Office of Billing Compliance 2017 Coding, Billing and Documentation Program. Department of Interventional Radiology
|
|
|
- Marcus Gilmore
- 6 years ago
- Views:
Transcription
1 Office of Billing Compliance 2017 Coding, Billing and Documentation Program Department of Interventional Radiology
2 Top Billed Non-E/M Codes CODE PROCEDURES 7697PR US GUIDE, VASCULAR ACCESS 4908PR ABDOM PARACENTESIS DX/THER W IMAGING GUIDANCE 76942PR SONO GUIDE NEEDLE BIOPSY 10022PR FINE NEEDLE ASP;W/IMAGING GUIDANCE 49424PR CONTRAST INJ,ABSCESS/CYST VIA CATH TUBE 49440PR INSERT GASTROSTOMY TUBE PERCUTANEOUS 76080PR X-RAY FISTULA,ABSCESS,SINUS TRACT 77001PR FLUOROGUIDE CNTRL VEN ACCESS,PLACE,REPLACE,REMOVE 99144PR MOD CONS SED BY SAME PHYS, 5+ YRS, 1ST 0 MIN 20206PR NEEDLE BIOPSY,MUSCLE 2555PR THORACENTESIS NEEDLE/CATH PLEURA W/IMAGING 2
3 All Billed E/M Codes Radiology Vascular Interventional CODE E&M 9921PR OFFICE/OUTPT VISIT,EST,LEVL III PR OFFICE/OUTPT VISIT,NEW,LEVL III PR OBSERVATION CARE DISCHARGE PR OFFICE/OUTPT VISIT,EST,LEVL IV PR SUBSEQUENT HOSPITAL CARE,LEVL II PR SUBSEQUENT HOSPITAL CARE,LEVL I PR OFFICE/OUTPT VISIT,NEW,LEVL IV PR OFFICE/OUTPT VISIT,EST,LEVL II PR OFFICE/OUTPT VISIT,NEW,LEVL II PR INITIAL HOSPITAL CARE,LEVL I PR HOSPITAL DISCHARGE DAY,<0 MIN 5 992PR SUBSEQUENT HOSPITAL CARE,LEVL III PR SUBSEQUENT OBSERVATION CARE,LEVEL I
4 Bell Curves of National E/M Services for IR New Office Visits Interventional Radiology Current Practice Dist. % Variance Practice vs. National E&M Code Count National Dist. % % 4.68% -4.68% % 1.10% -9.1% % 41.05% 4.81% % 0.99% % % 10.18% -9.55% Totals % % Established Office Visits Current Practice Dist. % Variance Practice vs. National E&M Code Count National Dist. % % 2.98% -2.80% % 16.0% -1.47% % 44.78% 5.% % 1.41% % % 4.80% -4.44% Totals % % 1% 0% 5% 4% New Office Visits 85% ` 41% 1% 11% 10% 1% Practice National Established Office Visits 80% 45% 1% ` 16% 17% 0% % % 0% 5% Practice National 4
5 Bell Curves of National E/M Services for IR Initial Hospital Visits Interventional Radiology Current Practice Dist. % Variance Practice vs. National E&M Code Count National Dist. % % 29.95% 57.55% % 40.18% % % 29.87% % Totals % % 88% 0% Initial Hospital Visits 40% 0% ` 1% 0% Practice National Subsequent Hospital Visits Current Practice Dist. % Variance Practice vs. National E&M Code Count National Dist. % % 4.27% -.96% % 4.54% 2.1% % 1.19% % Totals % % Subsequent Hospital Visits 67% 0% 4% 5% 1% ` % Practice National 5
6 2017 Code Changes 6
7 CPT 2017 New Codes Code Description Ultrasound, abdominal aorta, real time with image documentation, screening study for abdominal aortic aneurysm (AAA) Diagnostic mammography, including computer-aided detection (CAD) when performed; unilateral Diagnostic mammography, including computer-aided detection (CAD) when performed; bilateral Screening mammography, bilateral (2-view study of each breast), including computer-aided detection (CAD) when performed 7
8 CPT 2017 Revised Codes Code Description Fluoroscopic guidance for needle placement (eg, biopsy, aspiration, injection, localization device) (List separately in addition to code for primary procedure) 7700 Fluoroscopic guidance and localization of needle or catheter tip for spine or paraspinous diagnostic or therapeutic injection procedures (epidural or subarachnoid) (List separately in addition to code for primary procedure) 8
9 CPT 2017 Deleted Codes Code Description Crosswalk Code Angiography, arteriovenous shunt (eg, dialysis patient fistula/graft), complete evaluation of dialysis access, including fluoroscopy, image documentation and report (includes injections of contrast and all necessary imaging from the arterial anastomosis and adjacent artery through entire venous outflow including the inferior or superior vena cava), radiological S&I Transluminal balloon angioplasty, peripheral artery other than renal, or other visceral artery, iliac or lower extremity, radiological S&I Transluminal balloon angioplasty, each additional peripheral artery other than renal or other visceral artery, iliac or lower extremity, radiological S&I (List separately in addition to code for primary procedure) Transluminal balloon angioplasty, renal or other visceral artery, radiological S&I Transluminal balloon angioplasty, each additional visceral artery, radiological S&I (List separately in addition to code for primary procedure) Transluminal balloon angioplasty, venous (eg, subclavian stenosis), radiological S&I To report, see 6901, 6902, 690, 6904, 6905, 6906 To report, see 6902, 6905, 7246, 7247 To report, see 6902, 6905, 7246, 7247 To report, see 6902, 6905, 7246, 7247 To report, see 6902, 6905, 6907, 7248,
10 CPT 2017 Deleted Codes Code Description 77051Computer-aided detection (computer algorithm analysis of digital image data for lesion detection) with further review for interpretation, with or without digitization of film radiographic images; diagnostic mammography (List separately in addition to code for primary procedure) 77052Computer-aided detection (computer algorithm analysis of digital image data for lesion detection) with further review for interpretation, with or without digitization of film radiographic images; screening mammography (List separately in addition to code for primary procedure) Crosswalk Code To report, see 77065, To report, use
11 New Crosswalk Codes 6901 Introduction of needle(s) and/or catheter(s), dialysis circuit, with diagnostic angiography of the dialysis circuit, including all direct puncture(s) and catheter placement(s), injection(s) of contrast, all necessary imaging from the arterial anastomosis and adjacent artery through entire venous outflow including the inferior or superior vena cava, fluoroscopic guidance, radiological supervision and interpretation and image documentation and report 6902 Introduction of needle(s) and/or catheter(s), dialysis circuit, with diagnostic angiography of the dialysis circuit, including all direct puncture(s) and catheter placement(s), injection(s) of contrast, all necessary imaging from the arterial anastomosis and adjacent artery through entire venous outflow including the inferior or superior vena cava, fluoroscopic guidance, radiological supervision and interpretation and image documentation and report; with transluminal balloon angioplasty, peripheral dialysis segment, including all imaging and radiological supervision and interpretation necessary to perform the angioplasty 690 Introduction of needle(s) and/or catheter(s), dialysis circuit, with diagnostic angiography of the dialysis circuit, including all direct puncture(s) and catheter placement(s), injection(s) of contrast, all necessary imaging from the arterial anastomosis and adjacent artery through entire venous outflow including the inferior or superior vena cava, fluoroscopic guidance, radiological supervision and interpretation and image documentation and report; with transcatheter placement of intravascular stent(s), peripheral dialysis segment, including all imaging and radiological supervision and interpretation necessary to perform the stenting, and all angioplasty within the peripheral dialysis segment 6904 Percutaneous transluminal mechanical thrombectomy and/or infusion for thrombolysis, dialysis circuit, any method, including all imaging and radiological supervision and interpretation, diagnostic angiography, fluoroscopic guidance, catheter placement(s), and intraprocedural pharmacological thrombolytic injection(s) 6905 Percutaneous transluminal mechanical thrombectomy and/or infusion for thrombolysis, dialysis circuit, including all imaging and radiological supervision and interpretation necessary to perform the angioplasty 11
12 New Crosswalk Codes 6906 Percutaneous transluminal mechanical thrombectomy and/or infusion for thrombolysis, dialysis circuit with transcatheter placement of intravascular stent(s), peripheral dialysis segment, including all imaging and radiological supervision and interpretation necessary to perform the stenting, and all angioplasty within the peripheral dialysis circuit 7246 Transluminal balloon angioplasty (except lower extremity artery(ies) for occlusive disease, intracranial, coronary, pulmonary, or dialysis circuit), open or percutaneous, including all imaging and radiological supervision and interpretation necessary to perform the angioplasty within the same artery; initial artery 7247 Transluminal balloon angioplasty (except lower extremity artery(ies) for occlusive disease, intracranial, coronary, pulmonary, or dialysis circuit), open or percutaneous, including all imaging and radiological supervision and interpretation necessary to perform the angioplasty within the same artery; each additional artery (List separately in addition to code for primary procedure) 7248 Transluminal balloon angioplasty (except dialysis circuit), open or percutaneous, including all imaging and radiological supervision and interpretation necessary to perform the angioplasty within the same vein; initial vein 7249 Transluminal balloon angioplasty (except dialysis circuit), open or percutaneous, including all imaging and radiological supervision and interpretation necessary to perform the angioplasty within the same vein; each additional vein (List separately in addition to code for primary procedure) 12

13 New Moderate Sedation Codes (Deleted Previous CPT codes for moderate sedation, ) As a result of the 2017 Physician Fee Schedule, moderate sedation will be separately billed and paid starting in 2017 using new CPT codes. Services for which moderate sedation was previously considered inherent will be accordingly reduced. While this creates greater accuracy and prevents double-payment in instances where a moderate sedation service is provided by a second provider, it creates new billing and workflow requirements. Starting in 2017, Moderate Sedation CPT Codes 99151, 99152, 9915, 99155, 99156, should be used when administering moderate sedation with each procedure. Moderate (also known as conscious) sedation is a drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain cardiovascular function or a patent airway, and spontaneous ventilation is adequate. 1
14 Moderate Sedation Services Provided by the Same Physician Moderate sedation services provided by the same physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports, requiring the presence of an independent trained observer to assist in the monitoring of the patient s level of consciousness and physiological status; initial 15 minutes of intraservice time, patient younger than five years of age ; initial 15 minutes of intra- service time, patient age 5 years or older +9915* ; each additional 15 minutes of intra- service time (List separately in addition to code for primary service) An independent trained observer is an individual who is qualified to monitor the patient during the procedure, who has no other duties (eg, assisting at surgery) during the procedure. 14
15 Moderate Sedation Provided by a Different Physician Moderate sedation services provided by a physician or other qualified healthcare professional other than the physician or other qualified health-care professional performing the diagnostic or therapeutic service that the sedation supports; initial 15 minutes of intra-service time, patient younger than 5 years of age Moderate sedation services provided by a physician or other qualified health-care professional other than the physician or other qualified health-care professional performing the diagnostic or therapeutic service that the sedation supports; initial 15 minutes of intra-service time, patient age 5 years or older * Moderate sedation services provided by a physician or other qualified health care professional other than the physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports; each additional 15 minutes intra-service time (List separately in addition to code for primary service) 15
16 Moderate Sedation Notes Moderate sedation codes 99151, 99152, 9915, 99155, 99156, and G0500 are not used to report administration of medications for pain control, minimal sedation (anxiolysis), deep sedation, or monitored anesthesia care ( ). The new moderate sedation CPT codes published in CPT 2017 will be recognized by all payers. 16
17 Intraservice Time for Moderate Sedation Not the same as intraservice time for the endoscopic procedure. Intraservice time of moderate sedation is used to select the appropriate code(s) to report moderate sedation services: Begins with the administration of the sedating agent(s) (i.e., with the start of the first IV push of the sedating drug): Ends when the procedure is completed, the patient is stable for recovery status, and the physician or other qualified health care professional providing the sedation ends personal continuous face-to-face time with the patient; Includes ordering and/or administering the initial and subsequent doses of sedating agents; Requires continuous face-to-face attendance of the physician or other qualified health care professional; Requires monitoring patient response to the sedating agents, including: o Periodic assessment of the patient; o Further administration of agent(s) as needed to maintain sedation; and o Monitoring of oxygen saturation, heart rate, and blood pressure. 17
18 CPT Guidelines: Preservice Work Preservice Work : The following preservice work components are not included when determining intra-service time for reporting: Assessment of the patient's past medical and surgical history; Review of the patient's previous experiences with anesthesia and/or sedation; Family history of sedation complications; Summary of the patient's present medication list; Drug allergy and intolerance history; Focused physical examination of the patient with emphasis on: Mouth, jaw, oropharynx, neck and airway for Mallampati score assessment, chest and lungs; Heart and circulation; Vital signs, including heart rate, respiratory rate, blood pressure, and oxygenation with end tidal CO2 when indicated; Review of any pre-sedation diagnostic tests; Completion of a pre-sedation assessment form (with an American Society of Anesthesiologists [ASA] Physical Status classification); Patient informed consent; Immediate pre-sedation assessment prior to first sedating doses; and Initiation of IV access and fluids to maintain patency. 18
19 CPT Guidelines: Intraservice Work Intraservice Work: Intraservice time is used to determine the appropriate CPT code to report moderate sedation services. CPT indicates Intraservice time starts with the administration of the sedation agent(s), requires continuous face-to-face attendance, and ends at the conclusion of personal contact by the physician providing the sedation. In other words, the clock starts when the drug is administered and ends when the physician leaves the patient s room. If the physician or other qualified health care professional who provides the sedation services also performs the procedure supported by sedation (99151, 99152, 9915), the physician or other qualified health care professional will supervise and direct an independent trained observer who will assist in monitoring the patient's level of consciousness and physiological status throughout the procedure. throughout the procedure. 19
20 CPT Guidelines: Postservice Work Postservice Work: The postservice activities required for moderate sedation are included in the work described by each of these codes and are not reported separately. Once continuous face-to-face time with the patient has ended, additional face-to-face time with the patient is not added to the intraservice time, however, it is considered as part of the postservice work. The following postservice work components are not included, when determining intraservice time for reporting: Assessment of the patient's vital signs, level of consciousness, neurological, cardiovascular, and pulmonary stability in the postsedation recovery period; Assessment of the patient's readiness for discharge following the procedure; Preparation of documentation regarding sedation service; and Communication with family/caregiver regarding sedation service. Postservice work/times are not used to select the appropriate code. 20
21 Documentation Requirements Patient s age History, physical and diagnostic test(s) reviews, as appropriate when performing sedation. Duration of moderate sedation. Intraservice time should be documented based on the specific number of minutes, as opposed to a range of time, to meet all payer requirements. If the physician does not document his/her intraservice time or if the time is less than 10 minutes, the service is not reportable. Who provided the sedation and procedure(s). Pre- and post-sedation assessment and/or monitoring. Additionally, when the clinician is performing both the sedation and procedure, the medical record should reflect the identity of the trained observer who was present, when appropriate. It is also important that providers do not rely on the drug name to communicate whether moderate sedation was provided. Providers need to use the terms moderate or conscious sedation, in combination with intraservice time, to ensure the reader of the record understands moderate sedation was performed and the time recorded was intraservice. It is important to note here that deep sedation is not reportable for these codes. 21
22 RVU Values CPT Description Total RVUs Moderate Sedation, same physician performing the procedure, initial 15 minutes, < 5 years (Requires independent trained observer) Moderate Sedation, same physician performing the procedure, initial 15 minutes, 5 years or older (Requires independent trained observer) Moderate Sedation, same physician performing the procedure, each additional 15 minutes (Requires independent trained observer) Moderate Sedation, other physician performing the procedure, initial 15 minutes, < 5 years Moderate Sedation, other physician performing the procedure, initial 15 minutes, 5 years or older Moderate Sedation, other physician performing the procedure, each additional 15 minutes
23 Time Requirements To Bill Moderate Sedation Total Intraservice Time for Moderate Sedation Patient Age Moderate Sedation performed by the same provider performing the procedure that Moderate Sedation is supporting Code(s) Moderate Sedation performed by different provider performing the procedure that Moderate Sedation is supporting Code(s) Less than 10 Minutes Any Age Not Reported Separately Not Reported Separately Minutes < 5 Years Minutes 5 Years or > Minutes < 5 Years X X Minutes 5 Years or > X X Minutes < 5 Years X X Minutes 5 Years or > X X 2 2
24 Documentation When 2 nd Clinician As a result of the decreased threshold for the minimum time requirement and the RVU values the Centers for Medicare & Medicaid Services (CMS) assigned to the moderate sedation services, an increase in the volume reported is anticipated. Subsequently, with payments come heightened scrutiny regarding documentation, particularly when a second clinician is providing the sedation service. Given the substantial RVU variance when different providers are performing the sedation and related procedure, documentation must meet all requirements while simultaneously reflecting the medical necessity of having two clinicians involved. 24
25 Local Coverage Determinations (LCDs) 25
26 Creation and Purpose of LCD Local Coverage Determinations (LCDs) are created by the Medicare Administrative Contractor (MAC) Local contractor level Contractor Medical Directors responsibility May or may not be associated with a National Coverage Determination (NCD) Assist in determining reasonable and necessary criteria LCDs cannot restrict or conflict with an NCDs Or any CMS interpretive manuals 26

27 Locating LCDs 27
28 Local Coverage Determinations (LCDs) for First Coast Service Options, Inc. Id Title Effective Date Revision Effective Date End Dat e Last Updated Status Select All L256 D Interpretatio n and Reporting of Imaging Studies 10/01/15 10/01/16 N/A 09/28/16 Active D Interpretation and Reporting of Imaging Studies 28
29 On-going Inquiry By CMS 7676: D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality with image post-processing under concurrent supervision; not requiring image post-processing on an independent workstation 7677: D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality with image post-processing under concurrent supervision; requiring image post-processing on an independent workstation 29
30 7676 and LIMITATIONS In freestanding and independent diagnostic testing facilities, Medicare expects the referring physician to generate an appropriate written request indicating the clinical need for the additional D imaging, that a copy of that request be maintained by the interpreting physician and the interpreting physician s report addresses those specific clinical issues. In the event that a D interpretation is deemed urgently needed by the radiologist and the referring physician is not immediately available, the radiologist must document the time of the study, the specific need for the study, and a summary of the findings that were urgently transmitted to the practitioner named as the referring physician on the radiology report. CPT codes 7676 and 7677 may be considered medically unnecessary and denied if equivalent information obtained from the test has already been provided by another procedure (magnetic resonance imaging, ultrasound, angiography, etc.) or could be provided by a standard CT scan (two-dimensional) without reconstruction. Medicare expects that no more than 20 percent of the total Computerized Tomography (CT) and Magnetic Resonance (MR) imaging of any practice be submitted with -D rendering or interpretation, with or without image post-processing. However, for cancer evaluation applications, such as staging/monitoring for pulmonary metastases, this threshold may be often exceeded. Therefore, if data suggests providers are billing at higher rates for other indications for D rendering, then Medical Review may do pre or post pay reviews to validate the use and medical necessity of the test. All imaging studies will be subject to the American College of Radiology Guidelines for reporting. CPT code 7676 can be reported when D rendering is performed by a radiologist or a speciallytrained technologist at the acquisition scanner. However, CPT code 7677 is reported when the D post-processing images are reconstructed on an independent workstation with concurrent physician supervision. In order to report 7677, the supervising physician must provide concurrent supervision. 0
31 7676 and LIMITATIONS In order to report the correct CPT code for the D analysis (7676 or 7677), it should be documented within the radiology report as to whether the D was performed on an independent workstation or on the acquisition scanner. Making an explicit statement within the radiology report will avoid ambiguity, and aid the coder in accurately coding for the D reconstruction. Some practices may separately document this in the patient s electronic medical record, but not actually in the report. Imaging studies are complex with thousands of individual pictures. Beyond identifying a fracture in an emergency setting a discussion of treatment planning after the patient has left the department is common. D may be necessary to understand the anatomy for treatment planning. This discussion occurs after the acute event. Another vignette is an imaging study for stroke but later a seizure concern is identified subsequent to the emergency visit and D is applied to evaluate an anatomy of the hippocampus for a seizure focus. 1
32 ICD-10 Codes That Support Medical Necessity Group 1 Paragraph: Note: All primary diagnosis codes must be related to the primary procedural code when rendered for the -D reconstruction. The use of these diagnosis codes implies the medical necessity of the -D rendering and interpretation, as outlined in this LCD, is documented in the medical record. A written request for the study from the referring physician must also be in the medical record and made available upon request when performed in freestanding and independent diagnostic testing facilities. The following lists include only those secondary diagnoses for which the identified CPT/HCPCS procedures are covered. Note: If a covered secondary diagnosis is not on the claim, the edit will automatically deny the service as not medically necessary. 2
33 Covered ICD-10 Codes for 7676 & 7677 Group 1 ICD-10 Description R90.82 White matter disease, unspecified R91.8 Other nonspecific abnormal finding of lung field R9.0 Abnormal findings on diagnostic imaging of skull and head, not elsewhere classified R9.1 Abnormal findings on diagnostic imaging of heart and coronary circulation R9. Abnormal findings on diagnostic imaging of other parts of digestive tract R9.4 Abnormal findings on diagnostic imaging of urinary organs R9.5 Abnormal findings on diagnostic imaging of other abdominal regions, including retroperitoneum R9.6 Abnormal findings on diagnostic imaging of limbs R9.7 Abnormal findings on diagnostic imaging of other parts of musculoskeletal system R9.8 Abnormal findings on diagnostic imaging of other specified body structures
34 Covered ICD-10 Codes for 7676 & 7677: Group 2: Covered primary diagnosis for deep brain stem lead placement only. ICD-10 Codes Description G20 Parkinson's disease G21.4 Vascular parkinsonism G24.1 Genetic torsion dystonia G24. Spasmodic torticollis G24.9 Dystonia, unspecified G25.0 Essential tremor G25.1 Drug-induced tremor G25.2 Other specified forms of tremor 4
35 Documentation Requirements Documentation supporting the medical necessity should be legible, maintained in the patient s medical record and made available to Medicare upon request. Use of one of the secondary diagnosis codes in this LCD implies medical necessity for -D rendering and interpretation. Documentation supporting medical necessity must be maintained in the medical record along with the written request for the study from the referring physician. D Reconstruction services are to be reported by a separate report or in a separate section of the base service report. A permanent archive of D studies of CTA studies is suggested by the ACR. 5
36 Tips for Coding Selective Catheters The coding is extrapolated from practitioner documentation! First identify the point(s) of access where sheath has been placed (i.e., femoral, radial, jugular, brachial, etc.) Determine the approach (i.e., ipsilateral (same side) or contralateral (opposite sides)). Determine the point(s) of the highest level where the catheter was manipulated. The CPT code for selective catheterization supersedes CPT codes for non selective catheterization. Never code for both selective and non selective catheter placement from the same access and in the same vascular family. Code all imaging studies performed. Code for each vascular family separately. Code for each access separately. Code additional second or third order catheterizations within a family. Code for additional imaging studies within a family above the basic examination. 6
37 Additional Tips for Catheter Placement 1) Code to the highest order selective cath placement within each vascular family 2) Code the selective cath placement only if both nonselective & selective placements are performed from one access point ) Code each separate access site 4) All vessels imaged with documentation of findings in the report can be assigned the S&I codes more than once, even if they were not individually selected & if the code does not have the code narrative selective exceptions 5) Aorta takes precedence over other nonselective codes 6) Code each vascular family separately, using modifiers to distinguish the different vessels 7) Code to where the tip of the cath is, not to the tip of the wire 8) Do not code for injecting small amounts of contrast to localize a vessel for subsequent selection Coding Tips 7
38 Documentation of Device Position The final position of all devices inserted permanently or long-term with imaging guidance (eg, stents, endovascular grafts, central venous catheters, inferior vena cava filters, embolic agents, drainage catheters) should be documented with imaging. Benefits of documenting device position should be weighed against ionizing radiation risks of x-ray documentation (eg, in pregnancy). 8
39 ARCHIVING OF IMAGES General Principles All pertinent imaging data should be saved in permanently retrievable digital or hard-copy format. Examples of pertinent imaging data include: The relevant anatomy that will affect patient management, device position, complications, and transient adverse events (such as emboli) that might have been successfully treated during a given procedure. If ultrasound guidance is used to gain entry into a blood vessel, it is optional to save a sonographic image of this blood vessel. 9
40 Diagnosis Coding International Classification of Disease (ICD-10) ICD-10 compliance Relying on the information that comes across with each order to dictate the clinical information section of reports. Is that sufficient? Using report templates that pull this information directly from the order. For example, the text might read Special instructions: r/o pulmonary embolism along with the actual ICD-10 code. What is the best approach? 40
41 Choosing the Primary ICD-10 Code Confirmed Diagnosis Based on Results of Test Report any confirmed diagnosis Signs and/or symptoms may be reported as additional diagnoses Signs/Symptoms If the diagnostic test did not provide a diagnosis or was normal, the interpreting physician should code the sign(s) or symptom(s) that prompted the treating physician to order the study. On the rare occasion when the interpreting physician does not have diagnostic information as the reason for the test and the referring physician is unavailable to provide such information, it is appropriate to obtain the information directly from the patient or the patient s medical record if it is available. However, an attempt should be made to confirm any information obtained from the patient by contacting the referring physician. (Language removed in latest version of MCPM Chapter 2, Section
42 Choosing the Primary ICD-10 Code Uncertainty: Considered by the ICD-10-CM Coding Guidelines as unconfirmed and should not be reported Do not code the following diagnoses: Probable Suspected Questionable Rule out Working diagnosis Other similar terms indicating uncertainty. Code to the highest degree of certainty (symptoms, signs, abnormal test results, or other reason for the visit) 42
43 Modifiers
44 Consultation on Previous Interpretation 77 Repeat Procedure or Service by Another Physician or Other Qualified Health Care Professional: It may be necessary to indicate that a basic procedure or service was repeated by another physician or other qualified health care professional subsequent to the original procedure or service. This circumstance may be reported by adding modifier 77 to the repeated procedure or service. 44
45 Second Reads Reference Medicare Claims Processing Manual, Chapter 1, Radiology Services and Other Diagnostic Procedures ( Guidance/Guidance/Manuals/Downloads/clm104c1.pdf Generally, carriers must pay for only one interpretation of an EKG or x-ray procedure furnished to an emergency room patient. They pay for a second interpretation (which may be identified through the use of modifier -77 ) only under unusual circumstances (for which documentation is provided) such as a questionable finding for which the physician performing the initial interpretation believes another physician s expertise is needed or a changed diagnosis resulting from a second interpretation of the results of the procedure. - 45
46 Modifier 76 Fact Sheet Repeat Procedure by the Same Physician; use when it is necessary to report repeat procedures performed on the same day. Appropriate Usage On procedure codes that cannot be quantity billed Report each service on a separate line, using a quantity of one and append 76 to the subsequent procedures The same physician performs the services Inappropriate Usage Repeat services due to equipment or other technical failure For services repeated for quality control purposes Additional Information Medicare considers two physicians, in the same group with the same specialty performing services on the same day as the same physician 46
47 CPT Code 76140: Consultation on X-ray examination made elsewhere, written report You should only report if a physician from another institution requests your physician's opinion on a radiograph and you send that physician your interpretation. You should not report if a physician within your practice or hospital asks you to reread an x-ray that was primarily interpreted by another physician within the same practice. Instead, report when you interpret an imaging study that was primarily obtained and interpreted by a physician from a different practice and with a different provider number. Medicare and some private payers assign "0" relative value units to and will not reimburse you for this service. If your commercial insurer allows payment for this service, ask for the coverage guidelines in writing before billing to avoid unnecessary denials. Your practice should establish a policy related to billing the patient for reinterpretations of outside films. If you intend to bill for this service, you should obtain an advance beneficiary notice for patients whose payers do not provide payment for
48 Referring/Treating Physician and Orders Orders must be specific to the diagnostic test requested. Diagnostic tests require documentation of the name of the referring/ordering provider. Absent a valid ordering provider the claim will be denied. Notations such as Chest X-ray requested by Cardiology Service are not acceptable must be person specific 48
49 Treating Practitioner to Order all Tests Limited exceptions: Allows additional testing to be done by the radiologist prior to or without contacting the treating physician/practitioner, when the radiologist determines that based on the result of an ordered diagnostic test, an additional diagnostic test should be performed. All of the following criteria must be met: The diagnostic test ordered by the treating practitioner is performed; Radiologist determines and documents that, because of the abnormal result of the diagnostic test performed, an additional diagnostic test is medically necessary; A delay in additional diagnostic testing would have an adverse effect on the care of the patient; The result of the test is communicated to and is used by the treating practitioner in the treatment of the patient; and The radiologist documents in his/her report why additional testing was done. 49
50 The Interpreting Physician May: Determine the test design, unless specified in the order. The interpreting physician may determine, without notifying the treating physician/practitioner, the parameters of the diagnostic test (e.g., number of radiographic views obtained, thickness of tomographic sections acquired, use or non-use of contrast media). An order for MRI of orbit without a specific contrast component would allow the interpreting physician to determine if contrast was medically appropriate for that specific patient without obtaining an updated order. Modify, without notifying the treating physician/practitioner, an order with clear and obvious errors that would be apparent to a reasonable layperson, such as the patient receiving the test (e.g., x- ray of wrong foot ordered). 50
51 Conditional Orders CMS has approved the use of conditional orders as long as they are limited to a specific patient. Example: a patient-specific order reads: Diagnostic mammogram of right breast with ultrasound, as indicated, the radiologist may add the ultrasound to characterize the mass. A standing order for all patients of a given treating physician/practitioner (e.g., if gallbladder ultrasound for Dr. Smith is negative, do UGI ) is not acceptable. The conditional order process can be replicated across diagnostic testing modalities (i.e., CT; MRI; Ultrasound; etc) with the understanding that such conditional orders MUST BE patientspecific.
 Clinical signs or symptoms or personal history of")
52 Radiological Reports This becomes crucial in cases with negative or inconclusive findings! Elements of the report Clinical Information must include: Referring/ordering Physician Patient Demographics (unless readily available in the EMR) Clinical signs or symptoms or personal history of disease Body of the report should include Description of the procedure including anatomical area, modality, and use of contrast. Describes if and why additional testing was done. Impression Revises or confirms initial diagnosis If findings are negative coding is based on signs or symptoms All coding must be abstracted from the Body of the report and not from headers. 52

53 Teaching Physicians (TP) Guidelines Billing Services When Working With Residents Fellows and Interns All Types of Services Involving a resident with a TP Requires Appropriate Attestations In EHR or Paper Charts To Bill 5
54 High-Risk Procedures & Diagnostic Services Complex or high-risk procedures: Requires personal (in person) supervision of its performance by a TP and is billable only when the TP is present with the resident for the entire procedure. These procedures typically include cardiac and other interventional services. Example: Dr. TP (or I) was present for the entire (identify procedure). Diagnostic services with an interpretation: If documented by a resident to be billed by a TP requires that s/he personally document that s/he personally reviewed the images, tracing, slides etc. and the resident s interpretation and either agrees with it or edits the findings. Example: I personally reviewed the films (and/or slides etc.) and agree with the resident s findings. 54
55 Diagnostic Procedures RADIOLOGY AND OTHER DIAGNOSTIC TESTS General Rule: The Teaching Physician may bill for the interpretation of diagnostic Radiology and other diagnostic tests if the interpretation is performed or reviewed by the Teaching Physician with modifier 26 in the hospital setting. Teaching Physician Documentation Requirements: Teaching Physician prepares and documents the interpretation report. OR Resident prepares and documents the interpretation report The Teaching Physician must document/dictate: I personally reviewed the film/recording/specimen/images and the resident s findings and agree with the final report. A countersignature by the Teaching Physician to the resident s interpretation is not sufficient documentation. 55
56 Minor (< 5 Minutes): For payment, a minor procedure billed by a TP requires that s/he is physically present during the entire procedure. Example: I was present for the entire procedure. Major (>5 Minutes) TP Guidelines for Procedures SINGLE Procedure / Surgery When the teaching surgeon is present or performs the procedure for a single non-overlapping case involving a resident, he/she or the resident can document the TP s physical presence and participation in the surgery. Example: I was present for the entire procedure (or key and critical portions & description of the key and critical portions of the procedure and immediately available). Endoscopy Procedures (excluding Endoscopic Surgery): TP must be present during the entire viewing for payment. The viewing begins with the insertion and ends with the removal. Viewing of the entire procedure through a monitor in another room does not meet the presence requirement. Example: I was present for the entire viewing. 56
57 Evaluation and Management (E/M) E/M IP or OP: TP must personally document by a personally selected macro in the EMR or handwritten at least the following: That s/he was present and performed key portions of the service in the presence of or at a separate time from the resident; AND The participation of the teaching physician in the management of the patient. Initial Visit: I saw and evaluated the patient. I reviewed the resident s note and agree, except that the picture is more consistent with an upper respiratory infection not pneumonia. Will begin treatment with... Initial or Follow-up Visit: I saw and evaluated the patient. Discussed with resident and agree with resident s findings and plan as documented in the resident s note. Follow-up Visit: See resident s note for details. I saw and evaluated the patient and agree with the resident s finding and plans as written. Follow-up Visit: I saw and evaluated the patient. Agree with resident s note, but lower extremities are weaker, now /5; MRI of L/S Spine today. The documentation of the Teaching Physician must be patient specific. 57
58 Evaluation and Management (E/M) Time Based E/M Services: The TP must be present and document for the period of time for which the claim is made. Examples : Critical Care Hospital Discharge (>0 minutes) or E/M codes where more than 50% of the TP time spent counseling or coordinating care Medical Student documentation for billing only counts for ROS and PFSH. All other contributions by the medical student must be re-performed and documented by a resident or teaching physician. 58
59 Florida Medicaid Teaching Physician Guidelines TEACHING PHYSICIANS WHO SEEK REIMBURSEMENT FOR OVERSIGHT OF PATIENT CARE BY A RESIDENT MUST PERSONALLY SUPERVISE ALL SERVICES PERFORMED BY THE RESIDENT. PERSONAL SUPERVISION PURSUANT TO RULE 59G (276), F.C.A, MEANS THAT THE SERVICES ARE FURNISHED WHILE THE SUPERVISING PRACTITIONER IS IN THE BUILDING AND THAT THE SUPERVISING PRACTITIONER SIGNS AND DATES THE MEDICAL RECORDS (CHART) WITHIN 24 HOURS OF THE PROVISION OF THE SERVICE. 59
60 Modifier GC CMS Manual Part - Claims Process - Transmittal 172 Teaching Physician Services That Meet the Requirement for Presence During the Key Portion of the Service when working with a resident or fellow Teaching Physician Services that are billed using this modifier are certifying that they have been present during the key portion of the service. 60
61 Inpatient and Outpatient Evaluation and Management E/M Documentation and Coding 61
62 Putting The Puzzle Together 62




63 The Key Documentation Elements History Focus on HPI Physical Exam Medical Decision Making 6
64 Elements of an E/M History The extent of information gathered for history is dependent upon clinical judgment and nature of the presenting problem. Documentation of the patient s history includes some or all of the following elements: Chief Complaint (CC) & History of Present Illness (HPI) WHY IS THE PATIENT BEING SEEN TODAY Review of Systems (ROS) related to HPI, Past Family, Social History (PFSH) related to HPI. 64
 Detailed (D)")
65 EXAMINATION 4 TYPES OF EXAMS Problem focused (PF) Expanded problem focused (EPF) Detailed (D) Comprehensive (C) 65
66 1995: Physical Exam BODY AREAS (BA): Head, including face Neck Chest, including breast and axillae Abdomen Genitalia, groin, buttocks Back, including spine Each extremity CODING ORGAN SYSTEMS (OS): Constitutional/General Eyes Ears/Nose/Mouth/Throat Respiratory Cardiac GI GU Musculoskeletal Skin Neuro Psychiatric Hematologic/Lymphatic 66
67 PHYSICAL EXAM: General Multi-System Examination ( BA/OS) Elements of Examination BA Head, including the face BA Neck: neck (masses, symmetry, etc); thyroid BA Chest (Breasts): inspection breast; palpation breast/axillae BA Abdomen BA Genitalia, groin, buttocks BA Back, including spine BA Left upper extremity BA Right upper extremity BA Left lower extremity BA Right lower extremity OS Constitutional: vitals (sit/stand BP; sup BP; temp; pulse rate; resp; ht; wt) or General appearance OS Eyes: conjunctivae/lids; pupils/irises; optic discs OS Ears, Nose, Mouth/Throat: exam ears/ nose; exam auditory canal/tympanic membrane; hearing assessment; Exam nasal mucosa/septum/turbinates; exam lips/teeth/gums; exam oropharynx/palates OS Respiratory: respiratory effort; percussion of chest; palpation of chest; auscultation of lungs OS Cardiovascular: palpation heart; auscultation; Exam of: carotid; femoral arteries; abd aorta; pedal pulses; Exam extremities for edema/varicosities OS Gastrointestinal: exam of abd; exam liver/spleen; hernia +/-; exam anus, perineum, rectum; stool specimen if appropriate OS Genitourinary: Male: exam of scrotum; exam of penis; DRE of prostate; Female: exam ext genitalia, vagina, urethra, bladder, cervix, uterus, adnexa/parametria OS Musculoskeletal: gait/station; inspect digits/nails; inspect/rom/stability/strength of head/neck, spine/rib/pelvis (Rt upper, Lt upper, Rt lower, Lt lower extremities can be OS also) OS Skin: inspect skin/subcutaneous tissue; palpation skin/subcutaneous tissue OS Neurologic: test cranial nerves; deep tendon reflexes, sensations OS Psychiatric: judgment/ insight; orientation to person/place/time; recent/remote memory; mood & affect OS Hematological/lymphatic palpation of nodes neck, axillae, groin, other 67
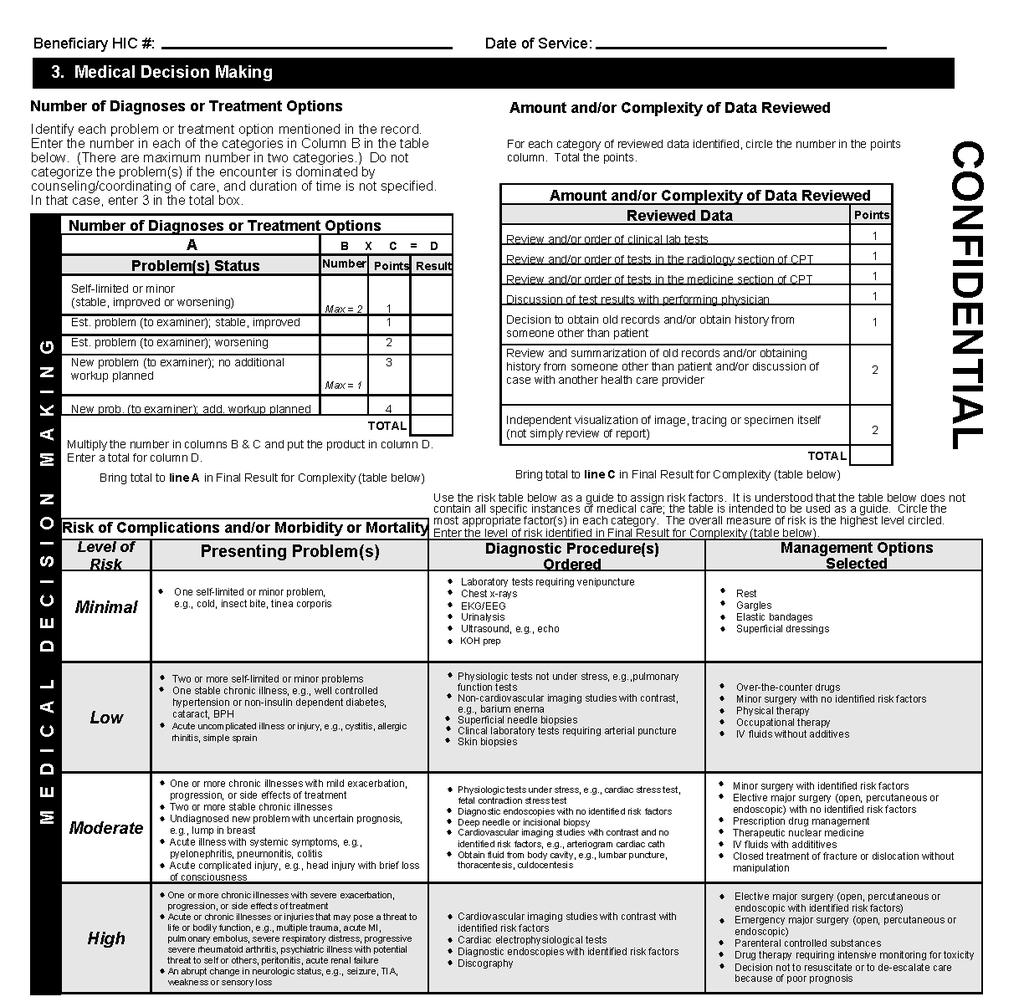
68 Medical Decision Making DOCUMENT EVERYTHING THAT EFFECTS YOUR SERVICE!! Include all diagnosis that impact the service. Exchange of clinically reasonable and necessary information and the use of this information in the clinical management of the patient Step 1: Number of possible diagnosis and/or the number of management options. Step 2: Amount and/or complexity of data reviewed, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed. Step : The risk of significant complications, morbidity, and/or mortality with the patient s problem(s), diagnostic procedure(s), and/or possible management options. Note: The 2 most complex elements out of will determine the overall level of MDM 68
69
70 Q&A From First Coast How to determine further work-up under number of diagnoses Q. In medical-decision making, how does one determine further work-up under number of diagnoses? A. A key element of the medical-decision making category includes management decisions made by the physician to determine a diagnosis and treatment. Evidence of further work-up within documentation would include: indicating a problem is worsening/probable and/or listing possible management options, advice sought, referrals or consultations, and the initiation of or change in treatment. 70
71 Using Time to Code an E/M Time shall be considered for coding an E/M in lieu of H-E-MDM when > 50% of the total billable practitioner visit time is counseling/coordination of care (CCC.) Time is only Face-to-face for OP setting Coding based on time is generally the exception & is typically used for: Exacerbation or change in the patient s condition or new diagnosis, Non-compliance with the treatment/plan, Counseling regarding previously performed procedures or tests to determine future treatment options Issues that may not lend themselves to typical E/M encounter. Examples: Behavior/school issues, ADHA Non-compliance with medications or treatments Introduction of new medications or treatments 71

72 Using Time to Code an E/M Required Documentation For Billing: 1. Total time of the encounter excluding separate procedure if billed 2. The amount of time dedicated CCC for that patient on that date of service.. A template statement would not meet the documentation requirements. 4. The documentation MUST be individualized for each patient visit! 5. Check boxes for time and check boxes for CCC are NOT acceptable for coding an E/M service based on time. 72
73 Counseling/Coordination of Care CCC Proper Language used in documentation of time: I spent minutes with the patient and family and over 50% was in counseling about her diagnosis, treatment options including and. I spent minutes with the patient and family more than half of the time was spent discussing the risks and benefits of treatment with (list risks and benefits and specific treatment) This entire minute visit I spent counseling the patient regarding and addressing their multiple questions. Total time spent and the time spent on counseling and/or coordination of care must be documented in the medical record. Documentation must reflect the specific issues discussed with patient present. Document the specific topics that were discussed during the counseling (i.e. diagnosis, prognosis, treatment options, medical management and side effects, etc). 7
74 Time-Based Billing for CCC Outpatient Counseling Time: min min min min min min min min min min min min min min min Inpatient Counseling Time: min min min min min min min min min min min 74
75 Observation Services The CMS Claims Processing Manual indicates that for a physician to bill the initial observation care codes, there must be a medical observation record for the patient which contains dated and timed physician s admitting orders to observation status. The observation record should reflect the care the patient receives while in observation, nursing notes, and progress notes prepared by the physician while the patient was in observation status. This record must be in addition to any record prepared as a result of an emergency department or outpatient clinic encounter. 75
76 Observation Services Documentation Requirements: If the patient requires to be admitted to observation, the physician must clearly document in the order place patient into observation status. The physician must also document the medical reasons why the patient requires to be admitted to observation on the physician s orders. The order must be signed and dated by the attending physician. The physician s order to admit the patient to observation must have the time the patient was admitted to observation and the time the patient is discharged from observation. 76
77 Observation Services Procedure Codes: 99218, 99219, 99220, and Outpatient observation services require monitoring by a physician and other ancillary staff, which are reasonable and necessary to evaluate the patient s condition. These services are only considered medically necessary when performed under a specific order of a physician. Outpatient observation services are not to be used for the convenience of the hospital, its physicians, patients, patients families, or while waiting placement to another facility. Outpatient observation services, generally, do not exceed 24 hours. Some patients may require a second day of observation up to a maximum of 48 hours. At 24 hours, the physician should evaluate patient s condition to decide if the patient needs to remain in observation for an additional 24 hours. 77
78 INITIAL OBSERVATION CARE SERVICES 99218, 99219, The codes to use when an observation stay spans more than one calendar date include: Initial observation care for problems of low severity. Documentation requires a detailed or comprehensive history, a detailed or comprehensive exam, and straightforward or low complexity MDM Initial observation care for problems of moderate severity. Documentation requires a comprehensive history, a comprehensive exam, and moderate complexity MDM Initial observation care for problems of high severity. Documentation requires a comprehensive history, a comprehensive exam, and high complexity MDM. PROCEDURE CODE HISTORY EXAMINATION MEDICAL DECISION- MAKING Detailed or Comprehensive Detailed or Comprehensive Straightforward or Low Complexity Comprehensive Comprehensive Moderate Complexity Comprehensive Comprehensive High Complexity 78
79 SUBSEQUENT OBSERVATION SERVICES All levels of Subsequent Observation Care ( ) include reviewing the medical record and reviewing the results of diagnostic tests and changes in the patient s status (i.e., changes in the history, physical condition and response to management) since the last assessment by the physician. Subsequent Observation Care Codes are TIME-BASED CODES and time spent at bedside and on Hospital floor unit must be documented by the physician. At 48 hours, the physician should re-evaluate patient s condition and decide if patient needs to be admitted to the hospital or discharged home. Outpatient observation time begins when the patient is physically placed in the observation bed. Outpatient observation time ends at the time it s documented in the physician s discharge orders. 79
