Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand
|
|
|
- Roxanne King
- 6 years ago
- Views:
Transcription

1 This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati, Ohio James Anderson Center for Health Systems Excellence


2 550 Bed Medical Center Admissions/Year 30,848 Opt Visits 1.02 M Surgical Procedures 32,000 cases 28 OR s, 2 IR suites, Hybrid Cath lab 8 OR Outpatient Surgery Center 1.4 M sq. ft. Research Space 15,000 Employees Cincinnati Children s Hospital
3 System Level Measures Health Care Delivery System Transformation Strategic Improvement Priorities and System Level Measures ACCESS FLOW PATIENT SAFETY CLINICAL EXCELLENCE REDUCE HASSLES TEAM WELLBEING FAMILY CENTERED CARE 3 rd Next available appointment % of eligible patients with delays Discharge Prediction and Execution Growth Prediction Adverse drug events (ADE) per 1,000 doses Nosocomial infection rates: Bloodstream infection rate Surgical site infection rate infection rates: VAP Safe Practices Serious Safety Events Codes outside the ICU rate/1000 days Standardized PICU Mortality Ratio Expected/ Actual % use of Evidence- Based Care for eligible patients Functional Health Status Touch Time for Providers Employee Satisfaction Staffing Effectiveness Staff Physician Satisfaction Voluntary staff turnover rate Accident rate for staff with Work days lost Overall Rating: Patient Experience Functional Health Status Risk Adjusted Cost per Discharge
4 What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver the Correct Therapy / Treatment Outcomes Prevent Complications or Errors in Care Deliver Safe Care regardless of the Inherent Risks Safety Get Me Home, Keep me at Home Respect my needs Give me my Money s Worth Patient / Family Experience Value This is all FLOW management it is essential for SAFETY, PATIENT / FAMILY EXPERIENCE and QUALITY DELIVERY
5 Flow is a Safety Initiative Prediction Framework for Safety Getting the Rights Right Right Diagnosis and Treatment Right Patient in Right Bed Location Right Nursing Staff and Staffing Expertise Disease Specific Expertise Equipment Expertise Best Care Model Requires ability to Predict future needs, and manage present capacity control variability Operations Management techniques to understand and manage variability are the key to success
6 Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor
7 10/5/ /12/ /19/ /26/ /2/ /9/ /16/ /23/ /30/ /7/ /14/ /21/ /28/2015 1/4/2016 1/11/2016 1/18/2016 1/25/2016 2/1/2016 2/8/2016 2/15/2016 2/22/2016 2/29/2016 3/7/2016 3/14/2016 3/21/2016 3/28/2016 4/4/2016 4/11/2016 4/18/2016 4/25/2016 5/2/2016 5/9/2016 5/16/2016 5/23/2016 5/30/2016 6/6/2016 6/13/2016 6/20/2016 6/27/2016 7/4/2016 7/11/2016 7/18/2016 7/25/2016 8/1/2016 8/8/2016 8/15/2016 8/22/2016 8/29/2016 9/5/2016 9/12/2016 9/19/2016 9/26/ /3/2016 # of New Patient Failures Total # of Bed Days Critical Flow Failure Recognition Weekly Critical Flow Failures Over the last 52 weeks Week Beginning # of New Failures Total Failures (Bed Days) Last Update: 2/2/2015 by Michael Ponti-Zins, for Data Source: MPS Type of Control Chart: P Chart

8 JUL AUG SEP OCT NOV DEC JAN FEB MAR APR MAY JUN # of Patients with a New Failure Our Growth Requires Efficiency Improvement 300 Critical Patient Flow Failures by Month Month of Fiscal Year Last Update: 3/4/2016 by M. Ponti-Zins, for Data Source: MPS
9 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, Predictive Risk Analysis
10 IHI Theory on Flow Outcomes Primary Drivers Secondary Drivers Specific Change Ideas Decrease overutilization of hospital services Shape or Reduce Demand Relocate care in ICUs in accordance with patients EOL wishes Relocate care in Med/Surg Units to community-based care settings Relocate low-acuity care in EDs to community-based care settings Decrease demand for hospital beds through delivering appropriate care Decrease demand for hospital beds by reducing hospital acquired conditions 1. Proactive advanced illness planning 2. Development of palliative care programs (hospital-based and community-based) 3. Reduce readmissions for high risk populations 4. Extended hours in primary care practices 5. Urgent Care and Retail Clinics 6. Enroll patients in community-based mental health services 7. Paramedics & EMTs triaging & treating patients at home 8. Greater use of clinical pathways and evidence-based medicine 9. Care management for vulnerable/high risk patient populations 10. Decrease complications/harm (HAPU, CAUTI, SSI, falls with harm) and subsequent LOS 11. Redesign surgical schedules to create an predictable flow of patients to downstream ICUs and inpatient units Optimize patient placement to insure the right care, in the right place, at the right time Increase clinician and staff satisfaction Demonstrate a ROI for the systems moving to bundled payment arrangements Match Capacity and Demand Redesign the System Decrease variation in surgical scheduling Oversight system for hospital-wide operations to optimize patient flow Real-time demand and capacity management processes Flex capacity to meet hourly, daily and seasonal variations in demand Early recognition for high census and surge planning Improve efficiencies and throughput in the OR, ED, ICUs and Med/Surg Units Service Line Optimization (frail elders, SNF residents, stroke patients, etc.) Reducing unnecessary variations in care James and managing M. Anderson LOS outliers Center 1. Assess seasonal variations and changes in demand patterns and proactively plan for variations 2. Daily flow planning huddles (improve predictions to synchronize admissions, discharges and discharges) 3. Real-time demand and capacity problem-solving (managing constraints and bottlenecks) 4. Planning capacity to meet predicted demand patterns 5. High census protocols to expedite admissions from the ED and manage surgical schedules. 1. Redesign surgical schedules to improve throughput and to improve smooth flow of patients to downstream ICUs and inpatient units 2. Separate scheduled and unscheduled flows in the OR 3. ED efficiency changes to decrease LOS 4. Decrease LOS in ICUs (timely consults, tests and procedures) 5. Decrease LOS on Med/Surg Units (case management for patients with complex medical and social needs) 6. Advance planning for transfers to community-based care settings 7. Cooperative agreements with rehab facilities, SNFs and nursing homes
11 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS/outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, Predictive Risk Analysis
12 Evidence Based Care Evidence Based Care Guidelines serve as an interface between rapidly evolving scientific information and busy clinical practices Developed by Inter-disciplinary teams experts Implementation Awareness of recommendation to facilitate change Easy access to the Evidence Feedback on Outcomes Feedback on further improvements Culture of Improvement / Evidence Based Care
13 Integration Priority Practice - Plan Prioritization Goal = Exceptional, Safe, Affordable Care Every Child Owner Executive Leadership Practice What we Do Essential Steps, Decisions and Actions Owner Clinical Leadership Teams Departments / Divisions Processes How we Do It Processes to execute to the goal Owner Operational Leaders Sites of Care Plan Implement the Processes - plan through application of process steps Owner Sites of Care leaders and clinical staff (MD / RN) Front Line Implementation Just Do It Every day for every child

14 Cytomegalovirus Prophylaxis 75% Decrease in CMV infection liver/intestine transplants Decreased IV-IGG expense Liver - Intestine Danziger-Isakov, Lara et al. CCHMC Integrated Solid Organ Transplant
15 Yearly SSI Patients - CCHMC Total SSI Pa ents Fiscal Year 1032 SSI s 12 Years 540 SSI s Prevented 492 SSI s



16 Yearly SSI Patients - CCHMC Total SSI Pa ents Case Average 10 days LOS $27, Business Case 5400 days LOS $145.8 million Fiscal Year 1032 SSI s 12 Years 540 SSI s Prevented 492 SSI s

17 Standardization for Outcomes Merging Evidence Based Care and Practice Focus on Excellence SSI Spines
18 SSI Accomplishments Baseline rate: 4.4 SSIs/100 procedures, Current Rate: 1.7 SSIs/100 procedures 60% reduction, 32% reduction in past 3 years - $17.4 Million from SSI alone Overall SPS - Estimated 6,686 fewer children harmed Since October $121.4 Million saved in SPS Network Toltzis P, O Riordan M, Cunningham DJ, Ryckman FC, Bracke TM, Olivea J, Lyren A. A statewide collaborative to reduce pediatric surgical site infections. Pediatrics :


19 Inflammatory Bowel Disease 92 Care Centers 26,000 patients 795 physicians
20 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, Predictive Risk Analysis
21 ICU Bed Availability ICU Scheduling Category Case Statistics by Category Total PICU Days Case Count ALOS Short (61%) 1.27 (27%) Medium (28%) 3.72 (37%) Long (11%) 9.76 (36%) Grand Total

22 ICU Admission Model Elective Cases Short Stay Cases Access Cap # Cases on Schedule / Day Long Stay Cases Fixed # Beds

23 Predicting ICU Discharge
24 7/16/2008 9/14/ /13/2008 1/12/2009 3/13/2009 5/12/2009 7/11/2009 9/9/ /8/2009 1/7/2010 3/8/2010 5/7/2010 7/6/2010 9/4/ /3/2010 1/2/2011 3/3/2011 5/2/2011 7/1/2011 8/30/ /29/ /28/2011 2/26/2012 4/26/2012 6/25/2012 8/24/ /23/ /22/2012 2/20/2013 4/21/2013 6/20/2013 8/19/ /18/ /17/2013 2/15/2014 4/16/2014 6/15/2014 8/14/ /13/ /12/2014 2/10/2015 4/11/2015 6/10/2015 8/9/ /8/ /7/2015 2/5/2016 4/5/2016 6/4/2016 8/3/ /2/ /1/2016 1/30/2017 3/31/2017 5/30/2017 7/29/2017 9/27/ /26/2017 1/25/2018 3/26/2018 # of Patients with a New Failure 7/16/2008 9/14/ /13/2008 1/12/2009 3/13/2009 5/12/2009 7/11/2009 9/9/ /8/2009 1/7/2010 3/8/2010 5/7/2010 7/6/2010 9/4/ /3/2010 1/2/2011 3/3/2011 5/2/2011 7/1/2011 8/30/ /29/ /28/2011 2/26/2012 4/26/2012 6/25/2012 8/24/ /23/ /22/2012 2/20/2013 4/21/2013 6/20/2013 8/19/ /18/ /17/2013 2/15/2014 4/16/2014 6/15/2014 8/14/ /13/ /12/2014 2/10/2015 4/11/2015 6/10/2015 8/9/ /8/ /7/2015 2/5/2016 4/5/2016 6/4/2016 8/3/ /2/ /1/2016 1/30/2017 3/31/2017 5/30/2017 7/29/2017 9/27/ /26/2017 1/25/2018 3/26/2018 # of Patients with a New Failure 7/16/ /14/2008 1/12/2009 4/12/2009 7/11/ /9/2009 1/7/2010 4/7/2010 7/6/ /4/2010 1/2/2011 4/2/2011 7/1/2011 9/29/ /28/2011 3/27/2012 6/25/2012 9/23/ /22/2012 3/22/2013 6/20/2013 9/18/ /17/2013 3/17/2014 6/15/2014 9/13/ /12/2014 3/12/2015 6/10/2015 9/8/ /7/2015 3/6/2016 6/4/2016 9/2/ /1/2016 3/1/2017 5/30/2017 8/28/ /26/2017 2/24/2018 7/16/ /14/2008 1/12/2009 4/12/2009 7/11/ /9/2009 1/7/2010 4/7/2010 7/6/ /4/2010 1/2/2011 4/2/2011 7/1/2011 9/29/ /28/2011 3/27/2012 6/25/2012 9/23/ /22/2012 3/22/2013 6/20/2013 9/18/ /17/2013 3/17/2014 6/15/2014 9/13/ /12/2014 3/12/2015 6/10/2015 9/8/ /7/2015 3/6/2016 6/4/2016 9/2/ /1/2016 3/1/2017 5/30/2017 8/28/ /26/2017 2/24/2018 # of Patients with a New Failure # of Patients with a New Failure Critical Flow Failures 24 Delayed or Canceled Surgery Due to Bed Capacity PICU Bed Not Available for Urgent Use Daily Failures Patients who Utilize an ICU bed b/c an Appropriate Bed is Not Available Daily Failures Psychiatry Patients Placed Outside of their Primary Unit Daily Failures
25 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, Predictive Risk Analysis

26 Strategies for Patient Placement Early Day Beds PICU, CICU Critical Units Later Day Beds All units Demand : Capacity Match Opportunistic with ethought Specific Bed D:C Match Unit Bed Awareness
27 Discharge Prediction P27 Various approaches to Discharge Management 1980 s Keep it a Secret 1990 s 2000 s Discharge goals AM before 11 > 30-40% Shift goals 4 hour time block goals with prediction of window Reactive Not Patient Centered Prediction Discharge when Medically Ready


28 Timeline for DC when Medically Ready Admission to Floor Discharge Criteria Set Treatment Protocol Followed Discharge Criteria Met Nurse Notifies Staff 2 Hrs Discharge Home Re-Adm & LOS Tracked Standardized Criteria Buy-In by Staff Standardized Protocols for most Tx Evaluation Criteria Modify Rounding Clear Discharge Criteria Communication Family Criteria established at admission Nurse at bedside notifies service when Medical discharge criteria are met Discharge from floor in < 2 hours Review Length of Stay and Re-Admissions as balancing measures Not about Speed Now about Efficiency
29 Discharge When Medically Ready Karen Tucker, Angela Statile, Diane Herzog, and Christy White Increase percentage of all HM patients who have met* Medically ready criteria who will be discharged within two hours of reaching that goal* on A6S, A6N, LA1W from 75%to 80% by June 30, 2014 Productivity: Optimize use of facilities and staff and improve patient flow to achieve 20% greater utilization of existing assets by June 30, 2015 Criteria for Medically Ready Defined at Admission Shared Ownership/ Accountability and Buy-In Among Physicians and Nurses Communication regarding prediction of discharge and defined goals is ongoing through the hospital stay Potential Barriers to Discharge are Clearly Articulated and Mitigation Plans Established Performance by team is transparent Evidence of Preoccupation with Failure Clear expectations for Parents/ Families Agreement among HM attendings and nursing staff of discharge criteria for order set diagnoses and general admissions (LOR 2) 1) 8 pm Huddle discussion re: early discharges (LOR 2) 2) 0630 notification of patients ready for discharge (LOR 1) Performance Management (LOR 1) Standardized and modifiable order sets (LOR 2) Identify and Mitigate Plans: 1) Transportation- census based (LOR 1) 2) Pharmacy- priority fills (LOR 2), Outpt delivery to patient room (LOR 1) 3) Consults- proactive evaluation (LOR 2) 4) RT- process in PICU (LOR 1) 5) Home Health Care Daily Feedback reports to RNs and MD s with ID and mitigation of process and outcome measure failures (LOR 2) Feedback of data by HM team In conference room and by (LOR 1) Auto notification to resident team that patient has met all criteria (LOR 2)

30 Discharge when Medically Ready All Units


31 Service Level DC when Medically Ready

32 Average Length of Stay (Days) Balancing Measures Length of Stay Hospital Medicine Average Length of Stay patients with selected diagnosis Unit 1 Unit 2 Unit 3 All FY11 FY13

33 Balancing Measures Readmission Rate
34 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, Predictive Risk Analysis

35 Predicting Future Programmatic Needs Environmental Impact Studies LUNG TRANSPLANTATION
 and the growth estimate.")


36 ICU Bed Needs Number of beds needed based on probability of having a full unit (5%, 2%, 1%, 0%) and the growth estimate. Low/Conservative Mid-Range/Most Likely High/Aggressive Growth 1 Yr 3 Yr 5 Yr 7 Yr 10 Yr 1 Yr 3 Yr 5 Yr 7 Yr 10 Yr 1 Yr 3 Yr 5 Yr 7 Yr 5% % % % Yr

37 Predicted to Actual ICU Bed Demand ICU Prediction Mid Level Conservative Aggressive Year Year Year Year Year Year ICU demand appears to be dependent on pre-transplant severity and much higher than originally anticipated Actual
38 Predicted to Actual Cardiology Bed Demand Heart Prediction Mid Level Conservative Aggressive Year Year Year Year Year Year Cardiology demand appears to be lower than original projections Actual

39 Predicted to Actual Pulmonary Bed Demand Pulmonary Prediction Mid Level Conservative Aggressive Year Year Year Year Year Year Pulmonary demand appears to be in line with original projections Actual
40 Outpatient Demand
41 Outcomes and Observations - Environmental Impact Assessment provided valuable information allowing for assessment and agreement across the hospital before program was initiated - Answer questions about patient flow and placement - Assess potential stress on existing resources - Quantify demand and capacity needs (staffing, beds, outpatient clinic rooms, PFT demand, OR demand) - Requires assumptions and research for new programs - As always your results are only accurate if your assumptions are correct

42 Staffing Prediction Proactive Planning Data to Front Line Leaders Updated daily Right Staff for the Right Patients Correct Number and Competency Flexible with Changing Environment Prediction of Needs Be Prepared Be Resilient
43 Staffing Prediction Proactive Planning
44 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, Predictive Risk Analysis
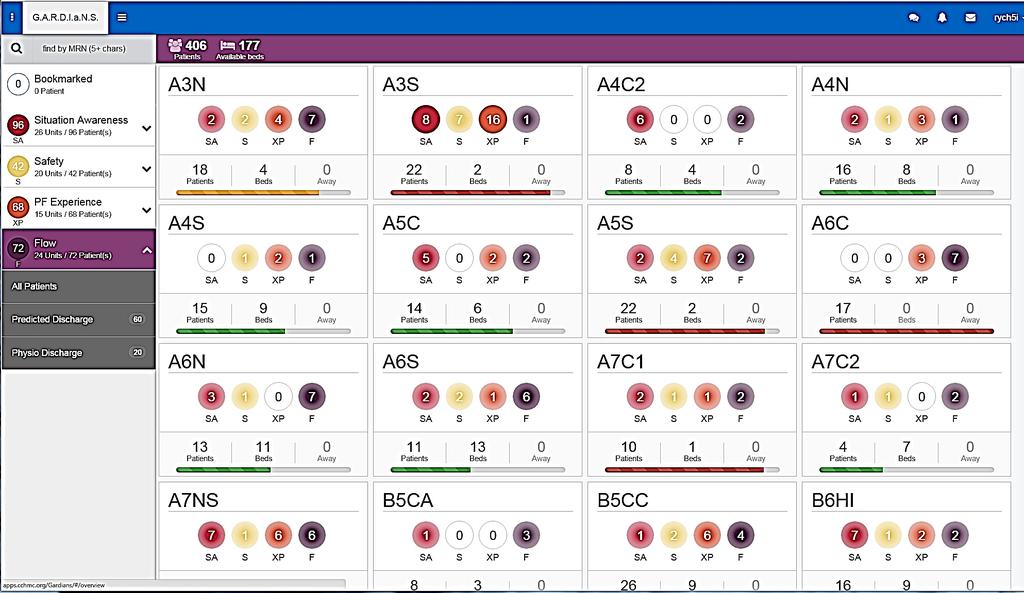
45 GARDiANS
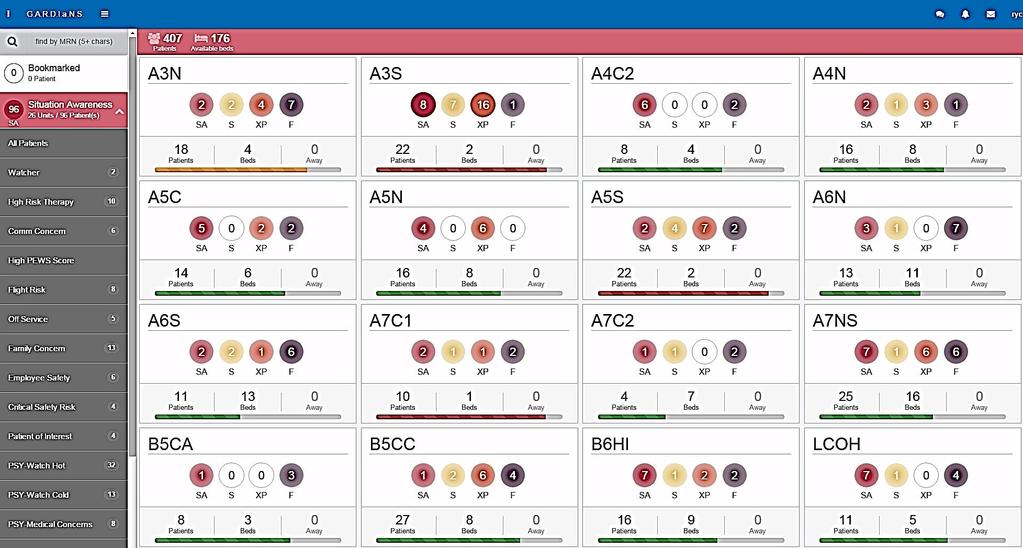
46 GARDiANS
47 Hospital Wide System for Safety 3 Times - Every Day Individual Room / Floor / System Predictions Capacity and Safety Floor Huddles PeriOp Huddle Outpt, Home, Psych ED Huddle ICU Huddles Institutional Wide Bed Huddle Capacity Management Pharmacy Pt. Transport Facilities Institutional Daily Operations Brief System Prediction Mitigation Strategy Security Housekeeping P.F.E.

48 Flow Dashboard Sites of Care

")

49 Patient Satisfaction Only 3-4% of 1 Million outpatient visitors rank our care in the lower half (0-6 of 10 pts) 35,000 patient per year Great American Ballpark Paul Brown Stadium 42,319 65,535
50 Understanding Outliers I thought: If I can get 80-85% of this under good control, that will solve at least 85% of the problem
51 N=297 cases < 62 days (85.6%) Total N=347 N=50 >62 Days N=25 >100 Days N=14 >200 Days N=6 >365 Days
52 1,795 bed days 1,339 bed days 2,131 bed days 2,340 bed days 7,595 Bed Days 50 Patients 342 Acute Care Beds 22.2 Days Total Hospital Census 6.08% Yearly Hospital Census
53 Observations on Outliers In these predictive models, it is important to be right. What is really important is the cumulative magnitude of your errors. The errors are often the result of big surprises, not multiple small issues. Failure to meet the predictive model leads to progressive and increasing cumulative error, (the more you are off, the more you are off.) It is hard to offset the surprise errors with great prediction of the expected.
54 Lessons Learned Building Will to work on Flow is a challenge When it works, it is not on anyone s radar If it works for me, your problem is not my problem. When it does not work, somebody else should solve it Linkage Safety and Flow Speed vs Efficiency Work Backwards not just ward Embrace Mathematics and Analytics Standardize processes and work flows

55 Make it Personal Don t let the Data Drown out the Dream Stories not Statistics Names and Faces Accountability is Personal & Group Responsibility Collective Mission/Vision Cincinnati Children s Hospital Medical Center 2013

56 Thanks!
Hospital Flow Case Study: Cincinnati Children s Hospital
 Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Right Care Right Place Right Time
 System Level Measures Right Care Right Place Right Time M15 I have nothing to disclose Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children
System Level Measures Right Care Right Place Right Time M15 I have nothing to disclose Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
Using Quality Improvement to Optimize Pediatric Discharge Efficiency
 This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
Why Do Flow? The Cincinnati Children s Hospital Journey. December 11, 2017
 December 11, 2017 Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation - Retired Sr. Vice President Medical Operations Cincinnati Children
December 11, 2017 Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation - Retired Sr. Vice President Medical Operations Cincinnati Children
Why Do Flow? The Cincinnati Children s Hospital Journey
 Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation Retired; Sr. Vice President Medical Operations, Cincinnati Children s Hospital, University
Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation Retired; Sr. Vice President Medical Operations, Cincinnati Children s Hospital, University
Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time
 This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Pat Rutherford Hospital Flow Professional Development
This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Pat Rutherford Hospital Flow Professional Development
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time
 This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Hospital Flow Professional Development Program
This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Hospital Flow Professional Development Program
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
4/12/2016. High Reliability and Microsystem Stress. We have no financial, professional or personal conflict of interest to disclose.
 High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance
 Directorate for Health Workforce and Performance") Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Page 347. Avg. Case. Change Length
 Page 345 EP 8 How nurses use trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery Model(s). The development of operational budgets
Page 345 EP 8 How nurses use trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery Model(s). The development of operational budgets
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
SFGH. Management System. Components. SFGH Management System. Improvement. Time. Strategic Planning True North. Value Streams: Rapid Improvement Events
 SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Value Equation for Healthcare
 Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver
Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo. Session ID: 325
 Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Taming Length of Stay Challenges Through Analytics
 Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Mark Stagen Founder/CEO Emerald Health Services
 The Value Proposition of Nurse Staffing September 2011 Mark Stagen Founder/CEO Emerald Health Services Agenda Nurse Staffing Industry Update Improving revenue trends in healthcare staffing 100% Percentage
The Value Proposition of Nurse Staffing September 2011 Mark Stagen Founder/CEO Emerald Health Services Agenda Nurse Staffing Industry Update Improving revenue trends in healthcare staffing 100% Percentage
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Self-assessment surveys details & definitions
 Self-assessment surveys details & definitions Completing the Paradigm self assessment surveys is the very first step in achieving the Paradigm Award. Only organizations who complete the self assessment
Self-assessment surveys details & definitions Completing the Paradigm self assessment surveys is the very first step in achieving the Paradigm Award. Only organizations who complete the self assessment
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Performance Improvement Bulletin
 SPECIAL DELIVERY UNIT/ NATIONAL TREATMENT PURCHASE FUND Issue No.1 08/12 Performance Improvement Bulletin Featured Work underway - Maximum Waiting Time Targets 2 Case Study No. 1 Galway & Roscommon University
SPECIAL DELIVERY UNIT/ NATIONAL TREATMENT PURCHASE FUND Issue No.1 08/12 Performance Improvement Bulletin Featured Work underway - Maximum Waiting Time Targets 2 Case Study No. 1 Galway & Roscommon University
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
1. November RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 12.5%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
Improve the Efficiency and Service of the Emergency Room at North Side Hospital
 Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Hip Today Home Tomorrow:
 Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
Accomplishments Fiscal Year UPMC Passavant
 Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
Integrating Quality Into Your CDI Program: The Case for All-Payer Review
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
Physician Performance Analytics: A Key to Cost Savings
 Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Tell Your Story with a Well- Designed Data Plan. Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System
 Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Transitions in Care. Discharge Planning Pathway & Dashboard
 Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Achieving Hospital-wide Patient Flow
 WHITE PAPER Achieving Hospital-wide Patient Flow The Right Care, in the Right Place, at the Right Time AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 ihi.org How to Cite This Paper: Rutherford
WHITE PAPER Achieving Hospital-wide Patient Flow The Right Care, in the Right Place, at the Right Time AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 ihi.org How to Cite This Paper: Rutherford
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Bold Goal PI Radar Dashboard
 Bold Goal PI Radar Dashboard Helen Macfie, Pharm.D., FABC Chief Transformation Officer Certified Lean Leader For IHI Patient Safety Executive Development Course, September, 2016 This presenter has nothing
Bold Goal PI Radar Dashboard Helen Macfie, Pharm.D., FABC Chief Transformation Officer Certified Lean Leader For IHI Patient Safety Executive Development Course, September, 2016 This presenter has nothing
Chest Pain Accredited. Transplant Program-Heart, Kidney, Liver. Hear Transplant Program serving San Antonio area for 25 years
 PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
1. March RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 13.8%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August 2016
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer,
 Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer, Professional Research Consultants and Executive Director, The
Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer, Professional Research Consultants and Executive Director, The
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PSYCHIATRY SERVICES UPDATE
 PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Harm Across the Board Reporting: How your Hospital Can Get There
 Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Meaningful Use: A Practical Approach. CSO HIMSS Spring Conference 2013
 CSOHIMSS 2013 Slide 0 May 17 th, 2013 Meaningful Use: A Practical Approach Jay Brown Sr. VP & CIO, UC Health Rick Haucke Manager, IS&T, PMO, UC Health Ajay Sharma FHIMSS, Sr. Manager, Sogeti USA, LLC CSO
CSOHIMSS 2013 Slide 0 May 17 th, 2013 Meaningful Use: A Practical Approach Jay Brown Sr. VP & CIO, UC Health Rick Haucke Manager, IS&T, PMO, UC Health Ajay Sharma FHIMSS, Sr. Manager, Sogeti USA, LLC CSO
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
New healthcare delivery models: Interprofessional, regional, international
 New healthcare delivery models: Interprofessional, regional, international Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu Center Timothy G. Buchman PhD, MD, FACS, FCCP, MCCM Founding Director, Emory
New healthcare delivery models: Interprofessional, regional, international Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu Center Timothy G. Buchman PhD, MD, FACS, FCCP, MCCM Founding Director, Emory
Hospital Flow: Right Care, in the Right Place, at the Right Time. Pat Rutherford, RN, MS Vice President, Institute for Healthcare Improvement
 Q11 This presenter has nothing to disclose Hospital Flow: Right Care, in the Right Place, at the Right Time Pat Rutherford, RN, MS Vice President, Institute for Healthcare Improvement IHI s National Forum
Q11 This presenter has nothing to disclose Hospital Flow: Right Care, in the Right Place, at the Right Time Pat Rutherford, RN, MS Vice President, Institute for Healthcare Improvement IHI s National Forum
8/31/2015. Session C826 Evidence-Based Staffing Strategies Support Healthy Work-Life Balance Rachael Schweikert, RN Kevin Schwedhelm MSN RN
 Session C826 Evidence-Based Staffing Strategies Support Healthy Work-Life Balance Rachael Schweikert, RN Kevin Schwedhelm MSN RN Nurse Staffing Core vs. Float Staff 30 years ago 20-10 years ago 5 yrs Prior
Session C826 Evidence-Based Staffing Strategies Support Healthy Work-Life Balance Rachael Schweikert, RN Kevin Schwedhelm MSN RN Nurse Staffing Core vs. Float Staff 30 years ago 20-10 years ago 5 yrs Prior
Use of TeleMedicine to Improve Clinical and Financial Outcomes
 Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Columbus Regional Hospital Pressure Ulcer Prevention
 Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
A21/B21: IHI 23rd Annual National Forum on Quality Improvement in Health Care
 A21/B21: IHI 23rd Annual National Forum on Quality Improvement in Health Care Carolyn Sanders, RN, PhD, NEA-BC Vice President, Patient Services & Chief Nursing Officer Lorna Prutzman, RN, MSN Executive
A21/B21: IHI 23rd Annual National Forum on Quality Improvement in Health Care Carolyn Sanders, RN, PhD, NEA-BC Vice President, Patient Services & Chief Nursing Officer Lorna Prutzman, RN, MSN Executive
? Prehab, immunonutrition. Safe surgical principles. Optimizing Preoperative Evaluation
 Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Riverside s Vigilance Care Delivery Systems include several concepts, which are applicable to staffing and resource acquisition functions.
 1 EP8: Describe and demonstrate how nurses used trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery System(s). Riverside Medical
1 EP8: Describe and demonstrate how nurses used trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery System(s). Riverside Medical
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
School of Nursing Applying Evidence to Improve Quality
 Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
The Case for Optimal Staffing: A Call to Action
 The Case for Optimal Staffing: A Call to Action 2015 ANCC National Magnet Conference October 7, 2015 2:30 3:30pm Session C721 Mary Jo Assi, DNP, RN, NEA BC, FNP BC Director of Nursing Practice and Work
The Case for Optimal Staffing: A Call to Action 2015 ANCC National Magnet Conference October 7, 2015 2:30 3:30pm Session C721 Mary Jo Assi, DNP, RN, NEA BC, FNP BC Director of Nursing Practice and Work
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving