Sepsis Collaborative: Simulation Outreach to Address Patient Safety (SOAPS) CAUTI, CLABSI and Sepsis Module
|
|
|
- Toby Washington
- 5 years ago
- Views:
Transcription
 CAUTI, CLABSI and Sepsis Module Author: Cathy")

1 Sepsis Collaborative: Simulation Outreach to Address Patient Safety (SOAPS) CAUTI, CLABSI and Sepsis Module Author: Cathy Buzbee, MHA, BSN, RNP, OCN Director of Accreditation and Compliance UAMS Office of Continuing Education 2/13/18 to 2/13/21
2 UAMS Disclosure Statement It is the policy of the University of Arkansas for Medical Sciences (UAMS) to ensure balance, independence, objectivity, and scientific rigor in all directly or jointly provided educational activities. All individuals who are in a position to control the content of the educational activity (course/activity directors, planning committee members, staff, teachers, or authors of CE) must disclose all relevant financial relationships they have with any commercial interest(s) as well as the nature of the relationship. Financial relationships of the individual s spouse or partner must also be disclosed, if the nature of the relationship could influence the objectivity of the individual in a position to control the content of the CE. The ACCME, ACPE, and ANCC describe relevant financial relationships as those in any amount occurring within the past 12 months that create a conflict of interest. Individuals who refuse to disclose will be disqualified from participation in the development, management, presentation, or evaluation of the CE activity.
3 Accreditation Statement and Disclosures from Planners and Authors In support of improving patient care, University of Arkansas for Medical Sciences is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the healthcare team. The following authors and planners of this CE activity have no relevant financial relationships with commercial interests to disclose: Travis Hill, M.Ed Cathy Buzbee, MHA, BSN, RNP, OCN Lea Mabry, M.Ed
4 Credit Designation Statements The University of Arkansas for Medical Sciences designates this enduring material for a maximum of 1.0 AMA PRA Category 1 Credits TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity. The University of Arkansas for Medical Sciences designates this enduring material for a maximum of 1.0 ANCC contact hours. Nursing contact hours will be awarded for successful completion of program components based upon documented attendance and completion of evaluation materials.
5 Target Audience Physicians, Nurses, Pharmacists and other Direct Patient Care Personnel.
6 Criteria for Successful Completion of this Module In order to receive Continuing Education Contact Hours or CME credit you must meet these conditions: View the entire module. Pass the post test with 80% or better score. Complete an evaluation of the module.
7 Objectives of this Module Describe and define Healthcare Associated Infection (HAI), Catheter Associated Urinary Tract Infection (CAUTI) and Catheter Associated Blood Stream Infection (CLABSI). Review the incidence, morbidity and mortality of CAUTI, CLABSI and sepsis. Discuss the precipitating factors that may lead to CAUTI, CLABSI and sepsis. Recognize the clinical presentation of CAUTI, CLABSI and sepsis. Discuss preventive measures for CAUTI, CLABSI and sepsis. Apply the goals of management for sepsis.
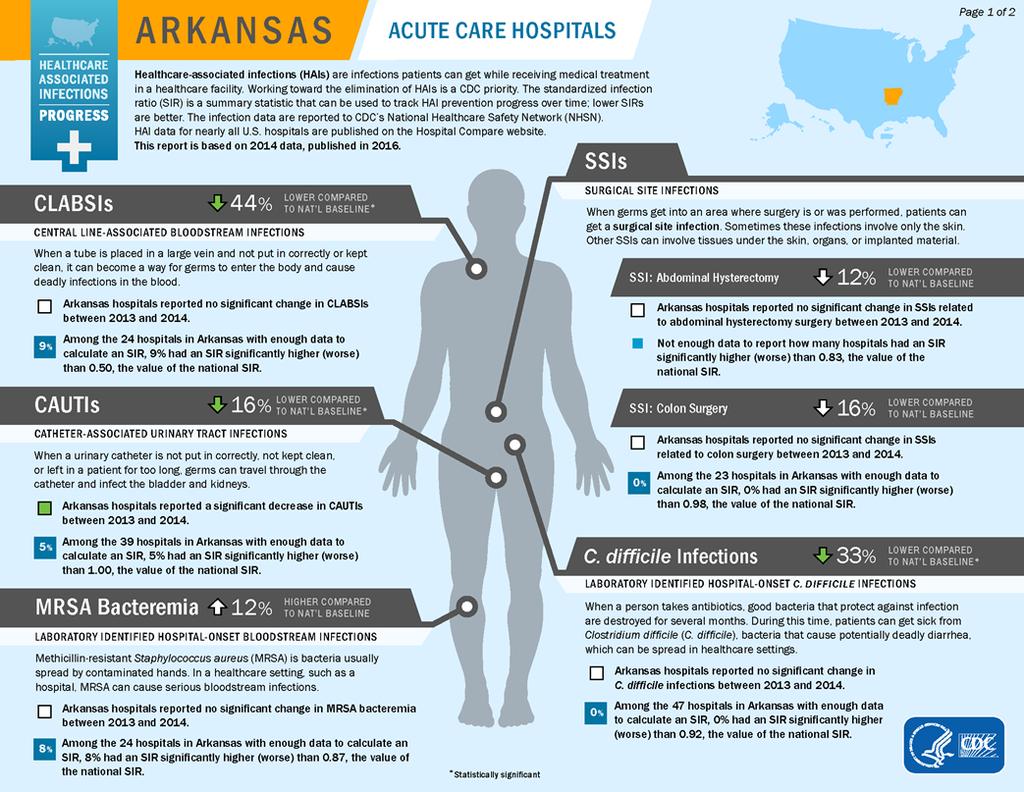
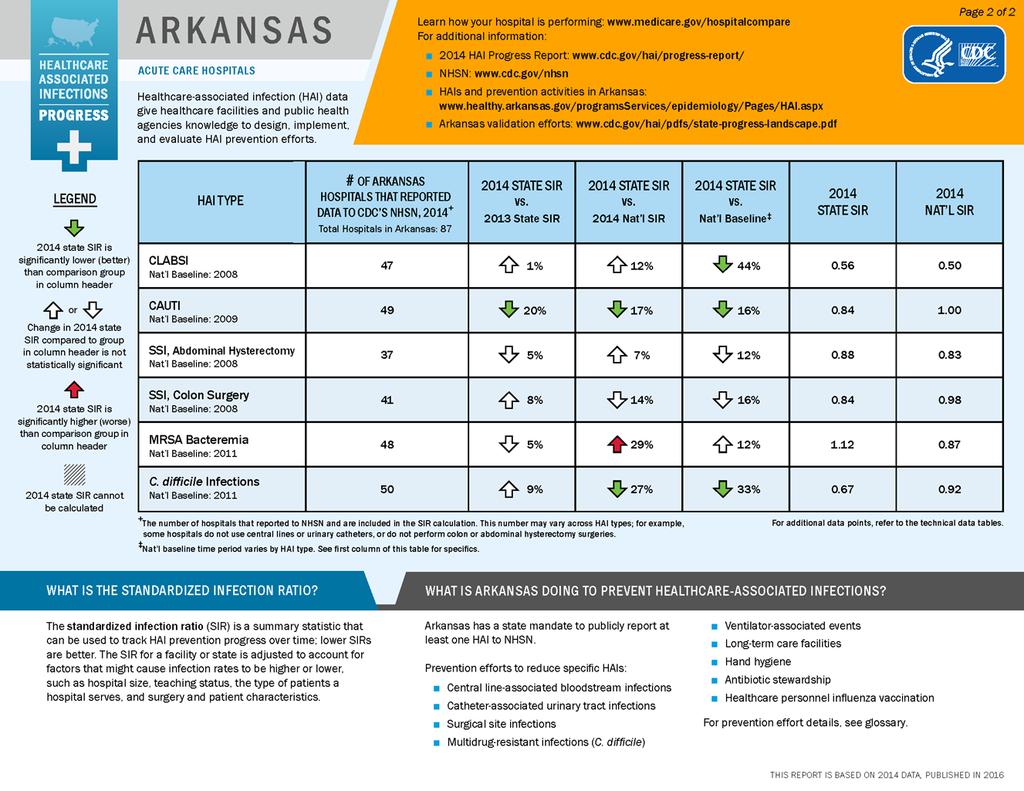
8 On the National level, between 2008 and 2013 the Healthcare Associated Infections (HAI) progress report found: A Few Statistics A 46% decrease in Central Line Associated Blood Stream Infections (CLABSI). A 19% decrease in Surgical Site Infections (SSI) related to the 10 select procedures. A 6% increase in Catheter Associated Urinary Tract Infections (CAUTI). An 8% decrease in hospital onset MRSA bacteremia. A 10% decrease in hospital onset C.difficile infections.

9 Centers for Disease Control Healthcare Associated Infection Data for Arkansas Click image to enlarge
10

11 Centers for Disease Control Healthcare Associated Infection Data for Arkansas Click image to enlarge
12

13 Catheter Associated Urinary Tract Infections (CAUTI)
14 Financial Impact of CAUTI Most common type of healthcare associated infection (HAI). Estimated to have more than 560,000 nosocomial UTI annually at an average cost of an additional $ per episode. Increased morbidity and mortality. Estimated to cause 13,000 attributable deaths annually. Leading cause of secondary Blood Stream Infections. Increased length of stay (LOS) 2 to 4 days per episode of CAUTI. Adding about 0.5 billion dollars per year. Unnecessary antimicrobial use.


15 A Few Statistics on CAUTI
16 All of these criteria must be met to be considered CAUTI Patient has an indwelling urinary catheter that has been in place for > 2 days on the date of event, OR removed the day before the date of event Criteria for CAUTI Patient has at least one of the following signs or symptoms: Fever (>38.0 C) Suprapubic tenderness Costovertebral angle pain or tenderness If catheter has been removed Urinary urgency Urinary frequency Dysuria Patient has a urine culture with no more than two species of organisms identified, at least one of which is a bacterium of 105 CFU/ml 1

17 Sources of CAUTI pdfs/maki.pdf



18 Extra-luminal Outside the Catheter Biofilm encrustation at the tip Organism migration Fecal incontinence and contamination Mechanism of CAUTI Intra-luminal Inside the Catheter Biofilm and encrustation inside the catheter Disconnection of catheter/drainage system Contamination at sample port
19 Indications for Use of an Indwelling Urinary Catheter Acute urinary retention/bladder outlet obstruction Peri-operative use in selected surgical procedures Assist in healing of open perineal and sacral wounds in incontinent patients Hospice/comfort/palliative care Prolonged immobilization for trauma or surgery Accurate measurement of urinary output in critically ill patients Chronic indwelling urinary catheter on admission from other healthcare facilities
20 Hand hygiene and standard (or appropriate isolation) precautions Insert catheters only for appropriate indications Core Prevention Strategies Leave catheters in place only as long as needed Ensure that only properly trained persons insert and maintain catheters Insert catheters using aseptic technique and sterile equipment Following aseptic insertion, always maintain a closed drainage system Maintain unobstructed urine flow at all times
21 Following aseptic insertion of the urinary catheter, maintain a closed drainage system Clinical Practice Pearls to Prevent CAUTI If breaks in aseptic technique, disconnection, or leakage occur, replace the catheter and collecting system using aseptic technique and sterile equipment Use urinary catheter systems with preconnected, sealed catheter-tubing junctions
22 Clinical Practice Pearls to Prevent CAUTI Maintain unobstructed urine flow Secure the catheter and collecting tube to keep free from kinking Keep the collecting bag below the level of the bladder at all times. Do not rest the bag on the floor Empty the collecting bag regularly using a separate, clean collecting container for each patient
23 Clinical Practice Pearls to Prevent CAUTI Care of the indwelling urinary catheter Routine hygiene (e.g., cleansing of the meatal surface during daily bathing or showering) is appropriate Do not clean the periurethral area with antiseptics to prevent CAUTI while the catheter is in place Routine change of indwelling catheters or drainage bags at fixed intervals is not recommended
 Click image to")
24 Central Line Associated Blood Stream Infections (CLABSI) Click image to enlarge
25
26 Major Veins Used for Central Venous Access Click image to enlarge
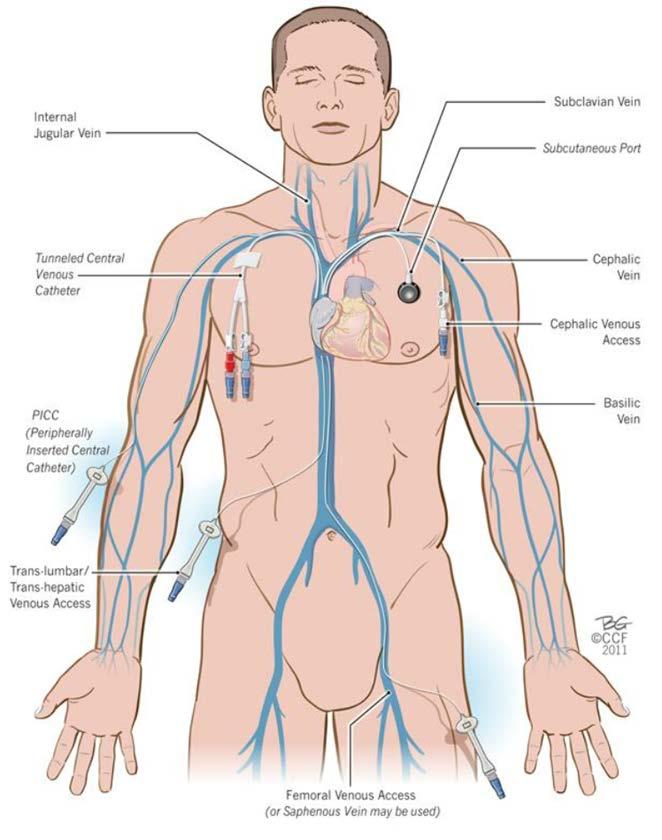
27


28 Types of Central Venous Access Devices: Tunneled and Non- Tunneled Tunneled: a catheter inserted into a central vein and the remainder is tunneled subcutaneously to a distant exit site. Subcutaneous cuff Non-Tunneled: a catheter inserted directly into a central vein
29 Types of Central Venous Access Devices: Peripherally Inserted Central Catheters (PICC) Click images to enlarge
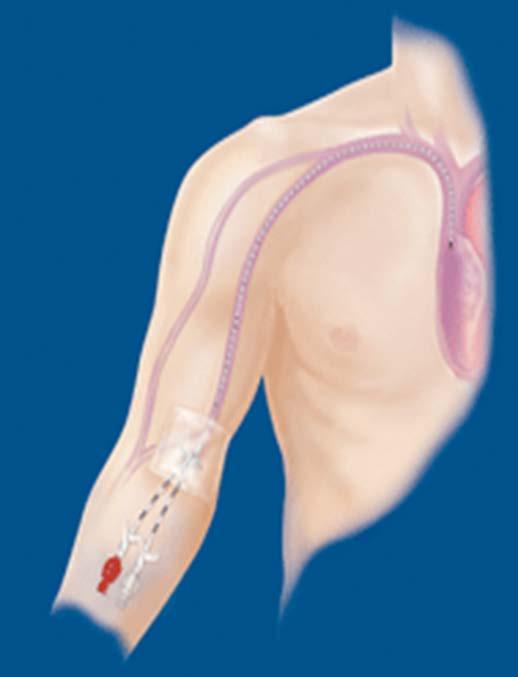
30

31
 Ports come in a variety of shapes and")
32 Click images to enlarge Types of Central Venous Access Devices: Implanted Venous Access Devices (I-Ports) Ports come in a variety of shapes and sizes.
33

34 Ports come in a variety of shapes and sizes.
35 A Few Facts About CLABSI Central Line Associated Blood Stream Infection (CLABSI) 80,000 reported in ICU patients per year. Estimated 250,000 cases outside ICU. Influencing factors for CLABSI Patient related: Severity of illness Type of illness Catheter related: Catheter type (tunneled, non-tunneled, midline) Conditions under which the catheter was placed Institutional Size of hospital Academic medical center
36 Routes of Contamination Migration of skin organisms at the insertion site into the catheter tract and along the surface of the catheter to the tip. Direct contamination of the catheter hub via contact with hands or contaminated fluids or devices. Catheter is seeded from another source of infection in the body. Very rarely contamination of the catheter from an infusate.
37 Guidelines for the Prevention of CLABSI Hand Hygiene before and after any inserting, palpating, replacing, accessing or dressing an intravascular catheter. Aseptic technique for insertion and care of a central venous catheter. Use of maximal sterile barrier precautions (gown, gloves, mask, patient drapes) for insertion of arterial, central and midline catheters.
38 Guidelines for the Prevention of CLABSI Dressing changes every 2 days for gauze dressings and weekly for transparent dressings, unless loose, torn or soiled. Sterile gloves and sterile kits for CVL dressings. Chlorhexidine swabs for cleaning and chlorhexidine impregnated sponges at exit site. Aseptic technique for CVL cap changes.


39 CVL Dressings: What s Wrong With These Pictures? Click here to enlarge and learn the answer
40 This CVL dressing 1. Exit site too close to edge of dressing, and edge is loose. 2. Exit site is reddened and has an exudate. 3. No CHG impregnated patch at exit site. 4. No date dressing was done.
41 This CVL dressing 1. Exit site in center of transparent dressing. Edges are sealed and secured. 2. CHG impregnated patch centered over exit site 3. Dressing is signed and dated.
42 Sepsis
43 A Few Statistics More than 1.5 million people are diagnosed with sepsis each year in the United States. Sepsis is responsible for 258,000 deaths in the United States each year and around 8 million deaths across the world. Leading cause of death in hospitals 1 of every 3 people that die in a hospital have sepsis Leading cause of hospital readmissions Biggest cost to hospitals at 24 billion dollars per year!
44 Arkansas ranks number 41 out of 50 for sepsis mortality 15.0 deaths per 100,000 total population Stats for Arkansas California is number 1, with the fewest deaths 3.5 deaths per 100,000 total population Mississippi is number 50 for the highest number of deaths 20.2 deaths per 100,000 total population NCHS-Septicemia Mortality by State
45 What is Sepsis? Sepsis is defined by the presence (probable or documented) of infection together with systemic manifestations of infection. Severe sepsis is sepsis plus sepsisinduced organ dysfunction or tissue hypoperfusion. International Guidelines for Management of Severe Sepsis and Septic Shock: 2012
46 Risk Factors for Sepsis People with chronic medical conditions Adults 65 or older People with weakened immune systems Children younger than 1 year of age
47 Risk Factors for Sepsis The four types of infections most often linked to sepsis: Pneumonia or other lung infections Urinary Tract Infections ( indwelling catheters, kidney disease) Infections from breaks in the skin (Central Venous Line, decubitus, surgical incisions or other wounds) Gastrointestinal infections The most common pathogens associated with sepsis: Staphylococcus aureus Escherichia coli Streptococcus strains
48 Definitions of Sepsis SIRS (Systemic Inflammatory Response Syndrome): An inflammatory state, affecting the whole body, frequently a response of the immune system to infection, but not necessarily so. Sepsis: SIRS that is due to a suspected infection, but has not been diagnosed clinically. Severe Sepsis: Sepsis plus signs of organ dysfunction, such as liver or kidney failure. Septic Shock: Severe Sepsis with cardiovascular system failure and refractory hypotension.
49 Subtle Signs of Sepsis Altered Mental Status Tachycardia (>90 beats per minute) Hypotension (SBP<9o, MAP<70, or a SBP drop of >40 mmhg) Cough, dyspnea and/or tachypnea> 22 breaths per minute Temperature 38.3 C (101 F) or below 36 C (96.8 F) Decreased capillary refill, cyanosis or mottling
50 Systemic Symptoms of Sepsis Inflammatory Symptoms Hemodynamic Organ Dysfunction Tissue Perfusion
51 Inflammatory Symptoms Systemic Symptoms of Sepsis Elevated WBC or Neutropenia WBC > 12,000 Elevated C-Reactive Protein (CRP) CRP>8 Elevated procalcitonin (PCT) PCT >0.5 ng/ml
52 Systemic Symptoms of Sepsis Hemodynamic Low Blood Pressure <90/60 or MAP<65 Low O2 saturation Tachypnea>20 bpm High Cardiac index Tachycardia >90 bpm
53 Systemic Symptoms of Sepsis Organ Dysfunction Low urine output <0.5ml/kg/hr x 2 hours High creatinine >2.0mg/dl Coagulation abnormalities INR>1.5 Low platelets <100,000 High bilirubin >2.0
54 Systemic Symptoms of Sepsis Tissue Perfusion High lactate >2.0 Decreased capillary filling or mottling

55 Screening for Sepsis
56 Screening for Sepsis Screening all patients for sepsis includes the following: Identifying patients at risk Assessment of changes in vital signs Assessment of changes in mental status Assessment of sites or potential sites of infection Assessment of lab results: WBC >12,000 or <4,000 If normal WBC, >10 % bands on differential Serum lactate (baseline and assess for elevations) Serum glucose >140mg/dl without a history of diabetes
57 Bundles are a small, straightforward set of evidencebased practices that, when performed collectively and reliably, have been proven to improve patient outcomes. Surviving Sepsis: Resuscitation Bundles There are 2 resuscitation bundles for sepsis: 3 Hour Bundle: actions to be taken within the first 3 hours of initial recognition of symptoms in adult patients and with within 60 minutes of initial recognition in pediatric patients. 6 Hour Bundle: actions to be taken within the first 6 hours of initial recognition of symptoms in adult patients and 60 minutes in pediatric patients.
58 Implementation of the 3 Hour Bundle: Triage Are two or more Sepsis criteria present? Is there a possible source of infection present? If the answer to these 2 questions is Yes then implement the 3 hour bundle. Nurses role Start two large bore IV s Draw blood cultures, CBC, electrolytes and serum lactate Physicians role Start broad spectrum antibiotics Initiate 2L Normal Saline bolus if SBP < 90 mmhg or initial lactate is > 4 mmol/l
59 The 3 hour bundle contains the following elements, and should be completed within 3 hours after presentation of severe sepsis symptoms: Components of the 3 Hour Bundle Measure the lactate level Obtain 2 sets of blood cultures prior to the administration of antibiotics Additional cultures to determine source of infection. Administer broad spectrum antibiotics Administer 30ml/kg of fluids (NS or RL) for hypotension (<90/60 or MAP <65) OR a lactate level 4mmol/L
60 After completing the steps of the 3 hour bundle: Components of the 6 Hour Bundle Apply vasopressors for hypotension that does not respond to initial fluid resuscitation, to maintain a Mean Arterial Pressure (MAP) 65mmHg. If hypotension persists after initial resuscitation (MAP < 65 mmhg) OR if initial lactate was 4 mmol/l, reassess volume status and tissue perfusion and document findings. Re-measure lactate if initial result was elevated.
61 Supportive Therapies for Sepsis Corticosteroids Blood Products RBC transfusion is recommended when the hemoglobin decreases to <7.0 g/dl Mechanical Ventilation Glucose Control Blood glucose should be maintained below 180mg/dl Nutrition Therapy Oral or enteral feedings as tolerated, avoid complete fasting
62 Long Term Effects of Sepsis Many people recover from sepsis completely and resume their normal lives. Some persons, especially with pre-existing conditions may have permanent organ damage. There is evidence that severe sepsis can disrupt the immune system and increase the risk for future infections and other medical conditions, even years later. Other long term effects of surviving sepsis include: Hospitalization for infections Cognitive impairment Cardiovascular complications
63 The Nurses Role in Triage and Treatment of Sepsis Early recognition of patients with signs and symptoms of sepsis Sepsis screening as part of routine assessment Early initiation of sepsis protocol Blood cultures, antibiotics, fluid resuscitation Prevention of Infections Central line associated blood stream infection (CLABSI), UTI, pressure sores Disposition of patient to higher level of care

64 So Remember SEPSIS
65 Sepsis Case Study Mr. B, 70 presents to the ED with a history of cutting his left hand with a knife while fishing 3 days ago. He stopped the bleeding with his handkerchief and put a bandage on it. His wife reports he is not feeling well for a couple of days and has been acting funny. The skin on his hand is warm to touch, swollen and has some erythema and some crusted matter around the wound. He can t remember the last time he urinated. He is being treated for COPD, Hypertension and Type 2 Diabetes by his PCP He is oriented to person, place and time, but does not know why he is in the ED. His vital signs are as follows: Oral temperature 101 F (38.3 C) Pulse 102, BP 88/42, Respirations 24 What is the presumed issue for Mr. B? What would you do next?
66 Triage What are the key pieces of information in his history and vital signs? 70 years old History of COPD, Hypertension and Type 2 Diabetes Infected wound on his hand Decreased urine output Altered mental status Temp 101 F Pulse 102 Blood Pressure 88/42 Respirations 24
67 Triage Ask the triage questions: Are there 2 or more risk factors for sepsis? YES! Age Chronic health conditions Is there a probable source of infection present? YES! Infected wound on hand Decreased urine output, possible Urinary Tract Infection


68 Next Steps Initiate 3 Hour Bundle
69 Sepsis Case Study Mr. B s history, symptoms and assessment indicate severe sepsis. Within an hour he has a set of aerobic and anaerobic blood cultures, CBC with diff, BMP, PT/PTT and lactate drawn. An IV is started and he receives a dose of a broad spectrum antibiotic and a NS IV bolus of 1000 ml every hour x 3. BP is assessed frequently and his MAP is 65. A Foley catheter is placed because he could not recall his last void. A urine specimen is obtained. Drainage from the wound is also collected for culture. The goals for his resuscitation at this point are a urine output of 0.5ml/kg/hr (or more) and a MAP of at least 65mmHg What would you expect to happen now?
70 Vital signs are monitored frequently What Happens Now? Fluid resuscitation continues Follow 6 hour bundle: Apply vasopressors if needed Reassess lactate
71 Sepsis Case Study At the 2 hour mark after severe sepsis was recognized, Mr. B s blood pressure is 92/36 (MAP 55), he has received his third bag of normal saline and has a urine output of 0.4mL/kg/hr. The initial lactate is 4.6 mmol/l. Because he is not responding to the initial fluid resuscitation, has a MAP < 65 and a low urine output, the physician decides to start him on a vasopressor. What is the next step the nurse should anticipate?
72 Next Step Patient should be moved to a higher level of care, such as the Intensive Care Unit for: Continued vital sign monitoring, especially blood pressure Respiratory assessment to evaluate for possible mechanical ventilation Evaluation for organ damage Monitoring lab results for kidney and liver abnormalities.
73 Sepsis Case Study Mr. B is transferred to the ICU, where the physician places a central venous catheter and a central venous pressure (CVP) of 5mmHg is obtained. Two hours after starting norepinephrine, Mr. B has a lactate level done, it is now 2.8mmol/L, his skin is warm and moist and urine output has increased to 0.7ml/kg/hr. He is more alert and is asking why he is in the hospital. His blood glucose is in the range. Blood gases are normal with a PO² of 98 on 2L of oxygen via nasal cannula.
74 Sepsis Case Study Mr. B continues to improve with fluid resuscitation, IV antibiotics and supportive care. His blood cultures are positive for S. aureus and the organism is sensitive to amoxicillin/clavulanic acid among several other antibiotics. He is afebrile, his hand wound is clean and healing and he is feeling back to his old self. He is discharged home on oral antibiotics and has an appointment to see his PCP in a few days. What are some take home messages for nurses in this case study?
75 Take Home Messages Screen all patients for sepsis using the 2 questions: Are there 2 or more risk factors for sepsis? Is there a probable source of infection present? If screening is positive-initiate the 3 hour bundle: Lab tests including lactate and blood cultures Fluid resuscitation Monitor vital signs and lactate levels Move to higher level of care Follow 6 hour bundle Vasopressors for continued hypotension Measure lactate again Assess for tissue perfusion.

76 Thank you for your participation in this educational module.
77 References Biomarkers of Sepsis gov/pmc/articles/pmc / Sepsis Alliance National Institute of General Medical Sciences v/education/pages/factshe et_sepsis.aspx For more information on accreditation contact : UAMS Office of Continuing Education 4301 W. Markham, #525 Little Rock, AR CDC Sites epsis/pdfs/life-aftersepsis-fact-sheet.pdf epsis/index.html epsis/get-ahead-ofsepsis/index.html hai/surveillance/index. html
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Current Status: Active PolicyStat ID: Guideline: Sepsis Identification And Management in Adults GUIDELINE: COPY
 Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
CAUTI reduction at Mayo Clinic
 CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
Joint Commission NPSG 7: 2011 Update and 2012 Preview
 Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Advanced Measurement for Improvement Prework
 Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
Course Outline and Assignments
 Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
ASEPTIC TECHNIQUE LEARNING PACKAGE
 ASEPTIC TECHNIQUE LEARNING PACKAGE Staff Name:... Date:... Table of Contents What is Aseptic technique? 3 Core infection control components 3 Key parts 5 References 6 Aseptic technique questionnaire 7
ASEPTIC TECHNIQUE LEARNING PACKAGE Staff Name:... Date:... Table of Contents What is Aseptic technique? 3 Core infection control components 3 Key parts 5 References 6 Aseptic technique questionnaire 7
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
2014 Maryland Patient Safety Center s Call for Solutions
 Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Infection Prevention & Control Orientation for Housestaff Welcome to Shands at UF!
 Infection Prevention & Control Orientation for Housestaff 2011 Welcome to Shands at UF! Hot Topics: Prevention Initiatives National Patient Safety Goal 07: Prevent Healthcare Associated Infections Prevent
Infection Prevention & Control Orientation for Housestaff 2011 Welcome to Shands at UF! Hot Topics: Prevention Initiatives National Patient Safety Goal 07: Prevent Healthcare Associated Infections Prevent
STANDARDIZED PROCEDURE LUMBAR DRAIN INSERTION (Adults, Peds)
") I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
Document Ratification Group Chairman s Action
 Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Section Z - Blood Culture Policy. Version 4
 Section Z - Blood Culture Policy Version 4 Important: This document can only be considered valid when viewed on the Trust s Intranet. If this document has been printed or saved to another location, you
Section Z - Blood Culture Policy Version 4 Important: This document can only be considered valid when viewed on the Trust s Intranet. If this document has been printed or saved to another location, you
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
E: Nursing Practice. Alberta Licensed Practical Nurses Competency Profile 51
 E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
STANDARDIZED PROCEDURE HEPATIC ARTERY INFUSION OF CHEMOTHERAPY (Adults, Peds)
") I. Definition Hepatic arterial infusion (HAI) of chemotherapy is accomplished by a small drug delivery system or pump that is implanted in a subcutaneous pocket in the lower abdomen. The pump reservoir
I. Definition Hepatic arterial infusion (HAI) of chemotherapy is accomplished by a small drug delivery system or pump that is implanted in a subcutaneous pocket in the lower abdomen. The pump reservoir
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012
 The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012 Objectives Discuss what is a Urinary Tract Infection (UTI) Reflect on current practices
The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012 Objectives Discuss what is a Urinary Tract Infection (UTI) Reflect on current practices
Healthcare-Associated Infections
 Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
STANDARDIZED PROCEDURE FEMORAL VENOUS BLOOD DRAW (Adult, Peds)
") I. Definition The Femoral venous blood draw (FVBD) is the procedure of performing a needle stick into the femoral vein for the purpose of drawing blood work that will assist in lab monitoring. II. Background
I. Definition The Femoral venous blood draw (FVBD) is the procedure of performing a needle stick into the femoral vein for the purpose of drawing blood work that will assist in lab monitoring. II. Background
Assisting with the Bedside (Percutaneous) Removal of Chronic Peritoneal Dialysis Catheters
 Removal of Chronic Peritoneal Dialysis Catheters") Assisting with the Bedside (Percutaneous) Removal of Chronic Peritoneal Dialysis Catheters ORIGIN DATE: APRIL 27, 2009 REVISED DATE: NOVEMBER 2013 This procedure is posted on the BC Provincial Renal Agency
Assisting with the Bedside (Percutaneous) Removal of Chronic Peritoneal Dialysis Catheters ORIGIN DATE: APRIL 27, 2009 REVISED DATE: NOVEMBER 2013 This procedure is posted on the BC Provincial Renal Agency
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers
 Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Burn Intensive Care Unit
 Purpose The burn wound is especially susceptible to microbial invasion because of loss of the protective integument and the presence of devitalized tissue. Reduction of the risk of infection is of utmost
Purpose The burn wound is especially susceptible to microbial invasion because of loss of the protective integument and the presence of devitalized tissue. Reduction of the risk of infection is of utmost
INFECTION PREVENTION AND CONTROL
 INFECTION PREVENTION AND CONTROL NATIONAL SYMPOSIUM ON ANTIBIOTIC STEWARDSHIP & INFECTION PREVENTION AND CONTROL - Right Drug, Right Dose, Right Duration, Right Frequency ASP 2016 January 23rd Hotel Crown
INFECTION PREVENTION AND CONTROL NATIONAL SYMPOSIUM ON ANTIBIOTIC STEWARDSHIP & INFECTION PREVENTION AND CONTROL - Right Drug, Right Dose, Right Duration, Right Frequency ASP 2016 January 23rd Hotel Crown
Northwell Sepsis Collaborative Evidence Based Best Practice
 Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
CENTRAL VENOUS LINES: REMOVAL
 [Type text] KINGSTON HEALTH SCIENCES CENTRE Kingston General Hospital site CENTRAL VENOUS LINES: REMOVAL LEARNING GUIDE FOR REGISTERED NURSES Prepared by: Nursing Education Services Date: 1993 December
[Type text] KINGSTON HEALTH SCIENCES CENTRE Kingston General Hospital site CENTRAL VENOUS LINES: REMOVAL LEARNING GUIDE FOR REGISTERED NURSES Prepared by: Nursing Education Services Date: 1993 December
Surgical Treatment. Preparing for Your Child s Surgery
 Surgical Treatment Preparing for Your Child s Surgery If your child needs an operation, it will be performed at a hospital that has special expertise in heart surgery for children. This may be a hospital
Surgical Treatment Preparing for Your Child s Surgery If your child needs an operation, it will be performed at a hospital that has special expertise in heart surgery for children. This may be a hospital
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa
 CENTRAL IOWA HEALTHCARE Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.37 Subject: Implanted Venous Access Device (Infus-A-Port), Nursing Management Of (Indwelling Vascular Access
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.37 Subject: Implanted Venous Access Device (Infus-A-Port), Nursing Management Of (Indwelling Vascular Access
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
2016 SUMMER STUDENT NURSE EXTERNSHIP PROGRAM SKILLS CHECK LIST
 2016 SUMMER STUDENT NURSE EXTERNSHIP PROGRAM SKILLS CHECK LIST STUDENT NURSE EXTERNNAME SCHOOL OF NURSING STUDENT AGREEMENT: I request the Clinical Skills Check list be released to (hospital/agency). I
2016 SUMMER STUDENT NURSE EXTERNSHIP PROGRAM SKILLS CHECK LIST STUDENT NURSE EXTERNNAME SCHOOL OF NURSING STUDENT AGREEMENT: I request the Clinical Skills Check list be released to (hospital/agency). I
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation
 Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
HHVNA Infusion Therapy MIDLINE CATHETER
 CONSIDERATIONS: 1. This midline procedure includes procedural steps for: a. Catheter Insertion b. Flushing c. Site care and dressing change d. Cap change e. Blood Draw f. Management of complications 2.
CONSIDERATIONS: 1. This midline procedure includes procedural steps for: a. Catheter Insertion b. Flushing c. Site care and dressing change d. Cap change e. Blood Draw f. Management of complications 2.
Recommendation II. Recommendation I. Who s on Your Team? Recommendation III
 Infection Prevention In the Surgical Suite Janie Kinsey, RN, CASC Administrator, St. Luke s South Surgery Center President, Kansas Association of Ambulatory Surgery Centers Objectives Recommendation I
Infection Prevention In the Surgical Suite Janie Kinsey, RN, CASC Administrator, St. Luke s South Surgery Center President, Kansas Association of Ambulatory Surgery Centers Objectives Recommendation I
STANDARDIZED PROCEDURE CENTRAL LINE PLACEMENT and TEMPORARY NONTUNNELLED CENTRAL VENOUS DIALYSIS CATHETER INSERTION (Adult, Peds)
") I. Definition: This protocol covers the task of central (venous) catheter placement and temporary nontunnelled central venous dialysis catheters by the Advanced Health Practitioner. The purpose of this
I. Definition: This protocol covers the task of central (venous) catheter placement and temporary nontunnelled central venous dialysis catheters by the Advanced Health Practitioner. The purpose of this
Returned Missionary Study Guide
 Returned Missionary Study Guide Skills to Refresh if Returning to Capstone: 1st Semester skills Head to Toe Assessment (Need to be able to document each of these.) o Vital Signs BP Pulse Respirations Temperature
Returned Missionary Study Guide Skills to Refresh if Returning to Capstone: 1st Semester skills Head to Toe Assessment (Need to be able to document each of these.) o Vital Signs BP Pulse Respirations Temperature
Welcome to the Cooper Infection Prevention Team
 Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Department of Public Health Infection Control Survey
 Patient Care Services, uality and Safety Being Ready for Every Patient Every Day Department of Public Health Infection Control Survey Resource Guide for Patient Care ssociates Excellence Every Day The
Patient Care Services, uality and Safety Being Ready for Every Patient Every Day Department of Public Health Infection Control Survey Resource Guide for Patient Care ssociates Excellence Every Day The
Reducing the risk of healthcare associated infection
 i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa
 MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.37 Subject: Implanted Venous Access Device (Infus-A-Port), Nursing Management Of (Indwelling
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.37 Subject: Implanted Venous Access Device (Infus-A-Port), Nursing Management Of (Indwelling
Hickman line insertion and caring for your line
 Hickman line insertion and caring for your line Information for patients This booklet explains how a Hickman line is put in, the benefits, the risks and the alternatives, as well as how to care for your
Hickman line insertion and caring for your line Information for patients This booklet explains how a Hickman line is put in, the benefits, the risks and the alternatives, as well as how to care for your
NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination.
 NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE. Early Recognition and Treatment of Severe Sepsis and Septic Shock
 SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
Supplementary Appendix
 Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
CENTRAL LINE ASSOCIATED BLOOD STREAM INFECTIONS (CLABSI)
") CENTRAL LINE ASSOCIATED BLOOD STREAM INFECTIONS (CLABSI) A Step-by- Step Approach 1 Evidence Based Recommendations for the Prevention of CLABSI 2013 CLABSI FACTS An estimated 41,000 central line-associated
CENTRAL LINE ASSOCIATED BLOOD STREAM INFECTIONS (CLABSI) A Step-by- Step Approach 1 Evidence Based Recommendations for the Prevention of CLABSI 2013 CLABSI FACTS An estimated 41,000 central line-associated
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION
 NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
SEPSIS RISK ASSESSMENT EVALUATION TOOL HEALTH QUALITY INNOVATORS
 Sepsis during hospital stay preceding this admission History of sepsis Renal concerns Respiratory Gastrointestinal Chronic renal failure History of stones Recent UTI Foley catheter during preceding hospital
Sepsis during hospital stay preceding this admission History of sepsis Renal concerns Respiratory Gastrointestinal Chronic renal failure History of stones Recent UTI Foley catheter during preceding hospital
When is it really a UTI?
 When is it really a UTI? Adrienne Mims, MD, MPH, FAAFP, AGSF VP, Chief Medical Officer Adrienne.Mims@AlliantQuality.org 2/19/2016 1 Disclosure This educational activity does not have commercial support
When is it really a UTI? Adrienne Mims, MD, MPH, FAAFP, AGSF VP, Chief Medical Officer Adrienne.Mims@AlliantQuality.org 2/19/2016 1 Disclosure This educational activity does not have commercial support
Laparoscopic Radical Nephrectomy
 Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Payment Model
 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Having a portacath insertion in the x-ray department
 Having a portacath insertion in the x-ray department This leaflet provides information about a portacath insertion, including the benefits, risks and any alternatives. It also explains what you can expect
Having a portacath insertion in the x-ray department This leaflet provides information about a portacath insertion, including the benefits, risks and any alternatives. It also explains what you can expect
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
PROCEDURAL SAFETY CHECKLIST
 PROCEDURAL SAFETY CHECKLIST Before any medical or patient care procedure, review checklist together with the other members of the procedural team. This checklist can be used by any health professional
PROCEDURAL SAFETY CHECKLIST Before any medical or patient care procedure, review checklist together with the other members of the procedural team. This checklist can be used by any health professional
Skills/Experience Checklist Home Health Registered Nurse
 This form is a self-assessment of your current skills and abilities. This form is also used to document skill demonstration. EMPLOYEE PROFILE Last Name First Name Middle Initial Employee Number Direct
This form is a self-assessment of your current skills and abilities. This form is also used to document skill demonstration. EMPLOYEE PROFILE Last Name First Name Middle Initial Employee Number Direct
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Chapter 10. medical and Surgical Asepsis. safe, effective Care environment. Practices that Promote Medical Asepsis
 chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
Reducing the risk of healthcare associated infection
 i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene 3. Isolation Precau
 Erlanger Infection Prevention Resident and df Fellow Orientation June 2011 1 Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene
Erlanger Infection Prevention Resident and df Fellow Orientation June 2011 1 Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene
Kansas Heart and Stroke Collaborative
 Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
From Defeating CAUTI to Preventing Urinary Catheter Harm
 From Defeating CAUTI to Preventing Urinary Catheter Harm Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University Senior Medical Director, Center of Excellence for Antimicrobial Stewardship
From Defeating CAUTI to Preventing Urinary Catheter Harm Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University Senior Medical Director, Center of Excellence for Antimicrobial Stewardship
Northeast Hospitals Infection Control Policy and Procedure Manual
 Northeast Hospitals Infection Control Policy and Procedure Manual Subject: Prevention/Control of Healthcare Associated Infections (HAI) Date Effective: 8/07 Date Revised: 3/11 Key Contact: Infection Prevention
Northeast Hospitals Infection Control Policy and Procedure Manual Subject: Prevention/Control of Healthcare Associated Infections (HAI) Date Effective: 8/07 Date Revised: 3/11 Key Contact: Infection Prevention
Management of Central Venous Access Devices. Institute for Healthcare Improvement (IHI)
") Management of Central Venous Access Devices Institute for Healthcare Improvement (IHI) Purpose The purpose of this e-learning module is to help educate patient care providers on the Institute for Healthcare
Management of Central Venous Access Devices Institute for Healthcare Improvement (IHI) Purpose The purpose of this e-learning module is to help educate patient care providers on the Institute for Healthcare
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
General information. Hospital type : Acute Care Hospitals. Provides emergency services : Yes. electronically between visits : Yes
 General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
Disclosure of Proprietary Interest. HomeTown Health HCCS
 HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
See Policy #1302 (Nursing Student Privileges and Limitations) for full details. Central Line dressing care, declotting and discontinuation may ONLY
 for full details. Central Line dressing care, declotting and discontinuation may ONLY") To assure a standardized knowledge base related to CVL Care and CLABSI prevention, ProMedica requires all Instructors/Faculty on adult and pediatric units to complete this educational module. This content
To assure a standardized knowledge base related to CVL Care and CLABSI prevention, ProMedica requires all Instructors/Faculty on adult and pediatric units to complete this educational module. This content
Unit 8 Med Surg Nursing Quiz
 Unit 8 Med Surg Nursing Quiz 1. How will the nurse assess the flank area of a patient with pyelonephritis for tenderness? a. Push gently into the two lowest intercostal spaces. b. Palpate along both sides
Unit 8 Med Surg Nursing Quiz 1. How will the nurse assess the flank area of a patient with pyelonephritis for tenderness? a. Push gently into the two lowest intercostal spaces. b. Palpate along both sides
Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT
, PREVENTION AND TREATMENT") COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
Prevention and Control of Infection in Care Homes. Infection Prevention and Control Team Public Health Norfolk County Council January 2015
 Prevention and Control of Infection in Care Homes Infection Prevention and Control Team Public Health Norfolk County Council January 2015 Content for today Importance of IPAC -refresher IPAC audits in
Prevention and Control of Infection in Care Homes Infection Prevention and Control Team Public Health Norfolk County Council January 2015 Content for today Importance of IPAC -refresher IPAC audits in
Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals. Bonnie M. Barnard, MPH, CIC
 Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals Bonnie M. Barnard, MPH, CIC Objectives Describe the features of critical access hospitals (CAHs) Describe
Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals Bonnie M. Barnard, MPH, CIC Objectives Describe the features of critical access hospitals (CAHs) Describe
STANDARDIZED PROCEDURE INTRAVENTRICULAR CHEMOTHERAPY VIA OMMAYA RESERVOIR (Adult, Peds)
") I. Definition The administration of chemotherapy via Ommaya Reservoir into cerebrospinal fluid (CSF) for treatment of previously diagnosed central nervous system (CNS) involvement by leukemia and lymphoma
I. Definition The administration of chemotherapy via Ommaya Reservoir into cerebrospinal fluid (CSF) for treatment of previously diagnosed central nervous system (CNS) involvement by leukemia and lymphoma
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Module 5.8: Pressure Ulcer Surgery Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module 5.8: Pressure
Pressure Ulcers ecourse Module 5.8: Pressure Ulcer Surgery Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module 5.8: Pressure
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
does staff intervene; used? If not, describe.
 Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
Direct cause of 5,000 deaths per year
 HOSPITAL ACQUIRED (NOSOCOMIAL) INFECTION Policies MRSA Policy Meningitis Policy Blood and body fluid Exposure Policy Disinfection Policy Glove Policy Tuberculosis Policy Isolation Policy DEFINITION: ANY
HOSPITAL ACQUIRED (NOSOCOMIAL) INFECTION Policies MRSA Policy Meningitis Policy Blood and body fluid Exposure Policy Disinfection Policy Glove Policy Tuberculosis Policy Isolation Policy DEFINITION: ANY
Prevention of Orthopaedic Surgical Site Infections in the Perioperative Setting. Disclosures. Objectives
 Prevention of Orthopaedic Surgical Site Infections in the Perioperative Setting Mary Atkinson Smith, DNP, FNP-BC, ONP-C, RNFA, CNOR & W. Todd Smith, MD, FAAOS Disclosures We hereby certify that, to the
Prevention of Orthopaedic Surgical Site Infections in the Perioperative Setting Mary Atkinson Smith, DNP, FNP-BC, ONP-C, RNFA, CNOR & W. Todd Smith, MD, FAAOS Disclosures We hereby certify that, to the
Overview of Revised LTC Surveillance Definitions
 Surveillance in Long-Term Care Facilities: Urinary Tract Infections (UTI) and Multidrug-Resistant Organisms (MDRO) Wisconsin Division of Public Health May-June 2014 Overview of Revised LTC Surveillance
Surveillance in Long-Term Care Facilities: Urinary Tract Infections (UTI) and Multidrug-Resistant Organisms (MDRO) Wisconsin Division of Public Health May-June 2014 Overview of Revised LTC Surveillance
If viewing a printed copy of this policy, please note it could be expired. Got to to view current policies.
 If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Entity: Fairview Pharmacy Services Department:
If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Entity: Fairview Pharmacy Services Department:
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.
 Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.") Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
Central Line Bundle Education. National Patient Safety Goal Preventing Central Line Infections 2010
 Central Line Bundle Education National Patient Safety Goal 07.04.01 Preventing Central Line Infections 2010 Central Line Associated Bloodstream Infections CAN and DO kill our patients. THE GOOD NEWS They
Central Line Bundle Education National Patient Safety Goal 07.04.01 Preventing Central Line Infections 2010 Central Line Associated Bloodstream Infections CAN and DO kill our patients. THE GOOD NEWS They