FLORIDA DEPARTMENT OF HEALTH (DOH) DOH
|
|
|
- Lionel Oliver
- 6 years ago
- Views:
Transcription
 FOR Broward School")
1 FLORIDA DEPARTMENT OF HEALTH (DOH) DOH INVITATION TO BID (ITB) FOR Broward School Health
2 TABLE OF CONTENTS SECTION 1.0: Introductory Materials... 4 SECTION 2.0: Procurement Process, Schedule, & Constraints... 6 SECTION 3.0: Instructions for Bid Submittal... 9 SECTION 4.0: Special Conditions ATTACHMENT A: Specifications or Scope of Services ATTACHMENT B: Price Page ATTACHMENT C: Reference Form ATTACHMENT D: Statement of Non-Collusion EXHIBIT 1: Skills Assessment Form EXHIBIT 2: Student Assessment Check List EXHIBIT 3: Individual Health Care Plan Asthma EXHIBIT 3A: Emergency Care Plan Asthma EXHIBIT 4: Individual Health Care Plan Diabetes EXHIBIT 4A: Emergency Care Plan Diabetes Hyperglycemia EXHIBIT 4B: Emergency Care Plan Diabetes Hypoglycemia EXHIBIT 5: Individual Health Care Plan Seizure Disorder EXHIBIT 5A: Emergency Care Plan Seizure Disorder EXHIBIT 6: Individual Health Care Plan Anaphylaxis/Allergy EXHIBIT 6A: Emergency Care Plan Anaphylaxis EXHIBIT 7: Authorization for Medication/Authorization for Treatment EXHIBIT 8: Student Medication Log EXHIBIT 9: Diabetes Medication/Treatment Authorization Solicitation Number: DOH Invitation to Bid Broward School Health Page 2
3 EXHIBIT 10: Daily Diabetes Log EXHIBIT 11: Daily Summary Log EXHIBIT 12: Unduplicated Log for Medications and Procedures EXHIBIT 13: Daily Clinic Log EXHIBIT 14: Monthly Summary Log EXHIBIT 15: School Monthly Data Collection Form by Grade Level EXHIBIT 16: In Kind Services EXHIBIT 17: School Health Room Review Sheet EXHIBIT 18: School Health Record Review Worksheet EXHIBIT 19: FTE Week Report EXHIBIT 20: RN School Visit Log EXHIBIT 21: School Health Services Plan Solicitation Number: DOH Invitation to Bid Broward School Health Page 3
4 SECTION 1.0: INTRODUCTORY MATERIALS 1.1 Statement of Purpose The purpose of this Invitation to Bid (ITB) is for the Department of Health to obtain competitive prices to provide basic school health services and track specialized services in designated schools during the public school calendar year. 1.2 Scope of Services Detailed scope of services for this solicitation are provided as Attachment A in this ITB. 1.3 Definitions Annual School Health Services Report: An annual report submitted to the State by August 15th of for the previous year that reflects reported health conditions, services provided, staffing and expenditures. The reporting period will cover July 1st through June 30th each year for the duration of this contract. Bid: The complete written response of the Provider to this ITB, including properly completed forms, supporting documents, and attachments. Business days: Monday through Friday, excluding state holidays. Business hours: 8 a.m. to 5 p.m., Eastern Time on all business days. Calendar days: All days, including weekends and holidays. Contract: The formal agreement or order that will be awarded to the successful Provider under this ITB, unless indicated otherwise. Contract Manager: The individual designated by the Department to be responsible for the monitoring and management of this contract. Department: The Department of Health; may be used interchangeably with DOH. Eligible Students: A student whose parent/guardian did not opt out of the required screenings (vision, hearing, BMI, and scoliosis). Fiscal Year: July 1st to June 30th. Health Management System (HMS): The Department s data system into which documented school health services are entered by service codes identified in the most current School Health Coding Manual, incorporated by reference. This data is used to provide a full accounting of school health services provided. Local Education Agency (LEA): As defined in the Elementary and Secondary Education Act, a public board of education or other public authority legally constituted within a State for either administrative control or direction of, or to perform a service function for, public elementary schools or secondary schools in a city, county, township, Solicitation Number: DOH Invitation to Bid Broward School Health Page 4
5 school district, or other political subdivision of a State, or for a combination of school districts or counties that is recognized in a State as an administrative agency for its public elementary schools or secondary schools. Minor Irregularity: As used in the context of this solicitation, indicates a variation from the ITB terms and conditions which does not affect the price of the Bid, or give the Provider an advantage or benefit not enjoyed by other Providers, or does not adversely impact the interests of the Department. Order: As used in the context of this solicitation refers to a Purchase Order or a Direct Order. Provider: The business entity that submits a Bid. This term also may refer to the entity awarded a contract by the Department in accordance with the terms of this ITB. Quarter: One-fourth (three months) of a fiscal year. The quarters are July 1 through September 30 (quarter 1); October 1 through December 31 (quarter 2); January 1 through March 31 (quarter 3); and April 1 through June 30 (quarter 4). School Health Services Plan: A document created by the Department, the Local Education Agency, and the local School Health Advisory Committee, that describes the school health services to be provided within the county, and the responsibility for provision of the services, as required by Section (4)(a), Florida Statutes. The School Health Services Plan is developed every two years. Vendor Bid System (VBS): Refers to the State of Florida internet-based vendor information system at: Solicitation Number: DOH Invitation to Bid Broward School Health Page 5
6 SECTION 2.0: PROCUREMENT PROCESS, SCHEDULE & CONSTRAINTS 2.1 Procurement Officer The Procurement Officer assigned to this solicitation is: Florida Department of Health in Broward County Attention: Marc Parkent 780 SW 24 th Street Fort Lauderdale, Florida Restriction on Communications 2.3 Term Respondents to this solicitation or persons acting on their behalf may not contact, between the release of the solicitation and the end of the 72-hour period following the agency posting the notice of intended award, excluding Saturdays, Sundays, and state holidays, any employee or officer of the executive or legislative branch concerning any aspect of this solicitation, except in writing to the procurement officer as provided in the solicitation documents. Violation of this provision may be grounds for rejecting a response. Section (23), Florida Statutes. It is anticipated that the Contract resulting from this ITB will be for a one year period from August 1, 2017 or the Contract execution date whichever is later, subject to renewal as identified in Section 4.2. The Contract resulting from this ITB is contingent upon availability of funds. Solicitation Number: DOH Invitation to Bid Broward School Health Page 6
7 2.4 Timeline EVENT DUE DATE LOCATION ITB Advertised / Released Questions Submitted in Writing 05/05/2017 Must be received PRIOR TO: 5:00 PM Posted to the Vendor Bid System at: Submit to: Florida Department of Health In Broward County Attention: Marc Parkent 780 SW 24 th Street Fort Lauderdale, FL marcus.parkent@flhealth.gov Non-mandatory Pre-Bid Conference 10:00 AM Florida Department of Health Broward County Administration Auditorium 780 SW 24 th Street Fort Lauderdale, FL Answers to Questions (Anticipated Date) Sealed Bids Due and Opened Anticipated Posting of Intent to Award 05/23/2017 Must be received PRIOR TO: 3:30 PM 06/13/2017 Posted to Vendor Bid System at: PUBLIC MEETING Submit to: Florida Department of Health Broward County Attention: Marc Parkent Administration Auditorium 780 SW 24 th Street Fort Lauderdale, FL Posted to the Vendor Bid System at: Solicitation Number: DOH Invitation to Bid Broward School Health Page 7
8 2.5 Addenda If the Department finds it necessary to supplement, modify, or interpret any portion of the solicitation during the procurement process, a written addendum will be posted on the MyFlorida.com Vendor Bid System, If the addendum alters the scope or specifications of the solicitation, the Provider will be required to sign the addendum acknowledging the changes and return it with the bid submittal. It is the responsibility of the Provider to be aware of any addenda that might affect their Bid. 2.6 Pre-Bid Conference A non-mandatory pre-bid conference will be held at the time and location indicated in the Timeline. Providers may ask questions and seek clarification during the pre-bid conference and submit written questions by the time set forth in the Timeline. The Department may answer any questions at the pre-bid conference or defer them to a later date as identified in the Timeline. Only written answers are binding. 2.7 Questions This provision takes precedence over General Instruction #5 in PUR1001. Questions related to this solicitation must be received, in writing (either via U.S. Mail, courier, , fax, or hand-delivery), by the Procurement Officer identified in Section 2.1, within the time indicated in the Timeline. Verbal questions or those submitted after the period specified in the Timeline will not be addressed. Answers to questions submitted in accordance with the ITB Timeline and during the prebid conference will be posted on the MyFlorida.com Vendor Bid System web site: Basis of Award A single award solicitation will be made to the responsive, responsible Provider offering the lowest grand total for the services requested in this ITB. 2.9 Identical Tie Bids Where there is identical pricing from multiple Providers, the Department will determine the order of award in accordance with Florida Administrative Code, Rule 60A Solicitation Number: DOH Invitation to Bid Broward School Health Page 8
9 SECTION 3.0: INSTRUCTIONS FOR BID SUBMITTAL 3.1 General Instructions to Respondents (PUR 1001) This section explains the General Instructions to Providers (PUR 1001) of the solicitation process, and is a downloadable document incorporated into this solicitation by reference. This document should not be returned with the Bid. The terms of this solicitation will control over any conflicting terms of the PUR Instructions for Submittal 1. Providers are required to complete, sign, and return the Price Page with the Bid submittal. (Mandatory Requirement) 2. Providers must submit all technical and pricing data in the formats specified in the ITB. 3. Submit one original Bid and one electronic copy of the Bid on CD or thumb drive. The electronic copy should contain the entire Bid as submitted, including all supporting and signed documents. Refer to Section 3.4 for information on redacting confidential information, if applicable. 4. Bids may be sent by U.S. Mail, Courier, or Hand Delivered to the location indicated in the Timeline. 5. Bids submitted electronically will not be considered. 6. Bids must be submitted in a sealed envelope/package with the solicitation number and the date and time of the Bid opening clearly marked on the outside. 7. The Department is not responsible for improperly marked Bids. 8. It is the Provider s responsibility to ensure its Bid is submitted at the proper place and time indicated in the ITB Timeline. 9. The Department s clocks will provide the official time for Bid receipt. Materials submitted will become the property of the State of Florida and accordingly, the State reserves the right to use any concepts or ideas contained in the response. 3.3 Cost of Preparation Neither the Department of Health nor the State is liable for any costs incurred by a Provider in responding to this solicitation. Solicitation Number: DOH Invitation to Bid Broward School Health Page 9
10 3.4 Public Records and Trade Secrets Notwithstanding any provisions to the contrary, public records must be made available pursuant to the provisions of the Public Records Act. If the Provider considers any portion of its Bid to this solicitation to be confidential, exempt, trade secret or otherwise not subject to disclosure pursuant to Chapter 119, Florida Statutes, the Florida Constitution or other authority, the Provider must segregate and clearly mark the document(s) as CONFIDENTIAL. Simultaneously, the Provider will provide the Department with a separate redacted paper and electronic copy of its Bid and briefly describe in writing the grounds for claiming exemption from the public records law, including the specific statutory citation for such exemption. This redacted copy must contain the solicitation name, number, and the name of the Provider on the cover, and must be clearly titled REDACTED COPY. The redacted copy must be provided to the Department at the same time the Provider submits its Bid and must only exclude or obliterate those exact portions which are claimed confidential, proprietary, or trade secret. The Provider will be responsible for defending its determination that the redacted portions of its Bid are confidential, trade secret or otherwise not subject to disclosure. Further, the Provider must protect, defend, and indemnify the Department for any and all claims arising from or relating to the determination that the redacted portions of its Bid are confidential, proprietary, trade secret or otherwise not subject to disclosure. If the Provider fails to submit a redacted copy with its Bid, the Department is authorized to produce the entire documents, data or records submitted by the Provider in response to a public records request for these records. 3.5 Price Page (Mandatory Requirement) The Price Page is Attachment B of this ITB. Providers must fill out the Price Page as indicated, sign it, and return it with their Bid. Providers must also complete and submit the renewal pricing section of the Price Page, Attachment B. 3.6 Documentation Providers must complete and submit the following information or documentation as part of their Bid: References Providers must have a minimum of 3 years of experience providing school health services. Providers must submit contact information for entities in which Provider provisioned school health services in a minimum of 30 schools per school year. Providers may use Attachment C, Reference Form of this ITB to provide the required information. The Department reserves the right to contact any and all entities in the course of this solicitation in order to verify experience. Information received may be considered in the Department s determination of the Provider s responsibility. The Department s determination is not subject to review or challenge. Solicitation Number: DOH Invitation to Bid Broward School Health Page 10
11 Organizational Profile Providers must submit responses to the following: Number of FTE personnel in your company. Number of years in business. Number of permanent certified and types of healthcare providers employed by your company. Provider must have a current State of Florida license and certification(s) to provide healthcare services as described in the ITB. Provider must submit a copy of their current State of Florida licenses and certification number(s) for healthcare services as indicated. State the name of the Director of Healthcare for your firm and submit a copy of the director s license as a registered healthcare provider Statement of Non-Collusion Providers must sign and return with their Bid the Statement of Non-Collusion form, Attachment D Licenses/Certifications Providers must submit the names and resumes of key healthcare staff that would be available to provide services during the term of this contract. Indicate and submit current State of Florida license and certification(s) and current CPR certification, as applicable, for all healthcare provider staff that may be assigned to this ITB Litigation History Providers must submit a statement of any litigation or regulatory action that has been filed or is pending against your company(s) in the last 3 years. If an action has been filed, state and describe the litigation or regulatory action filed, and identify the court or agency before which the action was instituted, the applicable case or file number, and the status or disposition for such reported action. If no litigation or regulatory action has been filed against your company(s), provide a statement to that effect. 3.7 Special Accommodations Any person requiring special accommodations at DOH Purchasing because of a disability should call DOH Purchasing at (850) at least five (5) work days prior to any pre-bid conference, Bid opening, or meeting. If hearing or speech impaired, please contact Purchasing by using the Florida Relay Service, at (TDD). Solicitation Number: DOH Invitation to Bid Broward School Health Page 11
12 3.8 Responsive and Responsible (Mandatory Requirements) Providers must complete and submit the following mandatory information or documentation as part of their Bid. Any Bid that does not contain the information below will be deemed non-responsive. Bids must be received by the time specified (Section 2.4). Attachment B: Price Page (as specified in Section 3.5). All documentation identified in Section Late Bids The Procurement Officer must receive Bids pursuant to this ITB no later than the date and time shown in the Timeline (Refer to Section 2.4). Bids that are not received by the time specified will not be considered. Solicitation Number: DOH Invitation to Bid Broward School Health Page 12
13 SECTION 4.0: SPECIAL CONDITIONS 4.1 General Contract Conditions (PUR 1000) The General Contract Conditions (PUR 1000) form is a downloadable document incorporated in this solicitation by reference, that contains general Contract terms and conditions that will apply to any Contract resulting from this ITB, to the extent they are not otherwise modified. This document should not be returned with the Bid. The terms of this solicitation will control over any conflicting terms of the PUR1000. Paragraph 31 of PUR 1000 does NOT apply to this solicitation or any resulting contract Renewal The Contract resulting from this solicitation may be renewed. Renewals may be made on a yearly basis or for a period that may not exceed three years or the term of the original Contract, whichever is longer. Renewals must be in writing, subject to the same terms and conditions set forth in the initial Contract and any written amendments signed by the parties. Renewals are contingent upon satisfactory fiscal and programmatic performance evaluations as determined by the Department and are subject to the availability of funds. 4.3 Conflict of Interest Section (17)(c), Florida Statutes, provides A person who receives a Contract that has not been procured pursuant to subsections (1)-(3) to perform a feasibility study of the potential implementation of a subsequent Contract, who participates in the drafting of a solicitation or who develops a program for future implementation, is not eligible to Contract with the agency for any other contracts dealing with that specific subject matter, and any firm in which such person has any interest is not eligible to receive such Contract. However, this prohibition does not prevent a vendor who responds to a request for information from being eligible to Contract with an agency. The Department of Health considers participation through decision, approval, disapproval, recommendation, preparation of any part of a purchase request, influencing the content of any specification or procurement standard, rendering of advice, investigation, or auditing or any other advisory capacity to constitute participation in drafting of the solicitation. Refer to Statement of Non-Collusion, Section Certificate of Authority All limited liability companies, corporations, corporations not for profit, and partnerships seeking to do business with the State must be registered with the Florida Department of State in accordance with the provisions of Chapters 605, 607, 617, and 620, Florida Statutes, respectively prior to Contract execution. The Department retains the right to ask for verification of compliance before Contract execution. Failure of the selected contractor to have appropriate registration may result in withdrawal of Contract award. Solicitation Number: DOH Invitation to Bid Broward School Health Page 13
14 4.5 Provider Registration Each Provider doing business with the State of Florida for the sale of commodities or contractual services as defined in section , Florida Statutes must register in the MyFloridaMarketPlace system, unless exempted under Florida Administrative Code Rule 60A State agencies must not enter into an agreement for the sale of commodities or contractual services as defined in section , Florida Statutes, with any Provider not registered in the MyFloridaMarketPlace system, unless exempted by rule. The successful Provider must be registered in the MyFloridaMarketPlace system within 5 days after posting of intent to award. Registration may be completed at: Providers lacking internet access may request assistance from MyFloridaMarketPlace Customer Service at or from State Purchasing, 4050 Esplanade Drive, Suite 300, Tallahassee, FL Minority and Service-Disabled Veteran Business-Participation The Department encourages Minority, Women, Service-Disabled Veteran, and Veteran- Owned Business Enterprise participation in all its solicitations 4.7 Financial Consequences Pursuant to section , Florida Statutes, the resulting Contract must contain financial consequences that will apply if the Provider fails to perform in accordance with the Contract terms. The financial consequences will be established based on final determination of the performance measures and Contract amount. 4.8 Standard Contract Providers must become familiar with the Department s Standard Contract which contains administrative, financial and non-programmatic terms and conditions mandated by federal laws, state statutes, administrative code rules, and directive of the Chief Financial Officer. Use of the Standard Contract is mandatory for Departmental contracts and the terms and conditions contained in the Standard Contract are non-negotiable. The Standard Contract terms and conditions are located at: department-of-health/about-us/administrative-functions/purchasing/_documents/doh- Standard-Contract.pdf 4.9 Conflict of Law and Controlling Provisions Any Contract resulting from this ITB, and any conflict of law issue, will be governed by the laws of the state of Florida. Venue must be Broward County, Florida Agency Inspectors General It is the duty of every state officer, employee, agency, special district, board, commission, contractor, and subcontractor to cooperate with the inspector general in Solicitation Number: DOH Invitation to Bid Broward School Health Page 14
15 any investigation, audit, inspection, review, or hearing pursuant to section , Florida Statutes Records and Documentation To the extent that information is used in the performance of the resulting Contract or generated as a result of it, and to the extent that information meets the definition of public record as defined in Section (12), Florida Statutes, said information is hereby declared to be and is hereby recognized by the parties to be a public record and absent a provision of law or administrative rule or regulation requiring otherwise, Provider must make the public records available for inspection or copying upon request of the Department s custodian of public records at cost that does not exceed the costs provided in Chapter 119, Florida Statutes, or otherwise, and must comply with Chapter 119 at all times as specified therein. It is expressly understood that the Provider s refusal to comply with Chapter 119, Florida Statutes, will constitute an immediate breach of the Contract resulting from this ITB and entitles the Department to unilaterally cancel the Contract agreement. Unless a greater retention period is required by state or federal law, all documents pertaining to the program contemplated by this ITB must be retained by the Provider for a period of six years after the termination of the resulting Contract or longer as may be required by any renewal or extension of the Contract. During the records retention period, the Provider agrees to furnish, when requested to do so, all documents required to be retained. Submission of such documents must be in the Department s standard word processing format. If this standard should change, it will be at no cost incurred to the Department. Data files will be provided in a format readable by the Department. The Provider must maintain all records required to be maintained pursuant to the resulting Contract in such manner as to be accessible by the Department upon demand. Where permitted under applicable law, access by the public must be permitted without delay Protests Failure to file a protest within the time prescribed in section (3), Florida Statutes, or failure to post a bond or other security required by law within the time allowed for filing a bond shall constitute a waiver of proceedings under Chapter 120, Florida Statutes. Only documents delivered by the U.S. Postal Service, a private delivery service, in person, or by facsimile during Business hours (Monday-Friday, 8:00 a.m. - 5:00 p.m., Eastern Time) will be accepted. Documents received after hours will be filed the following business day. No filings may be made by or any other electronic means. All filings must be made with the Agency Clerk ONLY and are only considered "filed" when stamped by the official stamp of the Agency Clerk. It is the responsibility of the filing party to meet all filing deadlines. Solicitation Number: DOH Invitation to Bid Broward School Health Page 15
16 DO NOT SEND BIDS TO THE AGENCY CLERK S OFFICE. Send all Bids to the Procurement Officer and address listed in the Timeline. The Agency Clerk's mailing address is: The Agency Clerk s physical address for hand deliveries is: Agency Clerk Agency Clerk, Department of Health Florida Department of Health 2585 Merchants Row Blvd Bald Cypress Way, BIN A-02 Tallahassee, Florida Tallahassee, Florida Fax No. (850) Telephone No. (850) Solicitation Number: DOH Invitation to Bid Broward School Health Page 16
17 ATTACHMENT A Scope of Services A. Service Tasks 1. Provider must provide basic school health services in 38 public schools to include 10 full service schools. In accordance with s , F.S., health services are conducted as a part of the total school health program and should be carried out to appraise, protect, and promote the health of students. Core program requirements, addressed in the School Health Services Plan (Exhibit 21) include: health appraisal, records review, nurse assessment, vision screening, hearing screening, scoliosis screening, growth and development screening, health counseling, referral and follow up of suspected or confirmed health problems, first aid and emergency needs in each school, medication administration and medical procedures, prevention of communicable diseases, referral of students to appropriate health treatment, consultation with students parent/guardian regarding need for health attention by an appropriate provider, and maintenance of student health information and records(s). 2. Provider must track specialized services that are provided in the full service schools in accordance with Section , Florida Statutes and as specified in the most recent version of the local School Health Services Plan. 3. Provider must perform the following screenings: a. Perform vision screenings each contract year for eligible students in kindergarten, first, third, and sixth grades who were absent on scheduled screening days or new to the school within 30 calendar days of scheduled screening date or school entry date. b. Contact the School Board of Broward County (SBBC) screening staff to schedule hearing screenings each contract year for eligible students in kindergarten, first, and sixth grades who were absent on scheduled screening days or new to the school within 30 calendar days of scheduled screening date or school entry date. c. Perform scoliosis screenings each contract year for eligible students in sixth grade who were absent on scheduled screening days or new to the school within 30 calendar days of scheduled screening date or school entry date. d. Perform growth and development screenings, which must include a body mass index (BMI) percentile calculation, each contract year for eligible students in first, third, and sixth grades who were absent on scheduled screening days or new to the school within 30 calendar days of scheduled screening date or school entry date. e. Refer all students with abnormal screening results to appropriate health care providers for further evaluation and or treatment within 45 calendar days of receiving an abnormal screening result. f. Follow-up with parents of students referred for further evaluation and or treatment to ensure the students received the necessary additional evaluation and or treatment within 30 calendar days of referral. g. Submit all service and screening data for each month to the Department Contract Manager within 10 calendar days following the end of each month. 4. Full Service Schools. Track provision of specialized services provided by SBBC or other community agencies, including but not limited to, nutritional services, economic and job Solicitation Number: DOH Invitation to Bid Broward School Health Page 17
18 ATTACHMENT A Scope of Services placement services, parenting classes, counseling for abused children, mental health and substance abuse counseling, and adult education for parents in accordance with Section , Florida Statutes and as specified in the most recent version of the local School Health Services Plan at designated full service schools. If provider becomes aware that a student is pregnant, provider must provide the student with information on interagency collaborations for assistance, counseling, education, and prenatal care. 5. By September 15 of each year, review each schools immunization compliance report and work with school personnel to obtain required student immunization documentation. 6. RN supervisors must conduct and document skills assessments every 90 days with health support technicians (HSTs) under their supervision utilizing the Skills Assessment Checklist (Exhibit 1). 7. By October 1 of each year, for all students, in all schools served by this contract, with: allergies, diabetes, asthma, seizure disorder, ADHD, autism, eating disorders, blood disorders, cardiac disorders, respiratory disorders, psycho/social issues, hearing impairment, visual impairment or other medical condition or a medical authorization, the RN must complete a Student Assessment Checklist (Exhibit 2). The Student Assessment Checklist will guide the RN supervisor and the RN in determining if an Individualized Health Care Plan (Exhibits 3-6) and if warranted an Emergency Care Plan should be written (Exhibits 3A-5A). 8. If during the completion of the Student Assessment Checklist it is determined that a student requires an Individualized Health Care Plan and if warranted, an Emergency Care Plan, it must be completed at that time for all students, in all schools served by this contract. Standardized Individual Health Care Plans and Emergency Care Plans are provided for use for the following health conditions: allergies, diabetes, asthma, and seizure disorder. Plans for all other health conditions are to be developed by the RN supervisor and/or the RN as needed. Individualized Health Care Plans should be developed in conjunction with the parent, staff, health care provider and student (as appropriate). 9. After October 1 when a new or newly diagnosed student with a chronic health condition is identified, a Student Assessment Checklist should be completed by the RN supervisor and/or the RN and if needed an Individualized Health Care Plan and, if warranted, an Emergency Care Plan should be completed within 30 calendar days as appropriate. 10. On school days at each school served by this contract, the RN and/or HST provides medication administration and treatment services, as prescribed by the student s healthcare provider on the Authorization for Medication (Exhibit 7) and documented on the Student Medication Log (Exhibit 8). 11. On each school day at each school served by this contract, the RN and/or HST provides diabetes medication and/or treatment services as prescribed by the student s healthcare provider on the Diabetes Medication /Treatment Authorization (Exhibit 9) form and documented on the Daily Diabetes Log (Exhibit 10). 12. As needed, child specific trainings should be completed and documented by the RN supervisor and the RN for all students with chronic health conditions requiring interventions at school. Trainings are to be provided to teachers, HSTs, and other school Solicitation Number: DOH Invitation to Bid Broward School Health Page 18
19 ATTACHMENT A Scope of Services staff who have interactions with the student. Trainings should be completed within 30 calendar days of the start of school or within 30 calendar days of notification of a new chronic health condition. 13. As needed, a chronic health condition overview will be provided and documented by the RN supervisor and the RN for teachers, HSTs and other school staff who have a need to know on the Emergency Care Plans. 14. On school days at each school, the RN and/or HST shall provide basic school health services. These services are to include, but not be limited to medication, First Aid, complex procedures and referrals, and should be documented on the Daily Summary Log (Exhibit 11). 15. Weekly at each school served by this contract, the RN and/or the HST shall monitor health room supplies and equipment for inventory and expiration. The AED machine should be checked bimonthly to ensure it is functional, along with the 911 posters, CPR certification, and medication administration certification to ensure they are present and current. 16. Weekly at each school served by this contract, the RN and/or the HST shall monitor medications and treatments for expiration, label, lock and quarantine expired medications, and work with SBBC Risk Management for expired medication pick up. 17. The Provider s Clinical Nurse Manager shall participate with the Department to develop and facilitate up to six (6) mandatory trainings per year on topics chosen by the Department in order to safely provide assigned health services. 18. All staff Provider shall participate in up to six (6) days of mandatory trainings per year, on topics chosen by the Department in order to safely provide assigned health services. These trainings shall be provided prior to and during the school year on days when students are not in school. 19. The Clinical Nurse Manager will complete and submit FTE Week Report (Exhibit 19) for each school according to the annual FTE week schedule. 20. Assist with communicable disease investigations and management. 21. Provider must complete and maintain the following documentation: a. Student Medication Log (Exhibit 8) b. Daily Diabetes Log (Exhibit 10) c. DOH-Broward Unduplicated Log (Exhibit 12) d. Daily Clinic Log (Exhibit 13) e. Daily Summary Log (Exhibit 11) f. Monthly Summary Log (Exhibit 14) g. School Monthly Data Collection Form by Grade Level (Exhibit 15) Solicitation Number: DOH Invitation to Bid Broward School Health Page 19
20 ATTACHMENT A Scope of Services h. RN Supervisor School Visit Log (Exhibit 20) i. Individual confidential student health records and individualized medication administration records, as provided by physicians, psychologists or other recognized health professionals and paraprofessionals, used in connection with the provision of medical treatment on school grounds, field trips, off-campus work, bus transportation j. Health records of individual students must be maintained in accordance with Section , Florida Statutes k. FTE Week report l. In-Kind Services in Full Service Schools (Exhibit 16) B. Deliverables 1. One hour or prorated partial hour (rounded up or down to the nearest quarter hour) of Clinical Nurse Manager services for a total of 40 hours per week year round. 2. One hour or prorated partial hour (rounded up or down to the nearest quarter hour) of Registered Nurse Supervisor services for a total of eight (8) hours per day for 189 days (180 days when students are present, up to 6 training days, 2 days prior to beginning of school year and 1 day after the end of the school year). 3. One hour or prorated partial hour (rounded up or down to the nearest quarter hour) of Registered Nurse services 6 hours per day for 180 school days (when students are present) and up to six (6) training days. 4. One hour or prorated partial hour (rounded up or down to the nearest quarter hour) of Health Support Technician services 6 hours per day for 180 school days (when students are present) and up to six (6) training days. 5. Submission of completed monthly summary logs and completed monthly data collection forms for each school to the Florida Department of Health in Broward County (DOH-Broward) Contract Manager by the 10th day of the month following the month being reported. 6. Clinical Nurse Manager is to conduct on-site quality assurance for each of the 38 schools one time per quarter utilizing the Health Room Review Sheet (Exhibit 17) and the Health Record Review Worksheet (Exhibit 18) and document findings. Upon completion of these forms they should be placed in the Health Room binder. 7. Submission of all information necessary for the completion of the Annual School Health Services Report to the DOH-Broward Contract Manager by July Submission of the In-Kind Services in Full Service Schools no later than July 15 to the DOH- Broward Contract Manager. 9. Provide a substitute HST/RN to a school within 2 hours of being advised of an HST/RN absence. If an HST cannot be substituted within the 2 hour time frame the RN supervisor must go to the HST s assigned school to provide coverage for that day/s. If an RN supervisor is absent the Program Manager must provide the Solicitation Number: DOH Invitation to Bid Broward School Health Page 20
21 ATTACHMENT A Scope of Services oversight of the absent RN supervisor s five (5) schools. C. Staffing Levels 1. Provider will maintain an administrative organizational structure sufficient to discharge its contractual responsibilities. The Provider shall assign Registered Nurses (RN) and Unlicensed Assistive Personnel (UAP) otherwise known as Health Support Technicians (HST) to specific schools with the expectation that the Provider s employee will remain assigned to that school absent the resignation or separation of the employee from the Provider or a request to move or remove the RN or HST from the school as determined by DOH-Broward. Provider must replace any employee whose continued presence would be detrimental to the success of the program with an employee of equal or superior qualifications. DOH-Broward will endeavor to provide no less than 3 days notice but, in any event, such replacement must be made immediately if such action is requested by the DOH- Broward Contract Manager. Information to document staffing configuration for basic school health services and full services school specialized services that may include: nutritional services, basic medical services, aid to dependent children, parenting skills, counseling for abused children, counseling for children at high risk for delinquent behavior and their parents, and adult education will be provided to the DOH-Broward Contract Manager for inclusion in the Annual School Health Services Report each year for the duration of this contract. There shall be one (1) FTE Clinical Nurse Manager to oversee the School Health Program and Staff, seven (7) RN Supervisors, three (3) RN s and 35 HST s. Each RN Supervisor shall supervise five HST s at five different schools as assigned by the department. If staff in any of these positions, with the exception of the HST s, is absent or the position is vacant, the direct supervisor of the person in that position will be responsible for covering the position until the return of staff or the position is filled. Solicitation Number: DOH Invitation to Bid Broward School Health Page 21
22 ATTACHMENT A Scope of Services 2. Number of Positions Position Title Education Experience Duties Days/Hours 1 Clinical Nurse Manager Registered Nurse, currently licensed under Chapter 464 F.S. with a Bachelor s Degree. School Health Program Management or similar experience. Two (2) years supervisory experience. Year Round Full See Roles Time Position. and Monday-Friday 40 Responsibilities hour work week. 7 Registered Registered Nurse, currently Nurse licensed under Supervisors Chapter 464 F.S. Full Time Position One (1) year experience as a Registered Nurse supervising an See 8 hours per day (180 days when students are present, up to 6 unlicensed assistive Roles and training days, 2 personnel or HST. School Health or pediatric nursing preferred. Responsibilities days prior to beginning of school year and 1 day after the end of the school year). 3 Registered Nurses Registered Nurses, currently licensed under Chapter 464 F.S. School Health or pediatric nursing preferred. 6 hours per day for 180 school days See (when students are Roles and present) and up to Responsibilities six (6) training days. 35 Health Support Technicians High School Diploma or GED. Certification in First Aid and Cardiopulmonary Resuscitation (CPR) per 64F F.A.C. One (1) year providing direct patient care services of a medical nature. See Roles and Responsibilities 6 hours per day for 180 school days (when students are present) and up to six (6) training days. Solicitation Number: DOH Invitation to Bid Broward School Health Page 22
23 ATTACHMENT B PRICE PAGE A single award solicitation will be made to the responsive, responsible Provider offering the lowest grand total for the services requested in this solicitation. Initial Year Term August July2018 Quantity Hours Per Description (Positions) Position Hourly Rate Total Clinical Nurse Supervisor Services 1 x x $ = $ RN Supervisor Services 7 x x $ = $ School Nurse services 3 x x $ = $ Health Support Technician (HST)* Services 35 x x $ = $ Initial Year Term Total: $ Renewal Term 1 August July 2019 Quantity Hours Per Description (Positions) Position Hourly Rate Total Clinical Nurse Supervisor Services 1 x x $ = $ RN Supervisor Services 7 x x $ = $ School Nurse services 3 x x $ = $ Health Support Technician (HST)* Services 35 x x $ = $ Solicitation Number: DOH Invitation to Bid Broward School Health Page 23
24 ATTACHMENT B PRICE PAGE Renewal Term 2 August July 2020 Quantity Hours Per Description (Positions) Position Hourly Rate Total Clinical Nurse Supervisor Services 1 x x $ = $ RN Supervisor Services 7 x x $ = $ School Nurse services 3 x x $ = $ Health Support Technician (HST)* Services 35 x x $ = $ Renewal Term 3 August July 2021 Quantity Hours Per Description (Positions) Position Hourly Rate Total Clinical Nurse Supervisor Services 1 x x $ = $ RN Supervisor Services 7 x x $ = $ School Nurse services 3 x x $ = $ Health Support Technician (HST)* Services 35 x x $ = $ Renewal Year Terms Total: $ **The estimated quantities in this Invitation to Bid are only to be used in determining bid prices and not to be considered as definite quantities to be ordered by the Department. The ordered quantities may be less than or greater than those stated in this solicitation at no penalty to the Department.** GRAND TOTAL $ (Initial Year Term plus Renewal Terms) Solicitation Number: DOH Invitation to Bid Broward School Health Page 24
25 ATTACHMENT B PRICE PAGE Provider Name: Provider Mailing Address: City-State-Zip: Telephone Number: Address: Federal Employer Identification Number (FEID): BY AFFIXING MY SIGNATURE ON THIS BID, I HEREBY STATE THAT I HAVE READ THE ENTIRE ITB TERMS, CONDITIONS, PROVISIONS AND SPECIFICATIONS AND ALL ITS ATTACHMENTS, INCLUDING THE REFERENCED PUR 1000 AND PUR I hereby certify that my company, its employees, and its principals agree to abide to all of the terms, conditions, provisions and specifications during the competitive solicitation and any resulting Contract including those contained in the Standard Contract Signature of Authorized Representative*: Printed (Typed) Name and Title: *An authorized representative is an officer of the Provider s organization who has legal authority to bind the organization to the provisions of the Bids. This usually is the President, Chairman of the Board, or owner of the entity. A document establishing delegated authority must be included with the Bid if signed by other than the President, Chairman or owner. Solicitation Number: DOH Invitation to Bid Broward School Health Page 25
26 ATTACHMENT C REFERENCE FORM Provider s Name: Providers must provide contact information for three references evidencing 3 years of experience in the last 5 years in basic school health services in a minimum of 30 schools per school year. Providers may use this reference form to provide the required information. The Department of Health will not be accepted as a reference for this solicitation. The Department reserves the right to contact any and all entities in the course of this solicitation in order to verify experience. Information received may be considered in the Department s determination of the Provider s responsibility. The Department s determination is not subject to review or challenge. Company/Agency Name: Address: City, State, Zip: 1. Contact Name: Contact Phone: Contact Address: General Description of Work: Service Dates: Approximate Contract Value: $ Company/Agency Name: Address: City, State, Zip: Contact Name: 2. Contact Phone: Contact Address: General Description of Work: Service Dates: Approximate Contract Value: $ Solicitation Number: DOH Invitation to Bid Broward School Health Page 26
27 ATTACHMENT C REFERENCE FORM Company/Agency Name: Address: City, State, Zip: Contact Name: 3. Contact Phone: Contact Address: General Description of Work: Service Dates: Approximate Contract Value: $ Solicitation Number: DOH Invitation to Bid Broward School Health Page 27
28 ATTACHMENT D STATEMENT OF NON-COLLUSION I hereby certify that my company, its employees, and its principals, had no involvement in performing a feasibility study of the implementation of the subject Contract, in the drafting of this solicitation document, or in developing the subject program. Further, my company, its employees, and principals, engaged in no collusion in the development of the instant Bid, proposal or reply. This Bid, proposal or reply is made in good faith and there has been no violation of the provisions of Chapter 287, Florida Statutes, the Administrative Code Rules promulgated pursuant thereto, or any procurement policy of the Department of Health. I certify I have full authority to legally bind the Provider, Respondent, or Vendor to the provisions of this Bid, proposal or reply. Signature of Authorized Representative* Date *An authorized representative is an officer of the Provider s organization who has legal authority to bind the organization to the provisions of the Bids. This usually is the President, Chairman of the Board, or owner of the entity. A document establishing delegated authority must be included with the Bid if signed by other than the President, Chairman or owner. Solicitation Number: DOH Invitation to Bid Broward School Health Page 28
29 Exhibit 1 Skills Assessment Form Health Support Technician: Date: Nurse Supervisor: School: Procedure ANAPHYLAXIS Administration of Epinephrine Auto Injector Caregiver Epi-Pen Kit List Performs activity in accordance with policy & procedure guidelines Does not perform activity in accordance with policy and procedure guidelines Requires further instruction & supervision ASTHMA Metered Dose Inhaler Administration Nebulizer Administration DIABETES Blood Glucose Monitoring Ketone Testing Carbohydrate Counting Insulin Injection via Pen or Syringe I n s u l i n Pump Procedures SEIZURES Diastat Administration Caregivers Diastat Kit List Seizure Log TRAINER CHILD ABUSE AND NEGLECT Recognizing Child Abuse Reporting Child Abuse
30 Student Assessment Check List School Year Exhibit 2 Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Other/Relationship: Contact #: Guidelines for Student Planning IHP will be developed for students with a significant chronic disease (i.e.: severe asthma, diabetes, seizure disorder, anaphylaxis, and psychotropic meds). ECP will be developed for students with a potential risk of emergency. Indications: Students with any of (but not limited to) the following condition(s) may need an IHP. Please check all that apply. Assessment Checklist. Does health problem require any of the following? Please check all that apply. Allergies Diabetes Asthma Seizure Disorder ADHD Autism Eating Disorder Blood Disorder Cardiac Disorder Respiratory Disorder Psycho/Social Issues Hearing Impairment Visual Impairment Other Special orders for care from a healthcare provider Medication and authorization Special training of school personnel Special diet Change in school environment Added safety measures Measures to relieve pain Self-care assistance Other Comments/History: Student needs IHP only Student needs IHP and ECP No plan required at this time RN signature: Date: DOH-Broward N-88 09/16
31 Individual Health Care Plan School Year Exhibit 3 Allergies: Previous Episode of Anaphylaxis: Describe Incident: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #: In Case of EMERGENCY Call 911 ASTHMA, check all that apply Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome Medication/ Treatment Authorization or Asthma Action Plan from Healthcare Provider. Yes No Medication to be administered by: Staff Student Risk for Ineffective Airway Clearance. Anxiety related to disease process. Knowledge deficit related to disease process. Avoid asthma and or allergy triggers. Provide and evaluate medication as ordered on Medication Authorization. Student will learn to identify early warning signs of asthma episode. Student will learn to utilize calming techniques. School staff will identify early warning signs of respiratory distress. School staff/school nurse will implement the Emergency Care Plan. Teachers and staff will be trained on recognizing signs and symptoms of Asthma and how/when to respond. Provide emotional support. Coach student to use relaxation techniques. Student s safety is maintained. Asthma medication is delivered efficiently and effectively. Name and date of staff members instructed: Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff Reviewed with parent/guardian: Name: in person by phone. Must make no less than two attempts to contact parents/guardian: ECP Completed. Date 1 Date 2 RN signature: Date: This plan is in effect for the current school year and summer school as needed. DOH-Broward N-92 09/16
: Student Asthma Symptom History Asthma Symptoms (please check medical history) : Exercise Stress Dust Pollen Smoke Mold Air pollution Animal hair/fur Change in")
32 Exhibit 3A School Year Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #: Asthma Asthma Triggers (please check all that apply): Student Asthma Symptom History Asthma Symptoms (please check medical history) : Exercise Stress Dust Pollen Smoke Mold Air pollution Animal hair/fur Change in Temp Seasonal Allergies Foods Other Changes in breathing: Coughing, Wheezing, Breathing through mouth, Shortness of breath Verbal reports of: Chest tightness, Doesn t feel well, Speaks quietly, Cannot catch breath, Dry mouth Appears: Anxious, Pale, Sweating, Nauseous, Fatigued, Shoulders hunched over, Difficulty walking and/or talking Green Zone, Mild Yellow Zone, Moderate Red Zone, Severe Doing well, no coughing or wheezing. Can work and play. Sleeps well at night. Some coughing or wheezing shortness of breath or chest tightness. Difficulty walking and/or talking. Quick relief medication: Difficulty breathing. Cannot work or play. Getting worse instead of better. Medication is not helping after min. Asthma Emergency Action Steps The severity of symptoms can change quickly. It is important that treatment is given immediately in the order that places the student s safety first. Stop activity immediately. Stay with student at all times. Stay calm. Help student assume a comfortable position (Sitting up is usually more comfortable). Notify School Nurse or Trained Personnel (see below). Call parent or guardian (listed above). Administer medication as ordered: o Medication stored: Health room Self Carries Other: Observe for relief of symptoms. If no relief noted in minutes, follow steps below for an asthma emergency. Encourage purse-lipped breathing. Encourage fluids to decrease thickness of lung secretions. Time, observe, and record what happens (note symptoms, over all appearance, skin color, respiratory rate and pattern of breathing). If symptoms don t improve: Call 911- Inform EMS that you have an Asthma Emergency. They will ask the student s name, age, physical symptoms, and what medications he/she takes daily and what has been given for this event (Medication Authorization form). Other instructions: Reviewed with parent/guardian: Name: in person by phone. ECP distributed to staff on a need to know basis. Personnel training date: Trained Personnel: Trained Personnel: RN signature: Date: This plan is in effect for the current school year and summer school as needed. DOH-Broward N/91 09/16
33 Individual Health Care Plan School Year Exhibit 4 Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #: In Case of EMERGENCY Call 911 DIABETES, please check all that apply Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome DMMP or Medication/Treatment Authorization on file. Exp. Date: Insulin to be given during school? Yes No Insulin pen: Insulin injection: Insulin pump: Insulin to be administered by: Staff Student Other medication: Glucagon kit In Health Room: With student: Other: Blood Sugar to be Checked by: Staff Student Target range: - Student is able to recognize risk factors for onset of elevated or low blood sugar. Yes No Risk for injury related to development of acute complications of hypo or hyperglycemia. Knowledge deficit related to disease process and emergency interventions related to hypo/hyperglycemia. Student will maintain a normal blood glucose level throughout the school day as per target range on DMMP. Student will notify staff/nurse if displaying signs and symptoms of hypo- or hyperglycemia. Student will learn and practice selfmanagement skills including blood glucose monitoring, carb counting & insulin administration. Staff will recognize signs/symptoms of hypo/hyperglycemia and verbalize understanding of emergency intervention in accordance to ECP. Nurse will reinforce diabetes education as per DMMP and appropriate for age level: blood glucose monitoring, carbohydrate counting, and insulin administration. Nurse will educate staff on recognizing signs and symptoms of hypo/hyperglycemia and provide appropriate response to the situation. Nurse will educate staff on the administration of Glucagon injection, in the event of severe hypoglycemia. Student will be an active participant in diabetes regimen. Staff and student will show proficiency operating the blood glucose meter. Staff and student will understand signs and symptoms and intervention for hypo/hyperglycemia. Staff will understand how and when to administer glucagon. Name and date of staff members instructed: Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff Reviewed with parent/guardian, Name: in person by phone. Must make no less than two attempts to contact parents/guardian: ECP Completed. Date 1 Date 2 RN signature: Date: DOH-Broward N/71 09/16 This plan is in effect for the current school year and summer school as needed.
34 Emergency Care Plan Exhibit 4A School Year Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #: Diabetes Hyperglycemia Causes of Hyperglycemia Too little insulin or other glucose lowering medication Too much food intake Decreased physical activity Illness, infection and or injury or emotional stress Insulin Pump malfunction The onset of Hyperglycemia happens over several hours or days and may progress rapidly Has the student experienced Hyperglycemia before? Yes No Most recent date:. What were his/her symptoms at the time of the event? Hyperglycemia Signs and Symptoms Please check what applies Increased thirst and or dry mouth Frequent or increased urination Change in appetite, nausea or vomiting Blurry vision Fatigue, lethargy Other: Ongoing Evaluation and Care for Hyperglycemia Recheck blood glucose every 1-2 hours to determine if it is decreasing to target range of - mg/dl. Check urine or blood for ketones if blood glucose levels are greater then: mg/dl If student uses a pump, check to see if pump is connected properly and functioning Review student s medication administration, food and liquid intake and activity for the last 24 hours Give extra water or non-sugary drinks (no fruit juices) Allow free and unrestricted access to the restroom. Restrict participation in physical activity Notify parents / guardian Actions for Treating Hyperglycemia Notify School Nurse or Trained Personnel as soon as you observe symptoms Check blood glucose level. The ideal target range for this student is - Give student water to drink (nothing with sugar/fructose) Accompany student to Health Room Hyperglycemia Emergency If student does not respond to treatment and blood glucose is still above target range If student is displaying any of the following: extreme thirst, nausea and/or vomiting, severe abdominal pain, weak or depressed level of consciousness Call 911 Notify parents/guardian Notify Healthcare Provider Stay with student till EMT arrives Reviewed with parent/guardian: Name: ECP distributed to staff on a need to know basis. Personnel training date: Trained Personnel: Trained Personnel: RN signature: Date: DOH-Broward N/63 09/16 This plan is in effect for the current school year and summer school as needed. in person by phone.
35 Emergency Care Plan Exhibit 4B School Year Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #: Diabetes Hypoglycemia Causes of Hypoglycemia Too much insulin Missing or delaying meals or snacks Not eating enough foods (carbohydrates) Getting intense or unplanned physical activity Being ill, particularly with gastrointestinal illness Does the student have Glucagon ordered by Healthcare Provider? Yes No, if yes, location of Glucagon: Trained personnel to administer Glucagon as ordered and Call 911 CALL 911 Special Instructions: Has the student experienced Hypoglycemia before? Yes No, most recent date: What were his or her symptoms at the time? Please check below. Hypoglycemia Signs and Symptoms Shaky or jittery Pale or sweaty Thirsty and/or hungry Headache, blurry vision Dizzy, confused, or disoriented Change in behavior, irritable, nervous or combative Weak, sleepy or lethargic Other: Ongoing Evaluation and Care for Hypoglycemia Recheck blood glucose levels every minutes Repeat quick acting glucose product or fruit juice or soda The onset of Hypoglycemia happens quickly and may progress rapidly. Actions for Treating Hypoglycemia School Nurse or Trained Personnel should come to the classroom to assist student. Always stay with student. Check blood glucose level. Ideal blood glucose level for this student is - Give student a quick acting glucose product such as: Contact the student s parents/guardian Other instructions: Treatment for Severe Hypoglycemia Position the student on his or her side Do not attempt to give anything by mouth If student is unable to eat or drink, unresponsive or having convulsions: Administer Glucagon injection as ordered by the Healthcare Provider While treating, have another person CALL 911 Notify parents / guardian of current situation Call student s Healthcare Provider Stay with student until EMT arrives Reviewed with parent/guardian: Name: in person by phone. ECP Distributed to staff on a need to know basis. Personnel training date: Trained Personnel: Trained Personnel: RN signature: Date: DOH-Broward N/64 09/16 This plan is in effect for the current school year and summer school as needed.
36 Individual Health Care Plan School Year Exhibit 5 Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #: In Case of EMERGENCY Call 911 SEIZURE DISORDER, Please check all that apply Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome Student has history of seizure disorder. Last episode(date and duration), triggers and description of seizure: Medication Orders from Physician: Yes No Based on seizure history: Risk of injury related to seizure activity. Yes No Potential for aspiration related to seizure activity. Yes No Importance of compliance with meds. Decreased self-esteem related to chronic illness. Train staff to identify and respond to seizure. Prevent injury during seizure. Prevent aspiration during seizure. Student receives medication as ordered by Healthcare Provider to reduce risk of seizure activity. Student will have increased knowledge base of disease process regarding prevention of seizure with medication compliance and recognizing the onset of a seizure to prevent injury. Train staff to protect, support and prevent injury. Position child on his/her side to prevent aspiration. Call for help. Maintain compliance with medications as ordered by Healthcare Provider. Increased self esteem by providing education and support for student to talk about issues related to illness. Student will not experience seizure. Staff will be well trained to provide care and support to the student. Staff will identify seizure and follow ECP and call for help. If a seizure occurs the student will not experience injury or aspirate during the seizure. Name and date of staff members instructed: Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff Reviewed with parent/guardian: Name: in person by phone. Must make no less than two attempts to contact parents/guardian: ECP Completed. Date 1 Date 2 RN signature: Date: DOH-Broward N/66 08/16 This plan is in effect for the current school year and summer school as needed
37 Emergency Care Plan Exhibit 5A School Year Allergies: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #: Seizure Disorder Basic Seizure First Aid If you see this: Symptoms of a seizure episode may include any or all of these. Temporary confusion, staring spell Convulsion lasting longer than minutes Uncontrollable jerking movements of the arms and legs Loss of consciousness or awareness Pale, clammy, nail beds pale/bluish gray in color Rapid heart rate or changes in breathing patterns Other symptoms: Do this: Stay calm. Remove bystanders Keep airway clear, turn on side if possible, nothing in mouth Keep safe, remove objects, do not restrain Time, observe, record what happens Stay with student until recovered from seizure Seizure Emergency Action Steps Call 911 Inform EMS that you have a Seizure Emergency. They will ask the student s name, age, physical symptoms and what medication he/she takes daily and what medication has been administered for this event. Notify School Nurse or Trained Personnel (see below). Administer medication as ordered. Location of medication: Clinic, Classroom, Self carries Medication: Dose: Route: Time Administered: Call parent or guardian (listed above) Other instructions: Reviewed with parent/guardian: in person by phone. Name: ECP Distributed to staff on a need to know basis. Personnel training date: Trained Personnel: Trained Personnel: RN signature: Date: DOH-Broward N/67 09/16 This plan is in effect for the current school year and summer school as needed
38 Individual Health Care Plan School Year Exhibit 6 Allergies: Previous episode of Anaphylaxis: Describe Incident: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #: In Case of EMERGENCY Call 911 Anaphylaxis / Allergy, Please check all that apply Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome Student has Medication/ Treatment Authorization. Yes No Events which may trigger an allergic response: Symptoms of student s allergic response (check those that apply): Itching or swelling of the mouth, lips, tongue, face, or extremities. Cough, tightness in throat, difficulty swallowing, wheezing, shortness of breath, difficulty breathing. Increased heart rate, weak pulse, dizziness, feeling faint. Skin redness, itchy hives/rash, pain at site of exposure. Nausea, vomiting, abdominal cramps, diarrhea. Potential for severe allergic reaction or life threatening episode. Knowledge Deficit related to disease process. Student will maintain optimum health and safety necessary for learning. Student and staff will understand the disease process of allergies/anaphylaxis and emergency interventions. Staff will be educated on the signs and symptoms of the early stages of anaphylaxis. Staff will be educated on emergency procedures for anaphylaxis. Student will have an Emergency Care Plan in place for severe allergy/anaphylaxis. Staff will be educated on use of Epinephrine. Staff will be educated on allergens and substances that can cause anaphylaxis and ways to avoid allergens. All substances causing anaphylaxis will be avoided and student will have an incident free learning experience. Staff will understand the emergency procedures and demonstrate competency regarding use of the Epinephrine. Student will participate in collaboration which facilitates optimum health and safety necessary for learning. Staff will understand the early stages of anaphylaxis and follow protocol to treat. Student is able to recognize risk factors for onset of anaphylaxis. Yes No Name and date of staff members instructed: Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff Reviewed with parent/guardian: Name: Must make no less than two attempts to contact parents/guardian: RN signature: in person by phone. ECP Completed Date 1 Date 2 Date: This plan is in effect for the current school year and summer school as needed. DOH-Broward N/62 09/16

39 Exhibit 6A School Year Allergies/triggers: nuts soy products wheat shellfish insects other: Date of previous episode of anaphylaxis: Describe Incident: Student s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #: Anaphylaxis Does the student have Asthma? Symptoms of an allergic reaction may include any/all of the following: If you see this: (Circle those that apply) Itching or swelling of lips, tongue or mouth. Hoarse, coughing, tightness in throat, difficulty swallowing, wheezing, shortness or difficulty breathing, increased heart rate, weak pulse. Redness, itchy hives, itchy rash, swelling of face and extremities. Nausea, vomiting, abdominal cramps, diarrhea. Dizziness, feeling faint, pain at site. Comment: Yes (increased risk for severe reaction) No Act Quickly! Follow the Medication / Treatment Authorization: (Check all that apply) Treatment should be initiated with symptoms Antihistamine ordered Epinephrine Auto Injector, follow instruction on devise Other: Medication in clinic Student self carries Other instructions: Call 911 after using Epinephrine Auto-Injector. Call School Nurse or Trained Personnel. Call parent/guardian (listed above). Stay with student at all times. Stay calm. Monitor student s reaction, respiratory and heart rate Special Instructions: Call 911- The severity of symptoms can change quickly It is important that treatment is given immediately in the order that places the student s safety first. Reviewed with parent/guardian: Name: in person by phone. ECP distributed to staff on a need to know basis. Personnel training date: Trained Personnel: Trained Personnel: RN signature: Date: DOH-Broward N/55 09/16 This plan is in effect for the current school year and summer school as needed.
40 THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDA Coordinated Student Health Services, 1400 NW 14 Court, Fort Lauderdale, FL Exhibit 7 AUTHORIZATION FOR MEDICATION: Prescription or Over-the-Counter Medication Student's Name: Date of Birth: Grade: School: Phone #: Fax#: *********************************************************************************************************************************** Allergies: Diagnosis: MEDICATION DOSAGE & ROUTE FREQUENCY SPECIFIC TIMES SPECIAL INSTRUCTIONS/ SIDE EFFECTS List any emergency precautions / health emergencies that should be anticipated for this student; e.g. allergy triggers, diabetic reactions, etc.) : There are no extraordinary emergency medical services available at school. Since only CPR and first aid are available until 911 arrive, is this adequate for student survival? YES NO, IF "NO", specifies: *********************************************************************************************************************************** Physician s Name (Printed) Physician s Signature Physician s Telephone & Fax Numbers Physician s Office Address Date Completed *********************************************************************************************************************************** This information will be obtained by School Board District Personnel PARENTAL PERMISSION FOR MEDICATION (TO BE COMPLETED BY THE STUDENT S PARENT / GUARDIAN) Student's Name: Date of Birth: Grade: I grant the principal or his / her designee the permission to assist or perform the administration of each medication to or for my child during the school day, including when he/she is away from school property for official school events. If my child has been authorized by his/her physician to self-administer their medication(s), I grant permission for my child to self-administer their medication at school and when they are away from school property for official school events. In the event that my child is unable to self-administer their medication, I give permission for the principal/designee to perform the administration of the prescribed medication. NOTE: Medications must be supplied in the original container. Ask the pharmacist to divide the medication into two completely labeled containers, providing one for home and one for school. School personnel may administer only medications authorized by a physician. It is your responsibility to notify the school when there is a change in medication regimen. Parent / Guardian Name (Printed) Date Signed Form #2240 Rev. 8/15 Signature of Parent / Guardian Home Phone Number Work/Cell Phone Number (Include Ext. if any) Page 1 of 2
41 THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDA Coordinated Student Health Services, 1400 NW 14 Court, Fort Lauderdale, FL Exhibit 7 AUTHORIZATION FOR TREATMENT Student's Name: Date of Birth: Grade: School: Phone #: Fax#: *********************************************************************************************************************************** Diagnosis: Allergies: TREATMENTS DURING SCHOOL HOURS Treatment Plan: PROCEDURE Catheterization Feedings Suctioning TYPE G-Tube J-Tube NG-Tube Special Oropharynx Tracheostomy Deep Surface Tracheostomy Tube Replacement Care (Cleaning) MEDS / FEEDING AMOUNT FREQUENCY SPECIFIC TIMES RATE / FLOW CPT Oxygen /Misting Ventilator Nebulizer Tx Pulse Oximeter Are any of the above procedures required for emergency care? YES NO, IF "YES", specify: List any procedures the student has been trained to perform List any limitations / precautionary measures that should be considered; e.g. physical education, outdoor activities, transporting, lifting, moving, special devices / equipment: List any emergency precautions / health emergencies that should be anticipated for this student; e.g. allergy triggers, diabetic reactions, etc.) : There are no extraordinary emergency medical services available at school. Since only CPR and first aid are available until 911 arrive, is this adequate for student survival? YES NO, IF "NO", specifies: Physician s Name (Printed) Physician s Signature Physician s Telephone & Fax Numbers Physician s Office Address Date Completed *********************************************************************************************************************************** This information will be obtained by School Board District Personnel PARENTAL PERMISSION FOR TREATMENT (TO BE COMPLETED BY THE STUDENT S PARENT / GUARDIAN) Student's Name: Date of Birth: Grade: I grant the principal or his / her designee the permission to assist or perform the administration of each treatment/procedure to or for my child during the school day, including when he/she is away from school property for official school events. If my child has been authorized by his/her physician to self-administer their medication(s), I grant permission for my child to self-administer their treatment at school and when they are away from school property for official school events. In the event that my child is unable to self-administer their treatment, I give permission for the principal/designee to perform the administration of the prescribed treatment. NOTE: school personnel may administer only treatments authorized by a physician. It is your responsibility to notify the school when there is a change in treatment regimen. Parent / Guardian Name (Printed) Signature of Parent / Guardian Date Signed Home Phone Number Work/Cell Phone Number (Include Ext. if any) Page 2 of 2
42 STUDENT MEDICATION LOG Allergies Exhibit 8 Student's Name: DOB: School: Hm Rm Teacher Doctor: Phone # Fax #: Diagnosis : Special Instructions: Side Effects: Month/Year: MEDICATION NAME DOSAGE TIME TO BE GIVEN ROUTE * Record the amount of Medication received (i.e. # of pills, amount of liquid) with each initial receipt in the Notes Section on the Reverse * Record Time Medication was given (or Reason not given) and Initials in the appropriate boxes * If medication is not given, please use one of the following abbreviations to indicate the reason why: A-absent O-out of medication F-field trip D-discontinued R-refused DW-dose wasted ER-early release day V-vacation/school closed S-Other and Provide explanation in the Notes Section on the Reverse side Date AM Initials PM Initials AM Initials PM Initials AM Initials PM Initials AM Initials PM Initials Signature/Initials/Date for each week. Signature/Initials: Signature/Initials:
43 Exhibit 8 STUDENT MEDICATION LOG NOTES DATE TIME DATE TIME DATE RECEIVED MEDICATION (Name and dosage) DOCUMENTATION OF RECEIPT OF MEDICATIONS AMOUNT (# of Tablets or amount of Liquid) PARENT/GUARDIAN SIGNATURE RECEIVED BY (SIGNATURE). 9/27/10 OP 151-O-PHN 45 Attachment 32 2
44 Exhibit 9 THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDA HEALTH EDUCATION SERVICES Diabetes Medication/Treatment Authorization Student s Name: School Name: Date of Birth: Date: Grade Homeroom CONTACT INFORMATION Parent/Guardian #1: Work Parent/Guardian #2: Work Physician/Healthcare Provider: Other Emergency Contact: Phone Number: Home Relationship: Phone Numbers: Home Cellular/Pager Phone Numbers: Home Cellular/Pager Phone Number Work/Cellular/Pager EMERGENCY NOTIFICATION: Notify parent/guardian of the following conditions If unable to reach parent/guardian: Notify healthcare provider and emergency contact listed above a. Loss of consciousness or seizure (convulsion) immediately after Glucagon given and 911 called. b. Blood sugars in excess of mg/dl c. Positive urine ketones. d. Abdominal pain, nausea/vomiting, diarrhea, fever, altered breathing, or altered level of consciousness. BLOOD GLUCOSE MONITORING: At school: Yes No Student has been trained by Healthcare Professional Yes No To ordinarily be performed by student: Yes No Type of Meter: Time to be performed: Before breakfast Before PE/Activity Time Mid-morning (before snack) After PE/Activity Time Before lunch Mid-afternoon Dismissal As needed for signs/symptoms of low/high blood glucose Place to be performed: Clinic/Health Room Classroom Other OPTIONAL: Target Range for blood glucose: mg/dl to mg/dl INSULIN INJECTIONS DURING SCHOOL:. Yes No Student has been trained by Healthcare Professional Yes No If yes, can student determine correct dose? Yes No Draw up correct dose? Yes No Give own injection? Yes No Insulin Delivery: Syringe/Vial Pen Pump (If pump worn, use Insulin Pump Medication/Treatment Plan ) Standard daily insulin at school: Yes No Type: Dose: Time to be given: Calculate insulin dose for carbohydrate intake: Yes No If yes use Regular Humalog Novolog #unit(s) per grams Carbohydrate Add carbohydrate dose to correction dose Correction dose of Insulin for High Blood Sugar: Yes No If yes, Regular Humalog Novolog Time to be given Time to be given: Determine dose per sliding scale below: Use formula Blood sugar: Insulin Dose: Blood Glucose - Blood sugar: Insulin Dose: Blood sugar: Insulin Dose: = Blood sugar: Insulin Dose: units of insulin OTHER ROUTINE DIABETES MEDICATIONS AT SCHOOL: Yes No Name of Medication Dose Time Route Possible Side Effects EXERCISE, SPORTS, AND FIELD TRIPS: Blood glucose monitoring and snacks as indicated. Easy access to sugar-free liquids, fast-acting carbohydrates, snacks, and blood glucose monitoring equipment. Child should not exercise if blood glucose level is below mg/dl OR if
45 Diabetes Medication/Treatment Authorization Page 2 MANAGEMENT OF HIGH BLOOD GLUCOSE ( over mg/dl) 4Usual signs/symptoms for this student: Indicate treatment choices: Increased thirst, urination, appetite Sugar-free fluids as tolerated Tired/drowsy Check urine ketones if blood glucose over mg/dl Blurred vision Notify parent if urine ketones positive. Warm, dry, or flushed skin May not need snack: call parent Nausea/Vomiting Frequent bathroom privileges Other See Insulin Injections: Extra Insulin for High Blood Glucose Other HES 1/02 Exhibit 9 MANAGEMENT OF LOW BLOOD GLUCOSE (below mg/dl) 4Usual signs/symptoms for this child Indicate treatment choices: Change in personality/behavior If student is awake and able to swallow, Pallor give grams fast-acting carbohydrate such as: Weak/shaky/tremulous _ 4oz. Fruit juice or non-diet soda or Tired/drowsy/fatigued _ 3-4 glucose tablets or Dizzy/staggering walk Concentrated gel or tube frosting or Headache _ 8 oz. Milk or Rapid heartbeat Other Nausea/loss of appetite Clammy/sweating Retest Blood Glucose 10-15minutes after treatment Blurred vision Repeat treatment until Blood Glucose over 80mg/dl Inattention/confusion Follow treatment with snack of Slurred speech if more than 1 hour till next meal/snack or if going to activity (i.e. P.E. or recess) Loss of consciousness Other Seizures Other If student is vomiting or unable to swallow, administer Glucose gel or Glucagon (See below for specific directions) IMPORTANT!! If student is unconscious or having a seizure, presume the student is experiencing a low blood glucose level and: Call 911 immediately and notify parents / guardian. Glucagon mg IM (injection) should be given by trained personnel Glucose gel 1 tube can be administered inside cheek and massaged from outside while waiting for help to arrive, or during administration of Glucagon by any trained staff member at scene. Student should be turned on his/her side and maintained in this recovery position till fully awake. Comments Physician /Healthcare Provider Signature: Date: Physician/Healthcare Provider Name Phone Number I grant the principal or his/her designee or a licensed nurse (RN/LPN) permission to assist with or perform the administration of each prescribed medication, including insulin either by injection or pump, and treatments/procedures for my child during the school day. This includes when he/she is away from school property for official school events. I have reviewed, understand and agree with the medications/treatments prescribed by the physician/healthcare provider on this form. It is my responsibility to notify the school if there is a change in the medication/treatment plan prior to its expiration date. Parent/Guardian Signature: Date: LOCATION OF SUPPLIES/EQUIPMENT: To be completed by school health personnel. Blood glucose testing equipment: Insulin administration supplies: Glucagon emergency kit: Glucose gel: Ketone testing supplies: Fast-acting carbohydrate: Snack foods: 3/04
46 Daily Diabetes Log Exhibit 10 Student s Name School Week of Doctor Phone # Fax # TYPE OF INSULIN GIVEN (H = Humalog R = Regular NP = NPH U = Ultra Lente) Given by (circle) PUMP INJECTION For Pump, give reason for insulin administration: B = Bolus C = Correction Dose A = absent V = no school S = other REMEMBER ADMINISTER INSULIN ONLY AT TIMES ORDERED DAY/DATE MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials Signature Signature Rev. 6/9/11
47 Daily Diabetes Log Exhibit 10 DATE TIME Initials DATE RECEIVED MEDICATION (Name and dosage) AMOUNT PARENT/GUARDIAN SIGNATURE RECEIVED BY (School designee signature) Rev 6/9/11 HES 4/05 PAGE 2
48 Daily Summary Log Exhibit 11 School Name/Level: Health Room Staff: Date: DAU #: Codes for Completing the Daily Clinic Log Table 1: Total Visits Table 2: Outcome Disposition Table 3: Procedure Table 4: Services provided by Table 5: Referral To 1 Non-Medication Visits Services 1 Medications (oral) 1 R.N. / A.R.N.P. 1 Abuse Registry 2 Medication Visits 2 Emergency Room 2 Medications (other) 2 L.P.N. 2 Dental Care TOTAL: 3 Returned to Class 3 Medications (Inhaler) 3 Health Support Tech 3 Guidance Counseling 4 Sent Home 4 Medications (Injection) 4 Clerical Support staff 4 Healthy Start 5 Other: 5 Insulin Adminstration 5 Kidcare TOTAL: 6 Intravenous Treatments 6 Medical / Nursing Care 7 Mental Health Coun. Complex Procedures 8 No Referral 7 Oxygen cont./intermittent 9 Nursing Assessment 8 Carbohydrate Counting 10 Social Work Services 9 Catheterization 11 Subst. Abuse Coun. 10 Ostomy care 12 Parent 11 Electronic Monitoring 12 Tube/PEG Feeding 13 Glucose Monitoring 14 Specimen Collect./testing 15 Tracheostomy Care 16 Ventilator Dependent Care 17 First Aid 18 Other DOH-Broward N-184a
49 Exhibit 12 DOH-Broward, School Health Services, Unduplicated Log for Medications and Procedures MEDICATIONS Insulin Administration Medications/Other Injections Medication/Intravenous Medications/Inhaler (or nebulizer) Medications/Oral (by mouth) Medications/Nasal Other Route-Specify: Other Route-Specify: Other Route-Specify: Subtotal: NUMBER OF STUDENTS PROCEDURES Carbohydrate Counting Glucose Monitoring Catheterization Colostomy, Ileostomy, Urostomy, Jejunostomy Care (site care) Electronic Monitoring (cardiac, oximetry, J, PEG, NG Tube Feeding Oxygen Continuous or Intermittent Specimen Collection or Testing Tracheostomy Care Ventilator Dependant Care Other Procedure-Specify: Other Procedure-Specify: Other Procedure-Specify: Subtotal: Total:
50 Exhibit 12 DOH-Broward, School Health Services UNDUPLICATED LOG Number of Students Needing Medications and/or Procedures During # STUDENTS NAME MEDICATION/PRODECURE Revised Page 1 OP 151-O-PHN 45 Attachment 22
51 Daily Clinic Log Exhibit 13 School: Health Room Staff: Date: DAU #: Table 1.a Table 1.b Table 2 Table 3 Table 4 Table 5 Time In Last Name First Name Grade Non- Medication Medication Outcome Disposition Procedure Service provided by Referral To Time Out Total: Total: Total: FDOH-Broward 184a, Rev. 9/2011 OP 151-O-PHN 45
 1 R.N. / A.R.N.P.")
52 Monthly Summary Log Exhibit 14 School Name/Level: Health Room Staff: Date: DAU #: Codes for Completing the Monthly Clinic Log Table 1: Total Visits Table 2: Outcome dispositon Table 3: Procedure Table 4: Services provided by Table 5: Referral To a Non-Medication Visits Services 1 Medications (oral) 1 R.N. / A.R.N.P. 1 Abuse Registry b Medication Visits 2 Emergency Room 2 Medications (other) 2 L.P.N. 2 Dental Care TOTAL: 3 Returned to Class 3 Medications (Inhaler) 3 Health Support Tech 3 Guidance Counseling 4 Sent Home 4 Medications (Injection) 4 Clerical Support staff 4 Healthy Start 5 Other: 5 Insulin Adminstration 5 Kidcare TOTAL: 6 Intravenous Treatments 6 Medical / Nursing Care 7 Mental Health Coun. Complex Procedures 8 No Referral 7 Oxygen cont./intermittent 9 Nursing Assessment 8 Carbohydrate Counting 10 Social Work Services 9 Catheterization 11 Subst. Abuse Coun. 10 Ostomy care 12 Parent 11 Electronic Monitoring 12 Tube/PEG Feeding 13 Glucose Monitoring 14 Specimen Collect./testing 15 Tracheostomy Care 16 Ventilator Dependent Care 17 First Aid 18 Other DOH-Broward N/184b
53 Exhibit 15 School: Month/Year: School Monthly Data Collection Form by Grade Level DAU # Grade Level: Description HMC PC # Pediculosus or Scabies screening, new Pediculosus or Scabies screening, repeat Pediculosus or Scabies screening, completed Student evaluation/intervention by a paraprofessional Student encounter by an LPN Physical activity referral RN nursing assessment / counseling RN nursing assessment / counseling postpartum Medication Administration First Aid Administration Complex Medical Procedures Immunization Follow-Up Counsultation with School Health staff / parent ESE staffing / screening Student Heatlh Care Plan developed Licensed Social Worker intervention Paraprofessional follow /up Health education, number of classes given Health education, number of participants Child specific training of school staff by RN Prepared by: *Note section above is not by grade level * Grade level is only for screenings Name/Title Agency Signed Date
54 2017 Annual School Health Report For: Exhibit 16 PART III: FULL SERVICE SCHOOLS III-A: IN-KIND SERVICES PROVIDED IN FULL SERVICE SCHOOLS BY COMMUNITY AGENCIES For in-kind hours and value of in-kind services, put annual totals (not weekly totals) and use only numbers (no text characters (i.e., per week). Type of Service ANNUAL Total Number Donated In-Kind Hours of ANNUAL Estimated Value of In-Kind Services Adult Education Basic Medical Services Case Management Child Protective Services Community Education Counseling Abused Children Counseling High-Risk Children Counseling High-Risk Parents Delinquency Counseling Dental Services Economic Services Healthy Start/Healthy Families Job Placement Services Mental Health Services Nutritional Services Parenting Skills Training Resource Officer School Health Nursing Services Social Work Services Substance Abuse Counseling TANF programs (job training) All Other TOTALS 0 0
55 Exhibit 17 School Health Room Review Sheet County: School: _Principal: _Date: Basic Comprehensive Full Service Number of Students: Reviewer: Legend: (F.S.)-Florida Statutes, (F.A.C)-Florida Administrative Code, (FSHAG)-Florida School Health Administrative Guidelines, (SREEF)-State Requirements for Existing Educational Facilities, (GS7)-General Records Schedule, (MUSRM)-Medication Use In Schools Resource Manual, (UAP)-Unlicensed Assistive Personnel, (AED)-Automated External Defibrillator, (ES)-Elementary School, (MS)-Middle School, (HS)-High School, (MAR)-Medication Administration Record, (RN)- Registered Nurse, (LPN)-Licensed Practical Nurse, (UAP)-Unlicensed Assistive Personnel, (FSS)-Full Service School I. Personnel Health Room staffed full time: Yes No If no, # hours/days staffed: # Designated School Staff: # of Health Room Staff by type: RN(s): LPN(s): UAP(s): RN supervisor: Frequency on site: FSHAG Sect. III, II. Health Room/Clinic Facilities Reference Items for Review Yes No Comments (A) Clinic Health treatment protocols for management of chronic and complex conditions, and emergency procedures are readily available, including communicable disease control protocols Administrative protocols and references are available Medication Administration Policy and Procedures s (1), F.S. School District Medication Policy available onsite & addresses: Ch. 64B9-14, F.A.C. School personnel designated by principal to assist in medication administration (list of designated staff available) Annual training of designated personnel with verification of delegate s understanding of assignment present and; Verification of periodic monitoring and supervision of delegated tasks present FSHAG III 4-3 Medication Errors with specific documentation required for reporting medication errors and: Medication Errors - notify supervising school nurse, school administrator, parent, prescribing MD, poison control if wrong student received medication GS7 - Item 120, FSHAG IV 18-5, Ch. 64F-6.005(1)(e), s , F.S. s (5b & 6c), F.S, FSHAG IV , SREEF 5-5 (13)(g) Pg. 35 SREEF (g)(1)(a & b) Ch. 64E (6), F.A.C. SREEF (g)(1)(c) SREEF (g)(1d), Ch. 64E F.A.C., SREEF (g)(2) SREEF (g)(2a) SREEF (g)(2b) SREEF (g)(3), (h)(3) SREEF (h)(4) FSHAG III-4-4 Pg. 36 SREEF (h)(5) SREEF 5-5 h)(5) SREEF (h)(6) SREEF (h)(6) Clinic Log Standardized clinic log (paper or electronic): student name, date, time in, reason for clinic visit, nurse/uap, time out, disposition. Clinic log concealed to protect student confidentiality. Clinic Physical Facilities School has adequate physical facilities for health clinic (reception/office/storage/toilet room/bed space present) Clinic toilet room(s) present: 1 for ES; 2 for MS/HS (1 male, 1 female) Clinic toilet room (sinks) have hot (temp 110 F) and cold water Toilet rooms functioning exhaust fan vented to exterior Clinic bed space (separated for male/female in MS/HS) Clean, plastic covered mattress & pillow per bed Clean, disposable mats for each patient Visual supervision of beds from reception area/office/nurses station (FSS) Lockable storage room with doors operable from the inside (for refrigerator, files, equipment, and supplies) (FSS) Data outlets for computer hookups & networking (FSS) Additional electric outlets for hearing/vision testing machines (FSS) Direct access to clinic from exterior (FSS) Direct access to from interior or connected by covered walk
56 SREEF 5-513(h)(7) (FSS) Designated parking adjacent to clinic (1 disabled accessible) (B) Emergency Supplies/Procedures Ch. 64F-6.004(1), F.A.C. Policies/Procedures for management of health emergencies in clinics, schools, etc. Ch. 64F-6.004(2) (3), F.A.C. Current First Aid/CPR certification-health room staff & 2 additional FSHAG III 7-3 school staff-copy in health room or office Ch. 64F-6.004(5)(6), F.A.C. First Aid supplies (band aids, gauze squares, elastic roller gauze, FSHAG III-4-1,2 cotton balls, cotton tipped applicators, tape, gloves, etc.), first aid kit FSHAG III-7-3&4 for use on other parts of campus, and emergency equipment are Ch. 64E (11), F.A.C. available and none are expired. Ch. 64F (1b)(2)(3), Locations of emergency supplies/aed/certified First Aid/CPR staff F.A.C., FSHAG III-7 s (1), F.S., SREEF-5-5 (10)(k)pg. 29, FSHAG IV, 21-3, Ch. 64J , F.A.C. s (2), F.S. Ch. 64J-1.023, F.A.C. posted - health room, cafeteria, gym, etc. AED required at schools in the Florida Athletic Assoc. only. If AED present, it is maintained in safe, secure, and usable condition. Location is registered with local EMS. Persons expected to use AED documented training/proficiency III. Medication Administration (A) Medications Reference Items for review Yes No Comments FSHAG III 4-1,2) Medication label (student name, med name, dosage & directions, times of admin., provider s name, date ( 1yr) s (1)(b-2) F.S. Medications received, counted (initially & refills) - stored in original FSHAG III -4-2 s (1)( c )(5)(a-1), F.S. s (3a,b), F.S., MUSRM page 72, FSHAG III 4-4 container, secured under lock and key when not in use OTC Meds labeled student specific Medications not expired (if expired meds present, quarantined from usable medications) Medications requiring refrigeration in locked fridge maintained at F (regularly documented) Assn. for Professionals. in Infection Control (APIC) (36-46) (B) Medication Administration Record (MAR) FSHAG III 4-5, IV 18-5 Demographics: student name, id, age, dob, grade, photo (if available) MUSRM page 47 Allergies (medication, food, environmental, etc.) Medication: name, dose, route, frequency, time Initials/name/signatures of persons authorized to administer Code (with explanation) for meds not administered s (1)(b)(1), F.S., Parental permission to administer med, statement of need for med & FSHAG III 4-1 known student-specific side effects to med Comments: Exhibit 17
57 Exhibit 18 School Health Record Review Worksheet School: RN Name/Signature: Student s name Contact Information Health Condition Immunization 680 Physical 3040 BMI Hearing Vision Scoliosis 504 IEP Comments DOH-Broward N/

58 FTE Week Report Exhibit 19 School: Agency: Counting School Health Encounters and Services at Your School during 2017 February FTE Week February 6-10, 2017 or other week in February specified by your County Health Department and/or School District School Health Coordinator. Count visits & health services to/by regular students, ESE students & students with 504 plans. (1) Student Visits to the School Health Room (Clinic) Count each time a student comes to the school health room (clinic) or other school location for health services (Medications Received or Self-Administered, Procedures, Counseling, Sick Care, First Aid, Other) Weekday Monday Tuesday Wednesday Thursday Friday Total Visit Totals (2) Medications Administered If a student receives more than one medication, count each medication separately. Weekday Monday Tuesday Wednesday Thursday Friday Total Insulin Administration Medications/Other Injections Medication/Intravenous Medications/Inhaler (or nebulizer) Medications/Oral (by mouth) Medications/Nasal Medication/Other Routes (specify): Medication/Other Routes (specify): Medication/Other Routes (specify): Medications Administered Totals (3) Health Procedures Performed If a student receives assistance with more than one procedure, count each procedure separately. Weekday Monday Tuesday Wednesday Thursday Friday Total Carbohydrate Counting Glucose Monitoring Catheterization Colostomy, Ileostomy, Urostomy, Jejunostomy Care (care to the site) Electronic Monitoring (cardiac, oximetry, other) J, PEG, NG Tube Feeding Oxygen Continuous or Intermittent Specimen Collection or Testing Tracheostomy Care Ventilator Dependent Care Other Procedure (specify): Other Procedure (specify): Other Procedure (specify): Procedures Performed Totals
59 RN School Visit Log Exhibit 20 RN Name: RN Signature: Dates: - Date School Visited Time In Time out Total Hours School Personnel Signature DOH-Broward
60 Exhibit 21

61 Exhibit 21
62 Exhibit 21
63 Exhibit 21
64 Exhibit 21
65 Exhibit 21

66 Exhibit 21
67 Exhibit 21
68 Exhibit 21

69 Exhibit 21

70 Exhibit 21

71 Exhibit 21

72 Exhibit 21

73 Exhibit 21
74 Exhibit 21
75 Exhibit 21
76 Exhibit 21

77 Exhibit 21
78 Exhibit 21

79 Exhibit 21

80 Exhibit 21

81 Exhibit 21

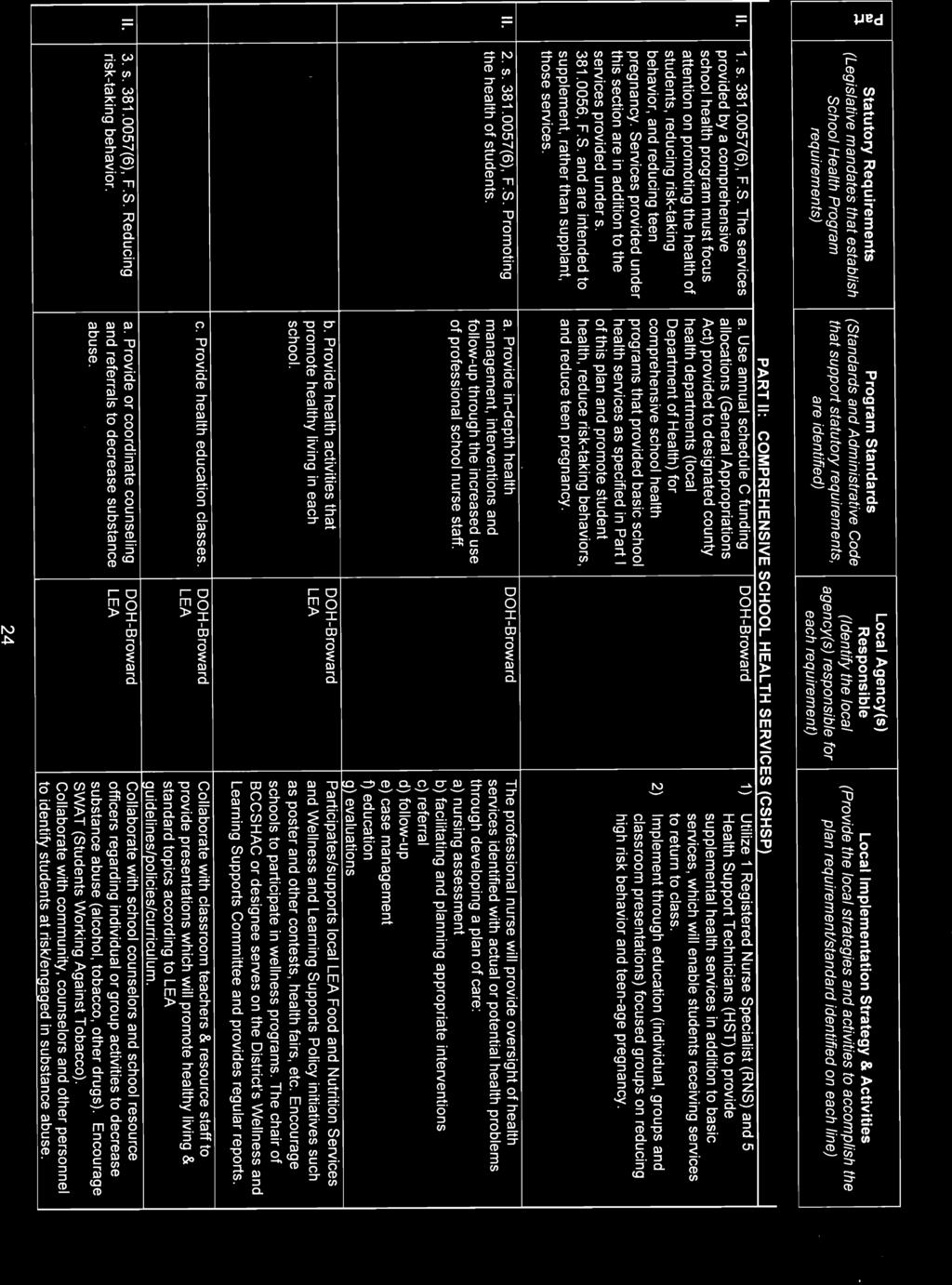
82 Exhibit 21

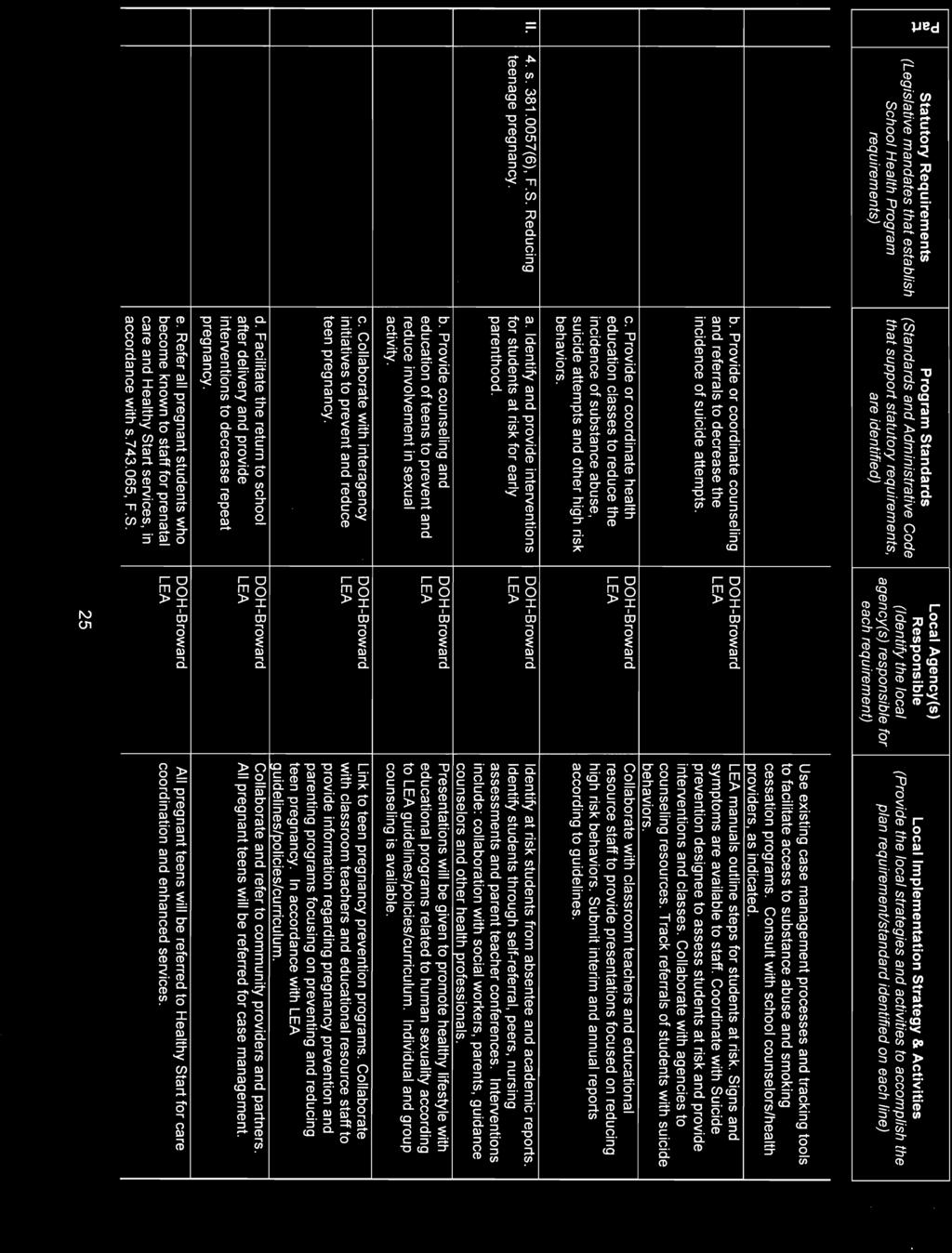
83 Exhibit 21
84 Exhibit 21
85 Exhibit 21

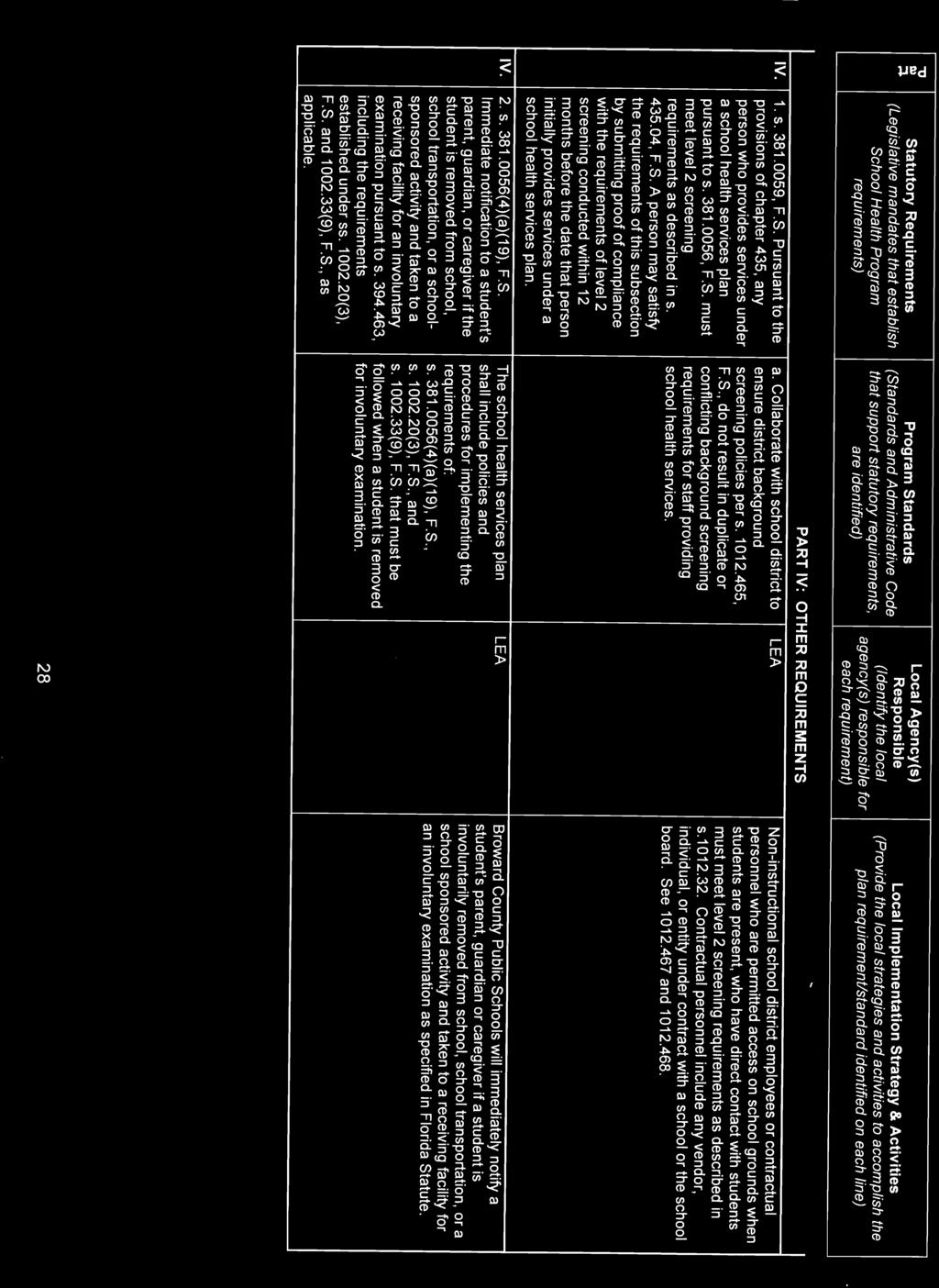
86 Exhibit 21
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH REQUEST FOR PROPOSALS (RFP) FOR Basic and Consultative School Health Services
 FOR Basic and Consultative School Health Services") TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 17-001 10-2016 REQUEST FOR PROPOSALS (RFP) FOR Basic and Consultative School Health Services Respondent Name: Respondent Mailing Address: City, State, Zip: Telephone:
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 17-001 10-2016 REQUEST FOR PROPOSALS (RFP) FOR Basic and Consultative School Health Services Respondent Name: Respondent Mailing Address: City, State, Zip: Telephone:
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH REQUEST FOR PROPOSALS (RFP) FOR Institutional Review Board (IRB) Application Management System
 FOR Institutional Review Board (IRB) Application Management System") TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 15-062 REQUEST FOR PROPOSALS (RFP) FOR Institutional Review Board (IRB) Application Management System Respondent Name: Respondent Mailing Address: City, State,
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 15-062 REQUEST FOR PROPOSALS (RFP) FOR Institutional Review Board (IRB) Application Management System Respondent Name: Respondent Mailing Address: City, State,
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD WELFARE
 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD WELFARE REQUEST FOR PROPOSALS ADOPTION AND INDEPENDENT LIVING SERVICES RFP# 07J15GN1 Commodity Code #: 93141505 1 TABLE OF CONTENTS
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD WELFARE REQUEST FOR PROPOSALS ADOPTION AND INDEPENDENT LIVING SERVICES RFP# 07J15GN1 Commodity Code #: 93141505 1 TABLE OF CONTENTS
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH INVITATION TO NEGOTIATE (ITN) for CMS Managed Care Plan
 for CMS Managed Care Plan") TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 17-026 10-2017 INVITATION TO NEGOTIATE (ITN) for Respondent Name: Respondent Mailing Address: City, State, Zip: Phone: ( ) Fax Number: ( ) E-Mail Address: Federal
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 17-026 10-2017 INVITATION TO NEGOTIATE (ITN) for Respondent Name: Respondent Mailing Address: City, State, Zip: Phone: ( ) Fax Number: ( ) E-Mail Address: Federal
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD WELFARE
 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD WELFARE REQUEST FOR PROPOSAL Child Welfare Training Proficiency Training Program RFP#: RFP05J26GN1 Release Date: June 1, 2017 COMMODITY
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD WELFARE REQUEST FOR PROPOSAL Child Welfare Training Proficiency Training Program RFP#: RFP05J26GN1 Release Date: June 1, 2017 COMMODITY
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH REQUEST FOR PROPOSALS (RFP) FOR Local Early Steps Program Offices
 FOR Local Early Steps Program Offices") TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 16-028 10-2016 REQUEST FOR PROPOSALS (RFP) FOR Local Early Steps Program Offices Respondent Name: Respondent Mailing Address: City, State, Zip: Telephone: (
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 16-028 10-2016 REQUEST FOR PROPOSALS (RFP) FOR Local Early Steps Program Offices Respondent Name: Respondent Mailing Address: City, State, Zip: Telephone: (
REQUEST FOR INFORMATION STAFF AUGMENTATION/IT CONSULTING RFI NO.: DOEA 14/15-001
 REQUEST FOR INFORMATION STAFF AUGMENTATION/IT CONSULTING RFI NO.: DOEA 14/15-001 I. INTRODUCTION The Florida Department of Elder Affairs (DOEA) hereby issues this Request for Information (RFI) to all interested
REQUEST FOR INFORMATION STAFF AUGMENTATION/IT CONSULTING RFI NO.: DOEA 14/15-001 I. INTRODUCTION The Florida Department of Elder Affairs (DOEA) hereby issues this Request for Information (RFI) to all interested
Exhibit Page 32 of 66. Exhibit 21
 Exhibit Page 32 of 66 Exhibit Page 33 of 66 Exhibit Page 34 of 66 Exhibit Page 35 of 66 Exhibit Page 36 of 66 Exhibit Page 37 of 66 Exhibit Page 38 of 66 Exhibit Page 39 of 66 Exhibit Page 40 of 66 Exhibit
Exhibit Page 32 of 66 Exhibit Page 33 of 66 Exhibit Page 34 of 66 Exhibit Page 35 of 66 Exhibit Page 36 of 66 Exhibit Page 37 of 66 Exhibit Page 38 of 66 Exhibit Page 39 of 66 Exhibit Page 40 of 66 Exhibit
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES. Substance Abuse and Mental Health Program Office. Certified Recovery Peer Specialist Training
 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Substance Abuse and Mental Health Program Office Certified Recovery Peer Specialist Training REQUEST FOR PROPOSAL COMMODITY CODE # 912-200 TABLE OF
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Substance Abuse and Mental Health Program Office Certified Recovery Peer Specialist Training REQUEST FOR PROPOSAL COMMODITY CODE # 912-200 TABLE OF
EXHIBIT A SPECIAL PROVISIONS
 EXHIBIT A SPECIAL PROVISIONS The following provisions supplement or modify the provisions of Items 1 through 9 of the Integrated Standard Contract, as provided herein: A-1. ENGAGEMENT, TERM AND CONTRACT
EXHIBIT A SPECIAL PROVISIONS The following provisions supplement or modify the provisions of Items 1 through 9 of the Integrated Standard Contract, as provided herein: A-1. ENGAGEMENT, TERM AND CONTRACT
STATE OF FLORIDA DEPARTMENT OF MANAGEMENT SERVICES DIVISION OF REAL ESTATE DEVELOPMENT AND MANAGEMENT PUBLIC ANNOUNCEMENT FOR CONSTRUCTION CONTRACTORS
 STATE OF FLORIDA DEPARTMENT OF MANAGEMENT SERVICES DIVISION OF REAL ESTATE DEVELOPMENT AND MANAGEMENT PUBLIC ANNOUNCEMENT FOR CONSTRUCTION CONTRACTORS TO PROVIDE CONSTRUCTION MANAGEMENT AT RISK SERVICES
STATE OF FLORIDA DEPARTMENT OF MANAGEMENT SERVICES DIVISION OF REAL ESTATE DEVELOPMENT AND MANAGEMENT PUBLIC ANNOUNCEMENT FOR CONSTRUCTION CONTRACTORS TO PROVIDE CONSTRUCTION MANAGEMENT AT RISK SERVICES
Request for Proposals City School District of Albany Empire State After-School Program Coordination and Programming June 14, 2017
 Request for Proposals City School District of Albany Empire State After-School Program Coordination and Programming June 14, 2017 Attention: Purchasing Agent Address: City School District of Albany 1 Academy
Request for Proposals City School District of Albany Empire State After-School Program Coordination and Programming June 14, 2017 Attention: Purchasing Agent Address: City School District of Albany 1 Academy
Request for Qualifications. Construction Management at Risk Services - William J. Rish Recreational Park Improvements RFQ-REDM17/ ADDENDUM #1
 Request for Qualifications Construction Management at Risk Services - William J. Rish Recreational Park Improvements RFQ-REDM17/18-005 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN
Request for Qualifications Construction Management at Risk Services - William J. Rish Recreational Park Improvements RFQ-REDM17/18-005 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN
REQUESTING QUALIFICATIONS FOR PROFESSIONAL SERVICES
 STATE OF FLORIDA, DEPARTMENT OF MILITARY AFFAIRS CONSTRUCTION & FACILITY MANAGEMENT OFFICE PUBLIC ANNOUNCEMENT REQUESTING QUALIFICATIONS FOR PROFESSIONAL SERVICES For PROJECT NUMBER: FEA 1802 Multi-Facility
STATE OF FLORIDA, DEPARTMENT OF MILITARY AFFAIRS CONSTRUCTION & FACILITY MANAGEMENT OFFICE PUBLIC ANNOUNCEMENT REQUESTING QUALIFICATIONS FOR PROFESSIONAL SERVICES For PROJECT NUMBER: FEA 1802 Multi-Facility
TOPIC: CONTRACTS STATE OF MISSISSIPPI DEPARTMENT OF EDUCATION SECTION 17.0 PAGE 1 OF 38 EFFECTIVE DATE: MAY 1, 2017 REVISION #4: MARCH 1, 2017
 SECTION 17.0 PAGE 1 OF 38 CONTRACT PROCUREMENT POLICY The Mississippi Department of Education (Department) Contract Procurement Policy set forth herein applies to the procurement, management, and control
SECTION 17.0 PAGE 1 OF 38 CONTRACT PROCUREMENT POLICY The Mississippi Department of Education (Department) Contract Procurement Policy set forth herein applies to the procurement, management, and control
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD CARE REGULATION AND BACKGROUND SCREENING
 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD CARE REGULATION AND BACKGROUND SCREENING REQUEST FOR PROPOSALS ACCREDITATION MANAGEMENT AND EDUCATIONAL SUPPORT SERVICES RFP-# 08C13AP1
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES OFFICE OF CHILD CARE REGULATION AND BACKGROUND SCREENING REQUEST FOR PROPOSALS ACCREDITATION MANAGEMENT AND EDUCATIONAL SUPPORT SERVICES RFP-# 08C13AP1
TOWN OF WINDERMERE REQUEST FOR PROPOSALS Race Timing & Event Services
 TOWN OF WINDERMERE REQUEST FOR PROPOSALS Race Timing & Event Services RESPONSES ARE DUE BY 5:00 PM December 12, 2014 MAIL OR DELIVER RESPONSES TO: ATT: Robert Smith, Town Manager 614 Main St. Windermere,
TOWN OF WINDERMERE REQUEST FOR PROPOSALS Race Timing & Event Services RESPONSES ARE DUE BY 5:00 PM December 12, 2014 MAIL OR DELIVER RESPONSES TO: ATT: Robert Smith, Town Manager 614 Main St. Windermere,
Request for Qualifications. North Broward Regional Service Center, Replace Columnade Roof Membrane RFQ-REDM17/ ADDENDUM #1
 Request for Qualifications North Broward Regional Service Center, Replace Columnade Roof Membrane RFQ-REDM17/18-012 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SECTION 120.57(3),
Request for Qualifications North Broward Regional Service Center, Replace Columnade Roof Membrane RFQ-REDM17/18-012 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SECTION 120.57(3),
Lyndon Township Broadband Implementation Committee Lyndon Township, Michigan
 Lyndon Township Broadband Implementation Committee Lyndon Township, Michigan Request for Proposal For Consulting Services For a Fiber-to-the-Home Network In Lyndon Township Proposals may be mailed or delivered
Lyndon Township Broadband Implementation Committee Lyndon Township, Michigan Request for Proposal For Consulting Services For a Fiber-to-the-Home Network In Lyndon Township Proposals may be mailed or delivered
REQUEST FOR PROPOSALS. For: As needed Plan Check and Building Inspection Services
 Date: June 15, 2017 REQUEST FOR PROPOSALS For: As needed Plan Check and Building Inspection Services Submit Responses to: Building and Planning Department 1600 Floribunda Avenue Hillsborough, California
Date: June 15, 2017 REQUEST FOR PROPOSALS For: As needed Plan Check and Building Inspection Services Submit Responses to: Building and Planning Department 1600 Floribunda Avenue Hillsborough, California
LIBRARY COOPERATIVE GRANT AGREEMENT BETWEEN THE STATE OF FLORIDA, DEPARTMENT OF STATE AND [Governing Body] for and on behalf of [grantee]
![LIBRARY COOPERATIVE GRANT AGREEMENT BETWEEN THE STATE OF FLORIDA, DEPARTMENT OF STATE AND [Governing Body] for and on behalf of [grantee]](/thumbs/87/96682002.jpg "LIBRARY COOPERATIVE GRANT AGREEMENT BETWEEN THE STATE OF FLORIDA, DEPARTMENT OF STATE AND [Governing Body] for and on behalf of [grantee]") PROJECT NUMBER _[project number]_ LIBRARY COOPERATIVE GRANT AGREEMENT BETWEEN THE STATE OF FLORIDA, DEPARTMENT OF STATE AND [Governing Body] for and on behalf of [grantee] This Agreement is by and between
PROJECT NUMBER _[project number]_ LIBRARY COOPERATIVE GRANT AGREEMENT BETWEEN THE STATE OF FLORIDA, DEPARTMENT OF STATE AND [Governing Body] for and on behalf of [grantee] This Agreement is by and between
STATE OF FLORIDA DEPARTMENT OF MANAGEMENT SERVICES REAL ESTATE DEVELOPMENT AND MANAGEMENT PUBLIC ANNOUNCEMENT FOR PROFESSIONAL SERVICES
 STATE OF FLORIDA DEPARTMENT OF MANAGEMENT SERVICES REAL ESTATE DEVELOPMENT AND MANAGEMENT PUBLIC ANNOUNCEMENT FOR PROFESSIONAL SERVICES FOR CONTINUING CONTRACTS MECHANICAL/ELECTRICAL/PLUMBING ENGINEERING
STATE OF FLORIDA DEPARTMENT OF MANAGEMENT SERVICES REAL ESTATE DEVELOPMENT AND MANAGEMENT PUBLIC ANNOUNCEMENT FOR PROFESSIONAL SERVICES FOR CONTINUING CONTRACTS MECHANICAL/ELECTRICAL/PLUMBING ENGINEERING
Integration of Substance Abuse, Mental Health And Child Welfare Services Pilot. Grant Solicitation # _LJZ63
 Application Instructions Integration of Substance Abuse, Mental Health And Child Welfare Services Pilot Grant Solicitation # _LJZ63 Offered by the Florida Department of Children and Families Office of
Application Instructions Integration of Substance Abuse, Mental Health And Child Welfare Services Pilot Grant Solicitation # _LJZ63 Offered by the Florida Department of Children and Families Office of
FLORIDA DEPARTMENT OF HEALTH (DOH) DOH16-069
 DOH16-069") FLORIDA DEPARTMENT OF HEALTH (DOH) DOH16-069 REQUEST FOR INFORMATION (RFI) CHILDREN S MEDICAL SERVICES HEALTH PLAN MODEL FOCUSED ON IMPROVING THE HEALTH OF CHILDREN AND YOUTH State of Florida Department
FLORIDA DEPARTMENT OF HEALTH (DOH) DOH16-069 REQUEST FOR INFORMATION (RFI) CHILDREN S MEDICAL SERVICES HEALTH PLAN MODEL FOCUSED ON IMPROVING THE HEALTH OF CHILDREN AND YOUTH State of Florida Department
201 North Forest Avenue Independence, Missouri (816) [September 25, 2017] REQUEST FOR PROPOSAL GRADUATION CAPS AND GOWNS
![201 North Forest Avenue Independence, Missouri (816) [September 25, 2017] REQUEST FOR PROPOSAL GRADUATION CAPS AND GOWNS](/thumbs/78/78017040.jpg "201 North Forest Avenue Independence, Missouri (816) [September 25, 2017] REQUEST FOR PROPOSAL GRADUATION CAPS AND GOWNS") 201 North Forest Avenue Independence, Missouri 64050 (816) 521-5300 [September 25, 2017] REQUEST FOR PROPOSAL GRADUATION CAPS AND GOWNS Sealed proposals will be received by the Independence School District
201 North Forest Avenue Independence, Missouri 64050 (816) 521-5300 [September 25, 2017] REQUEST FOR PROPOSAL GRADUATION CAPS AND GOWNS Sealed proposals will be received by the Independence School District
RFP No North Central Florida Regional Planning Council 2009 NW 67th Place Gainesville, FL
 RFP No. 2017-02 Request for Proposals for Community Transportation Coordinator Designation under Florida s Transportation Disadvantaged Program in Bradford County, Florida North Central Florida Regional
RFP No. 2017-02 Request for Proposals for Community Transportation Coordinator Designation under Florida s Transportation Disadvantaged Program in Bradford County, Florida North Central Florida Regional
Agency for Health Care Administration
 Page 57 of 174 requirements of an administrator pursuant to paragraph (1)(a) of this rule. Managers who attended the core training program prior to July 1, 1997, are not required to take the competency
Page 57 of 174 requirements of an administrator pursuant to paragraph (1)(a) of this rule. Managers who attended the core training program prior to July 1, 1997, are not required to take the competency
REQUEST FOR PROPOSALS. Design-Build of General Aviation Terminal Building. RFP# AIR/17-012, page 1
 REQUEST FOR PROPOSALS Design-Build of General Aviation Terminal Building RFP# AIR/17-012, page 1 RFP# AIR/17-012 REQUEST FOR PROPOSALS ISSUE DATE: November 22, 2017 TITLE: DUE: Design-Build of General
REQUEST FOR PROPOSALS Design-Build of General Aviation Terminal Building RFP# AIR/17-012, page 1 RFP# AIR/17-012 REQUEST FOR PROPOSALS ISSUE DATE: November 22, 2017 TITLE: DUE: Design-Build of General
Social Media Management System
 REQUEST FOR PROPOSAL No. DC177387P Social Media Management System PROPOSAL DUE DATE AND TIME August 25, 2015 (2:00 AM, PT) SUBMITTAL LOCATION Oregon State University Procurement, Contracts and Materials
REQUEST FOR PROPOSAL No. DC177387P Social Media Management System PROPOSAL DUE DATE AND TIME August 25, 2015 (2:00 AM, PT) SUBMITTAL LOCATION Oregon State University Procurement, Contracts and Materials
State of Florida Department of Children and Families
 State of Florida Department of Children and Families Rick Scott Governor Mike Carroll Secretary REQUEST FOR INFORMATION #23FS16006 Behavioral Health Training for the Child Protective Investigation Professional
State of Florida Department of Children and Families Rick Scott Governor Mike Carroll Secretary REQUEST FOR INFORMATION #23FS16006 Behavioral Health Training for the Child Protective Investigation Professional
INVITATION FOR BID Notice to Prospective Bidders IFB # Date Stamp Equipment Preventative Maintenance and Repair Services
 INVITATION FOR BID Notice to Prospective Bidders Date Stamp Equipment Preventative Maintenance and Repair Services June 1, 2011 You are invited to review and respond to this Invitation for Bid (IFB), entitled
INVITATION FOR BID Notice to Prospective Bidders Date Stamp Equipment Preventative Maintenance and Repair Services June 1, 2011 You are invited to review and respond to this Invitation for Bid (IFB), entitled
REQUESTING QUALIFICATIONS FOR PROFESSIONAL DESIGN SERVICES
 STATE OF FLORIDA, DEPARTMENT OF MILITARY AFFAIRS CONSTRUCTION & FACILITY MANAGEMENT OFFICE PUBLIC ANNOUNCEMENT REQUESTING QUALIFICATIONS FOR PROFESSIONAL DESIGN SERVICES For PROJECT NUMBER: 212060 BROOKSVILLE
STATE OF FLORIDA, DEPARTMENT OF MILITARY AFFAIRS CONSTRUCTION & FACILITY MANAGEMENT OFFICE PUBLIC ANNOUNCEMENT REQUESTING QUALIFICATIONS FOR PROFESSIONAL DESIGN SERVICES For PROJECT NUMBER: 212060 BROOKSVILLE
Arizona Department of Education
 State of Arizona Department of Education Request For Grant Application (RFGA) RFGA Number: ED07-0028 RFGA Due Date / Time: Submittal Location: Description of Procurement: February 9, 2007, at 3:00 P.M.
State of Arizona Department of Education Request For Grant Application (RFGA) RFGA Number: ED07-0028 RFGA Due Date / Time: Submittal Location: Description of Procurement: February 9, 2007, at 3:00 P.M.
CITY OF CAMARILLO AND CAMARILLO SANITARY DISTRICT WATER AND SEWER RATE STUDIES REQUEST FOR PROPOSAL
 CITY OF CAMARILLO AND CAMARILLO SANITARY DISTRICT WATER AND SEWER RATE STUDIES REQUEST FOR PROPOSAL 2011 PREPARED BY THE CITY OF CAMARILLO AND CAMARILLO SANITARY DISTRICT FINANCE DEPARTMENT Ronnie J. Campbell
CITY OF CAMARILLO AND CAMARILLO SANITARY DISTRICT WATER AND SEWER RATE STUDIES REQUEST FOR PROPOSAL 2011 PREPARED BY THE CITY OF CAMARILLO AND CAMARILLO SANITARY DISTRICT FINANCE DEPARTMENT Ronnie J. Campbell
Request for Qualifications. Parking Garage 50, Structural Repair - A/E RFQ-REDM17/ ADDENDUM #1
 Request for Qualifications Parking Garage 50, Structural Repair - A/E RFQ-REDM17/18-008 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SECTION 120.57(3), FLORIDA STATUTES, OR FAILURE
Request for Qualifications Parking Garage 50, Structural Repair - A/E RFQ-REDM17/18-008 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SECTION 120.57(3), FLORIDA STATUTES, OR FAILURE
SOLICITATION NO: 15-1 REQUEST FOR PROPOSALS (RFP) FOR ARCHITECTURAL SERVICES FOR NEW ELEMENTARY SCHOOL #3
 FOR ARCHITECTURAL SERVICES FOR NEW ELEMENTARY SCHOOL #3") SOLICITATION NO: 15-1 REQUEST FOR PROPOSALS (RFP) FOR ARCHITECTURAL SERVICES FOR NEW ELEMENTARY SCHOOL #3 BIBB COUNTY SCHOOL DISTRICT 484 Mulberry Street Macon, Georgia 31201 July 18, 2014 TIMELINE RFP
SOLICITATION NO: 15-1 REQUEST FOR PROPOSALS (RFP) FOR ARCHITECTURAL SERVICES FOR NEW ELEMENTARY SCHOOL #3 BIBB COUNTY SCHOOL DISTRICT 484 Mulberry Street Macon, Georgia 31201 July 18, 2014 TIMELINE RFP
State of Florida Department of Transportation District Four, Procurement Office 3400 West Commercial Boulevard Fort Lauderdale, FL 33309
 State of Florida Department of Transportation District Four, Procurement Office ITNSHELL. Revised 07/2017 INVITATION TO NEGOTIATE REGISTRATION ******************************************************************************
State of Florida Department of Transportation District Four, Procurement Office ITNSHELL. Revised 07/2017 INVITATION TO NEGOTIATE REGISTRATION ******************************************************************************
RESPECT of Florida. Proposal for Assignment. For RESPECT Grant for Micro Enterprise/Self Employment. Employment Center Name
 RESPECT of Florida Proposal for Assignment For 2016-18 RESPECT Grant for Micro Enterprise/Self Employment Employment Center Name Employment Center Mailing Address City-State-Zip Telephone Number Email
RESPECT of Florida Proposal for Assignment For 2016-18 RESPECT Grant for Micro Enterprise/Self Employment Employment Center Name Employment Center Mailing Address City-State-Zip Telephone Number Email
Request for Proposals. For RFP # 2011-OOC-KDA-00
 Request for Proposals For Issued by: Pennsylvania State System of Higher Education RFP # 2011-OOC-KDA-00 Issue Date: Month, Day, 2011 Response Date: Month, Day, 2011 Page 1 of 14 Table of Contents Page
Request for Proposals For Issued by: Pennsylvania State System of Higher Education RFP # 2011-OOC-KDA-00 Issue Date: Month, Day, 2011 Response Date: Month, Day, 2011 Page 1 of 14 Table of Contents Page
TENNESSEE CODE ANNOTATED 2008 by The State of Tennessee Title 49 Education Chapter 5 Personnel Part 4 --Employment and Assignment of Personnel
 TENNESSEE CODE ANNOTATED 2008 by The State of Tennessee Title 49 Education Chapter 5 Personnel Part 4 --Employment and Assignment of Personnel Tenn. Code Ann. 49-5-415 (2008) 49-5-415. Assistance in self-administration
TENNESSEE CODE ANNOTATED 2008 by The State of Tennessee Title 49 Education Chapter 5 Personnel Part 4 --Employment and Assignment of Personnel Tenn. Code Ann. 49-5-415 (2008) 49-5-415. Assistance in self-administration
REQUEST FOR PROPOSALS: AUDIT SERVICES. Issue Date: February 13 th, Due Date: March 22 nd, 2017
 REQUEST FOR PROPOSALS: AUDIT SERVICES Issue Date: February 13 th, 2017 Due Date: March 22 nd, 2017 In order to be considered, proposals must be signed and returned via email to rtan@wested.org by noon
REQUEST FOR PROPOSALS: AUDIT SERVICES Issue Date: February 13 th, 2017 Due Date: March 22 nd, 2017 In order to be considered, proposals must be signed and returned via email to rtan@wested.org by noon
TERREBONNE PARISH REQUEST FOR QUALIFICATIONS FOR ENGINEERING SERVICES. Generator Sizing and Installation
 TERREBONNE PARISH REQUEST FOR QUALIFICATIONS FOR ENGINEERING SERVICES Generator Sizing and Installation Proposal Due Date: June 26, 2017 Proposal Due Time: 2:00 P.M. Released May 23, 2017 Table of Contents
TERREBONNE PARISH REQUEST FOR QUALIFICATIONS FOR ENGINEERING SERVICES Generator Sizing and Installation Proposal Due Date: June 26, 2017 Proposal Due Time: 2:00 P.M. Released May 23, 2017 Table of Contents
INVITATION TO NEGOTIATE (ITN) ADDENDUM #1. July 21, 2017
 ADDENDUM #1. July 21, 2017") INVITATION TO NEGOTIATE (ITN) ADDENDUM #1 July 21, 2017 ITN Number: 10511 ITN Services: The Department seeks replies from qualified non-profit, for profit and government entities to serve as the single
INVITATION TO NEGOTIATE (ITN) ADDENDUM #1 July 21, 2017 ITN Number: 10511 ITN Services: The Department seeks replies from qualified non-profit, for profit and government entities to serve as the single
DISTRICT OF COLUMBIA WATER AND SEWER AUTHORITY (DC WATER) REQUEST FOR QUOTE RFQ 18-PR-DIT-27
 REQUEST FOR QUOTE RFQ 18-PR-DIT-27") DISTRICT OF COLUMBIA WATER AND SEWER AUTHORITY (DC WATER) REQUEST FOR QUOTE RFQ 18-PR-DIT-27 RFQ Number: RFQ 18-PR-DIT-27 Date Issued: Monday, March 5, 2018 Description: Headquarters (HQO) IT Hardware
DISTRICT OF COLUMBIA WATER AND SEWER AUTHORITY (DC WATER) REQUEST FOR QUOTE RFQ 18-PR-DIT-27 RFQ Number: RFQ 18-PR-DIT-27 Date Issued: Monday, March 5, 2018 Description: Headquarters (HQO) IT Hardware
Dakota County Technical College. Pod 6 AHU Replacement
 MINNESOTA STATE COLLEGES AND UNIVERSITIES Dakota County Technical College Pod 6 AHU Replacement REQUEST FOR PROPOSAL (RFP) FOR MECHANICAL ENGINEERING SERVICES JULY 16, 2018 SPECIAL NOTE: This Request for
MINNESOTA STATE COLLEGES AND UNIVERSITIES Dakota County Technical College Pod 6 AHU Replacement REQUEST FOR PROPOSAL (RFP) FOR MECHANICAL ENGINEERING SERVICES JULY 16, 2018 SPECIAL NOTE: This Request for
Request for Proposal Crisis Intervention Services
 Request for Proposal Crisis Intervention Services Issued by: Columbia County Health and Human Services Proposals must be submitted no later than 4:30pm CST Thursday, April 28, 2011 For further information
Request for Proposal Crisis Intervention Services Issued by: Columbia County Health and Human Services Proposals must be submitted no later than 4:30pm CST Thursday, April 28, 2011 For further information
LEXINGTON-FAYETTE URBAN COUNTY AIRPORT BOARD REQUEST FOR PROPOSALS. to provide INVESTMENT MANAGEMENT SERVICES. for BLUE GRASS AIRPORT
 LEXINGTON-FAYETTE URBAN COUNTY AIRPORT BOARD REQUEST FOR PROPOSALS to provide INVESTMENT MANAGEMENT SERVICES for BLUE GRASS AIRPORT DATED: March 5, 2017 TABLE OF CONTENTS 1. NOTICE AND REQUEST FOR PROPOSALS...
LEXINGTON-FAYETTE URBAN COUNTY AIRPORT BOARD REQUEST FOR PROPOSALS to provide INVESTMENT MANAGEMENT SERVICES for BLUE GRASS AIRPORT DATED: March 5, 2017 TABLE OF CONTENTS 1. NOTICE AND REQUEST FOR PROPOSALS...
WESTMINSTER SCHOOL DISTRICT NUTRITION SERVICES REQUEST FOR PROPOSAL FRESH PRODUCE 17/ For: July 1, 2018 to June 30, 2019
 WESTMINSTER SCHOOL DISTRICT NUTRITION SERVICES REQUEST FOR PROPOSAL FRESH PRODUCE 17/18-05 For: July 1, 2018 to June 30, 2019 DUE DATE OF PROPOSAL: MONDAY, APRIL 23, 2018-8:00 AM DROPPING OFF PROPOSAL:
WESTMINSTER SCHOOL DISTRICT NUTRITION SERVICES REQUEST FOR PROPOSAL FRESH PRODUCE 17/18-05 For: July 1, 2018 to June 30, 2019 DUE DATE OF PROPOSAL: MONDAY, APRIL 23, 2018-8:00 AM DROPPING OFF PROPOSAL:
RFP # Request for Proposal Grant Writing Services. Date: May 11, Proposals must be submitted by 3:00 PM: June 10, 2016
 RFP #0516-3 Request for Proposal Grant Writing Services Date: May 11, 2016 Proposals must be submitted by 3:00 PM: June 10, 2016 Purchasing Department Queens Borough Public Library 89-11 Merrick Boulevard
RFP #0516-3 Request for Proposal Grant Writing Services Date: May 11, 2016 Proposals must be submitted by 3:00 PM: June 10, 2016 Purchasing Department Queens Borough Public Library 89-11 Merrick Boulevard
B Request for Proposal for. Qualified Firms. Financial Advisory Services. Grossmont-Cuyamaca Community College District
 B17.045 Request for Proposal for Qualified Firms For Financial Advisory Services For the Grossmont-Cuyamaca Community College District Proposal Due Date August 18, 2017 4pm Return Proposals to: Grossmont-Cuyamaca
B17.045 Request for Proposal for Qualified Firms For Financial Advisory Services For the Grossmont-Cuyamaca Community College District Proposal Due Date August 18, 2017 4pm Return Proposals to: Grossmont-Cuyamaca
Request for Qualifications. Continuing Contracts Mechanical/Electrical/Plumbing Engineering Services, Central Florida Region RFQ-REDM17/18-001
 Request for Qualifications Continuing Contracts Mechanical/Electrical/Plumbing Engineering Services, Central Florida Region RFQ-REDM17/18-001 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED
Request for Qualifications Continuing Contracts Mechanical/Electrical/Plumbing Engineering Services, Central Florida Region RFQ-REDM17/18-001 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED
Request for Qualifications. Gadsden Correctional Facility Renovations, Quincy, Florida, Architecture-Engineering RFQ-REDM17/ ADDENDUM #1
 Request for Qualifications Gadsden Correctional Facility Renovations, Quincy, Florida, Architecture-Engineering RFQ-REDM17/18-011 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SECTION
Request for Qualifications Gadsden Correctional Facility Renovations, Quincy, Florida, Architecture-Engineering RFQ-REDM17/18-011 ADDENDUM #1 FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SECTION
Exhibit 1 Florida Minority Business Enterprise (MBE) Utilization Report 2
 Utilization Report 2") April 11, 2018 Subject: DJJ Solicitation Number RFP 10579 Request for Proposals (RFP): The Department of Juvenile Justice (Department or DJJ) is seeking a Respondent to conduct on-site monitoring visits
April 11, 2018 Subject: DJJ Solicitation Number RFP 10579 Request for Proposals (RFP): The Department of Juvenile Justice (Department or DJJ) is seeking a Respondent to conduct on-site monitoring visits
INVITATION TO NEOGOTIATE ISSUED DATE ITN #
 INVITATION TO NEOGOTIATE ISSUED DATE ITN # 14-0001 I. Introduction The Florida Alliance for Assistive Services and Technology, Inc. hereafter referred to as FAAST, is requesting sealed proposals from qualified
INVITATION TO NEOGOTIATE ISSUED DATE ITN # 14-0001 I. Introduction The Florida Alliance for Assistive Services and Technology, Inc. hereafter referred to as FAAST, is requesting sealed proposals from qualified
SOLICITATION FOR PARTICIPATION IN A REQUEST FOR PROPOSALS FOR CHIEF EXECUTIVE OFFICER (CEO) SEARCH SERVICES JACKSONVILLE, FL SOLICITATION NUMBER 94414
 SEARCH SERVICES JACKSONVILLE, FL SOLICITATION NUMBER 94414") SOLICITATION FOR PARTICIPATION IN A REQUEST FOR PROPOSALS FOR CHIEF EXECUTIVE OFFICER (CEO) SEARCH SERVICES JACKSONVILLE, FL SOLICITATION NUMBER 94414 PROPOSALS ARE DUE ON APRIL 27, 2018 BY 12:00 PM EST
SOLICITATION FOR PARTICIPATION IN A REQUEST FOR PROPOSALS FOR CHIEF EXECUTIVE OFFICER (CEO) SEARCH SERVICES JACKSONVILLE, FL SOLICITATION NUMBER 94414 PROPOSALS ARE DUE ON APRIL 27, 2018 BY 12:00 PM EST
REQUEST FOR PROPOSAL For East Bay Community Energy Technical Energy Evaluation Services
 REQUEST FOR PROPOSAL For East Bay Community Energy Technical Energy Evaluation Services RESPONSE DUE by 5:00 p.m. on April 24, 2018 For complete information regarding this project, see RFP posted at ebce.org
REQUEST FOR PROPOSAL For East Bay Community Energy Technical Energy Evaluation Services RESPONSE DUE by 5:00 p.m. on April 24, 2018 For complete information regarding this project, see RFP posted at ebce.org
REQUEST FOR PROPOSALS SELECTION OF EXECUTIVE SEARCH FIRM
 REQUEST FOR PROPOSALS SELECTION OF EXECUTIVE SEARCH FIRM Submitted By: Florida Memorial University Board of Trustees 15800 N.W. 42 nd Avenue Miami Gardens, FL 33054 Date: November 14, 2017 FLORIDA MEMORIAL
REQUEST FOR PROPOSALS SELECTION OF EXECUTIVE SEARCH FIRM Submitted By: Florida Memorial University Board of Trustees 15800 N.W. 42 nd Avenue Miami Gardens, FL 33054 Date: November 14, 2017 FLORIDA MEMORIAL
Florida International University Project Fact Sheet Construction Manager Continuing Services Contact
 PROJECT LOCATION: Modesto A. Maidique Campus (MMC), Biscayne Bay Campus (BBC), Engineering Center (EC) and other properties in South Florida managed by FIU. PROJECT DESCRIPTION: The Construction Manager
PROJECT LOCATION: Modesto A. Maidique Campus (MMC), Biscayne Bay Campus (BBC), Engineering Center (EC) and other properties in South Florida managed by FIU. PROJECT DESCRIPTION: The Construction Manager
Town of Derry, NH REQUEST FOR PROPOSALS PROFESSIONAL MUNICIPAL AUDITING SERVICES
 Town of Derry, NH Office of the Finance Department Susan A. Hickey Chief Financial Officer susanhickey@derrynh.org REQUEST FOR PROPOSALS PROFESSIONAL MUNICIPAL AUDITING SERVICES The Town of Derry, New
Town of Derry, NH Office of the Finance Department Susan A. Hickey Chief Financial Officer susanhickey@derrynh.org REQUEST FOR PROPOSALS PROFESSIONAL MUNICIPAL AUDITING SERVICES The Town of Derry, New
State of Florida Department of Transportation District Four, Procurement Office 3400 West Commercial Boulevard Fort Lauderdale, FL 33309
 State of Florida Department of Transportation District Four, Procurement Office 3400 West Commercial Boulevard Fort Lauderdale, FL 33309 REQUEST FOR PROPOSAL REGISTRATION ******************************************************************************
State of Florida Department of Transportation District Four, Procurement Office 3400 West Commercial Boulevard Fort Lauderdale, FL 33309 REQUEST FOR PROPOSAL REGISTRATION ******************************************************************************
REQUEST FOR PROPOSAL AUDITING SERVICES. Chicago Infrastructure Trust
 REQUEST FOR PROPOSAL AUDITING SERVICES Chicago Infrastructure Trust 10 August 2016 Table of Contents Background Information... 3 Objective and Scope of Services... 3 RFP Process and Submission Requirements...
REQUEST FOR PROPOSAL AUDITING SERVICES Chicago Infrastructure Trust 10 August 2016 Table of Contents Background Information... 3 Objective and Scope of Services... 3 RFP Process and Submission Requirements...
Students Controlled drugs means those drugs as defined in Conn. Gen. Stat. Section 21a-240.
 Students 5143 ADMINISTRATION OF STUDENT MEDICATIONS IN THE SCHOOLS A. Definitions Administration of medication means any one of the following activities: handling, storing, preparing or pouring of medication;
Students 5143 ADMINISTRATION OF STUDENT MEDICATIONS IN THE SCHOOLS A. Definitions Administration of medication means any one of the following activities: handling, storing, preparing or pouring of medication;
Agency for Health Care Administration
 Page 1 of 24 ST - Q0000 - Initial Comments Title Initial Comments Statute or Rule Type Memo Tag These guidelines are meant solely to provide guidance to surveyors in the survey process. ST - Q0100 - License
Page 1 of 24 ST - Q0000 - Initial Comments Title Initial Comments Statute or Rule Type Memo Tag These guidelines are meant solely to provide guidance to surveyors in the survey process. ST - Q0100 - License
TOWN AUDITING SERVICES
 REQUEST FOR PROPOSAL TOWN AUDITING SERVICES TOWN OF LONGMEADOW MASSACHUSETTS Saved as: RPF Acct Auditing Services FY 12-14 03/1/11 TOWN OF LONGMEADOW REQUEST FOR PROPOSALS FOR AUDITING SERVICES The Town
REQUEST FOR PROPOSAL TOWN AUDITING SERVICES TOWN OF LONGMEADOW MASSACHUSETTS Saved as: RPF Acct Auditing Services FY 12-14 03/1/11 TOWN OF LONGMEADOW REQUEST FOR PROPOSALS FOR AUDITING SERVICES The Town
REQUEST FOR PROPOSAL (RFP) # CONSULTANT SERVICES FOR DEVELOPMENT OF A DISTRICT SUSTAINABILITY PLAN
 # CONSULTANT SERVICES FOR DEVELOPMENT OF A DISTRICT SUSTAINABILITY PLAN") REQUEST FOR PROPOSAL (RFP) #1314-15 CONSULTANT SERVICES FOR DEVELOPMENT OF A DISTRICT SUSTAINABILITY PLAN Request for Proposal must be received no later than January 3, 2014 at 2:00 pm CARRI MATSUMOTO
REQUEST FOR PROPOSAL (RFP) #1314-15 CONSULTANT SERVICES FOR DEVELOPMENT OF A DISTRICT SUSTAINABILITY PLAN Request for Proposal must be received no later than January 3, 2014 at 2:00 pm CARRI MATSUMOTO
City of Malibu Request for Proposal
 Request for Proposal North Santa Monica Bay Coastal Watersheds Monitoring Services Date Issued: April 26, 2016 Date Due: May 17, 2016, 4:00 P.M. The Qualifications Proposal and Cost Proposal must be submitted
Request for Proposal North Santa Monica Bay Coastal Watersheds Monitoring Services Date Issued: April 26, 2016 Date Due: May 17, 2016, 4:00 P.M. The Qualifications Proposal and Cost Proposal must be submitted
Knights Ferry Elementary School District
 Knights Ferry Elementary School District REQUEST FOR PROPOSAL FOR THE IMPLEMENTATION OF ENERGY EFFICIENCY MEASURES FUNDED BY THE CLEAN ENERGY JOBS ACT - PROPOSITION 39 REQUEST FOR PROPOSAL SUBMITTAL DEADLINE
Knights Ferry Elementary School District REQUEST FOR PROPOSAL FOR THE IMPLEMENTATION OF ENERGY EFFICIENCY MEASURES FUNDED BY THE CLEAN ENERGY JOBS ACT - PROPOSITION 39 REQUEST FOR PROPOSAL SUBMITTAL DEADLINE
SCHOOL BOARD ACTION REPORT
 SCHOOL BOARD ACTION REPORT DATE: October 25, 2017 FROM: Executive Committee of the School Board For Introduction: November 15, 2017 For Action: November 15, 2017 1. TITLE Approval of a contract for an
SCHOOL BOARD ACTION REPORT DATE: October 25, 2017 FROM: Executive Committee of the School Board For Introduction: November 15, 2017 For Action: November 15, 2017 1. TITLE Approval of a contract for an
BOARD OF FINANCE REQUEST FOR PROPOSALS FOR PROFESSIONAL AUDITING SERVICES
 TOWN OF KILLINGWORTH BOARD OF FINANCE REQUEST FOR PROPOSALS FOR PROFESSIONAL AUDITING SERVICES DATE: February 14, 2018 1 I. INTRODUCTION A. General Information The Town of Killingworth is requesting proposals
TOWN OF KILLINGWORTH BOARD OF FINANCE REQUEST FOR PROPOSALS FOR PROFESSIONAL AUDITING SERVICES DATE: February 14, 2018 1 I. INTRODUCTION A. General Information The Town of Killingworth is requesting proposals
Grant Seeking Grant Writing And Lobbying Services
 REQUEST FOR PROPOSALS Grant Seeking Grant Writing And Lobbying Services FOR CITY OF SANGER, CALIFORNIA January 7, 2011 CITY OF SANGER TABLE OF CONTENTS This solicitation package includes the sections and
REQUEST FOR PROPOSALS Grant Seeking Grant Writing And Lobbying Services FOR CITY OF SANGER, CALIFORNIA January 7, 2011 CITY OF SANGER TABLE OF CONTENTS This solicitation package includes the sections and
SCHOOL BOARD OF BREVARD COUNTY OFFICE OF PURCHASING SERVICES 2700 JUDGE FRAN JAMIESON WAY VIERA, FL
 SCHOOL BOARD OF BREVARD COUNTY OFFICE OF PURCHASING SERVICES 2700 JUDGE FRAN JAMIESON WAY VIERA, FL 32940-6601 NON-COMPETITIVE SALES AND SERVICES AGREEMENT SSA #1213/JO Brevard County Health Department
SCHOOL BOARD OF BREVARD COUNTY OFFICE OF PURCHASING SERVICES 2700 JUDGE FRAN JAMIESON WAY VIERA, FL 32940-6601 NON-COMPETITIVE SALES AND SERVICES AGREEMENT SSA #1213/JO Brevard County Health Department
ISABELLA COUNTY REQUEST FOR PROPOSALS COMMISSION ON AGING CATV AND HEADEND EQUIPMENT
 ISABELLA COUNTY REQUEST FOR PROPOSALS COMMISSION ON AGING CATV AND HEADEND EQUIPMENT ISSUED BY ISABELLA COUNTY BOARD OF COMMISSIONERS ISSUE DATE: February 4, 2008 ISABELLA COUNTY REQUEST FOR PROPOSALS
ISABELLA COUNTY REQUEST FOR PROPOSALS COMMISSION ON AGING CATV AND HEADEND EQUIPMENT ISSUED BY ISABELLA COUNTY BOARD OF COMMISSIONERS ISSUE DATE: February 4, 2008 ISABELLA COUNTY REQUEST FOR PROPOSALS
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Office of Economic Self-Sufficiency
 STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Office of Economic Self-Sufficiency REQUEST FOR PROPOSAL Implementing Agency for SNAP-Ed, Nutrition Education RFP#: RFP10F16GS2 Release Date: NOVEMBER
STATE OF FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Office of Economic Self-Sufficiency REQUEST FOR PROPOSAL Implementing Agency for SNAP-Ed, Nutrition Education RFP#: RFP10F16GS2 Release Date: NOVEMBER
REQUEST FOR QUALIFICATIONS. Design Professional Services
 REQUEST FOR QUALIFICATIONS Design Professional Services Return Completed Qualifications To: Bonneville Joint School District No. 93 3497 North Ammon Road Idaho Falls, Idaho 83401 TO BE CONSIDERED, QUALIFICATIONS
REQUEST FOR QUALIFICATIONS Design Professional Services Return Completed Qualifications To: Bonneville Joint School District No. 93 3497 North Ammon Road Idaho Falls, Idaho 83401 TO BE CONSIDERED, QUALIFICATIONS
REQUEST FOR APPLICATION
 Florida Defense Infrastructure Grant Program REQUEST FOR APPLICATION Solicitation Acknowledgement Form Page 1 of 32 pages AGENCY RELEASE DATE: MAY 12, 2016 SOLICITATION TITLE: SUBMIT RESPONSE TO: Department
Florida Defense Infrastructure Grant Program REQUEST FOR APPLICATION Solicitation Acknowledgement Form Page 1 of 32 pages AGENCY RELEASE DATE: MAY 12, 2016 SOLICITATION TITLE: SUBMIT RESPONSE TO: Department
Consultant for Research and Design Services for Equipment and Systems for Unmanned Aerial Vehicle Drone (UAV) for OSU-Cascades
 for OSU-Cascades") INFORMAL REQUEST FOR PROPOSAL No. SF188885P Consultant for Research and Design Services for Equipment and Systems for Unmanned Aerial Vehicle Drone (UAV) for OSU-Cascades PROPOSAL DUE DATE AND TIME June
INFORMAL REQUEST FOR PROPOSAL No. SF188885P Consultant for Research and Design Services for Equipment and Systems for Unmanned Aerial Vehicle Drone (UAV) for OSU-Cascades PROPOSAL DUE DATE AND TIME June
Request for Qualifications CULTURAL COMPETENCY TRAINING
 Request for Qualifications CULTURAL COMPETENCY TRAINING RFQ #13-009 Deadline for Responses: 2 PM August 7, 2013 2300 High Ridge Road Boynton Beach, FL 33426 (561) 740-7000 www.cscpbc.org Table of Contents
Request for Qualifications CULTURAL COMPETENCY TRAINING RFQ #13-009 Deadline for Responses: 2 PM August 7, 2013 2300 High Ridge Road Boynton Beach, FL 33426 (561) 740-7000 www.cscpbc.org Table of Contents
Carey Park Playground Equipment. Submission Deadline July 13, :00 a.m. (CST)
") RFQ: 15-141 CITY OF HUTCHINSON, KANSAS REQUEST FOR QUALIFICATIONS City of Hutchinson Project Manager: Justin Combs, Director of Parks and Facilities 1500 S Plum Hutchinson, KS 67504 620-694-1912 Justin.combs@hutchgov.com
RFQ: 15-141 CITY OF HUTCHINSON, KANSAS REQUEST FOR QUALIFICATIONS City of Hutchinson Project Manager: Justin Combs, Director of Parks and Facilities 1500 S Plum Hutchinson, KS 67504 620-694-1912 Justin.combs@hutchgov.com
STANDARD PROCEDURE Number: S410.10
 Page: 1 of 8 PURPOSE: To establish procedures for the competitive procurement of goods and services utilizing an Invitation to Bid (ITB) or Invitation to Quote (ITQ) solicitation process or small purchase
Page: 1 of 8 PURPOSE: To establish procedures for the competitive procurement of goods and services utilizing an Invitation to Bid (ITB) or Invitation to Quote (ITQ) solicitation process or small purchase
FLORIDA DEPARTMENT OF LAW ENFORCEMENT
 FLORIDA DEPARTMENT OF LAW ENFORCEMENT REQUEST FOR INFORMATION (RFI) 1729 FOR Grant Management System Replacement April 4, 2017 Page 1 of 10 I. INTRODUCTION The Florida Department of Law Enforcement (FDLE),
FLORIDA DEPARTMENT OF LAW ENFORCEMENT REQUEST FOR INFORMATION (RFI) 1729 FOR Grant Management System Replacement April 4, 2017 Page 1 of 10 I. INTRODUCTION The Florida Department of Law Enforcement (FDLE),
Georgia Lottery Corporation ("GLC") PROPOSAL. PROPOSAL SIGNATURE AND CERTIFICATION (Authorized representative must sign and return with proposal)
 PROPOSAL. PROPOSAL SIGNATURE AND CERTIFICATION (Authorized representative must sign and return with proposal)") NOTE: PLEASE ENSURE THAT ALL REQUIRED SIGNATURE BLOCKS ARE COMPLETED. FAILURE TO SIGN THIS FORM AND INCLUDE IT WITH YOUR PROPOSAL WILL CAUSE REJECTION OF YOUR PROPOSAL. Georgia Lottery Corporation ("GLC")
NOTE: PLEASE ENSURE THAT ALL REQUIRED SIGNATURE BLOCKS ARE COMPLETED. FAILURE TO SIGN THIS FORM AND INCLUDE IT WITH YOUR PROPOSAL WILL CAUSE REJECTION OF YOUR PROPOSAL. Georgia Lottery Corporation ("GLC")
REQUEST FOR PROPOSAL (RFP) Concession Operations for Concession Stand at JOHNSTON HIGH SCHOOL ATHLETIC COMPLEX
 Concession Operations for Concession Stand at JOHNSTON HIGH SCHOOL ATHLETIC COMPLEX") REQUEST FOR PROPOSAL (RFP) Concession Operations for Concession Stand at JOHNSTON HIGH SCHOOL ATHLETIC COMPLEX The objective of this Request for Proposal is to award a Concession Agreement at Johnston
REQUEST FOR PROPOSAL (RFP) Concession Operations for Concession Stand at JOHNSTON HIGH SCHOOL ATHLETIC COMPLEX The objective of this Request for Proposal is to award a Concession Agreement at Johnston
PRACTICE PARTICIPANT AGREEMENT
 PRACTICE PARTICIPANT AGREEMENT this is an Agreement entered into on, 20, by and between Olathe LAD Clinic, LLC (Diana Smith RN, LPC, ARNP) a Kansas professional company, located at 1948 E Santa Fe, Suite
PRACTICE PARTICIPANT AGREEMENT this is an Agreement entered into on, 20, by and between Olathe LAD Clinic, LLC (Diana Smith RN, LPC, ARNP) a Kansas professional company, located at 1948 E Santa Fe, Suite
REQUEST FOR QUALIFICATIONS
 FACILITIES MANAGEMENT 4202 EAST FOWLER AVENUE / OPM 100 TAMPA, FL 33620-7550 EDITION: NOVEMBER 1, 2016 PHONE: (813) 974-2845 FAX: (813) 974-3542 REQUEST FOR QUALIFICATIONS PROJECT NAME: USF CPT REPLACE
FACILITIES MANAGEMENT 4202 EAST FOWLER AVENUE / OPM 100 TAMPA, FL 33620-7550 EDITION: NOVEMBER 1, 2016 PHONE: (813) 974-2845 FAX: (813) 974-3542 REQUEST FOR QUALIFICATIONS PROJECT NAME: USF CPT REPLACE
Request for Qualifications. Professional Design and Construction Services as a Design-Builder. For. Delhi Township Fire Station
 Request for Qualifications Professional Design and Construction Services as a Design-Builder For Submittal Due Date: August 4, 2015 Notice is hereby given that Delhi Township is seeking Statements of Qualification
Request for Qualifications Professional Design and Construction Services as a Design-Builder For Submittal Due Date: August 4, 2015 Notice is hereby given that Delhi Township is seeking Statements of Qualification
RFI /17. State of Florida Agency for Persons with Disabilities Request for Information
 RFI 001-16/17 State of Florida Agency for Persons with Disabilities Request for Information Intermediate Care Facilities for Individuals with Intellectual Disabilities Utilization & Continued Stay Review
RFI 001-16/17 State of Florida Agency for Persons with Disabilities Request for Information Intermediate Care Facilities for Individuals with Intellectual Disabilities Utilization & Continued Stay Review
REMINDER RFQ#: Administering Screens and Assessments: ASQ3 and ASQ-SE Training DEADLINE FOR SUBMISSION IS. July 24, PM
 1 P age REMINDER RFQ#: 12-005 Administering Screens and Assessments: ASQ3 and ASQ-SE Training DEADLINE FOR SUBMISSION IS July 24, 2012 2 PM REPLIES ARRIVING AFTER 2 PM ON JULY 24, 2012 WILL NOT BE ACCEPTED
1 P age REMINDER RFQ#: 12-005 Administering Screens and Assessments: ASQ3 and ASQ-SE Training DEADLINE FOR SUBMISSION IS July 24, 2012 2 PM REPLIES ARRIVING AFTER 2 PM ON JULY 24, 2012 WILL NOT BE ACCEPTED
Auditory Oral Early Education Program APPLICATION GUIDELINES FY
 Auditory Oral Early Education Program APPLICATION GUIDELINES FY 2017 2018 Florida Department of Health Division of Community Health Promotion Bureau of Chronic Disease Prevention May 8, 2017 RFA16 005
Auditory Oral Early Education Program APPLICATION GUIDELINES FY 2017 2018 Florida Department of Health Division of Community Health Promotion Bureau of Chronic Disease Prevention May 8, 2017 RFA16 005
Last updated on April 23, 2017 by Chris Krummey - Managing Attorney-Transactions
 Physician Assistant Supervision Agreement Instructions Sheet Outlined in this document the instructions for completing the Physician Assistant Supervision Agreement and forming a supervision agreement
Physician Assistant Supervision Agreement Instructions Sheet Outlined in this document the instructions for completing the Physician Assistant Supervision Agreement and forming a supervision agreement
Life Sciences Tax Incentive Program
 Life Sciences Tax Incentive Program Solicitation No. 2017 TAX-01 Program Manager: Cheryl Sadeli, Vice President of Finance Questions: Taxprogram@masslifesciences.com Solicitation Issued: December 4, 2017
Life Sciences Tax Incentive Program Solicitation No. 2017 TAX-01 Program Manager: Cheryl Sadeli, Vice President of Finance Questions: Taxprogram@masslifesciences.com Solicitation Issued: December 4, 2017
REQUEST FOR INFORMATION (RFI) DEP Posting Number:
 DEP Posting Number:") Request for Information Electronic Audio-Visual Beach Hazzard Warning System RFI No.: 2018003 REQUEST FOR INFORMATION (RFI) Electronic Audio-Visual Beach Hazard Warning System DEP Posting Number: 2018003
Request for Information Electronic Audio-Visual Beach Hazzard Warning System RFI No.: 2018003 REQUEST FOR INFORMATION (RFI) Electronic Audio-Visual Beach Hazard Warning System DEP Posting Number: 2018003
December 1, CTNext 865 Brook St., Rocky Hill, CT tel: web: ctnext.com
 December 1, 2016 CTNext, LLC is seeking proposals from qualified independent higher education institutions, policy institutes, or research organizations to conduct certain analyses of innovation and entrepreneurship
December 1, 2016 CTNext, LLC is seeking proposals from qualified independent higher education institutions, policy institutes, or research organizations to conduct certain analyses of innovation and entrepreneurship
REQUEST FOR PROPOSALS Thomas MacLaren State Charter School Classroom Furniture for K-5 School March 2, 2018
 REQUEST FOR PROPOSALS Thomas MacLaren State Charter School Classroom Furniture for K-5 School March 2, 2018 TO BE CONSIDERED, PROPOSALS MUST BE RECEIVED AT 1702 N MURRAY BLVD, COLORADO SPRINGS, CO 80915
REQUEST FOR PROPOSALS Thomas MacLaren State Charter School Classroom Furniture for K-5 School March 2, 2018 TO BE CONSIDERED, PROPOSALS MUST BE RECEIVED AT 1702 N MURRAY BLVD, COLORADO SPRINGS, CO 80915
Health-Related Website and Social Media Platform Services
 INFORMAL REQUEST FOR PROPOSAL No. DC188886IRFP Health-Related Website and Social Media Platform Services PROPOSAL DUE DATE AND TIME July 24, 2017 (2:00 PM, PT) SUBMITTAL LOCATION Oregon State University
INFORMAL REQUEST FOR PROPOSAL No. DC188886IRFP Health-Related Website and Social Media Platform Services PROPOSAL DUE DATE AND TIME July 24, 2017 (2:00 PM, PT) SUBMITTAL LOCATION Oregon State University
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH REQUEST FOR PROPOSALS (RFP) FOR Janitorial Services CMS
 FOR Janitorial Services CMS") TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 17-017 8-2017 REQUEST FOR PROPOSALS (RFP) FOR Janitorial Services CMS Respondent Name: Respondent Mailing Address: City, State, Zip: Telephone: Fax Number: E-Mail
TITLE PAGE FLORIDA DEPARTMENT OF HEALTH DOH 17-017 8-2017 REQUEST FOR PROPOSALS (RFP) FOR Janitorial Services CMS Respondent Name: Respondent Mailing Address: City, State, Zip: Telephone: Fax Number: E-Mail
SEALED PROPOSAL REQUEST FOR PROPOSAL. Professional Archaelogical Services
 Department of Forests, Parks & Recreation 1 National Life Drive, Davis 2 Montpelier, VT 05620-3801 www.vtfpr.org Agency of Natural Resources SEALED PROPOSAL REQUEST FOR PROPOSAL Professional Archaelogical
Department of Forests, Parks & Recreation 1 National Life Drive, Davis 2 Montpelier, VT 05620-3801 www.vtfpr.org Agency of Natural Resources SEALED PROPOSAL REQUEST FOR PROPOSAL Professional Archaelogical
STUDENTS Any school employee authorized in writing by the school administrator or school principal:
 Fremont School District No. 215 STUDENTS 3510 Student Medicines Assistance in Self Administration of Medicines to Students Any school employee authorized in writing by the school administrator or school
Fremont School District No. 215 STUDENTS 3510 Student Medicines Assistance in Self Administration of Medicines to Students Any school employee authorized in writing by the school administrator or school
WEB-BASED TRAINING RFI NO.: DMS 09/10-022
 Request for Information for Web-Based Training REQUEST FOR INFORMATION WEB-BASED TRAINING RFI NO.: DMS 09/10-022 The Department of Management Services (hereinafter DMS ) of the State of Florida (hereinafter
Request for Information for Web-Based Training REQUEST FOR INFORMATION WEB-BASED TRAINING RFI NO.: DMS 09/10-022 The Department of Management Services (hereinafter DMS ) of the State of Florida (hereinafter
RFP # November 24, To: Prospective Respondents. Subject: DJJ Solicitation Number RFP #10336
 November 24, 2015 To: Prospective Respondents Subject: DJJ Solicitation Number RFP #10336 Request for Proposals (RFP): The Department of Juvenile Justice (DJJ) is seeking proposals for a Respondent to
November 24, 2015 To: Prospective Respondents Subject: DJJ Solicitation Number RFP #10336 Request for Proposals (RFP): The Department of Juvenile Justice (DJJ) is seeking proposals for a Respondent to
REQUEST FOR PROPOSALS: PROFESSIONAL AUDITING SERVICES
 REQUEST FOR PROPOSALS: PROFESSIONAL AUDITING SERVICES Youth Co-Op, Inc. is a not-for-profit agency with a mission to promote the social wellbeing of South Florida residents through education, employment,
REQUEST FOR PROPOSALS: PROFESSIONAL AUDITING SERVICES Youth Co-Op, Inc. is a not-for-profit agency with a mission to promote the social wellbeing of South Florida residents through education, employment,