EAGLE RANCH ACADEMY, INC. Admissions / Enrollment Information
|
|
|
- Melvyn McCoy
- 6 years ago
- Views:
Transcription
1 EAGLE RANCH ACADEMY, INC. Admissions / Enrollment Information 2009

2 Our Goal is to Help YOU Help Your Child. Paul Arslanian - Executive Director ADMISSIONS / ENROLLMENT INFORMATION CONGRATULATIONS - Your Child has been accepted to one of the finest Youth Development Programs in the world. We look forward to working with your Child, and helping YOU help your Child begin to enjoy the benefits and opportunities of youth. Eagle Ranch Academy is proud to be able to bring families an upper level program at a more affordable price. ERA is not a Group Home with Students maintained in a confined space, nor a facility with a large enrollment where Students are just one of many. Our enrollment is limited, and our setting is a spacious residential campus in the heart of one of the favored locations in the USA. Our Team is committed to helping your Child benefit from this wholesome, healthy environment. We need your help to maximize the effects of our Staff. As we make our assessment of your Child during our Admissions/Intake Process, we will provide you with some very specific steps for you to take to help your Child progress in our Program. Our Program is unique among Youth Development Centers as your Child will be monitored and supervised by qualified therapists and professionals on a 24 hour 7 day a week basis. Thank you for completing the Application/Student Intake Assessment information, and we trust that it was as thorough as possible, as it will assist us in determining the appropriateness of our Program for your Child/Student. At Eagle Ranch Academy we provide the services necessary to assist each person in making the transition back to successful living. Now that your Child has been accepted, the accuracy of the information in each section of the Application will help us in effectively understanding your Child, and completing our Intake Assessment and Admissions Process. It is understood that upon physical admission to Eagle Ranch Academy, the admitting staff will do a complete assessment to ascertain whether or not the applicant/resident is sufficiently qualified (including detoxified) for admission. Eagle Ranch Academy is not a medical facility and in the event, during the Intake Process if the applicant does not meet the criteria for immediate admission, Eagle Ranch Academy will require immediate transportation to the necessary facility. Eagle Ranch Academy will assist you with this, but cannot assume responsibility for transportation, monitoring, or making arrangements for medical care prior to official admission. Additionally, it is understood if the applicant/resident is recalcitrant, refusing treatment, and unwilling to participate in the Program at anytime during residency, Eagle Ranch Academy reserves the right to immediately discharge, and although ERA will assist you with the following, it cannot assume responsibility for transportation, monitoring, or making arrangements for transfer to another facility. Eagle Ranch Academy is a voluntary program that challenges young adults to participate in the recovery process. We are committed to this process and the integrity of our community. Once again - Congratulations for the acceptance of your Child to Eagle Ranch Academy. Now, to complete the Admissions Process proceed to the next page, and follow the steps required. Eagle Ranch Academy - Admissions / Enrollment Information
3 List of steps to take for Admission: 1. Contact current counselor, therapist, etc., and let them know you are interested in placing your Child into Eagle Ranch Academy. It is important to sign the Release of Protected Health Information form (HIPAA) so we can discuss your Childs case with your Childs Clinician. 2. Provide ERA with copies of all Mental & Emotional Treatment Records including Discharge Summaries, Treatment Termination Summaries, Results of Psychological & Psychiatric Testing, Hospital Discharge Summaries, and Educational Testing Summaries. 3. Copy of Immunization Records. And, be sure to list any current and past medications. 4. Copy of Birth Certification. 5. Copies of all current School Transcripts and Records. Signed Permission Form so ERA can correspond directly with Childs current school officials. 6. Sign and have notarized the Power of Attorney form. 7. Current photograph of your Child. 8. If requested, provide a copy of Court Custody Agreements in case of divorced/separated Parents. 9. Work with ERA Admissions Director to arrange a date for your Child to be enrolled into ERA, and to help arrange for transportation. 10. Interstate Compact Agreement filled out, signed and returned to us. 11. Copy of Insurance Cards. 12. Pre-approved Insurance if benefits are available. 13. Review the Application / Student Intake Assessment form you previously filled out to make sure it is accurate, complete, and signed. We rely on this information in making our assessment. And finally - Secure the funds necessary for enrollment, sign the Enrollment Agreement, and send or bring everything requested to the Admissions Director at Eagle Ranch Academy. We are aware that it was a difficult decision for you to send your Child away from home. Your decision to do so was made after careful consideration and a great deal of anguish and pain. As you are realizing these specialized programs are not cheap. Most parents that enroll a child in a quality program such as Eagle Ranch Academy do so by making the personal sacrifice of dipping into the assets they have accumulated over the years or taking out a loan or second mortgage. We are unique in that we have a non-profit organization we work closely with to provide scholarships to you to help reduce the cost, and to your Child for long term benefit. We also have a full-time Insurance Specialist that will help guide you through the Insurance process, and our Admissions Staff will offer suggestions and advice on securing financing for the Tuition and Admission/Intake Assessment Fee. ERA provides assistance in billing your Insurance Company, and any reimbursement from your Insurance will be credited to your account or refunded to you if your Child has been discharged and your account is paid in full. Please note that this billing is a courtesy provided by ERA, and is for your convenience, but Parent/Guardians are still responsible for full payment via credit or debit card or check or cash, the 1 st of each month. Payment 6 months ahead will assist in scholarship benefit. Our monthly Tuition and Admission / Intake Assessment Fee are based on $350 per day. The Admission / Intake Assessment Process takes 20 days, and the Fee = $7,000 (20 days X $350). The monthly Tuition = $10,500 per month. Partial months are figured at $350 per day, and full months are billed at $10,500 per month. Before the Child can be brought to ERA, a payment of $7,000 (minimum) for 20 $350 per day must be sent to ERA. Once enrollment is secured, the monthly Tuition ($10,500) is due by the 1 st of each month, and full payment paid in advance can help in scholarship qualifications. Eagle Ranch Academy - Admissions / Enrollment Information
4 Payment Options include: - Tuition can be paid via debit or credit card or check prior to the 1 st of each month. - Pre-payment by check or cash for partial or full Tuition for anticipated length of stay. Any overpayment due to Students early or mid-month completion or discharge will be refunded. - Failure to pay Tuition will result in Students discharge; but, before this happens, please make arrangements with ERA to work with the personal advocate that we make available for funding consulting. The company is Solutions Financial, and due to a special arrangement with ERA, they will assist you in finding the most appropriate and cost efficient financing options. The Admission / Intake Assessment Fee includes the following: 1. Complete physical examination. 2. Dental examination if needed. 3. Psychiatric, psycho-social assessment. 4. Lab work. 5. Psychological/psychiatric and educational evaluation and testing as needed. 6. Academic assessment. 7. All academic books and supplies. 8. Complete student evaluation. 9. All clothing, sandals, coats, hats, etc. **Except for a pair of Athletic Shoes for hiking, basketball, soccer, active sports, etc. to be provided by Parent/Guardian. 10. All bedding needs (sheets, pillow case, blanket/comforter), linens, towels, and all personal hygiene items. 11. The Staff Physician administers a physical examination at admission, and the Staff Nurse monitors health issues thereafter. 12. The Staff Psychiatrist/Psychologist will complete a mental health examination and will provide ongoing psychiatric care thereafter, as needed; but please note that after the 2 initial visits, it will be billed as extra medical service, if necessary. ERA is not a medical facility, but if we can provide the appropriate level of care that your Child needs, we will do so at a much more cost efficient level than a medical facility is able to do. Eagle Ranch Academy - Admissions / Enrollment Information
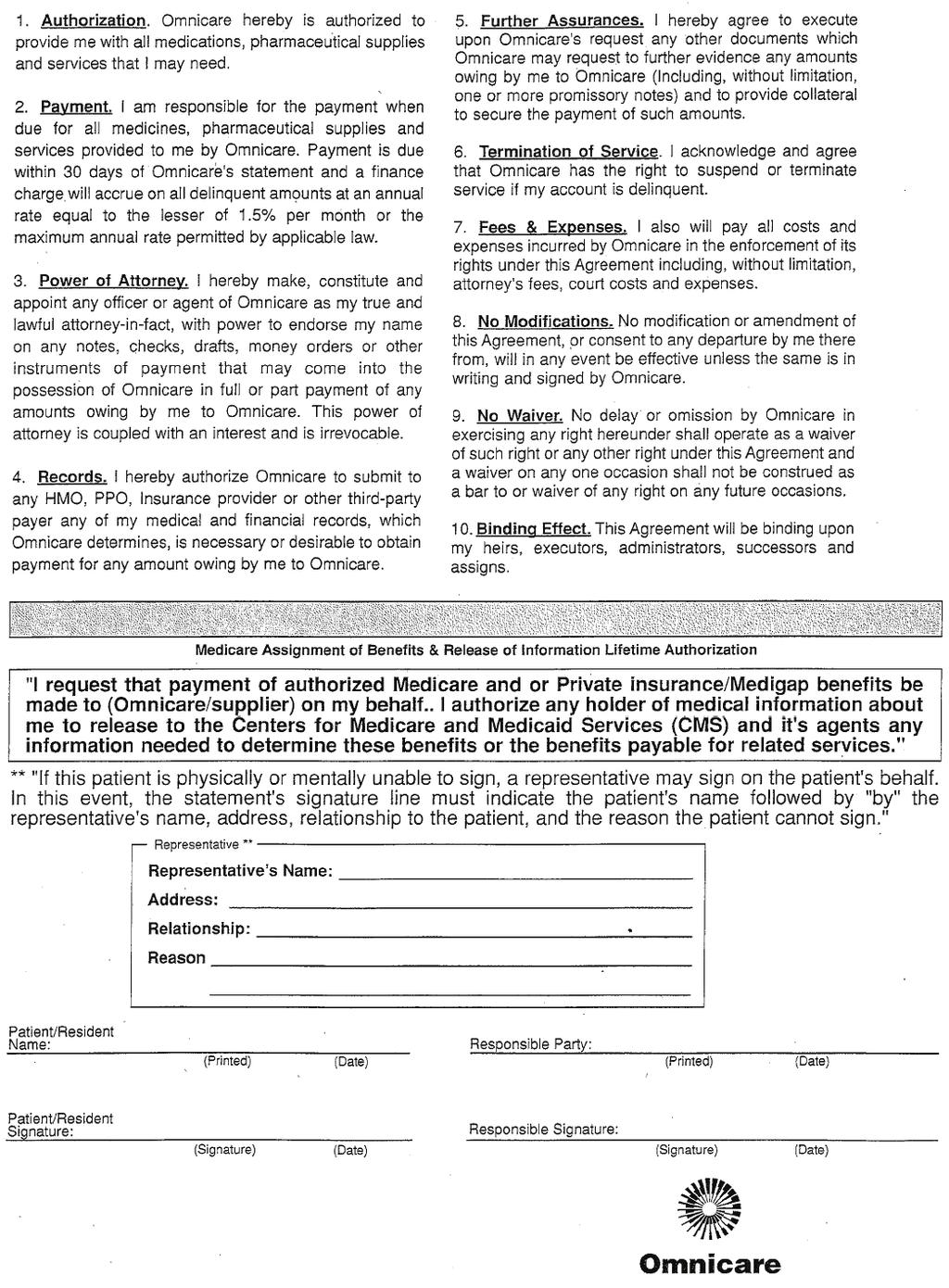
5 EAGLE RANCH ACADEMY - ADMISSIONS AND ENROLLMENT INFORMATION I. FORMS Complete and Sign before Student can be Admitted 1. Enrollment Agreement. 2. Power of Attorney (Must be Notarized). 3. Student Intake Assessment (previously filled out and sent to ERA during the Application Process). 4. Contact Information / Notification in case of Emergency. 5. Release of Protected Health Information - HIPAA. 6. Permission for Program Items. 7. Consent to Receive Psychoactive Medications. 8. Interstate Compact Law and Agreement. 9. Permission to Obtain School Records. 10. Assignment of Insurance Benefits & Omnicare Form. 11. Credit Card Policy and Authorization. 12. Academic Background. 13. Permission for Field Trips / Consent to Examination and Treatment. 14. Runaway Information. II. ITEMS TO INCLUDE Please include the following items with Admissions / Enrollment Information. 1. Current Picture of Student. 2. Copy of Students Birth Certificate. 3. Copy of Physical Exam if within last three months. AND, copies of all Mental and Emotional Treatment Records including Discharge Summaries, Treatment Termination Summaries, Psychological & Psychiatric Testing, Hospital Discharge Summaries, and Educational Testing. 4. Copy of Immunization Records. 5. Copy of Insurance Cards. 6. If Parents are divorced, include copy of Court Decree granting custody of the Student. III. TUITION AND FEES Tuition is $10, per month ($350 per day for partial months). Admissions / Intake Assessment Fee is $7, Initial payment is $7, for 1 st 20 days + $3,500 for next 10 days. Make payment to Eagle Ranch Academy, Inc. (The Admissions / Intake Assessment Fee is Non-Refundable). Credit or debit cards are accepted and billed monthly. Check or cash pre-paid for a minimum of 6 months will qualify for a Scholarship benefit. IV. ITEMS TO BRING The ONLY item you need to bring/send for your Child is a pair of Athletic Shoes for sports, hiking, everyday use. ALL other items are provided by ERA. All items brought to ERA by your Child, will be returned to you upon your first visit to ERA. Eagle Ranch Academy - Admissions / Enrollment Information
6 ENROLLMENT AGREEMENT ERA RECITALS AGREEMENT $5, Eagle Ranch Academy - Enrollment Agreement Page 1 of 9 / Sponsors Initials
7 $7, Eagle Ranch Academy - Enrollment Agreement Page 2 of 9 / Sponsors Initials
8 Eagle Ranch Academy - Enrollment Agreement Page 3 of 9 / Sponsors Initials
9 c) Eagle Ranch Academy - Enrollment Agreement Page 4 of 9 / Sponsors Initials
10 Eagle Ranch Academy - Enrollment Agreement Page 5 of 9 / Sponsors Initials
11 . Eagle Ranch Academy - Enrollment Agreement Page 6 of 9 / Sponsors Initials
12 Eagle Ranch Academy - Enrollment Agreement Page 7 of 9 / Sponsors Initials
13 Signatures on following page] Eagle Ranch Academy - Enrollment Agreement Page 8 of 9 / Sponsors Initials
14 EAGLE RANCH ACADEMY, INC. Eagle Ranch Academy - Enrollment Agreement Page 9 of 9 / Sponsors Initials
15 POWER OF ATTORNEY Eagle Ranch Academy, Inc. THE UNDERSIGNED (hereafter Sponsors ) hereby certify that I/We are the true and lawful attorney in-fact and legal guardians for (hereafter referred to as the Student ), and that the Student is my/our. I/We hereby execute this Power of Attorney for the purpose of appointing Eagle Ranch Academy, Inc., a Utah corporation (hereafter ERA ) as attorney-in-fact for the Student to provide him/her with custodial care, educational, therapeutic and clinical services in connection with his/her enrollment at ERA. Without limiting or qualifying the general Power of Attorney granted and delegated by Sponsor to ERA, Sponsor specifically grants to ERA the following powers: 1. To provide or obtain all medical records, dental, psychiatric treatment, and hospital care, and to authorize a physician to perform any and all procedures that may appear to be medically necessary for the well being of the Student. 2. To guide and discipline the Student as deemed necessary and reasonable by ERA (but not to include physical punishment). 3. To physically restrain the Student as deemed necessary should he/she become a danger to him/herself or to anyone else, as deemed necessary by ERA. 4. To allow the Student to participate in all activities. 5. To search the person and personal effects of the Student at any time, including but not limited to all mail sent to or by Student, and seize and confiscate any items deemed by ERA to be contraband or counterproductive to the Student s successful completion of the ERA Program. The search of the Student s person may require Student to remove all of his or her clothing and may include a strip search of all or any portions of Student s body, including cavities in which contraband could be hidden. 6. To restrict the Student s access to telephone calls, and visitors, and to otherwise monitor the Student s participation in telephone calls and visits when the same are allowed. 7. The enumeration of specific items, rights, acts or powers is not intended to, nor does it, limit or restrict, and is not to be construed as limiting or restricting, the powers herein granted to ERA under this Power of Attorney, but shall also include those rights, acts, or powers which relate to or are necessary to perform any of the foregoing items and those rights, acts, or powers which ERA deems necessary to the Student s advancement in ERA s program. [Signature And Notary On Following Page] Power of Attorney Page 1 of 2 / Sponsor Initials
16 This Power of Attorney shall be effective from the date of arrival, beginning 20 and shall terminate upon completion or termination of Student s enrollment at ERA. DATED this day of, 20. Father/Guardian Mother/Guardian Print Name Signature Print Name Signature STATE OF ) ): ss. COUNTY OF ) On the day of, 20, personally appeared before me, and duly acknowledged that he/she/they fully understand(s) the foregoing Power of Attorney, executed the same of his/here/their own volition and for the purposes set forth, and that he/she/they was acting under no constraint or undue influence whatsoever. Notary Public Residing at: My commission expires: ** Signature & Title of ERA Official receiving this document. Power of Attorney Page 2 of 2 / Sponsor Initials
17 EAGLE RANCH ACADEMY - CONTACT INFORMATION I hereby authorize Eagle Ranch Academy to keep me updated on the progress of my child through the use of the Parent Page and . Also, I give you permission to update the referral agent (if applicable) and my home therapist. In addition, the following is a list of names that I also want to receive these updates; and I verify that I have included any/all Parent/Guardians with Legal Custody rights that must be kept informed: Name Address Relationship Parent/Guardian Therapist Referral Agent Student Name Parent/Guardian Signature Date PERSONS TO NOTIFY IN CASE OF EMERGENCY Name Phone Number Relationship Eagle Ranch Academy - Contact Information / Person to Notify in case of Emergency
18 EAGLE RANCH ACADEMY - AUTHORIZATION FOR THE RELEASE OF PROTECTED HEALTH INFORMATION - HIPAA This authorization form has been specifically designed to comply with all state and federal regulations pertaining to the confidentially of health information. It must be filled out completely with respect to the required content. 1. THE PERSON WHO IS PROVIDING THE AUTHORIZATION: (Student Information) Name SS # Date of Birth Former Name(s) Home Phone No. Address City State / Zip 2. AUTHORIZATION IS HEREBY GRANTED FOR: (To be completed by ERA) Person / Agency Name Address City Phone No. State / Zip Attention to 3. THE SPECIFIC INFORMATION REQUESTED TO BE RELEASED: (Completed by ERA) E.R. Report Discharge Summary History and Physical Consultation X-Ray Report Pathology Report Lab Report Clinic/Progress Report Operative Status Evaluation Mental Status History and Other Date of Treatment(s) I acknowledge and hereby consent to such, that the released information may contain alcohol, drug abuse, psychiatric, HIV results, or Aids information. Initial Eagle Ranch Academy - HIPAA
19 4. PURPOSE OF DISCLOSURE: 5. RECORDS ARE TO BE RELEASED TO: Eagle Ranch Academy 115 West 1470 South St. George, UT office fax 6. REVOKING MY AUTHORIZATION AND WHEN IT WILL EXPIRE: I understand that I have the right to revoke this authorization at any time by sending a written request to the agency privacy officer prior to the expiration date. Revocation of this authorization shall not affect releases of information made prior to the revocation. Unless otherwise revoked, this authorization will expire on the following date or other/event. If I fail to specify an expiration date and/or event, the authorization will expire six (6) months from the date signed. Expires: Date or Other/Event (Discharge or Completion of ERA) 7. SIGNATURE TO GIVE MY AUTHORIZATION: I understand that authorizing the disclosure of my Protected Health Insurance is voluntary and that I need not sign this authorization in order to receive services. I further understand that the disclosure of this information carries with it the potential for authorized disclosure and the information may no longer be protected by Federal Confidentiality rules. Clients Signature Date Parent / Guardian / Personal Representative Signature: Date Relationship to Client I.D. Verification by Witness Signature Date Eagle Ranch Academy - HIPAA
20 EAGLE RANCH ACADEMY - PERMISSION FOR PROGRAM ITEMS Name of Student My Student has permission to attend any church of his/her choice. Yes No Eagle Ranch Academy has my permission to use name, photos, and audio-recordings of my Student in brochures or publicity. Yes No Eagle Ranch Academy has my permission to use my name for referrals to prospective Parents. Yes No I agree that my Student may be tested at any time that drugs or alcohol are suspected. Yes No I grant permission to staff at Eagle Ranch Academy to transport my Student to and from activities. Yes No I grant permission for a staff to dispense medications to my Student as prescribed by a Physician. Yes No I consent to having my Student photographed for the secured Parent Pages on the Eagle Ranch Academy website, and the Graduation DVD for the purpose of providing Parents with pictures of Activities that their Student is involved; and, I agree not to use or allow to be used any picture of other Students or Staff for any purpose outside of ERA. Yes No Signature Date Eagle Ranch Academy - Permission for Program Items
21 EAGLE RANCH - CONSENT TO RECEIVE PSYCHOACTIVE MEDICATIONS To: (Name of Patient) Your attending physician is M.D. State Department of Mental Health regulations require the treatment center to maintain a written record of your decision to consent to the administration of psychoactive medications. You may be treated with psychoactive medications only after you have been informed of your right to accept or refuse such medications, and you must be provided with sufficient information, which shall include the following: 1. The nature of your mental condition. 2. The reasons for your taking the medications, including the likelihood of your improving or not improving without the medications. 3. Reasonable alternative treatment available if any; the type, range of frequency and amount (including use of PRN orders), method (oral or injection), and duration of the probable side effects or these drugs known to commonly occur, any particular side effects likely to occur, and the possible additional side effects which may occur if you take such medication beyond three months. You should have been advised that such effects may include persistent involuntary movement of the face or mouth at times, and include similar movement of the hands and feet after medications have been discontinued. Your signature below constitutes your acknowledgment of the following: 1. That you have read and agree to the foregoing. 2. That the medications and treatment set forth below have been adequately explained and/or discussed with you by your supervising physician, and that you have received all of the information you desire concerning such medication and treatment. 3. That you authorize and consent to the administration of such medication. Medication and Treatment Date Time Student Signature Relationship Patient/Parent/Legal Guardian (Please circle) (If signed by other than patient) Witness Notations by Physician (if applicable) This form is in case the attending physician finds it necessary or advisable for the Student to receive psychotropic medication. This is in agreement with the Parent/Guardian as well as the Student. This form will/may be signed by the Student & Witness upon arrival at ERA. Eagle Ranch Academy - Consent to Receive Psychoactive Medications
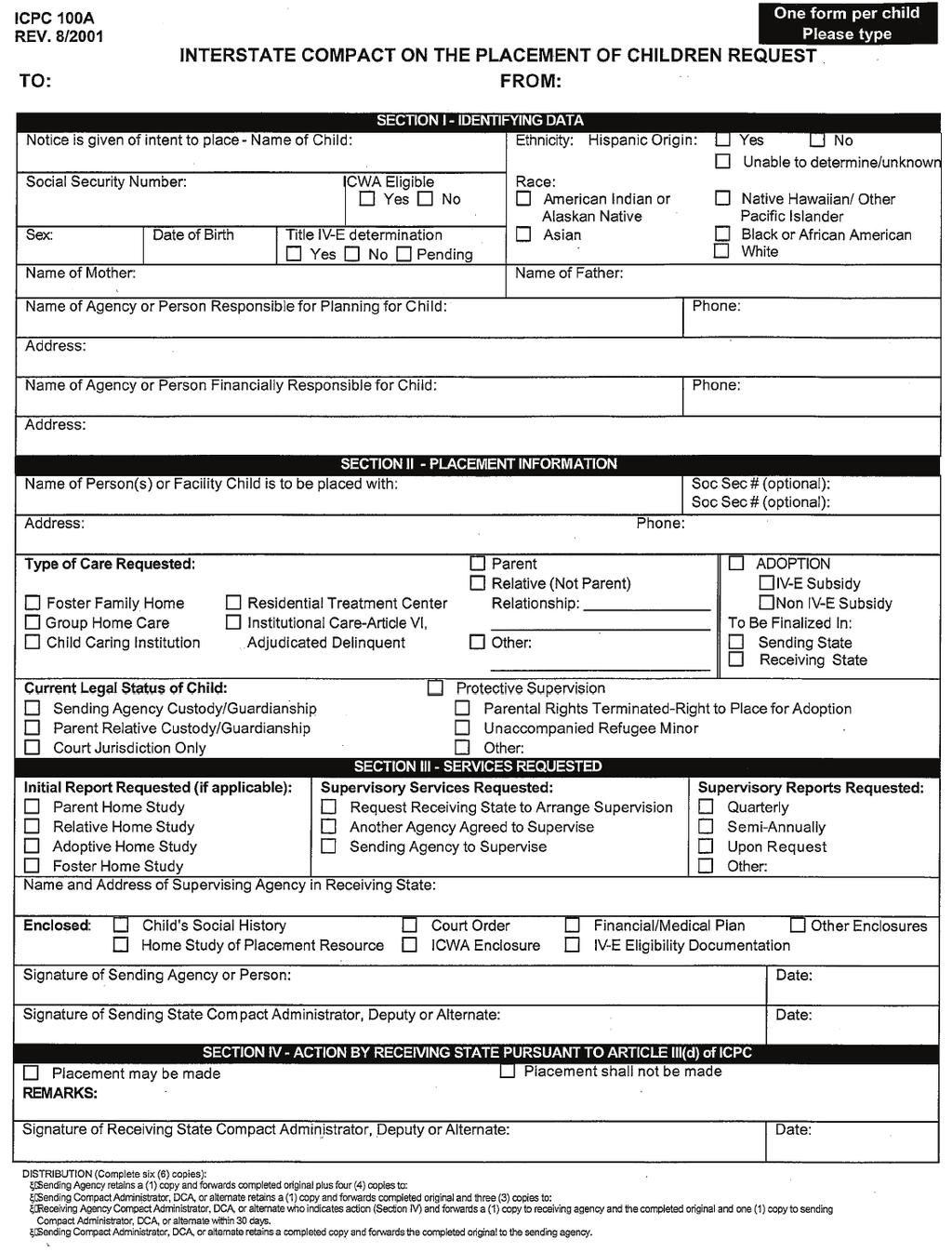
22 INTERSTATE COMPACT LAWS Dear Parent/Guardian: The Interstate Compact on the Placement of Children was established to protect parents and their children, and has been adopted in all 50 states. Federal Law requires that children cannot be placed into the care of an agency across state lines without the approval of the Interstate Compact Authorities in each state. This is intended to assure that children are placed into a licensed, safe and suitable environment with persons having appropriate qualifications and facilities to provide necessary and desirable care, and that the state laws in the sending and receiving states are followed. According to Utah State Law, no child can be sent to an agency in Utah from another state without prior approval from each state. In order to comply with the Utah law you must complete an Interstate Compact Placement Request form. After you have completed the Interstate Compact Placement Request, return it to Eagle Ranch Academy and we will forward it to the appropriate state. It is important to fill out and sign this form and return it to Eagle Ranch Academy immediately. Please feel free to call us with any questions you may have concerning filling out this form, Sincerely, Dave Arslanian Admissions Director Eagle Ranch Academy Important Items when filling out the attached Interstate Compact Request: - Section I - Name of Agency or Person Responsible for Planning for Child = Parent/Legal Guardian - Name of Agency or Person Financially Responsible for Child = Parent/Legal Guardian - Section II - Name of Person(s) or Facility Child is to be placed with = Eagle Ranch Academy - Section III - Name and Address of Supervising Agency in Receiving State = Eagle Ranch Academy - Signature of Sending Agency or Person = Parent/Legal Guardian Eagle Ranch Academy - Interstate Compact Laws
23
24 EAGLE RANCH ACADEMY - PERMISSION TO OBTAIN SCHOOL RECORDS To Principal, Counselor of Name of School Street Address City State Zip School Phone Number Fax Number Name of Student Date of Birth Date Requested Parent / Guardian / Personal Representative Signature The above named student has enrolled in Eagle Ranch Academy. I hereby request the release of his/her school records to be sent to our school at the following address: Eagle Ranch Academy 115 West 1470 South St. George, UT office fax Please include the following: 1. Transcripts. 2. Withdrawal Grades or Incomplete Classes. 3. Health and Immunization Records. 4. Counseling Information Including Psychiatric or Physiological Evaluations. 5. Special Education or Guidance Records. Name and Title of Person Requesting Sincerely, Eagle Ranch Academy Eagle Ranch Academy - Permission to Obtain School Records
25 EAGLE RANCH ACADEMY - ASSIGNMENT OF INSURANCE BENEFITS Patient Name Admit Date Insurance Company Address of Insurance Company Telephone Number of Insurance Company Group Number Policy Insured Name Insured SS # Insured Employer For the purpose of paying all or part monies owing to EAGLE RANCH ACADEMY for services it has or will render to the above patient, the undersigned hereby irrevocably assigns to EAGLE RANCH ACADEMY any benefit payments payable for the benefit of said patient by the above insurance company or companies and all rights and interest in said policy but only to the extent necessary to pay EAGLE RANCH ACADEMY in full. Undersigned hereby grants to EAGLE RANCH ACADEMY the right to bill the above insurance company at retail or at the contract rate. Undersigned acknowledges and agrees, however, that EAGLE RANCH ACADEMY is not obligated or required to bill the insurance company, and may choose to bill the undersigned directly notwithstanding any insurance coverage that may exist. Undersigned agrees to remain liable to pay the full amount of all monies billed by EAGLE RANCH ACADEMY as a result of rendering services to the above mentioned patient and undersigneds liability will only be reduced by the amount of benefit payments received by EAGLE RANCH ACADEMY from the above reference insurer. Notwithstanding the above, undersigneds liability will not be reduced until EAGLE RANCH ACADEMY has collected its full retail or contract rate. Undersigned understands that the nature of patients disability may be such that no benefit payments will be payable under the policy specified above. EAGLE RANCH ACADEMY verifies insurance as a courtesy to the undersigned, and is not responsible for any misinformation received from the insurance company regarding benefits. It is the responsibility of the insured to understand his/her benefits and allowable coverage under the policy. EAGLE RANCH ACADEMY may bill the insurance company as a courtesy only. To the extent necessary to determine liability for payment and to obtain reimbursement, the undersigned authorizes EAGLE RANCH ACADEMY to disclose information from the treatment received to persons or corporations that may be liable for all or any portion of the facilitys charges, including but not limited to insurance companies, health plans and Workers Compensation carriers. Such information may include psychiatric evaluations, diagnoses, history and physical examination reports, program notes, physicians orders and laboratory results, as well as school information. Such records may contain psychiatric or substance abuse information. Any monies owing by the undersigned under the terms of this Agreement shall be paid in full within thirty (30) days after billing by EAGLE RANCH ACADEMY unless other arrangements have been made. In the event that collection efforts are undertaken by EAGLE RANCH ACADEMY to enforce any of the terms of this Agreement, all expenses associated therewith, including attorneys fees, will be paid by the undersigned. The undersigned acknowledges that he or she is entitled to receive a copy of this assignment/authorization. POLICY HOLDER AND/OR PATIENT DATE Please attach a photocopy of the students medical insurance card in case of necessity. Eagle Ranch Academy - Assignment of Insurance Benefits
26 EAGLE RANCH ACADEMY - CREDIT CARD POLICY Eagle Ranch Academy is able to accept the following credit cards: Visa, Master Card, Discover, and American Express (plus 2.5% finance charge, which will be waived if payments are received on time). Credit cards can be used for the following: Initial Assessment Fees, Tuition, Medical Bills when insurance does not cover, and any miscellaneous costs incurred by your child. All credit cards are debited automatically on or around the 25 th of each month for the next month. If you are paying by credit card, please fill out the needed information, sign the authorization, and return to Eagle Ranch Academy. An itemized bill will be sent to you each month with all charges and credits that were applied that month. CREDIT CARD AUTHORIZATION I hereby give permission for Eagle Ranch Academy to debit my credit card monthly for tuition and other charges for my Student Name Credit Card Type Name on Card Credit Card Number Expiration Date Signature of Cardholder Date Day Phone No. Evening Phone No. Your Address where you receive your Credit Card Statement: Address City State Zip Eagle Ranch Academy - Credit Card Authorization
27
28
29 EAGLE RANCH ACADEMY - ACADEMIC BACKGROUND What are your childs current academic needs? What are your academic goals for your child while at ERA? At what age and with what class did your child begin school? In what grade did your child start to struggle (if any)? Has your child repeated any grade(s) If yes which grade(s) Has your child ever been suspended? Has your child ever been expelled? Explain: Explain: Has your child received Special Ed. or Resource Classes: What was the last grade your child completed? Last School Attended Counselor Classification? (i.e.. LD/BD): What grade is your child in? Extra Curricular Activities/Hobbies Has your child ever demonstrated violent behavior towards school staff, teachers, or other students? If yes Explain: Please attach a copy of your childs school transcript and immunization records to this form. Eagle Ranch Academy - Academic Background
30 EAGLE RANCH ACADEMY - PERMISSION FOR FIELD TRIPS I hereby give my permission for my child to participate in Eagle Ranch Academy sponsored excursions by car or van, supervised by school staff, away from school grounds to areas of interest or places for service projects. Yes, my child has my permission to go on school sponsored excursions. No, my child may not attend school sponsored excursions and is to remain at school in an alternative curriculum experience for the day as outlined by the Program Director. Student Name Parent/Guardian Signature Date EAGLE RANCH ACADEMY - CONSENT TO EXAMINATION AND TREATMENT Student Name Date of Birth I hereby authorize and consent to any x-ray examination, anesthetic, inoculation, vaccination, medical or surgical diagnosis or treatment and hospital care to be rendered to the above named minor under the general or special supervision and upon the advice of a licensed medical doctor. I hereby consent to x-ray examination, anesthetic, dental or surgical diagnosis or treatment and hospital care to be rendered to said minor by a licensed dentist. I hereby authorize and consent to any treatment and psychological testing from a licensed psychologist or psychiatrist to be rendered to the above named minor. I understand that I am responsible for all medical, dental and psychological expenses notwithstanding any health insurance I may have. I have read the foregoing and understand the same. Parent/Guardian Signature Date Eagle Ranch Academy - Consent for Field Trips / Examination and Treatment
31 EAGLE RANCH ACADEMY - RUNAWAY INFORMATION This information is to assist Eagle Ranch Academy in the event of a runaway or AWOL. Student Name SS# DOB Age Race Height Weight _ Hair Color Eye Color Describe any Birth marks, Tattoos, Scars, etc. Please give the name / relation, phone number and address of any individual(s) your child may contact to assist in the case of a runaway attempt Name / Relation Phone Number Address List the places your child may go to or where they may go to hang out How many times has your child runaway? How long was your child gone? Alone or with a Friend? Did your child return home? Describe any past runaway attempts, the methodology, the procedures and the mediums used (stolen car, bus, train, airplane, ride from a friend, hitchhiking,) Please Attach Current Photo of Your Child to This Form Eagle Ranch Academy - Runaway Information
YOUTH FOR TOMORROW NEW LIFE CENTER
 APPLICATION N YOUTH FOR TOMORROW NEW LIFE CENTER CHRISTIAN ACADEMCY AND THERAPEUTIC BOARDING SCHOOL 2016-2017 Revised 7/1/2016 Child s Name: Step 1 Application Process Date Once we receive all of the information
APPLICATION N YOUTH FOR TOMORROW NEW LIFE CENTER CHRISTIAN ACADEMCY AND THERAPEUTIC BOARDING SCHOOL 2016-2017 Revised 7/1/2016 Child s Name: Step 1 Application Process Date Once we receive all of the information
Langston University Returning Athlete Screening Form
 Langston University Returning Athlete Screening Form Name: Address: Social Security #: : Phone: Sport: DOB: M / D / Y 1. Have you had any injury since your last athletic screening here? Yes: No: If yes,
Langston University Returning Athlete Screening Form Name: Address: Social Security #: : Phone: Sport: DOB: M / D / Y 1. Have you had any injury since your last athletic screening here? Yes: No: If yes,
PATIENT ADVOCATE DESIGNATION FOR MENTAL HEALTH TREATMENT NOTICE TO PATIENT
 PATIENT ADVOCATE DESIGNATION FOR MENTAL HEALTH TREATMENT NOTICE TO PATIENT As the Patient you are using this Patient Advocate Designation for Mental Health Treatment to grant powers to another individual
PATIENT ADVOCATE DESIGNATION FOR MENTAL HEALTH TREATMENT NOTICE TO PATIENT As the Patient you are using this Patient Advocate Designation for Mental Health Treatment to grant powers to another individual
Basic Information. Date: Patient s Name: Address:
 1 Basic Information : Patient s Name: Address: Home Phone: Work Phone: Cell Phone: Email: Age: Birth : Marital Status: Occupation: Educational History: Name, Address and Phone of Child s School Counselor
1 Basic Information : Patient s Name: Address: Home Phone: Work Phone: Cell Phone: Email: Age: Birth : Marital Status: Occupation: Educational History: Name, Address and Phone of Child s School Counselor
Durable Health Care Power of Attorney and Appointment of Health Care Agent and Proxy
 Durable Health Care Power of Attorney and Appointment of Health Care Agent and Proxy NOTICE TO ADULT SIGNING THIS DOCUMENT: This is an important legal document. Before executing this document, you should
Durable Health Care Power of Attorney and Appointment of Health Care Agent and Proxy NOTICE TO ADULT SIGNING THIS DOCUMENT: This is an important legal document. Before executing this document, you should
We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal.
 Appointment Date: Appointment Time: Dear Orion Member, We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal. Enclosed
Appointment Date: Appointment Time: Dear Orion Member, We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal. Enclosed
Outpatient Wellness Clinic
 Outpatient Wellness Clinic Patient Name: Date of Birth: Address: Phone: Email: Emergency Contact: Relationship: Phone: What is the reason for the appointment? Who were you referred by? (Physician, agency/
Outpatient Wellness Clinic Patient Name: Date of Birth: Address: Phone: Email: Emergency Contact: Relationship: Phone: What is the reason for the appointment? Who were you referred by? (Physician, agency/
Albuquerque Police Department Applicant Additional Documents. Name: Page 1 of 9
 Albuquerque Police Department Applicant Additional Documents Name: Page 1 of 9 Additional Documents Needed Instructions You will need to locate/gather all of the following documents and bring them with
Albuquerque Police Department Applicant Additional Documents Name: Page 1 of 9 Additional Documents Needed Instructions You will need to locate/gather all of the following documents and bring them with
Children s Residential Treatment Center Medical Intake Information
 Children s Residential Treatment Center Medical Intake Information The following is required at/by intake: q Copy of Current Insurance Cards (Medical, Dental, or Medical Assistance) q Proof of Physical
Children s Residential Treatment Center Medical Intake Information The following is required at/by intake: q Copy of Current Insurance Cards (Medical, Dental, or Medical Assistance) q Proof of Physical
INFORMED CONSENT FOR TREATMENT
 INFORMED CONSENT FOR TREATMENT I (name of patient), agree and consent to participate in behavioral health care services offered and provided at/by Children s Respite Care Center, a behavioral health care
INFORMED CONSENT FOR TREATMENT I (name of patient), agree and consent to participate in behavioral health care services offered and provided at/by Children s Respite Care Center, a behavioral health care
Signature (Patient or Legal Guardian): Date:
: Date:") X-Ray Patient Information: [ ] Male [ ] Female Patient Name: Date of Birth: / / SS#: Mailing Address: City: State: Zip: Phone # s: (Home) (Work) (Cell) Referring Physician: Phone #: /Fax#: Additional Physician:
X-Ray Patient Information: [ ] Male [ ] Female Patient Name: Date of Birth: / / SS#: Mailing Address: City: State: Zip: Phone # s: (Home) (Work) (Cell) Referring Physician: Phone #: /Fax#: Additional Physician:
Written Financial Policy
 2316 South Mason Road Katy, TX 77450 Written Financial Policy Thank you for choosing Cinco Ranch Dental. Our primary mission is to deliver the best and most comprehensive dental care available. An important
2316 South Mason Road Katy, TX 77450 Written Financial Policy Thank you for choosing Cinco Ranch Dental. Our primary mission is to deliver the best and most comprehensive dental care available. An important
Printed from the Texas Medical Association Web site.
 Printed from the Texas Medical Association Web site. Medical Power of Attorney Patient and Health Care Provider Information September 1999 General Information To be read by the Patient and Health Care
Printed from the Texas Medical Association Web site. Medical Power of Attorney Patient and Health Care Provider Information September 1999 General Information To be read by the Patient and Health Care
Part One: Durable Power of Attorney for Health Care Decisions GRANT OF AUTHORITY TO AGENT. I,, (name) designate and appoint: (name of agent) (address)
 designate and appoint: (name of agent) (address)") INSTRUCTIONS KANSAS ADVANCE DIRECTIVE PAGE 1 OF 5 Part One: Durable Power of Attorney for Health Care Decisions GRANT OF AUTHORITY TO AGENT PRINT YOUR NAME PRINT THE NAME, ADDRESS, AND TELEPHONE NUMBERS
INSTRUCTIONS KANSAS ADVANCE DIRECTIVE PAGE 1 OF 5 Part One: Durable Power of Attorney for Health Care Decisions GRANT OF AUTHORITY TO AGENT PRINT YOUR NAME PRINT THE NAME, ADDRESS, AND TELEPHONE NUMBERS
INFORMATION CONCERNING THE MEDICAL POWER OF ATTORNEY
 INFORMATION CONCERNING THE MEDICAL POWER OF ATTORNEY THIS IS AN IMPORTANT LEGAL DOCUMENT. BEFORE SIGNING THIS DOCUMENT, YOU SHOULD KNOW THESE IMPORTANT FACTS: Except to the extent you state otherwise,
INFORMATION CONCERNING THE MEDICAL POWER OF ATTORNEY THIS IS AN IMPORTANT LEGAL DOCUMENT. BEFORE SIGNING THIS DOCUMENT, YOU SHOULD KNOW THESE IMPORTANT FACTS: Except to the extent you state otherwise,
To begin the application process, please complete the enclosed application and bring it with you to one of our weekly meetings.
 Dear Explorer Applicant, We are pleased that you have shown interest in the Miramar Police Department Explorer Program. The Explorer program is the best program that young men and women can become involved
Dear Explorer Applicant, We are pleased that you have shown interest in the Miramar Police Department Explorer Program. The Explorer program is the best program that young men and women can become involved
Family Care Health Centers
 Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Planning Ahead: How to Make Future Health Care Decisions NOW. Washington
 Washington Planning Ahead: How to Make Future Health Care Decisions NOW Your Questions Answered About Washington Living Wills and Powers of Attorney for Health Care Table of Contents P 1 What You Need
Washington Planning Ahead: How to Make Future Health Care Decisions NOW Your Questions Answered About Washington Living Wills and Powers of Attorney for Health Care Table of Contents P 1 What You Need
Claremont Police Department. Explorer Post #411. Application
 Claremont Police Department Explorer Post #411 Application 570 W. Bonita Ave. Claremont, CA 91711 (909) 399-5411 Dear Applicant, Thank you for your interest in the Claremont Police Explorer program. Please
Claremont Police Department Explorer Post #411 Application 570 W. Bonita Ave. Claremont, CA 91711 (909) 399-5411 Dear Applicant, Thank you for your interest in the Claremont Police Explorer program. Please
Rancho Cielo Culinary Academy ELIGIBILITY CHECKLIST
 ELIGIBILITY CHECKLIST NAME: HOME PHONE: SS#: CELL PHONE: AGE: DOB: HOME ADDRESS: Step 1 Please complete the following forms included in this packet. 1. Complete the John Muir Charter School Enrollment
ELIGIBILITY CHECKLIST NAME: HOME PHONE: SS#: CELL PHONE: AGE: DOB: HOME ADDRESS: Step 1 Please complete the following forms included in this packet. 1. Complete the John Muir Charter School Enrollment
INFORMED CONSENT FOR TREATMENT
 INFORMED CONSENT FOR TREATMENT I (name of client) agree and consent to participate in behavioral healthcare services offered and provided by Methodist Services - Community Counseling Services (CCS). I
INFORMED CONSENT FOR TREATMENT I (name of client) agree and consent to participate in behavioral healthcare services offered and provided by Methodist Services - Community Counseling Services (CCS). I
WELCOME. Payment will be expected at the time of service. Please remember our 24 hour cancellation notice.
 WELCOME Those of us at Crossroads Counseling want to thank you for choosing to work with us and we want to make your time with us as productive as possible. In order to expedite the intake process, please
WELCOME Those of us at Crossroads Counseling want to thank you for choosing to work with us and we want to make your time with us as productive as possible. In order to expedite the intake process, please
Cadenza Center for Psychotherapy & the Arts, Inc. ADULT INTAKE
 Cadenza Center for Psychotherapy & the Arts, Inc. ADULT INTAKE Date: / / Name: Date of Birth: / / Age: Sex: M F ETHNIC ORIGIN: White Hispanic Haitian African American Other: PRIMARY LANGUAGE: English Spanish
Cadenza Center for Psychotherapy & the Arts, Inc. ADULT INTAKE Date: / / Name: Date of Birth: / / Age: Sex: M F ETHNIC ORIGIN: White Hispanic Haitian African American Other: PRIMARY LANGUAGE: English Spanish
Affordable Concierge New Patient Registration
 Affordable Concierge New Patient Registration Patient Information Last name: First name: MI: DOB: [ ] Male [ ] Female Home address: City: State: Zip: Billing address: [ ] Same as home City: State: Zip:
Affordable Concierge New Patient Registration Patient Information Last name: First name: MI: DOB: [ ] Male [ ] Female Home address: City: State: Zip: Billing address: [ ] Same as home City: State: Zip:
East Baton Rouge Parish Junior Deputy
 East Baton Rouge Parish Junior Deputy 2018 Application Packet Sheriff Sid J. Gautreaux, III Captain Randy M. Aguillard Program Director raguillard@ebrso.org Junior Deputy Membership Rules All members of
East Baton Rouge Parish Junior Deputy 2018 Application Packet Sheriff Sid J. Gautreaux, III Captain Randy M. Aguillard Program Director raguillard@ebrso.org Junior Deputy Membership Rules All members of
Address: Phone: Alternate Agent: ADVANCED HEALTH-CARE DIRECTIVE. You have the right to give instructions about your own health care.
 Prepared by: Grantor: Agents: Alternate Agent: Name: Name: Address: Phone: Name: Address: Phone: ADVANCED HEALTH-CARE DIRECTIVE You have the right to give instructions about your own health care. You also
Prepared by: Grantor: Agents: Alternate Agent: Name: Name: Address: Phone: Name: Address: Phone: ADVANCED HEALTH-CARE DIRECTIVE You have the right to give instructions about your own health care. You also
ARSD 67 :42:07 : :42:07 :01. Definitions.
 ARSD 67 :42:07 :01 67 :42:07 :01. Definitions. Terms used in this chapter mean: (1) After-care services, supportive social services, as specified in the treatment plan, for the family after the child has
ARSD 67 :42:07 :01 67 :42:07 :01. Definitions. Terms used in this chapter mean: (1) After-care services, supportive social services, as specified in the treatment plan, for the family after the child has
RIVER CITY ADVOCACY COUNSELING SERVICES 145 Landa Street New Braunfels, TX (830)
") Date / / Client information: First name Middle initial Last name Parent/Legal Guardian (for 17 and under) Address Phone number Home Wk Cell Date of birth / / Sex Marital Status Ethnicity Employment status:
Date / / Client information: First name Middle initial Last name Parent/Legal Guardian (for 17 and under) Address Phone number Home Wk Cell Date of birth / / Sex Marital Status Ethnicity Employment status:
12 King Philip Rd. Sudbury, MA (585)
") Dear Parents, In order to get started with speech therapy services including screening, evaluation, and treatment, we ask that you submit the following registration paperwork to Sudbury Speech and Language
Dear Parents, In order to get started with speech therapy services including screening, evaluation, and treatment, we ask that you submit the following registration paperwork to Sudbury Speech and Language
Emergency Contact: Name Relationship Address
 Participant Information Name Treatment Start Date Address City State Zip Home/Cell Phone Work Phone Birth date Age SSN Marital Status Primary Insurance Provider Insurance ID # Primary Insured Name: Primary
Participant Information Name Treatment Start Date Address City State Zip Home/Cell Phone Work Phone Birth date Age SSN Marital Status Primary Insurance Provider Insurance ID # Primary Insured Name: Primary
Karen LeVasseur, LCSW Calm4Kids Therapy Center, LLC 514 Main Street Bradley Beach, NJ
 Karen LeVasseur, LCSW Calm4Kids Therapy Center, LLC 514 Main Street Bradley Beach, NJ 07720 732 272 8624 THERAPIST CLIENT SERVICE AGREEMENT/INFORMED CONSENT Welcome to my practice. This document contains
Karen LeVasseur, LCSW Calm4Kids Therapy Center, LLC 514 Main Street Bradley Beach, NJ 07720 732 272 8624 THERAPIST CLIENT SERVICE AGREEMENT/INFORMED CONSENT Welcome to my practice. This document contains
DURABLE POWER OF ATTORNEY FOR HEALTH CARE
 DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Please print or type required information) I. Appointment of Patient Advocate I, your name of full legal address hereby appoint name of your designated patient
DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Please print or type required information) I. Appointment of Patient Advocate I, your name of full legal address hereby appoint name of your designated patient
Application Requirements to be considered for Approval:
 338 Grapevine Hwy. Hurst, Texas 76054 phone: 817.503.1500 toll-free: 877.203.9111 fax: 817.503.1551 www.mhstx.org Application Requirements to be considered for Approval: Please print your answers using
338 Grapevine Hwy. Hurst, Texas 76054 phone: 817.503.1500 toll-free: 877.203.9111 fax: 817.503.1551 www.mhstx.org Application Requirements to be considered for Approval: Please print your answers using
DESIGNATION OF PATIENT ADVOCATE FORM
 DESIGNATION OF PATIENT ADVOCATE FORM AND DIRECTIONS for HEALTH CARE (Durable Power of Attorney for Health Care) NAME: DOB: This is an important legal document. You should discuss it with your doctor and
DESIGNATION OF PATIENT ADVOCATE FORM AND DIRECTIONS for HEALTH CARE (Durable Power of Attorney for Health Care) NAME: DOB: This is an important legal document. You should discuss it with your doctor and
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D KLONDIKE RD SW SUITE 205 CONYERS, GA TELEPHONE FAX
 PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
Glastonbury YMCA 29 Welles Street, Glastonbury CT Dear YMCA Family,
 s Dear YMCA Family, Thank you for choosing the Glastonbury Family YMCA Preschool for your early childhood child care needs. We are excited to welcome you and your family to our program! The Y s focus is
s Dear YMCA Family, Thank you for choosing the Glastonbury Family YMCA Preschool for your early childhood child care needs. We are excited to welcome you and your family to our program! The Y s focus is
New Patient Information
 New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
Patient Appointment Agreement
 Patient Appointment Agreement Welcome and thank you for choosing the East Carolina University School of Dental Medicine for your oral health care needs. We are committed to providing you with the best
Patient Appointment Agreement Welcome and thank you for choosing the East Carolina University School of Dental Medicine for your oral health care needs. We are committed to providing you with the best
PATIENT INFORMATION Please Print
 PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
Camp TOV Medical Form
 Mail: Fax: Please send these forms to us by either: Jewish United Fund/Jewish Federation of Metropolitan Chicago Attn: Camp TOV 30 South Wells Street, Room 5034 Chicago, IL 60606 Attn: Camp TOV 312-444-2086
Mail: Fax: Please send these forms to us by either: Jewish United Fund/Jewish Federation of Metropolitan Chicago Attn: Camp TOV 30 South Wells Street, Room 5034 Chicago, IL 60606 Attn: Camp TOV 312-444-2086
Youth Tomorrow New Life Center Application for Admission
 Youth Tomorrow New Life Center Application for Admission 12 VAC 35-46-710 & 12 VAC 35-45-90 Child s : Date Step 1 Application Process Once we receive all of the information listed in this section, our
Youth Tomorrow New Life Center Application for Admission 12 VAC 35-46-710 & 12 VAC 35-45-90 Child s : Date Step 1 Application Process Once we receive all of the information listed in this section, our
Friendswood Counseling Center, LLC Phone: (479) E. FM 528 Rd, Suite 200 Fax: (281) Client Registration
 E. FM 528 Rd, Suite 200 Fax: (281) Client Registration") Friendswood Counseling Center, LLC Phone: (479) 200-6034 3526 E. FM 528 Rd, Suite 200 Fax: (281) 819-7845 Friendswood, TX 77546 Email: kristi@friendswoodcc.com Website: www.friendswoodcc.com Client Registration
Friendswood Counseling Center, LLC Phone: (479) 200-6034 3526 E. FM 528 Rd, Suite 200 Fax: (281) 819-7845 Friendswood, TX 77546 Email: kristi@friendswoodcc.com Website: www.friendswoodcc.com Client Registration
SHERIFF OF GARFIELD COUNTY LOU VALLARIO
 SHERIFF OF GARFIELD COUNTY LOU VALLARIO 107 8 TH Street Glenwood Springs, CO 81601 Phone: 970-945-0453 Fax: 970-945-7700 106 County Road 333-A Rifle, CO 81650 Phone: 970-665-0200 Fax: 970-665-0253 Dear
SHERIFF OF GARFIELD COUNTY LOU VALLARIO 107 8 TH Street Glenwood Springs, CO 81601 Phone: 970-945-0453 Fax: 970-945-7700 106 County Road 333-A Rifle, CO 81650 Phone: 970-665-0200 Fax: 970-665-0253 Dear
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
*3ADV* Patient Rights & Responsibilities Advanced Directive Page 1 of 2. Patient Rights & Responsibilities. Patient Label
 PATIENT RIGHTS Portneuf Medical Center encourages respect for the personal preferences and values of each individual and supports the Rights of each patient and resident of the Center, or their representative
PATIENT RIGHTS Portneuf Medical Center encourages respect for the personal preferences and values of each individual and supports the Rights of each patient and resident of the Center, or their representative
HEALTH HISTORY QUESTIONNAIRE
 Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
Developmental Pediatrics of Central Jersey
 PATIENT INFORMATION: CLIENT INFORMATION Date: Name: (Last) (First) (M.I.) Birthdate: Sex: Race: Address: City: State: Zip: Phone: (Home) (Work) (Cell) Email Address: Regarding the office staff or physician
PATIENT INFORMATION: CLIENT INFORMATION Date: Name: (Last) (First) (M.I.) Birthdate: Sex: Race: Address: City: State: Zip: Phone: (Home) (Work) (Cell) Email Address: Regarding the office staff or physician
Adventure Club. Before and After School Care Enrollment Packet. Before and After School Care Mission:
 Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
2017 VENTURA COUNTY JUNIOR LIFEGUARD PROGRAM HELD ON SILVER STRAND BEACH IN OXNARD
 2017 VENTURA COUNTY JUNIOR LIFEGUARD PROGRAM HELD ON SILVER STRAND BEACH IN OXNARD Dear Junior Lifeguard Families and prospective Junior Lifeguards: Enclosed is your 2017 PROGRAM OUTLINE. Please retain
2017 VENTURA COUNTY JUNIOR LIFEGUARD PROGRAM HELD ON SILVER STRAND BEACH IN OXNARD Dear Junior Lifeguard Families and prospective Junior Lifeguards: Enclosed is your 2017 PROGRAM OUTLINE. Please retain
If you have any questions concerning the application process, do not hesitate to contact us soon.
 Cristo Vive International P.O. Box 527 Big Lake, MN 55309 Dear Applicant: Thank you for expressing an interest in joining the Cristo Vive Team as a participant with the camp ministries for children and
Cristo Vive International P.O. Box 527 Big Lake, MN 55309 Dear Applicant: Thank you for expressing an interest in joining the Cristo Vive Team as a participant with the camp ministries for children and
OSU Livestock Judging Camp 2009
 OSU Livestock Judging Camp 2009 July 7-9 Oklahoma State University Stillwater, Okla. Participants will have the unique opportunity to work one- on- one with 3 of the most elite and successful livestock
OSU Livestock Judging Camp 2009 July 7-9 Oklahoma State University Stillwater, Okla. Participants will have the unique opportunity to work one- on- one with 3 of the most elite and successful livestock
Psychological Services Agreement
 John A. Watterson, Ph.D. 4101 Parkstone Heights Drive, Suite 260 Austin, Texas 78746 Phone: 512-306-0663 Fax: 512-306-8086 Website: www.johnwatterson.com Psychological Services Agreement Welcome to my
John A. Watterson, Ph.D. 4101 Parkstone Heights Drive, Suite 260 Austin, Texas 78746 Phone: 512-306-0663 Fax: 512-306-8086 Website: www.johnwatterson.com Psychological Services Agreement Welcome to my
Form B - For those enrolled in other insurance
 Form B - For those enrolled in other insurance PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) Date of Birth
Form B - For those enrolled in other insurance PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) Date of Birth
Paragon Infusion Centers Patient Information
 Paragon Infusion Centers Patient Information Please complete the following form as accurately as you are able. Inaccurate and/or incomplete information can delay our ability to authorize your treatments,
Paragon Infusion Centers Patient Information Please complete the following form as accurately as you are able. Inaccurate and/or incomplete information can delay our ability to authorize your treatments,
(PLEASE PRINT) Sex M F Age Birthdate Single Married Widowed Separated Divorced. Business Address Business Phone Cell Phone
 Sex M F Age Birthdate Single Married Widowed Separated Divorced. Business Address Business Phone Cell Phone") (PLEASE PRINT) Emma Warner, MSW, LCSW, ACSW Tulsa, OK 74105 (918) 749-6935 Personal Information Name Address Last Name First Name Initial Home Phone Soc. Sec. # City State Zip Sex M F Age Birthdate Single
(PLEASE PRINT) Emma Warner, MSW, LCSW, ACSW Tulsa, OK 74105 (918) 749-6935 Personal Information Name Address Last Name First Name Initial Home Phone Soc. Sec. # City State Zip Sex M F Age Birthdate Single
2012/2013 ST. JOSEPH MERCY OAKLAND Pontiac, Michigan HOUSE OFFICER EMPLOYMENT AGREEMENT
 2012/2013 ST. JOSEPH MERCY OAKLAND Pontiac, Michigan SAMPLE CONTRACT ONLY HOUSE OFFICER EMPLOYMENT AGREEMENT This Agreement made this 23 rd of January 2012 between St. Joseph Mercy Oakland a member of
2012/2013 ST. JOSEPH MERCY OAKLAND Pontiac, Michigan SAMPLE CONTRACT ONLY HOUSE OFFICER EMPLOYMENT AGREEMENT This Agreement made this 23 rd of January 2012 between St. Joseph Mercy Oakland a member of
CORAZON PANES SANCHEZ., M.D., L.L.C.
 PERRYVILLE, MD 21903 Rising sun, MD 21911 BALTIMORE, MD 21221 PATIENT REGISTRATION NAME: DOB: SEX: ( ) MALE ( ) FEMALE SOCIAL SECURITY #: - - ADDRESS: CITY/STATE: ZIP:_ TELEPHONE #: MOTHER S NAME: FATHER
PERRYVILLE, MD 21903 Rising sun, MD 21911 BALTIMORE, MD 21221 PATIENT REGISTRATION NAME: DOB: SEX: ( ) MALE ( ) FEMALE SOCIAL SECURITY #: - - ADDRESS: CITY/STATE: ZIP:_ TELEPHONE #: MOTHER S NAME: FATHER
A PERSONAL DECISION
 A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. WHY ARE YOU GETTING
NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. WHY ARE YOU GETTING
Community Life Center
 Community Life Center- 2018-2019 Page 2 of 6 MEGA SPORTS CAMP- Waiver & Release Forms Effective Dates: January 1, 2018 January 1, 2019 CHILD S INFORMATION Name Grade Age DOB Male/Female Nickname School:
Community Life Center- 2018-2019 Page 2 of 6 MEGA SPORTS CAMP- Waiver & Release Forms Effective Dates: January 1, 2018 January 1, 2019 CHILD S INFORMATION Name Grade Age DOB Male/Female Nickname School:
12086 Ft. Caroline Road, Suite #401, Jacksonville, FL Phone: (904) Fax: (904) Patient Full Legal Name Date
 Fax: (904) Patient Full Legal Name Date") 12086 Ft. Caroline Road, Suite #401, Jacksonville, FL 32225 Phone: (904) 565-1271 Fax: (904) 645-7325 James A. Joyner, IV, MD, Kia M. Mitchell, MD, Thanh Nguyen, MD Dewey Lee, III, PA, Linda Rowan-Vander
12086 Ft. Caroline Road, Suite #401, Jacksonville, FL 32225 Phone: (904) 565-1271 Fax: (904) 645-7325 James A. Joyner, IV, MD, Kia M. Mitchell, MD, Thanh Nguyen, MD Dewey Lee, III, PA, Linda Rowan-Vander
Page 1 CHAPTER 31 SCREENING OUTREACH PROGRAM. 10: Screening process and procedures
 Page 1 CHAPTER 31 SCREENING OUTREACH PROGRAM 10:31-2.3 Screening process and procedures (a) The screening process shall involve a thorough assessment of the client and his or her current situation to determine
Page 1 CHAPTER 31 SCREENING OUTREACH PROGRAM 10:31-2.3 Screening process and procedures (a) The screening process shall involve a thorough assessment of the client and his or her current situation to determine
To ensure proper disclosure and release of Protected Health Information (PHI) Division/Department: All HealthPoint Policy/Procedure #:
 Division/Department: All HealthPoint Policy/Procedure #:") TITLE: Release of Medical Records Scope/Purpose: POLICY & PROCEDURE To ensure proper disclosure and release of Protected Health Information (PHI) Division/Department: All HealthPoint Policy/Procedure #:
TITLE: Release of Medical Records Scope/Purpose: POLICY & PROCEDURE To ensure proper disclosure and release of Protected Health Information (PHI) Division/Department: All HealthPoint Policy/Procedure #:
VOLUNTEER APPLICATION
 VOLUNTEER APPLICATION Name: Age: Date of Birth: Social Security : Address: City: State: Zip Phone: Work: Cell: Email Address: How can we reach you? Home phone Cell phone Text Email Work phone Employer/School:
VOLUNTEER APPLICATION Name: Age: Date of Birth: Social Security : Address: City: State: Zip Phone: Work: Cell: Email Address: How can we reach you? Home phone Cell phone Text Email Work phone Employer/School:
PATIENT RIGHTS TO ACCESS PERSONAL MEDICAL RECORDS California Health & Safety Code Section
 PATIENT RIGHTS TO ACCESS PERSONAL MEDICAL RECORDS California Health & Safety Code Section 123100-123149. 123100. The Legislature finds and declares that every person having ultimate responsibility for
PATIENT RIGHTS TO ACCESS PERSONAL MEDICAL RECORDS California Health & Safety Code Section 123100-123149. 123100. The Legislature finds and declares that every person having ultimate responsibility for
PROCEDURE-STUDENT RECORDS
 PROCEDURE-STUDENT RECORDS 3600P This procedure specifies the management of student records by the District. These procedures are aligned with the Family Educational Rights and Privacy Act (FERPA). Type
PROCEDURE-STUDENT RECORDS 3600P This procedure specifies the management of student records by the District. These procedures are aligned with the Family Educational Rights and Privacy Act (FERPA). Type
CITY OF MISSION CIVIL SERVICE APPLICATION
 CITY OF MISSION CIVIL SERVICE APPLICATION City of Mission Civil Service Department 1201 E. 8 th Street Mission, TX 78572 Applicant Name: Position Applying For: Police Officer Fire Fighter Page 1 of 15
CITY OF MISSION CIVIL SERVICE APPLICATION City of Mission Civil Service Department 1201 E. 8 th Street Mission, TX 78572 Applicant Name: Position Applying For: Police Officer Fire Fighter Page 1 of 15
Application. For The. Tyler Police Department Law Enforcement Explorer Program
 Application For The Tyler Police Department Law Enforcement Explorer Program Attached are the forms that are required to be completed to be admitted into the Law Enforcement Explorer Program at the Tyler
Application For The Tyler Police Department Law Enforcement Explorer Program Attached are the forms that are required to be completed to be admitted into the Law Enforcement Explorer Program at the Tyler
DURABLE POWER OF ATTORNEY FOR HEALTH CARE OF [NAME]
![DURABLE POWER OF ATTORNEY FOR HEALTH CARE OF [NAME]](/thumbs/78/77545542.jpg "DURABLE POWER OF ATTORNEY FOR HEALTH CARE OF [NAME]") DURABLE POWER OF ATTORNEY FOR HEALTH CARE OF [NAME] 1. DESIGNATION OF HEALTH CARE AGENT. (a) Pursuant to the Missouri Durable Power of Attorney for Health Act, Mo.Rev.Stat. 404.700-404.735 and 404.800-404.872,
DURABLE POWER OF ATTORNEY FOR HEALTH CARE OF [NAME] 1. DESIGNATION OF HEALTH CARE AGENT. (a) Pursuant to the Missouri Durable Power of Attorney for Health Act, Mo.Rev.Stat. 404.700-404.735 and 404.800-404.872,
Atascocita Counseling Associates Krissy Cotten, MA, LPC. Adult New Client Profile
 Adult New Client Profile Please complete the following as accurately and as completely as possible. Social Security Number is required only if you are filing with insurance. Today s Date: Name: Date of
Adult New Client Profile Please complete the following as accurately and as completely as possible. Social Security Number is required only if you are filing with insurance. Today s Date: Name: Date of
I. POLICY: DEFINITIONS:
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration {x} Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 11: HEALTH AND MEDICAL SERVICES Subject:
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration {x} Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 11: HEALTH AND MEDICAL SERVICES Subject:
Beck & Blackley Chiropractic Clinic
 Address City State Zip Code Home Phone Cell Phone Work Phone Email Address Sex: M F Marital Status: M S D W Date of Birth SS# Spouse Name How did you hear about our office? Employer Name/Occupation Emergency
Address City State Zip Code Home Phone Cell Phone Work Phone Email Address Sex: M F Marital Status: M S D W Date of Birth SS# Spouse Name How did you hear about our office? Employer Name/Occupation Emergency
St. Mary s Industrial Medicine 4017 Atlanta Hwy, Ste B Bogart, GA Phone: (706) Fax: (706)
 Fax: (706)") Please Fill Out Completely: St. Mary s Industrial Medicine Patient s Last Name First Name MI Social Security Number Date of Birth Age Gender Race Marital Status Ethnicity (Circle one): Language Latino
Please Fill Out Completely: St. Mary s Industrial Medicine Patient s Last Name First Name MI Social Security Number Date of Birth Age Gender Race Marital Status Ethnicity (Circle one): Language Latino
Singers ONSTAGE! Registration Form
 Singers ONSTAGE! Registration Form Student Information Full Name City State Zip Home Phone Date of Birth Grade (as of 9/1/15) Gender (circle one): Male Female Each registration includes two T-shirts, professional
Singers ONSTAGE! Registration Form Student Information Full Name City State Zip Home Phone Date of Birth Grade (as of 9/1/15) Gender (circle one): Male Female Each registration includes two T-shirts, professional
HEALTH CARE POWER OF ATTORNEY
 HEALTH CARE POWER OF ATTORNEY NOTE: YOU SHOULD USE THIS DOCUMENT TO NAME A PERSON AS YOUR HEALTH CARE AGENT IF YOU ARE COMFORTABLE GIVING THAT PERSON BROAD AND SWEEPING POWERS TO MAKE HEALTH CARE DECISIONS
HEALTH CARE POWER OF ATTORNEY NOTE: YOU SHOULD USE THIS DOCUMENT TO NAME A PERSON AS YOUR HEALTH CARE AGENT IF YOU ARE COMFORTABLE GIVING THAT PERSON BROAD AND SWEEPING POWERS TO MAKE HEALTH CARE DECISIONS
BANGOR REGION YMCA CHILDCARE REGISTRATION FORM
 On-Site Registration Required BANGOR REGION YMCA CHILDCARE REGISTRATION FORM Childcare Information & Program Attending - Please Print ( )Early Childhood Education ( )Y-Works ( )Before School ( )After School
On-Site Registration Required BANGOR REGION YMCA CHILDCARE REGISTRATION FORM Childcare Information & Program Attending - Please Print ( )Early Childhood Education ( )Y-Works ( )Before School ( )After School
Counselor Application 2018 July 9 th 13 th
 Counselor Application 2018 July 9 th 13 th Name Address City State & Zip Home Phone Cell Phone E-mail address Male Female Birth Date (mm/dd/yy) Age (at camp) Emergency Contact Name Phone Relation to Camper
Counselor Application 2018 July 9 th 13 th Name Address City State & Zip Home Phone Cell Phone E-mail address Male Female Birth Date (mm/dd/yy) Age (at camp) Emergency Contact Name Phone Relation to Camper
Application for Admission Instruction Sheet
 Application for Admission Instruction Sheet Thank you for your interest in Elk Hill and the programs we provide young people throughout central Virginia. To make a referral, please complete the Application
Application for Admission Instruction Sheet Thank you for your interest in Elk Hill and the programs we provide young people throughout central Virginia. To make a referral, please complete the Application
Massage Therapist License Application W 87 Street Pkwy Phone Lenexa, KS Fax
 Massage Therapist License Application 17101 W 87 Street Pkwy Phone 913-477-7725 Lenexa, KS 66109 Fax 913-477-7730 www.lenexa.com NOTE: Any failure to fully or truthfully answer any question or provide
Massage Therapist License Application 17101 W 87 Street Pkwy Phone 913-477-7725 Lenexa, KS 66109 Fax 913-477-7730 www.lenexa.com NOTE: Any failure to fully or truthfully answer any question or provide
The Salvation Army of Dane County Holly House Transitional Living for Women Application
 The Salvation Army of Dane County Holly House Transitional Living for Women Application Holly House is designed as an independent transitional housing program for women without children in their custody.
The Salvation Army of Dane County Holly House Transitional Living for Women Application Holly House is designed as an independent transitional housing program for women without children in their custody.
TOPS Piano and Creative Writing Camp Registration Form Summer 2018
 TOPS Piano and Creative Writing Camp Registration Form Summer 2018 Returning Camper New Camper Camper s Name Email(s) Address City Zip code Home phone Work phone(s) Cell phone(s) Parent/Guardian name Please
TOPS Piano and Creative Writing Camp Registration Form Summer 2018 Returning Camper New Camper Camper s Name Email(s) Address City Zip code Home phone Work phone(s) Cell phone(s) Parent/Guardian name Please
Michigan ADVANCE DIRECTIVE FOR MENTAL HEALTH CARE
 Michigan ADVANCE DIRECTIVE FOR MENTAL HEALTH CARE I I,, am of sound mind and (Print or type your full name) voluntarily make this designation. APPOINTMENT OF PATIENT ADVOCATE I designate, my, (Insert name
Michigan ADVANCE DIRECTIVE FOR MENTAL HEALTH CARE I I,, am of sound mind and (Print or type your full name) voluntarily make this designation. APPOINTMENT OF PATIENT ADVOCATE I designate, my, (Insert name
PATIENT REGISTRATION FORM (ecw)
") PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD
 PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD General Consent for Treatment I have the legal right to consent to medical and surgical treatment because (a) I am the patient
PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD General Consent for Treatment I have the legal right to consent to medical and surgical treatment because (a) I am the patient
Student T-shirt size is: Small Medium Large XLarge 2XLarge 3XLarge (Circle one)
") Participant Permission Form/ Release Waiver Form My child,, has my permission to attend. I understand this celebration is offered to all graduates who have signed and maintained both the Project Grad Participant
Participant Permission Form/ Release Waiver Form My child,, has my permission to attend. I understand this celebration is offered to all graduates who have signed and maintained both the Project Grad Participant
Medications List. Allergies. Drug Name Dosage Directions Reason Taking
 Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Saint Agnes Medical Center. Guidelines for Signers
 597 Saint Agnes Medical Center Page 1 Guidelines for Signers What is an Advance Health Care Directive? An "Advance Health Care Directive" is a document you can use to appoint another person, such as a
597 Saint Agnes Medical Center Page 1 Guidelines for Signers What is an Advance Health Care Directive? An "Advance Health Care Directive" is a document you can use to appoint another person, such as a
Application for Admission Instruction Sheet
 Application for Admission Instruction Sheet Thank you for your interest in Elk Hill and the programs we provide young people throughout central Virginia. To make a referral, please complete the Application
Application for Admission Instruction Sheet Thank you for your interest in Elk Hill and the programs we provide young people throughout central Virginia. To make a referral, please complete the Application
Welcome to University Family Healthcare, PA.
 Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Parma High School Washington, DC Trip 2018
 Parma High School Washington, DC Trip 2018 Dear Parents: Please find the attached Parents Approval Form Educational Trips Overnight / Out-of-State / Out-of-the-Country. Parents are asked to neatly print
Parma High School Washington, DC Trip 2018 Dear Parents: Please find the attached Parents Approval Form Educational Trips Overnight / Out-of-State / Out-of-the-Country. Parents are asked to neatly print
Julie Berger, MS, NCC, LPC HOLY FAMILY COUNSELING CENTER Peachtree Industrial Blvd. Suite 120, Duluth, GA INTAKE FORM
 INTAKE FORM We welcome you to our faith-based practice. It is our goal to help you through the difficulties you are experiencing by addressing the whole person and family with dignity. Our goal as your
INTAKE FORM We welcome you to our faith-based practice. It is our goal to help you through the difficulties you are experiencing by addressing the whole person and family with dignity. Our goal as your
Keene Family YMCA CAMP REGISTRATION PACKET 2018
 Keene Family YMCA CAMP REGISTRATION PACKET 2018 ONE PACKET PER CHILD. Please complete all pages of this registration packet. It is important that you fill out every field and provide complete contact information
Keene Family YMCA CAMP REGISTRATION PACKET 2018 ONE PACKET PER CHILD. Please complete all pages of this registration packet. It is important that you fill out every field and provide complete contact information
NAME SS# ADDRESS CITY STATE ZIP. TELEPHONE (home) (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE
 (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE") REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
CONTRACT OF AGREEMENT AND TERMS OF ADMISSION TO NEW LIFE USA RECOVERY CENTER
 Free Drug and Alcohol Recovery Center Page 1 of 8 CONTRACT OF AGREEMENT AND TERMS OF ADMISSION TO NEW LIFE USA RECOVERY CENTER 1. THE PARTIES The following contract (AGREEMENT, hereafter) represents an
Free Drug and Alcohol Recovery Center Page 1 of 8 CONTRACT OF AGREEMENT AND TERMS OF ADMISSION TO NEW LIFE USA RECOVERY CENTER 1. THE PARTIES The following contract (AGREEMENT, hereafter) represents an
OUTPATIENT SERVICES CONTRACT 2018
 1308 23 rd Street S Fargo, ND 58103 Phone: 701-297-7540 Fax: 701-297-6439 OUTPATIENT SERVICES CONTRACT 2018 Welcome to Benson Psychological Services, PC. This document contains important information about
1308 23 rd Street S Fargo, ND 58103 Phone: 701-297-7540 Fax: 701-297-6439 OUTPATIENT SERVICES CONTRACT 2018 Welcome to Benson Psychological Services, PC. This document contains important information about
NOTICE OF PRIVACY PRACTICES
 BUTTE COUNTY DEPARTMENT OF BEHAVIORAL HEALTH NOTICE OF PRIVACY PRACTICES Effective Date: 4/14/2003 THIS NOTICE DESCRIBES NOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
BUTTE COUNTY DEPARTMENT OF BEHAVIORAL HEALTH NOTICE OF PRIVACY PRACTICES Effective Date: 4/14/2003 THIS NOTICE DESCRIBES NOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
HOISINGTON POLICE DEPARTMENT 109 E. 1 st St. Hoisington, KS Telephone (620) Fax (620)
 Fax (620)") Chief of Police Kenton L. Doze HOISINGTON POLICE DEPARTMENT 109 E. 1 st St. Hoisington, KS 675440060 Telephone (620) 6534995 Fax (620) 6532422 Captain of Police Josh Nickerson Job : Police Officer Under
Chief of Police Kenton L. Doze HOISINGTON POLICE DEPARTMENT 109 E. 1 st St. Hoisington, KS 675440060 Telephone (620) 6534995 Fax (620) 6532422 Captain of Police Josh Nickerson Job : Police Officer Under
YOUTH ACTIVITIES REGISTRATION FORM
 YOUTH ACTIVITIES REGISTRATION FORM REGISTRATION FOR: Baseball, Basketball, Cheerleading, Flag Football, Soccer, Softball, CHILD S NAME: AGE: SEX: HEIGHT (INCHES): WEIGHT (POUNDS): D.O.B.: (YYYY/MM/DD)
YOUTH ACTIVITIES REGISTRATION FORM REGISTRATION FOR: Baseball, Basketball, Cheerleading, Flag Football, Soccer, Softball, CHILD S NAME: AGE: SEX: HEIGHT (INCHES): WEIGHT (POUNDS): D.O.B.: (YYYY/MM/DD)
Welcome to Baptist Medical Group - Westside. Please read the below information carefully to prepare for your upcoming appointment.
 BAPTISTMEDICALGROUP.ORG Westside Welcome to - Westside Please read the below information carefully to prepare for your upcoming appointment. Please arrive 15 minutes prior to your regularly scheduled appointment
BAPTISTMEDICALGROUP.ORG Westside Welcome to - Westside Please read the below information carefully to prepare for your upcoming appointment. Please arrive 15 minutes prior to your regularly scheduled appointment
Kairos Retreat Policies & Permission Forms Bring home to Parents TODAY!
 Kairos Retreat Policies & Permission Forms Bring home to Parents TODAY! ***Please Read All Information Carefully**** Complete & return all forms (retain first and back page) to the Reception Desk Main
Kairos Retreat Policies & Permission Forms Bring home to Parents TODAY! ***Please Read All Information Carefully**** Complete & return all forms (retain first and back page) to the Reception Desk Main