Quality Account 2016/17. Best care by the best people
|
|
|
- Lionel Morrison
- 6 years ago
- Views:
Transcription


1 Best care by the best people Quality Account 2016/17


2 NELFT NHS Foundation Trust Quality Account 2016/17
3 Contents Foreword from the chief executive Pages 4-5 Statement from the chief nurse 6 and executive director of integrated care (Essex) Introduction - what is a Quality Account? 8-9 Part A Our services 10 Our values 11 NELFT awards and achievements Sign up to safety campaign Looking forward Priorities for improvement 2017/2018 Development of our quality priorities 2017/2018 Brookside child and adolescent inpatient unit Priority 1 Safe Priority 2 Effective Priority 3 Responsive Priority 4 Well led Governors indicator How do our goals impact on patient safety, clinical effectiveness and patient experience? Looking back Review of our performance against our 2016/2017 priorities Priority 1 Working together for service users and patients Priority 2 Commitment to quality of care Priority 3 Respect and dignity Annual staff survey results Part B Statements of assurance from the board Participation in national clinical audit and confidential enquiries Learning from national clinical audits Learning from local clinical audits Participation in clinical research NICE compliance in NELFT CQUIN targets 2017/2018 Registration with the Care Quality Commission (CQC) NHS and general medical practice code validity Information governance assessment report Clinical coding error rate Audit - areas for improvement Reporting against our core indicators 2016/17 Appendix Appendix 1 - Governors selected indicator Rotational nurse programme Articles The enquirer, the Ilford Romford recorder Appendix 2a - National clinical audit and confidential enquiry - eligibility and participation Appendix 2b - National clinical audit and confidential enquiry - requirements and action taken Appendix 2c - Local clinical audit requirements and action taken Appendix 3 Royal College of Psychiatrists summary of NELFT s participation in national quality improvement projects Appendix 4 Quality Account governance structure Appendix 5 Statements from commissioners, local Healthwatch organisations and overview and scrutiny committees Appendix /17 Statement of directors responsibilities for the Quality Report Appendix 7 - Auditors limited assurance report Glossary 90 Useful contact numbers 91
4 Foreword Welcome to the latest Quality Account and our reflections on the last year of progress within NELFT and its service portfolios. These continue to be challenging times and this is characterised by our experience within the organisation, the economies in which we operate and of course nationally. The nature of the work we do is highly dependent on close and collaborative relationships with our partner organisations but particularly our local authority colleagues. They too are facing a high level of challenge and a huge amount of effort has gone in to seeking transformational approaches to maintaining and developing high quality treatment and care programmes for our patients. Whilst austerity has been a byword for much of what we do, our staff have maintained their efforts and innovative approach to continuously improve and develop services that meet the demands of our communities. Perhaps the biggest impact in this year was the Care Quality Commission conclusions and rating for our services. I know everyone was disappointed when we learned that the overall rating was that we require improvement. A good deal of time and effort went into preparation for the assessment and work to address the areas of concern identified within the final report. This has only served to motivate everyone and immediate efforts were made to address the areas of concern. I am particularly pleased to note for example that whilst Brookside was rated as inadequate our staff rallied round and addressed all of the concerns resulting in a revised rating across the board for all domains. This rating has now been adjusted to good. This is testament to the professionalism and commitment of our staff, of whom we should all be rightly proud, but at the same time recognise that we have much to learn and improve. Recruitment has consistently proved to be a challenge too but a great deal of effort has been put into improving our systems and performance and I am confident that we have begun to see some evidence of real improvement in this area. Despite these difficulties we have seen major change and development of new models of care. One good example of this is the work that has been done in Essex to embed and develop the Emotional Wellbeing Mental Health service which is getting positive recognition for its innovative approach in delivering care to young people. This no doubt will develop as a blueprint for many other service initiatives in the time ahead. NELFT NHS Foundation Trust Quality Account 2016/17

5 5 "Whilst accepting that we still have much to learn it would be wrong not to recognise that there are many areas of outstanding service provision across NELFT" John Brouder, Chief executive The CQC experience reminds us that there can be no room for complacency and the culture and leadership within the organisation must continue to learn and progress. Clinical leadership must be continuously developed and, like many other successful organisations, we have invested a lot of effort and focus in our own Quality Improvement programme. We have seen a number of cohorts going through the programme and they are generating exciting initiatives that will improve our patient and staff experience. As part of the KPMG audit this year they have highlighted some data quality issues around the home treatment team s record keeping. We have already responded to this and an action plan has been put in place. This will be overseen by the acute and rehabilitation integrated care director to ensure timely compliance. The Board continue to host a monthly patient journey. This is both inspiring and sobering and the initiative goes some way in ensuring the Board retain a close insight into what is happening within clinical services. Whilst accepting that we still have much to learn it would be wrong not to recognise that there are many areas of outstanding service provision across NELFT and a continued accumulation of awards received during the year. I hope that you enjoy reading about the detail of some of our achievements within this report and I sign off with a sense of confidence that NELFT will continue to grow, learn and improve the experience of the people that use our services and the staff that work within them. John Brouder Chief executive To the best of my knowledge the information presented to you in this account is accurate and provides a fair representation of the quality within the organisation.

6 Statement from the chief nurse and executive director of integrated care (Essex) Key to our success and achievement are our people; particularly as we continuously respond to the changing needs of the health of our communities, the remarkable and welcome improvement in the life expectancy of older people along with a changing social and financial landscape. The introduction of the CQC fundamental standards back in 2015 provided the framework we needed to monitor, review and transform the way we deliver care. With a greater focus on safety and quality at our Board we have ensured all our services are provided by caring staff, despite the increasing pressure and demand they face. As Chief Nurse I am proud of the achievements we have made following our CQC inspection in April 2016 and the challenging plans we have set for ourselves over the next year. The Quality Account sets out a number of areas that we need to focus on. These have been influenced and identified by our patients, staff and partner organisations; by listening to their views and comparing ourselves with others we ensure we focus on what matters to the people we serve. The Quality Account is a vital snapshot of our achievements and whilst it shows areas where we have progressed well; there are clearly areas where further improvement is still needed. For the coming year our priorities are aligned to the CQC as follows: Safety Ensuring all our patients and staff are protected from avoidable harm Effective Ensure all our patients receive evidence based treatments that achieves and supports good outcomes Responsive Ensure all our patients receive care and treatment organised to meet their needs We welcome all opportunities to provide feedback on the services we provide and the delivery of the fundamental standards. If you have used our services and wish to get involved in their further development we would be delighted to work with you. Stephanie Dawe Chief nurse and executive director of integrated care (Essex) NELFT NHS Foundation Trust Quality Account 2016/17


7 7
8 Introduction What is a Quality Account? Annually all NHS healthcare providers are asked to write a report about the quality of services they provide. This is called the Quality Account. The Quality Account enables us to engage with patients, service users, staff, stakeholders, partner organisations and the public in an open and transparent way. We look forward, identifying our key priorities for the year ahead and look back, showing the improvements we have made in the last year to improve the quality of care that we provide. This year the Quality Account will be split into two parts, part A and part B. Part A will provide an introduction to NELFT look at our awards and participation in the sign up to safety campaign look forward at our priorities for improvement 2017/18 look back on our progress in 2016/17 look at how we performed in the annual staff survey Part B will provide detailed information regarding our statements of assurance from the board inform you of our progress in regards to audit and data quality show performance data against our core indicators provide an appendix, glossary and useful contact numbers list Quality Account governance arrangements The chief nurse and executive director of integrated care (Essex) has overall responsibility for the NELFT Quality Account. Production of the Quality Account is the responsibility of the director of performance and business intelligence. Leads of our services are engaged in working with clinical and operational staff to deliver our key priorities. Progress reports on each of our priorities are reported to each leadership team on a bi-monthly basis and to our quality and safety committee, which is chaired by a nonexecutive director every 6 months. In addition, our chief nurse group oversee the Quality Account process and formally report once a quarter. This information is then reported to the executive management team, which reports to the NELFT board. Data quality is assured through NELFT s data quality group and through audit processes (both internal and external). NELFT NHS Foundation Trust Quality Account 2016/17
9 9 Our services Our values NELFT awards and achievements Sign up to safety campaign Looking forward Priorities for improvement 2017/2018 Priority 1: Safe Priority 2: Effective Priority 3: Responsive Priority 4: Well led How to provide feedback on this Quality Account We hope that you enjoy reading this year s Quality Account. If you would like to give us feedback on our Quality Account 2016/17, please contact: Julie Price, director of performance and business intelligence julie.price@nelft.nhs.uk Tel: ext Address: NELFT NHS Foundation Trust Suite 1, Phoenix House Christopher Martin Road Basildon, Essex SS14 3EZ. Looking back Review of our performance against our 2016/2017 priorities Priority 1: Working together for service users and patients Priority 2: Commitment to quality of care Priority 3: Respect and dignity Annual staff survey results Part A
10 1 Our services NELFT is a growing organisation serving a population of 2.8 million across north east London and Essex. We employ approximately 6000 staff and have an annual turnover in excess of 350 million. NELFT provides mental health and community services for people living in the London boroughs of Barking and Dagenham, Havering, Redbridge and Waltham Forest and people living in Essex. We provide these services in a range of settings including health centres, community hospitals and people s own homes. We work closely with a range of partners to provide the best care for our patients and service users. People first We remember that patients, service users and carers are our top priority, and treat others how we would like to be treated. Our values NELFT has a core set of values outlining what is important to our staff and the people who use our services. Our newest acquisition here at NELFT has been our Integrated Emotional Wellbeing and Mental Health Service in Essex. In 2016/17 this service has been given additional focus due to its transformational phase. In 2017/18 we will continue focusing on key areas such as clinical risk and quality governance and will continue to improve the quality of care we provide by delivering on our key priorities for the year ahead. NELFT NHS Foundation Trust Quality Account 2016/17
11 Prioritising quality We provide the best service possible, following best practice and national developments. 4Professional and honest We work to create relationships based on honesty, respect and trust, and meet the highest standards of professionalism and confidentiality. Progressive, innovative and continually improving We listen and continually improve our services for the benefit of our patients, service users and carers. 5Promoting what is possible independence, opportunity and choice We help people achieve the best quality of life possible, giving them the information and support they need.


12 NELFT awards and achievements In 2016/17 NELFT services have been recognised for the excellent care that they provide, winning some high profile external awards. Our equality and diversity manager Harjit Bansal and equality and diversity assistant manager Michael Beackon won the silver standards employer award at the Employers Network for Equality and Inclusion (ENEI) awards. The ENEI awards recognise and celebrate the achievements of organisations that have taken a lead in challenging discrimination and are working inclusively to tap into their talented workforce. NELFT was also nominated as the Diverse Company of the Year Award at the BEAM awards The Home Treatment Team (HTT) in Redbridge won an award at the Royal College of Psychiatrists annual awards ceremony in London. 10 members of the team were on hand to receive the award for the Psychiatric Team of the Year: Working-age Adults from Geraldine Strathdee, NHS England s National Clinical Director for Mental Health. The team was recognised for delivering high quality acute patient care and for their key role in keeping hospital admissions low. Equality and diversity manager Harjit Bansal and equality and diversity assistant manager Michael Beackon The Redbridge Home Treatment Team (HTT) NELFT NHS Foundation Trust Quality Account 2016/17

13 13 Home Treatment Team i The Home Treatment Team (HTT) is a community based treatment service which provides intensive support for service users who are in a mental health crisis providing an alternative to hospital admission. The NELFT dementia crisis support team won a prestigious Health Service Journal award for specialist service design. The team based at Brentwood Community Hospital has been responsible for reducing the amount of hospital admissions for those people suffering with dementia, seen a reduction in the length of stay for some patients and saved around a 1000 mental health bed days across Basildon and Brentwood CCG and Thurrock CCG over a 12 month period. Most recently NELFT has been shortlisted in two categories for this year s Patient Safety Awards both for Significant 7 - Signs of Deterioration for Care Homes. The project has been developed in collaboration with Barking and Dagenham, Havering and Redbridge CCGs. The awards ceremony will take place on July 4 at Manchester Central venue and the two nominations are in the Patient Safety in the Community and Care of Older People categories. NELFT won an award at last year s event for Patient Safety in Care of Older People. The dementia crisis support team


14 NELFT NHS Foundation Trust Quality Account 2016/17
15 15 Sign up to Safety is a national campaign which was launched on 24th June 2014 by the Secretary of State for Health. The ambition is to halve the amount of avoidable harm to patients and service users in the NHS over the next 3 years and strengthen patient safety across all services. NELFT signed up to the campaign and has committed to strengthen patient safety by signing up to the five pledges. Details of our patient safety improvement plan are listed under each of the pledges. This campaign is due to end in 2017, however progress against indicators such as pressure ulcers, falls and medication incidents will continue to be measured and reported to the trust board on a quarterly and annual basis. Corrective action will be taken as necessary and learning will be embedded throughout the organisation to keep our patients and service users safe. Put patients first Continue to progress the national harm-free care and zero tolerance campaign in relation to pressure ulcers; Reduce moderate/severe medication errors; Improve physical health care in mental health services; Improve diagnosis of bone fractures. Continually learn Improve services by listening to our patients; Reduce risk by learning from serious incidents. Honesty Promote and build on a culture of being open and honest. Collaborative Continue to be an active member of the University College London Partnership; Continue to share good practice with partners. Support Embed supervision to support staff; Develop annual staff awards to include specific patient safety award.
16 Looking forward Priorities for improvement 2017/18 Development of our quality priorities for 2017/18 Continuous improvement is a top priority for NELFT and our aim is to develop meaningful quality indicators that can be monitored, reported and scrutinised by all. In April 2016 NELFT was inspected by the Care Quality Commission (CQC), the independent regulator of health and social care in England. The CQC monitor, regulate and inspect health and social care services to ensure that fundamental standards of quality and safety are met. This includes inspecting services to see if they are safe, effective, compassionate and of a high quality. Findings are published nationally and include performance ratings to help patients and service users choose care. The trust was inspected and measured against five key questions/domains: are they safe? are they effective? are they caring? are they responsive? are they well-led? NELFT was rated good for many of our inspected service areas, achieving outstanding for our responsiveness in our forensic inpatient/ secure wards. For four out of the five domains NELFT was rated as requires improvement. Our priorities for the coming year therefore reflect the improvements required in these areas and form part of our action plan to ensure safe and high quality patient care is delivered across the trust. Views of patients, staff and the wider public have been taken into account when considering our priorities for the year ahead. During the inspection the CQC spoke to 265 patients and service users or their relatives and carers. They collated feedback from 339 patients, carers and staff using comment cards. The CQC also attended 43 multi-disciplinary meetings which included care reviews, and attended 18 focus groups that were attended by staff. NELFT has also run focus groups with managers and health professionals such as trainee doctors, mental health inpatient staff, community health care assistants and district nurses to gain feedback about the services we provide. NELFT NHS Foundation Trust Quality Account 2016/17

17 17 1. Safe 2. Effective 3. Responsive 4. Well led Brookside child and adolescent inpatient unit Back in April 2016, following the CQC comprehensive inspection, our child and adolescent mental health ward Brookside was rated inadequate. Brookside is an 18 bedded inpatient mental health unit for young people, providing 24 hour specialist care for those experiencing an acute mental health crisis and requiring inpatient care. Following the inspection NELFT made the decision to temporarily close Brookside to undertake an extensive refurbishment and recruitment programme. An action plan was co-produced with service users, clinicians and managers as part of the process, and the unit has since been fully refurbished and all recommendations to improve quality of care implemented. Brookside reopened in September 2016 with a transformed model of care providing greater treatment options for young people at home. We were delighted to welcome the CQC back for a re-inspection in October. The unit is now rated good across all five domains. The innovative model, developed in agreement with NHS England and local commissioners, provides both acute inpatient beds and a Young People s Home Treatment Team (YPHTT). The YPHTT is a 24/7 service designed to support young people in their own homes and ensures the maintenance of social networks, schooling and family connections. The trust would like to thank all the staff for their hard work. We look to continually improve our practice, undertaking quality visits to services to ensure learning and best practice is embedded. The table overleaf provides a summary of our latest inspection results. The latest inspection was carried out in September 2016.
18 Overall rating Inadequate Requires improvement Good Outstanding Acute wards for adults of working age and psychiatric intensive care units Safe Effective Caring Responsive Well led Overall Inadequate Requires improvement Requires improvement Requires improvement Requires improvement Requires improvement Child and adolescent mental health wards Good Good Good Good Good Good Community health inpatient services Requires improvement Good Good Good Good Good Community health services for adults Requires improvement Requires improvement Good Requires improvement Requires improvement Requires improvement Community health services for children, young people and families Requires improvement Requires improvement Good Good Requires improvement Requires improvement Community mental health services for people with learning disabilities or autism Community-based mental health services for adults of working age Requires improvement Good Good Good Good Good Requires improvement Good Good Good Good Good Community-based mental health services for older people Requires improvement Good Good Good Good Good Forensic inpatient/secure wards Good Good Good Outstanding Good Good Long stay/rehabilitation mental health wards for working age adults Good Good Good Good Good Good Mental health crisis services and health-based places of safety Good Requires improvement Good Good Good Good Specialist community mental health services for children and young people Good Requires improvement Good Good Good Good Wards for older people with mental health problems Requires improvement Requires improvement Good Requires improvement Requires improvement Requires improvement Wards for people with learning disabilities or autism Good Good Good Good Good Good NELFT NHS Foundation Trust Quality Account 2016/17

19 Looking forward Priorities for improvement 2017/18 19 Priority 1 Safe CQC definition: Are services safe? By safe, we mean that people are protected from abuse* and avoidable harm. *people are protected from physical, sexual, mental or psychological, financial, neglect, institutional or discriminatory abuse Aim To ensure that care plans and risk assessments are consistent across the trust to deliver safe and effective patient care. We want to strengthen the systems we already have in place and ensure that care plans and risk assessments are consistent and of a high quality so they support us to keep patients safe.
20 Priority 1: Safe Goal 1 To ensure that 85% of care plans and risk assessments are completed where applicable, and that all staff will be aware and deliver care in accordance with the plans and level of risk. Our aspiration is for all of our patients to have care plans and risk assessments completed when required. Area applicable to: acute wards for adults of working age and psychiatric intensive care unit wards for older people with mental health problems child and adolescent mental health wards community mental health services for adults of working age community mental health services for older people What do we expect to achieve? a) clinical risk assessment training to be made mandatory for all staff where applicable, achieving a compliance rate of 85% and above by quarter /18 b) risk assessments are monitored and updated when needed c) staff to use care plan checklist tool How progress will be monitored and measured a) through monthly mandatory training records b) through weekly care plan and risk assessment audit, managed through team meetings and supervision How progress will be reported reported monthly through directorate performance quality and safety group and leadership team meetings through trust quality improvement accelerator care planning programme NELFT NHS Foundation Trust Quality Account 2016/17
21 Looking forward Priorities for improvement 2017/18 21 Goal 2 To implement a system for monitoring and frequently auditing risk assessments ensuring consistency across services. Area applicable to: community health services for adults this was an area that was specifically highlighted by the CQC What do we expect to achieve? a) Director of nursing (clinical effectiveness) to review the clinical risk assessment policy to ensure it is fit for purpose by the end of quarter /18 b) to carry out an audit reviewing risk assessments in the clinical notes of patient records, achieving a compliance rate of 85% across 18 teams highlighted in the quality improvement programme by the end of quarter /18 How progress will be monitored and measured a) policy sign off through stakeholders, senior leadership and executive management team b) through clinical audit and quality improvement accelerator for care planning programme Risk assessment A risk assessment involves working with patients and service users to identify and investigate factors that may cause a specific risk to occur. It helps determine what the degree of the risk may be and also if it may pose problems at some point in the future for the patient or service user or the general public. Care plan i i A care/treatment plan is a personalised plan setting out how a patient or services users care and support needs will be met. How progress will be reported reported monthly through directorate performance quality and safety group and leadership team meetings reported through chief nurse group
22 Priority 1: Safe Goal 3 For patients over the age of 65 to automatically receive a falls risk assessment on admission to hospital Area applicable to: older adult s mental health wards What do we expect to achieve? a) a 50% reduction in the number of falls in the older adults inpatient wards by the end of quarter /18 b) a falls risk assessment to be completed for every patient who meets the threshold on admission to older adult mental health wards How progress will be monitored and measured a) through clinical audit and reporting of incidents b) through weekly clinical data audit and managed through supervision and staff team meetings How progress will be reported reported monthly through directorate performance quality and safety group and leadership team meetings bi-monthly through the harm free care strategy group In previous years, our performance regarding the completion of risk assessments and care planning has been measured in our annual record keeping audit. For each service trustwide, a sample of records is audited helping us to understand our compliance in certain areas of patient notes. The audit looks at the quality of our record keeping, from data capture through to the quality of clinical notes. The data overleaf gives an overview of our performance in regards to care plans and risk assessments for 2015 and During this time, services used both paper and electronic means for recording information. The trust now uses electronic patient record systems only. A total of 1,986 records were audited in 2015 and 1,995 records in Not all patients audited required a care plan or risk assessment to be completed. The results demonstrate the baseline from which we aim to improve. NELFT NHS Foundation Trust Quality Account 2016/17
23 Looking forward Priorities for improvement 2017/18 23 Is there evidence that an up to date risk assessment has been undertaken on the patient s needs where required? Electronic records Paper records % 85.0% 90.10% 89.04% Is there evidence of a current care plan/treatment plan/ treatment programme/goal setting agreed with the client or patient for this latest episode of care? Electronic records Paper records Adult 91.42% 92.0% 92.15% 93.93% Child / young person 81.98% 86.0% 87.43% 80.92% Has a discussion taken place regarding end of life care planning? Electronic and records records N/A 73.08% Has an individualised care plan for the last days of life been agreed? Electronic and records records N/A 50% Data taken from NELFT clinical record keeping audit 2016.

24 Priority 1: Safe NELFT NHS Foundation Trust Quality Account 2016/17

25 Looking forward Priorities for improvement 2017/18 25 Priority 2 Effective CQC definition: Are services effective? By effective, we mean that people s care, treatment and support achieves good outcomes, promotes a good quality of life and is based on the best available evidence. Aim To ensure that clinical staff are competent to deliver safe and effective patient care through the use of effective care planning. We want to ensure that everyone who requires a care plan receives one, that risk assessments are effective and that the people we see are involved in their care and treatment. We also want to ensure that our staff have the information they need to make informed decisions about patient care.
26 Priority 2: Effective Goal 1 That 85% of patient care plans include the 5 elements of care planning - consent and capacity, social situation, collaborative, risk assessment, recovery focused. Our aspiration is for all of our patients to have care plans that include the 5 elements of care planning. Area applicable to: acute wards for adults of working age and psychiatric intensive care unit child and adolescent mental health wards community mental health services for adults of working age How progress will be monitored and measured a) through audit of the quantity and quality of care plans supported by the trust quality improvement programme b) leads to be documented on a register c) by reviewing attendance records for the training programme How progress will be reported reported monthly through directorate performance quality and safety group and leadership team meetings through trust quality improvement programme What do we expect to achieve? a) all care plans include the 5 elements of care planning by the end of quarter /18. b) a lead to be identified for each of the teams requiring improvement in their care plans by end April c) leads to attend six fortnightly half day learning programmes about quality improvement methodology NELFT NHS Foundation Trust Quality Account 2016/17

27 Looking forward Priorities for improvement 2017/18 27
28 Priority 2: Effective Goal 2 All care plans for mental health patients are recovery orientated and reflect the personal views and preferences of patients. Area applicable to: acute wards for adults of working age and psychiatric intensive care unit child and adolescent mental health wards community mental health services for adults of working age What do we expect to achieve? a) that staff work collaboratively with patients to include their preferences and views in their care plan. b) that a broad range of recovery based goals are written into each care plan How progress will be monitored and measured through audit of the quality of care plans through the quality improvement accelerator programme How progress will be reported through chief nurse group NELFT NHS Foundation Trust Quality Account 2016/17
 waiting times are achieved.")
29 Looking forward Priorities for improvement 2017/18 29 Priority 3 Responsive CQC definition: Are services responsive to people s needs? By responsive, we mean that services are organised so that they meet people s needs. Aim To ensure that where appropriate, referral to treatment (RTT) waiting times are achieved. We want to ensure that all services are able to monitor and manage their own waiting lists. Using a performance monitoring tool, services will be able to identify those patients who have waited a long time and manage any risks accordingly. All services that have longer waits would carry out clinical risk assessments on each patient to ensure a longer wait does not cause any clinical harm. National guidance states that healthcare providers are to comply with maximum waiting times of 18 weeks. Here at NELFT, we want to go further and offer this waiting time management tool to all outpatient services supporting them to deliver high quality care in a timely fashion.
30 Priority 3: Responsive Goal To ensure an effective system of monitoring waiting times is embedded across NELFT for all patients attending outpatient type services. Area applicable to: NELFT wide What do we expect to achieve? a) by the end of quarter /18, training to be provided to service leads where the performance management tool has been newly rolled out, ensuring staff know how to use MIDAS effectively b) services where applicable, will effectively manage their waiting times through the performance management tool MIDAS How progress will be monitored and measured RTT monitored monthly through department patient and quality safety group and leadership meetings MIDAS training programme monitored quarterly by chief nurse group How progress will be reported reported monthly through directorate performance quality and safety group and leadership team meetings Referral to Treatment (RTT) i The NHS constitution gives patients in England the right to access services within maximum waiting times, or for the NHS to take all reasonable steps to offer patients a range of suitable alternative providers if this is not possible. Patients should wait no longer than 18 weeks from referral by a GP to treatment. MIDAS i MIDAS is a performance reporting tool to help integrate, validate and present data from multiple systems we use. Managers can see their team s performance in different areas, for example appraisal compliance or mandatory training. They can also look at the activity that is happening within the team to ensure that all patients are seen and they receive the right treatment in a timely fashion. MIDAS helps Managers to performance manage their services and enables us to extract data from a central source which can then be shared with our commissioners. NELFT NHS Foundation Trust Quality Account 2016/17

31 Looking forward Priorities for improvement 2017/18 31 Priority 4 Well led CQC definition: Are services wellled? By well-led, we mean that the leadership, management and governance of the organisation assure the delivery of high quality person centred care, supports learning and innovation, and promotes an open and fair culture. Aim To ensure that all leaders and managers within the trust have the tools required to lead and manage safe and effective services. We want to ensure that all of our staff at NELFT have the tools and training required to deliver excellent patient care.

