RADIATION SAFETY EMERGENCY CALL LIST. Work # or 2543 In-house pager B# Work # or 2543 In-house pager B# 32251
|
|
|
- Mildred Rosaline Pearson
- 6 years ago
- Views:
Transcription
1 1
2
3 Radiation Safety Office North Shore University Hospital Manhasset, New York RADIATION SAFETY EMERGENCY CALL LIST Name Working Hours On-Call Miyuki Yoshida-Hay (1 st call) Radiation Safety Officer Work # or 2543 In-house pager B# Long range pager or Contact hospital operator Cade Register (2 nd call) Radiation Safety Specialist Work # or 2543 In-house pager B# Contact hospital operator A backup service will be called if an emergency escalates beyond that which can be handled by local staff. The decision to call a backup service shall be made by the HICS Incident Commander in conjunction with the Radiation Safety Officer. The New York State Department of Health Bureau of Environmental Radiation Protection serves as the lead agency in New York State for radiological emergencies: New York State Department of Health Bureau of Environmental Radiation Protection Monday - Friday (9:00 a.m. to 5:00 p.m.) (518) Off - Hours (518) DOH Emergency Contact (866)
4 Radiation Safety Office North Shore University Hospital Manhasset, New York MISSION STATEMENT The purpose of Radiation Safety is to ensure that radiation is used and handled properly in accordance with State and Federal regulations and to minimize risk and exposure to patients, personnel, visitors and the environment. The Radiation Safety Office at North Shore University Hospital develops policies and executes programs to provide a safe environment. Essential components of the program include orientation and education of employees as to regulations, hospital policy, safety practices and overall awareness; continuous internal auditing of the program with regard to quality performance and improvement; and the support of Administration. 2
5 Radiation Safety Office North Shore University Hospital Manhasset, New York RADIATION SAFETY MANUAL PREFACE North Shore University Hospital (NSUH) is authorized to procure and use radioactive materials under a specific license of broad scope issued by the Bureau of Environmental Radiation Protection (BERP), New York State Department of Health (NYSDOH). This license is contingent upon the existence of a Radiation Safety Committee and a Radiation Safety Office which, among other requirements, shall: Assure that any physician or investigator using radioactive materials is qualified by training and experience; has the facilities to handle the materials safely; and proposes a use which is safe to all concerned. Assure observance of all safety standards established by the BERP and other regulatory or standards-setting agencies. These include requirements as set forth in Part 16, Chapter 1 of the State Sanitary Code and Broad license conditions. Copies of State Sanitary Code Part 16, the Hospital s Broad License and any notice of violation involving radiological working conditions are located and available for review in the Radiation Safety Office. Keep records of the receipt, storage, use, transfer, and ultimate disposal of all radioisotopes used at NSUH. Keep records of the monitoring of personnel and areas involved in the use of radionuclides and other sources of ionizing radiation. NSUH is subject to periodic inspections by the BERP to ensure that all requirements of the license are being met. These inspections are very thorough, including monitoring checks of laboratory areas, inspection of procurement and disposition records, records of the qualifications of individual users and records of administrations of radioactive materials to patients. Violations of license requirements can result in a loss of the license. All sources of ionizing radiation are not covered by the "broad" license which covers only radioactive materials. These sources are, however, controlled by regulations as prescribed in Part 16. Non-license sources include x-ray machines, high voltage accelerators and electron microscopes. This manual describes rules and regulations required of NSUH under the terms of licensure for the use of radioactive materials and non-licensed ionizing radiation sources as set forth by the State of New York. Radiation Safety Officer 3
6 RADIATION SAFETY MANUAL TABLE OF CONTENTS RADIATION SAFETY EMERGENCY CALL LIST Mission Statement Preface Page Introduction...7 Table of Organization...8 Radiation Safety Committee Responsibilities...9 Radiation Safety Office Responsibilities...10 Authorized User Responsibilities...12 Radioactivity Summary Sheet for Research Protocols...15 Individual User Responsibilities...16 Policies and Procedures for Radioisotope Areas...18 Rules for Safe Use of Radioactive Materials (Clinical Areas)...23 Rules for Safe Use of Radioactive Materials (Laboratories)...26 Spill Procedures (Posting)...28 Medical Emergencies in a Patient with Radioactive Sources...29 Radiation Safety Procedures Following Administrations of Diagnostic Radiopharmaceuticals...30 Radiation Safety Procedures During Radiopharmaceutical Therapy...31 Patient Care Instructions for Patients Treated with Iodine Digital Pocket Dosimeter Record...34 Instructions for Patients Treated with I-131 and Released from the Hospital...35 Procedure for the Release of a Room Occupied by an I-131 Therapy Patient...36 Patient Care Instructions Regarding Strontium-89 (Metastron) or Samarium-153 (Quadramet) Therapy Patients...37 Radiation Safety Procedures for Therapeutic Use of Sealed Sources...38 Patient Care Instructions for Patients Treated with Brachytherapy Sources...41 Patient Care Instructions Regarding Patients Treated with Permanent Prostate Implants...42 TURP Procedure on Patients with Prior Prostate Seed Implants...43 Radiological Procedures on Female Patients of Childbearing Age...44 Sentinel Node Radiation Safety Procedures
7 Table of Contents - Continued Radioactive Cadavers...46 Radiation Safety Report Accompanying Body to Funeral Director...47 Personnel Exposure Monitoring Program...48 Personal Dosimetry Badge Application Form...53 Level I Badge Notification Letter...54 Fluoroscopy Badge Notification Letter...55 Level II Personnel Monitor Radiation Exposure Investigation Form...56 Declared Pregnancy of a Radiation Worker/Badged Employee...57 Fetal Badge Notification Form...58 ALARA Program...59 Radiation Producing Equipment Operator s Responsibility...64 Policies for Radiation Producing Machines and Areas...65 Fluoroscopy Policy...67 Procedure for Obtaining Fluoroscopy Credentials...68 Policies and Procedures for Radiological Protective Garments...70 Care and Use of Radiological Protective Garments...71 Policy on Immobilization of Patients Undergoing X-ray Examination...72 Policy for Shielding Patients (Gonadal Shielding & CT Exams)...73 State of New York Notice to Employees Standards for Protection Against Radiation...74 NYSDOH Notice Unlicensed Operators of X-ray Equipment...75 Procedure for Obtaining an In-House Radioactive Materials Permit...76 Record Keeping Requirements for Research Labs...77 In-House Inspections of Department/Laboratories Utilizing Radioactive Materials...78 In-House Radiation Safety Inspection Outline for Laboratories...79 Procurement of Radioactive Materials and Radiation Sources...80 Procedure for Receipt of Packages Containing Radioactive Materials...82 Procedure for Safely Opening Packages Containing Radioactive Materials...83 Procedure for Area Surveys...85 Shipping Radioactive Materials
8 Table of Contents - Continued Research Centralized Radioactive Waste Handling Procedures...88 Clinical Radioactive Waste Handling Procedures...91 Guidelines for Investigators Using the Center of Comparative Physiology...92 Research Blood Irradiator Policies and Procedures...93 Operating Instructions for the RS 2000 X-ray Irradiator...94 Procedure for Leak Testing Sealed Sources...95 Procedure for Monitoring or Checking Gas and Aerosol Effluents...96 Procedure for the Operation and Maintenance of Fume Hoods Utilizing Radioactive Materials...98 Procedure for Monitoring for the Presence of Radioactivity in Hospital Waste Prior to Shipment for Disposal...99 Setup for Hospital Radiation Waste Monitors Record Retention Schedule Doses to Patients and the Fetus from Common Radiological Procedures Information Required for Submission of an RDRC Protocol Radioactive Drug Research Application Form Gliasite Therapy Procedure and Nursing Instructions Monitoring Dose in Interventional Radiology and Cardiology Bibliography / References
9 RADIATION SAFETY MANUAL INTRODUCTION Ionizing radiation sources and radioactive materials are among the most versatile and useful tools of modern medicine and biomedical research. Like many other modalities of medicine and research, ionizing radiation is potentially hazardous unless used with strict adherence to safety rules and procedures. The risks of exposure to low level radiation include carcinogenesis, damage to the embryo/fetus of a pregnant individual and genetic damage associated with exposure of germ cells. The U.S. Nuclear Regulatory Commission (NRC) has mandated limits of exposure to workers and members of the general public. The rules and procedures outlined in this manual are designed to limit exposure to levels far below these maximum permissible doses (MPD). The rules and procedures set forth in this manual have the purpose of protecting NSUH patients, employees and visitors against any unnecessary radiation exposures. Four levels of group and individual responsibilities are specified in the radiation safety program: Radiation Safety Committee: This committee is composed of physicians, scientists, administrators and patient care representatives appointed by the NSUH Medical Board and Administration to establish policies and regulations governing the use of ionizing radiation in the institution. Radiation Safety Office: A group of specially trained health physicists and technologists who are responsible for compliance with these policies and regulations; it also provides a variety of technical services necessary for achieving such compliance. The Radiation Safety Officer (RSO) is directly responsible to Administration. Authorized Users: Physicians and scientists whose training and experience are such that they have been authorized by the Radiation Safety Committee to use ionizing radiation in clinical care, clinical research, and laboratory research activities. Individual Users: Physicians, scientists, other professionals and workers engaged in patient care, clinical and laboratory research and research support activities which involve actual use and handling of materials and devices producing ionizing radiation. These personnel work under the supervision of Authorized Users. Detailed descriptions of the responsibilities of the individuals of these four levels regarding the safe use of radiation are given in the following pages. Information is also provided on policies, rules and procedures for various aspects of ionizing radiation source procurement, usage and disposal. Careful observance of responsibilities, rules and procedures set forth in this manual will help ensure protection against unnecessary exposure to ionizing radiation. 7
10 8
11 RADIATION SAFETY COMMITTEE RESPONSIBILITIES In carrying out the responsibilities and duties assigned by the Bureau of Environmental Radiation Protection (BERP) under the Hospital's Broad License, the Radiation Safety Committee (RSC) requires compliance with the following policies and procedures: The Committee is bound by the requirements of NY State Sanitary Code, Chapter I, Part 16 as well as requirements listed in the BERP Radiation Guide Copies of this guide are available for reference from the Radiation Safety Office. The Radiation Safety Committee (RSC) membership is appointed by the Medical Board and Administration of NSUH. It consists of such persons as the Radiation Safety Officer (RSO), at least one representative of Administration, one of patient care services, and technical persons representing the departments, groups or activities that will use radioactive materials or radiation producing equipment. Each technical member should have training and experience in the use of radioactive materials and radiation safety. Administrative members of the RSC need not have a background in radiation safety. The RSC shall meet as often as required to conduct its business, but not less than quarterly, and shall keep minutes of meetings and activities. The functions of the Committee are to: (a) (b) (c) (d) (e) (f) (g) (h) (i) Establish policies and overall guidelines for the radiation program. Review, approve and record safety evaluations of proposed uses of radioactive materials. Approve all authorized users of radioactive materials. Conduct periodic audits of the radiation safety program, review the activities of the RSO to include records that must be maintained to ensure compliance with Part 16. Review all instances of alleged infractions of use and safety rules with the RSO and authorized users prior to submitting reports or making recommendations. Review and prescribe training programs for the safe use of radioactive materials. Review annually, the diagnostic and therapeutic quality assurance programs for compliance with regulations. Maintain, in addition to the minutes, records of all applications and actions taken for the duration of the license. Evaluate personnel exposure records of occupationally exposed individuals with the goal of keeping all exposures As Low As Reasonably Achievable (ALARA). When considering a human use research study, the Committee will be guided in its decisions on whether it is subject to an IND (Investigational New Drug) application, NDA (New Drug Approval) or Radioactive Drug Research Committee (RDRC) approval. 9
12 RADIATION SAFETY OFFICE RESPONSIBILITIES The Radiation Safety Office, under the direction of the institution's Radiation Safety Officer, has supervisory responsibilities for: 1. General surveillance of all health physics activities including both personnel and environmental monitoring. Visual inspections, review of pertinent records, contamination sampling and radiation surveys of all radioactive material labs will be performed at least once per year. More frequent inspections will be made as required. 2. Furnishing consulting services to personnel at all levels of responsibility on all aspects of radiation protection. 3. Receiving and shipping of all radioactive materials coming into or going out from the premises. The RSO/Deputy, Nuclear Medicine Chief Technologist, or Radiation Medicine Physicist must approve all purchases of radioactive material by co-signing purchase requisitions. These requisitions will be compared to current inventory of radioactive materials to determine that the purchase will not exceed laboratory or institutional possession limits. 4. Distribution and processing of personnel monitoring equipment including the keeping of records of internal and external personnel exposure; notifying individuals and their supervisors of exposures above expected levels and recommending appropriate remedial action. Bioassays will be required for individuals performing dilutions and/or reactions using more than 100 mci of H-3 or 1 mci of I-125 or I-131 liquid in an open room. In a hood these amounts increase to 1000 mci of H-3 and 10 mci of I- 125 or I-131 liquid. 5. Instructing personnel in proper safety practices for the use of radioactive materials or radiation producing equipment in accordance with Part 16, paragraph Ancillary personnel will be included in the training programs. These programs are offered at least annually, and may be included as part of the mandatory topics program. 6. Supervision and coordination of the radioactive waste disposal program, including the keeping of waste storage and disposal records. 7. Storage of all radioactive materials not in current use. 8. Assuring that inventories of and leak tests on all sealed sources are performed. 9. Maintaining an inventory of all radionuclides at the institution and limiting the quantities of radionuclides to the amounts authorized by the license. The inventory record will include the name of the person responsible for each quantity of radionuclide, and where it will be used or stored. 10. Supervising decontamination in cases of contaminating accidents or major spills. 11. Maintaining a continuous program of environmental radiation hazard evaluation and hazard elimination. 10
13 12. Maintaining a reference library, radiation detecting equipment catalogue file and a list of suppliers of radioactive materials. 13. Performing calibration of radiation detection instruments, e.g. G-M detectors, ionization chambers, counting equipment (beta and gamma). 14. Establishing policies and procedures for the radiation safety aspects of patients on radiation isolation (brachytherapy, I-131 therapy) including training of patient care personnel, maintenance of survey records, ensuring that rooms are free of contamination prior to reassignment and ensuring the protection of other patients, patient care personnel and visitors. 15. Participating in institutional safety and quality assurance programs concerned with uses of radioactive materials or radiation producing equipment. 16. Reporting directly to a high level of administration any condition that threatens safety. 11
14 AUTHORIZED USER RESPONSIBILITIES Authorized Users of radioactive material are granted permits by the institutional radiation safety committee provided they demonstrate adequate training and experience in their proposed uses of radioactive materials and radiation safety. Two types of authorized use are granted: human use authorization and non-human use. Authorized users must also demonstrate that they have adequate facilities and equipment to carry out the proposed uses of radioactive materials. The authorized user/investigator has primary responsibility for the use of the radioactive material, for the protection of patients and employees and for the safe handling of all materials used under their tutelage. Any delegation of work does not shift responsibility. The widely accepted policy for medical uses of radioisotopes is that radioactive substances shall not be used in humans except when the investigation or treatment justifies the risk involved. It is NSUH policy to encourage use of the most sensitive instrumentation and assay procedures available, and to promote progressively better techniques aimed at reducing radiation doses. All research, diagnostic and therapeutic procedures should be designed with these policies in mind. The therapeutic use of radiation in other than malignant disease must be well justified. Applications for all use of radioactive materials will be reviewed by the Radiation Safety Committee in accordance with instructions from the Medical Board. In carrying out the responsibilities and duties assigned by the Bureau of Environmental Radiation Protection (BERP) under the Hospital's Broad License, the Radiation Safety Committee (RSC) requires compliance with the following policies and procedures: The Committee is bound by the requirements of NY State Sanitary Code, Chapter I, Part 16 as well as requirements listed in the BERP Radiation Guide Copies of this guide are available for reference from the Radiation Safety Office A separate application must be submitted to the RSC for each human use project that contemplates the use of radioactive materials. These protocol/proposal applications must have a completed "Radioactivity Summary Sheet for Protocols" (see sample in manual) attached to the protocol 'packet'. This radioactivity summary shall include: (a) (b) (c) Title of the project. A statement of the purpose and justification for the use of radionuclides. Description of the project; including methods and quantities of radioactive materials to be used. Reference to previous work published by the applicant or others concerning animal experimentation or human use should be carefully documented. The Committee requires a clear, concise calculation of the anticipated whole body and critical organ absorbed doses in rads (cgy). Published references may be used. Any references should be clearly stated. 12
15 (d) (e) (f) (g) Methods of waste disposal. Safety precautions for the protection of patients and employees. The application must specify whether children are included. In addition, the Radiation Safety Committee requires a short statement from the investigator regarding the information concerning radiation risks supplied to the research subject for obtaining consent. The Radiation Safety Committee follows FDA guidelines in limiting radiation doses to research subjects. Protocols that use novel radiopharmaceuticals in a limited number of research subjects must first be approved by the IRB and the Radioactive Drug Research Committee (RDRC). These protocols must be designed to obtain basic information on kinetics, distribution, dosimetry and localization of radioactive drugs. It must not be intended for immediate diagnostic or therapeutic use or for information obtained as part of a clinical trial. (See pages ). RDRC approved protocols require quarterly progress reports. In addition, the Authorized User is responsible for all individuals under their permit. They are specifically responsible for: 1. Adequate planning: Before a procedure is performed, the supervisor should determine the types and amount of radiation or radioactive material to be used. This will generally give a good indication of the protection required. The procedure must be well outlined. In many cases, before the procedure is actually performed with radiation, it should be rehearsed so as to preclude unexpected circumstances. In any situation where there is appreciable radiation hazard, the Radiation Safety Office shall be consulted before implementation. 2. Instructing those employees for whom they are responsible in the use of safe techniques and in the application of approved radiation safety practices. 3. Furnishing the Radiation Safety Office with information concerning individuals and activities in their areas, particularly pertinent changes in their personnel rosters. 4. Contacting the Radiation Safety Office when major changes occur in operational procedures, new techniques, alterations in physical plant (e.g., the removal of radiochemical fume hood), or when new operations that might lead to personnel exposure are anticipated. 5. Complying with the regulations governing the use of radioactive materials as established by the BERP and the Radiation Safety Committee for: (a) (b) The procurement of radioactive materials by purchase or transfer. Posting areas where radioisotopes are kept or used, or where radiation fields may exist. 13
16 (c) (d) (e) (f) (g). Recording the receipt, use and disposal of radioactive materials under the permit. This includes sealed sources such as those used for equipment calibration. The authorized user must submit monthly the required inventory data to the Radiation Safety Office. Assuring that all radioactive waste materials are consigned to the Radiation Safety Office for disposal. Surveying regular trash for presence of radioactivity prior to it leaving the laboratory for ultimate disposal. Taking steps to prevent the transfer of radioactive materials to unauthorized individuals. Monitoring of personnel and areas for radiation exposure/contamination when/where appropriate. 6. Keeping stocks of stored radioactive materials to a minimum within laboratory areas. 7. Complying with proper procedure for termination of work using radioactive materials. Under the terms and conditions of the license, the Authorized User must return to the Radiation Safety Office all radioactive materials and waste, all specialized equipment such as personnel monitoring devices (e.g., personal dosimetry badges), survey instruments and shielding materials. The Authorized User shall contact the Radiation Safety Office to arrange for a final termination survey if activities under the permit will cease. 14
17 Print or Type - Answer All Items: RADIOACTIVITY SUMMARY SHEET FOR PROTOCOLS 1) Title of Protocol: 2) New Protocol Protocol utilizing same methodologies, isotopes, etc., as a previously approved protocol. Change in previously approved protocol (i.e., increase in amount of radionuclide, etc.) 3) Protocol Abstract (Include how radioactivity is to be used, the method, how data will be collected and analyzed and why radioactivity is required - Do NOT state "See Attached Abstract") 4) Radioactive Materials Permit No.: Permit Holder: 5) Use of Radionuclide/Radiopharmaceuticals: Adult Subjects / Number of Subjects Minor Subjects / Number of Subjects Animals In Vitro 6) Radiopharmaceutical Isotope - Chemical Form Amount to be Used Per Study 7) Indicate any unusual radioactive waste handling situation: If Proposal is for Human Use, Answer the Following 8) Are these compounds: FDA Approved: YES / NO USP Approved: YES / NO 9) Route of Administration: 10) Number of Studies Per Subject: 11) Estimated Total Radiation Absorbed Dose in Rads Per Study: Total Body: Ovaries: Testes: Red Marrow: Lens of Eye: Target Organ(s): Dose: Dose: Dose: PRINT or TYPE: INVESTIGATOR SIGNATURE EXT. DATE PERMIT HOLDER S SIGNATURE EXT. DATE 15
18 INDIVIDUAL USER RESPONSIBILITIES Each individual at NSUH who has any contact with radioactive materials is responsible for: 1. Keeping exposures to radiation as low as possible, and specifically below the maximum permissible doses as listed in New York State Sanitary Code, Part 16. Laboratory air and sewage concentrations shall be maintained below the levels listed in 6 NYCRR Part 380. Radiation Office personnel will help in these assessments. 2. Wearing the prescribed monitoring equipment, such as personal dosimetry badges and pocket dosimeters, as outlined in this manual under Personnel Exposure Monitoring Program. 3. Surveying hands, shoes, and body for radioactivity, and performing any necessary decontamination before leaving the laboratory. 4. Utilizing all appropriate protective measures such as: (a) (b) (c) (d) (e) (f) Wearing protective clothing whenever contamination is possible and not wearing such clothing outside of the laboratory area. Wearing rubber or plastic gloves and respiratory protection when necessary. Using protective barriers and other shields whenever possible. Using mechanical devices whenever possible to reduce exposures. Using pipette filling devices. Never pipette radioactive solutions by mouth. Performing radioactive work with volatile materials within the confines of an approved hood or glove box. 5. No smoking, eating, drinking or applying cosmetics in radioisotope laboratories. 6. Maintaining good personal hygiene. Wash hands and forearms thoroughly after performance of a procedure with radioactive materials. 7. Checking the immediate areas for contamination, e.g., hoods, benches, etc., in which radioactive materials are being used on a periodic basis. A log record shall be maintained of these surveys including results that are negative. Any contamination that is observed shall be cleaned and documentation kept before and after decontamination. These records will be checked periodically by the Radiation Safety Office. 16
19 8. Keeping the laboratory neat and clean. The work area should be free from equipment and materials not required for the immediate procedure. Transport and store materials in such a manner as to prevent breakage or spillage (double container). Keep work surfaces covered with absorbent material, preferably in a tray or pan, to limit and collect spillage in case of accidents. 9. Labeling and isolating radioactive waste and equipment, such as glassware used in laboratories for radioactive materials. Once used for radioactive substances, equipment shall not be used for other work and shall not be sent from the area to central cleaning facilities, repair shops, or to surplus storage, until demonstrated to be free of contamination. Regular and biohazard waste shall be surveyed for the presence of radioactivity before it leaves the laboratory. 10. Requesting Radiation Safety Office supervision of any emergency repair of contaminated equipment in the laboratory by shop personnel or by commercial service contractors. At no time shall service personnel be permitted to work on equipment in radiation areas without the presence of a member of the laboratory staff to provide specific information concerning radiation levels. 11. Reporting to the supervisor and the Radiation Safety Office, incidents of inhalation, ingestion, or injury involving radioactive materials and carrying out their recommended corrective measures. The individual shall cooperate in any and all attempts to evaluate their exposure. 12. Carrying out decontamination procedures when necessary, and for taking the necessary steps to prevent the spread of contamination to other areas. 13. Complying with requests from the Radiation Safety Office for body burden measurements and the submission of urine samples for radioactivity assays. Requests for these tests will be made in the case of workers using significant quantities of certain radioisotopes. 17
20 POLICIES AND PROCEDURES FOR RADIOISOTOPE AREAS In addition to the regulations prescribed in Part 16, the following policies and procedures apply to the NSUH license: 1. Proper Marking of Laboratories, Areas, and Equipment. (a) (b) (c) (d) (e) A "CAUTION RADIOACTIVE MATERIALS" sign must be conspicuously posted on the doors to laboratory areas where radioactive materials are being used or stored. The name and phone number of the individual responsible for the posted area shall be known and available in case of an emergency. The supervisor shall be responsible for seeing that the information is current. In addition, containers in which materials are transported or stored shall bear a "CAUTION RADIOACTIVE MATERIALS" sign that states the quantities and kinds of isotopes in the containers and the date. A "CAUTION RADIATION AREA" sign must be conspicuously posted in areas where an individual could receive a dose equivalent in excess of 5 mrem in one hour at 30 cm from the source of radiation. A "CAUTION HIGH RADIATION AREA" or "DANGER HIGH RADIATION AREA" sign must be conspicuously posted in any area where an individual could receive a dose equivalent in excess of 100 mrem in one hour at 30 cm from the source of radiation. All equipment contaminated with radioactive material shall be marked with signs, decals, or other conspicuous means. Labeling is not required for laboratory containers such as beakers, flasks, and test tubes used transiently in laboratory procedures while in the presence of the user. A sign notifying women who are or may be pregnant or nursing must be posted and clearly visible to patients informing them to notify the staff before undergoing x-ray or radiopharmaceutical procedures. Signs must not be removed from any room except by Radiation Safety personnel following an inspection survey. 2. Shielding of Sources. (a) (b) Radioactive sources or stock solutions in the laboratory shall be shielded in such a manner that the radiation levels in any occupied area will not expose individuals in the area to more than 10 mrem in any seven consecutive days. Various shielding materials are available on loan from the Radiation Safety Office. 18
