UL Hospitals Group Operational Plan
|
|
|
- Catherine Conley
- 6 years ago
- Views:
Transcription
1 UL Hospitals Group Operational Plan 2017
2 arexecutive Summary Table of Contents Contents Operational Plan 2017 Acute Hospital Division... 2 INTRODUCTION... 2 ACUTE HOSPITAL DIVISION PRIORITIES UL Hospital Group... 3 INTRODUCTION... 3 UL HOSPITALS CEO PRIORITIES GOVERNANCE UL HOSPITALS... 6 ORGANISATIONAL CHART... 7 IMPACT OF DEMOGRAPHICS ON HOSPITALS ACTIVITY... 9 Unscheduled Care... 9 Scheduled Care Operational Framework Financial Plan Operational Framework Workforce Plan Cancer Services Quality and Patient Safety Performance and Accountability Framework Implementing Priorities Appendices APPENDIX 1 HUMAN RESOURCES APPENDIX 2: PERFORMANCE INDICATOR SUITE - DOP DETAILED ACTIVITY TARGETS BY HOSPITAL FOR INPATIENTS AND DAY CASES APPENDIX 3: CAPITAL PROJECTS
3 arexecutive Summary Operational Plan 2017 Acute Hospital Division Introduction The demand for acute hospital services continues to increase in line with a growing and ageing population. The Hospital Groups continue to implement the Securing the Future of Smaller Hospitals: A Framework for Development. This will ensure that all hospitals irrespective of size work together in an integrated way to meet the needs of patients and staff, with an increased focus on small hospitals managing routine or planned care locally and more complex care managed in the larger hospitals Available Budget 2016 Budget m m UL Hospitals Group m m Acute hospital services will continue to respond to demographic and demand driven cost pressures in An estimated increase of 1.7% in costs associated with increasing population and age profile is predicted for acute hospitals in 2017 compared with In addition, an increase in ED presentations of 5% is evident at the end of 2016, compared to the same period in The division will monitor this activity closely and manage the potential impact on elective services. Acute hospital services aims to provide safe, quality, effective patient centred care to all service users. Acute Hospital Division Priorities 2017 Embed robust structures within Hospital Groups to provide direct support to the smaller hospitals in the group in line with the development of the Hospital Group strategic plan Enhance and build capacity of quality and patient safety across hospitals Continue to develop a system to report hospital safety statements in conjunction with Hospital Group CEOs and Clinical Directors. 2

4 UL Hospital Group Introduction UL Hospitals Group Operational Plan 2017DarExecutive Summary University of Limerick (UL) Hospital Group is comprised of a group of six hospitals functioning collectively as a single hospital system in the Mid-West of Ireland. The six sites include: University Hospital Limerick is the Model 4 hospital for the region providing major surgery, cancer treatment and care, emergency department services, as well as a range of other medical, diagnostic and therapy services. It is where all critical care services are located in addition to a 24/7/365 Emergency Department and it is a designated cancer centre. UHL is one of the busiest Emergency Departments in Ireland with over 64,000 (new and return) patients annually. Emergency and complex surgeries are only undertaken at UHL. The hospital is the hub for Ennis hospital, Nenagh hospital and St. John s hospital which manage the majority of their local population through their medical assessment units and inpatient beds. Patients who require access to critical and complex care are seen at University Hospital Limerick and either stabilised and transferred to a local Model 2 hospital, namely Ennis or Nenagh or admitted to UHL if required. Croom Hospital is part of the UL Hospitals group. It is the dedicated orthopaedic hospital for adults and children in the Mid-West region. Croom hospital also accepts the transfer of Orthopaedic patients from UL hospital for post-acute. In addition to Orthopaedic services, Rheumatology and Pain Management services are also provided. University Maternity Hospital, Limerick is the second largest maternity hospital outside Dublin with approximately 4,500 births (2016) and the sole provider of obstetrical, midwifery and neonatal intensive care to the Mid-West region. It serves Limerick, Clare and Tipperary N.R. The maternity hospital also accommodates patients from outside the Mid-west region. These include women from North Cork, Tipperary, North Kerry and areas of Offaly. They also provide tertiary referral for smaller Neonatal Units from outside the region. 3
5 arexecutive Summary UL Hospitals CEO Priorities 2017 No. Priority Actions 1. Engage & Develop UL Hospitals next 3 year Strategy Set up Academic Hub with University of Limerick focusing on all Health Sciences. 3. Review Medicine Divisions and agree a new system of medical rotas and equal access. Persons Responsible CEO & Executive CEO & Executive CEO & CCD Target / Date Q1 Q2-Q3 Q2 4. Grow and flourish UL Hospitals Group that attracts and retains professionals with a focus on improving NCHD educational supports. CEO & DHR Q3 5. Open New Emergency Department that is aligned to new pathways that improves patient access across the services. CEO & COO Q3 6. Review Department of Radiology which enhances workflow across the Group and supports Diagnostic services. CEO & COO Q Review UL Hospitals approach to ehealth and enhance our ICT team function underpinned by a clear Strategy for ehealth. Progress Peri Operative Strategy to include: Increasing surgical procedures at Nenagh & Ennis Hospital Develop a National Centre for Robotic Surgery Open & develop the Vascular Hybrid Theatre CEO & Director of Informatics, Planning & Performance CEO & CCD Q3 Q3 & Q4 9. Progress Capital Planning Applications for: UL Hospitals New Maternity Hospital 96 bed block at University Hospital Limerick CEO Q4 10. Embed QRPS function across the Group with clear oversight and accountability on all aspects of QRPS. CEO/Director IPP Q4 11. Agree a clear approach to Research at UL Hospitals Group with the University of Limerick and seek Research Board funding and acknowledgement. CEO & CCD Q3-Q4 4
6 arexecutive Summary No. 12. Priority Actions Implement Accountability Framework across the Executive & Directorates in line with National Performance requirements. Persons Responsible CEO Target / Date Q1 13. Deliver on Pay & Numbers Strategy and manage costs in line with the budget. CEO & Executive 14. Progress the Values In Action Project across all MDT to improve culture. CEO & Executive Q1-Q2 15. Progress the National Maternity Strategy. CEO & DOM 16. Support and Lead out on the GE LEAF Project at UL Hospitals to improve efficiency. CEO,COO, CCD 5
 2017 and allocated Group budgets.")
7 arexecutive Summary Governance UL Hospitals The hospitals in Ireland are now organised into seven Hospital Groups (HGs). Each Group Chief Executive has full legal authority to manage the Group delegated to them under the Health Act 2004 in line with National Service Plan (NSP) 2017 and allocated Group budgets. The UL Hospitals Group Operational Plan 2017 is aligned with this Acute Hospitals Division overarching Operational Plan. The Group Chief Executives report to the National Director for Acute Services and are accountable for their planning and performance under the Performance and Accountability Framework of the HSE. All targets and performance criteria adopted in the service plan and the divisional Operational Plan will be reported through this framework. UL Hospitals is governed by an interim Board and an Executive Management Team led by a CEO who reports to the Board. Our services are delivered across the six sites under the leadership of five directorates namely, Medicine Directorate, Perioperative Directorate, Diagnostic Directorate, Maternal and Child Health Directorate and Facilities Directorate. Each Directorate is led by a team of staff bringing Clinical, Managerial and Financial expertise together to provide quality driven safe services, focused on the experience and outcomes for the patient. Back row left to right: Mr Jim Canny, Mr Graham Knowles, Mr Michael Mulcahy SC and, seated left to right, Dr Mary Gray, Prof Niall O Higgins (Chairman) and Mr Alec Gabbett. 6
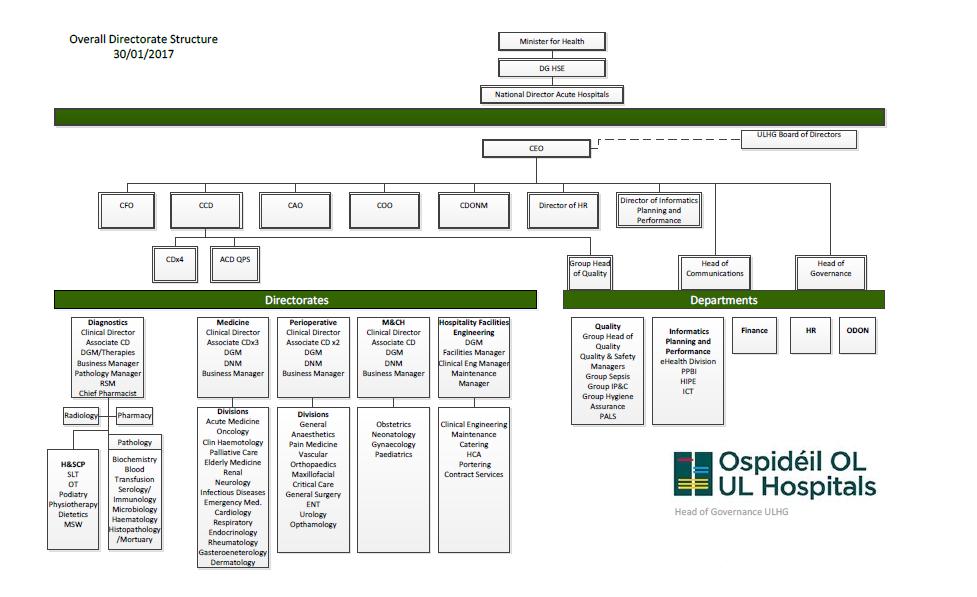
8 Organisational Chart 7
9 Impact of Demographics on Hospitals According to 2016 CSO Preliminary figures, the population of the Mid-West Region is 385,172. This is 1.5% higher than the 2011 reported figures. The biggest increase in population appeared to occur in Limerick City (2.1%). The population in Limerick County grew by 1.6%, North Tipperary by 1.5% and Clare saw an increase of 1.2%. The Hospital Group serves a socially diverse population including Limerick City which is the most deprived local authority nationally with 36.8% of its inhabitants either very disadvantaged or disadvantaged (Health Profile 2015 Limerick City). In sharp contrast to this, Limerick County is ranked as the eight most affluent local authority area nationally with 54% of its population either being marginally above affluence or affluent (Health Profile 2015 Limerick County). The national age profile particulary impacts on emergency services. Life expectancy at birth in Ireland has increased and is above the EU average of 80.9 years (Source: Eurostat). People are living longer through medical advances, technology along with an increased knowledge and focus on health and general well-being. According to the European Commission, ageing is one of the greatest social and economic challenges for all countries and by 2025 more than 20% of Europeans will be 65 or over with a particular rapid increase in the numbers of those aged 80 and above. Based on 2011 CSO figures, the population of over 65s was set to increase by 3.1% or 19,400 persons between 2015 and 2016 with an additional 2,900 persons over 85 years of age in Population Persons 2011 Persons 2016 * Actual change % change Limerick City 57,106 58,319 1, % Limerick County 134, ,856 2, % North Tipperary 70,322 71,370 1, % Clare 117, ,627 1, % Mid-West 379, ,172 5, % Ireland 4,588,252 4,757, , % * 2016 CSO figures are Preliminary The challenge remains to adapt health care services, settings and models of care to adequately meet the needs of an ageing population whilst providing a safe, dignified and patient centred service at all times within allocated budgets. In addition, chronic diseases (Cardiovascular disease, Cancer, Stroke, Respiratory Disease and Diabetes) are on the rise with population projections indicating that by 2021 a further 94,580 people will have at least one chronic condition (Tilda, 2010) representing a 20% increase. However, due to heightened awareness, a strong leaning towards more active and healthy lifestyles along with continuing focused clinical and academic research, surviorship of chronic diseases in Ireland is also increasing which is a postive and welcome transition. 8
10 2016 Activity Unscheduled Care In 2016 (December 2016 YTD) there was a 4.6% increase in the number of new patients presenting to the Emergency Department in University Hospital Limerick (59,950 YTD December 2016 up from 57,297 YTD December 2015). The Local Injury Units (LIU) within UL Hospitals Group also saw an overall increase in patients of 2.5% when compared to the same period last year (YTD Dec 2016 v YTD Dec 2015) New ED Attendances - UHL Emergency Discharges The result of this pressure on emergency services was a 16.9% year on year rise in the number of emergency discharges (YTD Nov 2015 v 2016) across the Group. (Nov 2016 most recent available data) Ennis Nenagh St. John's Hospital UHL Nov YTD 2015 Nov YTD 2016 LIU s now account for just over 30% of all emergency presentations for the Group. 9
11 Scheduled Care Inpatient Discharges Ennis Nenagh St. John's Hospital UHL Inpatient Discharges across the Group YTD December 2016 when compared to the same period in 2015 are showing an increase of 8.8% Outpatient attendances have grown by 1.5% across the Group year on year. UL Hospital Group has treated over 228,000 patients in all our outpatient centres this year to date (December 2016). Croom Ennis Nenagh St. John's Hospital Limerick UHL 2016 December YTD Outpatient Attendances 23, ,411 10,581 16,131 11,311 10,038 Day Cases Croom Ennis Nenagh St. John's Hospital UHL The 2016 Day Case Activity Based Funding (ABF) target was met
12 Operational Framework Financial Plan Introduction The University of Limerick Hospital Groups net budget allocation for 2017 amounts to m. Directorate/ St. John s Hospital Net Budget 2016 Indicative Net Budget 2017 NCG-Diagnostics 47,333,990 46,958,551 NCG-Peri-Operative Care 63,737,029 63,231,486 NCG-Medicine 75,470,496 74,871,886 NCG-Maternal & Child Health 26,369,084 26,159,932 NCG-Facilities & Hospitality 29,934,456 29,697,025 NCG-Acute Shared Services 18,695,927 18,547,637 St John's Hospital 17,998,937 18,264,136 Net Budget 279,539, ,730,652 Indicative Budgets for 2017, as based on a pro rata allocation over closing budgets 2016 Existing level of service The cost of maintaining existing services increase each year for all hospital groups due to a variety of factors including: Incremental costs of developments commenced during 2016 Impact of national pay agreements Increases in drugs and other clinical non pay costs Inflation related price increases Additional costs associated with demographic pressures Financial Approach Delivering the maximum amount of services, as safely as effectively as possible, within the limits of the funding available to the Group will remain a significant area of focus in There will be pressures within acute hospitals in the year ahead, in relation to responding to emergency presentations, costs of maintain appropriate staffing levels, the additional demands of treating an ageing population and the growing costs of drugs and medical technologies. The key components of ULHG approach to addressing its financial challenge, will involve pursing increased efficiency, value for money and budgetary control and it will include: Governance : continued focus of budgetary control through the Performance and Accountability Framework, which spans across the four domains of Access to services, Quality and Safety of those services, doing this within the Financial resources available and effectively harnessing the efforts of our Workforce Pay adherence to the Pay and Numbers Strategy for The Pay and Numbers Strategy 2017, is a continuation of the initial strategy approved in July 2016, which is compliance within allocated pay and expenditure budgets. Overall pay expenditure, which is made up of direct employment costs, overtime and agency will continue to be monitored, managed and controlled. Non Pay implement targeted cost improvement programmes for specific high growth areas Income, sustain and improve wherever possible the level on income generated in An accelerated income target has been assigned to ULHG for 2017, which will be a financial challenge. Activity, use the Activity Based Funding (ABF) model progressively as part of the management process within the Group. 11
13 Operational Framework Workforce Plan The Acute Hospital Division recognises and acknowledges its people as its most valuable assets and key to service delivery in The People Strategy Leaders in People Services underpins the wider health reform. It focuses on people services for the whole of the health services with the ultimate goal of delivering safer better healthcare. This is being achieved through leadership driving cultural change, enabled by staff engagement, workforce planning and adopting a partnering approach. The strategy is underpinned by a commitment to value and support the workforce. In particular, the role of HR Partner has been established as the link between National HR, the HR Leads in the Hospital Groups and the Acute Hospitals Division. The following are the HR priorities as identified in the National Service Plan for 2017: 1. Pay-Bill Management & Control - Compliance with the framework and the requirement for Hospital Groups to operate within the funded pay envelope continues to be a key priority for the Acute Hospital Division for 2017 alongside the management of risk and service implications. The monitoring of the funded workforce plans is a recurring agenda item of the monthly performance meetings held under the Performance and Accountability Framework. The Division is also partnering with National HR through the National Coordination Group. 2. Workforce Planning - The development of funded workforce plans at both Hospital and Hospital Group level requires alignment to the on-going review of skill mix requirements alongside effective staff deployment to manage workforce changes that are necessary in support of service delivery. The Division and Hospital Groups are partnering with HR Workforce Planning, Analytics, & Informatics in relation to the development of workforce planning and resourcing knowledge, skills and capability of local HR Managers and Service Managers. 3. Staff Engagement - All Acute Hospital employees are encouraged to complete in Staff Surveys to ensure that their views are considered to create circumstances where everyone s opinion can make a difference in providing guidance on what can be done to make the services better, both from the service user and staff perspective. There is also a need to take actions based on survey findings. 4. Workplace Health & Wellbeing - The implementation of the Healthy Ireland in the Health Services Policy is a priority to encourage staff to consider their own health and wellbeing to ensure a resilient and healthy workforce. 5. EWTD (European Work Time Directive) - Through the forum of the National EWTD Verification and Implementation Group, the Division continues to work collaboratively with Irish Medical Organisation (IMO), the Department of Health (DOH) and other key stakeholders to work towards the achievement of full compliance with the EWTD. The Division also collaborates with the DOH, the IMO and the National HR to facilitate a Learning Day to obtain progress to date from different experiences in relation to the implementation of measures in support of compliance. In 2017 detailed work plans across the following themes; Leadership and Culture; Staff Engagement; Learning and Development; Workforce Planning; Evidence and Knowledge; Performance; Partnering, and; Human Resource Professional Services are being further developed with a particular focus on leadership development and e-hrm, in addition to the work plans commenced in
14 Cancer Services UL Hospitals Group Operational Plan 2017D The National Cancer Control Programme will lead the implementation of the new cancer strategy in the HSE. This will involve providing leadership across the continuum of care, from diagnosis, treatment, to appropriate follow-up and support, in both the hospital and community setting. The main area of focus will continue to be the diagnosis and treatment of cancer. Further progress will be made in the consolidation of surgical oncology services into the cancer centres to ensure that optimal treatment is provided and outcomes are improved. Service improvements will be underpinned by evidence, best practice and continued development of further National Clinical Guidelines. Services will be monitored against agreed performance parameters. Quality and Patient Safety The Acute Hospital Division will prioritise the establishment of a robust governance and accountability structure for Quality and Patient Safety programmes within the Division during The division will work with the Hospital Groups including UL Hospitals to develop a model for patient safety and quality. The aim is to further enhance and build capacity of QPS departments across National Division, Hospital Groups and at hospital level and to focus on the following key areas of development: 1. The Division will continue to implement the Framework for Quality Improvement and National Patient Safety Programmes in partnership with NCSP, QAV and QID in the following areas: HCAI Decontamination Medication Safety Pressure Ulcers to Zero Sepsis and Early Warning Scores/ Systems Falls Prevention Clinical Handover Quality and Safety Governance e.g. Board on Board initiative. 2. Improve Risk and Patient Safety incident management Improve overall response to safety incidents by developing and streamlining processes and systems for managing, investigating, reviewing and learning from incidents Continue to put in place measures to improve reporting Implement revised Integrated Risk Management policy 3. Develop capacity to listen and learn from patients, public and staff Support and provide HSE project management for 2017 Patient Experience Programme- joint initiative with HIQA and DOH Develop project plan and lead the patient safety culture survey project Continue implementation and embed a culture of Open Disclosure across all services 4. Quality and Safety Performance Monitoring and Reporting Strengthen QPS monitoring and surveillance to ensure Patient Safety areas for improvement are identified and learning is shared Continue to publish monthly Maternity Safety Statements. Commence monthly Hospital Safety Statement monthly Reporting 13
15 UL Hospitals will support the Acute Hospital Division as they develop clinical and healthcare audit programmes. 14
16 Performance and Accountability Framework The Performance and Accountability Framework (PAF) sets out the process by which the National Divisions and Hospital Groups are accountable for improving their performance under four domains; Access to services, the Quality and Safety of those Services, doing this within the Financial Resources available and by effectively harnessing the efforts of the Workforce. Accountabilty Structure There are five main layers of acccountabilty in the HSE 1 Service Managers and the CEOs of Section 38 2 Hospital Group CEOs to the relevant National Directors 3 National Directors to the Director General 4 The Director General to the Directorate 5 The Directorate to the Minister The Accountable Officers have delegated responsibilty and accountabillity for all aspects of service delivery across the four domains outlined above. The Framework outlines what is expected of them and what happens if targets are not achieved. In this context, the individual hospital managers also have a responsibility for proactively identify issues of underperformance, to act upon them promptly and, to the greatest extent possible, to avoid the necessity for escalation. This performance review process is monitored and scrutinised by National Performance Oversight Group (NPOG) on behalf of the Director General and the Directorate in fulfilling their accountability responsibilities. Service Arrangements will continue to be the contractual mechanism governing the relationship between the HSE and Section 38 Agencies 1 to ensure delivery against targets. Performance management process Each level of management has a core responsibility to manage the delivery of services for which they have responsibility. This process involves; Keeping performance under constant review Having a monthly performance management process in place that will include formal performance meetings with their next line of managers Agreeing and monitoring actions at performance meetings to address underperformance Taking timely corrective actions to address any underperformance emerging Implementing a full Performance Improvement or Recovery Plan where significant and sustained underperformance has been identified and remedial actions have been unsuccessful. A formal escalation process can be applied at both the organsiation and the individual level where there is continued underperformance following monitoring and support. This can result in senior managers responsible for particular services attendance at relevant Oireachtas Committees to account for service delivery, quality and financial performance issues. The full text of Performance and Accountabililty Framework is available at 1 The HSE Acute Hospitals Division provides funding to 16 Voluntary Hospitals, known as Section 38 Agencies for the delivery of a range of healthcare services. 15
17 Implementing Priorities 2017 Priority Area Priority Actions Lead Governance and Compliance Embed robust structures within the hospital groups to facilitate effective managerial and clinical governance which will provide direct support to the smaller hospitals in the groups. CP Goal Date UL Hospitals 2 Control and Prevention of HCAIs Ensure governance structures are in place in Hospital Groups to drive improvement and monitor compliance with targets of HCAIs / AMR with a particular focus on antimicrobial stewardship and control measures for multiresistant organisms. UL Hospitals 2 Support of Surgical Clinical Programmes Refurbishment of Old ICU to accommodate POA/DOSA/SAU in line with Surgical Clinical Programme, Corporate strategic goal no 2 and the Peri-Operative Strategic Plan and The CSI programme Peri- Operative Directorate, UL Hospitals 2 Q1 Increase capacity/improve services in acute hospitals Newly Commissioned Units: Open new Emergency Department at University Limerick Hospital Medicine Directorate, UL Hospitals 2 Q2 Introduction of a Bed Bureau System to manager and triage all medical emergencies Medicine Directorate, UL Hospitals 2 Q1 Unscheduled Care: Implement the ED Task Force report recommendations Target a 5% improvement in PET (moving towards a 100% target). Implement the Patient Flow Project in pilot sites and implement the winter initiative 2016/2017 aimed at alleviating pressures on the hospital system over the winter period. Endeavour to eliminate ED waiting times of> 24hours for patients > 75 years. Co-operate with the roll-out of the Integrated Care Programme for Older People as appropriate, in acute hospital demonstrator sites UL Hospitals 2 Q1 16
18 Priority Area Priority Actions Lead Scheduled Care: Work with the National Treatment Purchase Fund (NTPF), in relation to the funding of 15m allocated nationally to the NTPF, to implement waiting list initiatives, to reduce waiting times and provide treatment to those patients waiting longest Waiting list management: actively manage waiting lists for inpatient and day case procedures by strengthening operational and clinical governance structures including chronological scheduling to ensure no patient is waiting longer than 18 months and achieve targets for patients waiting < 15 months. Implement the Strategy for Design of Integrated Outpatient Services on a phased basis under the direction of the outpatient services performance improvement programme. CP Goal Date UL Hospitals 2 Endoscopy Clinical Programme to develop guidelines and provide support to improve access to GI endoscopy Implementation of Maternity Strategy Provide dialysis in UHL, contracted units and in the home at 2016 funded levels Provide high level co-ordination of maternity, gynaecology and neonatal services and continue the implementation of the Maternity Strategy including the development of clinical maternity networks across the Hospital Groups Publish maternity safety statements for all maternity units/ hospitals. Roll-out the Maternal and Newborn Clinical Management System (MN-CMS) in phase 1 hospitals (Rotunda Hospital and National Maternity Hospital) and commence phase 2 preparation and roll-out. Progress plans for the relocation University of Limerick Maternity Hospital. Assist with the national implementation of a range of improvement actions based on the National Standards for Bereavement Care following Pregnancy Loss and Perinatal Death. UL Hospitals 2 17
19 Priority Area Priority Actions Lead Participate in the development of the Irish Maternity Indicator System (IMIS) Audit to facilitate assessment of quality of care in maternity services. CP Goal Date UL Hospitals 2 Quality and Patient Safety Continue to support the Guideline Development Group for NCEC Intra-partum Care Guidelines. Build Quality and Patient Safety capacity and capability at hospital group and divisional level to support Quality Improvement initiatives Monitor and support implementation of National Standards for Safer Better Healthcare Assist in the development and implementation of a quality and safety framework and programmes across the hospital groups. UL Hospitals 2 Continue to embed a culture of open disclosure. Work with the Acute Hospital Division to develop Group wide Clinical / Healthcare Audit Programme Work with the Acute Hospitals Division to endeavour to produce monthly Hospital Safety Statement monthly Reporting Co-operate with Quality Improvement Division in the Preventing VTE (blood clots) in Hospital Patients Improvement Collaborative Cancer Services and the National Cancer Control Programme NCCP will work with Hospital Groups to implement the recommendations of the KPI quality improvement plan for the Rapid Access Clinics Breast, Prostate and Lung Cancers. Roll out the Medical Oncology Clinical Information System on a phased basis (MOCIS) across the 26 systemic anticancer therapy hospital sites. UL Hospitals 2 National Services Prepare for the implementation of the policy in Trauma Systems for Ireland. UL Hospitals 2 Human Resources People Strategy Continue to work on implementing the People Strategy within acute hospitals. UL Hospitals 4 18
20 Priority Area Priority Actions Lead Employee Engagement: Use learning from the employee survey to shape organisational values and ensure that the opinions of staff are sought and heard. Workplace Health & Wellbeing: Implement the Healthy Ireland in the Health Services Policy supporting initiatives to encourage staff to look after their own health and wellbeing ensuring we have a resilient and healthy workforce Promote influenza vaccine uptake rates amongst staff in frontline settings European Working Time Directive (EWTD): Implement and monitor compliance with the EWTD National Policy Children First Compliance Support the Children First National Office in their Implementation, training and rollout of Children First across the Hospital Groups. Engage with the Children First National Office as reports are developed and tracked and monitored in relation to Child protection policies across the Hospital Groups. Patient Feedback Implement plans to build the capacity and governance structures needed to promote a culture of patient partnership across acute services and use patient insight to inform quality improvement initiatives and investment priorities which will include the completion of Patient Experience Surveys in all acute hospitals on a phased basis within available resources Internal Audit Ensure that processes in place at Group level to govern the oversight of Internal Audit recommendations. CP Goal Date UL Hospitals 4 UL Hospitals 4 UL Hospitals 4 UL Hospitals 3 UL Hospitals 3 UL Hospitals 3 19
21 Priority Area Priority Actions Lead Finance/ HR Employment Controls Ensure compliance with the Pay-bill Management and Control Framework within acute hospitals services. CP Goal Date UL Hospitals 3 Activity based funding UL Hospitals 5 Patient Charges Medicines Management Information Management Health and Wellbeing Support the next phase of ABF programme as per ABF Implementation Plan Ensure hospital activity and patient data is reported within 30 days. Ensure compliance with the terms of the MOU between the HSE, named hospitals and VHI Insurance DAC (March 2016) Hospital groups and hospitals to ensure billing is appropriate and current and that bed maps are accurate. Work on implementing the provisions of the Irish Pharmaceutical Healthcare Association Framework Agreement on the Pricing and Supply of New Medicines. Support the development of NQAIS Clinical to combine information from NQAIS Surgery and NQAIS Medicine. Support the continued development of the Irish National Orthopaedic Register. Support the development of TARN to evaluate the care of trauma patients. Healthy Ireland Implement Healthy Ireland in the Health Services National Implementation Plan across all hospital groups with local implementation of Hospital Group plans on a phased basis. Tobacco Free Ireland Complete planned Brief Intervention Training sessions for Smoking Cessation in line with existing programme and rollout of Making every contact count and Generic Brief intervention Training schemes by H&Wb Division. 5 5 UL Hospitals 5 3 UL Hospitals 3 UL Hospitals 5 UL Hospitals 1 UL Hospitals 1 20
22 Priority Area Priority Actions Lead Self- Management of Chronic Diseases Support the Implementation of the Self- Management Support (SMS) framework in all hospital groups on a phased basis CP Goal Date ULHG 1 21
23 Appendices Appendix 1: Human Resources University Limerick Hospital Group WTE December 2016 Hospital Group UL Hospitals Group Medical/ Dental Nursing Health & Social Care Management/ Admin General Support Staff Patient & Client Care Total 474 1, ,596 Hospital WTE December 2016 University Hospital Limerick 2,383 University Maternity Hospital 323 Croom Hospital 151 Ennis Hospital 220 Nenagh Hospital 218 St. John s Hospital 301 Total 3,596 22
24 Appendix 2: Performance Indicator Suite - DOP System-Wide Indicator Budget Management including savings Net Expenditure variance from plan (within budget) Pay Direct / Agency / Overtime Reporting Frequency NSP 2016 Expected Activity / Target M 0.33% Projected Outturn 2016 To be reported in Annual Financial Statements 2016 Expected Activity / Target % Non-pay M 0.33% 0.1% Income M 0.33% 0.1% Capital Capital expenditure versus expenditure profile Audit % of internal audit recommendations implemented by due date Q Q 100% 100% 100% 75% 75% 75% % of internal audit recommendations implemented, against total no. of Q 95% 95% 95% recommendations, within 12 months of report being received Service Arrangements / Annual Compliance Statement 100% 100% 100% % of number of Service Arrangements signed M % of the monetary value of Service Arrangements signed M 100% 100% 100% % of Annual Compliance Statements signed A 100% 100% 100% Workforce % absence rates by staff category M 3.5% 4.3% 3.5% % adherence to funded staffing thresholds M > 99.5% > 99.5% > 99.5% EWTD < 24 hour shift (Acute and Mental Health) M 100% 97% 100% < 48 hour working week (Acute and Mental Health) M 95% 82% 95% Health and Safety No. of calls that were received by the National Health and Safety Helpdesk Q 15% increase Service User Experience % of complaints investigated within 30 working days of being acknowledged by the complaints officer Serious Reportable Events % of Serious Reportable Events being notified within 24 hours to the Senior Accountable Officer and entered on the National Incident Management System (NIMS) % of investigations completed within 120 days of the notification of the event to the Senior Accountable Officer Safety Incident reporting % of safety incidents being entered onto NIMS within 30 days of occurrence by hospital group / CHO Extreme and major safety incidents as a % of all incidents reported as occurring 15% 10% increase M 75% 75% 75% M 99% 40% 99% M 90% 0% 90% Q 90% 50% 90% Q New PI 2017 New PI 2017 Actual results to be reported in
25 System-Wide Indicator % of claims received by State Claims Agency that were not reported previously as an incident HR Number of nurses and midwives with authority to prescribe medicines Number of nurses and midwives with authority to prescribe Ionising Radiation (X-Ray) Reporting Frequency A Annual Annual The expected Activity/target 2017 for this KPI is a national target i.e. inclusive of all divisions NSP 2016 Expected Activity / Target New PI 2016 New PI 2017 New PI 2017 Projected Outturn 2016 New PI 2017 New PI 2017 Expected Activity / Target % 40% Up to 940 Up to 310 Acute Hospitals Service Area New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Expected Activity/ Targets 2017 Activity University of Limerick Hospitals UHL UMHL CH SJL EH NH National Target Beds Available Inpatient beds ** Existing Monthly 10,643 10,681 Day Beds / Places ** Existing Monthly 2,150 2,150 Discharges Activity Inpatient Cases Existing Monthly 635,414 49,549 28,549 7,579 1,766 5,099 4,265 2, ,627 Inpatient Weighted Units Existing Monthly 632,282 42,958 26, , , , , , ,487 Day Case Cases ( includes Existing Monthly 1,044,192 57,730 34, ,164 5,362 6,606 7,652 1,062,363 Dialysis) Day Case Weighted Units ( includes Existing Monthly 1,030,918 67,007 37, , , , , ,028,669 Dialysis) Total inpatient and day case Cases Existing Monthly 1,679, ,279 63,336 7,738 4,930 10,461 10,871 9,943 1,702,990 Emergency Inpatient Discharges Existing Monthly 424,659 34,712 24, ,287 4,039 1, ,872 Elective Inpatient Discharges Existing Monthly 94,587 7,904 4, ,358 1, ,587 24
26 Acute Hospitals Service Area New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Expected Activity/ Targets 2017 Activity University of Limerick Hospitals UHL UMHL CH SJL EH NH National Target Maternity Inpatient Discharges Existing Monthly 116,168 6, , ,168 Emergency Care - New ED Existing Monthly 1,141,437 60,523 60,523 1,168,318 attendances -Return ED attendances Existing Monthly 94,483 4,159 4,159 94,225 - Injury Unit attendances Ω - Other emergency presentations New PI 2017 New PI 2017 Monthly 81,141 27,418 10,274 9,255 7,889 81,919 Monthly 49,029 48,895 Births: Total no. of births Existing Monthly 63,420 4,441 4,441 63,247 OPD: Total no. of new and return outpatient Existing Monthly 3,342, , ,643 25,507 11,287 10,644 17,399 12,134 3,340,981 attendances Outpatient attendances - New : Return Ratio (excluding obstetrics and warfarin haematology clinics) Existing Monthly 1:2.4 1:2 1:2 1:2 1:2 1:2 1:2 1:2 1:2 25
27 Detailed Activity targets by hospital for Inpatients and day cases Group Hospital Elective/ Emergency/ Maternity Inpatients Daycases Cases WU Cases WU 6. UL Group Maternity Limerick Elective UL Group Maternity Limerick Emergency 808 1, UL Group Maternity Limerick Maternity 6,761 3, UL Group Limerick Elective 4,042 5, ,772 37, UL Group Limerick Emergency 24,338 21, UL Group Limerick Maternity UL Group Croom Elective 1,358 2, ,164 5, UL Group Croom Emergency UL Group St Johns Limerick Elective 1,812 2, ,362 6, UL Group St Johns Limerick Emergency 3,287 1, UL Group Ennis Elective ,606 7, UL Group Ennis Emergency 4,039 2, UL Group Ennis Maternity UL Group Nenagh Elective ,652 9, UL Group Nenagh Emergency 1,832 1,
28 Service Area Performance Indicator Activity Based Funding (MFTP) model HIPE Completeness Prior month: % of cases entered into HIPE Acute Hospitals New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Expected Activity/ Targets 2017 Existing Monthly 96% 100% Dialysis New PI 2017 Number of Haemodialysis patients treated in Acute Hospitals New PI 2017 Bi-Annual ** Number of Haemodialysis patients treated in Contracted Centres ** New PI 2017 Bi-Annual New PI ,900 83,304 Number of Home Therapies dialysis Patients Treatments ** Existing Bi-Annual 89,815 90,400 98,215 Outpatient New OPD attendance DNA rates ** Existing Monthly 12.7% 12% % of Clinicians with individual OPD DNA rate of 10% or less ** Existing Monthly 36.5% 50% Inpatient, Day Case and Outpatient Waiting Times 90% % of adults waiting < 15 months for an elective procedure Existing Monthly 88.1% (inpatient) % of adults waiting < 15 months for an elective procedure (day case) Existing Monthly 92.2% 95% % of children waiting < 15 months for an elective procedure (inpatient) Existing Monthly 93% 95% % of children waiting < 15 months for an elective procedure (day case) Existing Monthly 96.8% 97% % of people waiting < 52 weeks for first access to OPD services Existing Monthly 84.3% 85% % of routine patients on Inpatient and Day Case Waiting lists that are chronologically scheduled ** Existing Monthly 75.8% 90% Elective Scheduled care waiting list cancellation rate)** Existing/ amended Monthly TBC TBC Colonoscopy / Gastrointestinal Service Number of people waiting greater than 4 weeks for access to an urgent colonoscopy New PI 2017 Monthly 0 0 % of people waiting < 13 weeks following a referral for routine colonoscopy or OGD Existing Monthly 51.5% 70% Emergency Care and Patient Experience Time % of all attendees at ED who are discharged or admitted within 6 hours of registration Existing Monthly 68% 75% % of all attendees at ED who are discharged or admitted within 9 hours of registration (goal is 100% performance with a target of improvement in 2017 against 2016 outturn) Existing Monthly 81.5% 100% % of ED patients who leave before completion of treatment Existing Monthly 5.2% <5% % of all attendees at ED who are in ED < 24 hours Existing Monthly 96.5% 100% % of patients attending ED aged 75 years and over ** Existing Monthly 11.4% 13% % of all attendees aged 75 years and over at ED who are discharged or admitted within six hours of registration Existing Monthly 44.5% 95% % of patients 75 years or over who were admitted or Existing Monthly 62.2% 100% 27
29 Service Area Performance Indicator discharged from ED within nine hours of registration Acute Hospitals New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Expected Activity/ Targets 2017 % of all attendees aged 75 years and over at ED who are discharged or admitted within 24 hours of registration New PI 2017 Monthly New PI % Ambulance Turnaround Times % of ambulances that have a time interval of 60 minutes from arrival at ED to when the ambulance crew declares the readiness of the ambulance to accept another call (clear and Existing Monthly 93.4% 95% available) Length of Stay ALOS for all inpatient discharges excluding LOS over 30 Existing Monthly days ALOS for all inpatients ** Existing Monthly Medical Medical patient average length of stay Existing Monthly % of medical patients who are discharged or admitted from AMAU within six hours AMAU registration Existing Monthly 63.7% 75% % of all medical admissions via AMAU Existing Monthly 35% 45% % of emergency re-admissions for acute medical conditions to the same hospital within 30 days of discharge New PI 2017 Monthly New PI % Surgery Surgical patient average length of stay Existing Monthly % of elective surgical inpatients who had principal procedure conducted on day of admission Existing Monthly 72.5% 82% % day case rate for Elective Laparoscopic Cholecystectomy Existing Monthly 43.6% > 60% Percentage bed day utilisation by acute surgical admissions 35.8% Existing Monthly 37.8% who do not have an operation** % of emergency hip fracture surgery carried out within 48 hours Existing Monthly 86.7% 95% % of surgical re-admissions to the same hospital within 30 days of discharge Existing Monthly 2.1% < 3% Delayed Discharges No. of bed days lost through delayed discharges Existing Monthly 200,774 < 182,500 No. of beds subject to delayed discharges Existing Monthly 630 < 500 (475) Health Care Associated Infections (HCAI) % compliance of hospital staff with the World Health Organisation s (WHO) 5 moments of hand hygiene using the national hand hygiene audit tool Existing Bi- Annual 89.2% 90% Rate of new cases of Hospital acquired Staph. Aureus bloodstream infection New PI 2017 Monthly New PI 2017 Rate of new cases of Hospital acquired C. difficile infection New PI 2017 Monthly New PI 2017 Mortality Standardised Mortality Ratio (SMR) for inpatient deaths by hospital and defined clinical condition ** Existing/ Modified Annual Data Not Yet Available < 1/10,000 Bed days used < 2/10,000 Bed days used N/A 28
30 Service Area Performance Indicator Acute Hospitals New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Quality Rate of slip, trip or fall incidents for as reported to NIMS that were classified as major or extreme New PI 2017 Monthly New PI 2017 Medication Safety Rate of medication error incidents as reported to NIMS that were classified as major or extreme New PI 2017 Monthly New PI 2017 Patient Experience % of hospital groups conducting annual patient experience surveys amongst representative samples of their patient population National Early Warning Score (NEWS) % of hospitals with implementation of NEWS in all clinical areas of acute hospitals and single specialty hospitals % of all clinical staff who have been trained in the COMPASS programme Existing Quarterly 64.5% Expected Activity/ Targets 2017 Reporting to commence in 2017 Reporting to commence in 2017 Existing Annual TBC 100% Existing Quarterly 96% 100% > 95% % of hospitals with implementation of PEWS (Paediatric Early Warning System) ** Existing Quarterly N/A 100% Irish Maternity Early Warning Score (IMEWS) % of maternity units / hospitals with full implementation of IMEWS Existing Quarterly 100% 100% % of hospitals with implementation of IMEWS for pregnant patients Existing Quarterly 84% 100% Clinical Guidelines % of maternity units / hospitals with an implementation plan for the guideline for clinical handover in maternity services New PI 2017 Quarterly New PI % % of acute hospitals with an implementation plan for the guideline for clinical handover New PI 2017 Quarterly New PI % National Standards % of hospitals who have completed first assessment against the NSSBH Existing Quarterly 90% 100% % of hospitals who have commenced second assessment against the NSSBH Existing Quarterly 50% 95% % maternity units which have completed and published Maternity Patient Safety Statement and discussed same at Hospital Management Team meetings each month Existing Monthly 100% 100% % of Acute Hospitals which have completed and published Patient Safety Statements and discussed at Hospital Management Team each month ** Existing Monthly N/A 100% Patient Engagement % of hospitals that have processes in place for participative engagement with patients about design, delivery & Existing Annual N/A 100% evaluation of health services ** Ratio of compliments to complaints ** Existing Quarterly 1:1 2:1 Stroke % acute stroke patients who spend all or some of their Existing Quarterly 56.2% 90% hospital stay in an acute or combined stroke unit ** 29
31 Service Area Performance Indicator Acute Hospitals New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Expected Activity/ Targets 2017 % of patients with confirmed acute ischaemic stroke who receive thrombolysis Existing Quarterly 10.5% 9% % of hospital stay for acute stroke patients in stroke unit who are admitted to an acute or combined stroke unit Existing Quarterly 65.9% 90% Acute Coronary Syndrome % STEMI patients (without contraindication to reperfusion therapy) who get PPCI Existing Quarterly 89.7% 90% % of reperfused STEMI patients (or LBBB) who get timely PPCI Existing Quarterly 70.8% 80% COPD Mean and median LOS for patients admitted with COPD ** Existing Quarterly % re-admission to same acute hospitals of patients with COPD within 90 days ** Existing Quarterly 27% 24% No. of acute hospitals with COPD outreach programme ** Existing Quarterly Access to structured Pulmonary Rehabilitation Programme in acute hospital services ** Existing Quarterly Asthma % nurses in secondary care who are trained by national asthma programme ** Existing Quarterly 1.3% 70% Number of bed days used by all emergency in-patients with a principal diagnosis of asthma** Number of bed days used by emergency inpatients < 6 years old with a principal diagnosis of asthma** Existing/ amended Existing/ amended Quarterly 11,394 3% Reduction Quarterly 1,650 5% Reduction Diabetes Number of lower limb amputations performed on Diabetic Existing Annual 449 <488 patients ** Average length of stay for Diabetic patients with foot ulcers ** Existing Annual days % increase in hospital discharges following emergency admission for uncontrolled diabetes. ** Existing Annual Data Not Available Until Q % increase Blood Policy No. of units of platelets issued in the reporting period ** Existing Monthly 20,704 21,000 % of units of platelets outdated in the reporting period ** Existing Monthly 5.1% <5% % of O Rhesus negative red blood cell units issued ** Existing Monthly 13.3% <14% % of red blood cell units rerouted ** Existing Monthly 3.4% <4% % of red blood cell units outdated out of a total of red blood cell units issued** Existing Monthly 0.5% <1% HR Compliance with EWTD European Working Time Directive compliance for NCHDs - < 24 hour shift Existing Monthly 97.1% 100% European Working Time Directive compliance for NCHDs - < 48 hour working week Existing Monthly 81% 95% 30
32 Service Area Performance Indicator Acute Hospitals New/ Existing KPI Reporting Frequency National Projected Outturn 2016 Expected Activity/ Targets 2017 Symptomatic Breast Cancer Services No. of patients triaged as urgent presenting to symptomatic breast clinics Existing Monthly 19,502 18,000 No. of non urgent attendances presenting to Symptomatic Breast clinics ** Existing Monthly 23,266 24,000 Number of attendances whose referrals were triaged as urgent by the cancer centre and adhered to the HIQA standard of two weeks for urgent referrals ** Existing Monthly 17,348 17,100 % of attendances whose referrals were triaged as urgent by the cancer centre and adhered to the national standard of two weeks for urgent referrals Existing Monthly 89% 95% Number of attendances whose referrals were triaged as nonurgent by the cancer centre and adhered to the HIQA standard of 12 weeks for non-urgent referrals (No. offered an Existing Monthly 18,468 22,800 appointment that falls within 12 weeks) ** % of attendances whose referrals were triaged as nonurgent by the cancer centre and adhered to the national standard of 12 weeks for non-urgent referrals (% offered an Existing Monthly 79.4% 95% appointment that falls within 12 weeks) Clinic Cancer detection rate: no. of new attendances to clinic, triaged as urgent, which have a subsequent primary diagnosis of breast cancer ** Existing Monthly 1,841 > 1,100 Clinical detection rate: % of new attendances to clinic, triaged as urgent, that have a subsequent primary diagnosis of breast cancer Existing Monthly 11% > 6% Lung Cancers Number of patients attending the rapid access lung clinic in designated cancer centres Existing Monthly 3,372 3,300 Number of patients attending lung rapid clinics who attended or were offered an appointment within 10 working days of receipt of referral in designated cancer centres ** Existing Monthly 2,796 3,135 % of patients attending lung rapid clinics who attended or were offered an appointment within 10 working days of receipt of referral in designated cancer centres Existing Monthly 81.2% 95% Clinic Cancer detection rate: Number of new attendances to clinic, triaged as urgent, that have a subsequent primary diagnosis of lung cancer ** Existing Monthly 1,030 > 825 Clinical detection rate: % of new attendances to clinic, triaged as urgent, that have a subsequent primary diagnosis of lung cancer Existing Monthly 32.4% > 25% Prostate Cancer Number of patients attending the rapid access prostate clinic in cancer centres Existing Monthly 2,626 2,600 Number of patients attending prostate rapid clinics who attended or were offered an appointment within 20 working Existing Monthly 1,366 2,340 days of receipt of referral in the cancer centres ** % of patients attending prostate rapid clinics who attended or were offered an appointment within 20 working days of Existing Monthly 52% 90% 31
Executive Summary. Children s Hospital Group Operational Plan Healthier children and young people throughout Ireland
 Children s Hospital Group Operational Plan Healthier children and young people throughout Ireland 2017 1 Children s Hospital Group Values, Vision and Mission Statements In living our values we will deliver
Children s Hospital Group Operational Plan Healthier children and young people throughout Ireland 2017 1 Children s Hospital Group Values, Vision and Mission Statements In living our values we will deliver
BIU Acute Hospital Division
 Health Service Executive BIU Acute Hospital Division Key Performance Indicator Health Service Executive Metadata BIU Acute 2016 Hospital Division Based on NSP and DOP 2016 KPIs Key Performance Indicator
Health Service Executive BIU Acute Hospital Division Key Performance Indicator Health Service Executive Metadata BIU Acute 2016 Hospital Division Based on NSP and DOP 2016 KPIs Key Performance Indicator
RCSI HOSPITALS GROUP. Introduction. RCSI Hospitals Group was established in The Group comprises of the following hospitals:
 RCSI HOSPITALS GROUP RCSI Hospitals Group Available Budget m 2015 Net Outturn m Total Spend 625.178 652.545 Percentage Difference -3.9% Introduction RCSI Hospitals Group was established in 2015. The Group
RCSI HOSPITALS GROUP RCSI Hospitals Group Available Budget m 2015 Net Outturn m Total Spend 625.178 652.545 Percentage Difference -3.9% Introduction RCSI Hospitals Group was established in 2015. The Group
Acute Hospitals Division
 Acute Hospitals Division Operational Plan 2016 Vision A healthier Ireland with a high quality health service valued by all Mission People in Ireland are supported by health and social care services to
Acute Hospitals Division Operational Plan 2016 Vision A healthier Ireland with a high quality health service valued by all Mission People in Ireland are supported by health and social care services to
National Service Plan Mr. Tony O Brien, Director General
 National Service Plan 2016 Mr. Tony O Brien, Director General Population Changes (2010 2015) Population has grown by 1.8% since 2010 and is projected to increase by 4% by 2021 Since 2010, 18% increase
National Service Plan 2016 Mr. Tony O Brien, Director General Population Changes (2010 2015) Population has grown by 1.8% since 2010 and is projected to increase by 4% by 2021 Since 2010, 18% increase
RCSI Hospital Group Operational Plan 2018
 RCSI Group Operational Plan 2018 Page 1 of 15 Contents 1. Introduction... 3 2. Financial Summary... 3 3. Population Health... 3 4. Financial Plan... 5 5. Capital Expenditure... 7 6. Workforce Plan... 8
RCSI Group Operational Plan 2018 Page 1 of 15 Contents 1. Introduction... 3 2. Financial Summary... 3 3. Population Health... 3 4. Financial Plan... 5 5. Capital Expenditure... 7 6. Workforce Plan... 8
National Service Plan
 2017 National Service Plan Contents Introduction... 1 Building a Better Health Service... 3 Finance... 7 Workforce... 13 Service Delivery... 15 Cross cutting priorities a multi-year system-wide approach...
2017 National Service Plan Contents Introduction... 1 Building a Better Health Service... 3 Finance... 7 Workforce... 13 Service Delivery... 15 Cross cutting priorities a multi-year system-wide approach...
Children s Hospital Group Operational Plan Healthier children and young people throughout Ireland
 Children s Hospital Group Operational Plan Healthier children and young people throughout Ireland 2018 1 The Children s Hospital Group Values, Vision and Mission were developed and agreed as part of the
Children s Hospital Group Operational Plan Healthier children and young people throughout Ireland 2018 1 The Children s Hospital Group Values, Vision and Mission were developed and agreed as part of the
Performance Report January/February 2016
 Building a high quality health service for a healthier Ireland Care ι Compassion ι Trust ι Learning Health Service Performance Report January/February 2016 Contents Key Performance Messages... 3 Quality
Building a high quality health service for a healthier Ireland Care ι Compassion ι Trust ι Learning Health Service Performance Report January/February 2016 Contents Key Performance Messages... 3 Quality
Health and Wellbeing Operational Plan 2017
 Health and Wellbeing Operational Plan Item type Authors Publisher Report Health and Wellbeing, Health Service Executive (HSE) Health Service Executive (HSE) Downloaded 2-May-2018 21:18:06 Link to item
Health and Wellbeing Operational Plan Item type Authors Publisher Report Health and Wellbeing, Health Service Executive (HSE) Health Service Executive (HSE) Downloaded 2-May-2018 21:18:06 Link to item
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Working together, Caring for the Mid-West UL HOSPITALS GROUP STRATEGIC PLAN
 Working together, Caring for the Mid-West UL HOSPITALS GROUP STRATEGIC PLAN 2018-2022 Belfast Ireland s Mid West Counties: Limerick, Clare, and North Tipperary Clare Galway Shannon Airport Dublin North
Working together, Caring for the Mid-West UL HOSPITALS GROUP STRATEGIC PLAN 2018-2022 Belfast Ireland s Mid West Counties: Limerick, Clare, and North Tipperary Clare Galway Shannon Airport Dublin North
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Quality and safety committee(s): guidance and sample terms of reference
: guidance and sample terms of reference") Quality and safety committee(s): guidance and sample terms of reference Item Type Report;Guideline Authors Health Service Executive (HSE);Quality and Patient Safety Publisher HSE Download date 04/10/2018
Quality and safety committee(s): guidance and sample terms of reference Item Type Report;Guideline Authors Health Service Executive (HSE);Quality and Patient Safety Publisher HSE Download date 04/10/2018
CHO CHO 3 Mid West CHO 3 Plan Operational Plan
 CHO CHO 3 Mid West CHO 3 Plan Operational Plan 2017 Contents Introduction... 1 Building a Better Health Service... 7 Finance... 11 Workforce... 14 Service Delivery... 18 Cross cutting priorities a multi-year
CHO CHO 3 Mid West CHO 3 Plan Operational Plan 2017 Contents Introduction... 1 Building a Better Health Service... 7 Finance... 11 Workforce... 14 Service Delivery... 18 Cross cutting priorities a multi-year
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Statement of Purpose Kerry General Hospital 2013
 Statement of Purpose Kerry General Hospital 2013 Table of Contents Introduction...3 Description of Services Provided...3 Kerry General Hospital Services...4 Models of service delivery and aligned resources
Statement of Purpose Kerry General Hospital 2013 Table of Contents Introduction...3 Description of Services Provided...3 Kerry General Hospital Services...4 Models of service delivery and aligned resources
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Board of Directors Meeting
 Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
National Waiting List Management Protocol
 National Waiting List Management Protocol A standardised approach to managing scheduled care treatment for in-patient, day case and planned procedures January 2014 an ciste náisiúnta um cheannach cóireála
National Waiting List Management Protocol A standardised approach to managing scheduled care treatment for in-patient, day case and planned procedures January 2014 an ciste náisiúnta um cheannach cóireála
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Health Information Exchange and Management: An EU/ Irish Perspective
 Health Information Exchange and Management: An EU/ Irish Perspective Gerry O Dwyer President European Association of Hospital Managers 25 Member Countries Group Chief Executive Officer, South/South West
Health Information Exchange and Management: An EU/ Irish Perspective Gerry O Dwyer President European Association of Hospital Managers 25 Member Countries Group Chief Executive Officer, South/South West
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Cork & Kerry CHO operational plan 2017
 Cork & Kerry CHO operational plan 2017 Item type Report Authors Community Health Organisation, Cork & Kerry Area 4. Health Service Executive Publisher Health Service Executive (HSE) Downloaded 5-May-2018
Cork & Kerry CHO operational plan 2017 Item type Report Authors Community Health Organisation, Cork & Kerry Area 4. Health Service Executive Publisher Health Service Executive (HSE) Downloaded 5-May-2018
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Summarise the Impact of the Health Board Report Equality and diversity
 AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Performance Improvement Bulletin
 SPECIAL DELIVERY UNIT/ NATIONAL TREATMENT PURCHASE FUND Issue No.1 08/12 Performance Improvement Bulletin Featured Work underway - Maximum Waiting Time Targets 2 Case Study No. 1 Galway & Roscommon University
SPECIAL DELIVERY UNIT/ NATIONAL TREATMENT PURCHASE FUND Issue No.1 08/12 Performance Improvement Bulletin Featured Work underway - Maximum Waiting Time Targets 2 Case Study No. 1 Galway & Roscommon University
Saolta University Health Care Group Operational Plan 2018
 Saolta University Health Care Group Operational Plan 2018 1 Saolta Vision Our Vision is to be a leading academic Hospital Group, providing excellent integrated patient-centred care delivered by skilled
Saolta University Health Care Group Operational Plan 2018 1 Saolta Vision Our Vision is to be a leading academic Hospital Group, providing excellent integrated patient-centred care delivered by skilled
Cork and Kerry Community Healthcare Organisation. Operational Plan 2015
 Cork and Kerry Community Healthcare Organisation Operational Plan 2015 Primary Care Services Social Care Services Mental Health Services Health and Wellbeing HSE Priorities 2015 HSE Priorities 2015 System
Cork and Kerry Community Healthcare Organisation Operational Plan 2015 Primary Care Services Social Care Services Mental Health Services Health and Wellbeing HSE Priorities 2015 HSE Priorities 2015 System
[Type text] Acute Hospital Services Divisional Plan
![[Type text] Acute Hospital Services Divisional Plan](/thumbs/79/80128651.jpg "[Type text] Acute Hospital Services Divisional Plan") [Type text] Acute Hospital Services Divisional Plan Acute Hospitals Division Draft Operational Plan 2018 [Type text] Contents Page Introduction: Acute Hospitals Introduction. 4 Section 1: Key Reform Themes..
[Type text] Acute Hospital Services Divisional Plan Acute Hospitals Division Draft Operational Plan 2018 [Type text] Contents Page Introduction: Acute Hospitals Introduction. 4 Section 1: Key Reform Themes..
STATEMENT OF PURPOSE August Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008)
") 1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
MENTAL HEALTH DIVISION
 MENTAL HEALTH DIVISION Operational Plan 2016 Values We will try to live our values every day and will continue to develop them Care Compassion Trust Learning Mission People in Ireland are supported by
MENTAL HEALTH DIVISION Operational Plan 2016 Values We will try to live our values every day and will continue to develop them Care Compassion Trust Learning Mission People in Ireland are supported by
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Sample CHO Primary Care Division Quality and Safety Committee. Terms of Reference
 DRAFT TITLE: Sample CHO Primary Care Division Quality and Safety Committee Terms of Reference AUTHOR: [insert details] APPROVED BY: [insert details] REFERENCE NO: [insert details] REVISION NO: [insert
DRAFT TITLE: Sample CHO Primary Care Division Quality and Safety Committee Terms of Reference AUTHOR: [insert details] APPROVED BY: [insert details] REFERENCE NO: [insert details] REVISION NO: [insert
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
National Service Plan 2018
 National Service Plan Contents Foreword from the Director General... 1 Section 1: Introduction and Key Reform Themes... 4 Section 2: Our Population... 9 Section 3: Building a Better Health Service...
National Service Plan Contents Foreword from the Director General... 1 Section 1: Introduction and Key Reform Themes... 4 Section 2: Our Population... 9 Section 3: Building a Better Health Service...
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Living Well with a Chronic Condition: Framework for Self-management Support
 Living Well with a Chronic Condition: Framework for Self-management Support National Framework and Implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular
Living Well with a Chronic Condition: Framework for Self-management Support National Framework and Implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular
Pre-hospital emergency care key performance indicators for emergency response times
 Pre-hospital emergency care key performance indicators for emergency response times Item Type Report Authors (HIQA) Publisher (HIQA) Download date 05/09/2018 21:43:37 Link to Item http://hdl.handle.net/10147/324297
Pre-hospital emergency care key performance indicators for emergency response times Item Type Report Authors (HIQA) Publisher (HIQA) Download date 05/09/2018 21:43:37 Link to Item http://hdl.handle.net/10147/324297
National Clinical Audit programme
 National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
Report of the unannounced monitoring assessment at University Hospital Limerick
 Report of the unannounced monitoring assessment at University Hospital Limerick Monitoring Programme for the National Standards for the Prevention and Control of Healthcare Associated Infections Date of
Report of the unannounced monitoring assessment at University Hospital Limerick Monitoring Programme for the National Standards for the Prevention and Control of Healthcare Associated Infections Date of
OP Action Plan Acute Hospital Outpatient Services. Outpatient Services Performance Improvement Programme
 OP Action Plan 2017 Acute Hospital Outpatient Services Outpatient Services Performance Improvement Programme 5 th May 2017 1. Introduction This action plan sets out the approach to outpatient waiting list
OP Action Plan 2017 Acute Hospital Outpatient Services Outpatient Services Performance Improvement Programme 5 th May 2017 1. Introduction This action plan sets out the approach to outpatient waiting list
Craigavon Area Hospital Profile
 Craigavon Area Hospital Profile 2012 Craigavon Area Hospital Profile Craigavon Area Hospital is located in Craigavon, County Armagh and is an essential part of the hospital network provided by the Southern
Craigavon Area Hospital Profile 2012 Craigavon Area Hospital Profile Craigavon Area Hospital is located in Craigavon, County Armagh and is an essential part of the hospital network provided by the Southern
Committee is requested to action as follows: Richard Walker. Dylan Williams
 BetsiCadwaladrUniversityHealthBoard Committee Paper 17.11.14 Item IG14_60 NameofCommittee: Subject: Summary or IssuesofSignificance StrategicTheme/Priority / Valuesaddressedbythispaper Information Governance
BetsiCadwaladrUniversityHealthBoard Committee Paper 17.11.14 Item IG14_60 NameofCommittee: Subject: Summary or IssuesofSignificance StrategicTheme/Priority / Valuesaddressedbythispaper Information Governance
Health Service Performance Report. December Performance Report
 Health Service Performance Report December Performance Report Contents Performance Overview... 3 Quality & Safety... 18 Accountability Framework... 21 Performance Overview by Service Provider... 36 Finance...
Health Service Performance Report December Performance Report Contents Performance Overview... 3 Quality & Safety... 18 Accountability Framework... 21 Performance Overview by Service Provider... 36 Finance...
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Ireland East Hospital Group Operational Plan 2018
 Ireland East Hospital Group Operational Plan 2018 Mission and Vision The Ireland East Hospital Group, together with our academic partner University College Dublin, will be a national leader in healthcare
Ireland East Hospital Group Operational Plan 2018 Mission and Vision The Ireland East Hospital Group, together with our academic partner University College Dublin, will be a national leader in healthcare
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Group Assistant Director of Nursing / Group Sepsis
 Job Description and Person Specification Group Assistant Director of Nursing / Group Sepsis Reference: IEHG/15/009 Permanent contract Closing Date: Monday, 7 th September 2015 Mary Day, Chief Executive
Job Description and Person Specification Group Assistant Director of Nursing / Group Sepsis Reference: IEHG/15/009 Permanent contract Closing Date: Monday, 7 th September 2015 Mary Day, Chief Executive
Health Service Performance Report. October Performance Report Supplementary Commentary
 Health Service Performance Report October Performance Report Supplementary Commentary Acute Services Contents Acute Services... 3 National Ambulance Service... 19 Health & Wellbeing... 24 Primary Care...
Health Service Performance Report October Performance Report Supplementary Commentary Acute Services Contents Acute Services... 3 National Ambulance Service... 19 Health & Wellbeing... 24 Primary Care...
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Aneurin Bevan University Health Board. Planning and Strategic Change Committee
 Aneurin Bevan University Health Board Planning and Strategic Change Committee A Meeting of the Planning and Strategic Change Committee was held on Tuesday, 19 th December 2014 in Seminar Room 4, Conference
Aneurin Bevan University Health Board Planning and Strategic Change Committee A Meeting of the Planning and Strategic Change Committee was held on Tuesday, 19 th December 2014 in Seminar Room 4, Conference
Key Objectives To communicate business continuity planning over this period that is in line with Board continuity plans and enables the Board:
 Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
CONTENTS. Introduction...1
 HSE Dublin Mid-Leinster Regional Service Plan 2013 CONTENTS Introduction...1 Resource Framework...7 Finance... 7 Human Resources... 11 Improving Performance Management... 15 Improving our Infrastructure...
HSE Dublin Mid-Leinster Regional Service Plan 2013 CONTENTS Introduction...1 Resource Framework...7 Finance... 7 Human Resources... 11 Improving Performance Management... 15 Improving our Infrastructure...
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST. PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control
 Documentation Control") NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
REFERRAL TO TREATMENT ACCESS POLICY
 Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Health Care Quality Indicators in the Irish Health System:
 Health Care Quality Indicators in the Irish Health System Examining the Potential of Hospital Discharge Data using the Hospital Inpatient Enquiry System - i - Health Care Quality Indicators in the Irish
Health Care Quality Indicators in the Irish Health System Examining the Potential of Hospital Discharge Data using the Hospital Inpatient Enquiry System - i - Health Care Quality Indicators in the Irish
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
Healthcare Audit Plan 2018/2019. Quality Assurance and Verification
 Healthcare Audit Plan 2018/2019 Quality Assurance and Verification Division 1 st March 2018 Table of Contents Page No 1. Method for selecting themes for HCA Plan 2018/2019 3 2. Key themes for HCA 3 3.
Healthcare Audit Plan 2018/2019 Quality Assurance and Verification Division 1 st March 2018 Table of Contents Page No 1. Method for selecting themes for HCA Plan 2018/2019 3 2. Key themes for HCA 3 3.
Powys Teaching Health Board. Respiratory Delivery Plan
 Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Our People/Our Workforce - Public Health Service
 Our People/Our Workforce - Public Health Service - 2016 Introduction In Ireland, at the end of 2016, the public health service is the largest employer in the state with over 128,000 personnel (including
Our People/Our Workforce - Public Health Service - 2016 Introduction In Ireland, at the end of 2016, the public health service is the largest employer in the state with over 128,000 personnel (including
Quality & Patient Safety Audit Service
 Quality & Patient Safety Audit Service End of Year Report 2014 Easy Access Public Confidence Staff Pride I. Introduction In 2014 Quality and Patient Safety Audit (QPSA) continued to build its profile and
Quality & Patient Safety Audit Service End of Year Report 2014 Easy Access Public Confidence Staff Pride I. Introduction In 2014 Quality and Patient Safety Audit (QPSA) continued to build its profile and
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
NATIONAL HEALTHCARE AGREEMENT 2011
 NATIONAL HEALTHCARE AGREEMENT 2011 Council of Australian Governments An agreement between the Commonwealth of Australia and the States and Territories, being: the State of New South Wales; the State of
NATIONAL HEALTHCARE AGREEMENT 2011 Council of Australian Governments An agreement between the Commonwealth of Australia and the States and Territories, being: the State of New South Wales; the State of
Midlands Louth Meath CHO Operational Plan 2018
 Midlands Louth Meath CHO Operational Plan 2018 Contents Foreword from the Chief Officer... Page 4 Section 1: Introduction and Key reform Themes... Page 9 Section 2: Our Population... Page 12 Section 3:
Midlands Louth Meath CHO Operational Plan 2018 Contents Foreword from the Chief Officer... Page 4 Section 1: Introduction and Key reform Themes... Page 9 Section 2: Our Population... Page 12 Section 3:
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Mental Health Services 2010 Mental Health Catchment Area Report
 Mental Health Services 2010 Mental Health Catchment Area Report MENTAL HEALTH CATCHMENT AREA (SUPER CATCHMENT AREA) HSE AREA MENTAL HEALTH SERVICES Limerick, North Tipperary, Clare West Limerick, Clare,
Mental Health Services 2010 Mental Health Catchment Area Report MENTAL HEALTH CATCHMENT AREA (SUPER CATCHMENT AREA) HSE AREA MENTAL HEALTH SERVICES Limerick, North Tipperary, Clare West Limerick, Clare,
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
Hospital Authority Key Performance Indicator Annual Review
 - 1 - For decision on 25.1.2018 AOM-P1352 Hospital Authority 2017 Key Performance Indicator Annual Review Purpose This paper informs Members of the progress of the 2017 Key Performance Indicator (KPI)
- 1 - For decision on 25.1.2018 AOM-P1352 Hospital Authority 2017 Key Performance Indicator Annual Review Purpose This paper informs Members of the progress of the 2017 Key Performance Indicator (KPI)
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Overview of Presentation
 Roscommon Hospital Overview of Presentation Governance Roscommon Hospital - a 2.5 year History Where is Roscommon Hospital now? Current Services at Roscommon Hospital Vision for Roscommon Hospital Roscommon
Roscommon Hospital Overview of Presentation Governance Roscommon Hospital - a 2.5 year History Where is Roscommon Hospital now? Current Services at Roscommon Hospital Vision for Roscommon Hospital Roscommon
Nursing and Midwifery Story. .Policy.Research.Practice.
 Nursing and Midwifery Story.Policy.Research.Practice. Dr Siobhan O Halloran Chief Nursing Officer @chiefnurseire Compassionate Mindful Healthcare Bon Secours September 2016 (Wilde) The significant problems
Nursing and Midwifery Story.Policy.Research.Practice. Dr Siobhan O Halloran Chief Nursing Officer @chiefnurseire Compassionate Mindful Healthcare Bon Secours September 2016 (Wilde) The significant problems
The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital
 The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital Introduction Supplementary Briefing Paper This paper provides more detailed
The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital Introduction Supplementary Briefing Paper This paper provides more detailed
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Health Service Executive CODE OF GOVERNANCE
 Health Service Executive CODE OF GOVERNANCE OCTOBER 2015 Health Service Executive Code of Governance 1 Contents 1 Introduction and Guiding Principles 2 2 Health Service Executive Governance 5 3 Health
Health Service Executive CODE OF GOVERNANCE OCTOBER 2015 Health Service Executive Code of Governance 1 Contents 1 Introduction and Guiding Principles 2 2 Health Service Executive Governance 5 3 Health
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome:
 TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board