.\ '1i. [21' Acceptable review with recommendation of reappointment to the clinical staff with clini~ar.prjvileges as requested. "-.
|
|
|
- Karin Horton
- 5 years ago
- Views:
Transcription
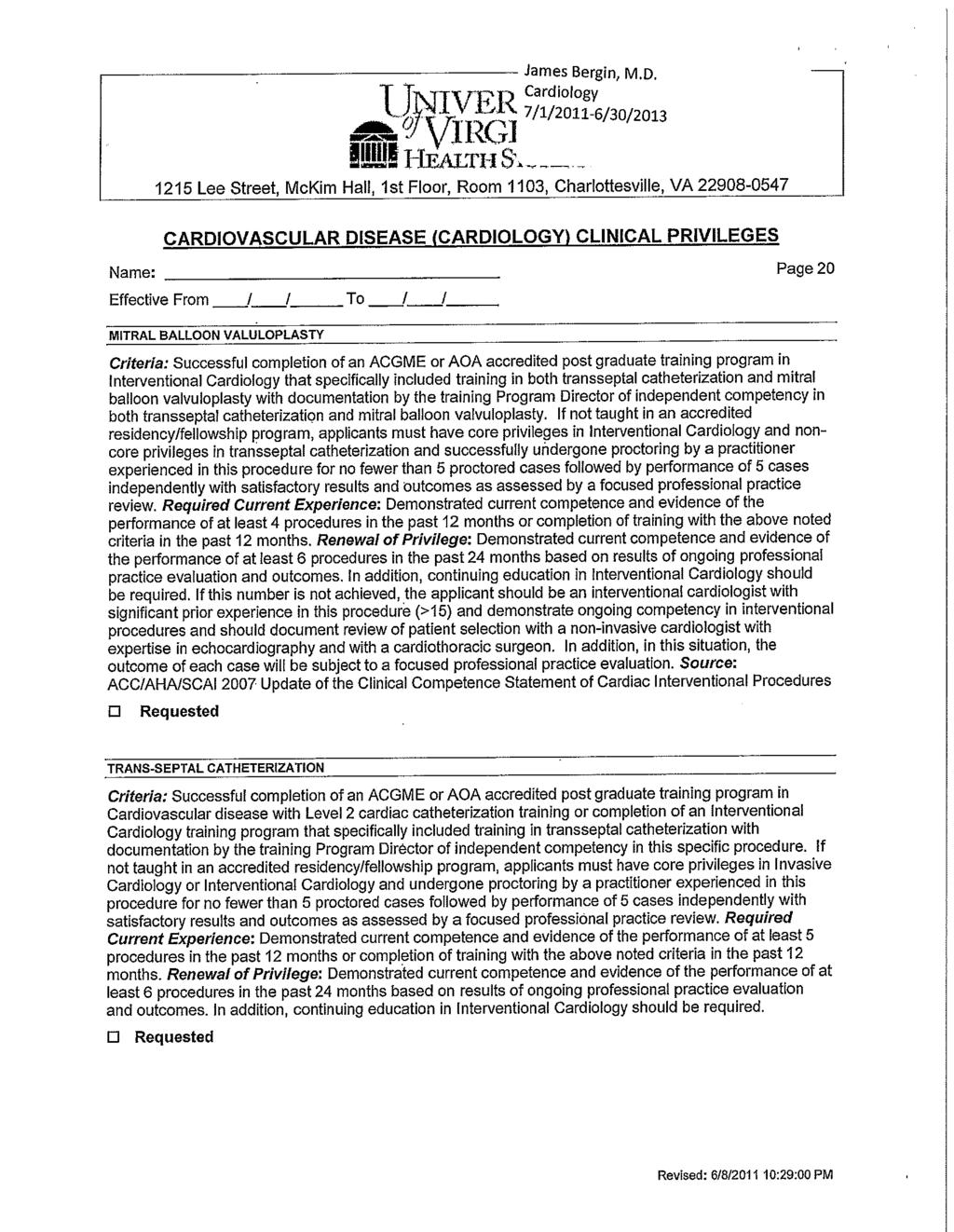
1 Clinical Privileges Update Form -"-~-""'-~-""'--l UNlVERSTIY q; VIRGINIA James Bergin Department of Medicine HEALTH SYsTEM I bave reviewed tbe privileges previously granted to me and request tbe following cbanges to include any new tberapies, procedures, or additional training necessary to perform new privileges requested. (please include supporting documentation to verify competency): New Privileges to be Added (please indicate category level and type of experience): ~~--~ _......_- Current Privileges not to be Renewed:* ~... --~ ~---~-~-~~-~ ~ l*~p;i;;il;ges~'not renewed are not reported as" bei';g' voi~"~xt;'~ily relin(i~ished unless is done you are under invhtig;i&;;;"'~' lor, in return for not conducting an investigation or proceeding. If privileges are to be reported as voluntarily relinquished you jwill be notified and receive a copy of the report to be filed with the National Practitioner Databank..\ '1i. DATE As the Division Head/QI Liaison and Department Chair/Medical Director, we have reviewed the abovenamed clinician's level ofexperience, past performance and quality indicators (if renewing privileges) as related to requested privileges and agree that the above named clinician's qualifications are appropriate. Sincefhe date of the last appointment, we have reviewed applicable information from the followin~ sources of quality and utilization data:., r " We r~""'ollows: 1 [21' Acceptable review with recommendation of reappointment to the clinical staff with clini~ar.prjvileges as requested. "-. ' Concerns noted on review with corrective action plan in place with recommendation of reappointment to the clinical staff with privileges as requested, but subject to a review in months. --_..._--_._-- DATE DEPARTMENT CHAIR SIGNATURE Revlo<d 3/1/2006
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29 Clinical Privileges Update Form James Bergin Department of Medicine I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures, or additional training necessary to perform new privileges requested. (Please include supporting documentation to verify competency): New Privileges to be Added (please indicate category level and type ofexperience): ---~ ~-~--~ -.-~~ ~~. Current Privileges not to be Renewed:'" ---_._ _---_..._--- j*privileges not renewed are not reported as voluntarily relinquished unless done while you are undlee;r:i;;~;e;tiigatio~; lor, in return for not conducting an investigation or proeeeding. If privileges are to be reported as voluntarily relinquished you iwill be notified and reeeive a copy of the report to be filed with the National Practitioner Databank. '2-( (3/" DATE ~. CL~CIAN~ATURE As the Division Head/QI Liaison and Department Chair/Medical Director, we have reviewed the above named clinician's level of experience, past performance and quality indicators (if renewing privileges) as related to requested privileges and agree that the above named clinician's qualifications are appropriate. Sinceihe date of the last appointment, we have reviewed applicable information from the following sources of quality and utilization data: We find as follows: ~ Acceptable review with recommendation of reappointment to the clinical staff with clinical privileges as requested ~_~)31" DATE DATE Concerns noted on review with corrective action plan in place with recommendation of reappointment to the clinical staff with privileges as requested, but subject to a review in months. Should have clinical privileges granted but restricted as follows: Lawrence Girnple, MD.~'-' J~~"L#~-=::::==:::::::: c-- Division Chief/Quality Liaison Mitchell Rosner, MD Interim Department Chair Revised lfl/loo6
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
~ ~..._..._...~..._ CLINICIAN SIGNATURE
 Clinical Privileges Update Form UNlVEHSrry qrvirginiau Barbara Wilson Department of Dermatology L--. HEALTH SYsTEM ~ ~ I have reviewed the privileges previously granted to me and request the following
Clinical Privileges Update Form UNlVEHSrry qrvirginiau Barbara Wilson Department of Dermatology L--. HEALTH SYsTEM ~ ~ I have reviewed the privileges previously granted to me and request the following
Clinical Privileges Update Form
 Clinical Privileges Update Form Mark Mendelsohn epartment of Pediatrics I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures,
Clinical Privileges Update Form Mark Mendelsohn epartment of Pediatrics I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures,
 Clinical Privileges Update Form Kenneth Liu Department of. Radiology I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures,
Clinical Privileges Update Form Kenneth Liu Department of. Radiology I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures,
 q' Clinical Privileges Update Form U~lVERSTY '!VRGNA Bhiken Naik Department of Anesthesiology HEALTH SYsTEM have reviewed the privileges previously granted to me and request the following changes to include
q' Clinical Privileges Update Form U~lVERSTY '!VRGNA Bhiken Naik Department of Anesthesiology HEALTH SYsTEM have reviewed the privileges previously granted to me and request the following changes to include
 ., Clinical Privileges Update Form Susan Modesitt Department of Obstetrics and I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures,
., Clinical Privileges Update Form Susan Modesitt Department of Obstetrics and I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures,
 X X AHP Clinical Privileges Update Form Joseph Fallon, PA Department of Radiology -------I have reviewed the privileges previously granted (COP)' attached) to me and request the following
X X AHP Clinical Privileges Update Form Joseph Fallon, PA Department of Radiology -------I have reviewed the privileges previously granted (COP)' attached) to me and request the following
BCBS NC Blue Medicare Credentialing Instructions
 BCBS C Blue Medicare Credentialing Instructions Licensed Certified Social Worker (LCSW) Certified Substance Abuse Counselor (CSAC) Licensed Clinical Addiction Specialist (LCAS) Licensed Marriage and Family
BCBS C Blue Medicare Credentialing Instructions Licensed Certified Social Worker (LCSW) Certified Substance Abuse Counselor (CSAC) Licensed Clinical Addiction Specialist (LCAS) Licensed Marriage and Family
CLINICAL STAFF CREDENTIALING AND PRIVILEGING MANUAL
 CLINICAL STAFF CREDENTIALING AND PRIVILEGING MANUAL January 20, 2012 TABLE OF CONTENTS Introduction...1 I. Clinical Staff Membership...1 II. Clinical Staff Privileges...2 III. Procedures for Initial Appointment
CLINICAL STAFF CREDENTIALING AND PRIVILEGING MANUAL January 20, 2012 TABLE OF CONTENTS Introduction...1 I. Clinical Staff Membership...1 II. Clinical Staff Privileges...2 III. Procedures for Initial Appointment
UNMH Psychologist Clinical Privileges
 o Initial privileges (initial appointment) o Renewal of privileges (reappointment) o Expansion of privileges (modification) All new applicants must meet the following requirements as approved by the UNMH
o Initial privileges (initial appointment) o Renewal of privileges (reappointment) o Expansion of privileges (modification) All new applicants must meet the following requirements as approved by the UNMH
TRINITY HEALTH Minot, North Dakota MEDICAL STAFF PRE-APPLICATION FORM
 TRINITY HEALTH Minot, North Dakota MEDICAL STAFF PRE-APPLICATION FORM Application Instructions: Complete the application in full. The application must be typed or neatly printed. Attach additional sheets
TRINITY HEALTH Minot, North Dakota MEDICAL STAFF PRE-APPLICATION FORM Application Instructions: Complete the application in full. The application must be typed or neatly printed. Attach additional sheets
Medical Genetics Clinical Privileges REAPPOINTMENT Effective from July 1, 2015 to June 30, 2016
 Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the Health Authority or Hospital, effective: 11/Dec2014.
Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the Health Authority or Hospital, effective: 11/Dec2014.
Department: Legal Department. Approved by:
 HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" Policies and Procedures Subject: Credentialing Requirements Department: Legal Department Issued by: Rene McWade, Esq. VP & General Counsel
HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" Policies and Procedures Subject: Credentialing Requirements Department: Legal Department Issued by: Rene McWade, Esq. VP & General Counsel
Name of Sex: M F Applicant: Last First Middle. Date of Birth: Social Security Number: Phone: ( ) City State Zip. Phone: ( ) City State Zip
 City State Zip. Phone: ( ) City State Zip") SCHNEIDER REGIONAL MEDICAL CENTER 9048 SUGAR ESTATE ST. THOMAS, U.S.V.I 00802 APPLICATION FOR TEMPORARY PRIVILEGES (USED FOR URGENT PATIENT NEED AND LOCUM TENENS) COMPLETE THE APPLICATION IN FULL. PRINT
SCHNEIDER REGIONAL MEDICAL CENTER 9048 SUGAR ESTATE ST. THOMAS, U.S.V.I 00802 APPLICATION FOR TEMPORARY PRIVILEGES (USED FOR URGENT PATIENT NEED AND LOCUM TENENS) COMPLETE THE APPLICATION IN FULL. PRINT
The University of Kansas Hospital POLICY AND PROCEDURE MANUAL Subject: Ongoing Professional Practice Evaluation
 The University of Kansas Hospital POLICY AND PROCEDURE MANUAL Subject: Ongoing Professional Practice Evaluation Signature Tammy Peterman, Executive VP COO and Chief Nursing Officer Formulation Revised
The University of Kansas Hospital POLICY AND PROCEDURE MANUAL Subject: Ongoing Professional Practice Evaluation Signature Tammy Peterman, Executive VP COO and Chief Nursing Officer Formulation Revised
Legal Last Name First Middle Professional Title/Degree
 IOWA STATEWIDE UNIVERSAL PRACTITIONER RECREDENTIALING APPLICATION Type or print responses in ink. A CV or See CV may not be use in lieu of completing any answers on this application. Review or complete
IOWA STATEWIDE UNIVERSAL PRACTITIONER RECREDENTIALING APPLICATION Type or print responses in ink. A CV or See CV may not be use in lieu of completing any answers on this application. Review or complete
YALE-NEW HAVEN HOSPITAL MEDICAL STAFF POLICY & PROCEDURE CONFLICT OF INTEREST
 YALE-NEW HAVEN HOSPITAL MEDICAL STAFF POLICY & PROCEDURE CONFLICT OF INTEREST Definitions External financial interests can create conflicts when they provide an incentive to a Medical Staff member to affect
YALE-NEW HAVEN HOSPITAL MEDICAL STAFF POLICY & PROCEDURE CONFLICT OF INTEREST Definitions External financial interests can create conflicts when they provide an incentive to a Medical Staff member to affect
SECTION ONE - PERSONAL INFORMATION SECTION TWO - EDUCATION INFORMATION
 Attachment H ALLIED HEALTH PROFESSIONALS INITIAL APPOINTMENT ADDENDUM TO THE TEXAS DEPARTMENT OF INSURANCE (TDI) STANDARDIZED CREDENTIALING APPLICATION SECTION ONE - PERSONAL INFORMATION Last Name: First
Attachment H ALLIED HEALTH PROFESSIONALS INITIAL APPOINTMENT ADDENDUM TO THE TEXAS DEPARTMENT OF INSURANCE (TDI) STANDARDIZED CREDENTIALING APPLICATION SECTION ONE - PERSONAL INFORMATION Last Name: First
WEST VIRGINIA BOARD OF OCCUPATIONAL THERAPY 1063 Maple Dr., Suite 4B Morgantown, WV
 WEST VIRGINIA BOARD OF OCCUPATIONAL THERAPY 1063 Maple Dr., Suite 4B Morgantown, WV 26505 304-285-3150 www.wvbot.org APPLICATION FOR TWO-YEAR RENEWAL OF LICENSE: OTR/L To renew your license for the coming
WEST VIRGINIA BOARD OF OCCUPATIONAL THERAPY 1063 Maple Dr., Suite 4B Morgantown, WV 26505 304-285-3150 www.wvbot.org APPLICATION FOR TWO-YEAR RENEWAL OF LICENSE: OTR/L To renew your license for the coming
APPLICATION FOR REAPPOINTMENT RESEARCH ASSOCIATE
 APPLICATION FOR REAPPOINTMENT RESEARCH ASSOCIATE Enclosed is an application for reappointment to the position of Research Associate. We ask that you review the shaded areas to assure that all current information
APPLICATION FOR REAPPOINTMENT RESEARCH ASSOCIATE Enclosed is an application for reappointment to the position of Research Associate. We ask that you review the shaded areas to assure that all current information
.0 Acceptable review with recommendation of reappointment to the clinical staff with clinical privileges as. Clinical Privileges Update Form
 Clinical Privileges Update Form ~, John Mason Department of Otolaryngology. U~-rr"tRSITY C!/ \lirgil\.;y\. HEALTH SYsTEM I have reviewed the privileges previously granted to me and request the following
Clinical Privileges Update Form ~, John Mason Department of Otolaryngology. U~-rr"tRSITY C!/ \lirgil\.;y\. HEALTH SYsTEM I have reviewed the privileges previously granted to me and request the following
Kalihi-Palama Health Center Hale Ho ola Hou. Policy and Procedure Manual
 Kalihi-Palama Health Center Hale Ho ola Hou Policy and Procedure Manual SUBJECT: Credentialing and Privileging of Licensed Staff SECTION OF MANUAL: Personnel DEPARTMENT/TEAM: All DATE: Effective: 9/06
Kalihi-Palama Health Center Hale Ho ola Hou Policy and Procedure Manual SUBJECT: Credentialing and Privileging of Licensed Staff SECTION OF MANUAL: Personnel DEPARTMENT/TEAM: All DATE: Effective: 9/06
UNM SRMC Nephrology Clinical Privileges. Name: Effective Dates: From To
 All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors, effective August 213, 2017 Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors, effective August 213, 2017 Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
APP PRIVILEGES IN RADIATION ONCOLOGY
 APP PRIVILEGES IN RADIATION ONCOLOGY Education/Training Licensure (Initial and Reappointment) Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the
APP PRIVILEGES IN RADIATION ONCOLOGY Education/Training Licensure (Initial and Reappointment) Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the
Network Participant Credentialing Application
 Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
Mount Sinai Health System
 Mount Sinai Health System Dear Doctor, The Chair of your department at a Mount Sinai Health System is currently reviewing your file for clinical reappointment. Because of your low level of practice volume,
Mount Sinai Health System Dear Doctor, The Chair of your department at a Mount Sinai Health System is currently reviewing your file for clinical reappointment. Because of your low level of practice volume,
FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE)
") A. Purpose: To establish a systematic process to evaluate and confirm the current competency of practitioners performance of privileges and professionalism at UCSF Medical Center.. This process is known
A. Purpose: To establish a systematic process to evaluate and confirm the current competency of practitioners performance of privileges and professionalism at UCSF Medical Center.. This process is known
CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process.
 CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process. PERSONAL IDENTIFICATION DATA Last Name: First: MI: Degree: Date of Birth: Social Security
CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process. PERSONAL IDENTIFICATION DATA Last Name: First: MI: Degree: Date of Birth: Social Security
DETROIT MEDICAL CENTER DEPARTMENT OF PSYCHIATRY DELINEATION OF PRIVILEGES IN PSYCHIATRY
 DETROIT MEDICAL CENTER DEPARTMENT OF PSYCHIATRY DELINEATION OF PRIVILEGES IN PSYCHIATRY Applicant Name: QUALIFICATIONS: Effective July 1, 2009, all new applicants to the DMC will be required to be board
DETROIT MEDICAL CENTER DEPARTMENT OF PSYCHIATRY DELINEATION OF PRIVILEGES IN PSYCHIATRY Applicant Name: QUALIFICATIONS: Effective July 1, 2009, all new applicants to the DMC will be required to be board
Regions Hospital Delineation of Privileges Certified Registered Nurse Anesthetist
 Regions Hospital Delineation of Privileges Certified Registered Nurse Anesthetist Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting.
Regions Hospital Delineation of Privileges Certified Registered Nurse Anesthetist Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting.
LIBERTY DENTAL PLAN. Provider Credentialing Application. (* Required Fields) *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )
 *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )") (Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
(Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
HONORHealth CREDENTIALING PROCEDURES MANUAL 2017
 HONORHealth CREDENTIALING PROCEDURES MANUAL 2017 Table of Contents Part 1 APPOINTMENT PROCEDURES 1.1 Application 1 1.2 Application Content 1 1.3 References 2 1.4 Effect of Application 2 1.5 Application
HONORHealth CREDENTIALING PROCEDURES MANUAL 2017 Table of Contents Part 1 APPOINTMENT PROCEDURES 1.1 Application 1 1.2 Application Content 1 1.3 References 2 1.4 Effect of Application 2 1.5 Application
UNMH Pediatric Nephrology Clinical Privileges
 ll new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 07/31/2015 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
ll new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 07/31/2015 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
LIBERTY DENTAL PLAN. Dental Hygienist - Credentialing Application. City: State: DEGREE: City: State: DEGREE:
 *Required Fields LIBERTY DENTAL PLAN Dental Hygienist - Credentialing Application Please complete one application per Dental Hygienist Demographic Information: Male Female *HYGIENIST NAME: RDH Other *DATE
*Required Fields LIBERTY DENTAL PLAN Dental Hygienist - Credentialing Application Please complete one application per Dental Hygienist Demographic Information: Male Female *HYGIENIST NAME: RDH Other *DATE
.11 Medical Director Qualifications.
 1/14/2011 10.07.02.11 10.07.02.11.11 Medical Director Qualifications. A. Medical Director Qualifications. The nursing facility shall: (1) Designate a medical director who has at least the following qualifications:
1/14/2011 10.07.02.11 10.07.02.11.11 Medical Director Qualifications. A. Medical Director Qualifications. The nursing facility shall: (1) Designate a medical director who has at least the following qualifications:
UNMH Nurse Practitioner (CNP) and Physician Assistant (PA) Ambulatory Special Non-Core Procedures (Appendix A) Name: Effective Dates: From To
 and Physician Assistant (PA) Ambulatory Special Non-Core Procedures (Appendix A) Name: Effective Dates: From To") All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective March 31, 2017: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective March 31, 2017: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
GENERAL INFORMATION. English Spanish Arabic Chinese French German Hmong Hindi Laotian Philippine Vietnamese Other
 **INCOMPLETE APPLICATIONS WILL DELAY THE CREDENTIALING PROCESS** 1. Please print or type ALL responses. 2. If you need additional space to complete a section, please attach additional sheets. 3. If you
**INCOMPLETE APPLICATIONS WILL DELAY THE CREDENTIALING PROCESS** 1. Please print or type ALL responses. 2. If you need additional space to complete a section, please attach additional sheets. 3. If you
DEPARTMENT OF SURGERY OTOLARYNGOLOGY-HEAD AND NECK SURGERY CLINICAL PRIVILEGES REQUEST FORM
 DEPARTMENT OF SURGERY OTOLARYNGOLOGY-HEAD AND NECK SURGERY CLINICAL PRIVILEGES REQUEST FORM Appointee: Date: NOTE: This request should be returned to: Medical Staff Affairs Office, Hershey Medical Center,
DEPARTMENT OF SURGERY OTOLARYNGOLOGY-HEAD AND NECK SURGERY CLINICAL PRIVILEGES REQUEST FORM Appointee: Date: NOTE: This request should be returned to: Medical Staff Affairs Office, Hershey Medical Center,
ATTENDING PHYSICIAN S STATEMENT CRITICAL ILLNESS (TERMINAL ILLNESS)
") ATTENDING PHYSICIAN S STATEMENT CRITICAL ILLNESS (TERMINAL ILLNESS) Name NRIC Number Policy Number Claim Number The abovenamed is insured with us against the happening of certain contingent events associated
ATTENDING PHYSICIAN S STATEMENT CRITICAL ILLNESS (TERMINAL ILLNESS) Name NRIC Number Policy Number Claim Number The abovenamed is insured with us against the happening of certain contingent events associated
SAMPLE Credentialing, Privileging and Peer Review Self-Evaluation
 1. The following professionals are credentialed: Physicians Residents Advanced Practice Providers (e.g., CRNA, PA, CMW) Dentists Podiatrists Chiropractors Others 2. The credentialing process includes the
1. The following professionals are credentialed: Physicians Residents Advanced Practice Providers (e.g., CRNA, PA, CMW) Dentists Podiatrists Chiropractors Others 2. The credentialing process includes the
MEDICAL STAFF BYLAWS
 MEDICAL STAFF BYLAWS, POLICIES, AND RULES AND REGULATIONS OF THE CHRIST HOSPITAL MEDICAL STAFF BYLAWS Adopted by the Medical Executive Committee: April 24, 2014 Adopted by the Medical Staff: May 13, 2014
MEDICAL STAFF BYLAWS, POLICIES, AND RULES AND REGULATIONS OF THE CHRIST HOSPITAL MEDICAL STAFF BYLAWS Adopted by the Medical Executive Committee: April 24, 2014 Adopted by the Medical Staff: May 13, 2014
APP PRIVILEGES IN UROLOGY
 APP PRIVILEGES IN UROLOGY Education/Training Licensure Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the state of CA Current certification as a
APP PRIVILEGES IN UROLOGY Education/Training Licensure Required Qualifications Successful completion of a PA or NP program Current Licensure as a PA or RN in the state of CA Current certification as a
Optima Health New Provider Application Packet
 Optima Health New Provider Application Packet Thank you for your interest in becoming a participating provider in the Optima Health Network. Please review the following instructions to ensure acceptance
Optima Health New Provider Application Packet Thank you for your interest in becoming a participating provider in the Optima Health Network. Please review the following instructions to ensure acceptance
MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD.
 MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD. APPLICANT NAME: SPECIALTY: In order to expedite the credentialing process, please complete every item
MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD. APPLICANT NAME: SPECIALTY: In order to expedite the credentialing process, please complete every item
SAMPLE - Verifying Credentialing Information Policy
 Subject: Number: Effective Date: Supersedes SPP# Approved by: (signature) Distribution: Verifying Credentialing Information Dated: Medical Staff, Credentialing Manual, Medical Staff Office I. STATEMENT
Subject: Number: Effective Date: Supersedes SPP# Approved by: (signature) Distribution: Verifying Credentialing Information Dated: Medical Staff, Credentialing Manual, Medical Staff Office I. STATEMENT
...,...,.., ,,...,...::.,-----'
 SANTA BARBARA COUNTY ~ DEPARTMENT OF Behavioral Wellness ~ ~ A System of Care and Recovery Pa g e 1 of 10 Departmental Policy and Procedure Section Sub-section Policy Quality Care Management General Policy#
SANTA BARBARA COUNTY ~ DEPARTMENT OF Behavioral Wellness ~ ~ A System of Care and Recovery Pa g e 1 of 10 Departmental Policy and Procedure Section Sub-section Policy Quality Care Management General Policy#
Credentialing Application for Hospitals and Facilities
 Instructions Credentialing Application for Hospitals and Facilities 1. Please accurately and legibly complete all sections of this Credentialing Application, and mark non-applicable fields with N/A. If
Instructions Credentialing Application for Hospitals and Facilities 1. Please accurately and legibly complete all sections of this Credentialing Application, and mark non-applicable fields with N/A. If
POLICY NO Volunteer Policy (Replaces Policy Adopted 1/26/1998)
") POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 1/26/1998) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 1/26/1998) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
WORK EXPERIENCE PLACEMENT - DESCRIPTION OF ACTIVITIES. Work Experience Placement, Psychological Assistant
 WORK EXPERIENCE PLACEMENT - DESCRIPTION OF ACTIVITIES 1 DETAILS TITLE: PLACEMENT LENGTH PAYMENT: LOCATION: HOURS: SESSIONS: BASE: ACCOUNTABLE TO: Work Experience Placement, Psychological Assistant Variable
WORK EXPERIENCE PLACEMENT - DESCRIPTION OF ACTIVITIES 1 DETAILS TITLE: PLACEMENT LENGTH PAYMENT: LOCATION: HOURS: SESSIONS: BASE: ACCOUNTABLE TO: Work Experience Placement, Psychological Assistant Variable
ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM
 ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM Independent Practitioners: Acupuncturist, Audiologist, Dietitian, Licensed Clinical Social Worker, Licensed Marriage and Family Therapist, Licensed
ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM Independent Practitioners: Acupuncturist, Audiologist, Dietitian, Licensed Clinical Social Worker, Licensed Marriage and Family Therapist, Licensed
Certified Registered Nurse Anesthetist (CRNA) Application. Full Name Nickname. Address. City State Zip County. Home Phone Cell Phone
 Application. Full Name Nickname. Address. City State Zip County. Home Phone Cell Phone") Certified Registered Nurse Anesthetist (CRNA) Application Date of Application: I. Personal Information: Full Name Nickname Address City State Zip County Home Phone Cell Phone Email Pager/Alt. Email Sex:
Certified Registered Nurse Anesthetist (CRNA) Application Date of Application: I. Personal Information: Full Name Nickname Address City State Zip County Home Phone Cell Phone Email Pager/Alt. Email Sex:
UNM SRMC CRITICAL CARE PRIVILEGES
 UNM SRMC INSTRUCTIONS All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective May 24, 2017 Applicant: Check off the "Requested" box for each privilege
UNM SRMC INSTRUCTIONS All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective May 24, 2017 Applicant: Check off the "Requested" box for each privilege
CREDENTIALING PROCEDURES MANUAL MEMORIAL HOSPITAL OF SOUTH BEND, INC. SOUTH BEND, INDIANA
 MEMORIAL HOSPITAL OF SOUTH BEND, INC. SOUTH BEND, INDIANA January 16, 1984 Revised: October 18, 1984 January 19, 1989 April 17, 1989 April 26, 1990 December 20, 1990 January 21, 1993 May 27, 1993 July
MEMORIAL HOSPITAL OF SOUTH BEND, INC. SOUTH BEND, INDIANA January 16, 1984 Revised: October 18, 1984 January 19, 1989 April 17, 1989 April 26, 1990 December 20, 1990 January 21, 1993 May 27, 1993 July
DEPARTMENT OF RADIOLOGY RULES AND REGULATIONS Effective May 31, 2014 TABLE OF CONTENTS
 DEPARTMENT OF RADIOLOGY Effective May 31, 2014 TABLE OF CONTENTS Page ARTICLE I Name 2 ARTICLE II Purpose 2 ARTICLE III Membership 2 ARTICLE IV Categories of the Radiology Staff 3 ARTICLE V Officers 3
DEPARTMENT OF RADIOLOGY Effective May 31, 2014 TABLE OF CONTENTS Page ARTICLE I Name 2 ARTICLE II Purpose 2 ARTICLE III Membership 2 ARTICLE IV Categories of the Radiology Staff 3 ARTICLE V Officers 3
PRACTICE INFORMATION AND LETTER AGREEMENT FORM. COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747
 PRACTICE INFORMATION AND LETTER AGREEMENT FORM COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747 PERSONAL DATA Last Name First Name License Number Tax I.D. Number for
PRACTICE INFORMATION AND LETTER AGREEMENT FORM COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747 PERSONAL DATA Last Name First Name License Number Tax I.D. Number for
10111 Richmond Avenue, Suite 400, Houston, Texas (713) / (866) (Toll Free) / (713) (Fax)
 / (866) (Toll Free) / (713) (Fax)") Application Date: \ \ Date Available: \ \ Provider s Name: O MD O DO O PA O NP SS # : City: State: Zip: Home Phone ( ) Work Phone ( ) Pager ( ) Cell Phone ( ) E-Mail address: Driver s Lic. # Expires: \
Application Date: \ \ Date Available: \ \ Provider s Name: O MD O DO O PA O NP SS # : City: State: Zip: Home Phone ( ) Work Phone ( ) Pager ( ) Cell Phone ( ) E-Mail address: Driver s Lic. # Expires: \
(Rev. 37, Issued: ; Effective/Implementation Date: ) Condition of Participation: Governing Body
 Condition of Participation: Governing Body") Verify that staff and personnel meet all standards (such as continuing education, basic qualifications, etc.) required by State and local laws or regulations. Verify that the hospital has a mechanism established
Verify that staff and personnel meet all standards (such as continuing education, basic qualifications, etc.) required by State and local laws or regulations. Verify that the hospital has a mechanism established
ELIGIBILITY INFORMATION DISCLOSURE AGREEMENT Shared Between Child Nutrition Program Sponsors. and. From to Effective Dates
 ELIGIBILITY INFORMATION DISCLOSURE AGREEMENT Determining Agency and Requesting Agency From to Effective Dates The agency which made free and reduced price meal or free milk eligibility determination (Determining
ELIGIBILITY INFORMATION DISCLOSURE AGREEMENT Determining Agency and Requesting Agency From to Effective Dates The agency which made free and reduced price meal or free milk eligibility determination (Determining
POLICY NO Volunteer Policy (Replaces Policy Adopted 12/13/2011)
") POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 12/13/2011) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 12/13/2011) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
CLINICAL PRIVILEGES- PEDIATRIC SEDATION SERVICE APP
 Name: Page 1 Initial Appointment Reappointment Department Specialty Area All new applicants must meet the following requirements as approved by the governing body effective: 8/7/2013 Applicant: Check off
Name: Page 1 Initial Appointment Reappointment Department Specialty Area All new applicants must meet the following requirements as approved by the governing body effective: 8/7/2013 Applicant: Check off
ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-8 ADVANCED PRACTICE NURSES: COLLABORATIVE PRACTICE TABLE OF CONTENTS
 Medical Examiners Chapter 540-X-8 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-8 ADVANCED PRACTICE NURSES: COLLABORATIVE PRACTICE TABLE OF CONTENTS 540-X-8-.01 540-X-8-.02 540-X-8-.03
Medical Examiners Chapter 540-X-8 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-8 ADVANCED PRACTICE NURSES: COLLABORATIVE PRACTICE TABLE OF CONTENTS 540-X-8-.01 540-X-8-.02 540-X-8-.03
MEDICAL STAFF BYLAWS Volume I: Governance, Structure and Function of the Medical Staff
 MEDICAL STAFF BYLAWS Volume I: Governance, Structure and Function of the Medical Staff January 2014 Table of Contents ARTICLE I - PURPOSE... 9 ARTICLE II - MEDICAL STAFF MEMBERSHIP, CATEGORIES, & RIGHTS...
MEDICAL STAFF BYLAWS Volume I: Governance, Structure and Function of the Medical Staff January 2014 Table of Contents ARTICLE I - PURPOSE... 9 ARTICLE II - MEDICAL STAFF MEMBERSHIP, CATEGORIES, & RIGHTS...
Social Circumstances (Community (CTO) patient - under 18) report for the Mental Health Tribunal/ Managers Panel* meeting to be held on (insert date)
 patient - under 18) report for the Mental Health Tribunal/ Managers Panel* meeting to be held on (insert date)") Appendix 9 Social Circumstances (Community (CTO) patient - under 18) report for the Mental Health Tribunal/ Managers Panel* meeting to be held on (insert date) *Please delete as applicable The content
Appendix 9 Social Circumstances (Community (CTO) patient - under 18) report for the Mental Health Tribunal/ Managers Panel* meeting to be held on (insert date) *Please delete as applicable The content
***CAPS will not begin processing your application until ALL of the above items (numbers 1-4) are returned***
 are returned***") As a service to providers and the community, the Greater Louisville Medical Society (GLMS) offers a Centralized Application Processing Service (CAPS). The GLMS CAPS department verifies: education, training,
As a service to providers and the community, the Greater Louisville Medical Society (GLMS) offers a Centralized Application Processing Service (CAPS). The GLMS CAPS department verifies: education, training,
Graduate Medical Education. Division of Cardiology Phone: Fax:
 Office of Graduate Medical Education Division of Cardiology Phone: 662-293-7687 Fax: 662-293-4347 Dear Doctor: Attached is an application for our Cardiology fellowship program. Please submit all information
Office of Graduate Medical Education Division of Cardiology Phone: 662-293-7687 Fax: 662-293-4347 Dear Doctor: Attached is an application for our Cardiology fellowship program. Please submit all information
Oncology Nurse Practitioner Fellowship Application
 Oncology Nurse Practitioner Fellowship Application I. General Information Use this form to apply for full time appointment to the Nurse Practitioner Fellowship in Oncology at Sylvester Comprehensive Cancer
Oncology Nurse Practitioner Fellowship Application I. General Information Use this form to apply for full time appointment to the Nurse Practitioner Fellowship in Oncology at Sylvester Comprehensive Cancer
Medical Staff Credentials Policy
 Medical Staff Credentials Policy MOUNT CARMEL HEALTH SYSTEM A Medical Staff Document \\Mcehemcshare\mchs med staff svcs$\misc\governing Documents\MCHS\Credentials Policy\MCHS Medical Staff Credentials
Medical Staff Credentials Policy MOUNT CARMEL HEALTH SYSTEM A Medical Staff Document \\Mcehemcshare\mchs med staff svcs$\misc\governing Documents\MCHS\Credentials Policy\MCHS Medical Staff Credentials
VNSNY CHOICE PRACTITIONER CREDENTIALING APPLICATION
 Attached please find an application for participation with VNSNY CHOICE. Upon completion, please forward this application to: VNSNY CHOICE Attn: Provider Relations Network Development 1250 Broadway - 11th
Attached please find an application for participation with VNSNY CHOICE. Upon completion, please forward this application to: VNSNY CHOICE Attn: Provider Relations Network Development 1250 Broadway - 11th
ASSEMBLY BILL No. 214
 AMENDED IN SENATE AUGUST, 00 AMENDED IN SENATE AUGUST, 00 AMENDED IN SENATE AUGUST, 00 AMENDED IN SENATE JULY, 00 AMENDED IN SENATE JUNE, 00 AMENDED IN SENATE JUNE, 00 AMENDED IN SENATE AUGUST 0, 00 california
AMENDED IN SENATE AUGUST, 00 AMENDED IN SENATE AUGUST, 00 AMENDED IN SENATE AUGUST, 00 AMENDED IN SENATE JULY, 00 AMENDED IN SENATE JUNE, 00 AMENDED IN SENATE JUNE, 00 AMENDED IN SENATE AUGUST 0, 00 california
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-5 ADVANCED PRACTICE NURSING COLLABORATIVE PRACTICE TABLE OF CONTENTS
 Nursing Chapter 610-X-5 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-5 ADVANCED PRACTICE NURSING COLLABORATIVE PRACTICE TABLE OF CONTENTS 610-X-5-.01 610-X-5-.02 610-X-5-.03 610-X-5-.04 610-X-5-.05
Nursing Chapter 610-X-5 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-5 ADVANCED PRACTICE NURSING COLLABORATIVE PRACTICE TABLE OF CONTENTS 610-X-5-.01 610-X-5-.02 610-X-5-.03 610-X-5-.04 610-X-5-.05
MEDICAL STAFF BYLAWS MCLAREN GREATER LANSING HOSPITAL
 MEDICAL STAFF BYLAWS MCLAREN GREATER LANSING HOSPITAL Final Document May 16, 2016 Horty, Springer & Mattern, P.C. 245957.7 MEDICAL STAFF BYLAWS TABLE OF CONTENTS PAGE 1. GENERAL...1 1.A. PREAMBLE...1 1.B.
MEDICAL STAFF BYLAWS MCLAREN GREATER LANSING HOSPITAL Final Document May 16, 2016 Horty, Springer & Mattern, P.C. 245957.7 MEDICAL STAFF BYLAWS TABLE OF CONTENTS PAGE 1. GENERAL...1 1.A. PREAMBLE...1 1.B.
The Who, What, When, and Wheres
 Ambulatory Care Program: The Who, What, When, and Wheres of Credentialing and Privileging The Who, What, When, and Wheres The Who, What, When, and Wheres Note that this was originally documented as a three-part
Ambulatory Care Program: The Who, What, When, and Wheres of Credentialing and Privileging The Who, What, When, and Wheres The Who, What, When, and Wheres Note that this was originally documented as a three-part
NASI Per Diem Malpractice
 Dear Nurse Anesthetist, We appreciate your interest in NASI s Per Diem Malpractice Insurance. This service is for those providers who need a supplemental policy for working an assignment outside of their
Dear Nurse Anesthetist, We appreciate your interest in NASI s Per Diem Malpractice Insurance. This service is for those providers who need a supplemental policy for working an assignment outside of their
CLINICAL PRIVILEGES- WOMEN S HEALTH NURSE PRACTITIONER
 Name: Page 1 Initial Appointment Department Reappointment Specialty All new applicants must meet the following requirements as approved by the governing body effective: March 4, 2015. Applicant: Check
Name: Page 1 Initial Appointment Department Reappointment Specialty All new applicants must meet the following requirements as approved by the governing body effective: March 4, 2015. Applicant: Check
MEDICAL STAFF CREDENTIALING MANUAL
 MEDICAL STAFF CREDENTIALING MANUAL 2016 MOUNT CLEMENS REGIONAL MEDICAL CENTER CREDENTIALING MANUAL TABLE OF CONTENTS I. PROCEDURES FOR APPOINTMENT 4 1. GENERAL PROCEDURE 4 2. APPLICATION FOR INITIAL APPOINTMENT
MEDICAL STAFF CREDENTIALING MANUAL 2016 MOUNT CLEMENS REGIONAL MEDICAL CENTER CREDENTIALING MANUAL TABLE OF CONTENTS I. PROCEDURES FOR APPOINTMENT 4 1. GENERAL PROCEDURE 4 2. APPLICATION FOR INITIAL APPOINTMENT
REQUIREMENTS TO QUALIFY AS A QUALIFIED MENTAL HEALTH PROFESSIONAL-CHILD (QMHP-C)
") REQUIREMENTS TO QUALIFY AS A QUALIFIED MENTAL HEALTH PROFESSIONAL-CHILD (QMHP-C) Qualified Mental Health Professional-Child or QMHP-C means a registered QMHP who is trained and experienced in providing
REQUIREMENTS TO QUALIFY AS A QUALIFIED MENTAL HEALTH PROFESSIONAL-CHILD (QMHP-C) Qualified Mental Health Professional-Child or QMHP-C means a registered QMHP who is trained and experienced in providing
MARYLAND BOARD OF PHYSICIANS P.O. Box 2571 Baltimore, Maryland
 MARYLAND BOARD OF PHYSICIANS P.O. Box 2571 Baltimore, Maryland 21215 www.mbp.state.md.us E-mail: mdh.mbppadispense@maryland.gov : ADDENDUM FOR PHYSICIAN ASSISTANT (PA) TO DISPENSE PRESCRIPTION DRUGS INSTRUCTIONS
MARYLAND BOARD OF PHYSICIANS P.O. Box 2571 Baltimore, Maryland 21215 www.mbp.state.md.us E-mail: mdh.mbppadispense@maryland.gov : ADDENDUM FOR PHYSICIAN ASSISTANT (PA) TO DISPENSE PRESCRIPTION DRUGS INSTRUCTIONS
Clinical Staffing. Primary Reviewer: Clinical Expert Secondary Reviewer: Governance/Administrative Expert, if needed
 Health Center Program Site Visit Protocol Clinical Staffing Primary Reviewer: Clinical Expert Secondary Reviewer: Governance/Administrative Expert, if needed Authority: Sections 330(a)(1), (b)(1)-(2),
Health Center Program Site Visit Protocol Clinical Staffing Primary Reviewer: Clinical Expert Secondary Reviewer: Governance/Administrative Expert, if needed Authority: Sections 330(a)(1), (b)(1)-(2),
TITLE 13 LEGISLATIVE RULE BOARD OF OCCUPATIONAL THERAPY SERIES 4 CONTINUING EDUCATION AND COMPETENCE
 TITLE 13 LEGISLATIVE RULE BOARD OF OCCUPATIONAL THERAPY SERIES 4 CONTINUING EDUCATION AND COMPETENCE 13-4-1. General. 1.1. Scope. -- This legislative rule establishes requirements for continuing education
TITLE 13 LEGISLATIVE RULE BOARD OF OCCUPATIONAL THERAPY SERIES 4 CONTINUING EDUCATION AND COMPETENCE 13-4-1. General. 1.1. Scope. -- This legislative rule establishes requirements for continuing education
Student Nurses Association Bylaws
 Student Nurses Association Bylaws ARTICLE I Section 1 The name of this organization shall be the Goodwin College Student Nurses Association. ARTICLE II Purpose and Function Section 1. Purpose A. To assume
Student Nurses Association Bylaws ARTICLE I Section 1 The name of this organization shall be the Goodwin College Student Nurses Association. ARTICLE II Purpose and Function Section 1. Purpose A. To assume
Initial Athletics Grant-in-Aid Offers to Prospective Student-Athletes
 Initial Athletics Grant-in-Aid Offers to Prospective Student-Athletes POLICIES Athletics grants-in-aid can only be offered to students for one year at a time. Coaches may state that it is Boston College
Initial Athletics Grant-in-Aid Offers to Prospective Student-Athletes POLICIES Athletics grants-in-aid can only be offered to students for one year at a time. Coaches may state that it is Boston College
WHITMAN COUNTY CIVIL SERVICE COMMISSION
 WHITMAN COUNTY CIVIL SERVICE COMMISSION In compliance with Federal and State equal employment opportunity guidelines, qualified applicants are considered for employment without regards to race, creed,
WHITMAN COUNTY CIVIL SERVICE COMMISSION In compliance with Federal and State equal employment opportunity guidelines, qualified applicants are considered for employment without regards to race, creed,
Massachusetts Integrated Application for Re-Credentialing/Re-Appointment
 Massachusetts Integrated Application for Re-Credentialing/Re-Appointment Name (Please type or print) Degrees MA License. Are you currently in the United States on a temporary visa? ** **Identify type of
Massachusetts Integrated Application for Re-Credentialing/Re-Appointment Name (Please type or print) Degrees MA License. Are you currently in the United States on a temporary visa? ** **Identify type of
ALABAMA~STATUTE. Code of Alabama et seq. DATE Enacted Alabama Board of Medical Examiners
 ALABAMA~STATUTE STATUTE Code of Alabama 34-24-290 et seq DATE Enacted 1971 REGULATORY BODY PA DEFINED SCOPE OF PRACTICE PRESCRIBING/DISPENSING SUPERVISION DEFINED PAs PER PHYSICIAN APPLICATION QUALIFICATIONS
ALABAMA~STATUTE STATUTE Code of Alabama 34-24-290 et seq DATE Enacted 1971 REGULATORY BODY PA DEFINED SCOPE OF PRACTICE PRESCRIBING/DISPENSING SUPERVISION DEFINED PAs PER PHYSICIAN APPLICATION QUALIFICATIONS
Proctoring and Observation for Credentialed Staff Medical Staff Policy
 Proctoring and Observation for Credentialed Staff Medical Staff Policy Approved by MEC 1/19/99 Revised 2/2003 Revised 5/2008 Approved SHMC MEC 2/2013 Approved HFH MEC 2/13 Approved PSHMC and PHFH MEC 3-2015
Proctoring and Observation for Credentialed Staff Medical Staff Policy Approved by MEC 1/19/99 Revised 2/2003 Revised 5/2008 Approved SHMC MEC 2/2013 Approved HFH MEC 2/13 Approved PSHMC and PHFH MEC 3-2015
REQUIREMENTS TO QUALIFY AS A QUALIFIED MENTAL HEALTH PROFESSIONAL-ADULT (QMHP-A)
") REQUIREMENTS TO QUALIFY AS A QUALIFIED MENTAL HEALTH PROFESSIONAL-ADULT (QMHP-A) Qualified Mental Health Professional-Adult or QMHP-A means a registered QMHP who is trained and experienced in providing
REQUIREMENTS TO QUALIFY AS A QUALIFIED MENTAL HEALTH PROFESSIONAL-ADULT (QMHP-A) Qualified Mental Health Professional-Adult or QMHP-A means a registered QMHP who is trained and experienced in providing
RULES/REGULATIONS FOR THE DEPARTMENT OF FAMILY MEDICINE AT STAMFORD HOSPITAL PURPOSE OBJECTIVE MEMBERSHIP
 RULES/REGULATIONS FOR THE DEPARTMENT OF FAMILY MEDICINE AT STAMFORD HOSPITAL PURPOSE The purpose of the Family Medicine Department is to provide family physicians with their own department for education
RULES/REGULATIONS FOR THE DEPARTMENT OF FAMILY MEDICINE AT STAMFORD HOSPITAL PURPOSE The purpose of the Family Medicine Department is to provide family physicians with their own department for education
Sherman and Lucille Tilney Euler Scholarship. Guidelines for Selection of Recipients and Use of Funds
 Sherman and Lucille Tilney Euler Scholarship Guidelines for Selection of Recipients and Use of Funds The Sherman and Lucille Tilney Euler Scholarship was established through Mrs. Euler s estate to prepare
Sherman and Lucille Tilney Euler Scholarship Guidelines for Selection of Recipients and Use of Funds The Sherman and Lucille Tilney Euler Scholarship was established through Mrs. Euler s estate to prepare
GLACIAL RIDGE HEALTH SYSTEM MEDICAL STAFF BYLAWS
 GLACIAL RIDGE HEALTH SYSTEM MEDICAL STAFF BYLAWS February 2016 Page 2 of 31 GLACIAL RIDGE HOSPITAL DISTRICT dba GLACIAL RIDGE HEALTH SYSTEM MEDICAL STAFF BYLAWS Index Preamble 3 Definitions 4 Article I:
GLACIAL RIDGE HEALTH SYSTEM MEDICAL STAFF BYLAWS February 2016 Page 2 of 31 GLACIAL RIDGE HOSPITAL DISTRICT dba GLACIAL RIDGE HEALTH SYSTEM MEDICAL STAFF BYLAWS Index Preamble 3 Definitions 4 Article I:
ADVANCED PRACTICE PROFESSIONAL STAFF
 Medical Staff Policy Governing Medical Practices POLICY NO: MS-001 Effective Date: 02/09/2012 Revision Dates: 07/24/2015 I. PURPOSE ADVANCED PRACTICE PROFESSIONAL STAFF This policy of the Medical Staff
Medical Staff Policy Governing Medical Practices POLICY NO: MS-001 Effective Date: 02/09/2012 Revision Dates: 07/24/2015 I. PURPOSE ADVANCED PRACTICE PROFESSIONAL STAFF This policy of the Medical Staff
TIFT REGIONAL MEDICAL CENTER MEDICAL STAFF POLICIES & PROCEDURES
 Title: Allied Health Professionals Approved: 2/02 Reviewed/Revised: 11/04; 08/10; 03/11; 5/14 Definition TIFT REGIONAL MEDICAL CENTER MEDICAL STAFF POLICIES & PROCEDURES P & P #: MS-0051 Page 1 of 7 For
Title: Allied Health Professionals Approved: 2/02 Reviewed/Revised: 11/04; 08/10; 03/11; 5/14 Definition TIFT REGIONAL MEDICAL CENTER MEDICAL STAFF POLICIES & PROCEDURES P & P #: MS-0051 Page 1 of 7 For
INTENT TO APPLY FOR PROVISIONAL PROVIDER LISTING VIA THE JUDICIAL RURAL INITIATIVE
 INTENT TO APPLY FOR PROVISIONAL PROVIDER LISTING VIA THE JUDICIAL RURAL INITIATIVE COLORADO DOMESTIC VIOLENCE OFFENDER MANAGEMENT BOARD COLORADO DEPARTMENT OF PUBLIC SAFETY DIVISION OF CRIMINAL JUSTICE
INTENT TO APPLY FOR PROVISIONAL PROVIDER LISTING VIA THE JUDICIAL RURAL INITIATIVE COLORADO DOMESTIC VIOLENCE OFFENDER MANAGEMENT BOARD COLORADO DEPARTMENT OF PUBLIC SAFETY DIVISION OF CRIMINAL JUSTICE
DELINEATION OF PRIVILEGES - PEDIATRICS AND PEDIATRIC SUBSPECIALTIES
 KALEIDA HEALTH Name Date DELINEATION OF PRIVILEGES - PEDIATRICS AND PEDIATRIC SUBSPECIALTIES The responsibility of Pediatrics begins with the newborn and continues through 21 years of age. There are special
KALEIDA HEALTH Name Date DELINEATION OF PRIVILEGES - PEDIATRICS AND PEDIATRIC SUBSPECIALTIES The responsibility of Pediatrics begins with the newborn and continues through 21 years of age. There are special
Emory Healthcare Quality Credentialing Process
 Emory Healthcare Quality Credentialing Process Dorothy Cook-Walter, JD Director System Credentialing & Medical Staff Services October 13, 2006 Mission Statement To provide a system-wide, efficient and
Emory Healthcare Quality Credentialing Process Dorothy Cook-Walter, JD Director System Credentialing & Medical Staff Services October 13, 2006 Mission Statement To provide a system-wide, efficient and
Credentialing Volunteer Licensed Independent Practitioners in the Event of Disaster
 Manual Medical Staff Effective Date 04/27/2006 Policy # 115 Date Revised 12/31/2008 Responsible Person Director, Medical Staff Services Next Scheduled Review 12/31/2017 PURPOSE Volunteer Licensed Independent
Manual Medical Staff Effective Date 04/27/2006 Policy # 115 Date Revised 12/31/2008 Responsible Person Director, Medical Staff Services Next Scheduled Review 12/31/2017 PURPOSE Volunteer Licensed Independent
SC Uniform Managed Care Provider Credentialing Application
 SC Uniform Managed Care Provider Credentialing Application I. PERSONAL INFORMATION Solo Practice Group Practice Name: Last First M.I. Suffix Degree Maiden and/or other name List W-9 name if different Place
SC Uniform Managed Care Provider Credentialing Application I. PERSONAL INFORMATION Solo Practice Group Practice Name: Last First M.I. Suffix Degree Maiden and/or other name List W-9 name if different Place
Credentialing Application
 Credentialing Application If you are active with CAQH it is not necessary for you to complete the application in this packet. In order for Meridian Health Plan to process your contract the following information
Credentialing Application If you are active with CAQH it is not necessary for you to complete the application in this packet. In order for Meridian Health Plan to process your contract the following information
Human Resources & Nursing
 2017 Hospital Breakfast Briefings Web-conference Series Human Resources & Nursing November 2, 2017 Faculty: Kathy Eichner, RN, MSN, CJCP Principal Consultant, Joint Commission Resources 1 Disclosure Statement
2017 Hospital Breakfast Briefings Web-conference Series Human Resources & Nursing November 2, 2017 Faculty: Kathy Eichner, RN, MSN, CJCP Principal Consultant, Joint Commission Resources 1 Disclosure Statement
Network Participation Agreement
 Network Participation Agreement This AGREEMENT is made and entered into as of, 201 by and between (Pharmacy), NABP # and Texas Pharmacy Association (Network Administrator). As providers in the Network,
Network Participation Agreement This AGREEMENT is made and entered into as of, 201 by and between (Pharmacy), NABP # and Texas Pharmacy Association (Network Administrator). As providers in the Network,
MEDICAL STAFF BYLAWS Volume I: Governance, Structure and Function of the Medical Staff Final Draft
 MEDICAL STAFF BYLAWS Volume I: Governance, Structure and Function of the Medical Staff Final Draft 5-15-13 DEFINITIONS ADVANCED PROFESSIONAL PRACTITIONER (APP): Advanced Practice Nurses, including advanced
MEDICAL STAFF BYLAWS Volume I: Governance, Structure and Function of the Medical Staff Final Draft 5-15-13 DEFINITIONS ADVANCED PROFESSIONAL PRACTITIONER (APP): Advanced Practice Nurses, including advanced
Certified Dangerous Goods Trainer Application
 GENERAL INFORMATION First Name: Last Name: Address: Certified Dangerous Goods Trainer Application Phone Number: Email: Employer: Employer Address: QUALIFICATIONS In order to qualify for the CDGT certification
GENERAL INFORMATION First Name: Last Name: Address: Certified Dangerous Goods Trainer Application Phone Number: Email: Employer: Employer Address: QUALIFICATIONS In order to qualify for the CDGT certification