Alex Smith explained that there are many QIPP plans and other programmes underway linked to prevention although recognised that much of the savings are longer term and difficult to define. Jo Sauvage asked that the more detailed discussion take place at the QIPP delivery Group and Julie Billett offered to attend to support the discussion. Alex Smith agreed to arrange for Julie Billett to attend the QIPP Delivery Group Rathini Ratnavel asked about the no cheaper stock issue and the increased cost associated with the overspend. Simon Goodwin reiterated that the increase in costs had impacted the CCG bottom line and as such had reduced the year end surplus Katie Coleman noted the comments regarding the 2.1M costs relating to primary care and asked if the detail could be further explained. Anthony Browne explained that this linked to the CCGs agreed underspend against the primary care budget. Katie Coleman asked if this could be made clearer, explaining that Islington CCG had agreed to defer any further spend against for in order to support the NCL positon. Simon Goodwin agreed that for month 11 and 12 that reporting would be much clearer Jess McGregor asked about the programme corporate costs and the inclusion of the Healthy London Partnership values. Anthony Browne explained that the full value related to the total London value and that other corporate costs included in the overall figure related to CCG staff and accommodation costs as well as other programme support costs ACTION: 14/03-05 Whilst it was noted that the Islington CCG financial performance was forecast to move into a year-end surplus positon, Lucy de Groot asked for transparency across NCL CCGs and requested the detail for the other forecast positons be shared with members. Simon Goodwin agreed to include this in future reporting. ACTION: 14/03-06 Karen Sennett asked how prevention should be included in QIPP plans. Alex Smith explained that there are many QIPP plans and other programmes 9 of 402
10 underway linked to prevention although recognised that much of the savings is longer term and difficult to define. Jo Sauvage asked that the more detailed discussion take place at the QIPP delivery Group and Julie Billett offered to attend to support the discussion. Alex Smith agreed to arrange for Julie Billett to attend the QIPP Delivery Group ACTION: 14/03 07 Katie Coleman noted the comments regarding the 2.1M costs relating to primary care and asked if the detail could be further explained. Anthony Browne explained that this linked to the CCGs agreed underspend against the primary care budget. Katie Coleman asked if this could be made clearer within the report, explaining that Islington CCG had agreed to defer any further spend against for in order to support the NCL positon. Simon Goodwin agreed that for month 11 and 12 that reporting would be much clearer The Governing Body NOTED the report. 3.2 Performance Report All referred to the Performance Report that was circulated ahead of the meeting. Alex Smith highlighted the following points in the report: Met the operational standard of 92% for referral to treatment (RTT) during November and December. On track for the full year performance delivery Cancer standards for October all met and six of the eight were met in November. Not met were 62 wait urgent GP referral and 62-day wait screening service. For December the forecast is for seven of eight standards to be met A&E performance in November was 90%, 87.7% in December and 87.6% in January, with the year to date performance at 90.5% for Islington CCG In the last six weeks Whittington Health has been at 86% and UCLH 83% although there have been days where performance has been significantly lower due to ongoing winter pressures Islington A&E Delivery Board will review the increase in ambulance conveyances at Whittington Health and the agreed actions implemented to help manage this, such as the fit to sit initiative where new equipment has been purchased and there is an increased focus on ambulatory care Ongoing focus on patient flows and the support provided by social services supporting transfer of care Mental health beds across London continue to be challenging with significant issues over recent weeks, specifically for female beds New LAS performance standards are indicating that for Islington, performance has been better than anticipated with a positive position noted on recruitment Community health services reporting is under review with Rachel Lissauer working with the Haringey and Islington CCG Chairs of sub-committees that focus on performance as part of a steering group to consider the options available to improve the activity reporting Mental health standards relating to improving access to psychological therapies (IAPT) five of the six standards met. No 12-hour mental health breaches at Whittington Health since the beginning of October 2017 and the recovery suite is scheduled to open in March 2018 Alex Smith concluded his update asking if there were any question relating to his report. Rosie Peregrine-Jones reiterated the excellent CQC reports for the trusts previously mentioned Karen Sennett asked if, as part of the Performance Report, information on the quality premium and CQUIN information could be included. Alex Smith agreed to review with the Head of Performance, what information could be included 10 of 402
11 Karen Sennett advised members that for Cancer, Islington s performance across a number of key areas has significantly improved Rathini Ratnavel asked how much focus was given to discussing community service performance. Rosie Peregrine-Jones confirmed that at the clinical quality review group (CQRG), specific areas of focus including those within community services were discussed and Rachel Lissauer explained that there was a review taking place of the performance dashboard, looking at routine and urgent performance and to see how this can be improved Rathini Ratnaval asked if the e-booking performance information could be included within the Performance Report. Alex Smith agreed to investigate what information was available that could be included. ACTION: 14/03 08 Karen Sennett asked if, as part of the Performance Report, information on the quality premium and CQUIN information could be included. Alex Smith agreed to review with the Head of Performance, what information could be included. ACTION: 14/03 09 Rathini Ratnaval asked if the e-booking performance information could be included within the Performance Report. Alex Smith agreed to investigate what information was available that could be included The Governing Body: 1. NOTED the content of the report 4 Strategy 4.1 Operating Plan Timetable and Governance All referred to the report that was circulated ahead of the meeting. Alex Smith highlighted the key points in the report: It was noted that some elements of the paper had already been covered within the meeting Key considerations relate to the tight timescales and the proposed method of governance regarding the review and submission of the operating plan It was proposed that the April 2018 Islington CCG seminar be used to provide an update on progress to members and that the Strategy and Finance Committee effectively review and sign off the plan on the 26 th April 2018 prior to submission on the 30 th April to NHSE Governing Body members would be invited to the April Strategy & Finance committee in order to review the plan. Karen Sennett also requested and it was agreed that those members unable to attend would be given the opportunity to provide feedback in advance Alex Smith concluded the update asking if there were any question relating to the report. Anthony Browne reiterated that a draft submission had previously been submitted and that the budgets linked to the operating plan continued to be reviewed and scrutinised carefully as part of the preparation for the final submission Jo Sauvage reiterated her support for the request for members to attend the April 2018 Strategy & Finance Committee and provide feedback if unable to do so. 11 of 402
12 4.1.1 The Governing Body: 1. NOTED the contents of this report and; 2. APPROVED the suggested 2018/19 Operating Plan sign off mechanism 5 Governance and Assurance 5.1 NCL Joint Commissioning Committee Terms of Reference All referred to the report that was circulated ahead of the meeting. Helen Pettersen highlighted the key points in the report: Noting the main changes to the terms of reference since they were last seen by members It was confirmed that the Enfield CCG lay member, Karen Trew continues to Chair the meeting supported by Kathy Elliott, Camden CCG lay member as Vice Chair Helen Pettersen concluded the update asking if there were any question relating to the report. Regarding the changes to the NCL Joint Commissioning Committee ToR, Sorrel Brookes asked if the membership could have roles and not individual names included. Helen Pettersen agreed to feedback the request. Deborah Snook asked if the section regarding questions from the public could be reviewed in order to ensure this allowed questions in advance and during the meeting. Helen Pettersen agreed to feedback the comment in order to ensure questions can be asked. ACTION: 14/03 10 Regarding the changes to the NCL Joint Commissioning Committee ToR, Sorrel Brookes asked if the membership could have roles and not individual names included. Deborah Snook asked if the section regarding questions from the public could be reviewed in order to ensure this allowed questions in advance and during the meeting. Helen Pettersen agreed to feedback the comment in order to ensure questions can be asked The Governing Body: 1. APPROVED the amended Terms of Reference and Standing Orders of the NCL Joint Commissioning Committee 5.2 Governing Body Risk Assurance Framework All referred to the report that was circulated ahead of the meeting. Alex Smith gave an overview of the risks highlighted within the report and noted the following: No new risks have been added to the RAF this month 434 re-development of St Pancras Hospital noted and mitigations to manage associated risk 205 Pressure on mental health acute beds risk has been downgraded given there has been a new psychiatric intensive care unit opened and there have been no further 12 hour breaches QIPP programme delivery has been downgraded given there are significant mitigations in place to achieve the Islington year end budget position 423 Lower Urinary Tract Symptoms (LUTS) risk has been increased to reflect the ongoing challenges and concern raised by local residents at the recent NCL Joint Commissioning Committee Two Islington risks were reported as closed A summary of the three NCL Joint Commissioning Committee risks that meet the RAF criteria was also provided 12 of 402
13 Alex Smith asked members if there were any questions relating to the report. Deborah Snook asked for clarity regarding the QIPP delivery risk and the year it referred to. Alex Smith explained that the risk related to the current year and not for Jo Sauvage noted the LUTS risk increase and reiterated the importance of the service to Islington residents and the desire to achieve an early resolution Karen Sennett noted the neurological pathways that are now in place across NCL practices and suggested that these may help alleviate the number of referrals going into the LUTs service although it was recognised that there would continue to be a cohort of patients that value the service Katie Coleman noted that the NCL Primary Care Committee risk relating to the Capita contract had remained at the same level and asked if this should be reviewed by the committee. Helen Pettersen explained that the contract is managed by NHSE and as such there is limited ability for us to directly influence mitigations, although she confirmed NHSE are aware that NCL have concerns. It was recognised that the risk would remain on the NCL Primary Care register in order to be monitored by the committee The Governing Body: 1. NOTED the content of the report 5.3 Minutes of the Quality and Performance Committee The Governing Body referred to the minutes that were circulated ahead of the meeting for assurance. Karen Sennett noted that the minutes supplied that had been approved by committees were always several months old and asked if it was possible for minutes to be circulated to members prior to the Governing Body so that they were more up to date. Jo Sauvage confirmed that this would be reviewed in order to ensure minutes were available earlier. ACTION: 14/03 11 Karen Sennett noted that the minutes supplied that had been approved by committees were always several months old and asked if it was possible for minutes to be circulated to members prior to the Governing Body so that they were more up to date. Jo Sauvage confirmed that this would be reviewed in order to ensure minutes were available earlier The Governing Body received ASSURANCE from the minutes. 5.4 Minutes of the Strategy & Finance Committee The Governing Body referred to the report that was circulated ahead of the meeting for assurance. There were no comments The Governing Body received ASSURANCE from the minutes. 6. For Information The Governing Body noted the minutes for the NCL Primary Care Joint Committee had been provided for information. 7. Any Other Business 7.1 No other business noted. These minutes are agreed to be a correct record of the Part 1 meeting of the Islington Clinical Commissioning Group Governing Body held on 9th May Signed: Date:. Dr Jo Sauvage, Chair, Islington Clinical Commissioning Group 13 of 402
14 Appendix ACTION LOG: Islington Clinical Commissioning Group Governing Body Meeting Date Action No. Minutes Reference Action Description Responsibility Target Date Progress details Jennie Hurley reiterated her request that when the CCG refer to the 'GP Five Year Forward View' that we also include the '10 Point Plan for general Practice Nursing' All Mar-18 Ongoing In respect to the ihub performance review and audit, Lucy de Clare Groot asked that this be noted as an action. Clare Henderson Henderson confirmed the review preparation was underway and that the Strategy and Finance committee would receive a report in June 2018 Jul-18 Strategy and Finance Committee to receive the report in June Alex Smith to find out from Enfield CCG, if they can provide information on the percentage of calls made to 111, as lead commissioner. Alex Smith May-18 Enfield CCG have recently asked for an enhanced data set of KPIs which includes this indicator it will be available from June Governing Bodies across NCL are in process of approving additional funding for additional clinical triage Lucy de Groot asked for a summary of the source of funding in relation to the new NCL post for Director of Acute Commissioning. Simon Goodwin May-18 The summary will be provided to the Governing Body once finalised Whilst it was noted that the Islington CCG financial performance was forecast to move into a year-end surplus positon, Lucy de Groot asked for transparency across NCL CCGs and requested the detail for the other forecast positons be shared with members. Simon Goodwin agreed to include this in future reporting. Simon Goodwin May-18 Completed - Reporting will reflect other NCL CCG positon. 14 of 402
15 Appendix ACTION LOG: Islington Clinical Commissioning Group Governing Body Meeting Date Action No. Minutes Reference Action Description Responsibility Target Date Progress details 14/ Karen Sennett asked how prevention should be included in QIPP plans. Alex Smith explained that there are many QIPP plans and other programmes underway linked to prevention although recognised that much of the savings is longer term and difficult to define. Jo Sauvage asked that the more detailed discussion take place at the QIPP delivery Group and Julie Billett offered to attend to support the discussion. Alex Smith agreed to arrange for Julie Billett to attend the QIPP Delivery Group Alex Smith May-18 Completed - Julie Billett is attending the QDG on 15th May Katie Coleman noted the comments regarding the 2.1M Anthony costs relating to primary care and asked if the detail could be Browne further explained. Anthony Browne explained that this linked to the CCGs agreed underspend against the primary care budget. Katie Coleman asked if this could be made clearer within the report, explaining that Islington CCG had agreed to defer any further spend against for in order to support the NCL positon. Simon Goodwin agreed that for month 11 and 12 that reporting would be much clearer May-18 Completed Reporting has been amended Karen Sennett asked if, as part of the Performance Report, information on the quality premium and CQUIN information could be included. Alex Smith agreed to review with the Head of Performance, what information could be included. Alex Smith tbc Completed. Included within GB Performance report Rathini Ratnaval asked if the e-booking performance information could be included within the Performance Report. Alex Smith agreed to investigate what information was available that could be included. Alex Smith May-18 Completed. Included within GB Performance report 15 of 402
16 Appendix ACTION LOG: Islington Clinical Commissioning Group Governing Body Meeting Date Action No. Minutes Reference Action Description Responsibility Target Date Progress details Regarding the changes to the NCL Joint Commissioning Committee ToR, Sorrel Brookes asked if the membership could have roles and not individual names included. Deborah Snook asked if the section regarding questions from the public could be reviewed in order to ensure this allowed questions in advance and during the meeting. Helen Pettersen agreed to feedback the comments in order to ensure the membership is appropriate noted and questions can be asked. Helen Pettersen May-18 Completed. The current Terms of Reference contain the roles of the members. Schedule 1 to the Terms of Reference contain the names and roles of Committee members. We have the ability in Schedule 1 to change the names of Committee members without the need to formally amend the Terms of Reference at Governing Body meetings. It is important that we retain this so that we have a clear and transparent understanding of who Committee members are. Questions from the public: In the Committee s Standing Orders (which form part of the Terms of Reference) there are comprehensive clauses on questions from the public and depositions. In addition, questions from the public is listed as a standing item twice on every meeting agenda. It is listed at the beginning and the end of the agenda so members of the public have the opportunity to ask questions at the beginning and at the end of meetings. In addition, as standard practice the Committee also receives questions in advance of meetings when these are submitted Karen Sennett noted that the minutes supplied that had been Vivienne approved by committees were always several months old Ahmad and asked if it was possible for minutes to be circulated to members prior to the Governing Body so that they were more up to date. Jo Sauvage confirmed that this would be reviewed in order to ensure minutes were available earlier. May-18 The Governing Body will continue to see approved minutes at each meeting. Those members who have asked to receive minutes earlier will receive minutes signed off by the relevant committee Chair in order to ensure they receive them earlier Karen Sennett amended the action relating to LAS. It was clarified that this was a request for information regarding the percentage of calls made to 111 that subsequently result in an ambulance conveyance that are assessed by a clinician. Alex Smith agreed to find out from Enfield CCG,if this information could be provided, as lead commissioners. Alex Smith May-18 Completed - LAS are attending the Haringey GB meeting where further discussion will take place. The request for data will be progressed 16 of 402
17 Appendix ACTION LOG: Islington Clinical Commissioning Group Governing Body Meeting Date Action No. Minutes Reference Action Description Responsibility Target Date Progress details Ian Huckle asked if we could see an average wait time for RTT as this may be more helpful. Alex Smith said that he would review this with his team to see if it could be easily provided. The action was updated at the March meeting to request if some regular data could be added to the performance report. Alex Smith May-18 Completed - RTT median waiting time information is routinely made available to CCG Performance teams through NELIE. Alex Smith agreed to incorporate some additional detail Paul Sinden to consider producing a synopsis of the key Paul Sinden May-18 The action remains whilst further consideration is given to areas for Katie Coleman to take to the UCLH Board in her the completion of an appropriate summary of key areas capacity as a new member of the UCLH Board of Governors. 17 of 402
18 Appendix ACTION LOG: Islington Clinical Commissioning Group Governing Body AWAITING OUTCOME Meeting Date Action No. Minutes Reference Action Description Responsibility Target Date Progress details Governing Body Seminar - Jo Sauvage agreed that it would be helpful to devote some time at a future seminar to focus on the complexities of the CCG finances. Anthony Browne Jul-18 Diarised Primary Care Delegated Budgets Anthony Browne May-18 Ongoing - Deborah Snook asked if spend for /18 along with could be provided in order to compare spend across the five CCGs In respect to the ihub Clare Henderson Jul-18 Strategy and Finance Committee to receive the performance review and audit, report in June 2018 Lucy de Groot asked that this be noted as an action. Clare Henderson confirmed the review preparation was underway and that the Strategy and Finance committee would receive a report in June of 402
19 Item: 2.1 MEETING: Islington Clinical Commissioning Group Governing Body DATE: Wednesday 9 May 2018 TITLE: Accountable Officer Report LEAD GOVERNING Helen Pettersen - Accountable Officer BODY MEMBER: AUTHOR: Helen Pettersen - Accountable Officer Tony Hoolaghan - Chief Operating Officer CONTACT t.hoolaghan@nhs.net DETAILS: SUMMARY: This paper provides the Governing Body with an update on key local developments and broader policy areas not otherwise covered on the agenda. This report contributes to: Ensuring every child has the best start in life, Preventing and managing long term conditions to extend both length and quality of life and reduce health inequalities, Improving mental health and wellbeing, and Delivering high quality, efficient services within the resources available. Prior consideration by Committees and other partners: This paper is for information only Patient & Public Involvement (PPI): This paper is for information only and is available on the CCG website for consideration by patients and the public. Equality Impact Assessment: Not applicable Risks: Not applicable RECOMMENDED ACTION: The Governing Body is asked to: 1. APPROVE the recommendations stated in item 12: Suspension and amendment of standing orders 2. NOTE and COMMENT on the rest of the items in this report. SUPPORTING PAPERS: None 19 of 402
20 Accountable Officer s Report 1. Introduction This report will focus on the key activities that the senior team and I have been involved in since the last Governing Body meeting degree CCG Feedback i. A survey is carried out every year by Ipsos Mori (on behalf of NHS England) to gauge whether CCGs have strong relationships in place with their local health and care partners. The survey allows a range of stakeholders to provide feedback on their working relationships with the CCG. Stakeholder groups include member GP practices, Healthwatch, the local authority, NHS provider trusts and other CCGs in north central London. The survey is now in its fifth year and the results for 2018 have just been released. I would like to thank all of our stakeholders who took the time to complete the survey. We use the survey responses every year to help us to inform our ongoing organisational development. ii. iii. iv. Islington CCG has received positive feedback about how we work in partnership with the council and health and wellbeing board. Positive results were also received from the majority of stakeholders who have confidence in the CCG s ability to commission high quality services. There have been improvements since last year in the majority of the questions asked about how people view the CCG s leadership. Member practices understanding of the CCG s finances and how things work could also continue to be developed. Areas of saving and investment are areas highlighted as being of key interest as in previous surveys. We have already looked at the results with our executive management team, who have made some helpful suggestions about how we could make improvements in certain areas to address the feedback. We will also be looking at the results in detail at our next Governing Body seminar in June. The results will be published on our website for Islington CCG. 3. Public Consultation on the Proposed Redevelopment of the St Pancras Hospital Site i. As previously reported to the Governing Body, we have been working closely with Camden CCG, NHS England and other partners (e.g. Healthwatch) on Camden and Islington Foundation Trust proposals to redevelop the St Pancras Hospital site. ii. iii. On today s agenda we have the Pre-Consultation Business Case (PCBC) for approval. The proposals include moving the mental health in patient wards from St Pancras Hospital to a brand new facility at the Whittington Hospital site, as well as developing two new community hubs (one in Camden and one in Islington). The PCBC is a required document that we must have completed prior to starting the public consultation. We are planning to hold a special joint Governing Body meeting 20 of 402
21 with Camden CCG in late June, where we can sign off the consultation document, consultation methodology, financial modelling and consider the findings of the London Clinical Senate Council review into the clinical case for the proposals. We will also take the consultation documents to the Camden and Islington Health Overview and Scrutiny Committees in mid-june when they will also meet jointly to consider the consultation documents. iv. The Governing Body will continue to be kept regularly updated on this public consultation and its findings will come back to the Governing Body for consideration in the autumn. 4. Public Consultation on the Proposed Move of Moorfield s Eye Hospital and Institute of Ophthalmology In late April 2018 we initiated the governance with Moorfield s Eye Hospital and NHS England to begin work on a public consultation on a proposal to relocate the Moorefield s Eye Hospital. This work is at an earlier stage than that reported above for St Pancras Hospital. We aim to adopt much of the learning and good practice from the St Pancras Hospital redevelopment public consultation, and plan to provide a more detailed update on the timetable for this public consultation at the July 2018 Governing Body meeting 5. CSU Transfer Update i. Governing Body members will recall that we are in the process of transferring a number of staff from NEL Commissioning Support Unit (NEL CSU) into the NCL CCGs. These staff work mainly on contracts with NHS Trusts (contract monitoring, finance, analytics, clinical quality, performance monitoring etc.). This work is progressing well. Having previously gained Governing Body approval to proceed with this project, and give notice to NEL CSU for some services, we are required to submit a Business Case to NHS England as part of the staff transfer approval process. ii. The business case was submitted the week of 9th April 2018 and we await feedback on it. We have NCL CCGs Governing Body members on the oversight group for this project, and we will continue to keep all Governing Body members updated on progress and confirm the precise transfer date when it is finalised. 6. Contracting i. The focus of our commissioning and finance teams has been on the 2018/19 contracting round with our acute, community and mental health provider organisations. This is due to be concluded by the end of April, with mediation meetings required for The Whittington Hospital NHS Trust, Royal Free London NHS Foundation Trust (RFL), North Middlesex Hospital NHS Trust and Central London Community Healthcare Trust (CLCH). ii. The main issue for the acute providers was the financial value of QIPP plans. A process is therefore being followed during April where clinicians from both parties review these plans again. The aim of this is to ensure all plans have been signed off as clinically appropriate and able to be delivered in year. This will be concluded by the end of April. All other areas, including growth, service developments and 21 of 402
22 planning assumptions for the Referral to Treatment target (RTT) have been agreed, subject to reaching overall contract agreement. iii. A lessons learnt exercise for the 2018/19 contracting round is underway. 7. Finance i. The focus of the CCG finance team has been year end accounts which have now closed. Subject to audit process, the CCG has been able to achieve our financial control target for 2017/18. ii. iii. I would like to acknowledge the hard work and effort of CCG staff during this year of substantial financial challenge for maintaining financial grip and focusing on delivery of the Quality, Innovation, Productivity and Prevention Plan (QIPP). The Executive Management team and Governing Body members have been involved with a substantial amount of planning for transformational priorities in 2018/19 and this work very much continues to be the focus of the CCG at present. 8. Operating Plan i. The operating plan is one of a number of planning returns (the other significant return being the financial plan) required by NHS England each year and captures a certain set of activity figures and performance trajectories that are used for in year monitoring and assurance. The activity figures have been prepared on the basis of historical trends, contractual negotiations and expected QIPP delivery. This plan has been prepared using the same assumptions as the financial plan. Performance trajectories have been built up in discussion with providers, based on the planning guidance and appropriate STP groups such as the A&E delivery board. ii. The plan has been signed off by the Strategy and Finance Committee to allow submission on 30th April in line with national deadlines. Governing body members were invited to attend to provide input. 9. Additional NCL Post i. At its meeting on 1 March 2018, a recommendation was put forward to the Remuneration Committee in Common for Barnet, Camden, Haringey, Enfield and Islington CCGs to split the role of the Director of Performance and Acute Commissioning, NCL CCGs into two roles. These are a Director of Performance, Planning and Primary Care and a Director of Acute Commissioning. ii. iii. The Governing Body is asked to note that the Remuneration Committees in Common approved the split of this role into two new posts. Paul Sinden will be the Director of Performance, Planning and Primary Care for the NCL CCGs. I am pleased to announce the appointment of Eileen Fiori to the post of Director of Acute Commissioning, NCL CCGs. Eileen has a strong provider and contracting background and is a qualified nurse. Eileen has most recently been working at NEL 22 of 402
23 CSU as a CSU POD Director and is experienced in leading transformational change. Eileen will start her new role on the 1st May Information Governance (IG) i. The IG toolkit process for has been submitted with a self-assessment rating of satisfactory. This reflects the CCGs ongoing performance of all IG related matters and includes staff training. ii. iii. The new General Data Protection Regulation (GDPR) comes into force on 25 th May 2018 and we are working with the CSU and NCL Corporate Services to ensure we meet the required standards and we will be providing governing Body members with some clear information and guidance on this. In addition, we are also liaising closely with our member practices to provide support and guidance to aid their preparation in relation to GDPR. 11. Suspension and amendment of standing orders We would like to make two changes to the CCG Governing Body that are in line with the Standing Orders. The reasons for requiring these proposed changes are summarised as follows: Quorum of the Governing Body Following the previous clinical Vice-Chair recently standing down from this role, and becoming a GP non-voting Governing Body member, we need to address potential quorum implications. For the Governing Body to be quorum we need to have at least 3 voting GPs present (excluding the GP Chair). However, our Standing Orders does allow us to make the GP Chair a voting member and whilst we do not have a clinical Vice Chair in place we are proposing that the GP Chair becomes a voting member. Elected members term length We are proposing that we use the flexibility our Standing Orders allows to extend the term of elected members to four years (from current two years). The rationale for this is that we are currently bringing our Governing Body Sub-Committees together with those in Haringey CCG. A number of the Islington Governing Body posts are due for re-election in June 2018 and given the current context and the need for continuity in leadership we feel now is not the right time to hold new elections and for the Governing Body membership to potentially change. The CCG Standing Orders technical details of what is proposed is given below. If Governing Body members approve these proposals we will take them to the CCG Remuneration Committee for final approval and following that we will also notify member practices via the weekly newsletter. Suspension and amendment of standing orders i. Suspension 23 of 402
24 Further to discussion at the Governing Body seminar in February, it was agreed that we would make some changes to support the working together collaboration between Haringey and Islington CCGs, avoiding unnecessary elections and the associated time and costs involved in managing these. This in part results from the Clinical Vice Chair stepping down, reducing voting GP attendance. With respect to the requirements for a quorum of the Governing Body: ii. The proposal is to suspend part of Standing Order (SO) 3.6.4(c) such that it will be amended (for the duration of the suspension) from "At least three voting GPs, not including the Chair" to "At least three voting GPs". This has the effect of allowing the Chair to be one of the three voting GPs (so that that number of GPs will be retained in the quorum). iii. iv. The recommendation is to amend to retain three voting GPs but to include the Chair Amendment to standing orders It is also proposed to amend SO 2.2.4(d) to provide that where it is considered appropriate the term of office of an elected member of the Governing Body may be extended so that in those circumstances no election will be called. As part of the amendment, paragraphs (i) and (ii), which concern past years, will be deleted. The proposed amendment is set out below. a) Subject to paragraph (ii) and SO 2.2.4(e), each elected member of the Governing Body will serve a term of office of four years. b) Where the Governing Body considers it appropriate to do so, any term of office of an elected member of the Governing Body may be extended by up to two years. The Governing Body should be advised on these matters by the Remuneration Committee. The recommendation is to amend so that elected members serve a four year term with an option for a two year extension. Current elected members will be eligible for the extension. Decision Required: The Governing Body are asked to APPROVE the recommendations. Helen Pettersen Accountable Officer, 9 May of 402

25 MEETING: Islington CCG Governing Body Item: 3.1 DATE: 9 th May 2018 TITLE: Finance Report Month /19 Draft Outturn LEAD COMMITTEE MEMBER: Simon Goodwin, NCL Chief Finance Officer AUTHOR: Anthony Browne Deputy Chief Finance Officer CONTACT anthony.browne@nhs.net DETAILS: SUMMARY: Pending final audit review and opinion, financial performance for the year 2017/18 can be summarised as: Islington CCG exceeded the in-year break-even control total by 2.5m and in addition to this, following NHS England instruction, released the 0.5% nonrecurrent reserve ( 1.7m) and Category M margin return ( 0.3m) to its bottom line at Month 12. This is in keeping with figures reported at Month 11 and resulted in the CCG delivering a combined final surplus of 4.5m for the year. Requirement to release 0.5% reserve (and the Category M Margin) was announced by NHS England on 20 th March 2018 and reported to Committee and Governing Body in Month 11. The conditions set by NHS England meant that this either increased surpluses or improved deficit positions across CCGs in England. For Islington CCG this meant increasing the surplus as set out in the table below. In total this increased the CCG s brought forward surplus from 7.3m to 11.8m (see table below). The opportunity to access this surplus in future years remains however special approval is required from NHS England. In usual circumstances the right to access this non-recurrent fund is retained for CCGs with lower levels of funding allocation growth and, at present, Islington CCG does not fall in to this category. Summary of Islington CCG Draft 17/18 Outturn Position (Month 12) m Islington CCG In-Year Surplus at Month Release of the system risk reserve at Month Category M drug margin rebate return to CCG at Month Revised in-year surplus at Month CCG Historic Brought Forward Surplus / (Deficit) 7.3 Revised (RAB) Cumulative Surplus / (Deficit) of 402
26 Aside from the reserve movements above the CCG reported a 0.7m reduction on in-sector contract costs between the month 11 forecasts and Month 12 draft outturn. This favourable movement is split between the Whittington ( 0.3m), UCLH ( 0.3m) and Royal Free ( 0.2m). The Barts position has remained materially unchanged from previous months. The draft Month 12 Agreement of Balances reconciliation has informed the final draft position for acute for which there is a 3.2m pressure at year end. As has been the case in previous years this was mainly realised in the UCLH contract ( 2.7m). The Whittington Health performed materially to contract however there were additional pressures against Moorfields ( 0.2m) and out of sector contracts (Barts 0.9m, Homerton 0.5m and Guys 0.4m). The Royal Free contract finished the year with a 1.1m underspend. Overall non-acute services were 1.4m underspent at year end. During the year there had been high profile pressures against Prescribing and although the return of the Category M margin return of 0.3m did see some benefit to the position the NCSO (no cheaper stock) budget pressures resulted in a 0.9m overspend at year end. Non-Acute pressures were also seen against Continuing Care ( 1.7m) and Learning Disability / Transforming Care budgets lines ( 0.7m). Offsetting underspends were seen against the Better Care Fund (see below) and Delegated Primary Care ( 2.6m). The latter outturn due to NCL wide risk management of primary care and the remaining headroom following CCG investments in 2017/18. Managing the CCG s overall financial pressure was achieved by: o Releasing the demand reserve and contingency balance, including an element of prior year accruals and provisions that were no longer required. o Freezing investment for part of the Better Care Fund due to nonelective pressures in acute contracting; o Holding a non-recurrent underspend against the Delegated Primary Care headroom in 2017/18. This was agreed by Governing Body during the year to balance the NCL Delegated Primary Care position and therefore reduced spend non-recurrently against Islington s bottom line. The CCG has approved plans to fully commit this headroom in 2018/19. As per previous reporting these mitigating items are all non-recurrent and the 2018/19 budget will require delivery of higher than previous QIPP programmes and robust financial management in order to control recurrent cost pressures. 26 of 402
27 During the year Islington CCG also provided direct and indirect support to the STP and other NCL CCGs in the following ways: o A contribution towards the costs of the STP programme management office ( 0.3m) which was hosted by Islington CCG; o A contribution to Islington s share of costs for the NCL Senior Management Team ( 0.3m) which was hosted by Islington CCG; The CCG s draft annual report was submitted to NHS England on the 20 th April in accordance with the national timetable. Draft annual accounts will follow on the 24 th April which will also see the commencement of the 2017/18 year-end audit. The external auditors (KPMG) are expected to finalise their work around the 15 th May with the final 2017/18 audit committee review scheduled for 22 nd May. The final draft annual report and accounts need to be signed and sent back to NHS England on the 29 th May The Operating Plan is not discussed in detail in this report and a separate presentation is to be provided discussing changes from the first draft submission made on the 8 March The final submission of the Operating Plan is due back to NHS England on 30 th April This report contributes to: Delivering high quality, efficient services within the resources available. Prior consideration by Committees and other partners: None specific Patient & Public Involvement (PPI): None specific Equality Impact Assessment: None specific Risks: This report is one element used to monitor the Clinical Commissioning Group s financial performance in terms of adherence to core statutory duties. RECOMMENDED ACTION: The Governing Body is asked to: CONSIDER the draft financial position for Islington Clinical Commissioning Group for the period 1 April 2017 to 31 March of 402
28 Islington Clinical Commissioning Group Finance Report: 1 April 2017 to 31 March 2018 (Month 12 Draft Outturn) 1. INTRODUCTION 1.1 This paper presents to Islington Clinical Commissioning Group s Governing Body, the financial position for the period to 31 March This represents the draft unaudited outturn for the CCG for the financial year 2017/ EXECUTIVE SUMMARY 2.1 Month 12 Draft Unaudited Financial performance for year ending 31 March 2018 can be summarised as follows: Month 12 Draft Outturn Budget Actual Variance '000 '000 '000 Resource Allocation (In-Year) (400,505) (400,505) 0 Acute Contracts (In and Out of Sector) 206, ,581 3,278 Other Acute 19,977 19,884 (93) Acute Commissioning 226, ,465 3,185 Mental Health 51,503 51, Continuing Care 9,289 11,008 1,719 Community Services 21,441 20,638 (804) Primary Care Prescribing 25,169 26, Primary Care 6,903 6,372 (530) PRC Delegated Co-Commissioning 35,408 32,709 (2,699) NHS 111 2,525 2, Non-Acute Commissioning 152, ,108 (1,130) Programme Corporate Cost 6,372 6,129 (243) Running Costs 5,037 4,759 (278) CCG Reserves (1% NR & 0.5% Contingency) 3,413 0 (3,413) Acute Demand Reserve 7,165 4,567 (2,598) In-Year Surplus / (Deficit) 0 4,477 (4,477) 28 of 402
29 2.2 The draft unaudited 2017/18 outturn position is reporting Islington CCG exceeding the in-year break-even control total by 2.5m and in addition to this, following NHS England instruction, released the 0.5% non-recurrent reserve ( 1.7m) and Category M margin return ( 0.3m) to its bottom line at Month 12. This is in keeping with figures reported at Month 11 and resulted in the CCG delivering a combined final surplus of 4.5m for the year. 2.3 Requirement to release 0.5% reserve (and the Category M Margin) was announced by NHS England on 20th March 2018 and reported to Committee and Governing Body in Month 11. The conditions set by NHS England meant that this either increased surpluses or improved deficit positions across CCGs in England. For Islington CCG this meant increasing the surplus as set out above. 2.4 In total this increased the CCG s brought forward surplus from 7.3m to 11.8m. The opportunity to access this surplus in future years remains however special approval is required from NHS England. In usual circumstances the right to access this non-recurrent fund is retained for CCGs with lower levels of funding allocation growth and, at present, Islington CCG does not fall in to this category. 2.5 Aside from the reserve movements above the CCG reported a 0.9m reduction in acute costs between the month 11 forecasts and Month 12 draft outturn. This favourable movement is split between the Whittington ( 0.3m), UCLH ( 0.3m) and Royal Free ( 0.2m). The Barts position has remained materially unchanged from previous months. 2.6 The draft Month 12 Agreement of Balances reconciliation has informed the final draft position for acute for which there is a 3.2m pressure at year end. As has been the case in previous years this was mainly realised in the UCLH contract ( 2.7m). The Whittington Health performed materially to contract however there were additional pressures against Moorfields ( 0.2m) and out of sector contracts (Barts 0.9m, Homerton 0.5m and Guys 0.4m). The Royal Free contract finished the year with a 1.1m underspend. 2.7 Overall non-acute services were 1.4m underspent at year end. During the year there had been high profile pressures against Prescribing and although the return of the Category M margin return of 0.3m did see some benefit to the position the NCSO (no cheaper stock) budget pressures resulted in a 0.9m overspend at year end. 2.8 Non-Acute pressures were also seen against Continuing Care ( 1.7m) and Learning Disability / Transforming Care budgets lines ( 0.7m). Offsetting underspends were seen against the Better Care Fund (see below) and Delegated Primary Care ( 2.6m). The latter outturn due to NCL wide risk management of primary care and the remaining headroom following CCG investments in 2017/ Managing the CCG s overall financial pressure was achieved by: 29 of 402
30 o Releasing the demand reserve and contingency balance, including an element of prior year accruals and provisions that were no longer required. o Freezing investment for part of the Better Care Fund due to non-elective pressures in acute contracting; o Holding a non-recurrent underspend against the Delegated Primary Care headroom in 2017/18. This was agreed by Governing Body during the year to balance the NCL Delegated Primary Care position and therefore reduced spend non-recurrently against Islington s bottom line. The CCG has approved plans to fully commit this headroom in 2018/ As per previous reporting these mitigating items are all non-recurrent and the 2018/19 budget will require delivery of higher than previous QIPP programmes and robust financial management in order to control recurrent cost pressures During the year Islington CCG also provided direct and indirect support to the STP and other NCL CCGs in the following ways: o A contribution towards the costs of the STP programme management office ( 0.3m) which was hosted by Islington CCG; o A contribution to the cost of the NCL Senior Management Team ( 0.3m) which was hosted by Islington CCG; 2.12 The CCG s draft annual report was submitted to NHS England on the 20 th April in accordance with the national timetable. Draft annual accounts will follow on the 24 th April which will also see the commencement of the 2017/18 year-end audit. The external auditors (KPMG) are expected to finalise their work around the 15 th May with the final 2017/18 audit committee review scheduled for 22 nd May. The final draft annual report and accounts need to be signed and sent back to NHS England on the 29 th May of 402
31 3. ACUTE ACTIVITY FINANCIAL PEFORMANCE 3.1. The table below summaries acute in and out of sector contract performance within the draft Month 12 position for 2017/18 for comparative purposes to Month 11 reporting. In Sector Agreements Full Year Budget Actual Variance '000 '000 '000 % Month 11 FOT Forecast Movement to M12 The Whittington Hospital 100, ,386 (14) (0%) 100,686 (300) UCLH NHS Foundation Trust 69,908 72,575 2,667 4% 72,903 (328) Royal Free Hampstead NHS Trust 13,216 12,088 (1,128) (9%) 12,302 (214) Moorfields Foundation Trust 4,392 4, % 4, North Middlesex University (23) (3%) 827 (2) Royal National Orthopaedic Hospital NHS Trust (50) (7%) 741 (34) Great Ormond Street Hospital % In Sector Total 189, ,654 1,660 1% 192,424 (771) Out of Sector Agreements Barts and The London NHS Trust 6,266 7, % 7, Homerton University Hospital FT 4,160 4, % 4, Imperial College Healthcare 1,620 1,515 (105) (6%) 1, Guys and St Thomas FT 2,364 2, % 2,856 (83) Chelsea and Westminster FT (196) (27%) Kings College Hospital FT % St George's Healthcare NHS Trust % 195 (9) North West London NHS Trust % 310 (29) Barking, Havering and Redbridge University Hospitals NHS Trust % 158 (15) Royal Brompton FT % The Royal Marsden NHS FT (17) (13%) Out of Sector Total 16,309 17,927 1,618 10% 17, Acute LAS 9,470 9,464 (5) (0%) 9,498 (33) Total 215, ,045 3,272 0% 219,744 (698) 3.2. The table below summarises the Forecast Outturn at PoD level for each of the CCG s main acute contracts. 31 of 402
32 3.3. Month 12 Acute Point of Delivery (PoD) Forecast Variance analysis ( 000 s): UCLH Whittington Health Royal Free London Moorfields Barts All other providers Total Accident and Emergency (118) (48) (7) (20) 51 Critical Care 322 (96) (891) (415) Diagnostic Imaging (373) (394) (77) 9 (33) (38) (906) Drugs and Devices (98) (12) 601 Elective 430 (231) (124) (47) 125 (29) 125 Maternity (186) (777) (860) Non-Elective 2, (434) ,189 Outpatients ,449 Other (880) ,667 (14) (1,128) , The most significant areas of pressure during the year were seen in Non- Elective, followed by Outpatients and drugs and decides. There were material underspends against Diagnostic Imaging, Maternity and Critical Care This same analysis, but by provider, shows that the Whittington realised most pressure against A&E, Non-Elective and Outpatients. At UCLH it is very apparent that there is a significant pressure within Non-Elective with additional over performance in Outpatients and Elective services. Royal Free underspending appears to be driven by reduced levels of spend in Critical Care and Non-Elective Within Out of Sector contracting there is a notable pressure against Non- Elective costs with Barts responsible for the majority of this activity. The Barts position also recorded pressures against Critical Care, Elective and Outpatient services. 32 of 402
33 4. NON-ACUTE Month 12 Draft Outturn Budget Actual Variance '000 '000 '000 Mental Health 51,503 51, Continuing Care 9,289 11,008 1,719 Community Services 21,441 20,638 (804) Primary Care Prescribing 25,169 26, Primary Care 5,617 5,120 (497) Delegated Primary Care 35,408 32,709 (2,699) GP Forward View 1,286 1,253 (33) NHS 111 2,525 2, Non-Acute Commissioning 152, ,108 (1,130) Programme Corporate Costs 6,372 6,129 (243) Non Acute Total 158, ,237 (1,373) 4.1. Non-Acute services were 1.4m underspent at year end. During the year there had been high profile pressures against Prescribing and although the return of the Category M margin return of 0.3m did see some benefit to the position the NCSO (no cheaper stock) budget pressures resulted in a 0.9m overspend at year end Non-Acute pressures were also seen against Continuing Care ( 1.7m) and Learning Disability / Transforming Care budgets lines ( 0.7m). Offsetting underspends were seen against the Better Care Fund (see below) and Delegated Primary Care ( 2.6m). The latter outturn due to NCL wide risk management of primary care and the remaining headroom following CCG investments in 2017/ Note that CCG Running costs reflected a 0.3m underspend against the 5.04m allocation. This was due to a presentational issue with where the Goswell Road to Laycock Street Provision needed to be released back to at the end of the year. 5. CONCLUSION 5.1. Pending final audit review and opinion, the CCG exceeded the in-year breakeven control total by 2.5m and following instruction from NHS England released the 0.5% non-recurrent reserve ( 1.7m) and Category M margin return ( 0.3m) to its bottom line at Month 12. This resulted in a revised final in-year surplus of 4.5m and a cumulative surplus of 11.8m at the end of financial year 2017/ The final outturn position will be confirmed through the annual accounts audit process which commences on 24 April 2018 and is due to be reported to the Audit Committee on 22 nd May The Governing Body is asked to: 33 of 402
34 CONSIDER the draft financial position for Islington Clinical Commissioning Group for the period 1 April 2017 to 31 March of 402
35 Appendix A - Islington CCG detailed year to date actual (Month /18 Draft Unaudited Position) 2017/18 Draft 2017/18 Budget Outturn Variance Variance '000 '000 '000 % Allocation In Year (365,097) (365,097) 0 0.0% Historic Underspend (7,295) (7,295) 0 0.0% Delegated Co-Commissioning (35,408) (35,408) 0 0.0% Revenue Resource Limit (407,800) (407,800) 0 0.0% Acute & Integrated Care NHS SLA - In Sector 189, ,654 1, % Acute & Integrated Care NHS SLA - Out of Sector 16,309 17,927 1, % SLA Exclusions 5,643 4,963 (680) -12.0% Acute Re-admissions & Threshold (5) -3.2% Acute LAS 9,470 9,464 (5) -0.1% Acute Planned Care 2,729 3, % Non Contracted Activity 1,985 2, % Acute & Integrated Care Total 226, ,465 3, % Mental Health 44,970 44,846 (124) -0.3% Mental Health - CAHMS 2,397 1,905 (492) -20.5% Learning Disabilities 4,136 4, % Continuing Care 9,289 11,008 1, % End of Life Care 1,353 1,322 (31) -2.3% Community Services 7,853 7, % Better Care Fund 11,508 10,753 (756) -6.6% Sexual Health (163) -22.4% NHS 111 2,525 2, % Primary Care - Prescribing 25,169 26, % Primary Care - Commissioning (81) -13.2% Primary Care - LCS 2,200 1,945 (255) -11.6% Delegated Primary Care 35,408 32,709 (2,699) -7.6% Primary Care - GP WIC & Interpreting 1,165 1, % Primary Care - GPIT (114) -15.0% 35 of 402
36 Primary Care - Development (83) -9.4% GP Forward View 1,286 1,253 (33) -2.6% Non Acute Total 152, ,108 (1,130) (1) London Healthy Living Partnerships 2,539 2, % Integrated Digital Care Record (IDCR) 11 0 (11) % Islington & Haringey Wellbeing Partnership % CSU Contract (Programme) (3) -0.4% Property Services (Programme) (197) -53.0% Commissioning Support % Project Management Office (14) -20.3% Nursing and Quality (169) -41.8% Safeguarding - Adults & Children (17) -5.2% Transforming Care Programme (5) -8.8% STP Support % Programme Corporate Costs Total 6,372 6,129 (243) -3.8% Total Programme Expenditure 384, ,702 1, % CCG Running Cost (Excl CSU) Pay 2,300 2,214 (87) -3.8% CCG Running Cost (Excl CSU) Non-Pay % CCG Running Cost (CSU) 1,853 1, % CCG Running Cost (PropCo) 257 (54) (312) % Operating Costs Total 5,037 4,759 (278) -5.5% Acute Demand Reserve 7,165 4,567 (2,598) CCG Reserves (0.5% Contingency) 1,734 0 (1,734) Non Recurrent Reserve (1%) 1,679 0 (1,679) Reserves and Contingencies Total 10,577 4,567 (6,011) Total Expenditure 400, ,028 (4,477) Cumulative (Surplus) / Deficit 7,295 11,772 (4,477) Removal of Cumulative (Surplus) / Deficit (7,295) (7,295) /18 Surplus (In-Year) 0 4,477 (4,477) 36 of 402
37 Appendix B Other Acute Point of Delivery (POD) Breakdown Month 12 Reporting ( ) Adjustment Description UCLH Whittington Health Royal Free London Moorfields Barts and London 17/18 Work in Progress movement (Maternity, Critical Care) (72,000) (60,949) (294,666) Prior Year Financial Impact (211,391) (16,795) (93,584) Intermediate Care (Evergreen Ward) 336,174 Neonatal Critical Care - Related Spells 139,872 Claims and Challenges (562,347) 514,649 (45,041) (13,135) Marginal Rate (703,141) (52,440) 354,024 QIPP STP 101,661 Readmissions to other Providers 48,358 Productivity metrics 125,180 (7,100) Patient Transport 122,659 Regular Day attendance 45,576 93,780 Ad-Hoc Items (218,693) (28,658) Patient Transport 38,858 Helicopter Emergency Medical Service (HEMS) 59,710 Other 192,778 (80,398) (22,243) 40,369 9,193 Total (880,055) 320,862 98, ,030 59, of 402
38 Item: 3.2 MEETING: Islington Clinical Commissioning Group Governing Body DATE: Wednesday 9th May 2018 TITLE: Performance Report LEAD COMMITTEE Alex Smith, Director of Planning, Performance & Delivery MEMBER: AUTHOR: Andrew Broddle, Head of Performance and Planning CONTACT DETAILS: SUMMARY: 1. Overview The Islington CCG Performance and Quality Summary produced by North East London Commissioning Support Unit (NEL CSU) details performance against constitution targets, locally agreed community targets as well as reporting on national and local quality standards. It should be noted that the performance and quality sections of the report contain different months activity, due to the reporting timetable. This is stated as clearly as possible within the report and near-time local intelligence is also included, where relevant. 2. Performance 2.1 ) 18 and 52-Week Referral to Treatment Time (RTT) Islington CCG met the operational standard (92%) in December 2017 but narrowly missed the standard in January 18 (91.8%) and February 18 (91.9%). In February the 92% standard was missed by just 18 patients from the 16,125 patients treated. The drop in performance has been associated with increased pressure during the winter period bewteen December 17 and February 18 and the proactive delaying of some outpatient appointments agreed across NCL to allow senior clinicians in relevant specialities to better support Emergency Care Departments. The drop in performance has been caused by increased pressure on University College London Hospitals, Whittington Health and the reporting issues at the Royal Free London Hospital which are being addressed by Camden CCG, NHS England and NHS Improvement. The year to date (April 17 February 18) performance (92.5%) is better than the 92% operational standard. The 52 week wait position at the end of February was that there were no patients who were waiting over 52 weeks for treatment. This is the first month since June 2017 that there have been no patients waiting over 52 weeks for treatment. The charts below show the changes in median waiting times for Islington patients at 38 of 402
39 Whittington Health (figure 1) and University College London Hospitals (figure 2) since January While waits have varied over time as of February 2018 the median waiting time at both providers is lower or comparable with year on year figures. Figure 1: Median Waiting Times: Whittington Health (Islington CCG patients) Figure 2: Median Waiting Times: University College London Hospitals (Islington CCG patients) Diagnostics Islington CCG met the operational standard (of 99%) for the percentage of patients waiting less than 6 weeks for a diagnostic tests continues to meet the operational standard with 99.4% of patients waiting less than 6 week for a diagnostic test in February. The year to date performance is meeting the standard at 99.2%. 2.2 ) Cancer Islington CCG met four of eight of the national cancer access standards in January 2018, narrowly missing two of the standards (2 week wait breast symptoms and 31 day wait to first definitive treatment). 39 of 402
40 The four standards which were not met in January were; 2 week wait breast symptoms (92.7% performance against the 93% target) There were three patient choice breaches from a total of 43 cases. 31 day wait to first definitive treatment (95.4% performance against the 96% target) There were three breaches from a total of 65 patients. The breaches were categorised into the following reasons for breach. One patient choice, one extremely complex diagnostic pathway and one due to a capacity issue. 62 day wait urgent GP referral (66.7% performance against the 85% target) There were nine breaches from 27 cases. The nine breaches were categorised into the following reasons for breach. Two were patient choice, one patient was unfit for treatment, three patients were on extremely complex diagnostic pathways, there was a delay in the work up of one patient and two patients did not have complete information on the inter-trust transfer form. University College London had the highest level of breaches of the 62 day wait standard. 62 day wait screening service (83.3% performance against the 90% target) There was one breach from six cases which was due to a complex diagnostic pathway. In total, of the 963 patients from Islington treated for cancer, breast symptoms or suspected cancer in January 2018, 912 (98%) were treated within national waiting time standards. This is an improvement on 97% for December The NCL Cancer Performance Leadership group meets fortnightly to review sector-wide cancer performance and hold each other to account regarding the achievement of improvement actions. These meetings support the London-wide regulatory process in providing assurance that Trusts and CCGs are taking all necessary steps to improve cancer performance. A number of actions to address the variable 62 day cancer performance are progressing. The UCLH Cancer Vanguard is also providing support. Key improvement actions have been agreed to further develop the urology one stop clinic model and straight to test which will reduce the waiting time for patients. 2.3 ) A&E Islington CCG performance against the 4-hour standard was 87.4% in February and 90.2% for the year to date. Overall 4-hour A&E performance at Whittington Health across February was 86.1%. All Trusts have been under significant pressure during the winter period All CCGs and provider organisations within North Central London are under scrutiny from NHS England and NHS Improvement, as performance has not matched trajectories agreed earlier in 2017/2018 which required 95% performance by March At the March 2018 A&E Delivery Board a renewed set of priorities were agreed to move the system towards consistently achieving 90% performance within six weeks. This included; Fit to Sit programme to improve ambulance handover times Maximising the use of Ambulatory Care Enhancing the Rapid Assessment and Treatment (RAT) model of care Expanding the Criteria Led Discharge Programme Further work on improving discharge arrangements between WH and LBI and 40 of 402
41 LBH Delayed transfers of care are where patients in acute hospitals are medically fit for discharge but are unable to be discharged. This can be due to delays in social care or when care in a more appropriate healthcare setting is not available. These delays create a poor patient experience and impact on the availability of acute beds for more acutely ill patients. The number of delayed transfers of care has been a continued area of focus by the A&E Delivery Board. The average number of delayed patients per day at Whittington Health has begun to reduce. In January there were average of 11 patients delayed per day which reduced to an average of 8.9 patients per day in February. This is approximately 3% of the bed base at Whittington Health which is lower (better) than the 3.3% target. Daily liaison between the hospital, CCG and Local Authorities continues to resolve obstacles that prevent the transfer of care. There are escalation processes for issues where progress is not being achieved quickly enough involving Director level support from all partner organisations. 2.4) Electronic referrals By 1 October 2018 all NHS Providers need to use e-referral as their only means of making and receiving referrals from GPs to consultant led first outpatient appointments. CCGs and providers are working together in partnership to make the changeover to an electronic only system. The North Central London e-referral Implementation and Steering Group has representation from commissioners and providers and is being chaired by Denise Pettit from Haringey CCG. The Whittington Hospital and North Middlesex Hospitals have paper switch over dates in April, while The Royal Free and University College London Hospitals have switch over dates in August. The latest available published (February) e- referral utilisation data for the Whittington hospital shows it was at 47%. During the last six weeks, intensive efforts have been accelerated to ensure all practices in Islington CCG receive training. NHS England and NHS Digital have been working in partnership with Whittington Health to ensure all suitable clinics are on the e-referrals system. Whittington Health remain on track for an April switch off. However, some services have been jointly agreed between regulators, CCG leads and the Whittington as excluded from e-rs due to alternative pathways being in operation (e.g. MSK) this impacts on utilisation data as reported by NHS Digital. 2.5) CQUIN As part of the Contract Round, two year CQUINs were agreed with all Providers. For Whittington Health all the CQUINs agreed were National CQUIN s for Acute and Community Providers as set out in the CQUIN Guidance. As at the end of Quarter 3, Whittington are forecasting delivery of all CQUIN targets other than CQUIN 8: Supporting proactive and safe discharge. The Trust have experienced technical difficulties and so are pushing back implementation of this CQUIN until Quarter 4. Final performance for 2017/18 will be available in July 2018 following validation of Quarter 4 achievement which will take place in June Figure 3 CQUIN Performance (Quarter /18) CQUIN Description Quarter 3 Comments 2017/18 Infections (AMR and Achieved Whittington Health achieved over the 90% 41 of 402
42 Sepsis) National 4: Improving services for people with mental health needs who present to ED National 6: Offering clinical advice and guidance Achieved Achieved target for both indicators and in some cases exceeded this target (notably reduction in antibiotic use and early identification of sepsis in clinical settings) The Trusts reviewed progress against Data Quality Improvement Plan (DQIP) and confirmed that systems are in place to ensure that coding of Mental Health via A&E HES data submissions are complete and accurate The patient cohort (people with mental health needs who present to ED) is discussed at frequent attenders meetings with Mental Health team. The coding system for A&E attendances will changing during Q4. A revised plan will be developed once the coding change has been implemented Data submitted via SDCS portal. Advice and & Guidance covers 35% of activity Timetable and implementation is aligned with the STP National 7: NHS e-referrals Achieved 90% of referrals to 1 st OP services able to be received through e-rs/on track with agreed trajectory (excluding agreed exclusions) National 8: Supporting proactive and safe discharge National 11:Personalised care and support In progress Whittington Health Trust Management Group have approved late implementation to enable testing, training and downtime of software implementation to be managed in a realistic manner Achieved 2.6) Integrated Urgent Care Service Haringey & Islington Community caseloads all had between % achievement. Generalist community matrons complete a personalised case plan for patients on their caseload (these are patients who have 2 or more long term conditions). The care plan will be shared with GPs and this will be recorded and saved on the patient electronic record (RIO). The integrated urgent care (IUC) service for North Central London (NCL) combines NHS 111 and GP out-of-hours services into a single integrated service operating a clinical hub with GP s, nurses, paramedics, and pharmacists, to offer direct access to assessment by a clinician, and a broader range of options for advice and treatment. It benefits all residents of Barnet, Camden, Enfield, Haringey and Islington by providing a more responsive model of care which avoids repetition of assessment and unnecessary steps in the patient s journey. Call waiting times (% within 60 seconds) deteriorated slightly in January and remain below the revised standard of 85%, agreed with Enfield CCG (as lead commissioners) as part of a recovery plan. 42 of 402
43 Figure 4: Integrated Urgent Care Service call waiting times Q1 Q2 Q3 Q4 Apr May Jun Jul Aug Sept Oct Nov Dec Jan 95.6% 91.0% 91.2% 86.3% 88.3% 81.6% 80.5% 73.3% 77.4% 76.7% Although the workforce plan is progressing to a planned trajectory, staffing levels still remain below the overall WTE target creating rostering challenges. 2.7) London Ambulance Service (LAS) LAS handover times Ambulance handover times remain a challenge across London s hospitals. At the Whittington site 15 minute handover performance worsened from 57.7% in December to 53.6% in January. However, this remains a significant improvement on October performance of 31.4%. The 30 minute handover time was 97.0% in December and 97.1% in January LAS Ambulance Response Programme (ARP) The new national ambulance response time standards were established under the Ambulance Response Programme Initiative (ARP) led by NHS England. The aim of the ARP is to ensure that: The sickest patients receive the fastest response All patients get the best response allocated to them No one is left waiting for and unacceptably long time for an ambulance to arrive Figure 5: London Ambulance performance against the national standards Category Measure National Standard December January February 1 Mean response time 7 minutes 00:07:24 00:07:09 00:07:28 90 th centile 15 minutes 00:12:04 00:11:43 00:11:48 2 Mean response time 18 minutes 00:24:11 00:20:23 00:23:21 90 th centile 40 minutes 00:51:11 00:42:05 00:49: th centile 120 minutes 02:58:56 02:25:11 02:59: th centile 180 minutes 02:51:49 02:19:17 02:34:17 The London Ambulance Service achieved the national standards for category 1 & 4 responses in February. February performance worsened slightly from January, in part due to the adverse weather conditions experienced across London and an increase in call volume across London. The London Ambulance service was ranked fourth of the ten ambulance trusts across England and performed within the England average by 50 seconds. Figure 6: London Ambulance Service performance by STP area February of 402
44 National Standard North Central North East North West South East South West C1 Mean C1 90 th Centile 7 15 minutes minutes (00:07:00) (00:15:00) C2 Mean 18 minutes (00:18:00) C2 90 th Centile 40 minutes (00:40:00) C3 90 th Centile 120 minutes (02:00:00) C4 90 th Centile 180 minutes (03:00:00) 00:07:37 00:12:24 00:24:31 00:51:25 03:42:28 03:17:46 00:07:45 00:11:50 00:25:45 00:54:23 03:14:55 02:49:53 00:07:34 00:11:47 00:23:51 00:51:18 03:12:56 02:42:06 00:07:14 00:11:33 00:19:55 00:40:43 02:18:08 02:06:48 00:06:35 00:11:27 00:21:56 00:45:05 02:36:10 02:01:38 2.8) Whittington Health (WH) Community Health Services (CHS) The new performance report for Community Services has been included within the P&Q report. This breaks down waiting time by routine, urgent and average. It showed that six of 30 services saw 95% of patients within target for routine services. Key highlights include: The podiatry service increased the number of patients meeting the routine target of six weeks from 24.8% in January to 53% in March 2018 The Bladder and Bowel adult service increased the number of patients meeting the routine target of twelve weeks from 54.8% in January to 72% in March 2018 Regular reports to the Islington Quality and Performance Committee are being made regarding the work of the Community Service Improvement Group which aims to improve performance standards. 2.9) Metal Health Standards Islington CCG met five of the six Improving Access to Psychological Therapies targets for the last reporting period. These were; The proportion of patients on CPA who were followed up within 7 days after discharge from psychiatric inpatient care. The proportion of admissions to acute wards that were gate kept by the CRHT teams. The percentage of RTT first episode psychosis (FEP) periods within 2 weeks of referral. The dementia diagnosis rate (Age 65+). Patients on a care programme approach who were followed up within 7 days of discharge from psychiatric inpatient care The standard which was narrowly missed was the proportion of children and young people with eating disorders (routine cases) that wait 4 weeks or less from referral to start of NICEapproved treatment. Performance in quarter 3 was 87.50% against the standard of 95%. 44 of 402
45 CIFT did not meet the standard in September of beginning 95% of mental health assessments within 1 hour within A&E departments at the Whittington, UCLH and the Royal Free (Performance was 88.6%, 86.2% and 91.9% respectively). CIFT did not meet the standard in September of beginning 95% of mental health assessments within 24 hours on wards at the Whittington (82.1%) or UCLH (90%) There have been no 12 hour mental health breaches at Whittington hospital since the beginning of October.. The new recovery lounge is due to open in the coming six weeks which will provide a better therapeutic environment for patient s in a crisis. 2.10) Continuing Health Care Figure 7: Percentage of decision support tool (DST) assessments carried out in an acute setting Period Number of DSTs carried out Number of DST carried out in an acute hospital setting % of DST carried out in an acute hospital setting Quarter % Quarter % Quarter % Quarter % The target for the percentage of Decision Support Tool (DST) assessments carried out in an acute setting is 15%. Two of the assessments in the acute setting in February were at hospitals which fall outside of our catchment area (one of the assessments was undertaken at Homerton Hospital and the other one was undertaken at the Royal London Hospital). The two hospitals have subsequently been contacted to discuss how CHC assessments in their settings can be avoided in the future for Islington patients. Two of the four assessments in March were completed in the acute setting as part of existing reviews. The target is that 80% of standard continuing health care referrals are completed within 28 days. Figure 8 shows that Islington met this standard in Quarter 2, 3 & 4. Figure 8: Percentage of continuing health care referrals are completed within 28 days. Period 2.11 Quality Premium Standard CHC referrals completed Number of referrals completed within 28 days % Standard CHC referrals completed within 28 days Quarter % Quarter % Quarter % Quarter % The Quality Premium (QP) is intended to reward CCGs for improvements in the quality of the services which they commission and for associated improvements in reductions in inequalities in access and in health outcomes. The QP award will be based on measures 45 of 402
46 that cover a combination of national and local priorities and will reflect the quality of the health services commissioned. The total value of the quality premium in 2017/18 was 1,145,905 The Quality Premium paid in 2018/19 will be based on the performance for 2017/18. There were five national measures (early cancer diagnosis, GP access and experience, continuing healthcare, bloodstream infections and mental health) and two local measures (one of which is the mental health measure and the other is the expected prevalence of chronic kidney disease). These measures are: 1. For CCGs to show an improvement in early cancer diagnosis (increase proportion diagnosed at stages 1 or 2) 2. That the GP survey indicates 85% of respondents said that they had a good experience of making an appointment or that there was a 3 percent increase (between July 17 and July 18 survey results) 3. For CCGs to ensure that in more than 80% of cases with a positive NHS Continuing Health Care (CHC) assessments took place within 28 days, and that less than 15% of all NHS Continuing Health Care assessments take place in an acute hospital. 4. For CCGs to demonstrate they are reducing Gram Negative Bloodstream Infections (GNBSIs) and inappropriate antibiotic prescribing in at risk groups 5. For CCGs to demonstrate a reduction in the number of out of area mental health placements The final data has not yet been confirmed for 2017/18. However, early indications are that at least three of the national improvement measures have not been met (early cancer diagnosis, overall experience of making a GP appointment, CHC assessments). Data for reductions in gram negative bloodstream infections and inappropriate antibiotic prescribing is still awaited. The value of the quality premium paid will be reduced by 25% for each of the constitutional measures which are not met. The constitutional measures are: The 18 week referral to treatment pathway; A&E four hour waits; the 62 day cancer waiting standard (urgent GP referral to first definitive treatment) and LAS performance for category A, red 1 ambulance calls. Of the four constitutional measure the latest data for 17/18 shows that at least three of these standards were not met. The only standard which may have been met when final data is published will be the 18 week referral to treatment pathway standard. This means that the payment any of the national or local measures which were met will be reduced by 75%. The current estimate of the likely quality premium payment is 129, of 402
47 This report contributes to: Delivering high quality, efficient services within the resources available. Prior consideration by Committees and other partners: not applicable Patient & Public Involvement (PPI): not applicable Equality Impact Assessment: not applicable Risks: not applicable RECOMMENDED ACTION: Islington Clinical Commissioning Group Governing Body is asked to: Note the report SUPPORTING PAPERS: Islington CCG Performance and Quality Summary April of 402

48 Appendix Islington CCG Performance and Quality Summary April of 402
49 Contents Item Page Islington CCG Performance and Quality Summary & Dashboards 3-6 Whittington Health NHS Trust Performance and Quality Summary 7-26 Moorfields Eye Hospital NHS Trust Performance and Quality Summary Camden & Islington NHS Foundation Trust Performance and Quality Summary University College London Hospitals NHS Foundation Trust Performance and Quality Summary NCL Integrated Urgent Care Services Summary London Ambulance Service Summary Quality Assurance Sign-off of 402 2
50 Executive Dashboard Performance Overview Reporting Month Islington CCG Trajectory Reporting Month Whittington RTT Admitted < 18 Weeks* Feb % Jan % 84.9% 74.8% 80.8% - RTT Non-Admitted < 18 Weeks* Feb % Jan % 90.4% 88.6% 94.0% - RTT Incomplete < 18 Weeks* Feb % Jan % 91.0% 83.0% 94.0% 92% Diagnostic Tests < 6 Weeks* Feb % Jan % 99.1% 99.3% 100.0% 99% Cancer Standards Met (Total 8 Standards) Jan-18 4 Jan UCLH Royal Free Moorfields Target IAPT - % Waited less than 6 weeks for a course of treatment (Islington CCG at C&I) Dec % 75% IAPT - % Waited less than 18 weeks for a course of treatment (Islington CCG at C&I) Dec % 95% A&E 4 Hour Waits* Feb % Feb % 86.0% 86.5% 99.3% 95% CAT 1 ARP 7 mins (London Wide LAS) - Mean Feb-18 00:07:26 ##### 00:07:00 CAT 1 ARP 15 mins (London Wide LAS) - 90th Centile Feb-18 00:11:48 00:15:00 00:15:00 CAT 2 ARP 18 mins (London Wide LAS) - Mean Feb-18 00:23:21 00:18:00 00:18:00 CAT 2 ARP 40 mins (London Wide LAS) - 90th Centile Feb-18 00:49:21 ##### 00:40:00 CAT 3 ARP 120 mins (London Wide LAS) - 90th Centile Feb-18 02:59:27 ##### 02:00:00 CAT 4 ARP 180 mins (London Wide LAS) - 90th Centile Feb-18 02:34:17 ##### 03:00:00 Ambulance Handover 15 Mins Feb % 35.6% 35.2% n/a 100% Ambulance Handover 30 Mins Feb % 83.4% 85.9% n/a 100% Key: Performance Performance is above Target Performance is below Target No Target Arrows indicate improvement or deteriorating performance on the previous month Notes: * Latest CCG data is provisional and unpublished. ** Moorfields only recorded activity for three cancer waiting time pathways in January 2018, and similarly Whittington Health NHS Trustittington Health NHS Trust recorded activity against six. 18 Weeks RTT Admitted and Non-Admitted Standards have been abolished, and the Incomplete Pathways Standard has become the sole measure of patients constitutional right to start treatment within 18 weeks. 50 of 402 ARP = Ambulance Response Programme 3
51 Islington CCG Performance and Quality Summary Key Messages CCG Performance - This slide is a brief summary of the overall CCG position for more detail on each provider see the relevant Provider Slides. Accident and Emergency Islington CCG performance against the four hour waiting time indicator in January 2018 was 87.4%. The main providers for Islington patients performed as below for February 2018: Whittington Health NHS Trust 86.1% University College London Hospitals NHS Foundation Trust 86.1% Royal Free London NHS Foundation Trust Hospitals 86.5% All CCGs and provider organisations within North Central London are under scrutiny from NHS England and NHS Improvement as performance has not matched trajectories agreed earlier in 2017/2018 which predicted 95% performance by March The Islington A&E Delivery Board Improvement Plan is under regular review and at the March 2018 A&E Delivery Board a renewed set of priorities were agreed to move they system towards 90% performance. The A&E Delivery Board Meeting in March 2018 identified increased numbers of patients presenting to A&E, the increased clinical needs of the patients presenting to A&E and to GP surgeries, the increased complexity of the needs of patients being discharged from hospital as factors contributing to A&E four hour wait performance being less than predicted. Cancer Islington CCG met four from the eight national cancer access standards in January The standards missed were: Two week wait symptomatic breast referrals three patient choice breaches from a total of 43 cases led to a performance of 92.7% against the 93% standard. 31 day diagnosis to treatment three breaches from a total of 65 patients one of which was patient choice, one clinical and one due to administrative delays led to a performance of 95.4% against the 96% standard. 62 day urgent GP referral to treatment nine breaches from 27 cases to give a performance of 66.8%. Six of the breaches 51 of were 402 due to patient choice or clinical reasons and three due to administrative or capacity delays. 4
52 Islington CCG Performance and Quality Summary Key Messages Cancer (continued) 62 day screening to treatment one breach from six cases which was due to complex clinical reasons led to a performance of 83.3% against the 90% standard In total, of the 963 patients from Islington treated for cancer, breast symptoms or suspected cancer in January 2018, 912 ( 98%) were treated within national waiting time standards. This is an improvement on 97% for December In summary Islington CCG performance on cancer access times improved overall but due to the small number of patients treated in specific areas four individual treatment targets were missed. Mental Health Indicators Islington CCG met all of the following standards for mental health access for the last relevant reporting period: Dementia Diagnosis Rate for February 2018 First Episode of Psychosis for February 2018 Gatekeeping of acute admissions by Crisis Resolution Home Treatment teams (CRHT) for Quarter Three 2017/2018 Care Programme Approach patients followed up within seven days of discharge for Quarter Three 2017/2018 The urgent referral waiting time standard for Children and Young People with Eating Disorders was met in Quarter /2018 but the routine waiting time standard of 95% of patients seen within four weeks was not met with the CCG performance at 87% as three from 24 patients waited longer than four weeks to be seen. Quarter Three Improving Access to Psychological Therapies data for Islington CCG shows a recovery rate of 47% which is below the standard of 50%. However, the most recent local monthly data shows the recovery rate has improved in January and February 2018 and Camden and Islington NHS Foundation Trust predict compliance with the 50% standard by the end of Quarter four. 52 of 402 5
53 Islington CCG Performance and Quality Summary Key Messages Referral to Treatment and Diagnostics Provisional data for February 2018 indicates that Islington CCG performance against the 18 week Referral to Treatment target was 91.9% against the 92% target. The overall Islington CCG 18 week Referral to Treatment standard was missed by 18 patients from a total of 16,125: Whittington Health (which accounts for 35% of all Islington patients on Referral to Treatment pathways) failed the standard for Islington by 65 patients while achieving the standard for all CCGs. University College London Hospitals (which accounts for 40% of all Islington patients on 18 week pathways) achieved the standard for Islington patients but failed to achieve the standard for all CCGs. Royal Free London Hospital (which accounts for 8% of all Islington patients on Referral to Treatment pathways) missed the standard for Islington by 104 patients and failed to achieve the standard for all CCGs. In summary, assuming provider trusts are not deliberately treating patients differently depending on their CCG of origin, the fact that Islington CCG has not met the 18 week Referral to Treatment Standard for the last two months is probably due to the increased pressure on University College London Hospitals and Whittington Health generally (as reflected across national performance) in meeting Referral to Treatment standards and the particular problems experienced by Royal Free London which are being addressed by Barnet CCG and NHS England and NHS Improvement. The charts below show the changes in median waiting times for Islington patients at Whittington Health and University College London Hospitals over the 14 months to February While waits have varied over time as at February 2018 median waiting time was lower for both providers than at January At CCG level 99.4% of patients were waiting less than six weeks for a diagnostic test at the end of February 2018 which is compliant with the 53 of 402 national standard. 6
54 Islington CCG Performance and Quality Dashboard Theme KPI / Measure Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb YTD A&E A&E All Types Performance 88.9% 89.7% 91.5% 92.6% 92.7% 91.4% 90.8% 90.1% 90.3% 90.0% 87.7% 87.6% 87.4% 90.2% 18 Weeks Referral to treatment and Diagnostics 18 Weeks RTT Admitted * 85.3% 84.6% 83.9% 84.6% 86.0% 81.3% 84.1% 82.4% 82.5% 84.9% 83.0% 86.0% 80.3% 83.6% 18 Weeks RTT Non-Admitted * 92.5% 94.1% 93.8% 93.9% 93.6% 91.9% 91.9% 92.3% 92.7% 91.2% 92.5% 92.0% 91.6% 92.5% 18 Weeks RTT Incomplete Pathways * 93.4% 93.6% 93.5% 93.4% 93.0% 92.2% 92.1% 92.1% 92.6% 92.7% 92.3% 91.8% 91.9% 92.5% RTT >52 week waits Incomplete * Weeks Diagnostic Waits * 0.2% 0.3% 0.6% 1.0% 0.9% 0.98% 0.99% 0.86% 0.70% 0.49% 0.89% 0.49% 0.57% 0.8% 2 Week Cancer Wait 96.7% 95.4% 92.9% 94.5% 96.7% 96.3% 93.8% 94.1% 95.1% 96.1% 96.9% 95.3% 95.2% Cancer Waits 2 Week Cancer Wait: Breast Symptoms 31 day Cancer Wait: 1st definitive treatment 31 Day Cancer Wait: Subsequent treatment (Surgery) 31 Day Cancer Wait: Subsequent treatment (Chemotherapy) 31 Day Cancer Wait: Subsequent treatment (Radiotherapy) 62 Day Cancer Wait: GP Referral 62 Day Cancer Wait: Screening service 62 Day Cancer Wait: Consultant Upgrade 94.4% 95.8% 93.6% 94.6% 95.9% 97.7% 98.3% 98.1% 95.7% 98.2% 96.6% 92.7% 96.2% 97.7% 97.2% 98.3% 96.8% 95.1% 100.0% 100.0% 95.2% 100.0% 97.3% 97.9% 95.4% 97.6% 100.0% 100.0% 100.0% 100.0% 100.0% 91.7% 100.0% 84.6% 100.0% 100.0% 100.0% 100.0% 96.6% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 94.7% 100.0% 100.0% 95.2% 92.9% 100.0% 100.0% 95.5% 100.0% 100.0% 100.0% 100.0% 98.5% 94.7% 65.4% 70.0% 92.6% 83.3% 85.2% 88.5% 85.7% 88.2% 80.6% 85.0% 66.7% 82.5% 100.0% 100.0% 100.0% 66.7% 50.0% 83.3% 85.7% 100.0% 81.8% 85.7% 83.3% 81.8% 100.0% 100.0% 80.0% 100.0% 100.0% 100.0% 100.0% 100.0% 80.0% 88.9% 100.0% 100.0% 93.5% MRSA reported infections Quality C. Difficile reported infections Mixed Sex Accommodation (MSA) (Number of breaches) of 402 7
55 Key Messages Whittington Health NHS Trust Provider Key Messages Accident and Emergency Whittington Health NHS Trust A&E four hour performance has been between 86.1% and 86.5% each month from December 2017 to February Performance was predicted to be 92% in February and reasons why performance has not been as predicted include increased cases of influenza, increased admissions in the over 75 s, increased ambulance presentations and increased numbers of complex discharges All of the above point to an increased acuity and complexity of cases Whittington Health NHS Trust which put pressure on acute and community capacity All A&E Delivery Board winter schemes are under regular review by the A&E Delivery Board. Progress on all these schemes is reviewed at the A&E Delivery Board and fortnightly calls with NHS England and NHS Improvement. Referral to Treatment Time and Diagnostics The percentage of patients waiting less than 18 weeks for treatment remains above the operational standard of 92% for January Whittington Health achieved the 99% of patients waiting less than six weeks for a diagnostic test in January 2018 but due to a reporting error by Whittington Health this is not reflected in the published data. At the end of January 2018 no patients were waiting over 52 weeks for treatment at Whittington Health while the number of patients waiting more than 18 weeks for treatment has remained fairly constant since September Cancer Services Whittington Health met all of its cancer access waiting time standards for January 2018 apart from the 62 day urgent GP referral to treatment target which was missed by 3% or one patient from 23 cases. The small number of cases seen by Whittington Health mean their performance can be significantly affected by small variations in numbers of patients attending or choosing to delay appointments. Community Services PA Consulting have been appointed by the Haringey and Islington Wellbeing Board to undertake a defined piece of project work with regard to Whittington Community Services to conclude in May The remit of the programme includes: Review of current service provision Format of performance reporting Recommendations for future strategy Based on current reporting overall Community Service waiting times have remained fairly constant between December 2017 and January of 402 apart from a significant improvement in District Nursing waiting times where of patients where over 90% of patients were seen within agreed waiting 8 times.
56 Whittington Health NHS Trust Performance Dashboard KPI/Threshold THE WHITTINGTON HOSPITAL NHS TRUST Jan-18 YTD KPI/Threshold THE WHITTINGTON HOSPITAL NHS TRUST Feb-18 YTD 18 Weeks RTT Admitted % 73.07% A&E All Types Performance 95% 86.10% 90.06% 18 Weeks RTT Non-Admitted % 89.74% 18 Weeks RTT Incomplete Pathways 92% 92.10% 92.16% >52 week waits Admitted >52 week waits Non Admitted >52 week waits Incomplete Weeks Diagnostic Waits 1% 1.01% 0.92% Cancelled Operations ( Q3) 100% % 97.33% THE WHITTINGTON HOSPITAL NHS KPI/Threshold TRUST Jan-18 YTD 2 Week Cancer Wait 93% 94.89% 94.64% No of waits from decision to admit to admission (Trolley waits - over 12 hours) KPI/Threshold % Ambulance Handovers within 15 mins: KPI 1 % Ambulance Handovers within 30 mins: KPI 2 Number of Ambulance Handover - 30 minute breaches Number of Ambulance Handover - 60 minute breaches % Patient Records Captured Electronically: KPI THE WHITTINGTON HOSPITAL NHS TRUST Feb-18 YTD 100% 52.80% 41.40% 100% 96.90% 97.40% % 92.70% 91.40% 2 Week Cancer Wait: Breast Symptoms 31 day Cancer Wait: 1st definitive treatment 31 Day Cancer Wait: Subsequent treatment (Surgery) 31 Day Cancer Wait: Subsequent treatment (Chemotherapy) 31 Day Cancer Wait: Subsequent treatment (Radiotherapy) 62 Day Cancer Wait: GP Referral 62 Day Cancer Wait: Screening service 62 Day Cancer Wait: Consultant Upgrade 93% 97.92% 97.97% 96% % % 94% % % 98% % % 94% 85% 82.22% 87.53% 90% % % 96.00% 56 of 402 9

57 57 of

58 58 of
59 Whittington Health NHS Trust Quality Dashboard Theme KPI/Measure Reporting Period Actual YTD Current Month and Previous Month's Trend Blue = Actual Red = Target SHMI rate - rolling 12 month average (received quarterly) Jul Jun Proportion of Patients New Pressure Ulcers (Safety Thermometer) Feb Proportion of Patients Falls With Severe Harm (as per NPSA definition - Safety Thermometer) Feb Number of Never Events Feb Serious Incidents (SIs) Reports Submitted Feb Number of MRSA Bacteraemia Jan Patient Safety Number of Clostridium Difficile Jan Mandatory Training rate Jan-18 81% Average fill rate - Registered nurses/midwives (Day) Jan-18 79% Average fill rate - Registered nurses/midwives (Night) Jan-18 89% Average fill rate - Care staff (Day) Jan % Average fill rate - Care staff (Night) Jan % 87% 86% 87% 86% 80% 85% 81% 81% 79% 94% 92% 92% 92% 103% 96% 91% 92% 89% 121% 111% 114% 111% 123% 133% 130% 136% 131% 124% 118% 128% 114% 137% 146% 144% 130% 148% 59 of
60 Theme KPI/Measure Reporting Period Actual YTD Current Month and Previous Month's Trend Blue = Actual Red = Target VTE - % patients who have had a VTE assessment within 24 hours of admission Dec % 95.7% 95% 95% 96% 95% 97% 96% 95% 96% 95% Clinical Effectiveness Cancelled operations - Number of patients not treated within 28 days of last minute elective cancellation Q Overall Maternity - C-Section rate (Trust Data) Feb % 25% 31% 28% 27% 33% 37% 28% 34% 34% Friends & Family test (FFT) - % Recommend Inpatients Jan % 94% 97% 96% 95% 98% 98% 98% 97% 97% Friends & Family test (FFT) - Response Rate % Inpatients Jan % 23% 20% 21% 15% 16% 18% 18% 16% 17% Friends & Family test (FFT) - % Recommend A&E Jan % 87% 84% 85% 83% 80% 82% 83% 83% 82% Friends & Family test (FFT) - Response Rate % A&E Jan % 16% 14% 13% 14% 13% 13% 12% 12% 13% Maternity Friends & Family test (FFT) - Question 1 % Recommend (Antenatal Care) Jan % 90% 100% 97% 100% 96% 100% 99% 97% Maternity Friends & Family test (FFT) - Score Question 2 % Recommend (Birth) Jan % 95% 89% 97% 93% 96% 96% 97% 98% Maternity Friends & Family test (FFT) - Score Question 3 % Recommend (Post Natal Ward) Jan % 81% 80% 84% 84% 86% 92% 93% 94% Maternity Friends & Family test (FFT) - Score Question 4 % Recommend (Post Natal Community Provision) Jan % 100% 98% 98% 94% 97% 100% 100% 98% Patient experience Friends & Family test (FFT) - % Recommended Outpatients Jan % 93% 94% 93% 91% 91% 93% 92% 92% 94% Friends & Family test (FFT) - Response Rate % Outpatients Jan % 3.60% 3.14% 2.80% 1.93% 2.47% 3.25% 3.40% 1.91% 2.39% Staff Friends & Family test (FFT) - % Recommended as a place to work Q2 53.3% 54% 53% Staff Friends & Family test (FFT) - % Not Recommended as a place to work Q2 34.2% 32% 34% Staff Friends & Family test (FFT) - % Recommended as a place for Care Q2 69.4% 69% 69% Staff Friends & Family test (FFT) - % Not Recommended as a place for Care Q2 13.0% 13% 13% Friends & Family test (FFT) - % Recommended Community Jan % Friends & Family test (FFT) - Response Rate % Community Jan % 95% 94% 95% 97% 96% 95% 95% 96% 95% 4% 3% 4% 3% 3% 3% 2% 2% 3% Mixed sex Accommodation - Breaches Feb Complaints - Number of formal complaints (Trust data) Feb of
61 Whittington Health NHS Trust Performance & Quality Summary Area Current Position/Risks Mitigating Actions Current level of Assurance / Recommendations Accident & Emergency Published performance against the four hour A&E target at Whittington Health was 86.1% in February From December 2017 to February 2018 performance has been around 86%. There are two factors impacting on the A&E performance: Flow through the A&E Department Flow through the hospital to allow admissions from the A&E Department In both areas performance has not been as predicted because of: Increased A&E attendances Increased acuity of attendances (as reflected by the number of occasions when the A&E resuscitation area is full) Increased complexity in medical management of patients admitted (as reflected in the increase in numbers of patients admitted for more than seven days) The continuing impact of influenza (consistently 20 beds occupied by patients with a confirmed laboratory diagnosis of flu) The Islington Discharge to Assess Programme has delivered or exceeded its trajectory for Pathways One, Two or Three for February 2018 Daily liaison between Whittington Health, CCG and Local Authorities takes place to resolve obstacles leading to delays to discharges. Weekly Multi-Agency Discharge Events (MADE) are held at Whittington Health to facilitate improved discharge flows. A recent review of the Islington A&E Delivery Board Improvement Plan identified the following areas for increased focus: Maximising rapid assessment and treatment utilisation Increasing Ambulatory Care presence in the Emergency Department Renewed focus on criterial led discharge Maintaining good ambulance handover performance through fit to sit A comprehensive A&E Delivery Board Improvement Plan incorporating actions from primary, community, acute mental health and social care providers is updated monthly and reviewed at A&E Delivery Board. Continued monitoring of performance at Contract Management Group and quality and safety implications of performance at Clinical Quality Review Group. 61 of
62 Whittington Health NHS Trust Performance & Quality Summary Area Current Position/Risks Mitigating Actions Current level of Assurance/ Recommendations Cancer In January 2018, Whittington Health achieved all relevant national cancer waiting time standards apart from the 62 day urgent GP referral to treatment standard. This standard was missed by one case from a total of 23. In all four cases breached the standard: two due to patient choice or clinical reasons, one due to internal delays at Whittington Health and one due to inter-trust referral delays. Low numbers of cases at Whittington Health mean that statistically insignificant variations in performance due to patient availability or complexity have a disproportionate impact on Whittington Health performance. Remedial measures to address the clinical and administrative challenges to gastroenterology and endoscopy services around two week waits reported earlier in the year have improved performance in this area from 39% in April 2017 to 87.2% for lower gastroenterology and 73.5% for upper gastroenterology for January Whittington Health predicts full compliance with all two week wait specialties in March Root cause analyses for all patients waiting longer than 62 days from referral to treatment are considered at the Clinical Quality Review Group Recommend monitoring of performance through Contract Monitoring Group, quality and patient safety implications of performance through Clinical Quality Review Group and application of contractual levers if appropriate. At specialty level upper and lower gastroenterology are the only areas failing to meet the two week wait urgent general practitioner referral to appointment standards. Data for January 2018, shows that two from five onward referrals from Whittington Health were made within 38 days of the original referral being received. 62 of
63 Whittington Health NHS Trust Performance & Quality Summary Area Current Position/Risks Mitigating Actions Current level of Assurance/ Recommendations Referral to Treatment Time and Diagnostics Whittington Heath met the headline 18 week incomplete referral to treatment standard for January 2018 with 92.10% of waiting patients waiting less than 18 weeks. No patients were identified as waiting more than 52 weeks for treatment at Whittington Health at the end of January The total number of patients waiting longer than 18 weeks for treatment (backlog) at the end of January 2018 was 1,202. This number has remained consistently around the 1,200 mark since September Whittington Health incorrectly reported their January 2018 diagnostic waiting time position as non-compliant with the 99% seen within six week standard. This was due to an error on the part of Whittington Health. Actual performance was that Whittington Health was compliant and 99.1% of patients were seen within six weeks for their test. For all diagnostic test categories 92% or more patients were tested within six weeks. Whittington Health has confirmed they have reviewed their reporting validation processes to prevent further errors occurring when uploading data to national reporting systems in the future. Nationally reported data will continue to be incorrect until NHS Digital refresh their reports for quarter four 2017/2018. Waiting times for colonoscopy, gastroscopy and flexisigmoidoscopy have been affected due to a vacant endoscopy nurse specialist post which has now been appointed to. Whittington Health had predicted these specialties would be compliant with the 99% within six week standard by January 2018 but this has been delayed until March 2018 as booking schedules and templates are reconfigured. Whittington Health has a record of sustained achievement of the 92% 18 week referral to treatment and six week diagnostic waiting time standards. At this stage no further action is recommended other than continued monitoring of Referral to Treatment Time and Diagnostic Performance at Contract Monitoring Group and Clinical Quality Review Group. 63 of
64 Whittington Health NHS Trust Performance & Quality Summary Area Current Position/Risks Mitigating Actions Current level of Assurance/ Recommendations Referral to Treatment Time and Diagnostics Backlog of Radiology Test Reporting In March 2018 Whittington Health reported that as part of a review exercise they had identified approximately 3000 radiology scans that had not been reported, some of which dated back to There is a project group that is reviewing the images weekly basis, and a weekly update is share with the Radiation Safety Committee. To date there have been no significant clinical findings or concerns raised by clinicians. The work to address the backlog is due to be completed by the end of April. Whittington Health have not declared this as a Serious Incident but have reviewed all Serious Incidents over the last year and themes from previous years and have found no connection between the reporting delays and serious incidents. Backlog of Radiology Test Reporting Project group set up and meeting weekly to review progress in reducing the backlog and ongoing clinical risk. Membership includes Consultant radiologists, radiographers, radiology information technology specialists and senior management. Whittington Health information team is generating weekly reports on backlog and supporting with system interrogation Processes around auto reporting are being strengthened within Whittington Health. Backlog of Radiology Test Reporting Update on review process due at both Clinical Quality Review Group and Contract Review Group in April Whittington Health are preparing a report on test to report waiting times which will be shared with Healthwatch Haringey and Haringey and Islington Quality Committees. 64 of
65 Whittington Health NHS Trust Performance & Quality Summary CQUINs (Commissioning for Quality and Innovation) CQUIN Infections (AMR and Sepsis) National 4: Improving Services for People with Mental Health Needs Who Present to ED National 6: Offering Advice and Guidance National 7: NHS e-referrals National 8: Supporting Proactive and Safe Discharge National 11: Personalised Care and Support Planning Quarter /2018 Status Comments Achieved Achieved Achieved Achieved In progress Achieved Data submitted via SDCS portal. A&G covers over 35% of activity Timetable and implementation aligned with STP - on track. 90% of Referrals to 1st O/P Services able to be received through e-rs ASIs reduced to 10% in line with agreed trajectory As discussed with CCGs - Whittington Health Trust Management Group have approved to delay implementation until April 2018 to enable the testing, training and downtime of software implmentation to be managed in a realistic manner. 65 of

66 Whittington Health NHS Trust Performance & Quality Summary E Referrals 2018/2019 NHS Standard Contract By 1 October 2018 all NHS Providers need to use E Referral as their only means of making and receiving referrals from GPs to consultant led first outpatient appointments This can only be achieved through joint working between CCGs and providers and is being led by the North Central London E Referral Implementation and Steering Group chaired by Denise Pettit from Haringey CCG. OP % Utilisation 60.0% 40.0% 20.0% 0.0% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 WHITTINGTON HEALTH NHS TRUST 66 of
67 Whittington Health NHS Trust Performance & Quality Summary Area Current Position/Risks Mitigating Actions Current level of Assurance/ Recommendations Community Services Two performance reports for Whittington Health Community services are included in this report. One replicates the 2016/2017 reporting format and the other is a work in progress report in which Whittington Health breaks down waiting time by routine and urgent and average waits. Within the 2016/2017 reporting format six of 31 services saw 95% of patients within six weeks and nine of 31 services saw 90% of patients within six weeks January Against the District Nursing target of 80% of urgent patients being seen within two hours Whittington Health achieved 83% in February Against the target of seeing 95% of patients within 48 hours Whittington Health achieved 91% in February PA Consulting have been appointed by the Haringey and Islington Wellbeing Board to undertake a defined piece of project work with regard to Whittington Health Community Services to conclude in May The remit of the programme includes: Review of current service provision Format of performance reporting Recommendations for future strategy A Task and Finish Group meets in April 2018 to consider future reporting arrangements and improvement trajectories and reports to the Community Services Improvement Group. Each community service provides an annual report (or more frequently if required) to the Whittington Health Clinical Quality Review Group including GP representatives from Haringey and Islington CCGs and a patients representative. The Community Service Improvement Group has been established, is chaired by the Chief Operating Officer for Whittington Health NHS Trust and Director of Haringey and Islington Wellbeing Board and includes GP and community service clinical representation. The Wellbeing Board will make regular reports to the relevant Haringey and Islington Quality and Performance Committees going forward regarding the work of the Community Service Improvement Group and the project work undertaken by PA Consulting. 67 of
68 Whittington Health NHS Trust Quality Summary Current Position/Risks Mitigating Actions Recommendations Cancer Quality Update Whittington Health was compliant for all cancer standards apart from 62 day which was 82.2% against a standard of 85%. Whittington Health was compliant for two week waits for January Colorectal and Upper Gastro-enterology did not meet the standard of 92% although the Trust was compliant overall. Colorectal and Upper Gastro-enterology operate a straight to test pathway. There is a plan in place where capacity has been identified in endoscopy so that there is sufficient capacity for these patients. This is demonstrating an improvement in March During 2017/18 NCL & NEL have been working to ensure that all inter trust tertiary referrals are sent from the original hospital by 38. The Trust has had a varied performance against this standard, which has been identified as a key indicator to delivery of 62 day standard. Work continues to improve this performance which is usually related to: Urology: issues with prostate patients being referred promptly to UCLH Gynaecology have been affected by one late referral, numbers are small Upper and Lower Gastro-enterolgoy: currently related to the delays in getting endoscopy procedures completed. This standard is being monitored closely across NEL and NCL. Quarterly Updates to Clinical Quality Review Group. 68 of
69 Whittington Health NHS Trust Quality Summary Area Current Position/Risks Mitigating Actions Recommendations Pressure Ulcers Comparing the avoidable pressure ulcers across the Trust between April January 2016/17 with the same period 2017/18 An increase in category 2 pressure ulcer by 12.8% (6), An increase in category 3 pressure ulcer by 17% (4) No increase in category 4 s Comparing the number of avoidable pressure ulcers within district nursing during the same period has seen: A 25% increase in Category 2 s (7) A 22.3% increase in category 3 s (4) No increase in avoidable Category 4 s. (Tissue Viability Nurse Report to CQRG March 2018) All pressure ulcers category 2 4, ungradable are reported as clinical incidents using the Datix system. Any Category 3, 4 or ungradable attributed to Whittington health is investigated using the pressure ulcer investigation tool. Key Themes from investigations: Shortfall in the assessment of patients (this includes skin assessment, Waterlow assessment), which can be attributed to the nursing skill mix, and changes to the skill mix. There have been an increase in the Band 4. The Trust have relooked at how the assessment are undertaken, and who can complete these, and the rollout of bespoke assessment training. The documentation is also being reviewed, with a plan to streamline the document. In district nursing that has been an increase in the caseload and number of patient contacts, highlighting the need for a review of the skill mix, as every patient on the caseload requires a skin bundle. There is a planned programme of training that will be rollout to all grades of staff to be competent to undertake these tasks. Quality Rounds, which includes spot check of the notes and a review of patient by the Tissue Viability service, has been introduced on one ward with a plan for this to be rollout. A regular Audit of Care Notes has also been launched. Update to Clinical Quality Review Group on implementation and outcomes of changes implemented June of
70 Whittington Health NHS Trust Quality Summary Area Current Position/Risks Mitigating Actions Recommendations Care Quality Committee Inspections Following an inspection of four of the Trust services in November 2018, the Trust has retained its overall rating of Good, from the previous inspection. The Trust were rated Outstanding in the Caring domain and Good in the Well Led domain, with both the Hospital and Community services rated as Good. There are four regulated activity actions from the CQC report including: Flow in ITU and delayed discharges Ligature risk in CAMHS Clinical Quality Review Group informed and will monitor progress of the improvement plan. The Trust provided a written response to the CQC in March The Trust reported that the actions have either been completed or will be completed within the next 3 months. Workforce Mandatory Training achievement is at 81% against a target of 90% Data on 9th February show 2.8% sickness rate and data on 19th February show 3.48% sickness rate.( February 2018 Trust Integrated Performance Report) Vacancy Rate against establishment 12.5% February 2018, the increase in vacancy factor is at least partially attributable to temporary increases in establishment in December to deal with winter pressures. (Trust Integrated Performance Report February 2018) Appraisals and statutory and mandatory training remains of concern that, despite modest improvements in both these indicators in this month, they remain below target; it is expected that reinforcing their priority in recent quarterly reviews will provide a renewed focus to improving ICSU performance. December sickness rate is 3.48% which is slightly above target. An issue in delayed recording of sickness has been identified which show a significant discrepancy. After a successful assessment centre for newly, qualified nurses the Trust have recruited over 50 nurses, who are due to start in September Clinical Quality Review Group informed and will monitor progress. 70 of
71 Moorfields Eye Hospital NHS Foundation Trust Provider Key Messages Key Messages Accident and Emergency Moorfields Eye Hospital performance against the four hour waiting time standard for February 2018 was 99.3% and there were no breaches of the 12 hour decision to admit to admission standard. Referral to Treatment Waiting Time and Diagnostic Waiting Times Moorfields Eye Hospital performance against the incomplete 18 week referral to treatment standard was 94.02% for January No patients at Moorfields Eye Hospital were waiting over 52 weeks for treatment at the end of December 2017 and no patients waited longer than six weeks for a diagnostic test. While the 18 week incomplete position remains good there has been an increase in the number of patients waiting more than 18 weeks for treatment from 601 patients to 1618 patients from March 2017 to January Moorfields Eye Hospital has provided the following statement: There are separate plans for the north, south and city road (and for their individual specialities), that are focusing around demand and capacity and long term solutions to improve our RTT performance rather than quick reductions in our breaching patients. The divisions are looking at job plans, clinic structures, theatre utilisation, booking practices and clinical engagement, as well as more service specific endeavours, to improve our RTT position percentage back to previous levels. To further understand the above plans and agree trajectories for performance a meeting has been convened for April 2018 with representatives from South West London commissioners and Islington CCG as lead commissioner. Cancer In January 2018 Moorfields Eye Hospital achieved all relevant national cancer access standards. Moorfields Eye Hospital monitors the percentage of patients seen within two weeks of referral to the NHS England commissioned specialist service. In February % of the 72 patients referred to the Ocular Oncology Service were seen within two weeks of referral. Of the ten patients not seen within two weeks eight were delayed due to patient choice or clinical reasons. These patients are not necessarily being referred for first treatment or diagnosis which can make co-ordinating appointments and persuading patients of the urgency of their case less straightforward than for traditional GP referred suspected cancer referrals. 71 of
 no more than 4% of completed referrals")
72 Moorfields Eye Hospital NHS Foundation Trust Provider Key Messages Key Messages E Referrals 2017/2018 CQUIN Ensure that 100% of GP Referrals to 1 st Outpatient Services can be made through E Referral by March 2018 Appointment Slot Issues (this is when a GP refers using E Referral but an appointment is not available electronically at the receiving provider) no more than 4% of completed referrals by March /2019 NHS Standard Contract By 1 October 2018 all NHS Providers need to use E Referral as their only means of making and receiving referrals from GPs to consultant led first outpatient appointments. This can only be achieved through joint working between CCGs and providers and is being led by the North Central London E Referral Implementation and Steering Group chaired by Denise Pettit from Haringey CCG % 50.0% OP % Utilisation 0.0% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST 72 of
73 Moorfields Eye Hospital NHS Foundation Trust Performance Dashboard Elective Care (RTT, Diagnostics & CWT) Non Elective (A&E) KPI/Threshold Moorfields Eye Hospital Jan-18 YTD KPI/Threshold Moorfields Eye Hospital Feb-18 YTD 18 Weeks RTT Admitted % 83.41% A&E All Types Performance 95% 99.30% 98.54% 18 Weeks RTT Non-Admitted % 94.82% 18 Weeks RTT Incomplete Pathways 92% 94.02% 95.50% >52 week waits Admitted >52 week waits Non Admitted >52 week waits Incomplete Weeks Diagnostic Waits 1% 0.00% 0.00% Cancelled Operations ( Q3) 100% 96.20% 97.47% No of waits from decision to admit to admission (Trolly waits - over 12 hours) KPI/Threshold % Ambulance Handovers within 15 mins: KPI 1 % Ambulance Handovers within 30 mins: KPI 2 Number of Ambulance Handover - 30 minute breaches Number of Ambulance Handover - 60 minute breaches % Patient Records Captured Electronically: KPI Moorfields Eye Hospital Feb-18 YTD 100% n/a n/a 100% n/a n/a 0 n/a n/a 0 n/a n/a 90% n/a n/a KPI/Threshold Moorfields Eye Hospital Jan-18 YTD 2 Week Cancer Wait 93% 100.0% 97.8% 31 day Cancer Wait: 1st definitive treatment 96% 100.0% 93.1% 31 Day Cancer Wait: Subsequent treatment (Radiotherapy) 94% 100.0% 31 Day Cancer Wait: Subsequent treatment (Surgery) 94% 100.0% 100.0% 62 Day Cancer Wait: GP Referral 62 Day Cancer Wait: Consultant Upgrade 85% 100.0% 73 of
74 Theme KPI/Measure Reporting Period Actual YTD Current Month and Previous Month's Trend Blue = Actual Red = Target Number of Never Events Feb Serious Incidents (SIs) Reports Submitted Feb Number of MRSA Bacteraemia Jan Number of Clostridium Difficile Jan Patient Safety Mandatory Training rate Jan-18 89% Average fill rate - Registered nurses/midwives (Day) Dec-17 98% Average fill rate - Registered nurses/midwives (Night) Dec % Average fill rate - Care staff (Day) Dec-17 85% Average fill rate - Care staff (Night) Dec % 99% 80% 103% 95% 90% 92% 95% 105% 100% 101% 97% 108% 98% 102% 104% 110% 109% 108% 90% 72% 83% 87% 98% 88% 103% 96% 94% 97% 83% 119% 100% 123% 110% 103% 113% 117% 74 of
75 Theme KPI/Measure Reporting Period Actual YTD Current Month and Previous Month's Trend Blue = Actual Red = Target Clinical Effectiveness VTE - % patients who have had a VTE assessment within 24 hours of admission Cancelled operations - Number of patients not treated within 28 days of last minute elective cancellation Dec % 98.7% Q % 99% 98% 99% 99% 98% 99% 99% 99% Friends & Family test (FFT) - % Recommend Inpatients Jan % 100% 99% 99% 99% 99% 99% 99% 99% 99% Friends & Family test (FFT) - Response Rate % Inpatients Jan % 59% 53% 57% 61% 58% 55% 51% 50% 56% Friends & Family test (FFT) - % Recommend A&E Jan % 95% 95% 95% 95% 96% 93% 92% 97% 95% Friends & Family test (FFT) - Response Rate % A&E Jan % 12% 17% 11% 14% 16% 16% 18% 07% 13% Friends & Family test (FFT) - % Recommended Outpatients Jan % 96% 97% 96% 97% 96% 96% 97% 97% 97% Patient Experience Friends & Family test (FFT) - Response Rate % Outpatients Staff Friends & Family test (FFT) - % Recommended as a place to work Jan % Q2 66.8% 12% 13% 12% 69% 65% 15% 14% 13% 10% 10% 15% 78% 70% 67% Staff Friends & Family test (FFT) - % Not Recommended as a place to work Staff Friends & Family test (FFT) - % Recommended as a place for Care Q2 15.8% Q2 95.4% 16% 17% 10% 13% 16% 94% 95% 95% 96% 95% Staff Friends & Family test (FFT) - % Not Recommended as a place for Care Q2 3.1% 2% 2% 3% 1% 3% Mixed sex Accommodation - Breaches Feb Complaints - Number of formal complaints (Trust data) Q of
76 Moorfields Eye Hospital NHS Foundation Trust Quality Summary Area Current Position/Risks Mitigating Actions Recommendations Duty of Candour Moorfields Eye Hospital needs to submit evidence of compliance with stage two for 2016/17. An audit of the Duty of Candour and Being Open process is to be carried out, to assure that the process is being followed through to completion. This retrospective review will seek to confirm that the process was followed appropriately and families were contacted directly, particularly where no written record exists for stage two The request was made at March 2017 Clinical Quality Review Group to submit required evidence for the previous year and how Moorfields has improved recording and implementation going forward. Moorfields Eye Hospital to report back to the Clinical Quality Review Group and via operational report once changes have been made and audit completed in March Update at July 2017 Clinical Quality Review Group was that Moorfields Eye Hospital is on track with compiling evidence of actions around Part Two despite logistic issues in obtaining evidence from patients and their families. Evidence to be submitted March 2018 Clinical Quality Review Group. Current status of audit progress discussed with Contracts team at NEL Commissioning Support Unit has contract implications. 76 of
77 Moorfields Eye Hospital NHS Foundation Trust Quality Summary Area Current Position/Risks Mitigating Actions Recommendations Workforce The rolling annual turnover rate is currently 17.4%, which is notably lower than it was a year ago. Stability remains well above our target minimum of 80%. Turnover hot spots include Clinical Support and Administrative staff. The vacancy rate is currently 13.4%. Hot spots include parts of Moorfields South and Theatres at City Road. The Appraisal rate and Statutory/Mandatory Training rate are both above our target threshold rates, at 84% and 88% respectively. Key Workforce Metrics: The rolling annual sickness rate has remained at 4.0% over the past quarter. However, a key contributing factor is the improved reporting and recording of sickness as e-rostering is being rolled out to more units across the trust. Sickness absence staff group hot spots include Clinical Support and Registered Nursing staff. Stress, Anxiety & Depression accounted for the most calendar days lost due to sickness over the past quarter, as well as the most episodes of longterm sickness. Clinical Quality Review Group to monitor monthly and quarterly. 73% of staff would recommend Moorfields as a place to work, and 92% would recommend Moorfields as a provider of care. Source: Moorfields Eye Hospital quarterly workforce report March of
78 Moorfields Eye Hospital NHS Foundation Trust Quality Summary Area Mitigating Actions Recommendations Care Quality Commission Update Care Quality Improvement Plan Update Moorfields Eye Hospital commissioned an internal audit review to test themselves on the implementation of the improvement plan; the initial feedback has been positive. The CQC improvement plan contained 78 recommendations in 50 actions. The Trust have made good progress with implementing the actions, and have completed 82% (41 actions). Clinical Quality Review Group to monitor monthly and quarterly. St Georges Hospital refurbishment is on track and with completion in 6-8 months. Duty of Candour in-house e-learning module is being developed with a filming date in April Children and Young Persons Strategy, has been developed and is in the consultation stage. A number of the Service Level Agreements have been signed off; however Mile End, Northwick Park, and St Georges remain outstanding. The Trust reported that for St Georges the principles are in place the financial agreement remains outstanding. 78 of
79 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = Actual Red = Target % Waited less than 6 weeks for a course of treatment (for those finishing a course of treatment) % Waited less than 18 weeks for a course of treatment (for those finishing a course of treatment) NHS Digital Dec % 75% NHS Digital Dec % 95% 80.00% 86.00% 81.00% 88.00% 88.00% 85.00% 87.00% 86.00% 84.00% 83.00% 84.00% 87.00% 88.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 97.00% 99.00% 99.00% 97.00% 99.00% 97.00% 97.00% 98.00% 98.00% 98.00% 98.00% 98.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Reliable Recovery Rate NHS Digital Dec % 42.00% 38.00% 40.00% 52.00% 55.00% 44.00% 49.00% 41.00% 46.00% 43.00% 42.00% 44.00% 43.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 ISLINGTON CCG IAPT Recovery Rate NHS Digital Dec % 50% Recovery Rate - QUARTERLY NHS Digital Q % 50.00% Access Rate NHS Digital Dec % 1.40% Access Rate - QUARTERLY NHS Digital Q3 4.23% 4.20% 47.00% 43.00% 44.00% 54.00% 58.00% 45.00% 53.00% 47.00% 49.00% 46.00% 46.00% 48.00% 47.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 46.67% 47.00% 48.00% 47.00% Q Q Q Q Q3 1.29% 1.63% 1.45% 1.54% 1.63% 1.42% 1.38% 1.41% 1.32% 1.14% 1.22% 1.36% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 4.50% 3.92% 3.87% 4.23% BME % of Numbers Entering Treatment - QUARTERLY NHS Digital Q % Q Q Q Q Q % 52.33% 48.18% 45.90% 45.32% Q Q Q Q Q3 NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE 79 of
80 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = Actual Red = Target Dementia Diagnosis Rate (Age 65+) NHS Digital Feb % 66.7% 96.41% 96.83% 92.70% 92.66% 92.06% 92.47% 92.04% 91.96% 91.32% 92.03% 92.17% 91.65% 91.16% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 ISLINGTON CCG MENTAL HEALTH The percentage of RTT First Episode Psychosis (FEP) periods within 2 weeks of referral. * Proportion of patients on CPA who were followed up within 7 days after discharge from psychiatric inpatient care Proportion of admissions to acute wards that were gate kept by the CRHT teams NHS Digital Feb % 50% NHS Digital Q % 95% NHS Digital Q % 95% Proportion of Children and Young people with eating disorders (routine cases) that wait 4 weeks or NHS Digital Q % 95% less from referral to start of NICEapproved treatment Proportion of Children and Young people with eating disorders (urgent cases) that wait 1 week or less from NHS Digital Q % 95% referral to start of NICE-approved treatment 80.00% 77.78% 80.00% 80.00% % 77.78% 50.00% 88.89% % 66.67% 90.00% 58.33% 77.78% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 98.63% 96.30% 94.59% Q Q Q Q % 99.21% 99.14% 99.13% Q Q Q Q % 87.50% 81.25% Q Q Q Q % % % Q Q Q Q3 *Latest data is provisional and unpublished NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE 80 of
81 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = Actual Red = Target % Waited less than 6 weeks for a course of treatment (for those finishing a course of treatment) % Waited less than 18 weeks for a course of treatment (for those finishing a course of treatment) NHS Digital Dec % 75% NHS Digital Dec % 95% 82.00% 83.00% 83.00% 86.00% 88.00% 89.00% 86.00% 87.00% 89.00% 89.00% 88.00% 84.00% 85.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 98.00% 97.00% 99.00% 98.00% 99.00% 99.00% 99.00% % 99.00% 99.00% 98.00% 97.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 43.00% 48.00% 45.00% 42.00% 40.00% 44.00% 46.00% 53.00% 45.00% 46.00% 40.00% 35.00% Reliable Recovery Rate NHS Digital Dec % Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 CAMDEN CCG IAPT Recovery Rate NHS Digital Dec % 50% Recovery Rate - QUARTERLY NHS Digital Q % 50.00% 48.00% 46.00% 51.00% 47.00% 47.00% 45.00% 49.00% 52.00% 54.00% 51.00% 48.00% 42.00% 40.00% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 48.00% 47.00% 44.00% 44.00% Q Q Q Q Q3 Access Rate NHS Digital Dec % 1.40% 1.30% 1.77% 1.49% 1.74% 1.46% 1.80% 1.61% 1.50% 1.27% 1.18% 1.27% 1.36% Access Rate - QUARTERLY NHS Digital Q3 3.54% 4.20% Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec % 5.00% 4.86% 3.96% 3.54% BME % of Numbers Entering Treatment - QUARTERLY NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE NHS Digital Q % Q Q Q Q Q % 51.39% 52.56% 46.32% 50.76% Q Q Q Q Q3 81 of
82 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = Actual Red = Target Dementia Diagnosis Rate (Age 65+) NHS Digital Feb % 66.7% 74.79% 75.37% 86.65% 86.41% 87.55% 87.22% 87.56% 88.04% 88.96% 88.51% 88.06% 88.38% 88.49% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 CAMDEN CCG MENTAL HEALTH The percentage of RTT First Episode Psychosis (FEP) periods within 2 weeks of referral. * Proportion of patients on CPA who were followed up within 7 days after discharge from psychiatric inpatient care Proportion of admissions to acute wards that were gate kept by the CRHT teams NHS Digital Feb % 50% NHS Digital Q % 95% NHS Digital Q % 95% Proportion of Children and Young people with eating disorders (routine cases) that wait 4 weeks or NHS Digital Q % 95% less from referral to start of NICEapproved treatment Proportion of Children and Young people with eating disorders (urgent cases) that wait 1 week or less from NHS Digital Q % 95% referral to start of NICE-approved treatment 91.67% % 70.00% 85.71% % 83.33% 80.00% 92.86% % 75.00% 75.00% % 81.82% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 98.41% 93.83% 92.41% Q Q Q Q % 98.50% 99.26% 98.64% Q Q Q Q % 75.00% 88.46% 86.96% Q Q Q Q % % % % Q Q Q Q3 *Latest data is provisional and unpublished NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE 82 of
83 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = NHS Digital Green = Local Data Red = Target % Waited less than 6 weeks for a course of treatment (for those finishing a course of treatment) NHS Digital Dec % Local Data Feb % 75% 84.02% 89.00% 87.79% 86.92% 88.28% 86.96% 83.26% 84.09% 84.90% 87.79% 89.08% 90.00% 84.58% 88.00% 89.00% 85.00% 87.00% 86.00% 84.00% 83.00% 84.00% 87.00% 85.71% 80.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 % Waited less than 18 weeks for a course of treatment (for those finishing a course of treatment) NHS Digital Dec % Local Data Feb % 95% % 98.70% 99.00% 99.00% 97.09% 97.00% 99.58% 99.00% 98.33% 98.70% 98.64% 99.09% 98.96% 99.06% 98.28% 97.00% 97.00% 98.00% 99.00% 98.00% 98.00% 97.14% % 99.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 ISLINGTON ICOPE IAPT Reliable Recovery Rate NHS Digital Dec % NHS Digital Dec % Recovery Rate 50.00% Local Data Feb % NHS Digital Q % Recovery Rate - QUARTERLY 50.00% Local Data Q % NHS Digital Dec Numbers entering into Treatment 434 Local Data Feb % 56.00% 40.00% 44.00% 49.00% 40.00% 46.00% 43.00% 42.00% 44.00% 43.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 60.81% 53.59% 60.00% 46.20% 46.41% 47.55% 50.00% 52.44% 47.37% 46.43% 46.99% 48.03% 47.43% 54.00% 53.00% 47.00% 49.00% 44.00% 45.00% 46.00% 46.00% 48.00% 47.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 49.17% 48.29% 47.12% 52.00% 48.00% 48.00% 47.00% Q Q Q Q Feb-17 Mar -17 Apr -17 May -17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Numbers entering into Treatment - Quarterly NHS Digital Q Local Data Q Q Q Q Q3 BME % of Numbers Entering Treatment - QUARTERLY NHS Digital Q % 51.99% 47.97% 46.31% 45.32% NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE Q Q Q Q3 83 of
84 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = NHS Digital Green = Local Data Red = Target % Waited less than 6 weeks for a course of treatment (for those finishing a course of treatment) NHS Digital Dec % Local Data Feb % 75% 89.21% 86.30% 82.57% 84.07% 84.64% 87.83% 88.05% 89.46% 86.90% 86.81% 87.37% 85.32% 82.79% 88.00% 81.00% 84.00% 85.00% 86.00% 89.00% 89.00% 88.00% 83.00% 84.00% 85.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 % Waited less than 18 weeks for a course of treatment (for those finishing a course of treatment) NHS Digital Dec % Local Data Feb % 95% 97.25% 96.00% 98.40% 98.35% 99.17% 99.06% 99.24% 99.66% 99.57% 98.98% 98.41% 97.98% 99.00% 99.00% 99.00% 99.00% % 99.00% 99.00% 98.00% 97.00% 97.00% 99.21% 96.31% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Reliable Recovery Rate NHS Digital Dec % 46.00% 43.00% 40.00% 40.00% 44.00% 47.00% 53.00% 46.00% 45.00% 39.00% 34.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 NHS Digital Dec % Recovery Rate 50.00% Local Data Feb % 50.80% 49.50% 50.00% 46.43% 50.00% 45.00% 44.00% 45.00% 51.64% 52.70% 55.27% 51.48% 50.00% 50.00% 52.00% 55.00% 51.00% 48.00% 42.79% 41.10% 42.00% 40.00% 49.52% 46.98% CAMDEN ICOPE IAPT NHS Digital Q % Recovery Rate - QUARTERLY 50.00% Local Data Q % NHS Digital Dec Numbers entering into Treatment 513 Numbers entering into Treatment - Quarterly Local Data Feb NHS Digital Q Local Data Q Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 53.16% 49.59% 45.07% 53.00% 47.00% 47.00% 44.00% Q Q Q Q Feb-17 Mar -17 Apr -17 May -17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb Q Q Q Q2 BME % of Numbers Entering Treatment - QUARTERLY NHS Digital Q % 46.15% 51.14% 52.56% 50.57% NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE Q Q Q Q3 84 of
85 Theme KPI/Measure Source Reporting Period Actual Standard Current Month and Previous Month's Trend Blue = NHS Digital Green = Local Data Red = Target The percentage of RTT First Episode Psychosis (FEP) periods within 2 weeks of referral. * NHS Digital Feb % 50% 86.36% 90.48% 72.22% 84.21% 93.75% 80.00% 75.00% 90.00% % 70.00% 78.95% 72.22% 78.95% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Proportion of patients on CPA who were followed up within 7 days after discharge from psychiatric inpatient care NHS Digital Q % 95% 96.30% 98.41% 95.52% 95.45% Q Q Q Q3 C&I MENTAL HEALTH TRUST Proportion of admissions to acute wards that were gate kept by the CRHT teams Whittington UCLH Royal Free % Assessments begun within 1 hour in A&E % Assessments begun within 4 hours in AMU % Assessments begun within 24 hours on wards % Assessments begun within 1 hour in A&E % Assessments begun within 24 hours on wards % Assessments begun within 1 hour in A&E % Assessments begun within 4 hours in AMU % Assessments begun within 24 hours on wards NHS Digital Q % 95% Local Data Sep % 95% Local Data Sep % 95% Local Data Sep % 95% Local Data Sep % 95% Local Data Sep % 95% Local Data Sep % 95% Local Data Sep % 95% Local Data Sep % 95% % 99.59% 99.12% 99.16% Q Q Q Q3 92.2% 90.8% 82.4% 79.6% 85.1% 87.6% 76.5% 88.6% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 97.9% 100.0% 100.0% 100.0% 98.1% 97.6% 98.8% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 95.65% 84.21% 83.33% 82.86% 82.35% 82.14% 70.73% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 93.0% 92.7% 88.9% 91.5% 90.7% 85.9% 86.2% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 90.00% 86.05% 91.18% 90.91% 89.19% 90.24% 90.00% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 91% 85.5% 86% 85% 88% 92% 83% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 100.0% 99% 98% 98% 99% 100% 100% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb % 96.36% 93.33% 96.08% 92.73% 94.74% 94.00% 96.23% Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 *Latest data is provisional and unpublished NHS Digital data published by NHS Digital Local data derived from Provider reports to NHSE 85 of
86 Camden & Islington NHS Foundation Trust Provider Key Messages Key Messages Improving Access to Psychological Therapies Access Rates Local data from Camden and Islington NHS Foundation Trust Improving Access to Psychological Therapies services shows that the number of patients entering treatment was: 440 for Islington against a target of 434 (101%) 489 for Camden against a target of 513 (98.9%) Waiting Times Camden and Islington NHS Foundation Trust report that the percentage of patients accessing treatment within 6 weeks and within 18 weeks was over the agreed standards of 75% and 99% respectively for Camden and Islington CCGs in February Recovery Rates Camden and Islington NHS Foundation Trust reported recovery rate data for February 2018 shows a recovery rate of 46.98% for Camden CCG and 47.43% for Islington CCG. The general downward trend in recovery rates for both CCGs that was seen prior to December 2017 has been reversed and for both CCGs Camden and Islington NHS Foundation Trust has assured it is on track to deliver its commitment of 50% recovery rate by Quarter Four 2017/2018. Other Performance Indicators - National Standards for treatment times for First Episode of Psychosis (FEP), follow up within seven days of discharge for Care Programme Approach patients and gatekeeping of acute admissions by Crisis Resolution Home Treatment teams were all met by Camden and Islington NHS Foundation Trust for the last relevant reporting period. Mental Health patients presenting to Accident and Emergency Departments A Recovery Suite for patients with mental health problems has been built at Whittington Health and is ready to open. Camden and Islington NHS Foundation Trust reported at the March Islington A&E Delivery Board that it did not expect to be in a position to open the unit until the end of April 2018 as staff were not in post for the unit. The Board asked Camden and Islington NHS Foundation Trust to expedite the opening of the unit if at all possible. Data for September 2017 shows that not all timescales for providing emergency liaison support to Emergency Departments (within one hour) and to inpatient wards (within 24 hours) were being met across the acute providers (University College London Hospitals, Royal Free London NHS Foundation Trust Hospitals and Whittington Health NHS). The contracts for this performance are held by the acute providers with Camden and Islington NHS Foundation Trust directly but the CCG and NEL CSU are supporting acute providers in their management 86 of 402 of these contracts. 39
87 Theme KPI/Measure Reporting Period Actual YTD Current Month and Previous Month's Trend Blue = Actual Red = Target Number of Never Events Feb Serious Incidents (SIs) Reports Submitted Feb Proportion of Patients New Pressure Ulcers (Safety Thermometer) Feb Proportion of Patients Falls With Severe Harm (as per NPSA definition - Safety Thermometer) Feb Patient safety Mandatory Training rate Q1 76% 83.10% 78.60% 77% 77% 80% 76% Average fill rate - Registered nurses/midwives (Day) Dec-17 99% 98% 97% 96% 96% 94% 94% 100% 98% 99% Average fill rate - Registered nurses/midwives (Night) Dec-17 99% 97% 98% 97% 96% 97% 95% 98% 100% 99% Average fill rate - Care staff (Day) Dec-17 99% Average fill rate - Care staff (Night) Dec % 116% 108% 110% 109% 109% 106% 98% 99% 99% 131% 115% 114% 119% 123% 116% 119% 123% 123% Friends & Family test (FFT) - % Recommend - Mental Health Jan % 90% 89% 93% 90% 89% 91% 88% 94% Friends & Family test (FFT) - Response Rate % Mental Health Jan % 9.60% 12.85% 13.71% 13.07% 13.33% 9.50% 7.83% 10.08% Staff Friends & Family test (FFT) - % Recommended as a place to work Q2 50.6% 68% 68% 67% 61% 51% Patient experience Staff Friends & Family test (FFT) - % Not Recommended as a place to work Q2 28.2% 20% 20% 20% 23% 28% Staff Friends & Family test (FFT) - % Recommended as a place for Care Q2 61.8% 71% 71% 60% 64% 62% Staff Friends & Family test (FFT) - % Not Recommended as a place for Care Q2 15.4% Complaints - Number of formal complaints (Trust data) Q % 12% 19% 13% 15% of
88 Camden & Islington NHS Foundation Trust Quality Summary Area Key Issues Key Actions Recommendations Care Quality Commission Improvement plan The Care Quality Commission (CQC) undertook their formal inspection in December Camden & Islington NHS Foundation Trust has been rated good which is an improvement on its previous rating of requires improvement. The final report was published 6th March 2018 and the organisation held a quality summit with its key partners on 8th March 2018 to identify its success and future developments required to achieve an outstanding rating at any future inspection. Camden & Islington NHS Foundation Trust was given 7 Must Do Actions and 56 should Do Actions. The 7 Must Do actions are attached to this report. The should do action plan is currently being drafted. Key points: Completion of mandatory training Sufficient staffing to cover shifts Comprehensive records keeping after restraint and rapid tranquilisation Appropriate care models to support and promote independent living and access to community services Sufficient Occupational Therapy on inpatient rehabilitation wards Clinical Quality Review Group continues to review and monitor progress.. High caseloads in Crisis Home Recovery Team 88 of
89 Camden & Islington NHS Foundation Trust Quality Summary Area Key Issues Key Actions Recommendations Serious Incidents Summary There were 22 open serious incident investigations. (21 level 1s and 1 level 2). There were 14 new serious incidents between 1 January and 28 February (7 in January and 7 in February). There are 8 serious incidents still open from the previous reporting period Camden & Islington Foundation Trust have made great effort to submit the overdue reports, and the current number of overdue reports are much lower than previously. Due to the ongoing delays in identifying Serious Incidents authors and investigators, and finalising the report for sending to the CSU means that the projection indicates ongoing delays. Camden & Islington NHS Foundation Trust are working to mitigate these. Clinical Quality Review Group to continue to monitor. There were 10 incident investigations completed and reported during this period. The most common serious incident category remains unexpected death in the community. (Serious Incidents and Complaints Report Summary for the period 1 st January 28th February 2018 Camden & Islington NHS Foundation Trust ) 89 of
90 Camden & Islington NHS Foundation Trust Quality Summary Area Key Issues Key Actions Recommendations Complaints Complaints Summary 12 new formal complaints received in January 2018, 7 in February 2018 The oldest complaint currently open was received in May This is a complex complaint involving the need to reassess the service user. 23 complaints were responded to during this period, 9 in January and 14 in February 12 complaints were not upheld, 6 were partially upheld and 3 fully upheld. 2 complaints were withdrawn. (Serious Incidents and Complaints Report Summary for the period 1 st January 28 th February 2018 Camden & Islington NHS Foundation Trust) Themes were: Communication with families and service users, including sharing information about decisions, continues to be raised frequently Discharge and assessment Waiting times for some services Staff attitudes Camden & Islington NHS Foundation Trust has continued to experience challenges in regards to complaint investigations being completed on time; the current year to date compliance rate is 57% completed on time against a target of 80%. With the aim of addressing this, the complaints policy has recently been revised to ensure that there is flexibility in timescales for addressing more complex complaints or where delays occur due to factors outside investigators control. The team has also been meeting with divisional leads to discuss the pressure points and how to address these, and has begun Clinical Quality Review Group to continue to monitor. 90 of
91 Camden & Islington NHS Foundation Trust Quality Summary Area Key Issues Key Actions Recommendations Workforce There were less staff leavers in Quarter Three 2017/2018 compared to Quarter Two shown by the reduced turnover rate at 4.8% in Quarter Three compared to 5.3% in Quarter Two; significant progress against Staff First programme in regards to internal promotions has contributed to this reduction. At the end of Quarter Three (1 April 2017 to 31 Dec 2017) The Budgeted Establishment Full Time Equivalent increased by in Q3 the rise was mainly in Acute Divisions. The increase in Full Time Equivalent mentioned above contributed to the vacancy rate rising from 12.0% in Q2 to 13.6% in Q3. A new criteria for requesting agency staff has been developed and is operational across Camden & Islington NHS Foundation Trust. A new dashboard showing temporary staffing usage has been developed and is in place. The dashboard will further help to surface usage by Division and cost centre level and support discussions and actions accordingly Core Skills compliance across Camden & Islington NHS Foundation Trust increased to 76.3% in Q3 from 63.4% in Q2, ongoing effort continues to reach the Trust set target of 80%. As part of the CQC action plan, Core Skills compliance is a must do action in Over the last four quarters Camden & Islington NHS Foundation Trust has seen a drop in the number of Black Minority Ethnic staff entering the formal stage of employment relationship process. Clinical Quality Review Group continues to monitor Serious Incidents monthly Temporary Workforce spend rose in Q3 by circa 316K compared to Q2. The rise in sickness absence rate to 3.8% in Q3 from 3.5% in Q2 may have resulted in the rise in spend. (Camden & Islington NHS Foundation Trust workforce Q3 Report April 2018) Camden & Islington NHS Foundation Trust has recently increased scrutiny on temporary workforce spend and a new criteria for requesting agency staff is in operation. In addition the Finance Director and HR Director have been meeting with each Division to review agency spend. 91 of
92 KPI/Threshold UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST KPI/Threshold Jan-18 YTD Feb-18 UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST YTD 18 Weeks RTT Admitted % 85.05% A&E All Types Performance 95% 86.05% 88.24% 18 Weeks RTT Non-Admitted % 92.51% 18 Weeks RTT Incomplete Pathways 92% 91.04% 91.48% >52 week waits Admitted >52 week waits Non Admitted >52 week waits Incomplete Weeks Diagnostic Waits 1% 0.94% 0.75% Cancelled Operations ( Q3) 100% 91.35% 91.60% KPI/Threshold UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST Jan-18 2 Week Cancer Wait 93% 92.99% 94.35% YTD KPI/Threshold No of waits from decision to admit to admission (Trolley waits - over 12 hours) % Ambulance Handovers within 15 mins: KPI 1 % Ambulance Handovers within 30 mins: KPI 2 Number of Ambulance Handover - 30 minute breaches Number of Ambulance Handover - 60 minute breaches % Patient Records Captured Electronically: KPI 4 UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST Feb-18 YTD % 35.60% 36.30% 100% 83.40% 84.30% % 91.80% 92.10% 2 Week Cancer Wait: Breast Symptoms 31 day Cancer Wait: 1st definitive treatment 31 Day Cancer Wait: Subsequent treatment (Surgery) 31 Day Cancer Wait: Subsequent treatment (Chemotherapy) 31 Day Cancer Wait: Subsequent treatment (Radiotherapy) 62 Day Cancer Wait: GP Referral 62 Day Cancer Wait: Screening service 62 Day Cancer Wait:. Consultant Upgrade 93% 84.52% 92.70% LONDON AMBULANCE SERVICE NHS TRUST KPI/Threshold 96% 90.44% 93.77% Feb-18 YTD 94% 90.12% 94.06% Category 1 Mean (min:sec) 0:07:00 0:07:26 0:07:16 98% % % Category 1 90th Centile (min:sec) 0:15:00 0:11:48 0:11:46 94% 97.50% 99.18% Category 2 Mean (min:sec) 0:18:00 0:23:21 0:21:36 85% 60.93% 68.14% Category 2 90th Centile (min:sec) 0:40:00 0:49:21 0:44:48 90% 81.25% 75.47% Category 3 90th Centile (min:sec) 2:00:00 2:59:27 2:39: % 81.53% Category 4 90th Centile (min:sec) 3:00:00 2:34:17 2:33:31 92 of
93 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations A&E (Accident & Emergency) In February 2018, University College London Hospital A&E performance was 86.1%, which is below the agreed trajectory of 91.0%, and below the 95% threshold. The projected March 2018 provisional A&E performance is 84.8%, and the projected 2017/18 provisional A&E performance is 87.9%. There were breaches of the 12 hour trolley wait standard at University College London Hospital in October 2017, January 2018 and February Camden CCG closed the 2016/17 A&E contract performance notice and issued a new 2017/18 contract performance notice on 12 April Performance remains at level 4 of the performance management framework. University College London Hospital has refreshed its Emergency Department recovery action plan and reprioritised the recovery actions which currently focuses on front door streaming, flow, better bed management and specialty and diagnostic improvements, and convening executive led daily meetings in January 2018.The recovery action plan and trajectories is discussed at A&E Delivery Board and at the Contract Review Group meetings. The University College London Hospital / Camden A&E system has: An internal exercise was conducted where all work packages on University College London Emergency Department Recovery and Improvement Plan have been reviewed and signed off at Emergency Care Recovery Board. This included updating the Red Amber and Green status of work packages, actions and timescales. The latest version was shared with Camden CCG on 13 February Continues to have bi-weekly escalation calls with NHS Improvement and NHS England. Opened the transition space in the emergency department to create 8/9 beds in January Convened executive led daily meetings since January University College London Hospital progresses with implementation of the revised A&E recovery actions derived from the jointly commissioned external review by McKinsey. Camden CCG continues to closely monitor University College London Hospital daily and weekly A&E performance via SIT REP reports and the weekly exception reports. Camden CCG monitors University College London Hospital A&E recovery action plan at the monthly Integrated Performance meetings. Camden CCG considers instigating a weekly conference call with University College London Hospital to discuss A&E under-performance and 93 of 402 issues with flow. 49
94 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject A&E (continued) Description of performance management issue Remedial actions undertaken As part of the recovery plan there are a number of actions that have a critical impact on delivering the A&E trajectory: Increasing the number of patients on acute frailty ambulatory pathways Development and implementation of Discharge to Assess pathways The actions from the review of internal discharge processes and clinical utilisation that include rolling out a new clinical utilisation tool and implementing criteria-led discharge across medical wards. NEL CSU recommendations University College London Hospital A&E Delivery Board to review the implementation and impact of the investment on A&E Performance. The University College London Hospital / Camden system has successfully bid for winter money ( 500,000) to: Enhance the RAPID service to support further admission avoidance and Discharge to Assess pathways 2 and 3 Support an electronic coordination centre to maximise patient flow over a seven day period Enhance the staffing in a surge area in the Emergency Department. 94 of
95 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations A&E (continued) The Monthly Integrated Performance meetings with University College London Hospital were set up by Camden CCG / NEL Commissioning Support Unit in June 2016 where the A&E performance, Sustainability and Transformation Fund trajectories and above listed recovery action plans are reviewed. Since February this has become a joint Camden CCG/University College London Hospital meeting. The A&E Delivery Board continues to monitor progress against the various work streams. With the added focus on Delayed Transfers of Care by NHS England and NHS Improvement, Camden CCG and University College London Hospital continue to work closely on a daily basis to ensure numbers of Delayed Transfer Of Care and Medically Optimised are kept within acceptable limits. Camden CCG supports University College London Hospital with the Discharge to Assess Sustainability and Transformation Plan work stream. A&E attendance analysis by practice has been requested by both University College London Hospital and Camden CCG and this constitutes to be one of the actions in the agreed Recovery Action Plan Camden CCG provides support for University College London Hospital in escalation of stroke repatriation issues and capacity issues with Mental Health beds. 95 of
96 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations Ambulance Handover London Ambulance Service handover overrides (activated when the Emergency Department has not received the PIN number regarding agreed handover time from London Ambulance Service) at University College London Hospital were 24.2% in February 2018, just below the whole of London figure of 25.4%. University College London Hospital are continuing to carry out a successful initiative to improve handover times. In February 2018, handovers within the fifteen minute threshold maintained their consistency with a performance of 35..6%. This is a continuing improvement on the January 2017 figure of 27.1%. Similarly, handovers within the thirty minute threshold were 83.4% in January 2018 against the January 2017 figure of 72.7%. A London Ambulance Service ambulance handover time improvement initiative is being undertaken as part of the University College London Hospital recovery action plan implementation. In February 2018, London Ambulance Service to Emergency Department handovers, University College London Hospital challenged 25 out of 226 thirty minute handover breaches. Last month, in January 2018, University College London Hospital had challenged 50 out of 284 thirty minute handover breaches. There were 61 sixty minute breaches in total in February 2018 of which six were challenged by University College London Hospital. Last month, in December 2017, University College London Hospital had 69 sixty minute breaches in total in January of which 15 were challenged. In December 2017 Camden CCG on behalf of the University College London Hospital A&E Delivery Board submitted a checklist to NHS Improvement. This is to support the recommended actions aimed to improve Ambulance Handover. The paper confirmed the recommended actions already taken and identified areas for further work. NEL CSU recommends that Camden CCG works with University College London Hospital to ensure that senior representatives interface with London Ambulance Service, to discuss the current A&E pressures, review data and implement action plans to minimise Ambulance Handover Breaches. Continuation of London Ambulance Service action plan to recruit staff, and hence improve service performance. Camden CCG/University College London Hospital A&E Delivery Board continues to develop, implement and review the impact of the recommended actions to improve ambulance 96 of 402 handover. 52
97 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations Diagnostics University College London Hospital again achieved the diagnostic target in January 2018 with a performance of 0.94%. There were a total of 68 patients waiting over six weeks and seven patients waited over 13 weeks from a total waiting list size of 7, 228. The non-compliant modalities this month were magnetic resonance imaging (1.4%), peripheral neurophys (1.7%), urodynamics (26.2%) and cystoscopy (3.7%). The year to date diagnostics performance at University College London Hospital is currently achieving the target at 0.75%. Camden CCG closed the 2016/17 diagnostics contract performance notice on the 31 March 2017 following University College London Hospital s compliance against the standard for three successive months. Actions include: Working group convened at Modality level Business case being prepared for improvement work in Peripheral Neurophysiology Increase in capacity for Urodynamics is being considered at University College London Hospital 2017/18 Diagnostics Sustainability and Transformation Fund trajectory indicates compliance across all months Zero tolerance allowed at modality level within University College London Hospital University College London Hospital completed the capacity and demand modelling for Magnetic Resonance Imaging, Computerised Tomography, Endoscopy and Non Obstetric US to better understand its demand and supply and engaged with the Transforming Cancer Services Team (TCST) who have led on this piece of work pan London. Endoscopy: University College London Hospital continues to deliver additional capacity, optimising in-house capacity and improving its booking processes. NEL CSU recommends that: Camden CCG continues to closely monitor University College London Hospital s weekly and monthly diagnostics performance. Camden CCG continues to review progress with the University College London Hospital diagnostics recovery action plans at the monthly Integrated performance meeting. 97 of
98 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations University College London Hospital has developed specialty level recovery action plans and trajectories were signed off on 16 October University College London Hospital continues to track backlog of affected specialties against a reduction trajectory. Camden CCG closely monitors University College Hospital London backlog clearing exercise for the challenged specialties at the monthly Integrated Performance meeting and Contract Review Group. Referral to Treatment In January 2018, UCLH was noncompliant against the 18 Weeks RTT Incompletes Target for the seventh consecutive month with performance of 91.0% against the 92% Target. This represents a small improvement in performance of (+0.3%) in performance when compared to December s performance of 90.7%. 37,939 patients were seen within 18 weeks from a total number of 41,671 incomplete pathways. Three 52 week long waiters were reported for January 2018 and have been reviewed for any clinical harm and discussed at Clinical Quality Review Group. Actions include: Orthodontics: Locum consultant started October 2017 Brought forward current booked patients into new capacity created by postgraduates started early in October Paediatric dentistry: New consultant started in October 2017 New specialty doctor fixed term started in September 2017 Replacement of lost post graduate appointments in November 2017 was closed as no longer required. Specialty on trajectory and continue to monitor Restorative dentistry: Review of waiting list management processes commenced in October 2017 Postgraduates commenced in post in November Deep dive meeting scheduled in December 2017 Camden CCG continues to review and monitor the Referral to Treatment patient tracking list snapshot received from University College London Hospital on a weekly basis. Camden CCG ensures that the 52 week long waiters are reviewed for any evidence of clinical harm and discussed at the Clinical Quality Review Group meetings monthly. Camden CCG requests additional information on the monthly report for patients waiting over 52 weeks to include assurance information requested by NHS England in relation to patient choice and offer 98 of for 402 the alternate provider. 54
99 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations Referral to Treatment The non-compliant specialties in January 2018 are as detailed below: Ear Nose and Throat (83.9%) 3,688 patients were seen within 18 weeks from a total of 4,395 incomplete pathways. Neurosurgery (78.9%) 637 patients were seen within 18 weeks from a total of 807 incomplete pathways. Neurology (90.5%) 1,961 patients were seen within 18 weeks from a total of 2,167 incomplete pathways Other (90.9%) 22, 373 patients were seen within 18 weeks from a total of 24,617 incomplete pathways University College London Hospital submitted a refreshed Referral to Treatment recovery action plan and trajectories to Camden CCG on 15 December 2017 and this continues to be monitored at the integrated UCLH/CCG performance meetings monthly. Women's Health Gynaecology: - Inpatient Waiting list initiative approved for uro-gynaecology commenced in August Additional weekend Out Patient clinics submitted to board - started September Gastro intestinal Services: - Plan to increase clinician capacity, includes consultant, Inflammatory Bowel Disease (IBD) fellow, physiology fellow and physiologist. Posts come online between June and October 2017 Medical Specialties: Locum employed to back fill lists to free up consultants with the relevant skills. Camden CCG requests additional information on the monthly UCL report for patients waiting over 52 weeks to include assurance information requested by NHS England in relation to patient choice and offer for the alternate provider. Camden CCG keeps University College London Hospital on level 1 of the NEL CSU Performance Management Framework. Backlog clearance continues and NEL CSU receives and reviews University College London Hospital s Referral to Treatment (Referral to Treatment) recovery tracker and board pack on a weekly basis. University College London Hospital had planned to return to overall compliance by January 2018 but this has been revised to March of
100 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Referral to Treatment Referral to Treatment Description of performance management issue Compliance for RTT forecast now for March albeit recent indication received that community ENT service remains a significant risk to compliance. As of 24 March 2018 University College London Hospital backlog position is as detailed below: Admitted backlog (922), Non-admitted backlog (3,562) and overall Incompletes backlog (4,484). Remedial actions undertaken Community Ear, Nose and Throat Services (ENT) - University College London Hospital One additional clinic per week started beginning of December 2017 New Information Technology (IT) System introduced in October to ensure that referrals will be listed in date order for booking team to book from Train new Royal National Throat, Nose and Ear validators Allergy Additional clinics through increase in utilisation of existing clinics and utilisation of telephone clinics. Service to hire an additional locum Sustaining Patient Tracking List management improvements NOTE: Allergy will not recover compliance at reporting unit level within the life cycle of this plan. Full recovery is likely to be summer Queen Square: Neurology: New dementia clinic commenced September 2017 (complete) - Additional epilepsy activity expected - September clinics (complete), October clinics complete - Additional headache activity started October Queens Square to provide timeline for additional 'super Saturday' clinics. These have not been factored into the current version of the plan but would accelerate recovery from the new year. NEL CSU recommendations If compliance is not attained in March 2018, recommend that Camden CCG applies formal contract levers. Camden CCG keeps University College London Hospital on Level 1 of the NEL CSU Performance Management Framework 100 of

101 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations Referral to Treatment Backlog clearance continues and NEL CSU receives and reviews University College London Hospital s Referral to Treatment recovery tracker and board pack on a weekly basis. Queen Square (continued): Neurosurgery: Consultants have returned from leave. - Aiming to provide 80 additional clinics before the end of March These clinics started in September NOTE: Neurosurgery will not achieve compliance within life of this plan. This is due to disruption of theatre redevelopment likely to complete in April Specialist Services: - Autonomics - maternity leave cover in place. Expected impact from November Neuropsychiatry - vacant Cognitive Behavioural Therapist post. Now recruited and starts October Functional Neuropsychology Services (FNS) pathway: ensure clocks are appropriate stopped at outpatient appointment - Uro-neurology: Ensuring clock stops appropriate documented in clinic letters - Pain: Return of clinician. Improved DNAs through nurse led pre-assessment calls. Maternity leave cover in place - Neuromuscular: additional Saturday clinic commenced in October Camden CCG keeps University College London Hospital on Level 1 of the NEL CSU Performance Management Framework Referral to treatment performance and issues continue to be discussed monthly at the integrated University College London Hospital/CCG Performance meeting and exceptions raised at CRG. 101 of
102 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations A 2017/18 contract performance notice for the Cancer 62 days Urgent GP referral was issued on 12 April 2017 as performance remains at level 4 of the performance management framework.. Urgent implementation of signed off 2017/18 Cancer recovery action plans and implementation of the recommendations following the external clinical review by NHS Improvements Team in November 2017 Attendance at University College London Hospital Patient Tracking list meetings Cancer Waiting Times University College London Hospital achieved three of the nine Cancer Waiting Times Standards in January 2018, which demonstrates a decline in cancer waiting time performance when compared to December 2017 performance. January 2018 performance decline was expected by University College London Hospital due to patient choice over December 2017 appointments, and a seasonal reduction in clinics at the Trust. In January 2018, the internal 62 Day Urgent GP referral Performance reduced to 68.2%, (from 88.1% last month) and University College London Hospital have attributed the drivers for non-compliance this month to: Patient choice, complex diagnostics, in the Urology Pathway. the two week wait median wait challenges remain in Children s, Gynaecology, Lower GI, and Upper GI, and Sarcoma tumour groups. NHS Improvement have convened a bi-weekly steering group meeting with the University College London Hospital to discuss cancer performance and review trajectories. A revised Cancer Recovery Action Plan and trajectories are expected to be agreed soon. Implementation of the 100+ Day Cancer Weekly review and sign off by Chief Executive University College London Hospital books all first out patient appointments by day seven across all tumour sites to reduce median waits Continuous review of e-referral appointments and achievement of the e-referral Commissioning for Quality and Innovation (CQUIN) Urgent work be carried out on the visibility of University College London Hospital cancer patient tracking list and Infoflex system Reinforcing Cancer escalation guidelines within University College London Hospital 102 of 402 Improvement of the Urology tumour sites performance 58
103 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations Cancer Waiting Times The underlying issues in January 2018: For the 62 day treatment standard, there were 29.5 breaches, out of 76 total treatment pathways. Tumour sites breakdown of breaches as follows: Breast (x2); Lung (x5.5); Haematology (x1.5); Upper GI (x1); Lower GI (x1.5); Gynaecology (x1.5); Urology (x11.5) Testicular (x0.5); Head and Neck (x4); Sarcomas (x0.5) Breach reasons were as follows: Patient Choice/Clinical Breaches: 3.5 due to Patient Choice 4.0 due to Patient Unfit 1.5 due to Other Medical Condition Prioritised 7.0 due to Exceptionally Complex Treatment Pathway Administrative/Capacity Breaches 0.5 due to Capacity 4.0 due to Delay in work up 2.0 due to Administrative issues 7.0 due to Intertrust with no Information Critical actions: Increase breast imaging capacity and improve imaging pathway due 30 November Improve head and neck Inter Trust Transfer (ITT) referral pathway, due 30 September This is now being picked up as part of the bilateral meetings across NCL. Ensure all escalation actions are reported as completed at trust Patient Tracking List Meetings (PTL s). All 62 day+ breaches, including all those over 100 day breaches have breach analysis undertaken and is analysed and reported together at Clinical Quality Review Group. Reduction of urology and lower gastro intestinal Patient Tracking List backlogs Urgent review of the 38 day Inter Trust Transfer NCL trajectories from referring providers into University College London Hospital for 2017/18 and monitoring of 24 day treatments within University College London Hospital Escalations to North Central London Sector Wide System Leadership Forum to discuss and review issues affecting NCL providers as a Cancer System University College London Hospital participates in the system wide bilateral meetings to improve Inter Trust Transfer pathways. 103 of
104 University College London Hospital - Performance Management Summary NEL CSU Performance Management Assessment Subject Description of performance management issue Remedial actions undertaken NEL CSU recommendations Cancer Waiting Times 62 Day Screening Standard: In January 2018, University College London Hospital achieved a performance of 81.3% against the 90% threshold 62 Day Consultant Upgrade Standard: University College London achieved a performance of 69.8% against Camden CCG set threshold of 90%. NCEL Actions: The North Central & East London Performance Leadership Group closely monitors provider cancer waiting lists, including performance against the intertrust transfer target of 38 days for onward referral and 24 days for treatment at a secondary Trust. Series of tumour specific bilateral meetings across NCEL commenced November 2017 Reduction of gynaecology 2 week wait to day 7 Reduction of skin 2 week wait to day 7 Delivery of treatment within 24 days of receipt of tertiary referral Continuous review of action plans submitted by University College London Hospital at the CCG / University College London Hospital monthly integrated performance meetings. Weekly attendance at University College London Hospital Cancer PTL Meetings or consider instigating weekly teleconference to discuss University College London Hospital PTL position and performance Delivery of neck lump ultrasound at first appointment Improving head and neck Inter Trust Transfer pathway Embedding Optimal Lung Timed Pathway Specialised commissioning to support Positron Emission Tomography and Computerised Tomography scan capacity in NCL. Increasing e-referral two week slots. 104 of
105 Theme UCLH: KPI/Measure Reporting Period Actual performance YTD Trend Blue = Actual Red = Target Number of complaints New Number of acquired pressure ulcers: Grades 3 & 4 (Safety Thermometer) Old Pressure ulcers that are present on admission 3 & 4 (Safety Thermometer) Quarter Feb Feb Patient Safety The number of patients falls with severe harm (target = 0) (as per NPSA definition - Safety Thermometer) Feb Number of Never Events (target = 0) Feb Serious Incidents (SIs) Number Reported (Provisional figures, due to potential de-escalation) Feb Number of MRSA Bacteriaemia Jan Number of Clostridium Difficile Jan Average fill rate - Registered nurses/midwives (Day) Dec % n/a 103.6% 100.2% 97.5% 94.06% 93.09% 94.6% 92.2% 92.02% 90.34% 95.6% 94.63% 93.26% 94.86% 96.07% 92.34% 95.08% 93.06% 93.28% 90.45% 91.61% 88.52% Average fill rate - Registered nurses/midwives (Night) Dec % n/a 105.6% 103.9% 104.1% 98.2% 98.4% 100.4% 98.83% 97.69% 99.87% 99.26% 97.75% 97.42% 96.70% 95.77% 96.30% 94.06% 94.17% 93.00% 94.28% 94.04% 92.22% Average fill rate - Care staff (Day) Dec % n/a % % % % % % % % % Average fill rate - Care staff (Night) Dec % n/a 156.7% 159.3% 150.3% 142.7% 147.0% 144.4% % % % % % % % % % % % % % 105 of % % 61
106 Theme Clinical Effectiveness UCLH: KPI/Measure Reporting Period Actual performance YTD VTE (% admitted patients assessed for VTE risk) Sep % 95.54% Trend Blue = Actual Red = Target 95.27% 96.12% 95.24% 96.04% Proportion of patients spending 90% of their stay on a stroke unit - HASU (Routinely admitting team) 60% of patients presenting with stroke with AF anti-coagulated on discharge HASU (Routinely admitting team) Stroke - 95% patients admitted to stroke unit within 4 hours - HASU (Routinely admitting team) 70% of applicable patients who were given a formal swallow assessment within 72h of clock start - HASU (Routinely admitting team) Apr to July 2017/18 Apr to July 2017/18 Apr to July 2017/18 Apr to July 2017/ % n/a % n/a 53.70% n/a 97.80% n/a Friends & Family test (FFT) - % Recommended - Inpatients Jan % n/a 77.7% 75.0% 84.3% 78.0% 71.20% 80.10% 68.40% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 56.20% 51.80% 61.50% 51.00% 55.90% 35.50% 45.90% 34.20% 66.90% 63.11% 71.20% 80.50% 81.70% 90.90% 91.30% 86.90% 82.10% 88.50% 94.00% 96.41% 95.50% 97.00% 93.57% 93.28% 92.28% 94.67% 93.52% 96.57% 94.97% 92.62% 93.21% 95.47% Friends & Family test (FFT) - Response Rate - Inpatients Jan % n/a 17.05% 19.48% 17.90% 18.83% 23.68% 19.82% 19.75% 18.88% 17.48% 19.09% Friends & Family test (FFT) - % Recommended -A&E Jan % n/a Friends & Family test (FFT) - Response Rate - A&E Jan % n/a Friends & Family test (FFT) - % Recommended - Out Patients Jan % n/a 93.93% 95.24% 94.41% 94.64% 94.15% 91.8% 89.58% 91.7% 91.4% 91.4% 80.39% 81.54% 80.35% 86.9% 87.0% 84.9% 85.7% 82.33% 84.03% 82.00% 83.10% 82.35% 18.25% 13.41% 11.93% 12.74% 11.34% 14.04% 14.45% 14.45% 13.05% 8.07% 33.9% 36.5% 30.3% 29.8% 31.02% 26.19% 29.40% 21.41% 18.5% 19.8% 19.5% 15.83% 18.50% 93.84% 90.39% 91.14% 93.52% 92.11% 92.36% 91.55% 91.38% 91.22% 90.97% Friends & Family test (FFT) - Response Rate - Outpatients Jan % n/a 18.50% 1.58% 1.92% 10.19% 12.36% 11.01% 22.80% 8.17% 6.41% 22.93% 9.70% 22.07% 19.77% Patient Experience Maternity Friends & Family test (FFT) - Question 1 % Recommended (Antenatal Care) Maternity Friends & Family test (FFT) - Score Question 2 % Recommend (Birth) Jan % n/a Jan % n/a 30.4% 34.5% 34.9% 31.1% 26.7% 25.4% 99.52% 97.81% 97.98% 23.90% 96.4% 96.1% 95.19% 93.86% 93.08% 26.8% 28.02% 94.9% 96.1% 97.0% 96.8% 88.89% 93.14% 98.25% 92.13% 91.67% 94.34% 0.00% 0.00% 0.00% 92.6% 94.1% 91.8% 91.7% 99.12% 90.34% 94.33% 92.86% 92.79% 90.63% 89.4% 99.01% 97.52% 88.3% 98.91% 87.9% 98.81% 87.50% 96.00% 97.14% 97.44% 0.00% Maternity Friends & Family test (FFT) - Score Question 3 % Recommend (Post Natal Ward) Jan % n/a 30.4% 34.5% 34.9% 31.1% 26.7% 25.4% 23.90% 26.8% 28.02% 32.82% 32.50% 39.14% 38.24% 97.8% 96.40% 93.7% 93.9% 93.81% 94.03% 93.58% 94.24% 93.6% 92.5% 89.8% 95.38% 87.88% 89.8% 92.91% 95.51% 93.02% 93.98% 98.59% 93.57% 0.00% 88.65% Maternity Friends & Family test (FFT) - Score Question 4 % Recommend (Post Natal Community Provision) Dec % n/a 30.4% 34.5% 34.9% 31.1% 26.7% 26.8% % % 95.24% % 91.67% 23.90% 32.50% 39.14% 38.24% 25.4% 28.02% 100% 100% 100% 100% % 98.0% 0.00% 95.5% 0.00% 100.0% 100.0% % 98.2% 98.2% 96.43% 97.30% Staff Friends & Family test (FFT) - % Recommended as a place to work Q2 2017/ % n/a 30.4% 72.9% 69.6% 34.5% 67.5% 34.9% 70.65% 31.1% 72.9% 60.34% 66.74% 32.82% 74.23% 71.43% 32.50% 66.67% 39.14% 70.86% 38.24% 70.97% 26.7% 28.02% 70.65% 69.6% 26.8% 25.4% 23.90% 67.5% Staff Friends & Family test (FFT) - % Not Recommended as a place to work Q2 2017/ % n/a 30.4% 34.5% 34.9% 31.1% 26.7% 25.4% 23.90% 16.99% 17.77% 17.12% 16.3% 20.97% 16.3% 12.78% 13.53% 12.59% 23.46% 26.8% 28.02% 12.3% 16.99% 17.12% 13.21% 12.3% Staff Friends & Family test (FFT) - % Recommended as a place for Q2 2017/ % n/a Care Staff Friends & Family test (FFT) - % Not Recommended as a Q2 2017/ % n/a place for Care Mixed sex Accomodation Breaches Jan % 26.7% 30.4% 88.5% 34.5% 90.1% 34.9% 92.39% 31.1% 87.71% 26.8% 88.22% 25.4% 32.82% 92.07% 28.02% 88.91% 32.50% 87.50% 39.14% 91.41% 38.24% 90.01% 23.90% 90.3% 88.5% 90.1% 92.39% 26.7% 3.3% 30.4% 6.1% 34.5% 4.1% 34.9% 4.08% 31.1% 6.1% 3.91% 26.8% 4.75% 25.4% 32.82% 3.52% 28.02% 3.50% 32.50% 6.52% 39.14% 38.24% 3.85% 23.90% 2.86% 3.3% 4.1% 4.08% of
107 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions and progress NEL CSU recommendations Serious Incidents (SIs) Two Serious Incidents were reported in February 2018 which related to: - Maternity/Obstetric incident meeting Serious Incident criteria: mother and baby (x1) - Sub-optimal care of the deteriorating patient (x1) Two Serious Incident investigation reports have not been submitted within deadline and are overdue as at the end of February University College London Hospitals NHS Foundation Trust provide a monthly Serious Incident report to the Clinical Quality Review Group The University College London Hospitals NHS Foundation Trust provide a quarterly assurance report against the Duty of Candour requirements NHS Improvement issued a revised Never Events Framework, effective from 01 February Assurances were provided to the Clinical Quality Review Group on 6 March 2018 that these changes have been cascaded to all clinical staff and the relevant policies have been updated as a result. NEL Commissioning Support Unit and Camden Clinical Commissioning Group to actively monitor progress against each Serious Incident and request status updates against the longest overdue Serious Incidents at Clinical Quality Review Group. 107 of
108 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions NEL CSU recommendations Meticillinresistant Staphylococcus aureus and Clostridium difficile Meticillin-resistant Staphylococcus aureus There has been one Meticillin-resistant Staphylococcus aureus bacteraemia against an ambition of zero for this financial year to date. The likely source was associated with a peripherally inserted central catheter and all recommendations and actions identified in the post infection review have been implemented. Clostridium difficile University College London Hospitals NHS Foundation Trusts latest validated position reports ten Clostridium difficile case in January The total trajectory for 2017/18 is 97. The year-to-date position is of 56 reported cases. Root cause analyses continue to be completed jointly with the multidisciplinary team within 10 days and are being discussed on a monthly basis with Camden Clinical Commissioning Group to identify any lapses in care. University College London Hospitals NHS Foundation Trust provide a quarterly assurance report to the Clinical Quality Review Group quarterly. University College London Hospitals NHS Foundation Trust and NEL Commissioning Support Unit / Camden Clinical Commissioning Group jointly agree the outcome of the Root Cause Analysis to determine lapse of care. All learning is reported at Clinical Quality Review Group as part of the quarterly agenda item. An example of changes from learning include the multidisciplinary C. difficile weekly ward round reviewing the progress of all C. difficile toxins and antigen cases admitted as inpatients. Identification of early signs of relapses and poor treatment response have been the key issues managed to date. Clinical Quality Review Group to continue to closely monitor Infection Control compliance and hold detailed quarterly discussions at Clinical Quality Review Group. 108 of
109 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions NEL CSU recommendations Mixed Sex Accommodation University College London Hospitals NHS Foundation Trust have reported 30 Mixed Sex Accommodation breaches in February of these breaches were reported for the University College Hospital site and four were reported at the Queen s Square site. Daily Site Management meetings take place, in which capacity and demand in relation to Mixed Sex Accommodation and preserving patients dignity is discussed. University College London Hospitals NHS Foundation Trust have not received any complaints or concerns from patients in relation to Mixed Sex Accommodation breaches. Commissioners / NEL Commissioning Support Unit to monitor monthly reports against Mixed Sex Accommodation breaches to Clinical Quality Review Group and any complaints relating to Mixed Sex Accommodation breaches. 109 of
110 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions NEL CSU recommendations Quarter 3 Patient Experience and Complaints The Quarter 3 report was presented to the March Clinical Quality Review Meeting. It is recognised that University College London Hospital have continued to make improvements in relation to patient experience, challenges remain in the following areas; - Communication - Waiting times - Hospital Transport Commissioners have identified issues with transport services as a recurring theme within complaints and incidents. There are a number of work streams in place to address the issues identified regarding communication and waiting times, which are monitored at Divisional level and reported into the Patient Experience Committee. Patients are reporting positive feedback on NHS Choices in relation to; - Clinical care and treatment - Staff attitude Transport services across the Trust are provided by a third party, G4S. The Trust executive team have reviewed these issues and in response, have strengthened key performance indicators (KPIs) and monitoring arrangements. Commissioners / NEL Commissioning Support Unit to seek assurance through quarterly patient experience reports to Clinical Quality Review Group 110 of
111 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions NEL CSU recommendation s Delay to Treatment: Clinical Harm Review Referral To Treatment January 2018: There were three patients waiting >52 weeks at January 2018 month end in Neurosurgery and one in Neurosurgery. Clinical harm reviews have not identified harm. To date no patient harm was identified relating to extended Referral To Treatment pathway waits. University College London Hospitals continues to track all patients waiting 35 weeks and above at the Patient Tracking List meetings in order to identify actions to prevent any patient reaching 40 weeks. Actions are followed up weekly with each service. All patients previously reported as having waited beyond 52 weeks have now received treatment. 62 Day Cancer standard December 2017 University College London Hospitals NHS Foundation Trust reported 14 breaches, five internal and nine external (which is 23 patients as each external treatment counts as a half). University College London Hospitals NHS Foundation Trust undertook RCAs and clinical harm reviews for all patients who experienced a delay to treatment. In all cases no harm has been identified. Agreed process in place to report assessment of clinical harm of patients that have extended waits for elective treatment. Each month University College London Hospitals undertake a root cause analysis and clinical harm review for every patient whose treatment breached the 62 day treatment standard. University College London Hospitals share the full anonymised versions of the reviews with Camden Clinical Commissioning Group and NEL Commissioning Support Unit on a monthly basis. Waiting times is a key risk noted on University College London Hospitals risk register for adequate monitoring. University College London Hospitals re monitoring their recovery plan through the Camden Clinical Commissioning Group Integrated Performance Meeting and Contract Review Group. Progress reporting on outcomes of the clinical harm review remains a substantive item for assurance on each Clinical Quality Review Group agenda. University College London Hospital undertake breach analyses and clinical harm reviews for all patients who experienced a delay in treatment. Monitor for clinical harm and adverse patient experience 111 of
112 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions NEL CSU recommendations Cancer Quarterly Discussion The Trust continue to be noncompliant with the 62-day standards (for GP referral all cancers and 62- day screening all cancers) across Q1, Q2 and Q3 2017/18. University College London Hospital has a low level of compliance against cancer staging data. Teams are not consistently providing updates leading to a potential source of errors and incorrect data reported via the Registry and on infloflex (cancer data system). The Trust state that all 62 day breaches including all breaches over 100 days have a breach analysis undertaken, as part of the Clinical Harm Review process. University College London Hospital have assured Clinical Quality Review Group that no clinical harm as a result of the breaches, has been identified to date. The Trust Quality and Safety team have reviewed the cancer clinical harm review guidelines to ensure a consistent approach is undertaken by all services. These guidelines are now being reviewed by senior management prior to signoff and implementation. Work on national best practice pathways is underway with work being led by the cancer vanguard. New timed pathways are being developed and implemented to support making a diagnosis by day 28 in line with the changes to cancer waiting standards. Clinical Quality Review Group to continue to closely monitor quality of Cancer services and hold detailed quarterly discussions at Clinical Quality Review Group. University College London Hospital have taken part in bilateral meetings with other providers for shared pathways with highest numbers of breach volumes. These have led to the production of bilateral action plans which are being overseen by the sector performance leadership group and a refreshed overall trajectory. 112 of
113 University College London Hospital Quality Summary NEL CSU Performance Management Assessment Subject Description of Issues Actions NEL CSU recommendations Cancer Quarterly Discussion 62 Day Standard Internal performance issues and risks: Medical complexity: This continues to be a cause of breaches and while we can reduce will still see some breaches. Patients choosing to delay diagnosis and treatment still continue to cause breaches. External performance issues and risks: Risks to achievement of the overall standard for shared pathways continue due the still receiving patients after day Day Standard - Internal Performance: Medical Complexity: UCLH continue to reduce this through close tracking and escalation especially in the early part of the pathway. Patients choosing to delay diagnosis and treatment: UCLH have identified actions such as extra support from members of the clinical team in decision making, patient leaflets on expectations within the urology pathway. UCLH have instigated a zero tolerance for breaches for avoidable reasons and have produced a number of operational reports to assist in identification of at risk patients lower down the pathway. 62 Day Standard - External performance issues and risks: University College London Hospital has taken part in bilateral meetings with other providers for shared pathways with highest numbers of breach volumes. These have led to the production of bilateral action plans which are being overseen by the sector performance leadership group and a refreshed overall trajectory. Clinical Quality Review Group to continue to closely monitor quality of Cancer services and hold detailed quarterly discussions at Clinical Quality Review Group. 113 of
114 NCL Integrated Urgent Care Service (IUC) Performance against Quality and Performance KPIs Quality and Performance Indicators KPI Type Qrt 1 Qrt 2 Qrt3 Qrt4 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 NCL-IUC NCL-IUCNCL-IUCNCL-IUC NCL-IUC NCL-IUC NCL-IUC NCL-IUC NCL-IUC NCL-IUC NCL-IUC Engaged calls Performance 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Abandoned calls Performance 0.4% 0.9% 0.8% 1.4% 1.5% 3.0% 3.2% 4.8% 3.5% 4.7% 8.5% Answer Time Performance 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Call waiting time Performance 95.6% 91.0% 91.2% 86.3% 88.3% 81.6% 80.5% 73.3% 77.4% 76.7% 62.6% Life threatening referrals Quality 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Meeting individuals needs Quality 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Safeguarding Quality 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Triage rate Quality 106.6% 108.1% 108.2% 106.4% 104.9% 104.0% 109.1% 106.8% 104.2% 104.4% 103.5% Transfer to 999 Performance 9.6% 9.7% 10.3% 10.4% 10.9% 11.7% 11.5% 11.6% 11.7% 12.0% 12.3% Attend Accident & Emergency Department Performance 9.4% 9.8% 10.1% 10.5% 9.4% 10.1% 10.0% 9.8% 9.0% 10.2% 10.3% Referred to Primary Care and other dispositions Performance 55.5% 52.8% 52.5% 52.9% 51.9% 51.0% 51.5% 51.9% 55.4% 55.3% 56.6% Warm Transfers Performance 68.1% 66.0% 68.0% 71.6% 73.8% 66.5% 73.3% 72.2% 72.4% 78.5% 80.7% Time taken for call back Performance 10.6% 13.1% 10.8% 54.6% 54.0% 53.5% 49.1% 48.7% 46.9% 44.8% 37.6% Notifications Quality 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Patient Education Quality 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Data Source: LCW Reports Types of activity by CCG Data Source: LCW Reports 114 of 402 There is a similar pattern to the types of call response for each CCG with most patients being supported by speaking to the call advisor. 70
115 NCL Integrated Urgent Care Service (IUC) IUC Activity Outcomes by Type and Patient Age Profile 9 IUC Outcomes 9.1 Count of outcomes of ambulance dispatch Count of outcomes of recommended to attend A&E Count of outcomes of recommended primary or community care Count of outcomes of recommended to contact primary medical care Count of outcomes of recommended to contact community care Count of outcomes of recommended to dental Count of outcomes of recommended to pharmacy Count of outcomes of recommended to attend other service Count of outcomes of not recommended to attend other service Count of outcomes of given health information Count of outcomes of home care recommend Count of outcomes of non-clinical Count of outcomes of mental health service 57 Data Source: LCW Reports Age profile of patients supported by LCW IUC service during February 2018 Caller Group Barnet Camden Enfield Haringey Islington Total Volume % Volume % Volume % Volume % Volume % Volume % Group 1 (total) SPNs % % % % % % Patients 80 years and older % % % % % % Patients under 5 years old % % % % % % All other patients % % % % % % Repeat callers % % % % % of % Data Source: LCW Reports 71
116 NCL Integrated Urgent Care Service (IUC) Key Issues A Serious Incident occurred at London Central West Unscheduled Care Collaborative in April An undercover journalist from The Sun newspaper made a number of allegations about the integrated urgent care service. London Central West Unscheduled Care Collaborative are meeting all of the agreed national and local key performance indicators apart from call waiting time (62.6%) and Abandoned Calls (8.5%). This is due to London Central West Unscheduled Care Collaborative having faced a number of staffing challenges following the April 2017 serious incident coupled with increased activity levels. There has not been any clinical risk to patients, however there have on some shifts been fewer staff resulting in call waiting times increasing above the agreed target, coupled with increased abandonment rates. It was agreed as part of the roadmap that the call waiting time key performance indicator is reduced to 85%, with a transition to average answer time. Priority Actions NHS England requested a commissioner initiated external review to investigate the serious incident. This was led by Professor David Colin Thome. An Extraordinary Clinical Quality Review Group took place on 16 February 2018 to review the findings of the report. It concluded that neither the internal investigation nor the Independent Investigation Team identified harm or detriment to patients; neither did the investigations reveal significant risks or issues relating to the delivery of ongoing services. London Central West Unscheduled Care Collaborative provided an update on the serious incident at Clinical Quality Review Group on 23 March 2018, advising that most actions are now closed. Enfield CCG have prepared a report to be shared with NCL and INWL CCGs at the appropriate Governing Body meetings. An update will be provided at the May 2018 Clinical Quality Review Group. London Central West Unscheduled Care Collaborative performance for the Call Waiting Time metric has dropped in February 2018, however this is an issue across London, with no London provider meeting this indicator or the abandoned calls indicator. London Central West Unscheduled Care Collaborative is carrying out further analysis to better understand the drivers of the increase in abandoned calls. They suggested that the data could be skewed by patients who end calls early to access the online service instead (Babylon) and are liaising with Health London Partnership to understand this. London Central West Unscheduled Care Collaborative analysis will be presented to commissioners at the April 2018 Clinical Quality Review Group. A Contract Technical Group has been set up to review finance and activity levels against the agreed contract baseline to understand the drivers of the increased activity. A finance & activity report is being developed to highlight London Central West Unscheduled Care Collaborative financial pressures. A Key Performance Indicator Task and Finish Group has been set up to review and agree the suite of national and local key performance indicators. The cost improvement roadmap has been progressing, with weekly meetings with commissioners and London Central West Unscheduled Care Collaborative. Current areas of focus include the closure of the Primary Care Centre bases at weekends and the deployment of black pear interface, to allow appointments to be booked directly into hubs. A paper is going to Senior Management Team 116 of 402 on 27 March 2018, to agree the next phases of the roadmap. 72
117 London Ambulance Service Performance The four new patient categories are: Category 1 Life Threatening (8% of calls) Category 3 Urgent (34% of calls) Category 2 Emergencies (48% of calls) Category 4 Less Urgent (10% of calls). 117 of
118 NCL Ambulance Service Quality and Performance Key Issues Priority Actions Following the introduction of the Ambulance Response Programme, performance reporting is under review across the organisation and in conjunction with commissioners. Due to this on-going review the new formal contract reports have not yet been formally agreed. A new Tri-Partite report will continue to measure activity by category and record hospital conveyances. Four key reports will contribute to data for the Tri-Partite. To be shared. NEL Commissioning Support Unit will continue to attend Contract and Performance meetings to activity monitor performance of the Ambulance Review Programme and other key KPI s. There are a small number of problems that will be shared with local management teams to decide/agree on resolution. Commissioners and NEL Commissioning Support Unit will continue to monitor and feedback on progress. 118 of
119 NCL Ambulance Service Quality and Performance Key Issues Priority Actions Ambulance Tethering The New Dispatch Model Trial was set up as part of a NCL improvement programme in response to an inequity of ambulance performance between sectors. The trial ran for nine weeks between 16 August 2017 and 17 October 2017 and consisted of three elements: North Central Dispatch Group: Dedicated allocators/dispatchers & a solo responder desk; Ambulance tethering: emergency ambulances based in North Central would only be dispatched to incidents occurring within their home sector (except Red 1 incidents); New Fast Response Unit end of shift process: Ambulance staff guaranteed a rest break during the course of their shift. The outcomes of the pilot were as follows: Category A response times were largely unchanged while Category C response times reduced; No significant association was found between the New Dispatch Model Trial and conveyance rates. A number of recommendations have been made by the New Dispatch Model Trial group which the Trust is currently considering. These include: The Emergency Operations Centre to be permanently reconfigured to align with the STP geographical boundaries; A formal end of shift process to be considered as part of new rest break arrangements; Ambulance tethering to be permanently implemented for Category 3 and Category 4 patients. For Category 2 patients, it is recommended that dispatchers should attempt to dispatch a local vehicle first, but if unable to assign after 8 minutes, any ambulance should be dispatched; Consideration to be given to extending the open channel function on Airwave radios taking into account cost, benefit and utility. While it had been hoped that the New Dispatch Model Trial would result in greater equity of performance between CCGs in North Central, this was not identified in the results. Job Cycle time remained largely unchanged in the New Dispatch Model Trial group with no clear change within any element. The end of shift trial was generally well received by solo responders with significant feedback citing that less late finishes and more rest breaks had a positive impact on morale. 119 of of 7272
120 Quality Assurance Sign-off Section Written By Performance Mark Bridgeford Quality Helena Sage NHS111, GP Out of Hours & LAS Contracts Greg Hudson/Emmet Masterson Final Sign Off By: Helen Boswell Date: 10/04/ of
121 To know more If you would like to discuss any elements of this presentation, please contact our Performance team on: of 402 Back to list 74
122 Item: 3.3 MEETING: Islington Clinical Commissioning Group Governing Body DATE: Wednesday 9 th May 2018 TITLE: St Pancras Hospital Estates Redevelopment LEAD GOVERNING Dr Rathini Ratnavel BODY MEMBER: AUTHOR: Jill Britton, Associate Director Joint Commissioning, Islington CCG CONTACT jill.britton2@nhs.net DETAILS: SUMMARY: Islington CCG is proposing a change to some services currently delivered on the St Pancras Hospital site, to modernise and improve the quality of care provided to local people. The changes will affect all inpatient services at St Pancras Hospital and some community services based both at St Pancras Hospital and other C&I Foundation Trust sites. The Pre-Consultation Business Case ( PCBC ) assesses the opportunity to deliver better outcomes for users of mental health services across Camden and Islington through the development of a high quality and accessible estate. It sets out a way forward for formal consultation on a preferred option which is demonstrably the best solution in terms of benefits and value for money. The objectives of the PCBC are to: Make the case for change for transformation and modernisation of the mental health services, delivered by Camden and Islington NHS Foundation Trust ( the Trust ) across its community estates, and specifically at the St Pancras Hospital ( SPH ) site, to set out proposals for the redevelopment of the estates required to enable the transformation; Describe how the transformation of mental health services contributes towards the STP objectives of improving overall mental health outcomes across North London and reducing inequalities for those with mental ill health; Describe the clinically developed model of care and specification for the movement of community services into community hubs and the movements of in-patient services from SPH to another site. Detail the process undertaken to engage the public, staff and other stakeholders in the pre-consultation phase and demonstrate how their feedback has shaped the development of the options as well as the proposed option to take forward; Set out how the development of the preferred options is compliant with the Secretary of State for Health and Social Care s ( SoS or Secretary of State ) four tests of service reconfiguration and NHSE s other tests; Make the case to NHS Islington Clinical Commissioning Group (CCG), NHS Camden CCG and NHS England ( NHSE ) to commence public consultation on the preferred option. The Governing Body are asked to approve the pre-consultation business case. If the Governing Body approve the PCBC, then the final version of the consultation documents 122 of 402
123 will come to the Board in June for approval to proceed to formal consultation. This report contributes to: Preventing and managing long term conditions to extend both length and quality of life and reduce health inequalities, Improving mental health and wellbeing Prior consideration by Committees and other partners: Elements of the pre-consultation business case have been approved by the Executive Management team; The PCBC was approved by the Strategy and Finance Group on 26 th April. The pre-consultation business case and the consultation documents were considered by Board members at the Islington CCG Governing Body seminar on 11 th April. The pre-consultation business case and consultation documents were also submitted to the NHS Camden CCG for its April Board seminar for consideration and comment. Patient & Public Involvement (PPI): A range of patient and public involvement activities have been undertaken in the development of the proposals, which has influenced the proposals and options appraisal. This includes meetings with HealthWatch in Camden and Islington, which have surveyed the inpatients units about the proposed developments. A wide range of community and voluntary organisations have also been engaged about the proposals, as well as service user and carer groups. Equality Impact Assessment: The EIA has been completed in two parts, with the initial phase completed prior to consultation and a second stage to be completed following the consultation outcomes. The majority of vulnerable or protected groups identified as part of the EIA have been judged as achieving greater equality, improved outcomes or increased accessibility through the proposal. For example, both inpatient and community developments will provide improved disabled access for service users, staff and visitors. For many other groups, the purpose built facilities offer an improvement in therapeutic environment, access to outdoor space and care delivered closer to home. At this stage, the EIA has identified the potential increased travel time for some disabled service users as the only vulnerable group that may experience a reduction in accessibility. In order to minimise this risk, route planning to the new site will be provided and shared with local community groups for individuals with disabilities. Risks: The major risk relating to this project is that the required consultation programme is not adequate or has not followed the prescribed process, which might lead to a Judicial Review or Independent Panel Review. To mitigate against this the following has been undertaken: 123 of 402
124 A Steering group has been established to oversee the process, which has membership from all key stakeholders including David Mallett, Head of Service Reconfiguration at NHS England, who is providing expert advice and assurance. Engagement with the Camden and Islington Health Overview and Scrutiny Committees; Expert advice commissioned for the consultation methodology and documentation Pre-consultation engagement with patients and carers (CIFT) Legal advice has been commissioned to ensure that the process is technically accurate. Additional management resources have been sourced to ensure that there is capacity to undertake the consultation effectively. RECOMMENDED ACTION: The Governing Body is asked to: Approve the pre-consultation business case. SUPPORTING PAPERS: The documents attached to this paper include: Draft pre-consultation business case 124 of 402
125 Appendix Pre-Consultation Business Case for the Redevelopment of the St Pancras Hospital site and Mental Health Com munit y Hub s Version April of 402
126 2 Glossary of Terms Term / Abbreviation Definition 5YFV Five Year Forward View A&E Accidents & Emergency ALoS Average Length of Stay CAMHS Child and Adolescents Mental Health Services Capex Capital Expenditure CBT Cognitive Behavioural Therapy CCCG Camden Clinical Commissioning Group CCG Clinical Commissioning Group CIM Capital Investment Manual CIP Cost Improvement Plan CMH Community Mental Health CNWL Central and North West London NHS Foundation Trust COIL Certificate Of Immunity from Listing COO Chief Operating Officer CQC Care Quality Commission CSF Critical Success Factors DHSC Department of Health and Social Care DMBC Decision-Making Business Case DQI Design Quality Indicator EAV Equivalent Annual Value EBITDA Earnings before Interest, Tax, Depreciation and Amortisation EA10 Equalities Act 2010 EIA Equality Impact Assessment FBC Full Business Case FSRR Financial Sustainability Risk Rating GB Green Book GEM General Economic Model GPs General Practitioner HMHC Highgate Mental Health Centre HMT HM Treasury HOSC Health Oversight and Scrutiny Committee HR & OD Human Resources & Organisational Development I&E Income and Expenditure IAPT Improved Access to Psychological Services ICCG Islington Clinical Commissioning Group ICT Information & Communication Technology IoMH Institute of Mental Health 126 of 402
127 3 IT ITFF JHOSC JHWS JSNA LCS LoS LTFM Moorfields NCL NHS FT NHSE NHSI NPC OBC OSC PBMH PCBC PDC PIA PICU PID PLACE PPE QIA R&R SAMH SMS SOC SoS SPH STF STP the Trust the Trust Two boroughs UCL UCLH UCLP VAT Information Technology Independent Trust Financing Facility Joint Health and Overview Scrutiny Committee Joint Health and Wellbeing Strategies Joint Strategic Needs Assessment London Clinical Senate Length of Stay Long Term Financial Model Moorfields Eye Hospital NHS Foundation Trust North Central London NHS Foundation Trust NHS England NHS Improvement Net Present Cost Outline Business Case Overview Scrutiny Committee Practice Based Mental Health Pre-Consultation Business Case Public Dividend Capital Privacy Impact Assessment Psychiatric Intensive Care Unit Patient Identifiable Data Patient Led Assessment of the Care Environment Property Plant and Equipment Quality Impact Assessment Rehabilitation and Recovery Services for Ageing and Mental Health Substance Misuse Service Strategic Outline Case Secretary of State St Pancras Hospital Sustainability and Transformation Fund Sustainability and Transformation Partnerships Camden and Islington NHS Foundation Trust Camden and Islington NHS Foundation Trust; the Trust The London Boroughs of Camden and Islington University College London University College London Hospital University College London Partners Value Added Tax 127 of 402
128 4 Contents Pre-Consultation Business Case for the Redevelopment of the St Pancras Hospital site and Mental Health Community Hubs 1 Foreword Introduction Case for change and care model Governance Stakeholder engagement Finance case Implementation The SoS s four tests and NHSE s other test Decision making and next steps 15 2 Introduction Overview PCBC objectives Background PCBC scope Parties involved in the production of this PCBC Proposal Development PCBC structure 21 3 Context The Population and Healthcare challenges Background to the Trust and CCGs 24 4 Case for Change Local Policy Framework National Policy Framework Regional Policy Framework of 402
129 5 4.4 Quality of Existing Estate Limitations of Current Service Provision 41 5 Care model and expected benefit Care Model Expected benefit Impact on service users and benefits Changes to travelling times and distances Public Sector Equality Duty 57 6 Governance Governance structure for the consultation process Roles and Responsibilities Information Governance Issues 61 7 Stakeholder engagement Legal Context Pre-consultation engagement on the case for change Options appraisal engagement Applying pre-consultation engagement findings to options appraisal Other pre-consultation engagement activity Consultation Plan 69 8 Options development, analysis and evaluation process Option development Appraisal 1: Feasibility Study Appraisal 2: Hurdle CSF Appraisal 3: Qualitative CSF Appraisal 4: Value for Money evaluation of options Combined appraisal Impact of the preferred option 82 9 Finance case Introduction Basis of preparation of 402
130 6 9.3 Financial projections Impact on financial sustainability risk rating (FSRR) Sensitivities Conclusions Implementation Post consultation process Programme management arrangements Project implementation plan Post project evaluation Approvals process for investment by the Trust The SoS s Four Tests Test 1: Strong public and patient engagement Test 2: Consistency with current and prospective need for patient choice Test 3: A clear clinical evidence base Test 4: Support for proposals from clinical commissioners NHSE s Bed Closures Test Decision making and next steps 117 Appendix Contents of 402
131 7 Forew ord North London Partners in Care share a vision for our community to be happier, healthier and to live longer in good health. We have a collective agenda and a commitment to transform the health and care services of North London. Our community has told us they want a more joined up and integrated health and care system, they want care closer to where they live and work, delivered by professional and compassionate health and care workforce. We are united in our commitment to transforming care to deliver the best possible health outcomes for our local population. This will be done by shifting our model of care so that more people are cared for in out of hospital settings, and through prevention, more proactive care, and new models of care delivery, we can reduce the reliance on secondary care and improve the way people access and receive care. We want to improve overall mental health outcomes across North London and reduce inequalities for those with mental ill health; enable more people to live well and receive services closer to home and ensure that we are treating both physical and mental ill health equally. Our ambition is that unless someone requires highly specialised care, they will be able to receive the care they need within North London, and not require an out of area placement. By investing in community based care, we aim to reduce demand on the acute sector and mitigate the need for additional mental health inpatient beds. To deliver our vision, we have designed a programme of transformation for mental health services based around these fundamental elements: Supporting people with mental ill health to live well, enabling them to receive care in the least restrictive setting for their needs; Raise mental health awareness to reduce stigma, ensuring that mental health is considered equally with physical health; Reduce reliance on inpatient care and expand community provision to support more people to spend more time at home, rather than in hospital; Ensuring more accessible and extensive mental health support is delivered locally within primary care services. We are developing our services in the community to make sure that health and care will be available closer to home for all, ensuring that people receive care in the best possible setting at a local level and with local accountability. At the heart of the care closer to home model is a place-based population health system of care delivery which draws together social, community, primary and specialist services underpinned by a systematic focus on prevention and supported self-care, with the aim of reducing unplanned hospital admissions. We believe that the changes proposed in this document provide an exciting opportunity to deliver on our ambition to improve the mental health and reduce the health inequalities of our communities. By delivering more care in community settings and working in a more joined up and integrated way with our health, social care and voluntary sector partners, we believe that we will be able to deliver better outcomes for our patients. By supporting people closer to their homes and embedding services in the community, our teams can help prevent 131 of 402
132 8 people becoming unwell, or help them earlier so that they require fewer hospital referrals and less crisis care. We know that services provided in the community for people who experience mental ill health bring many benefits and better health outcomes. Community service are less stigmatising and easier to access. People receiving their health care close to their homes can continue to receive the support of their families, friends and local community, which we know is vital to recovery. In order to realise our vision we need to be able to provide more specialist mental health services for all forms of mental health in the community, supporting the work of our GPs and community teams, so that we can support earlier discharge and reduce admissions and re-admissions. Sometimes people will need specialist support provided in a hospital environment and it is our aim that this is provided in environments that are safe, therapeutic and maintain individual privacy. Where care is underpinned by strong, integrated community services, people will be referred to hospital less often and will be discharged earlier following periods of illness. By providing treatment in the least restrictive environment possible, fewer people will be detained under the Mental Health Act and those that do can step down from a hospital environment as soon as possible. The community estate is key to delivering our vision. It can be brought together to help achieve these synergies between services and sectors, supporting joint and multi-agency working. The exact details of how all services may work together in the future is still to be developed through co-production with service users and carers and creating the space in Community Hubs is an enabler for this. The care that we provide to patients must be underpinned by the best practice and we want to be at the forefront of research developments to ensure that people who experience mental ill-health are receiving the best care possible. By working with our academic partners, we can ensure that every intervention is evidence based and so will be the least restrictive as possible. Helen Pettersen Accountable Officer North Central London CCGs Angela McNab Chief Executive Officer Camden & Islington NHS Foundation Trust 132 of 402
133 9 Executive summar y 1.1 Introduction The local health organisations are united in the commitment to transforming care to deliver the best possible health outcomes for the population of Camden and Islington. The local communities have voiced a need for a more joined up and integrated health and care systems. This will be done by shifting the model of care so that more people are cared for in out of hospital settings, and through prevention, more proactive care, and new models of care delivery, reliance on secondary care can be reduced and improve the way people access and receive care. This Pre-Consultation Business Case ( PCBC ) assesses the opportunity to deliver better outcomes for users of mental health services across Camden and Islington through the development of a high quality and accessible estate. It sets out a way forward for formal consultation on a preferred option which is demonstrably the best solution in terms of benefits and value for money. The objectives of the PCBC are to: Make the case for change for transformation and modernisation of the mental health services, delivered by Camden and Islington NHS Foundation Trust ( the Trust ) across its community estates, and specifically at the St Pancras Hospital ( SPH ) site, to set out proposals for the redevelopment of the estates required to enable the transformation; Describe the clinically developed model of care and specification for: The movement of community services into community hubs; and The movements of in-patient services from SPH to another site. Detail the process undertaken to engage the public, staff and other stakeholders in the pre-consultation phase and demonstrate how their feedback has shaped the development of the options as well as the proposed option to take forward; Set out how the development of the preferred options is compliant with the Secretary of State for Health and Social Care s ( SoS or Secretary of State ) four tests of service reconfiguration and NHSE s other tests; Make the case to Camden NHS Clinical Commissioning Group ( CCG ) ( Camden CCG ), Islington NHS CCG ( Islington CCG ), and NHS England ( NHSE ) to commence public consultation on the preferred option. The proposal set out in this document is to move the following: Services being provided from SPH that are moving into the community hubs Inpatient services being provided from SPH that are moving to another site that is 2.5 miles away from the current location; and A limited range of other NHS services that are currently delivered from a variety of Trust sites which will move as part of proposals. 133 of 402
134 Case for change and care model Context The current Joint Strategic Needs Assessments ( JSNAs ) for Camden and Islington produced by the respective Health and Wellbeing Boards outline a clear requirement for sustainable and high quality mental health service in the area. Both Camden and Islington have significantly higher rates of mental health diagnosis than other London Boroughs. Islington has the highest proportion of its population diagnosed with a psychotic disorder, with Camden third highest nationally. The proposed reconfigurations reflect Health and Well Being Board Strategies to achieve this goal. The Trust provides mental health services for people in the area. Almost 98% of services are commissioned by Islington CCG in their role as lead commissioner with Camden CCG as an associate commissioner. The SPH redevelopment programme and development of mental health Community Hubs enables an overarching transformation of the estate to enable effective delivery of the Trust s Clinical Strategy along with national and local health strategies through the development of a range of health services and research facilities. It puts service users at the centre, recognising there is a once in a lifetime opportunity to transform services across the London Boroughs of Camden and Islington, building more visible, more accessible and more integrated services for people locally alongside world class research driving the very best practice.the vision for the community hubs is that service users and carers will have a familiar, non-stigmatising, easily accessible place where they can access a variety of services that promote holistic care. Community services are being developed to make sure that health and care will be available closer to home for all, ensuring that people receive care in the best possible setting at a local level and with local accountability. At the heart of the care closer to home model is a placebased population health system of care delivery which draws together social, community, primary and specialist services underpinned by a systematic focus on prevention and supported self-care, with the aim of reducing unplanned hospital admissions. Parity of esteem for mental health through modern estate and integration of care with physical health is widely supported through national initiatives and within the local health system. This is a rare opportunity to make a step change in converting that concept into reality for service users in North Central London and is aligned to the wider Model of Care and goals in the local Sustainability and Transformation Plan ( STP ). To deliver the STP vision and the aims of the Five Year Forward View, a programme of transformation has been designed with four aspects: Prevention, Service transformation, Productivity and Enablers. The STP identifies the need to redevelop the estate at SPH, in conjunction with other redevelopments, in order to enable a range of initiatives across North Central London. Progress has been made against the STP plans through improving community resilience, increasing access to primary care mental health services, developing a women s psychiatric Intensive Care Unit ( PICU ), investing in a community perinatal service, investing mental health services delivered in A&E and increasing access to psychological therapies. The Trust s sites vary widely in terms of their distribution, age, condition and suitability and these extensive differences were noted in the 2016 Care Quality Commission ( CQC ) 134 of 402
135 11 inspection and whilst the 2018 inspection noted mitigations in place to address the concerns raised previously the overall rating for Safety remained as Required Improvement. Part of this is due to the inherent challenges of the estate such as visibility within the buildings. There is a potential time constraint on the ability to deliver the SPH transformation insofar as August 2015 the Trust were successful in their application for a Certificate of Immunity from Listing ( COIL ) that prevents the SPH site from becoming a listed building for five years Current and future care model The Trust s Care Model forms part of the broader NCL STP stepped model of care for mental health with goals around improved access to mental health services, improving the acute mental health pathway and improving patient pathways through practice based mental health teams and specialist care pathways. Following changes to the current care model, the workforce requirement will change in line with the NCL STP under this proposal to achieve portability, staff experience and career planning/development. Several initiatives have been developed that are specific to mental health, in conjunction with other NCL STP programmes, which include recruitment initiatives, rental initiatives development, and use of new roles and up-skilling current staff. The commercial structure around the payments to the Trust from the CCGs is such that there would be no negative financial impact on the CCGs as a direct result of the proposed service changes. The Trust currently has 235 beds (84 on the SPH site) used for acute admissions, treatment of adults and older people. Over the last couple of years the Trust has experienced consistent pressure on its remaining beds and an increase in numbers of peopl e admitted and those treated by the Crisis system. The STP mental health work stream is to a large extent based on reducing the demand for in-patient beds and meeting people s needs in the community. The Trust has undertaken a range of changes to bed management that has reduced admissions, reduced bed utilisation so reduce private sector admissions, and reduced length of stay. Consequently the CCGs are confident that maintaining the current bed base at 235, will be sufficient to meet demand in 2025, the new build will actually allow one additional bed to 236 due to the removal of the estate compromise that saw one bed close in Expected benefit The service user benefits depend on the service they access: Community based care: The relocation of some services to the Camden hub offers the opportunity to access services at a welcoming community based, non-acute setting. Improved therapeutic environment: For inpatients at SPH, moving to a new facility ensures they receive care in a high quality, specialised building with modern facilities. Improved access: Relocating to a newly built site that meets modern accessibility requirements, this will increase equality of access for users, staff and visitors. There will need to be a focus on supporting disabled service users with accessibility to the new site as identified in the Equality Impact Assessment. Parity of esteem for mental and physical health: By co-locating the new purpose built facility alongside the Whittington Acute Hospital, service users are able to receive specialist mental health treatment from the same site as users of the acute service. 135 of 402
136 12 Improved integration between acute and mental health services: It is expected that users transferring between mental health inpatient and acute facilities on the same site will receive a quicker and more streamlined transition. Better working initiatives for staff: By developing new facilities and implementing the workforce plan as per the STP, the local health organisations are more likely to attract a higher quality staff by providing a high level of staff support. Improved research opportunities: Leading to long term improvements in mental health care and outcomes. 1.3 Governance The consultation phase of the redevelopment of the St Pancras site is being overseen by the St Pancras Hospital Redevelopment Oversight Group and led by the Chief Operating Officer of Islington CCG. This group is reporting to both of the CCGs, in addition to providing assurances to NHS England and be supported by three sub-groups: Clinical Senate Liaison Group, Public Consultation Working Group and Financial Modelling Group. In order to proceed to public consultation, the process requires approval from the CCGs Governing Bodies and NHS England. Camden and Islington Health and Overview Scrutiny Committees will be also be provided an opportunity to review and comment on the consultation prior to launch. As a part of the proposed relocation, the Trust is not proposing to change the use, storage or accessibility of any Patient Identifiable Data it holds. 1.4 Stakeholder engagement Under section 242 of the NHS Act 2006 and section 142Z of the Health and Social Care Act 2012, NHS Trusts and CCGs have a legal duty to make arrangements for individuals to whom the services are being or may be provided, to be involved throughout the process. All public consultations should adhere to the Gunning Principles Pre-consultation engagement on the case for change The local health organisations have engaged with inpatient service users, community service users, carers, staff and other stakeholders as part of pre-consultation engagement work for the development of the plans. Pre-consultation engagement including as part of the STP included service users and carers, employees, GPs, the JHOSC and other local stakeholders Options appraisal engagement As part of the options development a series of meetings were held to get input and understand the needs of stakeholders. The following options appraisal engagement was incorporated into the options appraisal process up to the point of selecting the preferred option. Shortlisted options for inpatients included: A1 Do minimum - The Trust would carry out the minimum works necessary to improve the quality of their existing estate to enable the Trust to deliver a higher quality of care. 136 of 402
137 13 A2 Re-provide inpatients at SPH - A new mental health inpatient facility would be built on the existing SPH site. A3 Re-provide inpatients at Whittington Hospital - The Whittington Hospital is located in Islington but on the border road between Camden and Islington to the North of both Borough s. It is an acute hospital with land available for the Trust to build a new inpatient facility. A4 Re-provide inpatients at St Ann s Hospital - St Ann s Hospital was identified during the Strategic Outline Case ( SOC ) stage as having the potential to host a new inpatient facility for the Trust. Each option had the same proposal for community services and other services which is why they are not explicitly mentioned under each option above. A summary of the areas considered following this engagement included: The need for adequate consultation with service users, which would include the formal consultation process itself; Preference for inpatient beds to remain within or close to Camden; Preference for inpatient beds not to shift to the St Ann s site due to travel and accessibility issues; Noting the proposal land disposal of the SPH site; and Preference the provision of appropriate services from the community hubs. Following this the preferred option was agreed to be to move inpatient beds from SPH to a site in Camden and Islington, invest in community services through the two community hubs and bring researchers and academics together on a single site at SPH. The Whittington site was selected as the preferred option for inpatients and there has since been further engagement undertaken in the form of regular meetings with service users, carers, Trust staff, JHOSC updates and meetings with NHS Improvement ( NHSI ) and NHSE by the local health organisations Consultation Plan In light of the service changes under this proposal, Islington CCG is proposing to run a public consultation for 12 weeks starting from July 2018 to September As part of the formal consultation process, the group of stakeholders who will be engaged will be widened. Accordingly the range of methodologies will also be expanded to cover targeted and ongoing engagement, across a range of channels. The concerns raised through the pre-consultation engagements will be incorporated in the consultation as follows: Consulting with current and ex-service users; Keeping the provision of services within Islington or Camden; Undertaking further travel time analysis; Be clear about strategy of sale of NHS Resources; and Opportunity to input on which services are provided in the Community Hubs. The channels used to share the consultation and gather as many views as possible will include website/online media, paper copies, public meetings, focus groups, staff engagement, NHS provider roadshows, targeted interventions and local networks. 137 of 402
138 14 The CCGs will appoint an independent partner to evaluate the consultation responses and analyse the results of the consultation. This will inform proposals in a Decision-Making Business Case ( DMBC ) that will validate the consultation outcomes. Following the closure of the consultation on 30 th September 2018, the evaluation team will have a period to analyse the results and present these to both of the CCG Governing Bodies ( CCG CBs ). Islington CCG will then make a recommendation on the redevelopment proposals to NHSE and both of the Overview and Scrutiny Committees ( OSCs ) for Islington and Camden. 1.5 Finance case As previously detailed, the amount of spending planned by both CCGs with the Trust will not negatively change as a direct result of these proposals because of the contract arrangements in place, whereby the Trust receive a negotiated fixed amount per period from CCGs to provide services to the local population this is not directly linked to volume of service users unlike Payment by Results approaches for many physical care services. The Chief Financial Officer for both Camden CCG and Islington CCG corroborated the financial information presented below with the Director of Finance for the Trust and both individuals have reached an agreed position. As a result the main impact of the proposals is on the Trust. The preferred option does provides a sustainable solution for the SPH site, eliminates backlog maintenance and enables the Trust to procure alternative accommodation which will directly support and enable implementation of the Trust s Clinical Strategy. Due to the high value of estate at St Pancras, the capital receipt from the redevelopment of the SPH site is expected to be greater than the total capital cost of the transformation. In the Trust s Outline Business Case ( OBC ), a red book valuation has been undertaken as per NHSI and HM Treasury guidance which presents a prudent value. Therefore, the risk of not achieving a level of capital receipt to cover the costs of the redevelopment is low. As above, there is no request for funding associated with this programme of work, with any shortfall from land sales being initially met through the Trust s internally generated reserves and to be recovered through the benefits in future periods. There will, however, likely be a requirement for interim financing arrangements for the Trust to manage the timing of cash flows. 1.6 Implementation Following the close of the consultation and decision-making process the CCGs will hand back decision making responsibility to the Trust. The Trust will implement the proposal, having already factoring in considerations from the consultation process. The Trust has developed a robust programme management and governance structure which ensures accountability through clear allocation of responsibilities, and provides assurance through regular reporting, enabling quick identification and addressing any issues as they arise. The Trust implementation team will comprise approximately 4-6 people on a whole time equivalents ( WTE ) basis to be engaged at various points during the implementation. The function requirements during the implementation include: Programme Director; Project 138 of 402
139 15 Director; Project Managers: Finance Support; HR and Workforce Support; Clinical Support; and Administration. A detailed project plan exists that sets out milestones which will be updated on a regular basis as more information becomes available and the project develops. There is also an existing risk management process in place for the Programme, and this process will continue throughout the implementation and delivery phase of the programme to ensure that risks are identified, monitored and where possible, mitigated. NHSI also require Trusts to submit a SOC, OBC and Final Business Case ( FBC ) for approval for capital investment proposals of this value. 1.7 The SoS s four tests and NHSE s other test The 2014/15 mandate from the Secretary of State to NHS England, outlines that proposed service changes should be able to demonstrate evidence to meet four tests before they can proceed: 1) Strong public and patient engagement: There has been extensive stakeholder engagement to date as described in Section 7 of this document including presentations, discussions, surveys, meetings and s. This will continue during the Consultation. 2) Patient choice: There will no change in the number of providers serving the local area, whilst choice will be improved through the offer of a fit for purpose mental health facilities for local service users. 3) Clinical evidence base: There is a clear case for change insofar as the existing estate is ageing and inflexible with multiple ligature points and blind spots where staff cannot easily observe service users. A wide range of clinicians have been engaged and consulted throughout to ensure patient outcomes are central to plans with feedback showing a strong level of support. The Clinical Senate will also provide feedback prior to formal consultation commencing. 4) Support from clinical commissioners: Both CCGs support and have helped to develop the proposals in this document. CCG Governing Body leads have been involved in the process throughout alongside member GPs. It is also noted that NHS England have also introduced an additional test but as it only relates to circumstances where there are proposals to reduce bed numbers it is not applicable here. 1.8 Decision making and next steps Following consultation, the St Pancras Hospital Redevelopment Oversight Group will review consultation responses received from members of the public and organisations. The committee will then consider the views of the participants and the effect these may have on the decision-making process. However, to give an indicative timeline, the programme expects the following milestones for this process. These may be subject to change, as described above: Formal public consultation 5 th July 2018 to 30 th September 2018 (12 weeks). External analysis of consultation responses October Final business case preparation November of 402
140 Each CCG GB to consider the final business case document November 2018 Each CCG GB make a decision on the final business case November of 402
141 17 2 Introduction This section provides an overview of the purpose and development of the Pre-Consultation Business Case ( PCBC ), as well as a description of the contents of the PCBC. 2.1 Overview The local health organisations are united in the commitment to transforming care to deliver the best possible health outcomes for the population of Camden and Islington. The local communities have voiced a need for a more joined up and integrated health and care systems. This will be done by shifting the model of care so that more people are cared for in out of hospital settings, and through prevention, more proactive care, and new models of care delivery, reliance on secondary care can be reduced and improve the way people access and receive care. This PCBC sets out the proposal to develop a fit for purpose and cost-effective service transformation that delivers a high quality and accessible estate for patients with mental health needs across the London Boroughs of Camden and Islington. The new estate, combined with the service transformation, will enable Camden and Islington NHS Foundation Trust ( the Trust ) to deliver high quality integrated health and social care services, whilst supporting the Trust s research objectives. As set out in the Trust s Estates Strategy, it is necessary to release value from the St Pancras Hospital ( SPH ) site to enable the delivery of the broader transformation of mental health facilities in the area. This PCBC sets out a way forward for full public consultation on a preferred option which is demonstrably the best solution in terms of benefits and value for money. 2.2 PCBC objectives The objectives of this PCBC are to: Make the case for change for transformation and modernisation of the current services delivered at the SPH site and the community sites of Greenland Road and Lowther Road and detail the proposal for redevelopment that enable these changes to happen; Describe the clinically developed model of care and specification for the re-provision of: Inpatient services from SPH to a new site; The re-provision and alignment of some community services into newly developed community settings; and Detail the services that are remaining on SPH, albeit in new facilities. Detail the process undertaken with stakeholders to inform, develop and evaluate viable options for the redevelopment of the SPH site and re-provision of services elsewhere; Detail the process undertaken to engage the public, staff and other stakeholders in the pre-consultation phase and demonstrate how their feedback has shaped the development and selection of the preferred option; 141 of 402
142 18 Set out how the development of the preferred options is compliant with the Secretary of State for Health and Social Care s ( SoS or Secretary of State ) four tests of service reconfiguration and NHSE s other tests; Make the case to Camden NHS Clinical Commissioning Group ( CCG ) ( Camden CCG ), Islington NHS CCG ( Islington CCG ), and NHS England ( NHSE ) to commence public consultation on the preferred option. 2.3 Background The existing mental healthcare estate at SPH is not fit for purpose it is in part converted from Victorian workhouses and was simply not designed to meet modern health and safety requirements or provide an optimal environment for delivering healthcare. The latest Care Quality Commission ( CQC ) inspection published in March 2018 noted that the Trust had sufficient mitigations in place to address the concerns raised previously. However the overall rating for Safety remained as Required Improvement. The previous The CQC report (June 2016) highlighted that the Trust s acute wards (for adults of working age) and psychiatric intensive care units require significant improvement. This judgement was based in part on the breach of guidance on single sex accommodation, the physical ward layout which prevented staff observation of all areas and the presence of a number of ligature risks that were insufficiently managed; with the risk either not consistently recognised or mitigated or the unavailability of ligature cutters. As well as failing to meet modern standards, the location itself is no longer fit for purpose as it does not provide therapeutic value for people who may be resident for many weeks or months. For example, the estate lacks space for physical activity, monitoring of service user wellbeing is impeded by the layouts, and there are significant commercial developments in the area surrounding St Pancras that infringe on the privacy and therapeutic environment of service users. Significant investment would be required to maintain and upgrade the current premises to meet modern standards, and it would require significant disruption to services during a transition period with several stages of decanting services from one site to another. Even then, in some cases, the Trust would still be unable to satisfy the standards prescribed by Department of Health best practice guidance (Health Building Notes). The Trust has, however, identified an opportunity to transform the estate to provide a fit for purpose, cost-effective, integrated, accessible estate to enable the delivery of high quality health and social care services. This is set out in subsequent sections of this document. 2.4 PCBC scope Islington CCG, Camden CCG and the Trust have carefully considered what needs to be consulted on. It has been decided that the following services will be publicly consulted on: Inpatient services being provided from SPH that are moving to another site that is 2.5 miles away from the current location; Services being provided from SPH that are moving into the community hubs; and A limited range of other mental health services that are currently delivered from a variety of sites which will move as part of proposals. A complete list of the Trust s services that are moving can be found in Appendix [1]. 142 of 402
143 19 Services that are not moving will not form part of this consultation, but for completeness this document does set out the NHS services that will be staying on the SPH site. The following NHS organisations who are currently providing services on SPH will continue to do so in new buildings: Royal Free NHS Foundation Trust; and King s Cross Surgery and London Central and West Unscheduled Care Collaborative. Central North West London NHS Foundation Trust and University College London Hospital, who are currently providing services out of the South Wing building at SPH, will continue to do so from existing facilities: All of these organisations have been consulted with as part of the production of PCBC and will have the opportunity to feed into the consultation. It is not currently envisaged that services will have to move off the SPH site during the redevelopment process. However, there is a possibility that the GP out of Hours service and GP practice may need to temporarily move within the SPH site. If this is the case, every effort will be made to reduce disruption and inconvenience to patients, staff and the public. Furthermore, during this redevelopment period every effort will be made to ensure disruption is kept to a minimum for users of the site and surrounding area. Where development is required alongside existing services, all regulatory processes will be followed to ensure development areas are sectioned off and safe for public passage in line with best practice for construction contractors. In particular, current plans for access for contractors will be through the eastern end of the SPH site, away from South Wing and residential areas of Somerfield, thereby not obstructing access, limiting noise impacts and retaining ambulance access. Trust services that are not provided on SPH site and are not moving, as well as back office support services will not form part of the consultation. A complete list of other provider services that are staying at SPH can be found in Appendix [2]. 2.5 Parties involved in the production of this PCBC The PCBC has been produced following engagement throughout the process with the following parties: NHS England ( NHSE ); The local CCGs, specifically Camden NHS CCG and Islington NHS CCG; The local Health Trusts, specifically Camden & Islington NHS Foundation Trust ( the Trust ); London Health and Care Devolution; Other primary care providers; including those on site (King s Cross Surgery and London Central and West Unscheduled Care Collaborative); and Local Authorities, specifically Islington London Borough Council and Camden London Borough Council including through the Joint Health Oversight and Scrutiny Committee ( JHOSC ), as set out in Section [7]. 143 of 402
144 Proposal Development The Trust proposal set out in this document is to invest in new facilities for community services provided on the SPH site, plus one site in Islington and one in Camden, whilst reproviding the working age acute and rehabilitation inpatient facilities at SPH to a site adjacent to HMHC. These new facilities in Camden and Islington are described as community hubs. The new facilities provided at the SPH site will also accommodate a new Institute for Mental Health ( IoMH ) on behalf of Universities College London ( UCL ). Development of the proposed changes has been ongoing since early 2016 by the local health organisations. This includes work on the pre-consultation activities, stakeholder engagement and options development. Further detail of the options development is set out in Section [8]. The SPH redevelopment programme and development of mental health Community Hubs enables an overarching transformation of the estate to enable effective delivery of the Trust s Clinical Strategy along with national and local health strategies through the development of a range of health services and research facilities. It puts service users at the centre, recognising there is a once in a lifetime opportunity to transform services across the London Boroughs of Camden and Islington, building more visible, more accessible and more integrated services for people locally alongside world class research driving the very best practice. The opportunity is time limited because of the Certificate of Immunity from Listing ( COIL ) that is set out in more detail in Section [4.1.3]. The SPH redevelopment programme is an opportunity to reshape the services themselves delivering high class local, integrated care, meet leading 21 st century standards in facilities and develop a world class research institute. As part of this transformation, the Trust will: Build the community hubs, as part of the wider SPH transformation programme, where people can access local integrated health and social care; Deliver innovative wellbeing and recovery services, with improved visibility with the local population, colleges, universities, and employers; and Create an attractive setting that combines physical and mental health provision alongside a vibrant new development of residential, restaurant and leisure uses. The SPH and Community Hubs programme will deliver: 1) Community hubs that support integrated care The vision for the community hubs is that service users and carers will have a familiar, nonstigmatising, easily accessible place where they can access a variety of services that promote holistic care. There is a programme of transformation for mental health services based around these fundamental elements: Supporting people with mental ill health to live well, enabling them to receive care in the least restrictive setting for their needs; Raise mental health awareness to reduce stigma, ensuring that mental health is considered equally with physical health; Reduce reliance on inpatient care and expand community provision to support more people to spend more time at home, rather than in hospital; 144 of 402
145 21 Ensuring more accessible and extensive mental health support is delivered locally within primary care and other community services. Community services are being developed to make sure that health and care will be available closer to home for all, ensuring that people receive care in the best possible setting at a local level and with local accountability. At the heart of the care closer to home model is a placebased population health system of care delivery which draws together social, community, primary and specialist services underpinned by a systematic focus on prevention and supported self-care, with the aim of reducing unplanned hospital admissions. The plan is to develop community hubs as follows: A 4 storey community hub at the Trust s existing site in Greenland Road, in the London Borough of Camden; and A 4 storey community hub at the Trust s existing site at Lowther Road in the London Borough of Islington, replacing the existing building. What this means for residents is that some services will move from their current locations the final details for some of these services are yet to be fully determined. However, the local health organisations are confident that by co-locating clinical teams, giving access to joinedup care will have significant benefits for residents. 2) The SPH Site The St Pancras Hospital site will be redeveloped to provide a total of 2,187m 2 of accommodation for the Trust including, out of a total current Trust occupied area of 12,117m 2 : New community facilities that will include consulting rooms, meeting rooms, training facilities and the Recovery College. The Recovery College includes space for both clinical delivery and support facilities for the clinical teams; In addition, a new Institute of Mental Health ( IoMH ) in partnership with University College London will provide an opportunity to improve mental health outcomes over the long term; and New facilities for the other NHS services. 3) High quality inpatient facilities A new build inpatient facility located at Whittington Hospital ( the Whittington ). The inpatient facility will be a three storey new build surrounded by landscaped gardens with car parking available at our neighbouring Highgate Mental Health Centre ( HMHC ); The new facility will have 84 single bed rooms, supported by 606 m of support space, an 2 external courtyard or garden space and consulting rooms for each ward; The new facility will be fully accessible, and present an attractive, therapeutic and welcoming environment for staff and service users; and The facility will be designed to be future proof allowing reconfiguration in use as requirements change over the next decades. 2.7 PCBC structure This PCBC was developed in line with the NHSE guidance Planning, assuring and delivering service change for patients published on 1 November 2015 and the update in 145 of 402
146 22 March 2018, and HM Treasury Green Book guidance in relation to the capital investment decisions involved to support that service change. It includes the following sections: Executive summary: Summarises the key findings from the PCBC. Introduction (this section): Provides an overview of the project s objectives, background, scope, parties involved in the production and the proposal. Context: This section sets the background of the parties involved, the current healthcare challenges faced by the commissioners and providers, and the commissioning arrangements between the CCGs and Trust. Case for change: This section details the rationale and key drivers for changing the way services are delivered including from a national and local strategic context. Care model: This section sets out the model of care and details how the model of care is changing and the proposal facilitates delivery of this. It highlights the expected benefits and also how the model meets the needs identified in the Case for Change section. Governance: This section documents the governance structure that has been put in place to ensure the consultation process is robust, accommodates relevant stakeholder views and who is responsible for making decisions and who is responsible for approvals. Stakeholder engagement: This section sets out the engagement undertaken to date, how this has informed the consultation proposed and how the consultation will be run. Options for consultation: This section documents the process for options generation and evaluation. Finance case: This section sets out the financial impact of the selected option on the CCGs, Trust and any other relevant parties. Implementation: This section sets out the practice steps needed to deliver the option identified in the Options for consultation, including project team, governance, risk management and timelines. The SoS s Four Tests: This section sets out how the consultation process has met the Secretary of State s four tests and NHSE s other tests. Decision making and next steps: This section identifies next steps for the consultation process and wider development programme. 146 of 402
147 23 3 Context 3.1 The Population and Healthcare challenges The healthcare challenges set out below are in line with those presented in each of the borough s Joint Strategic Needs Assessments (JSNAs) and latest published Annual Report and Accounts Health and well-being challenges in the borough of Islington Islington borough is London s fifth most deprived borough and the fourteenth most deprived in England, which contributes to poor health and wellbeing outcomes. The borough is one of London s most mobile populations with approximately 20% of residents entering and leaving the borough each year. This results with challenges in identifying health issues and monitoring improvement in health outcomes. At least 44,000 registered service users have one long term condition such as diabetes. It is also assumed that many more long term conditions may be undiagnosed. Islington has the highest prevalence of psychotic disorders in England, nearly double the national average. In addition, 10% of registered service users has a diagnosis of depression which is amongst the highest in London. It is estimated that about 31,000 people in Islington suffer with depression or anxiety. The suicide rate has been reducing since 2001 and in it was below the national average and slightly above the London average. The relatively younger population explains a lower prevalence of dementia. Islington is the 14th most deprived Local Authority in England. The borough has a few small pockets of higher financial capability, with the rest of the population having low financial capability Health and well-being challenges in the borough of Camden Camden is ranked the 15 th most deprived borough in London (out of 33). Within Camden there are areas that are within the 10% most deprived areas in England. Poverty is a key determinant of poor outcomes in health and wellbeing and higher levels of deprivation are linked to numerous health problems such as chronic illness. Camden has the third highest diagnosed prevalence of serious mental illness in the country and the 8 th highest diagnosed prevalence of depression in London. One in seven GP registered adults in Camden have been diagnosed with one or more mental health conditions. Camden experience a higher rate of alcohol specific hospital admissions than England and London. Three quarters of the adult population in Camden drink alcohol and of those who drink an estimated 34% drink at levels that cause risk of harm to physical and mental health. Life expectancy in the borough of Camden is higher than the average life expectancy in London and England. While the life expectancy is higher, on average the last 20 years of 147 of 402
148 24 their life is spent in poor health. There is also a stark difference in the life expectancy between the most and least deprived boroughs. The JSNA s published in October 2016 estimate that the population is due to rise by 9% over 10 years. Although older people make up a relatively small proportion of Camden s population (approximately 11.5% are aged 65 and over), the highest percentage growth (41%) in the 10 years commencing 2016 will be seen in those aged 75 years and older, resulting with exacerbation of health challenges Background to the Trust and CCGs The services provided by the Trust are primarily commissioned by Islington CCG in their role as lead commissioner for mental health services, with Camden CCG as a significant Associate commissioner to the Islington CCG contract. This account for 98% of services commissioned. As such, the Chief Accountable Officer for both organisations will be the decision maker for this proposal; this position is held by the same person across both organisations Islington NHS CCG Islington CCG is the lead commissioner for mental health services provided by the Trust, accounting for 98% of services commissioned. Islington CCG has 33 member GP practices, serving a population of nearly 250,000. The CCG spent a total of million in 2016/17 and achieved an in year surplus of 9.7 million 2. The majority of the CCG s services are provided by local NHS organisations such as Whittington Health, Moorfields NHS Foundation Trust, Camden and Islington NHS Foundation Trust, University College London Hospital NHS Foundation Trust and Royal Free London NHS Foundation Trust. Services are also commissioned from not-for-profit organisations based in the local community and other providers. As part of taking forward the Haringey and Islington Wellbeing Partnership, the executive management team of the CCG operates jointly with neighboring Haringey CCG. The two CCGs are led by a single Chief Operating Officer. Islington CCG received a Good rating at the 2016/17 annual assessment Camden NHS CCG Camden CCG is a significant Associate to the Islington CCG contract. Camden CCG has 35 member GP practices and serves a slightly smaller population than Islington of 280,000 residents. The CCG spent million in 2016/17 and achieved an inyear surplus of 476k 3. Similarly for Camden CCG, the majority of services commissioned are provided by local NHS organisations, including Camden and Islington NHS Foundation Trust, University College London Hospital NHS Foundation Trust and Royal Free London NHS Foundation Trust, Whittington Health and Moorfields NHS Foundation Trust. Camden CCG also 1 Camden JSNA 2015/16 (October 2016) 2 Islington CCG Annual Report and Accounts 2016/17 3 Camden CCG Annual Report and Accounts 2016/ of 402
149 5 commissions services from not-for-profit organisations based in the local community and other providers Background to the Trust The Trust provides mental health services for people with psychoses, complex psychological conditions such as personality disorders, substance misuse, acute and crisis care, common mental health disorders and dementia care. In addition, the Trust has a number of specialist programmes such as mental health care for veterans living in London which is commissioned by NHSE, this will not form part of this consultation as these services are not moving, as set out in Section [2.4]. The Trust is the main provider of mental health services for people living in Camden and Islington and also provides statutory social work and social care services on behalf of the London Boroughs of Islington and Camden. Services are provided for adults of working age, adults with learning difficulties and older people in the London area, either in a community or inpatient setting. The Trust has approximately 1,700 staff and provides services to approximately 30,000 people per year. This includes a significant minority of people who are not local residents, but are temporarily based here, such as students, asylum seekers and visitors to the capital. Services at the Trust are managed in the following five operational divisions: Acute and Crisis Care (Urgent care); Recovery and Rehabilitation (Psychosis); Services for Ageing and Mental Health (Older people and Dementia); Substance Misuse Services (Alcohol and drugs); Community Mental Health (Complex psychological and common mental health conditions). The Trust does not provide child and adolescent mental health services (which is provided by the Tavistock and Portman in Camden and Whittington Health in Islington) and has relatively few specialist services. The Trust is a member of University College London Partners ( UCLP ), one of the world s leading academic health science partnerships, and has a strong reputation for supporting world-class quality research in to mental health. The Trust has around 30 sites across Camden and Islington, as follows: Inpatient beds are accommodated at two significant hospital sites in Camden (SPH and HMHC) providing 235 beds; Community beds (residential) are provided across several sites, accommodating 78 beds; Community clinical services are delivered from a number of buildings, spread across Camden and Islington. The Trust s Head Office is located at SPH, located within Camden. This occupies the former St Pancras Workhouse and Infirmary and comprises 17 separate buildings and structures. The site is located north of Kings Cross and St Pancras Station and west of the mainline railway tracks. The Grand Union Canal is located just to the north and east of the site. St 149 of 402
150 26 Pancras Gardens forms the southern boundary to the site. In addition, the South Wing of the hospital is located just to the south fronting onto St Pancras Way. Adjacent developments around Kings Cross and St Pancras have transformed the area and attracted significant inward investment. A number of large-scale housing developments, a feature of the regeneration of the area, overlook the site which is not seen as conductive to mental health recovery. The proposal is in line with the Trust s clinical strategy, which highlights some particular demands on the estates of the Trust. The focus of the Trust s Clinical Strategy is to promote recovery, resilience and independence via easy to access community-based services and specialist care-pathways. This is based on: Expanding capacity by integrating more staff into primary care and community settings; Integrating physical and mental health; Reducing the physical and psychological barriers to entry (through more local provision, better access for those with disabilities and more generally through greater awareness in the community); Improving lives and wellbeing through wider integration of social and mental health support. The Clinical Strategy is consistent with national policy and the North Central London ( NCL ) Sustainability and Transformation Plan ( STP ), which aims to increase early intervention and support through primary care, join up social care and health services and ensure mental health has parity with physical health. This is outlined in further detail in the regional policy case for change in Section [4] below. 150 of 402
151 27 4 Case for Change There are five categories of drivers for change to the current service delivery: The local policy framework drivers for change delivering on the objectives set out in the Trust s clinical and estates strategies by providing more care in the community, developing research capabilities and leading on equality and diversity; The national policy framework drivers for change focusing on prevention, achieving parity for mental health and physical health care provision and integration of physical and mental care; The regional policy drivers for changes implementing the NCL STP plan; The poor quality of existing estate at SPH; and The limitations on the current service provision at SPH; 4.1 Local Policy Framework The Trust s Clinical Strategy This proposal is in line with the Trust s clinical strategy, which highlights some particular demands on the estates of the Trust. The Trust s Clinical Strategy represents a vision for the transformation of mental health and substance misuse services. It is aimed at addressing the challenges for mental health services of: Increasing demand; Historic underfunding in comparison with physical health services; Difficulties with accessing timely interventions due to stigma; and Poor awareness and services often not being joined up or accessible particularly for vulnerable communities. The strategic priorities of the Trust are: Early and effective intervention; Helping people to live well; and Research and innovation. It focuses on increasing services based in primary care and the community, improving access to services and integrating physical and mental health. The Clinical Strategy recognises that health and wellbeing are shaped by individual characteristics, lifestyle choices and environmental influences. So instead of attempting to fix people and their problems, or do things to them rather than with them, recovery-orientated services look at individual needs and help people reach their potential. The Trust aims to provide services that are accessible, person-centred and responsive to the often complex needs of individuals. It is also recognised that the main determinants of health are socio-economic. In order to promote good health, prevent ill health and reduce inequalities in health, the Clinical 151 of 402
152 28 Strategy promotes ongoing joint working with our partner organisations to act on the social determinants that are likely to impair people s health. A key component of the Clinical Strategy is the development of Practice Based Mental Health. Practice-based teams work locally with GPs and other services in primary care. Offering rapid assessments near to where people live, by senior clinicians who can make decisions about treatments, access services in the community or, if needed, refer to our specialist care-pathways. They will link people into the local community resources and services as they are better placed to see people who won t engage with secondary care mental health services. They will support GPs in managing people with chronic mental illnesses who are stable. Along with acute services, the practice-based teams are the entry point into our specialist care-pathways. Development of specialist care-pathways that deliver treatment and support to people with similar needs due to mental illness is another priority. The focus of these services is to help people achieve their recovery goals and link into their local social networks and community resources. Access to these pathways is based on risk, intensity and the need for specialist treatment. The Trust has won awards for the development of an Integrated Practice Unit for people with psychosis, which brings together partner organisations to improve the physical health of those with psychosis. This is done with an aim to close the health inequality and lost years of life for people with this condition experience. Bringing together all the providers who deliver care to people with psychosis and coordinate their treatment and support will deliver a better quality service and better outcomes, especially physical health outcomes. Through community teams, and work with partners the Clinical Strategy sets out the vision to offer high quality and comprehensive care and treatment. This is to ensure that service users have access to high quality supported housing and are helped where necessary into education and employment, and to develop social networks. Community services and support help people to continue their recovery and maintain their independence locally, and help reduce the length of time people need to spend in hospital, when they are very unwell, to a minimum. The Trust is committed to offering world class, safe inpatient services in therapeutic environments. The focus of the Trust s Clinical Strategy is to promote recovery, resilience and independence via easy to access community-based services and specialist care-pathways. It is clear that in order to meet this clinical vision, the Trust needs an estate that enables Practice Based Mental Health to work locally and effectively with GPs and other services in primary care. It also needs an estate that allows the early successes of Integrated Practice Units to expand and bring physical health and mental health services together to meet health in-equalities. The development of Community Hubs, rather than multiple sites for small teams, allows a bringing together of services and providers to enable the coordination of treatment to deliver care closer to people s homes, a better quality service and better outcomes. Finally, the Trust needs an estate that can provide a safe and therapeutic environment to those requiring inpatient care. 152 of 402
153 29 The Clinical Strategy was approved and adopted by the Trust Board in November The Clinical Strategy Programme Board was set up to oversee and monitor the delivery of the Clinical Strategy. The Clinical Strategy is in line with the NCL STP, which aims to increase early intervention and support through primary care, joined up social care and health services and ensure mental health has parity with physical health The Trust s Estate Strategy The overarching aims of the Estate Strategy are to: Provide modern, therapeutic mental health facilities across Camden and Islington; Move more of our services into the community; Build high quality, up-to-date, warm and welcoming inpatient facilities; and Create world-class research facilities to help us deliver the very best care. The Estates Strategy sets out the Trust s vision for an overarching transformation of the estate to enable effective delivery of national and local health strategies. It covers the period 2017 to 2022 and it is based on the Trust s assessment of the present estate to establish the scale of investment required to achieve the desired transformation. It has been developed in consultation with Trust Clinicians and the Estates Team, and was approved by the Board in April In summary, the Estates strategy: Highlights the significant shortcomings of the present Trust estate and the need for wholesale estate change to meet service transformation; Sets out an estate transformation strategy for the next five years that enables the intentions of the Trust s Clinical Strategy to be delivered; Illustrates the opportunity that exists through a comprehensive approach to the St Pancras site and wider estate to enable the creation of community hubs (buildings that bring together a range of services for mental and physical health and social care) in local settings across both boroughs, supporting the local CCGs and Local Authorities strategies for locally based services in defined geographical patches; Creating centralised high quality clinical, education and research, facilities, integrated primary care and the development of key worker and social housing for staff and local communities; Improving access for all to services both through the location of services and by addressing EA10 compliance both of which are currently difficult to achieve within the existing estate; and Improving the efficiency and environmental impact of buildings alongside critically ensuring we create environments that are therapeutic supporting people s wellbeing and recovery. The Trust s vision is: 153 of 402
154 30 Our vision is to provide a fit for purpose, therapeutic, cost-effective, integrated and accessible estate which enables the delivery of high quality health and social care services for our local population Equality and Diversity Policy The Trust s Equality and Diversity Policy sets out how the Trust will demonstrate that it is planning and delivering services in a fair and equitable manner to all sections of the community, free from discrimination, and with dignity and respect. Tackling health inequalities and social exclusion is an important priority for the Trust and it is committed to taking positive steps to ensure fair and equitable access to services for all. As a major provider of services, the Trust recognises the need to be pro-active so that it can meet the changing needs of diverse communities, and provide fair access for all in an environment where dignity, equality, diversity and human rights are respected and promoted. In this respect, the proposed redevelopment will provide fit for purpose, accessible facilities and support improved access to services for all users Global Leader in research The SPH site has a strategic importance due to its proximity to Kings Cross Station, Euston Station and St Pancras Station representing a major national and international transport hub. There is also a Health and Life Sciences Cluster around Euston and Kings Cross that already includes The Trust, UCL, University College London Hospital NHS FT, the Francis Crick Institute, the Wellcome Trust and the London BioScience Innovation Centre. The Trust already has one of the strongest records and reputations in UK mental health research. That is why the vision for the SPH site includes the establishment of an IoMH in partnership with UCL who have the highest number of mental health academic citations in the UK so that the Trust can build on this strength and be a world leader. For every 1 invested in mental health research, economic benefits are estimated to be 37p 4 per year in perpetuity, so this is an initiative that supports not only better care for service users but also the Mental Health Taskforce 5YFW (2016) objectives and broader economic sustainability. 4.2 National Policy Framework Figure [4.1] summarises a number of relevant national policies and guidelines for mental health and also for healthcare more broadly. These policies and guidelines have guided and informed the proposal in a number of ways; Services should be delivered to a local population footprint, rather than an organisational footprint; Access to mental health must be improved to meet the rising demand for services; Mental health must have parity of esteem to physical health to improve outcomes; 4 Health Economics Research Group, Office of Health Economics, RAND Europe. Medical Research: What s it worth? Estimating the economic benefits from medical research in the UK. London: UK Evaluation Forum; of 402
155 31 The barriers between primary and secondary care must be reduced to improve outcomes and reduce costs; Services should be delivered as close to user s homes as possible and supporting primary care; The NHS Estate Policy highlights the importance of the estate as an enabler to these changes. Figure [4.1]: Key National Policy Frameworks 5 Year Forward view and New Models of Care Improving mental health provision is a central theme in NHS England s 2014 Five Year Forward View ( 5YFV ) alongside mental health specific policies, such as the Mental Health Growth Strategy and the NHS Mental Health Policy, which sets out the need for change in how the NHS delivers services in the future. The strategy includes a focus on prevention, allowing people more control over their care, better use of technology and so-called triple integration: between primary and secondary care, between mental health and physical health and between health and social care. The 5YFV suggests that mental health outcomes can improve by better prevention, increasing early access to effective treatments and crisis care and integrating care to reduce mortality. It challenges the NHS to develop new models of care to better provide for the needs of people and the increasing demand on health services. North London Partners in Health and Care (NLP) has produced a five year Sustainability and Transformation Plan (STP) which drives the implementation of the 5YFV. This focuses on planning by place for local populations rather than individual organisations. Incorporating the STP plans, the Trust has developed an ambitious, innovative and robust Clinical Strategy in line with the 5YFV, evidencing the Trust s willingness to adopt new models of care to transform outcomes. This includes using Practice-Based Mental Health Teams to provide mental health services from local GP Surgeries; allowing service users to be seen directly in Primary Care and facilitating early diagnosis and intervention. Having Multidisciplinary Teams removes organisational and specialty barriers between primary and secondary care and also any perceived divisions between mental and physical health. The Trust have developed an ambitious, innovative and robust Clinical Strategy in line with these principles from the 5YFV, evidencing the Trust s willingness to adopt new models of care to transform outcomes. This not only aligns local planning to national policy, but supports mental health specific guidance around increasing access to services by reducing stigma, putting mental health within reach of local communities and allowing access through primary care. This is often 155 of 402
156 32 5YFV for Mental Health NHS Mental Health Policy referred to as getting parity for mental health services and is important to this case for change, as that is precisely what the SPH redevelopment facilitates. In January 2016 the UK Prime Minister announced proposals to increase spending on mental health by 1bn. This was followed by the publication of the Five Year Forward View for Mental Health in February 2016 from an independent national taskforce. Relevant areas of growth for the Trust include: Access New access targets to reduce waiting lists and address the pressures between demand and current capacity. This has been announced in Early Intervention in psychosis and will extend into other areas. Integration of physical health and mental health Services which support integration with physical health care and acute Trust efficiencies such as comprehensive liaison services, specifically in A&E, but also including areas such as support to people with dementia to reduce Average Length of Stay (ALoS). The Trust already provides services in these areas, and has evaluated pilot projects to expand them in new models of delivery. It is therefore expected that the Trust will be successful in extending its services in this area in the next few years and this has formed part of the service reconfiguration plans. The government plans to continue to prioritise improvements to mental health services, building on the policy priorities of the last coalition government. This was further reinforced by the Prime Minister s statement on 9 January The government wants public services to reflect the importance of mental health in their planning, putting it on a par with physical health. This is often referred to as getting parity for mental health services and is important to this case for change as that is precisely what the SPH redevelopment will allow, particularly in enabling better access to mental health services. The key priorities that are relevant to this PCBC are: Enabling better access to mental health services and shorter waiting times a priority for NHS England; Making reducing mental health problems a priority for Public Health England, the new national public health service; Making mental health part of the new national measure of wellbeing, so it is more likely to be taken into account when government creates policy; Providing 400m between 2011 and 2015 to give more people access to psychological therapies - including adults with depression, and children and young people; and 156 of 402
157 33 Providing up to 16m of funding over four years for Time to Change, the campaign against mental health stigma and discrimination. Other policies and frameworks that would affect the strategic decision making of the Trust are: The current national strategy for mental health in England: No Health without Mental Health. A new national strategy up to 2020 for mental health in England is currently being developed by the Crisis Care Concordat, which the Trust signed up to in 2014 together with many of its partners in the two boroughs (Camden and Islington). The CQC 2015 Report Right Here Right Now. Recent reports such as Transforming Care (2012) and the Confidential Inquiry into the Premature Deaths of People with Learning Disabilities (2013). The Care Act Guidance from The Department of Health states the environment provided by acute mental health services is a crucial element in the delivery of positive therapeutic outcomes for service users, their safety and the safety of staff and the wider community. The environment in which care is delivered is a dynamic of the care itself and plays a crucial role in supporting the delivery of higher-quality and more cost-effective care. In particular for mental health facilities, a superior and sympathetically designed therapeutic environment has the power to alleviate stress and provide comfort to peoples at times of acute distress and vulnerability. By continuing to deliver services in sub-par facilities, the Trust is failing to deliver an optimal service and the projected improvements to quality as laid out in the STP are unlikely to be achieved. By moving a number of services currently provided at the SPH site to facilities in the community, the Trust will be able to increase access and provision to the local population. The associated reduction in cost of delivering services in the community also supports this strategy, allowing the CCGs to deliver better value services. NHS Estates Policy The Trust is required to reach an agreement on an outcome that works in the interests of all interested providers, commissioners (local CCGs and NHSE) and regulators (NHS Improvement). As above, the Trust has already started this process through its bilateral agreements as described in Section [4.5]. 157 of 402
158 Regional Policy Framework NCL STP (January 2017) background The Camden and Islington CCGs are part of the grouping of commissioners and providers in the North Central London region, which incorporates Barnet, Enfield, Haringey, Camden and Islington health, social care and public health commissioners, as well as all NHS Providers in the sub-region. This group is now referred to as North London Partners in Health and Care (NLP). North London Partners in Health and Care has worked together to develop an North Central London (NCL) wide STP which sets out how local health and care services will transform and over the next five years, build and strengthen local relationships and ultimately deliver the Five Year Forward View vision. The STP Vision is as follows: Our vision is for North Central London to be a place with the best possible health and wellbeing, where no-one gets left behind A set of core principles to support delivery of the vision has been developed, along four themes. 1. Prevention: increased efforts on prevention and early intervention to improve health and wellbeing outcomes for the whole population, to reduce health inequalities, and help prevent demand for more expensive health and care services in the longer term. 2. Service transformation: service transformation to meet the changing needs of the population and bring care into the community, closer to home. This includes taking a population health approach by strengthening the offering in the community by closely integrating with primary care. 3. Productivity: identifying areas to drive down unit costs, remove unnecessary costs and achieve efficiencies to ensure sustainability. For providers, this includes implementing recommendations from the Carter Review and working together across organisations to identify opportunities to deliver better productivity at scale. 4. Enablers: a focus on delivering capacity in key areas that will support the delivery of transformed care across NLP. This includes digital, workforce, estates, and new commissioning and delivery models NCL STP: Plan for Mental Health The STP proposes a stepped model of care supporting people with mental ill health to live well, enabling them to receive care in the least restrictive setting for their needs. The aim is to reduce demand on the acute sector and mitigate the need for additional mental health inpatient beds. 158 of 402

159 35 Figure [4.2]: Stepped Model of Care for Mental Health, NCL STP Initiatives include: Improving community resilience through specific initiatives supported by NHSE, such as helping service users get back into work, which have been shown to reduce cost and activity; Increasing access to primary care mental health services: ensuring more accessible mental health support is delivered locally within primary care services; Improving the acute mental health pathway: developing alternatives to admission by strengthening crisis and home treatment teams; Developing a Woman s Psychiatric Intensive Care Unit ( PICU ): ensure local provision of inpatient services to female service users requiring psychiatric intensive care, where currently there is none; Investing in mental health liaison services: scaling up 24/7 all-age comprehensive liaison to more wards and Emergency Departments; Investing in a dementia friendly NCL: looking at prevention and early intervention, supporting people to remain at home longer and supporting carers to ensure that we meet national standards around dementia. In addition to the alignment with the STP plan indicated in Section [4.1], the reconfiguration of services directly addresses the building of community resilience, improving access to primary care mental health services and the development of a women s PICU. The subsequent section set out the current model of care at the Trust and its relation to the STP model of care in more detail. 159 of 402
160 Progress on STP mental health initiatives in Camden and Islington There has been significant progress made in Camden and Islington since the STP was written with the boroughs on track to deliver the STP mental health vision. The mental health STP was driven by care models to improve patient outcomes, care and treat people in the least restrictive environment, thus mitigating the need to expand the in-patient facilities Improving community resilience Camden and Islington have implemented new employment schemes based on Integrated Personal Support which is an evidence based type of employment support to help those with mental health conditions back into work. These initiatives are specifically supported by NHS England and have been shown to reduce activity, and also cost to, health services as people gain employment. Mental Health First aid is also widely rolled out to Camden and Islington Council and voluntary sector services. This initiative is aimed at non-specialist front line services helping them identify mental health concerns and support people to access mental health services. Similarly suicide prevention training is also being commissioned to support early identification and intervention with people who may be at risk of suicide but not in contact with mental health services Increasing access to primary care mental health services The rollout and increased access to Practice Based Mental Health ( PBMH ) has been mentioned as a part of the health organisation s vision and transformation strategy specifically ensuring more accessible and extensive mental health support is delivered locally within primary care services. This will help the population get local care with local accountability that is integrated with social, community and specialist services underpinned by a systematic focus on prevention and supported self-care, with the aim of reducing unplanned hospital admissions. In addition Camden and Islington CCG are on target to increase access to IAPT services to 25% by Islington CCG has also invested in integrated IAPT which specifically targets people with long-term physical health conditions who may otherwise not recognise and come forward for help with depression and anxiety associated with their conditions, but which nevertheless make their condition more difficult to live with. Initially this is targeted at those with diabetes and chronic pulmonary respiratory disorder Improving the acute mental health pathway Camden and Islington both have Crisis Home Recovery Teams that can respond to individuals in the community who feel in crisis and without immediate support would need to attend an Emergency Department. All acute admissions for mental health are agreed by the Crisis Team to ensure that no one who could be supported at home or in a Crisis House is admitted. There is also a 24-hour crisis line that the public and professionals can call to get 160 of 402
161 37 advice and support over the phone. Camden and Islington residents can also access Crisis Houses across the boroughs to help avoid inpatient admissions where possible. These teams will be reviewed in 18/19 to ensure that they are being efficiently used and working to ensure that they are working to fully support people in the community, able to respond in a timely way, working closely with voluntary sector and social care; in order to support people s needs in the least restrictive setting. Islington and Camden CCGs are early implementers of the Serenity Integrated Mentoring ( SIM ) programme, which brings together police and care co-ordinators around a specific cohort of patients who are repeatedly admitted to Health Based Paces of Safety under S136 of the Mental Health Act. In pilots elsewhere, this has resulted in a 50% decline in attendance at Health Based Places of Safety and impacted on subsequent admissions Developing a Woman s Psychiatric Intensive Care Unit ( PICU ) In November 2017 the Trust launched an 11 bed Women s PICU, which is a shared resource for North London Partners; however the majority of admissions will be from Camden and Islington due to the higher acuity of need in these boroughs. The service is already demonstrating significant improvement to patient care, not only are patients now able to be provided with services in the NHS and within their local area enabling visits from relatives and better joined up care, but length of stay has also reduced to an average of 27 days from previous average in the private sector of 45 days. It is too early to say but it is hoped that this locally provided more joined up care, as well as reduced length of stay on the PICU, will impact on the overall length of stay in in-patient care for these women Investing in mental health liaison services The Trust provides mental health liaison services in UCLH, Royal Free London and Whittington Hospitals which are the main Emergency Departments attended by Camden and Islington residents. The services there operate 24/7 and provide in-reach to the wards to support training of staff, early discharge and reduced re-admission. The services provided at these hospitals can be described at meeting many of the Core 24 requirements. In addition a new mental health suite is being implemented in Whittington Hospital, which will provide a safe and therapeutic environment for patients who have attended Emergency Departments to be assessed and cared for prior to admission or discharge. It is expected that the mental health suite will provide a calming environment which will support more people to be able to access services at Crisis Houses, or in the community with support from community teams and thereby reduce admissions to acute inpatient mental health settings New model of care for Child and Adolescents Mental Health Services ( CAMHS ) and perinatal services The Trust does not provide CAMHS services and therefore this proposal will not impact on CAMHS services. However in 2016 the Trust launched a new Community Specialist Perinatal Service. This service is a NLP resource and builds upon the small services that 161 of 402
162 38 were already operating in Islington, Camden and Haringey. The new service works across maternity units and peripatetically in the community to support the needs of pregnant women and those with babies under one year old. This multi-disciplinary specialist service ensures that the top 3-5% of women with severe mental health needs are provided with specialist care and support, to better anticipate potential decompensation of mental health and to support better treatment in the community Investing in a dementia friendly NCL Islington and Camden achieve high rates of dementia diagnosis for their estimated dementia population; the NHSE target is for two-thirds of those estimated to have dementia to have received a diagnosis. As of March 2017 Camden s diagnosis rate was 75.4% and Islington s 96.8%. This means that people in Camden and Islington can access support and services early in their diagnosis thus reducing crisis and inpatient care and supporting more people in their homes. The mental health for older people pathway will also be reviewed in 18/19 to ensure that services are best supporting people s needs The Health Estate as an Enabler The STP states that: An important enabler of a number the initiatives is the redevelopment of both the Barnet, Enfield and Haringey Mental Health Trust St Ann s site and the Camden and Islington Foundation Trust St Pancras site. Furthermore, the STP confirms that the proposed developments at the St Ann s and St Pancras sites would: Transform the current inadequate acute mental health inpatient environments on both sites; Provide more therapeutic and recovery-focused surroundings for service users and staff; Improve clinical efficiency and greater integration of physical and mental health care; Release estate across the Trusts, to enable development of community-based integrated physical and mental health facilities; Develop world class research facilities for mental health and ophthalmology enabling practice to reflect the best evidence; and Provide land for both private and affordable housing, as well as supported housing for service users and housing for key workers. At a local level there is also alignment towards the health estate as an enabler for broader transformation. Both Islington CCG and Camden CCG, have overarching visions to improve access to appropriate and effective mental health services and to ensure services are integrated to enable a much more seamless experience for service users. This vision will be enabled through the provision of fit for purpose, cost-effective, integrated, accessible estate which enables the delivery of high quality services. This is covered in more detail in Section [4.5]. 162 of 402
163 Links to Joint Strategic Needs Assessments ( JSNA ) The current JSNAs for Camden and Islington produced by the respective Health and Wellbeing Boards with input from the local authorities, CCGs and other public sector parties further outline the requirements for a sustainable and high quality mental health service in the area. Both Camden and Islington have significantly higher rates of mental health diagnosis than other London Boroughs, with Islington holding the highest percentage of psychotic disorder diagnoses and Camden 3 rd on that list. This has significant impacts for the overall health and wellbeing of residents across the boroughs; the Camden JSNA (2016) reveals that of those receiving incapacity benefits in Camden, mental ill health and behavioural disorders accounts for the largest proportion of claims. Consequently, the proposals to dramatically improve the quality of services to promote recovery and outcomes alongside improved access for users in the community are essential to meeting local needs. a service model that systematically promotes integration of physical and mental health across primary and secondary care services and including self-management is required. Additionally, as articulated in the extract above from the Camden JSNA (2016) and, as stated in the most recent Islington JSNA (2016) the strong link between mental and physical health warrants a more joined up model of care that addresses mental and physical health together; providing further support for a model that aligns these services Joint Health and Wellbeing Strategies ( JHWS ) Both the Camden JHWS (2016) and the Islington JHWS (2017) identify mental health as one of their key priorities to improve health and wellbeing in their Borough over the next few years. There are similar strategies proposed in these documents to deliver this goal, such as improving access to community based interventions and improving attitudes towards mental health by developing understanding and reducing stigma. The proposed reconfigurations reflect these broader strategies. 4.4 Quality of Existing Estate CQC reports The Trust delivers the majority of its care to residents in the London Boroughs of Camden and Islington, including from its two acute sites at St Pancras Hospital (SPH) and the HMHC. The sites vary widely in terms of their distribution, age, condition and suitability and these extensive differences were noted in the June 2016 CQC report. The report highlighted that the SPH acute wards and psychiatric intensive care units required significant improvement. Therefore, it is a priority for the Trust to update the facilities within which these services are delivered to enable better outcomes for service users. The latest CQC inspection published in March 2018 it was noted that the Trust had sufficient mitigations in place to address the concerns raised previously. However the overall rating for Safety remained as Required Improvement. Furthermore this most recent report highlights the staffing difficulties facing the St Pancras site, with the vacancy rate of over 20% on all 163 of 402
164 40 wards. This not only increases workload for staff but also increases the reliance on agency and bank staff, which increases the likelihood of protocol not being followed and staff training shortfalls Backlog maintenance As may be expected, there is a considerable amount of backlog maintenance, particularly at SPH, to the value of 10 million. Many of the buildings are inefficient, do not provide a therapeutic inpatient environment, lack modern safety features and make it difficult to bring together a full range of services (physical and mental health, and social care). Beyond the 10 million of backlog maintenance, an estimate of approximately 175 million has been quoted to re-provide services at the St Pancras site that meet modern standards. A significant proportion (c.73%) of the Trust s backlog maintenance requirement relates to the SPH site Time bound opportunity Critically, the opportunity to transform the mental health services in the area through the St Pancras redevelopment is potentially time bound insofar as the Trust were successful in their application for a Certificate of Immunity from Listing (COIL) and this is valid for a 5-year period running to The importance of this to the scheme is that it means that no further buildings on the site can become listed in this period, enabling the Trust to consider alternative uses for the current site Accessibility In addition, whilst SPH does meet the Disability access requirements under Equalities Act 2010 ( EA10) ) compliance, the issues highlighted above, due to the age and consequent design of the estate, leave room for improvement as they do not inherently meet the requirements Patient assessment The 2016 Patient Led Assessment of the Care Environment (PLACE) scores, shown in Figure [4.3], demonstrates the challenges the Trust has on the SPH site. This clearly evidences that SPH needs improvements within the Condition, Appearance and Maintenance section and is a significant outlier on both the Dementia Friendly and Disability Access sections. Figure [4.3]: 2016 PLACE assessment scores for SPH Site Assessed Cleanliness 2016 Food & Hydration (Ward) 2016 Privacy, Dignity & Wellbeing 2016 Condition, Appearance & Maintenance 2016 Dementia Friendly 2016 Disability Access 2016 St Pancras Hospital Average score C&I 99.51% 86.26% 87.28% 91.4% 68.28% 65.57% 99.51% 93.54% 89.43% 96.35% 82.07% 83.87% 164 of 402
165 41 National average 98.1% 89% 84.2% 93.4% 75.3% 78.8% Comparative MH Trusts 99.6% 84.83% 96.24% 97.84%* 94.96% 93.32% *SLAM spent a considerable sum in environmental works prior to the PLACE inspections 4.5 Limitations of Current Service Provision Parity of esteem for mental health Parity of esteem for mental health is widely supported as a concept across the health and social care system, reflecting the fact that mental health can be more debilitating than most physical conditions as well as the enormous social and economic costs of untreated conditions (only 25% of those with depression are diagnosed). Similarly, for inpatients that are admitted to the service at SPH, there is an associated stigmatism with the facility which could be addressed through moving to a new, modern site rather than staying at SPH. By exploring options to deliver inpatient facilities at a site that also has physical health acute wards, there is an opportunity to develop closer collaboration in meeting mental and physical health needs. This supports the wider new Model of Care as set out in Section [5] and STP goals for mental health provision that is integrated and viewed as equal to physical health provisions Integration of care This is a rare opportunity to make a step change in converting that concept into reality for service users in North Central London. The proposal for the development of community hubs brings the potential for significant strategic benefit for the broader health and social care system as this hub will allow service users to have their physical and mental health conditions considered on a single site through cross organisational working. The local health organisations know that those living with psychosis on average die 20 years earlier than average, but often this is due to poor management of preventable physical health and wellbeing such as weight, diabetes and substance abuse. So this will enhance the delivery of whole health and social care system transformation that is already underway. As this way of working is embedded across the community, there may also be opportunities for workforce diversification, allowing staff to work more holistically than ever before with service users. By bringing facilities and workforce together, collaborative working and smoother transitions between services can achieved, which could not be achieved at SPH. For example an inpatient on a mental health ward could be visited on-site by a cardiologist or diabetic nurse without significant travel or time delays. Similarly, an individual receiving treatment on an acute ward may be recommended for swift assessment by a member of the mental health team to best meet their needs. 165 of 402
166 42 5Care model and expected benefit 5.1 Care Model The Trust s Clinical Strategy sets out the clinical model for services provided at the Trust, both currently and in the future. This model has been designed to keep community teams at the heart of service delivery; ensuring care is provided as close to patients homes as possible. This model and its constituent parts are unchanged by the proposed relocations, however its delivery will be greatly enhanced by the improved quality and location of services, as evidenced below. As described in the previous section, the Trust s Care Model forms part of the broader NCL STP stepped model of care for mental health. This overarching model supports the focus of services wrapped around individuals within their communities, with increasing levels of more intensive, specialist care provided according to increasing need. The development of a new inpatient facility 2.5 miles away from the existing site, alongside new community facilities on the existing site and development of two new community hubs, supports the improved delivery of the North Central London STP in a number of ways: Improving facilities Due to current inadequacy of the facilities at the St Pancras site, and the location of some community services at this site, the Trust is unable to sufficiently deliver on a number of aspects of the STP Model. This includes the delivery of high quality specialist services close to home (Step 3) and elements of the more intensive levels that stipulate services should support recovery at home and in the community (Step 4). Furthermore, one of the enablers of the STP is the estates strategy, which lists the redevelopment as key to delivering more therapeutic and recovery focussed surroundings Increasing access to mental health services The STP s focus on delivering more accessible and extensive mental health support within primary care services is aligned to the planned roll out of the practice-based mental health (PBMH) to all practices and increased access to Improved Access to Psychological Services (IAPT) to 25% of the indicated population by All Islington CCG registered patients are now able to access PBMH service. However some patients need to be seen at an alternative venue to their GP practice due to the limitations of this estate. Camden CCG will expand their residents access to PBMH by building on their current Team Around the Practice model from 18/19, which too will add pressure on the primary care estate. Currently there are a high number of secondary care community teams located across multiple sites, which includes some teams based on the St Pancras site. The development of Community Hubs will allow the re-location of some of these services into more accessible local sites for residents, away from hospital and closer to home. It also brings teams from the same Division onto a single site which improves closer working between professionals. Community delivered services are expected to increase in levels of contact time with 166 of 402
167 43 patients as care is re-directed away from inpatient services, this requires a larger community estate to accommodate additional activity. Community Hubs may also be able to bring opportunities for a wider range of in-reach work for physical health services to patients with mental health to help improve accessibility to physical health services Improvements to access within Camden South Camden icope (IAPT) and Assessment and Advice Team moving from St Pancras to Greenland Road; South Camden Recovery Team to move into Greenland Road; Community Recovery Service for Older People to Lowther Road in Islington (most patients are seen at home) Improvements to access within Islington Islington Practice Mental Health Team (where there is no capacity for patients to be seen at their GP practice) to move to Lowther Road; Islington Assertive Outreach Team to move to Lowther Road; Islington North icope Team to move to Lowther Road; Community Recovery Service for Older People to Lowther Road (most patients are seen at home) Moves from St Pancras to sites other than the community hubs Rivers Crisis House is likely to be moved off the St Pancras site, however plans for where this will be located are not finalised; Pharmacy services to move to HMHC to support inpatients at both inpatient sites Improving the acute mental health pathway The proposed relocation and development of Community Hubs does not involve the provision of any extra inpatient beds, which aligns with the STP vision to develop alternatives to hospital admission by strengthening crisis and home treatment teams. As part of the acute pathway improvements, the STP also identifies the investment needed in supported living arrangements, providing users with a supported, and longer term arrangement for effective discharge Patient pathways Practice Based Mental Health Teams PBMH based in primary care is a key component of the NCL STP, the Trust s Clinical Strategy and the CCG commissioning intentions. PBMH was piloted in Barnet and found to reduce the need for referral to specialist care pathways by 60-65%. Subsequently it has been operating across nine of the 34 practices in Islington for two years and has been rolled out to all practices in 17/18, and across Camden from 18/ of 402
168 44 Service users are able to access locality based services, which include consultant psychiatrists, psychologists, social workers and nurses. These services aim to: Increase access to high quality assessment and early intervention; Provide a supporting role to GPs and primary care staff to help manage patients at the primary care level, avoiding deterioration of health and the need to refer to secondary services; and Reduce demands on a range of secondary services including Crisis Teams, secondary care teams, and acute inpatient admissions. Healthy London Partnership has commissioned an economic evaluation of PBMH models used across London. Islington PBMH service will be one of the sites which is expected to deliver its findings in summer of The economic evaluation will look at a range of factors including the impact of the service on secondary care and acute bed utilisation. PBMH also helps to reduce the stigma of accessing services specifically for mental health and they have been found to be effective in managing mental health in Primary Care settings. By continuing to invest in PBMH, more individuals requiring mental health services can be identified and supported early on, thereby reducing the impact of undiagnosed and untreated conditions on long term health and wellbeing. For the majority of service users, PBMH will be the entry point to more specialist support, however other entry points include the Urgent Care/Acute pathway and A&E. PBMH complements IAPT services where people with common mental health services can access care and support without the need to meet secondary care thresholds of care Specialist Care Pathways Service user access to specialist care pathways depends on a number of factors, including; risk level, intensity of interventions required and the need for a specialist treatment only available via these pathways. There are four divisions currently in place focused on particular user cohorts and providing specialised, tailored support depending on user need and these continue to be developed by the Trust. Community Mental Health (CMH) Division; Rehabilitation and Recovery (R&R) Division; Services for Ageing and Mental Health (SAMH) Division; Substance Misuse Service (SMS) Division. In addition to these four divisions, the Trust also provides an Urgent Care/Acute Pathway (Figure [5.1]) that service users may enter if they are experiencing a crisis in their mental health. For some service users this may be their initial entry pathway to services. However service users on this pathway are moved as soon as possible onto less intensive and more tailored pathways. A service user will often move among or between pathways and specialist sub-divisions as part of their therapeutic journey and teams work collaboratively across pathways to ensure users are supported throughout by a team that knows and understands their needs. 168 of 402

169 45 Figure [5.1] The Trust s Clinical Model Following changes to the current care model, the workforce requirement will change in line with the NCL STP; under this proposal this is related to greater expansion of community staff. The NCL STP Mental Health Workforce programme recognises that all NCL mental health providers will face the following key issues: Care closer to Home: to provide more care from integrated primary and community settings; and Workforce: to ensure the workforce can meet the above expectations. The aims of the programme are: Portability to enable staff to work across traditional boundaries (organisational and health and care settings); Improving staff experience of providing care; and To provide analytical support in designing the workforce elements across workstreams to address the key issues above, including providing an understanding of the impacts and benefits of introducing new roles and ways of working; 169 of 402
170 46 To provide a common approach to recruitment across the 10 NHS Trusts in NLP which will cover common recruitment policy and processes that will support collaborative recruitment and retention initiatives for provider trusts; and Enable portability of staff between providers and into primary and community care settings. To deliver these aims and address the issues, the NCL STP proposes a range of measures which will impact the workforce considered as a part of this proposal: Recruitment initiatives General STP workforce recruitment initiatives are: The CapitalNurse (CN) programme is trialling a joint approach across NCL and NEL by giving an employment guarantee to all locally educated student nurses in September This will provide a core offer to all students including access to a CN branded preceptor ship programme. The NLP are keen to understand whether this approach would be of value to other staff groups. There will be a joint approach and a common policy to facilitate collaboration in NCL to training Nursing Associates, and using apprenticeships to grow the workforce. NCL has led the way in identifying overseas educated nurses who do not have a UK registration but are working in support roles in the NHS and social care in NCL. Whilst the new funding arrangements at HEE mean that the funding approach will change this is a great route to identifying more new nurses. The development of a shared staff bank in NCL. Some mental health specific initiatives that are directly applicable to the Trust are: International nurse recruitment from the Philippines. Participating in local, London-wide and national careers fairs as well as engaging with local schools. Streamlined recruitment process has improved time to hire and had a positive impact on our vacancy rate. Retention initiatives: A Retention Study is being conducted across the STP by IPSOS Mori, with the results available in May Once the retention issues have been identified initiatives can be designed and delivered to tackle those problems. Reviewing flexible working and flexible retirement options and introducing new package of non-pay benefits for staff. Buddy scheme for new starters. Current action planning to address issues identified in staff survey. Over 30 Quality Improvement projects focussing on staff wellbeing, reducing violence and aggression in wards, improving patient experience. Identifying training needs across NCL in order to inform a programme of joint training that can be utilised across the STP. This has recently been done with Dialectical Behaviour Training running across NCL. Training to be provided for adult MH colleagues in CAMHS and vice versa in order to enhance skills and enable a more joined up workforce across the sectors. 170 of 402
171 47 Development and use of new roles: Piloted nursing associates in 2017/18 and seeking to expand cohort in 18/19. Working with Skills for Health to identify new roles/existing roles suitable to be adapted to our workforce and activities (e.g. advanced practitioner) Working in partnership with Inclusion Barnet to identify roles, which benefit from being held by people with lived experience of mental health issues. This follows a two year experience of employing community engagement workers who all have lived experience. The development of Children and Young People crisis services that will work across NCL a children and young people s Out of Hours crisis team and bid to develop a new Health Based Place of Safety at HMHC will create new roles and posts. The potential devolution of Tier 4 CAMHS and the development of the acute care pathway across NCL will result in further enhancement of the workforce and create new roles by 2020/21. Expansion of IAPT services is seeing a growing workforce that requires better career development and support. Up-skilling current staff: Recruited Physical Health Leads to improve skills of our mental health workforce. Apprenticeship programme to enhance technical and management skills of staff. Nursing associate and nurse degree apprenticeships commencing autumn Dialectical behaviour therapy ( DBT ) training is being undertaken by 23 staff across NCL to further enhance the acute care pathway. The development of a CAMHs Out of Hours crisis team will create opportunities for staff to work in different settings and developing their skill set. Opportunities are being explored to develop joint training across adult mental health and CAMHS in order to upskill staff in both sectors. Mental Health First Aid Training for 200 non-mental health staff and current Peer Support Workers to be delivered by June Primary Care and Social Care Staff to receive Suicide Prevention Training A further 250 primary care and community staff will receive training through integrated IAPT programme. In accordance with the care model, many staff at the Trust are already more community based than they have been previously, and the preferred option does not call for any staff to transfer out of the Boroughs of Camden and Islington. These proposals are not expected to have negative impacts on the workforce. Any workforce changes will be consulted on in-line with the Trust s agreed Change Management Policy and sufficient time will be allowed to ensure appropriate notice is given of any changes. Furthermore, the Trust s devolved structure encourages clinically led divisional autonomy, within the Trust s overarching policies, procedures and values. Each division will be responsible for managing their workforce changes, supported by the Human Resources & Organisational Development Team. The Trust Strategic Development Committee will have oversight of workforce plans, with ultimate accountability being held by the Trust Board. 171 of 402
172 Commercial principles There is no activity shift expected between the different providers of the services being consulted on. In fact, the commercial structure around the payments to the Trust from the CCGs is such that there would be no negative financial impact on the CCGs as a result of the proposed service changes. This is because of the block grant payment mechanism which is set out in more detail in Section [9]. As a result, the CCGs will not be conducting any further consideration of impact on other providers Activity, Volume and Capacity Modelling The table below sets out the overarching activity figures for the Trust over the period April 2014 to March Figure [5.2]: Trust Total Activity and Admissions April 2012 to March / / / / /17 Admissions 1,216 1,316 1,315 1,397 1,363 Inpatient and Community Episode Caseload (Total distinct patients) 20,020 21,567 22,584 23,274 23,823 The Trust currently has 235 beds (84 on the St Pancras Hospital site) used for acute admissions, treatment of adults and older people. Over the past decade or more, changes in the way mental health services are delivered have consistently reduced the use of inpatient beds. The Trust has closed approximately 130 beds (acute and continuing care) in the past 10 years, through the development of increased alternatives to hospital care and improvements to the arrangements and working practices in inpatient care. Over the last couple of years the Trust has experienced consistent pressure on its remaining beds and an increase in numbers of people admitted and those treated by the Crisis system. This reflects both demographic growth and the nature of the local demographic, which is highly transient and includes many people accessing mental health services for the first time (and who therefore often require greater support). There has been an increasing number of Overseas Visitors to the UK who require urgent and emergency care, often resulting in an inpatient admission, before they can be re-patriated to their home country. In 2016, commercial advisors were commissioned by NCL STP to undertake bed modelling for the area. The advisors predicted an increase in the overall requirement of inpatient beds to increase from 236 to 268 in the Trust by 2021, an increase of 32 beds based on an 8% demographic growth if services remained as they were with no operational efficiencies or clinical improvements. The advisors also suggested that if the STP mental health work stream was delivered, it would remove the need for many of the additional inpatient beds 172 of 402
173 49 required estimating that the Trust bed base would need to increase to 246, a much smaller growth of 10 beds. The STP mental health work stream and progress on it in Camden and Islington is detailed in section [4.4.2], these are to a large extent based on reducing the demand for inpatient beds and meeting people s needs in the community. In addition to this there have been a range of changes to the Trust bed utilisation since the commercial advisors modelling as the STP initiatives and Trust initiatives have advanced Trust initiatives on inpatient beds usage In 2017, the bed situation specifically length of stay had worsened for Male PICU and acute wards. Due to this and the already high length of stay for older people and rehabilitation wards, the Trust embarked on an ambitious plan to reduce the length of stay of all of its wards which is showing real progress and has enabled some significant changes. The commercial advisors review detailed that the average length of stay in 2015 for acute wards was around 49 days, and 55 for male PICU. The Trust acknowledged that they were an outlier compared to other Trusts for length of stay, which contributed to high occupancy levels and meant that they often had to use private beds to accommodate needs; this included a length of stay for older adults of 135 days. The commercial advisor found that bed occupancy was at 97-98% for acute and 99% for older adults, the Trust s ambition is to achieve 95% by March To achieve the overall aim of 95% bed occupancy by March 2018 the Trust programme was to: Free up 12 beds across the system by 31 July 2017 to enable the opening of a Women s PICU by 1 November 2017; Fully utilise new community resource to step down some long staying rehabilitation patients by September 2017; Reduce the number of people staying beyond the agreed median Length of Stay (LoS) by 50% by the end of 2017; Convert 4 older people s continuing care beds to acute beds by 31 March This was achieved in a range of ways including: Re-assessment of number of patients who were outliers in terms of LoS; Closer links with Islington s voluntary sector Crisis House to better utilise this service, the Trust is a partner in the newly re-commissioned service which started in April 2018; Greater social care presence in acute wards to strengthen links to the community and supported accommodation to facilitate move on; Senior clinical review of patients to support reduction in LoS, including older adults with a target of reducing stays to 60 days; Introduction of Red to Green which is a daily analysis of the treatment and care delivered to inpatients; red days being days where the treatment given could have been provided in the community. Therefore working towards ensuring that every inpatient day is fully utilised and that patients are supported to discharge ensuring that they are treated in the least restrictive setting. 173 of 402
174 50 The Trust has made significant progress on these targets with the following having been achieved: Reconfiguration of bed base to allow the opening of an 11 bed women s PICU (this included one bed closure due to the restrictions of the SPH estate); Reduction in Continuing Health Care beds by four as planned, but increases acute bed base to support demand; Increased flow to rehabilitation beds which in turn supports reduction in length of stay in acute beds; Utilisation of all types of beds has reduced in the last year (Appendix [25]) Utilisation of acute beds has reduced from 99% to 96% in the last year, a reduction of 3%; Length of stay for acute beds for 17/18 is 67 days including PICU wards; Utilisation of older adult beds has reduced from a high of 648 bed days in June 2017 to 502 in March 2018, a reduction of 33% Length of stay for older adult for 17/18 is 118 days; Utilisation of rehabilitation beds has reduced from 99% to 97% over the last year a reduction of 2%; Length of stay for rehabilitation for 17/18 is 721 days; Occupied bed days (OBD) for private sector placement for acute care and PICU are now on a significant downward trajectory, following sharp peaks between July Dec , and are now on a zero trajectory by March 2021 (submission to NHSE) (Appendix [25]) 6 ; Total OBDs for private sector placement acute and PICU placements fell from a high of 2065 in quarter three of 2017/18 to 330 in the following quarter; New admissions have reduced from 591 to 474 between 15/16 and 17/18 representing a 20% reduction Refreshed bed modelling Further bed modelling has been developed for the Trust which forecasts further in to the future. In this updated bed modelling local demographic trends have been extrapolated into short term and long term growth scenarios. The forecast suggests population growth of 8.29% in the years 2017 to 2025 with the population of Camden and Islington rising from 509,594 in 2017 to 551,855 in Growth in Islington is forecast to be higher that Camden over this period (9.24% compared to 7.43%). The trajectory of demographic growth from on the projected bed requirement in would be 254 beds from the current bed base of 235, with no mitigation of efficiency or service development. In short there would be a requirement of 19 additional beds. 5 This was due to closure of a 12 bedded acute ward during the re-configuration to women s PICU, since opening of the PICU (November 2017) both PICU and acute bed admissions to private sector have fallen to under 100 per month, compared with highs of 500 (PICU) and 400 (acute) per month. 6 STP trajectory is not zero but C&I trajectory is and this is likely to be achieved ahead of schedule. 174 of 402
175 51 The Trust has the second highest number of acute beds per head of population, and is within the upper quartile of mental health trusts for acute admissions and length of stay (Appendix [24]). The Trust has around 70 beds more than the crude arithmetic mean. 40 of these beds result from a higher than average propensity to admit. 30 of these beds result from a higher than average length of stay. There are some local factors that account for a proportion of this higher admission and length of stay, such as the need for higher dependency bed usage, and for admissions of people with a diagnosis of psychosis (above upper quartile for Cluster 10-16, and near to it for Cluster 17). London similarly has much higher proportion of psychosis patients. However, figures suggest that this may account for as many as 29 beds. There are high relative levels of homelessness in Camden that analysis suggests could account for 8 beds, plus the ongoing need of high levels of funded overseas visitors, again an additional 8 beds. Thus 45 excess beds can be explained by clinical need, (from the identified 70), leaving opportunity for improving bed utilisation that could result in bed savings of 25. This reflects the difference between the existing and remodel of care figures, and mitigates against the 19 forecast additional beds demographic change suggest should the care model not change. The Trust has around the median number of older adult beds per head of population, and is in the lowest quartile of mental health trusts for older adult admissions (Appendix [24]). Both Camden and Islington have relatively young populations compared to London and England. Length of stay in the Trust is fifth highest nationally and the longest in London. The Trust has a much lower propensity to admit but a higher length of stay, with overall fewer than average beds (c. 2 beds) per head of relevant population. Analysis suggests that the lower propensity to admit accounts for 12 beds fewer than the mean, whilst the higher than average length of stay accounts for about 10 beds. There is little to suggest any capacity to reduce the bed base in this area 7 and would need to reflect demographic growth in the future. With regard to rehabilitation beds there is a predicted growth of eight beds. However, significant work has been done to reduce the length of stay for these patients including the opening of a new resource which has allowed the opportunity for patients to step out of rehabilitation that had previously had very long stays. Thus the need for additional beds is mitigated, and a further review of rehabilitation across inpatient and community wards will be undertaken in 2018/19 to ensure optimised care pathway to reduce length of stay where possible. The evidence above with regard to the progress made so far both in terms of delivery of the STP and Trust initiatives suggests that this requirement will not be needed. For example, through earlier diagnosis and intervention; and greater support and capacity to enable patients to receive care in the community, as well as continuation of the Length of Stay project to absorb demand as admission and treatment length are reduced. Some of these initiatives are difficult to quantify exactly, for example, there is yet to be an established evidence base on the impact of PBMH on inpatient beds. However this, combined with 7 Source: 2016 NHS Mental Health providers benchmarking club 175 of 402
176 52 initiatives in crisis services, is the prevailing good practice model and one being followed by all mental health Trusts. Consequently the CCGs are confident that maintaining the current bed base at 235, will be sufficient to meet demand in 2025, and the new build will actually allow one additional bed to 236 due to the removal of the estate compromise that saw one bed close in CCG believe that this is a conservative proposal based on the clinical efficiencies postulated within the STP, the service development being delivered in the Trust s Clinical Strategy and improved practice that is already in track. These movements are set out in more detail in Figure [5.3]. 176 of 402
177 53 Figure [5.3]: Bed modelling Type of Bed Current Location No of Beds (Feb 16) No of Beds Predicted by STP due to demographic growth and no service developments (Feb 21) McKinsey No of Beds Predicted in STP with demographic growth and Service Developments (Feb 21) McKinsey Mitigation Current No of beds (Feb 18) No of Beds Predicted in OBC due to 8% demographic growth and no community developments (Feb 25 ) No of Beds Predicted in OBC due to demographic growth with Clinical Strategy implemented community developments (Feb 25) Service Developments Assumed / Delivered (15/16) full year data available to McKinsey Assumptions are 13.3% demographic growth from 15/16-20/21 (5 years) steady length of stay and occupancy As detailed in the STP Increased CRHT Teams / Perinatal/Primary Care Service Developments from Feb 17 include: Women's PICU N/A As detailed in the Clinical Strategy Men s PICU Total Length of stay MPICU Women PICU Total Length of stay WPICU 36 Acute Total Length of stay Acute Older Adult Total Length of stay Older Adult Rehabilitation Total Length of stay Rehab Total number of beds of 402
178 Expected benefit The benefit impact of the proposed development of facilities is focused around the improved therapeutic environment for service users. This is in line with the current clinical strategy to promote recovery, resilience and independence via easy access to community-based services and specialist care-pathways. The main benefits that have been identified are as follows: Improve quality of care by enabling transformation of service models; Support the delivery of the Trust s clinical strategy and STP by increasing accessibility to community services; To create fit for purpose, therapeutic inpatient wards; Enable the Trust to fully comply with CQC requirements without the need for high numbers of adaptations both hospital regulations and standards and statutory regulations; Improve the Trust s status as a research and development centre of excellence through e.g. better facilities and partnerships with other organisations; Promote equality through improved access to disability friendly facilities; Improve sustainability through improved efficiency of facilities and enablement of better and more efficient care models; Enable greater alignment of Trust services with the needs of service users through improved access to safer facilities; Reduce stigmatisation of Mental Health service users by facilitating easy access to new facilities and open spaces; Improve service user experience with the ability to access integrated physical and mental health services in line with the 5YFV and national NHS Mental Health strategy No Health without Mental Health ; Enable greater proximity to services for a high proportion of service users by locating services in Camden and Islington; Attract and retain high quality staff by providing a high level of staff support including improved engagement and facilities; Contribute to the local community by promoting community health services and improving staff s workplace; Support the movement or maintenance of the current location of others Trusts as set out in the STP; and To allow the development of joint Mental and Physical health care by the proximity of the Whittington health site. 5.3 Impact on service users and benefits Of the 25,000-30,000 people seen by the Trust on average per year, just under 9,000 were seen at the St Pancras site last year. Of these 9,000 users, over half were visiting services that will remain at the St Pancras site and so the number of users expected to be affected is around 3,100 (see Figures below). 178 of 402
179 55 Figure [5.3]: Affected service users by service - Inpatients Name of service Proposed new location Number of service users affected (based on attendances 1 Jan-31Dec 2017) Dunkley Ward (mixed sex with 4 learning disability beds) New in-patient facility 165 Laffan Ward (mixed acute mental health) New in-patient facility 168 Ruby Ward (female PICU) 8 New in-patient facility 20 Rosewood Ward (female acute mental health) New in-patient facility 115 Montague Ward (mixed high dependency rehab ward) New in-patient facility 32 Sutherland Ward (mixed longterm complex care ward) New in-patient facility 27 Total number of service users 527 Note: The Approved Mental Health Professional Service and Pharmacy services are addition to those listed above that form part of the proposal (see Appendix [1]). However, these two services support services listed above and are therefore covered in their numbers of service users. Figure [5.4]: Affected service users by service - Community Name of service Proposed new location Number of service users affected (based on attendances 1 Jan-31Dec 2017) Camden Mental Health Camden Hub 720 Assessment and Advice Team Islington Practice Mental Health Team 9 Islington Hub 15 Islington Assertive Outreach Islington Hub 101 South Camden Recovery Team Camden Hub 720 icope North Islington Team Islington Hub 2,179 Community Recovery Service for Older People (Camden and Islington) Islington Hub 99 South Camden icope Camden Hub 2,450 Total number of service users 6,284 These users will see a number of significant benefits depending on the service they access: Community based care Over two-thirds of the users likely to be impacted are attributed to the South Camden icope service, which is a low intensity service providing guided self-help interventions alongside psychological interventions such as Cognitive Behavioural Therapy (CBT). For these users, 8 Part year effect opened in November Those not able to be seen in GP surgeries figure based on March 18 only when full roll-out was achieved. 179 of 402
180 56 the relocation of this service to the Camden hub offers the opportunity to access services at a more welcoming community based, non-acute setting. This will not only provide easier, more direct access to services but also reduce the stigma attached with accessing mental health services Improved therapeutic environment For inpatients at the St Pancras site, moving to a newly built facility ensures they receive care in a high quality, specialised building with state of the art facilities. The current site was deemed unfit for purpose following a CQC report in June 2016, with some wards having serious health and safety concerns, including ligature points and blind spots. The latest CQC inspection published in March 2018 noted that the Trust had sufficient mitigations in place, however the overall rating for Safety remained as Required Improvement. Furthermore this most recent report highlights the staffing difficulties facing the St Pancras site, with the vacancy rate over 20% on all wards. This not only increases workload for staff but also increases the reliance on agency and bank staff, which increases the likelihood of protocol not being followed and staff training shortfalls. By transferring these services to a purpose-built facility, critical safety improvements will be seen alongside drastic improvements to the general therapeutic environment. For example, the new site will improve on the poor quality of available outside space at the St Pancras site and improve lines of sight for monitoring of patients Improved access When rated for disability access, the current site s 2016 PLACE rating is a significant outlier at only 65.57% accessible when compared to the national average of 78.8%, and the even higher rating for comparative MH Trusts at 93.32% accessible. By relocating to a newly built site that meets modern accessibility requirements, this will increase equality of access for users, staff and visitors Parity of esteem for mental and physical health By co-locating the new purpose built facility alongside the Whittington Acute Hospital, service users are able to receive specialist mental health treatment from the same site as users of the acute physical health care service. This helps reduce the stigma attached to mental health facilities and is a key aim of both the Trust and the STP clinical aims Improved integration between acute and mental health services In addition to the reduced stigma, by having mental health inpatient and acute facilities on the same site, it is expected that users transferring between the two services will receive a quicker and more streamlined transition. For service users being stepped-up or steppeddown from the acute pathway, there will be a minimal physical transfer required and this will be able to occur more quickly between the two providers, improving treatment and service user experience. By continuing to deliver a model of care that is primary care and community focused, the proposed relocation of some services does not impact upon the majority of service users access to services. The ongoing roll out of practice-based teams ensures all service users are able to access mental health professionals and receive treatment and support close to their homes. 180 of 402
181 Better working initiatives for staff: By developing new facilities and implementing the workforce plan as per the STP, it is expected that the local health organisations are more likely to attract a higher quality staff by providing a high level of staff support including improved engagement and facilities. There will also be a naturally higher retention rate due to the higher quality buildings. 5.4 Changes to travelling times and distances The travel time analysis and presentation is being developed into maps. It sets out lower super output areas using the Transport for London travel tool. Analysis and maps will be presented in the form of heat maps and demonstrate the impact on services users and populations for the change in travel times by differing modes of transport for the following scenarios: For all postcodes - a map showing the change in time due to relocation of beds from St Pancras to the Whittington. For those showing an improvement (meaning a reduction in travel time) of greater than 5 minutes a shading of green. For those showing an improvement reduction of 5 minutes or less or an increased time up to and including 5 minutes, a shading of Amber. For those postcodes where there is an increase in time of over 5 minutes a shading or red. For Islington Postcodes a map showing change in time due to relocation of community services from St Pancras to Lowther Rd For those showing an improvement (meaning a reduction in travel time) of greater than 5 minutes a shading of green. For those showing an improvement reduction of 5 minutes or less or an increased time up to and including 5 minutes, a shading of Amber. For those postcodes where there is an increase in time of over 5 minutes a shading or red. For Camden Postcodes - Map showing change in time due to relocation of community services from St Pancras to Greenland Rd For those showing an improvement (meaning a reduction in travel time) of greater than 5 minutes a shading of green. For those showing an improvement reduction of 5 minutes or less or an increased time up to and including 5 minutes, a shading of Amber. For those postcodes where there is an increase in time of over 5 minutes a shading or red.] The Figure below provides a summary of this analysis, with supporting information in Appendix [3]. Figure [5.5]: Summary of travel time analysis [x] 5.5 Public Sector Equality Duty The Equality Impact Assessment (EIA) process is designed to ensure that a project, policy or scheme does not discriminate against any disadvantaged or vulnerable people or groups. This ensures CCGs pay due regard to the Public Sector Equality Duty. The EIA will be completed in two parts, with the initial phase completed prior to consultation and a second stage to be completed following the consultation outcomes. The initial phase EIA focused on: How the services will impact on protected and vulnerable groups in the community; 181 of 402
182 58 How the CCGs and providers must ensure equality and fairness in terms of access to these services- and appropriate provision for all patients based on their clinical, personal, cultural and religious needs; and How the CCGs will work together with local providers and patients and carers to ensure a high quality of services that all patients can experience. The majority of vulnerable or protected groups identified as part of the EIA have been judged as achieving greater equality, improved outcomes or increased accessibility through the proposal. For example, both inpatient and community developments will provide improved disabled access for service users, staff and visitors. For many other groups, the purpose built facilities offer an improvement in therapeutic environment, access to outdoor space and care delivered closer to home. At this stage, the EIA has identified the potential increased travel time for some disabled service users as the only vulnerable group that may experience a reduction in accessibility. In order to minimise this risk, route planning to the new site will be provided and shared with local community groups for individuals with disabilities. 182 of 402
183 59 6Governance 6.1 Governance structure for the consultation process The consultation phase of the redevelopment of the St Pancras site is being overseen by the St Pancras Hospital Redevelopment Oversight Group and led by the Chief Operating Officer of ICCG (Figure [6.1]). This group is reporting to both of the CCGs in addition to providing assurances to NHS England. NHSE representatives also have positions within a number of the groups relevant to the redevelopment to ensure adherence to rigorous NHSE guidelines for consultation. These arrangements are for the consultation phase only, with full project governance details being set out in Section [9]. In order to proceed to public consultation, the process requires approval from the CCGs Governing Bodies and NHSE. To support this decision, the CCG Governing Bodies will review the proposed consultation document, consultation methodology (including the Equality Impact Assessment (EIA) and Quality Impact Assessment (QIA)), financial modelling and consider the response from the Clinical Senate. Camden and Islington Local Authority s Heath and Care Overview and Scrutiny Committees will be also be provided an opportunity to review and comment on the consultation prior to launch. Figure [6.1] Public Consultation Governance Structure A full break down of these consultation groups is provided below. Figure [6.2] Membership of consultation groups Group Lead Members Reporting to St Pancras Hospital Redevelopment Oversight Group Chief Operating Officer, Islington CCG Transformation Programme Director, the Trust Islington CCG Camden CCG NHSE CCG Governing Bodies and NHSE Clinical Senate Liaison Associate Director of Joint Commissioning for Islington CCG Camden CCG Islington CCG Medical Director, the Trust NHSE St Pancras Hospital Redevelopment Oversight Group 183 of 402
184 60 Public Consultation Working Group Financial Modelling Workstream Senior Engagement Manager, Islington and Haringey CCGs Chief Finance Officer, North Central London CCGs Camden CCG Engagement Lead Head of Communications and Engagement, the Trust HealthWatch Camden and Islington Service users Trust Director of Finance NHSE Finance lead St Pancras Hospital Redevelopment Oversight Group St Pancras Hospital Redevelopment Oversight Group St Pancras Hospital Redevelopment Oversight Group The overall redevelopment programme is managed by the St Pancras Hospital Redevelopment Oversight Group and chaired by the Chief Operating Officer for Haringey and Islington CCGs. This group has representation from the Trust, the CCGs (including Engagement leads from each CCG) and NHSE. This group reports to CCG Governing Bodies and in turn to NHSE Clinical Senate Liaison The Clinical Senate Liaison group is led by the Associate Director of Joint Commissioning for Islington CCG and is responsible for co-ordinating activities with the London Clinical Senate (LCS). This group includes the CCG GP leads for Mental Health from Camden and Islington and clinical representatives from CCGs, the Trust and NHSE. This group reports to the St Pancras Hospital Redevelopment Oversight Group which in-turn reports to the NHSE locally established Clinical Senate panel Public Consultation Working Group The primary purpose of this group is to facilitate strong public engagement and ensure a thorough and rigorous consultation is undertaken. All public consultation activities are being managed by this group. The group is led by the Senior Engagement Manager for Islington and Haringey CCGs and has support from the Camden CCG Engagement lead and the Trust. Members from Healthwatch Camden and Healthwatch Islington and two service users are members of this group. This group has inputted into the consultation document itself and methodology Financial Modelling Work stream This small working group consists of representatives from the Trust and NHSE and is led by the Chief Financial Officer for the North Central London CCGs. This group is responsible for providing financial insight and recommendations for funding of the redevelopment and also report to the St Pancras Hospital Redevelopment Oversight Group. 184 of 402
185 Roles and Responsibilities The CCGs Approximately 98% of services provided at the St Pancras site are commissioned by Islington CCG in their role as lead commissioner, with Camden CCG being a significant Associate to the Islington CCG contract. As such, these CCGs will be the ultimate decision making authority for the programme The Trust The Trust is leading on the SPH redevelopment proposal and working with stakeholders such as NHSI, London Devo, NHSE, the Local Authorities, Service Users, staff and other interested public bodies, including the CCGs to ensure plans are in line with individual commissioner intentions and fit for purpose NHS England NHSE are providing assurances and support at all levels of the programme, including representation on many of the programme working groups. 6.3 Information Governance Issues The Trust stores data about its patients that could identify each patient. This Patient Identifiable Data (PID) can be classed as any information, electronic or paper format that would allow a third party to identify the patient. As a part of the proposed relocation, the Trust is not proposing to change the use, storage or accessibility of any PID it holds. A Privacy Impact Assessment (PIA) screening questions form was completed by the Trust (Appendix [4]) whereby the result indicated that a PIA was not required. The principal reasons include: 1. Trust staff will still be able to access data in the usual way via Carenotes and N3 secure connection to digital records 2. Trust staff will still be able to access paper records through the Iron Mountain procedures Should there be any changes to information privacy as a part of this proposal in the future; the Trust will re-complete the PIA screening questions form to determine whether a PIA is needed. The Trust s Head of Information Governance and Security will be consulted closer to the relocation to discuss shredding bins, privacy displays, and photocopier / scanner / medical device locations. 185 of 402
186 62 7 Stakeholder engagement This section sets out the engagement that has been undertaken to date regarding the relocation of some services away from the St Pancras site and the development of community hubs. This includes the stakeholder groups who have been included as a part of the pre-consultation process, engagement activities undertaken and the findings from those activities. Moreover, it explains how this feedback has been used to develop the options detailed in Section [8] of this PCBC. 7.1 Legal Context Under section 242 of the NHS Act 2006 and section 142Z of the Health and Social Care Act 2012, NHS Trusts and CCGs have a legal duty to make arrangements for individuals to whom the services are being or may be provided, to be involved. Individual involvement includes participation in consultation, information sharing, or in other ways, such as: Planning of the provision of those services; Developing and considering proposals for changes to the way services are provided; and Influencing decisions which affect operation of those services. In order to meet these legislative requirements and the four tests outlined in the Mandate from the Secretary of State to NHS England and NHSE s other tests, public involvement must be an integral part of the service change process. Engagement should be early and ongoing throughout the process using a broad range of engagement activities. The Clinical Commissioning Group (CCG) must make arrangements to secure that individuals to whom the services are being or may be provided are involved (whether by being consulted or provided with information or in other ways): In the planning of the commissioning arrangements by the group; In the development and consideration of proposals by the group for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which the services are delivered to the individuals or the range of health services available to them; and In decisions of the group affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact. All public consultations should adhere to the Gunning Principles, which are: Consultation must take place when the proposal is still at a formative stage; Sufficient reasons must be put forward for the proposal to allow for intelligent consideration and response; Adequate time must be given for consideration and response; and The product of consultation must be conscientiously taken in to account. 186 of 402
187 Pre-consultation engagement on the case for change The local health organisations have engaged with inpatient service users, community service users, carers and staff as part of pre-consultation engagement work for the development of the plans. The local health organisations have met regularly as part of the Stakeholder Reference Group, which is made up of senior representatives from the Trust, both CCGs and both Councils. This group provides oversight and maintains responsibility for the pre-consultation activities, consultation programme and implementation programme, including the review and approval of business cases developed by member organisations. See Appendix [5] for a full list of meetings conducted and pre-consultation engagement activities undertaken to date Pre-consultation engagement with service users and carers The local health organisations have held a number of pre-consultation engagement events to listen to the views of existing and previous service users and carer representation groups. This has included: The Trust s medical director attending existing service user meetings to explain proposals and take questions; The Nubian Service Users Forum and the Women s Strategy Group are among the existing groups the Trust has engaged with; A two borough community hubs event in March 2018, which attracted a diverse audience; A Service User Alliance meeting on 31 March 2017; and A Service User Conference on 13 April At these meetings, senior leaders from the Trust provided information on the outline plan and long list of options. Time was allocated for full debate, questions and feedback and this has been logged and passed on for consideration. In addition, a survey was developed to better understand the clinical and service priorities of service users in both the community and inpatient settings. This was sent to all service users via and copies were made available in paper form at key meetings. Feedback from this survey is set out in Section [7.3] below. Some groups were asked to feedback on the positive aspects of the community services they currently use, what could be improved, if they envisaged any problems if some community services were based in the new hubs and if any problems were identified, what the Trust could do to mitigate or minimise impact. Carers in both Camden and Islington have been given opportunities to hear more about the proposals, to provide feedback and ask questions through a number of meetings throughout This includes the Islington Carers Hub and Camden Carers Hub. Healthwatch Camden was also commissioned to attend the Camden and Islington carers meetings to engage carers and listen to feedback. Healthwatch interviewed 55 individuals comprised of current and former inpatients at SPH, Highgate, staff and carers during February and March of 402
188 Pre-consultation engagement with employees Due to the potential workforce implications, the Trust have also completed initial consultations with their staff and governors. This includes meetings with trade union representatives and Governors and staff at key sites including St Pancras, HMHC, Lowther Road and the Peckwater Centre. Five clinical and technical design review workshops were also held to secure input from approximately 30 clinicians on the optimal design of the estate in terms of both community and inpatient facilities. See Appendix [5] for a full list of these meetings Pre-consultation engagement undertaken as a part of the STP As a part of the STP process, a wide array of stakeholders were engaged that included CCG Chairs, CCG Members, Clinical Cabinet, GPs, LINKs Local Healthwatch, Local Authorities Health and Wellbeing Boards, Local Authorities Lead Officers and Members, Provider Trusts, OSC/JHOSCs and voluntary and community groups. Appendix [6] sets out how these parties were engaged with and continue to contribute to the development and implementation of the STP Pre-consultation engagement with GPs The Trust s Clinical Director and SPH programme director presented at a Camden CCG GB seminar on 26 July 2017 and to Islington GB in July The Camden GB included the GP chair of the locality meetings and an elected GP representative. The Islington GB includes the GB Clinical Lead for Mental Health. A written briefing was shared with Camden GPs in November 2017 and the medical director is scheduled to present the Trust s proposals at the CCG s April 2018 locality meetings. In March 2018 proposals were presented to the Islington GP Forum by the CCGs Clinical Lead for Mental Health Pre-consultation engagement with the JHOSC The London Boroughs of Camden and Islington are on the same committee of the North Central London Joint Health and Overview Scrutiny Committee ( JHOSC ). The JHOSC undertook a review of the SPH proposal in April 2017, September 2017 and March At the 19 September 2017 JHOSC meeting, the redevelopment at the St Pancras site was discussed, as part of the wider NHS Estates strategy. This meeting provided an opportunity for the JHOSC to question and challenge current plans. A copy of the full minutes from this meeting is in Appendix [7]. A summary of the points raised at this meeting includes: Overall members welcomed the proposal to move inpatient facilities to the Whittington and agreed with the suitability of this site; Councillors would appreciate the opportunity to view the current site to assess the opportunities for Social Housing development and this was agreed at the meeting; Following concerns raised that sale proceeds would be used for revenue spending, members were assured this would not happen; The opportunity for surplus land to be used for GP surgery sites was raised as desirable; 188 of 402
189 65 Concerns were raise that the number of inpatient beds was not increasing. The Trust should ensure the justification for this is clear in the consultation; and It was agreed that the Full Business Case would be presented to the JHOSC when appropriate. The SPH Project Director presented at the JHOSC on 23 March 2018 with an update on the SPH redevelopment project. The following was noted in the minutes which are yet to be formally agreed: It was agreed that further information would be provided at the June 2018 Camden and Islington OSCs by the Trust; The London Estates Devolution team have been engaged and are being consulted but the SPH redevelopment would not require their approval; It was agreed that the Chair of the Camden HOSC would be invited to the next SPH redevelopment programme board meeting, which for the first time would combine the separate boards of stakeholders and providers; and There were no further concerns or issues raised about the proposal. All review points raised by the JHOSC have been addressed and it should be noted that the SPH redevelopment is implementing the STP plan, to which the JHOSC contributed to Pre-consultation engagement with local people The Trust has shared its proposals with local people through the St Pancras Community Association and the Somers Town Neighbourhood Forum. Local people asked that consideration is paid to what young people may need and the provision of jobs Pre-consultation engagement with other local stakeholders The Trust has engaged with a number of local organisations including Healthwatch, Citizen s Advice Bureau, Voluntary Action Camden, the Old St Pancras Church, Octopus Communities and the Holy Cross Centre Trust who provide support for people who are socially excluded, for example, homeless. 7.3 Options appraisal engagement As part of the options development (Section [8]), a series of meeting were held to get input and understand the needs of stakeholders. The following options appraisal engagement was incorporated into the options appraisal process, as set out in the next section, up to the point of selecting the preferred option. A brief summary of the options are set out below: Re-provide inpatients at SPH; Re-provide inpatients at Whittington site; or Re-provide inpatients at St Ann s Hospital. Each option had the same proposal for community services and other services as set out in Appendix [10] which is why they are not explicitly mentioned under each option above. 189 of 402
190 Overview Key findings included: Concerns over adequate consultation with service users; Concerns over inpatient beds moving out of Camden; Concerns over inpatient beds moving to St Ann s site due to travel and accessibility issues; Concerns over land disposal proposals of the SPH site; and Concerns over the provision of appropriate services from the community hubs. However, a consensus was reached on the preferred option: Moving the inpatient beds from St Pancras to a site in Camden or Islington, invest in community services through the two community hubs, build new facilities, and bring researchers and academics together on a single site at SPH. Specifically, the Healthwatch feedback indicated a unanimous agreement that the existing facilities at St Pancras Hospital are not fit for the purpose and the majority were in favour of the proposal Consulting with the service users Local Healthwatch teams identified that service users felt strongly that there needed to be a focus on consulting with current and ex-service users as part of the consultation Inpatient beds moving out of Camden Concerns were raised in some service user groups about inpatient beds being moved away from St Pancras and out of Camden whether that be to Whittington Hospital or to St Ann s Hospital. The trade-off, which reached a general consensus to be accepted by the majority of service users, is that to resource the building of new warm, welcoming and therapeutic inpatient spaces, beds would need to move from the high cost St Pancras site to one where a new inpatient facility could be affordably built with additional revenue being directed towards improving community services. The Healthwatch engagement found a small minority said they would prefer to retain the existing St Pancras Hospital. The central location and good transport links at St Pancras are highly valued by many. However, depending on the specific circumstances for the individual, a roughly equal number of respondents said a Whittington location would be easier for them personally. Many people said they thought that the potential benefits of a new purpose built hospital would outweigh any disadvantages associated with the re-location of the new site to Whittington. The concerns about the Whittington location are almost exclusively related to transport links and the walking distance to shops which in both cases are less convenient than for St Pancras Inpatient beds moving to St Ann s Some service users with direct experience of the St Ann s site raised concerns about the possibility of inpatient beds moving there. There was concern mainly focused on the travel challenges and general accessibility of the St Ann s site. This concern is analysed in more detail through the travel analysis undertaken in Section [5.4] and also factored into the options evaluation process in Section [8.4]. 190 of 402
191 67 It was explained that the Trust would create its own buildings and deliver its own services. It was also emphasised that the purchase of land at St Ann s would be cheaper, enabling more resources to be channelled into our community services. Relocating inpatient beds to St Ann s next to Barnet, Enfield and Haringey s mental health inpatient site might allow for the sharing of some facilities, such as an on-site gymnasium for example Land disposal proposal for SPH Concerns were raised over the irreversible selling-off of precious NHS resources, namely the St Pancras site. The mitigation includes the plan to offer some of the land to another NHS provider, as well as sell a portion of the estate for the creation of affordable accommodation with an element being key-worker staff, potentially including Trust staff. It was explained that all existing services remaining on the St Pancras site would no longer be viable beyond a certain point in time, because without a substantial additional and continuing stream of finance it would become unaffordable to either maintain and or replace existing St Pancras facilities to ensure they were safe and fit-for-purpose Community care delivery Service users highlighted confusion at the term community hub, confusing it with a community centre. Part of the session was used to identify more suitable terms for the new hubs. Going forwards, further engagement will be sought to define the community hubs in a clear and consistent manner. A need for a non-stigmatising and respectful environment that is considerate to different cultures was highlighted. It was generally felt that more interventional services were required to prevent a mental health crisis, namely a drop-in facility that is accessible to service users so they have a place to go when they begin to feel unwell. It was felt that A&Es are inappropriate and terrifying when suffering a mental health crisis with a preference for a different first port of call option. Equally, it was felt that more support is needed when an individual is out of crisis which the Trust needed to be more proactive rather than reactive. Although one service user stated that some of the Trust s proposed new locations could be more difficult for those with mobility issues, if they did have to travel further, the majority view was that location was less of an issue if services were good, improved and inclusive. Some group members were particularly interested in the design of the buildings asking that they are Obsessive Compulsive Disorder friendly, not anxiety provoking in terms of design or layout and present a more therapeutic environment with the right colours and plants. Others said that there was a need to ensure the Trust had staff to support these new buildings people who have experience of the issues to talk to service users. Most service users were generally positive about the proposed new facilities. The strongest views were based on wanting services that were inclusive, resourced with knowledgeable and compassionate staff and a non-stigmatising and welcoming environment. One service user said: Buildings need to feel more vibrant, don t want to feel that we re going to that place. 191 of 402
192 Applying pre-consultation engagement findings to options appraisal As part of the formal consultation process, the group of stakeholders who will be engaged will be widened to include commentators and influencers such as local media, ward councillors, NHS pressure groups and heritage bodies, as well as the wider local community, including residents and businesses. Furthermore, Camden Healthwatch and Islington Healthwatch will be commissioned to engage local people covering the nine protected characteristics and other vulnerabilities. Accordingly the range of methodologies will also be expanded to cover targeted and ongoing engagement, across a range of channels, as shown in Section [7.5.3]. Stakeholder mapping has been completed to ensure all interested and relevant groups are captured. The concerns raised through the pre-consultation engagement highlight the requirement for full and contextual information to be provided alongside the options when undertaking the formal consultation. Specific concerns raised will be incorporated in the consultation as follows: Consulting with current and ex-service users The Trust s Clinical Director will speak at all of the Trust s service users groups to introduce the consultation, taking questions and letting people know how to fill it in (along with taking some hard copies). Further targeted engagement using the consultation survey with service users across all five of the Trust s divisions Acute, Services for Ageing and Mental Health, Recovery and Rehabilitation, Substance Misuse Services and Community Mental Health. This will include both current service users of inpatient services and community services Moving services out of Camden This stresses the importance of ensuring the case for change is clear in all consultation materials; emphasising not only the inadequate provision currently at the St Pancras site and the premium paid on land here, but also the added value of the public pound when looking at the alternative sites. The strategic case must be accessible to all stakeholders to ensure this message is understood thoroughly. Moving inpatient beds to the St Ann s Hospital site in Tottenham, would mean moving them out of the boroughs of Camden and Islington. The majority of pre-consultation engagement activity points to individuals being not in favour of St Ann s, saying it is a harder-to-reach location for most people than the HMHC. We are therefore proposing we move our inpatient beds to a new site at Whittington opposite the HMHC. This is consistent with the qualitative scoring undertaken in Section [8] of the St Ann s option and therefore will not form part of the consultation Travel challenges The concerns raised around travel times and access highlights the need for clear distance and travel time information. To this end, travel analysis has been completed (see Section [5.3]) and provides interested parties the opportunity to understand the direct impact of a move. This information will also be included in the consultation document and materials, including publication on the CCGs and Trust s websites. 192 of 402
193 Sale of NHS Resources This common concern is particularly emotive, and this issue must be handled sensitively during the wider consultation to ensure the underlying strategy behind the move of some services is clear. This also highlights that there should be some emphasis placed on the number of services that will remain at the St Pancras site, alongside the proposed use of the redeveloped space for NHS use; such as supported living accommodation, the Institute of Mental Health and any space that will be utilised by other NHS healthcare providers Services in the Community Hubs There will be opportunities for broader input on a range of issues. For example, to agree a new name for the community hubs, ideas to generate this include a board where service users can post suggestions and vote on a range of names. It will be a number of years before community hubs opened, should the proposal go ahead, so there is ample time to develop this with services users. 7.5 Other pre-consultation engagement activity Following on from the above engagement activity, the Whittington site was selected as the preferred option as set out in Section [8]. There has since been further engagement undertaken in the form of regular meetings with service users, carers, Trust staff, JHOSC updates and meetings with NHSI and NHSE by the local health organisations. 7.6 Consultation Plan This section provides an outline of the plan for public consultation on the proposal. This plan is in the process of review and is subject to change. The full consultation plan can be found in Appendix [8] Overview of the consultation plan In line with statutory duties, both CCGs are required to consult on the redevelopment proposals, ensuring local people are given the opportunity to share their views on the redevelopment of the St Pancras Hospital site and all of the services affected. The redevelopment of the site will affect the inpatient facility, the community services both on the site and on additional Trust sites, along with NHS services which are delivered on the St Pancras Site by other NHS Providers such as the Royal Free Hospital. A summary of service changes can be seen in Section [1] Summary of planned activities In light of these plans, Islington CCG is proposing to run a public consultation for 12 weeks starting in early July 2018 to the end of September A draft consultation document, questionnaire and Frequently Asked Questions have been developed and can be found in Appendix [9]. These will be finalised and approved by CCG GBs in June 208. The consultation aims to: Understand the views of the local community on the development of two new mental health community hubs, one in Camden and another in Islington. 193 of 402
194 70 Understand the views of the local community on the relocation and development of new Camden and Islington NHS Foundation Trust mental health inpatient services from the St Pancras Hospital site to a site by HMHC and Whittington Hospital; and The CCGs will speak to as many people in the local community as possible, ensuring they hear from a wide range of service users of all of the services proposed for relocation, the local community, local voluntary organisations and the two local Healthwatch, as well as other key stakeholders such as local Councillors and MPs Consultation communications and engagement channels The channels used to share the consultation and gather as many views as possible are set out in Figure [7.1]. Figure [7.1]: Communication channels for the consultation Channels Websites/online media Paper copies Implementation assumptions A full consultation document containing a survey about the proposals will be available on Islington CCG, Camden CCG, the Trust and Healthwatch websites. Prompts placed on the Trust social media channels will advise on how to leave feedback and join the public consultation meetings Copies of the full consultation will be available at each service affected by the St Pancras redevelopment, at other Camden and Islington Foundation Trust sites and upon request. Posters and leaflets in all 30 Trust sites will advise on the consultation and opportunities for feedback. Paper copies of the survey will also be available at each site. All paper publications will be in an easy to read format, with copies available in large print, easy read, community languages, braille and audio on request. Public meetings There will be a dedicated telephone line for local people either requesting the consultation documents or any questions they may have. Held at easily accessible sites for people in Camden and Islington to discuss and provide feedback on the consultation. 194 of 402
195 71 Focus groups Staff Engagement NHS Provider Roadshows Targeted Interventions There will be a drop-in session with the Trust s Clinical Director. Healthwatch Camden and Healthwatch Islington will be commissioned to undertake targeted research with groups that face barriers to accessing services and do not traditionally have their views heard in service redevelopment. Trust and CCG staff will be updated on the consultation via staff meetings and staff newsletters. GP member practices will also receive regular updates in GP forums, locality meetings and GP newsletters. Targeted engagement using the consultation document and survey with the services users of the other NHS providers affected by the proposed redevelopment. Using the EIA to identify disadvantaged or vulnerable groups, the Trust will support the CCGs to consult with these groups. Local networks Further targeted engagement using the consultation survey with service users across all five of the Trust s divisions Acute, Services for Ageing and Mental Health, Recovery and Rehabilitation, Substance Misuse Services and Community Health. This work will be carried out by Healthwatch Camden. The consultation document and survey will be shared with local groups for distribution amongst their members, including Islington Patient and Community Groups, Trust Service User Groups, Patient representatives, local voluntary and community sector groups. As mentioned in Section [7.4], following pre-consultation engagement feedback, the Trust s Clinical Director will attend all service user groups to introduce the consultation, and service users across the Trust s five divisions will be targeted with surveys Proposed consultation timeline The table below (Figure [7.2]) provides an overview of the primary consultation activities and communications planned. 195 of 402
196 72 Figure [7.2]: Timeline for Consultation Activities Action Lead Date Consultation documents and methodology sign off Islington CCG Governing Body June 2018 Camden CCG Governing Body June 2018 Consultation documents and methodology reviewed by Camden and Islington Health and Overview Scrutiny Committees ICCG and CCCG June 2018 Public consultation goes live ICCG early July 2018 to end September 2018 Evaluation of responses External agency October 2018 Results of consultation published and shared Islington CCG, Camden CCG, the Trust and partners November 2018 Final Business Case prepared Islington CCG November 2018 Consideration of Final Business case by Islington CCG Governing Body Islington CCG November 2018 Consideration by Camden CCG Governing Body Camden CCG November 2018 A decision is made by Camden and Islington CCGs on the final Business Case Camden and Islington CCG November 2018 The decision is communicated with the local community, OSCs, HealthWatch and partners Islington CCG / Camden CCG / The Trust November Results, feedback and analysis The CCGs will appoint independent partner (third party agent) to evaluate the consultation responses and to analyse the results of the consultation. The partner will develop a process and infrastructure that reassures stakeholders of the independent nature of the evaluation. This will inform proposals in a Decision-Making Business Case ( DMBC ) that will validate the consultation outcomes. Following the closure of the consultation on in September 2018, the evaluation team will have a period to analyse the results and present these to both of the CCG GBs. 196 of 402
197 73 Islington and Camden CCGs will then make a recommendation on the redevelopment proposals to NHS England and both OSCs for Islington and Camden. The results will be available publically, which will include, sharing on CCG and Trust websites and sharing through other stakeholders networks, such as Healthwatch Islington and Camden. 197 of 402
 for the identification of a preferred option from a long list of options.")
198 74 8 Options development, analysis and evaluation process This section sets out the range of options identified to address the objectives set out in the Case for Change and documents the appraisal process used to evaluate these. The local health organisations have developed a four-stage process (Figure [8.1]) for the identification of a preferred option from a long list of options. This includes: 1. An initial feasibility study; 2. The development and application of a set of hurdle Critical Success Factors (CSF) to create a short list of options; 3. The development and application of a more detailed set of qualitative CSFs to appraise short-listed options; and 4. A value for money assessment of the short-listed options. The outcome of this process is to enable the local health organisations, through the St Pancras Hospital Redevelopment Oversight Group, to determine preferred options for each area that will be subject to full public consultation. Figure [8.1]: Overview of option evaluation process 8.1 Option development In advance of developing options for the St Pancras site, a process was run by the local health organisations, incorporating service user input, to decide the appropriate setting for its services; see a summary in Appendix [10]. This work concluded: 198 of 402
199 75 Set 1: Certain services, as set out in Appendix [10], should be provided in community hubs off site (including on existing Trust owned sites at Greenland Road and Lowther Road); Set 2: Other services, again as set out in Appendix [10], should be provided on the St Pancras site to maintain a presence in the area and to enable the Institute of Mental Health; and Set 3: Inpatient services should be re-provided on or off site. Therefore, all options to be developed, bar the do minimum benchmark option, will include the Set 1 services being provided off the St Pancras site and all options include the Set 2 services being provided on the St Pancras site. The key variable between options is therefore the location of the re-provision of inpatient services (Set 3). 8.2 Appraisal 1: Feasibility Study As lead comissioner, 98% of services provided at the SPH are comissioned by Islington CCG, for the population of the London Boroughs of Camden and Islington, where the majority of patients come from. Therrefore, the focus of the sites search was primarily within the Camden and Islington boroughs to ensure continuity of provision, access for service users and building on the support gained to date from the two councils for this propoal. This is consistent with the pre-consultation engagement feedback receied as set out in Section [7] which detailed concerns around time travel to a new location. To allow the Trust to support its current cohort of service users effectively, sites were only considered if they were within the boroughs of Camden or Islington, unless there was an exceptional reason for their inclusion. For example, St Ann s Hospital was included at Strategic Outline Case (SOC) stage as it was identified that the Trust who owns that site (Barnet Enfield and Haringey Mental Health Trust) had land available next to their existing mental health facilities which are located approximately two miles away from the Islington boundary. The following types of site were considered: Surplus council owned land in Camden or Islington; Sites owned by other government bodies which are being decommissioned; Sites owned by neighbouring NHS providers; and Privately owned sites. Following identification of the long list of options, these were then screened for viability and site availability. This process was led by the Project Director and Transformation Programme Director in dialogue with local stakeholders and GL Hearn. This assessment was presented to the Boards of the local health organisations for consideration and approval as summarised in Appendix [11]. The boards reviewed the proposed screening of the long list and validated the options to be taken forward to the next stage of evaluation via the CSF process. A detailed description of the options considered can be seen in Appendix [12]. 199 of 402
200 Appraisal 2: Hurdle CSF The purpose of Hurdle CSFs is to eliminate options that are not able to satisfy any one of the three hurdles, using a binary pass/fail process. As such the hurdle objectives are CSFs that must be delivered for the project to succeed. These were developed with service users and carers, and were enhanced following pre-consultation engagement feedback around the need to minimise disruption for any inpatients. Figure [8.2] sets these CSFs out in more detail. Figure [8.2]: Hurdle Critical Success Factors (CSFs) # CSF Key points 1 CQC requirements The option provides a safe environment for service users and staff. Facilities must as a minimum meet all CQC requirements, and ideally exceed them. 2 Minimise service user disruption 3 Research and development The option does not require inpatient facilities to be moved more than once and minimises disruption to services users. This is critical due to the nature of the services delivered. The option supports and facilitates the creation and successful operation of a research and development institute closely integrated with a top research university. The four options were then assessed against the three hurdle CSFs as shown below. Figure [8.3]: Results of Hurdle CSF evaluation # Option Name A1 A2 A3 A4 Do minimum with inpatients Re-provide inpatients at SPH Re-provide inpatients at Whittington Re-provide inpatients at St Ann s Hospital Hurdle CSF 1 CQC requirements Hurdle CSF 2 Minimise service user disruption Hurdle CSF 3 Research and development Progressio n to qualitative CSFs For comparison only For Net Present Cost (NPC) comparison only Yes Yes As shown above, the following decisions were made about which options to take forward to the qualitative CSF appraisal: 200 of 402
201 77 Option A1, (Do minimum with inpatients) is not a viable option on the basis that it failed to meet any of the hurdle criteria. However as this provides the baseline comparison it was progressed to the shortlist for evaluation purposes only as a benchmark for the other options in line with NHS capital business case requirements. Option A2, (Re-provide inpatients at SPH), failed to meet the hurdles as it will cause significant disruption to service users during construction, particularly the large amount of eavy traffic movements and demolition that would be required. There is also concern that privacy and dignity could be compromised on St Pancras for inpatient services, as there are approved development plans around St Pancras are for tall residential blocks (up to 12 storeys) with balconies overlooking the site, and therefore over any inpatient facilities gardens or outdoor areas. In addition the reduction in value of the St Pancras site under this option was found to make it the least affordable and to provide the worst value for money. This option will be considered in the quantitative analysis of net present costs for comparison purposes only in line with an approach agreed with NHS Improvement (NHSI). Option A3, (Re-provide inpatients at Whittington), was progressed based on meeting all of the hurdle criteria. Option A4, (Re-provide inpatients at St Ann s Hospital), was progressed based on meeting all of the hurdle criteria. 8.4 Appraisal 3: Qualitative CSF A total of nine further qualitative CSFs were jointly identified and agreed between the local health organisations, service users and carers. These criteria were judged to be important to the provision of mental health services but would not cause the project to be unachievable in their own right. Figure [8.4]: Qualitative Critical Success Factors (CSFs) # CSF Key points 4 Quality of service user care The option enables the Trust to deliver the highest possible standards of care quality to service users. 5 Aligned to service user need and supportive of the clinical strategy The option enables alignment of clinical service location to the needs of the population it serves. The option supports the Trust and the wider STP objectives for early intervention in a community settings. 6 Destigmatise mental health 7 Promotes equality The option enables services to be provided in a setting which destigmatises mental health services, creating an attractive welcoming environment for service users. The option provides facilities which are accessible to all users and helps to promote equality for service users, staff and wider stakeholders. 8 Integrated care The option enables integration of mental health service provision with other healthcare provision. 201 of 402
202 78 9 Located with inborough or close to Camden and Islington 10 Support staff wellbeing 11 Consistent with the NCL STP 12 Consistent with plans for local community and place development The option provides new facilities which are based in either the London Borough of Camden or the London Borough of Islington, or if this is not possible, as close as possible to the Boroughs. The option supports staff health and wellbeing, including the onsite provision of staff wellness services (e.g. fitness classes, changing rooms and staff faith rooms). The option aligns with the plans set out in the STP and facilitates delivery of the STP. It supports and enables wider plans for other Trusts in NCL including proposed relocation of Moorfields The option aligns with local authority and community plans for place and area development, including the provision of housing for local people, employment opportunities and environmental benefits The agreed list of CSFs were evaluated by the local health organisations to establish the appropriate weighting. It concluded that all CSFs should carry equal weighting as there were no mutually exclusive or conflicting factors. The CSFs which were regarded as constituting an absolute requirement were additionally designated as hurdles Application of the Qualitative CSF The key themes from the quality assessment scoring workshops can be seen in Appendix [13]. The scores across the workshops were averaged to establish a total overall ranking. The detailed option scores arrived at during each workshop is also set out in Appendix [14]. The qualitative options evaluation was carried out by scoring each of the four options against the CSFs, including the hurdles. The option scoring was carried out by the following three groups, for which further information on the members is included in Appendix [15]. The Clinical Reference Group; The Trust Board; and The Trust Governors. On each occasion the committees carrying out the scoring were briefed on the options under consideration and provided with a summary of the options. The scoring was carried out in small groups and the options were scored between 0 and 4, with 4 being the highest score. This was done for the three Hurdle CSFs and the nine other CSFs (12 in total). The scores were then averaged across the different groups to give an average score out of Pre-consultation feedback As laid out in Section [7], the local health organisations completed a range of preconsultation engagement with key stakeholder groups, such as service user and carer representative groups and Healthwatch teams since March 2017 and will continue to do so throughout the pre-consultation phase. The findings of these preliminary consultations will be used to further shape options, as a good indicator of user and public acceptability of options. 202 of 402
203 79 Of the three key themes identified during the consultation activities was a particular concern over the St Ann s site in terms of accessibility for service users and staff and also the potential loss of identity by moving alongside another mental health Trust. We understand from this that for service users and staff, the integrity of the service s identity can be an emotive and important factor. Consequently, when measuring the St Ann s site against the Whittington site, the Whittington site was preferred as a direct result of pre-consultation engagement activities Summary qualitative evaluation of options Overall, option A3 (rebuild at the Whittington) has the highest average score, and therefore highest rank, leading it to being selected as the preferred option from a quality perspective. The key drivers of this are: Whittington is more accessible and geographically better located for service users, their families and staff; Whittington will deliver significant benefits to service users through delivering a better clinical environment and a more relaxed suburban community with green space; Whittington has good transport connections; The Whittington site is located close to the existing HMHC which provides opportunity for a stronger staff community and joint training; The Whittington is an inpatient community hospital, with acute services and an A&E. This means that service users will benefits from comprehensive holistic care on one site; Whittington is in the borough of Islington, with other current in-patient beds located at HMHC in the borough of Camden, and is therefore supported by both the local authorities and the STP; and The Whittington site enables the construction of the Institute of Mental Health on the SPH site and maintains close links with the Community Hubs. 8.5 Appraisal 4: Value for Money evaluation of options CCG impact The financial appraisal was undertaken by the Financial Modelling Work stream that is led by the Chief Financial Officer of the North Central London CCGs, (Section [6.1]). The impact was found to not be significant as the commissioning arrangement between the CCGs and the Trust is not one that is directly impacted by any changes in activity (such as Payment by Results arrangements) and instead is based on an agreed settlement for providing mental health services in the region ( block payments). There is no change expected therefore in the financial forecast of either of the CCGs as a result of these proposals Trust Impact Economic assessment of options The quantitative evaluation of the options was carried out by KPMG and a specialist long term financial model consultant ( Assista ). They worked with the finance team from the Trust to verify the current financial status of the Trust, as the starting point for the model. 203 of 402
204 80 The Trust s finance department worked with Assista to understand what the income and cost of providing services would be going forward, without any changes to the delivery model. This analysis was based on information in the STP and the Trust s understanding of future funding and likely demand for the Trust s services as described below. They worked together to understand the implications of each options, including the do minimum option. This included an evaluation of the risk that a forecast benefit was only partially delivered or not delivered at all Outcome of quantitative assessment of options For the quantitative assessment, the project costs (capital, revenue and lifecycle), benefits and risks were calculated for the Trust cash flows under the different options in accordance with relevant guidance by independent technical consultants (Turner and Townsend (T&T)) Net present cost (NPC) assumptions The Department of Health and Social Care template Generic Economic Model ( GEM ) was used to generate the Net Present Cost ( NPC ) and Equivalent Annual Value ( EAV ) Capital Costs The Trust and its technical consultants have developed a schedule of accommodation and functional requirements based on the scope agreed with the board to deliver the vision and consistent with the analysis of the bed requirement in Section [5.1.9] of the model of care. This has supported the development of initial designs for the four options being considered in this phase. The capital costs of all options have been developed by T&T and are summarised in the figure below. Option A1 (Do Minimum) has been based upon the latest estimate of backlog maintenance which is attached at Appendix [16]; therefore, no specific additional capital has been considered. Figure [8.7]: Capital costs for each option Reconciliation of costs from LTFM to GEM Option A1 Option A2 Option A3 Option A4 Reprovide IP Reprovide at Reprovide at Do minimum 000s at SPH Whittington St Anns Total incremental capital cost per LTFM - 124, , ,693 Less: transitional fees capitalised - (4,852) (4,852) (4,852) Less: land acquisitions - - (14,460) (4,000) Less: decant costs - (589) - - Nominal capital investment (nominal) - 118, , ,841 Discount nominal to real (17/18 prices) - (10,036) (8,501) (7,923) Less: Planning contingency (real) - (7,371) (7,555) (7,123) Less: VAT (real) - (18,145) (18,005) (16,820) Real capital investments (less contingency and VAT) - 83,353 82,472 76,975 Discount real to NPC - (9,580) (8,228) (7,664) Capital investment NPC per GEM - 73,773 74,243 69, of 402
205 Operating costs and lifecycle An LTFM has been produced for each option that covers the period from 2017/18 to 2025/26. This was used as the basis of the operating cost assumptions for that period. Beyond that period it was assumed that costs were flat in real terms Quantifiable benefits The Trust has sought to quantify the public benefits that the proposed development will deliver to the local and wider community as well as NHS. To do this, members of the project team reviewed the benefits identified to set out those benefits that were able to be quantified. The Trust worked through the list of potential benefits with input from clinicians delivering the services. Once benefits were identified as quantifiable, they were considered either as a reduction in cost or an increase in income. Where benefits were reducing costs, full consideration was given to the cost at present and to the impact that the change would have on that cost. Where an additional income stream was identified this was valued based on past experience and current benchmarks. Once the benefit was identified the period when it is most likely to have an impact was agreed an applied to the model, there were then discounted where appropriate in the model. Appendix [17] summarises the benefits identified, the value of those benefits and the key assumptions associated with those benefits Net Present Cost summary The figure below sets out the outputs of the assumptions given above for the four options. As described above, Option A1 and Option A2 are only provided for comparative purposes as both have failed the Trust s Hurdle CSFs. Figure [8.9]: NPC calculations of the options Net Present Cost (NPC) Option A1 Option A2 Option A3 Option A4 Reprovide IP Reprovide at Reprovide at Do minimum 000s at SPH Whittington St Anns Property and opportunity cost 71,770 36,781 34,963 25,827 Initial capital investment - 73,773 74,243 69,311 Other capex Lifecycle and business as usual capex 59,413 59,413 59,413 59,413 Total capex 131, , , ,551 Fees - 4,349 4,349 4,349 Total transitional costs - 4,349 4,349 4,349 Operating costs 3,078,767 2,978,245 2,958,380 2,973,361 Working capital adjustments (6,875) (7,616) (7,635) (7,635) Total opex 3,071,893 2,970,630 2,950,746 2,965,727 Externalities Total NPC (unadjusted) 3,203,076 3,144,946 3,123,715 3,124,627 Total Risk Adjustment 73,370 90,625 92,407 93,219 Trust total (risk adjusted) 3,276,446 3,235,572 3,216,121 3,217,846 Rank of 402
206 82 As shown above, Option A3 (rebuild at Whittington) has the lowest net present cost, slightly ahead of Option A4 (rebuild at St Ann s) and therefore is ranked as the preferred option from a NPC perspective. Whilst the initial capital investment is slightly higher for this option the operational savings delivered through co-location with both mental health and acute facilities at the Whittington has driven this outcome (see benefits above). 8.6 Combined appraisal The quality ranking has been averaged with the quantitative NPC ranking in the figure below. This resulted in option A3 (build a new inpatient facility at Whittington) being identified as the preferred option. Figure [8.10]: Combined rankings of the Options Preferred option analysis Option A1 Option A3 Option A4 Reprovide at Reprovide at Do minimum Whittington St Anns Quantifiable appraisal Total risk adjusted NPC ( m) 3, , ,217.8 Total risk adjusted EAC ( m) Qualitative benefits (weighted scores) Weighted benefits score Quality points per EAC Quantifiable appraisal Qualitative appraisal Points per EAC Preferred option The option to build a new inpatient hospital facility on land vacated by the Whittington Hospital is the preferred option from both the quantifiable and qualitative appraisal. Trust clinicians also believe that the Whittington option delivers the closest alignment to the clinical objectives of the STP and the Trust s Clinical Strategy. 8.7 Impact of the preferred option Quality Impact Assessment A Quality Impact Assessment (QIA) process was developed and led by the Clinical Workstream Group for the preferred option to evaluate the impact on quality of care. This was developed in partnership with clinicians at the Trust to ensure it provides an accurate reflection of the changes to service delivery. Specifically, the QIA of the proposed redevelopment will provide assurance that any resultant reconfiguration services will not adversely affect the quality of service user care. 206 of 402
207 83 This is defined by NHS England as care that is clinically effective, safe and that provides as positive an experience for service users as possible Independent review The Clinical Senate Liaison Group was established as part of the pre-consultation phase to ensure proposals are independently reviewed and guided by NHSE Clinical Senate. Clinical Senates provide independent strategic advice and guidance to commissioners and stakeholders regarding healthcare provision. A request for advice from the London Clinical Senate (LCS) was requested on 29 February 2018 by Islington CCG, with support from both the Trust and Camden CCG. The LCS request sought guidance on: Whether the change of environment will improve clinical care for inpatient and community services Whether the proposals for changes to inpatient and community mental health services: o will enable improvements in clinical care and quality benefits for patients o are informed by best practice o align with national policy and are supported by STP plans and commissioning intentions Whether the approach ensuring the inpatient demand of population growth is absorbed by the development of mental health community services. The Local Clinical Senate will complete its work in June The recommendations will be shared with the CCG GBs for to ensure recommendations are addressed. NHSE conducts a series of assurance tests including financial assurance which will be required before CCGs can launch the public consultation. 207 of 402
208 84 9 Finance case 9.1 Introduction The purpose of the financial case is to set out the impact of the preferred option on the CCGs and Trust s financial performance and position and to show the impact of the key financial risks. This is important as it demonstrates the options being considered for consultation are sustainable financially CCG impact The CCG s current spending plans with the Trust will not significantly change as a result of these proposals directly because of the contract arrangements in place between the CCGs and the Trust. Specifically, the Trusts receive a fixed amount per period from each CCG to provide mental health services to the local population. Unlike tariff arrangements this is not directly correlated to changes in activity by volume or type, therefore any service expansion requiring investment will need to be agreed in advance by CCGs. Both of the CCGs have reviewed the activity and financial modelling undertaken by the Trust. The CCGs are assured that the underlying assumptions behind the activity and income are consistent with their own projections, and the wider STP expectations. Specifically, the Chief Financial Officer for both Camden CCG and Islington CCG corroborated the financial information presented below with the Director of Finance for the Trust. Most of the commentary in the section below therefore focuses on the impact on the affordability of the proposals to the Trust as a provider the Trust will see substantive impacts on its cost base, balance sheet and cashflows as a result of the proposals in this document Provider impact The impacts of the proposals impact almost exclusively on the Trust in terms of providers and therefore the system affordability of the proposals can be shown by setting out the position for the Trust. This section sets out what those impacts are from a financial perspective and that the preferred option is affordable for the Trust. For the purposes of this analysis, affordability is defined as: ensuring that the Trust has the cash required to complete the estates programme; having sufficient cash to cover the Trust s working capital requirement throughout the ten year period (assumed to be two months of operating costs, circa 20.0m); the Trust being forecast to have a sustainable positive net surplus position by the end of the period considered; and the Financial Sustainability Risk Rating (FSRR) will be at least 3 in all years when appropriate adjustments are made for the impact of bridge financing. This section of the business case: Shows the financial forecast of the investment case, with an analysis of the incremental impact against the baseline (do minimum) case; 208 of 402
209 85 Shows that the preferred option is affordable in the base case. 9.2 Basis of preparation The projections in this section have been prepared on the following basis: The Trust has completed NHSI s 10 year Long Term Financial Model (LTFM). In line with the approach agreed with NHSI, 2016/17 was the outturn year used based on the forecast outturn at month 11 that had been submitted to NHSI. Separate models were populated for the baseline and the preferred option and a comparison of the outputs was used to assess the incremental impact. The assumptions for the baseline case (do minimum) were based on a revised version of the Trust s annual operating plan over the ten-year LTFM period. The costs of the investment and associated operating and financing costs were obtained from the Trust s facilities building cost model. 9.3 Financial projections A series of assumptions have been used to forecast the Trust s Income & Expenditure (I&E), Balance Sheet and Cash Flow statements. These are set out in Appendix [18]. The figures presented in the financial case may differ from those presented in the economic case due to discounting. The financial case figures are all nominal and not discounted, whereas the economic case figures are discounted Income and expenditure The Figure below sets out the Trust s projected income and expenditure under the investment case. This covers the period of construction (from 2018/19 to 2021/22) and the following three years of steady state operations. The incremental impact of the investment over the baseline is shown further below (the full baseline income and expenditure is set out in Appendix [19]). A bridge is also included, which shows the incremental impact of the investment on the first full year of operation (2022/23). 209 of 402
210 86 Figure [9.1]: Projected income and expenditure for the investment case m 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Income Clinical income Research & training Other income Total income Operating costs Pay (97.0) (97.0) (98.1) (99.6) (101.2) (101.8) (103.4) (105.3) (107.3) (109.4) Non-pay (29.0) (27.6) (27.4) (27.1) (26.0) (23.1) (22.4) (21.7) (21.3) (20.8) Total operating expenses (126.1) (124.6) (125.4) (126.7) (127.3) (124.9) (125.8) (127.0) (128.6) (130.2) EBITDA Impairment (8.2) Depreciation & amortisation (4.7) (5.2) (5.4) (5.4) (5.4) (6.4) (7.9) (7.9) (7.9) (7.9) Financing (3.5) (3.5) (3.2) (2.8) (2.4) (2.0) PDC (4.3) (4.3) (4.7) (4.8) (2.9) (4.2) (3.9) (3.5) (3.1) (2.2) Surplus/(deficit) (0.1) (7.1) The projected investment case income and expenditure shows that: Income growth is driven principally by the underlying growth in contractual income from clinical services (from the CCGs), with inflation accounting for 33% of the increase. This growth is partially offset by the assumed loss of 0.8m Sustainability and Transformation Fund (STF) funding from 2019/2020. Pay costs are forecast to remain at 97.0m in 2017/18, due to the underlying growth being matched by the Trust s CIP programme (3.2% of pay costs in that year). In subsequent years pay CIPs are projected at between 1.2% and 1.5%, thereby only partially offsetting the underlying pay cost growth. The investment is projected to reduce substantive and agency staff costs by 1.6m from 2021/22. Any increases above this amount in line with recent government announcements are assumed to be funded and it is therefore assumed would not have an impact on affordability. This will be modelled at FBC stage. Non-pay costs are projected to fall from 29.0m in 2016/17 to 27.6m in 2017/18 due to recurrent CIP savings of 2.2m in other expenses (8.4% of other expenses). The CIP target for other expenses is 0.8m per year thereafter. The investment is projected to generate savings in other expenses of 3.5m in 2021/22, increasing to 4.4m in 2025/26). An impairment of 8.2m is projected upon completion of the building works in 2021/22. This is the result of the requirement to change the valuation method of the new building from a cost basis to depreciated replacement cost upon its completion. As shown above the Trust remains in surplus throughout the projection period except for two years: 2020/21: the (0.1)m deficit is projected due to the increased finance costs incurred during construction, with the benefits not being realised until the building is completed in the following year. 2021/22: the (7.1) m deficit is projected due to the one-off impairment charge described above of 402
211 211 of 402
212 Figure [9.2]: Incremental impact of the investment on income and expenditure m 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Income Protected revenue Research & training Other Total income Operating costs Pay Non-pay Total operating expenses Earnings before Interest, Tax, Depreciation and Amortisation (EBITDA) Impairment (8.2) Depreciation & amortisation (1.0) (2.5) (2.5) (2.5) (2.5) Financing - (0.0) (0.0) (0.1) (3.7) (3.6) (3.3) (2.9) (2.6) (2.1) Public Dividend Capital (PDC) - (0.3) (0.6) (1.3) 0.5 (0.9) (0.7) (0.4) Surplus/(deficit) - (0.3) (0.6) (1.4) (2.0) (8.7) (0.8) of
213 The incremental impact of the investment on income and expenditure described above shows: The investment is projected to generate a marginal increase in income ( 30,000 per year) from research and development and other income. Pay and non-pay cost reductions are described above. The investment is projected to increase EBITDA by 6.3m (recurrently) by the end of the projection period. The impairment relates to the revaluation of the new building, as described above. Depreciation on the new building is projected to start from 2021/22, as the building is brought into use. The investment is projected to cause an increase in financing costs throughout the construction and operating phases. This relates to the cost of financing the bridging loan described above in Figure [9.2]. This is a short term loan that could be substantially repaid within five years but to be prudent the Trust has modelled as having a ten year term. The net impact of the investment is a deficit through construction from 2017/18 and into the first year of full operation (2022/23). As loan repayments reduce the financing cost, the investment is projected to yield a surplus from 2023/ of 402
214 Figure [9.3]: Net deficit/surplus bridge between the baseline and investment cases at 2025/26 8.0m 7.0m 6.0m 4.4m (2.5)m 5.0m 4.0m (2.1)m 3.0m 2.0m 1.9m 0.9m 2.2m 1.0m - (1.0)m (0.3)m Baseline case 2025/26 deficit Pay costs Non-pay costs Depreciation & amortisation Financing PDC Investment case 2025/26 surplus The (0.3)m net deficit forecast in 2025/26 for the baseline case is significantly improved in the investment case to a 2.2m net surplus. As noted above, the additional financing cost is expected to fall to nil from 2026/27, further improving the investment case position over the baseline case Statement of financial position The investment case statement of financial position is set out below, along with the incremental impact assessed against the baseline case (the statement of financial position for the full baseline case is included in Appendix [20]). 214 of 402
215 Figure [9.4]: Projected statement of financial position for the investment case m Property, plant and equipment 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Trade receivables Other current assets Cash and cash equivalents Total assets Trade payables (6.8) (6.9) (6.9) (7.0) (6.8) (6.1) (6.0) (5.9) (5.8) (5.7) Loans: current (12.5) (12.5) (12.5) (12.5) (12.5) (12.5) Other current liabilities (18.1) (12.4) (11.2) (11.2) (11.2) (11.2) (11.2) (11.2) (11.2) (11.2) Loans: non-current (112.5) (100.0) (87.5) (75.0) (62.5) (50.0) Other non-current liabilities (0.0) (0.0) (0.0) (0.0) (0.0) (0.0) (0.0) (0.0) (0.0) (0.0) Total liabilities (24.9) (19.4) (18.2) (18.2) (143.0) (129.9) (117.2) (104.6) (92.0) (79.4) Net assets PDC Retained earnings Revaluation reserve Total equity The investment case projected statement of financial position shows: The property, plant and equipment balance is projected to increase significantly in the construction phase from 2017/18 to 2021/22. An impairment of the new building of 8.2m is projected in 2021/21 as set out in the assumptions above. The sale of the St Pancras site is projected to be phased between 2022/23 and 2025/26, reducing the property, plant and equipment balance significantly in each of these years. The trade receivables balance is projected to remain fairly constant, as no significant changes in trade receivables days are assumed. Cash is projected to remain above the Trust s requirement of 20.0m, which is sufficient to meet its working capital requirements. Cash is discussed further in the following section. 215 of 402
216 The fall in the trade payables balance of around 1.1m between 2017/18 and 2025/26 is driven by the reduction in other expenses which form part of CIP savings. There are no significant changes in trade payables days assumed over this period. A loan of 125.0m is projected to be drawn down in 2020/21 (current element: 12.5m, non-current element: 115.5m). As noted in the assumptions table, this is the amount required for the Trust to maintain a minimum cash balance of 20m, required for working capital. As shown below the Trust s cash balance presents an opportunity to optimise these loan arrangements to improve the net surplus position and this will be considered further throughout the Trust s business case process as part of the commercial dialogue with the Independent Trust Financing Facility (ITFF). The capital receipt from the redevelopment of the SPH site is expected to be greater than this. In the Trust s OBC, a red book valuation has been undertaken as per NHSI and HMT guidance which presents a prudent value. Therefore, the risk of not achieving a level of capital receipt to cover the costs of the redevelopment is low. Figure [9.5]: Incremental impact on the projected statement of financial position m Property, plant and equipment 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Cash and cash equivalents - (15.6) (18.8) (37.2) 13.7 (27.5) (19.7) (10.4) (0.2) 25.5 Total assets - (0.3) (0.9) (2.2) Trade payables Loans: current (12.5) (12.5) (12.5) (12.5) (12.5) (12.5) Loans: non-current (112.5) (100.0) (87.5) (75.0) (62.5) (50.0) Total liabilities (124.8) (111.7) (99.1) (86.6) (74.0) (61.5) Net assets - (0.3) (0.9) (2.2) (4.3) (13.0) (13.8) (13.5) (12.4) (9.8) Retained earnings - (0.3) (0.9) (2.2) (4.3) (13.0) (13.8) (13.5) (12.4) (9.8) Total equity - (0.3) (0.9) (2.2) (4.3) (13.0) (13.8) (13.5) (12.4) (9.8) The incremental impact of the investment on the statement of financial position shows the following: The property, plant and equipment balance increases during the construction phase, subsequently falling as the St Pancras site is sold. The negative impact on the cash balance is managed through the projected loan draw down, so that the Trust maintains sufficient cash for its working capital requirement. 216 of 402
217 The trade payables balance is projected to decrease by 1.0m as a result of the CIPs enabled by the investment that reduce other expenses. Loans are drawn down and repaid. Retained earnings is lower in the investment case, principally due to the additional financing costs ( 21.1m), additional depreciation ( 11.1m) and impairment of the new building ( 8.2m), which is partially offset by the improved underlying cost base ( 30.6m) Cash flows Figure [9.6] below sets out the sources and uses of funding for the proposal on the Trust for the scheme. It can be seen that the funding is provided through a source of land value from SPH, Tottenham Mews and Trust reserves. [Figure 9.6]: Source and uses of funds excluding external financing Sources of funds Uses of funds SPH Land value 95.4 Land receipt for Trust space 5.0 Tottenham Mews 12.0 Land purchase 14.5 Hanley Road 1.0 New inpatient facility 59.0 Trust reserves 32.0 Community hubs 40.6 SPH hub 16.4 Fees 4.9 Total Total Figure [9.7] below shows the cash flow statements for the investment case. The incremental impact of the investment against the baseline case is shown on the following figure and the full baseline cash flow statement is included in Appendix [21]. 217 of 402
218 Figure [9.7]: Projected cash flow statement for the investment case m 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Surpus from operations Movement in working capital (Inc)/dec in NHS trade receivables (1.3) (0.0) (0.0) (0.1) (0.1) (0.1) (0.1) (0.1) (Inc)/dec in non-nhs trade receivables (0.0) (0.0) (Inc)/dec in other receivables (Inc)/dec in prepayments (0.2) Inc/(dec) in deferred income Inc/(dec) in provisions (0.3) Inc/(dec) in trade payables (0.0) 0.1 (0.2) (0.6) (0.1) (0.1) (0.1) (0.1) Inc/(dec) in other payables (2.1) Inc/(dec) in accruals 2.7 (5.7) (1.2) Net cash inflow/(outflow) from operating activities Capital expenditure (4.2) (20.7) (7.3) (21.2) (76.0) (32.7) (4.5) (4.1) (4.1) (4.1) Proceeds on disposal of PPE Net cash inflow/(outflow) (4.2) (20.7) (7.3) (8.2) (76.0) (32.7) from investing activities Dividends paid (4.1) (4.3) (4.7) (4.8) (2.9) (4.2) (3.9) (3.5) (3.1) (2.2) Net interest (paid)/received (3.5) (3.5) (3.2) (2.8) (2.4) (2.0) Drawdown/(repayment) of loans (12.5) (12.5) (12.5) (12.5) (12.5) Net cash inflow/(outflow) (4.0) (4.3) (4.6) (4.8) (20.2) (19.6) (18.8) (18.0) (16.6) from financing activities Net cash inflow/(outflow) 2.9 (19.1) (1.2) (1.9) 54.3 (38.6) Opening cash balance Closing cash balance The cash flow statements show the following: Surplus from operations corresponds to the EBITDA shown in Figure [9.1]. 218 of 402
219 Working capital movements are as described below. These show minimal projected movements in the working capital requirement, apart from accruals. Capital expenditure includes the capital investment, as well as ongoing maintenance capped at between 2.3m and 2.7m per year. Proceeds on the disposal of Property Plant and Equipment (PPE) includes the sale of Tottenham Mews ( 12.0m) and Hanley Road ( 1.0m) in 2019/20 and receipts relating to the sale of St Pancras of 19.1m each year from 2022/23 to 2024/25 and a final receipt of 33.2m in 2025/26. The increase in interest costs relate to the financing of the bridge loan, which is due to be fully repaid by the end of 2025/26. The projections show a minimum cash balance of 21.8m in 2019/20, which is sufficient to cover its working capital position. Figure [9.8]: Incremental impact of the investment on the cash flow statement m 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Surplus from operations Movement in working capital (Inc)/dec in non-nhs trade receivables (0.0) (0.0) Inc/(dec) in trade payables (0.2) (0.6) (0.1) (0.1) (0.0) (0.0) Net cash inflow/(outflow) from operating activities Capital expenditure - (15.4) (2.5) (17.1) (71.9) (28.6) (0.4) Proceeds on disposal of PPE Net cash inflow/(outflow) - (15.4) (2.5) (17.1) (71.9) (28.6) from investing activities Dividends paid - (0.3) (0.6) (1.3) 0.5 (0.9) (0.7) (0.4) Net interest (paid)/received - (0.0) (0.0) (0.1) (3.7) (3.6) (3.3) (2.9) (2.6) (2.1) Drawdown/(repayment) of loans (12.5) (12.5) (12.5) (12.5) (12.5) Net cash inflow/(outflow) - (0.3) (0.6) (1.4) (17.1) (16.5) (15.8) (15.1) (13.8) from financing activities Net cash inflow/(outflow) - (15.6) (3.1) (18.4) 50.9 (41.3) Opening cash balance - - (15.6) (18.8) (37.2) 13.7 (27.5) (19.7) (10.4) (0.2) Closing cash balance - (15.6) (18.8) (37.2) 13.7 (27.5) (19.7) (10.4) (0.2) of 402
220 The incremental impact of the investment on the Trust s cash flows over the baseline shows: An improvement in surplus from operations, resulting from the CIPs that are enabled by the investment. A slight decrease in trade payables, driven by the reduction in other expenses CIPs. apital expenditure relating to the investment. Proceeds from the sale of the St Pancras site. Note that the sale of Tottenham Mews and Hanley Road in 2019/20 are assumed in both baseline and investment cases and therefore does not form part of the incremental impact. The million bridging loan (assumed to be ITFF) is projected to be drawn down in 2020/21 and repaid at 12.5m per year over 10 years by The net impact on cash of the investment is projected to be a cash outflow in each year of the projections except 2020/21, due to the loan receipt, and in 2025/26, when the final payment for the St Pancras site is assumed to be received. There is no assumed income statement impact from the disposals at this stage. The Trust will formally review this treatment at FBC stage once the development partner is identified as in the commercial case. This will not impact on affordability insofar as it does not impact on cash and would be treated as an exceptional item if a gain were recognised. The principal factors of the investment that impact the cash balance at 2025/26 are illustrated in Figure [9.9] below. 220 of 402
221 Figure [9.9]: 2025/26 cash bridge from the baseline to the investment case 200.0m 125.0m 150.0m 100.0m 30.6m (1.0)m (62.5)m 97.1m 71.5m (18.3)m 90.4m 50.0m (2.8)m - (50.0)m Baseline case 2025/26 cash Operating surplus Working capital differences (135.8)m Capital expenditure Proceeds on disposal of PPE PDC dividend paid Loans drawndown Loans repaid Net interest Investment case 2025/26 cash The main differences in cash between the baseline and investment cases arise from the following cumulative impacts: Operating surplus: 30.6m, of which 21.0m relates to other expenses, 9.4m relates to reduced pay costs and 0.2m relates to additional income. Capital expenditure of 131.0m is set out in the capital bridge above. The drawdown of a 125.0m loan to bridge the temporary cash shortfall 10. Loans repaid of 62.5m. 221 of 402
222 10 The Trust have assumed a 125m facility is available at ITFF rates. There is a risk that this funding will not be available at the time it is needed or altogether which could delay the project timescales. 222 of 402
223 Net interest paid increases by 21.1m, relating to the bridging loan described above. 9.4 Impact on financial sustainability risk rating (FSRR) The financial sustainability risk rating (FSRR) is NHSI s view of the level of financial risk a Trust is exposed to and is a therefore key metric to consider for this transaction. Ratings go from 1 to 4, where 1 is the highest risk and 4 is the lowest risk. The FSRR scores for the investment and baseline cases are set out in Appendix [22]. The FSRR calculation performed by the LTFM yield a capital service cover risk rating of 1 for the investment case, as the bridge loan repayments are included in the debt service total 9.5 Sensitivities The Trust has run a number of sensitivities to understand the impact of different risks on the project: 1. Construction programme delay by one year: This has an initial I&E and cash benefit, but worsens the position by 2025/26 as the benefits are also delayed. 2. Development/capital cost increase by 10%: This has a limited impact on the net surplus (decreasing it by 0.8m by 2025/26) but it reduces the forecast cash balance by 15.3m by 2025/ Land value at Whittington 50% higher: This has a limited I&E impact (decreasing it by 0.5m by 2025/26), but reduces forecast cash by 10.0m by 2025/ Land value at SPH 10% lower: This has a limited I&E impact (decreasing it by 0.4m by 2025/26), but reduces forecast cash by 11.6m by 2025/ Benefits delivered at 50% below plan: This reduces the recurrent net surplus by 3.8m 2.3m and cash by 16.6m at 2025/ Benefits delivered at 30% below plan: This reduces the recurrent net surplus by 2.3m and cash by 10.0m at 2025/ Recurrent CIP 30% lower than plan: This reduces the recurrent net surplus by 5.7m and cash by 21.3m at 2025/ Pay costs 5% higher than plan: This reduces the recurrent net surplus by 6.7m and cash by 40.2m at 2025/26. As this sensitivity is also considered in the baseline case analysis, it has no impact on the incremental impact of the transaction. 9. Pay costs 2.5% higher than plan: This reduces the recurrent net surplus by 3.4m and cash by 20.2m at 2025/26. As this sensitivity is also considered in the baseline case analysis, it has no impact on the incremental impact of the transaction. The sensitivities set each have minimal or no impact on the forecast FSRR score when considered individually. A combined downside case will be considered in the Trust s FBC along with the impact on the FSRR, including the impact of delays in land receipts. 223 of 402
224 9.6 Conclusions The projections show that the Trust will have sufficient cash to implement the investment, while maintaining sufficient headroom for the working capital requirement. The adjusted FSRR scores also imply an acceptable level of financial risk. The projections require that a bridge loan of 125.0m is made available by the ITFF from 2020/21. The Trust will need to secure a commitment on this loan or to make alternative funding arrangements in order to proceed with the investment. There is no financial impact on any other parties, including both of the CCGs due to the block-payment contract provided to the Trust for the delivery of mental health services. 224 of 402
225 10 Implementation This sections sets out what happens after the consultation phase, namely, how the Trust plans to manage the project and sets out in more detail the actions that will be required to ensure the successful delivery of the scheme in accordance with best practice Post consultation process Following the close of the consultation and decision-making process as set out at the end of Section [7], the CCGs will hand back decision making responsibility to the Trust. The Trust will implement the proposal, having already factoring in considerations from the consultation process, as set out in subsequent sections Programme management arrangements The Trust has implemented a robust programme management and governance structure which ensures accountability through clear allocation of responsibilities, and provides assurance through regular reporting, enabling quick identification and addressing any issues as they arise. This section describes the following programme management arrangements: Programme management approach; Project implementation budget; Risk Management Arrangements; and Benefits management Programme management approach The Trust will follow the PRINCE2 principles in their approach to project management to ensure the delivery of the project. This is the de facto standard in use in the public sector in the UK. Project implementation budget The implementation costs for the project are expected to be 4.9m in nominal terms over the project implementation period and are inclusive of costs associated with the programme team, town planning and technical support. 225 of 402
226 Risk Management The risk management strategy is in line with the HM Treasury Green Book and NHS guidance for capital projects. There is an existing risk management process in place for the Programme, and this process will continue throughout the implementation and delivery phase of the programme to ensure that risks are identified, monitored and where possible, mitigated. The overarching risk management policy is based on an iterative process of: Identifying and prioritising the risks to the achievement of the Programme aims and objectives; Evaluating the likelihood of those risks being realised and the impact should they be realised; Managing the risks efficiently, effectively and economically. The Programme Office maintains the Risk Register for the Programme. Project risks registers are maintained by the project manager/work stream lead and risks escalated where necessary via reporting Programme governance structure The key elements of the programme governance structure include: A clear governance and delivery structure from operational workstreams to the Trust Board. The structured relationship between programme management and delivery. The interface between the Programme Board and its assurance mechanism. The interface between the Trust Board and its assurance mechanism. 226 of 402
227 The programme governance structure surrounding this project is illustrated in the diagram below: Figure [10.1]: Project Governance Structure The day to day development of the case is delivered by a series of project workstreams within which the membership will vary in line with the specific needs of the workstream and the phase of the business case. Finance and Procurement 227 of 402
228 Lead: Director of Finance, the Trust or nominee To monitor the development expenditure and advice on elements such as cash flow, VAT and compliance with finance requirements. Procurement should advise on best practice for contracts and equipping new schemes. Workforce Lead: Director of HR & OD, the Trust Review the project for any impact on the workforce that creates change, and set out the process for achieving this within the business case. Estates Lead: Director of Estates and Facilities, the Trust To review the proposals for Estates issues and advise and provide solutions. Operational Lead: Chief Operating Officer, the Trust or nominee To review the design proposals, advise on operation issues such as compliance and working with Trust objectives and policies. Clinical Lead: Medical Director, the Trust or nominee Review the clinical implications of the design proposals. IM & T Lead: Associate Director of ICT, the Trust Review the design proposals against the Trust IT strategy and advice how this can be best delivered. Partnership Lead: Transformation Programme Director, the Trust 228 of 402
229 To work closely with the Trust partners to keep them informed and understand and report on any deliverables, groups include: On Site Partner, Stakeholders Holder Reference Group, Council of Governors Site Development Working Group. Communication Lead: Head of Communications and Engagement, the Trust To set out the communication strategy to deliver and monitor the plan Trust implementation team The Trust implementation team will comprise approximately 4-6 people on a whole time equivalents (WTE) basis to be engaged at various points during the implementation. The function requirements during the implementation include: Programme Director; Project Director; Project Managers: Main Inpatient Build; Community Projects; St Pancras Hub and Disposal; Finance Support; HR and Workforce Support; Clinical Support; and Administration. Figure [10.2]: Trust implementation team Role 2017/ / / / / /23 Programme Management Office WTE WTE WTE WTE WTE WTE 229 of 402
230 Role 2017/ / / / / /23 Leadership ¼ Management 1 ¼ 2 1 ¾ ½ Activity Modelling ½ ½ Financial HR support ¾ ½ ½ Project Support Total 4 ½ 5 ¼ 4 ¼ 5 ½ 5 ¼ 2 ¾ This proposed staffing profile for the implementation team has been informed by the recommendations of the Project Director based on experience of similar schemes Project implementation plan The key milestones for implementation are set out in Figure [10.3] below. These milestones will be updated on a regular basis as more information becomes available and the project develops. For further details on the consultation phase and approval timeline, see Section [7.5]. Figure [10.3]: Project milestones Date TBC Key item Approval of OBC 230 of 402
231 Date TBC TBC TBC TBC TBC TBC TBC TBC TBC June 2022 February 2022 August 2023 TBC Key item Go to market for Development Partner Appointment of Development Partner Planning application for new inpatient facility Planning application for community facilities Planning Application for SPH Completion of FBC Approval of FBC Construction of new inpatient facility completed Decant of inpatients into new inpatient facility Community hubs operational Redevelopment of SPH site begins SPH site operational (for C&I) Post project evaluation 10.4 Post project evaluation The Trust has developed a high level post project evaluation plan which identifies the mechanisms that would enable monitoring and review of performance at different stages of the project. These are to be shared with and approved by the Trust at each key milestone. 231 of 402
232 A thorough and robust post project evaluation will: Facilitate continual learning from the project to be implemented at subsequent stages as well as future projects. Ensure that the project adheres to the project plan/ milestones and review of project risks Enable measuring of project performance against project aims including the realisation of benefits Provide useful feedback and knowledge that can be shared with key stakeholders as well as the NHS as a whole. The key components of the Trust s post project evaluation arrangements are: A review of performance against Project Programme throughout the life of the project; A review of actual performance toward achieving the benefits detailed in the Benefits Realisation Plan and confirmation that they have been met; A review of project implementation to learn lessons for future; and A review of the FBC capital and revenue costs to assess their robustness and accuracy. At the OBC stage, Design Quality Indicator (DQI) workshops have been conducted to review and improve the design and construction approach based on input from a range of stakeholders. Going forward, service users, staff and the project team will be asked to evaluate the project through the use of questionnaires, stakeholder consultation meetings, staff focus groups and benefits realisation data. The arrangements for the Post Project Evaluation will be established in accordance with best practice. The Trust will identify responsibilities and resource requirements for management of the Post Project Evaluation during the FBC development period, and Post Project Evaluation will be an integral part of the post implementation operating model Approvals process for investment by the Trust NHS Improvement require Trusts to submit a SOC, OBC and FBC for approval for capital investment proposals of this value (i.e. > 50m). The SOC submitted to NHSI in November 2016 has already been approved, while the OBC was submitted in June 2017 and is currently going through approvals with an open dialogue with NHSI. The FBC may take between 3-6 months to gain approval. The process for approval of each case is shown in figure [10.3]. 232 of 402
233 Figure [10.3]: Capital Business Case Approval Process HM Treasury Consultation with DHSC NHS Improvement Resources Committee Approval NHS Improvement Board Approval DHSC Approval HM Treasury Approval Source: Capital Regime, Investment and Property Business Case Approval Guidance for Trusts and Foundation Trusts, NHS Improvement, of 402
234 11The SoS s Four Tests NHS England, in Planning and delivering service changes for service users published in December 2013, outlined good practice for commissioners on the development of proposals for major service changes and reconfigurations. Building on this, the 2014/15 mandate from the Secretary of State to NHS England, outlines that proposed service changes should be able to demonstrate evidence to meet four tests: 1. Strong public and patient engagement; 2. Consistency with current and prospective need for patient choice; 3. A clear clinical evidence base; and 4. Support for proposals from clinical commissioners. Reconfiguration proposals must meet the four tests before they can proceed. These tests are designed to demonstrate that there has been a consistent approach to managing change, and therefore build confidence within the service, and with service users and the public Test 1: Strong public and patient engagement This test evaluates how service users and the public have been involved in the development of the proposals for the redevelopment of the St Pancras site. The extensive stakeholder engagement undertaken to date and that which is proposed over the course of the project is laid out in detail in Section [7] of this document. The methods and approaches for consultation have included presentations, discussions, surveys, meetings and s. A summary of these activities includes; 15 Service User engagements; 5 Staff engagements; 5 Carer engagements; 5 for senior stakeholders; 2 Governor engagements; 5 Healthwatch engagements; 234 of 402
235 5 local community engagements; 1 local resident engagement. The figure below lists each of the committees who have considered the pre-consultation plan and associated engagement activities. Figure [11.1]: Staff Engagement Meeting/approach Date How were participants informed Staff-side meeting 14 March 2017 Peckwater Centre staff 28 March 2017 Highgate Mental Health staff 04 April 2017 Presentation St Pancras staff 05 April 2017 Lowther Road staff 05 April 2017 C&I Senior Leadership Team Meeting 24 April 2017 Presentation St Pancras and Greenland Road staff 11 May 2017 Presentation Highgate Mental Health staff 12 May 2017 Presentation All-staff briefing 24 May update for staff 02 February 2018 Update C&I staff briefing, Greenland Road 30 April 2018 Presentation C&I staff briefing, St Pancras 01 May 2018 Presentation C&I staff briefing, Lowther Road 03 May 2018 Presentation C&I staff briefing, Highgate 04 May 2018 Presentation Figure [11.2]: Service User and Carer Engagement Meeting/approach Date How were participants informed cbug, ibug, Nubian Users Forum, Women s Strategy Group 24 March 2017 Service User Alliance 31 March 2017 Service Users Conference at St Pancras 13 April 2017 Presentation followed by Q&A session cbug 25 April 2017 Islington Carers Hub 28 April 2017 Discussion Camden Carers Hub 19 May of 402
236 ibug 27 June 2017 Nubian Users Forum 18 July 2017 Presentation Service User Alliance 22 September 2017 Briefing SMS Service Users at Margarete Centre 28 September 2017 Frontline Service Users 02 November 2017 Meeting of CPPEG 06 November 2017 icope Islington 15 November 2017 Carers Partnership Meeting 09 January 2018 Discussion and Q&A session Healthwatch inpatient survey 24 January 2018 Verbally by Healthwatch and then asked a series of questions Healthwatch inpatient survey 26 January 2018 Verbally by Healthwatch and then asked a series of questions Healthwatch inpatient survey 30 January 2018 Verbally by Healthwatch and then asked a series of questions Extraordinary Service Users Forum 02 February 2018 Update presentation followed by Q&A session Islington Carers Meeting 06 February 2018 Verbally by Healthwatch and then asked a series of questions Camden Carers Meeting 16 February 2018 Verbally by Healthwatch and then asked Previous inpatients Through March 2018 a series of questions Verbally by Healthwatch and then asked a series of questions St Pancras Redevelopment Consultation Review Group 07 March 2018 Papers and verbally Two borough community hubs engagement event 15 March 2018 Presentation Communications meeting with Paul Ware 19 March 2018 Verbally Meeting with Paul Ware 18 April 2018 Verbally Nubian Service Users' Forum 09 May 2018 Presentation Figure [11.3]: Senior Stakeholder Engagement Meeting/approach Date How were participants informed Stakeholder Reference Group meeting 27 July 2016 Discussion 236 of 402
237 Stakeholder Reference Group meeting 05 October 2016 Discussion Stakeholder Reference Group meeting 26 January 2017 Discussion Stakeholder Reference Group meeting 27 February 2017 Discussion Stakeholder Reference Group meeting 29 March 2017 Discussion JHOSC 21 April 2017 Presentation North Central London JHOSC 19 September 2017 Presentation Stakeholder Reference Group meeting 24 October 2017 Discussion Knowledge Quarter 01 November 2017 Presentation followed Clinicians community hubs meeting 26 January 2018 Discussion North Central London Joint Health Overview Scrutiny Committee 23 March 2018 Presentation Stakeholder Reference Group meeting 24 April 2018 Discussion Figure [11.4]: Governor Engagement Meeting/approach Date How were participants informed Council of Governors 09 May 2017 Presentation update for governors 02 February 2018 Update C&I Council of Governors 08 May 2018 Presentation 11.2 Test 2: Consistency with current and prospective need for patient choice This test is to illustrate whether the proposed redevelopment will maintain the availability of service user choice. For most service users that currently access mental health services in the Borough of Camden and Islington, the entry pathway will remain the same following the proposed redevelopment. As the clinical model remains unchanged, with the majority of services continuing to be delivered in the community and via primary care, the range of service user choice is unaffected. For service users of the inpatient facilities at St Pancras, the proposed changes will have minimal impact on the choices available due to the fact that there is no change in the number of providers serving the local area and the Trust s own services are moving 2.5 miles further away. 237 of 402
238 Currently the closest alternative provider of inpatient mental health is at Gordon Hospital (operated by CNWL and 3.7 miles from St Pancras and 5.8 miles from the Whittington site). In respect of the fact that many users of this service are admitted to the facility under the Mental Health Act, the relocation would be insignificant in terms of impact on patient choice. In addition, the travel time identified, there should not be any services users that, following the relocation of services to the Whittington site, would find the travel time an issue or that their choice of provider has substantively diminished. This will be discussed further with service users as part of the consultation phase following approval of the PCBC. Patient choice would also be improved from a quality perspective as with the proposed redevelopment, service users would have a purposebuilt, higher quality, and safer facility from which to receive care than is available currently. This increase in the quality is in line with the CCGs and the Trust s vision to deliver their vision of excellence; We will continually improve the quality and safety of service delivery, service user experience and improve outcomes Test 3: A clear clinical evidence base This test is to demonstrate sufficient clinical evidence and clarity on the case for change. This is clearly outlined in Section [4]. The independent verification of this case for change will be gained through submission for consideration by the London Clinical Senate, engagement with a range of clinicians as detailed below, and using reports from the CQC reports. The model of care and proposals to relocate certain services have the support of the CCG GP mental health leads and were developed by the Trust s Medical Director and Director of Nursing. CQC Report The Trust s most recent CQC report was published in March 2018, where the Trust received an overall rating of Good. The previous report, published in June 2016 identified the deteriorating St Pancras Hospital site compared to the refurbished HMHC. Due to the ageing and inflexible site at St Pancras, there is a clinical need to move service users to a site without multiple ligature points and multiple blind spots from where staff cannot easily observe service users. After publication of the 2016 report, the CQC was briefed on the Trust s plans to review the entire St Pancras estate. London Clinical Senate The Clinical Senate Liaison group contacted the London Clinical Senate for advice on: Whether the change of environment will improve clinical care for inpatient and community services 238 of 402
239 Whether the proposals for changes to inpatient and community mental health services: o will enable improvements in clinical care and quality benefits for patients o are informed by best practice o align with national policy and are supported by STP plans and commissioning intentions Whether the approach ensuring the inpatient demand of population growth is absorbed by the development of mental health community services. The LCS will provide feedback after submission of the PCBC to the CCG GBs. However, consultation will not commence unless LCS have approved the consultation plan. Clinical engagement A wide range of clinicians have been engaged and consulted throughout the process to ensure proposals have patient outcomes central to plans. There has been broad and varied communication with a range of clinical staff, further details of which can be found in Figures 7.3 and 7.3. Of particular note are the GB Seminars, which the Trust presented the redevelopment plans. CCG GB leads have been involved in the process throughout, alongside the member GPs. Furthermore, a meeting of clinical leads from the local health organisations was held on 26 January 2018 to discuss the community hubs. The Trust is scheduled to attend the Camden GP locality meetings in April 2018 and Islington GPs were updated in March A number of engagement events for Trust staff have been held at various Trust locations where clinicians have attended. Trust clinicians also continue to be kept informed through existing internal meeting structures. Feedback provided demonstrated a strong level of support for the proposal with a consensus that the changes identified would improve services for service users. A letter of support from the Trust s Director of Nursing, dated June 13 th 2017, provides this assurance on behalf of the clinicians at the Trust, stating that considering the environmental challenges around access, ligature management, the privacy and dignity of our service users and infection control, we believe that the proposal reflects the collective view on how our local services should be configured. This can be found in Appendix [23] Test 4: Support for proposals from clinical commissioners. This test is to provide assurance that the proposals have the approval of local commissioners. 239 of 402
240 Both of the CCGs have been involved and provided their support for the proposed redevelopment as joint commissioners of the Trust. The Chief Operating Officer for Haringey and Islington CCG has led the engagement on behalf of Camden and Islington CCGs and been the primary communicator to senior stakeholders. They also lead the St Pancras Hospital Redevelopment Oversight Group, providing guidance over the Consultation work stream and with representation from Camden CCG and Islington CCG. Figure [11.5]: Meeting/approach Islington GP Forum South Camden GP Locality meeting North Camden GP Locality meeting West Camden GP Locality meeting Date 22 March April April April 2018 How were participants informed Presentation Target audience s GPs Presentation GPs 16 Presentation GPs 10 Presentation GPs 13 Number of attendees/num ber of hits or users 11.5 NHSE s Bed Closures Test From 1 April 2017, NHSE introduced a new test to evaluate the impact of any proposal that includes a significant number of bed closures and to ensure commissioners are able to evidence that one of the following three conditions have been met; Sufficient alternative provisions have been made, such as increased GP or community services; New treatments or therapies will reduce specific categories of admissions, or; Where a hospital has been using beds less effectively than the national average, that there is a credible plan to improve performance without affecting patient care. This test is only applied where the proposal includes plans to significantly reduce bed numbers. As this proposal maintains the current inpatient bed provision following activity and bed modelling, as outlined in further detail in section 5, this test is not applicable. 240 of 402
241 241 of 402
242 12 Decision making and next steps Following consultation, the St Pancras Hospital Redevelopment Oversight Group will review consultation responses received from members of the public and organisations. The committee will then consider the views of the participants and the effect these may have on the decisionmaking process. At this stage of the development of options, it is not possible to fully detail the timescales in which decisions will be taken and when subsequent implementation could take place. This is due to a number of factors, including: The quantity and detail of consultation responses received, and timescales required to analyse those responses; The consideration of consultation responses by the St Pancras Hospital Redevelopment Oversight Group and subsequent update of analysis and evaluation of options as required; The development of a decision making business case and confirmation by the St Pancras Hospital Redevelopment Oversight Group; and The development of detail implementation plans between providers and commissioners on the basis of the decision made by the St Pancras Hospital Redevelopment Oversight Group. However, to give an indicative timeline, the programme expects the following milestones for this process. These may be subject to change, as described above: Formal public consultation July September 2018 (12 weeks). External analysis of consultation responses October Final business case preparation November 2018 Each CCG GB to consider the final business case document November 2018 Each CCG to make a decision on the final business case November of 402
243 Appendix Contents Appendix Name Number 1 Trust services provided at SPH relocation summary 2 Other Provider s services at SPH 3 Travel time report 4 Privacy Impact Assessment (PIA) screening questions form 5 Pre-consultation engagement meetings 6 NCL STP stakeholder engagement summary 7 JHOSC meeting minutes 8 Consultation plan 9 Consultation document, questionnaire and FAQs 10 Options development summary 11 Feasibility Study 12 Options considered 13 Qualitative assessment workshop summary 14 Qualitative assessment scoring 15 Qualitative scores of each option 16 Backlog maintenance 17 Quantifiable benefits 18 Trust s Income & Expenditure assumptions 19 Baseline income and expenditure 20 Baseline statement of financial position 21 Baseline cash flow statement 22 Trust FSRR scores for the investment and baseline cases 243 of 402
244 23 Letter of support from the Trust s Director of Nursing 24 Bed modelling benchmarking 25 Occupied Bed Days Trend Analysis 244 of 402
245 Appendix 1 Trust services provided at SPH relocation summary Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road ST PANCRAS Dunkley Ward (16 bed mixed sex with 4 learning disability beds) ACUTE Laffan Ward (16 bed mixed acute mental health) ACUTE Rosewood Ward (12 bed female acute mental health) ACUTE Ruby Ward (11 bed female PICU) ACUTE Montague Ward (14 mixed high dependency rehab ward) R&R Sutherland Ward (14 mixed long-term complex care ward) R&R Complex Depression, Anxiety and Trauma Service COMMUNITY Camden & Islington Psychodynamic Psychotherapy Service COMMUNITY 245 of 402
246 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road Sexual Problems Team COMMUNITY South Camden icope COMMUNITY Traumatic Stress Clinic COMMUNITY NHS Transition, Intervention and Liaison Veterans Mental Health Service (formally known as LVS) COMMUNITY ADHD Team Attention Deficit Hyperactivity Disorder COMMUNITY Adult Autism Clinic COMMUNITY Camden Mental Health Assessment and Advice Team COMMUNITY Islington Practice Mental Health Team COMMUNITY South Camden Crisis Resolution Home Treatment ACUTE Acute Day Unit (Jules Thorn) ACUTE 246 of 402
247 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road The Rivers Crisis House (subject to separate review) Approved Mental Health Professional Service ACUTE Recovery College COMMUNITY Pharmacy ACUTE Clozapine Clinic COMMUNITY HIGHGATE Sapphire Ward (16 bed mixed acute mental health) ACUTE Emerald Ward (15 bed mixed acute mental health) ACUTE Opal Ward (16 bed mixed acute mental health) ACUTE Jade Ward (16 bed mixed acute mental health) ACUTE 247 of 402
248 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road Amber Ward (16 bed mixed acute mental health) ACUTE Topaz Ward (16 bed acute mental health) ACUTE Pearl Ward (14 bed mixed older people with mental illness) SAMH Highgate Day Centre R&R Malachite Ward (16 bed mixed high dependency rehabilitation) R&R Coral Ward (12 bed male PICU) ACUTE Garnet Ward (14 bed mixed dementia care) SAMH Personality Disorder Therapies Team COMMUNITY Personality Disorder Community Team COMMUNITY Accommodation Team R&R 248 of 402
249 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road GREENLAND ROAD Camden Assertive Outreach Team R&R Islington Assertive Outreach Team R&R COMMUNITY Camden Early Intervention Team R&R Islington Early Intervention Team R&R Focus Homeless Outreach COMMUNITY LOWTHER ROAD North Islington Rehabilitation and Recovery Team R&R Cornwallis Outreach Project R&R Islington Mental Health Re-ablement Service R&R PECKWATER CENTRE 249 of 402
250 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road Camden Community Team SAMH Camden Memory Service SAMH Care Home Liaison Team SAMH South Camden Recovery Team R&R BLENHEIM COURT (NON-CLINICAL SITE) Dementia Navigators SAMH Home Treatment Team SAMH Islington Community Mental Health Team SAMH Islington Memory Team SAMH Care Home Liaison Team SAMH 250 of 402
251 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road MARGARETE CENTRE South Camden Drug Centre SMS ARLINGTON ROAD Camden Alcohol Service SMS THE HOO North Camden Recovery Team R&R DALEHAM GARDENS North Camden Drug Service SMS North Camden Recovery Centre R&R SOUTHWOOD SMITH CENTRE Accommodation Team R&R 251 of 402
252 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road South Islington Recovery Team R&R DRAYTON PARK Islington Learning Disabilities Service COMMUNITY MANOR GARDENS icope - North Islington Team COMMUNITY CAMDEN MEWS Community Recovery Service for Older People - covering both Camden and Islington SAMH Mental Health Liaison Team ACUTE OTHER SITES Aberdeen Park R&R Highview R&R 252 of 402
253 Current locations and services No move (staying as is) Move to new site Move to Greenland Road Move to Lowther Road Stacey Street (subject to separate review) Raglan Day Centre SAMH Whittington Hospital Mental Health Liaison Assessment Team (ILAT), Key: Acute: Acute and Crisis Care (Urgent care) R&R: Recovery and Rehabilitation (Psychosis) SAMH: Services for Ageing and Mental Health (Older people and Dementia) SMS: Substance Misuse Services (Alcohol and drugs) Community: Community Mental Health (Complex psychological and common mental health conditions) 253 of 402
254 Appendix 2 Other Provider s services at SPH NHS Services & description of service Current address Future location Rehabilitation inpatient wards (Central and North West London Foundation Trust) Provides treatment and support for patients whose physical abilities have been reduced through illness, such as a stroke, or a fall or a musculoskeletal condition. Evergreen Ward (University College London Hospital) A ward predominantly for care of the elderly Kidney dialysis clinic (Royal Free Hospital) Ophthalmology clinic (Royal Free Hospital) GP out of hours service (London Central & West Unscheduled Care Collaborative) Kings Cross GP Practice (AT Medics) South Wing South Wing St Pancras Hospital St Pancras Hospital St Pancras Hospital St Pancras Hospital To remain in current building To remain in current building To remain but in a new building To remain but in a new building To remain but in a new building To stay but in a new building 254 of 402
255 Appendix 3 Travel time report Postcode Travel Times by TFL net changes are from SPH to alternative locations Travel times (in minutes) from centre of 4 Fig Postcode to: St Pancras Hospital Proposed site at Whittington Hospital Net change Lowther Road Net change Greenland Road Net Change Location reference (coordinates of centre of post code) EC1Y EC1V EC1R WC1N WC1N WC1X N N N N N , N , N , N , N , N , N , N , N , N , of 402
256 N N NW NW NW NW NW NW NW NW NW NW N N N N N N N NW NW NW NW NW NW NW NW , , , , , , , , , , , , , , , , , , , , , , , , , , , of 402
257 NW NW NW NW NW , , , , , of 402
258 Appendix 4 Privacy Impact Assessment (PIA) screening questions form Documenting here which of the screening questions are applicable to your initiative will help to draw out the particular privacy considerations that will help formulate your risk register later in the template. This will also assist in ensuring that the investment the organisation makes is proportionate to the risks involved: Remember! imagine this initiative involved the use of your own information or that of a relative Yes No Unsure Comments i ii iii iv v vi vii Is the information about individuals likely to raise privacy concerns or expectations e.g. health records, criminal records or other information people would consider particularly private? Will the initiative involve the collection of new information about individuals? Are you using information about individuals for a purpose it is not currently used for, or in a way it is not currently used? Will the initiative require you to contact individuals in ways which they may find intrusive 11? Will information about individuals be disclosed to organisations or people who have not previously had routine access to the information? Does the initiative involve you using new technology which might be perceived as being privacy intrusive e.g. biometrics or facial recognition? Will the initiative result in you making decisions or taking action against individuals in ways which can have a significant impact on them? No change will be made to the way staff access patient information electronically. The Trust stores paper records in a central off-site facility. No new information will be collected. There are no changes to the way data is used. Stakeholders, including patients have been publically and privately engaged throughout. There are no staff changes and data remains with the Trust. There are no new technologies used. No impact of the initiative on decision making. 258 of 402
259 Appendix 5 Pre-consultation engagement meetings Pre-consultation engagement activities Service users and carers Service User Engagement 24-Mar-17 cbug, ibug, Nubian Users Forum, Women s Strategy Group 31-Mar-17 Service User Alliance 13-Apr-17 Service Users Conference at St Pancras 25-Apr-17 cbug 27-Jun-17 ibug 18-Jul-17 Nubian Users Forum 22-Sep-17 Service User Alliance 28-Sep-17 Briefing SMS Service Users at Margarete Centre 02-Nov-17 Frontline Service Users 06-Nov-17 Meeting of CPPEG to road-test Public Consultation document and survey 15-Nov-17 icope Islington 24-Jan-18 Healthwatch inpatient survey 26-Jan-18 Healthwatch inpatient survey 30-Jan-18 Healthwatch inpatient survey 02-Feb-18 Extraordinary Service Users 15-Mar-18 Community hubs engagement event Pre-consultation engagement activities - Staff Staff Engagement 14-Mar-17 StaffSide 28-Mar-17 Peckwater Centre staff 4-Apr-17 Highgate Mental Health staff 5-Apr-17 St Pancras staff 5-Apr-17 Lowther Road Staff 11-May-17 St Pancras and Greenland Road staff 12-May-17 Highgate Mental Health staff 24-May-17 C&I All-staff briefing 24-Jan Jan Jan Feb-18 update for all C&I staff Pre-consultation engagement activities Broader Engagement Broader Engagement 20-Mar-17 Islington and Camden Healthwatch 21-Apr-17 Joint Health Oversight Scrutiny Committee (JHOSC) (elected representatives from local Health Oversight Scrutiny Committees (HOSC)) 28-Apr-17 Islington Carers Hub 09-May-17 Council of Governors 259 of 402
260 19-May Aug Sep Sep Sep Sep Oct Nov Nov Dec Dec Dec Jan Jan Jan Feb Feb Feb-18 Camden Carers Hub St Pancras Community Association Islington Healthwatch Voluntary Action Camden Camden Healthwatch Service User Conference Camden and Islington Healthwatch Knowledge Quarter (DS) Margie Butler, CEO at Camden Citizen s Advice Bureau (MM) Julie Parish, Operational Lead, Octopus Communities (MM) Saul Gallick, Operational Lead and Sam Hopely, Chief Executive, Holy Cross Centre Trust (MM) Carers Partnership Meeting Somers Town Neighbourhood Forum Clinicians community hubs meeting (Trust and CCG clinical leads) update for governors Islington Carers Meeting (Healthwatch) Camden Carers Meeting (Healthwatch) 260 of 402
261 Appendix 6 NCL STP stakeholder engagement summary We have developed a governance structure to enable NHS and local government partners to work together in new ways. The objectives of our governance arrangements are to: Support effective collaboration and trust between commissioners, providers, political leaders and the general public to work together to deliver improved health and care outcomes more effectively and reduce health inequalities across the North London system; Provide a robust framework for system level decision making, and clarity on where and how decisions are made on the development and implementation of the North London STP; Provide greater clarity on system level accountabilities and responsibilities for the North London STP; Enable opportunities to innovate, share best practice and maximise sharing of resources across organisations in North London; and Enable collaboration between partner organisations to achieve system level financial balance over the remaining 3 years of the Five Year Forward View timeframe and deliver the agreed system control total, while safeguarding the autonomy of organisations. The North London Programme Delivery Board oversees delivery of the plan. This is an executive steering group made up of a cross section of representatives from across North London. This group is specifically responsible for providing accountability for the implementation of the workstream plans. Membership includes the Senior Responsible Officers (SRO) of each workstream and SRO leads for CCGs, Providers and Local Authorities. Two subgroups provide advice to the Programme Delivery Board: the Health and Care Cabinet (formerly the Clinical Cabinet) and the Finance and Activity Modelling Group. The Health and Care Cabinet meets monthly to provide clinical and professional steer, input and challenge to each of the workstreams as they develop. Membership consists of the five CCG Chairs, the eight Medical Directors, clinical leads from across the workstreams, three nursing representatives from across the footprint, Pharmacy and Allied Health Professions representatives, a representative for the Directors of Public Health and representatives for the Directors of Adult Social Services and the Directors of Children s Services respectively. The Finance and Activity Modelling Group is attended by the Finance Directors from all organisations (commissioners and providers). This group currently meets fortnightly, to oversee the finance and activity modelling of the workstream plans as they develop. The workstreams are responsible for developing proposals and delivery plans in the core priority areas and feed into the overarching governance framework. Every workstream has its own governance arrangements and meeting cycles which have been designed to meet their respective specific requirements, depending on the core stakeholders involved. 261 of 402

262 The STP Advisory Board enables a collective partnership approach, and acts as the sounding board for the implementation of the STP plans. The membership of this group includes Local Authority leaders, NHS Chairs, and Healthwatch. In addition to the above governance groups, CEOs and other relevant executive directors and stakeholder representatives will meet quarterly for executive leadership events to enable continued engagement and momentum, regular communication, and to assist with resolving any programme delivery issues identified by the programme delivery board. Follow this link to view a detailed governance handbook including the terms of reference for all of the governance groups. Link: of 402
263 Appendix 7 JHOSC meeting minutes Meeting on 19 th September 2017 Consideration was given to an amended presentation from the Camden and Islington Foundation Trust. Malcolm McFrederick, the Project Director, was the lead presenter. He explained that they were not as far in the process for the St Pancras site as the Barnet, Enfield and Haringey Mental Health Trust were for St Ann s. They had submitted an outline business case to NHS Improvement and were waiting for it to be approved. They were anticipating it would be approved in October. If approval was granted, there would be a full CCG-led public consultation. Mr McFrederick highlighted that the existing buildings were not fit for purpose and it was not viable to bring the St Pancras buildings up to date. They wanted to see good and vibrant community facilities and mental health research taking place. A modern therapeutic environment would be good for patients and safer for staff. Inpatient beds would be moved from the St Pancras site and there would be two new community hubs. Mr McFrederick said there had been consultation with service user groups, CCGs and local councils. Members were informed that the preferred option of moving inpatient beds to the Whittington, establishing community hubs and bringing researchers and academics onto one site had been reached by considering it against 12 Quality Critical Success Factors. There were benefits from co-locating mental and physical health services. They had also researched the travel patterns of their patients, and had wanted to find a site which was easily accessible to those who used public transport and did not have a car. There was discussion about what would be in community hubs. There would be an office area, clinical space (for mental health services and for other health services), and a community space. The community space could include a café or gallery for service users to spend time in and for voluntary sector organisations to operate in. The Chair mentioned that the Adult Education strategy made mention of community hubs. She asked whether the Trust were working with Camden and Islington on this. Mr McFrederick said that they had spoken to Islington about this and would also speak to Camden in future. Trust officers said that they wished to align their plans for the surplus land in the St Pancras site with the borough s plans for housing. Members asked how the redevelopment would fit in with wider STP matters. The Trust felt that community hubs would help with the linking of mental and physical health services. The Chair asked where the revenue from estates disposals would go. Mr McFrederick said that the sales proceeds would be used to fund the redevelopment plans. The Trust would be selling 80% of the St Pancras site and retaining 20%. Some of the land would be used for housing and some would be used by Moorfields Eye Hospital. 263 of 402
264 Members sought clarification that sales proceeds would not be used for revenue spending. They were assured that this would not be the case. The Trust representatives were asked if a developer had been appointed. They said that this would take place after the outline business case was approved and would then go through the OJEU process. Members asked about the progress Moorfields were making in terms of their business case for locating on part of the St Pancras site. The Trust representatives said that the two bodies were working together in terms of the timing of their work and submissions. However, they were two distinct schemes and not integrated. Angela McNab, the Trust Chief Executive, confirmed that land which was surplus to Camden & Islington Foundation Trust requirements would be offered to other health bodies. Members said that there was pent-up demand for GP surgery sites in the area, and they hoped that some of the surplus land could be used for this. Councillor Connor asked if the number of beds would increase following the move of inpatient facilities from St Pancras to the Whittington. She was informed that they would not decrease, however there had been no indication from commissioners that they would purchase enough beds to allow for the creation of a whole new ward. She expressed disappointment at this and felt it was important to ensure there were more inpatient facilities available for mental health patients, as demand for these had not fallen. Members also wished to avoid patients having to be placed out of area. Officers said that, on average, the number of Camden and Islington patients who had to be placed outside of those boroughs was low. Ms McNab said the Trust had noted that people were being kept in beds here long than elsewhere and that they could be moved into intermediate care. Councillor Khatoon, who was a ward councillor for the area, addressed the meeting. She wanted to see consultation with local residents and attention given to how more social housing could be provided on the site and if employment opportunities could be created for local residents. Trust officers agreed to arrange an opportunity for Councillor Khatoon to have a walkabout around the site. Members expressed concern about the availability of key worker housing, and they felt that this was important to recruit and retain staff. Members welcomed the proposals to move beds to the Whittington and felt that it was a suitable site. They wished the final business case to come back to the Committee at a future date. Meeting on 23 March 2018 Draft Minutes Malcolm McFrederick, the Project Director (Camden & Islington Foundation Trust), addressed members on the St Pancras hospital plans. He said that they were planning on selling their site and moving the inpatient facilities to the Whittington site. They were looking to develop two new hubs on Lowther Road and Greenland Road and they were considering whether a third site would be required. 264 of 402
265 Mr McFrederick said that the Trust were going to go out for tender for a development partner. This could be on a long lease basis rather than for sale. The matter was also complicated by the fact the Department of Health had a historic interest in the site. Mr McFrederick explained that the site could possibly be sold to Moorfields Eye Hospital as a replacement for their old site. The Trust wanted to involve local communities in consultation on the future of the site. Mr McFrederick said that further information would come to both the Camden and Islington health scrutiny committees in June. Members asked whether London Estates Devolution would apply to the schemes. They were informed that they were not at the stage where estates devolution would apply. The Chair voiced concerns about the development board for St Pancras not meeting. Mr McFrederick said that the two development boards one involving stakeholders and one involving providers were being amalgamated. He assured the Chair that she would be invited to the next meeting. 265 of 402
266 Appendix 8 Consultation plan Consultation methodology: St Pancras Site Redevelopment Islington Clinical Commissioning Group, together with Camden Clinical Commissioning Group is leading a consultation on the proposals for the redevelopment of the St Pancras Hospital site of which Camden and Islington NHS Foundation Trust is the landlord. These changes will affect the inpatient facility and community mental health services currently delivered on the site and on additional Trust sites. The other NHS services which are delivered on the St Pancras Hospital Site by other NHS Providers such as the Royal Free Hospital and a Camden GP practice will remain on the site. In some cases these services will be delivered in newly refurbished buildings, as part of the redevelopment process. In line with our statutory duties, the CCGs will consult on the redevelopment proposals, ensuring local people are given the opportunity to share their views on the services affected by the redevelopment of the St Pancras Hospital site. The statutory duties are: Section 242 of the NHS Act 2006 states: Each relevant English body must make arrangements, as respects health services for which it is responsible, which secure that users of those services, whether directly or through representatives, are involved (whether by being consulted or provided with information, or in other ways) in: The planning of the provision of those services The development and consideration of proposals for change in the way those services are provided, and Decisions to be made by that body affecting the operation of those services Section 14Z2 of the Health & Social Care Act 2012 states: The Clinical Commissioning Group (CCG) must make arrangements to secure that individuals to whom the services are being or may be provided are involved (whether by being consulted or provided with information or in other ways): a) In the planning of the commissioning arrangements by the group, b) In the development and consideration of proposals by the group for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which the services are delivered to the individuals or the range of health services available to them, and c) In decisions of the group affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact In light of these plans, Islington and Camden CCGs are proposing to run a public consultation for 12 weeks starting from 5 h July to end of September A consultation document, questionnaire and Frequently Asked Questions have been developed. 266 of 402
267 Aims of the Consultation: To understand the views of the local community on the relocation and development of new Camden and Islington NHS Foundation Trust mental health inpatient services from the St Pancras Hospital site to a site by Highgate Mental Health Centre and Whittington Hospital. To understand the views of the local community on the development of two new mental health community hubs, one in Camden and another in Islington. The CCGs, with support from Camden and Islington NHS Foundation Trust, will speak to as many people in the local community as possible, ensuring they hear from a wide range of service users of all of the services proposed for relocation, the local community, local voluntary organisations and HealthWatchs, as well as other key stakeholders such as local Councillors and MPs. Communications and engagement channels The channels we will use to share the consultation and gather as many views as possible are: General Population and Service Users: A full consultation document with a survey about the proposals will be available on Islington Clinical Commissioning Group, Camden Clinical Commissioning Group, Camden and Islington NHS Foundation Trust and Healthwatch websites There will be hard copies available of the above with a freepost addressed envelope at Camden and Islington Foundation Trust sites, on request Posters/ flyers across the Trust s 30 sites advertising the consultation Prompts on social media, encouraging people to join one of the consultation meetings or provide their feedback online Public meetings on XXXX dates at venues that are easily accessible to people in Camden and Islington A drop-in session with CIFT Trust Clinical Director - Vincent Kirchner Sharing the consultation document and survey through our local networks, this includes to the Islington and Camden patient and community groups and Trust service user groups, our patient representatives and our local voluntary and community sector groups Sharing information on the consultation through the GP newsletters and at the GP Forums Sharing information on the consultation through our staff newsletters and at our staff briefings (CCGs and Trust) Promoting the consultation survey to seek input from groups who traditionally face barriers to accessing services or having their voice heard Availability of the consultation document and survey questions in audio, braille, large print, easy read and in languages other than English, upon request. There will be a dedicated telephone line for local people either requesting the consultation documents or any questions they may have. Service Users Specific It was felt strongly by local HealthWatches and Service Users that there needed to be a focus on consulting with current and ex Service Users as part of the consultation. The points below specifically cover how we will work with service users: 267 of 402
268 Attendance (with Clinical Director Vincent Kirchner) to speak at all of the Trust s service users groups introducing the consultation, taking questions and letting people know how to fill it in (along with taking some hard copies) Further targeted engagement using the consultation survey with service users across all five of the Trust s divisions Acute, Services for Ageing and Mental Health, Recovery and Rehabilitation, Substance Misuse Services and Community Mental Health. This will include both current service users of inpatient services and community services. This work will be carried out by HealthWatch Camden and Islington with Trust service users. Results, analysis and feedback Camden & Islington Clinical Commissioning Groups will appoint an independent partner to evaluate the consultation process and analyse the results of the consultation. The partner will develop a process and infrastructure that reassures stakeholders of the independent nature of the evaluation. Following the closure of the consultation on 30 th September 2018, the evaluation team will have a period to analyse the results and present these to Islington and Camden Clinical Commissioning Group Governing Bodies. Islington Clinical Commissioning Group will then make a recommendation on the redevelopment proposals to NHS England and Council Overview and Scrutiny Committees for Islington and Camden. The results will be available publically, which will include, sharing on CCG and CIFT websites and sharing through other stakeholders networks, such as Healthwatch Islington and Camden. Decision making process 7. Proposed consultation timeline Action Lead Date Consultation documents and methodology sign off Consultation documents and methodology reviewed by Camden and Islington Health and Overview Scrutiny Committees Islington CCG Governing Body Camden CCG Governing Body Islington CCG and Camden CCG June 2018 June 2018 June 2018 Public consultation goes live Islington CCG 5 th July 2018 to 30 th September 2018 Evaluation of responses External agency October 2018 Results of consultation Islington CCG, Camden November 2018 published and shared CCG, the Trust and partners Final Business Case prepared Islington CCG November of 402
269 Consideration of Final Business case by Islington CCG Governing Body Consideration by Camden CCG Governing Body A decision is made by Camden and Islington CCGs on the final Business Case The decision is communicated with the local community, OSCs, HealthWatch and partners Islington CCG November 2018 Camden CCG November 2018 Camden and Islington CCGs Islington CCG / Camden CCG / The Trust November 2018 November of 402
270 Appendix 9 Consultation document, questionnaire and FAQs Draft Consultation document Transforming mental health services in Camden and Islington: Proposals for change to the Camden and Islington NHS Foundation Trust Estate Date: July of 402
271 Contents 1. Foreword 2. Who we are 3. Introduction 4. Section 1: Inpatient beds 5. Section 2: Community services and development of Community Hubs 6. Section 3: Other non-camden and Islington NHS Foundation Trust services providing services on the St Pancras Site 7. What will happen to the St Pancras site if the redevelopment happens? 8. Table of all NHS services of the St Pancras site and how they are affected by the redevelopment 9. Consultation details 271 of 402
272 Foreword by Clinical Directors from all three organisations To be written Camden and Islington Clinical Commissioning Groups (CCGs) are the local organisations with responsibility for planning, buying and monitoring local primary care, hospital services, mental health care, children's services and community services, with a clear vision and shared priorities for commissioning the best health services for our local community. The two CCGs commission mental health services provided by Camden and Islington NHS Foundation Trust, on behalf of local people. The Trust provides mental health care to service users in their homes, in the community, and in hospital. They provide services for adults of working age, adults with learning difficulties, and older people. The CCGs and the Trust want to ensure local people have the opportunity to shape their healthcare services. Introduction: We are proposing a change to some services, currently delivered on Camden and Islington NHS Foundation Trust s St Pancras Hospital site, to modernise and improve the quality of care provided to local people. The changes will affect all inpatient services at St Pancras and some community services, based at St Pancras and other Trust sites, will also be affected. These proposals do not include a cut to services. Other NHS organisations, such as the Royal Free Hospital and a GP practice, also provide services from the St Pancras Hospital site. They will all remain onsite and in some cases, these services will be delivered in newly refurbished buildings, as part of the redevelopment process. Before any changes are agreed or made we need to speak with you, our local community and our partners and stakeholders, to listen to views, ideas and concerns about the proposals. There are two sections in this document on which we are seeking your views. These are: 1. The move of the Mental health inpatient beds currently on the St Pancras Hospital site and their proposed relocation and development on the new site by the Whittington Hospital 2. The proposed relocation of some of Camden and Islington NHS Foundation Trust s community mental health services, and the development of two community hubs with one in Camden and another in Islington Section 3 of this document gives additional information on the services provided by other NHS organisations that will remain at the St Pancras Hospital site. We have also included some additional information on how the St Pancras Hospital site will be redeveloped if plans go ahead (on page XXX). The present inpatient mental health services at St Pancras Hospital are provided in buildings that are not designed to meet modern health and safety needs, nor do they provide an ideal therapeutic environment; the site was previously a Victorian workhouse. A Care Quality 272 of 402
273 Commission report, published in June 2016, highlighted that the Trust s inpatient wards require significant improvement. This document explains why we think the proposed changes will lead to better quality services which improve the quality of care provided to our local residents and the way in which the different NHS services currently delivered on the St Pancras Hospital site will be affected by the redevelopment plans. There is a survey attached which we ask you to complete, to let us know what you think about the proposals. If you are only interested in one area of the proposals, please feel free to only answer this section of the survey. We have also developed some Frequently Asked Questions which you can refer to. 273 of 402
274 Section 1: Inpatient Beds Introduction Camden and Islington NHS Foundation Trust has around 30 sites in total. The majority of services are based in the community with an inpatient facility at Highgate Mental Health Centre and another at St Pancras Hospital. We are proposing to move 84 mental health inpatient beds from the St Pancras Hospital site to a new purpose built site on land purchased adjacent to Whittington Hospital and next to Camden and Islington Foundation Trust s Highgate Centre for Mental Health (which also has inpatient facilities). The St Pancras Hospital site is a Victorian building (previously a workhouse) and the inpatient units are no longer fit for purpose and are outdated and unsafe. We are acting now to address issues that we know will become increasingly problematic in years to come. These are: The St Pancras area has changed considerably over the years. The site is already overlooked by tall and high rise buildings and with building work set to continue, inpatient privacy and dignity will be compromised more and more. Alongside this, there is little outdoor space for patients and the space that is there is not of the quality that we would strive for. Some of the structural issues from the building include no clear line of sight to all areas of the wards, thus mirrors have to be installed and there are ligature risks throughout the building which cannot be changed. This clearly has significant impact on the patients. Significant investment would be required to maintain and upgrade the current premises to meet modern standards. In addition, due to the basic structure of the buildings, in some cases, we would still be unable to satisfy the standards prescribed by the Department of Health best practice guidance. Benefits for the proposal: A new building will mean we can design a space which is both welcoming and safe for patients The new building will exactly meets the needs of patients, as the Trust will develop it with them The proposed site by the Whittington Hospital will mean that mental health patients have easy access to physical health services. The new site will have more outdoor space with a designed garden area Initial engagement with service users, staff and carer groups showed the vast majority of service users, staff and carers were in support of the move of the inpatient beds. Whilst some concerns were raised by people about inpatient beds being moved from the familiar environment of the St Pancras Hospital site, most people agreed that continuing to maintain the buildings was not an option long-term. There was recognition that the St 274 of 402
275 Pancras Hospital site buildings are not as good as they could be and a new modern environment, with therapeutic inpatient spaces was welcomed. There was also a desire to move to a more peaceful location than St Pancras Hospital site. There are no plans to cut any inpatient beds from Camden and Islington as part of the proposals; the aim of the proposal is to strengthen current services. We have done an analysis of the number of inpatient beds needed by service users up to 2025, in tandem with the ambition of providing greater services in the community, and we are confident that there will not be an increase in demand for inpatient beds. The St Pancras Hospital site is located in the London Borough of Camden. The proposed new site would be located in the London Borough of Islington and inpatients, and their families and friends, may therefore have a greater distance to travel. The newly developed Inpatient Unit: We are proposing that the new inpatient facility will be located on land bought from Whittington Hospital. It will comprise a three-storey new build surrounded by landscaped gardens. The new facility would be designed to have 84 bedrooms across five wards, there will be 17 beds in four wards and 16 beds in the other ward, with 11.8sqm room space and 3.1 sqm en-suites.. However the configuration of each of the wards can be managed flexibly to accommodate clinical need e.g. a ward could be split into two wards. No ward will be over 18 beds in line with national guidance. At the St Pancras Hospital site there are currently six wards including two with 12 beds, two with 14 beds and two with 16 beds. There is a mix of bedrooms at St Pancras Hospital, based in Ash House and the Huntley Centre. Single rooms vary between 10.4m2 to 13.3m2 and not all bedrooms in the Huntley Centre have en-suite facilities, a limited number are shared. 61 rooms currently have en-suite facilities. The drawing below shows the layout of two of the new proposed wards. 275 of 402

276 Each ward will have two consulting rooms, communal lounges and a garden or outdoor terrace area. The new building would be fully accessible, with disability access. It would present a warm, therapeutic and welcoming environment, in line with what service users have told us they want from a building. The new buildings would be developed to the highest standards. Criteria will be based upon sustainability, carbon emission reduction, design, durability, adaptation to climate change, ecological value and biodiversity protection. So you can get a visual idea of the difference between the current inpatient units and the proposed new site we have included some pictures below. 276 of 402




277 Pictures of the current inpatient wards at St Pancras Hospital Pictures of a newly designed inpatient ward. Please note this is not the proposed inpatient ward but is the quality, style and standard that we will meet. If the proposals are agreed, the Trust will be working with service users to design the new wards and space: 277 of 402

278 Travel: The new location of the inpatient unit will mean that Camden residents will have to travel further to reach it, while the current St Pancras Hospital site is located between Camden Town Station and Kings Cross tube and rail Station, the new site is by the Whittington Hospital which is in Archway. Map: Travel: The Whittington site is served by 8 bus routes, as well as the Northern Line (Archway) and London Over-ground (Upper Holloway). By tube: Northern line to Archway British Rail: the nearest station is Upper Holloway (Barking to Gospel Oak line). By Bus: 143, 210, 263, W5 and 271 stop outside the Archway Campus on Highgate Hill. 134, 43 and 264 stop alongside the Archway Road. 278 of 402
279 Section 2: Camden and Islington Foundation Trust Community services and the development of Mental Health Community Hubs Alongside the move of inpatient beds, we are also proposing to make significant investment into community services and move some mental health community services (please see the table on page 14) from the St Pancras Hospital site and other Trust sites, into newly developed community centres. Our ambition is that the investment in new community hubs will allow the Trust staff to deliver improved mental health and wellbeing care in the local community. The hubs model has been designed to keep community teams at the centre of mental health service delivery; ensuring care is provided as close to patients homes as possible. Currently there are a high number of community services located across multiple sites, which includes some teams based on the St Pancras site. The development of Community Hubs will allow the relocation of some of these services into more accessible local sites for service users, away from hospital and closer to home. It also brings teams from the same service into one location which improves closer working between professionals. Community Hubs may also be able to bring opportunities for a wider range of physical health services for service users with mental health needs, to help improve accessibility to physical health services. These community hubs will be located at Lowther Road (Islington) and Greenland Road (Camden). This should ensure community services are more accessible to Camden and Islington residents and will be provided in a local community setting. Benefits for redeveloping community services and the community hubs: Future mental health care will need more services in the community to help manage people s conditions in the least restrictive environment, with a greater focus on prevention and early intervention. Developing community care will allow us to work in a more joined-up way across Camden and Islington, with physical health and social care partners, removing the barriers to personalised and coordinated services that our community need Local people have told us they would prefer more services in the community and our mental health community have highlighted that they need more support to look after their physical health. The Trust has a number of small buildings that are not used very much. Moving services based in these buildings to one of the new community hubs will allow the Trust to be more effective and efficient with its money. Although this would mean fewer buildings overall, patients, families, carers and staff would benefit from more community mental health services in the same place and working closely together. 279 of 402

280 In March 2018 the Trust held an engagement event for service users and carers to carry out further engagement on the proposed new community hubs. Most service users were generally positive about the proposed new facilities. The strongest views were based on wanting services that were inclusive, resourced with knowledgeable and compassionate staff and a non-stigmatising and welcoming environment. Although, it was highlighted that some of the proposed new locations could be more difficult for those with mobility issues, if they did have to travel further, the majority view was that location was less of an issue if services were good, improved and inclusive. Islington: It is proposed the site for the Islington community hub would be at a Trust s existing site on Lowther Road. It would be developed into a four storey community centre. There will also be additional community space, which could be used for more wellbeing or health focused activities such as exercises classes or art classes and office space on the upper levels for Trust support staff. Lowther Road offers excellent access to the Piccadilly Line at Holloway Road. Map of where Lowther Road is and travel options. Map of Lowther Road Travel options: By Tube: Close to Holloway Tube station (Piccadilly Line) By bus: 43, 153, 263, 271, 393 Camden: 280 of 402

281 It is proposed the site for the Camden community hub will be at Greenland Road, which is an existing Trust site. Greenland Road will also be developed into a four storey community centre by developing the existing building. This would consist of consulting rooms, community space and office space on the upper floors for Trust support staff. Map of Greenland Road and Travel Options Map of Greenland Road Travel Options: By tube: Adjacent to Camden Town tube station (Northern Line) By bus: 24, 27,29, 88,134,168,214,253,274,C2 281 of 402
282 The services in each community hub: Below we have pulled together a table which shows which community services are proposed to move into the Lowther Road and Greenland community centres and where the community services are currently located. Table of community services that are proposed to move into the new community hubs: Current locations and services Move to Greenland Road Move to Lowther Road St Pancras Hospital Site South Camden icope Camden Mental Health Assessment and Advice Team Islington Practice Mental Health Team (where there is no GP practice capacity but if you are seen in your practice this will remain) The Rivers Crisis House Pharmacy Approved Mental Health Professional Service There will be a separate consultation on this Highgate Centre for Mental Health: The Pharmacy is currently connected with the St Pancras Hospital site inpatient unit and, therefore, would move with the inpatient facilities to Highgate if the proposals are agreed. Highgate Centre for Mental Health: Most service users are seen in the community or in hospital settings. Greenland Road Islington Assertive Outreach Team Peckwater Centre 282 of 402
283 South Camden Recovery Team Manor Gardens icope - North Islington Team Camden Mews Community Recovery Service for Older People - covering both Camden and Islington Below we have highlighted which community services are already based at St Pancras Hospital site, Greenland Road and Lowther Road and will remain at these locations: Current locations and services No move (staying as is) St Pancras Complex Depression, Anxiety and Trauma Service Camden & Islington Psychodynamic Psychotherapy Service Sexual Problems Team Traumatic Stress Clinic NHS Transition, Intervention and Liaison Veterans Mental Health Service (formally known as LVS) ADHD Team Attention Deficit Hyperactivity Disorder Adult Autism Clinic South Camden Crisis Resolution Home Treatment COMMUNITY COMMUNITY COMMUNITY COMMUNITY COMMUNITY COMMUNITY COMMUNITY 283 of 402
284 Acute Day Unit (Jules Thorn) Community Recovery College Clozapine Clinic Greenland Road Camden Assertive Outreach Team Camden Early Intervention Team Islington Early Intervention Team Islington Early Intervention Service 35+: These are highly specialist services and so it is important that the Islington Early Intervention and Camden Early Intervention teams are located together in the same building. This enables them to work together more closely and improve care for services users through sharing learning and best practices. By being located together in this way, both teams also have access to a lead psychologist for support and supervision with complex cases. Some service users are seen onsite but the teams also work with service users in their own homes and in community locations across Islington. Focus Homeless Outreach Lowther Road North Islington Rehabilitation and Recovery Team Cornwallis Outreach Project Islington Mental Health Reablement Service 284 of 402
285 Section 3: Other NHS services which are currently delivered from St Pancras Hospital site There are additional services, located on the St Pancras Hospital site and are delivered by other NHS providers. All of these services will stay on the St Pancras Hospital site and depending on the service, it could be housed in a refurbished building. As these services are not moving, they will not form part of this consultation. However, for you to fully understand the redevelopment plans we have included information in this document on the NHS services which will be staying on the St Pancras Hospital site. It is intended that the GP out of Hours service and GP practice will be delivered in a newly refurbished building. We do not envisage the services will have to move at any point during the redevelopment process. However, there is a possibility that we will need to temporarily house the GP out of Hours service and GP practice on the St Pancras Hospital site. If this is the case we will ensure disruption to the service is as limited as possible. Table of services which are staying NHS Services & description of service Rehabilitation inpatient wards (Central and North West London Foundation Trust) Provides treatment and support for patients whose physical abilities have been reduced through illness, such as a stroke, or a fall or a musculoskeletal condition. Evergreen Ward (University College London Hospital) A ward for predominantly care of the elderly Kidney dialysis clinic (Royal Free Hospital) Ophthalmology clinic (Royal Free Hospital) GP out of hours service (London Central & West Unscheduled Care Collaborative) Kings Cross GP Practice (AT Medics) Current address South Wing South Wing St Pancras Hospital St Pancras Hospital St Pancras Hospital St Pancras Hospital Future location There will be no change to the site or location of this service There will be no change to the site or location of this service New building on St Pancras Hospital site New building on St Pancras Hospital site New building on St Pancras Hospital site New building on St Pancras Hospital site 285 of 402
286 What will happen to the St Pancras Hospital site if it is redeveloped? In order to finance the changes to mental health inpatient and mental health community services, a significant portion of the St Pancras Hospital site, which is owned by Camden and Islington NHS Foundation Trust, would need to be redevelopment. Redevelopment of the land will free the necessary funds to build a new inpatient unit in the more therapeutic setting near Highgate Centre for Mental Health and to invest in community mental health hubs. The St Pancras Hospital site is 5.4 acres in size and the Trust currently leases out about a third of it. Most of the space the Trust occupies is for inpatient beds. Moorfields Eye Hospital want to purchase two acres to replace their existing Victorian buildings. The Trust is hopeful this will happen, however the redevelopment of the land can happen with or without Moorfields buying a section. Camden and Islington NHS Foundation Trust will retain a presence on the site. The Trust s new accommodation at St Pancras will occupy the same amount of space as the existing East Wing. The remaining land would be redeveloped and a minimum of 35% of any housing generated would be for social and affordable housing. The Trust s accommodation at St Pancras would consist of consulting rooms, meeting rooms, training facilities and the Recovery College. The Recovery College will include space for both clinical delivery and support facilities for the clinical teams. In the same building the Trust intends to host the new Institute of Mental Health with UCL partners, which will take up approximately the same space. The Trust already has one of the strongest records and reputations in UK mental health research. That is why the vision for the St Pancras site includes the establishment of an Institute of Mental Health, bringing together the Trust s research facilities and staff. This will enable research departments to collaborate more effectively, making it easier to run world-class research into tailored treatment plans for every individual, ensuring the best treatment and care for local people. The new plans also mean there will be fewer buildings overall and the new buildings will be modern and energy efficient, helping to reduce running costs for the NHS to further protect services. The buildings delivering other NHS services will remain (please see Section 3, page XXX for more details). 286 of 402
287 The consultation details: The consultation will begin on [xxx June 2018] and run until [xx August 2018 *tbc]. Public meetings will be held in Camden and in Islington [DATE, LOCATION HERE] [DATE, LOCATION HERE] All opportunities to get involved in this consultation will be advertised on Islington and Camden CCGs, Camden and Islington NHS Foundation Trust and Camden and Islington Councils websites; as well as in local media in both boroughs to encourage participation from those affected by these proposed changes including service users, stakeholders, and the public. We will also be attending service user groups and speaking directly with those patients who currently use the services. We are keen to hear your views on our proposals and to listen to any suggestions about how we can improve our services in future. If you have any queries about this consultation or you require this document in an alternative format such as Easy Read, large print, audio, braille, and in languages other than English please CCG address Or call XXXXX You can fill in the consultation survey online or send the completed survey back to: FREE POST Address will be an evaluation company 287 of 402
288 Appendix 1 Travel in more detail Below we have calculated the travel from three fixed points across Camden and two fixed points across Islington to the new inpatient unit which will be located by Highgate Mental Health Centre, for anyone interested in further information about travel to the site. Travel times to Highgate Mental Health Centre Camden St Pancras Hospital Site Between St Pancras Hospital and Whittington Health, Magdala Avenue, N19 5NF. Distance: 2.5 miles Drive: 14 minutes Tube: 25 minutes Mornington Crescent to Archway on Northern Line followed by a 7 minute walk. Bus: 36 minutes 214 from bus stop N (Royal College St Crowndale Road) to William Ellis School, bus stop GF. From here bus C11 towards Archway and get off at bus stop HQ, Magdala avenue Dartmouth park hill and followed by an approximately 2 minute walk to the site. West Hampstead Station: Distance: 3.5 miles Drive 20 minutes Tube: 29 minutes East London and city line (toward Stratford) to Gospel Oak. Gospel oak (toward Barking) to Upper Holloway and followed by an approximately 13 minute walk Bus and train: 25 minutes West Hampstead to Gospel Oak. Go to bus stop GC and get the C11 bus toward Archway, get off at Magdala Avenue Dartmouth Park Hill, followed by a 2 minute walk Bus: 46 minutes get the C11 bus (toward Archway) from bus stop W, West Hampstead underground station and alight at Magdala Avenue Dartmouth Park Hill, followed by an approximately 2 minute walk Highgate Station Distance: 1.1 miles Drive 6 minutes Tube: 10 minutes, Northern line (southbound to Kennington or Morden) to Archway and followed by an approximately 7 minute walk from the Station. Bus: 18 minutes,134, 43 or 364 from bus stop T to Archway station bus stop W followed by an approximately 7 minute walk. Travel times to Highgate Mental Health Centre Islington Highbury and Islington station: 288 of 402
289 Distance: 2.6 miles Drive: 16 minutes Tube: 23 minutes, Victoria line (toward Brixton) to Euston, northern line (toward high barnet) to Archway, followed by approximately 7 minute walk. Bus: 30 minutes, 263 or 271 toward Archway station Stop D followed by an approximately 8 minute walk Farringdon station: Distance: 4.8 miles Drive: 29 minutes Tube: 28 minutes, catch the Hammersmith & city, circle or metropolitan line to Kings Cross station, transfer to the northern line (toward high Barnet) to Archway, followed by an approximately 7 minute walk. Bus: 44 minutes, catch the 63 bus (toward Kings Cross) from bus stop C, Clerkenwell Road Farringdon Road, change at bus stop G, Kings Cross Station York Way and catch the 390 bus (toward Archway) to bus stop U, Archway Station, followed by an approximately 7 minute walk. Community Hubs Travel times Below we have calculated the travel time to Lowther Road from two fixed points across Islington: Travel times Islington, Lowther Road Farringdon Station Distance: 2.4 miles Drive: 18 minutes Tube: 22 minutes, Metropolitan line to Kings Cross, change to Piccadilly line to Caledonian Road, followed by an approximately 9 minute walk Bus: 32 minutes, 153 directly to Lowther Road, bus stop SR, followed by an approximately 3 minute walk Or the number 19 or 38 from bus stop Tysoe Street to Highbury Corner, Stop F from here pick up the 43 to Liverpool Road Stop SV, from here there is an approximately 4 minute walk. Highbury & Islington station Distance: 0.5 miles Drive 5 minutes Bus: 10 minutes 43, 271, 263 to bus stop Liverpool Road, followed by an approximately 1 minute walk Walk: 11 minutes Below we have calculated the travel to Greenland Road from three fixed points across Camden: Travel times Camden, Greenland Road St Pancras Hospital 289 of 402
290 Distance: 0.7 miles Drive 8 minutes Buses: 11 minutes 214 to Camden T own bus stop Y and walk approx. 3 minutes to hub Walk: 14 minutes West Hampstead station Distance: 2.8 miles Drive: 16 minutes Bus: 31 minutes C11 toward Archway to Elsworthy Rise stop M, from here bus 31 toward Camden Town to Stop Z, followed by an approximately 1 minute walk. Tube: 20 minutes East London and City Line Train from West Hampstead station to Camden Road, followed by an approximately 7 minute walk from Camden Road Highgate Station: Distance: 3.3 miles Drive: 20 minutes Bus: 30 minutes, 134 towards Camden Town, to Stop S followed by an approximately 3 minute walk Tube: 13 minutes Highgate underground to Camden Town station followed by an approximately 3 minute walk 290 of 402
291 ADD FREEPOST ADDRESS HERE. will be evaluation company Survey questions 1. Do you have any concerns about the proposed move (to opposite Highgate Mental Health Centre): Travel (my travel to the centre) Travel (for family and friends) Familiarity: I have been going to St Pancras Hospital for a number of years The location Other: Other free text box Please give any further comments on your concerns 2. Are there any ways you feel your concerns could be eased? 3. People have told us travel was an area of concern. What, if any, is your biggest concern about travelling to a new site (opposite the Highgate mental health centre)? The cost of travel Additional travel time A more complex travel journey (i.e. I now have to get more than one mode of transport such as a bus and tube, I have to change tubes twice, I have to get two buses etc.) 291 of 402
292 I have to walk further My family have to travel further There won t be any parking I don t know the journey and may get lost or confused I am not concerned about travel to the new site Other: free text box 4. What do you think are the good things about the proposed move (to opposite Highgate Mental Health Centre). A quieter and therapeutic setting Newly designed wards, bedrooms and shared spaces Being near the Whittington Hospital The location Quality of care Green Space Other free text Please give any further comments 5. Please tell us if you support the move of inpatient beds from the St Pancras Hospital site to a new and purpose-built facility by Whittington Hospital and opposite Highgate Mental Health Centre Strongly support Support Neutral Against Strongly against Not sure Please add any further comments you have. 292 of 402
293 Community Hubs: 1. Are you a Camden or Islington resident? Camden Islington Other 2. Which, if any, community services do you use? Please tick every one you use List of services to tick None 3. Do you have any concerns about the proposed move of the community services to new locations? Travel (my travel to the new hub) Familiarity: I have been going to my current location for a number of years I might not see the same member of staff I am concerned about the range of services being delivered from the same site Other: Other free text box Please give any further comments on your concerns Are there any ways you feel your concerns could be eased? 293 of 402
294 4. What do you think are the good things about the proposed move of the community services to new locations? A newly designed space A range of community services being located together The location Quality of care The new location is easier for me to travel to Other free text Please give any further comments 6. Please tell us if you support the proposed move of the community services to new locations? Strongly support Support Neutral Against Strongly against Not sure Please add any further comments you have. 294 of 402
295 About you Camden and Islington NHS Foundation Trust is committed to promoting equality of opportunity, to ensure everyone has the chance to participate fully in the activities and decisions of the organisation. By completing this information you will help us understand who we are reaching and how to better serve everyone in our community. 1) Which age group are you in? 18 or under Prefer not to say 2) What is your postcode? 3) Which of the following options best describes how you think of yourself? Female (including trans woman) Male (including trans man) Non-binary In another way Prefer not to say 4) Is your gender identity the same as the gender you were given at birth? 295 of 402
296 Yes No Prefer not to say 5) Do you consider yourself to have a disability? Definition of disability under the Equality Act 2010: if you have a physical or mental impairment that has a 'substantial' and 'long-term' negative effect on your ability to do normal daily activities. Yes No Prefer not to say 6) Please select what you consider your ethnic origin to be. Ethnicity is distinct from nationality. White: Welsh/English/Scottish/Northern Irish/British White: Irish White: Gypsy or Irish Traveller White: Any other White background Mixed: White and Black Caribbean Mixed: White and Black African Mixed: White and Asian Mixed: Any other mixed background Asian/Asian British: Indian Asian/Asian British: Pakistani Asian/Asian British: Bangladeshi Asian/Asian British: Any other Asian background Black or Black British: Black - Caribbean Black or Black British: Black - African Black or Black British: Any other Black background Other ethnic background: Chinese 296 of 402
297 Other ethnic background: Any other ethnic group Please indicate your religion or belief. 7) Please indicate which option best describes your religion or belief. No religion Buddhist Christian Hindu Jewish Muslim Sikh Atheist Any other religion Prefer not to say 8) Please indicate the option which best describes your sexual orientation. Heterosexual Gay Lesbian Bisexual Prefer not to say 9) In what capacity are you responding to the consultation? Current or former service user Carer/family member Member of the public Voluntary organisation/charity Clinician NHS provider organisation 297 of 402
298 Private provider organisation NHS commissioner Industry other public body Do we want to add an option for resident close to St Pancras site? 298 of 402
299 Appendix 10 Options development summary Service Location Review by Camden and Islington Foundation Trust April 2017 Background As part of the Outline Business Case one of the options under consideration is the redevelopment of St Pancras with services moving to new community facilities funded through the business case. In order for the Trust to make a decision on the services to remain on St Pancras a process was agreed with the board for criteria for services to be reviewed. The criteria is noted below CQC requirements met in full by facilities Patient disruption must be minimised inpatients moved once only Research and innovation supported alongside wider learning/ knowledge focus Staff wellbeing supported Enabling of the Sustainability and Transformation Plan (STP) ambitions Enabling wider healthcare transformation across North Central London (NCL) Affordability and value for money achieved St Pancras site to be symbolic of our vision for mental health e.g. visibly demonstrating integration, recovery, research etc. Workshops Two workshops were arranged by Operations to be undertaken on the 24 th and 31 st March 2017, the attendees at these meetings were Clinical Directors, Consultants, Divisional Directors and Service Managers, a full list of attendees can be seen in the Appendix 2. The Outcome Stays at SPH Adult autism ADHD team London Veteran s Service / traumatic stress clinic Medical education Head Quarters & Staff Facilities? Could be SPH / Could be somewhere else (academic) Recovery College (Community feel) Sexual Problems Clinic Moves with inpatient Adult inpatient Inpatient rehabilitation and recovery service Volunteers 299 of 402
300 Advocacy Moves to community Approved Mental Health Professionals Assessment and Advice Team Acute Day Unit (one of two facilities) Phlebotomy - building must have good access, as currently an issue Could go to community but want to be in one place Complex Depression Anxiety and Trauma Services (Acute Day Unit, Crisis House, Crisis Team) exists in Daleham Gardens would be good to replicate for Rivers Crisis centre Community / mainly primary care some admin ICOPE Psychological Therapies Service (Consider future need for TMS machines) A full table is noted below of the preferences, along with comments made during the two meetings. The next stage The work needs to be ratified by a number of groups before being presented to Executive for agreement, so far it has been suggested that this is reviewed by the academics group held at UCL, and the consultants group held at St Pancras. In addition, Operations have been requested to review other services not currently provided at St Pancras. 300 of 402
301 The review output Service CQC requiremen ts met in full by facilities Patient disruption must be minimised; inpatients moved once only Research and innovation supported alongside wider learning/ knowledge focus Staff wellbeing supported Enabling of the Sustainability and Transformation Plan (STP) ambitions Enabling wider healthcare transformation across North Central London (NCL) Affordability and value for money achieved St Pancras site to be symbolic of our vision for mental health e.g. visibly demonstrating integration, recovery, research etc. Adult Autism Diagnostic and Consultation Service x x x x x x x Adult services inpatient x x x x x x x Approved Mental Health Professionals Team (AMHPs) x x x x x Assessment Advice Team and x x x x x Attention Deficit Hyperactivity Disorder (ADHD) Team x x x x x x 301 of 402
302 Camden and Islington Psychodynamic Psychotherapy Services x x x x x Complex Depression Anxiety and Trauma Service (CDAT) x x x x x ICOPE Psychological Therapies Service x x x x x London Service Veteran s x x x x x x x Rehabilitation and Recovery Service Inpatients x x x x x x x Sexual Clinic Problems x x x x x Acute Day Unit Jules Thorn x x x x x South Camden Crisis Team x x x x x 302 of 402
303 The Rivers House Crisis x x x x x x Traumatic Clinic Stress x x x x x 303 of 402
304 The attendees 24 th March 2017 Ian Griffiths Clinical Director Acute Suzanne Joel Clinical Director SAMH Gina Waters Consultant psychiatrist Acute Liz McGrath Clinical Director SMS Gillian Paterson Service Manager SMS Dominic O Ryan Clinical Psychologist STIS Aisling Clifford Divisional Director Acute Adele McKay Senior Service Manager Acute Diana Brown Social Worker CDAT Allison Arekion Service Manager CDAT Matt Allin Psychiatrist RR R&R Robert Murray Divisional Director R&R Neill Wells Senior Service Manager R&R Roger Evans Service Dev. Manager Ops Emily van de Pol Divisional Director CMH Ian Prenelle Clinical Director R&R Chris Dunbar KPMG Neil Turvey Project Director Andy Stopher Acting Director of Ops 31 st March 2017 Connor McIntyre Service Manager North Islington R&R Druid Fleming Sen. Service Manager Camden R&R Neill Well Sen. Service Manager R&R Adele McKay Sen. Service Manager Acute James Wakefield Asst. Psychologist CDAT Alison Areilion Service Manager CDAT Emily van de Pol Divisional Director Community Matt Allin Clinical Director SMS Dominic O Ryan Clinical Psychologist STIS Andy Stopher Acting Director of Ops Chris Dunbar KPMG Lauren Oxley KPMG Additional Comments Acute Acute all on one site would be preferable Retain Crisis hub on St Pancras? 12 bed Crisis House Acute day units - Doesn t need to be on St Pancras, but does function better when collocated with inpatient acute. In patient facility - Library for head office / back office? Acute could be some value in collocation (acute day units, crisis house, crisis team) Acute day units need large group rooms and consulting rooms Community Hubs 304 of 402
305 CRTs predominantly mobile working need hot desking space and car parking need cars Direction of travel is that crisis teams staffing might grow slightly ADUs should not grow but should develop to do prevention / step down join up with CRTs (acute service is currently 9-5) Social housing to supported accommodation (One Housing and Circle Housing) currently there is a lack of move on/step down. Residential development could provide an opportunity for the Trust to incorporate MH focussed social housing/step down facilities. East London has a step down unit with roadside exits (i.e. access directly from the street) this represents the next level of step down housing. Rehab wards remain with acute wards R&R 2 EIS teams (need to be collocated) 2 AOT teams (could be incorporated into community R&R teams) Focus team (should stay in Camden Town) Community Rehab teams may not need 2 where do we co-locate? HOO? HOO currently difficult to maintain and a long way away. Could be an opportunity. What do we do whilst rebuilding takes place? Need a solution Always need co-location for a particular cohort with long term needs (AOT and rehab) Clinical strategy sees movement into GP surgeries but will be an ongoing need for central spaces for communication / to allow practice based teams to come together all grades of staff, regular team meetings. Technology will help, but it won t eliminate the need for a home space. Hot Desking Reasons this might not work for specific teams / individuals: Special physical / OH requirements OH quiet space Professions requiring dedicated space (i.e. Doctors need dedicated space although could possibly hot desk within the dedicated area) Confidentiality / noise distraction Managers confidential/sensitive discussions Culturally inequitable if not required at all levels (i.e. including Executive) Other considerations Lowther Road pleased to see something being done with this When you create community hubs need to consider what happens to staff in the interim as interim accommodation costs can be expensive 154 Camden Mews could we be doing more with that site? we need the beds and the day service Aged Mental Health: We are very happy with Peckwater in Camden very happy with it as a community site integrated with primary care and CNWL In Islington we are happy with Brewery Road but we don t like that we can t see patients there. D1 declined. Means Brewery Road could be a possible location for cheap back office space. Would mean we need another community site in Islington. Southwood not much opportunity to expand and surrounded by residential development. 305 of 402
306 See most people in own homes need some group rooms and clinic space (can be shared with other services) Expect to slowly expand service over coming years. Substance Misuse Holloway Road is not fit for purpose Would be happy for substance misuse to be part of a larger community hub Critical to have dispensing pharmacy in each hub Would like to be more integrated with R&R teams Key things to consider: 1. Future of Margaret Centre Site (HS2 / underutilised) 2. Redevelopment / alternative use of Holloway Road site 3. Daleham site tenant (GP) dominates could expand 4. Future of Grays in Road site? should we keep it 5. Need more flexible space for day programmes / web based delivery 6. Do we want medically assisted detox beds (e.g. upstairs at Daleham?) commercial opportunity as no other providers of this service 7. Conference facilities would be beneficial (i.e. for 40/50 people to come together) could be provided within community hubs 8. Opportunity for community use of Conference facilities come in and use (nice quality) 9. Hubs should have a site coordinator / manager to make the building work 10. Section 75 review in Camden currently don t know the outcome but will impact the role of social workers and level of integration more focused space Support social enterprises support GP surgeries link to physical care currently no facilities for online therapy (either public / treatment room or social enterprise use) We are not really engaging the younger population. Community Mental Health We need to integrate with primary care, and also with other teams Our services (CDAT, PD, traumatic stress) work across boroughs ICOPE benefits in combining across boroughs (call centre / admin space) More and more wanting to see patients within primary care space but this is dependent on timescales for expanding GP estate / facilities Many consultation rooms (high volume services) Need group space Need IT capacity / workstations Further comments for considerations - Where community services are located at the St Pancras site, it is positive when they can be easily accessed without passing through the hospital e.g. Camden icope is easily reached via the new entrance. Clients can be deterred from engaging with community services if they find that attending the service means they are in contact with clients who are more unwell. - Crisis teams at hospital locations: on occasion clients are anxious to attend a crisis service at a hospital due to fear of being sectioned. As such being in the community can help de-stigmatize. - Crisis houses that are not so medicalised in appearance have received positive feedback from clients. 306 of 402
307 Appendix 11 Feasibility Study Option Name Option Description Option Evaluation Option Outcome Camden Council Site Make use of council land which is either vacant or due to become vacant in the near future in the London Borough of Camden. Camden Council has recently consolidated its estate and built a new head office near St Pancras. It has advised the Trust that is has no suitable land available. Islington Council Site Make use of council land which is either vacant or due to become vacant in the near future in the London Borough of Islington Islington Council has confirmed that it has no suitable land available. Pentonville Prison Site Pentonville Prisons is located near to the western edge of the London Borough of Islington and is due to close in the near future. The agent responsible for the redevelopment has confirmed they intend to make use of the land for residential development and the timetable is uncertain at this stage as the prison has no close date. Holloway Prison Site Holloway Prison is located just to the North of Pentonville Prison and was closed in The site may therefore be available in the near future. The agent responsible for the redevelopment has confirmed they intend to make use of the land for residential development and the timetable for works is too short for this project as the prison is closed and negotiations on its redevelopment already well advanced. Royal Free Site The Royal Free s main hospital site is located roughly in the centre of the London Borough of Camden. As the Trust would like to co-locate with an acute hospital Trust this would provide an ideal location. The Royal Free is landlocked and has no surplus available space. Moorfields Hospital Site (Moorfields) Moorfields Eye Hospital NHS FT (Moorfields) is located in the south eastern corner of the London Borough of Islington. Moorfields is a specialist eye hospital. Moorfields Eye Hospital has its own plans to relocate away from its current site at the North Eastern Edge of the City of London. Their project is reliant on a significant capital windfall as a result of the sale and is therefore not a suitable site for the new inpatient facility. University College London Hospital UCLH s main hospital is located in the south of London Borough of Camden. As the Trust would like to co-locate with an acute hospital UCLH is landlocked and has no surplus available space. 307 of 402
308 Option Name Option Description Option Evaluation Option Outcome (UCLH) Trust this would provide an ideal location. UCLH also has excellent links with University College London (UCL) for the development of a research centre. Vacant Private Sector Land Any vacant private land of a suitable size that is identified in the area has the potential to be used to deliver the new hospital facility. No private sector vacant land has been identified. St Ann s St Ann s Hospital was identified during the SOC stage as having the potential to host a new inpatient facility for the Trust. It is located in the London Borough of Haringey, but has been included as it was identified as the best site during the SOC stage and is a mental health Trust and is within two miles of the Islington border. There is land available to deliver the project and early discussions have taken place. Whittington The Whittington Hospital is located on the border between Camden and Islington to the North of both Borough s. It is an acute hospital with land available for the Trust to build a new inpatient facility. The Whittington Hospital has land available as part of their ongoing capital strategy and is an acute hospital so has the potential to provide a full range of care for service users as part of the collaboration. It is also close to the existing Highgate mental health facility. Do minimum Under this option the Trust would carry out the minimum works necessary to improve the quality of their existing estate to enable the Trust to deliver a higher quality of care. This option requires the minimum amount of capital as the land is available and buildings are already built. Rebuild at SPH A new mental health inpatient facility would be built on the existing SPH site. The land at SPH is currently occupied by the Trust s existing facilities and therefore these will need to be relocated or worked around while the new site is being built. However the land is the Trust s to use as required. 308 of 402
309 Appendix 12 Options considered Inpatient options Option name Option description and key observations A1 A2 A3 Do minimum (Continue to provide inpatient services in existing buildings). Re-provide inpatients at SPH Re-provide inpatients at Whittington Hospital The configuration of the SPH site will remain unchanged. We will continue to maintain the facilities. As care will still be provided in old buildings, there will be a number of challenges with providing modern facilities. Due to space constraints on the current site there will be no Institute of Mental Health and the ability to fundamentally transform care will be limited. A new inpatient facility will be built on the SPH site. This will provide a modern clinical space which is disability friendly and enable the Trust to deliver a safe service for service users and staff. This would however be on a site that would offer limited ability to offer privacy and dignity to the inpatients. The only location available to enable the build (without the decant of one or two inpatient facilities) would be on the site adjacent to Granary Street, where a recent development scheme has achieved planning permission for up to 13 stories on the opposite side of the road, so this significantly reduces the value that can be realised from the site for reinvestment back into developing sustainable high quality facilities. In addition the Trust is aware of development plans for the so called Ugly Brown Building at the south of St Pancras of up to 12 stories directly overlooking the site, therefore a new inpatient facility could be overlooked in two directions, and only a double carriageway apart which is not seen as a desirable environment for delivering mental health inpatient services. The inpatient facilities would also restrict the density of development adjacent to them, if inpatient facilities are to be delivered on the SPH site, to ensure the wellbeing of service users. The Trusts capital receipt will also be affected by the lower density. The Trust would receive less capital receipt due to selling less land and less receipt because of the reduced density on the site; this results in a considerable reduction in the overall capital receipt for the site. This will undermine the Trust s ability to deliver the requirements of this business case. A new inpatient facility will be built adjacent to the Whittington Hospital in Archway, Islington. This will provide a modern clinical space that is disability friendly and enable the Trust to deliver a safe service for service users and staff. Disruption to service users will be minimised during the construction phase as significant work will not commence at SPH until inpatients are moved to the new site. The Institute of Mental Health can be delivered at the SPH site, but there will also be potential to sell some of the site for 309 of 402
310 Inpatient options A4 Option name Re-provide inpatients at St Ann s Hospital Option description and key observations residential development, releasing funds for the rest of the project. The new inpatient facility will continue to be located in the London Boroughs of Camden and Islington. A new inpatient facility will be built adjacent to the St Ann s Hospital, Haringey. This will provide a modern clinical space, which is disability friendly and enable the Trust to deliver a safe service for service users and staff. Disruption to service users will be minimised during the construction phase as significant work will not commence at SPH until inpatients are moved to the new site. The Institute of Mental Health can be delivered at the SPH site, but there will also be potential to sell some of the site for residential development, releasing funds for the rest of the project. The new inpatient facility will not to be located in the London Boroughs of Camden and Islington. 310 of 402
311 Appendix 13 Qualitative assessment workshop summary Forum Date of Workshop Key themes Senior Leadership Team Clinical Reference Group Council of Governors 26 April 2017 Key themes from the Senior Leadership Team included: The benefits of remaining in the London Boroughs of Camden and Islington to ensure they remain close to their communities was considered an issue for the St Ann s site particularly as transport links are not as good as for the other options. There should be good transport links for service users and staff. Support for improved links between the community and inpatient services offered by the C&I. There will be long term clinical benefits for service users from developing a new research facility Whittington option allows for the co-location of a new Whittington Facility with the existing Highgate Mental Health Centre Co-location with Whittington also provides acute and mental health care on the same site 25 April 2017 Key themes from the Clinical Reference Group included: Refurbishing the existing facilities at SPH will not ensure they meet CQC guidelines and will continue to impact the care delivered to service users. Travelling between St Ann s and SPH would be a significant challenge for C&I personnel. Staff wellbeing facilities can be incorporated into the new site, improving staff morale. 9 May 2017 The council of governors identified: The need to do more work to establish the impact on service users, staff and other stakeholders of increased travel to the preferred option chosen if moving from SPH. It was confirmed that further work on this will be completed as part of the FBC stage. 311 of 402
312 Appendix 14 Qualitative assessment scoring Option A1 Option A3 Option A4 Summary of comments made by each of the groups when scoring against the critical success factors Do Whittington St Ann's minimum CSF CSF CSF CSF CSF CSF CSF CSF CSF CSF CSF CSF Overall Score The two new build inpatient facilities will meet CQC requirements. However the St Ann s option creates travel challenges for service users and staff due to limited public transport links and will make co-ordination between inpatient and community activity more difficult. There will be significant disruption at St Pancras during the refurbishment work over an extended period of time. There will also be some disruption for service users during the transition to either St Ann s or Whittington although for service users and their families when visiting St Ann's this will be more challenging due to the relative inaccessibility of the site. The do minimum option does not make any land available for the new research facility. The new inpatient facility at St Ann s would be considerably more remote from the research hub than an inpatient facility at Whittington. Only new facilities can have a significant impact on the quality of care. Travel time for carers and family when visiting at St Ann's will have a significant impact on those individuals. Only new facilities are aligned to the service user needs and enable the clinical strategy. Travel time for carers and family when visiting at St Ann's will have a significant impact on those individuals. The current SPH cannot support the de-stigmatisation of mental health. Putting the new inpatient site next to an existing mental health site will allow the internal changes to be made but will not support the external perception, which would be supported by co-locating with the Whittington (an acute physical health hospital). The ability to make changes to SPH to meet the requirements of the Equalities Act 2010 is limited. St Ann's is not as good for the service user cohort due to accessibility. Whittington is the only site that provides the potential for an integrated whole person health solution (i.e. integrated physical and mental health). St Ann's is out of area whereas SPH and Whittington are within the borough. The is concern that staff travelling St Ann's will have a lifestyle impact due to the additional travel time. Whittington has the critical mass of staff to provide more support. Do minimum, prevents delivery of the NCL STP as it continues to occupy SPH, it doesn't encourage community care and continues to provide care in substandard, high cost facilities. Whittington meets the STP most closely, while the St Ann's option is outside the borough. Both Whittington and St Ann s enable delivery of the local plans, in particular delivery of new housing. SPH in its current form does not allow housing on the land it occupies. Option A3 (Rebuild at Whittington) has the highest score in the qualitative assessment and therefore is the preferred option. 312 of 402
313 Overall Rank of 402
314 Appendix 15 Qualitative scores of each option Senior Leadership Team and Board Scores Critical Success Factor Option A1 Option A3 Option A4 Notes 1) CQC requirements Community inpatient link weaker at 3 compared to 2 due to location 2) Minimise service user disruption ) Research and development It was noted that a new research facility could not be constructed under option 1 4) Quality of service user care Again the community - inpatient link was emphasised, hence 2 scoring greater than 3 5) Aligned to service user need and supportive of the clinical strategy Yet again the community - inpatient link was emphasised, hence 2 scoring greater than 3 6) De-stigmatise mental health A view that option 3 creates a large mental health facility compared to a mental health facility collocated with physical health in option 2. Options 2 and 3 will both facilitate new facilities on the St Pancras site 7) Promotes equality The accessibility of option 3 was a concern, as was the accessibility for the current buildings in Option 1 8) Integrated care Option 2 provides colocation with physical health that the other options do not. 9) Located with inborough or close to Camden and Islington ) Support staff wellbeing The effective creation of a larger mass of staff in option 2 gives this option the extra point 11) Consistent with the NCL STP of 402
315 12) Consistent with plans for local community and place development of 402
316 Council of Governors Scores Critical Success Factor Option A1 Option A3 Option A4 Notes 1) CQC requirements St Pancras doesn't meet the criteria 2) Minimise service user disruption St Ann's impact on friends and family travelling to see admitted patients 3) Research and development St Pancras already undertakes this 4) Quality of service user care ) Aligned to service user need and supportive of the clinical strategy 6) De-stigmatise mental health St Pancras is a good location, St Ann's is too far Whittington does put all our beds close together, and concentration of patients 7) Promotes equality ) Integrated care ) Located with inborough or close to Camden and Islington 10) Support staff wellbeing 11) Consistent with the NCL STP St Ann's is out of area Don't need a building to support staff development, this is cultural, but longer travel could affect staff Not all members of the group scored this CSF, which has distorted the average. 12) Consistent with plans for local community and place development Some people will want to keep SPH beds 316 of 402
317 Clinical Reference Group Scores Critical Success Factor Option A1 Option A3 Option A4 Notes 1) CQC requirements New facilities will meet the criteria, existing unlikely too due to the age of the building and the lack of amenity space and the ability to put adequate accessibility into buildings designed in the C18th. Concern was noted that the location of St Ann s would meet the accessibility criteria for service users due to the lack of close tube or train service directly to the site and it being only on one bus route 2) Minimise service user disruption The greatest known disruption would be at St Pancras given the planning approvals around the site but also noting the other options also have building plans 3) Research and development Under option 1 there will be no available space for an IoMH on the St Pancras site, as services will continue to be delivered in the same way. Locating Institute of mental health at St Pancras with easy link to Archway will be better than having our main facilities at St Ann s due to the difficulty of access between the St Pancras and St Ann s as whilst the nearest tube to St Ann s is Seven Sisters a further walk of c20mins is needed to get to the site. 4) Quality of service user care Only new facilities can ensure this criteria but travel difficulties to St Ann s noted in scoring The travel relates to carers of those being in the trust premises, as St Ann s is not as easy to get to as Archway which is accessible on buses as well as the tube for our Camden and Islington residents, whereas as St Ann s is not on many bus routes is difficult to get to from Camden and Islington and only with substantial walking 5) Aligned to service user need and supportive of the clinical strategy As with the CSF above the same reasoning 6) Destigmatise mental health St Pancras Hospital does not achieve this in current layout, all options with community hubs improve this aside from St Ann s being similar to St Pancras as being recognised as a specific mental health 317 of 402
318 hospital site, not a general hospital site as the Whittington 7) Promotes equality St Pancras has poor EA10 compliance new builds should be better but transport links to St Ann s are poor 8) Integrated care Only the Whittington options provides fully integrated care with inpatient and community hubs located within Camden and Islington, and the inpatient facilities colocated with acute facilities, whilst St Ann s option will provide the community hubs, the inpatient facility is not located in Camden or Islington or on an acute site but a mental health site. 9) Located with inborough or close to Camden and Islington 10) Support staff wellbeing 11) Consistent with the NCL STP The 3rd option only has community hubs in borough, St Ann s is close but not within The new facilities can provide a higher level of staff wellbeing, but the score also reflects staff being isolated at St Ann s Only options 2 &3 support this and option 2 is more aligned to closer to home 12) Consistent with plans for local community and place development Options 2 &3 enable this to be delivered at St Pancras 318 of 402
319 Appendix 16 Backlog maintenance Capital 2016/17 Capital 2017/18 Capital 2018/19 Capital 2019/20 Capital 2020/21 Building External Internal M&E External Internal M&E External Internal M&E External Internal M&E External Internal M&E Total Comments Ash House - SPH 48,900 75, , ,100 Bloomsbury Building - SPH 211,931 13,600 75,000-50, ,531 Boiler House - SPH 35, , , ,300 East Wing - SPH 100, ,000 47, ,950 Camley Centre/Estates Office - SPH - 300,000 50, ,000 Jules Thorn Day Hospital - SPH - 44, , , ,348 Gate House Building - SPH 58,132 75,000 75,000 16,650-27, , ,082 Huntley Centre - SPH 350,000 97, ,000-10, ,051 Former Kitchen - SPH , , ,000 Cost to bring building back to beneficial use Former Mortuary Building - SPH - 50,000 50, ,000 North East Building - SPH 199, , ,000 24,365 20, ,838 North Wing - SPH - 114,201-11, , ,901 This is RF cost under lease but shown to indicate extent of BLM Post Room Building - SPH - 65,000 47, ,000 Former Residence Building - SPH - 400, , , , ,450,000 Cost to bring building back to beneficial use River Crisis House - SPH - - 1,800 20, ,800 South Wing - SPH 100,000 97, , , ,000 56,200-3,200 1,198,068 The Well - SPH 36,305 1,276 1,225-4,000 1,739 6, ,888 West Wing - SPH 10, , , , ,000 13,350 56,350-1,061,720 SPH Site Infrastructure & Services 1,218, ,000 1,761,000 HMHC M Block 100,000 47,760 3, ,000 7,000-20, , Daleham Gardens 8,140 7,678 2,850 10,469 20,000-6,962 3,500-5,441 15,000-80, Aberdeen Park 4,600 2,940 7,540 2,226 10,000 4,475 15, ,819 Camden Mews - 100,000 1, ,000 4, , Camden Road ,000 1,200-4, ,980 Drayton Park 7,872-1,400 50,463 2,320 5, ,145 Greys Inn Road 9, ,850-2, ,500-20,494 Greenland Road , , ,000 5, , , Hanley Road 60, , , ,000 BLM liability assuming retention Hornsey Lane Leased to third party - no residual BLM liability The Hoo 20, , ,298 14,000 2, ,000 9,900 41,807 20,222 5,000 3, , ,876 Holloway Road 5,784 3,698 2, ,000-2, ,582 2,500-53,730 Lowther Road 19, , ,000 1,200 6, ,580 Margarete Centre - - 7, ,000 50, ,939 Southwood Smith Building 2, ,660 10, ,087 Stacey Street 13,557 5,868 2,050 2,987 3,500 3, ,000-28, ,287 Highview Residential - 3,000 1, ,242 9,418 5, ,150 Blenheim Court Brewery Road Leased but no BLM liability beyond repairing covenants Caledonian Road Not owned by C&I - no BLM liability Finsbury Health Centre Not owned by C&I - no BLM liability Raglan St Not owned by C&I - no BLM liability Hanley Gardens Not C&I properties - no backlog liability Highgate Road Not owned by C&I - no BLM liability Hunter Street Leased building no residual BLM liability - possible vacation Isledon Road Not owned by C&I - no BLM liability Manor Gardens Leased but no BLM liability beyond repairing covenants Netherwood St Not owned by C&I - no BLM liability Peckwater Leased building no residual BLM liability - possible vacation Simmons House Leased and sublet - no residual BLM liability Tottenham Mews Derelict Building surplus to requirements - potential disposal 71, ,000 1,107,835 2,034,640 2,300,332 1,830,552 1,977,847 1,685, ,060 57, ,618 90, , ,000-13,705,054 Annual Total 2,129,181 Annual Total 6,165,525 Annual Total 4,408,054 Annual Total 348,444 Annual Total 653,850 13,705,054 St Pancras Hospital - 850, ,641 1,666,370 1,373,276 1,675,333 1,096,225 1,200, ,800 15, ,693 25, , ,000-9,999,578 HMHC - 100,000 47, , ,000-7, , ,260 Community Sites 71, , , , , , ,147 59,260 42,457 87,925 45,130 53, ,000-2,977,216 Total 71, ,000 1,107,835 2,034,640 2,300,332 1,830,552 1,977,847 1,685, ,060 57, ,618 90, , ,000-13,705, of 402
320 Appendix 17 Quantifiable benefits Type of Benefit Activity (less acute because more community intervention / early intervention / less duplication) Staffing (reduced staff costs through less agency, more productive and happier staff) Benefit Quicker service user recovery frees up bed capacity and reduced cost (noncash releasing, recurrent) Reduced cost of physical healthcare through co-location of mental and physical healthcare services (non-cash releasing, recurrent) Reduced agency staffing, so reducing cost, through improved staff working conditions and therefore retention (cash releasing, recurrent) Reduced costs due to new build wards, with large bed capacity and better layout (cash releasing, recurrent) Reduced cost of staff training due to co-location of the site with other similar medical facilities (non-cash releasing, recurrent) Option A1 Do Minimum N/a Option A2 Rebuild SPH 1.5m per annum (from 2023/24) Option A3 Whittington 1.5m per annum (from 2023/24) N/a N/a 70k per annum (from 21/22) N/a N/a 800k per annum 800k per annum 800k per annum 800k per annum N/a N/a 80k per annum (from 2021/22) Option A4 St Ann s 1.5m per annum (from 2023/24) N/a 800k per annum 800k per annum 80k per annum (from 2021/22) Assumptions Improving the environment for service will mean they make a quicker recovery. Identifying service users earlier, means that the severity of their conditions is reduced. Costs of care for the Trust will reduce as a result of co-locating with an acute Trust. Costs of service user transport will reduce The new facility will improve staff morale. The new facility will therefore encourage staff to stay in post, reducing vacancies and therefore agency staffing costs. Reducing the number of wards by one but maintaining the number of beds means that the number of senior staff required on each shift will reduce. By training staff in larger groups or being able to offer more training on site will reduce costs. 320 of 402
321 Staff progression and therefore satisfaction will increase due to increased opportunity Admin staff flexibly located to increase operational efficiency (non-cash releasing, recurrent) N/a 100k per annum (from completio n of the project) 100k per annum (from completio n of the project) 100k per annum (from completio n of the project) Admin staff are more accessible to clinical staff, reducing inefficiency. By making effective use of flexible working arrangements less space is required. Overheads Operating costs of a new building are lower than those of an old building (cash releasing, recurrent) N/a 1.8m per annum (from 2021/22) 1.8m per annum (from 2021/22) 1.8m per annum (from 2021/22) Lifecycle cost report provided by T&T shows a significantly reduced costs from a more efficient new building. Energy and utility costs (cash releasing, recurrent) N/a 360k per annum (from 2021/22) 360k per annum (from 2021/22) 360k per annum (from 2021/22) The new building will be more efficient due to using better building design / materials. Renegotiation of existing FM contracts (cash releasing, recurrent) N/a 575k per annum (from 2018/19) N/a N/a Based on benchmarking data the existing FM costs can be reduced by renegotiating the contract. Other Increased research income from working closely with the Institute of Mental Health (IoMH) (cash releasing, recurrent) N/a 10k per annum (from 2021/22) 10k per annum (from 2021/22) 10k per annum (from 2021/22) IoMH works closely with the Trust and therefore benefits from some research grants. Sub-let consultancy rooms (cash releasing, recurrent) N/a 20k per annum 20k per annum 20k per annum 2% of consultancy rooms sublet on a regular basis to enable the provision of other services. Uptake of these rooms will be high. Realisation of land proceeds from access community and hospital estate. (cash releasing, non-recurrent) N/a 66.3m (between 90.4m (between 90.4m (between Land which is surplus to requirements in both the 321 of 402
322 2017/ / /18 community estate and inpatient and and and estate can be sold at market 2026/27) 2026/27) 2026/27) value to realise a financial gain 322 of 402
323 Appendix 18 Trust s Income & Expenditure assumptions Area Income Expenditure: Pay costs Assumption Baseline and investment case Contractual income from clinical services with Camden CCG and Islington CCG is assumed to grow at an average rate of 0.7% and 1.7% per year between 2016/17 and 2025/26 (before inflation). Income from other contracts for clinical services is assumed to fall from 13.3m in 2016/17 to 11.7m in 2017/18 (an 11.5% decrease) and then grow by 0.8% per year (before inflation). Non-contract activity income is assumed to remain at the 2016/17 level of 1.3m per year throughout. Section 75 income is assumed to remain at 12.7m per year throughout. A reduction in income reflecting the risk of funding from parity of esteem has been applied from 2019/20 at 0.7m, increasing to 1.9m by 2025/26. STF funding has been assumed at 0.8m per year for 2016/17, 2017/18 and 2018/19. No funding has been assumed thereafter. Investment case The investment case is assumed to increase research and development and other revenue by 10k (from 2021/22) and 21k (from 2020/21) respectively. Baseline and investment case Activity growth is assumed to increase pay costs across all staff groups by 1.0% in 2017/18 and 0.6% per year thereafter. Pay-related CIPs are assumed at 3.3% of total pay costs in 2017/18 and between 1.5% and 1.2% per year thereafter. The impact of agenda for change (AfC) pay rates is assumed to be an annual increase of 1.2% in pay costs across all staff groups. The cost associated with additional parity of esteem funding is assumed at 0.3% for 2019/2020, around 0.7% for 2020/21 and 0.5% per year thereafter. Investment case The investment is assumed to reduce spend on substantive nursing staff by 0.9m per year from 2021/22. This is a CIP plan to reduce the number of staff by one ward, made possible by the larger modern wards in the new building. CIP plans to further reduce agency staff costs through: more efficient staff rotas, better staff retention and co-locating admin staff with community hubs is assumed to reduce agency costs by: o 0.3m in 2020/21 o 0.6m in 2021/22 o 0.9m per year thereafter 323 of 402
324 Area Expenditure: Non-pay costs Cost improvement plans Interest expense Assumption Baseline and investment case Activity growth is assumed to increase drug costs, clinical supplies and directly managed staff costs by 0.7% in 2017/18 and is assumed to have no further impact thereafter. Parity of esteem funding is assumed to increase drug costs by 0.4% in 2019/20, 0.9% in 2020/21 and 0.6% thereafter. Other expenses (general supplies, establishment costs, premises and plant costs and other costs) are assumed to fall slightly from 27.1m in 2016/17 to 27.4m in 2017/18 and in each year thereafter (before CIP and inflation). Other expenditure CIPs are assumed to be achieved recurrently at 2.2m in 2017/18, with a further 0.8m assumed recurrently each year thereafter. Investment case The investment is assumed to reduce other expenses by 0.8m in 2020/21 and around 3.5m per year thereafter. This is the result of three CIP schemes: o o o 1.8m from the reduced operating costs of the new building; 1.5m from reducing the length of stay (LOS) resulting from the improved therapeutic environment; and 0.4m from reduced energy costs of the new building. Baseline and investment case The assumptions underlying the pay and non-pay CIPs are set out in the relevant sections above. All CIPs are assumed to be recurrent. No income CIPs are assumed. CIPs are assumed at, as a percentage of operating expenditure: o 4.1% for 2017/18 o 1.8% from 2018/19 to 2019/20 o 1.7% from 2020/21 to 2023/24 o 1.6% from 2024/25 to 2025/26 Investment case The investment is assumed to generate pay cost savings of 1.8m by 2022/23, as set out in the pay costs section above. Other expenses CIPs are assumed at 3.5m from 2021/22, as set out in the non-pay costs section above. Baseline case No interest costs are included in the baseline case. Investment case Interest costs under the investment case are assumed to be 2.9%. 324 of 402
325 Area Inflation Assumption Baseline and investment case Inflation has been assumed at the following rates: 2018/ / / / /23+ Income 0.1% 0.3% 0.3% 0.3% 0.3% Pay costs 1.0% 1.0% 1.0% 1.0% 1.0% Drug costs 3.5% 3.5% 3.5% 3.5% 3.5% Other expenses 2.0% 2.0% 2.0% 2.0% 2.0% Capex 3.0% 3.0% 3.0% 3.0% 3.0% The above inflation rates are consistent with the Trust s Sustainability & Transformation Plan (STP) assumptions Note, in addition to the inflation rates above, the Trust has assumed a 1.2% AfC increase that whilst not technically inflation will compound with the inflation rates above to increase wages in cash terms. Transitional support The Trust has not assumed that it will receive any transitional support funding as part of its affordability assessment. Funding for the clinical transformation and estates strategy will be from land sales and internally generated reserves. As described above, due to the timing of the major cashflows (construction cost and land purchases coming before land sales), the Trust has assumed a bridging loan to ensure that it can maintain sufficient working capital over the LTFM period. 325 of 402


326 Appendix 19 Baseline income and expenditure 326 of 402

327 Appendix 20 Baseline statement of financial position 327 of 402

328 Appendix 21 Baseline cash flow statement 328 of 402
329 Appendix 22 Trust FSRR scores for the investment and baseline cases The financial sustainability risk rating (FSRR) is NHSI s view of the level of financial risk a trust is exposed to and is a therefore key metric to consider for this transaction. The FSRR is a combination of the following four metrics: Liquidity: days of operating costs held in cash or cash equivalents Capital servicing capacity: the degree to which the organisation s generated income covers its interest and debt repayments. Note that this may exclude repayment of bridging debt at NHSI s discretion (discussed further below). Income and expenditure (I&E) margin: the degree to which the organisation is operating a surplus/deficit with respect to its total operating and non-operating income. Surplus/(deficit) is calculated before impairments and gains/losses on asset disposal. Variance from plan in relation to I&E margin: the variance between a trust s planned and actual I&E margin. Each of the metrics yields a score between 1 (greatest risk) and 4 (least risk). An overall FSRR score is calculated from the average of the four metrics, although this is capped at 2 if one of the metrics is a 1. Trusts that score a 1 or 2 may be subject to an investigation by NHSI. The details of the FSRR calculations criteria are shown in Table F1 below. Table F1: FSRR criteria Financial criteria Metric Risk categories Balance sheet sustainability Capital service capacity (times) < >2.5 Liquidity Liquidity (days) <(14) (14)-(7) (7)-0 >0 Underlying performance I&E margin (%) <(1) (1) >1 Variance from plan Notes: Variance in I&E margin as % of income <(2) (2)-(1) (1)-0 >0 The metrics are weighted equally (i.e. averaged), then rounded to produce a single FSRR If the trust scores 1 on any metric, the overall rating will be capped at a of 402
330 The FSRR scores for the investment and baseline cases are set out in Tables F2 to F4 below. The FSRR calculation performed by the LTFM yield a capital service cover risk rating of 1 for the investment case, as the bridge loan repayments are included in the debt service total. This significantly distorts the position as the Trust has sufficient cash to make these repayments as shown in the tables above. The LTFM itself provides an area where adjustments can be made to reverse out the impact of bridge loan financing from the FSRR analysis and that is deemed appropriate here. These repayments are excluded for bridge loans and the impact of this is shown in Table F3 below. Table F2: FSRR scores for the investment case (unadjusted) Risk score 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Capital service capacity Liquidity I&E margin Variance in I&E margin n/a Overall FSRR n/a As noted above, the inclusion of the bridge debt repayments as debt service in the capital service capacity calculation causes this metric to become 1. Table F3 below presents the FSRR scores after these payments have been excluded from the calculation. Table F3: FSRR scores for the investment case (adjusted for debt repayments) Risk score 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Capital service capacity Liquidity I&E margin Variance in I&E margin n/a Overall FSRR n/a The adjusted FSRR shows an I&E margin rating of 2 in 2020/21, as the projections show a small net deficit in this year of (0.1)m. The overall rating remains at 3 for this year and at 4 for all other years. 330 of 402
331 Table F4: FSRR scores for the baseline case Risk score 2016/ / / / / / / / / /26 Outturn Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Capital service capacity Liquidity I&E margin Variance in I&E margin n/a Overall FSRR n/a Under the baseline case, the FSRR remains at 4 throughout, although the declining net surplus position causes the I&E margin score to fall to a 2 by 2025/26. The sensitivities set out in the previous section each have minimal or no impact on the forecast FSRR score when considered individually. A combined downside case will be considered in the FBC along with the impact on the FSRR. 331 of 402
332 Appendix 23 Letter of support from the Trust s Director of Nursing 332 of 402


333 Appendix 24 Bed modelling benchmarking On the graphs below, the Trust is identified as M11. Adults 333 of 402

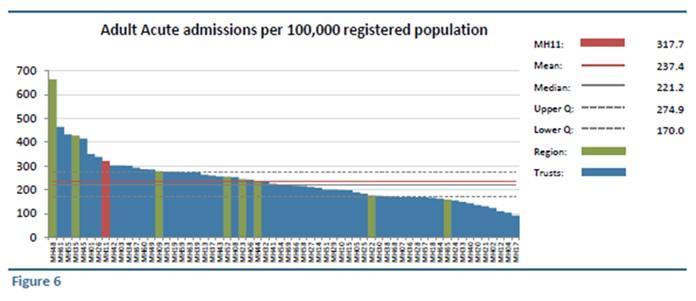
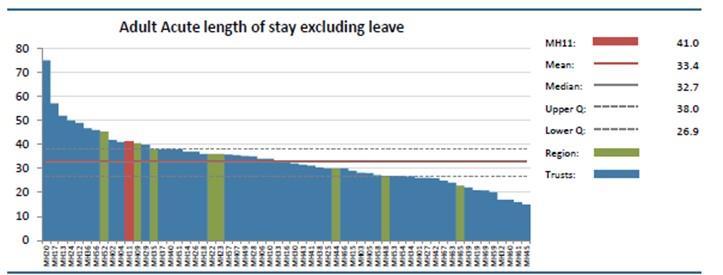
334 Acute 334 of 402


335 Length of Stay 2015/ /18 Length of stay MPICU Length of stay WPICU 36 Length of stay Acute Length of stay Older Adult Length of stay Rehab of 402
336 Appendix 25 Bed occupancy Bed Occupancy Acute: Reduction approx. 3% R&R: Reduction approx. 2% SAMH:33% reduction in usage 336 of 402
337 Number of Out of Area Placements (OAPs) Reduction in ECR th 5 April zero ECR bed 337 of 402
338 MEETING Islington CCG Governing Body Item: 3.4 DATE 9th May 2018 REPORT LEAD DIRECTOR AUTHOR CONTACT DETAILS Request to Delegate Authority for Approval of the Annual Report and Accounts to the Islington CCG Audit Committee Tony Hoolaghan, Chief Operating Officer Emer Delaney, Head of Communications and Engagement, Haringey CCG and Islington CCG Karl Thompson, NCL Head of Corporate Services EXECUTIVE SUMMARY All NHS bodies have a statutory requirement to produce an Annual Reports and Accounts (ARA) as a single document. Islington CCG has adopted the template issued by NHS England (NHSE) for the financial year, which contains the following required sections. 1. The Performance Report: an overview and a performance analysis. 2. The Accountability Report: Corporate Governance Report, Remuneration and Staff Report and a Parliamentary Accountability and Audit Report. 3. The Annual Accounts: including financial statements. Draft submissions of the ARA were required by 20 th April The Haringey and Islington Executive Management team reviewed the organisation s draft ARA at its meeting on 18 th April. The meeting agreed a number of changes, and members along with CCG lay members have been given until 4 th May to make any further comments (see Table 1 for the drafting and approval timeline). As in previous years, it is proposed that authority to approve the final submission is delegated to the CCG Audit Committee; to be discharged at is meeting on 22 nd May Table 1: National and Local Timelines Date April 2018 Actions Friday 20 April (noon) CCGs to submit: Draft annual report as approved by the Accountable Officer (and passed to appointed auditors for audit). A full copy of the draft Head of Internal Audit Opinion statement as issued by the CCG s internal auditors. To include a list of all audit reviews undertaken, and the level of assurance assigned to each review. Completed NAO disclosure checklist 2017/18 for draft submission May May Final draft of the ARA to be considered by the CCG Audit Committee Tuesday 29 May (noon) Note: Monday 28 May is CCGs to submit: Full audited ARA, signed and dated by the Accountable Officer and appointed auditors, as one composite document. A full copy of the final Head of Internal Audit Opinion statement as issued by the CCG s internal auditors. Submitted a separate document. Summary version included in the ARA. Completed NAO disclosure checklist 2017/18 for final submission 338 of 402
339 a Bank holiday June 2018 By 15 June CCGs to publish their ARA in full on their public website. September 2018 By 29 Sept The ARA will be presented in public at a Islington CCG Annual General Meeting Member statement As part of our preparation and sign off of the annual report and accounts, whilst the Governing Body have delegated responsibility for the documentation to be signed off at the Audit Committee, each individual who is a member of the Governing Body at the time the Members Report is approved, is asked to confirm the following: so far as the member is aware, there is no relevant audit information of which the CCG s auditor is unaware that would be relevant for the purposes of their audit report the member has taken all the steps that they ought to have taken in order to make him or herself aware of any relevant audit information and to establish that the CCG s auditor is aware of it. Governing Body Members are asked to confirm they are happy to support this statement. RECOMMENDED ACTION: The Governing Body is asked to: DELEGATE authority for the approval of the final ARA submission to the CCG Audit Committee. NOTE members response to the disclosure to auditors statement Patient & Public Participation (PPP): Audit Committee membership includes lay members. Equality Impact Assessment: Not required Risks: As outlined in the CCG s assurance framework and risk register Resource Implications: None identified at present 339 of 402
340 Item: 4.1 MEETING: Islington CCG Governing Body DATE: 9 May 2018 TITLE: LEAD COMMITTEE MEMBER: AUTHOR: CONTACT DETAILS: RAF Report Alex Smith Director Planning Performance and Delivery Haringey and Islington (H&I) CCGs Vivienne Ahmad, Board Secretary, Islington CCG v.ahmad@nhs.net SUMMARY: This report presents the Risk Assurance Framework (RAF) following an alignment of the current risks into Islington CCG s Objectives and clarifies movement with key strategic risks during Quarter 1, providing an insight in to the current level of risk likely to impact on the achievement of Islington CCG s strategic objectives: Ensuring every child has the best start in life; Preventing and managing long term conditions to extend both length and quality of life and reduce health inequalities; Improving mental health and wellbeing; Delivering high quality, efficient services within the resources available. This framework should be considered in conjunction with the: NCL (North Central London CCGs) Strategic Risk Register PCCC (Primary Care Committee in Common) Risk Register NCL JCC (Joint Commissioning Committee) Risk Register Prior consideration by Committees and other partners: Specific elements of the RAF were considered by the Strategy and Finance Committee on 24 April 2018 and the Quality and Performance Committee on 26 April Patient & Public Involvement (PPI): This paper will be available on the CCG website for consideration by patients and public. Relevant risks will be reviewed by the PPP Committee on 3 May 2018 and further reviewed by the Chair of the PPP Committee and the Chief Operating Officer. Equality Impact Assessment: not required for summary report. 340 of 402
341 Risks: N/A RECOMMENDED ACTION: The Governing Body is asked to: NOTE and COMMENT on the latest iteration of the RAF document SUPPORTING PAPERS: Islington CCG Risk Assurance Framework - April NCL Joint Commissioning Committee Risk Register - April Primary Care Committee in Common Risk Register April NCL Risk Register - April Risk Scoring Key 341 of 402
342 Islington CCG Audit Committee Risk Assurance Framework BACKGROUND & CONTEXT Principal Risks The RAF document is focused on the principal risks to the achievement of our strategic objectives, by this we are referring to risks that if not managed effectively will result in our failure to deliver against each objective. Principal risks have therefore been defined as those with an inherent risk score (before mitigation) of 15+ (red risks). It can be assumed that risks with inherent risk scores lower than 15 are not on their own likely to result in our failure to achieve an objective. These risks are still important though and will be managed through our corporate risk register but will not feature in the RAF. High Residual Risks There may be instances where risks not inherently scored as high escalate due to further circumstances arising. Once these risks are reassessed as high risk, they are brought in to the RAF for consideration by the Governing body. LATEST MOVEMENT IN THE RISK ASSURANCE FRAMEWORK New Risks There was one new risk added to the RAF since the last meeting. Risk 437 (score 15) 2018/19 QIPP Programme Delivery Previous QIPP risk of 2017/18 was risk ID 409 which has been recommended to close. This new risk 437 would be discussed at Strategy and Finance Committee on 26 April Risk Movement Risk 428 (score 12) Medicines Management - The recommendation is to reduce the risk rating from 16 to 12 given that recent reporting has shown a decline in the financial impact of NCSOs. Risks Closed The following risk is proposed for closure: Risk 409 (score 12) 2017/18 QIPP Programme Delivery - It is recommended to close this risk as the new 2018/19 QIPP Risk has been opened - risk number of 402
343 NCL Joint Commissioning Committee Risk Register The NCL Joint Commissioning Committee ( NCL JCC ) risk register has 7 risks with a current risk score of 15 or higher and therefore are reporting them to the Governing Body to ensure visibility and oversight. These risks are from a pan NCL perspective and therefore there is some overlap with Barnet CCG only risks. Key Highlights JCC 1- Delivery of Cancer 62-day waiting time standard (Threat): NCL as a system delivered the standard in December 2017 but additional work is required for this to be sustainable. However, the individual recovery plan from UCLH defers their recovery of the standard from March 2018 to June Internal pathways are expected to be compliant in April JCC 10- Mobilisation of STP and QIPP plans (Threat): The in-housing of functions from NEL CSU into the CCGs is underway. This will provide greater support and capacity to deliver STP interventions. However, additional capacity is needed to progress the work on alternative contract forms. JCC 11- Managing Acute Contracts within Contract Baselines (Threat): Signed contracts with acute providers in place for 2017/18 and 2018/19 with respect to all the main contract terms other than baseline. Baselines predicated on growth have been agreed but discussions on STP interventions are on-going with providers until end of April The contracts operate under a marginal rate basis against the agreed baseline. This helps to mitigate risk for both providers and commissioners from variances in activity levels and incentivises both sides to reduce unnecessary and avoidable activity. NCL Primary Care Co-Commissioning Risk Register The NCL Primary Care Co-Commissioning Committee in Common ( NCL PCC ) risk register has 1 risks with a residual risk score of 15 or higher and therefore this risk is being reported to the Governing Body to ensure visibility and oversight. Risks from the NCL PCC can be from either a local perspective or a pan NCL perspective depending on the risk. Risk 18- Primary Care Support England (Threat): The NHS England primary care support functions provided by NHS England and contracted to Capita have been significantly underperforming. This has led to a disruption in GP business continuity and potential cost pressures to CCGs. This risk is primarily managed by NHS England. NHS England meet with Capita regularly to try to resolve the issues and the NCL CCGs raise issues with NHS England at London primary care meetings. 343 of 402
344 NCL Risk Register The NCL Risk Register captures the key pan NCL risks that are not captured by our other risk registers. The NCL Risk Register contains ten risks which include NCL and STP risks. The NCL Risk Register will be reviewed regularly by the NCL Senior Management Team, the STP PMO and the assurance process will be overseen by the NCL audit committees. Key Highlights NCL 4- Failure to Effectively Engage with Patients and the Public (Threat): A new Head of Communications for the STP has been recruited and will start in May NCL 8- Recruitment and Retention a High Performing Workforce (Threat): The NCL HR team has been fully recruited to with all team members being in place by end of June Recruitment for the Organisational Development roles is under way. NCL 9- Delivering Financial Balance across NCL CCGs (Threat): budget planning is underway and QIPP plans will be implemented throughout the year. 344 of 402
345 GOVERNING BODY RISK ASSURANCE FRAMEWORK SUMMARY April 2018 Risk Ref Review Committee Objective 1 Ensuring every child has the best start in life Description Inherent Risk Score 17/18 18/19 Q4 Q1 Q2 Q3 Q4 Risk Movement since last Qtr No principal risks have currently been identified for this objective based on the criteria defined (15+ risk score) Objective 2 Preventing and Managing Long Term Conditions to extend both length and quality of life and reduce health inequalities No principal risks have currently been identified for this objective based on the criteria defined (15+ risk score) Objective 3 Improving Mental Health and Wellbeing 205 Strategy & Finance Pressure on mental health acute beds If pressure/demand exceeds the current bed base provided by our commissioned services then The CCG may not be able to meet its obligation to commission effectively to meet the health needs of our residents in terms of safety through delayed admission and risk of stay on an excessively high occupancy ward Clinical effectiveness: care not based on health need or poor continuity of care Poor patient experience. This could also adversely affect the CCG s reputation. Objective 4 Delivery of High Quality, Efficient Services Within Available Resources Strategy & Finance NCL Commissioning Arrangements & Local Change Process Uncertainty over the NCL commissioning arrangements and change process involving Haringey CCG, may occur as a result of a lack of clarity and tranparency over the organisation structure and impact on individuals and teams. This could lead to loss of organisational knowledge from increased staff absenteeism/leaving and also the over reliance on interim staff due to higher levels of vacancies Quality & Performance Whittington Health - Quality of Community Service Provision There are a number of community services which are performing poorly against current contract specifications relating to access.this increases the likelihood of harm, discomfort and poor quality outcomes as a result of the longer waits Quality & Performance Moorfields - standardisation of service provision The lack of formally agreed service level (SLA) contracts acorss satelitte sites potentailly leads to poor service provision resulting from ineffective quality governance systems. This inturn restricts the drive for improvement, standardising of practices and influencing of change which can lead to poor patient outcome and experience Quality & Performance Moorfields - Safer Surgery checklist (WHO) The failure to utilise the WHO safer surgery checklist may lead to inconsistent practices across sites which in turn increases the chances of never events occuring and patients being exposed to harm or clinical incidents Quality & Performance Moorfields - SI system adherence A lack of adherence to the 2015/16 serious incident framework and failure to provide evidence over the completion of part 2 Duty of Candour, will lead to poor learning from incidents and an increased likelihood of repeat occurrences. The likely result is a detrimental impact on the reputation of the CCG through a lack of feedback around meeting Duty of Candour and an increase in poor patient outcomes of 402
346 Risk Ref Review Committee Description Inherent Risk Score 17/18 18/19 Risk Movement Q4 Q1 Q2 Q3 Q4 since last Qtr 423 Quality & Performance Whittington Health - Lower Urinary Tract Symptoms (LUTS) The Trust and Commissioners have agreed a phased reopening of the LUTs clinic as a tertiary service for adult patients subject to conditions set out by the NCL Joint CCG Commissioning Committee in April There is a risk that the agreed specifcation for 2018/19 may not be met Patient and Public Participation STP engagement The STP covers a wider footprint with an increased number of partners. This could lead to engagement becoming less effective, with groups that experience high levels of deprivation and inequalities potentially not being heard. This could jeopodise the relationship with the community and cause significant reputational damage for the CCG Quality & Performance Camden & Islington FT - Mr G external investigation outcome Failure to deliver recommendations within the action plan, increases the likelihood of similar incidents occuring, with the potential for further safeguarding concerns Quality & Performance Other 409 Strategy & Finance Islington (Borough Council and NHS Trust) and Camden and Islington FT Adult Safeguarding Process The electronic drive is held by the Local Authority (London Borough of Islington) and shared with the Trust (Camden and Islington NHS Foundation Trust). In November 2017, it became apparent that the drive contains lists of names, including safeguarding concerns, police referrals etc and the Trust were not accessing the list and were not aware of the list. There is no electronic link between the LA and Trust system for safeguaridng adults. This could result in patients falling through the system unmanged, increasing the chances of safeguarding concerns materialising. Statutory Obligations and Core Business 17/18 QIPP Programme Delivery The QIPP target is set at m, 5.2m of which is expected to be delivered through the STP. The STP QIPP programme is largely transformation which requires substantial changes to models of care. Any slippage in QIPP (or unidentified QIPP) will need an action plan in plan to recover the position and mitigate financial and performance risks to the organisation. Failure to achieve the CCG QIPP plan is likely to impact on the organisation's ability to meet its financial control total for the year and, as a result, the NCL Financial Control Total Strategy & Finance 108 Strategy & Finance 434 Strategy & Finance Medicines Management A significant national increase in the number of short supply high volume generic medicines (categorised as No Cheaper Stock Obtainable, NCSO in the Drug Tariff) has created an unpredictable rise month on month in the cost of these items. As a result, the CCG has predicted a potential additional overspend for these medicines in excess of 1.4m. This is a national issue being managed by NHS England and the Department of Health. NHS England has published the guidance ''Refreshing NHS plans for 2018/19", which makes it clear that CCGs should assume that the high level of discretionary prices for generic drugs in short supply will not persist in 2018/19. Primary care workforce development If the CCG is ineffective in developing the primary care workforce then this may have an adverse impact on the delivery of the primary care strategy. This could mean for example, patients with long term conditions are not fully supported in primary care and require more frequent hospital care. Re-development of St Pancras site Delayed start of consultation, failure to gain assurance from NHSE on process, threat of judicial review, not enough capacity to carry out a more thorough public consultation and currently no support from Clinical Senate for clinical proposals, means the whole re-development of the St Pancras site is at risk Strategy & Finance 2018 / 19 QIPP Programme Delivery The QIPP target is set at 12.6m net savings. The QIPP programme is largely transformational which requires substantial changes to models of care. Agreement as to the level of QIPP contained within provider contracts as part of STP initiatives has not concluded in March 2018 and the contract with Whittington Health is subject to mediation. The outcome of mediation is that Clinical Review sessions are taking place between commissioners and providers to be concluded by 30/4/18. Contractual agreement regarding levels of QIPP within provider contracts is one of the key mechanisms to delivering QIPP savings. Any slippage in QIPP, will need an action plan in place to recover the position and mitigate financial and performance risks to the organisation. Failure to achieve the CCG QIPP plan is likely to impact on the organisation's ability to meet its financial control total for the year, and as a result, impact on the NCL Financial Control Total of 402
347 Objective 1 Ensuring every child has the best start in life No principal risks have currently been identified for this objecitve based on the criteria defined (15+ risk score) 347 of 402
348 Objective 2 Preventing and Managing Long Term Conditions to extend both length and quality of life and reduce health inequalities No principal risks have currently been identified for this objecitve based on the criteria defined (15+ risk score) 348 of 402
349 Objective 3 Improving Mental Health and Wellbeing Date Risk Added: RAF Ref: 205 Risk: Pressure on mental health acute beds If pressure/demand exceeds the current bed base provided by our commissioned services then The CCG may not be able to meet its obligation to commission effectively to meet the health needs of our residents in terms of safety through delayed admission and risk of stay on an excessively high occupancy ward Clinical effectiveness: care not based on health need or poor continuity of care Poor patient experience. This could also adversely affect the CCG s reputation. Risk Owner Director of Commissioning Risk Lead Senior Commissioning Manager Mental Health and Continuing Healthcare Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively Evidence what was received and where was it presented Date Strength 1=red 2=amber 3=green Internal / External STP work on overall capacity including development of St Anne's A new women's PICU has been opened to improve acute pathway for Islington Quarterly reports to Quality & patients. The acute pathway remains a focus for the STP Mental Health work performance committee Additional beds are now available as part of a risk share agreement stream. C1 2 Readmission rates are Feb-18 2 Internal with Camden and Islington Foundation Trust (CIFT) There have been no further 12 hour breaches in finding mental health acute beds. Risk has therefore been downgraded from 12 to 9. reported to Contract review group STP, through Healthy London Partnerships, created service specification for mental health place of safety outside of A&E. Quarterly reports to Quality & performance committee Risk share arrangement includes monthly meeting with CIFT to During March increased demand on acute beds, as well as reduced discharges C2 3 Readmission rates are Apr-17 2 Internal monitor bed occupancy, identify issues and solve problems resulted in long delays in A&E and on wards for patients waiting admission. Gold command at CIFT was put in place which has brought the situation back under control but capacity remains high at %. reported to Contract review group Quarterly reports to Quality & C3 performance committee The National Crisis Concordat has led to a local action plan to 3 Regular performance reports to committee. Readmission rates are enhance admission avoidance capability reported to Contract review Mar-17 2 Internal group Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 17/04/2018 Committee Feedback There had been no further 12 hour breaches in finding Mental Health acute beds. Risk was therefore downgraded from 12 to 9 in February Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 349 of 402
350 Objective 4 Delivery of High Quality, Efficient Services Within Available Resources Date Risk Added: RAF Ref: 408 Risk: NCL Commissioning Arrangements & Local Change Process Uncertainty over the NCL commissioning arrangements and change process involving Haringey CCG, may occur as a result of a lack of clarity and tranparency over the organisation structure and impact on individuals and teams. This could lead to loss of organsiational knowledge from increased staff absenteeism/leaving and also the over reliance on interim staff due to higher levels of vacancies. Risk Owner Chief Operating Officer Risk Lead Director of Commissioning Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the principal risks. Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively Evidence what was received and where was it presented Date Strength 1=red 2=amber 3=green Internal / External NCL and COO now in post and attending key committees. Appointments to key posts across NCL and the CCG CCG meeting records of C1 3 May-17 2 Internal attendance Turnover of staff during the past 3 months (20%) C2 Fortnightly briefings to staff 2 Updates and presentations from Chief Officer and key individuals on programmes of work. Wellbeing partnership, I Hub learning disabilities etc. Meetings moved to Thursdays to improve attendance. Regular updates on structure changes and plans. Staff feedback at fortnightly briefings on issues concerning the changes Schedule of staff briefings planned ansd delivered. Record of staff feedback at group session Feb 2017 fortnightly meetings 2 Internal Weekly newsletters via . C3 Weekly Friday staff newsletter 2 record of staff newletters issued. weekly 2 Internal Updates on intranet Joint Haringey and Islington Executive Management Team meetings Schedule of meetings and papers distributed to members and actions resulting C4 3 Minutes of previous meetings weekly 2 Internal weekly from meetings ciruclated to key officers. 350 of 402
351 Objective 4 Delivery of High Quality, Efficient Services Within Available Resources New Joint Management Operating Model for Haringey and Islington Details of period of engagement and the new perating model are available to staff Friday News provides link to C5 CCGs on 22/9/17. Period of engagement and 'Go Live' date 16th 2 Sep-17 2 Internal through the intranet. documents. October. All new EMT directors appointed and in post bar Programme Director C6 3 Directors in post and starting to attend meetings. N/A N/A 2 Internal for Care Closer to Home who starts on 16/10/17 Pro-active recruitment to vacancies previously filled with interims to Number of new starters have commenced recently increasing the compliment of Introductions at staff briefing C7 2 2 Internal give stability and promote continuity. permanent recruits in post. sessions OD programme being taken forward that includes mixed staff groups C8 doing task and finish work on flexible and SMART working in response 2 2 Internal to the staff survey. C9 Haringey and Islington CCGs all staff away day booked for 30th Away day joint working group met for its first meeting on Monday 25th October - mixed group of staff to help co-design programme for the 2 September day. record of meeting held. Sep-17 2 Internal Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 17/04/2018 Committee Feedback This risk went through a review in February and since then there has been no change since last review. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 351 of 402
352 Objective 4 Delivery of High Quality, Efficient Services Within Available Resources Date Risk Added: RAF Ref: 419 Risk: Whittington Health - Quality of Community Service Provision There are a number of community services which are performing poorly against current contract specifications relating to access.this increases the likelihood of harm, discomfort and poor quality outcomes as a result of the longer waits. Risk Owner Director of Quality Risk Lead Assistant Director of Nursing Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Strength Strength Controls 1=red Assurances Evidence 1=red Specific tasks and measure implemented to mitigate the effect of the Date 2=amber Reports/information received that confirms controls listed are working effectively what was received and where was 2=amber Internal / pricipal risks. Control Ref: 3=green it presented 3=green External 1. Community disagregation to understand capacity and demand has started with focus on specific services with long waits. ie how much 1.Minutes of the meetings for each of the community disagregation workstreams C1 each service costs / is invested in. 2 Copies of Minutes 2 Internal 2.The CCG ensures the Trust provides the minimum data to provide 2. CQRG papers and minutes demonstrate review and discussion of key quality C2 assurance that services remain safe and issues relating to the quality 2 CQRG minutes and papers monthly 3 Internal and safety metrics relating to the community contract. of services are being addressed. 3.The CCG uses contractural levers where quality and performce fails C3 3 3.Minutes from Contract Review Meetings and Contract Query Notices Meeting minutes and papers monthly 2 Internal below the standard required. 4. CQRG will recieve assurance that quality of care is being protected 4.During 2017/18 the CQRG workplan will require the Trust to present focussed C4 3 CQRG minutes and papers monthly 3 Internal in services where access is underperforming. items on community services. Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: None identified Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance None identified Review Committee Quality and Performance Committee Date Committee Feedback Draft dashboard has been developed and agreed by CCGs and Trust. For presentation to CCG committees in April & May /04/2018 Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 352 of 402
353 Objective 4 Delivery of High Quality, Efficient Services Within Available Resources Date Risk Added: RAF Ref: 420 Risk: Moorfields - standardisation of service provision The lack of formally agreed service level (SLA) contracts acorss satelitte sites potentailly leads to poor service provision resulting from ineffective quality governance systems. This inturn restricts the drive for improvement, standardising of practices and influencing of change which can lead to poor patient outcome and experience. Risk Owner Director of Quality Risk Lead Assistant Director of Nursing Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively Evidence what was received and where was it presented 1. The CCG has reviewed the Trust improvement plan addressing every" Must do" and "Should do action" and there will be a robust Copies of CQRG Minutes 1a. CQRG minutes will demonstrate that the CCG is provided with near time mechanism in place to review implementation updates on the progress made by the Trust in delivering improvements. Insight visit action plans to CQRG meetings 1b. The CCG will undertake insight visits to key services requring "Must do C1 2 Monthly 3 Internal actions" where assurance given at CQRG requires follow up. F&F Test, SI, Complaints Reports to CQRG and Q&P 1c.Reports on friends and family test, patient experience, complaints and SI's. committee (minutes and papers) Date Strength 1=red 2=amber 3=green Internal / External 2. The CCG is assured that the Trust is resolving the SLA contract C2 2 2.Minutes of CQRG and Trust Board minutes will show resolution of SLA issues CQRG minutes and papers monthly 2 Internal issues identified by the CQC. Actions Cross Ref: actions taken to directly improve the effectiveness of controls or assurances Type Delivery Date Owner Ref: None identified Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance None identified Review Committee Quality and Performance Committee Date 18/04/2018 Committee Feedback There was no further update since last review. Risk Conclusion Risk currently being managed within agreed tolerance levels 353 of 402
354 Objective 4 Delivery of High Quality, Efficient Services Within Available Resources Date Risk Added: Risk: Moorfields - Safer Surgery checlkist The failure to utilise the WHO safer surgery checklist may lead to inconsistent practices across sites which in turn increases the chances of never events occuring and patients being exposed to harm or clinical incidents.. Risk Owner Director of Quality Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total RAF Ref: 421 Risk Lead Assistant Director of Nursing Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. 1. There are CQC "Must do" actions relating to the WHO checklist.action plan in place Strength 1=red 2=amber 3=green C1 2 Assurances Reports/information received that confirms controls listed are working effectively 1a. CQRG minutes demonstrate close oversight of the "Must do " actions including the WHO checklist. 1b.The outcome of audits demonstrating compliance with WHO checklist is presented at CQRG. Evidence what was received and where was it presented 1a CQRG minutes and papers 1b Audit reports to CQRG Date 1a Monthly 1b Periodically Strength 1=red 2=amber 3=green Internal / External 3 Internal 2. Monthly Internal audits by Trust quality leads taking place 2. Results from monthly audits demonstrate positive progress to date. C2 2 Audit Reports monthly 3 Internal Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Similar visit to the one at City Road Theatres is planned for the St C1 assurance Jan-18 Director of Quality Georges site. Review Committee Quality and Performance Committee Date 18/04/2018 Committee Feedback The current controls and planned controls continue. The visit planned to St Georges has not yet taken place. Risk rating remains the same. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 354 of 402
355 Objective 4 Delivery of High Quality, Efficient Services Within Available Resources Date Risk Added: RAF Ref: 422 Risk: Moorfields - SI system adherence A lack of adherence to the 2015/16 serious incident framework and failure to provide evidence over the completion of part 2 Duty of Candour, will lead to poor learning from incidents and an increased likelihood of repeat occurrences. The likely result is a detrimental impact on the reputation of the CCG through a lack of feedback around meeting Duty of Candour and an increase in poor patient outcomes. Risk Owner Director of Quality Risk Lead Assistant Director of Nursing Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Strength Strength Controls 1=red Assurances Evidence 1=red Specific tasks and measure implemented to mitigate the effect of the Date 2=amber Reports/information received that confirms controls listed are working effectively what was received and where was 2=amber Internal / pricipal risks. Control Ref: 3=green it presented 3=green External 1. The CCG holds the Trust to account for adhering to the national 1&3.CQRG minutes will demonstrate close oversight of the Trust's adherence to C1 guidance on the management of serious incidents (SIs) 2 the national guidance. Copies of CQRG Minutes monthly 3 Internal C2 2.The Trust is conducting 72 hour reviews of all serious incidents 2 2. Minutes of the NCL SI panel will provide assurance that 72 hour reports become NCL SI Panel minutes and business as usual in the management of SIs. The Interim Director of Quality will papers request sight of 72 hour reports monthly 3 Internal CQRG minutes will demonstrate that quarterly SI assurance reports generated for the CCG by the CSU are presented, discussed and appropriate actions agreed with C3 3. There is appropriate scrutiny of SIs reported by the Trust 3 the Trust. CQRG minutes and papers monthly 2 Internal Currently no assurance on the Trust's compliance with part 2 Duty of Candour requirements. Actions Cross Ref: actions taken to directly improve the effectiveness of controls or assurances Type Delivery Date Owner Ref: None identified Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance None identified Review Committee Quality and Performance Committee Date 18/04/2018 Committee Feedback The risk is to be reviewed following May's CQRG. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 355 of 402
356 Objective 4 Date Risk Added: 30/6/17 RAF Ref: 423 Risk: Delivery of High Quality, Efficient Services Within Available Resources Whittington Health - LUTS The Trust and Commissioners have agreed a phased reopening of the LUTs clinic as a tertiary service for adult patients subject to conditions set out by the NCL Joint CCG Commissioning Committee in April There is a risk that the agreed specifcation for 2018/19 may not be met. Risk Owner Director of Quality Risk Lead Assistant Director of Nursing Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line Strength Strength Controls 1=red Assurances Evidence 1=red Specific tasks and measure implemented to mitigate the effect of the Date 2=amber 2=amber Internal / Reports/information received that confirms controls listed are working effectively what was received and where was Control Ref: pricipal risks. 3=green it presented 3=green External 1. The Trust is not accepting new patients in to the service until the The NCL Director of Commissioning and CCG Director of Quality are in attendance RCP recommendations have been fully implemented. at paitent group meetings. C1 2 Patient Group meeting minutes monthly 2 Internal 2. The NCL Director of Commissioning and the CCG Director of Quality are attending meetings with the Trust Deputy Chief Executive to C2 monitor delivery of the action plan including the succession plan and Notes of patient group meetings provided to the Chieft Operating Officer and 2 work towards the service being delivered within a teriary setting Accountable Officer. Patient Group meeting minutes monthly 2 Internal External review of service C3 3.CCG Director of Quality and Head of Medicines Management attend 3 External report monthly 3 Internal 2 stakeholder assurance meetings held. Evidence has been received but not yet the MDT meetings to be assured of the safety of the service.. full assurance. Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Desk top review being undertaken Jan-18 Director of Quality None identified Review Committee Quality and Performance Committee Date 18/04/2018 Committee Feedback Reviewed risk in April. Updated assurance and mitigations. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 356 of 402
357 Objective 4 Date Risk Added: 17/8/17 RAF Ref: 425 Risk: Delivery of High Quality, Efficient Services Within Available Resources STP engagement The STP covers a wider footprint with an increased number of partners. This could lead to engagement becoming less effective, with groups that experience high levels of deprivation and inequalities potentially not being heard. This could jeopodise the relationship with the community and cause significant reputational damage for the CCG. Risk Owner Director of Quality Risk Lead Assistant Director of Nursing Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line Strength Strength Controls 1=red Assurances Evidence 1=red Specific tasks and measure implemented to mitigate the effect of the Date 2=amber Reports/information received that confirms controls listed are working effectively what was received and where was 2=amber Internal / pricipal risks. Control Ref: 3=green it presented 3=green External Patient Voice delivers a broad reach Regular updates feed in to the Patient and Public Participation Committee PPP Meeting minutes bimonthly C1 2 bi monthly 2 Internal Developed engagement approach for Wellbeing Partnership which C2 has been signed up to and also engagement approach for STP. 2 Signed engagement agreement 3 Internal CCG Engagement Lead feeds in to the STP on what engagement C3 should look like. Wellbeing Partnership 2 meetings 2 Internal Joint Engagement and Communications working Group for the STP. Joint engagement and communication meeting papers and minutes although Joint meeting papers and C4 2 current concerns exist over the gravitas of the groups which are often poorly 2 Internal minutes attended. The corporate services review is proposing to move communications Copy of Agreement with the C5 and engagement under the performance and delivery directorate. 3 3 Internal council Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: C1 None identified as yet. Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance None identified Review Committee Patient and Public Participation Committee Date 18/04/2017 Committee Feedback No change since last review. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 357 of 402
358 Objective 4 Date Risk Added: 31/01/18 Risk: Delivery of High Quality, Efficient Services Within Available Resources Camden & Islington FT - Mr G external investigation oucome Failure to deliver recommendations within the action plan, increases the likelihood of similar incidents occuring, potentially leading to further harm to patients or members of the public. Risk Owner Director of Quality before we consider any mitigation Risk after consideration of controls The level of risk the CCG will tolerate in line Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total RAF Ref: 426 NHSE commissioned an independent investigation in to the organisations management of a service user who committed homicide whilst under the care of the Trust. Risk Lead Assistant Director of Nursing Controls Strength 1=red Control Ref: Specific tasks and measure implemented to mitigate the effect of the 2=amber pricipal risks. 3=green Stakeholder meeting to be held involving Islington CCG, Camden CCG, C1 NHSE, C&I FT to review in detail evidence to support the impementation of agreed actions. 2 Assurances Reports/information received that confirms controls listed are working effectively Output from the stakeholder evidence review meeting fed in to the January and February CQRG meetings will provide assurances over the current level of implementation of actions. Evidence trail. Evidence what was received and where was it presented CQRG minutes and papers Date monthly Strength 1=red 2=amber 3=green Internal / External 2 Internal Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance C1 None identified None identified Review Committee Quality and Performance Committee Date 18/04/2018 Committee Feedback No change since last review. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 358 of 402
359 Objective 4 Date Risk Added: 31/01/18 RAF Ref: 427 Risk: Delivery of High Quality, Efficient Services Within Available Resources Islington (Borough Council and NHS Trust) and Camden and Islington FT Adult Safeguarding Process The electronic drive is held by the Local Authority (London Borough of Islington) and shared with the Trust (Camden and Islington NHS Foundation Trust). In November 2017, it became apparent that the drive contains lists of names, including safeguarding concerns, police referrals etc and the Trust were not accessing the list and were not aware of the list. There is no electronic link between the LA and Trust system for safeguaridng adults. This could result in patients falling through the system unmanged, increasing the chances of safeguarding concerns materialising. Risk Owner Director of Quality Risk Lead Assistant Director of Nursing Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Risk Tolerance The level of risk the CCG will tolerate in line Strength Strength Controls 1=red Assurances Evidence 1=red Specific tasks and measure implemented to mitigate the effect of the Date 2=amber Reports/information received that confirms controls listed are working effectively what was received and where was 2=amber Internal / pricipal risks. Control Ref: 3=green it presented 3=green External The Local Authority and Trust to meet and look at a way forward and Meeting to take place C1 to look at the drive. 2 Minutes 2 Internal Trust is currently doing checks against names to confirm that all are Internal review of names being completed to check no one falling through the gap. being managed correctly. Discussions taking place with LA around This will likely result in an improvement action plan. C2 improving the linkage between the two systems. Report is due back to 1 Improvement plan 1 Internal the CQRG (date to be confirmed). Actions Cross Ref: actions taken to directly improve the effectiveness of controls or assurances Type Delivery Date Owner Ref: C1 None identified Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance None identified Review Committee Quality and Performance Committee Date 18/04/2018 Committee Feedback No change since last review. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 359 of 402
360 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Date Risk Added: 26/6/2017 Risk: 2017/18 QIPP Programme Delivery The QIPP target is set at m, 5.2m of which is expected to be delivered through the STP. The STP QIPP programme is largely transformation which requires substantial changes to models of care. Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total Any slippage in QIPP (or unidentified QIPP) will need an action plan in plan to recover the position and mitigate financial and performance risks to the organisation. Failure RAF Ref: to achieve the CCG QIPP plan is likely to impact on the organisation's ability to meet its financial control total for the year and, as a result, the NCL Financial Control Total. Risk Owner Director of Planning, Performance and Delivery Risk Lead Acute Contracts & QIPP Consultant Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Strength 1=red 2=amber 3=green A monthly dashboard highlighting current and FOT QIPP achievement C1 2 against planned outcomes. C2 Senior management and clinical leads for each QIPP schemes. 2 Assurances Reports/information received that confirms controls listed are working effectively Monthly QIPP Reports to Exec Management Group, Strategy and Finance, & Governing Body Month 8 reports show slippage of 2.9m against forecast Monthly QIPP Reports to Exec Management Group, Strategy and Finance, & Governing Body STP/CSU reporting performance against STP QIPP Evidence what was received and where was it presented QIPP reports QIPP reports The frequency of the QIPP delivery group has been increased to C3 fortnightly to drive the pace of change and ensure any barriers are 2 STP reports to CCG Fortnightly 2 escalated to EMT members for resolution. Providers report Fortnightly meetings are in place with providers to drive change (i.e. C4 2 Provider report Fortnightly 2 local delivery team meetings) Date Monthly Monthly Strength 1=red 2=amber 3=green 2 2 Internal / External Internal Internal Internal Internal C5 Financial and Activity reporting on STP QIPP via CSU and STP PMO 2 STP/CSU reporting performance against STP QIPP QIPP reports Fortnightly 2 Internal C6 Finance Budget Monitoring Meetings for Non-STP QIPP monitoring 2 STP/CSU reporting performance against STP QIPP QIPP reports Fortnightly 2 Internal 360 of 402
361 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Actions actions taken to directly improve the effectiveness of controls or assurances Cross Ref: received Type Delivery Date Owner Ref: C1 No further actions agreed. Risk Tolerance Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 17/04/2018 Committee Feedback This risk is recommended for closure as the new 2018/19 QIPP Risk has been opened - Risk ID 437. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 361 of 402
362 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Risk Tolerance Date Risk Added: 20/10/2017 Risk: Medicines management A significant national increase in the number of short supply high volume generic medicines (categorised as No Cheaper Stock Obtainable, NCSO in the Drug Tariff) has created an unpredictable rise month on month in the cost of these items. As a result, the CCG has predicted a potential additional overspend for these medicines in excess of 1.4m. Risk Owner Director of Planning and Delivery Risk Lead Head of Medicines Management Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total This is a national issue being managed by NHS England and RAF Ref: the Department of Health. NHS England has published the guidance ''Refreshing NHS plans for 2018/19", which makes it clear that CCGs should assume that the high level of discretionary prices for generic drugs in short supply will not persist in 2018/19. Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively Evidence what was received and where was it presented The London Pharmacy leads meet regularly to consider options in There has been some positive movement in respect of Olanzapine coming off Report to S&F Committee C1 respect of this issue and have escalated the issue to Department of 2 Monthly 2 the list although there are a significant number of other drugs currnetly being Internal December 2017 Health and NHS England. reviewed for inclusion on the NCSO list. Date Strength 1=red 2=amber 3=green Internal / External The Pharmaceutical Services Negotiating Committee have made strong representations to the Department of Health regarding the potential The financial impact of the lack fo supply is estimated to fall between 1.3m impact for patients and community pharmacies of continuing shortages. and 1.8m. However this cannot be predicted with any certainty due to the Report to S&F Committee C2 2 Monthly 2 Internal December 2017 situation/?utm_source=psnc+newsletter&utm_campaign=0f5496bc48- _CAMPAIGN_2017_09_25&utm_medium= &utm_term=0_b5 ca69e1d1-0f5496bc possibility of additional medicines being added to the shortage list or of medicines coming back into supply and the risk reducing. Category M generic drug prices designed to recover excess community pharmacy margin from previous years (i.e. the Cat M clawback will not continue beyond 2017/18). CCGs should assume that the current high level of discretionary prices for generic drugs in short supply will not persist in 2018/19. In 2018/19, CCGs will Refreshing NHS plans for 2018/19' guidance has made it clear that CCGs s.uk/wpcontent/uploads/2018/0 2 Internal receive the remaining period of temporary benefit from changes made to C3 should assume that the high level of discretionary prices for generic 2 drugs in short supply will not persist in 2018/19. 2/planning-guidance pdf 362 of 402
363 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Cross Ref: Actions actions taken to directly improve the effectiveness of controls or assurances received No further actions agreed. Type Delivery Date Owner Ref: Risk Tolerance Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 17/04/2018 Committee Feedback The recommendation is to reduce that risk rating from 16 to 12 given that recent reporting has shown a decline in the financial impact of NCSOs. Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. Date Risk Risk: Primary care workforce development Risk Owner Risk Tolerance Added: If the CCG is ineffective in developing the primary care Inherent risk score Residual Risk score The level of risk the CCG will tolerate in 20/10/2017 workforce then this may have an adverse impact on the Director of Commissioning before we consider any mitigation Risk after consideration of controls line with the risk appetite delivery of the primary care strategy This could mean that for example, patients with long term Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total conditions are not fully supported in primary care and Risk Lead RAF Ref: require more frequent hospital care. Assistant Director of Primary 108 Care Commissioning Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively Existing Assurance CCG Workforce working group reviews the workforce development aspects of the primary care strategy Evidence what was received and where was it presented The education programme for GPs, practice nurses and practice staff The primary care team is now fully established Development funding in primary care strategy for practice managers, practice nurse and practice-based pharmacists C1 Creation of blended roles for urgent care developed through CEPN 2 Monthly 2 Internal Primary Care monires used to establish practice based pharmacists and potential for physiotherapists too subject to NHSE release of investment monies. Date Strength 1=red 2=amber 3=green Internal / External Planned Mitigation A programme for practice nurses to enhance deliver of the '6 C' strategy is being scoped. Existing Assurance C2 2 CCG Workforce working group reviews the workforce development aspects of Monthly 2 Internal the primary care strategy 363 of 402
364 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Risk Tolerance Gaps in Mitigation The CCG could consider the global recruitment of practice nurses funded C3 in part through the strategy fund but this would require joint working and consultation with the LMC and practices. 2 2 Internal Opportunity to build resilience in primary care through the uplift in funding for primary medical services in 2016/17 and 2017/18 Cross Ref: Actions actions taken to directly improve the effectiveness of controls or assurances received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 17/04/2018 Committee Feedback This was in the process of being reviewed in February and since then there has been no change since last review. Risk Conclusion 364 of 402
365 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Date Risk Added: 31/01/2018 Risk: Re-development of St Pancras site Risk Owner Chief Operating Officer Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Risk Tolerance Risk Tolerance The level of risk the CCG will tolerate in Delayed start of consultation, failure to gain assurance from NHSE on process, threat of judicial review, not enough Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total capacity to carry out a more thorough public consultation Risk Lead RAF Ref: 434 and currently no support from Clinical Senate for clinical proposals, means the whole re-development of the St Associate Director of Joint Commissioning Pancras site is at risk. Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Planned Controls Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively St Pancras Fortnightly Steering group. David Mallet is attending. Evidence what was received and where was it presented Date Strength 1=red 2=amber 3=green Internal / External - liaising with Camden and Islington OSCs to ensure consultaiton documentation and methodology is approved before going to consultation -Working on service models with CIFT C1 - NHSE London Clinical Senate reviewing PCBC, consultaiton documents and clinical case for change on 15th May, which is part of the NHSE 2 In progress for review Monthly 2 Internal assurance programme - Ensuring robust project planning - Obtaining legal advice to ensure that PCBC and consultation documents are fit for purpose - Commissioned advice from the OCnsulation Institute to ensure best practice on methodology and process C2 2 Monthly 2 Internal C3 2 2 Internal Cross Ref: Actions actions taken to directly improve the effectiveness of controls or assurances received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 19/04/2018 Committee Feedback In progress for review Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 365 of 402
366 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Date Risk Added: 17/04/18 Risk: 2018/19 QIPP Programme Delivery Risk Owner Director of Planning, Performance and Delivery Inherent risk score before we consider any mitigation Residual Risk score Risk after consideration of controls Risk Tolerance Risk Tolerance The level of risk the CCG will tolerate in line with the risk appetite The QIPP target is set at 12.6m net savings. The QIPP programme is largely transformational which requires substantial changes to models of care. Agreement as to the Impact Likelihood Total Impact Likelihood Total Impact Likelihood Total level of QIPP contained within provider contracts as part of Risk Lead STP initiatives has not concluded in March 2018 and the Acute Contracts & QIPP contract with Whittington Health is subject to mediation. The Consultant outcome of mediation is that Clinical Review sessions are taking place between commissioners and providers to be RAF Ref: 437 concluded by 30/4/18. Contractual agreement regarding levels of QIPP within provider contracts is one of the key mechanisms to delivering QIPP savings. Control Ref: Controls Specific tasks and measure implemented to mitigate the effect of the pricipal risks. Strength 1=red 2=amber 3=green Assurances Reports/information received that confirms controls listed are working effectively Evidence what was received and where was it presented Date Strength 1=red 2=amber 3=green Internal / External 366 of 402
367 4.1.1 RAF Format ICCB GB April 2018 Other Statutory Obligations and Core Business Weekly QIPP Reports to Exec Management group Risk Tolerance Monthly QIPP Reports to Strategy and Finance, S29& Governing Body Current controls - Clinical review meetings are taking place with Whittington Health to STP/CSU reporting performance against STP QIPP agree the extent of QIPP which is included in the 2018/19 provider contract. These are being jointly led by the QIPP lead for Islington CCG, Monthly Financial performance reporting the Clinical Chair of Islington CCG and the Director of Planning, Performance and Primary Care for NCL CCGs and the process will be Haringey and Islington Joint QIPP delivery group meets on a fortnightly basis. concluded by 30/4/18. - A monthly dashboard highlighting current and FOT QIPP achievement against planned outcomes is in place. - Senior management and clinical leads are in place for each QIPP team. - The frequency of the QIPP delivery group is continuing fortnightly to drive the pace of change and ensure senior directors and Governing Body members are able to support the unblocking of any barriers. The C1 focus of the group is on ensuring large transformational schemes are 2 In progress for review Monthly 2 Internal delivered on time. - Financial and Activity reporting on STP QIPP is in place via the CSU and STP PMO to a consistent standard across CCGs. - Finance Budget Monitoring Meetings for Non-STP QIPP monitoring are in place. - Lessons learned from 17/18 and the NHSE QIPP Review (February 2018) have been incorporated into 2018/19 delivery planning and the programme is much more evenly phased than 2017/18. Planned controls - There is continued Pan NCL collaborative working to identify further opportunities and standardise pathway changes to best ensure the engagement of providers across NCL C2 2 Monthly 2 Internal C3 2 2 Internal Cross Ref: Actions actions taken to directly improve the effectiveness of controls or assurances received Type Delivery Date Owner Ref: Gaps In Control / Assurance Aread requiring improvement where we lack control or assurance Review Committee Strategy and Finance Committee Date 17/04/2018 Committee Feedback New Risk. Risk was discussed at the Strategy & Finance on 26 April Risk Conclusion Further mitigation of risk is required to bring In line with the defined risk appetite. 367 of 402
368 GOVERNING BODY RISK ASSURANCE FRAMEWORK Review Risk Ref Committee Objective 3 Delivery of High Quality, Efficient Services Within Available Resources RISKS REMOVED FROM THE RAF DURING 2017/18 Description Oversight of quality and safety issues An undetected and unaddressed failure in a commissioned service due to poor performance or quality of services could result in poor patient experience potential patient harm missed targets 105 Quality & Performance Resulting in Failure to meet our statutory and strategic obligations Damage to CCG s reputation The CCG is the lead commissioner for the Whittington, Moorfields, Camden and Islington Foundation Trust (for mental health), Care UK GP out of hours services, and the local NHS 111 service. Inherent Risk Score 2016/17 Q2 Q3 Q4 Q1 Q2 Q3 Q /18 Risk Movement since last Qtr Reasons for removal This risk is now superseeded by additional rquality risks added. Workforce and succession planning 215 Quality & Performance If the CCG does not effectively recruit, retain or plan for succession for its workforce it may not deliver on its local leadership role, key projects, overall strategy and statutory obligations The failure to deliver community services in line with historical investment and the specifications agreed within the Community Services Contract leads to concerns over the quality and 410 Quality & Performance timeliness of services being escalated and formal contract notices being issued. 414 Strategy & Finance 406 Strategy & Finance Impact of Extended Access Services ICCG has recently contracted for Extended Access services as a 2+1 year contract that commenced in April The STP plan indicates a substantial reduction of A&E attendances as a result of the succesful implementation of this service. The risk is that this expected impact is not delivered. As this is a relatively recently developed service, the national evidence around the expected impact on A&E attendances is limited, and locally we have not been able to identify a clear impact from the pilot to date. There are operational and financial risks relating to continuing health care occuring from the backlog of follow up assessments. This excludes the national rate increase for funded nursing care which is now closed. The new 2018/19 AQP is being drawn upand the new contracts should promote innovation and quality This risks has been superseeded by risk 408 This risk has been superseeded by risk 42 Now covered as part of STP management The risk has been fully mitigated and is unlikely to reoccur. 305 Strategy & Finance Implementation of Integrated Digital Care Record If the CCG does not manage the implementation stage of this programme effectively, then there may be cost overrun, late delivery, poor functionality or a failure to realise the intended benefits of the programme. Potential adverse consequences include Inability to introduce new care models Poor return on investment Commissioning and contract delivery impeded Inability to benchmark CCG Knock-on effect on other projects Development of clinical pathways affected Patient & public engagement affected Damage to CCG reputation and relations with stakeholders The IDCR project has now closed and will be replaced by an NCL wide HIE. Camden and Islington FT - CQC Compliance 416 Quality & Performance The failure to deliver month on month service improvements in the areas specified by the CQC following a "requires improvement" rating could lead to a deterioration in the quality of care delivered and poor patient experience. Camden & Islington FT - Mr T external investigation outcome 424 Quality & Performance Failure to deliver recommendations within the action plan, increases the likelihood of similar incidents occuring, potentially leading to further harm to patients or members of the public It has been stable all year and therefore has been removed from the RAF At Quality & Performance Committee on 13/02/18, it was felt that this is no longer a risk and the Committee agreed to close and remove this risk. 368 of 402
369 North Central London CCG Risk Register as at April 2018 App ID Director Objective Risk Controls in place Evidence of Controls Overall Strength of Controls in Place Rating (Current) Likelihood (Current) Consequence Risk level (Current) Controls Needed Evidence of Controls Needed Actions Action Completion Date Update on Actions Likelihood (Target) Consequence Rating (Target) Risk level (Target) RISKS FROM THE NCL JOINT COMMISSIONING COMMITTEE JCC 1 Paul Sinden, NCL Director of Performance and Acute Commissioning 62 Days Waiting Time Standard is Met Delivery of Cancer 62-day waiting time standard (Threat) Cause: There may be insufficient capacity within the system, and inefficiencies along pathways in particular for inter-provider transfers. Effect: There is a risk that the system may be unable to cope with the level of demand and has limited resilience to unexpected events. Impact: This may result in people not receiving treatment within 62 days with potential adverse impact on their health outcome. C1. North Central London ('NCL') cancer governance arrangements established to cover both performance and transformation. C2. Improvement trajectory agreed with NHS England and NHS Improvement. C3. Remedial Action Plans in place with providers that are not meeting the 62 day standard. Updated plan received from Royal Free London. C4. 38 day transfer protocol in place for inter-provider transfers from district general hospitals to tertiary services with the 38 day standard compatible with treatment commencing within 62 days. C5. Trajectory agreed with providers to meet the 38-day standard for transfers of care C6. Recovery plan received from UCLH, with overall compliance by June 2018 and compliance on internal pathways by April 2018 C1. Meeting papers and notes. C2. Plans and trajectories in place with providers to allow NCL to meet the standard overall. Backlog analysis indicates reduction towards sustainable level. Progress most marked at Royal Free London in October and November. C3. Plans. C4. Transfer protocol document. C5. Provider trajectories C6. Provider recovery plan Average Very High CN1. Arrangement to be put into place to ensure all providers are abiding by the inter-provider transfer protocol. CN2. Individual providers to resolve internal pathway issues to ensure they meet the 62 day target. CN3. Backlog reduction by providers to level consistent with delivery of the waiting time standard. CN1. Improvements delivered inline with agreed trajectories and contained in reports. CN2. Improvements delivered inline with agreed trajectories and contained in reports. CN3. Analysis agreed with NHS Improvement indicates maximum backlog level to deliver the standard A1. Continue to work with providers on delivering the trajectories. A2. Continue to work with providers to ensure sustainable delivery and includes work through the cancer vanguard. A3. NCL recovery of the 62 day standard by December A4. UCLH recovery of the 62 day standard by end of March 2018 and is consistent with system recovery by December Updated recovery plan required from the Trust. A A A A A1. Provider meetings continue on a fortnightly basis on recovering the trajectories. A2. Cancer vanguard meetings in place with provider and commissioner representation which meet monthly. A3. NCL delivered the standard in December 2017 but further work is required for sustainability. This work is being undertaken and is reflected in action A4. A4. UCLH recovery plan received but defers recovery to June 2018 from expected recovery by March Internal pathways are expected to be compliant by April High JCC 10 Paul Sinden, NCL Director of Performance and Acute Commissioning Effective mobilisation of Sustainability and Transformati on (STP) plans and CCG QIPP plans to ensure contracts remain within resource envelopes Mobilisation of STP and QIPP plans (Threat) Cause: if we do not ensure that STP and QIPP plans are delivered in accordance with planning assumptions Effect: There is a risk that contracts will not be delivered within resource envelopes for 2017/18 Impact: This may result in delays to service changes, higher contract baselines for 2018/19 than anticipated in financial plans for CCGs, and a wider system financial gap. C1. Signed contracts in place for 2017/18 and 2018/19 C2. Contract frameworks in place with each provider including Local Delivery Teams to support the STP C3. In-year contract variances subject to marginal rates rather than full tariff adjustments C4. Collaborative arrangements in place through Finance and Activity Modelling (FAM) Group as part of STP governance framework C5. Sustainability and Transformation Plan governance and supporting work streams with commissioner and provider membership in place C6. Development of schemes for 2018/19 underway. Project initiation documents shared with providers for planned care, care closer to home, and urgent and emergency care C1. Signed contracts C2. Meeting minutes and papers C3. Signed contracts C4. Meeting minutes and papers C5. Meeting papers C6. Meeting papers and project initiation documents Average Very High CN1. CCG and CSU redirection of CN1. Realigned CCG and CSU capacity to support mobilisation of STP teams for contract frameworks interventions that release resources to support CN2. Collaborative work with the STP providers to realign system incentives, CN2. Proposals for alternative and contract form, to support STP contract form delivery A1. Finalise proposals to A increase support for STP work A streams A2. Progress the work of the acute contract modelling group to consider alternative contract forms A1. In-housing of NELCSU to provide greater support and capacity for delivery of STP interventions is underway. A2. Work is progressing but needs additional capacity to put into place shadow proposals for High JCC11 Paul Sinden, NCL Director of Performance and Acute Commissioning Management of acute contracts to ensure contracts are delivered within contact baselines (CCG resource envelopes) Managing acute contracts within contract baselines (Threat) Cause: if expenditure on acute contracts exceeds planned contract baselines Effect: There is a risk that CCGs will not meet their financial duties and/or investment is withheld to support delivery of the Sustainability and Transformation Plan Impact: This may result in delays to investing in primary care and community capacity and perpetuate the risk over performance on acute hospital contracts C1. Signed contracts in place for 2017/18 and 2018/19 C2. Contracts include marginal rate payments/deductions for variances from plan and 3% growth (higher than historic growth trends) C3. Contract management framework in place with providers C4. Issue of contract notices in line with contact provisions C5.. Mobilisation of STP and QIPP plans (see JCC10) C6. North Central London Finance and Activity Modelling (FAM) Group, with commissioner and provider membership. that oversees system financial position C7. Work on alternative contract forms to support the Sustainability and Transformation Plan (STP) through the Acute Contract Modelling Group (with commissioner and provider membership) C8. Quarter one reconciliation agreed with providers as a precursor to establishing the opening contract baseline for 2018/19 C9. Agreement of treatment of disputed items with Royal Free London in 2017/18 reached C1. Signed contracts C2. Signed contracts C3. Meeting minutes and papers C4. Contract documentation and correspondence including remedial action plans C5. See JCC10 C6. Meeting minutes and papers C7. Meeting minutes and papers C8. Meeting minutes and papers Average Very high CN1. Development of system intentions for 2018/19 CN2. Develop proposals to realign system incentives including new contract forms for hospital contracts CN1. CCG system leadership for commissioning. Contract requirement to signal major contact/service changes CN2. Proposals for realigning system incentives. A1. Develop and sign-off system intentions for 2018/19 A2. Develop, in co-production, with providers, proposals for alternative contract forms for hospital providers A3. Development of planning assumptions for 2018/19 with providers. A A A A1. Action completed. System intentions issued to providers. A2. Consideration of models used elsewhere - Aligned Incentive Contract in Bolton; Accountable Care models. Work has commenced on this and is continuing. A3. Planning assumptions are being developed through STP finance meetings following publication of national planning guidance High 369 of 402
370 ID Director Objective Risk Controls in place Evidence of Controls JCC 13 Paul Sinden, NCL Director of Performance and Acute Commissioning Management of winter pressures to support recovery of A&E waiting time standard and protect capacity for delivery of cancer and referral-totreatment waiting time standards Ensuring that management of winter pressures supports recovery of waiting time standards for A&E and cancer and protects capacity for elective pathways (Threat) Cause: if we are unable to manage non-elective flows within planned hospital and community capacity to meet winter pressures Effect: There is a risk that patients may receive suboptimal care and long waiting times leading to the local system missing waiting time standards for A&E and referral-to-treatment. Historically capacity to meet cancer waiting time standards has been successfully ring-fenced. Impact: Patients may remain in inpatient placements longer than anticipated as community care packages are developed. C1. Establishment of A&E Delivery Boards with representation across health and care system C2. Establishment of NCL Urgent and Emergency Care (UEC) Board C3. STP work streams for urgent and emergency care established for long-term sustainability. C4. Winter plans for 2017/18 prepared by each A&E Delivery Board C5. Recovery plans submitted by each A&E Delivery Board to regain A&E four-hour waiting time standard C6. See JCC2 - recovery of A&E four-hour waiting time standard C7. Supplementary winter plans submitted by each A&E Delivery Board to NHS England and NHS Improvement in December 2017 C1. Meeting papers and minutes from A&E Delivery Boards C2. Meeting papers and minutes from UEC Board. C3. Work streams plans and QIPP monitoring reports C4. Plans submitted and reports/dashboards monitoring progress. C5. Plans submitted and reports/dashboards monitoring progress. C6. See JCC2 C7. Funding confirmation for priority supplementary schemes from NHS England Overall Strength of Controls in Place Average Rating (Current) Likelihood (Current) Consequence Risk level (Current) Very high Controls Needed Evidence of Controls Needed Actions Action Completion Date Update on Actions CN1. Development of NCL-wide escalation process for winter 2017/18 CN2. NCL winter workshop on 27 September to align plans across A&E Delivery Boards. CN3. Development of further plans for winter 2017/18 to ensure resilience CN1. NCL wide escalation process; CN2. Notes of workshop; CN3. Plans. A1. Agree escalation process for NCL with NHS England and NHS Improvement A2. Hold winter workshop on 27 September A3. Identification of further recover plans through winter workshop and A&E Delivery Boards A4. Provider mutual aid plans developed for January 2018 to free up clinical time from elective care pathways to support emergency patient flows A5. Each A&E deliver board to complete an after action review process for winter A6. Plans for winter to be submitted to NHS England by end of April A A A A A A A1. Action completed. NCL approach to escalation agreed in principle with NHS England. All A&E Delivery Boards have agreed escalation protocols to respond to surges in pressure and/or demand A2. Action completed. Actions from winter workshop were actioned through A&E Delivery Boards A3. Additional plans submitted by A&E deliver boards in December A4. Action completed. A5. Work is progressing on this. A6. Work is progressing on this. Likelihood (Target) Consequence Rating (Target) Risk level (Target) Very high JCC 14 Paul Sinden, NCL Director of Performance and Acute Commissioning Mobilising STP schemes that shifts activity away from acute providers in a way that allows those providers to release capacity and costs, and thereby reduce overall system costs STP and local plans target the shift of care from hospital into community settings, to reduce the overall system financial deficit this needs to be done in a way that allows hospital providers to reduce capacity and costs. This risk follows on from the initial risk of mobilising STP and local plans in JCC10 (Threat) Cause: if we are unable to shift care from hospital to community settings that allow providers to make a stepchange in capacity Effect: There is a risk that hospital providers are left with stranded costs and we do not reduce overall system costs Impact: STP and local interventions do not help reduce the system financial deficit in the anticipated way. C1. Signed contracts for 2017/18 and 2018/19 that include the impact of STP interventions C2. System intentions for 2018/19 that seek to align intentions across CCGS so we commission at scale C3. Agreement of approach to planning round for 2018/19 with providers through STP finance meetings. Contract baselines for 2018/19 to include the impact of STP interventions. C4. Work with providers on alternative contract forms to support STP delivery, with the work informed by provider cost profiles. C5. STP Finance meetings with commissioners and providers that has a common understanding of financial position in NCL system C6. STP interventions for 2018/19 developed and shared with providers C1. Contract documentation C2. NCL Systems Intentions letter C3. Meeting paper and notes. C4. Meeting papers and notes. C5. Meeting papers and notes C6. Meeting papers and project initiation documents. Average Very high CN1. Development of STP work streams interventions plans for 2018/19 CN2. Agreement of contract baselines for 208/19 CN3. Development of alternative contract models and incentive systems CN1. Interventions impacts need to be planned and agreed for incorporation into contracts CN2. Signed contracts for require the negotiation of contact baselines for 2018/19 CN3. Alternative contract forms need to be shadow run in 2018/19 to be used in contracts from 2019/20 onwards A1. Work streams development of STP plans for 2018/19. A2. Agree option for setting contract baselines for 2018/19. A3. Negotiation of contract baselines for 2018/19 incorporating 2017/18 plan/outturn, growth and impact of interventions. A4. Agree models for alternative contract forms to be shadow run in 2018/19 A5. Create finance and activity schedules that support the shadow running od the alternative contract forms. A A A A A A1. Plans submitted to STP finance group in November A2. Options being refreshed following issue of national planning guidance. A3. Negotiations are underway with completion targeted in line with national timetable. A4. Work is progressing but needs additional capacity to put into place shadow proposals for A5. Open book approach to provider cost profiles agreed and work is underway to provide the information High JCC 18 Paul Sinden, NCL Director of Performance Reducing the system financial NCL is a system in deficit. One of the aims of our Sustainability and Transformation Plan is to deliver financial recovery and maintain and sustainable health and care system. The STP sets out the challenges to financial recovery from demographic and demand trends. (Threat) Cause: if our plans do not deliver financial balance Effect: There is a risk that additional savings plans will need to be developed that have a greater impact on service delivery and access than current plans, and the local system comes under greater scrutiny from regulators. C1. STP finance meeting established that has a common view of system deficit C2. Collaborative approach to contracting round for 2017/18 and 2018/19 C3. Work on alternative contract forms for future years to support cost reduction C4. Monthly reporting cycle and monitoring C5. Working groups established for areas of pressure and with scope for cost reduction - estates, continuing healthcare, demand management etc. C6. Iterative CCG QIPP plans C1. Meeting papers and minutes from STP Average finance group C2. Contract documentation; notes from STP finance group. C3. Notes from acute contract modelling group C4. Reports C5. Meeting notes C6. Reports Very CN1. Identify opportunities for yearend settlements with providers to allow planning certainty and focus on cost reduction CN2. Identification of further savings opportunities for the system CN3. Ensure mobilisation of STP and local interventions (see JCC 10) CN1. Quarter one reconciliation process. Both CCGs and providers under financial pressure CN2. CCG finance reports - risks outweigh opportunities in 2017/18 CN3. See JCC10 A1. Finalise quarter one reconciliation process to identify opportunities for yearend settlements A2. Continue to identify further savings opportunities A /19 planning round to set contract baselines for 2018/19 A4. Greater alignment of CCG QIPP and provider cost improvement programmes (CIP) for 2018/19 A A A A A1. Action completed. A2. Work is on-going. Opportunities are being developed through STP finance group and locally by CCGs A3. Process for planning round agreed through STP finance group and work is on-going. A4. QIPP/CIP meeting held in January Very 370 of 402
371 ID Director Objective Risk Controls in place Evidence of Controls JCC 18 Performance deficit in line and Acute with planning Impact: Delivery of our STP developments is slowed Commissioning assumptions down and impact reduced. Greater local resource is taken up with assurance processes Overall Strength of Controls in Place Rating (Current) Likelihood (Current) Consequence Risk level (Current) high Controls Needed Evidence of Controls Needed Actions Action Completion Date Update on Actions Likelihood (Target) Consequence Rating (Target) Risk level (Target) high JCC week Paul Sinden, NCL Director of Performance and Acute Commissioning referral-totreatment waiting time standard is met Delivery of referral-to-treatment (RTT) waiting time standard (Threat) Cause: There may be insufficient capacity within the system, and inefficiencies along pathways. Effect: There is a risk that the system may be unable to cope with the level of demand and has limited resilience to unexpected events. Impact: This may result in people not receiving treatment within 18 weeks of referral from their GP with potential adverse impact on their health outcome. C1. Contract governance arrangements established to C1. Meeting papers and notes. cover performance. C2. Agreed remedial action plan C2. Remedial action plan agreed with UCLH. C3. STP Project Initiation Documents (PIDs) C3. Planned Care work stream considering demand C4. Draft remedial action plan management schemes to support RTT delivery including Clinical Advice and Navigation. C4. Remedial action plan received from Royal Free London but with recovery of the waiting time standard targeted by August CCGs and NHS Improvement are challenging the Trust for a faster recovery. Average Very High CN1. Receipt of Royal Free London remedial action plan CN2. Build more effective early warning system for long waits CN3. Development of planned care initiatives in the STP to support delivery of elective pathways CN4. Agreement of contract terms including tariff for Clinical Advice and Navigation. CN5. Ensure payment for waiting list backlog consistent with marginal rates set in the contract CN6. Understand impact of winter planning mutual aid on elective waiting time performance CN1. Plan; CN2. Growth in long waits including waits over 52 weeks (for which clinical harm reviews are undertaken) CN3. STP service developments offset demographic growth CN4. Clinical Advice and Navigation requires a different tariff to outpatient referral CN5 Under performance in 2017/18 due to backlog recouped at marginal rate, pay for backlog clearance at marginal rate if falls into 2018/19 CN6. Trust plans to free-up clinical capacity from elective pathways to support winter pressures A1. Continue to work with UCLH and Royal Free London on delivery of remedial action plans A2. Continue to work with providers to ensure sustainable delivery including work through the STP A3. Develop activity plans for 2018/19 for sustainable delivery A4. Develop tariff arrangements for Clinical Advice and Navigation A A A A A1. Updated Remedial Action Plan received from Royal Free London in March Continuing to monitor remedial action plans through contract meetings. A2. Action completed. Development of planned care initiatives for 2018/19 are completed. A3. Development of activity plans for 2018/19 underway taking into account national planning guidance that waiting lists should be maintained at current levels as a minimum. A4. Draft tariff agreed by commissioners which will be shared with providers High 371 of 402
372 North Central London Primary Care Joint Committee Risk Register as at April 2018 APPENDIX Ref Risk Category Potential impact Co-Commissioning Conflicts of Interest Risk that there may be an actual or perceived conflict of interest. This is particularly the case for GP members of the Committee where their judgements as a commissioner could be, or be perceived to be, unduly influenced and impaired by their own concerns and obligations as a provider. Date Inherent Inherent Inherent Opened Likelihood Impact Risk Score Mitigation 15-Jul A register of interest is in place and is published with the papers for every Committee meeting. Declarations of interest requested at start of each Committee and recorded in formal minutes. The Committee is only quorate if it has a lay member and officer majority. Quoracy is supported by options for cooption to avoid conflicts of interest. The NCL Conflicts of Interest Policy was updated to reflect this new guidance in November Owner NHS England / CCGs Residual Residual Residual Likelihood Impact Risk Score Next action / comments NHS England have published new conflicts of interest guidance for CCGs (June 2016). Completion of mandatory training by Committee members. 2 Co-Commissioning Governance and Operations Cause and Effect 1) NHSE financial responsibilities may cause cost pressures on CCG budgets. 2) Risk of additional work without correlating resources correctly identified and aligned to the activity. 3) Unintended change to CCGs relationship with member practices where CCG becomes a decision maker over contractual matters for practices 06-Mar Full delegation for all five CCGs from April Memorandum of Understanding between NHSE and CCGs drafted to support delegation of primary medical services budgets. Memorandum sets out responsibilities for CCGs and NHSE under delegated conditions. Robust representation on Committee from all CCGs enables management of risk resources. Bi-monthly update to CCG Governing Bodies through minutes of the meetings and Governing Body and Committee membership overlap Finance reports to the Joint Committee established, reporting on fully delegated budgets. Headroom in financial position across the five CCGs in 2017/18, although differential across the CCGs. Director of Performance and Acute Commissioning Standard Operating Procedure developed between NHSE and London STPs Developing NCL commissioning arrangements will need to take account of local resources for primary care development. Agreement of local budget setting and risk-share arrangements to Governing Bodies in November Primary Care Provision Loss of Service Provider without notice due to lack of notice or regulatory intervention (CQC, GMC, NHSE) There is a risk that patients will not be able to receive services or that they will seek care from other providers including - U&EC service providers -other GP practices this is unsafe and has system and financial impact for commissioners and providers London Primary Care Board established to align work of 01-May CCG d NHS E l d NHSE undertakes assessment of practice resilience to identify those at risk of failure Resilience support built into CCG primary care commissioning plans for 2017/18 and beyond NHSE shall accelerate normal list dispersal arrangements to support registration NHSE and CCGs can accelerate processes to appoint a caretaker or "step-in" provider Terms of reference for the Committee include provision for urgent and immediate decision-making between Committee meetings NHS England / CCGs Development of plans for primary care at scale for 2018/19 to develop the Resilience Programme. Plans will be supported by GP Forward View monies. Development of a standard operating procedure (SOP) to address financial support that can be offered. CCGs may develop solutions as part of their provider development and commissioning intentions, including through development of GP Federations To work with NHS and Capita to reinstate a process of allocation for vulnerable patients Development of IT solutions to allow for service provision from other sites 372 of 402
373 Ref Risk Category Potential impact 12 Primary Care Provision Variation in Primary Care Quality & Performance Across NCL Lack of granularity in current standard report to Primary Care Joint Committee makes it difficult to understand areas of concern in a meaningful way. There is a risk that the current variation in the quality and performance of primary care services in NCL will not be addressed effectively and in a timely manner. Date Inherent Inherent Inherent Mitigation Owner Opened Likelihood Impact Risk Score 01-May An NCL Sustainability and Transformation Plan has been NHS England / developed as part of a 5 year plan to reduce variation across CCGs NCL and to improve the quality of care provided to patients. NHSE identifies poor performance using published data on performance and works with CQC and CCG's to performance manage practices where safety is a concern The NCL Primary Care Joint Committee has agreed the establishment of a working group to review 'what good looks like' with regards to how quality and performance is monitored across NCL. NHSE has established a London working group to improve the information provided to decision makers (Committees, providers and commissioners) 06-Mar The education programme for GPs, practice nurses and practice staff. Residual Residual Residual Likelihood Impact Risk Score Next action / comments Implementation of Care Closer to Home Integrated Networks (CHINs) and Quality Improvement S Teams (QISTs) through the Care Closer to Home STP workstream. Development of performance report to incorporate qualitative aspects of performance. London QSAG report adopted for Primary Care Committee-in- Common this will be further developed by adding local reports. Development of refreshed primary care strategy for NCL has a focus on reducing unwarranted variation and reducing inequalities Plans for utilising primary care growth monies in 2018/19 being developed and will come to the Committee in June Islington CCG A programme for practice nurses to enhance deliver of the '6 C' strategy is being scoped. 13 Primary Care Provision Primary care workforce development If the CCGs are ineffective in developing the primary care workforce then this may have an adverse impact on the delivery of the primary care strategy This could mean that for example, patients with long term conditions are not fully supported in primary care and require more frequent hospital care. The primary care team is now fully established, and Assistants Director (8d) post recruited to. Development funding in primary care strategy for practice managers, practice nurse and practice-based pharmacists. Creation of blended roles for urgent care developed through Community Education Provider Networks (CEPN) Primary Care monies used to establish practice based pharmacists and potential for physiotherapists too subject to NHSE release of investment monies. The emergence of the GP federation and a review of locally commissioned services will help meet the development and support needs of member practices and enable a streamline of commissioning to ensure resilience and equity. Develop framework for CCGs to work with respective Federations. Development of the refreshed primary care strategy has a focus on workforce including retention, skillmix, and portfolio careers Establishment of STP workforce workstream 02-Mar NHSE undertakes an assessment of patient impact and risk 14 Primary Care Provision Alternative Primary Medical Service Cause: A temporary provider for services in Camden, Enfield, Haringey and Islington has not been commissioned as planned in March A procurement to secure a permanent NCL provider with effect from 01/04/17 has not yet commenced as planned in March Effect: Although less than 100 patients are affected, there is a risk and impact of no service being available for these patients. Impact: There is current no provider of services in Camden and Islington. The Haringey provider has no premises from which to deliver the service and the Enfield provider will cease providing services on 31/03/17. NHSE and CCGs to accelerate processes to appoint a caretaker or "step-in" provider for Camden. Haringey and Islington Implement communication and engagement plan Temporary service in place for Camden, Islington and Haringey residents. Notify relevant patients of mobilising interim service for the three CCGs (service in place for Barnet and Enfield) NHS England / CCGs NCL CCG procurement underway based on Londonwide service specification. 03-Mar NCL CCGs to complete a baseline assessment of impact on practices. NCL CCGs Work with PMS practices to secure contract variation sign-off by the end of May Primary Care Provision PMS Review Cause: Responsibility for completing PMS Reviews now delegated to CCGs to complete by 1st October Effect: There is a risk that there is insufficient time and capacity to complete the PMS review process by the 1st October 2017 deadline. There is also a risk that the funding required to deliver an equitable offer in general practice will not be available leading to the destabilisation of practices. Impact: CCG implementation of SCF and STP proposals are compromised due to delay in releasing premium GMS practices and their patients are not able to access premium funding. This may create uncertainty for practices and delay additional investment in primary care. Baseline assessment to inform financial modelling of impact on PMS practices and future commissioning intentions. PMS Oversight Group established for NCL CCGs. Transition period for PMS and GMS equalisation agreed. NCL CCGs commissioning intentions will aim to minimise impact of PMS reviews on practices while delivering equalisation across GMS and PMS. Commissioning intentions for all 5 CCGs signed off by primary care committee-in-common, and by NHS England and Local Medical Committee through London-wide process. Contract variations sent to all PMS practices for signature by end of May Agreed that the PMS transition process will commence on 1 April Implement commissioning intentions for 2018/19 across all practices in North Central London PMS transition to start across NCL CCGs in April of 402
374 Ref Risk Category Potential impact 16 Fully Delegated Commissioning Embedding of NHSE Team into STP The impact of new NCL commissioning arrangements and embedding of the NHSE team with a vacant Head of Primary Care role may result in the loss of its core knowledge base and continuity. This could significantly reduce the effectiveness of the Primary Care Committee and how the committee works with the NHSE Primary Care Commissioning Team. Date Inherent Inherent Inherent Opened Likelihood Impact Risk Score Mitigation 19-Apr Only one change in Primary Care Commissioning team means that continuity and knowledge base of team is preserved. Recruitment to Head of Primary Care for NCL team completed Establishment of Primary Care Committee-in-Common Joint workshop for primary care held on 14 December 2017 Residual Residual Owner Likelihood Impact Director of PCC (NHSE)/NCL Director of Performance and Acute Commissioning Enfield Commissioning Workstream Lead Residual Risk Score Next action / comments Develop work programme that better aligns intentions for core and enhanced primary care: - Primary care team support for care closer to home strategy; - Opportunity to better align incentives for primary care Quality Outcomes Framework (QOF), Locally Commissioned Services (LCS), and GP Forward View: - Stronger links into London-wide work on primary care. 17 Fully Delegated Commissioning Committee in common Quoracy In light of the changes to the terms of reference for the Primary Care Committee in common that require quoracy attendance to be met for all 5 CCGs, there is an increased chance of the meeting being inquorate and therefore unable to make decisions. This will result in an increase in urgent decisions being taken outside of the committee forum reducing the transparency and scrutiny of decisions and potentially impacting on the consistent approach proposed across the 5 CCGs. 19-Apr Committee membership has been formally defined in advance and approved by CCG Governing Bodies. Terms of reference incudes provision for co-option to support quoracy 2 Independent GPs have been included in the membership to provide co-option arrangements for CCGs unable to field a clinical representative who wish to delegate this responsibility to an alternative clinical lead. Committee meeting schedules are reviewed at each meeting to identify in advance issues in attendance. NCL Director of Performance and Acute Commissioning can act as Executive lead for any of the 5 CCGs. Committee Secretary CCGs to clarify deputies to attend for members. Permanent recruitment to CCG Primary Care Commissioning Teams provides a more stable Executive Officer presence. Schedule of meetings agreed for 2018/19 to maximise attendance. Dates for 2018/19 meetings set to support quoracy 18 Fully Delegated Commissioning Primary Care Support England There is a risk that the NHS England Primary Care Support Services functions (commissioned and managed by NHS England) result in impact on business continuity of GP services, quality of service to primary care users and cost pressures to fully delegated CCGs 19-Apr Inclusion of independent contractors in operational review group for London. Monthly report by independent contractor groups (LMC) to NHS England-London primary care team on recurrent issues being reported by contractors in relation to PCSE Increasing scrutiny and validation of this action on a case by case basis by NHS England Director of Primary Care Commissioning (NHS England) Standing agenda item on PCCCC agenda comprising regular update from risk owner on current issues/cases for NCL and progress to date with resolution of these. 374 of 402
375 10 11 Ref Risk Category Potential impact Date Opened Primary Care Provision Primary Care Provision PMS Contract Review Risk of delays due to ongoing negotiations with key stakeholders. CCG implementation of SCF and STP proposals are compromised due to delay in releasing premium GMS practices and their patients are not able to access premium funding This may create uncertainty for practices and delay additional investment in primary care. PMS Review (Threat) Cause: If NHS England fail to successfully complete the PMS Review. Effect: There is a risk that the funding required to deliver an equitable offer in general practice will not be available leading to the destabilisation of practices. Impact: This may impact on core PMS funding resulting in CCGs being unable to deliver the Primary Care Mandate commitment - a consistent offer for patients in general practice in Camden. North Central London Primary Care Joint Committee Closed Risks Inherent Likelihoo d Inherent Impact Inherent Risk Score Mitigation 01-May Extension to the deadline has been agreed by NHS England which will support alignment with the NCL Sustainability and Transformation Plan. National guidance issued to CCGS Owner NHS England / CCGs Residual Likelihoo d Residual Impact Residual Risk Score Next action / comments Ongoing discussions are underway with key stakeholders regarding the timeline for completing PMS contract reviews. Risk superseeded by Risk no. 15 Risk superseeded by Risk no Service Transformation / STP Regeneration projects Impact on local population and practices' ability to absorb increase in population. Issues: 1. Alignment of NHS strategic planning with LA planning timescales 2. Affordability of new premises which will initially have void capacity 01-May CCG Estates Strategies in place - Engagement with local stakeholders, developers and council planners. - Impact assessment and review of GP services in the area. - CCGs have recently submitted bids for additional funding through the Estates and Technology Transformation Fund (June 2016). 01-May Processes in place to: 1. identify vulnerable patients who can be allocated to a new practice CCGs CCGs are awaiting outome of recently submitted bids for additional funding through the Estates and Technology Transformation Fund. 6 Primary Care Provision Resignation of a provider where premises will not be available to reprovide the service resulting in a list dispersal Impact to registered patients and the local population. Issues: 1. Possible disruption of service continuity for patients who need to register with a new practice 2. Increased workload for receiving practices who may already be under strain 2. provide information to patients to support re-registration 3. additional capitation payments for new patients 4. implement communication and engagement with patients and other stakeholders NHS England/C CG Options and decisions relating to resignation of providers are brought to the NCL Primary Care Joint Committee. Where required, an urgent decision making process is in place. Resilience Programme is considering how receiving practices can be supported in the future. CCG's may address sucession planning as part of STP and provider development Development of IT solutions to allow for service reprovision from other sites 7 Primary Care Provision Resignation of a provider with insufficient notice to appoint a new provider under long term APMS arrangements The current lead time to appoint under competitive procurement is circa 12 months whilst notice periods are either 3 or 6 months. If this is not addressed there will be a service gap necessitating the need for high cost care-taking arrangements and uncertainty for patients 01-May Joint commissioners should ensure that care-taking arrangements are for fixed term whilst a procurement is initiatied. Where possible caretaking providers should be directed to improve the quality and/or viability of the service. Implement Communication and engagement plan NHS England/C CG CCG's may address via provider development workstreams to promote new operational models that enhance viability. Development of IT solutions to allow for service reprovision for other sites 8 Primary Care Provision Resignation of a strategically essential provider with a small list The list size means that procurement is likely to be unsuccessful due to the viability of the service 01-May London APMS programme undertakes a strategic assessment and a viability assessment of all proposed procurements. This will establish whether there is a need to maintain the service and if so, the viability under APMS arrangements. Where viability is an issue but can be addressed through service growth or development, then support payments may be offered to the bidders. NHS England/C CG CCG's to address via provider development workstreams to promote new operational models that enhance viability 375 of 402
376 NCL Risk Register April 2018 App ID Director Objective Risk Controls in place Evidence of Controls Overall Strength of Controls in Place Consequence Likelihood Rating (Current) Risk level Controls Needed Evidence of Controls Needed Actions Action Completion Date Update on Actions Consequence Likelihood Rating (Target) Risk level (Target) NCL Risk Register NCL 1 Will Huxter, NCL Director of Strategy Successful delivery of the STP transformation agenda Delivery of the Transformation Agenda (Threat) Cause: If the STP does not have sufficient clinican and political support and suitable capacity and resources Effect: There is a risk that the STP will not deliver the expect financial or quality benefits and that services are not appropriately integrated Impact: This may result in a system wide financial deficit and deterioration in clinical quality which will negatively impact on patient care and reputational damage. C1. Clinical leaders are in place across workstreams; C2. NCL wide Health and Care Cabinet established to oversee plans; C3. Recruitment to STP programme team is in progress; C4. QIPP Planning processes in NCL aligned with STP; C5. On-going senior enagement with local councillors and with the Joint Health and Overview Scrutiny Committee C6. STP programme infrastructure in place including programme board with senior representation from parter organisations and a sector wide finance group; C7. Robust planning process in place including regular reviews with NHS England and NHS Improvement; C8. Commissioning intentions; C9. Service business cases and project plans; C10. CCG commissioning teams and Provider teams in place; C11. Clinically led STP delivery plans in place. C1. Terms of reference and project documentation; C2. Papers; C3. Job adverts and employment contracts; C4. Finance reports, CCG QIPP plans. C5. Meeting papers. C6. Terms of reference and meeting papers. C7. Programme delivery plans, notes and minutes from meetings; C8. Governing Body papers; C9. Business case and project plan papers; C10. Employment contracts; C11. Documents and papers. Average High CN1. On-going work to link to new CCG operating models is in progress. CN2. Scope and develop provider focussed efficiency workplan; CN3. Complete recruitment to STP programme team. CN4. Strengthen Health and Care Cabinet and link back to partner organisations CN5. Improve tracking of benefits across programmes. CN1. Papers, Standing Operating Procedures; CN2. Provider focussed delivery plan; CN3. Employment contracts; CN4. Refreshed Terms of Reference and communications plans; CN5. Benefit tracker. A1. Continue to work with CCGs on linking CCG operating models to STP plans. A2. Scope and develop provider focussed efficiency workplan; A3. Complete recruitment to STP programme team; A4. Revise terms of reference for Health and Care Cabinet; A5. Develop communications plan; A6. Develop new programme highlight reports containing benefits tracker. A A ; A ; A ; A ; A A1. Alignment on QIPP is completed. Alignment on risk management is underway; A2. SRO appointed and areas of scoping chosen; A3. 80% posts recruited to substantively; A4. Terms of reference under review; A5. Communication manager recruitment in progress; A6. A review of this is in progress High NCL 2 Paul Sinden, Director of Maintaining Performance System Stability and Acute Commissioning Sustainability of Fragile Services (Threat) Cause: If the STP does not recognise the need for system stability across services and providers Effect: There is a risk that smaller and fragile services become unsustainable Impact: This may result in disruption to patient services and system instability. C1. NCL Joint Commissioning Committee in place which considers issues of system stability; C2. Relevant STP programme boards feed into service plans where appropriate; C3. CCGs have commissioning teams in place; C4. Governing Bodies focus on issues when they arise; C5. CCG commissioning intentions; C6. Commissioners feed into development of workstream plans. C1. Terms of reference and committee papers; Average C2. Minutes and notes of programme board meetings; C3. Stuffing structure and employment contracts; C4. Governing Body and committee meeting papers and minutes; C5. Document; C6. Minutes and notes of programme board meetings High CN1. Strengthened oversight of totality of provider contracts: CN2. Centrally held registers of contracts in each CCG; CN3. Overview of fragile services CN1. Completed register of contracts, named leads; CN2. Completed register of contracts; CN3. Notice from providers on service cessation for unsustainable services. A1. Development of contract registers A2 Identification of fragile services A A A1. CCGs developing contract registers and identifying small contracts rolled forward year-on-year A2. STP planned care workstream identifying fragile and at-risk services in providers Moderate NCL 3 Failure to Develop an Effective STP Estates Strategy Cause: If the STP partners do not develop an effective estates strategy for the STP which takes into account the resources within the system and the current limitations of national legislation Effect: There is a risk that the Estates Strategy does not deliver Development of the most effective use of resources and impacts on services and Simon Goodwin, an Effective STP staff NCL CCGs CFO Estates Strategy Impact: This may result in wasted resources, opportunity costs, reputational damage and difficulties in recruiting and retaining high quality staff. C1. STP Estates Board established; C2. STP SRO appointed; C3. Working with STP partners, regulators and the London Estates Board to understand the key objectives. C1. Terms of Reference, meeting papers and notes; C2. Papers and notes of meeting; C3. s, papers and notes. Average High CN1. Develop STP estates strategy CN2. Ensure appropriate link between STP Estates Board and NCL CCG Governing Bodies. CN1. Estates Strategy paper; CN2. Governance chart, Governing Body papers and reports. A1. Develop draft STP estates strategy for engagement with key partners; A2. Establish appropriate governance arrangements for the STP Estates Board A ; A A1. Initial draft NCL estates workbook completed system engagement underway with next draft due A2. Strategy outlines proposed Terms of Reference and governance Moderate NCL 4 Helen Pettersen, NCL CCGs Accountable Officer Effective Engagement with Patients and the Public Failure to Effectively Engage with Patients and the Public (Threat) Cause: If the STP partner organisations do not effectively engage with patients and the public as part of the STP process Effect: There is a risk that the STP process is not properly understood by patients, the public and their representatives causing them to disengage Impact: This may result in service design not taking proper account of the needs of local people, reputational damage and a blcokage to integrated services. C1. STP governance structure which includes significant clinical and public oversight; C2. Health and Well Being Boards; C3. Joint Health Overview and Scritiny Committee; C4. CCG Governing Bodies; C5. Provder Board of Directors and Council of Governors where appropriate; C6. Local Councils and Councillors; C7. NCL Advisory Board including councillors, Healthwarch and the Chairs of STP partner organisations; C8. Health and Care Cabinet with extensive clinical leadership; C9. CCGs and Providers have their own communications and engagement teams and local patient and public engagement mechanisms and meetings; C10. Named Communications Lead in each CCG. C1. STP plan; C2. Papers and minutes of meetings; C3. Papers and minutes of meetings; C4. Papers and minutes of meetings; C5. Papers and minutes of meetings; C6. Papers and minutes of meetings; C7. Papers and minutes of meetings; C8. Papers and minutes of meetings; C9. Contracts of employment, meeting papers and notes; C10. Employment contracts. Average High CN1. Recruit to Head of STP Communications role; CN2. STP communications and engagement plan; CN1. Employment contract; CN2. Finalised STP communications and engagement plan. A1. Recruit Head of STP Communications A2. Draft STP Communcations and Engagement Plan. A ; A A1. A1. Head of Ccomms due to start in May 2018; A2. This will begin once the Head of STP Communications is in role High NCL 5 Helen Pettersen, NCL CCGs Accountable Officer Achievement of STP Year 2 Objectives Purdah Period and the Impact of Local Elections (Threat) Cause: If there is an inability for decision making at the local Councils due to the Purdah period or if there is signficant change of policial leadership and direction of travel due to local council elections in 2018 Effect: This is a risk that the Council cannot make key decisons as an STP partner organisation and/or that a change in personnel and policy within one of more local councils Impact: This may result in a delay in the implemntation of the STP workstreams and/or the need to develop and strengthen new relationships to preservice continuity of delivery. C1. Continued work with the Joint Health Oversight and Scrutiny Committee; C2. Continue to work with local authroity partner organisations; C3. Continue to work with and strengthen relationships with local councillors; C4. Continue to effectively engage. C1. Papers and minutes of meetings; C2. Papers and minutes of meetings; C3. Papers and minutes of meetings; C4. Papers and minutes of meetings, communications, s. Average High CN1. An STP induction programme CN2. Ensure clearer narrative between STP programmes and postive impact on local people; CN3. STP Communications and Engagement Plan; CN4. Quickly build relationships with new local councillors; CN5. Involve existing and new local councillors in on-going development of STP. CN1. Register of attendance, induction pack; CN2. Communications; CN3. STP Communications and Engagement Plan document; CN4. s and correspondence; CN5. s, correspondence and papers. A1. Create STP indiction pack; A ; A2. Develop KPIs for workstreams which demonstrate positive impact A ; on local people; A ; A3. Draft STP Communcations and Engagement Plan; A A4. Identify and make contact with new councillors after local elections in 2018; A1. Action in progress; A2. Action in progress; A3. This in being developed; A4. This will be completed after the results of the local elections are announced High NCL 6 Will Huxter, NCL Ensuring CCG Director of Effective Strategy Lack of Clarity on STP and NCL CCG Governance Arrangements (Threat) Cause: If there is a lack of clarity on STP and NCL CCGs' governance arrangements; Effect: There is a risk of confusions as to where decisions are made and that decisions are not made in the correctly or at all Decision Making Impact: This may result in decision freeze or in decisions being made ultra vires which may result in signficant delay in delivering integrated services due to an inability to act or legal challenge. C1. STP Head of Programme Management in place; C1. Employment contract; Average C2. Interim NCL Head of Governance and Risk in place for the NCL C2. Employment contract; CCGs; C3. STP governance structure in place; C4. CCG and Provider organisations' governance structures in place; C5. STP website containing STP structure and minutes of STP C3. STP Plan, structure chart and papers and minutes of meetings; C4. Governance documentation, structure charts, papers and minutes of meetings; C5. Webiste; C6. Document. Programme Delivery Board and Health and Care Cabinet meetings; C6. STP governance handbook in place High CN1. STP Communications and Engagement Plan; CN2. Recruit to Head of STP Communications role; CN3. A document clearly outlining STP governance and how it links with STP partners' governance structures; CN4. Recruitment to all governance and Board Secretary posts on NCL CCG Corporate Services structure. CN1. STP Communications and Engagement Plan document; CN2. Employment contract; CN3. Governance document. CN4. Contracts of employment. A1. Draft STP Communcations and Engagement Plan; A ; A2. Recruit Head of STP Communications; A ; A3. Create document setting out STP governance and how its links A with STP partner organisations' governance structures. A A4. Complete recruitment to NCL CCG Corporate Services governance roles. A1. This is being developed; A2. Head of Communications due to start in May 2018; A3. This work is due to begin. A4. Board Secretaries recruitment completed. Interim NCL Risk Manager is in role and interviews are being held for interim Governance Lead Moderate 376 of 402
377 NCL 7 Will Huxter, NCL Delivery of the CCG Director of STP Digital Strategy Agenda Failure to Deliver the Digital Agenda Across the STP (Threat) Cause: If the STP partners do not deliver the digaital agenda across the STP; Effect: There is a risk that the STP partners will not be able to deliver the Five Year Forward View and the underlying digital infrastructure such as integrated ditigal care records and will be unable to deliver the required QIPP savings Impact: This may result in a negative impact on investments across the STP partners, a negaitve impact on the quality of patient care, reputational damage and an inability to meet the required national targets. C1. Ditigal Programme Board in place; C2. Digital road map between STP partner organisations; C3. NCL IG Group in place; C4. Health Information Exchange ('HIE') delivery plan and Population Health Management ('PHM') delivery plan being developed; C5. Priorities for agreed with SRO being Health Information Exchange ('HIE') and population health management. C1. Terms of Reference, meeting papers; C2. Terms of Reference, meeting papers; C3. Terms of Reference, meeting papers; C4. Papers; C5. Minutes from February 2018 STP Delivery Board. Average CN1. STP Digital Strategy; CN1. Digital Strategy paper; CN2. Clear digital governance structure; CN2. Digital governance structure paper; CN3. Clear differentiation between commissioner and provider digital CN3. Agreement between STP partner orgsnisations showing clear roles and responsibilities. responsibilities. High A1. Develop Digital Strategy; A2. Continue to develop HIE and PHM Delivery Plan; A3. Develop Digital governance structure; A4. Develop agreement between STP partners on responsibilities; A5. HIE and PHM delivery plan to be presented to May 2018 STP Delivery Board. A ; A ; A ; A ; A A1. This work is due to begin; A2. This work is being developed; A3. This work is being developed; A4. This work is due to begin; A5. PHM delivery plan is being drafted Moderate NCL 8 Ian Porter, NCL Recruit and CCG Director of Retain a High Corporatre Performing Servces Workforce Recruitment and Retention a High Performing Workforce (Threat) Cause: If the NCL CCGs are unable to recruit and retain a high performing workforce; Effect: The NCL CCGs will be unable to deliver their stategic objectives and operational goals; Impact: This may result in a negivtive impact on the delivery of CCG workstreams, integrated care and patient services. C1. STP is developing priorities for key clinical and staff providing care; C2. NCL CCG wide Senior Management Team in post; C3. Chief Operating Officer for each CCG in post; C4. Chief Operating Officers are recruiting to vacant posts on the establishment; C5. NCL SMT are fostering a culture of openness and transparency; C6. Executive leadership development is under way; C7. NHS Staff Survey and acting on the results; C8. NCL HR Team to support the NCL SMT and CCG Chief Operating Officers; C9. Recruiting to NCL HR roles; C10. NCL wide HR policies; C11. Increased focus on Organisational Development; C12. HR and OD groups operating locally in some CCGs and are being developed for all CCGs; C13, Equality, Diversity and Inclusion work is being developed across NCL; C1. Papers; C2. Employment contracts; C3. Employment contracts; C4. Job adverts, employment contracts; C5. Papers, communications; C6. Papers; C7. Results paper and plans; C8. Employment contracts; C9. Job adverts and Job Descriptions; C10. Policy documents; C11. Papers, communications; C12. Meeting papers and notes; C13. Papers. Strong Moderate CN1. Develop NCL Organisational Development strategy; CN2. Develop specific workforce strategy/plans for each CCG which includes talent management and succession planning; CN3. Develop organisational development strategic plan; CN4. Develop Equality, Diversity and Inclusion Strategy for ; CN5. Complete HR recruitment. CN1. NCL Organisational Development strategy document; CN2. Strategy/plan documents; CN3. Strategic plan document; CN4. Equality, Diversity and Inclusion Strategy document; CN5. Employment contract. A1. Develop NCL Organisational Development strategy; A ; A2. Develop specific workforce strategies/plans for each CCG; A ; A3. Develop organisational development strategic plan; A ; A4. Develop Equality, Diversity and Inclusion Strategy for ; A ; A5. Continue to recruit to HR and Organisational Developlment roles. A A1. This work is due to begin; A2. This work is due to begin; A3. This work is due to begin; A4. This was is being developed; A5. The HR team has been fully recruited to with all team members being in place by end of June Recruitment for the Organisational Development roles is under way Low NCL 9 Simon Goodwin, NCL CCGs CFO Achiement of Finance Balance Across NCL CCGs Delivering Financial Balance Across NCL CCGs (Threat) Cause: If the five CCGs in North Central London fail to deliver their QIPP targets and achieve financial balance by the end of the financial year Effect: There is a risk that the NCL CCGs will fails to meet the collective NHS England control total. Impact: This may result in one or more CCGs being placed under legal directions or special measures, destbilisation of one or more CCGs, a negative impact on the local health economy and loss of influence of quality of patient care. C1. Each CCG has QIPP schemes in place and delivery plans; C2. QIPP planning and delivery is overseen and scrutinised by Governing Bodies and relevant committees; C3. NCL Senior Management Team are QIPP focussed; C4. QIPP managers are in role; C5. Deloitte review of QIPP completed; C6. CCGs working with providers through the STP to deliver QIPP savings; C7. Contractual levers and sanctions; C8. Addtional strategic QIPP capacity in place; C9. Single NCL CFO in place; C10. Financial planning undertaken at NCL level using consistent methology; C11. NCL finance leads meet on a monthly basis; C12. CCG Finance and Performance Committees (and equivalent) C1. QIPP plans and papers; C2. Governing Body and committee papers and minutes; C3. Meeting papers, minutes and notes; C4. Contracts of employment; C5. Review outcomes document; C6. STP QIPP plans, meeting notes and minutes; C7. Contracts with providers; C8. Contract for services; C9. Employment contract; C10. Plans; C11. Papers; C12. Papers and minutes of meetings. Average Veery High CN1. Develop and implement a budget to offset potential unmitigated financial risks within each CCG; CN2. Implement QIPP plans. CN1. Agreed budgets and papers; CN2. In year QIPP moniroing reports. A1. Develop and agree the budgets; A2. Implent QIPP plans. A ; A A budget planning is underway; A2. This will start at the beginning of the financial year High NCL 10 Paul Sinden, NCL Director of Performance and Acute Commissioning Successful inhousing of the multidisciplinary contract team from North East London Commissioning Support Unit (NELCSU) CSU In-Housing of Services (Threat) Cause: If we do not manage the in-housing of the contract team from NELCSU successfully Effect: There is a risk that business continuity is disrupted which may have a significant negative impact on services, staffing, organisational stability, finance, performance, and contract delivery. Impact: This may result in a reduction in contract delivery. an increase in costs, downturn in performance, reputational damage and a potential negative impact on patient services. C1. Senior Management Team with a high degree of experience and expertise in CSU contracting. C2. Programme Director in place; C3. Working Group in place with Governing Body oversight; C4. Project Plan in place. C5. Contingency for additional support if needed. C6. Signed SLA in place for 2017/18 and 2018/19 as a baseline C1. Employment contracts. C2. Service Agreement. C3. Minutes and papers of meetings. C4. Project plan document. C5. WAP Process. C6. Signed service level agreement Strong High CN1. Business case for NHS England to be developed. CN2. Business case to be approved by NHS England. CN3. HR engagement process; CN4. Communications and engagement plan. CN1. Business case a formal part of process to in-house CSU services; CN2. Approval from NHS England required before HR consultation process can begin. A1. Continue to implement the project plan; A2. Draft the business case for NHS England; A3. Present the business case to NHS England; A4. Develop supporting HR engagement process to start on approval of business case by NHS England; A5. Development of communications and engagement plan to support the HR process; A6. Continue to refine stranded costs included by NELCSU in the business case. A A A A A A1. Weekly project team meetings are held and going to plan; A2. Draft business case circulated; A3. Business case is on track for submission by revised target date; A4. Development of HR process underway; A5. Plan in development; A6. Negotiations overseen by weekly project group meeting Low 377 of 402
378 Appendix: Risk Scoring Key This document sets out the key scoring methodology for risks and risk management. 1. Overall Strength of Controls in Place There are four levels of effectiveness: Level Criteria Zero The controls have no effect on controlling the risk. Weak The controls have a 1-60% chance of successfully controlling the risk. Average The controls have a 61 79% chance of successfully controlling the risk Strong The controls have a 80%+ chance or higher of successfully controlling the risk 2. Risk Scoring This is separated into Consequence and Likelihood. Consequence Scale: Level of Impact on the Objective Descriptor of Level of Impact on the Objective Consequence the Objective 0-5% Very low impact Very Low % Low impact Low % Moderate impact Medium % High impact High 4 76%+ Very high impact Very High 5 Likelihood Scale: Level of Likelihood the Risk will Occur Descriptor of Level of Likelihood the Risk will Occur for Likelihood the Risk will Occur 0-5% Highly unlikely to Very Low 1 occur 6-25% Unlikely to occur Low % Fairly likely to occur Medium % More likely to occur High 4 than not 76%+ Almost certainly will Very High 5 occur Consequence Score Likelihood Score 378 of 402
379 3. Level of Risk and Priority Chart This chart shows the level of risk a risk represents and sets out the priority which should be given to each risk: LIKELIHOOD CONSEQUENCE Very (1) Low Low (2) Medium (3) High (4) Very High (5) Very Low (1) Low (2) Medium (3) High (4) Very High (5) Low Priority Moderate Priority High Priority Very High Priority 379 of 402
380 Item: 4.2 MEETING NHS Islington CCG Governing Body DATE Wednesday 9 May 2018 REPORT LEAD DIRECTOR / GOVERNING BODY MEMBER AUTHOR CONTACT DETAILS NCL Audit Committee in Common and Individual CCG s Audit Committees Ian Porter, Director of Corporate Services for NCL CCGs Andrew Spicer, NCL Head of Governance and Risk Andrew.spicer1@nhs.net EXECUTIVE SUMMARY This paper sets out revisions to the Terms of Reference for each CCG s audit committee and the NCL Audit Committee in Common. It also sets out the proposed membership and asks the Governing Body to approve these and delegate the power to appoint future members of the CCG s audit committee to the Chair of the Governing Body. RECOMMENDED ACTION The Governing Body is asked to approve: 1. The amended Terms of Reference; 2. The membership of the CCG s audit committee; 3. The Chair and Vice Chair of the NCL Audit Committee in Common; 4. Delegation of the power to appoint members of the CCG s audit committee in line with the membership requirements set out in the Terms of Reference to the Chair of the Governing Body. Objective(s) / Plans supported by this paper: (How does this report help to deliver the CCG Strategic Goals and Quality Strategy?) This report supports the CCG in achieving all of its strategic goals by ensuring that robust governance processes are in place at the CCG. Audit Trail: This report builds on the work approved by Governing Bodies in November 2016 to support the development and delivery of their Sustainability and Transformation Plan and integrated working arrangements. A report on the NCL Audit Committee in 380 of 402
381 Common was presented to the Governing Bodies of Camden, Enfield, Haringey and Islington CCG in January 2018 and to the Barnet CCG Governing Body in March Patient & Public Involvement (PPI): This report is being presented to the Governing Bodies of the five CCGs in North Central London which include lay members and elected clinicians. In addition, the lay members for governance and audit in each of the five North Central London Clinical Commissioning Groups were consulted. Equality Impact Assessment: This report was written in accordance with the provisions of the Equality Act Risks: This report helps to maximise the opportunities for strategic collaboration across the five North Central London Clinical Commissioning Groups and strengthens oversight and assurance of our internal control mechanisms. Conflicts of Interest: Conflicts of Interest have been managed in accordance with the NCL Conflicts of Interest Policy. Resource Implications: This report if approved will: Reduce duplication of effort across the five North Central London Clinical Commissioning Groups; Reduce the amount of internal and external auditor resource needed to carry out effective scrutiny of our internal control mechanisms; Better deploy resources and increase expertise, effectiveness and learning through information, knowledge and skills sharing. Provide the flexibility to work together or individually when it best suits the needs of an effective audit function. Next Steps: If the recommendations in the report are approved the next step is to mobilise the NCL Audit Committee in Common with the first meeting due to take place in July of 402
382 Appendix: NCL Audit Committee in Common and Individual CCG s Audit Committees Introduction This paper sets out revisions to the Terms of Reference for each CCG s audit committee and the NCL Audit Committee in Common. It also sets out the proposed membership and asks the Governing Body to approve these and delegate the power to appoint future members of the audit committee to the Chair of the Governing Body. Background In January and March 2018 the Governing Bodies of the five North Central London Clinical Commissioning Groups approved the harmonisation of their audit committee s Terms of Reference, approved the formation of an audit committee in common known as the NCL Audit Committee in Common, and approved Terms of Reference for each. However, membership of these committees had not been agreed and lay members requested some additional amendments to the Terms of Reference to strengthen the quorum requirements and clarify the importance of individual audit committees in terms of accountabilities. Terms of Reference The revised Terms of Reference contain the following amendments: Paragraph Amendment Reason 1.3, 5.1, 6.1, 7.1, 8.1, 9.1, 10.1, 10.2, 11.1, 11.2, , 13.1, 13.3 Minor amendments to wording. To emphasise the importance of individual audit committees and their accountabilities Inclusion of a paragraph setting out that the lay member for audit and governance from another NCL CCG will be appointed to the audit committee on a non-remunerated basis. 17.1, 17.2 Amended the quorum requirements so that at least one member of the audit committee must be from the respective CCG for a meeting to be quorate. 18.1, 18.2 Minor amendments to simplify the drafting. To clarify to basis on which the lay member for audit and governance from another CCG is appointed onto the audit committee. This removes any risk of an audit committee being quorate without a member of the respective CCG being present. To make the Terms of Reference easier to read. 382 of 402
383 31.2 Minor amendment so Terms of Reference are reviewed annually. To increase committee effectiveness and ensure ease of operations. Membership Under the agreed Terms of Reference the membership of each CCG s audit committee comprises of three people who are: The CCG s Governing Body lay member for audit and governance; A Governing Body lay member for audit and governance from another NCL Clinical Commissioning Group; An additional member who is either: o A Governing Body member who is not the NCL Accountable Officer nor the NCL Chief Finance Officer nor the Chair of the CCG Governing Body; or o A second Governing Body lay member for audit and governance from another NCL Clinical Commissioning Group who is a different person that that referred to above. In this regard the Governing Body is asked to formally appoint their members of their audit committee. The proposed membership of each audit committee is as follows: CCG CCG s Lay Member A Lay Member for Additional Member for Audit and Audit and Governance Governance from another NCL CCG Barnet Dominic Tkaczyk Karen Trew Ian Bretman Camden Richard Strang Dominic Tkaczyk TBC Enfield Karen Trew Adam Sharples TBC Haringey Adam Sharples Lucy De Groot TBC Islington Lucy De Groot Richard Strang TBC Governing Bodies are not asked to approve the membership of other CCG s audit committees. Chair and Vice Chair of the NCL Audit Committee in Common The Chair and Vice Chair of the NCL Audit Committee in Common are important as they act as convenors of the meeting and help ensure meetings run smoothly. The Chair and Vice Chair only have voting rights on the individual audit committees that they are appointed to. It is proposed that the Chair and Vice Chair of the NCL Audit Committee in Common are: Name Role CCG Adam Sharples Chair Haringey Dominic Tkaczyk Vice Chair Barnet The NCL Audit Committee in Common will review the Chairing arrangements after 12 months. When CCG audit committees meet individually the Chair shall be the Lay Member for Audit and Governance from that respective CCG. 383 of 402
384 Delegation to the Governing Body Chair It is a requirement that the members of the audit committee are formally appointed by the Governing Body as set out above. To maximise operational flexibility, effectiveness and preserve current practices whilst ensuring that our governance processes remain robust Governing Bodies are requested to delegate to the Chair of the Governing Body the power to appoint future members of the CCG s audit committee in line with the membership requirements set out in the Terms of Reference. Recommendations The Governing Body is asked to approve: The amended Terms of Reference; The membership of the CCG s audit committee; The Chair and Vice Chair of the NCL Audit Committee in Common; Delegation of the power to appoint members of the CCG s audit committee in line with the membership requirements set out in the Terms of Reference to the Chair of the Governing Body. 384 of 402
 have each established their own audit committees to critically review and report to their respective")
385 Appendix: NCL Audit Committee in Common and Individual Audit Committees Terms of Reference 1. Introduction 1.1 The Governing Bodies of the five Clinical Commissioning Groups in North Central London ( NCL ) have each established their own audit committees to critically review and report to their respective Governing Body on the relevance and robustness of the governance and assurance processes on which each relies. 1.2 The five NCL Clinical Commissioning Groups are: NHS Barnet Clinical Commissioning Group ( Barnet CCG ); NHS Camden Clinical Commissioning Group ( Camden CCG ); NHS Enfield Clinical Commissioning Group ( Enfield CCG ); NHS Haringey Clinical Commissioning Group ( Haringey CCG ); NHS Islington Clinical Commissioning Group ( Islington CCG ). 1.3 The NCL Clinical Commissioning Groups are working together to form and operate with a common set of controls. To support this and provide strengthened oversight the NCL Clinical Commissioning Groups have agreed to hold their audit committees together at the same time, in the same place, with a common agenda and a common chair as a committee in common. This is known as the NCL Audit Committee in Common. 1.4 The NCL Clinical Commissioning Groups have also agreed to retain the flexibility for their individual audit committees to meet by themselves where doing so best achieves an effective audit committee function. 1.5 These Terms of Reference set out the membership, remit, responsibilities and reporting arrangements of both the individual Clinical Commissioning Group ( CCG ) audit committees and the NCL Audit Committee in Common. 2. Committees in Common 2.1 The following committees form the NCL Audit Committee in Common: NHS Barnet CCG Audit Committee; NHS Camden CCG Audit Committee; NHS Enfield CCG Audit Committee; NHS Haringey CCG Audit Committee; NHS Islington CCG Audit Committee. 3. Statutory Framework 3.1 The four key statutory requirements for Clinical Commissioning Group audit committees are: Provision Section 14(M) of the NHS Act 2006 (as amended) Requirement A governing body of a clinical commissioning group must have an audit committee 385 of 402
NORTH CENTRAL LONDON ( NCL ) JOINT COMMISSIONING COMMITEE
 JOINT COMMISSIONING COMMITEE") NORTH CENTRAL LONDON ( NCL ) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 3 rd August 2017 from 3pm - 4.20pm Seminar Room 2, Resource for London, 356 Holloway Road, London
NORTH CENTRAL LONDON ( NCL ) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 3 rd August 2017 from 3pm - 4.20pm Seminar Room 2, Resource for London, 356 Holloway Road, London
Commissioning Arrangements in North Central London
 Commissioning Arrangements in North Central London 1 Summary The NHS 5 Year Forward View sets out the direction for the NHS In response, 44 areas across England have been developing Sustainability and
Commissioning Arrangements in North Central London 1 Summary The NHS 5 Year Forward View sets out the direction for the NHS In response, 44 areas across England have been developing Sustainability and
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Governing Body Vice Chair and Lay Member, Camden CCG. Governing Body Lay Member, Barnet CCG
 Present: NORTH CENTRAL LONDON (NCL) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 5 October 2017, 15:00-17:00 Conference Hall Cypriot Community Centre Earlham Grove London
Present: NORTH CENTRAL LONDON (NCL) JOINT COMMISSIONING COMMITEE Minutes of the meeting held in public on Thursday 5 October 2017, 15:00-17:00 Conference Hall Cypriot Community Centre Earlham Grove London
Haringey CCG Governing Body 9 November STP 6 month progress report
 Haringey CCG Governing Body 9 November 2017 STP 6 month progress report Helen Pettersen Accountable Officer & STP Convenor Will Huxter Director of Strategy North Central London CCGs Ambition of the STP
Haringey CCG Governing Body 9 November 2017 STP 6 month progress report Helen Pettersen Accountable Officer & STP Convenor Will Huxter Director of Strategy North Central London CCGs Ambition of the STP
North Central London Medicines Optimisation Network. Terms of Reference. North Central London Medicines Optimisation Network 1 of 8
 North Central London Medicines Optimisation Network Medicines Optimisation Committee Terms of Reference North Central London Medicines Optimisation Network 1 of 8 Document control Date Version Amendments
North Central London Medicines Optimisation Network Medicines Optimisation Committee Terms of Reference North Central London Medicines Optimisation Network 1 of 8 Document control Date Version Amendments
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
APPROVED MINUTES OF THE NCL STP PROGRAMME DELIVERY BOARD
 P a g e 1 APPROVED MINUTES OF THE NCL STP PROGRAMME DELIVERY BOARD 15:00-17:00 on Tuesday 10 July 2018 Room 11.10-11.12, 5 Pancras Square, London, N1C 4AG Members PDB role / job title Attended Deputy Apologies
P a g e 1 APPROVED MINUTES OF THE NCL STP PROGRAMME DELIVERY BOARD 15:00-17:00 on Tuesday 10 July 2018 Room 11.10-11.12, 5 Pancras Square, London, N1C 4AG Members PDB role / job title Attended Deputy Apologies
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
1.1.1 Apologies were received from Dr Dina Dhorajiwala, David Graham, Tony Hoolaghan, and Rachel Lissauer.
 Minutes Meeting of the Haringey Clinical Commissioning Group Finance and Performance Committee 14 December 2017 at 1.00pm Room 7, Level 4, River Park House Present: Dr John Rohan JR GP Governing Body Member,
Minutes Meeting of the Haringey Clinical Commissioning Group Finance and Performance Committee 14 December 2017 at 1.00pm Room 7, Level 4, River Park House Present: Dr John Rohan JR GP Governing Body Member,
Appendix 5.5. AUTHOR & POSITION: Jill Shattock, Director of Commissioning CONTACT DETAILS:
 Appendix 5.5 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE Wednesday, 30 July 2014 TITLE: North Central London (NCL) NHS 111 and GP Out of Hours LEAD GOVERNING Jill Shattock,
Appendix 5.5 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE Wednesday, 30 July 2014 TITLE: North Central London (NCL) NHS 111 and GP Out of Hours LEAD GOVERNING Jill Shattock,
Professional Interests Non-Financial. Personal Interests Is the interest direct or indirect? X Direct Practice Partner
 Haringey CCG Declarations 7.3.18 Name Current position (s) held- i.e. Governing, Member practice, Employee or other Declared Interest- (Name of the organisation and nature of business) Financial Interests
Haringey CCG Declarations 7.3.18 Name Current position (s) held- i.e. Governing, Member practice, Employee or other Declared Interest- (Name of the organisation and nature of business) Financial Interests
Appendix 5.2 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Thursday, 15 March 2018 TITLE: LEAD DIRECTOR:
 Appendix 5.2 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Thursday, 15 March 2018 TITLE: LEAD DIRECTOR: AUTHOR: CONTACT DETAILS: Performance & Quality Summary (P&Q) Alex
Appendix 5.2 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Thursday, 15 March 2018 TITLE: LEAD DIRECTOR: AUTHOR: CONTACT DETAILS: Performance & Quality Summary (P&Q) Alex
The North Central London Sustainability and Transformation Plan. and. Camden Local Care Strategy. Caz Sayer Chair, Camden CCG
 The North Central London Sustainability and Transformation Plan and Camden Local Care Strategy Caz Sayer Chair, Camden CCG About the Sustainability & Transformation Plan (STP) N C L North Central London
The North Central London Sustainability and Transformation Plan and Camden Local Care Strategy Caz Sayer Chair, Camden CCG About the Sustainability & Transformation Plan (STP) N C L North Central London
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April The Broadway, Wimbledon, SW19 1RH
 MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body Vice Chair and Lay Member, Camden. Governing Body Chair, Camden CCG
 NCL Joint Commissioning Committee Thursday 5 th October 2017 3-5pm Main Conference Hall Cypriot Community Centre Earlham Grove London N22 5HJ Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel
NCL Joint Commissioning Committee Thursday 5 th October 2017 3-5pm Main Conference Hall Cypriot Community Centre Earlham Grove London N22 5HJ Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
MINUTES OF THE NORTH LONDON STP HEALTH AND CARE CABINET
 MINUTES OF THE NORTH LONDON STP HEALTH AND CARE CABINET 17:00-19:00 ON WEDNESDAY 20 SEPTEMBER 2017 HOLBROOK HOUSE, ENFIELD Members Role Attended Deputy Apologies sent Jo Sauvage Co-Chair and Clinical Lead
MINUTES OF THE NORTH LONDON STP HEALTH AND CARE CABINET 17:00-19:00 ON WEDNESDAY 20 SEPTEMBER 2017 HOLBROOK HOUSE, ENFIELD Members Role Attended Deputy Apologies sent Jo Sauvage Co-Chair and Clinical Lead
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016
 Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
AGENDA Lead Action required Appendices
 Meeting in Public of the Enfield Clinical Commissioning Group Governing Body 11 May 2016 2.30pm to 5pm Millfield House Silver Street Edmonton N18 1PJ AGENDA Lead Action required Appendices 1. Welcome and
Meeting in Public of the Enfield Clinical Commissioning Group Governing Body 11 May 2016 2.30pm to 5pm Millfield House Silver Street Edmonton N18 1PJ AGENDA Lead Action required Appendices 1. Welcome and
Item Title Lead Action Papers Page No. 1. INTRODUCTION 1.1 Welcome and Apologies Chair To note Oral -
 Haringey Clinical Commissioning Group Governing Body Meeting Thursday, 13 September 2018 2.00pm 4.30pm Cypriot Centre Earlham Grove London N22 5HJ Item Title Lead Action Papers Page No. 1. INTRODUCTION
Haringey Clinical Commissioning Group Governing Body Meeting Thursday, 13 September 2018 2.00pm 4.30pm Cypriot Centre Earlham Grove London N22 5HJ Item Title Lead Action Papers Page No. 1. INTRODUCTION
Engagement Summary. North London Partners Urgent and Emergency Care Programme. Camden Barnet Enfield Haringey Islington
 Engagement Summary North London Partners Urgent and Emergency Care Programme Camden Barnet Enfield Haringey Islington Introduction This report summarises a year-long programme of engagement undertaken
Engagement Summary North London Partners Urgent and Emergency Care Programme Camden Barnet Enfield Haringey Islington Introduction This report summarises a year-long programme of engagement undertaken
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Contract Award Recommendation for NCL Direct Access Diagnostics Service Tim Deeprose/Leo Minnion
 Appendix 5.4 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Wednesday, 26 March 2014 TITLE: LEAD DIRECTOR/ MANAGER: CLINICAL LEADS AUTHORS: CONTACT DETAILS: Contract Award
Appendix 5.4 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE: Wednesday, 26 March 2014 TITLE: LEAD DIRECTOR/ MANAGER: CLINICAL LEADS AUTHORS: CONTACT DETAILS: Contract Award
Chair: Anne Rainsberry, Regional Director (London Region), NHS England (AR)
, NHS England (AR)") COMMISSIONER MEETING IN COMMON SPECIALIST CANCER AND CARDIOVASCULAR SERVICES FOR NORTH AND EAST LONDON AND WEST ESSEX Minutes of the meeting held on Friday 9 May 2014 14.00-16.00 Portland House, Bressenden
COMMISSIONER MEETING IN COMMON SPECIALIST CANCER AND CARDIOVASCULAR SERVICES FOR NORTH AND EAST LONDON AND WEST ESSEX Minutes of the meeting held on Friday 9 May 2014 14.00-16.00 Portland House, Bressenden
Governing Body Vice Chair and Lay Member, Enfield CCG. Governing Body Lay Member, Camden CCG
 NCL Joint Commissioning Committee Thursday 5 th April 2018 3-5pm Hendon Town Hall Committee Room 1 The Burroughs London NW4 4BG Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel Brookes Dr Peter
NCL Joint Commissioning Committee Thursday 5 th April 2018 3-5pm Hendon Town Hall Committee Room 1 The Burroughs London NW4 4BG Voting Members Ms Karen Trew (Chair) Dr Mo Abedi Ms Sorrel Brookes Dr Peter
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
MINUTES OF THE THIRTY-SECOND MEETING OF THE GOVERNING BODY OF KINGSTON CLINICAL COMMISSIONING GROUP HELD ON TUESDAY
 GOVERNING BODY LEAD: Chair ATTACHMENT: Agenda item: A ACTION: For Approval MEETING DATE: 5 th September 2017 MINUTES OF THE THIRTY-SECOND MEETING OF THE GOVERNING BODY OF KINGSTON CLINICAL COMMISSIONING
GOVERNING BODY LEAD: Chair ATTACHMENT: Agenda item: A ACTION: For Approval MEETING DATE: 5 th September 2017 MINUTES OF THE THIRTY-SECOND MEETING OF THE GOVERNING BODY OF KINGSTON CLINICAL COMMISSIONING
Therefore to accommodate these conflicting issues, the following contracting arrangements are proposed:
 Appendix: 3.3b North Central London CCGs Collaboration Arrangements for Contracting 22-1-13 Introduction Across the 5 CCGs in North Central London, the total value of all contracts excluding non clinical
Appendix: 3.3b North Central London CCGs Collaboration Arrangements for Contracting 22-1-13 Introduction Across the 5 CCGs in North Central London, the total value of all contracts excluding non clinical
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
NWL STP plans for the last phase of life
 NWL STP plans for the last phase of life Dr Tim Spicer, GP & Chair of Hammersmith & Fulham CCG & Toby Hyde, Head of Strategy Hammersmith & Fulham CCG NW London Sustainability & Transformation Plan Improving
NWL STP plans for the last phase of life Dr Tim Spicer, GP & Chair of Hammersmith & Fulham CCG & Toby Hyde, Head of Strategy Hammersmith & Fulham CCG NW London Sustainability & Transformation Plan Improving
CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow
 CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow Present In Attendance Prash Gupta (PG) HCCG (Chair) Natasha Malhotra (NM)
CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow Present In Attendance Prash Gupta (PG) HCCG (Chair) Natasha Malhotra (NM)
PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE
 PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE Page 1 DOCUMENT CONTROL SHEET Name of Document: Patient Safety and Quality Committee Terms of Reference Version: 5 File Location / Document Name:
PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE Page 1 DOCUMENT CONTROL SHEET Name of Document: Patient Safety and Quality Committee Terms of Reference Version: 5 File Location / Document Name:
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Chief Accountable Officer Director Transformation and Quality. Director Transformation and Quality Chief Accountable Officer
 Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Croydon Clinical Commissioning Group Clinical Leadership Meeting Minutes
 Attachment 16 Appendix 1 Date: 13 July 2012 Time: 13 30 15 30 Location: Room 11.4, Leon House Present: Dev Malhotra, GP Board Member Bobby Abbot, GP Dipti Gandhi, Clinical Leader Brian Okumu, GP Clinical
Attachment 16 Appendix 1 Date: 13 July 2012 Time: 13 30 15 30 Location: Room 11.4, Leon House Present: Dev Malhotra, GP Board Member Bobby Abbot, GP Dipti Gandhi, Clinical Leader Brian Okumu, GP Clinical
Present: Also in Attendance: Mrs Karen Ball (Minute taker) LR PA to the Chief Finance Officer Welcome
 LR PA to the Chief Finance Officer Welcome") Telford and Wrekin Clinical Commissioning Group Governance Board Minutes of the Meeting held on Tuesday 9 th June 2015 The Temperton Room, Harper Adams University, Edgmond, Newport, TF10 8NB Present: Dr
Telford and Wrekin Clinical Commissioning Group Governance Board Minutes of the Meeting held on Tuesday 9 th June 2015 The Temperton Room, Harper Adams University, Edgmond, Newport, TF10 8NB Present: Dr
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
Update on NHS Central London CCG QIPP schemes
 Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY. TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10. Chair Dr Tony Martin
 - 13:00-13:10. Chair Dr Tony Martin") NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY HELD IN THE HARBOUR SANDS MEETING ROOM, 3 RD FLOOR, THANET DISTRICT COUNCIL TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10 Chair
NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY HELD IN THE HARBOUR SANDS MEETING ROOM, 3 RD FLOOR, THANET DISTRICT COUNCIL TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10 Chair
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Quality Account 2016/17 & 2017/18 Quality Priorities
 Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Integrated Care Systems. Phil Richardson NHS Dorset CCG
 Integrated Care Systems Phil Richardson NHS Dorset CCG Integrated care system? ICS were previously called accountable care systems Take the lead in planning and commissioning care for their populations
Integrated Care Systems Phil Richardson NHS Dorset CCG Integrated care system? ICS were previously called accountable care systems Take the lead in planning and commissioning care for their populations
Kingston Clinical Commissioning Group Report Summary
 Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 9 th January 2018 Report Title Minutes of the 34 th Meeting held on 7 th November 2017 Agenda Item 3 Attachment
Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 9 th January 2018 Report Title Minutes of the 34 th Meeting held on 7 th November 2017 Agenda Item 3 Attachment
OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING
 22 September Month 2016 2017-2019 OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING Today the national bodies NHS England (NHSE) and NHS Improvement (NHSI) have published their planning
22 September Month 2016 2017-2019 OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING Today the national bodies NHS England (NHSE) and NHS Improvement (NHSI) have published their planning
PRESENT ACTION OPENING ADMINISTRATION
 PRESENT NHS Barnet Clinical Commissioning Group Governing Body Meeting held in Public Thursday 26 January 2017 09:30 to 12:00 Committee Room One, Hendon Town Hall Debbie Frost DF NHS Barnet CCG Chair (West
PRESENT NHS Barnet Clinical Commissioning Group Governing Body Meeting held in Public Thursday 26 January 2017 09:30 to 12:00 Committee Room One, Hendon Town Hall Debbie Frost DF NHS Barnet CCG Chair (West
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
WORKFORCE RACE EQUALITY STANDARD (WRES)
") WORKFORCE RACE EQUALITY STANDARD (WRES) NHS Barnet CCG NHS Camden CCG NHS Enfield CCG NHS Haringey CCG NHS Islington CCG Report 2016 WRES report produced by NEL CSU for North Central London (NCL) Clinical
WORKFORCE RACE EQUALITY STANDARD (WRES) NHS Barnet CCG NHS Camden CCG NHS Enfield CCG NHS Haringey CCG NHS Islington CCG Report 2016 WRES report produced by NEL CSU for North Central London (NCL) Clinical
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
10.1 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING A&E DELIVERY BOARD UPDATE. Date of the meeting 19/07/2017 Author
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING A&E DELIVERY BOARD UPDATE Date of the meeting 19/07/2017 Author Sponsoring Board member Purpose of Report M Wood, Director of Service Delivery
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING A&E DELIVERY BOARD UPDATE Date of the meeting 19/07/2017 Author Sponsoring Board member Purpose of Report M Wood, Director of Service Delivery
Minutes: Quality and Safety Committee (QSC) Date Wednesday 20 May 2015 Time 10:00-13:00 Venue. 5.3, 15 Marylebone Road, London, NW1 5JD
 Date Wednesday 20 May 2015 Time 10:00-13:00 Venue. 5.3, 15 Marylebone Road, London, NW1 5JD") Minutes: Quality and Safety Committee (QSC) Date Wednesday 20 May 2015 Time 10:00-13:00 Venue 5.3, 15 Marylebone Road, London, NW1 5JD Present Dr Neville Purssell NP GP, CLCCG and Governing Body Member
Minutes: Quality and Safety Committee (QSC) Date Wednesday 20 May 2015 Time 10:00-13:00 Venue 5.3, 15 Marylebone Road, London, NW1 5JD Present Dr Neville Purssell NP GP, CLCCG and Governing Body Member
CONTINUING HEALTHCARE POLICY
 BEFORE USING THIS POLICY ALWAYS ENSURE YOU ARE USING THE MOST UP TO DATE VERSION CONTINUING HEALTHCARE POLICY 1 SUMMARY This policy describes the way in which the five Primary Care Trusts in NHS North
BEFORE USING THIS POLICY ALWAYS ENSURE YOU ARE USING THE MOST UP TO DATE VERSION CONTINUING HEALTHCARE POLICY 1 SUMMARY This policy describes the way in which the five Primary Care Trusts in NHS North
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
With these corrections made, it was agreed that the Minutes be approved as a correct record.
 Agenda item 14 CCG Operational Leadership Team 18 July 2013, 8.30 11.30am Board Room, Trust HQ, St Martin s Hospital In Attendance: Simon Douglass (Chair) (SD) Hester McLain (For Item 10) Tracey Cox (Chair)
Agenda item 14 CCG Operational Leadership Team 18 July 2013, 8.30 11.30am Board Room, Trust HQ, St Martin s Hospital In Attendance: Simon Douglass (Chair) (SD) Hester McLain (For Item 10) Tracey Cox (Chair)
Ambulatory emergency care Reimbursement under the national tariff
 HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years
 Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
Continuing Healthcare Policy
 Continuing Healthcare Policy 1 SUMMARY This policy describes the way in which Haringey Clinical Commissioning Group (HCCG) will make provision for the care of people who have been assessed as eligible
Continuing Healthcare Policy 1 SUMMARY This policy describes the way in which Haringey Clinical Commissioning Group (HCCG) will make provision for the care of people who have been assessed as eligible
Seeking your views on transforming health and care in Bedfordshire, Luton and Milton Keynes. March 2017
 Seeking your views on transforming health and care in Bedfordshire, Luton and Milton Keynes March 2017 Agenda 1. STP update October submission, feedback so far, about the March 2017 Discussion Paper 2.
Seeking your views on transforming health and care in Bedfordshire, Luton and Milton Keynes March 2017 Agenda 1. STP update October submission, feedback so far, about the March 2017 Discussion Paper 2.
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Time No. Item Lead Action OPENING ADMINISTRATION Declarations of Interest Chair, Dr Debbie Frost Note 5-8
 Barnet Clinical Commissioning Group Governing Body Meeting in Public Thursday 11 January 2018 09.00 to 12.00 Committee Room 1 Hendon Town Hall, The Borroughs, Hendon, London NW4 4BG Time No. Item Lead
Barnet Clinical Commissioning Group Governing Body Meeting in Public Thursday 11 January 2018 09.00 to 12.00 Committee Room 1 Hendon Town Hall, The Borroughs, Hendon, London NW4 4BG Time No. Item Lead
NHS North West London
 NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper. 2.0 Delegated Opportunities, Benefits and Risks
 Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Joint Committee of Clinical Commissioning Groups. Meeting held 21 February 2017, 9:30 11:30 am, Barnsley CCG Decision Summary for CCG Boards
 Paper A Joint Committee of Clinical Commissioning Groups Meeting held 21 February 2017, 9:30 11:30 am, Barnsley CCG Decision Summary for CCG Boards 1 Minutes of the Joint Committee of Clinical Commissioning
Paper A Joint Committee of Clinical Commissioning Groups Meeting held 21 February 2017, 9:30 11:30 am, Barnsley CCG Decision Summary for CCG Boards 1 Minutes of the Joint Committee of Clinical Commissioning
Draft Minutes. Agenda Item: 16
 Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July C Hickson, Head of Management Accounts
 NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July 2013 9.4 Date of the meeting 18/09/2013 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July 2013 9.4 Date of the meeting 18/09/2013 Author Sponsoring GB member Purpose of report Recommendation Resource
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
CCG Annual General Meeting (AGM) AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs
 AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs") CCG Annual General Meeting (AGM) AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs Riverside Centre, The Quay, Newport, Isle of Wight, PO30 2QR Item Item Title/Heading Initial Paper No /Attachment 1.
CCG Annual General Meeting (AGM) AGENDA Thursday 19 July 2018, 17:30hrs to 19:00hrs Riverside Centre, The Quay, Newport, Isle of Wight, PO30 2QR Item Item Title/Heading Initial Paper No /Attachment 1.
REFERRAL TO SECRETARY OF STATE FOR HEALTH Report by Devon County Council Health and Wellbeing Scrutiny Committee Torrington Community Hospital
 The Rt Hon Jeremy Hunt MP Secretary of State for Health Richmond House 79 Whitehall London SW1A 2NS 6 th Floor 157 197 Buckingham Palace Road London SW1W 9SP 23 September 2016 Dear Secretary of State REFERRAL
The Rt Hon Jeremy Hunt MP Secretary of State for Health Richmond House 79 Whitehall London SW1A 2NS 6 th Floor 157 197 Buckingham Palace Road London SW1W 9SP 23 September 2016 Dear Secretary of State REFERRAL
Lincolnshire County Council: Councillors Mrs W Bowkett, R L Foulkes, C R Oxby and N H Pepper
 1 PRESENT: COUNCILLOR MRS S WOOLLEY (CHAIRMAN) LINCOLNSHIRE HEALTH AND WELLBEING BOARD Lincolnshire County Council: Councillors Mrs W Bowkett, R L Foulkes, C R Oxby and N H Pepper Lincolnshire County Council
1 PRESENT: COUNCILLOR MRS S WOOLLEY (CHAIRMAN) LINCOLNSHIRE HEALTH AND WELLBEING BOARD Lincolnshire County Council: Councillors Mrs W Bowkett, R L Foulkes, C R Oxby and N H Pepper Lincolnshire County Council
Governing Body meeting in public
 Present Minutes Name Role/ organisation Initials Dr Fiona Butler GP, CCG Chair FB Clare Parker Chief Officer CP Dr OisÍn Brannick GP member, Clinical Lead for North Kensington Recovery OB Neil Ferrelly
Present Minutes Name Role/ organisation Initials Dr Fiona Butler GP, CCG Chair FB Clare Parker Chief Officer CP Dr OisÍn Brannick GP member, Clinical Lead for North Kensington Recovery OB Neil Ferrelly
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10. Date of Meeting: 31 st August 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
1.1. Apologies for absence had been received from Professor Dame Glynis Breakwell (Non-Executive Director and Senior Independent Director).
.") MINUTES OF A MEETING OF THE NHS IMPROVEMENT BOARD MEETING HELD ON THURSDAY 24 MAY 2018 AT 15.30 AT SKIPTON HOUSE, 80 LONDON ROAD, LONDON SE1 6LH SUBJECT TO APPROVAL AT THE MEETING OF THE BOARD ON 26 JULY
MINUTES OF A MEETING OF THE NHS IMPROVEMENT BOARD MEETING HELD ON THURSDAY 24 MAY 2018 AT 15.30 AT SKIPTON HOUSE, 80 LONDON ROAD, LONDON SE1 6LH SUBJECT TO APPROVAL AT THE MEETING OF THE BOARD ON 26 JULY
Integrated Care in North Central London
 Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way