80 SUBSEQUENT OBSERVATION CARE SERVICES, CONTINUED Two out of the three components must be documented. Time spent must be documented. PROCEDURE CODE HISTORY EXAMINATION MEDICAL DECISION- MAKING Detailed or Comprehensive Detailed or Comprehensive Straightforward or Low Complexity 15 Min Comprehensive Comprehensive Moderate Complexity 25 Min Comprehensive Comprehensive High Complexity 5 Min. 80
81 OBSERVATION CARE DISCHARGE Observation care discharge includes services on the date of observation discharge (can only be used on a calendar day other than the initial day of observation). These services include a final exam, discussion of the observation stay, follow-up instructions, and documentation. 81
82 OBSERVATION CARE SERVICES ADMISSION AND DISCHARGE SAME DAY The codes for same day observation admit and discharge include: 9924-Observation or inpatient hospital care for problems of low severity. Documentation requires a detailed or comprehensive history, a detailed or comprehensive exam, and straightforward or low complexity MDM Observation or inpatient hospital care for problems of moderate severity. Documentation requires a comprehensive history, a comprehensive exam, and moderate complexity MDM Observation or inpatient hospital care for problems of high severity. Documentation requires a comprehensive history, a comprehensive exam, and high complexity MDM. 82
83 OBSERVATION CARE SERVICES Admission and Discharge on the Same Calendar Date PROCEDURE CODE 9924 Detailed or Comprehensive HISTORY EXAMINATION MEDICAL DECISION-MAKING Detailed or Comprehensive Straightforward or Low Complexity 9925 Comprehensive Comprehensive Moderate Complexity 9926 Comprehensive Comprehensive High Complexity 8
84 OBSERVATION CARE SERVICES Hospital observation services should be coded and billed according to the time spent in observation status as follows: 8 Hours or Less > 8 Hours < 24 Hours 24 Hours or More (Initial Observation Care) (Observation or Inpatient Care) (Initial Observation Care) Subsequent Day different calendar day Same Calendar Date Admission paid o Discharge not paid separately Same Calendar Date Admission and Discharge Included Same Calendar Date Admission paid o Discharge not paid separately Different Calendar Date Admission and Discharge (99217) paid separately Different Calendar Date Use codes Discharge (99217) paid separately Different Calendar Date Admission and Discharge paid separately 84
85 Outpatient Surgeries Observation Services Coverage of outpatient observation services are restricted to situations where a patient exhibits an uncommon or unusual reaction or complication after a surgical procedure is performed such as: The inability to urinate (requiring catheterization) The inability to keep solids or liquids down (requiring continued intravenous feeding) The inability to control pain (requiring intramuscular or intravenous analgesics) The inability to move the lower extremities and safely ambulate after spinal anesthesia (requiring continued bed rest and sensation assessment and monitoring) Unexpected surgical bleeding (requiring frequent dressing changes, and/or dressing reinforcement) Unstable vital signs (requiring continued monitoring and/or drug intervention) and the patient s condition requires monitoring or treatment beyond the treatment customarily provided in the immediate postoperative period. OUTPATIENT OBSERVATION SERVICES SHOULD BE ORDERED AT THAT TIME. The order should never be performed and signed by the attending physician prior to the surgical procedure. Four (4) to six (6) hours is used as a guideline for a normal recovery period. Observation would be appropriate when the recovery of the patient exceeds the normal recovery period. 85
86 OBSERVATION CARE SERVICES Below there is a list of issues to consider when billing for observation services: Only the physician who admits the patient to observation status and is responsible for his/her stay in observation may bill using observation codes. All other physicians who see the patient in observation must bill E/M outpatient service codes or outpatient consultation codes, as appropriate. The initial observation care code is the initial day of care. This is determined by calendar date, not 24-hour period. Therefore, any time spent in observation until midnight of the first day is considered as one day. If patient is evaluated after midnight or any time on the day following the initial evaluation a subsequent observation care code is to be used A patient should not stay in an observation longer than 48 hours. A decision should be made by the attending physician to either admit or discharge the patient home. At 24 hours, the physician should evaluate patient s condition to decide if the patient needs to remain in observation for an additional 24 hours. At 48 hours, the physician should re-evaluate patient s condition and decide if patient needs to be admitted to the hospital or discharged home. 86
87 OBSERVATION CARE SERVICES Q & As Q: How should we bill for a patient admitted to observation status by a resident on day 1 at 9:00 p.m. but not seen by an attending until day 2 at 8:00 a.m.? (The patient is ready for discharge on day 2 as well.) The attending saw the patient only that one calendar date. Should the attending bill the second day as a same-day admit and discharge ( )? Or as initial observation care ( ) on that second day and an observation discharge (99217)? A: You must base your claim on the attending physician s date of service, so you can t bill for the first day when only the resident saw the patient. Use the observation admit and discharge same-day codes ( ) and bill day 2 as the only date of service. 87
88 OBSERVATION CARE SERVICES Q & As Q: How should I code services rendered to a patient admitted to observation status on one date, then admitted as an inpatient for two additional days? A: Bill an initial observation care code, , on the first date, when the patient is in observation status. Any evaluation and management services in another setting, such as the office or an emergency department, that are related to the admission to observation status cannot be billed separately, as they are considered part of the initial observation care service. Bill an initial inpatient hospital care code, , on the second date, on which you admit the patient to the hospital inpatient setting. You cannot report the observation care discharge service code, 99217, in conjunction with a hospital admission. All related evaluation and management services are part of the initial hospital care service, regardless of the setting. Bill a hospital discharge service code, , for the third date. 88
89 OBSERVATION CARE SERVICES Q & As Q: What about admission and discharge from observation to home on the same date? A: Bill a CPT Observation or Inpatient Care Services (Including Admission and Discharge Services) code, These codes are to be used for a samedate admission and discharge in the observation status or inpatient setting. For billing Medicare patients a minimum of 8 hours in observation status is required. Q: What if I admit a patient to observation status and then send him or her home the next day? A: If the patient is admitted to observation status on one calendar date and discharged on the next date, bill an initial observation care code, , for the first date of service and the observation care discharge service code, 99217, for the second. 89
90 OBSERVATION CARE SERVICES Q & As Q: Does Medicare require a minimum number of hours on observation status before a physician can bill ? A: Yes. A patient must be in observation status at least eight hours for a physician to bill a same-date admission and discharge code. Medicare rules differ from the instructions in the CPT code book for this scenario and, thus, are more likely to differ from private-payer billing rules. For Medicare: If the patient is admitted to observation status and is then discharged home on the same date of the observation stay that lasted at least eight hours (but fewer than 24 hours, since it must be on the same date), bill a code from the range. If the patient is discharged home after fewer than eight hours in observation status, bill only an initial observation care code, The Medicare eight-hour minimum rule for observation status pertains to same-date admission and discharge only. If, as happens rarely, a Medicare patient is admitted to observation status and is discharged in fewer than eight hours on a different date, bill an initial observation care code, , for the first date of service and the observation care discharge service code, 99217, on the second date. 90
91 Completing the Puzzle 91

92 Evaluation & Management Coding Card 92

93 Evaluation & Management Coding 9
Office of Billing Compliance 2016 Coding, Billing and Documentation Program. Diagnostic Radiology
 Office of Billing Compliance 2016 Coding, Billing and Documentation Program Diagnostic Radiology Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide you with every tool you
Office of Billing Compliance 2016 Coding, Billing and Documentation Program Diagnostic Radiology Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide you with every tool you
Changes in Coding 2017 Presented by: Cynthia Robinson, RT, CPC
 Changes in Coding 2017 Presented by: Cynthia Robinson, RT, CPC All Rights Reserved 2 Overview of ICD-10 Over 69,000 codes ( ICD-9 had approximately 17,000) Codes start with an alpha character, except U
Changes in Coding 2017 Presented by: Cynthia Robinson, RT, CPC All Rights Reserved 2 Overview of ICD-10 Over 69,000 codes ( ICD-9 had approximately 17,000) Codes start with an alpha character, except U
Anesthesia Services Policy
 Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Office of Billing Compliance 2015 Coding, Billing and Documentation Program. Interventional Radiology
 Office of Billing Compliance 2015 Coding, Billing and Documentation Program Interventional Radiology 2015 Code Changes 2 Interventional Radiology Interventional Radiology saw the majority of changes in
Office of Billing Compliance 2015 Coding, Billing and Documentation Program Interventional Radiology 2015 Code Changes 2 Interventional Radiology Interventional Radiology saw the majority of changes in
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Moderate Sedation PAYMENT POLICY ID NUMBER: Original Effective Date: 12/22/2009. Revised: 03/15/2018 DESCRIPTION:
 Private Property of Florida Blue. This payment policy is Copyright 2018, Florida Blue. All Rights Reserved. You may not copy or use this document or disclose its contents without the express written permission
Private Property of Florida Blue. This payment policy is Copyright 2018, Florida Blue. All Rights Reserved. You may not copy or use this document or disclose its contents without the express written permission
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Genetics
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Genetics Top Billed Non-E/M Codes CODE PROCEDURES UNITS 9780PR MED NUTR THER, SUBSQ, INDIV, EA
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Genetics Top Billed Non-E/M Codes CODE PROCEDURES UNITS 9780PR MED NUTR THER, SUBSQ, INDIV, EA
The ASA defines anesthesiology as the practice of medicine dealing with but not limited to:
 1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Programming a Spinal Cord Neurostimulator
 Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
LOUISIANA MEDICAID PROGRAM ISSUED: 02/01/12 REPLACED: 02/01/94 CHAPTER 5: PROFESSIONAL SERVICES SECTION 5.1: COVERED SERVICES PAGE(S) 11
 11") Anesthesia Services Surgical anesthesia services may be provided by anesthesiologists or certified registered nurse anesthetists (CRNAs). Maternity-related anesthesia services may be provided by anesthesiologists,
Anesthesia Services Surgical anesthesia services may be provided by anesthesiologists or certified registered nurse anesthetists (CRNAs). Maternity-related anesthesia services may be provided by anesthesiologists,
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES
 GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES") PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
2. This additional imaging modality applied to a base procedure, must meet but, not exceed the patient s medical need; and
 3D Interpretation and Reporting of Imaging Studies [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr. Go to Comunicados a Proveedores, and click Cartas
3D Interpretation and Reporting of Imaging Studies [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr. Go to Comunicados a Proveedores, and click Cartas
Basic Teaching Physician Presence and Documentation
 Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Diagnostic Radiology
 Diagnostic Radiology Caren Swartz, CPC-I, CPC-H, CPMA, CIC Caren@practiceintegrity.com Overview Terminology Associated with Diagnostic Radiology Proper Reporting CPT Challenges CMS Issues 1 Have fun! Diagnostic
Diagnostic Radiology Caren Swartz, CPC-I, CPC-H, CPMA, CIC Caren@practiceintegrity.com Overview Terminology Associated with Diagnostic Radiology Proper Reporting CPT Challenges CMS Issues 1 Have fun! Diagnostic
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
Anesthesia Policy REIMBURSEMENT POLICY CMS Reimbursement Policy Oversight Committee. Policy Number. Annual Approval Date. Approved By 2018R0032B
 REIMBURSEMENT POLICY CMS-1500 Policy Number 2018R0032B Annual Approval Date Anesthesia Policy 3/14/2018 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
REIMBURSEMENT POLICY CMS-1500 Policy Number 2018R0032B Annual Approval Date Anesthesia Policy 3/14/2018 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that apply)
: (Check all that apply)") POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Regions Hospital Delineation of Privileges Nurse Practitioner
 Regions Hospital Delineation of Privileges Nurse Practitioner Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Regions Hospital Delineation of Privileges Nurse Practitioner Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
MEDICARE RULE FOR TEACHING PHYSICIANS Effective July 1, 1996.
 MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
Radiology Services INDIANA HEALTH COVERAGE PROGRAMS. Copyright 2017 DXC Technology Company. All rights reserved.
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Radiology Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 4 P U B L I S H E D : D E C E M B E R 1 2, 2 0 1 7 P O L
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Radiology Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 4 P U B L I S H E D : D E C E M B E R 1 2, 2 0 1 7 P O L
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES. SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION
 NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
JOHNS HOPKINS HEALTHCARE Physician Guidelines
 Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
 Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Post-Op hemorrhage repair. Is it billable?
 Post-Op hemorrhage repair. Is it billable? August 10, 2017 Can I bill for taking the patient back to the OR to explore and repair post-op hemorrhage on day post-op? I heard that all complications are included
Post-Op hemorrhage repair. Is it billable? August 10, 2017 Can I bill for taking the patient back to the OR to explore and repair post-op hemorrhage on day post-op? I heard that all complications are included
Resident Core Curriculum Vascular and Interventional Radiology
 Resident Core Curriculum Vascular and Interventional Radiology General Goals: The specific goals include objectives required for every level of training with graduated levels of supervision and responsibility.
Resident Core Curriculum Vascular and Interventional Radiology General Goals: The specific goals include objectives required for every level of training with graduated levels of supervision and responsibility.
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Welcome To The Digital Learning Center. Billing Compliance: Today s Presentation. Course Faculty. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation Billing liance: Avoiding Fraud & Abuse in Your Medical/Surgical Practice Course
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation Billing liance: Avoiding Fraud & Abuse in Your Medical/Surgical Practice Course
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Anesthesia Policy. Approved By 3/08/2017
 REIMBURSEMENT POLICY Anesthesia Policy Policy Number 2018R0032B Annual Approval Date 3/08/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are
REIMBURSEMENT POLICY Anesthesia Policy Policy Number 2018R0032B Annual Approval Date 3/08/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are
Protocol/Procedure XX. Title: Procedural Sedation/Moderate Sedation
 Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
HC 1930 HC 1930 ICD-9-CM III/CPT Coding II
 South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Element(s) of Performance for DSPR.1
 of Performance for DSPR.1") Prepublication Issued Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Prepublication Issued Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
VAMC Interventional Radiology Goals & Objectives
 VAMC Interventional Radiology Goals & Objectives Introduction: During the time allotted for the interventional radiology (IR) service, radiology residents can expect to become proficient in all major aspects
VAMC Interventional Radiology Goals & Objectives Introduction: During the time allotted for the interventional radiology (IR) service, radiology residents can expect to become proficient in all major aspects
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Modifier -25 Significant, Separately Identifiable E/M Service
 Manual: Policy Title: Reimbursement Policy Modifier -25 Significant, Separately Identifiable E/M Service Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM028 Last Updated:
Manual: Policy Title: Reimbursement Policy Modifier -25 Significant, Separately Identifiable E/M Service Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM028 Last Updated:
E/M Fast Finder. CPT only 2012 American Medical Association. 1 All Rights Reserved.
 E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Coding Companion for Primary Care. A comprehensive illustrated guide to coding and reimbursement
 Coding Companion for Primary Care A comprehensive illustrated guide to coding and reimbursement 2009 Contents Getting Started with Coding Companion... i Integumentary...1 Breast...67 General Musculoskeletal...68
Coding Companion for Primary Care A comprehensive illustrated guide to coding and reimbursement 2009 Contents Getting Started with Coding Companion... i Integumentary...1 Breast...67 General Musculoskeletal...68
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
UniCare Professional Reimbursement Policy
 UniCare Professional Reimbursement Policy Subject: Anesthesia Services Policy #: UniCare 0020 Adopted: 02/03/2009 Effective: 02/07/2017 Coverage is subject to the terms, conditions, and limitations of
UniCare Professional Reimbursement Policy Subject: Anesthesia Services Policy #: UniCare 0020 Adopted: 02/03/2009 Effective: 02/07/2017 Coverage is subject to the terms, conditions, and limitations of
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Patient Age Group: ( ) N/A (X) All Ages ( ) Newborns ( ) Pediatric ( ) Adult
 N/A (X) All Ages ( ) Newborns ( ) Pediatric ( ) Adult") Title: Documentation of Clinical Activities by UNMH Medical Staff and House Staff Applies To: UNM Hospitals Responsible Department: Office of Clinical Affairs Updated: 05/2016 Policy Patient Age Group:
Title: Documentation of Clinical Activities by UNMH Medical Staff and House Staff Applies To: UNM Hospitals Responsible Department: Office of Clinical Affairs Updated: 05/2016 Policy Patient Age Group:
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Global Days Policy. Approved By 7/12/2017
 Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Evaluation & Management Documentation Training Tool
 Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Anthem Blue Cross and Blue Shield Professional Reimbursement Policy
 Subject: Anesthesia CT Policy: 0020 Effective: 08/01/2014 01/31/2015 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria listed
Subject: Anesthesia CT Policy: 0020 Effective: 08/01/2014 01/31/2015 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria listed
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018
 Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Global Period for Surgery. Is it billable?
 Global Period for Surgery. Is it billable? August 10, 2017 Question: My patient presented to the ED with an infection at the incision site from a surgery that I did 4 weeks ago. It has a 90 day global.
Global Period for Surgery. Is it billable? August 10, 2017 Question: My patient presented to the ED with an infection at the incision site from a surgery that I did 4 weeks ago. It has a 90 day global.
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Family Medicine
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Family Medicine 2017 Code Changes 2 Medicine: New Vaccine 90674 Influenza virus vaccine, quadrivalent
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Family Medicine 2017 Code Changes 2 Medicine: New Vaccine 90674 Influenza virus vaccine, quadrivalent
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Patient Care. Medical Knowledge
 Interventional Radiology (First Year, First Block) This rotation involves performance and interpretation of diagnostic and therapeutic angiograms and venograms, dialysis access, line placement, drainage
Interventional Radiology (First Year, First Block) This rotation involves performance and interpretation of diagnostic and therapeutic angiograms and venograms, dialysis access, line placement, drainage
today! Visit or call 800/
 The bestselling Certified Coder Boot Camp is now available online! Register today! Visit www.hcprobootcamps.com or call 800/750-0584. Register 30 days in advance and save $200! Call HCPro at 800/750-0584
The bestselling Certified Coder Boot Camp is now available online! Register today! Visit www.hcprobootcamps.com or call 800/750-0584. Register 30 days in advance and save $200! Call HCPro at 800/750-0584
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Clinical Privileges Profile Family Medicine. Kettering Medical Center System
 Clinical Privileges Profile Kettering Medical Center Sycamore Medical Center Kettering Medical Center System Applicant: Check off the Requested box for each privilege requested. Applicants have the burden
Clinical Privileges Profile Kettering Medical Center Sycamore Medical Center Kettering Medical Center System Applicant: Check off the Requested box for each privilege requested. Applicants have the burden
Corporate Reimbursement Policy
 Corporate Reimbursement Policy Code Bundling Rules Not Addressed in ClaimCheck or Correct File Name: code_bundling_rules_not_addressed_in_claim_check Origination: 6/2004 Last Review: 12/2017 Next Review:
Corporate Reimbursement Policy Code Bundling Rules Not Addressed in ClaimCheck or Correct File Name: code_bundling_rules_not_addressed_in_claim_check Origination: 6/2004 Last Review: 12/2017 Next Review:
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
Empire BlueCross BlueShield Professional Reimbursement Policy
 Subject: Anesthesia Services NY Policy: 0020 Effective: 01/01/2015 11/30/2015 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
Subject: Anesthesia Services NY Policy: 0020 Effective: 01/01/2015 11/30/2015 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Quarterly CERT Error Findings Report WPS GHA Part B J8 MAC ~ Indiana and Michigan ~
 Quarterly CERT Error Findings Report WPS GHA Part B J8 MAC ~ Indiana and Michigan ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed April 1, 2017, through June 30,
Quarterly CERT Error Findings Report WPS GHA Part B J8 MAC ~ Indiana and Michigan ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed April 1, 2017, through June 30,
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program. Medicine Cardiology
 Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Medicine Cardiology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Medicine Cardiology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and
Evaluation & Management Documentation Training Tool
 A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
Corporate Medical Policy Bundling Guidelines
 Corporate Medical Policy Bundling Guidelines File Name: bundling_guidelines Policy Number: ADM9020 Origination: 1/2000 Last Review: 03/2006 Next Review: 03/2007 Discussion Related to Blue Care, Blue Choice,
Corporate Medical Policy Bundling Guidelines File Name: bundling_guidelines Policy Number: ADM9020 Origination: 1/2000 Last Review: 03/2006 Next Review: 03/2007 Discussion Related to Blue Care, Blue Choice,
(1) Ambulatory surgical center--a facility licensed under Texas Health and Safety Code, Chapter 243.
 Ambulatory surgical center--a facility licensed under Texas Health and Safety Code, Chapter 243.") RULE 200.1 Definitions The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise. (1) Ambulatory surgical center--a facility
RULE 200.1 Definitions The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise. (1) Ambulatory surgical center--a facility
UPMC 1 Delineation of Privileges Request Criteria Summary Sheet. Facility: UPMC Shadyside. Specialty: MEDICINE
 1 Facility: Shadyside Specialty: MEDICINE KNOWLEDGE Successful Completion of an ACGME/AOA, accredited program TRAINING The successful completion of an approved (ACGME/AOA) post graduate residency program
1 Facility: Shadyside Specialty: MEDICINE KNOWLEDGE Successful Completion of an ACGME/AOA, accredited program TRAINING The successful completion of an approved (ACGME/AOA) post graduate residency program
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (Revised )
") RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (Revised 12-31-2011) Section I. Introduction The Urology Department has adopted the general supervision policy as provided by the UTHSCSA-GMEC. A link to the
RESIDENT SUPERVISION DEPARTMENT OF UROLOGY (Revised 12-31-2011) Section I. Introduction The Urology Department has adopted the general supervision policy as provided by the UTHSCSA-GMEC. A link to the
CHAP2-CPTcodes _final doc Revision Date: 1/1/2017
 CHAP2-CPTcodes00000-01999_final103116.doc Revision Date: 1/1/2017 CHAPTER II ANESTHESIA SERVICES CPT CODES 00000-09999 FOR NATIONAL CORRECT CODING INITIATIVE POLICY MANUAL FOR MEDICARE SERVICES Current
CHAP2-CPTcodes00000-01999_final103116.doc Revision Date: 1/1/2017 CHAPTER II ANESTHESIA SERVICES CPT CODES 00000-09999 FOR NATIONAL CORRECT CODING INITIATIVE POLICY MANUAL FOR MEDICARE SERVICES Current
POLICY AND PROCEDURE
 AND PROCEDURE NUMBER: 0020 PAGE NUMBER: 1 of 7 I. PURPOSE: To ensure compliance with Federal and State billing and documentation guidelines of all UMMG billing providers. II. SCOPE: University of Miami
AND PROCEDURE NUMBER: 0020 PAGE NUMBER: 1 of 7 I. PURPOSE: To ensure compliance with Federal and State billing and documentation guidelines of all UMMG billing providers. II. SCOPE: University of Miami
SNF Consolidated Billing Exclusions/Inclusions
 SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
Procedure Codes Assigned to Surgical Benefit Categories
 Manual: Policy Title: Reimbursement Policy Procedure Codes Assigned to Surgical Benefit Categories Section: Surgery Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM023 Last Updated: 4/5/2017
Manual: Policy Title: Reimbursement Policy Procedure Codes Assigned to Surgical Benefit Categories Section: Surgery Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM023 Last Updated: 4/5/2017
Regions Hospital Delineation of Privileges Physician Assistant Emergency Medicine
 Regions Hospital Delineation of Privileges Physician Assistant Emergency Medicine Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting.
Regions Hospital Delineation of Privileges Physician Assistant Emergency Medicine Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting.
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Anesthesiology
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Anesthesiology Top Billed Non-E/M Codes Procedure Procedure Code Procedure Quantity % of Total
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Anesthesiology Top Billed Non-E/M Codes Procedure Procedure Code Procedure Quantity % of Total
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Sample page. Contents
 CODING COMPANION 2018 Oncology/Hematology A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
CODING COMPANION 2018 Oncology/Hematology A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
SPECIALTY TIP #13 Evaluation and Management (E&M)
") ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
APP PRIVILEGES IN SURGERY
 APP PRIVILEGES IN SURGERY Education/Training Licensure (Initial and Reappointment) Required Qualifications Successful completion of a PA or NP program Current licensure as a PA or RN in the state of California
APP PRIVILEGES IN SURGERY Education/Training Licensure (Initial and Reappointment) Required Qualifications Successful completion of a PA or NP program Current licensure as a PA or RN in the state of California
The presenter has owns Kelly Willenberg, LLC in relation to this educational activity.
 Kelly M Willenberg, MBA, BSN, CCRP, CHC, CHRC 1 The presenter has owns Kelly Willenberg, LLC in relation to this educational activity. 2 1 Medical Necessity when you submit claims Coding for qualifying
Kelly M Willenberg, MBA, BSN, CCRP, CHC, CHRC 1 The presenter has owns Kelly Willenberg, LLC in relation to this educational activity. 2 1 Medical Necessity when you submit claims Coding for qualifying
Billing and Compliance Guide for Anesthesia Providers
 INTRODUCTION Anesthesia is one of the most complex medical specialties from a billing standpoint. When you send a claim to a payer, you are attesting that all services on that claim are true and appropriate,
INTRODUCTION Anesthesia is one of the most complex medical specialties from a billing standpoint. When you send a claim to a payer, you are attesting that all services on that claim are true and appropriate,