CMS Innovation and Health Care Delivery System Reform
|
|
|
- Ashlyn Taylor
- 5 years ago
- Views:
Transcription


1 CMS Innovation and Health Care Delivery System Reform Maine Chapter of the American Health Information Management Association March 17, Andy Finnegan CMS RO1
2 Better. Smarter. Healthier. So we will continue to work across sectors and across the aisle for the goals we share: better care, smarter spending, and healthier people.
3 CMS support of health care Delivery System Reform will result in better care, smarter spending, and healthier people Historical state Evolving future state Public and Private sectors Key characteristics Producer-centered Incentives for volume Unsustainable Fragmented Care Systems and Policies Fee-For-Service Payment Systems Key characteristics Patient-centered Incentives for outcomes Sustainable Coordinated care Systems and Policies Value-based purchasing Accountable Care Organizations Episode-based payments Medical Homes Quality/cost transparency 3
4 Delivery System Reform requires focusing on the way we pay providers, deliver care, and distribute information { } Improving the way providers are incentivized, the way care is delivered, and the way information is distributed will help provide better care at lower cost across the health care system. FOCUS AREAS Pay Providers Deliver Care Distribute Information Source: Burwell SM. Setting Value-Based Payment Goals HHS Efforts to Improve U.S. Health Care. NEJM 2015 Jan 26; published online first. 4
5 What is MACRA? The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is a bipartisan legislation signed into law on April 1 6, What does Title I of MACRA do? Repeals the Sustainable Growth Rate (SGR) Formula Changes the way that Medicare rewards clinicians for value over volume Streamlines multiple quality programs under the new Merit- Based Incentive Payments System (MIPS) Provides bonus payments for participation in eligible alternative payment models (APMs) 5

6 CMS has adopted a framework that categorizes payments to providers Category 1: Fee for Service No Link to Value Category 2: Fee for Service Link to Quality Category 3: Alternative Payment Models Built on Fee-for-Service Architecture Category 4: Population-Based Payment Description Payments are based on volume of services and not linked to quality or efficiency At least a portion of payments vary based on the quality or efficiency of health care delivery Some payment is linked to the effective management of a population or an episode of care Payments still triggered by delivery of services, but opportunities for shared savings or 2-sided risk Payment is not directly triggered by service delivery so volume is not linked to payment Clinicians and organizations are paid and responsible for the care of a beneficiary for a long period (e.g., 1 year) Medicare Fee-for- Service examples Limited in Medicare feefor-service Majority of Medicare payments now are linked to quality Hospital valuebased purchasing Physician Value Modifier Readmissions / Hospital Acquired Condition Reduction Program Accountable Care Organizations Medical homes Bundled payments Comprehensive Primary Care initiative Comprehensive ESRD Medicare-Medicaid Financial Alignment Initiative Fee-For- Service Model Eligible Pioneer Accountable Care Organizations in years 3-5 Maryland hospitals Source: Rajkumar R, Conway PH, Tavenner M. CMS engaging multiple payers in payment reform. JAMA 2014; 311:


7 During January 2015, HHS announced goals for value-based payments within the Medicare FFS system 7
8 Target percentage of payments in FFS linked to quality and alternative payment models by 2016 and 2018 Alternative payment models (Categories 3-4) FFS linked to quality (Categories 2-4) All Medicare FFS (Categories 1-4) % ~20% 30% 50% ~70% >80% 85% 90% Historical Performance Goals 8

9 CMS will achieve Goal 1 through alternative payment models where providers are accountable for both cost and quality Major APM Categories Accountable Care Organizations Medicare Shared Savings Program ACO* Pioneer ACO* Comprehensive ESRD Care Model Next Generation ACO Bundled Payments Bundled Payment for Care Improvement* Specialty Care Models Advanced Primary Care Comprehensive Primary Care* Multi-payer Advanced Primary Care Practice* Other Models Maryland All-Payer Hospital Payments* ESRD Prospective Payment System* Model completion or expansion CMS will continue to test new models and will identify opportunities to expand existing models * MSSP started in 2012, Pioneer started in 2012, BPCI started in 2013, CPC started in 2012, MAPCP started in 2011, Maryland All Payer started in 2014 ESRD PPS started in
10 CMS is aligning with private sector and states to drive delivery system reform CMS Strategies for Aligning with Private Sector and states Convening Stakeholders Incentivizing Providers Partnering with States 10
11 The Health Care Payment Learning and Action Network will accelerate the transition to alternative payment models Medicare alone cannot drive sustained progress towards alternative payment models (APM) Success depends upon a critical mass of partners adopting new models Network Objectives Match or exceed Medicare alternative payment model goals across the US health system -30% in APM by % in APM by 2018 The network will Convene payers, purchasers, consumers, states and federal partners to establish a common pathway for success Identify areas of agreement around movement to APMs Collaborate to generate evidence, shared approaches, and remove barriers Develop common approaches to core issues such as beneficiary attribution Create implementation guides for payers and purchasers Shift momentum from CMS to private payer/purchaser and state communities Align on core aspects of alternative payment design 11

12 Accountable Care Organizations: Participation in Medicare ACOs growing rapidly 423 ACOs have been established in the MSSP and Pioneer ACO programs* 7.9 million assigned beneficiaries This includes 89 new ACOS covering 1.6 million beneficiaries assigned to the shared saving program in 2015 ACO-Assigned Beneficiaries by County * April
13 Medicare Shared Savings Program: Results to date Financial Results In 2014: 92 ACOs (28%) held spending $806 million below their targets and earned performance payments of more than $341 million In : 58 ACOs (26%) held spending $705 million below their targets and earned performance payments of more than $315 million Quality Results ACOs that reported in both 2013 and 2014 improved average performance on 27 of 33 quality measures Quality improvement was shown in such measures as patients ratings of clinicians communication, beneficiaries rating of their doctor, screening for tobacco use and cessation, and screening for high blood pressure figures include both 2012 and 2013 savings / loss generated for some ACOs that started mid-year in 2012 (these were the first ACOs in the program) 13

14 Pioneer ACOs meet requirement for expansion after two years and continued to generate savings in performance year 3 Pioneer ACOS were designed for organizations with experience in coordinated care and ACO-like contracts Pioneer ACOs generated savings for three years in a row Total savings of $92 million in PY1, $96 million in PY2, and $120 million in PY3 Average savings per ACO increased from $2.7 million in PY1 to $4.2 million in PY2 to $6.0 million in PY3 Pioneer ACOs showed improved quality outcomes Mean quality score increased from 72% to 85% to 87% from Average performance score improved in 28 of 33 (85%) quality measures in PY3 Elements of the Pioneer ACO have been incorporated into track 3 of MSSP 19 ACOs operating in 12 states (AZ, CA, IA, IL, MA, ME, MI, MN, NH, NY, VT, WI) reaching over 600,000 Medicare fee-for-service beneficiaries Duration of model test: January 2012 December 2014; 19 ACOs extended for 2 additional years Results from actuarial analysis 14
15 Independence at Home (IAH) Demonstration saves more than $3,000 per beneficiary IAH tests a service delivery and shared savings model using home-based primary care to improve health outcomes and reduce expenditures for highrisk Medicare beneficiaries In year 1, demo produced more than $25 million in savings, an average of $3,070 per participating beneficiary per year CMS will award incentive payments of $11.7 million to nine practices that produced savings and met the designated quality measures for the first year All 17 participating practices improved quality in at least three of the six quality measures There are 17 total practices, including 1 consortium, participating in the model Approximately 8,400 patients enrolled in the first year Duration of initial model test:
16 Multi-payer Advanced Primary Care Practice (MAPCP) Demonstration has generated net savings Medicare participated in 8 state-led multi-payer patient centered medical home (PCMH) initiatives in partnership with Medicaid and commercial payers CMS supports these multi-payer PCMH initiatives through: Enhanced, non-visit-based payments to practices, community-based support teams, and states Quarterly data feedback Gross savings of $40.3 million and net savings of $4.2 million were observed Initially 8 states (ME, MI, MN, NC, NY, PA, RI, VT) encompassing more than 4,000 providers, 700 practices, and 350,000 Medicare fee-for-service beneficiaries participating in the first year Duration of initial model test: July 2011 December 2014 ME, MI, NY, RI, VT were extended through Dec


17 Comprehensive Primary Care (CPC) is showing early positive results CMS convenes Medicaid and commercial payers to support primary care practice transformation through enhanced, non-visit-based payments, data feedback, and learning systems In program year 1 across all 7 regions, CPC reduced Medicare Part A and B expenditures per beneficiary by $14 or 2%* Reductions appear to be driven by initiative-wide impacts on hospitalizations, ED visits, and unplanned 30-day readmissions 7 regions (AR, OR, NJ, CO, OK, OH/KY, NY) encompassing 31 payers, nearly 500 practices, and approximately 2.5 million multi-payer patients Duration of model test: Oct 2012 Dec 2016 * Reductions relative to a matched comparison group and do not include the care management fees (~$20 pbpm) 18


18 Partnership for Patients contributes to quality improvements Data shows Leading Indicators, change from 2010 to 2013 Ventilator- Associated Pneumonia Early Elective Delivery Central Line- Associated Blood Stream Infections Venous thromboembolic complications Readmissions 62.4% 70.4% 12.3% 14.2% 7.3% 18


 If a model meets one of these three criteria and other statutory")
19 The CMS Innovation Center was created by the Affordable Care Act to develop, test, and implement new payment and delivery models The purpose of the [Center] is to test innovative payment and service delivery models to reduce program expenditures while preserving or enhancing the quality of care furnished to individuals under such titles Section 3021 of Affordable Care Act Three scenarios for success 1. Quality improves; cost neutral 2. Quality neutral; cost reduced 3. Quality improves; cost reduced (best case) If a model meets one of these three criteria and other statutory prerequisites, the statute allows the Secretary to expand the duration and scope of a model through rulemaking 19
20 The Innovation Center portfolio aligns with delivery system reform focus areas Focus Areas Pay Providers CMS Innovation Center Portfolio* Test and expand alternative payment models Accountable Care Pioneer ACO Model Medicare Shared Savings Program (housed in Center for Medicare) Advance Payment ACO Model Comprehensive ERSD Care Initiative Next Generation ACO Primary Care Transformation Comprehensive Primary Care Initiative (CPC) Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration Independence at Home Demonstration Graduate Nurse Education Demonstration Home Health Value Based Purchasing Medicare Care Choices Bundled payment models Bundled Payment for Care Improvement Models 1-4 Oncology Care Model Comprehensive Care for Joint Replacement (proposed) Initiatives Focused on the Medicaid Medicaid Incentives for Prevention of Chronic Diseases Strong Start Initiative Medicaid Innovation Accelerator Program Dual Eligible (Medicare-Medicaid Enrollees) Financial Alignment Initiative Initiative to Reduce Avoidable Hospitalizations among Nursing Facility Residents Medicare Advantage (Part C) and Part D Medicare Advantage Value-Based Insurance Design model Part D Enhanced Medication Therapy Management Deliver Care Distribute Information Support providers and states to improve the delivery of care Learning and Diffusion State Innovation Models Initiative Partnership for Patients SIM Round 1 Transforming Clinical Practice SIM Round 2 Community-Based Care Transitions Maryland All-Payer Model Health Care Innovation Awards Million Hearts Cardiovascular Risk Reduction Model Increase information available for effective informed decision-making by consumers and providers Health Care Payment Learning and Action Network Information to providers in CMMI models Shared decision-making required by many models * Many CMMI programs test innovations across multiple focus areas 23
21 Next Generation ACO Model builds upon successes from Pioneer and MSSP ACOs Designed for ACOs that are experienced in coordinating care for populations of patients These ACOs will assume higher levels of financial risk and reward than the Pioneer or MSSP ACOS Model Principles Prospective attribution Financial model for longterm stability Reward quality The model will test how strong financial incentives for ACOs can improve health outcomes and reduce expenditures Greater opportunities to coordinate care (e.g., telehealth and skilled nursing facilities) More predictable financial targets Benefit enhancements that improve patient experience Protect freedom of choice Allow beneficiaries to choose alignment with ACO Smooth ACO cash flow and improved investment capabilities 25
22 Bundled Payments for Care Improvement is also growing rapidly The bundled payment model targets 48 conditions with a single payment for an episode of care Incentivizes providers to take accountability for both cost and quality of care Four Models - Model 1: Retrospective acute care hospital stay only - Model 2: Retrospective acute care hospital stay plus post-acute care - Model 3: Retrospective post-acute care only - Model 4: Acute care hospital stay only 360 Awardees and 1755 Episode Initiators in Phase 2 as of July 2015 Duration of model is scheduled for 3 years: Model 1: April 2013 to present Models 2, 3, 4: October 2013 to present * Current until July
23 Oncology Care Model: new emphasis on specialty care 1.6 million people annually diagnosed with cancer; majority are over 65 years Major opportunity to improve care and reduce cost Model Objective: Provide beneficiaries with higher intensity coordination to improve quality and decrease cost Key features Implement 6 part practice transformation Create two part financial incentive with $160 pbpm, payment and performance based payment Institute robust quality measurement Engage multiple payers Practice Transformation 1.Patient navigation 2.Care plan with 13 components based on IOM Care Management Plan 3.24/7 access to clinician and real time access to medical records 4.Use of therapies consistent with national guidelines 5.Data driven continuous quality improvement 6.ONC certified electronic health record and stage 2 meaningful use by year 3 27
24 Proposed Comprehensive Care for Joint Replacement would test a bundled payment model across a broad cross section of hospitals The proposed model tests bundled payment of lower extremity joint replacement Payment model would apply to most Medicare LEJR procedures within select geographic areas with few exceptions Payment model would be implemented through rulemaking Participants would include Inpatient Prospective Payment System Hospitals in selected Metropolitan Statistical Areas (MSA) not participating in phase II of the Bundled Payment for Care Improvement model Participating areas were selected in a two-step randomization process MSAs were placed into five groups based on their historic LEJR episode payment and population size MSAs were then randomly selected within each group * Current until October
25 Comprehensive ESRD Care will improve patient centered coordination of care ESRD patients represent 1% of Medicare beneficiaries but account for 8% of payments ESRD PPS accounts for approximately 33% of total cost of care for ESRD patient Opportunity exist to improve patient centered care that coordinates dialysis care with care outside of dialysis CEC model will improve care coordination through the creation of ESRD Seamless Care Organizations (ESCO) that will include dialysis providers, nephrologist, and other medical providers ESCOs can be formed by Medicare certified dialysis facilities, nephrologist, certain other Medicare enrolled providers and suppliers Care Model Improve care coordination Clinical and support services Data driven, population care management Enhance communication between providers Whole-patient care management EHR information exchange among providers Increase access to care After hours call-in line; extended business hours Enhanced convenience through on-site rounding 25
26 Medicare Advantage Value Based Insurance Design Model offers more flexibility to Medicare Advantage Plans Allows MA plans to structure enrollee cost-sharing and other health plan design elements to encourage enrollees to use clinical services that have the greatest potential to positively impact on enrollee health Will begin on January 1, 2017 and run for 5 years Plans in 7 states will be eligible to participate Arizona, Indiana, Iowa, Massachusetts, Oregon, Pennsylvania, and Tennessee Eligible Medicare Advantage plans in these states, upon approval from CMS, can offer varied plan benefit design for enrollees who fall into certain clinical categories identified and defined by CMS Changes to benefit design made through this model may reduce cost-sharing and/or offer additional services to targeted enrollees 26
27 Part D Enhanced Medication Therapy Management (MTM) Model Enhanced MTM, when implemented correctly, can improve health care and outcomes for patients and has the potential to lower overall health costs The model will assess whether additional incentives and flexibilities to design and implement programs will achieve improving compliance with medication protocols reducing medication-related problems increasing patients knowledge of their medications improving communication among prescribers, pharmacists, caregivers and patients Will begin January 1, 2017 with a 5 year performance period CMS will test the model in 5 part D regions Region 7 (Virginia) Region 11 (Florida), Region 21 (Louisiana), Region 25 (Iowa, Minnesota, Montana, Nebraska, North Dakota, South Dakota, Wyoming) Region 28 (Arizona). 27
28 Million Hearts Cardiovascular Disease Risk Reduction Model will reward population-level risk management Heart attacks and strokes are a leading cause of death and disability in the United States Prevention of cardiovascular disease can significantly reduce both CVD-related and all-cause mortality Participant responsibilities Systematic beneficiary risk calculation* and stratification Shared decision making and evidence-based risk modification Population health management strategies Reporting of risk score through certified data registry Eligible applicants General/family practice, internal medicine, geriatric medicine, multi-specialty care, nephrology, cardiology Private practices, community health centers, hospital-owned practices, hospital/physician organizations Payment Model Pay-for-outcomes approach Disease risk assessment payment - One time payment to risk stratify eligible beneficiary - $10 per beneficiary Care management payment - Monthly payment to support management, monitoring, and care of beneficiaries identified as high-risk - Amount varies based upon population-level risk reduction *Uses American College of Cardiology/American Heart Association (ACA/AUA) Atherosclerotic Cardiovascular Disease (ASCVD) 10-year pooled cohort risk calculator 32
29 Medicare Care Choices Model (MCCM) provides new options for hospice patients MCCM allows Medicare beneficiaries who qualify for hospice to receive palliative care services and curative care at the same time. Evidence from private market that can concurrent care can improve outcomes, patient and family experience, and lower costs. Services The following services are available 24 hours a day, 7 days a week Nursing MCCM is designed to Increase access to supportive care services provided by hospice; Improve quality of life and patient/family satisfaction; Inform new payment systems for the Medicare and Medicaid programs. Model characteristics Hospices receive $400 PBPM for providing services for 15 days or more per month 5 year model Model will be phased in over 2 years with participants randomly assigned to phase 1 or 2 Social work Hospice aide Hospice homemaker Volunteer services Chaplain services Bereavement services Nutritional support Respite care 29


30 State Innovation Model grants have been awarded in two rounds CMS is testing the ability of state governments to utilize policy and regulatory levers to accelerate health care transformation Primary objectives include Improving the quality of care delivered Improving population health Increasing cost efficiency and expand value-based payment Six round 1 model test states Eleven round 2 model test states Twenty one round 2 model design states 30

31 Round 1 states are testing and Round 2 states are designing and implementing comprehensive reform plans Round 1 States testing APMs Round 2 States designing interventions Arkansas Maine Patient centered medical Health Accountable homes homes care Episodes Near term CMMI objectives Establish project milestones and success metrics Support development of states stakeholder engagement plans Massachusetts Support development and refinement of operational plans Minnesota Oregon Vermont 31

32 Round 1 of the Health Care Innovation Awards tested a broad range of delivery system innovations Awards tested service delivery and payment models that improved quality and decreased cost in communities across the U.S. 107 projects awarded Ideas tested include - Enhancing primary care - Coordinating care across multiple settings - New types of health care workers - Improving decision making - Testing new service delivery technologies Approximately 575,000 Medicare, Medicaid, and CHIP beneficiaries served Projects were funded in all 50 states* Awards ranged from ~$1 M to $30 M * Darker colors on map represent more HCIA projects in that state 32

33 Round 2 of the Health Care Innovation Awards shared goals with Round 1 but focused on four themes 39 projects awarded Increase focus on four areas that have high likelihood of driving health care system transformation and delivering better outcomes 1. Reduce Medicare, Medicaid, and CHIP expenditure in outpatient and/or post-acute settings 2. Improve care for populations with specialized needs 3. Transform the financial and clinical models for specific types of providers and suppliers 4. Improve the health of populations 27 states and the District of Columbia* Awards ranged from ~$2 M to $24 M * Darker colors on map represent more HCIA projects in that state 33
 Practice Transformation Networks: peer-based learning networks designed to")
34 Transforming Clinical Practice Initiative is designed to help clinicians achieve large-scale health transformation The model will support over 150,000 clinician practices over the next four years to improve on quality and enter alternative payment models Two network systems will be created Phases of Transformation 1) Practice Transformation Networks: peer-based learning networks designed to coach, mentor, and assist 2) Support and Alignment Networks: provides a system for workforce development utilizing professional associations and publicprivate partnerships 34
35 Alternative Payment Models (APMs) APMs are new approaches to paying for medical care through Medicare that incentivize quality and value. According to MACRA law, APMs include: CMS Innovation Center model (under section 1115A, other than a Health Care Innovation Award) MSSP (Medicare Shared Savings Program) Demonstration under the Health Care Quality Demonstration Program Demonstration required by Federal Law MACRA does not change how any particular APM rewards value. APM participants who are not QPs will receive favorable scoring under MIPS. Only some of these APMs will be eligible APMs. 35
36 How does MACRA provide additional rewards for participation in APMs? Most physicians and practitioners who participate in APMs will be subject to MIPS and will receive favorable scoring under the MIPS clinical practice improvement activities performance category. APM participants Those who participate in the most advanced APMs may be determined to be qualifying APM participants ( QPs ). As a result, QPs: 1. Are not subject to MIPS 2. Receive 5% lump sum bonus payments for years Receive a higher fee schedule update for 2026 and onward QPs 36
37 What is an eligible APM? Eligible APMs are the most advanced APMs that meet the following criteria according to the MACRA law: Base payment on quality measures comparable to those in MIPS Require use of certified EHR technology Either (1) bear more than nominal financial risk for monetary losses OR (2) be a medical home model expanded under CMMI authority 37

38 How do I become a qualifying APM participant (QP)? QPs are physicians and practitioners who have a certain % of their patients or payments through an eligible APM. eligible APM QP Beginning in 2021, this threshold % may be reached through a combination of Medicare and other non-medicare payer arrangements, such as private payers and Medicaid. QPs: 1. Are not subject to MIPS 2. Receive 5% lump sum bonus payments for years Receive a higher fee schedule update for 2026 and onward 38
39 Potential value-based financial rewards APMs and eligible APMs in particular offer greater potential risks and rewards than MIPS. In addition to those potential rewards, MACRA provides a bonus payment to providers committed to operating under the most advanced APMs. MIPS only MIPS adjustments APMs APM-specific rewards + MIPS adjustments eligible APMs eligible APMspecific rewards + 5% lump sum bonus 39
 and favorable scoring in MIPS for")
40 Recall: How MACRA get us closer to meeting HHS payment reform goals The Merit-based Incentive Payment System helps to link fee-for-service payments to quality and value. New HHS Goals: The law also provides incentives for participation in Alternative Payment Models via the bonus payment for Qualifying APM Participants (QPs) and favorable scoring in MIPS for APM participants who are not QPs. 30% 85% 50% 90% All Medicare fee-for-service (FFS) payments (Categories 1-4) Medicare FFS payments linked to quality and value (Categories 2-4) Medicare payments linked to quality and value via APMs (Categories 3-4) Medicare payments to QPs in eligible APMs under MACRA 40
41 How will MACRA affect me? Am I in an eligible APM? Yes No Do I have enough payments or patients through my eligible APM? Yes No Am I in an APM? Yes No Is this my first year in Medicare OR am I below the low-volume threshold? Yes Not subject to MIPS No Subject to MIPS Qualifying APM Participant 5% lump sum bonus payment Higher fee schedule updates APM-specific rewards Excluded from MIPS Subject to MIPS Favorable MIPS scoring APM-specific rewards Bottom line: There are opportunities for financial incentives for participating in an APM, even if you don t become a QP.
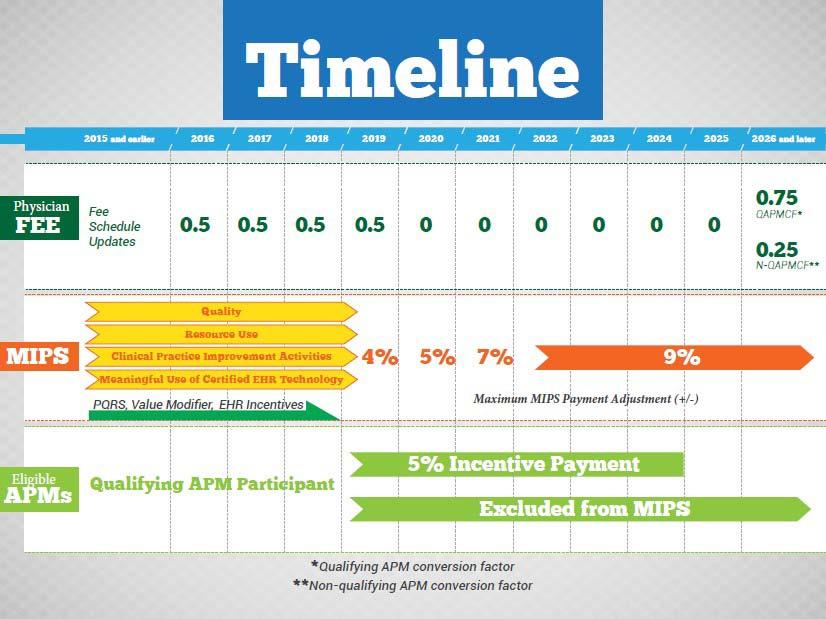
42 How will physicians and practitioners be scored under MIPS? A single MIPS composite performance score will factor in performance in 4 weighted performance categories: MIPS Composite Performance Score Quality Resource use Clinical practice improvement activities Meaningful use of certified EHR technology 4

43 How much can MIPS adjust payments? Based on the MIPS composite performance score, physicians and practitioners will receive positive, negative, or neutral adjustments up to the percentages below. MIPS adjustments are budget neutral. A scaling factor may be applied to upward adjustments to make total upward and downward adjustments equal. MAXIMUM Adjustments 4% 5% 7% 9% -4% -5% -7% -9% onward Merit-Based Incentive Payment System (MIPS) Adjustment to provider s base rate of Medicare Part B payment 4
44 18
45 MACRA Goals Through MACRA, HHS aims to: Offer multiple pathways with varying levels of risk and reward for providers to tie more of their payments to value. Over time, expand the opportunities for a broad range of providers to participate in APMs. Minimize additional reporting burdens for APM participants. Promote understanding of each physician s or practitioner s status with respect to MIPS and/or APMs. Support multi-payer initiatives and the development of APMs in Medicaid, Medicare Advantage, and other payer arrangements. 45
46 Disclaimers This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose obligations. Although every reasonable effort has been made to assure the accuracy of the information within these pages, the ultimate responsibility for the correct submission of claims and response to any remittance advice lies with the provider of services. This presentation is a general summary that explains certain aspects of the Medicare Program, but is not a legal document. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings. Medicare policy changes frequently, and links to the source documents have been provided within the document for your reference The Centers for Medicare & Medicaid Services (CMS) employees, agents, and staff make no representation, warranty, or guarantee that this compilation of Medicare information is error-free and will bear no responsibility or liability for the results or consequences of the use of this guide.. 46
Alternative Payment Models and Health IT
 Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act
 Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Value based care: A system overhaul
 Value based care: A system overhaul Lee A. Fleisher, M.D. Robert D. Dripps Professor and Chair of Anesthesiology Perelman School of Medicine at the University of Pennsylvania Email: lee.fleisher@uphs.upenn.edu
Value based care: A system overhaul Lee A. Fleisher, M.D. Robert D. Dripps Professor and Chair of Anesthesiology Perelman School of Medicine at the University of Pennsylvania Email: lee.fleisher@uphs.upenn.edu
CMS Priorities, MACRA and The Quality Payment Program
 CMS Priorities, MACRA and The Quality Payment Program Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services Presentation on behalf of HSAG November 16, 2016
CMS Priorities, MACRA and The Quality Payment Program Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services Presentation on behalf of HSAG November 16, 2016
ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT
 ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT The Centers for Medicare and Medicaid Services Kate Goodrich, MD MHS Director, Clinical Standards & Quality Chief Medical Officer 1 DISCLAIMERS
ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT The Centers for Medicare and Medicaid Services Kate Goodrich, MD MHS Director, Clinical Standards & Quality Chief Medical Officer 1 DISCLAIMERS
Healthcare Transformation and the Affordable Care Act David Nilasena, MD, MSPH, MS Chief Medical Officer, CMS Region VI
 National Readmission Prevention Collaborative Dallas, TX October 22, 2015 Healthcare Transformation and the Affordable Care Act David Nilasena, MD, MSPH, MS Chief Medical Officer, CMS Region VI Disclaimers
National Readmission Prevention Collaborative Dallas, TX October 22, 2015 Healthcare Transformation and the Affordable Care Act David Nilasena, MD, MSPH, MS Chief Medical Officer, CMS Region VI Disclaimers
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
What Have we Learned from the Pioneer ACO Model?
 What Have we Learned from the Pioneer ACO Model? Sherly Binu, CMMI December 7, 2016 Disclaimers 2 This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose
What Have we Learned from the Pioneer ACO Model? Sherly Binu, CMMI December 7, 2016 Disclaimers 2 This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose
Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems
 Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems Dr. Ashby Wolfe, Chief Medical Officer Centers for Medicare and Medicaid Services,
Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems Dr. Ashby Wolfe, Chief Medical Officer Centers for Medicare and Medicaid Services,
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
The Quality Payment Program Overview Fact Sheet
 Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
QUALITY PAYMENT PROGRAM
 NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
Volume to Value Transition in the USA
 Volume to Value Transition in the USA Lee A. Fleisher, M.D. Robert D. Dripps Professor and Chair of Anesthesiology Perelman School of Medicine at the University of Pennsylvania Email: lee.fleisher@uphs.upenn.edu
Volume to Value Transition in the USA Lee A. Fleisher, M.D. Robert D. Dripps Professor and Chair of Anesthesiology Perelman School of Medicine at the University of Pennsylvania Email: lee.fleisher@uphs.upenn.edu
MACRA, MIPS, and APMs What to Expect from all these Acronyms?!
 MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA Implementation: A Review of the Quality Payment Program
 MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
Future of Patient Safety and Healthcare Quality
 Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Health System Transformation. Discussion
 Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Kate Goodrich, MD MHS. Director, Center for Clinical Standards & Quality. Center for Medicare and Medicaid Services (CMS) May 6, 2016
 May 6, 2016") Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
Innovative Coordinated Care Delivery
 Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
The Role of Pharmacy in Alternative Payment Models
 The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
MIPS, MACRA, & CJR: Medicare Payment Transformation. Presenter: Thomas Barber, M.D. May 31, 2016
 MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
MACRA and the Quality Payment Program. Frequently Asked Questions Edition
 MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA MACRA MACRA 9/30/2015. From the Congress: A New Medicare Payment System. The Future of Medicare: A Move Toward Value Driven Healthcare W20.
 W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Moving To Value-Based Payment: What Are The New Models In Medicaid & Medicare?
 Moving To Value-Based Payment: What Are The New Models In Medicaid & Medicare? #OMPerformance The 2017 OPEN MINDS Performance Management Institute Thursday, February 16, 2017 11:30am 12:45am Athena Mandros,
Moving To Value-Based Payment: What Are The New Models In Medicaid & Medicare? #OMPerformance The 2017 OPEN MINDS Performance Management Institute Thursday, February 16, 2017 11:30am 12:45am Athena Mandros,
CMS: Delivery System Reform
 CMS: Delivery System Reform Session #6, February 20, 2017 Pierre Yong, Director, Quality Measurement and Value-Based Incentives Group, Centers for Clinical Standards and Quality, Centers for Medicare &
CMS: Delivery System Reform Session #6, February 20, 2017 Pierre Yong, Director, Quality Measurement and Value-Based Incentives Group, Centers for Clinical Standards and Quality, Centers for Medicare &
Objectives. Preparing for Value-Based Reimbursement 3/28/2016
 Preparing for Value-Based Reimbursement Tracy Bird, FACMPE, CPC, CPMA, CPC-I, CEMC Sr. Advisor Education and Consulting KaMMCO April 12, 2016 1 2 Objectives A look back - how did we get here Existing and
Preparing for Value-Based Reimbursement Tracy Bird, FACMPE, CPC, CPMA, CPC-I, CEMC Sr. Advisor Education and Consulting KaMMCO April 12, 2016 1 2 Objectives A look back - how did we get here Existing and
Primary Care Transformation in the Era of Value
 Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Centers for Medicare & Medicaid Services: Innovation Center New Direction
 Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
The Quality Payment Program: Overview & Roles and Responsibilities
 The Quality Payment Program: Overview & Roles and Responsibilities National Tribal Health Conference Susy Postal DNP, RN-BC Chief Health Informatics Officer September 27, 2017 INDIAN HEALTH SERVICE / OFFICE
The Quality Payment Program: Overview & Roles and Responsibilities National Tribal Health Conference Susy Postal DNP, RN-BC Chief Health Informatics Officer September 27, 2017 INDIAN HEALTH SERVICE / OFFICE
Episode Payment Models:
 Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Overview of Quality Payment Program
 Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
VALUE BASED ORTHOPEDIC CARE
 VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
Patient-Centered Primary Care
 Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
MACRA Fall into Place. By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof
 MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
Getting Ready for the Post-SGR World. Presented by: Sybil R. Green, JD, RPh, MHA. West Virginia Oncology Society Spring Meeting May 5, 2016
 Getting Ready for the Post-SGR World Presented by: Sybil R. Green, JD, RPh, MHA West Virginia Oncology Society Spring Meeting May 5, 2016 CME/CE Information For Physicians: This activity has been planned
Getting Ready for the Post-SGR World Presented by: Sybil R. Green, JD, RPh, MHA West Virginia Oncology Society Spring Meeting May 5, 2016 CME/CE Information For Physicians: This activity has been planned
MACRA The shift to Value Based Care and Payment. Michael Munger, M.D., FAAFP
 MACRA The shift to Value Based Care and Payment Michael Munger, M.D., FAAFP Current State Silos of Care Over Utilization Volume over Value Push Towards Value and Quality 85% Medicare Payments tied to quality
MACRA The shift to Value Based Care and Payment Michael Munger, M.D., FAAFP Current State Silos of Care Over Utilization Volume over Value Push Towards Value and Quality 85% Medicare Payments tied to quality
Understanding Medicare s New Quality Payment Program
 Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
MACRA-Impacts on Primary
 MACRA-Impacts on Primary Care Providers and Practices Jennifer Bell, MS, Chamber Hill Strategies Mara McDermott, JD, CAPG Shari Erickson, MPH (Moderator), American College of Physicians Macaran Baird,
MACRA-Impacts on Primary Care Providers and Practices Jennifer Bell, MS, Chamber Hill Strategies Mara McDermott, JD, CAPG Shari Erickson, MPH (Moderator), American College of Physicians Macaran Baird,
Advancing Care Coordination Proposed Rule
 Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
HIMSS Southern California David Sayen March 28, 2017
 HIMSS Southern California David Sayen March 28, 2017 You re cured! 4 3 3 2 2 1 1 - Government Non-Government Medicare Group Practice Demo Physician Quality Reporting Initiative Premier Hospital P4P
HIMSS Southern California David Sayen March 28, 2017 You re cured! 4 3 3 2 2 1 1 - Government Non-Government Medicare Group Practice Demo Physician Quality Reporting Initiative Premier Hospital P4P
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
Glossary of Acronyms for the Quality Payment Program
 The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Glossary of Acronyms for the Quality Payment Program 1 P a g e MEDICARE QPP PHYSICIAN EDUCATION
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Glossary of Acronyms for the Quality Payment Program 1 P a g e MEDICARE QPP PHYSICIAN EDUCATION
Value-Based Psychiatric Care
 Value-Based Psychiatric Care North Carolina Psychiatric Association Annual Meeting September 15, 2017 Grace E. Terrell, MD Mission: To be your medical home Vision: To be the model for physician-led health
Value-Based Psychiatric Care North Carolina Psychiatric Association Annual Meeting September 15, 2017 Grace E. Terrell, MD Mission: To be your medical home Vision: To be the model for physician-led health
ALLIANCE FOR ACADEMIC INTERNAL MEDICINE
 Academic Internal Medicine Week Baltimore, MD March 19, 2017 ALLIANCE FOR ACADEMIC INTERNAL MEDICINE KATE GOODRICH, M.D., MHS CHIEF MEDICAL OFFICER DIRECTOR, CENTER FOR CLINICAL STANDARDS & QUALITY DISCLAIMERS
Academic Internal Medicine Week Baltimore, MD March 19, 2017 ALLIANCE FOR ACADEMIC INTERNAL MEDICINE KATE GOODRICH, M.D., MHS CHIEF MEDICAL OFFICER DIRECTOR, CENTER FOR CLINICAL STANDARDS & QUALITY DISCLAIMERS
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix
: The Doc Fix") April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians
 Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
What s Next for CMS Innovation Center?
 What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Elizabeth Mitchell December 1, Transforming Healthcare in an Uncertain Environment
 Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Is HIT a Real Tool for The Success of a Value-Based Program?
 Is HIT a Real Tool for The Success of a Value-Based Program? Sally Montes, MPH, RHIA, CCHP President, SM & Associates, Inc. smontes@sm-asociados.com (787) 306-1149 President, PR HFMA Chapter INTRODUCTION
Is HIT a Real Tool for The Success of a Value-Based Program? Sally Montes, MPH, RHIA, CCHP President, SM & Associates, Inc. smontes@sm-asociados.com (787) 306-1149 President, PR HFMA Chapter INTRODUCTION
Person-Centered Accountable Care
 Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care
 MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care AMERICAN NEUROLOGICAL ASSOCIATION October 17, 2017 Marc R. Nuwer, MD PhD Professor and Vice Chair UCLA Lyell K. Jones,
MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care AMERICAN NEUROLOGICAL ASSOCIATION October 17, 2017 Marc R. Nuwer, MD PhD Professor and Vice Chair UCLA Lyell K. Jones,
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012
 Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation
 New Member Orientation") SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Transforming Payment for a Healthier Ohio
 Transforming Payment for a Healthier Ohio Greg Moody, Director Governor s Office of Health Transformation Legislative Joint Medicaid Oversight Committee August 20, 2014 www.healthtransformation.ohio.gov
Transforming Payment for a Healthier Ohio Greg Moody, Director Governor s Office of Health Transformation Legislative Joint Medicaid Oversight Committee August 20, 2014 www.healthtransformation.ohio.gov
Are physicians ready for macra/qpp?
 Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
MACRA Quality Payment Program
 The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Understanding the... 3 Navigating MIPS in 2017... 4 MIPS Reporting: Individuals or Groups... 6 2017: The
The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Understanding the... 3 Navigating MIPS in 2017... 4 MIPS Reporting: Individuals or Groups... 6 2017: The
Quality Payment Program October 14, 2016
 Executive Summary Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 414 and 495 [CMS-5517-FC] RIN 0938-AS69 Medicare Program; Merit-based Incentive Payment System
Executive Summary Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 414 and 495 [CMS-5517-FC] RIN 0938-AS69 Medicare Program; Merit-based Incentive Payment System
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Global Budget Revenue. October 8, 2015
 Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Frequently Asked Questions
 Frequently Asked Questions What is the Compass Practice Transformation Network (Compass PTN)? The Compass Practice Transformation Network (Compass PTN) was founded by the Iowa Healthcare Collaborative
Frequently Asked Questions What is the Compass Practice Transformation Network (Compass PTN)? The Compass Practice Transformation Network (Compass PTN) was founded by the Iowa Healthcare Collaborative
Where We re Heading in Health Care. Grace Terrell, MD Founder & Strategist CHESS
 Where We re Heading in Health Care Grace Terrell, MD Founder & Strategist CHESS Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician
Where We re Heading in Health Care Grace Terrell, MD Founder & Strategist CHESS Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician
Thank You to Our Sponsor!
 AMCP Webinar Emerging Physician Payment Models: What Does it Mean for AMCP Members and Medication Management? April 19, 2017 Thank You to Our Sponsor! 1 Disclaimer Organizations may not re use material
AMCP Webinar Emerging Physician Payment Models: What Does it Mean for AMCP Members and Medication Management? April 19, 2017 Thank You to Our Sponsor! 1 Disclaimer Organizations may not re use material
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Integrating Population Health into Delivery System Reform
 Integrating Population Health into Delivery System Reform Population Health Roundtable IOM Jim Hester Washington DC June 13, 2013 Theme The health care system is transitioning from payment rewarding volume
Integrating Population Health into Delivery System Reform Population Health Roundtable IOM Jim Hester Washington DC June 13, 2013 Theme The health care system is transitioning from payment rewarding volume
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
INTRODUCTION TO POPULATION HEALTH. Kathy Whitmire, Vice President
 INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
Practice Transformation Networks
 Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
Centers for Medicare and Medicaid CMS Updates. Christol Green, Anthem Inc.
 Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Statement for the Record. American College of Physicians. Hearing before the House Energy & Commerce Subcommittee on Health
 Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the
 published in the Federal Register the") MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed criteria for the Quality Payment Program as prescribed
MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed criteria for the Quality Payment Program as prescribed
Statement for the Record. American College of Physicians. U.S. House Committee on Ways and Means Subcommittee on Health
 Statement for the Record American College of Physicians U.S. House Committee on Ways and Means Subcommittee on Health Hearing on Implementation of MACRA s Physician Payment Policies March 21, 2018 The
Statement for the Record American College of Physicians U.S. House Committee on Ways and Means Subcommittee on Health Hearing on Implementation of MACRA s Physician Payment Policies March 21, 2018 The
MACRA: Disrupting the health care system at every level
 Health Policy Brief MACRA: Disrupting the health care system at every level Produced by the Deloitte Center for Health Solutions and the Deloitte Center for Regulatory Strategies Executive summary The
Health Policy Brief MACRA: Disrupting the health care system at every level Produced by the Deloitte Center for Health Solutions and the Deloitte Center for Regulatory Strategies Executive summary The
VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY
 VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY Danielle Hansen, DO, MS (Med Ed), MHSA Healthcare Quality/ Value Challenge 1 Value-Based Programs Supports the IHI Triple Aim: 1. Better
VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY Danielle Hansen, DO, MS (Med Ed), MHSA Healthcare Quality/ Value Challenge 1 Value-Based Programs Supports the IHI Triple Aim: 1. Better
Alternative payment models in Medicaid Could MACRA be a catalyst for states value-based care efforts?
 Health Policy Brief Alternative payment models in Medicaid Could MACRA be a catalyst for states value-based care efforts? Executive summary Many states have been experimenting with Medicaid alternative
Health Policy Brief Alternative payment models in Medicaid Could MACRA be a catalyst for states value-based care efforts? Executive summary Many states have been experimenting with Medicaid alternative
The Future of Healthcare Delivery; Are we ready?
 The Future of Healthcare Delivery; Are we ready? Lisa K. Saladin, PT, PhD, FAPTA Dean and Professor Medical University of South Carolina copyright LisaSaladin 2016 Objectives 1. Discuss 5 of the projected
The Future of Healthcare Delivery; Are we ready? Lisa K. Saladin, PT, PhD, FAPTA Dean and Professor Medical University of South Carolina copyright LisaSaladin 2016 Objectives 1. Discuss 5 of the projected
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Prior to implementation of the episode groups for use in resource measurement under MACRA, CMS should:
 Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov