2014 AANAC 9_30_ AANA C AANA
|
|
|
- Albert Pearson
- 6 years ago
- Views:
Transcription

1 AANAC AANAC 9_30_14
2 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT
3 Requirements for Successful Completion 1 Contact hour will be awarded for this continuing nursing education activity The American Association of Nurse Assessment Coordination is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on accreditation (ANCC). Criteria for successful completion includes purchase of and attendance for at least 80% of the entire event. Partial credit may not be awarded. Approval of this continuing education activity does not imply endorsement by AANAC or ANCC of any commercial products or services.
4 Conflict of Interest Disclosure Judi Kulus, NHA, RN, MAT, RAC-MT, C-NE Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT There are no conflicts of interest to disclose with this presentation.
5 Poll Question Tell us who you are: MDS Coding Nurse Other IDT MDS Clinician DON Nurse Manager Administrator Corporate Consultants Other
6 Learning Objectives Describe the most recent updates to the MDS, sections A Z Explain items added and deleted from the Item Sets Detail clarification to Change of Therapy (COT) assessments Review End of Therapy (EOT) examples









7
8 Maintaining RAI Records in the Clinical Record Update Federal regulation requires that 15 months of RAI information be kept in the active clinical record After 15 months have passed, RAI information can be thinned. The exception is that demographic information (Items A0500-A1600) from the most recent Admission assessment must be maintained in the active clinical record until the resident is discharged return not anticipated or is discharged return anticipated but does not return within 30 days (p. 2-6). 8
9 Assessment Types and Definition There are 10 nursing home and 8 swing bed item sets, listed on pages 2-10 through 2-12, that will become effective October 1, 2014 (v ) Printed layouts for the item sets are available in Appendix H of this manual (p. 2-12) The item sets can be downloaded on the CMS MDS 3.0 technical information page Update 9
10 Deletion of Readmission/Return Assessments Update Effective October 1, 2014, A0310B (06) has been deleted from all item sets and the manual For all providers, including Swing bed providers, the first required Medicare assessment is always the Medicare-required 5-Day assessment (Item A0310B = 01) as long as the resident is eligible for Medicare Part A services, requires and receives skilled services and has days remaining in the benefit period. (p. 2-73) 10
11 Scheduled PPS Assessments SNF PPS Assessment Type Reason for Assessment (A0310B code) Assessment Reference Date Window Assessment Reference Date Grace Days Applicable Medicare Payment Days 5-day* 01 Days through day 02 Days through day 03 Days through day 04 Days through day 05 Days through 100 *Columns 3, 4, and 5 of this row also apply to Readmission/Return Assessment (A0310B code = 06) related to days of the readmission 11
12 SECTION A IDENTIFICATION INFORMATION 12
13 Discharge Assessments Update When a resident is transferred from a Medicareand/or Medicaid-certified bed to a noncertified bed, a Discharge assessment is required (p. 2-10). 13
14 Discharge Assessments Example: Mr. K. was transferred from a Medicare-certified bed to a noncertified bed on December 12, 2013 and plans to remain long term in the facility. Code the December 12, 2013 Discharge assessment as follows: A0310F=10 A2000= A2100=2 Update 14
15 Unit Certification or Licensure Designation (A0410) Update Coding instructions: Code 1, Unit is neither Medicare nor Medicaid certified and MDS data is not required by the State: if the MDS record is for a resident on a unit that is neither Medicare nor Medicaid certified, and the state does not have authority to collect MDS information for residents on this unit, the facility may not submit MDS records to QIES ASAP. If any records are submitted under this certification designation, they will be rejected by the QIES ASAP system. 15
16 Unit Certification or Licensure Designation (A0410) Update Coding instructions: Code 2, Unit is neither Medicare nor Medicaid certified but MDS data is required by the State: if the nursing home resident is on a unit that is neither Medicare nor Medicaid certified, but the state has authority under state licensure to collect MDS information for residents on such units, the facility should submit the resident s MDS records per the state s requirement to QIES ASAP or directly to the state. Note that this certification designation does not apply to swing-bed facilities. Assessments for swing-bed residents on which A0410 is coded 2 will be rejected by the QIES ASAP system. 16
17 Unit Certification or Licensure Designation (A0410) Update Coding instructions: Code 3, Unit is Medicare and/or Medicaid certified: if the resident is on a Medicare and/or Medicaid certified unit, regardless of payer source (i.e., even if the resident is private pay or has his/her stay covered under e.g., Medicare Advantage, Medicare HMO, private insurance, etc.), the facility is required to submit these MDS records to QIES ASAP. Consult Chapter 5, page 5-1 of this Manual for a discussion of what types of records should be submitted to the QIES ASAP system. (p. A-8) 17
18 Medicare Advantage Assessments that are completed for purposes other than OBRA and SNF PPS reasons are NOT to be submitted, e.g., private insurance, including but not limited to Medicare Advantage plans (p. 5-1) 18
19 Medicare Advantage Managed Care transition to traditional Med A When a resident goes from Medicare Advantage to Medicare Part A start scheduled assessment over with a 5 -day PPS assessment (2-46) Begin submitting PPS assessments to the QIES ASAP system starting with the 5-Day assessment The current benefit period continues Resident does not get another 100 days after transition
20 Entry Date (A1600) Update This item is the initial date of admission to the facility, or the date the resident most recently returned to your facility after being discharged. Capture the date by using the following format: Month-Day-Year: XX-XX-XXXX. Example: October 12, 2010, would be entered as (p. A-22). 20
21 Type of Entry (A1700) Update The admission (A1700 = 1) is coded when a resident is: admitted for the first time to this facility; OR Is readmitted after a discharge return not anticipated; OR Is readmitted after a discharge return anticipated when return was not within 30 days of discharge (p. 2-33). 21
22 Type of Entry (A1700) Update Reentry (A1700 = 2) is checked when a resident is: Readmitted to this facility, AND Was discharged return anticipated from this facility, AND Returned within 30 days of discharge. Note: When either and entry or reentry occurs, an Entry Tracking Record should be completed (A0310F = 01) (see 2-33) 22
23 Admission Date (A1900) Update New Coding Item! This new item on the item sets is to indicate when the current admission (or episode of care) in this facility began (p. A-25). While the RAI User s Manual does not define an episode of care, the MDS 3.0 Quality Measures User s Manual defines an episode as a period of time spanning one or more stays (p. 1). 23
24 Admission Date (A1900) Update QM Glossary: An episode is a period of time spanning one or more stays An episode begins with an admission Entry record (A0310F = 01 and A1700 = 1) 24
25 QM Glossary: Episode An episode ends with the earliest of the following: Discharge assessment with return not anticipated (A0310F = 10) or Discharge assessment with return anticipated (A0310F = 11) but the resident did not return within 30 days of discharge or A death-in-facility tracking record (A0310F = 12) or The end of the target period (the 3-month reporting period for the report) 25
26 QM Glossary: Episode Example 2 3 Stay Episode Admission Reentry Reentry Stay 1 Stay 2 Stay 3 Admission Date (A1900) Entry Date (A1600) Entry Date (A1600) D/C Return Anticipated (Out <31 days) End: Discharge Return Not Anticipated Discharge Return Anticipated but gone at least 31 days Death End of Target Period D/C Return Anticipated (Out <31 days)
27 SIGNIFICANT CHANGE IN STATUS ASSESSMENT (SCSA) 27
28 Hospice and SCSA A SCSA is required when a terminally ill resident enrolls in a hospice program and remains a resident of the nursing facility Must be completed regardless of whether an assessment was recently conducted on the resident must be within 14 days from the effective date of hospice 28
29 Hospice and SCSA If a resident is admitted on the hospice benefit (i.e. the resident is coming into the facility having already elected hospice), or elects hospice on or prior to the of the Admission assessment, the facility should complete the Admission assessment, checking the Hospice Care item, O0100K. Completing an Admission assessment followed by a SCSA is not required. Where hospice election occurs after the Admission assessment but prior to its completion, facilities may choose to adjust the to the date of hospice election so that only the Admission assessment is required. In such situations, an SCSA is not required. (p. 2-21) Update 29
30 Hospice and SCSA If a resident is admitted on the hospice benefit but decides to discontinue it prior to the of the Admission assessment, the facility should complete the Admission assessment, checking the Hospice Care item, O0100K. Completing an Admission assessment followed by a SCSA is not required. Where hospice revocation occurs after the Admission assessment but prior to its completion, facilities may choose to adjust the to the date of hospice revocation so that only the Admission assessment is required. In such situations, an SCSA is not required. (p. 2-22) Update 30
31 Hospice and SCSA Update The must be less than or equal to 14 days after the IDT s determination that the criteria for a SCSA are met (determination date + 14 calendar days). (p. 2-22) 31
32 SECTION K SWALLOWING / NUTRITIONAL STATUS 32

33 Percent Intake by Artificial Route (K710) K0710 (Percent Intake by Artificial Route):
34 Coding Average Fluids (K0710B) Mon Tues Wed Thurs Fri Sat Sun Total Hospital Hospital Hospital Hospital Nursing Home Nursing Home Nursing Home 400cc 520cc 500cc 480cc 510cc 520cc 490cc 7 days Hospital Total Update = 1900 Nursing =1520 = /4 Home 1520/3 3420/7 Total
35 Coding Average Fluids (K0710B) Mon Tues Wed Thurs Fri Sat Sun Total Hospital Hospital Hospital Hospital Nursing Home Nursing Home Nursing Home 400cc 520cc 500cc 480cc 510cc 520cc 490cc 7 days Hospital Total Update = 1900 Nursing =1520 = /4 Home 1520/3 3420/7 Total
36 Coding Average Fluids (K0710B) Mon Tues Wed Thurs Fri Sat Sun Total Hospital Hospital Hospital Hospital Nursing Home Nursing Home Nursing Home 400cc 520cc 500cc 480cc 510cc 520cc 490cc 7 days Hospital Total Update = 1900 Nursing =1520 = /4 Home 1520/3 3420/7 Total

37 Coding Average Fluids (K0710B) Mon Tues Wed Thurs Fri Sat Sun Total Hospital Hospital Hospital Hospital Nursing Home Nursing Home Nursing Home 400cc 520cc 500cc 480cc 510cc 520cc 490cc 7 days Hospital Total Update = 1900 Nursing =1520 = /4 Home 1520/3 3420/7 Total
38 SECTION O SPECIAL TREATMENTS, PROCEDURES, AND PROGRAMS 38
39 Ventilator or Respirator (O0100F) Update This item s definition was expanded to include residents receiving closed-system ventilation... via an endotracheal tube (e.g., nasally or orally intubated) as well as those residents with a tracheostomy (p. O-3). 39
40 Influenza Vaccine (O0250) Once the influenza vaccination has been administered to a resident for the current influenza season, this value is carried forward until the new influenza season begins (p. O-8). CMS also instructs that residents should be immunized as soon as the vaccine becomes available and continue until influenza is no longer circulating in your geographic area (p. O-8). Update Info about current flu season can be obtained at 40
41 Chapter 5: Correcting Errors Update According to the update to this section of the manual, facility staff should correct any errors noted on a submitted record within 3 years of the target date of the record for facilities that are still open. If a facility is terminated, then corrections must be submitted within 2 years of the facility termination date (p. 5-10). Note that even with the timeframes listed above, Errors identified in QIES ASAP system records must be corrected within 14 days after identifying the errors (p. 5-10) 41
42 CHANGE OF THERAPY (COT) OMRA Other Medicare Required Assessments 42
43 Change of Therapy OMRA Required when Resident is receiving therapy and The intensity of therapy increases or decreases to the extent that the RUG in effect is no longer an accurate reflection of the intensity of therapy received Informal evaluation of therapy RUG required essentially every 7 days 43
44 Change of Therapy OMRA Change may be due to increase/decrease in: Reimbursable Therapy Minutes (RTM) Days of therapy Number of disciplines Restorative Nursing ADL score is not taken into account COT OMRA also applies when index maximized RUG is non-rehab but resident is receiving enough therapy to classify into a therapy RUG 44
45 Change of Therapy OMRA Actual number of minutes resident spends in therapy should be documented in chart RTM for calculating the RUG = sum of 100% of individual minutes from chart 50% of concurrent minutes from chart 25% of group minutes (not to exceed 25% cap per discipline) from chart 45
46 Change of Therapy OMRA Facility monitoring of therapy intensity COT observation - successive 7-day windows Begin day after of most recent PPS assessment If COT OMRA not required, next COT observation starts day 1 after 7th day of COT observation When EOT-R has been completed, COT observation starts the day therapy resumes Must evaluate rehab intensity after each 7th day until COT OMRA or other PPS scheduled or unscheduled assessment is completed 46
47 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 47
48 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 48
49 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 49
50 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 3 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 50
51 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 3 Day 4 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 51
52 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 3 Day 4 Day 5 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 52
53 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 53
54 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 7 COT Check Date Day 27 54
 is")
55 Change of Therapy OMRA Rolling Observation and Check Date Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day Day Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 7 COT Check Date Day 27 Day 7 COT Check Date Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Explanation: The COT check date after an unscheduled or scheduled assessment (with the exception of the EOT-R) is the plus SEVEN days. 55
56 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 56
57 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Therapy Resumes Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 57
58 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 58
59 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 2 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 59
60 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 2 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Day 3 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 60
61 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 2 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Day 3 Day 4 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 61
62 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 2 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Day 3 Day 4 Day 5 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 62
63 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 2 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Day 3 Day 4 Day 5 Day 6 Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 63
64 Change of Therapy OMRA COT Observation After EOT-R Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Last Day of Therapy EOT Day 1 EOT Day 2 EOT Day 3 Day 1 Therapy Resumes Day 2 Day 42 Day 43 Day 44 Day 45 Day 46 Day 47 Day 48 Day 3 Day 4 Day 5 Day 6 Day 7 COT Check Date Explanation: The COT check date after an EOT-R is the resumption date plus SIX days. 64
65 Change of Therapy OMRA Facility monitoring of therapy intensity COT observation required following all PPS assessments that calculate a therapy RUG Required even if the therapy RUG is not going to be billed because the assessment also qualifies for a nursing RUG that will pay more Due to index maximization, the software will assign the RUG with the higher rate 65
66 Change of Therapy OMRA Update A COT OMRA may only be completed when a resident is currently classified into a RUG-IV therapy group (regardless of whether or not the resident is classified into this group for payment), based on the resident s most recent assessment used for payment. 66
67 Change of Therapy OMRA Update The COT OMRA may be completed when a resident is not currently classified into a RUG-IV therapy group, but only if both of the following conditions are met: 1. Resident has been classified into a RUG-IV therapy group on a prior assessment during the resident s current Medicare Part A stay, and 2. No discontinuation of therapy services (planned or unplanned) occurred between Day 1 of the COT observation period for the COT OMRA that classified the resident into his/her current non-therapy RUG-IV group and the of the COT OMRA that reclassified the resident into a RUG-IV therapy group. Under these circumstances, completing the COT OMRA may be considered optional. (p. 2-52) 67
68 Change of Therapy OMRA Example: Mr. T classified into the RUG group RUA on his 30-day assessment with an set for Day 30 of his stay. On Day 37, the facility checked the amount therapy provided to Mr. T. and found that while he did receive the requisite number of therapy minutes to qualify for this RUG category, he only received therapy on 4 distinct calendar days, which would make it impossible for him to qualify for an Ultra-High Rehabilitation RUG group. Due to lack of 5 distinct calendar days of therapy and a lack of restorative nursing services, Mr. T. did not qualified for a therapy RUG group. Mr. T. s rehabilitation regimen has continued throughout this time period. The facility may complete a COT OMRA with an of Day 44 to reclassify Mr. T. back into RUA. 68 Update
69 Scheduling Tracking Systems Resource available at: 69
70 END OF THERAPY (EOT) Other Medicare Required Assessments (OMRAs) 70
71 End of Therapy OMRA Used to establish a non-therapy payment rate when: A resident is being discharged from therapy but will continue on Medicare Part A for a nontherapy reason for at least three (3) days A resident who is receiving therapy has a break in the furnishing of therapy for at least three (3) consecutive days regardless of reason 71
72 End of Therapy OMRA Update When determining whether a resident missed a day of therapy, a treatment day is defined the same way as in Chapter 3, Section O, 15 minutes of therapy a day. If a resident receives less than 15 minutes of therapy in a day, it is not coded on the MDS and it cannot be considered a day of therapy (p. 2-48). 72

73 EOT-R Resumption of Therapy May be used When a skilled resident resumes therapy within 4 5 days of the last therapy treatment Resumes at the same RUG-IV classification level that had been in effect prior to the EOT OMRA Resumes with the same therapy plan of care that had been in effect prior to the EOT OMRA 73
74 EOT-R Resumption of Therapy If therapy is not provided for more than 5 days, or therapy resumes within 5 days but the therapy RUG or treatment plan changes, EOT-R OMRA not applicable EOT OMRA required When therapy restarts, do SOT OMRA or wait until next scheduled assessment New therapy evaluation and care plan required 74
75 EOT-R Resumption of Therapy If the resumption occurs after the start of next billing period, resumed RUG continues in effect until next PPS assessment takes effect Last tx Day 10 Day 11 Day 12 Day 13 Day 14 Resumed Day 15 Day 16 Non-Therapy RUG Resumed RUG 14-day assessment RUG would not be used
76 EOT-R Resumption of Therapy Update In all cases where an EOT-R would be completed, the resident must resume therapy at the same RUG-IV therapy level as had been in effect prior to the break in therapy It is possible that the for an EOT OMRA reporting resumption may be set for the first grace day of the allowable grace days for a scheduled PPS assessment, while the for the scheduled assessment was set for a day within the normal window In this case, the resumption of therapy should occur using the previous RUG-IV therapy level (which should be the same as the therapy level determined on the scheduled PPS assessment if the resumption is appropriate) but using the Activities of Daily Living (ADL) score from the most recent PPS assessment (ch. 6-12) 76
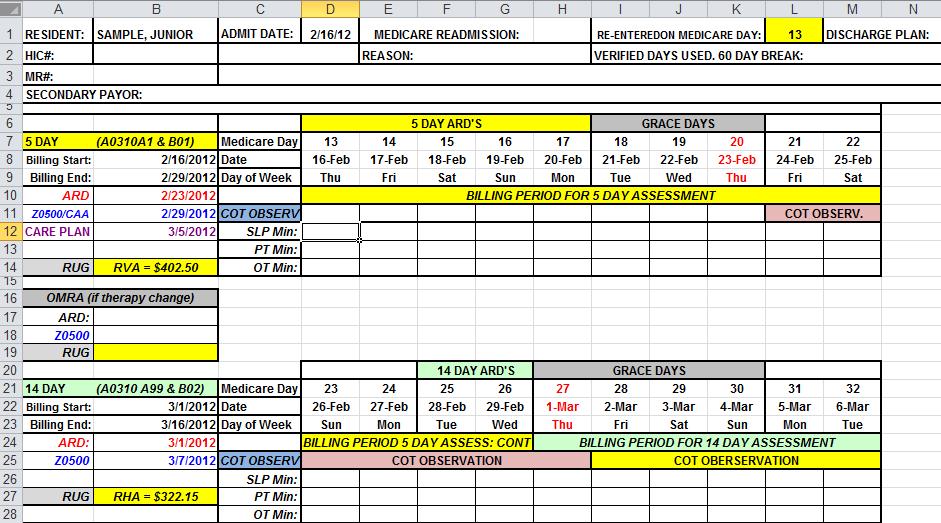
77 EOT-R Resumption of Therapy: Example Example: Mrs. Smith, is admitted on 10/01/14. The of the 5-day assessment for Mrs. Smith is set for 10/07/14 (Day 7) and the RUG assigned to Mrs. Smith is RVB. The of the 14- day assessment is set for 10/14/14 (Day 14) and the RUG assigned to Mrs. Smith is again RVB. The of the 30-day assessment is set for 10/28/14 (Day 28) and the RUG assigned to Mrs. Smith is now RVA. Due to an acute illness, Mrs. Smith is unable to receive therapy services from 10/29/14 through 10/31/14, but is expected to resume therapy on 11/2/14 under the same therapy regimen. The facility completes an EOT for Mrs. Smith with an of 10/31/14 and reports that the resumption of therapy will occur on 11/2/14. The EOT OMRA assigns Mrs. Smith a nontherapy RUG of CE2. Mrs. Smith is discharged from the facility on 11/12/14. 77
78 EOT-R Resumption of Therapy: Example RAI Example Answer: Assuming no intervening assessments were necessary, the facility would bill in the following manner. Days 1-14 would be billed under HIPPS code RVB10. Days would be billed under HIPPS code RVB20. Days would be billed under HIPPS code CE20A. Days would be billed under HIPPS code RVA0A. This represents the one and only occasion where the three character RUG-IV therapy RUG code may differ from that which was billed prior to the break in therapy, and the difference may only be in the third character in the therapy RUG code related to the resident s ADL score. (pp ) 78
79 EOT-R Resumption of Therapy: Example SUN MON TUES WED THU FRI SAT Day 27 Day 28 Day 29 Day 30 Day 31 Day 32 Day Day RUG (RVB) 30-Day Window 79
80 EOT-R Resumption of Therapy: Example SUN MON TUES WED THU FRI SAT Day 27 Day 28 Day 29 Day 30 Day 31 Day 32 Day Day RUG (RVB) 30-Day (RVA) 30-Day Window 80
81 EOT-R Resumption of Therapy: Example SUN MON TUES WED THU FRI SAT Day 27 Day 28 Day 29 Day 30 Day 31 Day 32 Day 33 No Therapy 14-Day RUG (RVB) 30-Day (RVA) 30-Day Window 81
82 EOT-R Resumption of Therapy: Example SUN MON TUES WED THU FRI SAT Day 27 Day 28 Day 29 Day 30 Day 31 Day 32 Day 33 No Therapy 14-Day RUG (RVB) 30-Day (RVA) EOT (CE2) 30-Day Window 82
83 EOT-R Resumption of Therapy: Example SUN MON TUES WED THU FRI SAT Day 27 Day 28 Day 29 Day 30 Day 31 Day 32 Day Day RUG (RVB) 30-Day (RVA) No Therapy EOT (CE2) Therapy Resumes 30-Day Window 83
 No Therapy EOT (CE2) Therapy Resumes 30-Day Window Rehab RUG RVA 14-Day Rehab RUG pays from day 32, with the ADL score from the 30-day")
84 EOT-R Resumption of Therapy: Example SUN MON TUES WED THU FRI SAT Day 27 Day 28 Day 29 Day 30 Day 31 Day 32 Day Day RUG (RVB) 30-Day (RVA) No Therapy EOT (CE2) Therapy Resumes 30-Day Window Rehab RUG RVA 14-Day Rehab RUG pays from day 32, with the ADL score from the 30-day RUG 84
85 Resources AANAC cm/ RAI User s Manual for MDS Patient-Assessment- Instruments/NursingHomeQualityInits/MDS30RAIManu al.html SNF Proposed Rule FY /pdf/ pdf

86 QUESTIONS? Join us directly after the webinar in the AANAConnect community. Check your confirmation for the link!
5/11/2017. Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC. It s official!
 Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC It s official! 2 1 Capturing the services and resident characteristics provided to Medicare A residents in specific timeframes. Determining the Medicare payment
Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC It s official! 2 1 Capturing the services and resident characteristics provided to Medicare A residents in specific timeframes. Determining the Medicare payment
The Prospective Payment System
 Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com The Prospective Payment System January 2018 NC & VA Source: Current RAI Manual, Chapter 2 & 6
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com The Prospective Payment System January 2018 NC & VA Source: Current RAI Manual, Chapter 2 & 6
Medicare Scheduled and Unscheduled MDS Assessment Schedule for SNFs (cont.)
") 2 2.5 2-8 Except for the OBRA admission assessment, assessments must be completed within 14 days after the ARD of the assessment. Completion requirements are dependent on the assessment type and timing
2 2.5 2-8 Except for the OBRA admission assessment, assessments must be completed within 14 days after the ARD of the assessment. Completion requirements are dependent on the assessment type and timing
Changes to the RAI manual effective October 1, 2013
 Changes to the RAI manual effective October 1, 2013 CMS released on Friday, September 27 an updated version of the RAI manual that became effective October 1, 2013. The manual is found here> http://www.cms.gov/medicare/quality-initiatives-patient-assessment-
Changes to the RAI manual effective October 1, 2013 CMS released on Friday, September 27 an updated version of the RAI manual that became effective October 1, 2013. The manual is found here> http://www.cms.gov/medicare/quality-initiatives-patient-assessment-
5DAY = 1 AND
 July 2008 Revision Table CH. Sect. Pg. July 2008 Revision NA Title Page NA Change the revised date to July 2008 CH 2 2.2 2-11 Revise as follows: Delete the second sentence of the second paragraph, The
July 2008 Revision Table CH. Sect. Pg. July 2008 Revision NA Title Page NA Change the revised date to July 2008 CH 2 2.2 2-11 Revise as follows: Delete the second sentence of the second paragraph, The
5/26/2016. What's New? What's Changed? Urgent Updates QM Manual v10. Faculty Disclosure. Requirements for Successful Completion
 What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
11/23/2011. Proactive vs. Reactive Relationship
 Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
11/18/2013 MDS 3.0 RAI MANUAL CHAPTER 1 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18
 MDS 3.0 CHANGES EFFECTIVE 10-1-2013 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18 Support Agency Contractors to assist in accomplishment of a CMS function. To assist another Federal or SA.for purposes of
MDS 3.0 CHANGES EFFECTIVE 10-1-2013 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18 Support Agency Contractors to assist in accomplishment of a CMS function. To assist another Federal or SA.for purposes of
All Medicare Advantage Organizations (MAOs), PACE Organizations, Cost Plans, and certain Demonstrations
, PACE Organizations, Cost Plans, and certain Demonstrations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
CMS Updates RAI User s Manual
 CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS
 CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit Omnibus Budget Reconciliation Act required (OBRA) MDS records for all residents in Medicare- or Medicaid-certified
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit Omnibus Budget Reconciliation Act required (OBRA) MDS records for all residents in Medicare- or Medicaid-certified
All Medicare Advantage Organizations (MAOs), PACE Organizations, Cost Plans, and certain Demonstrations
, PACE Organizations, Cost Plans, and certain Demonstrations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS)
") CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1)
") CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS
 CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit MDS records for all residents in Medicare- or Medicaidcertified beds regardless of the pay source. Skilled
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit MDS records for all residents in Medicare- or Medicaidcertified beds regardless of the pay source. Skilled
AANAC Education Advancement. MDS Essentials: An Introduction. Learning Objectives 3/22/2017. Education Advancement
 AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
6/12/2017. The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group
 The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
Section A Identification Information
 r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES
 COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
The Prospec1ve Payment System May What is SNF PPS? HIPPS & MDS 3.0 4/17/17. Wilhide Consul1ng, Inc. (c) 1. Source: Source:
 1. Source: Source:") Source: The Prospec1ve Payment System May 2016 Current RAI Manual, Chapter 2 & 6 ( resources www.judywilhide.com) Chapter 2: 2.8: The SNF PPS Assessment Schedule 2.9: MDS Medicare Assessments for SNFs
Source: The Prospec1ve Payment System May 2016 Current RAI Manual, Chapter 2 & 6 ( resources www.judywilhide.com) Chapter 2: 2.8: The SNF PPS Assessment Schedule 2.9: MDS Medicare Assessments for SNFs
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
100 Days Out: What's Changing with the MDS 3.0 Item Set on October 1, 2018
 100 Days Out: What's Changing with the MDS 3.0 Item Set on October 1, 2018 June 22, 2018 Learning Objectives/Outcomes Locate the current DRAFT MDS 3.0 Item Sets as well as the Item Set Change History document
100 Days Out: What's Changing with the MDS 3.0 Item Set on October 1, 2018 June 22, 2018 Learning Objectives/Outcomes Locate the current DRAFT MDS 3.0 Item Sets as well as the Item Set Change History document
Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report. User s Guide Sixth Edition. Prepared by
 Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report User s Guide Sixth Edition Prepared by Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report
Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report User s Guide Sixth Edition Prepared by Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report
CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Housekeeping. Harmony Healthcare International, Inc. The Devils in The Details: RUG Intimacy. Objectives. Copyright 2012 All Rights Reserved
 The Devils in The Details: RUG Intimacy Harmony University The Provider Unit of (HHI) Presented by: Caroline Mullin, OTR/L Corporate Consultant/Denial Manager Housekeeping Sign In and Sign Out Contact
The Devils in The Details: RUG Intimacy Harmony University The Provider Unit of (HHI) Presented by: Caroline Mullin, OTR/L Corporate Consultant/Denial Manager Housekeeping Sign In and Sign Out Contact
SECTION A: IDENTIFICATION INFORMATION. A0100: Facility Provider Numbers. Item Rationale. Coding Instructions
 SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Countdown to MDS Section GG: Collaboration Between Nursing and Therapy
 Countdown to MDS Section GG: Collaboration Between Nursing and Therapy Presented in Collaboration with NASL: Joanne M. Wisely, MA CCC/SLP, VP Legislative Advocacy Genesis Rehab Services/Respiratory Health
Countdown to MDS Section GG: Collaboration Between Nursing and Therapy Presented in Collaboration with NASL: Joanne M. Wisely, MA CCC/SLP, VP Legislative Advocacy Genesis Rehab Services/Respiratory Health
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
OASIS ITEM ITEM INTENT TIME POINTS ITEM(S) COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES
 COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES") (M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
(M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
QIES Help Desk. Objectives. Nursing Home Quality Initiatives and Five-Star Quality Rating System
 Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
Wilhide Consulting, Inc. (c) 1
 1") Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
Medicare Program Integrity Manual Chapter 6 - Intermediary MR Guidelines for Specific Services
 Medicare Program Integrity Manual Chapter 6 - Intermediary MR Guidelines for Specific Services Transmittals for Chapter 6 Table of Contents (Rev. 475, 07-19-13) 6.1 - Medical Review of Skilled Nursing
Medicare Program Integrity Manual Chapter 6 - Intermediary MR Guidelines for Specific Services Transmittals for Chapter 6 Table of Contents (Rev. 475, 07-19-13) 6.1 - Medical Review of Skilled Nursing
Carol Maher, RN-BC, RAC-CT. Long-Term Care MDS Coordinator s Field Guide
 Carol Maher, RN-BC, RAC-CT Long-Term Care MDS Coordinator s Field Guide Long-Term Care MDS Coordinator s Field Guide Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Long-Term Care MDS Coordinator s Field Guide
Carol Maher, RN-BC, RAC-CT Long-Term Care MDS Coordinator s Field Guide Long-Term Care MDS Coordinator s Field Guide Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Long-Term Care MDS Coordinator s Field Guide
Mds 3.0 caas cheat sheet
 Mds 3.0 caas cheat sheet Search MDS Tools for MDS Coordinator documentation in long term care. MDS scheduling tools and forms for MDS 3. 0 and. MDS Data Collection Cheat Sheet. MDS. MDS Cheat Sheets. Below
Mds 3.0 caas cheat sheet Search MDS Tools for MDS Coordinator documentation in long term care. MDS scheduling tools and forms for MDS 3. 0 and. MDS Data Collection Cheat Sheet. MDS. MDS Cheat Sheets. Below
August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]
![August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]](/thumbs/83/88557772.jpg "August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]") Bridgepoint 1, Suite 300 5918 West Courtyard Drive, Austin TX 78730-5036 August 30, 2013 [Contact Name] SNF Name, 009168 [Address Line 1] [Address Line 2] [City], B8 [ZIP] RE: Program for Evaluating Payment
Bridgepoint 1, Suite 300 5918 West Courtyard Drive, Austin TX 78730-5036 August 30, 2013 [Contact Name] SNF Name, 009168 [Address Line 1] [Address Line 2] [City], B8 [ZIP] RE: Program for Evaluating Payment
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #21 Compliance = Confidence! Tuesday, August 6 2:30 to 4:30 p.m. Diplomat 1 & 2 Upon completion of this presentation,
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #21 Compliance = Confidence! Tuesday, August 6 2:30 to 4:30 p.m. Diplomat 1 & 2 Upon completion of this presentation,
LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI)
") LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI) v 2018 0614 Contents Learning Objectives...1 Sequencing of Documents...2 Admission
LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI) v 2018 0614 Contents Learning Objectives...1 Sequencing of Documents...2 Admission
Transitioning to the New IRF-PAI
 Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
Goodbye PPS: Hello RCS!
 Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
2. D Mood E Behavior F Preferences for Customary Routine and Activities G Functional Status H Bladder and Bowel
 Newslet ter Title R A I C o o r d i n a t or 1-7 1 7-7 8 7-1 8 1 6 q a - m d s @ s t a t e. p a. u s RAI Spotlight MDS 3.0 Training R AI C o o r d i n a t o r 1-7 1 7-7 8 7-1 8 1 6 q a -m ds @ state.p
Newslet ter Title R A I C o o r d i n a t or 1-7 1 7-7 8 7-1 8 1 6 q a - m d s @ s t a t e. p a. u s RAI Spotlight MDS 3.0 Training R AI C o o r d i n a t o r 1-7 1 7-7 8 7-1 8 1 6 q a -m ds @ state.p
Medicare PPS Report. Self Guided Tutorial
 Medicare PPS Report Self Guided Tutorial 1 Tutorial Objectives After completing this tutorial, you will be able to: Identify the purpose of the Medicare PPS Report Access the Medicare PPS Report Customize
Medicare PPS Report Self Guided Tutorial 1 Tutorial Objectives After completing this tutorial, you will be able to: Identify the purpose of the Medicare PPS Report Access the Medicare PPS Report Customize
Patient-Driven Payment Model
 Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
SECTION A: IDENTIFICATION INFORMATION. A0050: Type of Record. Coding Instructions for A0050, Type of Record
 SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
SNF proposed rule revisions to case-mix methodology
 SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
MDS 3.0 RAC-CT. Certification Program. July 17, 18 & 19, Maine Health Care Association 317 State Street, Augusta, Maine
 MDS 3.0 RAC-CT Certification Program July 17, 18 & 19, 2012 Maine Health Care Association 317 State Street, Augusta, Maine Presented by Official Training Partner BECOME MDS 3.0 RAC-CT CERTIFIED IN 3 DAYS
MDS 3.0 RAC-CT Certification Program July 17, 18 & 19, 2012 Maine Health Care Association 317 State Street, Augusta, Maine Presented by Official Training Partner BECOME MDS 3.0 RAC-CT CERTIFIED IN 3 DAYS
Clinical and Compliance Bulletin
 Clinical and Compliance Bulletin 877.799.9595 www.evergreenrehab.com 2011 Quarter 3 Coding Corner FAQ 1. How do I bill for group speech therapy treatment? There are two group therapy CPT codes that are
Clinical and Compliance Bulletin 877.799.9595 www.evergreenrehab.com 2011 Quarter 3 Coding Corner FAQ 1. How do I bill for group speech therapy treatment? There are two group therapy CPT codes that are
2/20/2018. Resident Classification System RCS-1. CMS Proposal
 Resident Classification System RCS-1 CMS Proposal Resident Classification System I (RCS-I) Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2017 CMS released an Advance
Resident Classification System RCS-1 CMS Proposal Resident Classification System I (RCS-I) Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2017 CMS released an Advance
The Shift is ON! Goodbye PPS, Hello RCS
 The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
Sneak Peak: MDS 3.0 Changes & New QRP s. Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma
 Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Section GG GG 1. MDS Coding Essentials: Section GG and Function. MDS Essentials. Section GG Assessment Types. Content 4/24/2017.
 Section GG GG 1 MDS Coding Essentials: SECTION GG: FUNCTIONAL ABILITIES AND GOALS Intent: This section assesses the need for assistance with self care and mobility activities. Sections GG and K 1 4 MDS
Section GG GG 1 MDS Coding Essentials: SECTION GG: FUNCTIONAL ABILITIES AND GOALS Intent: This section assesses the need for assistance with self care and mobility activities. Sections GG and K 1 4 MDS
MDS 3.0: What Leadership Needs to Know
 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
The Finalized MDS 3.0 RAI Manual: What you need to know about the new item set, new section, and more!
 The Finalized MDS 3.0 RAI Manual: What you need to know about the new item set, new section, and more! Presented by: Amy Franklin RN, RAC-MT, DNS-MT, QCP-MT AANAC Curriculum Development Specialist 1 Faculty
The Finalized MDS 3.0 RAI Manual: What you need to know about the new item set, new section, and more! Presented by: Amy Franklin RN, RAC-MT, DNS-MT, QCP-MT AANAC Curriculum Development Specialist 1 Faculty
MDS 3.0/RUG IV Distance Learning Series January - May 2016
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
What Did Your PEPPER Tell CMS?
 What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
Patient Driven Payment Model 101
 Patient Driven Payment Model 101 MARK MCDAVID, OTR, RAC-CT Presented by Why a New Payment Model? MedPAC has raised concerns about: Provider advantage Payment inequities for different patient types Patient
Patient Driven Payment Model 101 MARK MCDAVID, OTR, RAC-CT Presented by Why a New Payment Model? MedPAC has raised concerns about: Provider advantage Payment inequities for different patient types Patient
Medicaid RAC Audit Results
 Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Clinical RUG-IV. RUG Qualifiers & Length of Stay. Part 1. for clients of: Content developed and presented by:
 Clinical RUG-IV RUG Qualifiers & Length of Stay Part 1 for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252
Clinical RUG-IV RUG Qualifiers & Length of Stay Part 1 for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Compliance Issues under Medicare Prospective Payment for Nursing Facilities. Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group
 Compliance Issues under Medicare Prospective Payment for Nursing Facilities Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group Anyplace where there is no PPS Risk Areas Physician Certification
Compliance Issues under Medicare Prospective Payment for Nursing Facilities Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group Anyplace where there is no PPS Risk Areas Physician Certification
MDS Inaccuracy: Forecast for Failure!
 MDS Inaccuracy: Forecast for Failure! PRESENTED FOR KHCA BY: BECKY LABARGE, RN, RAC-CT, RAC-MT MDS Inaccuracy: Forecast for Failure! OBJECTIVES: oreview RAI Manual updates for FY2016 ouncover common MDS
MDS Inaccuracy: Forecast for Failure! PRESENTED FOR KHCA BY: BECKY LABARGE, RN, RAC-CT, RAC-MT MDS Inaccuracy: Forecast for Failure! OBJECTIVES: oreview RAI Manual updates for FY2016 ouncover common MDS
Navigating the New CMS Quality Measures
 Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Changes in the CMI Report Process and Updates from OLTL
 Changes in the CMI Report Process and Updates from OLTL Ruth Anne Barnard, B.S.N., R.N. MDS/OBRA Coordinator for Nursing Facility Field Operations Catharine B. Petko, B.S.N., R.N. Senior Nurse Consultant,
Changes in the CMI Report Process and Updates from OLTL Ruth Anne Barnard, B.S.N., R.N. MDS/OBRA Coordinator for Nursing Facility Field Operations Catharine B. Petko, B.S.N., R.N. Senior Nurse Consultant,
Set Yourself Up for Success: How VBP is Changing the Game NYSHFA January 26, 2018 Presented by, Maureen McCarthy, RN, BS, RAC-MT, QCP-MT
 Set Yourself Up for Success: How VBP is Changing the Game NYSHFA January 26, 2018 Presented by, Maureen McCarthy, RN, BS, RAC-MT, QCP-MT 1 Maureen McCarthy, RN, BS, RAC-MT, QCP-MT 2 Maureen is the President
Set Yourself Up for Success: How VBP is Changing the Game NYSHFA January 26, 2018 Presented by, Maureen McCarthy, RN, BS, RAC-MT, QCP-MT 1 Maureen McCarthy, RN, BS, RAC-MT, QCP-MT 2 Maureen is the President
A1600 A1800: Most Recent Admission/Entry or Reentry into this Facility
 A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
CMS OASIS Q&As: CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 CMS OASIS Q&As: CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q1. [Q&A RETIRED 09/09; Outdated] Q2. When integrating the OASIS data items into an HHA's assessment
CMS OASIS Q&As: CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q1. [Q&A RETIRED 09/09; Outdated] Q2. When integrating the OASIS data items into an HHA's assessment
The RoPs are here! Do you know what s changing?
 The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
10/22/2012. Discharge, Revocation and Transfer: Process, ABN and Appeals. Discharge the regulations. Objectives for Today s Session
 Discharge, Revocation and Transfer: Process, ABN and Appeals Jennifer Kennedy, MA, BSN, CHC, LNC National and Palliative Care Organization Patricia Smith Putzbach, RN, BSN, MBA, CHPN Life Choice Discharge
Discharge, Revocation and Transfer: Process, ABN and Appeals Jennifer Kennedy, MA, BSN, CHC, LNC National and Palliative Care Organization Patricia Smith Putzbach, RN, BSN, MBA, CHPN Life Choice Discharge
OASIS QUALITY IMPROVEMENT REPORTS
 6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
CRITICAL ACCESS HOSPITAL SWING BED PROGRAM
 CRITICAL ACCESS HOSPITAL SWING BED PROGRAM Operational and Management Strategies March 1, 2016 Andrea Elliott, CPA Senior Managing Consultant aelliott@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing Consultant
CRITICAL ACCESS HOSPITAL SWING BED PROGRAM Operational and Management Strategies March 1, 2016 Andrea Elliott, CPA Senior Managing Consultant aelliott@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing Consultant
Thank you for joining us!
 Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the SNF Training and Resources section. A recording of
Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the SNF Training and Resources section. A recording of
THE ART OF DIAGNOSTIC CODING PART 1
 THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
P&NP Computer Services: Page 1. UPDATE for Version
 P&NP Computer Services: 585.637.3240 Page 1 THIS UPDATE INCLUDES SOME VERY IMPORTANT CHANGES TO YOUR RESIDENT MANAGEMENT SYSTEM ADT AND CENSUS MODULE CHANGES 1. Changes to Diagnoses Diagnoses can be entered,
P&NP Computer Services: 585.637.3240 Page 1 THIS UPDATE INCLUDES SOME VERY IMPORTANT CHANGES TO YOUR RESIDENT MANAGEMENT SYSTEM ADT AND CENSUS MODULE CHANGES 1. Changes to Diagnoses Diagnoses can be entered,
More than a Century of Legal Experience
 Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Long Term Care User Guide for Hospice Providers
 Long Term Care User Guide for Hospice Providers v 2018 0802 Contents Learning Objectives...1 Forms to be Submitted...2 Hospice Form 3071 Election/Cancellation/Discharge Notice...2 How to Submit Form 3071...3
Long Term Care User Guide for Hospice Providers v 2018 0802 Contents Learning Objectives...1 Forms to be Submitted...2 Hospice Form 3071 Election/Cancellation/Discharge Notice...2 How to Submit Form 3071...3
RAC Audits and Denials Management WHCA Fall Conference September 9, 2014
 JoLynn Munro, MS,OTR/L, Regional Vice President Infinity Rehab Carolyn Staples, CCC/SLP, Area Rehab Director Infinity Rehab RAC Audits and Denials Management WHCA Fall Conference September 9, 2014 Objectives
JoLynn Munro, MS,OTR/L, Regional Vice President Infinity Rehab Carolyn Staples, CCC/SLP, Area Rehab Director Infinity Rehab RAC Audits and Denials Management WHCA Fall Conference September 9, 2014 Objectives
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Building A Successful MDS Program
 Building A Successful MDS Program Nadine Olness RN, RAC-CT MN State RAI Coordinator March 12, 2018 Objectives Acquire essential knowledge about what is required in order for MDS coordinators to be successful.
Building A Successful MDS Program Nadine Olness RN, RAC-CT MN State RAI Coordinator March 12, 2018 Objectives Acquire essential knowledge about what is required in order for MDS coordinators to be successful.
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT
 A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
Upcoming Seminars for the Illinois Health Care Association and the Illinois Council on Long Term Care
 February 8, 2011 Number 47 Upcoming Seminars for the Illinois Health Care Association and the Illinois Council on Long Term Care Seminars included in this issue: MDS 3.0 RAC-CT Certification and Recertification
February 8, 2011 Number 47 Upcoming Seminars for the Illinois Health Care Association and the Illinois Council on Long Term Care Seminars included in this issue: MDS 3.0 RAC-CT Certification and Recertification
Section O Special Treatments, Procedures and Programs. Presented for the DOH by Catharine B. Petko, RN BSN Myers and Stauffer LC April 7, 2016
 Section O Special Treatments, Procedures and Programs Presented for the DOH by Catharine B. Petko, RN BSN Myers and Stauffer LC April 7, 2016 Updates July 1, 2016: Mandatory submission of staffing and
Section O Special Treatments, Procedures and Programs Presented for the DOH by Catharine B. Petko, RN BSN Myers and Stauffer LC April 7, 2016 Updates July 1, 2016: Mandatory submission of staffing and
Downtime Viewer User Guide for All Users
 Downtime Viewer User Guide for All Users Overview... 1 Logging into Downtime Viewer... 1 Opening a Patient Chart in Downtime Viewer... 2 Patient Lists... 2 Clinics... 4 Navigating in the Patient s Chart...
Downtime Viewer User Guide for All Users Overview... 1 Logging into Downtime Viewer... 1 Opening a Patient Chart in Downtime Viewer... 2 Patient Lists... 2 Clinics... 4 Navigating in the Patient s Chart...
Payment Methodology. Acute Care Hospital - Inpatient Services
 Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance
 PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
State FY2013 Hospital Pay-for-Performance (P4P) Guide
 Guide") State FY2013 Hospital Pay-for-Performance (P4P) Guide Table of Contents 1. Overview...2 2. Measures...2 3. SFY 2013 Timeline...2 4. Methodology...2 5. Data submission and validation...2 6. Communication,
State FY2013 Hospital Pay-for-Performance (P4P) Guide Table of Contents 1. Overview...2 2. Measures...2 3. SFY 2013 Timeline...2 4. Methodology...2 5. Data submission and validation...2 6. Communication,
QAPI: Not too early to begin. Section M: Is your assessment system up to par?
 LTC LEADER jul112013 www.aanac.org Section M: Is your assessment system up to par? Caralyn Davis, Staff Writer When the Centers for Medicare and Medicaid Services (CMS) updates the RAI User s Manual for
LTC LEADER jul112013 www.aanac.org Section M: Is your assessment system up to par? Caralyn Davis, Staff Writer When the Centers for Medicare and Medicaid Services (CMS) updates the RAI User s Manual for
SAVE $50 SAVE $100. Medicare Boot Camp. Long-Term Care Version classes forming now!
 Medicare Boot Camp Long-Term Care Version *cannot be combined with any other discounts Register up to 90 days before course start date and SAVE $100 Coupon code: bcsave100 Register up to 60 days before
Medicare Boot Camp Long-Term Care Version *cannot be combined with any other discounts Register up to 90 days before course start date and SAVE $100 Coupon code: bcsave100 Register up to 60 days before
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling. Speaker: Thomas Martin November 2014
 Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across