32 Priority 4: Well led i Goal 1 To ensure that all staff are up to date with mandatory training, including clinical risk assessment and mental health act training where applicable Area applicable to: NELFT wide What do we expect to achieve? to achieve a compliance rate of 85% for all mandatory training by the end of quarter /18. Mental Health Act In most cases people are treated in hospital or a mental health service and they are known as a voluntary patient as they have agreed to attend. However, there are cases when a person has to be detained under the Mental Health Act (1983) and they are provided treatment without their consent. This is sometimes referred to as being sectioned. The Mental Health Act is legislation that covers the assessment and treatment of people and helps them to understand their rights when detained. How progress will be monitored and measured monitored monthly through directorate performance quality and safety group and leadership team meetings measured through monthly training compliance reports How progress will be reported through monthly leadership team, senior leadership team and executive management team meetings NELFT NHS Foundation Trust Quality Account 2016/17
33 Looking forward Priorities for improvement 2017/18 33 Goal 2 To ensure that teams have access to MIDAS to support their management of services. Area applicable to: older adult wards this was an area that was specifically highlighted by the CQC What do we expect to achieve? a) 85% of managers working on older adult wards to have received MIDAS training by the end of quarter /18 b) in addition, MIDAS training to be rolled out to all managers NELFT wide, achieving a compliance rate of 75% or above by the end of quarter /18 How progress will be monitored and measured through review of business intelligence training records How progress will be reported through monthly directorate performance quality and safety group and leadership meetings Goal 3 To develop an effective performance analytical tool which provides the executive management team with forecasting information and highlights any risks or areas of underperformance. Area applicable to: NELFT wide What do we expect to achieve? a) to develop a heatmap performance tool which demonstrates key safety and quality measures for services. Pilot to be completed by the end of quarter /18 b) the heatmap will show us areas of best practice, enabling the trust to develop consistent quality of care across the organisation c) the heatmap will provide forecasting information to help us identify risks early on How progress will be monitored and measured a) through heatmap and performance data eg: appraisal compliance, fire risk training, delayed transfers of care b) through the performance team, leadership teams meetings and monthly senior leadership meetings How progress will be reported through monthly senior leadership and executive management team meetings
34 Governors indicator The Friends and Family Test has been implemented nationally across all mental health and community services since January This involves our services contacting a minimum of five patients, service users or carers on a monthly basis and asking them about their experience of care with NELFT. The Friends and Family Test asks the following questions: how likely is it that you would recommend this service to friends and family if they needed similar care or treatment? did you find it easy to get care, treatment or support from this service? did staff introduce themselves to you? did the service you receive meet your expectations? did you feel you were involved in your care as much as you would have liked? Feedback from our patients and service users is important as it helps us to understand what we are doing well and how we can improve. The table overleaf provides an overview of our results for NELFT overall, our community and mental health services for the last financial year. Each year the governor s indicator is audited. This indicator has been selected for audit by KPMG to evaluate: that the collection and collation methods we use for 5x5 are sound that patient feedback is appropriately disseminated throughout the organisation and action is taken if needed that the demographics of respondents are representative of the communities that we serve How do our goals impact on patient safety, clinical effectiveness and patient experience? Patient safety will be enhanced through: comprehensive care plans and risk assessments being completed for patients, where applicable, both in the community and on inpatient wards NELFT monitoring and auditing risk across the trust ensuring consistency of standards across services falls assessments being completed for all patients over the age of 65 on admission to hospital Clinical effectiveness will be enhanced through: staff being up to date with mandatory training, including clinical risk assessment and mental health act training care plans containing the five elements of care planning consent and capacity, social inclusion, collaborative, risk assessment, recovery focused care plans reflecting the personal views and preferences of patients Patient experience will be enhanced through: the review of the friends and family test, ensuring that feedback collated is appropriately disseminated through the organisation and used to help inform service delivery services have an effective system of monitoring wait times through the MIDAS performance management tool care plans are recovery orientated and reflecting the personal views and preferences of patients, ensuring their voice is heard and care is tailored to their individual needs NELFT NHS Foundation Trust Quality Account 2016/17
35 Looking forward Priorities for improvement 2017/18 35 How likely is it that you would recommend this service to friends and family if they needed similar care or treatment? Survey name Date Survey returns Would recommend Would not recommend NELFT overall Q1 2016/ % 2% Q2 2016/ % 2% Q3 2016/ % 2% Q4 2016/ % 2% Community services Q1 2016/ % 1% Q2 2016/ % 1% Q3 2016/ % 1% Q4 2016/ % 1% Mental health Q1 2016/ % 6% Q2 2016/ % 5% Q3 2016/ % 4% Q4 2016/ % 4% Statements of assurance from the board The statements of assurance from the board for our trust are in part B of this document. Please therefore refer to part B where you will see information regarding our registration, participation and progress in these areas.
36 Looking back Progress against each of our 2016/17 priorities Considerable progress has been achieved against our targets for 2016/17 and our achievements are noted over the following pages. Last year NELFT s priorities focused on: 1. Working together for service users and patients 2. Commitment to quality of care 3. Respect and dignity NELFT NHS Foundation Trust Quality Account 2016/17
37 37 Priority 1: Working together for service users and patients Goal 1 To ensure duty of candour is embedded in practice ensuring we are providing openness and transparency in care delivery. That any patient harmed by the provision of a healthcare service is informed of the fact and offered an appropriate remedy, regardless of whether a complaint has been made or a question asked about it.' What we achieved At NELFT we openly support duty of candour and encourage our staff to be truthful in their dealings with patients. To raise awareness of the duty of candour a news article has been published to improve staff knowledge and better reporting of incident categories. A video link and case studies are also used in communication about the duty of candour amongst staff, helping to generate awareness. Duty of candour training has also been disseminated to our front line staff. Our monthly duty of candour report evidences our continuing work with community staff caring for patients who develop avoidable pressure ulcers. All duty of candour incidents are also reported monthly to commissioning groups and through our department and locality patient and quality safety group meetings. Goal 2 The patient record and duty of candour letters to provide additional assurance that professionals are exercising the duty in accordance with professional codes. What we achieved The duty of candour templates for our patient record systems have been finalised and were launched in March This will provide assurance that professionals are exercising the duty in accordance with the General Medical Council (GMC) and the Nursing and Midwifery Council (NMC). By using these forms it will help evidence our duty of candour work. Going forward we will continue to audit our practice in this area to ensure it is embedded throughout the organisation. i Duty of candour The duty of candour is a legal duty for hospital, community and mental health trusts to inform and apologise to patients if mistakes have been made in their care that have led to significant harm. Any patient harmed by health service provision should be informed of the fact and offered an appropriate remedy.
38 Priority 1: Working together for service users and patients Goal 3 NELFT trust board to review the monthly duty of candour performance data and to be informed of any gaps in assurance that are creating significant risk or issues. What we achieved Each month the trust board receive data regarding duty of candour. This is also reviewed at a locality level. Each year we are including duty of candour in our clinical audit enabling us to measure and reflect on our practice. The duty of candour risk action plan continues to be monitored monthly through our chief nurse group. The following tables show data collected from our annual clinical record keeping audit. Data shows our performance in 2015 and 2016 for both electronic and paper patient records. We expect the results of our 2017 annual record keeping audit to show improvement, thus reflecting our embedding of practice throughout the 2016/17 year and the many initiatives we have put in place with our staff. Have duty of candour discussions been documented on the clinical record? Electronic records Paper records % 53.78% 84.85% 75.00% Did this take place within 10 days? Electronic records Paper records % 96.92% 96.43% 94.44% Duty of candour incidents are also reported in our monthly performance reporting to locality based clinical commissioning groups (CCGs). Within NELFT this is monitored and reported on a monthly basis to department patient and quality safety group, leadership and executive management team meetings. NELFT NHS Foundation Trust Quality Account 2016/17
39 39 Looking back Progress against each of our 2016/17 priorities Priority 2: Commitment to quality of care Goal 1 To use an agreed logo to flag learning disability patients to our services so we can make reasonable adjustments to their care. What we achieved The learning disability logo has now been piloted on some of our inpatient wards. 100% of patients during the pilot were in favour of using the logo with 67% of patients reporting that communication was better with staff in regards to their care. NELFT are now rolling out the initiative across other inpatient wards within the trust. The progress made last year against our 2015/16 priority will enable staff to clearly identify these patients and tailor their care accordingly.
40 Priority 2: Commitment to quality of care Goal 2 To improve end of life care experience for patients, running an educational session for staff focusing on managing difficult conversations and access to support mechanisms across NELFT. What we achieved An initial training programme was designed for London and Essex and end of life champions were selected from respective services. A range of internal training has been delivered to NELFT staff including difficult communication, advance care planning, use of the individualised care plan for last days of life and T34 syringe pump updates. In Essex, external education has been provided to 180 learners across Basildon, Brentwood and Thurrock care homes. The programme covers foundation level introduction to palliative and end of life care. 9 social workers working at Essex County Council have also worked with the NELFT team to understand more about end of life care. In London, 24 staff received 2 day palliative care training. This included information on pain and symptom management, syringe driver medication, communication skills, advance care planning and recognising a dying patient including the use of the individualised care plan for last days of life. Nursing home training was delivered to 20 qualified staff and included grief, loss and bereavement, drug considerations at the end of life, feeding and hydration, planning for end of life care and advance care planning. An all of me - personalised end of life care workshop was delivered to 65 staff from acute and community sectors within health, social services and the voluntary sector. Personalised end of life care was explored using a filmed case study. In addition a health and social services (HASS) end of life seminar training was delivered at each of the 4 HASS localities to 54 allied healthcare professionals and social worker s. End of life care needs were discussed using 2 case studies and incorporated difficult conversations and advance care planning. In order to reach a wider audience, NELFT has decided to develop an end of life e-learning training module in 2017/18 which will fall under essential training for staff, (for those it is applicable to) in the end of life teams. This e-learning provides training in line with NICE clinical standards and ambitions for end of life. This will continue to support staff to deliver high quality personalised care. Staff education also forms part of our 2016/2021 end of life clinical strategy. This helps to develop staff member s competence and confidence in delivering care. This strategy is based on the ambitions for palliative and end of life care; a national framework for local action, five priorities for the care of dying people and together for short Lives standards framework for children s palliative care (2015). Progress against the end of life clinical strategy will be reported bi-monthly through the end of life group, bi-monthly through the harm free care strategy group and quarterly to the quality patient safety committee. NELFT NHS Foundation Trust Quality Account 2016/17

41 Looking back Progress against each of our 2016/17 priorities 41 i NICE The National Institute for Health and Care Excellence (NICE) provides national guidance and advice to improve health and social care. This includes developing quality standards that providers should adhere to. Participant feedback from training delivered in Essex Improved my knowledge about palliative care and learned some new information. I have learnt multiple pieces of information that has aided in my knowledge, and hopefully ability, to deliver better end of life care not only to the person but also their family/friends. Very informative and interesting, very well communicated by all staff.
42 Priority 2: Commitment to quality of care I have gained so much from the process and have tried to relay this in how I treat my patients. Doing this certificate has changed my thought process on how the patient should be treated. We all take so much for granted when a patient comes to our door; we assume that all is well in their lives and treat as a matter of routine, asking the same questions going through the same process. This certificate teaches you to look outside the box and see beyond what is required and how to deliver the requirements that each individual needs. NELFT Dental Nurse Team Leader I felt really proud of myself, but most important I felt valued and I would like to thank the trust for the opportunities given to staff to progress, improve skills, and develop our career as a Health Care Professional. NELFT Healthcare Support Worker Goal 3 To ensure that all Health Care Support Worker s (HCSW s) are competent to deliver safe patient care. 90% of all newly recruited HCSW's to have completed the care certificate training within 12 months of joining NELFT. 100 existing HCSW's to be trained per quarter. What we achieved The care certificate was launched in April It provides clear evidence to employers, service users and patients and people who receive care that the HCSW's have the skills, knowledge and behaviours to provide compassionate and high quality care. It also offers the opportunity to both new and existing staff to improve and refresh their knowledge. The care certificate is completed by clinical staff bands 1-4 who are completing clinical duties and has two main elements; training and assessment. Between April 2016 and March 2017 there were a total of 87 new starters. 100% of new starters have therefore either completed, or are in the process of completing the care certificate. The total number of existing staff in post applicable to complete the care certificate training in April 2016 was staff completed the training by the end of quarter 4; therefore the total of 400 existing HCSW s to be trained by the end of 2016/17 was achieved. The training is provided on a rolling programme, so new starters and existing staff are already booked or completing training on the programme for completion in 2017/18. As part of the HCSW development, 12 staff that successfully completed the care certificate have now started clinical apprenticeships. NELFT NHS Foundation Trust Quality Account 2016/17



43 Looking back Progress against each of our 2016/17 priorities 43 Priority 3: Respect and dignity Goal To have a dementia friendly environment in our in-patient areas helping to deliver person centred care. What we achieved A document called this is me has been created for each dementia patient. This document is created in conjunction with family members and helps staff to understand what patients specific needs may be. This document can include information such as how the patient likes their tea, so staff do not repeatedly ask the same questions. It can also provide information as to why the patient may behave in a certain way, for example if they are frequently walking around do they need to use the toilet? To further enhance care delivered to dementia patients NELFT has launched John s campaign. This is where family or carers are able to visit day or night, helping to settle the patient whilst Carers welcome here We welcome the carers of our patients in the ward and would like to work in partnership with you. If you are a carer, please ask for a Care passport and let the staff know who you are. Supporting Johns Campaign John's campaign poster on an inpatient ward. A pilot has been successful at the Ainslee unit in Waltham Forest improving communication and increasing patient and carer satisfaction. The campaign will be rolled out to other wards in 2017/18 such as Stage ward in our acute and rehabilitation integrated care directorate and Thordon ward in Essex. Three of our inpatient wards have recently undergone refurbishment to improve the environment for dementia patients. In Stage ward the lighting has been changed to make the environment brighter. The walls have been painted and new flooring has been laid. Revised signage has also been put up, and feedback about the changes from staff and patients has been positive. Stage ward before and after refurbishment Internally, to help staff gain a better understanding of dementia, training has been provided to staff through an e-learning programme. Community practice subgroups also meet on a monthly basis to discuss themes around dementia such as research. Local events have been held with staff and external agencies to raise the awareness of dementia in the local community and NELFT continue to actively promote awareness of dementia through our live twitter chat and conference participation.
44 Governors selected local indicator: Rotational nurse competencies Goal Newly qualified nurses to undertake rotational nurse training to help build a sustainable workforce and address vacancy gaps. What we achieved NELFT now has a total of 12 nurses taking part in the rotational nurse training programme in the trust. Each nurse spends an initial 6 months in the area they trained in, either community health services or mental health services. In the first 6 months, nurses are expected to achieve 100% of the competencies. These are listed below. This is known as rotation 1. Mental health Ethical practice Knowledge Process/care Interventions Physical health Continence Personal care Nutrition Observations Pressure ulcer care Specialist placement (as part of rotation 3) Next is rotation 2. This is when the nurse spends the next 6 months of the programme in an area opposite to where they completed their training. For example a community health nurse will spend time working in mental health services and vice versa. The nurses are expected to achieve 85% of the competencies. Finally a nurse takes part in rotation 3. This is where nurses then spend time in a specialist area before returning to their original role. This may be for a registered community health nurse to work in a specialist memory service or for a registered mental health nurse to work in district nursing. During this time nurses are expected to achieve 50% of the competencies. In 2015/16 NELFT conducted a pilot of the rotational nurse programme. This was a small pilot set up to test the competencies required for the programme. The competencies were developed as the project moved forward. In 2016/17 we have had the second generation of the rotational nurse programme. Currently we have 4 nurses in rotation in Essex. NELFT nurses from the integrated health care teams in Basildon and Brentwood are spending time gaining experience, by rotating with nurses from Basildon hospital accident and emergency (A&E) and the accident and emergency ward (AMU). In September the nurses will rotate again. NELFT NHS Foundation Trust Quality Account 2016/17
45 Looking back Progress against each of our 2016/17 priorities 45 In London we have 8 nurses currently on rotation: 2 adult nurses and 6 mental health nurses. They are currently rotating between services within NELFT. The rotational nurse programme has made good progress in 2016/17 and the profile of the programme has risen. Throughout the year we have had articles featured: in the Nursing Times in August 2016, the Enquirer in October 2016 and the Ilford Romford Recorder in December Copies of the Enquirer and Ilford Romford Recorder articles can be found in appendix 1. For 2017/18 we intend to continue recruiting more nurses onto the programme. We currently have a waiting list of nurses ready to join and through twitter we have received many expressions of interest. You can join us on our journey by NELFT also continues to work with other health professionals helping them to gain experience. In 2017/18 we have 110 paramedics gaining mental health experience within the trust. We have also had excellent feedback from first year adult student nurses who have joined NELFT for 6 weeks to gain experience. A reflection of a placement is featured on the right. One important reflection was realising how much an interaction with a patient can mean to them. Choosing words very carefully is so important because of the impact it can have in their care. The same goes with first impressions and introducing oneself. I have realised these things are also very applicable for general nursing. Any patient could be anxious or scared in the same way that an acute patient could be. This is technically a mental health issue, so it is important for me to remember that mental health is part of holistic care. I have realised physical and mental health have a symbiotic relationship and cannot both exist without the other. The training I was given in the first week was very useful and I can now understand the rationale behind why it is given at the end of the first week. Having one days training after a few days of practical experience is very beneficial, as it allows you to touch base first then understand how that theory applies to the placement. I have not come across a situation where I have felt unsafe or did not have enough skills. I have always been supervised and have had to show competence before doing any task on my own. I am very impressed with the new set of skills I have learned as a result. I have learned that interacting with patients to improve their care is the most important thing about patient care. It applies to both fields of nursing, so it is great I have started to practice all of my communication skills at the start of my degree rather than closer to the end. First year adult nurse who came to NELFT on a 6 week placement in mental health

46 NELFT NHS Foundation Trust Quality Account 2016/17
47 Looking back Progress against each of our 2016/17 priorities 47 Annual Staff Survey 2016 Each year, NHS England asks NHS providers to complete a staff survey. This survey gives staff an opportunity to feedback about their experience working for the trust. From the survey results, we will then put together local improvement plans to help better the staff experience and wellbeing. The information taken from the survey also enables us to review our performance against other NHS providers and how we compare nationally. We value the feedback from our staff and the national staff survey is one of numerous ways of gauging their opinions. We pride ourselves on an open and honest culture that embeds the trust values in everything that we do. This has been a challenging year for the trust in terms of uncertainty about the potential changes the sustainability transformation plan agenda may bring, as well as the impact of the CQC inspection and subsequent report. We were disappointed that some of the results have not shown significant improvement on the previous year; however we do remain committed to engage positively with staff to act upon the recommendations contained within the report. A communications plan is being developed to share the results across the organisation and ensure that all staff have the opportunity to participate in making improvements to their working lives. Overleaf is a sample of some of the questions asked during this year s annual survey and our results. Percentage scores are from 0-100%. A full copy of our annual staff survey results can be found on the National NHS Staff Survey Co-ordination Centre website Sustainability transformation plan (STP) A sustainability transformation plan (STP) is a five year plan which outlines how services are going to improve health and wellbeing, improve quality and develop new models of care and improve efficiency of services. The plans cover all areas of NHS spending, and focuses on the better integration with social care and local authority services. i
48 Average (median) score for sector NELFT 2015 NELFT 2016 Q21a Care of patients / service users is my organisation's top priority Q21b My organisation acts on concerns raised by patients/ service users Q21c I would recommend my organisation as a place to work Q21d If a friend or relative needed treatment, I would be happy with the standard of care provided by this organisation KF3 Percentage of staff agreeing that their role makes a difference to patients/service users 73% 66% 68% 75% 71% 71% 57% 48% 50% 66% 57% 55% 89% 89% 90% KF11 Percentage of staff appraised in the last 12 months 92% 90% 90% KF15 Percentage of staff satisfied with opportunities for flexible working patterns KF18 Percentage of staff attending work in the last 3 months despite feeling unwell because they felt pressure from their manager, colleagues or themselves KF20 Percentage of staff experiencing discrimination at work in the last 12 months KF21 Percentage of staff believing that the organisation provides equal opportunities for career progression or promotion KF25 Percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in the last 12 months KF26 Percentage of staff personally experiencing harassment, bullying or abuse from staff in the last 12 months KF29 Percentage of staff reporting errors, near misses or incidents witnessed in the last month 58% 54% 59% 55% 68% 67% 11% 17% 15% 88% 83% 83% 28% 32% 28% 21% 25% 23% 93% 92% 90% Data is taken from (March 2017) NELFT NHS Foundation Trust Quality Account 2016/17
49 49 Statements of assurance from the board Participation in national clinical audit and confidential enquiries Learning from national clinical audits Learning from local clinical audits Participation in clinical research NICE compliance in NELFT CQUIN targets 2017/2018 Registration with the Care Quality Commission (CQC) NHS and general medical practice code validity Information governance assessment report Clinical coding error rate Audit - areas for improvement Reporting against our core indicators 2016/17 Appendix Glossary Useful contact numbers Part B
50 Welcome to part B of the Quality Account. As outlined in part A, part B provides statements of assurance from the board regarding the review of our services. We highlight our contributions to data quality and clinical audit and provide you with some detailed information in our appendices. Should you wish to provide feedback on our Quality Account, please refer to part A where our contact details for feedback are provided. Statement of assurance from the board During 2016/17 NELFT provided and/or subcontracted 110 relevant health services (provided across multiple localities). NELFT has reviewed all the data available to them on the quality of care in 110 of these relevant health services. The income generated by the relevant health services reviewed in 2016/17 represents 100% of the total income generated from the provision of relevant health services by NELFT for 2016/17. Participation in national clinical audit and confidential enquiries During 2016/17 9 national clinical audits and 1 national confidential enquiry covered relevant health services that NELFT provides. During that period NELFT participated in 100% national clinical audits and 100% national confidential enquiries of the national clinical audits and national confidential enquiries which it was eligible to participate in. The national clinical audits and national confidential enquiries that NELFT was eligible to participate in during 2016/17 are listed in appendix 2a. The national clinical audits and national confidential enquiries that NELFT participated in during 2016/17 are also listed in appendix 2a. The national clinical audits and national confidential enquiries that NELFT participated in, and for which data collection was completed during 2016/17, are listed in appendix 2a, alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry. Learning from national clinical audits The reports of 9 national clinical audits were reviewed by NELFT in 2016/17 and NELFT intends to take the following actions to improve the quality of healthcare provided, as listed in appendix 2b. Learning from local clinical audits The reports of 19 local clinical audits were reviewed by NELFT in 2016/17 and NELFT intends to take the following actions to improve the quality of healthcare provided, as listed in appendix 2c. Participation in clinical research The number of patients receiving relevant health services provided or sub-contracted by NELFT in 2016/17 that were recruited during that period to participate in research approved by a research NELFT NHS Foundation Trust Quality Account 2016/17
51 51 ethics committee was This figure relates to recruitment activity on NIHR portfolio studies from 01 April NICE compliance in NELFT The trust has an efficient and demonstrable process for the dissemination of NICE guidance in place, which ensures monthly review and determination of the applicability of NICE guidance to services. Further, there is an efficient operational process in place which ensures on a monthly basis, that all relevant NICE Baseline Assessment Tools and guidelines are made available to the appropriate service leads, which in turn provides the status of NICE compliance within the said service. All processes and systems are therefore in place to ensure a level of NICE compliance within services. CQUIN targets 2017/18 Commissioning for quality and innovation (CQUIN) is a payment framework enabling commissioners to award excellence by linking a proportion of the income they give to providers such as NELFT to the achievement of national and local quality improvement goals. A proportion of NELFT income in 2016/17 was conditional on achieving quality improvement and innovation goals agreed between NELFT and any person or body that they entered into a contract, agreement or arrangement with for the provision of relevant health services, through the Commissioning for Quality and Innovation payment framework. Further details of the agreed goals for 2016/17 and for the following 12 month period are available on request from: Special projects performance team specialprojects@nelft.nhs.uk Tel: Address: NELFT NHS Foundation Trust, Suite 1, Phoenix House, Christopher Martin Road, Basildon, Essex SS14 3EZ The total amount of income in 2016/17 conditional upon achieving quality improvement and innovation goals was 5,508k. The monetary total for achievement in goals for 2015/16 was 5,095k. Registration with the Care Quality Commission (CQC) NELFT is required to register with the Care Quality Commission and its current registration status is that it is registered to carry out the following regulated activities: Assessment or medical treatment of people detained under the Mental Health Act Diagnostic and screening procedures Treatment of disease, disorder or injury Family planning Surgical (application to cancel this regulated activity was made to the CQC on 1/3/2017 in advance of the planned decommissioning of community dental services on 1/4/2017) NELFT has no conditions on registration.
52 The Care Quality Commission has taken enforcement action against NELFT during 2016/17 across three core services. An extensive improvement plan has been developed and agreed with the CQC and is due to be completed by 31/03/17. NELFT has not participated in any special reviews or investigations by the CQC during this period. NHS number and general medical practice code validity NELFT submitted records during 2016/17 to the Secondary Uses Service for inclusion in the Hospital Episode Statistics which are included in the latest published data. The percentage of records in the published data which included the patient s valid NHS number was: 98.3% for admitted patient care 98.3% for accident and emergency care which included the patient s valid General Medical Practice Code was: 99.9% for admitted patient care 99.8% for accident and emergency care Information governance assessment report NELFT s information governance assessment report overall score for 2016/17 was 71% and was graded green (satisfactory on all requirements). Clinical coding error rate NELFT was not subject to the Payment by Results clinical coding audit during 2016/17 by the Audit Commission. Audit areas for improvement NELFT will be taking the following actions to improve data quality: All staff receive training on electronic recording systems prior to being given access. E-learning packages are being developed to provide more timely and efficient access to systems and will support the face to face learning that is available. The data quality / information governance mandatory e-learning programme that is now an annual requirement is being revised to include further guidance. This will include guidance around the registration of death and associated record management, synchronisation of records and recording of diagnosis, particularly within inpatient records applicable to Secondary Uses Service submissions. A data quality responsibilities document is currently under development and will be circulated to staff reminding them that they each have an individual responsibility to ensure that they complete all of their required mandatory training and that they are aware of the key trust policies that influence their role. This will assist in promoting and producing good quality data. Data quality prompts are being developed within the electronic patient records highlighting missing high priority information such as demographics and equalities data to enhance data collection and recording. The data quality guidance is being amended to consolidate agreed new and revised requirements identified over the last year and will be available via the trust intranet. The 2016/17 annual healthcare records audit included an increased focus on the assessment of data quality practices and those areas that impact on them. More use was shown of electronic systems for recording activity and clinical information as well as increased access via mobile devices. This information informs an action plan for improvement of data quality and record keeping across the trust which is reviewed by the trust on a regular basis. Data quality issues are identified and reported on a monthly basis, highlighting areas where improvement is required. The use of data quality information to support individual teams and individual practitioners is an area of development that will further support progress in completing the minimum required data. Data quality information is available to all staff through both the clinical activity reports and performance dashboards produced on the business intelligence tool, MIDAS. Maintenance and improvement of data quality across both clinical and corporate services is a function of the data quality action group who report to senior leadership team on a monthly basis via the Chairperson. The group identify priorities to target in the coming financial year, review the impact to financial performance in regards to data quality issues and agree the annual healthcare records audit, corporate records audit and information governance toolkit clinical coding audit. NELFT NHS Foundation Trust Quality Account 2016/17
53 Information assurance framework assessment and spot checks are agreed each year to monitor the quality and accuracy of our reported data against source data. In addition to the above, NELFT continues to monitor the capture and quality of information submitted as part of datasets and commissioned activity. Reporting against our core indicators 2016/17 Monitor, known as NHS Improvement since April 2016, require foundation trusts to report on a set of quality indicators. These were known as the risk assessment framework. From 1st October 2016 the single oversight framework was introduced, which replaced the risk assessment framework. For 2016/17 we have therefore reported on our indicators across both of these. Performance against our core set of quality indicators using data made available by the health and social care information centre (HSCIC) are summarised overleaf with detailed analysis of each indicator in the following pages. 53
54 Indicator Measure 2015/ /2017 The percentage of patients on Care Programme Approach (CPA) who were followed up within 7 days after discharge from psychiatric inpatient care during the reporting period Percentage 97.9% 95.8% The percentage of admissions to acute wards for which the Crisis Revolution Home Treatment Teams (HTT) acted as a gatekeeper during the reporting period The percentage of patients aged: (i) 0-15 and Percentage 98.1% 98.5% 16% (4 of 25) 5.88% (1 of 17) (ii) 16 or over readmitted to a hospital which forms part of the trust within *30 days of being discharged from a hospital which forms part of the trust during the reporting period Percentage 3.8% (157 of 4115) 5.13% (201 of 3917) *The national indicator states a 28 day readmission rate, however NELFT works and reports data on a 30 day readmission rate The trusts 'Patient experience of community mental health services' indicator score with regard to a patient's experience of contact with a health or social care worker during the reporting period Patient safety incidents Number Number ** Rate per 100,000 population N/A Patient safety incidents that resulted in severe harm or death Number ** Percentage 0.9% 0.5% ** ** April 2016 Sep 2016 verified data only available at time of print NELFT NHS Foundation Trust Quality Account 2016/17
55 1. The percentage of patients on Care Programme Approach (CPA) who were followed up within 7 days after discharge from psychiatric inpatient care during the reporting period / /2017 NELFT 97.9% 95.8% National Target 95% 2016/ / / /2017 Quarter 1 Quarter 2 Quarter 3 Quarter 4 National Target 95% NELFT 97% 97% 96% 94% National average 96.2% 96.8% 96.7% 96.7% NHS trusts/foundation trusts with highest 100% 100% 100% 99.4% and lowest for the same 28.6% 76.9% 73.3% 84.6% CPA is a framework designed to promote the effective co-ordination of care for those people suffering from complex mental health issues and those being treated within secondary mental health services. Services users on CPA must be contacted by a mental health professional, ideally face to face within a maximum seven days from discharge. NELFT considers that this data is as described for the following reason: both internal and external audits have taken place on a regular basis over the year and no significant issues have been found. NELFT intends to take the following actions to improve this percentage, and so the quality of its services by: continuing to monitor this indicator monthly via leadership team to maintain the high level of performance and quality of its services. 2. The percentage of admissions to acute wards for which the Crisis Resolution Home Treatment Team (HTT) acted as a gatekeeper during the reporting period 2015/ /2017 NELFT 98.1% 98.5% National Target 95% 2016/ / / /2017 Quarter 1 Quarter 2 Quarter 3 Quarter 4 National Target 95% NELFT 97.8% 99.4% 97.9% 98.9% National average 98.1% 98.4% 98.7% 98.8% NHS trusts/foundation trusts with highest 100% 100% 100% 100% and lowest for the same 78.9% 76% 88.3% 90%
56 NELFT acute and crisis care pathway provides people with an integrated single point of access to all acute mental health services for adults. Aside from providing a single point of access, NELFT drives towards strong HTTs to provide care alternatives to inpatient care. The Trust has a very high ratio of acute home treatment to inpatient care, as well as a low acute bed base. The Trust s acute mental health services are made up of five acute recovery wards, four frail wards, one male PICU, three adult HTTs and one older adult HTT. NELFT considers that this data is as described for the following reason: The teams have been able to effectively gate keep admissions into inpatient beds, thus resulting in more people being cared for closer to home, fewer admissions to inpatient services and elimination of out of area placements for a number of years. The teams have achieved this by being involved in all assessments including mental health act assessments and also HTTs attending daily reviews for all the patients on the acute wards, which enables them to identify people who could qualify for early discharge, whenever appropriate. Both the inpatients wards and HTTs have dedicated consultants working as part of the integrated acute mental health care pathway and this reduces delays in decision making. NELFT intends to take the following actions to improve this percentage, and so the quality of its services by: continuing to monitor this indicator monthly via leadership team to maintain the high level of performance and quality of its services. 3. The percentage of patients aged: (i) 0-15 years and (ii) 16 years or over readmitted to a hospital which forms part of the trust within *30 days of being discharged from a hospital which forms part of the trust during the reporting period *The national indicator states a 28 day readmission rate, however NELFT works and reports data on a 30 day readmission rate 2015/ /2017 Percentage of patients 0-15 years 16% (4 of 25) 5.88% (1 of 17) Percentage of patients 16 years or over 3.8% (157 of 4115) 5.13% (201 of 3917) NELFT considers that this data is as described for the following reason: The rates for readmission within a 30 day period have significantly improved, this relates to strengthened care co-ordination by clinicians in the community as well as a more integrated approach to supporting service users within their own home from a health and social care perspective as well as involving primary care. Service users have realistic rehabilitation goals set to support their recovery and sustained independence via a multidisciplinary approach including physiotherapists, occupational therapists, nurses, medical staff, social workers and pharmacists. Staff are also supporting those with long term conditions with the skills to manage their own condition during times of crisis for example COPD. Service users are supported to have their rehabilitation within an average of 21 days therefore minimising the amount of time spent within a clinical setting and therefore minimising the risks associated with hospitalisation (infection, immobility depression and loss of independence). NELFT intends to take the following actions to improve this percentage, and so the quality of its services by: Essex reviewing the pathway for intermediate care following a public consultation by developing a model of care (The Intensive Rehabilitation Service ) that delivers rehabilitation in the patient s own home moving away from a bed based model. 30 beds have been replaced with the introduction of the community model. Rehabilitation will be more focused around the service user (care closer to home). Length of stay within the existing bed base will decrease as patients will be discharged earlier on in their treatment so as to complete care in their own home. NELFT NHS Foundation Trust Quality Account 2016/17
57 4. The trusts patient experience of community mental health services indicator score with regard to a patients experience of contact with a health or social care worker during the reporting period 57 Patients experience of contact with a health or social care worker 2015/ /2017 NELFT Score NELFT considers that this data is as described for the following reason/s: This is a CQC managed survey which is overseen by an independent company Quality Health and has strict sampling and administration processes. The results are in the public domain on the CQC website. This is an improving picture since last year and NELFT is rated by the CQC as about the same as other mental health trusts. NELFT has taken the following actions to improve this percentage and so the quality of its services by introducing a Quality Improvement (QI) programme in relation to care planning, to ensure patients are always actively involved in decisions about their own care. 5. The number, and where available, rate of patient safety incidents reported within the trust during the reporting period, and the number and percentage of such patient safety incidents that resulted in severe harm or death Number of patient safety incidents reported 2015/ /2017 Quarter 1 and 2 Quarter 3 and 4 (Quarter 1 and 2 only) NELFT ** National average NHS trusts/foundation trusts with highest and lowest for the same Number of patient safety incidents that resulted in severe harm or death 2015/ /2017 Quarter 1 and 2 Quarter 3 and 4 (Quarter 1 and 2 only) NELFT ** National average NHS trusts/foundation trusts with highest and lowest for the same * April 2016 Sep 2016 verified data only available at time of print NELFT considers that this data is as described for the following reason/s: The data is taken from information that is published by NHS Improvement and is available to the general public. This information indicates that NELFT is higher than the national average for the number of patient safety incidents reported and sits within the top 25% of reporters for mental health trusts. NHS Improvement acknowledges that organisations that report more incidents usually have a better and more effective safety culture. The number of incidents NELFT report as severe harm or death is significantly lower than the national average. NELFT has taken the following actions to improve this percentage, and so the quality of its services by encouraging reporting through communication with staff through the weekly intranet update, the delivery of training sessions across the organisation and acting on feedback.
58 NELFT also report on the following indicators. Our performance for 2015/16 and 2016/17 is reported below: Indicator Measure Target 2015/ /2017 Maximum time of 18 weeks from point of referral to treatment (RTT) in aggregate patients on an incomplete pathway Percentage 92% 81% 100% A&E: maximum waiting time of four hours from arrival to admission/transfer/discharge Percentage 95% 99.51% 98.3% Care programme approach (CPA) patients (I), comprising: receiving follow-up contact within 7 days of discharge Percentage 95% 97.9% 95.8% having formal review within 12 months 98.1% 96.8% Admissions to inpatient services had access to crisis resolution/home treatment teams Percentage 95% 98.1% 98.5% Early intervention in psychosis (EIP): people experiencing a first episode of psychosis treated with a NICE-approved care package within two weeks of referral (added from quarter /16) Percentage 50% 83.2% (Quarter 4 only) 76% Improving access to psychological therapies (IAPT) (N): Percentage people with common mental health conditions referred to the IAPT programme will be treated within 6 weeks of referral 75% 98.3% 98.9% people with common mental health conditions referred to the IAPT programme will be treated within 18 weeks of referral 95% 100% 100% C. difficile meeting the C. difficile objective Number NELFT NHS Foundation Trust Quality Account 2016/17

59 Appendix 1 Looking back 2016/17 - Governors selected indicator - rotational nurse programme 59 The Enquirer Nurses get the chance to try hospital and community work


60 Ilford Romford Recorder New nursing scheme breaks down barriers NELFT NHS Foundation Trust Quality Account 2016/17
61 Appendix 2a National clinical audit and confidential enquiries - eligibility and participation 61 National audit/enquiry Early Intervention in Psychosis audit (EIP) National Chronic Obstructive Pulmonary Disease (COPD) Cases submitted 100 cases 134 cases submitted for the cumulative ( ) second NDFA annual report. 1 case in 2014/15 and 133 cases during 2015/16. Multiple participating sites have registered for integrated care directorates as follows: Waltham Forest - hawkwell court chingford, langthorne health centre and forest road medical centre Dagenham - porters avenue health centre Redbridge diabetes centre Havering - harold hill health centre The data collection period for both organisational and clinical audit components is January to July 2017 POMH-UK QIP Topic 11c - Prescribing antipsychotic medication for people with dementia (1st supplementary) POMH-UK QIP Topic 7e - Monitoring of patients prescribed lithium (3rd supplementary) POMH-UK QIP Topic 16a - Rapid Tranquilisation (Baseline audit) Sentinel Stroke National Audit Programme (SSNAP) CQUIN Mental Health 16/17 (Inpatients & Community) National Diabetes Foot Care Audit (NDFA) National Confidential Enquiry into Patient Outcome and Death (NCEPOD): Mental Health Conditions in Young People 576 cases 147 cases 45 cases 43 cases for Barking and Dagenham. Quarterly reporting audit throughout the year 150 cases 134 cases. The second annual report will include all foot ulcers where the first assessment was prior to 8 April This report is due for publication in spring cases for the prospective data collection in March 2016 National confidential enquiries National Confidential Enquiry into Suicide and Homicide for people with mental illness (NCISH) 2016/17 100%
62 Appendix 2b National clinical audit and confidential enquiry - requirements and actions taken Early Intervention in Psychosis (EIP) audit Improving access to evidence-based care for people with a first episode of psychosis is a national priority. A new access and waiting time standard has been set and additional funding has been made available to deliver better services. As part of this initiative, NHS England commissioned an audit to establish a baseline position regarding services ability to provide timely access to NICE recommended interventions across England. All NHS mental health providers were asked to submit retrospective data on a sample of up to 100 patients accepted onto the caseload of EIP services between 30/06/2014 and 31/12/2014 and the treatment they received over the following six months. They were also asked to provide service-level information for each of their EIP teams. Actions taken: 1) Offers and update will be monitored as part of Service Development & Improvement Plan (SDIP) for Waltham Forest and other boroughs. 2) The full work plan for physical health CQUIN will be implemented. National Chronic Obstructive Pulmonary Disease (COPD) (Pulmonary Rehab Work stream) The core aim of the programme is to drive improvements in the quality of care and services provided for COPD patients. The pulmonary rehabilitation audit 2017 will be running a snapshot audit of organisation and resources of pulmonary rehabilitation services, as well as a snapshot audit of clinical care. These will take place concurrently in the first half of Multiple participating sites have registered for their integrated care directorates as follows: Waltham Forest - hawkwell court chingford, langthorne health centre and forest road medical centre Dagenham - porters avenue health centre Redbridge - diabetes centre Havering - harold hill health centre Data collection period for both organisational and clinical audit components is January to July POMH-UK QIP Topic 11c - Prescribing antipsychotic medication for people with dementia (1st supplementary) The Prescribing Observatory for Mental Health (POMH-UK) runs audit-based Quality Improvement Programmes (QIPs) that focus on discrete areas of prescribing practice. During April and May 2016, 58 specialist Mental Health Trusts or healthcare organisations within the UK participated in this supplementary audit of prescribing antipsychotics for people with dementia. NELFT NHS Foundation Trust Quality Account 2016/17
63 Actions taken: 63 1) The clinical indications (target symptoms) for antipsychotic treatment will be clearly documented in the clinical records. 2) Before prescribing antipsychotic medication for behavioural and psychological symptoms in dementia (BPSD), likely factors that may generate, aggravate or improve such behaviours will be considered 3) The potential risks and benefits of antipsychotic medication will be considered and documented by the clinical team prior to initiation. 4) The potential risks and benefits of antipsychotic medication will be discussed with the patient and/or carer(s) prior to initiation. 5) Medication will be regularly reviewed, and the outcome of the review will be documented in the clinical records. The medication review should take account of a) therapeutic response b) possible adverse effects. POMH-UK QIP Topic 7e - Monitoring of patients prescribed lithium (3rd supplementary) POMH-UK aims to help specialist mental health trusts/healthcare organisations improve their prescribing practice. Organisations are able to benchmark their performance against one another and identify where their prescribing practice meets nationally agreed standards and where it falls short. The on-line data submission period was August The national report has been published in January The national report has been received by POMH-UK and a local summary and action plan is under development. POMH-UK QIP Topic 16a - Rapid Tranquilisation (Baseline audit) The on-line data submission period was July to November The national report is due to be published in June NELFT will review this report and take action accordingly. Sentinel Stroke National Audit Programme (SSNAP) The SSNAP clinical audit collects a minimum dataset for every stroke patient, including acute care, rehabilitation, 6-month follow-up, and outcome measures in England, Wales and Northern Ireland. The aims of the audit are: 1) To benchmark services regionally and nationally 2) To monitor progress against a background of organisational change to stroke services and more generally in the NHS 3) To support clinicians in identifying where improvements are needed, planning for and lobbying for change and celebrating success 4) To empower patients to ask searching questions.
64 There is a quarterly reporting audit throughout the year. Data collection for the period August to November 2016 ended on 9th January A report with an action plan for the trust is currently under development. UK Parkinson s Audit (previously known as National Parkinson) The 2017/18 UK Parkinson's Audit aims to provide a clear picture of the state of Parkinson's services, showcasing good practice but highlighting many areas for improvement. It was the first to include a Patient Reported Experience Measure (PREM), giving people with Parkinson's a stronger voice in rating the services they receive. Registration opened in February National Diabetes Foot Care Audit (NDFA) The National Diabetes Foot Care Audit (NDFA) enables all diabetes foot care services to measure their performance against NICE clinical guidelines and peer units, and to monitor adverse outcomes for people with diabetes who develop diabetic foot disease. The NDFA is a continuous collection audit. The on-line data submission period closed on 29th July The second annual report will include all foot ulcers where the first assessment was prior to 8 April This report is due for publication in spring National Confidential Enquiry into Patient Outcome and Death (NCEPOD): Mental Health Conditions in Young People This study has been commissioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the Clinical Outcome Review Programme into Child Health, under a contract awarded in The audit aims to: 1) Identify the remediable factors in the quality of care provided to young people treated for mental health disorders; with specific reference to: -Depression and anxiety -Eating disorders and -Self harm 2) To examine the interface between different care settings 3) To examine the transition of care The national report is due for publication in Autumn/Winter 2017 National Confidential Enquiry National Confidential Enquiry into Suicide and Homicide for people with mental illness (NCISH) 2016/17 The enquiry examines suicide and homicide committed by people who had been in contact with secondary and specialist mental health services in the previous 12 months and publishes this in an annual report. Between , the enquiry was notified of 49,269 NELFT NHS Foundation Trust Quality Account 2016/17
65 deaths in England that were registered as suicide or undetermined, an average of 4,479 per year. In , the enquiry was notified of 6,241 homicide convictions, an average of 567 per year. 65 Actions taken: 1) Mental health services are to be aware of the changing nature of patients at risk of suicide, i.e. economic problems, recent immigration, isolation. 2) Crisis teams are unlikely to be a safe setting for patients at high risk or who live alone. The use of crisis teams or Crisis Resolution Home Treatment Team (CRHT) is to be kept under regular review in such cases. 3) Services are to ensure that patients are followed up within 2-3 days of hospital discharge and that care plans are in place
66 Appendix 2c Local clinical audit - requirements and actions to be taken Re-audit to assess the completeness of referrals to the Nutrition & Dietetic (N&D) service from care homes across Havering This re-audit aims to investigate the effectiveness of providing referral guidance trainings/ referral guidance packs to care homes and whether this plan of action has had an impact on the quality (assessed by the completeness) of referrals received in NELFT. All 83 referrals received for patients in care homes for the period of June to September 2016 were collected and data was entered onto the online SNAP database. Actions: Malnutrition Universal Screening Tool (MUST) and Referral Guidance Training to be delivered in the Havering Care Homes. More time to be allocated in the training sessions to focus on how to manage patients that do not meet the N&D s criteria (the inappropriate referrals). Single Point of Access (SPA) has been designed to restrict inappropriate referrals made for the care home patients. Improving service provision for children with Attention Deficit Hyperactivity Disorder (ADHD) in ADHD follow-up clinic The audit aims to: Ascertain child/young person and parents/carer s satisfaction, who are accessing the ADHD Follow up clinic at Havering Children and Adolescents Mental Health Service (CAMHS). Evaluate the overall standard of service quality and ongoing service development. Improve the patient experience and continuity of care. A number of assessments are carried out at Havering CAMHS, including assessment and management of ADHD. This was a cross sectional survey which was undertaken by a questionnaire to the patient/carer accessing the ADHD clinic over two consecutive clinics during November A one page questionnaire (of 10 questions) was designed and distributed to patients/ carers attending ADHD follow up clinics on two consecutive clinics, during November 2016 in Havering CAMHS. The questionnaire was designed to be user friendly given the client group it was representing (0-18years). Simple non-medical terminology was used and anonymised and no person identifiable information was requested to maintain participant s confidentiality. Actions: Patients to be involved in the service design which will lead to positive impact. Clinicians making collective decisions to improve compliance and enhancing patient experience. NELFT NHS Foundation Trust Quality Account 2016/17
67 Demonstrating compliance with assessment and management of challenging behaviour NICE guidance across community and inpatient Learning Disability services (NG11) 67 The audit aims at comparing local practice both community based and in-patient based against the standards recommended by NICE in NG11: Challenging behaviour and learning disabilities: prevention and interventions for people with learning disabilities whose behaviours challenge. Retrospective audit of case notes (RIO/ paper notes) was conducted for 10 new patients with a diagnosis of autism spectrum disorder. Actions: Functional analysis / psychosocial intervention considered as the first line in management of challenging behaviour in people with autism. An autism-specific referral proforma to be introduced to encourage the completion of full functional analysis/psychosocial intervention and compliance with NICE. On-going recording of patients open to psychiatry with a co morbid diagnosis of autism. Carer intervention to be incorporated with the care pathway of assessment and diagnosis of people with intellectual disabilities and autism. End of life care plan (EOL) audit The aim of the audit is to establish that the end of life care plan meets the standards set by the leadership alliance and that it is completed. The leadership alliance for care of dying people following the Neuberger report on the Liverpool Care Pathway, recommended that organisations develop person centred end of life care plans. The NELFT end of life care plan was originally piloted in Havering last year and has been extended to all four boroughs. All areas require a further audit. Actions: Recording of conversations related to end of life care will be established to meet the priorities of care for dying people. This will be achieved by using the EOL care plan A review to be undertaken for the care of the dying leaflet through consultation with all community nurses on whether the current document is fit for purpose. A bereavement survey to be undertaken across NELFT with consultation through community staff and Barking and Dagenham, Havering and Redbridge University Trust (BHRUT) staff who already undertake a bereavement survey to identify if the service provided is effective. Dementia & End of Life Care The aim of the audit is to improve in the quality of care for people with dementia in care homes and to avoid unnecessary admissions to hospital for people with advanced dementia. The Human Rights Act imposes an obligation to facilitate a good death. This audit used the National Gold Standards Framework which is a systematic, evidence-based approach to optimise care for patients nearing the end of life. Actions:
68 Staff to be advised about the importance of meeting the Gold Standards Framework (GSF) when patients first arrive. Information will be provided to staff about appropriate and inappropriate admissions to general hospital. GPs to be actively involved in care planning, do not resuscitate (DNR) status and gatekeeping admissions. Mental health inpatient and acute services administration and indication of PRN (on a when required basis) Lorazepam is documented in the patient s clinical notes to closely monitor and ensure safe prescribing of rapid tranquilizers. NELFT have achieved an overall 4.1% improvement in compliance of nurses to documentation. Community Recovery Team Services Regular monitoring of lithium levels and blood test has been set up by the community teams. Blood test forms are sent routinely at 3 monthly intervals to all patients by the secretaries. Children s Targeted Services The quality of the Initial Health Assessments (IHA) process is being reviewed by evaluating information available prior to assessment, looking at the quality of assessments and reviewing the quality of the reports. All IHA s for the Looked After Children are completed within 28 days of referral. Long Term Conditions Services The community diabetes service has had better attendance of patients with poorly controlled Type 2 diabetes (HbA1c 65mmols) on 2 or more diabetes medication after setting up pilot clinics in GP practices with practice and Diabetes Specialist Nurses. Nutrition and Dietetics Service (N&D) - Malnutrition Universal Screening Tool (MUST) and referral guidance training is to be delivered and more time is to be allocated in the training sessions to focus on how to manage patients that do not meet the N&D s criteria. Older Adults Mental Health & Memory Service The Human Rights Act imposes an obligation to facilitate a good death. The audit used the National Gold Standards Framework which is a systematic, evidence-based approach to optimise care for patients nearing the end of life. Staff are to be advised about the importance of meeting the Gold Standards Framework (GSF) when patients first arrive for appointments and information is to be provided to staff about appropriate and inappropriate admissions to general hospital. Quality & Patient Safety - Following an action from the CQC initial findings which referred to 3 core services not always implementing the lone working policy, an audit to increase staff awareness of safety issues relating to lone working and to ensure managers are aware of the support available was undertaken. As a result, further support is to be provided to ensure all managers are aware of the lone working policy and procedure. All lone working team risk assessments will be made suitable and sufficient to include controls and further actions to reduce risk to staff. The risk assessment is to be reviewed to ensure that outstanding actions are completed. Child & Adolescent Mental Health Services (CAMHS) A robust multi-agency pathway for children and adolescents presenting with harmful sexual behaviour is to be implemented and training needs of the workforce are to be reviewed to ensure we can provide more effective and highly specialist interventions to young people with harmful sexual behaviour. NELFT NHS Foundation Trust Quality Account 2016/17
69 Health Visiting & School Nursing Services Identifying further training requirements for new staff and mentoring them during their induction period enables them to achieve the skills and competence to record information correctly using the safeguarding palette protocol. Staff champions who are confident and competent in recording on System One are available to mentor new staff and support existing staff to record safeguarding concerns. 69 Safeguarding Adult Services The adult safeguarding duty desk is the single point of contact for NELFT staff requiring safeguarding adults advice and support. Team members within the safeguarding adults team adhere to legislation, local and national guidance when providing safeguarding advice to frontline staff across NELFT and the use of a single telephone number for contact has ensured a prompt and timely response to enquiries to operational staff working in any area within the Trust. A&E Liaison Services - The Older Adults Psychiatry Liaison Service (PLS) team at whipps cross university hospital will play an integral role in the multi-disciplinary team in the hospital settings, facilitating safe discharge where possible, and avoiding unnecessary re-admissions in those with psychiatric co-morbidities. Early involvement of different professionals is helping in preventing un-necessary re-admissions. Health & Safety - Robust systems are implemented for the dissemination of alerts and the completion of action plans, as a requirement of the Central Alerting System (CAS) policy. Alerts are acknowledged and recorded on the safety alerts module of Datix and are then cascaded to central alerting system assessors as per the trust s policy. Pharmacy Services - The covert administration of medicines should only be used in exceptional circumstances when such a means of administration is judged necessary, in accordance with the Mental Capacity Act All staff continue to work within the legal and ethical framework for the covert administration of medicine and ensure that the pharmacist is consulted before covert administration of medicines. Practice Improvement Practitioners Services (PIPs) - Every service user admitted to an inpatient ward is issued with a care plan. Further monitoring is undertaken by operational staff via weekly audits to review the quality of care plans, ensuring service users are issued a copy of the agreed care plan
70 Appendix 3 Royal College of Psychiatrists summary of NELFT's participation in national quality improvement projects NELFT NHS Foundation Trust Quality Account 2016/17
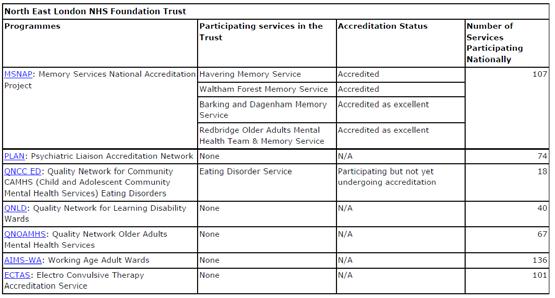
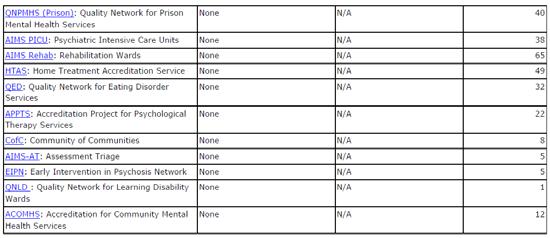
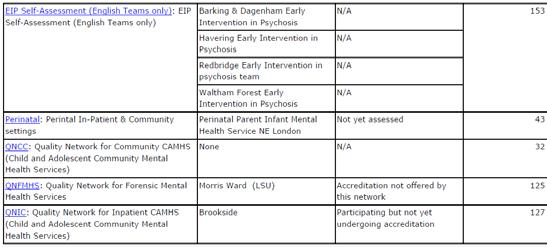
71 71
72 Appendix 4 Quality Account governance structure NELFT board/emt Reports to NELFT board ( Half yearly Stephanie Dawe) Quality and safety committee (Half yearly Stephanie Dawe) Data quality group Chief nurse group (Quarterly Julie Price) Basildon and Brentwood LT* (Monthly service director) Thurrock LT (Monthly service director) Barking and Dagenham LT (Monthly service director) Havering LT (Monthly service director) Redbridge LT (Monthly service director) Waltham Forest LT (Monthly service director) Acute and Rehab LT (Monthly service director) Basildon and Brentwood DPQSG** (Monthly assistant service director) Thurrock DPQSG (Monthly assistant service director) Barking and Dagenham DPQSG (Monthly assistant service director) Havering DPQSG (Monthly assistant service director) Redbridge DPQSG (Monthly assistant service director) Waltham Forest DPQSG (Monthly assistant service director) Acute and Rehab DPQSG (Monthly assistant service director) Local Improvement priorities/leads Patient and service user involvement * LT - Local leadership team meeting ** DPQSG - Directorate performance and quality safety group NELFT NHS Foundation Trust Quality Account 2016/17
73 Appendix 5 Statements from commissioners, local Healthwatch organisations and overview and scrutiny committees 73 Quality Account distributed for comment to: Healthwatch Barking and Dagenham Havering Redbridge Thurrock Waltham Forest Health and wellbeing boards Barking and Dagenham Basildon Havering Redbridge Thurrock Waltham Forest Local authority Barking and Dagenham Basildon Essex County Council Havering Redbridge Thurrock Waltham Forest Local authority health and overview scrutiny committees Barking and Dagenham Essex Havering Redbridge Thurrock Waltham Forest Clinical commissioning chair groups Barking and Dagenham, Havering & Redbridge (BHR CCG) Basildon & Brentwood Thurrock Waltham Forest West Essex NELFT Staff Trust board members Governors
74 Statement from Healthwatch Havering Dear John, Thank you for providing Healthwatch Havering with the opportunity to comment on your Quality Accounts. Although we understand that the CQC report did not provide the much hoped for continuation of NELFT's previous ratings, the positive approach taken in the Quality Account to responding to the challenges of the CQC report is very welcome and very much in keeping with the attitude that we have consistently seen from the NELFT team. Again, the staff of NELFT have shone and proved to be excellent ambassadors for the organisation by winning nationally recognised awards - well done. We also know from talking to patients that 'in the day to day' caring that NELFT staff give, services are very valued and appreciated such as the Ambulance Care Service and the Home Treatment team. We were also impressed by the Street Triage Scheme for mental health patients, worked in conjunction with the police and LAS. We have recommended to the Police, LAS and the CCGs that it be continued and developed. Reviewing the programme set out in the Quality Accounts we are pleased to note the investment in staff in supporting their education and training. The Rotational Nurse programme, staff education in 'End of Life' strategy and encouraging staff such as the Health Care Support Workers, the majority of whom complete their care certificates in a year, to invest further in themselves and the organisations by starting clinical apprenticeships. In respect of the delivery of care we are pleased to note the monitoring of the Duty of Candour responsibility will be reviewed by the Trust board monthly. The response to RTT and the additional tools to help staff closely monitor their own patients on the waiting list both ensures patients care is a priority but empowers staff to monitor and manage the care more closely. Also the goal to achieve 95% compliance with care plans and risk assessments to be completed where applicable gives patients and carers confidence and also a better understanding of the up to date care management programme being designed for that individual patient. Two initiatives that directly improve, support and enable patients are, * 'this is me' project for patients with dementia and * the logo designed for learning disability patients, both of these initiatives have caught our imagination and we look forward to receiving more information about these. We look forward to working with you and the team in 2017/18 Best Anne-Marie Dean Chairman Havering Healthwatch Limited Registered in England & Wales no Address and Registered Office: Morland House, Eastern Road, Romford RM1 3PJ Telephone (24hr voic ) Chairman Havering Healthwatch Limited Registered in England & Wales no Address and Registered Office: Morland House, Eastern Road, Romford RM1 3PJ Telephone (24hr voic ) NELFT NHS Foundation Trust Quality Account 2016/17

75 Statement from Barking and Dagenham CCG written in collaboration with Havering CCG, Redbridge CCG and colleagues from the North and East London Commissioning Support Unit 75

76 NELFT NHS Foundation Trust Quality Account 2016/17
77 77

78 Statement from Thurrock CCG NELFT NHS Foundation Trust Quality Account 2016/17
79 79

80 NELFT NHS Foundation Trust Quality Account 2016/17

81 Statement from West Essex CCG 81
82 NELFT NHS Foundation Trust Quality Account 2016/17

83 Statement from Waltham Forest CCG 83

84 NELFT NHS Foundation Trust Quality Account 2016/17
85 Appendix 6 Statement of directors' responsibilities for the Quality Account 85 The directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each financial year. NHS Improvement has issued guidance to NHS foundation trust boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that NHS foundation trust boards should put in place to support the data quality for the preparation of the Quality Report. In preparing the Quality Report, directors are required to take steps to satisfy themselves that: the content of the Quality Report meets the requirements set out in the NHS foundation trust annual reporting manual 2016/17 and supporting guidance the content of the Quality Report is not inconsistent with internal and external sources of information including: o board minutes and papers for the period April 2016 to 23/05/2017 o papers relating to quality reported to the board over the period April 2016 to 23/05/2017 o feedback from commissioners dated 04/05/2017, 08/05/2017 and 25/05/2017 o feedback from governors dated 26/04/2017 o feedback from local Healthwatch organisations dated 29/04/2017 o feedback from Overview and Scrutiny Committee dated 10/04/2017 o the trust s complaints report published under regulation 18 of the Local Authority Social Services and NHS Complaints Regulations 2009, dated 01/06/2016 o the latest national patient survey 25/10/2016 o the latest national staff survey 25/04/2017 o the Head of Internal Audit s annual opinion over the trust s control environment included within the Internal Audit Annual Report and Annual Statement of Assurance presented to the 25/4/2017 Audit Committee o CQC inspection report dated 27/09/2016 the Quality Report presents a balanced picture of the NHS foundation trust s performance over the period covered the performance information reported in the Quality Report is reliable and accurate there are proper internal controls over the collection and reporting of the measures of performance included in the Quality Report, and these controls are subject to review to confirm that they are working effectively in practice the data underpinning the measures of performance reported in the Quality Report is robust and reliable, conforms to specified data quality standards and prescribed definitions, is subject to appropriate scrutiny and review the Quality Report has been prepared in accordance with NHS Improvement s annual reporting manual and supporting guidance (which incorporates the Quality Accounts regulations) as well as the standards to support data quality for the preparation of the Quality Report The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the Quality Report.
86 By order of the Board Date: 25 May 2017 Signature Chairman Date: 25 May 2017 Signature Chief Executive NELFT NHS Foundation Trust Quality Account 2016/17

87 Appendix 7 Auditors limited assurance report 87

88 NELFT NHS Foundation Trust Quality Account 2016/17
89 89
Best Care Clinical Strategy Principles for the next 10 years of Best Care. Dr Caroline Allum, Executive Medical Director
 Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Specialist mental health services
 How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy
 Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
Action required: To agree the process by which Governors will meet with the inspection team.
 Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
BEST CARE BY THE BEST PEOPLE. Quality Account 2015/16. Best care by the best people
 BEST CARE BY THE BEST PEOPLE Quality Account 2015/16 Best care by the best people 2 Page 2 NELFT NHS Foundation Trust I Quality Account 2015/16 Contents Foreword from the chief executive 4 Statement from
BEST CARE BY THE BEST PEOPLE Quality Account 2015/16 Best care by the best people 2 Page 2 NELFT NHS Foundation Trust I Quality Account 2015/16 Contents Foreword from the chief executive 4 Statement from
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Improvement and assessment framework for children and young people s health services
 Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Annual Quality Account 2015/2016
 Annual Quality Account 2015/2016 Summary Quality at CityCare Everyone at CityCare is passionate and committed to ensuring our patients receive the best care at all times and we continue to build on the
Annual Quality Account 2015/2016 Summary Quality at CityCare Everyone at CityCare is passionate and committed to ensuring our patients receive the best care at all times and we continue to build on the
Whittington Health Trust Board
 Executive Offices Direct Line: 020 7288 3939/5959 www.whittington.nhs.uk The Whittington Hospital NHS Trust Magdala Avenue London N19 5NF Whittington Health Trust Board Title: 4 th March 2015 Sign up to
Executive Offices Direct Line: 020 7288 3939/5959 www.whittington.nhs.uk The Whittington Hospital NHS Trust Magdala Avenue London N19 5NF Whittington Health Trust Board Title: 4 th March 2015 Sign up to
SOMERSET PARTNERSHIP NHS FOUNDATION TRUST QUALITY ACCOUNT PRIORITIES 2016/17. Report to the Trust Board 22 March 2016
 SOMERSET PARTNERSHIP NHS FOUNDATION TRUST QUALITY ACCOUNT PRIORITIES 2016/17 Report to the Trust Board 22 March 2016 Sponsoring Director: Author: Purpose of the report: Key Issues and Recommendations:
SOMERSET PARTNERSHIP NHS FOUNDATION TRUST QUALITY ACCOUNT PRIORITIES 2016/17 Report to the Trust Board 22 March 2016 Sponsoring Director: Author: Purpose of the report: Key Issues and Recommendations:
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
PAHT strategy for End of Life Care for adults
 PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
5 Boroughs Partnership NHS Foundation Trust. Quality Account Version: QA FINAL
 5 Boroughs Partnership NHS Foundation Trust Quality Account 2016-2017 Version: QA FINAL 1 Contents Part 1- Our Commitment to Quality 1.1 Our Quality Report / Quality Account 2016-17...5 1.2 Chief Executive
5 Boroughs Partnership NHS Foundation Trust Quality Account 2016-2017 Version: QA FINAL 1 Contents Part 1- Our Commitment to Quality 1.1 Our Quality Report / Quality Account 2016-17...5 1.2 Chief Executive
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting
 Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
The new inspection process for End of Life Care. Dr Stephen Richards GP Advisor - London Care Quality Commission
 The new inspection process for End of Life Care Dr Stephen Richards GP Advisor - London Care Quality Commission Our purpose and role Our purpose We make sure health and social care services provide people
The new inspection process for End of Life Care Dr Stephen Richards GP Advisor - London Care Quality Commission Our purpose and role Our purpose We make sure health and social care services provide people
Our Achievements. CQC Inspection 2016
 Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
NHS Equality Delivery System for Isle of Wight NHS Trust. Interim baseline assessment against the
 Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Direct Commissioning Assurance Framework. England
 Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Nursing Strategy
 Nursing Strategy 2016-2018 At The Royal Marsden, we deal with cancer every day, so we understand how valuable life is. And when people entrust their lives to us, they have the right to demand the very
Nursing Strategy 2016-2018 At The Royal Marsden, we deal with cancer every day, so we understand how valuable life is. And when people entrust their lives to us, they have the right to demand the very
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT
 KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
Delivering the Five Year Forward View. through Business Intelligence
 Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
End of Life Care Strategy PROUD TO MAKE A DIFFERENCE
 End of Life Care Strategy 2017-2019 PROUD TO MAKE A DIFFERENCE Background Sheffield Teaching Hospitals NHS Trust is committed to delivering high quality care to patients and those identified as important
End of Life Care Strategy 2017-2019 PROUD TO MAKE A DIFFERENCE Background Sheffield Teaching Hospitals NHS Trust is committed to delivering high quality care to patients and those identified as important
PATIENT AND SERVICE USER EXPERIENCE STRATEGY
 PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
End Of Life Care Strategy
 End Of Life Care Strategy Document Control: Document Author: Director of Nursing Document Owner: Board Of Directors Electronic File Name: End of Life Care Strategy dated June 2016 Document Type: Corporate
End Of Life Care Strategy Document Control: Document Author: Director of Nursing Document Owner: Board Of Directors Electronic File Name: End of Life Care Strategy dated June 2016 Document Type: Corporate
Responding to a risk or priority in an area 1. London Borough of Sutton
 Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Your guide to the CQC Fundamental Standards
 Your guide to the CQC Fundamental Standards RDaSH Introduction In order to get to the heart of people s experiences of care and support, the focus of the Care Quality Commission (CQC) Regulatory Framework
Your guide to the CQC Fundamental Standards RDaSH Introduction In order to get to the heart of people s experiences of care and support, the focus of the Care Quality Commission (CQC) Regulatory Framework
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
4 Year Patient and Public Involvement Strategy
 4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
TITLE OF REPORT: Looked After Children Annual Report
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Nursing Strategy Nursing Stratergy PAGE 1
 Nursing Strategy 2016-2021 Nursing Stratergy 2016-2021 PAGE 1 2 PAGE Nursing Stratergy 2016-2021 foreword Welcome to Greater Manchester West Mental (GMW) Health NHS Trust s Nursing Strategy. This document
Nursing Strategy 2016-2021 Nursing Stratergy 2016-2021 PAGE 1 2 PAGE Nursing Stratergy 2016-2021 foreword Welcome to Greater Manchester West Mental (GMW) Health NHS Trust s Nursing Strategy. This document
Quality Improvement Strategy 2017/ /21
 Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
York Teaching Hospital NHS Foundation Trust. Caring with pride. The Nursing and Midwifery Strategy
 York Teaching Hospital NHS Foundation Trust Caring with pride The Nursing and Midwifery Strategy 2017-2020 1 To be a nurse, a midwife or member of care staff is an extraordinary role. What we do every
York Teaching Hospital NHS Foundation Trust Caring with pride The Nursing and Midwifery Strategy 2017-2020 1 To be a nurse, a midwife or member of care staff is an extraordinary role. What we do every
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
Quality Strategy
 Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Developing the culture of compassionate care: creating a new vision for nurses, midwives and care-givers
 Developing the culture of compassionate care: creating a new vision for nurses, midwives and care-givers Organisation: Sue Ryder Author: Lotte Good, Senior Policy and Campaigns Officer Email: Charlotte.good@sueryder.org
Developing the culture of compassionate care: creating a new vision for nurses, midwives and care-givers Organisation: Sue Ryder Author: Lotte Good, Senior Policy and Campaigns Officer Email: Charlotte.good@sueryder.org
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Learning from Deaths Policy
 Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Quality Strategy (Refreshed March 2015)
") Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
How do you demonstrate effectiveness?
 How do you demonstrate effectiveness? Demonstrating Effectiveness Conference 25 November 2014 Professor Edward Baker Deputy Chief Inspector Our purpose and role Our purpose We make sure health and social
How do you demonstrate effectiveness? Demonstrating Effectiveness Conference 25 November 2014 Professor Edward Baker Deputy Chief Inspector Our purpose and role Our purpose We make sure health and social
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Mental Health Crisis Care: Essex Summary Report
 Mental Health Crisis Care: Essex Summary Report Date of local area review: Onsite 16-17 December 2014 Date of publication: June 2015 This inspection was carried out under section 48 of the Health and Social
Mental Health Crisis Care: Essex Summary Report Date of local area review: Onsite 16-17 December 2014 Date of publication: June 2015 This inspection was carried out under section 48 of the Health and Social
A fresh start for registration. Improving how we register providers of all health and adult social care services
 A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
OUR COMMITMENTS TO CARE A STRATEGY FOR NURSES & ALLIED HEALTH PROFESSIONALS
 OUR COMMITMENTS TO CARE A STRATEGY FOR NURSES & ALLIED HEALTH PROFESSIONALS Version: 2 Ratified by: Trust Board Date ratified: January 2014 Name of originator/author: Acting Head of Nursing Nursing & AHP
OUR COMMITMENTS TO CARE A STRATEGY FOR NURSES & ALLIED HEALTH PROFESSIONALS Version: 2 Ratified by: Trust Board Date ratified: January 2014 Name of originator/author: Acting Head of Nursing Nursing & AHP
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Overall rating for this trust Requires improvement. Inspection report. Ratings. Are services safe? Requires improvement
 Bradford District Care NHS Foundation Trust Inspection report SBS New Mill Victoria Road, Saltaire Shipley West Yorkshire BD18 3LD Tel: 01274228300 www.bdct.nhs.uk Date of inspection visit: October 4th
Bradford District Care NHS Foundation Trust Inspection report SBS New Mill Victoria Road, Saltaire Shipley West Yorkshire BD18 3LD Tel: 01274228300 www.bdct.nhs.uk Date of inspection visit: October 4th
The Care Values Framework
 The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
Quality Account 2016/17 & 2017/18 Quality Priorities
 Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
East Lancashire Clinical Commissioning Group. Quality Strategy
 East Lancashire Clinical Commissioning Group Quality Strategy 2016 21 1 CONTENTS Foreword 3 Executive Summary 4 Introduction 6 Local Context 7 National Context 8 What is Quality? 9 The Five Dimensions
East Lancashire Clinical Commissioning Group Quality Strategy 2016 21 1 CONTENTS Foreword 3 Executive Summary 4 Introduction 6 Local Context 7 National Context 8 What is Quality? 9 The Five Dimensions
Mental health and crisis care. Background
 briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
Strategy for Delivery of Clinical Quality and Patient Safety. North Norfolk Clinical Commissioning Group
 Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
talkmagazine ouryear Celebrating the achievements and reflecting on the challenges of 2016/17
 Trust talkmagazine s p e c i a l e d i t i o n a n n u a L r e p o r t ouryear Celebrating the achievements and reflecting on the challenges of 2016/17 Chair & Chief Executive Welcome Our full Annual Report
Trust talkmagazine s p e c i a l e d i t i o n a n n u a L r e p o r t ouryear Celebrating the achievements and reflecting on the challenges of 2016/17 Chair & Chief Executive Welcome Our full Annual Report
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Mortality Policy. Learning from Deaths
 Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Harnessing the commitment of staff across the NHS in England to make care safer.
 SIGN UP PACK Welcome to Sign up to Safety Harnessing the commitment of staff across the NHS in England to make care safer. Our vision is for the whole NHS to become the safest healthcare system in the
SIGN UP PACK Welcome to Sign up to Safety Harnessing the commitment of staff across the NHS in England to make care safer. Our vision is for the whole NHS to become the safest healthcare system in the
The NHS Constitution
 2 The NHS Constitution The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot
2 The NHS Constitution The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot
IT ALL STARTS WITH YOU
 Email: jo.curtis@nhs.net IT ALL STARTS WITH YOU Tell us about your experience Help us improve NHS services This guide takes you through the different ways you can tell the NHS about your experiences, so
Email: jo.curtis@nhs.net IT ALL STARTS WITH YOU Tell us about your experience Help us improve NHS services This guide takes you through the different ways you can tell the NHS about your experiences, so
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Lancashire Care NHS Foundation Trust
 Lancashire Care NHS Foundation Trust Contents Part 1: Quality Statement Statement on Quality from the Chief Executive Page 2 Part 2: Priorities for Improvement and Statements of Assurance from the Board
Lancashire Care NHS Foundation Trust Contents Part 1: Quality Statement Statement on Quality from the Chief Executive Page 2 Part 2: Priorities for Improvement and Statements of Assurance from the Board
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
PALLIATIVE AND END OF LIFE CARE EDUCATION PROSPECTUS 2018/19
 #wearenhft Northamptonshire Healthcare NHS Foundation Trust PALLIATIVE AND END OF LIFE CARE EDUCATION PROSPECTUS 2018/19 DELIVERED BY: THE NORTHAMPTONSHIRE END OF LIFE CARE PRACTICE DEVELOPMENT TEAM Working
#wearenhft Northamptonshire Healthcare NHS Foundation Trust PALLIATIVE AND END OF LIFE CARE EDUCATION PROSPECTUS 2018/19 DELIVERED BY: THE NORTHAMPTONSHIRE END OF LIFE CARE PRACTICE DEVELOPMENT TEAM Working
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Patient Experience Strategy
 Patient Experience Strategy Published: June 2017 Find us online at cornwallft 1.Introduction At Cornwall Partnership NHS Foundation Trust (CFT) we believe in delivering high quality care. We care deeply
Patient Experience Strategy Published: June 2017 Find us online at cornwallft 1.Introduction At Cornwall Partnership NHS Foundation Trust (CFT) we believe in delivering high quality care. We care deeply
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
Admiral Nurse Standards
 Admiral Nurse Standards Foreword The last few years have seen many new government directives and policy initiatives. Plans for enhancing the quality of care in the NHS have been built around national standards
Admiral Nurse Standards Foreword The last few years have seen many new government directives and policy initiatives. Plans for enhancing the quality of care in the NHS have been built around national standards
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Debbie Edwards Interim Deputy Director of Nursing Gail Naylor- Executive Director of Nursing & Midwifery. Safety & Quality Committee
 Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Your Guide to the proposed NHS Constitution
 Your Guide to the proposed NHS Constitution I like to feel that I am making a difference We want to start looking after our own health Everybody should be treated as an individual It s your NHS. Know your
Your Guide to the proposed NHS Constitution I like to feel that I am making a difference We want to start looking after our own health Everybody should be treated as an individual It s your NHS. Know your