2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES
|
|
|
- Millicent Cora O’Brien’
- 6 years ago
- Views:
Transcription
1 2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES
2 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality Measure Reporting 3. Alignment with Quality Payment Program 4. Beneficiary Preferences and ACO Assignment 5. Chronic Care Management (CCM) Updates
3 ACO Participants who report PQRS measures separately REGULATORY UPDATES
4 ACO Participants who report PQRS quality measures separately After consideration of the comments received regarding CMS proposed policies for EPs and group practices participating in ACOs that report PQRS quality measures separately from the ACO, CMS is finalizing the policies as proposed. At (j)(1)(ii), CMS is finalizing its proposal to establish a secondary PQRS reporting period for the 2017 PQRS payment adjustment for individual EPs or group practices who bill under the TIN of an ACO participant if the ACO failed to report on behalf of such individual EPs or group practices during the previously established reporting period for the 2017 PQRS payment adjustment.
5 ACO Participants who report PQRS quality measures separately This option is limited to EPs and group practices that bill through the TIN of an ACO participant in an ACO that failed to satisfactorily report on behalf of its EPs and would not be available to EPs and group practices that failed to report for purposes of PQRS outside the Shared Savings Program; e.g. not in an ACO. CMS is finalizing its proposal that these affected EPs may utilize the secondary reporting period either as an individual EP or as a group practice using one of the registry, QCDR, direct EHR product, or EHR data submission vendor reporting options. CMS is are also finalizing its proposal that such EPs do not need to register for the PQRS GPRO for the 2017 PQRS payment adjustment.
6 ACO Participants who report PQRS quality measures separately In addition, CMS is finalizing at (j)(4)(v) its proposal that sections (j)(8)(ii), (iii), and (iv) would apply to affected EPs reporting as individuals using this secondary reporting period for the 2017 PQRS payment adjustment. Further, CMS is finalizing at (j)(7)(viii) its proposal that sections (j)(9)(ii), (iii), and (iv) would apply to affected EPs reporting as group practices using this secondary reporting period for the 2017 PQRS payment adjustment.
7 ACO Participants who report PQRS quality measures separately CMS is finalizing its proposal that the secondary reporting period for the 2017 PQRS payment adjustment would coincide with the reporting period for the 2018 PQRS payment adjustment (that is, January 1, 2016 through December 31, 2016). In addition, CMS is finalizing a policy under which CMS will assess the individual EP or group practice s 2016 data using the applicable satisfactory reporting requirements for the 2018 PQRS payment adjustment (including, but not limited to, the applicable PQRS measure set). If an affected individual EP or group practice decides to use the secondary reporting period for the 2017 PQRS payment adjustment, the EP or group practice should expect to receive a PQRS payment adjustment for services furnished in 2017 until CMS is able to determine that the EP or group practice satisfactorily reported for purposes of the 2017 PQRS payment adjustment. Further, CMS is finalizing its proposal that the informal review submission periods for these EPs or group practices would occur during the 60 days following the release of the PQRS feedback reports for the 2018 PQRS payment adjustment.
8 2017 ACO Quality Measure Reporting REGULATORY UPDATES
9
10
11
12 GPRO Web Interface Added/Removed Added: Medication Reconciliation Post Discharge Removed: Removed: Removed: Removed: Medication Documentation PREV -11 Blood Pressure Coronary Artery Disease (CAD) Heart Failure (HF)
13 Medication Reconciliation Post Discharge NQF #0097 The percentage of discharges from any inpatient facility (e.g. hospital, skilled nursing facility, or rehabilitation facility) for patients 18 years and older of age seen within 30 days following discharge in the office by the physician, prescribing practitioner, registered nurse, or clinical pharmacist providing on-going care for whom the discharge medication list was reconciled with the current medication list in the outpatient medical record. file:///c:/users/administrator/downloads/2016_pqrs_measure_046_11_17_2015.pdf.pdf
14 Medication Reconciliation Post Discharge Definition: Medication Reconciliation A type of review in which the discharge medications are reconciled with the most recent medication list in the outpatient medical record. Documentation in the outpatient medical record must include evidence of medication reconciliation and the date on which it was performed.
15 Medication Reconciliation Post Discharge Any of the following evidence meets criteria: (1) Documentation of the current medications with a notation that references the discharge medications (e.g., no changes in meds since discharge, same meds at discharge, discontinue all discharge meds), (2) Documentation of the patient s current medications with a notation that the discharge medications were reviewed, (3) Documentation that the provider reconciled the current and discharge meds, (4) Documentation of a current medication list, a discharge medication list and notation that the appropriate practitioner type reviewed both lists on the same date of service, (5) Notation that no medications were prescribed or ordered upon discharge
16 Claims Based Added/Removed Added: ACO-44 Use of Imaging Studies for Low Pack Pain Added: ACO-43 Ambulatory Sensitive Condition Acute Composite Removed: ACO 9 Ambulatory Sensitive Conditions Admissions: COPD or Asthma in Older Adults Removed: ACO 10 Ambulatory Sensitive Conditions Admissions: Heart Failure (HF)
17
18 Prevention Quality Acute Composite Description Prevention Quality Indicators (PQI) composite of acute conditions per 100,000 population, ages 18 years and older. Includes admissions with a principal diagnosis of one of the following conditions: dehydration, bacterial pneumonia, or urinary tract infection.
19 Numerator Discharges, for patients ages 18 years and older, that meet the inclusion and exclusion rules for the numerator in any of the following PQIs: PQI #10 Dehydration Admission Rate PQI #11 Bacterial Pneumonia Admission Rate PQI #12 Urinary Tract Infection Admission Rate Discharges that meet the inclusion and exclusion rules for the numerator in more than one of the above PQIs are counted only once in the composite numerator. Denominator Population ages 18 years and older in metropolitan area or county. Discharges in the numerator are assigned to the denominator based on the metropolitan area or county of the patient residence, not the metropolitan area or county of the hospital where the discharge occurred. Conditions treatable in outpatient setting
20
21 ACO Alignment with Quality Payment Program WHAT YOUR MEDICARE ACO NEEDS TO KNOW ABOUT MACRA 11/14/
22 Quality Payment Program The Quality Payment Program will reform Medicare Part B payments for more than 600,000 clinicians. Clinicians will choose how they want to participate in the Quality Payment Program based on their practice size, specialty, location or patient population. Alternative Payment Model (APM) Advanced APM Merit-based Incentive Payment System (MIPS) 11/14/
23 MIPS or APM or Advanced APM 11/14/
24 MIPS 11/14/
25 Who participates in MIPS? MIPS Participants Medicare Part B clinicians billing more than $30,000 a year AND providing care for more than 100 Medicare patients per year Physicians Nurse Practitioners Physician Assistants Clinical Nurse Specialists Certified Registered Nurse Anesthetists 11/14/
26 Who is excluded from MIPS? Excluded from MIPS Clinicians below the low-volume threshold Medicare Part B clinicians billing less than or equal to $30,000 a year OR 100 or fewer Medicare Part B patients. Clinicians in an Advanced APM Newly-enrolled Medicare clinicians. Clinicians who enroll in Medicare for the first time during a performance period are exempt from reporting on measures and activities for MIPS until the following performance year. 11/14/
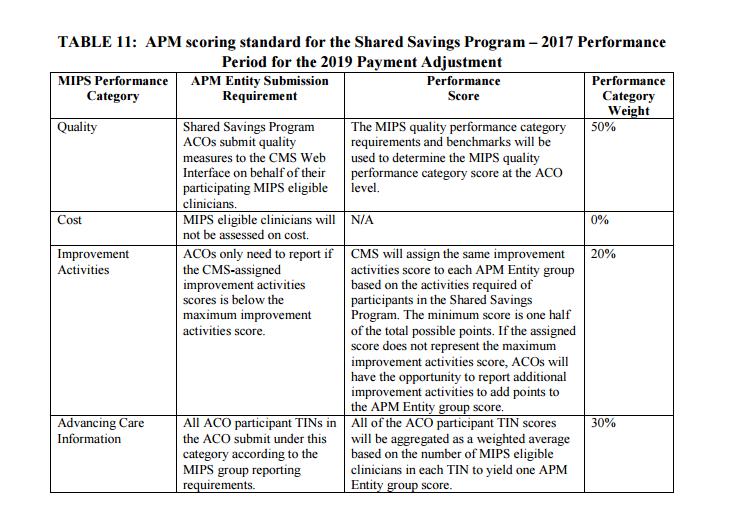
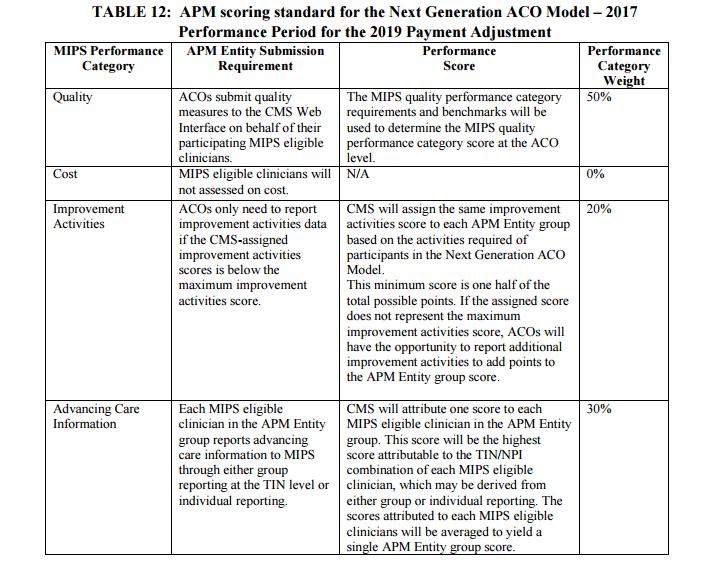
27 What are Medicare ACOs? APM Shared Savings Program Track 1 Shared Savings Program Track 2 and 3 Advanced APM Next Generation ACO Advanced APM MIPS eligible clinicians in ACOs are subject to MIPS under the APM scoring standard All MIPS eligible clinicians in the APM Entity are considered a group and will receive the same score Participating eligible clinicians who are determined to be Qualifying APM Participants are exempt from MIPS. Participating eligible clinicians who are determined to be Qualifying APM Participants are exempt from MIPS. 11/14/
28 Pick your pace for participation in the MIPS transitional year 2017 Participate in an Advanced Alternative Payment Model [Excluded from MIPS] Comprehensive List: ced_apms_in_2017.pdf Test Pace MIPS Partial Year MIPS Full Year Submit some data after January 1, Neutral or small payment adjustment Report for 90 day period after January 1, 2017 Small positive payment adjustment Fully participate starting January 1, 2017 Modest positive payment adjustment Not participating in the Quality Payment Program for the transition year 2017 will result in a negative 4% payment adjustment 11/14/
29 11/14/
30 11/14/
31 11/14/
32 11/14/
33 11/14/
34 11/14/

35 11/14/
36 11/14/
37 11/14/
38 11/14/
39 11/14/
40 11/14/
41 11/14/
42 11/14/
43 11/14/
44 11/14/
45 Table 14: APM Entity Submission Method for each MIPS Performance Category Quality Cost Improvement Activities APM Entity group submits quality measure data to CMS as required under the APM. ACOS use GPRO No data submitted by APM Entity group to MIPS No data submitted by APM Entity group to MIPS UNLESS the assigned score at the MIPDS APM level does not represent the maximum improvement activities score, in which case the APM Entity may report additional improvement activities using a MIPDS data submission mechanism. Advancing Care Information Shared Savings Program ACO participant TINs submit data using a MIPS data submission mechanism. Next Generation ACO Model and other MIPS APM eligible clinicians submit data at either the individual level or at the TIN level using the MIPS data submission mechanism. 11/14/
46 11/14/
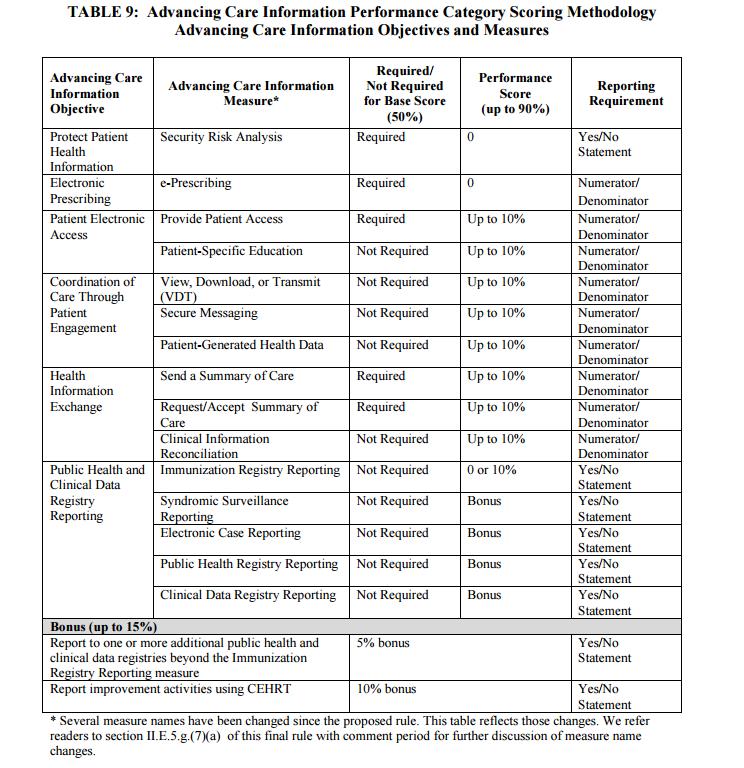
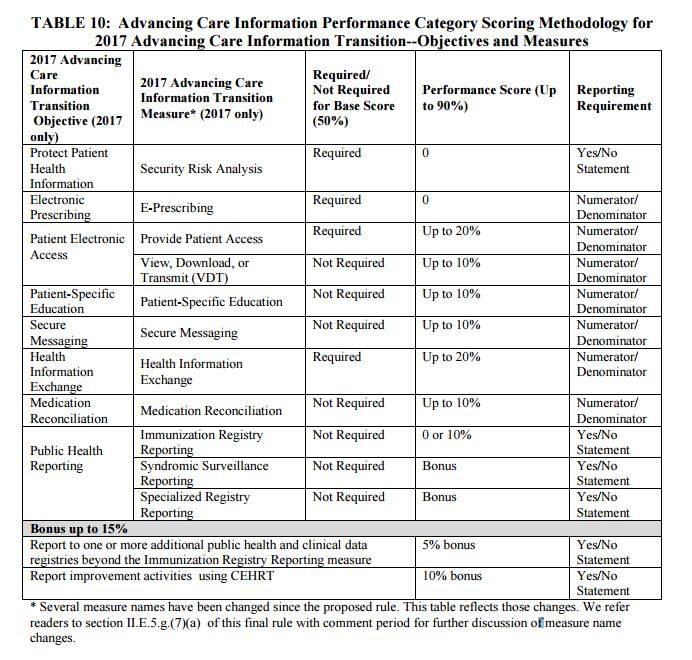
47 Advancing Care Information Performance Category 1. CEHRT. Use CEHRT for the performance period. 2. Report MIPS Advancing Care Information Objectives and Measures. Report the numerator (of at least one) and denominator, or yes/no statement as applicable, for each required measure; or Report a null value for each required measure that includes a null value as an acceptable result in the measure specification. 3. Support information exchange and the prevention of health information blocking and engage in activities related to supporting providers with the performance of CEHRT. 4. Implemented in a manner that allowed for the timely, secure and trusted bi-directional exchange of structured electronic health information with other health care providers, including unaffiliated providers, and with disparate certified EHR technology and health IT vendors. 11/14/
48 11/14/

49 11/14/

50 11/14/
51 11/14/
52 11/14/
53 11/14/
54 11/14/
55 11/14/
56 11/14/
57 11/14/
58 11/14/
59 How does Health Endeavors help MIPS APMs with MACRA? Quality Group Practice Reporting Option (GPRO) Advancing Care Clinical Information Reconciliation Chronic Care Management (CCM) Patient-Generated Health Data Chronic Care Management (CCM) Patient Empowerment Portal Patient-Specific Education Patient Empowerment Portal Provide Patient Access Patient Empowerment Portal Secure Messaging Patient Empowerment Portal Send a Summary of Care Record Request/Accept Summary of Care Measure Chronic Care Management (CCM) Patient Empowerment Portal View, Download and Transmit (VDT) Chronic Care Management (CCM) Patient Empowerment Portal 11/14/
60 Beneficiary Preferences and ACO Assignment PATIENT ALIGNMENT 11/14/
61 Beneficiary Preferences and ACO Assignment Because of uncertainty inherent in FFS Medicare where there is no beneficiary lock-in or enrollment, both patient advocacy groups and ACOs have expressed interest in and support for enhancing claimsbased assignment of beneficiaries to ACOs by taking into account beneficiary attestation regarding the healthcare provider that they consider to be responsible for coordinating their overall care.
62 Basic assignment methodology. * * * * * (e) For performance year 2018 and subsequent performance years, if a system is available to allow a beneficiary to designate a provider or supplier as responsible for coordinating their overall care and for CMS to process the designation electronically, CMS will supplement the claims-based assignment methodology described in this section with information provided by beneficiaries regarding the provider or supplier they consider responsible for coordinating their overall care. Such designations must be made in the form and manner and by a deadline determined by CMS. (1) Notwithstanding the assignment methodology under paragraph (b) of this section, beneficiaries who designate an ACO professional participating in an ACO as responsible for coordinating their overall care are prospectively assigned to that ACO, regardless of track, annually at the beginning of each benchmark and performance year based on available data at the time assignment lists are determined for the benchmark and performance year.
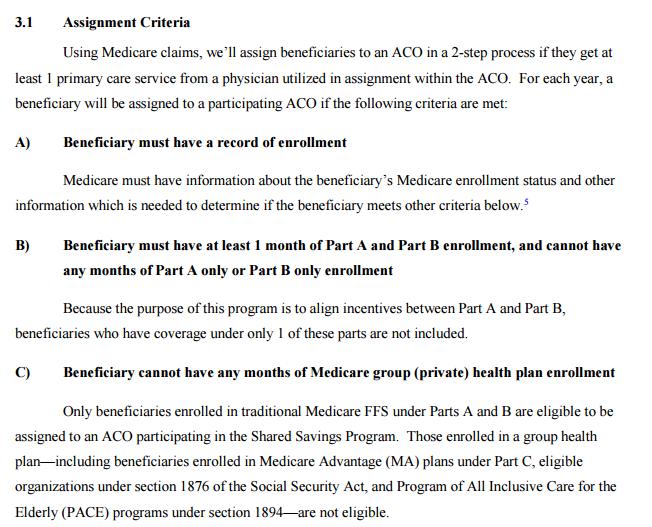
63 (2) Beneficiaries will be added to the ACO s list of assigned beneficiaries if all of the following conditions are satisfied: The beneficiary must have had at least one primary care service during the assignment window as defined under with a physician who is an ACO professional in the ACO who is a primary care physician as defined under or who has one of the primary specialty designations included in paragraph (c) of this section. The beneficiary meets the eligibility criteria established at (a) and must not be excluded by the criteria at (b). The exclusion criteria at (b) apply for purposes of determining beneficiary eligibility for alignment to ACOs under all tracks based on the beneficiary s designation of an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section
64
65 (2) Beneficiaries will be added to the ACO s list of assigned beneficiaries if all of the following conditions are satisfied: The beneficiary must have designated an ACO professional who is a primary care physician as defined at , a physician with a specialty designation included at paragraph (c) of this section, or a nurse practitioner, physician assistant, or clinical nurse specialist as responsible for coordinating their overall care. If a beneficiary has designated a provider or supplier outside the ACO who is a primary care physician as defined at , a physician with a specialty designation included at paragraph (c) of this section, or a nurse practitioner, physician assistant, or clinical nurse specialist, as responsible for coordinating their overall care, the beneficiary will not be added to the ACO s list of assigned beneficiaries for a performance year under the assignment methodology in paragraph (b) of this section.
66 (3) The ACO, ACO participants, ACO providers/suppliers, ACO professionals, and other individuals or entities performing functions and services related to ACO activities are prohibited from providing or offering gifts or other remuneration to Medicare beneficiaries as inducements for influencing a Medicare beneficiary s decision to designate or not to designate an ACO professional under paragraph (e) of this section. The ACO, ACO participants, ACO providers/suppliers, ACO professionals, and other individuals or entities performing functions and services related to ACO activities must not, directly or indirectly, commit any act or omission, nor adopt any policy that coerces or otherwise influences a Medicare beneficiary s decision to designate or not to designate an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section, including but not limited to the following: (i) Offering anything of value to the Medicare beneficiary as an inducement to influence the Medicare beneficiary s decision to designate or not to designate an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section. Any items or services provided in violation of paragraph (e)(3) will not be considered to have a reasonable connection to the medical care of the beneficiary, as required under (a)(2). (ii) Withholding or threatening to withhold medical services or limiting or threatening to limit access to care.
67 2017 Chronic Care Management (CCM) Program REGULATORY UPDATES & HEALTH ENDEAVORS CCM PROGRAM

68 New Medicare Payment for CCM Beginning January 1, 2015, Medicare now pays for chronic care management, or CCM. As detailed below, CCM payments will reimburse practitioners for furnishing specified non-face-to-face services to qualified beneficiaries over a calendar month. Specifically, CMS has adopted CPT for Medicare CCM services, which is defined in the CPT Professional Codebook as follows: Chronic care management services, at least 20 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month, with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient; chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline; comprehensive care plan established, implemented, revised, or monitored.
69 E/M Visit G0506 Add-on Code OR G0505 Add-on Code AND Prolonged Service Codes Total Billing Initiating Visit Start Face-to-Face Initiating Visit Initiation during an Annual Wellness Visit (AWV), Initial Preventive Physical Examination (IPPE or Welcome to Medicare Visit), face-to-face E/M visit (Level 4 or 5 visit not required), for new patients or patients not seen within 1 year prior to the commencement of chronic care management (CCM) services. The face-to-face visit is NOT a component of the CCM service, and thus may be billed separately. G0506 Add-on Code. Comprehensive assessment of and care planning by the physician or other qualified health care professional for patients requiring chronic care management services, including assessment during the provision of a face-toface service. This add-on code is to be listed separately in addition to the primary service and billed separately from monthly care management services. The projected payment rate for G0506 is $63.68 (non-facility) and $46.15 (facility).
70 E/M Visit G0506 Add-on Code OR G0505 Add-on Code AND Prolonged Service Codes Total Billing Initiating Visit Add-On Code G0506 Additional work of the billing practitioner in personally performing a faceto-face assessment Acknowledging complaints that the time spent developing the CCM-required care plan currently is not reimbursed, CMS proposes to pay physicians for care plan development under a new code, G0506. The agency proposes the following description for this code: Comprehensive assessment of and care planning by the physician or other qualified health care professional for patients requiring chronic care management services, including assessment during the provision of a face-to-face service. This add-on code is to be listed separately in addition to the primary service and billed separately from monthly care management services. The projected payment rate for G0506 is $63.68 (non-facility) and $46.15 (facility).
71 E/M Visit G0506 Add-on Code OR G0505 Add-on Code AND Prolonged Service Codes Total Billing Initiating Visit Prolonged Prolonged E/M Service Codes CCM and Complex CCM reimburse providers for clinical staff time spent providing care management services, not time spent by physicians. Recognizing the additional resource costs involved in spending an extraordinary amount of time outside the office visit caring for an individual patient s needs, CMS proposes to make payment under two codes: CPT Prolonged E/M service before and/or after direct patient care, first hour CPT Prolonged E/M service before and/or after direct patient care, each additional 30 minutes (listed separately in addition to CPT 99358) In discussing these services, CMS warns the time counted for these codes must be beyond the usual service time for the primary or companion E/M code that is also billed; no time can be counted more than once toward the provision of CPT 99358, 99359, and any other service reimbursable under the Medicare Physician Fee Schedule. The projected payment rate for is $ (facility and non-facility); for 99359, it is $54.38 (facility and non-facility).
72 Care Plan Development Addon Code G0506 Payment to physicians for care plan development under new code, G0506. G0505 companion code plus Non-Face-to-Face Prolonged E/M Services and Extraordinary amount of time outside the office visit caring for an individual patient s needs. Comprehensive assessment of and care planning by the physician or other qualified health care professional for patients requiring CCM services, including assessment during the provision of a faceto-face service. The projected payment rate is $63.68 (non-facility) and $46.15 (facility) prolonged E/M service before and/or after direct patient care, 60 minutes prolonged E/M service before and/or after direct patient care, each additional 30 minutes after Same or different day Projected payment rate for is $ (facility and non-facility and for is $54.38 (facility and non-facility) Same or different day
73 E/M Visit G0506 Add-on Code $63.68 Total Billing Initiating Visit Same Day or Different Day E/M Visit G0505 Addon Code $ minutes $ each additional 30 minutes $54.38 Total Billing Initiating Visit
74 Next Confirm Patient CCM Eligible 2+ Chronic Conditions expected to last at least 12 months (or until death that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline. CMS has not mandated a definitive list of chronic conditions for purposes of CCM. Health Endeavors generally uses
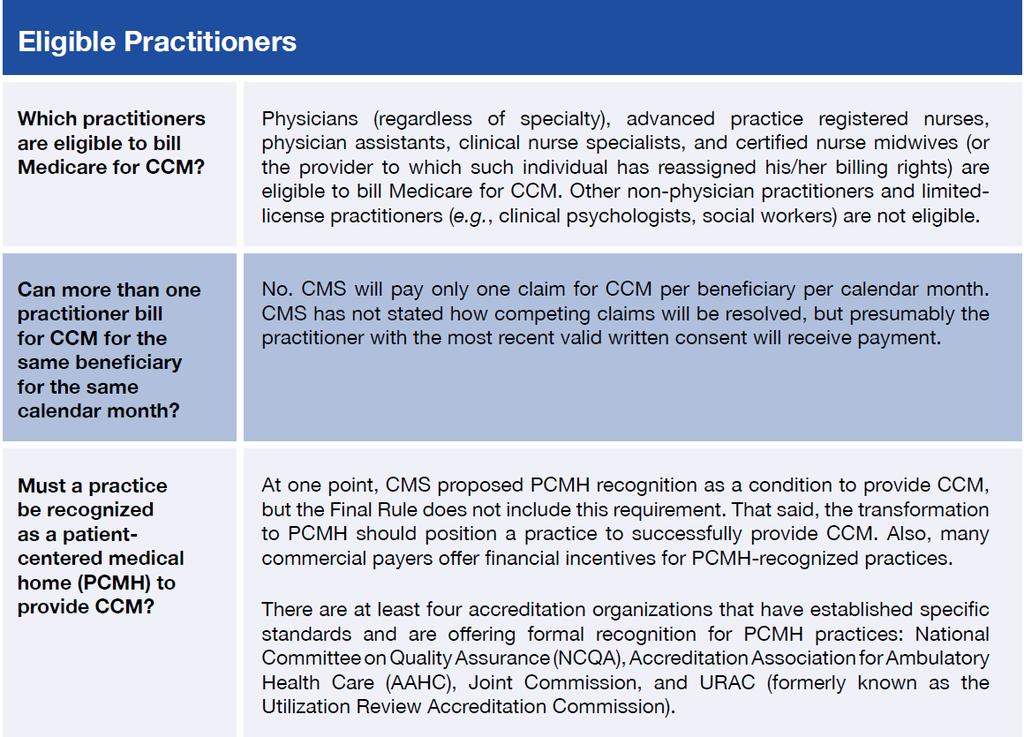
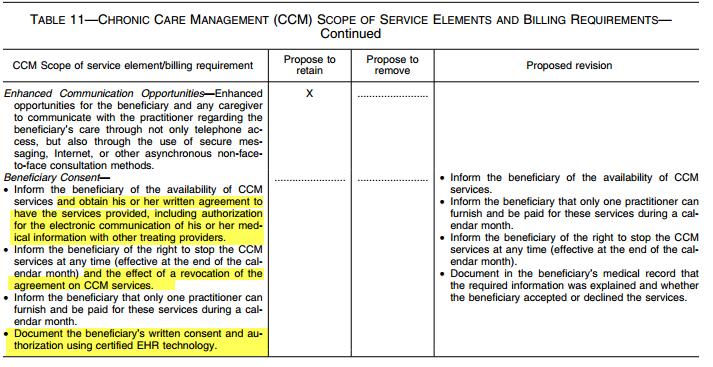
75 Next Verbal Consent Documented Inform the beneficiary of the availability of CCM services; that only one practitioner can furnish and be paid for these services during a calendar month; and of their right to stop the CCM services at any time (effective at the end of the calendar month) Document in the beneficiary s medical record that the required information was explained and whether the beneficiary accepted or declined the services. Next Co-pay Discussion Verify Supplement Payment Collect Monthly Waiver of Co-pay for indigent patients
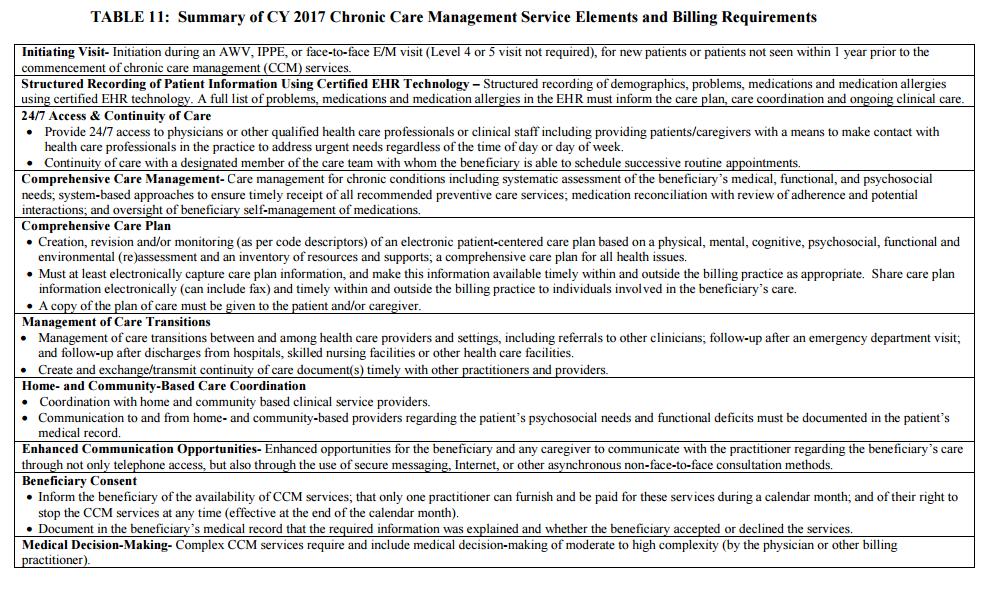
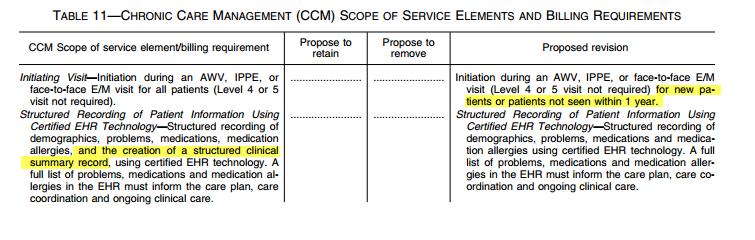
76 Structured EHR Technology Structured Recording of Patient Information Using Certified EHR Technology Structured recording of demographics, problems, medications and medication allergies using certified EHR technology. A full list of problems, medications and medication allergies in the EHR must inform the care plan, care coordination and ongoing clinical care
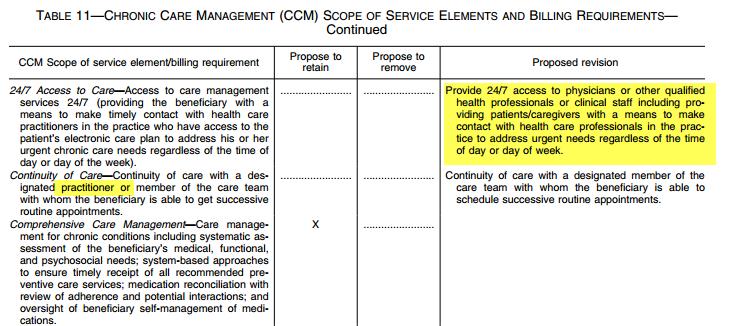
77 24/7 Access 24/7 Access & Continuity of Care Provide 24/7 access to physicians or other qualified health care professionals or clinical staff including providing patients/caregivers with a means to make contact with health care professionals in the practice to address urgent needs regardless of the time of day or day of week. Continuity of care with a designated member of the care team with whom the beneficiary is able to schedule successive routine appointments.
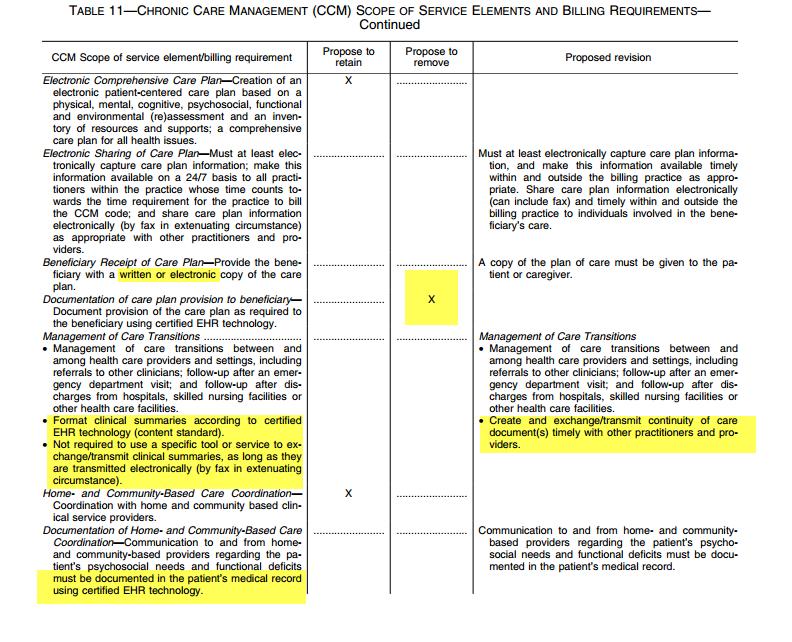
78 Initial Care Plan Initial Care Plan developed by billing practitioner Comprehensive Care Plan Creation, revision and/or monitoring (as per code descriptors) of an electronic patient-centered care plan based on a physical, mental, cognitive, psychosocial, functional and environmental (re)assessment and an inventory of resources and supports; a comprehensive care plan for all health issues. Must at least electronically capture care plan information, and make this information available timely within and outside the billing practice as appropriate. Share care plan information electronically (can include fax) and timely within and outside the billing practice to individuals involved in the beneficiary s care. A copy of the plan of care (in any form) must be given to the patient and/or caregiver.

79 Request Staffing Request Patient Case Management Services
80 minutes Chronic care management (CCM) services under CPT code (Chronic care management services, at least 20 minutes of clinical staff time directed by a physician or other qualified health professional, per calendar month, with the following required elements: Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient; Chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline; Comprehensive care plan established, implemented, revised, or monitored.
81
82 99487 Complex CCM 60 minutes CPT code Complex chronic care management services, with the following required elements: Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient; Chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline; Establishment or substantial revision of a comprehensive care plan; Moderate or high complexity medical decision making; 60 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month.
83 99489 Complex CCM Each additional 30 minutes after initial 60 minutes CPT code Each additional 30 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month (List separately in addition to code for primary procedure).
84 RHC RHC Supervision After considering the comments, we are finalizing this policy to revise (a)(5) and (a)(5) to state that services and supplies furnished incident to CCM and TCM services can be furnished under general supervision of a RHC or FQHC practitioner.
85
86


87

88
89
90 Operational Workflow #1 Schedule face-to-face initiating visit. Check for 2+ chronic conditions and identify chart as CCM Eligible with sticker or electronic methodology. Include Health Endeavors CCM Patient Brochure in chart for visit. #6 Health Endeavors verify no other provider billing or transitional care codes using claims data. #7 Health Endeavors commence CCM Basic (20 minutes) and Complex Services (60 minutes plus 30 minutes). #2 At face-to-face initiating visit obtain patient verbal consent and conduct copay discussion using Health Endeavors CCM Patient Brochure to guide the conversation. Note the verbal consent in patient chart. #5 Request Health Endeavors CCM Services via Health Endeavors Portal. Must complete all mandatory fields. #8 Health Endeavors staff onsite in clinic or offsite call centers located in Omaha, NE and Phoenix, AZ Must have at least 100 consents and 500 total potential eligible patients for Health Endeavors to staff program. #3 Conduct and bill face-to-face initiating E/M visit and Add-On or Prolonged Service Codes (depending on time spend with patient. #4 Create plan of care in EHR. Health Endeavors must have access to EHR for each CCM patient. #9 For clinic staff access to Health Endeavors events and reporting tools setup patient match API/Single Sign-On.
91 Conduct Monthly Assessment Identify patient needs on a monthly basis for Referrals/Orders, Appointments and Prescription Renewal using Care Coordination Patient Needs Assessment Template (Monthly Assessment). Health Endeavors communicate Monthly Assessment to clinic nurse manager via fax or secure on a daily basis. Alternative clinic provide point of contact to set appointments, provider referrals/orders and prescription renewal. Health Endeavors may be granted access to schedule appointments in clinic scheduling system (optional). Patient Phone Intervention with clinical staff Review Monthly Assessment with Patient. Complete assigned template for month; e.g. Fall Screening, medication reconciliation, immunization reminder, etc. 3 attempts made each month. Voice message left with #800 return number. Call made on behalf of Assigned Provider. Area Code masking to local area code available upon request. Patient Empowerment Portal (MACRA Compliance) Online Chat with clinical staff Monthly Things to Complete - Online Screenings (Customizable Templates) Things to Complete /Text Message reminders Patient Disease-Specific Education with interactive quizzes Measurable Goal Setting Templates (Intervention Templates) Continuity of Care Record/Document transfer from EHR to patient (Clinical Summary)
92
93
94
95
96
97 Benefits of CCM Patient Case Management Quality Measure Completion ACO Shared Savings Revenue Generation Improve Patient Experience Improve Patient Health Value-Based Medicine
98
99
100
101
102
103 Request Patient Case Management Services TRAINING GUIDE CURRENT VERSION V HEALTH ENDEAVORS 2016

104 HEALTH ENDEAVORS 2016
105 Health Endeavors CCM Consent Health Endeavors Clinic Contact HEALTH ENDEAVORS 2016
106 Mandatory Mandatory Mandatory Mandatory HEALTH ENDEAVORS 2016
107 Mandatory only if patient has an authorized delegate for care Mandatory only if patient has an authorized delegate for care Mandatory only if patient has an authorized delegate for care Mandatory only if patient has an authorized delegate for care Click Save (DO NOT CLICK Save and Close) HEALTH ENDEAVORS 2016
108 Request Patient Case Management Services TRAINING GUIDE NEW RELEASE DECEMBER, 2016 V HEALTH ENDEAVORS 2016
109 Updates Find Patient Add Patient Select Payor Type Select Program Type Coming Soon - Edit Patient launches patient portal - Myhe.com patient portal
110
111 Health Endeavors CCM Consent Health Endeavors Clinic Contact HEALTH ENDEAVORS 2016
112 Mandatory Mandatory Mandatory Mandatory HEALTH ENDEAVORS 2016
113 Mandatory only if patient has an authorized delegate for care Mandatory only if patient has an authorized delegate for care Mandatory only if patient has an authorized delegate for care Mandatory only if patient has an authorized delegate for care Click Save (DO NOT CLICK Save and Close) HEALTH ENDEAVORS 2016
114 Contact Us Kris Gates, CEO 11/14/
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
MACRA Frequently Asked Questions
 Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation
 New Member Orientation") SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
2017 Transition Year Flexibility Advancing Care Information (ACI) Category Options
 Category Options") The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2017 Transition Year Flexibility Advancing Care Information (ACI) Category Options Ad 1 P a g e
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2017 Transition Year Flexibility Advancing Care Information (ACI) Category Options Ad 1 P a g e
MACRA Implementation: A Review of the Quality Payment Program
 MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
Strategic Implications & Conclusion
 Kelly Court Chief Quality Officer Wisconsin Hospital Association Brian Vamstad Government Relations Consultant Gundersen Health System Overview and Key Takeaways of the Medicare Quality Payment Program
Kelly Court Chief Quality Officer Wisconsin Hospital Association Brian Vamstad Government Relations Consultant Gundersen Health System Overview and Key Takeaways of the Medicare Quality Payment Program
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
Advancing Care Information- The New Meaningful Use September 2017
 Advancing Care Information- The New Meaningful Use September 2017 ACO Announcements Reminders: ACO Notifications PECOS-Maintain active enrollment 2017 Patient Prospective Lists Upcoming provider/office
Advancing Care Information- The New Meaningful Use September 2017 ACO Announcements Reminders: ACO Notifications PECOS-Maintain active enrollment 2017 Patient Prospective Lists Upcoming provider/office
MIPS Checkpoint. Beth Hickerson Quality Improvement Advisor. PHA Lunch and Learn May 19, Value Driven. Health Care. Solutions.
 MIPS Checkpoint Beth Hickerson Quality Improvement Advisor PHA Lunch and Learn May 19, 2017 Check Your MIPS Eligibility QPP.CMS.GOV 2 MIPS Category Weights Over Time : Quality Advancing Care Information
MIPS Checkpoint Beth Hickerson Quality Improvement Advisor PHA Lunch and Learn May 19, 2017 Check Your MIPS Eligibility QPP.CMS.GOV 2 MIPS Category Weights Over Time : Quality Advancing Care Information
2017 Transition Year Flexibility Improvement Activities Category Options
 The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2017 Transition Year Flexibility Improvement Activities Category Options 1 P a g e Ad MEDICARE
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2017 Transition Year Flexibility Improvement Activities Category Options 1 P a g e Ad MEDICARE
The Quality Payment Program Overview Fact Sheet
 Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
Quality Payment Program MIPS. Advanced APMs. Quality Payment Program
 Proposed Rule: Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models The Department
Proposed Rule: Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models The Department
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Physician Quality Reporting System & VBPM, 2015
 Physician Quality Reporting System & VBPM, 2015 Andrew Bienstock Transformation Support Services Manager 1 Agenda 1. PQRS Penalty 2. PQRS Eligibility 3. PQRS Reporting Options 4. Value Based Payment Modifier
Physician Quality Reporting System & VBPM, 2015 Andrew Bienstock Transformation Support Services Manager 1 Agenda 1. PQRS Penalty 2. PQRS Eligibility 3. PQRS Reporting Options 4. Value Based Payment Modifier
MIPS Program: 2018 Advancing Care Information Category
 MIPS Program: 2018 Advancing Care Category The 2018 Quality Payment Program (QPP) Year Two final rule continues to implement the programs authorized under the Medicare and CHIP Reauthorization Act of 2015
MIPS Program: 2018 Advancing Care Category The 2018 Quality Payment Program (QPP) Year Two final rule continues to implement the programs authorized under the Medicare and CHIP Reauthorization Act of 2015
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs. September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto
 2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
Quality Payment Program: The future of reimbursement
 Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
Strategies for Coding, Billing and Getting Paid Appropriately
 Strategies for Coding, Billing and Getting Paid Appropriately 2015 Monograph Update California Academy of Family Physicians Another new year and time to make sure your practice is doing everything possible
Strategies for Coding, Billing and Getting Paid Appropriately 2015 Monograph Update California Academy of Family Physicians Another new year and time to make sure your practice is doing everything possible
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Travis Broome AMIA
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Travis Broome AMIA 9-20-2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New clinical quality measures
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Travis Broome AMIA 9-20-2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New clinical quality measures
Sevocity v Advancing Care Information User Reference Guide
 Sevocity v.12 User Reference Guide 1 877 877-2298 support@sevocity.com Table of Contents About Advancing Care Information... 3 Setup Requirements... 3 Product Support Services... 3 About Sevocity v.12...
Sevocity v.12 User Reference Guide 1 877 877-2298 support@sevocity.com Table of Contents About Advancing Care Information... 3 Setup Requirements... 3 Product Support Services... 3 About Sevocity v.12...
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
From Surviving to Thriving in the QPP World
 From Surviving to Thriving in the QPP World Today s Objectives Brief MACRA Overview Where are we going?: Advanced Alternative Payment Models (APMs) Where are we now? Merit Incentive-Based Payment System
From Surviving to Thriving in the QPP World Today s Objectives Brief MACRA Overview Where are we going?: Advanced Alternative Payment Models (APMs) Where are we now? Merit Incentive-Based Payment System
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Meaningful Use 2016 and beyond
 Meaningful Use 2016 and beyond Main Street Medical Consulting May 12, 2016 Meaningful use, MACRA, MIPS? Whaaaaat? 1 Reporting Period and Timeline In 2016 all providers are required to use CEHRT versions
Meaningful Use 2016 and beyond Main Street Medical Consulting May 12, 2016 Meaningful use, MACRA, MIPS? Whaaaaat? 1 Reporting Period and Timeline In 2016 all providers are required to use CEHRT versions
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
Registering for PQRS Reporting and Understanding the Implications and Proposed Policies for the Value based Payment Modifier
 Registering for PQRS Reporting and Understanding the Implications and Proposed Policies for the Value based Payment Modifier Presented by: Centers for Medicare and Medicaid Services Performance Based Payment
Registering for PQRS Reporting and Understanding the Implications and Proposed Policies for the Value based Payment Modifier Presented by: Centers for Medicare and Medicaid Services Performance Based Payment
QUALITY PAYMENT PROGRAM
 NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
Beyond Meaningful Use: Driving Improved Quality. CHCANYS Webinar #1: December 14, 2016
 Beyond Meaningful Use: Driving Improved Quality CHCANYS Webinar #1: December 14, 2016 Agenda The Current State Measuring Monitoring & Reporting Quality. Meaningful Use 2018 and Beyond The New Quality Payment
Beyond Meaningful Use: Driving Improved Quality CHCANYS Webinar #1: December 14, 2016 Agenda The Current State Measuring Monitoring & Reporting Quality. Meaningful Use 2018 and Beyond The New Quality Payment
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
Stage 3 and ACI s Relationship to Medicaid MU Massachusetts Medicaid EHR Incentive Program
 Stage 3 and ACI s Relationship to Medicaid MU Massachusetts Medicaid EHR Incentive Program September 19 & 20, 2017 Today s presenters: Brendan Gallagher Thomas Bennett Agenda Stage 3 Meaningful Use (MU)
Stage 3 and ACI s Relationship to Medicaid MU Massachusetts Medicaid EHR Incentive Program September 19 & 20, 2017 Today s presenters: Brendan Gallagher Thomas Bennett Agenda Stage 3 Meaningful Use (MU)
Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP)
") Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP) 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois
Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP) 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Overview of Quality Payment Program
 Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Michelle Brunsen & Sandy Swallow May 25, , Telligen, Inc.
 MIPS Survive and Thrive: Advancing Care Information Michelle Brunsen & Sandy Swallow May 25, 2017 2016, Telligen, Inc. Objectives Quality Payment Program Updates Advancing Care Information (ACI) Category
MIPS Survive and Thrive: Advancing Care Information Michelle Brunsen & Sandy Swallow May 25, 2017 2016, Telligen, Inc. Objectives Quality Payment Program Updates Advancing Care Information (ACI) Category
Disclosure Statement
 2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
Quality Payment Program Year 2: 2018 MIPS Participation. An Introductory Guide for CRNAs in 2018
 Quality Payment Program Year 2: 2018 MIPS Participation An Introductory Guide for CRNAs in 2018 Quality Payment Program (QPP) The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) established
Quality Payment Program Year 2: 2018 MIPS Participation An Introductory Guide for CRNAs in 2018 Quality Payment Program (QPP) The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) established
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017
 Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
MIPS Advancing Care Information: Tips, Tools and Support Q&A from Live Webinar March 29, 2017
 MIPS Advancing Care Information: Tips, Tools and Support Q&A from Live Webinar March 29, 2017 Below are questions that were submitted during the Quality Insights Advancing Care Information webinar on March
MIPS Advancing Care Information: Tips, Tools and Support Q&A from Live Webinar March 29, 2017 Below are questions that were submitted during the Quality Insights Advancing Care Information webinar on March
WHITE PAPER. Taking Meaningful Use to the Next Level: What You Need to Know about the MACRA Advancing Care Information Component
 Taking Meaningful Use to the Next Level: What You Need to Know Table of Contents Introduction 1 1. ACI Versus Meaningful Use 2 EHR Certification 2 Reporting Periods 2 Reporting Methods 3 Group Reporting
Taking Meaningful Use to the Next Level: What You Need to Know Table of Contents Introduction 1 1. ACI Versus Meaningful Use 2 EHR Certification 2 Reporting Periods 2 Reporting Methods 3 Group Reporting
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Decoding the QPP Year 2 Quality Measure Benchmarks and Deciles to Maximize Performance
 Decoding the QPP Year 2 Quality Measure Benchmarks and s to Maximize Performance Leila Volinsky, MHA, MSN, RN, PCMH CCE, CPHQ Senior Program Administrator New England Regional Lead Quality Payment Program
Decoding the QPP Year 2 Quality Measure Benchmarks and s to Maximize Performance Leila Volinsky, MHA, MSN, RN, PCMH CCE, CPHQ Senior Program Administrator New England Regional Lead Quality Payment Program
MIPS (Merit-based Incentive Payment System) Clinical Practice Improvement Activities
 Clinical Practice Improvement Activities") MIPS (Merit-based Incentive Payment System) Clinical Practice Improvement Activities Today we will cover: 2 General review of the Quality Payment Programs as per the final rule. Who is Eligible/Exceptions
MIPS (Merit-based Incentive Payment System) Clinical Practice Improvement Activities Today we will cover: 2 General review of the Quality Payment Programs as per the final rule. Who is Eligible/Exceptions
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule
 Final Rule") Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Centers for Medicare and Medicaid CMS Updates. Christol Green, Anthem Inc.
 Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
The MIPS Survival Guide
 The MIPS Survival Guide The Definitive Guide for Surviving the Merit-Based Incentive Payment System TABLE OF CONTENTS 1 An Introduction to the Merit-Based Incentive Payment System (MIPS) 2 Survival Tip
The MIPS Survival Guide The Definitive Guide for Surviving the Merit-Based Incentive Payment System TABLE OF CONTENTS 1 An Introduction to the Merit-Based Incentive Payment System (MIPS) 2 Survival Tip
Transitional Care Management We provide these services a-la-carte...
 Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013 What is in the Rule Changes to Stage 1 of meaningful use Stage
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013 What is in the Rule Changes to Stage 1 of meaningful use Stage
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference
 Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference June 22, 2017 Michael J. Sexton, MD Catherine I. Hanson, JD COI Disclosure To assure the highest quality of CME programming, the OMA
Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference June 22, 2017 Michael J. Sexton, MD Catherine I. Hanson, JD COI Disclosure To assure the highest quality of CME programming, the OMA
MEANINGFUL USE 2015 PROPOSED 2015 MEANINGFUL USE FLEXIBILITY RULE
 MEANINGFUL USE 2015 PROPOSED 2015 MEANINGFUL USE FLEXIBILITY RULE *Please note, the below guidelines are currently proposed. ASCRS will let you know if and when they are finalized through regulatory alerts
MEANINGFUL USE 2015 PROPOSED 2015 MEANINGFUL USE FLEXIBILITY RULE *Please note, the below guidelines are currently proposed. ASCRS will let you know if and when they are finalized through regulatory alerts
MACRA and MIPS. How Medicare Meaningful Use and PQRS are Changing
 MACRA and MIPS How Medicare Meaningful Use and PQRS are Changing Link to recorded session: https://attendee.gotowebinar.com/recording/1305549490878052097 Presenting Today: Molly Goodhart Joined Quatris
MACRA and MIPS How Medicare Meaningful Use and PQRS are Changing Link to recorded session: https://attendee.gotowebinar.com/recording/1305549490878052097 Presenting Today: Molly Goodhart Joined Quatris
during the EHR reporting period.
 CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
Understanding Medicare s New Quality Payment Program
 Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
WHY SHOULD A CHC/FQHC CARE?
 Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
EHR/Meaningful Use
 EHR/Meaningful Use 2015-2017 The requirements for Meaningful Use attestation have changed due to the recently released Medicare and Medicaid Programs: Electronic Health Record Incentive Program Stage 3
EHR/Meaningful Use 2015-2017 The requirements for Meaningful Use attestation have changed due to the recently released Medicare and Medicaid Programs: Electronic Health Record Incentive Program Stage 3
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
Preparing for the 2018 EHR Medicaid Incentive Payment Program
 Preparing for the 2018 EHR Medicaid Incentive Payment Program 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois Health Information
Preparing for the 2018 EHR Medicaid Incentive Payment Program 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois Health Information
Agenda. Surviving the New Program Requirements and the Financial Penalties Under MIPS 9/9/2016. Steps to take to prepare for MIPS
 Surviving the New Program Requirements and the Financial Penalties Under MIPS September 2016 Selena Hood Agenda Steps to take to prepare for MIPS Introduction and Evaluation of the Merit-Based Incentive
Surviving the New Program Requirements and the Financial Penalties Under MIPS September 2016 Selena Hood Agenda Steps to take to prepare for MIPS Introduction and Evaluation of the Merit-Based Incentive
Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care
 Small Rural Hospital Transition (SRHT) Project HELP Webinar Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care Paul Kleeberg, MD, FAAFP, FHIMSS Aledade Medical Director
Small Rural Hospital Transition (SRHT) Project HELP Webinar Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care Paul Kleeberg, MD, FAAFP, FHIMSS Aledade Medical Director
FAQ s from TRAKnet webinar MIPS/MACRA: The most up-to-date information and what you need to know in TRAKnet to comply in 2017
 FAQ s from TRAKnet webinar MIPS/MACRA: The most up-to-date information and what you need to know in TRAKnet to comply in 2017 Do we have to do the quality measures that we have previously done from the
FAQ s from TRAKnet webinar MIPS/MACRA: The most up-to-date information and what you need to know in TRAKnet to comply in 2017 Do we have to do the quality measures that we have previously done from the
Meaningful Use CHCANYS Webinar #1
 Meaningful Use 2016 CHCANYS Webinar #1 Ekem Merchant -Bleiberg, Director of Implementation Services Alliance of Chicago Wednesday February 24, 2016 Agenda 2016 Meaningful Use Guidelines Timelines & Deadlines
Meaningful Use 2016 CHCANYS Webinar #1 Ekem Merchant -Bleiberg, Director of Implementation Services Alliance of Chicago Wednesday February 24, 2016 Agenda 2016 Meaningful Use Guidelines Timelines & Deadlines
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
MIPS Program: 2017 Advancing Care Information Category (formerly known as Meaningful Use) Proposed Rule Guide
 Proposed Rule Guide") MIPS Program: 2017 Advancing Care Information Category (formerly known as Meaningful Use) Proposed Rule Guide On April 27, 2016, CMS released a proposed rule on the Quality Payment Program, which includes
MIPS Program: 2017 Advancing Care Information Category (formerly known as Meaningful Use) Proposed Rule Guide On April 27, 2016, CMS released a proposed rule on the Quality Payment Program, which includes
How to Participate Today 4/28/2015. HealthFusion.com 2015 HealthFusion, Inc. 1. Meaningful Use Stage 3: What the Future Holds
 Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
The History of Meaningful Use
 A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
EHR Incentive Programs: 2015 through 2017 (Modified Stage 2) Overview
 Overview") EHR Incentive Programs: 2015 through (Modified Stage 2) Overview CMS recently released a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and critical access hospitals
EHR Incentive Programs: 2015 through (Modified Stage 2) Overview CMS recently released a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and critical access hospitals
Eligibility. Program Structure and Process for Receiving Incentives
 Overview of Medicare Incentives in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use of Certified Electronic Health Records 1 Eligibility Medicare Eligibility: For Medicare
Overview of Medicare Incentives in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use of Certified Electronic Health Records 1 Eligibility Medicare Eligibility: For Medicare
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018
 Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018 NOTE: These policies have only been proposed. No policies are final
Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018 NOTE: These policies have only been proposed. No policies are final
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Medical Practice Executive Insights
 Proposed 2019 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
Proposed 2019 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage
 PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2016 Tipsheet
 EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2016 Tipsheet CMS published a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and
EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2016 Tipsheet CMS published a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals, and
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
The AAAAI Quality Clinical Data Registry: What the office staff needs to know
 The AAAAI Quality Clinical Data Registry: What the office staff needs to know Today We ll Cover The AAAAI Allergy, Asthma & Immunology Quality Clinical Data Registry I. Defining a Qualified Clinical Data
The AAAAI Quality Clinical Data Registry: What the office staff needs to know Today We ll Cover The AAAAI Allergy, Asthma & Immunology Quality Clinical Data Registry I. Defining a Qualified Clinical Data
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians
 Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems
 Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems Dr. Ashby Wolfe, Chief Medical Officer Centers for Medicare and Medicaid Services,
Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems Dr. Ashby Wolfe, Chief Medical Officer Centers for Medicare and Medicaid Services,
Medicare and Medicaid EHR Incentive Program. Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment
 Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
American Recovery & Reinvestment Act
 American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
2014 CMS PROPOSED PHYSICIAN FEE SCHEDULE OVERVIEW & ANALYSIS
 2014 CMS PROPOSED PHYSICIAN FEE SCHEDULE OVERVIEW & ANALYSIS OVERVIEW: The Centers for Medicare and Medicaid Services (CMS) released the proposed 2014 Medicare Physician Fee Schedule in July. Final code
2014 CMS PROPOSED PHYSICIAN FEE SCHEDULE OVERVIEW & ANALYSIS OVERVIEW: The Centers for Medicare and Medicaid Services (CMS) released the proposed 2014 Medicare Physician Fee Schedule in July. Final code
MIPS eligibility lookup tool (available in Spring 2018): https://qpp.cms.gov/participation-lookup
: https://qpp.cms.gov/participation-lookup") 2018 MIPS Roadmap Under the Quality Payment Program launched in 2017, the Centers for Medicare and Medicaid Services (CMS) evaluates all eligible clinicians based on one of two tracks. The Academy expects
2018 MIPS Roadmap Under the Quality Payment Program launched in 2017, the Centers for Medicare and Medicaid Services (CMS) evaluates all eligible clinicians based on one of two tracks. The Academy expects