PROGRAM AND HEALTH REQUIREMENTS FOR BSN STUDENTS
|
|
|
- Gloria Greene
- 6 years ago
- Views:
Transcription


1 PROGRAM AND HEALTH REQUIREMENTS FOR BSN STUDENTS Cleveland State University Advancing Excellence in Nursing Professionals 1
2 2
3 PROGRAM AND HEALTH REQUIREMENTS FOR STUDENTS This packet contains information and forms which must be completed. Please adhere to the appropriate deadlines for submission of the forms to the School of Nursing: o Basic BSN Program (Early Decision) Before May 15 th o Basic BSN Program Before June 15 th o Accelerated BSN Program Before October 30 th o RN to BSN Fall Program Before September 30 th o RN to BSN Spring Program Before January 30 th Student Handbook: Go to the School of Nursing Home page at Download the Undergraduate Student Handbook and read completely Print and sign the following sheets: Memorandum of Understanding Informed Consent Program and Health Documentation Required: Ability to Perform Nursing Tasks Health Examination Medical Forms with TDap Booster Varicella (Chicken Pox) Titer Measles Mumps Rubella (MMR) Titer Tuberculin Mantoux Skin Test or Chest X-Ray Verification Seasonal Influenza Vaccination Hepatitis B Titer Vision Screening Dental Exam Form (optional but recommended) Other Information Required: Health Insurance Verification Automobile Information Fingerprinting and Background Check Information CPR Certification Information Agency Confidentiality and related forms Uniform Dress Code Requirements (ABSN & BSN only) 1. Before you submit the documents indicated above- make a copy for your records. 2. Faxed documents cannot be accepted. 3. NOTE: The original documentation should be submitted to the School of Nursing The CSU Health & Wellness Services Department provides medical services and immunizations inexpensively and most health insurance is accepted. For an appointment, please call 216/ The Department is located at 2112 Euclid Avenue, Room 205 (IM Building). 3
4 Ability to Perform Nursing Tasks Please consider carefully any physical limitations you might have. If you have a diagnosed disability that may prevent you from carrying out any of these physical expectations, please discuss your situation with the School of Nursing Undergraduate Program Director/Advisor. Students who enter the program do so with the understanding that they will be expected to meet course requirements, with or without any reasonable accommodations. Students who have a disability will be referred to the Office of Disability Services for determination of the reasonable accommodation that can be made.* Inability to carry out any of these activities while in the program may prevent completion of the program. Students Please place a checkmark next to the items that you are unable to perform. 1. Work for hours in a standing position and do frequent walking and stair climbing. 2. Independently lift and transfer an adult patient up to 6 inches from a stooped position; then, push or pull the adult up to 3 feet. 3. Independently lift and transfer an adult patient while you move from a stooped to an upright position to accomplish bed-tochair and chair-to-bed transfers. 4. Physically apply up to 10 pounds of pressure to bleeding sites or in performing CPR. 5. Immediately respond and react to auditory instructions/requests, monitor equipment and perform auditory auscultation without auditory impediment. 6. Perform a clinical/laboratory experience for up to 12-hour duration, including standing for up to 4 hours straight at a time. 7. Perform close and distant visual activities involving objects, persons, and paperwork, as well as discriminate depth and color perception (If need accommodation, i.e. glasses or contacts, check line). 8. Discriminate between rough/smooth and hot/cold when using hands. 9. Manipulate small objects in precise movements; for example, prepare and administer injectable medications. 10. Communicate intelligibly, both orally and in writing. 11. Use products containing natural rubber latex due to allergy. STUDENT STATEMENT PLEASE SIGN ONE OF THE FOLLOWING STATEMENTS: 1. I am able to perform the unchecked tasks without accommodation. Student Signature Date 2. I am able to perform the checked tasks only with accommodation. Student Signature Date If you have a disability that requires accommodation, please have your physician/nurse practitioner verify the disability. PHYSICIAN STATEMENT I have examined the above student and hereby verify that she or he has a physical disability (# above) that will require accommodations in order to carry out activities. Physician/Nurse Practitioner Signature Physician/Nurse Practitioner Name Date (Please print name) This information must be legible and include professional credentials. * The University Office of Disability Services will determine if an accommodation is reasonable in accordance with applicable law. To be completed by a physician/nurse practitioner. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH
5 Health Examination Medical Form A physical examination is required for all students upon admission to the Nursing Program. The student may have a physical examination performed by his/her private physician/nurse practitioner or at CSU Health & Wellness Services Department. Complete this page and give to your physician/nurse practitioner when the physical examination is done. This information will be treated confidentially. Last First M. I. CSU I.D. Number Street Address: (City) (State) (Zip) ( ) ( ) / / (Home Phone with Area Code) (Cell Phone with Area Code)( (Date of Birth) HEALTH HISTORY (COMPLETE BEFORE VISIT WITH PHYSICIAN/NURSE PRACTITIONER) Have you had, or do you now have, any of the following: (Please check all YES answers.) Allergies High Blood Pressure Scarlet Fever Anemia Joint Pains Seizures Asthma Kidney Pain Shortness of Breath on Exertion Cancer Liver Disease Sickle Cell Disease/Trait Cold Sores (frequent) Migraine Headaches Strep Throat Cough (persistent) Mononucleosis Stroke Diabetes Psychological/Psychiatric Problems Heart Trouble Rheumatic Fever Do you use tobacco in any form? If yes, specify type: Amount: Do you have any physical impairment that limits your activity? No Yes (If yes, please explain) Do you have any other health or medical problems not listed? No Yes ( If yes, please explain) Are you presently taking any kind of medication(s) No Yes (If yes, name drug(s) and how often taken) Do you have any allergies (food, medicine, environmental)? No Yes (If yes, please list) I hereby certify that I have read and understand all of the above questions, and have responded to them to the best of my knowledge. I also consent to the release of medical information to the Program and clinical site. Student s Signature Date 5
6 Student Name: CSU I.D. Number: Date: PHYSICAL EXAMINATION *ABNORMAL HEIGHT WEIGHT PULSE B/P General Appearance Skin PHYSICIAN S NOTE ON PHYSICAL & SUMMARY OF SIGNIFICANT FINDINGS*Abnormal finds must have documentation. Eyes, include Fundus Ears /Hearing Nose/Sinuses Mouth, Throat Neck, include Thyroid Chest, include Breasts Heart Vascular System Lymphatic System Abdomen, Include Inguinal Genitourinary System Nervous System Extremities Spine, Other Musculoskeletal Anus, Rectum DISTANT VISION URINE HEARING Right 20/ Left 20/ Both 20/ Corrected to 20/ Corrected to 20/ Corrected to 20/ Glucose Protein Right: Passed Left: Passed Failed Failed IMMUNIZATIONS/INFECTIOUS DISEASE EVALUATION REQUIRED Tetanus/Diphtheria Boosters required every 10 years. (Original Series may be DPT or Td) Date of Original Series Date of Last Boster Tuberculin (TB) Skin Test Complete Form on Page 9 *TB (Mantoux Only... 2 Step Process) NOTE: Chest x-ray required if Mantoux positive (CHEST X-RAY: Date & Results) Hepatitis B Complete Form on Page 10 MMR (Measles, Mumps, Rubella) Complete Form on Page 10 Varicella Complete Form on Page 8 Seasonal Flu Required By October 15 th, Complete Form on Page 10 Physician/Nurse Practitioner s Name (Please Print) Office Address City, State Zip Code This information must be legible and include professional credentials. Examining Physician or Nurse Practitioner Signature Date Phone # including area code Place Physician s Office Stamp in the Box on the Right for Validation*: *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 6
7 IMMUNIZATION STATUS Students must provide documentation of satisfactory immunization status for the following: a. Tetanus-Diphtheria Toxoid - Most students will have completed their original DPT (Diphtheria, Pertussis or "Whooping Cough" and Tetanus) series during their childhood. If the student was older than six years, the primary immunization series required three injections of TD. The date of completion of either series and the date of a TD (Tetanus-Diphtheria) booster within the past ten years must be recorded on the Health Examination Form Please indicate number of immunizations received in the series and dates of the boosters. If the student is due for a TD booster at this time, he/she should have it administered at least two month prior to classes, with the scheduled date of the immunization noted on the form. b. MMR (Measles, Mumps, Rubella) Students must show proof of a positive titer. If titer is negative, student must be re-immunized and retested with blood titer results showing immunity recorded on the Measles, Mumps, Rubella Form. Rubella also known as German Measles Rubeola also known as English Measles c. Varicella - Students are required to submit proof from a physician or health institution of having a positive titer. If titer is negative, student must be re-immunized and retested with result recorded on the Verification of Having Varicella (Chicken Pox) Illness, Immunization, and Blood Titer Test Form. d. TB Mantoux Test - The two-step TB Mantoux Test or QuantiFERON report is required for all students admitted to the Nursing Program and a one-step or QuantiFERON is required for every subsequent year in the program. A physician will determine the appropriate follow-up for positive results. The results of the TB Mantox Test or Chest X-Ray should be indicated on the TB Mantoux Skin Test or Chest X-Ray Form. The PPD and/or Chest X-Ray can be administered by your private physician or at the County Tuberculosis Clinic located on the ground floor of the Bell Greve Building at Cleveland MetroHealth Medical Center. The telephone number is (216) An appointment is required. The PPD is also available at the CSU Health & Wellness Services Department. e. Hepatitis B The School of Nursing requires that all nursing students receive the Hepatitis B Vaccine. This is to be administered as a series of three. The date of each dose is to be recorded on the Verification of Completed Hepatitis B Immunization Form and submitted after each injection. Documentation of a positive titer is required to show immunity. The vaccine is also available at the CSU Health & Wellness Services Department. f. Seasonal Influenza (Flu Shot) Vaccination - The Centers for Disease Control established the requirement that anyone working in any health care setting must receive a Flu Shot every year. Documentation must be recorded on the Seasonal Influenza (Flu Shot) Vaccination Form and submitted by October 15 th ANNUALLY to be qualified to continue or begin clinical. To be completed by physician or nurse. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH
8 HEPATITIS B IMMUNIZATION Student Name: CSU ID Number: Have you completed a series of Hepatitis B immunization? 1. If so, have a titer drawn and complete the following: Titer Result: Positive Negative Physician/Nurse Practitioner Name & Credentials (Please Print): (Date of Titer) (Physician/Nurse Practitioner Signature) Place Physician s Stamp in the Above Box for Validation* If your results are positive, you are done! 2. If not, one full series of re-immunization is required followed by a second titer to confirm immunization. 1 st Vaccination Date Physician/Nurse Practitioner Signature Place Physician s Stamp in this Box for Validation* 2nd Vaccination Date Physician/Nurse Practitioner Signature Place Physician s Stamp in this Box For Validation* 3 rd Vaccination Date Physician/Nurse Practitioner Signature Place Physician s Stamp in this Box For Validation* 3. Upon completion of the full series, a second titer to confirm immunization is required. Titer Result: Positive Negative Physician/Nurse Practitioner Name & Credentials (Please Print): (Date of Titer) (Physician/Nurse Practitioner Signature) Place Physician s Stamp in the Above Box for Validation* 4. Please note, if the titer remains negative, the physician/nurse practitioner will need to determine follow up as appropriate and provide the School of Nursing with the plan. * * * EVIDENCE OF EACH DOSE/TITER RESULT MUST BEAR A VALIDATION STAMP AND BE SUBMITTED TO THE SCHOOL OF NURSING ONCE IT IS ADMINISTERED. *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 8
9 To be completed by physician or nurse. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH MEASLES MUMPS RUBELLA (MMR) IMMUNIZATION Student Name: CSU ID Number: Have you received your MMR immunization? 1. If so, have a titer drawn and complete the following: Measles (Rubeola) Mumps Rubella (Measles) Titer Result: Positive Negative Titer Result: Positive Negative Physician/Nurse Practitioner Name & Credentials (Please Print): Titer Result: Positive Negative (Date of Titer) (Physician/Nurse Practitioner Signature) Place Physician s Stamp in the Above Box for Validation* If your results are positive, you are done! 2. If any of the results are negative, re-immunization is required followed by a second titer to confirm immunization: Measles Mumps Rubella (MMR) Booster Physician/Nurse Practitioner Name & Credentials (Please Print): Place Physician s Stamp in this Box for Validation* (Date of MMR Booster) (Physician/Nurse Practitioner Signature) 3. Upon completion of re-immunization, a second titer to confirm immunization is required: Measles (Rubeola) Mumps Rubella (Measles) Titer Result: Positive Negative Titer Result: Positive Negative Physician/Nurse Practitioner Name & Credentials (Please Print): Titer Result: Positive Negative (Date of Titer) (Physician/Nurse Practitioner Signature) Place Physician s Stamp in the Above Box for Validation* 4. Please note, if the titer remains negative, the physician/nurse practitioner will need to determine follow up as appropriate and provide the School of Nursing with the plan. * * * * EVIDENCE OF EACH DOSE/TITER RESULT MUST BEAR A VALIDATION STAMP AND BE SUBMITTED TO THE SCHOOL OF NURSING ONCE IT IS ADMINISTERED. *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 9
10 To be completed by physician or nurse. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH VARICELLA (CHICKEN POX) IMMUNIZATION Student Name: CSU ID Number: Have you received the Varicella (Chicken Pox) immunization or had chicken pox? 1. If so, have a titer drawn and complete the following: Titer Result: Positive Negative Physician/Nurse Practitioner Name & Credentials (Please Print): (Date of Titer) (Physician/Nurse Practitioner Signature) Place Physician s Stamp in the Above Box for Validation* If your result is positive, you are done! 2. If the above result is negative, re-immunization is required followed by a second titer to confirm immunization: Varicella (Chicken Pox) Booster Physician/Nurse Practitioner Name & Credentials (Please Print): Place Physician s Stamp in this Box for Validation* (Date of Varicella Booster) (Physician/Nurse Practitioner Signature) 3. Upon completion of the full series, a second titer to confirm immunization is required. Titer Result: Positive Negative Physician/Nurse Practitioner Name & Credentials (Please Print): (Date of Titer) (Physician/Nurse Practitioner Signature) Place Physician s Stamp in the Above Box for Validation* 4. Please note, if the titer remains negative, the physician/nurse practitioner will need to determine follow up as appropriate and provide the School of Nursing with the plan. * * * EVIDENCE OF EACH DOSE/TITER RESULT MUST BEAR A VALIDATION STAMP AND BE SUBMITTED TO THE SCHOOL OF NURSING ONCE IT IS ADMINISTERED. *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 10
11 To be completed by a physician/nurse practitioner after the test has been read. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH QUANTIFERON OR TUBERCULIN MANTOUX SKIN TEST (OR CHEST X-RAY WHEN NECESSARY) Student Name: CSU ID Number: STEP ONE: Date administered: Date read: Results: Positive Negative To be performed 1 3 weeks after Step One. STEP TWO: Date administered: Date read: Results: Positive Negative Physician s/nurse Practitioner s Name (Please Print) Office Address City, State Zip Code This information must be legible and include professional credentials. Physician/Nurse Signature Date The Quantiferon or two-step TB Mantoux Test report is required for all students admitted to the Nursing Program and the Quantiferon or one-step TB Mantoux Test must be performed ANNUALLY throughout the program. If chest x-ray is needed, you must attach a copy of the results with this form. Documentation must include date X-ray was read and the name and credentials of the individual who read the X-Ray. Place Physician s Office Stamp in the Box on the Right for Validation*: *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 11
12 To be completed by Optometrist. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH Student Name: CSU ID Number: Vision Screening* *Only needs to be done if the Ability to Perform Nursing Tasks (page 4) shows you need accommodation. Optometrist Statement Vision Right 20/ Corrected to 20/ Left 20/ Corrected to 20/ Both 20/ Corrected to 20/ This individual last visited my office on. This patient has acceptable vision either by nature or by the use of corrective vision wear. If vision deficits have not all been taken care of, please explain what still needs to be done: Optometrist Name (Please Print) Office Address City, State Zip Code This information must be legible and include professional credentials. Optometrist s Signature Date Place Physician s Office Stamp in the Box on the Right for Validation*: *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 12
13 To be completed by Dentist. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH Dental Exam Although this is optional, a dental examination is strongly recommended for all students at the time of admission to the Nursing Program. This information is strictly confidential. Name (Last, First, M.I.) CSU I.D. No. The above named student is a candidate for admission into the Cleveland State University School of Nursing. Dentist s Statement This individual last visited my office on. At that time all necessary (Date) dental corrections were made. If they have not all been taken care of, please explain what still needs to be done: Dentist/Nurse Practitioner Name (Please Print) Office Address City, State Zip Code This information must be legible and include professional credentials. Dentist s Signature Place Physician s Office Stamp in the Box on the Right for Validation*: *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. Date 13
14 To be completed by a physician/nurse practitioner. Please return to: School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH SEASONAL INFLUENZA (FLU SHOT) VACCINATION *STUDENTS BEGINNING SPRING SEMESTER MUST HAVE THIS COMPLETED BEFORE START OF SEMESTER. FLU SEASON TYPICALLY BEGINS MID SEPTEMBER. VACCINATIONS ARE NOT AVAILABLE BEFORE THIS TIME. Student Name: CSU ID Number: Please provide the following: Date Administered Lot # Exp. Date Site of Injection: Left Deltoid Right Deltoid Administered by Place Physician s Stamp in this Box for Validation* (Signature) (Please Print Name) Office Address: City, State Zip Code This information must be legible and include professional credentials Documentation must be submitted to the School of Nursing by October 15 th Annually. *An Official Letter from the Physician/Nurse Practitioner detailing the above may be substituted for a validation stamp. 14
15 Insurance Requirements and Forms: Student Liability Insurance Cleveland State University covers students through a blanket student liability insurance plan when they are enrolled in the nursing program while participating in clinical experiences under the direction, supervision, and control of the Cleveland State University School of Nursing. The limits of liability are $1,000,000 each claim, $3,000,000 aggregate. o All students enrolled in a CSU Baccalaureate Nursing Program will be covered with this insurance when the Semester registration is paid. Health Insurance Verification Each student must carry some form of health insurance for his/her own protection. The student may obtain insurance from a private agency or participate in CSU s Student Health Insurance Plan. Insurance plan brochures are available in the Health & Wellness Services Department, 2112 Euclid Avenue, Room 205 (IM Building), or on their website: Please document below information related to your Health Insurance coverage. Student s Name (Last, First, M.I.) CSU I.D. Number Policy Holder s Name (if different from Student): Company Name: Dates of Coverage: Policy Number: Group Number: Automobile Information for Parking at Clinical Sites Student Name: Vehicle Year: Vehicle Plate # CSU ID Number Make/Model: State Issued: 15
16 Additional Clinical Agency Requirements: 1. Proof of a clean background check. Third party background checks are not accepted. 2. Current CPR Certification Basic Life Support for Health Care Provider. Fingerprinting and Background Check - BOTH a Civilian (BCI) Check & Federal (FBI) Check Results are required. It is in your best interest to complete your background check screening in the School of Nursing Main Office as early as possible. It can take as many as 30 days for the results to return to School of Nursing. Fingerprinting Locations On CSU Campus School of Nursing Main Office, Julka Hall, Room 238, (216) No appointment is necessary, however, we would like to know that you are coming to campus. Bring your Proof of Payment, Driver s License/State ID, and Request for Background Check Form (page 17). The Combined cost of BCI & FBI Screenings is $ Ways to Pay: Monday Friday 9:00 am 4:00 pm Results are sent directly to the School of Credit/Debit Card ~ ShopNet: Cash/Check Payments: Bring this page to the Office of Treasury Services in Main Classroom, 1899 East 22 nd Street, room 115 and pay the $60 fee. Your payment must be applied to the following: ACCOUNT #: LAB_FEES Off Campus/In-State Identify fingerprint locations on National WebCheck or call Off Campus/Out-of-State Identify fingerprint locations on the internet Google where to get fingerprinted in {enter your city/state}. Contact your state s authorized Civilian and Federal Background Check Center If you are printed at an agency other than the School of Nursing, DO NOT use page 17. You will be responsible for providing the agency with the EXACT responses as listed below. Results not received within 30 days are your responsibility to check the status. Q: Reason for background check: (Be Specific) Q: Address for results to be mailed to: A: Student Entering Nursing School A: CSU School of Nursing 2121 Euclid Avenue, JH 238 Cleveland, OH
17 For Fingerprinting Use On CSU Campus ONLY: Request for a Background Check via Electronic Fingerprinting () Graduate (X) Undergraduate () Faculty (X) BCI and FBI Personal Information (please print) Name Date of Birth SSN Address City State/Province Zip/Postal Code Phone# Driver License Exp. Date: This portion only is needed for FBI background check: Sex Race Height Weight Hair Eyes Reason for background check ( ): Address for results to be mailed to: (X) New Admit Nursing Student CSU School of Nursing Graduating Nursing Senior Ohio Board of Nursing Faculty Other print address below: Other: if checked must complete (This section may be used if you would like a copy) a different form I certify that the personal identifiers provided on this form are accurate and I voluntarily and knowingly authorize the Ohio Bureau of Criminal Identification & Investigation to conduct a criminal records check for the information relating to me. I also voluntarily and knowingly authorize BCI&I to disseminate criminal arrest, conviction and juvenile delinquency adjudication records to Cleveland State University. I voluntarily and knowingly release and discharge the Ohio Attorney General s Office, BCI&I and their employees from all claims and liability related to this authorized criminal record review and dissemination. Signature: Date: 17
18 Cardiopulmonary Resuscitation CLEVELAND STATE UNIVERSITY SCHOOL OF NURSING All students are required to maintain CPR certification Basic Life Support (BLS) for the Healthcare Provider. You may complete the course through any provider authorized by the American Heart Association. Two sources are listed below for your convenience: o You must submit documentation of current CPR certification. o If you have already completed the correct course within the past twelve months, please provide documentation (24 months from the date of certification it must be renewed). o Your CPR certification for Healthcare Provider MUST BE renewed every twenty four (24) months throughout the program. A copy of your two-year re-certification card must be submitted upon completion of the course biennially. CPR Course Locations On CSU Campus Sigma Theta Tau, International Nu Delta Chapter (216) Off Campus (Ohio) CPR Ohio Register online or by phone: (216) East: Landerwood Plaza North, Pinetree, Suite 225, Pepper Pike, OH West: Emerald Crossing, 4760 Grayton Road, Suite 3, Cleveland, OH Off Campus (Outside Ohio) Contact any local provider authorized by the American Heart Association. Agency Confidentiality and Related Forms Signed forms are required to be assigned for clinical experiences. The attached form must be completed, signed and submitted with the other documents and forms described in this packet. Other hospitals, such as Cleveland Clinic Hospitals, MetroHealth Medical Center, and University Hospitals have an on-line system for signing their confidentiality form. o St. Vincent Charity Hospital -- ID Badge Form fill in name and automobile information 18
19 STUDENT I.D. BADGE DATA SHEET FIRST NAME LAST NAME SCHOOL Cleveland State University Job Title: STUDENT Dept: Expiration Date: Clinical Rotation Period FROM: / / TO: / / Clinical Instructor: VEHICLE REGISTRATION Year: Make: Model: License Plate #: Vehicle Color: >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> The following to be completed by Protective Services <<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<<< BADGE # BADGE DESIGN: STUDENT VEHICLE REG.# DATABASE GROUP: STUDENT ACCESS Building 24 HR General Parking Radiology 24 HR PED Access 4A 4B ANC Access Any other access required to perform within Department assigned 19
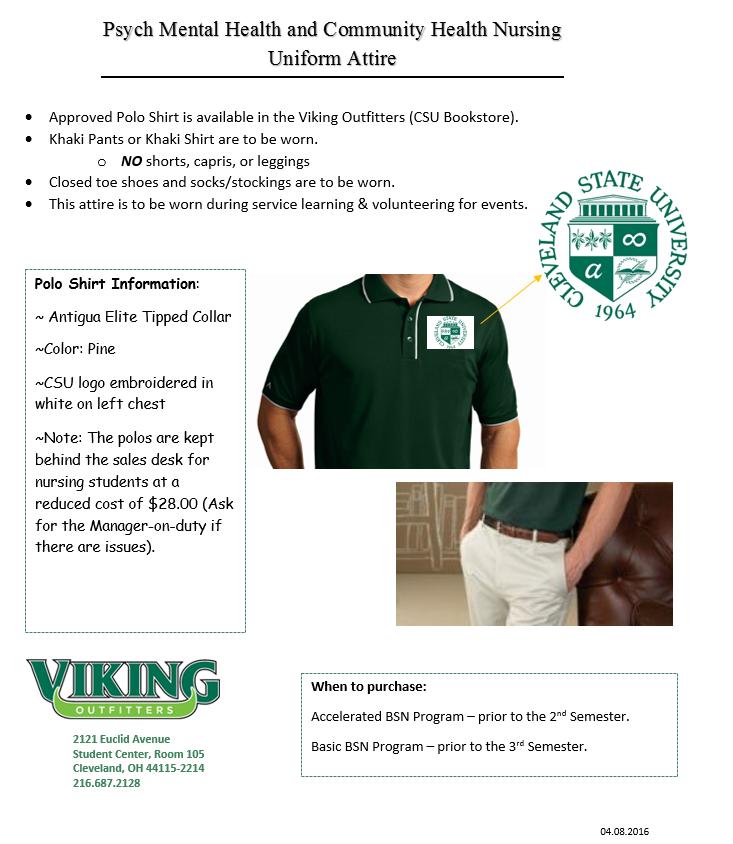
20 Uniform Information Basic and Accelerated Students will need to have a lab coat and full uniform. The lab coat and uniforms must be ordered from Affordable Uniforms. Please contact store to check for current hours. Both must be ordered at least 6 weeks prior to clinical orientation. They are located at: 4916 Turney Road Garfield Hts., OH (216) Mentor Avenue Mentor, OH (440) Lorain Road North Olmsted, OH (440) You will need to purchase the following items. Those with a * must be purchased through Affordable Uniforms. Other items can be purchased from the company or through your own sources. WOMEN *Uniform (either skirt or pant suit style). * Lab coat MEN *Uniform shirt and white trousers * Lab coat BOTH *CSU Name Pin *CSU Student Nurse Patch (one for each uniform and lab coat) Stethoscope White Nurse s Shoes (No canvas tennis shoes, open heel, or clogs may be worn. All white leather tennis shoes without color markings are allowed. Shoes must have closed toe and heel to meet OSHA requirements.) Please Note: Your uniform and lab coat do not come with the CSU patch sewn on. You will need to purchase separate patches and sew them on the upper left sleeve of each uniform and lab coat. Affordable Uniforms will sew on the patches for an extra charge. Be sure to allow plenty of room in your tops to be able to move your arms freely, even if wearing a sweater. Uniforms are paid for at the time you place your order. Also note, NUR 313 Psych Mental Health and NUR 414 Community Health Nursing have separate uniform attire that is to be worn while participating in Service Learning Activities in the Community. The approved Polo Shirt is available at CSU Bookstore (refer to page 24 for details). 20
21 For use by ABSN and BSN Students Only: CLEVELAND STATE UNIVERSITY SCHOOL OF NURSING 21

22 Prices effective January, 2016 and are subject to change. Please call store for hours of operation and current prices. 22
23 23
24 Student Checklist to Ensure Health Data is Up To Date Hep B Documentation of a positive titer Flu Vaccine Documentation of completion each year Varicella Documentation of a positive titer MMR Documentation of a positive titer TB Documentation of the 2-step on admission and a 1-step every year thereafter T-Dap/DT Documentation of Immunization complete Polio Vaccine Documentation of Immunization complete Health Exam Documentation complete Eye Exam Documentation complete (see page 12) Dental Exam Documentation complete (see page 13) Checklist to Ensure Other Requirements Have Been Met CPR (BLS) is up to date and remains current ~ Copy Attached Background Check Health Insurance Verification Complete CSU Uniform Order Completed Affiliate Hospital Confidentiality Forms Completed (highlighted section only) Ability to Perform Nursing Tasks Form completed Student Handbook ~ Memorandum of Understanding Student Handbook ~ Informed Consent Keep this page and a copy of your documents for your records. 24
PROGRAM AND HEALTH REQUIREMENTS FOR BSN STUDENTS
 PROGRAM AND HEALTH REQUIREMENTS FOR BSN STUDENTS Cleveland State University Advancing Excellence in Nursing Professionals 1 2 PROGRAM AND HEALTH REQUIREMENTS FOR STUDENTS This packet contains information
PROGRAM AND HEALTH REQUIREMENTS FOR BSN STUDENTS Cleveland State University Advancing Excellence in Nursing Professionals 1 2 PROGRAM AND HEALTH REQUIREMENTS FOR STUDENTS This packet contains information
FirstName: MiddleInitial: LastName: Student ID# LEHMAN COLLEGE DEPARTMENT OF NURSING READ ME FIRST
 FirstName: MiddleInitial: LastName: Student ID# Program: Generic/Accelerated (B.S.) RN-B.S Master s/post-master s Certificate Cohort/Online/Offsite: RN-BS MD-RN Master s ANNUAL HEALTH CLEARANCE REQUIREMENTS
FirstName: MiddleInitial: LastName: Student ID# Program: Generic/Accelerated (B.S.) RN-B.S Master s/post-master s Certificate Cohort/Online/Offsite: RN-BS MD-RN Master s ANNUAL HEALTH CLEARANCE REQUIREMENTS
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS
 NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
Student Health Form Howard Community College Health Science Division
 Name: HCC ID#: Student Health Form Howard Community College Health Science Division Student- Check program: Nursing: Fall: PN RN Day E/W Spring Accelerated Pathways (NURS-103) CVT: Dental Hygiene: MLT:
Name: HCC ID#: Student Health Form Howard Community College Health Science Division Student- Check program: Nursing: Fall: PN RN Day E/W Spring Accelerated Pathways (NURS-103) CVT: Dental Hygiene: MLT:
Student Health Form Howard Community College Health Science Division
 Name: HCC ID#: Student Health Form Howard Community College Health Science Division HEALTH FORM DEADLINES Completed Health Form must be submitted prior to the following dates. Late submissions may result
Name: HCC ID#: Student Health Form Howard Community College Health Science Division HEALTH FORM DEADLINES Completed Health Form must be submitted prior to the following dates. Late submissions may result
MOUNTAIN VIEW COLLEGE Health Record
 MOUNTAIN VIEW COLLEGE Health Record Date Name: DOB: Last First Middle Month Day Year Address: Street City & State Zip Telephone: Home Work Cell or VM I certify that I have: Health Questionnaire: To be
MOUNTAIN VIEW COLLEGE Health Record Date Name: DOB: Last First Middle Month Day Year Address: Street City & State Zip Telephone: Home Work Cell or VM I certify that I have: Health Questionnaire: To be
Health & Safety Packet for Incoming Students
 Health Occupations Division 707-256-7600 Health & Safety Packet for Incoming Students This packet has been designed to help Health Occupations students comply with CPR and health/physical documentation
Health Occupations Division 707-256-7600 Health & Safety Packet for Incoming Students This packet has been designed to help Health Occupations students comply with CPR and health/physical documentation
Nurse Aide. We reserve the right to cancel any class due to insufficient enrollment.
 Nurse Aide We reserve the right to cancel any class due to insufficient enrollment. **All clinical dates may vary according to site and instructor availability ABOUT THE NURSE AIDE PROGRAM The Nurse Aide
Nurse Aide We reserve the right to cancel any class due to insufficient enrollment. **All clinical dates may vary according to site and instructor availability ABOUT THE NURSE AIDE PROGRAM The Nurse Aide
VILLANOVA UNIVERSITY COLLEGE OF NURSING GRADUATE PROGRAM DIRECTIONS TO COMPLETING PRACTICUM APPLICATION
 VILLANOVA UNIVERSITY GRADUATE PROGRAM DIRECTIONS TO COMPLETING PRACTICUM APPLICATION DUE DATE Dates for submission of Practicum applications vary depending on the semester in which you plan to enroll in
VILLANOVA UNIVERSITY GRADUATE PROGRAM DIRECTIONS TO COMPLETING PRACTICUM APPLICATION DUE DATE Dates for submission of Practicum applications vary depending on the semester in which you plan to enroll in
MOLLOY COLLEGE THE BARBARA H. HAGAN SCHOOL OF NURSING. CHECKLIST Everything must be completed
 : MOLLOY COLLEGE CHECKLIST Everything must be completed 1. PHYSICAL EXAMINATION, completed on a School of Nursing Physical Form. Must be signed, stamped and dated by a Health Care Provider and include:
: MOLLOY COLLEGE CHECKLIST Everything must be completed 1. PHYSICAL EXAMINATION, completed on a School of Nursing Physical Form. Must be signed, stamped and dated by a Health Care Provider and include:
SOUTHWESTERN MICHIGAN COLLEGE NURSING PROGRAM
 Office Use Only Date Submitted to Nursing Office SOUTHWESTERN MICHIGAN COLLEGE NURSING PROGRAM Application to Begin the Nursing Program Complete and return to the Nursing Department Electronic signatures
Office Use Only Date Submitted to Nursing Office SOUTHWESTERN MICHIGAN COLLEGE NURSING PROGRAM Application to Begin the Nursing Program Complete and return to the Nursing Department Electronic signatures
MOLLOY COLLEGE Barbara H. Hagan School of Nursing
 New Clinical Student Checklist MOLLOY COLLEGE Barbara H. Hagan School of Nursing The following is a checklist of requirements for attending clinical practice Hospitals and Community Agencies. Each item
New Clinical Student Checklist MOLLOY COLLEGE Barbara H. Hagan School of Nursing The following is a checklist of requirements for attending clinical practice Hospitals and Community Agencies. Each item
Middle Tennessee State University Master of Science in Nursing Health History and Physical Examination Form
 1 Middle Tennessee State University Master of Science in Nursing Health History and Physical Examination Form HEALTH HISTORY To be completed by student and/or health care provider include immunization
1 Middle Tennessee State University Master of Science in Nursing Health History and Physical Examination Form HEALTH HISTORY To be completed by student and/or health care provider include immunization
Disclosure and Release of Health History and Immunization Requirements
 TO BE COMPLETED BY THE STUDENT: NURSING AND HEALTH OCCUPATIONAL PROGRAMS Disclosure and Release of Health History and Immunization Requirements Student s Name: Birth date: Last First Middle Month/Day/Year
TO BE COMPLETED BY THE STUDENT: NURSING AND HEALTH OCCUPATIONAL PROGRAMS Disclosure and Release of Health History and Immunization Requirements Student s Name: Birth date: Last First Middle Month/Day/Year
CRITICAL REQUIREMENTS FAQs Press control and click on the question to follow the link to the answer.
 CRITICAL REQUIREMENTS FAQs Press control and click on the question to follow the link to the answer. Table of Contents 1) What are the changes to the critical requirements?... 3 2) What cohorts are affected?...
CRITICAL REQUIREMENTS FAQs Press control and click on the question to follow the link to the answer. Table of Contents 1) What are the changes to the critical requirements?... 3 2) What cohorts are affected?...
RUTGERS SCHOOL OF NURSING - CAMDEN STUDENT HEALTH RECORDS PACKET
 School of Nursing-Camden Rutgers, The State University of New Jersey Residence Hall 215 North 3 rd Street Camden, NJ 08102-1405 nursing.camden.rutgers.edu nursecam@camden.rutgers.edu Phone: 856-225-6226
School of Nursing-Camden Rutgers, The State University of New Jersey Residence Hall 215 North 3 rd Street Camden, NJ 08102-1405 nursing.camden.rutgers.edu nursecam@camden.rutgers.edu Phone: 856-225-6226
Hinds Community College Nursing and Allied Health Programs Clinical Record Packet
 Clinical Record Packet General Directions & Information All clinical requirements must be submitted by the health profession program s designated due date. Failure to submit Clinical Record Packet requirements
Clinical Record Packet General Directions & Information All clinical requirements must be submitted by the health profession program s designated due date. Failure to submit Clinical Record Packet requirements
Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM
 Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM TO THE PHYSICIAN: Southwestern College requires a physical examination for students enrolling in the Nursing and Health
Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM TO THE PHYSICIAN: Southwestern College requires a physical examination for students enrolling in the Nursing and Health
CRAFTON HILLS COLLEGE PARAMEDIC PROGRAM Fall 2016 Application
 CRAFTON HILLS COLLEGE PARAMEDIC PROGRAM Fall 2016 Application TO: FROM: Prospective EMT-Paramedic Student Dan Word MSHS, EMT-P Director Paramedic Education SUBJECT: Fall 2016 Paramedic Program (Class 87)
CRAFTON HILLS COLLEGE PARAMEDIC PROGRAM Fall 2016 Application TO: FROM: Prospective EMT-Paramedic Student Dan Word MSHS, EMT-P Director Paramedic Education SUBJECT: Fall 2016 Paramedic Program (Class 87)
Jacksonville State University Lurleen B. Wallace College of Nursing and Health Sciences Health Appraisal Form
 Jacksonville State University Lurleen B. Wallace College of Nursing and Health Sciences Health Appraisal Form Welcome to the Lurleen B. Wallace College of Nursing and Health Sciences at Jacksonville State
Jacksonville State University Lurleen B. Wallace College of Nursing and Health Sciences Health Appraisal Form Welcome to the Lurleen B. Wallace College of Nursing and Health Sciences at Jacksonville State
HEALTH PROFESSIONS PROGRAM Physical Examination Form
 TIDEWATER COMMUNITY COLLEGE HEALTH PROFESSIONS PROGRAM Physical Examination Form Diagnostic Medical Sonography Emergency Medical Services Health Information Management Medical Laboratory Technology Occupational
TIDEWATER COMMUNITY COLLEGE HEALTH PROFESSIONS PROGRAM Physical Examination Form Diagnostic Medical Sonography Emergency Medical Services Health Information Management Medical Laboratory Technology Occupational
LONE STAR COLLEGE-TOMBALL DOCUMENTATION OF REQUIRED IMMUNIZATIONS Please Print
 LONE STAR COLLEGE-TOMBALL DOCUMENTATION OF REQUIRED IMMUNIZATIONS Please Print Name: (Last) (First) (MI) of Birth ID# Enrollment All students enrolled in health related courses who have or will have any
LONE STAR COLLEGE-TOMBALL DOCUMENTATION OF REQUIRED IMMUNIZATIONS Please Print Name: (Last) (First) (MI) of Birth ID# Enrollment All students enrolled in health related courses who have or will have any
Middle Tennessee State University School of Nursing Undergraduate Program Clinical Policy
 Middle Tennessee State University School of Nursing Undergraduate Program Clinical Policy The Middle Tennessee State University School of Nursing has one undergraduate degree seeking program. Tracks in
Middle Tennessee State University School of Nursing Undergraduate Program Clinical Policy The Middle Tennessee State University School of Nursing has one undergraduate degree seeking program. Tracks in
University of South Alabama College of Nursing Bachelor of Science in Nursing
 ADMISSIONS POLICY Enrollment into the University (pre-professional component) as a nursing major does not assure the student admission to the Professional Component. Enrollment in the Professional Component
ADMISSIONS POLICY Enrollment into the University (pre-professional component) as a nursing major does not assure the student admission to the Professional Component. Enrollment in the Professional Component
DEPN AND GRADUATE NURSING MANDATORIES INFORMATION
 DEPN AND GRADUATE NURSING MANDATORIES INFORMATION INITIAL MANDATORIES DUE AUGUST 15, 2018 Pre Clinical Mandatories Form If you have a first time positive PPD, include a radiology report If you have a history
DEPN AND GRADUATE NURSING MANDATORIES INFORMATION INITIAL MANDATORIES DUE AUGUST 15, 2018 Pre Clinical Mandatories Form If you have a first time positive PPD, include a radiology report If you have a history
Cisco College Surgical Technology Program Application for Admission and Student Health Record
 Cisco College does not discriminate on the basis of race, color, creed, national origin, religion, age, gender, sexual orientation, political affiliation, or physical disability Applications to Health
Cisco College does not discriminate on the basis of race, color, creed, national origin, religion, age, gender, sexual orientation, political affiliation, or physical disability Applications to Health
Marian University Leighton School of Nursing-Bachelor of Science in Nursing Program Clinical Application-Spring 2017 CAMPUS BASED ACCELERATED
 Marian University Leighton School of Nursing-Bachelor of Science in Nursing Program Clinical Application-Spring 2017 CAMPUS BASED ACCELERATED Only completed applications will be accepted in the Nursing
Marian University Leighton School of Nursing-Bachelor of Science in Nursing Program Clinical Application-Spring 2017 CAMPUS BASED ACCELERATED Only completed applications will be accepted in the Nursing
ATHLETIC TRAINING MANDATORIES INFORMATION
 ATHLETIC TRAINING MANDATORIES INFORMATION FIRST YEAR MANDATORIES (DUE DATE WILL BE ANNOUNCED IN CLASS) HIPAA/OSHA Training You will complete your training through the Evolve e-learning Solutions website.
ATHLETIC TRAINING MANDATORIES INFORMATION FIRST YEAR MANDATORIES (DUE DATE WILL BE ANNOUNCED IN CLASS) HIPAA/OSHA Training You will complete your training through the Evolve e-learning Solutions website.
Guide to CastleBranch
 Guide to CastleBranch CastleBranch / CB: https://www.castlebranch.com/ Prior to beginning practicum courses, students must provide documentation that they have met certain requirements through CastleBranch,
Guide to CastleBranch CastleBranch / CB: https://www.castlebranch.com/ Prior to beginning practicum courses, students must provide documentation that they have met certain requirements through CastleBranch,
HEALTH REQUIREMENTS AND OTHER DOCUMENTATION Required for RN Mobility Students
 HEALTH REQUIREMENTS AND OTHER DOCUMENTATION Required for RN Mobility Students 1. Health and physical exam form (Form 1) 2. Student Immunization form requiring verification of completed immunizations (Form
HEALTH REQUIREMENTS AND OTHER DOCUMENTATION Required for RN Mobility Students 1. Health and physical exam form (Form 1) 2. Student Immunization form requiring verification of completed immunizations (Form
ATHLETIC TRAINING MANDATORIES INFORMATION
 ATHLETIC TRAINING MANDATORIES INFORMATION FIRST YEAR MANDATORIES (DUE DATE WILL BE ANNOUNCED IN CLASS) HIPAA/OSHA Training You will complete your training through the Evolve e-learning Solutions website.
ATHLETIC TRAINING MANDATORIES INFORMATION FIRST YEAR MANDATORIES (DUE DATE WILL BE ANNOUNCED IN CLASS) HIPAA/OSHA Training You will complete your training through the Evolve e-learning Solutions website.
If you would like to volunteer in the Gift Shop as part of the Hospital Auxiliary, please call for additional information.
 Dear Prospective Volunteer. Thank you for your interest in the volunteer program at Robert Wood Johnson University Hospital Rahway. We are happy to know that you are considering becoming a part of the
Dear Prospective Volunteer. Thank you for your interest in the volunteer program at Robert Wood Johnson University Hospital Rahway. We are happy to know that you are considering becoming a part of the
New Student Information for Licensed Undergraduate Registered Nurse (RN) to Bachelor of Science in Nursing (BSN) Students
 to Bachelor of Science in Nursing (BSN) Students") New Student Information for Licensed Undergraduate Registered Nurse (RN) to Bachelor of Science in Nursing (BSN) Students 1. Orientation a. New Student Orientation is mandatory for all new undergraduate
New Student Information for Licensed Undergraduate Registered Nurse (RN) to Bachelor of Science in Nursing (BSN) Students 1. Orientation a. New Student Orientation is mandatory for all new undergraduate
STUDENT NAME: Date Completed:
 WINONA STATE UNIVERSITY College of Nursing and Health Sciences Graduate Programs in Nursing HEALTH INFORMATION AND REQUIREMENTS FOR PARTICIPATION IN THE GRADUATE PROGRAMS IN NURSING STUDENT NAME: Date
WINONA STATE UNIVERSITY College of Nursing and Health Sciences Graduate Programs in Nursing HEALTH INFORMATION AND REQUIREMENTS FOR PARTICIPATION IN THE GRADUATE PROGRAMS IN NURSING STUDENT NAME: Date
MEDICAL LABORATORY SCIENCE MANDATORIES INFORMATION
 MEDICAL LABORATORY SCIENCE MANDATORIES INFORMATION FIRST YEAR MANDATORIES HIPAA/OSHA Training You will complete your training through the Evolve e Learning Solutions website. You will receive an email
MEDICAL LABORATORY SCIENCE MANDATORIES INFORMATION FIRST YEAR MANDATORIES HIPAA/OSHA Training You will complete your training through the Evolve e Learning Solutions website. You will receive an email
Golden West College School of Nursing Medical Exam Information Sheet
 Golden West College School of Nursing Medical Exam Information Sheet History and Physical Clearance A report, signed by the physician, physician s assistant, or nurse practitioner, shall be provided to
Golden West College School of Nursing Medical Exam Information Sheet History and Physical Clearance A report, signed by the physician, physician s assistant, or nurse practitioner, shall be provided to
Please review the information in this packet. If you have any questions, please contact me at (310) or me at
 or me at") WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH Nursing Assistant /Home Health Aide & Acute Care Programs 9000 OVERLAND AVE., CULVER CITY, CA 90230-3519 (310) 287-7226 Fax (310) 287-4352 Summer 2017
WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH Nursing Assistant /Home Health Aide & Acute Care Programs 9000 OVERLAND AVE., CULVER CITY, CA 90230-3519 (310) 287-7226 Fax (310) 287-4352 Summer 2017
Paramedic Program Roseville, CA
 Paramedic Program Roseville, CA Dear Applicant: We appreciate your interest in the Roseville Paramedic Program and the following is attached: 1. Application Checklist 2. Application Forms 3. Medical History
Paramedic Program Roseville, CA Dear Applicant: We appreciate your interest in the Roseville Paramedic Program and the following is attached: 1. Application Checklist 2. Application Forms 3. Medical History
COLUMBUS STATE COMMUNITY COLLEGE Dental Hygiene
 1 Dental Hygiene HEALTH HISTY To be completed by the Student: PLEASE PRINT ALL INFMATION COUGAR I.D. Name: SS#: Last First Middle Address: Street City State Zip Date of Birth: Phone: Month/Day/Year Home
1 Dental Hygiene HEALTH HISTY To be completed by the Student: PLEASE PRINT ALL INFMATION COUGAR I.D. Name: SS#: Last First Middle Address: Street City State Zip Date of Birth: Phone: Month/Day/Year Home
Department of State Academic Exchanges Participant Medical History and Examination Form
 Department of State Academic Exchanges Participant Medical History and Examination Form Having been selected to participate in a U.S. Department of State educational exchange program, you are required
Department of State Academic Exchanges Participant Medical History and Examination Form Having been selected to participate in a U.S. Department of State educational exchange program, you are required
Health Record Health Services 1025 North Broadway, K-254 Milwaukee, Wisconsin Phone: Fax:
 For office use only: Jenzabar: / / MM DD YY (Initial) Revision date: 7/10/17 Health Record Health Services 1025 North Broadway, K-254 Milwaukee, Wisconsin 53202 Phone: 414-277-7333 Fax: 414-277-2897 Student
For office use only: Jenzabar: / / MM DD YY (Initial) Revision date: 7/10/17 Health Record Health Services 1025 North Broadway, K-254 Milwaukee, Wisconsin 53202 Phone: 414-277-7333 Fax: 414-277-2897 Student
Ambassador Program Application Packet
 Ambassador Program Application Packet Thank you for your interest in becoming an Ambassador at Centinela Hospital Medical Center. Please complete the attached forms and then contact the Centinela Hospital
Ambassador Program Application Packet Thank you for your interest in becoming an Ambassador at Centinela Hospital Medical Center. Please complete the attached forms and then contact the Centinela Hospital
EMS Paramedic Program Application. Copies of the following: Completed Paramedic Application Due Date April 25, 2018
 EMS Paramedic Program Application Student Application Personal Health History Physical Examination Form Student s Work Reference Copies of the following: High School Diploma/GED or equivalent College transcripts
EMS Paramedic Program Application Student Application Personal Health History Physical Examination Form Student s Work Reference Copies of the following: High School Diploma/GED or equivalent College transcripts
NURSING ASSISTANT ADVANCED PLACEMENT PROGRAM REGISTRATION PACKET AND INFORMATION
 NURSING ASSISTANT ADVANCED PLACEMENT PROGRAM REGISTRATION PACKET AND INFORMATION Classes are offered at the following locations: Superstition Mountain Campus Signal Peak Campus Maricopa Campus San Tan
NURSING ASSISTANT ADVANCED PLACEMENT PROGRAM REGISTRATION PACKET AND INFORMATION Classes are offered at the following locations: Superstition Mountain Campus Signal Peak Campus Maricopa Campus San Tan
College of Sequoias Physical Therapist Assistant Program Student Health Release Form
 Part A: College of Sequoias Physical Therapist Assistant Program Student Health Release Form To be completed by the Student Name: Telephone: Cell Number: Address: City: ZIP Code: Birth Date: Family Health
Part A: College of Sequoias Physical Therapist Assistant Program Student Health Release Form To be completed by the Student Name: Telephone: Cell Number: Address: City: ZIP Code: Birth Date: Family Health
BINGHAMTON UNIVERSITY DECKER SCHOOL OF NURSING Student Health Requirements
 BINGHAMTON UNIVERSITY DECKER SCHOOL OF NURSING Student Health Requirements This document includes information regarding: Student health evaluation form Documentation of immunity to communicable diseases
BINGHAMTON UNIVERSITY DECKER SCHOOL OF NURSING Student Health Requirements This document includes information regarding: Student health evaluation form Documentation of immunity to communicable diseases
APPLICATION FOR VOLUNTEER AMBASSADOR (18 yrs and older)
") APPLICATION F VOLUNTEER AMBASSAD (18 yrs and older) Date Name Mailing Address City Zip Telephone Cell Phone E-mail Address EMERGENCY CONTACT EDUCATION: High School College Other Schools/Training REFERENCES:
APPLICATION F VOLUNTEER AMBASSAD (18 yrs and older) Date Name Mailing Address City Zip Telephone Cell Phone E-mail Address EMERGENCY CONTACT EDUCATION: High School College Other Schools/Training REFERENCES:
MSU-Crowder Bachelor of Science in Nursing (BSN-C) Scholars Program.
 Scholars Program.") Dear Prospective Student: Thank you for your inquiry regarding the MSU-Crowder Bachelor of Science in Nursing (BSN-C) Scholars Program. This program is the result of an exciting collaboration between Crowder
Dear Prospective Student: Thank you for your inquiry regarding the MSU-Crowder Bachelor of Science in Nursing (BSN-C) Scholars Program. This program is the result of an exciting collaboration between Crowder
Clinical Education Policies
 1 Clinical Education Policies Table of Contents Assignment of Students Page 1 Student Information Page 1 Student Information Form Page 2 Reasonable Accommodations Request Student Health Form Pages 3-5
1 Clinical Education Policies Table of Contents Assignment of Students Page 1 Student Information Page 1 Student Information Form Page 2 Reasonable Accommodations Request Student Health Form Pages 3-5
FALL Juan Carlos Castillo
 WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH Nursing Assistant /Home Health Aide & Acute Care Programs 9000 OVERLAND AVE., CULVER CITY, CA 90230-3519 (310) 287-7226 Fax (310) 287-4352 FALL 2017 Dear
WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH Nursing Assistant /Home Health Aide & Acute Care Programs 9000 OVERLAND AVE., CULVER CITY, CA 90230-3519 (310) 287-7226 Fax (310) 287-4352 FALL 2017 Dear
NURSING ASSISTANT PROGRAM REGISTRATION PACKET AND INFORMATION
 NURSING ASSISTANT PROGRAM REGISTRATION PACKET AND INFORMATION Must be received 10 days prior to the start of class to be admitted for the semester. Classes are offered at the following locations: Superstition
NURSING ASSISTANT PROGRAM REGISTRATION PACKET AND INFORMATION Must be received 10 days prior to the start of class to be admitted for the semester. Classes are offered at the following locations: Superstition
** Clinical Training Requirements Checklist for Conditionally Accepted EMS Students**
 1 ** Clinical Training Requirements Checklist for Conditionally Accepted 2017-18 EMS Students** The following checklist outlines required documentation for conditionally accepted 2016-17 EMS and Paramedic
1 ** Clinical Training Requirements Checklist for Conditionally Accepted 2017-18 EMS Students** The following checklist outlines required documentation for conditionally accepted 2016-17 EMS and Paramedic
WELCOME BACHELOR OF SCIENCE IN RADIOLOGICAL SCIENCE
 WELCOME BACHELOR OF SCIENCE IN RADIOLOGICAL SCIENCE SUMMER 2017 RADIOLOGICAL SCIENCE ORIENTATION SUMMER 2017 IMPORTANT INFORMATION & DATES Please complete and submit the information noted below to the
WELCOME BACHELOR OF SCIENCE IN RADIOLOGICAL SCIENCE SUMMER 2017 RADIOLOGICAL SCIENCE ORIENTATION SUMMER 2017 IMPORTANT INFORMATION & DATES Please complete and submit the information noted below to the
** Clinical Training Requirements Checklist for Conditionally Accepted Allied Health Students**
 1 ** Clinical Training Requirements Checklist for Conditionally Accepted 2016-17 Allied Health Students** The following checklist outlines required documentation for conditionally accepted 2016-17 Allied
1 ** Clinical Training Requirements Checklist for Conditionally Accepted 2016-17 Allied Health Students** The following checklist outlines required documentation for conditionally accepted 2016-17 Allied
DMACC INSTRUCTIONS FOR COMPLETING STUDENT HEALTH AND IMMUNIZATION RECORD
 DMACC DES MOINES AREA COMMUNITY COLLEGE INSTRUCTIONS FOR COMPLETING STUDENT HEALTH AND IMMUNIZATION RECORD Health and Public Service Department Students need to complete and submit the Student Health and
DMACC DES MOINES AREA COMMUNITY COLLEGE INSTRUCTIONS FOR COMPLETING STUDENT HEALTH AND IMMUNIZATION RECORD Health and Public Service Department Students need to complete and submit the Student Health and
Allan Hancock College 2019 Licensed Vocational Nursing Program Application Period: April 1 st June 30 th, 2018
 *This application is for applicants who currently have an LVN waitlist number* It is the responsibility of the student to complete this application packet and turn it into the Health Sciences Department
*This application is for applicants who currently have an LVN waitlist number* It is the responsibility of the student to complete this application packet and turn it into the Health Sciences Department
1419 Salt Springs Road Syracuse, NY (Health Office)
") 1419 Salt Springs Road Syracuse, NY 13214-1301 315-445-4440 (Health Office) Dear FAMILY NURSE PRACTITIONER Student: Congratulations! As Nurse Manager of the Wellness Center I would like to welcome you
1419 Salt Springs Road Syracuse, NY 13214-1301 315-445-4440 (Health Office) Dear FAMILY NURSE PRACTITIONER Student: Congratulations! As Nurse Manager of the Wellness Center I would like to welcome you
Applicant Name (Please print) Last First MI. Northeast State Community College assigned Student ID Number: City: State: Zip Code:
 Last First MI. Northeast State Community College assigned Student ID Number: City: State: Zip Code:") Applicant Information (Please note application must be completed in ink.) Applicant Name (Please print) Last First MI Northeast State Community College assigned Student ID Number: Street Address: PO Box:
Applicant Information (Please note application must be completed in ink.) Applicant Name (Please print) Last First MI Northeast State Community College assigned Student ID Number: Street Address: PO Box:
Policy S-4 FLORIDA STATE UNIVERSITY COLLEGE OF NURSING CLINICAL CLEARANCE
 Policy S-4 FLORIDA STATE UNIVERSITY COLLEGE OF NURSING Page 1 of 2 TITLE: POLICY: RATIONALE: PROCEDURE: CLINICAL CLEARANCE Clinical Clearance is required for a student to participate in a required clinical
Policy S-4 FLORIDA STATE UNIVERSITY COLLEGE OF NURSING Page 1 of 2 TITLE: POLICY: RATIONALE: PROCEDURE: CLINICAL CLEARANCE Clinical Clearance is required for a student to participate in a required clinical
PROCEDURE: 1. Prospective students are required to obtain the Pre-Entrance Physical Examination Form from the Nursing Program office.
 Policy # S-11 POLICY: PRE-ENTRANCE PHYSICAL EXAM POLICY: It is the Policy of the at the University of Pittsburgh at Titusville to require students seeking admission to the to submit documentation of a
Policy # S-11 POLICY: PRE-ENTRANCE PHYSICAL EXAM POLICY: It is the Policy of the at the University of Pittsburgh at Titusville to require students seeking admission to the to submit documentation of a
POLICY TITLE: STUDENT CLINICAL REQUIREMENTS PART ONE
 Page 1 of 6 STUDENT CLINICAL REQUIREMENTS PART ONE Policy Number: S101 POLICY TITLE: STUDENT CLINICAL REQUIREMENTS PART ONE The College of Nursing (CON) is committed to ensuring that all nursing students
Page 1 of 6 STUDENT CLINICAL REQUIREMENTS PART ONE Policy Number: S101 POLICY TITLE: STUDENT CLINICAL REQUIREMENTS PART ONE The College of Nursing (CON) is committed to ensuring that all nursing students
BEFORE COMPLETING THIS PACKET
 Baton Rouge Community College Medical Assistant Certificate of Technical Studies MEDICAL ASSISTANT ADMISSION PACKET BEFORE COMPLETING THIS PACKET 1. Complete and Submit MEDICAL ASSISTANT PROGRAM APPLICATION
Baton Rouge Community College Medical Assistant Certificate of Technical Studies MEDICAL ASSISTANT ADMISSION PACKET BEFORE COMPLETING THIS PACKET 1. Complete and Submit MEDICAL ASSISTANT PROGRAM APPLICATION
Proof of current (within 1 year) Tuberculin PPD or skin test administration. If PPD result is positive a negative chest x-ray is required.
 Tuberculin PPD or skin test administration. If PPD result is positive a negative chest x-ray is required.") Failure to submit all documents will result in an INCOMPLETE application. FAMU SCHOOL OF NURSING PROFESSIONAL LEVEL APPLICATION CHECKLIST For admission to the Professional Nursing Program, applications
Failure to submit all documents will result in an INCOMPLETE application. FAMU SCHOOL OF NURSING PROFESSIONAL LEVEL APPLICATION CHECKLIST For admission to the Professional Nursing Program, applications
CNA CERTIFICATE PROGRAM APPLICATION PACKET
 CNA CERTIFICATE PROGRAM APPLICATION PACKET Application Instructions Thank you for your interest in the Certified Nursing Assistant Certificate Program at the College of Continuing and Professional Education
CNA CERTIFICATE PROGRAM APPLICATION PACKET Application Instructions Thank you for your interest in the Certified Nursing Assistant Certificate Program at the College of Continuing and Professional Education
RDA Registered Dental Assisting
 Verified by Dawn Brewster, RDA Coordinator: RDA Registered Dental Assisting HEALTH SCIENCES PROGRAM HEALTH REQUIREMENTS To be filled out by Health Care Provider (HCP) STUDENT NAME: DATE OF BIRTH: Applicants
Verified by Dawn Brewster, RDA Coordinator: RDA Registered Dental Assisting HEALTH SCIENCES PROGRAM HEALTH REQUIREMENTS To be filled out by Health Care Provider (HCP) STUDENT NAME: DATE OF BIRTH: Applicants
RN Refresher Program Information Packet
 MESA COMMUNITY COLLEGE RN Refresher Program Information Packet 2017-2018 Mesa Community College Nursing Department, Health & Wellness Building #8 (480) 461-7104 Fax (480) 461-7821 NONDISCRIMINATION POLICY
MESA COMMUNITY COLLEGE RN Refresher Program Information Packet 2017-2018 Mesa Community College Nursing Department, Health & Wellness Building #8 (480) 461-7104 Fax (480) 461-7821 NONDISCRIMINATION POLICY
IMPORTANT Instructions for Incoming First Semester ADN Students Spring 2018
 IMPORTANT Instructions for Incoming First Semester ADN Students Spring 2018 Congratulations and welcome to first semester of the ADN Program! My name is Laura DeFreitas. I am course coordinator for first
IMPORTANT Instructions for Incoming First Semester ADN Students Spring 2018 Congratulations and welcome to first semester of the ADN Program! My name is Laura DeFreitas. I am course coordinator for first
BROOKLINE COLLEGE PHYSICAL THERAPIST ASSISTANT PROGRAM APPLICATION REQUIREMENTS
 BROOKLINE COLLEGE PHYSICAL THERAPIST ASSISTANT PROGRAM APPLICATION REQUIREMENTS 2017-2018 Lynn E. Bagnull, PT, MBA Program Director lynn.bagnull@brooklinecollege.edu James Mulroy, PT, MS Academic Coordinator
BROOKLINE COLLEGE PHYSICAL THERAPIST ASSISTANT PROGRAM APPLICATION REQUIREMENTS 2017-2018 Lynn E. Bagnull, PT, MBA Program Director lynn.bagnull@brooklinecollege.edu James Mulroy, PT, MS Academic Coordinator
Checklist for Nursing Program Students
 Checklist for Nursing Program Students It is recommended that students make copies of all documents for your personal record prior to submitting. Complete and upload the following forms to CastleBranch
Checklist for Nursing Program Students It is recommended that students make copies of all documents for your personal record prior to submitting. Complete and upload the following forms to CastleBranch
CRAFTON HILLS COLLEGE PARAMEDIC PROGRAM Spring 2019 Application
 CRAFTON HILLS COLLEGE PARAMEDIC PROGRAM Spring 2019 Application To: FROM: Prospective Paramedic Student Kathy Crow, BVE, EMT- P Director, Paramedic Education SUBJECT: Spring 2019 Paramedic Program (Class
CRAFTON HILLS COLLEGE PARAMEDIC PROGRAM Spring 2019 Application To: FROM: Prospective Paramedic Student Kathy Crow, BVE, EMT- P Director, Paramedic Education SUBJECT: Spring 2019 Paramedic Program (Class
OBSERVER APPLICATION
 OBSERVER APPLICATION Application Instructions: Please type all responses. Review and complete the application and required attachments following the application. A submission checklist is provided to ensure
OBSERVER APPLICATION Application Instructions: Please type all responses. Review and complete the application and required attachments following the application. A submission checklist is provided to ensure
Clinical Pre-Placement Health Form
 Clinical Pre-Placement Health Form Program Name : Practical Nursing-IEN Fast Track Due Program Code (#) 9352 Program Year Program Descriptor Fast Track Student Last Name: Student First Name: Student I.D.
Clinical Pre-Placement Health Form Program Name : Practical Nursing-IEN Fast Track Due Program Code (#) 9352 Program Year Program Descriptor Fast Track Student Last Name: Student First Name: Student I.D.
NURSING AND HEALTH OCCUPATION PROGRAMS
 TO BE COMPLETED BY STUDENT: Statement of Health and Immunization Records (pages 1 & 2) Student s Name: Birth date: Last First Middle Month/Day/Year Address: Street City, State Zip Code Telephone: ( ) E-mail
TO BE COMPLETED BY STUDENT: Statement of Health and Immunization Records (pages 1 & 2) Student s Name: Birth date: Last First Middle Month/Day/Year Address: Street City, State Zip Code Telephone: ( ) E-mail
Santa Rosa Junior College Health Sciences Department Health Evaluation Form. STUDENT NAME: Last First MI BIRTHDATE: SRJC ID # GENDER: M F
 Santa Rosa Junior College Health Sciences Department Health Evaluation Form STUDENT NAME: Last First MI BIRTHDATE: SRJC ID # GENDER: M F ADDRESS: Street City State Zip Code Home Phone ( ) - Mobile Phone
Santa Rosa Junior College Health Sciences Department Health Evaluation Form STUDENT NAME: Last First MI BIRTHDATE: SRJC ID # GENDER: M F ADDRESS: Street City State Zip Code Home Phone ( ) - Mobile Phone
JOHNS HOPKINS SCHOOL OF NURSING PRE-ENTRANCE HEALTH FORM
 JOHNS HOPKINS SCHOOL OF NURSING PRE-ENTRANCE HEALTH FORM Master s Entry into Nursing MSN Advanced Practice MSN/MPH Post Graduate Certificate DNP Advanced Practice DNP Executive PhD CHECK ( ) PROGRAM OF
JOHNS HOPKINS SCHOOL OF NURSING PRE-ENTRANCE HEALTH FORM Master s Entry into Nursing MSN Advanced Practice MSN/MPH Post Graduate Certificate DNP Advanced Practice DNP Executive PhD CHECK ( ) PROGRAM OF
Monday through Thursday 9:30am 11:30am And 2pm 4pm
 Dear Applicant: Thank you for your interest in the Stony Brook University Hospital Volunteer Program. To expedite the application process, please carefully review the information below. All applicants
Dear Applicant: Thank you for your interest in the Stony Brook University Hospital Volunteer Program. To expedite the application process, please carefully review the information below. All applicants
ADN Program Application Packet
 ADN Program Application Packet New Associate Degree Nursing (ADN) students are admitted each Spring and Fall semester. Space in the ADN program is limited; therefore, admission is competitive and applicants
ADN Program Application Packet New Associate Degree Nursing (ADN) students are admitted each Spring and Fall semester. Space in the ADN program is limited; therefore, admission is competitive and applicants
Wabash Student Health Center
 Wabash Student Health Center Information and Instructions for Completing the Student Health Record Dear Incoming Wabash Student: Welcome to Wabash College! In order to make your experience at Wabash a
Wabash Student Health Center Information and Instructions for Completing the Student Health Record Dear Incoming Wabash Student: Welcome to Wabash College! In order to make your experience at Wabash a
Middle Tennessee State University MSN Program. Clinical/Student Requirements- Admission to MSN Program
 Middle Tennessee State University MSN Program Clinical/Student Requirements- Admission to MSN Program The following are required documents that MUST be uploaded in Medatrax prior to beginning the MSN program.
Middle Tennessee State University MSN Program Clinical/Student Requirements- Admission to MSN Program The following are required documents that MUST be uploaded in Medatrax prior to beginning the MSN program.
Shadow-a-Professional Program 2016 Application
 Thank you for your interest in The Shadow-A-Professional program that allows high school junior and senior students interested in the hospital industry to explore career options and/or gain experience
Thank you for your interest in The Shadow-A-Professional program that allows high school junior and senior students interested in the hospital industry to explore career options and/or gain experience
VOLUNTEER APPLICATION
 Please return to: Mount Nittany Medical Center Volunteer Services Department 1800 East Park Avenue State College, PA 16803 814.234.6170 VOLUNTEER APPLICATION Application Date Assignment Interview Date!
Please return to: Mount Nittany Medical Center Volunteer Services Department 1800 East Park Avenue State College, PA 16803 814.234.6170 VOLUNTEER APPLICATION Application Date Assignment Interview Date!
Health Requirements for Students. Updated 1/23/18
 Health Requirements for Students Updated 1/23/18 1 Health Requirements Table of Contents Health Requirements for Students... 3 Instructions on Getting Started... 4 Instructions on Uploading Documents...
Health Requirements for Students Updated 1/23/18 1 Health Requirements Table of Contents Health Requirements for Students... 3 Instructions on Getting Started... 4 Instructions on Uploading Documents...
PRE-CLINICAL HEALTH REQUIREMENTS (PCHR) GRADUATE NURSING
 GRADUATE NURSING") PRE-CLINICAL HEALTH REQUIREMENTS (PCHR) GRADUATE NURSING PCHR Guidelines and General Information Academic Programs with PCHR: Duquesne University School of Pharmacy Duquesne School of Nursing Undergraduate
PRE-CLINICAL HEALTH REQUIREMENTS (PCHR) GRADUATE NURSING PCHR Guidelines and General Information Academic Programs with PCHR: Duquesne University School of Pharmacy Duquesne School of Nursing Undergraduate
The Clinical Practicum: Guidelines for Success
 ! School&of&Nursing& The Clinical Practicum: Guidelines for Success Adult-Gerontology Clinical Nurse Specialist & Primary Care Adult-Gerontology Nurse Practitioner 2016-2017 1 ! Table of Contents 1.Introduction...
! School&of&Nursing& The Clinical Practicum: Guidelines for Success Adult-Gerontology Clinical Nurse Specialist & Primary Care Adult-Gerontology Nurse Practitioner 2016-2017 1 ! Table of Contents 1.Introduction...
WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH MEDICAL ASSISTING PROGRAM 9000 OVERLAND AVE
 WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH MEDICAL ASSISTING PROGRAM 9000 OVERLAND AVE., CULVER CITY, CA 90230-3519 Phone: (310) 287-7226 Fax: (310) 287-4352 Dear Applicant, FOR FALL 2017 Thank
WEST LOS ANGELES COLLEGE DIVISION OF ALLIED HEALTH MEDICAL ASSISTING PROGRAM 9000 OVERLAND AVE., CULVER CITY, CA 90230-3519 Phone: (310) 287-7226 Fax: (310) 287-4352 Dear Applicant, FOR FALL 2017 Thank
DMACC INSTRUCTIONS FOR COMPLETING STUDENT HEALTH AND IMMUNIZATION RECORD. Questions about uploading the form or CastleBranch?
 DMACC DES MOINES AREA COMMUNITY COLLEGE INSTRUCTIONS FOR COMPLETING STUDENT HEALTH AND IMMUNIZATION RECORD Health and Public Service Department students need to complete and submit the Student Health and
DMACC DES MOINES AREA COMMUNITY COLLEGE INSTRUCTIONS FOR COMPLETING STUDENT HEALTH AND IMMUNIZATION RECORD Health and Public Service Department students need to complete and submit the Student Health and
2016 Health History and Enrollment for Sam Davis Youth Camp for Youth and Adults
 2016 Health History and Enrollment for Sam Davis Youth Camp for Youth and Adults Complete this form in ink answering all questions. Please print legibly The parent/guardian and camper both must sign this
2016 Health History and Enrollment for Sam Davis Youth Camp for Youth and Adults Complete this form in ink answering all questions. Please print legibly The parent/guardian and camper both must sign this
Patient Care Technician Certificate. Career Talk and Program Requirements
 Patient Care Technician Certificate Career Talk and Program Requirements Welcome to the PCT Career Talk! Completion of this Career Talk is a requirement for all students prior to registration for PCT courses.
Patient Care Technician Certificate Career Talk and Program Requirements Welcome to the PCT Career Talk! Completion of this Career Talk is a requirement for all students prior to registration for PCT courses.
Sexual Assault Nurse Examiner Job Description
 Sexual Assault Nurse Examiner Job Description Job Title: Forensic Examiner/SANE Reports to: Executive Director Functions Summary: A SANE provides timely and accurate medical assessments and injury identification/documentation
Sexual Assault Nurse Examiner Job Description Job Title: Forensic Examiner/SANE Reports to: Executive Director Functions Summary: A SANE provides timely and accurate medical assessments and injury identification/documentation
APPLICATION PACKET All students enrolling in HCNA 1215 must complete application packet
 Baton Rouge Community College Nurse Assisting (HCNA 1215) Program APPLICATION PACKET All students enrolling in HCNA 1215 must complete application packet INCOMPLETE OR LATE APPLICATIONS WILL NOT BE ACCEPTED
Baton Rouge Community College Nurse Assisting (HCNA 1215) Program APPLICATION PACKET All students enrolling in HCNA 1215 must complete application packet INCOMPLETE OR LATE APPLICATIONS WILL NOT BE ACCEPTED
ADMISSION PACKET. School of Nursing BSN - DNP Program
 ADMISSION PACKET School of Nursing BSN - DNP Program The Doctor of Nursing Practice (DNP) program at Kentucky State University is a 72 credit hours (9 semesters) BSN-DNP online program with emphasis in
ADMISSION PACKET School of Nursing BSN - DNP Program The Doctor of Nursing Practice (DNP) program at Kentucky State University is a 72 credit hours (9 semesters) BSN-DNP online program with emphasis in
ADVANCED C.N.A Registration Process Check Sheet
 ADVANCED C.N.A Registration Process Check Sheet DATE COMPLETED 1. Complete an online DMACC application and select one of the following: (1) Nurse Aide as your major if you only plan on taking C.N.A classes
ADVANCED C.N.A Registration Process Check Sheet DATE COMPLETED 1. Complete an online DMACC application and select one of the following: (1) Nurse Aide as your major if you only plan on taking C.N.A classes
Student Pre-Clinical Requirements 2017
 BACHELOR OF NURSING (COLLABORATIVE) PROGRAM Student Pre-Clinical Requirements 2017 Memorial University School of Nursing Centre for Nursing Studies Western Regional School of Nursing INTRODUCTION TO STUDENT
BACHELOR OF NURSING (COLLABORATIVE) PROGRAM Student Pre-Clinical Requirements 2017 Memorial University School of Nursing Centre for Nursing Studies Western Regional School of Nursing INTRODUCTION TO STUDENT
Middle Tennessee State University MSN Program. Clinical/Student Requirements- Admission to MSN Program
 Middle Tennessee State University MSN Program Clinical/Student Requirements- Admission to MSN Program The following are required documents that MUST be uploaded in Medatrax prior to beginning the MSN program.
Middle Tennessee State University MSN Program Clinical/Student Requirements- Admission to MSN Program The following are required documents that MUST be uploaded in Medatrax prior to beginning the MSN program.
APPLICATION FOR ADMISSION TO THE EMT-PARAMEDIC PROGRAM FALL 2018
 APPLICATION FOR ADMISSION TO THE EMT-PARAMEDIC PROGRAM FALL 2018 Pre-Admission Session for Allied Health NAME JC STUDENT ID NUMBER ADDRESS CITY STATE ZIP HOME PHONE CELL PHONE EMAIL ADDRESS The following
APPLICATION FOR ADMISSION TO THE EMT-PARAMEDIC PROGRAM FALL 2018 Pre-Admission Session for Allied Health NAME JC STUDENT ID NUMBER ADDRESS CITY STATE ZIP HOME PHONE CELL PHONE EMAIL ADDRESS The following
Monday, July 23, 2018*
 The Department of Nursing and Health Sciences requires that students registered in the BN program complete the following by: Monday, July 23, 2018* To be completed by First Year students: Register for
The Department of Nursing and Health Sciences requires that students registered in the BN program complete the following by: Monday, July 23, 2018* To be completed by First Year students: Register for
OWENS COMMUNITY COLLEGE DENTAL ASSISTING CERTIFICATE ORIENTATION
 OWENS COMMUNITY COLLEGE DENTAL ASSISTING CERTIFICATE ORIENTATION CHECKLIST WHAT MUST BE DONE BEFORE STARTING THE DENTAL ASSISTING CERTIFICATE PROGRAM Register as soon as possible and scheduled in the class
OWENS COMMUNITY COLLEGE DENTAL ASSISTING CERTIFICATE ORIENTATION CHECKLIST WHAT MUST BE DONE BEFORE STARTING THE DENTAL ASSISTING CERTIFICATE PROGRAM Register as soon as possible and scheduled in the class
Separate instructions on how to open an account with American Databank and upload the documents are on pg. 2
 Dear Graduate Nursing Student: Students who are registered for NURS 640: Advanced Physical Assessment, for fall are required to complete the first step in their clinical clearance process between and August
Dear Graduate Nursing Student: Students who are registered for NURS 640: Advanced Physical Assessment, for fall are required to complete the first step in their clinical clearance process between and August
Mission Statement and Goals of the Diagnostic Medical Sonography Program
 Mission Statement and Goals of the Diagnostic Medical Sonography Program The Quinnipiac University Diagnostic Medical Sonography Program supports the mission statement of both Quinnipiac University and
Mission Statement and Goals of the Diagnostic Medical Sonography Program The Quinnipiac University Diagnostic Medical Sonography Program supports the mission statement of both Quinnipiac University and
MOODY BIBLE INSTITUTE HEALTH SERVICE DEPARTMENT
 HEALTH SERVICE DEPARTMENT Welcome to Moody! Congratulations on your acceptance to the Moody Bible Institute! Health Service is available to assist you with health concerns you may have as a student here
HEALTH SERVICE DEPARTMENT Welcome to Moody! Congratulations on your acceptance to the Moody Bible Institute! Health Service is available to assist you with health concerns you may have as a student here