Data Quality and Clinical Coding for Improvement What happens when the data are wrong? The key responsibilities for Clinicians and Managers
|
|
|
- Gwendolyn Benson
- 6 years ago
- Views:
Transcription
1 Data Quality and Clinical Coding for Improvement Data Quality and Clinical Coding for Improvement What happens when the data are wrong? The key responsibilities for Clinicians and Managers 19 th November :45 am Hallam Conference Centre Brian Jarman Imperial College,
2 Subjects I have been asked to cover learning from Mid Staffordshire clinical coding: understanding the data and what the data is telling you how Dr Foster use the data to identify outliers and produce alerts case studies and examples in practice
3 Mid Staffs Independent Inquiry, 24 Feb 2010, p366, 46 Furthermore, the maintenance, certification and submission of accurately recorded data to the regulatory authorities are ultimately the responsibility of Trust leadership.
4 Data covered Hospital Standardised Mortality Ratios (HSMRs) methodology from Dr Foster unit (DFU) at Imperial College HSMR published annually from 2001 by Dr Foster Intelligence (DFI) main national press Data Quality Summary from DFI Monthly mortality alerts - used the Dr Foster Unit (DFU) at Imperial College to identify outliers and produce alerts
5 Variables for HSMR logistic regression adjustment Age group (<1, then 5-year bands to 90+) Sex Admission method/type (emergency, elective etc) Admission source (home, transfers etc) Deprivation quintile (based on postcode) Diagnosis subgroup (CCS sub-groups within each CCS group) Comorbidity (Charlson score) Emergency admissions in previous 12 months Palliative care (any episode that has a treatment function code 315 or any Z515 ICD10 diagnosis code) Month of admission Year of discharge (Day cases are excluded from the risk models ~ 70 deaths/year)
6 Data Quality Summary DFU monthly checks on reords: Duplicate record Admission/Appointment date Episode order Admission method/appointment type Sex Date of birth Provider Episode start Episode end Episode duration Postcode NHS Number GP Practice Local patient ID Age Day case Deprivation Provider + Local patient ID Consultant Ethnicity Elective/Referral date Discharge/Outcome Diagnosis Procedure Procedure date Spell overlaps Missing first episode Missing last episode Inconsistent bed-days/los Age group Sex (spell) Admission (spell) Episode order (spell) Invalid LOS Invalid HRG
7 Effect of coding of variables in model Direct vs indirect standardisation Comorbidity (Charlson Index) Palliative care Admission vs patient All in-hospital deaths vs 30-days inhospital deaths HSMR covering 80% deaths (56 CCS) vs HSMR all IP deaths (259 CCS gps)
8 Indirectly standardised HSMR Comparison of indirect vs direct standardisation 2005 HSMR (simple model) 150% 140% 130% 120% 110% 100% Trusts Identical match 25% more than directly standardised 10% more than directly standardised 10% less than directly standardised 25% less directly standardised 90% 80% 70% 60% 60% 70% 80% 90% 100% 110% 120% 130% 140% 150% Directly standardised HSMR
9 HSMR without Charlson Charlson co-morbidity index Comparison of HSMR calculated with and without Charlson English Acute Trusts 2008/ y = x R² = Salford Royal NHS Foundation Trust Trusts Identical match 25% more than standard HSMR 10% more than standard HSMR 10% less than standard HSMR 25% less than standard HSMR HSMR
10 HSMR excluding paliative care Palliative care y = x R² = Comparison of HSMR calculated using adjustment or exclusion to account for palliative care English Acute Trusts 2008/9 Trusts Identical match 25% more than standard HSMR 10% more than standard HSMR 10% less than standard HSMR 25% less than standard HSMR Medway NHS Trust 60 Walsall Hospitals NHS Trust HSMR adjusting for palliative care
11 HSMR based on last admission in financial year Admissions versus Patients y = x R² = Comparison of HSMR calculated using admissions and based on last admission in financial year English Acute Trusts 2008/9 Trusts Identical match 25% more than standard HSMR 10% more than standard HSMR 10% less than standard HSMR 90 Trafford Healthcare NHS Trust 25% less than standard HSMR HSMR
12 HSMR in-hospital 30 day deaths HSMR (all in-hospital deaths) vs. all in-hospital 30 day deaths y = x R² = Comparison of HSMR calculated using 30 day in-hospital deaths with HSMR using all in-hospital eaths English Acute Trusts 2008/9 130 Trusts Identical match 25% more than in-hospital deaths HSMR 10% more than in-hospital deaths HSMR 10% less than in-hospital deaths HSMR 25% less than in-hospital deaths HSMR Linear (Trusts) HSMR (all in-hospital deaths)
13 HSMR all 30 day deaths HSMR 30 day in-hospital deaths vs 30 day all deaths y = x R² = Comparison of HSMR calculated using 30 day in-hospital deaths with HSMR using all 30 day deaths English Acute Trusts 2004/5 120 Trusts Identical match Bradford Teaching Hospitals NHS Foundation Trust 25% more than in-hospital deaths HSMR 10% more than in-hospital deaths HSMR 10% less than in-hospital deaths HSMR 25% less than in-hospital deaths HSMR HSMR in-hospital 30 day deaths
14 HSMR based on all diagnosis groups 56 diagnosis group HSMR vs. all 259 CCS diagnoses Comparison of HSMR calculated using 56 diagnoses compared with all 259 diagnoses English Acute Trusts 2008/ y = x R² = Trusts Identical match 25% more than standard HSMR 10% more than standard HSMR 10% less than standard HSMR 25% less than standard HSMR Linear (Trusts) HSMR
15 The changes of palliative care coding by CfH rules. Changes at Medway, Mid Staffs and Basildon = effect on HSMRs March Medway From March 2007 CfH Coding Clinic permitted non-curable illnesses to be coded as palliative care secondary diagnosis Z51.5 (not just terminal illnesses under consultant) Imperial College was persuaded to introduce a palliative care adjustment Medway increased % deaths coded Z51.5 from <1% to 37% and HSMR value decreased (advised by CHKS). Only trust in England at that time to make those changes CHKS, Dec 2008: Our review of coding at Medway NHS Foundation Trust found that end-of-life care was recorded for only eight per cent of deaths, when the actual proportion should have been 37 per cent. We believe that the hospital mortality index should exclude these cases and, by making this adjustment, Medway's mortality index reduced by just over a third. March Mid Staffs Mid Staffs made similar changes and HSMR reduced by ~7% Two other West Midlands SHA trusts made similar changes later in 2008 We publicised the effect of Z51.5 changes on HSMR values ( doesn t save lives ) Mid Basildon & Thurrock Made similar changes to starting mid 2009 June 2010 CfH Coding Clinic reverted to ~pre 2007
16 Changes in coding at Medway, Mid Staffs and Basildon Mid Staffs and Basildon In 2005/06 had the highest HSMR (lower 95% CI above 100) In 2007 had the largest number of mortality alerts from Imperial College Had had significantly high HSMRs for about 10 years First major palliative care coding change was at Medway NHS Foundation Trust in was advised would reduce its HSMR value.

17 CHKS 11 Dec 2008 press release re HSJ article (exh BJ87)
18 2004-Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q1 % deaths coded as palliative care HSMR Medway coding of palliative care vs HSMR 60% 50% MEDWAY HSMR % England % deaths coded as palliative care 30% 20% MEDWAY %deaths Z51.5 ENGLAND % deaths Z Medway NHS Foundation Trust (RPA) % deaths coded as palliative care HSMR Medway NHS Foundation Trust 10% 20 0% 0
19 Happenings re Mid Staffs in February & March Feb 2008 Mid Staffs was formally awarded Foundation Trust status by Monitor 1 Feb 2008 A group of local patients told the local PCT about complaints from patients that had come to the HCC independently through its helpline 14 Feb 2008 Healthcare Commission Investigations Committee met to discuss concerns about the Trust 15 Feb 2008 Mid Staffs increased the % cases coded as palliative care and coder started coding all deaths herself. Large increase % deaths coded palliative care Z51.5 from March March 2008 Healthcare Commission investigation
20 Healthcare Commission investigation at Mid Staffordshire NHS Foundation Trust - press release 18 March 2008 Healthcare Commission press release 18/3/08 The Healthcare Commission has also recently received a number of concerns from individual patients and relatives, about standards of care at ward level. The Healthcare Commission is therefore launching an investigation at Mid Staffordshire NHS Foundation Trust. The trust s data on outcomes for patients has also recently caused the Dr Foster Unit at Imperial College London to bring concerns to the attention of the trust and the Healthcare Commission.
21 2004-Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q1 % deaths coded as palliative care HSMR Mid Staffs coding of palliative care vs HSMR 40% 35% 30% 25% England % deaths coded as palliative care 20% 15% 10% 5% Mid Staffordshire NHS Foundation Trust (RJD) % deaths coded as palliative care HSMR Mid Staffordshire NHS Foundation Trust 0% 0
22 2004-Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q1 % deaths coded as palliative care HSMR Basildon & Thurrock coding of palliative care vs HSMR 40% 35% England % deaths coded as palliative care 30% % 20% 15% 10% 5% Basildon and Thurrock University Hospitals NHS Foundation Trust (RDD) % deaths coded as palliative care HSMR Basildon and Thurrock University Hospitals NHS...tion Trust 0% 0
 Healthcare Commission first report")
23 37. Mid Staffordshire NHS Hospitals Trust HSMRs follow-up after mortality reduction programme (as at 16 Dec 2010) Healthcare Commission first report 18/03/2008
24 John Holden, Director of system regulation Department of Health; former head of foundation trust team. Mid Staffs Public Inquiry 14-Sep2011, Exhibit JH6 DH 04/03/2009 Subject: Re: Mid staffs lines to take etc During the period of SHA and DH assessment (ie up to SoS support) the first Dr Foster report had only just been published, April 2007). The SHA had set in place a process for the findings to be validated and supported the trust in developing an action plan. At this time, the issue was thought to be largely one of clinical coding. It was only after further Dr Foster reports were published, from July2007, focusing on specific patient groups was it recognised (including by HCC) that there was potentially greater cause for concern. Even so the HCC did not launch its investigation until March 2008.
25 John Holden 09 March 2009 exhibit JH9 DH 09/03/2009: Subject Urgent-Mid Staffs. "Miranda, further to our discussion, the Secretary of State is tomorrow briefing the Cabinet on the issues arising at Mid Staffs. The key issue being considered is how regulation is working in the NHS, and whether the difficulties at Mid Staffs are evidence that more needs to be done. In order to brief Secretary of State we need to establish the extent to which standardised mortality rates feature in Monitor s compliance regime and application assessment process. Looking at Monitor s Board Minutes for January 2008 re consideration of Mid Staffs, it is noted that the Trust received a 127 mortality rate for2005/06 from Dr Foster. This has reduced to c. 101 between May and August 2007/08 as a result of significant improvements to coding for co-morbidities; This figure 101 is incorrect (exhibit BJ83). The HSMR at Mid Staffs May-Aug 2008 = ( )
26 Mid Staffs Public Inquiry, 20-Sep-2011 PROFESSOR SIR BRUCE KEOGH, NHS Medical Director, Department of Health from November 2007 DH briefing to Minister on Mid staffs lines to take etc Exhibits BK49, JH6 "In April 2007, the Dr Foster s Good Hospital Guide classified the Trust as having a High Hospital Standardised Mortality Rate. (The Good Hospital Guide was first published in 2001) [DH witnesses to Mid Staffs Public Inquiry said HSMRs were only available from 2007]
27 HEALTHCARE COMMISSION, INVESTIGATION INTO MID STAFFORDSHIRE NHS FOUNDATION TRUST, 18 MARCH 2009 The trust assumed that the raised mortality was primarily due to poor coding of information, but could not substantiate its claim... The default position appeared to be that the deaths had been inevitable and there were no problems with the care of the patients.
28 Mid Staffs Public Inquiry oral evidence observed minus expected deaths 2005/6-2007/8 was not Approx 500, range 400 to 600, over 3 years, 95% Conf Ints Exact 492, range , over 3 years, 95% Conf Intervals 2023 mentions of mortality 1018 mentions of HSMR 458 mentions of hindsight 799 mentions of coding
29 Some of the problems at Mid Staffordshire. Professor Sir George Alberti. 29 April 2009 Understaffing of A&E - too few consultants, middle-grade doctors and nurses Initial patient assessment by untrained receptionists Poor supervision of junior doctors Weak leadership of nurses and inadequate nurse training Poor equipment in A&E Long delays and tendency to move patients to the Emergency Assessment Unit (EAU), Clinical Decision Unit (CDU) and assess and treat area in order to meet the 4 hour target before they had been investigated or any diagnosis made Lack of protocols and clear pathways Chaotic, large, understaffed EAU with little training for the nurses Poorly equipped EAU. Poor handover from EAU to medical and surgical wards Insufficient beds for coronary care or strokes Major delays for emergency operations Inadequate numbers of experienced surgeons with poor 24/7 cover Poor post-operative care Very poor patient care on the medical and surgical wards Inadequate handling of patient complaints
30 Healthcare Commission report on Mid Staffordshire NHS Hospitals Trust 18 March data/assets/pdf_file/0004/234976/healthcare_commission_report.pdf The SHA was not aware of any concerns regarding the quality of services provided by the trust before Dr Foster Intelligence published its Hospital Guide in April [Note: HSMRs published annually in the Dr Foster Good Hospital Guide had shown Mid Staffs to have significantly high HSMRs for 9 years before 2007/8. Mortality alerts were sent by Imperial College to the hospital and the Care Quality Commission from July 2008]
31 Mid Staffs Public Inquiry 26-Sep-2011 Sir Hugh Taylor's statement, ex-permanent Secretary, DH, Statement Paragraph 54: "In terms of the role of the SHA in relation to the situation at the Trust, at the time of publication of the report, my view is that it probably became too defensive, having been drawn too far into the issue of poor coding rather than seeing the mortality information as a basis for further investigation."
32 Bill Moyes, ex-chair Monitor Evidence to the HoC Health Select Committee, 5 March 2009 "We also relied on the extensive work that had been done by the trust itself to try and understand its high mortality rates. It was not that we did not know about them, but we were persuaded by the external scrutiny of SHAs, by the work that the SHA did, by the PCT's view that this was a coding problem and not an indicator of really seriously deficient care."
33 Mid Staffs Public Inquiry 20-Sep-11 PROFESSOR SIR BRUCE KEOGH, NHS Medical Director, Department of Health from November 2007 The trust..."had little focus on outcomes before the publication [of the HSMRs]..." It considered that poor coding was a likely explanation.'
34 Mid Staffs Public Inquiry, 2-Mar-11 DR PHILIP COATES, Consultant physician at Mid Staffs Trust from 1996, NICE guideline and Clinical Governance lead Q. We'll come on to this in a little more detail later, but you, I think, are fairly frank in your statement in saying that it was wrong to latch on to this coding explanation, rather than fully exploring whether there were clinical deficiencies. A. It was -- it was absolutely wrong to focus on it as a sole cause for the abnormal HSMR, and it was only much later that we began to realise that we had -- we should be looking at clinical quality. Q. Was Monitor wrong to accept what you were saying? A. I would have to say yes.
35 Mid Staffs Public Inquiry Dr Suarez, Medical Director Mid Staffs, statement, Paragraph 122 "CKS [sic] offered to look at our data to see if they could demonstrate the same high mortality figures that Dr Fosters did; however they could not. CKS identified that there were coding issues, but I believe they were very reassuring in that they said we did not have a problem with mortality."
36 Telegraph publication 24 April 2007 showed Mid Staffs HSMR significantly high The Department of Health asked for the following statement from them to go at the end of the publication: We would strongly advise against patients using these figures to make decisions about the relative safety of hospitals. Inquiry Counsel oral Closing Submission 9 December 2011: "What of the HSMR statistics published in April 2007? Why, we ask rhetorically, wasn't more attention paid to them? May 2007 University of Birmingham review of Imperial College methodology commissioned by West Midlands SHA.
37 Mid Staffs Independent Inquiry, 24 Feb Harvard external experts opinion (endorsed in Inquiry report) " the University of Birmingham reports, though probably wellintentioned, were distractions. They used the Mid Staffordshire issue as a context for discrediting the Dr. Foster methodology. the [HSMR] rates published in the Good Hospital Guide alone obviously required extremely serious consideration,
38 Mid Staffs Independent Inquiry, published 24 Feb 2010, pp 336 and 446 Section G Mortality statistics Harvard independent experts opinion We also agree that every statistical quality monitoring algorithm, including Dr Foster, should be critically examined by experts to determine its validity. However, we believe that in the case of Mid-Staffordshire, there were so many different warning flags from different entities, using different approaches, and over multiple time periods, that it would have been completely irresponsible not to aggressively investigate further.
39 Sir Bruce Keogh, Medical Director of the NHS in England, statement to the Mid Staffs Public Inquiry, para 219: "I am reasonably confident that the process which is now in place would have picked up the situation at the trust before it was granted Foundation Trust status. The HSMR information and the question in the staff survey about whether the member of staff would be happy for someone in their family to be treated at the hospital are two examples..."
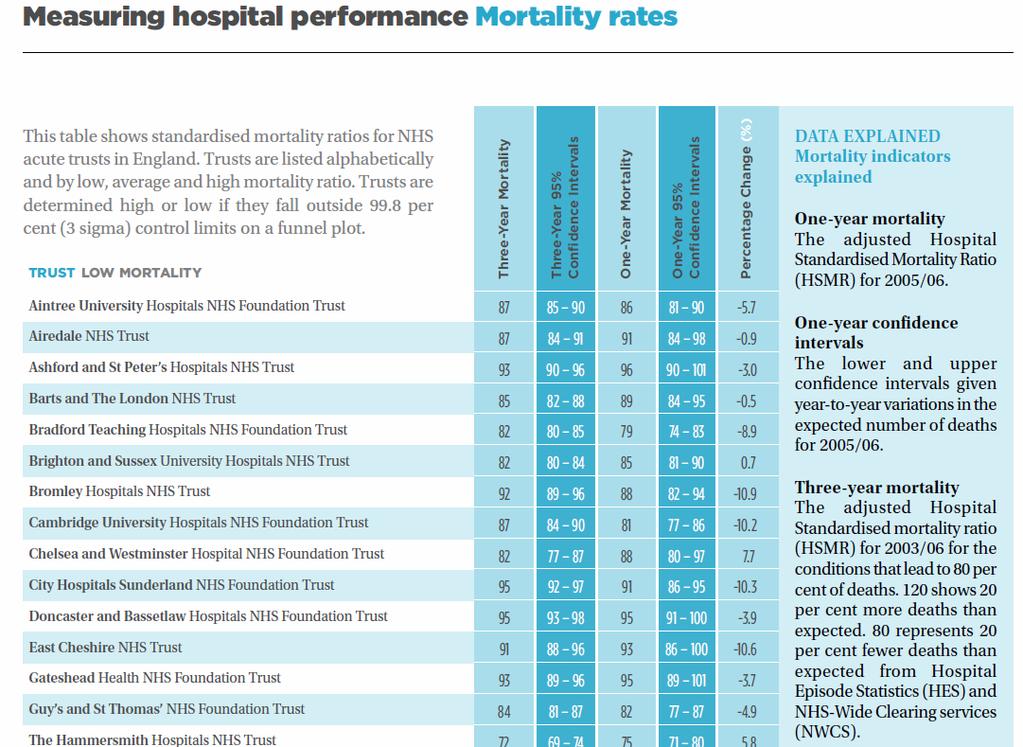
40 Criticisms of HSMRs ranking and league tables Sir Bruce Keogh statement para 139: I have major reservations with the presentation of simplistic league tables of HSMRs (such as those presented in the 2007 Dr Foster Hospital Guide) Professor David Spiegelhalter [MSInq D135/P88/15] "I had considerable misgivings about Dr Foster's work for the Good Hospital Guide, particularly their insistence on ranking hospitals and their use of HSMR." The HSMRs were in fact published in 2007, (as Sir Bruce Keogh suggested that they should be in paragraph 133 of his statement), in alphabetical order in three bands, 'low', 'average' and 'high'.
41
42 INQUIRY REPORT PRESENTATION TO SoS BY ROBERT FRANCIS, QC Finally and perhaps of most concern, I found a widespread culture of denial. The then Board s reaction to the HCC report was individually and collectively one of denial. It should have been one of searching self-criticism. The high HMSR at Mid Staffs, however provided compelling grounds for an investigation of the type carried out by the HCC. It became apparent throughout the inquiry that many staff during the period under investigation did express concern about the standard of care being provided to patients. The tragedy was that they were ignored. The staff evidence persuaded me that a culture of bullying and fear was prevalent in the Trust among staff. I heard of a fear of bullying being a possible explanation for more staff not coming forward with concerns. What this investigation has uncovered is a scale of failure which I believe to be greater than that revealed by the HCC report.
43 Monthly mortality alerts NHS hospital trusts are sent a confidential letter when an alert occurs on a series of statistical process control charts (cumulative sum analysis, CUSUM) that are run each month designed to detect a doubling, over the preceding 3 months, of the odds of death for a number of diagnosis and procedure groups that cover all IP deaths in England. Alerts are filtered to include only signals with a probability of a false alarm less than 0.1% and other restrictions are also applied to exclude some diagnoses including cancer, and vague symptoms and signs. Diagnostic procedures such as endoscopies are also excluded. The mortality alerts are copied to the Care Quality Commission (before 01 April 2009 to the Healthcare Commission) First alerts sent to a trust in May 2007 Excluding other diagnoses and cancer we currently use 43 diagnoses, 79 procedures for the alerts Our letter to the CE of a Trust notes that alerts could be due to: Poor coding Inadequate case-mix adjustment Quality of care

44 Monthly alerts sent to hospitals: Example diagnosis = Acute MI
45 Anonymised version of a monthly alert letter Sent to trust Chief Executive (copied to the CQC)
46 Imperial DFU (& HCC) Mortality alerts Jul to Nov 2007 Operations on jejunum Aortic, peripheral and visceral artery aneurysms Peritonitis and intestinal abscess Other circulatory disease HCC alerts Diabetes (HCC) Epilepsy and convulsions (HCC) Repair abdominal aortic aneurysm (HCC)

47 Mortality alert from Imperial College to CE Mid Staffs 29 June 2007
48 Royal College of Surgeons invited review of Mid Staffs surgical department 2007 & 2009 (Ch 18 Closing Submission 2/12/11] The Royal College of Surgeons conducted two invited reviews of the Trust, one in 2007 and one in The review team was asked to advise whether the complication rate following colorectal surgery was acceptable and whether any change of practice needed to be adopted.
49 Royal College of Surgeons invited review of Mid Staffs surgical department 2007 & 2009 (Ch 18 Closing Submission 2/12/11] There was reference within the [2009] report to the Trust providing care that was "grossly negligent". Notwithstanding the seriousness of that finding Mr Black gave evidence that in line with usual practice the College did not report it to the GMC. The Case Review Report refers to so many badly managed cases that it would be difficult to single out any particular surgeon. The review team found that the service provided by the general surgical unit was inadequate, unsafe and at times, dangerous.
50 Royal College of Surgeons invited review of Mid Staffs surgical department 2007 & 2009 (Ch 18 Closing Submission 2/12/11] Mr Black was asked about the College s failure to follow up the recommendations in his oral evidence: Q. How did you follow up that the trust had acted upon the recommendations that the reviewers made? A. I believe we wrote to them, and we never subsequently made sure that the recommendations had been carried out. Q. Do you recognise that for a member of the public listening to that, that is to say unacceptable, to put it mildly? A. I would accept that. The strong recommendations were made to the trust. The college has no statutory power to enforce those recommendations. We did follow up by letter. We did not follow it up any more than that, and I wish we had done.

51 Richard Hamblin, Director of Intelligence CQC, Slide 58 of PPT Institute of Health Economics 9 April 2010 as example of CQC alert

52 Imperial College alert for complications of surgical procedures or medical care we sent to the Healthcare Commission on 31/08/2007

53 The CQC website - Mortality outliers programme example (accessed 16/04/2010):- Our data is therefore more specific and more timely than HSMR.

54 Imperial College alert for Excision of the lung we sent to the Healthcare Commission on 17/01/2009
.")
55 HCC: Following up mortality 'outliers, Dec 2008 We have established a new programme of work to identify and follow up concerns about apparently high rates of mortality in the NHS. Over the 12 month period considered by this report, we have considered 85 alerts, relating to 56 acute trusts (one out of three acute trusts in England). After analysing the data, we concluded that 42 of these alerts (relating to 29 or 17% of acute trusts in England), needed to be pursued by the Commission. There is clear evidence that our follow-up action has led directly to improvements in clinical practice, and in the use of clinical data in NHS trusts. We expect this to have led to direct improvements in the care provided to patients, but acknowledge that further evaluation is necessary to understand the extent to which this may have happened.
 Intervention reduce adm to op time & appoint orthopaedic")
56 50. Example for Royal Bolton: #nof Apr 2004 Aug 2008 (1899 admissions) Intervention reduce adm to op time & appoint orthopaedic geriatrician
57 2004-Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q3 Crude death rate 51. Royal Bolton: fractured neck of femur Apr 2004 Jul 2010 Reduction of crude death rate after intervention Intervention 30% 25% 20% Crude death rate 15% 10% 5% 0%
58 2004-Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q3 Cumulative sum obs - exp deaths 52. Royal Bolton: #nof Apr 2004 Jul 2010 Cumulative sum of actual deaths expected deaths if 2004-Q3 SMR had persisted Intervention Cusum of Observed -Expected deaths if 2004-Q3 SMR had persisted -200
59 2004-Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q Q3 % LoS values > 75th %ile for England (for #nof) 53. Change of length of stay (leads to reduced costs % LoS values > 75th %ile for England (for #nof) Intervention Long LoS = % LoS values greater than 75th percentile patient in England for #nof Linear (Long LoS = % LoS values greater than 75th percentile patient in England for #nof)
 Robb, E. et al.")
60 Fig 3 Hospital standardised mortality rates (HSMR) in acute hospitals in England, , and change in position of North West London Hospitals NHS Trust (NWLH) Robb, E. et al. BMJ 2010;340:c1234 Copyright 2010 BMJ Publishing Group Ltd.
61 Hero of the Hudson Capt. Chesley Sullenberger s From 1967 to 1976, the chances of dying in a large U.S. jetliner crash were roughly 1 in 2 million. Today it s closer to 1 in 20 million thanks to tightened safety standards and a massive culture change in the industry...
62 Hero of the Hudson Capt. Chesley Sullenberger s We still think of these [patient deaths] as an unavoidable consequence of providing care and sometimes that s true, but not always, Sullenberger said. We must stop thinking about them as unavoidable and start thinking about them as unthinkable.


63 Paediatric cardiac surgical mortality in England after Bristol: BMJ 2004; 329 : 7 October 2004

64 Paediatric cardiac surgical mortality in England after Bristol: BMJ 2004; 329 : 7 October 2004 External inspection Intervention
65 Paediatric Cardiac Surgery in England age 0-5 From 1991/95 to 1999/02 PCS mortality at Bristol reduced from 29% to 3.5% ie 8 times From 1991/95 to 2008/12 PCS mortality in England reduced from 12% to 2% ie 6 times From 1967 to 1976, mortality in large U.S. jetliner crashes reduced from 1 in 2 million to 1 in 20 million i.e. 10 times.

66 Nobel prizes vs chocolate consumption - correlation
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Monitoring hospital mortality A response to the University of Birmingham report on HSMRs
 Monitoring hospital mortality A response to the University of Birmingham report on HSMRs Dr Paul Aylin Dr Alex Bottle Professor Sir Brian Jarman Dr Foster Unit at Imperial, Department of Primary Care and
Monitoring hospital mortality A response to the University of Birmingham report on HSMRs Dr Paul Aylin Dr Alex Bottle Professor Sir Brian Jarman Dr Foster Unit at Imperial, Department of Primary Care and
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
Learning from Deaths; Mortality Review Policy
 Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Focus on hip fracture: Trends in emergency admissions for fractured neck of femur, 2001 to 2011
 Focus on hip fracture: Trends in emergency admissions for fractured neck of femur, 2001 to 2011 Appendix 1: Methods Paul Smith, Cono Ariti and Martin Bardsley October 2013 This appendix accompanies the
Focus on hip fracture: Trends in emergency admissions for fractured neck of femur, 2001 to 2011 Appendix 1: Methods Paul Smith, Cono Ariti and Martin Bardsley October 2013 This appendix accompanies the
Reducing In-hospital Mortality
 Advancing Quality Alliance Reducing In-hospital Mortality Observations arising from AQuA s work May 2013 Contents Introduction and background Understanding mortality rates Mortality rates SMR methodologies
Advancing Quality Alliance Reducing In-hospital Mortality Observations arising from AQuA s work May 2013 Contents Introduction and background Understanding mortality rates Mortality rates SMR methodologies
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Using the structured judgement review method
 National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
O U T C O M E. record-based. measures HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT
 HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Special measures: one year on. A report into progress made at 11 NHS trusts that were put into special measures in July 2013
 Special measures: one year on A report into progress made at 11 NHS trusts that were put into special measures in July 2013 August 2014 Contents 1. Summary 2 2. Background 4 The Keogh Review 4 What the
Special measures: one year on A report into progress made at 11 NHS trusts that were put into special measures in July 2013 August 2014 Contents 1. Summary 2 2. Background 4 The Keogh Review 4 What the
Overview of a new study to assess the impact of hospice led interventions on acute use. Jonathan Ellis, Director of Policy & Advocacy
 Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Assessing Quality of Hospital Services - the importance of national clinical audits
 Assessing Quality of Hospital Services - the importance of national clinical audits Professor Sir Mike Richards Chief Inspector of Hospitals November 2015 1 Overview CQC s role and purpose Our approach
Assessing Quality of Hospital Services - the importance of national clinical audits Professor Sir Mike Richards Chief Inspector of Hospitals November 2015 1 Overview CQC s role and purpose Our approach
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Hospital Standardised Mortality Ratios
 Hospital Standardised Mortality Ratios Quarterly Release Publication date 15 May 2018 A National Statistics publication for Scotland This is a National Statistics Publication National Statistics status
Hospital Standardised Mortality Ratios Quarterly Release Publication date 15 May 2018 A National Statistics publication for Scotland This is a National Statistics Publication National Statistics status
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Monthly and Quarterly Activity Returns Statistics Consultation
 Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
London CCG Neurology Profile
 CCG Neurology Profile November 214 Summary NHS Hammersmith And Fulham CCG Difference from Details Comments Admissions Neurology admissions per 1, 2,13 1,94 227 p.1 Emergency admissions per 1, 1,661 1,258
CCG Neurology Profile November 214 Summary NHS Hammersmith And Fulham CCG Difference from Details Comments Admissions Neurology admissions per 1, 2,13 1,94 227 p.1 Emergency admissions per 1, 1,661 1,258
Is the quality of care in England getting better? QualityWatch Annual Statement 2013: Summary of findings
 Is the quality of care in England getting better? QualityWatch Annual Statement 2013: Summary of findings October 2013 About QualityWatch QualityWatch is a major research programme providing independent
Is the quality of care in England getting better? QualityWatch Annual Statement 2013: Summary of findings October 2013 About QualityWatch QualityWatch is a major research programme providing independent
EuroHOPE: Hospital performance
 EuroHOPE: Hospital performance Unto Häkkinen, Research Professor Centre for Health and Social Economics, CHESS National Institute for Health and Welfare, THL What and how EuroHOPE does? Applies both the
EuroHOPE: Hospital performance Unto Häkkinen, Research Professor Centre for Health and Social Economics, CHESS National Institute for Health and Welfare, THL What and how EuroHOPE does? Applies both the
NHS Patient Survey Programme 2016 Emergency Department Survey
 NHS Patient Survey Programme 2016 Emergency Department Survey Identifying outliers within trust-level results Published October 2017 Contents Summary... 2 Outlier analysis and trust-level benchmark reports...
NHS Patient Survey Programme 2016 Emergency Department Survey Identifying outliers within trust-level results Published October 2017 Contents Summary... 2 Outlier analysis and trust-level benchmark reports...
Emergency readmission rates
 Emergency readmission rates Further analysis 1 Emergency readmission rates DH INFORMATION READER BOX Policy Estates HR / Workforce Commissioning Management IM & T Clinical Planning / Finance Clinical Social
Emergency readmission rates Further analysis 1 Emergency readmission rates DH INFORMATION READER BOX Policy Estates HR / Workforce Commissioning Management IM & T Clinical Planning / Finance Clinical Social
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
National Trends Winter 2016
 National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance
 Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Improving Patient Outcomes
 Agenda Item No: 8 PURPOSE: To highlight to the Board the importance of reducing avoidable mortality and to propose a series of evidence based measures that could significantly improve patient safety. IMPLICATIONS:
Agenda Item No: 8 PURPOSE: To highlight to the Board the importance of reducing avoidable mortality and to propose a series of evidence based measures that could significantly improve patient safety. IMPLICATIONS:
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Researcher: Dr Graeme Duke Software and analysis assistance: Dr. David Cook. The Northern Clinical Research Centre
 Real-time monitoring of hospital performance: A practical application of the hospital and critical care outcome prediction equations (HOPE & COPE) for monitoring clinical performance in acute hospitals.
Real-time monitoring of hospital performance: A practical application of the hospital and critical care outcome prediction equations (HOPE & COPE) for monitoring clinical performance in acute hospitals.
Increased mortality associated with week-end hospital admission: a case for expanded seven-day services?
 Increased mortality associated with week-end hospital admission: a case for expanded seven-day services? Nick Freemantle, 1,2 Daniel Ray, 2,3,4 David Mcnulty, 2,3 David Rosser, 5 Simon Bennett 6, Bruce
Increased mortality associated with week-end hospital admission: a case for expanded seven-day services? Nick Freemantle, 1,2 Daniel Ray, 2,3,4 David Mcnulty, 2,3 David Rosser, 5 Simon Bennett 6, Bruce
Indicator Specification:
 Indicator Specification: CCG OIS 3.2 (NHS OF 3b) Emergency readmissions within 30 days of discharge from hospital Indicator Reference: I00760 Version: 1.1 Date: March 2014 Author: Clinical Indicators Team
Indicator Specification: CCG OIS 3.2 (NHS OF 3b) Emergency readmissions within 30 days of discharge from hospital Indicator Reference: I00760 Version: 1.1 Date: March 2014 Author: Clinical Indicators Team
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
4 CM/02/18/04. Chief Executive s report to the Board David Behan, Chief Executive Kate Eisenstein, Special Policy Advisor to the Chief Executive
 Meeting PUBLIC BOARD MEETING Date 21 February 2018 Agenda item Paper Number 4 CM/02/18/04 Item title Sponsor Author Chief Executive s report to the Board David Behan, Chief Executive Kate Eisenstein, Special
Meeting PUBLIC BOARD MEETING Date 21 February 2018 Agenda item Paper Number 4 CM/02/18/04 Item title Sponsor Author Chief Executive s report to the Board David Behan, Chief Executive Kate Eisenstein, Special
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust
 A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
Hospital Mortality Monitoring. May 2015
 Hospital Mortality Monitoring Report 24: Oct 213 to Sep 214 May 215 undertaken by North East Quality Observatory System on behalf of All North East Subscribers to NEQOS Services NEQOS is jointly operated
Hospital Mortality Monitoring Report 24: Oct 213 to Sep 214 May 215 undertaken by North East Quality Observatory System on behalf of All North East Subscribers to NEQOS Services NEQOS is jointly operated
Finalised Patient Reported Outcome Measures (PROMs) in England Data Quality Note
 in England Data Quality Note") Finalised Patient Reported Outcome Measures (PROMs) in England Data Quality Note April 2015 to Published 10 August 2017 This data quality note accompanies the publication by NHS Digital of finalised data
Finalised Patient Reported Outcome Measures (PROMs) in England Data Quality Note April 2015 to Published 10 August 2017 This data quality note accompanies the publication by NHS Digital of finalised data
Society for Cardiothoracic Surgery in Great Britain and Ireland
 Notes on Divergence in the Lung Cancer Surgery Consultant Outcomes Publication (LCCOP) (1) Summary The Lung Cancer Surgery Consultant Outcomes Publication (LCCOP) publishes data on resection rates and
Notes on Divergence in the Lung Cancer Surgery Consultant Outcomes Publication (LCCOP) (1) Summary The Lung Cancer Surgery Consultant Outcomes Publication (LCCOP) publishes data on resection rates and
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Francis Report: Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry 1 A carer s response
 : Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry 1 A carer s response Laurie Beed June 2013 As a former carer I looked forward to reading the Francis report with great interest and
: Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry 1 A carer s response Laurie Beed June 2013 As a former carer I looked forward to reading the Francis report with great interest and
Hospital Standardized Mortality Ratios, Edmonton, Canada: A Tale of Two Sites Lessons Learned from the UK
 Hospital Standardized Mortality Ratios, Edmonton, Canada: A Tale of Two Sites Lessons Learned from the UK Joanne Zaborowski Performance Advisor Provincial Projects Clinical Quality Metrics Healthcare Quality
Hospital Standardized Mortality Ratios, Edmonton, Canada: A Tale of Two Sites Lessons Learned from the UK Joanne Zaborowski Performance Advisor Provincial Projects Clinical Quality Metrics Healthcare Quality
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Ambulatory emergency care Reimbursement under the national tariff
 HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
Boarding Impact on patients, hospitals and healthcare systems
 Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Results of censuses of Independent Hospices & NHS Palliative Care Providers
 Results of censuses of Independent Hospices & NHS Palliative Care Providers 2008 END OF LIFE CARE HELPING THE NATION SPEND WISELY The National Audit Office scrutinises public spending on behalf of Parliament.
Results of censuses of Independent Hospices & NHS Palliative Care Providers 2008 END OF LIFE CARE HELPING THE NATION SPEND WISELY The National Audit Office scrutinises public spending on behalf of Parliament.
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Delivering a Paperless NHS by Dr Masood Nazir General Practitioner Clinical Informatics Advisor NHS England
 Delivering a Paperless NHS by 2018 Dr Masood Nazir General Practitioner Clinical Informatics Advisor NHS England About us The NHS Commissioning Board (NHS CB): was established as a special health authority
Delivering a Paperless NHS by 2018 Dr Masood Nazir General Practitioner Clinical Informatics Advisor NHS England About us The NHS Commissioning Board (NHS CB): was established as a special health authority
Health Care Quality Indicators in the Irish Health System:
 Health Care Quality Indicators in the Irish Health System Examining the Potential of Hospital Discharge Data using the Hospital Inpatient Enquiry System - i - Health Care Quality Indicators in the Irish
Health Care Quality Indicators in the Irish Health System Examining the Potential of Hospital Discharge Data using the Hospital Inpatient Enquiry System - i - Health Care Quality Indicators in the Irish
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System
 Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
NHS Outcomes Framework 2014/15:
 NHS Outcomes Framework 2014/15: Domain 3 Helping people to recover from episodes of ill health or following injury Indicator specifications Version: 1.2 Date: August 2014 Author: Clinical Indicators Team
NHS Outcomes Framework 2014/15: Domain 3 Helping people to recover from episodes of ill health or following injury Indicator specifications Version: 1.2 Date: August 2014 Author: Clinical Indicators Team
National Cancer Patient Experience Survey National Results Summary
 National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
Supplemental materials for:
 Supplemental materials for: Ricci-Cabello I, Avery AJ, Reeves D, Kadam UT, Valderas JM. Measuring Patient Safety in Primary Care: The Development and Validation of the "Patient Reported Experiences and
Supplemental materials for: Ricci-Cabello I, Avery AJ, Reeves D, Kadam UT, Valderas JM. Measuring Patient Safety in Primary Care: The Development and Validation of the "Patient Reported Experiences and
National Clinical Audit & Patient Outcome Programme: An update
 National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Pricing and funding for safety and quality: the Australian approach
 Pricing and funding for safety and quality: the Australian approach Sarah Neville, Ph.D. Executive Director, Data Analytics Sean Heng Senior Technical Advisor, AR-DRG Development Independent Hospital Pricing
Pricing and funding for safety and quality: the Australian approach Sarah Neville, Ph.D. Executive Director, Data Analytics Sean Heng Senior Technical Advisor, AR-DRG Development Independent Hospital Pricing
Tele Stroke ( Telemedicine in Practice)
") Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Commissioning for Value insight pack
 Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB)
") Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Executive Summary 10 th September Dr. Richard Wagland. Dr. Mike Bracher. Dr. Ana Ibanez Esqueda. Professor Penny Schofield
 Experiences of Care of Patients with Cancer of Unknown Primary (CUP): Analysis of the 2010, 2011-12 & 2013 Cancer Patient Experience Survey (CPES) England. Executive Summary 10 th September 2015 Dr. Richard
Experiences of Care of Patients with Cancer of Unknown Primary (CUP): Analysis of the 2010, 2011-12 & 2013 Cancer Patient Experience Survey (CPES) England. Executive Summary 10 th September 2015 Dr. Richard
TRUST BOARD SEPTEMBER Surgical Services Reconfiguration
 def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
North West COPD Report Nov 2011
 North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
Do quality improvements in primary care reduce secondary care costs?
 Evidence in brief: Do quality improvements in primary care reduce secondary care costs? Findings from primary research into the impact of the Quality and Outcomes Framework on hospital costs and mortality
Evidence in brief: Do quality improvements in primary care reduce secondary care costs? Findings from primary research into the impact of the Quality and Outcomes Framework on hospital costs and mortality
Using mortality data to improve the quality and safety of patient care December 2015
 Using mortality data to improve the quality and safety of patient care December 2015 Version Date Published Notes 12.0 18/12/2015 12 th publication 11.0 18/09/2015 11 th publication 10.0 19/06//2015 10
Using mortality data to improve the quality and safety of patient care December 2015 Version Date Published Notes 12.0 18/12/2015 12 th publication 11.0 18/09/2015 11 th publication 10.0 19/06//2015 10
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
National Cancer Patient Experience Survey National Results Summary
 National Cancer Patient Experience Survey 2015 National Results Summary Introduction As in previous years, we are hugely grateful to the tens of thousands of cancer patients who responded to this survey,
National Cancer Patient Experience Survey 2015 National Results Summary Introduction As in previous years, we are hugely grateful to the tens of thousands of cancer patients who responded to this survey,
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Predict, prevent & manage AKI: A UK collaboration to detect a devastating condition AKI
 Predict, prevent & manage AKI: A UK collaboration to detect a devastating condition AKI Case Study Acute kidney injury (AKI) is a potentially devastating condition, thought to contribute to the deaths
Predict, prevent & manage AKI: A UK collaboration to detect a devastating condition AKI Case Study Acute kidney injury (AKI) is a potentially devastating condition, thought to contribute to the deaths
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST. Quarterly Clinical Effectiveness and Outcomes Report:
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Quarterly Clinical Effectiveness and Outcomes Report: Report to Trust Board 27 th September 2011 Report from Sponsoring Executive Aim of Report Jane Druce, Quality
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Quarterly Clinical Effectiveness and Outcomes Report: Report to Trust Board 27 th September 2011 Report from Sponsoring Executive Aim of Report Jane Druce, Quality
Implementation of the right to access services within maximum waiting times
 Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Community Pharmacy in 2016/17 and beyond
 Community Pharmacy in 2016/17 and beyond Stakeholder briefing sessions 1 CONTENTS Contents This presentation describes our vision for community pharmacy, and outlines proposals for achieving that vision,
Community Pharmacy in 2016/17 and beyond Stakeholder briefing sessions 1 CONTENTS Contents This presentation describes our vision for community pharmacy, and outlines proposals for achieving that vision,
Implementing NHS Services Seven Days a Week
 Implementing NHS Services Seven Days a Week Deborah Williams 7 Day Services Programme Manager NHS England November 2015 NHS Five Year Forward View To reduce variations in when patients receive care, we
Implementing NHS Services Seven Days a Week Deborah Williams 7 Day Services Programme Manager NHS England November 2015 NHS Five Year Forward View To reduce variations in when patients receive care, we
Current policy context of safe staffing in A&E Departments
 Current policy context of safe staffing in A&E Departments Howard Catton, Head of Policy and International Affairs Hallam Conference Centre, London -18 th May 2015 Why is safe staffing so important? Right
Current policy context of safe staffing in A&E Departments Howard Catton, Head of Policy and International Affairs Hallam Conference Centre, London -18 th May 2015 Why is safe staffing so important? Right
Improving Health Services for Carers
 Improving Health Services for Carers A carer is someone who, without payment, looks after or provides help and support to somebody who could not manage otherwise due to age, physical or mental illness,
Improving Health Services for Carers A carer is someone who, without payment, looks after or provides help and support to somebody who could not manage otherwise due to age, physical or mental illness,
Reference costs 2016/17: highlights, analysis and introduction to the data
 Reference s 2016/17: highlights, analysis and introduction to the data November 2017 We support providers to give patients safe, high quality, compassionate care within local health systems that are financially
Reference s 2016/17: highlights, analysis and introduction to the data November 2017 We support providers to give patients safe, high quality, compassionate care within local health systems that are financially
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE HEALTHCARE GOVERNANCE COMMITTEE HELD ON 25 NOVEMBER 2013
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY E REPORT TO THE HEALTHCARE GOVERNANCE COMMITTEE HELD ON 25 NOVEMBER 2013 Subject Supporting TEG Member Author Status Care Quality Commission
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY E REPORT TO THE HEALTHCARE GOVERNANCE COMMITTEE HELD ON 25 NOVEMBER 2013 Subject Supporting TEG Member Author Status Care Quality Commission
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Innovation Series Move Your DotTM. Measuring, Evaluating, and Reducing Hospital Mortality Rates (Part 1)
") Innovation Series 2003 200 160 120 Move Your DotTM 0 $0 $4,000 $8,000 $12,000 $16,000 $20,000 80 40 Measuring, Evaluating, and Reducing Hospital Mortality Rates (Part 1) 1 We have developed IHI s Innovation
Innovation Series 2003 200 160 120 Move Your DotTM 0 $0 $4,000 $8,000 $12,000 $16,000 $20,000 80 40 Measuring, Evaluating, and Reducing Hospital Mortality Rates (Part 1) 1 We have developed IHI s Innovation
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
National Mortality Case Record Review Programme. Using the structured judgement review method A guide for reviewers (England)
") National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
Prof. Helen Ward Profesora clínica de Salud Pública y Directora PATIENT EXPERIENCE RESEARCH CENTRE (PERC) IMPERIAL COLLEGE
 IMPERIAL COLLEGE") Prof. Helen Ward Profesora clínica de Salud Pública y Directora PATIENT EXPERIENCE RESEARCH CENTRE (PERC) IMPERIAL COLLEGE LONDON @profhelenward Imperial NIHR Biomedical Research Centre Translating research
Prof. Helen Ward Profesora clínica de Salud Pública y Directora PATIENT EXPERIENCE RESEARCH CENTRE (PERC) IMPERIAL COLLEGE LONDON @profhelenward Imperial NIHR Biomedical Research Centre Translating research
Hospital at home or acute hospital care: a cost minimisation analysis Coast J, Richards S H, Peters T J, Gunnell D J, Darlow M, Pounsford J
 Hospital at home or acute hospital care: a cost minimisation analysis Coast J, Richards S H, Peters T J, Gunnell D J, Darlow M, Pounsford J Record Status This is a critical abstract of an economic evaluation
Hospital at home or acute hospital care: a cost minimisation analysis Coast J, Richards S H, Peters T J, Gunnell D J, Darlow M, Pounsford J Record Status This is a critical abstract of an economic evaluation
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Recommendations of the NH Strategy
 Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Continuously Measuring Patient Outcome using Variable Life-Adjusted Displays (VLAD)
") Continuously Measuring Patient Outcome using Variable Life-Adjusted Displays (VLAD) Mr. Steve GILLETT Ms. Kian WONG Dr. K.H. LEE HAHO Casemix Office Acknowledgements : 1. Queensland Health Department (VLAD
Continuously Measuring Patient Outcome using Variable Life-Adjusted Displays (VLAD) Mr. Steve GILLETT Ms. Kian WONG Dr. K.H. LEE HAHO Casemix Office Acknowledgements : 1. Queensland Health Department (VLAD
New foundations: the future of NHS trust providers
 RCN Policy Unit Policy Briefing 05/2010 New foundations: the future of NHS trust providers April 2010 Royal College of Nursing 20 Cavendish Square London W1G 0RN Telephone 020 7647 3754 Fax 020 7647 3498
RCN Policy Unit Policy Briefing 05/2010 New foundations: the future of NHS trust providers April 2010 Royal College of Nursing 20 Cavendish Square London W1G 0RN Telephone 020 7647 3754 Fax 020 7647 3498
NHS Wiltshire PCT Programme Budgeting fact sheet /12 Contents
 PCT Programme Budgeting fact sheet - 2011/12 Contents Introduction... 2 Methodology and caveats... 3 Key facts... 4 Relative expenditure by programme... 6 Relative expenditure by setting... 7 The biggest
PCT Programme Budgeting fact sheet - 2011/12 Contents Introduction... 2 Methodology and caveats... 3 Key facts... 4 Relative expenditure by programme... 6 Relative expenditure by setting... 7 The biggest
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives
 NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect