Behavioral Health Integration and the Psychiatric NP Role. Manuel A. Castro, MD, Medical Director of BHI Kathleen Peniston, PMHNP-BC
|
|
|
- Cynthia Tucker
- 5 years ago
- Views:
Transcription

1 Behavioral Health Integration and the Psychiatric NP Role Manuel A. Castro, MD, Medical Director of BHI Kathleen Peniston, PMHNP-BC
2 Objectives Understand the growing need to integrate behavioral health into Primary Care Provider s Office. Understand the CHS Virtual Model for BH Integration Understand how standardization of screening tools and treatment algorithms are critical to improving patient care within ambulatory care settings. Identify tools and measurements for evaluating the effectiveness of an integrated behavioral health program. Understand and describe the role of the Psychiatric NP as part of the BH Integration Team.
3 Behavioral Health Integration at CHS wmz0wjw2i
4 Our Story Clinically Integrated Why? The Case for Virtual Care Virtual Care Models in Hospital Acute Care Behavioral Health Primary Care Integration Outcomes Lessons Learned and Next Steps
5 Achieving the Triple Aim Carolinas HealthCare System will develop a transformative, clinically integrated and sustainable system of high quality, patient and family centered care to serve the behavioral health needs of patients, their families and the community. 5

6 Carolinas HealthCare System 39 hospitals and 900+ care locations in North Carolina, South Carolina and Georgia More than 7,800 licensed beds More than 11 million patient encounters in ,000+ system-employed physicians, 14,000+ nurses and more than 60,000 employees $1.5 billion in community benefit in 2013 More than $8 billion in annual revenue The region s only Level I trauma center One of five academic medical centers in North Carolina One of the largest HIT and EMR systems in the country Cerner s largest contract
7 The State of Behavioral Health One in five adults suffers from a diagnosable mental disorder. The average annual Medicaid spend per person is only $4,000, but that jumps to $38,000 annually with one mental health and one substance use diagnosis. Untreated mental health and substance abuse disorders cost the US $250-$500 billion per year. $193 billion per year in lost workplace earnings due to untreated mental illness. Even beyond the United States, mental illness is the #1 cause of disability life years worldwide, vastly outnumbering those caused by cardiovascular disease and cancer. With proposer diagnosis and effective treatment, the recovery rate for patients with mental illness is 60-80%. But in today s environment, the effective recovery rate is only 5-10% due to such limited resources and infrastructure.


8 All Healthcare Spending $2.7 Trillion Behavioral Health $ Billion
9 1971 Spending on behavioral health is shrinking relative to overall healthcare spending Share of national health spending

10 Psychiatry Workforce US: 40,000 Psychiatrist 9,000 Psychiatric NPs Most are located in Urban Areas Half of all the counties in the US don t have a single practicing Mental Health professional Psychiatrists." U.S. Bureau of Labor Statistics. U.S. Bureau of Labor Statistics, n.d. Web. 30 Nov AANP National NP Database
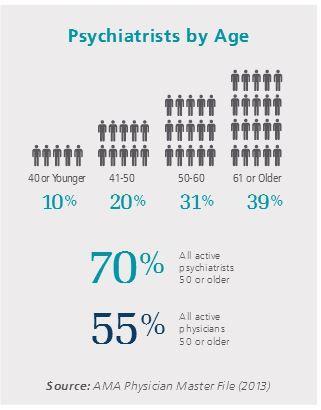
11 Psychiatry Workforce
12 Psychiatric Facilities - Nationwide 12

13 NC Mental Health Workforce Shortage 95 counties have no addiction psychiatrist, 87 without any MD with addiction specialty. 70 counties have no Child and Adolescent Psychiatrist. 60 counties across North Carolina nave no practicing Psychiatric NPs. 28 counties across North Carolina have no practicing Psychiatrist. 18 counties across North Carolina have only one. NC Health Professions Data System, with data from the NC BON 13
14 Fragmented System Unique emr Referral Coordinat or PCP Patient Medic al ED Psyc h ED Psychiatri st Transpor t 13


15 Crisis = Call to Action

16 Why Primary Care? Stigma is lower Roughly 80% of all antidepressants are prescribed by non-psychiatrists 70% of visits are Psycho-Socially related 1 Million Active Patients Annals of General Psychiatry. 14 (13) 2015,WJM Jan 170, No.1, 1999 Psychosomatics 41:5 Sept 2000, Psychiatric Services Jan 2006

17 We couldn t get a psychiatrist, but perhaps you d like to talk about your skin. Dr. Perry here is a dermatologist. 2/3 of PCP s report poor access to mental health services for their patients
18 PERCENT Prevalence of Major Depressive Disorder in Chronic Disease 60% 50% 51% 40% 42% 30% 20% 10% 11% 17% 23% 27% 0% Alzheimer's Cardiovascular Cerebrovascular Diabetes Cancer Parkinson's National Center for Chronic Disease Prevention and Health Population. Published 2012
19 Cost of a Chronic Disease with a Mental Illness Absent Comorbity $18,870 $17,200 $10,030 $3,730 $11,650 $9,770 $10,980 $12,280 $3,840 $5,480 A STHMA CA NCER CHF COPD D IABETES
20
21 40,000 suicides annually 64% of these patients saw their Primary Care Provider within 30 days. 38% people made a healthcare visit the previous week. Estimated cost of each Suicide $1 million American Foundation for Suicide Prevention:

22 Behavioral Health Integration: IMPACT PCP Patient BHP/Care Manager New Roles Core Program Consulting Psychiatrist Other Behavioral Health Clinicians Additional Clinic Resources Substance Treatment, Vocational Rehabilitation, CMHC, Other Community Resources Outside Resources 22
23 BHP Deconstructing the BHP by Function BH Screener BH Diagnoser BH Treater BH Navigator BH Coach/Activator BH Communicator
24 IMPACT / Collaborative Care Model 2 year Randomized Control Trial: 1801 Adults with Depression 12 months-50% reduction of depressive symptoms 45% IMPACT model 19% usual care participants 4 years $3,300 in savings in health care spend per patient Repeated in 80 Randomized Trials
25 24-Month Health Care Costs IMPACT Enrollees vs. Control Patients

26 Going Virtual 26


 rather than have to")




27 Consumerism Patient feedback: I appreciate having this service available at my primary care. I would much rather get taken care of at one place (my PCP office) rather than have to drive especially to Charlotte. This is the coolest thing ever! Virtual Heart Success CMC Lincoln HF 30 Day All Cause Readmission Rate ytd Readmissi on Observed
 Currently offering Virtual Care services in 21 Emergency Departments")
28 Virtual Team in ED 4,688 patients received a Telepsych consult in 2014 (75% increase) Currently offering Virtual Care services in 21 Emergency Departments 28
29 CHS Telepsychiatry Growth and Projected Volume for
30 BHI Team Call Back Protocol Motivational Interviewing Symptom Management Mindfulness Chart Reviews Patient Education Online Therapy Health Coach BHP (LCSW, LPC) Patient Education Psych Assessments Diagnostic Clarification Crisis Intervention Tx Planning Psychoeducation Practice Onboarding Educational Services Chart Reviews Clinical support and oversight for team Evidenced Based Medication Algorithm Psychiatrist ACP Pharm D Patient and Provider Education Access to Medication Chart Review Evidenced Based Medication Algorithm


31 Why a Psychiatric Nurse Practitioner
32 Our Model We ve got your back The key to making teambased medical care work is helping the patient feel that his or her relationship with the primary-care provider is at its center. What we want to accomplish: Improve early detection Timely access to services Referrals to the right level of care Drive cost effective & clinically effective treatment Support the Primary Care Provider Support the Patient Suzanne Koven is a primary care doctor at Massachusetts General Hospital in Boston and writes the column "In Practice" at the Boston Globe.

33 Screening is the Driver



34 Treatment and Patient Engagement Evidenced Based Treatment Standardized tools in the PCP setting enhances screening diagnosis, and treatment planning Patient Engagement Recovery



35 Technology Utilized
36 Program Outcomes: Return on Investment Disease Severity Clinical Outcomes Healthcare Utilization Cost of Care Depression symptoms Weight/BMI Inpatient visits Overall Anxiety symptoms Suicide ideations HgB A1C Cholesterol (Total, triglycerides, LDL, HDL) Inpatient days ED visits Inpatient Ambulatory Ambulatory visits (Primary/specialty) ED Avoidable ED/IP visits
37 Evaluation Framework P R E P O S T Clinical Indicators (labs) were compared at baseline and 12 months after enrollment. If patient had multiple clinical test results the score closest to baseline (but prior to BHI enrollment) was considered a baseline measurement and score closest to the end of 1-year mark was considered as post measurement. Healthcare utilization and charges were also compared for 1-year pre and 1-year post- enrollment time windows
 ** Patient who had at least 6 months follow-up,")
38 Depression Compares baseline and the latest reported PHQ-9 scores *p-value <.05 indicates statistically significant change within the same patients overtime (Pre-post analysis using paired t-test procedure) ** Patient who had at least 6 months follow-up, started out with elevated PHQ-9 score (>=10) and had at least 30 days between the first and last assessment 38
39 Anxiety Compares baseline and the latest reported GAD-7 scores *p-value <.05 indicates statistically significant change within the same patients overtime (Pre-post analysis using paired t-test procedure) ** Patient who had at least 6 months follow-up, started out with elevated GAD-7 score (>=10) and had at least 30 days between the first and last assessment 39
40 Suicidal Ideations* Compares baseline and the latest reported PHQ-9 (Q9) or CSSRS assessments * Based on Question 9 on the PHQ-9 Scale and CSSRS Assessments ** Patient who had at least 6 months follow-up and at least 30 days between the first and last assessment ***p-value <.05 indicates statistically significant change 40
41 Weight n=980 Mean (± Standard Deviation) Mean change p-value* Baseline (±57.8) 6 months (±57.7) 2.0 (±18.4) p=.0006 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 41
42 BMI Mean (± Standard Deviation) Mean change p-value* Baseline 30.9 (±8.7) 1-year 31.2 (±8.6) 0.32 (±2.8) p=.0006 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 42
43 HgB A1C Mean (± Standard Deviation) Mean change p-value* Baseline 7.8 (±2.3) 1-year 7.4 (±1.8) 0.4 (±1.8) p=.013 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 43
44 Lipids: Total Cholesterol Mean (± Standard Deviation) Mean change p-value* Baseline (±53.4) 1-year 179 (±43.4) 11.5 (±41.9) p=.009 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 44
45 Lipids: Triglycerides Mean (± Standard Deviation) Mean change p-value* Baseline (±106.9) 1-year (±123.7) 6.2 (±88.7) p=.5 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 45
46 Lipids: LDL Mean (± Standard Deviation) Mean change p-value* Baseline (± 44) 1-year 98 (± 37.9) 11.7 (±31.2) p=.0007 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 46
47 Lipids: HDL Mean (± Standard Deviation) Mean change p-value* Baseline 47.3 (± 13.9) 1-year 46.4 (± 14.2) 0.87 (±8.5) p=.32 *p-value <.05 indicates statistically significant change (statistical significance doesn t necessarily indicate clinical significance) NOTE: To allow for pre-post comparison patients had to have at least 2 measurements (explains decrease in sample size) 47
48 Healthcare Utilization: Inpatient Care 12% of patients had at least one IP admission 1-year prior or 1-year post-enrollment (averaging 0.2 visits per patient) Only 3% of patients had more than 1 IP stay Overall length of IP stay was 1285 days pre- and 1433 days post-intervention, respectively There was a $930,050 increase in overall billed charges that could have been caused by increase in total IP days in the year after intervention 48
 methodology 49 The decrease in avoidable visits resulted in $130,833 savings in total billed charges")
49 Healthcare Utilization: Avoidable Inpatient Care There was 25% reduction in avoidable inpatient visits (from 53 visits pre- to 38 visits post-intervention). Inpatient visits were classified as avoidable using AHRQ Prevention Quality Indicator (PQI) methodology 49 The decrease in avoidable visits resulted in $130,833 savings in total billed charges (average of $8722 saved per patient)
50 Healthcare Utilization: ED Avg $480 per person Avg $690 per person Total number of ED only visits that did not result in admission decreased by ~ 8% (109 less visits) 36% of the patients had at least one ED visit 1-year before the program start date averaging 1(± 2.6) visits per person 34% had at least one ED visit 1-year after the program start date averaging 0.9 (± 2.3) visits per person About 10% of the patients had 3 or more visit a year Although number of overall ED visits decreased the complexity of these visit must have increased resulting in of average billed charges of $690 per visit 1-year after intervention compared to $480 1-year before intervention 50
51 Healthcare Utilization: Ambulatory Overall billed charges associated with ambulatory care have increased by $470,077 averaging $343 increase per patient Increase in total charges concurred with the rise in total patient visits. Average ambulatory charge per person Mean (± Standard Devition) 1-year PRE $2534 (±3708) 1-year POST $2877 (±4193) Mean change $343 (± 4619) p-value* p=.006 *p-value <.05 indicates statistically significant change (statistical significance doesn t always indicate clinical significance) 51

52 System Investment Incremental Salary Expense 1,268,791 salary and benefits BHI by the Numbers 7,049 Unique Patients 64,299 Patient Encounters 2,392 Patients currently under active mgmt. 21 Primary Care Practices 4 Pediatric Clinics 70 Care Management Clinics Teammate Interventions 2016 Health Coach [VALUE] Total Patient Interventions 64,299 MD/ACP [VALUE] BHP [VALUE] Existing Resources Utilized 1 Manager 1 Program Coordinator 1 On Boarding Specialist 12 BHPs + 2 PRN 13 Health Coaches Per Patient Expense = $ PharmD/BHI Support 0.2%
53 Next Steps / Lessons Learned Next Steps: Expansion into Pediatrics Standardize screenings across Pediatric and OB/GYN clinics. Increase patients enrolled by expanding the program to incorporate additional CHS Pediatric Clinics Capture Parent depression screenings to provide services to the entire family. Incorporate other tools, such as texting to engage patients in our Patient Outreach Program. Virtual Therapy, Transition Clinics and Virtual BH Outpatient Sites. Lessons Learned: Leadership support. One EMR is very helpful. Standardize screenings Who When Screener in the EMR It Takes a Village!!!
54

55 Contact Information NPSS ASHEVILLE, NC
Session 84X Integrating Behavioral Health into Primary Care and Care Management
 Prepared for the Foundation of the American College of Healthcare Executives Session 84X Integrating Behavioral Health into Primary Care and Care Management Presented by: Martha J. Whitecotton, RN, FACHE
Prepared for the Foundation of the American College of Healthcare Executives Session 84X Integrating Behavioral Health into Primary Care and Care Management Presented by: Martha J. Whitecotton, RN, FACHE
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Mental Health at Mercy Health: Treating the Whole Person. David E. Blair, MD Mercy Health Physician Partners President and CMO
 Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Integrated Behavioral Health Services
 Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Beacon Health Strategies Primary Care Provider Training
 Beacon Health Strategies Primary Care Provider Training REFERRAL AND RESOURCE GUIDE Updated June 2015 BEACON HEALTH STRATEGIES beaconhealthstrategies.com June 15, 2015 1 Agenda 1. Review Medi-Cal Managed
Beacon Health Strategies Primary Care Provider Training REFERRAL AND RESOURCE GUIDE Updated June 2015 BEACON HEALTH STRATEGIES beaconhealthstrategies.com June 15, 2015 1 Agenda 1. Review Medi-Cal Managed
Collaborative Care (IMPACT)- An Overview June 11, 2015
- An Overview June 11, 2015") Collaborative Care (IMPACT)- An Overview June 11, 2015 1 2 Mental Health in the US Depression is the leading cause of disability worldwide ~7% of US adults experienced major depression at least once during
Collaborative Care (IMPACT)- An Overview June 11, 2015 1 2 Mental Health in the US Depression is the leading cause of disability worldwide ~7% of US adults experienced major depression at least once during
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
 Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Turning Big Data Into Better Care
 Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Integrated Mental Health Care. Questions
 Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
THE AFFORDABLE CARE ACT: OPPORTUNITIES FOR SOCIAL WORK PRACTICE IN INTEGRATED CARE SETTINGS. Suzanne Daub, LCSW April 22, 2014
 THE AFFORDABLE CARE ACT: OPPORTUNITIES FOR SOCIAL WORK PRACTICE IN INTEGRATED CARE SETTINGS Suzanne Daub, LCSW April 22, 2014 Agenda Why integrate primary care and behavioral health? Define integrated
THE AFFORDABLE CARE ACT: OPPORTUNITIES FOR SOCIAL WORK PRACTICE IN INTEGRATED CARE SETTINGS Suzanne Daub, LCSW April 22, 2014 Agenda Why integrate primary care and behavioral health? Define integrated
Best Management Practices In Integrated Behavioral Health/Primary Care Programs
 Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Transdisciplinary Care: Opportunities and Challenges for Behavioral Health Providers
 Transdisciplinary Care: Opportunities and Challenges for Behavioral Health Providers Virna Little Journal of Health Care for the Poor and Underserved, Volume 21, Number 4, November 2010, pp. 1103-1107
Transdisciplinary Care: Opportunities and Challenges for Behavioral Health Providers Virna Little Journal of Health Care for the Poor and Underserved, Volume 21, Number 4, November 2010, pp. 1103-1107
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Overview of New Nursing Roles in Whole Person Care. Session 1
 Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Resident Rotation: Collaborative Care Consultation Psychiatry
 Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD James Basinski, MD With contributions from: Jurgen Unutzer, MD, MPH, MA Jennifer Sexton, MD, Catherine Howe, MD, PhD
Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD James Basinski, MD With contributions from: Jurgen Unutzer, MD, MPH, MA Jennifer Sexton, MD, Catherine Howe, MD, PhD
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Residential Treatment Facility TRR Tool 2016
 Provider Name: Address: Provider Type: Name of Reviewer: Date of Review: Residential Treatment Facility TRR Tool 2016 Member ID Auth Dates 1 Initial Assessment Areas of Review Reference Record 1 Record
Provider Name: Address: Provider Type: Name of Reviewer: Date of Review: Residential Treatment Facility TRR Tool 2016 Member ID Auth Dates 1 Initial Assessment Areas of Review Reference Record 1 Record
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers. Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW
 Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Intensive In-Home Services (IIHS): Aligning Care Efficiencies with Effective Treatment. BHM Healthcare Solutions
: Aligning Care Efficiencies with Effective Treatment. BHM Healthcare Solutions") Intensive In-Home Services (IIHS): Aligning Care Efficiencies with Effective Treatment BHM Healthcare Solutions 2013 1 Presentation Objectives Attendees will have a thorough understanding of Intensive
Intensive In-Home Services (IIHS): Aligning Care Efficiencies with Effective Treatment BHM Healthcare Solutions 2013 1 Presentation Objectives Attendees will have a thorough understanding of Intensive
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
FOLLOW UP STUDY OF HEALTHFIRST SENIOR MEMBERS WITH DIAGNOSES OF DIABETES AND DEPRESSION
 FOLLOW UP STUDY OF HEALTHFIRST SENIOR MEMBERS WITH DIAGNOSES OF DIABETES AND DEPRESSION Deborah Brotman, MD, FACP Chief Medical Officer FEGS Health & Human Services Monday, November 4, 2013 Inspiring Success
FOLLOW UP STUDY OF HEALTHFIRST SENIOR MEMBERS WITH DIAGNOSES OF DIABETES AND DEPRESSION Deborah Brotman, MD, FACP Chief Medical Officer FEGS Health & Human Services Monday, November 4, 2013 Inspiring Success
CCBHC Standards of Care
 CCBHC Standards of Care Mark Disselkoen, MSW, LCSW, LADC CASAT March 7, 2017 Disclaimer The views, opinions, and content expressed in this presentation do not necessarily reflect the views, opinions, or
CCBHC Standards of Care Mark Disselkoen, MSW, LCSW, LADC CASAT March 7, 2017 Disclaimer The views, opinions, and content expressed in this presentation do not necessarily reflect the views, opinions, or
Using the BHI model in the Health Care for the Homeless Clinic utilizing a Team Approach
 Using the BHI model in the Health Care for the Homeless Clinic utilizing a Team Approach Lincoln Community Health Center Health Care for the Homeless Clinic 412 Liberty Street Durham NC, 27701 2015 National
Using the BHI model in the Health Care for the Homeless Clinic utilizing a Team Approach Lincoln Community Health Center Health Care for the Homeless Clinic 412 Liberty Street Durham NC, 27701 2015 National
Transforming Healthcare Delivery, the Challenges for Behavioral Health
 Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
What s the BIG DEAL? Behavioral Health Integration Throughout the Continuum
 What s the BIG DEAL? Behavioral Health Integration Throughout the Continuum NCAHQ April 5, 2017 Monica Cooke MA, RNC, CPHQ, CPHRM, FASHRM Quality Plus Solutions LLC Objectives Describe the prevalence of
What s the BIG DEAL? Behavioral Health Integration Throughout the Continuum NCAHQ April 5, 2017 Monica Cooke MA, RNC, CPHQ, CPHRM, FASHRM Quality Plus Solutions LLC Objectives Describe the prevalence of
Drug Medi-Cal Organized Delivery System
 Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
Integration Improves the Odds: Lessons Learned. Monday, December 18 th, 2017
 Integration Improves the Odds: Lessons Learned Monday, December 18 th, 2017 Julie Cornell, North America Regional Manager, Global Community Impact INTEGRATION IMPROVES THE ODDS Lessons Learned Webinar
Integration Improves the Odds: Lessons Learned Monday, December 18 th, 2017 Julie Cornell, North America Regional Manager, Global Community Impact INTEGRATION IMPROVES THE ODDS Lessons Learned Webinar
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
Opportunities and Issues Related to BH Services in Primary Care
 Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Risk Stratification: Necessary Tool for Value-Based Payments
 Risk Stratification: Necessary Tool for Value-Based Payments Presenters: Jolene Rasmussen, Texas Council of Community Centers Tim Markello, Gulf Coast Center Mary Duffy, Bluebonnet Trails Community Services
Risk Stratification: Necessary Tool for Value-Based Payments Presenters: Jolene Rasmussen, Texas Council of Community Centers Tim Markello, Gulf Coast Center Mary Duffy, Bluebonnet Trails Community Services
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
BHS Policies and Procedures
 BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and
 Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
Using Innovation to Maximize Behavioral Health Accommodations. Regions Hospital Case Study
 Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Community Care of North Carolina
 Community Care of North Carolina 2007 Community Care of North Carolina Mail Service Center 2009 Raleigh, NC 27699-2009 (919) 715-1453 www.communitycarenc.com Background Several networks in the Community
Community Care of North Carolina 2007 Community Care of North Carolina Mail Service Center 2009 Raleigh, NC 27699-2009 (919) 715-1453 www.communitycarenc.com Background Several networks in the Community
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Robert N. Cuyler, Ph.D., Senior Associate, OPEN MINDS The 2014 OPEN MINDS Planning & Innovation Institute June 3, :15am 12:30pm
 Robert N. Cuyler, Ph.D., Senior Associate, OPEN MINDS The 2014 OPEN MINDS Planning & Innovation Institute June 3, 2014 11:15am 12:30pm I. Overview Of The Current Telehealth Market II. Telehealth In An
Robert N. Cuyler, Ph.D., Senior Associate, OPEN MINDS The 2014 OPEN MINDS Planning & Innovation Institute June 3, 2014 11:15am 12:30pm I. Overview Of The Current Telehealth Market II. Telehealth In An
Evidence Based Practice: The benefits and challenges of behavioral health services in primary care settings.
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Evidence Based Practice: The benefits and challenges of behavioral health services in primary care settings.
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Evidence Based Practice: The benefits and challenges of behavioral health services in primary care settings.
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Quality Management and Improvement 2016 Year-end Report
 Quality Management and Improvement Table of Contents Introduction... 4 Scope of Activities...5 Patient Safety...6 Utilization Management Quality Activities Clinical Activities... 7 Timeliness of Utilization
Quality Management and Improvement Table of Contents Introduction... 4 Scope of Activities...5 Patient Safety...6 Utilization Management Quality Activities Clinical Activities... 7 Timeliness of Utilization
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Mission: Providing excellent health care to American Indians. Vision: To be the national model for American Indian Health Care
 Mission: Providing excellent health care to American Indians Vision: To be the national model for American Indian Health Care Core Values: Patient First, Quality, Integrity, Professionalism and Indian
Mission: Providing excellent health care to American Indians Vision: To be the national model for American Indian Health Care Core Values: Patient First, Quality, Integrity, Professionalism and Indian
VSHP/ Behavioral Health
 VSHP/ Behavioral Health Deb Dukes & Dr Kelly Askins The contact numbers in the presentation apply to WEST Member Services ONLY. New numbers for EAST Member Services will be published and distributed by
VSHP/ Behavioral Health Deb Dukes & Dr Kelly Askins The contact numbers in the presentation apply to WEST Member Services ONLY. New numbers for EAST Member Services will be published and distributed by
Partial Hospitalization. Shelly Rhodes, LPC
 Partial Hospitalization Shelly Rhodes, LPC Shelly.Rhodes@beaconhealthoptions.com Transition and Certification 2 Transition and Certification Current Rehabilitative Services for Persons with Mental Illness
Partial Hospitalization Shelly Rhodes, LPC Shelly.Rhodes@beaconhealthoptions.com Transition and Certification 2 Transition and Certification Current Rehabilitative Services for Persons with Mental Illness
CONTROLLING MENTAL HEALTH COSTS THROUGH EAP PROGRAMS. Sean Fogarty, Curalinc Healthcare
 CONTROLLING MENTAL HEALTH COSTS THROUGH EAP PROGRAMS Sean Fogarty, Curalinc Healthcare Using EAPs to Control the Cost of Mental Health April 5, 2016 Introduction Sean Fogarty, President and CEO, CuraLinc
CONTROLLING MENTAL HEALTH COSTS THROUGH EAP PROGRAMS Sean Fogarty, Curalinc Healthcare Using EAPs to Control the Cost of Mental Health April 5, 2016 Introduction Sean Fogarty, President and CEO, CuraLinc
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 SERIOUS MENTAL ILLNESS SPECIALTY PLAN
 ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 SERIOUS MENTAL ILLNESS SPECIALTY PLAN The provisions in Attachment II and the MMA Exhibit apply to this Specialty Plan, unless otherwise specified
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 SERIOUS MENTAL ILLNESS SPECIALTY PLAN The provisions in Attachment II and the MMA Exhibit apply to this Specialty Plan, unless otherwise specified
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER
 PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
Peripheral Arterial Disease: Application of the Chronic Care Model. Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario
 Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Blending Behavioral Health and Primary Care. Cherokee Health Systems Clinical Model
 Blending Behavioral Health and Primary Care Cherokee Health Systems Clinical Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Our Mission To improve the quality
Blending Behavioral Health and Primary Care Cherokee Health Systems Clinical Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Our Mission To improve the quality
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division
 Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Psychiatric Mental Health Nurse Practitioner (PMHNP) Graduate Certificate DESCRIPTION
 Graduate Certificate DESCRIPTION") PROGRAM CERTIFICATE NAME OF: Program/Certificate COLLEGE OF GRADUATE STUDIES AND RESEARCH POST-BACCALAUREATE OR POST-MASTER S CERTIFICATE PROPOSAL PROGRAM/CERTIFICATE COVER SHEET Nursing Psychiatric Mental
PROGRAM CERTIFICATE NAME OF: Program/Certificate COLLEGE OF GRADUATE STUDIES AND RESEARCH POST-BACCALAUREATE OR POST-MASTER S CERTIFICATE PROPOSAL PROGRAM/CERTIFICATE COVER SHEET Nursing Psychiatric Mental
BEHAVIORAL HEALTH Section 13. Introduction. Behavioral Health Benefit Overview
 Introduction Ohana Health Plan s Clinical Services Program is designed to coordinate medically necessary care at the most appropriate level of service. The goal is to provide the right service in the right
Introduction Ohana Health Plan s Clinical Services Program is designed to coordinate medically necessary care at the most appropriate level of service. The goal is to provide the right service in the right
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies
 Improvement Strategies") Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Social Innovation Fund (SIF)
") Welcome & Social Innovation Fund (SIF) Pre-Launch Training John A. Hartford Foundation Seattle, Washington September 14-15, 2013 Welcome & Implementing IMPACT University of Washington AIMS Center 1. Lay
Welcome & Social Innovation Fund (SIF) Pre-Launch Training John A. Hartford Foundation Seattle, Washington September 14-15, 2013 Welcome & Implementing IMPACT University of Washington AIMS Center 1. Lay
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Overview. Improving Chronic Care: Integrating Mental Health and Physical Health Care in State Programs. Mental Health Spending
 Improving Chronic Care: Integrating Mental Health and Physical Health Care in State Programs Barbara Coulter Edwards bedwards@healthmanagement.com NCSL Winter CHAPS Meeting December 4, 2006 Overview Current
Improving Chronic Care: Integrating Mental Health and Physical Health Care in State Programs Barbara Coulter Edwards bedwards@healthmanagement.com NCSL Winter CHAPS Meeting December 4, 2006 Overview Current
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Appendix 4. PCMH Distinction in Behavioral Health Integration
 Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes. UB-04 Revenue Codes
 Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
The CCBHC: An Innovative Model of Care for Behavioral Health
 The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
COMMUNITY HEALTH IMPLEMENTATION PLAN
 COMMUNITY HEALTH IMPLEMENTATION PLAN 2017 2017-2020 Table of Contents Letter from Jeff Feasel, President & CEO 1 About Halifax Health 3 Executive Summary 6 Halifax Health Community Health Plan 2017-2020
COMMUNITY HEALTH IMPLEMENTATION PLAN 2017 2017-2020 Table of Contents Letter from Jeff Feasel, President & CEO 1 About Halifax Health 3 Executive Summary 6 Halifax Health Community Health Plan 2017-2020
Developing a Behavioral Health Care Service Line at a Small Rural Hospital
 Developing a Behavioral Health Care Service Line at a Small Rural Hospital Mike Glenn, CEO, Jefferson Healthcare Joe Mattern, MD, CMO, Jefferson Healthcare Sue Ehrlich, MD, Medical Director, Discovery
Developing a Behavioral Health Care Service Line at a Small Rural Hospital Mike Glenn, CEO, Jefferson Healthcare Joe Mattern, MD, CMO, Jefferson Healthcare Sue Ehrlich, MD, Medical Director, Discovery
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Programs and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance Program
 s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions
 Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Alternative or in Lieu of Service Description Alliance Behavioral Healthcare
 Alternative or in Lieu of Service Description Alliance Behavioral Healthcare 1. Service Name and Description: Rapid Response Crisis Services for Children and Youth Service Name: Rapid Response Procedure
Alternative or in Lieu of Service Description Alliance Behavioral Healthcare 1. Service Name and Description: Rapid Response Crisis Services for Children and Youth Service Name: Rapid Response Procedure
Mary Hoefler, MS, LCSW Office of Behavioral Health Office
 Mary Hoefler, MS, LCSW Office of Behavioral Health mary.hoefler@state.co.us 303.866.7518 Office Senate Bill 266 Components of the BH crisis response system will reflect a continuum of care from crisis
Mary Hoefler, MS, LCSW Office of Behavioral Health mary.hoefler@state.co.us 303.866.7518 Office Senate Bill 266 Components of the BH crisis response system will reflect a continuum of care from crisis
SECTION 3. Behavioral Health Core Program Standards. Z. Health Home
 SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
Integrating Behavioral Health into the Primary Care Visit for Co-Morbid Disease. Kari B. Kirian, Ph.D.
 Integrating Behavioral Health into the Primary Care Visit for Co-Morbid Disease Kari B. Kirian, Ph.D. Objectives Integrated Care 101 Primary Care Behavioral Health (PCBH) PCBH at ECU Family Medicine Defining,
Integrating Behavioral Health into the Primary Care Visit for Co-Morbid Disease Kari B. Kirian, Ph.D. Objectives Integrated Care 101 Primary Care Behavioral Health (PCBH) PCBH at ECU Family Medicine Defining,
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System
 Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans
 Training Presentation for Managed Medical Assistance Specialty Plans") Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Outline 11/17/2014. Overview of the Issue Program Overview Program Components Program Implementation
 Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of