Measure #138: Melanoma: Coordination of Care National Quality Strategy Domain: Communication and Care Coordination
|
|
|
- Candice Paul
- 6 years ago
- Views:
Transcription
1 Measure #138: Melanoma: Coordination of Care National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage of patient visits, regardless of age, with a new occurrence of melanoma that have a treatment plan documented in the chart that was communicated to the physician(s) providing continuing care within one month of diagnosis INSTRUCTIONS: This measure is to be reported at each denominator eligible visit occurring during the performance period ending November 30 th for melanoma patients seen during the performance period. It is anticipated that eligible clinicians providing care for patients with melanoma will submit this measure. Measure Reporting: The listed denominator criteria is used to identify the intended patient population. The numerator options included in this specification are used to submit the quality actions allowed by the measure. The quality-data codes listed do not need to be submitted for registry-based submissions; however, these codes may be submitted for those registries that utilize claims data. THERE ARE TWO REPTING CRITERIA F THIS MEASURE: 1) All visits for patients, regardless of age, diagnosed with a new occurrence of melanoma during excision of malignant lesion 2) All visits for patients, regardless of age, diagnosed with a new occurrence of melanoma evaluated in an outpatient setting REPTING CRITERIA 1: ALL VISITS F PATIENTS, REGARDLESS OF AGE, DIAGNOSED WITH A NEW OCCURRENCE OF MELANOMA DURING EXCISION OF MALIGNANT LESION DENOMINAT (REPTING CRITERIA 1) All visits for patients, regardless of age, diagnosed with a new occurrence of melanoma Denominator Criteria (Eligible Cases) 1: Diagnosis for melanoma (ICD-10-CM): C43.0, C43.10, C43.11, C43.12, C43.20, C43.21, C43.22, C43.30, C43.31, C43.39, C43.4, C43.51, C43.52, C43.59, C43.60, C43.61, C43.62, C43.70, C43.71, C43.72, C43.8, C43.9, D03.0, D03.10, D03.11, D03.12, D03.20, D03.21, D03.22, D03.30, D03.39, D03.4, D03.51, D03.52, D03.59, D03.60, D03.61, D03.62, D03.70, D03.71, D03.72, D03.8, D03.9 AND Patient encounter for excision of malignant melanoma (CPT): 11600, 11601, 11602, 11603, 11604, 11606, 11620, 11621, 11622, 11623, 11624, 11626, 11640, 11641, 11642, 11643, 11644, 11646, 14000, 14001, 14020, 14021, 14040, 14041, 14060, 14061, 14301, 17311, of 10 12
2 NUMERAT (REPTING CRITERIA 1): Patient visits with a treatment plan documented in the chart that was communicated to the physician(s) providing continuing care within one month of diagnosis Numerator Instructions: A treatment plan should include the following elements: diagnosis, tumor thickness, and plan for surgery or alternate care. Definition: Communication Communication may include: documentation in the medical record that the physician(s) treating the melanoma communicated (e.g., verbally, by letter, copy of treatment plan sent) with the physician(s) providing the continuing care a copy of a letter in the medical record outlining whether the patient was or should be treated for melanoma. Numerator Options: Performance Met: Denominator Exception: Denominator Exception: Performance Not Met: Treatment plan communicated to provider(s) managing continuing care within 1 month of diagnosis (5050F) Documentation of patient reason(s) for not communicating treatment plan to the Primary Care Physician(s) (PCP)(s) (eg, patient asks that treatment plan not be communicated to the physician(s) providing continuing care) (5050F with 2P) Documentation of system reason(s) for not communicating treatment plan to the PCP(s) (eg, patient does not have a primary care physician or referring physician) (5050F with 3P) Treatment plan not communicated, reason not otherwise specified (5050F with 8P) REPTING CRITERIA 2: ALL VISITS F PATIENTS, REGARDLESS OF AGE, DIAGNOSED WITH A NEW OCCURRENCE OF MELANOMA EVALUATED IN AN OUTPATIENT SETTING DENOMINAT: (REPTING CRITERIA 2) All visits for patients, regardless of age, diagnosed with a new occurrence of melanoma Denominator Criteria (Eligible Cases) 2: Diagnosis for melanoma (ICD-10-CM): C43.0, C43.10, C43.11, C43.12, C43.20, C43.21, C43.22, C43.30, C43.31, C43.39, C43.4, C43.51, C43.52, C43.59, C43.60, C43.61, C43.62, C43.70, C43.71, C43.72, C43.8, C43.9, D03.0, D03.10, D03.11, D03.12, D03.20, D03.21, D03.22, D03.30, D03.39, D03.4, D03.51, D03.52, D03.59, D03.60, D03.61, D03.62, D03.70, D03.71, D03.72, D03.8, D03.9 AND Patient encounter during the performance period (CPT): 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, WITHOUT Telehealth Modifier: GQ, GT NUMERAT (REPTING CRITERIA 2): Patient visits with a treatment plan documented in the chart that was communicated to the physician(s) providing continuing care within one month of diagnosis 2 of 12
3 Numerator Instructions: A treatment plan should include the following elements: diagnosis, tumor thickness, and plan for surgery or alternate care. Definition: Communication Communication may include: documentation in the medical record that the physician(s) treating the melanoma communicated (e.g., verbally, by letter, copy of treatment plan sent) with the physician(s) providing the continuing care a copy of a letter in the medical record outlining whether the patient was or should be treated for melanoma. Numerator Options: Performance Met: Denominator Exception: Denominator Exception: Performance Not Met: Treatment plan communicated to provider(s) managing continuing care within 1 month of diagnosis (5050F) Documentation of patient reason(s) for not communicating treatment plan to the Primary Care Physician(s) (PCP)(s) (eg, patient asks that treatment plan not be communicated to the physician(s) providing continuing care) (5050F with 2P) Documentation of system reason(s) for not communicating treatment plan to the PCP(s) (eg, patient does not have a primary care physician or referring physician) (5050F with 3P) Treatment plan not communicated, reason not otherwise specified (5050F with 8P) RATIONALE: Perceived lack of follow-up with primary care providers which is reinforced in the Institute of Medicine (IOM) report on patient errors. The intention of this measure is to enable the primary care provider to support, facilitate, and coordinate the care of the patient. Deficits in communication have clearly been shown to adversely affect post-discharge care transitions. A recent summary of the literature found that direct communication between hospital physicians and primary care physicians occurs infrequently (in 3%-20% of cases studied), the availability of a discharge summary at the first post-discharge visit is low (12%-34%) and did not improve greatly even after 4 weeks (51%-77%), affecting the quality of care in approximately 25% of follow-up visits. This systematic review of the literature also found that discharge summaries often lack important information such as diagnostic test results, treatment or hospital course, discharge medications, test results pending at discharge, patient or family counseling, and follow-up plans. CLINICAL RECOMMENDATION STATEMENTS: Each local skin cancer multi-disciplinary team (LSMDT) and specialist skin cancer multi-disciplinary team (SSMDT) should have at least one skin cancer clinical nurse specialist (CNS) who will play a leading role in supporting patients and caregivers. There should be equity of access to information and support regardless of where the care is delivered. A checklist may be used by healthcare professionals to remind them to give patients and caregivers the information they need in an appropriate format for pre-diagnosis, diagnosis, treatment, follow-up, and palliative care. This may also include a copy of the letter confirming the diagnosis and treatment plan sent by the consultant to the general practitioner (GP). Provide a rapid referral service for patients who require specialist management through the LSMDT/SSMDT. Be responsible for the provision of information, advice, and support for patients managed in primary care and their care givers. 3 of 10 12
4 Maintain a register of all patients treated, whose care should be part of a regular audit presented to the LSMDT/SSMDT. Liaise and communicate with all members of the skin cancer site-specific network group. Ensure that referring GPs are given prompt and full information about their patients diagnosis or treatment in line with national standards on communication to GPs of cancer diagnoses. Collect data for network-wide audit. (NICE, 2006) Communication and information exchange between the medical home and the receiving provider should occur in an amount of time that will allow the receiving provider to effectively treat the patient. This communication and information exchange should ideally occur whenever patients are at a transition of care; eg, at discharge from the inpatient setting. The timeliness of this communication should be consistent with the patient s clinical presentation and, in the case of a patient being discharged, the urgency of the follow-up required. Communication and information exchange between the MD and other physicians may be in the form of a call, voic , fax or other secure, private, and accessible means including mutual access to an EHR. The TOCCC proposed a minimal set of data elements that should always be part of the transition record and be part of any initial implementation of this standard. That list includes the following: Principle diagnosis and problem list Medication list (reconciliation) including over the counter/ herbals, allergies and drug interactions Clearly identifies the medical home/transferring coordinating physician/institution and their contact information Patient s