21 3. Aerosols, Dusts, and Gaseous Products. (a) (b) (c) (d) Procedures involving aerosols, dusts or gaseous products, or procedures which might produce airborne contamination shall be conducted in a hood, glove box, or other suitable closed system. All releases from such systems shall not exceed the maximum permissible concentration in air for the nuclide in question. (See 6 NYCRR Part 380 for appropriate values.) However, where practical, traps should be incorporated in the experimental set-up to insure that environmental releases are as low as possible. Radioactive gases or materials with radioactive gaseous daughters must be stored in gas-tight containers and must be kept in areas having approved ventilation. Hoods to be used for radioisotope work should be tested by the Maintenance and Engineering Department to insure that they meet the minimum requirements for air velocity at the face of the hood. 4. Sealed Radioactive Sources. (a) (b) (c) (d) All sealed radioactive sources must be registered with the Radiation Safety Office. Sealed sources shall be leak tested by Radiation Safety personnel or designee prior to initial use. Subsequent to the initial leak test, wipe tests will be required at least every six months by the personnel using it. Reports shall then be sent to the RSO. For those sources that may change location frequently, the Radiation Safety Office in cooperation with individual users shall establish strict accountability procedures. 5. Radioactive Materials in Gas Chromatography Equipment. All gas chromatography units in which radioactive materials are to be used are regulated as follows: (a) (b) As is true with other radioactive shipments, radioactive foils to be used in gas chromatography cells must be shipped to the Radiation Safety Office. Each foil must be registered with the Radiation Safety Office. In addition, each cell containing a radioactive foil must have a "CAUTION RADIOACTIVE MATERIAL" label and the identity and activity of the radioactive material. The radioactive foil shall not be removed from its identifying cell except for cleaning and shall not be transferred to other cells. 19
22 (c) (d) (e) The following notice shall appear in a conspicuous location on the outside of each gas chromatography unit: "This equipment contains a radioactive source registered with the Radiation Safety Office as required by license from the BERP. Notify the Radiation Safety Office before removing the source from this room or area or upon any change in custodial responsibility." These notification tags are available from the Radiation Safety Office. Individuals using radioactive components in gas chromatography equipment must vent the cell-exhaust through plastic tubing into a hood, room exhaust, or Radiation Safety approved trap, to avoid contamination of work areas from the release of radioactive samples introduced into the system or from the accidental overheating of radioactive foils in the cells. The Radiation Safety Office will perform periodic leak tests, store radioactive foils when not in use, and maintain the necessary records on such tests and storage. 6. Work Surfaces. All work areas (bench tops, hood floors, etc.) as well as storage areas and areas adjacent to permanent set-ups and sinks should be covered at all times with stainless steel or plastic trays, un-cracked glass plates, or other impervious materials. For some purposes a plasticbacked absorbent paper (e.g., "chux", available from the Central Storeroom) will be satisfactory. However, if such paper is used, it should be changed frequently to prevent active materials from dusting off the surface. 7. Periodic Surveys of Radiation Areas. The immediate areas (e.g., hoods, bench tops) in which radioactive materials are being used should be checked for contamination and excessive radiation levels at least once daily by the radiation workers in that laboratory. In addition, these areas should be inspected each and every time there is reason to suspect a contamination incident. Records of wipe test results and both positive and negative survey results shall be kept in the authorized user's laboratory logs. Consult the Radiation Safety Office for the appropriate schedule for performing these tests. 8. Laboratory Monitors. Each laboratory or area other than those where H-3 is used exclusively or where only exempt quantities of other radionuclides are handled shall be equipped with a portable or semi-portable monitoring device to be used for personnel and area monitoring. 9. Removal of Equipment from the Laboratory. Once used for radioactive substances, equipment shall not be used for other work, or sent from the area to central cleaning facilities, repair shops, surplus storage, or returned to the source of supply, until demonstrated to be free of contamination. Equipment to be removed from the laboratory must be cleared through the Radiation Safety Office. 20
23 10. Repair and Maintenance of Equipment in the Laboratory. Equipment to be repaired by shop and maintenance personnel or by commercial service contractors shall be demonstrated to be free of contamination. The work will be supervised by a member of the Radiation Safety Office staff or designee, who will assure that the necessary safeguards are taken. It is the responsibility of the laboratory personnel to request this supervision from the Radiation Safety Office. 11. House Vacuum Lines. House vacuum lines are vulnerable to contamination. If house vacuum lines are to be used, the withdrawn gas must be demonstrated to the Radiation Safety Office to be free of radioactivity. It is advisable to use a separate vacuum system whenever possible, such as a separate vacuum pump exhausting into a hood. 12. Radioactive Contamination of Areas. In general, no radioactive contamination can be tolerated. Exceptions to this will include certain hood trays, glove boxes, stainless steel trays, surfaces covered with chux, or other equipment which is used frequently for active work and which will be clearly marked with the standard radiation caution signs or stickers. Any contamination that is not confined to protected surfaces should be reported immediately to the Radiation Safety Office. The Radiation Safety staff will supervise the decontamination of such areas or equipment. 13. Decontamination of Areas Contaminated with Radioactivity. Preparations for decontamination should begin promptly. Determine the extent and hazard of contamination. The Radiation Safety Office staff will assist in this evaluation. The individual responsible for the contamination will be expected to do most of the cleanup under the supervision of the Radiation Safety staff. After decontamination, the area or equipment shall be considered contaminated until proven otherwise by Radiation Safety personnel. 14. Decontamination of Personnel Contaminated with Radioactivity. (a) (b) (c) Notify supervisor immediately after contamination occurs. Wash involved body area thoroughly for 2 or 3 minutes, repeatedly "soaping" and rinsing. Consideration should be given to the chemistry of the contaminant and an attempt made to find a suitable agent for dissolving it. Any cleansing agent may be used, but synthetic detergents are preferred to soaps. Avoid prolonged use of any one decontamination procedure. Irritation of the skin may impede the success of more suitable procedures. Avoid the use of organic solvents as they may make the skin more permeable to radioactive contaminants. Do not use abrasive brushes as this will break down the skin barrier. If this procedure is not immediately and completely effective, notify the Radiation Safety Office. 15. Prophylactic Thyroid Blocking Agents in Laboratories using Radioiodine. 21
24 Individuals utilizing greater than 10 mci of liquid radioiodine should consult with and follow the recommendations of the Radiation Safety Officer prior to the use of prophylactic thyroid blocking agents. Such individuals are reminded that the use of these blocking agents in no way reduces the need to take all other precautions in the safe handling of radioiodine. 16. Emergency Procedures. Emergency procedures shall be prominently posted in all controlled areas, radioactive material laboratories and storage areas. 22
25 RULES FOR SAFE USE OF RADIOACTIVE MATERIAL (For Clinical Areas - Nuclear Medicine, Nuclear Cardiology, PET, & Radiation Medicine) 1. Wear laboratory coats or other protective clothing at all times in areas where radioactive materials are used. 2. Wear disposable gloves and laboratory coats at all times while handling radioactive materials. 3. Hands, shoes and clothing must be frequently monitored for evidence of contamination, after each procedure and before leaving the area. Do this in an area away from radiation sources using a thin window probe G.M. counter with the audio function turned on. An area monitor may also be used. 4. Use syringe shields for routine preparation of radiopharmaceuticals and administration to patients, except in circumstances such as pediatric cases when their use would compromise the patient's well-being. In these exceptional cases, use other protective methods such as remote delivery of the dose (i.e. through use of an IV line). 5. a. Do not eat, drink, smoke, or apply cosmetics in any room or area where radioactive material is stored or used. b. Storage of food and drink is prohibited in refrigerators, freezers and cold rooms used for work with radioactive materials or storage of such materials. Store radioactive materials requiring refrigeration only in refrigerators or freezers labeled for radioactive material storage. 6. a. Assay each patient dose in the dose calibrator prior to administration. Do not use any doses that differ from the prescribed dose by more than 10 percent. b. Check the patient's name and identification, the radionuclide, the chemical form, and the activity against the order written by the professional practitioner before administration. All such orders must be approved by a physician authorized on the Radioactive Materials permit. Do not administer therapy doses of radiopharmaceuticals or quantities of Iodine-131 or Iodine-125 in the form of sodium iodide in excess of 30 microcuries, except in accordance with a written order by a physician authorized on the permit or a physician under the supervision of a physician authorized on the permit for these uses. In lieu of a written order, the authorized physician may be present during the administration. c. Identify all patients by two different means before administering a dose. For inpatients: always check the I.D. bracelets and/or bands and ask the patient his/her name. If an I.D. band is missing do not perform the procedure. For out-patients: Ask for identification by name and double check for identification with any relatives who may accompany the patient. This is particularly important for infirm or confused patients. If there is still doubt, ask for positive identification such as a Medicare card or driver's license. 23
26 7. Wear prescribed personnel monitoring devices (personal dosimetry badges). Wear TLD finger badges during elution of generator and preparation, assay, and injection of radiopharmaceuticals. Follow procedures outlined under Personnel Monitoring Program in this manual. 8. Dispose of radioactive waste only in specifically designated and properly shielded receptacles. 9. Never pipette by mouth. 10. Segregate pipetting devices used with radioactive materials from those used with nonradioactive solutions. 11. Confine radioactive solutions in shielded containers that are clearly labeled and store gaseous or volatile materials in a properly ventilated area. Multi-dose vials and therapy vials should be plainly identified and labeled with name of compound, radionuclide, date, time of receipt or preparation, activity, and radiation level, if applicable. Radioactive solutions for therapy should be stored in double containment with enough absorbent material to absorb the volume of liquid. 12. Always keep flood sources, syringes, waste, and other radioactive material in shielded containers. 13. Use a cart to move flood sources, syringes, waste, and other radioactive material. Always transport radioactive material in shielded containers. 14. Use radioactive aerosol devices on surfaces covered with plastic-backed absorbent pads so that any aerosol that escapes, especially through the exhaust port, will not contaminate surfaces under and around the unit. 15. If generators are used, for each elution of technetium-99m from a molybdenum- 99/technetium-99m generator: a. Assay the eluate for technetium-99m in a dose calibrator; record the results and retain the record for 3 years after the assay. b. Test for molybdenum-99 concentration; record the results and retain the record for 3 years after the test. c. Do not use technetium-99m for human use if the technetium-99m contains more than 0.15 microcurie of molybdenum-99 per millicurie of technetium-99m. The concentration of molybdenum-99 must be far enough below this limit so that it will not exceed the above limit at any time up to and including the expiration date and time shown on the package label. 24
27 16. Monitoring of radiopharmaceutical preparation areas shall be performed at least once each day in laboratories where this work is undertaken. In addition, daily surveys (with survey meter), and weekly wipe tests must be performed and recorded for review by the Radiation Safety personnel. Laboratory personnel must survey their non-radioactive waste at the end of each day prior to disposal. 17. Work with volatile radionuclides (e.g., I-131) or with radioactive materials that may otherwise become airborne must be performed in a hood approved for low-level radioactive materials use. Notify the Radiation Safety Office prior to working with volatile radionuclides. Bioassays must be performed on individuals working with more than 1 millicurie of a radioiodine or 100 millicuries of H-3. These quantities increase to 10 millicuries and 1000 millicuries respectively when work is performed in a hood. 18. Dispose of dry (solid) radioactive waste and dry materials suspected of being contaminated (i.e. chux, gloves, paper towels, etc.) in labeled dry radioactive waste containers, never in ordinary waste baskets. Do not use dry waste containers for sharp objects (i.e. glass pipettes, pipette tips, glass vials, needles, etc.) -- use properly labeled sharps containers. 19. Clean up of contaminated equipment or areas is the responsibility of the person(s) working with the equipment and of the designated user. It may not be assigned or delegated to staff outside the laboratory such as housekeeping or maintenance workers. Radiation Safety personnel will supervise decontamination or provide advice upon request. 20. Report incidents of inhalation, ingestion, skin contamination or spills of radioactive materials to the Radiation Safety Office. 21. Maintain good personal hygiene. Keep fingernails short and clean. If there is a break in the skin below the wrist, use double gloves or do not work with radioactive materials. Wash hands frequently and thoroughly when routinely handling radioactive materials. 22. For further information contact the Radiation Safety Office, Biomedical Research Building, Room Extension 2543 or
28 RULES FOR SAFE USE OF RADIOACTIVE MATERIAL (For Laboratories) 1. Wear laboratory coats or other protective clothing at all times in areas where radioactive materials are used. 2. Wear disposable gloves and laboratory coats at all times while handling radioactive materials. 3. Hands, shoes and clothing must be frequently monitored for evidence of contamination, after each procedure and before leaving the area. Do this in an area away from radiation sources using a thin window probe G.M. counter with the audio function turned on. An area monitor may also be used. 4. Do not eat, drink, smoke, or apply cosmetics in any room or area where radioactive material is stored or used. 5. Storage of food and drink is prohibited in refrigerators, freezers and cold rooms used for work with radioactive materials or storage of such materials. Store radioactive materials requiring refrigeration only in refrigerators or freezers labeled for radioactive material storage. 6. Dispose of radioactive waste only in specifically designated and properly shielded receptacles. 7. Never pipette by mouth. 8. Segregate pipetting devices used with radioactive materials from those used with nonradioactive solutions. 9. Confine radioactive solutions in shielded containers that are clearly labeled and store gaseous or volatile materials in a properly ventilated hood. 10. Always keep source vials, waste and other radioactive materials in shielded (i.e., plastic for beta emitters, lead for gamma emitters) containers. 11. Use a cart to transport waste, and other radioactive material. Always transport radioactive material in shielded containers. 12. Monitoring of radioactive material use areas shall be performed after each use in laboratories where this work is undertaken. In addition, weekly surveys (with survey meter), and monthly wipe tests must be performed and recorded for review by Radiation Safety personnel. Laboratory personnel must survey their non-radioactive waste at the end of each day prior to disposal. Weekly surveys are not required in laboratories using exclusively H-3. 26
29 13. Work with volatile radionuclides (iodinations) or with radioactive materials that may otherwise become airborne must be performed in a hood approved for low-level radioactive materials use. Notify the Radiation Safety Office prior to working with volatile radionuclides. Bioassays must be performed on individuals working with more than 1 millicurie of a radioiodine or 100 millicuries of H-3. These quantities increase to 10 millicuries and 1000 millicuries respectively when work is performed in a hood. 14. Dispose of liquid radioactive waste in properly labeled plastic containers. Label each container with the isotope the date the container was closed, and the activity of the container (mci or uci). Contact the Radiation Safety Office to arrange for disposal. 15. Liquid scintillation (LSC) vials containing H-3 and C-14 with quantities less than 0.05 uci/ml of medium must be tightly capped and placed in designated 55-gallon barrels. All other isotopes must be segregated for decay. Contact the Radiation Safety Office to arrange for disposal. 16. Dispose of dry (solid) radioactive waste and dry materials suspected of being contaminated (i.e. chux, gloves, paper towels, etc.) in labeled dry radioactive waste containers, never in ordinary waste baskets. Use double containers for sharp objects (i.e. glass pipettes, pipette tips, glass vials, etc.). 17. Clean up of contaminated equipment or areas is the responsibility of the person(s) working with the equipment and of the designated user. It may not be assigned or delegated to staff outside the laboratory such as housekeeping or maintenance workers. Radiation Safety personnel will supervise decontamination or provide advice upon request. 18. Report incidents of inhalation, ingestion, skin contamination or spills of radioactive materials to the Radiation Safety Office. 19. Maintain good personal hygiene. Keep fingernails short and clean. If there is a break in the skin below the wrist, use double gloves or do not work with radioactive materials. Wash hands frequently and thoroughly when working with radioactive materials. 20. For further information contact the Radiation Safety Office, Biomedical Research Building, Room Extension 2543 or
30 SPILL PROCEDURES MINOR SPILLS - Quantities less than 1 millicurie (mci) of radioiodines or cobalt-60; less than 10 mci of other radionuclides or less than 30 mci of a diagnostic radiopharmaceutical. 1. NOTIFY: Notify persons in the area that a spill has occurred. 2. PREVENT THE SPREAD: Cover the spill with absorbent paper. 3. CLEAN UP: Use disposable gloves and remote handling tongs. Carefully fold the absorbent paper and pad and insert into a plastic bag and dispose of in the radioactive waste container. Also insert into the plastic bag all other contaminated materials such as disposable gloves. 4. SURVEY: With a low-range thin-window GM survey meter, check the areas around the spill, hands, and clothing for contamination. Perform a wipe test to ensure that no removable contamination remains. 5. REPORT: Report incident to the Radiation Safety Officer. MAJOR SPILLS - Quantities greater than or equal to minor spills (above). 1. CLEAR THE AREA - NOTIFY all persons not involved in the spill to vacate the room. 2. PREVENT THE SPREAD: Cover the spill with absorbent pads, but DO NOT attempt to clean it up. Confine the movement of all personnel potentially contaminated to prevent the spread. 3. SHIELD THE SOURCE: If possible, the spill should be shielded, but only if it can be done without further contamination or without significantly increasing your radiation exposure. 4. CLOSE THE ROOM: Leave the room and lock the door(s) to prevent entry. 5. CALL FOR HELP: Notify the Radiation Safety Officer immediately. 6. PERSONNEL DECONTAMINATION: Contaminated clothing should be removed and stored for further evaluation by the Radiation Safety Officer. If the spill is on the skin, flush thoroughly and then wash with mild soap and lukewarm water. 7 The Radiation Safety Officer will supervise the clean-up of the spill and will complete a report. RADIATION SAFETY OFFICE: FEINSTEIN INSTITUTE (ROOM 3155) Phone: 3895 or
31 MEDICAL EMERGENCIES IN A PATIENT WITH RADIOACTIVE SOURCES The following is the policy regarding a patient who has radioactive sources in place and experiences a cardiac arrest or other medical emergency: 1. All necessary medical emergency procedures are to be taken regardless of the radioactive sources that are in place. 2. The radioactive sources are not to be removed by anyone other than an authorized user. This means that the house staff, attending physicians, patient care personnel, etc. cannot remove the radioactive devices or sources. 3. The responsible radiation oncologist, as well as the radiation safety officer, are to be notified immediately. 4. As soon as the radiation oncologist arrives, he/she will remove the sources, if it is a temporary implant. If it is a permanent implant where the sources cannot be removed, the radiation oncologist and radiation safety officer should still be notified so that they can evaluate the situation. 5. If needed, the patient can be transferred with the radioactive sources in place to the appropriate intensive care unit. 29
32 RADIATION SAFETY PROCEDURES FOLLOWING ADMINISTRATION OF DIAGNOSTIC RADIOPHARMACEUTICALS Since there is minimal external hazard to others from routine diagnostic doses of radionuclides, there are no restrictions on the patient's activities or contacts with other people. Patient care personnel are not required to wear personnel monitoring devices. Should questions arise, call the Radiation Safety staff for assistance. 30
33 RADIATION SAFETY PROCEDURES DURING RADIOPHARMACEUTICAL THERAPY 1. The patient s room will be as far away from the nursing station and heavy traffic hallways as is consistent with good medical care. It will be a private room with private sanitary facilities and should be without carpeting. The door of the room will be posted with a "Caution-Radiation Area" sign. The shield, patient s wrist band and chart will also be posted. 2. The room shall be prepared for the procedure as follows: a. Leak-proof absorbent material shall be used to cover surfaces including the floor around the toilet and small items (telephone, door knobs, bed remote control, television control, and nurse call cord) that are likely to be contaminated. A shield will be placed in front of the door. b. Linens and disposable waste shall be deposited in plastic bags in special containers and kept in the room for the duration of treatment. c. Urine shall not be collected nor bloods drawn for the duration of the treatment. If physician's written order contradicts this, consult with the Radiation Safety Officer or designee for specific instructions with regard to radiation safety precautions. If specimens from such patients are to be sent to a laboratory they must be labeled "Radioactive". Preferably, the laboratory should be called in advance to give them additional information, such as the amount of activity and special handling instructions required, if any. d. Additional stock of disposable gloves, absorbent material, and radioactive labels shall be on hand for use as necessary by nuclear medicine and radiation safety personnel. 3. Disposable table service shall be ordered for the precaution period. Environmental Services shall be informed that they should stay out of the room until otherwise notified. 4. Patient care personnel assigned to the patient will be supplied with digital pocket dosimeters. When using a digital pocket dosimeter, record the required information on the Digital Pocket Dosimeter Record form supplied for that purpose. 5. Patient care personnel will be briefed on radiation safety precautions. A written copy of the radiation safety precautions (see nursing instruction form following this section) shall be posted on the patient's door and a radiation precaution sticker shall be attached to the patient's chart. Instructions for nurses caring for the patient will be written in the patient s chart. 6. The patient shall be briefed on radiation safety procedures regarding the dosage administration, visitor control, segregation of radioactive waste (i.e., linens, garbage, trash, etc.), and other items as applicable. 7. Only personnel needed for medical, safety, or training purposes shall be present during the administration. Personnel shall wear gloves when opening containers of 31
34 radiopharmaceuticals such as I-131. Doses of therapeutic I-131 are generally supplied in capsule form only. 8. Visitors must remain behind the shield at all times. 9. Following administration of the dosage, the exposure rate in mr/hr is measured at the bedside, 3 feet and 6 feet from the patient, at the room entrance and in the surrounding hallways and rooms (the last rates must conform to requirements in New York State Sanitary Code Part 16). This and any other necessary information shall be recorded on the nursing instructions form. 10. Waste shall remain in patient's room until the end of the therapy at which time it will be removed to the designated storage shed for decay-in-storage. If the waste becomes problematic (i.e., overflow or odorous), it shall be removed to the storage shed, as soon as possible, by Nuclear Medicine or Radiation Safety personnel. 11. Patients in general are not released until retained radioactivity is less than 30 millicuries. A measurement performed with a portable ionization chamber at 6 feet indicates the retained activity. 12. Before the room may be used for general occupancy, it must be decontaminated by nuclear medicine or radiation safety personnel and approved for release to the Admitting Office. (See procedure on page 37) 13. Each patient must be advised of radiation safety precautions to be followed after discharge and provided with written instructions. An example of the instruction form is appended. 14. In case of emergency, the Nuclear Medicine physician in charge and Radiation Safety Office personnel must be notified. Consult the call list included at the beginning of this manual. 32
35 PATIENT CARE INSTRUCTIONS FOR PATIENTS TREATED WITH IODINE-131 Patient Name: Patient I.D. #: Patient Room/Location: Physician: Dose: mci of as was administered at : am/pm on (date) / / Signature: Exposure Rates Date Time Bedside 3 ft from bed Door Other / / : am/pm mr/hr mr/hr mr/hr mr/hr Visitor Restrictions No visitors under 18 or pregnant. minutes each day maximum for each visitor. Visitors must stay behind shield at all times Nursing Guidelines Patient is restricted to room. No nurses who are pregnant may render care. Nurses shall minimize time spent in patient's room. Wear disposable gloves. Wash your hands after caring for patient. Discard linen/bedclothes, plates/utensils, dressings, etc. in separate containers. All waste must remain in room. Discard urine and feces in toilet. Flush three times. Environmental Services personnel are not permitted in the room. Only the Radiation Safety Officer or designee may release room to Admitting Office. Wear the radiation monitor (digital dosimeter) when caring for patient. Record all results on dosimeter record sheet. Leave the dosimeter at designated location at the end of your shift. Any questions, please contact the Radiation Safety Office **IN CASE OF EMERGENCY: CONTACT: EXT. 33
36 NORTH SHORE UNIVERSITY HOSPITAL Manhasset, New York RADIATION SAFETY OFFICE DIGITAL POCKET DOSIMETER RECORD PATIENT: RADIOACTIVE SOURCE: PATIENT ROOM #: AMOUNT: Treatment Duration: hours From: To: *** FILL IN THE FOLLOWING INFORMATION ONLY IF YOU RECEIVE A READING*** (Note: 1 mrem (10 usv) is equivalent to background radiation you are exposed to in single day, and 5 mrem (50 usv) is approximately equivalent to a chest x-ray.) If you receive a dose greater than 5 mrem or 50 usv per shift Contact the Radiation Safety Office at x 3895, DATE PRINT Employee Name (Last, First) Time IN Pre-Dosimeter Reading Time OUT Post- Dosimeter Reading Net Dosimeter Reading (mrem or usv) Rev 5/
37 INSTRUCTIONS FOR PATIENTS TREATED WITH I-131 AND RELEASED FROM THE HOSPITAL Patient Name: MR #: Date of Treatment: Treatment Dose: mci Check ONE of the following Patient Classifications Patient treated with I-131 and is self sufficient Patient treated with I-131 and requires extended care Patient treated with I-131 and requires custodial care It is necessary for you to remain in isolation (and follow these instructions) until: You may drive home with another (non-pregnant) adult no more than one hour. Going to work, shopping and other public places is PROHIBITED. You must remain in separate quarters and at least 10 feet from all other household members at all times. You are permitted to go outside in your backyard (Private homes only). It is a good idea to cover telephone mouthpiece during the isolation period. Maintaining salivary flow is important. This can be aided by sucking on lemons or sour candy during this period. In addition the following radiation precautions must be followed: The greater the distance you remain from others the less radiation exposure they will receive. Minimize the amount of time you remain in close proximity to others. Avoid direct contact with the neck. Incidental contact is permitted. Flush toilet two or three times after using the bathroom. Wash your hands thoroughly and routinely. It is recommended to shower or bathe daily. Restrict fluids for 24 hours after treatment. After 24 hours, drink fluids to help flush any extra radioiodine from your body. Launder clothing separately from other household members. Use separate eating utensils and wash them separately. NOTE: Do not use paper plates or disposable cups or flatware. Avoid foods that come into contact with saliva and are subsequently disposed (e.g., corn on the cob, barbecue ribs, apples, chicken on the bone, etc.). Tissues and paper napkins should be flushed in the toilet if plumbing allows. For other articles contaminated with body fluids that cannot be washed or disposed in the toilet, contact the Nuclear Medicine Dept. or the Radiation Safety Office for special instructions. Discard toothbrush at the end of the precaution period. An unborn child s thyroid can be harmed by radioiodine, therefore before attempting to get pregnant, consult your physician. Refrain from breast-feeding until a sample of breast milk is tested in one month. Sleep alone until: Avoid social contact with children and pregnant women until: May resume physical contact with infants: May take airline or long car trip: Contamination precautions are no longer necessary after: Return to the Nuclear Medicine Dept. for scanning on: I have read and understand the above instructions, which have been explained to me, and I agree to abide by them. Patient Signature: Witness: Date: Date: If you have additional questions: Contact NUCLEAR MEDICINE: (516) or RADIATION SAFETY OFFICE (516)
38 PROCEDURE FOR THE RELEASE OF A ROOM OCCUPIED BY AN I-131 THERAPY PATIENT 1. After the patient is discharged, personnel from Nuclear Medicine or Radiation Safety will check the room for contamination with a G.M. or scintillation survey meter. 2. Areas likely to be contaminated such as bed, bed rail, chairs, tables, telephone, bed control, nurse's call button, doors, windowsill, floors, sinks, toilet seat, toilet bowl, flush handle, light switches, etc., will be washed down with bleach and/or "Radiacwash" (or equivalent). 3. Area surveys and wipe tests will then be performed on all such areas. 4. Repeat steps 2 and 3 if results of wipe tests exceed 200 dpm per 100 cm 2 of removable contamination. In general, area surveys should be below 0.2 mr/hr. Contact the Radiation Safety Office if higher levels exist. 5. When acceptable limits have been reached, the charge nurse will be notified and the room will be released to Environmental Services for terminal cleaning. 6. The room may then be returned to the Admitting list. 36
39 PATIENT CARE INSTRUCTIONS REGARDING STRONTIUM-89 (METASTRON) OR SAMARIUM-153 (QUADRAMET) THERAPY PATIENTS Strontium-89 (Metastron) or Samarium-153 (Quadramet), used for palliative treatment of metastatic bone pain, is administered intravenously. Urine will be radioactive for about one week. Radiations from Metastron and Quadramet are primarily absorbed within the patient s body and therefore do not represent an external hazard to patient care personnel, ancillary personnel or other patients. Treatments may be performed on an outpatient basis. There are no special radiation precautions for continent patients other than routine personal hygiene. Patients who are incontinent are placed on radiation precautions because of the handling of radioactive urine and concerns associated with waste disposal. Such precautions may include the following: 1. Patient may require a private room. 2. Urine must frequently be emptied into the toilet. Flush at least 3 times. 3. When Foley catheter is discontinued, contact Nuclear Medicine for proper disposal x4400. On weekends the Nuclear Medicine technologist on call may be reached through the page operator. Personnel caring for these in-house incontinent patients will be briefed on a case by case basis by Nuclear Medicine and Radiation Safety personnel. IN THE EVENT OF A URINE SPILL FROM A PATIENT RECEIVING A METASTRON OR QUADRAMET TREATMENT FOLLOW THE STEPS BELOW: 1. Using standard precautions absorb any visible liquid (e.g. chux, paper towels). 2. Cover the area with absorbent material (e.g. chux). 3. Leave all potentially contaminated waste and laundry in the patient s room. 4. Contact the Radiation Safety Office immediately (x3895) for any further instructions. 5. Do not attempt to decontaminate the spill as this will be done by Nuclear Medicine or Radiation Safety Office personnel. 37
40 RADIATION SAFETY PROCEDURES FOR THERAPEUTIC USE OF SEALED SOURCES 1. All patients treated with brachytherapy sources will be placed in a private room that has a toilet. The room will be as far away from the nursing station and heavy traffic hallways as is consistent with good medical care. 2. The patient's room will be properly posted and shall conform to the requirements of New York State Department of Health Sanitary Code Part Visitors must remain behind the portable shield placed in the room at all times. 4. For Temporary Implants: Surveys of the patient's room and surrounding areas will be conducted as soon as practicable after sources are implanted. Exposure rate measurements will be taken at 3 feet (or 1 m) from the patient, at the patient's bedside and behind the shield. The Radiation Safety Officer or designee will post the exposure rate at 3 feet (or 1 m) from the patient on the patient's chart. The measured exposure rate at 1 meter will be compared to the expected calculated value. For Permanent Implants: If the implant is performed other than in the patients room, the area used for the procedure will be surveyed immediately afterward. In the case of seeds, any area where the seeds are handled (i.e. sterilization area, operating room, source storage room) will be surveyed immediately after use. 5. Radiation levels in unrestricted areas will be maintained less than the limits specified in New York State Department of Health Sanitary Code Part 16 (2 mr/hr). 6. Immediately after sources are implanted, a form for nursing instructions for patients treated with brachytherapy sources will be completed and posted on the patient room door. (See Nursing Instruction Form) 7. Nurses caring for brachytherapy patients will be assigned personnel monitoring devices, i.e., digital pocket dosimeters. (See Digital Pocket Dosimeter Record) 8. A survey will be performed at the conclusion of treatment to ensure that all sources other than permanent implants have been removed from the patient and that no sources remain in the patient's room or in any other area occupied by the patient. At the same time, all radiation signs will be removed. 38
41 9. Instructions to Patient Care Personnel a. Special restrictions may be noted on the precaution sheet. Personnel should read these instructions before attending to the patient. The Radiation Safety Officer should be contacted to answer any questions about the care of these patients in regard to radiation safety precautions. b. Personnel should minimize the time spent near a patient for routine nursing care. c. When patient care personnel are assigned to a therapy patient, a personnel monitor should be obtained. Personnel shall record the required information on the pocket dosimeter record form and return the dosimeter at the end of the shift. d. Pregnant individuals should not be assigned to the personal care of these patients. e. Never touch needles, capsules, or containers holding brachytherapy sources. If a needle becomes dislodged, use the long forceps that are provided, and place it in the shielded empty source container provided by Radiation Medicine. Contact the Radiation Oncologist in charge and the Radiation Safety Officer. f. Bed bath should be discontinued while the sources are in place. g. Perineal care is not given during gynecologic treatment; the perineal pad may be changed when necessary unless orders to the contrary have been written. h. Surgical dressings and bandages used to cover the area of the needle insertion may be changed only by the attending physician or radiation oncologist and MAY NOT BE DISCARDED until directed by the radiation oncologist or RSO. Dressings should be kept in a basin until checked by the RSO or designee. i. No special precautions are needed for sputum, urine, vomitus, stools, dishes, or utensils unless specially ordered. j. All bed linens must be checked with a radiation survey meter before being removed from the patient's room to ensure that no dislodged sources are inadvertently removed. k. These patients must stay in bed unless orders to the contrary are written. In any event, patients will remain in their assigned rooms during the treatment period. l. Visitors will be limited to those 18 years of age or older unless other instructions are noted on the precaution sheet. 39
42 m. Visitors should stay behind the shield and should remain no longer than the time specified on the form posted on the patient's door. n. No personnel or visitors who are pregnant should be permitted in the room of a patient while brachytherapy sources are implanted in the patient. Female visitors should be asked whether or not they are pregnant. o. Emergency Situations If an implant source becomes loose or separated from the patient, or if the patient dies, or if the patient requires emergency care, immediately call the Radiation Oncologist on call and the Radiation Safety Officer. Patient care requirements always take precedence over radiation safety concerns. 10. At the conclusion of treatment, the Radiation Safety Officer/designee or Radiation Oncologist will: a. Survey the patient and room; b. Count the radiation sources to be sure that all temporary implants have been removed prior to discharging the patient; and c. Record a summary of the final survey results on the patient's precaution sheet that shall be returned to the Radiation Medicine Department. If any permanent implants are to remain in the patient, the Radiation Safety Officer or designee will brief the patient on the precautions for minimizing radiation exposure to others after discharge from the hospital (see sample forms). Each patient is evaluated before discharge and given appropriate instructions to minimize exposures to other individuals. 40
43 Patient Care Instructions for Patients Treated with Brachytherapy Sources Patient Name: MR #: Room No: Isotope: Activity:(mCi): Length of Implant (hrs): Date & Time of Administration: / /, : AM PM Date & Time of Removal: / /, : AM PM Exposure rates in mr/hr Bedside 1 meter from Bed Behind Shield Comply with the following items: Wear a personal dosimetry badge or digital dosimeter, available at the nurse s station, when in the room. Record any dosimeter readings on the digital pocket dosimeter record form. Whenever possible, care for patient from behind the shield. Patient may not have visitors under 18 years of age or visitors who are pregnant. Visitors must remain behind shield at all times. Environmental Services personnel may not enter the room. All items (linens/waste) must remain in the room until approved for disposal by the Radiation Safety Office or designee. A dismissal survey must be performed by the RSO or designee, before the patient is discharged. IN AN EMERGENCY, CONTACT THE RADIATION ONCOLOGIST ON CALL Dismissal Survey Date: Instrument Used: Performed by: Bkg (mr/hr): Pt.(mR/hr): Bed (mr/hr): Linen (mr/hr): Trash (mr/hr): Comments: 41
44 PATIENT CARE INSTRUCTIONS REGARDING PATIENTS TREATED WITH PERMANENT PROSTATE IMPLANTS Permanent prostate implants are a type of brachytherapy used in the treatment of prostate cancer. These radioactive implants contain either Iodine-125 (I-125) or Palladium-103 (Pd- 103) in the form of encapsulated seeds and are placed in the prostate gland permanently. Since these seeds are sealed sources the patient s bodily fluids will NOT become radioactive. These patients do not represent an external exposure hazard to patient care or ancillary personnel or to other patients. In accordance with NYS Department of Health regulations, inventory control must be maintained of all radioactive sources. 1. Following the implant procedure, the patient s linens, urine and Foley catheter are to be held until the next day for survey by Radiation Medicine Physics or Radiation Safety personnel. Urine may be strained and poured into the toilet, in lieu of collection. These surveys are performed to ensure that any seeds that may have been passed are recovered. If a seed is found in the interim, use tweezers and carefully place it into a specimen cup, leave it in the patient s bathroom and notify Radiation Medicine Physics or Radiation Safety. 2. Prior to discharge of the patient, a member of Radiation Medicine Physics or Radiation Safety will discuss and give written instructions to the patient concerning radiation precautions to be followed at home (see attached instructions). A copy of the instructions will be placed in the patient s hospital chart. 3. Radiation Medicine Physics or Radiation Safety personnel will perform a survey of the room and notify the patient care personnel when the room may be released. 42
45 POLICY FOR TRANS URETHRAL RESECTION OF THE PROSTATE (TURP) PROCEDURES ON PATIENTS WITH PRIOR PROSTATE SEED IMPLANTS The radioactive seeds used for prostate implantation remain radioactive for 6 months to 2 years depending upon the radioisotope used. Palladium seed implants older than 6 months or iodine seed implants older than 2 years do not require any radiation precautions. At NSUH Manhasset, patients are given a card with information about the date of implant, isotope used and length of time various precautions are required. Whenever a TURP procedure is planned on a patient with prior seed implantation, concerns exist about specimens which will be obtained during the TURP procedure. If the seeds are still hot as determined by the date of the implant then the steps outlined below should be followed. Procedure for Removing Seeds from Specimens 1. The following items will be needed: a Geiger counter, a scalpel, a forceps and a specimen cup half filled with saline solution. 2. Carefully using the scalpel and the forceps remove the seeds from the specimen and place them in the specimen container. 3. Use the Geiger counter to determine that the remaining specimens are free of radioactive seeds. Survey the area to make sure that no seeds are lost. 4. Label the specimen container with the date, isotope, # of seeds and activity. Place a radioactive materials label on the container. 5. Store the seeds for at least 10 half-lives. Prior to disposal as non-radioactive waste, survey the seeds with a Geiger counter to insure that they are no longer radioactive. The following resources are recommended for obtaining information about the specifics of dealing with a patient s implant. Contact the RSO or Radiation Medicine Department of the institution where the implant procedure was performed. Patients usually receive instructions and information regarding their implants upon discharge from the hospital. If questions still remain contact the Radiation Safety Office (extension 3895) 43
46 POLICIES FOR RADIOLOGICAL PROCEDURES ON FEMALE PATIENTS OF CHILDBEARING AGE Radiopharmaceuticals in Female Patients of Childbearing Age: 1. Signs must be posted in the waiting area and injection area, notifying patients to inform the technologist or nurse if they are or could be pregnant or nursing. 2. In addition, the technologist shall ask all female patients of childbearing age if they are or could be pregnant or nursing before any radiopharmaceutical is administered. 3. The decision to perform a procedure involving radiopharmaceuticals on a pregnant patient is a medical decision and shall be made by the nuclear medicine physician in consultation with the referring physician and the patient. If the procedure is to be performed, the department physician must explain the risks to the patient, provide informed consent and the appropriate consent form shall be signed. 4. In general, only emergency scans are performed on pregnant patients. 5. Nursing patients who receive Tc-99m should abstain from nursing for 48 (forty-eight) hours. 6. Patients who receive long-lived radioisotopes who are nursing shall consult with the Radiation Safety Officer concerning resumption of nursing activities. X-Ray Procedures in Female Patients of Childbearing Age: 1. Signs must be posted in the department, notifying patients to inform the technologist or nurse if they are or could be pregnant. 2. Technologists shall ask each female of childbearing age if they are or could be pregnant before commencing any radiological examination/procedure. Follow departmental procedures 3. The decision to perform a radiological examination/procedure on a patient who could be pregnant is a medical decision and shall be made by a physician in consultation with the patient. If the procedure is to be performed, the department physician must explain the risks to the patient, provide informed consent and the appropriate consent form shall be signed. 4. Shielding shall be used to shield the abdomen from radiation provided it does not interfere with the procedure. 5. Medical emergency radiological procedures take precedence over pregnancy status. Also refer to Radiology Services, Policy # RAD Pregnancy Screening for Radiology Procedures posted on Health port. 44
47 SENTINEL NODE RADIATION SAFETY PROCEDURES PURPOSE: To promote safe and proper handling of radioactive materials and to avoid the potential for any hazardous conditions during the clinical sentinel node procedures. POLICY: Personnel handling radioactive materials will assure compliance with all safety procedures and will complete all training requirements prior to and during the practice. New physicians (surgeons) will be trained/observed by a senior physician (surgeon) prior to performing procedures. All related records and list of authorized physicians (surgeons) will be kept by the Department of Surgery. 1. Approximately 0.5 to 1.6 mci of Tc-99m is administered to a tumor site for a sentinel node procedure. 2. Whole body radiation exposure to personnel is negligible from this procedure. Pregnant individuals may perform the procedure without concern. 3. Hand exposure may be minimized by handling directly injected specimens with forceps or tongs. Specimens, which do not contain the injected activity, may be handled without concern. 4. Use standard precautions (gloves) to prevent hand contamination. 5. Specimens may be sent directly to Pathology. 6. Syringes, that are used to inject radioactive material, must be transported back to Nuclear Medicine in shielded containers. 7. Surgeons who have not performed sentinel node procedures previously must be observed for radiation safety technique for 1 to 3 cases before being permitted to perform procedures on their own. 8. Radiation surveys are generally no longer required for the operating rooms where procedures are performed. New sentinel node procedures may have surveys instituted for a limited number of cases to ensure that contamination control is appropriate. 9. Pathologists may handle specimens without concern since the short half-life of the radioactive material reduces exposure significantly. 10. In case of a spill: cover the area with an absorbent material and clean with a damp gauze. Discard cleaning materials in the transport container so that they can be returned to Nuclear Medicine. Contact Nuclear Medicine (x4400) or Radiation Safety (x3895, Beepers or 31238) for a survey to insure that the area is decontaminated. I have read the material presented above and will abide by these procedures. Print Name Signature 45
48 RADIOACTIVE CADAVERS 1. If any patient containing radioactive material for therapeutic purposes dies, it is the responsibility of the physician who pronounces the patient as dead to immediately notify the physician in charge of the case or designated representative. 2. No person shall commence an autopsy on any cadaver that contains therapeutic radioactive material in any quantity that exceeds five (5) millicuries, without first having consulted with and being advised by the Radiation Safety Officer of the hospital or, if the RSO is not available, the physician responsible for the administration of the radioactive material. If neither is available, a designated representative may serve. 3. A radioactivity report on every cadaver containing more than five (5) millicuries of therapeutic radioactive material will be completed by the Radiation Safety Officer or the physician responsible for the administration of the radioactive material or a designated representative, in conformance with a form prescribed by the RSO. This report will accompany the body (whether autopsied or not) when it is surrendered to the funeral director. A copy of the report must be sent to the New York State Department of Health BERP. 4. The report (see sample form) must include: the name and address of the hospital; the name of the deceased; the name, address and telephone number of the next of kin; the name, address and telephone number of the funeral home to which the deceased will be sent; the radionuclide involved; the approximate activity; the physical form; the location of radioactive material; external exposure rate closest to the source; precautions to be observed in handling of the body by the funeral director and the name of the person who prepared the form. 5. All patients discharged with permanent implants are discharged with instruction forms specifying the radioactive material, activity and date of the implant. Any patient subsequently readmitted would be identified as having an implant. 46
49 Radiation Safety Office North Shore University Hospital Manhasset, New York RADIATION SAFETY REPORT ACCOMPANYING BODY TO FUNERAL DIRECTOR Name of the Deceased: Last First I.D. (number, if any): Next of Kin Name: Last First Relationship: Address: Telephone: ( ) Funeral Home: Address: Telephone ( ) Radioactive Material: Form: Location of Radioactive Material: Approximate Activity: Exposure Rate Closest to the Source: The following precautions are to be observed: Print Name: Date Radiation Safety Officer or Designee Signature 47
50 I. Annual Limits on Exposure PERSONNEL EXPOSURE MONITORING PROGRAM The Nuclear Regulatory Commission imposes limits on the amount of radiation an individual may receive while performing occupational duties. These limits are in addition to any radiation one receives for medical diagnoses or treatment or from background sources. They are designed to limit risks from occupation exposure to be equivalent to risks in other safe industries. The table below lists annual occupational exposure limits as well as the exposure amount from natural background sources, excluding radon, as a reference value. Type of Exposure Total Body Deep Dose Any Organ Lens of the Eye Skin or Extremity Natural Background Amount 5 rem 50 rem 15 rem 50 rem 0.1 rem In addition to the above, limits are also applied to the embryo/fetus of a declared pregnant radiation worker. In order for these limits to be applied the pregnant worker must declare the pregnancy in writing (see Declared Pregnancy form) to her supervisor who will then notify the Radiation Safety Office. The table below lists the specific limits for the embryo/fetus: Period of Exposure Entire Gestation Each Month During Gestation Amount 0.5 rem 0.05 rem When a declared pregnancy form is submitted to the Radiation Safety Office the employee's job duties will be reviewed and if the limits indicated above are likely to be exceeded, recommendations will be made to ensure that these limits are adhered to during the course of the pregnancy. II. Requirements for Monitoring In accordance with NYSDOH Part 16.11, only those individuals who, during the performance of normal occupational duties, are likely to exceed 10% of the limits described in Section I above shall be monitored for external exposure. In addition, anyone who enters a high or very high radiation area (i.e., HDR, linear accelerator rooms, cyclotron vaults) during the course of their duties shall be monitored. The Radiation Safety Officer in conjunction with the Radiation Safety Committee decides if a group of workers require monitoring. Based on the above requirements, the following is a list of workers who require individual monitoring: Individuals routinely involved in fluoroscopy; Nuclear Medicine technical personnel and physicians; Radiation Safety personnel; Radiopharmacy personnel; Individuals routinely involved with brachytherapy; Individuals involved with cyclotron production of radioisotopes; Radiation Medicine technologists, nurses, physicians and physics staff; and declared pregnant individuals working in radiation or radioisotope areas. 48
51 If indicated and at the discretion of the Radiation Safety Officer, quarterly area monitors will be installed as necessary to evaluate areas where individuals could be receiving exposure. The Radiation Safety Office conducts on-going evaluations of personnel monitoring and requirements. Individuals who mishandle radiation monitors/personnel badges and/or who are noncompliant with the policies and procedures described herein will be reported to their department head and/or hospital administration as violating safety rules and regulations. III. Types of External Monitors The types of radiation monitors routinely employed in this institution are listed below: Whole body monitor Ring or finger monitor Collar/shield monitor (fluoroscopy) Pocket dosimeter (a temporary whole body monitor) Whole body monitors are to be worn on the portion of the body expected to receive the highest exposure. Ring or finger monitors are worn by individuals who handle radioactive material or sources. Ring monitors shall be worn on the hand expected to get the largest exposure and oriented inward to best measure that exposure. Physicians performing fluoroscopy may be assigned two monitors. The whole body badge shall be worn beneath the lead apron at the waist and the collar badge shall be worn outside of the protective apron attached to the thyroid shield. Pocket dosimeters are supplied to nurses who occasionally care for patients receiving therapeutic radioactive materials. Whole body monitors shall be worn by declared pregnant workers at waist level. IV. Internal Radiation Monitoring Thyroid counts are performed on the following groups of employees: 1) Nuclear medicine personnel who dispense radioiodine capsules (I-131) for diagnostic or therapeutic purposes. These employees are monitored quarterly. 2) Radiation safety personnel who monitor therapeutic I-131 patients and handle I- 125 and I-131 radioactive waste. These employees are monitored quarterly. 3) Laboratory personnel who perform radio-iodination with I-125 or I-131. These employees are monitored 24 to 48 hours after each procedure. 4) Nuclear medicine or radiation safety personnel that administer liquid I-131 doses to patients shall be monitored 24 to 48 hours after each procedure. 49
52 V. Handling Radiation Monitors and Personnel Badges and Records 1) Area monitors and personnel badges shall be ordered, changed and cancelled by the Radiation Safety Office 2) Each badge account must appoint a coordinator to coordinate the requirements of this section. These individuals will meet with Radiation Safety Office personnel to discuss their duties and assist in maintaining departmental compliance with the regulations including obtaining and coordinating necessary information with the Radiation Safety Office. Badge coordinators are also responsible for the distribution and return of personnel monitors for their department/division. 3) Personnel badges must be exchanged monthly for processing by the contract service company. All old badges must be returned to the service company during the first week of every month. 4) Control badges shall be kept in a low background area and must be returned with personnel monitors for accurate processing of badges. 5) Personnel badges shall not be shared -- they must be worn only by the individual to whom they are assigned. Personnel badges must not be taken home nor used outside this institution. Personnel badges shall not be intentionally exposed. 6) If an employee is aware that their personnel badge has been exposed by other than normal working conditions, it is the employee s responsibility to immediately inform their supervisor of such an event who will then notify the Radiation Safety Office. Employees shall cooperate in investigations conducted by the Radiation Safety Office (i.e., investigations into high or unusual readings). 7) Employees assigned personnel badges who were monitored at previous employment must submit their occupational radiation exposure history to the Radiation Safety Office or they must submit the information about their previous employer so their occupational dose histories can be obtained (see personal dosimetry badge application form). 8) The Radiation Safety Office will place and retrieve area monitors. Area monitors shall not be handled or moved by anyone other than Radiation Safety personnel. 9) The radiation monitor and personnel badge processing company sends the radiation exposure reports to the Radiation Safety Office where they are reviewed and then forwarded to respective accounts -- if necessary, notations will be written on the report. Each account shall post reports accessible for employees to review. 50
53 VI. Maintaining ALARA NSUH is committed to the implementation of a program to maintain radiation exposures as low as reasonably achievable. The program is implemented through monthly and quarterly audits of personnel monitoring records by the Radiation Safety Office. Results of these audits are reviewed by the Radiation Safety Committee and recommendations are made to maintain ALARA. The table below summarizes the ALARA review process: Radiation Exposure Levels Per Month Type Level I Level II Whole Body 50 mrem (DDE) 150 mrem (DDE) Ring/Wrist 500 (SDE) 1,500 (SDE) Fluoro/Collar Badge 150 (DDE) 450 (DDE) DDE = Deep Dose Equivalent SDE = Shallow Dose Equivalent Whole body maximum for pregnant worker: 50 mrem/month Physicians who perform a high workload of fluoroscopic procedures may be issued both a whole body badge to be worn beneath the lead apron and a fluoro/collar badge to be worn external to any lead protection. Note: Level I: Each incident will be noted on the personnel badge report by the Radiation Safety Office. A notification letter is sent to the employee. (See Level I Notification Letter). No specific investigation will occur unless a trend is noted or unless the hospital Radiation Safety Committee requests one. Level II: The Radiation Safety Office will investigate each such incident. A report will be generated and the results of each investigation will be presented to the hospital Radiation Safety Committee. (See Level II Investigation Form). Physicians performing fluoroscopy that receive Level II collar badge readings will get a notification letter that includes their effective dose. (See Fluoroscopy Notification Letter). 51
54 VII. Policy on Pregnant Employees 1. If a pregnant employee working in a radiation or radioisotope area chooses to formally disclose a pregnancy she must do so in writing as required by New York State Department of Health Sanitary Code Part The Radiation Safety Office supplies forms for this purpose (See Declared Pregnancy form). The employee should submit the form to her supervisor who in turn will forward it to the Radiation Safety Office. 2. The maximum permissible whole body (deep dose) exposure to a pregnant individual shall be less than 50 mrem per month throughout the declared pregnancy. If necessary, the pregnant employee shall be reassigned to other tasks to stay within these limits. 3. Upon receipt of a Declared Pregnancy form, the Radiation Safety Officer will review the job duties, make necessary recommendations and sign the form. A copy will be sent to the employee s supervisor. 4. If the employee does not have an existing personal dosimetry badge, one will be issued to her for the duration of the pregnancy. During such time it is the employee s responsibility to exchange the personal dosimetry badge each month. 52
55 North Shore University Hospital (Manhasset) Radiation Safety Office PERSONAL DOSIMETRY BADGE APPLICATION RETURN COMPLETED FORM TO THE RADIATION SAFETY OFFICE TYPE or PRINT Today's Date: Name: Last: First: Maiden Name: Sex: Female Male Date of Birth: Month: Day: Year: 19 Soc. Sec. No.: - - Position: Lab/Division: Ext. Print Name of Employee s Supervisor or Film Badge Coordinator: Signature of Employee s Supervisor or Film Coordinator: Request pertains to: Body Badge Ring Badge Fluoro/Collar Badge Discontinue Badge Number: Customer Number: Transfer From: To: Lab / Division / Customer Number Lab/Division / Customer Number Reinstate Badge (state badge number, if known): Customer Number: Add Badge(s) for Badge Number: to Customer Number: (DO NOT WRITE IN THIS SPACE) FOR RSO USE ONLY: Complete this section ONLY IF YOU WERE ASSIGNED A RADIATION MONITORING BADGE in the past - INCLUDING at a North Shore University Hospital campus: PRINT OR TYPE Radiation Exposure History Employee Name: Employer / Institution: Address: ZIP CODE: Department Employed In: For the Period: FROM: TO: Month/Year Month/Year I hereby request and authorize the release of my occupational radiation exposure history to North Shore University Hospital, 300 Community Drive, Manhasset, New York Employee Signature Date 53
 mrem This is to notify you of a Level I ALARA reading on your badge.")
56 Radiation Safety Office (516) Level I Badge Notification Letter Employee Name: Department / Unit: Badge No.: Badge Date: Body Badge Reading: Collar Badge Reading: Ring Badge Reading: mrem mrem (*Calculated EDE = mrem) mrem This is to notify you of a Level I ALARA reading on your badge. The ALARA program is a program for maintaining occupational exposure As Low As Reasonably Achievable. Part of this program requires workers to be notified when their exposure exceeds certain predetermined levels. Those pre-determined levels are as follows: *Body Badge: 50 mrem Collar Badge: 150 mrem Ring Badge: 500 mrem In order to adequately protect yourself follow TIME, DISTANCE and SHIELDING principles: Decrease the time spent near radiation sources, increase distance and/or use shielding barriers wherever possible. If you have any questions regarding this notification, please contact the Radiation Safety Office at (516) No formal response to this letter is required., Radiation Safety Office Date: 54
57 Radiation Safety Office (516) Fluoroscopy Badge Notification Letter Employee Name: Department / Unit: Badge No.: Badge Date: Collar Badge Reading: Body Badge Reading: mrem mrem This is to notify you of a Level II ALARA reading on your collar badge. However, your effective dose equivalent (EDE) associated with this reading has been evaluated to be mrem. (Note: Less than 50 mrem is below ALARA Level I and less than 150 mrem is below ALARA Level II.) In order to adequately protect yourself, it is mandatory that you utilize proper eye protection (leaded glasses of 0.5 mm lead equivalent with side shields). If you have any questions regarding this notification, please contact the Radiation Safety Office at (516) No formal response to this letter is required., Radiation Safety Office Date: Please note: The effective dose equivalent (EDE) for: A one-badge (collar badge) user is calculated as follows: EDE = (Collar Badge Reading) x 0.3 A two-badge (collar and body badge) user is calculated as follows: EDE = (Body Badge Reading x 1.5) + (Collar Badge Reading x 0.04) 55
58 Radiation Safety Office (516) Return completed and signed form to the Radiation Safety Office within one week. Date sent to employee/department: Level II Personnel Monitor Radiation Exposure Investigation Form Employee Name: Badge No.: Employee Social Security Number: Date of Birth: Department / Unit: Badge Date Badge Account No.: Exposure Report Process No: Badge Type: Badge Type: Reading: mrem Reading: mrem EDE: mrem Explanation: Aforementioned reading(s) to be removed and/or corrected from my (employee) official radiation exposure record: WRITE Yes or No As required by NYSDOH regulations, we are required to determine total radiation exposure for badged individuals. In an effort to comply with this requirement, if you are currently badged at other facilities please list them below: Employee Signature Supervisor Signature Radiation Safety Office Date: Date: Date: [Revised 01/11] 56
59 Radiation Safety Office North Shore University Hospital - Manhasset, New York DECLARED PREGNANCY OF A RADIATION WORKER/BADGED EMPLOYEE In accordance with NRC regulations, the maximum permissible whole body occupational radiation exposure (deep dose) to a pregnant individual must be less than 50 mrem per month and less than a total of 500 mrem throughout the gestation period. The radiation monitor must be placed at the abdomen to best measure the dose. TYPE or PRINT Employee Name: Last: First: Social Security Number: Date of Birth Laboratory/Division/Department: Position: For the purpose of closer monitoring occupational radiation exposure throughout my pregnancy, I am at this time voluntarily formally declaring that I am pregnant. Approximate date of conception is: Month Day Year I understand universal radiation safety procedures regarding my job duties and specifically the additional recommendations (if any) during my declared pregnancy as they were reviewed with me by the Radiation Safety Officer (RSO). RSO recommendation(s) during the pregnancy, if any: Employee Signature: Date: Employee Supervisor: Name: Signature: Date: RSO Signature: Date: Radiation Safety Office Use Only: Landauer Acct #: Series Code: Participant Number: cc: Lab/Department Supervisor Rev: 08/17/
60 Radiation Safety Office (516) Fetal Badge Notification Attached is your monthly fetal badge report. This report is based upon the whole body dosimeter worn closest to the fetus. The fetal dose is reported for the current wear period, plus the estimated dose from conception to declaration and the total dose from declaration to present. Fetal Badge Limit is 50 mrem per month and 500 mrem for the entire gestation period This badge report indicates fetal doses below regulatory limits and considered to be safe. If you have any questions regarding this notification, please contact the Radiation Safety Office at (516) No formal response to this letter is required., Radiation Safety Office Date: 58
61 1. Management Commitment ALARA Program (Program for Maintaining Occupational Radiation Exposure As Low As Reasonably Achievable) a. We, the management of this medical facility, are committed to keeping personnel exposures and environmental releases as low as reasonably achievable (ALARA). In accordance with this commitment, we hereby describe an administrative organization for radiation safety and have developed the necessary written policy, procedures and instructions to foster the ALARA concept within our institution. The organization includes a Radiation Safety Committee (RSC) and a Radiation Safety Officer (RSO). b. We perform a formal annual review of the radiation safety program, including ALARA considerations. This includes reviews of operating procedures and exposure records, inspections etc., and consultations with the radiation safety staff or outside consultants. c. Modification to operating and maintenance procedures and to equipment and facilities will be made where they will reduce exposures or environmental releases unless the cost, in our judgment, is considered to be unjustified. We will demonstrate, if necessary, those improvements have been sought, that modifications have been considered, and that they have been implemented where reasonable. Where modifications have been recommended but not implemented, we will be prepared to describe the reasons for not implementing them. d. In addition to maintaining doses to individuals as far below the limits as reasonably achievable, the sum of the doses received by all exposed individuals will also be maintained at the lowest practicable level. It would not be desirable, for example, to hold the highest doses to individuals to some fraction of the applicable limit if this involved exposing additional people and significantly increasing the sum of radiation doses received by all involved individuals. 2. Radiation Safety Committee (RSC) a. The RSC will encourage all users to review current procedures and develop new procedures as appropriate to implement the ALARA concept. b. The RSC will perform reviews of occupational radiation exposure with particular attention to instances where investigational levels are exceeded. The principal purpose of these reviews is to assess trends in occupational exposure as an index of the ALARA program quality and to decide if action is warranted when investigational levels are exceeded. (The New York State Department of Health has emphasized that the Investigational Levels in this program are not new dose limits but, as noted in ICRP Report 26, "Recommendations of the International Commission on Radiological Protection," serve as checkpoints above which the results are considered sufficiently important to justify further investigation). 59
62 c. The RSC will evaluate our institution's overall efforts for maintaining exposures ALARA on an annual basis. This review will include the efforts of the RSO, authorized users, and workers as well as those of management. 3. Radiation Safety Officer (RSO) a. Safety Reviews 1) The RSO will perform an annual review of the radiation safety program for adherence to ALARA concepts. Reviews of specific procedures may be conducted on a more frequent basis. 2) The RSO will review at least quarterly the external radiation exposures of authorized users and workers to determine that their exposures are ALARA in accordance with the provisions of this program. 3) The RSO will review radiation levels in unrestricted and restricted areas to determine that they are at ALARA levels whenever changes to the physical plant might affect radiation levels. 4) The RSO will monitor environmental releases in accordance with the regulations of the NYS Department of Environmental Conservation (Part 380). b. Education Responsibilities for ALARA Program 1) The RSO will schedule briefings and educational sessions to inform workers of ALARA program efforts. 2) The RSO will ensure that authorized users, workers and ancillary personnel who may be exposed to radiation will be instructed in the ALARA philosophy and informed that management, the RSC and the RSO are committed to implementing the ALARA concept. c. Cooperative Efforts for Development of ALARA Procedures Radiation workers will be given opportunities to participate in formulation of the procedures that they will be required to follow. 1) The RSO will be in close contact with all users and workers in order to develop ALARA procedures for working with radioactive materials and radiation producing machines. 2) The RSO will establish procedures for receiving and evaluating the suggestions of individual workers for improving health physics practices and will encourage the use of those practices. 60
63 4. Authorized Users a. New Procedures Involving Potential Radiation Exposures 1) The authorized user will consult with, and receive the approval of, the RSO and RSC during the planning stage before using radioactive materials for a new procedure. 2) The RSO will evaluate all procedures before allowing the use of radioactive materials to ensure that exposures will be kept ALARA. This may be satisfied through the application of trial runs. b. Responsibility of Authorized User to Persons Under His/Her Supervision 1) The authorized user will explain the ALARA concept and his/her commitment to maintain exposures ALARA to all persons under his/her supervision. 2) The authorized user will ensure that persons under his/her supervision who are subject to occupational radiation exposure are trained and educated in good health physics practices and in maintaining exposures ALARA. 5. Persons Who Receive Occupational Radiation Exposure a. The worker will be instructed in the ALARA concept and its relationship to working procedures and work conditions. b. The worker will know what recourse is available if he/she feels that ALARA is not being promoted on the job. 6. Establishment of Investigational Levels in Order to Monitor Individual Occupational External Radiation Exposures. This institution hereby establishes Investigational Levels for occupational external radiation exposure that, when exceeded, will initiate review or investigation by the RSC and/or the RSO. The Investigational Levels that we have adopted are listed in Table 1 (below). These levels apply to the exposure of individual workers. 61
64 TABLE 1 Investigational Levels (mrems) Exposure Levels: Quarterly Level I Quarterly Level II Overexposure (Body) (Collar) (Body) (Collar) Deep Dose (DDE) 125 or 375 mrem 375 or 1,125mrem 5,000 mrem/year Lens Dose (LDE) 375 1,125 15,000 Shallow Dose (SDE) 1,250 3,750 50,000 Extremity 1,250 3,750 50,000 a. Quarterly exposure of individuals less than investigational Level I. Except when deemed appropriate by the RSO, no further action will be taken in those cases where an individual's exposure is less than Table 1 values for the investigational level I. b. Personnel exposures equal to or greater than investigational Level I, but less than investigational Level II. The RSO will review the exposure of each individual whose exposures equal or exceed investigational Level I and will report the results of the reviews at the first RSC meeting following the quarter when the exposures were recorded. If the exposure does not equal or exceed investigational Level II, no action related specifically to the exposure is required unless deemed appropriate by the Committee. The Committee will, however, consider each such exposure in comparison with those of others performing similar tasks as an index of ALARA program quality and will record the review in the committee minutes. c. Exposures equal to or greater than investigational Level II The RSO will investigate in a timely manner the cause(s) of all personnel exposures equaling or exceeding investigational Level II and, if warranted, will take action. A report of the investigation, actions taken, if any, will be presented to the RSC at the first RSC meeting following completion of the investigation. The details of these reports will be recorded in the RSC minutes. Committee minutes will be sent to the management of this institution for review. The minutes, containing details of the investigation, will be made available to Health Department inspectors for review at the time of the next inspection. d. Re-establishment of occupational workers Investigational Levels to levels above those listed in Table 1. In cases where a worker's or a group of workers exposures need to exceed investigational levels, new, higher investigational levels may be established on the basis that it is consistent with good ALARA practices for that individual or group. Justification for new investigational levels will be documented. 62
65 The RSC will review the justification for, and will approve, all revisions of investigational levels. In such cases, when the exposure equals or exceeds the newly established investigational levels, actions listed in the paragraphs above will be followed. In no case are investigational levels allowed to exceed an overexposure. 7. Discharges to the Environment a. NSUH is committed to operational procedures which minimize discharge of radioactive materials to the environment. Discharges are regulated by the Department of Environmental Conservation under NYCRR Part 380. Discharges of radioactive liquids are monitored by the Radiation Safety Officer and are maintained below maximum permissible concentrations. Discharges of radioactive gases are maintained below 10% of permissible airborne effluent concentrations for all discharge points that are not specifically under permit of the Department of Environmental Conservation. All potential effluent sources will be monitored and evaluated by the Radiation Safety Office and results reported to the Radiation Safety Committee. b. For DEC permitted discharge points (stacks) investigational levels are established whenever a discharge exceeds 50 % of DEC annual permit limits. c. Procedures involving aerosols, dusts or gaseous products, or procedures which might produce airborne contamination shall be conducted in a hood, glove box, or other suitable closed system. All releases from such systems shall be maintained in accordance with ALARA guidelines and, where practical, traps and filters shall be incorporated in experimental set-ups. Hoods used for radioisotope work shall be tested at least annually by the Maintenance and Engineering Department to ensure that they meet the specifications for air velocity at the face of the hood. d. Surveys and effluent monitoring of all areas with potential for release of airborne radioactive materials shall be performed at least annually for compliance with Department of Environmental Conservation regulations. e. The implementation of the discharge minimization program will be reviewed annually by the Radiation Safety Officer, Radiation Safety Committee and Administration. 63
66 RADIATION PRODUCING EQUIPMENT OPERATOR S RESPONSIBILITY The operator of any radiation producing equipment is responsible for: 1. Notifying Radiation Safety/Medical Physics when there is any change in the setup, i.e., new equipment installed, changes in shielding, change in output of radiation, or change in usage of the unit. 2. Requesting and wearing appropriate monitoring devices. Whenever protective lead aprons are worn, a radiation monitor will be worn outside the apron attached to the thyroid collar to monitor dose to unprotected body parts. In addition, ring badges may be worn if the unprotected hands and forearms must come in close proximity to the beam. Some physicians may be assigned two badges, one to be worn beneath the lead apron and one to be worn attached to the thyroid shield. These badges, if assigned, must never be reversed. 3. Keeping exposure as low as possible. The operator must never expose himself to the direct beam, and must not stand within two meters of the tube or irradiated target while the unit is in operation unless adequately shielded. Make full use of protective barriers, lead aprons, gloves and goggles. 4. Clearing the area of all nonessential personnel. The operator should insist that all nonessential personnel leave the exposure area before operating the unit and that all essential personnel be adequately shielded. 5. Observing any restrictions on the use of the unit recommended by the Radiation Safety/Medical Physics staff. 6. Using minimum exposure factors. Fluoroscopic work shall be performed in the minimum time possible using the lowest dose rate and smallest aperture consistent with clinical requirements. 7. Visually monitoring tube current and voltage of fluoroscopic equipment with image intensifiers at frequent intervals because, under automatic brightness control, these variables can rise to high values. 8. Notifying the supervisor and the Radiation Safety Officer immediately of any accidental exposures to radiation. 9. Keeping x-ray units disconnected or locked when not in actual use. 10. Gonadal shielding of 0.5mm lead equivalent shall be used for patients of reproductive age during radiographic procedures in which the gonads are in the useful beam unless this would interfere with the diagnostic procedure. Gonadal shielding is not required for fluoroscopic procedures. Patients undergoing a scoliosis series (usually pediatrics) will have a specifically designed gonadal shield attached to the collimator housing. The light field will be utilized to insure that the gonads are protected before x-rays are taken. 64
67 POLICIES FOR RADIATION PRODUCING MACHINES AND AREAS The operator of any radiation producing equipment shall ascertain that the following activities are enforced: 1. A "CAUTION RADIATION AREA" sign must be conspicuously posted in areas where an individual could receive a dose equivalent in excess of 5 mrem in one hour at 30 cm from the source of radiation. A "CAUTION HIGH RADIATION AREA" or "DANGER HIGH RADIATION AREA" sign must be conspicuously posted in any area where an individual could receive a dose equivalent in excess of 100 mrem in one hour at 30 cm from the source of radiation. In addition, the controls shall bear a decal with the statement: CAUTION RADIATION - This Equipment Produces Radiation When Energized. Exception: Diagnostic and patient treatment areas where portable units are utilized need not be so marked, provided that a person is charged with the responsibility for protection of employees, patients, and visitors against radiation exposure, and for the execution of radiation safety recommendations. 2. The structural shielding requirements of any new installations, or an existing one in which changes are contemplated, shall be discussed with Radiation Safety / Medical Physics staff. 3. A semi-annual survey of all radiation producing equipment used on patients shall be made by medical physics personnel. In addition, radiation surveys shall be made of all new installations and all existing installations after every change that might increase the radiation hazard (e.g., replacement of an x-ray tube, changes in filtration of beam.) 4. Protective aprons shall be worn by the physician, nurse, technologist, and all other persons within the room or area whenever radiation-producing equipment is energized. 5. Dose rates for the beam shall be determined for all units used on humans and shall be reported to the operator in milliroentgens per milliampere-second or milliroentgens per minute. 6. In the operation of mobile and dental units, the operator should stand as far away as possible from the tube and patients during exposure. He/she should also wear a protective apron or step behind an adequate shield. 7. The hand of the fluoroscopist should never be placed in the useful beam unless the beam is attenuated by the patient or a protective glove of at least 0.5 mm lead equivalent. 65
68 8. No person shall be regularly employed to hold patients during exposure. Any person holding the patient shall wear protective gloves and a protective apron, and no part of that person s body should be in the un-attenuated useful beam. Exceptions may occur if ordered by a physician when required for good medical practice. All such instances that are exceptions must be reported to a supervisor and the Radiation Safety Officer. 9. If safe use of the installation depends upon mechanical restriction of the orientation of the radiation beam, or upon limitations (voltage, current, time, permanent filter, and maximum aperture) in the output of the unit, then these restrictions shall be rigidly followed. 10. Shutter mechanisms and interlocking devices should not be tampered with and shall be inspected at frequent intervals to insure proper operation. 11. A manual reset cumulative timing device shall be used during fluoroscopy that will either indicate elapsed time or turn off the apparatus when the total exposure reaches a certain previously determined limit. 12. In cine-radiography, tube currents and potentials are often higher than those used in fluoroscopy. Thus, special care should be taken to limit patient exposure. The exposure rates on these cine-radiography units shall be determined during the semi-annual survey. 13. For large, individually licensed irradiators and accelerators, specific operating and emergency procedures shall be established and posted. All users of this equipment shall operate it in compliance with these posted instructions and must have appropriate security clearance. 14. All interlocks, visual and audible warning devices, and monitoring equipment shall be inspected for proper operation at prescribed intervals by Radiation Safety / Medical Physics personnel. 15. A sign notifying women who are or may be pregnant must be posted and clearly visible to patients informing them to notify the staff before undergoing a radiological procedure. 66
69 FLUOROSCOPY POLICY Physician Credentialing: The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) requires that physicians who use or operate fluoroscopic x-ray systems be properly credentialed. The hospital shall delineate clinical privileges based on evidence of completion of specific training as conferred by appropriate board certification or other equivalent process. This training shall include radiation safety, management of fluoroscopic radiation, and operation of the specific fluoroscopic x-ray system(s) used by the physician. Training in radiation safety and fluoroscopic radiation management is in addition to any clinical training or qualifications required to perform the specific clinical diagnostic or therapeutic procedures for which the fluoroscopic systems are used. The hospital must require specific documentation of appropriate training before granting fluoroscopic privileges. The North Shore University Hospital Radiology Department has implemented a presentation for fluoroscopy safety training. This teaching tool is available on the hospital s Healthport website, so that physicians have an opportunity to become credentialed. After completing the online training document, each physician will need to complete an attestation. An attestation certificate will be available for printing. This certificate must be presented to the physician s department chairperson for recording the successful completion of the fluoroscopy safety requirement. It is up to the individual departments to establish other training and education requirements needed to obtain fluoroscopy privileges. Monitoring Fluoroscopy Time: The Food and Drug Administration (FDA) has reported that serious skin injuries to patients may occur following prolonged fluoroscopically guided interventional procedures. In its 2006 standards, the JCAHO has defined prolonged fluoroscopy with cumulative dose > 1500 rads to a single field as a potential sentinel event. Consequently, monitoring of the fluoroscopy time for extended procedures is an appropriate patient safety precaution. Procedures that exceed 1 hour of fluoroscopy shall be recorded and reported to the radiation safety committee. The following departments/areas need to consider which procedures could entail extended use of fluoroscopy: Interventional Radiology Cardiology Gastroenterology (Endoscopy) Surgery Sentinel Events: If a fluoroscopic procedure exceeds five hours, the following sequence of events must take place: 1. Notify the radiation safety officer who will investigate details of the procedure to determine if the dose delivered to the patient exceeded the 1,500 rad threshold required for investigation as a sentinel event. 2. Should this dose threshold be exceeded, Quality Management will be immediately notified to review the case under the JCAHO sentinel event policy. 67
: http://www.northshorelij.")
70 PROCEDURE FOR OBTAINING FLUOROSCOPY CREDENTIALS Go to: Click on Healthport (upper right hand corner): 68

71 Click on Fluoroscopy Credentialing and proceed with training. After you have completed the training, complete the Physician s Attestation Form. This attestation form must be presented to and filed with the department chairman who privileges physicians to perform specific fluoroscopic procedures. The responsibility for delineation of clinical privileges ultimately lies with the department chairman. If you have any questions, please contact the Radiation Safety Office: (516)
72 POLICY AND PROCEDURES FOR RADIOLOGICAL PROTECTIVE GARMENTS Background: The proper use of x-ray protective garments, gloves and eye shields is regulated by the New York State Department of Health, Bureau of Environmental Radiation Protection under the State Sanitary Code, Part 16 on ionizing radiation. The regulations require that only persons required for a radiographic or fluoroscopic procedure be present in the room during an x-ray exposure. In addition, all such persons must be equipped with appropriate shielding devices such as lead aprons, thyroid collars, gloves and eyewear with a least 0.25 mm lead equivalent. Acquisition: The North Shore / LIJ Radiation Safety Committee requires all x-ray protective devices, e.g., aprons, gloves, thyroid shields and eyewear to be at least 0.35 mm lead equivalent. Employees involved in the performance of extended procedures using fluoroscopy should use 0.5 mm lead equivalent protection. Aprons made of composite materials represent the best tradeoff between weight and durability. The Radiation Safety Office will provide consultative services to aid in the ordering of new devices. Gonadal shielding of not less than 0.5 mm lead equivalent shall be used for patients who have not passed the reproductive age during radiographic procedures in which the gonads are in the useful beam, except for cases in which this would interfere with the diagnostic procedure. Protective garments shall be obtained from Radiation Safety Committee approved vendors. Use: Any person required to be in the procedure room during radiographic or fluoroscopic exposure must wear a protective apron. If a person is positioned within one meter (3 feet) from the axis of the radiation beam, that person should also wear a thyroid shield and protective eyewear. Lead aprons should never be folded. Cracks in the lead lining can develop at the fold, reducing the useful life of the apron. When not in use, aprons shall be hung appropriately on a hanger. Inspection: Personnel that use protective garments should inspect them prior to each use. The inspection should include both a thorough visual as well as physical assessment of the garment. Closely inspect each item for breaks, cracks, creases and irregularities. Run your hands over the surface of the item pressing firmly. You may feel damage that you cannot readily see. If any item is suspected of being defective, it must be brought to the attention of a supervisor and, if confirmed, either discarded or repaired. In addition, protective garments must be formally inspected every six months by a departmental supervisor. Documentation will include the date and initials of the person performing the inspection. It is advisable to maintain an inventory of all items in the department. Disposal Protective garments cannot be disposed as regular trash because of their lead content. They can either be exchanged through the apron vendor (preferred) or disposed through a licensed commercial vendor. 70
73 CARE AND USE OF RADIATION PROTECTION GARMENTS INSPECTION Visually and physically inspect your aprons on a regular basis. STORAGE Hang aprons up by the shoulders or on an approved apron hangar. In the case of kilts, use the attached reinforced hanging straps. Do not fold or crease the apron, as repeated actions may cause damage. Do not lay or store aprons on a flat surface - e.g. floor, table Do not expose aprons to extreme temperatures. FITTING Make sure that the Velcro is lined up correctly; failure to do so may cause fraying of the binding and the embroidery. Do not use excessive force when closing kilt straps. This can cause tearing of fabric at seams. Do not sit while wearing your apron. This can stretch and damage the apron. CLEANING Clean and deodorize by scrubbing with a soft bristle brush and a colloidal based cleaner. Rinse thoroughly with water to remove residue of cleaner. Hang to dry. Do not use products containing bleach. Test cleaner on a small section before cleaning. Do not machine launder or dry-clean the apron. For more information contact your vendor. 71


74 POLICY ON IMMOBILIZATION OF PATIENTS Whenever a patient requires immobilization for a radiological exam, mechanical means such as immobilization devices, tape and sandbags are used. Only when all means of immobilization fail may another individual be used to help immobilize the patient. This other individual may be a relative. The oldest available person should be utilized in descending order of age. The holder must be supplied with a lead apron, lead gloves and a digital dosimeter. All holding must be logged into a book and maintained for a period of three years. The information entered into the holding log book must include: Date Name of the patient and medical record # Name of the holder and relationship to the patient Type of exam Pre-exposure dosimeter reading including units (see Step 3 below). Post-exposure dosimeter reading including units How to use the ALOKA PDM-117 Digital Dosimeter Power Switch 1. Turn ON by firmly pressing the power switch for approximately 3 seconds. Use thumb pads-never use nails or pointed tools (i.e., pens). 2. Display indicates: 8888 for 3 seconds as an initial test which will then switch to (Note: The dosimeter will not automatically reset to zero. Accumulated doses will remain in memory until it is reset see Step 7.) 3. Record this initial (usv) reading on the log. (This is your pre-exposure reading.) 4. Securely fix the dosimeter to the holder s clothing by using the clip and neck strap to prevent dropping the unit. 5. When the exam is completed, remove the dosimeter and record (usv) reading on the log. (This is your post-exposure reading.) 6. The difference between post and pre exposure reading will be the dose received by the holder. 7. REMEMBER to turn the dosimeter OFF by pressing power switch for approximately 3 seconds after each use. 8. To RESET the unit to 0000 press the power switch again from approximately 10 seconds. The display will change from the stored value to 0000 with the following displays: 0clr. 72
75 POLICY ON SHIELDING OF PATIENTS Use of Gonadal Shielding: 1. Gonadal shielding of 0.5mm lead equivalent shall be used for patients of reproductive age during radiographic procedures in which the gonads are in the useful beam unless this would interfere with the diagnostic procedure. 2. Gonadal shielding is not required for fluoroscopic procedures. 3. Patients undergoing a scoliosis series (usually pediatrics) will have a specifically designed gonadal shield attached to the collimator housing. The light field will be utilized to insure that the gonads are protected before x-rays are taken. Undergoing CT Examination: It has been traditional to shield the torso of patients undergoing radiological procedures. This makes sense from the point of view of radiation protection when the x-ray beam is onedirectional. In CT examinations, the x-ray tube rotates about the patient making it impossible to use traditional lead aprons to shield patients from radiation. It would be necessary to place the patient in a lead tube to achieve protection and that is not practical. Therefore the policy for CT examinations is not to use traditional lead aprons for shielding body parts outside the scanner. 73
76 74
77 75
78 PROCEDURE FOR OBTAINING AN IN-HOUSE RADIOACTIVE MATERIALS PERMIT The use of radioactive materials under the North Shore University Hospital (Manhasset) Broad License is restricted to individuals who are designated as Authorized Users on a radioactive materials permit or who work under the direct supervision of an Authorized User. These in-house permits are not transferable to other institutions. As a general policy, permits are not given to students, interns, residents, or fellows. To obtain an in-house radioactive materials permit, you must: 1. Obtain a radioactive materials permit application from the Radiation Safety office. 2. Return completed application to the Radiation Safety Office with the following: * A copy of your curriculum vitae * A copy of your board certification and medical license where applicable * Documentation of adequate training in the use of radioactive materials for Authorized User status * A detailed sketch of your facility indicating work areas, radioactive materials storage, radioactive waste storage, fume hoods, etc. 3. The completed application will be reviewed by the Radiation Safety Officer. 4. The application is then presented to the full Radiation Safety Committee and Administration for final approval. 5. Permits are issued by the Radiation Safety Office. A conditional permit may be granted on the basis that certain requirements will be met within a given time frame. Such conditions could involve obtaining necessary equipment or training by completing an inhouse Authorized Users course. 6. Once a permit is issued, it may be revoked by the Radiation Safety Committee or Administration at any time if hospital or New York State regulations and guidelines are not being followed. 76
79 RECORDKEEPING POLICIES FOR RESEARCH LABORATORIES HAVING RADIOACTIVE MATERIALS PERMITS Active Laboratories: Laboratories that frequently order and use radioactive materials (RM) (e.g. monthly): 1. These labs must perform monthly surveys and wipe tests as required by radioactive materials licensing guidelines. 2. Orders for new RM must be submitted to the radiation safety office together with the following documentation: a. Surveys / wipe test results obtained within the past month. b. A current summary of RM stock vial inventory possessed by the lab Partially Active Laboratories: Laboratories that maintain an inventory of long-lived isotopes but use them infrequently (e.g. quarterly): 1. These labs must perform quarterly surveys and wipe tests of storage and use areas in the laboratory. The results must be submitted by the end of each calendar quarter to the Radiation Safety Office. 2. Current RM stock vial inventories also must also be submitted quarterly to the Radiation Safety Office. Inactive Laboratories: Laboratories that have a RM permit but neither have inventory nor presently use radioactive materials. 1. No records are required while a lab is on inactive status. 2. Laboratories designated as having inactive status must inform and obtain approval from the Radiation Safety Office before resuming experiments with RM. 3. Inactive status can only be maintained for five years. After that, the permit will be revoked and a new permit must be applied for. 77
80 IN-HOUSE INSPECTIONS OF DEPARTMENTS/LABORATORIES UTILIZING RADIOACTIVE MATERIALS Under conditions of the institutional broad license, the Radiation Safety Office routinely inspects all radioactive materials permit holders' facilities for compliance with radiation safety rules and regulations. The following inspection schedule will be maintained for all active labs: Clinical laboratories will be inspected 3x per year. Research laboratories will be inspected 1x per year. Centralized waste storage areas under control of the Radiation Safety Office will be inspected monthly. The scope of permit inspections is covered on the next page. Non-compliance issues are handled in various ways depending upon the severity of the issue: 1. Immediate Safety Issues - The Radiation Safety Office, in conjunction with laboratory personnel, will correct these issues during the inspection. If this cannot be achieved, the issue will be immediately reported to Administration who will take any necessary action to correct the problem. 2. ALARA Violations - If the Radiation Safety Office determines that laboratory conditions are such that exposures are not as low as reasonably achievable, a citation will be issued and reported to the Radiation Safety Committee. A follow-up inspection will occur within three months to see if the citation issues have been corrected. If the citation has not been addressed and corrected, the Radiation Safety Committee will be notified for further action. The Radiation Safety Committee and Administration have the authority to suspend use of radioactive materials or terminate a permit. 3. Record Keeping Violations - Upon the first occurrence, a recommendation to correct the condition will be made. If corrections are not made, they will be handled in the same manner as ALARA violations. 4. General Recommendations - These are made to help a laboratory maintain compliance. Authorized Users are ultimately responsible for compliance in their laboratory and individual users working under their permit. 78
81 IN-HOUSE RADIATION SAFETY INSPECTION OUTLINE FOR DEPARTMENTS/LABORATORIES UTILIZING RADIOACTIVE MATERIALS In-house inspections include the following areas: General Radioactive Materials Permit Requirements: - Personnel: Authorized users, current staff, and training. - Previous violations/citations and corrective actions. Record Keeping: - Isotope inventory; receipt log (lot numbers, date of receipt, activity, volume); use log (amount, date, balance remaining and employee's initials); disposal log (type - liquid/dry; amount, date and manner of disposal); maximum possession limit - monthly inventory. Surveys: - Area Surveys: correct meter, performed on schedule, documented, area mapped, regular trash checked, areas above action levels noted and corrected. - Wipe Tests (DPM, background sample counted, calibrated equipment; proper efficiency used; performed on scheduled basis; corrective action documented. - Personnel: hands, gloves, lab coats free from contamination. Radiation Monitoring Badges: - Records available; three months posted. - Status as per radiation safety office audits, i.e., compliance issues. Physical Lab Inspection: - Posting requirements: notice to employees, emergency procedures and all other pertinent signs. Contamination Prevention: working area condition (neatness, chux, etc.); personnel lab attire (lab coats, gloves); no drinking or eating in lab areas; availability of decontamination kits. - Nuclide storage: shielding (< 2mR/hr); space (centralized, properly segregated); labeling (specific location; no unnecessary labels); adequate security. - Waste: labels clearly visible; shielding (< 2mR/hr); adequate space (not overflowing; centralized); segregation (clearly labeled, liquid vs. dry, by isotopes). - Equipment: survey meters operational, calibrated, adequate; beta/gamma counters calibrated; check sources (for meters, counters); hoods (calibrated). RSO Section: - Sealed sources: physical inventory (quarterly); leak test (semi-annual). - Bioassays (as needed). - In-service as necessary. - Final summation (violations, opportunities for improvement). 79
82 PROCUREMENT OF RADIOACTIVE MATERIALS AND RADIATION SOURCES The following procedures for the procurement of radioactive materials and radiation sources are intended to insure compliance with the terms and conditions of the license and regulations. 1. Radioactive Materials Prerequisite Individuals ordering radioactive materials must have an in-house radioactive materials permit and be authorized by an authorized user to do so. The Radiation Safety Office must approve each order of radioactive materials and ensure that the requested materials and quantities are authorized by the permit and that the possession limits are not exceeded. When the receipt of radioactive materials is contemplated through other means, such as transfers from other institutions, the Radiation Safety Office must be notified in advance. Ordering Procedure a. Orders for radioactive materials must be written on a regular requisition form with the words "RADIOACTIVE MATERIALS" and the permit number printed or typed across the top of the form and shall indicate the isotope, compound, activity catalog number and supplier. All required approvals must be present on the requisition. These requisitions must be forwarded directly to the Radiation Safety Office. DO NOT send to Purchasing. Non-radioactive materials MUST NOT be ordered on the same form. b. The Radiation Safety Office will enter a Peoplesoft order and place the order by telephone as prearranged with the Materials Support Services Department. The order will be kept in the Radiation Safety Office and will be used to verify the incoming packages. c. Radioactive materials will be accepted by the Receiving Department and then delivered to the Radiation Safety Office (during regular hours) for distribution. Packages will be checked for leakage and external package surveys will be performed in the Radiation Safety Office Laboratory. The package will then be picked up by the user. It is the responsibility of the person who ultimately receives the package to place it in proper storage. 80
83 d. Radioactive materials in the form of therapeutic sealed sources, i.e., Ir-192 and I- 125 seeds, etc., will be ordered by the Radiation Medicine physicists and delivered directly to them under authorized physicians authorization. e. Radiopharmaceuticals will be ordered by Nuclear Medicine or Nuclear Cardiology under authorized physicians authorization. 2. X-Ray Generators and Radionuclide Irradiators a. The Radiation Safety Office must be notified in advance of the procurement of all ionizing radiation producing machines and radionuclide irradiators. b. Provisions must be made to notify the Facilities Department so that a properly shielded installation is planned. Shielding designs must be approved by the Radiation Safety Officer or the Medical Physics consultant for diagnostic x-ray equipment. 81
84 PROCEDURE FOR RECEIPT OF PACKAGES CONTAINING RADIOACTIVE MATERIALS During Normal Working Hours (Receiving Department Open) 1. Radioactive materials (RM) packages are delivered to the hospital Materials Operations Department. 2. If the package appears to be damaged, immediately contact the Radiation Safety Office. Ask the carrier to remain at the hospital until it can be determined that neither the driver nor the delivery vehicle is contaminated. 3. RM packages are to be delivered to the Radiation Safety Office, Nuclear Medicine, Nuclear Cardiology or Radiation Medicine as soon as possible. During Non-Working Hours (Receiving Department Closed) 1. The security personnel on duty at the Hospital s Main Security Desk shall sign for any packages containing radioactive material that arrive during non-working hours. Packages should be placed on a cart and taken immediately to the Nuclear Pharmacy in Nuclear Medicine. Unlock the door, place the package on top of the counter and relock the door. 2. If the package appears to be damaged, immediately contact the Radiation Safety Officer (see Radiation Safety Emergency Call List). Ask the carrier to remain at the hospital until it can be determined that neither the driver nor the delivery vehicle is contaminated. 82
85 PROCEDURES FOR SAFELY OPENING PACKAGES CONTAINING RADIOACTIVE MATERIAL 1. Special requirements shall be followed for packages containing quantities of radioactive material in excess of the Type A quantity limits as referred to in Part (e.g. more than 20 curies for Mo-99, or 30 curies of Cs-137). Type A packages shall be monitored for contamination and external radiation levels within 3 hours after receipt if received during working hours or within 18 hours if received after working hours. The New York State Department of Health will be notified in accordance with the regulations if removable contamination exceeds 0.01 uci/100 cm 2 (22,000 dpm) or if external radiation levels exceed 200 mr/hr at the package surface or 10 mr/hr at 3 feet (1 m). 2. The following procedures shall be carried out when opening all packages containing radioactive materials: a. Wear gloves to prevent hand contamination. b. Visually inspect package for any sign of damage (i.e. wetness, crushed). If damage is noted, stop and notify the Radiation Safety Officer. c. Measure exposure rate at the package surface and 3 feet (1 m) from package surface and record. If it is higher than indicated on the transport index, stop and notify the Radiation Safety Officer. d. Open the package with the following precautionary steps: - Open the outer package (following manufacturer's directions, if supplied) and remove packing slip. - Open inner package and verify that contents agree with those on packing slip. Compare requisition, packing slip and label on bottle (in the case of special orders, i.e. therapy doses, also compare with physician's written request). - Check integrity of final source container (i.e. inspect for breakage of seals or vials, loss of liquid, or discoloration of packaging material). e. If there is any reason to suspect contamination, wipe external surface of final source container. Assay the wipe and record amount of removable radioactivity (i.e. dpm/100 cm 2 etc.). Take precautions against the spread of contamination as necessary. f. Monitor the packing material and packages for contamination before discarding. If contaminated, treat as radioactive waste. If not contaminated, deface radiation labels before discarding in regular trash. 83
86 3. Example of information to be recorded when receiving packages containing radioactive materials.: Lab/Dept.: PO #: Surveyor: (Please Print) A) Condition of Package: OK Punctured Wet B) Measured Radiation Levels: Package Surface: mr/hr 3 feet from Surface: mr/hr C) Do Packing Slip and Vial Contents Agree? Yes No If not, explain discrepancy: D) Wipe Test Results: Background: cpm (if necessary) Outer: net dpm Inner: net dpm Signature Date 84
87 Ambient Exposure Rate Surveys 1. Survey Areas PROCEDURE FOR AREA SURVEYS a. In radiopharmaceutical elution, preparation and administration areas, survey at the end of each day of use with a low-range survey meter. If diagnostic administrations are occasionally made in patients' rooms and special care is taken to remove all paraphernalia, these rooms need not be surveyed. b. In laboratories where only small quantities of gamma or beta emitting (excluding H-3) radioactive material are used (less than 200 microcuries at a time), survey monthly with a low-range survey meter. c. In centralized radioactive materials waste storage areas, survey monthly with an ionization chamber survey meter. d. In sealed source and brachytherapy storage areas, survey quarterly with an ionization chamber survey meter. 2. Immediately notify the Radiation Safety Office if unexpected high levels are observed. Removable Contamination Surveys 1. Survey Areas a. In radiopharmaceutical elution, preparation, and administration areas, survey weekly for removable contamination. If diagnostic administrations are occasionally made in patients' rooms and special care is taken to remove all paraphernalia, these rooms need not be surveyed. b. In laboratories where only small quantities of gamma or beta emitting (including H-3) radioactive material are used (less than 200 microcuries at a time), survey monthly for removable contamination. c. In centralized radioactive materials waste storage areas, survey monthly for removable contamination. d. In sealed source and brachytherapy storage areas, survey semi-annually all source drawers for removable contamination (evidence of sealed source leakage). 2. The wipe sample assay procedure should be sufficiently sensitive to detect the presence of 200 dpm/100 cm 2 of removable contamination. A standard source with associated efficiency is used convert sample measurements (usually in counts per minute) to dpm. Radiopharmaceutical preparation and injection areas must be below 1,000 dpm/100 cm 2. Clean areas must be below 200 dpm/100 cm Immediately notify the Radiation Safety Office if unexpectedly high levels are noted. 85
88 4. The Radiation Safety Office calibrates all gamma and beta counters annually and supplies efficiency factors for all commonly used radioisotopes. Records 1. Keep a record of exposure rate and contamination survey results. It must include the following information: a. The date, area surveyed, and equipment used. b. The name or initials of the person who made the survey. c. A drawing of the areas surveyed and contamination and exposure rate action levels as established by the Radiation Safety Officer. d. Measured exposure rates in mr/hr or contamination levels in dpm/100 cm 2. Only count rates above twice background need to be converted to dpm. A zero may be entered for any area with a count rate less than twice background since the level is below the minimum detectable activity. e. Actions taken in the case of excessive exposure rates or contamination and follow-up survey information. 2. These records will be reviewed during Radiation Safety inspections. 86
89 SHIPPING RADIOACTIVE MATERIALS 1. The Radiation Safety Office must be contacted when the shipping of radioactive materials from NSUH is considered. Before shipment can be made, the recipient must provide the Radiation Safety Office with a copy of their current radioactive materials license indicating that they are authorized to receive the material. Noncompliance with this requirement is a violation of regulations. Check with the radiation safety staff to see if the recipient's license is already on file. If not, request a copy from the recipient in order to fulfill this requirement. 2. The radiation safety staff will supervise the shipping. The description of articles must include radionuclide, chemical and physical form and activity. Nuclear Medicine, Nuclear Cardiology, Radiation Medicine and Cyclotron/PET personnel may return sources to the manufacturer for repair or disposal but must follow exclusively the manufacturer s instructions. 3. Radiation Safety personnel will assist with Department of Transportation (DOT) labeling of outgoing packages and with drawing up the appropriate manifests. Transportation of radioactive materials must be done by properly trained individuals. Re-training is required every three years. DOT Type III packages may only be transported in placarded vehicles. 87
90 RESEARCH CENTRALIZED RADIOACTIVE WASTE HANDLING PROCEDURES 1. Preparation Instructions for Waste Disposal There are essentially three methods for disposing of radioactive waste: a. Pouring of liquids into the sewerage system. b. Decay-in-storage and ultimate release as regular trash. c. Disposal by commercial means. Disposal into the sewerage system shall be done only by Radiation Safety personnel and in accordance with NYSDEC Part 380 regulations. Liquids are assayed prior to pouring. Decay-in-storage and commercial disposal will be handled by the Radiation Safety staff after all packaging and storage requirements have been met. Under no circumstances will radioactive materials be incinerated. No radioactive waste shall be released from a laboratory area for disposal until it has been deactivated of infectious agents. Radionuclides shall be separated according to isotope; i.e. H-3, P-32, S-35, etc. unless otherwise instructed by the RSO. This is particularly important for decay-in-storage and for commercial disposal. Whatever means of disposal is utilized, records shall be kept and labels shall be generated showing the physical and chemical description of the waste, its volume, the radionuclide identity, date and total radioactivity. Heavy-duty plastic bags should be used for most of the non-liquid waste. Bags shall be securely tied and labeled. Call the Radiation Safety Office when you are ready to transfer the waste. 2. Waste Containers To insure that solid and liquid wastes are kept separate, each laboratory having radioactive waste must be equipped with at least one container for solid dry waste and one for liquid waste. Additional waste containers may be requested as needed and must be labeled with the isotopes being used. a. Solid dry waste containers: Must be kept fitted with a disposable waterproof polyethylene liner. b. Liquid waste containers: Plastic carboys and jars are suitable for storage of liquid wastes. These liquid containers must have securely fitting covers and must be tightly closed. In addition, they shall be conspicuously marked with appropriate radiation labels. 88
91 c. Liquid scintillation media: Liquid scintillation vials and plates are handled as radioactive waste unless they conform to the special exemption described in paragraph 6 below. 3. Waste Disposal Request for disposal of radioactive waste may be made by telephone to the Radiation Safety Office. The investigator must comply with packaging instructions. 4. Radioactive Animal Carcasses a. Carcasses must be covered and dusted generously with slaked lime to retard decay. Slaked lime will be supplied by the Radiation Safety Office. b. Each carcass must be wrapped neatly and tightly in absorbent paper with plastic backing (chux) and taped closed. c. Place the packaged carcass into zip-lock/sealable plastic bags supplied by the Radiation Safety Office. d. Each bag shall be labeled with a Radioactive Materials sign/tag stating type and amount of radioisotope. Only one type of radionuclide shall be placed in each bag. Exception to this rule will be made if an animal contains more than one radionuclide. e. Call the Radiation Safety Office for arrangements to deliver carcasses. Animal carcasses must be frozen. The Radiation Safety staff will make arrangements to store the animal carcasses in a freezer designated for this purpose. f. Animal carcasses containing less than 0.05 uci of H-3 or C-14 per gram of animal may be disposed of without regard to radioactivity. 5. Unusual Waste Disposal Problems Plans for proper disposal of infectious agents or highly toxic or hazardous substances containing radioactivity shall be made early in the design stage of the experiment. Proposed procedures involving unusual waste disposal problems will be considered individually by the Radiation Safety Office staff. 89
92 6. Special Disposal Instructions for Isotopes in Liquid Scintillation Vials When the concentration of these isotopes is less than 0.05 uci per milliliter of scintillation fluid, the vials may be disposed of without regard to radioactivity. Complete records will be kept of this disposal. In all cases, liquid scintillation vials should be kept separate from other radioactive waste. Special barrels are available for this purpose. 7. Centralized Decay in Storage Decay-in-storage will be provided by the Radiation Safety staff in the central storage facilities. Users must make sure that the radionuclides for this method of disposal have halflives less than 90 days, that each radionuclide is packaged separately and that it is clearly labeled as described in paragraph 1. Quality assurance of radioactive waste records is maintained through the periodic inspections of laboratories and the maintenance of a database for centralized waste disposal. Laboratory inspections include a review of inventory sheets that show how waste is generated. The Radiation Safety Office performs annual calculations based on disposal assays to make sure that sanitary sewer limits are not exceeded. 90
93 CLINICAL RADIOACTIVE WASTE HANDLING PROCEDURES Nuclear Medicine and Nuclear Cardiology: Waste is segregated by isotope and type. The major categories are as follows: 1) Short lived waste (e.g., Tc-99m). Category 1 waste is generally stored for decay in the lab where the waste is generated. 2) Long-lived waste (e.g., Ga-67, Tl-201, I-131, I-123, In-111). 3) In-vitro wastes (e.g., I-125, Cr-51). 4) Therapeutic wastes (e.g., Sr-89, Sm-153, Y-90). Categories 2 through 4 wastes are temporarily stored by the laboratory where generated and transferred to the Radiation Safety storage shed for complete decay. 5) I-131 therapy room waste. Category 5 waste is stored for decay in the Radiation Safety storage shed. 6) Mo-99/Tc-99m generators. Category 6 waste is returned to the manufacturer in accordance with the manufacturer s instructions. Radiation Medicine: The medical physicists in Radiation Medicine are responsible for returning to the manufacturer the low dose rate Ir-192 sources after removal from the patient. Pd-103 and I-125 seeds are generally stored for decay in specially designated areas of the Radiation Medicine Hot Lab. On occasion, they are also shipped back to the manufacturer. High dose rate afterloader sources (Ir-192) are exchanged periodically by the manufacturer of the device. NSUH has adopted a policy regarding procurement of long-lived sources. Whenever possible, the user must arrange an exchange for a spent source when a replacement source is ordered. This policy is designed to eliminate the storage of long-lived sources which are difficult to dispose of. Nuclear Medicine, Nuclear Cardiology and Radiation Medicine personnel maintain records of their own radioisotope waste disposal and transfers. These records are checked by Radiation Safety personnel during their periodic inspections. 91
94 GUIDELINES FOR INVESTIGATORS USING THE CENTER FOR COMPARATIVE PHYSIOLOGY 1. Animals that have been given radioactive materials should be isolated from other animals. 2. Cages housing animals containing radioactive materials shall be labeled with appropriate radioactive materials warning signs. 3. The bottom of the cages shall be lined with absorbent paper pads with plastic backing (i.e., chux, etc.). 4. For radioactive waste disposal, a 30-gallon can with an appropriate radioactive sign shall be placed in the area where the animals are located when cleaning the cages. This can shall be used for radioactive waste only and must be double-lined with red plastic bags. The removal of these bags is the responsibility of the investigator. At the time of removal, the investigator shall tag the bags with the following information: Type of radioactive material, estimated amount of radioactive material (mci or uci) contained in waste, date and investigator s name and laboratory. Tags may be obtained from the Radiation Safety Office. At the completion of a study, the investigator shall decontaminate the cages using Radiacwash or similar detergent. Bags of waste shall be brought to the centralized storage facility after prearrangement with the Radiation Safety Office. 5. After the cages have been washed, contamination checks (wipe tests) shall be performed by the investigator to detect any residual contamination. Contamination checks shall also be performed in areas of the animal shelter where radioactive materials have been used. The results of these checks shall be documented and sent to the Radiation Safety Office. 6. The Notice to Employees and Spill Procedures shall be posted in a conspicuous place within the shelter. 7. Call the Radiation Safety Office for assistance or information. 92
95 RESEARCH BLOOD IRRADIATOR POLICY & PROCEDURE In order for us to comply with the new guidelines set forth by the Nuclear Regulatory Commission (Effective June 1 st, 2006) 1. All users must receive prior authorization from their Lab Head, Radiation Safety Office and Human Resources. NRC fingerprint clearance is also required. 2. All users must sign the user attestation form. 3. Use of the blood irradiator is allowed only to trained individuals. 4. Formal training in the use of the blood irradiator and emergency procedures must be conducted by a member of the Radiation Safety Office or authorized laboratory person. 5. The use of this room must be scheduled through the Feinstein security desk. Security will have you sign out the key to the irradiator. When you are finished with the irradiator, you must immediately return the key back to the security desk. USE OF ANIMALS IN THE BLOOD IRRADIATOR 1. Notify the CCP Manager and the Radiation Safety Office at least TWO WEEKS prior to the initial irradiation of the animals. This will allow the CCP to set aside a quarantine room to house the animals after irradiation. All individuals must be trained by the Radiation Safety staff in the proper use and emergency procedures of the irradiator. NOTE: No animals will be allowed to be irradiated on the holidays/weekends. 2. A secure container (less than 6 inches high / 2.5 inches diameter) with air holes on top must be approved by the CCP Manager or Veterinarian and the Radiation Safety Office prior to initial use. 3. Keys to the irradiator will be signed out from the Feinstein security desk and returned immediately after use. 4. Animals will be transported in covered cages via the freight elevator to the 2 nd floor and will be transported directly back to the quarantine room after irradiation. These animals MUST remain in the quarantine room for the duration of the study. 5. Report any problems encountered to the CCP Manager at x 1061 or the Radiation Safety Office at x An x-ray irradiator is available for use in the CCP. To schedule use of the x-ray rradiator, contact the CCP manager and the Radiation Safety Office for appropriate training. 93
96 94
97 PROCEDURE FOR LEAK-TESTING SEALED SOURCES 1. Make a list of all sources to be tested. This should include the isotope, the activity on a specified date, and the physical form. 2. If you will be testing high-activity sources, set out a survey meter, preferably with audio, so you can monitor your exposure rate. 3. Prepare a separate wipe sample for each source. A cotton swab, alcohol prep pad, filter paper or tissue paper is suitable. Number each wipe so you will know for which source it is to be used. Samples should be taken as follows: a. For small sealed sources, it is easiest to wipe the entire accessible surface area. Pay particular attention to seams and joints. However, do not wipe the port of beta applicators. Storage containers should also be wiped since contamination can accumulate there. b. For larger sealed sources and devices (survey meter calibrator, irradiators), take the wipe near the radiation port and on the activating mechanism. c. If you are testing radium sources, they should also be checked for radon leakage. This can be done by submerging the source in a vial of fine-grained charcoal or cotton for a day. Then remove the source and analyze the absorbent sample as described below. A survey should be done to be sure the sources are adequately shielded during the leak-test period. 4. The samples are to be analyzed as follows: Select a suitable detector that is sufficiently sensitive to detect microcuries (10,000 dpm). For beta sources, a liquid scintillation counter will be used. For gamma sources, an auto gamma counter will be used. 5. Only sealed sources with activity greater than 100 uci must be checked for contamination. 6. Leak tests must be performed semi-annually. 7. Sealed source inventories must be performed quarterly. 95
98 PROCEDURE FOR MONITORING OR CHECKING GAS AND AEROSOL EFFLUENTS Charcoal traps can significantly reduce air contamination. They can also become saturated or be spoiled by improper use, humidity, chemicals or inadequate maintenance. 1. If the trap effluent is monitored by a radiation detector designed to monitor effluent gas, check the detector according to the manufacturer's instructions and keep a record of the checks. 2. If you do not routinely monitor the trap effluent, check it upon receipt and after every 10 patient studies. Collect the effluent from the trap during one patient study in a plastic bag and then monitor the activity in the bag by holding the bag against a gamma camera, with the camera adjusted to detect the gas, and compare its counts per minute (cpm) to background cpm with no other radioactivity in the area. Keep a record of the date, background cpm, and bag cpm. 3. The Radiation Safety Officer will establish an action level based on cpm or a multiple of background cpm. If you measure a significant increase in the bag cpm, the trap is breaking down and must be replaced. 4. Follow the trap manufacturer's instructions for replacing the charcoal. Procedure for Calculating Worker Dose from Concentrations of Aerosols in Work Areas 1. Collect the following data: a. Estimate the number of studies performed per year. b. Determine the activity administered to patients per study. c. Estimate the activity released to the room (assume a 20% loss). d. Measure air flow supply and exhaust in each imaging room. All rooms must be negative pressure and exhaust cannot be re-circulated within the facility. e. The estimated average annual concentration is calculated as follows: C = ( released activity) (# of studies) annual room exhaust volume e. The maximum permissible concentration levels (Tc-99m) for occupational and effluent air are as follows (6 NYCRR Part 380): Occupational: 6 x 10-5 uci/ml Effluent: 2 x 10-7 uci/ml Concentrations should be kept as far below permissible levels as practical. 96
99 Procedure for Calculating Spilled Gas Clearance Time 1. Collect the following data: a. Highest activity of gas in a single container (A) in millicuries; b. Measured airflow supply from each vent in the room (if different during heating and cooling seasons, use the greater value); c. Measured airflow exhaust to each plenum in the room (the exhaust should be vented and not re-circulated within the facility); this may be either the normal air exhaust or a specially installed gas exhaust system. The exhaust rate for the room must be greater than the supply (negative pressure). Determine the total room exhaust rate in cubic feet per minute (cfm) (F); d. Maximum permissible air concentrations in restricted and unrestricted areas; for Xe-133 the maximum permissible values are 1x10-4 uci/ml in restricted areas and 5x10-7 uci/ml in unrestricted areas (C). 2. For each room make the following calculation: a. Decide whether you will control the room as a restricted or an unrestricted area. b. Divide the largest single container activity by the total room volume in cubic feet (V); c. Compute the time required in minutes (t) to reach permissible concentration levels from the following equation: C = V A exp 28.3 F V t 97
100 PROCEDURE FOR THE OPERATION AND MAINTENANCE OF FUME HOODS UTILIZING RADIOACTIVE MATERIALS Operation of Hood: Before working in a fume hood with radioactive materials, the following precautions must be observed: 1. There shall be adequate air flow into the hood. The air flow should be approximately 120 feet per minute through a vertical opening of about 1 foot. The hood shall have been calibrated within the past 1 year and the sash shall be maintained at the height prescribed during calibration. 2. The bottom of the hood shall be covered with an absorbent material backed with an impermeable layer (i.e., chux). 3. Stainless steel or polyethylene type plastic trays shall cover the chux and any handling of radioactive materials shall take place in the tray. 4. A Geiger counter or scintillation survey meter shall be available to check for contamination. 5. Wipe tests shall be performed at the end of the procedure and/or at the end of the day. 6. All radioactive waste shall be handled in accordance with radioactive waste handling procedures and not left in the hood. 7. Bioassays shall be performed within 48 hours of completion of any iodinations. Maintenance of Hood: The operator of the hood or maintenance personnel shall inform the Radiation Safety Office before service or maintenance on the hood is performed. A radiation safety staff member or other qualified individual will supervise the procedure and evaluate any potential hazards. The following steps should be taken: 1. Monitor the hood with a radiation survey meter (G.M. or scintillation type) for contamination. 2. If there is any dismantling, wear disposable gloves and lab coat and check components for contamination. 3. Check filters for contamination and replace if necessary. Contaminated filters must be treated as radioactive waste. 4. Decontaminate hood areas as necessary. 5. When free of contamination, service and maintenance personnel may proceed with their work in the normal manner. If there are any questions or problems concerning this procedure, contact the Radiation Safety Office. 98
101 PROCEDURE FOR MONITORING FOR THE PRESENCE OF RADIOACTIVITY IN HOSPITAL WASTE PRIOR TO SHIPMENT FOR DISPOSAL Waste is collected at the hospital loading dock where it is packaged and sent via commercial carrier to an authorized location for ultimate disposal. Prior to this waste leaving the hospital, it must be surveyed for the presence of radioactivity as follows: 1. Personnel engaged in monitoring procedures will receive in-service training by Radiation Safety staff or by Environmental Service supervisors. 2. The waste shall be surveyed by Environmental Services at the main Hospital and at the Research Building. 3. At the main hospital, all waste passes through the fixed radiation detection system located on the loading dock. If radioactivity is present in the waste, the alarm will be triggered. If the alarm is triggered: Pull the cart back away from the detectors. The audible alarm will reset automatically. Proceed through the detectors again. If the alarm does not trigger a second time then the waste may be disposed of in a routine manner. If the alarm is triggered a second time: Hand scan and try to isolate the bag containing contamination using the portable survey meter. Place the waste in the designated holding area. Re-check the waste after 48 hours and dispose of if cold. If it is still hot after one week, notify the Radiation Safety Office (x 3895). 4. In the research building, waste is surveyed by using a hand-held monitor. 5. Waste found to contain detectable amounts of radioactivity (above background levels) shall be set aside and the Radiation Safety staff shall be notified for evaluation and disposal. Should this occur over a weekend or during off hours, place the waste in a designated holding area and notify the Radiation Safety Office on the next working day. 99
102 SETUP FOR HOSPITAL RADIATION WASTE MONITORS FIXED LOADING DOCK DETECTORS Two fixed detectors are mounted at the hospital exit so that all waste passes through them. The system is setup to alarm at two times background. Operational status is checked monthly by the Radiation Safety Office using 10 microcurie Cesium-137 button sources. Once per year the system has a full sensitivity check using multiple radioactive sources of cobalt-57, barium-133 and cesium-137. Significant sensitivity variations initiate an entire recalibration of the system. HAND HELD MONITORS Hand held monitoring is performed with ultra-high sensitivity survey meters. Meters should be used on the 50 ur/hour scale. Any full scale deflection (3x background) of the meter indicates hot waste. Hand held monitors are checked monthly by the Radiation Safety Office using 1 microcurie Cs-137 button sources. It should be noted that two times background is approximately equivalent to the sensitivity set for detectors located at waste transfer stations 100
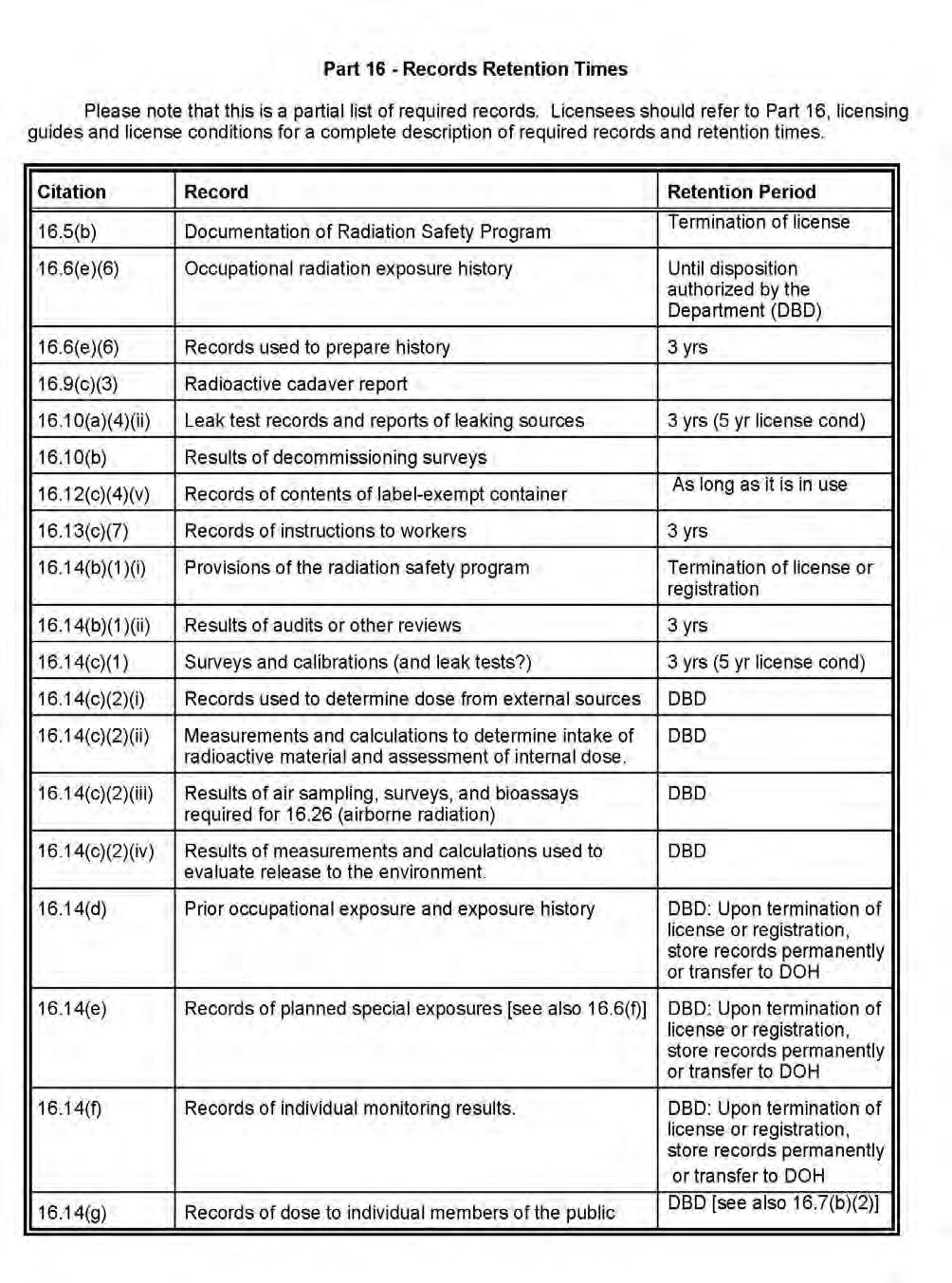
103 101
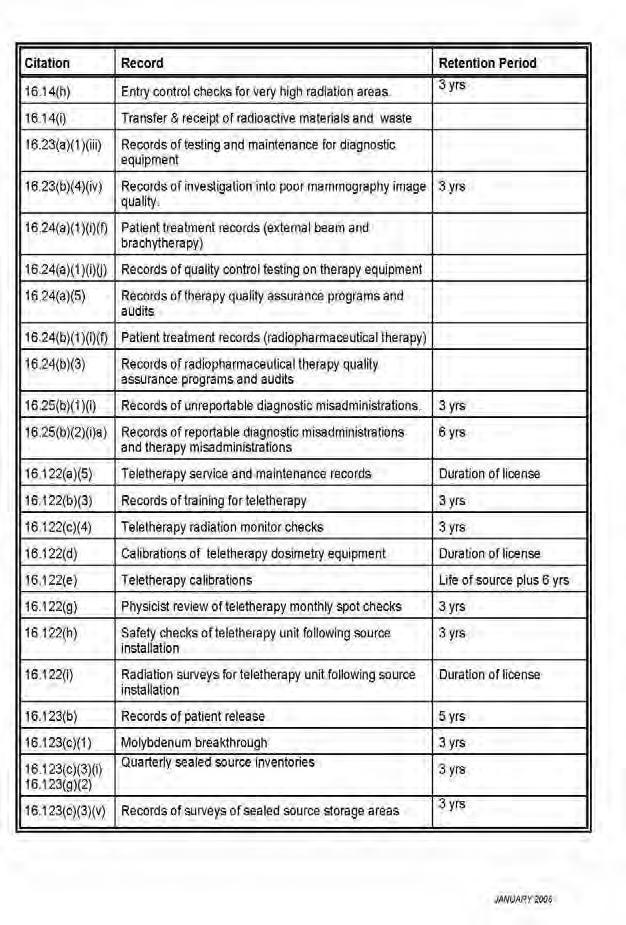
104 102
105 Doses to Patients and the Fetus from Common Radiological Procedures Examination Effective Dose (msv) Fetal Dose (mgy) Chest x-ray 0.05 to 0.10 < 0.01 Thoracic spine 0.3 to 0.6 < 0.01 Abdomen 0.4 to Lumbar spine 0.8 to Screening mammogram max CT head 1 to 2 < 0.1 CT chest 5 to 10 <0.1 CT abdomen/pelvis 4 to to 20 Bone scan 4.2 to to 5.6 Lung scan 1.6 to to 1.1 Cardiac scan (Tc99m MIBI stress and Tl201 rest) 18.5 to to 27.7 Hepatobiliary scan 3.2 to to 3.8 PET scan (FDG) 7.0 to to 12.0 References: Patient Dose in Radiology Walter Huda Fetal Radiation Dose Estimates Duke University Radiation Safety Division The Essential Physics of Medical Imaging Jerrold Bushberg et.al. Tables of Radiation Absorbed Dose to the Embryo/Fetus from Radiopharmaceuticals RIDIC Oak Ridge Associated Universities 103
106 Information Required for Submission of an RDRC protocol The Radioactive Drug Research Committee (RDRC) provides oversight to protocols that use novel radiopharmaceuticals in a limited number of research subjects. The protocols must be designed to obtain basic information on kinetics, distribution, dosimetry and localization of radioactive drugs. It must not be intended for immediate diagnostic or therapeutic use or for information obtained as part of a clinical trial. The following information must be included in any protocol submitted to the RDRC: 1. Prior Research Experience a. Evidence must be presented from other institutions that have used the research drug that it is safe. Site appropriate references. b. What is the sum total of experience with the drug? How many subjects has it been used in? c. Have there been any adverse reactions? What is the nature of those reactions? How is the present protocol designed to monitor for and handle reactions? 2. Pharmacological Dose a. What is the specific activity? Has this been adequately documented on-site? b. Is the specific activity adequate and consistent with prior formulations at other institutions? 3. Radiation Dose a. Are there references to available radiation dosimetry? b. Does the intended protocol meet FDA dose limits? All associated radiopharmaceuticals and x-ray procedures must be considered in the protocol. c. Confirm that the protocol will specifically exclude children and pregnant women. 4. Research Subjects a. Does the protocol limit the number of subjects to less than 30? 5. Radioactive Drug Safety a. Has the formulation on-site been adequately tested for radionuclidic purity, radiochemical purity, apyrogenicity, sterility? In order for a protocol to be approved, all of the above items must be adequately addressed in the contents of the submission. 104
107 Print or Type - Answer All Items: North Shore University Hospital - Manhasset, New York RADIOACTIVE DRUG RESEARCH APPLICATION 1) Title of Protocol: 2. Has this protocol been approved by the IRB? Yes No Approval date: (Protocols submitted without a copy of the IRB approval will be returned without review.) IRB Protocol #: 3) Protocol abstract: 4) Principal investigator: Radioactive materials permit #: ) Number of subjects: 6) Radiopharmaceuticals Activity (mci) per study Annual # of studies 7) Are these compounds: FDA approved: YES / NO USP approved: YES / NO 8) Associated radiological procedures Radiation dose # per year 9) Estimated total radiation absorbed dose in rads per study: (Attach worksheet) Effective dose: Ovaries: Testes: Red Marrow: Target organ(s): Dose: Dose: Dose: 10) Estimated total radiation absorbed dose in rads per year: Effective dose: Ovaries: Testes: Red Marrow: Target organ(s): Dose: Dose: Dose: 105
108 Page 2 11) Active ingredients Pharmacologic dose per injection 12) References Maximum permissible pharmacologic dose: 13) Is the study limited to subjects 18 years or older? YES NO 14) Is pregnancy a contraindication to the study? YES NO How will pregnancy status be determined? 15) Study subject monitoring Symptoms YES NO Vital signs YES NO EKG YES NO Other (specify) All adverse reactions must be reported to the RDRC within 7 days. 16) Radiopharmaceutical quality control: All radiopharmaceutical quality control is performed in accordance with USP monograph # 823. Sterility Method: Apyrogenicity Method: Minimum radiochemical purity: Method: Minimum specific activity: 17) Attach a sample radiopharmaceutical label below. Investigator Name Investigator signature Telephone. Date [Revised 06/10] 106
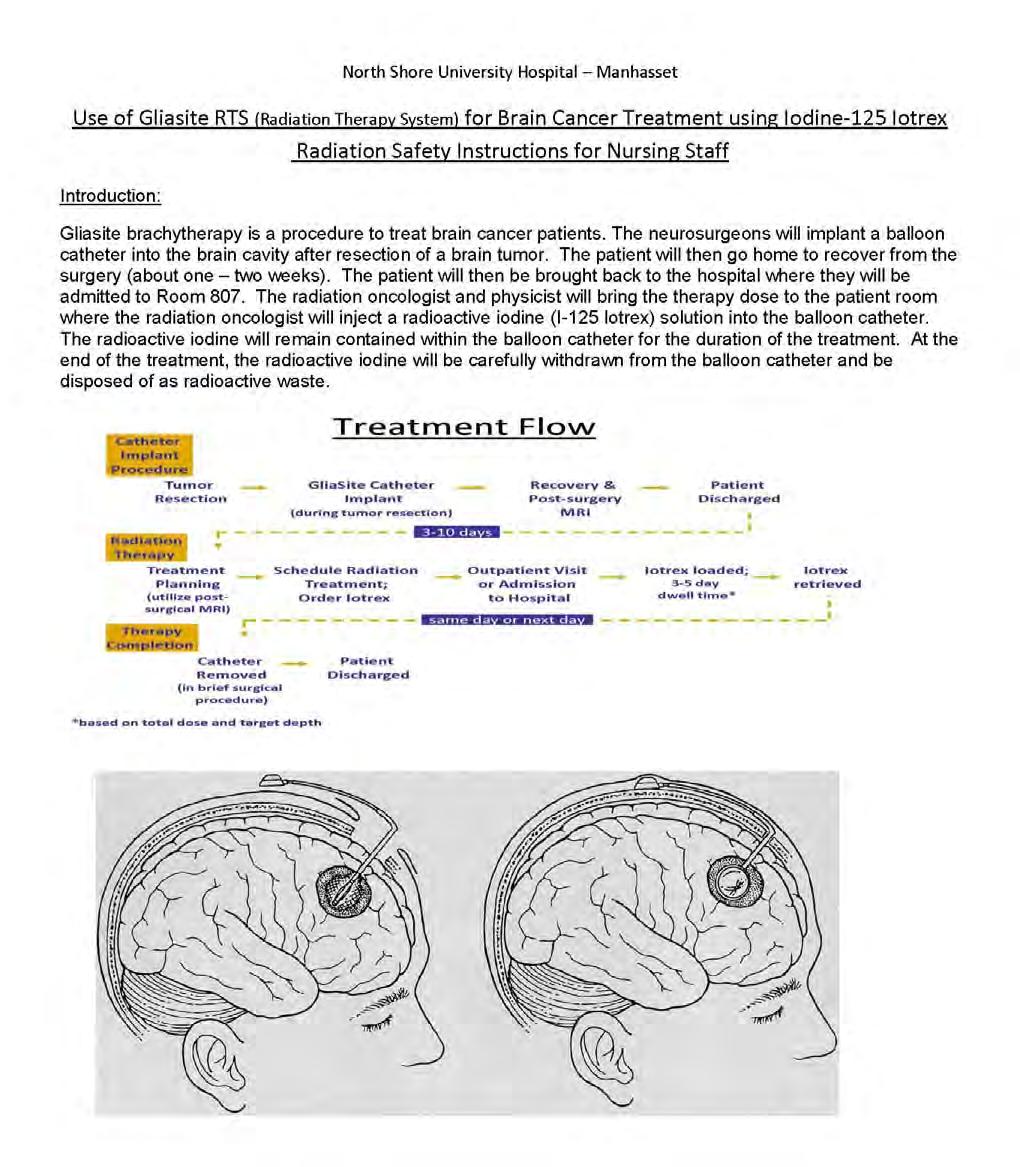
109 107
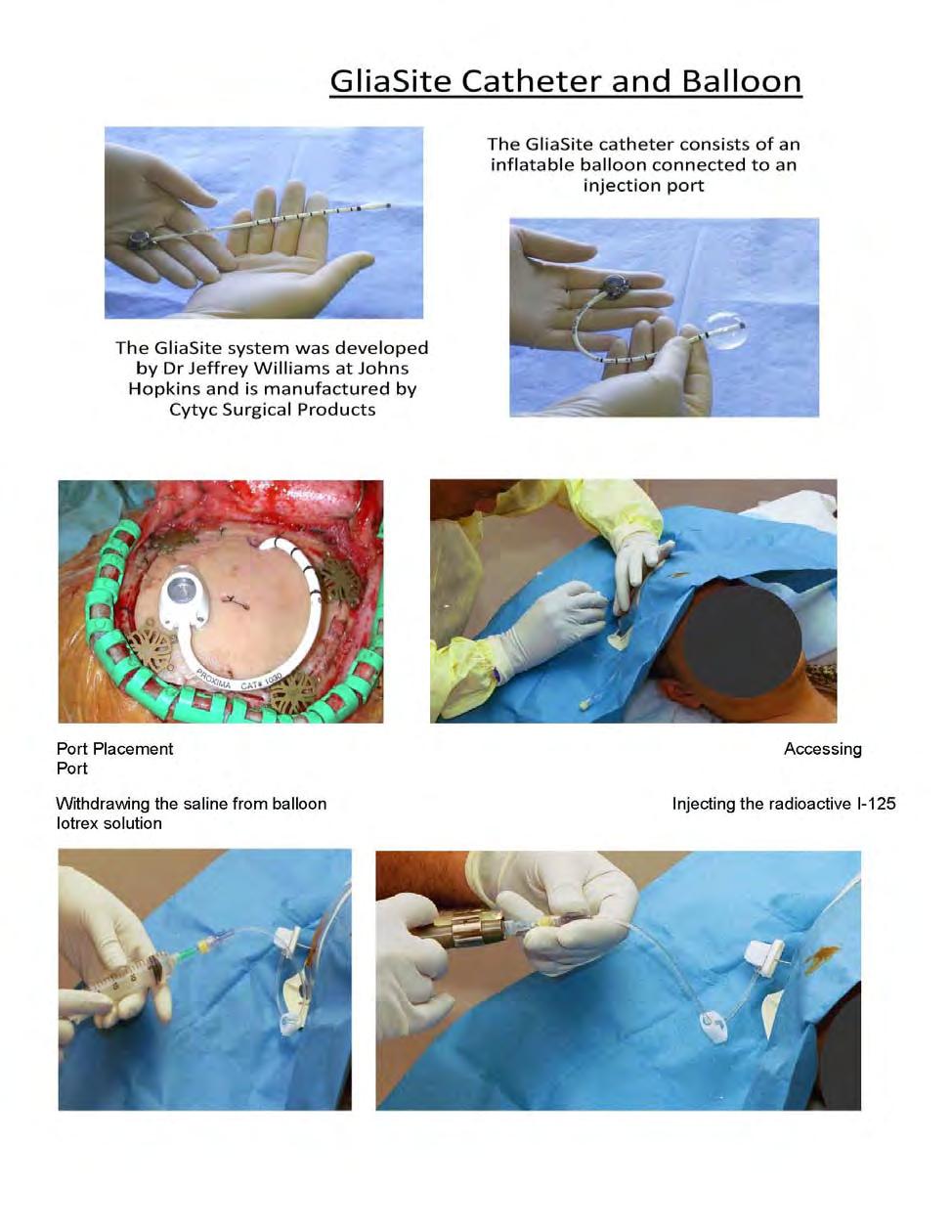
110 108
111 109
VAMC Radiation Safety Refresher Training March 2011
 VAMC Radiation Safety Refresher Training March 2011 The University of Iowa Radiation Safety Program 1 Taking The Course and Receiving Credit Who Should Complete This Course? You should complete this course
VAMC Radiation Safety Refresher Training March 2011 The University of Iowa Radiation Safety Program 1 Taking The Course and Receiving Credit Who Should Complete This Course? You should complete this course
Radiation Safety Manual
 Environmental Health and Safety Division Radiation Safety Office September 29, 2016 Intentionally Blank ii Table of Contents Chapter Title Page Table of Contents...iii-v 1. Radiation Safety Program...
Environmental Health and Safety Division Radiation Safety Office September 29, 2016 Intentionally Blank ii Table of Contents Chapter Title Page Table of Contents...iii-v 1. Radiation Safety Program...
RADIATION SAFETY MANUAL
 THE UNIVERSITY OF TEXAS MEDICAL BRANCH RADIATION SAFETY MANUAL ENVIRONMENTAL HEALTH AND SAFETY Revised: April, 2016 RADIATION SAFETY MANUAL Table of Contents Chapter 1 : General Information... 1-1 Radiation
THE UNIVERSITY OF TEXAS MEDICAL BRANCH RADIATION SAFETY MANUAL ENVIRONMENTAL HEALTH AND SAFETY Revised: April, 2016 RADIATION SAFETY MANUAL Table of Contents Chapter 1 : General Information... 1-1 Radiation
University of Maryland Baltimore. Radiation Safety Procedure
 University of Maryland Baltimore Procedure Number: 4.4 Radiation Safety Procedure Title: Radiation Safety During Therapeutic Radiopharmaceutical Procedures Revision Number: 0 Technical Review and Approval:
University of Maryland Baltimore Procedure Number: 4.4 Radiation Safety Procedure Title: Radiation Safety During Therapeutic Radiopharmaceutical Procedures Revision Number: 0 Technical Review and Approval:
HUMAN USE RADIATION SAFETY MANUAL
 February 2, 1999 (Revised February 27, 2001) DEPARTMENT OF ENVIRONMENTAL HEALTH AND SAFETY Office of Radiation Safety 852-5231 I. INTRODUCTION 1 II. CHARTER FOR THE UNIVERSITY RADIATION SAFETY 2 COMMITTEE
February 2, 1999 (Revised February 27, 2001) DEPARTMENT OF ENVIRONMENTAL HEALTH AND SAFETY Office of Radiation Safety 852-5231 I. INTRODUCTION 1 II. CHARTER FOR THE UNIVERSITY RADIATION SAFETY 2 COMMITTEE
MINNESOTA DEPARTMENT OF HEALTH
 MINNESOTA DEPARTMENT OF HEALTH REGULATORY GUIDE FOR GAS CHROMATOGRAPHS AND X-RAY FLUORESCENCE ANALYZERS Radioactive Materials Unit Minnesota Department of Health 625 Robert Street North P.O. Box 64975
MINNESOTA DEPARTMENT OF HEALTH REGULATORY GUIDE FOR GAS CHROMATOGRAPHS AND X-RAY FLUORESCENCE ANALYZERS Radioactive Materials Unit Minnesota Department of Health 625 Robert Street North P.O. Box 64975
Regulatory Issues Licensure by State Department of Nuclear Safety/Homeland Security or NRC Current License required or a "Timely Filed Notice"
 After reviewing this tutorial, participants should Know the basics of licensure by the NRC and State regulatory agencies Be able to state the difference between agreement states and non-agreement states
After reviewing this tutorial, participants should Know the basics of licensure by the NRC and State regulatory agencies Be able to state the difference between agreement states and non-agreement states
Radiation Safety Initial Training Module 3 Policies and Procedures
 In This Module Radiation Safety Initial Training Module 3 Policies and Procedures In order to work with or around radioisotopes at UAB, you should have a clear understanding of the policies and procedures.
In This Module Radiation Safety Initial Training Module 3 Policies and Procedures In order to work with or around radioisotopes at UAB, you should have a clear understanding of the policies and procedures.
(2) Ensure measures are established to control health and safety hazards from ionizing radiation sources and radioactive material.
 Ensure measures are established to control health and safety hazards from ionizing radiation sources and radioactive material.") Chapter 11 Radiation Safety Program 11-1. General a. Command policies and procedures for the procurement, production, transfer, storage, use, and disposal of radioactive material and ionizing and non-ionizing
Chapter 11 Radiation Safety Program 11-1. General a. Command policies and procedures for the procurement, production, transfer, storage, use, and disposal of radioactive material and ionizing and non-ionizing
Radiation Licensure and Management (RS100) Course
 Course") Intro/Opening Welcome to the Radiation Licensure and Management course. This training is designed and required for anyone who is requesting a Radiation License at UAB. The intent of this course is to inform
Intro/Opening Welcome to the Radiation Licensure and Management course. This training is designed and required for anyone who is requesting a Radiation License at UAB. The intent of this course is to inform
OH&S Radiation Safety Refresher Course Materials
 OH&S Radiation Safety Refresher Course Materials Note: This information is almost the same as the Flash file in the course. Some of it has been modified for reading purposes. Other information was not
OH&S Radiation Safety Refresher Course Materials Note: This information is almost the same as the Flash file in the course. Some of it has been modified for reading purposes. Other information was not
Republic of the Philippines Department of Science and Technology PHILIPPINE NUCLEAR RESEARCH INSTITUTE Don Mariano Marcos Avenue Diliman, Quezon City
 Republic of the Philippines Department of Science and Technology PHILIPPINE NUCLEAR RESEARCH INSTITUTE Don Mariano Marcos Avenue Diliman, Quezon City LICENSES TO MANUFACTURE AND DISPENSE RADIOPHARMACEUTICALS
Republic of the Philippines Department of Science and Technology PHILIPPINE NUCLEAR RESEARCH INSTITUTE Don Mariano Marcos Avenue Diliman, Quezon City LICENSES TO MANUFACTURE AND DISPENSE RADIOPHARMACEUTICALS
Radiation Safety Handbook
 Radiation Safety Handbook The University of Texas Health Science Center at San Antonio April 2006 Revision 5 TABLE OF CONTENTS PAGE # 1.0 Introduction 1 1.1 Purpose 1 1.2 Emergency Telephone Numbers 2
Radiation Safety Handbook The University of Texas Health Science Center at San Antonio April 2006 Revision 5 TABLE OF CONTENTS PAGE # 1.0 Introduction 1 1.1 Purpose 1 1.2 Emergency Telephone Numbers 2
RADIATION PROTECTION PROGRAM FOR USE OF RADIATION GENERATING MACHINES IN THE HEALING ARTS, RESEARCH AND EDUCATION
 RADIATION PROTECTION PROGRAM FOR USE OF RADIATION GENERATING MACHINES IN THE HEALING ARTS, RESEARCH AND EDUCATION Radiation Safety Office 629 Wareham Parkway Criss I, Room 213 Omaha, NE 68178 Phone: 402-280-5570
RADIATION PROTECTION PROGRAM FOR USE OF RADIATION GENERATING MACHINES IN THE HEALING ARTS, RESEARCH AND EDUCATION Radiation Safety Office 629 Wareham Parkway Criss I, Room 213 Omaha, NE 68178 Phone: 402-280-5570
Effective Date: 6/15/77. Date Reviewed:
 Classification: Radiology Policy Number: 668.027 Subject: ALARA Program for Radiation Exposure Contact Position: Radiology Director Effective Date: 6/15/77 Date Reviewed: Page: 1 of 5 Date Revised: 7/02,
Classification: Radiology Policy Number: 668.027 Subject: ALARA Program for Radiation Exposure Contact Position: Radiology Director Effective Date: 6/15/77 Date Reviewed: Page: 1 of 5 Date Revised: 7/02,
Health & Safety Policy and Procedures Manual SECTION 31 CADMIUM
 SECTION 31 CADMIUM 1. CADMIUM A. Scope: This written compliance program applies to all Maul Electric, Inc employees or employees of Maul Electric, Inc subcontractors who may be exposed to cadmium at or
SECTION 31 CADMIUM 1. CADMIUM A. Scope: This written compliance program applies to all Maul Electric, Inc employees or employees of Maul Electric, Inc subcontractors who may be exposed to cadmium at or
Radiation Safety in the Hospital for Housekeeping Personnel
 Radiation Safety in the Hospital for Housekeeping Personnel Presented By: Walter L. Robinson, M.S., A.B.S.N.M. & A.B.M.P. Consultant Certified Medical Radiation Health & Diagnostic Imaging Physicist Areas
Radiation Safety in the Hospital for Housekeeping Personnel Presented By: Walter L. Robinson, M.S., A.B.S.N.M. & A.B.M.P. Consultant Certified Medical Radiation Health & Diagnostic Imaging Physicist Areas
Fifty Shades Of Gray A Medical Physicists Guide as RSO. Kevin Nelson, Ph.D, CHP Mayo Clinic Florida
 Fifty Shades Of Gray A Medical Physicists Guide as RSO Kevin Nelson, Ph.D, CHP Mayo Clinic Florida nelson.kevin2@mayo.edu Objectives Review training and education requirements for a Radiation Safety Officer
Fifty Shades Of Gray A Medical Physicists Guide as RSO Kevin Nelson, Ph.D, CHP Mayo Clinic Florida nelson.kevin2@mayo.edu Objectives Review training and education requirements for a Radiation Safety Officer
THE UNIVERSITY OF AKRON
 THE UNIVERSITY OF AKRON Radiation-Generating Equipment Quality Assurance Program INDEX I. Design of the Radiation-Generating Equipment Quality Assurance (QA) Program..... 1 A. Purpose of the QA Safety
THE UNIVERSITY OF AKRON Radiation-Generating Equipment Quality Assurance Program INDEX I. Design of the Radiation-Generating Equipment Quality Assurance (QA) Program..... 1 A. Purpose of the QA Safety
RADIOACTIVE MATERIALS REGULATORY GUIDE
 RADIOACTIVE MATERIALS REGULATORY GUIDE ANNUAL AUDIT CHECKLIST FOR MEDICAL FACILITIES Radioactive Materials Unit 625 Robert Street North PO Box 64975 St. Paul, Minnesota 55164-0975 February 13, 2009 TABLE
RADIOACTIVE MATERIALS REGULATORY GUIDE ANNUAL AUDIT CHECKLIST FOR MEDICAL FACILITIES Radioactive Materials Unit 625 Robert Street North PO Box 64975 St. Paul, Minnesota 55164-0975 February 13, 2009 TABLE
Access to the laboratory is restricted when work is being conducted; and
 APPENDIX E-2: Biosafety Level 2 (BSL-2) The following is taken from the Biosafety in Microbiological and Biomedical Laboratories (BMBL) 5 th Edition, February 2009 Centers for Disease Control and Prevention
APPENDIX E-2: Biosafety Level 2 (BSL-2) The following is taken from the Biosafety in Microbiological and Biomedical Laboratories (BMBL) 5 th Edition, February 2009 Centers for Disease Control and Prevention
UNIVERSITY OF SOUTH ALABAMA RADIATION SAFETY PROCEDURES MANUAL
 UNIVERSITY OF SOUTH ALABAMA RADIATION SAFETY PROCEDURES MANUAL The University of South Alabama was granted a radioactive materials license to possess and use radioactive material for purposes of research
UNIVERSITY OF SOUTH ALABAMA RADIATION SAFETY PROCEDURES MANUAL The University of South Alabama was granted a radioactive materials license to possess and use radioactive material for purposes of research
RADIATION PROTECTION
 RADIATION PROTECTION Students entering the Program must be advised of the radiation protection precautions prior to being clinically assigned to a location where ionizing radiation is produced. Responsibility:
RADIATION PROTECTION Students entering the Program must be advised of the radiation protection precautions prior to being clinically assigned to a location where ionizing radiation is produced. Responsibility:
RMM 700 Radiation Safety Program for University Laboratories
 Submitted: Senior Health Physicist Approved: Chair, HPAC Approved: Vice President, Administration Page: 1 of 27 Authorized: President and Vice-Chancellor 1 PURPOSE 1.1 Under the Radiation Protection Regulations
Submitted: Senior Health Physicist Approved: Chair, HPAC Approved: Vice President, Administration Page: 1 of 27 Authorized: President and Vice-Chancellor 1 PURPOSE 1.1 Under the Radiation Protection Regulations
Mobile Positron Emission Tomography
 Mobile Positron Emission Tomography PURPOSE This procedure provides general instructions for developing, maintaining, and documenting radiation protection procedures for preparation, calibration and administration
Mobile Positron Emission Tomography PURPOSE This procedure provides general instructions for developing, maintaining, and documenting radiation protection procedures for preparation, calibration and administration
RADIATION SAFETY PROGRAM
 RADIATION SAFETY PROGRAM THE UNIVERSITY OF MARYLAND BALTIMORE (UMB) Revision Number: 1 Technical Review and Approval: Radiation Safety Officer Date: Radiation Safety Committee Approval: Chair, Radiation
RADIATION SAFETY PROGRAM THE UNIVERSITY OF MARYLAND BALTIMORE (UMB) Revision Number: 1 Technical Review and Approval: Radiation Safety Officer Date: Radiation Safety Committee Approval: Chair, Radiation
Yale University ALARA (AS LOW AS REASONABLY ACHIEVABLE) PROGRAM
 PROGRAM") Yale University ALARA (AS LOW AS REASONABLY ACHIEVABLE) PROGRAM 1. Management Commitment a. The goal of the ALARA program is to maintain ionizing radiation exposures to individuals and releases to the
Yale University ALARA (AS LOW AS REASONABLY ACHIEVABLE) PROGRAM 1. Management Commitment a. The goal of the ALARA program is to maintain ionizing radiation exposures to individuals and releases to the
NRC INSPECTION MANUAL
 NRC INSPECTION MANUAL MSSA/RMSB INSPECTION PROCEDURE 87132 BRACHYTHERAPY PROGRAMS PROGRAM APPLICABILITY: 2800 87132-01 INSPECTION OBJECTIVES 01.01 To determine if licensed activities are being conducted
NRC INSPECTION MANUAL MSSA/RMSB INSPECTION PROCEDURE 87132 BRACHYTHERAPY PROGRAMS PROGRAM APPLICABILITY: 2800 87132-01 INSPECTION OBJECTIVES 01.01 To determine if licensed activities are being conducted
NRC INFORMATION NOTICE 91-71: TRAINING AND SUPERVISION OF INDIVIDUALS SUPERVISED BY AN AUTHORIZED USER
 Page 1 of 5 UNITED STATES NUCLEAR REGULATORY COMMISSION OFFICE OF NUCLEAR MATERIALS SAFETY AND SAFEGUARDS WASHINGTON, D.C. 20555 NRC INFORMATION NOTICE 91-71: TRAINING AND SUPERVISION OF INDIVIDUALS SUPERVISED
Page 1 of 5 UNITED STATES NUCLEAR REGULATORY COMMISSION OFFICE OF NUCLEAR MATERIALS SAFETY AND SAFEGUARDS WASHINGTON, D.C. 20555 NRC INFORMATION NOTICE 91-71: TRAINING AND SUPERVISION OF INDIVIDUALS SUPERVISED
Walter L. Robinson & Associates Presents..
 Walter L. Robinson & Associates Presents.. Copyright, 2006 Walter L. Robinson & Associates Note This presentation is intended for annual in-services or initial radiation safety orientations What Every
Walter L. Robinson & Associates Presents.. Copyright, 2006 Walter L. Robinson & Associates Note This presentation is intended for annual in-services or initial radiation safety orientations What Every
BLOODBORNE PATHOGENS EXPOSURE PREVENTION POLICY AND PROCEDURE BLOODBORNE PATHOGENS EXPOSURE CONTROL PLAN
 BLOODBORNE PATHOGENS EXPOSURE PREVENTION POLICY AND PROCEDURE This sample plan is provided only as a guide to assist in complying with the OSHA Bloodborne Pathogens standard 29 CFR 1910.1030, as adopted
BLOODBORNE PATHOGENS EXPOSURE PREVENTION POLICY AND PROCEDURE This sample plan is provided only as a guide to assist in complying with the OSHA Bloodborne Pathogens standard 29 CFR 1910.1030, as adopted
University of Pennsylvania Environmental Health and Radiation Safety. Diagnostic Energized Equipment Radiation Safety Manual
 University of Pennsylvania Environmental Health and Radiation Safety Diagnostic Energized Equipment Radiation Safety Manual (Reviewed: September 2012) I. Proper Operating Procedures A. Radiographic Units
University of Pennsylvania Environmental Health and Radiation Safety Diagnostic Energized Equipment Radiation Safety Manual (Reviewed: September 2012) I. Proper Operating Procedures A. Radiographic Units
University of Maryland Baltimore. Radiation Safety Procedure
 University of Maryland Baltimore Radiation Safety Procedure Procedure Number: 4.5 Title: Radiation Safety During Y-90 Microsphere Treatment Revision Number: 0 Technical Review and Approval: Radiation Safety
University of Maryland Baltimore Radiation Safety Procedure Procedure Number: 4.5 Title: Radiation Safety During Y-90 Microsphere Treatment Revision Number: 0 Technical Review and Approval: Radiation Safety
RADIATION SAFETY COMMITTEE
 RADIATION SAFETY COMMITTEE PURPOSE This procedure defines the membership, authority, responsibilities and operating rules of the University's Radiation Safety Committee. POLICY The Radiation Safety Committee
RADIATION SAFETY COMMITTEE PURPOSE This procedure defines the membership, authority, responsibilities and operating rules of the University's Radiation Safety Committee. POLICY The Radiation Safety Committee
Guidelines for Biosafety in Teaching Laboratories Using Microorganisms
 Guidelines for Biosafety in Teaching Laboratories Using Microorganisms Prepared February, 2013 (Adapted from the American Society for Microbiology Guidelines for Biosafety in Teaching Laboratories, 2012)
Guidelines for Biosafety in Teaching Laboratories Using Microorganisms Prepared February, 2013 (Adapted from the American Society for Microbiology Guidelines for Biosafety in Teaching Laboratories, 2012)
BLOODBORNE PATHOGENS EXPOSURE CONTROL PLAN
 BLOODBORNE PATHOGENS EXPOSURE CONTROL PLAN School Name: Eastern Local School District Date of Preparation: August 2, 2000 (Revised August 22, 2002) In accordance with the PERRP Bloodborne Pathogens standard,
BLOODBORNE PATHOGENS EXPOSURE CONTROL PLAN School Name: Eastern Local School District Date of Preparation: August 2, 2000 (Revised August 22, 2002) In accordance with the PERRP Bloodborne Pathogens standard,
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6055.8 March 31, 1989 SUBJECT: Occupational Radiation Protection Program Administrative Reissuance Incorporating Change 1, May 6, 1996 USD(A&T) References: (a)
Department of Defense INSTRUCTION NUMBER 6055.8 March 31, 1989 SUBJECT: Occupational Radiation Protection Program Administrative Reissuance Incorporating Change 1, May 6, 1996 USD(A&T) References: (a)
University of Maryland Baltimore. Radiation Safety Procedure
 University of Maryland Baltimore Procedure Number: 1.1 Radiation Safety Procedure Title: Radiation Safety Program Organization and Administration Revision Number: 0 Technical Review and Approval: Radiation
University of Maryland Baltimore Procedure Number: 1.1 Radiation Safety Procedure Title: Radiation Safety Program Organization and Administration Revision Number: 0 Technical Review and Approval: Radiation
RADIATION POLICY Page 1 of 5 Reviewed: August 2017
 Page 1 of 5 Policy Applies to: All Mercy Hospital staff, who work with (or work in the vicinity of) radiological equipment. Compliance by credentialed specialists and visitors will be facilitated by Mercy
Page 1 of 5 Policy Applies to: All Mercy Hospital staff, who work with (or work in the vicinity of) radiological equipment. Compliance by credentialed specialists and visitors will be facilitated by Mercy
Formaldehyde Exposure Control Plan
 A. Purpose To maintain formaldehyde exposure below the limits established by the Occupational Safety and Health Administration s (OSHA) Formaldehyde Standard 29 CFR 1910.1048. These limits are the Action
A. Purpose To maintain formaldehyde exposure below the limits established by the Occupational Safety and Health Administration s (OSHA) Formaldehyde Standard 29 CFR 1910.1048. These limits are the Action
Appendix AX: B Occupational Exposure to Bloodborne Pathogens Exposure Control Plan
 Occupational Exposure to Bloodborne Pathogens Exposure Control Plan Employer: Nevada State Health Division Effective Date: May 5, 1992 Compliance Statement: In accordance with OSHA Bloodborne Pathogens
Occupational Exposure to Bloodborne Pathogens Exposure Control Plan Employer: Nevada State Health Division Effective Date: May 5, 1992 Compliance Statement: In accordance with OSHA Bloodborne Pathogens
Mandatory Licensure for Radiologic Personnel. Christopher Jason Tien
 Mandatory Licensure for Radiologic Personnel Christopher Jason Tien Licensure Permission to perform a given occupation 3 rd party examinations State hands out licenses Occupations licensed: teachers, architects,
Mandatory Licensure for Radiologic Personnel Christopher Jason Tien Licensure Permission to perform a given occupation 3 rd party examinations State hands out licenses Occupations licensed: teachers, architects,
QUALITY MANAGEMENT PROGRAM FOR HUMAN RESEARCH SUBJECT UNIVERSITY OF CINCINNATI
 Effective January 27, 1992 Modified: August 10, 1993; March 8, 1994; August 11, 1994; July 18, 1995; September 23, 1997, November 14, 2001, May 19, 2004, June 17, 2006 and (November 8, 2006) I. Purpose
Effective January 27, 1992 Modified: August 10, 1993; March 8, 1994; August 11, 1994; July 18, 1995; September 23, 1997, November 14, 2001, May 19, 2004, June 17, 2006 and (November 8, 2006) I. Purpose
Allied Health Department. Radiation Protection Program (RPP) Policies & Procedures
 Policies & Procedures") Allied Health Department Radiation Protection Program (RPP) Policies & Procedures REVISION: 12/12/2017 Allied Health- Radiologic Technology Kevin D. Yow, MHA., R.T. (R), Radiation Safety Officer (619)
Allied Health Department Radiation Protection Program (RPP) Policies & Procedures REVISION: 12/12/2017 Allied Health- Radiologic Technology Kevin D. Yow, MHA., R.T. (R), Radiation Safety Officer (619)
CHEMICAL HYGIENE PLAN ENVIRONMENTAL HEALTH AND SAFETY 72 ONYX BRIDGE
 CHEMICAL HYGIENE PLAN ENVIRONMENTAL HEALTH AND SAFETY 72 ONYX BRIDGE 541-346-3192 Environmental Health and Safety Staff and Services Waste Collection Request ----------------------------- 541-346-3192
CHEMICAL HYGIENE PLAN ENVIRONMENTAL HEALTH AND SAFETY 72 ONYX BRIDGE 541-346-3192 Environmental Health and Safety Staff and Services Waste Collection Request ----------------------------- 541-346-3192
RADIOACTIVE MATERIALS REGULATORY GUIDE DIAGNOSTIC AND THERAPEUTIC MEDICAL PROCEDURES
 RADIOACTIVE MATERIALS REGULATORY GUIDE DIAGNOSTIC AND THERAPEUTIC MEDICAL PROCEDURES Radioactive Materials Unit 625 Robert Street North P.O. Box 64975 St. Paul, MN 55164-0975 July 2007 TABLE OF CONTENTS
RADIOACTIVE MATERIALS REGULATORY GUIDE DIAGNOSTIC AND THERAPEUTIC MEDICAL PROCEDURES Radioactive Materials Unit 625 Robert Street North P.O. Box 64975 St. Paul, MN 55164-0975 July 2007 TABLE OF CONTENTS
Brachytherapy-Radiopharmaceutical Therapy Quality Management Program. Rev Date: Feb
 Section I outlines definitions, reporting, auditing and general requirements of the QMP program while Section II describes the QMP implementation for each therapeutic modality. Recommendations are expressed
Section I outlines definitions, reporting, auditing and general requirements of the QMP program while Section II describes the QMP implementation for each therapeutic modality. Recommendations are expressed
Radiation Safety Manual
 OFFICE OF RESEARCH Radiation Safety Manual RADIATION SAFETY OFFICE 1 UNIVERSITY OF NEW MEXICO MSC 08-4560 ALBUQUERQUE, NM 87131 (505) 272-4607 (505) 925-0745 The University of New Mexico Health Sciences
OFFICE OF RESEARCH Radiation Safety Manual RADIATION SAFETY OFFICE 1 UNIVERSITY OF NEW MEXICO MSC 08-4560 ALBUQUERQUE, NM 87131 (505) 272-4607 (505) 925-0745 The University of New Mexico Health Sciences
REGULATORY GUIDE 4.3 TEXAS DEPARTMENT OF STATE HEALTH SERVICES RADIATION SAFETY LICENSING BRANCH (RSLB) P.O. Box Austin, Texas
 P.O. Box Austin, Texas") I. Introduction REGULATORY GUIDE 4.3 TEXAS DEPARTMENT OF STATE HEALTH SERVICES RADIATION SAFETY LICENSING BRANCH (RSLB) P.O. Box 149347 Austin, Texas 78714-9347 GUIDE FOR THE PREPARATION OF OPERATING AND
I. Introduction REGULATORY GUIDE 4.3 TEXAS DEPARTMENT OF STATE HEALTH SERVICES RADIATION SAFETY LICENSING BRANCH (RSLB) P.O. Box 149347 Austin, Texas 78714-9347 GUIDE FOR THE PREPARATION OF OPERATING AND
NUCLEAR MEDICINE RESIDENT DUTIES
 NUCLEAR MEDICINE RESIDENT DUTIES General The American Board of Radiology requires four months training in Nuclear Medicine. Residents will be assigned at least 4 rotations on service. Rotations will be
NUCLEAR MEDICINE RESIDENT DUTIES General The American Board of Radiology requires four months training in Nuclear Medicine. Residents will be assigned at least 4 rotations on service. Rotations will be
Radiation Protection Procedures for the Cincinnati Proton Therapy Center (CPTC)
") Radiation Protection Procedures for the Cincinnati Proton Therapy Center (CPTC) Ver 1.3 1 Cincinnati Children s Medical Center University of Cincinnati Revision Number Original- Ver 1 Date of Revision
Radiation Protection Procedures for the Cincinnati Proton Therapy Center (CPTC) Ver 1.3 1 Cincinnati Children s Medical Center University of Cincinnati Revision Number Original- Ver 1 Date of Revision
CHEMICAL HYGIENE PLAN
 SAMPLE WRITTEN CHEMICAL HYGIENE PLAN For Compliance With 29 CFR 1910.1450 Wyoming General Rules and Regulations Wyoming Department of Workforce Services OSHA Division Consultation Program ACKNOWLEDGEMENTS
SAMPLE WRITTEN CHEMICAL HYGIENE PLAN For Compliance With 29 CFR 1910.1450 Wyoming General Rules and Regulations Wyoming Department of Workforce Services OSHA Division Consultation Program ACKNOWLEDGEMENTS
RADIOACTIVE MATERIAL LICENSE
 Page 1 of 7 pages Pursuant to the California Code of Regulations, Division 1, Title 17, Chapter 5, Subchapter 4, Group 2, Licensing of Radioactive Material, and in reliance on statements and representations
Page 1 of 7 pages Pursuant to the California Code of Regulations, Division 1, Title 17, Chapter 5, Subchapter 4, Group 2, Licensing of Radioactive Material, and in reliance on statements and representations
We are very excited to provide this update for your Radiation for Dental Safety Manual.
 Dear TMC Radiation Client: We are very excited to provide this update for your Radiation for Dental Safety Manual. Several sections in the manual were updated. Each section with changes is listed below
Dear TMC Radiation Client: We are very excited to provide this update for your Radiation for Dental Safety Manual. Several sections in the manual were updated. Each section with changes is listed below
Massey University Radiation Safety Plan Version
 Massey University Radiation Safety Plan Version 2007.4 CONTENTS Radiation Safety Policy...1 Purpose:...1 Policy:...1 Audience:...2 Relevant legislation:...2 Related Polices and Procedures:...2 Document
Massey University Radiation Safety Plan Version 2007.4 CONTENTS Radiation Safety Policy...1 Purpose:...1 Policy:...1 Audience:...2 Relevant legislation:...2 Related Polices and Procedures:...2 Document
Radiologic Technology Program. Radiation Safety and Protection Program
 Radiologic Technology Program Radiation Safety and Protection Program Name of Program: Charles R. Drew University of Medicine and Science College of Science and Health Program Number: 1029 Name of Program
Radiologic Technology Program Radiation Safety and Protection Program Name of Program: Charles R. Drew University of Medicine and Science College of Science and Health Program Number: 1029 Name of Program
CHEMICAL HYGIENE PLAN
 CHEMICAL HYGIENE PLAN The SDSU Laboratory Chemical Safety Program for Compliance with 29 CFR 1910.1450 and 8 CCR 5191: Occupational Exposure to Hazardous Chemical in Laboratories Prepared by San Diego
CHEMICAL HYGIENE PLAN The SDSU Laboratory Chemical Safety Program for Compliance with 29 CFR 1910.1450 and 8 CCR 5191: Occupational Exposure to Hazardous Chemical in Laboratories Prepared by San Diego
Formaldehyde Exposure Control Policy
 Formaldehyde Exposure Control Policy POLICY AND PROCEDURES FOR WORKING WITH FORMALDEHYDE Policy: It is Columbia University (CU) policy to maintain formaldehyde exposure below the action level (AL) 0.5
Formaldehyde Exposure Control Policy POLICY AND PROCEDURES FOR WORKING WITH FORMALDEHYDE Policy: It is Columbia University (CU) policy to maintain formaldehyde exposure below the action level (AL) 0.5
Administrative Safety
 Administrative Safety Environmental Health and Safety Department 800 West Campbell Rd., SG10 Richardson, TX 75080-3021 Phone 972-883-2381/4111 Fax 972-883-6115 http://www.utdallas.edu/ehs Modified: March
Administrative Safety Environmental Health and Safety Department 800 West Campbell Rd., SG10 Richardson, TX 75080-3021 Phone 972-883-2381/4111 Fax 972-883-6115 http://www.utdallas.edu/ehs Modified: March
Radiation Safety Refresher (OHS_RS103) Course Material
 Course Material") (OHS_RS103) Course Material Introduction Welcome to the Course (OHS_RS103). The UAB OH&S Radiation Safety Program, which is licensed by the State of Alabama, requires that any UAB employees who work with
(OHS_RS103) Course Material Introduction Welcome to the Course (OHS_RS103). The UAB OH&S Radiation Safety Program, which is licensed by the State of Alabama, requires that any UAB employees who work with
Regulations that Govern the Disposal of Medical Waste
 Regulations that Govern the Disposal of Medical Waste In Louisiana, there are three (3) sources of regulations for medical wastes: OSHA, the Louisiana Department of Health and Hospitals, and the Louisiana
Regulations that Govern the Disposal of Medical Waste In Louisiana, there are three (3) sources of regulations for medical wastes: OSHA, the Louisiana Department of Health and Hospitals, and the Louisiana
Radiation Safety Code of Practice
 Radiation Safety Code of Practice 2017 Contents REVISION HISTORY... II DEFINITIONS... 1 1 PURPOSE... 3 2 SCOPE... 3 3 REGULATORY CONSIDERATIONS... 3 4 ALARA PRINCIPLE... 4 5 PROGRAM AUTHORITY ROLES AND
Radiation Safety Code of Practice 2017 Contents REVISION HISTORY... II DEFINITIONS... 1 1 PURPOSE... 3 2 SCOPE... 3 3 REGULATORY CONSIDERATIONS... 3 4 ALARA PRINCIPLE... 4 5 PROGRAM AUTHORITY ROLES AND
Local Government Records Control Schedule
 Local s Control Schedule 1. Page 58 of 116 PS4525-01 HR4750-01 EMERGENCY MEDICAL SERVICE TRAINING RECORDS HEALTH SERVICES APPOINTMENT RECORDS s relating to the training (including continuing education)
Local s Control Schedule 1. Page 58 of 116 PS4525-01 HR4750-01 EMERGENCY MEDICAL SERVICE TRAINING RECORDS HEALTH SERVICES APPOINTMENT RECORDS s relating to the training (including continuing education)
Radiotherapy Licence Application Form
 Radiotherapy Licence Application Form Section A Applicant A1 Type of request Construction Renewal Operating to commission Decommissioning Routine operation (amendment) Current licence # A2 Language of
Radiotherapy Licence Application Form Section A Applicant A1 Type of request Construction Renewal Operating to commission Decommissioning Routine operation (amendment) Current licence # A2 Language of
Rice University Exposure Control Plan
 Rice University Exposure Control Plan Environmental Health and Safety MS 123 P.O. Box 1892 Houston, TX 77251-1892 713 348 4444 February 2015 1 Rice University Exposure Control Plan Rice University is committed
Rice University Exposure Control Plan Environmental Health and Safety MS 123 P.O. Box 1892 Houston, TX 77251-1892 713 348 4444 February 2015 1 Rice University Exposure Control Plan Rice University is committed
HOWARD UNIVERSITY Position Description. POSITION TITLE: Radiation Safety Officer SALARY GRADE: HU-13. DATE REVISED: December 01, 2014 EEO CODE: 02
 DEPARTMENT: POSITION NO: REPORTS TO: GRANT: No Yes BASIC FUNCTION: SUPERVISORY ACCOUNTABILITY: NATURE AND SCOPE: PRINCIPAL ACCOUNTABILITIES: Directs, develops and maintains a comprehensive radiological
DEPARTMENT: POSITION NO: REPORTS TO: GRANT: No Yes BASIC FUNCTION: SUPERVISORY ACCOUNTABILITY: NATURE AND SCOPE: PRINCIPAL ACCOUNTABILITIES: Directs, develops and maintains a comprehensive radiological
Biology 100, 101, 102, 105 Laboratory Safety Agreement
 Biology 100, 101, 102, 105 Laboratory Safety Agreement In the interest of safety and accident-prevention, there are regulations to be followed by all credit students in designated science laboratory rooms
Biology 100, 101, 102, 105 Laboratory Safety Agreement In the interest of safety and accident-prevention, there are regulations to be followed by all credit students in designated science laboratory rooms
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Neurology (Hemby Lane) Date Originated: 2/20/14 Date Reviewed: 6.5.18 Date Approved: 6/3/14 Page 1 of 7 Approved by: Department Chairman Administrator/Manager
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Neurology (Hemby Lane) Date Originated: 2/20/14 Date Reviewed: 6.5.18 Date Approved: 6/3/14 Page 1 of 7 Approved by: Department Chairman Administrator/Manager
CORPORATE SAFETY MANUAL
 CORPORATE SAFETY MANUAL Procedure No. 27-0 Revision: Date: May 2005 Total Pages: 9 PURPOSE To make certain that our employees are duly aware of the hazards of blood exposure or other potentially infectious
CORPORATE SAFETY MANUAL Procedure No. 27-0 Revision: Date: May 2005 Total Pages: 9 PURPOSE To make certain that our employees are duly aware of the hazards of blood exposure or other potentially infectious
Infection Control Safety Guidance Document
 Infection Control Safety Guidance Document Lead Directorate and Service: Corporate Resources - Human Resources, Safety Services Effective Date: June 2014 Contact Officer/Number Garry Smith / 01482 391110
Infection Control Safety Guidance Document Lead Directorate and Service: Corporate Resources - Human Resources, Safety Services Effective Date: June 2014 Contact Officer/Number Garry Smith / 01482 391110
Ch. 129 NUCLEAR MEDICINE SERVICES CHAPTER 129. NUCLEAR MEDICINE SERVICES GENERAL PROVISIONS
 Ch. 129 NUCLEAR MEDICINE SERVICES 28 129.1 CHAPTER 129. NUCLEAR MEDICINE SERVICES GENERAL PROVISIONS Sec. 129.1. Principle. 129.2. Organizational options. 129.3. Organization and staffing. 129.4. Director.
Ch. 129 NUCLEAR MEDICINE SERVICES 28 129.1 CHAPTER 129. NUCLEAR MEDICINE SERVICES GENERAL PROVISIONS Sec. 129.1. Principle. 129.2. Organizational options. 129.3. Organization and staffing. 129.4. Director.
Infection Control Policy and Procedure Manual. Post-Anesthesia Care Unit (Recovery Room) Page 1 of 6
 Page 1 of 6") (Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
(Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
FIRST AID POLICY. (to be read in conjunction with Administration of Medicines Policy) CONTENTS
 CONTENTS") FIRST AID POLICY (to be read in conjunction with Administration of Medicines Policy) CONTENTS Authority & circulation... 2 Definitions...... 2 Aims of this policy...... 2 Who is responsible...... 3 First
FIRST AID POLICY (to be read in conjunction with Administration of Medicines Policy) CONTENTS Authority & circulation... 2 Definitions...... 2 Aims of this policy...... 2 Who is responsible...... 3 First
MODULE 22: Contingency Planning and Emergency Response to Healthcare Waste Spills
 MODULE 22: Contingency Planning and Emergency Response to Healthcare Waste Spills Module Overview Present examples of contingencies related to HCWM Describe steps in developing a contingency plan Describe
MODULE 22: Contingency Planning and Emergency Response to Healthcare Waste Spills Module Overview Present examples of contingencies related to HCWM Describe steps in developing a contingency plan Describe
105 CMR: DEPARTMENT OF PUBLIC HEALTH
 120.440: continued (1) If commercial software is used to generate shielding requirements, also identify the software used and the version/ revision date. (2) If the software used to generate shielding
120.440: continued (1) If commercial software is used to generate shielding requirements, also identify the software used and the version/ revision date. (2) If the software used to generate shielding
Medical Response To Radiation Incidents
 Medical Response To Radiation Incidents Kevin Nelson, Ph.D., CHP Health Physics Society President-Elect nelson.kevin2@mayo.edu (904) 953-8978 HPS Items HPS Membership benefits HPS Committee assignments
Medical Response To Radiation Incidents Kevin Nelson, Ph.D., CHP Health Physics Society President-Elect nelson.kevin2@mayo.edu (904) 953-8978 HPS Items HPS Membership benefits HPS Committee assignments
Houston Controls, Inc Safety Management System
 Preparation: Safety Mgr Authority: Dennis Johnston Issuing Dept: Safety Page: Page 1 of 8 Purpose This Bloodborne Pathogen Exposure Control Plan has been established to ensure a safe and healthful working
Preparation: Safety Mgr Authority: Dennis Johnston Issuing Dept: Safety Page: Page 1 of 8 Purpose This Bloodborne Pathogen Exposure Control Plan has been established to ensure a safe and healthful working
To provide information about the role of the pharmacy in Infection Prevention and Control.
 TITLE/DESCRIPTION: Pharmacy DEPARTMENT: Pharmacy PERSONNEL: Pharmacy Personnel EFFECTIVE DATE: 1/97 REVISED: 4/97, 7/08, 12/11, 1/15 I. PURPOSE To provide information about the role of the pharmacy in
TITLE/DESCRIPTION: Pharmacy DEPARTMENT: Pharmacy PERSONNEL: Pharmacy Personnel EFFECTIVE DATE: 1/97 REVISED: 4/97, 7/08, 12/11, 1/15 I. PURPOSE To provide information about the role of the pharmacy in
Urinalysis and Body Fluids
 Urinalysis and Body Fluids Unit 1 A Safety in the Clinical Laboratory Types of Safety Hazards Physical risks Sharps hazard Electrical hazard Radioactive hazard Chemical exposure risk Fire / explosive hazards
Urinalysis and Body Fluids Unit 1 A Safety in the Clinical Laboratory Types of Safety Hazards Physical risks Sharps hazard Electrical hazard Radioactive hazard Chemical exposure risk Fire / explosive hazards
Bloodborne Pathogens Exposure Control Plan. Approved by The College at Brockport, Office of Environmental Health and Safety, February 2018
 Kinesiology, Sport Studies and Physical Education Athletic Training Program Bloodborne Pathogens Exposure Control Plan Approved by The College at Brockport, Office of Environmental Health and Safety, February
Kinesiology, Sport Studies and Physical Education Athletic Training Program Bloodborne Pathogens Exposure Control Plan Approved by The College at Brockport, Office of Environmental Health and Safety, February
RP COP001 Radiation Protection Supervisors
 RP COP001 Radiation Protection Supervisors 1. Introduction This Code of Practice (CoP) concerns University staff or postgraduate students who are, or are about to be, appointed as Radiation Protection
RP COP001 Radiation Protection Supervisors 1. Introduction This Code of Practice (CoP) concerns University staff or postgraduate students who are, or are about to be, appointed as Radiation Protection
Doing Business As name (if applicable): 2. Mailing Address: (Street Address/City/State/Zip) 3. Physical Location: (Street Address/City/State/Zip)
: 2. Mailing Address: (Street Address/City/State/Zip) 3. Physical Location: (Street Address/City/State/Zip)") ZZ113-120 REGISTRATION APPLICATION FOR USERS OF RADIATION MACHINES HEALING ARTS, DENTAL, VETERINARY MEDICINE AND MEDICAL ACADEMIC FACILITIES TEXAS DEPARTMENT OF STATE HEALTH SERVICES (DSHS) RADIATION SAFETY
ZZ113-120 REGISTRATION APPLICATION FOR USERS OF RADIATION MACHINES HEALING ARTS, DENTAL, VETERINARY MEDICINE AND MEDICAL ACADEMIC FACILITIES TEXAS DEPARTMENT OF STATE HEALTH SERVICES (DSHS) RADIATION SAFETY
POLICY & PROCEDURES MEMORANDUM
 Policy No. *SF-1373.6 POLICY & PROCEDURES MEMORANDUM TITLE: BLOODBORNE PATHOGENS: EXPOSURE CONTROL PLAN (ECP) EFFECTIVE DATE: November 25, 2002* (*ORM Regulations Update 9/24/12; Title Updates 5/7/05)
Policy No. *SF-1373.6 POLICY & PROCEDURES MEMORANDUM TITLE: BLOODBORNE PATHOGENS: EXPOSURE CONTROL PLAN (ECP) EFFECTIVE DATE: November 25, 2002* (*ORM Regulations Update 9/24/12; Title Updates 5/7/05)
University of Cincinnati
 University of Cincinnati Quality Assurance and Radiation Protection Manual For Human-Use Radiation Generating Equipment (QA&RP MANUAL FOR HUMAN-USE RGE) RECORD OF REVISION PAGE Revision # Date of Revision
University of Cincinnati Quality Assurance and Radiation Protection Manual For Human-Use Radiation Generating Equipment (QA&RP MANUAL FOR HUMAN-USE RGE) RECORD OF REVISION PAGE Revision # Date of Revision
UNIVERSITY OF VICTORIA X-RAY EQUIPMENT SAFETY POLICIES AND PROCEDURES
 UNIVERSITY OF VICTORIA X-RAY EQUIPMENT SAFETY POLICIES AND PROCEDURES Department of Occupational Health, Safety and Environment November 2009 TABLE OF CONTENTS 1.0 PURPOSE 2 2.0 SCOPE AND APPLICATION 2
UNIVERSITY OF VICTORIA X-RAY EQUIPMENT SAFETY POLICIES AND PROCEDURES Department of Occupational Health, Safety and Environment November 2009 TABLE OF CONTENTS 1.0 PURPOSE 2 2.0 SCOPE AND APPLICATION 2
Laboratory Chemical Hygiene Plan Research Lab
 Laboratory Chemical Hygiene Plan Research Lab A chemical hygiene plan is a written program developed to establish procedures, protective equipment requirements and standard work practices that promote
Laboratory Chemical Hygiene Plan Research Lab A chemical hygiene plan is a written program developed to establish procedures, protective equipment requirements and standard work practices that promote
Qualifications for University Radiation Safety Officer
 Standards of Qualification and Practice (SQ/P) Qualifications for University Radiation Safety Officer RSO Section American Academy of Health Physics and Radiation Safety Operations Section of the Health
Standards of Qualification and Practice (SQ/P) Qualifications for University Radiation Safety Officer RSO Section American Academy of Health Physics and Radiation Safety Operations Section of the Health
Oklahoma State University Policy and Procedures INSTITUTIONAL RADIATION SAFETY POLICY
 Oklahoma State University Policy and Procedures INSTITUTIONAL RADIATION SAFETY POLICY 4-0302 RESEARCH December 2014 PURPOSE 1.01 The purpose of this policy is to formalize Oklahoma State University s (hereinafter
Oklahoma State University Policy and Procedures INSTITUTIONAL RADIATION SAFETY POLICY 4-0302 RESEARCH December 2014 PURPOSE 1.01 The purpose of this policy is to formalize Oklahoma State University s (hereinafter
The Alphabet Soup of Regulatory Compliance: Being Prepared for Inspections. Objectives. Inspections are often unannounced, so DOCUMENTATION
 The Alphabet Soup of Regulatory Compliance: Being Prepared for Inspections Linda Kroger, MS UC Davis Health System Objectives Recognize the various regulatory bodies and organizations with oversight or
The Alphabet Soup of Regulatory Compliance: Being Prepared for Inspections Linda Kroger, MS UC Davis Health System Objectives Recognize the various regulatory bodies and organizations with oversight or
NORTH CAROLINA A&T STATE UNIVERSITY Chemical Hygiene Plan
 North Carolina Agricultural and Technical State University OFFICE OF ENVIRONMENTAL HEALTH & SAFETY Safety Manual Subject: Chemical Hygiene Plan Number: 5-1 Date February 1, 2009 Amends: None Supersedes:
North Carolina Agricultural and Technical State University OFFICE OF ENVIRONMENTAL HEALTH & SAFETY Safety Manual Subject: Chemical Hygiene Plan Number: 5-1 Date February 1, 2009 Amends: None Supersedes:
TEMPLE UNIVERSITY ENVIRONMENTAL HEALTH AND RADIATION SAFETY
 Page 1 of 12 ISSUED: 6/94 REVISED: 06/07 Introduction: Purpose The purpose of this program is to ensure the protection of all employees from respiratory hazards through the proper use of respirators. Respirators
Page 1 of 12 ISSUED: 6/94 REVISED: 06/07 Introduction: Purpose The purpose of this program is to ensure the protection of all employees from respiratory hazards through the proper use of respirators. Respirators
Swedish Radiation Safety Authority Regulatory Code
 Swedish Radiation Safety Authority Regulatory Code ISSN: 2000-0987 SSMFS 2008:26 The Swedish Radiation Safety Authority s Regulations on Radiation Protection of Individuals Exposed to Ionising Radiation
Swedish Radiation Safety Authority Regulatory Code ISSN: 2000-0987 SSMFS 2008:26 The Swedish Radiation Safety Authority s Regulations on Radiation Protection of Individuals Exposed to Ionising Radiation
King Abdulaziz University Faculty of Dentistry. Radiology Policy & Procedure Clinical Manual
 King Abdulaziz University Faculty of Dentistry Radiology Policy & Procedure Clinical Manual October 2009 ORAL RADIOLOGY CLINICS DIVISION This division shall be operated by the radiology division of the
King Abdulaziz University Faculty of Dentistry Radiology Policy & Procedure Clinical Manual October 2009 ORAL RADIOLOGY CLINICS DIVISION This division shall be operated by the radiology division of the
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 911 AIRLIFT WING 911 AIRLIFT WING INSTRUCTION 40-102 22 JANUARY 2014 Certified Current, 28 FEBRUARY 2018 Medical Command RADIATION SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
BY ORDER OF THE COMMANDER 911 AIRLIFT WING 911 AIRLIFT WING INSTRUCTION 40-102 22 JANUARY 2014 Certified Current, 28 FEBRUARY 2018 Medical Command RADIATION SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
Formaldehyde Program. For Compliance with Federal and State Regulated Carcinogen Regulations
 Formaldehyde Program For Compliance with Federal and State Regulated Carcinogen Regulations Approved by Safety Committee April 20, 2017 Table of Contents PURPOSE... 1 AUTHORITY CITATIONS... 1 DEFINITIONS...
Formaldehyde Program For Compliance with Federal and State Regulated Carcinogen Regulations Approved by Safety Committee April 20, 2017 Table of Contents PURPOSE... 1 AUTHORITY CITATIONS... 1 DEFINITIONS...
LAW ON RADIATION PROTECTION AND SAFETY
 LAW ON RADIATION PROTECTION AND SAFETY I. GENERAL PROVISIONS Article 1 This Law shall regulate the system of control of all ionizing radiation sources, as well as the protection of population and environment
LAW ON RADIATION PROTECTION AND SAFETY I. GENERAL PROVISIONS Article 1 This Law shall regulate the system of control of all ionizing radiation sources, as well as the protection of population and environment
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER MACDILL AIR FORCE BASE MACDILL AIR FORCE BASE INSTRUCTION 48-100 23 JANUARY 2015 Aerospace Medicine INSTALLATION RADIATION SAFETY PROGRAM COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
BY ORDER OF THE COMMANDER MACDILL AIR FORCE BASE MACDILL AIR FORCE BASE INSTRUCTION 48-100 23 JANUARY 2015 Aerospace Medicine INSTALLATION RADIATION SAFETY PROGRAM COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
RMM # 500 Title: Designated Substances Control Program Approved: Karen Belaire Vice President, Administration
 McMaster University Risk Management Manual Submitted: Risk Management Support Group RMM # 500 Title: Designated Substances Control Program Approved: Karen Belaire Vice President, Administration Date: July
McMaster University Risk Management Manual Submitted: Risk Management Support Group RMM # 500 Title: Designated Substances Control Program Approved: Karen Belaire Vice President, Administration Date: July
MEDICAL-TECHNICAL SPECIALIST: BIOLOGICAL/INFECTIOUS DISEASE
 BIOLOGICAL/INFECTIOUS DISEASE Mission: Advise the Incident Commander or Section Chief, as assigned, on issues related to biological or infectious disease emergency response. Position Reports to: Incident
BIOLOGICAL/INFECTIOUS DISEASE Mission: Advise the Incident Commander or Section Chief, as assigned, on issues related to biological or infectious disease emergency response. Position Reports to: Incident
Title: Radioactive Material Storage
 Environmental Standard Operating Procedure Originating Office: Revision: Prepared By: Approved By: MCAS Miramar Environmental Original Waste Management Division William Moog Management Department File
Environmental Standard Operating Procedure Originating Office: Revision: Prepared By: Approved By: MCAS Miramar Environmental Original Waste Management Division William Moog Management Department File