Department of Radiation Oncology
|
|
|
- Quentin Maxwell
- 6 years ago
- Views:
Transcription


1 Department of Radiation Oncology Final Report Department Analysis Management Systems Department Chad Cleveringa Chad Dejong Chris Gannon 19 April 1994
2 EXECUTIVE SUMMARY

3 EXECUTIVE SUMMARY EXECUTIVE SUMMARY Introduction The Department of Radiation Oncology (DRO) at the University of Michigan Medical Center (UMMC) is at the forefront of the technological and clinical advances that are revolutionizing the field of therapeutic radiology. Innovation has been a hallmark of the DRO throughout its history. The department continues to grow in size, activity, and stature, and is dedicated to the maintenance of clinical and academic excellence and to the exploration and application of new ideas in the field of therapeutic radiology. To continue this tradition there is an increasing need for greater efficiency and a continual pursuit of quality care. Through obtaining an efficient system in which to work, the activities of patient care, research, and teaching will be able to continually meet new demands and flourish. Recognizing this need is the first step in continued improvement. However, more than recognition is necessary to attain the high level of excellence desired. To meet this need, the DRO has teamed up with the Management Systems Department (MSD) to conduct a study of the current system and determine a procedure for continual improvement. Purpose This study was conducted to improve the overall efficiency of the clinic in DRO by minimizing patient waiting times and achieving the highest possible quality care. Goal The goals of the study were the following: To offer scheduling and practice recommendations which will decrease cost and increase efficiency. To enable the DRO to achieve continual improvement. This will increase the quality of service delivered to patients. The study findings were as follows The present scheduling system is very inefficient. Appointments take longer than scheduled. Physicians are expected to be in more than one place at a time. Dr. Howard Sandier is most efficient overall. Saw the most patients during data collection. Spent as much time with patients as other


4 EXECUTIVE SUMMARY physicians on average. He compartmentalizes his schedule. He uses time management tools. Having one physician see patient during Follow-Up and On-Treatment visits decreases first physician encounter until checkout time by 9 minutes and 6 minutes respectively. However, the wait time in the lobby increases by 6 minutes and 8 minutes respectively. Patients for 8:30 appointments wait for 38 minutes to be seen by physician. Clinic schedules are created too far in advance Physicians in lab most have longest overall wait times. Present schedule (April-June) is over-scheduled on Wednesday and Thursday, and under-scheduled on Friday. Present notification process of patient arrival and exam room placement to the physicians is very inefficient. Having all required materials (charts, x-rays, etc.) present before patients arrive is a significant problem. 30 percent of consent forms for Simulation not signed during Consult visit. Exam rooms are being used as waiting rooms. Patients arrive early, however close to their scheduled appointments. Overall room utilization is 54 percent. Recommendations Compartmentalize the schedule. That is, schedule certain types of treatments on the same day and other treatments on the other days. Schedule by the shortest service time first. Increase the allotted time for Consult visits to one and one half hours. During busy times, a Follow-Up patient should be seen by just the staff physician. For On-Treatment patients, have just the resident or staff physician see the patient during busy times. To maximize this effect, the

5 EXECUTIVE SUMMARY decision to do so must be made earlier, not after the patient has already waited excessively. Schedule patients at 9:15 A.M. as opposed to 8:30 A.M.. At least one physician should not attend the conference each day of the week, and schedule On-Treatment patients as early as possible. Tighter conference schedule. Start on time. Finish on time. Develop new clinic schedules every one or two months. Use the utmost discretion in canceling clinic days. At least one physician from Wednesday or Thursday morning should be rescheduled for Friday morning. Make use of present computer system for notification of patient arrival and placement in an exam room, as well as for data collection. Designate specific responsibifities to a position that can effectively find charts, x-rays, relevant history, etc.. Have all the materials collected and prepared so that the physician has little if any pre-visit paperwork to complete. Also possible for physician to review prior to start of clinic. Have the search and the gathering of materials begin at least one day before the patients scheduled visit. Get consent form for Simulation signed during Consult visits.

6


7 Table of Contents INTRODUCTION AND BACKGROUND 1-1 DEFINITION OF TERMS 2-1 APPROACH & METHODOLOGY 3-1 DESCRIPTION OF CURRENT SYSTEM 4-1 FINDINGS & CONCLUSIONS 5-1 RECOMMENDATIONS 6-1 ACTION & IMPLEMENTATION PLAN 74 RECOMMENDATIONS FOR FURTHER STUDY 8-1 APPENDICES Appendix A - DRO Clinic Layout Appendix B - DRO Micro Flow Diagram Appendix C - Data Collection Forms Appendix D - Memorandum to DRO patients Appendix E - Questionnaire Appendix F - Current Clinic Schedule Appendix G - Graphs
8
9 INTRODUCTION & BACKGROUND

10 INTRODUCTION AND BACKGROUND Introduction INTRODUCTION AND BACKGROUND The Department of Radiation Oncology (DRO) at the University of Michigan Medical Center (UMMC) is at the forefront of the technological and clinical advances that are revolutionizing the field of therapeutic radiology. Innovation has been a hallmark of the DRO throughout its history. The department continues to grow in size, activity, and stature, and is dedicated to the maintenance of clinical and academic excellence and to the exploration and application of new ideas in the field of therapeutic radiology. To continue this tradition there is an increasing need for greater efficiency and a continual pursuit of quality care. Through obtaining an efficient system in which to work, the activities of patient care, research, and teaching will be able to continually meet new demands and flourish. Recognizing this need is the first step in continued improvement. However, more than recognition is necessary to attain the high level of excellence desired. To meet this need, the DRO has teamed up with the Management Systems Department (MSD) to conduct a study of the current system and determine a procedure for continual improvement. Purpose This study was conducted to improve the overall efficiency of the clinic in the DRO by minimizing patient waiting times and achieving the highest possible quality care. Goal To offer scheduling and practice recommendations which will decrease cost and increase efficiency. To enable the DRO to achieve continual improvement. This will increase the quality of service delivered to patients. Background To make these recommendations, MSD has gathered data and collected information concerning patieit flow times and operating procedures. MSD, physicians, nurses, and patients were all responsible for collecting data and information. This was accomplished during operating clinic sessions without impacting clinic operations. In addition, root cause analysis of data was performed through the use of statistics, spreadsheets, flowcharts, and graphics. A simulation model using the GPSS/H language was developed of the clinic to perform analysis of physician assigned rooms (current method) versus the use of pooled rooms (proposed method). Refer to the Approach and Methodology section for a further expansion of study procedures.

11

12 DEFINITION OF TERMS

13 Note: Refer to Appendix A for clinic layout. DEFINITION OF TERMS Type of visit where a patient is seen to discuss type of treatment modality which will be Type of visit where the patient attends to exam the effectiveness of past treatment and desk, schedules patients, and answers various general patient questions. have. Aides in all areas of patient care. Consult Visit Follow-Up Simulation Unscheduled Lobby/waiting room, and reception area Eight exam rooms used to service cancer patients Physician work room Bathrooms Social Work room On-Treatment Nurse/Nurse Aide station Two simulation rooms Consult The clinic is the location where cancer patients come to for five types of visits: The boundaries of the clinic are defined as: Part of the Department of Radiation Oncology (DRO) staff. Supervises the reception DEFINITION OF TERMS 2-i Clerk Clinic used. Patient is informed of clinic and radiation processes. Patient was previously Follow-Up Visit discuss any future needs. physician. Asks pertinent background questions. Answers any questions patient may Part of DRO staff. Brings patients to exam rooms. Prepares patients to be seen by diagnosed with cancer. Nurse
14 DEFINITION OF TERMS 2-2 Nurse Aid Part of the DRO staff. Brings patients to exam rooms, helps the nurses with daily activities, and answers various general patient questions. On-Treatment Visit Type of visit in which patient is seen weekly by his/her physician during the course of radiation therapy. Patient Flow The process which patient goes through within clinic from checking in at the reception desk until checking out of the system. Resident Physician Member of RadOnc staff. Recent graduate of medical school. Receiving training (residency) in RadOnc. Residents assist staff physicians with all clinical care. Simulation Visit Visit which determines general area of radiation therapy and simulates final treatment set-up. Staff Physician Part of the DRO staff. Primarily responsible for the care and treatment of patients and the training and education of the resident physicians. Unscheduled Visit Visit where patients comes to clinic because of urgent needs for care while under treatment. The patient does not have an appointment.
15
16 APPROACH & METHODOLOGY
 clinic.")



17 APPROACH AND METHODOLOGY 3-1 APPROACH AND METHODOLOGY Several technology and application oriented methodologies presented below were used by the Management Systems Department (MSD). These methodologies were applied to develop a deep fundamental understanding of the Department of Radiation Oncology (DRO) clinic. The basic goal, in utilizing these methodologies, was to develop an understanding of the current system, define areas of improvement, and make suggestions for improvement. Methods: * Flow Diagram Analysis Interviews Data Collection Sensitivity Analysis Decision Analysis Questionnaire Organizational Analysis Simulation Program * Please note that these methods are not mutually exclusive. Rather they are quite interdependent. Flow Diagram Analysis MSD performed an analysis of the DRO Micro Flow Diagram (Appendix B). This enabled MSD to obtain a broad overview and understanding of the current clinic system. In addition, MSD was able to determine possible bottlenecks and areas of investigation. Interviews MSD conducted weekly interviews of: administrators, staff physicians, resident physicians, nurses, nurse aides, and clerks. This enabled MSD to obtain a sound understanding of the flow process, the overall system, and the problems confronting the department and personnel on a daily basis. Data Collection Forms Patient data collection forms (see Appendix C) were developed on 2/20/94 to collect data on patient processing times. It was determined that a month long study was necessary to obtain at least 20 to 25 data points for each physician for the given type


18 APPROACH AND METHODOLOGY 3-2 of visits under study. Furthermore, these forms were designed to have the actual clinic patients fill them out. This was done for three reasons. First, Health Care has traditionally been a non-interactive environment. In the past, patients passively sat and waited for treatment, while having little impact on overall visit. In an effort to change this situation and allow communication from actual patients, MSD decided to ask the patients to complete a portion of the data collection forms. Furthermore, patients know that a problem existed within the department. By acknowledging that the problem existed and allowing the patient to aid in its correction, patients feel more comfortable within the current system Second, MSD felt that patients would be able to fill out the forms more accurately. This is because patients have more time to fill out the data collection forms, while the DRO staffs time is limited. By having the data collected by the patients, MSD was successful in obtaining more accurate data than what would have been collected otherwise. Third, DRO has long been known as an innovator in all respects. Having patients fill out data collection forms has never been done before. By enabling the patients to fill out the data forms, an innovative approach has been undertaken. This process could form a new approach to further study within the Healthcare field. The month long data collection process began on 2/24/94 and ended on 3/25/94. Accompanying the data collection forms was a memorandum to the DRO patients (see Appendix D). This memorandum explained the reasons for the current study and the process in filling out the data collection forms. Sensitivity Analysis MSt) utilized this approach to analyze the system input variables to determine changes in system output. Because of uncertainty in input data, it is useful to know over what range the solution of a problem remains unchanged. This method allowed MSD to visualize how changing one parameter out of a given set of inputs affects the output. By determining which inputs are sensitive and insensitive, MSD was able to evaluate which inputs are most important and which are limiting factors. This method was utilized throughout the entire project.
. Identify the likelihood and magnitude of changes.")


19 APPROACH AND METHODOLOGY 3..3 Decision Analysis Decision analysis is a powerful analytical tool used to support and aid the decisionmaking process. MSD utilized this method to: Identify problems and aid in the structuring of the simulation model (discussed in detail later in this section). Identify the likelihood and magnitude of changes. Perform sensitivity analysis of system to determine the robustness of recommendations. Evaluate the implementation of strategies suggested. Questionnaire MSD utilized this technique to gather additional information from the DRO staff. A questionnaire was distributed to all staff which stated general questions and asked for input from the individuals within the department (see Appendix E). The questionnaire had the following advantages. Permitted the creation of a group larger than would have otherwise been possible. This enabled MSD to obtain everyone s input. Many times people have suggestions, but these suggestions are never voiced. Participants were not subject to social pressure, due to the anonymity of the summarized information. Therefore, the responses were more reliable. Organizational Analysis Everything mentioned thus far has been a form of organizational analysis. The goal of organizational analysis is to design and structure individual jobs and the relationship among these jobs. Ultimately, the goal of organizational analysis is to create the framework for positive group and individual behavior. This will allow an entity (staff physician, resident physician, nurse, etc.) to function and accomplish its objective effectively and efficiently within the department. MSD has made suggestions regarding job descriptions and lines of communication that will provide an effective approach to aid DRO in its transition process. In addition, DRO will be in a position to better adapt to problem solving for current and/or new circumstances.


20 APPROACH AND METHODOLOGY 3.4 Simulation Program Simulation is a decision making tool used to imitate the real-world (DRO, in this case). This tool enables the analysis of system reactions to various operational changes without interfering with people, places, and/or things. The behavior of a system as it evolves over time is studied by developing a simulation model. This model usually takes the form of a set of assumptions concerning the operation of the system. A system is the collection of objects forming a whole with relationships between them which interact for the purpose of accomplishing objectives according to a plan. A set of limiting boundaries are placed around this system to define the scope and purpose of the model. The simulation model was formulated to analyze the impact of switching from the current physician allocated room system to the use of physician pooled rooms.
21
22 DESCRIPTION OF CURRENT SYSTEM


23 DESCRIPTION OF CURRENT SYSTEM 4-1 DESCRIPTION OF CURRENT SYSTEM Scheduling Practices The Department of Radiation Oncology (DRO) schedules four types of visits: On- Treatment, Follow-Up, Consult, arid Simulation. Clinic schedules are created quarterly within DRO. These schedules list which staff physicians see patients in clinic for each day and how many of each type of visit they see throughout the day. See Appendix F for a copy of the current April - June clinic schedule. Currently only one physician schedules patients on Fridays. Four physicians are scheduled on Mondays and Tuesdays, and five physicians are scheduled on Wednesdays and Thursdays. A summary of the current scheduling practices are given in Table 1. Table 1 - Scheduling Practice for Each Physician 1st Patient I2nd Patient l3rd Patient 14th Patient On Treatment Patients scheduled every 15 minutes. Scheduling starts at 7:00 am Consult 8:00 AM 10:30 PM 1:00 PM 2:30 PM ollow Up 9:00/9:30 10:00/10:30 11:00 AM 1:00 PM Further scheduling until 3:30 PM every 30 minutes Simulation Scheduled from 8:00 am until 3:30 PM Scheduled approximately every 60 minutes Jnscheduled Patients arrive at random Approximately four patients per day (one per physician) Clinic Rooms There are eight exam rooms within the clinic. The exam rooms are used to see the five types of patients listed in the above table. All exam rooms are equally equipped, except for minor variations in two of the rooms. One exam room is typically reserved for unscheduled visits or other similar events. There is also a physician workroom in which the physicians study their patients charts, and anything related to their work. At the front of the clinic is the social work room, in which the social worker meets with patients regarding any financial matters, personal problems, etc.


24 nurse aides, clerical staff, and administration. There are eight staff physicians and patients and events, work practices, and resident physician education. the conference room each morning at 7:30 am where the physicians discuss daily numerous resident physicians within the clinic. There is a physicians meeting in Staff The DRO clinic staff consists of the staff physicians, resident physicians, nurses, purpose for which the computer system is used. After this, patient flow is recorded Physician Workroom. by writing down patient arrivals to the exam rooms on a piece of paper in the Patient flow within DRO is communicated primarily by means of paper and little by computer. DRO uses their computer information system to record patient arrival by placing an asterisk next to the patients name. However, this is currently the only Patient Flow Communication general or specific job requirements for each staff position. There has been no nurse aides and physicians. This has resulted from no formal policy stating the consistent practice which the staff uses to perform duties within the clinic. There is presently no exact job description for the nursing staff in relation to the DESCRIPTION OF CURRENT SYSTEM 4-2
25 3 )
")
26 SNOISIYDNOD S SNIGNH ) )


.")

27 FINDINGS AND CONCLUSIONS 5-1 FINDINGS AND CONCLUSIONS Finding 1 The present scheduling system is not accurate. Physicians are expected to be in two to five places at any given time. Obviously this is impossible. However, the schedule does not currently account for this, which is a major reason why patients have excessive waiting times. Furthermore, Management Systems Department (MSD) has found that certain types of visits take x+y minutes, when they are only scheduled for x minutes. One such example is that of the Consult Visit, which is scheduled for 1 hour. However, our data shows that these visits take significantly longer than this. Conclusion 1 An improvement to the scheduling system is definitely needed. Any improvement in this system will have the biggest impact on the patient waiting times. Finding 2 Dr. Howard Sandler is the overall most efficient physician in the Department of Radiation Oncology (DRO). He serviced the most patients during the data collection period while spending on average the same amount of time with each patient as the rest of the clinic. He compartmentalizes his schedule and uses time management tools. Conclusion 2 Compartmentalizing the schedule by scheduling only certain types of visits on some days and other types of visits on other days reduces wait time. In addition, any type of time management tool is beneficial to the physician, which in turn benefits the customer. However, the choice to do so is personal preference. Finding 3 Physicians in Lab most often (in clinic least), which are U and ER, have the longest wait times. Appendix G - Graphs contains this data in Graphs 8,9, and 10. Conclusion 3 The current scheduling practices for these physicians must be changed to accomodate their limited time in clinic. Finding 4 When only the staff physician sees the patient during a Follow-Up visit, the time from first physician encounter until checkout decreases by nine minutes. Furthermore, when only one physician (resident or staff) sees the patient in an On Treatment visit, the time from first physician encounter until checkout decreases by




28 FINDINGS AND CONCLUSIONS 5-2 six minutes. However, the wait in the lobby increases by six minutes for a Follow- Up visit, and eight minutes for an On-Treatment visit, when only one physician sees the patient. Conclusion 4 The increase in wait time for the patient that only sees one physician indicates that the physician is making the decision to see a patient by oneself too late. In addition, the practice of having only one physician see the patient on these particular visits does not sacrifice a large amount of educational value, especially since the resident physician can see the On-Treatment patients by themselves. MSD believes that the decrease in waiting time to the patient outweighs the educational value that may be lost. Finding 5 Each morning between 7:30 and 8:30 A.M. a physician conference is scheduled to discuss: The days planning and events. Past events/problems and resolutions of problems. Future events and needs planning. Resident education Patient scheduling begins at 8:30 A.M. However, the conference rarely finishes at 8:30 A.M., and once the conference ends physicians typically become involved in other areas outside clinic: Dosimetry Simulation Treatment Rooms This causes patients scheduled at 8:30 A.M. to wait for extended periods of time before being seen. In addition, this wait time (queue) perpetuates throughout the rest of day, backing up the entire system. Conclusion 5 This is a major problem area. The 38 minutes that a patient has to wait for the first appointment of the day is unnecessary. This 38 minutes perpetuates through the system the entire day, causing excessive wait times. Finding 6 Currently schedules are created every three months. This increases the possibility for ineffective communication between physicians and the clinic. Also, physicians can cancel clinic appointment times easily, with very little notice. Conclusion 6


, the clinic is overscheduled on Wednesday s and Thursday s. Furthermore, only one physician is currently scheduled in clinic on Friday.")
29 FINDINGS AND CONCLUSIONS 53 Better coordination should be undertaken by physician to inform clinic far in advance of absence. Cancellations bring about extra costs since clerical staff must spend time notifying and rescheduling patients. However, a time frame for scheduling should be developed, as it is rather difficult to determine ones schedule three months in advance. MSD realizes that many unexpected responsibilities occur with little notice. Finding 7 Physician schedules were overloaded in morning during the data collection period. This caused early back-up in the system. This was further perpetuated by the lateness of physicians to clinic. In the present schedule (April-June, see Appendix F), the clinic is overscheduled on Wednesday s and Thursday s. Furthermore, only one physician is currently scheduled in clinic on Friday. Conclusion 7 A scheduling system should be developed which addresses the issue of overloading schedules in morning. Patient scheduling should be made evenly throughout the day. Some physicians should switch days in clinic from Tuesday and Thursday to Monday and Friday. This will alleviate some of the scheduling problems experienced on Tuesday and Thursday. Furthermore, with more physicians in clinic on Fridays, utilization of staff and clinic will increase. This will also alleviate pressure from other scheduled days, thus reducing the average wait time while also decreasing costs, as less overtime will be needed on the busy days. Finding 8 The nursing staff presently lets the physicians know when the patients arrive by writing the information on a piece of paper in the Physician Workroom. Furthermore, the nurses occasionally do not promptly put the information on the paper. Consequently, there are times when the physicians can see the patient but have no idea that they are even present, or in an exam room waiting to be seen. Furthermore, there is presently a computer scheduling system that can give updated information about patient status to all interested parties. However, this system is not being utilized other than to determine if a patient has arrived at the clinic. Conclusion 8 This is an area of technological improvement, or just implementation of present technology within the department.




30 FINDINGS AND CONCLUSIONS 54 Finding 9 Like in most healthcare settings, having charts and x-rays present when the patient arrives is a significant problem. Conclusion 9 Consequently, every step possible should be taken to reduce or eliminate this problem. Any improvement is an obvious decrease in waiting time for the patient, while also increasing the utilization of the staff. Finding 10 The following table illustrates who places the patient into the exam rooms for Consult, Follow-Up, and On-Treatment visits. Distribution of Patient Placement Into Exam Rooms by Nurses and Nurse Aides Consult Follow-Up On-Treatment Nurse 20% 35% 70% Nurse Aide 80% 65% 30% Conclusion 10 These percentages show that more definition is needed in their respective job descriptions. Having this much overlap in tasks creates room for frustration and miscommunication and confusion between the two positions. Finding 11 The Simulation consent form is supposed to be signed by the physician during the patient Consult visit. However, frequently the consent form is not signed during this visit. In fact, 30 percent of the time the consent form is not signed until right before simulation. Conclusion 11 Once again this causes excess waiting time for every patient of that particular physician. Thus, a few minutes spent getting the consent form signed during the Consult visit is a reduction in overall wait time. The physician will not be spending time on unscheduled tasks when there are scheduled tasks to be completed.


 Arrival pattern = Appointment Time - 2) Not applicable to unscheduled visits.")
31 FINDINGS AND CONCLUSIONS 55 Finding 12 Exam rooms are being utilized as waiting rooms through the shifting of patients from the lobby to the exam room. A graphical representation showing time waiting in an exam room until first physician encounter is given in Graph 6 in Appendix G. Conclusion 12 The current system is hiding the work-in-process by using the exam room as another waiting room. Finding 13 Patients on average arrive early, however they are close to arriving at their scheduled appointments. For a Simulation visit, the patients arrive significantly early for their appointments. Graphs 3 and 4 in Appendix G illustrate the overall wait times in the lobby along with the arrival patterns of the patients for each type of visit. Note: 1) Arrival pattern = Appointment Time - 2) Not applicable to unscheduled visits. Arrival Time Conclusion 13 The arrival pattern of patients is not a significant factor in their overall wait time. Finding 14 The overall utilization of rooms is 54 percent. The breakdown by day of the week is given as Graph 1 in Appendix G. Furthermore, the results of the simulation program show no difference in exam room utilization when using the present system of physician-allocated exam rooms compared with using a pooled exam room system (the pooled exam room system is where the physician sees the patient in the first exam room available). Conclusion 14 The calculations show that the bottleneck of patient flow within the clinic is not the number of exam rooms. Thus, there are presently enough exam rooms available, and few changes need to be made at this point in time. The reason the utilization percentages for the exam rooms did not change in the simulation program is because the exam rooms are currently so under-utilized that it doesn t matter which exam room system is used. However, MSD feels that after exam room utilization percentages increase (to approximately 80% or better), DRO should use the pooled exam room system rather than the current physician-allocated system. MSD feels that this common sense method would only further increase exam room utilization.


32 FINDINGS AND CONCLUSIONS 5-6 Finding 15 Patients consistently need their blood drawn prior to being seen by a physician. However, this is consistently not done nor realized until the patient arrives for their appointment. This is another area where the patient flow process can be slowed significantly. Conclusion 15 Further investigation into the possible solutions for this problem is necessary. See the Recommendations for Further Study section. Finding 16 There is no discernable decision process for the assignment of rooms by the nurses with respect to the physicians or to the patients. Conclusion 16 Further investigation into this decision making process is needed. However, if appointments are scheduled by shortest service time first, the only guideline to follow would be to place patients in exam rooms by appointment time. Patients arriving late should be seen in the first available exam room after being notified of their tardiness and how it causes increased waiting times for all patients.x

33
34 RECOMMENDATIONS


 Put simply, itis a tool for effective time management. This enables one to have an Dr. Howard Sandier presently compartmentalizes his schedule. He is also one of the Follow-Ups. e.g. Schedule Follow-Ups before Consults.")
35 and schedule On-Treatments and Follow-Ups the another day. Recommendations for Finding 1 Compartmentalizing the schedule smoothes the daily tasks of the physician. By doing this one naturally becomes more efficient. This also simplifies the decision Sheduling by the shortest service time first will significantly decrease the overall wait time of the patient. Furthermore, use any time management tools such as placing a hardcopy of the Increasing the alotted time for Consult visits will smooth the daily schedule. most efficient physicians in the clinic with respect to wait times. used by other physicians. It is an obvious benefit, illustrated by Dr. Sandler s preference. efficiency. However, such a policy cannot be implemented as this is personal Support Recommendations for Finding 2 Compartmentalize the schedule. (See part one of Recommendations for Finding 1.) Put simply, itis a tool for effective time management. This enables one to have an Dr. Howard Sandier presently compartmentalizes his schedule. He is also one of the Follow-Ups. e.g. Schedule Follow-Ups before Consults. Schedule On-Treatments before 2) Schedule by the shortest service time first whenever possible. 3) Increase the alotted time for Consult visits from one hour to one and a half hour. 1) Compartmentalize the schedule. Schedule Consults and Follow-Ups on one day RECOMMENDATIONS RECOMMENDATIONS 6-1 Benefits process by which nurses place patients into exam rooms. Overall patient wait times will be reduced. Data collection. Interviews. Questionnaires. Observation. Benefits overall picture of the schedule and allows one to plan accordingly. This also helps make decisions about busy times earlier. Any advantage such as this one should be physician s schedule in a visible place.

 For an On-Treatment visit, have just the resident physician or just the staff 3) When recommendations 3 and 4 are done, the decision to do so must be made See graphs 14 and 15 in Appendix G.")

36 Support Support Support Benefits Benefits Dr. Sandier s lower than average wait times and service times with respect to the clinic wait times, while seeing the most patients during data collection. Data collection. Interviews. Observation. afternoons in the same fashion. clinic for 1.5 days. However, this can still be done by dividing up the mornings and See above benefits for Finding 1. See graphs 8, 9, and 10 in Appendix G 1) For a Follow-Up visit, have just the staff physician see the patient in busy times. 2) For an On-Treatment visit, have just the resident physician or just the staff 3) When recommendations 3 and 4 are done, the decision to do so must be made See graphs 14 and 15 in Appendix G. Data collection. Interviews. Questionnaires. This is presently done by some of the physicians in the clinic. Having only one physician see the patient during busy times for both a Follow-Up wait time will decrease significantly. The early decision will eliminate the longer wait time that a patient experiences in the lobby when they are only seen by one physician than when they are seen by more than one physician. and On-Treatment visit will make up for excessive waiting by the patient. If the decision to see a patient by oneself is made when the patient arrives, the overall earlier, not after the patient has already waited excessively. See graphs 15 and 16 in Appendix G. physician see the patient during busy times. Recommendations for Finding4 Data collection. compartmentalize types of treatments is limited since these physicians are only in Need extended appointment times for research-focused physicians. The ability to Recommendations for Finding 3 RECOMMENDATIONS 6-2
 Tighter conference schedule. Start on time. Finish on time. Benefits Physicians can be involved with other necessary areas outside the clinic without making a patient wait.")
 Develop new clinic schedules every one or two months.")
37 RECOMMENDATIONS 6-3 Recommendations for Finding 5 1) Schedulue patients at 9:15 A.M. as opposed to 8:30 A.M.. 2) At least one physician should not attend the conference each day of the week 3) Schedule On-Treatment patients as early as possible. 4) Tighter conference schedule. Start on time. Finish on time. Benefits Physicians can be involved with other necessary areas outside the clinic without making a patient wait. Eliminates the 38 minute wait at the start of the day that perpetuates through the system the entire day. Support Data collection. Interviews. Questionnaire responses. Dr. Lori Pierce presently schedules On-Treatment visits at 7:00 A.M. Recommendations for Finding 6 1) Develop new clinic schedules every one or two months. 2) Use the utmost discretion in cancelling clinic days. Benefits Will decrease the amount of wasted time rescheduling appointments. Subsequently, the clerks will have more time to spend preparing charts, x-rays, etc.. Most importantly, the customer will experience fewer inconviences. Support Interviews. Questionnaires. Recommendations for Finding 7 1) At least one physician from Wednesday or Thursday morning should be rescheduled on Friday morning. 2) Smooth the schedule. e.g. Switch two of AE s Follow-Ups from Wednesday afternoon to Monday afternoon. Benefits Moving at least one physician to Friday morning will smooth the schedule dramatically. A decrease in overtime, an increase in physician efficiency, and most importantly, a decrease in wait time for patients will result. This will also utilize the staff more efficiently on Friday morning, since the work schedule is the same regardless of the number of physicians in the clinic.
 Recommendations for Finding 8 1) The nurse or nurse aid should enter into the existing computer system the exam room number, time")
 Possibly purchase a larger monitor to place in the Physician Workroom so that a visible tracking system is at their disposable.")
38 RECOMMENDATIONS 6-4 Support Data collection. Expected room requirements for April schedule (see Appendix F - Clinic Schedule). Current exam room utilization percentages (see Graph 1 in Appendix G) Recommendations for Finding 8 1) The nurse or nurse aid should enter into the existing computer system the exam room number, time of placement, etc. of the patient at the appropriate time. 2) Hook up terminals into areas or rooms where they are necessary. 3) Possibly purchase a larger monitor to place in the Physician Workroom so that a visible tracking system is at their disposable. Benefits By the increased use of the computer system, the paper methods should be gradually eliminated. The computer tracking system will give real time status of patients, such as arrival time, what exam room they were placed in and what time, overall cumulative waiting time, diagnosis, type of appointment, and much other important information. Displaying such information will reduce the risk of miscommunication between the clinic staff and the physicians. It will also give administrators the opportunity to see the patient flow process at any time, thus giving them a beneficial tool to improve the patient flow process. They will be able to prevent problems from occurring, while also enabling them to find the root cause of problems, since they wifi realize the problems when they occur as opposed to a few hours or a day later. The computer system will also enable them to chart their progress towards continually reducing the overall patient wait time by recording the patient service and wait times. In addition, using this system will eliminate the excessive time nurses presently use to inform the physicians of patient status. Finally, the physicians will always be able to know when there is a patient waiting for them. Support Observation. Interviews. Questionnaires. Recommendations for Finding 9 1) Designate specific responsibilities to a position that can effectively find charts, x rays, relevant history, etc., and that can also follow through to ensure the materials arrival to the clinic. 2) Have all the materials collected and prepared so that the physician has little if any pre-visit paperwork to complete.
 should perform which tasks. Support else.")

39 Take every step possible to have the consent form signed during the Consult visit, Will eliminate the excess waiting time that arises when the physician has to leave also eliminate time spent in an exam room if the patient is waiting for the signature NOTE: Define what position (nurse or nurse aide) should perform which tasks. Support else. Starting the search on the previous day will increase the percentage of Benefits possibilities for miscommurtication. Eliminates the overlapping searching for materials. If all materials are prepared before the physician is set to see the patient, the physician s time will not be spent on tasks that can be completed by someone complete materials by the appointment time. patients scheduled visit. Interviews. Questionnaires. Observation. Eliminates miscommunication between the two positions. Eliminating Data collection. Interviews. Questionnaires. unless the patient can not sign it at that time. Otherwise, do not let the physician be the reason for an unsigned consent form. Data collection. Interviews. Questionnaires. Observation. Support Support Will eliminat the time someone has to spend to tracking the physician down. Will Having one position responsible for the collection of materials will eliminate the Recommendations for Finding 10 miscommunication ultimately results in higher quality service delivered to the patient. However, please note that help from one another is necessary during busy times. Recommendations for Finding 11 scheduled tasks to complete an unscheduled task. Will enable smoother clinic flow. 3) Have the search and the gathering of materials begin at least one day before the RECOMMENDATIONS 6-5 Benefits Benefits in an exam room. There are no recommendations for Findings 12 - due to their nature. 16
40
41 ACTION & IMPLEMENTATION PLAN

42 Two months. When new schedule is developed in June. in a visible place. Two months. When new schedule is developed in June. Clerks Administration Physicians Implementation Responsibility Follow the recommendations, and schedule accordingly. 3. Increase the allotted time for Consult visits from one hour to one and a hail hour. 2. Schedule by the shortest service time first whenever possible. e.g. Schedule Follow- 1. Compartmentalize the schedule. Schedule Consults and Follow-Ups one day and Recommendation for Finding 1 ACTION & IMPLEMENTATION PLAN Ups before Consults. Schedule On-Treatments before Follow-Ups. Time Horizon use any time management tools such as placing a hard copy of the physician s schedule Time Horizon Clerks Administration Physicians Follow the recommendations, and schedule accordingly. Implementation Responsibility ACTION & IMPLEMENTATION PLAN 7-1 schedule On-Treatments and Follow-Ups the another day. Recommendations for Finding 2 Compartmentalize the schedule. (See Recommendations for Finding 1.) Furthermore, Recommendations for Finding 3 Implement all recommendations for finding 1. The ability to compartmentalize types of treatments is limited since these physicians are only in clinic for


43 ACTION & IMPLEMENTATION PLAN 7-2 one and a half days. However, this can still be done by dividing up the mornings and afternoons in the same fashion. Implementation Makes changes when the schedule is developed. Discuss possible solutions among responsible parties. Responsibility Dr. Lawrence and Dr. Radney Chairman Associate Chairman Administration Clerks Time Horizon Immediately discuss possible alternatives. Two months. When new schedule is developed in June. Recommendation for Finding 4 1. For a Follow-Up visit, have just the staff physician see the patient during busy times. 2. For an On-Treatment visit, have just the resident physician or just the staff physician see the patient during busy times. 3. When recommendations 1 and 2 are done, the decision to do so must be made earlier, not after the patient has already waited excessively. Implementation Discuss the advantages and reasons for these recommendations to all the staff and resident physicians. Responsibility Chairman Associate Chairman Physicians Time Horizon Immediately Recommendations for Finding 5 1. Schedule patients at 9:15 A.M. as opposed to 8:30 A.M.. 2. At least one physician should not attend the conference each day of the week




44 Two months for parts 1 and 2. When new schedule is developed in June. Immediately for part 3. Reclarify in meetings the importance of being in clinic. Two months. When new schedule is developed in June. Take the necessary steps given in the recommendations, and schedule accordingly. Physicians Administration Clerks having these schedule changes. Then schedule accordingly. Implementation Responsibility Implementation Responsibility Implementation 1. Develop clinic schedules every one or two months. Administration 1. Take one physician from Wednesday or Thursday morning and schedule them for Physicians Clerks Recommendations for Finding 6 4. Tighter conference schedule. Start on time. Finish on time. 2. Use the utmost discretion in canceling clinic days. 3. Schedule On-Treatment patients as early as possible. ACTION & IMPLEMENTATION PLAN 73 Have a meeting between physicians and remaining staff to discuss the advantages of Prepare the schedules monthly if possible, if not, schedule every two months. Recommendations for Finding 7 Wednesday afternoon to Monday afternoon. 2. Take steps to smooth the clinic schedule. e.g. Switch two of AEs Follow-Ups from Time Horizon Time Horizon Friday morning.



45 Consultation with a management systems, engineer, the staff programmer within DRO, patients scheduled visit. Administration 2. Hook up terminals into areas or rooms where they are necessary. Administration Nurses 3. Have the search and the gathering of materials begin at least one day before the 2. Have all the materials collected and prepared so that the physician has little if any clinic. 1. Designate specific responsibilities to a position that can effectively obtain charts, x 1. Have the nurse or nurse aide enter into the present scheduling system the exam Recommendations for Finding 8 Recommendations for Finding 9 visible tracking system is at their disposable. The paper method should be sooner, depending on the commitment and priorities of the responsible parties. Staff Programmer 3. Possibly purchase a larger monitors to place in the Physician Workroom so that a V Two months when the new schedule is made. this recommendation. Physicians Clerks V Physicians Responsibility Implementation Responsibility ACTION & IMPLEMENTATION PLAN 74 Time Horizon room number, time of placement, etc. of the patient at the appropriate time. eliminated. nurses, physicians, and administration, about the possible alternatives in implementing Time Horizon rays, relevant history, etc., and foilow through to ensure the materials arrival to the Immediately. However, a few months until a bug free system is in place. Possibly pre-visit paperwork to complete.
 should perform what tasks.")


46 ACTION & IMPLEMENTATION PLAN 75 Time Horizon Clerks Time Horizon input from the physicians, determine who can fit this role most effectively. Immediately. Responsibility Discuss what position can most effectively deal with these tasks. Implementation Define what position (nurse or nurse aid) should perform what tasks. Recommendations for Finding 10 Time Horizon Immediately. Administration Nurses Nurse Aids Administration Nurses Nurse Aides Take every step possible to have the consent form signed during the Consult visit, Administration Physicians, Nurses, Nurse Aides Responsibility recommendation will contribute to this goal. Discuss the importance of reducing overall patient wait times, and how this Implementation reason for an unsigned consent form. unless the patient can not sign it at that time. Otherwise, do not let the physician be the Recommendations for Finding 11 Immediately. Responsibility Have a meeting among administration, nurses, nurses aides, and clerks, coupled with Implementation
47 p ID 0

48 RECOMMENDATIONS FOR FURTHER STUDY

49 The spreadsheets can be easily manipulated to gather such information as wait DRO should analyze what information would be beneficial and can be obtained with Computer SystemlNetwork Information from the data collection sheets gathered can be continuously analyzed Data Collection Information and each day. to gather relevant information regarding their patient and clinic flow processes. Radiation Oncology (DRO) can refer to these spreadsheets at any time in the future RECOMMENDATIONS FOR FURTHER STUDY RECOMMENDATIONS FOR FURTHER STUDY 8-1 from the spreadsheets containing all of their information. The Department of times, service times, and other patterns for each type of patient visit, each physician, staff to make improvements to the system so that everyone within the department can use the system efficiently and understand it (i.e., make the system user can be made to the current staffing levels of nurses and nurse aides within DRO. Job Descriptions It is the opinion of Management Systems Department (MSD) that improvements friendly ). made policy. This will reduce confusion and miscommunication among staff Staffing of Nurses and Nurse Aides A more detailed job description for all staff members should be determined and within the department. This will require working with the programmer and the to insure that all members of the staff are committed to using the computer system the existing and/or revised computer system. DRO should take any steps necessary benefits can also be realized through this study. Descriptions ). Cost benefits can be realized by having a fewer number of more staff to more accurately reflect clinic operating hours. This will reduce the amount staff members and decreased waiting times for the patients on the average. analyzing the patients particular service needs, their physician s work practices and productive staff members. DRO should also investigate rescheduling the nursing Patient Exam Room Assignments Currently there is no sound decision making process in determining the order in of overtime paid to the nursing staff while reducing the amount of regular time can be done by the nurse aides just as well and just as efficiently (see Job MSD feels that much of the work that the higher salaried nurses currently perform members, as well as decrease frustration for the patients and staff members. Cost being paid during less busy times (such as Friday afternoons). which certain patients should be seen. Nurses, nurse aides, and clerks should all be aware of the most efficient means of servicing any variation of a group of patients by schedule, the current clinic schedule, etc. This will result in less confusion for all

50 Hiring of a Phiebotumist when necessary. If the frequency of this need increases, DRO should make an and future benefits to determine if hiring a phlebotamist would be beneficial. analysis of the situation in regards to patient waiting times, costs, and DRO present DRO should consider hiring an in-house phiebotumist to draw patients blood Communication between Staff Clerks problem between the clerks at DRO. This was in response to the questionnaire that determine what changes can be made to rectify the situation. this matter to determine the severity of the miscommunication problem and MSD distributed to the DRO staff to complete and return. DRO should investigate It has come to the attention of MSD that there is currently a communication RECOMMENDATIONS FOR FURTHER STUDY 8-2

51 name or position. information such as paperwork, charts, x-rays, etc. Please list any I complete anonymity and no effort will be made to tie your responses to your flow and scheduling practices. The Management Systems Department would greatly appreciate your comments so that we may use this information to improve the overall service delivered to the patients. Once again, we assure The following is a confidential questionnaire regarding your views on clinic 1. Please give your view concerning the current patient scheduling 2. Please give your view regarding the present system of obtaining patient 1 possible changes you feel could be made to improve this system. patient scheduling practices. practices and list any changes you feel could be made to the current Questionnaire Department of Radiation Oncology
52 3. Please give any views regarding the current use and/or allocation of exam rooms. Please list any possible changes you feel could be made to improve the current use and/or allocation of exam rooms. 4. Please give any input or comments you may have regarding anything within Department of Radiation Oncology. 2
53 Appendix F: Current Clinic Scheduk

 TL (2) RS (2) DT (4) T ER (2) AL(2) H (2) LP (3) DT (12)* TL (2) C cn AE (2) TL (1) AE (2) DT (2) (BC (Co1water MDC AL (BCC) AB (Lymph) HS (FCC) Dr ER AL OTV AE ii HS.")
54 ER V V LP V JR(2) V HS Ut V V U ER(4) 0 R 3rd Tues) LP. AM Monday Tuesday Wednesday Thursday Friday Multidisciplinary Clinic; BCC - Breast Care Clinic; ENT - Oto Clinic; PCC - Prostate Cancer Clinic CN - Consults; FU - Followup; OTV - On Treatment visit; MDC - Radiation Oncology ATT/ne o REVISED March 8, 1994 * Only after clearance through LIT/Nurse MDC AE(ENT) LP LIT AL LI OTV AE TL HS JR N A AE (2) JR (4) AE (4) TL (4) LP (3) V (2)* AL (4) R PU as <3) TL (2) RS (2) DT (4) T ER (2) AL(2) H (2) LP (3) DT (12)* TL (2) C cn AE (2) TL (1) AE (2) DT (2) (BC (Co1water MDC AL (BCC) AB (Lymph) HS (FCC) Dr ER AL OTV AE ii HS. JR JR(4) AL(4) ER (4) AE (2) LP (1) ER (4) DT (4) FtJ HS (3) TL (2) AE(4) AL (4) JR (4) JR (2) AL (2) ER (2) AE (2) LF (1.) ER (2) AL (2) (N HS (2) TL (1) AE (2) DT (2) JR (2). Apiil 1994 clinicsëhedul
55 Appendix G: Graphs

56 LIST OF GRAPHS Average Utilization Percent by Day - All Visits 1 Time Patient in Exam Room and Time Patient Serviced in Exam Room Percent Utilization vs. Day of Week Average Utilization Exam Room Hours by Day - All Visits 2 Time Patient in Exam Room and Time Patient Serviced in Exam Room Average Utilization Hours vs. Day of Week Average Arrival Pattern - All Visits 3 Average Time per Patient vs. Type of Visit Average Wait Time in Lobby - All visits 4 Average Time per Patient vs. Type of Visit Time in System - All Visits 5 Total Time in System and Arrival Time until Leave System Average Time per Patient vs. Type of Visit Time Patient Waits in Exam Room vs. 1st Phvs. Encounter until Leave - All Visits 6 Average Time per Patient vs. Type of Visit 1st Physician Encounter until Leave vs. Current Scheduled Time 7 Times for Consult, Follow Up, and On Treatment Visits Average Time per Patient vs. Type of Visit Consult Visit 8 Enter Exam Room until Leave and 1st Physician Encounter until Leave Average Time per Patient vs. Type of Visit Follow-Up Visit 9 Enter Exam Room until Leave and 1st Physician Encounter until Leave Average Time per Patient vs. Type of Visit On-Treatment Visit 10 Enter Exam Rooni until Leave and 1st Physician Encounter until Leave Average Time per Patient vs. Type of Visit Consult Visit 11 Total Time in System and Arrival until Leave System Average Time per Patient vs. Type of Visit

57 Follow-Up Visit 12 Total Time in System and Arrival until Leave System Average Time per Patient vs. Type of Visit On-Treatment Visit 13 Total Time in System and Arrival until Leave System Average Time per Patient vs. Type of Visit Follow-Up Visit 14 Total Time when Res. & Staff see patient and when only Staff sees patient Average Time per Patient vs. Type of Visit Comparisons of 3 Times with RP/SP vs. SF only - Follow-Up Visit 15 Enter Exam Room until Leave, 1st Phys. Encounter until Leave, and Arrival until Enter Exam Room Average Time per Patient vs. Treatment Provider Comparisons of 3 Times with RP/SP vs. SF only vs. RP Only - On Treatment Visit 16 Enter Exam Room until Leave, 1st Phys. Encounter until Leave, and Arrival until Enter Exam Room Average Time per Patient vs. Treatment Provider Simulation Visit - Arrival Until Leave 17 Average Time per Patient vs. Physician Name Simulation Visit - Exam Room Until Leave 18 Average Time per Patient vs. Physician Name Simulation Visit - Total Time in System 19 Average Time per Patient vs. Physician Name

58 L1 Time Patient In Exam Room Patient Serviced In Exam Room Overall Average Utilization Percent by Day - All Visits o a) Monday Tuesday Wednesday Thursday Day of Week Friday NOTFS; All Days Utilization : Patient in any one of eight exam rooms Utilization Percent = (Avg. serve time for each visi[)(total II of each type of visit) / Total U exam room hours per day Total II exam room hours per day = 72 for Mon. - Thurs., 32 for Fri.
 (Avg.")
59 Patient Serviced in Exam Room 4 Average Utilized Exam Room Hours by Day All Visits ii - Time Patient In Exam Room f\) a) bo Monday Tuesday Wednesday Thursday 8 kc1 Friday NOTPth Day of Wecic Utilization Patient in any one of the eight exam rooms Utilization = (Avg. service time for each visit) (Avg. I visits day of each type of visit) Full Utilization for Mon. - Thurs. based on 8 exam rooms at 9 hours/day = 72 hours Full Utilization for Friday based on 8 exam rooms at 4 hours/day = 32 hours
 Not applicable to Unscheduled Visits")
60 Average Arrival Pattern - All Visits ci ai ci H ci CU -4 ci 7 12 On Treatment I Consull Follow Up Simulation -10 Type of Visit NOT1S; Arrival Pattern Appointment Time - Arrival Time (Negative value Indicates late patients) Not applicable to Unscheduled Visits






61 Consult Follow Up On Treatment Simulation Unscheduled 4 Average Wait Time in Lobby - All Visits Ui c U Type of Visit Wait Time iu Lobby = Time enter exam room Appointment time
a1iets appointment time if (hey arrive early and their arrival time if they")
62 1i1 Total Time In System Arrival Time until Leave System Time in System - All Visits Consult Follow Up On Treatment Simulation Unscheduled NOTh Type of Visit Total time in system is calculated by using the l)a1iets appointment time if (hey arrive early and their arrival time if they arrive late
 bo Cu 0) 100 80 60 40 20 0 NOTES: 80 59 Consult Follow Up (Enter exam room Lime) - 37 On Treatment Type of Visit a).0 Cu Simulation (1st phys.")
63 Enter Exam Boom until Leave 1st PhysIcian Encounter until Leave Time Patient Waits in Exam Room vs. 1st Physician Encounter until Leave for all Visits Cu p ) 0)1::.. 0) bo Cu 0) NOTES: Consult Follow Up (Enter exam room Lime) - 37 On Treatment Type of Visit a).0 Cu Simulation (1st phys. encounter) Time exam room = is used as additional waiting room Simulation Visit : Patient does not encounter physician C) z Unscheduled

 - I c1-4 0) 50 40 30 20")
64 1st Physician Encounter uiti1 Leave vs. Current Scheduled Time li1 1st Physician Encounter until Leave 4-. LU Practiced Shecluled Time -4 a) - I c1-4 0) Consult Follow Up On Treatment Type of Visit



65 Enter Exam Room until Leave Consult Visit st PhysIcian Encounter until Leave 100 I60 80 Ii AE AL DT TL LI F3 I-- -I- JR LP Physician Name
 40 20 0- AE AL DT ER TL Physician Name")
66 71 Follow Up Visit Enter Exam Room until Leave 100 1st PhysIcian Encounter until Leave (1 a) AE AL DT ER TL Physician Name 1-6 LP


67 1 On-Treatment Visit iii1 Enter Exam Room until Leave 1st PhysIcian Encounter until Leave Gi 40 - I-. ( AE AL DT FR TL H3 LP Physician Name

68 180 Consult Visit Total Time In System E Arrival until Leave System cli I. I-. p cli H cli Cd 1-4 cli AE AL DT ER TL Physician Name JI LP





69 Follow Up Visit ToLal Time in System U. Arrival until Leave System I-. -l - AL DT ± ER Physician Name TL US JR LP




70 AE AL DT TL IE LP On Treatment Visit Total Time In System Arrival until Leave System I I Physician Name


71 ki Total Time when Resident & Staff sees Patient 80 Follow Up Visit Total Time when only Staff sees Patient F4 2O -I-- - I- I AE AL DT TL HS LP Physician Name


72 C C U Enter Exam Room until Leave 1st Phys. Encounter until Leave U Arrival until Enter Exam Room Patients spend approximately the same amount of time waiting to enter exam room and waiting in exam room as they do seeing the physician. Staff physicians should see the patient by themselves if the patient has been waiting for an excessive amount of time Comparison of 3 Times with RP/SP vs. SP only - Follow Up Visit 4-. Ci i P Ci I (C 1-4 Ci 10 0 NflTFS RP/SP average SP average Treatment Provider

")

73 Enter Exam until Leave 1st Phys. Encounter until Leave Comparison of 3 Times wi[h RP/SP vs. SP On Treatment Visit only vs. RP only - Qi (U $ Arrival until Enter Exam Room a) bo CU a) RP/SP average SPaverage RPaverage 18 Treatment Provider NOTE Treatment times are lower when staff or resident physician work alone Staff and resident physicians currenly only work alone if patient has been waiting in lobby for long time






74 AE AL DT TL KS JR Simulation Visit - Arrival until Leave ra ti 60 1-i Physician Name
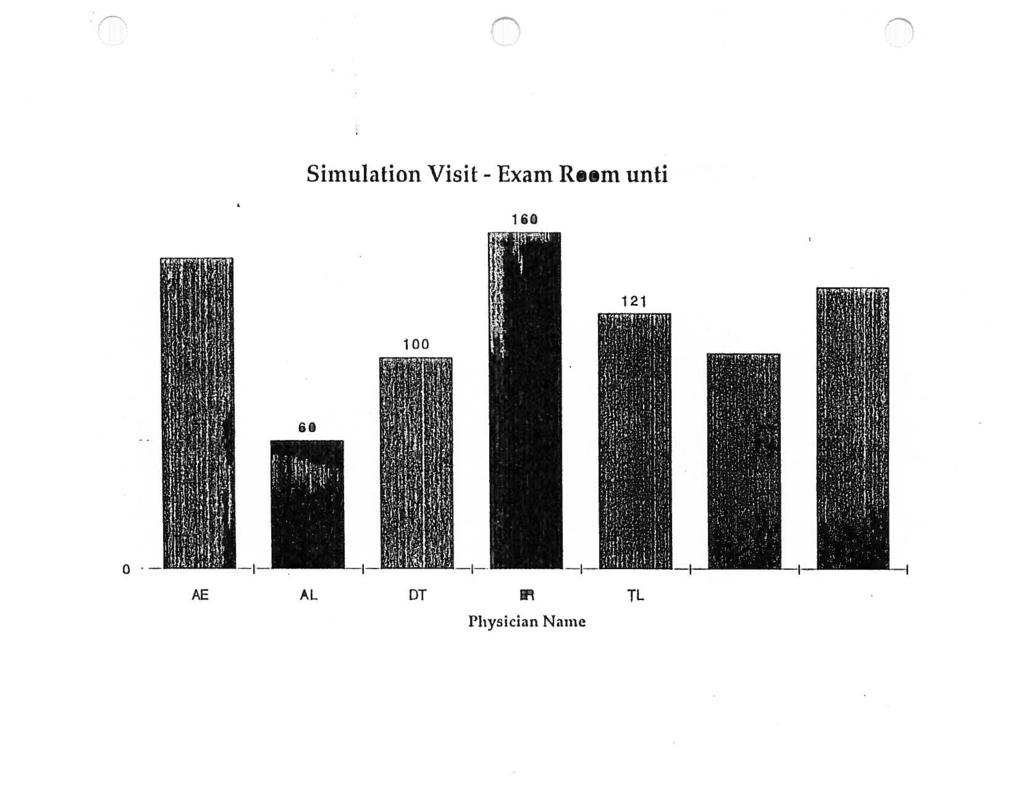



75 Simulation Visit - Exam Room until Leave I 120 I 00 H AE AL DT TL KS Physician Name


76 AE AL DT ER TL I-IS JR Sinnilation Visit - Total Time in System I 100 oi 80. to -4 ci Physician Name

77 1) D
78 APPENDICES

79 Appendix A: DRO Clinic Layout


80 Th /,(\ : I1t 1-4
81 Appendix B: DRO Micro Flow Diagram

82 Radiation Oncoi Reception Oe l*1u 3 e_fl_l I ZZL. Receptionist asks for pt.s name C pertinent data such as films C slides. Does pt. have a valid registration card? 2 8 BLUE noje de 1 10utJ Receptionist hits the find key on the computer keyboard. Receptionist calls billing office, glues pt. name C phone #, tells them pt. refused to complete insurance form. Jee detain 1.reakouj 1ou.J JalT yes Billing Offlce/insurance Forms yes Receptionist hits FiB (Star Key) on the computer keyboard. Pt. given insurance C database forms to complete. Box 8 BLUE Stamp wi reg. card consult packet (BRRF form, blue database sheet, PRO, RT checklist). Write Initials of attending MO C date only on PRO. Carry packet C outside Information such as slides C films to clinic desk.

83 Ooes.pts name appear on compute Send pt awa ues Send pt awag.




84 bhh iocm tilu, ULL., I I U.O n19 IS BHRF Form complete? 2-H H-BLUE no i Clerk check consultation form to see If appt. is correct. Check HIS to see if pt is scheduled in another clinic. Is pt. appt. form? no- Page resident. V Send pt. to other clinic. yes fisk the resident if we should add pt. to clinic schedule. Type pt. appt. in computer. 4 Pt. given insurance data form to complete.


85 film: to lntc desk. on SRRF farm data onij on PRO. nforrnatlan suez as slide: D CarrLJ packet D outside Initial: of ttendlng MU D date packet (SRRF farm, blue database sheet, PRO, Rr ciac1istl Write Stamp wi reg. card, car1t = pt. haue a ualld registration card? Patient Consult Master Flow Cria/IJoes stern. N Into Rad. Oncciogg chedullng 4- computer. Receptionist enter: Receptionist enter: registration Receptionist gets to Tautman to register. Receptionist sand: pt. Receptionist gets pt. computer. registration I off of V Ijee T ue I Tue, Sep 22, %j scheduling sustem. registration I Into RU registration I off of registration number aft of computer. Receptionist gets pt.

86 Radiation Oncology Reception Dells pt. non-hmo? u-lu, uct i, is rri limo notification sheet put an NT chart Nurse Ride tell: Or. about sheet. Reception clerk checks far signature: an form:.

87 lissembie lit shadow 3-fl-P INK sheet. HO s, pathology C race dictation from other chart; RHO notification, w/chart or look on HIS Call med records or unit ci original In lit for location of chart documents, put chart, copies on before p1 arriues. to pathology. C send w/sildes Copy tilde report Copy all referring Desk

88 yes yes know where 1 database. chart; HMO notification, dictation from other information on desk, for H-rays. Rssemble fit shadow Clerk puts 3-fl-PINK sheet. MD s, pathology, face be seen? needed befor thsre? oes Radiology 4 film jacket. yes H rag. I yes!jes green sticker on jacket? um? the pt. s H-ray no from wi flo assemble RT Shadow Chart 1 Copy face sheet for Do we have films oes the pt. e outside y lcail Radiology for 1 Complete outside film card C put H rays. n ) fire H-rays Nurse Ride puts pt. in exam roam. Send transporter InciudIng chart C

89 s pt. a candidate for treatment? 4-fl-GREEN Pt. leaves department with paperwork. 1an gets I consent form I signed/nurse Stop at clinic desk to drop off paperwork. Pt. Is seen by nursing -nurse Introduces self enplains role to pt.lfamlly nurse glues pt.j family their business card nursing may assess the chtlds cooperativeness need for sedation. mop t. Slide tape reviewed it time allows or nurse reviews simulation preparation D t. Info, as well as lit t. routines. Pt. Is seen by nursing -nurse Introduces self epla1ns role to pt./!amlig nurse glues pt./r;mily their business card -reviews protocol, th. planning coordinates apt s. ay assess housing D.ransportatlon needs D makes referrals as appropriate -may fill out BRRF sheet glue to clerk n Pt. simulated treated. Pt./famiiy routed to reception desk for parking sticker. Nursing may participate In obtaining release of medical Info. r is papeork Clinic cie needs to given to clerk at no find nursing or staff clinic desk? H.U. while pt.. waits. Schedule appointments. (see 5-VEI.LOW) L Pt. Ieaues department.



90 are I*ing p11(1. It D What ICtl.,h1 _1J tile Wile,, Ilfa (uric It(e It I: allallable. cj pobbij until r,em Pr. Waits lit the meg get tiling peeler nag gel films aviilible ha get chart liurle Ride nag Valuntlif, It nag call Cr.: iectstar er (ilnic alt the Pt. where itt Sill cietz.141 finds cut :9(141 train faildent Itatiflul (UrIC Ride heel Pete_J IC let hect page. na-utan Set detail time. meat wipt. i 2nd RinIlliat 9 limit a ruialagg IC lie flint. anetiler M.,, need II tiitlnetrlj. leti Ii call gill, called Ii (lu. be lit mimer p1... DC called I: I leildint m3 list II CI Pt. Wilt, lit elm,m. he tidieiegg tine. claimer H.L, heed he ge d.ilme2rg aced IS call aim, Ulied ha OTV, be 1st mitether pt., be called be R.ildhil mag lead II CU Pt. with In acm flit.


, thighs, leg, hand,")
91 Patient out of room Wed, Mar 16, :29 PM noh Page Dr. complete missing info (area, ports, machine, name, reg.) Check computer for sim auailability on neht day Dr. is in clinic. LS area other than ped brain, CNS, 3 or 4 port breast, lung C brain, rectum, whole abdomen, (ouary), thighs, leg, hand, feet, 3 or port boneg mets, orbit, parotid, mantle, para aortics

92 5 A YELLOW checkout desk paperwork to Pt. brings Wed, Mar 16, :46PM
..I%àSl?.Jil. d. Will pt.")
93 EOH em 11 em. Thurs or Fri between 7 efter sim 0 not on Tues, no sooner then dej 1Ler tim. CT euelleblllty on d Cteck computer for no cluii7 ied? Cell Molt CT. Schedule CT. )..I%àSl?.Jil. d. Will pt. be
 efter")





94 euthleblllty ot leest 3 Enter speclel Fri) efter CT (or sim II no working dejs (ehcluding Check computer for sim Schedule CT no pege II em notes (Ecatinued on Initlels Enter schedulers V no elter sirn no on jes sooner then deg between 7 em O Cell Hott CT. Dr. Is in clinic CT I: scheduled) when The:, Thurs or Fri

95 ( sctir.duler s initiqis
96 Appendix C: Data Collection Forms
 and improving the overall department structure.")

97 Consult/Follow-Up Juformati on Form Department of Radiation Oncology This information form is part of a combined effort between the Department of Radiation Oncology and the Management Systems Department of the UM Hospital to enhance the patient flow. This will be accomplished through decreasing patient wait time(s) and improving the overall department structure. The information you present on this form is in no way related to your name. Accurate information is greatly appreciated. Date: Physician: Diagnosis: Type of Visit: D Consult Follow-Up Appointment Time: Arrival Time: I I I I TO BE FILLED-OUT BY PAITENT Exam Room Number: Time Enter Exam Room: I I I. I Check All Providers Involved In Encounter Encounter 1 Provider Type; Staff Physician D Resident Physician D Nurse Nurse Aide Time In TI Time Out Encounter 2 Provider Type; D Stat! Physician D Resident Physidan 0 Nurse Q Nurse Aide Time Iii I Time Out Did anyone check on you while waiting: Yes D No If yes, who performed check:: Staff Physician D Resident Physician 0 Nurse 0 Nurse Aide Time performed check Encounter 3 Provider Type; D Stat! Physician D Resident Physician D Nurse Nurse Aide Time In F Time Out rovider T)pe; 0 Staff Physidan 0 0 Resident Physician Nurse 0 Nurse Aide Check Out Time: Time In I 1 Please write any comments you may have on the backo this form. Also, please return this form to the Check-Out Desk before Leaving. Thank you for your assistaucel Time Out II,
 and improving the overall department structure.")
98 On-Treatment Visit Information Form Department of Radiation Oncology This information form is part of a combined effort between the Department of Radiation Oncology and the Management Systems Department of the UM Hospital to enhance the patient flow. This will be accomplished through decreasing patient wait time(s) and improving the overall department structure. The information you present on this form is in no way related to your name. Accurate information is greatly appreciated. Date: Physician: Diagnosis: Appointment Time: I. I Arrival Time: Exam Room Number: I I Time Enter I I Exam Room: TO BE Fll.dLED-OUT BY PATENT Check All Providers Involved In Encounter Encounter 1 Provider Type; Staff Physician Resident Physician Nurse Nurse Aide I Time In Time Out Encounter 2 Provider Type; Staff Physician Resident Physician D Nurse Nurse Aide Time In Time Out [1 Encounter 3 Provider Type; St.aff Physician Resident Physician Nurse Nurse Aide I Time In lime Out e Patient Leaves Exam Room: F Check Out Time: Ii Please return this form to the Check-Out Desk before Leaving. Please additional comments on back of sheet. Thank you for your assistance and have a nice day!





99 I Staff Physician F If yes: Date: Physician: present on this form is in no way related to your name. Accurate iaformation is greatly appreciated. Tnis infom2ation form is part of a combined effort between the Department of Radiation Oncology and the Management Systems Department of the UM Hospital to enhance the patient flow. This will be accomplished through decreasing patient wait time(s) and improving the overall department structure. The information you Thank you for your assistance! Please return this form to the Check-Out Desk before Leaving. Check Out Time: I I Please give any additional C Simulation: Time Began Time Ended Resident Physician Nurse Aide Nurse If yes, who was present: Did you sign a Patient Consent Form: Time Signed Resident Physician Nurse Aide Staff Physician Nurse If yes, who conducted: Was there further education after viewing slide tape: Time Began Time Ended I I Did you see the Radiation Oncology Slide Tape: Time Began Time Ended Check All Providers Involved In Encounter I TO BE FELLED-OUT BY PA Arrival Time: LI Time Enter Exam Room: I Appointment Time: Exam Room Number: Diagnosis: Department of Radiation Oncology Simulation Information Form
 and improving the overall department structure. The information you Management Systems Department of the UM Hospital to enhance the patient flow.")

100 Date: Physician: present on this form is in no way related to your name. Accurate information is greatly appreciated. through decreasing patient wait time(s) and improving the overall department structure. The information you Management Systems Department of the UM Hospital to enhance the patient flow. This will be accomplished This information form is part of a combined effort between the Department of Radiation Oncology and the Thank you for your assistance! Please return this form to the Check-Out Desk before Leaving. Check Out Time: Comments: Time Physician Enter: Time Physician Leave: J Nurse Only Visit: Physician who saw patient: ResideuL Physician Nurse Aide ) StaftPhysician Nurse Who placed patient in room: Exam Room Number: Time Enter Exam Room: Nature of Visit: Arrival Time: I I Diagnosis: Department of Radiation Oncology Unscheduled Clinic Visit Information Form
101 Appendix D: Memorandum to DRO Patients



102 The University of Michigan Medical School Department of Radiation Oncology o)a February 23, 1994 TO: PROM: SUBJECT: Radiation Oncology Patients. University of Michigan Hospital Department of Radiation Oncology Management Systems Department Study of patient flow within the Department of Radiation Oncology. The Department of Radiation Oncology is committed to Total Quality Health Care. We continually look for ways to improve our service. With the assistance of the Hospital Management Systems Department we are studying this area. The purpose of this memo is to ask you to assist us in finding ways to improve your care. If you are here for a consult or follow-up visit, an on-treatment visit, and/or a simulation visit, you will be given an information form pertaining to your treatment and asked to complete the TO BE FILLED OUT BY FAUENT section. Your name is not recorded in this study, and the information that you provide will in no way be tied to your identity. In order to best serve your needs, we ask that you be honest in your comments, and try to give complete and accurate information concerning the service you receive. Thank you for your time, Department of Radiation Oncology Management Systems Department ino i1 ojrv, /,
103 aajtuuo9sano :a xjpuadd j
104

105 .:. Department CD of Radiation Oncology Department Analysis Graphics from Presentation 19 April1994 Management Systems Chad Cleveringa Chad Dejong Chris Cannon




106 n C) C Department_of Radiation_Oncology Clinic Analysis Performed by Management Systems Department Chad Cleveringa Chad DeJong Chris Gannon




107 Improve overall efficiency of clinic through: 7Th Purpose of Clinic Analysis - Improved scheduling practices - Improved clinic care decisions Increase quality of patient care




108 n Clinic Analysis Approach Analysis of Clinic Flow Diagram Interviewed Clinic Patients - Clinic Staff - Data Collection Forms Patients Filled Out - Questionnaire Clinic Flow Simulation Model





109 0 Description of Current System Scheduling for 4 types of Visits - Consult - Follow-Up - On-Treatment - Simulation Eight Exam Rooms - Equally - One Supplied Room Typically Reserved for Unscheduled Visits Social Work Room



110 . X cont. :ci Description of Current System -..M Physician meeting every morning Patient Flow communication by paper One Physician in Clinic on Friday



111 . n Finding 1 Present Scheduling System Inefficient - Physicians - Clinic - Inefficient scheduled to be in more than one place at a time visits take significantly longer than scheduled - Consult Visit in particular utilization of Exam Rooms

 70-60 - 60 Lifl until")
 50 40-30 - 30 3.")

112 1st Physician Encounter until Leave vs. Current Scheduled Time G) Lifl 1st Physician Encounter until Leave Practiced Sheduled Time 3.4 r) I Consult Follow Up On Treatment Type of Visit



113 fl Recommendation 1 Compartmentalize schedule - Consults - On-Treatment and Follow-Ups same day and Follow-Ups same day Schedule by shortest service time first Increase allotted time for consult visits - From one hour to one and a half hour


114 .1 n Finding 2 Staff Physician Howard Sandier Most efficient in clinic Saw highest number of patients Time spent with patient follows departmental average Compartmentalizes schedule Uses time management tools


115 Total Time in System AE AL DT ER TL HS JR LP 106 Follow Up Visit 180 TI Arrival until Leave System j Physician Name


116 (Th Recommendation 2 Compartmentalize schedule Use time management tools



117 n Finding 3 Staff Physician/Resident Physician vs. One Physician Service time for One Physician faster - - Wait time in lobby higher for One Physician


")
 (U 0) 0) bo (U 31 0) 80 70 60 50 40 30 20 10 0 71 RP/SP")
118 I Enter Exam Room until Leave 1St Phys. Encounter until Leave I Arrival until Enter Exam Room Patients spend approximately the same amount of time waiting to enter exam room and waiting in exam room as they do seeing the physician. Staff physicians should see the patient by themselves if the patient has been waiting for an excessive amount of time n N C) Comparison of 3 Times with RP/SP Follow Up Visit vs. SP only - 4.J 0) (U 0) 0) bo (U 31 0) RP/SP average SP average Treatment Provider NOTES:

 bo 40 35 30 25 20 15 10 5 0 NOTES: 39 33 21 U Arrival until Enter Exam")

119 U Enter Exam until Leave F 1st Phys. Encounter until Leave C Comparison of 3 Times with RP/SP vs. SP only vs. RP only - On Treatment Visit 0) 3-4 a).. 0) bo NOTES: U Arrival until Enter Exam Room RP/SP average SP average RP average Treatment Provider Treatment times are lower when staff or resident physician work alone Staff and resident physicians currenly only work alone if patient has been waiting in lobby for long time


120 Recommendation 3 a.... Follow-Up Visit Staff Physician see patient during busy times - On-Treatment Visit Either Staff or Resident Physician see patient during - busy times Make decision early as possible



121 (fl 0 Finding 4 Physician Conference every morning between 7:30 and 8:30 Patient Scheduling begins at 8:30 Pre-visit Activities Dosimetry Simulation Radiation Treatment Rooms Conference rarely finishes on time Causes patient wait for extended periods of time Wait perpetuates throughout day

122 ( rj) r-- I 1. C.? 5 r(



123 Physician forego Conference on days in clinic n C Recommendation 4 Alternative 1: Begin scheduling patients at 9:15 AM Alternative 2 Tighten Conference schedule Alternative 3:


124 (fl n Finding 5 Schedules created every 3 months - Creates inefficient coordination between Physicians and clinic Physicians can cancel appointment very little notice - Creates times easily, with extra costs to notify and reschedule patients

125 Develop clinic schedule every one to two months Physicians should use discretion in cancelling clinic CD Recommendation 5
,")

126 C Finding 6 Physicians in lab most (clinic least), have longest patient wait times Physicians TL and ER -

 40")
127 Consult Visit Total Time In System TiI Arrival until Leave System IH 60 0) I AE AL DT FR TL Physician Name KS LP

128 .... Recommendation 6 Smooth schedules to reflect extra time See patients with shortest service time first See Follow-Up and On-Treatment visits before Consult visits


129 n C Finding 7 Wednesday and Thursday over scheduled One Physician scheduled in clinic on Friday - Under utilization of clinic



130 n Expected Room Requirements for Changes in Number of Visits Using April Schedule Expected Total Room Requirement Actual Available Time (1) Room Time (2) Monday Tuesday Wednesday Thursday Friday Monday Tuesday Wednesday Thursday Friday


131 Recommendation 7 Physician from Wednesday or Thursday mornings - Place - Or on Friday morning adjust work schedule of staff Smooth schedule - Example: Switch two of AE s Follow-Ups from Wednesday to Monday





132 C n fl Finding 8 Notification of patient arrival by Nurses through paper in Physician work room Notification of patient arrival sometimes late Physicians not informed of patient arrival - Computer system available Not currently used - - Programmer on staff


133 .... Recommendation 8.. Use existing computer system Eliminate paper method - Place computer terminals in areas and rooms where necessary Nurses - Physicians - Administrative - or Nurse Aides use terminal to update patient information use computer terminal purposes o Flag System on exam room doors L.IE Quality



134 C) Finding Charts and X-Rays not always present when patients arrive - Significant problem


135 Recommendation 9 Designate specific responsibility to staff member to: Obtain - Ensure - Collect - Charts and X-Rays their arrival all materials and prepare for Physician - Little pre-visit paperwork to complete Begin search and gathering day before patient visit - check into system used in Hospital
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic. Final Report
 Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
The University of Michigan Health System. Geriatrics Clinic Flow Analysis Final Report
 The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience
 University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System
 University of Michigan Health System Program and Operations Analysis Analysis of the Orthopedic Surgery Taubman Clinic Final Report To: Andrew Urquhart, MD: Orthopedic Surgeon Patrice Seymour, Administrative
University of Michigan Health System Program and Operations Analysis Analysis of the Orthopedic Surgery Taubman Clinic Final Report To: Andrew Urquhart, MD: Orthopedic Surgeon Patrice Seymour, Administrative
Final Report. Karen Keast Director of Clinical Operations. Jacquelynn Lapinski Senior Management Engineer
 Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Analysis of Room Allocation in the Taubman Center Clinic of Internal Medicine
 University of Michigan Health System Program and Operations Analysis Analysis of Room Allocation in the Taubman Center Clinic of Internal Medicine Final Report To: Cherie Freed, Administrative Associate
University of Michigan Health System Program and Operations Analysis Analysis of Room Allocation in the Taubman Center Clinic of Internal Medicine Final Report To: Cherie Freed, Administrative Associate
Pediatric Hematology / Oncology Clinic
 Pediatric Hematology / Oncology Clinic Final Report for Analysis of Operations April 13, 1995 Program and Operations Analysis Project Team Cristina Bermudez Katherine Horvath Julie Pinsky Seth Roseman
Pediatric Hematology / Oncology Clinic Final Report for Analysis of Operations April 13, 1995 Program and Operations Analysis Project Team Cristina Bermudez Katherine Horvath Julie Pinsky Seth Roseman
RADIATION ONCOLOGY RESIDENCY SUPERVISION POLICY
 RADIATION ONCOLOGY RESIDENCY SUPERVISION POLICY This policy is intended to guide the activities of radiation oncology residents in insuring that patient care activities in which residents participate are
RADIATION ONCOLOGY RESIDENCY SUPERVISION POLICY This policy is intended to guide the activities of radiation oncology residents in insuring that patient care activities in which residents participate are
Online library of Quality, Service Improvement and Redesign tools. Process templates. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Process templates collaboration trust respect innovation courage compassion Process templates What is it? Process templates provide a visual
Online library of Quality, Service Improvement and Redesign tools Process templates collaboration trust respect innovation courage compassion Process templates What is it? Process templates provide a visual
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process. Final Report
 University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
ORTHODONTIST. Scheduling Coordinator Manual
 ORTHODONTIST Scheduling Coordinator Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
ORTHODONTIST Scheduling Coordinator Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
SCHEDULING COORDINATOR MANUAL GENERAL DENTIST. Scheduling Coordinator Manual
 GENERAL DENTIST Scheduling Coordinator Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing
GENERAL DENTIST Scheduling Coordinator Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing
Emergency Services. Time Study
 Prepared for: Peter Forster Management Systems University of Michigan Hospitals December 18,1991 by: Associate Hospital Administrator Emergency Services Ann Arbor, MI Don Suffivan Jeremy Roberts Lisa Clayton
Prepared for: Peter Forster Management Systems University of Michigan Hospitals December 18,1991 by: Associate Hospital Administrator Emergency Services Ann Arbor, MI Don Suffivan Jeremy Roberts Lisa Clayton
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE SURGICAL SUITE OPERATING ROOM. Sarah M. Ballard Michael E. Kuhl
 Proceedings of the 2006 Winter Simulation Conference L. F. Perrone, F. P. Wieland, J. Liu, B. G. Lawson, D. M. Nicol, and R. M. Fujimoto, eds. THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE
Proceedings of the 2006 Winter Simulation Conference L. F. Perrone, F. P. Wieland, J. Liu, B. G. Lawson, D. M. Nicol, and R. M. Fujimoto, eds. THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE
University of Michigan Health System. Current State Analysis of the Main Adult Emergency Department
 University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
University of Michigan Health System. Program and Operations Analysis. CSR Staffing Process. Final Report
 University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
CHAPTER 1. Documentation is a vital part of nursing practice.
 CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
EXECUTIVE SUMMARY. Introduction. Methods
 EXECUTIVE SUMMARY Introduction University of Michigan (UM) General Pediatrics offers health services to patients through nine outpatient clinics located throughout South Eastern Michigan. These clinics
EXECUTIVE SUMMARY Introduction University of Michigan (UM) General Pediatrics offers health services to patients through nine outpatient clinics located throughout South Eastern Michigan. These clinics
VENICE FAMILY CLINIC: Improving capacity and managing patient lead times
 CASE STUDY, 4/12 VENICE FAMILY CLINIC: Improving capacity and managing patient lead times PREPARED BY Professor Kumar Rajaram, UCLA Anderson School of Management Karen Conner, MD, UCLA David Geffen School
CASE STUDY, 4/12 VENICE FAMILY CLINIC: Improving capacity and managing patient lead times PREPARED BY Professor Kumar Rajaram, UCLA Anderson School of Management Karen Conner, MD, UCLA David Geffen School
Work Effort Analysis
 Coordinator: Dolorese Umar The University of Michigan, Ann Arbor Special Projects in Hospital Systems Client: Karolyn Brewer Industrial and Operations Engineering 481 Vivek Gupta Sonia Raheja Julie Simmons
Coordinator: Dolorese Umar The University of Michigan, Ann Arbor Special Projects in Hospital Systems Client: Karolyn Brewer Industrial and Operations Engineering 481 Vivek Gupta Sonia Raheja Julie Simmons
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
uncovering key data points to improve OR profitability
 REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
Scheduling & Physician/Staff Utilization
 Scheduling & Physician/Staff Utilization Presented By Economedix Your Partner In Building High Performance Practices Today s Course Practice Management Seminar Series First of Four Patient Flow & Marketing
Scheduling & Physician/Staff Utilization Presented By Economedix Your Partner In Building High Performance Practices Today s Course Practice Management Seminar Series First of Four Patient Flow & Marketing
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012
 HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
Minnesota Adverse Health Events Measurement Guide
 Minnesota Adverse Health Events Measurement Guide Prepared for the Minnesota Department of Health Revised December 2, 2015 is a nonprofit organization that leads collaboration and innovation in health
Minnesota Adverse Health Events Measurement Guide Prepared for the Minnesota Department of Health Revised December 2, 2015 is a nonprofit organization that leads collaboration and innovation in health
The ASRT is seeking public comment on proposed revisions to the Practice Standards for Medical Imaging and Radiation Therapy titled Medical Dosimetry.
 The ASRT is seeking public comment on proposed revisions to the Practice Standards for Medical Imaging and Radiation Therapy titled Medical Dosimetry. To submit comments please access the public comment
The ASRT is seeking public comment on proposed revisions to the Practice Standards for Medical Imaging and Radiation Therapy titled Medical Dosimetry. To submit comments please access the public comment
Patient Navigation: A Multidisciplinary Team Approach
 Patient Navigation: A Multidisciplinary Team Approach by David Nicewonger, MHA MultiCare Health System is a community-based healthcare organization based in Tacoma, Washington, that includes four hospitals,
Patient Navigation: A Multidisciplinary Team Approach by David Nicewonger, MHA MultiCare Health System is a community-based healthcare organization based in Tacoma, Washington, that includes four hospitals,
Managing Queues: Door-2-Exam Room Process Mid-Term Proposal Assignment
 Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean
 LEAN CASE STUDY: Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean In healthcare today, having to do more with less goes with the territory. Volumes are increasing
LEAN CASE STUDY: Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean In healthcare today, having to do more with less goes with the territory. Volumes are increasing
Uses a standard template but may have errors of omission
 Evaluation Form Printed on Apr 19, 2014 MILESTONE- BASED FELLOW EVALUATION Evaluator: Evaluation of: Date: This is a new milestone-based evaluation. To achieve a level, the fellow must satisfy ALL the
Evaluation Form Printed on Apr 19, 2014 MILESTONE- BASED FELLOW EVALUATION Evaluator: Evaluation of: Date: This is a new milestone-based evaluation. To achieve a level, the fellow must satisfy ALL the
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
HOW TO USE THE WARMBATHS NURSING OPTIMIZATION MODEL
 HOW TO USE THE WARMBATHS NURSING OPTIMIZATION MODEL Model created by Kelsey McCarty Massachussetts Insitute of Technology MIT Sloan School of Management January 2010 Organization of the Excel document
HOW TO USE THE WARMBATHS NURSING OPTIMIZATION MODEL Model created by Kelsey McCarty Massachussetts Insitute of Technology MIT Sloan School of Management January 2010 Organization of the Excel document
The Practice Standards for Medical Imaging and Radiation Therapy. Medical Dosimetry Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Medical Dosimetry Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
The Practice Standards for Medical Imaging and Radiation Therapy Medical Dosimetry Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
NHS Dental Services Quarterly Vital Signs Reports
 NHS Dental Services Quarterly Vital Signs Reports Dental Services Gateway ref: NHSBSA/DSD/0008 Introduction The NHS Dental Services (NHS DS) has been working closely with the Department of Health (DH)
NHS Dental Services Quarterly Vital Signs Reports Dental Services Gateway ref: NHSBSA/DSD/0008 Introduction The NHS Dental Services (NHS DS) has been working closely with the Department of Health (DH)
Simulering av industriella processer och logistiksystem MION40, HT Simulation Project. Improving Operations at County Hospital
 Simulering av industriella processer och logistiksystem MION40, HT 2012 Simulation Project Improving Operations at County Hospital County Hospital wishes to improve the service level of its regular X-ray
Simulering av industriella processer och logistiksystem MION40, HT 2012 Simulation Project Improving Operations at County Hospital County Hospital wishes to improve the service level of its regular X-ray
practice standards CFP CERTIFIED FINANCIAL PLANNER Financial Planning Practice Standards
 practice standards CFP CERTIFIED FINANCIAL PLANNER Financial Planning Practice Standards CFP Practice Standards TABLE OF CONTENTS PREFACE TO THE CFP PRACTICE STANDARDS............................................................................
practice standards CFP CERTIFIED FINANCIAL PLANNER Financial Planning Practice Standards CFP Practice Standards TABLE OF CONTENTS PREFACE TO THE CFP PRACTICE STANDARDS............................................................................
Applying Toyota Production System Principles And Tools At The Ghent University Hospital
 Proceedings of the 2012 Industrial and Systems Engineering Research Conference G. Lim and J.W. Herrmann, eds. Applying Toyota Production System Principles And Tools At The Ghent University Hospital Dirk
Proceedings of the 2012 Industrial and Systems Engineering Research Conference G. Lim and J.W. Herrmann, eds. Applying Toyota Production System Principles And Tools At The Ghent University Hospital Dirk
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
10 Things To Know About
 10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
A Measurement Guide for Long Term Care
 Step 6.10 Change and Measure A Measurement Guide for Long Term Care Introduction Stratis Health, in partnership with the Minnesota Department of Health, is pleased to present A Measurement Guide for Long
Step 6.10 Change and Measure A Measurement Guide for Long Term Care Introduction Stratis Health, in partnership with the Minnesota Department of Health, is pleased to present A Measurement Guide for Long
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
May Improving Strategic Management of Hospitals: Addressing Functional Interdependencies within Medical Care Paper 238
 A research and education initiative at the MIT Sloan School of Management Improving Strategic Management of Hospitals: Addressing Functional Interdependencies within Medical Care Paper 238 Masanori Akiyama
A research and education initiative at the MIT Sloan School of Management Improving Strategic Management of Hospitals: Addressing Functional Interdependencies within Medical Care Paper 238 Masanori Akiyama
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
FundsforNGOs. Resource Guide: Questions Answered on How to Write Proposals A Basic Guide on Proposal Writing for NGOs
 FundsforNGOs Resource Guide: Questions Answered on How to Write Proposals A Basic Guide on Proposal Writing for NGOs Contents 1. Introduction... 2 2. What is a Proposal?... 3 3. How to start writing a
FundsforNGOs Resource Guide: Questions Answered on How to Write Proposals A Basic Guide on Proposal Writing for NGOs Contents 1. Introduction... 2 2. What is a Proposal?... 3 3. How to start writing a
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Improving Patient Throughput in the Emergency Department
 University of Michigan Health System Program and Operations Analysis Improving Patient Throughput in the Emergency Department To: Jennifer Holmes, Director of Operations, Emergency Department Sam Clark,
University of Michigan Health System Program and Operations Analysis Improving Patient Throughput in the Emergency Department To: Jennifer Holmes, Director of Operations, Emergency Department Sam Clark,
Customer Situation Solution Benefits
 Trident Case Study GE Centricity * Imaging Analytics Real-time Dashboard helps Trident Medical Center improve radiology department efficiency and productivity Customer Trident Medical Center is a 296-bed
Trident Case Study GE Centricity * Imaging Analytics Real-time Dashboard helps Trident Medical Center improve radiology department efficiency and productivity Customer Trident Medical Center is a 296-bed
Example 1: Self-Management: Development of a Self-Management form, Part 1
 PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Blue Care Network Physical & Occupational Therapy Utilization Management Guide
 Blue Care Network Physical & Occupational Therapy Utilization Management Guide (Also applies to physical medicine services by chiropractors) January 2016 Table of Contents Program Overview... 1 Physical
Blue Care Network Physical & Occupational Therapy Utilization Management Guide (Also applies to physical medicine services by chiropractors) January 2016 Table of Contents Program Overview... 1 Physical
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Grants to Institutions
 Grants to Institutions A Guide to Administrative Procedures Grant Administration Division Introduction IDRC accountability Management philosophy Recipient accountability Technical reporting Financial reporting
Grants to Institutions A Guide to Administrative Procedures Grant Administration Division Introduction IDRC accountability Management philosophy Recipient accountability Technical reporting Financial reporting
HEALTH WORKFORCE SUPPLY AND REQUIREMENTS PROJECTION MODELS. World Health Organization Div. of Health Systems 1211 Geneva 27, Switzerland
 HEALTH WORKFORCE SUPPLY AND REQUIREMENTS PROJECTION MODELS World Health Organization Div. of Health Systems 1211 Geneva 27, Switzerland The World Health Organization has long given priority to the careful
HEALTH WORKFORCE SUPPLY AND REQUIREMENTS PROJECTION MODELS World Health Organization Div. of Health Systems 1211 Geneva 27, Switzerland The World Health Organization has long given priority to the careful
National Cancer Patient Experience Survey National Results Summary
 National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
EHR Implementation Best Practices. EHR White Paper
 EHR White Paper EHR Implementation Best Practices An EHR implementation that increases efficiencies versus an EHR that is underutilized, abandoned or replaced. pulseinc.com EHR Implementation Best Practices
EHR White Paper EHR Implementation Best Practices An EHR implementation that increases efficiencies versus an EHR that is underutilized, abandoned or replaced. pulseinc.com EHR Implementation Best Practices
Real-time adjudication: an innovative, point-of-care model to reduce healthcare administrative and medical costs while improving beneficiary outcomes
 Real-time adjudication: an innovative, point-of-care model to reduce healthcare administrative and medical costs while improving beneficiary outcomes Provided by Conexia Inc Section 1: Company information
Real-time adjudication: an innovative, point-of-care model to reduce healthcare administrative and medical costs while improving beneficiary outcomes Provided by Conexia Inc Section 1: Company information
Administrative Form 1 4/20/2013 Version 1.1
 TRINITY ALLERGY, ASTHMA AND IMMUNOLOGY CARE, P.C. NATARAJAN ASOKAN, M.D. 3931 Stockton Hill Road, Suite D, Kingman, AZ 86409 Tel. 928-681-5800 Fax. 928-681-5801 1971 Highway 95, Bullhead City, AZ 86442
TRINITY ALLERGY, ASTHMA AND IMMUNOLOGY CARE, P.C. NATARAJAN ASOKAN, M.D. 3931 Stockton Hill Road, Suite D, Kingman, AZ 86409 Tel. 928-681-5800 Fax. 928-681-5801 1971 Highway 95, Bullhead City, AZ 86442
National Patient Experience Survey UL Hospitals, Nenagh.
 National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Chubb Healthcare Physician Office Practice Self-Assesment Tool
 1 Chubb Healthcare Physician Office Practice Self-Assesment Tool As the delivery of healthcare continues to change and evolve, physician office practices are increasingly being acquired and integrated
1 Chubb Healthcare Physician Office Practice Self-Assesment Tool As the delivery of healthcare continues to change and evolve, physician office practices are increasingly being acquired and integrated
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
University of Michigan Health System
 University of Michigan Health System Program and Operations Analysis Utilization Study of Linear Accelerators in the Radiation Oncology Department Project Report To: Kathy Lash: Director of Operations
University of Michigan Health System Program and Operations Analysis Utilization Study of Linear Accelerators in the Radiation Oncology Department Project Report To: Kathy Lash: Director of Operations
Michigan Medicine--Frankel Cardiovascular Center. Determining Direct Patient Utilization Costs in the Cardiovascular Clinic.
 Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
ESSAYS ON EFFICIENCY IN SERVICE OPERATIONS: APPLICATIONS IN HEALTH CARE
 Purdue University Purdue e-pubs RCHE Presentations Regenstrief Center for Healthcare Engineering 8-8-2007 ESSAYS ON EFFICIENCY IN SERVICE OPERATIONS: APPLICATIONS IN HEALTH CARE John B. Norris Purdue University
Purdue University Purdue e-pubs RCHE Presentations Regenstrief Center for Healthcare Engineering 8-8-2007 ESSAYS ON EFFICIENCY IN SERVICE OPERATIONS: APPLICATIONS IN HEALTH CARE John B. Norris Purdue University
2013 Call for Proposals. Canadian Breast Cancer Foundation (CBCF) Canadian Institutes of Health Research (CIHR)
 Canadian Institutes of Health Research (CIHR)") 2013 Call for Proposals Canadian Breast Cancer Foundation (CBCF) Canadian Institutes of Health Research (CIHR) Breast Cancer in Young Women Research Program Overview The Canadian Breast Cancer Foundation
2013 Call for Proposals Canadian Breast Cancer Foundation (CBCF) Canadian Institutes of Health Research (CIHR) Breast Cancer in Young Women Research Program Overview The Canadian Breast Cancer Foundation
Maryland MOLST FAQs. Maryland MOLST Training Task Force
 Maryland MOLST FAQs Maryland MOLST Training Task Force October 2017 Frequently Asked Questions About Maryland MOLST What does MOLST stand for? MOLST is an acronym that stands for Medical Orders for Life-Sustaining
Maryland MOLST FAQs Maryland MOLST Training Task Force October 2017 Frequently Asked Questions About Maryland MOLST What does MOLST stand for? MOLST is an acronym that stands for Medical Orders for Life-Sustaining
Occupation Description: Responsible for providing nursing care to residents.
 NOC: 3152 (2011 NOC is 3012) Occupation: Registered Nurse Occupation Description: Responsible for providing nursing care to residents. Key essential skills are: Document Use, Oral Communication, Problem
NOC: 3152 (2011 NOC is 3012) Occupation: Registered Nurse Occupation Description: Responsible for providing nursing care to residents. Key essential skills are: Document Use, Oral Communication, Problem
PANELS AND PANEL EQUITY
 PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
GP appointments systems in Coventry
 GP appointments systems in Coventry Good practice examples October 2010 Tel: 024 7622 0381. Fax: 024 7625 7720 Email coventrylink@vacoventry.org.uk Website: www.coventrylink.org.uk Contents Introduction
GP appointments systems in Coventry Good practice examples October 2010 Tel: 024 7622 0381. Fax: 024 7625 7720 Email coventrylink@vacoventry.org.uk Website: www.coventrylink.org.uk Contents Introduction
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
4.09. Hospitals Management and Use of Surgical Facilities. Chapter 4 Section. Background. Follow-up on VFM Section 3.09, 2007 Annual Report
 Chapter 4 Section 4.09 Hospitals Management and Use of Surgical Facilities Follow-up on VFM Section 3.09, 2007 Annual Report Background Ontario s public hospitals are generally governed by a board of directors
Chapter 4 Section 4.09 Hospitals Management and Use of Surgical Facilities Follow-up on VFM Section 3.09, 2007 Annual Report Background Ontario s public hospitals are generally governed by a board of directors
INFUSION CENTER OPERATIONAL IMPROVEMENT: MAXIMIZING THE PATIENT THROUGHPUT OF INFUSION CENTERS
 THOUGHT LEADERSHIP SERIES TACTICAL REPORT INFUSION CENTER OPERATIONAL IMPROVEMENT: MAXIMIZING THE PATIENT THROUGHPUT OF INFUSION CENTERS The demand for cancer services has never been higher, and is expected
THOUGHT LEADERSHIP SERIES TACTICAL REPORT INFUSION CENTER OPERATIONAL IMPROVEMENT: MAXIMIZING THE PATIENT THROUGHPUT OF INFUSION CENTERS The demand for cancer services has never been higher, and is expected
GENERAL DENTIST. Dental Receptionist Manual
 GENERAL DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
GENERAL DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
PEDIATRIC DENTIST. Dental Receptionist Manual
 PEDIATRIC DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
PEDIATRIC DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
ORAL EXAMINATION CANDIDATE GUIDELINES AMERICAN BOARD OF OTOLARYNGOLOGY
 ORAL EXAMINATION CANDIDATE GUIDELINES AMERICAN BOARD OF OTOLARYNGOLOGY INTRODUCTION The purpose of the oral examination is to evaluate the candidate s knowledge and reasoning skills to obtain and interpret
ORAL EXAMINATION CANDIDATE GUIDELINES AMERICAN BOARD OF OTOLARYNGOLOGY INTRODUCTION The purpose of the oral examination is to evaluate the candidate s knowledge and reasoning skills to obtain and interpret
SPECIALIZED FOSTER CARE GUIDELINES MANUAL
 DEPARTMENT OF MENTAL HEALTH CHILD WELFARE DIVISION SPECIALIZED FOSTER CARE GUIDELINES MANUAL SECTION 4: DMH PARTICIPATION IN THE DCFS CSAT PROCESS I. PURPOSE This release issues procedural guidelines for
DEPARTMENT OF MENTAL HEALTH CHILD WELFARE DIVISION SPECIALIZED FOSTER CARE GUIDELINES MANUAL SECTION 4: DMH PARTICIPATION IN THE DCFS CSAT PROCESS I. PURPOSE This release issues procedural guidelines for
Smethwick & Hollybush Medical Centres Patient Participation Report 2012/2013
 Smethwick & Hollybush Medical Centres Patient Participation Report 2012/2013 Under initiatives issued by the Department of Health in 2011, GP Practices were asked to form Patient Participation Groups (PPGs
Smethwick & Hollybush Medical Centres Patient Participation Report 2012/2013 Under initiatives issued by the Department of Health in 2011, GP Practices were asked to form Patient Participation Groups (PPGs
A Publication for Hospital and Health System Professionals
 A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
ROTATION DESCRIPTION - PGY1 Adult Internal Medicine
 ROTATION DESCRIPTION - PGY1 Adult Internal Medicine PURPOSE The IM rotation provides the opportunity for PGY1 residents to improve their knowledge base and pharmacotherapeutic skills while enhancing care
ROTATION DESCRIPTION - PGY1 Adult Internal Medicine PURPOSE The IM rotation provides the opportunity for PGY1 residents to improve their knowledge base and pharmacotherapeutic skills while enhancing care
Full-time Equivalents and Financial Costs Associated with Absenteeism, Overtime, and Involuntary Part-time Employment in the Nursing Profession
 Full-time Equivalents and Financial Costs Associated with Absenteeism, Overtime, and Involuntary Part-time Employment in the Nursing Profession A Report prepared for the Canadian Nursing Advisory Committee
Full-time Equivalents and Financial Costs Associated with Absenteeism, Overtime, and Involuntary Part-time Employment in the Nursing Profession A Report prepared for the Canadian Nursing Advisory Committee
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
Pennsylvania Patient and Provider Network (P3N)
") Pennsylvania Patient and Provider Network (P3N) Cross-Boundary Collaboration and Partnerships Commonwealth of Pennsylvania David Grinberg, Deputy Executive Director 717-214-2273 dgrinberg@pa.gov Project
Pennsylvania Patient and Provider Network (P3N) Cross-Boundary Collaboration and Partnerships Commonwealth of Pennsylvania David Grinberg, Deputy Executive Director 717-214-2273 dgrinberg@pa.gov Project
ADMINISTRATIVE SUMMARY OF INVESTIGATION BY THE VA OFFICE OF INSPECTOR GENERAL IN RESPONSE TO ALLEGATIONS REGARDING PATIENT WAIT TIMES
 ADMINISTRATIVE SUMMARY OF INVESTIGATION BY THE VA OFFICE OF INSPECTOR GENERAL IN RESPONSE TO ALLEGATIONS REGARDING PATIENT WAIT TIMES VA Medical Center in Wilmington, Delaware March 1, 2016 1. Summary
ADMINISTRATIVE SUMMARY OF INVESTIGATION BY THE VA OFFICE OF INSPECTOR GENERAL IN RESPONSE TO ALLEGATIONS REGARDING PATIENT WAIT TIMES VA Medical Center in Wilmington, Delaware March 1, 2016 1. Summary
The Practice Standards for Medical Imaging and Radiation Therapy. Quality Management Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Quality Management Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
The Practice Standards for Medical Imaging and Radiation Therapy Quality Management Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care. Harold D. Miller
 Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
INTEGRATION OF PRIMARY HEALTH CARE NURSE PRACTITIONERS INTO EMERGENCY DEPARTMENTS
 INTEGRATION OF PRIMARY HEALTH CARE NURSE PRACTITIONERS INTO EMERGENCY DEPARTMENTS Section I Facilitators Reasons for integrating the Nurse Practitioner into the Emergency Department 1. Please consider
INTEGRATION OF PRIMARY HEALTH CARE NURSE PRACTITIONERS INTO EMERGENCY DEPARTMENTS Section I Facilitators Reasons for integrating the Nurse Practitioner into the Emergency Department 1. Please consider
Using discrete event simulation to improve the patient care process in the emergency department of a rural Kentucky hospital.
 University of Louisville ThinkIR: The University of Louisville's Institutional Repository Electronic Theses and Dissertations 6-2013 Using discrete event simulation to improve the patient care process
University of Louisville ThinkIR: The University of Louisville's Institutional Repository Electronic Theses and Dissertations 6-2013 Using discrete event simulation to improve the patient care process
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
UWDRO RESIDENT SUPERVISION POLICY
 Roles, Responsibilities and Patient Care Activities of Residents UNIVERSITY OF WASHINGTON RADIATION ONCOLOGY RESIDENT EDUCATION PROGRAM UNIVERSITY OF WASHINGTON MEDICAL CENTER HARBORVIEW MEDICAL CENTER
Roles, Responsibilities and Patient Care Activities of Residents UNIVERSITY OF WASHINGTON RADIATION ONCOLOGY RESIDENT EDUCATION PROGRAM UNIVERSITY OF WASHINGTON MEDICAL CENTER HARBORVIEW MEDICAL CENTER
The Practice Standards for Medical Imaging and Radiation Therapy. Radiation Therapy Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Radiation Therapy Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
The Practice Standards for Medical Imaging and Radiation Therapy Radiation Therapy Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
Lily M. Gutmann, Ph.D., CYT Licensed Psychologist 4405 East West Highway #512 Bethesda, MD (301)
") Lily M. Gutmann, Ph.D., CYT Licensed Psychologist 4405 East West Highway #512 Bethesda, MD 20814 (301) 996-0165 www.littlefallscounseling.com PRACTICE POLICIES AND CONSENT TO TREATMENT WELCOME Welcome
Lily M. Gutmann, Ph.D., CYT Licensed Psychologist 4405 East West Highway #512 Bethesda, MD 20814 (301) 996-0165 www.littlefallscounseling.com PRACTICE POLICIES AND CONSENT TO TREATMENT WELCOME Welcome
Lean Options for Walk-In, Open Access, and Traditional Appointment Scheduling in Outpatient Health Care Clinics
 Lean Options for Walk-In, Open Access, and Traditional Appointment Scheduling in Outpatient Health Care Clinics Mayo Clinic Conference on Systems Engineering & Operations Research in Health Care Rochester,
Lean Options for Walk-In, Open Access, and Traditional Appointment Scheduling in Outpatient Health Care Clinics Mayo Clinic Conference on Systems Engineering & Operations Research in Health Care Rochester,
Accreditation Beta Test Quality Improvement Project CENTRAL VALLEY HEALTH DISTRICT ENVIRONMENTAL HEALTH SERVICES IMPROVEMENT
 ENVIRONMENTAL HEALTH SERVICES IMPROVEMENT This report was completed by: Robin Iszler, Kali Lautt, Brenton Nesemeier EXECUTIVE SUMMARY Central Valley Health District (CVHD) is a two-county health department
ENVIRONMENTAL HEALTH SERVICES IMPROVEMENT This report was completed by: Robin Iszler, Kali Lautt, Brenton Nesemeier EXECUTIVE SUMMARY Central Valley Health District (CVHD) is a two-county health department