SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST. Clinical Governance Performance Report: Outcomes Nov 2010
|
|
|
- Jody Booker
- 6 years ago
- Views:
Transcription
1 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Clinical Governance Performance Report: Outcomes Nov 2010 Report to: Trust Board 23 rd November Report from: Sponsoring Executive: Aim of Report: Jane Druce, Quality Contract Manager David Weeden, Associate Director Patient Safety Martin Stephens, Associate Medical Director, Clinical Effectiveness Derek Waller, Deputy Medical Director Michael Marsh, Medical Director 1) To brief Trust Board on performance against patient improvement targets (PIF) relating to outcome measures. 2) To highlight areas of progress and challenge, and identify the work streams in place to address these. Review History to Date: This report on Patient Outcomes covers the quarter 2 period July-Sept Presented at Quality Governance Steering Group (QGSG) 20 th October 2010 Presented at Trust Executive Committee (TEC) 3 rd November Strategic Objectives Ref: SO1- Trusted on Quality Recommendations: Trust Board is asked to: 1. To support the QGSG proposal as agreed at TEC; of a rota of clinicians to validate and upload TARN data in a timely manner due to its impact on the new trauma centre developments. 2. QGSG recommendations to be taken forward by the Associate Medical Director (Patient Safety). 3. To develop the CQuins report section to include specialist services contracts requirements when agreed (released October 2010). 4. Identify any areas where further assurance is required. 5. To note the key issues below discussed at QGSG and TEC Summary Patient Outcome (PIF) Priorities Priority Work Stream Target set Q1 Target Achievement Q2 Target Achievement Section Reference Hospital Standardised Mortality Rate (HSMR) Patient reported Outcome Measures (PROMS) (first questionnaire) (Commissioning for Quality and Innovation (CQUINs) Clinical Effectiveness Trauma Audit and Research Network (TARN) 90 (reporting Q4) % Not released 100% Green:7/ 14 (Reporting Q1) Broadly on track, national average performance Green: 7/9 (AQx5 elements under review). New report. Above national average performance. Section A Page 3-7 Section B Page 8-9 Section C Page Section D Page
2 1. Context and key changes 1.1. This governance report for quarter 2 supports the priorities identified for the 2010/11 PIF Outcomes theme (Appendix A), our 2010/11 Quality Account priorities and our contracted quality requirements including CQuins The Department of Health (DH) Transparency in Outcomes proposals for NHS reporting were published following the NHS White paper, for consultation in July The final version will be due for implementation in April 201. This governance report makes links from our existing priorities to those proposed in the new framework in readiness for next years requirements. The DH proposed framework is structured around five high level outcome domains being: Effectiveness preventing people from dying prematurely enhancing the quality of life for people with long-term conditions helping people to recover from episodes of ill health or following injury Patient experience ensuring people have a positive experience of care Safety treating and caring for people in a safe environment and protecting them from avoidable harm 1.3. The detail to support this framework will be discussed further following the consultation result publication. The outcome themes already reflect our current quality governance reports for experience outcomes and safety currently in place at SUHT. In preparing for the new Outcomes reporting proposed above, this governance quality performance report includes: Section A - Preventing people from dying prematurely (DH Outcome 1) Mortality reports via Dr Foster HSMR dataset have been established as part of the core Trust Board reporting system since summer Section B - Enhancing the quality of life for people with long-term conditions (DH Outcome 2) The national report for PROMS was published on 16th September 2010 for the period April 2009 to April The Trust had 1112 episodes eligible for inclusion and 646 pre-operative questionnaires were completed (58.1%). The four procedures are hip replacement, knee replacement, groin hernia repair and varicose vein surgery. The joint replacements are those with greater than 30 records completed for the Trust [where follow up questionnaires were completed, required to allow analysis] The additional sections of this report complete our local, PIF and Quality Account priorities, being: Section C Our outcomes required by our local PCT commissioner contract schedule 3.4 and CQuins Schedule 18, quarterly update. From quarter three onwards, negotiations for next years quality contract content will begin. The feedback from our performance to date will inform this. Section D - helping people to recover from episodes of ill health or following injury (DH Outcome 3) Clinical effectiveness underpins our success in outcomes and is now integrated to this report. As well as being improvement processes, national and local audits help identify our outcomes. The Quality Account and clinical audit reports address the broad range of audits we undertake, for this report we focus TARN, the national audit that detail our performance in trauma. 2
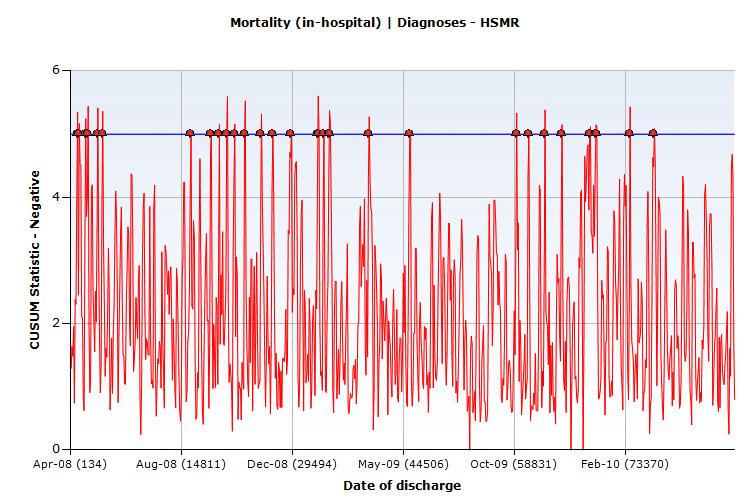
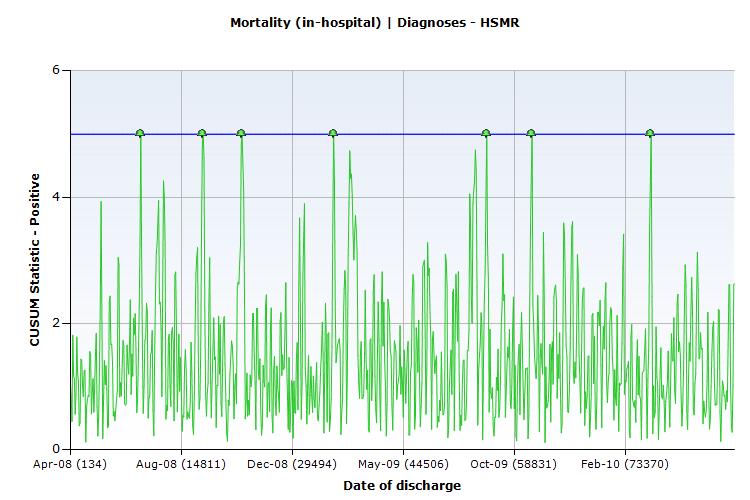
3 Section A HSMR: Preventing people from dying prematurely (DH Outcome 1) 2. Context and Overview: All HSMR figures in this report are benchmarked to the The impact of the national re-benchmarking on the 1st September 2010 has moved the Trust s HSMR for the period April 2009 to March 2010 from 94.3 to (see section 2.2) The Princess Anne Hospital (PAH) HSMR is high because of a cluster of neonatal deaths (see section 2.3) The Countess Mountbatten House (CMH) HSMR remains stable but high following the introduction of the 24-hour rule for non-elective admission (see section 2.4) We are waiting for the Care Quality Commission (CQC) to comment on our response to their Alert relating to Post Partum Haemorrhage (see section 2.7) Recommendations (see section 2.9) Overall Trust s HSMR (56 basket) and cumulative sum control chart (CUSUM), all Diagnoses trends HSMR PERFORMANCE BY YEARS SUHT SGH PAH CMH Apr 08 Mar Apr 09 Mar Apr June SUHT SGH PAH CMH HSMR PERFORMANCE BY QUARTERS Oct-Dec 2009 Q3 Jan-Mar 2010 Q4 Apr-Jun 2010 Q For the period April 2009 to March 2010 the annual revision of the benchmarking has changed the Trust s overall HSMR from 94.3 to 105.2, which is numerically on the predicted value but more Trust s managed to lower their HSMRs by data revision than us so we have not managed to stay within the as expected group but are just within the worse than expected group. From April 2009 to June 2010 the HSMR run chart for the whole Trust simply shows random change Negative (red plot) and positive (green plot) CUSUM charts show trends in HSMR for All Diagnoses and where the trace crosses the upper control limit it is very likely that real change has occurred. The Trust s negative CUSUM showed 16 peaks in the year April 2008 to March 2009 and 10 peaks in the year April 2009 to March There remains a less impressive improvement in the positive CUSUM (4 peaks in the year April 2008 to March 2009 and 3 peaks in the year April 2009 to March 2010). 3

4 4

5 2.3 SGH HSMR The HSMR trends for the SGH site are similar to those for the whole Trust but exclude the unusual problems related to the higher than expected HSMRs at PAH and CMH and more accurately reflect the results of the majority of the elective and emergency care provided by the Trust PAH HSMR The HSMR fell slightly last year (230.5 in April 08 to March 09, in April 2009 to March 2010) but has risen since April 2010 (342.3). From April to June 2010 there have been 11 deaths (6 Obstetric (stillbirths), 3 Neonatal, 1 Well Baby and 1 Gynaecology). The rise in HSMR is almost entirely due to the neonatal deaths (clinical review of their care has shown no cause for concern). The one Gynaecological death (a rare event) requires clinical review as does the one Well Baby death (to check this is not a stillbirth). Level 3 Obstetric & Neonatal Units Chelsea & Westminster University Hospitals of Leicester University College London Leeds Teaching Guy s and St Thomas Southampton University Average for Group CMH HSMR The number of non-elective admissions using the 24 hour rule has remained stable (April 2008 to March %, April 2009 to March %, April to June %). I am still waiting for the result of the investigation into Primary Diagnosis (reason for admission) and Secondary Diagnoses (co-morbidities) that has been carried out. We may need to reconsider the definition of a non-elective admission to extend the period to 48 hours if the delay was for non-clinical reasons. 5
6 2.5. Peer Groups Our Current Hospitals Peer HSMR HSMR Group St George s University Hospitals Coventry Central Manchester University Oxford Radcliffe Sheffield Teaching University Hospitals of Leicester University Hospitals Bristol Nottingham University Guy s and St Thomas Southampton University Leeds Teaching University Hospital Birmingham Brighton & Sussex University Average for Peer Group Hampshire Acute Hospitals HSMR HSMR Basingstoke & N Portsmouth Hampshire Winchester & Eastleigh Isle of Wight Dr Foster Patient Safety Indicators The rate for Obstetric Trauma in vaginal delivery without instruments remains slightly above the national average and continued monitoring is required. The rate of Post-operative Sepsis remains high. However, in the broader Diagnostic Group Septicaemia the HSMR was A detailed case note review is underway CQC Alert SUHT National 22/10/ Death in low risk HRGs Pressure Ulcers Retained foreign body during surgery Obstetric trauma Caesarean Section Obstetric trauma instrumented vaginal delivery Obstetric trauma non-instrumented vaginal delivery Post-operative hip fracture Post-operative sepsis Selected infection due to medical care We have changed our definition of PPH to a loss of over 1000ml in line with the RCOG recommendation. Our calculations show that this reduces our PPH rate to the expected level and we are waiting for the CQC s response to our submission. No further action is required at present Investigations (January to August 2010) Investigation Status CMH -1ry & 2ry Diagnosis Notes review Completed Post-partum Haemorrhage high rate Coding practice review and revision of Completed coding guidance Death in low risk HRG for Clinical notes review On-going Post-operative sepsis for Clinical notes review On-going Trust HSMR for April June 2010 Targeted notes review On-going 6
7 2.9. Summary of Key issues relating to HSMR and conclusions To ensure that all current planned changes relating to clinical information in Discharge Summaries on e-docs being developed by Derek Waller are introduced as soon as possible Consider with DCDs then CGCLs systems to ensure Consultants are actively involved in the decisions and accurate recording of: a. Primary Diagnosis (reason for admission); b. Secondary Diagnosis (co-morbidity); c. End-of-life care (withdrawal of active treatment) and Palliative Care; d. Interventional procedure recording (this may already be accurate enough for the purposes of HSMR calculation and HRG designation). All these could be achieved by a front sheet for each admission capturing this information from Consultants or on Consultant Ward Rounds. This might ease the problems of multi-spell admissions Case note review by the Consultant providing care at the time of death or care for the majority of the final admission if more appropriate in the period April to June 2010 for: a. 8 Diagnostic Groups (DGs) with the highest Observed Mortality (DG and deaths for Pneumonia 56, Acute cerebrovascular disease 40, Ca lung 26, Congestive cardiac failure (non-hypertensive) 21, Urinary tract infection 16, Cardiac arrest & Ventricular fibrillation 15, Secondary malignancy 13, Coronary atherosclerosis & Other heart disease 12); b. Relevant DGs in 8 highest volume of Spells (admissions) (Abdominal pain 695 patients but only 2 deaths as this is a symptom description not a diagnosis, Chronic obstructive pulmonary disease & Bronchiectasis 8 deaths, UTI and CA&OHD included in a.; c. All DGs with HSMR above 120 (DGs and HSMRs for Other perinatal conditions - 371, Other circulatory disease 253, Ca ovary 236, Ca prostate 210, Ca oesophagus 206, Chronic ulcer of skin 177, Ca stomach 177, Non-infectious gastroenteritis 169, Ca bladder 165, Ca breast 162, Ca pancreas 159, Syncope 154 (sometimes a symptoms not a diagnosis), Gastrointestinal haemorrhage 148, Non-Hodgkin s lymphoma 145, Other fractures 140, Ca lung 139 (in a.), Chronic renal failure 137, Pulmonary heart disease 133, Ca colon 133, Cardiac arrest & VF 131 (in a.), UTI 130 (in a. and b.) and Intra-cranial injury (126) Case note review by the Consultant providing care at the time of death or care for the majority of the final admission if more appropriate in the period June 2009 to June 2010 for: a. Death in low risk HRGs 28 deaths, and; b. Death from Post-operative sepsis 31 deaths Carry out a detailed review of 50 deaths randomly drawn from Divisions A, B and D every six months Linked to recommendation 4.2 consider the feasibility of local review (Care Group or Subspecialty Group) for all deaths. 7
8 Section B PROMS: Enhancing the quality of life for people with long-term conditions (DH Outcome 2) 3. PROMS - Patient Report Outcome Measures From April 2009, trusts were required to recruit patients across four procedures into this outcome measurement scheme. The four procedures are hip replacement, knee replacement, groin hernia repair and varicose vein surgery. The Trust has relatively few hernia and varicose vein cases, joint replacements are the area for attention The first year s report was published on 16th September The results included in this report are based on these data and are yet to be given detailed scrutiny. It is understood that the data used are provisional The methodology is to administer pre- and post- operative health related quality of life questionnaires. The EQ5D questionnaire is used. This asks patients how they are doing across 5 health related dimensions, it is a well accepted tool in economic evaluation, it is not condition specific. For joint replacements, the condition specific Oxford knee or hip assessment was used in addition. The Trust s role is to ensure the pre-operative questionnaire is completed if patients are happy to participate the rest is undertaken nationally. The second questionnaire is administered several months after the operation Participation number of pre-operative questionnaires submitted All procedures: SUHT had 1112 eligible cases, 646 Q s were submitted 58.1%, English average was 60.0% Groin hernia Hip replacement Knee replacement Varicose Vein Cases Q s % Cases Q s % Cases Q s % Cases Q s % done done done done SUHT English average % Outcomes the impact we made on health of patients The EQ5D asks the patient to score their health state across the dimensions of mobility, selfcare, ability to undertake usual activities, pain & discomfort, anxiety & depression. Each dimension has three possible answers in essence: no problems, some problems, severe problems, for example no pain or discomfort, moderate pain or discomfort, extreme pain or discomfort. This is an internationally accepted tool and is used as the go to assessment for economic analysis. It allows us to generate the cost per QALY (quality adjusted life year), non-health economists tend to be wary of its non-specific nature, but that is the reason it allows comparison of very different health interventions For PROMS, pre and post operative administration of EQ5D allows us to estimate the impact on health related quality of life it asks did the operation improve your health related quality of life and by how much. In addition to the 5 domain questionnaire a visual analogue scale is used patients give a score pre and post operation to their health related quality of life Data are available for individual organisations shown as: unadjusted pre and post scores; proportions where change occurred; case mix adjusted health gains Similarly, analysis of the changes on the condition specific Oxford hip and Oxford knee assessment tools are provided. Of course for both Oxford scores and EQ5D any patients who did not survive or were too ill to complete post operative assessments are omitted. 8
9 Hip replacement England SUHT Knee replacement England SUHT Cases included 14, , EQ5D unadjusted scores Pre op Post op Change [index 0 to 1 used] Numbers showing Health gain No change Health worsening Case mix adjusted EQ5D scores Post op , ,483 1,776 1, Gain Confidence interval given Case mix adjusted Oxford score (condition specific) Gain made by post op Confidence interval ( to 0.413) ( to ) ( to 0.478) ( to ) ( to 0.298) ( to ) ( to 0.361) ( to ) 3.4. Summary of key issues relating to PROMS, and conclusions The most obvious point is that too few data are available from SUHT to identify whether we do better or worse than the national average in terms of health gain. However, we do appear to follow a similar pattern as the national average for those completing both questionnaires: Health related quality of life (HrQoL) improves meaningfully for most patients who undergo hip or knee replacement HrQoL is, on average, worse in patients requiring hip replacements than those requiring knee replacements and gains are greater for those having h9)ips replaced A higher proportion of patients having knee replacements have no improvement in HrQoL than those having hip replacements, similarly a high proportion have a reduction in HrQoL The key questions are can we predict which patients are likely to do less well, though even if this was possible patients may wish to proceed; and secondly, can we increase the health gains for any or all of these patients? 9
10 Section C Schedule 3.4 -Quality outcomes, and Schedule 18- CQuins for Quarter 2 (Due to PCT by 9 th November 2010) 4. Schedule 3.4 -Quality outcomes The standard contracts Schedule 3.4a includes an outcomes element and supports the framework for our Outcomes reports local measures. Contract detail is now managed through divisional governance systems and processes prior to divisional sign-off for submission to PCTs. The dashboard approach to data management is overseen at the quarterly divisional performance Boards for exception reporting and management assurance Early data trends, that may warrant further divisional follow up prior to PCT submission, are highlighted in appendix B Divisions are asked to support target setting their metrics to support RAG rating assignment for easier follow up CQuin Schedule 18: The CQuin requirements for 2010/11 are detailed in schedule 18 held at O:\PCT Quality Contracts\The 2010 contract. This report supports the quarterly update to be provided to PCTs on our progress on all CQuins CQuin schedule for Southampton, Hampshire Isle of Wight and Portsmouth (SHIP) commissioners, South West commissioners and South West specialist services commissioners were agreed jointly in Q1 as a common schedule. South Central specialist services commissioning group CQuin has been released separately for discussion and agreement in mid October 2010 and will be integrated when agreed into the dashboard approach for management The CQuin programme for 2010/11 carries 1.5% of contract value. Financial weighting has been mitigated with the commissioners as part of the financial envelope agreements process. However it is in our best interests to get CQuin delivery right as finance will apply next year Progress All our CQuins are performance managed by our PCT commissioners. Quarterly milestones are largely focused on setting up systems and processes in-year, with delivery of data outcomes by year-end. This is reflected in the style of reporting on progress. An update to PCTs is required each quarter metrics are at Amber rating for Q2, and 5 at Amber or Red for year end achievement Divisional and Trust Management process Where possible existing steering groups have been used to adopt and drive delivery of relevant CQuin measures. This applies for VTE, patient experience, pressure ulcers, enhanced recovery, end of life The exception is Advancing quality which has required a separate project structure set up for its delivery. The Advancing Quality programme is currently under review by the SHA following feedback from all Trusts on the Q1 feasibility study results. A separate paper (ref: TEC 6th October) outlining our findings and recommendations for Advancing Quality has been shared in draft to support PCTs and the St SHA in developing an appropriate way forward Division D has a majority of the AQ project leads, and regular divisional performance meetings to oversee progress are in place. All divisions have included CQuin progress updates at their divisional board meetings A progress report for each CQuin for Quarter 2 is provided below. 10
11 RAG Key- Green: On Track/ Amber: Broadly on track, known Issue with action plan./ Red: Off track, issues not resolved. Note that RAGs relate to CQuin Q2 requirements only. These may differ from other targets set or reported separately eg via performance. SUMMARY OF KEY ISSUES RELATING TO CQUIN FOR SUHT 2020/11 QUARTER 2 Q2 Required Q2 Progress (RAG) / Key Issues (text) Next Steps: Q3 Fye Q4 VTE Q2: 50% data collection Data completeness 46.8 % to date, by admissions date 60 VTE Data Completeness Target: 75% data, Q4 Target : 100% data, We are on trajectory for DH target and correct Thromboprophylaxis % Apr May Jun Jul Aug Sep 2010 Q2: 50% VTE risk assessment. Patient Experience PDA/Picker reports AQ: Heart Failure Acute MI Community acq. pneumonia Hip/Knee rep t CABG Pressure Ulcers Q2: Report on delivery against end of year target 88 = 53 ytd. Targeted data completion review is n place. Further detail see patient safety report (TEC October) Risk assessed 78% Further detail see patient safety report (TEC October) Picker reports in place to support monthly. First reports received but data required on discharge, so small numbers to date. Further detail see patient experience report (TEC September) All projects- Further detail see AQ Briefing (TEC October) Under SHA review Under SHA review Under SHA review Under SHA review Under SHA review Reporting requirement achieved, Further detail see patient safety report (TEC October) /11 Newly Acquired Pressure Ulcers Grade 3&4 75% patients assessed Monthly PDA/Picker reports SHA-wide CEO and PCT CEO Boards, and CIS to review October. Q3: Provider report on delivery against end of year target. Q4 Target: 90% assessed. Q4 Target: 8 point improvement TBC Unknown delivery requirement for Q4, SHA to confirm following agreement by key Trust leads Q4 Target: < 88 New grade 3&4. -Currently not on trajectory to reach Q4 target, as IQI implementation and the Turnaround project has raised awareness and reporting levels Commissioners are aware of this effect Jan Feb Mar Apr May Jun Jul Aug Sep (to date) Oct Nov Dec Jan Feb Mar Grade 3&4 Target
12 End of Life 1a) Q2 Training needs analysis report, action plan. Final Q4 target still in negotiation with PCTs. Action plan in place to deliver for Q2 requirement by submission date to PCT Training plan includes use of SHA roll-out plan in November for SUHT trainers, with cascade to National Core Competency Category A and identified Category B staff. IMT support development to begin in February Further detail see patient experience report (TEC September) 1a) Q3 provide training needs data Q4 Target: -detail still under negotiation with PCT. 1b) Q2: Number placed on LCP as proportion deaths Further detail see patient experience report (TEC September) 50.00% CQUIN % Deaths placed on LCP or equivalent 1b) Number placed on LCP as proportion deaths Q4 Target: 25% deaths on LCP 45.00% 40.00% 35.00% 30.00% 25.00% 20.00% 15.00% 10.00% 5.00% 0.00% Apr-10 May-10 Jun-10 Jul-10 Aug-10 % of Deaths on LCP Target Enhanced Recovery Q2: Update on delivery plan Smoking Cessation Q2: Audit: 50% elective admission smokers receive advice Q2: Audit: 50% antenatal smokers receive advice SHA review held on Sept 22nd with updates and discussion for further developments, from lead clinicians Positive report feedback received. 200 pts/ week surgery, T&O, At 100% relevant advice at pre-assessment by practice. -Audit requirement not yet in place. Roll-out plan to cardio, gynae, neuro. Currently paper based, IMT solution proposed, to be prioritised at ISSG (date tbc). 100% achieved. This is automated on HICSS & reported for all relevant patients Q1 284 patients (100%) Q2 276 patients (100%) Q3 Update on delivery plan Audit: 75% smokers receive advice Audit: 75% smokers receive advice Q4 Target: 90% pts receive ERP for 6 procedures, Plan for Knee & Hip Q4 target: 95% elective admission smokers receive advice: Requires IMT support, date tbc. - Patient experience survey required. Mechanism to be identified. Q4: 95% antenatal smokers advised- Patient experience survey required. Mechanism to be identified Summary of Key issues relating to Quality Contract & CQUIN and conclusions Actions required to mitigate these are summarised as: o VTE- Divisions to support the targeted reviews for data completion o AQ- Executive team to support appropriate future planning agreements with SHA and subsequently with SUHT IM&T team o Pressure ulcers- Divisions to maintain support for the new processes in place to manage improved patient outcomes. o End Of Life- To complete the Q2 action plan to enable the training needs analysis report. o Smoking Cessation- Divisions to support audit of elective smoker advice for Q2 and 3, and to agree a process for the required patient experience survey, due Q4. 12
13 Section D Clinical Effectiveness: TARN, trauma 5. Introduction The Trauma Audit and Research Network (TARN) provides a national framework for the collection, submission and scrutiny of trauma survival data by hospitals and, crucially, supports comparison with other hospitals. The framework allows a common approach across different centres, which supports systematic process for clinical audit SUHT first joined TARN in 1989 when it was set up. Data collection continued for a number of years until SUHT re-joined TARN in January Data are submitted retrospectively, reports are received regularly and these reports are used in morbidity and mortality meetings Data collection Data for severely injured patients are collected from the patients healthcare records and entered on the Electronic Data Collection and Reporting system (EDCR). The patients are identified through ICD10, S and T codes, the list provided by TARN. The inclusion criteria are defined in the TARN user manual, fractured neck of femur in the over 65s are excluded. Submissions include data gathered from ambulance sheets, radiology reports, post mortems, hospital notes, trauma sheets, operative notes and discharge summaries The patients are identified once they have left hospital and been coded. Bearing in mind the varying length of stay for severely injured patients, the data are always recorded in a retrospective manner. The TARN organisation reviews all the data submitted, checking it and approving the data. They then assign each approved case with an Abbreviated Injury Score (AIS), based on all of the detail inputted. Then a Probability of Survival (PS) score is calculated. These ratings then permit summary and review providing the headline: based on our case mix and numbers we would expect N patients to survive, whilst in fact M actually survived. To oversimplify: if actual survivors are greater than predicted it indicates the Trust is achieving better outcomes than the whole group s average Reports and publications Each quarter TARN publishes a series of reports on the public website, including a report showing the trust s position benchmarked against other trusts using the survival/outcomes results Themed quarterly reports are produced by TARN and cover the following themes: Thoracic (Issue 1 - February) Orthopaedic injuries (Issue 2 - May) Abdominal/spinal (Issue 3 - August) Head injuries (Issue 4 - November) These reports include process measures monitoring standards set out in the Royal College of Surgeons and British Orthopaedic Association report of 2000 "Standards of Care for the Severely Injured" Since SUHT re-joined TARN in January 2009, care groups have used these reports at their morbidity and mortality meetings SUHT data report September Southampton University Hospitals NHS Trust (HES data indicates 546 expected admissions p.a.) The data are for the period 1/08/2009 to 31/7/2010. The bands are based on chance of survival, for example band groups all patients who, based on their injuries, co-morbidities and so on, are predicted as having between 25 and 50 % chance of survival [at time of writing how those precisely at 25.00% or other boundaries are categorised is not understood]
14 Bands of Number in that Predicted Actual Difference Weighted chance of survival chance survivors survivors between difference survival band predicted and (%) actual (%) Total Unexpected deaths in minor/moderate injury Usually due to poor management of comorbidity and/or complications Unexpected survivors with more serious injury Usually indicates good initial resuscitation and the treatment of head injury in Neurological Centres SUHT has 4.4 additional survivors per 100 patients (based on data submitted up to September 2010; since then a further 80 cases have been added). NB The weighted difference (known in TARN as adjusted difference) provides a summary of each band s contribution to our overall additional survivorship 5.5. Comparator Trust : Addenbrooke s Hospital (HES data indicates 555 expected admissions p.a.) Bands of Number in that Predicted Actual Difference chance of survival chance survivors survivors between survival band predicted and (%) actual (%) Total Addenbrooke s has 3.7 additional survivors per 100 patients. Weighted difference 5.6. Data completeness Trusts are also rated on their data completeness full submissions made compared to expected number of submissions. A tick rating is used with 1 tick the weakest performance and a threshold of 65% of all cases submitted for the four tick score. SUHT submitted 51% in and, at September we have submitted sufficient for one tick we expect to achieve above 50% very soon Addenbrooke s have a strong track record of submission though they have invested in an additional data processing staff Southampton Addenbrooke s We are not aware of any selection bias in our data submission but clearly our confidence in the survival comparison would be enhanced if we significantly increased our submissions Some other hospitals do not use consultant or nursing staff to validate their data and some only input the minimum dataset. TARN measures completeness of data by the number of submissions to the TARN database, compared to the expected submissions. Expected submissions are calculated by taking the average of the previous four-year s HES data Whole cohort comparators The following three figures are extracts from the TARN website. They plot Southampton s survival scores against all other participants They show historic performance line plot at left of each chart and performance at time of plot. SUHT are not shown in historic data. We can see that as additional data are submitted confidence intervals shorten but we also improve our relative position. {Southampton is plotted as the red dot larger central dot]. 14
15 Plot as at February 2010 Plot as at May
16 Plot as at August Summary of Key issues relating to TARN (Clinical Effectiveness) and conclusions SUHT has 4.4 additional survivors per 100 patients seen - based on data submitted up to September The Trust s position has remained amongst the top third of organisations for additional survivors IT solutions are currently being explored with the TARN organisation, to save up to 30% of manual data collection by developing methods of extracting data for TARN submissions from existing hospital electronic data To Support the QGSG proposal agreed at TEC; of a rota of clinicians to help ensure TARN data is validated and uploaded in a timely manner due to its impact on the new Trauma Centre developments This and other QGSG recommendations to be taken forward by the Associate Medical Director (Patient Safety). 6. Outcome Report Conclusion and summary Trust Board is asked to 6. To support the QGSG proposal as agreed at TEC; of a rota of clinicians to validate and upload TARN data in a timely manner due to its impact on the new trauma centre developments. 7. QGSG recommendations to be taken forward by the Associate Medical Director (Patient Safety). 8. To develop the CQuins report section to include specialist services contracts requirements when agreed (released October 2010). 9. Identify any areas where further assurance is required. 10. Note the key issues discussed at QGSG and TEC for: HSMR (page 7) PROMS (page 9) CQuin (Page 12) TARN (page 16) 16

17 Appendix A
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST. Quarterly Clinical Effectiveness and Outcomes Report:
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Quarterly Clinical Effectiveness and Outcomes Report: Report to Trust Board 27 th September 2011 Report from Sponsoring Executive Aim of Report Jane Druce, Quality
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Quarterly Clinical Effectiveness and Outcomes Report: Report to Trust Board 27 th September 2011 Report from Sponsoring Executive Aim of Report Jane Druce, Quality
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Quarter /13 Quality Account (Quality and Safety)
") Airedale NHS Foundation Trust Board of Directors:23 rd January 213 Title: Quarter 2 212/13 Quality Account (Quality and Safety) Author: Alison Fuller, Assistant Director Healthcare Quarter 2 212/13 Quality
Airedale NHS Foundation Trust Board of Directors:23 rd January 213 Title: Quarter 2 212/13 Quality Account (Quality and Safety) Author: Alison Fuller, Assistant Director Healthcare Quarter 2 212/13 Quality
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER
 Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
Patient Reported Outcome Measures Frequently Asked Questions (PROMs FAQ)
") Patient Reported Outcome Measures Frequently Asked Questions (PROMs FAQ) Author: Secondary Care Analysis (PROMs), NHS Digital Responsible Statistician: Jane Winter 1 Copyright 2016 Health and Social Care
Patient Reported Outcome Measures Frequently Asked Questions (PROMs FAQ) Author: Secondary Care Analysis (PROMs), NHS Digital Responsible Statistician: Jane Winter 1 Copyright 2016 Health and Social Care
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB)
") Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST National Inpatient Survey Report July 2011
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 2010 National Inpatient Survey Report July 2011 Report to: Trust Board - 2 nd August 2011 Report from: Sponsoring Executive: Aim of Report: Joanne Dimmock, Head
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 2010 National Inpatient Survey Report July 2011 Report to: Trust Board - 2 nd August 2011 Report from: Sponsoring Executive: Aim of Report: Joanne Dimmock, Head
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Learning from Deaths; Mortality Review Policy
 Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Finalised Patient Reported Outcome Measures (PROMs) in England Data Quality Note
 in England Data Quality Note") Finalised Patient Reported Outcome Measures (PROMs) in England Data Quality Note April 2015 to Published 10 August 2017 This data quality note accompanies the publication by NHS Digital of finalised data
Finalised Patient Reported Outcome Measures (PROMs) in England Data Quality Note April 2015 to Published 10 August 2017 This data quality note accompanies the publication by NHS Digital of finalised data
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Hospital Mortality Monitoring. May 2015
 Hospital Mortality Monitoring Report 24: Oct 213 to Sep 214 May 215 undertaken by North East Quality Observatory System on behalf of All North East Subscribers to NEQOS Services NEQOS is jointly operated
Hospital Mortality Monitoring Report 24: Oct 213 to Sep 214 May 215 undertaken by North East Quality Observatory System on behalf of All North East Subscribers to NEQOS Services NEQOS is jointly operated
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Richard Wilson, Quality Insight and Intelligence Director
 To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
Paper 8 DECISION NOTE. Recommendation
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
National Clinical Audit & Patient Outcome Programme: An update
 National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
NHS Dental Services Quarterly Vital Signs Reports
 NHS Dental Services Quarterly Vital Signs Reports Dental Services Gateway ref: NHSBSA/DSD/0008 Introduction The NHS Dental Services (NHS DS) has been working closely with the Department of Health (DH)
NHS Dental Services Quarterly Vital Signs Reports Dental Services Gateway ref: NHSBSA/DSD/0008 Introduction The NHS Dental Services (NHS DS) has been working closely with the Department of Health (DH)
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Mortality Report. 1. Introduction / Background
 Mortality Report 1. Introduction / Background 1.1 The Board is reminded of the findings from the CQC review in December 2016, 'Learning, candour and accountability: a review of the way trusts review and
Mortality Report 1. Introduction / Background 1.1 The Board is reminded of the findings from the CQC review in December 2016, 'Learning, candour and accountability: a review of the way trusts review and
Outcomes benchmarking support packs: CCG level
 Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Pain Management HRGs
 The NHS Information Centre is England s central, authoritative source of health and social care information The Casemix Service designs and refines classifications that are used by the NHS in England to
The NHS Information Centre is England s central, authoritative source of health and social care information The Casemix Service designs and refines classifications that are used by the NHS in England to
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
National Clinical Audit programme
 National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
Authors: Head of Outcomes & Effectiveness, Quality Project Manager and Deputy MD, Sponsor: Medical Director
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
TRUST BOARD/DIRECTORS GROUP 2016 Key Performance Indicators
 TRUST BOARD/DIRECTORS GROUP 2016 Key Performance Indicators Introduction This paper provides an update on our progress towards our vision to be England s best acute teaching trust in 2016 and beyond. The
TRUST BOARD/DIRECTORS GROUP 2016 Key Performance Indicators Introduction This paper provides an update on our progress towards our vision to be England s best acute teaching trust in 2016 and beyond. The
Elaine Andrews, Assistant Director of Nursing & Safety and Caroline Booton Quality Analyst Jill Asbury, Acting Director of Nursing
 Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Integrated Performance Report. NHS Rotherham Board 6 July 2011
 Integrated Performance Report NHS Rotherham Board 6 July 2 CONTENTS Introduction Pg 2 Efficiency Pg 3-6 Rotherham Outcomes Pg 7- Contract Performance Pg -13 Finance Pg 14-15 1 INTRODUCTION Report format..
Integrated Performance Report NHS Rotherham Board 6 July 2 CONTENTS Introduction Pg 2 Efficiency Pg 3-6 Rotherham Outcomes Pg 7- Contract Performance Pg -13 Finance Pg 14-15 1 INTRODUCTION Report format..
North West COPD Report Nov 2011
 North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
O U T C O M E. record-based. measures HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT
 HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
NHS Outcomes Framework 2014/15:
 NHS Outcomes Framework 2014/15: Domain 3 Helping people to recover from episodes of ill health or following injury Indicator specifications Version: 1.2 Date: August 2014 Author: Clinical Indicators Team
NHS Outcomes Framework 2014/15: Domain 3 Helping people to recover from episodes of ill health or following injury Indicator specifications Version: 1.2 Date: August 2014 Author: Clinical Indicators Team
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
CQUIN Supplement Quality Account
 CQUIN Supplement Quality Account 2011-2012 Introduction The CQUIN framework was introduced in April 2009 as a National Framework for locally agreed quality improvement schemes. It enables commissioners
CQUIN Supplement Quality Account 2011-2012 Introduction The CQUIN framework was introduced in April 2009 as a National Framework for locally agreed quality improvement schemes. It enables commissioners
Clinical Use of Blood The AIM II Trial. Challenges of Near-Live Organisational Blood Use Monitoring
 Clinical Use of Blood The AIM II Trial Challenges of Near-Live Organisational Blood Use Monitoring Goals for AIM Assist hospitals in complying with timely metric driven standards Create an inclusive approach
Clinical Use of Blood The AIM II Trial Challenges of Near-Live Organisational Blood Use Monitoring Goals for AIM Assist hospitals in complying with timely metric driven standards Create an inclusive approach
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals
 A Guide for Healthcare Professionals") Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
The Royal Wolverhampton NHS Trust
 Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Tele Stroke ( Telemedicine in Practice)
") Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Understanding and promoting good outcomes
 Understanding and promoting good outcomes PROMs in the Best Practice Tariff for hip and knee replacement Jake Gommon (Pricing Team, NHS England) & Rafael Goriwoda (Patient & Information analytical team,
Understanding and promoting good outcomes PROMs in the Best Practice Tariff for hip and knee replacement Jake Gommon (Pricing Team, NHS England) & Rafael Goriwoda (Patient & Information analytical team,
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Serious Incident Report Public Board Meeting 26 November 2015
 Serious Incident Report Public Board Meeting 26 November 2015 Presented for: Presented by: Author Previous Committees Governance Yvette Oade, Chief Medical Officer Craig Brigg, Director of Quality None
Serious Incident Report Public Board Meeting 26 November 2015 Presented for: Presented by: Author Previous Committees Governance Yvette Oade, Chief Medical Officer Craig Brigg, Director of Quality None
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Clinical Audit for Improvement: HQIP update
 Clinical Audit for Improvement: HQIP update Mirek Skrypak @MirekSkr Associate Director for Quality and Development National Clinical Audit and Patient Outcomes Programme Healthcare Quality Improvement
Clinical Audit for Improvement: HQIP update Mirek Skrypak @MirekSkr Associate Director for Quality and Development National Clinical Audit and Patient Outcomes Programme Healthcare Quality Improvement
Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September 2009
 Summary Report Q2 July September 2009") Agenda 24/1 Public Board Meeting, 28 JAN 21 Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September Presented by: Colin Johnston, Medical Director 1. Purpose The following CLIP
Agenda 24/1 Public Board Meeting, 28 JAN 21 Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September Presented by: Colin Johnston, Medical Director 1. Purpose The following CLIP
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Using the structured judgement review method
 National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
Emergency readmission rates
 Emergency readmission rates Further analysis 1 Emergency readmission rates DH INFORMATION READER BOX Policy Estates HR / Workforce Commissioning Management IM & T Clinical Planning / Finance Clinical Social
Emergency readmission rates Further analysis 1 Emergency readmission rates DH INFORMATION READER BOX Policy Estates HR / Workforce Commissioning Management IM & T Clinical Planning / Finance Clinical Social
Ensuring quality outcomes
 Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Paediatric Critical Care and Specialised Surgery in Children Review. Paediatric critical care and ECMO: interim update
 Gateway Reference: 06662 Paediatric Critical Care and Specialised Surgery in Children Review Paediatric critical care and ECMO: interim update June 2017 Contents Executive summary 1. Introduction 2. Context
Gateway Reference: 06662 Paediatric Critical Care and Specialised Surgery in Children Review Paediatric critical care and ECMO: interim update June 2017 Contents Executive summary 1. Introduction 2. Context
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Clinical Commissioning Group Governing Body Paper Summary Sheet Date of Meeting: 26 September 2017
 Clinical Commissioning Group Governing Body Paper Summary Sheet Date of Meeting: 26 September 2017 For: PUBLIC session PRIVATE Session For: Decision Discussion Noting Agenda Item and title: Author: GOV/17/09/15
Clinical Commissioning Group Governing Body Paper Summary Sheet Date of Meeting: 26 September 2017 For: PUBLIC session PRIVATE Session For: Decision Discussion Noting Agenda Item and title: Author: GOV/17/09/15
Aneurin Bevan University Health Board. Professional Revalidation
 28 th January 20 Aneurin Bevan University Health Board Professional Revalidation Purpose of the Report: The purpose of this paper is to provide the Board with an update in relation to the Nursing Revalidation
28 th January 20 Aneurin Bevan University Health Board Professional Revalidation Purpose of the Report: The purpose of this paper is to provide the Board with an update in relation to the Nursing Revalidation
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Commissioning for Value insight pack
 Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Powys Teaching Health Board. Respiratory Delivery Plan
 Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
THE LOGICAL RECORD ARCHITECTURE (LRA)
") THE LOGICAL RECORD ARCHITECTURE (LRA) Laura Sato KITH Conference 27 September 2011 Presentation Overview NHS (England) Informatics NHS Data Standards & Products develops and delivers UK terminologies and
THE LOGICAL RECORD ARCHITECTURE (LRA) Laura Sato KITH Conference 27 September 2011 Presentation Overview NHS (England) Informatics NHS Data Standards & Products develops and delivers UK terminologies and
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Monthly and Quarterly Activity Returns Statistics Consultation
 Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September Executive Summary from CEO
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST PAGE 1 OF 2 Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September 2017 Executive Summary from CEO Paper
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST PAGE 1 OF 2 Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September 2017 Executive Summary from CEO Paper
Reducing Elective Waits: Delivering 18 week pathways for patients. Programme Director NHS Elect Caroline Dove.
 Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COLLABORATIVE SERVICES SHOW POSITIVE OUTCOMES FOR END OF LIFE CARE
 Art & science The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON COLLABORATIVE SERVICES SHOW POSITIVE OUTCOMES FOR END OF LIFE CARE Jennifer Garside and colleagues
Art & science The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON COLLABORATIVE SERVICES SHOW POSITIVE OUTCOMES FOR END OF LIFE CARE Jennifer Garside and colleagues
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep