Good Shepherd Centres Youth Services. Community Mental Health Liaison: Program Evaluation PHASE II
|
|
|
- Alannah Gregory
- 5 years ago
- Views:
Transcription
1 Good Shepherd Centres Youth Services Community Mental Health Liaison: Program Evaluation PHASE II A Report to: Children s Hospital of Eastern Ontario Submission Date: April 30, 2007 Submitted by: Good Shepherd Centres 143 Wentworth Street South Hamilton, ON L8N 2Z1 Tel: Fax
2 For more information contact: Loretta Hill-Finamore Director, Youth Services, Good Shepherd Centres Tel: x LorettaHillFinamore@GoodShepherdCentres.ca Kristin Cleverley McMaster University, School of Nursing St. Joseph s Hospital, Acute Mental Health cleverk@mcmaster.ca Carrie Bullard Mental Health Liaison Nurse, Good Shepherd Centres-Youth Services McMaster University, School of Nursing CarrieBullard@GoodShepherdCentres.ca 2
3 Table of Contents EXECUTIVE SUMMARY... 4 BACKGROUND... 5 Description of the Program... 5 Purpose of the Evaluation... 5 Literature Review... 6 METHODOLOGY... 8 Outcome Refinement... 8 Tool Development... 8 Design (Sampling and Data Collection)... 9 Sources of Information Evaluation Limitations Analysis RESULTS Demographic Information Outcomes Results CONCLUSIONS Recommendations Knowledge Exchange Plan APPENDICES Appendix A. Phase One Logic Model Appendix B. Phase One Youth Core Indicators and Outcomes Appendix C. Community Mental Health Liaison Program Minimum Data Set (MDS-MH) Appendix D. BPRS Symptoms
4 EXECUTIVE SUMMARY The community mental health liaison program (CMHLP) is an outreach program that provides early mental health intervention, including, counseling and advocacy to street involved and homeless youth. This program is unique as it is integrated within existing youth services in the downtown core and acts to bridge the gap in services for this vulnerable population. It was identified that there was a need to evaluate and determine outcomes of this program early on. In 2006, The Provincial Centre of Excellence for Child and Youth Mental Health (CHEO) funded Phase One of this evaluation project which entailed developing broad based indicators and outcomes. The purpose of this evaluation project was to prioritize the outcomes and develop a method of evaluating these outcomes. Guided by the outcomes from Phase 1 an evaluation tool was developed using previous psychometric instruments, data collection tools and by developing a series of items. Data was collected using the identical tool over 2 time points; time 1 involved a chart audit of the initial assessment/interview of the youth and time 2 was the most recent contact/assessment. The results showed that for most outcomes, the street involved and homeless youth were doing better following initiation in the mental health liaison program. Area of particular improvement was an ability of youth to engage and maintain services, build social networks, set and attain goals, and control their mental health symptoms. The findings of this evaluation will be used to evaluate the program, improve systems and processes, and begin to advocate for system changes where warranted. Based on this evaluation a series of recommendations were developed and focused on improving the program and its delivery, investigating future research and evaluation, and further development of community/research alliances. 4
5 BACKGROUND Description of the Program 1 The community mental health liaison program (CMHLP) is an outreach program that was initiated by two well established community-based organizations - Good Shepherd Centres and Wesley Urban Ministries, both of whom serve street involved and homeless youth. The CMHLP provides early mental health intervention, including, counseling and advocacy to street involved youth. This program is unique as it is integrated within existing youth services in the downtown core and acts to bridge the gap in services for this vulnerable population. Through referrals from staff at youth agencies, a mental health nurse provides a basic triage assessment to help identify and respond to youth s mental health needs. The nurse conducts a holistic assessment before providing services and linkages to meet the needs of the youth. This assessment is done through an informal process over a period of time as the relationship builds. The target population for this program include youth within the Hamilton community between the ages of who are street involved (hard to reach, homeless, living in shelters) and dealing with mental health issues (i.e. depression, anxiety, self harm). Purpose of the Evaluation A recent review of best practices for street involved youth was completed in 2005 by the Street Involved Youth Managers and the Social Planning and Research Council, this report Addressing the Needs of Street Involved and Homeless Youth in Hamilton described the best approach to evaluation with this population is outcomes based. Last 1 Description of Program based in part on CHEO Phase 1 Report. 5
6 year CHEO funded Phase One of this evaluation project which entailed developing broad based indicators and outcomes. The logic model from Phase One can be found in Appendix A. The purpose of this evaluation project was to prioritize the outcomes and develop a method of evaluating these outcomes. This involved refining and prioritizing the outcomes and searching out measurement tools that could be implemented within the program. The goal of this evaluation was to begin to measure the activities and outcomes of this program and to use these findings to begin to evaluate the program, improve systems and processes, and begin to advocate for system changes where warranted. Literature Review Homelessness is a serious social issue, particularly with children and youth who often (up to 70%) leave abusive homes for the street (Mayor s Homelessness Task Force, 1999). Although there is no accurate way of counting the amount of youth that are homeless at any given time, local estimates are that there were up to 600 youth living on the streets of Hamilton in 2004 (Vengris, 2005) and the estimates for Toronto range from 5,000 to 12,000 on any given night (Caputo, Wieler and Andreson, 1997). Emotional and mental health problems, often diagnosed concurrently with drug and alcohol addictions, are quite common in street-involved and homeless youth (Craig and Hodson, 1998; Cleverley, 2005; Teesson, Hodder and Buhrich, 2004). However, this population reports extremely low levels of health and social service utilization (Buckner and Bassuk, 1997; Smart and Adlaf, 1991) as these youth face several barriers to receiving comprehensive health care. Youth have identified barriers such as lack of transportation, not knowing where to go, inconvenient clinic hours, lack of proper identification, and the negative attitudes of health professionals (Farrow, Deisher, Brown, Kulig and Kipke, 1992; Geber, 1997). In order to provide youth-friendly programming 6
7 recent recommendations have centred on the importance of linking health services to programs seeking to meet the needs of homeless and street-involved youth (Barry, Ensign and Lippek, 2002; Klein et al, 2000). Furthermore, Klein et al (2000) point to outreach programming, which includes direct services and providing information and referrals, to be the most effective in reducing the barriers homeless and street-involved youth face. The Community Mental Health Liaison Program is an important building block in Hamilton to creating an integrated mental health system for homeless and streetinvolved youth. It involves early mental health intervention through a collaborative model of existing street involved youth programs. However, as this is an innovative program, there is a lack of outcomes and evidence-based research with this population and program. With the need to evaluate the current program and to develop outcomes to disseminate to other regions, Phase Two of the evaluation was undertaken with funding from CHEO. 7
8 METHODOLOGY Outcome Refinement Prior to the development of the instrument the outcomes developed in Phase One were refined and prioritized. This was accomplished through several lengthy meetings between the manager, mental health nurse and clinical research team. The outcomes were refined to include those that were measurable, were useful for program evaluation and planning, fundamental to future research and will guide program revisions. The final list of outcomes is listed in Appendix B. Once the outcomes and indicators were refined the majority of the project focused on locating and/or developing an appropriate measurement tool. Tool Development Items were generated for the tool from a variety of sources. A focus group with individuals who work with the population of interest (homeless youth) took place; this included the Director, Case Workers, Mental Health Nurse and Manager. This was an extremely informative meeting for outcome refinement and item generation. A significant amount of time was then spent locating appropriate measures of the outcomes. Initially it was thought that most measures could come from previous questions/items/tools published in the literature, however, due to the relatively little amount of research published in this area this became extremely difficult. A series of questions came from the Ministry of Children and Youth services reporting tool (i.e. demographic questions) and a questions on drug use and psychiatric hospitalizations were modified from the Residence Assessment Index-Mental Health (RAI-MH) which is currently used as a reporting tool for mental health units in Ontario (Hirdes et al, 2000). However, most questions were developed by the team using the guidance and scales of McDowell (2006) and Streiner and Norman (2005). 8
