Our Healthier South East London Consolidated Strategy. Draft v1.0 June 2015
|
|
|
- Elizabeth Waters
- 6 years ago
- Views:
Transcription

1 Our Healthier South East London Consolidated Strategy Draft v1.0 June 2015
2 Section Page No. Executive Summary 3 Purpose of the document 35 Introduction to south east London 38 Introduction to the Our Healthier South East London Strategy and the approach taken to developing it Stakeholder communications and engagement 45 The case for change 54 Vision for the future of health and care in south east London 62 Proposed model(s) of care: Delivering better care for our populations 65 Community Base Care Planned Care Maternity Children & Young People Urgent Emergency Care Model Cancer Benefits/ outcomes of achieving our vision 136 Financial impact and affordability 149 What is needed to deliver our vision? 154 Infrastructure & Estates Supporting Strategy Workforce Supporting Strategy Information Management and Technology Supporting Strategy Risks and challenges 169 Delivering the strategy 172 Appendices Commissioning Groups and NHS England Draft in progress 2
3 Draft in progress 3
4 Executive Summary Overview This executive summary provides an overview of the Our Healthier South East London Commissioning Consolidated Strategy. It will summarise and provide key highlights from the programme. This section provides: 1. Introduction and Purpose 2. Introduction to south east London 3. Introduction to the Our Healthier South East London Strategy and the approach taken to developing it 4. Stakeholder Communications and Engagement 5. The case for change 6. Vision for the future of health and care services in south east London 7. The strategy proposed model(s) of care: Delivering better care for our south east London populations 8. The approach to identifying the outcomes the strategy aims to achieve 9. Financial impact and affordability 10. What is needed to deliver our vision for south east London 11. Risks and Challenges 12. Delivering the strategy and next steps Commissioning Groups and NHS England Draft in progress 4
5 Executive Summary Introduction Purpose of this document In south east London, we have some very good health services. People are living longer and many people are healthier. But we also have some services that could be better. We have services that people find hard to access and some people do not get the help they need to keep themselves and their families well. We also have wide varieties in life expectancy and too many people die early from preventable diseases. Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark CCGs, working with NHS England as co-commissioner, are working in partnership with local authorities, local providers and other key stakeholders to define a five-year strategy for health and integrated care services across south east London. The strategy complements and builds on local work and has a particular focus on those areas where improvement can only be delivered by collective action or where there is added value from working together. It seeks to respond to local needs and aspirations, to improve the health of people in south east London, to reduce health inequalities and to deliver a health care system which is clinically and financially sustainable. The approach is commissioner led and clinically driven, and informed by wide engagement with local communities, patients and the public. It brings together the context of the south east London health and social care economy and details the potential initiatives that could be implemented to have transformational impact. Every CCG in the country is required to produce a strategy. In south east London, commissioners want to make sure that the strategy reflects local needs and aspirations. The first draft of the south east London strategy was sent to NHS England for review on 20 June This was a national deadline. The strategy runs for five years, so it is very much a work in progress. Through local and wider clinical and public engagement, potential ways to improve services have been identified, but considerable further work and engagement on the thinking and implementation of these plans is now taking place. This version has developed significantly since June 2014 and brings together the proposed initiatives and their potential impact. It remains a work in progress and is under review by a wide range of stakeholders. Commissioning Groups and NHS England Draft in progress 5
6 Executive Summary Introduction to south east London This commissioning strategy focuses on six NHS Clinical Commissioning Groups in south east London covering a population of approximately 1.8 million people: Bexley CCG Bromley CCG Greenwich CCG Lambeth CCG Lewisham CCG Southwark CCG Each of these CCGs works in partnership with a number of organisations and providers. In particular the key providers which the CCGs have worked with to develop the strategy are: King's College Hospital NHS Foundation Trust Guy's and St Thomas' NHS Foundation Trust Lewisham and Greenwich NHS Trust Dartford and Gravesham NHS Trust South London and Maudsley NHS Foundation Trust Oxleas NHS Foundation Trust Bromley Healthcare Community Interest Company To develop the best possible care models and interventions for the strategy it is important to understand the current health of the population of south east London. To do this a model called the Christmas tree was used. The segmentation model summarises the population segments which are detailed below: You can view the diagram on page 36. Approximately 16% of people in south east London are in the health and wellbeing group Approximately 50% of people in south east London are experiencing inequalities or putting their health at risk. For example this could be people who drink too much or don t take enough exercise or are living in poverty. Approximately 25% of people in south east London are in the early stages of long term conditions. For example, a long term condition could be, diabetes, poor mental health or high blood pressure. Approximately 9% of people in south east London are living with 3 or more long term conditions. Approximately 1% of people in south east London are at the end of their life Through understanding our population better the strategy is able to focus on developing care models and innovations that best address the needs of the people in south east London. A key component of this is to develop a strong foundation of Community Based Care to support people to live healthier lives and reduce the number of people exposed to risk factors either by birth or behaviour. A central part of the vison for the strategy is to be able to provide person centred care in a proactive and integrated way. In order to do this Local Care Networks are being developed across south east London. These Local Care Networks will deliver community based care to local populations through patient focused, proactive, accessible, coordinated services and through making every contact count. Further detail of Local Care Networks are provided in the following slides and on pages 66 onwards. Commissioning Groups and NHS England Draft in progress 6
7 Executive Summary Introduction to the Our Healthier South East London Strategy and the approach taken to developing the strategy This programme is led by the six NHS Clinical Commissioning Groups in the south east London with commissioners from NHS England (London), working in close partnership with local authorities, local providers of care and other partners. They have identified six priorities for improvement to deliver better care for the south east London population. These are referred to as Clinical Leadership Groups and focus on: Community based care Planned care Urgent and emergency care Maternity Children and young people Cancer The groups are formed from clinicians, commissioners, social care leads and other experts, Healthwatch representatives and other patient and public voices from across south east London. Each of these groups has developed a model of care which forms part of the integrated whole system model described on page 13. Each Clinical Leadership Group has developed a number of interventions and assessed the impacts of these interventions in terms of delivering improved quality, better and less variable outcomes for people across south east London, and that they provide value for money and support a sustainable whole system health and care economy. Aligning our Strategy with London and National Policy Agendas We know that a 'one size fits all' model will not work for the NHS, which is why we are responding to local needs. However, we have taken the insight, evidence and direction provided by London and national policy agendas and embedded this into our design. This includes the: NHS Five Year Forward view Better Health for London South east London leads are represented across the 13 London Transformation Programmes and our work is enabled by the learning from others and our collaborative work on a "once-for-london basis, where appropriate. Principles and governance In addition, as part of implementing and developing the strategy, the programme follows a number of principles which have been reflected in the governance and delivery structure. This structure entails the five key governance elements of the programme : Senior joint forum for strategic direction and decision making (equivalent to a Programme Board) the Clinical Commissioning Board Collaborative forum for partnership working the South East London Partnership Group Clinical forum to guide design work the Clinical Executive Group Delivery focused forum to manage design and implementation activities the Implementation Executive Group. Collective forum for patients and public voices to contribute to shaping the strategy s content Public and Patient Advisory Group Draft in progress 7
8 Executive Summary Stakeholder Communications and Engagement is a core part of the strategy development process Our approach to developing the strategy has been strongly focused around communicating and engaging and working in partnership with our stakeholders. Commissioners continue to design and develop the strategy with partners, patients, local people and key stakeholders, with thinking and planning being developed and amended through the engagement process. The strategy is clinically-led and developed, with over 300 clinicians, nurses, allied health professionals, social care staff, commissioners and others developing ideas through the six Clinical Leadership Groups. These Clinical Leadership Groups also include Patient and Public Voices and Healthwatch representatives to make sure that these voices are heard at all points in the development of the strategy. In addition to ensuring that patient and public voices feed directly into the Clinical Leadership Groups and supporting work streams, commissioners have been engaging widely from the beginning by building on existing local borough-level work. A series of deliberative events were held in June 2014, December 2014 and February 2015 looking at people s current experiences of care and particularly at the more recent events, how people s experiences might be enhanced in the future by these new models of care. Capturing feedback from engagement activities is systematic and transparent. All contributions are recorded and fed back into the strategy via programme managers - ensuring that local views influence strategy development. Examples of feedback and how it is being used are published via You Said, We Did reports which are published on the website as well as the full reports of deliberative events and other activity. Engagement and communication is led by Clinical Commissioning Groups via the Communications and Engagement Steering Group which has met at least monthly since May The group consists of Clinical Commissioning Groups Communications and Engagement leads. Leads from NHS providers and local councils have also been invited to attend. Engagement at local level and through local channels is on-going. This was primarily focused on the case for change during 2014, with a wider focus on the whole system model and emerging ideas in the spring of This included gathering patient stories and using materials developed by engagement partners, the Innovation Unit, Local engagement on the Issues Paper commenced in May A variety of methods have, and will be, used to gather the views of a broad spectrum of patients and the public. Activities will include: borough level deliberative events focus groups with specific communities utilising the existing mechanisms and opportunities identified through our Clinical Commissioning Groups engagement colleagues. Commissioning Groups and NHS England Draft in progress 8
9 Executive Summary There is a strong case for changing the way current health and care services are provided in south east London This strategy identifies that outcomes in south east London are not as good as they should be: The longer we leave these problems, the worse they will get. We therefore recognise that we all need to change what we do and how we do it. The case for change has identified and investigated these problems, helping to target our aims. Nine key issues have been identified as detailed below: Too many people live with preventable ill health or die too early About 11,000 people died prematurely across south east London between 2009 and 2011, with four of our boroughs being classed in the worst category for premature death in England. The outcomes from care in our health services vary significantly and high quality care is not available all the time Too often, the quality of care that patients receive and the outcome of their treatment depend on when and where they access health services. We don t always treat people early enough to have the best results Our services are often not set up to detect problems soon enough, meaning that people with long term conditions or mental illness often have to be admitted to hospital in crisis. People s experience of care is very variable and can be much better While patients are very happy with some services, surveys tell us that their experience of the NHS is inconsistent and that they do not always receive the care they want. Patients tell us that their care is not joined up between different services Patients and carers find it frustrating to have to continually provide the same information to different people. This is because different parts of the NHS do not always communicate effectively with each other or with social services The social care system is under increasing pressure Many Local Authorities are facing unprecedented pressures due to growing demand in some areas, with increasing numbers of older residents, residents living much longer with complex care and health needs and increased mental health needs. New laws and duties are also leading to additional implications and uncertainty for councils. The money to pay for the NHS is limited and need is continually increasing NHS funding currently increases in line with inflation each year. However, the costs of providing care are rising much faster because the NHS is now treating more people with more complex conditions than ever before and the costs of care often grow faster than consumer inflation It is taxpayers money and we have a responsibility to spend it well We know that by providing services in a different way, it is possible to improve outcomes, to help people to live healthier lives, to deliver services which are consistently of high quality and get more for our money South east London s acute, community and mental health providers face a similar and interrelated set of challenges and drivers Providers in south east London share key issues and drivers, such as workforce and regulatory requirements and London s ambulance service is facing increasing and changing needs for care. Commissioning Groups and NHS England Draft in progress 9
10 Executive Summary Vision for the future of health and care services in south east London To solve the problems outlined in the case for change, we have developed a collective vision for south east London. In south east London we spend 2.3billion in the NHS. Over the next five years we aim to achieve much better outcomes than we do now by: Supporting people to be more in control of their health and have a greater say in their own care Helping people to live independently and know what to do when things go wrong Helping communities to support one another Making sure primary care services are consistently excellent and have an increased focus on prevention Reducing variation in healthcare outcomes and addressing inequalities by raising the standards in our health services to match the best Developing joined up care so that people receive the support they need when they need it Delivering services that meet the same high quality standards whenever and wherever care is provided Spending our money wisely, to deliver better outcomes and avoid waste. Commissioning Groups and NHS England Draft in progress 10
11 Executive Summary The strategy proposes model(s) of care: to deliver better care for our south east London populations Care Model Design To develop the initiatives to focus on these aims, the Clinical Commissioning Groups and NHS England London region have identified the six Clinical Leadership Groups to deliver better care for our population. Each of these groups has developed a model of care which forms part of the integrated whole system model described on page 13. Each Clinical Leadership Group has developed a number of interventions and assessed the impacts of these interventions in terms of delivering improved quality, better and less variable outcomes for people across south east London and that they provide value for money and support a sustainable whole system health and care economy. Local Care Networks Local Care Networks are the centrepiece of the strategy and sit within Community Based Care. The Community Based Care Clinical Leadership Group aims to support people to live healthier lives and reduce the number of people exposed to risk factors either by birth or behaviour. For people with a long term condition, Community Based Care will take a rehabilitative/ re-ablement approach, supporting people to manage their own health positively, prevent deterioration wherever possible and reduce risks on these people. For those people with complex long term conditions or who are in the last year of life, support will be available to enable them to continue to lead as full and active life as possible. Community based care will be delivered through Local Care Networks. The services available will be proactive, accessible, coordinated and provide continuity; with a flexible, holistic approach to ensure every contact counts. This will be primary care delivered to geographically coherent populations, at scale, whilst still encouraging self-reliance. 24 local care networks are being developed to support whole populations across south east London. This will be a universal service covering the whole population cradle to grave. A local care network will involve primary, community and social care colleagues working together and drawing on others from across the health, social care and the voluntary sector to provide proactive patient centred care. Services will be delivered in ways that respond to the varied needs and characteristics of our communities. Clinical Leadership Group initiatives In addition to the Local Care Networks, each Clinical Leadership Group proposes further initiatives. These are summarised in the following slides. Commissioning Groups and NHS England Draft in progress 11
12 Executive Summary The Community Based Care Target Model The strategy sets out an agreed target model for local care networks that will deliver community based care. It is intended that each Local Care Network across south east London delivers the target model. However, the target model will have to be tailored to the local community that it serves. Integrated Single System Leadership and Management Serving geographically coherent populations between 50, ,000 Southwark Lambeth Lewisham Greenwich Bromley Bexley The Core (as a minimum all LCNs should encompass) Leadership team All general practices working at scale (federated with single IT system and leadership) All community pharmacy Voluntary and community sector Community nursing for adults and children Social care Community Mental Health Teams Community therapy Community based diagnostics Patient and carer engagement groups Working with Strong and confident communities Accessible hospital outpatient treatment clinics and acute oncology (urgent and emergency and cancer care) Specialist opinion (not face to face) and clear specialist service pathways Pathways to Multi Disciplinary Teams Integrated 111, London Ambulance Service and Out of Hours system (interface with Urgent care centres co-located with emergency department model) Housing, education and other council services Community based midwifery teams Private and voluntary sector e.g. care homes and domiciliary care Cancer services Children s integrated community team and short stay units Rapid response services Carers And there will be others.. Big hitters Supporting patients to manage their own health (Asset Mapping, Social Prescribing, education, community champions etc Prevention Obesity, Alcohol and Smoking Improved Core general practice access plus 8-8, 365 Enhanced call and recall improves screening and early identification and management of long term conditions Reduction in gap between recorded and expected prevalence in long term conditions Supporting vulnerable people in the community including those in care homes and domiciliary care Reduction in variation (level up) primary care management of long term conditions Reablement Admissions avoidance and effective discharge Multi Disciplinary Team configuration main long term conditions groups (incl. mental health) and Frail elderly End of Life Care Integrated Pathways of care Commissioning Groups and NHS England Draft in progress 12

13 Executive Summary Community Based Care delivered by Local Care Networks Commissioning Groups and NHS England Draft in progress 13
14 Executive Summary Our integrated whole system model Community Based Care delivered by Local Care Networks is the foundation of the integrated whole system model that has been developed for south east London. This diagram provides an overview of the whole system model, incorporating initiatives from all 6 Clinical Leadership Groups. Commissioning Groups and NHS England Draft in progress 14
15 Executive Summary Planned care model Key Features of the model 1 Standardisation Reducing variation across the planned care pathway from referral practice to discharge through to co-development of high level standards. 2 Diagnostics Person 2 Diagnostics 3 Elective Care Centres H Enhance patient management by GPs Rapid access to diagnostics for GP s Evidence based standardised Clinical pathways Shared results across the system supported by integrated IT systems 3 Elective Care Centres Provider collaboration to create centres of excellence for high volume specialities that drive up quality of service provision and improve outcomes for patients Orthopaedic (hips and knees) Ophthalmology 4 Pathway Review Urology Neurosurgery Nephrology Gynaecology Dermatology Commissioning Groups and NHS England Draft in progress 15
16 Executive Summary Maternity model Key Features of the model 1 Primary prevention and targeted wellness programmes within the Local Care Network 2 Assessment of pregnancy risk before 10 weeks to assign the most appropriate midwife team from the outset: 1. Local Care Network community based midwife teams for low risk 2. Specialist condition focused teams for high risk Person 1 Geographic midwife teams for low risk mothers 6 2 Condition focused midwife cohorts for high risk mothers 3 DAU & 24/7 Triage 5 H 4 3 Easy access to acute assessment clinic for unexpected problems during pregnancy and assessment unit for assessment of onset of labour 4 Culture of birthing units to encourage straightforward birth and improve the experience for low risk women 5 Achieve the London Quality Standards 6 Better co-ordination through postnatal and neonatal phase to improve mother and baby flows and experience 7 Smooth handover to Local Care Network with continuing advice and support on healthy choices. It is our intention that through this strategy we will meet the London quality standards. The above interventions aim to address this. Commissioning Groups and NHS England Draft in progress 16
17 Executive Summary Children and Young People model Key Features of the model 1 Primary prevention and wellness: Within the local care network, focusing on the well child. In the context of the family setting, looking after the child or young person s physical, social, emotional and mental well being. Person Children s Integrated Community Team 4 5 ACUTE CYP SS PAU H 2 Children s integrated community team delivering: A range of proactive services for children with long-term conditions and care needs Early intervention for acute illness and supported early discharge Management of short-term conditions Signposting and navigation through the system and navigate through the system 3 Extended GP hours For general practice from 8 to 8 With closer links to short stay paediatric units and emergency departments, to enable better co-ordination and to help prevent unnecessary hospital admissions To be delivered via the Community Based Care model. 4 Short stay paediatric units Designed to ensure that children and young people are returned to the community as quickly as possible and unnecessary hospital stays are avoided With close links with the Children s integrated community team 5 Planned care pathways With referral advice and guidance tools Specialist advice and support back into the community 6 Supported transition to adult services As part of community based care, within the local care network It is our intention that through this strategy we will meet the London quality standards. The above interventions aim to address this. Commissioning Groups and NHS England Draft in progress 17
18 Executive Summary Urgent and emergency care model Person A Rapid response Home Ward C Specialist Response Clinic B E D Enhance d Front Door H Key Features of the model Achieving the London Quality Standards in all areas: Acute medicine Emergency general surgery Emergency departments Critical care Fractured neck of femur A B C D Improving access in Primary Care, in hours and out of hours, to unscheduled care. GPs, UCC and ED functioning in a closely linked co-ordinated way; responsive community care, including specialist response teams, will prevent un-necessary hospital admissions with easy access to specialist advice for GPs as an alternative to ED referral 1. 8am 8pm 7 days a week 2. Standalone Urgent Care Centres with the same standards 3. Community based rapid access teams including a home ward. Specialist advice and referral 4. Access to specialist advice 5. Access to a specialist response clinic Improved 111 capability and LAS onward referral 6. LAS will be able to redirect to appropriate services, such as the rapid access team, home ward or hospital based specialist clinics and excel in navigating patients to the right part of the system are able to give advice, provide internal triage and coordinate onward referral to other parts of the system other than the ED An enhanced single front door to the Emergency Department. 8. Bringing together UCCs and the ED in a single governance structure and providing expert streaming across all sites E Emergency Department interface with Mental Health services 9. This will also allow for earlier identification of MH cases (including Dementia) reducing length of stay and enabling quicker streaming to specialities for mental health patients by having Psychiatric Liaison nurse (PLNs) and Triage joint assessments. 10. Quicker interface with specialist services like drug and alcohol 11. Quicker interface with under 18 mental health liaison teams Commissioning Groups and NHS England Draft in progress 18
19 Executive Summary Cancer model Key Features of the model A Primary prevention: Best delivered in the Local Care Network Early detection 1. Increased screening rates to national benchmark through targeted engagement 2. Diagnostics: Pilot project serious but unspecific symptoms pathway 3. Promotion of early diagnosis and equal access to treatment for older people 4. Professional development for all staff within Primary Care Person 4 End of Life 1 2 Early detection 3 Living with & Beyond Cancer Treatment H B C Treatment Provider collaboration to create networked centres of excellence: 5. Non complex cancer treatments and support closer to home 6. Access to appropriate information and support for patients and carers 7. Acute Oncology Services networked and supported by integrated IT 8. Consistently meet the access time scales on our cancer services 9. Routine use of the recovery package Living with and Beyond Cancer 10. Stratified follow-up 11. Support for people living with the adverse consequences of cancer treatments 12. Comprehensive support for carers 13. Psychological support for people living with Cancer 14. Inclusion of Cancer as a criteria for referral to exercise/physical activity on prescription schemes 15. Support to return to work, study or volunteering 16. Routine use of the recovery package D End of Life: Best Delivered in the Local Care Network 17. Ensure a dignified death irrespective of setting 18. Ensure consistent use of coordinate my care 19. Advance Care planning Commissioning Groups and NHS England Draft in progress 19
20 Executive Summary Approach to identifying the outcomes the strategy aims to achieve The primary aim of delivering the Our Healthier South East London strategy and vision is to develop ways to improve the health and care outcomes for south east London communities and people. A framework which sets out measures to monitor the impact of the strategy and interventions on outcomes has been developed through engaging with our partners across health and care providers, Public Health, clinicians and public and patients. This framework sets out the measures that demonstrate the effectiveness of the strategy in achieving the outcomes allowing us to quantify the strategy s impact. Focusing on the achievement of outcomes By implementing the strategy and its care models the aim is to reduce the variability in outcomes we see today as outlined in the case for change and to improve the overall health and care outcomes for people across south east London. Structure of the framework The framework is made up of the following core elements: Domains: The high-level grouping or classification of outcomes that are measuring similar things. There are a number of existing outcome frameworks which were reviewed and based on those frameworks, four domains that are common across them were selected. Outcomes: The overall impact of the strategy on the health and well-being of our populations and individuals in south east London Indicators: The measures selected to demonstrate the achievement of the outcome. These are as outcome focused as possible but in some cases a process/structure measure has been used as a proxy. Eight outcomes have been identified Preventing people from dying prematurely and can live longer and healthier lives Reducing differences in life expectancy and healthy life expectancy between communities People are independent, in control of their health, and able to access personalised care to suit their needs Health and care services enable people to live a good quality of life with their long term condition Treatment is effective and delivers the best results for patients and service users Delivering the right care, at right place, at the right time along the whole cycle of care Commitment to people having a positive experience of care Caring for people in a safe environment and protecting them from avoidable harm Indicators There are a number of indicators that have been identified and these are still undergoing review from stakeholders and Public Health Commissioning Groups and NHS England Draft in progress 20
21 System wide income/expenditure ( millions) Executive Summary The NHS faces a growing affordability challenge NHS funding currently increases in line with inflation each year. However, the costs of providing care are rising much faster because the NHS is now treating more people with more complex conditions than ever before and the costs of care often grow faster than consumer inflation. The NHS Five Year Forward View outlines a 30 billion financial challenge nationally by 2020/21. Consistent with this, in the absence of action, the scale of the affordability challenge in south east London is forecast to grow to over 1 billion by 2019/20. The graph to the right and the table below demonstrate how this challenge grows over this period. Local authorities, who are responsible for social care services, are also looking to save over 30% of their current expenditure over the next 3-4 years. Therefore we need to get better value for money for all that is done in the NHS and social care services. We need to get the best possible outcomes for patients and make the most of resources that are under increasing pressure. This means we need a more integrated approach between different services. 5,900 5,903 5,400 4,900 4,812 4,400 Expenditure (Do Nothing) Revenue 3, / / / / / / /20 Absolute challenge Annual challenge Percentage challenge Over the period from 2014/15 to 2019/20, the south east London expenditure (without efficiencies) will grow by just over 1 billion more than the projected budget of 5 billion. This is comparable with the 30 billion national challenge set out in NHS England s Five Year Forward View. On average, the south east London healthcare system will need to make efficiencies of 218m each year (from a budget which will grow to 4.8bn) between 2014/15 and 2019/20. An estimated breakdown is shown below. On average, the south east London healthcare system will need to make efficiencies of 4.2% each year between 2014/15 and 2019/20. An estimated annual breakdown is shown below. 14/15 15/16 16/17 17/18 18/19 19/20 14/15 15/16 16/17 17/18 18/19 19/20 251m 228m 154m 162m 141m 156m 6.0% 5.3% 3.4% 3.5% 3.0% 3.2% Commissioning Groups and NHS England Draft in progress 21
22 System wide income/expenditure ( millions) Affordability challenge ( millions) Executive Summary Closing the affordability challenge The graphs on this page demonstrates how the benefits from the programme can be combined with savings within individual organisations to close a substantial amount of the 1.1 billion affordability challenge. The benefits shown are as follows: 1. Programme central case (gross benefit): As described previously. 2. Provider efficiencies at 2.5%: The provider finance leads feel that a 2.5% CIP may be reasonable in addition to efficiencies generated through the programme. 1,200 1, , ,900 5, ,400 4,900 4,400 5,672 5,078 4,812 Expenditure (Do Nothing) Expenditure (Strategy) Expenditure (Residual) Revenue 3, / / / / / / /20 NB: Profiling of benefits shown above may significantly change as implementation plans are developed. It is important to note that both of these savings are presented gross of investment requirements (which total 90 million in the programme central case). It is expected that these investment requirements will, at least in part, be satisfied through additional funding requested through the Five Year Forward View and committed by the Government. Taking south east London s proportionate share of the 8 billion committed would imply that 248 million is available for this purpose. The resultant position is a 266 million affordability challenge for the South East London health care economy. Commissioning Groups and NHS England Draft in progress Affordability challenge (2019/20) Programme central case (gross benefit) Provider efficiencies at 2.5% 266 Residual challenge (2019/20)
23 Executive Summary Initial estimate of acute bed requirement Using historical NHS bed occupancy data for the acute providers and our projections of bed demand considering demographic/nondemographic growth assumptions we have estimated the bed gaps/increases show in the table below. We have modelled the impact of the strategy on overnight bed days to be a net reduction of 140,000 and a net increase in day case bed days of 25,000. This translates directly to a number of beds using various occupancy rates as shown in the table below. This only relates to acute beds and we would expect a proportion of this activity to be provided within community beds. Also note that the do nothing position does not reflect any potential reductions associated with QIPP delivery post 2014/15 plans or Better Care Fund related non-elective admission reductions. Baseline bed days/beds Strategic impacts bed days/beds 2013/14 Growth (2019/20)*** Gross change (2019/20) Net change (2019/20) Overnight Day case Total Overnight bed days 1,178, ,000 (339,000) (140,000) Overnight beds (current occupancy rates*) 3, (1,015) (414) Overnight beds (85% occupancy rates) 3, (1,092) (231) Day case bed days 181,000 30,000 (5,000) 25,000 Day case beds (current occupancy rates*) (15) 84 Day case beds (68% occupancy rates) (19) 235 Total bed days 1,359, ,000 (343,000) (115,000) Total beds (current occupancy rates*) 4, (1,030) (330) Total beds (revised occupancy rates****) 4,166 1,115 (1,111) 4 * Bed occupancy source: Bed occupancy for the year estimated using the average of KH03 quarterly returns from NHS England for Q4 2013/14 Q3 2014/15. (GSTT: 81%, KCHT: 94%, LGT: 94%, DGT: 95%, weighted average: 90.5%). ** These figures have been fixed at current occupancy levels and 2013/14 activity. *** These figures relate to a level of increased demand as shown above and an additional number of beds due to requiring lower occupancy levels. **** The total revised occupancy rates are blended across the inpatient overnight bed and day case bed rates shown earlier in the table. Commissioning Groups and NHS England Draft in progress 23
24 Executive Summary Summary of where we have reached in developing the strategy The aims of the consolidated strategy are to make a difference to the health and well-being outcomes of the people and communities in south east London and to create a sustainable health and care system as a foundation for the future. To date, the consolidated strategy brings together the case for change, the care models and their anticipated impacts on outcomes for the people and communities in south east London. This is combined with an assessment of the potential impact these models may have on how people use services and the extent to which it will support the future financial sustainability of the system. Taking into consideration growth assumptions over the next 5 years, and not changing our clinical models of care would mean that too many people would continue to be admitted to hospital where better Community Based Care models could provide improved outcomes. We have calculated the increase in bed capacity that would be needed across south east London to respond to the rise in population and aging population using our current approaches to delivering care. The projected demand would increase so much that the number of beds needed would be enough to fill a new hospital site and this is not possible or affordable. Applying the initial impact of the strategy s care models work on the projected demand levels for hospital beds, shows that by implementing the care models in the strategy, we would reduce the need for additional hospital beds by providing an alternative high quality model of care that is focussed on improved outcomes for the population we serve. This is because, The care models are focused on prevention and early intervention and keeping people healthy. Therefore keeping people out of hospital Community Based Care is the foundation of the whole system and is intended to keep people closer to home, treating them in the community and enabling people to only visit hospital when they really need to Pathways and professionals will be more integrated Productivity is expected to increase and there will be greater efficiency in the south east London system The plan will be for bed occupancy to meet the national guidance (which is not the case now) which will improve safety, quality and efficiency Recent programme updates include; The whole system affordability gap has been defined The Clinical Leadership Groups design guides are being finalised and potential impacts of the care models reviewed Supporting strategies of Estates, Workforce and IT continue to be developed Whilst the strategy programme has progressed a long way to achieve its aim, there is still much work to do Further work is required on Ensuring that progress and plans for the London Quality Standards are embedded into the strategy and exploring options on how they can be achieved Further developing the supporting strategies of Workforce, IM&T and Estates Refining the indictors for the Outcomes to make sure the best possible ones have been selected so we can measure the benefits or not of the strategy Engagement on the options appraisal methodology Ongoing communications and engagement Commissioning Groups and NHS England Draft in progress 24
25 Executive Summary How will we deliver the strategy? Part of the Clinical Leadership Groups work is to develop the plans to deliver the care models. In addition, three supporting strategies are being developed to support the overall delivery of the care models and changes at a whole system level. The three supporting strategies are Infrastructure & Estates Workforce Information Management and Technology Infrastructure & Estates The Estates Supporting Strategy is an essential element of the strategy programme to support the delivery of our new models of care in a way which ensures they deliver the outcomes we aim to achieve. We must understand the capacity of our capital assets, estates and facilities across south east London to utilise, reduce or develop these in the most appropriate way to meet the needs of our population. There is a clear synergy between the south east London need to reconsider estates and the national and London wide direction of travel. The five year forward view sets out an integrated agenda and new care models over the next five years. In addition, Better Health for London outlines the evidence base for re-evaluating the utilisation and value of NHS estate in London. (The Healthy London Partnership Estates Programme). Therefore, our Estates Supporting Strategy has made clear links with the work being delivered at a London wide level by the Our Healthy London Partnership - Estates Programme being led by London CCGs and NHS England. The Estates Supporting Strategy aims to address specific requirements that provide additional support to facilitate delivery of the strategy, building upon London wide programme delivery where the time scales allow. The estates strategy will be built into the delivery programmes for all models of care as appropriate and financial impacts further detailed within the Financial modelling. The three stages of the Estates Supporting Strategy is are as follows: Understanding the baseline Understanding the requirement Addressing the gap Commissioning Groups and NHS England Draft in progress 25
26 Executive Summary Workforce Better Health for London, the Five Year Forward View and Our Healthier South East London have all identified the need to focus on developing a modern workforce in order to support the delivery of innovative new models of care. Workforce is therefore a key enabler of the Our Healthier South East London strategy. The supporting strategy is identifying the key actions that should take place in order to move the workforce in south east London from where it is today to where it needs to be in the future. For instance, we know that the future care delivery will involve empowering patients and promoting independence; making every contact count; and fostering an environment where colleagues engage with each other rather than refer and handover. With these significant changes on the horizon, understanding what patients will require in the future and challenging existing ways of working will allow us to plan for a workforce that is fit for purpose and sustainable. The workforce supporting strategy will need to clearly articulate how the workforce is going to deliver what south east London needs. This will include new ways of working (i.e. flexibility, rotations, different staff groups doing different tasks to today, team work and collaboration) and different working locations (i.e. more staff working in the community as opposed to acute settings). For this purpose the programme has so far established: A baseline of the current workforce A methodology to define characteristics of the required new workforce These will support the next steps which will take the workforce where it needs to be in the future. These steps include: Articulating the workforce strategy Reaching out to the workforce Commissioning Groups and NHS England Draft in progress 26
27 Executive Summary Information Management & Technology Information and IT will be a key enabler for the strategy. Specifically, it can support staff in new ways of working and empower patients to be active participants in their care. Key considerations for understanding the IM&T requirements to support the strategy and any gaps are: National and London initiatives and policies: There are a number of National and local initiatives and policies that may support the implementation of the strategy. CCG IM&T strategies: Each CCG has its own IM&T strategy and implementation plans, which have been reviewed and initial assessments made to determine support for the strategy. Identifying uniformities at a south east London level so there are consistent ways of working. For example, adopting the same data quality standards, and staff identification processes for who should be viewing/editing data and design principles Gaps and any investment costs: Understanding where these are not currently accounted for in CCG and or provider plans, and are needed to implement the strategy. A primary requirement to enable the strategy is for health and care systems across south east London to be interoperable Why is interoperability Important? Interoperability is important because it will enable south east London health information systems and professionals to work together within and across organizational boundaries in order to more effectively deliver healthcare to people and communities. Key ways in which interoperability will support the delivery of the vision and care models in the consolidated strategy are: Care Quality Improves the quality of patient care by providing access to complete, accurate, timely information in one location. Provides visibility into the whole patient by sharing basic medical information across a patient s care providers Care Efficiency Saves time previously used to look for information, i.e. lab results, or repeat tests that have already been performed in another care setting Patient Safety Makes life-saving information available 24-hours-a-day for clinical decision support Our findings so far indicate that primary key requirements of interoperability between GP systems and primary and secondary care are planned and/or being implemented at various speeds. All CCGs are moving to GP systems that will enable sharing of records across GP practises supporting Local Care Networks and will be interoperable with acute To various extents CCGs have plans in place to align with some of the key IT/Digital guidance in the 5YFP IT/Digital, London Transformation Programme, 2020 Personalised Health and Care and Implementing these guidelines would meet many of the strategy requirements. However, additional transformation initiatives that may require agreement and funding at a south east London level have not been explored or agreed at this stage. Commissioning Groups and NHS England Draft in progress 27
28 Executive Summary There are risks to delivering the Strategy which are closely monitored and assessed for impact The following high level risks have been identified to the implementation of the strategy. This list will be reviewed regularly through the Clinical Executive Group, Implementation Executive Group and Clinical Commissioning Board. Title Risk Impact Mitigations 1. Information Systems 2. Workforce Capability 3. Delivery Timeframe 4. Delivery Timeframe Lack of integrated or interoperable information systems undermines ability to integrate services across the health system in south east London Existing workforce skills or capability to deliver new models of care It may be challenging to complete required activities and assurances in time to go to consultation, if required, in December, particularly as a result of needing to engage patients and service users in the process Insufficient time for good processes in terms of governance, decision making and ownership Possible duplication of system, process or information, resulting in poorer patient experience, poor quality of services across integrated pathways and additional cost New models of care may not be implemented Services may not be delivered safely Patient satisfaction Staff satisfaction issues Quality and effectiveness of care Delay to programme implementation for those elements which might require formal consultation or loss of support from partners and stakeholders for some or all of the strategy The strategy and associated documents are not owned by all stakeholders across SEL IM&T supporting strategy workstream established. Utilising existing integration initiatives across SEL to support strategy Workforce supporting strategy workstream established Work in hand to identify gaps between capabilities required to deliver new models of care and those available in current workforce Key characteristics and skills being identified for training purposes On-going dialogue with NHSE to agree assurance process and detailed communications and engagement plan to test critical path We will maintain four key activities: intensive engagement with partners and stakeholders; ensuring NHS England is engaged; careful mapping of governance and decision making; and meeting with NHSE by mid-june to review the approach Commissioning Groups and NHS England Draft in progress 28
29 Executive Summary Title Risk Impact Mitigations 5. Clinical Leadership Group Impact Analysis Modelling: Finance and Activity The impact analysis does not fully close the identified affordability gap but does make significant progress towards doing so. It is not yet clear if this is sufficient Explore and incorporate additional QIPP and CIP opportunities and continue to explore options with NHSE 6. Financial sustainability of health system 7. Patient / Public Resistance to Change New service models do not deliver reduced demand for hospital care or hospital capacity does not reduce in line with demand If partners and stakeholders are not sufficiently engaged throughout the development of the five year strategy or if the case for change is not sufficiently convincing - any proposed service change could be subject to significant local opposition Potential increased system costs through duplication of services System may not be sustainable Further engagement required Possible legal challenge Delays to implementation of changes leading to increased cost and delay Need to amend strategy in response to concerns Making sure there are clinical input into the design of care models and that they have sufficient impact on activity Engagement activities will be undertaken with a broad range of partners and stakeholders throughout the development and implementation of the strategy Dedicated communications and engagement enabling workstream to coordinate these activities Patient and Public voices in all key groups to help shape strategy Strategy reflects input from partners and stakeholders Commissioning Groups and NHS England Draft in progress 29
30 Executive Summary Delivering the strategy and next steps A number of interventions have been defined and agreed and now the strategy programme must start to consider how these will be implemented and delivered. For most interventions implementation planning can commence immediately. There are some interventions where care model delivery options need to be considered. These interventions will have to undergo a robust options appraisal process. Implementation planning The development and implementation of the strategy has involved consideration of options for care model design from the outset. This is an iterative process which reviews the range of interventions to produce best outcomes for south east London. It considers ways to formulate the care models to produce these best outcomes based on a range of qualitative and quantitative evidence. Implementing some of the interventions will require consideration of care model delivery options and these will either be implemented at a local level or at a south east London level. It is proposed that the filtering of options will occur through two gateways of assessment against criteria; hurdle criteria and evaluation criteria (the diagram on the following page provides an overview of the methodology). The criteria against which the options will be assessed will be agreed before commencing the appraisal. Moreover, the likelihood of optimal implementation of options is increased by gathering wide ranging stakeholder contribution to the formation and specificity of criteria. Although some interventions do not in their own right require a detailed options appraisal (those that start implementation planning), the result of implementing those interventions could impact on the appraisal of other interventions because they will lead to shifts in settings of care and volumes of activity. As a result, it is important to consider the scope of a detailed options appraisal and how to account for whole system changes within the appraisal of individual interventions.. Options appraisal process This approach aims to identify the best way or way(s) of delivering the overarching strategy and realise its full benefits. It filters the many potential options for how the system can be implemented and is designed to identify options that are recommended for further work. Commissioning Groups and NHS England Draft in progress 30
31 Executive Summary Options for appraisal methodology Case for Change Agreed whole system outcomes Finance and activity baseline Future demand and funding envelope Current health outcomes Proposed care models and interventions Agreed scale of affordability challenge Options appraisal Evaluation Criteria: These will be used to develop a short list of options. They will be used to assess the options in terms of impact and feasibility, helping to identify realistic options and those with potentially the best outcomes. Model the interventions Activity shifts identified through a triangulation process using benchmarking, academic evidence and clinical judgement Define scope Agree hurdle and evaluation criteria Estate and service baseline Apply hurdle criteria Hurdle Criteria: Tests that options either pass or fail. They provide a sense check of the full list of options, identifying options that are feasible. Long List Apply evaluation criteria Short List CLG consideration of options for delivery leading to agreed care models and interventions Split interventions by implementation or options appraisal Implementation planning Commissioning Groups and NHS England Draft in progress 31
32 Executive Summary High level programme plan The high level plan on the next page shows at high level the next stages of the plan for implementation, option appraisal and consultation if required. It is ambitious and dependent on partners and key stakeholders continuing to engage with and support the work as it develops. Over the next few weeks, CCGs will be testing this with their governing bodies and membership and with key partners and stakeholders. There will be a formal stocktake in late July and the plan will be confirmed or amended. Further stocktakes will be scheduled as appropriate. The case for change is pressing and there is much that can be implemented at pace, but it is important to keep the high levels of engagement and support which we have had so far. Commissioning Groups and NHS England Draft in progress 32
33 Key Outputs Key Activities Executive Summary High level programme plan Phase 1 (January May 2015) Phase 2 (May August 2015) Programme Plan Phase 3 Phase 4 Phase 5 (September November 2015) (December 2015 March 2016) (April September 2016) Phase 1 Phase 2 Phase 3 Phase 4 Phase 5 Further refinement of the Whole System Model and the models of care, including testing with providers, partners and wider stakeholders Building greater detail into the care models so their impact can be modelled Modelling expected impacts for providers and commissioners Further development of the supporting strategies Clinical model implementation Workshops CO discussion on commissioner models, Provider and CLG Identification of potential for significant service change. Create options appraisal methodology Develop options Appraise options Modelling to support option appraisal and decision making Short list of options Further support to implementation Continued work with partners to ensure ownership and wider engagement to test and develop Development of business cases. There will need to be agreement as to the business cases required and who will lead them (commissioners or providers). Modelling to support development/review of business cases Decisions making processes for business cases Continued wide engagement Implementation and continuous quality improvement Any consultation, if required. Note: In the event that consultation is not required, and for any elements of implementation where consultation is not required, the timetable will be shortened, but for planning purposes this paper assumes that there will be some formal consultation, although the subject of such consultation has yet to be established. Conclusion of any consultation Further modelling if required Decision making Implementation Continuous quality improvement Detailed implementation plan Presentation to NHSE Provider outline of steps required to operationalise the Whole System Model Development of the supporting strategies Equality Impact Assessment Modelling Impact Assessment Publish Equalities Impact Assessment and action plan Refinement of implementation plan Options analysis Refinement of detailed implementation plan Gateway review Business Case sign off Monitoring, evaluation, reporting and improvement frameworks established Live implementation and continuous quality improvement Governance Groups Comms & Engagement Finance & Modelling Continuous input throughout the process with regular meetings Continued aligned plan to ensure the programme continues with a high level of engagement Modelling to establish the baseline position, required investment and quantify benefits to be realised Supporting Strategies Continue the commissioning framework, LCN, workforce, IM&T systems and estates configuration needed to realise the change Commissioning Groups and NHS England Draft in progress 33
34 Full Strategy Section Page No. Purpose of the document 35 Introduction to south east London 38 Introduction to the Our Healthier South East London Strategy and the approach taken to developing it Stakeholder communications and engagement 45 Case for change 54 Vision for the future of health and care in south east London 62 Proposed model(s) of care: Delivering better care for our populations 65 Benefits/ outcomes of achieving our vision 136 Financial impact and affordability 149 What is needed to deliver our vision? 155 Risks and Challenges 179 Delivering the strategy 172 Appendices Draft in progress 34
35 Draft in progress 35
36 Purpose of the document Introduction In south east London, we have some very good health services. People are living longer and many people are healthier. But we also have some services that could be better. We have services that people find hard to access and some people do not get the help they need to keep themselves and their families well. We also have wide varieties in life expectancy and too many people die early from preventable diseases. Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark CCGs, working with NHS England as co-commissioner, are working in partnership with local authorities, local providers and other key stakeholders to define a five-year strategy for health and integrated care services across south east London. The strategy complements and builds on local work and has a particular focus on those areas where improvement can only be delivered by collective action or where there is added value from working together. It seeks to respond to local needs and aspirations, to improve the health of people in south east London, to reduce health inequalities and to deliver a health care system which is clinically and financially sustainable. The approach is commissioner led and clinically driven, and informed by wide engagement with local communities, patients and the public. Purpose of this document It brings together the context of the south east London health and social care economy and details the potential initiatives that could be implemented to have transformational impact. Every CCG in the country is required to produce a strategy. In south east London, commissioners want to make sure that the strategy reflects local needs and aspirations. The first draft of the south east London strategy document was sent to NHS England for review on 20 June This was a national deadline. The strategy runs for five years, so it is very much a work in progress. Through local and wider clinical and public engagement, potential ways to improve services have been identified, but considerable further work and engagement on the thinking and implementation of these plans is now taking place. This version has developed significantly since June 2014 and brings together the proposed initiatives and their potential impact, but it remains a work in progress and is under review by a wide range of stakeholders. Commissioning Groups and NHS England Draft in progress 36
37 Purpose of the document Overview This document sets out: 1. Introduction to south east London 2. Introduction to the Our Healthier South East London Strategy and the approach taken to developing it 3. Stakeholder Communications and Engagement 4. The case for change 5. Vision for the future of health and care services in south east London 6. The strategy proposed model(s) of care: Delivering better care for our south east London populations 7. Benefits/outcomes of achieving our vision 8. Financial impact and affordability 9. What is needed to deliver our vision? 10. Risks and Challenges 11. Delivering the strategy 12. Appendices This document steps through each of the above sections. Firstly providing context and an overview of the programme, before detailing the reasons for the strategy and the initiatives developed to support this. Commissioning Groups and NHS England Draft in progress 37
38 Draft in progress 38

 and is made up of 44 local GP practices NHS Bexley CCG: services 238,446 (in 2014) NHS Bromley CCG: Services 320,460 (in 2014) and is made up of 47")
39 Introduction to south east London Overview of the NHS in south east London There are a number of organisations across south east London who commission and deliver health services. These are summarised below: Commissioning organisations There are 6 Clinincal Commissioning Groups in south east London. These organisation are co-terminus with London Boroughs and commission the majority of services people receive. The CCGs are: NHS Greenwich CCG: 265,995 (in 2014) and is made up of 44 local GP practices NHS Bexley CCG: services 238,446 (in 2014) NHS Bromley CCG: Services 320,460 (in 2014) and is made up of 47 local GP practices. NHS Southwark CCG: Services 302,290 (in 2014) and is made up of 44 local GP practices. NHS Lambeth CCG: Services 317,738 (in 2014) and is made up of 47 local GP practices. NHS Lewisham CCG: Services 289,794 (in 2014) and is made up of 44 local GP practices South London and Maudsley NHS Foundation Trust (Mental Health) Oxleas NHS Foundation trust (Mental Health) In addition to the organisations set out above people in south east London receive care from a number of other organisations including NHS trusts located in other areas, community health providers and third sector organisations. Main acute and mental health providers There are a number of provider organisations located in and delivering health services in south east London. These include: King's College Hospital NHS Foundation Trust Guy's and St Thomas' NHS Foundation Trust Lewisham and Greenwich NHS Trust Commissioning Groups and NHS England Draft in progress 39
40 Introduction to south east London Population of south east London For south east London, we have used a segmentation model to understand the population: Public Health have developed a model of the south east London population based on the use of the Kernow Model of population demographics developed in Cornwall and a well evidenced Scottish model of long term conditions prevalence. The south east London population has been segmented here to show those people living healthy lives, those with risks of developing long term conditions and those who are living with long term conditions. These segments of the population are demonstrated, based on their size, as the segmentation model. Community Based Care (CBC) aims to support people to live healthier lives and reduce the number of people exposed to risk factors either by birth or behaviour. For people with a long term condition Community Based Care will take a rehabilitative/ reablement approach supporting people to manage their own health positively, prevent deterioration wherever possible and reduce risks on these people. For those people with complex long term conditions or who are in the last year of life, support will be available to enable them to continue to lead as full and active life as possible. Community Based Care will be delivered through Local Care Networks. The services available will be proactive, accessible, coordinated and provide continuity; with a flexible, holistic approach to ensure every contact counts. This will be primary care delivered to geographically coherent populations, at scale, whilst still encouraging self-reliance. EoL Early (1%) stages of LTC (25%) 3+ LTC (9%) Early stages of LTC (25%) People experiencing inequalities or putting their health at risk (50%) Health and wellbeing group (16%) Costs People with multiple complex needs where standard services are not effective who need personalised care Note: Total equals 101% due to rounding Draft in progress 40
41 Draft in progress 41
42 Introduction to the Our Healthier South East London Strategy and the approach taken to developing it Overview of the programme Our Healthier South East London is a five year commissioning strategy which aims to improve health, reduce health inequalities and ensure all health services in south east London meet safety and quality standards consistently whilst being sustainable in the longer term. The way health services are delivered needs to change in order to meet the emerging needs of an ageing population in which many more people live with long term conditions. This means that more resources must be directed towards services based in the community, keeping people out of hospital unless they really need to be there. Commissioners have already made progress on improving care outside hospital in south east London, and the strategy aims to build on that by delivering better integrated care outside hospital, meaning less care delivered in hospitals and more in the community. For this purpose, six priorities for local healthcare have therefore been identified for improvement. These are: Community based care Planned care Urgent and emergency care Maternity Children and young people Cancer The programme is being shaped by six Clinical Leadership Groups (one for each of the priorities above). Each of these groups includes clinicians, commissioners, social care leads and other experts, Healthwatch representatives and other patient and public voices from across south east London. Each of these groups has developed a model of care which forms part of the integrated whole system model described on page 64. Each Clinical Leadership Group has developed a number of interventions and assessed the impacts of these interventions in terms of delivering improved quality, better and less variable outcomes for people across south east London and that they provide value for money and support a sustainable whole system health and are economy NHS Five Year Forward View and Better Health for London We know that a 'one size fits all' model will not work for the NHS, which is why we are responding to local needs. Our vision for the future is also in line with the NHS Five Year Forward view and the aspirations and recommendations of the London Health Commission.(Better Health for London) The NHS Five Year Forward View starts the move towards a different NHS, recognising the challenges and outlining potential solutions to the big questions facing health and care services in England. The London Health Commission (now known as Better Health for London) in November 2014 reported ten aspirations for the capital, with the main aim of making London the healthiest major city in the world. The report made a series of recommendations, including measures to tackle childhood obesity, encouraging healthier lives, better support for people with mental illness, improving GP access and more community support for people with long term conditions. Commissioning Groups and NHS England Draft in progress 42
43 Introduction to the Our Healthier South East London Strategy and the approach taken to developing it Programme Principles For the purposes of identifying and implementing this strategy, the Commissioning Strategy Programme approach has been based on the following principles, which have additionally been reflected in the governance and delivery structure: Being based on local needs and aspirations, listening to local voices and building on work at borough level, whilst taking into account national and London policies Focusing on improving health outcomes and reducing inequalities Employing a strong partnership approach, led by NHS commissioners and involving closely a wide range of local partners, including patients and communities, local authorities and NHS partners, to build agreement on priorities, strategic goals and outcomes Creating solid foundations by ensuring all stakeholders have a common understanding of the scale of the challenge and then a shared vision and ambition for the next five years Being open and transparent throughout the process, from identification of need, to implementation of the strategy Engaging broadly, building on existing borough-level work with wider engagement activity to complement this as appropriate Programme governance structure The Commissioning Strategy Programme governance has been designed to sit within the existing governance and decision making structures of the CCGs and NHSE. It also provides new formal forums to undertake the five key governance elements of the programme: Senior joint forum for strategic direction and decision making (equivalent to a Programme Board) the Clinical Commissioning Board Collaborative forum for partnership working the South East London Partnership Group Clinical forum to guide design work the Clinical Executive Group Delivery focused forum to manage design and implementation activities the Implementation Executive Group. Collective forum for the patients to contribute to shaping the strategy s content Public and Patient Advisory Group These functions are supported by a programme management structure to support clinical design and implementation activities. The Clinical Commissioning Board provides the link between programme governance and business as usual governance within commissioning bodies: NHS England governance for direct commissioning and the CCG Governing Bodies. Working with the Health and Wellbeing Board in each borough. The Clinical Commissioning Board currently reports via the existing Clinical Strategy Committee to the CCG Governing Bodies, who are responsible for making formal decisions in public relating to the proposed Commissioning Strategy. The CCGs have now proposed to establish a committee in common for Strategic Decision Making for collaborative decision making on strategic issues. This arrangement also provides the link, through existing local arrangements, to the Health and Wellbeing Boards to ensure alignment with their strategies and obtain agreement for Commissioning Groups and NHS England the Better Care Plans. Draft in progress 43
44 Introduction to the Our Healthier South East London Strategy and the approach taken to developing it Overview of the programme The diagram below summarises the governance structure for the five year commissioning strategy. However, it should be noted that a Committee in Common is currently being proposed as an additional decision making body. Commissioning Groups and NHS England Draft in progress 44
45 Draft in progress 45
46 Stakeholder Communications and Engagement South east London providers and partners Working on behalf of the six CCGs and NHS England, the programme engages and works in partnership with a wide range of stakeholders and organisations. Providers Across south east London the six CCGs work with seven main providers as demonstrated on slide 31. These are: King's College Hospital NHS Foundation Trust - a local and specialised acute hospital Guy's and St Thomas' NHS Foundation Trust - local and specialised acute hospital focusing on residents of Lambeth and Southwark Lewisham and Greenwich NHS Trust a local acute hospital with some specialised acute services and community care services Dartford and Gravesham NHS Trust a local acute trust South London and Maudsley NHS Foundation Trust a mental health trust focusing on residents of Lambeth, Lewisham and Southwark Oxleas NHS Foundation Trust a mental health trust focusing on residents of Bexley, Bromley and Greenwich Bromley Healthcare Community Interest Company In addition to the six acute providers there are also: GP practices Voluntary and third sector organisations Local authority social care services England and London wide partners The CCGs also work closely with NHS organisations in London and across England These organisations include: London Ambulance Service Department of Health NHS England Neighbouring CCGs NHS South East Commissioning Support Unit Public Health England Local authority partners The CCGs have strong partnerships with local authorities to take into account the various health and wellbeing groups that operate within local authorities. Commissioning Groups and NHS England Draft in progress 46
47 Stakeholder Communications and Engagement Overview and approach Our approach to developing the strategy has been strongly focused around communicating and engaging and working in partnership with our stakeholders. Commissioners continue to design and develop the strategy with partners, patients, local people and key stakeholders, with thinking and planning being developed and amended through the engagement process. The strategy is clinically-led and developed, with over 300 clinicians, nurses, allied health professionals, social care staff, commissioners and others developing ideas through the six Clinical Leadership Groups. These Clinical Leadership Groups also include Patient and Public Voices and Healthwatch representatives to ensure that a patient voice is heard at all points in the development of the strategy. In addition to ensuring that patient and public voices feed directly into the Clinical Leadership Groups and supporting work streams, commissioners have been engaging widely from the beginning by building on existing local borough-level work. A series of deliberative events were held in June 2014, December 2014 and February 2015 looking at peoples current experiences of care and particularly at the more recent events, how peoples experiences might be enhanced in the future by these new models of care. Capturing feedback from engagement activities is systematic and transparent. All contributions are recorded and fed back into the strategy via programme managers - ensuring that local views influence strategy development. Examples of feedback and how it is being used are published via You Said, We Did reports which are published on the website as well as the full reports of deliberative events and other activity. Engagement and communication is led by CCGs via the Communications and Engagement Steering Group which has met at least monthly since May The group consists of CCG Communications and Engagement leads. Leads from NHS providers and local councils have also been invited to attend. Engagement at local level and through local channels is on-going. This was primarily focused on the case for change during 2014, with a wider focus on the whole system model and emerging ideas in the spring of This included gathering patient stories and using materials developed by engagement partners Innovation Unit, Local engagement on the Issues Paper commenced in May A variety of methods have, and will be, used to gather the views of a broad spectrum of patients and the public. Activities will include: borough level deliberative events focus groups with specific communities utilising the existing mechanisms and opportunities identified through our Clinical Commissioning Groups engagement colleagues. Commissioning Groups and NHS England Draft in progress 47
48 Stakeholder Communications and Engagement Direct involvement of patient and public voices Patient and public voices (PPVs) and Patient and Public Advisory Group (PPAG) Patient and public voices have been involved in the Clinical Leadership Groups since June Each of the Clinical Leadership Groups has at least three patient and public voices and one Healthwatch representative, who are supported by the Patient and Public Voice Project Manager and the Programme Manager in each area. The PPVs come together in a Patient and Public Advisory Group (PPAG) forum for peer support and to strengthen public and patient voices across the strategy, which meets every 6-8 weeks. The PPAG enables members to explore a range of issues not covered within the individual Clinical Leadership Groups; review key draft documents from the south east London commissioning strategy programme, advising on clarity of message and the development of plain English versions; and contribute to engagement plans and activities, complementing the advisory role of the South East London Stakeholder Reference Group. The PPAG has undertaken a number of deep dive sessions into each of the Clinical Leadership Groups, the workforce supporting strategy, whole systems model and whole systems outcomes enabling members to contribute to all the areas of the programme. The PPAG has also reviewed the first Equalities Impact Assessment and identified priority areas for the next Equalities Analysis. PPAG has formed a reading group to review public facing documents to ensure that the language is suitable for the public to understand. This has included the Case for Change summary for the programme; website; the Issues Paper; and newsletters. Changes were made to all of these documents following feedback from the Reading Group, including the addition of questions to the Frequently Asked Questions (FAQ) list; changes to terminology; reordering of contents; use of simpler English; and addition of information. The Patient and Public Advisory Group members themselves suggested that we should not rely wholly on the Reading Group. We have therefore committed to ensuring that key materials will be sent to the external Plain English campaign to be kite-marked with their plain English mark, although this will depend on timescales and other practical considerations. Members of PPAG have been involved in discussions to shape the short film to introduce Our Healthier South East London and have been included in the film itself. They have also been involved in the procurement of: external support for the programme and for workforce development. Commissioning Groups and NHS England Draft in progress 48
49 Stakeholder Communications and Engagement Wider engagement Early engagement activities and feedback - Case for Change for south east London The early public engagement on the strategy focused on testing the draft case for change via CCG engagement routes. The Case for Change was developed by local clinicians, social care and public health professionals. It looked at the most important health issues for people in south east London. It is based on local needs and aspirations and builds on work carried out already at borough level, while also taking into account national and London-wide policies. Dedicated engagement events: Wider testing of the work of the Clinical Leadership Groups and the overall shaping of the strategy has also been carried out to further test developing ideas. These have included: Deliberative events (June 2014) Two south east London-wide engagement events involving more than 100 invited representatives of voluntary and public stakeholder groups, the public and patients The events were led by clinicians, social care professionals and CCG commissioning leads. Rich feedback was provided and participants welcomed the overall direction of the strategy. Detailed feedback was gathered and used directly to shape strategy development and engagement. The headline reports from these meetings are available at Key messages and comments included: Participants agreed with most of what they had seen of the draft strategy. A need for more detail on some of the aims was expressed, with helpful suggestions for additional focus areas Participants broadly agreed the case for change reflected their experiences. Participants broadly agreed with the strategy s clinical themes which they explored. However it was felt that there is a need for further detail and more focus on certain elements. Additional helpful suggestions were made. Participatory workshops (December 2014 and February 2015) Four workshops were held across south east London - for the boroughs of Lambeth and Southwark; Bromley; Bexley; and the boroughs of Greenwich and Lewisham. 110 people participated across the four workshops. The aims of the workshops were to: Familiarise people with the purpose and main messages of the strategy Listen to people s experiences and thoughts about current services Gather feedback on behalf of the programme team to be fed into the further development of the strategy Commissioning Groups and NHS England Draft in progress 49
50 Stakeholder Communications and Engagement The events were led by CCG chief officers and the programme team. A number of members of the programme s Public and Patient Advisory Group attended. Detailed feedback was gathered and four overarching themes connected all the comments: Person-centred care: people talked about the importance of building relationships of trust with health and care professionals, of getting support that takes account of their wider health and social needs, of feeling listened to and respected Seamless and continuous care: people talked of the lack of coordination between services and the need for better ways of sharing information about patients and connecting provision, so that patients do not have to knock on multiple doors to get the right help, or indeed fall into gaps between services The importance of support networks in the community: being connected to networks of support in the community makes a vital difference on people s health, quality of life and how much they need to rely on formal health and care services The need for better information and signposting: people recognised that there is a wealth of services, which are perhaps not being used to their full potential because of lack of clarity on what is available and how to access it, from alternative options to ambulance and A&E, to support services in the community. All of this feedback has been shared with the programme and the Clinical Leadership Groups to consider as part of the development of the plans. Reports on these are available including format, agenda and responses and can be found in Appendix C Market research: An independently-run telephone survey with a representative sample of local populations to gain deeper insight into local people s views on priority areas for the strategy s Clinical Leadership Groups was carried out in July and August This was supplemented with more in-depth face-to-face surveys with groups of people with those protected characteristics for which it would not be realistic to obtain a statistically valid sample through the telephone survey. These individuals were contacted via local community groups and surveyed in July and August 2014 via in-depth interviews by an independent research company. This research fed into the development of the programme s Clinical Leadership Groups to consider as part of the development of the strategy and the emerging clinical models. A report on findings can be found in Appendix C. Commissioning Groups and NHS England Draft in progress 50
51 Stakeholder Communications and Engagement Community research A number of drop-in sessions were held during November and December 2014 with the aim of talking to people in different groups about their experiences of care, to provide richer insights to support the work that Clinical Leadership Groups are doing to design new models of care. The sessions focused on maternity, children and young people, urgent care and Local Care Networks. 5 November Community research with new or expectant parents. Drop-in session at Northend Children s Centre, Bexley 6 November Community research with new or expectant parents. Drop-in session at St Augustine s Children s Centre, Bexley 11 November Community research with people with cancer a drop-in session at Greater London Support Group (part of Prostate Cancer Support Federation), Lambeth 13 November Community research with families, children and young people. Drop-in session at Kaleidoscope, Lewisham 25 November - Community research with people with cancer a drop-in session at St Christopher s Hospice, Bromley 29 November Community research with families, children and young people. Drop-in session at Lewisham paediatric A&E 8 December Community research with people with cancer. Drop-in session at Waterloo Action Centre, Lambeth Altogether 59 people and families were involved in this research, representing a range of backgrounds. The key insights about what excellent services look and feel like and what outcomes are most valued have been used as part of the Care Design Guides produced by the Clinical Leadership Groups, which set out proposed models and interventions. The research also led to the development of a set of case studies showing current patient journeys and key points where the future journey will improve the health and the experience of patients. These case studies are being used in on-going engagement work and have been used to bring the abstract ideas to life. In-depth case study research Alongside the drop-in sessions, a number of detailed case studies were produced to be used by Clinical Leadership Groups to explore what their planned models might mean for patients; and for further engagement research. The case studies and engagement materials have been tested with patients through local engagement events in March and April Details on the case studies can be found in Appendix C Commissioning Groups and NHS England Draft in progress 51
52 Stakeholder Communications and Engagement You said, we did reports Communications As part of the programme, You Said, We Did reports are produced that summarise our engagement work and include samples of the feedback that we have received along with our responses to the feedback. All feedback and responses to the programme are logged centrally and shared with the appropriate groups for action and response. Some specific examples are below: Local Care Networks: more person-centred care and focusing on keeping well You said: People who live alone are much less likely to come forward for screening, so campaigns should be targeted at them There should be more proactive care to stop greater needs arising down the line. This doesn t need to be provided by a highly-paid professional, they could be a volunteer. I found I ended up having to coordinate medical staff, and I think this was particularly hard as I have other health conditions as well as cancer. We did: A key element of the Local Care Networks is to support people to live healthier lives. There will be a greater focus on prevention as well as advice and treatment. Local Care Networks will draw on a range of specialists, service providers and community groups including those in the voluntary sector to help people stay well and/or manage their conditions. Care navigators will help ensure care is co-ordinated with the patient at the centre. Targeted wellness programmes are a key part of this (and specifically for cancer), which will take into account current research on what campaigns are most effective and how to target people. Regular communications with programme stakeholders is fundamental to ensuring that there is an awareness and understanding of the strategy. This includes: Monthly updates to Governing Bodies Updates to Health and Well Being Boards at programme milestones Monthly public-facing updates, shared via CCGs and the programme website Weekly s to CCGs and members of the programme groups Programme website, launched October 2014 Twitter stream launched May 2015 Working with CCGs to ensure patients and residents know initiatives currently underway Commissioning Groups and NHS England Draft in progress 52
53 Stakeholder Communications and Engagement Accessible materials Equalities analysis We are committed to ensuring that our public facing documents are understandable. As such we work with the PPAG reading group to shape and improve all public facing documents. Their input has enabled us to produce a number of materials in plain English, such as a summary of the strategy and the case for change (August 2014); Issues Paper and summary Issues Paper (March 2015); and Easy Read versions of the Issues Paper. In order to ensure that our strategy is informed by the diverse population in south east London and to enable us to fully understand the potential impact on communities with protected characteristics (as well as complying with the Equalities act 2010) we have, and will, conduct equalities analyses throughout the programme. An initial equalities impact assessment was carried out at the beginning of the programme. Building on this, the programme has commissioned a second equalities analysis to be conducted in June 2015 and to influence the focus of pre-consultation engagement work (if consultation goes ahead). Commissioning Groups and NHS England Draft in progress 53
54 Draft in progress 54
55 The case for Change Outline of the case for change: Why we are developing the strategy Our health outcomes in south east London are not as good as they should be. Too many people live with preventable ill health or die too early The outcomes from care in our health services vary significantly and high quality care is not available all the time We don t always treat people early enough to have the best results People s experience of care is very variable and can be much better Patients tell us that their care is not joined up between different services The social care system is under increasing pressure The money to pay for the NHS is limited and need is continually increasing It is taxpayers money and we have a responsibility to spend it well South east London s acute, community and mental health providers face a similar and interrelated set of challenges and drivers The longer we leave these problems, the worse they will get. There is a need to change what we do and how we do it. The rest of this section describes the above points in more detail and sets out our case for change in south east London. The full case for change is available on our website It is currently being updated to include the latest figures and supporting information. Too many people live with preventable ill health or die too early In south east London premature death and differences in life expectancy are both significant issues. There is a difference in life expectancy between the best and worst wards in south east London of 11.8 years for women and 11.4 years for men (data for years ). About 11,000 people died prematurely across south east London between 2009 and 2011, with four of our boroughs being classed in the worst category for premature death in England. The biggest causes of early death are heart disease, cancer and respiratory diseases. While the mortality rates for these illnesses have decreased significantly in our area in recent years, they are still considerably higher than the London average. To address this problem, we need to improve the health of people who live in south east London. From a UK wide perspective, the health of our population is poor and worse than comparable countries. The UK is ranked 10th out 11 countries for people living health lives. Our poor health is a major factor in generating the demand for care which is putting the NHS and social care under such well publicised pressure. People are living longer than ever before, but this means many more people are also living with long term conditions such as diabetes, high blood pressure and mental illnesses. Commissioning Groups and NHS England Draft in progress 55
56 The case for Change The diagram opposite breaks the population into five broad groups; people known to be nearing the end of life (1%), people with three or more long term conditions (9%), people in the early stages of a long term condition (25%), people experiencing inequalities or putting their health at risk (50%) and people who are healthy and well (16%). The higher up the tree the more money is spent on that group. The major causes of health inequalities between people in south east London and elsewhere in the UK are smoking, excess alcohol and drug use, not enough exercise and obesity, and poor mental health. Our aim is to help people move towards the trunk and into the healthy and well group. To do this we must support the 50% of the population who are affected by inequalities and who are at risk of developing long term conditions due to inequalities or lifestyle factors. The outcomes from care in our health services vary significantly and high quality care is not available all the time. Too often, the quality of care that patients receive and the outcome of their treatment depend on when and where they access health services. For example, we do not always provide the recommended level of cover by senior doctors in services dealing with emergency care, maternity or children. People taken ill at weekends or in the evenings are less likely to see a senior doctor in hospital. EoL Early (1%) stages of LTC (25%) 3+ LTC (9%) Early stages of LTC (25%) People experiencing inequalities or putting their health at risk (50%) Health and wellbeing group (16%) Costs People with multiple complex needs where standard services are not effective who need personalised care Note: Total equals 101% due to rounding Commissioning Groups and NHS England Draft in progress 56
57 The case for Change We don t always treat people early enough to have the best results Our services are often not set up to detect problems soon enough, meaning that people with long term conditions or mental illness often have to be admitted to hospital in crisis. Earlier diagnosis and support could have helped them to get better sooner or prevented their illness becoming so serious. In this respect, we are not putting enough emphasis or resources into services based in the community, to prevent people becoming ill or encourage them to take responsibilities in managing their own health. People s experience of care is very variable and can be much better While patients are very happy with some services, surveys tell us that their experience of the NHS is inconsistent and that they do not always receive the care they want. Patient satisfaction in south east London is generally low compared to national benchmarks. Four of our boroughs scored in the bottom 25% for patient satisfaction in hospital care and three of four trusts were in the bottom 25% for the Friends and Family Test, which tests whether patients would recommend the trust to friends and family. Therefore it is crucial that we provide consistent, high quality services for everyone in south east London. Patients tell us that their care is not joined up between different services Patients and carers find it frustrating to have to continually provide the same information to different people. This is because different parts of the NHS do not always communicate effectively with each other or with social services. This results in patients with complex conditions often being passed from one service to another. In particular, patients sometimes stay longer in hospital because joined up arrangements for their care in the community on and after discharge have not been put in place. Commissioning Groups and NHS England Draft in progress 57
58 The case for Change The social care system is under increasing pressure Many local authorities face unprecedented pressures on their resources and in some instances are looking to save over 30% of their current expenditure over the next 3-4 years. Demand in services is growing in some areas with increasing numbers of older residents, residents living much longer with complex care and health needs, increased mental health service demand alongside the continued need to support those with lifelong health and care needs to live as independently and as full a life as possible. Council investment is increasingly focused on statutory provision, thus reducing any ability to work creatively with universal and preventative services. In due course, this could have further significant impacts on demand for health and care services. Added to this, requirements on social care providers continue to increase (examples include minimum wage increases and statutory holiday increases) without increases in funding - yet the level of complexity that we expect these organisations to support continues to rise. If we are to provide high quality community based care, we need to further develop and value this workforce. The implementation of the Care Act 2014 places new duties on local authorities and partners to promote wellbeing and prevention within communities to help reduce or delay the need for care. From April 2016, there will be a cap on individual contributions to the cost of their care. Although welcome, this focus comes without any certainty on the costs associated with these new duties, nor of the increased demands from people who use services and their carers. Furthermore, developing implications of case law with regard to the Mental Capacity Act and Deprivation of Liberty Safeguards (DoLS) are adding significant new duties and pressures on adult social care, putting additional pressures on care homes and hospitals to ensure that people are not illegally deprived of their liberty. A focus on care at home can best reduce the trauma of change for those with impaired capacity and consequently help reduce the need for DoLS assessments. Commissioning Groups and NHS England Draft in progress 58
59 System wide income/expenditure ( millions) The case for Change The NHS faces a growing affordability challenge NHS funding currently increases in line with inflation each year. However, the costs of providing care are rising much faster because the NHS is now treating more people with more complex conditions than ever before and the costs of care often grow faster than consumer inflation. The NHS Five Year Forward View outlines a 30 billion financial challenge nationally by 2020/21. Consistent with this, in the absence of action, the scale of the affordability challenge in south east London is forecast to grow to 1 billion by 2019/20. The graph to the right and the table below demonstrate how this challenge grows over this period. Local authorities, who are responsible for social care services, are also looking to save over 30% of their current expenditure over the next 3-4 years. Therefore we need to get better value for money for all that is done in the NHS and social care services. We need to get the best possible outcomes for patients and make the most of resources that are under increasing pressure. This means we need a more integrated approach between different services. 5,900 5,903 5,400 4,900 4,812 4,400 Expenditure (Do Nothing) Revenue 3, / / / / / / /20 Absolute challenge Annual challenge Percentage challenge Over the period from 2014/15 to 2019/20, the south east London expenditure (without efficiencies) will grow by just over 1 billion more than the projected budget of 5 billion. This is comparable with the 30 billion national challenge set out in NHS England s Five Year Forward View. On average, the south east London healthcare system will need to make efficiencies of 218m each year (from a budget which will grow to 4.8bn) between 2014/15 and 2019/20. An estimated breakdown is shown below. On average, the south east London healthcare system will need to make efficiencies of 4.2% each year between 2014/15 and 2019/20. An estimated annual breakdown is shown below. 14/15 15/16 16/17 17/18 18/19 19/20 14/15 15/16 16/17 17/18 18/19 19/20 251m 228m 154m 162m 141m 156m 6.0% 5.3% 3.4% 3.5% 3.0% 3.2% Commissioning Groups and NHS England Draft in progress 59
60 The case for Change It is taxpayers money and we have a responsibility to spend it well We know that by providing services in a different way, it is possible to improve outcomes, to help people to live healthier lives, to deliver services which are consistently of high quality and get more for our money. As an example, changes have been made in the acute treatment of stroke, major trauma and heart attacks in London: services are now provided in a small number of specialist centres rather than in every hospital and this has transformed outcomes. More people now survive strokes, major trauma injuries and heart attacks in London than ever before. In bypassing their local hospitals to these centres, the care they receive is much better. These changes have also saved money for the NHS so we know that such cost effective changes are possible. A study showed that the changes to stroke services saved 12% more lives (around 400 lives a year) and 811 per patient, in spite of the costs of setting up the new system. Nationally 16 million people attend A&E each year, but 40% needed no treatment or could have been managed by their GP. This adds unnecessary costs to the system and create delays in planned hospital care. Additionally there are problems of access to GP appointments which can put added pressure on the system; in producing meaningful discharge and care plans; and in producing better outcomes after surgery and cancer treatments. Changes are needed to reduce unnecessary costs in order to get more value for the limited money available to the NHS. Commissioning Groups and NHS England Draft in progress 60
61 The case for Change South east London s acute, community and mental health providers face a similar and interrelated set of challenges and drivers A number of drivers and issues are shaping the strategic context for provider organisations in south east London. The key issues and drivers for providers include the following: A constrained financial environment The implications of regulatory changes and recent key recommendations in relation to safety, quality and patient care (including the Francis Report, the Berwick Report, recommendations as a result of Winterbourne View, the Urgent and Emergency Care review, and the Future Hospitals Commission) Uncertainty in the system about the long term provider landscape and future patient flows Local service integration including primary care and integrated community care Emergency centre designation Specialist service consolidation / designation in line with the national strategic direction New workforce models in response to the need for ambulatory upskilling and staff shortages within the existing workforce Information Management and Technology, which will be a key enabler of change for providers, but will also demand time and investment. In addition, London s ambulance services are facing increasing and changing needs for care. Some of the key factors affecting the service include: Increasing demand, whereby over the last three years there have been significant changes in the health needs and expectations of Londoners, with a total increase in incidents of 5% between 2011 and Changing profile of demand by illness, including an 11% increase in alcohol related calls between 2011 and 2013; a 19% increase in chest pain related calls between 2011 and 2013; and an 11% increase in dyspnoea calls between 2011 and 2013 Diversion between demand growth and level of funding Changing patient needs including those on an ageing population, high and increasing diversity of population, increasing issues as a result of population not registered with a GP, and the need to address the symptoms of mental illness Utilisation of staff significantly above the rest of the country. Commissioning Groups and NHS England Draft in progress 61
62 Draft in progress 62
63 Vision for the future of health and care services in south east London Vision for the case for change To solve the problems outlined in the case for change, we have developed a collective vision for south east London. In south east London we spend 2.3billion in the NHS. Over the next five years we aim to achieve much better outcomes than we do now by: Supporting people to be more in control of their health and have a greater say in their own care Helping people to live independently and know what to do when things go wrong Helping communities to support one another Making sure primary care services are consistently excellent and have an increased focus on prevention Reducing variation in healthcare outcomes and addressing inequalities by raising the standards in our health services to match the best Developing joined up care so that people receive the support they need when they need it Delivering services that meet the same high quality standards whenever and wherever care is provided Spending our money wisely, to deliver better outcomes and avoid waste. Commissioning Groups and NHS England Draft in progress 63
64 Vision for the future of health and care services in south east London Our integrated whole system model Community Based Care delivered by Local Care Networks is the foundation of the integrated whole system model that has been developed for south east London. This diagram provides an overview of the whole system model, incorporating initiatives from all 6 Clinical Leadership Groups. Commissioning Groups and NHS England Draft in progress 64
65 Draft in progress 65
66 Proposed model(s) of care: Delivering better care for our south east London populations Introduction to the care models Purpose To develop the initiatives to focus on these aims, the Clinical Commissioning Groups and NHS England London region have identified the six priority areas to deliver better care for our population. These are: Community based care Planned care Urgent and emergency care Maternity Children and young people Cancer The programme is being shaped by six Clinical Leadership Groups (one for each of the priorities above) which form part of the integrated whole system model and have developed. They have each developed a number of interventions and assessed the impacts of these interventions in terms of delivering improved quality, better and less variable outcomes for people across south east London and that they provide value for money and support a sustainable whole system health and are economy. This section provides an overview of how these interventions have been developed through engagement with wider stakeholders and the public. We then provide an overview of the Community Based Care model followed by more detail on the remaining Clinical Leadership Groups. Each of the CLGs provides a high level summary of the Clinical Leadership Group s proposed interventions. This is followed by more detailed information on each individual intervention for the care model. This provides: The purpose of the intervention A detailed summary of the proposed intervention Each of the Clinical Leadership Groups includes clinicians, commissioners, social care leads and other experts, Healthwatch representatives and other patient and public voices from across south east London who have worked together to develop these initiatives. Further information on each of the care models is provided in each of the Clinical Leadership Group Design Guides. Commissioning Groups and NHS England Draft in progress 66
67 Proposed model(s) of care: Delivering better care for our south east London populations Engagement and input into the Clinical Leadership Groups Our Healthier South East London overarching programme has encouraged and supported engagement from a wide range of stakeholders and patients. In particular, the Clinical Leadership Group membership comprises representatives from CCGs, Local authorities, patient and public voices, the voluntary sector, public health and clinicians. Their insight has been woven into the care models and their design. This was via events that created an opportunity for communities and patients to explore proposed changes to the models and find solutions together to meet specific challenges identified in the case for change. In addition, we recognise that the experience and perspectives of patients and others are integral to the development of a truly service user centred model. Service users, patients and members of our local communities have therefore been engaged through a variety of mechanisms. The programme has engaged a large group of public and patient voice (PPV) representatives with a growing focus on ensuring they represent the needs of the whole population including those who experience inequalities. The programme has an active Patient and Public Advisory Group (PPAG) and each model of care has been developed with the input of a small group of PPVs. In addition, patient stories have been gathered from across south east London to help groups think through what elements of a new model of care could be of benefit to individuals and any current barriers to receiving effective quality care we should consider changing for the future. The aim is also for these patient stories to facilitate wider discussions with partners, patients and the public about their own experiences of health and social care in order to encourage and facilitate discussion to inform service development in the strategy. The following two pages summarise patient views on the Community Based Care model and the overarching system model. Importantly, the model design recognises the need for a continuous quality improvement culture during implementation and delivery whereby providers and commissioners act as system stewards facilitating a feedback and improvement cycle underpinned by the voice of the patient. Engagement to date Specific engagement for the Clinical Leadership Groups has been managed through the Innovation Unit as co-design sessions held different locations to reach the population of the six boroughs. The sessions targeted a mixed group of participants (including community, patients, carers, clinicians, provider representatives and representatives of care homes). This engagement is in addition to those led by individual CCGs and is in addition to the involvement of Patient and Public Voices in the Clinical Leadership Group membership and through workshop attendance. Commissioning Groups and NHS England Draft in progress 67
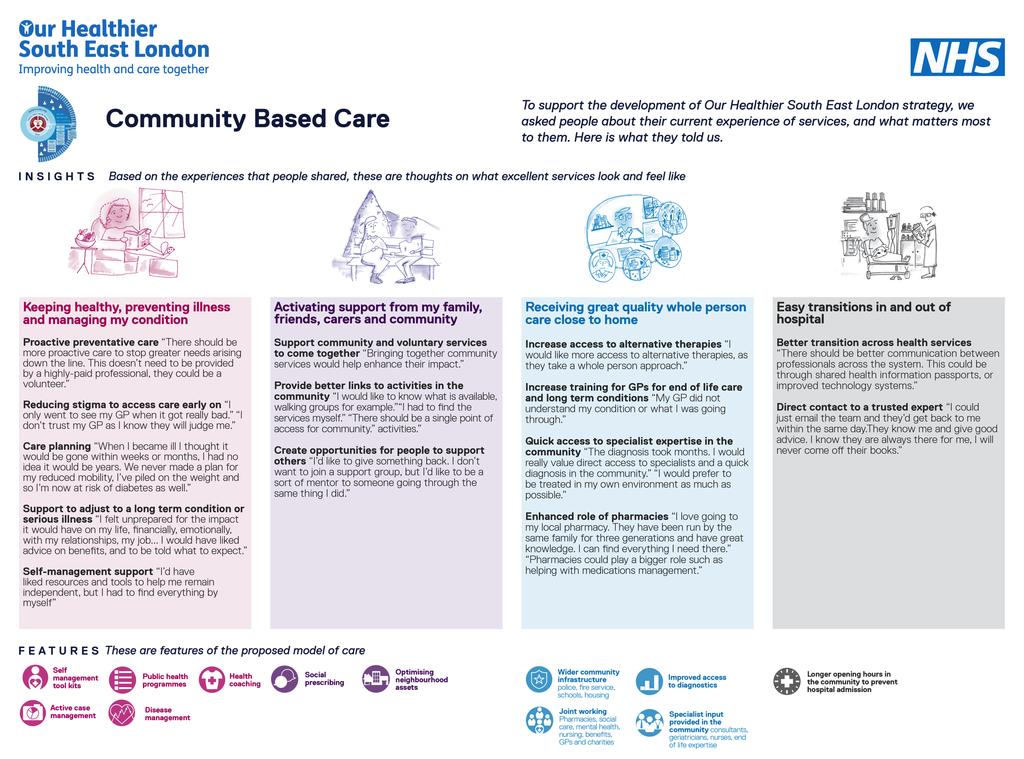
68

69 Proposed model(s) of care: Delivering better care for our south east London populations Engagement to date Commissioning Groups and NHS England Draft in progress 69
70 Draft in progress 70
71 Community Based Care The vision for Community Based Care Community Based Care aims to focus on the following: Strong and confident communities supporting people to maintain and regain health and social wellbeing and to continue to live at home. Delivery of primary and community based care in the broadest sense, to geographically coherent populations and at a scale that respond to the varied needs and characteristics of our communities with a focus on reducing inequalities. A broadly defined integrated care team for the population, including community physical & mental health, social care, housing, voluntary sector and specialists services coming together around the holistic needs of the person. Primary, community and social care that focuses on delivering proactive prevention, equitable and timely access, effective coordination and continuity of professional accountable services for individual s care. A systematic risk stratification and problem solving approach to identify people who require additional co-ordinated multidisciplinary and multi agency assessment, support and treatment to improve their quality of life, live more independently and have rapid access to specialist community based support when needed, including those requiring support within an end of life pathway. Involved and informed patients and carers, with care plans developed by and with them, to support them to stay independent and active and encourage self-management. Adaptable and capable staff working together between hospital and community services, mental health, social care and the voluntary sector to provide joined up, flexible assessments and care packages to provide a seamless service from a patient s perspective. Responsive services providing access from 8am 8pm seven days a week, so that patients are confident they will receive a prompt assessment if they are at risk of admission to hospital, and proactively planned discharge from hospital to ensure re-ablement care and follow up is provided. Delivery of consistently high standards of care with clear outcome measures that can demonstrate improvements in population health, quality of life, quality for care and effectiveness of care across south east London. For those with multiple complex needs or long term conditions, a focus on secondary prevention with the aim of improving underlying conditions and preventing deterioration or development of further long term conditions. Recognition that the future healthcare needs to be sustainable, with a shift in spend towards prevention and care delivered outside of hospital. Connected and intelligent IT that shares health information not just data. Use of technology in people s home that allows the delivery of healthrelated services and information via telecommunications technologies to support self-management and independence. A relentless focus on the physical health and wellbeing of people with enduring and significant mental health problems. Commissioning Groups and NHS England Draft in progress 71
72 Community Based Care Characteristics of Community Based Care Delivery of community based care through the platform of Local Care Networks will be achieved in line with seven Characteristics of Care: More accessible primary and community care Timely and prompt assessment Enhanced health promotion and disease prevention Proactive and empowering care Seamless co-ordinated care Multidisciplinary holistic care Continuity of care professional Local Care Networks Local Care Networks are a key characteristic and centrepiece of the strategy and sits within Community Based Care (CBC) The CBC Clinical Leadership Group aims to support people to live healthier lives and reduce those people exposed to risk factors either by birth or behaviour. For people with a long term condition, Community Based Care will take a rehabilitative/ re-ablement approach enabling people to manage their own health positively and to prevent deterioration wherever possible. For those people with complex long term conditions or who are in the last year of life, support will be available to enable them to continue to lead as full and active life as possible. Community Based Care will be delivered through Local Care Networks. The services available will be proactive, accessible, coordinated and provide continuity; with a flexible, holistic approach to ensure every contact counts. This will be primary care delivered to geographically coherent populations, at scale, whilst still encouraging self-reliance 24 local care networks are being developed to support whole populations across south east London. This will be a universal service covering the whole population cradle to grave. A local care network will involve primary, community and social care colleagues working together and drawing on others from across the health, social care and the voluntary sector to provide proactive patient centred care. Services will be delivered in ways that respond to the varied needs and characteristics of our communities. This is core to the Community Based Care Target Model which provides a summary of the central community based care services which are part of the Local Care Network and how they work with other services in the system. This also summarises how these services are 'big hitters' for the whole system. More detail on the Community Based Care Target Model is provide on the following slide. Commissioning Groups and NHS England Draft in progress 72
73 Community Based Care The Community Based Care Target Model The strategy sets out an agreed target model for local care networks that will deliver community based care. It is intended that each Local Care Network across south east London delivers the target model. However, the target model will have to be tailored to the local community that it serves. Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with Big hitters Serving geographically coherent populations between 50, ,000 Southwark Lambeth Lewisham Greenwich Bromley Bexley Leadership team All general practices working at scale (federated with single IT system and leadership) All community pharmacy Voluntary and community sector Community nursing for adults and children Social care Community Mental Health Teams Community therapy Community based diagnostics Patient and carer engagement groups Strong and confident communities Accessible hospital outpatient treatment clinics and acute oncology (urgent and emergency and cancer care) Specialist opinion (not face to face) and clear specialist service pathways Pathways to Multi Disciplinary Teams Integrated 111, London Ambulance Service and Out of hours system (interface with Urgent care centres colocated with emergency department model) Housing, education and other council services Community based midwifery teams Private and voluntary sector e.g. care homes and domiciliary care Cancer services Children s integrated community team and short stay units Rapid response services Carers And there will be others.. Supporting patients to manage their own health (Asset Mapping, Social Prescribing, education, community champions etc Prevention Obesity, Alcohol and Smoking Improved Core general practice access plus 8-8, 365 Enhanced call and recall improves screening and early identification and management of long term conditions Reduction in gap between recorded and expected prevalence in long term conditions Supporting vulnerable people in the community including those in care homes and domiciliary care Reduction in variation (level up) primary care management of long term conditions Reablement Admissions avoidance and effective discharge Multi Disciplinary Teams configuration main long term conditions groups (incl. mental health) and Frail elderly End of Life Care Integrated Pathways of care Commissioning Groups and NHS England Draft in progress 73

74 Community Based Care Community Based Care delivered by Local Care Networks Commissioning Groups and NHS England Draft in progress 74
75 Community Based Care Local Care Network Development & Mobilisation Local Care Networks form the core of the Community Based Care model. The proposed high-level approach to implementation of Local Care Networks across south east London is therefore central to the strategy. It has been described as: The case for change and outcomes Identify why we need to change and what we want to achieve. Design Agree the Target Model ( the core, working with and big hitters ) Strategic impact assessment Demonstrate the activity & finance implications for the Target Model assessing the value equation; patient outcomes over cost Local interpretation Using the target model to articulate shared design principles, interpret these to meet the needs of local communities Provider models Looking at the localised Target Model, outline options and select provider model (for example the provider models described in the Five Year Forward View) Contracting and business models With a preferable provider model selected, commissioners consider the contracting models, and providers the business model, that enables them to deliver GP federation Determination of core services and shared leadership Determination of services that link into the Local Care Network Population and outcomes Value realisation = health outcomes achieved true cost of achieving those outcomes Commissioning Groups and NHS England Draft in progress 75
76 Draft in progress 76
77 Planned Care Planned care model Key Features of the model 1 Standardisation Reducing variation across the planned care pathway from referral practice to discharge through to co-development of high level standards. 2 Diagnostics Person 2 Diagnostics 3 Elective Care Centres H Enhance patient management by GPs Rapid access to diagnostics for GP s Evidence based standardised Clinical pathways Shared results across the system supported by integrated IT systems 3 Elective Care Centres Provider collaboration to create centres of excellence for high volume specialities that drive up quality of service provision and improve outcomes for patients Orthopaedic (hips and knees) Ophthalmology 4 Pathway Review Urology Neurosurgery Nephrology Gynaecology Dermatology Commissioning Groups and NHS England Draft in progress 77
78 Planned Care Intervention 1: Standardisation The case for change Patients do not receive the same standard of care across south east London. In particular, there is variation in patient experience and procedure outcomes for Planned Care. The proposal To co-develop high level standards across the planned care pathway from referral to discharge. Standardisation means patients can expect to receive the same standard of care at every point on the planned care pathway. This initiative therefore proposes to develop high level standards across the planned care pathway from referral through to discharge. Through this we recognise that standardisation is one of the primary methods to reduce variation in a system* and that it is the foundation upon which improvement in quality and costs is built** References: *Kohn LT, Corrigan JM. Donaldson MS, editors. To err is human: building a safer health system. A report of the Committee on Quality of Health Care in America, Institute of Medicine. Washington, DC: National Academy Press; 2000) **1IHI: 1. Standardization as a mechanism to improve safety in health care. Rozich JD1, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK) Commissioning Groups and NHS England Draft in progress 78
79 Planned Care Intervention 2: Diagnostics The case for change NHS Atlas of Variation in Diagnostic Services have highlighted variation in the provision of healthcare. In particular, there is variation in GP access to diagnostics and access to rapid diagnostic pathways across south east London Non standardised diagnostic pathways leads to costly waste and inefficiency in the system, delays and unnecessary duplication of tests all impacting on patient experience and patient outcomes. This initiative therefore aims to address this problem. The proposal Diagnostic services underpin the effective and efficient management of patient pathways and ensure that decisions made about patient care can be made as quickly and accurately as possible*. Two models have been proposed to provide this service. 1. Evidence based standardised clinical pathways: Explore potential and impact of local innovation programmes such as Transforming Outcomes and Health Economics Through Imaging (TOHETI) GSTT & KHP. Patient outcomes are negatively affected by inefficient and late diagnosis. The TOHETI programme aims to improve patient outcomes and health sector cost-effectiveness by changing the way in which imaging is used as a diagnostic and therapeutic tool. This model could be considered for wider use across south east London 2. Serious but unspecific symptom pathway - international case study: Danish Model (Dr P Vedsted) This model uses a "3 legged diagnostic strategy based on: 1. Alarm Symptoms - urgent suspected cancer referral indicated 2. Non Specific, serious symptoms (the difficult ones) referral to a Diagnostic centre - fast multidisciplinary assessment 3. Vague Symptoms ( the common) If the GP cannot allocate the patient to an alarm pathway e.g. weight loss, fatigue, cough etc, then the GP performs a filter function - imaging and bloods within 2 days, e.g. CT body cavity with electronic transmission of results to practice within 2 days. If no diagnosis is reached following this initial set of tests, then the next step is referral to a diagnostic centre which involves a single responsible clinician working with a team of co-ordinators and imaging specialists. References: *NHS Atlas of Variation in DS 2003 Commissioning Groups and NHS England Draft in progress 79
80 Planned Care Intervention 3: Elective Care Model - Orthopaedics: Hips & Knees Case for change The Briggs Report (March 2015) states that the population is living longer and by 2030 over 15.3 million people in the UK will be over the age of 65 years. As a consequence, we will see an ever increasing demand on our health resources which are already stretched (such as orthopaedic referrals from GPs to secondary care providers which are currently increasing by 7-8% per annum). Variation in practice is therefore unsustainable and needs addressing urgently. A more cost effective, patient outcome driven and coordinated Planned Care Model is needed The proposal New provider models of partnership Elective Care models are cost effective and deliver a multitude of benefits for staff, patients & the organisations they serve. This initiative therefore focuses on elective care centres for high volume specialities. which would: Consolidate service configuration across south east London Provide a standardised pathway of planned care which: o o Reduces variation in the quality of care and clincial outcomes for patients Minimises negative risk and error thus improving patient safety As an example. the benefits and outcomes evidenced by south west London Elective Orthopaedic Centre (SWLEOC) are: Improved quality of care seen in reduced waiting times from 7.3 to 5.2 months. Patients achieved their estimated date for discharge 90% patients achieved their estimated date for discharge (the national average is 50%) Average lengths of stay reduced from 6.2 days to 4.9 days Cancellation rates at 1.86% (the national average is 4.3%) Reduction in procurement costs resulting in an annual saving for London of c. 3m Reduction in post operative complications, saving over 700 per patient compared to UK averages. If replicated nationally, this could save up to 92m across England and Wales. Positive patient feedback Commissioning Groups and NHS England Draft in progress 80
81 Planned Care Intervention 4: Clinical pathway review Case for change Across south east London there is variation in service provision and patient outcomes. The proposal The Planned Care Clinical Leadership Group has requested data pertaining to the following 5 specialities: Urology Neurosurgery Nephrology Gynaecology Dermatology This data will enable a clinical pathway review of each speciality to highlight whether there are opportunities for standardisation, consolidation or to test new models of patient care. Commissioning Groups and NHS England Draft in progress 81
82 Draft in progress 82
83 Maternity Maternity model Key Features of the model 1 Primary prevention and targeted wellness programmes within the Local Care Network 2 Assessment of pregnancy risk before 10 weeks to assign the most appropriate midwife team from the outset: 1. Local Care Network community based midwife teams for low risk 2. Specialist condition focused teams for high risk Person 1 Geographic midwife teams for low risk mothers 6 2 Condition focused midwife cohorts for high risk mothers 3 DAU & 24/7 Triage 5 H 4 3 Easy access to acute assessment clinic for unexpected problems during pregnancy and assessment unit for assessment of onset of labour 4 Culture of birthing units to encourage straightforward birth and improve the experience for low risk women 5 Achieve the London Quality Standards 6 Better co-ordination through postnatal and neonatal phase to improve mother and baby flows and experience 7 Smooth handover to Local Care Network with continuing advice and support on healthy choices. It is our intention that through this strategy we will meet the London quality standards. The above interventions aim to address this. Commissioning Groups and NHS England Draft in progress 83
84 Maternity Intervention 1: Pre-conceptual care The case for change There are increasing numbers of women with more complicated health needs due to obesity and diabetes and a range of other long term conditions as well as lifestyle choices that impact on pregnancy and long term health outcomes for mothers and babies. This initiative aims to address these issues. The proposal This proposal includes access within the Local Care Network to provide advice on lifestyle and pre-pregnancy support to optimise pregnancy. It is important to improve the health of women before they conceive in order to increase their outcomes and experience of pregnancy and birth. This links with initiatives such as making every contact count which states that every contact an individual makes with a healthcare professional is also used where possible to maintain or improve their health and wellbeing. Commissioning Groups and NHS England Draft in progress 84
85 Maternity Intervention 2: Access to Midwifery Antenatal Support by 10 weeks The case for change Due to a lack of early access a number of issues have been identified. These include: Late access to maternity care can have an impact on outcomes for mothers and babies leading in some cases leading to poorer outcomes and increased mortality rates. Delaying the first antenatal appointment stops a women making an informed choice of all the available antenatal screening services, such as screening for infectious diseases, including HIV and hepatitis B, as well as for haemoglobin disorders such as sickle cell disease and thalassaemia. Nutritional supplements such as folic acid are most effective early in pregnancy and women could be given early advice on diet and exercise. Earlier engagement also enables an early risk assessment. Whilst the majority of women do have their first antenatal assessment in the first few weeks of pregnancy up to 12% of women in some parts of SEL do not come into the service early on in their pregnancies. The proposal This initiative focuses on access to midwifery antenatal support by 10 weeks. Currently the national standard for antenatal support is 12 weeks and 6 days and so this proposal will achieve compliance with standards (e.g. sickle cell) and enable informed choice through prenatal screening. This model supports direct-access to maternity care or access via a GP referral, following which the women should be seen within a maximum of 2 weeks. Commissioning Groups and NHS England Draft in progress 85
86 Maternity Intervention 3: Continuity of Midwife-led Care The case for change Midwifery led care has a number of benefits, for example: Midwifery care is important for high quality and safe care Women who receive midwife continuity of care are less likely to experience preterm birth or lose their baby before 24 weeks gestation and overall it is associated with several benefits for mothers and their babies. The proposal This initiative proposes that every woman will have a named midwife to improve women s experience of maternity care. For example, this will prevent women repeating themselves at each visit to maternity services, particularly if they have mental health, physical health or social care issues. The development of a core and standardised offering for every woman with a named midwife will provide continuity and co-ordination of care antenatally and postnatally in community and hospital settings including for high risk and specialist pathways. This will provide continuity and safety for women. In particular through providing further support, women will feel more comfortable to disclose domestic abuse or mental health problems as a result of knowing the midwife. This also makes appointments more effective and reduces duplication. There are a number of benefits associated with midwifery-led continuity of care and no adverse effects compared with models of medical-led and shared care, including for example a reduction in epidurals and instrumental births and increased chances of a straightforward birth. This reflects the importance of the maternity workforce and how their interventions at each stage can contribute to the achievement of high quality and safe maternity care. The model also includes the availability of high quality information to support women to make informed decisions / choices which lead in turn to better outcomes and enables informed choice of place of birth. Continuity links with early access and identification of risk factors, enabling referral to more specialist maternity care pathways if required this includes early access to community based antenatal services and empowering women through ease of access, enabling triage where required to more specialist obstetric or multidisciplinary services. Sharing these pathways with continuity of midwife care will help to normalise birth and increase choices on care and place of birth for women on these pathways. References: Midwife-led continuity models versus other models of care. Cochrane Review. Sandall et al (2013) The contribution of midwifery care to high quality maternity care. Royal College of Midwives. Sandall J. Discussion of findings from a Cochrane review of midwife-led versus other models of care. Sandall et al (2009) Can we prevent postnatal depression? A randomised control trial. Marks et al (2013) DH (2007) Maternity Matters Commissioning Groups and NHS England Draft in progress 86
87 Maternity Intervention 4: Continuity of Care (cont.) - Obstetric and Specialist Care The case for change This initiative highlights: The importance of clinical leadership and multidisciplinary working to ensure safe, high quality and effective care for all women. It is important that all within the multidisciplinary team recognise each others responsibilities to improve safety. More senior obstetrician cover on labour wards has been shown to reduce both caesarean section rates and complications. The proposal This initiative involves an early identification of risk factors, streaming into high/low risk, social/medical risk pathways this includes the initial risk assessment with a midwife and early risk stratification so that the woman can be directed to the right support and specialist / multidisciplinary team as well as triage to the right midwifery team. Multiple pathways by condition are shared where appropriate with other services such as primary care which will enable the centring of pregnancy within the wider social infrastructure and developing sustainable and long term relationships within the local care network. The proposal also involves a multidisciplinary team and step up to condition specific care includes continuity of midwife care. The named midwife providing continuity is kept throughout the pregnancy although the woman may see other midwives and professionals as part of her care. This means that the named midwife will have an operational / organisational aspect to her role in supporting the woman. Continuity enables ease of step-up at any stage during pregnancy to obstetric care so that the woman can be maintained on her maternity pathway but with specialist input when required. References: DH (2007) Maternity Matters Society for Maternal-Fetal Medicine: Safe Prevention for the Primary Caesarean Delivery (March 2014) Evidence-based strategies for reducing caesarean section rates: a meta analysis, Chaillet et al (2007) Commissioning Groups and NHS England Draft in progress 87
88 Maternity Intervention 5: Increasing Out of Labour Ward births The case for change This initiative highlights that: It is important to give low risk women information and advice about all available birth settings, so they can make a fully informed decision. The care a woman receives during labour can affect her, emotionally and physically in the short and long term, as well as the health of her baby. It is important to enable a woman to feel in control of what is happening and to have her wishes respected as well as focusing on contributing to a positive birth experience, good communication and support and care from staff. The proposal This initiative focuses on women and their families receiving the best possible information and communication to ensure that they are able to make an informed decision about where to have their babies at home, in a hospital alongside birth centre or in a hospital obstetric unit. This involves explaining to both new mothers and women who already have children that they may choose any birth setting and that they will be supported in their choice of birth setting. However it is important that the best guidance from the National Institute for Clinical Excellence (NICE) recommendations are: Advise low risk multiparous women (women who have previously had children) that a home birth or a birth centre birth is particularly suitable for them because the rate of interventions is lower and the outcomes for the baby is no different. Advise low risk nulliparous women (women who have not given birth before) that planning to give birth in a midwifery led birth centre is particularly suitable for them because the rate of interventions is lower and the outcome for the baby is no different compared with an obstetric unit. If they plan birth at home there is a small increase in the risk of adverse outcomes for their baby. The maternity model supports increasing the rate of out of obstetric unit births in SEL. Each maternity service have alongside birth centres, which are beginning to prove popular with women suitable for this option. The rate of home births in SEL is low and the maternity model supports an increase from current rates in home birth where appropriate. The findings show that women who choose and are suitable for home and midwife-led birth centre births, have birth experience that are positive and lead to high quality emotional and psychological outcomes for both mother and baby with a low risk of adverse outcomes. In addition studies have shown that there are economic (financial) advantages of providing more care in out of obstetric unit settings for low risk women. References: DH (2007) Maternity Matters Society for Maternal-Fetal Medicine: Safe Prevention for the Primary Caesarean Delivery (March 2014) Evidence-based strategies for reducing caesarean section rates: a meta analysis, Chaillet et al (2007) Commissioning Groups and NHS England Draft in progress 88
89 Maternity Intervention 6: Postnatal and neonatal care The case for change This initiative highlights that: Postnatal (after birth) support should be based on the individual needs of women and families. Breastfeeding initiation and continuation should be a priority.. The proposal This initiative focuses on developing postnatal care to improve access to support for women and babies ensuring that there are sufficient postnatal options in the community and hospital for women and that continuity of midwife led care continues. In addition, it aims to develop better communications and information sharing with primary care and health visiting to enable a smoother transition from maternity services to primary care and health visiting support in local care networks. For neonatal care the model supports better co-ordination through both the postnatal and neonatal phases in particular in relation to the examination of new born babies within 72 hours of birth. This can become a bottleneck within maternity services with mothers waiting for this examination before discharge and for those out of area. It is proposed that this check if necessary could be performed at home by a midwife, thus reducing length of stay for some women. The model supports services working collaboratively in the postnatal phase (including maternity, health visiting, children s centres and primary care) to support women initiating and continuing breastfeeding. The aim is to achieve the level 3 (the best) Unicef Baby Friendly Initiative standards to support women in recognising the importance of breastfeeding and to enable mothers to continue breastfeeding for as long as they wish. References: Unicef UK (2013) The Evidence and Rationale for the Unicef UK Baby Friendly Initiative Standards. NHS Commissioning Board: (July 2012): Commissioning Maternity Services NICE Clinical Guidelines (2006). Routine postnatal care of women and their babies Commissioning Groups and NHS England Draft in progress 89
90 Maternity Intervention 7: The London Quality Standards The case for change This initiative highlights that Midwives should be the main care-giver for normal labour and birth and form partnerships with obstetricians and other clinicians for women with complex labours. Multi-disciplinary team working and excellent clinical leadership should be developed in all services. One-to-one midwifery care should be provided for all women during established labour. There should be increased involvement of consultant obstetricians on the labour ward in the care of women with complex pregnancies and in the supervision and training of medical staff. Postnatal support should be arranged in line with NICE guidance on postnatal support The proposal The initiative focuses on the achievement of the London maternity quality standards, which is ongoing and integral to the maternity model. One of the key issues for the maternity strategy will require an assessment of the impact of achieving the requirement for 24/7 consultant presence on labour ward, this involves the setting of a trajectory and timeframe and developing a quality framework or criteria around the agreed solution. To achieve this requirement, additional consultant obstetricians will be required and a stepped approach and trajectory is being developed. References: The London Health Programmes (2013), The London Quality Standards NHS Commissioning Support for London (2011), A framework for developing services Commissioning Groups and NHS England Draft in progress 90
91 Draft in progress 91
92 Children and Young People Children and Young People model Key Features of the model 1 Primary prevention and wellness: Within the local care network, focusing on the well child. In the context of the family setting, looking after the child or young person s physical, social, emotional and mental well being. Person Children s Integrated Community Team 4 5 ACUTE CYP SS PAU H 2 Children s integrated community team delivering: A range of proactive services for children with long-term conditions and care needs Early intervention for acute illness and supported early discharge Management of short-term conditions Signposting and navigation through the system and navigate through the system 3 Extended GP hours For general practice from 8 to 8 With closer links to short stay paediatric units and emergency departments, to enable better co-ordination and to help prevent unnecessary hospital admissions To be delivered via the Community Based Care model. 4 Short stay paediatric units Designed to ensure that children and young people are returned to the community as quickly as possible and unnecessary hospital stays are avoided With close links with the Children s integrated community team 5 Planned care pathways With referral advice and guidance tools Specialist advice and support back into the community 6 Supported transition to adult services As part of community based care, within the local care network It is our intention that through this strategy we will meet the London quality standards. The above interventions aim to address this. Commissioning Groups and NHS England Draft in progress 92
93 Children and Young People Intervention 1: Primary prevention and wellness The case for change This initiatives highlights that: Social deprivation is high in some areas of south east London; c. 27.8% of our young people are living in poverty compared to a national average of 17.1%. It is estimated that less than 50% of our children and young people are living healthy lives and that 44% of our young people experience inequalities or are putting their health at risk Compared nationally, five out of six CCGs in south east London are in the bottom 25% for childhood obesity (year 6 pupils). Levels range from 17.3% to 26%, which is consistently higher than the London average and significantly above the England average Toxic stress (where children in families experience stress due to parental mental health issues, domestic violence and/or substance abuse) has a high incidence of prevalence in south east London and is predictive of poor health and mental health outcomes In the context of the family setting, we need to ensure that every child s or young person s physical, social and emotional well being are looked after. The proposal This initiative focuses on: A holistic approach which needs to be adopted by health, social care and education services to ensure that every child s or young person s physical, social and emotional well being is looked after. We need our communities to be resilient in order to help our children and young people and their families and carers - remain healthy; championing healthy living that will support their long-term health and well being both physical and emotional. Supporting self-care, through proposing that Community Champions should be appointed across south east London. Provided by the voluntary sector, these individuals will help to deliver health care promotion and prevention. For example, they could lead community food and exercise programmes or help to develop parenting skills to help Tackle Toxic Stress. Community champions providing a better link between service providers, helping to signpost children and young people to the appropriate services; helping to ensure that the first contact is the right contact. Commissioning Groups and NHS England Draft in progress 93
94 Children and Young People Intervention 2: Children s integrated community team The case for change Children, young people and their families/carers tell us that: knowing which service to access and how to access them can be confusing and the process is very complicated. referrals take too long and appointments are hard to get service provision is not joined up; they feel that the services do not talk to each other they have to repeat the same information over and over again they want access to paediatric specialists who take their concerns more seriously and communicated better with children GPs tell us that they would value access to specialist advice The proposal This initiative therefore focuses on developing Children s Integrated Community Teams that will: deliver better integration of services for children and young people; Improve care co-ordination bring together a core group of paediatric services; improve Mental Health Integration; and improve in-reach and out-reach. As a result the model defines a Children s Integrated Community Teams as providing a range of proactive services for children with long-term conditions and care needs; early intervention for acute illness; supported early discharge; safeguarding; and management of short-term conditions for children with and without a long-term condition Given the number of children and young people in each borough is less than 75,000 it is not viable to establish a Children s Integrated Community Team in every Local Care Network. It is envisioned that there will be one team, working closely with each of the Local Care Networks within that locality. Commissioning Groups and NHS England Draft in progress 94
95 Children and Young People Intervention 3: Extended GP hours for general practice The case for change This initiative identifies that: Many of the families/parents we spoke to highlighted the difficulties of accessing GP appointments. Families wanted flexibility of when they could visit care professionals - children and babies can have strict routines so appointments can be very disruptive: : I want flexibility and ease of access to care at times convenient for me Families/parents are often risk averse: you can t take any risks with children; they seek reassurance quickly when their child is ill The proposal Local Care Networks will provide extended hours from 8am to 8pm and out of hours cover to help provide 24/7 cover to improve urgent care. This will help to reduce the lack of access to timely care in the community The service will be staffed by GPs and emergency nurses. They will have rapid access to paediatric specialists for children and young people with long term conditions, including both physical and mental health. Extended hours will also enable better co-ordination of care and help prevent unnecessary hospital admissions Commissioning Groups and NHS England Draft in progress 95
96 Children and Young People Intervention 4: Short stay specialist paediatric assessment units The case for change Unnecessary admissions are to be avoided; and so as far as possible, children and young people need to be treated in the community. Care in the community is not only better for their physical well being but also for their emotional well being. However, there are times when a child or young person needs urgent care, either due to an unforeseen incident or to a change in a previously well-managed long-term condition. In these cases, they need to be assessed by a paediatric specialist as quickly as possible. Such crises can happen at any time; not just in working hours. Once assessed, there needs to be a coordinated and rapid response to the child s or young person s care, especially in cases where there may be an underlying but unrelated condition - such as mental health. The proposal This proposal focuses on the development of a short stay paediatric assessment unit (the Unit) that will hold children and young people for assessment for no longer than 24 or 48 hours. Such Units will operate seven days a week on a 24/7 basis. The Unit will be co-located with emergency departments to ensure safety and increase effectiveness and easy access to diagnostics. Senior clinical staff will be available at times of peak demand, including during evenings and weekends. Bed numbers will be determined by local demand but need to allow for variable demand. As required, staff will be able to access other specialities quickly; for instance, mental health. Ultimately, the expectation is that the child or young person will be discharged at the end of 24/48 hours; staff will work closely with community nursing teams to facilitate early discharge and on-going care in the community. Commissioning Groups and NHS England Draft in progress 96
97 Children and Young People Intervention 5: Planned care pathways The case for change This initiative identifies that: Not every child and young person in south east London receives the same standard of care; there is variation in experience and outcomes. There are unnecessary delays in the patient journey; time from first appointment, to test, to getting results and receiving treatment which could be quicker and more efficient. Delays in discharge to home from hospital can mean poorer outcomes, with increased risk of poor physical and emotional well being. Extended hospital stays can have an adverse effect on the wider family; a carer s loyalties can be divided and a sibling can be upset if his/her routine is upset. The proposal The initiative aims to develop a coordinated approach to planned care - both admittance and discharge managed through the Children s Integrated Community Team and the child s/young person s Local Care Network. A coordinated approach will ensure that there is less duplication of effort and that the well being of the child and his/her family are taken into consideration. For instance, better planning will take account of the impact on the young person s schooling. The approach will also allow for safe discharge planning, taking into account the support the child or young person will need once home to ensue full re-enablement. In taking this proposal forward, there will be closer working with the Planned Care Clinical Leadership Group. Commissioning Groups and NHS England Draft in progress 97
98 Children and Young People Intervention 6: Supported transition to adult services The case for change Our young people are ill prepared for transition to adult services. Even the well young person may not know how to book an appointment with a GP or where else they might go to for medical advice. We need to start preparing them earlier to take care of their own health and well being; as early as Year 9. Those young people with more complex needs require continuity of care for longer and when they do transition to adult services there is often a passing over rather than a dialogue between parties. Young people with mental health issues can often fall between two stools. CAMHS will work with them until they are 16 but they are not covered by adult services until they are 18. At an age when young people are particularly vulnerable, there could be a lost year that could have a damaging effect not only on their mental health but their overall health and well being. GPs complain that they are not always included in the care planning of young people with more complex conditions, yet are expected to organise their care at 18 with no previous insight or knowledge. Although effective transition is recognised as vitally important, experiences across south east London are variable. Such variability fails to take account on individual need. The initiative aims to improve transition services across all conditions to reduce variability imbedded in the Local Care Networks and in the Children s Integrated Community Teams. Services will put the young person at the centre of their transition plan. There will be greater collaboration and communication with the young person; taking into account their views and aspirations. Transition will be coordinated by a transition coordinator who may come from either the community or acute setting, depending on where the young person has received most of their care. All transition coordinators will work closely with the young person; for instance, taking them to clinics in the adult setting. They will also organise meetings between the relevant paediatric and adult clinicians to agree the future care plan. They will ensure that the GP now looking after the young person is aware of their history. The coordinator will also remain in contact with the young person for a period of time after they have moved to adult services in order to provide the individual with support at a time when they may feel quite vulnerable. The duration will vary from patient to patient, according to the complexity of their case but could be for as long as a year. Transition coordinators will need to be well informed about generic teenage health issues such as skin problems, worries about weight, puberty and sexuality. They will also need to understand the psychological and social difficulties that are common among adolescents such as depression, anger, risk taking behaviour and non adherence to treatment. They will have close links to the Children s community integrated health team to help support these wider issues. Commissioning Groups and NHS England Draft in progress 98
99 Draft in progress 99
100 Executive Summary Urgent and emergency care model Person A Rapid response Home Ward C Specialist Response Clinic B E D Enhance d Front Door H Key Features of the model Achieving the London Quality Standards in all areas: Acute medicine Emergency general surgery Emergency departments Critical care Fractured neck of femur A B C D Improving access in Primary Care, in hours and out of hours, to unscheduled care. GPs, UCC and ED functioning in a closely linked co-ordinated way; responsive community care, including specialist response teams, will prevent un-necessary hospital admissions with easy access to specialist advice for GPs as an alternative to ED referral 1. 8am 8pm 7 days a week 2. Standalone Urgent Care Centres with the same standards 3. Community based rapid access teams including a home ward. Specialist advice and referral 4. Access to specialist advice 5. Access to a specialist response clinic Improved 111 capability and LAS onward referral 6. LAS will be able to redirect to appropriate services, such as the rapid access team, home ward or hospital based specialist clinics and excel in navigating patients to the right part of the system are able to give advice, provide internal triage and coordinate onward referral to other parts of the system other than the ED An enhanced single front door to the Emergency Department. 8. Bringing together UCCs and the ED in a single governance structure and providing expert streaming across all sites E Emergency Department interface with Mental Health services 9. This will also allow for earlier identification of MH cases (including Dementia) reducing length of stay and enabling quicker streaming to specialities for mental health patients by having Psychiatric Liaison nurse (PLNs) and Triage joint assessments. 10. Quicker interface with specialist services like drug and alcohol 11. Quicker interface with under 18 mental health liaison teams Commissioning Groups and NHS England Draft in progress 100
101 Urgent and Emergency Care Model Intervention 1: 8am 8pm 7 days a week The case for change Local Care Networks with extended staffing and hours to reduce the lack of access to timely care in the community The proposal LCNs will: Provide extended hours from 8am-8pm and out of hours cover so there is 24/7 cover to provide improved urgent care Be staffed by GPs and nurse practitioners Link to rapid access services to support the frail, elderly and those patients with long term conditions. This will include mental health liaison for patients in crisis such as perinatal, drugs & alcohol, children & young people and older people & dementia patients. Intervention 2: Standalone Urgent Care Centres with the same standards The case for change The current points of access for care can be confusing for the public and health care professionals and lack a single clinical governance structure. Opening times can differ as well as the type of care that can be received. All the public want to know is that if an urgent care problem ever arises, they can access a service that will ensure they get the right care when they need it. They do not want to decide whether they should go to an major injuries unit, a walk in centre or A&E, or whether they should ring their GP, 111 or 999. We shouldn t expect people to make informed, rational decisions at a crisis point in their lives: the system should be intuitive, and should help people to make the right decision. We have created a complicated system which in itself has contributed to increasing demand by sending people around various services, confused about who to call and where to go. (Transforming Urgent and Emergency care services in England NHSE). The proposal In order to provide consistent and less confusing points of care in the community setting we propose standalone Urgent Care Centres which will: be integrated over time with the Local Care Network service model and be part of the Emergency Department clinical network to improve safety and quality have longer opening hours, improved access for unregistered patients and reduce the need to go to the Emergency Department work closely with Rapid Access Services in the community and in the hospital setting Urgent Care Centres could encompass all existing urgent care facilities which are not Emergency Departments such as Walk-in Centres, Minor Injuries Units and Darzi Centres. There will be clear standards for all Urgent Care Centres, for example in relation to opening hours and staffing, and an expectation that they will work within the Urgent Care Network to broaden their role in providing timely access to services. All Emergency Departments should have a co-located Urgent Care Centre, wherever possible. (Professor Jonathan Benger, National Clinical Director for Urgent Care for NHS England, updates on the Urgent and Emergency Care Review) In south east London we want existing standalone urgent care centres to be seen as a service rather than a location. There could be co-location with GP practices and potentially other services such as dermatologists for example. We also want social care to be part of the urgent care centre service. Commissioning Groups and NHS England Draft in progress 101
102 Urgent and Emergency Care Model Intervention 2: Community based teams including a homeward (urgent care in the home) The case for change Currently the only service available 24/7 is the Emergency Department. Stable short term medical needs are met by admissions to hospital due to a risk averse culture and lack of confidence in community skills to support patients in a home setting. In addition, currently one trust is not meeting the standard for Timely access, seven days a week to, and support from, onward referral clinics and efficient procedures for discharge from hospital and one trust at weekend. The proposal We propose a rapid access team that will: Be a single point of access providing navigation for GPs, clinical advice and supporting cross boundary working and speeding up discharge with more care packages for the elderly away from the Emergency Department. Direct patients onto the Home Ward or other specialist teams. Risk stratify patients with enhanced/faster access for very vulnerable patients. Have integrated IT that is also patient held to support cross boundary and service working Be consistently capable of assessing and treating people in their own home or nearby. Give all settings the confidence they need to hold patients safely until they are able to move to the next part of the system. Enable care homes in particular to be capable of holding onto the patient, assessing and treating those with long term conditions and mental health conditions. Commissioning Groups and NHS England Draft in progress 102
103 Urgent and Emergency Care Model Intervention 3: Access to specialists advice The case for change The initiative aims to better manage risk by enabling GPs to feel more supported and reduce Emergency Department attendance. The proposal The initiative aims to: Have easy access to specialist advice and enable referrals directly to specialist care rather than having to access a specialist through A&E. This could be made available through telemedicine, telephone lines or community based consultants. Provide advanced access to local urgent care for minor illnesses/injuries for vulnerable patients and a prioritising of over 75s. Contract incentives to make this happen as currently this takes place by goodwill. As an example a trial in Bristol has an advice line which is working using smart technology. Previously the GPs spent half the patient appointment time going through the hospital switchboard to be directed to an answer phone. Or if they did speak to the emergency team it could be a less experienced doctor answering who might err on the side of caution. GPs were unsure whether to make an urgent referral to outpatients or ask for an emergency cardiac admission. With the new telephone advice line GPs now get through to a consultant cardiologist in less than 15 seconds and agree a decision on how to manage the patient while they are still in the building. The service gets GPs straight through to a senior grade doctor during the actual patient consultation. GP Care now plans to extend the service to other specialties - with gynaecology, paediatrics and general medicine the next likely options. The organisation also plans to include specialists from other hospitals so that GPs receive advice from their local consultant teams. The software has been developed to allow practices to shape the list of specialists according to their own preference as the system expands. Commissioning Groups and NHS England Draft in progress 103
104 Urgent and Emergency Care Model Intervention 4: Specialist response clinic (located in hospital) The case for change Currently the Emergency Department can be the only route to assess and treat patients directly referred from GPs and community services. As a result a large number of patients are turning up at the front door of the emergency department with a GP letter because of a lack of access to hot clinics. The proposal A specialist response clinic and team will be established that will provide: A community service in a hospital that can carry out diagnostics such as blood and urine testing, X-Rays, Examination couches, but not beds as patients will not be admitted to be assessed and treated within the clinic. Rapid response times and a multi-disciplinary service Supported discharge home Specialist Gerontology, mental health A fast track OP clinic Potential links to faster than a 2WW referral for Cancer Patients with long term conditions who experience an urgent care need are seen by someone who knows them. In addition, the service will allow for GP and carer referral. The model will not require new staff but will expect staff to be used in the clinics rather than ward rounds as short term medical needs are met in clinic rather than being admitted. The initiative will encompass a consistent approach to service across elderly/mental health/social care pathway and will be co- located with the emergency department as the optimum location in the hospital. In addition follow up clinics will be available during the week. Commissioning Groups and NHS England Draft in progress 104
105 Urgent and Emergency Care Model Intervention 5: London Ambulance Service (LAS) refers to the most appropriate pathway The case for change There is a lack of understanding about parts of the system, other than the Emergency Department, that London Ambulance Service could refer into. Pathways do exist, but these vary across SE London which can be confusing and the turnaround time to respond can be inconsistent. This can also mean crews from out of area are reluctant to use these pathways. GPs are also not easily available during hours to support alternative pathways for patients. Therefore this initiative aims to alleviate these problems. The proposal Under this initiative London Ambulance Service will be able to: Operate an internal triage approach to improve directing patients to best access points and appropriate services, such as the rapid access team, home ward (remove -or hospital based specialist clinics - until this is clearer) and excel in navigating patients to the right part of the system Operate a call ahead system to the emergency department triage nurse for mental health patients to enable a parallel assessment to take place at triage (see mental health interventions). This may mean a Mental Health assessment en route. Navigate the system easier through a simplified, accurate and up-todate Directory of Services combined referral pathways and one book for all pathways. Better communication of pathways and hospital liaison officers to challenge crews if alternative pathways available. Use the London Ambulance Service control room to put more calls through to 111 (not just during surge periods) and give patients the confidence that they will have good outcomes from using this service rather than 999. Have rapid access to information and specific patient plans with a possible link to GPs during In hours to enable alternative pathways for patients with long term conditions and frequent callers. Implement alternative care pathways through integrated working (and attitudinal changes). Use SEL wide pathways that avoid complexity and confusion and consider using technology better to support this smart phones so that ambulances crews can call to easily check pathways and a way of storing pathways so they can be accessed and updated quickly. Tackle the reactive risk averse culture, seeing rates of acceptance as a joint problem between the referrer and the receiver and consider building in consequences for not accepting a referral. Once a service doesn t accept a referral it may prevent further referrals to that service. Commissioning Groups and NHS England Draft in progress 105
106 Urgent and Emergency Care Model Intervention 6: Enhanced 111 capability The case for change There is a lack of understanding about parts of the system, other than the Emergency Department, that 111 could refer into. The proposal To improve this we propose that 111: Call handlers are educated/trained in the new models for SEL Are able to give advice, provide internal triage and coordinate onward referral to other parts of the system other than the Emergency Department Operate 24/7 managing appointments to Out-Of-Hours services or Emergency Department to support demand management Use clinicians to make decisions Provide a simplified DOS An Enhanced 111 service will be provided. This will be a smart call to make, helping people get the right advice or treatment in the right place, first time. This service will: Be an integral part of the Urgent Care Network Have knowledge about you and your medical problems, so the staff advising you can help you make the best decisions; Allow you to speak directly to a wider range of professionals (e.g. a nurse, doctor, paramedic, member of the mental health team, pharmacist or other healthcare professional); If needed, directly book you an appointment at whichever urgent or emergency care service can deal with your problem, as close to home as possible; Still provide you with an immediate emergency response if your problem is more serious, with direct links to the 999 ambulance service, and the enhanced ability to book appointments at Emergency Centres. Commissioning Groups and NHS England Draft in progress 106
107 Urgent and Emergency Care Model Intervention 7: Urgent care centre and the emergency department in a single governance structure and providing expert streaming across all sites The case for change This initiative recognises that: There is a need to reduce emergency department waits, allow patients to be re-directed immediately, and be seen and treated through rapid, expert early assessment. The points of access for care need to be less confusing for the public and health care professionals. Better value comes with co location There is currently no streaming at the PRUH for C&YP The proposal This initiative proposes: A single clinical governance structure for urgent care centres and emergency departments A single front door for urgent care centres and emergency departments. GP led minors service PALs with same 8-8 hours of operation. Cross working and training of ENPs and GPs across the emergency department and urgent care centre to improve capacity and capability of injury and illness. An appropriately qualified streaming decision maker that will stream patients at the front door to get the initial decision right and direct patients to the correct department - Majors, Minors, the urgent care centre or back to their GP Decisions are made with the correct pathway and outcome in mind to avoid unnecessary delays when the patient is ready to go home Earlier identification of Mental Health cases (including Dementia) with quicker and direct streaming to PNL for mental health patients+ The role is not covered by bank or agency staff Access to paediatric specialists at front door and other specialist services such as Drug and Alcohol. Commissioning Groups and NHS England Draft in progress 107
108 Urgent and Emergency Care Model Intervention 7: Urgent care centre and the emergency department in a single governance structure and providing expert streaming across all sites The proposal cont/d Suggested competencies for front door streamer Uses active listening skills, to establish an accurate history from the patient. Effectively acquires and utilises the signs and symptoms presented by the patient and acts accordingly. Demonstrates an ability to prioritise the patient s condition, in relation to actual/potential severity of injury/illness. Adheres to presentations listed when using triage bypass form. Requests appropriate x-rays. Provides analgesia where appropriate. Allocates patient to the appropriate stream, taking into account departmental workload. Is able to list patient presentations not to be redirected according to the policy. Requests all redirected patients to complete patient redirection form. Provides directions to locations away from the emergency department. Utilises the PALS officer appropriately. Asks for guidance if unsure regarding patient redirection. Streams patients for further assessment who are a potential for redirection. Streams patients who could be redirected into the emergency department if appropriate. Commissioning Groups and NHS England Draft in progress 108
109 Urgent and Emergency Care Model Intervention 8: Parallel assessments The case for change The current model of clinical triage with a separate Psychiatric Liaison Nurse assessment is often the cause of a long waits and breaching of emergency department targets. This can result in patients absconding and re-attending. The prevalence of mental health conditions amongst older people inpatient in the general hospital is estimated at 60% (Parsonage et al, 2012). The use of acute hospital services by people with dementia is rising and emergency admissions for people with dementia account for nearly 10% of all hospital admissions. 95% of acute hospital admissions for people with dementia occur in an emergency, with over 60% of these coming through emergency departments, even though 25% of all emergency presentations in people with dementia are preventable (Parsonage et al, 2012). In emergency departments, the main focus of liaison psychiatry work is on self-harm, severe mental illness and alcohol-use for adults of working age, and delirium and dementia for older adults. The high number of selfharm presentations in England each year means that this should therefore be a key focus for hospital-based services. There has been a 50% increase in the use of Emergency Care in the last decade, and there is evidence that the urgent and emergency care system is finding it increasingly difficult to meet indicators such as the four hour wait time in Emergency Departments and ambulance handover targets. The literature suggests that there is a need to find solutions that will increase the flow of patients through the health and care system (The King s Fund, 2013). The proposal To reduce these waits for mental health patients there will be: Experts streaming at the front door (see Enhanced Front Door) to allow for earlier identification of mental health cases (including Dementia) with quicker streaming to specialities for mental health patients. This means training the emergency department nurses on the front door to better recognise mental health needs and refer to mental health services faster. The potential for mental health screening to be carried out during the ambulance journey Parallel working of the Psychiatric Liaison nurse within the emergency department at an early stage ensuring rapid intervention and moving away from the medical model of clearance. Enabling of the police to better recognise mental health needs and being able to refer to mental health services rather than bringing patients to the emergency department. A Dr and Nurse mental health professional in the emergency department at peak times. There is therefore clear demand for a service such as liaison psychiatry that will help support the movement of patients through the system. (Developing models for Psychiatry liaison models). Commissioning Groups and NHS England Draft in progress 109
110 Urgent and Emergency Care Model Intervention 8: Parallel assessments The proposal cont/d Specification and Guidance on levels of Liaison Psychiatry Services - Developing Models for Liaison Psychiatry Services Guidance 2013 recommend four levels: Core Liaison Psychiatry Services - These services have the minimum specification likely to offer the benefit suggested by the literature. Core will serve acute health care systems with or without minor injury or emergency department environments where there is variable demand across the week, including periods of no demand where a 24-hour staffed response would be uneconomical. This model mainly serves emergency and unplanned care pathways and will provide a timely response to all mental health presentations in the emergency department within one hour between 9-5 M-F. Core24 Liaison Psychiatry Services - These services have the minimum specification likely to offer the benefit suggested by the literature where there is sufficient demand across the 24 hours period to merit a full service. Typically these acute health care systems are hospital based in urban or suburban areas with a busy emergency department. This model mainly serves emergency and unplanned care pathways. Enhanced 24 Liaison Psychiatry Services - These services have enhancements to the minimum specification to fit in with gaps in existing pathways and services. Often they have additional expertise in addictions psychiatry and the psychiatry of intellectual disability. Demography and demand may suggest additional expertise with younger people, frail elderly people or offenders, crisis response or social care. This may extend to support for medical outpatients. This model mainly serves emergency and unplanned care pathways but extends to support elective and planned care pathways where mental health problems co-exist. Comprehensive Liaison Psychiatry Services - Comprehensive services are required at large secondary care centres with regional and supra-regional services. These services include Core24 level services but will have additional specialist consultant liaison psychiatry, senior psychological therapists, specialist liaison mental health nursing, occupational and physiotherapists. They support inpatient and outpatient areas such as neurology, gastroenterology, bariatric surgery, plastic and reconstructive surgery, pain management and cancer services. They may support other condition specific elements such as chronic fatigue / ME and psychosexual medicine. Comprehensive services run over office and extended hours supported by the core service running twenty four hours, seven days a week. They may include specialist liaison psychiatry inpatient beds. This model serves emergency and unplanned care pathways as well as elective and planned care pathways where mental health problems co-exist. Commissioning Groups and NHS England Draft in progress 110
111 Urgent and Emergency Care Model Intervention 8: Parallel assessments The proposal cont/d The benefits we might expect from an effective model of liaison psychiatry service? There is now growing evidence for the impact of liaison psychiatry services. Descriptive evidence shows a list of benefits including: decreased length of stay, reduction in psychological distress, improved service user experience, improved dementia care And enhanced knowledge and skill of general hospital clinicians (Parsonage et al, 2012). Benefits apparent in the literature include: Improved service user experience Increased knowledge and understanding of mental health issues amongst general hospital staff Improved care outcomes Reduced emergency department waiting times Reduced admissions, re-admissions and lengths of stay Reduced use of acute bed by patients with dementia Reduced risk of adverse events Improved compliance of acute trusts with legal requirements under the Mental Health Act (2007) and Mental Capacity Act (2005) Reducing psychological distress following self-harm, and reducing suicide Improved compliance with NHS Litigation Authority Risk Management Standards and the Clinical Negligence Scheme for Trusts (CNST) (Joint Commissioning Panel for Mental Health, 2012). Commissioning Groups and NHS England Draft in progress 111
112 Urgent and Emergency Care Model Intervention 9: Specialist service interface D&A The case for change Currently two out of our five hospitals (2013/14 data) are not meeting the London Quality Standards for the following: Emergency departments to have a policy in place to access support services seven days a week including: Alcohol liaison, Mental health Older people s care Safeguarding Social services There are often delays to other specialist services such as Drug and alcohol teams due to the drop off between the patient taking themselves from the emergency department to the drugs and alcohol service. In South London the impact of alcohol is significant. The recent Screening and brief Intervention Programme for Sensible drinking study (SIPS) found that 40% of attendances at King s College and St Thomas s Hospital emergency department were alcohol related. Alcohol related inpatient admissions to acute care have doubled in the past 8 years in England and now account for 14% of all acute admissions in King s Health Partners (KHP). A study in South West London found that 50% of adult mental health admissions were alcohol related. During 2011, emergency department attendances at St Thomas Hospital and Kings College Hospital, coded with apparently drunk, alcohol dependent or alcohol cited on the GP letter totalled 400 patients per month. In outer London, the Sutton Health Profile 2011 indicates an above national value for rates of Increasing and higher risk drinking. Although hospital stays for alcohol related harm were below average at 1,523 admissions per 100,000 population. The case for action in South London is strong, six out of 12 South London Health and Wellbeing Boards have prioritised alcohol harm reduction, and most others have priorities that are affected by alcohol. There are early gains that can be made to reduce the burden on the health and social care system by addressing service access, early interventions and prevention approaches. The proposal This initiative proposes: Drug and Alcohol professionals and a rapid access to the drugs and alcohol service from the emergency department to reduce the drop off between the patient taking themselves from the emergency department to the drugs and alcohol service Low cost interventions Having Drug & Alcohol professionals sited in the emergency department. Commissioning Groups and NHS England Draft in progress 112
113 Urgent and Emergency Care Model Intervention 10: Specialist service interface for paediatric mental health The case for change For paediatric mental health patients there can be significant periods of time between both: Arrival in the emergency department to the referral being made And from referral being made to being seen There are four key issues for paediatric mental health patients that present in the Emergency Department that can lead to the waits described above: 1. In hours cover for paediatric mental health liaison is variable across SEL. Both in and out of hours there is a wide variation of resource particularly in those trusts where there is no in-house paediatric mental health provision 2. Out of hours paediatric mental health provision is poor in some trusts, and even in those trusts with in-house provision, is less out of hours than in hours. This means the waiting time can be more than twice as long out of hours. Typically the majority of paediatric deliberate self harm (DSH) cases attend out of hours. 3. The policies on admitting paediatric mental health patients to paediatric beds vary across hospitals. This may lead to patients in some hospitals suffering far more significant delays in admission than those elsewhere. Any admission requiring a child or adolescent psychiatric bed invariably suffers significant delay, whatever the originating emergency department, because of the national bed crisis. 4. Whilst the lack of paediatric mental health staff cause some delays, (for example a child may have to wait overnight in the emergency department until CAMHS can send a liaison nurse), the longest emergency department breaches are typically due to the difficulty in accessing paediatric mental health inpatient beds. Children may occasionally be admitted to an adult mental health ward or otherwise remain in the emergency department. Data from repeat audits carried out by the KCH paediatric liaison service for under 18s presenting to the emergency department over a three month period confirmed the two stages of delay arrival to referral and referral to being seen. Out of hours the waiting time can be more than twice as long as in hours. Data for St.Thomas is expected to reveal that patients are seen quicker for the initial assessment, but this is still longer out of hours. However the significant delay is in accessing inpatient beds. In the PRUH, Lewisham and QEW site emergency departments it is expected there may be only limited family therapist sessions or potentially no service provision as well as difficulties accessing inpatient paediatric mental health beds NICE Clinical Guidance 16: : states all children or young people who have self-harmed should normally be admitted overnight to a paediatric ward and assessed fully the following day before discharge or further treatment and care is initiated. Alternative placements may be required, depending upon the age of the child, circumstances of the child and their family, the time of presentation to services, child protection issues and the physical and mental health of the child; this might include a child or adolescent psychiatric inpatient unit where necessary. Commissioning Groups and NHS England Draft in progress 113
114 Urgent and Emergency Care Model Intervention 10: Specialist service interface for paediatric mental health The proposal In order to meet NICE guidance this initiative proposes to: Provide specialist input at an early stage to avoid long waits especially in the year age range. Provide an increase in specialist services within the emergency department according to level of need across SEL Aim for entry to referral within 1 hour from streaming or Triage nurse to the paediatric mental nurse (more triage nurses and medics, as well as slicker IT (King s College Hospital and, possibly, Guy s and St Thomas Trust use paper) Build in Nice guidance being mindful that the DOH or Government don t state NICE is mandatory and CQC don t penalise for being non-compliant. There are several models for providing out of hours emergency department based services for children and young people: Core trainee in psychiatry with access to CAMHS on call ST and consultant (this is the model SLaM use); Core trainee with access to consultant CAP telephone supervision and multispecialty consultant cover; multi-professional out of hours CAMHS professional with ST/Consultant CAP cover; Multi-professional out of hours CAMHS professional with multispeciality ST/consultant cover. There are also a range of models in terms of how much emergency cover is provided (e.g. only till rather than overnight). Commissioning Groups and NHS England Draft in progress 114
115 Draft in progress 115
116 Cancer Cancer model Person 4 End of Life 1 2 Early detection 3 Living with & Beyond Cancer Treatment H Key Features of the model 1 Primary prevention: Best delivered in the Local Care Network Early detection 1. Increased screening rates to national benchmark through targeted engagement 2. Diagnostics: Pilot project serious but unspecific symptoms pathway 3. Promotion of early diagnosis and equal access to treatment for older people 4. Professional development for all staff within Primary Care 2 Treatment Provider collaboration to create networked centres of excellence: 5. Non complex cancer treatments and support closer to home 6. Access to appropriate information and support for patients and carers 7. Acute Oncology Services networked and supported by integrated IT 8. Consistently meet the access time scales on our cancer services 9. Routine use of the recovery package 3 Living with and Beyond Cancer 10. Stratified follow-up 11. Support for people living with the adverse consequences of cancer treatments 12. Comprehensive support for carers 13. Psychological support for people living with Cancer 14. Inclusion of Cancer as a criteria for referral to exercise/physical activity on prescription schemes 15. Support to return to work, study or volunteering 16. Routine use of the recovery package 4 End of Life: Best Delivered in the Local Care Network 17. Ensure a dignified death irrespective of setting 18. Ensure consistent use of coordinate my care 19. Advance Care planning Commissioning Groups and NHS England Draft in progress 116
117 Cancer Intervention 1: Increase screening rates to national benchmark through targeted engagement The case for change Taking a south east London view, rates of screening for Breast, Cervical and Bowel screening, with the exception of Bromley and Bexley Clinical Commissioning Group for Breast Screening, do not currently meet the national benchmark as shown in the tables below. Cervical Ages National Benchmark Bexley 77% 80.00% Bromley 76.60% 80.00% Greenwich 71.30% 80.00% Lambeth 71% 80.00% Lewisham 72.70% 80.00% Southwark 72.30% 80.00% Breast Ages Ages Bexley 59% 73% 70% Bromley 63% 72% 70% Greenwich 51% 63% 70% Lambeth 49% 58% 70% Lewisham 52% 62% 70% Southwark 51% 61% 70% National Benchmark Bowel Ages Bexley 47.00% 60% Bromley 48.70% 60% Greenwich 41.10% 60% Lambeth 34.90% 60% Lewisham 39.30% 60% Southwark 34.60% 60% National Benchmark Source: London Cancer Alliance Q Metrics Pack (Produced June 2014) The proposal The Cancer Clinical Leadership Group propose a suite of evidence based interventions to improve screening rates which focus on targeted engagement work within the local care network. These include: Opportunistic face-to-face health promotion within the GP practices Telephone out-reach offered by multi-lingual staff Tackling DNA through o o o Reminder letters Flags on IT systems to identify patients who DNA screening Actively working with did not attend to support and encourage participation Home testing kits coordinated by the hub Catch all automated letter system on 60th Birthday s Communication of eligibility for breast screening to women aged 73+ years Targeted prevention conversations with patients and carers Commissioning Groups and NHS England Draft in progress 117
118 Cancer Intervention 2: Diagnostics (sits in the Planned care Clinical Leadership Group) Pilot project: Patients with serious but unspecific symptoms The case for change Cancer Research UK (CRUK) has very persuasive economic analysis showing potential savings in treatment costs if there s a shift in the percentage of patients detected at early stages. Delivery of this vision will mean a 10% increase in those patients diagnosed early which is equivalent to about 8,000 more patients living longer than five years after diagnosis. It has been shown that the GP indicates potential alarm symptoms in up to 12% (Ingebrigsten et al, 2013) of all consultations and suspects a serious disease in need of further elucidation in 6% of consultations (Hjertholm et al, 2014) (Figure 1). A study showed that 10% of these patients had a new serious diagnosis within 2 months. This means that when the GP suspects serious illness there are reasons to support the GP in having access to relevant investigations (Nylenna, 1986). The proposal This initiative is a three-legged strategy in diagnosing cancer taken from the example pathway trialled in Denmark. This model includes urgent referral pathways for suspicious symptoms of a specific cancer, urgent referral to diagnostic centres when we need quick and profound evaluation of patients with nonspecific, serious symptoms and finally easy and fast access to No-Yes-Clinics' for cancer investigations for those patients with common symptoms in whom the diagnosis of cancer should not be missed. References: (Br J Cancer Mar 31; 112(Suppl 1): S65 S69. Published online 2015 Mar 3. doi: /bjc PMCID: PMC A differentiated approach to referrals from general practice to support early cancer diagnosis the Danish three-legged strategy P Vedsted1,* and F Olesen1) Commissioning Groups and NHS England Draft in progress 118
119 Cancer Intervention 3: Promotion of early detection and equal access to treatment for older people The case for change Macmillan reports that the UK has some of the worst cancer survival rates in Europe for older people. Every year there are around 14,000 avoidable cancer deaths in people over 75. One of the reasons for this is that they are sometimes not offered the right treatment. Studies have shown that inequalities exist in terms of access to and outcomes from treatment for older people, for example, breast cancer patients over 70 are much less likely to receive surgery than those under 70. Older people often present with cancers at a later stage and are more likely to have their cancers diagnosed through emergency routes. Cancer treatment rates are thus lower in older people both factors have an impact on survival rates. In addition cancer mortality rates for older people in the UK are improving at a much slower rate than in the younger population. As a result, this initiative aims to promote early detection and treatment in older people. The proposal For this purpose, this initiative aims to: Raise awareness and promote early detection for older people Encourage collaborative working in secondary care In addition research undertaken by Macmillan and the Department of Health recommended the following interventions to address inequalities in care and improve the older patient outcomes and experience: Engage elderly care specialists as active part of the cancer care team & adopt a Multi Disciplinary Team approach to assessment & management of patients Have early appropriate assessment Ensure patients have maximum benefit for treatment Manage other health conditions Link with voluntary sector agencies Support staff through training and access to resources. Commissioning Groups and NHS England Draft in progress 119
120 Cancer Intervention 4: Professional development for Primary Care Staff The case for change Cancer Research UK (CRUK) has very persuasive economic analysis showing potential savings in treatment costs if there s a shift in the percentage of patients detected at early stages. Delivery of this vision will mean a 10% increase in those patients diagnosed early which is equivalent to about 8,000 more patients living longer than five years after diagnosis. Community-based healthcare staff and local volunteers are ideally placed to promote cancer awareness in their local area. The proposal To enable recognition of early signs and symptoms, three interventions are proposed: 1. Promote implementation of the Cancer Decision Support (CDS) Tool to support early detection in General Practice. CDS is an electronic tool developed by Macmillan. It is designed to be used as part of every day GP practice and assess the risk of a patient having an existing, undiagnosed cancer and will help GPs assess patients with possible cancer more effectively thus supporting early detection. 2. Significant Event Audit (SEA) - which promotes good practice through learning from significant events 3. Making every contact count; training for staff to promote and support early detection including: o o o o Pharmacists Practice nurses Macmillan practice nurse course Roll out of Very Brief Advice (VBA) for all professionally trained staff Front line primary care staff in CRUK Talk Cancer package Commissioning Groups and NHS England Draft in progress 120
121 Cancer Intervention 5: Provider collaboration to create networked centres of excellence The case for change There is a an opportunity to reduce variation in patient experience, patient care and outcomes through better coordinated services and standardised patient pathways across south east London. Across south east London, we are not consistently meeting the access time scales on our cancer services. Outcomes in SEL lag behind national and international comparators and there is variation in rates and quality of 2WW referral The proposal For this purpose, this initiative aims to provide networked cancer services supported by integrated IT systems, to include the following suite of interventions: Acute Oncology Services Non Complex chemotherapy treatment options closer to home Consistently met cancer standard wait times o o o A detailed review of any patient waiting over 100 days South east London 62 day cancer waits group which provide a system wide approach to speed treatment pathways Implementation of 2WW NICE Guidance Access to appropriate information and support for Patients and Carers Routine use of the Cancer Recovery Package. Commissioning Groups and NHS England Draft in progress 121
122 Cancer Intervention 6: Non complex chemotherapy treatment options closer to home The case for change Many of the drugs used to treat cancer can be safely delivered away from major cancer centres. Community chemotherapy are where patients receive their chemotherapy treatment outside of the accredited cancer centres and cancer units in facilities nearer to home such as a GP surgery or in their own homes. The key drivers for delivering chemotherapy services in the community are improved patient choice and experience and managing the on-going increasing demand for chemotherapy. Additionally, in some circumstances there is the potential for it to deliver efficiencies, particularly where physical expansion is required. The proposal This next step for this intervention will be to agree a south east London model for delivering non-complex treatment options closer to home. Commissioning Groups and NHS England Draft in progress 122
123 Cancer Intervention 7: Access to appropriate information & support for patients and carers The case for change The NHS Five Year forward view outlines that patients don t always have the information they need and, crucially, the support to understand the issues. 87% of people affected by cancer want to know more about their disease, 50% of cancer patients forget most of the information given to them within minutes of their consultation (Macmillan). Various studies have shown that 16% who would like to receive information about their condition do not receive any at all and 43% would like more information than they are given. Macmillan funded research has shown that 37% of people with cancer found the whole cancer support system confusing and would benefit from structured support and guidance on managing their condition. 43% of people use the internet to access cancer information. For people living with something as life changing as cancer, speaking to others in the same position can be a vital way to deal with emotions (Macmillan). The proposal This initiative includes: A Care/Case navigator role which will be able to provide information on where/how to access appropriate information for patients and carers such as psychological support, An acute oncology services 24/7 advice line Support to facilitate patients and carers to access existing on-line support services Support to signpost patients and carers to Cancer advice and support centres Commissioning Groups and NHS England Draft in progress 123
124 Cancer Intervention 8: Acute Oncology Services (AOS) The case for change There are a high percentage of patients first presenting in A&E with a previously unidentified cancer diagnosis, cancer patients also present with chemotherapy and radiotherapy complications as well as progressive disease symptoms. This leads to inappropriate admissions via A&E to non specialist treatment and care with extended length of stay in general medicine beds as patients wait for specialist care. This impacts on patient experience and potentially can have adverse clinical outcomes. The five year Cancer commissioning (p29) states that whilst AOS has been introduced and currently exists within south east London, there is variation in provision and failures to comply with AOS metrics. The proposal This initiative proposes coordinated and consistent Acute Oncology Services networked and supported by integrated IT systems. National expectation NCAG report and Cancer Reform Strategy recommended the establishment of an acute oncology service in all hospitals by 2011, at the latest, for quality and safety reasons: To provide early recognition, better treatment, fast referral to appropriate team, earlier discharge To enable close integration with the Clinical Haematology team, as well as Palliative Care, acute Medicine, acute Surgery, Radiology, Pathology etc. and to lead chemotherapy and oncology services at hospital level To provide chemotherapy in appropriate local settings Coordinated Acute Oncology Services provide consistent standards of care and improved access to oncology specialists supported by integrated IT systems for sharing patient records. Early review provides a member of the Acute Oncology Team: 24/7 access to telephone advice from an Oncologist Fast track clinic access from A&E/MAU Access to information on individual patients across the Trust/Trusts Protocols for the management of oncological emergencies and referral pathways from A&E and MAU Specific pathways for the investigation and treatment of malignant spinal cord compression (MSCC). Commissioning Groups and NHS England Draft in progress 124
125 Cancer Intervention 9: Routine use of the Cancer Recovery Package The case for change There is a need for better coordination across primary, secondary care and the third sector to achieve seamless service provision and support patients to transition home. The proposal Routine use of the Cancer Recovery Package will ensure care is coordinated, transition home is supported and patients are empowered to take good life style choices. The Recovery Package is a combination of different interventions, which when delivered together, will greatly improve the outcomes and coordination of care for people living with and beyond cancer. These are: A Holistic Needs Assessments and care planning at key points of the care pathway, A Treatment Summary completed at the end of each acute treatment phase, sent to patient and GP and in secondary care A Cancer Care Review completed by GP or practice nurse to discuss the person s needs, and A patient education and support event, such as a Health and Wellbeing Clinic, to prepare the person for the transition to supported self management, which will include advice on healthy lifestyle and physical activity. The Recovery Package has been developed and tested by the National Cancer Survivorship Initiative (NCSI) (NHS Improvement 2012) to assist people living with a diagnosis of cancer to prepare for the future, identify their individual needs and support rehabilitation to enable people to return to work and or a near normal lifestyle. The Recovery Package has been designed to complement the stratified care pathway (NHS Improvement 2012) which enables individualised follow-up care as a supported self management programme, shared care or complex care. Reference: National Cancer Survivorship initiative Macmillan, Department of Health, NHS England Commissioning Groups and NHS England Draft in progress 125
126 Cancer Intervention 10: Implement stratified pathways of care The case for change There were 186,000 people living with and beyond cancer in London in 2010, it is estimated that there will be 364,000 in London by 2030 (Macmillan). Currently there is not enough personalised care for patients and patients needs change over time (Macmillan) Tailored care is required to support individual needs, to support healthy life style choices and transition back into their lives. The proposal Stratified means that the clinical team and the person living with cancer make a decision about the best form of aftercare based on their knowledge of the disease, the treatment and the person and how much support that they feel they need (National Cancer Survivor initiative). There are three forms of aftercare: Supported Self Management where patients are given the information about self management support programmes or other types of available support, the signs and symptoms to look out for and who to contact if they notice any, what scheduled tests they may need such as annual mammograms, and how they get in touch with professionals if they have any concerns. Shared Care where patients continue to have face to face, phone or contact with professionals as part of continuing follow up. Complex Case Management where patients are given intensive support to manage their cancer and/or other conditions. Reference: National Cancer Survivorship initiative Macmillan, Department of Health, NHS England Commissioning Groups and NHS England Draft in progress 126
127 Cancer Intervention 11: Better management and support for people living with the adverse consequences of Cancer treatments The case for change Given the growing number of people who are living with cancer, there has been a shift from seeing it as a fatal illness to a chronic one, where people may be in one of a number of possible stages, ranging from diagnosis, active treatment, remission and relapse to end of life. This shift has led to a growing focus on survivorship, and on the long-term needs of those living with and after cancer. Evidence shows that many of these cancer survivors have unmet needs particularly at the end of treatment, whilst others are struggling with consequences of treatment that could be either avoided or managed (Macmillan) % of patients receiving anti-cancer treatments are affected by fatigue that may persist for years (National Cancer Action). 30% of cancer patients have unmet needs after treatment for cancer, which could be addressed by rehabilitation (National Cancer Action) Late effects of radiotherapy and chemotherapy leads to a raised risk of heart disease and diabetes (TCST) The proposal The initiative includes: Greater access to physical health support for people who experience the unwanted consequences of treatment pathways Enabling access to Social Care aids/services to facilitate independent living, social support - Citizens Advice Practice nurse training up-skilling the generalist workforce to support patients Developing a strategy for lymphedema based on best practice examples Rehabilitation pathways (National Cancer Action Team guidance) Linking patients with right services for support: o o Access to specialist services for lymphedema and pelvic radiation disease Access to generalist services for Sexual dysfunction (men and women) Psychological support Chronic Fatigue Pain management Sleep management Commissioning Groups and NHS England Draft in progress 127
128 Cancer Intervention 12: Comprehensive Support for Carers The case for change Across the UK, at least 1.1 million people are currently caring for a friend or family member with cancer. As the number of people living with and beyond cancer continues to rise, from two million to four million by 20302, the number of carers is also rising. Sadly, many people caring for someone with cancer remain hidden. They care in isolation, unaware of support services that may be available to them. Carers in the UK make a major contribution to society. Their care is invaluable to the person who needs it, and the economic value for health and social care is an estimated 119 billion each year. Cancer carers provide care worth at least 14.5 billion each year. The proposal The initiative includes early identification of carers to support them in their own needs as well as signpost them to information, support and advice. Carers should also be included in advanced care and discharge planning which can ensure that the person with cancer will be supported at home. The model encourages: Adopting Macmillan s guidance outlined in Identifying cancer carers and signposting them to support Enabling and supporting carers in their care giving roles with access to range of support options group, on-line etc. The provision of training in which carers can train alongside professionals to support them in their care giving roles Offering carers needs assessment as routine Reference: Macmillan do you care making identification and support for carers a priority Commissioning Groups and NHS England Draft in progress 128
129 Cancer Intervention 13: Psychological Interventions The case for change In the first year after cancer diagnosis about 25 per cent of people experience psychological distress, with symptoms of anxiety and depression severe enough to affect their quality-of-life. There is however, variation in the provision of emotional and psychological support services across London. The government s mental health outcomes strategy No Health Without Mental Health places considerable emphasis on the connections between mental and physical health. The proposal The initiative includes: Early identification of carers to support individuals. Considering a persons mental wellbeing at all stages of their journey Facilitating greater access to Psychological interventions to promote mental health & well-being o Access to psychological support: during treatment phase - Level 2 CNS, Level 3/4 psychiatric liaison services o o Access to psychological support post treatment (patient and carer) IAPT (self/gp referral). Reviewing outcomes and learning from the London Cancer Alliance ehna pilot model pathway for Mental Health and Psychological support services for adults In addition, the London Mental Health Strategic Clinical Network in partnership with the Transforming Cancer Services Team for London has produced guidance to support commissioners and service providers in improving psychological support across the cancer pathway. The south east London programme proposes to follow these recommendations upon publication. Reference: National Institute for Clinical Excellence (2004) Guidance on Improving Support and Palliative Care for Adults with Cancer. Commissioning Groups and NHS England Draft in progress 129
130 Cancer Intervention 14: Inclusion of Cancer as a criteria for referral to exercise/physical activity on prescription schemes The case for change Evidence shows that physical activity can reduce the risk of developing breast, bowel or womb cancer preventing an estimated 3,400 cases of cancer every year in the UK. Aerobic exercise like running, cycling or swimming can help alleviate fatigue during or following cancer treatment (Macmillan). The proposal The initiative includes: Physical activity to be prescribed to patients by their GP s following cancer treatment where appropriate A named professional to encourage and facilitate access to opportunities to undertake physical activity both Cancer and noncancer specific options/schemes. Commissioning Groups and NHS England Draft in progress 130
131 Cancer Intervention 15: Support to return to work, study or volunteering The case for change Macmillan states that over a third of the two million people living with cancer in the UK are of working age (18 64 years). Work is an integral part of helping people get back to normality and for many, it can also be a financial necessity. However, the reality is that those who want to return to work don t always receive the support they need, thus preventing them from benefiting both employers and making a significant contribution to the UK economy. The proposal This models proposes adopting a new model for vocational rehabilitation services. Macmillan, as part of the National Cancer Survivorship Initiative (NCSI), piloted a new model of vocational rehabilitation services for people with cancer. The evaluation identified three different levels of work support to be offered as routine: Level 1 Open access to information and support: o All service providers and health professionals should ask people living with cancer who are in work or have the potential to work about their employment situation. Level 2 Active support for self-management: o Health professionals and other support staff with some specialist knowledge of work-related cancer issues should provide resources to help people self manage so they can return to work. Level 3 Specialist vocational rehabilitation: o People who have complex needs should be referred to a vocational rehabilitation service for specialist case management support. (Making the shift - Providing specialist work support to people with cancer) Commissioning Groups and NHS England Draft in progress 131
132 Cancer Intervention 16: Implementation of the Cancer Recovery Package The case for change There is a need for better coordination across primary, secondary care and the third sector to achieve seamless service provision and support patients to transition home. The proposal Routine use of the Cancer Recovery Package will ensure care is coordinated, transition home is supported and patients are empowered to take good life style choices. The Recovery Package is a combination of different interventions, which when delivered together, will greatly improve the outcomes and coordination of care for people living with and beyond cancer. These are: A Holistic Needs Assessments and care planning at key points of the care pathway, A Treatment Summary completed at the end of each acute treatment phase, sent to patient and GP and in secondary care A Cancer Care Review completed by GP or practice nurse to discuss the person s needs, and A patient education and support event, such as a Health and Wellbeing Clinic, to prepare the person for the transition to supported self management, which will include advice on healthy lifestyle and physical activity. The Cancer Care review and patient well being event can take place in the local care network. The Recovery Package has been developed and tested by the National Cancer Survivorship Initiative (NCSI) (NHS Improvement 2012) to assist people living with a diagnosis of cancer to prepare for the future, identify their individual needs and support rehabilitation to enable people to return to work and or a near normal lifestyle. The Recovery Package has been designed to complement the stratified care pathway (NHS Improvement 2012) which enables individualised follow-up care as a supported self management programme, shared care or complex care. Reference: National Cancer Survivorship initiative Macmillan, Department of Health, NHS England Commissioning Groups and NHS England Draft in progress 132
133 Cancer Intervention 17: Ensuring a dignified death irrespective of setting The case for change There is potential to improve the experience of care in the last year and months of life. The Parliamentary and Health Service Ombudsman report Dying without dignity (p4) states that: the experience of people who are dying and their loved ones of the care provided by the NHS is a recurring theme in complaints Key themes and issues were identified as: Not recognising that people are dying and not responding to their needs Poor symptom control Poor communication Inadequate out-of-hours service Poor care planning Delays in diagnosis & referral for treatment b The proposal The initiative therefore support improved patient experience at end of life through Implementing the 5 priorities outlined by the Leadership Alliance for the Care of Dying People One Chance To Get it Right (June 2014). These include: o o o o o The possibility that a person may die within the next few days or hours is recognised and communicated clearly, decisions are made and actions taken in accordance with the person s needs and wishes Sensitive communication takes place between health care professionals and the dying person, and those identified as important to them The dying person, and those identified as important to them, are involved in decisions about treatment and care The needs of families and others identified as important to the dying person are actively explored, respected and met as far as possible An individual plan of care, which includes symptom control and psychological, social and spiritual support, is agreed, coordinated and delivered with compassion. Promoting autonomy at end of life to facilitate dying in a place of choice. Reference: NHS England (Nov2014) Actions for End of Life Care Commissioning Groups and NHS England Draft in progress 133
134 Cancer Intervention 18: Ensuring a dignified death irrespective of setting The case for change Coordinate My Care (CMC) is a service dedicated to preserving dignity and autonomy at the end of life. Its care pathways enable health professionals from primary and secondary care to put the patient at the centre of health care delivery. This service is underpinned by an electronic solution. The CMC record can be accessed 24/7 by all health and social care professionals who have a legitimate relationship with the patient. The record can display diagnosis, prognosis, advanced care plan, resuscitation status and patients wishes for end of life. A patient can access and contribute to their own record. The proposal The initiative proposes: Implementation of Coordinate My Care Support for professionals to access and use CMC Ensuring consistent use of Coordinate My Care across south east London monitor and audit. References: BMJ - Coordinate My Care: a clinical service that coordinates care, giving patients choice and improving quality of life Clare Smith,1 Libby Hough,1 Chi-Chi Cheung,2 Catherine Millington-Sanders,3 Eileen Sutton,4 Joy R Ross,1,5 Michael Thick,5 Julia Riley1,5 December 6, Published by group.bmj.com Commissioning Groups and NHS England Draft in progress 134
135 Cancer Intervention 19: Advance Care Planning The case for change A diagnosis of cancer may prompt planning for future care. Planning future care is important in case a person becomes ill unexpectedly and becomes unable to make choices and decisions about treatment, healthcare or make financial plans for their loved ones (Macmillan). The proposal The initiative recognises the need to: Start conversations early to facilitate greater choice and control over care options Advance care planning to promote early assessment of end of life needs, advance care planning, including the following suite of interventions: o o o o Living wills, advance decisions and advance statements Advance decision to refuse treatment Your wishes for future care Lasting Power of Attorney. Commissioning Groups and NHS England Draft in progress 135
136 Draft in progress 136
137 Benefits/outcomes of achieving our vision Purpose of the Outcomes Framework The primary aim of delivering the Our Healthier South East London strategy and vision is to develop ways to improve the health and care outcomes for south east London communities and people. A framework which sets out measures to monitor the impact of the strategy on outcomes has been developed through engaging with our partners across health and care providers, Public Health, clinicians and public and patients. This framework sets out the measures that demonstrate the effectiveness of the strategy in achieving the outcomes allowing us to quantify the strategies impact. Focusing on the achievement of outcomes By implementing the strategy and its care models the aim is to reduce the variability in outcomes we see today as outlined in the case for change and to improve the overall health and care outcomes for people across south east London. Our outcomes aim to improve health, reduce health inequalities and make sure that services are consistently of a high standard both in terms of clinical outcomes and patient experience. Inputs/ process measures may be used as proxies to identify these. Approach to selecting indicators to measure the performance of the strategy To measure if the strategy is delivering the outcomes a number of indicators were selected that will demonstrate the strategies performance against the outcomes. Hundreds of indicators exist across health and social care, however a small number is required in order to remain focused. These will be complex and more focused on care models than at a CCG or Local Care Network level. The aim for this process was to strike a balance between an appropriate number of measures by applying the following principles to selecting the indicators and through feedback from stakeholder groups including public health: Principles applied for selecting indicators: outcome focused where possible addresses the challenges set out in the Case for Change reflect the new clinical models of care reflect the whole pathway of health and care, including mental health indicators that predominately come from existing sources drawing on national frameworks, emerging frameworks from other parts of the country and local data sources. It should be noted that a number of placeholders have been included where indicators are being developed nationally. By following these principles it will be possible to measure the impact of the strategy and be able to measure and compare south east London with other health and care economies. Commissioning Groups and NHS England Draft in progress 137
138 Benefits/outcomes of achieving our vision Structure of the framework The framework is made up of the following core elements: Domains: The high-level grouping or classification of outcomes that are measuring similar things. There are a number of existing outcome frameworks which were reviewed and based on those frameworks, four domains that are common across them were selected. Outcomes within these domains will represent performance across the system and for different population groups. Outcomes: The overall impact of the strategy on the health and wellbeing of our populations and individuals in south east London Indicators: The measures selected to demonstrate the achievement of the outcome. These are as outcome focused as possible but in some cases a process/structure measure has been used as a proxy. It should be noted that, while indicators are aligned with certain domains, many of them could be included in a number of different areas. Measuring outcomes at different levels Outcome measures for Our Healthier South East London can be used in a number of different ways and at different levels. While the outcome framework below focuses on the achievement of the overall strategy at a south east London level, they can be applied at different levels in the system as set out below: South East London Whole System Outcomes: A small, focused, number of outcome indicators at a system level to demonstrate the overall impact of the strategy as outlined on the following pages. CCG outcomes: CCGs already have a large number of outcomes and measures, both local and national; these will remain There will be alignment with the whole system model outcomes for those outcomes and measures where the 6 CCGs can achieve greater impact together Local Care Network outcomes: Over time, Local Care Networks will be measured on their performance in a number of ways; 1. At a strategic level a common set of measures across the Local Care Networks that demonstrate the performance of the Local Care Network linked to the whole system outcomes 2. Local level measures for areas of concern /improvement that may vary between boroughs and Local Care Network areas, for example because of demographic differences (set by individual CCGs) and 3. Contractual performance measures that will link to both strategic and local outcomes Commissioning Groups and NHS England Draft in progress 138
139 Benefits/outcomes of achieving our vision is possible to measure many of the indicators in the framework at all levels. However, in some instances local measures and methodologies will need to be defined in order to routinely capture and monitor performance. Measuring performance at a local level will also be supported by the development of patient-linked data sets where possible. These have been highlighted as TBC in the framework. System transformation measures In addition to the whole system outcomes, a number of system transformation measures can be applied to demonstrate how organisations across south east London are implementing the strategy. Many of these measures will be linked to outcomes and will be able to act as proxy indicators until outcomes are realised. These measures will be developed as we move towards implementation and will be led by the clinical and operational teams developing these models. For example; Outputs and processes: Care models will begin to define how certain interventions will be delivered. Through this process a range of outputs and process measures will be defined. For example, the number of patients who have a care plan. Financial: It is anticipated that, by delivering care in a more integrated way and with greater emphasis on prevention, there will follow a range efficiency and financial benefits across the system. These are articulated as part of the financial impact assessment. Developing a baseline Once the framework has been agreed a baseline will be developed to understand current performance and agree the scale of improvement the strategy is expected to deliver. This will take place from June to August. Whole System Outcome Framework The following pages set out the whole system Outcome Framework. This includes supporting information: The definition and rationale for each indicator Method of collection, Frequency of collection Readiness of the data to be collected and measured The level at which it can or potentially can be measured Quality: A core component of the strategy is improving the quality of care and, in particular, supporting providers to achieve the London Quality Standards. Many of these measure are, not directly measuring outcomes but rather look at the standards that should be in place in order to improve outcomes. Through the development and implementation of the care models, it will be important to monitor performance against national and regional quality standards such as the London Quality Standards. Commissioning Groups and NHS England Draft in progress 139
140 Population Health Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Potential Years of Life Lost (PYLL) from causes considered amenable to healthcare NHSOF 1a, CCGOF 1.1 Potential years of life lost (PYLL) rate from causes considered amenable to healthcare. To ensure that the NHS is held to account for doing all that it can to prevent amenable deaths. Deaths from causes considered amenable to healthcare are premature deaths that should not occur in the presence of timely and effective healthcare. Each CCG has were required to set out a level of ambition to improve this in their 3 and 5 year plans. Data Annual X X Preventing people from dying prematurely and can live longer and healthier lives Disease Burden: Incidence and/or prevalence of major chronic conditions - Diabetes - Obesity (adult and 16-18) - Chronic Obstructive Pulmonary Disorder - Cardiovascular Disease Premature mortality (under 75) from the major causes of death in SEL: - Cardiovascular diseases, - Cancers - Respiratory diseases (COPD) - Alcohol specific mortality QOF HSCIC / CCG OF Analysis based on QOF data which can be used to determine impact on prevalence at a local level. Notes (1) QOF measures Obesity from 16 (2) some of these may increase if there is an increase in reporting and/or early detection - this should be recognised as positive. A measure of the likelihood of dying of CVD, Cancer or COPD under the age of 75, which allows for comparisons between populations with different age profiles and over time. A number of health issues in the case for change have been identified as a high burden of ill health across south east London where the trend or outlook is worsening Premature mortality and differences in life expectancy are both significant issues. There is a difference in life expectancy between the most and least deprived wards of 8.7 years for women and 9.3 years for men. About 11,000 people died prematurely across south east London over the period 2009 to 2011, with four boroughs being classified in the worst category for premature mortality outcomes in England. Data TBC X X X Data Quarterly X X T B C The biggest causes of premature mortality are cardiovascular diseases, cancers and respiratory diseases. Mortality rates for these diseases have decreased significantly over recent years, but rates continue to be considerably above London average (SEL Case for Change) KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 140
141 Population Health Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Reduction in gap in life expectancy between the most and least deprived ONS, PHOF, GLA data store Life expectancy at birth: the average number of years a person would expect to live based on contemporary mortality rates. Figures calculated by Office for National Statistics using ONS mortality data and midyear population estimates The average number of years a person would expect to live based on contemporary mortality rates. For a particular area and time period, it is an estimate of the average number of years a new-born baby would survive if he or she experienced the agespecific mortality rates for that area and time period throughout his or her life. Data Annually X X Reducing differences in life expectancy and healthy life expectancy between communities There is a difference in life expectancy between the most and least deprived wards of 8.7 years for women and 9.3 years for men. About 11,000 people died prematurely across south east London over the period 2009 to 2011, with four boroughs being classified in the worst category for premature mortality outcomes in England. Major causes of death between communities linked to level of deprivation. Mortality rates for: - Circulatory, cancer, and respiratory conditions (need to confirm for each borough) HSCIC (Primary Care Mortality Database) There are a number of contributing factors to the life-expectancy gap. One of the major factors is the major causes of death. For example, in Lambeth, the major contributing factors are Circulatory, cancer and respiratory conditions ( s/ssh-lambeth-life-expectancy-2014.pdf). Capturing this information at a local level could act as a proxy for health inequalities See above. Data Quarterly (TBC) Local analysis required X X X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 141
142 Quality of Life Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Permanent admissions to residential and care homes, per 100,000 population (both over 65 and 18-65) (All admissions) ASCOF 2A, BCF (just over 65) This is a two part-measure reflecting the number of admissions of younger adults (part 1) and older people (part 2) to residential and nursing care homes relative to the population size of each group. The measure compares council records with ONS population estimates. The working group also agreed that it would be necessary to capture admissions from different parts of the system. Avoiding permanent placements in residential and nursing care homes is a good indication of delaying dependency, and local health and social care services will work together to reduce avoidable admissions. Research suggests where possible people prefer to stay in their own home rather than move into residential care. Data 6 monthly X X T B C People are independent, in control of their health, and able to access personalised care to suit their needs Proportion of people who use services who have control over their daily life ASCOF 1B This measure shows the proportion of service users who have control over their daily life, and is calculated from data collected in the Adult Social Care Survey. The relevant question drawn from the Adult Social Care Survey is Question 3a: "Which of the following statements best describes how much control you have over your daily life?" Control is one of the key outcomes for individuals derived from the policy on personalisation. Part of the intention of personalised services is to design and deliver services more closely matching the needs and wishes of the individual, putting them in control of their care and support. This measure is one means of determining whether that outcome is being achieved Survey Annual X X Unplanned hospitalisation for chronic ambulatory care sensitive conditions HES, CCG 2.6, NHSOF 2.3i Directly age and sex standardised rate of unplanned hospitalisation admissions for chronic ambulatory care sensitive conditions for persons of all ages. These conditions include, for example, diabetes, epilepsy and high blood pressure. This outcome is concerned with how successfully the NHS manages the conditions through looking at unnecessary hospital admissions. Data Quarterly (rolling) X X Complications associated with diabetes CCG OF 2.8 Indirectly age and sex standardised rate for complications associated with diabetes, per 100 people with diabetes. This is an outcome measure that captures exacerbations in existing conditions. This should promote preventative activities to reduce the occurrence of complications. Data Annual X X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 142
143 Quality of Life Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Employment of people with long-term conditions NHSOF 2.2 The percentage point difference between the rate of employment in the general working age population (aged 16-64) and the rate of employment amongst those working age adults self reporting a mental illness. Both component employment rates are reported alongside the indicator. This indicator measures the extent to which people with long-term conditions are able to live as normal a life as possible by looking at their levels of employment. Data Annual X X Health and care services enable people to live a good quality of life with their long term condition Health-related quality of life for people with a long-term mental health condition Proportion of adult carers who have as much social contact as they would like CCG OF 2.16 ASCOF / PHOF 1.18ii Average adjusted health status (EQ-5D ) score for individuals reporting that they have a longterm mental health condition, based on responses to a question from the GP Patient Survey. This measure shows the proportion of carers who reported that they have as much social contact as they would like. The measures are calculated from data collected in the Adult Social Care Survey and the Carers Survey. The question from the Carers Survey is Question 11; Thinking about social contact you ve had with people you like, which statement best describes your present social situation? There is a clear link between loneliness and poor mental and physical health. A key element of the Government s vision for social care is to tackle loneliness and social isolation, supporting people to remain connected to their communities and to develop and maintain connections to their friends and family. This measure will draw on self-reported levels of social contact as an indicator of social isolation for both users of social care and carers. Survey Annual X X Survey TBC X X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 143
144 Effectiveness of Care Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Treatment is effective and delivers the best results for patients and service users Emergency readmissions within 30 days of discharge from hospital all admissions CCGOF 3.2 Total number of emergency admissions episodes for people of all ages where an acute condition that should not usually require hospital admission was the primary diagnosis. The indicator shows information on the number of emergency admissions per 100,000 population. This indicator has been indirectly age and sex standardised. To measure the progress in helping people to recover as effectively as possible. This is a short-term outcome measure. Data Annual X X Patient Reported Outcome Measures for elective care services PROM data The EQ-5D index case mix adjusted average and total health gain from patients reported improvement in health status following elective procedures. To ensure elective care is covered by the NHS Outcomes Framework. Over time the number of PROMS may be increased. Survey Annual X Proportion of older people (65 and over) who where still at home 91 days after discharge from hospital into reablement/rehabilitation services NHSOF 3.6i, ASCOF 2B Proportion of older people (65 and over) who where still at home 91 days after discharge from hospital into reablement/rehabilitation services This measures the benefit to individuals from reablement, intermediate care and rehabilitation following a hospital episode, by determining whether an individual remains living at home 91 days following discharge the key outcome for many people using reablement services. It captures the joint work of social services and health staff and services commissioned by joint teams, as well as adult social care reablement. Data Annual (can be produced monthly locally) X X T B C Survival rates for cancer in the effectiveness of care outcome (1 and 5 years) NHSOF 1.4 / CCG OF / ONS One-year and five-year net survival for adults suffering from cancer. A measure of the number of adults diagnosed with any type of cancer in a year who are still alive five years after diagnosis. ONS still publish survival percentages for individual types of cancers. These can be found at: and-followed-up-to-2012/index.html Data Annual KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 144
145 Effectiveness of Care Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N A reduction in the average length of stay (acute bed days) SUS data A reduction in the average length of stay from an agreed baseline position The length of time patients spend in hospital for specific conditions has a large impact on overall health system costs. It also impacts on the quality of patient care exposing them to potentially negative risks such as increased frailty. A reduction in the length of stay will demonstrate a system that is working well and that supports patients along the pathway of care. Data Quarterly (potential for more frequent measurement) X X T B C Delivering the right care, at right place, at the right time along the whole cycle of care Delayed transfers of care from hospital per 100,000 population (18+) ASCOF and Existing Data A delayed transfer of care occurs when a patient is ready for transfer from a hospital bed, but is still occupying such a bed. This is also a core BCF measure This measures the impact of hospital services (acute, mental health and nonacute) and community-based care in facilitating timely and appropriate transfer from all hospitals for all adults. This indicates the ability of the whole system to ensure appropriate transfer from hospital for the entire adult population, and is an indicator of the effectiveness of the interface within the NHS, and between health and social care services. Minimising delayed transfers of care and enabling people to live independently at home is one of the desired outcomes of social care. Data Quarterly (potential for more frequent measurement) X X T B C Emergency admissions for acute conditions that should not usually require hospital admission CCGOF 3.1, NHSOF 3.3a Total number of emergency admissions episodes for people of all ages where an acute condition that should not usually require hospital admission was the primary diagnosis. The indicator shows information on the number of emergency admissions per 100,000 population. This indicator has been indirectly age and sex standardised. To measure the progress in helping people to recover as effectively as possible. This is a short-term outcome measure. Data Quarterly X X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 145
146 Quality of Care Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Commitment to people having a positive experience of care Patient experience of hospital care (composite measure of inpatient, outpatient and A&E) Patient experience of GP services Patients experience of Integrated Care (Placeholder currently under development) NHSOF 4b NHSOF 4a NHSOF and ASCOF Patient experience measured by scoring the results of a selection of questions from the national inpatient survey looking at a range of elements of hospital care. Patient experience of GP services, measured by scoring the results of one question from the GP Patient Survey To capture the experience of patients who have recently received medical treatment in hospital. Over time it may be possible to move to a single measure of satisfaction for all health and care services. All south east London CCGs have lower than average GP access (Case for Change) Survey Annual X Survey Annual X X TBC TBC TBC TBC Caring for people in a safe environment and protecting them from avoidable harm Proportion of people who use [social care] services who feel safe Percentage of professionals who report they are satisfied or very satisfied with their job ASCOF 4A Provider staff surveys This measure shows the proportion of people who use services who feel safe, and is calculated from data collected in the Adult Social Care Survey. The relevant question drawn from the Adult Social Care Survey is Question 7a: Which of the following statements best describes how safe you feel? Exact definition and method TBC Based on recent research the satisfaction levels among a hospital's staff are closely linked to the quality of healthcare it provides. As such, staff satisfaction can be included as a proxy for the quality of care. ( /early/2013/02/20/bmjqs full) Survey TBC X X Survey TBC X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 146
147 Quality of Care Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Caring for people in a safe environment and protecting them from avoidable harm NHS safety thermometer (for all settings within scope): - pressure ulcers - falls - urinary tract infections (UTIs) in patients with a catheter - new venous thromboembolisms (VTEs) Reduction in the variation of care across SEL(1): To demonstrate the variations in care a number of measures can be used that are consistent across all 24 Local Care Networks. Measures could include: - Emergency department attendances - Emergency admissions - Emergency readmissions - Referrals HSCIC SUS data The NHS Safety Thermometer is the measurement tool for a programme of work to support patient safety improvement. It is used to record patient harms at the frontline, and to provide immediate information and analyses for frontline teams to monitor their performance in delivering harm free care. Measurement is across care settings including; Acute Hospital Ward, Community, Community Hospital Ward, Hospice, Mental Health Community, Nursing Home, Other, Own Home, Residential Care Home. Providers should be measured against all settings within scope of the contract. A number of indicators, linked to the case for change, that will demonstrate key variations in care across SEL. The exact detail for these will be determined through community based care implementation group and agreed across SEL. For many of these indicators it will be possible to build these from existing data sets on a quarterly basis. This would require the combination of SUS, ONS deprivation and Exeter Registrations Together these measures will ensure that providers are delivering safe care and protecting patients and service users from harm. There is variation in the quality of care across SEL. As LCNs are developed they should be able to impact on some of the core measures that indicate quality of care. Activity measures are used as a proxy in this instance to highlight potential variations based on need. For example, the kings fund have identified that the rate of emergency admissions in the most deprived areas is more than twice the rate in the least deprived areas in England. Conversely referrals for some procedures are lower in areas of greater deprivation. - - X X X X X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 147
148 Quality of Care Benefits/outcomes of achieving our vision Whole System Outcome Framework Outcome framework to monitor the impact of the strategy Outcome Indicator Indicator Source Definition Rationale Type Frequency Readiness S E L L A L C N Caring for people in a safe environment and protecting them from avoidable harm Reduction in the variation of care across SEL(2): To demonstrate the variations capture the % of GP practices 'achieving' or 'higher achieving' against the GP outcomes framework GP Outcome Standards The Quality and Outcomes Framework (QOF) is the annual reward and incentive programme detailing GP practice achievement results. QOF awards surgeries achievement points for: managing some of the most common chronic diseases, e.g. asthma, diabetes; implementing preventative measures, e.g. regular blood pressure checks; the extra services offered such as child health care and maternity services; the quality and productivity of the service, including the avoidance of emergency admissions to hospital; compliance with the minimum time a GP should spend with each patient at each appointment There is significant variation in achievement of GP outcomes, both within and between boroughs. Best performance against GP outcomes across south east London was Bromley where 54% of practices are achieving or higher achieving practices; the worst performance was in Lambeth where this figure is only 12%. The equivalent England average is 62%. (SEL Case for Change) Data TBC X X X KEY South east London (SEL) Local Authority (LA) Local Care Network (LCN) Commissioning Groups and NHS England Draft in progress 148
149 Draft in progress 149
150 Financial impact and affordability Introduction In estimating the affordability challenge facing south east London and the impact of proposals in this consolidated strategy, we have undertaken a number of pieces of analysis. Given the timescales we were working to and the developmental status of the proposals developed by the Clinical Leadership Groups, it would not have been practical or cost efficient to construct a sophisticated bottom up model of the health and social care economy before and after the proposed changes. Rather, our approach was to provide an indication of the expected impact of our interventions on the financial challenges facing the health and social care economy making use of the best available data from a range of publicly available sources and information provided to us by the participating parties. While our findings will need to be revisited and tested in detail at the design phase, we believe that the results provide a clear and robust indication of the benefits and costs associated with the proposals in the strategy. Approach Throughout our analysis, our estimates of impacts take a system-wide view. That is to say that they consider the impact of solutions in terms of cost of provision given the limited funding coming into the system (i.e. through CCG allocations). As such, at this stage, our impacts are not considered on an individual organisation basis (i.e. how much more or less commissioners would have to pay for the new services under the existing tariff payment structure). This reflects that: Clinical models should provide value for money for the entire system rather than individual organisations. It may be necessary to share benefits between organisations in order to encourage change. Existing payment structures may no longer be the best method to enable change. Data sources The primary data sources used in our analysis are as follows: Reference costs (2013/14) with significant adjustments (agreed with local providers) to allow for the dissolution of South London Healthcare NHS Trust. CCG five year financial plans. Provider long term financial models or annual plan templates. Hospital Episode Statistics (HES) data using the Healthcare Evaluation Data (HED) tool ( Engagement We have developed strong local engagement from Finance Leads across the south east London health economy as evidenced by very good attendance/participation at monthly meetings, an agreed memorandum of understanding for information, setting out data sharing principles and rapid responses to any data requests. Commissioning Groups and NHS England Draft in progress 150
151 Financial impact and affordability Overall impact The overall savings presented below are system-wide cost savings, i.e. they relate to reductions in the cost of provision following the changes in activity. Thus they can be counted against the 1.1bn affordability challenge. Further to these savings, individual organisations will still be required to achieve their own efficiency savings. This is true both of providers (in terms of traditional CIP efficiencies) and commissioners (i.e. prescribing QIPPs, which will continue regardless). Therefore it is important not to count the saving presented below as the only effort to close the affordability gap. In making this saving we must take account of the impact it has on other organisations to achieve their own efficiency targets. For example acute providers may struggle to achieve the same levels of CIP savings as forecast if they are attempting to do so on a smaller overall cost base. Clinical Leadership Group Scenario 1 Net benefit (2019/20) ( m) The table below shows the potential impact of the proposed changes under three investment scenarios: 1. Scenario 1: 30% of gross benefits reinvested. 2. Scenario 2: 40% of gross benefits reinvested. 3. Scenario 3: 50% of gross benefits reinvested. In the table below, a positive number is a net benefit to the system, while a negative number is a net investment. However, given the strong links between Community Based Care and the other Clinical Leadership Groups, the segmentation below is somewhat arbitrary, reflecting that an investment in Local Care Networks may be required in order to derive a saving elsewhere. Further detail on impacts for each Clinical Leadership Group can be found in Appendix E. Scenario 2 Net benefit (2019/20) ( m) Scenario 3 Net benefit (2019/20) ( m) Urgent & Emergency Care Children & Young People Planned Care Maternity Cancer Community Based Care* (12) (12) (12) Total Commissioning Groups and NHS England Draft in progress 151
152 System wide income/expenditure ( millions) Affordability challenge ( millions) Financial impact and affordability Closing the affordability challenge The graph to the right demonstrates how the benefits from the programme can be combined with savings within individual organisations to close a substantial amount of the 1.1 billion affordability challenge. The benefits shown are as follows: 1,200 1, Programme central case (gross benefit): As described previously. 2. Provider efficiencies at 2.5%: The provider finance leads feel that a 2.5% CIP may be reasonable in addition to efficiencies generated through the programme , ,900 5,400 4,900 4,400 5,903 5,672 5,078 4,812 Expenditure (Do Nothing) Expenditure (Strategy) Expenditure (Residual) Revenue 3, / / / / / / /20 NB: Profiling of benefits shown above may significantly change as implementation plans are developed. Commissioning Groups and NHS England Draft in progress Affordability challenge (2019/20) Programme central case (gross benefit) Provider efficiencies at 2.5% 266 Residual challenge (2019/20) It is important to note that both of these savings are presented gross of investment requirements (which total 90 million in the programme central case). It is expected that these investment requirements will, at least in part, be satisfied through additional funding requested through the Five Year Forward View and committed by the Government. Taking south east London s proportionate share of the 8 billion committed would imply that 248 million is available for this purpose. The resultant position is a 266 million affordability challenge for the South East London health care economy.
153 Financial impact and affordability Initial estimate of acute bed requirement Using historical NHS bed occupancy data for the acute providers and our projections of bed demand considering demographic/nondemographic growth assumptions we have estimated the bed gaps/increases show in the table below. We have modelled the impact of the strategy on overnight bed days to be a net reduction of 138,000 and a net increase in day case bed days of 25,000. This translates directly to a number of beds using various occupancy rates as shown in the table below. This only relates to acute beds and we would expect a proportion of this activity to be provided within community beds. Also note that the do nothing position does not reflect any potential reductions associated with QIPP delivery post 2014/15 plans or Better Care Fund related non-elective admission reductions. Baseline bed days/beds Strategic impacts bed days/beds 2013/14 Growth (2019/20)*** Gross change (2019/20) Net change (2019/20) Overnight Day case Total Overnight bed days 1,178, ,000 (339,000) (140,000) Overnight beds (current occupancy rates*) 3, (1,015) (414) Overnight beds (85% occupancy rates) 3, (1,092) (231) Day case bed days 181,000 30,000 (5,000) 25,000 Day case beds (current occupancy rates*) (15) 84 Day case beds (68% occupancy rates) (19) 235 Total bed days 1,359, ,000 (343,000) (115,000) Total beds (current occupancy rates*) 4, (1,030) (330) Total beds (revised occupancy rates****) 4,166 1,115 (1,111) 4 * Bed occupancy source: Bed occupancy for the year estimated using the average of KH03 quarterly returns from NHS England for Q4 2013/14 Q3 2014/15. (GSTT: 81%, KCHT: 94%, LGT: 94%, DGT: 95%, weighted average: 90.5%). ** These figures have been fixed at current occupancy levels and 2013/14 activity. *** These figures relate to a level of increased demand as shown above and an additional number of beds due to requiring lower occupancy levels. **** The total revised occupancy rates are blended across the inpatient overnight bed and day case bed rates shown earlier in the table. Commissioning Groups and NHS England Draft in progress 153
154 Draft in progress 154
155 Draft in progress 155
156 Infrastructure & Estates Supporting Strategy Summary The Estates Supporting Strategy is an essential element of Our Healthier South East London strategy programme if we are to be able to support the delivery of our new models of care in a way which ensures they deliver the outcomes we aim to achieve. We must understand the capacity of our capital assets, estates and facilities across south east London to utilise, reduce or develop these in the most appropriate way to meet the needs of our population. There is a clear synergy between the south east London need to reconsider estates and the national and London wide direction of travel. The five year forward view sets out an integrated agenda and new care models over the next five years. In addition, Better Health for London outlines the evidence base for re-evaluating the utilisation and value of NHS estate in London. (The Healthy London Partnership Estates Programme). Therefore, our Estates Supporting Strategy has made clear links with the work being delivered at a London wide level by the Our Healthy London Partnership - Estates Programme being led by London CCGs and NHS England. Scope The Estates Supporting Strategy will: Support development and utilise the London wide outputs of the Our Healthy London Partnership Estates Programme; Reference the TSA Transaction Agreement including the review of Orpington hospital required to be completed by October 2016; Establish an estates and assets database and the current level of investment and capital developments already in process; Consider all new models of care to determine the characteristics of any estate needed and how best to utilise current estate in order to deliver optimal utilisation and functionality; Encourage Clinical Leadership Groups to examine non-nhs estate solutions for delivery of new models of care in the community, when NHS estate is not fit for purpose or available. These could be community assets (libraries, leisure centres, church halls), social care or voluntary sector facilities or commercial arrangements. This may support the integration of NHS services with other wellness services, encourage engagement from those who may not traditionally attend NHS services and re-frame NHS services as part of the local community and not as an institution of illness; Work cohesively with all supporting strategies to fully understand the need for physical buildings and assets in line with other options proposed to support delivery of services, specifically IT and workforce; Establish a joint working group with providers (including primary care general practice), commissioners, Community Health Partnership (CHP), NHS Property Services (NHSPS) and NHS England in order to identify potential reconfiguration options. Implementation may require public consultation on the options. Requirement The Estates Supporting Strategy aims to address specific requirements for Our Healthier South East London that provide additional support to facilitate delivery of the strategy, building upon London wide programme delivery where the time scales allow. The estates strategy will be built into the delivery programmes for all models of care as appropriate and financial impacts further detailed within the Financial modelling. Commissioning Groups and NHS England Draft in progress 156
157 Key Enablers Infrastructure & Estates Supporting Strategy Approach The below diagram details the approach for the estates supporting strategy. High level approach to developing estate plans to support the implementation of the strategy. Central programme- working with CCGs and providers Assess (baseline & new models) Gaps Options Delivered by CCGs/Providers Detailed Design The baseline Identify the configuration of the current estate (including major assets / capital equipment), how it is used and for what purpose it is best suited. Research New models of care Determine the type, scale and characteristics of estate and major assets that south east London will need to deliver the new models of care identified within Our Healthier South East London. Gap Analysis Identify difference between the requirement and the baseline Proposals Identify actions needed to be taken to reach the desired future state Challenges and Opportunities Identify the challenges that any reconfiguration of estate may have alongside opportunities Design and Deliver Address specific requirements of the strategy Working in collaboration with NHS England, NHS Property Services and Community Health Partnership National and London policies and initiatives Plans from the workforce and IM&T supporting strategies Stakeholder Engagement Commissioning Groups and NHS England Draft in progress 157
158 Infrastructure & Estates Supporting Strategy Next steps Establish the baseline Identify the configuration of the current estate (including major assets / capital equipment), how it is used and for what purpose it is best suited. Are there opportunities for co-locating delivery of health services in nonhealth estate? Work with Our Healthy London asset database Source any additional available information on relevant estate and assets (Update of TDA) including other community buildings Gain information on the purpose current estate can be used for Identify ownership of estate Identify capital developments already in progress Identify policy changes that could impact estate changes Establish baseline of current investment: financial and resource Understand the requirement Determine the type, scale and characteristics of estate and major assets that south east London will need to deliver the new models of care identified within Our Healthier South East London. Clinical Leadership Groups to establish the needs of their interventions from estates and major assets Working in collaboration with the Clinical Leadership Groups determine the type, scale and design of estate required for the new models Assess the functionality and utilisation of estate needed (hot desks / Scanning equip / theatres / diagnostics / Local Care Network hubs?) Consider requirements in light of workforce and IM&T supporting strategies Establish estate standards to improve equality of health and care provision and outcomes in south east London Addressing the gap Focusing on the difference between the requirement and the baseline, what actions need to be taken to reach the desired future state? Identify the challenges that any reconfiguration of estate may have Conduct gap analysis between the outcomes of stage 1 and 2 Identify potential challenges to be addressed as work progresses: financial; equipment; environmental; resource; skills; engagement. Identify options for estates reconfiguration Understand the organisation specific impact of estate change as linked to commissioning Understand elements of estate change that will impact on implementation and those that may need wider consultation Test and refine options with key stakeholders to gain a consensus on the estates requirements and how this can be delivered Commissioning Groups and NHS England Draft in progress 158
159 Draft in progress 159
160 Workforce Supporting Strategy Summary Better Health for London, the Five Year Forward View and Our Healthier South East London have all identified the need to focus on developing a modern workforce in order to support the delivery of innovative new models of care. The workforce in south east London will be a key enabler of the Our Healthier South East London strategy Scope Our workforce supporting strategy is identifying the key actions that should take place in order to move the workforce in south east London from where it is today to where it needs to be in the future. For instance, we know that the future care delivery will involve empowering patients and promoting independence, making every contact count and fostering an environment where colleagues engage with each other rather than refer and hand-over. With these significant changes on the horizon, understanding what patients will require in the future and challenging existing ways of working, will allow us to plan for a workforce that is fit for purpose and sustainable. The workforce supporting strategy will need to clearly articulate how the workforce is going to deliver what south east London needs; this will include new ways of working (i.e. flexibility, rotations, different staff groups doing different tasks to today, team work & collaboration) and different working locations (i.e. more staff working in the community as opposed to acute settings). Requirements Delivery will also require significant cultural and behavioural changes; for instance, we need the entire workforce to make every contact count and to appreciate that patients want more say in the care they receive. The workforce will also need to work differently with each other; there needs to be greater integration and more dialogue between parties - rather than a simple passing on of information and/or a patient. Not only do commissioners and providers need to work more closely together but there also needs to be greater cooperation and integration across pathways. Whilst it is acknowledged that it is for the providers to determine their actual workforce requirements, as a programme we need to model the whole system s future requirements across south east London in sufficient detail to inform a possible pre-consultation business case. For instance, we need to understand the likely shifts in activity from acute to primary care and the consequent impact on where our workforce will need to be located. The workforce supporting strategy also needs to take account of the London Transformation Group s work and we are part of the pan-london network. In summary, the workforce supporting strategy will support providers and commissioners as required and hold a system-wide view of the future workforce for south east London. The strategy will feed into the overall Our Healthier South East London strategy, as well as any potential Pre- Consultation Business Case. Commissioning Groups and NHS England Draft in progress 160
161 Workforce Supporting Strategy Findings to date and next steps Findings to date With funding from Health Education South London, we have: A baseline of the current workforce in south east London established This demonstrates that c.62k FTEs are employed across a range of settings of care in south east London. Approximately 40% of these work in the acute sector. Nurses are the largest cohort in acute, community and mental health settings; c. 13K FTEs. The social care workforce numbers c 19K FTES, of whom c. 11K are unpaid carers. The recruitment and retention of quality nursing staff is a key challenge. Nursing vacancy rates range between 14% and 16% across providers. This compares to vacancy rates for medical staff of 6% - 12%. Vacancy rates in social care are reportedly low; 2% - 6% across all staff groups. These vacancy rates mean that there is a significant cost in using agency staff and locums. Overall, the workforce in south east London, the workforce is projected to grow by 1.3% year on year to 2019/20. The largest area of projected growth will be in nursing within the acute sector which is projected to grow by 19% as providers seek to fill vacancies and reduce their dependency on agency staff. Workforce numbers in Primary Care and Community Pharmacy are estimated to grow by 22%. This reflects an anticipated demographic changes; primarily in response to an aging population and an increase in the numbers of those with long-term conditions. Given the mismatch between the increasing demand and low growth in supply, we need to consider how things could be done differently. For instance, are there roles that could be filled Third Sector resources or community volunteers? We also need to look closely at retention and the secondary care providers are already meeting to consider this. A methodology to define the characteristics of the new workforce developed This is being used by our Clinical Leadership Groups, which include PPV representation, to identify the characteristics of the workforce required to develop their new schemes and interventions. The methodology is allowing each Clinical Leadership Groups to map skills and experience to the new interventions and identify where capability gaps lie. Each Clinical Leadership Group will also consider an indicative number of staff in each group required to deliver the models of care. In turn this will inform wider workforce planning and identify where training and development will be required. Commissioning Groups and NHS England Draft in progress 161
162 Key Enablers Workforce Supporting Strategy Approach The below diagram details the approach for the workforce supporting strategy. High level approach to developing workforce supporting strategy to support the implementation of the strategy. Central programme- working with CCGs and providers Assess Gaps Options Delivered by CCGs/Providers Detailed Design A baseline of the current workforce in south east London established Identify current different in supply and demand Vacancy rates Growth in workforce A methodology to define the characteristics of the new workforce developed Map skills to interventions Articulate the workforce supporting strategy Clinical Leadership Group driven workforce challenges and plan Assessment against London quality standards Reach out to the workforce Working in collaboration with Heath Education South London Stakeholder Engagement National and London policies and initiatives Commissioning Groups and NHS England Draft in progress 162
163 Workforce Supporting Strategy Next steps Articulate the workforce supporting strategy The work being carried out by each Clinical Leadership Group will inform the content for the workforce supporting strategy across south east London; both at Clinical Leadership Group and at system-wide level. The outputs from each Clinical Leadership Group will be consolidated into a document that describes the system-wide workforce challenges and required actions, as well as those that are specific and unique to individual Clinical Leadership Group s. This will also require input from both commissioners and providers. The workforce supporting strategy will need to include the planned approach for realising the change needed. Given this, the input from each Clinical Leadership Group on the level of change required will help to describe the short/medium/long-term actions that are needed to deliver the workforce of the future in south east London. From a whole system point of view, the strategy also needs to consider where south east London is failing to meet the London Quality Standards and whether workforce is a key contributor. If it is, the strategy needs to consider how this might be addressed. Stakeholder management will also be a component of the workforce supporting strategy in terms of how the enablers will be delivered (e.g. Royal Colleges, Deaneries, Health Education South London). In describing the enablers, the workforce supporting strategy will need to identify at a system-wide level where investment will be required; for instance, in new roles, training or development. This will require input from commissioners, providers and Health Education South London and will be fed into the financial model. Reach out to the workforce If the workforce owns the new models of care, implementation will be more successful and staff satisfaction higher. Workforce representatives will be helping to define the characteristics of the workforce that will be required to deliver the new models of care but we need to involve more frontline staff as the work progresses. There are compelling examples of where the involvement of workforce in a co-design relationship has delivered significant benefit; for example, the experience in Greenwich regarding integration. We also need to ensure that the workforce understand what is being undertaken and why. Therefore, the strategy team is working closely with the Programme s communication team to develop key messages that will help to secure commitment to the new models of care and reassure them that the changes will be positive not only for the communities and patients we serve but for them as well. A key aim of the Programme is to increase staff satisfaction; we are considering how best to gauge staff satisfaction both today and as a consequence of implementation of the strategy. Commissioning Groups and NHS England Draft in progress 163
164 Draft in progress 164
165 Information Management and Technology Supporting Strategy Summary Our Healthier South East London aims to improve health, reduce inequalities and ensure that local services consistently meet safety and quality standards and are clinically and financially sustainable. The strategy proposes a whole system model with Community Based Care delivered by Local Care Networks, as the foundation for the whole system model providing person centred service to geographically coherent populations and five high priority pathways providing services to cohorts of people. Information and IT will be a key enabler for the strategy. Specifically it can support staff in new ways of working and empower patients to be active participants in their care. Key considerations for understanding the IM&T requirements to support the strategy and any gaps are National and London initiatives and policies: There are a number of National and local initiatives and policies that may support the implementation of the strategy. These are: o o Five year forward view London Health Commission o Personalised Health and Care 2020 CCG IM&T strategies: Each CCG has its own IM&T strategy and implementation plans, which have been reviewed and initial assessments made to determine support for the strategy. Identifying uniformities at a south east London level so there are consistent ways of working. For example, adopting the same data quality standards, and staff identification processes for who should be viewing/editing data and design principles Gaps and any investment costs: Understanding where these are not currently accounted for in CCG and or provider plans, and are needed to implement the strategy. Scope To enable the Our Healthier South East London whole system model and pathways, the work has considered; Information exchange and interoperability across south east London health and care organisations and patients, and the systems and tools that support this. Benefits that may arise from collective agreement at a south east London level, for example: Identifying design principles and ways of working Identifying areas where a collective IT/digital investment could have greater impact. For example in enabling self-care and prevention, pregnancy support, developing digital Local Care Networks Commissioning Groups and NHS England Draft in progress 165
166 Key Enablers Information Management and Technology Supporting Strategy High level overview of the method used for the IM&T supporting strategy High level approach to developing IM&T plans to support the implementation of the strategy. Central programme- working with CCGs and providers Assess Gaps Options Delivered by CCGs/Providers Detailed Design Current plans CCG Plans London wide and national strategies & policies Clinical Leadership Groups requirements Agreed Prioritised Requirements Clinical Leadership Groups and whole system model Initiatives that Support the requirements Gap Analysis Solution options and examples from elsewhere High level Roadmap and Implementatio n Costs Transition Plan Detailed Requirements Transition Costs Target Operating Model Research Information Governance Stakeholder Engagement National and London policies and initiatives Commissioning Groups and NHS England Draft in progress 166



167 Information Management and Technology Supporting Strategy Understanding the IM&T Requirements of the Care Models and Whole System Model The requirements that could support the strategy on the following slides have been gathered in a number of ways: Through the 6 Clinical Leadership Group workshops and planning meetings 1. Cancer 2. Planned Care 3. Urgent and Emergency Care 4. Maternity 5. Children's and Young People 6. Community Based Care Considering case studies and evidence of what has worked elsewhere, for example Looking at system level initiatives that have supported similar strategies (integrating primary, secondary, community and social care information to enable new ways of working and in particular enabling Local Care Networks and multidisciplinary teams Pathway specific initiatives to enable key interventions The IT/digital guidance direction setting from National and London initiatives, specifically NHS Five Year Forward View NHS England Personalised Health and Care 2020 National Information Board Better Health For London London Health Commission Commissioning Groups and NHS England Draft in progress 167
168 Information Management and Technology Supporting Strategy Summary of IM&T findings to date and next steps The primary key requirements of interoperability between GP systems and primary and secondary care are planned and/or being implemented at various speeds with all CCGs moving to GP systems that will enable sharing of records across GP practises supporting Local Care Networks and will be interoperable via the Medical Interoperability Gateway with Acute led portal solutions, KHP online and Connect Care at Lewisham. To various extents CCGs have plans in place to align with some of the key IT/Digital guidance in the 5YFP IT/Digital, London Transformation Programme, 2020 Personalised Health and Care and Implementing these guidelines would meet many of the strategy requirements. However additional transformation initiatives that may require agreement and funding at a south east London level have not been explored or agreed at this stage. Gaps for the strategy identified to date Interoperability with Local Authorities will be needed to fully enable the strategy and plans for this are not well understood at the time of writing but form part of the next steps of work 2 separate interoperability solutions: KHP online (Lambeth, Southwark, Bromley) Connect Care (Bexley, Lewisham, Greenwich) Ability of CCGs to meet the guidelines set out in National and London initiatives (funding) Possible funding/investment case needed to speed up support for key parts of the strategy, for example for Multi Disciplinary Teams working in Local Care Networks and LA integration South east London Whole System Outcomes. There is a requirement to set up a monitoring and reporting service. This service will need to be agreed and procured on behalf of the 6 CCGs. is it part of the transformation cost or business as usual costs? There is no central capital funding pot to fund any SPG IM&T initiatives. Capital funding pot from NHSE but application would be for 16/17 Staff Training will be required as new systems and ways of working are introduced. Further work to understand what training is included in CCG and provider plans and costs of training to CCGs Considerations for next stage of work KHP online and Connect Care timelines for going live could be after some federations/local Care Networks are up and running Further work to asses if there are confirmed plans for KHP online and Connect Care solutions to integrate with Local Authorities and if there are any associated costs for CCGs Interoperability between KHP online and Orion Connect Care connect could resolve boundary issues across south east London. An assessment is needed to understand impact of this, for example number of patients that cross over and the costs vs benefits case ( is it worth doing?). Additional transformation initiatives that may require agreement and funding at a south east London level have not been discussed. For example, could moving to a more mature Digital solution to enable Local Care Networks and Community Based Care provide greater benefit? Investment may be needed to implement key parts of the strategy and or to ensure consistency in implementation timelines across the six CCGs, for example, to enable the Community Based Care and Local Care Networks Capital funding: if any investment is required, a business funding case will need to be developed for 2016/17 Revenue costs such as licencing, staff training and project management, yearly service management for KHP online and Connect care. Part of the next steps is to understand if these costs are picked up in CCG planning Understanding the IT investment set out in CCG and provider financial plans. Once we have done this, determine costs associated with: Any planned IT changes that are not included in the plans. Any further changes that we are proposing through the programme to improve consistency of IT provision across the system. Southwark Greenwich Lambeth Bexley Lewisham Bromley Commissioning Groups and NHS England Draft in progress 168
169 Draft in progress 169
170 Risks and Challenges Risks to implementation of the Strategy There are risks to delivering the Strategy which are closely monitored and assessed for impact The following are high level risks which have been identified to the implementation of the strategy. This list will be reviewed regularly through the Clinical Executive Group, Implementation Executive Group and Clinical Commissioning Board. Title Risk Impact Mitigations 1. Information Systems 2. Workforce Capability 3. Delivery Timeframe 4. Delivery Timeframe Lack of integrated or interoperable information systems undermines ability to integrate services across the health system in south east London Existing workforce skills or capability to deliver new models of care It may be challenging to complete required activities and assurances in time to go to consultation, if required, in December, particularly as a result of needing to engage patients and service users in the process Insufficient time for good processes in terms of governance, decision making and ownership Possible duplication of system, process or information, resulting in poorer patient experience, poor quality of services across integrated pathways and additional cost New models of care may not be implemented Services may not be delivered safely Patient satisfaction Staff satisfaction issues Quality and effectiveness of care Delay to programme implementation for those elements which might require formal consultation or loss of support from partners and stakeholders for some or all of the strategy The strategy and associated documents are not owned by all stakeholders across SEL IM&T supporting strategy workstream established. Utilising existing integration initiatives across SEL to support strategy Workforce supporting strategy workstream established Work in hand to identify gaps between capabilities required to deliver new models of care and those available in current workforce Key characteristics and skills being identified for training purposes On-going dialogue with NHSE to agree assurance process and detailed communications and engagement plan to test critical path We will maintain four key activities: intensive engagement with partners and stakeholders; ensuring NHS England is engaged; careful mapping of governance and decision making; and meeting with NHSE by mid-june to review the approach Commissioning Groups and NHS England Draft in progress 170
171 Risks and Challenges Title Risk Impact Mitigations 5. Clinical Leadership Group Impact Analysis Modelling: Finance and Activity The impact analysis does not fully close the identified affordability gap but does make significant progress towards doing so. It is not yet clear if this is sufficient Explore and incorporate additional QIPP and CIP opportunities and continue to explore options with NHSE 6. Financial sustainability of health system 7. Patient / Public Resistance to Change New service models do not deliver reduced demand for hospital care or hospital capacity does not reduce in line with demand If partners and stakeholders are not sufficiently engaged throughout the development of the five year strategy or if the case for change is not sufficiently convincing - any proposed service change could be subject to significant local opposition Potential increased system costs through duplication of services System may not be sustainable Further engagement required Possible legal challenge Delays to implementation of changes leading to increased cost and delay Need to amend strategy in response to concerns Making sure there are clinical input into the design of care models and that they have sufficient impact on activity Engagement activities will be undertaken with a broad range of partners and stakeholders throughout the development and implementation of the strategy Dedicated communications and engagement enabling workstream to coordinate these activities Patient and Public voices in all key groups to help shape strategy Strategy reflects input from partners and stakeholders Commissioning Groups and NHS England Draft in progress 171
172 Draft in progress 172
173 Delivering the strategy Care model design process The interventions within the Our Healthier South East London Strategy have been designed by Clinical Leadership Groups and the detail of these are set out in the Proposed models of care section. The overarching process undertaken by the Clinical Leadership Groups to design and deliver their respective care models is shown below. Along this process is continual decision making and iteration using a range of qualitative and quantitative evidence, including local clinical judgement. Importantly, we need to decide what is implemented at south east London and what is implemented locally; in addition to the process for appraising care model design and delivery options. Case for Change Finance and activity baseline Future demand and funding envelope Current health outcomes Agreed scale of affordability challenge Agreed whole system outcomes Proposed care models and interventions Model the interventions Activity shifts identified through a triangulation process using benchmarking, academic evidence and clinical judgement Detailed options appraisal CLG consideration of options for delivery leading to agreed care models and interventions Implementation planning Commissioning Groups and NHS England Split interventions by implementation or detailed options appraisal Draft in progress 173
174 Delivering the strategy Localising the interventions Implementation of the models may happen at both CCG and south east London level. In order to provide the right support to CCGs and provider organisations, Clinical Leadership Group working groups will need to consider the level at which each intervention should be implemented. There are two broad routes for taking interventions forward which reflect the different characteristics of the care models. Depending on the route the programme team may offer a different level of support. This is set out below: Route Characteristics of intervention Type of support offered by the programme team Local implementation: CCGs lead the detailed design and development of the care models Will benefit from local implementation Less need for standardisation Primarily out of hospital Implementation toolkit development Implementation advice and guidance SPG implementation: Detailed design and development of model takes place at an SPG level with involvement of impacted CCGs Directly impacts one or more providers delivering services across CCGs Requires a high-level of standardisation Involves/impacts a number of CCGs Hands on project management support Regardless of the route, a central reporting process will be established to track the implementation of schemes. This will support the monitoring of benefits and anticipated impact. Implementation plans are currently being developed which will set out the required support to deliver these interventions. This process will confirm the implementation route, required level of support and supporting governance. Commissioning Groups and NHS England Draft in progress 174
175 Delivering the strategy Process for appraising options In order to identify the best way or way(s) of delivering the overarching strategy, an options appraisal process is required to realise its full benefits. This focuses on those options which may lead to significant service change. This approach filters the many potential options for how the system can be implemented and is designed to identify options that are recommended for further work It is proposed that the filtering of options will occur through two gateways of assessment against criteria; hurdle criteria and evaluation criteria (the diagram on the following page provides an overview of the methodology). The criteria against which the options will be assessed should be agreed before commencing the appraisal. Moreover, the likelihood of optimal implementation of options is increased by gathering wide ranging stakeholder contribution to the formation and specificity of criteria. Although some interventions do not in their own right require a detailed options appraisal, the result of implementing those interventions could impact on the appraisal of other interventions because they will lead to shifts in settings of care and volumes of activity. As a result, it is important to consider the scope of a detailed options appraisal and how to account for whole system changes within the appraisal of individual interventions. Commissioning Groups and NHS England Draft in progress 175

176 Delivering the strategy Options for appraisal methodology Case for Change Agreed whole system outcomes Finance and activity baseline Future demand and funding envelope Current health outcomes Proposed care models and interventions Agreed scale of affordability challenge Options appraisal Evaluation Criteria: These will be used to develop a short list of options. They will be used to assess the options in terms of impact and feasibility, helping to identify realistic options and those with potentially the best outcomes. Model the interventions Activity shifts identified through a triangulation process using benchmarking, academic evidence and clinical judgement Define scope Agree hurdle and evaluation criteria Estate and service baseline Apply hurdle criteria Hurdle Criteria: Tests that options either pass or fail. They provide a sense check of the full list of options, identifying options that are feasible. Long List Apply evaluation criteria Short List CLG consideration of options for delivery leading to agreed care models and interventions Split interventions by implementation or options appraisal Implementation planning Commissioning Groups and NHS England Draft in progress 176
177 Delivering the strategy High level programme plan The high level plan on the next page shows at high level the next stages of the plan for implementation, option appraisal and consultation if required. It is ambitious and dependent on partners and key stakeholders continuing to engage with and support the work as it develops. Over the next few weeks, CCGs will be testing this with their governing bodies and membership and with key partners and stakeholders. There will be a formal stocktake in late July and the plan will be confirmed or amended. Further stocktakes will be scheduled as appropriate. The case for change is pressing and there is much that can be implemented at pace, but it is important to keep the high levels of engagement and support which we have had so far. Commissioning Groups and NHS England Draft in progress 177
178 Key Outputs Key Activities Delivering the strategy High level programme plan Phase 1 (January May 2015) Phase 2 (May August 2015) Programme Plan Phase 3 Phase 4 Phase 5 (September November 2015) (December 2015 March 2016) (April September 2016) Phase 1 Phase 2 Phase 3 Phase 4 Phase 5 Further refinement of the Whole System Model and the models of care, including testing with providers, partners and wider stakeholders Building greater detail into the care models so their impact can be modelled Modelling expected impacts for providers and commissioners Further development of the supporting strategies Clinical model implementation Workshops CO discussion on commissioner models, Provider and CLG Identification of potential for significant service change. Create options appraisal methodology Develop options Appraise options Modelling to support option appraisal and decision making Short list of options Further support to implementation Continued work with partners to ensure ownership and wider engagement to test and develop Development of business cases. There will need to be agreement as to the business cases required and who will lead them (commissioners or providers). Modelling to support development/review of business cases Decisions making processes for business cases Continued wide engagement Implementation and continuous quality improvement Any consultation, if required. Note: In the event that consultation is not required, and for any elements of implementation where consultation is not required, the timetable will be shortened, but for planning purposes this paper assumes that there will be some formal consultation, although the subject of such consultation has yet to be established. Conclusion of any consultation Further modelling if required Decision making Implementation Continuous quality improvement Detailed implementation plan Presentation to NHSE Provider outline of steps required to operationalise the Whole System Model Development of the supporting strategies Equality Impact Assessment Modelling Impact Assessment Publish Equalities Impact Assessment and action plan Refinement of implementation plan Options analysis Refinement of detailed implementation plan Gateway review Business Case sign off Monitoring, evaluation, reporting and improvement frameworks established Live implementation and continuous quality improvement Governance Groups Comms & Engagement Finance & Modelling Continuous input throughout the process with regular meetings Continued aligned plan to ensure the programme continues with a high level of engagement Modelling to establish the baseline position, required investment and quantify benefits to be realised Supporting Strategies Continue the commissioning framework, LCN, workforce, IM&T systems and estates configuration needed to realise the change Commissioning Groups and NHS England Draft in progress 178
179 Draft in progress 179
180 Draft in progress 180
181 Appendices Introduction Principles The Our Healthier South East London governance is designed to ensure a partnership approach to design and delivery, while remaining commissioner-led and clinically-driven and ensuring that the needs of local people are at the heart of the strategy. The governance structure has been designed to be consistent with the NHS England Strategic Planning guidelines to support joint commissioning and strategic planning, building on well established collaborative relationships within the six boroughs and NHS England. The structure will enable effective decision-making and oversight and clear ownership of deliverables and benefits at all stages of the programme. It will operate in an open and transparent manner, and takes account the voices of stakeholders across the south east London community. The purpose of this section of the document is to outline the following aspects of the governance of the programme: Principles Structure and high-level memberships Key roles and functions Arrangements that will be put in place for collaboration and advice The governance approach is based on a number of overarching principles and assumptions: It must ensure the Commissioning Strategy is based on local needs and aspirations, listening to local voices and building on work at borough level, whilst taking into account national and London policies It must be open and transparent throughout the process, from identification of need, to implementation of the strategy, with opportunity for challenge by patients and the public Patient safety and quality must be at the heart of decision making Decisions should take into account patient, carer and community voice The roles, responsibilities and accountabilities of the CCGs, NHS England and all partner organisations must be explicitly defined There should be clear points of accountability for all deliverables Programme governance should provide assurance that the anticipated benefits of the programme will be delivered The core programme will be responsible for ensuring that contributing projects and programmes deliver the planned benefits of the programme in line with the critical path and overall timetable Duplication of effort should be minimised across the health system Commissioning Groups and NHS England Draft in progress 181
182 Appendices Commissioning Groups and NHS England Draft in progress 182
183 Appendices Key roles and elements The roles and elements of the Our Healthier South East London specific governance bodies are outlined below. The overall structure reflects initial planning guidance (NHSE, LGA, TDA and Monitor - 04 November 2013) including approach to joint working and units of planning. Structure and membership have been designed to best support the development of the Commissioning Strategy and it is likely that this will need to be revisited at key points in the programme lifecycle in particular when the programme moves on to a delivery footing. In south east London the function of the Strategic Planning Group is being delivered primarily through the Clinical Commissioning Board, supported by South East London Partnership Group and the Implementation Executive Group. The programme is led by the Clinical Commissioning Board (CCB), which acts as the overall programme board. The CCB is commissionerled and clinically-driven and steers and makes decisions on the development and delivery of the strategy. Members of the CCB have the authority to make decisions on the scope of the programme on behalf of their respective organisations. All workstream SROs within the programme are accountable to the CCB for delivering their agreed share of the benefits of the programme. The South East London Partnership Group is the strategic and partnership forum for the programme. The group is clinically-led and will frame and shape the commissioning strategy on behalf of the CCB, providing collective system leadership and oversight to the programme. Key programme decisions require the support of the Partnership Group. The Clinical Executive Group (CEG) brings together clinical leaders (including social care professional leaders), patient and public voices and Healthwatch representation from across south east London to frame and provide oversight of clinical design work by providing guidance and assurance to the individual clinical leadership groups and managing interdependencies across the group. It also acts as a conduit for the management and escalation of clinical risks. The Implementation Executive Group (IEG) is the executive group supporting the CCB, providing oversight of planning, implementation, benefits realisation and assurance. The IEG also steers the mobilisation workstream, and has a continuing responsibility to make recommendations to the CCB on the optimal structure and scope of the programme. The Public and Patient Advisory Group (PPAG) is the collective forum for the strategy s patient and public voices to contribute to shaping the strategy s content and the programme s processes, to share learning, provide peer support, facilitate wider engagement and disseminate messages and provide feedback on key programme materials. Programme design and delivery is undertaken by combination of contributing clinical groups, projects and programmes at varying points in their lifecycle, each requiring the appropriate treatment from a governance and operating perspective. Commissioning Groups and NHS England Draft in progress 183
184 Appendices Collaboration and advice The programme links to a number of existing advisory and collaborative bodies. Relationships have been established with these groups as appropriate as part of mobilisation and ongoing delivery. Health and Wellbeing Boards (HWBs) provide oversight, advice and input into the programme at borough level, focused on improvement of the health and wellbeing of their local populations, reducing health inequalities, and encouraging joined up working across commissioners. As well as being engaged and involved in the co-development of the Commissioning Strategy, ensuring alignment with local Health and Wellbeing Strategies, Health and Wellbeing Boards have agreed Better Care Fund plans Health Overview and Scrutiny Committees (HOSCs) will provide local scrutiny and review in line with statutory requirements under the Local Government Act 2000 and Health and Social Care Act 2012 The programme links to the South East London CCG Stakeholder Reference Group for advice and oversight in relation to engagement on the development of the Commissioning Strategy, in order to ensure that the views of patients, service users, the public and their representatives are heard and acted upon The programme links to local Healthwatch teams in each borough to ensure that proposals developed as part of the Commissioning Strategy take account of the voices of consumers and those who use local health and social care services. An external Clinical Advisory Group will be established, if and as required at later stages in the programme, to ensure that any proposed clinical changes are designed in a manner which ensures wide ranging clinical engagement in service design and alignment with national and London-wide quality standards; and that clinical services will be safe and sustainable both during transition and post implementation. Commissioning Groups and NHS England Draft in progress 184
185 Draft in progress 185
186 Appendices Terms of Reference Clinical Commissioning Board Terms of reference The Clinical Commissioning Board (CCB) acts as the overall programme board. The CCB is commissioner-led and clinically-driven. It steers and makes decisions on the development and delivery of the strategy. Members of the CCB have the authority to make decisions on the scope of the programme on behalf of their respective organisation. All workstream SROs within the programme are accountable to the CCB for delivering their agreed share of the benefits of the programme. The role of the Clinical Commissioning Board is to: Agree the 5-year commissioning strategy for south east London for final approval by CCG Governing Bodies and NHSE Act as the decision-making authority regarding the objectives, scope and benefits of the programme Commission and be assured of clinical and partnership-focused input from the South East London Partnership Group Be the forum where the CCGs and NHSE can hold themselves and each other collectively to account Ensure that the programme delivers on its objectives of safety, quality and clinical and financial sustainability Seek assurance of and approve the progress of the programme against its objectives and plans Agree actions and make decisions to resolve escalated risks, issues and dependencies from the programme Remove obstacles preventing or hampering development and successful implementation Approve the funding and structure of support for the programme, and monitor and make decisions on spend Set the parameters for other groups within the governance structure based on recommendations from the Implementation Executive Group Chairing and facilitation Membership Quorum Frequency & duration Secretariat Co-chairs: 1 Clinical Chair or other senior clinician from within south east London CCGs and NHSE Medical Director for South London CCG Chief Officers (x6) CCG Clinical Chairs (x6) NHSE Direct Commissioning Leads NHSE Director of Delivery, South London Non-voting: Representation from local authorities (up to 3 chief executives) Healthwatch (1 Member on behalf of the 6 south east London Healthwatch organisations) Patient and Public Voice (x2) A CCG Chief Officer/Clinical Chair or nominated deputy from each CCG NHS England Representation Usually bi-monthly meetings, but additional meetings may be convened as required for the effective management of the programme Our Healthier South East London programme team Commissioning Groups and NHS England Draft in progress 186
187 Appendices Terms of Reference South East London Partnership Group Terms of reference The South East London Partnership Group is the strategic and partnership forum for the programme. It is clinically-led and frames and shapes the commissioning strategy on behalf of the Clinical Commissioning Board, providing collective system leadership and oversight to the programme. Key programme decisions will require the support of the Partnership Group. The role of the South East London Partnership Group is to Ensure that the programme recognises the public health challenges across south east London and is developed to reflect the needs of the local population in south east London Provide clinical and local leadership and oversight to the programme on behalf of the south east London health system, ensuring that innovative whole system solutions are developed in line with programme objectives Shape and agree the Vision, Case for Change Clinical Models and Outcomes for the Commissioning Strategy and shape options for implementation Provide oversight to the Clinical Executive Group and Clinical Leadership Groups in ensuring that all elements of the strategy: reflect national and London clinical quality standards are sustainable clinically and financially Resolve strategic issues between the Commissioning Strategy Programme and other projects, programmes and strategies within partner organisations Provide commitment and endorsement in support of the programme objectives across the local health system and provide visible leadership for implementing agreed initiatives Ensure effective communication and engagement takes place regarding the programme within stakeholder organisations and with other partners Chairing Membership Chair:1 CCG Clinical Chair CCG Chief Officers (x6) CCG Clinical Chairs (x6) Provider CEOs (x7) Provider Medical Directors (x7) Local Authority CEOs (x6) Representation from NHS Trust Development Authority Representation from NHS England Representation from London Ambulance Service Representation from Health Education South London (HESL) Representation from South London Health Innovation Network/Academic Health Science Networks Representation from Public Health In attendance: Our Healthier South East London and programme team members as required Quorum Frequency & duration Secretariat CCG Clinical Chairs over 50% (3/6 organisations) Provider Trust Representation over 50% (4/7 organisations) including nominated deputies. To include minimum 1 provider of acute services, 1 provider of mental health services and 1 provider of community services Local Authority Representation over 50% (3/6 organisations) NHS England Representation Usually meetings every two months, but more frequently if required Our Healthier South East London programme team Commissioning Groups and NHS England Draft in progress 187
188 Appendices Terms of Reference Clinical Executive Group Terms of reference The Clinical Executive Group supports the Partnership Group by providing oversight of clinical design work, providing assurance and managing interdependencies across the individual clinical leadership groups. It acts as a conduit for the management and escalation of clinical risks across the programme. The role of the Clinical Executive Group is to: Provide collective clinical leadership for the strategy s development and delivery Provide clinical assurance and oversight of all clinical design work within the programme Ensure that clinical interdependencies have been fully recognised and risks mitigated/managed appropriately Define the tasks and membership for Clinical Leadership Groups based on the direction set by the Partnership Group Oversee the development of models of care and key interventions by Clinical Leadership Groups Ensure that the models of care developed, and associated hospital and community based interventions: reflect national and London clinical quality standards meet the ambitions of the CCGs and NHS England for the strategy for south east London are sustainable clinically and financially Consider the workforce implications and provide recommendations to the workforce enabling workstream Contribute to shaping options for implementation Ensure that clinical redesign projects have plans in place to deliver safe services during any transition and change Act as the conduit for the management and where appropriate escalation of any clinical risks identified across the programme Chairing and facilitation Membership Quorum Frequency & duration Secretariat Co-chairs:1 CCG Clinical Chair plus 1 secondary care clinical leader CCG Clinical Chairs (x6) Provider Medical Directors (x7) NHS England (South London) Medical Director Local Authority Representation: Senior children s and adults social care professional leaders (x2) Representation from other clinical and social care professions as needed Our Healthier South East London Programme Director and other programme team members as required CCG Clinical Chairs over 50% (3/6 organisations) Provider representation over 50% (4/7 organisations) including nominated deputies. To include minimum 1 provider of acute services, 1 provider of mental health services and 1 provider of community services NHS England representation Local Authority representation Usually every 6 weeks, but may meet more frequently in line with the needs of the programme Our Healthier South East London programme team Commissioning Groups and NHS England Draft in progress 188
189 Appendices Terms of Reference Implementation Executive Group Terms of reference The Implementation Executive Group (IEG) is the executive group supporting the CCB, providing oversight of planning, implementation, benefits realisation and assurance. The IEG also steers the mobilisation workstream, and has an ongoing responsibility to make recommendations to the CCB on the optimal structure and scope of the programme. This forum is accountable directly to the Clinical Commissioning Board. Its role is: To hold programme workstreams to account for delivering against their agreed scope and benefits To act as an acceptance gateway for projects, programmes and other schemes of work moving from the design stage into implementation, and from implementation into business as usual To act as the conduit for programme functions such as tracking of progress, monitoring benefits realisation, managing dependencies and interdependencies, identifying mitigating actions for issues and risks, identifying issues and risks that need to be escalated and identifying workstream resource requirements/constraints To support the Clinical Commissioning Board with executive input and oversight across the workstreams of the programme as needed To guide the programme through OGC Gateway reviews pre-consultation engagement and formal consultation, as appropriate The remit of the IEG includes all workstreams within the Our Healthier South East London Programme Chairing Co-chairs: NHS England Director of Delivery for South London and 1 CCG Chief Officer Membership Quorum Frequency & duration Secretariat CCG Chief Officers NHS England Medical Director for South London NHS England Representation (Specialised and Primary Care) Chair of Chief Financial Officers Group Chair of Directors of Commissioning Group Workstream SROs (where not COs) Our Healthier South East London Programme Director Where a member is unable to attend, they will usually nominate a deputy CCG COs over 50% (3/6 organisations) Local Authority Representation NHS England Representation Usually fortnightly meetings of 1.5 hours, but may meet more frequently in line with the needs of the programme Our Healthier South East London programme team Commissioning Groups and NHS England Draft in progress 189
190 Draft in progress 190
191 Appendices Case Study: St Christopher's Bromley Care Coordination Service (BCC) Patient-centred end of life care in Bromley Overview The final days of life are very important. For people with advanced illness or frailty the type of care they receive and where they receive it has an enormous impact on their experience. It creates long lasting memories for their loved ones too positive and negative. St Christopher's Bromley Care Coordination Service (BCC) is rising to the challenge of making sure people can spend their final days in the place of their choice which is usually at home. The team cares for people in their own homes and supports family members and carers so they can make decisions that reflect patients' preferences. It's just one of the ways NHS Bromley Clinical Commissioning Group is investing in services that make a real impact on older people and their carers and families. Dr Mandy Selby, GP and Clinical Lead at NHS Bromley CCG, said, "Most of the patients who are referred to the service are elderly and need to be registered with a Bromley GP and thought to be living in their final year. The service has been specifically designed to pick up individuals who normally would not be referred for specialist palliative care." The service is staffed by nurses who have a wide range of experience spanning heart failure, dementia, respiratory disease, and palliative care. The service operates from the St Christopher's Bromley site in Orpington and receives management support from St Christopher's. Bromley Care Coordination has now been operating for a year. It was short listed for a Health Service Journal award and recently won a Hospice UK Innovation award. Users of the service have given it high praise: "My GP discussed this new service with me and I was very happy for my mother to be referred. The first visit was lovely. It put a new emphasis on the care for my mother and showed me that it was no longer just about the practical matters but she allowed me to see this time as a truly special time with my mother. It was amazing really. I know I wouldn't have been able to do that on my own. This service has given me huge confidence that I can cope and I can care for my mother at home knowing that I have back up 24 hours a day." - Cecilia Willatt, carer for her mother Dorothy, aged 94 who has Parkinson's disease Service Model The model looks to enable people with progressive and advanced illness or frailty to: receive timely, well-coordinated care in the final year if life die with dignity in a place of their choice It also looks to: provide support to their families: and reduce unnecessary hospital admissions Commissioning Groups and NHS England Draft in progress 191
192 Appendices Case Study: St Christopher's Bromley Care Coordination Service (BCC) Unique Features Case-finding patients in the final year of life Nurse specialist assessment Advanced care planning and Coordinate My Care record Referral and engagement of other services to support integrated care (including four hour direct access to community equipment) Delivery of care with 24 hours access to advice and support Assigned key workers Monitoring and review with rapid response for those whose conditions change Personal care service up to 6 weeks post-hospital discharge (Potential ) Impact High proportion (83%) of patients dying at home. Avoiding unplanned admissions in the final year of life - two of on average 3 admissions costing 6.5k. Estimated cost of new service supporting a caseload of up to K Increased CMC utilisation - patients have an agreed & accessible plan for the end of their lives from 25 to 51% of expected prevalence and from 64 to 644 recorded deaths in 12 months. 30% of caseload live alone 55% of caseload not known to community or social care at time of referral Challenges Hospital referrals lower than planned (staff now seconded into secondary care) Many patients not known to other services so the BCC nurse Commissioning Groups and NHS England Draft in progress 192
193 Appendices Case Study: NHS Greenwich Clinical Commissioning Group Integration - that s what you need NHS Greenwich Clinical Commissioning Group has found innovative ways to integrate healthcare services. It was once the case that older patients in the Royal Borough of Greenwich faced long stays in hospital. Health services were not integrated with social care teams and, as a result, the over-65s spent too long awaiting community support. Today, the story is very different. Gone is this silo approach where different departments operate independently and, in its place, NHS Greenwich Clinical Commissioning Group (CCG) has created an efficient, streamlined service. We used to have a lot of fragmentation, which led to delays in people getting care packages so they stayed in hospital longer, says Dr Rebecca Rosen, GP Clinical Commissioner at the CCG. Now the approach is joined up and quick. Integration has led to significant reductions in hospital admissions and delayed hospital discharges, and a range of rehabilitation services being provided at home or in intermediate care facilities. Caring outside of hospital There will always be health emergencies at care homes, GP surgeries and A&E units. What Greenwich CCG has done is ensure that teams of nurses, social workers, occupational therapists and physiotherapists work together to respond within 24 hours. The Joint Emergency Team (JET) liaises with GPs and identifies people who need help but don t necessarily need admission to a hospital or a care home. Instead, patients are assessed and treated at home or through short-term residential care in the community. The Hospital Integrated Discharge Team enables people to leave hospital safely more quickly by organising the support they need and Community Assessment and Rehabilitation Teams (CAR) provide rehab and support to aid their recovery. Care navigators have meaningful conversations with people to understand the whole picture and what it would take to improve a person s health and wellbeing. From this a personalised plan is co-produced. Some people, for example, might prefer their partner to get them ready instead of being assisted by a stranger. This is all about supporting people to stay at home for as long as they can, says Jane Wells, Oxleas Director of Adult Community Services. People can regain their independence where possible without assumptions being made about their needs. Transforming health and social care through partnership has won the teams national praise. In 2013, Greenwich was selected by the government as a pioneer in the world of integration. Chosen from 100 applicants, Greenwich Coordinated Care (GCC) was recognised for saving nearly 1 million from the social care budget and allowing people to be cared for in the community rather than in hospital. Making services more responsive to local people won the GCC the top award for innovation in social care at the Municipal Journal Achievement Awards The transformation has been achieved through a partnership between the CCG, the Royal Borough of Greenwich, Oxleas NHS Foundation Trust, local GPs and the local voluntary sector. Commissioning Groups and NHS England Draft in progress 193
194 Appendices Case Study: Lewisham Community Connections - Asset mapping supporting social prescribing Service Model Community Connections Open to all Lewisham residents 18+ deemed vulnerable Funded by LA: 600k for 18 months (9 staff) Delivered by a consortium of charity organisations Facilitators see clients in the community (e.g. home, coffee shop, library) and deliver a person centred approach to understanding personal needs and wants Signpost and support clients to attend local groups and organisations Development workers mapped all groups in Lewisham incl. those only found by getting on foot and looking Engage with groups and organisations to develop their delivery of support for local people s needs Unique Features Referrals from GPs, hospitals, word of mouth, community groups/orgs., hairdressers, shopkeepers etc. The community is involved in looking after itself Information sharing on everything available Facilitators and volunteers support clients to attend groups Established befrienders for housebound clients Arranges transport to get to groups for those less able Has set up forums between local organisations to engage them in tackling issues together Breakfast group in South Lewisham (GPs, Counsellor and local organisations) Overcoming these: Working with the community to establish new groups Highlighting the needs of the diverse community. Commissioning Groups and NHS England Draft in progress 194 Impact Impacts expected: Reduced A&E attendances, admissions and GP appointments (system is being put in place to monitor this) Improves quality of life and prevents deterioration of health 600+ clients have been supported by the team (in 18 months) 160+ local organisations accepting referrals (in 18 months) 40+ local groups have been supported to develop plans to increase what they can deliver (in 18 months) Clients previously supported are now volunteering, supporting new clients to attend groups (in 18 months) Anecdotal evidence of a reduction in GP appointments. for those supported(in 18 months) Challenges Buy in GP and hospital departments buy in variable Very variable referral rates from different practices Meeting certain needs in Lewisham: Dementia support in the community Support specifically for men Support specifically catering for those aged Groups and activities for young adults with learning or physical disability that meet their needs as young people Evening & weekend groups Groups/services with transport provided Wheelchair/stokes/mobility require an escort
195 Appendices Case Study: Bromley - Prevention Obesity, Alcohol and Smoking Service Model Targeting the pre-diabetic population with an intensive lifestyle support programme to prevent the onset of Type 2 Diabetes (one of two pilots in Europe) following NICE PH Guidance 38. Unique Features Primary Care to identify pre-diabetic patients (targeting priority communities) through the Health Checks and Diabetes Audit and refer for intervention: practical, tailored advice, support & encouragement to help people be more physically active, achieve and maintain a healthy weight and eat a healthier diet for 12 months. Quarterly monitoring by Primary Care and Weight Watchers as well as 24 month follow up. (Potential ) Impact Impacts expected: Treating 100 adults who are high risk of Type 2 diabetes, with an intensive lifestyle intervention can. Prevent 15 new cases of type 2 diabetes1 Prevent 162 missed work days2 Avoid the need for BP/Cholesterol pills in 11 people3 Add the equivalent of 20 good years of health4 Avoid 57,000 in healthcare costs5 There are approx. 11.5k people in Bromley who are deemed high risk and Challenges Lack of referral capacity in comparison to need - most at risk to be referred. Others at high risk can be referred to the Walking Away from Diabetes 3hr intervention. Potential high drop out rates - Primary Care to receive motivational skills training. 1. Knolwer et al (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med; 7: 346(6): DPP Research Group (2003) Within-trial cost-effectiveness of lifestyle intervention or metformin for the primary prevention of type 2 diabetes. Diabetes Care;26(9): Ratner et al (2005) Impact of Intensive Lifestyle and Metformin Therapy on Cardiovascular Disease Risk Factors in the Diabetes Prevention Program. Diabetes Care 28 (4): Herman et al (2005) The cost-effectiveness of lifestyle modification or metformin in preventing type 2 diabetes in adults with impaired glucose tolerance. Ann Intern Med. 2005;142: Ackermann et al (2008) Translating the DPP into the community. Am J Prev Med 35 (4), pp ; estimates scaled to 2008 could benefit Commissioning Groups and NHS England Draft in progress 195
196 Appendices Case Study: Bromley - Prevention Obesity, Alcohol and Smoking Primary Care Identify pre-diabetic patients through the NHS Health Checks and Diabetes Audit Refer patients using the eligibility criteria Referral includes starting blood measurements, repeated blood test at 6, 12 and 24 months (including a weight measurement at 24 months) Referral includes starting blood pressure measurement, repeated at 3, 6, 9, 12 and 24 months. Undertake Motivational Interviewing training, utilising techniques to support and motivate patients throughout the process. Provide feedback through the qualitative monitoring interview process Weight Watchers Implement the Weight Watchers Diabetes Prevention Pilot Programme Manage the referral hub Deliver objective data to PH team for quantitative data collection Deliver self reported data to PH for evaluation Qualitative evaluation of outcomes Gaining consent to share data and secure data transfer Deliver the information session and continued support for all partners Commissioning Groups and NHS England Draft in progress 196
197 Appendices Case Study: Southwark - Improved Core general practice access plus 8-8, 365 Service Model Two clinics accessible via general practice or GP out of hours service. All patients will be telephone managed by a senior clinician. The service in the south (replacing a walk in centre) will offer same day/next day appointments The service in the north will provide a mixture of routine and urgent appointments. This vision is to put GPs at the heart of providing local health services Unique Features Shared patients record system Service model co-designed with practices and patients Delivering services through a practice-led federated model Telephone management by a senior clinician (Potential ) Impact Reducing variability in quality, access and patient outcomes Supporting patients to find the right service at the right time Improve and increase primary care capacity Promote consistency of care across general practice. Reducing reliance on unscheduled care services. Challenges Keeping everyone engaged whilst working at pace Working with new provider organisations Delegated APMS contract Provider ability to work with ambiguity within a negotiated framework Ability to collect data to evaluate integrated pathway due to overlap with core contract Ensuring consistent application of pathway at practice level. Commissioning Groups and NHS England Draft in progress 197
198 Appendices Enhanced call and recall improves screening and early identification and management of long term conditions Service Model Intervention to improve awareness and uptake of bowel cancer screening in ethnically-diverse areas Unique Features Face-to-face health promotion on bowel cancer screening to invitees in 9 GP Practices; Health promotion delivered by telephone only to patients of 9 other GP practices 24 practices of similar size as comparators (Potential ) Impact Median gfobt kit uptake in the target population (aged 59 70) was 46.7% in the telephone practices, 43.8% in the face-to-face practices and 39.1% in the comparison practices Personally delivered health promotion improved uptake of bowel cancer screening in areas of low socio-economic status and high ethnic diversity with telephone intervention most effective Commissioning Groups and NHS England Draft in progress 198
199 Appendices Lewisham Neighbourhood Primary Care Improvement Scheme - Reduction in gap between recorded / actual prevalence of long term conditions Service Model The scheme enables primary care to target its efforts/resources to achieve specific indicators over a range of priority clinical areas including diabetes, cancer, COPD, hypertension, PPI, flu, pneumococcal and childhood immunisations Unique Features GP practices are encouraged to advance care through a variety of means, including working collaboratively in Neighbourhoods. Neighbourhoods have begun to establish their own mechanisms to deliver the scheme, for example through sharing dedicated admin resource or appointing leads for clinical areas across all practices (Potential) Impact Increased self-management for people with long term conditions A positive impact on access to primary care To build on the collaborative working within Neighbourhoods Reduced variation Improved health outcomes for people with long term conditions To provide a platform for the delivery of population based care Since September 2014: 574 cases of newly recorded / diagnosed Type 2 diabetes 220 newly diagnosed COPD patients 758 newly diagnosed hypertensive patients Challenges Data quality (coding) issues consistency and accuracy Commissioning Groups and NHS England Draft in progress 199
200 Appendices Lambeth (& Southwark) Diabetes Modernisation Initiative - Reduction in variation (level up) primary care management of long term conditions Service Model Intermediate multi-disciplinary team clinics Structured education & self-management support for patients Improving primary care management of diabetes Unique Features Telephone/ support by DSN Joint in-practice patient clinics run in practices by DSN & practice staff Virtual clinics by DSN-led review of patients on diabetes registers Intensive support of DSN and GPWSI for practices with lowest HbA1c control, blood pressure control & detection rates (Potential) Impact Improved management and control leading to better outcomes and reduction in hospital activity The overall spend on planned diabetes care per person on the diabetes register has reduced Improvements in biological outcomes for targeted practices High levels of patient satisfaction Challenges Increasing complexity being managed out of hospital including: increasing follow-ups need to review specialist clinical capacity Increasing demands on primary care Commissioning Groups and NHS England Draft in progress 200
201 Appendices Greenwich - Re-ablement Admissions avoidance and effective discharge Service Model The Community Assessment and Rehabilitation teams work in partnership with Greenwich Council to provide community-based assessment, rehabilitation and prevention services for people over 18 years of age. Referrals are taken directly from patients who need the service and from health and social care professionals. Unique Features Neuro-rehabilitation, for injuries and conditions including head injuries, Stroke, Parkinsons, Cerebral Palsy and MS and MND Dietetics, for people require dietary/ nutritional advice/support Mobility assessments and intervention Assessment and rehabilitation of activity of daily living (ADL), with a reablement focus Falls intervention Help to manage a long-term condition. (Potential) Impact Reductions in DTOC s. Improvement in A&E attendances and admissions avoided. 64% assisted require no ongoing support from LA (London average is 50%). 7 % reduction in clients needing long-term care. Increased use of assistive technology (up by 21 %), and a reduction in the number of service users requiring home care Savings of 900,000 to the local authority's care budget, and of 5.5 % to NHS community health budgets Challenges Demand through A&E/ACUTE Discharges Workforce Increase in frailty Financial balance across health and social care system Commissioning Groups and NHS England Draft in progress 201
202 Appendices Bexley Case Management Multi Disciplinary Team configuration main long term condition groups (incl. mental health) and Frail elderly Service Model GP-led model of an integrated multi-disciplinary team approach using innovative models of communication, to planning care for patients with complex needs, and monitoring outcomes Unique Features Holding multi-disciplinary team meetings to plan patients care in an integrated and holistic way whereby effectiveness is maximised through: Greater use of risk stratification to identify patients to be discussed Involving the social workers Enabling all professionals to identify patients that they are concerned about Circulating/sharing the patient list prior to the meeting so that professionals have the opportunity to review their own care records Using conference call facilities to enable professionals to dial in when they are unable to attend meetings (Potential) Impact The benefits of this approach include: better coordinated care for patients avoidance of admissions to care homes and hospital improved medicine management As part of the overall Integrated Care Older People programme: 1,867 admissions can be prevented (approximately 5 per day) 13,130 acute bed days saved (reduction of approximately 37 beds) Disinvesting 4.02m from the acute sector. Commissioning Groups and NHS England Draft in progress 202

203 Appendices Bexley Case Management Multi Disciplinary Team configuration main long term condition groups (incl. mental health) and Frail elderly Commissioning Groups and NHS England Draft in progress 203
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
The Community Based Target Model
 1 The Community Based Target Model Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with High Impact Changes Lambeth Serving geographically coherent
1 The Community Based Target Model Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with High Impact Changes Lambeth Serving geographically coherent
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
South East London: Sustainability and Transformation Plan
 South East London: Sustainability and Transformation Plan 21 October 2016 Key information details Name of footprint and no: South east London; no. 30 Region: South east London (Bexley; Bromley; Greenwich;
South East London: Sustainability and Transformation Plan 21 October 2016 Key information details Name of footprint and no: South east London; no. 30 Region: South east London (Bexley; Bromley; Greenwich;
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Richmond Clinical Commissioning Group
 Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
NHS LEWISHAM CLINICAL COMMISSIONING GROUP. COMMISSIONING INTENTIONS 2014/15 and 2015/16
 NHS LEWISHAM CLINICAL COMMISSIONING GROUP COMMISSIONING INTENTIONS 2014/15 and 2015/16 1 CONTENTS Introduction 1. Who We Are p5-6 1.1 CCG s Responsibilities p5 1.2 Partnership Working p6 2. CCG s Strategic
NHS LEWISHAM CLINICAL COMMISSIONING GROUP COMMISSIONING INTENTIONS 2014/15 and 2015/16 1 CONTENTS Introduction 1. Who We Are p5-6 1.1 CCG s Responsibilities p5 1.2 Partnership Working p6 2. CCG s Strategic
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
NHS Ayrshire and Arran. 1. Which of the following performance frameworks has the most influence on your budget decisions:
 A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
South West London Commissioning Intentions 2015/16
 Attach 5 NHS SOUTH WEST LONDON COMMISSIONING COLLABORATIVE South West London Commissioning Intentions 2015/16 Draft v0.7 8/21/2014 Document version Date of revision Document Iterations made Status v0.1
Attach 5 NHS SOUTH WEST LONDON COMMISSIONING COLLABORATIVE South West London Commissioning Intentions 2015/16 Draft v0.7 8/21/2014 Document version Date of revision Document Iterations made Status v0.1
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
The North Central London Sustainability and Transformation Plan. and. Camden Local Care Strategy. Caz Sayer Chair, Camden CCG
 The North Central London Sustainability and Transformation Plan and Camden Local Care Strategy Caz Sayer Chair, Camden CCG About the Sustainability & Transformation Plan (STP) N C L North Central London
The North Central London Sustainability and Transformation Plan and Camden Local Care Strategy Caz Sayer Chair, Camden CCG About the Sustainability & Transformation Plan (STP) N C L North Central London
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Summary annual report 2014/15
 1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
A new mindset: the Five Year Forward View for mental health
 A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
Greenwich Clinical Commissioning Group. Patient and Public Engagement Strategy ( )
") Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP)
") Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP) UPDATE Toby Sanders, STP Lead 13 September, 2016 What is the STP? Health and care place based plan for Leicester, Leicestershire
Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP) UPDATE Toby Sanders, STP Lead 13 September, 2016 What is the STP? Health and care place based plan for Leicester, Leicestershire
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
Five year strategy for Leeds A view from the Leeds Unit of Planning June submission.
 Five year strategy for Leeds A view from the Leeds Unit of Planning June submission. Background - Leeds Leeds has an ambition to be internationally renowned for its excellent health and social care economy
Five year strategy for Leeds A view from the Leeds Unit of Planning June submission. Background - Leeds Leeds has an ambition to be internationally renowned for its excellent health and social care economy
Southwark s Primary and Community Care Strategy
 Southwark s Primary and Community Care Strategy 2013/2014 2017/2018 Southwark Primary and Community Care Strategy 2013/2014 2017/2018 Table of Contents Section Page Number Executive Summary 3 1. Introduction,
Southwark s Primary and Community Care Strategy 2013/2014 2017/2018 Southwark Primary and Community Care Strategy 2013/2014 2017/2018 Table of Contents Section Page Number Executive Summary 3 1. Introduction,
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
Our vision. Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey
 Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS
 THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
August Planning for better health and care in North London. A public summary of the NCL STP
 August 2017 Planning for better health and care in North London A public summary of the NCL STP Planning for better health and care in North London North London NHS organisations are working together with
August 2017 Planning for better health and care in North London A public summary of the NCL STP Planning for better health and care in North London North London NHS organisations are working together with
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
1. Introduction FOR SIGN OFF BY CCG CHAIRS - PENDING
 DRAFT consultation document Improving planned orthopaedic care in south east London --- Tell us what you think and help us to shape the future of these services CONTENTS 1. Introduction 2. What is orthopaedic
DRAFT consultation document Improving planned orthopaedic care in south east London --- Tell us what you think and help us to shape the future of these services CONTENTS 1. Introduction 2. What is orthopaedic
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
ANSWERS TO QUESTIONS YOU MAY HAVE
 ANSWERS TO QUESTIONS YOU MAY HAVE What is Better Care Together really all about? Better Care Together is about ensuring that health and social care services in Leicester, Leicestershire and Rutland are
ANSWERS TO QUESTIONS YOU MAY HAVE What is Better Care Together really all about? Better Care Together is about ensuring that health and social care services in Leicester, Leicestershire and Rutland are
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
TRUST BOARD TB(16) 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals
 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals") TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Child Health 2020 A Strategic Framework for Children and Young People s Health
 Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS. September 2014
 OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
A consultation on the Government's mandate to NHS England to 2020
 A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Sustainability and transformation plan (STP)
") Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
LEARNING FROM THE VANGUARDS:
 LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Stockport Strategic Vision. for. Palliative Care and End of Life Care Services. Final Version. Ratified by the End of Life Care Programme Board
 Stockport Strategic Vision for Palliative Care and End of Life Care Services Final Version Ratified by the End of Life Care Programme Board on 8 th February 2012 Clinical Commissioning Pathfinder Contents
Stockport Strategic Vision for Palliative Care and End of Life Care Services Final Version Ratified by the End of Life Care Programme Board on 8 th February 2012 Clinical Commissioning Pathfinder Contents
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
NHS Lambeth Clinical Commissioning Group and Guy s & St Thomas NHS Foundation Trust
 and Guy s & St Thomas NHS Foundation Trust Summary of proposed changes to: inpatient intermediate care services at Lambeth Community Care Centre and Pulross and rehabilitation services for people who have
and Guy s & St Thomas NHS Foundation Trust Summary of proposed changes to: inpatient intermediate care services at Lambeth Community Care Centre and Pulross and rehabilitation services for people who have
Annual Report Summary 2016/17
 Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...