PATIENT INFORMATION:
|
|
|
- Geraldine Lloyd
- 6 years ago
- Views:
Transcription
1 NEW PATIENT INFORMATION DATE: / / HOME PHONE: NAME: (First) (MI) (Last) ADDRESS: CITY: STATE: ZIP CODE: BIRTHDATE: / / Sex: Male Female Marital Status: S M D W Occupation: Work Phone: Employer: City & State: Social Security: Address: Cell Phone: PATIENT INFORMATION: Spouse Name: Occupation: Work Phone: Employer: City & State: Social Security: Date of Birth: SPOUSE INFORMATION: How did you find out about us? TV (Channel?) Website Internet Facebook Trib OTHER Referral from a physician Referral from a friend/family (Name) (Name) Have you had Physical Therapy this year? (Circle one) YES NO If yes, where Have you been or are you on Home Health Care? (Circle one) YES NO Is this related to a Workman s Comp Case or Auto Accident Case? (Circle one) YES NO If YES, please provide Workman s Comp/Auto Accident information to Front Desk. Please note: We do not accept third party payments. It is the patient s responsibility to pay for therapy charges. Primary Care Physician: (If other than the referring physician) Address: City: State: Zip Code: Specialty: Telephone: Pharmacy: Phone: Insurance Information: Primary: Group or ID#: Insured s Name: Secondary: Group or ID#: Insured s Name: In Case of Emergency, Contact: Phone: Assignment of Benefits/Release of Information: I authorize payment of insurance benefits directly to Illinois Back Institute. I authorize to execute any documents necessary to secure the payment of benefits and obtain any records from any other source necessary for the course of my treatment. I agree to be financially responsible for all charges incurred during treatment by Illinois Back Institute including my insurance deductible co-payment, and services not covered by my insurance carrier or paid in full through any settlement or court case. Any remaining balances I will pay in full per the policies of Countryview Medical Center dba Illinois Back Institute. Signature: Date: MRI No Yes Disc Films Cleared for Vibration: No Yes
2 NAME: AGE: DATE: WHAT IS YOUR REASON FOR YOUR VISIT TODAY? Primary Care Physician: DATE OF LAST PHYSICAL EXAM: HEALTH STATUS (please circle): For Women Date of Last Menstrual Period: Last Pap Smear: Date of Last Mammogram: Pregnant Yes / No No. of Children Complications, (if any) with childbirth? Have you experienced (please circle): Abnormal Pap Smear Abnormal Bleeding Breast Lump/Pain Vaginal Discharge HEALTH HISTORY (please circle): Patient History Chills Poor Appetite Chest Pain Itching Depression Bloating High/Low Blood Pressure Changes In Moles Dizziness/Fainting Bowel Changes Swelling in Ankles Rash Fever Constipation Varicose Veins Scars Sweats Diarrhea Blurred/Double Vision Sore (non- healing) Forgetfulness Excessive Hunger/Thirst Earache/Ringing In Ears Low Back Pain Headaches/Migraines Gas Sinus Problems Neck Pain Sleep Loss Indigestion Allergies Leg/Arm Pain Weight Loss Nausea/Vomiting Nosebleeds Other: Nervousness Difficulty Swallowing Persistent Cough Numbness Rectal Bleeding Bruise Easily AIDS Chicken Pox Hernia Polio Tonsilitis Alcoholism Diabetes High Cholesterol Prostate Problems Typhoid Fever Anemia Emphysema Kidney/Liver Disease Psychiatric Care Ulcers Appendicitis Epilepsy Measles Rheumatic Fever Vaginal Infections Bronchitis Gout Miscarriage Scarlet Fever Venereal Disease Cancer Heart Disease Pacemaker Stroke Other: Cataracts Hepatitis Pneumonia Thyroid Problems
3 Name: Date: / / Please List Prescriptions and OTC Medications: (Use back if needed) Please List Medical Allergies: Family Health History Relation Age Status of Health Age of Death Cause of Death Father Mother Brother (s) Sister (s) Family History (please check below if any applies) Check Condition Relationship Arthritis, Gout Asthma, Hay Fever Cancer Chemical Dependency Diabetes Heart Disease, Strokes High Blood Pressure Kidney Disease Tuberculosis Other Health Habits (please mark if using the following) Caffeine: How much? Tobacco: How much? Drugs: Water: Surgeries and Hospitalizations Date Reason for Hospitalization/Type of Surgery Outcome/Results How much? How much? Other: I certify that the above information is correct to the best of my knowledge. I will not hold my doctor or any member of his/her staff responsible for any errors or omissions that I may have made in the completion of this form. / / Patient Signature Date / / Reviewed By Date
4 Name: Date: / / Please state your initial problem and/or reason for visiting today? Date Condition/Problem began? What is the frequency of your symptoms? Constant Frequent Intermittent Occasional SCALE of 0 to 10; 0 representing no pain and 10 the most severe pain, please circle the appropriate number below. Please rate your pain today? Since your pain started, how would you rate your least pain level? Since your pain started, how would you rate your worst pain level? If your initial pain is a pain complaint, does it radiate? YES No If yes, where to? Please check if your initial complaint effects your movement by the following: Inflexibility Stiffness Spasm Cramp If your initial complaint gives you sensations, please check from the following: Crawling Pins & Needles Burning Stinging Tingling Stabbing Shooting Excruciating Deadness Hurting Throbbing Dull Prickly Pulsating Aching Pounding What aggravates your complaint? Flashing Lights Looking Up/Down Looking side to side Driving Pushing Carrying Getting in/out of Car What relieves you initial complaint? Resting Sitting Tylenol Sneezing Lifting Coughing Sitting Anger Standing Stress Walking Emotional Upset Pulling Straining at BM Climbing Stairs Other Sleeping Shower Pain Pills Cold Advil Treatment Heat Aspirin Mineral Ice Exercising Stooping Depression Getting out of Bed Repetitive Movements Walking up hill Other
5 Patient Name: Date: / / Please Circle the correct answer for each question: 1. Have you ever had blood clots? Yes No 2. Have you ever had a hernia? Yes No a. If yes, How long ago? 3. Do you have Spondylolisthesis? Yes No 4. Have you ever had a compression fracture? Yes No 5. Have you ever had a hip, knee or foot implant (artificial)? Yes No 6. Are you pregnant? Yes No 7. Do you have a pacemaker? Yes No 8. Do you have any metal in your body (Plates or screws)? Yes No 9. Do you have an infection? Yes No 10. Do you have diabetes? Yes No 11. Do you have any stents for your Heart or Arteries? Yes No 12. Do you have a severe heart problem? Yes No 13. Do you have epilepsy? Yes No 14. Do you or have you had cancer? Yes No
6 NOTICE OF PRIVACY PRACTICES In compliance with a newly enacted Federal Law, the Health Insurance Portability and Accountability Act (HIPAA), The Illinois Back Institute is informing you of your privacy rights. Please review this notice carefully. What is HIPAA? HIPAA is a law passed by Congress in 1996 to improve the efficiency and effectiveness of the healthcare system. It requires health care professionals to adhere to privacy and security standards in order to protect their patient s Personal Health Information (PHI). PHI is confidential information about a patient, including demographic information. What are my rights under HIPAA? Under HIPAA you have a right to request the following as long as a request is made in writing to the attention of the Privacy Officer and applicable fees are paid. There is a possibility that your request may be denied. If your request is denied we will explain why it was denied in writing. You have a right to inspect and obtain a copy of your PHI. We will respond to your request within 30 days. In most cases your request will be honored and a copy of your PHI will be mailed to you. You have a right to request an amendment of PHI. If you feel that your PHI is inaccurate or incomplete, you may request an amendment to your PHI. We will respond to your request within 60 days. If we honor your request we will amend your PHI and notify you and applicable parties. We will deny your request if we determine your PHI to be correct or complete, if your request was not created by us, or if PHI is not available for inspection. You have the right to know what disclosure(s) of your PHI have been made. You have a right to request a listing of who your PHI was sent to, when it was sent, what content of your PHI was sent and for what purpose. We will respond to your request within 60 days. There will be no charge to you for an initial request. Additionally, your request may not include disclosures made for national security reasons, to law enforcement officials/correctional facilities, or disclosures made prior to June 1, 2004 Updated: October 14, You have a right to request confidential communications of PHI. We will honor all reasonable requests to keep communications confidential. A reasonable request is one that specifies an alternative address, gives other means of contact and provides detailed information on how payment will be handled. You have a right to request restrictions on the use and disclosure of PHI, however we are not required to agree to your request. Your request must state specific restrictions requested and to whom the restrictions would apply. You have a right to receive a hard copy of this notice. This notice can also be accessed on our website How will The Illinois Back Institute Use and Disclose PHI under HIPAA? HIPAA allows us to use and disclose your PHI for the purposes of Treatment, Payment and Healthcare Operations. We will specifically use and disclose your PHI to communicate with your physician and to, upon request, assist your insurance company with the processing of your claims. Additionally, we will use your basic demographic information to notify you of new services or facilities. Your authorization is not required for Use and Disclosure of PHI for the purposes of Treatment, Payment and Healthcare Operations. Listed are other instances in which Use and Disclosure of your PHI is allowed without your authorization. Disclosure to those Involved in the Individual s Care when necessary, we will make a professional decision to disclose PHI to family members, close friends or other persons involved in and assisting in your care when you approve or when are not able or present to approve. Uses and Disclosures Required by Law as required by law we are required to use and disclose PHI for the following reasons: Use and Disclose PHI for Public Health Activities Examples include: communicable diseases, sexually transmitted diseases, lead poisoning, Reyes Syndrome, etc., to public health officials. Disclose PHI about Victims of Abuse, Neglect, or Domestic Violence - Examples include: child abuse and neglect; an abused or neglected nursing home resident; a patient over 60 years old involved in elder abuse. Uses and Disclosure of Health Oversight Activities we may use and release PHI to be used for audits, investigations, licensure issues, etc.
7 Disclosure for Judicial and Administrative Proceedings we may disclose limited PHI to the appropriate authorities as a result of a court order subpoena, discovery request, etc. Disclosure for Law Enforcement Purposes we may disclose reasonably necessary PHI to law enforcement officials to identify or locate a suspect, fugitive, material witness or missing person. Uses and Disclosures Related to Decedents we may use and disclose PHI to a coroner or medical examiner and funeral directors as required by law. Uses and Disclosures Related to Cadaveric Organ, Eye or Tissue Donations we may use and release PHI in order to facilitate organ, eye or tissue donations. Uses and Disclosures to Avert a Serious Threat to Health or Safety we may use and release PHI to public health and other authorities required by law in order to prevent a serious threat to your health or safety. Uses and Disclosures for Specialized Government Functions we may use and release PHI for military/veterans activities and national security/intelligence activities. Use and Disclosure of PHI in Emergency Situations - in the event of an eminent threat to the safety of a patient, we may disclose PHI to prevent or lessen the threat. Uses and Disclosures of PHI for Marketing Purposes - The Illinois Back Institute will notify you of new services and facilities unless you specify otherwise. Unless you authorize such a disclosure we will not disclose your PHI for marketing purposes. Uses and Disclosures of PHI for Research Purposes we do not use or disclose identifiable PHI for research purposes, unless you authorize such use and disclosure. Uses and Disclosures requiring the Patients Authorization - we must obtain your written authorization if we are interested in using and or disclosing your PHI for reasons other than treatment, payment and health care operations. You may revoke your authorization at any time. What does HIPAA require of The Illinois Back Institute? The Illinois Back Institute must maintain the privacy of PHI, abide by the terms of this notice and provide patients with a revised notice, if necessary. Where can I file a privacy complaint? If you feel your privacy rights have been violated, contact The Illinois Back Institute s Privacy Officer, or contact the regional Department of Health and Human Services at or Receipt of Notice of Privacy Practices Form Effective June 1, 2004 Updated: October 14, 2009 I,, hereby acknowledge receipt of The Illinois Back Institute s Notice of Privacy Practices. The Illinois Back Institute will use or disclose my PHI for the purposes of carrying out treatment, payment and health care operations. The Notice of Privacy Practices provides detailed information about how the practice may use and disclose my confidential information. I understand The Illinois Back Institute has reserved a right to change its privacy practices that are described in the Notice. I also understand a copy of any Revised Notice will be provided to me or made available at my next office visit. I give my consent for The Illinois Back Institute to notify me of new facilities or services. I understand that I may revoke this consent at any time by giving written notice of my desire to do so, to The Illinois Back Institute. Signed: Date: If you are not the patient, please specify your relationship to the patient.

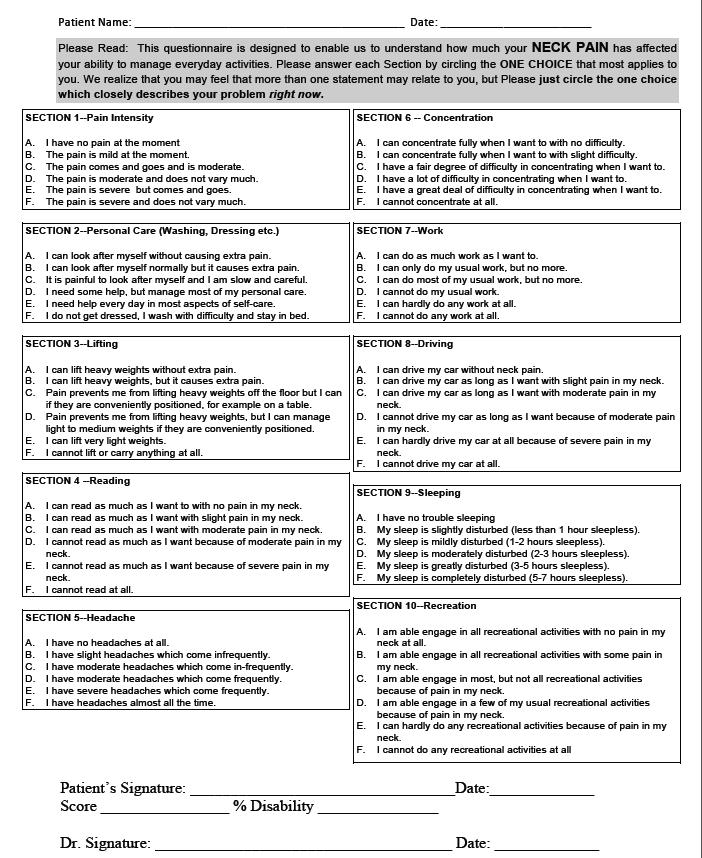
8 Oswestry Pain Questionnaire THE NECK DISABILITY INDEX QUESTIONNAIRE PATIENT NAME: DATE: How long have you had neck pain? years months weeks On the diagram below, please indicate where you are experiencing pain or other symptoms, right now. Please complete both sides of this form. A = ACHE P = PINS & NEEDLES B = BURNING N = NUMBNESS S = STABBING O = OTHER
9
10
11
12
Age: Birthdate: Date of Last Physical exam:
 Name: : Age: Birthdate: of Last Physical exam: SYMPTOMS: Check symptoms you currently have OR have had within the past YEAR. General Fever Chills Weight loss Weight Gain Headache Depression Vertigo Ringing
Name: : Age: Birthdate: of Last Physical exam: SYMPTOMS: Check symptoms you currently have OR have had within the past YEAR. General Fever Chills Weight loss Weight Gain Headache Depression Vertigo Ringing
Dear Patient, Sincerely, Gastroenterology Associates of North Jersey
 GASTROENTEROLOGY ASSOCIATES OF NORTH JERSEY, P.A. Doctors Park 369 West Blackwell Street, Dover, NJ 07801 16 Pocono Road, Suite 210, Denville, NJ 07834 Tel (973) 361-7660 Fax (973) 361-0455 Tel (973) 627-7600
GASTROENTEROLOGY ASSOCIATES OF NORTH JERSEY, P.A. Doctors Park 369 West Blackwell Street, Dover, NJ 07801 16 Pocono Road, Suite 210, Denville, NJ 07834 Tel (973) 361-7660 Fax (973) 361-0455 Tel (973) 627-7600
GRAHAM CHIROPRACTIC CENTER, INC. BRYAN GRAHAM, DC, CCSP
 New Patient Intake Form Patient Information Thank you for choosing our practice for your chiropractic needs. Please fill out this form as completely as possible. If you have any questions or concerns,
New Patient Intake Form Patient Information Thank you for choosing our practice for your chiropractic needs. Please fill out this form as completely as possible. If you have any questions or concerns,
Patient Communication Request
 Patient Communication Request Name: Date of Birth: Address: ZIP: Home Phone: Work Phone: Cell Phone: E-mail address: It is the policy of Capstone Family Practice to contact patients for any lab results.
Patient Communication Request Name: Date of Birth: Address: ZIP: Home Phone: Work Phone: Cell Phone: E-mail address: It is the policy of Capstone Family Practice to contact patients for any lab results.
Patients Name. Insurance policy holders name and Social security number. Address. Home Phone number. Work Phone Number
 Patient Registration Form Print out this form and also the Health History Form. Bring both fully completed forms and your insurance card with you and give them to our staff as you check in for your appointment.
Patient Registration Form Print out this form and also the Health History Form. Bring both fully completed forms and your insurance card with you and give them to our staff as you check in for your appointment.
May Family Chiropractic Health Information and Health History Patient Name: Gender: Male Female
 1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
The process has been designed to be user friendly and involves a few simple steps.
 HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
PATIENT INFORMATION. Last Name: First Name: MI: Date of Birth: SS #: Gender: Male Female. City: State: Zip Code:
 PATIENT DEMOGRAPHIC FORM PATIENT INFORMATION Last Name: First Name: MI: Date of Birth: _ SS #: Gender: Male Female Address: Apt. #: City: State: Zip Code: Home Phone: ( ) - Cell Phone: ( ) - E-mail: Marital
PATIENT DEMOGRAPHIC FORM PATIENT INFORMATION Last Name: First Name: MI: Date of Birth: _ SS #: Gender: Male Female Address: Apt. #: City: State: Zip Code: Home Phone: ( ) - Cell Phone: ( ) - E-mail: Marital
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Name DOB / / SS# / / Street Address City/State/Zip. Home ( ) - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -
 - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -") Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
PATIENT DEMOGRAPHICS. Age: Date of Birth: S.S#:
 WORKERS COMPENSATION PATIENT DEMOGRAPHICS Name: Date: Age: Date of Birth: S.S#: Email: Address: Street Name & Number City State Zip Home Phone #: Cellular #: Wk #: Marital Status: S M W D HOW DID YOU HEAR
WORKERS COMPENSATION PATIENT DEMOGRAPHICS Name: Date: Age: Date of Birth: S.S#: Email: Address: Street Name & Number City State Zip Home Phone #: Cellular #: Wk #: Marital Status: S M W D HOW DID YOU HEAR
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group
 DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Patient Intake Form. Address City State and Zip
 Patient Intake Form Patient Information First Name Last Name Sex: Male Female Birthday Address City State and Zip May we send you text reminders of future appointments? Yes / No Email Phone Number If yes,
Patient Intake Form Patient Information First Name Last Name Sex: Male Female Birthday Address City State and Zip May we send you text reminders of future appointments? Yes / No Email Phone Number If yes,
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL
 Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Office Hours Our office hours are Monday through Friday 7:30 am to 5:30pm. Our office is closed on all major Holidays.
 Dear New Patient: We would like to welcome you to our practice. Our goal is to make your experience with us as pleasant as possible. In order to help us meet this goal we have listed some helpful hints
Dear New Patient: We would like to welcome you to our practice. Our goal is to make your experience with us as pleasant as possible. In order to help us meet this goal we have listed some helpful hints
POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX
 Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient Registration. City, State & Zip Code Date of Birth Age. Occupation: Family Physician: Married Single Other Spouse's Name
 *SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
*SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
ALFRED ALINGU, MD INTERNAL MEDICINE
 Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
ADULT PATIENT INFORMATION. Patient Name: Last Name First Name Address: City: State: Zip Code: Phone #: Cell Phone #: Social Security:
 716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
Dear New Patient. Tarrant County Medical Institute values its patients and is committed to providing them with the highest of quality care.
 Dear New Patient Tarrant County Medical Institute values its patients and is committed to providing them with the highest of quality care. You have made us aware that you will be the responsible party
Dear New Patient Tarrant County Medical Institute values its patients and is committed to providing them with the highest of quality care. You have made us aware that you will be the responsible party
2017 Medi-Slim Weight Loss Patient Information Form
 Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
991 Van Houten Avenue Clifton, NJ Phone: Fax: Website: DrLouisVita.com
 Louis R. Vita, D.D.S., F.A.G.D. Angelo Colavita D.C., BCAO 991 Van Houten Avenue Clifton, NJ 07013 Phone: 973-777-1933 Fax: 973-777-4727 Website: DrLouisVita.com Email: Vitaoffice991@gmail.com Welcome!
Louis R. Vita, D.D.S., F.A.G.D. Angelo Colavita D.C., BCAO 991 Van Houten Avenue Clifton, NJ 07013 Phone: 973-777-1933 Fax: 973-777-4727 Website: DrLouisVita.com Email: Vitaoffice991@gmail.com Welcome!
The Home Doctor. Registration Checklist
 The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
DENTAL PATIENT APPLICATION CHECKLIST
 Robert S. Peterson Building 45580 Woodward Ave Pontiac, MI 48341 248-309-3752-Phone 248-309-3835-Fax www.garyburnsteinclinic.org DENTAL PATIENT APPLICATION CHECKLIST In order to become a patient at the
Robert S. Peterson Building 45580 Woodward Ave Pontiac, MI 48341 248-309-3752-Phone 248-309-3835-Fax www.garyburnsteinclinic.org DENTAL PATIENT APPLICATION CHECKLIST In order to become a patient at the
PATIENT HISTORY. Name Last First Middle/Maiden Name you Prefer. Address Street City State/Zip. Address
 PATIENT HISTORY GENERAL INFORMATION Name Last First Middle/Maiden Name you Prefer Address Street City State/Zip Home Phone ( ) - Cell Phone ( ) - E-Mail Address Age Sex Date of Birth / / Social Security#
PATIENT HISTORY GENERAL INFORMATION Name Last First Middle/Maiden Name you Prefer Address Street City State/Zip Home Phone ( ) - Cell Phone ( ) - E-Mail Address Age Sex Date of Birth / / Social Security#
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
TOS Health Questionnaire
 Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
CURE CARDIOVASCULAR CONSULTANTS
 NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W
 CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W") PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
Allergies Drug Food Environmental. Previous Surgeries & Hospitalizations (Please list date, reason, and hospital)
") Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Patient Health Information Consent Form
 Patient Health Information Consent Form We want you to know how your Patient Health Information (PHI) is going to be used in this office and your rights concerning those records. Before we will begin any
Patient Health Information Consent Form We want you to know how your Patient Health Information (PHI) is going to be used in this office and your rights concerning those records. Before we will begin any
HEALTH. CENTER Main St NE, Suite 101 PO Box 507 Duvall, WA ph fax Dr. Jeffrey P. Metcalf
 Welcome To Our Office Name I prefer to be called First MI Last Home Address: Street City Zip Mailing Address: Street City Zip Phone: ( ) ( ) ( ) Home Cell Work E-mail: Birth : / / Age: Male / Female Marital
Welcome To Our Office Name I prefer to be called First MI Last Home Address: Street City Zip Mailing Address: Street City Zip Phone: ( ) ( ) ( ) Home Cell Work E-mail: Birth : / / Age: Male / Female Marital
PATIENT INFORMATION Indiana Plastic Surgery Center, PC
 PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
NEW PATIENT REGISTRATION FORM
 A New Approach to Healthy Living NEW PATIENT REGISTRATION FORM TODAY S DATE: NAME: MALE FEMALE ADDRESS: CITY: STATE ZIP H ( ) C ( ) W ( ) BEST NUMBER TO REACH YOU? WOULD YOU LIKE APPT REMINDERS TO YOUR
A New Approach to Healthy Living NEW PATIENT REGISTRATION FORM TODAY S DATE: NAME: MALE FEMALE ADDRESS: CITY: STATE ZIP H ( ) C ( ) W ( ) BEST NUMBER TO REACH YOU? WOULD YOU LIKE APPT REMINDERS TO YOUR
Medical History. Patient Information. Dental History. Your current physical health is: Good Fair Poor
 Medical History Your current physical health is: Good Fair Poor Cruse Dental Center complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin,
Medical History Your current physical health is: Good Fair Poor Cruse Dental Center complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin,
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip
 PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
Patient Name:,, Address: Phones:,, Home Work Cell. Primary Physician: Emergency Contact: Phone#:
 Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Columbia Medical Practice- Pediatrics Ken Klebanow M.D. and Associates
 HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
Welcome to our office! Please fill out this form as completely as possible and return it to the desk.
 Welcome to our office! Please fill out this form as completely as possible and return it to the desk. Name of Doctor you wish to see: Today's Date Name Email Address Address Home Male Female Cell City
Welcome to our office! Please fill out this form as completely as possible and return it to the desk. Name of Doctor you wish to see: Today's Date Name Email Address Address Home Male Female Cell City
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
Workers Compensation Demographic
 Workers Compensation Demographic Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg. Cell Phone o OK to Leave Msg. Email Do
Workers Compensation Demographic Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg. Cell Phone o OK to Leave Msg. Email Do
*Family Chiropractic Care* New Patient Information Worksheet*
 *Family Chiropractic Care* New Patient Information Worksheet* Name: SSN: Age: Address: City: State: Zip: Phone Hm: Wk: Date of Birth: E-Mail Employer: Insurance: Policy/I.D. # : Spouses Name: Marital Status:
*Family Chiropractic Care* New Patient Information Worksheet* Name: SSN: Age: Address: City: State: Zip: Phone Hm: Wk: Date of Birth: E-Mail Employer: Insurance: Policy/I.D. # : Spouses Name: Marital Status:
Patient Information. Address: City: State: Zip: Spouse/Guardian s Last 4 Digits S.S. #: Phone: ( ) Cell Phone: ( ) Emergency Contact Information
 Cell Phone: ( ) Emergency Contact Information") Patient Information Patient Name: D.O.B: Marital Status: Age: Address: Gender: Male Female City: State: Zip: Last 4 Digits S.S #: Home: ( ) Cell Phone: ( ) E-mail Address: Patient Occupation: Phone: (
Patient Information Patient Name: D.O.B: Marital Status: Age: Address: Gender: Male Female City: State: Zip: Last 4 Digits S.S #: Home: ( ) Cell Phone: ( ) E-mail Address: Patient Occupation: Phone: (
Norman H. Anderson M.D., P.A. Robert Boissoneault Oncology Institute INSURANCE AUTHORIZATION
 Norman H. Anderson M.D., P.A. D/B/A Robert Boissoneault Oncology Institute 2020 SE 17 th Street Ocala, Fl 34471 522 N. Lecanto Highway Lecanto, FL 34461 605 W. Highland Blvd. Inverness, FL 34452 9401 SW
Norman H. Anderson M.D., P.A. D/B/A Robert Boissoneault Oncology Institute 2020 SE 17 th Street Ocala, Fl 34471 522 N. Lecanto Highway Lecanto, FL 34461 605 W. Highland Blvd. Inverness, FL 34452 9401 SW
PATIENT INFORMATION & CONDITION FORM
 PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
Patient Health Questionnaire - PHQ ACN Group, Inc. - Form PHQ-202 ACN Group, Inc. Use Only rev 7/18/05
 Patient Health Questionnaire - PHQ ACN Group, Inc. - Form PHQ-202 ACN Group, Inc. Use Only rev 7/18/05 Patient Name 1. Describe your symptoms a. When did your symptoms start? b. How did your symptoms begin?
Patient Health Questionnaire - PHQ ACN Group, Inc. - Form PHQ-202 ACN Group, Inc. Use Only rev 7/18/05 Patient Name 1. Describe your symptoms a. When did your symptoms start? b. How did your symptoms begin?
Symptoms and Ill Health (Present State)
") Name Date Address City State Zip Home Phone ( ) Work Phone ( ) Cell ( ) Date of Birth Age ( ) Referred by Friend/Family Yelp Google Other Search Engine Facebook Instagram Groupon Event PhoneBook Occupation
Name Date Address City State Zip Home Phone ( ) Work Phone ( ) Cell ( ) Date of Birth Age ( ) Referred by Friend/Family Yelp Google Other Search Engine Facebook Instagram Groupon Event PhoneBook Occupation
9129 Dickey Drive Mechanicsville, VA 23116
 WELCOME TO STOVER CHIROPRACTIC, P.C. Congratulations on your decision to join the millions of people who are enhancing their lives through regular chiropractic care. We, at, welcome you and will strive
WELCOME TO STOVER CHIROPRACTIC, P.C. Congratulations on your decision to join the millions of people who are enhancing their lives through regular chiropractic care. We, at, welcome you and will strive
Pain Specialists of Greater Chicago Notice of Privacy Practices
 1 Pain Specialists of Greater Chicago Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please
1 Pain Specialists of Greater Chicago Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please
Welcome to the Southeastern Urology Associates meridianemr Patient Portal
 New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
PATIENT APPLICATION FOR TREATMENT
 PATIENT APPLICATION FOR TREATMENT First Name: M.I.: Last Name: What do you prefer to be called: DOB: Age: Address: City: State: Zip Code: Home #: Cell#: Other: SS#: Sex: Single\Married\Divorced\Widow Spouse
PATIENT APPLICATION FOR TREATMENT First Name: M.I.: Last Name: What do you prefer to be called: DOB: Age: Address: City: State: Zip Code: Home #: Cell#: Other: SS#: Sex: Single\Married\Divorced\Widow Spouse
Anne C. Roulo, DC 7501 Murdoch Ave, Shrewsbury, MO, Patient Data Sheet
 Anne C. Roulo, DC 7501 Murdoch Ave, Shrewsbury, MO, 63119 314.484.0690 Patient Data Sheet Date Name: Address: City: State: Zip: Social Security Number: - - Email: Home Phone: ( ) Cell Ph.: ( ) Work Ph.:
Anne C. Roulo, DC 7501 Murdoch Ave, Shrewsbury, MO, 63119 314.484.0690 Patient Data Sheet Date Name: Address: City: State: Zip: Social Security Number: - - Email: Home Phone: ( ) Cell Ph.: ( ) Work Ph.:
Body Basics Physical Therapy Medical History
 Body Basics Physical Therapy Medical History Name Date Age Height Weight Hand Dominance: Right/Left Primary Language Do you require an interpreter? Yes/No How did you hear about us? Doctor s First and
Body Basics Physical Therapy Medical History Name Date Age Height Weight Hand Dominance: Right/Left Primary Language Do you require an interpreter? Yes/No How did you hear about us? Doctor s First and
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c
 W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
BETHESDA DENTAL GROUP
 PLEASE COMPLETE ALLINFORMATION THAT APPLIES TO YOU - THANK YOU PATIENT LAST NAME: FIRST: INITIAL How did you hear about us? Whom may we thank for your referral? Date of Birth: Single: Married: Divorced:
PLEASE COMPLETE ALLINFORMATION THAT APPLIES TO YOU - THANK YOU PATIENT LAST NAME: FIRST: INITIAL How did you hear about us? Whom may we thank for your referral? Date of Birth: Single: Married: Divorced:
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
City. Whom may we thank for referring you to us?
 CAMBRIDGE DENTAL CENTER - PATIENT REGISTRATION Date Patient's Last Name First :Kame MI Age Soc. Sec. No.: Home Work Phone: Home rujul
CAMBRIDGE DENTAL CENTER - PATIENT REGISTRATION Date Patient's Last Name First :Kame MI Age Soc. Sec. No.: Home Work Phone: Home rujul
Patient s Name Home Phone # Last First Middle Would you like reminders sent here? Y N Cell # Address City State Zip
 PLEASE PRINT PATIENT REGISTRATION DATE: Patient s Name Home Phone # Last First Middle E-mail: @ Would you like reminders sent here? Y N Cell # Address City State Zip Social Security # Birthdate Sex Marital
PLEASE PRINT PATIENT REGISTRATION DATE: Patient s Name Home Phone # Last First Middle E-mail: @ Would you like reminders sent here? Y N Cell # Address City State Zip Social Security # Birthdate Sex Marital
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Ivis M. Getz, D.M.D. Caring For Kids Pediatric Dentistry, P.C. 140 Lockwood Avenue, Suite 315, New Rochelle, NY 10801
 How did you hear of our office? New Patient Registration SECTION 1: PATIENT INFORMATION Patient Name: M / F Date of Birth: Address: City: State: Zip Code: SECTION 2: PARENT / GUARDIAN / INSURANCE Name:
How did you hear of our office? New Patient Registration SECTION 1: PATIENT INFORMATION Patient Name: M / F Date of Birth: Address: City: State: Zip Code: SECTION 2: PARENT / GUARDIAN / INSURANCE Name:
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
PATIENT INFORMATION. Address: Sex: City: State: address: Cell Phone: Home Phone: Work Phone: address: Cell Phone:
 PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
MAIN STREET RADIOLOGY
 MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
PS CHIROPRACTIC PATIENT CASE HISTORY
 PS CHIROPRACTIC PATIENT CASE HISTORY Personal Information Last Name First Name Middle Initial Address: City: State: Zip: Home Phone: - - Work Phone: - - Cell Phone: - - Date of Birth: age Social Security
PS CHIROPRACTIC PATIENT CASE HISTORY Personal Information Last Name First Name Middle Initial Address: City: State: Zip: Home Phone: - - Work Phone: - - Cell Phone: - - Date of Birth: age Social Security
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT INFORMATION FORM
 PATIENT INFORMATION FORM Name: E-Mail: New Patient? Previous Patient? Previous name if different: Age: Date of Birth: Social Security #: Sex: Female Male Marital Status: S M W D Home Address: City: State:
PATIENT INFORMATION FORM Name: E-Mail: New Patient? Previous Patient? Previous name if different: Age: Date of Birth: Social Security #: Sex: Female Male Marital Status: S M W D Home Address: City: State:
Cooley Chiropractic. Date of Birth. Married Single Spouse Name. Street City State Zip. . Name. Occupation. Current Symptoms. When Symptoms began
 Please Print Clearly Date NAME: Date of Birth Male Female Married Single Spouse Name Address: Street City State Zip Home Phone Cell Phone E-mail In Case of Emergency please contact: Name Phone Relationship
Please Print Clearly Date NAME: Date of Birth Male Female Married Single Spouse Name Address: Street City State Zip Home Phone Cell Phone E-mail In Case of Emergency please contact: Name Phone Relationship
Patient Information. Address: City: State: Zip: Spouse/Guardian s Last 4 Digits S.S. #: Phone: ( ) Cell Phone: ( ) Emergency Contact Information
 Cell Phone: ( ) Emergency Contact Information") Patient Information Patient Name: D.O.B: Marital Status: Age: Address: Gender: Male Female City: State: Zip: Last 4 Digits S.S #: Home: ( ) Cell Phone: ( ) E-mail Address: Patient Occupation: Phone: (
Patient Information Patient Name: D.O.B: Marital Status: Age: Address: Gender: Male Female City: State: Zip: Last 4 Digits S.S #: Home: ( ) Cell Phone: ( ) E-mail Address: Patient Occupation: Phone: (
Welcome and thank you for choosing Jerman Family Dentistry
 Welcome and thank you for choosing Jerman Family Dentistry We provide dental services for the entire family. The following is helpful information to serve you better as a patient. If there are questions
Welcome and thank you for choosing Jerman Family Dentistry We provide dental services for the entire family. The following is helpful information to serve you better as a patient. If there are questions
NORTHSIDE PARK GASTROENTEROLOGY & ENDOSCOPY CENTER, PLLC
 NORTHSIDE PARK GASTROENTEROLOGY & ENDOSCOPY CENTER, PLLC PATIENT REGISTRATION Today s Date: / / Birthdate: / / S.S. # / / Patient Name: Age: Sex: Last First MI Address: City: State: Zip Code: Home Phone:
NORTHSIDE PARK GASTROENTEROLOGY & ENDOSCOPY CENTER, PLLC PATIENT REGISTRATION Today s Date: / / Birthdate: / / S.S. # / / Patient Name: Age: Sex: Last First MI Address: City: State: Zip Code: Home Phone:
Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care
 Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care We are dedicated to providing the highest quality chiropractic health care
Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care We are dedicated to providing the highest quality chiropractic health care
Last Name: First Name: Sex: Male Female. Birth Date: / / Age: Home Address: Home Phone #: Cell Phone #: Work Phone #:
 Today s Date: / / Last Name: First Name: Sex: Male Female Birth Date: / / Age: Email: Home Address: City: State: Zip Code: Home Phone #: Cell Phone #: Work Phone #: Which is the best number to reach you?
Today s Date: / / Last Name: First Name: Sex: Male Female Birth Date: / / Age: Email: Home Address: City: State: Zip Code: Home Phone #: Cell Phone #: Work Phone #: Which is the best number to reach you?
Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION. Cell Phone ( ) Employer s Name
 Employer s Name") Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION Name Last First M.I. Social Security. Home Address Street City State Zip Mailing Address
Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION Name Last First M.I. Social Security. Home Address Street City State Zip Mailing Address
Entrance Case History (Please write or print clearly)
") Stony Brook Medical Park 2500 Nesconset Highway Suite 4-A Stony Brook, NY 11790 (631) 675-9000 Fax (631) 675-9002 www.naturalapproach.us Entrance Case History (Please write or print clearly) Today s Date
Stony Brook Medical Park 2500 Nesconset Highway Suite 4-A Stony Brook, NY 11790 (631) 675-9000 Fax (631) 675-9002 www.naturalapproach.us Entrance Case History (Please write or print clearly) Today s Date
MOTOR VEHICLE COLLISION QUESTIONNAIRE
 Patient Name: _ : Address: _ City: _ State: Zip Code: Home Ph #: Work Ph #: Cell Ph #: Email: Sex: M F Marital Status: M S D W of Birth: _ Age: _ Occupation: _ Employer: Your Prior Doctor of Chiropractic:
Patient Name: _ : Address: _ City: _ State: Zip Code: Home Ph #: Work Ph #: Cell Ph #: Email: Sex: M F Marital Status: M S D W of Birth: _ Age: _ Occupation: _ Employer: Your Prior Doctor of Chiropractic:
Naturopathic Wellness Center
 Naturopathic Wellness Center Ashley G. Lewin, N.D. Erica Waters, ND Mychael Seubert, ND Pediatric Intake Birth to 3 years Name Sex Date of Birth / / Age Parent(s)/Guardian(s) Address City/State/Zip Telephone
Naturopathic Wellness Center Ashley G. Lewin, N.D. Erica Waters, ND Mychael Seubert, ND Pediatric Intake Birth to 3 years Name Sex Date of Birth / / Age Parent(s)/Guardian(s) Address City/State/Zip Telephone
Patient Demographic Sheet
 Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
History Form. PAST SURGICAL HISTORY Surgeries/Hospitalizations Year Complications/Problems with anesthesia
 History Form Name: Date of Birth: Today's Date: Height: Weight: Date of Injury: Primary Care Physician: Address Who recommended this office? Address CHIEF COMPLAINT Why are you seeing the doctor today?
History Form Name: Date of Birth: Today's Date: Height: Weight: Date of Injury: Primary Care Physician: Address Who recommended this office? Address CHIEF COMPLAINT Why are you seeing the doctor today?
Practice Limited to Infants, Children, & Adolescents
 Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
(Please Print) PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )
 PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )") (Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
(Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
South Florida Neurosurgery REGISTRATION FORM
 MF South Florida Neurosurgery REGISTRATION FORM Today s Date: Primary Care Physician: PATIENT INFORMATION Patient s last name: First: Middle: Marital status: Birth date: Age: Sex: Social Security no.:
MF South Florida Neurosurgery REGISTRATION FORM Today s Date: Primary Care Physician: PATIENT INFORMATION Patient s last name: First: Middle: Marital status: Birth date: Age: Sex: Social Security no.:
Don't forget to bring the following items to your appointment (if available):
:") Dear Thank you for choosing our office. We are EXCITED about helping you enjoy life again without the painful symptoms of peripheral neuropathy! We currently have you scheduled on NOTE: We do our very
Dear Thank you for choosing our office. We are EXCITED about helping you enjoy life again without the painful symptoms of peripheral neuropathy! We currently have you scheduled on NOTE: We do our very
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
School Based Health Consent for Services Grace Community Health Center, Inc.
 School Based Health Consent for Services Grace Community Health Center, Inc. Please read carefully: In order for us to see your child in school based clinics, all pages of this form must be completed by
School Based Health Consent for Services Grace Community Health Center, Inc. Please read carefully: In order for us to see your child in school based clinics, all pages of this form must be completed by
Senior Care Pharmacy Wichita
 Senior Care Pharmacy Wichita 1402 S.RIDGE ROAD WICHITA, KS, 67209 Phone: 316-945-7455 Fax: 316-945-7457 Contact:- Carol Parsons Dear patient/responsible party, Effective immediately, each patient/responsible
Senior Care Pharmacy Wichita 1402 S.RIDGE ROAD WICHITA, KS, 67209 Phone: 316-945-7455 Fax: 316-945-7457 Contact:- Carol Parsons Dear patient/responsible party, Effective immediately, each patient/responsible
WELCOME TO OUR OFFICE!
 WELCOME TO OUR OFFICE! Name Date: / / Address City State Zip Home Phone Cell Phone E-Mail Birthdate Age SS# Race: Marital Status: M W D S Employer Work Phone Occupation Name & Birthdate of Primary Insured
WELCOME TO OUR OFFICE! Name Date: / / Address City State Zip Home Phone Cell Phone E-Mail Birthdate Age SS# Race: Marital Status: M W D S Employer Work Phone Occupation Name & Birthdate of Primary Insured
NEW PATIENT INFORMATION Primary Care Physician
 Last Name NEW PATIENT INFORMATION Primary Care Physician Date: First Name MI Referring Provider Previous Name Date of Birth (mm/dd/yyyy) Address City Gender Male Female Marital Status Single Divorced Married
Last Name NEW PATIENT INFORMATION Primary Care Physician Date: First Name MI Referring Provider Previous Name Date of Birth (mm/dd/yyyy) Address City Gender Male Female Marital Status Single Divorced Married
Name (First): (MI) (Last) Date: Address: City: State: Zip: Home Phone: Cell Phone: Driver s License #: Driver s License State: Occupation:
: (MI) (Last) Date: Address: City: State: Zip: Home Phone: Cell Phone: Driver s License #: Driver s License State: Occupation:") Board Certified & Fellowship Trained in Sports Medicine & Orthopaedic Arthroscopic Surgery 9980 Central Park Blvd North, Suite 222 Boca Raton, FL 33428 Please Print: Name (First): (MI) (Last) Date: Address:
Board Certified & Fellowship Trained in Sports Medicine & Orthopaedic Arthroscopic Surgery 9980 Central Park Blvd North, Suite 222 Boca Raton, FL 33428 Please Print: Name (First): (MI) (Last) Date: Address:
Burton M. Sundin, M.D. / Reps B. Sundin, M.D. Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: address:
: Address: Zip, City, State: Home#: Work#: Cell#: address:") Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
Form B - For those enrolled in other insurance
 Form B - For those enrolled in other insurance PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) Date of Birth
Form B - For those enrolled in other insurance PATIENT REGISTRATION Please print clearly so that we can process your information quickly and efficiently. Thank you! Name (First, M.I., Last) Date of Birth
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with?
 Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
Welcome To Health First Chiropractic
 Welcome To Health First Chiropractic Dear Patient: Please complete this questionnaire. Your answers will help us determine if chiropractic can help you. If we do not sincerely believe your condition will
Welcome To Health First Chiropractic Dear Patient: Please complete this questionnaire. Your answers will help us determine if chiropractic can help you. If we do not sincerely believe your condition will
Spine Solutions By Donald Mackenzie, MD Relieving the pain Healing the spine Rejuvenating the person
 Welcome to by Donald Mackenzie, M.D. Dear Friend, Thank you for choosing me as your spine surgeon. I will personally do everything possible to deserve your trust. I see this as the beginning of a great
Welcome to by Donald Mackenzie, M.D. Dear Friend, Thank you for choosing me as your spine surgeon. I will personally do everything possible to deserve your trust. I see this as the beginning of a great
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W