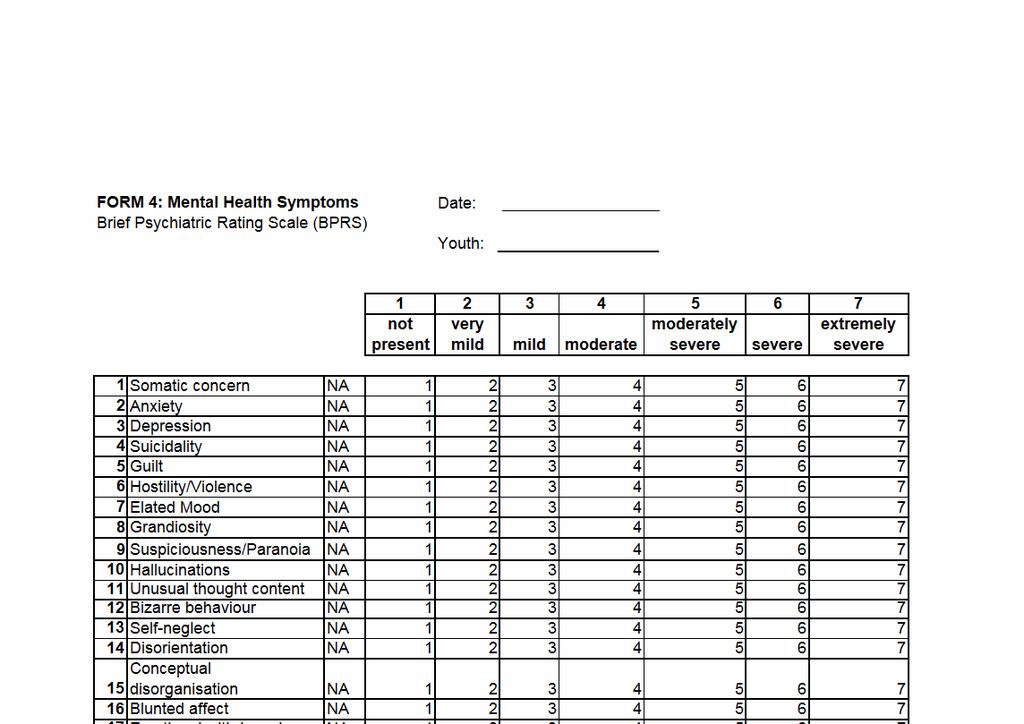
9 The initial tool was developed and refined through a series of meetings completed with clinical staff consultation and research team meetings. A variety of questions were added to the tool that did not directly relate to a specific outcome, however added to the ability to further evaluate and develop the mental health liaison program. This included the Brief Psychiatric Rating Scale (BPRS) which was added to determine baseline and concluding symptoms of mental illness homeless youth endorse that are served by this service (Ventura, Green, Shaner and Liberman, 1993). The BPRS has been validated in a variety of settings and more recently has been recommended by the Community Mental Health Evaluation Initiative in Ontario as a useful tool in community evaluations (see The final tool included 22 demographic questions, 28 mental health evaluation questions and the 24-item BPRS (see Appendix C). As well, a concluding interview was added to determine length of service use, reason for noncompletion, referrals, youth s satisfaction with the service and the overall client outcome since initiation. Design (Sampling and Data Collection) A repeated measures design was used to assess change in outcomes attributed to the mental health liaison program. The measurement tool was completed by the mental health nurse who was familiar with all youth in the program. A pilot test of 5 youth was completed using the measurement tool. Once the pilot test was completed the tool was refined, items were rewritten for readability, several not applicable choices had to be added, questions on self harm and violence were added, and a friendship scale was removed. The youth used in the pilot test were not used for the final evaluation. The tool was then completed on 23 homeless and street-involved youth served by the program in the last 18 months. Thus, a purposeful sample of 23 youth who had program files (including an intake assessment) and where also familiar to the mental health nurse were used for this evaluation. The initial data was collected the last week of 9
10 March based on several sources of information (described in detail below). The initial data was based on the baseline information of the youth when they were first referred to the program and initially assessed by the mental health nurse. The resurvey captured the current functioning of the 23 youth and was based on the latest contact/assessment the mental health nurse had with the youth. This data collection took place 3 weeks after the initial, enough time to ensure there was minimal to no contamination of the answers provided for the initial tool (Streiner and Norman, 2005). In summation, this evaluation involved collecting data on 23 youth at 2 times points, intake and last contact. Sources of Information The evaluation tool was completed at both time points by the Mental Health Liaison nurse using primarily chart review. Extensive information and assessments is collected on the youth in the program, although this made data extraction tedious, it also made for relatively little missing data. As well, the mental health liaison nurse also used information from the youth and case workers from the youth-serving programs to fill in incomplete information. Evaluation Limitations Although using a single individual to collect the data and complete the evaluation tools was helpful in reducing the amount of missing data, it also has the potential to introduce a significant amount of bias. While having a single rater (mental health liaison nurse) could not be avoided (as there is only one nurse in this program) it might have also introduced bias in that the ratings are based on a single rater. The use of chart review may have worked to reduce this bias. A logical next step would be to further test this tool for reliability using generalizability theory (see Streiner and Norman, 2005). As well, completing chart reviews opposed to completing the tool at the time of the interview may be effected by retrospective recall, as some questions (especially those related to 10
11 decision making capabilities) were based more on opinion than actual assessments from the chart. This bias will be reduced with future use as the plan is to integrate this tool into the regular intake of youth into this program. Thus it will be completed at the point of contact rather than some time later. Analysis The data were entered into SPSS Descriptive statistics (mean, frequencies) were generated on the demographic variables and items. T-tests were utilized to determine mean change in the core items as well as change in the BPRS. Significance was set at the 0.05 level. The analysis will be presented and linked back to the outcomes where possible. 11
12 RESULTS Demographic Information The instrument was completed on 15 females (65.2%) and 8 males. The average age was years, ranging from years 2. Most of the youth had not completed high school (82.6%) and only 1 youth was currently employed. Most youth had no source of income (30.4%) or their income was from Ontario Works (34.8%), ODSP (13.0%) and Children s Aid Society (13.0%). At intake into the program youth were living in a variety of settings, including, in a shelter (17.4%), with a partner or friends (34.8%), in their own apartment (17.8%), transitional housing (8.7%), on the street (8.7%), correctional facility (4.3%) and other (4.3%). The majority (69.4%) of youth wanted their family involved in their life, specifically for financial and emotional support. All but 2 youth reported having at least one support person at intake; this was typically a family member or friend. At the point of intake approximately a third (34.8%) of the youth had no previous contact with a mental health professional/agency, while 39.1% had contact greater than 30 days ago, and 21.7% had contact recently (within 30 days). Youth had very few diagnosed medical problems (30.4%) and most of the issues related to asthma. However, all but one youth had a (reported) past psychiatric illness and the majority (56.5%) reported multiple diagnoses, with mood disorders (i.e. depression, bipolar, etc) being reported by all youth. The majority of youth (78.7%) had used marijuana in the past year and most (80.5%) youth had drunk alcohol. At the resurvey (latest contact) youth reported extremely high numbers of significant live events (questions MH28a-l) with most reporting they had been robbed or assaulted (74.4%), experienced the death of family member (82.6%), had witnessed 2 Although the mental health liaison program s mandate is year old youth, one of the referring programs works with youth up to 25 years of age. This is reflected in the current sample. 12
13 violence (95.7%), reported sexual abuse (56.5%) physical abuse (78.3%) and/or emotional abuse (91.3%). Outcomes Results 1. The first outcome was increasing access to timely mental health support. In this sample, the time from intake to initial contact with the mental health liaison nurse was 8 days (0-32 days). There is no current information on the length of time youth currently wait in Hamilton for mental health services however, 8 days is extremely short and can be used in the future as a benchmark for future program planning. 2. The second outcome was the increased engagement of youth in planning and directing their recovery. At the resurvey, after youth had the opportunity to engage with the mental health nurse in planning their care, 61.9% of the youth were dependable to carry out the recommended mental health plan (Question MH12a). All 23 youth that were included in this sample were referred and subsequently became program clients. However, this is not representative of all program clients over the past 18 months. This tool has allowed for the initiation of collection of data on this outcome. For all referrals that do not become program clients the mental health nurse will now complete a concluding interview form to determine percentage of noninitiators and possible reasons for non-initiation. 3. The third outcome of this project was the ability to increasingly engage and maintain services with the mental health nurse. At the end of the data collection period, according to the concluding interview tool a total of 5 (21.7%) youth had dropped out of the program prior to completion. However, all of these youth were referred to/connected with other mental health services prior to disengagement. Using this concluding interview form more data will be collected on this outcome to determine 13
14 benchmarks for this program. Although, given the transient nature of this population, maintaining almost 80% of the population is excellent. 4. The fourth outcome was improving relationships. This was measured using Questions MH6 and MH7 on social effectiveness and social networking. Question MH6 (How effectively does the youth interact with others) was measured using a 6 item likert scale with 1 being very ineffectively and 5 being very effectively. the mean score increased from 2.30 to 3.13 and was significant (p=0.01). Question MH7 (How extensive is the youths social network) was measured on a 5 point likert scale with 1 being very limited to 5 being very extensive. The mean score increased from 1.78 to 2.57 and was significant (p=0.002). The ability for youth to engage with peers and interact with health service providers is an essential outcome of the mental health program, the increase in their ability to do this is an excellent outcome of this program. 5. The ability of youth to set and attain goals was the fifth outcome for this project. Four questions were included on goals setting and attainment in this tool (MH8-11). Questions MH8, 9, and 11 were measured using a 5 point likart scale with 1 being all of the time and 5 being none of the time. All three of these questions showed significant (p 0.001) improvement between the intake assessment and the last contact. Question MH10 was used to determine the amount of guidance the youth requires from the mental health nurse in identifying goals, with 1 = nurse required to identify, 2 = significant prompting required, 3=minimal guidance required and 4 no guidance required. On the 4 point scale, the average score went from 1.30 to 2.09 and was significant (p 0.001). 6. An important aspect of the mental health program is to work with youth to increase their ability to control the symptoms of their mental illness. Questions MH12a was regarding the youths ability to follow through on the mental health plan and was 14
15 measured on a 4 point likart scale. Question 12b was regarding the youths compliance with medication. Neither question changed significantly over the two time points. This will be explored further with the research team and program. Other indicators of symptom control were elicited using the BPRS. Selected results can be found in Appendix D. Of interest is that symptoms of depression, anxiety, suicidality, violence, distractibility and mannerisms got significantly better between the intake assessment and the latest contact assessment. 7. One of the primary purposes of the mental health liaison program is to connect youth with appropriate support systems (outcome 7). At the resurvey (latest contact) youth had been connect with an average of 2 other community/mental health services. Most youth had been connected with a psychiatrist or family physician as well as supportive housing programs (ie. the Good Shepherd Centres HOMES program). An area that will be explored further using this evaluation tool is the development of appropriate family and peer supports. 8. Another primary role of the mental health liaison program is education, to provide youth with the resources to increase their knowledge and understanding of symptoms of mental illness and the impact mental illness has on their life (outcome 8). Questions MH14-15d focused on assessing the knowledge and understanding of the youth. Question 14 determined what level of insight (1=full, 2=limited, 3=none) the youth had into their current mental health functioning. The average score youth received changed significantly (p=0.001) from 2.35 to This shows that over the course of the program youth were getting more insight into their mental health functioning, with most youth moving from limited insight to full insight. Questions 15a- 15d were measured on a 5 point likert scale (1=all of the time; 5=none of the time) and measured the youths understanding of the effect of mental illness on their functioning. There was significant improvement in the youths understanding of the 15
16 effect of mental illness on their activities of daily living (p 0.001) and on the impact of attaining and maintaining housing (p=0.01). However, there was not a significant effect on understanding the impact on employment and education. This may have been related to the fact that most youth were not employed or enrolled in school at the time of the program. 9. A final outcome of this project was the youths satisfaction with the program (outcome 9). A decision was not to develop a separate self-report survey for youth to complete on program satisfaction; this was mostly due to the timing of the project (as several youth were no longer in the program). However, the mental health liaison nurse was collecting information at the concluding interview on whether youth were satisfied with the services received. This information was extracted for 10 youth which completed the program (excluding those who dropped out as a concluding interview was not completed). Of the 10 youth; one youth felt none of their needs were met, 2 thought only a few of their needs were met; 6 (60%) felt most of their needs were met and 1 thought all of their needs were met. As well the low drop out rate (~20%) is also a measure of program satisfaction. This component of the outcome evaluation program will be further developed, with more time devoted to developing reliable measures of evaluating program satisfaction with this population. In the future, a self-report survey may be developed to capture this outcome. 16
17 CONCLUSIONS This project is the first step in developing a sustainable outcomes evaluation of the mental health liaison program in Hamilton. The goal of this project was to develop a tool that would be used to capture realistic outcomes of the program to use to guide future research, program revisions, and development. The results of this initial evaluation are promising. The majority of the indicators of the outcomes show significant improvement. In the future, this tool will be refined based on the current project and will be implemented as part of the current intake and ongoing assessment. As well, it is also a goal of this program to develop an online version of this assessment, as the mental health nurse is mobile and this will aid in the collection of data and information. Recommendations Based on the results of this evaluation, the following are recommended: 1. Develop an outline and benchmark what a mental health plans consists of. 2. Explore in more depth what relationships between youth and their supports (ie. family and friends) consists of. Specifically how to measure these supports and how youth engage with these supports. 3. Explore the need for program expansion to serve a larger population, specifically the need for an interdisciplinary team. 4. Continue to develop a collaborative relationship with researchers and other community programs. 5. Develop education/information sessions on mental health and core competencies based on the trends developed from this project and the program in the future. 6. Explore funding opportunities for purchasing software that will be useful for ongoing data collection and analysis. 7. Explore funding opportunities for ongoing research and evaluation. 17
18 8. Investigate funding opportunities for developing youth-driven evaluation initiatives and involving youth in the development and revisions of youth-friendly programming. 9. Improve access to data sets and results for mental health researchers and community members. 10. Continue to explore the effect that mental illness and substance use has on street-involved and homeless youth and how best to serve this population. 11. Contribute to teaching programs (ie. college, undergraduate and graduate programs) on mental health and street-involved. Knowledge Exchange Plan The knowledge exchange process has begun through providing mentorship to new researchers (i.e. McMaster University, Nursing Research Student). This nursing student aided in the collection of measurement tools and literature. In collaboration with the research team and mental health liaison nurse this student presented the preliminary findings of this report at the annual student nursing research day at McMaster in April. The project has also provided opportunity to collaborate with other expert researchers in a consultation capacity who have specialized in street involved and homeless youth and mental health. The plan is to use this project as a starting point for communicating the outcomes of the mental health liaison program to community members, specifically through local forums and meetings. In particular the project will be presented to the Street Involved Youth Managers meeting, the Street Involved Youth Network, Cleghorn Program: Early Intervention Community advisory group, the Children s Community Services Committee, and Hospital Advisory groups. Finally results from this project will be submitted to local research meetings for presentation (ie. McMaster Nursing Research Day and Grand Rounds). This will aid in developing and 18
19 maintaining collaborative projects and development of reports with McMaster University, other community programs and Good Shepherd Centres. These reports will be made available through our web site and other appropriate venues. 19
20 REFERENCES Barry, P., Ensign, J. & Lippek, S. (2002). Embracing street culture: Fitting health care into the lives of street youth. Journal of Transcultural Nursing, 13(2), Caputo, T., Weiler, R., & Anderson, J. (1997). The street lifestyle study. Ottawa, ON: Minister of Public Works and Government Services Canada. Cleverley, K. (2005). Homeless youth: The prevalence of psychiatric disorder and the change seen in psychiatric symptoms over time. Unpublished Master s Thesis. Hamilton, ON: McMaster University. Craig, T & Hodson, S. (1998). Homeless youth in London: I. Childhood antecedents and psychiatric disorder. Psychological Medicine, 28, Farrow, J., Deisher, R., Brown, R., Kulig, J. & Kipke, M. (1992). Health and health needs of homeless and runaway youth: A position paper for the Society of Adolescent Medicine. Journal of Adolescent Health 13(8), Geber, G.M. (1997). Barriers to health care for street youth. Journal of Adolescent Health, 21(5), Hirdes, J., Marhaba, M., Smith, T., Clyburn, L., Mitchell, L., Lemick, R. et al (2000/2001). Development of the resident assessment instrument-mental health. Hospital Quarterly, Winter, Klein, J., Woods, K., Wilson, K., Pospero, M., Greene, J. and Ringwalt, C. (2000). Homeless and runaway youths access to health care. Journal of Adolescent Health 27(5), Mayor s Homelessness Action Task Force (1999). Taking responsibility for homelessness: An action plan. Toronto, Ontario: City of Toronto. Smart, R. & Adlaf, E. (1991). Substance use and problems among Toronto street youth. British Journal of Addiction 86,
21 Streiner, D. and Norman, G. (2003). Health measurement scales: A practical guide to their development and use (3 rd ed.). New York, NY: Oxford University Press. Teesson, M., Hodder, T. and Buhrich, N. (2004). Psychiatric disorders in homeless men and women in Sydney. Australian and New Zealand Journal of Psychiatry, vol.38 pp Vengris, J. (2005). Addressing the needs of street-involved and homeless youth in Hamilton. Report prepared for: Social Planning and Research Council of Hamilton. Ventura, M., Green, M., Shaner, A and Liberman, R. (1993). Training and quality assurance of the brief psychiatric rating scale: The drift buster. International Journal of Methods in Psychiatric Research, 3,
22 APPENDICES Appendix A. Phase One Logic Model Appendix B. Phase One Youth Core Indicators and Outcomes Appendix C. Community Mental Health Liaison Program Minimum Data Set (MDS-MH) Appendix D. BPRS Symptoms 22
23 Appendix A. Phase One Logic Model Inputs Activities Outputs Participants Outcomes - Impact Short Term Medium Term Long Term Impact Street-Involved Youth Individual/Youth Level Counseling Education Safety Planning Advocacy Transitional support for housing and health care Mental Health Assessments Information, Referral and Linkage Street-involved youth in Hamilton Increased access to timely mental health support Increased engagement in planning and directing their own recovery Increased ability to obtain/maintain appropriate mental health services Improved retention within youth programs Increased ability to form therapeutic relationships/ communicate Decreased hopelessness through empowering youth Improved symptom control Increased psychosocial functioning Increased self esteem Increased knowledge and understanding of mental illness and health Improved utilization of appropriate housing Youth satisfaction with program Mental Health Liaison Nurse Materials (i.e. Supplies, space) Community Partners (including SIYN/SIYM) Resources (including SIYM/SPRC report) Staff Level Mental Health Consultation and Training Support Mentoring Attend community meetings/committees Advocacy Share mental health information Promote networking/ collaboration among partners Community Level Program/Agency Level Staff working with streetinvolved youth Program and community partners Increased awareness of Mental Health Liaison program Greater awareness of community resources and the system of services Bridged gap in youth mental health services Illuminate trends in street-involved youth population Increased ability to effectively communicate with youth with mental illness Better able to collaborate with Mental Health Liaison Nurse re: developing customized plans of care for youth Decreased anxiety Increased understanding of mental health and illness More efficient use of mental health services Increased familiarity of mental health program Staff Community Increased core competencies related to working with street-involved youth with mental illness Increased confidence in working with street-involved youth with mental illness Increased dialogue among community partners about the mental health issues of street-involved youth The ultimate outcome of the program is that youth are self sufficient and as adults are productive contributing members of society. Provide program support for street-involved and homeless youth Good Shepherd Centres Increased capacity to meet the needs of youth and staff Contribution to wider knowledge e.g., best practice Program/Agency Leader in quality mental health service delivery for street involved and homeless youth 23
24 Appendix B. Phase One Youth Core Indicators and Outcomes 1. Increased access to timely mental health support a. Length of time to initial contact with mental health services 2. Increased engagement in planning and directing own recovery a. Percent of outreach referrals that subsequently become program clients b. Percent of clients that follow through with some or all of the recommended program s services 3. Increased ability to engage with and maintain appropriate mental health services with mental health liaison nurse a. Percent of youth that drop out, and non-initiate 4. i) Improved peer relationships ii) Improved communication with health/social service workers a) Increase in appropriate communication strategies (i and ii) b) Improvement in social skills (i and ii) c) Increase in socializing behaviour and decrease in isolative behaviour (ii) 5. Decreased hopelessness a. Increased ability to set goals b. Increased ability to attain goals c. Increased ability to make decisions 6. Increased symptom control (i.e. adherence re: meds) a. Youth self-report improved symptom control b. Nurses report improved client functioning/symptom control 7. Improved network of supports a. Youth identify and connect with appropriate family supports b. Youth identify and connect with appropriate peer supports 8. Increased knowledge and understanding of mental illness a. Youth accurately describe symptoms of mental illness b. Youth clearly describe the impact of their mental illness 9. Youths satisfaction with the program at discharge a. Youth self report program met their needs 24
25 Appendix C. Community Mental Health Liaison Program Minimum Data Set (MDS-MH) 25
26 26
27 27
28 28
29 29
30 30
31 31
32 Appendix D. BPRS Symptoms Symptom Time N Mean (SD) P-value (change) Depression Initial (0.85) Current (0.87) Anxiety Initial (1.07) Current (0.63) 0.01 Suicidality Initial (1.40) Current (0.99) Hostility/Violence Initial (1.90) Current (1.20) 0.01 Distractibility Initial (1.90) Current (1.10) 0.02 Mannerisms Initial (1.30) Current (0.52) selected results 32
Macomb County Community Mental Health Level of Care Training Manual
 1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
Patients satisfaction with mental health nursing interventions in the management of anxiety: Results of a questionnaire study.
 d AUSTRALIAN CATHOLIC UNIVERSITY Patients satisfaction with mental health nursing interventions in the management of anxiety: Results of a questionnaire study. Sue Webster sue.webster@acu.edu.au 1 Background
d AUSTRALIAN CATHOLIC UNIVERSITY Patients satisfaction with mental health nursing interventions in the management of anxiety: Results of a questionnaire study. Sue Webster sue.webster@acu.edu.au 1 Background
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Benchmarking across sectors: Comparisons of residential dual diagnosis and mental health programs
 University of Wollongong Research Online Faculty of Health and Behavioural Sciences - Papers (Archive) Faculty of Science, Medicine and Health 2009 Benchmarking across sectors: Comparisons of residential
University of Wollongong Research Online Faculty of Health and Behavioural Sciences - Papers (Archive) Faculty of Science, Medicine and Health 2009 Benchmarking across sectors: Comparisons of residential
The Way Forward. Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador
 The Way Forward Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador 2 Table of Contents Introduction... 2 Background... 3 Vision and Values... 5 Governance... 6
The Way Forward Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador 2 Table of Contents Introduction... 2 Background... 3 Vision and Values... 5 Governance... 6
PROGRAM EVALUATION GRANT AWARD 2006 GOAL SETTING AND CAFAS EVALUATION Program Evaluation Grant #
 1 Program Description: PROGRAM EVALUATION GRANT AWARD 2006 GOAL SETTING AND CAFAS EVALUATION Program Evaluation Grant # 162606-051 As a non-profit Children s Mental Health Center with a long history of
1 Program Description: PROGRAM EVALUATION GRANT AWARD 2006 GOAL SETTING AND CAFAS EVALUATION Program Evaluation Grant # 162606-051 As a non-profit Children s Mental Health Center with a long history of
The Art and Science of Evidence-Based Decision-Making Epidemiology Can Help!
 The Art and Science of Evidence-Based Decision-Making Epidemiology Can Help! Association of Public Health Epidemiologists in Ontario The Art and Science of Evidence-Based Decision-Making Epidemiology Can
The Art and Science of Evidence-Based Decision-Making Epidemiology Can Help! Association of Public Health Epidemiologists in Ontario The Art and Science of Evidence-Based Decision-Making Epidemiology Can
Outcome and Process Evaluation Report: Crisis Residential Programs
 FY216-217, Quarter 4 Outcome and Process Evaluation Report: Crisis Residential Programs April Howard, Ph.D. Erin Dowdy, Ph.D. Shereen Khatapoush, Ph.D. Kathryn Moffa, M.Ed. O c t o b e r 2 1 7 Table of
FY216-217, Quarter 4 Outcome and Process Evaluation Report: Crisis Residential Programs April Howard, Ph.D. Erin Dowdy, Ph.D. Shereen Khatapoush, Ph.D. Kathryn Moffa, M.Ed. O c t o b e r 2 1 7 Table of
Community-Based Psychiatric Nursing Care
 Community-Based Psychiatric Nursing Care 1 The goal of the mental health delivery system is to help people who have experienced a psychiatric illness live successful and productive lives in the community
Community-Based Psychiatric Nursing Care 1 The goal of the mental health delivery system is to help people who have experienced a psychiatric illness live successful and productive lives in the community
3.12. Specialty Psychiatric Hospital Services. Chapter 3 Section. 1.0 Summary. Ministry of Health and Long-Term Care
 Chapter 3 Section 3.12 Ministry of Health and Long-Term Care Specialty Psychiatric Hospital Services 1.0 Summary There are about 2,760 long-term psychiatric beds in 35 facilities (primarily hospitals)
Chapter 3 Section 3.12 Ministry of Health and Long-Term Care Specialty Psychiatric Hospital Services 1.0 Summary There are about 2,760 long-term psychiatric beds in 35 facilities (primarily hospitals)
Position Number(s) Community Division/Region(s) Inuvik
 Community Division/Region(s) Inuvik") IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Child, Youth and Family Counsellor Position Number(s) Community Division/Region(s) 47-90057 Inuvik Inuvik
IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Child, Youth and Family Counsellor Position Number(s) Community Division/Region(s) 47-90057 Inuvik Inuvik
David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health
 David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation,
David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation,
Long-Stay Alternate Level of Care in Ontario Mental Health Beds
 Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Request for Applications (RFA) HBCU Mental Health Pilot Program
 HBCU Mental Health Pilot Program") Request for Applications (RFA) 2008-2009 HBCU Mental Health Pilot Program Background and Instructions A 2006 national survey conducted by the Substance Abuse Mental Health Services Administration (SAMHSA)
Request for Applications (RFA) 2008-2009 HBCU Mental Health Pilot Program Background and Instructions A 2006 national survey conducted by the Substance Abuse Mental Health Services Administration (SAMHSA)
TOGETHER We Make it Work:
 TOGETHER We Make it Work: Mental Health and Addictions (MHA) Nurses in School Boards for Student Well-Being Toronto, ON June 20 21, 2014 2 A Joint Presentation of Mississauga Halton CCAC Cynthia Johnston
TOGETHER We Make it Work: Mental Health and Addictions (MHA) Nurses in School Boards for Student Well-Being Toronto, ON June 20 21, 2014 2 A Joint Presentation of Mississauga Halton CCAC Cynthia Johnston
Position Number(s) Community Division/Region(s) Fort Simpson
 Community Division/Region(s) Fort Simpson") IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Mental Health/Addictions Counsellor Position Number(s) Community Division/Region(s) 37-11334 Fort Simpson
IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Mental Health/Addictions Counsellor Position Number(s) Community Division/Region(s) 37-11334 Fort Simpson
Submission to the South Australian Child and Adolescent Mental Health Service Re: CAMHS Review. August 2014
 Submission to the South Australian Child and Adolescent Mental Health Service Re: CAMHS Review August 2014 Australian Association of Social Workers National Office Canberra Level 4, 33-35 Ainslie Place
Submission to the South Australian Child and Adolescent Mental Health Service Re: CAMHS Review August 2014 Australian Association of Social Workers National Office Canberra Level 4, 33-35 Ainslie Place
Situation Analysis Tool
 Situation Analysis Tool Developed by the Programme for Improving Mental Health CarE PRogramme for Improving Mental health care (PRIME) is a Research Programme Consortium (RPC) led by the Centre for Public
Situation Analysis Tool Developed by the Programme for Improving Mental Health CarE PRogramme for Improving Mental health care (PRIME) is a Research Programme Consortium (RPC) led by the Centre for Public
Aboriginal and Torres Strait Islander mental health training opportunities in the bush
 Aboriginal and Torres Strait Islander mental health training opportunities in the bush Warren Bartik, Hunter New England Health, Angela Dixon, Children s Hospital at Westmead INTRODUCTION Aboriginal and
Aboriginal and Torres Strait Islander mental health training opportunities in the bush Warren Bartik, Hunter New England Health, Angela Dixon, Children s Hospital at Westmead INTRODUCTION Aboriginal and
Addressing the Employability of Australian Youth
 Addressing the Employability of Australian Youth Report prepared by: Dr Katherine Moore QUT Business School Dr Deanna Grant-Smith QUT Business School Professor Paula McDonald QUT Business School Table
Addressing the Employability of Australian Youth Report prepared by: Dr Katherine Moore QUT Business School Dr Deanna Grant-Smith QUT Business School Professor Paula McDonald QUT Business School Table
INTEGRATED CASE MANAGEMENT ANNEX A
 INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
Mental Health Accountability Framework
 Mental Health Accountability Framework 2002 Chief Medical Officer of Health Report Injury: Predictable and Preventable Contents 3 Executive Summary 4 I Introduction 6 1) Why is accountability necessary?
Mental Health Accountability Framework 2002 Chief Medical Officer of Health Report Injury: Predictable and Preventable Contents 3 Executive Summary 4 I Introduction 6 1) Why is accountability necessary?
2.0 APPLICABILITY OF THIS PROTOCOL AGREEMENT FRAMEWORK
 Roles and Responsibilities of the Director (Child, Family and Community Service Act) and the Ministry Of Health: For Collaborative Practice Relating to Pregnant Women At-Risk and Infants At-Risk in Vulnerable
Roles and Responsibilities of the Director (Child, Family and Community Service Act) and the Ministry Of Health: For Collaborative Practice Relating to Pregnant Women At-Risk and Infants At-Risk in Vulnerable
National review of NHS acute inpatient mental health services in England: implications for psychiatric intensive care units
 National review of NHS acute inpatient mental health services in England: implications for psychiatric intensive care units Nicola Vick, Project lead September 2008 Outline of presentation 1. Overview
National review of NHS acute inpatient mental health services in England: implications for psychiatric intensive care units Nicola Vick, Project lead September 2008 Outline of presentation 1. Overview
Te Ao Māramatanga New Zealand College of Mental Health Nurses
 Te Ao Māramatanga New Zealand College of Mental Health Nurses Mental Health and Addictions Credential in Primary Care (Nursing) Monitoring and Evaluation Handbook - ABRIDGED 19 April 2013 Jointly prepared
Te Ao Māramatanga New Zealand College of Mental Health Nurses Mental Health and Addictions Credential in Primary Care (Nursing) Monitoring and Evaluation Handbook - ABRIDGED 19 April 2013 Jointly prepared
UnitedHealthcare Guideline
 UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
AOPMHC STRATEGIC PLANNING 2018
 SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
Improving Outcome and Efficiency with. Service Delivery
 Transforming Public Behavioral Health Care: Improving Outcome and Efficiency with Consumer-Driven, Outcome-Informed (CDOI) Service Delivery Scott D. Miller, Ph.D. http://twitter.com/scott_dm http://www.linkedin.com/in/scottdmphd
Transforming Public Behavioral Health Care: Improving Outcome and Efficiency with Consumer-Driven, Outcome-Informed (CDOI) Service Delivery Scott D. Miller, Ph.D. http://twitter.com/scott_dm http://www.linkedin.com/in/scottdmphd
HIV HEALTH & HUMAN SERVICES PLANNING COUNCIL OF NEW YORK Mental Health Service Directive - Tri-County Approved by the HIV Planning Council 3/31/16
 Goals: 1) Provide treatment and counseling services to individuals living with HIV and mental illness, with or without cooccurring substance use disorders, that aim to improve quality of life and mental
Goals: 1) Provide treatment and counseling services to individuals living with HIV and mental illness, with or without cooccurring substance use disorders, that aim to improve quality of life and mental
Reporting to: Director, Settlement Orientation Services (SOS) Location: # West Hastings, Vancouver
 Location: # West Hastings, Vancouver") Community Case Manager 10 September, 2015 Reporting to: Director, Settlement Orientation Services (SOS) Location: #207 744 West Hastings, Vancouver About SOS SOS is a community-based organization that
Community Case Manager 10 September, 2015 Reporting to: Director, Settlement Orientation Services (SOS) Location: #207 744 West Hastings, Vancouver About SOS SOS is a community-based organization that
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/22/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/22/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Working in the NHS: the state of children s services. Report prepared by Charlie Jackson, Research Fellow (BACP)
") Working in the NHS: the state of children s services Report prepared by Charlie Jackson, Research Fellow (BACP) 1 Contents Contents... 2 Context... 3 Headline Findings... 4 Method... 5 Findings... 6 Demographics
Working in the NHS: the state of children s services Report prepared by Charlie Jackson, Research Fellow (BACP) 1 Contents Contents... 2 Context... 3 Headline Findings... 4 Method... 5 Findings... 6 Demographics
The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus
 University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
The Way Forward. Report Card: The First Six Months Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador
 The Way Forward Report Card: The First Six Months Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador Measuring Progress On June 27, 2017, the Government of Newfoundland
The Way Forward Report Card: The First Six Months Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador Measuring Progress On June 27, 2017, the Government of Newfoundland
DRAFT. An Introduction to The ASAM Criteria for Patients and Families. What is The ASAM Criteria?
 An Introduction to The ASAM Criteria for Patients and Families This document has been created to provide you information about how some of the decisions regarding your available treatment or service options
An Introduction to The ASAM Criteria for Patients and Families This document has been created to provide you information about how some of the decisions regarding your available treatment or service options
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers
 Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Central East LHIN Strategic Aims
 Central East LHIN Strategic Aims Mental Health and Addictions Strategic Aim Update December 16, 2015 Presented By: Dr. Ian Dawe, Jai Mills and Marilee Suter Agenda Background and Overview Aim Metrics Update
Central East LHIN Strategic Aims Mental Health and Addictions Strategic Aim Update December 16, 2015 Presented By: Dr. Ian Dawe, Jai Mills and Marilee Suter Agenda Background and Overview Aim Metrics Update
Mental Health Atlas Questionnaire
 Mental Health Atlas - 2014 Questionnaire Department of Mental Health and Substance Abuse World Health Organization Context In May 2013, the 66th World Health Assembly adopted the Comprehensive Mental Health
Mental Health Atlas - 2014 Questionnaire Department of Mental Health and Substance Abuse World Health Organization Context In May 2013, the 66th World Health Assembly adopted the Comprehensive Mental Health
Behavioral Health Services. San Francisco Department of Public Health
 Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Collaborative. Decision-making Framework: Quality Nursing Practice
 Collaborative Decision-making Framework: Quality Nursing Practice December 7, 2016 Please note: For consistency, when more than one regulatory body is being discussed in this document, the regulatory bodies
Collaborative Decision-making Framework: Quality Nursing Practice December 7, 2016 Please note: For consistency, when more than one regulatory body is being discussed in this document, the regulatory bodies
Child and Family Development and Support Services
 Child and Services DEFINITION Child and Services address the needs of the family as a whole and are based in the homes, neighbourhoods, and communities of families who need help promoting positive development,
Child and Services DEFINITION Child and Services address the needs of the family as a whole and are based in the homes, neighbourhoods, and communities of families who need help promoting positive development,
The Hamilton Family Health Team. Program Evaluation. The Primary Care Child & Youth Mental Health. Initiative
 The Hamilton Family Health Team Program Evaluation The Primary Care Child & Youth Mental Health Initiative Submitted to: The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO Evaluation
The Hamilton Family Health Team Program Evaluation The Primary Care Child & Youth Mental Health Initiative Submitted to: The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO Evaluation
Monadnock Community Hospital Community Health Needs Assessment Implementation Plan:
 Monadnock Community Hospital Community Health Needs Assessment Implementation Plan: 2016-2018 Working with, and for, our community to address today s healthcare needs Background - Compliance The Community
Monadnock Community Hospital Community Health Needs Assessment Implementation Plan: 2016-2018 Working with, and for, our community to address today s healthcare needs Background - Compliance The Community
Request for Proposals (RFP) for. School-Based Prevention Programs. As issued by Montgomery County Alcohol, Drug Addiction, & Mental Health Services
 for. School-Based Prevention Programs. As issued by Montgomery County Alcohol, Drug Addiction, & Mental Health Services") Request for Proposals (RFP) for School-Based Prevention Programs As issued by Montgomery County Alcohol, Drug Addiction, & Mental Health Services Released: March 12, 2018 Deadline: May 1, 2018 1 TABLE
Request for Proposals (RFP) for School-Based Prevention Programs As issued by Montgomery County Alcohol, Drug Addiction, & Mental Health Services Released: March 12, 2018 Deadline: May 1, 2018 1 TABLE
Program Design: Mental Health and Addiction Nurses in District School Board Program
 Program Design: Mental Health and Addiction Nurses in District School Board Program September 6, 2011 Table of Contents Program Design: Mental Health and Addiction Nurses in District School Boards Program
Program Design: Mental Health and Addiction Nurses in District School Board Program September 6, 2011 Table of Contents Program Design: Mental Health and Addiction Nurses in District School Boards Program
Defining the Nathaniel ACT ATI Program
 Nathaniel ACT ATI Program: ACT or FACT? Over the past 10 years, the Center for Alternative Sentencing and Employment Services (CASES) has received national recognition for the Nathaniel Project 1. Initially
Nathaniel ACT ATI Program: ACT or FACT? Over the past 10 years, the Center for Alternative Sentencing and Employment Services (CASES) has received national recognition for the Nathaniel Project 1. Initially
Wisconsin State Plan to Serve More Children and Youth within Medical Homes
 Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Report of the Auditor General to the Nova Scotia House of Assembly
 November 22, 2017 Report of the Auditor General to the Nova Scotia House of Assembly Performance Independence Integrity Impact November 22, 2017 Honourable Kevin Murphy Speaker House of Assembly Province
November 22, 2017 Report of the Auditor General to the Nova Scotia House of Assembly Performance Independence Integrity Impact November 22, 2017 Honourable Kevin Murphy Speaker House of Assembly Province
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
IMPACT OF SIMULATION EXPERIENCE ON STUDENT PERFORMANCE DURING RESCUE HIGH FIDELITY PATIENT SIMULATION
 IMPACT OF SIMULATION EXPERIENCE ON STUDENT PERFORMANCE DURING RESCUE HIGH FIDELITY PATIENT SIMULATION Kayla Eddins, BSN Honors Student Submitted to the School of Nursing in partial fulfillment of the requirements
IMPACT OF SIMULATION EXPERIENCE ON STUDENT PERFORMANCE DURING RESCUE HIGH FIDELITY PATIENT SIMULATION Kayla Eddins, BSN Honors Student Submitted to the School of Nursing in partial fulfillment of the requirements
Mission: Providing excellent health care to American Indians. Vision: To be the national model for American Indian Health Care
 Mission: Providing excellent health care to American Indians Vision: To be the national model for American Indian Health Care Core Values: Patient First, Quality, Integrity, Professionalism and Indian
Mission: Providing excellent health care to American Indians Vision: To be the national model for American Indian Health Care Core Values: Patient First, Quality, Integrity, Professionalism and Indian
Moving forward on mental health and substance abuse: The time is now!
 CNA Webinar Series: Progress in Practice Moving forward on mental health and substance abuse: The time is now! Louise Bradley President & CEO, Mental Health Commission of Canada Michel Perron Chief Executive
CNA Webinar Series: Progress in Practice Moving forward on mental health and substance abuse: The time is now! Louise Bradley President & CEO, Mental Health Commission of Canada Michel Perron Chief Executive
Primary Health Tasmania Primary Mental Health Care Activity Work Plan
 Primary Health Tasmania Primary Mental Health Care Activity Work Plan 2016-2018 Primary Health Networks - Primary Mental Health Care Funding Activity Work Plan 2016-2018 Primary Health Tasmania t: 1300
Primary Health Tasmania Primary Mental Health Care Activity Work Plan 2016-2018 Primary Health Networks - Primary Mental Health Care Funding Activity Work Plan 2016-2018 Primary Health Tasmania t: 1300
Original Article Rural generalist nurses perceptions of the effectiveness of their therapeutic interventions for patients with mental illness
 Blackwell Science, LtdOxford, UKAJRAustralian Journal of Rural Health1038-52822005 National Rural Health Alliance Inc. August 2005134205213Original ArticleRURAL NURSES and CARING FOR MENTALLY ILL CLIENTSC.
Blackwell Science, LtdOxford, UKAJRAustralian Journal of Rural Health1038-52822005 National Rural Health Alliance Inc. August 2005134205213Original ArticleRURAL NURSES and CARING FOR MENTALLY ILL CLIENTSC.
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and
 Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Fostering Effective Integration of Behavioral Health and Primary Care in Massachusetts Guidelines. Program Overview and Goal.
 Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Intensive Psychiatric Care Units
 NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
Level 3 Certificate in Working in Community Mental Health Care ( )
") Level 3 Certificate in Working in Community Mental Health Care (3561-03) Qualification handbook for centres 501/1157/7 www.cityandguilds.com October 2010 Version 1.1 About City & Guilds City & Guilds is
Level 3 Certificate in Working in Community Mental Health Care (3561-03) Qualification handbook for centres 501/1157/7 www.cityandguilds.com October 2010 Version 1.1 About City & Guilds City & Guilds is
Denise Figueroa. Gurabo Community Health Center, Inc. Gurabo, Puerto Rico
 The One Stop Shop: An Integrated t Model of Early Intervention Services in HIV Care Denise Figueroa HIV Program Director Gurabo Community Health Center, Inc. Gurabo, Puerto Rico G URABO * SA N LO R ENZO
The One Stop Shop: An Integrated t Model of Early Intervention Services in HIV Care Denise Figueroa HIV Program Director Gurabo Community Health Center, Inc. Gurabo, Puerto Rico G URABO * SA N LO R ENZO
Consumer Perception of Care Survey 2015
 Maryland s Public Behavioral Health System Consumer Perception of Care Survey 2015 EXECUTIVE SUMMARY MARYLAND S PUBLIC BEHAVIORAL HEALTH SYSTEM 2015 CONSUMER PERCEPTION OF CARE SURVEY ~TABLE OF CONTENTS~
Maryland s Public Behavioral Health System Consumer Perception of Care Survey 2015 EXECUTIVE SUMMARY MARYLAND S PUBLIC BEHAVIORAL HEALTH SYSTEM 2015 CONSUMER PERCEPTION OF CARE SURVEY ~TABLE OF CONTENTS~
Quality Management and Improvement 2016 Year-end Report
 Quality Management and Improvement Table of Contents Introduction... 4 Scope of Activities...5 Patient Safety...6 Utilization Management Quality Activities Clinical Activities... 7 Timeliness of Utilization
Quality Management and Improvement Table of Contents Introduction... 4 Scope of Activities...5 Patient Safety...6 Utilization Management Quality Activities Clinical Activities... 7 Timeliness of Utilization
Psychological therapies for common mental illness: who s talking to whom?
 Primary Care Mental Health 2005;3:00 00 # 2005 Radcliffe Publishing Research papers Psychological therapies for common mental illness: who s talking to whom? Ruth Lawson Specialist Registrar in Public
Primary Care Mental Health 2005;3:00 00 # 2005 Radcliffe Publishing Research papers Psychological therapies for common mental illness: who s talking to whom? Ruth Lawson Specialist Registrar in Public
EVALUATION OF THE CARE MANAGEMENT OVERSIGHT PROJECT. Prepared By: Geneva Strech, M. Ed., MHR Betty Harris, M. A. John Vetter, M. A.
 University of Oklahoma College of Continuing Education EVALUATION OF THE CARE MANAGEMENT OVERSIGHT PROJECT June 30, 2011 Prepared By: Geneva Strech, M. Ed., MHR Betty Harris, M. A. John Vetter, M. A. Funding
University of Oklahoma College of Continuing Education EVALUATION OF THE CARE MANAGEMENT OVERSIGHT PROJECT June 30, 2011 Prepared By: Geneva Strech, M. Ed., MHR Betty Harris, M. A. John Vetter, M. A. Funding
Institute Presenters. Objectives: Participants Will Learn. Agenda 6/27/2014
 Continuous Quality Improvement (): Assessing System of Care Implementation and Expansion Georgetown Training Institutes July 16 20, 2014 Washington, D.C. Funded by the Substance Abuse and Mental Health
Continuous Quality Improvement (): Assessing System of Care Implementation and Expansion Georgetown Training Institutes July 16 20, 2014 Washington, D.C. Funded by the Substance Abuse and Mental Health
Covered Service Codes and Definitions
 Covered Service Codes and Definitions [01] Assessment Assessment services include the systematic collection and integrated review of individualspecific data, such as examinations and evaluations. This
Covered Service Codes and Definitions [01] Assessment Assessment services include the systematic collection and integrated review of individualspecific data, such as examinations and evaluations. This
Innovative and Outcome-Driven Practices and Systems Meaningful Prevention and Early Intervention Wellness, Recovery, & Resilience Focus
 Our Mission: To provide a culturally competent system of care that promotes holistic recovery, optimum health, and resiliency. Our Vision: We envision a community where persons from diverse backgrounds
Our Mission: To provide a culturally competent system of care that promotes holistic recovery, optimum health, and resiliency. Our Vision: We envision a community where persons from diverse backgrounds
Rapid Intervention Service Kenora (RISK) Table Report May May 2017
 Table Report May May 2017") Rapid Intervention Service Kenora (RISK) Table Report May 2016 - May 2017 Rapid Intervention Service Kenora (RISK) Table Report May 2016 - May 2017 Table of Contents Background... p3 Introduction.... p4
Rapid Intervention Service Kenora (RISK) Table Report May 2016 - May 2017 Rapid Intervention Service Kenora (RISK) Table Report May 2016 - May 2017 Table of Contents Background... p3 Introduction.... p4
Agenda Item 6.7. Future PROGRAM. Proposed QA Program Models
 Agenda Item 6.7 Proposed Program Models Background...3 Summary of Council s feedback - June 2017 meeting:... 3 Objectives and overview of this report... 5 Methodology... 5 Questions for Council... 6 Model
Agenda Item 6.7 Proposed Program Models Background...3 Summary of Council s feedback - June 2017 meeting:... 3 Objectives and overview of this report... 5 Methodology... 5 Questions for Council... 6 Model
NURSING FACILITY ASSESSMENTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Executive Summary. An Evaluation of Staffordshire and Stoke on Trent Partnership NHS Trust s Anxiety Management Programme (AMP) at HMP Stafford
 at HMP Stafford") An Evaluation of Staffordshire and Stoke on Trent Partnership NHS Trust s Anxiety Management Programme (AMP) at HMP Stafford Executive Summary Prepared by Dr Martin Glynn and Professor Laura Serrant The
An Evaluation of Staffordshire and Stoke on Trent Partnership NHS Trust s Anxiety Management Programme (AMP) at HMP Stafford Executive Summary Prepared by Dr Martin Glynn and Professor Laura Serrant The
Evaluation of the Brant Community Response Team Initiative: Six-month Report. Alexey Babayan, Ph.D. Tamara Landry-Thompson, Ph.D.
 Evaluation of the Brant Community Response Team Initiative: Six-month Report Alexey Babayan, Ph.D. Tamara Landry-Thompson, Ph.D. Adam Stevens, MSc October 30, 2015 Suggested Citation: Babayan A, Landry-Thompson
Evaluation of the Brant Community Response Team Initiative: Six-month Report Alexey Babayan, Ph.D. Tamara Landry-Thompson, Ph.D. Adam Stevens, MSc October 30, 2015 Suggested Citation: Babayan A, Landry-Thompson
Mental / Behavioral Health Screening in Pediatric Primary Care OVERVIEW OF THE PEDIATRIC PSYCHIATRY COLLABORATIVE PROGRAM
 Mental / Behavioral Health Screening in Pediatric Primary Care OVERVIEW OF THE PEDIATRIC PSYCHIATRY COLLABORATIVE PROGRAM 1 Co-Presenters Ray Hanbury, Ph.D., A.B.P.P. Chief Psychologist, Dept. of Psychiatry
Mental / Behavioral Health Screening in Pediatric Primary Care OVERVIEW OF THE PEDIATRIC PSYCHIATRY COLLABORATIVE PROGRAM 1 Co-Presenters Ray Hanbury, Ph.D., A.B.P.P. Chief Psychologist, Dept. of Psychiatry
SERVICE SCHEDULE FOR CLINICAL PSYCHIATRIC SERVICES CONTRACT NO: «Contract_»
 SERVICE SCHEDULE FOR CLINICAL PSYCHIATRIC SERVICES CONTRACT NO: «Contract_» A. QUICK REFERENCE INFORMATION 1. TERM FOR PROVIDING CLINICAL PSYCHIATRIC SERVICES The Term for the provision of Clinical Psychiatric
SERVICE SCHEDULE FOR CLINICAL PSYCHIATRIC SERVICES CONTRACT NO: «Contract_» A. QUICK REFERENCE INFORMATION 1. TERM FOR PROVIDING CLINICAL PSYCHIATRIC SERVICES The Term for the provision of Clinical Psychiatric
Building Bridges to Improve Care in First Nations Communities
 Building Bridges to Improve Care in First Nations Communities Contact: M. Janet Kasperski RN, MHSc, CHE The Ontario College of Family Physicians 340 Richmond St. W., Toronto, Ontario M5V 1X2 Telephone
Building Bridges to Improve Care in First Nations Communities Contact: M. Janet Kasperski RN, MHSc, CHE The Ontario College of Family Physicians 340 Richmond St. W., Toronto, Ontario M5V 1X2 Telephone
IV. Clinical Policies and Procedures
 A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
Care Programme Approach Policies and Procedures. Choice, Responsiveness, Integration & Shared Care
 Care Programme Approach Policies and Procedures Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose:
Care Programme Approach Policies and Procedures Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose:
Profile: Integrating the Patient Activation Measure Into Health Coaching to Improve Patient Engagement
 MEASURING PATIENT ENGAGEMENT: HOW IS CAPACITY AND WILLINGNESS TO ENGAGE IN HEALTH CARE ASSESSED? 75 Profile: Integrating the Patient Activation Measure Into Health Coaching to Improve Patient Engagement
MEASURING PATIENT ENGAGEMENT: HOW IS CAPACITY AND WILLINGNESS TO ENGAGE IN HEALTH CARE ASSESSED? 75 Profile: Integrating the Patient Activation Measure Into Health Coaching to Improve Patient Engagement
A SURVEY OF THE USE OF AN ASSESSMENT AND TREATMENT UNIT FOR ADULTS WITH LEARNING DISABILITY IN LANARKSHIRE OVER A SIX YEAR PERIOD ( )
") The British Journal of Developmental Disabilities Vol. 54, Part 2, JULY 2008, No. 107, pp. 89-99 A SURVEY OF THE USE OF AN ASSESSMENT AND TREATMENT UNIT FOR ADULTS WITH LEARNING DISABILITY IN LANARKSHIRE
The British Journal of Developmental Disabilities Vol. 54, Part 2, JULY 2008, No. 107, pp. 89-99 A SURVEY OF THE USE OF AN ASSESSMENT AND TREATMENT UNIT FOR ADULTS WITH LEARNING DISABILITY IN LANARKSHIRE
STROKE REHAB PROGRAM
 STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
Ryan White Part A. Quality Management
 Quality Management Mental Health Services Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part A grant
Quality Management Mental Health Services Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part A grant
Interactive Voice Registration (IVR) System Manual WASHINGTON STREET, SUITE 310 BOSTON, MA
 System Manual WASHINGTON STREET, SUITE 310 BOSTON, MA") Interactive Voice Registration (IVR) System Manual 1000 WASHINGTON STREET, SUITE 310 BOSTON, MA 02118-5002 1-800-495-0086 www.masspartnership.com TABLE OF CONTENTS INTRODUCTION... 3 IVR INSTRUCTIONS...
Interactive Voice Registration (IVR) System Manual 1000 WASHINGTON STREET, SUITE 310 BOSTON, MA 02118-5002 1-800-495-0086 www.masspartnership.com TABLE OF CONTENTS INTRODUCTION... 3 IVR INSTRUCTIONS...
4.09. Hospitals Management and Use of Surgical Facilities. Chapter 4 Section. Background. Follow-up on VFM Section 3.09, 2007 Annual Report
 Chapter 4 Section 4.09 Hospitals Management and Use of Surgical Facilities Follow-up on VFM Section 3.09, 2007 Annual Report Background Ontario s public hospitals are generally governed by a board of directors
Chapter 4 Section 4.09 Hospitals Management and Use of Surgical Facilities Follow-up on VFM Section 3.09, 2007 Annual Report Background Ontario s public hospitals are generally governed by a board of directors
Maine s Co- occurring Capability Self Assessment 1
 Maine s Co- occurring Capability Self Assessment August 2009 Version 3.3 Date: Rater(s): Time Spent: Agency Name: Program Name: Program Type(s): Level of Care: Address: Contact Person: Title: Telephone:
Maine s Co- occurring Capability Self Assessment August 2009 Version 3.3 Date: Rater(s): Time Spent: Agency Name: Program Name: Program Type(s): Level of Care: Address: Contact Person: Title: Telephone:
Provider Documentation and High Risk Cases
 Provider Documentation and High Risk Cases For Audio Call: (877) 563-4796 Enter Code: 7771224# *Phones are muted due to the large number of attendees Welcome and Introductions Presenter Douglas Briskman,
Provider Documentation and High Risk Cases For Audio Call: (877) 563-4796 Enter Code: 7771224# *Phones are muted due to the large number of attendees Welcome and Introductions Presenter Douglas Briskman,
EVALUATION OF THE CARE MANAGEMENT OVERSIGHT PROJECT. June 30, 2011 Prepared By: Geneva Strech, M. Ed., MHR Betty Harris, M. A. John Vetter, M. A.
 University of Oklahoma College of Continuing Education EVALUATION OF THE CARE MANAGEMENT OVERSIGHT PROJECT June 30, 2011 Prepared By: Geneva Strech, M. Ed., MHR Betty Harris, M. A. John Vetter, M. A. Funding
University of Oklahoma College of Continuing Education EVALUATION OF THE CARE MANAGEMENT OVERSIGHT PROJECT June 30, 2011 Prepared By: Geneva Strech, M. Ed., MHR Betty Harris, M. A. John Vetter, M. A. Funding
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
FRENCH LANGUAGE HEALTH SERVICES STRATEGY
 FRENCH LANGUAGE HEALTH SERVICES STRATEGY 2016-2019 Table of Contents I. Introduction... 4 Partners... 4 A. Champlain LHIN IHSP... 4 B. South East LHIN IHSP... 5 C. Réseau Strategic Planning... 5 II. Goal
FRENCH LANGUAGE HEALTH SERVICES STRATEGY 2016-2019 Table of Contents I. Introduction... 4 Partners... 4 A. Champlain LHIN IHSP... 4 B. South East LHIN IHSP... 5 C. Réseau Strategic Planning... 5 II. Goal
September Sub-Region Collaborative Meeting: Bramalea. September 13, 2018
 September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
The University of Ioannina Counselling Centre
 SUMMER UNIVERSITY 2011 Thematic Symposium The Present and the Future of Students Psychological Counselling: Meeting the challenges, discussing the prospects. The University of Ioannina Counselling Centre
SUMMER UNIVERSITY 2011 Thematic Symposium The Present and the Future of Students Psychological Counselling: Meeting the challenges, discussing the prospects. The University of Ioannina Counselling Centre
Children s Senior Psychotherapist. Therapeutic Services GRADE: 05. Context and Purpose of the Job
 JOB TITLE: TEAM: GROUP: LOCATION: REPORTS TO: Children s Psychotherapist Therapeutic Services Operations Luton Children s Senior Psychotherapist GRADE: 05 HOURS: 21 hours per week Context and Purpose of
JOB TITLE: TEAM: GROUP: LOCATION: REPORTS TO: Children s Psychotherapist Therapeutic Services Operations Luton Children s Senior Psychotherapist GRADE: 05 HOURS: 21 hours per week Context and Purpose of
CE LHIN Board Ontario Shores Update January 19, Glenna Raymond, President and CEO
 CE LHIN Board Ontario Shores Update January 19, 2010 Glenna Raymond, President and CEO Ontario Shores: The Journey Begins 2 Divestment from Government March 27, 2006 a standalone public hospital Creation
CE LHIN Board Ontario Shores Update January 19, 2010 Glenna Raymond, President and CEO Ontario Shores: The Journey Begins 2 Divestment from Government March 27, 2006 a standalone public hospital Creation
Recommendations for Adoption: Major Depression. Recommendations to enable widespread adoption of this quality standard
 Recommendations for Adoption: Major Depression Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
Recommendations for Adoption: Major Depression Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS)
") NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS) Perception of Care Survey of Alliance Consumers Fiscal Year 2014 Background Information The Division
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS) Perception of Care Survey of Alliance Consumers Fiscal Year 2014 Background Information The Division
Managing deliberate self-harm in young people
 Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
CASE MANAGEMENT POLICY
 CASE MANAGEMENT POLICY Subject: Acuity Scale Determination Effective Date: March 21, 1996 Revised: October 25, 2007 Page 1 of 1 PURPOSE: To set a minimum standard across Cooperative agencies regarding
CASE MANAGEMENT POLICY Subject: Acuity Scale Determination Effective Date: March 21, 1996 Revised: October 25, 2007 Page 1 of 1 PURPOSE: To set a minimum standard across Cooperative agencies regarding
SECTION 3. Behavioral Health Core Program Standards. Z. Health Home
 SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
Ontario Systems Projects
 Drug Treatment Funding Program () Delivered by Project Leads at the Launch Event October 13 th and 14 th, 2011, Toronto Investment areas The supports sustainable improvement in the quality and organization
Drug Treatment Funding Program () Delivered by Project Leads at the Launch Event October 13 th and 14 th, 2011, Toronto Investment areas The supports sustainable improvement in the quality and organization