ECRI Patient Safety Organization HFACS and Healthcare
|
|
|
- Sheila Woods
- 6 years ago
- Views:
Transcription
1 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health
2 Learning Objectives Understand the human factors errors for a large health system. Understand lessons learned from the roll out of HFACS across two healthcare systems.
3 Current Quality Approach Good Quality is Assumed to Equal Safe Patient Care Quality Improvement is Project Based Examples Core Measures, CLABSI, Hand Hygiene, etc. Too Many Things to Do!!! Not Sustainable!!! PI Methods are Inadequate Copy what someone else did and replicate it. Use of simple PI methods (PDCA, Best Practice, etc.). Failure to identify specific causes for performance and fix them. Reactive, rather than Proactive We will be talking about the same errors with the next case. Punitive approach, rather than a system s based approach.


4 The pursuit of mediocrity is always successful. Karl Albrecht
5 Event Opportunity Continuum Customer Complaints Patient driven reporting Focus is on immediate mitigation and patient satisfaction Currently difficult to obtain systematic information Occurrences Staff reported events and near misses Identifies areas for process improvement Captured in database, but <10% of events are reported Adverse Events Intense investigation of adverse events Identifies both process and behavioral root causes Malpractice Claims Limited data with several year lag time Generally it is about money, not about process or behavior
6 Traditional Healthcare Root Cause Analysis Heavily focused on TJC Sentinel Events Focused primarily on actual harm, rather than the risk of harm. Facilitates a Culture of Blame Find out Who did What, rather than Why an event occurred. Flawed Investigation Process Identification of risk events is not optimal. The RCA process is not standardized leading to inconsistent investigation processes and thus findings. The Root Causes are Usually High Level and Not Actionable Events are managed individually without a systematic assessment of risk. We can t improve poor communication. Corrective Actions Do Not Solve the Problems, which then Recur Many corrective actions are relatively weak. Find who is at fault and punish them. Change a policy or process with variable outcomes. More education and training. Try Harder!!!
7

8 Error Causation James Reason University of Manchester Organizations create redundant system defense barriers to prevent error. Each defense barrier has its own inherent weakness. Failure or error occurs when the system defense barrier weaknesses accumulate and align. The failures can be due to latent or system failures, or can be due to active or human failures. Thus, usually adverse events have more than one cause. Used with Permission of HPI


9 Greenville Health System P9 5 Medical Campuses with 1268 Beds GMH = 750 Bed Tertiary Center 2 Community Hospitals Acute Surgical Hospital LTACH > 10,000 Employees > 1,250 Medical Staff 731 Employed / Contracted Physicians $1.5B Net Revenue > 42,000 Discharges > 2.3 M Outpatient Visits ~ 170,000 ETS Visits USC School of Medicine Greenville 7 Residencies / 7 Fellowships > 5,000 Health Care Students
10 Greenville Health System Process Centralized Risk Management Department Fully trained in methodology (helped develop it) Monitored occurrence reports to identify potential and actual harm events Led investigations and analytics Academic Health System Vice Chairs of Quality all trained in HFACS 2 Vice Chairs of Quality assisted in the development of the methodology Vice Chairs of Quality partnered with Risk Management in the conduction of the investigation and review of findings They were typically accountable for fixes
11
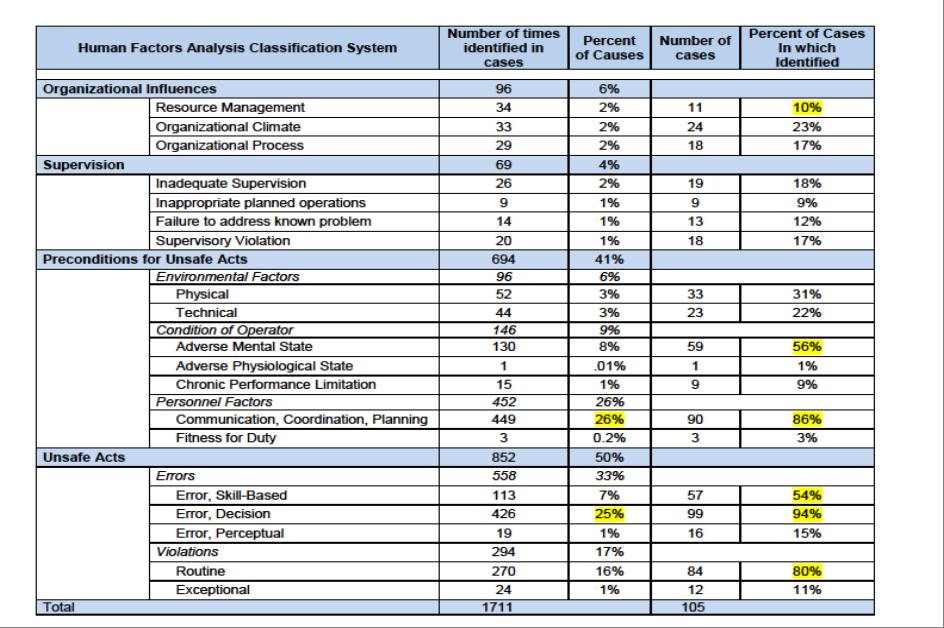
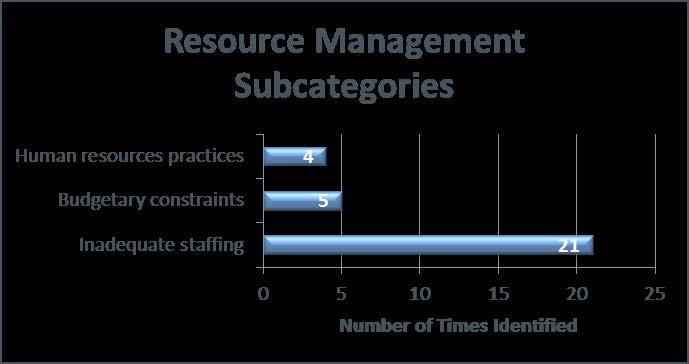
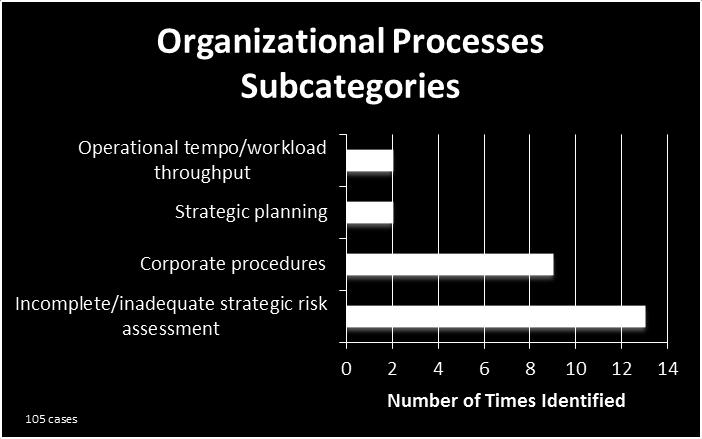
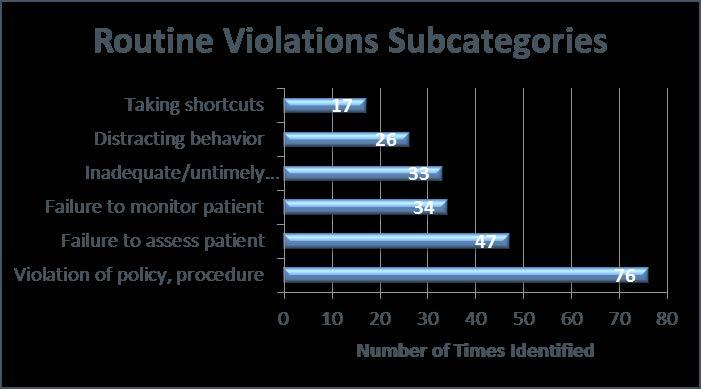
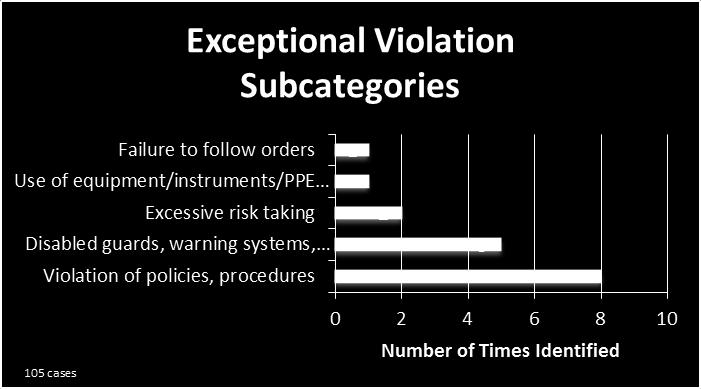
12 Human Factors Analysis Classification System (HFACS) Framework Organizational Influences Supervision Resource Management Organizational Climate Organizational Process Inadequate Supervision Inappropriate Planned Operations Failure to Address a Known Problem Supervisory Violation Preconditions for Unsafe Acts Environmental Factors Personnel Factors Conditions of the Operator Physical Environment Technological Environment Communication / Coordination / Planning Fitness for Duty Adverse Mental State Adverse Physiological State Chronic Performance Limitation Unsafe Act Errors Violations Skill-Based Error Decision Error Perceptual Error Routine Exceptional
13

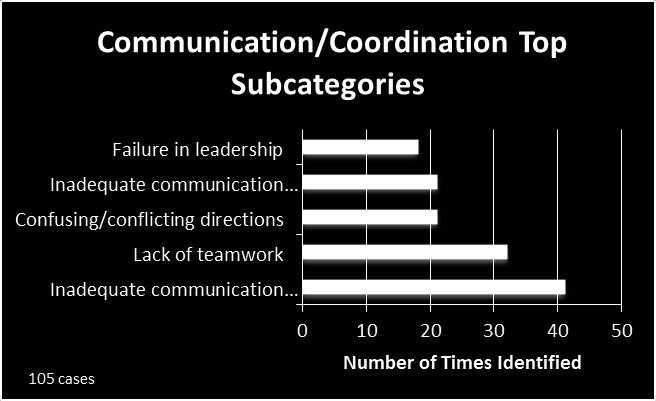
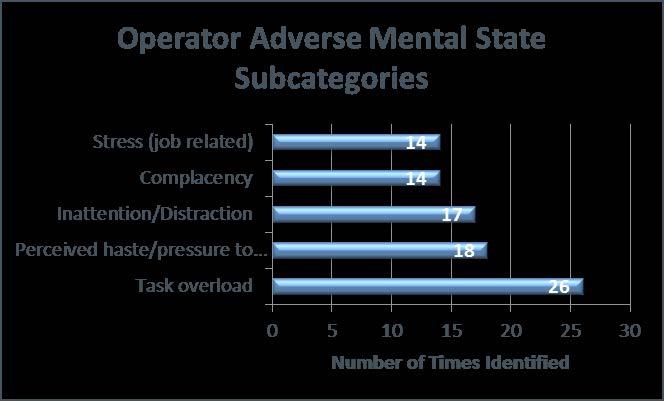
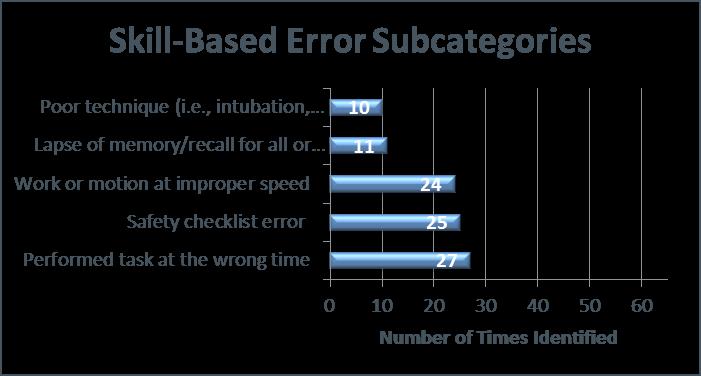
14 HFACS 500 Causal Categories Most Common in Adverse Events Number of Cases Percent of Cases coded cases Personnel, Communication, Coordination, Planning Error, Decision Violation, Routine Operator, Adverse Mental State General Causal Category Error, Skill-Based 0.00 P14
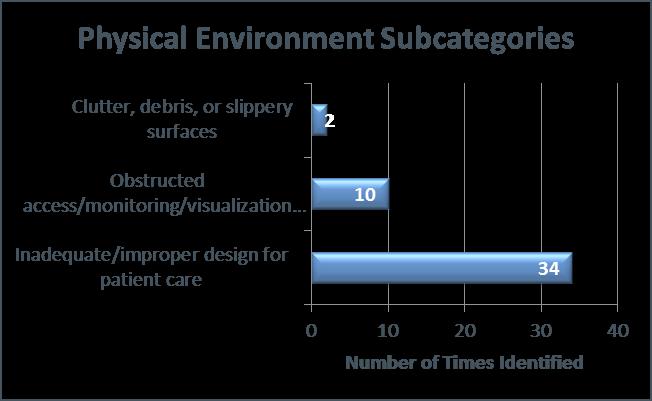
15 HFACS 60 Causal Categories Most Common in Adverse Events Number of Cases Percent of Cases coded cases Environment, Physical Organization, Organizational Climate Environment, Technical Supervision, Inadequate General Causal Category Organization, Organizational Processes Supervision, Inappropriate planned operations 0.00 P15
16 Organizational Influences
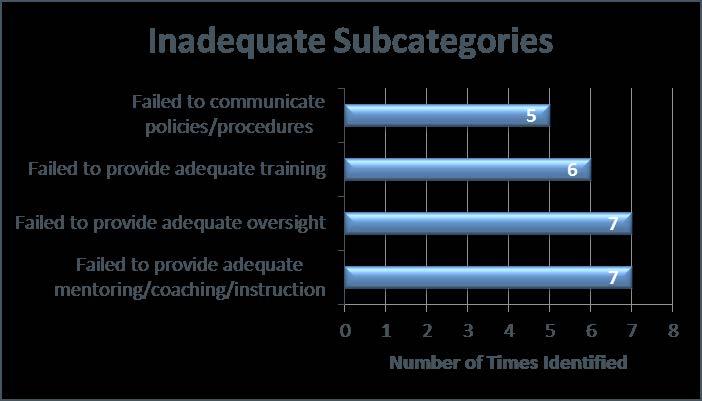
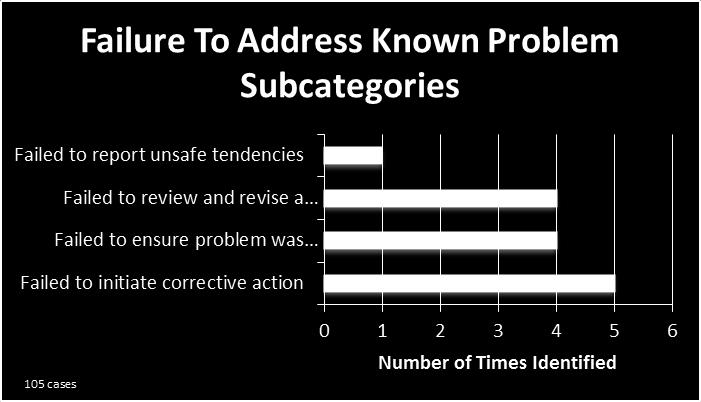
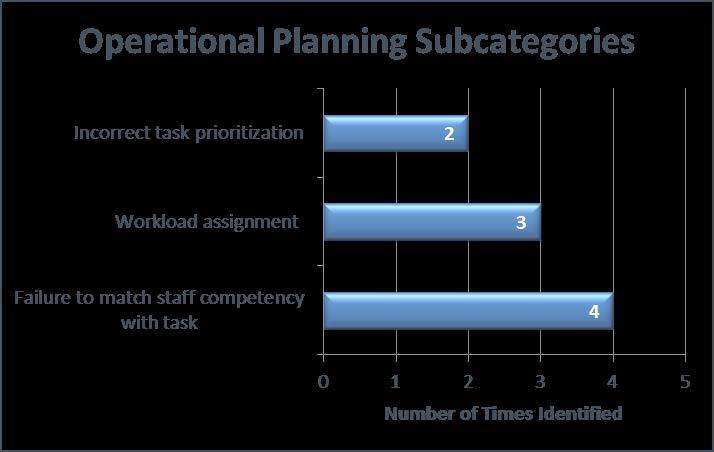
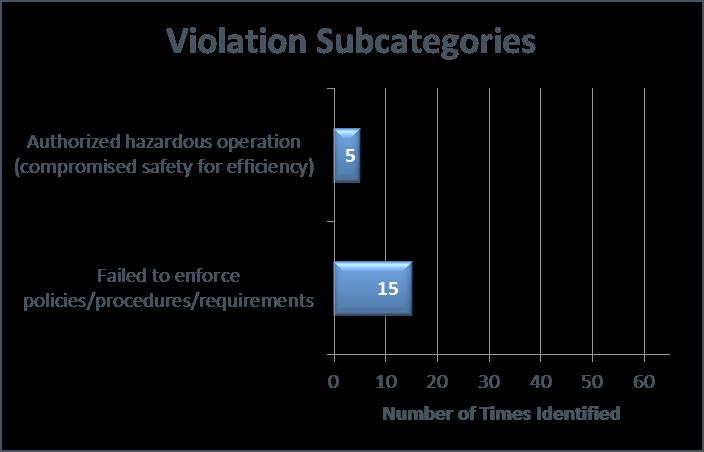
17 Supervision
18 Preconditions for Unsafe Acts

19 Unsafe Acts
20 Findings Comparison Source Pt. Safety Survey Occurrence Reports HFACS Adverse Mental State No No Yes Communication Yes Yes Yes Errors (Decision / Skill Based) Handoffs and Transitions Organizational Learning Staffing (Resource Management) No No Yes Yes Yes Yes Yes No No Yes +/- +/- Violations No No Yes P20
21 Findings Comparison Prior to HFACS No preceding cause Lack of sufficient information May have failed to address root causes Non-actionable Root Causes With use of HFACS Actionable Common Causes identified Avoid unintended consequences Identify commonalities across departments/services/units System solutions P21
22 Lessons Learned HFACS required refining for the healthcare industry Resource intensive and took over two years of adjustments Future refinements should be expedited Retrospective application of HFACS was ineffective Traditional reviews failed to address multiple failure modes or preceding causes Training for key staff (physician leaders and risk managers) is essential Excel database works well Identification of causes is only the beginning; appropriate solutions are essential P22
23 CHRISTUS Health Catholic Health Care System Top 15 Health System by Size ~25 Hospitals in the U.S. in TX, LA, NM ~11 Hospitals in Mexico / Chile $4.5B in Net Revenues ~30,000 Employees Non-academic, community based
24 Root Cause Analysis Transition Roll out HFACS as the system-wide standard for the conduction of RCAs. Standardize the process for the conduction of an RCA. Requires substantial education and reinforcement. Focus RCAs on events with both harm and the potential risk of harm. Develop an HFACS database to analyze adverse events / potential events and identify specific opportunities for systemwide and local mitigation of risk. Link performance improvement activity, training including simulation and clinical policies to system-wide risk mitigation.
25 CHRISTUS Health System Roll Out Process 4 Two day training sessions with Dr. Shappell. Focus on Regional CMOs / CNOs / Quality / Risk / Clinical Education System office key clinical leaders (CCO / CMO / CNO / CQO / CMIO) ~130 key individuals trained Clinical Risk Management Developed a Go Team to assist regions in processes Senior Clinical Leadership Introduced over time as part of a cultural transformation discussion Reinforced including in novel settings capital equipment acquisition
26 CHRISTUS Health Adverse Event Workflow Potential Risk Event Occurs Actual Risk Event Occurs Front Line Staff Enter Event into Event System Service Recovery / Mitigation Mgr. Reviews Event (24 hrs.) Service Recovery / Mitigation Investigates, Clarifies & CRM Reviews Risk Based Prioritization (48 72 hrs.) High Low Track and Trend Identifies as High Risk Event Identifies as High Risk Event Identifies as High Risk Event Implement Corrective Action Plan Patient Safety Officer Reviews Track and Trend Review Findings Conduct Investigation Assign a Team RCA 2 Process Initiated
27 CHRISTUS Health Lessons Learned Roll Out Training was spread out over 4 months, needed to be more compact Have regional people come in teams, rather than as individuals Training of senior clinical leaders (CMOs, CNOs) was critical ~12 Adverse Event Investigations To Date All have numerous decision and skill based errors Resource management (staffing) is a concern Fitness for duty (primarily sleep deprivation from more than 1 job)
28 Questions / Discussion Tom Diller, MD, MMM Thomas.Diller@christushealth.org
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Operational Excellence at Lifespan. Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence
 Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
A26/B26: Goal Zero: South Carolina s Commitment to Safety
 A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
Creating Exceptional Physician-Nurse Partnerships
 1 Creating Exceptional Physician-Nurse Partnerships Using Collaborative Partnerships to Raise the Standard of Care and Improve the Overall Patient Experience Your Speakers 2 Alan J. Conrad, MD, MMM,CPE,
1 Creating Exceptional Physician-Nurse Partnerships Using Collaborative Partnerships to Raise the Standard of Care and Improve the Overall Patient Experience Your Speakers 2 Alan J. Conrad, MD, MMM,CPE,
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI)
") United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
Quality Improvement Overview. Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International
 Quality Improvement Overview Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International The History of Improving We are perfect! Get rid of the bad apples! System
Quality Improvement Overview Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International The History of Improving We are perfect! Get rid of the bad apples! System
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
VA Radiotherapy Incident Reporting and Analysis System (RIRAS)
") VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
Revolutionizing Patient Safety through Organizational Certification Anne Arundel Medical Center
 Revolutionizing Patient Safety through Organizational Certification Anne Arundel Medical Center 1 Anne Arundel Medical Center 1 Learning Objectives Established the Patient Safety Officer (PSO) as the focal
Revolutionizing Patient Safety through Organizational Certification Anne Arundel Medical Center 1 Anne Arundel Medical Center 1 Learning Objectives Established the Patient Safety Officer (PSO) as the focal
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES. James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Quality Management and Accreditation
 Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model
 Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
QAPI Plan QAPI Plan. snits: Sanitas, Denver, CO. Effective Date: 01-Jan-2018
 QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
Steven Sutlief, PhD UC San Diego February 13 th, 2015
 Corrective Actions Steven Sutlief, PhD UC San Diego February 13 th, 2015 Objectives By the end of this presentation, the listener should gain A vocabulary to discussing and thinking about corrective actions,
Corrective Actions Steven Sutlief, PhD UC San Diego February 13 th, 2015 Objectives By the end of this presentation, the listener should gain A vocabulary to discussing and thinking about corrective actions,
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
Evaluating Your Anesthesia Services What to Expect From Your Anesthesia Team
 Evaluating Your Anesthesia Services What to Expect From Your Anesthesia Team Tuesday, May 8, 2012, 2:15pm EST Today s Speakers Syed Ishaq VP, Client Development Somnia Anesthesia David Perlstein, MD, MBA
Evaluating Your Anesthesia Services What to Expect From Your Anesthesia Team Tuesday, May 8, 2012, 2:15pm EST Today s Speakers Syed Ishaq VP, Client Development Somnia Anesthesia David Perlstein, MD, MBA
MEDMARX ADVERSE DRUG EVENT REPORTING
 MEDMARX ADVERSE DRUG EVENT REPORTING Comparative Performance Reporting Helps to Reduce Adverse Drug Events Are you getting the most out of your adverse drug event (ADE) data? ADE reporting initiatives
MEDMARX ADVERSE DRUG EVENT REPORTING Comparative Performance Reporting Helps to Reduce Adverse Drug Events Are you getting the most out of your adverse drug event (ADE) data? ADE reporting initiatives
Targeted Solutions Tools
 TARGETED SOLUTIONS TOOL NOW AVAILABLE FOR OUR INTERNATIONAL CUSTOMERS! Joint Commission Center for Transforming Healthcare Targeted Solutions Tools Hand Hygiene Safe Surgery Hand-off Communications Preventing
TARGETED SOLUTIONS TOOL NOW AVAILABLE FOR OUR INTERNATIONAL CUSTOMERS! Joint Commission Center for Transforming Healthcare Targeted Solutions Tools Hand Hygiene Safe Surgery Hand-off Communications Preventing
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Washington Patient Safety Coalition December 10, 2014
 Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Quality Improvement/Systems-based Practice. Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery
 Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement Program
 Introduction Molina Healthcare of Michigan serves Michigan members in counties throughout Michigan since 2000. For all plan members, Molina Healthcare emphasizes personalized care that places the physician
Introduction Molina Healthcare of Michigan serves Michigan members in counties throughout Michigan since 2000. For all plan members, Molina Healthcare emphasizes personalized care that places the physician
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Problem Solving Tools
 Problem Solving Tools Report 162 Self Assessment of Radiation Safety Programs (2009) Report 173 - Investigation of Radiological Incidents (2012?) Mary L. Birch NC HPS Meeting October 4, 2012 Problem Solving
Problem Solving Tools Report 162 Self Assessment of Radiation Safety Programs (2009) Report 173 - Investigation of Radiological Incidents (2012?) Mary L. Birch NC HPS Meeting October 4, 2012 Problem Solving
NERC Improving Human Performance
 NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD
 Polskie Towarzystwo Medycyny Ubezpieczeniowej IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD Warsaw, 23.09.2016
Polskie Towarzystwo Medycyny Ubezpieczeniowej IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD Warsaw, 23.09.2016
Standards of Practice for Professional Ambulatory Care Nursing... 17
 Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting
 patients from the Acute Care Setting to the Ambulatory Setting") Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting American College of Medical Practice Executives Case Study Submitted by Chantay Lucas,
Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting American College of Medical Practice Executives Case Study Submitted by Chantay Lucas,
The Healthcare Executive Handbook for Organizational Resilience
 The Healthcare Executive Handbook for Organizational Resilience Session #203, February 22,2017 @ 4:00 PM Paul E. Seale, Managing Director Hospital Operations, Milton S. Hershey Medical Center Scott Ream,
The Healthcare Executive Handbook for Organizational Resilience Session #203, February 22,2017 @ 4:00 PM Paul E. Seale, Managing Director Hospital Operations, Milton S. Hershey Medical Center Scott Ream,
EpiCenter and Target Population Initiative. Better Health For All
 EpiCenter and Target Population Initiative Better Health For All Background on the EpiCenter The Need: Large integrated health and hospital systems like the Santa Clara Valley Health and Hospital System
EpiCenter and Target Population Initiative Better Health For All Background on the EpiCenter The Need: Large integrated health and hospital systems like the Santa Clara Valley Health and Hospital System
PANELS AND PANEL EQUITY
 PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
PREPARING FOR THE CLER SITE VISIT FOR BEN TAUB GENERAL HOSPITAL
 PREPARING FOR THE CLER SITE VISIT FOR BEN TAUB GENERAL HOSPITAL 1 Goals and Objectives Overview the Clinical Learning Environment Review (CLER) program Discuss the concept of maintaining a culture of readiness
PREPARING FOR THE CLER SITE VISIT FOR BEN TAUB GENERAL HOSPITAL 1 Goals and Objectives Overview the Clinical Learning Environment Review (CLER) program Discuss the concept of maintaining a culture of readiness
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment. MEDCOM PS Center
 ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
CPPS RECERTIFICATION HANDBOOK
 CBPPS Certification Board for Professionals in Patient Safety 268 Summer Street, Sixth Floor Boston, MA 02210 info@cbpps.org CPPS RECERTIFICATION HANDBOOK Recertification Guidelines The Certified Professional
CBPPS Certification Board for Professionals in Patient Safety 268 Summer Street, Sixth Floor Boston, MA 02210 info@cbpps.org CPPS RECERTIFICATION HANDBOOK Recertification Guidelines The Certified Professional
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Root Cause Analysis. Responding to a Sentinel Event
 2.1 HOURS Root Cause Analysis Responding to a Sentinel Event Brenda M. Ewen, MSN, RN, CPHRM, and Gale Bucher, MSN, RN, COS-C rors. Root cause analysis (RCA) provides an evidence-based structure for methodical
2.1 HOURS Root Cause Analysis Responding to a Sentinel Event Brenda M. Ewen, MSN, RN, CPHRM, and Gale Bucher, MSN, RN, COS-C rors. Root cause analysis (RCA) provides an evidence-based structure for methodical
Towards Quality Care for Patients. Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care
 Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
2014 QAPI Plan for [Facility Name]
![2014 QAPI Plan for [Facility Name]](/thumbs/74/70066237.jpg "2014 QAPI Plan for [Facility Name]") presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
Using Transparency to Drive Patient Safety
 Session Code These presenter s have nothing to disclose Using Transparency to Drive Patient Safety Doug Salvador, MD MPH Chief Quality Officer, Baystate Health Chief Medical Officer, Baystate Medical Center
Session Code These presenter s have nothing to disclose Using Transparency to Drive Patient Safety Doug Salvador, MD MPH Chief Quality Officer, Baystate Health Chief Medical Officer, Baystate Medical Center
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
HOW MUCH MONEY ARE YOU LEAVING ON THE TABLE WITH FRAGMENTED QUALITY PROGRAMS?
 HOW MUCH MONEY ARE YOU LEAVING ON THE TABLE WITH FRAGMENTED? HIGHLIGHTS As healthcare organizations consolidate, the result is a fragmented quality program with variability in reporting and objectives.
HOW MUCH MONEY ARE YOU LEAVING ON THE TABLE WITH FRAGMENTED? HIGHLIGHTS As healthcare organizations consolidate, the result is a fragmented quality program with variability in reporting and objectives.
QUALITY OPERATIONALIZED! Is your facility prepared?
 Performance Improvement Boot Camp For Assisted Living QUALITY OPERATIONALIZED! Is your facility prepared? Presented by: Barb Jezorski, RN, MSN & Brian R. Purtell WiCAL Executive Director 1 Objectives Describe
Performance Improvement Boot Camp For Assisted Living QUALITY OPERATIONALIZED! Is your facility prepared? Presented by: Barb Jezorski, RN, MSN & Brian R. Purtell WiCAL Executive Director 1 Objectives Describe
Clinical Audit: Legal Medicine Service and clinical risk management R. Giannini*, G. Terranova**
 Clinical Audit: Legal Medicine Service and clinical risk management R. Giannini*, G. Terranova** In Italian National Health System Legal Medicine Service, officially assigned by Regional laws to Prevention
Clinical Audit: Legal Medicine Service and clinical risk management R. Giannini*, G. Terranova** In Italian National Health System Legal Medicine Service, officially assigned by Regional laws to Prevention
MHA Patient Safety Organization
 MHA Patient Safety Organization Membership Benefits 2014 Copyright ECRI Institute PSO MHA PSO does more than analyze reported events and near misses. They provide members with tools and resources to help
MHA Patient Safety Organization Membership Benefits 2014 Copyright ECRI Institute PSO MHA PSO does more than analyze reported events and near misses. They provide members with tools and resources to help
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The Conceptual Framework for the International Classification for Patient Safety. An Overview
 The Conceptual Framework for the International Classification for Patient Safety An Overview Action by the WHO 2002 World Health Assembly Resolution WHA55.18 2003 WHO commissions work to explore the state
The Conceptual Framework for the International Classification for Patient Safety An Overview Action by the WHO 2002 World Health Assembly Resolution WHA55.18 2003 WHO commissions work to explore the state
HALF YEAR REPORT ON SENTINEL EVENTS
 HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Community Health Centre Program
 MINISTRY OF HEALTH AND LONG-TERM CARE Community Health Centre Program BACKGROUND The Ministry of Health and Long-Term Care s Community and Health Promotion Branch is responsible for administering and funding
MINISTRY OF HEALTH AND LONG-TERM CARE Community Health Centre Program BACKGROUND The Ministry of Health and Long-Term Care s Community and Health Promotion Branch is responsible for administering and funding
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
EP7f, CN III OB Hemorrhage.pdf OBSTETRIC HEMORRHAGE. Amelia Indig RN Clinical Nurse III Candidate December 17, 2009
 OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety
 Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety MaryPat Sullivan, CNO and Chief Experience Officer, Overlook Medical Center, Atlantic Health System, Summit, NJ Jacalyn
Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety MaryPat Sullivan, CNO and Chief Experience Officer, Overlook Medical Center, Atlantic Health System, Summit, NJ Jacalyn
A Publication for Hospital and Health System Professionals
 A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
Catherine Porto, MPA, RHIA, CHP Executive Director HIM. Madelyn Horn Noble 3M HIM Data Analyst
 1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Where There s a Spark
 Where There s a Spark Counties Manukau District Health Board THERE S A WAY FORWARD Changing our Game Geraint Martin, CEO, Counties Manukau District Health Board Ron Pearson, Deputy CEO, Counties Manukau
Where There s a Spark Counties Manukau District Health Board THERE S A WAY FORWARD Changing our Game Geraint Martin, CEO, Counties Manukau District Health Board Ron Pearson, Deputy CEO, Counties Manukau
Creating a Learning Health System: Translating Research into the Standard of Care
 Creating a Learning Health System: Translating Research into the Standard of Care William E. Smoyer, M.D. C. Robert Kidder Chair, Vice President and Director, Center for Clinical and Translational Research
Creating a Learning Health System: Translating Research into the Standard of Care William E. Smoyer, M.D. C. Robert Kidder Chair, Vice President and Director, Center for Clinical and Translational Research
LEADERSHIP CHALLENGES IN PATIENT SAFETY
 LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
The Role of Health IT in Quality Improvement. P. Jon White, MD Health IT Director Agency for Healthcare Research and Quality
 The Role of Health IT in Quality Improvement P. Jon White, MD Health IT Director Agency for Healthcare Research and Quality and I m Here to Help NOTICE Persons attempting to find a motive in this narrative
The Role of Health IT in Quality Improvement P. Jon White, MD Health IT Director Agency for Healthcare Research and Quality and I m Here to Help NOTICE Persons attempting to find a motive in this narrative
12.01 Safety Management Plan UWHC Administrative Policies
 Page 1 of 7 12.01 Safety Management Plan Category: UWHC Administrative Policy Policy Number: 12.01 Effective Date: October 8, 2013 Version: Revision Section: Environmental Safety (Hospital Administrative)
Page 1 of 7 12.01 Safety Management Plan Category: UWHC Administrative Policy Policy Number: 12.01 Effective Date: October 8, 2013 Version: Revision Section: Environmental Safety (Hospital Administrative)
Statewide Patient Safety Culture: North Carolina HSOPS and Medical Office SOPS
 Statewide Patient Safety Culture: North Carolina HSOPS and Medical Office SOPS What is safety culture? The safety culture of an organization is the product of individual and group values, attitudes, perceptions,
Statewide Patient Safety Culture: North Carolina HSOPS and Medical Office SOPS What is safety culture? The safety culture of an organization is the product of individual and group values, attitudes, perceptions,
Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program
 Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program Initial assessment by: Date: In consultation with: Date of previous assessment: The success of a health information
Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program Initial assessment by: Date: In consultation with: Date of previous assessment: The success of a health information
Implementation Strategy FY Building on a Solid Foundation
 Implementation Strategy FY 2013-2015 The CentraCare Health Melrose Implementation Strategy is a roadmap for how community benefit resources will be used to address the health needs identified through the
Implementation Strategy FY 2013-2015 The CentraCare Health Melrose Implementation Strategy is a roadmap for how community benefit resources will be used to address the health needs identified through the
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference
 Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
Quality Assurance and Performance Improvement (QAPI)
") Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Joint Commission introduces patient safety chapter CAMH addition turns focus on leadership involvement
 Joint Commission introduces patient safety chapter CAMH addition turns focus on leadership involvement WHITE PAPER Editor s note: The following white paper is excerpted from the HCPro newsletter Briefings
Joint Commission introduces patient safety chapter CAMH addition turns focus on leadership involvement WHITE PAPER Editor s note: The following white paper is excerpted from the HCPro newsletter Briefings
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Communication Among Caregivers
 Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
From Private Practice to an Integrated Health System: Playing to Your Strengths
 From Private Practice to an Integrated Health System: Playing to Your Strengths Mark Schickendantz, MD Director, Cleveland Clinic Center for Sports Health Associate Professor of Surgery, Cleveland Clinic
From Private Practice to an Integrated Health System: Playing to Your Strengths Mark Schickendantz, MD Director, Cleveland Clinic Center for Sports Health Associate Professor of Surgery, Cleveland Clinic