cognitive status Test results/pending results The TOCCC recommended the following additional elements that should be included in an ideal transition record in addition to the above: Emergency plan and contact number and person Treatment and diagnostic plan Prognosis and goals of care Advance directives, power of attorney, consent Planned interventions, durable medical equipment, wound care, etc. Assessment of caregiver status Patients and/or their family/caregivers must receive, understand and be encouraged to participate in the development of their transition record which should take into consideration the patient s health literacy, insurance status and be culturally sensitive. (ACP, SGIMSHM, AGS, ACEP, SAEM, 2009) (Consensus Policy Statement) COPYRIGHT: This Measure is not a clinical guideline, does not establish a standard of medical care, and has not been tested for all potential applications. This Measure, while copyrighted, can be reproduced and distributed, without modification, for noncommercial purposes, e.g., use by health care providers in connection with their practices. Commercial use is defined as the sale, license, or distribution of the Measure for commercial gain, or incorporation of the Measure into a product or service that is sold, licensed or distributed for commercial gain. Commercial use of this measure requires a license agreement between the user and the American Academy of Dermatology (AAD). Neither the AAD nor its members shall be responsible for any use of the Measure. AAD encourages use of this Measure by other health care professionals, where appropriate. THE MEASURES AND SPECIFICATIONS ARE PROVIDED AS IS WITHOUT WARRANTY OF ANY KIND. 4 of 10 12
5 2014 American Medical Association and the American Academy of Dermatology. All Rights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use. Limited proprietary coding is contained in the Measure specifications for convenience. Users of the proprietary code sets should obtain all necessary licenses from the owners of these code sets. The AAD and its members disclaim all liability for use or accuracy of any Current Procedural Terminology (CPT ) or other coding contained in the specifications. CPT contained in the Measures specifications is copyright American Medical Association. LOINC copyright Regenstrief Institute, Inc. SNOMED CLINICAL TERMS (SNOMED CT ) copyright College of American Pathologists. All Rights Reserved. 5 of 10 12
6 6 of 12
7 7 of 12
8 68 of 10 12
9 2017 Registry Individual Measure Flow #138: Melanoma: Coordination of Care Please refer to the specific section of the Measure Specification to identify the denominator and numerator information for use in reporting this Individual Measure. Reporting Criteria One 1. Start with Denominator 2. Check Patient Diagnosis: a. If Diagnosis of New Occurrence of Melanoma as Listed in the Denominator equals No, do not include in Eligible Patient Population. Stop Processing. b. If Diagnosis of New Occurrence of Melanoma as Listed in the Denominator equals Yes, proceed to check Excision of Malignant Melanoma as listed in the denominator. 3. Check Excision of Malignant Melanoma as Listed in the Denominator: a. If Excision of Malignant Melanoma as Listed in the Denominator equals No, do not include in Eligible Patient Population. Stop Processing. b. If Excision of Malignant Melanoma in the Denominator equals Yes, include in the Eligible population. 4. Denominator Population: a. Denominator population is all Eligible Patients in the denominator. Denominator is represented as Denominator in the Sample Calculation listed at the end of this document. Letter d1 equals 8 visits in the sample calculation. 5. Start Numerator 6. Check Treatment Plan Communicated to Provider Managing Continuing Care within 1 Month of Diagnosis: a. If Treatment Plan Communicated to Provider Managing Continuing Care within 1 Month of Diagnosis equals Yes, include in Data Completeness Met and Performance Met. b. Data Completeness Met and Performance Met letter is represented in the Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter a1 equals 4 visits in Sample Calculation. c. If Treatment Plan Communicated to Provider Managing Continuing Care within 1 Month of Diagnosis equals No, proceed to Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s). 7. Check Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s): a. If Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s)equals Yes, include in Data Completeness Met and Denominator Exception. b. Data Completeness Met and Denominator Exception letter is represented in the Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter b1 equals 1 visit in the Sample Calculation. 9 of 12
10 c. If Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s)equals No, proceed to Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s). 8. Check Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s): a. If Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s) equals Yes, include in Data Completeness Met and Denominator Exception. b. Data Completeness Met and Denominator Exception letter is represented in the Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter b2 equals 0 visits in the Sample Calculation. c. If Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s) equals No, proceed to Treatment Plan Not Communicated, Reason Not Specified. 9. Check Treatment Plan Not Communicated, Reason Not Specified: a. If Treatment Plan Not Communicated, Reason Not Specified equals Yes, include in the Data Completeness Met and Performance Not Met. b. Data Completeness Met and Performance Not Met letter is represented in the Data Completeness in the Sample Calculation listed at the end of this document. Letter c1 equals 2 visits in the Sample Calculation. c. If Treatment Plan Not Communicated, Reason Not Specified equals No, proceed to Data Completeness Not Met. 10. Check Data Completeness Not Met: a. If Data Completeness Not Met equals No, Quality Data Code or equivalent not reported. 1 visit has been subtracted from the data completeness numerator in the sample calculation. 10 of 12
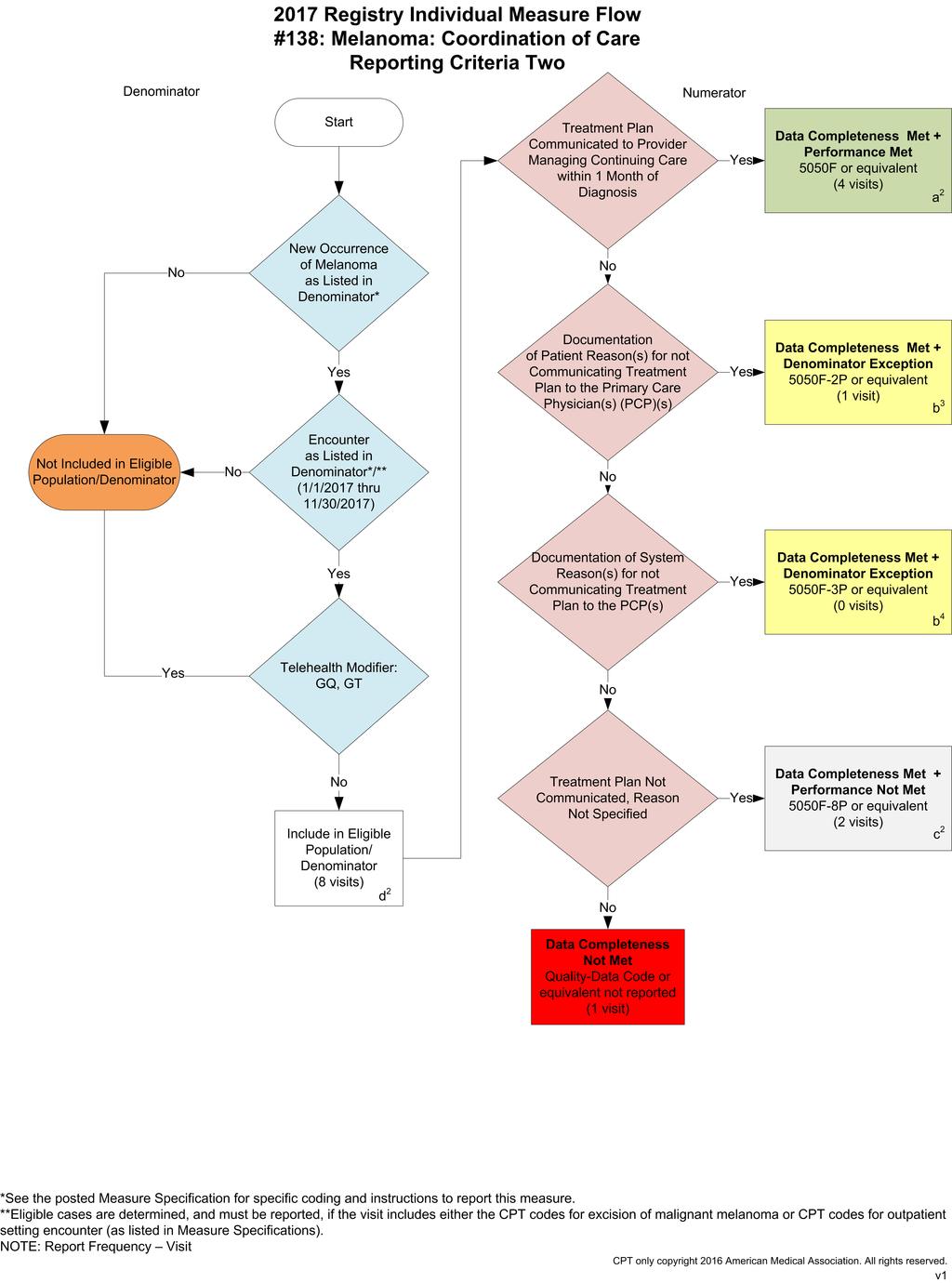
11 2017 Registry Individual Measure Flow #138: Melanoma: Coordination of Care Please refer to the specific section of the Measure Specification to identify the denominator and numerator information for use in reporting this Individual Measure. Reporting Criteria Two 1. Start with Denominator 2. Check Patient Diagnosis: a. If New Occurrence of Melanoma as Listed in the Denominator equals No, do not include in Eligible Patient Population. Stop Processing. b. If New Occurrence of Melanoma as Listed in the Denominator equals Yes, proceed to check Encounter Performed. 3. Check Encounter Performed: a. If Encounter as listed in the denominator equals No, do not include in Eligible Patient Population. Stop Processing. b. If Encounter as listed in the denominator equals Yes, check Telehealth Modifier. 4. Check Telehealth Modifier: a. If Telehealth Modifier equals Yes, do not include in Eligible Patient Population. Stop Processing. b. If Telehealth Modifier equals No, include in the Eligible population. 5. Denominator Population: a. Denominator population is all Eligible Patients in the denominator. Denominator is represented as Denominator in the Sample Calculation listed at the end of this document. Letter d2 equals 8 visits in the sample calculation. 6. Start Numerator 7. Check Treatment Plan Communicated to Provider Managing Continuing Care within 1 Month of Diagnosis: a. If Treatment Plan Communicated to Provider Managing Continuing Care within 1 Month of Diagnosis equals Yes, include in Data Completeness Met and Performance Met. b. Data Completeness Met and Performance Met letter is represented in the Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter a1 equals 4 visits in Sample Calculation. c. If Treatment Plan Communicated to Provider Managing Continuing Care within 1 Month of Diagnosis equals No, proceed to Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s). 8. Check Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s): 119 of 10 12

12 a. If Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s)equals Yes, include in Data Completeness Met and Denominator Exception. b. Data Completeness Met and Denominator Exception letter is represented in the Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter b1 equals 1 visit in the Sample Calculation. c. If Documentation of Patient Reason(s) for not Communicating Treatment Plan to the Primary Care Physician(s) (PCP)(s)equals No, proceed to Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s). 9. Check Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s): a. If Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s) equals Yes, include in Data Completeness Met and Denominator Exception. b. Data Completeness Met and Denominator Exception letter is represented in the Data Completeness and Performance Rate in the Sample Calculation listed at the end of this document. Letter b2 equals 0 visits in the Sample Calculation. c. If Documentation of System Reason(s) for not Communicating Treatment Plan to the PCP(s) equals No, proceed to Treatment Plan Not Communicated, Reason Not Specified. 10. Check Treatment Plan Not Communicated, Reason Not Specified: a. If Treatment Plan Not Communicated, Reason Not Specified equals Yes, include in the Data Completeness Met and Performance Not Met. b. Data Completeness Met and Performance Not Met letter is represented in the Data Completeness in the Sample Calculation listed at the end of this document. Letter c1 equals 2 visits in the Sample Calculation. c. If Treatment Plan Not Communicated, Reason Not Specified equals No, proceed to Data Completeness Not Met. 11. Check Data Completeness Not Met: a. If Data Completeness Not Met equals No, Quality Data Code or equivalent not reported. 1 visit has been subtracted from the data completeness numerator in the sample calculation of 10 12
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination
: Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination") Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #137 (NQF 0650): Melanoma: Continuity of Care Recall System National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #288: Dementia: Caregiver Education and Support National Quality Strategy Domain: Communication and Care Coordination
 Quality ID #288: Dementia: Caregiver Education and Support National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #288: Dementia: Caregiver Education and Support National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #286: Dementia: Safety Concerns Screening and Mitigation Recommendations or Referral for Patients with Dementia National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #286: Dementia: Safety Concerns Screening and Mitigation Recommendations or Referral for Patients with Dementia National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #374: Closing the Referral Loop: Receipt of Specialist Report National Quality Strategy Domain: Effective Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Quality ID #374: Closing the Referral Loop: Receipt of Specialist Report National Quality Strategy Domain: Effective Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Measure #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
Measure #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
Quality ID #427: Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU) National Quality Strategy Domain: Communication
Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination
: Care Plan National Quality Strategy Domain: Communication and Care Coordination") Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Quality ID#141 (NQF 0563): Primary Open-Angle Glaucoma (POAG): Reduction of Intraocular Pressure (IOP) by 15% OR Documentation of a Plan of Care National Quality Strategy Domain: Communication and Care
Quality ID#141 (NQF 0563): Primary Open-Angle Glaucoma (POAG): Reduction of Intraocular Pressure (IOP) by 15% OR Documentation of a Plan of Care National Quality Strategy Domain: Communication and Care
DENOMINATOR: All final reports for patients, regardless of age, undergoing a CT procedure
 Quality ID #361: Optimizing Patient Exposure to Ionizing Radiation: Reporting to a Radiation Dose Index Registry National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #361: Optimizing Patient Exposure to Ionizing Radiation: Reporting to a Radiation Dose Index Registry National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
DENOMINATOR: All final reports for patients, regardless of age, undergoing a CT procedure
 Quality ID #362: Optimizing Patient Exposure to Ionizing Radiation: Computed Tomography (CT) Images Available for Patient Follow-up and Comparison Purposes National Quality Strategy Domain: Communication
Quality ID #362: Optimizing Patient Exposure to Ionizing Radiation: Computed Tomography (CT) Images Available for Patient Follow-up and Comparison Purposes National Quality Strategy Domain: Communication
Quality ID #424 (NQF 2681): Perioperative Temperature Management National Quality Strategy Domain: Patient Safety
: Perioperative Temperature Management National Quality Strategy Domain: Patient Safety") Quality ID #424 (NQF 2681): Perioperative Temperature Management National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #424 (NQF 2681): Perioperative Temperature Management National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Note: This is an outcome measure and will be calculated solely using registry data.
 Quality ID #304: Cataracts: Patient Satisfaction within 90 Days Following Cataract Surgery National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL
Quality ID #304: Cataracts: Patient Satisfaction within 90 Days Following Cataract Surgery National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL
Quality ID #426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 537 of 593
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
Measure #389: Cataract Surgery: Difference Between Planned and Final Refraction - National Quality Stategy Domain: Effective Clinical Care
 Measure #389: Cataract Surgery: Difference Between Planned and Final Refraction - National Quality Stategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #389: Cataract Surgery: Difference Between Planned and Final Refraction - National Quality Stategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety
: Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety") Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Note: This is an outcome measure and will be calculated solely using registry data.
 Measure #384: Adult Primary Rhegmatogenous Retinal Detachment Surgery: No Return to the Operating Room Within 90 Days of Surgery National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS
Measure #384: Adult Primary Rhegmatogenous Retinal Detachment Surgery: No Return to the Operating Room Within 90 Days of Surgery National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS
Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure National Quality Strategy Domain: Effective Clinical Care
 Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
American College of Physicians Council of Subspecialty Societies (CSS) Patient-Centered Medical Home (PCMH) Workgroup
 Patient-Centered Medical Home (PCMH) Workgroup") American College of Physicians Council of Subspecialty Societies (CSS) Patient-Centered Medical Home (PCMH) Workgroup PRINCIPLES OF SERVICE AGREEMENTS BETWEEN PATIENT CENTERED MEDICAL HOMES (PCMH) AND
American College of Physicians Council of Subspecialty Societies (CSS) Patient-Centered Medical Home (PCMH) Workgroup PRINCIPLES OF SERVICE AGREEMENTS BETWEEN PATIENT CENTERED MEDICAL HOMES (PCMH) AND
Measure #181: Elder Maltreatment Screen and Follow-Up Plan National Quality Strategy Domain: Patient Safety
 Measure #181: Elder Maltreatment Screen and Follow-Up Plan National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients
Measure #181: Elder Maltreatment Screen and Follow-Up Plan National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients
ED Transfer Communication
 ED Transfer Communication USING DATA TO DRIVE IMPROVEMENT! EDTC-4: Medication information June 16 th 2016 Presented By: Shanelle Van Dyke Agenda EDTC 4 Measure Overview Review of Data Results Discussion
ED Transfer Communication USING DATA TO DRIVE IMPROVEMENT! EDTC-4: Medication information June 16 th 2016 Presented By: Shanelle Van Dyke Agenda EDTC 4 Measure Overview Review of Data Results Discussion
2011 Melanoma Physician Quality Reporting (PQRS): FREQUENTLY ASKED QUESTIONS
: FREQUENTLY ASKED QUESTIONS") Q: What is the Physician Quality Reporting System? A: The Physician Quality Reporting System, formerly known as PQRI, is a program developed by the Centers for Medicare and Medicaid Services (CMS) to provide
Q: What is the Physician Quality Reporting System? A: The Physician Quality Reporting System, formerly known as PQRI, is a program developed by the Centers for Medicare and Medicaid Services (CMS) to provide
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification. 001 Service Commissioner Lead Contracting Lead Provider Lead Period Teledermoscopy Service Dr Nicholas Rayner and Dr Andrew Yager
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification. 001 Service Commissioner Lead Contracting Lead Provider Lead Period Teledermoscopy Service Dr Nicholas Rayner and Dr Andrew Yager
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Quality Data Model December 2012
 Quality Data Model December 2012 Chris Millet, MS Senior Project Manager, Health IT Juliet Rubini, RN-BC, MSN, MSIS Senior Project Manager, Health IT Agenda 12:00 pm Welcome and Introductions 12:05 pm
Quality Data Model December 2012 Chris Millet, MS Senior Project Manager, Health IT Juliet Rubini, RN-BC, MSN, MSIS Senior Project Manager, Health IT Agenda 12:00 pm Welcome and Introductions 12:05 pm
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Possible Denominator Codes Applicable to OMS * Le Fort Fractures 21346, 21347, 21348, 21422, 21423, 21432, 21433, 21435, 21436
 Individual PQRS s Eligible OMS #20: #22: Perioperative Care: Timing of Antibiotic Prophylaxis Ordering Physician. Percentage of surgical patients aged 18 years and older undergoing procedures with the
Individual PQRS s Eligible OMS #20: #22: Perioperative Care: Timing of Antibiotic Prophylaxis Ordering Physician. Percentage of surgical patients aged 18 years and older undergoing procedures with the
2011 Electronic Prescribing Incentive Program
 2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
2010 PQRI REPORTING OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #193: Perioperative Temperature Management 2010 PQRI REPTING OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients, regardless of age, undergoing surgical or therapeutic
Measure #193: Perioperative Temperature Management 2010 PQRI REPTING OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients, regardless of age, undergoing surgical or therapeutic
Quality Data Model (QDM) Style Guide. QDM (version MAT) for Meaningful Use Stage 2
 Style Guide. QDM (version MAT) for Meaningful Use Stage 2") Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Terminology in Healthcare and
 Terminology in Healthcare and Public Health Settings Unit 17-Clinical Vocabularies This material was developed by The University of Alabama at Birmingham, funded by the Department of Health and Human Services,
Terminology in Healthcare and Public Health Settings Unit 17-Clinical Vocabularies This material was developed by The University of Alabama at Birmingham, funded by the Department of Health and Human Services,
Physician Hospital/SNF Collaborative Guidelines
 Overview Physician Hospital/SNF Collaborative Guidelines Effective coordination of care is an essential element in any successful health care system and this element requires the willingness of specialists,
Overview Physician Hospital/SNF Collaborative Guidelines Effective coordination of care is an essential element in any successful health care system and this element requires the willingness of specialists,
I. LIVE INTERACTIVE TELEDERMATOLOGY
 Position Statement on Teledermatology (Approved by the Board of Directors: February 22, 2002; Amended by the Board of Directors: May 22, 2004; November 9, 2013; August 9, 2014; May 16, 2015; March 7, 2016)
Position Statement on Teledermatology (Approved by the Board of Directors: February 22, 2002; Amended by the Board of Directors: May 22, 2004; November 9, 2013; August 9, 2014; May 16, 2015; March 7, 2016)
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
SURGICAL ONCOLOGY MCVH
 SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
Stage 1 Meaningful Use Objectives and Measures
 Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Chronic Care Management Services. Presented by Noridian Part B Medicare Provider Outreach and Education April 2015
 Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
EMERGENCY CARE DISCHARGE SUMMARY
 EMERGENCY CARE DISCHARGE SUMMARY IMPLEMENTATION GUIDANCE JUNE 2017 Guidance for implementation This section sets out issues identified during the project which relate to implementation of the headings.
EMERGENCY CARE DISCHARGE SUMMARY IMPLEMENTATION GUIDANCE JUNE 2017 Guidance for implementation This section sets out issues identified during the project which relate to implementation of the headings.
Quality ID #348: HRS-3 Implantable Cardioverter-Defibrillator (ICD) Complications Rate National Quality Strategy Domain: Patient Safety
 Complications Rate National Quality Strategy Domain: Patient Safety") Quality ID #348: HRS-3 Implantable Cardioverter-Defibrillator (ICD) Complications Rate National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #348: HRS-3 Implantable Cardioverter-Defibrillator (ICD) Complications Rate National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Medication Reconciliation
 Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016
 Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Stage 2 Eligible Hospital and Critical Access Hospital Meaningful Use Core Measures Measure 12 of 16 Date issued: May 2013
 Summary of Care Objective Measure Exclusion Stage 2 Eligible Hospital and Critical Access Hospital Meaningful Use Core Measures Measure 12 of 16 Date issued: May 2013 The eligible hospital or CAH who transitions
Summary of Care Objective Measure Exclusion Stage 2 Eligible Hospital and Critical Access Hospital Meaningful Use Core Measures Measure 12 of 16 Date issued: May 2013 The eligible hospital or CAH who transitions
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Consultations IN, KY, MO, OH, WI Policy: 0030 Effective: 12/01/2016 Coverage is subject to the terms, conditions, and limitations of an individual member
Subject: Documentation and Reporting Guidelines for Consultations IN, KY, MO, OH, WI Policy: 0030 Effective: 12/01/2016 Coverage is subject to the terms, conditions, and limitations of an individual member
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals
 The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
Telemedicine and Telehealth Services
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
Medicare and Medicaid EHR Incentive Program. Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment
 Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
during the EHR reporting period.
 CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
Definition. Competency
 Description of Work: NURSE PRACTITIONER This class provides patient care, including performing assessment, determining diagnosis, developing treatment plans, prescribing medication, engaging in research
Description of Work: NURSE PRACTITIONER This class provides patient care, including performing assessment, determining diagnosis, developing treatment plans, prescribing medication, engaging in research
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
The Care Compact. 11 PCPI All rights reserved.
 The Care Compact There are several change package ideas provided in this tool kit and none were more important than the Care Compact during the pilot project. It will be your starting point. So, what is
The Care Compact There are several change package ideas provided in this tool kit and none were more important than the Care Compact during the pilot project. It will be your starting point. So, what is
Quanum Electronic Health Record Frequently Asked Questions
 Quanum Electronic Health Record Frequently Asked Questions Table of Contents... 4 What is Quanum EHR?... 4 What are the current capabilities of Quanum EHR?... 4 Is Quanum EHR an EMR?... 5 Can I have Quanum
Quanum Electronic Health Record Frequently Asked Questions Table of Contents... 4 What is Quanum EHR?... 4 What are the current capabilities of Quanum EHR?... 4 Is Quanum EHR an EMR?... 5 Can I have Quanum
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013
 GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
AQI48a: Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia care
 Measure Title AQI48: Patient-Reported Experience with Anesthesia Measure Description Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia
Measure Title AQI48: Patient-Reported Experience with Anesthesia Measure Description Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Chapter 2 Provider Responsibilities Unit 6: Behavioral Health Care Specialists
 Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
Medical Staff Rules & Regulations Last Updated: October University Hospital Medical Staff. Rules & Regulations
 University Hospital Medical Staff Rules & Regulations 1 UNIVERSITY HOSPITAL MEDICAL STAFF RULES AND REGULATIONS The Medical Staff shall adopt Rules and Regulations as may be necessary to implement the
University Hospital Medical Staff Rules & Regulations 1 UNIVERSITY HOSPITAL MEDICAL STAFF RULES AND REGULATIONS The Medical Staff shall adopt Rules and Regulations as may be necessary to implement the
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Third Party Payer Days. IMGMA February 25, 2015
 Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1
 Services 1") GE Healthcare Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
GE Healthcare Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
HIE Implications in Meaningful Use Stage 1 Requirements
 s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
Primary Care Specialist Physician Compact
 I. Purpose To provide optimal health care for our patients. To provide a framework for better communication and safe transition of care between primary care and specialty care providers. II. Principles
I. Purpose To provide optimal health care for our patients. To provide a framework for better communication and safe transition of care between primary care and specialty care providers. II. Principles
Health Informatics. Health Informatics professionals treat technology as a tool that helps patients and healthcare professionals.
 Health Informatics Health Informatics professionals treat technology as a tool that helps patients and healthcare professionals. 3.02 Understand health informatics 2 Health Informatics A career area that
Health Informatics Health Informatics professionals treat technology as a tool that helps patients and healthcare professionals. 3.02 Understand health informatics 2 Health Informatics A career area that
Telemedicine Policy Annual Approval Date
 Policy Number 2017R0046A Telemedicine Policy Annual Approval Date 7/13/2016 Approved By REIMBURSEMENT POLICY CMS-1500 Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You
Policy Number 2017R0046A Telemedicine Policy Annual Approval Date 7/13/2016 Approved By REIMBURSEMENT POLICY CMS-1500 Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You
Medical-legal Issues in Pathology
 Medical-legal Issues in Pathology Kathryn Reducka MD, Physician Risk Manager, CMPA Pathology Update 2015 Toronto, ON November 14, 2015 Faculty / Presenter Disclosure Faculty: Employee of: Dr Kathryn Reducka
Medical-legal Issues in Pathology Kathryn Reducka MD, Physician Risk Manager, CMPA Pathology Update 2015 Toronto, ON November 14, 2015 Faculty / Presenter Disclosure Faculty: Employee of: Dr Kathryn Reducka
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
9/28/2011. Learning Agenda. Meaningful Use and why it s here. Meaningful Use Rules of Participation. Categories, Objectives and Thresholds
 Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
HEALTH DEPARTMENT BILLING GUIDELINES
 HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
Module 1 Program Description and Metrics
 Module 1 Program Description and Metrics Outpatient Clinic / Office-based Program Description 1. Is this program serving an urban, suburban or rural community? Urban Suburban Rural 2. Who administers your
Module 1 Program Description and Metrics Outpatient Clinic / Office-based Program Description 1. Is this program serving an urban, suburban or rural community? Urban Suburban Rural 2. Who administers your
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Eligible Professional Core Measure Frequently Asked Questions
 Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
Meaningful Use Stage 2 Clinical Quality Measures Are You Ready?
 22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Meaningful Use Stage 2 Clinical Quality Measures Are You Ready? Tuesday, June 4, 1:00 pm The transition from chart-abstracted legacy core
22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Meaningful Use Stage 2 Clinical Quality Measures Are You Ready? Tuesday, June 4, 1:00 pm The transition from chart-abstracted legacy core
2017 National Survey of Canadian Nurses: Use of Digital Health Technology in Practice Final Executive Report May, 2017
 2017 National Survey of Canadian Nurses: Use of Digital Health Technology in Practice Final Executive Report May, 2017 Table of contents Section Heading Background, methodology and sample profile 3 Key
2017 National Survey of Canadian Nurses: Use of Digital Health Technology in Practice Final Executive Report May, 2017 Table of contents Section Heading Background, methodology and sample profile 3 Key
CMS has finalized its proposal to eliminate Medicare payment for consultations and use the money from
 Consultation Services and Transfer of Care CMS has finalized its proposal to eliminate Medicare payment for consultations and use the money from these services to increase payments for visits, including
Consultation Services and Transfer of Care CMS has finalized its proposal to eliminate Medicare payment for consultations and use the money from these services to increase payments for visits, including
REPORT OF THE COUNCIL ON MEDICAL SERVICE
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Telemedicine Policy. Approved By 4/08/2015
 Telemedicine Policy Policy Number 2016R0046B Annual Approval Date 4/08/2015 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
Telemedicine Policy Policy Number 2016R0046B Annual Approval Date 4/08/2015 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission