Demonstrating the Chain of Medical Necessity. Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President
|
|
|
- Gordon Nichols
- 6 years ago
- Views:
Transcription

1 Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1
 - AAPC Certified Chiropractic Professional Coder (CCPC) - AAPC Qualified Chiropractic Coder (QCC) - ChiroCode Certified")
2 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting - Brigham Young University Master s of Business Administration - Broadview University Doctor of Chiropractic, Valedictorian - Palmer College of Chiropractic Certifications Certified Professional Coder (CPC) - AAPC Certified Chiropractic Professional Coder (CCPC) - AAPC Qualified Chiropractic Coder (QCC) - ChiroCode Certified Professional Coder Instructor (CPC-I) - AAPC Medical Compliance Specialist Physician (MCS-P) - MCS Certified Professional Medical Auditor (CPMA) AAPC, NAMAS Certified ICD-10 Trainer AAPC Certified MIPS Healthcare Professional (CMHP) 4Med Fellow AAPC 2
3 Take-away Document the entire Episode of Care Learn to use the Chain of Medical Necessity Create powerful diagnostic statements Use a solid diagnostic code hierarchy Create meaningful goals Know how to convey Medical Necessity through E/M codes 3

4 Episode of Care 4
5 Episode of Care

6 From the new and improved documentation chapter in the 2018 DeskBook

7 7
8 Medical Necessity Services or items reasonable and necessary for the diagnosis or treatment of illness or injury, or to improve the functioning of a malformed body member -CMS How can you prove medical necessity?
9 Chain of Medical Necessity 1. History of onset 2. Patient complaint 3. Exam findings 4. Diagnosis 5. Treatment plan 6. Progress
10 Chain of Medical Necessity 1. History of onset Explain why the patient has a complaint Document mechanism of trauma for acute patients For chronic patients, try to establish why the patient decided to come in today, rather than another time
11 Chain of Medical Necessity 2. Patient complaint 3. Exam findings Relate exam findings to complaint Functional loss should be documented in the complaint (ADLs) and consistent with the exam findings.
12 Chain of Medical Necessity 4. Diagnosis The diagnosis should provide a plausible explanation for the symptoms. Clinical criteria from the history and exam should match up with the diagnosis.
13 5. Treatment Plan Should be appropriate for the diagnosis. Care given because of provider technique, philosophy, or just routine is not medically necessary. Treatment should transition from passive to active. Avoid cookie cutter care. Plans should vary for different ages and different diagnoses. Chain of Medical Necessity

14 Chain of Medical Necessity 6. Progress Goals should be specific to each patient and measurable Outcomes Assessment Tools are the best way to quantify functional progress Goals must be evaluated and updated over time See chapter 4.4 of the 2018 DeskBook for more on goals
15 Chain of Medical Necessity 1. History of onset 2. Patient complaint 3. Exam findings 4. Diagnosis 5. Treatment plan 6. Progress
16 Does you care plan answer these questions? 1. Why are you treating the patient? 2. What are you going to do with the patient? 3. How long and how often are you going to see the patient? 4. What are you and the patient trying to accomplish? 5. How do you know when you have accomplished the goals?
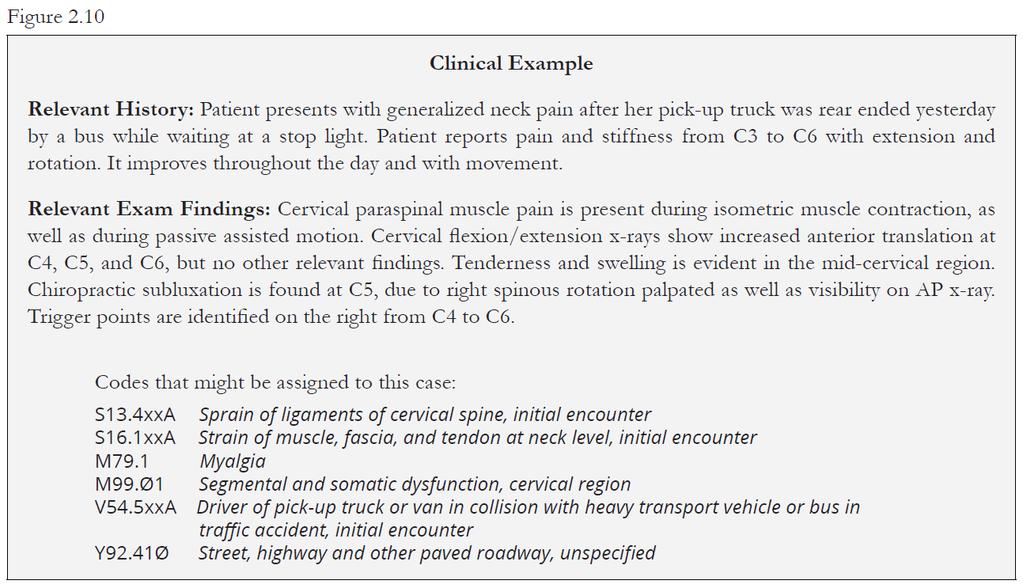
17 ICD-10 Heirarchy 1. Nerve-related disorders (e.g. radiculopathy) 2. Acute injuries (e.g. sprains and strains) 3. Structural diagnoses (e.g. degenerative disc disease) 4. Functional diagnoses (e.g. difficulty with walking) 5. Soft tissue problems (e.g. myalgia) 6. Symptoms (e.g. neck pain) 7. Complicating factors/comorbidities (e.g. diabetes) 8. External causes (e.g. place and activity)
18 ICD-10 Tips Follow ICD-10 guidelines (Excludes1, NOS) When coding for symptoms, add the phrase due to for better specificity. Complicating factors may also be coded, if relevant. Learn to document a Diagnostic Statement or Clinical Impression that matches the code requirements. 18

19 ICD-10 Guidelines

20
21 Functional Goals 1. What is the activity (sleep, walk) the patient will be able to perform? 2. Under what conditions (how far or for how long) will they be able to do it? 3. How well will they be able to do it (without assistance, without increased pain)? 4. When will this be accomplished (2 weeks, 2 months)? Keep them patient-centered! 21
22 Weak Care Plans Only address frequency and duration of visits, and neglect goals entirely OR Include goals, but o They are only subjective o They do not address function o They are not measurable 22
23 Short term goals restated: 1. Reduce pain 2. Increase pain-free ROM 3. Restore normal vertebral segmental motion 4. Increase ability to move affected area Short term goals improved: 1. Reduce VNRS from 8/10 to 5/10 within 2 weeks 2. Increase pain-free ROM by 50% within 2 weeks 3. If you restore normal vertebral segmental motion, you can t adjust anymore, right? 4. Same as number 2? 23
24 Two weeks later Assessment should discuss progress towards goals Were goals achieved? If not, why? Patient went on vacation Patient fell down the stairs How will the care plan change to adapt to goals that were not met? Easier or harder exercises? More or fewer visits? Referral or new diagnostic test? 24
25 Short term goals restated: 1. Reduce pain by 10% 2. Increase strength (Is there documented loss of strength?) 3. Increase endurance (How do you measure this?) 4. Increase ability to move affected area (Measurable?) 5. Increase ability to exert force to affected area AND (these are better) 1. Get 5-6 hours of quality sleep (within what time frame?) 2. Stand for more than 20 minutes (Is this from Oswestry?) 3. Sit for more than 20 minutes pain free 4. Walk for more than 1 block pain free 5. Lift more than 20 pounds from off the floor 25
26 Evaluation & Management Office/Outpatient New Patient Office/Outpatient Established Patient *A new patient is one who has not received any professional services from the physician.within the past three years.
27 Evaluation & Management Three Key Components: History Physical Examination Medical Decision Making Contributing Factors: Nature of Presenting Problem Time Counseling Coordination of Care
28 Nature of the Presenting Problem Medical necessity is the overarching criterion for payment. Medicare will not cover services that are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member. -Social Security Act 1862 (a)(1)(a)
29 Nature of the Presenting Problem A presenting problem is a disease, condition, illness, injury, symptom, sign, finding, complaint, or other reason for encounter, with or without a diagnosis being established at the time of the encounter. The E/M codes recognize five types of presenting problems that are defined as follows: Minimal: A problem that may not require the presence of the physician or other qualified health care professional, but service is provided under the physician s or other qualified health care professional s supervision. Self-limited or minor: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status OR has a good prognosis with management/compliance.
30 Nature of the Presenting Problem Low severity: A problem where the risk of morbidity without treatment is low; there is little to no risk of mortality without treatment; full recovery without functional impairment is expected. Moderate severity: A problem where the risk of morbidity without treatment is moderate; there is moderate risk of mortality without treatment; uncertain prognosis OR increased probability of prolonged functional impairment. High severity: A problem where the risk of morbidity without treatment is high to extreme; there is a moderate to high risk of mortality without treatment OR high probability of severe, prolonged functional impairment.
31 Nature of the Presenting Problem New Patient E/M Self-limited or minor Low to Moderate severity Moderate severity Moderate to High severity Moderate to High severity

32 The NEW ChiroCode DeskBook is available at ChiroCode.com Most of this presentation is covered in Chapters 4 and 5.
33 Take-away Document the entire Episode of Care Learn to use the Chain of Medical Necessity Create powerful diagnostic statements Use a solid diagnostic code hierarchy Create meaningful goals Know how to convey Medical Necessity through E/M codes 33
Chiropractic Record Keeping
 Chiropractic Record Keeping (DeskBook Chapter 4.1) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting
Chiropractic Record Keeping (DeskBook Chapter 4.1) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting
Quality Payment Program: The future of reimbursement
 Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
Medical Necessity: Not just LCD. Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC
 Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Under the Magnifying Glass
 5 6 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
5 6 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
Advanced E/M Auditing: Secrets to Success
 Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Under the Magnifying Glass
 5 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
5 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
Risk Adjustment and Hierarchial Condition Category Coding and Auditing
 December 2, 2016 Risk Adjustment and Hierarchial Condition Category Coding and Auditing Risk Adjustment (RA) and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997,
December 2, 2016 Risk Adjustment and Hierarchial Condition Category Coding and Auditing Risk Adjustment (RA) and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997,
PSYCHIATRY SERVICES: MD FOCUSED
 PSYCHIATRY SERVICES: MD FOCUSED CY2013 Risk Based Scheduled Review Agenda 2 Overview of New Risk Based Scheduled Reviews Initial review findings PhD summary MD summary Examples Template/Psychotherapy Time
PSYCHIATRY SERVICES: MD FOCUSED CY2013 Risk Based Scheduled Review Agenda 2 Overview of New Risk Based Scheduled Reviews Initial review findings PhD summary MD summary Examples Template/Psychotherapy Time
Implementation Date: January 2018 Clinical Operations
 Magellan Healthcare Clinical guidelines RECORD KEEPING AND DOCUMENTATION STANDARDS Original Date: November 2015 Page 1 of 11 Physical Medicine Clinical Decision Making Last Review Date: June 2017 Guideline
Magellan Healthcare Clinical guidelines RECORD KEEPING AND DOCUMENTATION STANDARDS Original Date: November 2015 Page 1 of 11 Physical Medicine Clinical Decision Making Last Review Date: June 2017 Guideline
ICD-9 (Diagnosis) Coding
 Coding") 1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
ICD Codes health health health
 1-10-2017 Encounter for screening for malignant neoplasm of cervix. 2016 2017 2018 Billable/Specific Code Female Dx POA Exempt. Z12.4 is a billable/specific ICD-10. ICD-10 is the 10th revision of the International
1-10-2017 Encounter for screening for malignant neoplasm of cervix. 2016 2017 2018 Billable/Specific Code Female Dx POA Exempt. Z12.4 is a billable/specific ICD-10. ICD-10 is the 10th revision of the International
Coding Complexities of Critical Care
 Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care. Excerpts from:
 FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care Excerpts from: Practical E/M: Documentation and Coding Solutions for Quality Patient Care by Dr. Stephen R. Levinson To
FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care Excerpts from: Practical E/M: Documentation and Coding Solutions for Quality Patient Care by Dr. Stephen R. Levinson To
BHS Policies and Procedures
 BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
This Material is Copyright Protected
 ICD-10 Utilization in the NEW World With Mario Fucinari DC, CCSP, CPCO, MCS-P, MCS-I Presented by NCMIC The information contained in these notes is for educational purposes and is not intended to be and
ICD-10 Utilization in the NEW World With Mario Fucinari DC, CCSP, CPCO, MCS-P, MCS-I Presented by NCMIC The information contained in these notes is for educational purposes and is not intended to be and
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Transitioning to ICD-10: An Action Plan for Practices
 Transitioning to ICD-10: An Action Plan for Practices By Nancy M Enos, FACMPE, CPMA, CPC-I, CEMC 1 viterahealthcare.com/icd10 The Four T s of Transition to ICD-10: Timing, Training, Testing and Technology
Transitioning to ICD-10: An Action Plan for Practices By Nancy M Enos, FACMPE, CPMA, CPC-I, CEMC 1 viterahealthcare.com/icd10 The Four T s of Transition to ICD-10: Timing, Training, Testing and Technology
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
Coding for the Practitioner
 Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
Medical Appropriateness and Risk Adjustment
 Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Crash Course in Medical Necessity for E/M Coders
 Crash Course in Medical Necessity for E/M Coders Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions
Crash Course in Medical Necessity for E/M Coders Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions
Crash Course in Medical Necessity for E/M Coders. Regional Conference
 Crash Course in Medical Necessity for E/M Coders Regional Conference About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions that allow coders
Crash Course in Medical Necessity for E/M Coders Regional Conference About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions that allow coders
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC
 The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC Chiropractic Training from CMS In April of last year Congress repealed the SGR formula. As part of that law, CMS was to provide
The Physician Quality Reporting System 2016 By Dr. Ron Short, DC, MCS-P, CPC Chiropractic Training from CMS In April of last year Congress repealed the SGR formula. As part of that law, CMS was to provide
Preparing for ICD 10 Compliance While Living in ICD 9 A Challenge to Overcome
 Preparing for ICD 10 Compliance While Living in ICD 9 A Challenge to Overcome Betty B. Bibbins, MD, BSN, CHC, C CDI, CPEHR, CPHIT President & Chief Medical Officer Physician Executive Educator DocuComp
Preparing for ICD 10 Compliance While Living in ICD 9 A Challenge to Overcome Betty B. Bibbins, MD, BSN, CHC, C CDI, CPEHR, CPHIT President & Chief Medical Officer Physician Executive Educator DocuComp
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
HEALTH DEPARTMENT BILLING GUIDELINES
 HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
CRASH COURSE MEDICAL NECESSITY SKILLS FOR NON PROVIDERS
 CRASH COURSE MEDICAL NECESSITY SKILLS FOR NON PROVIDERS PRESENTED BY: MAGGIE MAC CPC, CEMC, CHC, CMM, ICCE, AHIMA APPROVED ICD 10 CM/PCS TRAINER STEPHANIE CECCHINI, CPC, CEMC, CHISP, APPROVED ICD 10 TRAINER
CRASH COURSE MEDICAL NECESSITY SKILLS FOR NON PROVIDERS PRESENTED BY: MAGGIE MAC CPC, CEMC, CHC, CMM, ICCE, AHIMA APPROVED ICD 10 CM/PCS TRAINER STEPHANIE CECCHINI, CPC, CEMC, CHISP, APPROVED ICD 10 TRAINER
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
9 TIPS FOR SURVIVING AFTER THE ICD-10 GRACE PERIOD ENDS. By Aine Cryts
 9 TIPS FOR SURVIVING AFTER THE ICD-10 GRACE PERIOD ENDS By Aine Cryts BE SPECIFIC IN YOUR CODING "Specificity in documentation and diagnosis coding since the ICD-10 implementation is to be encouraged.
9 TIPS FOR SURVIVING AFTER THE ICD-10 GRACE PERIOD ENDS By Aine Cryts BE SPECIFIC IN YOUR CODING "Specificity in documentation and diagnosis coding since the ICD-10 implementation is to be encouraged.
CREATING AN AUDIT PLAN FOR PHYSICIAN OFFICES. Katherine Abel, CPC, CPB, CPMA, CPPM, CPC-I, AAPC Fellow Director of Curriculum AAPC
 CREATING AN AUDIT PLAN FOR PHYSICIAN OFFICES Katherine Abel, CPC, CPB, CPMA, CPPM, CPC-I, AAPC Fellow Director of Curriculum AAPC OIG Compliance Guidance Implementing written policies, procedures and standards
CREATING AN AUDIT PLAN FOR PHYSICIAN OFFICES Katherine Abel, CPC, CPB, CPMA, CPPM, CPC-I, AAPC Fellow Director of Curriculum AAPC OIG Compliance Guidance Implementing written policies, procedures and standards
Providing and Documenting Medically Necessary Behavioral Health Services
 Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Audit Scope and Sampling. AAPC HealthCon 2017 Las Vegas Jaci J Kipreos CPC COC CPMA CEMC CPCI
 Audit Scope and Sampling AAPC HealthCon 2017 Las Vegas Jaci J Kipreos CPC COC CPMA CEMC CPCI About the Presenter Jaci J Kipreos CPC, COC CPMA, CPC-I, CEMC Jaci has been working in the field of medical
Audit Scope and Sampling AAPC HealthCon 2017 Las Vegas Jaci J Kipreos CPC COC CPMA CEMC CPCI About the Presenter Jaci J Kipreos CPC, COC CPMA, CPC-I, CEMC Jaci has been working in the field of medical
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Psychosocial Rehabilitation Medical Necessity Criteria
 Program Description Psychosocial Rehabilitation Medical Necessity Criteria Psychosocial Rehabilitation (PSR) is a community-based program that promotes recovery, community integration, and improved quality
Program Description Psychosocial Rehabilitation Medical Necessity Criteria Psychosocial Rehabilitation (PSR) is a community-based program that promotes recovery, community integration, and improved quality
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Clinical Utilization Management Guideline
 Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims
 March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Macomb County Community Mental Health Level of Care Training Manual
 1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Getting Paid for What You Do! Coding 2010
 Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
HMSA Physical and Occupational Therapy Utilization Management Guide
 HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
Few non-clinical issues have created as
 from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
AAPC Webinar 3/28/2016
 Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Section 7: Core clinical headings
 Section 7: Core clinical headings Core clinical heading standards: the core clinical headings are those that are the priority for inclusion in EHRs, as they are generally items that are the priority for
Section 7: Core clinical headings Core clinical heading standards: the core clinical headings are those that are the priority for inclusion in EHRs, as they are generally items that are the priority for
Optum Physical Health Clinical Forms Instruction Manual
 Optum Physical Health Clinical Forms Instruction Manual OptumHealth Care Solutions Physical Health includes OptumHealth Care Solutions, LLC, ACN Group IPA of New York, Inc., Managed Physical Network, Inc.,
Optum Physical Health Clinical Forms Instruction Manual OptumHealth Care Solutions Physical Health includes OptumHealth Care Solutions, LLC, ACN Group IPA of New York, Inc., Managed Physical Network, Inc.,
Home Health Eligibility Requirements
 Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
Presented By: Melinda A. Gaboury, COS-C Chief Executive Officer Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com Home Health Eligibility Requirements Meets eligibility for home health
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments
 Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
DRGs & MS-DRGs. System that takes into consideration the role that a hospitals case mix plays in influencing costs
 DRGs & MS-DRGs What are DRGs? System that takes into consideration the role that a hospitals case mix plays in influencing costs Relates the type of patients a hospital treats (case mix) to the costs incurred
DRGs & MS-DRGs What are DRGs? System that takes into consideration the role that a hospitals case mix plays in influencing costs Relates the type of patients a hospital treats (case mix) to the costs incurred
Electronic Health Records - Advantages and Pitfalls of Documentation
 Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
8/19/2017. The OIG Report
 This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
Quincy Bay Coders Professional Development Workshop & Job Fair
 Quincy Bay Coders Professional Development Workshop & Job Fair June 2012 June 2012 **Consider using the chapter logo 1 The $64,000 Question: What kinds of jobs are out there for professional coders? 2
Quincy Bay Coders Professional Development Workshop & Job Fair June 2012 June 2012 **Consider using the chapter logo 1 The $64,000 Question: What kinds of jobs are out there for professional coders? 2
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Chapter 9 Worksheet Code It
 Class: Date: Chapter 9 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. Notes located beneath headings and/or subheadings apply to all codes in the categories or subcategories.
Class: Date: Chapter 9 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. Notes located beneath headings and/or subheadings apply to all codes in the categories or subcategories.
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Modern Optometric Staff BILLING & CODING THE MEDICAL EYE EXAMINATION. I m From The Government. The HIPPA Act of And I m Here To Help
 BILLING & CODING THE MEDICAL EYE EXAMINATION Modern Optometric Staff Ask the right questions, take the right actions Follow HIPPA guidelines Craig Thomas, O.D. 3900 West Wheatland Road Dallas, Texas 75237
BILLING & CODING THE MEDICAL EYE EXAMINATION Modern Optometric Staff Ask the right questions, take the right actions Follow HIPPA guidelines Craig Thomas, O.D. 3900 West Wheatland Road Dallas, Texas 75237
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
RISK ADJUSTMENT CONCEPTS AN INTRODUCTION AND DISCUSSION
 RISK ADJUSTMENT CONCEPTS AN INTRODUCTION AND DISCUSSION HFMA Maine Chapter Physician Practice Management Seminar March 16, 2017 AGENDA Risk Adjustment How Risk Adjustment Works Comprehensive Annual Visits
RISK ADJUSTMENT CONCEPTS AN INTRODUCTION AND DISCUSSION HFMA Maine Chapter Physician Practice Management Seminar March 16, 2017 AGENDA Risk Adjustment How Risk Adjustment Works Comprehensive Annual Visits
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Informed Consent for Chiropractic Care
 Informed Consent for Chiropractic Care When a patient seeks chiropractic health care and we accept a patient for such care, it is essential for both of us to be working toward the same objective. This
Informed Consent for Chiropractic Care When a patient seeks chiropractic health care and we accept a patient for such care, it is essential for both of us to be working toward the same objective. This
Tennessee Health Link Guidelines: Adults Medical Necessity Criteria
 Tennessee Health Link Guidelines: Adults Medical Necessity Criteria https://providers.amerigroup.com Program description The Health Link service model is a program created to address the diverse needs
Tennessee Health Link Guidelines: Adults Medical Necessity Criteria https://providers.amerigroup.com Program description The Health Link service model is a program created to address the diverse needs
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System
 Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES Table of Contents GENERAL INFORMATION AND INSTRUCTIONS... 3 MMIS MODIFIERS... 12 LABORATORY SERVICES PERFORMED IN A PODIATRIST'S OFFICE... 13 MEDICAL
NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES Table of Contents GENERAL INFORMATION AND INSTRUCTIONS... 3 MMIS MODIFIERS... 12 LABORATORY SERVICES PERFORMED IN A PODIATRIST'S OFFICE... 13 MEDICAL
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness. October 12, 2009
 Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
ORIGINAL ARTICLE. Prevalence of nonmusculoskeletal versus musculoskeletal cases in a chiropractic student clinic
 ORIGINAL ARTICLE Prevalence of nonmusculoskeletal versus musculoskeletal cases in a chiropractic student clinic Bruce R. Hodges, DC, MS, Jerrilyn A. Cambron, DC, PhD, Rachel M. Klein, DC, Dana M. Madigan,
ORIGINAL ARTICLE Prevalence of nonmusculoskeletal versus musculoskeletal cases in a chiropractic student clinic Bruce R. Hodges, DC, MS, Jerrilyn A. Cambron, DC, PhD, Rachel M. Klein, DC, Dana M. Madigan,
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES. SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION
 NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
The Business of Medicine
 The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
Today s educational presentation is provided by. The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE
 Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered
 CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
Basic Training in Medi-Cal Documentation
 Basic Training in Medi-Cal Documentation Sara Kashing, J.D. Staff Attorney The Therapist May/June 2012 Since 1998, Medi-Cal mental health services have been provided through county-based Mental Health
Basic Training in Medi-Cal Documentation Sara Kashing, J.D. Staff Attorney The Therapist May/June 2012 Since 1998, Medi-Cal mental health services have been provided through county-based Mental Health
AAPC Richardson, TX Chapter. Monthly Meeting. 6pm. Location:
 AAPC Richardson, TX Chapter Monthly Meeting 4/17/2017 @ 6pm Location: Methodist Richardson/Renner Medical Center-Physician Pavilion I 2821 E President George-Physician Services Building, 2nd floor Conference
AAPC Richardson, TX Chapter Monthly Meeting 4/17/2017 @ 6pm Location: Methodist Richardson/Renner Medical Center-Physician Pavilion I 2821 E President George-Physician Services Building, 2nd floor Conference
ICD-CM Coding The Structural Considerations
 The Challenge ICD-CM Coding The Structural Considerations Hospices are being called upon to 1. Start using ICD-9 CM coding on its claims 2. Be prepared to transition to ICD-10-CM by 10/1/2014 Complicating
The Challenge ICD-CM Coding The Structural Considerations Hospices are being called upon to 1. Start using ICD-9 CM coding on its claims 2. Be prepared to transition to ICD-10-CM by 10/1/2014 Complicating
BEFORE THE ALASKA OFFICE OF ADMINISTRATIVE HEARINGS ON REFERRAL FROM THE COMMISSIONER OF HEALTH AND SOCIAL SERVICES
 BEFORE THE ALASKA OFFICE OF ADMINISTRATIVE HEARINGS ON REFERRAL FROM THE COMMISSIONER OF HEALTH AND SOCIAL SERVICES In the Matter of: ) ) FAMILY MEDICAL CLINIC ) OAH No. 10-0095-DHS ) DECISION I. INTRODUCTION
BEFORE THE ALASKA OFFICE OF ADMINISTRATIVE HEARINGS ON REFERRAL FROM THE COMMISSIONER OF HEALTH AND SOCIAL SERVICES In the Matter of: ) ) FAMILY MEDICAL CLINIC ) OAH No. 10-0095-DHS ) DECISION I. INTRODUCTION
Inpatient IOC Checklist Clinical Record Review
 Date of Review Reason for Review: Inspection of Care Action Plan Follow-up (Focus of Follow-up: ) Beneficiary Record ID: Beneficiary Age: Custody: DCFS DYS Provider Name: Acute RTC PRTF Date of Admission:
Date of Review Reason for Review: Inspection of Care Action Plan Follow-up (Focus of Follow-up: ) Beneficiary Record ID: Beneficiary Age: Custody: DCFS DYS Provider Name: Acute RTC PRTF Date of Admission: