NBER WORKING PAPER SERIES THE EFFECT OF OEF/OIF DEPLOYMENT INTENSITY ON THE RATE OF POSTTRAUMATIC STRESS DISORDER AMONG ACTIVE DUTY POPULATION
|
|
|
- Roxanne Nicholson
- 5 years ago
- Views:
Transcription
1 NBER WORKING PAPER SERIES THE EFFECT OF OEF/OIF DEPLOYMENT INTENSITY ON THE RATE OF POSTTRAUMATIC STRESS DISORDER AMONG ACTIVE DUTY POPULATION Yu-Chu Shen Jeremy Arkes Boon Wah Kwan Lai Yee Tan Thomas V. Williams Working Paper NATIONAL BUREAU OF ECONOMIC RESEARCH 1050 Massachusetts Avenue Cambridge, MA July 2009 Shen and Arkes thank GSBPP DFR program and N1 MPT&E for financial support. From the Center for Healthcare Management Studies, Office of the Assistant Secretary of Defense, Health Affairs (OASD (HA)), TRICARE Management Activity (TMA), Falls Church, VA. We thank Dennis Mar, Wendy Funk and the staff at DMDC and TMA for assisting with data extraction. The opinions or assertions herein are those of the authors and do not necessarily reflect the view of the United States Department of Defense and any of the affiliated institutions. This work received IRB approvals from NPS, DMDC, TMA, and the Office of Navy Medicine. The views expressed herein are those of the author(s) and do not necessarily reflect the views of the National Bureau of Economic Research by Yu-Chu Shen, Jeremy Arkes, Boon Wah Kwan, Lai Yee Tan, and Thomas V. Williams. All rights reserved. Short sections of text, not to exceed two paragraphs, may be quoted without explicit permission provided that full credit, including notice, is given to the source.
2 The Effect of OEF/OIF Deployment Intensity on the Rate of Posttraumatic Stress Disorder Among Active Duty Population Yu-Chu Shen, Jeremy Arkes, Boon Wah Kwan, Lai Yee Tan, and Thomas V. Williams NBER Working Paper No July 2009 JEL No. I1 ABSTRACT This study estimates the effect of deployment location and length on the risk of developing PTSD, relative to what it would be from the normal military operations. We use a random sample of activity-duty enlisted personnel serving between 2001 and We identify PTSD cases from TRICARE medical records and link deployment information from Contingent Tracking System. Comparing to those in other duties around the world, deployment to Iraq/Afghanistan increases the odds of developing PTSD substantially, with the largest effect observed for the Navy (OR=9.06, p<0.01) and the smallest effect for the Air Force (OR=1.25, p<0.01). A deployment longer than 180 days increases the odds of PTSD by 1.11 times to 2.84 times, depending on the service, compared to a tour under 120 days. For Army and Navy, a deployment to Iraq/Afghanistan further exacerbates the adverse effect of tour length. Our research identifies the extent of PTSD across services and quantifies the risks associated with OEF/OIF deployment intensity. Further research is needed for effective monitoring and preventive measures of PTSD on the active duty population. Yu-Chu Shen Graduate School of Business and Public Policy Naval Postgraduate School 555 Dyer Road Monterey, CA and NBER yshen@nps.edu Jeremy Arkes Graduate School of Business and Public Policy Naval Postgraduate School 555 Dyer St Monterey, CA jaarkes@nps.edu Lai Yee Tan Naval Postgraduate School 555 Dyer Road, Monterey CA irenetanly@hotmail.com Thomas V. Williams TRICARE 5111 Leesburg Pike, Suite 810 Falls Church, VA thomas.williams@tma.osd.mil Boon Wah Kwan Naval Postgraduate School 555 Dyer Road, Monterey CA bw_kwan@yahoo.com
3 Introduction Recent research suggests that the wars in Afghanistan and Iraq, also known as Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF), pose substantial mental health challenges to U.S. military service members and mental health systems (Hoge, Castro et al. 2004; Hoge, Auchterlonie et al. 2006; Erbes, Westermeyer et al. 2007; Rosenheck and Fontana 2007; Seal, Bertenthal et al. 2007; Tanielian and Jaycox 2008). Post-traumatic stress disorder (PTSD), in particular, has risen steadily, with heavy combat typically being cited as a leading cause of PTSD (Helzer, Robins et al. 1987; CDC 1988; The Iowa Persian Gulf Study Group 1997; Prigerson, Maciejewski et al. 2002; Kang, Natelson et al. 2003; Hoge, Castro et al. 2004). A recent comprehensive review of the literature by Rand found a wide range of PTSD rates among those serving in Iraq and Afghanistan, with estimates ranging from 4% to 45%, depending on the samples and how PTSD was measured (Tanielian and Jaycox 2008). Many studies used anonymous survey responses from convenience samples of Army soldiers who were deployed in either Iraq or Afghanistan from 2003 to 2005 (Helzer, Robins et al. 1987; Hoge, Castro et al. 2004; Grieger, Cozza et al. 2006; Vasterling, Proctor et al. 2006; Erbes, Westermeyer et al. 2007). Some analyzed the mental health issues using post-deployment health assessment surveys collected by the Mental Health Advisory Team (MHAT), which measured PTSD by primary-care PTSD screening questions (U.S. Army 2003; U.S. Army 2005; Hoge, Auchterlonie et al. 2006; U.S. Army 2006; U.S. Army 2006; Shen, Arkes et al. 2009), while a few used actual medical records from the VA health care system. With the Global War on Terrorism (GWOT) going into its 8 th year and with a planned surge of forces in Afghanistan, it is critical to evaluate the prevalence of PTSD among the active duty population and how the deployment intensity in OEF/OIF affect the mental health readiness of the Armed Forces. While previous studies have provided important information on PTSD in the current operations, they have several shortcomings. First, the previous studies have been descriptive 3
4 analyses except for a study analyzing UK solders and one focusing on the US Navy (Rona, Fear et al. 2007; Shen, Arkes et al. 2009). Second, most studies focus on just the Army and Marine Corps. Yet the rates of PTSD among those deployed in Iraq and Afghanistan could be different across services because of different types of assignments, and such differences are important to identify in evaluating total force readiness. Third, most studies used convenience samples on those returning from OEF/OIF, without a comparable control group of personnel who were not deployed under OEF/OIF. Thus, while these studies indicate the frequency of PTSD for those deployed under OEF/OIF, they cannot speak to the effect of being deployed under OEF/OIF relative to their risk of PTSD under other military operations. Fourth, studies using surveys often had to rely on screening questions (such as PCL-DSM IV), which are typically short and simple to administer but likely miss some cases of PTSD and misdiagnose PTSD in other cases (Kimerling, Ouimette et al. 2006; Ramchand, Karney et al. 2008). Finally, previous studies focus on the effect of the deployment location (i.e, Iraq or Afghanistan) with little attention paid to the duration of deployment or the cumulative effect of multiple deployments on the PTSD occurrence. However, deployment duration and frequency are equally important deployment dimensions to consider when designing the optimal deployment strategy. In this study, we address the shortcomings of the previous literature with a random sample based on all active duty enlisted personnel serving between 2001 and We merge data on PTSD diagnoses from the TRICARE medical records and deployment records from the Contingency Tracking System. We then examine the effects of OEF/OIF deployment intensity for enlisted personnel separately for the four services (Army, Marines, Navy, and Air Force). We analyze two dimensions of deployment intensity: location and duration. Specifically, we address the following research questions: 1. What are the rates of PTSD among all active duty enlisted personnel and how do the rates 4
5 differ by service and deployment location? 2. How do deployment location and length of deployment affect the probability of being diagnosed with PTSD? 3. Is there an interactive effect between a deployment s length and location? In particular, do longer deployments to Iraq or Afghanistan exacerbate the risk of PTSD? Data and Methods Methods Overview. Our sample is based on all individuals who were active duty enlisted service members of the US Armed Forces between 2001 and The outcome of interest is whether the individual was diagnosed with PTSD within the TRICARE system. We first use a descriptive analysis to compare the rate of PTSD among different branches of the Armed Services by deployment location. We then estimate two multivariate models using logistic regressions to assess the effect of deployment intensity (location, duration) under OEF/OIF on the rate of PTSD. These regression models address the policy question of how much an Iraq/Afghanistan (or other OEF/OIF) deployment increases the risk of developing PTSD relative to the risk military personnel would have had if they had not been deployed to OEF/OIF missions. We estimate our models separately for each service (Army, Air Force, Marines, and Navy). We provide more details on the model specifications below. Data and Sample. We use a random sample of activity-duty enlisted personnel serving between 2001 and 2006 because the GWOT started in 2001 and 2006 is the year for which the latest data are available. We combine several data sources from TRICARE and the Defense Manpower Data Center (DMDC) to form the basis of our analysis. First, we identify the active duty personnel population and obtain demographic and service information (such as age, gender, race, rank) from 5
6 the Defense Enrollment Eligibility Reporting System (DEERS). Second, depending on where PTSD was diagnosed (military treatment facility or TRICARE civilian provider) and whether it was identified from inpatient or outpatient claims, we identify the date that PTSD was first diagnosed and related health information from the following sources: the Standard Inpatient Data Record, the Standard Ambulatory Data Record, and the TRICARE Encounter Data. Third, we obtain OEF/OIF deployment characteristics and military occupational specialty (MOS) codes between 2001 and 2006 from the Contingency Tracking System (CTS). The CTS Deployment Files were used to track personnel involved in contingency operations and report all personnel who have been deployed in support of the Global War on Terror (GWOT) since September 11, CTS data contain information on deployment location, start and end dates of the deployment. A person would have multiple sets of deployment records in CTS if he were deployed multiple times during the study period. The study received expedited IRB approval. Each observation in our data represents unique enlisted personnel. Based on the TRICARE medical records and monthly DEERS records, we first identify all personnel who were diagnosed with PTSD and take their demographic and rank information from DEERS the month they were diagnosed. Next, for the remaining active duty population (those without PTSD), we randomly select a month from each individual s monthly DEERS records for their demographic and rank information. We then draw a 25 percent random sample of this population from each service (regardless of whether they used TRICARE services). At the end, our data consist of 678,227 unique enlisted personnel from all services. This represents a 25% random sample of the active population without PTSD and 100% of the PTSD population. We weight all of our comparisons and empirical models to reflect this sampling scheme so our estimated numbers are representative of all personnel from each service. For all personnel in our sample, we extract complete deployment information from CTS. 6
7 Outcome measures. The dependent variable in our analysis is whether an enlisted person was diagnosed with PTSD anytime between 2001 and 2006 (i.e., if the ICD-9 code of the principal diagnosis is )(American Psychiatric Association 2000). Statistical Models. After an initial set of descriptive analyses for raw comparisons of PTSD rates for different types of deployments across services, we conduct regression models in order to control for relevant factors. Because our outcome is binary, we estimate logistic regression models. In the primary models, we focus on deployment characteristics of the last deployment. For example, if a person was included in the analytical sample on March 2004 and his/her most recent deployment prior to this date was July 2003, we would use deployment information from the July 2003 deployment in this set of models. Our key variables of interest in Model 1 are the deployment location and duration (details below). In Model 2, we estimate an interaction effect between deployment duration and deployment location (in particular, Iraq and Afghanistan) to test whether longer deployments as a result of OIF and OEF magnifies the effect of such a deployment on the probability of being diagnosed with PTSD. As a sensitivity analysis on the location effect, we also estimate a model based on all past deployments locations, since PTSD is not necessarily triggered by the last deployment and often emerges after a long delay. Specifically, if a person was included in the sample on March 2004, we identify the locations for all deployments between 2001 and March The key variable of interest in this sensitivity model is whether a person was ever deployed to a given location (details below). In all models, we control for service and demographic characteristics as explained below. 7
8 Explanatory variables. There are three categories of variables that we include in the models: deployment characteristics, service characteristics, and demographic information. Summary statistics of these measures are presented in Table 1. We describe here the different types of variables. We classify three categories of deployment locations: not deployed under OEF or OIF (the reference group), deployed to Iraq/Afghanistan, deployed on other OEF/OIF missions (such as Kuwait, Quatar, Saudi Arabia, Turkey). 1 For the duration of the last deployment, we classify the deployment length into three categories: short if the length of the last deployment is less than 120 days (the reference group), medium if the length of last deployment is between 120 and 180 days, and long if the duration is greater than 180 days. In the sensitivity analysis, we define four mutually exclusive categories of all past deployment location indicators: ever deployed to Iraq or Afghanistan (but not other locations), ever deployed on other OEF/OIF missions, ever deployed to Iraq/Afghanistan as well as other OEF/OIF missions, and never deployed on any OEF/OIF mission (the reference group). For service characteristics, we include rank and military occupation specialty (MOS) categories. Studies have shown that soldiers in combat divisions and those in medical service tend to have different rates of PTSD than non-combat specialties (Martin 2007; Tanielian and Jaycox 2008). We categorize military occupational specialty codes into the following categories: Combat arms (reference group), combat support, combat service support, aviation, medical, and other MOS. 2 To control for demographic characteristics, we include the following demographic 1 We do not define more detailed location categories because sample size would be too small for the finer categorization. 2 The four service branches use different sets of military occupation codes. The Army and Marine Corps use a Military Occupational Specialty (MOS) code, while a system of Air Force Specialty Codes (AFSC) is used in the Air Force. The Navy uses a system of naval ratings and designators along with the Naval Enlisted Classification (NEC) system. For some service branches, some of the categories are merged due to small numbers of observations in the individual categories and some categories are missing (for example, Marines and Air Force do not have medical MOS) 8
9 information in the models: gender, race (with White as the reference group, African-American, Hispanic, Asian, and other races), marital status (single or married), and age. Lastly, we include year indicators to control for possible macro trends in PTSD rate in the general active duty population. Results Table 1 presents the descriptive statistics of the sample by service branches. We focus our discussion on the deployment characteristics. The majority of the active duty personnel were not deployed under OEF/OIF: the percentages range from 61.5% in Air Force to 78% in Army. However, while not shown, this rate did vary by year as increasing numbers of Army and Marine Corps personnel were deployed under OEF/OIF in later years. Not surprisingly, the service with the highest share of its enlisted members sent to Iraq/Afghanistan is the Army (11.3%), follow by the Marines (8.6%). The Navy and Air Force appear to serve a more supporting role, with 35% and 33%, respectively, of their enlisted population being sent on OEF/OIF missions other than Iraq/Afghanistan. Among those deployed, large proportions of Army and Marine Corps personnel had been deployed more than 180 days in their most recent deployment prior to being included in the sample (58% and 48%, respectively), whereas 65% of deployed Air Force personnel had a tour length under 120 days. The next set of summary statistics report the proportions of those ever deployed under OEF/OIF who were ever deployed to a given location since September 11, We categorize the past deployment location indicators into three mutually exclusive categories to allow for easier comparison (i.e., the three rows add up to 100%). With the Army, for example, 31% of solders ever deployed under OEF/OIF were sent to Iraq/Afghanistan (but not on other OEF/OIF missions), 45% were sent on other OEF/OIF missions, and the remaining 24% have been to Iraq/Afghanistan as well as other OEF/OIF missions. The rest of Table 1 provides summary statistics of service and demographic characteristics, which are representative of the US 9
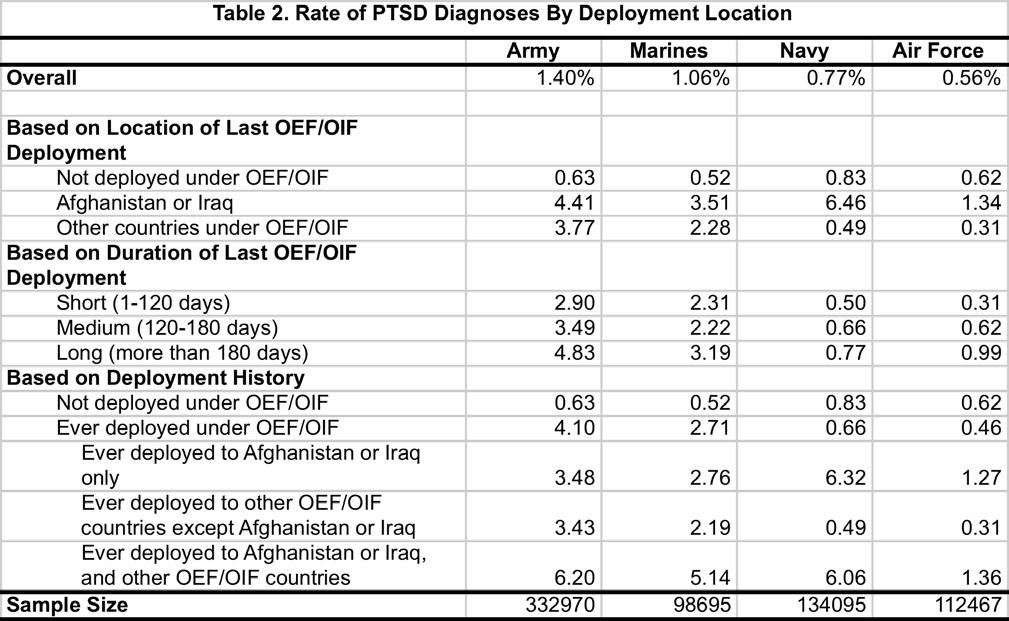
10 Armed Forces active duty population. Table 2 reports the proportion of the active duty population who were diagnosed with PTSD for each service. The first row presents the PTSD percentage for the entire active duty population, regardless of their deployment status, and ranges from 0. 6% for Air Force to 1.4% for Army. The next set reports the PTSD rate by the last deployment location. People deployed to Iraq/Afghanistan had much higher rates of being diagnosed with PTSD compared to those not deployed under OEF or OIF (4.4% vs. 0.6% for the Army, 3.5% vs. 0.5% for the Marines, 6.5% vs. 0.5% for the Navy, and 1.3% vs. 0.6% for the Air Force; p<0.01 for statistical tests of all of these differences). Army and Marine Corps personnel deployed to other OEF/OIF missions also have higher rates of PTSD compared to those not deployed under OEF/OIF (3.8% for Army, 2.3% for Marines), but the opposite is the case for the Navy and Air Force. Among those deployed under OEF/OIF, the PTSD rate increases as the tour length increases. With the Army, for example, the proportion of enlisted personnel who were later diagnosed with PTSD is 2.9% among those with a short tour length (1-120 days), and the rate increases to 3. 5% in the medium length category ( days) and to 4.8% for long tours (>180 days). We observe similar, but not as stark, patterns for the other three services. The last set of statistics in Table 2 reports the PTSD rate by whether a person was ever deployed to a given location. With the Army, the proportion of people ever deployed to Iraq/Afghanistan (but not other OEF/OIF missions) who were diagnosed with PTSD is 3.5%. The number is slightly lower for those who were deployed elsewhere except for Iraq/Afghanistan (3.4%). The rate of PTSD is even higher (6.2%) for those who have been to Iraq/Afghanistan, as well as other OEF/OIF missions. We observe similar pattern for the other three branches. The raw proportions of personnel being diagnosed with PTSD shown in Table 2 provide a good comparison across services of the prevalence of PTSD based on types of deployments. We 10
11 next report, in Table 3, the logistic regression results that compare, across services, the effect of the OEF/OIF deployment on the risk of developing PTSD relative to the risk enlisted personnel would have had in the more typical military missions around the world. We present the results in terms of odds ratios and focus only on the effect of deployment characteristics in Table 3 (the complete regression results for Model 1 are included in the Appendix). The top panel of Table 3 reports the main effect of the last deployment s location and duration. With the Army, the first row indicates that the odds of being diagnosed with PTSD is 3.96 times higher among those deployed to Iraq/Afghanistan compared to those not deployed under OEF/OIF (p<0.01). Being deployed on other OEF/OIF missions also increases the odds of PTSD by the same magnitude (OR=3.97, p<0.01). The effects of being deployed to Iraq/Afghanistan and on other OEF/OIF missions are comparable for the Marines, as it increases the odds of developing PTSD by 4.57 and 3.51 times (p<0.01 for both), respectively. For the Navy, being deployed to Iraq/Afghanistan also carries a very high risk of developing PTSD (OR=9.06, p<0.01) compared to those not deployed under OEF/OIF. Iraq/Afghanistan missions appear to have the smallest impact for Air Force, as the odds of developing PTSD among those deployed to Iraq/Afghanistan is only 1.25 times higher than those not deployed (p<0.05). For the Navy and Air Force, the risk of being deployed on other OEF/OIF missions is actually lower than for those not deployed on an OEF/OIF mission (OR=0.54 and 0.44, respectively, both p<0.01). Model 1 also shows that the tour length matters. Compared to those who have a short tour length (<120 days), Army soldiers whose last deployment was between days are 1.18 times more likely to get PTSD (p<0.01) and those whose last deployment was more than 180 days have an odds ratio of 1.62 (p<0.01). Similar adverse effects of longer tours are observed for the Navy and Air Force. For the Marine Corps, the duration effect only shows up if they have been deployed 11
12 more than 180 days (OR=1.11, p<0.10). It is worth noting that the adverse effects of deployment location and length are present even after we control for MOS, and not surprisingly, those in combat arms specialty (the reference group) have the highest odds of developing PTSD (Appendix). For Model 2, presented in the lower panel of Table 3, we add an interaction effect between the Iraq/Afghanistan location and the tour duration variables to test whether long tour exacerbate the effects of deployments to these two countries. For the Army, the 1.53 odds ratio on the long duration variable itself now indicates that those whose OEF/OIF deployment to locations other than Iraq/Afghanistan lasted more than 180 days are 1.53 times more likely to be diagnosed with PTSD than those whose last tour to those locations were under 120 days. The odds ratio on the Iraq/Afghanistan indicator now essentially compares the rate of PTSD between those deployed to Iraq/Afghanistan under 120 days and those not deployed to OEF/OIF missions. Even with a short tour, deployment to Iraq still results in an odds ratio of 3.70 (p<0.01). The same applies to the Marine Corps and Navy, but the Air Force still has a smaller effect of an Iraq/Afghanistan deployment. The key variables are the last two rows. Among soldiers whose last deployment was to Iraq/Afghanistan, those that lasted more than 180 days had a 1.15 times higher risk of developing PTSD (p<0.10) compared to those with a short (less than 120-day) deployment, which is in addition to the main Iraq/Afghanistan effect of 3.96). For the Army, a medium-length deployment had no additional effect on the risk of developing PTSD. We observe additive effects for the Navy (OR for the interactive terms on medium and long duration are 2.50 and 2.47, respectively, p<0.01), but not for Marines or Air Force. As a sensitivity analysis, we estimate Model 3, which captures whether the individual was ever deployed to a given location. The results in Table 4 are similar to Model 1 (where we only capture the location of last deployment). The odds ratio of developing PTSD for those deployed to Iraq/Afghanistan (but not other OEF/OIF locations) compared to those never deployed under 12
13 OEF/OIF ranges from 1.85 times for the Air Force to times for the Navy (p<0.01 for all services). The highest odds belong to those who were deployed to Iraq/Afghanistan as well as other OEF/OIF locations (essentially, deployed at least twice): the odds ratio of developing PTSD ranges from 1.92 for the Air Force to 9.65 for the Navy (p<0.01 for all services) compared to those never sent on an OEF/OIF missions. In another sensitivity analysis, we address the empirical issue that the year variables could be highly correlated with the -OEF/OIF missions, thus causing multicollinearity and perhaps leading to an underestimation of the deployment effect on the risk of developing PTSD. Thus we estimated models that excluded the year dummies, and the estimated effects of an Iraq/Afghanistan deployment on the risk of developing PTSD were about percent higher than our main models. Comments In this study, we link deployment information and TRICARE health records to examine the relationship between deployment intensity and PTSD. We find that the percentage of PTSD diagnoses among the active duty population varies by service, but are all below one percent among those not deployed on OEF/OIF missions. But, those deployed to Iraq/Afghanistan have a much higher probability of developing PTSD, with the percentages ranging from 1.3% for the Air Force to 6.5% for the Navy. Those deployed on other OEF/OIF missions, on the other hand, have higher PTSD rates relative to those not deployed on such missions only for the Army and Marines. While those comparisons describe the actual rates of PTSD across the services for different types of deployments, our regression models further explore how the deployment location and duration affect the risk of developing PTSD, relative to what it would have been in other typical world-wide missions of the U.S. military. A deployment to Iraq/Afghanistan increases the odds of 13
14 developing PTSD substantially, with the largest effect observed for the Navy (OR=9.06) and the smallest effect for the Air Force (OR=1.25). The tour length also matters, as a deployment lasting longer than 180 days increases the odds of PTSD by 1.11 times to 2.84 times, depending on the service, compared to a short tour. Furthermore, for the Army and Navy, a deployment to Iraq/Afghanistan further exacerbates the adverse effect of tour length. The sizable adverse effect of deployment location persists when we considered all past deployments, not just the previous deployment. Our overall rates of PTSD are much lower than previously reported based on surveys or on VA data (Ramchand, Karney et al. 2008). There are several important factors that contribute to the differences. First, our sample is active duty personnel who are still deemed fit to serve in the military, whereas people who show up in the VA health care system are those who had left the military because they have serious physical or mental health problems that prevent them from continuing to serve. Second, compared to PTSD rates reported in anonymous surveys, which lack clinical details in the screening questions, our PTSD rates are based on clinical diagnoses. The enlisted person may be more willing to admit to PTSD symptoms, even if they were mild, on an anonymous survey than they would to military health officials. Third, for people who have the desire to continue serving (and thus stay within the TRICARE system), the stigma of PTSD often prevents them from seeking care when needed since this information would then go on the service person s record. It is also important to keep in mind the following limitations of this study. First, even though we were able to include military occupational specialty categories, we do not have details on the specific assignments. The lack of details on assignments might contribute to the lower odds ratios we observe among Navy and Air Force personnel who were deployed to OEF/OIF locations 14
15 that are not in Iraq or Afghanistan. 3 Second, since our intention is to look at the prevalence of PTSD among the population of personnel who are still in service, we most likely miss severe cases of PTSD since those would show up in the VA system unless they were first diagnosed inside the TRICARE system. With these caveats in mind, there are several important policy implications from our findings. While the adverse effects of Iraq/Afghanistan deployments across all services is expected, it might be surprising that such deployments cause the highest PTSD rates for the Navy. This might be due to many sailors deployed to Iraq or Afghanistan being what the military calls Individual Augmentees (IA), who are those deployed individually or in a small group to assist Army and Marines. The IAs are subject to additional stress as they are thrust into an unfamiliar environment away from their parent command. It may be important to train these personnel for not just the additional physical skills but also mental health readiness for such assignments. In addition, the adverse effect of tour length is observed across all services and for the Air Force, longer durations are more likely to lead to PTSD than being deployed in Afghanistan/Iraq. While a recommendation of the optimal tour length for each branch is beyond the scope of this study, our findings do suggest that efforts to keep OEF/OIF deployments to reasonable lengths could help reduce PTSD rates. Given the continuing nature of the Global War on Terror, it is unavoidable that many enlisted personnel will be subjected to multiple deployments to OEF/OIF locations. We can expect thousands of new cases of PTSD, and it is imperative to monitor these soldiers mental health. The DoD has begun to address this issue by introducing the Post-Deployment Health Reassessment (PDHRA, DD2900) in March 2005, and mandates the completion of this re-assessment at days after a deployment (US Department of Defense 2008). However, our data show that almost 75 3 For example, in the Navy the reference group is mostly people on routine shipboard operation (although they might also be on their shore rotation). Personal communications with the sailors reveal that the living condition on ship is usually horrendous, and a ground OIF assignment in places like Quatar or Kuwait might actually be better compared to life on ship. 15
16 percent of the PTSD population in our sample did not get diagnosed with PTSD until 200 days after their last deployment the average lapse between the last deployment and the first diagnosis of PTSD is 291 days. Further research effort should look into the extent of the effect due to repeated deployments and explore how effective PDHRA is in identifying PTSD cases, as well as more effective monitoring methods beyond the 180 day mandated surveys. PTSD leads to a host of long-term family and workplace problems and is often comorbid with other psychiatric and physical disorders. Our research identifies the extent of the PTSD problem within the active duty population and highlights how certain enlisted personnel, based on their deployment characteristics, are at higher risks of developing this disorder. Further research into preventive measures and effective treatments of PTSD on the active duty population, especially the higher risk groups, needs to remain a focus within the Department of Defense. In addition, while PTSD remains the focus of media attention, other mental health illness such as depression and substance abuse have higher prevalence in the active duty population, and are just as costly to the individuals, military health system, and the society. A comprehensive analysis of other mental health illness would help the evaluation of total force readiness. 16
17 Reference American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR. CDC (1988). "Health status of Vietnam veterans. I. Psychosocial characteristics. The Centers for Disease Control Vietnam Experience Study." JAMA 259(18): Erbes, C., J. Westermeyer, et al. (2007). "Post-traumatic stress disorder and service utilization in a sample of service members from Iraq and Afghanistan." Military medicine 172(4): Grieger, T. A., S. J. Cozza, et al. (2006). "Posttraumatic stress disorder and depression in battleinjured soldiers." The American journal of psychiatry 163(10): ; quiz Helzer, J. E., L. N. Robins, et al. (1987). "Post-traumatic stress disorder in the general population. Findings of the epidemiologic catchment area survey." N Engl J Med 317(26): Hoge, C. W., J. L. Auchterlonie, et al. (2006). "Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan." JAMA 295(9): Hoge, C. W., C. A. Castro, et al. (2004). "Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care." N Engl J Med 351(1): Kang, H. K., B. H. Natelson, et al. (2003). "Post-traumatic stress disorder and chronic fatigue syndrome-like illness among Gulf War veterans: a population-based survey of 30,000 veterans." Am J Epidemiol 157(2): Kimerling, R., P. Ouimette, et al. (2006). "Brief report: Utility of a short screening scale for DSM-IV PTSD in primary care." Journal of general internal medicine 21(1): Martin, C. (2007). "Routine screening and referrals for PTSD after returning from Operation Iraqi Freedom in 2005." U.S. Armed Forces Medical Surveillance Monthly Report 14(6): 2-7. Prigerson, H. G., P. K. Maciejewski, et al. (2002). "Population attributable fractions of psychiatric disorders and behavioral outcomes associated with combat exposure among US men." American journal of public health 92(1): Ramchand, R., B. R. Karney, et al. (2008). Prevalence of PTSD, Depression, and TBI among Returning Service members. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. T. Tanielian and L. H. Jaycox. Santa Monica, Rand Corporation: Rona, R. J., N. T. Fear, et al. (2007). "Mental health consequences of overstretch in the UK armed forces: first phase of a cohort study." BMJ 335(7620): 603. Rosenheck, R. A. and A. F. Fontana (2007). "Recent trends In VA treatment of post-traumatic stress disorder and other mental disorders." Health affairs (Project Hope) 26(6):
18 Seal, K. H., D. Bertenthal, et al. (2007). "Bringing the war back home: mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs facilities." Arch Intern Med 167(5): Shen, Y. C., J. Arkes, et al. (2009). "The effects of deployment intensity on post-traumatic stress disorder: " Military medicine 174(3): Tanielian, T. and L. H. Jaycox (2008). Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery, Rand Corporation. The Iowa Persian Gulf Study Group (1997). "Self-reported illness and health status among Gulf War veterans. A population-based study. The Iowa Persian Gulf Study Group." JAMA 277(3): U.S. Army (2003, Jan 1). "Operation Iraqi Freedom (OIF) Mental Health Advisory Team (MHAT) Report." Retrieved May 11, 2009, from U.S. Army (2005, January 30, 2005). "Operation Iraqi Freedom (OIF) Mental Health Advisory Team (MHAT-II) Report." Retrieved May 11, 2009, from U.S. Army (2006, May 29, 2006). "Operation Iraqi Freedom (OIF) Mental Health Advisory Team (MHAT-III) Report." Retrieved May 11, 2009, from Redacted.pdf. U.S. Army (2006, November 17, 2006). "Operation Iraqi Freedom (OIF) Mental Health Advisory Team (MHAT-IV) Report." Retrieved May 11, 2009, from US Department of Defense (2008, October 14, 2008). "Post-Deployment Health Reassessment (PDHRA) Program (DD Form 2900)." Retrieved October 14, 2008, from Vasterling, J. J., S. P. Proctor, et al. (2006). "Neuropsychological outcomes of army personnel following deployment to the Iraq war." JAMA 296(5):
19 19
20 20
21 21
22 22
23 23
Effects of Iraq/Afghanistan Deployments on PTSD Diagnoses for Still Active Personnel in All Four Services
 MILITARY MEDICINE, 175, 10:763, 2010 Effects of Iraq/Afghanistan Deployments on PTSD Diagnoses for Still Active Personnel in All Four Services Yu-Chu Shen, PhD * ; Jeremy Arkes, PhD * ; MAJ Boon Wah Kwan,
MILITARY MEDICINE, 175, 10:763, 2010 Effects of Iraq/Afghanistan Deployments on PTSD Diagnoses for Still Active Personnel in All Four Services Yu-Chu Shen, PhD * ; Jeremy Arkes, PhD * ; MAJ Boon Wah Kwan,
Analysis of VA Health Care Utilization Among US Global War on Terrorism (GWOT) Veterans
 Veterans") Analysis of VA Health Care Utilization Among US Global War on Terrorism (GWOT) Veterans Operation Enduring Freedom Operation Iraqi Freedom VHA Office of Public Health and Environmental Hazards May 2008
Analysis of VA Health Care Utilization Among US Global War on Terrorism (GWOT) Veterans Operation Enduring Freedom Operation Iraqi Freedom VHA Office of Public Health and Environmental Hazards May 2008
Analysis of VA Health Care Utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans
, Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans") Analysis of VA Health Care Utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans Cumulative from 1 st Qtr FY 2002 through 1 st Qtr FY
Analysis of VA Health Care Utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans Cumulative from 1 st Qtr FY 2002 through 1 st Qtr FY
Comparison of Select Health Outcomes by Deployment Health Assessment Completion
 MILITARY MEDICINE, 181, 2:123, 2016 Comparison of Select Health Outcomes by Deployment Health Assessment Completion Tina M. Luse, MPH; Jean Slosek, MPH; Christopher Rennix, ScD, MS, CIH Abstract The Department
MILITARY MEDICINE, 181, 2:123, 2016 Comparison of Select Health Outcomes by Deployment Health Assessment Completion Tina M. Luse, MPH; Jean Slosek, MPH; Christopher Rennix, ScD, MS, CIH Abstract The Department
Supplementary Online Content
 Supplementary Online Content Ursano RJ, Kessler RC, Naifeh JA, et al; Army Study to Assess Risk and Resilience in Servicemembers (STARRS). Risk of suicide attempt among soldiers in army units with a history
Supplementary Online Content Ursano RJ, Kessler RC, Naifeh JA, et al; Army Study to Assess Risk and Resilience in Servicemembers (STARRS). Risk of suicide attempt among soldiers in army units with a history
Health on the Homefront:
 Health on the Homefront: Formation of a Wounded, Ill, and Injured Registry for USN and USMC Service Members Dagny Magill, MPH, Epidemiologist Deployment Health Division, Epidemiology Data Center Department
Health on the Homefront: Formation of a Wounded, Ill, and Injured Registry for USN and USMC Service Members Dagny Magill, MPH, Epidemiologist Deployment Health Division, Epidemiology Data Center Department
Suicide Among Veterans and Other Americans Office of Suicide Prevention
 Suicide Among Veterans and Other Americans 21 214 Office of Suicide Prevention 3 August 216 Contents I. Introduction... 3 II. Executive Summary... 4 III. Background... 5 IV. Methodology... 5 V. Results
Suicide Among Veterans and Other Americans 21 214 Office of Suicide Prevention 3 August 216 Contents I. Introduction... 3 II. Executive Summary... 4 III. Background... 5 IV. Methodology... 5 V. Results
from March 2003 to December 2011,
 Medical Evacuations from Operation Iraqi Freedom/Operation New Dawn, Active and Reserve Components, U.S. Armed Forces, 23-211 From January 23 to December 211, over 5, service members were medically evacuated
Medical Evacuations from Operation Iraqi Freedom/Operation New Dawn, Active and Reserve Components, U.S. Armed Forces, 23-211 From January 23 to December 211, over 5, service members were medically evacuated
Fleet and Marine Corps Health Risk Assessment, 02 January December 31, 2015
 Fleet and Marine Corps Health Risk Assessment, 02 January December 31, 2015 Executive Summary The Fleet and Marine Corps Health Risk Appraisal is a 22-question anonymous self-assessment of the most common
Fleet and Marine Corps Health Risk Assessment, 02 January December 31, 2015 Executive Summary The Fleet and Marine Corps Health Risk Appraisal is a 22-question anonymous self-assessment of the most common
MINISTERIAL SUBMISSION
 200847 Ref: CJHLTH/OUT/20 10lAF5992222 Requested Australian Government Department of Defence MINISTERIAL SUBMISSION To: Mr Snowdon CC: Senator Feeney Copies to: Secretary, CDF, FASMSPA, CN, CA, CAF. Timing:
200847 Ref: CJHLTH/OUT/20 10lAF5992222 Requested Australian Government Department of Defence MINISTERIAL SUBMISSION To: Mr Snowdon CC: Senator Feeney Copies to: Secretary, CDF, FASMSPA, CN, CA, CAF. Timing:
Operational Stress and Postdeployment Behaviors in Seabees
 CAB D0017113.A2/Final April 2008 Operational Stress and Postdeployment Behaviors in Seabees Neil B. Carey James L. Gasch David Gregory Cathleen McHugh 4825 Mark Center Drive Alexandria, Virginia 22311-1850
CAB D0017113.A2/Final April 2008 Operational Stress and Postdeployment Behaviors in Seabees Neil B. Carey James L. Gasch David Gregory Cathleen McHugh 4825 Mark Center Drive Alexandria, Virginia 22311-1850
Patterns of Ambulatory Mental Health Care in Navy Clinics
 CRM D0003835.A2/Final June 2001 Patterns of Ambulatory Mental Health Care in Navy Clinics Michelle Dolfini-Reed 4825 Mark Center Drive Alexandria, Virginia 22311-1850 Approved for distribution: June 2001
CRM D0003835.A2/Final June 2001 Patterns of Ambulatory Mental Health Care in Navy Clinics Michelle Dolfini-Reed 4825 Mark Center Drive Alexandria, Virginia 22311-1850 Approved for distribution: June 2001
Outreach. Vet Centers
 26-06 October 6, 2006 STATEMENT OF CATHLEEN C. WIBLEMO, DEPUTY DIRECTOR VETERANS AFFAIRS AND REHABILITATION DIVISION COMMISSION THE AMERICAN LEGION TO THE SUBCOMMITTEE ON HEALTH COMMITTEE ON VETERANS AFFAIRS
26-06 October 6, 2006 STATEMENT OF CATHLEEN C. WIBLEMO, DEPUTY DIRECTOR VETERANS AFFAIRS AND REHABILITATION DIVISION COMMISSION THE AMERICAN LEGION TO THE SUBCOMMITTEE ON HEALTH COMMITTEE ON VETERANS AFFAIRS
Assessing the Effects of Individual Augmentation on Navy Retention
 Assessing the Effects of Individual Augmentation on Navy Retention Ron Fricker & Sam Buttrey Eighth Annual Navy Workforce Research and Analysis Conference May 7, 2008 What is Individual Augmentation? Individual
Assessing the Effects of Individual Augmentation on Navy Retention Ron Fricker & Sam Buttrey Eighth Annual Navy Workforce Research and Analysis Conference May 7, 2008 What is Individual Augmentation? Individual
APNA 28th Annual Conference Session 2034: October 23, 2014
 Mary Ann Boyd, PhD, DNS, PMHCNS BC Wanda Bradshaw, RN BC, MSN Marceline Robinson, MSN, PMHCNS BC American Psychiatric Nurses Association Annual Meeting October 23, 2014 Indianapolis, IN Describe the military
Mary Ann Boyd, PhD, DNS, PMHCNS BC Wanda Bradshaw, RN BC, MSN Marceline Robinson, MSN, PMHCNS BC American Psychiatric Nurses Association Annual Meeting October 23, 2014 Indianapolis, IN Describe the military
In Press at Population Health Management. HEDIS Initiation and Engagement Quality Measures of Substance Use Disorder Care:
 In Press at Population Health Management HEDIS Initiation and Engagement Quality Measures of Substance Use Disorder Care: Impacts of Setting and Health Care Specialty. Alex HS Harris, Ph.D. Thomas Bowe,
In Press at Population Health Management HEDIS Initiation and Engagement Quality Measures of Substance Use Disorder Care: Impacts of Setting and Health Care Specialty. Alex HS Harris, Ph.D. Thomas Bowe,
PREPARED FOR: U.S. Army Medical Research and Materiel Command Fort Detrick, Maryland
 AD Award Number: W81XWH-10-1-0810 TITLE: Adaptive Disclosure: A Combat-Specific PTSD Treatment PRINCIPAL INVESTIGATOR: Brett Litz, Ph.D. CONTRACTING ORGANIZATION: VA Research Institute, MA 02130 REPORT
AD Award Number: W81XWH-10-1-0810 TITLE: Adaptive Disclosure: A Combat-Specific PTSD Treatment PRINCIPAL INVESTIGATOR: Brett Litz, Ph.D. CONTRACTING ORGANIZATION: VA Research Institute, MA 02130 REPORT
NAVAL POSTGRADUATE SCHOOL THESIS
 NAVAL POSTGRADUATE SCHOOL MONTEREY, CALIFORNIA THESIS ANALYSIS OF SUICIDE BEHAVIORS IN THE NAVY ACTIVE DUTY AND RESERVE COMPONENT POPULATION by Neeta Serena Blankenship Kristin M. Shepherd March 2015 Thesis
NAVAL POSTGRADUATE SCHOOL MONTEREY, CALIFORNIA THESIS ANALYSIS OF SUICIDE BEHAVIORS IN THE NAVY ACTIVE DUTY AND RESERVE COMPONENT POPULATION by Neeta Serena Blankenship Kristin M. Shepherd March 2015 Thesis
June 25, Honorable Kent Conrad Ranking Member Committee on the Budget United States Senate Washington, DC
 CONGRESSIONAL BUDGET OFFICE U.S. Congress Washington, DC 20515 Douglas Holtz-Eakin, Director June 25, 2004 Honorable Kent Conrad Ranking Member Committee on the Budget United States Senate Washington,
CONGRESSIONAL BUDGET OFFICE U.S. Congress Washington, DC 20515 Douglas Holtz-Eakin, Director June 25, 2004 Honorable Kent Conrad Ranking Member Committee on the Budget United States Senate Washington,
Patterns of Reserve Officer Attrition Since September 11, 2001
 CAB D0012851.A2/Final October 2005 Patterns of Reserve Officer Attrition Since September 11, 2001 Michelle A. Dolfini-Reed Ann D. Parcell Benjamin C. Horne 4825 Mark Center Drive Alexandria, Virginia 22311-1850
CAB D0012851.A2/Final October 2005 Patterns of Reserve Officer Attrition Since September 11, 2001 Michelle A. Dolfini-Reed Ann D. Parcell Benjamin C. Horne 4825 Mark Center Drive Alexandria, Virginia 22311-1850
Navy and Marine Corps Public Health Center. Fleet and Marine Corps Health Risk Assessment 2013 Prepared 2014
 Navy and Marine Corps Public Health Center Fleet and Marine Corps Health Risk Assessment 2013 Prepared 2014 The enclosed report discusses and analyzes the data from almost 200,000 health risk assessments
Navy and Marine Corps Public Health Center Fleet and Marine Corps Health Risk Assessment 2013 Prepared 2014 The enclosed report discusses and analyzes the data from almost 200,000 health risk assessments
Traumatic Brain Injury: Care and Treatment of Operation Enduring Freedom and Operation Iraqi Freedom Veterans
 Traumatic Brain Injury: Care and Treatment of Operation Enduring Freedom and Operation Iraqi Freedom Veterans Amalia K. Corby-Edwards Analyst in Public Health and Epidemiology November 25, 2009 Congressional
Traumatic Brain Injury: Care and Treatment of Operation Enduring Freedom and Operation Iraqi Freedom Veterans Amalia K. Corby-Edwards Analyst in Public Health and Epidemiology November 25, 2009 Congressional
ECHCS Eligibility Training. VA Medical Benefits and Eligibility
 ECHCS Eligibility Training VA Medical Benefits and Eligibility Overview Establishing Eligibility Health Service Priority Groups Copays Additional Services Where to Seek More Information Establishing Eligibility
ECHCS Eligibility Training VA Medical Benefits and Eligibility Overview Establishing Eligibility Health Service Priority Groups Copays Additional Services Where to Seek More Information Establishing Eligibility
-name redacted- Information Research Specialist. August 7, Congressional Research Service RS22452
 A Guide to U.S. Military Casualty Statistics: Operation Freedom s Sentinel, Operation Inherent Resolve, Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom -name redacted- Information
A Guide to U.S. Military Casualty Statistics: Operation Freedom s Sentinel, Operation Inherent Resolve, Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom -name redacted- Information
U.S. Military Casualty Statistics: Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom
 U.S. Military Casualty Statistics: Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom Hannah Fischer Information Research Specialist February 5, 2013 CRS Report for Congress Prepared
U.S. Military Casualty Statistics: Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom Hannah Fischer Information Research Specialist February 5, 2013 CRS Report for Congress Prepared
REPORT OF THE COUNCIL ON MEDICAL SERVICE. Acceptance of TRICARE Health Insurance
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report - I-0 Subject: Presented by: Referred to: Acceptance of TRICARE Health Insurance David O. Barbe, MD, Chair Reference Committee J (Jack J. Beller, MD,
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report - I-0 Subject: Presented by: Referred to: Acceptance of TRICARE Health Insurance David O. Barbe, MD, Chair Reference Committee J (Jack J. Beller, MD,
Officer Retention Rates Across the Services by Gender and Race/Ethnicity
 Issue Paper #24 Retention Officer Retention Rates Across the Services by Gender and Race/Ethnicity MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training
Issue Paper #24 Retention Officer Retention Rates Across the Services by Gender and Race/Ethnicity MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training
Long-Stay Alternate Level of Care in Ontario Mental Health Beds
 Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Population Representation in the Military Services
 Population Representation in the Military Services Fiscal Year 2008 Report Summary Prepared by CNA for OUSD (Accession Policy) Population Representation in the Military Services Fiscal Year 2008 Report
Population Representation in the Military Services Fiscal Year 2008 Report Summary Prepared by CNA for OUSD (Accession Policy) Population Representation in the Military Services Fiscal Year 2008 Report
Manpower System Analysis Thesis Day Brief v.3 / Class of March 2014
 Calhoun: The NPS Institutional Archive Graduate School of Business and Public Policy (GSBPP) Thesis Day Programs and Documents 2014-03 Manpower System Analysis Thesis Day Brief v.3 / Class of March 2014
Calhoun: The NPS Institutional Archive Graduate School of Business and Public Policy (GSBPP) Thesis Day Programs and Documents 2014-03 Manpower System Analysis Thesis Day Brief v.3 / Class of March 2014
MEDICAL SURVEILLANCE MONTHLY REPORT
 VOL. 14 NO. 4 JULY 27 msmr A publication of the Armed Forces Health Surveillance Center MEDICAL SURVEILLANCE MONTHLY REPORT INSIDE THIS ISSUE: Mental health encounters and diagnoses following deployment
VOL. 14 NO. 4 JULY 27 msmr A publication of the Armed Forces Health Surveillance Center MEDICAL SURVEILLANCE MONTHLY REPORT INSIDE THIS ISSUE: Mental health encounters and diagnoses following deployment
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6490.3 August 7, 1997 SUBJECT: Implementation and Application of Joint Medical Surveillance for Deployments USD(P&R) References: (a) DoD Directive 6490.2, "Joint
Department of Defense INSTRUCTION NUMBER 6490.3 August 7, 1997 SUBJECT: Implementation and Application of Joint Medical Surveillance for Deployments USD(P&R) References: (a) DoD Directive 6490.2, "Joint
Authors alone are responsible for opinions expressed in the contribution and for its clearance through their federal health agency, if required.
 ORIGINAL ARTICLES Authors alone are responsible for opinions expressed in the contribution and for its clearance through their federal health agency, if required. MILITARY MEDICINE, 179, 9:964, 2014 Determinants
ORIGINAL ARTICLES Authors alone are responsible for opinions expressed in the contribution and for its clearance through their federal health agency, if required. MILITARY MEDICINE, 179, 9:964, 2014 Determinants
Lawrence A. Allen, MBA, CPC
 Lawrence A. Allen, MBA, CPC This presentation is based on the presenter s perspective and views and does not represent official policy, guidance, or opinions of the Department of Defense (DoD) or the U.S.
Lawrence A. Allen, MBA, CPC This presentation is based on the presenter s perspective and views and does not represent official policy, guidance, or opinions of the Department of Defense (DoD) or the U.S.
WikiLeaks Document Release
 WikiLeaks Document Release 2, 2009 Congressional Research Service Report RS22452 United States Military Casualty Statistics: Operation Iraqi Freedom and Operation Enduring Freedom Hannah Fischer, Knowledge
WikiLeaks Document Release 2, 2009 Congressional Research Service Report RS22452 United States Military Casualty Statistics: Operation Iraqi Freedom and Operation Enduring Freedom Hannah Fischer, Knowledge
CHARLES L. RICE, M.D.
 HOLD UNTIL RELEASED BY THE COMMITTEE STATEMENT BY CHARLES L. RICE, M.D. PRESIDENT, UNIFORMED SERVICES UNIVERSITY OF THE HEALTH SCIENCES, PERFORMING THE DUTIES OF THE ASSISTANT SECRETARY OF DEFENSE, HEALTH
HOLD UNTIL RELEASED BY THE COMMITTEE STATEMENT BY CHARLES L. RICE, M.D. PRESIDENT, UNIFORMED SERVICES UNIVERSITY OF THE HEALTH SCIENCES, PERFORMING THE DUTIES OF THE ASSISTANT SECRETARY OF DEFENSE, HEALTH
Medical Requirements and Deployments
 INSTITUTE FOR DEFENSE ANALYSES Medical Requirements and Deployments Brandon Gould June 2013 Approved for public release; distribution unlimited. IDA Document NS D-4919 Log: H 13-000720 INSTITUTE FOR DEFENSE
INSTITUTE FOR DEFENSE ANALYSES Medical Requirements and Deployments Brandon Gould June 2013 Approved for public release; distribution unlimited. IDA Document NS D-4919 Log: H 13-000720 INSTITUTE FOR DEFENSE
 Joint Medical Readiness Oversight Committee Annual Report to Congress On the Health Status and Medical Readiness of Members of the Armed Forces May 2008 TABLE of CONTENTS Background... 1 Action 1, Ronald
Joint Medical Readiness Oversight Committee Annual Report to Congress On the Health Status and Medical Readiness of Members of the Armed Forces May 2008 TABLE of CONTENTS Background... 1 Action 1, Ronald
VE-HEROeS and Vietnam Veterans Mortality Study
 VE-HEROeS and Vietnam Veterans Mortality Study Review of Health Effects in Vietnam Veterans of Exposure to Herbicides: Eleventh Biennial Update Health and Medicine Division, National Academy of Science,
VE-HEROeS and Vietnam Veterans Mortality Study Review of Health Effects in Vietnam Veterans of Exposure to Herbicides: Eleventh Biennial Update Health and Medicine Division, National Academy of Science,
MICHAEL E. KILPATRICK, M.D. DEPUTY DIRECTOR, DEPLOYMENT HEALTH SUPPORT BEFORE THE VETERANS AFFAIRS COMMITTEE U.S. HOUSE OF REPRESENTATIVES
 MICHAEL E. KILPATRICK, M.D. DEPUTY DIRECTOR, DEPLOYMENT HEALTH SUPPORT BEFORE THE VETERANS AFFAIRS COMMITTEE U.S. HOUSE OF REPRESENTATIVES POST TRAUMATIC STRESS DISORDER July 27, 2005 Mr. Chainnan and
MICHAEL E. KILPATRICK, M.D. DEPUTY DIRECTOR, DEPLOYMENT HEALTH SUPPORT BEFORE THE VETERANS AFFAIRS COMMITTEE U.S. HOUSE OF REPRESENTATIVES POST TRAUMATIC STRESS DISORDER July 27, 2005 Mr. Chainnan and
In , an estimated 181,500 veterans (8% of
 U.S. Department of Justice Office of Justice Programs Bureau of Justice Statistics Special Report DECEMBER 2015 NCJ 249144 Veterans in and, 2011 12 Jennifer Bronson, Ph.D., E. Ann Carson, Ph.D., and Margaret
U.S. Department of Justice Office of Justice Programs Bureau of Justice Statistics Special Report DECEMBER 2015 NCJ 249144 Veterans in and, 2011 12 Jennifer Bronson, Ph.D., E. Ann Carson, Ph.D., and Margaret
Soldier Attitudes toward Mental Health Screening and Seeking Care upon Return from Combat
 MILITARY MEDICINE, 173, 6:563, 2008 Soldier Attitudes toward Mental Health Screening and Seeking Care upon Return from Combat MAJ Christopher H. Warner, MC USA*; LTC George N. Appenzeller, MC USA*; CPT
MILITARY MEDICINE, 173, 6:563, 2008 Soldier Attitudes toward Mental Health Screening and Seeking Care upon Return from Combat MAJ Christopher H. Warner, MC USA*; LTC George N. Appenzeller, MC USA*; CPT
Reenlistment Rates Across the Services by Gender and Race/Ethnicity
 Issue Paper #31 Retention Reenlistment Rates Across the Services by Gender and Race/Ethnicity MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training
Issue Paper #31 Retention Reenlistment Rates Across the Services by Gender and Race/Ethnicity MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training
DEFENSE HEALTH CARE. DOD Is Meeting Most Mental Health Care Access Standards, but It Needs a Standard for Followup Appointments
 United States Government Accountability Office Report to Congressional Committees April 2016 DEFENSE HEALTH CARE DOD Is Meeting Most Mental Health Care Access Standards, but It Needs a Standard for Followup
United States Government Accountability Office Report to Congressional Committees April 2016 DEFENSE HEALTH CARE DOD Is Meeting Most Mental Health Care Access Standards, but It Needs a Standard for Followup
Prevalence and Screening of Mental Health Problems Among U.S. Combat Soldiers Pre- and Post- Deployment
 Principal Author: Charles W. Hoge, MD, COL, MC, U.S. Army Chief Department of Psychiatry and Behavioral Sciences Division of Neuropsychiatry Walter Reed Army Institute of Research 503 Robert Grant Ave,
Principal Author: Charles W. Hoge, MD, COL, MC, U.S. Army Chief Department of Psychiatry and Behavioral Sciences Division of Neuropsychiatry Walter Reed Army Institute of Research 503 Robert Grant Ave,
Development of Houston Veterans Court
 Development of Houston Veterans Court Incarcerated Veterans Suicide Rates in Returning Veterans PTSD in Returning Veterans Why we need Veterans Courts Importance of Community Partnerships Unique Features
Development of Houston Veterans Court Incarcerated Veterans Suicide Rates in Returning Veterans PTSD in Returning Veterans Why we need Veterans Courts Importance of Community Partnerships Unique Features
Tri-service Disability Evaluation Systems Database Analysis and Research
 Tri-service Disability Evaluation Systems Database Analysis and Research Prepared by Accession Medical Standards Analysis and Research Activity Division of Preventive Medicine Walter Reed Army Institute
Tri-service Disability Evaluation Systems Database Analysis and Research Prepared by Accession Medical Standards Analysis and Research Activity Division of Preventive Medicine Walter Reed Army Institute
Report on DoD-Funded Service Contracts in Forward Areas
 Report on DoD-Funded Service Contracts in Forward Areas July 2007 REPORTABLE INFORMATION This report provides the information required by section 3305 of the Fiscal Year (FY) 2007 Supplemental Appropriations
Report on DoD-Funded Service Contracts in Forward Areas July 2007 REPORTABLE INFORMATION This report provides the information required by section 3305 of the Fiscal Year (FY) 2007 Supplemental Appropriations
Mental Health Advisory Team 9 (MHAT 9) Operation Enduring Freedom (OEF) 2013 Afghanistan. 10 October 2013
 Operation Enduring Freedom (OEF) 2013 Afghanistan. 10 October 2013") Mental Health Advisory Team 9 (MHAT 9) Operation Enduring Freedom (OEF) 2013 Afghanistan 10 October 2013 Office of The Surgeon General United States Army Medical Command and Office of the Command Surgeon
Mental Health Advisory Team 9 (MHAT 9) Operation Enduring Freedom (OEF) 2013 Afghanistan 10 October 2013 Office of The Surgeon General United States Army Medical Command and Office of the Command Surgeon
Criminal justice involvement. Risk of Incarceration and Other Characteristics of Iraq and Afghanistan Era Veterans in State and Federal Prisons
 Risk of Incarceration and Other Characteristics of Iraq and Afghanistan Era Veterans in State and Federal Prisons Jack Tsai, Ph.D. Robert A. Rosenheck, M.D. Wesley J. Kasprow, Ph.D. James F. McGuire, Ph.D.
Risk of Incarceration and Other Characteristics of Iraq and Afghanistan Era Veterans in State and Federal Prisons Jack Tsai, Ph.D. Robert A. Rosenheck, M.D. Wesley J. Kasprow, Ph.D. James F. McGuire, Ph.D.
Pursuant to Section 1073b(a) of Title 10, United States Code
 of Title 10, United States Code") Report to Committees on Armed Services of the Senate and House of Representatives on the Calendar Year 2016 Activities of the Force Health Protection Quality Assurance Program of the Department of Defense
Report to Committees on Armed Services of the Senate and House of Representatives on the Calendar Year 2016 Activities of the Force Health Protection Quality Assurance Program of the Department of Defense
Veterans and the Justice System: The Next Forensic Frontier
 EDITORIAL Veterans and the Justice System: The Next Forensic Frontier Debra A. Pinals, MD J Am Acad Psychiatry Law 38:163 7, 2010 On most days in the United States, stories appear in the media related
EDITORIAL Veterans and the Justice System: The Next Forensic Frontier Debra A. Pinals, MD J Am Acad Psychiatry Law 38:163 7, 2010 On most days in the United States, stories appear in the media related
Determining Patterns of Reserve Attrition Since September 11, 2001
 CAB D0011483.A2/Final June 2005 Determining Patterns of Reserve Attrition Since September 11, 2001 Michelle A. Dolfini-Reed Ann D. Parcell Dave Gregory Benjamin C. Horne 4825 Mark Center Drive Alexandria,
CAB D0011483.A2/Final June 2005 Determining Patterns of Reserve Attrition Since September 11, 2001 Michelle A. Dolfini-Reed Ann D. Parcell Dave Gregory Benjamin C. Horne 4825 Mark Center Drive Alexandria,
Mental Health Follow-up Care Post Inpatient Hospitalization in the Military Health System
 Mental Health Care Post Hospitalization in the Military Health System Prepared by the Deployment Health Clinical Center Released January 2017 by Deployment Health Clinical Center, a Defense Centers of
Mental Health Care Post Hospitalization in the Military Health System Prepared by the Deployment Health Clinical Center Released January 2017 by Deployment Health Clinical Center, a Defense Centers of
Demographic Profile of the Active-Duty Warrant Officer Corps September 2008 Snapshot
 Issue Paper #44 Implementation & Accountability MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training Branching & Assignments Promotion Retention Implementation
Issue Paper #44 Implementation & Accountability MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training Branching & Assignments Promotion Retention Implementation
Prepared Statement. Captain Mike Colston, M.D. Director, Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury.
 Prepared Statement of Captain Mike Colston, M.D. Director, Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury and Captain Walter Greenhalgh, M.D. Director, National Intrepid
Prepared Statement of Captain Mike Colston, M.D. Director, Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury and Captain Walter Greenhalgh, M.D. Director, National Intrepid
2013 Workplace and Equal Opportunity Survey of Active Duty Members. Nonresponse Bias Analysis Report
 2013 Workplace and Equal Opportunity Survey of Active Duty Members Nonresponse Bias Analysis Report Additional copies of this report may be obtained from: Defense Technical Information Center ATTN: DTIC-BRR
2013 Workplace and Equal Opportunity Survey of Active Duty Members Nonresponse Bias Analysis Report Additional copies of this report may be obtained from: Defense Technical Information Center ATTN: DTIC-BRR
Hannah Fischer Information Research Specialist. August 7, Congressional Research Service RS22452
 A Guide to U.S. Military Casualty Statistics: Operation Freedom s Sentinel, Operation Inherent Resolve, Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom Hannah Fischer Information
A Guide to U.S. Military Casualty Statistics: Operation Freedom s Sentinel, Operation Inherent Resolve, Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom Hannah Fischer Information
United States Military Casualty Statistics: Operation Iraqi Freedom and Operation Enduring Freedom
 Order Code RS22452 Updated 9, United States Military Casualty Statistics: Operation Iraqi Freedom and Operation Enduring Freedom Summary Hannah Fischer Information Research Specialist Knowledge Services
Order Code RS22452 Updated 9, United States Military Casualty Statistics: Operation Iraqi Freedom and Operation Enduring Freedom Summary Hannah Fischer Information Research Specialist Knowledge Services
MSMR. Women s Health Issue JULY 2012
 JULY 2012 Volume 19 Number 7 MSMR M E D I C A L S U R V E I L L A N C E M O N T H L Y R E P O R T Women s Health Issue P A G E 2 Health of women after wartime deployments: correlates of risk for selected
JULY 2012 Volume 19 Number 7 MSMR M E D I C A L S U R V E I L L A N C E M O N T H L Y R E P O R T Women s Health Issue P A G E 2 Health of women after wartime deployments: correlates of risk for selected
Summary of Key Findings from the Mental Health Advisory Team 6 (MHAT 6): OEF and OIF
: OEF and OIF") Summary of Key Findings from the Mental Health Advisory Team 6 (MHAT 6): OEF and OIF Presented to the DoD Task Force on the Prevention of Suicide by Members of the Armed Forces MAJ Jeffrey L. Thomas, Ph.D.
Summary of Key Findings from the Mental Health Advisory Team 6 (MHAT 6): OEF and OIF Presented to the DoD Task Force on the Prevention of Suicide by Members of the Armed Forces MAJ Jeffrey L. Thomas, Ph.D.
TBI and PTSD - The Impact of Invisible War Wounds in the Academic Environment. With Rick Briggs, Major, U.S. Air Force (Ret), Veteran Program Manager
, Veteran Program Manager") TBI and PTSD - The Impact of Invisible War Wounds in the Academic Environment With Rick Briggs, Major, U.S. Air Force (Ret), Veteran Program Manager Since its founding in 2007, most all of the BIAMI Veterans
TBI and PTSD - The Impact of Invisible War Wounds in the Academic Environment With Rick Briggs, Major, U.S. Air Force (Ret), Veteran Program Manager Since its founding in 2007, most all of the BIAMI Veterans
NAVAL POSTGRADUATE SCHOOL THESIS
 NAVAL POSTGRADUATE SCHOOL MONTEREY, CALIFORNIA THESIS THE EFFECTS OF INDIVIDUAL AUGMENTATION (IA) ON NAVY JUNIOR OFFICER RETENTION by Michael A. Paisant March 2008 Thesis Advisor: Second Reader: Samuel
NAVAL POSTGRADUATE SCHOOL MONTEREY, CALIFORNIA THESIS THE EFFECTS OF INDIVIDUAL AUGMENTATION (IA) ON NAVY JUNIOR OFFICER RETENTION by Michael A. Paisant March 2008 Thesis Advisor: Second Reader: Samuel
Department of Defense INSTRUCTION. Counseling Services for DoD Military, Guard and Reserve, Certain Affiliated Personnel, and Their Family Members
 Department of Defense INSTRUCTION NUMBER 6490.06 April 21, 2009 Incorporating Change 2, March 31, 2017 USD(P&R) SUBJECT: Counseling Services for DoD Military, Guard and Reserve, Certain Affiliated Personnel,
Department of Defense INSTRUCTION NUMBER 6490.06 April 21, 2009 Incorporating Change 2, March 31, 2017 USD(P&R) SUBJECT: Counseling Services for DoD Military, Guard and Reserve, Certain Affiliated Personnel,
NAVAL POSTGRADUATE SCHOOL THESIS
 NAVAL POSTGRADUATE SCHOOL MONTEREY, CALIFORNIA THESIS CASUALTY PROFILE OF THE UNITED STATES ARMY IN AFGHANISTAN AND IRAQ by Sezgin Ozcan Thesis Advisor: Second Reader: June 2012 Samuel E. Buttrey Chad
NAVAL POSTGRADUATE SCHOOL MONTEREY, CALIFORNIA THESIS CASUALTY PROFILE OF THE UNITED STATES ARMY IN AFGHANISTAN AND IRAQ by Sezgin Ozcan Thesis Advisor: Second Reader: June 2012 Samuel E. Buttrey Chad
The Persian Gulf Veterans Coordinating Board Fact Sheet
 The Persian Gulf Veterans Coordinating Board Fact Sheet Persian Gulf Veterans' Health Problems An interagency board - the Persian Gulf Veterans Coordinating Board - was established in January 1994 to work
The Persian Gulf Veterans Coordinating Board Fact Sheet Persian Gulf Veterans' Health Problems An interagency board - the Persian Gulf Veterans Coordinating Board - was established in January 1994 to work
Invisible Wounds of War
 Invisible Wounds of War Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery TERRI TANIELIAN AND LISA H. JAYCOX, EDITORS Sponsored by the California Community Foundation
Invisible Wounds of War Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery TERRI TANIELIAN AND LISA H. JAYCOX, EDITORS Sponsored by the California Community Foundation
APPENDIX A: SURVEY METHODS
 APPENDIX A: SURVEY METHODS This appendix includes some additional information about the survey methods used to conduct the study that was not presented in the main text of Volume 1. Volume 3 includes a
APPENDIX A: SURVEY METHODS This appendix includes some additional information about the survey methods used to conduct the study that was not presented in the main text of Volume 1. Volume 3 includes a
Admissions and Readmissions Related to Adverse Events, NMCPHC-EDC-TR
 Admissions and Readmissions Related to Adverse Events, 2007-2014 By Michael J. Hughes and Uzo Chukwuma December 2015 Approved for public release. Distribution is unlimited. The views expressed in this
Admissions and Readmissions Related to Adverse Events, 2007-2014 By Michael J. Hughes and Uzo Chukwuma December 2015 Approved for public release. Distribution is unlimited. The views expressed in this
DHCC Strategic Plan. Last Revised August 2016
 DHCC Strategic Plan Last Revised August 2016 Table of Contents History of DHCC... 3 Executive Summary... 4 DHCC Mission and Vision... 5 Mission... 5 Vision... 5 DHCC Strategic Drivers... 6 Strategic drivers
DHCC Strategic Plan Last Revised August 2016 Table of Contents History of DHCC... 3 Executive Summary... 4 DHCC Mission and Vision... 5 Mission... 5 Vision... 5 DHCC Strategic Drivers... 6 Strategic drivers
National Guard Personnel and Deployments: Fact Sheet
 Order Code RS22451 Updated November 20, 2007 National Guard Personnel and Deployments: Fact Sheet Summary Michael Waterhouse and JoAnne O Bryant Information Research Specialists Knowledge Services Group
Order Code RS22451 Updated November 20, 2007 National Guard Personnel and Deployments: Fact Sheet Summary Michael Waterhouse and JoAnne O Bryant Information Research Specialists Knowledge Services Group
Dr. Mark Reger, Ph.D.
 AD AWARD NUMBER: W81XWH-09-1-0540 TITLE: The Association Between Suicide and OIF/OEF Deployment History PRINCIPAL INVESTIGATOR: Dr. Mark Reger, Ph.D. RECIPIENT: The Geneva Foundation Tacoma, WA 98402 REPORT
AD AWARD NUMBER: W81XWH-09-1-0540 TITLE: The Association Between Suicide and OIF/OEF Deployment History PRINCIPAL INVESTIGATOR: Dr. Mark Reger, Ph.D. RECIPIENT: The Geneva Foundation Tacoma, WA 98402 REPORT
The views expressed in this research are those of the authors and do not necessarily reflect the official policy or position of the Department of the
 The views expressed in this research are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Army, Department of the Air
The views expressed in this research are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Army, Department of the Air
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Alpert Medical School of Brown University Clinical Psychology Internship Training Program Rotation Description
 Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
UNDER SECRETARY OF DEFENSE 4000 DEFENSE PENTAGON WASHINGTON, DC
 UNDER SECRETARY OF DEFENSE 4000 DEFENSE PENTAGON WASHINGTON, DC 203014000 PERSONNEL AND READINESS The Honorable Howard P. "Buck" McKeon Chairman Committee on Armed Services U.S. House of Representatives
UNDER SECRETARY OF DEFENSE 4000 DEFENSE PENTAGON WASHINGTON, DC 203014000 PERSONNEL AND READINESS The Honorable Howard P. "Buck" McKeon Chairman Committee on Armed Services U.S. House of Representatives
Demographic Profile of the Officer, Enlisted, and Warrant Officer Populations of the National Guard September 2008 Snapshot
 Issue Paper #55 National Guard & Reserve MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training Branching & Assignments Promotion Retention Implementation
Issue Paper #55 National Guard & Reserve MLDC Research Areas Definition of Diversity Legal Implications Outreach & Recruiting Leadership & Training Branching & Assignments Promotion Retention Implementation
Re-Engineering Healthcare Integration Programs (REHIP)
") Re-Engineering Healthcare Integration Programs (REHIP) Planning for Primary Care & Psychological Health Care Integration A DCoE-Funded Tri-Service Demonstration Project Report Documentation Page Form Approved
Re-Engineering Healthcare Integration Programs (REHIP) Planning for Primary Care & Psychological Health Care Integration A DCoE-Funded Tri-Service Demonstration Project Report Documentation Page Form Approved
THE COURTS AND MILITARY FAMILIES: URGENT ACTION NEEDED
 POLICY BRIEF FEBRUARY 2011 THE COURTS AND MILITARY FAMILIES: URGENT ACTION NEEDED KATHLEEN M. WEST DEMOGRAPHICS OF INTEREST The Military Health System has among the most reliable data available to describe
POLICY BRIEF FEBRUARY 2011 THE COURTS AND MILITARY FAMILIES: URGENT ACTION NEEDED KATHLEEN M. WEST DEMOGRAPHICS OF INTEREST The Military Health System has among the most reliable data available to describe
Using Secondary Datasets for Research. Learning Objectives. What Do We Mean By Secondary Data?
 Using Secondary Datasets for Research José J. Escarce January 26, 2015 Learning Objectives Understand what secondary datasets are and why they are useful for health services research Become familiar with
Using Secondary Datasets for Research José J. Escarce January 26, 2015 Learning Objectives Understand what secondary datasets are and why they are useful for health services research Become familiar with
131,,000 homeless veterans on any given night 300,000 homeless veterans during the year 23% of the total number of homeless people are veterans
 131,,000 homeless veterans on any given night 300,000 homeless veterans during the year 23% of the total number of homeless people are veterans Vietnam era--97% are men 3% are women OEF/OIF 89% are men
131,,000 homeless veterans on any given night 300,000 homeless veterans during the year 23% of the total number of homeless people are veterans Vietnam era--97% are men 3% are women OEF/OIF 89% are men
How Does Sea Duty Affect First-Term Reenlistment?: An Analysis Using Post-9/11 Data
 CRM D0013608.A2/Final May 2006 How Does Sea Duty Affect First-Term Reenlistment?: An Analysis Using Post-9/11 Data Diana S. Lien Cathleen M. McHugh with David Gregory 4825 Mark Center Drive Alexandria,
CRM D0013608.A2/Final May 2006 How Does Sea Duty Affect First-Term Reenlistment?: An Analysis Using Post-9/11 Data Diana S. Lien Cathleen M. McHugh with David Gregory 4825 Mark Center Drive Alexandria,
June 25, Shamis Mohamoud, David Idala, Parker James, Laura Humber. AcademyHealth Annual Research Meeting
 Evaluation of the Maryland Health Home Program for Medicaid Enrollees with Severe Mental Illnesses or Opioid Substance Use Disorder and Risk of Additional Chronic Conditions June 25, 2018 Shamis Mohamoud,
Evaluation of the Maryland Health Home Program for Medicaid Enrollees with Severe Mental Illnesses or Opioid Substance Use Disorder and Risk of Additional Chronic Conditions June 25, 2018 Shamis Mohamoud,
Hospital Discharge Data, 2005 From The University of Memphis Methodist Le Bonheur Center for Healthcare Economics
 Hospital Discharge Data, 2005 From The University of Memphis Methodist Le Bonheur Center for Healthcare Economics August 22, 2008 Potentially Avoidable Pediatric Hospitalizations in Tennessee, 2005 Cyril
Hospital Discharge Data, 2005 From The University of Memphis Methodist Le Bonheur Center for Healthcare Economics August 22, 2008 Potentially Avoidable Pediatric Hospitalizations in Tennessee, 2005 Cyril
VA Overview and VA Psychosocial Programming
 VA Overview and VA Psychosocial Programming August 2014 Organizational Structure of VA Department of Veterans Affairs (VA) Veterans Health Administration (VHA) Veterans Benefits Administration (VBA) National
VA Overview and VA Psychosocial Programming August 2014 Organizational Structure of VA Department of Veterans Affairs (VA) Veterans Health Administration (VHA) Veterans Benefits Administration (VBA) National
Last Revised March 2017
 DHCC Strategic Plan Last Revised March 2017 Released January 2017 by Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury Center. This
DHCC Strategic Plan Last Revised March 2017 Released January 2017 by Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury Center. This
GAO. DEFENSE BUDGET Trends in Reserve Components Military Personnel Compensation Accounts for
 GAO United States General Accounting Office Report to the Chairman, Subcommittee on National Security, Committee on Appropriations, House of Representatives September 1996 DEFENSE BUDGET Trends in Reserve
GAO United States General Accounting Office Report to the Chairman, Subcommittee on National Security, Committee on Appropriations, House of Representatives September 1996 DEFENSE BUDGET Trends in Reserve
PROFILE OF THE MILITARY COMMUNITY
 2004 DEMOGRAPHICS PROFILE OF THE MILITARY COMMUNITY Acknowledgements ACKNOWLEDGEMENTS This report is published by the Office of the Deputy Under Secretary of Defense (Military Community and Family Policy),
2004 DEMOGRAPHICS PROFILE OF THE MILITARY COMMUNITY Acknowledgements ACKNOWLEDGEMENTS This report is published by the Office of the Deputy Under Secretary of Defense (Military Community and Family Policy),
Expanding Access to Help for Veterans in Crisis: The Veterans Online Self-Check Quiz & the Interactive Screening Program
 Expanding Access to Help for Veterans in Crisis: The Veterans Online Self-Check Quiz & the Interactive Screening Program Meeting the Needs of SUNY Veterans May 24 th, 2013 Maggie Mortali Manager of the
Expanding Access to Help for Veterans in Crisis: The Veterans Online Self-Check Quiz & the Interactive Screening Program Meeting the Needs of SUNY Veterans May 24 th, 2013 Maggie Mortali Manager of the
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
Impact of Combat Duty in Iraq and Afghanistan on Family Functioning: Findings from the Walter Reed Army Institute of Research Land Combat Study
 Impact of Combat Duty in Iraq and Afghanistan on Family Functioning: Findings from the Walter Reed Army Institute of Research Land Combat Study Charles W. Hoge, MD, COL, MC, U.S. Army Director, Division
Impact of Combat Duty in Iraq and Afghanistan on Family Functioning: Findings from the Walter Reed Army Institute of Research Land Combat Study Charles W. Hoge, MD, COL, MC, U.S. Army Director, Division
Working document to be approved. Working Document To Be Approved
 1 Working Document To Be Approved Welcome and Introduction 2 What You Need to Know about Veterans Disability Appeals Presented by Brett Buchanan VA-Accredited Claims Agent Brett Buchanan bio 3 Attended
1 Working Document To Be Approved Welcome and Introduction 2 What You Need to Know about Veterans Disability Appeals Presented by Brett Buchanan VA-Accredited Claims Agent Brett Buchanan bio 3 Attended
Subj: ADMINISTRATIVE SEPARATIONS FOR CONDITIONS NOT AMOUNTING TO A DISABILITY
 DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY 7700 ARLINGTON BOULEVARD FALLS CHURCH VA 22042 Canc: Jun 2019 IN REPLY REFER TO BUMEDNOTE 1900 BUMED-M3 BUMED NOTICE 1900 From: Chief, Bureau of Medicine
DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY 7700 ARLINGTON BOULEVARD FALLS CHURCH VA 22042 Canc: Jun 2019 IN REPLY REFER TO BUMEDNOTE 1900 BUMED-M3 BUMED NOTICE 1900 From: Chief, Bureau of Medicine
The Prior Service Recruiting Pool for National Guard and Reserve Selected Reserve (SelRes) Enlisted Personnel
 Enlisted Personnel") Issue Paper #61 National Guard & Reserve MLDC Research Areas The Prior Service Recruiting Pool for National Guard and Reserve Selected Reserve (SelRes) Enlisted Personnel Definition of Diversity Legal
Issue Paper #61 National Guard & Reserve MLDC Research Areas The Prior Service Recruiting Pool for National Guard and Reserve Selected Reserve (SelRes) Enlisted Personnel Definition of Diversity Legal
journal of medicine The new england Combat Duty in Iraq and Afghanistan, Mental Health Problems, and Barriers to Care abstract
 The new england journal of medicine established in 1812 july 1, 2004 vol. 351 no. 1 Combat Duty in Iraq and Afghanistan, Mental Health Problems, and Barriers to Care Charles W. Hoge, M.D., Carl A. Castro,
The new england journal of medicine established in 1812 july 1, 2004 vol. 351 no. 1 Combat Duty in Iraq and Afghanistan, Mental Health Problems, and Barriers to Care Charles W. Hoge, M.D., Carl A. Castro,
Study of female junior officer retention and promotion in the U.S. Navy
 Calhoun: The NPS Institutional Archive DSpace Repository Theses and Dissertations Thesis and Dissertation Collection 2016-03 Study of female junior officer retention and promotion in the U.S. Navy Mundell,
Calhoun: The NPS Institutional Archive DSpace Repository Theses and Dissertations Thesis and Dissertation Collection 2016-03 Study of female junior officer retention and promotion in the U.S. Navy Mundell,
Effects of Overweight and Obesity on Recruitment in the Military
 Effects of Overweight and Obesity on Recruitment in the Military Tracey J. Smith, PhD, RD Military Nutrition Division U.S. Army Research Institute of Environmental Medicine Roundtable on Obesity Solutions
Effects of Overweight and Obesity on Recruitment in the Military Tracey J. Smith, PhD, RD Military Nutrition Division U.S. Army Research Institute of Environmental Medicine Roundtable on Obesity Solutions
The Price of Freedom. Robert Williamson. abroad. When combat veterans return home, many have a difficult time transitioning back to
 Course: English 102 Instructor: Mr. Christopher Genre Assignment: Proposing Solutions Essay The Price of Freedom Robert Williamson America is on the verge of a domestic crisis brought about by seven years
Course: English 102 Instructor: Mr. Christopher Genre Assignment: Proposing Solutions Essay The Price of Freedom Robert Williamson America is on the verge of a domestic crisis brought about by seven years
What Counts in Mental Health and What We Are Counting? Our Performance Measures and Other Metrics
 What Counts in Mental Health and What We Are Counting? Our Performance Measures and Other Metrics Dan Kivlahan, PhD Acting National Mental Health Program Director, Addictive Disorders Katy Lysell, Psy.D.,
What Counts in Mental Health and What We Are Counting? Our Performance Measures and Other Metrics Dan Kivlahan, PhD Acting National Mental Health Program Director, Addictive Disorders Katy Lysell, Psy.D.,
GAO MILITARY PERSONNEL. Number of Formally Reported Applications for Conscientious Objectors Is Small Relative to the Total Size of the Armed Forces
 GAO United States Government Accountability Office Report to Congressional Committees September 2007 MILITARY PERSONNEL Number of Formally Reported Applications for Conscientious Objectors Is Small Relative
GAO United States Government Accountability Office Report to Congressional Committees September 2007 MILITARY PERSONNEL Number of Formally Reported Applications for Conscientious Objectors Is Small Relative