ED Care Coordination Pathway Partnership
|
|
|
- Trevor O’Neal’
- 6 years ago
- Views:
Transcription
1 ED Care Coordination Pathway Partnership 1 SUPER UTILIZER INTERVENTION FOR QUALITY IMPROVEMENT THE HEALTH COLLABORATIVE HEALTH CARE ACCESS NOW UNIVERSITY OF CINCINNATI MEDICAL CENTER MAY 29, 2013


2 Cincinnati Partnership for ED Care Management 2
3 Snapshot of Greater Cincinnati Region 2011 ED Utilization Emergency Visits.1,084,212 Avoidable ED Visit..182,193 Percent Avoidable % Top 5 Communities With ED Visits Fairfield Liberty Township..35,319 Liberty Township..34,466 Provider Information Covington..34,421 Total Milleville Rossville 30,846 Hospital/Ed.. 25 Cincinnati Mt. Healthy. 24,659 Total Licensed Beds..6,526 Neighborhoods Total Population in SW Ohio counties: 1.1 Served..3,624 million people 3 Top 5 Payers for ED Visits Medicaid HMO.197,371 Self Pay.. 181,171 Medicare 180,419 Commercial Ins.127,142 Medicaid 115,270
4 University Hospital General Information 2012 AVOIDABLE* ED VISITS (Treat/Released) Total ED Visits = 9287 ALL ED VISITS Total ED Visits = 85,979 Admitted/Observation = 19,722 Treated/Released = 66,257 Total Charges = $790 M Admitted/Observation = $669 M Treated/Released = $121M Average Charge per Visit = $9,187 Admitted/Observation = $33,921 Treated/Released = $1,833 Total Charges = $14.2 M Average Charge per Visit = $1, % Of ED Visits at University Hospital were Avoidable ED Visits Source: HCAN/UCMC ED Data Analysis * Avoidable as defined by AHRQ Ambulatory Sensitive Conditions 4

5 HCAN ED Care Coordination Pathway 5
6 Analysis of 2009 Patient Cohort Patient cohort 434 pts./1037 visits & uninsured adults who were interviewed by Community Health Worker Record review six month pre & post sentinel visit (CHW interview) Patient ED Utilization Results 6 60% decrease in utilization (from 1.77 visit/patient to 0.73 visits/patient) 77% decrease in visits, 15% no change and 9% increase in visits Largest reduction in ED visits = 6; largest increase in ED visits = 4
7 Super User Case Finding Strategy Inclusion Criteria: 20 ED visits in past 12 months, Hamilton County resident Exclusion Criteria: sickle cell, cancer, psychiatric primary diagnosis, and pregnant patients Patient identification tactics: mainly data driven, also accepting physician referrals Coordination with Behavioral Health ED pilot Keys to Health Patient Alert technology HealthBridge (RHIE) 7
8 Initial Super Utilizer Patient Profile 14 patients: Female = 9; Male = 5 White = 3; African American = 11 Inclusion Criteria/Primary Diagnoses ED Visits (2/2010 2/2012) = 1201 ED Charges = $1,426,333 Admission Charges = $2,829,210 Hospital Admissions = 145 Hospitalization LOS = 584 days Payer Sources = Medicare/Medicaid -4, Self-Pay -3, Medicaid (including managed care plans) -7 8
9 Super User Demographics Number of clients enrolled: 15 Females - 8, Males - 7 African American - 11, White - 4 Median Age: 46 yrs. Ranging from yrs. No zip code clustering - 12 different zip codes PCP status: yes 8; no -7 Employment status: unemployed - 13; disability 8; employed - 2 9
10 Current Patients (15) Utilization Information AVOIDABLE* ED VISITS Total Avoidable ED Visits = 50 ALL ED VISITS Total ED Visits = 504 Admitted/Observation = 23 Treated/Released = 481 Total Charges = $957K Admitted/Observation = $197K Treated/Released = $660K Average Charge per Visit = $1,899 Admitted/Observation = $12,916 Treated/Released = $1,372 Total Charges = $117K Average Charge per Visit = $2,237 ~10% of ED Visits were avoidable Source: HCAN/UC ED Data Analysis * Avoidable as defined by AHRQ Ambulatory Sensitive Conditions 10
11 Super User Workflow: High Touch/High Tech Community Health Worker Role 11 Data management Role: patient identification, utilization history verification, reporting, etc. Clinical Role ED coordination and linkages with hospital-based services Community Connections: medical, behavioral health and social/environmental


12 Top Ten Diagnoses for ED Visit 12


13 Insurance Status of Current Clients 13


14 Type of ED Visit 14
15 Pre/Post Intervention Utilization 15 Patient ED Visits 12 Month Prior ED Charge 12 Month Prior M.O. 34 $ 22,807 A.G. 45 $ 83,455 C.B. 54 $ 38,434 ED Visits since enrollment ED Charge since Enrollment 4 in 4 months $ 4,501 Reduction in ED Visits Reduction in ED Charge 65% 41% 4 in 5 months $ 26,502 79% 24% 27 in 5 months $ 18, 233 no reduction no reduction Note: C.B. was non-responsive after several contacts.
16 Qualitative Results Complicated patients but health seeking behaviors can be changed Prioritize social/environmental challenges and logistical barriers issues Eliminate duplication of services across case managers/duplication Determine patient readiness to engage and manage crises 16


17 Maslow Hierarchy of Needs 17

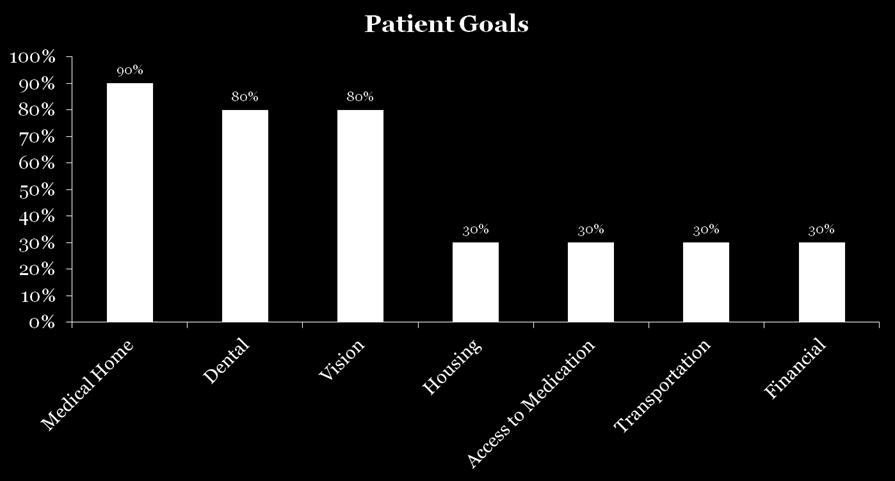
18 Patient Goals 18
19 ED Care Coordination Pathway Goals Identify resources to increase service capacity among relevant providers and CBOs Develop an Integrated Ambulatory Services Community Network within UCHealth to address the ED capacity and referral needs Improve care coordination for patients with for chronic illness; improve inter-system collaboration
20 Value Proposition Providers & Payors 20 HCAN & UH process improvements: internal operations & communication; paperwork reduction; dedicated data management infrastructure Silo- busting Leverage seed money from grant to build a better system of coordination and access to care for high cost/unmanaged patients Medicaid requirements for 1% high cost patients
21 Policy Opportunities 21 State Medicaid role challenges with negotiating 1:1 with each Medicaid plan; Medicaid expansion and impact on payment to hospitals Payment for CHW interventions Regional spread of program into other hospitals Dissemination of results to inform local policymakers
22 For More Information: Judith Warren, MPH Chief Executive Officer Health Care Access Now 22 Kim Vance, RN, MSN, NE-BC Assistant Chief Nursing Officer Emergency Services UC Health University Medical Center
Communities to Improve Health. through the Pathways HUB Model Second level
 PREGNANT Unleashing CLIENT the Power of Communities to Improve Health Click to edit Master text styles through the Pathways HUB Model Second level Third level Fourth level Fifth level Judith Warren, Healthcare
PREGNANT Unleashing CLIENT the Power of Communities to Improve Health Click to edit Master text styles through the Pathways HUB Model Second level Third level Fourth level Fifth level Judith Warren, Healthcare
Improving Health Outcomes with Pathways. November 28, 2012
 Improving Health Outcomes with Pathways November 28, 2012 2 Do we serve the most at-risk? Why should we? Pregnant Client at-risk: 5% of population uses 56% of health care resources Most at-risk are often
Improving Health Outcomes with Pathways November 28, 2012 2 Do we serve the most at-risk? Why should we? Pregnant Client at-risk: 5% of population uses 56% of health care resources Most at-risk are often
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Hospitals Collaborating to Assess and Address Changing Community Health Needs
 Hospitals Collaborating to Assess and Address Changing Community Health Needs MARGARET DROZD, MSN, RN, APRN-BC DIRECTOR COMMUNITY MOBILE HEALTH SERVICES SAINT PETER S UNIVERSITY HOSPITAL Hospitals Collaborating
Hospitals Collaborating to Assess and Address Changing Community Health Needs MARGARET DROZD, MSN, RN, APRN-BC DIRECTOR COMMUNITY MOBILE HEALTH SERVICES SAINT PETER S UNIVERSITY HOSPITAL Hospitals Collaborating
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Check Hep B Patient Navigation Program
 Check Hep B Patient Navigation Program Nirah Johnson, LCSW Director, Capacity Building & Program Implementation Viral Hepatitis Program New York City Department of Health Hepatitis B in NYC Estimated 100,000
Check Hep B Patient Navigation Program Nirah Johnson, LCSW Director, Capacity Building & Program Implementation Viral Hepatitis Program New York City Department of Health Hepatitis B in NYC Estimated 100,000
Reports Glossary. Enhanced Personal Health Care
 Enhanced Personal Health Care Reports Glossary This glossary is a reference for providers participating in Enhanced Personal Health Care. It is organized to allow the user to quickly find the definition
Enhanced Personal Health Care Reports Glossary This glossary is a reference for providers participating in Enhanced Personal Health Care. It is organized to allow the user to quickly find the definition
Connect the Dots in Community Services
 LEVERAGING THE POWER OF CARE MANAGEMENT Connect the Dots 2016 Population Health Colloquium Helen Dunkle MSN RN-BC Agenda in Community Services Caring for High-Need, High-Cost Patients: What Makes for a
LEVERAGING THE POWER OF CARE MANAGEMENT Connect the Dots 2016 Population Health Colloquium Helen Dunkle MSN RN-BC Agenda in Community Services Caring for High-Need, High-Cost Patients: What Makes for a
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Learning Briefs: Equity in Specialty Care
 Learning Briefs: Equity in Specialty Care LAUREN SMITH, MD, MPH, MANAGING DIRECTOR APRIL 2016 1 About FSG About FSG FSG is a mission-driven consulting firm that supports leaders to create large-scale,
Learning Briefs: Equity in Specialty Care LAUREN SMITH, MD, MPH, MANAGING DIRECTOR APRIL 2016 1 About FSG About FSG FSG is a mission-driven consulting firm that supports leaders to create large-scale,
Caring for the most complex and high-utilizing patients Emerging program models in California primary care clinics
 Caring for the most complex and high-utilizing patients Emerging program models in California primary care clinics Melissa Barajas, RN, BSN, PHN and Loreta Villemez, Neighborhood HealthCare Fern Ebeling,
Caring for the most complex and high-utilizing patients Emerging program models in California primary care clinics Melissa Barajas, RN, BSN, PHN and Loreta Villemez, Neighborhood HealthCare Fern Ebeling,
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
OPERATIONS MANUAL CARE CONNECTIONS PROGRAM LOS ANGELES COUNTY DEPARTMENT OF HEALTH SERVICES
 OPERATIONS MANUAL CARE CONNECTIONS PROGRAM LOS ANGELES COUNTY DEPARTMENT OF HEALTH SERVICES SECTION: PATIENT REFERRAL and INTAKE PROCEDURES 1 P age 1 CCP Referral Procedure Referrals for the Care Connections
OPERATIONS MANUAL CARE CONNECTIONS PROGRAM LOS ANGELES COUNTY DEPARTMENT OF HEALTH SERVICES SECTION: PATIENT REFERRAL and INTAKE PROCEDURES 1 P age 1 CCP Referral Procedure Referrals for the Care Connections
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
Pathways Community HUB overview September Sarah Redding, MD, MPH Pathways Community HUB Institute (PCHI)
") Pathways Community HUB overview September 2016. Sarah Redding, MD, MPH Pathways Community HUB Institute (PCHI) The HUB model is all about risk. It is about the comprehensive identification and reduction
Pathways Community HUB overview September 2016. Sarah Redding, MD, MPH Pathways Community HUB Institute (PCHI) The HUB model is all about risk. It is about the comprehensive identification and reduction
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential
 A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Innovative Community Based Care Community Transitional Care Team
 Innovative Community Based Care Community Transitional Care Team Canadian Association of Nurses in AIDS Care April 2007 CTCT Homelike community transitional residence for IDU s requiring long-term IV antibiotics
Innovative Community Based Care Community Transitional Care Team Canadian Association of Nurses in AIDS Care April 2007 CTCT Homelike community transitional residence for IDU s requiring long-term IV antibiotics
Organizational Changes to Promote Health Literacy and Cultural Competency: The NewYork-Presbyterian Hospital Experience
 Organizational Changes to Promote Health Literacy and Cultural Competency: The NewYork-Presbyterian Hospital Experience Roundtable on Health Literacy and Cultural Competency Institute of Medicine J. Emilio
Organizational Changes to Promote Health Literacy and Cultural Competency: The NewYork-Presbyterian Hospital Experience Roundtable on Health Literacy and Cultural Competency Institute of Medicine J. Emilio
LEARNING ABOUT CAREERS USING AND ADAPTING TEXTS FROM THE OCCUPATIONAL OUTLOOK HANDBOOK
 LEARNING ABOUT CAREERS USING AND ADAPTING TEXTS FROM THE OCCUPATIONAL OUTLOOK HANDBOOK 1. SELECT THE MATERIAL FOR YOUR LEARNERS LEVEL 2. REFLECT: Would this material be relevant to your learners? Why or
LEARNING ABOUT CAREERS USING AND ADAPTING TEXTS FROM THE OCCUPATIONAL OUTLOOK HANDBOOK 1. SELECT THE MATERIAL FOR YOUR LEARNERS LEVEL 2. REFLECT: Would this material be relevant to your learners? Why or
L3: Developing a Portfolio of Projects to Support a Triple Aim Strategy. Faculty Disclosures
 L3: Developing a Portfolio of Projects to Support a Triple Aim Strategy IHI National Forum December 4, 2011 1:00 4:30 Carol Beasley, Institute for Healthcare Improvement Rebecca Ramsay, CareOregon Trissa
L3: Developing a Portfolio of Projects to Support a Triple Aim Strategy IHI National Forum December 4, 2011 1:00 4:30 Carol Beasley, Institute for Healthcare Improvement Rebecca Ramsay, CareOregon Trissa
Highline Health Connections: Care Navigation for Vulnerable Populations
 Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Nursing Leadership Drives Implementation of Community Health Needs Assessment and Best Practice Strategies Session Number: C512
 Nursing Leadership Drives Implementation of Community Health Needs Assessment and Best Practice Strategies Session Number: C512 2016 ANCC National Magnet Conference Wednesday, October 5, 2016 11:30 AM
Nursing Leadership Drives Implementation of Community Health Needs Assessment and Best Practice Strategies Session Number: C512 2016 ANCC National Magnet Conference Wednesday, October 5, 2016 11:30 AM
Hennepin Health. People.Care.Respect. Super Utilizer Summit February 2013 Jennifer DeCubellis. Hennepin County, MN
 Hennepin Health People.Care.Respect Super Utilizer Summit February 2013 Jennifer DeCubellis Hennepin County, MN What is Hennepin Health? Minnesota Department of Human Services (DHS) & Hennepin County Collaborative
Hennepin Health People.Care.Respect Super Utilizer Summit February 2013 Jennifer DeCubellis Hennepin County, MN What is Hennepin Health? Minnesota Department of Human Services (DHS) & Hennepin County Collaborative
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017
 Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura
Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura
EHR Report Implementation Training September 26, 2016
 EHR Report Implementation Training September 26, 2016 The McSilver Institute for Poverty Policy and Research at New York University Silver School of Social Work is committed to creating new knowledge about
EHR Report Implementation Training September 26, 2016 The McSilver Institute for Poverty Policy and Research at New York University Silver School of Social Work is committed to creating new knowledge about
Leveraging Managed Care to Support Community Health Workers and Promote Population Health
 Leveraging Managed Care to Support Community Health Workers and Promote Population Health Association of State and Territorial Health Officials (ASTHO) September 9, 2015 9:30 AM 10:45 AM ET Thomas Pryor
Leveraging Managed Care to Support Community Health Workers and Promote Population Health Association of State and Territorial Health Officials (ASTHO) September 9, 2015 9:30 AM 10:45 AM ET Thomas Pryor
2015 Hospital Inpatient Discharge Data Annual Report
 2015 Hospital Inpatient Discharge Data Annual Report Health Systems Epidemiology Program Epidemiology and Response Division New Mexico Department of Health 2015 Hospital Inpatient Discharge Data Report
2015 Hospital Inpatient Discharge Data Annual Report Health Systems Epidemiology Program Epidemiology and Response Division New Mexico Department of Health 2015 Hospital Inpatient Discharge Data Report
FLPPS Projects Roles & Responsibilities 6/15/2015 Project Hospital PCP/Pediatrician FQHC Health Home/Care Management
 FLPPS Projects Roles & Responsibilities 6/15/2015 Project Hospital PCP/Pediatrician FQHC Health Home/Care 2.a.i-Create Integrated Delivery System THIS PROJECT IS MANDATORY FOR ALL PARTICIPATING PROVIDERS
FLPPS Projects Roles & Responsibilities 6/15/2015 Project Hospital PCP/Pediatrician FQHC Health Home/Care 2.a.i-Create Integrated Delivery System THIS PROJECT IS MANDATORY FOR ALL PARTICIPATING PROVIDERS
Paying for HIV Prevention: Reimbursement & Sustainable Payer Sources
 Paying for HIV Prevention: Reimbursement & Sustainable Payer Sources About the Primary Care Development Corporation (PCDC) Founded in 1993, PCDC s mission is to catalyze excellence in primary care through
Paying for HIV Prevention: Reimbursement & Sustainable Payer Sources About the Primary Care Development Corporation (PCDC) Founded in 1993, PCDC s mission is to catalyze excellence in primary care through
Pathways in Washington
 Pathways in Washington What do you most want to know about Pathways? Relationship to Medicaid Demonstration Project? How it works? What training is like for the Care Coordinators? Medicaid Transformation
Pathways in Washington What do you most want to know about Pathways? Relationship to Medicaid Demonstration Project? How it works? What training is like for the Care Coordinators? Medicaid Transformation
Bronx Health REACH Vegetable and Fruit Rx Program at 3 IFH s FQHCs in the South Bronx: Design, Implementation & Evaluation
 Bronx Health REACH Vegetable and Fruit Rx Program at 3 IFH s FQHCs in the South Bronx: Design, Implementation & Evaluation Rachel Ingram, Joseph Ellis, Mubashir Mohi-ud-Din, Margaret Paul Institute for
Bronx Health REACH Vegetable and Fruit Rx Program at 3 IFH s FQHCs in the South Bronx: Design, Implementation & Evaluation Rachel Ingram, Joseph Ellis, Mubashir Mohi-ud-Din, Margaret Paul Institute for
Integrating social determinants of health in population health case
 Integrating social determinants of health in population health case Amanda Parsons MD, MBA management LEARNING OBJECTIVES Describe the relationship between physical health and the social needs of a high
Integrating social determinants of health in population health case Amanda Parsons MD, MBA management LEARNING OBJECTIVES Describe the relationship between physical health and the social needs of a high
CareConcepts Integrating Payor Sponsored Disease Management into Primary Care Practice
 Integrating Payor Sponsored Disease Management into Primary Care Practice Physicians Foundation for Health Systems Excellence Grant # 9600013 (2005 PFHSE Grantees) January 2006 June 2009 PO Box 762, Farmington,
Integrating Payor Sponsored Disease Management into Primary Care Practice Physicians Foundation for Health Systems Excellence Grant # 9600013 (2005 PFHSE Grantees) January 2006 June 2009 PO Box 762, Farmington,
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
AN EIGHT COUNTY COMMUNITY NEEDS ASSESSMENT (CNA) UNDERTAKEN IN COLLABORATION WITH: WESTCHESTER MEDICAL CENTER, MONTEFIORE MEDICAL CENTER, REFUAH
 UNDERTAKEN IN COLLABORATION WITH: WESTCHESTER MEDICAL CENTER, MONTEFIORE MEDICAL CENTER, REFUAH") AN EIGHT COUNTY COMMUNITY NEEDS ASSESSMENT (CNA) UNDERTAKEN IN COLLABORATION WITH: WESTCHESTER MEDICAL CENTER, MONTEFIORE MEDICAL CENTER, REFUAH HEALTH CENTER AND HEALTH ALLIANCE OF THE HUDSON VALLEY 1
AN EIGHT COUNTY COMMUNITY NEEDS ASSESSMENT (CNA) UNDERTAKEN IN COLLABORATION WITH: WESTCHESTER MEDICAL CENTER, MONTEFIORE MEDICAL CENTER, REFUAH HEALTH CENTER AND HEALTH ALLIANCE OF THE HUDSON VALLEY 1
Comparison of Care in Hospital Outpatient Departments and Physician Offices
 Comparison of Care in Hospital Outpatient Departments and Physician Offices Final Report Prepared for: American Hospital Association February 2015 Berna Demiralp, PhD Delia Belausteguigoitia Qian Zhang,
Comparison of Care in Hospital Outpatient Departments and Physician Offices Final Report Prepared for: American Hospital Association February 2015 Berna Demiralp, PhD Delia Belausteguigoitia Qian Zhang,
Council on Aging. Independence. Resources. Quality of Life. Guide to Programs and Services
 Council on Aging Independence. Resources. Quality of Life Guide to Programs and Services About Council on Aging As the Area Agency on Aging for Butler, Clermont, Clinton, Hamilton and Warren counties,
Council on Aging Independence. Resources. Quality of Life Guide to Programs and Services About Council on Aging As the Area Agency on Aging for Butler, Clermont, Clinton, Hamilton and Warren counties,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Cultivating External Partners as a Strategy in Achieving Your Hospital s Community Benefit Goals
 Cultivating External Partners as a Strategy in Achieving Your Hospital s Community Benefit Goals Association for Community Health Improvement Annual Conference March 2010 This work may be reproduced without
Cultivating External Partners as a Strategy in Achieving Your Hospital s Community Benefit Goals Association for Community Health Improvement Annual Conference March 2010 This work may be reproduced without
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Brian Sheitman MD
 Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Frequently Asked Questions
 Frequently Asked Questions Q: What is a clinically integrated network? A: Clinically integrated (CI) networks are integrated systems of hospitals, physicians and other medical facilities that collaborate
Frequently Asked Questions Q: What is a clinically integrated network? A: Clinically integrated (CI) networks are integrated systems of hospitals, physicians and other medical facilities that collaborate
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Financial Disclosure. Learning Objectives. None. Using Technology to Build a Grassroots Approach to A Community Needs Assessment
 Using Technology to Build a Grassroots Approach to A Community Needs Assessment Tim Mullett, MD Joan Scales, LCSW University of Kentucky, Lexington, Kentucky None Financial Disclosure Learning Objectives
Using Technology to Build a Grassroots Approach to A Community Needs Assessment Tim Mullett, MD Joan Scales, LCSW University of Kentucky, Lexington, Kentucky None Financial Disclosure Learning Objectives
Comprehensive Primary Care: Our Success Story
 Comprehensive Primary Care: Our Success Story March 2, 2016 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell,
Comprehensive Primary Care: Our Success Story March 2, 2016 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell,
New Facts and Figures on Hospice Care in America
 New Facts and Figures on Hospice Care in America NHPCO has just released the 2010 edition of NHPCO Facts and Figures: Hospice Care in America. Through an easy-to-read narrative that is written for the
New Facts and Figures on Hospice Care in America NHPCO has just released the 2010 edition of NHPCO Facts and Figures: Hospice Care in America. Through an easy-to-read narrative that is written for the
Articles of Importance to Read: UnitedHealthcare Goes Live With 13th Edition of Milliman Care Guidelines. Summer 2009
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
A Collaborative Approach to Integrating Mental Health Services with Pediatrics and Obstetrics for an Urban Population
 Mercy St. Vincent Medical Center Healthy Connections A Collaborative Approach to Integrating Mental Health Services with Pediatrics and Obstetrics for an Urban Population Healthy Connections: Multi-disciplinary
Mercy St. Vincent Medical Center Healthy Connections A Collaborative Approach to Integrating Mental Health Services with Pediatrics and Obstetrics for an Urban Population Healthy Connections: Multi-disciplinary
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013
 National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013 Understand the potential strengths of family- and patient-centered Medical
National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013 Understand the potential strengths of family- and patient-centered Medical
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Using An APCD to Inform Healthcare Policy, Strategy, and Consumer Choice. Maine s Experience
 Using An APCD to Inform Healthcare Policy, Strategy, and Consumer Choice Maine s Experience What I ll Cover Today Maine s History of Using Health Care Data for Policy and System Change Health Data Agency
Using An APCD to Inform Healthcare Policy, Strategy, and Consumer Choice Maine s Experience What I ll Cover Today Maine s History of Using Health Care Data for Policy and System Change Health Data Agency
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Improving Access in Infusion Therapy
 Improving Access in Infusion Therapy Timmi Anne Boesken, MHA, CPhT Medication Access Services Coordinator Kathryn Clark McKinney, PharmD, MS, BCPS, FACHE Director of Pharmacy Services Michelle Dusing Wiest,
Improving Access in Infusion Therapy Timmi Anne Boesken, MHA, CPhT Medication Access Services Coordinator Kathryn Clark McKinney, PharmD, MS, BCPS, FACHE Director of Pharmacy Services Michelle Dusing Wiest,
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Approaches to Extending Complex Care Models into the Community: Emerging Evidence
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
2018 DOM HealthCare Quality Symposium Poster Session
 Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:
 Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:") 2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
The Camden Coalition of Healthcare. Management
 Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
9/23/2015. Jackie F. Webb, DNP, FNP-BC Assistant Professor Linfield College
 Jackie F. Webb, DNP, FNP-BC Assistant Professor Linfield College Participants will understand differences between traditional care vs. group care Participants will describe effective components of group
Jackie F. Webb, DNP, FNP-BC Assistant Professor Linfield College Participants will understand differences between traditional care vs. group care Participants will describe effective components of group
Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population Health
 Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population Health B C Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population
Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population Health B C Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population
Medicaid and the. Bus Pass Problem
 Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Pathways Community HUB Certification Standards Background/Rational and Requirements
 1600 Research Blvd Rockville, MD 20850 240-314-2594 Pathways Community HUB Certification Standards Background/Rational and Requirements HUB PREREQUISITES PREREQUISITE #1 The HUB is an independent legal
1600 Research Blvd Rockville, MD 20850 240-314-2594 Pathways Community HUB Certification Standards Background/Rational and Requirements HUB PREREQUISITES PREREQUISITE #1 The HUB is an independent legal
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
11/18/2016. A Regional Medicaid Accountable Care Organization (ACO) that would leverage the existing behavioral health managed care foundation.
 that would leverage the existing behavioral health managed care foundation.") This collaborative effort gained momentum and resulted in the release of a white paper, which proposed a solution to the vision of the Governor and General Assembly for integrated care in a capitated environment.
This collaborative effort gained momentum and resulted in the release of a white paper, which proposed a solution to the vision of the Governor and General Assembly for integrated care in a capitated environment.
Billing Information. Patient Billing Information Patient Demographic Client / Ordering Physician Information Ordering Tests/Panels
 Billing Information Patient Billing Information Patient Demographic Client / Ordering Physician Information Ordering Tests/Panels This section provides instructions on how to process a patient and fill
Billing Information Patient Billing Information Patient Demographic Client / Ordering Physician Information Ordering Tests/Panels This section provides instructions on how to process a patient and fill
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
Care Redesign and Population Health
 Care Redesign and Population Health Care Redesign Amendment At stakeholder request, we asked CMS to approve an amendment to our All-Payer Model (Model) to obtain comprehensive patient level Medicare data
Care Redesign and Population Health Care Redesign Amendment At stakeholder request, we asked CMS to approve an amendment to our All-Payer Model (Model) to obtain comprehensive patient level Medicare data
The Memphis Model: Building Webs of Trust at Community Scale
 The Memphis Model: Building Webs of Trust at Community Scale Rev. Bobby Baker: Director of Faith and Community Partnerships & Dr. Teresa Cutts : Director of Research for Innovation The White House Sept.
The Memphis Model: Building Webs of Trust at Community Scale Rev. Bobby Baker: Director of Faith and Community Partnerships & Dr. Teresa Cutts : Director of Research for Innovation The White House Sept.
SUSAN G. KOMEN FOR THE CURE Greater Cincinnati Affiliate. Grant Writing Workshop December 8, 2011
 SUSAN G. KOMEN FOR THE CURE Grant Writing Workshop December 8, 2011 Workshop Goals 1. Familiarize applicants with the Greater Cincinnati Affiliate of Susan G. Komen for the Cure 2. Inform potential applicants
SUSAN G. KOMEN FOR THE CURE Grant Writing Workshop December 8, 2011 Workshop Goals 1. Familiarize applicants with the Greater Cincinnati Affiliate of Susan G. Komen for the Cure 2. Inform potential applicants
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
The National Association of Clinical Nurse Specialists (NACNS)
") The National Association of Clinical Nurse Specialists (NACNS) Response to the Institute of Medicine s Future of Nursing Report This document was prepared by an NACNS appointed task force that was tasked
The National Association of Clinical Nurse Specialists (NACNS) Response to the Institute of Medicine s Future of Nursing Report This document was prepared by an NACNS appointed task force that was tasked
5/5/2014. A National Best Practice Overview May Lauran Hardin MSN, RN CNL
 A National Best Practice Overview May 2014 Lauran Hardin MSN, RN CNL lauran@octoberday.com Disclosure Lauran Hardin I have no financial relationships with commercial interests with products or services
A National Best Practice Overview May 2014 Lauran Hardin MSN, RN CNL lauran@octoberday.com Disclosure Lauran Hardin I have no financial relationships with commercial interests with products or services
The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care
 Partnership to Improve Dementia Care") The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care Ohio Psychotropic Medication Nursing Facility Quality Improvement Project Ohio KePRO Nursing Home Quality Care Collaborative
The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care Ohio Psychotropic Medication Nursing Facility Quality Improvement Project Ohio KePRO Nursing Home Quality Care Collaborative
Partners Against Trafficking in Humans Project
 Partners Against Trafficking in Humans Project Fanell Williams, MSW, LSW Project Coordinator University of Toledo Human Trafficking and Social Justice Institute Photo credit: http://www.simpleimarketingsolutions.com/
Partners Against Trafficking in Humans Project Fanell Williams, MSW, LSW Project Coordinator University of Toledo Human Trafficking and Social Justice Institute Photo credit: http://www.simpleimarketingsolutions.com/
2016 Social Service Funding Application Non-Alcohol Funds
 2016 Social Service Funding Application Non-Alcohol Funds Applications for 2016 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
2016 Social Service Funding Application Non-Alcohol Funds Applications for 2016 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
2012 Community Health Needs Assessment
 Indiana University Health Goshen 2012 Community Health Needs Assessment A Report on Implementation Strategies to Address Community Health Needs Summary Report Our Commitment to You We are here for you,
Indiana University Health Goshen 2012 Community Health Needs Assessment A Report on Implementation Strategies to Address Community Health Needs Summary Report Our Commitment to You We are here for you,
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Community Health Needs Assessment Implementation Strategy Adopted by St. Vincent Charity Medical Center Board of Directors on April 5, 2017
 St. Vincent Charity Medical Center Community Health Needs Assessment Implementation Strategy Adopted by St. Vincent Charity Medical Center Board of Directors on April 5, 2017 Introduction In 2016, St.
St. Vincent Charity Medical Center Community Health Needs Assessment Implementation Strategy Adopted by St. Vincent Charity Medical Center Board of Directors on April 5, 2017 Introduction In 2016, St.
Advanced Medical Homes: Bending the Trend. Alan Glaseroff, MD Co-Director Stanford Coordinated Care
 Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Healthcare Reform & Role of the Nurse: Preparing for the Brave New World
 Healthcare Reform & Role of the Nurse: Preparing for the Brave New World Nena Bonuel, PhD, RN, CCRN-E, CNS, ACNS-BC Director, Nursing Strategic Initiatives, Harris Health System, Ambulatory Care Services
Healthcare Reform & Role of the Nurse: Preparing for the Brave New World Nena Bonuel, PhD, RN, CCRN-E, CNS, ACNS-BC Director, Nursing Strategic Initiatives, Harris Health System, Ambulatory Care Services
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Mental Health Engagement Network (MHEN): Facilitating Mobile Patient Centric Care
: Facilitating Mobile Patient Centric Care") Mental Health Engagement Network (MHEN): Facilitating Mobile Patient Centric Care Presentation Outline MHEN Project Context MHEN Project Results and Findings Lessons Learned and Implications Sandbox Mental
Mental Health Engagement Network (MHEN): Facilitating Mobile Patient Centric Care Presentation Outline MHEN Project Context MHEN Project Results and Findings Lessons Learned and Implications Sandbox Mental
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Central Iowa Healthcare. Community Health Needs Assessment
 Central Iowa Healthcare Community Health Needs Assessment October 20, 2016 Table of Contents Executive Summary 1 Introduction 3 Summary Observations from Current CHNA 5 Information Sources and Data Collection
Central Iowa Healthcare Community Health Needs Assessment October 20, 2016 Table of Contents Executive Summary 1 Introduction 3 Summary Observations from Current CHNA 5 Information Sources and Data Collection
Health Information Technology and Coordinating Care in Ohio
 Health Information Technology and Coordinating Care in Ohio 1 Dan Paoletti, CEO Ohio Health Information Partnership CliniSync Health Information Exchange Health Information Technology in Ohio HITECH Federal
Health Information Technology and Coordinating Care in Ohio 1 Dan Paoletti, CEO Ohio Health Information Partnership CliniSync Health Information Exchange Health Information Technology in Ohio HITECH Federal
School of Public Health University at Albany, State University of New York
 2017 A Profile of New York State Nurse Practitioners, 2017 School of Public Health University at Albany, State University of New York A Profile of New York State Nurse Practitioners, 2017 October 2017
2017 A Profile of New York State Nurse Practitioners, 2017 School of Public Health University at Albany, State University of New York A Profile of New York State Nurse Practitioners, 2017 October 2017
Turning Big Data Into Better Care
 Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
A Care Coordination Model for Value-Based Performance Programs
 A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
Tufts Health Unify. A One Care plan (Medicare-Medicaid) for people ages March 16, /27/2017 1
 for people ages March 16, /27/2017 1") Tufts Health Unify A One Care plan (Medicare-Medicaid) for people ages 21-64 March 16, 2017 3/27/2017 1 About Tufts Health Plan Founded in 1979, Tufts Health plan is a nonprofit organization nationally
Tufts Health Unify A One Care plan (Medicare-Medicaid) for people ages 21-64 March 16, 2017 3/27/2017 1 About Tufts Health Plan Founded in 1979, Tufts Health plan is a nonprofit organization nationally
2018 IMPLEMENTATION PLANS. of the 2016 Community Health Needs Assessment
 2018 IMPLEMENTATION PLANS of the 2016 Community Health Needs Assessment After examining the range of services currently available, significance, impact ability, relevance to the population served, and
2018 IMPLEMENTATION PLANS of the 2016 Community Health Needs Assessment After examining the range of services currently available, significance, impact ability, relevance to the population served, and
The MetroHealth System
 The MetroHealth System June 16, 2016 Presentation to Ohio Joint Medicaid Oversight Committee Dr. James Misak, Vice Chair of Community and Population Health, Department of Family Medicine Susan Mego, Executive
The MetroHealth System June 16, 2016 Presentation to Ohio Joint Medicaid Oversight Committee Dr. James Misak, Vice Chair of Community and Population Health, Department of Family Medicine Susan Mego, Executive