North Carolina College of Emergency Physicians Standards Policy Air Transport
|
|
|
- Lynn Griffin
- 6 years ago
- Views:
Transcription

1
2 Policy: North Carolina College of Emergency Physicians Air Transport Trauma system patients should be transported to the closest trauma center by the most effective means, as specified in this policy. Air transport should be utilized whenever patient care can be improved by decreasing transport time to the closest trauma center. Improve patient outcome by means of effective and timely transport to the most appropriate medical facility. Allow for expedient transport in serious, mass casualty settings. Trauma patients who meet one or more of the following triage criteria should be transported to the closest trauma center (CaroMont Regional Medical Center, Carolinas Medical Center, or Cleveland Regional Medical Center): Physiologic criteria: o Glasgow Coma Scale of less than 14. o Systolic BP of less than 90. o Respiratory rate of less than 10 or greater than 29, or less than 20 in an infant under 1 year old. Anatomical criteria: o Penetrating injuries to the head, neck, torso, or extremities proximal to the elbow or knee. o Flail chest. o Two or more proximal long bone fractures. o Crushed, degloved, or mangled extremity. o Amputation proximal to the wrist or the ankle. o Pelvic fracture. o Open or depressed skull fracture. o Paralysis. Mechanism of Injury criteria: o Falls greater than 20 feet (adult). o Falls greater than 10 feet or 2-3 times patient height (child). o MVC: Intrusion greater than 12 inches into patient side of the vehicle or greater than 18 inches into any side of the vehicle. Ejection (partial or complete) from a vehicle. Death of an occupant in the same passenger compartment. Vehicle telemetry data consistent with high risk injury. Auto vs. pedestrian, Bicyclist thrown, Patient run over, OR significant (>20 mph) impact. Motorcycle crash >20 mph Other criteria for Trauma Center transport: o Age less than 12 or greater than 55. o Anticoagulation and bleeding disorders. o Burns. o Time sensitive extremity injury. o End stage renal disease requiring dialysis. o Pregnancy greater than 20 weeks. o EMS provider judgment. Policy 1 (Page 1 of 2)
3 Transport method: North Carolina College of Emergency Physicians Air Transport Patients will be transported to the closest Trauma Center by ground ambulance if that Trauma Center can be reached in less than 60 minutes. Air Medical Transport should be utilized if the closest Trauma Center cannot be reached by ground in less than 60 minutes and pre-hospital time would be reduced. Air Medical Transport may also be used for medical or trauma patients during a multiple casualty incident with multiple patients triaged red. Policy 1 (Page 2 of 2)
4 Policy: North Carolina College of Emergency Physicians Child Abuse Recognition and Reporting Child abuse is the physical and mental injury, sexual abuse, negligent treatment, or maltreatment of a child under the age of 18 by a person who is responsible for the child s welfare. The recognition of abuse and the proper reporting is a critical step to improving the safety of children and preventing child abuse. Assessment of a child abuse case based upon the following principles: Protect the life of the child from harm, as well as that of the EMS team from liability. Suspect that the child may be a victim of abuse, especially if the injury/illness is not consistent with the reported history. Respect the privacy of the child and family. Collect as much evidence as possible, especially information. 1. With all children, assess for and document psychological characteristics of abuse, including excessively passivity, compliant or fearful behavior, excessive aggression, violent tendencies, excessive crying, fussy behavior, hyperactivity, or other behavioral disorders 2. With all children, assess for and document physical signs of abuse, including especially any injuries that are inconsistent with the reported mechanism of injury. 3. With all children, assess for and document signs and symptoms of neglect, including inappropriate level of clothing for weather, inadequate hygiene, absence of attentive caregiver(s), or physical signs of malnutrition. 4. Immediately report any suspicious findings to both the receiving hospital (if transported) and Gaston County DSS Child Protective Services. After office hours, the child protective services worker on call can be contacted by the EMS System s 911 communications center. While law enforcement may also be notified, North Carolina law requires the EMS provider to report the suspicion of abuse to DSS. EMS should not accuse or challenge the suspected abuser. This is a legal requirement to report, not an accusation. In the event of a child fatality, law enforcement must also be notified. After transfer of patient to facility, crew must contact On Duty Operations Supervisor to advise them of the situation. Policy 2
5 Policy: North Carolina College of Emergency Physicians Child with Special Health Care Needs (NC Kidbase) Medical technology, changes in the healthcare industry, and increased home health capabilities have created a special population of patients that interface with the EMS system. It is important for EMS to understand and provide quality care to children with special health care needs. The purpose of this policy is to: Provide quality patient care and EMS services to children with special health care needs. Understand the need to communicate with the parents and caregivers regarding healthcare needs and devices that EMS may not have experience with. Promote, request, and use the Kidbase form, which catalogs the health care problems, needs, and issues of each child with a special healthcare need. 1. Caregivers who call 911 to report an emergency involving a child with special health care needs may report that the emergency involves a Kidbase child (if they are familiar with the NC Kidbase program) or may state that the situation involves a special needs child. 2. Responding EMS personnel should ask the caregiver of a special needs child for a copy of the Kidbase Form, which is the North Carolina terminology for the Emergency Information Form (EIF). 3. EMS personnel may choose to contact the child s primary care physician for assistance with specific conditions or devices or for advice regarding appropriate treatment and/or transport of the child in the specific situation. 4. Transportation of the child will be made to the hospital appropriate for the specific condition of the child. In some cases this may involve bypassing the closest facility for a more distant yet more medically appropriate destination (with Medical Control authorization.) Policy 3
6 Policy: North Carolina College of Emergency Physicians Criteria for Death / Withholding Resuscitation CPR and ALS treatment are to be withheld only if the patient is obviously dead or a valid North Carolina MOST and/or Do Not Resuscitate form (see separate policy) is present. The purpose of this policy is to: Honor those who have obviously expired prior to EMS arrival. 1. If a patient is in complete cardiopulmonary arrest (clinically dead) and meets one or more of the criteria below, CPR and ALS therapy need not be initiated: Body decomposition Rigor mortis Dependent lividity Blunt force trauma with high mechanism of injury Injury not compatible with life (i.e., decapitation, burned beyond recognition, massive open or penetrating trauma to the head or chest with obvious organ destruction) 2. If a bystander or first responder has initiated CPR or automated defibrillation prior to an EMS paramedic s arrival and any of the above criteria (signs of obvious death) are present, the paramedic may discontinue CPR and ALS therapy. All other EMS personnel levels must communicate with medical control prior to discontinuation of the resuscitative efforts. 3. If doubt exists, start resuscitation immediately. Once resuscitation is initiated, continue resuscitation efforts until either: a) Resuscitation efforts meet the criteria for implementing the Discontinuation of Prehospital Resuscitation Policy (see separate policy) b) Patient care responsibilities are transferred to the destination hospital staff. Policy 4
7 North Carolina College of Emergency Physicians Deceased Subjects Policy: EMS will handle the disposition of deceased subjects in a uniform, professional, and timely manner. All personnel must follow the procedures outlined in GEMS SOP The purpose of this policy is to: Organize and provide for a timely disposition of any deceased subject Maintain respect for the deceased and the family Allow EMS to return to service in a timely manner. 1. Do not remove lines or tubes from unsuccessful cardiac arrests/codes unless directed below. 2. Notify the law enforcement agency with jurisdiction if applicable. 3. If subject was found deceased by EMS, the scene is turned over to law enforcement. 4. If EMS has attempted to resuscitate the patient and then terminated the resuscitative efforts, the EMS personnel should contact the family physician (medical cases) or medical examiner (traumatic cases or family physician unavailable) to provide information about the resuscitative efforts. 5. Transport arrangements should be made in concert with law enforcement and the family s wishes. 6. If the deceased subject s destination is other than the county morgue, any line(s) or tube(s) placed by EMS should be removed prior to transport. 7. Document the situation, name of Physician or Medical Examiner contacted, the agency providing transport of the deceased subject, and the destination on the patient care report form (PCR). Policy 5
8 Policy: North Carolina College of Emergency Physicians Discontinuation of Prehospital Resuscitation Unsuccessful cardiopulmonary resuscitation (CPR) and other advanced life support (ALS) interventions will be discontinued prior to transport when this procedure is followed. The purpose of this policy is to: Allow for discontinuation of prehospital resuscitation after the delivery of adequate and appropriate ALS therapy. 1. Discontinuation of CPR and ALS intervention may be implemented AFTER contact with Medical Control if ALL of the following criteria have been met: Patient must be 18 years of age or older Adequate CPR has been administered Airway has been successfully managed with verification of device placement. Acceptable management techniques include orotracheal intubation, nasotracheal intubation, Blind Insertion Airway Device (BIAD) placement, or cricothyrotomy IV or IO access has been achieved No evidence or suspicion of any of the following: -Drug/toxin overdose -Active internal bleeding -Hypothermia -Preceding trauma Rhythm appropriate medications and defibrillation have been administered according to local EMS Protocols for a total of 3 cycles of drug therapy without return of spontaneous circulation (palpable pulse) All EMS paramedic personnel involved in the patient s care agree that discontinuation of the resuscitation is appropriate 2. The Deceased Subjects Policy should be followed. Document all patient care and interactions with the patient s family, staff, personal physician, medical examiner, law enforcement, and medical control in the EMS patient care report (PCR). Policy 6
9 Policy: North Carolina College of Emergency Physicians Disposition (Patient Instructions) All patient encounters responded to by EMS will result in the accurate and timely completion of: The Patient Care Report (PCR) for all patients transported by EMS The Patient Disposition Form for all patients not transported by EMS To provide for the documentation of: The evaluation and care of the patient The patient s refusal of the evaluation, treatment, and/or transportation The patient s disposition instructions The patient s EMS encounter to protect the local EMS system and its personnel from undue risk and liability. 1. All patient encounters, which result in some component of an evaluation, must have a Patient Care Report completed. 2. All patients who refuse any component of the evaluation or treatment, based on the complaint, must have a Gaston County EMS refusal/well uninjured form completed. (See Appendix R) 3. All patients who are NOT transported by EMS must be given a Gaston County EMS Non-Transport Disposition Instructions. (See Appendix S) Policy 7
10 Policy: North Carolina College of Emergency Physicians North Carolina Do Not Resuscitate and MOST Form Any patient presenting to any component of the EMS system with a completed North Carolina Do Not Resuscitate (DNR) form (yellow form) and/or MOST (Medical Orders for Scope of Treatment) form (bright pink form) shall have the form honored. Treatment will be limited as documented on the DNR or MOST form. To honor the terminal wishes of the patient To prevent the initiation of unwanted resuscitation 1. When confronted with a patient or situation involving the NC DNR and/or MOST form(s), the following form content must be verified before honoring the form(s) request. The form(s) must be an original North Carolina DNR form (yellow form - not a copy) and/or North Carolina MOST form (bright pink not a copy) The effective date and expiration date must be completed and current The DNR and/or MOST Form must be signed by a physician, physician s assistant, or nurse practitioner. 2. A valid DNR or MOST form may be overridden by the request of: The patient The guardian of the patient An on-scene physician If the patient or anyone associated with the patient requests that a NC DNR and/or MOST form not be honored, EMS personnel should contact Medical Control to obtain assistance and direction 3. A living will or other legal document that identifies the patient s desire to withhold CPR or other medical care may be honored with the approval of Medical Control. This should be done when possible in consultation with the patient s family and personal physician. Policy 8
11 Page Intentionally Left Blank
12 Policy: North Carolina College of Emergency Physicians EMS Documentation and Data Quality The complete EMS documentation associated with an EMS events service delivery and patient care shall be electronically recorded into a Patient Care Report (PCR) within 24 hours of the completion of the EMS event with an average EMS Data Score of 5 or less. Definition: The EMS documentation of a Patient Care Report (PCR) is based on the appropriate and complete documentation of the EMS data elements as required and defined within the North Carolina College of Emergency Physician s EMS Standards ( Since each EMS event and/or patient scenario is unique, only the data elements relevant to that EMS event and/or patient scenario should be completed. The EMS Data Score is calculated on each EMS PCR as it is electronically processed into the North Carolina PreHospital Medical Information System (PreMIS). Data Quality Scores are provided within PreMIS and EMS Toolkit Reports. The best possible score is a 0 (zero) and with each data quality error a point is added to the data quality score. A complete Patient Care Report (PCR) must contain the following information (as it relates to each EMS event and/or patient): Service delivery and Crew information regarding the EMS Agency s response Dispatch information regarding the dispatch complaint, and EMD card number Patient care provided prior to EMS arrival Patient Assessment as required by each specific complaint based protocol Past medical history, medications, allergies, and DNR/MOST status Trauma and Cardiac Arrest information if relevant to the EMS event or patient All times related to the event All procedures and their associated time All medications administered with their associated time Disposition and/or transport information Communication with medical control Appropriate Signatures (written and/or electronic) The purpose of this policy is to: Promote timely and complete EMS documentation. Promote quality documentation that can be used to evaluate and improve EMS service delivery, personnel performance, and patient care to the county s citizens. Promote quality documentation that will decrease EMS legal and risk management liability. Provide a means for continuous evaluation to assure policy compliance. Policy 9 (Page 1 of 2)
13 North Carolina College of Emergency Physicians EMS Documentation and Data Quality The following procedures shall be implemented to assure policy compliance: 1. The EMS Patient Care Report (PCR) shall be completed as soon as possible after the time of the patient encounter. Documentation should be completed prior to leaving the destination facility unless call demand dictates otherwise, in which case documentation must be completed prior to the end of the personnel s shift. 2. A copy of the patient care report form SHOULD be provided to the receiving medical facility. If the final PCR is not available at the time the patient is left with the emergency department or other healthcare facility, an interim report such as the PreMIS Preliminary Report Form MUST be provided. 3. The PCR must be completed in the PreMIS System or electronically submitted to the PreMIS System within 24 hours of the EMS event or patient encounter s completion. The EMS data quality feedback provided at the time of the electronic submission into PreMIS should be reviewed and when possible any identified errors will be corrected within each PCR. Each PCR may be electronically resubmitted to PreMIS as many times as needed. 4. The EMS Data Quality Scores for the EMS System, EMS Agency, and individual EMS personnel will be reviewed regularly within the EMS System Peer Review Committee. Policy 9 (Page 2 of 2)
14 Policy: North Carolina College of Emergency Physicians Documentation of Vital Signs Every patient encounter by EMS will be documented. Vital signs are a key component in the evaluation of any patient and a complete set of vital signs is to be documented for any patient who receives some assessment component. To insure: Evaluation of every patient s volume and cardiovascular status Documentation of a complete set of vital signs 1. An initial complete set of vital signs includes: Pulse rate Manual systolic AND diastolic blood pressure Respiratory rate Pain / severity (when appropriate to patient complaint) GCS for Injured Patients 2. When no ALS treatment is provided, palpated blood pressures are acceptable for REPEAT vital signs. 3. Based on patient condition and complaint, vital signs may also include: Pulse Oximetry Temperature End Tidal CO2 Breath Sounds Level of Response 4. If the patient refuses this evaluation, the patient s mental status and the reason for refusal of evaluation must be documented. A Gaston County refusal/well uninjured form must be completed and a Gaston County Non-Transport Disposition Instructions Form must be given. 5. Document situations that preclude the evaluation of a complete set of vital signs. 6. Complete set of Vital Signs MUST be obtained at least every 5 minutes for unstable patients and at least every 15 minutes for stable patients. Record the time that each set of vital signs are obtained. 7. Any abnormal vital sign should be repeated and monitored closely. Policy 10
15 Policy: North Carolina College of Emergency Physicians Domestic Violence (Partner and/or Elder Abuse) Recognition and Reporting Domestic violence is physical, sexual, or psychological abuse and/or intimidation, which attempts to control another person in a current or former family, dating, or household relationship. The recognition, appropriate reporting, and referral of abuse is a critical step to improving patient safety, providing quality health care, and preventing further abuse. Elder abuse is the physical and/or mental injury, sexual abuse, negligent treatment, or maltreatment of a senior citizen by another person. Abuse may be at the hand of a caregiver, spouse, neighbor, or adult child of the patient. The recognition of abuse and the proper reporting is a critical step to improve the health and wellbeing of senior citizens. Assessment of an abuse case based upon the following principles: Protect the patient from harm, as well as protecting the EMS team from harm and liability. Suspect that the patient may be a victim of abuse, especially if the injury/illness is not consistent with the reported history. Respect the privacy of the patient and family. Collect as much information and evidence as possible and preserve physical evidence. 1. Assess the/all patient(s) for any psychological characteristics of abuse, including excessive passivity, compliant or fearful behavior, excessive aggression, violent tendencies, excessive crying, behavioral disorders, substance abuse, medical non-compliance, or repeated EMS requests. This is typically best done in private with the patient. 2. Assess the patient for any physical signs of abuse, especially any injuries that are inconsistent with the reported mechanism of injury. Defensive injuries (e.g. to forearms), and injuries during pregnancy are also suggestive of abuse. Injuries in different stages of healing may indicate repeated episodes of violence. 3. Assess all patients for signs and symptoms of neglect, including inappropriate level of clothing for weather, inadequate hygiene, absence of attentive caregiver(s), or physical signs of malnutrition. 4. Immediately report any suspicious findings to both the receiving hospital (if transported). If an elder or disabled adult is involved, also contact the Gaston County DSS Adult Protective Services. After office hours, the adult protective services worker on call can be contacted by the 911 communications center. 5. EMS personnel should attempt in private to provide the patient with the phone number of the local domestic violence program, or the National Hotline, SAFE. Policy 11
16 Policy: North Carolina College of Emergency Physicians EMS Back in Service Time All EMS Units transporting a patient to a medical facility shall transfer the care of the patient and complete all required operational tasks to be back in service for the next potential EMS event within 20 minutes of arrival to the medical facility. (Goal is 90% of the time.) Definition: The EMS Back in Service Time is defined as the time interval beginning with the time the transporting EMS Unit arrives at the medical facility destination and ending with the time the EMS Unit checks back in service and available for the next EMS event. The purpose of this policy is to: Assure that the care of each EMS patient transported to a medical facility is transferred to the medical facility staff in a timely manner. Assure that the EMS unit is cleaned, disinfected, restocked, and available for the next EMS event in a timely manner. Assure that an interim or complete EMS patient care report (PCR) is completed and left with the receiving medical facility documenting, at a minimum, the evaluation and care provided by EMS for that patient (It is acceptable to leave the PreMIS Preliminary Report or equivalent if the final PCR cannot be completed before leaving the facility). Provide quality EMS service and patient care to the county s citizens. Provide a means for continuous evaluation to assure policy compliance. The following procedures shall be implemented to assure policy compliance: 1. The EMS Unit s priority upon arrival at the medical facility will be to transfer the care of the patient to medical facility staff as soon as possible. 2. EMS personnel will provide a verbal patient report on to the receiving medical facility staff. 3. EMS personnel will provide an interim (PreMIS Preliminary Report or equivalent) or final Patient Care Report (PCR) to the receiving medical facility staff, prior to leaving the facility, that documents at a minimum the patient s evaluation and care provided by EMS prior to arrival at the medical facility. A complete PCR should be completed as soon as possible but should not cause a delay in the EMS Back in Service Time. 4. The EMS Unit will be cleaned, disinfected, and restocked (if necessary) during the EMS Back in Service Time interval. 5. Any EMS Back in Service Time delay resulting in a prolonged EMS Back in Service Time will be documented in Patient Care Report (PCR) as an EMS Turn-Around Delay as required and defined in the North Carolina College of Emergency Physicians (NCCEP) EMS Dataset Standards Document. 6. All EMS Turn-Around Delays will be reviewed regularly within the EMS System Peer Review Committee. Policy 12
17 Page Intentionally Left Blank
18 Policy: North Carolina College of Emergency Physicians EMS Dispatch Center Time The EMS Dispatch Center Time will be less than 90 seconds for all events identified and classified as an emergent or hot (with lights and siren) response. (Goal is 90% of the time) Definition: The EMS Dispatch Center Time is defined as the time interval beginning with the time of the initial 911 phone pickup at the 911 Communications Center requesting emergency medical services and ending with the dispatch time of the EMS Unit responding to the event. The purpose of this policy is to: Provide the safest and most appropriate level of response to all EMS events within the EMS System. Provide a timely and reliable response for all EMS events within the EMS System. Provide quality EMS service and patient care to the county s citizens. Provide a means for continuous evaluation to assure policy compliance. The following procedures shall be implemented to assure policy compliance: 1. A public calls into the 911 Communications Center requesting emergency medical assistance will never be required to speak with more than two persons before a formal EMS Unit is dispatched. 2. In EMS Dispatch Centers where Emergency Medical Dispatch (EMD) has been implemented, EMS Units will be dispatched by EMD certified personnel in accordance with the standards developed by the Medical Director and the Emergency Medical Dispatch Protocols. 3. EMS Units will be dispatched hot (with lights and sirens) or cold (no lights and sirens) by the 911 Call Center based on predetermined criteria. If First Responders are dispatched as a component of the EMS response, they should typically be dispatched hot (with lights and sirens). 4. Without question, exception, or hesitation, EMS Units will respond as dispatched (hot or cold). This includes both requests to respond on active calls and requests to move-up to cover areas of the System that have limited EMS resources available. 5. EMS Units may, at their discretion, request for a First Responder on Non-First Responder calls in situations where additional resources are required such as manpower, extreme response time of the EMS Unit, need for forcible entry, etc. Policy 13 (Page 1 of 2)
19 North Carolina College of Emergency Physicians EMS Dispatch Center Time 6. EMS Units dispatched with a cold (no lights and sirens) response, will not upgrade to a hot (with lights and sirens) response UNLESS: Public Safety personnel on-scene requests a hot (with lights and sirens) response. Communications Center determines that the patient s condition has changed, and requests you to upgrade to a hot (with lights and sirens) response. 7. An EMS Unit may divert from a current cold (no lights and sirens) call to a higher priority hot \ (with lights and sirens) call ONLY IF: The EMS Unit can get to the higher priority call before it can reach the lower priority call. Examples of High Priority Calls: Chest Pain, Respiratory Distress, CVA, etc. The diverting EMS Unit must notify the EMS Dispatch Center that they are diverting to the higher priority call. The diverting EMS Unit ensures that the EMS Dispatch Center dispatches an EMS Unit to their original call. Once a call has been diverted, the next EMS Unit dispatched must respond to the original call. A call cannot be diverted more than one (1) time. 8. Any EMS Dispatch Center Time delays resulting in a prolonged EMS Dispatch Center Time for emergent hot (with lights and sirens) events will be documented in Patient Care Report (PCR) as an EMS Dispatch Delay as required and defined in the North Carolina College of Emergency Physicians (NCCEP) EMS Dataset Standards Document. 9. All EMS Dispatch Delays will be reviewed regularly within the Gaston County EMD Audit Review Process. Policy 13 (Page 2 of 2)
20 Policy: North Carolina College of Emergency Physicians EMS Wheels Rolling (Chute) Time The EMS Wheels Rolling (Chute) Time will be less than 60 seconds for all events identified and classified as an emergent or hot (with lights and siren) response. (Goal is 90% of the time.) Definition: The EMS Wheels Rolling (Chute) Time is defined as the time interval beginning with the time the EMS Dispatch Center notifies an EMS Unit to respond to a specific EMS event and ending with the time the EMS Unit is moving en route to the scene of the event. The purpose of this policy is to: Provide a timely and reliable response for all EMS events within the EMS System. Provide quality EMS service and patient care to the county s citizens. Provide a means for continuous evaluation to assure policy compliance. The following procedures shall be implemented to assure policy compliance: 1. In EMS Dispatch Centers where Emergency Medical Dispatch (EMD) has been implemented, EMS Units will be dispatched by EMD certified personnel in accordance with the standards developed by the Medical Director and the Emergency Medical Dispatch Protocols. 2. The EMS Unit Wheels Rolling (Chute) time will be less than 60 seconds from time of dispatch, 90% of the time. If a unit fails to check en route, the next available EMS unit will be dispatched. 3. Without question, exception, or hesitation, EMS Units will respond as dispatched (hot or cold). This includes both requests to respond on active calls and requests to move-up to cover areas of the System that have limited EMS resources available. 4. An EMS Unit may divert from a current cold (no lights and sirens) call to a higher priority hot (with lights and sirens) call ONLY IF: The EMS Unit can get to the higher priority call before it can reach the lower priority call. Examples of High Priority Calls: Chest Pain, Respiratory Distress, CVA, etc. The diverting EMS Unit must notify the EMS Dispatch Center that they are diverting to the higher priority call. The diverting EMS Unit ensures that the EMS Dispatch Center dispatches an EMS Unit to their original call. Once a call has been diverted, the next EMS Unit dispatched must respond to the original call. A call cannot be diverted more than one (1) time. 5. Any EMS Wheels Rolling (Chute) Time delay resulting in a prolonged EMS Response Time for emergent hot (with lights and sirens) events will be documented in Patient Care Report (PCR) as an EMS Response Delay as required and defined in the North Carolina College of Emergency Physicians (NCCEP) EMS Dataset Standards Document. 6. All EMS Response Delays will be reviewed regularly within the EMS System Peer Review Committee. Policy 14
21 North Carolina College of Emergency Physicians Infant Abandonment Policy: The North Carolina Infant Homicide Prevention Act provides a mechanism for unwanted infants to be taken under temporary custody by a law enforcement officer, social services worker, healthcare provider, or EMS personnel if an infant is presented by the parent within 7 days of birth. Emergency Medical Services will accept and protect infants who are presented to EMS in this manner, until custody of the child can be released to the Department of Social Services. A law enforcement officer, a department of social services worker, a health care provider as defined in G.S at a hospital or local or district health department, or an emergency medical technician at a fire station shall, without a court order, take into temporary custody an infant under 7 days of age that is voluntarily delivered to the individual by the infant's parent who does not express an intent to return for the infant. An individual who takes an infant into temporary custody under this subsection shall perform any act necessary to protect the physical health and well-being of the infant and shall immediately notify the department of social services. Any individual who takes an infant into temporary custody under this subsection may inquire as to the parents' identities and as to any relevant medical history, but the parent is not required to provide this information. To provide: Protection to infants that are placed into the custody of EMS under this law Protection to EMS systems and personnel when confronted with this issue 1. Initiate the Pediatric Assessment Procedure. 2. Initiate Newly Born Protocol as appropriate. 3. Initiate other treatment protocols as appropriate. 4. Keep infant warm. 5. Call Gaston County Department of Social Services as soon as infant is stabilized. 6. Transport infant to medical facility as per local protocol. 7. Assure infant is secured in appropriate child restraint device for transport. 8. Document protocols, procedures, and agency notifications in the PCR. Policy 15
22 North Carolina College of Emergency Physicians Patient Without a Protocol Policy: Anyone requesting EMS services will receive a professional evaluation, treatment, and transportation (if needed) in a systematic, orderly fashion regardless of the patient s problem or condition. To ensure the provision of appropriate medical care for every patient regardless of the patient s problem or condition. 1. Treatment and medical direction for all patient encounters, which can be triaged into an EMS patient care protocol, is to be initiated by protocol. 2. When confronted with an emergency or situation that does not fit into an existing EMS patient care protocol, the patient should be treated by the Universal Patient Care Protocol and a Medical Control Physician should be contacted for further instructions. Policy 16
23 North Carolina College of Emergency Physicians Physician on Scene Policy: The medical direction of prehospital care at the scene of an emergency is the responsibility of those most appropriately trained in providing such care. All care should be provided within the rules and regulations of the state of North Carolina. To identify a chain of command to allow field personnel to adequately care for the patient To assure the patient receives the maximum benefit from prehospital care To minimize the liability of the EMS system as well as the on-scene physician 1. When a non medical-control physician offers assistance to EMS or the patient is being attended by a physician with whom they do not have an ongoing patient relationship, EMS personnel must review the On-Scene Physician Form with the physician.(see Appendix P) All requisite documentation must be verified and the physician must be approved by on-line medical control. 2. When the patient is being attended by a physician with whom they have an ongoing patient relationship, EMS personnel may follow orders given by the physician if the orders conform to current EMS guidelines, and if the physician signs the PCR. Notify medical control at the earliest opportunity. Any deviation from local EMS protocols requires the physician to accompany the patient to the hospital. 3. EMS personnel may accept orders from the patient s physician over the phone with the approval of medical control. The paramedic should obtain the specific order and the physician s phone number for relay to medical control so that medical control can discuss any concerns with the physician directly. Policy 17
24 North Carolina College of Emergency Physicians State Poison Center Policy: The state poison center should be utilized by the 911 centers and the responding EMS services to obtain assistance with the prehospital triage and treatment of patients who have a potential or actual poisoning. The purpose of this policy is to: Improve the care of patients with poisonings, envenomations, and environmental/biochemical terrorism exposures in the prehospital setting. Provide for the most timely and appropriate level of care to the patient, including the decision to transport or treat on the scene. Integrate the State Poison Center into the prehospital response for hazardous materials and biochemical terrorism responses 1. The 911 call center will identify and if EMD capable, complete key questions for the Overdose/ Poisoning, Animal Bites/Attacks, or Carbon Monoxide/Inhalation/HazMat emergency medical dispatch complaints and dispatch the appropriate EMS services and/or directly contact the State Poison Center for consultation. 2. If no immediate life threat or need for transport is identified, EMS personnel may conference the patient/caller with the Poison Center Specialist at the State Poison Center at If possible, dispatch personnel should remain on the line during conference evaluation. 3. The Poison Center Specialist at the State Poison Center will evaluate the exposure and make recommendations regarding the need for on-site treatment and/or hospital transport in a timely manner. If dispatch personnel are not on-line, the Specialist will recontact the 911 center and communicate these recommendations. 4. If the patient is determined to need EMS transport, the poison center Specialist will contact the receiving hospital and provide information regarding the poisoning, including treatment recommendations. EMS may contact medical control for further instructions or to discuss transport options. 5. If the patient is determined not to require EMS transport, personnel will give the phone number of the patient/caller to the Poison Center Specialist. The Specialist will initiate a minimum of one follow-up call to the patient/caller to determine the status of patient. 6. Minimal information that should be obtained from the patient for the state poison center includes: Name and age of patient Substance(s) involved Time of exposure Any treatment given Signs and symptoms 7. Minimal information which should be provided to the state poison center for mass poisonings, including biochemical terrorism and HazMat, includes: Substance(s) involved Time of exposure Signs and symptoms Any treatment given Policy 18
25 North Carolina College of Emergency Physicians Safe Transport of Pediatric Patients Policy: Without special considerations children are at risk of injury when transported by EMS. EMS must provide appropriate stabilization and protection to pediatric patients during EMS transport. To provide: Provide a safe method of transporting pediatric patients within an ambulance. Protect the EMS system and personnel from potential harm and liability associated with the transportation of pediatric patients. 1. Drive cautiously at safe speeds observing traffic laws. 2. Tightly secure all monitoring devices and other equipment. 3. Insure that all pediatric patient less than 40 lbs are restrained with an approved child restraint device secured appropriately to the stretcher or captains chair. 3. Insure that all EMS personnel use the available restraint systems during the transport. 4. Transport adults and children who are not patients, properly restrained, in an alternate passenger vehicle, whenever possible. 5. Do not allow parents, caregivers, or other passengers to be unrestrained during transport. 6. NEVER attempt to hold or allow the parents or caregivers to hold the patient during transport. Policy 19
26 North Carolina College of Emergency Physicians Transport Policy: All individuals served by the EMS system will be evaluated, treated, and furnished transportation (if indicated) in the most timely and appropriate manner for each individual situation. To provide: Rapid emergency EMS transport when needed. Appropriate medical stabilization and treatment at the scene when necessary Protection of patients, EMS personnel, and citizens from undue risk when possible. 1. All trauma patients with significant mechanism or history for multiple system trauma will be transported as soon as possible. The scene time should be 10 minutes or less. 2. All acute Stroke and acute ST-Elevation Myocardial Infarction patients will be transported as soon as possible. The scene time should be 10 minutes or less for acute Stroke patients and STEMI patients. 3. Other Medical patients will be transported in the most efficient manner possible considering the medical condition. Advanced life support therapy should be provided at the scene if it would positively impact patient care. Justification for scene times greater than 20 minutes should be documented. 4. In unusual circumstances, transport in other vehicles may be appropriate when directed by EMS management. Policy 20
27 North Carolina College of Emergency Physicians Cardiac Arrest Management in Residential Healthcare Facilities Policy: Unsuccessful cardiopulmonary resuscitation (CPR) and other advanced life support (ALS) interventions can be discontinued prior to transport when patient meets the criteria of this policy. Residential Healthcare Facilities, such as skilled nursing facilities or nursing homes, are defined as: 1) patient resides at the facility, 2) there is nursing care available, and 3) facility has oversight by a physician. This policy does not apply to facilities classified as hospitals or freestanding Emergency Departments. The purpose of this policy is to: Allow for discontinuation of prehospital resuscitation after the delivery of adequate and appropriate ALS therapy. All indicated procedures and ALS interventions will be performed and aggressive attempts at resuscitation will be provided on scene until the criteria below are met. 1. Personnel should aggressively attempt resuscitation and follow all protocols that are applicable to the patient in cardiac arrest. ALL of the the following MUST be completed in order to follow this policy: Adequate CPR has been administered Airway has been successfully managed with verification of device placement. Acceptable management techniques include orotracheal intubation, nasotracheal intubation, Blind Insertion Airway Device (BIAD) placement, or cricothyrotomy IV or IO access has been achieved Rhythm appropriate medications have been administered according to local EMS Protocols for a total of 3 cycles of drug therapy without return of spontaneous circulation (palpable pulse) 2. Discontinuation of CPR and ALS intervention may be implemented AFTER contact with Medical Control if ALL of the following criteria are also met: Patient is 18 years of age or older Patient has an initial rhythm of Asystole or PEA on arrival of ALS personnel No evidence or suspicion of any of the following: -Drug/toxin overdose -Active internal bleeding -Hypothermia -Preceding trauma All EMS paramedic personnel involved in the patient s care agree that discontinuation of the resuscitation is appropriate 3. Paramedic personnel must contact Medical Control and receive an order from the physician to discontinue resuscitation attempts. 4. The Deceased Subjects Policy must be followed. ALS personnel will work with staff to ensure that they have a physician to sign the death certificate and that funeral home arrangements have been made. EMS personnel will remove any line(s) or tube(s) placed by EMS and the decedent will be left with staff at the facility until funeral home transportation arrives. Document all patient care and interactions with the patient s family, staff, personal physician, medical examiner, law enforcement, and medical control in the EMS patient care report (PCR). Policy 21
28 North Carolina College of Emergency Physicians Interfacility Transports Interfacility Transports Transporting a patient from a medical facility to another medical facility that requires Advanced Life Support care during transport and the facility does not send a registered nurse to attend the patient. Policy: 1. The transporting paramedic may maintain any infusion approved by the North Carolina Medical Board for Interfacility transport by an EMT-Paramedic provided. 2.. The transporting paramedic should ensure that all appropriate documentation accompanies the patient. 3. While in transit to the receiving facility, all appropriate Gaston County EMS Protocols shall remain in place. 4. If the patient deteriorates, the sending facility should be notified via radio. 5. If additional ALS orders are needed the attendant will act at their certification level and function under the Gaston County EMS Protocols or under the direction of the physician at the sending medical facility. Policy 22
29 North Carolina College of Emergency Physicians Patient Hand Off and Continuum of Care Patient Hand Off and Continuum of Care All Gaston County EMS system agencies shall hand off care to appropriate system providers in a manner that ensures a safe and expedient transfer and continuum of care throughout the call. The purpose of this treatment policy is to provide a simple and efficient method of patient handover in the event of multi agency response. Policy: 1. The initial agency on scene, which has been properly dispatched to the call, shall be responsible for the patient until another agency that has been properly dispatched and has greater capability and arrives. 2. Greater capability is defined as a higher functional level of certification, or transport capability, or both. 3. When another agency that has been properly dispatched and has authority to receive the patient arrives, the initial agency on scene shall transfer care of the patient to the arriving agency after giving a full turnover report. 4. Patients shall not be turned over to agencies with less training than that of the previous agency, unless they are capable of providing the appropriate level of patient care. 5. At no time shall any agency block or prevent properly dispatched agencies from accessing the patient unless there are hazards that would endanger them. Policy 23
30 North Carolina College of Emergency Physicians Patient Self Medication Patient Self Medication All levels of certification. Indication: A patient who wishes to take his or her own medication or prescription. Policy: We should not administer anything to a patients that is not part of the 2009 NCCEP Standards for Medication Formulary. We should not advise any patient to take something they have in their possession (prescription or over the counter) that is not part of the 2009 NCCEP Standards for Medication Formulary. We should not advise a patient NOT to take something that is not part of the 2009 NCCEP Standards for Medication Formulary, however, if it is medically contraindicated, we should advise them of that and advise them to contact their prescribing physician. Policy 24
31 North Carolina College of Emergency Physicians Non-Transport Patients Policy: A PCR will be completed for all responses regardless of disposition. For any patient encounters in which the subject is well and uninjured, a well and uninjured form will also be completed. If there are any signs or symptoms of any trauma or medical complaint, or if any treatment beyond BLS assessment has been rendered, a refusal form will also be completed. In either case, Non-transport Disposition Instructions will be given to each subject or patient encountered. All levels of Certification Competent patients maintain the right to refuse care and/or transport. If unsure, contact Medical Control. All patients refusing service will be: o Informed of the availability of service and offered treatment and transport in a nonconfrontational, polite manner. o Advised to call 911 for emergency service if desired, and o Advised that they accept full responsibility for their actions. Contact Medical Control if ALS has been started and patient declines transport. Give the Medical Control Physician an explanation by recorded device of the situation and request permission to discontinue ALS. The name of the physician who gave the order must be documented in the PCR. When making contact with the physician, the contact should be done on a recorded device. Calling the hospital direct will not record the call. Documentation: o In the report narrative, describe he patient encounter, vital signs, advice given, that the patient is alert and oriented to person, place, and time and that the patient understands instructions given to them. o Have the patient sign a refusal form and have a third party witness the signature. Give the patient a copy of the Gaston County EMS System HIPAA form. o Complete all necessary documentation in the EPCR. If orders were received to discontinue ALS care by a physician, have the physician sign the PCR. At no time will MS professionals mention cost of transport, patients insurance status, hospital billing or insurance practices, status of system/unit availability, or any other non-clinical subject in an attempt to influence a patients decision to accept or decline transport. Policy 25
32 North Carolina College of Emergency Physicians Maintenance of Blood or Blood Products Establish guidelines for the maintenance of blood or blood products. 1. Type and Cross Matched Packed Red Blood Cells and administration orders should be obtained from referring facility prior to departure. 2. The referring physician should inform the patient or responsible party of the indications and risks and benefits of blood transfusion. The only exception is in an emergency. The nature of the emergency and/ or consent must be documented in the patient s medical record and/or documented in the transfer record. Verify with primary RN that blood tubing and blood products will not exceed recommended time frame during transport period. 3. Assure that the patient is wearing an ID bracelet with his/her name and hospital ID number from the referring hospital. Confirm the patient s name and date of birth match those on the unit of blood, and verify the patient s identity and matching numbers with two providers. 4. Blood transfusions must be administered through a blood filter and through a primary infusion of Normal Saline. 5. Obtain a complete set of vital signs. 6. Vital signs are monitored 5 minutes after the start of each unit of blood and at least every 15 minutes thereafter unless needed more often as dictated by the clinical situation. 7. Paramedics may monitor and maintain pre established blood or blood products infusions during inter facility transfer. 8. If additional non-hanging units are to be administered during transport, the attending paramedic will spike and run the remaining unit(s) of blood that has been ordered by the sending facility. 9. Once the last bag of blood has infused, paramedics will: a. Spike a bag of Normal Saline. b. Infuse the bag of normal Saline at KVO or a rate that will maintain patient s hemodynamic status. c. Document time of re-spiking of the bag, and amount of Saline that infused into the patient. d. Upon arrival at the receiving facility give used blood bag(s) to receiving facility staff. e. The following documentation shall be provided for each bag of blood administered: a. Beginning Time b. Ending Time c. Lot number 10. Identification and Management of Complications : Contact Medical Control for consultation immediately. Hemolytic Transfusion Reaction Signs and Symptoms: facial flushing, hyperventilation, tachycardia, hives, chest pain, wheezing, fever chills, cyanosis, dark urine, sense of impending doom. Management 1. Stop transfusion, change all tubing, infuse normal saline, collect blood bags for lab analysis. 2. Maintain normovolemia with normal saline. Policy 26
33 Page Intentionally Left Blank
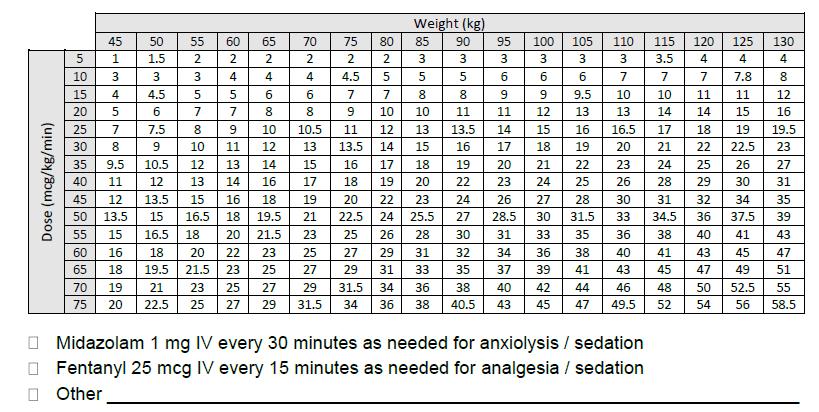
34 North Carolina College of Emergency Physicians Maintenance of Propofol Infusions Policy: Patients receiving a propofol infusion during interfacility transport must be cared for by a Paramedic-level provider who has 1) received education on propofol and 2) has shown proficiency in the operation of the IV pump to be used. Propofol is only administered during interfacility transports and is not carried on the ambulance. This policy and the accompanying GEMS Transfer Orders Form only apply to intubated adult patients. (Age of at least 15 years or body weight of at least 50kg.) Propofol must always be administered by IV pump and can NEVER be administered by IV bolus. Establish guidelines for the safe maintenance of propofol infusions during interfacility transport. 1. Propofol infusions must be ordered by a physician at the sending facility and initiated prior to EMS transport. 2. Patient must be receiving propofol infusion for at least 10 minutes prior to EMS transport with no episodes of irreversible hypotension. Any reactions to propofol must be reported to the transport crew. 3. Receive patient report from primary RN, including the dose and concentration of propofol that is being infused and any patient reactions to the medication prior to time of transport. Verify settings on the IV pump with the primary RN or ED Pharmacist. This verification must occur at bedside by visualizing the IV pump settings and must be documented in the PCR. 4. Assure that the patient is wearing an ID bracelet with his/her name from the sending facility and confirm the name and date of birth with the primary RN. 5. Obtain a complete set of vital signs and document patient s level of responsiveness. 6. Place patient on waveform capnography. Waveform capnography is required throughout transport. 7. Vital signs MUST be monitored and documented every 10 minutes during transport. 8. Titration of the propofol dose can only occur with a Medical Control Order from the sending facility. All patients receiving propofol must have a signed GEMS Transfer Order Form. -The attending paramedic should monitor vital signs, capnography, and overall patient condition closely in order to anticipate and prepare for adequate sedation. -If patient has systolic BP 110 and needs additional sedation, Midazolam may be administered per protocol at dose of 1 mg IV/IO. -If patient has systolic BP < 110 and needs additional sedation, Medical Control must be consulted regarding propofol rate and further sedation. If patient has a sudden hemodynamic deterioration (severe hypotension, severe bradycardia, or arrythmias), immediately stop propofol infusion and contact Medical Control. If patient goes into cardiac arrest, immediately stop propofol infusion and administer fluid boluses per protocol. 9. On arrival at the receiving facility, handoff report to the primary RN must include the dose and rate of current propofol infusion, any reactions or dosing changes that occurred during transport, and any changes in patient condition. For any patient receiving propofol: A copy of the PCR MUST be delivered within 24 hours to the Training Coordinator for Quality Management, either by hard copy or electronically. This is an NCOEMS requirement. All PCRs involving patients who receive propofol will be reviewed by GEMS Training and QI, GEMS Medical Director, and CRMC ED Pharmacist. Policy 27
35
North Carolina College of Emergency Physicians Standards Policy Table of Contents
 Policy North Carolina College of Emergency Physicians Standards Policy Table of Contents Disposition Policy Section 1. Criteria for Death or Withholding Resuscitation 2. Deceased Subjects 3. Discontinuation
Policy North Carolina College of Emergency Physicians Standards Policy Table of Contents Disposition Policy Section 1. Criteria for Death or Withholding Resuscitation 2. Deceased Subjects 3. Discontinuation
POLICIES AND PROCEDURES
 POLICIES AND PROCEDURES POLICY: 553.25 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 5 I. AUTHORITY Division 2.5, California Health and Safety
POLICIES AND PROCEDURES POLICY: 553.25 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 5 I. AUTHORITY Division 2.5, California Health and Safety
interventional cardiac facility (see Appendix 2). Notify receiving hospital, as soon as possible of impending arrival of the patient and give ETA.
. Notify receiving hospital, as soon as possible of impending arrival of the patient and give ETA.") Page 1 of 9 Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure
Page 1 of 9 Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure
Oakland County Medical Control Authority System Protocols Transportation Protocol Section Transportation Protocol.
 Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure A.
Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure A.
Emergency Medical Services Program
 County of Santa Cruz HEALTH SERVICES AGENCY 1080 EMELINE AVENUE, SANTA CRUZ, CA 95060 (831) 454-4120 FAX: (831) 454-4272 TDD: (831) 454-4123 EMERGENCY MEDICAL SERVICES PROGRAM Policy No. 7000 Reviewed
County of Santa Cruz HEALTH SERVICES AGENCY 1080 EMELINE AVENUE, SANTA CRUZ, CA 95060 (831) 454-4120 FAX: (831) 454-4272 TDD: (831) 454-4123 EMERGENCY MEDICAL SERVICES PROGRAM Policy No. 7000 Reviewed
DEATH IN THE FIELD. Escambia County, Florida - ALS/BLS Medical Protocol
 This protocol is divided into separate sections that cover the different situations of death in the field that the paramedic will be presented with. All patients found in cardiac arrest will receive cardiopulmonary
This protocol is divided into separate sections that cover the different situations of death in the field that the paramedic will be presented with. All patients found in cardiac arrest will receive cardiopulmonary
WESTCHESTER REGIONAL
 WESTCHESTER REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL POLICY STATEMENT Supersedes/Updates: New Policy No. 11-02 Date: February 8, 2011 Re: EMS System Resource Utilization Pg(s): 5 INTRODUCTION The Westchester
WESTCHESTER REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL POLICY STATEMENT Supersedes/Updates: New Policy No. 11-02 Date: February 8, 2011 Re: EMS System Resource Utilization Pg(s): 5 INTRODUCTION The Westchester
North Carolina College of Emergency Physicians Standards for the Selection and Performance of EMS Performance Improvement
 Performance Improvement North Carolina Performance Improvement Guidelines The purpose of this guideline is to provide direction to Agencies with respect to patient care based quality management performance
Performance Improvement North Carolina Performance Improvement Guidelines The purpose of this guideline is to provide direction to Agencies with respect to patient care based quality management performance
Determination of Death in the Prehospital Setting
 Determination of Death in the Prehospital Setting Supersedes: 02-03-09 Effective: 12-01-16 PURPOSE The purpose of this procedure is to establish guidelines for the withholding or termination of resuscitation
Determination of Death in the Prehospital Setting Supersedes: 02-03-09 Effective: 12-01-16 PURPOSE The purpose of this procedure is to establish guidelines for the withholding or termination of resuscitation
South Cook County Policies and Procedures. September, 2015
 South Cook County Policies and Procedures September, 2015 Objectives Upon completion of the program, the participant will be able to: 1.Understand the transport guidelines for emotionally disturbed patients
South Cook County Policies and Procedures September, 2015 Objectives Upon completion of the program, the participant will be able to: 1.Understand the transport guidelines for emotionally disturbed patients
TITLE: Trauma Triage and Patient Destination EMS Policy No. 5210
 PURPOSE: The purpose of this policy is to establish triage criteria for trauma patients, identify appropriate receiving hospital destinations for trauma patients, and direct the actions of the prehospital,
PURPOSE: The purpose of this policy is to establish triage criteria for trauma patients, identify appropriate receiving hospital destinations for trauma patients, and direct the actions of the prehospital,
San Joaquin County Emergency Medical Services Agency Policy and Procedure Manual
 Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
San Joaquin County Emergency Medical Services Agency Policy and Procedure Manual
 Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2010-04 Bariatric Patient Transports 12/17/2010 2012-01 DNR and POLST
Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2010-04 Bariatric Patient Transports 12/17/2010 2012-01 DNR and POLST
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy
 Policy") Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #501: Hospital Radio Reports HOSPITAL RADIO REPORTS Effective: February 12, 2015 Replaces: January 22, 2008 Review: November 12, 2018 Resources:
County of Santa Clara Emergency Medical Services System Policy #501: Hospital Radio Reports HOSPITAL RADIO REPORTS Effective: February 12, 2015 Replaces: January 22, 2008 Review: November 12, 2018 Resources:
San Joaquin County Emergency Medical Services Agency Policy and Procedure Manual
 Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
CONNECTICUT STATE BLS GUIDELINES GUIDELINES FOR WITHHOLDING RESUCITATION ADULT - AGE 18 AND OVER
 CONNECTICUT STATE BLS GUIDELINES GUIDELINES FOR WITHHOLDING RESUCITATION ADULT - AGE 18 AND OVER Purpose: To provide specific instruction regarding the protocols used to withhold or withdraw resuscitation
CONNECTICUT STATE BLS GUIDELINES GUIDELINES FOR WITHHOLDING RESUCITATION ADULT - AGE 18 AND OVER Purpose: To provide specific instruction regarding the protocols used to withhold or withdraw resuscitation
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject References Emergency Medical Services Administrative Policies and Procedures Title
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject References Emergency Medical Services Administrative Policies and Procedures Title
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DESTINATION POLICY
 SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY I. PURPOSE DESTINATION POLICY Policy Reference No.: 5000 Supersedes: February 1, 2015 A. To identify the approved ambulance-transport destinations for the
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY I. PURPOSE DESTINATION POLICY Policy Reference No.: 5000 Supersedes: February 1, 2015 A. To identify the approved ambulance-transport destinations for the
South Central Region EMS & Trauma Care Council Patient Care Procedures
 South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
POLICY SUMMARIES and HOSPITAL REFERENCES
 Base Hospital and Receiving Facilities Burn Centers Burn Patient Destination Burn Surface Area - Rule of Nines Declining Medical Care or Transport (AMA) Destination Determination Destination - 5150 and
Base Hospital and Receiving Facilities Burn Centers Burn Patient Destination Burn Surface Area - Rule of Nines Declining Medical Care or Transport (AMA) Destination Determination Destination - 5150 and
HOSPITALS TO ENTER PATIENTS INTO THE
 PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
Wadsworth-Rittman Hospital EMS Protocol
 Wadsworth-Rittman Hospital EMS Protocol Prehospital Advanced Life Support Protocol Revised: May 2004 Version 04.1 DISCLAIMER Every attempt has been made to reflect sound medical guidelines and protocols
Wadsworth-Rittman Hospital EMS Protocol Prehospital Advanced Life Support Protocol Revised: May 2004 Version 04.1 DISCLAIMER Every attempt has been made to reflect sound medical guidelines and protocols
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DOCUMENTATION, EVALUATION AND NON-TRANSPORTS
 SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DOCUMENTATION, EVALUATION AND NON-TRANSPORTS Policy Reference No.: 4040 Review Date: February 1, 2011 Supersedes: August 1, 2008 TABLE OF CONTENTS I. PURPOSE
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DOCUMENTATION, EVALUATION AND NON-TRANSPORTS Policy Reference No.: 4040 Review Date: February 1, 2011 Supersedes: August 1, 2008 TABLE OF CONTENTS I. PURPOSE
The Trauma System. Prevention Pre-hospital care and transport Acute hospital care Rehab Research
 An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
Modesto Junior College Course Outline of Record EMS 390
 Modesto Junior College Course Outline of Record EMS 390 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 390 Emergency Medical Technician 1 6 Units Limitations on Enrollment:
Modesto Junior College Course Outline of Record EMS 390 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 390 Emergency Medical Technician 1 6 Units Limitations on Enrollment:
PARAMEDIC STUDENT FIELD INTERNSHIP GUIDE
 Through field experience in the emergency ambulance, the paramedic student will develop a more comprehensive understanding of the pathophysiology of disease and trauma, rationale for treatments rendered,
Through field experience in the emergency ambulance, the paramedic student will develop a more comprehensive understanding of the pathophysiology of disease and trauma, rationale for treatments rendered,
Chapter 59. Learning Objectives 9/11/2012. Putting It All Together
 1 Chapter 59 Putting It All Together 2 Learning Objectives Discuss how assessment based management contributes to effective patient and scene assessment. Describe factors that affect assessment and decision
1 Chapter 59 Putting It All Together 2 Learning Objectives Discuss how assessment based management contributes to effective patient and scene assessment. Describe factors that affect assessment and decision
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
2011 Guidelines for Field Triage of Injured Patients
 2011 Guidelines for Field Triage of Injured Patients Slide 1 Welcome! Today, we are going to discuss the 2011 Guidelines for Field Triage of Injured Patients (2011 Guidelines). This presentation and the
2011 Guidelines for Field Triage of Injured Patients Slide 1 Welcome! Today, we are going to discuss the 2011 Guidelines for Field Triage of Injured Patients (2011 Guidelines). This presentation and the
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency Acute Care
 Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
Standard Operating Procedure Hospital Pre-alert & Patient Handover
 Standard Operating Procedure Hospital Pre-alert & Patient Handover No of Pages: 6 Unique reference No: Implementation date: 17 th May 2010 Version: Final Version 2.0 Next review date: May 2013 Title of
Standard Operating Procedure Hospital Pre-alert & Patient Handover No of Pages: 6 Unique reference No: Implementation date: 17 th May 2010 Version: Final Version 2.0 Next review date: May 2013 Title of
Chapter 1. Learning Objectives. Learning Objectives 9/11/2012. Introduction to EMS Systems
 Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
RECEIVING HOSPITALS. APPROVED: EMS Administrator
 Page 1 RECEIVING HOSPITALS APPROVED: EMS Administrator EMS Medical Director Assistant EMS Medical Director 1. Purpose: To provide paramedics and EMT-1's with information and guidance about the capability
Page 1 RECEIVING HOSPITALS APPROVED: EMS Administrator EMS Medical Director Assistant EMS Medical Director 1. Purpose: To provide paramedics and EMT-1's with information and guidance about the capability
PARAMEDIC REFRESHER COURSE
 Essential Medical Training, LLC Providing Quality, Professional Training PARAMEDIC REFRESHER COURSE 48 hours of Continuing Education This course is approved by the Florida Bureau of EMS for continuing
Essential Medical Training, LLC Providing Quality, Professional Training PARAMEDIC REFRESHER COURSE 48 hours of Continuing Education This course is approved by the Florida Bureau of EMS for continuing
Nassau Regional Medical Advisory Committee
 Nassau Regional Medical Advisory Committee Advisories Advisory# Subject Issued Effective 07-02.1 BLS Assisted Medications 2/7/07 2/7/07 07-06.1 BLS Use of Pulse Oximeters 6/6/07 6/6/07 08-12.1 Incident
Nassau Regional Medical Advisory Committee Advisories Advisory# Subject Issued Effective 07-02.1 BLS Assisted Medications 2/7/07 2/7/07 07-06.1 BLS Use of Pulse Oximeters 6/6/07 6/6/07 08-12.1 Incident
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES Manual Subject Emergency Medical Services Administrative Policies and Procedures First Responder Prehospital Care Report - BLS Policy Page 1 of 13 References
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES Manual Subject Emergency Medical Services Administrative Policies and Procedures First Responder Prehospital Care Report - BLS Policy Page 1 of 13 References
Northwest Community EMS System POLICY MANUAL
 Policy Title: ILLINOIS POLST forms and Advance Directive Guidelines No. D - 5 Board approval: 11/10/16 Effective: 12/1/16 Supersedes: 1/30/15 Page: 1 of 9 References: Public Act 094-0865 that amends the
Policy Title: ILLINOIS POLST forms and Advance Directive Guidelines No. D - 5 Board approval: 11/10/16 Effective: 12/1/16 Supersedes: 1/30/15 Page: 1 of 9 References: Public Act 094-0865 that amends the
0031 MESA COUNTY EMS SYSTEM PROTOCOLS: PCRs
 PATIENT CARE REPORTS POLICY 1. At least one provider will complete and file a patient care report (PCR), and any required data reports, for each patient contact. 2. If the author of the PCR is not the
PATIENT CARE REPORTS POLICY 1. At least one provider will complete and file a patient care report (PCR), and any required data reports, for each patient contact. 2. If the author of the PCR is not the
Clinical Guideline Trauma Care: Accessing Trauma Services
 Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
SKILLS CHECKLIST FOR RECERTIFICATION
 NAME 2012 CBT 434-EMT12 Cardiovascular Emergencies EMERGENCY MEDICAL SERVICES (11/22/2011) MH PRINT STUDENT S NAME SKILLS CHECKLIST FOR RECERTIFICATION ID # DATE Objective: Given a partner, appropriate
NAME 2012 CBT 434-EMT12 Cardiovascular Emergencies EMERGENCY MEDICAL SERVICES (11/22/2011) MH PRINT STUDENT S NAME SKILLS CHECKLIST FOR RECERTIFICATION ID # DATE Objective: Given a partner, appropriate
EMERGENCY MEDICAL SERVICES (EMS)
") Bismarck State College 2018-2019 Catalog 1 EMERGENCY MEDICAL SERVICES (EMS) EMS 110. Emergency Medical Technician Credits: 4 Prerequisite: Completion of a healthcare provider level CPR (BLS) Course. Corequisites:
Bismarck State College 2018-2019 Catalog 1 EMERGENCY MEDICAL SERVICES (EMS) EMS 110. Emergency Medical Technician Credits: 4 Prerequisite: Completion of a healthcare provider level CPR (BLS) Course. Corequisites:
Standard Policies Policy 4002
 I. PURPOSE This policy identifies the procedure for determining the appropriate receiving facility for patients transported by ground ambulance to the Emergency Department (ED) of an acute care hospital.
I. PURPOSE This policy identifies the procedure for determining the appropriate receiving facility for patients transported by ground ambulance to the Emergency Department (ED) of an acute care hospital.
Modesto Junior College Course Outline of Record EMS 350
 Modesto Junior College Course Outline of Record EMS 350 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 350 First Responder with Healthcare Provider CPR 3 Units Formerly
Modesto Junior College Course Outline of Record EMS 350 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 350 First Responder with Healthcare Provider CPR 3 Units Formerly
Standard Policies Reference
 Policy Index 1000 System Organization, Management and Operations 1001 EMS System Medical Direction and Oversight 1002 Prehospital Transfer of Care 1003 Do Not Resuscitate Orders 1004 Determination of Death
Policy Index 1000 System Organization, Management and Operations 1001 EMS System Medical Direction and Oversight 1002 Prehospital Transfer of Care 1003 Do Not Resuscitate Orders 1004 Determination of Death
Emergency Medical Technician
 PRECISION EXAMS Emergency Medical Technician EXAM INFORMATION Items 100 Points 100 Prerequisites NONE Grade Level 11-12 Course Length ONE YEAR DESCRIPTION The Emergency Medical Technician (EMT) course
PRECISION EXAMS Emergency Medical Technician EXAM INFORMATION Items 100 Points 100 Prerequisites NONE Grade Level 11-12 Course Length ONE YEAR DESCRIPTION The Emergency Medical Technician (EMT) course
EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN
 EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN Approved by East Alabama Regional Trauma Advisory Council On 11.20.2008 EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN TABLE OF CONTENTS BACKGROUND 3 TRAUMA SYSTEM GOALS.
EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN Approved by East Alabama Regional Trauma Advisory Council On 11.20.2008 EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN TABLE OF CONTENTS BACKGROUND 3 TRAUMA SYSTEM GOALS.
Field Triage Decision Scheme: The National Trauma Triage Protocol
 Field Triage Decision Scheme: The National Trauma Triage Protocol U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Injury Prevention and Control
Field Triage Decision Scheme: The National Trauma Triage Protocol U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Injury Prevention and Control
Destination & Diversion Guidelines
 Date: October 15, 2012 Page 1 of 5 Destination & Diversion Guidelines Purpose: To define the decision-making process regarding the destination of EMS patients. To provide a guideline and policy regarding
Date: October 15, 2012 Page 1 of 5 Destination & Diversion Guidelines Purpose: To define the decision-making process regarding the destination of EMS patients. To provide a guideline and policy regarding
Ontario Ambulance. Documentation. Standards
 Ontario Ambulance Documentation Standards Ministry of Health and Long-Term Care Emergency Health Services Branch April 2000 Ontario Ambulance Documentation Standards Part I - GENERAL For all Parts of the
Ontario Ambulance Documentation Standards Ministry of Health and Long-Term Care Emergency Health Services Branch April 2000 Ontario Ambulance Documentation Standards Part I - GENERAL For all Parts of the
Grey Nuns Community Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency Acute Care
 Grey Nuns Community Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene If the First Person On-Scene is able to proceed
Grey Nuns Community Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene If the First Person On-Scene is able to proceed
EMS Subspecialty Certification Review Course. Learning Objectives
 EMS Subspecialty Certification Review Course Mass Gatherings: 4.3 Disaster Planning and Operations: 4.3.1 Human Resource Needs in Disaster Response 4.3.2 Care Teams 4.3.2.1 Physician Placement 4.3.2.2
EMS Subspecialty Certification Review Course Mass Gatherings: 4.3 Disaster Planning and Operations: 4.3.1 Human Resource Needs in Disaster Response 4.3.2 Care Teams 4.3.2.1 Physician Placement 4.3.2.2
Occupational First Aid Attendants and Services are required as per WorkSafe BC Regulations.
 SAFETY & SECURITY PROTOCOL Title: Occupational First Aid Protocol Category: Safety No.: CS&S-3-2012 Replaces: Applicability: Campus Effective Date: September, 25, 2012 INTENTION This protocol is intended
SAFETY & SECURITY PROTOCOL Title: Occupational First Aid Protocol Category: Safety No.: CS&S-3-2012 Replaces: Applicability: Campus Effective Date: September, 25, 2012 INTENTION This protocol is intended
DEPARTMENT OF PUBLIC HEALTH
 DEPARTMENT OF PUBLIC HEALTH Emergency Medical Services Agency POLICY #542.00 TITLE: PATIENT REFUSAL OF EMERGENCY MEDICAL SERVICE, REFUSAL AGAINST MEDICAL ADVICE (AMA) & QUALIFY FOR RELEASE AT SCENE (RAS)
DEPARTMENT OF PUBLIC HEALTH Emergency Medical Services Agency POLICY #542.00 TITLE: PATIENT REFUSAL OF EMERGENCY MEDICAL SERVICE, REFUSAL AGAINST MEDICAL ADVICE (AMA) & QUALIFY FOR RELEASE AT SCENE (RAS)
Chapter 190 Emergency Medical Service: Overview and Ground Transport
 Chapter 190 Emergency Medical Service: Overview and Ground Transport Episode Overview There are multiple designs for EMS systems, including public and private services, those operating at basic and advanced
Chapter 190 Emergency Medical Service: Overview and Ground Transport Episode Overview There are multiple designs for EMS systems, including public and private services, those operating at basic and advanced
Chapter 4. Objectives. Objectives 01/08/2013. Documentation
 Chapter 4 Documentation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 4 Documentation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
2015 CPR / Resuscitation Skills EMERGENCY MEDICAL SERVICES
 2015 CPR / Resuscitation Skills EMERGENCY MEDICAL SERVICES SKILL CHECKLIST Cardiac Arrest NAME PRINT NAME EMS # DATE Objective: Given a multi-person company, BLS/ALS equipment and manikin: demonstrate
2015 CPR / Resuscitation Skills EMERGENCY MEDICAL SERVICES SKILL CHECKLIST Cardiac Arrest NAME PRINT NAME EMS # DATE Objective: Given a multi-person company, BLS/ALS equipment and manikin: demonstrate
Many who are interested in medicine, palliative care and hospice and bioethics have been
 NEW "DNR" RULES WENT INTO EFFECT MAY 20, 1999 Many who are interested in medicine, palliative care and hospice and bioethics have been carefully following the progress of the legislation on "portable DNR"
NEW "DNR" RULES WENT INTO EFFECT MAY 20, 1999 Many who are interested in medicine, palliative care and hospice and bioethics have been carefully following the progress of the legislation on "portable DNR"
CASEY COUNTY HOSPITAL EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA )
") CASEY COUNTY HOSPITAL EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA ) SCOPE: This Policy and Procedure applies to the hospital and rural health clinics including Casey County Primary Care and
CASEY COUNTY HOSPITAL EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA ) SCOPE: This Policy and Procedure applies to the hospital and rural health clinics including Casey County Primary Care and
Patient Restraint 1. INTRODUCTION
 Patient Restraint Supersedes: 09-13-13 Effective: 12-14-15 1. INTRODUCTION 1.1. Patients have the right to refuse treatment and/or transport if they are of legal age and are competent. Competence is defined
Patient Restraint Supersedes: 09-13-13 Effective: 12-14-15 1. INTRODUCTION 1.1. Patients have the right to refuse treatment and/or transport if they are of legal age and are competent. Competence is defined
Ethics in EMS. Presented by: Dwayne Cottel ACP Jeff Conway ACP, LLB
 Ethics in EMS Presented by: Dwayne Cottel ACP Jeff Conway ACP, LLB Objectives Define Ethics, Morals and Ethical Dilemmas Review of Legal and Ethical Accountability in EMS Describe common Ethical Dilemmas
Ethics in EMS Presented by: Dwayne Cottel ACP Jeff Conway ACP, LLB Objectives Define Ethics, Morals and Ethical Dilemmas Review of Legal and Ethical Accountability in EMS Describe common Ethical Dilemmas
Overview. Overview. Chapter 3. Medicolegal and Ethical Issues 9/11/2012. Consent for Treatment and Transport. Scope of Practice
 Chapter 3 Medicolegal and Ethical Issues Slide 1 Overview Scope of Practice Legal Duties to the Patient, Medical Director, and Public Ethical Responsibilities Duty to Act Slide 2 Overview Consent for Treatment
Chapter 3 Medicolegal and Ethical Issues Slide 1 Overview Scope of Practice Legal Duties to the Patient, Medical Director, and Public Ethical Responsibilities Duty to Act Slide 2 Overview Consent for Treatment
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221. I. Title Trauma team Activation Protocol/Roles & Responsibilities of the Trauma Team
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Objectives. Emergency Medicine Risk Factors
 The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
MASS CASUALTY INCIDENTS. Daniel Dunham
 MASS CASUALTY INCIDENTS Daniel Dunham WHAT IS A MASS CASUALTY INCIDENT? Any time resources required exceed the resources available. The number of patients is not necessarily large or small, and may be
MASS CASUALTY INCIDENTS Daniel Dunham WHAT IS A MASS CASUALTY INCIDENT? Any time resources required exceed the resources available. The number of patients is not necessarily large or small, and may be
SMO: School Bus Accident Response/ Alternative Transport Vehicle
 OSF NORTHERN ILLINOIS EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS BLS, ILS, ALS SMO: School Bus Accident Response/ Alternative Transport Vehicle Overview: This policy was developed to assist in
OSF NORTHERN ILLINOIS EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS BLS, ILS, ALS SMO: School Bus Accident Response/ Alternative Transport Vehicle Overview: This policy was developed to assist in
Section 1: County Operating Procedures
 Section 1: County Operating Procedures Pend Oreille County Presented by S. Ragsdale 2017-05-30 Page 1 of 53 Abandoned Babies Newborn Safety Act If a parent wishing to leave a newborn at a fire station
Section 1: County Operating Procedures Pend Oreille County Presented by S. Ragsdale 2017-05-30 Page 1 of 53 Abandoned Babies Newborn Safety Act If a parent wishing to leave a newborn at a fire station
Attachment B ORDINANCE NO. 14-
 ORDINANCE NO. 14- AN ORDINANCE OF THE COUNTY OF ORANGE, CALIFORNIA AMENDING SECTIONS 4-9-1 THROUGH 4-11-17 OF THE CODIFIED ORDINANCES OF THE COUNTY OF ORANGE REGARDING AMBULANCE SERVICE The Board of Supervisors
ORDINANCE NO. 14- AN ORDINANCE OF THE COUNTY OF ORANGE, CALIFORNIA AMENDING SECTIONS 4-9-1 THROUGH 4-11-17 OF THE CODIFIED ORDINANCES OF THE COUNTY OF ORANGE REGARDING AMBULANCE SERVICE The Board of Supervisors
EL PASO COUNTY HOSPITAL POLICY: P-2 DISTRICT POLICY EFFECTIVE DATE: 02/05 LAST REVIEW DATE: 03/17
 POLICY The policy of the El Paso County Hospital District (EPCHD) is to provide services in compliance with applicable federal and state laws, rules and regulations regarding the appropriate medical screening
POLICY The policy of the El Paso County Hospital District (EPCHD) is to provide services in compliance with applicable federal and state laws, rules and regulations regarding the appropriate medical screening
EMS System for Metropolitan Oklahoma City and Tulsa 2017 Medical Control Board Treatment Protocols
 PROTOCOL 17A: Adult General Medical s Adult General Medical s Four (4) Levels of General Medical s Priority I and II Priority III No Will time and distance to the hospital of choice be detrimental to the
PROTOCOL 17A: Adult General Medical s Adult General Medical s Four (4) Levels of General Medical s Priority I and II Priority III No Will time and distance to the hospital of choice be detrimental to the
Chapter 3. Objectives. Objectives 01/07/2013. Medical, Legal, and Ethical Issues
 Chapter 3 Medical, Legal, and Ethical Issues Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 3 Medical, Legal, and Ethical Issues Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Declining Emergency Medical Care or Transport
 I. PURPOSE This policy defines the requirements for patients with decision making capacity to decline medical care/ This policy is applicable to all EMS providers. Providers should recognize these situations
I. PURPOSE This policy defines the requirements for patients with decision making capacity to decline medical care/ This policy is applicable to all EMS providers. Providers should recognize these situations
Paramedic First Responder Policies and Procedures December 1, 2015
 Emergency Medical Services Division Paramedic First Responder Policies and Procedures December 1, 2015 Kern County Fire Department Station 58 Pine Mountain Club Edward D. Hill EMS Director Kristopher Lyon,
Emergency Medical Services Division Paramedic First Responder Policies and Procedures December 1, 2015 Kern County Fire Department Station 58 Pine Mountain Club Edward D. Hill EMS Director Kristopher Lyon,
If you do not have a chart already created Click Create blank chart to create a new chart. The Dispatch screen will appear
 Let s Get Started!!! Click on incomplete chart to finish a previously started chart. Example of Patient Records Page If you do not have a chart already created Click Create blank chart to create a new
Let s Get Started!!! Click on incomplete chart to finish a previously started chart. Example of Patient Records Page If you do not have a chart already created Click Create blank chart to create a new
MEDICAL EMERGENCIES WHAT YOU NEED TO KNOW IS IT AN EMERGENCY? FROM AMERICA S EMERGENCY PHYSICIANS. Is It An. Emergency?
 MEDICAL EMERGENCIES WHAT YOU NEED TO KNOW FROM AMERICA S EMERGENCY PHYSICIANS IS IT AN EMERGENCY? Is It An Emergency? www.emergencycareforyou.org Uncontrolled bleeding Severe or persistent vomiting or
MEDICAL EMERGENCIES WHAT YOU NEED TO KNOW FROM AMERICA S EMERGENCY PHYSICIANS IS IT AN EMERGENCY? Is It An Emergency? www.emergencycareforyou.org Uncontrolled bleeding Severe or persistent vomiting or
Best Practice Guideline #5. Management of Deaths Occurring Outside of Health Care Facilities
 Best Practice Guideline #5 Management of Deaths Occurring Outside of Health Care Facilities Introduction Emergency Medical Services (EMS) personnel and police officers are most often the first to respond
Best Practice Guideline #5 Management of Deaths Occurring Outside of Health Care Facilities Introduction Emergency Medical Services (EMS) personnel and police officers are most often the first to respond
Dr. Darrell Nelson, FACEP, FAAEM Medical Director Stokes County EMS
 Dr. Darrell Nelson, FACEP, FAAEM Medical Director Stokes County EMS Steven Roberson, EMT-P Fire Chief City of King Fire Department Brian Booe, EMT-P Training Officer Stokes County EMS AHA changes from
Dr. Darrell Nelson, FACEP, FAAEM Medical Director Stokes County EMS Steven Roberson, EMT-P Fire Chief City of King Fire Department Brian Booe, EMT-P Training Officer Stokes County EMS AHA changes from
Trauma Logistics: The things to know ED Charge RN
 The University East Bank Campus is verified by the American College of Surgeons as a Level II Trauma Center. We serve the metro and referring areas as a definitive care trauma center for our patients.
The University East Bank Campus is verified by the American College of Surgeons as a Level II Trauma Center. We serve the metro and referring areas as a definitive care trauma center for our patients.
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: MEDICAL/LEGAL ISSUES Revised: 11/2013
 SCOPE OF PRACTICE Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: MEDICAL/LEGAL ISSUES Revised: 11/2013 The action and care that an EMT is legally
SCOPE OF PRACTICE Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: MEDICAL/LEGAL ISSUES Revised: 11/2013 The action and care that an EMT is legally
AKRON POLICE DEPARTMENT PROPOSED EMERGENCY MENTAL ILLNESS PROCEDURE INTRODUCTION
 INTRODUCTION AKRON POLICE DEPARTMENT Police officers are often called upon to respond to incidents involving persons who are known to be or suspected of suffering from a mental illness. The degree of police
INTRODUCTION AKRON POLICE DEPARTMENT Police officers are often called upon to respond to incidents involving persons who are known to be or suspected of suffering from a mental illness. The degree of police
VERIFICATION OF LIFE EXTINCT POLICY DECEMBER Verification of Life Extinct Policy December 2009 Page 1 of 18
 VERIFICATION OF LIFE EXTINCT POLICY DECEMBER 2009 Page 1 of 18 POLICY TITLE: Verification of Life Extinct Policy POLICY REFERENCE NUMBER: Med01/009 IMPLEMENTATION DATE: December 2009 REVIEW DATE: December
VERIFICATION OF LIFE EXTINCT POLICY DECEMBER 2009 Page 1 of 18 POLICY TITLE: Verification of Life Extinct Policy POLICY REFERENCE NUMBER: Med01/009 IMPLEMENTATION DATE: December 2009 REVIEW DATE: December
GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE The Georgia General Assembly has long recognized the right of individuals to control all aspects of their personal care and medical treatment, including the
GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE The Georgia General Assembly has long recognized the right of individuals to control all aspects of their personal care and medical treatment, including the
EMT Basic. Course Outcome Summary. Western Technical College. Course Information. Course History. Bibliography
 Western Technical College 10531109 EMT Basic Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 5.00 Total Hours 180.00 Designed to train the student
Western Technical College 10531109 EMT Basic Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 5.00 Total Hours 180.00 Designed to train the student
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES Manual Subject Emergency Medical Services Administrative Policies and Procedures Patient Care Report Policy Page 1 of 20 References Title 22, Division 9, Chapter
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES Manual Subject Emergency Medical Services Administrative Policies and Procedures Patient Care Report Policy Page 1 of 20 References Title 22, Division 9, Chapter
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX
 Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Department of Emergency Medical Services
 MIAMI DADE COLLEGE MEDICAL CENTER CAMPUS SCHOOL OF HEALTH SCIENCES Department of Emergency Medical Services CLINICAL COURSE OUTLINE EMS 1431 EMERGENCY MEDICAL TECHNICIAN BASIC 1 EMS 1431 EMERGENCY MEDCIAL
MIAMI DADE COLLEGE MEDICAL CENTER CAMPUS SCHOOL OF HEALTH SCIENCES Department of Emergency Medical Services CLINICAL COURSE OUTLINE EMS 1431 EMERGENCY MEDICAL TECHNICIAN BASIC 1 EMS 1431 EMERGENCY MEDCIAL
First Aid, CPR and AED
 First Aid, CPR and AED Training saves lives! If you observe someone who requires medical attention as a result of an accident, injury or illness, it is very important for you to understand your options.
First Aid, CPR and AED Training saves lives! If you observe someone who requires medical attention as a result of an accident, injury or illness, it is very important for you to understand your options.
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC CONDUCT TRIAGE
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
Base Hospital Advanced Life Support Program for Durham Region
 Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
Sierra Sacramento Valley EMS Agency Program Policy. EMT Training Program Approval/Requirements
 Sierra Sacramento Valley EMS Agency Program Policy EMT Training Program Approval/Requirements Effective: 07/01/2017 Next Review: As Needed 1002 Approval: Troy M. Falck, MD Medical Director Approval: Victoria
Sierra Sacramento Valley EMS Agency Program Policy EMT Training Program Approval/Requirements Effective: 07/01/2017 Next Review: As Needed 1002 Approval: Troy M. Falck, MD Medical Director Approval: Victoria
TRANSPORT POLICY. F. Pediatric: Consult Mary Bridge if unsure as to where to transport the patient. Include parents in care as much as possible.
 I. Transport Criteria. II. A. ALS versus BLS transport: TRANSPORT POLICY 1. If the patient meets ALS criteria, they must be transported by the crew of a licensed, verified ALS ambulance agency; with at
I. Transport Criteria. II. A. ALS versus BLS transport: TRANSPORT POLICY 1. If the patient meets ALS criteria, they must be transported by the crew of a licensed, verified ALS ambulance agency; with at
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) This advance directive for health care has four parts: PART ONE HEALTH CARE AGENT. This part allows you to choose
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) This advance directive for health care has four parts: PART ONE HEALTH CARE AGENT. This part allows you to choose
Introduction to the EMS System
 Because of permissions issues, some material (e.g., photographs) has been removed from this chapter, though reference to it may occur in the text. The omitted content was intentionally deleted and is not
Because of permissions issues, some material (e.g., photographs) has been removed from this chapter, though reference to it may occur in the text. The omitted content was intentionally deleted and is not
Middlesex Hospital EMS Department Basic Life Support Guidelines
 EMS Department May 1, 2012 Table of Contents Section 1 General Clinical 1.01 Introduction 1.02 Medical Control 1.03 Patient Destination 1.04 Assessment 1.05 Mass Casualty Incidents 1.06 Refusal of Medical
EMS Department May 1, 2012 Table of Contents Section 1 General Clinical 1.01 Introduction 1.02 Medical Control 1.03 Patient Destination 1.04 Assessment 1.05 Mass Casualty Incidents 1.06 Refusal of Medical
GEORGIA Advance Directive Planning for Important Health Care Decisions
 GEORGIA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
GEORGIA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
State of Alaska Department of Corrections Policies and Procedures Chapter: Subject: Health Examinations
 Index #: 807.14 Page 1 of 8 I. Authority In accordance with 22 AAC 05.155, the Department will maintain a manual comprised of policies and procedures established by the Commissioner to interpret and implement
Index #: 807.14 Page 1 of 8 I. Authority In accordance with 22 AAC 05.155, the Department will maintain a manual comprised of policies and procedures established by the Commissioner to interpret and implement