Three Pillars of Long Term Care Strategy: Quality/Data, Compliance, Customer Service/Engagement
|
|
|
- Rudolph Cook
- 6 years ago
- Views:
Transcription


1 Three Pillars of Long Term Care Strategy: Quality/Data, Compliance, Customer Service/Engagement Susan LaGrange, RN. BSN, NHA Director of Education, Pathway Health 1 Objectives Upon Completion of this program, attendees will be able to: Review the health care shifts and initiatives driving change in post-acute care Understand the Three Pillars of tomorrow s health care and the leader s role for positive outcomes Describe the push for data-driven quality outcomes, compliance history, and consumer engagement, all of which will shape your position in the long term care profession 2 1


2 Objectives (continued) Discuss the impact on hospital readmission, falls, infection control and pain management on quality Identify five leadership strategies to implement change for positive outcomes and improved operations 3 Health Care Shifts To Post Acute Care 4 2


3 The Journey Begins 7/24/12 It is time for CHANGE! All rights reserved. Copy with permission only. 6 3

4 Leadership Strategies 7 4


5 THE COURSE HAS BEEN SET! Industry Landscape Trends and Health Care Reform Post Acute Care Impact Reality Check Operational Challenges Impact on Consumers Examples of Redesign in new environment 10 5


6 Challenges - Post Acute Care Government Unrest Reform of Health Care as we know Reimbursement Changes Increased Costs Regulatory Changes External Oversight 11 Challenges Post Acute Care 6


7 Health Care Climate 14 7


8 Challenges - Post Acute Care 15 Government Response Need to Reform Health Care! Decrease Costs Decrease Reimbursement Increase Quality Increase Access 16 8
9 Government Response Patient Protection and Affordable Care Act (PPACA) Signed into effect March 23, 2010 Reform Private Insurance Reform Public Insurance Improve coverage to those with pre-existing conditions Expand access to care Reduce long term costs of health care Health Care Reform Outcomes Accountable Care Act (ACA) Link reimbursement to quality outcomes Move from Fee for Service to Bundled Payment methods Person Centered Care Consumer engagement and access to data 18 9

10 Destination: Quality + Value = Lower Cost Start 2010 Arrival 2015 and beyond 19 KNOWLEDGE AND RESOURCES 10




11 Complex Health Care Environment 21 National Positioning of HealthCare Delivery Innovation Center A new engine for revitalizing and sustaining the Medicare, Medicaid and CHIP programs and ultimately to help to improve the healthcare system for all Americans. Flexibility and resources Test innovative care models Test innovative payments models Accountable Care Organizations 22 11





12 Dual Eligible Initiative Reforming Medicaid Accountable Care Initiatives CMS Strategic Plan 2014 CMS Triple AIM 12
 to establish a national strategy that will improve: The delivery of health care services Patient health outcomes Population")
13 HEALTH CARE QUALITY National Quality Strategy Introduction The Affordable Care Act (ACA) requires the Secretary of the Department of Health and Human Services (HHS) to establish a national strategy that will improve: The delivery of health care services Patient health outcomes Population health 13


14 The strategy is to concurrently pursue three aims: Better Care Healthy People/Healthy Communities Affordable Care National Quality Strategy From the National Strategy for Quality Improvement in Health Care gforquality/nqs/nqs2013an nlrpt.htm Guiding force in quality improvement efforts across the nation and health care entities Develop a national QAPI model 14

 National Quality")
15 National Quality Strategy Adopts unified measures Across federal government, private sector, States, health systems and providers Guage performance outcomes Create continuity Consistency between providers Creates a buying Value initiative (VBP) National Quality Strategy 15
16 Priority 1: Making care safer by reducing harm caused in the delivery of care LONG-TERM GOALS 1. Reduce preventable hospital admissions and readmissions. 2. Reduce the incidence of adverse health care-associated conditions. 3. Reduce harm from inappropriate or unnecessary care. 31 Priority 2: Ensuring that each person and family members are engaged as partners in their care LONG-TERM GOALS 1. Improve patient, family, and caregiver experience of care related to quality, safety, and access across settings. 2. In partnership with patients, families, and caregivers and using a shared decisionmaking process develop culturally sensitive and understandable care plans. 3. Enable patients and their families and caregivers to navigate, coordinate, and manage their care appropriately and effectively


17 Priority 3: Promoting effective communication and coordination of care LONG-TERM GOALS 1. Improve the quality of care transitions and communications across care settings. 2. Improve the quality of life for patients with chronic illness and disability by following a current care plan that anticipates and addresses pain and symptom management, psychosocial needs, and functional status. 3. Establish shared accountability and integration of communities and health care systems to improve quality of care and reduce health disparities. 33 Priority 6: Making quality care more affordable for individuals, families, employers, and governments by developing and spreading new health care delivery models LONG-TERM GOALS 1. Ensure affordable and accessible high-quality health care for people, families, employers, and governments. 2. Support and enable communities to ensure accessible, high-quality care while reducing waste and fraud. Reducing costs must be considered hand-in-hand with the aims of better care, healthier people and communities, and affordable care. The National Quality Strategy will foster strategies that reduce waste from undue administrative burdens and make health care costs and quality more transparent to consumers and providers, so they can make better choices and decisions


18 New Health Care Environment INITIATIVES IN MOTION 36 18

19 37 Accountable Care Act Initiatives Remember Still in Effect Sequestration Across the board federal budget reductions March 1/2013 State Survey Agencies are affected S&C Memo ALL Revisit survey protocols Special Focus Facility Last chance FINAL survey Home Health Targeted Surveys Complaint Investigations 38 19
20 Accountable Care Act Initiatives Initiatives currently in motion Hospital Readmission Reduction Program Fraud and Abuse QAPI Corporate Compliance Bundle Payment Demonstration Community Based Services Enhancing Patient Safety Accountable Care Act Initiatives Initiatives in motion Dementia Initiative Unnecessary Medications - Antipsychotic Abuse prevention training updates National program for background checks Person Centered Care Equalize certain payments between Inpatient Rehab and SNF Health Information Technology 20
21 CMS and OIG Updates NEW! CMS QAPI Development POC to be aligned with QAPI approach Surveyors, regulatory guidance and QAPI next steps Involve residents and families with QAPI CMP Analytical Tool Per day vs. per instance Abuse and Neglect clarification Electronic POCs OIG Work Plan 2014 Medicare Part A Billing ¼ of all claims billed in error High Therapy RUGs vs Resident characteristics Medicare Part B Billing State Agency Verification of Deficiency Outcomes QoC and Safety Verifying POCs and actual quality outcomes National Background Checks Hospitalizations of nursing home residents for manageable and preventable conditions 25% of SNF Med A beneficiaries were hospitalized as a result of condition that to be manageable or preventable in SNF indicates QoC problems in SNF Plan-2014.pdf Accountable Care Act Initiatives Initiatives in motion Expand Medicare and Medicaid sharing of information between entities DATA! Quality Initiatives Benchmark data, standards of practice, compliance and set expectations for reimbursement Bundle Payment methodology by 2017! Medicare Value Based Purchasing Performance based pay Quality metrics P4P 21
22 ICD 9 to ICD 10 Transition Education Implementation Preparation Operational Readiness H.R Protecting Access to Medicare 2014 Sustainable Growth Rate SRG Doc fix repeals the 24% cut for Physicians Extension of Therapy Caps Extension of the two midnight rule for acute care Skilled Nursing Facility Readmission Measure (10/1/15 All Cause All condition hospital readmission factor) must be specified by the Secretary phase in 2016 and beyond Public Reporting of SNF Readmission and other performance measures 22



23 NEW Initiative! Value based purchasing - VBP HR 4302 full implementation 10/2019 Drivers and Effects of Value-Based Care Kaufman Figure 1. Source: Kaufman, Hall & Associates, Inc. 23

 Specific Dx and Bundled/Episodic payment http://www.cms.")
24 New Era of Healthcare Quality and Efficiency VBP Acute care and SNF Initiatives Acute Care "Affects payment for inpatient stays in 2,985 hospitals across the country Quality Measures Clinical Processes of Care Outcomes of Care Patient Care Experience Satisfaction Mortality Efficiency Penalties (HRRP, HAI, QM, Care Transitions, more) Specific Dx and Bundled/Episodic payment 24

25 VBP It s Not Going Away Acute Care and SNF SNF VBP Premise Quality Oversight Broad infrastructure exists to support quality oversight SNF prospective payment system (PPS), Based on costs and resources Does not provide strong incentives for furnishing high quality care CMS views implementation of a SNFVBP program as an important step in revamping how Medicare pays for health care services, Move Medicare towards rewarding better value, outcomes, and innovations instead of the volume of services provided. Payment/SNFPPS/Downloads/SNF-VBP-RTC.pdf VBP Acute Care and SNF Initiatives SNF VBP Premise Using financial incentives to reward quality and improvement in health care VBP programs aim to hold providers accountable for the quality of care they provide to Medicare beneficiaries, Promote more effective, efficient and high quality care processes, and address the variation in quality across care settings. Payment/SNFPPS/Downloads/SNF-VBP-RTC.pdf 25
26 VBP Acute care and SNF Initiatives SNFVBP program will align with many of the Department of Health and Human Services (HHS) and CMS s efforts to improve coordination of care. CMS s plan to implement a SNFVBP - consistent with the National Quality Strategy to promote health care that is focused on the needs of patients, families, and communities. Better Care: Improve the overall quality of the health care system, by making health care more patient-centered, reliable, accessible, and safe. Healthy People and Communities: Improve the health of the United States population by supporting proven interventions to address behavioral, social, and environmental determinants of health in addition to delivering higher-quality care. Affordable Care: Reduce the cost of quality health care for individuals, families, employers, and government. HR 4302 Components For SNF VBP SNF Performance Scores SNF Ranking Based on Performance Scores Readmission Rate first measure Quality Measures alignment with health care providers Value Based Incentive Payment Public Reporting 26
27 Steps to Design SNF VBP PER CMS 1. Continuous Quality Improvement Framework - QAPI 2. Consider adoption of Structural measures related to E H R 3. Defining SNFVBP Population (Medicare, Medicaid and other) 4. Enhanced Data Infrastructure and Validation process 5. Performance Scoring and Evaluation Model considerations(specific targets and overall improvement) a. MDS Measures b. Survey and Certification c. Staffing Steps to Design SNF VBP PER CMS 5. Performance Scoring and Evaluation Model (continued) a. Readmission rates b. Satisfaction Surveys c. Five Star Quality Rating 6. Funding Source/Performance Incentive Funds 7. Transparency and Public Reporting 8. Coordination across Medicare Payment System Align with all other VBP programs 27


28 VBP is Around the Corner 28
29 INTERNAL REVIEW Assess Organizational Readiness Assess Organization Systems Corporate Programs and Outcomes Facility specific protocols Assess need to change Benchmark internal systems for review Current status Industry standards Best practice approach Identify opportunities 29

30 Assess Organizational Readiness Assess Clinical Readiness Your Role Industry initiatives Market initiatives and expectations Quality Outcomes Payer and External Expectations Consequences Internal competency process Right People and Right Roles 30
31 Leadership Implementation Strategies 1. Clarify Change Clear about why change is needed and being implemented Work through with your team Will change? Require unknown tasks New relationships New methods of working Threats to current operations New training or retraining Right people in right roles (Resources and Capabilities) Leadership Implementation Strategies 2. Build a case for change Outline what organization will look like at end of change Outline clear case - quantitative and qualitative needs Assess Drivers for Change Business as usual? Impact? Barriers Performance metrics in terms of business objectives Link to vision of future if change is successful 31
32 Leadership Implementation Strategies 3. Communicate Need for Change Your team at ALL levels needs to understand the need for change and respective roles Communicate clear vision Current State of organization Desired future state Define, document and specify the change Anticipate and address staff responses to change Leadership Strategies Ownership Acceptance Resistance Denial Time Anxiety Executives Managers Employees 32


33 Leadership Implementation Strategies 4. Develop Teams Action oriented team Mix of technical competencies, expertise, levels of seniority and informal leaders Engage Mavericks Appoint leads to streamline plan and actions for implementation Leadership Implementation Strategies 5. Identify Barriers Acknowledge and address barriers Organizational Operational Clinical Organization Readiness Training, Knowledge, Resources Talent Management Obstacles to Opportunities 33


34 Internal Review and Implementation After Internal Review, Determination of Readiness and Communicating Change. Develop Quality and Implementation Strategy Goals Prioritize Impact Systems and tools needed to change processes Resources applied or needed Time frames Approval/Agreement QUALITY OUTCOMES AND DATA: FUTURE OF HEALTHCARE 34



35 Quality Outcomes: Data We are transforming Medicare from a passive payer, to an active purchaser of value Tom Valuck Assistant CMS Administrator Quality Care + Data = Reimbursement 35

36 One thing you can control to some degree is performance! Quality Outcomes: Data Outcome data and performance Industry and Regional Trends Consumer Satisfaction Quality Measures MDS 3.0, OASIS C, Quality Initiatives Hospital, Nursing Home, Home Care Compare websites Regulatory data Re admission Rates 36


37 Current #1 Data Source Quality Outcomes: Data Data and Performance Who is measuring your performance? Customers, consumers, the facility State, consumers, press/media How are you measuring your performance? Quality Improvement processes Consumer Surveys External Surveys Compliance History 7/24/12 37
38 Organizational Data: The New Path to Value Determine Quality Profile: Assess Organization Data Review Internal Processes: Optimize Data Establish an Information Agenda for Planning Leadership today Data Driven Decisions! Your data is key to positive outcomes. 21 st Century Leadership Data Driven Decisions Understand what the real business question is. (Who, What, Why, When, How) Create an analysis plan with hypotheses. Collect or review the right data Gather insights Make recommendations Take action 38



39 PREPARATION AND PREPAREDNESS 78 39




40 Preparedness and Protection Preparedness and Protection 40


41 Preparedness and Protection Preparedness and Protection 41
42 Preparedness and Protection High Risk Areas Sudden changes in billing Spikes in billing Compromised identities (provider/beneficiary) High error rates RUG changes or discrepancies Overpayments/underpayments Preparedness and Protection Negative Outcomes Administrative Actions Suspension of payments Exclusion from participation Criminal action 42

43 Preparedness and Protection Strategies Internal and External monitoring Education/Knowledge Documentation Policies and Procedures Staffing Right Roles Preparedness and Protection 43


44 Preparedness and Protection INNOVATION AND IMPLEMENTATION 88 44


45 Find Your Organization s Position on the New Health Care Map! Implementation and Innovation 45

46 Specialty Units Partnership s Adult Day Services Senior Services Implementation Facility Overall Goals Increase communication Efficiency and effectiveness Collaboration with partners Reduce redundancy Determine roles and anticipated processes Improve patient outcomes Care Transitions 46
47 Implementation Facility Strategic Positioning Readiness Benchmark Data Compare Data Nursing Home Compare Hospital Compare: Home Health Compare: Implementation and Innovation For Sustainability Preparation Operational Readiness Assessment Services Internal Systems Team composition Increase clinical competencies Validation and benchmark data Excellent outcomes quality and financial Evaluate, reposition, partner and implement 94 47


48 The Three Pillars 1. QUALITY AND PERFORMANCE 2. CUSTOMER ENGAGEMENT AND SATISFACTION 3. COMPLIANCE 96 48

49 Quality and Performance Consumer Engagement and Satisfaction Compliance 5/21/2014 Three Pillars of The Future of Health Care Affordable Care Act National Quality Strategy HR 4302 QAPI HHS/CMS Strategic Plan/Triple Aim /Work Plans OIG - Work Plans/Compendium Fraud Prevention System Hospital Readmission Reduction Program 49

50 Challenges Post Acute Care Government Unrest Reform of Health Care as we know Reimbursement Changes Increased Costs Regulatory Changes External Oversight 99 Government Response Reform Health Care Decrease Costs Decrease Reimbursement Increase Quality Increase Access
 must be specified by the Secretary phase in 2016 and beyond Public Reporting of SNF Readmission and")
51 H.R Protecting Access to Medicare 2014 Sustainable Growth Rate SRG Doc fix repeals the 24% cut for Physicians Extension of Therapy Caps Extension of the two midnight rule for acute care Skilled Nursing Facility Readmission Measure (10/1/15 All Cause All condition hospital readmission factor) must be specified by the Secretary phase in 2016 and beyond Public Reporting of SNF Readmission and other performance measures 101 HR 4302 Section 215, Skilled Nursing Facility Value- Based Purchasing: (1) READMISSION MEASURE,-Not later than October 1, 2015, the Secretary shall specify a skilled nursing facility allcause all-condition hospital readmission measure (or any successor to such measure) (2) RESOURCE USE MEASURE.- Not later than October 1, 2016, the Secretary shall specify a measure to reflect an all condition risk-adjusted potentially preventable hospital readmission rate for skilled nursing facilities
52 HR 4302 Beginning October 1, 2016, and with each quarter thereafter, the Secretary will provide confidential feedback reports to SNF s on the performance of the Readmission Measure Public reporting: the Secretary will establish procedures for public reporting of the measures on Nursing Home Compare SNF s will have opportunity to review and submit corrections prior to information becoming public 103 HR4302 You can access H.R at: 113hr4302enr/pdf/BILLS- 113hr4302enr.pdf
53 (Once Again) Assess Organizational Readiness Assess Clinical Readiness Your Role Industry initiatives Market initiatives and expectations Quality Outcomes Payer and External Expectations Consequences Internal competency process Right People and Right Roles 105 Hospital Readmission Reduction Program Medicare spends > $25 billion/year on unnecessary readmissions from SNFs and other post-acute care providers About 18% of all Medicare hospitalizations are rehospitalizations. Being admitted to the same or to a different hospital within 30 days of discharge, for certain applicable conditions Goal Reduce hospital readmission rates Reduce rates by 25% and save over $2 billion annually
54 Hospital Readmission Reduction Program If You Remember.Effective October 1, 2012 Diagnoses and conditions 258 reviewed First 3 to be monitored Heart Failure (CHF) Pneumonia Heart Attack (AMI) NOW Septicemia UTI FUTURE: All-Cause 107 Hospital Readmission Reduction Program CMS will recover/reduce payments for readmissions 2013 up to 1% total Medicare billings up to 2% 2015 up to 3%

55 Co-ordination Counts For fully integrated providers that form accountable care organizations teams of providers that coordinate care payments will be bundled to cover all of a patient s care. But for most providers which are not integrated payments must be bundled for an episode of care, with providers dividing the payment among themselves Accountable Care Organizations Variety of Health Care Providers working together As a Group Accountable for the quality and the $$ of care Quality outcomes will be rewarded Will choose providers wisely! Will evaluate your quality data Goal: Better Outcomes at a Lower Cost


56 CMS Action Plan 3 Part AIM 1. Improving the individual experience of care; 2. Improving the health of populations; and 3. Reducing the per capita cost of care for populations. 111 SUCCESSFUL PLANNING


57 Next Steps Begin a Quality Assurance/Performance Improvement project on re-hospitalization. Begin gathering and analyzing data Identify trends Search for gaps in care Review any advanced care planning steps. 113 Operations People Human Resources Re hospitalization Supplies and Equipment Methods Policies and Procedures
58 Care Transition Management Comprehensive Communication Coordination of Care Resident/Family Teaching with evidence of understanding Will work towards: Decreased chance of medication errors Hospital readmissions GREAT resource-amda Clinical Practice Guideline: Transitions of Care in the Long-Term Care Continuum: Process Investigation and Correction Are Weekends a Problem? Ask WHY - Common causes include: Changes in MD coverage - alternate unfamiliar with resident Nurse Practitioner less available Unfamiliar weekend staff Staffing levels Assessment skill levels fewer nursing leadership staff available for direction & decision making
59 Medical Director or Extender Staff Is there trust in the skills of corresponding staff? If not, WHY? Common causes include: Lack of assessment skill Lack of thorough communication of details and analysis at facility level Call without enough data accessible to answer questions 117 Resident and Family Incomplete advance directives Lack of trust in facility staff Poor communication of options Uninformed about risks/benefits Unresolved acute care or transition problems **Cover all bases with family in person or by phone find out fears and expectations
60 INTERACT Program Designed to improve the quality of nursing home care Provides tools, resources to staff to reduce avoidable acute care transfers Supported by Centers for Medicare and Medicaid Services Early identification of change in resident status Improved documentation 119 INTERACT Program Enhances communication Guides nursing home staff when there is a change in the resident status. Provides an opportunity to improve quality of care Advanced care planning
61 Reducing Unnecessary Hospitalizations Successfully integrate a system to improve care Reduce hospital admissions when possible Develop a win-win relationship with strategic partners Utilize system management for marketing strategies 121 Get It Together Establish a core committee Develop and reinforce communication with referral sources Establish your mutual goals patient stability and management without readmission to hospital Meet face to face to identify what each of you need to do to make it happen
62 Team Work & Collaboration Medical Director to assist with training Facility review of Interact clinical pathways Pharmacy management and training on high risk medications Additional education provided by Lab, therapy, or physician extenders The complexity of services provided and the skill level of nursing. 123 SBAR and Communication SBAR was developed by our United States Navy. Submariners use this communication tool. It was adopted by the airline industry after investigations of crashes in the 70 s showed the main cause was a breakdown in communication between the pilots in the cockpit. Works well in their stressful, time-critical, emergency situations
63 SBAR The SBAR technique provides a framework for communication between members of the health care team about a patient's condition. It allows for an easy and focused way to set expectations for what will be communicated and how between members of the team, which is essential for developing teamwork and fostering a culture of patient safety. 125 Situation The situation describes the problem It is a to-the-point punch-line Communicated in 5-10 seconds to get the attention of the receiver. Included are: Identification of yourself your name and unit Patient s name, physician, and room number Brief and to-the-point statement of your concern
64 Background Prior to speaking with the other person: Anticipate what information the receiving person needs. Have all the relevant information in front of you. Have the medical record / electronic record open to that patient. Using SBAR notepad, write down all information. Practice conversation if uncomfortable with the situation. 127 SBAR Prior to calling the physician Have I seen and assessed the patient myself before calling? Has the situation been discussed with resource nurse Review the chart for appropriate physician to call. Know the admitting diagnosis and date of admission. Have I read the most recent MD progress notes and notes from the nurse who worked the shift ahead of me?

65 SBAR Have available the following when speaking with the physician: Resident chart List of current medications, allergies, IV fluids, and labs Most recent vital signs Reporting lab results: provide the date and time test was done and results of previous tests for comparison Code status 129 SBAR Once Again - When calling the physician : Situation: What is the situation you are calling about? Identify self, unit, patient, room number. Briefly state the problem, what is it, when it happened or started, and how severe
66 SBAR Background: Pertinent background information related to the situation could include the following: The admitting diagnosis and date of admission List of current medications, allergies, IV fluids, and labs Most recent vital signs Lab results: provide the date and time test was done and results of previous tests for comparison Other clinical information Code status 131 SBAR Assessment: What is the nurse s assessment of the situation? Be precise on the assessment Review the advanced care plan Recommendation: What is the nurse s recommendation or what does he/she want? Examples: Notification that patient has been admitted Patient needs to be seen now Order change
67 The Benefits of SBAR (SBAR) provides a standardized way of communicating. It promotes patient safety through efficient and accurate communication. It helps facilitate a shared set of expectations. Staff and physicians can use SBAR to share patient information in a concise and structured format. 133 Why Physicians Like SBAR The nurse gets straight to the point, It has essential pieces of information The guessing game is eliminated Nurses are trained to write care plans more Narrative in nature. Physicians, however, are trained to use headlines or bullet point notations. SBAR gets to the point
68 First Steps with Implementation Review your current communication systems. Complete an analysis of problem areas with the current communication. Review your current documentation systems. Identify any opportunities for improvement prior to initiating the SBAR form. 135 First Steps with Implementation Take the opportunity to participate in daily report and shift to shift report for at least 7 days on all shifts. Review the 24-hour report. Complete walking rounds with the nursing assistants. Develop an interdisciplinary team of nurses from all shifts to review the current gaps in communication
69 ACTION PLAN Determine which tools you will use Interact Facility Specific designated tools Staff Education Implementation of Program Evaluation 137 Policy and Procedure From Preadmission to Discharge! Assessment Forms (Preadmission -> Discharge) Monitoring requirements Staff Training Care Planning Documentation Notifications


70 Auditing Tools Preadmission Audits Admission Documentation Audits Assessment Audits Rehospitalization Root Cause Audits Documentation Audits Care Planning Audits 139 Quality Mapping Assess need to change Benchmark internal systems for review Current status Industry standards Best practice approach Identify opportunities

71 Action Plan AREA OF CONCERN RECOMMENDATIONS GOAL DATE RESPONSIBLE PERSON Lung Assessment not completed with resident s/s productive cough (Pneumoni a dx) 1. Nurse re-educated in assessment process with return demonstration of lung assessment. 2. Nurse re-education in documentation requirements. 3. Follow up review of assessment and documentation each shift 6/5/14 6/5/14 Beginning 6/5/14 DON or Nurse Manager DON or Nurse Manager DON or Nurse Manager 141 Quality Mapping Develop quality strategy Goals Prioritize Impact Systems and tools needed to change processes Resources applied or needed Time frames Approval/Agreement
72 Quality Mapping Training Plan Educate all levels Why change is needed Process changes Roles and Responsibilities Measurement and Communication of Success Not a quick fix 143 QAPI Together, Quality Assessment and Process Improvement provide the model for: effective problem identification root cause analysis system and culture changes Establish care delivery improvements to realize healthcare consumer defined goals
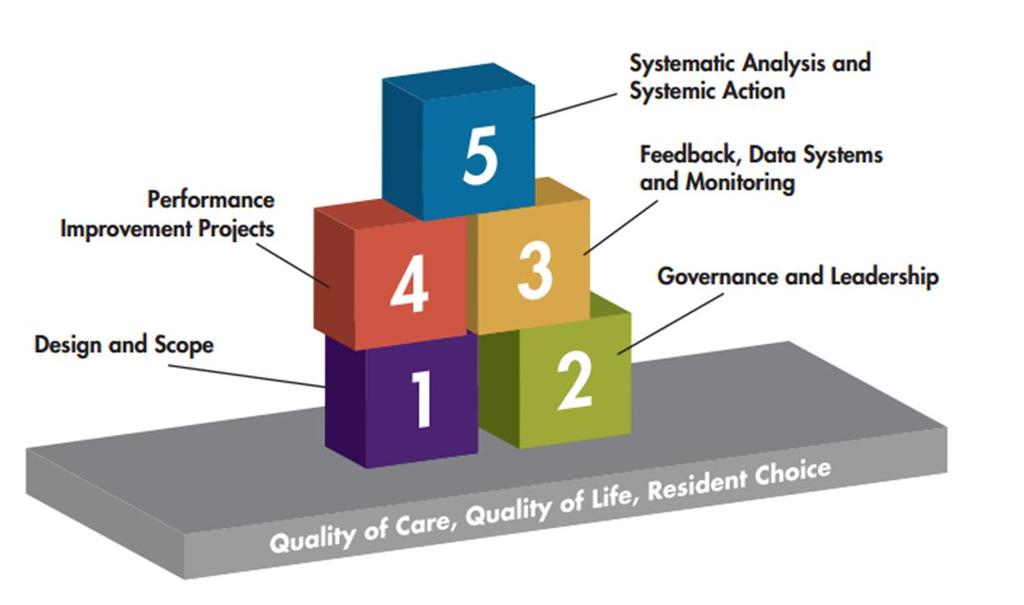
73 Establish Leadership Accountability Establish commitment of: Executive leadership, including the board of directors in non-profit homes, owners of other homes, and the directors of publicly traded nursing homes. Corporate leadership personnel set a climate and provide resources to help leadership flourish in each home. 145 QAPI must include: Ongoing & organized use of data and feedback from multiple sources Approach to early problem identification Root Cause Analysis Performance Improvement projects Understanding how systems of care might affect quality outcomes Systemic Action Involvement of all staff in quality mission University of MN, Division of Health Policy and Management and Stratus Health

74 Rewards of QAPI Competencies that equip you to solve quality problems and prevent further occurrences Competencies that allow you to seize opportunities to achieve new goals Staff fulfillment when goals are achieved Better Care for residents Better quality of life for residents University of MN, Division of Health Policy and Management and Stratus Health 147 Keep the team informed Celebrate small successes Post the data Keep accountability by ongoing review. Develop a standard of excellence
75 Consequences for SNF s HR 4302 Value-Based Incentive Payment Percentage Based on the SNF performance score of the skilled nursing facility Value-based incentive payment Quality Performance Standards = $$ **Hospital Readmissions will be part of this! 149 In Summary: Prepare ALL staff now! Look at your data Develop an Action Plan Consider a QAPI, PIP Involve the ENTIRE team! Ongoing re-evaluation Monitor Data Ongoing Communication Always Follow up! Position Yourself Successfully for the Future


76 FALLS MANAGEMENT PROGRAM FOR QUALITY A Culture of Safety?

77 F323 Intent is that the facility provides an environment that is free from hazards over which the facility has control and Provides appropriate supervision to each resident to prevent avoidable accidents. 153 F323 This includes systems and processes to: Identify hazard(s) and risk(s); Evaluate and analyze hazard(s) and risk(s); Implement interventions to reduce hazard(s) and risk(s); and Monitor for effectiveness and modify approaches as indicated. Residents receive supervision and assistive devices to prevent avoidable accidents
78 Definition: Unavoidable Accident Accident occurred when: Environmental hazards had been identified Resident risks were identified Hazards & risks were assessed Interventions were implemented to decrease hazards and risk Effectiveness of interventions were being monitored and modified as needed 155 Definition: Avoidable Accident Accident occurred related to failure to: Identify environmental hazard Identify individual resident risk factors Evaluate/analyze hazards & risks Implement interventions to reduce an accident Monitor and modify interventions as needed

79 Definition: Adequate Supervision An intervention to decrease the risk of an accident. Adequate supervision must be based on individual resident s needs and identified hazards in the resident s environment. 157 Fall Definition Unintentional change in position coming to rest on the ground, floor or onto the next lower surface (e.g. onto a bed, chair, or bedside mat). The fall may be witnessed, reported by the resident or an observer or identified when a resident is found on the floor or ground. Falls include any fall, no matter whether it occurred at home, while out in the community, in an acute hospital or a nursing home. Falls are not a result of an overwhelming external force (e.g. a resident pushes another resident). An intercepted fall occurs when the resident would have fallen if he or she had not caught him/herself or had not been intercepted by another person this is still considered a fall. -MDS 3.0 RAI Manual

80 Steps for System Overview: Resident Risk Identification Resident Assessment Risk Factors Resident Vulnerabilities Realistic Goals INVESTIGATION and Root Cause Analysis Fall Prevention Interventions Creative Individualized 159 Steps for System Overview: Assistive Devices Hazards and/or Positioning Devices Unsafe Wandering &/or Elopement Resident Smoking Chemicals Oxygen Use
 Policies and Procedures Culture of Safety, Prevention, Quality Assessment Process Hazard Identification")
81 Environmental Rounds Hazards Electrical cords Beds by heat registers Carpet condition Handrails secure Sharp edges on furniture Chemicals secured Sharps secured Equipment working properly 161 Operational Updated Policies and Procedures for Accident Prevention Staff Education (examples) Policies and Procedures Culture of Safety, Prevention, Quality Assessment Process Hazard Identification Equipment Use Consistent Implementation of Care Plan Interventions Safe Lifting and Transfers Investigation and Root Cause Analysis Communication

82 QAPI QUALITY ASSURANCE AND PERFORMANCE IMPROVEMENT 163 QAPI QA Quality Assurance (F520 QA&A, Quality assessment & assurance) Identifies and corrects quality issues Retrospective Focus on outliers or individuals Efforts end once achieved DON, Physician and 3 staff members Meet quarterly

 Systematic, Comprehensive, Data-driven, Proactive approach QAPI System")
83 Performance Improvement PI - Performance Improvement Proactive approach Efforts are on-going Focus on system changes Plan involves input from staff representing all roles and disciplines within the organization Meet at more frequent intervals 165 QAPI QAPI (Quality Assurance & Performance Improvement) Systematic, Comprehensive, Data-driven, Proactive approach QAPI System Changes 83

84 What is Your Commitment? It must include: Blameless problem-solving Involvement of those most affected by the issue Willingness & means to coach & mentor after training Person-centered care 167 QAPI is resident-centered yet built on systems thinking. QAPI involves everyone who works in your facility
85 Making Data Meaningful Without a baseline or point of comparison, it is hard to judge your own performance. QAPI uses performance indicators to monitor care processes and outcomes. It reviews findings against benchmarks, or targets the facility has established for performance. Objective data (Numbers) will give you concrete information on improvement, decline or maintenance of goals! 169 Benchmarking Identifying a standard against which facility processes can be measured - Benchmarking is the process of comparing your results to best practices & the performances of your peers
86 PIP Process Improvement Projects examine performance & make improvements In any area needing attention Found to be a high priority based on the needs of the residents. Or ACCIDENT PREVENTION is an EXCELLENT PIP! 171 Let s Look at Fall Prevention Where could the problem start? How effective is your restorative program? Do residents lose function through reduced mobility? Could you review ambulation status to find out?
87 Use Your Data MDS 1. Run a report of Current Mobility Status for this quarter and last quarter walk in room, walk in corridor 2. Compare it to report from last quarter 3. Have there been changes, declines? 173 What to Look For - Trending Look for trends in conjunction with wing, diagnosis, falls, behaviors the more granular, the more effective your root cause analysis will be. Location - room, hallway, bathroom Devices in use, call lights, alarms, etc
88 Questions Reasons for the mobility decline-root Cause Analysis Interview direct care-giving staff, family, resident for their perspectives regarding why the decline happened Document interview results & analyze 175 Employee Participation Include staff members at all levels, all departments, in program development, implementation & support. Leaders facilitate, provide resources, and coach- ALWAYS include your care giving staff in decision making

89 Resident/Family Alliances Establish commitment to Falls and Injury Prevention Market your commitment Pre-admission considerations Admission assessment in-put ALWAYS include the resident/family in assessment findings & Education if responsible, or with resident permission 177 Risk Assessment Tools Risk assessment tools by themselves do not prevent patient falls - they predict them * *National Patient Safety Foundation Professional Learning Series


90 When to Assess? On admission* Upon transfer from one unit to another* With any status change* Following a fall* At regular intervals* *How soon?
91 Assessment Recommendations History & Root Causes Documentation Current Status Footwear Seating Standing Transfers Toileting status Ability to understand safety needs 181 Past & Current H & P s Read it all, look for: Differences from current presentation Medications Safety measures Resident & Family Impressions Past care giver perspectives

92 RAI PROCESS CARE PLAN CAA SUMMARY CAAs CATs MDS CARE ASSESSMENTS RESIDENT INTERVIEWS Seating Challenges Ideal sitting posture is unnatural. People slide into a position of comfort and support. However... everyone fatigues out of the ideal sitting posture. Body type and disability often prevent ideal sitting posture



93 Pain Untreated, pain leads to: Restlessness Irritability Depression Reduced mobility Atrophy 185 What s Your Response to Alarms? Remain in place, wait for direction? Get up to see what s wrong? See what you can do to help?
94 Critical Investigation Elements Environmental review at the time of the event by onshift staff: Make immediate modifications Add to care plan immediately Communicate interventions & rationales immediately 187 Safety Rounds Everyone s responsibility What do you see? Are you really LOOKING for unsafe conditions? Who will be responsible to correct? How are we making changes to the culture of the facility? 94


95 Anticipate Medication Risks Do not wait until a fall happens to check for: Effects Side effects Interactions Plan for Falls Prevention! 189 Root Cause Analysis Root Cause Analysis: Does your staff understand how to immediately begin a RCA investigation with resultant pertinent interventions?
96 Resident Fall at 3am: C.N.A. reported to the nurse, He didn t use his call light New intervention on the Care Plan, Remind resident to use call light for assistance during the night. **Does this happen?? More often than you think! 191 Steps to Root Cause Analysis 1. Immediate Investigation 2. Include information from anyone that could possibly have knowledge 3. Step back and look at the whole picture 4. Where is the concern? 1. Resident Need? 2. Staff Error? 3. Resident Noncompliance? 4. Medical Condition? 5. Equipment Failure? 6. Environmental Concerns? 7. Other?

97 Examples: Let s go back to the resident who fell out of bed at 3am. Why did the resident fall? What was the resident doing? Where did the resident fall? When did the resident fall Who observed or has direct knowledge of the resident fall? How did the resident fall? 193 KEY POINT How can we put sensible, realistic interventions into place, if we don t dig deep enough for the information! **The interventions should match the need!

98 Documentation Necessary We need to substantiate that we have thoroughly investigated with Root Cause Analysis by: (Immediate investigation following resident stabilization) Assessing the situation Environment Devices and/or equipment Etc. Interviewing The resident All Staff with possible knowledge Roommate Visitors/family 195 Investigation: Resident Activity Underlying changes of condition? Contributing Factors (i.e. medications, eyeglasses not on, etc.) Staff involved Presence of hazards?


99 DOCUMENTATION Giving yourself CREDIT for Investigation Remember: If you didn t chart it Documentation Assessment Process Environmental Assessment Interviews Resident All staff with possible knowledge Families/visitors Roommate Identification of Hazards Change in Condition Contributing Factors
100 What NOT to document Impressions Assumptions It is wise not to document in the nurse s notes that you completed an Incident Report (Check your facility Policy and Procedures) Staff concerns (they do not belong in the resident record) Other resident s names 199 Care Plan Updates: Need to be based on the root cause analysis identification of the REASON for the fall/accident Include revised interventions to prevent further avoidable accidents Identified potential hazards and risks Individualized to each resident to address the current need for prevention Communicated to all staff caring for the resident!

101 Care Planning REALISTIC goals for resident s with a history of falling Decrease the number of falls by: Individualized environmental adjustments Resident Directed Care Removal of identified hazards Minimize Injury: Decreasing any contributing factors ***TIMELY Care Plan Updates are Essential!!! 201 Teach Staff - Begin Immediately To get the most out of critical times around an event Staff on the scene must be coached in: skills of observation critical thinking
102 Don t Wait! Delaying the investigation until morning or Monday, or whenever the DON or Risk Manager gets around to it will not improve your outcomes or statistics. 203 Assemble Key Players Assigned nurse & care assistants Others on duty Supervisor Dining Housekeeping/Maintenance Administrator/Clinical Managers More eyes & ears = more thorough perspectives
103 Observations + Questions Placement of the person s body at the time of the fall What was the person trying to do? Was it unusual or typical has it happened before? 205 What Exactly Happened? Person needed to use bathroom Urgently? Why? Does this follow their usual pattern Do they usually call for help? If they do, but didn t, what happened this time? If they did, why didn t they wait?

104 And Then What? If they don t, or didn t wait what makes them unsafe to do it independently - weakness, stiffness, dizziness? 207 Compensation VS Restriction If they are known not to call for help, what are you doing to make it safer for them? Strengthen, loosen up, address causes of dizziness
105 Plan of Care RAI Process Updates based on changes, assessment and root cause analysis investigation Documented Communicated 24 hour report Nurse to Nurse Nurse to C.N.A. Nurse to IDT Consistently Implemented Care Plan Interventions You can keep a list at the nursing station of a variety of ideas to help with the thought process after assessment! Individualized toileting Plan -Removing foot pedals Assistive devices in reach -Corner guards on tables Adequate Footwear -Cordless phones Low Bed -Bedspread material Environmental adaptions -Low rods in closet Individualized Monitoring schedules Resident centered activities Floor Mats Room Arrangements Lighting Music Medication change
106 Implementation of Interventions The process includes communication of the new interventions to all relevant caregivers 24 hour report Verbal report C.N.A. Care Card/Care Plan/Care Record Nurse Manager Rounds DON Rounds Fall Team Meeting Assigning Responsibility Providing training and resources if necessary Consistent Implementation of interventions Documentation 211 Analyze the Trends! As the Leader get involved! Be part of the falls team/committee to review accidents/incidents each week to determine: Time of day/shift Location Resident Activity at time of accident Personnel working Environmental Conditions

107 Example: 60% of falls occur between 6pm and 7pm 80% of these falls occur on one unit 75% of these falls occurred while resident was attempting to self toilet 213 Example-continued Investigation of trends: Observations that multiple staff members were taking breaks immediately following supper meal for residents Observations included multiple call lights that took extended periods of time for response due to staff breaks Observations and resident interviews indicated that residents would attempt to self toilet rather than wait for staff following the meal
108 Example: Interventions/Correction Staff breaks would not be allowed until all residents were toileted following meals Activities would provide an activity in the dining room following the meal to engage residents while staff were able to manage each resident s toileting needs 215 Audit Audit your system for success: F323 Rounds by the IDT Hazard Identification Fall Audits Incident/Accident Reports * Use these audits to correct the system through your QA process for success!
109 AUDIT-Example Area of Review YES NO Recommended Action Hazards Observation -Are chemicals accessible to residents? -Are staff promptly responding to alarms? -Is the environment safe for residents? Record review: -Resident is assessed for unsafe wandering and/or elopement -Risk of falls is assessed and care plan is individualized Following a Fall/Accident -The incident/accident was investigated (Root cause analysis) -Interventions were put into place based on investigation and are individualized -The Plan of Care was promptly updated -Hazards and risks were identified -Staff consistently implement new Staff Responsible/Date 217 INFECTION CONTROL FOR QUALITY 109


110 Overview Infections are a significant source of morbidity and mortality for nursing home residents Account for up to half of all nursing home resident transfers to hospitals. Infections occur an average of 2 to 4 times per year for each nursing home resident. 219 F441 Federal Regulation In the TOP 3 Citations Nationwide Infection Control The facility must establish and maintain an Infection Control Program designed to provide a safe, sanitary and comfortable environment and to help prevent the development and transmission of disease and infection
111 Infection Control Program The facility must establish an Infection Control Program under which it 1)Investigates, controls, and prevents infections in the facility; 2)Decides what procedures, such as isolation, should be applied to an individual resident; and 3) Maintains a record of incidents and corrective actions related to infections. 221 Intent of F441 The intent of this regulation is that the facility: Develops, implements and maintains an Infection Prevention and Control Program in order to Prevent, recognize and control, to the extent possible, the onset and spread of infection within the facility. **No longer control Now PREVENTION

112 Recent Survey Citations Pathway Health Services, Inc Survey Citations for F441 Hand-washing Peri-care Tracking of staff attendance when calling in (actually wanted a log of all call-ins and when they came back to work) Mapping of infections on a facility grid Proper storage of items in the dietary refrigerators

113 F441 Survey Citations Wiping down of equipment, including med carts, when used on an area that had known infections (like Influenza A) Proper use and changing of gloves Dating items used for med-pass Disinfection of equipment Proper disinfection 225 Survey Citations for F441 Blood Glucose Monitors not disinfected between each use. (In accordance with manufacturers recommendations) Catheter drainage bag on floor Gait belt used resident on isolation Dressing changes- technique Periwipes and skin cream contaminated Failure to have an IC Program Did not clean and disinfect electric razors

114 Recent Survey Citations Did not clean resident s finger before using lancet Did not have an assigned person for infection control program Lack of surveillance and analysis of data to determine clusters, prevalent organisms, or rate of infections Did not wash hands between each resident at med pass Dumping soiled water into sink 22 7 COMPONENTS OF A COMPREHENSIVE INFECTION PREVENTION AND CONTROL PROGRAM
115 Components of the Program Program Development and Oversight Policies and Procedures Infection Preventionist Surveillance Documentation Monitoring Data Analysis Communicable Disease Reporting Education Antibiotic Review 229 Development and Oversight Facility program oversight should collaboratively include: Infection Preventionist Administrator Medical Director (or a designee) Director of Nursing Other staff as appropriate

116 Medical Director Oversight Advisory Criteria for identifying infections How to distinguish facility acquired from community-acquired Appropriate surveillance activities Data collection instruments Antibiotic usage Surveillance forms Policy and Procedures 231 Policies and Procedures When was the last time your Infection Control Policies and Procedures were reviewed and revised? If you have revised the P&P s, how have we educated the staff? Have we audited the system?

117 Policies and Procedures Consistent with regulations and standards of practice Provide guidance to staff on steps to follow Should be in a place where easily accessible to all staff New changes in the industry should be researched and included in the P&P 233 Policy & Procedures Examples Use of standard precautions facility-wide Use of transmission-based precautions when indicated Define surveillance activities Require that staff use accepted hand hygiene after each direct resident contact for which hand hygiene is indicated Prohibit direct resident contact by an employee who has an infected skin lesion or communicable disease Housekeeping, Laundry, Dietary policies

118 Infection Preventionist F441: A facility may designate an IP to serve as the coordinator of an Infection Prevention and Control Program. Responsibilities may include collecting, analyzing, and providing infection data and trends to nursing staff and health care practitioners; consulting on infection risk assessment, prevention, and control strategies; providing education and training; and implementing evidence-based infection control practices, including those mandated by regulatory and licensing agencies, and guidelines from the Centers for Disease Control and Prevention. Will need a good job description and resources 235 Surveillance There are no magic buttons


119 Surveillance Cornerstone of IC Program The primary purpose of infection control surveillance is the collection of information for action. 237 Surveillance Two Types Process Outcome
 Do your policies work? 239 Outcome Surveillance Identifies and reports evidence of an infectious disease.")
120 Process Surveillance Identifies whether the practices are compliant with established prevention, control and policies based on recognized guidelines. Audit- (hand washing, environmental rounds) Do your policies work? 239 Outcome Surveillance Identifies and reports evidence of an infectious disease. The outcome surveillance process consists of collecting/documenting data on individual cases and comparing the collected data to standard written definitions (criteria) of infections. (See McGeers) Data- Analysis

121 Surveillance Consideration All symptoms must be new or acutely worse. Many residents have chronic symptoms, such as cough or urinary urgency, that are not associated with infection; However, a new symptom or a change from baseline may be an indication that an infection is developing. 241 Surveillance Consideration Alternative noninfectious causes of signs and symptoms (eg, dehydration, medications) Should generally be considered and evaluated before an event is deemed an infection

122 Surveillance Consideration Identification of infection should not be based on a single piece of evidence Always consider the clinical presentation and any microbiologic or radiologic information Microbiologic and radiologic findings should not be the sole criteria 243 Surveillance Consideration Diagnosis by a physician alone is not sufficient for a surveillance definition of infection and must be accompanied by documentation of compatible signs and symptoms
123 Surveillance Consideration Infections should be attributed to a LTCF onset If there is no evidence of an incubating infection at the time of admission to LTC (on the basis of clinical documentation of appropriate signs and symptoms and not solely on screening microbiologic data) and Onset of clinical manifestation occurs >2 calendar days after admission - McGeer Infection Rates Calculated monthly, quarterly, & annually Health facility acquired infections (HAIs) HAI rates are calculated as infections per 1000 resident days A standard infection report form facilitates reporting of surveillance information Tables, graphs, and charts may be used and facilitate education of personnel
 are calculated.")
124 Infection Calculations Infections are counted in the statistics only once. An infection lasting over more than one reporting period reported only oncein the period it had its onset. Incidence rated (the number of new cases of infection during a defined time period ) are calculated. 247 Calculation Formula Formula for calculation: Number of new HAI s infections* X 1000 Number of resident days in a month Nosocomial Infections are known as Healthcare Associated Infection (HAI s)
 3.")
125 Documentation and Data Documentation should include written definitions of infections Concurrent surveillance is preferable to retrospective surveillance Surveillance at least weekly (APIC) is need to collect timely data 249 Use of Tracking Tools 1. Identification of all infections in the facility 2. Detection of types of infections and location in the facility. (Use McGeer Criteria) 3. Determination of prevalence of infections 4. Determine trends 5. Information will assist the facility in the development of an effective Action Plan 6. Are you MAPPING your infections?
126 Documentation and F441 You can use whatever approach works for your facility for gathering, documenting and listing surveillance data. You will need reports to describe the types of infections and to identify any trends and patterns. You can summarize observations of staff practices, infection causes and any RCA investigation into infections. You will need to define how often and how your data will be collected. 251 Monitoring The Infection Preventionist and all others assigned to monitor the program will need to monitor: Implementation of P&P Condition of resident(s) with infection(s) Outbreaks Compliance with facility practices to ensure consistent implementation of the program

127 Data Collection Data is collected from: Communication with staff Walking rounds Review of MD progress notes Lab/X-ray review Treatment records MAR Nurse notes Information from hospital transfers 253 Analysis of the Data Includes the following elements on each infection to detect clusters and trends: Resident identifier Type of infection Date of onset Location in the facility Appropriate lab information

128 Data Analysis Determination of the origin of infections Reviewing and comparing facility surveillance data over time Determination of trends, patterns, unusual situations or performance concerns Evaluation and Action Planning Communicable Disease Reporting The Infection Preventionist is responsible for reporting to the state Department of Health Infectious Disease Division, cases of specific conditions (Refer to your State Specific Disease Reporting Requirements)
 and we are responsible to communicate results")

129 Antibiotic Review Ongoing review and oversight Medical Director involvement Consultant Pharmacist Compare antibiotic with lab C&S report The physician is responsible to review (and prescribe) and we are responsible to communicate results The consultant pharmacist will also review during the medication regimen review and give recommendations as appropriate **Due to the increase in MDRO s, review of antibiotic use is crucial 257 EDUCATION AND ACCOUNTABILITY INFECTION CONTROL 129


130 Staff Education Orientation and Yearly Policies and Procedures Hand Hygiene (return demonstration) Personal Protective Equipment Transmission Based Precautions Standard Precautions Linen Handling Identification of signs/symptoms of infection Communicating, Documentation, Reporting Staff illness/signs and symptoms and when they can and cannot work Infection Criteria 259 INTERDISCIPLINARY INVOLVEMENT ALL disciplines need to be involved in Infection Control Nursing Social Services Activities Dietary Administration Therapy Physicians or other practitioners Lab and/or X-ray Spiritual

 are identified and")

131 Staff Education On-The-Spot When break in procedures/technique or practice is observed either through audit or observation. When an infection (or infections) are identified and procedures/techniques need to be reinforced. New information needs to be addressed. Do you hold your staff accountable? 261 AUDITING FOR COMPLIANCE 131

132 Audits Hand Hygiene Audits Food Preparation Audits Personal Protective Equipment Audits Water Pass Audits Med Pass Audits Catheter Care Audits Peri-Care Audits Room Sanitization Audits Environmental Audits Dining Room Audits Linen Handling Audits 263 Well-trained and dedicated employees are the only sustainable source of competitive strength. -Robert Reich


133 PAIN MANAGEMENT FOR QUALITY Pain Management Pain management means that nursing homes will implement a comprehensive system to address issues related to pain. This system involves assessing and managing pain in residents, both long and short term, so that all residents have individualized, personcentered care plans. Nursing home residents will receive appropriate care to prevent and minimize episodes of moderate to severe pain. Less than adequate pain management can affect residents daily activities and quality of life. It can also cause depression, sleeplessness, restlessness, or decline in appetite and unintentional weight loss. -Advancing Excellence in America s Nursing Homes ontrols=decreasesymptomsofpain 133
134 Focus Considerations for long stay and short stay residents. Timely assessment/recognition and management of pain as well as monitoring and managing side effects of medications utilized. 5_Pain_TAW_Guide.pdf Quality Measures Percent of Residents Who Self-Report Moderate to Severe Pain (Short Stay) Percent of Residents Who Self-Report Moderate to Severe Pain (Long Stay) 134

135 F309 Quality of Care Each resident must receive and the facility must provide the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being, in accordance with the comprehensive assessment and plan of care. Policies and Procedures Is your system: Current? Evidence Based? Consistent with F309? 135
136 Introduction to Pain Introduction: To help a resident attain or maintain his/her highest practicable level of well-being and to prevent or manage pain, to the extent possible, the facility: Recognizes when the resident is experiencing pain and identifies circumstances when pain can be anticipated; Evaluates the existing pain and the cause(s); and Manages or prevents pain, consistent with the resident s goals, the comprehensive assessment and plan of care, and current clinical standards of practice. F309 Pain Management Process Screening to determine if the resident has been or is experiencing pain; Comprehensively assessing the pain; Identifying circumstances when pain can be anticipated; and 136
137 F309 Pain Management Process Developing and implementing a plan, using pharmacologic and/or nonpharmacologic interventions to manage the pain and/or try to prevent the pain consistent with the resident s goals Monitor and evaluate outcomes Myth 1: Fact: Pain is a normal part of aging Pain is common in older adults, but it is not part of normal aging. Older adults tend to have more pain because they have chronic diseases. Understanding Pain in Frail Elders Karen S. Feldt, PhD, GNP U of MN School of Nursing Center for Nursing Research 137

138 Myth 2: Elders get adequate pain treatment Fact: Studies in several settings indicate under-treatment of pain Studies have also shown that persons with dementia receive less analgesia for similar conditions Understanding Pain in Frail Elders Karen S. Feldt, PhD, GNP U of MN School of Nursing Center for Nursing Research Pain and Aggressive Behavior Research on 38 aggressive cognitively impaired nursing home residents families suspected pain in 44% of subjects CNAs suspected pain in 66% of subjects For residents for whom CNAs suspected pain, 56% had received no analgesic in the previous month Feldt, Warne, & Ryden, (1998) 138
139 Pain and Aggressive Behavior Residents with > 1 pain-related diagnosis were significantly more aggressive than residents with one or no pain-related diagnosis (13.9 incidents/day vs 8.2/day) Residents with arthritis had significantly higher aggression scores than those without arthritis (14.1/day vs. 8.6/day) Identification of Pain Inadequately treated pain can lead to: decreased functioning, sleep disturbances, depression, and decreased emotional well-being. Acute pain may indicate a new and potentially life-threatening disease process. It is important, that a resident s reports of pain be taken seriously and be evaluated comprehensively. 139

140 Pain Misconceptions Some common misconceptions contribute to the inadequate management of pain include: viewing pain as a sign of weakness or a mechanism for getting attention; believing that older or cognitively impaired residents have a higher tolerance for pain; or a concern that residents may become addicted to pain medication. Screening Interview- preadmission Resident interview Family interview Friends, responsible party Observe body language Monitoring for pain is part of the IDT process 140
141 Assessment-Frequency Recognize and address pain promptly Screening for pain at admission helps identify the resident who is experiencing pain or for whom pain may be anticipated during specific procedures, care, or treatment. Admission screening Screened periodically (Quarterly MDS) Change in condition Anytime pain is suspected As with many symptoms, pain in residents with moderate to severe cognitive impairment may be more difficult to recognize and assess Pain Assessment Location (where?)* Onset, progression (when did it start?) Precipitating factors (what sets it off?) Quality and characteristics (describe) Duration, intensity, severity (how bad?)* Alleviating factors (what helps?) Associated symptoms (what else?) * required documentation for JCAHO 141
142 Pain Assessment Items to consider on Assessment: History of Pain Review of Diagnoses- Acute and Chronic concerns Resident History-previous pain management needs/treatment (What works? What hasn t worked?) Resident Interview- Is resident verbalizing pain? If new admission, were they medicated prior to leaving the hospital? Assessment-Verbal Words used to report or describe pain may differ by culture and/or region of the country. Examples of descriptions may include heaviness or pressure, stabbing, throbbing, aching, gnawing, cramping, burning, numbness, tingling, shooting spasms, soreness, tenderness, discomfort, pins and needles, feeling rough, tearing or ripping. Verbal descriptions of pain can help a practitioner identify the source, nature, and other characteristics of the pain. 142

143 Pain Assessment Does your Pain Assessment include: Pain Location Pain Scale Description of Pain Pain Frequency Pain Goal What has worked? Medications Non-pharmacological interventions Pain Assessment Continued- Breakthrough pain? Pain with activity? Does pain interfere with sleep? Activities? New health concerns? Signs/Symptoms? Non-verbal indicators of pain? Type of Pain? 143
144 Non-Verbal Indicators Need to be viewed in the context of the whole picture of the resident with consideration given to pain as well as other clinically pertinent explanations. Examples of symptoms may include: Negative verbalizations and vocalizations (e.g., groaning, moaning crying/whimpering, stop, ouch that hurts, or screaming); Facial expressions (e.g., grimacing, frowning, fright, or clenching of the teeth or jaw, wincing); Non-Verbal continued: Changes in gait (e.g., limping), skin color, vital signs (e.g., increased heart rate and blood pressure) A change in behavior (e.g., resisting care, distressed pacing, withdrawing, inability to perform ADLs, rubbing a specific location of the body, or guarding or protecting a limb or other body parts); Weight loss; and Difficulty sleeping (insomnia). 144
, since you received your pain medicine? Where do you want your pain to be?")
145 Intensity Quantitative measurement scales Numeric Rating Scale (NRS) Verbal Descriptor Scale (VDS) Faces Scales (Wong-Baker, Bieri) Pain Thermometer Questions to ask If 0 is no pain and 10 is the worst possible pain, what is your pain right now, in the past 24 hours (since lunch time yesterday), since you received your pain medicine? Where do you want your pain to be? Pain Assessment and Management: Strategies & Techniques for Nursing Facilities; Stratis Health 2003 Pain Assessment and Management: Strategies & Techniques for Nursing Facilities; Stratis Health
146 The Process Pre-Screen Pre-Admission Admission Assessment Reassessment RAI Progress Towards Goals Care Plan Interpretation of Pain Multiple barriers to the evaluation and management of pain exist, such as: language and cultural barriers, co-existing illness (co-morbidities), and cognitive impairment. The use of multiple medications may affect a resident s ability to interpret or report pain, may modify his or her response to pain, and may make it harder to identify pain symptoms 146

147 Overcoming Barriers Pain Identification Education Staff Resident Medication Management Non-pharmacological interventions Documentation Nonverbal Pain Indicators Facility System Management PROACTIVE APPROACH Anticipating Pain Education for staff and resident on medications and non-pharmacological interventions that can be utilized when pain can be anticipated. A good assessment will determine what activities are associated with pain and the interventions that have been successful and can be care planned! 147

148 Care Planning The goal: To provide effective pain management that results in a constant level of comfort while maintaining as much function as possible. Care Planning Successful intervention starts with a clear statement of the problem. The problem: Etiology of the problem what is the pain due to? Exacerbation of the pain what makes it worse? Example: Alteration in comfort related to acute pain due to right hip surgery and exacerbated by therapeutic exercises **Do you use your CAA to individualize your care plan? 148
149 Care Planning Interventions should be: Specific to the individual resident s assessed problems Interdisciplinary Medications + non-pharmacologic Assessed for effectiveness within a reasonable amount of time after implementation Include resident preferences Coordinated Plan of Care When hospice services are involved, the facility and hospice are jointly responsible for developing a coordinated plan of care for the resident that guides both providers and is based upon their assessments and the resident s needs and goals. The coordinated plan of care must identify which provider (hospice or facility) is responsible for various aspects of care
150 Coordinated Care Planning The care plan will incorporate the Hospice philosophy of care to include pain management both pharmacological and non-pharmacological in nature and the Hospice will collaborate with facility to train staff. 299 Medication Adverse Effects Monitor for adverse effects of the medication Constipation Sedation Nausea/Vomiting Pruritis Confusion/Delirium Myoclonic jerking Respiratory Depression (sedation precedes) 150
151 Pain and Resident Function F309: Actual or potential harm/negative outcome for F309 related to pain assessment and management may include, but is not limited to: Persisting or recurring pain and discomfort related to failure to recognize, assess, or implement interventions for pain; and Decline in function resulting from failure to assess a resident after facility clinical staff became aware of new onset of moderate to severe pain. Pain and Resident Function Areas for consideration: Pain Management prior to cares Pain Management prior to Restorative Programs Pain Management prior to meals Medication side effects and nonpharmacological interventions 151
152 Summary Review your system for pain management Policies and Procedures Assessments and Screenings Staff implementation of interventions Documentation Review Education (staff, resident, family, practitioners) Care Planning Auditing Review of Quality Measures Quality Assurance COMPLIANCE 152

153 Compliance Survey State and Federal regulations Reimbursement-Medicaid and Medicare 305 Federal Top 10 F323: Prevention of Accidents F441: Infection Control F309: Quality of Care F371: Food Sanitation F279: Care Plans F281: Services that Meet Professional Standards F514: Clinical Records F225: Employ Individuals Guilty of Abuse F329: Unnecessary Drugs F241: Dignity 153
154 Compliance Ensure systems are in place! Updated and appropriate policies and procedures Ongoing employee education and engagement Resource management Corporate Compliance Program Oversight QA and QAPI Compliance - Education All policy, procedure or protocol changes need to be communicated with education to all staff PRIOR to date of implementation. There should be a system for evidence of training It is a good idea to use a variety of training methods Lecture - Skills Checklists Handouts - Return Demonstration Etc

155 Compliance - Education What is your system for staff that do not attend your educational programs? Do you have an evaluation system for staff to determine effectiveness of educational activity? Have you considered including staff in the process? Compliance Do you have an ongoing and meaningful audit system? How are you ensuring sustained compliance? What is your process? 155


156 Verification of Compliance and Satisfaction Audit System Facility Rounds Documentation Evaluation Staff Interviews Resident Interviews Family/Visitor Interviews Medical Director Discussion 311 Example F309 Each resident must receive and the facility must provide the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being, in accordance with the comprehensive assessment and plan of care

157 F309 Includes: Care of a resident with dementia End of Life Diabetes Resdent receiving dialysis services Non-pressure related skin ulcers Pain 313 Providing care and services to keep residents at their highest level of functioning in conjunction with the plan of care for: Fractures Congestive heart failure Fecal Impaction F309 **F309 indicates that Surveyors should consider any quality of care issue that is not covered in a specific Quality of Care tag to be covered under this tag, 314 F
158 Examples of Survey Deficiencies Lack of Evidence for Proper Pain Management Failure to show evidence of care and services for non-pressure related wounds Failure to evidence of care plan coordination with Hospice Dialysis: No evidence of adequate communication and lack of emergency procedures 315 Examples of Survey Deficiencies Prompt physician notification and action for residents with low blood sugars Insulin given when resident documentation indicates poor intake Staff indicates to surveyor that they are not aware of non-pharmacological interventions on the care plan for behaviors to be utilized prior to medication use Resident with dementia and new onset of behaviors without assessment to determine 316 reason for behavior 158
 Dementia Care Care Plans Individualized Consistent Implementation Updates Communication Notifications Quality of Care 318 Education")
159 EDUCATIONAL NEEDS OF EMPLOYEES 317 Areas for staff education include: Policies and Procedures (examples) Pain Management (including documentation, forms) Dialysis Care (arrangements and emergency P&P) Dementia Care Care Plans Individualized Consistent Implementation Updates Communication Notifications Quality of Care 318 Education 159
160 Manager Oversight Regular oversight on F309 will be crucial for compliance -Daily Rounds -Chart reviews Ongoing audits (can include nurse managers in the process for both compliance and learning) Action Planning based on results 319 QA and QAPI F309 Quality of Care AUDIT Area of Review YES NO Recommended Action Assessment includes history, medical and psychological diagnoses, physical, cognitive and functional status, psychological and concerns Non-pharmacological interventions for behaviors are in the care plan and observed to be implemented with resident with dementia When a resident elects Hospice a Significant Change of Condition MDS is present in the record Hospice and Facility have collaborated in a Plan of care There is evidence of monitoring for Bowel Movements for all residents in the facility Residents who are not eating with orders for insulin: -There is an assessment documented -Blood Glucose Monitoring completed -Physician 320 is notified if blood glucose result is outside parameters -Insulin is held as indicated Staff Responsible/Date 160
161 F309 Quality of Care AUDIT Area of Review YES NO Recommended Action There is evidence in the medical record of communication between the dialysis facility and the LTC facility: -Medication Administration times -Weights -Labs -New medical concerns An updated Pain Assessment is located in the medical record Staff Responsible/Date Documentation for prn pain medication administration includes: -Time and Date -Location of pain -Pain intensity (scale) -Medication Administered -Non-pharmacological Interventions -Effectiveness 321 of Pain Medication including intensity Audits You can develop your own based on findings Can use the information to measure compliance Can be used as a PIP for QAPI Can include staff at all levels Will help in determining education and oversight needs of the department

162 COMPLIANCE HOW will compliance problems affect your facility? 323 CUSTOMER SERVICE/ENGAGEMENT
163 Consumer Engagement What successful processes do you have in place for successful consumer engagement? Preadmission Admission Ongoing Formal Informal 325 Consumer Engagement How have you prepared ALL staff for customer service? Have you conducted satisfaction surveys? How is your relationship with other health care entities? (What are they telling your potential or current customers?) What IS the culture of your facility? Do you truly practice Person Centered Care?
164 Let s Keep Our Staff Informed! Well-trained and dedicated employees are the only sustainable source of competitive strength. -Robert Reich 327 Consumer Engagement Provide an environment for success Quality Care is essential in the process! Listen, Listen and Listen again! Provide multiple opportunities and platforms for the sharing of information Employee education and ongoing involvement will be crucial

165 Communication Every week, any new regulatory updates should be addressed with the Department Managers All Staff Involvement as necessary Residents Families Medical Director Pharmacy Consultant 329 In Conclusion LEADERSHIP STRATEGIES

166 Leadership Strategies to Implement Change for Successful Outcomes 1. The Course has been set-road Map! Affordable Care Act HR 4302 OIG Workplan OIG Compendium CMS S&C Memo s OIG Memos Leadership Strategies to Implement Change for Successful Outcomes 2. Arm yourself with knowledge and resources on the initiatives 166
167 Leadership Strategies to Implement Change for Successful Outcomes 3. Review your systems and the culture of your facility for compliance and satisfaction! Review systems Engage and include all employees in the process Resident/family engagement Expect quality, compliance and satisfaction as a way of doing business! Leadership Strategies to Implement Change for Successful Outcomes 4. Position yourself for success Data, Data, Data!!! Objective Accurate Meaningful 167


168 Leadership Strategies to Implement Change for Successful Outcomes 5. Preparedness and Protection- Preparing yourself for audits and surveys Situate yourself for quality and prepare for Value Based Purchasing Leadership Strategies to Implement Change for Successful Outcomes 6. Innovation: Roll out your process delivery to meet the demands of the new consumer and dynamic health care environment! 168
169 Resources CMS (QAPI): Certification/QAPI/NHQAPI.html QAPI News Brief Volume1, 2013; Certification/QAPI/Downloads/QAPINewsBrief.pdf State Operations Manual: Guidance/Guidance/Manuals/downloads/som107ap_pp_gui delines_ltcf.pdf Resources Advancing Excellence in America s Nursing Homes CDC-Falls in Nursing Homes sing.html NCOA Excellent Resources- Falls Prevention Day September 22,
170 Resources Veteran s Administration projects Institute for Person Centered Care Sue Ann Guildermann, RN, BA, MA. Effective Fall Prevention Strategies Without Physical Restraints or Personal Alarms Empira, 4/24/2012 Webinar for Stratis Health Resources Vibrant Living Concepts Willy BA; Wheelchair Seating for Elders; On line pamphlet prepared under contract for Mountain Pacific Quality Health Wyoming %20for%20EldersPPoutline.pdf
171 Resources SHEA/CDC Position Paper Surveillance Definitions of Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria Resources Surveillance: AJIC_Surveillance_2007.pdf Guideline for disinfection and sterilization: wledg.html APIC (Association for Professionals in Infection Control and Epidemiology):
172 Resources CDC: utions.html html 343 Resources s_ pdf spx?controls=decreasesymptomsofpain nicpain llenges-pain-management-long-termcare?page=0,0 172



173 Resources Some additional clinical resources available for guidance regarding the management of pain include: American Geriatrics Society at American Academy of Hospice and Palliative Medicine at American Academy of Pain Medicine at American Pain Society at Hospice and Palliative Nurses Association at Partners Against Pain at Sustainability and the future 173
174 Quality and Performance Consumer Engagement and Satisfaction Compliance 5/21/2014 Three Pillars of The Future of Health Care Affordable Care Act National Quality Strategy HR 4302 QAPI HHS/CMS Strategic Plan/Triple Aim /Work Plans OIG - Work Plans/Compendium Fraud Prevention System 174


175 QUESTIONS?

176 THANK YOU Susan LaGrange, RN, BSN, NHA Director of Education Pathway Health 176
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
LeadingAge New York Technology Solutions
 LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC-CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC-CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
Restorative Nursing: The NHA s Role and Organizational Outcomes
 Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
9/8/2017. Making the Connection: Linking the Facility Assessment and QAPI Plan. Cindy Mason VP Provider Services. Final Rule. Providigm, LLC,
 Making the Connection: Linking the Facility Assessment and QAPI Plan Cindy Mason VP Provider Services Final Rule Providigm, LLC, 2017 1 Final Rule Effective Date These regulations are effective as of November
Making the Connection: Linking the Facility Assessment and QAPI Plan Cindy Mason VP Provider Services Final Rule Providigm, LLC, 2017 1 Final Rule Effective Date These regulations are effective as of November
LeadingAge New York Technology Solutions
 LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
The New Survey Process What To Expect Paula G. Sanders, Esq.
 PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
Succeeding in Value-Based Care CareConnect Journey
 Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Observations for all areas: What type of supervision is provided to the resident and by whom? How are care-planned interventions implemented?
 Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
The Impact of Health Care Reform on Long- Term Care
 The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT
 A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
QAPI - What Is It All About? Rebecca McMinn, RN, BSN, MBA New Century Hospice
 QAPI - What Is It All About? Rebecca McMinn, RN, BSN, MBA New Century Hospice CMS Quality Initiatives CMS has encouraged Healthcare to monitor itself and gather data Standard measures of quality care are
QAPI - What Is It All About? Rebecca McMinn, RN, BSN, MBA New Century Hospice CMS Quality Initiatives CMS has encouraged Healthcare to monitor itself and gather data Standard measures of quality care are
Goodbye Grace Period. What will be expected from your Facility Assessment in the Coming Year. Ellen Kuebrich Chief Strategy Officer, Providigm
 Goodbye Grace Period What will be expected from your Facility Assessment in the Coming Year Ellen Kuebrich Chief Strategy Officer, Providigm Final Rule Final Rule Effective Date These regulations are effective
Goodbye Grace Period What will be expected from your Facility Assessment in the Coming Year Ellen Kuebrich Chief Strategy Officer, Providigm Final Rule Final Rule Effective Date These regulations are effective
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
PBS Support within Nursing Homes. Dave Mackowski. Warren Bird M.S. State of Oregon Department of Human Services March, 2011.
 PBS Support within Nursing Homes Dave Mackowski Warren Bird M.S. State of Oregon Department of Human Services March, 2011 Before we begin We are going to talk today about how a behavior specialist: Can
PBS Support within Nursing Homes Dave Mackowski Warren Bird M.S. State of Oregon Department of Human Services March, 2011 Before we begin We are going to talk today about how a behavior specialist: Can
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES. James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications
 Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Psychotropic Drug Use To Medicate or Not to Medicate?
 Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement. Patty Austin, RN, CPHQ Project Coordinator
 QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Accountable Care and Governance Challenges Under the Affordable Care Act
 Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
7/1/2011 EVERYTHING YOU NEED TO KNOW TO SUCCEED WITH THIS NEW PROCESS ABOUT LEAH I FOCUS ON LEARNING, NOT TEACHING
 BIP-PITY BOB-PITY BOO!!!!!! MAKE THE MDS 3.0 WORK FOR YOU IT IS NOT MAGIC!!!!!! Leah Klusch, RN, BSN, FACHCA EVERYTHING YOU NEED TO KNOW TO SUCCEED WITH THIS NEW PROCESS ABOUT LEAH I FOCUS ON LEARNING,
BIP-PITY BOB-PITY BOO!!!!!! MAKE THE MDS 3.0 WORK FOR YOU IT IS NOT MAGIC!!!!!! Leah Klusch, RN, BSN, FACHCA EVERYTHING YOU NEED TO KNOW TO SUCCEED WITH THIS NEW PROCESS ABOUT LEAH I FOCUS ON LEARNING,
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Using Quality Data to Market to Referral Sources BUSINESS OF HEALTHCARE
 Using Quality Data to Market to Referral Sources Cindy Mason Change as a Matter of Survival BUSINESS OF HEALTHCARE 2 National Transformation of Healthcare the Affordable Care Act provides CMS the flexibility
Using Quality Data to Market to Referral Sources Cindy Mason Change as a Matter of Survival BUSINESS OF HEALTHCARE 2 National Transformation of Healthcare the Affordable Care Act provides CMS the flexibility
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care
 The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Quality Assurance and Performance Improvement (QAPI)
") Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Checklist: What Can My Organization Do?
 Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
10/22/2015. QIO Program Restructures. QIO Program Restructures ANHA Activities/Social Services Convention Person-Centered Care
 2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
Presentation Objectives
 Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
INFORMATION ABOUT YOUR OXFORD COVERAGE REIMBURSEMENT PART I OXFORD HEALTH PLANS OXFORD HEALTH PLANS (NJ), INC.
, INC.") OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
Home Health Eligibility Requirements
 Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
Hot Survey Topics. Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health
 Hot Survey Topics Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health Objectives Upon completion of this presentation, attendees should be able to: 1. Identify the top
Hot Survey Topics Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health Objectives Upon completion of this presentation, attendees should be able to: 1. Identify the top
9/27/2017. Getting on the Path to Excellence. The path we are taking today! CMS Five Elements
 Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017
 NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
Improving Nursing Home Compare for Consumers. Five-Star Quality Rating System
 Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Chances are.. Based on my experience MDS 3.0 Update for Long Term Care PRESENTED BY 2/13/2017. New focus on Data by CMS and Regulatory Agencies
 PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
2014 QAPI Plan for [Facility Name]
![2014 QAPI Plan for [Facility Name]](/thumbs/74/70066237.jpg "2014 QAPI Plan for [Facility Name]") presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
QAPI Quality Assurance Process Improvement
 QAPI Quality Assurance Process Improvement Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC 2017 Final Rule in the Federal Register of January 13, 2017
QAPI Quality Assurance Process Improvement Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC 2017 Final Rule in the Federal Register of January 13, 2017
Review of F323 Related to Falls. Marilyn Hirsch Region V December 16, 2015
 Review of F323 Related to Falls Marilyn Hirsch Region V December 16, 2015 Objectives Describe Region V F323 Project Review F323 Regulation Review and discuss citations History At our meeting two years
Review of F323 Related to Falls Marilyn Hirsch Region V December 16, 2015 Objectives Describe Region V F323 Project Review F323 Regulation Review and discuss citations History At our meeting two years
QAPI Plan QAPI Plan. snits: Sanitas, Denver, CO. Effective Date: 01-Jan-2018
 QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Session #8. The Key to Preventing Immediate Jeopardies. Speaker: Janine Lehman 4/17/2013 KBN:
 2013 KAHCF Spring Education Conference Session #8 The Key to Preventing Immediate Jeopardies Speaker: Janine Lehman 4/17/2013 KBN: 5-0002-707-041-1217 The Key to Preventing Immediate Jeopardies Janine
2013 KAHCF Spring Education Conference Session #8 The Key to Preventing Immediate Jeopardies Speaker: Janine Lehman 4/17/2013 KBN: 5-0002-707-041-1217 The Key to Preventing Immediate Jeopardies Janine
Phase 2: 4/24/2017. Implementation Phases. Objectives. Phase 1: November 28, Phase 3: November 28, 2019
 NEW Requirements for Participation for Skilled Nursing Facilities The Elements of Compliance for Phase 2 April 28, 2017 1:30pm 2:45pm Objectives Identify the new and revised regulations in the Final Rule
NEW Requirements for Participation for Skilled Nursing Facilities The Elements of Compliance for Phase 2 April 28, 2017 1:30pm 2:45pm Objectives Identify the new and revised regulations in the Final Rule
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
The Patient Protection and Affordable Care Act (Public Law )
") Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Person-Centered Accountable Care
 Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care
 Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
QAPI: Quality Assurance Performance Improvement - Meeting the Requirements of Participation. PADONA 2017 Annual Convention Hershey, PA.
 PADONA Annual Convention 2017 QAPI: Quality Assurance Performance Improvement - Meeting the Requirements of Participation PADONA 2017 Annual Convention Hershey, PA March 29, 2017 Your presenter today is:
PADONA Annual Convention 2017 QAPI: Quality Assurance Performance Improvement - Meeting the Requirements of Participation PADONA 2017 Annual Convention Hershey, PA March 29, 2017 Your presenter today is:
MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW
 MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW LIBBY YOUSE, LNHA Long Term Care Leadership Coach OBJECTIVES Understanding factors why MDS s are so important in your home Identify the effects it places
MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW LIBBY YOUSE, LNHA Long Term Care Leadership Coach OBJECTIVES Understanding factors why MDS s are so important in your home Identify the effects it places
Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS
 PROVIDERS") Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS Navigation To Start the training, please press Function + F5 To advance through each slide use the icon located at the
Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS Navigation To Start the training, please press Function + F5 To advance through each slide use the icon located at the
Preventing Falls in the Home
 ~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Pitch Perfect: Selling Your Services to LTC Facilities
 Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Disclaimer. Learning Objectives
 Data Analysis in Today s Skilled Nursing Facilities: How Data is Driving Reimbursement and 5-Star Ratings Presented by: Reinsel Kuntz Lesher Senior Living Services Consulting 0 Disclaimer The information
Data Analysis in Today s Skilled Nursing Facilities: How Data is Driving Reimbursement and 5-Star Ratings Presented by: Reinsel Kuntz Lesher Senior Living Services Consulting 0 Disclaimer The information
Infection Control, Still the Most Commonly Cited Tag in Texas
 July 2016 Commitment to Care Quality Topic Infection Control, Still the Most Commonly Cited Tag in Texas F -441 continues to show up on the list of top 10 deficiencies every quarter here in Texas. During
July 2016 Commitment to Care Quality Topic Infection Control, Still the Most Commonly Cited Tag in Texas F -441 continues to show up on the list of top 10 deficiencies every quarter here in Texas. During
The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool
 The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool Myth: The Centers for Medicare and Medicaid Services (CMS) 5 Star Nursing Home Quality rating system provides a useful
The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool Myth: The Centers for Medicare and Medicaid Services (CMS) 5 Star Nursing Home Quality rating system provides a useful
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care. Harold D. Miller
 Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
2/13/2017. SNF Requirements for Participation. Facility Wide Resource Assessment
 Objectives SNF Requirements for Participation Facility Wide Resource Assessment Recognize the key concepts of the new facility wide resource assessment in the new regulations for skilled nursing facilities
Objectives SNF Requirements for Participation Facility Wide Resource Assessment Recognize the key concepts of the new facility wide resource assessment in the new regulations for skilled nursing facilities
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
HealthStream Ambulatory Regulatory Course Descriptions
 This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many