Physician, Health Care Professional, Facility and Ancillary. Provider Manual.
|
|
|
- Melina Foster
- 6 years ago
- Views:
Transcription

1 Physician, Health Care Professional, Facility and Ancillary Provider Manual New Jersey 2011
2 Welcome to New Jersey s State Government Health Care Benefits Program otherwise known as UnitedHealthcare Community Plan (UnitedHealthcare), the government programs division of UnitedHealth Group. UnitedHealthCare has focused solely on this complex and dynamic market since its founding 20 years ago. Today, we serve 3 million beneficiaries of public sector health care programs in more than 25 states across the country. This administrative guide is designed as a comprehensive reference source for the information you and your staff need to conduct your interactions and transactions with us in the quickest and most efficient manner possible. Much of this material, as well as operational policy changes and additional electronic tools, are available on our web site at Our goal is to ensure our members have convenient access to high quality care provided according to the most current and efficacious treatment protocols available. We are committed to working with and supporting you and your staff to achieve the best possible health outcomes for our members. If you have any questions about the information or material in this administrative guide or about any of our policies or procedures, please do not hesitate to contact the Provider Services Line at We greatly appreciate your participation in our program and the care you provide to our members. Important Information regarding the use of this Manual In the event of a conflict or inconsistency between your participation agreement and this Manual, the terms of the participation agreement shall control. In the event of a conflict or inconsistency between your participation agreement, this Manual and applicable federal and state statutes and regulations, applicable federal and state statutes and regulations will control. UnitedHealthcare reserves the right to supplement this Manual to ensure that its terms and conditions remain in compliance with relevant federal and state statutes and regulations. This Manual will be amended as operational policies change.
3 Table of Contents HOW TO CONTACT US SECTION 1 UNITEDHEALTHCARE PRODUCTS SECTION 2 COVERED AND NON-COVERED SERVICES UnitedHealthcare NJ FamilyCare/Medicaid UnitedHealthcare Dual Complete (Medicare) SECTION 3 PRIOR AUTHORIZATION Determination of Medical Necessity Prior Authorization Fax Form Hysterectomy Consent Form Sterilzation Consent Form SECTION 4 REFERRALS Healthy First Steps (OB Program) SECTION 5 CLAIMS POLICIES AND PROCEDURES Electronic Claims Submission NPI Claim Adjustments Provider Claim Payment Appeal Processes Provider Service Appeals Provider Central Service Unit (PCSU) Provider Complaints or Grievances Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Services Coordination of Benefits How to Change Provider Information & Provider Information Update Form SECTION 6 HOSPITALS AND HOSPITALIZATION Elective Admissions & Same Day Surgery Emergency Admissions Maternity and Obstetrical Admissions Newborn Admissions Enrollment of Newborns (Medicaid) SECTION 7 PERSONAL CARE MODEL (CARE MANAGEMENT) New Jersey County Case Management Units SECTION 8 PHARMACY SECTION 9 BEHAVIORAL HEALTH Behavioral Health Toolkit for Primary Care Providers Mental Health/Substance Abuse Screening Tool i
4 SECTION 10 MEMBER INFORMATION Member ID Cards Member Eligibility Verification Member Rights and Responsibilities Member Appeals and Grievances SECTION 11 PARTICIPATING PROVIDER RESPONSIBILITIES Provider Office Standards Timeliness Standards for Appointment Scheduling Medical Record Documentation Standards Medical Record Review Tool SECTION 12 PRIMARY CARE PHYSICIANS STANDARDS & POLICIES PCPs as Specialists Vaccine for Children Program (VFC) Pediatric Primary Care Medical Record and Charting Standards SECTION 13 SPECIALIST PHYSICIANS STANDARDS & POLICIES Specialists as PCPs SECTION 14 PREVENTIVE HEALTH & CLINICAL PRACTICE GUIDELINES SECTION 15 UTILIZATION MANAGEMENT APPEALS Types of Internal UM Appeals Expedited Appeals for Medicaid and NJ FamilyCare External Appeal Process for Medicaid and NJ FamilyCare (Stage 3) UnitedHealthcare Dual Complete (Medicare) Appeals Medicare 72-Hour Expedited Appeal Process Medicare 14-Day Extension Appeals of Pharmacy Denials SECTION 16 QUALITY MANAGEMENT PROGRAM Monitoring and Improving Quality of Care Quality Concerns and Corrective Action Sanctions for Quality Concerns Termination and Appeal Process ii
5 How to contact us EDI Provider Services Line Health Services Special Needs and Care Management Referral Hotline Pharmacy Services Medical Professional Line (877) (800) , select option 1 (888) (888) (800) Fax (877) Extension (800) (800) (800) Fax (800) Fax for injectable drugs only To review a patient s eligibility or benefits, check claims status, submit claims or review the physician and provider directory To register for UnitedHealthcareOnline, ask questions about online capabilities or receive assistance To review the online physician and provider directory if not a registered user of UnitedHealthcareOnline EDI Support Services provides support for all electronic transactions involving claims, electronic remittances and eligibility. Please call us for assistance with any of these transactions. To inquire about a patient s eligibility or benefits or check claim status To notify us of the procedures and services that require prior authorization, as outlined in the prior authorization section of this Manual For providers to refer high-risk members to the Care Management Program. To view the Preferred Drug List (PDL) Pharmacy Help Desk for claims issues For medications requiring prior authorization Mental Health, Substance Abuse Vision Radiology Prior Authorization (888) (888) or Fax (888) To inquire about a patient's behavioral health, vision All MRIs, MRAs, CTs, PETs and nuclear studies require prior authorization through MedSolutions 1
6 SECTION 1 UNITEDHEALTHCARE PRODUCTS Product Overview In New Jersey, UnitedHealthcare offers the following products: NJ FamilyCare (including Medicaid) UnitedHealthcare Dual Complete (Medicare) NJ FamilyCare NJ FamilyCare, a state and federally funded program, offers free or low cost health insurance for uninsured children 18 years old or younger and certain low-income parents who live in New Jersey. The program is available to families who do not have or cannot afford employer-funded or private insurance. Who is Eligible? Children and parents must live in New Jersey. Lawful permanent residents or those in a qualified immigrant status may be eligible regardless of their date of entry into the United States. Eligibility is based on family size and income only. Assets are not counted. The income eligibility level for children's coverage is 350% of the federal poverty level. For example, children in a family of four with a monthly income of up to $6,519 could be eligible for coverage. For parents, the income eligibility level is 133% of the federal poverty level, or $2,478 for a family of four.* What does it cost? For many families, it costs nothing; no monthly premiums or copayments. For families with higher incomes, there is a sliding scale for small copayments and monthly premiums may be required. What does it cover? NJ FamilyCare has four different plans (A, B, C & D). Enrollment in the plan is based on the family s income and household size. Please see Section 2: Covered and Non-Covered Services for a detailed list of services covered under each plan. If applicable, premiums and copays associated with each plan will be identified on the member s UnitedHealthcare ID card. Are there any restrictions? Applicants will be eligible for NJ FamilyCare only if they have been uninsured for a period of three months or more. However, there are exceptions to this rule; such as if you lost your insurance because your place of work went out of business or you were laid off. Depending on income, other exceptions may apply for families privately paying for health insurance or for COBRA benefits. Pre-existing conditions do not affect eligibility. *January 1, 2011 Gross Income Levels 2
7 UnitedHealthcare Dual Complete (Medicare) UnitedHealthcare Dual Complete is a Special Needs Plan (SNP) for people with Medicare (Parts A & B) and Medicaid eligibility under Title XIX. This program, which is approved by the federal government, is available to individuals who reside in Atlantic, Bergen, Essex, Hudson, Mercer, Middlesex, Monmouth, Passaic, Ocean and Union counties. UnitedHealthcare Dual Complete offers qualified individuals all of the benefits of Medicaid and Medicare; plus, extra services at no additional costs. A few examples include: Access to a Personal Care Specialist who will help manage members benefits and coordinate their care no cost to the member The security of a Personal Medical Emergency Response System that lets members call for help when they can t get to a phone no cost to the member Comprehensive dental services The member pays a $0 copayment for comprehensive dental services such as implants, fixed prosthetics and bleaching. Coverage for dental services is limited to $2,500 per calendar year for any combination of the dental services listed above. Prior authorization is required for comprehensive dental Routine eye wear (eyeglasses and contact lenses) The member is covered up to $150 for one pair of eyeglasses (lenses and frames) or $150 for contact lenses every 2 year(s). Transportation (12 round trips or 24 one-way routine medical trips) for visits to any health care appointment, including trips to the pharmacy no cost to the member Up to $55 every quarter in benefit credits to choose from over 150 health care products from our Personal Health Care Catalog. Credits can be used to order vitamins, bandages, aspirin, blood pressure monitors, digital thermometers, bath safety items and much more no cost to the member 3
8 SECTION 2 COVERED AND NON-COVERED SERVICES How Benefits Vary Under UnitedHealthcare Products From the provider s perspective, the list of covered services is important in developing treatment plans and in obtaining prior authorization when necessary. For a list of services that must be given prior authorization, refer to the Benefits for UnitedHealthcare Products and the 2010 UnitedHealthcare Dual Complete Cost Sharing and Prior Authorization for Contracted Providers charts in this section. Benefits for Division of Developmental Disabilities (DDD) Clients The benefits for DDD clients are displayed separately on the following pages because of the differences in how benefits are managed for DDD clients in contrast to other Medicaid and NJ FamilyCare members. Dual Eligibles (Medicare/Medicaid) In New Jersey, an individual who is dually eligible for Medicare and Medicaid may enroll in one of the following UnitedHealthcare of New Jersey Plans: UnitedHealthcare Community Plan- Medicaid Managed Care Plan and Traditional Medicare Fee-for- Service Medicare is the primary payer for these members. UnitedHealthcare Medicaid supplements the traditional Medicare benefit package. See the UnitedHealthcare Medicaid benefits chart. UnitedHealthcare Dual Complete- Special Needs Plan To be enrolled in this Plan, the individual must have Medicare Parts A and B and Medicaid eligibility under Title XIX. NOTE: Beginning January 1, 2009, the State of NJ no longer is involved in the Medicare SNP program. As a result of this change, members have several options as to how they can enroll in the UnitedHealthcare Dual Complete product, and a member s cost sharing depends on the member s level of dual eligibility with Medicaid and Medicare. There are two categories that an UnitedHealthcare Dual Complete member with Medicaid may be enrolled with UnitedHealthcare Community Plan: 1) Member is enrolled in both UnitedHealthcare Dual Complete product and UnitedHealthcare Community Plan Medicaid Managed Care Plan product. UnitedHealthcare coordinates both the Medicare and Medicaid benefits for these members. UnitedHealthcare Medicaid supplements the UnitedHealthcare Dual Complete (Medicare) benefit package. To have a full picture of the covered benefits for members, first review the chart displaying UnitedHealthcare Dual Complete (Medicare) benefits. Then refer to the UnitedHealthcare Medicaid benefits chart, column titled Medicaid & NJ FamilyCare A. 2) Member is enrolled in UnitedHealthcare Dual Complete and has fee-for-service (FFS) Medicaid (QMB* or full Medicaid). UnitedHealthcare reimburses the provider for the Medicare portion of the claims, minus deductibles and coinsurance (copays). The provider must bill Medicaid directly for the Medicaid portion of the claim. *Qualified Medicare Beneficiary (QMB or QMB Only): Entitled to Medicare Part A, income does not exceed 100% of the Federal Poverty Level (FPL) and resources do not exceed twice the Supplemental Security Income (SSI) limit. QMB is eligible for Medicaid payment of Medicare premiums, deductibles, coinsurance and copays (except Part D). 4
9 Medicaid law and regulation require that when an enrollee is eligible for both Medicare and Medicaid benefits (i.e., dually eligible), the Provider must first bill UnitedHealthcare Community Plan for covered services prior to submitting a claim to the State Medicaid Agency for coinsurance and deductible. If the dual eligible member is not in a dual eligible category for which the State provides cost sharing coverage, you are only permitted to collect the cost sharing from the member that the State would ordinarily pay. You may not collect amounts that exceed what you would receive from Medicaid. Note: UnitedHealthcare Community Plan does have some members who do not have Medicaid who are enrolled in the UnitedHealthcare Dual Complete Plan. These members were enrolled prior to January 2006 and are considered grandfathered in for this Plan. These members are subject to copays, deductibles and/or coinsurance and do not receive any Medicaid benefits. Interpreter Services UnitedHealthcare provides members with access to interpreter services including the deaf or hard of hearing or those who have need of interpreter services due to language barriers. Language services can be accessed via UnitedHealthcare s contract with a telephone language service or can be provided via in-person assistance. Call the Member Helpline ( ) or Care Management ( ) for additional information or to arrange for services. Family members, especially children, should not be used as interpreters in assessments, therapy or other situations where impartiality is critical. Benefits Under UnitedHealthcare Community Plan Products The benefits covered under Medicaid, NJ FamilyCare, and Medicare are displayed on the following pages. If further information is needed, providers can call DOC-DENT ( ). 5
10 Benefits for UnitedHealthcare Products The following charts display UnitedHealthcare of New Jersey, Inc. products/services. Prior authorization is indicated where required. If you have any questions about whether a service may require prior authorization, call BENEFITS (Subject to UnitedHealthcare MEDICAID & NJ FAMILYCARE policies and procedures) NJ FAMILYCARE A DDD CLIENTS B & C NJ FAMILYCARE D Abortion Medicaid FFS Medicaid FFS Medicaid FFS Medicaid FFS Acupuncture COVERED COVERED COVERED NOT COVERED (Except when performed as a form of Anesthesia in conjunction with approved surgery) Allergy Testing COVERED COVERED COVERED COVERED with PCP Referral with PCP Referral with PCP Referral with PCP Referral Audiology COVERED COVERED COVERED NOT COVERED, except for children under the age of 16 years Blood &Plasma COVERED COVERED COVERED NOT COVERED Products Except for administration and processing of blood including fees for autologous blood donation Bone Mass COVERED COVERED COVERED COVERED Measurement with PCP Referral with PCP Referral with PCP Referral with PCP Referral (Bone Density) Care Management COVERED COVERED COVERED COVERED Chiropractor Services COVERED COVERED COVERED NOT COVERED (Manual Manipulation with PCP Referral with PCP Referral with PCP Referral of Spine) Colorectal/Prostate COVERED COVERED COVERED COVERED Screening Exams Court Ordered COVERED Contact COVERED Contact COVERED Contact NOT COVERED Services UnitedHealthcare for UnitedHealthcare for UnitedHealthcare for additional information additional information additional information Dental Services COVERED COVERED COVERED COVERED to age 19. Preventive & routine Preventive & routine Preventive & routine Preventive & routine services - services member may services member may services member may member may Self Refer to Self Refer to network Self Refer to network Self Refer to network network providers providers providers providers Medicaid FFS The member is COVERED using his/her Medicaid or NJ FamilyCare card. Services are provided by a Medicaid Participating Provider. Member May Self Refer The member may choose a doctor from the UnitedHealthcare Provider Network 6
11 BENEFITS (Subject to UnitedHealthcare MEDICAID & NJ FAMILYCARE policies and procedures) NJ FAMILYCARE A DDD CLIENTS B & C NJ FAMILYCARE D Diabetic Education COVERED COVERED COVERED COVERED Diabetic Supplies COVERED COVERED COVERED COVERED and Equipment with PCP Referral with PCP Referral with PCP Referral with PCP Referral Durable Medical COVERED COVERED COVERED COVERED Equipment (DME)/ Prior Authorization Prior Authorization Prior Authorization for limited items as identified Assistive Technology required if greater required if greater required if greater on NJ State's DME list effective Devices than $500 than $500 than $500 7/1/2010. Prior Authorization required for DME greater than $500. Contact Provider Services Helpline at for assistance. DYFS Residential Medicaid FFS Medicaid FFS Medicaid FFS NOT COVERED Treatment Educational or Medicaid FFS Medicaid FFS Medicaid FFS NOT COVERED Special Remedial Services Early and Periodic COVERED COVERED COVERED with EPSDT is NOT COVERED. Screening, Diagnostic, and limitations Well child visits are covered. Treatment (EPSDT) Immunizations are covered. Services/Immunizations (0 through 20 yrs of age) Emergency Room Care COVERED COVERED COVERED COVERED Emergency Medical COVERED COVERED COVERED COVERED Transportation (Ambulance) Routine Eye Exams COVERED COVERED COVERED COVERED Member may Self Refer Member may Self Refer Member may Self Refer Member may Self Refer Enterals COVERED WITH PRIOR COVERED WITH PRIOR COVERED WITH PRIOR NOT COVERED AUTHORIZATION AUTHORIZATION AUTHORIZATION Family Planning Basic COVERED COVERED COVERED COVERED Services (Self Referral Member may Self Member may Self Member may Self Member may Self Reproduction Health Refer to participating Refer to participating Refer to participating Refer to participating (Procedures/Devices) OB/GYN OB/GYN. OB/GYN. OB/GYN Medicaid FFS when Medicaid FFS when Medicaid FFS when Obtaining Family furnished by a non- furnished by a non- furnished by a non- Planning services participating doctor participating doctor participating doctor outside of UnitedHealthcare s network is not available to Plan D members, except for those with a PSC 380. Family Planning COVERED WITH PRIOR COVERED WITH PRIOR COVERED WITH PRIOR COVERED WITH PRIOR Genetic Testing and Counseling AUTHORIZATION AUTHORIZATION AUTHORIZATION AUTHORIZATION Hearing Exams COVERED COVERED COVERED COVERED with PCP Referral with PCP Referral with PCP Referral as part of physician s screening Medicaid FFS The member is COVERED using his/her Medicaid or NJ FamilyCare card. Services are provided by a Medicaid Participating Provider. Member May Self Refer The member may choose a doctor from the UnitedHealthcare Provider Network. 7
12 BENEFITS (Subject to UnitedHealthcare MEDICAID & NJ FAMILYCARE policies and procedures) NJ FAMILYCARE A DDD CLIENTS B & C NJ FAMILYCARE D Hearing Aids and COVERED COVERED COVERED NOT COVERED, except for Batteries with PCP Referral with PCP Referral with PCP Referral children under the age of Prior Authorization Prior Authorization Prior Authorization 16 years. required if greater required if greater required if greater than $500 than $500 than $500 Hemodialysis COVERED COVERED COVERED COVERED with PCP Referral with PCP Referral with PCP Referral with PCP Referral HIV/AIDs Testing COVERED COVERED COVERED COVERED Member may Self Refer Member may Self Refer Member may Self Refer Member may Self Refer Home Health Care & COVERED with Prior COVERED with Prior COVERED COVERED Infusion Therapy Authorization Authorization with Prior limited to skilled (except for ABD (except for ABD Authorization nursing and medical members who are members who are social services with Covered by Covered by Prior Authorization Medicaid FFS) Medicaid FFS) Hospice Care COVERED COVERED COVERED COVERED with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization Immunizations COVERED COVERED COVERED COVERED Infertility Testing & Services NOT COVERED NOT COVERED NOT COVERED NOT COVERED Inpatient Hospitalization COVERED COVERED COVERED COVERED (acute care, rehabilitation special hospitals) Lab Tests and X-Rays COVERED COVERED COVERED COVERED with PCP Referral with PCP Referral with PCP Referral with PCP Referral Mammograms COVERED COVERED COVERED COVERED (Screening) Member may Self Refer. Member may Self Refer. Member may Self Refer. Baseline for women Baseline for women Baseline for women and annual for and annual for and annual for women 40+ women 40+ women 40+ Medical Day Care Medicaid FFS Medicaid FFS Not Covered FFS Not Covered Medical Supplies COVERED COVERED COVERED NOT COVERED* Limited to Diabetic Supplies *Effective 7/1/2010: Only medical supplies on the NJ State's DME list will be covered for NJ FamilyCare D members. Methadone & Methadone for pain Methadone for pain Methadone for pain Methadone for pain Methadone management is COVERED by management is COVERED by management is COVERED by management is COVERED by Maintenance UnitedHealthcare; Methadone UnitedHealthcare; Methadone UnitedHealthcare; Methadone UnitedHealthcare; Methadone maintenance for substance maintenance for substance maintenance for substance maintenance for substance abuse treatment is covered abuse treatment is covered abuse treatment is covered abuse treatment is NOT by Medicaid FFS. by Medicaid FFS. by Medicaid FFS. COVERED. Obstetrical/Maternity COVERED COVERED COVERED COVERED Care Member may Self Refer Member may Self Refer Member may Self Refer Member may Self Refer Optical Appliances COVERED COVERED COVERED COVERED $100 allowance $100 allowance $100 allowance $100 allowance Age <19 and >59: new Age <19 and >59: new NJ FamilyCare B New Pair of glasses or pair of glasses every pair of glasses every Age Under age 19: contact lenses every year. Age 19-59: new year. Age 19-59: new new pair of glasses 2 years. Member may pair of glasses or pair of glasses or every year. Under age 19: Self Refer. contact lenses every contact lenses every new pair of glasses or 2 years. Member 2 years. Member contact lenses every may Self Refer. may Self Refer. 2 years. Member may self refer. Plan C - Age <19: new pair of glasses every year or contact lenses every 2 years. Member may Self Refer. Organ Transplant COVERED COVERED COVERED COVERED Evaluation with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization Medicaid FFS The member is COVERED using his/her Medicaid or NJ FamilyCare card. Services are provided by a Medicaid Participating Provider. Member May Self Refer The member may choose a doctor from the UnitedHealthcare Provider Network 8
13 BENEFITS (Subject to UnitedHealthcare MEDICAID & NJ FAMILYCARE policies and procedures) NJ FAMILYCARE A DDD CLIENTS B & C NJ FAMILYCARE D Organ Transplants COVERED COVERED COVERED COVERED (Includes donor and with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization recipient costs unless individuals were already placed on a transplant list while in Medicaid FFS or another HMO prior to initial enrollment in UnitedHealthcare. In those cases, members are covered by FFS or the original HMO. If a member was placed on a transplant list while a member of UnitedHealthcare, and then moves to FFS or a different HMO, UnitedHealthcare is responsible for covering that service within two months of the transplant. UnitedHealthcare is responsible for cost for those members enrolled in UnitedHealthcare who briefly, i.e. less than 60 days, return to FFS, for any reason.) Orthodontia COVERED BY EXCEPTION COVERED BY EXCEPTION COVERED BY EXCEPTION BY EXCEPTION ONLY- Limited to when ONLY- Limited to when ONLY- Limited to when ONLY- Limited to when medical necessity can be medical necessity can be medical necessity can be medical necessity can be proven and Requires Prior proven and Requires Prior proven and Requires Prior proven and Requires Prior Authorization Authorization Authorization Authorization Orthopedic Shoes COVERED COVERED COVERED NOT COVERED with PCP Referral with PCP Referral with PCP Referral Outpatient Hospital Services Covered with Prior Covered with Prior Covered with Prior Covered with Prior Authorization Authorization Authorization Authorization. Exception Mental Health Visits are not covered. Outpatient Surgery, COVERED COVERED COVERED COVERED Same Day Surgery, with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization Ambulatory Surgical Center Pain Management COVERED COVERED COVERED COVERED Services with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization Pap Smears and COVERED COVERED COVERED COVERED Pelvic Exams Member may Self Refer Member may Self Refer Member may Self Refer Member may Self Refer Parenterals COVERED WITH PRIOR COVERED WITH PRIOR COVERED WITH PRIOR Effective 7/1/2010, COVERED AUTHORIZATION AUTHORIZATION AUTHORIZATION WITH PRIOR AUTHORIZATION Parenting/Child Birth COVERED COVERED COVERED COVERED Education Member may Self Refer Member may Self Refer Member may Self Refer Member may Self Refer Personal Care (in Medicaid FFS Medicaid FFS NOT COVERED NOT COVERED home)/aide Services Podiatry Care COVERED COVERED COVERED COVERED Medically Necessary with PCP Referral with PCP Referral with PCP Referral with PCP Referral (Office-Based, Non- Surgical) Podiatry Care- NOT COVERED NOT COVERED NOT COVERED NOT COVERED Routine Preventive (Office-Based, Non- Surgical) Prescription Drugs COVERED COVERED COVERED COVERED Drug Formulary Drug Formulary Drug Formulary Drug Formulary OTC & Legend drugs OTC & Legend drugs OTC & Legend drugs OTC excluded (Medicaid FFS for (Medicaid FFS for ABD population) ABD population) Post-Acute Care COVERED COVERED COVERED COVERED Preventive Health COVERED COVERED COVERED COVERED Care & Counseling/ Health Promotion Medicaid FFS The member is COVERED using his/her Medicaid or NJ FamilyCare card. Services are provided by a Medicaid Participating Provider. Member May Self Refer The member may choose a doctor from the UnitedHealthcare Provider Network. 9
14 BENEFITS (Subject to UnitedHealthcare MEDICAID & NJ FAMILYCARE policies and procedures) NJ FAMILYCARE A DDD CLIENTS B & C NJ FAMILYCARE D Primary Care Physician COVERED COVERED COVERED COVERED Private Duty or Skilled COVERED COVERED COVERED NOT COVERED Nursing Care If related to EPSDT If related to EPSDT If related to EPSDT (unless authorized screening screening screening by UnitedHealthcare) Prostate Cancer COVERED COVERED COVERED COVERED Screening Exams Member may Self Refer Member may Self Refer Member may Self Refer Member may Self Refer Prosthetics & COVERED COVERED COVERED Prosthetics Limited Orthotics with PCP Referral with PCP Referral with PCP Referral Benefits - COVERED Prior authorization Prior authorization Prior authorization with Prior Authorization required if greater required if greater required if greater Orthotics - NOT than $500 than $500 than $500 COVERED Radiation/Chemotherapy/ COVERED COVERED COVERED COVERED Hemodialysis with PCP Referral with PCP Referral with PCP Referral with PCP Referral Radiology Scans COVERED With COVERED With COVERED With COVERED With (MRI, MRA, PET) Prior Authorization Prior Authorization Prior Authorization Prior Authorization Second Medical/ COVERED COVERED COVERED COVERED Surgical Opinions with PCP Referral with PCP Referral with PCP Referral with PCP Referral Rehabilitation Medicaid FFS Medicaid FFS Medicaid FFS Medicaid FFS (Outpatient Limited to 60 days of Limited to treatment for a Occupational Therapy/ therapy per year 60 (business) day consecutive Physical Therapy/ period per incident of Speech Therapy, illness or injury beginning Inpatient RHCF) with the first day of treatment per contract year. Sex Abuse Medicaid FFS Medicaid FFS Medicaid FFS Medicaid FFS Examinations Skilled Nursing COVERED COVERED Coverage limited to NOT COVERED Facility Care (LTC) Limited to first 30 days of Limited to first 30 days of Rehabilitation services admission to a nursing admission to a nursing only for NJ FamilyCare facility. facility. B and C enrollees. (no 30-day limit) Sleep Apnea Studies COVERED COVERED COVERED COVERED with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization Sleep Therapy COVERED COVERED COVERED NOT COVERED with Prior Authorization with Prior Authorization with Prior Authorization Smoking Cessation COVERED COVERED COVERED COVERED Products with Prior Authorization with Prior Authorization with Prior Authorization with Prior Authorization Specialty Physician COVERED COVERED COVERED COVERED Services (except OB with PCP Referral with PCP Referral with PCP Referral with PCP Referral which member may Self Refer) Speech Tests COVERED COVERED COVERED COVERED with PCP Referral with PCP Referral with PCP Referral with PCP Referral Thermograms & COVERED COVERED COVERED NOT COVERED Thermography with PCP Referral with PCP Referral with PCP Referral Transportation Emergency COVERED COVERED COVERED COVERED Ambulance, MICU Transportation Non- COVERED COVERED COVERED NOT COVERED Emergency Ambulance, with Prior with Prior with Prior Invalid Coach Authorization Authorization Authorization Transportation Medicaid FFS Medicaid FFS NOT COVERED NOT COVERED Lower Mode Urgent Care COVERED COVERED COVERED COVERED Care required within Care required within Care required within Care required within 24 hours 24 hours 24 hours 24 hours Waiver and Medicaid FFS Medicaid FFS NOT COVERED NOT COVERED Demonstration Program Services Medicaid FFS The member is COVERED using his/her Medicaid or NJ FamilyCare card. Services are provided by a Medicaid Participating Provider. Member May Self Refer The member may choose a doctor from the UnitedHealthcare Provider Network. 10
15 BENEFITS (Subject to UnitedHealthcare MEDICAID & NJ FAMILYCARE policies and procedures) NJ FAMILYCARE A DDD CLIENTS B & C NJ FAMILYCARE D BEHAVIORAL HEALTH Atypical Medicaid FFS Medicaid FFS Medicaid FFS Medicaid FFS Antipsychotic Drugs within the specific therapeutic drug classes H7T and H7X Inpatient Psychiatric Medicaid FFS COVERED Medicaid FFS Medicaid FFS Hospital Services with Prior Authorization Limited to 35 days for individuals under per year 21 or 65 and over Inpatient Substance Medicaid FFS COVERED Medicaid FFS Limited to detox only Abuse (diagnosis, with Prior Authorization treatment and detoxification) Intermediate Care Medicaid FFS Medicaid FFS NOT COVERED NOT COVERED Facilities Mental Retardation (ICF/MR) Outpatient Medicaid FFS 1st visit COVERED Medicaid FFS Medicaid FFS Substance Abuse, Member may Self Refer. Limited to detox only (diagnosis, treatment After 1st visit covered and detoxification) with Prior Authorization Inpatient & Outpatient Medicaid FFS COVERED Medicaid FFS Medicaid FFS Mental Health, including with Prior Authorization Hospital Services: any testing limited to 35 days per year. Outpatient benefits for short-term, outpatient evaluation and crisis intervention or home health mental health services: limited to 20 visits per year. No limit for those under 19. Partial Care Medicaid FFS Medicaid FFS Medicaid FFS Medicaid FFS for Mental Health Partial Hospitalization Medicaid FFS Medicaid FFS Medicaid FFS Medicaid FFS for Mental Health Medicaid FFS The member is COVERED using his/her Medicaid or NJ FamilyCare card. Services are provided by a Medicaid Participating Provider. Member May Self Refer The member may choose a doctor from the UnitedHealthcare Provider Network. 11
16 The following services are not covered by either Medicaid or UnitedHealthcare for clients of Medicaid and NJ FamilyCare A, B and C programs: Services not medically necessary Cosmetic surgery, except when medically necessary and with prior approval Experimental organ transplants and investigational services Infertility treatment services Rest cures, personal comfort, convenience items and custodial care Respite Care Services involving the use of equipment in facilities, the purchase, rental or construction of which has not been approved by applicable laws of the State of New Jersey and regulations issued pursuant thereto All claims arising directly from services provided by or in institutions owned or operated by the federal government such as Veterans Administration hospitals Services provided in an inpatient psychiatric institution, that is not an acute care hospital, to individuals under 65 years of age and over 21 years of age. Services provided to all persons without charge. Services and items provided without charge through programs of other public or voluntary agencies (for example, New Jersey Department of Health and Senior Services, New Jersey Heart Association, First Aid Rescue Squad and so forth) shall be utilized to the fullest extent possible. Services or items furnished for any sickness or injury occurring while the covered person is on active duty in the military. Services provided outside the United States and territories. Services or items furnished for any condition or accidental injury arising out of and in the course of employment for which any benefits are available under the provisions of any workers compensation law, temporary disability benefits law, occupational disease law, or similar legislation, whether or not the Medicaid beneficiary claims or receives benefits thereunder and whether or not any recovery is obtained from a third-party for resulting damages. That part of any benefit which is covered or payable under any health, accident, or other insurance policy (including any benefits payable under the New Jersey no-fault automobile insurance laws), any other private or governmental health benefit system, or through any similarly third-party liability, which also includes the provision of the Unsatisfied Claim and Judgment Fund. Any service or items furnished for which the provider does not normally charge. Services furnished by an immediate relative or member of the Medicaid beneficiary s household. Services billed for which corresponding health care records do not adequately and legibly reflect the requirements of the procedure code utilized by the billing provider. Services or items reimbursed based upon submission of a cost study when there are no acceptable records or other evidence to substantiate either the costs allegedly incurred or beneficiary income available to offset those costs. In the absence of financial records, a provider may substantiate costs or available income by means of other evidence acceptable to the Division. 12
17 NJ FamilyCare D Exclusions The following services are not covered by either Medicaid or UnitedHealthcare for clients enrolled in NJ FamilyCare D program: Non-medically necessary services Intermediate Care Facilities/Mental Retardation Private duty nursing unless authorized by the contractor Personal Care Assistant Services Medical Day Care Services Chiropractic Services Orthotic devices Targeted Care Management for the chronically ill Residential treatment center psychiatric programs Religious non-medical institutions care and services Durable Medical Equipment except for specific items ( Contact Provider Services Helpline at for assistance) EPSDT except for well-child care including immunizations and lead screening and treatments Transportation Services including non-emergency ambulance, invalid coach and lower mode transportation Hearing Aid Services except for children under 16 Blood and Blood Plasma, except administration of blood, processing of blood, processing fees and fees related to autologous blood donations are covered Cosmetic Surgery Custodial Care Special Remedial and Educational Services Experimental and Investigational Services Medical Supplies, except diabetic supplies Infertility Services Rehabilitative Services for Substance Abuse Weight reduction programs or dietary supplements, except surgical operations, procedures or treatment of obesity when approved by the contractor Acupuncture and acupuncture therapy, except when performed as a form of anesthesia in connection with covered surgery Temporomandibular joint disorder treatment, including treatment performed by prosthesis placed directly in the teeth Recreational Therapy Sleep Therapy Court-ordered services Thermograms and thermography Biofeedback Radial keratotomy Respite Care Nursing facility services Audiology services, except for children under 16 years 13
18 2010 UnitedHealthcare Dual Complete Member Cost Sharing for Services All member cost sharing in the UnitedHealthcare Dual Complete Plan depends on the members level of dual eligibility, and some members may have out-of-pocket costs for premiums, copayments and coinsurance. It is important to note that there is a small subset of members enrolled in UnitedHealthcare Dual Complete plan who do not have Medicaid coverage. These members are responsible for all deductibles, copayments and coinsurance amounts outlined in the 2010 Summary of Benefits. All other members enrolled in UnitedHealthcare Dual Complete Plan have either full or partial Medicaid coverage. The State is responsible for cost sharing for those members who have full Medicaid coverage (Qualified Medicare Beneficiary - QMB). All other partial duals will be subject to the same cost sharing as the members who do not have Medicaid. Please note that generally, the State is not required to provide any payment for any expenses incurred relating to payment for deductibles, coinsurance or copayment for Medicare cost sharing to the extent that payment under Medicare for the service would exceed the payment amount that otherwise would be made under the State Medicaid plan. Explanation of Cost Sharing: UnitedHealthcare Dual Complete member with no Medicaid member is responsible for cost sharing. UnitedHealthcare Dual Complete member and UnitedHealthcare Medicaid Managed Care Plan member UnitedHealthcare responsible for most cost sharing. Provider must bill Fee-for-Service (FFS) Medicaid for those services that are carved out i.e. inpatient mental health care beyond 190 days. UnitedHealthcare Dual Complete member who has FFS Medicaid (QMB or full Medicaid) State Medicaid responsible for all cost sharing. Provider must bill State for cost sharing. UnitedHealthcare Dual Complete member FFS Medicaid (non-qmb or partial Medicaid) State Medicaid is not liable; member responsible for cost sharing. Cost-Sharing for Dual Eligible Members Provider will not bill, charge, collect a deposit from, seek compensation, remuneration or reimbursement from, or have any recourse against any UnitedHealthcare Dual Complete member who is eligible for both Medicare and Medicaid, or his or her representative, or the UnitedHealthcare Dual Complete organization for Medicare Part A and B cost sharing (e.g., copays, deductibles, coinsurance) when the state is responsible for paying such amounts. Provider will either: (a) accept payment made by or on behalf of the UnitedHealthcare Dual Complete organization as payment in full; or (b) bill the appropriate state source for such cost sharing amount. 14
19 2010 UnitedHealthcare Dual Complete Cost Sharing and Prior Authorization for Contracted Providers January 1, December 31, 2010 Atlantic, Bergen, Essex, Hudson, Mercer, Middlesex, Monmouth, Passaic, Ocean, and Union Counties, New Jersey (Note: Non-Contracted providers always require prior authorization for all Personal Care Plus covered services.) Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 1. Premium and Other Important Information $110.50* monthly Medicare Part B. $155 yearly Medicare Part B deductible. If a doctor or supplier does not accept assignment, Member s costs are often higher, which means Member pays more. *Most people will continue to pay the 2009 Part B premium of $96.40 in If a member has questions about Part B premium, they should call Social Security at TTY users should call General All cost sharing in this summary of benefits is based on Member s level of Medicaid eligibility. In-Network $0 yearly deductible. Contact the plan for services that apply. Out-of-Network unless otherwise noted, out-of-network services are not covered. General All cost sharing in this summary of benefits is based on Member s level of Medicaid eligibility. In-Network $155 yearly deductible. Contact the plan for services that apply. Out-of-Network unless otherwise noted, outof-network services are not covered. N/A 2. Doctor and Hospital Choice (For more information, see Emergency - #15 and Urgently Needed Care #16.) Member may go to any doctor, specialist or hospital that accepts Medicare. In-Network Member must go to network doctors, specialists, and hospitals. Referral required for network specialists (for certain benefits). In-Network Member must go to network doctors, specialists, and hospitals. Referral required for network specialists (for certain benefits). No Member may have to pay separate copay for certain doctor office visits. Member may have to pay separate copay for certain doctor office visits. 15
20 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 3. Inpatient Hospital Care (including Substance Abuse & Rehabilitation Services) For each benefit period: Days 1-60: $1100 deductible Days 61-90: $275 per day Days : $550 per lifetime reserve day Please call MEDICARE ( ) for information about lifetime reserve days. Lifetime reserve days can be only used once. A benefit period starts the day Member goes into a hospital or skilled nursing facility. It ends when Member goes for 60 days in a row without hospital or skilled nursing care. If Member goes into the hospital after one benefit period has ended, a new benefit period begins. Member must pay the inpatient hospital deductible for each benefit period. There is no limit to the number of benefit periods Member can have. In-Network $0 yearly deductible For Medicare-covered hospital stays $0 or: Days 1-60: $0 copay per day Days 61-90: $0 copay per day Plan covers 60 lifetime reserve days. Cost per lifetime reserve day; $0 or: Days 1-60; $0 copay per day. Plan covers 90 days each benefit period. Except in an emergency, Member s provider must obtain authorization from UnitedHealthcare Dual Complete. In-Network $1100 yearly deductible For Medicare-covered hospital stays $0 or: Days 1-60: $0 copay per day Days 61-90: $275 copay per day Days (or 60 lifetime reserve days): $550 copay per day. Medicare benefit periods apply Plan covers 90 days each benefit period. Plan covers 60 lifetime reserve days. Cost per lifetime reserve day; $0 or: Days 1-60; $550 copay per day. Plan covers 90 days each benefit period. Except in an emergency, Member s provider must obtain authorization from UnitedHealthcare Dual Complete. Yes 16
21 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 4. Inpatient Mental Health Care Same deductible and copay as inpatient hospital care (see Inpatient Hospital Care above). 190 day limit in a Psychiatric Hospital. In-Network $0 yearly deductible For Medicare-covered hospital stays $0 or: Days 1-60: $0 copay per day Days 61-90: $0 copay per day Plan covers 60 lifetime reserve days. Cost per lifetime reserve day; $0 or: Days 1-60; $0 copay per day. Member gets up to 190 days in a Psychiatric Hospital in a lifetime. Except in an emergency, Member s provider must obtain authorization from UnitedHealthcare Dual Complete. In-Network $1100 yearly deductible For Medicare-covered hospital stays $0 or: Days 1-60: $0 copay per day Days 61-90: $275 copay per day Plan covers 60 lifetime reserve days. Cost per lifetime reserve day; Days 1-60; $550 copay per day. Member gets up to 190 days in a Psychiatric Hospital in a lifetime. Except in an emergency, Member s provider must obtain authorization from UnitedHealthcare Dual Complete. Yes 17
22 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 5. Skilled Nursing Facility (in a Medicare-certified skilled nursing facility) For each benefit period after at least a 3-day covered hospital stay: Days 1-20: $0 per day Days : $ per day 100 days for each benefit period. A benefit period starts the day you go into a hospital or SNF. It ends when you go for 60 days in a row without hospital or skilled nursing care. If you go into the hospital after one benefit period has ended, a new benefit period begins. You must pay the inpatient hospital deductible for each benefit period. There is no limit to the number of benefit periods you can have. General Prior authorization is required. In-Network $0 or: Days 1-20: $0 per day Days : $0 per day 100 days covered for each benefit period No prior hospital stay is required. General Prior authorization is required. In-Network $0 or: Days 1-20: $ 0 per day Days : $ per day 100 days covered for each benefit period No prior hospital stay is required. Yes 6. Home Health Care (Includes medically necessary intermittent skilled nursing care, home health aide services, and rehabilitation services, etc.) $0 copay. General Authorization rules may apply. In-Network $0 copay for each Medicare-covered home health visit. General Authorization rules may apply. In-Network $0 copay for each Medicarecovered home health visit. Member pays 20% of the Medicare-approved amount for durable medical equipment. Yes 7. Hospice Member pays part of the cost for outpatient drugs and inpatient respite care. Member must receive care from a Medicarecertified hospice and meet medical criteria. In-Network Member must receive care from a Medicarecertified hospice. In-Network Member must receive care from a Medicare-certified hospice. Yes (Provider must bill Original Medicare Feefor-Service) 18
23 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 8. Doctor Office Visits 20% coinsurance In-Network 0% of the cost for each primary care doctor office visit for Medicarecovered benefits. 0% of the cost for each specialist visit for Medicare-covered benefits. In-Network 20% of the cost for each primary care doctor office visit for Medicare-covered benefits. 20% of the cost for each specialist visit for Medicarecovered benefits. No 9. Chiropractic Services 20% coinsurance Routine care not covered 20% coinsurance for manual manipulation of the spine to correct subluxation, if Member gets it from a chiropractor or other qualified provider. In-Network 0% of the cost for Medicare-covered visits. Medicare-covered chiropractic visits are for manual manipulation of the spine to correct a displacement or misalignment of a joint or body part. In-Network 20% of the cost for Medicarecovered visits. Medicare-covered chiropractic visits are for manual manipulation of the spine to correct a displacement or misalignment of a joint or body part. No 10. Podiatry Services 20% coinsurance Routine care not covered. 20% coinsurance for medically necessary foot care, including care for medical conditions affecting the lower limbs. General Authorization rules may apply. In-Network 0% of the cost for each Medicare-covered visit. 0% of the cost for each routine visit up to 4 visits every year. Medicare-covered podiatry benefits are for medically-necessary foot care. General Authorization rules may apply. In-Network 20% of the cost for each Medicare-covered visit. 0% of the cost for each routine visit up to 4 visits every year. 20% of the cost for each routine visit after the 4th visit every year. Medicare-covered podiatry benefits are for medicallynecessary foot care. No 11. Outpatient Mental Health Care 45% coinsurance for most outpatient mental health services. In-Network 0% of the cost for each Medicare-covered individual or group therapy visit. In-Network 45% of the cost for each Medicare-covered individual or group therapy visit. No 19
24 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 12. Outpatient Substance Abuse Care 20% coinsurance General Authorization rules may apply. In-Network 0% of the cost for Medicare-covered individual or group visits. General Authorization rules may apply. In-Network 20% of the cost for Medicarecovered individual or group visits. Yes 13. Outpatient Services/Surgery 20% coinsurance for the doctor 20% of outpatient facility General Authorization rules may apply. In-Network 0% of the cost for each Medicare-covered ambulatory surgical center visit. 0% of the cost for each Medicare-covered outpatient hospital facility visit. General Authorization rules may apply. In-Network 20% of the cost for each Medicare-covered ambulatory surgical center visit. 20% of the cost for each Medicare-covered outpatient hospital facility visit. Additional facility charges may apply. Yes Additional facility charges may apply. 14. Ambulance Services (medically necessary ambulance services) 20% coinsurance General Authorization rules may apply. In-Network 0% of the cost for each Medicare-covered ambulance benefits. General Authorization rules may apply. In-Network 20% of the cost for each Medicare-covered ambulance benefits. Yes, for nonemergency ambulance services. 20
25 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 15. Emergency Care (You may go to any emergency room if you reasonably believe you need emergency care.) 20% coinsurance for the doctor 20% of facility charge, or a set copay for emergency room visit Member doesn t have to pay the emergency room copay if admitted to the hospital for the same condition within 3 days of the emergency room visit. NOT covered outside the U.S. except under limited circumstances. In-Network $0 for Medicare-covered emergency room visits. This amount applies toward Member s innetwork plan deductible. Out-of-Network Worldwide coverage. In and Out-of-Network If Member is admitted to the hospital within 24- hour(s) for the same condition, Member pays pay $0 for the emergency room visit. In-Network $50 copay for Medicarecovered emergency room visits. This amount applies toward Member s in-network plan deductible. Out-of-Network Worldwide coverage. In and Out-of-Network If Member is admitted to the hospital within 24-hour(s) for the same condition, Member pays $0 for the emergency room visit. No 16. Urgently Needed Care (This is NOT emergency care, and in most cases, is out of the service area.) 20% coinsurance, or set a copay NOT covered outside the U.S. except under limited circumstances. General 0% of the cost for Medicare-covered urgently needed care visits. General 20% of the cost for Medicarecovered urgently needed care visits. No 17. Outpatient Rehabilitation Services (Occupational Therapy, Physical Therapy, Speech and Language Therapy) 20% coinsurance General Authorization rules may apply. In-Network 0% of the cost for Medicare-covered Occupational Therapy visits. 0% of the cost for Medicare-covered Physical Therapy and /or Speech/ Language Therapy visits. General Authorization rules may apply. In-Network 20% of the cost for Medicarecovered Occupational Therapy visits. 20% of the cost for Medicarecovered Physical Therapy and/or Speech/ Language Therapy visits. Yes, after 6 visits. 18. Durable Medical Equipment (Includes wheelchairs, oxygen, etc.) 20% coinsurance General Authorization rules may apply. In-Network 0% of the cost for Medicare-covered items. General Authorization rules may apply. In-Network 20% of the cost for Medicarecovered items. Yes, if greater than $500 per item. NJ UnitedHealthcare Provider Manual 4/09 21
26 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 19. Prosthetic Devices (Includes braces, artificial limbs and eyes, etc.) 20% coinsurance General Authorization rules may apply. In-Network 0% of the cost for Medicare-covered items. General Authorization rules may apply. In-Network 20% of the cost for Medicarecovered items. Yes 20. Diabetes Self-Monitoring Training and Supplies (includes coverage for glucose monitors, test strips, lancets, screening tests and self-management training) 20% coinsurance In-Network 0% of the cost for Diabetes self-monitoring training. 0% of the cost for Nutrition Therapy for Diabetes. 0% of the cost for Diabetes supplies. In-Network 20% of the cost for Diabetes self-monitoring training. 20% of the cost for Nutrition Therapy for Diabetes. 20% of the cost for Diabetes supplies. No, except if done in home. 21. Diagnostic Tests, X-Rays, and Lab Services 20% coinsurance for diagnostic tests and x- rays $0 copay for Medicarecovered lab services Lab Services: Medicare covers medically necessary diagnostic lab services that are ordered by Member s treating doctor when they are provided by a Clinical Laboratory Improvement Amendments (CLIA) certified laboratory that participates in Medicare. Diagnostic lab services that are done to help Member s doctor diagnose or rule out a suspected illness or condition. Medicare does not cover most routine screening tests, like checking Member s cholesterol. In-Network 0% of the cost for Medicare-covered lab services. 0% of the cost for Medicare-covered diagnostic procedures and tests. 0% of the cost for Medicare-covered X-rays. 0% of the cost for Medicare-covered diagnostic radiology services. 0% of the cost for Medicare-covered therapeutic radiology services. In-Network 0% of the cost for Medicarecovered lab services. 20% of the cost for Medicarecovered diagnostic procedures and tests. 20% of the cost for Medicarecovered X-rays. 20% of the cost for Medicarecovered diagnostic radiology services. 20% of the cost for Medicarecovered therapeutic radiology services. No 22
27 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 22. Bone Mass Measurement (For people with Medicare who are at risk) 20% coinsurance Covered once every 24 months (more often if medically necessary) if Member meets certain medical conditions. In-Network 0% of the cost for Medicare-covered Bone Mass Measurement. In-Network 20% of the cost for Medicarecovered Bone Mass Measurement. No 23. Colorectal Screening Exams (For people with Medicare age 50 and older) 20% coinsurance Covered when Member is at high risk or is age 50 and older. In-Network 0% of the cost for Medicare-covered colorectal screenings. In-Network 20% of the cost for Medicarecovered colorectal screenings. No 24. Immunizations (Flu vaccine, Hepatitis B vaccine - for people with Medicare who are at risk, Pneumonia vaccine) $0 copay for Flu and Pneumonia vaccines 20% coinsurance for Hepatitis B vaccine. Member may only need the Pneumonia vaccine once in their lifetime. In-Network $0 copay for Flu and Pneumonia vaccines. No referral needed for Flu and Pneumonia vaccines. 0% of the cost for Hepatitis B vaccine. In-Network $0 copay for Flu and Pneumonia vaccines. No referral needed for Flu and Pneumonia vaccines. 20% of the cost for Hepatitis B vaccine. No 25. Mammograms- Annual Screening (For women with Medicare age 40 and older) 20% coinsurance No referral needed. Covered once a year for all women with Medicare age 40 and older. One baseline mammogram covered for women with Medicare between age 35 and 39. In-Network 0% of the cost for Medicare-covered screening mammograms. In-Network 20% of the cost for Medicarecovered screening mammograms. No 26. Pap Smears and Pelvic Exams $0 copay for Pap smears Covered once every 2 years. Covered once a year for women with Medicare at high risk. 20% coinsurance for Pelvic Exams. In-Network 0% of the cost for Medicare-covered pap smears. 0% of the cost for Medicare-covered pelvic exams. In-Network 0% of the cost for Medicarecovered pap smears. 20% of the cost for Medicarecovered pelvic exams. No 23
28 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 27. Prostate Cancer Screening Exams (For men with Medicare age 50 and older) 20% coinsurance for the digital rectal exam. $0 for the PSA test; 20% coinsurance for other related services. In-Network 0% of the cost for Medicarecovered prostate cancer screening. In-Network 20% of the cost for Medicarecovered prostate cancer screening. No Covered once a year for all men with Medicare over age ESRD 20% coinsurance for dialysis In-Network 0% of the cost for in and outof-area dialysis In-Network 20% of the cost for in and outof-area dialysis Yes 0% of the cost for Nutrition Therapy for Renal Disease. 20% of the cost for Nutrition Therapy for Renal Disease. 29. Outpatient Prescription Drugs Most drugs not covered. (Member can add prescription drug coverage to Original Medicare by joining a Medicare Prescription Drug Plan.) General 0% of the cost for Part B- covered drugs (not including Part B-covered chemotherapy drugs). 0% of the cost for Part B- covered chemotherapy drugs. General 20% of the cost for Part B- covered drugs (not including Part B-covered chemotherapy drugs). 20% of the cost for Part B- covered chemotherapy drugs. Yes, if Rx is non-formulary. Yes, if Rx is in Formulary and requires Prior Authorization. See Formulary. Drugs Covered under Medicare Part D Drugs Covered under Medicare Part D General This plan uses a formulary. The plan sends the Member the formulary. Member can also see the formulary at on the web. The plan offers national in-network prescription coverage. This means that the Member will pay the same amount for their prescription drugs if they get them at an in-network pharmacy outside of the plan s service area (for instance when Member travels). General This plan uses a formulary. The plan sends the Member the formulary. Member can also see the formulary at on the web. The plan offers national in-network prescription coverage. This means that Member will pay the same amount for their prescription drugs if they get them at an in-network pharmacy outside of the plan s service area (for instance when Member travels). Total yearly drug costs are the total drug costs paid by both Member and the plan. Total yearly drug costs are the total drug costs paid by both Member and the plan. 24
29 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization continued 29. Outpatient Prescription Drugs Most drugs not covered. (Member can add prescription drug coverage to Original Medicare by joining a Medicare Prescription Drug Plan.) The plan may require the Member to first try one drug to treat their condition before it will cover another drug for that condition. Some drugs have quantity limits. Member s provider must get prior authorization from Personal Care Plus for certain drugs. In-Network $0 or $56 yearly deductible (amount depends on Member s income). Initial Coverage Depending upon Member's income and institutional status, they pay the following: For generic drugs (including brand drugs treated as generic), either: A $0 copay or A $1.10 copay or A $2.50 copay For all other drugs, either: A $0 copay or A $3.30 copay or A $6.30 copay. Retail Pharmacy Member can get drugs the following way (s): -one-month (31-day) supply The plan may require the Member to first try one drug to treat their condition before it will cover another drug for that condition. Some drugs have quantity limits. Member s provider must get prior authorization from Personal Care Plus for certain drugs. In-Network $0 or $56 yearly deductible (amount depends on Member s income). Initial Coverage Depending upon Member's income and institutional status, they pay the following: For generic drugs (including brand drugs treated as generic), either: A $0 copay or A $1.10 copay or A $2.50 copay For all other drugs, either: A $0 copay or A $3.30 copay or A $6.30 copay. Retail Pharmacy Member can get drugs the following way (s): -one-month (31-day) supply -three month (90-day) supply Long Term Care Pharmacy Member can get drugs the following way (s): Yes, if Rx is non-formulary. Yes, if Rx is in Formulary and requires Prior Authorization. See Formulary. -three month (90-day) supply Long Term Care Pharmacy Member can get drugs the following way (s): -one-month (31-day) supply Catastrophic Coverage after the Member s yearly outof-pocket costs reach $ 4550, they pay the following (amount depends on their income): UnitedHealthcare Provider Manual 12/10 25
30 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization continued 29. Outpatient Prescription Drugs Most drugs not covered. (Member can add prescription drug coverage to Original Medicare by joining a Medicare Prescription Drug Plan.) -one-month (31-day) supply Catastrophic Coverage After the Member s yearly out-of-pocket costs reach $4550, they pay the following (amount depends on their income): -$0 copay for any drugs; or Depending on Members income and institutional status, they will be reimbursed by UnitedHealthcare Dual Complete (HMO) up to the full cost of the drug minus the following: Yes, if Rx is non-formulary. Yes, if Rx is in Formulary and requires Prior Authorization. See Formulary. -$0 copay for any drugs; or Out-of-Network Plan drugs may be covered in special circumstances, for instance, illness while traveling outside of the plan s service area where there is no network pharmacy. Member may pay more than the copay if they get their drugs at an out-of-network pharmacy. Out-of-Network Initial Coverage Depending on Members income and institutional status, they will be reimbursed by UnitedHealthcare Dual Complete (HMO) up to the full cost of the drug minus the following: For generic drugs purchased out-of-network (including brand For generic drugs purchased out-of-network (including brand drugs treated as generic), either: A $0 copay or A $1.10 copay or A $2.50 copay For all other drugs purchased out-of-network, either: A $0 copay or A $3.30 copay or A $6.30 copay. Out-of-Network Plan drugs may be covered in special circumstances, for instance, illness while traveling outside of the plan s service area where there is no network pharmacy. Member may pay more than the copay if they get their drugs at an out-of-network pharmacy. Out-of-Network Initial Coverage Depending on Members income and institutional status, they will be reimbursed by UnitedHealthcare Dual Complete (HMO) up to the full cost of the drug minus the following: 26
31 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization continued 29. Outpatient Prescription Drugs For generic drugs purchased out-of-network (including brand drugs treated as generic), either: A $0 copay or A $1.10 copay or A $2.50 copay For all other drugs purchased out-of-network, either: A $0 copay or A $3.30 copay or A $6.30 copay. Yes, if Rx is non-formulary. Yes, if Rx is in Formulary and requires Prior Authorization. See Formulary. Out-of-Network Catastrophic Coverage After the Member s yearly outof-pocket costs reach $4550, they pay the following (amount depends on their income): -$0 copay for any drugs; or Out-of-Network Catastrophic Coverage Depending on Members income and institutional status, they will be reimbursed by UnitedHealthcare Dual Complete (HMO) up to the full cost of the drug minus the following: For generic drugs purchased out-of-network (including brand 27
32 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 30. Dental Services Preventative dental services (such as cleaning) not covered. In-Network Comprehensive dental services- The member pays a $0 copayment for comprehensive dental services such as implants, fixed prosthetics and bleaching. Coverage for dental services is limited to $2,500 per calendar year for any combination of the dental services listed above. Prior authorization is required for comprehensive dental 0% of the cost for Medicarecovered dental benefits. In-Network Comprehensive dental services-the member pays a $0 copayment for comprehensive dental services such as implants, fixed prosthetics and bleaching. Coverage for dental services is limited to $2,500 per calendar year for any combination of the dental services listed above. Prior authorization is required for comprehensive dental 20% of the cost for Medicarecovered dental benefits. Yes 31. Hearing Services Routine hearing exams and hearing aids not covered. 20% coinsurance for diagnostic hearing exams. In-Network In general, routine hearing exams and hearing aids not covered. -0% of the cost for diagnostic hearing exams In-Network In general, routine hearing exams and hearing aids not covered. -20% of the cost for diagnostic hearing exams No, for hearing exams. Yes, for hearing aids. 32. Vision Services 20% coinsurance for diagnosis and treatment of diseases and conditions of the eye. Routine eye exams and glasses are not covered. Medicare pays for one pair of eyeglasses or contact lenses after cataract surgery. In-Network Non-Medicare-covered eye exams and glasses are not covered. $0 copay for -one pair of eyeglasses or contact lenses after cataract surgery -The member is covered up to $150 for one pair of eyeglasses (lenses and frames) or $150 for contact lenses every 2 year(s). -0% of the cost for exams to diagnose and treat diseases and conditions of the eye. In-Network Non-Medicare-covered eye exams and glasses are not covered. $0 copay for -one pair of eyeglasses or contact lenses after cataract surgery -The member is covered up to $150 for one pair of eyeglasses (lenses and frames) or $150 for contact lenses every 2 year(s). -20% of the cost for exams to diagnose and treat diseases and conditions of the eye. No 28
33 Benefit Category Traditional Medicare Fee-for-Service What Member Will Pay If Member Has UnitedHealthcare Dual Complete SNP (Has Both Medicaid and Medicare Coverage) What Member Will Pay If Member Has UnitedHealthcare Dual Complete (Medicare Coverage Only and No Medicaid Coverage) Services That Require Prior Authorization 33. Physical Exams 20% coinsurance for one exam within the first 6 months of Member s new Medicare Part B coverage When Member gets Medicare Part B, they can get a one time physical exam within the first 6 months of their new Part B coverage. The coverage does not include lab tests. In-Network When the Member gets Medicare Part B, they can get a one time physical exam within the first 6 months of their new Part B coverage. The coverage does not include lab tests. Routine exams are covered. In-Network When the Member gets Medicare Part B, they can get a one time physical exam within the first 6 months of their new Part B coverage. The coverage does not include lab tests. Routine exams are not covered. No 34. Health/Wellness Education Not covered. In-Network This plan covers health/wellness education benefits. In-Network This plan covers health/wellness education benefits. No -Written health education materials, including -Newsletters -Nutritional Training -Smoking Cessation -Other Wellness Services -Written health education materials, including -Newsletters -Nutritional Training -Smoking Cessation -Other Wellness Services 35. Transportation (Routine) Not covered. General Authorization rules apply. In-Network $0 copay for up to 12 round trip(s) to planapproved location every year. General Authorization rules apply. In-Network $0 copay for up to 12 round trip(s) to plan-approved location every year. No, for transportation to Medically Necessary Appointments. Yes, for nonemergency ambulance. 29
34 The following additional benefits are available to all UnitedHealthcare Dual Complete Members to help keep them healthy. Personal Care Specialist (PCS) Health Care Products Transportation Personal Medical Emergency Response System Comprehensive Dental Services When members join UnitedHealthcare Dual Complete, they are assigned their own Personal Care Specialist (PCS). The PCS is responsible for coordinating all member services and care on behalf of plan enrollees. An allowance of up to $55 every quarter for non-prescription, health related items purchased from a plan approved catalog. The catalog includes such items as vitamins, first aid kits, bandages, disposable wash cloths, poligrip, denture cleaning tablets, digital thermometers, humidifiers, cough, cold and allergy medicines, ben-gay, skin lotion, chair cushions, and more. Up to 12 round-trips to plan approved locations, including the doctor s office and laboratories, at no cost to the member. A dedicated personal emergency response system that allows members to call for help even if they can t get to the phone; this is available at no cost to members for the installation and monthly monitoring. The member pays a $0 copayment for comprehensive dental services such as implants, fixed prosthetics and bleaching. Coverage for dental services is limited to $2,500 per calendar year for any combination of the dental services listed above. Prior authorization is required for comprehensive dental 30
35 SECTION 3 PRIOR AUTHORIZATION Responsibility for Requesting Prior Authorization The PCP or specialist referring a patient for an elective admission or same day surgery is responsible for contacting UnitedHealthcare for prior authorization. UnitedHealthcare recommends calling at least 5 days, but not later than 48 hours, in advance of the admission or surgery. Requests for prior authorization are prioritized according to level of medical exigency. Certain cases are reviewed under emergency guidelines. For prior authorizations, providers should call or fax the appropriate number listed below. If faxing, use the UnitedHealthcare forms. Prior Authorization 24 hrs / 7 days a week Listen to prompts Phone Fax Medical/Surgical Maternity/Newborn Behavioral Health Pharmacy Prior Authorization (Mon Fri, 9:00 AM 9:00 PM) The following information is required: Patient s Name and UnitedHealthcare ID number PCP s name and UnitedHealthcare Provider ID number Attending MD s name and UnitedHealthcare Provider ID number Facility name Expected date of admission or service Diagnosis(es) or reason for treatment Planned procedures, services, or medications Other insurance information for Coordination of benefits (COB) Once the Service Center receives the complete information to review the request according to Milliman USA Healthcare Guidelines, the Service Center makes a determination. If approved, UnitedHealthcare assigns an authorization number to the elective admission or same day surgery and enters the authorization number into UnitedHealthcare s information system. UnitedHealthcare then informs the requesting physician s office of the authorization number. This authorization number references the admission or procedure. Determination of Medical Necessity Medically necessary services or supplies are those services required to identify and treat a member s illness or injury and which, as determined by the Medical Director, are: Appropriate and necessary for the diagnosis, prevention, quantification, cure or treatment of the member s medical condition, illness, disease, or injury; Appropriate with regard to standards of UnitedHealthcare and good medical practice as recommended and accepted by the medical community; 31
36 Not solely for the convenience of the provider, the member, or the member s family; and The most appropriate supply or level of service which can be safely provided to the member. When specifically applied to an inpatient, it further means that the member s medical symptoms or conditions require that the member cannot be treated as an outpatient. Criteria and Guidelines UnitedHealthcare uses Milliman USA Healthcare Guidelines for determinations of appropriateness of care. UnitedHealthcare has written policies and procedures specifying responsibilities and qualifications of staff that authorize admissions, services, procedures, or extensions of stay. UnitedHealthcare makes determinations on a timely basis, as required by the exigencies of the situation. The Care Manager can authorize, but not deny, an admission, service, procedure, or extension of stay. If the Care Manager is unable to determine by chart documentation, documentation from the facility utilization review department, or discussion with the PCP or attending physician, the need for admission, surgical or diagnostic procedure, or continued stay, the case is referred to a Medical Director or a Physician Advisor under the direction of a Medical Director. If, after reviewing all documentation of clinical information, a Medical Director/ Physician Advisor determines that the admission, service, procedure, or extension of stay is reasonable, the Care Manager notifies the provider by phone or fax, assigns an authorization number, and sets the next review date. If a Medical Director/ Physician Advisor makes a determination to deny or limit an admission, service, procedure, or extension of stay, UnitedHealthcare notifies the facility s utilization review department, which is responsible for notifying the attending physician. UnitedHealthcare informs the facility of a Medical Director/ Physician Advisor s name and contact information. The attending physician or designee may contact a Medical Director/ Physician Advisor to have the decision reconsidered, based on medical information. A Medical Director/ Physician Advisor is available immediately in urgent or emergency cases and on a timely basis for all other cases. If, after discussion with the attending physician or designee, a Medical Director/ Physician Advisor determines the admission, service, procedure, or extension of stay is reasonable, a Medical Director/ Physician Advisor notifies the Care Manager, who notifies the facility s utilization review department by phone or fax. UnitedHealthcare will not retroactively deny reimbursement for a covered service provided to a member by a provider who relied upon the written or oral authorization of UnitedHealthcare prior to providing the service to the member, except in cases where there was material misrepresentation or fraud. Prior authorization for an inpatient stay does not mean authorization for continued inpatient stays. After giving prior authorization for an admission, service, or procedure, UnitedHealthcare conducts concurrent review to determine whether the stay continues to meet Milliman USA Healthcare Guidelines for determinations of appropriateness of care. UnitedHealthcare approves or denies continuation of the stay in accordance with the criteria and guidelines described in this section. In the case of a denial, UnitedHealthcare notifies the facility by phone or fax within one working day, followed by written notification from the UnitedHealthcare UM Appeals Department within 15 working days. The PCP, specialist, attending physician, or the facility may appeal any adverse decision, according to the procedures in Section Utilization Management Appeals. 32
37 Provider s Responsibility to Verify Prior Authorization All physicians, facilities, and agencies providing services that require prior authorization should call the Prior Authorization Department at DOC-DENT ( ) in advance of performing the procedure or providing service(s) to verify that UnitedHealthcare has issued an authorization number. Continuity of Care When Provider Leaves Network Upon termination by provider or UnitedHealthcare of the provider agreement for any reason, other than UnitedHealthcare s insolvency, provider shall continue to furnish covered services to members and UnitedHealthcare shall continue to compensate provider in accordance with the provisions of the provider agreement: For any member who is registered as an inpatient of provider as of the date of termination, coverage shall continue until the member is transferred or discharged from provider. If provider is a health care professional, for any member under provider s care who, at the time of termination of the provider agreement, is a registered bed patient at a hospital or other institution, coverage shall continue until such member s discharge therefrom. Where it is medically necessary for the member to continue treatment with provider, coverage shall continue for up to four (4) months. In cases of the pregnancy of a member, medical necessity shall be deemed to have been demonstrated and coverage by provider shall continue to postpartum evaluation of a member, up to six (6) weeks after delivery. In cases of post-operative care, coverage by provider shall continue for up to six (6) months. In cases of oncological treatment, coverage by provider shall continue for up to one (1) year. In cases of psychiatric treatment, coverage by provider shall continue for up to one (1) year. In the case of a hospital provider whose contract is not renewed or terminated by either party, provider and UnitedHealthcare agree to continue to abide by the terms of the most current contract for a period of four months from the contract termination date, or some other mutually agreed upon date. UnitedHealthcare members must be permitted to continue to receive nonemergency services from the hospital during the four-month period. Emergency services will continue to be available to UnitedHealthcare members after the four-month period expires. The determination as to the medical necessity of a member s continued treatment with provider shall be subject to appeal. UnitedHealthcare shall not be required to continue coverage by provider if the reason for termination was: (i) that provider is an imminent danger to members or public health, safety, and welfare; (ii) a determination of fraud; or (iii) provider is subject to disciplinary action by the State Board of Medical Examiners. Authorization of Care for New Members UnitedHealthcare will honor plans of care (including prescriptions, DME, medical supplies, prosthetic and orthotic appliances, and any other ongoing services) initiated prior to a new member s enrollment until the PCP evaluates the member and establishes a new plan of care. Referrals to Non-Participating Providers All referrals to non-participating providers must receive prior authorization from UnitedHealthcare. If you need to verify a provider s participation in UnitedHealthcare, call DOC-DENT ( ). 33
38 Assure required services are furnished; Enrollees with Special Needs: Are those individuals with complex/chronic medical conditions requiring specialized health care services, including persons with physical, mental, substance abuse, and for developmental disabilities, including such people who are homeless. Methods to identify those at risk who should be referred for a Complex Needs Assessment Members with Special Needs are identified in the following ways: State Enrollment File Call Center Providers Member/guardian Utilization reports Census reports Pharmacy Plan Selection Form (PSFs) Methods and guidelines of determining specific needs of referred individuals Members who are designated as having special needs should be referred to Care Management for a Comprehensive Health Status Assessment by calling X A plan of care will be developed in conjunction with the provider, the member, and/or the member s family/guardian. Allow for continuation of existing relationships with non-par providers Additionally, UHCCP will provide for specialty care, diagnostic, and interventional strategies, as well as long term management of medical conditions, as well as continuation of out of network providers when considered to be in the best medical interest of the member. Referrals to special care facilities for highly specialized care UnitedHealthcare will provide access to specialty centers for diagnosis and treatment of rare disorders. Standing referrals for long-term specialty care UnitedHealthcare Community Plan realizes that some care exceeds the capabilities of the Primary Care Provider (PCP) therefore, UnitedHealthcare Community Plan allows qualified specialists who meet the credentialing criteria of the plan to serve as the overall coordinator of all medically necessary care for members with complex conditions. Responding to crisis situations after hours for enrollees with special needs All medical emergencies should be handled by contacting 911. Members or Providers may reach their Personal Care Manager by directly phone during normal business hours. After hours messages may be left on the automated voice messaging system. The Special Needs Hot Line X5260 is also available for messages; these messages will be returned in one (1) business day. Provision for dental services for enrollees with developmental disabilities UnitedHealthcare will provide access for comprehensive, quality dental services for the special needs enrollee. Emphasis will be placed on providing coordinated care managed dental services with the goal of decreasing the member susceptibility to caries and periodontal disease. 34
39 Program Goals: Improve special needs members access to quality comprehensive dental care through a network of providers with expertise with developmental disabilities. Coordination of access and delivery with Primary Care Provider(s) linkages and community based organizations. Creation of dental management services and expanded benefits for comprehensive dental care within the framework of comprehensive total treatment planning and preventive care delivery. Objectives: The dental care management coordinator will monitor linkages with care managers, community based organizations and the Primary Care Provider to emphasize preventive education Quality utilization management and improvement of the program using national and internally developed benchmark standards will be monitored by the Chief Dental Officer. Provider directories will identify dentists that meet the treatment requirements of the special needs member. The special needs dental coordinator will assist members with special needs in all aspects of dental treatment. Requirements: The provider network includes dentists that offer expertise in the dental management of enrollees with developmental disabilities. In addition to the covered services offered by UnitedHealthcare, special needs enrollees have the following benefit of increased frequency of visits based on the dental risk assessment. The standard allows up to four visits annually without prior authorization. All other quality utilization management and improvement benchmark standards are in effect. Emphasis is placed on establishing linkages with the Primary Care Physician, care manager, and community organizations. Informed Consent is required from all patients with developmental disabilities or authorized legal representative/guardian before all surgical cases are treated in the operating room. The care manager of an enrollee shall coordinate authorizations for dental required hospitalizations in conjunction with the UnitedHealthcare dental consultant team. The special needs program will be reviewed, audited and monitored using the utilization management and quality improvement measures established by UnitedHealthcare. Dentists Management Fee - Providers are paid a dental management fee for initial and fol 35
40 FAX:
41 B.4.15 Hysterectomy and Sterilization Procedures and Consent Forms HYSTERECTOMY RECEIPT OF INFORMATION FORM FD-189 Federally prescribed documentation regulations for hysterectomies are extremely rigid. Specific Medicaid requirements must be met and documented on the Hysterectomy Receipt of Information Form (FD-189). Any claim (hospital, operating physician, anesthesiologist, clinic, etc) involving hysterectomy procedures must have a properly completed FD-189 form attached when submitted for payment. Hysterectomy claims are hard copy restricted; electronic billing is not permitted. Additional information concerning Medicaid policy governing hysterectomy procedures may be found in Title 10, Subchapter 54, Section V Physicians Services, included with your manual. Providers may obtain additional copies of the FD-189 form from the Fiscal Agent; however, photocopies of the FD-189 are acceptable. A sample of the Hysterectomy Receipt of Information Form and instructions for the form s proper completion are included for reference. 37
42 State of New Jersey Department of Human Services Division of Medical Assistance and Health Services HYSTERECTOMY RECEIPT OF INFORMATION FORM A woman who has a hysterectomy can never again get pregnant. When you have a hysterectomy, the doctor removes your uterus (womb). You cannot have a baby after your uterus is removed and you will not have menstrual periods anymore. I received the above information orally and in writing from name of clinic or physician before my operation was performed. I talked to about a hysterectomy. name of responsible person(s) she/he/they discussed it with me and gave me a chance to ask questions and answered them for me before the operation. I have read all of this notice. I agree that it is a true description of what was explained to me by of and that name of staff member clinic/hospital/physician all my questions were answered to my satisfaction. I,, hereby consent (or did consent) of my own free name of recipient will to have a hysterectomy done by and/or physician associate(s) or assistant(s) of his or her choice. I consent (or did consent) to any other medical treatment that the doctor thinks is (was) necessary to preserve my health. I also consent to the release of this form and other medical records about the operation to representatives of the United States Department of Health and Human Services or employees of programs or projects funded by that Department but only for purpose of determining if Federal laws were observed. Recipient s Signature Date: Month/Day/Year FD-189 (Rev 7/83) 7472 M ED 7/83 38
43 Item-By-Item Instructions for Completing the Hysterectomy Receipt of Information Form FD-189 (Rev 3/91) 1) Name of Clinic or Physician: Enter the name of the clinic or physician who provided the information. 2) Name of Responsible Person(s): Enter the name of the individual who discussed the procedure with the recipient. 3) She/He/They: Enter appropriate selection. 4) Name of Staff Member: Enter the name of the individual who explained the procedure to the recipient. 5) Clinic/Hospital/Physician: Enter the name of the clinic/hospital or physician s office in which the individual who explained the procedure is affiliated. 6) Recipient s Name: Copy the recipient s name as printed on the Medicaid Eligibility Identification Card. First name must be entered first. 7) Name of Physician: Enter the physician s name. 8) Recipient s Signature and Date: Recipient must personally sign and hand date the completed form. 39
44 Consent Form 7473 M ED Federally prescribed documentation regulations for sterilization procedures are extremely rigid. Specific Medicaid requirements must be met and documented on the Consent Form prior to the sterilization of an individual. The Consent Form is a replica of the form contained in the Federal Regulations and must be utilized by providers when submitting claims for sterilization procedures. Any claim (hospital, operating physician, anesthesiologist, clinic, etc) involved in a sterilization procedure must have a properly completed Consent Form attached when it is submitted for payment. Sterilization claims are hard copy restricted; electronic billing is not permitted. Additional information concerning Medicaid policy governing sterilization procedures may be found in Title 10, Subchapter 54, Section V Physicians Services, included with your manual. Providers may obtain additional copies of the Consent Form from the Fiscal Agent; however, photocopies of the Consent Form are acceptable. A sample of the Consent Form and instructions for the form s proper completion are provided for reference. 40
45 41
46 Item-By-Item Instructions for Completing the Sterilization Consent Form Section 1 Consent to Sterilization 1) Doctor or Clinic: Enter the name of the physician or clinic. 2) Sterilization Procedure: Enter the name of the sterilization procedure. 3) Recipient s Date of Birth: Enter recipient s date of birth in month, day, and year sequence (mm/dd/yy). 4) Recipient s Name: Copy the recipient s name as printed on the Medicaid Eligibility Identification Card. First name must be entered first. 5) Doctor: Enter physician s name who is performing the procedure. 6) Type of Sterilization: Enter the method of sterilization chosen. 7) Recipient s Signature and Date: Recipient must personally sign and hand date form at least thirty (30) days, but not more than 180 days prior to surgery. Section II Race and Ethnicity Designation: 8) Race and Ethnicity Designation: OPTIONAL INFORMATION requested by the Federal Government, but is NOT required. Section III Interpreter s Statement: To be used only when the Recipient does not speak English 9) Language Used: Enter language used. 10) Interpreter s Signature: Interpreter must sign and date form at least thirty (30) days, but not more than 180 days prior to the sterilization procedure. Section IV Statement of Person Obtaining Consent 11) Name of Individual: Enter the name of the recipient as it appears in Section I, item 4. 12) Sterilization/Operation: Enter the name of the sterilization procedure. 13) Signature of Person Obtaining Consent: Signature and date of the person who explains the procedure to the recipient and obtains the recipient s consent. Must be completed at least thirty (30) days, but not more than 180 days prior to the sterilization procedure. 14) Facility s Name and Address: Enter the name and address of the facility or physician s office with which the person obtaining the consent is affiliated. 15) Name of Individual to be Sterilized: Enter the recipient s name as it appears in Section I, item 4. 16) Date of Sterilization: Enter the date of the sterilization in month, day, and year sequence (mm/dd/yy). 42
47 17) Specify Type of Operation: Enter the name of the sterilization procedure. 18) Paragraphs 1) and 2): The physician must indicate the paragraph that applies to recipient s situation. Paragraph 1) states that at least thirty (30) days have passed between the date of the individual s signature on the consent form and the date the sterilization was performed. Paragraph 2) states that the sterilization was performed less than thirty (30) days, but more than 72 hours after the date of the individual s signature on the consent form. The circumstances are premature delivery (state the expected date of delivery) or emergency abdominal surgery (describe the emergency). 19) Physician s Signature and Date: Physician must sign and date form after the surgery has been performed. 43
48 SECTION 4 REFERRALS Primary Care Provider The Entry Point to Health Care Services The Primary Care Physician (PCP) is the physician care manager for all members on the PCP s roster. The PCP s role is to ensure that members receive the most appropriate care, at the most appropriate time, at the most appropriate level of care during an episode of illness or injury. The PCP is the member s point of entry into the delivery system, except for services allowing selfreferral, emergencies, and out-of-area urgent care. UnitedHealthcare expects PCPs to communicate with specialists in writing (e.g., prescription or letter) the reason for the referral and to note this in the patient s medical record. UnitedHealthcare expects specialists to communicate to the PCP via consultation report significant findings and recommendations for continuing care. A specialist may refer the patient directly to another specialist. Referral Guidelines Written referrals from the PCP using prescription form or letterhead are recommended for most care delivered by other providers. The guidelines for referrals are as follows: Refer only to UnitedHealthcare participating laboratories. Referrals to non-participating laboratories require prior authorization. Refer only to UnitedHealthcare participating specialists. Referrals to non-participating specialists require prior authorization (needs to be called in by the PCP). Initial referrals should be limited to 1 2 visits. Subsequent referrals are usually up to 3 visits. For chronic dialysis, referrals will be valid for 6 months. Referrals are not required for out-of-area dialysis for ESRD. Referrals should indicate all services requested including frequency and duration of each service. Services Not Requiring a Referral (Self-Referral Services) Please refer to the member benefit grid that begins on page 6. PCP Referrals PCPs can issue referrals by completing a prescription or written note on the PCP s letterhead. In addition to clearly noting that the patient is an UnitedHealthcare member, include the following information: Member Name, Address, Date of Birth PCP Name, UnitedHealthcare Provider ID Number, and Telephone Number Specialist/Ancillary Provider Name, UnitedHealthcare Provider ID Number, Address, and Telephone Number The PCP should record the referral in the member s medical record and give the prescription or letter to the member to take to the specialist at the time of the appointment. 44
49 Standing referral to a specialist UnitedHealthcare has a provision for allowing for standing referrals when on-going, long-term specialty care is required. The referring provider is required to consult the UnitedHealthcare medical director and specialist to determine if the standing referral is appropriate. Approval of the referral is pursuant to a treatment plan approved by UnitedHealthcare in consultation with the primary care provider, the specialist, the care manager, and the member (or authorized person). The standing referral may be limited to a specific number of visits or the period during which visits are authorized. Special Needs UnitedHealthcare has a provision to allow enrollees with special needs that require highly complex, specialized health care services over a prolonged period of time, to be referred to a physician specialist (where available) in lieu of a traditional PCP. The referral to a physician specialist may be made when the member s condition is at a level of complexity would be difficult for a traditional PCP to manage. The physician specialist is required to be specially credentialed demonstrating they have the clinical skills, capacity, accessibility, and availability to ensure the member receives all necessary specialty care related to their special need. The physician specialist is also contractually obligated to assume the responsibility for the member s overall health care coordination which includes all routine preventive care and health maintenance services. For further information providers may contact UnitedHealthcare Special Needs and Care Management Hot Line at Extension Elective Admissions and Same Day Surgery The PCP or specialist referring a patient for an elective admission or same day surgery is responsible for contacting UnitedHealthcare for prior authorization. UnitedHealthcare recommends that information should be submitted no less than 5 business days prior to the expected date of service. Consideration will be given for less notice on a case by case basis. Notification to UnitedHealthcare may be via fax, telephone, iexchange or mail. Requests for prior authorization are prioritized according to level of medical exigency. Certain cases are reviewed under emergency guidelines. The prior authorization process can move promptly and efficiently by phone if physicians ensure that: A clinical person, familiar with medical terminology, calls UnitedHealthcare The caller is prepared in advance with all the necessary information (see list below) The physician s office can also fax the information to: Prior Authorization 24 hrs / 7 days a week Listen to prompts Phone Fax Medical/Surgical Maternity/Newborn Behavioral Health The following information is required to receive authorization for an admission or procedure: Patient s name and UnitedHealthcare ID number Referring Physician and UnitedHealthcare Provider ID number 45
50 Physician referred to and UnitedHealthcare Provider ID number Facility name Expected date of admission or service Diagnosis(es) Code(s) Planned procedure(s) Procedure code(s) Type of service (e.g., outpatient, inpatient admission, home care, DME) Other insurance information for Coordination of benefits (COB) The Service Center will contact the physician if there are questions or more information is needed. Once the Service Center receives the complete information to review the request according to Milliman USA Healthcare Guidelines, the Service Center makes a determination. If approved, UnitedHealthcare assigns an authorization number to the elective admission or same day surgery and enters the authorization number into UnitedHealthcare s information system. UnitedHealthcare then informs the requesting physician s office of the authorization number. This authorization number references the admission or procedure. Pharmacy Prior Authorization Pharmacy Prior Authorization (Mon Fri, 9:00 AM 9:00 PM) UnitedHealthcare provides clients with a 72-hour supply of medication, whether on or off the formulary, while awaiting a prior authorization determination. Existing UnitedHealthcare members may continue taking a medication that has been removed from the formulary for as long as that member is enrolled in UnitedHealthcare (unless the medication has been deemed unsafe) with valid medical reasoning from the member s prescribing provider, and with the member s consulation and agreement. A member may change his or her medication to a medication that is on UnitedHealthcare s formulary only if the prescribing provider and member agree to that change. Members new to therapy will be required to use a medication on the formulary. Referrals to Nonparticipating Providers A participating physician must initiate requests for referrals to nonparticipating providers. Providers should not ask members to contact UnitedHealthcare to initiate requests for non-participating provider referrals. Members may initiate requests for services allowing self-referrals. If the PCP has difficulty locating a participating provider, the Service Center can assist the PCP. Call PCPs Acting as Specialists If a physician is credentialed as a specialist as well as a PCP, the physician can accept referrals from other PCPs. If the PCP wants to provide specialty services to members on his or her own panel, the PCP can contact a Medical Director to discuss arrangements for providing these services. The PCP should call DOC-DENT ( ) and explain what he/she wants to do with his/her patients and ask to speak with a Medical Director. Second Opinions 46
51 UnitedHealthcare does not require a second opinion for any specific services or procedures. However, all UnitedHealthcare members are entitled to a second opinion from an UnitedHealthcare participating provider prior to initiating any recommended treatment plan or undergoing any surgical procedure. The member must have seen his/her PCP, or a participating specialist to whom the PCP referred the member, for initial evaluation or treatment prior to requesting a second opinion consultation. Normally, the PCP, upon the request of the member, will initiate a referral to the second opinion physician. If the UnitedHealthcare network does not include specialists in the specialty needed, the PCP should call DOC-DENT ( ) to request authorization for a second opinion by an out-ofplan specialist. UnitedHealthcare will contact the PCP and specialist within 72 hours with referral information, including the authorization number. The member and his/her family, after considering the recommendation of the second opinion physician and evaluation of alternatives, will make the final decision regarding the course of treatment. Healthy First Steps (HFS) UnitedHealthcare has developed a national model for maternal care. Implementation of this National Healthy First Steps (HFS) program is a strategy to leverage best practices across the organization to improve maternal and infant outcomes and care. HFS has proven its efficacy over the years. Many providers have partnered with this program to enhance member and provider relationships. We urge your support and partnership with Healthy First Steps and would welcome the opportunity to discuss the Program in more detail at your convenience. The Healthy First Steps (HFS) program is available for all pregnant members. While the HFS program is a voluntary program; all pregnant members are encouraged to participate. Members may selfrefer, be referred by their provider or be identified by eligibility or claims data. Program Referral Providers are requested to make Healthy First Steps referrals as soon after the member s first prenatal office visit as possible. Please submit the designated enclosed form for your Heath Plan. The New HFS Referral fax number is The New HFS Telephone number is Enrollment and Follow up Process Once identified, a Healthy First Steps staff member will contact the member and provide a program overview, enrollment opportunity and discussion of their past and current health care and psychosocial needs. Level of risk is ascertained with assignment to either a Health Coach or Care Manager for telephonic followup. Risk levels are evaluated throughout the pregnancy. All OB Care Managers are Registered Nurses with extensive obstetrical backgrounds. 47
52 Program Goals The ultimate goal of the HFS program is to improve pregnancy outcomes by: Facilitating early entry into medical care and program enrollment Providing education related to self care, physical and emotional changes related to pregnancy, recognition of complications, and preparation for labor, delivery and infant care Improving provider visit compliance during pregnancy with return for post partum exam Partnering with Providers to manage co-morbid conditions, pregnancy complications and specialty provider identification and referral as indicated Identification and referral to community resources Providing a multidisciplinary team to address medical, social and behavioral needs Inpatient Stays and Discharge Hospital admissions are reviewed and authorized by the Healthy First Steps Inpatient Care Managers. Communication within the HFS team related to discharge planning, home care needs and required education facilitates continuity of care for members. Discharge from the HFS program occurs two months after delivery. If additional medical needs are identified, the member will be referred for continued care management services. Infants requiring NICU admission are also managed by the Healthy First Steps team. Inpatient authorizations, family education and discharge planning occur while the infant is hospitalized. Infants are followed for 30 days after NICU discharge within the HFS team. If additional care management needs are identified, the infant will be referred to a Pediatric Care Manager within the Plan. 48
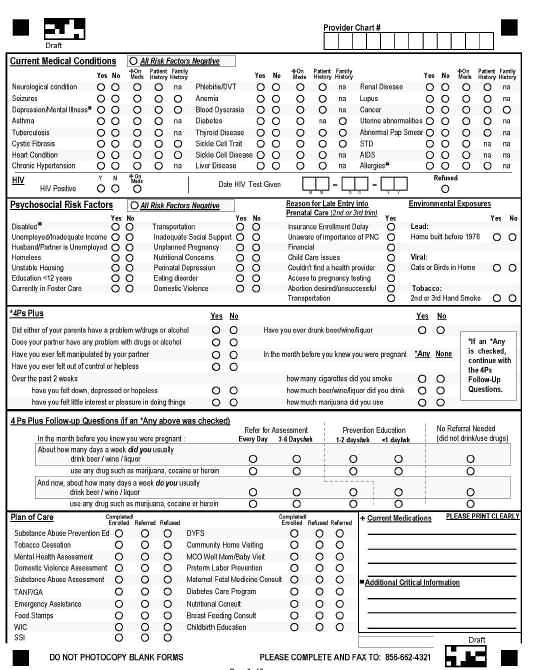
53 49
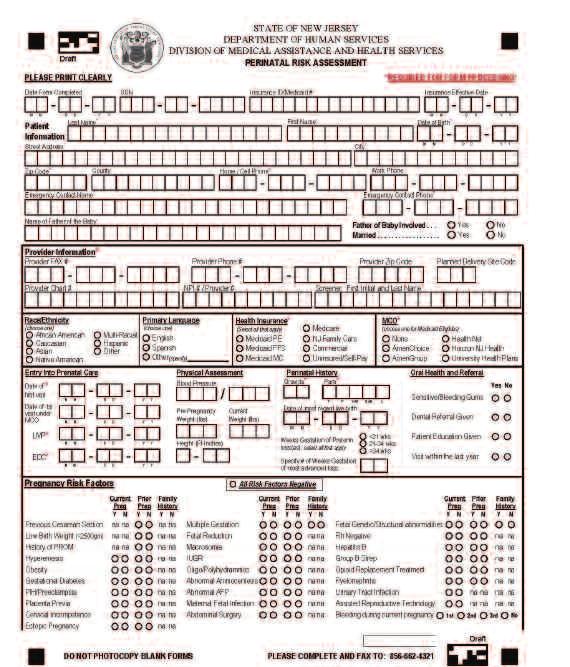
54 50
55 SECTION 5 CLAIMS POLICIES AND PROCEDURES Our claims process To be paid promptly for the services you provide, please follow these procedures: Claims must be submitted within 90 days of the date of service or as otherwise described in your Provider Agreement. After we receive your claim, if we request additional information in order to process your claim, you must submit this additional information within 60 days of our request. Register for UnitedHealthcareOnline ( our free Web site for network physicians and health care professionals. At UnitedHealthcareOnline, you can check eligibility, claims status, and adjustment requests and submit claims electronically, for faster claims payment. To register, follow the instructions on the UnitedHealthcareOnline Web site. Once you ve registered, review the patient s eligibility on the Web site at To check patient eligibility by phone, call Provider Services. Notify us of planned procedures and services on our notification list. Prepare a complete and accurate claim form. Electronic Claims Submission Submit the claim online at OR Submit via Emdeon or another clearinghouse vendor If you currently use Emdeon or another vendor to submit claims electronically, be sure to use the correct UnitedHealthcare electronic payer ID to submit claims to us. Payer ID Plan Description UnitedHealthcare of New Jersey: Medicaid, NJ FamilyCare UnitedHealthcare of New Jersey: UnitedHealthcare Dual Complete (Medicare) For more information, contact your vendor or the UnitedHealthcare EDI Support Group at (800) To become a registered user of Emdeon, call (800) Paper Claims Submission In the event that a provider is unable to submit medical, professional or facility claims electronically, or is submitting a claim requiring invoice documentation, or as a contingency when the electronic system is not available, paper claims may be submitted to the following addresses: Medicaid and NJ FamilyCare: UnitedHealthcare of New Jersey P.O. Box 5250 Kingston, NY UnitedHealthcare Dual Complete (Medicare): UnitedHealthcare of New Jersey P.O. Box 5250 Kingston, NY
56 Medicare claims must be separated from all other claims. Refer to section on Coordination of Benefits for more instructions. For dual eligibles (Medicare / Medicaid), submit Medicare claims first. Claims sent to the wrong lock box will be denied. Do not send claims to UnitedHealthcare of New Jersey offices. Do not send claims to any New Jersey PO box. Instructions for completing the CMS 1500 for Medical and Professional claims can be found at: Providers can use Item 33 on the form to record the provider number and Item 19 for the authorization number. Instructions for completing the UB-04 for Hospital Inpatient claims can be found at Complete Claims Whether you use an electronic or a paper form, complete a CMS 1500 (formerly HCFA 1500) or UB-04 (formerly UB-92) form. A complete claim includes the following information; additional information may be required by us for particular types of services or based on particular circumstances or state requirements. Patient s name, sex, date of birth and relationship to subscriber Member ID Number This must be the member identification number as it appears on the member s UnitedHealthcare ID card. For UnitedHealthcare Dual Complete (Medicare) claims, use the UnitedHealthcare member ID number. Do not use the member s Medicare ID from his/her Medicare card or Medicaid number (if dually eligible on Medicare/Medicaid). Subscriber s name, address and ID number Subscriber s group name and group number Name, signature, remit to address and phone number of physician or provider performing the service, as in your contract document National Provider Identifier (NPI) number Physician s or provider s federal tax ID number Date of service(s), place of service(s) and number of services (units) rendered Current CPT-4 and HCPCS procedure codes with modifiers where appropriate Current ICD-9 diagnostic codes by specific code to the highest level of specificity (e.g ) Referring physician s name (if applicable) Charges per service and total charges Information about other insurance coverage, including job-related, auto or accident information, if available Attach operative notes for claims submitted with modifiers 22, 62, 66 or any other team surgery modifiers as well as CPT (physician standby) Attach an anesthesia report for claims submitted with a 23, QS, G8 or G9 modifier Attach a detailed description of the procedure or service provided for claims submitted with unlisted medical or surgical CPT or other revenue codes as well as experimental or reconstructive services 52
57 For hysterectomy and sterilization procedures, provider must submit paper claims with the appropriate Consent Form attached. Purchase price for DME rental claims exceeding $500 If you need to correct and re-submit a claim, submit a new CMS 1500 or UB-04 indicating the correction being made. Hand corrected claim re-submissions will not be accepted. Additional information needed for a complete UB-04 form: Date and hour of admission and discharge as well as patient status-at-discharge code Type of bill code Type of admission (e.g. emergency, urgent, elective, newborn) Current revenue code and description Current principal diagnosis code (highest level of specificity e.g ) with the applicable Present on Admission (POA) indicator on hospital inpatient claims. Current other diagnosis codes, if applicable (highest level of specificity e.g ), with the applicable Present on Admission (POA) indicator on hospital inpatient claims. Attending physician ID Bill all outpatient surgeries with the appropriate revenue and CPT code if reimbursed according to ambulatory surgery groupings Provide specific CPT and appropriate revenue code (e.g. laboratory, radiology, diagnostic or therapeutic) for services reimbursed based on a contractual fee maximum Attach an itemized list of services or complete box 45 for physical, occupational or speech therapy services (revenue code ) submitted on a UB-04 Submit claims according to any special billing instructions that may be indicated in your agreement (or letter of contract) If patient is seen in the ER and the inpatient admission is denied or not authorized, when submitting the claim, be sure to add the revenue codes of for the ER services rendered. This will ensure that Claims pays the ER portion as required by law. If you have questions about submitting claims to us, please contact Provider Services. National Provider Identifier (NPI) The Health Insurance Portability and Accountability Act (HIPAA), federal Medicare regulations, and many state Medicaid agencies mandate the adoption and use of a standardized National Provider Identifier (NPI) for all health care professionals. In compliance with HIPAA, all covered health care providers and organizations must obtain an NPI for identification purposes in standard electronic transactions. To avoid payment delays or denials, please include a valid NPI on all Medicare and Medicaid claims submitted to UnitedHealthcare for processing. A valid NPI is required for all covered claims. It is important that in addition to the NPI you continue to submit your Tax Identification Number (TIN) on all electronic and paper professional medical claims. Please continue to submit complete claims to comply with complete claim billing requirements as published in the UnitedHealthcare New Jersey Provider Manual. The NPI information that you report to us now and on all future claims is essential in allowing us to efficiently process claims. View How to Submit NPI, TIN and Taxonomy on Paper and Electronic Claims for more information. To ensure effective and efficient processing of transactions, companion documents should also be referenced. These documents include company-specific details for Electronic Data Interchange 53
58 transactions. These companion documents contain only supplementary instructions for the ASC X12 implementation guides, and they do not replace or modify the implementation guides, but should be used in conjunction with them. For more information, please visit A covered health care provider is any provider who transmits health information in electronic form in connection with a transaction for which standards have been adopted. These covered health care providers must obtain an NPI and use this number in all HIPAA transactions, in accordance with the instructions in the Implementation Guides. How do I submit an NPI, TIN and Taxonomy on a claim? UnitedHealthcare New Jersey is able to accept NPI on the UB-04 and CMS 1500 (08-05) paper and HIPAA 837 professional and institutional claim submissions. It is important that all electronic and paper claims include the TIN in addition to the NPI. In addition, we are requesting the billing provider NUCC taxonomy code be submitted on institutional claims. Any changes to our NPI policy will be preceded with communications to physicians, health care professionals, organizations and trading partners. Such communications will express when we will reserve the right to no longer accept HIPAA transactions which do not contain a valid NPI in the fields specified by our HIPAA-adopted implementation guides. The information below identifies the location for NPI, TIN and Taxonomy on paper and electronic claims in accordance with HIPAA NPI compliance effective May 23, 2008: HIPAA 837P (Professional) Claim Transaction (for enumerated providers) Billing Provider Identifier Location Primary Identifier NPI Loop 2010AA, NM109 / NM108=XX Secondary Identifier TIN Loop 2010AA, REF02 (REF01=EI or SY) Pay-To Provider Primary Identifier NPI Loop 2010AB, NM109 (NM108=XX) Secondary identifier TIN Loop 2010AB, REF02 (REF01=EI or SY) Referring Physician Primary Identifier NPI Loop 2310A, NM109 (NM108=XX) Rendering Physician Primary Identifier NPI Loop 2310B, NM109 (NM108=XX) HIPAA 837I (Institutional) Claim Transaction (for enumerated providers) Billing Provider Identifier Location Primary Identifier NPI Loop 2010AA, NM109 (NM108=XX) Secondary Identifier TIN Loop 2010AA, REF02 (REF01=EI or SY) Taxonomy NUCC Code Loop 2000A, PRV03 (PRV01=BI) Pay-To Provider Primary Identifier NPI Loop 2010AB, NM109 (NM108=XX) Secondary identifier TIN Loop 2010AB, REF02 (REF01=EI or SY) Taxonomy NUCC Code Loop 2000A, PRV03 (PRV01=PT) Attending Physician Primary Identifier NPI Loop 2310A, NM109 (NM108=XX) Taxonomy NUCC Code Loop 2310A, PRV03 Note: refer to the Implementation Guides at for additional 837I/P rules regarding the above identifiers. Taxonomy is mutually exclusive. 54
59 CMS 1500 (08-05) Professional Claim Form (for enumerated providers) Billing Provider NPI Field 33a Billing Provider TIN Field 25 Referring Provider NPI Field 17b Rendering Provider NPI Field 24j Service Facility Location NPI Field 32a Important: Make sure that your claim software supports the revised 1500 claim form (08-05). Reference the 1500 Reference Instruction Manual at for specific details on completing this form. UB-04 Paper Institutional Claim Form (for enumerated providers) Billing Provider NPI Locator 56 Billing Provider TIN Locator 05 Billing Provider Taxonomy Code Locator 81 Attending Provider NPI Locator 76 Operating Provider NPI Locator 77 Other Provider NPI Locator See definitions in the UB-04 Data Specifications Manual available at Claim Adjustments If you believe you were underpaid, you may submit an adjustment request at or call the Provider Services Line at If you or our staff identifies a claim where you were overpaid, we ask that you send us the overpayment within 30 calendar days from the date of your identification of the overpayment or our request. If your payment is not received by that time, we may apply the overpayment against future claim payments. We typically make claim adjustments without requesting additional information from the network physician. You will see the adjustment on the Explanation of Benefits (EOB) or Provider Remittance Advice (PRA). When additional or correct information is needed, we will ask you to provide it. If you disagree with a claim adjustment, you can appeal the determination as described in the following processes: 1. Provider Claim Payment Appeal Processes Claim payment disputes are disputes that do not require any action by the UnitedHealthcare member. The claim payment appeal process is a procedure to resolve billing, payment, and other administrative disputes between the health care provider and UnitedHealthcare for any reason including, but not limited to: lost or incomplete claim forms or electronic submissions; requests for additional explanation as to services or treatment rendered by a health care provider; inappropriate or unapproved services initiated by the providers; or any other reason for billing disputes. There are two types of claim payment appeals: Informal and Formal. A. Informal Claim Appeals Informal claim payment appeals are claim resubmissions in order to revise a previously submitted claim and obtain payment. Claim disputes can be handled through this process if additional administrative information is submitted for payment such as proof of timely filing. If you are disputing a claim that was denied because filing was not timely, please include the following: 55
60 Electronic claims include confirmation that UnitedHealthcare or one of its affiliates received and accepted your claim. Paper claims include a copy of a screen print from your accounting software to show the date you submitted the claim. Requests for informal claim payment appeals must be submitted within ninety (90) days from the receipt of the EOB/PRA. They can be submitted online at by calling the Provider Service Center at , or in writing to the following address: UnitedHealthcare of New Jersey Attention: Claim Administrative Appeals P.O. Box 5250 Kingston, NY Please note that clinical information will not be reviewed for appeals based on medical necessity, experimental or investigational services through the informal claim payment appeal process. If you are dissatisfied with the claim payment appeal outcome and would like to submit a formal claim payment appeal, the formal appeal must be done within ninety (90) days of the original date of denial on your EOB/PRA on a Health Care Provider Application to Appeal a Claims Determination (HCAPPA) form. Please be advised that you do not receive an additional ninety (90) days from the date of the decision of the informal claim payment appeal. B. Formal Claim Appeals Formal claim payment appeals must be submitted to UnitedHealthcare utilizing the Department of Banking and Insurance approved form, Health Care Provider Application to Appeal a Claims Determination (HCAPPA) which is located on the UnitedHealthcare.com website. If you submit a claim payment appeal using this form within 90 days following receipt of the EOB/PRA, you will have the right to access the New Jersey Department of Banking and Insurance arbitration process in the event that you are not satisfied with the decision made by UnitedHealthcare. If you are not satisfied with the appeal decision made by UnitedHealthcare, and filed your initial appeal utilizing the Health Care Provider Application to Appeal a Claims Determination (HCAPPA) form, you may initiate the New Jersey Department of Banking and Insurance arbitration process by writing to the address shown below on or before the 90th calendar day following the receipt of the claim payment determination. Attn: NJPICPA MAXIMUS 50 Square Drive, Suite 210 Victor, NY Providers can also access and submit the request online at: 2. Provider Service Appeals Claim appeals based on UnitedHealthcare s adverse determination regarding medical necessity, experimental or investigational services should be processed under the Utilization Management (UM) appeal process within 60 days from receipt of the original UM denial letter. According to New Jersey Administrative Code 11:24-8.4, any provider appealing on behalf of a member must have the member s written consent in order to request a Utilization Management (UM) appeal. To proceed with a Stage 1 Utilization Management Appeal, include a copy of the 56
61 original UM denial letter, the member s written consent, a copy of the medical record, and any additional information which supports the need for medical necessity on the denied date (s) of services. Utilization Management Appeals should be mailed to the following address: UnitedHealthcare of New Jersey Attention: UM Appeals Coordinator P.O. Box Salt Lake City, UT To ensure all required medical information is reviewed with your appeal, it is important to send the necessary medical records with the initial appeal request. The appeal process will start in the absence of necessary medical records. Note: If a provider submits a UM appeal on behalf of a member with clinical information and without member written consent, the appeal will be considered a provider service appeal. Although clinical information may be reviewed for medical necessity, the provider appealing on behalf of a member is not entitled to a Stage II UM appeal nor the New Jersey Department of Banking and Insurance arbitration process. See Section 15: Utilization Management Appeals for additional information. 3. Provider Central Service Unit (PCSU) To improve our business interactions with our providers, UnitedHealthcare of New Jersey, Inc (UnitedHealthcare) offers providers access to our Provider Central Service Unit (PCSU). The focus of the PCSU is to resolve claims payment issues for UnitedHealthcare NJ FamilyCare/Medicaid members that have not been resolved to your satisfaction only after utilizing standard avenues of resolution. Before contacting the PCSU, UnitedHealthcare would like to remind you that the following resources should be utilized if you ve submitted a claim and received either a payment or a denial for payment that you do not agree with: Visit our secure website for physicians and other health care professionals at This is your best source for checking member eligibility information, claim status, and filing claim adjustment requests. Many of the same transactions can also be completed by calling our toll free provider service line at If you call about a claim issue, be sure to have the supporting documentation needed for prompt resolution. If you disagree with our determination after using the on-line tools or calling our service center, an additional review may be requested by contacting the PCSU at The PCSU staff has a special team dedicated to address NJ FamilyCare/Medicaid claims issues. 4. Provider Complaints or Grievances If you have a complaint or grievance, you may call the Provider Service Center at and speak to a Customer Center Professional (CCP). Hours of operation are 8 A.M. to 6 P.M. EST, Monday through Friday. If we are not able to resolve your inquiry during the initial call, a written response will be sent to you within thirty (30) days of your call. 57
62 If you have a provider complaint related to a payment issue, you will be advised to follow the procedure for Provider Claim Payment Appeal process outlined below, which does not require any action by an UnitedHealthcare member. If you have already submitted the payment appeal and are not aware of the status, the CCP can provide you with the status of the appeal. You may also utilize the Provider Portal to review the status of a claim/payment appeal if the claim was originally submitted electronically. Coding Standards UnitedHealthcare uses the most recent versions of the following codes: Current Procedural Terminology, 4th edition (CPT-4) Health Care Financing Administration Common Procedure Coding System (HCPCS) International Classification of Diseases, 9th revision, Clinical Modifications (ICD-9-CM) Submittal of claims without the most current set of codes will result in delayed payment or denial. The U.S. Department of Health and Human Services (DHHS) and the American Medical Association (AMA) annually publish industry standard codes that are essential for prompt and accurate payment of provider claims. All providers are encouraged to obtain the most current version of CPT-4, HCPCS,and ICD-9-CM codes. Each new version becomes effective on January 1 of the current year and expires on December 31. Providers must use codes for data items with a schedule of codes. No narratives are accepted for data items where codes are available. Providers must state ICD-9-CM codes to the highest level of specificity stated in the current version. Providers must add whatever modifier is stated in the current version. Providers should not rely on the index, which only lists family of codes and not the highest level of specificity. Claims lacking codes with the highest level of specificity will be denied. Capitated Primary Care Provider and EPSDT Encounters PCPs must report all encounters, especially Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) encounters and those covered by capitated payment. Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Early and Periodic Screening, Diagnostic and Treatment (EPSDT) is a Title XIX mandated program that covers screening and diagnostic services to determine physical and mental defects in enrollees under the age 21, and health care, treatment, and other measures to correct or ameliorate any defects and chronic conditions discovered, pursuant to Federal Regulations found in TITLE XIX of the Social Security Act. UnitedHealthcare monitors pediatric preventive care according to the EPSDT guidelines and the American Academy of Pediatrics Recommendations for Preventive Care. In addition, UnitedHealthcare makes incentive payments to PCPs for providing EPSDT services. All well-child visits and immunizations must be documented on CMS 1500 claim forms and only ONE date of service should be recorded on each form. To ensure appropriate incentive payments, PCPs must record their NPI and tax ID numbers on the claim forms. UnitedHealthcare reimburses for the administration of immunizations included under the VFC Program. To ensure payment, PCPs must submit appropriate CPT 4 Codes for the vaccines given, as well as the administration code. 58
63 EPSDT GUIDE FOR EPSDT VISIT CODES FOR CHILDREN 0-21 YEARS EPSDT VISIT CODES Age and Status CPT4 Code Age and Status CPT4 Code Normal Newborn Care Established Patient (Under One Year) New Patient (Under One Year) Established Patient (Ages 1-4 Years) New Patient (Ages 1-4 Years) Established Patient (Ages 5-11 Years) New Patient (Ages 5-11) Established Patient (Ages Years) New Patient (Ages 12-17) Established Patient (Ages Years) EP New Patient (Ages 18-21) EP IMMUNIZATION & LEAD SCREENING Description CPT4 Code Lead Screening , , (finger stick) HPV Hep A-Adult Hep-A Ped/Adol Hep A-Hep B (Adult) Hib PRP-OMP Hib PRP-T Flu (Split Virus) Flu (Split Virus) Flu (Split Virus) Flu (Split Virus) Flu (Intranasal) Pneumococcal Conjugate - 7 valent Pneumococcal Conjugate - 13 valent Rotavirus - 3 Dose Series Rotavirus - 2 Dose Series DTaP MMR MMRV E-IPV Td Tdap Varicella Tetanus & Diphtheria (Td) for 7 y/o or older
64 Description CPT4 Code Diptheria, tetanus, acellular pertussis and Hemophilus influenza B vaccine (DTaP-Hib) DTaP/HepB/IPV Pneumococcal (Polysaccharide) Meningococcal Hep B - Adol Hep B Hep B- Adult Hep B/Hib PRP-OMP DTaP/Hib/IPV DTaP-IPV Administration Codes* 90465, 90466, 90471, 90472, 90467, 90468, 90473, ICD-9 Diagnosis Codes** V V20.2 * Admin codes should not be submitted to UnitedHealthcare for EPSDT visits **Denotes primary diagnosis whenever well-child care and immunizations are rendered 60
65 Encounter Data UnitedHealthcare is contractually obligated to submit accurate, detailed, and complete encounter information to Centers for Medicare and Medicaid (CMS) and the NJ Department of Human Services (DHS). Consequently, UnitedHealthcare participating providers are required to submit accurate, detailed, and complete encounter information to UnitedHealthcare. Claims submission constitutes the provider s certification of the submitted data. Coordination of benefits Coordination of benefits (COB) is used when a member is covered by more than one insurance policy. By coordinating benefit payments, the member receives the maximum benefits allowable under each plan. The most common COB issue among UnitedHealthcare members arises with persons who have traditional Medicare Fee-for-Service (FFS) and are enrolled in UnitedHealthcare Medicaid Managed Care. In New Jersey, an individual who is dually eligible for Medicare and Medicaid may be enrolled in one of the following combinations: Enrolled in UnitedHealthcare Dual Complete Special Needs Plan (SNP Medicare) and UnitedHealthcare Medicaid Managed Care Enrolled in traditional Medicare and UnitedHealthcare Medicaid Managed Care Enrolled in UnitedHealthcare Dual Complete Special Needs Plan (SNP-Medicare) and Medicaid Fee For-Service For members who have both Medicare and Medicaid, Medicare is always primary and should be billed first. The provider should bill either traditional Medicare or UnitedHealthcare Dual Complete (Medicare), depending on the member s coverage for Medicare. If the member is enrolled in UnitedHealthcare Dual Complete (Medicare), the provider should submit the Medicare claim to UnitedHealthcare. Because both the primary and secondary payers are UnitedHealthcare, UnitedHealthcare will do the COB. If the member is enrolled in traditional Medicare and UnitedHealthcare Medicaid is secondary, the provider should first submit the claim to Medicare. Then the secondary claim must be submitted on paper with the Medicare EOB attached to UnitedHealthcare. The only exception is for a working Medicare beneficiary who has health coverage through his or her employer, in which case the commercial insurance is primary. However, members in this category are rarely enrolled in the UnitedHealthcare Dual Complete Program. If COB is involved, the provider should attach evidence of payment from the first payer (traditional Medicare or commercial insurance) when billing UnitedHealthcare as the second payer. The 90-day and 180-day periods for claims submission begin from the date of payment denial from the first payer. In New Jersey, some individuals in the Aged, Blind, and Disabled (ABD) category, including Division of Developmental Disabilities (DDD) clients, may be enrolled in UnitedHealthcare and also have commercial health insurance coverage as a dependent through a parent or guardian s health plan. In these cases, the commercial plan is primary and must be billed first. Unless UnitedHealthcare has given prior authorization for services that require prior authorization, UnitedHealthcare shall not be liable for payment if the other payer refuses payment due to a determination that the services provided were not medically necessary. If UnitedHealthcare gives 61
66 prior authorization for services for UnitedHealthcare members and another payer denies the authorized services, UnitedHealthcare will pay according to the terms of its contractual agreement with the provider. With respect to Medicaid members, the provider shall maintain and make available to UnitedHealthcare records reflecting collection of benefits by the provider and amounts paid directly to Medicaid members by other payers. AmerChoice shall maintain or have immediate access to records concerning collection of benefits. UnitedHealthcare members should NEVER receive a bill or a balance bill for covered services. Sending bills or balance bills to UnitedHealthcare members for covered services is a violation of your Participating Provider Agreement with UnitedHealthcare and violates New Jersey law and regulation. Instruct office staff to ask for appropriate documentation of a patient s insurance coverage and accurately maintain this information in all billing systems. If your office has not received payment for covered services provided to an UnitedHealthcare member, call DOC-DENT ( ). Subrogation and Tort Policy To the extent permitted by applicable law, the provider shall cooperate with subrogation procedures in instances where the member is covered by automobile insurance or worker s compensation. In the event that UnitedHealthcare is notified of a legal action being taken by, or on behalf of, a member in connection with an illness or injury, UnitedHealthcare may contact the provider to make available information related to the services provided in connection with the illness or injury. With respect to Medicaid members, the provider shall maintain and make available to UnitedHealthcare records reflecting collection of benefits by the provider and amounts paid directly to Medicaid members by other payers. AmerChoice shall maintain or have immediate access to records concerning collection of benefits. All providers are required to notify UnitedHealthcare when an UnitedHealthcare member presents with an illness or injury that is related to an automobile accident or employment. Notification can be made on a standard claim form. Providers are also required to notify UnitedHealthcare if they become aware of any litigation on behalf of the member resulting from the member s injuries. Providers should call DOC-DENT ( ). How to Change Provider Information To notify UnitedHealthcare of any provider changes, complete and fax the following Provider Information Update Form. 62
67 RETURN FORM BY FAX TO Ox HPDemo: PROVIDER INFORMATION UPDATE FORM UnitedHealthcare Region PROVIDER NAME: Unitedhealthcare ID# National Provider ID (NPI) # Individual Organization Dear AmerChoice Provider: In order to ensure prompt service, in the space below please fill out all information concerning your practice. (Please Print or type) Is this an additional location? Y N Effective Date: Is this a change to an existing location? Y N Effective Date: Specialty at this location: If you are requesting a change to an existing location, please indicate only the information to be updated. If this is a new location, please complete the entire form. Site Name (If different from Provider) Site Address Medical Group Name Office Manager Office Phone ( ) Fax ( ) Gender of Provider M F Wheelchair Accessible Y N Languages Age Range of patient s served to Specify any additions or deletions to your practice s health care services provided at this site: Payee Tax ID# (Attach a copy of a W-9 form if your tax id has changed) Make check payable to (if different from provider name) Billing Address City/State/Zip Billing Contact Billing Billing Phone ( ) Billing Fax ( ) 63
68 PROVIDER INFORMATION UPDATE FORM Office Hours: Sunday Monday Tuesday Wednesday Thursday Friday Saturday From: To: Hospital Privileges Yes No Name of Hospital Hospital Address Covering Physician (Must be an UnitedHealthcare contracted provider): Name Provider ID# Address Phone ( ) Provider s Signature Date / / Contact Name of person who completed this form Contact Phone of person who completed this form ( ) Internal Use Only: Reviewed by Date / / 64
69 Newborn Claims for Outpatient Visits There may be newborn outpatient visits in the 60 days before a Medicaid number is assigned to the newborn. If no member identification number has been issued for the newborn, report the following information on the electronic claim or the CMS 1500 form for services eligible for reimbursement: the mother s identification number in Section 1A the newborn s name in Section 2 the newborn s date of birth in Section 3 the mother s name in Section 4 Fraud, Waste, and Abuse There is no single definition of "fraud" in the health care industry. Generally speaking, fraud as a legal concept involves an intentional misrepresentation of a material fact made to induce detrimental reliance by another. A misrepresentation can entail an affirmative false statement or the omission of a material fact. Moreover, fraud can be both intentional (knowing), reckless, or negligent. Intentional or knowing fraud can include both misrepresentations made to deceive and induce reliance, and those made with the knowledge that they are substantially likely to induce reliance. Federal and state statutes and regulations variously define fraud (e.g., 42 C.F.R defines fraud as "an intentional deception or misrepresentation made by a person with the knowledge that the deception could result in some unauthorized benefit to himself or some other person."). For the purposes of this Program, PSMG construes health care fraud liberally in its broadest sense. "Waste and abuse" in the context of health care claims are generally broader concepts than fraud. They include over-utilization of services and provider and member practices inconsistent with sound fiscal, business, or medical practices that cause unnecessary costs or fail to meet professionally recognized health care standards. Some typical general categorical examples of provider health care fraud, waste and abuse include: Billing for services/goods never provided Billing for services/goods not medically necessary Billing for services/goods not covered (e.g., experimental services) and/or for services to ineligible members Duplicative billing for the same services/goods Billing without adequate supporting documentation Billing for more costly/complex services/goods than those actually provided ("upcoding") Billing separately services/goods required to be billed collectively ("unbundling") Improper modifications of billing codes Billings by fictitious, sanctioned, and/or unqualified providers Excessive fees charged for services/goods Poor quality services that are tantamount to no services provided Provider/member identity theft 65
70 Provider waiver of patient co-payments Misrepresentations in cost reports Unlawful referrals of patients to related providers Some examples of member/beneficiary health care fraud, waste and abuse include: Selling/loaning member identification information Intentional receipt of unnecessary/excessive services/goods Unlawful sales of prescriptions and/or prescription medications Misrepresentations to establish program/plan eligibility (e.g., non-disclosure of income/assets) Reporting Fraud, Waste, and Abuse If you suspect a provider or member has committed fraud, waste, or abuse, you have a responsibility and a right to report it. Reports of suspected fraud, waste, or abuse can be made in several ways. Go to unitedhealthcare.com and select Contact Us to report information relating to suspected fraud or abuse. Call the UnitedHealthcare Special Investigations Unit Fraud Hotline at Mail the information listed below to: UnitedHealthcare Special Investigations Unit Four Gateway Center 100 Mulberry Street - 4th Floor Newark, New Jersey For Provider related matters (e.g. doctor, dentist, hospital, etc) please furnish the following: Name, address and phone number of provider Medicaid number of the provider Type of provider (physician, physical therapist, pharmacist, etc.) Names and phone numbers of others who can aid in the investigation Dates of events Specific details about the suspected fraud or abuse For Member related matters (beneficiary/recipient) please furnish the following: The person s name, date of birth, Social Security number, ID number The person s address Specific details about the suspected fraud, waste, or abuse 66
71 SECTION 6 HOSPITALS AND HOSPITALIZATION General Requirements The standards, policies and procedures described in this section of the manual apply to participating hospitals unless they specifically address another type of provider, e.g. Primary Care Providers (PCPs). For additional information about the Utilization Management process, see Section Prior Authorization of Services. Elective Admissions and Same Day Surgery The PCP or specialist referring a patient for an elective admission or same day surgery is responsible for contacting UnitedHealthcare for prior authorization. UnitedHealthcare recommends calling at least 5 days, but not later than 48 hours, in advance of the admission or surgery. Requests for prior authorization are prioritized according to level of medical exigency. Certain cases are reviewed under emergency guidelines. Nurses in the Service Center can authorize admissions and procedures, but may not deny authorization. All cases that do not meet Milliman USA Healthcare Guidelines or are clinically questionable are referred to a Medical Director or Physician Advisor who renders a medical necessity determination. Once the Service Center receives the complete information to review the request according to Milliman USA Healthcare Guidelines, the Service Center makes a determination. If approved, UnitedHealthcare assigns an authorization number to the elective admission or same day surgery and enters the authorization number into UnitedHealthcare s electronic clinical documentation system. UnitedHealthcare then informs the requesting physician s office of the authorization number. This authorization number references the admission or procedure. The hospital learns of requests for elective admissions or same day surgeries from several sources: the PCP, specialist, or attending physician. UnitedHealthcare recommends that the hospital contact the appropriate unit listed below in advance of performing the procedure or providing service(s) to verify that UnitedHealthcare has issued an authorization number for the procedure or service. The authorization is valid only if the patient is an UnitedHealthcare member on the date of service. Prior Authorization 24 hrs / 7 days a week Listen to prompts Phone Fax Medical/Surgical Maternity/Newborn Behavioral Health Pharmacy Prior Authorization (Mon Fri, 9:00 AM 9:00 PM) UnitedHealthcare provides clients with a 72-hour supply of medication, whether on or off the formulary, while awaiting a prior authorization determination. Admissions are subject to concurrent review for medical necessity of continued stays after the initial authorization. 67
72 The PCP, specialist, attending physician, or facility may appeal any adverse decision made by UnitedHealthcare. Procedures for filing an appeal are in Section Utilization Management Appeals. Emergency Admissions Prior authorization is not required for emergency services. Emergency care should be rendered at once, with notification by the hospital of any admission to the Service Center at DOC-DENT ( ) within 24 hours or by 5:00 PM the next business day. Nurses in the Health Services Department review emergency admissions within one working day of notification. UnitedHealthcare uses Milliman USA Healthcare Guidelines for determinations of appropriateness of care. Care in the Emergency Room UnitedHealthcare members who present at an emergency room should be screened to determine whether a medical emergency exists. Prior authorization is not required for the medical screening. UnitedHealthcare provides coverage for these services without regard to the emergency care provider s contractual relationship with UnitedHealthcare. Emergency services, i.e. inpatient and outpatient services furnished by a qualified provider necessary to treat an emergency medical condition, are covered both within and outside UnitedHealthcare s service area. An emergency medical condition is defined as a medical condition manifesting itself by acute symptoms of sufficient severity, including severe pain, such that a prudent layperson who possesses an average knowledge of health and medicine, could reasonably expect in the absence of immediate medical attention to result in: Placing the health of the individual afflicted with such condition in serious jeopardy (or, with respect to a pregnant woman, the health of the woman or her unborn child); Serious impairment to the individual s bodily functions; or Serious dysfunction of any bodily organ or part. Maternity Care and Obstetrical Admissions Maternity Care Pregnant UnitedHealthcare members should receive care from UnitedHealthcare participating providers only. UnitedHealthcare will consider exceptions to this policy if 1) the woman was in her second trimester of pregnancy when she became an UnitedHealthcare member, and 2) if she has an established relationship with a non-participating obstetrician. UnitedHealthcare must approve all out-of-plan maternity care. Providers should call to obtain approval. Physicians should notify UnitedHealthcare immediately of a member s confirmed pregnancy to ensure appropriate follow-up and coordination by the UnitedHealthcare Maternal Care Manager. Providers should call or fax a prior authorization form to The following information must be provided to UnitedHealthcare within one business day of the visit when the pregnancy is confirmed: Patient s name and UnitedHealthcare ID number Obstetrician s name, phone number, and UnitedHealthcare ID number 68
73 Facility name Expected date of confinement (EDC) Planned vaginal or cesarean delivery Any concomitant diagnoses that could affect pregnancy or delivery Obstetrical risk factors Gravida Parity Number of living children Previous care for this pregnancy An UnitedHealthcare member does not need a referral from her PCP for prenatal care provided by participating obstetricians. An obstetrician does not need approval from the member s PCP for prenatal testing or obstetrical procedures. Obstetricians may give the pregnant member a written prescription to present at any of the UnitedHealthcare participating radiology and imaging facilities listed in the provider directory. Perinatal home care services are available for UnitedHealthcare members when medically necessary. In addition, UnitedHealthcare has community-based outreach and social service support programs specific to the needs of pregnant women. The UnitedHealthcare Maternal Care Manager can assist obstetricians and PCPs with referrals to these services. Members or providers can call the Healthy First Steps program at to speak with a Maternal Care Manager. Obstetrical Admissions UnitedHealthcare considers all full-term maternity admissions to be scheduled admissions. Obstetricians and PCPs are expected to notify UnitedHealthcare as soon as a pregnancy is confirmed. Newborn Admissions The hospital must notify UnitedHealthcare at prior to or upon the mother s discharge, if the baby stays in the hospital after the mother is discharged. The Health Services Department will conduct concurrent review of the newborn s extended stay. The hospital should make available the following information: Date of birth Birth weight Gender Any congenital defect Name of attending neonatalogist Enrollment of Newborns (Medicaid) Participating hospitals can facilitate the enrollment of newborns on Medicaid by advising each new mother covered by Medicaid to report the birth of her baby to her Medical Assistance Customer Center (MACC). Once reported, the MACC will have the baby enrolled in Medicaid and accreted to the Medicaid eligibility file and subsequently to UnitedHealthcare's enrollment file. If the mother does not report the birth of her baby to the MACC, UnitedHealthcare must wait 60 days before notifying the state of the baby s birth. The state then notifies the appropriate MACC to have the baby enrolled in Medicaid and accreted to the Medicaid eligibility file and subsequently to UnitedHealthcare's enrollment file. This process can take several weeks. 69
74 Concurrent Review UnitedHealthcare performs concurrent review on all hospitalizations for the duration of the stay based on contractual arrangements with the hospital. UnitedHealthcare performs the reviews telephonically or on site whenever possible. UnitedHealthcare uses Milliman USA Healthcare Guidelines for determinations of appropriateness of care. The Care Manager may certify extension of the length of stay, but may not deny any portion of the stay. Only a Medical Director or Physician Advisor can deny an extension of the length of stay. If a Medical Director or Physician Advisor determines that the extended stay is not justified, UnitedHealthcare will notify the facility of its decision. The PCP, attending physician, or the facility may appeal any adverse decision, according to the procedures in Section 15 Utilization Management Appeals. Discharge Planning and Continuing Care The Care Manager contacts the PCP, attending physician, member, Hospital Discharge Planner and member s family to assess needs and develop a plan for continuing care beyond discharge, if medically necessary. UnitedHealthcare Care Managers manage each patient across the continuum of care. The Care Managers work with the member, family members, physicians, hospital discharge planners, rehabilitation facilities, and home care agencies. They evaluate the appropriate use of benefits, oversee the transition of patients between levels of care, and refer to community-based services as needed. 70
75 SECTION 7 UNITEDHEALTHCARE PERSONAL CARE MODEL (PCM) The Personal Care Model is a holistic approach to care for members with complex needs and chronic conditions. The goal of the Personal Care Model is to maintain the member in his or her community whenever possible with the resources necessary to provide the highest functional status. Because early identification and intervention are key to the program, UnitedHealthcare encourages providers to identify and refer high-risk members to the Care Management Program. To refer members, providers may contact UnitedHealthcare of NJ Special Needs and Care Management Hotline at (877) Ext Providers may contact Care Management to refer high-risk members. Once enrolled, members become the focus of a concerted, hands-on outreach effort. UnitedHealthcare clinical staff develops and implements a comprehensive treatment plan based on the evaluation of the member s health and living conditions. Members are identified for the program by review of data from assessments, inpatient census data, review of claims and pharmacy data, and by referrals from Primary Care Physicians, other providers, community groups, social service agencies, claims, utilization data and member self referrals. A registered nurse or a graduate level social worker conducts a comprehensive needs assessment and develops a plan to address the member s needs. The assessment considers all clinical and socio-economic factors. Additional information is gathered from the member s family and physicians. Staff from the Member Service Department, with contacts in the community, are also an integral component of both the planning and implementation of the member s care. The Personal Care Model provides the following: Personal contact with the member and the development of ongoing relationships between Care Managers and members. Intervention can be telephonic care management, home visits or face-to-face in facilities. Disease Management programs (Asthma, Diabetes, and Congestive Heart Failure) in addition to the management of special needs diagnoses (HIV/AIDS, DYFS, DDD and Lead). An educational component with mailings of health education materials and other outreach activities. Member evaluation stratifies members according to diagnosis and severity of the member s medical and psychosocial conditions. Involvement of family members, community-based organizations and government social service programs as elements of a comprehensive support structure for members. Standing referral to a specialist UnitedHealthcare has a provision for allowing for standing referrals when on-going, long-term specialty care is required. The referring provider is required to consult the UnitedHealthcare medical director and specialist to determine if the standing referral is appropriate. Approval of the referral is pursuant to a treatment plan approved by UnitedHealthcare in consultation with the primary care provider, the specialist, the care manager, and the member (or authorized person). The standing referral may be limited to a specific number of visits or the period during which visits are authorized. 71
76 Medicare Personal Care Specialist For members of our Medicare plan, a Personal Care Specialist is available to help with access to care (including transportation to doctor s appointments, adult day care, home-delivered meals, and assistance from community organizations). The Medicare Personal Care Specialists can be reached at New Jersey Early Intervention Services NEW JERSEY DEPARTMENT OF HEALTH AND SENIOR SERVICES SPECIAL CHILD, ADULT AND EARLY INTERVENTIONS SERVICES COUNTY CASE MANAGEMENT UNITS Atlantic County SCHS-Case Management Unit Department of lntergenerational Services 101 South Shore Road Northfield, NJ PHONE: (609) ext FAX: (609) Bergen County SCHS-Case Management Unit Bergen County Department of Health Services 327 E. Ridgewood Avenue, Rm. 206 Paramus, NJ PHONE: (201) FAX: (201) Burlington County SCHS-Case Management Unit Community Nursing Services Raphael Meadow Health Center Woodlane Road PO Box 287 Mount Holly, NJ PHONE: (609) FAX: (609) Camden County SCHS-Case Management Unit Camden County Division of Health Jefferson House-Lakeland Road PO Box 9 Blackwood, NJ PHONE: (856) or (800) FAX: (856) Cape May County SCHS-Case Management Unit Cape May Department of Health 6 Moore Rd. Crest Haven Complex Cape May Court House, NJ PHONE: (609) FAX: (609) Cumberland County SCHS-Case Management Unit Cumberland County Department of Health 790 East Commerce Street Bridgeton, NJ PHONE: (856) FAX: (856)
77 Essex County SCHS Case Management Unit Essex County Department of Health and Rehabilitation Division of Community Health Services Unit of Special Child Health Services 160 Fairview Avenue, Rawson Hall, Bldg. #37 Cedar Grove, NJ PHONE: (973) FAX: (973) Gloucester County SCHS-Case Management Unit Gloucester County Health Department 160 Fries-Mill Road Turnersville, NJ PHONE: (856) ext FAX: (856) Hudson County SCHS-Case Management Unit Jersey City Medical Center 50 Baldwin Avenue, Department th Floor Clinic Bldg. Jersey City, NJ PHONE: (201) FAX: (201) Hunterdon County SCHS-Case Management Unit Hunterdon Medical Center 2100 Wescott Drive Flemington, NJ PHONE: (908) FAX: (908) Mercer County SCHS-Case Management Unit Sypek Center 129 Bull Run Road Pennington, NJ PHONE: (609) or FAX: (609) Middlesex County SCHS-Case Management Unit Middlesex County Department of Health John F. Kennedy Square, 5th Floor New Brunswick, NJ PHONE: (732) FAX: (732) Monmouth County SCHS-Case Management Unit Special Child Health Services/Early Intervention Monmouth County 141 Bodman Place Red Bank, NJ PHONE: (732) FAX: (732) Morris County SCHS-Case Management Unit Morristown Memorial Hospital 100 Madison Avenue, Box 99 Morristown, NJ PHONE: (973) FAX: (973)
78 Ocean County SCHS-Case Management Unit Ocean County Department of Health PO Box 2191 Sunset Avenue Toms River, NJ PHONE: (732) ext FAX: (732) Passaic County SCHS-Case Management Unit Catholic Family and Community Services 279 Carroll Street Paterson, NJ PHONE: (973) FAX: (973) Salem County SCHS-Case Management Unit Salem County Department of Health 98 Market Street Salem, NJ PHONE: (856) ext FAX: (856) Somerset SCHS-Case Management Unit Somerset Handicapped Children s Treatment Center 377 Union Avenue P.O. Box 6824 Bridgewater, NJ PHONE: (908) FAX: (908) Sussex County SCHS-Case Management Unit Sussex County Health Department Division of Public Health Nursing 129 Morris Turnpike Newton, NJ PHONE: (973) ext. 62 FAX: (973) Union County SCHS-Case Management Unit 328 South Avenue Fanwood, NJ PHONE: (908) FAX: (908) Warren County SCHS-Case Management Unit Warren County Health Department Special Child Health Services 162 East Washington Avenue Washington, NJ PHONE: (908) ext. 258 FAX: (908) wcschs(@netscape.net 74
79 SECTION 8 PHARMACY Pharmacy Benefit Management Medicaid and NJ FamilyCare members receive their outpatient prescription drugs through UnitedHealthcare, with the following two exceptions: FamilyCare Plan D parents and adults on General Assistance who need AIDS drugs receive them through the AIDS Drug Distribution Program (ADDP). The UnitedHealthcare HIV/AIDS case manager identifies the members who qualify for this program and assists with their application. The following drugs are obtained through the Medicaid fee-for-service program: > Clozaril > Risperdal > Geodon > Zyprexa > Seroquel > Methadone maintenance cost and administration > Generically equivalent drug products of the above. Member ID Cards for Prescription benefits All UnitedHealthcare members must use their UnitedHealthcare member ID card to obtain covered prescription drugs. Prescription Drug Coverage Coverage for outpatient prescription drugs varies by UnitedHealthcare product: UnitedHealthcare Product Medicaid NJ FamilyCare A NJ FamilyCare B NJ FamilyCare C NJ FamilyCare D UnitedHealthcare Dual Complete Outpatient Prescription benefit Prescription and over-the-counter drugs covered by the Medicaid program No cap. No copayments. Eligible parents and adults receive protease inhibitors and certain antiretrovirals solely through the AIDS Drug Distribution Program Prescription and over-the-counter drugs covered by the Medicaid program. No cap. $1 copay for generic drugs $5 copay for brand name drugs Prescription drugs covered. No cap $5 copay for brand and generic drugs. If greater than a 34-day supply of a prescription drug, $10 copay applies. Over-the-counter drugs excluded; Eligible parents, adults, and members with program status codes of 380 receive protease inhibitors and certain anti-retrovirals solely through the AIDS Drug Distribution Program Prescriptions covered by the Medicare Part B & Care Plus (Medicare) D program. No cap. Deductibles and copayments may apply. For details regarding drugs covered under the UnitedHealthcare pharmacy benefit and the list of drugs that require prior authorization, providers can go to the UnitedHealthcare Web site at 75
80 Prescriptions Requiring Prior Authorization For Pharmacy Prior Authorization, including injectable drugs, call or fax the prior authorization request to the following: For injectable drugs (800) For all other drugs (800) Physicians should consult the UnitedHealthcare Drug Formulary to identify the drugs that require prior authorization to verify if prior authorization is necessary. Physicians should receive prior authorization before giving an UnitedHealthcare member a prescription for a medication that requires prior authorization. UnitedHealthcare makes prior authorization determinations within 24 hours of receiving all the necessary information from the provider. The member is entitled to a 72-hour supply of most medications while awaiting the prior authorization determination. Pharmacy Network Most chain pharmacies and many independent pharmacies fill prescriptions for UnitedHealthcare members. To locate a pharmacy that is convenient for a member, call DOC-DENT ( ). Generic Drugs Generic drugs are provided when available as required by State mandatory generic substitution regulations. Generic drugs are approved by the Food and Drug Administration (FDA) to be equivalent to their brand name counterparts. If a generic drug is available, a brand name drug will not be provided to the member. However, if a physician provides information that documents why a brand name drug is medically necessary and submits a prior authorization. Exception: No generic substitutions will be made for mental health/substance abuse prescriptions written by psychiatrists or mental health/substance abuse providers. Physicians submitting a request for prior authorization for brand name drugs should contact the Pharmacy Prior Authorization service at to present the information supporting the medical necessity of the brand drug. Pharmacy Benefit Exclusions Certain drugs are not covered by the pharmacy benefit. Drugs that are not covered include: Drugs that are used for weight loss or appetite suppression Drugs that are used for cosmetic purposes Drugs used to treat infertility Drugs used to stimulate hair growth or prevent hair loss Investigational and experimental drugs, unless a Medical Director gives prior authorization DESI drugs Existing UnitedHealthcare members may continue taking a medication that has been removed from the formulary for as long as that member is enrolled in UnitedHealthcare (unless the medication has been deemed unsafe) with valid medical reasoning from the member s prescribing provider, and with the member s consultation and agreement. A member may change his or her medication to a medication that is on UnitedHealthcare s formulary only if the prescribing provider and member agree to that change. Members new to therapy will be required to use a medication on the formulary, unless otherwise authorized. 76
81 SECTION 9 NJ Behavorial Health Screening for Behavioral Health Problems Primary Care Providers (PCPs) are required to screen UnitedHealthcare members for behavioral health problems, using the Screening Tool for Substance Abuse and Mental Health found at the end of this section. PCPs should file the completed screening tool in the patient s medical record. In addition, please refer to the section titled "Behavioral Health Toolkit for the PCP" found in this section to assist the PCP in referring members for behavioral health services. Behavioral Health Services for UnitedHealthcare Members Only UnitedHealthcare Medicaid members who are registered clients of the NJ Division of Developmental Disabilities (DDD) receive mental health and substance abuse services, including Partial Hospitalization, through UnitedHealthcare. The exception is Partial Care which is covered for DDD clients through the State s Medicaid Fee-For-Service program. All other Medicaid and NJ FamilyCare members receive mental health and substance abuse services through the State of New Jersey feefor-service program. DDD members must use UnitedHealthcare participating providers listed in the provider directory. UnitedHealthcare Dual Complete (Medicare) members receive mental health and substance abuse services through UnitedHealthcare. Role of the Behavioral Health Unit UnitedHealthcare s Behavioral Health Unit is an important resource to all providers when members experience mental health or substance abuse problems. Providers call DOC-DENT ( ). The Behavioral Health Unit: Operates 9:00 AM - 5:00 PM, weekdays Responsible for member emergencies and requests for inpatient behavioral health admissions 24 hours, 7 days a week Fully supports primary care providers with assessment and referrals to mental health and chemical dependence services Provides behavioral health care management Reviews, monitors, and authorizes behavioral health care Responsible for provider relations for behavioral health providers Staffed by professionals with extensive experience in mental health and chemical dependence services Behavioral Health Emergencies for DDD Members If a provider believes the DDD member is having a psychiatric emergency, the provider should either call 911 or direct the member to the designated county screening center or nearest hospital emergency room. If the provider is unsure about the member s mental status, call the UnitedHealthcare Behavioral Health Unit at DOCDENT ( ). 77
82 Referrals for Behavioral Health Services for Medicaid DDD and UnitedHealthcare Dual Complete (Medicare) Members PCPs and behavioral health providers should communicate with the Behavioral Health Unit by calling DOC-DENT ( ). Providers can also send requests via the Behavioral Health confidential fax at Providers should note the referral or request in the patient s medical record. A DDD member can self-refer to a participating behavioral health provider for the first outpatient visit at a participating provider. The Behavioral Health Unit generally approves a maximum of six initial outpatient visits to allow for full clinical evaluation. The initial treatment assessment must include a full psychosocial history, a mental status examination, and M.D. psychiatric evaluation. The assessment and development of a comprehensive treatment plan must be developed within the first 30 days of treatment. Authorization for Continuation of Outpatient Behavioral Health Services for Medicaid DDD and UnitedHealthcare Dual Complete (Medicare) Members Behavioral health providers can fax ( ) their requests for continued treatment to the Behavioral Health Unit. Providers can utilize either the UnitedHealthcare Behavioral Health Treatment Plan Form or their own treatment plan form, as long as the provider s form covers all the elements in the UnitedHealthcare form. The Behavioral Health Unit evaluates the treatment plan for quality assurance. The Behavioral Health Unit forwards the treatment plan review to the member s PCP to assure coordination of care. UnitedHealthcare authorizes outpatient treatment for a 3-6 month period depending on treatment intensity. Behavioral Health Guidelines and Standards UnitedHealthcare utilizes the following diagnostic assessment tools and placement criteria guidelines, consistent with current standards of care: DSM-IV (Diagnostic and Statistical Manual of Mental Disorders), 4th edition ASAM PPC-2 (American Society of Addiction Medicine) UnitedHealthcare uses Milliman USA Healthcare Guidelines for appropriateness of care and discharge reviews. Behavioral health providers may not refer patients to another provider without notifying the Behavioral Health Unit and obtaining prior authorization. UnitedHealthcare expects behavioral health providers to comply with Section Timeliness Standards for Appointment Scheduling. Providers referring members for Behavioral Health Services need to provide a copy of the medical consultation and diagnostic results to the MH/SA provider. You must notify an enrollee s mental health/substance abuse provider of the findings of his/her physical examination and laboratory/radiological tests within 24 hours of receipt for urgent cases and within five (5) business days in non-urgent cases. Notification should be made by phone with follow-up in writing when feasible. Documentation is required when notifying a member s MH/SA provider of the findings of his/her physical examination and laboratory/radiological tests within twenty-four (24) hours of receipt for urgent cases and within five business days in non-urgent cases. Notification should be made by phone with follow-up in writing when feasible. 78
83 Behavioral Health Toolkit for the Primary Care Provider (PCP) Purpose: This toolkit was created to assist the PCP in identifying Integrated Care Program (ICP) members who may be in need of Behavioral Health services, to supply both the PCP and Integrated Care Program member with helpful resources links containing important information about common Behavioral Health conditions and their treatment, and to assist the PCP in obtaining consultation and/or referral services for Integrated Care Program members with Behavioral Health conditions. Clinical Practice Guidelines (CPGs): The following links will enable the PCP to access CPGs for the commonly seen Behavioral Health conditions. For CPGs pertaining to Bipolar Disorder, Schizophrenia, Depression, Substance Use Disorders, follow this link (the American Psychiatric Association CPG website): For the ADHD CPG, follow this link (the American Academy of Pediatrics): Screening Tools for PCPs (scoring methodologies are included in the screening tools themselves): 1. Substance Abuse (Project Cork website): 2. Depression (Pfizer Patient Health Questionnaire, aka PHQ-9): In those situations where a member screens positive for a Behavioral Health condition, or you otherwise suspect the presence of a Behavioral Health condition needing further assessment and/or treatment, please refer the member as appropriate to an UnitedHealthcare Behavioral Health Provider. For assistance in identifying a behavioral health provider please contact the UnitedHealthcare Physician Helpline: (888) For provider and member related resources for Behavioral Health conditions affecting adults follow this link (Substance Abuse and Mental Health Services Administration): or (National Alliance on Mental Illness): For member related resources for Behavioral Health conditions affecting Children and Adolescents, follow this link (Illinois Federation of Families): 79
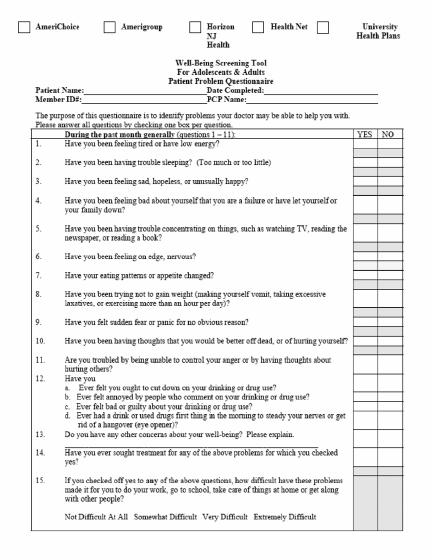
84 80
85 Specialty/Biotech Products UnitedHealthcare will coordinate with a specialty supplier to arrange delivery of specialty products covered under the pharmacy benefit to a provider s office or a member s home, as appropriate. Providers can call (800) to request an authorization for these products, as well as to arrange delivery. Pharmacy Lock-In Program If a provider suspects that a member is misusing or abusing the prescription benefit by obtaining prescriptions from multiple providers or requesting controlled substances for questionable indications, the provider should call the UnitedHealthcare Fraud and Abuse Hotline at In addition, episodes of stolen prescription pads and suspected forged prescriptions should be reported to UnitedHealthcare. UnitedHealthcare will investigate the issues and take the appropriate action, which will include, but is not limited to, reporting the member to the State, enrolling the member in the pharmacy lock-in program, and informing the pharmacy network of the activity. The pharmacy lock-in program restricts a member to a single pharmacy for obtaining prescriptions. AIDS Drug Distribution Program (ADDP) UnitedHealthcare will facilitate the enrollment of qualified NJ FamilyCare parents and adults into ADDP. This program, administered by the NJ DHSS, provides protease inhibitors and certain antiretrovirals. Enrollees in ADDP receive these drugs solely through ADDP, not UnitedHealthcare. 81
86 SECTION 10 MEMBER INFORMATION Member ID Cards UnitedHealthcare issues a member identification (ID) card to each member enrolled in the plan. Even when more than one member of a family enrolls, UnitedHealthcare issues a separate ID card to each family member. All member ID cards display the UnitedHealthcare logo and the UnitedHealthcare toll-free Member Services number. The member ID card also displays: The member s Primary Care Provider s (PCP s) name and telephone number The member s name and UnitedHealthcare ID number Co-payment requirements for members if applicable. The back of the member ID card has the following information: Instructions for members on how to access care Instructions for providers on how to verify eligibility and obtain prior authorization Mailing address for claims Pharmacy Help Desk phone number for pharmacy claim issues A statement allowing release of medical information (Medicaid and NJ FamilyCare card only) The member should present his or her member ID card whenever seeking UnitedHealthcare covered services. See Member ID Cards for Prescription Benefits. No member should be denied services because of failure to have a member ID card at the time of service. Providers can call DOC-DENT ( ) to verify eligibility. If a PCP believes that an incorrect PCP name is listed on the member card, he or she should call DOC-DENT ( ), option 1, to verify the member s eligibility and to confirm the PCP s name. 82
87 UnitedHealthcare Member ID Cards PLEASE NOTE: New Claims Address P.O. Box 5250 Kingston, NY NJ FamilyCare C NJ FamilyCare B NJ FamilyCare A Medicaid 83



88 UnitedHealthcare Member ID Cards (cont.) PLEASE NOTE: New Claims Address P.O. Box 5250 Kingston, NY UnitedHealthcare Dual Complete NJ FamilyCare D 84
FREEDOM BLUE PPO R CO 307 9/06. Freedom Blue PPO SM Summary of Benefits and Other Value Added Services
 FREEDOM BLUE PPO R9943 2007 CO 307 9/06 Freedom Blue PPO SM Summary of Benefits and Other Value Added Services Introduction to Summary of Benefits for Freedom Blue January 1, 2007 - December 31, 2007 California
FREEDOM BLUE PPO R9943 2007 CO 307 9/06 Freedom Blue PPO SM Summary of Benefits and Other Value Added Services Introduction to Summary of Benefits for Freedom Blue January 1, 2007 - December 31, 2007 California
Correction Notice. Health Partners Medicare Special Plan
 Correction Notice Special Plan Following are corrections that apply to both the English and Spanish versions of the 2015 for Special (HMO SNP): Original Information Page 1, under the heading SECTIONS IN
Correction Notice Special Plan Following are corrections that apply to both the English and Spanish versions of the 2015 for Special (HMO SNP): Original Information Page 1, under the heading SECTIONS IN
Freedom Blue PPO SM Summary of Benefits
 Freedom Blue PPO SM Summary of Benefits R9943-206-CO-308 10/05 Introduction to the Summary of Benefits for Freedom Blue PPO Plan January 1, 2006 - December 31, 2006 California YOU HAVE CHOICES IN YOUR
Freedom Blue PPO SM Summary of Benefits R9943-206-CO-308 10/05 Introduction to the Summary of Benefits for Freedom Blue PPO Plan January 1, 2006 - December 31, 2006 California YOU HAVE CHOICES IN YOUR
Summary of Benefits. January 1, 2018 December 31, Providence Medicare Dual Plus (HMO SNP)
") Summary of Benefits January 1, 2018 December 31, 2018 Providence Medicare Dual Plus (HMO SNP) This plan is available in Clackamas, Multnomah and Washington counties in Oregon for members who are eligible
Summary of Benefits January 1, 2018 December 31, 2018 Providence Medicare Dual Plus (HMO SNP) This plan is available in Clackamas, Multnomah and Washington counties in Oregon for members who are eligible
2018 CareOregon Advantage Plus (HMO-POS SNP) Summary of Benefits
 Summary of Benefits") 2018 CareOregon Advantage Plus (HMO-POS SNP) Summary of Benefits For Oregon counties: Clackamas, Clatsop, Columbia, Jackson, Josephine, Multnomah, Tillamook, Washington and Yamhill H5859_1099_CO_1018 CMS
2018 CareOregon Advantage Plus (HMO-POS SNP) Summary of Benefits For Oregon counties: Clackamas, Clatsop, Columbia, Jackson, Josephine, Multnomah, Tillamook, Washington and Yamhill H5859_1099_CO_1018 CMS
MEDICARE CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS.
 ine 1-800-544-0088 www.care1st.com CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS MEDICARE 2009 COUNTIES: LOS ANGELES - ORANGE - SAN BERNARDINO - SAN DIEGO H5928_09_004_SNP_SB 10/2008 Section I Introduction
ine 1-800-544-0088 www.care1st.com CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS MEDICARE 2009 COUNTIES: LOS ANGELES - ORANGE - SAN BERNARDINO - SAN DIEGO H5928_09_004_SNP_SB 10/2008 Section I Introduction
Summary of Benefits. New York: Bronx, Kings, New York, Queens and Richmond Counties
 Summary of Benefits New York: Bronx, Kings, New York, Queens and Richmond Counties January 1, 2006 - December 31, 2006 You ve earned the right to live life on your own terms. And that includes the right
Summary of Benefits New York: Bronx, Kings, New York, Queens and Richmond Counties January 1, 2006 - December 31, 2006 You ve earned the right to live life on your own terms. And that includes the right
special needs plan (hmo snp) MEDICARE advantage plan summary of benefits Serving Members in Douglas & Klamath Counties
 MEDICARE advantage plan summary of benefits Serving Members in Douglas & Klamath Counties") special needs plan (hmo snp) 2017 MEDICARE advantage plan summary of benefits Serving Members in Douglas & Klamath Counties Table of Contents About the Summary of Benefits... 2 Who Can Join?... 2 Which
special needs plan (hmo snp) 2017 MEDICARE advantage plan summary of benefits Serving Members in Douglas & Klamath Counties Table of Contents About the Summary of Benefits... 2 Who Can Join?... 2 Which
Summary of benefits Health Net. seniority plus green. Benefits effective January 1, 2009 H0562 Medicare Advantage HMO
 2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
FREQUENTLY ASKED QUESTIONS (FAQS) FOR PROVIDER INDUSTRY
 FOR PROVIDER INDUSTRY") FREQUENTLY ASKED QUESTIONS (FAQS) FOR PROVIDER INDUSTRY 1. What changes are proposed for the Medicaid Program in the State Fiscal Year 2012 budget? Will clients be notified if these changes are not approved
FREQUENTLY ASKED QUESTIONS (FAQS) FOR PROVIDER INDUSTRY 1. What changes are proposed for the Medicaid Program in the State Fiscal Year 2012 budget? Will clients be notified if these changes are not approved
2017 Summary of Benefits
 H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
Information for Dual-Eligible Members with Secondary Coverage through California Regular Medi-Cal (Fee-for-Service)
") Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2011 December 31, 2011 Los Angeles County This publication is a supplement to the 2011 Positive (HMO SNP) Evidence
Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2011 December 31, 2011 Los Angeles County This publication is a supplement to the 2011 Positive (HMO SNP) Evidence
First Look: Plan Benefit Filings
 July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
Y0021_H4754_MRK1427_CMS File and Use PacificSource Community Health Plans, Inc. is a health plan with a Medicare contract
 Y0021_H4754_MRK1427_CMS File and Use 08262012 PacificSource Community Health Plans, Inc. is a health plan with a Medicare contract Section I - Introduction to Summary of s Thank you for your interest in.
Y0021_H4754_MRK1427_CMS File and Use 08262012 PacificSource Community Health Plans, Inc. is a health plan with a Medicare contract Section I - Introduction to Summary of s Thank you for your interest in.
SUMMARY OF BENEFITS 2009
 HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
HealthPartners Freedom Plan (Cost) 2011 Medical Summary of Benefits Wisconsin
 2011 Medical Summary of Benefits Wisconsin") HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
Your Out-of-Pocket Type of Service
 Calendar Year Deductible (CYD) 1 $0 single/ 3x family Out-of-Pocket Maximum - Deductibles, coinsurance and copays all accrue toward the outof-pocket maximum. With respect to family plans, an individual
Calendar Year Deductible (CYD) 1 $0 single/ 3x family Out-of-Pocket Maximum - Deductibles, coinsurance and copays all accrue toward the outof-pocket maximum. With respect to family plans, an individual
Your Out-of-Pocket Type of Service
 Calendar Year Deductible (CYD) 1 $3,000 single/ 3x family Out-of-Pocket Maximum - Deductibles and copays all accrue towards the out-of-pocket $6,200 single/ 2x family maximum. With respect to family plans,
Calendar Year Deductible (CYD) 1 $3,000 single/ 3x family Out-of-Pocket Maximum - Deductibles and copays all accrue towards the out-of-pocket $6,200 single/ 2x family maximum. With respect to family plans,
Summary of Benefits for SmartValue Classic (PFFS)
") Summary of Benefits for SmartValue Classic (PFFS) Available in Select Counties in Nevada A health plan with a Medicare contract. Rocky Mountain Hospital and Medical Service, Inc. has contracted with the
Summary of Benefits for SmartValue Classic (PFFS) Available in Select Counties in Nevada A health plan with a Medicare contract. Rocky Mountain Hospital and Medical Service, Inc. has contracted with the
CLASSIC BLUE SECURE/BLUE CROSS BLUE SHIELD COMPLEMENTARY Monroe County Benefit Summary/Comparison (Over 65 Retirees)
") WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
2015 Summary of Benefits
 2015 Summary of Benefits Health Net Cal MediConnect Plan (Medicare-Medicaid Plan) Los Angeles County, CA H3237_2015_0291 CMS Accepted 09082014 Health Net Cal MediConnect Summary of Benefits! This is a
2015 Summary of Benefits Health Net Cal MediConnect Plan (Medicare-Medicaid Plan) Los Angeles County, CA H3237_2015_0291 CMS Accepted 09082014 Health Net Cal MediConnect Summary of Benefits! This is a
Basic Covered Benefits and Services
 Basic Covered Benefits and A prior authorization is when UnitedHealthcare Community Plan gives the doctor permission to perform certain services. Bed Liners Coverage Covered for members age 4 and up; Prior
Basic Covered Benefits and A prior authorization is when UnitedHealthcare Community Plan gives the doctor permission to perform certain services. Bed Liners Coverage Covered for members age 4 and up; Prior
Summary Of Benefits. WASHINGTON Pierce and Snohomish
 Summary Of Benefits WASHINGTON Pierce and Snohomish 2018 Molina Medicare Choice (HMO SNP) (800) 665-1029, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local time H5823_18_1099_0007_WAChoSB Accepted 9/26/2017
Summary Of Benefits WASHINGTON Pierce and Snohomish 2018 Molina Medicare Choice (HMO SNP) (800) 665-1029, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local time H5823_18_1099_0007_WAChoSB Accepted 9/26/2017
2016 Summary of Benefits
 2016 Summary of Benefits Health Net Jade (HMO SNP) Kern, Los Angeles and Orange counties, CA Benefits effective January 1, 2016 H0562 Health Net of California, Inc. H0562_2016_0175 CMS Accepted 09082015
2016 Summary of Benefits Health Net Jade (HMO SNP) Kern, Los Angeles and Orange counties, CA Benefits effective January 1, 2016 H0562 Health Net of California, Inc. H0562_2016_0175 CMS Accepted 09082015
Summary of Benefits Advantra Freedom PEBTF
 Advantra Freedom is a Medicare Advantage Private Fee-For-Service (PFFS) Plan. This Summary of Benefits tells you some features of our Plan. It doesn't list every service that we cover or list every limitation
Advantra Freedom is a Medicare Advantage Private Fee-For-Service (PFFS) Plan. This Summary of Benefits tells you some features of our Plan. It doesn't list every service that we cover or list every limitation
Benefits are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
2018 Summary of Benefits
 2018 Summary of Benefits H5209-004_MDASB 9-13-17 Accepted 9/18/2018 DHS Approved 09/13/2017 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP)
2018 Summary of Benefits H5209-004_MDASB 9-13-17 Accepted 9/18/2018 DHS Approved 09/13/2017 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP)
SmartSaver. A Medicare Advantage Medical Savings Account Plan. Summary of Benefits and Other-Value Added Services. From Blue Cross of California
 SmartSaver From Blue Cross of California A Medicare Advantage Medical Savings Account Plan Service Area C Summary of Benefits and Other-Value Added Services H5769 2007 CO 415 09/22/06 Introduction to the
SmartSaver From Blue Cross of California A Medicare Advantage Medical Savings Account Plan Service Area C Summary of Benefits and Other-Value Added Services H5769 2007 CO 415 09/22/06 Introduction to the
Summary of Benefits 2018
 SM Summary of Benefits 2018 bluecareplus.bcbst.com H3259_18_SB Accepted 08282017 This is a summary of drug and health services covered by BlueCare Plus (HMO SNP) SM health plan January 1, 2018 - December
SM Summary of Benefits 2018 bluecareplus.bcbst.com H3259_18_SB Accepted 08282017 This is a summary of drug and health services covered by BlueCare Plus (HMO SNP) SM health plan January 1, 2018 - December
Amherst Central School District First Choice Health Plan. Non-First Choice Providers and Out-of-Network Providers
 Health: Hospital Services provided by First Choice Preferred Provider Network Medical Services Radiology, Ultrasounds 20% after $500 individual or Laboratory Testing 20% after $500 individual or MRI and
Health: Hospital Services provided by First Choice Preferred Provider Network Medical Services Radiology, Ultrasounds 20% after $500 individual or Laboratory Testing 20% after $500 individual or MRI and
PLAN DESIGN AND BENEFITS - PA POS 4.2 with $5/$15/$30 RX PARTICIPATING PROVIDERS
 PLAN FEATURES Deductible (per calendar year) PHYSICIAN SERVICES Primary Care Physician Visits Specialist Office Visits Maternity OB Visits Allergy Treatment Allergy Testing PREVENTIVE CARE Routine Adult
PLAN FEATURES Deductible (per calendar year) PHYSICIAN SERVICES Primary Care Physician Visits Specialist Office Visits Maternity OB Visits Allergy Treatment Allergy Testing PREVENTIVE CARE Routine Adult
Blue Cross Premier Bronze
 An individual PPO health plan from Blue Cross Blue Shield of Michigan. You will have a broad choice of doctors and hospitals within BCBSM s unsurpassed statewide PPO network including nationwide coverage.
An individual PPO health plan from Blue Cross Blue Shield of Michigan. You will have a broad choice of doctors and hospitals within BCBSM s unsurpassed statewide PPO network including nationwide coverage.
Summary of Benefits for Anthem MediBlue Dual Advantage (HMO SNP)
") Summary of Benefits for Available in: Select Counties* in Maine *See Page 2 for a list of counties. Plan year: January 1, 2018 December 31, 2018 In this section, you ll learn about some of the benefits
Summary of Benefits for Available in: Select Counties* in Maine *See Page 2 for a list of counties. Plan year: January 1, 2018 December 31, 2018 In this section, you ll learn about some of the benefits
OF BENEFITS. Cigna-HealthSpring TotalCare (HMO SNP) H Cigna H3949_15_19921 Accepted
 H Cigna H3949_15_19921 Accepted") agesummary OF BENEFITS Cover erage Cigna-HealthSpring TotalCare (HMO SNP) H3949-009 2014 Cigna H3949_15_19921 Accepted SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get
agesummary OF BENEFITS Cover erage Cigna-HealthSpring TotalCare (HMO SNP) H3949-009 2014 Cigna H3949_15_19921 Accepted SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get
Schedule of Benefits
 Schedule of Benefits ANTHEM Small Business Health Options Program (SHOP) This is a brief schedule of benefits. Refer to your Anthem Certificate of Coverage (Booklet) for complete details on benefits, conditions,
Schedule of Benefits ANTHEM Small Business Health Options Program (SHOP) This is a brief schedule of benefits. Refer to your Anthem Certificate of Coverage (Booklet) for complete details on benefits, conditions,
2017 Comparison of the State of Iowa Medicaid Enterprise Basic Benefits Based on Eligibility Determination
 General Plan Provisions Benefits Available from Out-of-Network Providers 2017 Comparison of the State of Iowa Enterprise Cost Sharing: A variety of methods are used to share expenses between the state
General Plan Provisions Benefits Available from Out-of-Network Providers 2017 Comparison of the State of Iowa Enterprise Cost Sharing: A variety of methods are used to share expenses between the state
2012 Summary of Benefits
 2012 Summary of Benefits San Francisco County, CA Benefits effective January 1, 2012 H0562 Health Net of California, Inc. Material ID # H0562_2012_0055 CMS Approved 08122011 SECTION I Introduction to
2012 Summary of Benefits San Francisco County, CA Benefits effective January 1, 2012 H0562 Health Net of California, Inc. Material ID # H0562_2012_0055 CMS Approved 08122011 SECTION I Introduction to
Kaiser Permanente (No. and So. California) 2018 Union
 2018 Union") Kaiser Permanente (No. and So. California) General Information Lifetime Maximum Benefit Annual Maximum Benefit Coinsurance Percentage Precertification Requirements Precertification Penalty Health Savings
Kaiser Permanente (No. and So. California) General Information Lifetime Maximum Benefit Annual Maximum Benefit Coinsurance Percentage Precertification Requirements Precertification Penalty Health Savings
Services Covered by Molina Healthcare
 Services Covered by Molina Healthcare As a Molina Healthcare member, you will continue to receive all medically-necessary Medicaid-covered services at no cost to you. The following list of covered services
Services Covered by Molina Healthcare As a Molina Healthcare member, you will continue to receive all medically-necessary Medicaid-covered services at no cost to you. The following list of covered services
SUMMARY OF BENEFITS. Hamilton County Department of Education Network Copay Plan. Connecticut General Life Insurance Co.
 SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Hamilton County Department of Education Annual deductibles and maximums Lifetime maximum Pre-Existing Condition Limitation (PCL) Coinsurance All
SUMMARY OF BENEFITS Connecticut General Life Insurance Co. Hamilton County Department of Education Annual deductibles and maximums Lifetime maximum Pre-Existing Condition Limitation (PCL) Coinsurance All
Extra Value Summary YOU HAVE CHOICES ABOUT HOW TO GET YOUR MEDICARE BENEFITS TIPS FOR COMPARING YOUR MEDICARE CHOICES
 INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2016 - December 31, 2016 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2016 - December 31, 2016 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
Cigna Health and Life Insurance Company. Plan Benefits. Unlimited. Unlimited. Not applicable. Not applicable. Not applicable
 SUMMARY OF BENEFITS Client Name: Washington County Public Schools Benefit Option Name: Medicare Supplement Effective: July 1, 2018 through June 30, 2019 1 Benefit Description Lifetime Maximum Applies to
SUMMARY OF BENEFITS Client Name: Washington County Public Schools Benefit Option Name: Medicare Supplement Effective: July 1, 2018 through June 30, 2019 1 Benefit Description Lifetime Maximum Applies to
$10 copay. $10 copay. $10 copay $5 copay $10 copay $5 copay. $10 copay. No charge. No charge. No charge
 PLAN FEATURES * ** Deductible (per calendar ) Member Coinsurance Copay Maximum (per calendar ) Lifetime Maximum Unlimited Primary Care Physician Selection Required Upon enrollment to a Vitalidad Plus plan,
PLAN FEATURES * ** Deductible (per calendar ) Member Coinsurance Copay Maximum (per calendar ) Lifetime Maximum Unlimited Primary Care Physician Selection Required Upon enrollment to a Vitalidad Plus plan,
January 1, 2015 December 31, Maintenance Organization (HMO) offered by HEALTHNOW NEW YORK INC. with a Medicare contract)
 offered by HEALTHNOW NEW YORK INC. with a Medicare contract)") BLUECROSS BLUESHIELD SENIOR BLUE 601 (HMO), BLUECROSS BLUESHIELD SENIOR BLUE HMO SELECT (HMO) AND BLUECROSS BLUESHIELD SENIOR BLUE HMO 651 PARTD (HMO) (a Medicare Advantage Health Maintenance Organization
BLUECROSS BLUESHIELD SENIOR BLUE 601 (HMO), BLUECROSS BLUESHIELD SENIOR BLUE HMO SELECT (HMO) AND BLUECROSS BLUESHIELD SENIOR BLUE HMO 651 PARTD (HMO) (a Medicare Advantage Health Maintenance Organization
True Blue Special Needs Plan (HMO SNP)
") True Blue Special Needs Plan (HMO SNP) 2012 Summary of Benefits You think about finding the perfect health insurance plan. We think about providing you with seamless service and affordable benefits. Serving
True Blue Special Needs Plan (HMO SNP) 2012 Summary of Benefits You think about finding the perfect health insurance plan. We think about providing you with seamless service and affordable benefits. Serving
OVERVIEW OF YOUR BENEFITS
 OVERVIEW OF YOUR BENEFITS IMPORTANT PHONE NUMBERS Member Services Department (646) 473-9200 For answers to questions about your benefits or to be referred to another Benefit Fund department. Program for
OVERVIEW OF YOUR BENEFITS IMPORTANT PHONE NUMBERS Member Services Department (646) 473-9200 For answers to questions about your benefits or to be referred to another Benefit Fund department. Program for
The MITRE Corporation Plan
 Benefit Type Plan Year Type Calendar Year Annual Medical Out of (for certain services) Employee Employee + 1 Family Annual Prescription Drug Out of Employee Employee + 1 Family Copayments: One copay per
Benefit Type Plan Year Type Calendar Year Annual Medical Out of (for certain services) Employee Employee + 1 Family Annual Prescription Drug Out of Employee Employee + 1 Family Copayments: One copay per
Medicaid Benefits at a Glance
 Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
Information for Dual-Eligible Members with Secondary Coverage through California Regular Medi-Cal (Fee-for-Service)
") Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2015 December 31, 2015 Los Angeles County This publication is a supplement to the 2015 Evidence of Coverage and
Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2015 December 31, 2015 Los Angeles County This publication is a supplement to the 2015 Evidence of Coverage and
Telemedicine services $0 copay Not applicable Primary care provider (PCP) CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance
 CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance") Calendar Year Deductible (CYD) 2 Plan includes an embedded individual deductible provision. An embedded deductible combines individual and family deductibles in $4,000 Single / $8,000 Family $12,000 Single
Calendar Year Deductible (CYD) 2 Plan includes an embedded individual deductible provision. An embedded deductible combines individual and family deductibles in $4,000 Single / $8,000 Family $12,000 Single
INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS
 INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS January 1, 2015 - December 31, 2015 CARE1ST HEALTH PLAN California: Fresno, Merced, Stanislaus and San Joaquin Counties H5928_15_029_SB_CTCA_2
INTRODUCTION TO SUMMARY OF BENEFITS SECTION 1 SUMMARY OF BENEFITS January 1, 2015 - December 31, 2015 CARE1ST HEALTH PLAN California: Fresno, Merced, Stanislaus and San Joaquin Counties H5928_15_029_SB_CTCA_2
CA Group Business 2-50 Employees
 PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Member Coinsurance Copay Maximum (per calendar year) Lifetime Maximum Referral Requirement PHYSICIAN SERVICES Primary
PLAN FEATURES Network Primary Care Physician Selection Deductible (per calendar year) Member Coinsurance Copay Maximum (per calendar year) Lifetime Maximum Referral Requirement PHYSICIAN SERVICES Primary
Summary Of Benefits. CALIFORNIA Imperial, Los Angeles, Riverside (partial), San Bernardino (partial), and San Diego
, San Bernardino (partial), and San Diego") Summary Of Benefits CALIFORNIA Imperial, Los Angeles, Riverside (partial), San Bernardino (partial), and San Diego 2018 Molina Medicare Options Plus (HMO SNP) (800) 665-0898, TTY/TDD 711 7 days a week,
Summary Of Benefits CALIFORNIA Imperial, Los Angeles, Riverside (partial), San Bernardino (partial), and San Diego 2018 Molina Medicare Options Plus (HMO SNP) (800) 665-0898, TTY/TDD 711 7 days a week,
Covered Benefits Rhody Health Partners
 Covered s Rhody Health Partners s Covered by UnitedHealthcare Community Plan As member of UnitedHealthcare Community Plan, you are covered for the following services. (Remember to always show your current
Covered s Rhody Health Partners s Covered by UnitedHealthcare Community Plan As member of UnitedHealthcare Community Plan, you are covered for the following services. (Remember to always show your current
GIC Employees/Retirees without Medicare
 GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
CALIFORNIA Small Group HMO Aetna Health of California, Inc. Plan Effective Date: 04/01/2007. Aetna Value Network* HMO $30/$40
 PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral Requirement PHYSICIAN SERVICES CALIFORNIA Small Group HMO Primary Care Physician
PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral Requirement PHYSICIAN SERVICES CALIFORNIA Small Group HMO Primary Care Physician
Our service area includes the following county in: Delaware: New Castle.
 2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Dual Complete (HMO SNP) H3113-011 Look inside to learn more about the health services and drug coverages the plan provides. Call Customer
2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Dual Complete (HMO SNP) H3113-011 Look inside to learn more about the health services and drug coverages the plan provides. Call Customer
Summary of Benefits Prominence HealthFirst Small Group Health Plan
 POS Triple Choice 3000 Summary of Benefits Calendar Year Deductible (CYD) $3,000 Single / $9,000 Family $7,000 Single / $21,000 Family $21,000 Single / $63,000 Family Coinsurance 40% coinsurance 50% coinsurance
POS Triple Choice 3000 Summary of Benefits Calendar Year Deductible (CYD) $3,000 Single / $9,000 Family $7,000 Single / $21,000 Family $21,000 Single / $63,000 Family Coinsurance 40% coinsurance 50% coinsurance
Select Summary YOU HAVE CHOICES ABOUT HOW TO GET YOUR MEDICARE BENEFITS TIPS FOR COMPARING YOUR MEDICARE CHOICES
 INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2015 - December 31, 2015 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR January 1, 2015 - December 31, 2015 Central Alabama and Mobile Area SECTION I INTRODUCTION TO THE SUMMARY OF BENEFITS This booklet gives you a summary of what
2018 SUMMARY OF BENEFITS
 2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Senior Care Options (HMO SNP) H2226-001 Look inside to learn more about the plan and the health and drug services it covers. Call Customer
2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Senior Care Options (HMO SNP) H2226-001 Look inside to learn more about the plan and the health and drug services it covers. Call Customer
Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx]
![Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx]](/thumbs/86/94175655.jpg "Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx]") Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx] Group Plan HMO Benefit
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx] Group Plan HMO Benefit
WILLIS KNIGHTON MEDICAL CENTER S2763 NON GRANDFATHERED PLAN BENEFIT SHEET
 BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Customized COB Dependents Children birth to 26 Filing Limit 12 months For employees that work in a WKHS location within the primary HealthPlus
BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Customized COB Dependents Children birth to 26 Filing Limit 12 months For employees that work in a WKHS location within the primary HealthPlus
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
Services Covered by Molina Healthcare
 Services Covered by Molina Healthcare Because you are covered by Medicaid, you pay nothing for covered services. As a Molina Healthcare member, you will continue to receive all medically necessary Medicaid-covered
Services Covered by Molina Healthcare Because you are covered by Medicaid, you pay nothing for covered services. As a Molina Healthcare member, you will continue to receive all medically necessary Medicaid-covered
Summary of Benefits. New Mexico Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, Sandoval, San Juan, Santa Fe, Sierra, Torrance and Valencia
 Summary of Benefits New Mexico Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, Sandoval, San Juan, Santa Fe, Sierra, Torrance and Valencia 2016 Molina Medicare Options Plus HMO SNP Member Services
Summary of Benefits New Mexico Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, Sandoval, San Juan, Santa Fe, Sierra, Torrance and Valencia 2016 Molina Medicare Options Plus HMO SNP Member Services
For full details of services and costs for each plan, please consult the Evidence of Coverage at GeisingerGold.com or call us for more information.
 This Summary of Benefits contains 2018 plan information for: Geisinger Gold Secure Rx (HMO SNP) For full details of services and costs for each plan, please consult the Evidence of Coverage at GeisingerGold.com
This Summary of Benefits contains 2018 plan information for: Geisinger Gold Secure Rx (HMO SNP) For full details of services and costs for each plan, please consult the Evidence of Coverage at GeisingerGold.com
Summary Of Benefits. Molina Medicare Options Plus (HMO SNP) (866) , TTY/TDD days a week, 8 a.m. 8 p.m. local time
 (866) , TTY/TDD days a week, 8 a.m. 8 p.m. local time") Summary Of Benefits OHIO Brown, Butler, Clark, Clermont, Clinton, Columbiana, Delaware, Fairfield, Fayette, Franklin, Greene, Hamilton, Highland, Hocking, Lake, Madison, Miami, Montgomery, Morrow, Perry,
Summary Of Benefits OHIO Brown, Butler, Clark, Clermont, Clinton, Columbiana, Delaware, Fairfield, Fayette, Franklin, Greene, Hamilton, Highland, Hocking, Lake, Madison, Miami, Montgomery, Morrow, Perry,
Summary of Benefits. for Blue Medicare Access Value SM (Regional PPO) Available in Ohio
 Available in Ohio") Summary of Benefits for SM Available in Ohio Anthem Blue Cross and Blue Shield is a Health plan with a Medicare contract.anthem Insurance Companies, Inc. (AICI) is the legal entity that has contracted
Summary of Benefits for SM Available in Ohio Anthem Blue Cross and Blue Shield is a Health plan with a Medicare contract.anthem Insurance Companies, Inc. (AICI) is the legal entity that has contracted
Summary of Benefits Report SENIOR CARE PLUS: VALUE BASIC PLAN (HMO)-009 January 1, 2015 December 31, 2015 WASHOE COUNTY, NEVADA
-009 January 1, 2015 December 31, 2015 WASHOE COUNTY, NEVADA") SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get your Medicare benefits One choice is to get your Medicare benefits through Original Medicare (fee-for-service Medicare).
SECTION I - INTRODUCTION TO SUMMARY OF BENEFITS You have choices about how to get your Medicare benefits One choice is to get your Medicare benefits through Original Medicare (fee-for-service Medicare).
Summary of Benefits For Advantage Health NY - SNP (HMO SNP)
") Summary of Benefits For Advantage Health NY - SNP January 1, 2014 December 31, 2014 Summary of Benefits, H2773-003 Advantage Health NY - SNP H2773_QHPNY0658 Accepted Advantage Health NY - SNP 1 SECTION
Summary of Benefits For Advantage Health NY - SNP January 1, 2014 December 31, 2014 Summary of Benefits, H2773-003 Advantage Health NY - SNP H2773_QHPNY0658 Accepted Advantage Health NY - SNP 1 SECTION
RSNA EMPLOYEE BENEFIT TRUST PLAN II S2502 NON GRANDFATHERED PLAN BENEFIT SHEET
 BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Standard COB Dependents Children birth to age 26 Filing Limit 1 year from date of service Mailing Address & PPO Company. Remit claims to:
BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Standard COB Dependents Children birth to age 26 Filing Limit 1 year from date of service Mailing Address & PPO Company. Remit claims to:
Summary Of Benefits. NEW MEXICO Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, San Juan, Sandoval, Santa Fe, Sierra, Torrance, and Valencia
 Summary Of Benefits NEW MEXICO Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, San Juan, Sandoval, Santa Fe, Sierra, Torrance, and Valencia 2018 Molina Medicare Options Plus (HMO SNP) (866) 440-0127,
Summary Of Benefits NEW MEXICO Bernalillo, Chaves, Dona Ana, Luna, McKinley, Otero, San Juan, Sandoval, Santa Fe, Sierra, Torrance, and Valencia 2018 Molina Medicare Options Plus (HMO SNP) (866) 440-0127,
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network & Out-of- Annual Deductible This is the amount you have to pay out of pocket before the plan will pay
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network & Out-of- Annual Deductible This is the amount you have to pay out of pocket before the plan will pay
Summary of Benefits Platinum Full PPO 0/10 OffEx
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Full PPO 0/10 OffEx Group Plan PPO Benefit Plan This Summary of Benefits shows the amount
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Full PPO 0/10 OffEx Group Plan PPO Benefit Plan This Summary of Benefits shows the amount
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA HEALTH PLANS INC.
 Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network Providers Annual Maximum Out-of-Pocket Amount $2,500 The maximum out-of-pocket limit applies to all
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network Providers Annual Maximum Out-of-Pocket Amount $2,500 The maximum out-of-pocket limit applies to all
Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Deductible
 $200 Deductible") BENEFIT HIGHLIGHTS 1 Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Group Effective Date December 1, 2017 Benefit Period (used for and Coinsurance limits) January 1 through December
BENEFIT HIGHLIGHTS 1 Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Group Effective Date December 1, 2017 Benefit Period (used for and Coinsurance limits) January 1 through December
Summary of Benefits Platinum Trio HMO 0/25 OffEx
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Trio HMO 0/25 OffEx Group Plan HMO Benefit Plan This Summary of Benefits shows the amount
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Trio HMO 0/25 OffEx Group Plan HMO Benefit Plan This Summary of Benefits shows the amount
Section I Introduction to Summary of Benefits
 Section I Introduction to Summary of Benefits Thank you for your interest in + Rx Classic (PPO) and. Our plans are offered by Regence BlueShield, a Medicare Advantage Preferred Provider Organization (PPO)
Section I Introduction to Summary of Benefits Thank you for your interest in + Rx Classic (PPO) and. Our plans are offered by Regence BlueShield, a Medicare Advantage Preferred Provider Organization (PPO)
Benefits. Benefits Covered by UnitedHealthcare Community Plan
 Benefits Covered by UnitedHealthcare Community Plan UnitedHealthcare provides all medically necessary covered services under Medicaid SSI. Some services may require a prior authorization. Specific covered
Benefits Covered by UnitedHealthcare Community Plan UnitedHealthcare provides all medically necessary covered services under Medicaid SSI. Some services may require a prior authorization. Specific covered
Summary of Benefits Prominence Preferred Health Insurance Small Group Health Plan
 Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family $3,000 Single / $9,000 Family Coinsurance - Member responsibility 20% coinsurance 50% coinsurance Out-of-Pocket Maximum 3 - Deductibles, coinsurance
Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family $3,000 Single / $9,000 Family Coinsurance - Member responsibility 20% coinsurance 50% coinsurance Out-of-Pocket Maximum 3 - Deductibles, coinsurance
Summary Of Benefits. FLORIDA Broward, Hillsborough, Miami-Dade, Palm Beach, Pinellas, and Polk
 Summary Of Benefits FLORIDA Broward, Hillsborough, Miami-Dade, Palm Beach, Pinellas, and Polk 2018 Molina Medicare Options Plus (HMO SNP) (866) 553-9494, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local
Summary Of Benefits FLORIDA Broward, Hillsborough, Miami-Dade, Palm Beach, Pinellas, and Polk 2018 Molina Medicare Options Plus (HMO SNP) (866) 553-9494, TTY/TDD 711 7 days a week, 8 a.m. 8 p.m. local
Covered Benefits Rhody Health Partners ACA Adult Expansion
 Covered s Rhody Health Partners ACA Adult Expansion Abortion Services Adult Day Services AIDS Medical and Non-Medical Case Management Alcohol and Substance Abuse Treatment Cosmetic Surgery Dental Care
Covered s Rhody Health Partners ACA Adult Expansion Abortion Services Adult Day Services AIDS Medical and Non-Medical Case Management Alcohol and Substance Abuse Treatment Cosmetic Surgery Dental Care
Highlights of your Health Care Coverage
 Highlights of your Health Care Coverage Any deductibles, copays, and coinsurance percentages shown are amounts for which you're responsible. Medical Benefits apply after the calendar-year deductible is
Highlights of your Health Care Coverage Any deductibles, copays, and coinsurance percentages shown are amounts for which you're responsible. Medical Benefits apply after the calendar-year deductible is
Excellus Blue PPO Signature Hybrid 1
 Excellus Blue PPO Signature Hybrid 1 Drug Coverage Excluded Benefit Time Period: 03/01/2018-12/31/2018 Trinity Health - Syracuse Traditional General Cost Sharing Expenses Deductible - Single $250 $750
Excellus Blue PPO Signature Hybrid 1 Drug Coverage Excluded Benefit Time Period: 03/01/2018-12/31/2018 Trinity Health - Syracuse Traditional General Cost Sharing Expenses Deductible - Single $250 $750
Excellus BluePPO Signature Deduct 3
 Excellus BluePPO Signature Deduct 3 Drug Coverage Excluded Benefit Time Period: 03/01/2018-12/31/2018 Trinity Health - Syracuse HSA General Cost Sharing Expenses - Single $1,500 $2,500 $3,500 - Two Person
Excellus BluePPO Signature Deduct 3 Drug Coverage Excluded Benefit Time Period: 03/01/2018-12/31/2018 Trinity Health - Syracuse HSA General Cost Sharing Expenses - Single $1,500 $2,500 $3,500 - Two Person
UNIVERSITY OF THE CUMBERLANDS MEDICAL BENEFITS SCHEDULE
 November 1, 2016 UNIVERSITY OF THE CUMBERLANDS MEDICAL BENEFITS SCHEDULE NETWORK NON-NETWORK Lifetime Maximum Benefit Unlimited Unlimited Annual Deductible (Single/Family) $500/$1,000 $1,000/$2,000 Maximum
November 1, 2016 UNIVERSITY OF THE CUMBERLANDS MEDICAL BENEFITS SCHEDULE NETWORK NON-NETWORK Lifetime Maximum Benefit Unlimited Unlimited Annual Deductible (Single/Family) $500/$1,000 $1,000/$2,000 Maximum
Summary Of Benefits. IDAHO Ada, Bannock, Bingham, Bonner, Bonneville, Canyon, Kootenai, Nez Perce, and Twin Falls
 Summary Of Benefits IDAHO Ada, Bannock, Bingham, Bonner, Bonneville, Canyon, Kootenai, Nez Perce, and Twin Falls 2018 Molina Medicare Options Plus (HMO SNP) (844) 239-4913, TTY/TDD 711 7 days a week, 8
Summary Of Benefits IDAHO Ada, Bannock, Bingham, Bonner, Bonneville, Canyon, Kootenai, Nez Perce, and Twin Falls 2018 Molina Medicare Options Plus (HMO SNP) (844) 239-4913, TTY/TDD 711 7 days a week, 8
WHAT DOES MEDICALLY NECESSARY MEAN?
 WHAT DOES MEDICALLY NECESSARY MEAN? Your Primary Care Provider (PCP) will help you get the services you need that are medically necessary as defined below. Medically Necessary means appropriate and necessary
WHAT DOES MEDICALLY NECESSARY MEAN? Your Primary Care Provider (PCP) will help you get the services you need that are medically necessary as defined below. Medically Necessary means appropriate and necessary
Summary of Benefits. for Anthem Medicare Preferred Premier (PPO)
") Summary of Benefits for Available in Androscoggin, Cumberland, Franklin, Hancock, Kennebec, Lincoln, Oxford, Penobscot, Piscataquis, Sagadahoc, Somerset, Waldo, and Washington Counties, ME Anthem Blue
Summary of Benefits for Available in Androscoggin, Cumberland, Franklin, Hancock, Kennebec, Lincoln, Oxford, Penobscot, Piscataquis, Sagadahoc, Somerset, Waldo, and Washington Counties, ME Anthem Blue
Benefits are effective January 01, 2017 through December 31, 2017
 Benefits are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of- Annual Deductible $0 This is the amount
Benefits are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of- Annual Deductible $0 This is the amount
CONRAD INDUSTRIES, INC. S2489 NON GRANDFATHERED PLAN BENEFIT SHEET
 BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Standard COB Dependents Children to age 26 Filing Limit 12 months from date of service Mailing Address & PPO Company. PPO Co.: PPO CIGNA
BENEFIT SHEET GENERAL PLAN INFORMATION Coordination of Benefits Standard COB Dependents Children to age 26 Filing Limit 12 months from date of service Mailing Address & PPO Company. PPO Co.: PPO CIGNA
BCBSM provides administrative claims services only. Your employer or plan sponsor is financially responsible for claims.
 Michigan Catholic Conference Group Number: 71755 Package Code(s): 010 Section Code(s): 1000, 2000 PPO - PPO1, Hearing, Vision ( Exam only) Effective Date: 01/01/2018 Benefits-at-a-glance This is intended
Michigan Catholic Conference Group Number: 71755 Package Code(s): 010 Section Code(s): 1000, 2000 PPO - PPO1, Hearing, Vision ( Exam only) Effective Date: 01/01/2018 Benefits-at-a-glance This is intended
Select Summ ary. VIVA MEDICARE Plus Select (HMO) INTRODUCTION TO THE SUMMARY OF BENEFITS FOR. You have choices in your health care.
 INTRODUCTION TO THE SUMMARY OF BENEFITS FOR. You have choices in your health care.") INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE Plus January 1, 2013 - December 31, 2013 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc./,
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE Plus January 1, 2013 - December 31, 2013 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc./,
Aetna Health of California, Inc.
 Easily locate PrimeCare participating providers at www.aetna.com/docfind/primecare PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral
Easily locate PrimeCare participating providers at www.aetna.com/docfind/primecare PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral
2018 Summary of Benefits Eon Deluxe (HMO SNP) GEORGIA / SOUTH CAROLINA
 GEORGIA / SOUTH CAROLINA") 2018 Summary of Eon Deluxe (HMO SNP) GEORGIA / SOUTH CAROLINA For more information, call 1-844-895-8643 Y0122_0172 Accepted DSNP This page intentionally left blank 2018 Summary of Eon Deluxe (HMO SNP)
2018 Summary of Eon Deluxe (HMO SNP) GEORGIA / SOUTH CAROLINA For more information, call 1-844-895-8643 Y0122_0172 Accepted DSNP This page intentionally left blank 2018 Summary of Eon Deluxe (HMO SNP)
VIVA MEDICARE Select (HMO)
") INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE January 1, 2014 - December 31, 2014 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc., which
INTRODUCTION TO THE SUMMARY OF BENEFITS FOR VIVA MEDICARE January 1, 2014 - December 31, 2014 Central Alabama and Mobile Area Thank you for your interest in. Our plan is offered by Viva Health, Inc., which
Explorer Plan (HMO-POS) SunSaver Plan (HMO-POS)
 SunSaver Plan (HMO-POS)") January 1, 2016 December 31, 2016 Explorer Plan SunSaver Plan SECTION I INTRODUCTION This booklet gives you a summary of what we cover and what you pay. It doesn't list every service that we cover or list
January 1, 2016 December 31, 2016 Explorer Plan SunSaver Plan SECTION I INTRODUCTION This booklet gives you a summary of what we cover and what you pay. It doesn't list every service that we cover or list
Our service area includes these counties in: Texas: Aransas, Kleberg, Nueces, San Patricio.
 2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Dual Complete Focus (HMO SNP) H4527-004 Look inside to learn more about the health services and drug coverages the plan provides. Call Customer
2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Dual Complete Focus (HMO SNP) H4527-004 Look inside to learn more about the health services and drug coverages the plan provides. Call Customer
CO-PAYMENT BOOK Las Vegas Blvd. South Suite 107 Las Vegas, NV
 CO-PAYMENT BOOK 1901 Las Vegas Blvd. South Suite 107 Las Vegas, NV 89104 702-733-9938 www.culinaryhealthfund.org Revised January 2018 (Replaces Co-Payment Book dated June 2017) TABLE OF CONTENTS 4 5 6
CO-PAYMENT BOOK 1901 Las Vegas Blvd. South Suite 107 Las Vegas, NV 89104 702-733-9938 www.culinaryhealthfund.org Revised January 2018 (Replaces Co-Payment Book dated June 2017) TABLE OF CONTENTS 4 5 6
H1463-HMO 20 (HMO) HMO 20 (HMO) / HMO 20Rx (HMO) Summary of Benefits
 HMO 20 (HMO) / HMO 20Rx (HMO) Summary of Benefits") H1463- / Summary of Benefits January 1, 2014 December 31, 2014 Call us 8 a.m. to 8 p.m. daily Toll-free 1-800-965-4022 TTY/TDD 1-800-526-0844 www.healthalliancemedicare.org med-hmo20sob-0713 H1463_14_8837
H1463- / Summary of Benefits January 1, 2014 December 31, 2014 Call us 8 a.m. to 8 p.m. daily Toll-free 1-800-965-4022 TTY/TDD 1-800-526-0844 www.healthalliancemedicare.org med-hmo20sob-0713 H1463_14_8837