North Simcoe Muskoka Local Health Integration Network (LHIN) Board of Directors Meeting Monday, June 26, 2017
|
|
|
- Prudence Baldwin
- 5 years ago
- Views:
Transcription

1 ITEM SUB ITEM North Simcoe Muskoka Local Health Integration Network (LHIN) Board of Directors Meeting Monday, June 26, :00 p.m. 1:00 p.m. Board Education Session 1:00 p.m. 4:00 p.m. Board Meeting Boardroom 210 Memorial Ave., Suite 128, Orillia, ON A G E N D A TOPIC PRESENTER OUTCOME REQUIRED I I/D M/R 1.0 Convening the Meeting 1.1 Call to Order Notice and Quorum Kirsten Parker 1.2 Approval of the Agenda* Motion: That the NSM LHIN Board of Directors approve the agenda of June 26, Kirsten Parker 1.3 Declaration of Conflict of Interest Kirsten Parker 1.4 Delegations to the Board There are no delegations to the board for the meeting of June 26, Kirsten Parker 2.0 Presentation / Board Education Session Primary Care and Health Links* 3.0 By Consent 3.1 Meeting Minutes* Approval NSM LHIN Board of Directors Meeting May 29, Board Meeting Evaluation May 29, 2017* Information 3.3 Action Log* Information 3.4 CEO Monthly Report* Information 3.5 Meeting Minutes* Information DRAFT Committee of the Whole June 12, New Funding Update* Information 3.7 Quality Improvement Plan and Patient Safety Dashboard* Information 3.8 Annual Business Plan 2017/18* Approval 3.9 Psychogeriatric Resource Consultants Integration by Funding* Approval 3.10 Broader Public Sector Accountability Act (BPSAA) Reporting Requirements* Approval Motion: That the NSM LHIN Board of Directors approve the Consent Agenda of June 26, M
2 4.0 Reports 4.1 Report of the Chair Kirsten Parker 4.2 Report of the Directors Board Members 4.3 Report of the Chief Executive Officer Jill Tettmann 5.0 Business Arising 6.0 Committee Business 7.0 New Business 7.1 NSM CCAC 2016/17 Audit Report and Draft Financial Statements* 7.2 Status of Audit Recommendations Office of Auditor General of Ontario, CCAC Audits, 2015* 7.3 Status of Audit Recommendations Office of Auditor General of Ontario, LHIN Audits, 2015* Jeff Kwan Guest - BDO Debbie Roberts Jeff Kwan 7.4 Supportive Housing Case Management* Neil Walker M 8.0 Standing Items 8.1 System Transformation Kirsten Parker Jill Tettmann 9.0 For Information 10.0 Break Followed By In-Camera Session 10.1 Report on In-Camera Session Kirsten Parker 11.0 Meeting Evaluation and Adjournment 11.1 Meeting Adjournment Motion: That the NSM LHIN Board of Directors meeting of June 26, 2017 be adjourned. Kirsten Parker M Legend: I (Information) / I/D (Input/Direction) / M/R (Motion / Resolution) *Attachment 2
3 North Simcoe Muskoka Health Links NSM LHIN Board of Directors June 26, 2017
4 Purpose: It has been estimated that 2/3 of the health care budget in Ontario is spent on 5% of the people of the province, representing the most medically and socially complex, challenging and vulnerable. The Health Links (HL) approach is a collaborative endeavour of the Ministry of Health and Long Term Care (MOHLTC), LHINs, Health Quality Ontario (HQO) and local Health Links teams. The goal is to coordinate care for the person across their journey through our health care system in a holistic way. 2

5
6 Core Features Person Centred (individual goals and care plan). Local Focus (bringing together providers within a community around an individual). Voluntary Partnerships (supported by Partnership Agreements/Memorandum of Understanding). Strengthened by: Robust Primary Care involvement, Measurement focus and Outcome orientation, Visionary leadership. 4
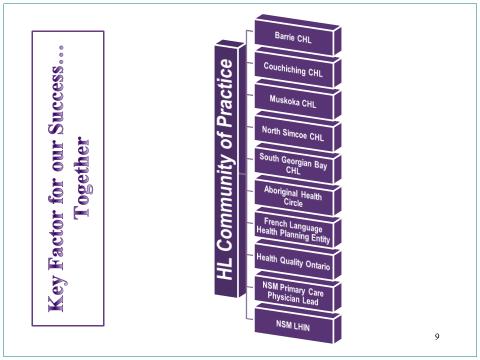
7 LHIN s Role in Health LINKS The LHIN provides leadership. Primary Care Lead, Dr. Van Iersel Sub-regional Director at each HLs Steering Committee Table HL Community of Practice The LHIN is responsible for the development, monitoring and tracking of the LHIN Funding Accountability Framework. The LHIN provides guidance on provincial and Ministerial initiatives and funding. 5
8 Ministry Role in Health LINKS The MOHLTC provided start up funding (project funding) for potential HLs to prepare a business case. Templates were created that all potential HLs completed with the support of the LHIN. These templates were submitted to the MOHLTC and approval was required for all HLs, and funding was provided. There is a provincial LHIN HL Leads table to support knowledge exchange. The Ministry funded Care Coordination Tool pilot projects with 3 HLs participating in our region. The MOHLTC has facilitated regular HLs provincial meetings and conferences to spread the successes. 6
9 HQO Role in Health Links Supporting data collection, timely reports and analysis. Leading systematic identification of emerging innovations and best practices. Accelerating progress through standardization of best practices across all Health Links. Supporting inter-health Links sharing of lessons learned on regional or pan-provincial basis. Connecting LHIN Health Links leads with other relevant provincial quality initiatives. 7
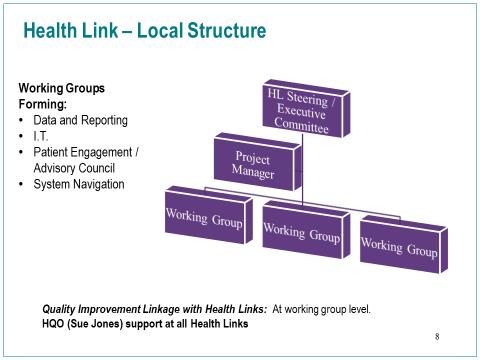
10 8
11 9
12 10
13 Defining High Users of the Local Health System ICES has identified 23,320 individuals who meet the definition or criteria of a High User in NSM, individuals who have a high frequency of system utilization. Utilizes high costs resources in the local health system. These individuals have complex needs requiring support from many health and social care resources including housing and income supports. Utilization of health resources typically used across one s journey of care might include: Primary care Services and programs received through connection with primary care such as Congestive heart failure (CHF), Diabetes, social work, dietitian, physiotherapy Acute care and admissions to hospital Emergency department visits Home care Mental Health 11
14 About Barrie HL Provincial Early Adopter. HL Steering Committee comprised of key partners in the Barrie Area. Barrie uses a clinic, the LINK, located at the Barrie and Community Family Health Team (BCFHT) building to provide primary care to unattached HL patients. Has partnered with Simcoe County s Emergency Management Services (EMS) to identify patients. 12
15 About South Georgian Bay HL Provincial Early Adopter. Built upon the Home for Life work occurring locally. Use a Patient Think Tank-a weekly team meeting which wraps service around the most medically complex HL patient. Utilizes a Patient Portal (launched 2016). All Primary Care Health Service Providers (HSPs) are on the same electronic medical system. Strong governance structure. 13
16 About North Simcoe (NS) HL Only HL with a co-chair role shared between the Family Health Team (FHT) and Community Health Centre (CHC). Indigenous System Navigator working out of Georgian Bay General Hospital (GBGH) providing direct service for those individuals coming from Beausoliel First Nation (FN). Chigamik Community Health Centre (CHC) has a regional, Francophone system navigator providing support to all HLs patients across the LHIN. Strong data sharing agreement with the hospital and means of data analysis at the individual, patient level to demonstrate efficiency and financial savings to the health system as a result of the NS HL work. Strong focus on the social determinants of health. Canadian Index of Wellbeing, sense of belonging 14
17 About Couchiching HL Has a strong system navigation team and great working relationship with the hospital and community partners. Via the Orillia Soldiers Memorial Hospital (OSMH) Transitions of Care Committee, patient needs have been addressed in a timely way. reducing alternate level of care (ALC) and emergency department (ED) visits/admissions. Embedded Quality Improvement methodology early. Improving & Driving Excellence Across Sectors (IDEAS) cohort 15
18 About Muskoka HL Only HL in the province led by a municipality. Developed a novel navigation approach in which the case conference occurs using flash cards which depict various social and health related aspects of life and these are then prioritized by the client. Inclusive engagement of primary care. Active partnership with Nurse Practitioner Led Clinic (NPLC) and health hubs in their community. 16
19 NSM HLs Spotlights Four of five HLs have a community collaborative Quality Improvement Plan aligning with the NSM Regional Quality Advisory Council area of focus (improving transitions in care). Provincial Leading Practice First Nations Metis Inuit (FNMI) and Francophone navigation. Brenda Jackson of Barrie and Area Native Advisory Council (BANAC) assists in regional coordination of care and education as relates to Indigenous individuals. All are working on the development of patient level data which can be used to demonstrate the efficiencies in the health system of this model of care. 17
20 Health Links and the Sub-Region Transformation Population Based Patient-centred medical home Sub-region Planning tables journey journey journey 1-5% Health Links Health Link Steering Committee
21 Primary Care NSM LHIN Board of Directors June 26, 2017
22 Definition pri ma ry care noun health care at a basic rather than specialized level for people making an initial approach to a doctor or nurse for treatment. 2
23 Definition Secondary Care: Medical care provided by a consultant physician Tertiary Care: care received in a center that has personnel and facilities for special investigation and treatment. (acute care) Quaternary Care: Advanced levels of medicine which are highly specialized and not widely accessed. 3


24 Primary Care in Ontario Ontario s primary care system is made up of a wide range of provider groups and clinicians, each with their own funding and accountability relationships. 94% of Ontarians have a regular health care provider 25% of Ontarians have access to interdisciplinary teams 4
25 Who delivers primary care services? Family Physician Nurse Practitioner Allied team members/interdisciplinary Health Professional TEAM BASED CARE 5
26 Practice Models of Care Solo Physician Group practice (non FHT) FHT CHC Ministry funded TEAM BASED CARE NPLC 6
 s are practice")

27 Family Health Team (FHT) Family Health Teams are practice models NOT physician funding models 7



28 Payment Models for Primary Care Fee For Service FFS Fee For Service Capitation Based FHN Family Health Network Salary Based CHC Community Health Centre CCM Comprehensive Care Model FHO Family Health Organization BSM Blended Salary Model FHG RNPGA Family Health Group Rural & Northern 8
 in NSM RNPGA 0% CCM 1% CHC 3% FHG 7% FHN 12% FHO")
29 Primary Care Physicians by Physician Enrollment Model (PEM) in NSM RNPGA 0% CCM 1% CHC 3% FHG 7% FHN 12% FHO 77% 9
30 Primary Care Accountability Layers of accountabilities Complex Competing 10
31 Team based Primary Care Accountability Varies depending upon Model of Care FHTs; Executive Director accountable to Board, Service Agreement with MOHLTC CHCs; Executive Director accountable to Board, Service Agreement with LHINs NPLCs; Executive Director accountable to Board, Service Agreement with MOHLTC 11
32 Professional Accountability Physician The Patient The Profession [College of Physicians and Surgeons of Ontario (CPSO), College of Family Physicians of Canada/Ontario College of Family Physicians (CCFP/OCFP), PEM Group Board) The Business (MOHLTC, PEM Group Board, employees) Other Professional (NP, allied) The Patient The Profession (respective colleges) The Business (employing body, CHC, FHT, NPLC) 12
33 Governance Variable Board composition Voluntary positions PEMs almost exclusively physicians FHTs vary with some having community and patient reps CHCs more likely to have community 13
34 Future of Primary Care Proposed role in: Health Human Resource Planning* Contract Management* Funding Performance Accountability Awaiting legislation/regulation/direction for clarity 14
35 Approved: Minutes of the North Simcoe Muskoka Local Health Integration Network Board Meeting held on Monday, May 29, :00 p.m. 4:00 p.m. at the NSM LHIN office in the Simcoe Georgian Room in Barrie. Present: Robert Morton, Chair Barbara Dickson Ernie Vaillancourt Larry Saunders Ewelina Chwilkowska Ellen Mary Mills Andy Ott Tim Withey Jacques Boulet Andrea Butcher-Milne Jill Tettmann, CEO Leanne Vincent, Recording Secretary Regrets: Colleen Geiger Staff: Neil Walker, Vice President, System Transformation Rebecca Van Iersel, Vice President, Clinical Jeff Kwan, Vice President, Financial Health & Accountability Karen Taillefer, Vice President, Home & Community Care Debbie Roberts, Vice President, Quality & Performance Kathleen Bain, Director, Communications Public in Attendance: There were several members of the public in attendance throughout the meeting. 1.0 Convening of the Meeting 1.1 Call to Order The Board meeting of May 29, 2017 was called to order at 12:00pm with the meeting being legally constituted, with Board members having received adequate notice in accordance with the guidelines, with adequate posting to the public of the meeting and with a quorum present. Roundtable introductions were completed. 1.2 Approval of Agenda Motion: T. Withey Seconded: E. M. Mills That the agenda of the NSM LHIN Board Meeting of May 29, 2017, be approved. carried 1.3 Declaration of Conflicts
36 There were no declarations of conflict noted. 1.4 Delegations to the Board There are no delegations to the board for the meeting of May 29, Presentation/Board Education Session: Capital Overview & Orillia Soldiers Memorial Hospital Strategic Plan B. Sibrohvan, Board Member, P. Campbell, President & CEO, Doug Murray, Executive Vice President Corporate Services & CFO, and Nina Lowe, Project Manager, Orillia Soldiers Memorial Hospital joined that meeting for the board education session. N. Walker provided an overview of the capital planning process. B. Sibrohvan provided an overview of the agenda for the OSMH presentation. P. Campbell provided an overview of OSMH highlighting recent accomplishments, regional role and strategic plan. D. Murray provided an overview of OSMH capital planning and the principles developed for capital planning. It was noted that the development of a clinical services plan will help to determine where and how services should be delivered in the future. The LHIN Board expressed their appreciation to OSMH for the presentation and their leadership. ACTION: It was requested that a more fulsome review of acute care planning occur as a future discussion by the NSM LHIN Board. 3.0 By Consent The below items were included in the consent agenda of the NSM LHIN Board Meeting of <Date>. Note: Italicized items were removed from the consent agenda. 3.1 Approval of Minutes NSM LHIN Board of Directors Meeting April 24, 2017* 3.2 Board Meeting Evaluation April 24, 2017* 3.3 Action Log* 3.4 CEO Monthly Report* 3.5 Meeting Minutes Draft Committee of the Whole May 15, 2017* 3.6 Meeting Minutes Draft Audit Committee May 15, 2017* 3.7 Annual Report on Use of Consultants April 1, 2016 March 31, 2017* 3.8 New Funding Update* 3.9 Hospital Sector Funding* Motion: B. Dickson Seconded: L. Saunders That the NSM LHIN Board of Directors approve the Consent Agenda of May 29, carried 4.0 Reports 4.1 Report of the Chair R. Morton circulated a written report on his involvement in the following meetings and engagements since the Board of Directors meeting on April 24, 2017:
37 April 25 April 27 May 1 May 2 May 3 May 4 May 5 May 6 May 8 May 9 May 12 May 15 May 18 May 19 May 24 May 25 May 26 Third Age Barrie: HQO Josh Tepper Alliston Matthews House Hospice groundbreaking Governance Work Stream GBGH Penetang site visit Third Age Barrie: Rethinking Aging Brenda Elias Transition Day Small Urban Municipalities Association conference at Blue Mountain Seven South Street HSP Board New Board Member Orientation (JB) New Board member Orientation (CG, ABM) CEO Evaluation Children s Mental Health Collaborative Governance Forum CARF Accreditation LHIN Chairs tc Victoria Village LTC Board of Directors Ontario Community Support Association Leading Change Forum Committee meetings Chairs and CEOs meeting with Deputy and ADM Pan LHIN Leadership Council and Chairs Council SGB CHC Chair Peter Preager debrief meeting CEO Evaluation Board Advance planning Mill Creek LTC Board of Directors Deloitte re LHIN Board training MAHST Stakeholder Engagement Forum R. Morton noted his attendance at the Children s Mental Health Collaborative Governance Forum and requested a board member volunteer to be the LHINs point person when this collaborative comes together which is anticipated to be in September R. Morton provided an overview of the meeting with the LHIN Chairs and Ministry on May 18. R. Van Iersel provided an overview of the Opioid Strategy Forum held on May Report of the Directors L. Saunders noted continued meetings with MAHST and that the group is currently focusing on engagement. E. M. Mills noted attendance at the HSSO Audit Committee meeting on May 24. E. Vaillancourt noted receiving an invitation to the Entite 4 AGM R. Morton requested that E. Vaillancourt and J. Boulet attend. A. Butcher-Milne noted a meeting with Gary Machan of the Association of Ontario Health Centres, about the Canadian Index of Wellbeing project through the Barrie Community Health Centre. 4.3 Report of the CEO
38 J. Tettmann noted this is the first Board meeting since transition and provided an update on transition of other LHINs. It was noted that further discussion about transition will occur at the Committee of the Whole in June. An update was provided on a culture project underway. An update was provided about the Canadian Red Cross divestment of services. R. Morton provided background and history on Red Cross. 5.0 Business Arising 5.1 Digital Health N. Walker introduced M. Moland to provide information on the ehealth Portfolio within NSM LHIN. An explanation of the three ehealth clusters was provided. An overview was provided on digital health within NSM LHIN noting that 91% of family physicians in NSM use a certified Electronic Medical Record system. NSM ehealth Innovations were explained including an overview of the ehealth Advisory Committee, Telemedicine and Telehomecare initiatives, ecredentialing, and eprescribing. Health Information Systems were explained including the recommendations of the HIS Renewal Advisory Panel. Coordinated Care planning for Health Links was explained. An overview of econsult was provided noting we are doing well with implementation but not adoption. An explanation of ereferral was provided. 6.0 Committee Business 6.1 NSM LHIN 2016/17 Audit Report and Draft Financial Statements B. Dickson provided remarks about the audit report. Motion: B. Dickson Seconded: J. Boulet That the NSM LHIN Board of Directors approve the 2016/17 audited financial statements and authorize the Chair and the Vice-Chair of the Board to sign the audited financial statements on behalf of the Board. carried It was noted that the CCAC Audit will come to the June Board of Directors meeting for information. 6.2 Priorities for Investment and Allocation Process B. Dickson provided an overview of the priorities for investment and allocation process. There was discussion about priorities and it was requested the word local be removed from system alignment. It was noted that LHIN Board priorities are the local priorities. Motion: B. Dickson Seconded: E. M. Mills That the NSM LHIN Board of Directors approve the revised process for allocation of discretionary funds for fiscal year carried
39 7.0 New Business 7.1 Advance Planning L. Saunders provided an overview of work underway to plan a June Board Advance. There was discussion about facilitation for the day and noted the facilitation has not been confirmed. 7.2 Action Log There was discussion about how items are identified on the action log noting that a sustainability plan for Health Links is due to the LHIN in December. It was requested that Health Links be added to the education session for June. ACTION: Health Links to be added to June education session. 7.3 Consultants Report It was questioned if the amount spent on consultants was comparable to previous years or if there were additional expenses due to transition and confirmed that the amount spent was comparable to previous years. It was requested that a briefing note be included with the consultant s report moving forward Standing Items System Transformation For Information Break Followed By In-Camera Session (if required) Report on In-Camera Session (if required) Meeting Evaluation and Adjournment Meeting Adjournment R. Morton was acknowledged for his contributions as Chair of LHIN Board. Motion: T. Withey Seconded: L. Saunders That the NSM LHIN Board of Directors meeting, of May 29, 2017, be adjourned. carried NEXT MEETING: Monday June 26, 2017 (12:00 p.m. 4:00 p.m.) NSM LHIN, 210 Memorial Avenue, Suite 128, Boardroom Robert Morton, Board Chair Jill Tettmann, Chief Executive Officer
40
41 Item 3.2 Board Meeting Monthly Evaluation 1. Date of Board Meeting Answer Options Date / Time Response Percent Response Count 100.0% 6 answered question skipped question 6 0 Number Response Date Date / Time Categories 1 Jun 6, :23 PM 05/29/ Jun 4, :40 PM 05/29/ Jun 1, :31 PM 05/29/ Jun 1, :35 PM 05/29/ May 31, :17 AM 05/29/ May 30, :01 PM 05/29/ Overall, I felt good about the meeting today Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count The agenda was balanced on strategic and fiduciary/operational/management matters Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question 6 0
42 Item Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count Education Session - The content was valuable, pertinent, timely and appropriately linked to the Board's strategic directions Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count Time was used effectively Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count 0 0 6
43 Item We had enough insight and understanding about a question, problem, challenge or an opportunity in order to make an informed decision or recommendation. Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count Board members were frank, open and effective in their communication with each others priorities Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count I had the opportunity to express my views on the agenda items at this meeting Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question 6 0
44 Item Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count Suggestions or ideas raised by Board members were fully discussed and resolved Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count We adhered to the spirit of transparency of the LHIN mode Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count 0 0 6
45 Item Discussion was focused on the Board's mandate and strategic priorities Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count We are making an impact with respect to improving health care in our LHIN Answer Options Strongly Agree Agree Neither Agree or Disagree Disagree Strongly Disagree Rating Average Response Count answered question skipped question Comments (required when answering "Strongly Agree" or "Strongly Disagree") Answer Options answered question skipped question Response Count Number Response Date Response Text Categories 1 Jun 6, :25 PM NSM LHIN is recognized as a leader in Ontario 24. Additional comments Answer Options answered question skipped question Response Count 0 0 6
46 North Simcoe Muskoka LHIN Action Log Committee of the Whole and Board of Directors Item 2.2 Meeting Date In Progress CoW / Board Agenda Item # Description of item June CoW 4.0 Governance Date for September or October Board Advance to be identified May Priorities for Investment and Allocation Process Jan Board Risk Oversight Effectiveness Survey Response Responsible Date to be Complete By Board to provide direction for Q3 surplus reallocation Risk definition and framework be reviewed in transition planning Complete *reflects items as of June 2017 May Board 7.2 Action Log Health Links to be added to June E June CoW 5.1 Annual Business Plan Clarification about active offer for French language services to be included in the annual business plan June CoW 2.2 Action Log Action Log to be updated to include items from Committee and Board Action/Status L. Vincent June 2017 In Progress J. Kwan Fall 2017 In Progress N. Walker D. Roberts Ongoing In Progress L. Vincent June 2017 Complete M. Wilkinson June 2017 Complete L. Vincent June 2017 Complete Board of Directors Committee of the Whole: Action Log as of June 21, 2017
47 Approved: Minutes of the NSM LHIN Committee of the Whole Meeting Monday June 12, :30a.m. to 2:00p.m. NSM LHIN Boardroom, Orillia, ON Present: Andrea Butcher-Milne Andy Ott Barbara Dickson Colleen Geiger Ellen Mary Mills Ernie Vaillancourt Ewelina Chwilkowska Jacques Boulet Kirsten Parker Larry Saunders Tim Withey Jill Tettmann, CEO Leanne Vincent, Recording Secretary Staff: Neil Walker, Vice President, System Transformation Jeff Kwan, Vice President, Financial Health and Accountability Rebecca Van Iersel, Vice President, Clinical Debbie Roberts, Vice President, Quality and Performance Karen Taillefer, Vice President, Home and Community Care Kathleen Bain, Director, Communications 1.0 Convening the Meeting 1.1 Call to Order Notice & Quorum The meeting was called to order at 9:35 a.m. with a quorum noted. The Committee members received adequate notice of the meeting. 1.2 Approval of the Agenda Motion: E. Vaillancourt Seconded: A. Ott That the agenda for the Committee of the Whole meeting of June 12, 2017 be approved. carried 1.3 Declarations of Conflict There were no conflicts declared. 2.0 By Consent The below items were included in the consent agenda of the NSM LHIN Committee of the Whole Meeting of June 12, 2017: Note: Italicized items were removed from the consent agenda. 2.1 Meeting Minutes Committee of the Whole May 15, Action Log 1 P a g e
48 Approved: Motion: C. Geiger Seconded: L. Saunders That the Committee of the Whole approve the Consent Agenda of June 12, carried It was noted that the Action Log will be updated to include items from Board and Committee of the Whole. ACTION: Action Log to be updated to include items from Board and Committee of the Whole 3.0 Transition 3.1 LHIN Renewal Post Transition Update Chris Archer, Project Manager joined the meeting. J. Tettmann introduced M. Wilkinson and C. Archer to provide an update on post transition activities noting that we are focusing on activities thru to the end of the second quarter. C. Archer provided an overview of the transition work underway noting that some deliverables are common provincially while others are local priorities. A review of the post transition structure was provided. It was questioned how frequently this information would be provided to the Board and noted that as we develop a new Committee structure we will have to understand where transition activities should be reported within the new structure. 4.0 Governance L. Saunders provided an update on the planning underway for a Board Advance on June 16. The importance of getting together as a board to begin the relationship building and team development was highlighted. It was noted that a fall session will follow to further the conversation and that we should receive the mandate letter for 2018/19 prior to this session. ACTION: Date for September / October advance to be identified. 5.0 Health System Improvement 5.1 Annual Business Plan 2017/18 E. Vaillancourt introduced M. Wilkinson to provide an overview of the annual business plan. M. Wilkinson provided an overview of the annual business plan purpose, planning cycle, and process and ministry feedback on the annual business plan was reviewed. An overview of the revisions to the annual business plan since the draft originally presented to the Board was provided. There was discussion about French Language Services for home and community care. An explanation of supportive housing was provided noting there is additional volumes being introduced this year. It was questioned if initiatives identified are dependent on new funding and clarified that actions and initiatives identified in the annual business plan have funding allocated to them. It was requested that clarification on active offer be included in the annual business plan. ACTION: Clarification about active offer for French language services be included in the annual business plan. Motion: A. Ott Seconded: L. Saunders That the NSM LHIN Committee of the Whole recommend to the Board of Directors approval of the North Simcoe Muskoka Local Health Integration Network s Annual Business Plan for 2017/18. carried 2 P a g e
49 Approved: 5.2 Psychogeriatric Resource Consultants Integration by Funding M. Wilkinson introduced L. Byrch to provide an overview of the integration proposal. L. Byrch explained various types of integration with Integration by funding explained as the most efficient type of integration. There was a discussion about the risks associated with this integration. It was noted that both Collingwood General & Marine Hospital and Waypoint Centre for Mental Health Care have agreed to this integration. Moved: L. Saunders Seconded: T. Withey That the NSM LHIN Committee of the Whole recommend to the Board of Directors support for an integration by funding of the Psychogeriatric Resource Consultant program that would result in the permanent transfer of all associated program resources, including $208,258 in LHIN funding, from Collingwood General and Marine Hospital Community Mental Health Service to Waypoint s regional Specialized Geriatric Services program effective October 1, carried /18 Quality Improvement Plans E. Vaillancourt introduced V. Armstrong to provide an overview of the Quality Improvement Plans. V. Armstrong provided an overview of Excellent Care for all Act, 2010 and the system approach to health care quality. It was noted that Health Quality Ontario has provided a definition for quality and that Quality Improvement Plans are public information. An overview of the role of the LHIN Board in Quality Improvement Plans was explained. The analysis of QIPs was reviewed and it was clarified that quality indicators are developed by HQO. 5.4 Broader Public Sector Accountability Act (BPSAA) Reporting Requirements J. Kwan provided an overview of the requirement for public disclosure of expenses. Moved: E.M. Mills Seconded: T. Withey That the NSM LHIN Committee of the Whole recommend to the Board of Directors approval of the 2016/17 Public Disclosure of Expenses report as outlined in Section 2. carried 5.5 Verbal Update on LHIN Initiatives J. Tettmann provided an update on the current financial position of the hospitals within North Simcoe Muskoka. An update was provided on the work of MAHST noting that they are working towards a June 30 date for submission of a report to the LHIN. It was noted that there is broad awareness of the work of MAHST. An update was provided on staffing at GBGH noting that a new interim CEO is in place. There was discussion about the GBGH partial designation for French language services. 6.0 Home and Community Care 6.1 Quality Improvement Plan and Patient Safety Dashboard C. Geiger introduced the Quality Improvement and Patient safety dashboard and highlighted historical process for the CCAC Board to receive this information. 3 P a g e
50 Approved: An overview of the patient safety dashboard was provided as well as an explanation on how risks are identified and defined. It was noted that the former CCAC had developed a patient safety culture that encouraged timely and accurate reporting of risk events. It was requested that total number of visits be included in the report moving forward. The complaints process was explained. An overview of the Quality Improvement Plan dashboard was provided and it was explained that the two five day wait time indicators on the QIP are also MSAA performance targets. 7.0 Standing Items 8.0 In-Camera Session 8.1 Report on In-Camera Session 9.0 Adjournment Motion: E. Vaillancourt Seconded: A. Ott That the Committee of the Whole meeting of June 12, 2017 be adjourned at 2:00p.m. carried Chair 4 P a g e
51 Briefing Note Title: 2017/18 Allocations by Sector May 31, 2017 Update Agenda Item: 3.6 Meeting Date: June 26, 2017 Item For: Information Submitted By: Brenda Drinkle Input/Direction Approved By: Jeff Kwan Decision Attachment(s): Yes (list below) No - New Funding Update Schedule Issue/Context: To provide the NSM LHIN Board of Directors with an overview of the NSM LHIN 2017/18 Allocations by Sector (also known as the New Funding Update schedule). Background: The NSM LHIN 2017/18 Allocations by Sector New Funding Update schedule is a monthly Board/Committee meeting agenda item. The purpose of the schedule is to inform the Board of the funding allocations by sector and provide regular updates regarding new funding announcements and / or NSM LHIN discretionary funding allocations. The information, presented by health care sector in both numerical and pie-chart format, provides an overview of the current health care financial allocations in the NSM LHIN. Below is an outline of the type of care delivered and providers in each sector: Sector Hospitals Long Term Care Homes Services Includes 5 Community, 1 Private and 1 Specialty Psychiatric Hospital Includes 26 Long Term Care Homes operated by 21 unique Health Service Providers CCAC / Home Care Includes 1 CCAC - transitioned to Home Care LHIN Delivered Service May 3, 2017 Community Support Service (Includes Acquired Brain Injury Services) Assisted Living Services in Supportive Housing Community Mental Health Addictions Program Initiative Funding Includes 28 Unique Health Service Providers funded to provide Community Support Services (i.e. meal delivery, transportation, homemaking, adult day programs, etc.) Includes 6 Health Service Providers funded to provide assisted living services, accessible on a 24-hour basis Includes 10 Health Service Providers funded to provide community mental health programs Includes 4 Health Service Providers funded to provide substance abuse and problem gambling programs Ministry funding used to support Ministry defined priorities (i.e. Community Investments, PSS Wage Enhancement, Community Paramedicine, etc.) The NSM LHIN Ministry-LHIN Performance Agreement (MLPA) Funding Envelope schedule provides additional details, by sector, of the funded programs / initiatives and identifies the funding as base (ongoing) or one-time. The schedule represents the current funding amounts as per the NSM LHIN Ministry-LHIN Performance Agreement (MLPA). Current Status: The current report, for the period ended May 31, 2017, reflects new funding of $3,302,100 received since April 30, The new funding is for the CCAC / Home Care LHIN Delivered Service sector for the provision of the following services: Levels of Care, Caregiver Support and for High Needs Clients.

52 Item 3.6 North Simcoe Muskoka LHIN 2017/18 Allocations by Sector For the Period ending May 31, 2017 Sectors May /18 Allocations April /18 Allocations Variance Hospital Operations $ 580,289,138 $ 580,289,138 $ Explanation Long Term Care Homes $ 146,452,434 $ 146,452,434 $ Community Care Access Centres / Home Care LHIN Delivered Services $ 107,622,417 $ 104,320,317 $ 3,302,100 Community Investment: Home Care Services LHIN Delivered Services: Levels of Care $2,184,400; Caregiver Support $728,100; High Needs Clients $389,600 Community Support Services (includes ABI) $ 17,497,310 $ 17,497,310 $ Assisted Living Services in Supportive Housing $ 9,038,527 $ 9,038,527 $ Community Health Centres $ 11,836,192 $ 11,836,192 $ Community Mental Health $ 28,206,935 $ 28,206,935 $ Addictions Program $ 5,265,330 $ 5,265,330 $ Initiative Funding: (Community Investment, Urgent Priority Fund) $ 624,677 $ 624,677 $ GRAND TOTAL $ 906,832,960 $ 903,530,860 $ 3,302, /18 Allocations by Sector $906,832,960 as of May 31, 2017 Community Health Centres, $11,836,192, 1% Community Mental Health, $28,206,935, 3% Assisted Living Services in Supportive Housing, $9,038,527, 1% Community Support Services (includes ABI), $17,497,310, 2% Addictions Program, $5,265,330, 1% Initiative Funding: (Community Investment, Urgent Priority Fund), $624,677, 0% Community Care Access Centres / Home Care LHIN Delivered Services, $107,622,417, 12% Long-Term Care Homes, $146,452,434, 16% Hospital Operations, $580,289,138, 64%
53 North Simcoe Muskoka LHIN 2017/18 Ministry LHIN Performance Agreement Funding Envelope For the Period ending May 31, 2017 Sector Month Funding Type Base One Time Hospitals 2017/2018 Opening Annualized Base Allocation April Operating 432,107,447 Child & Youth Mental Health RVH April Ministry 3,200,000 Preschool Speech Language Recovery & Transfer to MCYS RVH April Ministry (453,323) Health System Funding Reform & Other Hospital Funding April Ministry 13,111,202 2,443,154 Emergency Department Pay for Results April Ministry 4,217,600 Sexual Assault & Domestic Violence Treatment Centres OSMH April Ministry 34,200 Sector Reallocation to CMH: Telemedicine Nurses April LHIN Strategic (85,020) Sector Reallocation from CCAC: Support to Achieve FLS Designation GBGH April LHIN Strategic 72,750 Large Community & Private Hospitals 447,880,306 6,767, /2018 Opening Annualized Base Allocation April Operating 123,177,528 Health System Funding Reform & Other Hospital Funding April Ministry 2,463,600 Specialty Psych Hospitals Total 125,641,128 Hospital Total 573,521,434 6,767,704 Long Term Care Homes 2017/18 Opening Annualized Base Allocation April Operating 143,623,308 Sector Reallocation & UPF:36 CCP Beds IOOF (20), Muskoka Shores (12) and Collingwood NH (4) April LHIN Strategic 2,282,014 Ministry Top Up for 32 CCP Beds IOOF (20), Muskoka Shores (12) April Ministry 422,112 Sector Realloc from CSS: Health Links Ongoing Operational Support (Muskoka) April LHIN Strategic 125,000 Long Term Care Homes Total 146,327, ,000 Community Care Access Centres / Home Care LHIN Delivered Services 2017/2018 Opening Annualized Base Allocation April Operating 104,772,667 Sector Reallocation from CSS: Regional Palliative Care Program April LHIN Strategic 70,000 Community Investment: Regional Palliative Care Program Top Up April LHIN Strategic 35,000 CCAC/LHIN Delivered Services Funding Adjustment (8% Savings) April Ministry (484,600) Sector Reallocation to HOSPITAL: Support to Achieve FLS Designation GBGH April LHIN Strategic (72,750) Community Investment: Home Care Services LHIN Delivered Services May Ministry 3,302,100 Community Care Access Centres / Home Care LHIN Delivered Services Total 107,695,167 (72,750) Community Support Services (CSS) 2017/2018 Opening Annualized Base Allocation April Operating 16,771,294 Community Investment: FNMI System & Health Link Lead April LHIN Strategic 120,000 Community Investment: Health Link Ongoing Operational Support (Couchiching) April LHIN Strategic 125,000 Community Investment: Enhanced SMART VON April LHIN Strategic 327,000 Sector Realloc to LTC: CCP Beds Muskoka Shores (12) and Collingwood NH (4) April LHIN Strategic (907,074) Sector Realloc to LTC: Health Links Ongoing Operational Support April LHIN Strategic (125,000) Community Support Services Total 16,771,294 (460,074) Acquired Brain Injury (ABI) 2017/2018 Opening Annualized Base Allocation April Operating 1,186,090 Acquired Brain Injury Total 1,186,090 Community Support Services including ABI Total 17,957,384 (460,074) Assisted Living Services Supportive Housing (ALSSH) 2017/18 Opening Annualized Base Allocation April Operating 9,904,012 Sector Reallocation to LTC: CCP Beds IOOF (20) April LHIN Strategic (865,485) Assisted Living Services Supportive Housing Total 9,904,012 (865,485) Community Health Centres (CHC) 2017/2018 Opening Annualized Base Allocation April Operating 11,461,192 Community Investment: Health Link Ongoing Operational Support (Barrie, North Simcoe, South Georgian Bay) April LHIN Strategic 375,000 Community Health Centres Total 11,461, ,000 Community Mental Health (CMH) 2017/2018 Opening Annualized Base Allocation April Operating 28,121,915 Sector Reallocation from HOSPITAL: Telemedicine Nurses April LHIN Strategic 85,020 Community Mental Health Total 28,206,935 Addictions Program 2017/2018 Opening Annualized Base Allocation April Operating 5,265,330 Addictions Program Total 5,265,330 Sector Subtotal excluding Initiative Funding 900,338,888 5,869,395 Initiative Funding Non Sector Specific Urgent Priorities Funds May Initiatives Non Sector Specific Prior Years Residual Community Investments May Initiatives Non Sector Specific Community Investments 2017/18 May Initiatives Non Sector Specific Community Paramedicine May Initiatives Initiative Funding Total Grand Total
54 Title: Quality Improvement Plan and Patient Safety Dashboards Agenda Item: 3.7 Meeting Date: June 26, 2017 Item For: Information Submitted By: Valerie Armstrong Input/Direction Approved By: Debbie Roberts Decision Attachment(s): Yes (list below) No - Patient Safety Dashboard and Narrative - QIP Dashboard and Narrative Key Highlights from Committee: Colleen Geiger introduced the Quality Improvement and Patient Safety dashboard and highlighted the process for the former NSM CCAC Board to receive this information. An overview of the Patient Safety dashboard was provided. Noted that in Home and Community Care, patient choice is a factor which may impact on patient safety. Within the NSM CCAC Enterprise Risk Management Framework, patient choice and patient safety are risk categories. Clarification was provided that these reported events are specific to CCAC patients who are in our care but are not necessarily events that CCAC or its contracted service providers have witnessed or were involved in. It was requested that with the future data, the number total number of visits be provided so as to provide context as to the incidence of these events. It was questioned if the number of reported events is increasing and if this is a reflection of the understanding of a patient safety culture. Discussion as to the importance of a culture of patient safety and quality that encourages the reporting of patient safety/risk events. As well, it was noted that software improvements in 15/16 have made the event management system much easier to utilize. Unexpected deaths and medication errors noted as previous areas of focus for the CCAC Board. Clarification that complaints data reflects both verbal and written complaints. An overview of the Quality Improvement Plan dashboard was provided. Discussion as to indicators that are present on both the QIP dashboard as well as MSAA. The two five day wait times within the QIP are also MSAA performance indicators. These two indicators have been on the QIP for 3 years pushing to the 95% target that is in the MSAA. Considerations for the Board: Quarterly reporting will continue on these two dashboards; however, future reconfigurations regarding the dashboard formats may occur as part of organizational realignment activities. In addition, the indicators will be refreshed taking into consideration organizational performance data/information, organizational improvement priorities, industry standards and trends and leading practices in governance reporting for patient safety and quality. Proposed Motion (if required): None required Information as submitted to the Committee of the Whole on June 12, 2017: Issue/Context: To provide updated data for Q4 2016/17 from two legacy dashboards previously provided to the Patient Services and Quality Committee of the Board and the full Board of Directors of the former Community Care Access Centre (CCAC). Background: Prior to the transfer of Home and Community Care Service Delivery to the North Simcoe Muskoka Local Health Integration Network (NSM LHIN), the former North Simcoe Muskoka Community Care Access Centre (CCAC) created a set
55 of quarterly deliverables comprised of multiple dashboards and scorecards. While some of these dashboards were related to operational monitoring, specific dashboards were prepared in support of Board level oversight. The dashboards reported for oversight purposes include the following: 1. Strategic Scorecard 2. Patient Safety Dashboard 3. Quality Improvement Plan (QIP) Dashboard 4. Multi-Sector Accountability Agreement (MSAA) Dashboard In prior years, the four oversight dashboards would normally have been generated in April for Q4 and gone through a review process involving management committees before being reported to the Patient Service and Quality Committee of the Board and the full Board of Directors. However due to LHIN transition activities and personnel changes, there was a delay in preparing the information. In order to ensure that appropriate accountability measures are reviewed, a data refresh has been prepared to provide a baseline from which to inform and plan future quarterly reporting to the new LHIN board and Executive Team. This briefing note focuses specifically on the results from the Patient Safety Dashboard and the Quality Improvement Plan (QIP Dashboard). A visual summary of the Patient Safety Dashboard is provided in Appendix 1 followed by narrative commentary on each of the indicators. Similarly the visual summary and accompanying narrative of the QIP Dashboard is provided in Appendix 2. Considerations: Quarterly reporting will continue on these two dashboards; however, future reconfigurations regarding the dashboard formats may occur as part of organizational realignment activities. For example, future reporting will be re-branded to include LHIN logos instead of CCAC logos. In addition, the indicators will be refreshed taking into consideration organizational performance data/information, organizational improvement priorities, industry standards and trends and leading practices in governance reporting for patient safety and quality. Recommendation: None Proposed Motion: Not Required Page 2 of 2
56 APPENDIX 1 Patient Safety Dashboard Page 3 of 6
57 Appendix 1a- Patient Safety Dashboard Narrative Commentary All Risk Events: The number of risk events reported in Q4 decreased significantly from 468 events reported in Q3 to only 307 events in Q4. Critical Patient Safety Events: There were 9 Critical Patient Safety events identified in Q4. Unexpected Deaths: Six (6) unexpected patient deaths occurred in Q4. Four (4) died from natural causes. One incident involved a wound care patient who passed away in hospital. Critical Patient Safety Events (Excluding Unexpected Deaths): There were three (3) other critical patient safety events reported in Q4. One incident was related to a patient in long term care setting fire to their room resulting in significant injuries. Another event was concerning the improper pain and symptom management of an End-of-Life (EOL) patient's symptoms. The third event involved the lack of communication specific to a patient s deterioration and symptom management. High Risk Falls: The number of High/Critical risk patient falls increased slightly in Q4. Similar to the previous quarter, all eight (8) falls were high risk and occurred while no CCAC or Contracted Service Provider was present. High and Critical Medication Errors: There were five (5) High risk medication errors in Q4, a small increase over Q3. One event was related to a missed dose and a second to an incorrect dose. In the third event, a patient's pain pump was not programmed properly resulting in the patient experiencing significant pain. Two events were concerning lack of communication between the service provider and the CCAC and the incorrect processing of medical orders resulting in the patient receiving the wrong concentration of pain medication. *Two events involved the same patient and were entered for this one issue as this was regarding both a Service Provider Organization (SPO) and the CCAC. Medium and High Risk Complaints: The number of Medium/High risk complaints decreased by 6 in Q4. Only one complaint was high risk and related to the quality of care a patient was receiving in the home. High Risk Privacy Events: There were no high risk privacy events reported in Q4. Missed Care: Missed Care data is reported by the service providers beginning January 31 st, The rate of missed care remains at less than one quarter of one percent (Q3 = 0.25%, Q4 = 0.23%). Page 4 of 6
58 APPENDIX 2 Quality Improvement Plan (QIP) Dashboard Page 5 of 6
59 Appendix 2a- Quality Improvement Plan (QIP) Dashboard Narrative Commentary Long Stay Home Care Falls: The percentage of long-stay home care patients reporting a fall has increased since Q3 by 3.2%. This is the highest percentage of falls that NSM has seen since Provincially the number of reported falls also reached a peak. It is important to note that this measure is a lagging indicator. Patients may only be reassessed as per standards on an annual basis. Safety: This indicator identifies the percent of home care clients who responded "Yes" to specific questions on a Client Experience Survey relating to setting up the home for safety. The Q4 results reflect the reporting from Q1-Q2 of and indicate that 91.4% of respondents responded positively about safe setup in the home. However, due to changes in the specific questions asked on the survey that occurred for , the data cannot be compared to previous years or the Q1 result (which reflects data). Unplanned Emergency Department Visits and Hospital Readmission: Hospital indicator data is very lagging and data will be updated as it becomes available. The data provided relates to results from Q , which shows little change in the rate of unplanned Emergency Department visits and a slight improvement (+0.6%) for hospital readmissions in Q compared to Q This is normal quarter over quarter variation Visiting Nursing - Five-Day Wait Time 1 : Nursing results in Q4 have increased slightly (+0.7%) since Q3 and remain consistent with the variation seen throughout the last fiscal year. NSM has remained +/- 1.5% since the beginning of 2015/16. This indicator continues to be closely monitored and shared with staff and service providers. Personal Support Five-Day Wait Time 1 : Complex Personal Support continues to improve, exceeding our 2016/17 target again in Q4, thanks to an exceptional March with over 90% of patients seen in 5 days or less. In Q1 NSM will roll out a process to ensure that we are able to explain the difference between our current performance and our stretch targets for the 2017/18 year. This indicator continues to be closely monitored and shared with staff and service providers. Overall Experience: Q4 data reflects Q1-Q2 cumulative , which shows a slight decrease from the year. This data will continue to be monitored as we move into the 17/18 fiscal year with a continued focus on improving patient experience. Dying in Preferred Place of Death: In Q4 palliative care coordinators continued to document their initial conversation with the patient/family concerning preferred place of death at both initial assessment and reassessment. An audit occurred in Q4 to ensure accurate entry of discharge dispositions in the electronic patient record (CHRIS) as well as accurate use of referral discharge codes. A resource was shared with staff to assist them in determining the most appropriate discharge disposition code to improve accuracy of documentation. Audits will continue into 2017/18 to ensure the discharge dispositions match the patients last known preferred place of death. 1 Beginning Q1 17/18, this indicator will change and now measure wait time from patient available date to first visit (currently measures from authorization to first visit) this will give a more accurate picture of wait times experienced by patients. Page 6 of 6
60 Briefing Note Title: 2017/2018 Annual Business Plan Agenda Item: 3.8 Meeting Date: June 26, 2017 Item For: Information Submitted By: Maureen Wilkinson / Erin Salkeld Input/Direction Approved By: Neil Walker Decision Attachment(s): Yes (list below) No /2018 Annual Business Plan Key Highlights from Committee: The LHIN submitted our draft Annual Business Plan (ABP) to the Ministry of Health and Long-Term Care (MOHLTC) for review in mid-april, and received feedback on May 26. This feedback has been incorporated into the final version of the ABP and was reviewed by the Committee of the Whole on June 12, Based on Committee of the Whole feedback, additional language to describe the principles of active offer in relation to French Language Services has been added. This revision has been highlighted in yellow in the document. Considerations for the Board: Once approved by the Ministry, the ABP becomes a public document and must be posted on the LHIN website in both official languages. A communication plan will be developed to support public posting of the ABP. Proposed Motion: That the NSM LHIN Board of Directors approves the North Simcoe Muskoka Local Health Integration Network s Annual Business Plan for 2017/18. Information as submitted to the Committee of the Whole on June 12, 2017: Issue/Context: The LHIN submitted our draft ABP to the Ministry of Health and Long-Term Care (MOHLTC) for review in mid-april, and received feedback on May 26. This feedback has been incorporated into the final version of the ABP submitted today for the review by the Committee of the Whole. Board approval of the Annual Business Plan will be requested at the June 26 Board of Directors meeting. Revisions to the Annual Business Plan from the draft previously submitted to the NSM LHIN Board of Directors have been highlighted in yellow. Background: The Local Health System Integration Act (LHSIA) requires LHINs to produce an annual plan for spending the funding that the network receives, which spending shall be in accordance with the appropriation from which the Minister has provided the funding to the network (LHSIA 2006, c.4, s.18(2)). The Ministry s LHIN Liaison Branch provided a guide to assist LHINs in the development of their respective 2017/18 ABPs. Following these guidelines ensured that the plan met the obligations of the Local Health System Integration Act (LHSIA), the Agencies and Appointments Directive (AAD), and other obligations. The LHIN s ABP is also a key component of the Ministry-LHIN Accountability framework and as such demonstrates consistency with the Patients First: Action Plan for Health Care. The 2017/18 ABP aligns with both the Integrated Health Service Plan (IHSP) and the priorities identified in the Minister s mandate letter. The 2017/18 ABP is the operational plan for the second year of the IHSP. The draft ABP was presented at the Committee of the Whole and Board meetings in March for information and discussion prior to
61 submission to the Ministry. The Board is required to approve the final ABP prior to submission to the Ministry. The highlevel timelines for the ABP process, as defined by the LHIN Liaison Branch, are as follows: Steps Timelines (estimated) LHINs submit 2017/2018 draft ABP April 18, 2017 Budget announcement April 27, 2017 Ministry feedback to LHIN on draft ABP May 26, 2017 Budget announcement updates to draft ABP TBD ABP submitted to the LHIN CoW June 12, 2017 Board approval of ABP June 26, 2017 ABP submitted to MOHLTC June 28, 2017 Obtain Minister s Approval Minister s Approval Letter to LHINs LHINs post Minister Approved ABP Within 120 days of the date a budget motion (April 27, 2017) is approved by the Ontario Legislature for the fiscal year TBC (dependent on timing of Minister s signing of approval) Within 30 days of the Minister approving the ABP. Considerations: Once approved by the Ministry, the ABP becomes a public document and must be posted on the LHIN website in both official languages. A communication plan will be developed to support public posting of the ABP Proposed Motion: That the NSM LHIN Board of Directors approves the North Simcoe Muskoka Local Health Integration Network s Annual Business Plan for 2017/18. Page 2 of 2



62 2017/2018 Annual Business Plan June 16, 2017
63 Table of Contents Introduction 3 Setting Context 4 Mandate and Strategic Directions... 4 Overview of Current and Forthcoming Programs and Activities... 5 Environmental Scan... 8 Successes French Language Services (FLS) 13 Indigenous and Métis Peoples Improve Access to Appropriate Care 17 Goal 1.1: Enhance access to timely and appropriate primary care Goal 1.2: Improve access to high-quality acute and specialty care Goal 1.3: Promote health equity and enable access to appropriate and culturally safe care Build Capacity and Enhance Coordination 30 Goal 2.1: Enable consistent and coordinated home and community care Goal 2.2: Establish infrastructure to improve care for seniors and older adults Goal 2.3: Strengthen partnerships at the community and sub-regional levels Goal 2.4: Improve patient flow, transitions of care, and coordination between providers Drive System Sustainability 45 Goal 3.1: Advance quality, best practice, and innovation across the local health care system Goal 3.2: Ensure accountability for current investments and evaluate opportunities to improve capacity Conclusion 52
64 Table of Appendices Appendix A: Integrated Communications Strategy A-1 Appendix B: Community Engagement Strategy B-1 Appendix C: LHIN Operations Spending Plan C-1 Appendix D: LHIN Staffing Plan (Full-Time Equivalents) D-1 2
65 Introduction The North Simcoe Muskoka LHIN s Annual Business Plan (ABP) for 2017/18 serves as the operational plan for the LHIN to deliver on the second year of its Integrated Health Service Plan (IHSP). The 2017/18 ABP also reflects the LHIN s enhanced role in the health care system following the passage of the Patients First Act, 2016 (the Act). 1 The NSM LHIN s 2017/18 ABP builds upon achievements to date, aligned with the three strategic priorities outlined in the LHIN s IHSP: Improve Access to Appropriate Care Build Capacity and Enhance Coordination Drive System Sustainability These three strategic priorities were developed with the Board of Directors in alignment with the Ministry of Health and Long-Term Care s Patients First: Action Plan for Health Care 2. To reflect the LHINs expanded mandate, the NSM LHIN revised its IHSP goals to bring together existing areas of focus with new priority areas from the Patients First Act. For each of these goals, the Annual Business Plan identifies specific actions and associated indicators of success that will be measured to demonstrate accountability for results. Development and monitoring of the Annual Business Plan are key in ensuring transparency for stakeholders and LHIN accountability for deliverables. Over the coming months, the NSM LHIN and its Board of Directors will work with local stakeholders to refresh its existing Mission, Vision and Values to better reflect the role of the renewed LHIN. This work will take place through an iterative process with input from a broad group of stakeholders including health service providers, the public, the LHIN s Patient Caregiver Family Advisory Panel, local municipalities, Public Health colleagues, Indigenous and Métis partners, and representatives of the Francophone community. We value the input of these partners as we work to develop a common vision for the transformation of the LHIN that is reflective of both local realities and provincial direction. The work required to operationalize changes supported by the new legislation will take place over the next several planning cycles. The NSM LHIN and its Board of Directors will continue to work collaboratively with local communities, health service providers and other system partners to leverage their collective expertise as we work towards delivering on our strategic priorities and our collective vision for the system. These partnerships will be key as we move forward to evolve the local health care system towards the vision of Patients First. 1 Patients First Act, Office of the Minister, Ministry of Health and Long-Term Care. Patients first: action plan for health care. Ministry of Health and Long-Term Care;
66 Setting Context Mandate and Strategic Directions It is the mandate of the North Simcoe Muskoka LHIN to plan, integrate and fund local health care. We also deliver and coordinate home and community care. In consultation with patients, health service providers and other stakeholders, the NSM LHIN considered the following four strategic goals of the Patients First: Action Plan for Health Care 3 in the local context: ACCESS CONNECT INFORM PROTECT Improve access provide faster access to the right care Connect services deliver better coordinated and integrated care in the community, closer to home Support people and patients provide the education, information and transparency they need to make the right decisions about their health Protect the public health care system make decisions based on value and quality, to sustain the system for generations to come The result of the analysis of local needs in the context of provincial direction led to the identification of three strategic priorities for the North Simcoe Muskoka LHIN s Integrated Health Service Plan: 1.0 Improve Access to Appropriate Care 2.0 Build Capacity and Enhance Coordination 3.0 Drive System Sustainability The priorities of the NSM LHIN and the goals that cascade from them reflect both the strategic goals of Patients First and the priorities of the Ministry of Health and Long-Term Care. These priority areas include home and community care, relationships with primary care and public health, community-based planning and integration in geographically defined sub-regions, expanded digital health, and capacity building. Equity, quality, community engagement, collaboration and patient-centred care continue to be a lens for work now and in the future. 3 Office of the Minister, Ministry of Health and Long-Term Care. Patients first: action plan for health care. Ministry of Health and Long-Term Care;
67 Overview of Current and Forthcoming Programs and Activities Across NSM s five communities, the NSM LHIN will allocate over $850 million to 60 LHIN-funded health service provider organizations that deliver services across the continuum of care. Several of these organizations have multiple homes, programs or branches in North Simcoe Muskoka, which brings the total to 70. Many of the LHIN-funded health service provider organizations offer different services and hold more than one type of agreement with the LHIN. Table 1 lists the LHIN-funded organizations in NSM and identifies the sectors among which their services fall. Table 1: LHIN-Funded Service Providers in North Simcoe Muskoka HEALTH SERVICE PROVIDERS 5 Hospital Sector Long Term Care Community Health Centre Community Support Services Mental Health & Addictions Collingwood General and Marine Hospital HOSP CSS MH&A Waypoint Centre for Mental Health Care HOSP CSS MH&A Orillia Soldiers' Memorial Hospital HOSP MH&A Royal Victoria Regional Health Centre HOSP MH&A Beechwood Private Hospital HOSP Georgian Bay General Hospital HOSP Muskoka Algonquin Healthcare HOSP Corporation of the County of Simcoe (including Georgian, Sunset and Trillium Manors) LTC CSS Grove Park Home for Senior Citizens LTC CSS IOOF Senior Homes Inc. LTC CSS Bay Haven Senior Care Community LTC Coleman Care Centre (Schlegel Villages Inc.) LTC Collingwood Nursing Home Limited LTC District Municipality of Muskoka (The Pines Long-Term Care Home) LTC Hillcrest Village Inc. LTC Huntsville District Nursing Home Inc. (Fairvern Nursing Home) LTC Leacock Care Centre (Orillia Long-Term Care Centre Inc.) LTC Mill Creek Care Centre LTC Muskoka Landing (Huntsville Long-Term Care Centre Inc.) LTC Ontario Mission of the Deaf Incorporated, The LTC Revera Long-Term Care (including Oak Terrace and Sara Vista Long-Term Care Centres) LTC Roberta Place (Barrie Long-Term Care Centre Inc.) LTC Sienna Senior Living (including Creedan Valley, Muskoka Shores and Owen Hill Care Communities) LTC Spencer House Inc. LTC Stayner Care Centre (Stayner Care Centre Inc.) LTC Victoria Village Inc. LTC Villa Care Centre (Jarlette Limited) LTC Woods Park Care Centre Inc. LTC Wendat Community Programs CSS MH&A Alzheimer Society of Muskoka CSS Alzheimer Society of Simcoe County CSS Barrie Area Native Advisory Circle CSS Beausoleil First Nation CSS Brain Injury Services of Simcoe County Inc. CSS Breaking Down Barriers - An independent Living Centre Inc CSS Canadian National Institute for the Blind, The - Simcoe Branch CSS Canadian Red Cross Society (Muskoka, Northumberland, Simcoe County Branches) CSS Chippewas of Rama First Nation CSS Deaf Access Simcoe-Muskoka Inc. CSS CCAC
68 HEALTH SERVICE PROVIDERS Gravenhurst Senior Citizens Club Inc Helping Hands, Orillia Hospice Georgian Triangle Hospice Huronia Hospice Simcoe Huntsville Meals-on-Wheels Inc. Independent Living Services of Simcoe County and Area Moose Deer Point First Nation Muskoka Seniors Home Assistance Hospital Sector Long Term Care Community Health Centre Community Support Services CSS CSS CSS CSS CSS CSS CSS CSS CSS Mental Health & Addictions CCAC North Simcoe Muskoka Hospice Palliative Care Network CSS Victorian Order of Nurses for Canada - Ontario Branch, Simcoe County Wahta Mohawks Barrie Community Health Centre Centre de santé communitaire CHIGAMIK Community Health Centre Inc. South Georgian Bay Community Health Centres, The Canadian Mental Health Association, Muskoka-Parry Sound Branch Canadian Mental Health Association, Simcoe County Branch Enaahtig Healing Lodge and Learning Centre Huronia Transition Homes Mental Health Consumer Survivor Project of Simcoe County Seven South Street Treatment Centre CHC CHC CHC CSS CSS MH&A MH&A MH&A MH&A MH&A MH&A In 2015/16, the NSM LHIN provided $550 million in base funding to support the region s five community hospitals, one specialty mental health facility, and one private hospital. In total, the funding supported delivery of approximately 377,000 days of patient care, 263,000 emergency department visits, 55,000 surgeries and 317,000 outpatient clinical visits. The LHIN also has 26 long-term care homes with 2,956 long stay, 19 priority access/veterans, 18 interim, 16 short stay/respite, and 56 convalescent care beds. The region s average occupancy rates are approximately 98% for long stay residents and 80% for convalescent care beds. As the LHIN mandate has expanded to include both home and community care management and service delivery and more formal relationships with public health and primary care, the NSM LHIN will be further enabled to support system transformation in alignment with provincial priorities. Funded health service providers in the community sector include community support service (CSS) providers, community mental health and addiction (CMHA) service providers and community health centres (CHCs). In fiscal 2015/16, NSM s community sector health service providers utilized $170 million of LHIN funding to provide 2.6 million units of care (visits, hours, attendance days, meals, etc.) to a combined 29,000 CSS clients, 11,500 CMHA consumers, 5,000 CHC patients and 25,500 Community Care Access Centre (CCAC) patients. North Simcoe Muskoka LHIN includes organizations that are either fully or partially designated to provide health care services in French. In the North Simcoe sub-region, Beechwood Private Hospital is a designated agency while the Chigamik Community Health Centre has applied for partial designation, and Georgian Bay General Hospital is awaiting final approval for partial designation. Agencies identified to deliver health care in French include the Canadian Mental Health Association Simcoe Branch, Georgian Manor Long-Term Care Home, Orillia Soldiers Memorial Hospital, Royal Victoria Regional Health Centre, Waypoint Centre for Mental Health Care, and Wendat Community Programs. 6

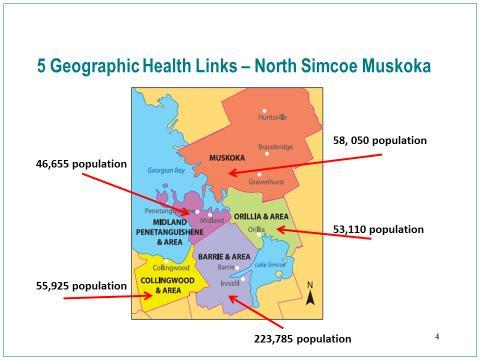
69 The LHIN also funds a variety of services through six organizations specifically serving the Indigenous population. All four of the First Nations communities in the region have LHIN-funded services. These communities include Beausoleil First Nation, Chippewas of Rama First Nation, Wahta Mohawks First Nation, and Moose Deer Point First Nation. The Barrie Area Native Advisory Circle and Enaahtig Healing Lodge and Learning Centre also deliver LHIN-funded programs in the region. North Simcoe Muskoka LHIN includes five sub-regions. These sub-regions have been the foundation of community planning for many years in the region. The Ministry of Health and Long-Term care has approved NSM sub-region boundaries which include only slight realignments to better reflect patient access patterns. These sub-regions are as follows: Barrie and Area Couchiching (previously referred to as Orillia and Area) Muskoka North Simcoe (previously referred to as Midland Penetanguishene and Area) South Georgian Bay (previously referred to as Collingwood, Wasaga Beach and Area) Figure 1: Sub-regions of North Simcoe Muskoka LHIN There are five approved Health Links in North Simcoe Muskoka, which align to the five geographic sub-regions. These Health Links have been in place for more than two years. North Simcoe Muskoka LHIN was one of the first regions in the province to have an approved Health Link within each of its geographic sub-regions. The Health Links have been extremely successful in creating partnerships across both funded and non-funded organizations and each has a range of service providers committed to the partnership. These partnerships continue to be the basis of subregional planning going forward. 7
70 Environmental Scan There are a number of local issues that impact the planning and delivery of health services in North Simcoe Muskoka. Although some of these are trends that are reflected in other regions, others are specific to the unique characteristics of the NSM LHIN population or to the unique geography of the region. These local considerations are essential in ensuring that system planning is responsive to the needs of NSM s residents and communities. Access to Appropriate Levels of Care Primary care access is key in ensuring that patients receive care in the most appropriate setting for their needs. Local data on primary care attachment includes both a patient self-report measure and a measure of continuity in primary care utilization. According to data from the Canadian Community Health Survey, approximately 96.5% of NSM adults report having access to a regular medical doctor. 4 By contrast, an analysis of utilization data indicates that 87.4% of NSM residents are either attached to a primary care physician or Nurse Practitioner-Led Clinic (NPLC), or are regularly accessing the same family physician. 5 Regardless of how it is measured, this equates to a large majority of NSM residents being attached to a primary care provider. Despite the high primary care attachment rate, utilization of NSM emergency departments (EDs) for less urgent / non urgent conditions and for conditions better treated in a primary care setting exceed those of the province. Based on 2016/17 data, the rate of ED visits for CTAS IV and V conditions best managed elsewhere was 6.95 per 1000 population. 6 Data also shows that local patients frequently remain in hospital while awaiting placement in a more appropriate setting, which is reflected in the alternate level of care (ALC) rate. The ALC rate represents the proportion of inpatient days in acute and/or post-acute care settings that are spent as ALC. In North Simcoe Muskoka, the proportion of patients designated ALC who are occupying acute care beds (20.6% in Q2 16/17) is consistently among the highest in the province. 7 The ALC rate for post-acute services including rehab, mental health and complex continuing care is significantly lower (6.4% in the same data period), resulting in an all-service ALC rate of 15.0%. Aging Population North Simcoe Muskoka currently ranks in the top three LHINs in terms of its relative proportion of seniors aged 65 and older. In 2015, seniors represented 18.8% of the NSM population. As is the case in other regions across the province, forecasted growth for seniors greatly exceeds that of other age groups. By 2020, seniors are expected to comprise 21.3% of the NSM population and by 2025 this will increase to 24.3%. 8 Data from the Canadian Institute for Health Information shows that seniors are high users of the health care system, including the hospital, continuing care, home care, and primary care sectors. 9 Provincial data shows a clear association between older age and the rates of both scheduled and unscheduled emergency department (ED) visits and ED visits for potentially preventable conditions. 10 Between 2010 and 2012, seniors accounted for approximately 22.4% of all NSM emergency department visits. 11 Seniors also account for a significant proportion of patients designated as ALC; based on 2015/16 4 Health Analytics Branch. Environmental scan integrated health service plans Ministry of Health and Long-Term Care; Internal analysis up to March 31, 2016 based on Corporate Provider Database (CPDB), Claim History Database (CHDB), Registered Persons Database (RPDB), Client Agency Program Enrolment (CAPE). Accessed June North Simcoe Muskoka LHIN. Ministry-LHIN quarterly stocktake report, May NSM LHIN; Access to Care. North Simcoe Muskoka LHIN monthly alternate level of care performance summary, December Cancer Care Ontario; Health Analytics Branch. Environmental scan integrated health service plans Ministry of Health and Long-Term Care; Canadian Institute for Health Information. Health care in Canada 2011 A focus on seniors and aging. CIHI; Bronskill SE, Carter MW, Costa AP, Esensoy AV, Gill SS, Gruneir A et al. Aging in Ontario: an ICES chartbook of health service use by older adults. Institute for Clinical Evaluative Sciences; North Simcoe Muskoka LHIN Senior s Strategy Task Group. Strategy for a specialized geriatric services program in North Simcoe Muskoka. North Simcoe Muskoka LHIN;
71 data, seniors aged 65 and older accounted for 85% of patients who were in acute care and designated ALC long waiters (ALC lengths of stay greater than 30 days). 12 Complexity and Chronic Disease Prevalence Data indicates that the prevalence of chronic disease in NSM is the second highest in the province and that the rate of multiple chronic conditions is increasing over time. Specifically, in 2013, 43.5% of North Simcoe Muskoka residents reported having a chronic condition and 18.3% reported having multiple chronic conditions. High blood pressure is the most prevalent chronic condition in the region, followed by arthritis and asthma. Related to this are high rates of health system utilization and increased rates of mortality. Relative to the province, residents of this region had higher rates of both hospitalization and mortality from cancer, Chronic Obstructive Pulmonary Disease (COPD), diabetes, ischemic heart disease, and stroke. Further, in this region, nine chronic conditions accounted for more than 60% of all deaths and nearly a quarter of acute hospitalizations in Based on the Ministry of Health and Long-Term Care s definition, a patient is identified as being complex and chronic if that patient has three or more comorbid chronic conditions. Based on internal analysis of 2013/14 data, the largest proportion of chronic and complex patients in NSM are those between 75 and 84 years of age. However, the prevalence of chronic and complex conditions begins to increase after the age of 55. Among chronic and complex patients in NSM, the top five most prevalent conditions are hypertension, diabetes, ischemic heart disease, arthritis disorders and pneumonia. Mental health and addiction conditions are included in the Ministry s definition of chronic disease. Utilization rates for designated mental health beds among NSM residents are among the highest in the province. Specifically, in 2013/14, the rates of active cases, admissions and discharges per 100,000 population among NSM residents were the second-highest in the province. This is consistent with the overall trend of higher utilization rates in LHINs with tertiary psychiatric beds, and may reflect the drift of individuals with severe persistent mental illness to regions with specialized resources. Among active cases in NSM LHIN hospitals, short stay, mood disorders, and schizophrenia / psychotic disorders accounted for the largest proportions of patients. Emergency department utilization for mental health and substance abuse conditions in NSM is, however, well below the provincial average, which may reflect recent efforts to implement community-based approaches to care in the region. 14 The exception to this is emergency utilization for children and youth with mental health or addiction conditions. In 2014/15, the NSM LHIN had the third-highest ED visit rate in the province for children and youth with a primary diagnosis of mental health or addiction, which may reflect the lack of inpatient mental health services for children and youth at that time. 15 This gap has been addressed through the Ministry s recent investment in a regional Child and Youth Mental Health program for NSM. Rural Geography and Seasonal Variability Nearly one-third (32%) of NSM residents live in a rural area, making the region home to the third largest proportion of rural residents in the province. This is notable given the significant urban-rural gap on a number of health-related measures, including both risk factors like obesity and smoking, and outcomes, such as mortality from injury and certain chronic diseases. 16 NSM also experiences significant seasonal variation in population and demand for related health services including a significant impact on NSM emergency departments. The data showing NSM s high proportion of seniors is in part due to its 12 Access to Care. North Simcoe Muskoka LHIN monthly alternate level of care performance summary, December Cancer Care Ontario; Ministry of Health and Long-Term Care, Health Analytics Branch. Environmental scan Integrated Health Service Plans Ministry of Health and Long-Term Care; North Simcoe Muskoka LHIN. Ministry-LHIN quarterly stocktake report, February NSM LHIN; Royal Victoria Regional Health Centre (RVH) analysis of National Ambulatory Care Reporting System (NACRS) and 2013 Ministry of Finance data. Accessed July DesMeules M, Pong R, Lagacé C, Heng D, Manuel D, Pitblado R et al. How healthy are rural Canadians? An assessment of their health status and health determinants. Canadian Institute for Health Information;
72 popularity as a retirement destination. Given the increased health needs of the senior s population, this impacts utilization of health services across sectors, including acute care, home and community care, and long-term care. Palliative and End-of-Life Care In calendar year 2012, there were 3,702 deaths among NSM LHIN residents. Of these, 51.2% occurred in hospital, 20.6% in other health care facilities (e.g., long-term care homes), 9.5 % in other non-health related facilities (e.g., hospices and group homes), and 18.7% in the patient s home. Over the five-year time period including 2008 to 2012, the number of deaths in hospital decreased while the number of deaths at home or in other non-health related facilities increased. In particular, in 2008 there were 62 deaths in other non-health facilities but five years later in 2012, there were 350 deaths in other nonhealth care facilities. In the same period, deaths at home increased from 570 to Palliative care patients are more likely than other types of patients to be designated as ALC. Specifically, 14.7% of palliative care patients in the province had at least one ALC day in 2010/11 compared to 5.4% in other patients. In North Simcoe Muskoka, 21.5% of palliative patients had at least one ALC day versus 6.6% in other patients. This is of particular importance given the high rate of ALC utilization in the region. 18 Successes ALC Review The NSM LHIN initiated a region-wide ALC review in 2015/16, including stakeholder interviews, a review of data, a retrospective chart audit, and a review of both ALC long-stay outliers and patients with behavioural needs. The review resulted in 24 recommendations addressing discharge planning, communication, education, advocacy, standardization, resources, and home care. NSM s ALC Steering Committee was kicked off in the Fall of 2016 and is intended to provide system oversight on the implementation of the recommendations as well as lead the change management process. An ALC Standardization Task Force was also established to support implementation of recommendations aligned with the development and adoption of regional standards. Two remaining proposed working groups, Information Technology and Legal Advisory, will be addressed in future years. Since project initiation, the LHIN ALC rate has decreased from 16.20% in the third quarter of 2015/16 to 14.60% in the third quarter of 2016/17. Further improvements are anticipated as the LHIN moves forward in implementing the recommendations of the review. Transitional Bed Pilot Program In 2015/16, the NSM LHIN funded a three-year regional Transitional Bed Pilot Program, which is currently offered through one of the region s CSS providers. The program supports seniors and adults requiring community-based assisted living and additional services such as personal support and care coordination. Through the program, individuals have access to transitional bed support 24 hours per day, for up to six months. Clients also have access to both CCAC nursing and therapy support and the potential for symptom management for palliative care. The waitlist ranking criteria for the program prioritizes patients who are in hospital with an ALC designation, therefore supporting system flow. Since opening approximately six months ago, the six-bed program has had an average occupancy rate of 92% and an average length of stay of 36 days. As a regional program, the transitional beds have had referrals from 17 Internal analysis based on 2012 Vital Statistics data. Accessed via IntelliHealth, December Ministry of Health and Long-Term Care. Analysis based on 2010/11 data extracted from the DAD. MOHLTC;
73 each of the five acute care facilities in NSM. Findings from the LHIN s ALC review indicate that the program has already had an impact on ALC days. In the fourth quarter of 2016/17, the program was provided funding for an additional three beds to bring this three-year pilot program to a total of nine beds. An evaluation framework is currently being finalized and will be used to assess the impact of the program going forward. Child and Youth Mental Health Program In November 2016, the Ministry of Health and Long-Term Care announced that it would invest $3.2 million in annual operating funds for a regional Child and Youth Mental Health program in NSM. The investment will enable Royal Victoria Regional Health Centre to establish a comprehensive regional program, including an eight-bed inpatient unit and a day hospital program that will have capacity for approximately 3,000 outpatient visits annually. This program addresses a significant gap in that North Simcoe Muskoka was the only LHIN in the province without dedicated inpatient beds for children and youth with acute mental health issues. Services provided through the new program will include prevention and health promotion, assessment, and specialized treatment based on individual needs ranging from moderate to severe and complex conditions. The program will increase services available in the region, help to reduce wait times for children and youth suffering from mental health challenges and ensure that high quality mental health treatment can be accessed in one location. Muskoka and Area Health System Transformation Council In June 2016, the NSM LHIN Board of Directors approved the formation of the Muskoka and Area Health System Transformation (MAHST) Council as the next step in developing an integrated health care model for Muskoka and the surrounding area. The LHIN appointed a local Chair for the Council and has secured Dr. Adalsteinn Brown to serve as Co-Chair and Special Advisor to the Council. Executive and General Councils have been formed for MAHST and these are supported by five working groups dedicated to programs and services, funding and governance, information management and technology, wayfinding, and stakeholder relations. The Council has established its project scope for the near and longer term and will report back to the LHIN in 2017/18 with a recommended framework for the design of a transformed local health system. The comprehensive model will be evidence-based, aligned with the LHIN s strategic plan, and will serve the best interests of the people of Muskoka and area. The framework will then be implemented in phases as part of a ten-year plan for the Muskoka sub-region. Health Based Allocation Model Working Group As one component of Health System Funding Reform (HSFR), a portion of hospital funding is allocated using the Health Based Allocation Model (HBAM), which is an evidence-based formula that uses demographic and clinical data to inform funding. In 2016/17, the Ministry provided funding of $139 million for hospitals under HBAM to support the delivery of patient care. The HBAM formulary is complex, with one of the required inputs being an annual data submission from each hospital provider. A local working group was established in 2016 to review the financial data submissions of NSM hospitals to improve the quality of financial reporting, share learnings among providers and to identify opportunities for increased funding. Recommendations to improve alignment of financial costs and patient activity with the HBAM formula were identified and are expected to increase the NSM LHIN share of provincial HBAM funding in 2018/19 and future years. The recommendations were endorsed by the HSFR Local Partnership committee with implementation completed by the end of fiscal year 2016/17 as appropriate to each hospital. 11
74 Quality Based Procedures Optimization Under Health System Funding Reform (HSFR), the Ministry currently provides funding of $46 million for NSM hospitals to provide Quality Based Procedures (QBPs), such as hip and knee replacements, cataract surgery, and stroke care. Recommendations to improve utilization of QBPs were identified by hospital partners and later endorsed by the HSFR Local Partnership committee. The recommendations supported a reallocation approach for one-time and permanent QBP volumes to optimize services available to patients in the LHIN, in accordance with Ministry volume management principles. The recommendations have been approved by the Ministry and appropriate funding reallocations of $700,000 within the LHIN were completed. This work demonstrated strong collaboration and system-level thinking among NSM s individual hospital providers to ensure full utilization of funding within the region. Telemedicine Telemedicine is an ongoing area of focus within North Simcoe Muskoka, with quarterly performance monitoring taking place using customized NSM reporting templates and clear accountability agreements. In August 2016, funding was reallocated from a program that was closing and divided between two programs which have seen a large demand for care via telemedicine. In 2015/16, this funding served a total of 183 patients using a 0.7 full time equivalent (FTE) Registered Nurse. Using the same funding resources, the new program is expected to deliver 600 clinical events for patients, which represents an increase of 417 patients served. In the third quarter, 2016/17 community investment base funding was allocated towards 2.0 additional FTE Registered Nursing resources to add to the existing 10 FTEs received from the Ministry as part of the 9,000 Nurses Initiative. The additional resources were provided to fill the gap in programs which were operating with only partial FTEs and challenged to meet patient needs as a result. It is expected that in 2017/18, these additional resources will allow 2,150 more patients to be served closer to home via telemedicine. Between the reallocation of funds and the addition of new community funds, a total of 2,567 patients are targeted for service in 2017/18 beyond current service levels. ereferral to CCAC During 2016/17, the NSM LHIN worked closely with its five acute care hospitals, the NSM CCAC and the Ontario Association of Community Care Access Centres (OACCAC) to build an electronic solution for referral from hospital to home care services and from hospital to long-term care placement. In collaboration with the vendors of the hospitals Health Information Systems, Cerner and Meditech, four electronic interfaces were built to automate the referral process. In the past, paper referrals were often sent incomplete, which resulted in either rework to complete the information or inadequate information for placement, allocation of services, or clinical decision making. The new system, implemented at the end of 2016/17, will improve patient quality of care and clinical outcomes as well as ensuring efficient access to patient data through the use of mandatory fields. Through the electronic system, no incomplete referral will be sent and the risk of a misplaced referral is avoided. Based on the referrals sent in 2014/15, it is estimated that 12,000 referrals which have previously been paper-based will be sent and managed through the new ereferral process. Work will continue in 2017/18 to ensure hospital referrals to home care services and LTC are embedded into clinical practice and adoption of the new system is effective. 12
75 French Language Services (FLS) Approximately half a million Francophones reside in Ontario. This represents Canada's largest Frenchspeaking community outside of the province of Quebec. The provision of services in French is provincially directed by the French Language Services Act (FLSA). 19 The FLSA guarantees an individual's right to receive services in French from Government of Ontario ministries and agencies in 26 designated areas. North Simcoe Muskoka is home to three of the 26 provincially designated areas. LHINs are responsible for ensuring that Ontario s Francophone population has equitable access to a full range of health services in French. The LHIN has overall responsibility for identifying health service providers, or specific services within a given HSP, for potential designation under the French Language Services Act. In this context, designation refers to legal recognition by the government of Ontario of an agency s ability to offer French language services in accordance with criteria established by the Office of Francophone Affairs. There are currently eight health service providers in North Simcoe Muskoka that are identified and one that is designated to provide health care services in French. The NSM LHIN and the local French Language Health Planning Entity actively support health service providers with the implementation of French language services required to achieve designation. Improved access to French language services requires concerted efforts by all major stakeholder groups, including LHINs, health service providers, health care professionals, political decision-makers, training institutions and communities. In 2015, the Ministry of Health and Long-Term Care renewed the mandate with the Francophone planning entity for North Simcoe Muskoka. The local French Language Health Planning Entity, Entité 4, works collaboratively with the LHIN to ensure a Francophone perspective is included in the planning and integration of health services in the region. A joint action plan among the North Simcoe Muskoka, Central, and Central East LHINs and Entité 4 has been developed with the objective to improve access to the right French language care, at the right place and at the right time within the following priority sectors: care for seniors, mental health and addiction services, primary care, and patients with chronic conditions. Entité 4 is represented at NSM LHIN planning tables aligned with the priority sectors identified above and at NSM s Leadership Council, which helps in ensuring that issues relevant to our Francophone population are reflected in the LHIN s planning. With the integration of home and community care, the NSM LHIN will continue to strengthen the delivery of French language services based on the principle of an active offer. An active offer of service in French is extended by the health service provider so that the onus is not on the patient or client to make the request. 20 According to the Joint Position Statement on the Active Offer of French Language Health Services in Ontario, an active offer respects the principle of equity; aims for service quality comparable to that provided in English; is linguistically and culturally appropriate to the needs and priorities of Francophones; is inherent in the quality of the services provided to people (patients, residents, clients) and an important contributing factor to their safety. 21 The NSM LHIN continues to provide French language services in compliance with the FLSA, including local FLS obligations in service accountability agreements of identified and designated providers. The LHIN 19 Ontario, French Language Services Act, R.S.O. 1990, c. F Office of Francophone Affairs. Practical guide for the active offer of French-language services in the Ontario Government. Office of Francophone Affairs; French Language Health Planning Entities and French Language Health Networks of Ontario. Joint position statement on the active offer of French language health services in Ontario. French Language Health Planning Entities and French Language Health Networks of Ontario;
76 requires that all health service providers (including contracted service providers) submit an annual FLS report, which is based on the criteria developed by the Office of Francophone Affairs. The LHIN uses this information to assess HSP capacity to offer and plan for the provision of French language services based on community need. The NSM LHIN and Entité 4 have maintained a strong working relationship and have pursued a number of collaborative initiatives aligned with the joint action plan. In 2015/16 and 2016/17, the LHIN and the Entité partnered with NSM s Mental Health and Addictions Coordinating Council to provide the Mental Health Commission of Canada s Mental Health First Aid program in French to health service providers and the general public. The aim of the program is to improve mental health literacy and provide the requisite skills and knowledge to help participants better manage potential or developing mental health problems in themselves or others. The LHIN and the Entité also partnered to establish a French Language Services Patient Navigator position at Centre de Santé Communautaire CHIGAMIK CHC in November 2016 based on an earlier pilot program. The FLS Patient Navigator provides health system navigation and case management support to Francophone clients within the region. As noted above, the LHIN and Entité 4 also work collaboratively to support health service providers in meeting the criteria required to achieve designation under the FLSA. The LHIN and the Entité are currently working to formalize a new support process for identified HSPs to help them move forward in implementing French language services. The Entité also continues to support Francophone community engagement in collaboration with the NSM LHIN, including co-chairing the NSM French Language Services Community of Practice (FLS COP). The NSM FLS COP includes all identified and designated health service providers in the region and serves as a forum for sharing best practices and resources to support French language service provision. The LHIN and the Entité also participate in the Community Partners with Schools (COMPASS) meetings, which are attended by elementary and secondary school representatives and community mental health service providers. These partnerships support the development of French language mental health and addiction services for Francophone youth. In addition to these ongoing partnerships, the LHIN and Entité 4 collaborate throughout the year to support Francophone community engagements related to new LHIN initiatives, such as regional palliative care and the implementation of the new personal support services guidelines. The continued partnership between the LHIN and Entité 4 demonstrates a joint commitment to improving access to French language health services for the local Francophone and French-speaking populations. 14
77 Indigenous and Métis Peoples There are four First Nations communities in North Simcoe Muskoka, including Beausoleil First Nation, Chippewas of Rama First Nation, Wahta Mohawks First Nation, and Moose Deer Point First Nation. There are also many individuals living outside of these communities who self-identify as Indigenous or Métis. The LHIN funds a variety of services through six organizations whose main focus is the provision of services for individuals who identify as Indigenous. Consultation with NSM s local Indigenous and Métis communities occurs through a number of engagements and through the region s Aboriginal Health Circle (AHC). NSM s Aboriginal Health Circle aims to work in partnership with the LHIN to improve the health status of Aboriginal people in the region. The Aboriginal Health Circle includes representation from 12 local communities and organizations that work collaboratively to address Aboriginal community health issues in system coordination and integration. The NSM LHIN provides direct and indirect support to the Aboriginal Health Circle in the implementation of its objectives and deliverables, as articulated in the AHC s workplan. In 2016/17, the LHIN worked closely with the Aboriginal Health Circle to expand Indigenous and Métis representation at LHIN planning tables, including Specialized Geriatrics Services, Palliative Care, Mental Health and Addictions, and Home and Community Care. The AHC is also represented at NSM s Leadership Council, which in combination with representation at the planning tables, helps to ensure that Indigenous and Métis perspectives are reflected in the LHIN s planning. In partnership with the Aboriginal Health Circle, NSM LHIN leadership, the LHIN Aboriginal Lead, and NSM s First Nation, Métis, Inuit (FNMI) Health System Coordinator meet annually with the Chiefs and Councils of each of the First Nations communities in the region. These meetings provide the LHIN with a better understanding of local needs, priorities and opportunities within each of the communities, which in turn supports annual and strategic planning. The visits also help to strengthen existing relationships between the LHIN and the First Nations Chiefs and Councils. Through community engagement with local Indigenous and Métis communities, the need for improved system navigation was identified. In 2016/17, the LHIN allocated base funding to the Beausoleil First Nation to fund a navigator to support, advocate, facilitate and coordinate access for Indigenous patients and their families. Also based on community input, the LHIN provided base funding to the Moose Deer Point First Nation to support a transportation program and expand its existing meals on wheels and adult day programs. The LHIN has also committed to support Indigenous Cultural Safety Training for all local planning tables, LHIN staff, and Board members to further enable respectful and positive partnerships. The NSM LHIN and the Aboriginal Health Circle jointly hosted an Annual Forum in March 2017, supporting provincial direction regarding collaboration with Indigenous and Métis partners. The forum included invited experts from the Southcentral Foundation in Alaska to share their knowledge and experience with the Nuka model of care. Nuka is an integrated system that provides medical, dental, behavioural, traditional and health care support services to more than 65,000 Alaska Native and American Indian people in its catchment. The experience of the Southcentral Foundation in transforming their local health care system to a more holistic, patient-centred model was the theme running through this joint event. The NSM LHIN s Aboriginal Lead also participates in the Provincial Aboriginal LHIN Network (PALN), which is a shared community of practice for Aboriginal LHIN Leads from the 14 LHINs. The network serves to facilitate knowledge transfer, share promising practices, engage and develop relationships with provincial 15
78 and federal stakeholders, and increase awareness surrounding Indigenous and Métis health priorities. Since 2011, the PALN and the LHIN CEOs have met on an annual basis to share information and best practices and further their learning about Ontario s Indigenous and Métis communities. The annual meetings have provided a forum for discussion on system-level issues and opportunities related to advancing the health status of Ontario s Indigenous and Métis residents and have served as an important input to the NSM LHIN s planning process. Improved access to culturally safe care for the region s Indigenous and Métis residents remains a key goal for the NSM LHIN in 2017/18. Meaningful engagement and continued partnership with the Aboriginal Health Circle and the region s Indigenous and Métis communities will be crucial in achieving this and in advancing the LHIN s post-transition role. The LHIN will continue to leverage these partnerships and will look to the province for direction as it continues to engage in the parallel process with Indigenous and Métis partners. 16

79 Integrated Health Services Plan Strategic Priority: 1.0 Improve Access to Appropriate Care Description of the Priority The priority to improve access to appropriate care reflects the importance of ensuring that residents have timely access to the best possible care, in the most appropriate setting, in order to optimize health outcomes. Local data indicates that NSM residents are not always accessing care that is appropriate for their needs. Current Status Primary Care Primary care attachment data includes a patient self-report measure, which cites approximately 96.5% of NSM adults as having access to a regular medical doctor. 22 Data on continuity of primary care utilization indicates that 87.4% of NSM residents are attached to a primary care physician or Nurse Practitioner-Led Clinic, or are regularly accessing the same family physician. 23 Despite high overall patient attachment, timely access to primary care remains a challenge in NSM. Only 29.4% of adults in NSM report being able to see their doctor or nurse practitioner either the same day or next day when ill, and 61.1% of NSM patients report having difficulty accessing after-hours care without visiting an emergency department. Further to this, in 2013/14, only 33.3% of NSM LHIN patients discharged from hospital for an acute illness saw their physician within seven days following discharge. 24 Acute and Specialty Care Challenges in accessing primary care, can also mean that emergency departments (EDs) are left managing conditions that would be best treated elsewhere. In NSM, the rate of emergency visits for conditions that could be treated in alternative primary care settings consistently exceeds that of the province. The rate of ED visits for conditions best managed elsewhere in the first quarter of 2016/17 was 6.27 per 1,000 population, versus the provincial average of 4.16 visits per 1, Further, the proportion of visits to NSM EDs (43.4%) that were classified as CTAS IV and V (less urgent / non-urgent), was also higher than the corresponding proportion for Ontario. 26 However, data shows that both ED visits for conditions best treated in primary care and the proportion of lower acuity visits have decreased over time. 27 With respect to utilization related to chronic disease, the most recent Ontario Stroke Report Card indicates that only 5.8% of NSM patients had access to a specialized stroke unit in 2014/15, as compared to a provincial benchmark of 72.3%. Data also shows that wait times in NSM for stroke rehabilitation exceed those of the province, with a median wait time of 12.0 days versus the provincial benchmark of 6.0 days. 28 NSM is also currently the only LHIN in the province without advanced cardiac care services. In fiscal year 2015/16, there were 2,459 cardiac catheterization visits by NSM LHIN residents outside of the 22 Health Analytics Branch. Environmental scan integrated health service plans Ministry of Health and Long-Term Care; Internal analysis up to March 31, 2016 based on Corporate Provider Database (CPDB), Claim History Database (CHDB), Registered Persons Database (RPDB), Client Agency Program Enrollment (CAPE). Accessed June Ministry of Health and Long-Term Care Health Analytics Branch. Environmental scan Integrated Health Service Plans Ministry of Health and Long-Term Care; North Simcoe Muskoka LHIN. Ministry-LHIN quarterly stocktake report, November NSM LHIN; Health Analytics Branch. Environmental scan integrated health service plans Ministry of Health and Long-Term Care; Ministry of Health and Long-Term Care Health Analytics Branch. Environmental scan integrated health service plans Ministry of Health and Long-Term Care; Ontario Stroke Network. Ontario stroke evaluation report card Institute for Clinical Evaluative Sciences;
80 LHIN. Of these visits, 85.4% were to Southlake Regional Health Centre. 29 The additional travel poses a risk in that some NSM residents are unable to access percutaneous coronary intervention (PCI) within standard targets for myocardial infarctions. Royal Victoria Regional Health Centre is in the late stages of the Ministry s capital approval process to bring an Advanced Cardiac Centre to the region. Health Equity According to Census data, 2.8% of NSM LHIN residents identify French as their mother tongue. 30 Among the NSM LHIN s five sub-regions, the North Simcoe area has the highest proportion of residents who reported French as their mother tongue. 31 There are 26 areas in the province that are designated under the French Language Services Act, meaning that Francophones comprise at least 10% of the population. In North Simcoe Muskoka, the Town of Penetanguishene and both Essa and Tiny Townships are considered to be designated areas under the Act. Based on the 2011 Census, 4.3% of NSM residents self-identify as Aboriginal, which is the third highest proportion among the 14 LHINs. 32 In addition to those who live off reserve, Indigenous people reside in four First Nations communities within the region. Among NSM s five sub-regions, the North Simcoe area is home to the largest proportion of residents who self-identify as Aboriginal. 33 The significant Indigenous population in the region is an important planning consideration as First Nations, Métis and Inuit people in general experience a greater burden of morbidity and mortality than the general population Internal analysis of 2015/16 data from the National Ambulatory Care Reporting System (NACRS). Accessed via IntelliHealth, January Ministry of Health and Long-Term Care Health Analytics Branch. Environmental scan Integrated Health Service Plans Ministry of Health and Long-Term Care; Ministry of Health and Long-Term Care Health Analytics Branch. Health Link demographic, census and utilization profile. Ministry of Health and Long-Term Care; Ministry of Health and Long-Term Care Health Analytics Branch. Environmental scan integrated health service plans Ministry of Health and Long-Term Care; Ministry of Health and Long-Term Care Health Analytics Branch. Health Link demographic, census and utilization profile. Ministry of Health and Long-Term Care; Garner R, Carrière G, Sanmartin C and the Longitudinal Health and Administrative Data Research Team. The health of Inuit, Métis, and First Nations adults living off-reserve in Canada: the impact of socio-economic status on inequalities in health. Statistics Canada;
81 Goal 1.1: Enhance access to timely and appropriate primary care. Consistency with Government Priorities A focus on enhancing access to primary care has been of paramount importance across Ontario for some time now. Over the last decade, significant change in primary care has taken place. The creation of new models of care, changes to contracts and funding reform have resulted in fewer unattached patients. Since 2004, the government has created 200 Family Health Teams, 25 Nurse Practitioner-Led Clinics and supported a significant expansion of Ontario s Community Health Centres. 35 While there are fewer unattached patients, timely access to primary care continues to be a challenge. Ontario s overall ranking relative to international comparators for primary care indicators is increasingly lagging despite significant change over recent years. 36 The Auditor General of Ontario s 2015 Annual Report, identified the need for the Ministry of Health and Long-Term Care to determine how best the LHINs can support primary care to meet the mandate of system integration. 37 The Patients First Act, 2016 will help the province improve access to family doctors and nurse practitioners, by supporting the province's commitment that all Ontarians who want one will have a primary care provider. 38 North Simcoe Muskoka also has a tradition of building strong relationships among providers and engaging the community in joint decision making and collaborative planning. It is within this tradition that work will continue in the shared interest of improving patient care. Action Plans and Interventions Action Plans and Interventions Strengthen relationships with provincial primary care associations and regulatory bodies and their local representatives to ensure alignment in transformation efforts In collaboration with HealthForceOntario (HFO) and through sub-regional clinical leadership, develop a primary care health human resources capacity plan. Build the foundation to ensure that every patient who would like the support of a primary care providers can access one Foster sub-regional collaboration with primary care to consider innovative ways to improve access to comprehensive primary care for the population, inclusive of after-hours care Connect unattached Health Links patients with a primary care provider at discharge. 2017/ / /20 Status % Status % Status % Not yet started Not yet started Not yet started Not yet started 33 In progress 80 In progress 25 In progress 33 In progress 33 To be completed 10 To be completed 50 To be completed 33 To be completed Ministry of Health and Long-Term Care. News release: Ontario passes legislation that delivers better health care for families. Queen s Printer for Ontario; Steering Committee for the Ontario Primary Care Performance Measurement Initiative. A primary care performance measurement framework for Ontario. Report of the steering committee for the Ontario primary care performance measurement initiative: phase one. Health Quality Ontario; Auditor General of Ontario. Annual report Office of the Auditor General of Ontario; Ministry of Health and Long-Term Care. The Patients First Act frequently asked questions. Queen s Printer for Ontario;
82 Measuring Success Most of the initiatives supporting access to primary care are foundational and as such will be measured by output indicators and/or level of completion. Metrics reflecting patient access to care are currently under development at a provincial level. Indicators that will be measured to reflect progress in this area include: Number of engagements with primary care associations and regulatory bodies Number of engagements with LHIN participation specific to access Percentage of Health Links patients with regular and timely access to a primary care provider (Target: 95%) Percentage of NSM residents attached to a primary care provider Readmissions within 30 days for selected HIG conditions (MLAA Target: 15.50%) Rate of emergency visits for conditions best managed elsewhere Risks and Mitigation Strategies Risks Level of physician support could create a risk to initiatives intended to improve access to primary care. Access to human resources to support and manage the accountability mechanisms for primary care are uneven and may negatively impact some providers. If timely and valid data relating to access and patient outcomes is difficult to collect, analyze and share across providers, then it also becomes difficult to plan based on evidence and to provide the appropriate level of monitoring and oversight. Mitigation Strategy Reduce likelihood through change management, engagement and strengthening relationships with broad stakeholders including primary care, provincial associations and regulatory bodies within NSM sub-regions, NSM-wide and across Ontario. Avoid risk by collaborating to maximize the use of existing resources and develop contingency plans to move forward without additional funding. Reduce the likelihood by collaborating with the Ministry of Health and Long-Term Care, the five regional Health Links and primary care and local partners to simplify data collection, improve sharing across providers, and strengthen data quality. Key Enablers Homogeneity across Provider Models Over half of all primary care physicians in the LHIN are working as part of a Family Health Team (FHT). Each of the LHIN s five sub-regions has an established FHT located within its geographic boundaries. This homogeneity streamlines the connections between physician groups and all of the other care providers and stakeholders in the system. Local Physician Leadership The NSM LHIN has been a forerunner in clinical leadership by having a family physician as a member of NSM LHIN staff whose role is to lead clinical planning and system integration. This role is key to facilitating relationships, and acting as a champion and subject matter expert. In 2017/18, LHIN clinical leadership will expand and this level of expertise will be brought to enable work with and engage primary care providers within the LHIN sub-regions. Partnerships with HealthForceOntario The local HealthForceOntario representative is closely tied to the LHIN and collaborates regularly on projects with shared objectives. This relationship with HFO allows the NSM LHIN to broaden and build upon its relationship with academic centres, residency programs and primary care providers. 20
83 Goal 1.2: Improve access to high-quality acute and specialty care. Consistency with Government Priorities Ensuring timely and appropriate access to high-quality acute and speciality care is an important element of many provincial initiatives, which are reflected in the regional work taking place in North Simcoe Muskoka. These programs and services include emergency department (ED) and critical care, as well as speciality services for patients with chronic disease and those requiring end of life care. Provincial direction for emergency care is provided by Ontario s Emergency Room Wait Times Strategy, which supports enhancing alternatives to emergency services, improving capacity and operating processes in the ED, and supporting discharges by increasing home and community supports. 39 Critical Care Services Ontario (CCSO) is responsible for the overall implementation and evolution of the initiatives under Ontario s Critical Care Strategy. CCSO has recently developed the Ontario Critical Care Plan and has identified strategic goals that inform the activities of the local Critical Care Network. 40 Provincial leadership for Ontario's cardiac, vascular and stroke services is now provided by a single entity under the corporate structure of the Cardiac Care Network (CCN), following an integration with the Ontario Stroke Network. In alignment with national and provincial best practice recommendations, the NSM LHIN is working towards regionalizing stroke care through an integrated model. North Simcoe Muskoka is also working to develop a regional advanced cardiac program that will align with the core competencies and functions defined by the CCN. The Rehabilitative Care Alliance (RCA) is a province-wide collaborative that was established by the 14 LHINs in 2013 to strengthen and standardize rehabilitative care across the province. In accordance with LHIN CEO endorsement of the RCA's Definitions Frameworks for Bedded and Community-Based Levels of Rehabilitative Care, the NSM LHIN will move towards re-aligning existing rehabilitative care resources with the levels of care defined in the frameworks. 41,42 The Declaration of Partnership and Commitment to Action that was provincially established in 2011 provides a common vision for palliative and end of life care in Ontario based on optimizing quality of life, comfort, dignity and respect. 43 The Ontario Palliative Care Network (OPCN) was established in March 2016 following extensive stakeholder consultation and the release of the province s Palliative and End-of- Life Care Provincial Roundtable Report. 44 Aligned with the expectations of the OPCN, NSM s Regional Palliative Care Network (NSM RPCN) is responsible for planning a regional palliative care program and supporting the alignment of local services and performance with provincial standards. Both Open Minds, Healthy Minds: Ontario s Comprehensive Mental Health and Addictions Strategy and the Patients First: Action Plan for Health Care, highlighted the provision of the right care for those living with mental health and addiction as critical to health system performance. 45, 46 More recently, the key findings of Ontario s Mental Health and Addictions Leadership Advisory Council, as outlined in its 2015 and 2016 annual reports, identify recommendations on the development of a person-centred system that 39 Ministry of Health and Long-Term Care. Ontario s emergency room wait times strategy. Queen s Printer for Ontario; Critical Care Services Ontario. Ontario critical care plan CCSO; Rehabilitative Care Alliance. Definitions framework for bedded levels of rehabilitative care. RCA; Rehabilitative Care Alliance. Definitions framework for community based levels of rehabilitative care. RCA; Local Health Integration Networks and Quality Hospice Palliative Care Coalition of Ontario. Advancing high quality, high value palliative care in Ontario: declaration of partnership and commitment to action. Queen s Printer for Ontario; Fraser J. Palliative and end-of-life care provincial roundtable report. Queen s Printer for Ontario; Ministry of Health and Long-Term Care. Open minds, healthy minds. Ontario s comprehensive mental health and addictions strategy. Ministry of Health and Long-Term Care; Ministry of Health and Long-Term Care. Patients first: action plan for health care. Officer of the Minister, Ministry of Health and Long-Term Care;
84 is equitable, accessible, high-performing and recovery-oriented. 47, 48 Efforts continue within the NSM LHIN to align policies, programming and funding with this provincial direction. Current examples include, but are not limited to, the development of a regional opioid strategy and the implementation of a regional working group on information and information management. Action Plans and Interventions Action Plans and Interventions Monitor and support the scheduled hospital implementation of standardized electronic triage (e-ctas) in emergency departments Establish Pay-for-Results target setting by initiative as part of the Action Plan submission from the participating hospitals to improve overall performance of emergency departments and quality of patient experience Work with emergency department leadership and Access to Care to develop a process for regional review of ED Return Visit Program amalgamate data Establish a working group in collaboration with hospital sector partners to investigate centralized scheduling, evaluate options to improve efficiencies and establish best practices to improve access to CT and MRI scans Establish a Collaborative that will focus on integrated critical care services across the LHIN Execute the phased implementation plan to support realignment of rehabilitative care resources with the RCA Definitions Framework for Bedded and Community Levels of Rehabilitative Care. Ensure alignment with Ministry reporting requirements for rehabilitation as they are developed Develop and implement the required elements of an Integrated Regional Stroke Program including an integrated funding bundle, the transitional stroke care and rehabilitative care pathway, and evaluation framework Develop and implement inpatient and outpatient rehabilitation services for stroke Develop and implement the required elements of a Regional Advanced Cardiac Program, including prevention and health promotion, and the acute, postacute and rehabilitative phases of cardiac care Develop and implement inpatient and outpatient rehabilitation services for cardiac care Facilitate the establishment of a regional Musculoskeletal Central Booking Task Force Promote the expansion, adoption, enhancement, and evaluation of Telemedicine enabled models of care including Telehomecare. 2017/ / /20 Status % Status % Status % To be completed To be completed Not yet started Not yet started Not yet started Not yet started In progress In progress In progress In progress Not yet started To be completed In progress 15 To be completed In progress 45 To completed 50 In progress 25 To be completed 30 To be completed 33 To be completed 25 To be completed To be completed In progress 50 To be completed Ontario s Mental Health & Addictions Leadership Advisory Council. Moving forward: Better mental health means better health. Ontario s Mental Health & Addictions Leadership Advisory Council; Ontario s Mental Health & Addictions Leadership Advisory Council. Moving forward: Better mental health means better health. Ontario s Mental Health & Addictions Leadership Advisory Council;
85 Action Plans and Interventions Promote the increased adoption of econsult by engaging local primary care providers and specialists and supporting business process redesign and change management Develop a North Simcoe Muskoka Regional Palliative Care Program aligned with the OPCN and in collaboration with Cancer Care Ontario Coordinate, in collaboration with public health, the development of a comprehensive, cross sector, regional opioid strategy aligned with the Provincial Opioid Strategy Develop and implement a regional working group on information and information management focused specifically on mental health and addictions Work with health service providers to assess and develop opportunities to implement enhanced structured psychotherapy services within the LHIN, in alignment with Ministry direction. 2017/ / /20 Status % Status % Status % To be completed In progress In progress To be completed Not yet started To be completed 75 To be completed In progress 33 To be completed 34 Measuring Success A number of initiatives supporting the provision of acute and specialty services are foundational and as such will be measured by level of completion. Others, such as palliative care, are provincial programs for which performance frameworks are under development. Indicators that will be measured to reflect progress in this area include: Number of hospitals implementing e-ctas (Target: implemented in all 5 NSM hospitals in fiscal 2017/18) ED length of stay for admitted patients (Target: at or below provincial average) ED length of stay for non-admitted complex patients (Target: at or below provincial average) ED length of stay for non-admitted minor patients (Target: at or below provincial average) Time to physician initial assessment for ED patients (Target: at or below provincial average) Time to inpatient bed for ED patients (Target: at or below provincial average) Ambulance offload time for ED patients (Target: at or below provincial average) Percentage of return ED visits within 72 hours of discharge from initial ED visit resulting in an admission on the second presentation (No target audit program) Percentage of return ED visits within 7 days from initial ED visit resulting in admission with a sentinel event (No target audit program) Percentage of priority 2, 3, and 4 cases completed within access targets for MRI scans (MLAA Target: 90.00%) Percentage of priority 2, 3, and 4 cases completed within access targets for CT scans (MLAA Target: 90.00%) Readmissions to an Intensive Care Unit within 48 hours Proportion of stroke/tia patients treated on a stroke unit at any time during their inpatient stay Median number of days between stroke (excluding TIA) onset and admission to stroke inpatient rehabilitation Percentage of priority 2, 3 and 4 cases completed within access target for hip replacement (MLAA Target: 90.00%) Percentage of priority 2, 3 and 4 cases completed within access target for knee replacement (MLAA Target: 90.00%) Number of direct and indirect clinical events delivered via Telemedicine (Target: increase of 2,567 direct and indirect clinical events over 2016/17 service levels) Number of patients enrolled in Telehomecare (Target: 240 patients enrolled in the coaching stream, and 320 patients enrolled in the monitoring stream during 2017/18) Number of providers signed up for OTN HUB (Target: improve over baseline of 120 providers) Repeat unscheduled emergency visits within 30 days for substance abuse conditions (MLAA Target: 22.40%) 23
86 Risks and Mitigation Strategies Risks The process of establishing initiative-specific Pay-for-Results targets is new to the NSM LHIN and may require some initial change management efforts. Currently the availability of community resources to enable early supported discharge for stroke varies between communities. As such, early supported discharge programs may look substantially different in each of the three phases of the project. Cardiac rehabilitation programs will vary across the region as community-based rehab programs are currently offered in partnership with the YMCA and not all communities have access to a YMCA. There is some degree of misalignment between current reporting mechanisms and the RCA framework, which may be a source of concern for participating hospitals. Mitigation Strategy The LHIN will continue to engage with the ED Steering Committee and look to provincially successful initiatives to help drive improved performance across the six P4R indicators. Continue to work with service providers to better understand available community resources to address rehabilitation needs for stroke patients. Continue to work with service providers to determine if other community resources could be leveraged to address rehabilitation needs for cardiac patients in communities without access to a YMCA. There may also be a need to consider structural changes to the Integrated Vascular Committee to include community providers. Leverage learning from the acute care facility in the region that has already begun working towards alignment with the RCA definitions. Key Enablers Stroke Steering Committee - The NSM Stroke Steering Committee is comprised of hospitals that provide stroke care in NSM, partners from other acute care facilities in the region, emergency medical services (EMS), local physicians, home care, and other community organizations. The committee enables collaboration in establishing standards, benchmarks and guidelines that support the realization of an integrated stroke program. NSM Local Critical Care Network - The Local Critical Care Network includes representatives from NSM s acute care facilities. Their role is to collaborate and support the implementation of the Ontario Critical Care Plan The key goal is to provide standard and consistent care across the region despite the differing capacities to deliver critical care services at each facility. NSM Critical Care Environmental Scan - The NSM LHIN has secured subject matter expertise in the area of critical care to inform strategy development. This resource has mapped out current state of the ICU and critical care services including the Level 2 and level 3 centres and the allocation of beds. Triggers of patient transfer between centres have also been identified and recommendations have been formulated around guidelines for patient transfer and return between centres. Emergency Department Steering Committee - North Simcoe Muskoka s Emergency Department Steering Committee includes both administrative and clinical leaders in emergency medicine. The committee enables the spread of successful initiatives to improve emergency department flow and quality. The structure of physician leadership within the NSM LHIN allows for improved integration between access to primary care and ED utilization. 49 Critical Care Services Ontario. Ontario critical care plan CCSO;
87 NSM Regional Palliative Care Network (NSM RPCN) The NSM Regional Palliative Care Network Steering Committee was established in December 2016 and includes key regional health care and community stakeholders and providers as well as patients/family members. The NSM RPCN is aligned with the Ontario Palliative Care Network (OPCN) and will be guiding palliative care within NSM. The NSM RPCN will continue to work with regional providers, stakeholders and communities to support the development of a high-quality, coordinated hospice palliative care system. Existing Telemedicine Resources The Ontario Telemedicine Network (OTN) and telemedicine assets held by NSM providers continue to enable care provision across a range of clinical areas. Telemedicine services have been incorporated into the models being developed for stroke, cardiac, and critical care by enabling access to specialists, increasing provider capacity through education, and facilitating care in the patient s home. LHIN-funded Telemedicine nurse resources are also embedded in hospitals, long-term care homes, home and community care services and primary care settings across the region. 25
88 Goal 1.3: Promote health equity and enable access to appropriate and culturally safe care. Consistency with Government Priorities The Local Health System Integration Act (LHSIA), 2006, requires that the province s health care system be guided by a commitment to equity and respect for diversity in communities in serving the people of Ontario and respect the requirements of the French Language Services Act in serving Ontario s Frenchspeaking community. LHSIA also mandates that LHINs recognize the role of First Nations and Aboriginal peoples in the planning and delivery of health services in their communities. 50 Further to these provisions, the Patients First Act, 2016 includes a requirement for LHINs to to promote health equity, including equitable health outcomes, to reduce or eliminate health disparities and inequities, to recognize the impact of social determinants of health, and to respect the diversity of communities and the requirements of the French Language Services Act in the planning, design, delivery, and evaluation of health services. This obligation strengthens the provisions of LHSIA as it relates to health equity and recognizes a broader definition of health that includes the social determinants of health. The Patients First Act also builds upon existing provisions with respect to FLS and reinforces access to and integration of health services for Ontario s Francophone population as key objectives of the LHIN s planning. The NSM LHIN s ongoing partnership with the local French Language Health Planning Entity, Entité 4, aims to ensure that issues relevant to the Francophone population are reflected in system level planning. With the release of Patients First: A Proposal to Strengthen Patient-Centred Health Care in Ontario, the Ministry of Health and Long-Term Care also committed to meaningful engagement with the province s Indigenous and Métis partners. This engagement is occurring through a parallel process that aims to increase Indigenous and Métis inclusion in the health care system and improve access to culturally appropriate services. The NSM LHIN s initiatives align with the provincial commitment, as well as reflecting the ongoing work of the region s Aboriginal Health Circle. The requirement under the Patients First Act to promote health equity, reduce health disparities and recognize the social determinants of health requires a broader consideration of the health of the population. This is aligned with the efforts of other ministries including the Ministry of Housing and the Minister Responsible for the Poverty-Reduction Strategy, as articulated in Realizing Our Potential: Ontario s Poverty Reduction Strategy. 51 The provincial strategy has led to the release of a discussion paper Finding a Better Way: A Basic Income Pilot Project for Ontario 52 and in turn this paper has become the focus of local work led by the Simcoe Muskoka District Health Unit and endorsed by the NSM LHIN. The NSM LHIN is an active participant in extensive collaborative efforts at the local level to measure and address issues related to basic needs. Current state and many of the services currently offered are described in Simcoe Muskoka s Vital Signs report. 53 The NSM LHIN continues to strengthen relationships with multiple stakeholders including the Simcoe Muskoka District Health Unit. 50 Ontario, Local Health System Integration Act, 2006, S.O. 2006, c Government of Ontario. Realizing our potential: Ontario s poverty reduction strategy. Queen s Printer for Ontario; Segal, H.D. Finding a better way: A basic Income pilot project for Ontario; Queen s Printer for Ontario; Simcoe Muskoka s Vital Signs Project Team. Simcoe Muskoka s vital signs. Huronia Community Foundation and United Way Simcoe Muskoka;
89 Action Plans and Interventions Action Plans and Interventions Conduct an environmental scan with primary care in NSM regarding experience addressing poverty, including available resources, supports, tools, as well as barriers Develop and implement an outreach strategy to enhance primary care providers knowledge, attitudes and comfort towards supporting patients living in poverty, Support the integration of the Ontario Poverty Tool into primary care clinical practice Develop a project evaluation plan for the Poverty in Primary Care Project including measures of primary care provider knowledge, use of the Ontario Poverty Tool, and patient experience Develop a working collaborative and framework with the Simcoe Muskoka District Health Unit for enhanced integrated planning to better meet Public Health service needs Develop a collaborative plan between home care providers, community support services and Indigenous and Métis communities aimed at enhancing home and community care services for the Indigenous and Métis population Support health service providers to develop, implement and monitor Indigenous self-identification policy Develop a plan to support the provision of Indigenous Cultural Safety training in health service provider organizations Support the work of the Aboriginal Health Circle in its proposal of a regional First Nation, Métis, and Inuit Residential Treatment Centre Support the implementation of the Aboriginal Health Circle objectives and deliverables of the LHIN s strategic priorities, in the context of improving the health status of Indigenous and Métis people Deliver Indigenous Cultural Safety training for local planning tables, all LHIN staff and Board members Partner with Entité 4 to deliver on the Joint Action Plan and implement performance indicators on French Language Services linked to the plan Support health service providers to collect data on patients linguistic identity Develop enhanced intake processes to fully appreciate the linguistic needs of home and community care patients and support access to services in French Support agencies seeking identification or designation to ensure they meet the required standards Promote the implementation of and compliance with "Active Offer" guidelines Establish a French Language Services Committee to support planning, monitoring and reporting on the provision of services in French for the renewed LHIN, including home and community care services. 2017/ / /20 Status % Status % Status % To be completed To be completed To be completed To be completed To be completed Not yet started In progress In progress In progress In progress In progress In progress In progress Not yet started In progress In progress Not yet started In progress 25 In progress 60 To be completed 30 In progress 30 In progress 25 In progress 40 To be completed 30 In progress 25 In progress 30 In progress 30 In progress To be completed 25 To be completed To be completed 30 To be completed 25 To be completed To be completed 25 To be completed 30 To be completed 30 To be completed
90 Action Plans and Interventions Develop and monitor an internal human resources plan that includes FLS requirements and strategies to support the recruitment of French speaking staff to meet local needs. 2017/ / /20 Status % Status % Status % Not yet started 50 To be completed 50 Measuring Success The NSM LHIN s collaborative work with Public Health is foundational and as such will be measured by level of completion. A number of indicators are monitored to measure progress towards the goals related to access for Indigenous and Métis patients/people, and FLS including: Number of HSP agencies that have implemented an Indigenous self-identification policy (Currently establishing baseline) Number of Indigenous clients served (Currently establishing baseline) Number of staff at HSP organizations who have been trained in Indigenous Cultural Safety (Currently establishing baseline) Number of HSP agencies collecting data related to clients identified as Francophone (Target: improve over baseline of 6 agencies) Number of Francophone clients served (Currently establishing baseline) Number of health care staff members within identified and non-identified HSPs who are able to provide services in French at an advanced level (Target: improve over baseline of 385 staff) Risks and Mitigation Strategies Risks Health service providers are managing multiple competing priorities, which may impact resources dedicated to French language service requirements. Challenges in recruiting and retaining adequate French speaking staff may impact identification or designation of HSPs. Health service providers level of knowledge and capacity may not be sufficient to provide culturally safe care and services to Indigenous and Métis patients. Complexity of potential funding mechanisms for residential treatment services involve various ministries as funding partners and can therefore be difficult to navigate. Indigenous patients may not be identified at intake points, as effective mechanisms may not be in place. Mitigation Strategy Reduce impact by encouraging participation of health service providers at the NSM FLS Community of Practice to improve the sharing of strategies and resources. Leverage FLS Community of Practice to share best practices for recruitment of bilingual staff. Build knowledge and capacity through continued partnership with the Aboriginal Health Circle and by supporting cultural safety training for health service providers. Improve likelihood of accessing funding by investigating all alternate sources. Submitting an Indigenous Report is included as a Service Accountability Agreement (SAA) obligation. Through SAAs and quarterly/annual reports, develop a baseline for number of Indigenous clients served and then measure and monitor annually (maintain service levels or increase). Key Enablers Close Alignment of LHIN and Public Health Boundaries The Simcoe Muskoka District Health Unit (SMDHU) is the only Health Unit within NSM LHIN boundaries. The NSM LHIN and SMDHU are therefore well positioned to collaborate on joint initiatives and to begin advancing integrated planning to meet both LHIN and public health service needs. 28
91 NSM Chronic Disease Prevention and Management (CDPM) Steering Committee The CDPM Steering Committee is jointly led by the LHIN and the Simcoe Muskoka District Health Unit (SMDHU) and leverages the evidence-based Ontario Chronic Disease Prevention Management framework. The deliverables of the committee aim to further integrate the prevention of chronic disease into the delivery of integrated services across the health system continuum. To effectively accomplish this, building relationships and communication across the sectors is essential. Efforts have been made to ensure membership on the committee from each of the five sub-regions, multiple sectors, primary care, patients, families and caregivers. The Ontario Poverty Tool The Ontario Poverty Tool Poverty: A Clinical Tool for Primary Care Providers was originally developed by the Centre for Effective Practice (CEP) and has now been expanded by the CEP in cooperation with the College of Family Physicians of Canada (CFPC). The tool provides guidance on screening for and responding to poverty concerns with patients who may be underserved, vulnerable or at risk. The creation and availability of a tool that is endorsed by the CFPC and its provincial chapters enables local work by providing a standardized high-quality resource for clinicians. Partnership with Entité 4 - Ongoing partnership with the French Language Health Planning Entity (Entité 4) is key in ensuring that a Francophone perspective is included in the planning and integration of health services in the region. The primary role of Entité 4 is to support the engagement of the Francophone population by soliciting feedback regarding health needs and priorities, increasing awareness of health services available, and supporting potential identification of organizations for French language services. Entité 4 is also represented at NSM LHIN planning tables aligned with priority sectors and at NSM s Leadership Council to ensure that issues relevant to the Francophone population are reflected in the LHIN s planning. Aboriginal Health Circle The Aboriginal Health Circle works in partnership with the NSM LHIN to improve the health status of Aboriginal people in the NSM region. The Aboriginal Health Circle includes representation from 12 local communities and organizations that work collaboratively to address Aboriginal community health issues in system coordination and integration. Engagement of representatives of the Indigenous and Métis communities helps ensure that LHIN work continues to be informed by the needs and perspectives of these populations. 29

92 Integrated Health Services Plan Strategic Priority: 2.0 Build Capacity and Enhance Coordination Description of the Priority The priority to build capacity and enhance coordination reflects the importance of ensuring that patients receive high-quality, integrated care from providers across the continuum. Given the high proportions of individuals in the region who are aging and/or live with chronic disease, highly coordinated care is critical. It is not only important to coordinate points of care to streamline access, but also to better integrate the clinical data that informs high-quality care. Current Status Home and Community Care In 2015/16, North Simcoe Muskoka s community support services and CCAC sectors served 29,000 and 25,500 patients respectively. Home care performance is measured provincially via three indicators included in the current Ministry-LHIN Accountability Agreement, reflecting waits for nursing and personal support services and waits from community referrals for in-home services. Current data indicates that 85.23% of complex home care clients in NSM received their personal support visit within 5 days of authorization, versus an average of 87.09% across the province. For those receiving nursing services, 92.85% of NSM clients received their visit within 5 days of authorization, as compared to 94.93% for the province. Local data also indicates that the 90 th percentile wait time from community for in-home services is currently days relative to the provincial average of days. 54 Seniors and Older Adults The relative proportion of seniors residing in North Simcoe Muskoka is among the highest in the province. Seniors represented 18.8% of the NSM population in Similar to other regions across the province, forecasted growth for seniors greatly exceeds that of other age groups. This means that those aged 65 and older are expected to account for 21.3% of the population by 2020 and 24.3% by This demographic shift has a number of implications on the delivery of health care services in the region. In fiscal 2015/16, seniors aged 65 and older accounted for approximately 85.0% of patients designated as ALC long waiters (ALC length of stay greater than 30 days). 55 Further to this, the largest proportion of ALC days were spent waiting for long-term care, where the median wait time as of July 2015 was 226 days for patients waiting in acute care beds. Current wait list data indicates that there are significantly more people waiting for long term care placement in NSM than there are beds to accommodate. For example, in the Barrie area, the wait list for placement is approximately double the number of funded beds in that community. The wait list numbers for basic accommodations significantly exceed those for either semiprivate or private rooms for most facilities North Simcoe Muskoka LHIN. Ministry-LHIN quarterly stocktake report, February NSM LHIN; Access to Care. North Simcoe Muskoka LHIN monthly alternate level of care performance summary, December Cancer Care Ontario; NSM CCAC; North Simcoe Muskoka long-term care home wait time report. NSM CCAC; November
93 Sub-Region Planning A sub-regional approach to health service planning and evaluation has been in place for many years in North Simcoe Muskoka. NSM s sub-regions have now been formalized in alignment with the Patients First Act, and are coterminous with those of the five existing Health Links, with the exception of areas outside of overall LHIN boundaries. NSM s five geographic sub-regions include: Barrie and Area Couchiching (previously referred to as Orillia and Area) Muskoka North Simcoe (previously referred to as Midland, Penetanguishene and Area) South Georgian Bay (previously referred to as Collingwood, Wasaga Beach and Area) Each of the sub-regions includes one of NSM s five acute care hospitals and is aligned with one single Board of Health, the Simcoe Muskoka District Health Unit. Care Transitions and Patient Flow Alternate level of care (ALC) remains a significant issue in North Simcoe Muskoka and reflects challenges in capacity and coordination across the continuum of care. The proportion of patients designated ALC occupying NSM acute care beds is consistently among the highest in the province (20.6% in Q2 2016/17). However, the ALC rate for post-acute services including rehab, mental health and complex continuing care is significantly lower (6.4% in the same data period), resulting in an all-service ALC rate of 15.0%. Seniors aged 65 and older represent the majority of acute care patients designated as ALC, which is of particular importance given the projected rate of growth for the senior s population in North Simcoe Muskoka. Coordination of care can also be measured by hospital readmission rates, which are influenced by factors such as the quality of hospital care, care transition and coordination processes, and the availability and use of community resources. The 30-day hospital readmission ratio for selected HBAM Inpatient Grouper (HIG) conditions is included as a performance indicator in the Ministry-LHIN Accountability Agreement. Current performance for 30-day readmissions to NSM hospitals is 15.83%, which is less than the provincial average of 16.66%. 57 Care transitions and hospital readmissions have been identified as a key area of focus for North Simcoe Muskoka s Regional Quality Advisory Council. 57 North Simcoe Muskoka LHIN. Ministry-LHIN quarterly stocktake report, May NSM LHIN;
94 Goal 2.1: Enable consistent and coordinated home and community care. Consistency with Government Priorities Strengthening home and community care has been an evolving provincial priority for some time. In 2014, regulatory changes enabled LHINs to fund designated community agencies to deliver personal support services. In March 2015, the Report of the Expert Group on Home and Community Care, Bringing Care Home identified challenges which informed the development of the MOHLTC s Patients First: A Roadmap to Strengthen Home and Community Care. 58,59 The provincial roadmap outlined the plan to improve quality, consistency, and integration in the home and community care sector. In September 2015, the Auditor General of Ontario called for further reform in the manner in which home and community care was delivered in the Special Report on the Community Care Access Centres. 60 The Ministry endorsed the report and the recommendations within it, which called for greater standardization of care, increased accountability, and improved cost effectiveness. This was followed by the Auditor General s 2015 Annual Report which further identified geographic inequities in the availability of supports, inconsistencies in care coordination, and a lack of oversight. 61 One of the four pillars of the Patients First: Action Plan for Health Care is to deliver better coordinated and integrated care in the community, closer to home. 62 The Patients First Act operationalizes and legislates these principles to enable the health care system to build on progress and further advance system transformation. In 2016, the LHIN CEO Council approved the recommendation of the pan-lhin Personal Support Services Implementation group to bring their work within the Home and Community work stream aligned with the implementation of the Patients First Act. The NSM LHIN, like all LHINs across the province, work diligently to ensure that the CCAC transition to the LHIN did not interrupt continuity of care for clients, and that system transformation in the longer term works to optimize patient outcomes and protect system sustainability. Action Plans and Interventions Action Plans and Interventions Develop a regional strategy for Personal Support Services within the Home and Community sector aligned with provincial standards and guidelines for PSS implementation Plan and implement the Canadian Red Cross Integration within the NSM LHIN supporting a sub-regional approach that prioritizes continuity of care Plan and implement the expanded caregiver respite program inclusive of nursing and PSW support for medically complex children and end-of-life patients Develop and communicate a new system vision for the renewed LHIN. Build upon the foundational work done related to Care Connections, Care Connections Second Curve and the 2017 NSM LHIN Visioning Day. 2017/ / /20 Status % Status % Status % In progress To be completed To be completed To be completed 40 To be completed Donner G, Fooks C, McReynolds J, Sinha S, Smith K, Thomson D. Report of the expert group on home and community care, bringing home care. Expert Group on Home and Community Care; Ministry of Health and Long-Term Care. Patients first: A roadmap to strengthen home and community care. Office of the Minister, Ministry of Health and Long-Term Care; Auditor General of Ontario. Special report on Community Care Access Centres: Financial operations and service delivery. Office of the Auditor General of Ontario; Auditor General of Ontario. Annual report Office of the Auditor General of Ontario; Office of the Minister, Ministry of Health and Long-Term Care. Patients first: action plan for health care. Ministry of Health and Long-Term Care;
95 Action Plans and Interventions Establish clinical, home and community, and sub-regional leads to work as a triad with health system partners in acute care, primary care, municipalities, social services and community partners to support care at the sub-regional level Assess leading practices and identify opportunities to strengthen patient centred care at the community level between primary care and home and community care services Complete the operational elements required to deliver on the LHIN s expanded mandate to manage and deliver home and community care through transition Apply the locally developed change management framework to support transition and transformation in home and community care Complete environmental scan and use results to map information management and technology assets and initiatives to sub-regions. 2017/ / /20 Status % Status % Status % To be completed In progress To be completed In progress To be completed In progress In progress To be completed 30 To be completed Measuring Success A number of initiatives supporting transition and transformation in home and community care are foundational and as such will be measured by level of completion. There are also three indicators included in the Ministry-LHIN Accountability Agreement that will be closely monitored to ensure that the transition of home care services to the LHIN does not adversely affect client wait times. Indicators that will be measured to reflect progress toward this goal include: Percentage of home care clients with complex needs who received their personal support visit within five days of the date they were authorized for PSS (MLAA Target: 95.00%) Percentage of home care clients who received their nursing visit within five days of the date they were authorized for nursing services (MLAA Target: 95.00%) 90th percentile wait time from community for CCAC in home services: Application from community setting to first CCAC service (excluding case management) (MLAA Target: days) CCAC client experience (KPI 1) In addition to these currently tracked indicators, the provincial work related to CCAC transition to the LHIN has a dedicated work stream for performance. This group is currently defining the indicators to measure the success of CCAC transition to the LHINs and the success of system transformation in the longer term. Once the indicators are defined by the work stream, the NSM LHIN will work to align with measurement of, and accountability for, these indicators. 33
96 Risks and Mitigation Strategies Risks There is a need to ensure that changes related to PSW utilization in Home and Community Care are aligned with the broader system transformation. There may be challenges in personal support capacity in North Simcoe Muskoka (and elsewhere in the province) that could negatively impact drivers of system transformation and key indicators such as the ALC rate. Separation of the services between home and community and the community services sector may not take into account the manner in which the patient flows in and out of the system and often accesses services at different times by different providers. The divestment of services by the Canadian Red Cross could create a risk to continuity of care. Stakeholder expectations regarding the pace of change may not be aligned with the work required to support sustainable system change. CCAC/LHIN transition period could lead to client confusion about their care or lack of clarity among providers related to patient referrals and navigation. Mitigation Strategy Changes with respect to PSW utilization will be considered in the context of Patients First. The LHIN has undertaken a personal support capacity project to understand key drivers and identify actions that can be taken locally (and perhaps provincially) to mitigate this potential issue. Reduce this risk through the continued focus on the initial spirit of the policy change which is to keep the patient at the centre and create a one-sector experience for patients. This risk to continuity of care will be decreased by moving quickly and ensuring the services to be deployed back into community are done as efficiently and effectively as possible. Manage stakeholder expectations through a comprehensive communications strategy, including extensive engagement targeting all stakeholders. The importance of sustainable change and the value of quality evidence to inform change efforts will be critical components embedded in the strategy. Reduce the likelihood by ensuring timely and consistent communication and key messages. Ensure all transition activities remain focused on continuity of care for clients. This focus will ensure that all current points of access continue to be operational on and after transition day (i.e., intake phone numbers, referral fax lines etc.) Key Enablers Shared Vision for Home and Community Care A shared vision for the delivery of Personal Support Services (PSS) within NSM was developed by a collaborative working group, comprised of CCAC and CSS providers. The visioning process facilitated stronger relationships and increased trust amongst the providers within the NSM home and community sector. This mutual trust will continue to be fostered through the implementation of the vision. The shared vision combined with the collaborative approach to its development, will support a stronger and more patient-centred home and community sector in regards to PSS and system transformation more broadly. Existing Collaboration between the former CCAC and LHIN The NSM LHIN and the former CCAC had a longstanding and positive relationship that served to enable the successful implementation of the CCAC transition and continues to support the broader transformation in home and community care. There is a broad cross pollination of staff at both the LHIN and former CCAC who have previously worked for the other organization and continue to have close working relationships. This strong foundation ensures a collaborative approach toward addressing new challenges and shared objectives in the new organization. Foundational Work in Change Management In anticipation of the upcoming change to the system, NSM led the creation of a change management framework to guide the local work related to transition activities. This framework will continue to guide the collective work of both the LHIN and CCAC as readiness for transition is determined and implementation of transition occurs. This Change Management Framework has also been shared at the provincial level and is being adopted more broadly to enable provincial system transformation. 34
97 Establishment of Future Organizational Culture A Request for Information (RFI) was initiated, followed by a Request for Proposals (RFP) to support organizational culture development in preparation for the LHIN and CCAC integration. This work includes assessing current state and moving organizational culture towards a common desired state for the new organization. Creating the right organizational culture will be critical to the success of the integration and to operationalizing the requirements of the Patients First Act with respect to managing the delivery of services in home and community care. Collaborative Approach to the Design of the LHIN Vision The NSM LHIN has always taken a collaborative approach to the development of a shared vision of care in the region. This began years ago with the input of many stakeholders to develop the initial Care Connections: Partnering for Health Communities framework for regional planning. While the Care Connections model has been in place, the vision for services in the region has continued to evolve. This evolution is continually informed by the input of patients, care providers and health service organizations. Two years ago, the regional approach to integrated services was further developed with the Care Connections Second Curve work. This new vision was intended to align with the vision for Designing and Creating Second Curve Healthcare Systems. 63 Most recently, the LHIN facilitated a visioning day related to home and community transition and system transformation. The products of this day will be taken back to the community in accordance with the communications and community engagement plan to enable the creation of a new LHIN vision, mission and values in 2017/ Ball T, Merry MD, Verlaan-Cole L. Designing and creating second curve healthcare systems. Quantum Transformation Technologies. 35
98 Goal 2.2: Establish infrastructure to improve care for seniors and older adults. Consistency with Government Priorities A number of provincial policies and directives guide the provision of care and services for the senior s population. Taken together, these policies highlight the need to strengthen services across the continuum from low- to moderate- and high-risk seniors. Within this context, it is imperative that the LHIN ensure better integration and coordination of services to support this growing population. In 2011, the Ministry of Health and Long-Term Care (MOHLTC) approved the Assisted Living Services for High Risk Seniors Policy, which was developed to support high-risk seniors remaining safely at home with improved access to personal support and homemaking services. 64 The NSM LHIN continues to evaluate the outcomes of its existing model and operational framework for the provision of assisted living services for high-risk seniors. In 2013, the MOHLTC released its action plan for seniors entitled Independence, Activity and Good Health, identifying seniors as a key area of focus for the Ministry. The plan was informed by Dr. Samir Sinha s Living Longer, Living Well report, which included 166 recommendations regarding senior s health, ranging from wellness and housing to specialized geriatric services and end-oflife care. 65,66 In alignment with provincial direction, the NSM LHIN developed its Strategy for a Specialized Geriatric Services (SGS) Program, focusing on SGS and frail seniors as the first building block of an integrated regional senior s health program. The Ministry has since released the Assess and Restore Guideline, which supports an approach that includes short-term rehabilitative and restorative care treatments for the frail elderly. 67 In alignment with this approach, the NSM LHIN established and continues to fund the Enhanced SMART program, which is designed to support frail seniors with restorative potential through community-based classes and inhome services. Also supporting a continuum of care for seniors, the Ministry established the Enhanced Long-Term Care Home Renewal Strategy in 2014, which will enable the redevelopment of approximately 900 beds across 12 long-term care homes in North Simcoe Muskoka. The primary role of the LHIN in supporting this provincial initiative will be to analyze the need for long-term care beds at the regional and community levels and to support equitable distribution of these beds in the future state. Most recently, the Ministry has released a discussion paper to inform the development of a provincial dementia strategy. In releasing this report, Developing Ontario s Dementia Strategy: A Discussion Paper, the Ministry aimed to consult with the public and service providers to better understand existing capacity, current best practices, and required improvements to service delivery. 68 The NSM LHIN will align its efforts to support people living with dementia with provincial direction, as it evolves. Action Plans and Interventions Action Plans and Interventions Facilitate the continued implementation of a Specialized Geriatrics Service Program. 2017/ / /20 Status % Status % Status % In progress 30 In progress 30 To be completed Ministry of Health and Long-Term Care. Assisted living services for high risk seniors policy, An updated supportive housing program for frail or cognitively impaired seniors. Ministry of Health and Long-Term Care; Ontario Seniors Secretariat. Independence, activity and good health. Ontario s action plan for seniors. Queen s Printer for Ontario; Sinha SK. Living longer, living well. Report submitted to the Minister of Health and Long-Term Care and the Minister Responsible for Seniors on recommendations to inform a seniors strategy for Ontario Ministry of Health and Long-Term Care. Assess and restore guideline. Ministry of Health and Long-Term Care; Developing Ontario s Dementia Strategy: A Discussion Paper. September Queen s Printer for Ontario. 36
99 Action Plans and Interventions Develop a redesign of a regional behavioural support system including a capacity and resource plan, system-wide education and improved integration Liaise, facilitate and coordinate the implementation of the provincial Dementia Strategy in partnership with the Specialized Geriatrics Program Monitor the implementation of the current Assess & Restore projects as a means of improving community capacity to support frail seniors Evaluate the Assisted Living Services for High Risk Seniors (ALS-HRS) program to assess outcomes of the existing model and make recommendations to LHIN leadership regarding suitability for spread Review and provide endorsement or feedback on redevelopment applications submitted by long-term care homes. Oversee capital planning process as homes are approved Continue analysis of the need for long term-care beds at the regional and sub-regional levels to support redevelopment planning Support long-term care home operators and the Ministry of Health and Long-Term Care to facilitate the redevelopment of 900 LTC beds in 12 long-term care homes across the region. (Completion date 2025). 2017/ / /20 Status % Status % Status % To be completed Not yet started To be completed In progress In progress In progress In progress To be completed To be completed 10 In progress 10 In progress 10 In progress In progress 10 In progress 10 In progress Measuring Success Many of the initiatives related to seniors are aimed at establishing program infrastructure and/or integration and redesign of services, and as such will be measured by level of completion. Other indicators that will be used to measure progress towards this goal include: Number of group education events provided by the SGS program Number of individuals supported by Behavioural Support initiatives Number of high-risk seniors receiving ALS-HRS services Number of clients put on ALS-HRS service from hospital with ALC designation Number of emergency department visits by ALS-HRS clients (reported by CTAS) Number of hospital admissions for ALS-HRS clients Number of unique individuals served by Enhanced SMART (Target: 225) Percentage of unplanned admissions to hospital within 30 days of admission to Enhanced SMART program Percentage of unplanned, less urgent ED visits within 30 days of admission to Enhanced SMART program Percentage of unplanned, less urgent ED visits within 90 days of admission to Enhanced SMART program ALC Rate (MLAA Target: 12.70%) Risks and Mitigation Strategies Risks Redesign of existing programs and services could lead to loss of services for some organizations and augmentation of services in others. The affected organizations could experience spin-off effects to other programs in terms of service reduction. There may also be potential impacts on continuity of care or service quality for patients. Mitigation Strategy Reduce likelihood by engaging stakeholders including seniors, caregivers, and health service providers in planning and implementation. Map programs as well as program strengths during planning to ensure that opportunities to leverage existing resources and lessons learned are maximized. 37
100 Risks Implementing the Specialized Geriatrics Services Program may have resource reallocation implications that should be considered during planning. There are no new net long-term care beds available provincially, which may pose a challenge for facilities eligible to redevelop in that they must rely on current system capacity to do so. The redevelopment plans of long-term care homes as submitted may not align with the needs of the LHIN. The interest of each long-term care home to protect its own resources at times can create a risk or disincentive for homes to plan collaboratively with the needs of the population as a whole within the community. Mitigation Strategy Avoid risk via LHIN review and approval of all proposed changes that impact funding and service volumes for seniors programs and services through the implementation of SGS. Mitigate risk by working collaboratively with redeveloping long-term care homes to ensure a systems approach to planning is achieved, and to support a sustainable system that protects client safety and improved outcomes. The NSM LHIN will continue to work collaboratively with the ministry to review redevelopment plans to ensure that local needs are being considered as redevelopment moves forward. Avoid risk by ensuring LHIN oversight of the planning submissions of the local long-term care homes. Ensure that each has considered the needs of the broad community beyond their own specific interests as a requirement for LHIN proposal endorsement. This risk will be further mitigated by collaborative planning meetings or sessions involving all operators, and facilitated or supported by the LHIN. The LHIN will encourage information sharing and facilitate discussions among long-term care homes when issues are present. The NSM LHIN will also continue to work collaboratively with the ministry to review redevelopment plans to ensure that local needs are being considered as redevelopment moves forward. Key Enablers SGS Lead Agency A lead agency for the Specialized Geriatric Services Program was selected in 2015 to co-lead planning and implementation of the program with the NSM LHIN. Clinical and administrative leadership for SGS has been established and relevant working groups and committees have been formed to support the work. The LHIN continues to have a Planning Lead assigned to the SGS work. Progress related to planning and implementation of the SGS work is reported to the LHIN CEO, the LHIN Board of Directors, and Leadership Council. Senior s Health Project Team The Project Team, as advisory to the LHIN and Specialized Geriatric Services Lead Agency, is accountable for regional system recommendations and ensuring planning and implementation aligns with relevant project charter(s). Comprised of strategic leaders from within and outside the health sector, this team will use best evidence and system knowledge to inform recommendations that take into consideration the perspective of NSM seniors and their caregivers, health service providers, as well as the health system, including value for money. ALS-HRS Steering Committee The existing ALS-HRS Steering Committee will continue to support LHIN efforts to evaluate the provision of ALS-HRS services in NSM. A comprehensive evaluation framework was established for the program with the support of the Steering Committee. The evaluation framework will enable an assessment of the outcomes of the existing program and support the direction of planning for ALS-HRS in North Simcoe Muskoka. Ministry of Health and Long-Term Care, Long-Term Care Renewal Branch The MOHLTC has created a Long-Term Care Renewal Branch to support long term care home redevelopment. Individual project managers have been assigned to long-term care homes requiring redevelopment, and LHINs will work closely with these project managers to support movement and ensure a collaborative approach to planning. The NSM LHIN continues to work with individual homes to understand their needs and assist with a system approach to planning. 38
101 Technical Subject Matter Expertise Improving care for seniors within NSM will require an integrated and collaborative approach, supported and enabled through technology. As the Specialized Geriatric Services Program evolves, systems will be needed to process referrals and manage client health information. Existing services and partner organizations will be engaged to determine if there are opportunities to leverage systems used in other organizations or build upon existing digital assets. 39
102 Goal 2.3: Strengthen partnerships at the community and sub-regional levels. Consistency with Government Priorities The North Simcoe Muskoka LHIN has worked towards care that was better integrated at the community level for many years through strong community-centred planning based on geographically defined areas. Community-centred planning is patient-focused, as most individuals seek out and receive care from providers closest to their homes. Collaborative community based planning has been operational under NSM s Care Connections model and more recently Health Links. NSM was one of the first regions in the province to have an approved Health Link in all of its sub-regional communities. The NSM LHIN decisionmaking framework also focuses on supporting innovative projects which are informed and supported by multiple organizations. Not only is the approach in NSM consistent with the priority of community-based planning, but was very likely evidence in the determination of the provincial priority. The Patients First Act will enable North Simcoe Muskoka to continue collaborative work but also enable transformation at an even faster pace. Redefining existing community partnerships as formal integrated networks of care will further improve multidisciplinary patient care in the community. Clinical leadership, shared governance, and mutual accountability are elements that will allow common goals to be strengthened and achievements to be shared. Patients First formally broadens the concept of the local health community, with the inclusion of primary care and public health, into the collaborative work already taking place between home and community services, agencies supporting those with mental health and addictions, acute care, community health centres, long term care homes, the French Language Health Planning Entité and Indigenous and Métis communities. Action Plans and Interventions Action Plans and Interventions Recruit clinical leadership as well as developing informal leadership in each LHIN sub-region Continue to develop the LHIN sub-regional lead roles to work closely with their sub-regional clinical leads, home and community leads and other sub regional partners Build upon the collaborative planning taking place in the Muskoka and South Georgian Bay sub-regions and facilitate sharing opportunities to support the other three sub-regions in their movement towards an integrated plan inclusive of primary care, acute, home and community care and public health Refine and develop sub-regional scorecards as provided by the Ministry Develop a framework between the North East and NSM LHINs to describe how the LHINs will work with health service providers in Muskoka and Parry Sound on matters related to planning, funding, accountability and communication Support North Simcoe health service providers to develop a proposal for a Community Health Hub in the Penetanguishene community Develop a high-level implementation plan for a future model of health care for Muskoka and Area. 2017/ / /20 Status % Status % Status % To be completed In progress Not yet started Not yet started In progress To be completed To be completed To be completed 33 In progress 60 To be completed 25 To be completed To be completed
103 Measuring Success The initiatives related to strengthening partnerships at the community and sub-regional levels are foundational in nature. It is anticipated that early in 2017/18, five part-time clinical leads will be hired, along with the appointment of five Sub-Regional Directors and five Home and Community Care Directors. The remaining five actions will be measured by level of completion and are anticipated to be complete by the end of the fiscal year. Risks and Mitigation Strategies Risks Depending on the content of the scorecard, some data is significantly lagged such that it is reactive rather than proactive in nature. There is also a risk that the Ministry will not provide scorecards or templates. Risk to the development of a Community Health Hub in Penetanguishene relates to the need for a timely decision to be made regarding ownership of the current hospital site to allow time for potential tenants to make the necessary arrangements. The augmented workload for both the NSM and North East LHINs related to the implementation of Patients First adds a schedule and resource risk for the development of a framework for matters related to funding, communication, training, and planning in West Parry Sound. Mitigation Strategy Open communication with the Ministry, providing feedback on suggested dashboards and content Mitigate risk by supporting the partnership of funded and non-lhin funded programs in collaboration with Georgian Bay General Hospital to make the Penetanguishene General Hospital site financially viable for ownership by a not-for-profit agency. In order to mitigate this risk, an effort will be made to initiate this work early in As well, the NSM LHIN Mental Health and Addiction Lead, and the Lead for the North East, will work to keep the framework concise and focused in order to avoid delay or deference. Key Enablers Existing partnerships with Public Health, Primary Care and other non-lhin funded organizations Opportunities remain to strengthen partnerships and the definition of common objectives with organizations outside of the narrow definition of health care. NSM is eager to continue to broaden and strengthen existing partnerships at the local level to including those with the Simcoe Muskoka District Health Unit and primary care providers in the region. Well established sub-regions Five well-established and clearly distinguishable sub-geographies have been in place for many years in NSM. The recently approved sub-regional boundary alignment represented a fine-tuning of existing sub-regional boundary lines rather than a creation of new subregions. This need for fine-tuning was based on patterns of patient movement and alignment with municipal boundaries. Aligning with municipalities allows for cleaner data collection and use of Census and other data for evidence-based decision making. Planning according to sub-regions is a well-accepted practice in the region and this comfort will enable sub-regional success moving forward. Health Links - The lessons learned with Health Links over the past two years will be leveraged to further sub-regional collaborative work. Health Links has led health system providers and partners to better understand necessary improvements and where efficiencies need to be realized to ensure sustainability. Health Links patients are often challenged not only in the narrowest definition of their health but also often experience mental health and addiction issues, social isolation and/or multiple chronic conditions which are poorly managed. They are also often under-housed or have housing issues, poor nutrition and income supports. Improvement of physical health does not come without these broader determinants of health being addressed. Relationships that have arisen between health care providers and non-lhin funded organizations has been a first step to a more integrated and inter-professional circle of care. 41
104 Goal 2.4: Improve patient flow, transitions of care, and coordination between providers. Consistency with Government Priorities Improving patient flow, communication and coordination of care can be addressed by taking action in many project areas. The intended result will be a better patient experience, system efficiency and interprofessional collaboration all supported by the Patients First Act. Patients who remain in hospital waiting for placement in a more appropriate setting are reflected in the alternate level of care (ALC) rate. The ALC rate is a key indicator of patient flow and access to appropriate care in the health care system and as such is included in the Ministry-LHIN Accountability Agreements (MLAA) as a key indicator. Alternate level of care is a longstanding provincial priority, reflected in the establishment of the ALC Expert Panel in 2006 and the release of Dr. David Walker s report, Caring for our Aging Population and Addressing Alternate Level of Care in In North Simcoe Muskoka, the ALC rate is consistently among the highest rates in the province and as a result represents both a local and provincial priority area. Coordinating care for individuals after an emergency department visit, or planning for hospital surges before they happen are also project areas that can improve the patient experience and bring savings to the system. Care coordination and sharing of data needed for clinical decision-making can be enabled through technology. The Ministry of Health and Long-Term Care is taking steps to ensure that existing investments in digital health advance the provincial priorities through the development of the provincial Digital Health Strategy. Work at the local level reflects both the principles of the provincial Digital Health Strategy while also taking into consideration the priorities of provincial delivery partners such as ehealth Ontario, Ontario MD and the Ontario Telemedicine Network. Action Plans and Interventions Action Plans and Interventions Continue to develop a regional integrated LHIN-wide Surge Plan and revise existing sub-regional surge capacity plans in the context of integrated networks of care Support the activities of the ALC Standardization Task Force in the implementation of the five high priority recommendations from the NSM LHIN ALC Strategy Develop Patient Flow Scorecards tracking resource usage and patient movement within and out of the NSM LHIN to support service planning Increase the number of complex patients who receive coordinated care through the NSM Health Links Work with OntarioMD to implement enotification and seek opportunities to better integrate notifications into clinical workflows Use Integrated Assessment Record (IAR) data and stakeholder feedback to determine next steps to improve record sharing between providers and avoid unnecessary reassessments. 2017/ / /20 Status % Status % Status % In progress In progress Not yet started In progress In progress To be completed 50 To be completed 60 To be completed 50 To be completed 25 In progress 30 In progress To be completed 40 To be completed Walker D. Caring for our aging population and addressing alternate level of care. Report submitted to the Minister of Health and Long-Term Care. Queen s Printer for Ontario;
105 Action Plans and Interventions Implement Ontario Laboratory Information Systems (OLIS) in the remaining two NSM hospitals sites that are not yet fully contributing and promote ehealth Ontario s clinical integration initiatives Support needs of Health Links in the local implementation of provincial recommendations relating to electronic Care Coordination Solutions Identify which organizations locally are registered with ehealth Ontario s OneID and any opportunities locally to enable access to provincial solutions by increasing provider registration Support regional electronic integration by implementing and adopting connectingontario according to sub-regional planning areas and individual organizational readiness Support and monitor change management related to the implementation of the Acute to CCAC/LTC ereferral. Align with provincial direction around ereferral pathways and projects. 2017/ / /20 Status % Status % Status % To be completed To be completed To be completed To be completed To be completed Measuring Success Several of the initiatives related to patient flow and transitions are foundational and as such will be measured by level of completion. Other indicators that will be used to measure progress towards this goal include: ED length of stay for admitted patients (Target: at or below provincial average) ALC rate (MLAA Target: 12.70%) Number of patients with a Coordinated Care Plan developed through the Health Link (Target: 750) Readmissions within 30 days for selected HIG conditions (MLAA Target: 15.50%) Number of hospitals live and fully contributing to OLIS (Target: all 5 NSM hospitals) Number of OneID registered users sponsored by organizations located within NSM (Target: increase over baseline of 2028) Percent of referrals sent and managed electronically via the ereferral process (Target 80% of the 12,000 paper referrals sent via paper in 2013/14) Risks and Mitigation Strategies Risks Capacity issues can become a risk once patient flow is optimized and barriers are identified for organizations that have not traditionally planned around expected surge periods. Linkages to ALC work and capacity for surge must also be identified. Capacity is a risk that will interfere with the Health Links ability to take on and support more patients. Continuous evolution and improvement related to technology can lead to change fatigue which in turn can become a risk to the level of clinician engagement and system adoption. Mitigation Strategy Capacity risks are mitigated by working with organizations to develop a variable planning cycle based upon predictable surge capacities, inclusive of primary and community care to ensure that capacity exists in all sectors to respond. Actively connect work to ALC work for solutions when capacity is the root cause of the surge Risk will be mitigated through broader support of the most complex patients. Expanding the approach to care beyond Health Links and creating shared responsibility will increase system capacity and decrease the burden on the Health Links. Reduce likelihood through effective community engagement and change management. 43
106 Risks Information gaps between different sectors of the health care system can be a risk to continuity of care and create gaps in the patient s journey. Inclusion of local organizations in provincial ehealth projects according to interest rather than appropriateness could create a risk to project success, change management and future adoption. Mitigation Strategy Existing CCAC and IAR systems will be leveraged as much as possible to mitigate risks in the availability of the patient data. In addition, a number of the projects within this goal area are focused on building the technological infrastructure needed to improve the flow of patient information between providers. Mitigate the likelihood of the risk occurring by implementing criteria, based on lessons learned in other regions, which will inform which organizations are more appropriate to be included in pilot projects. Close alignment between the LHIN and provincial delivery partners will ensure that projects are rolled out locally according to local needs and priorities. Key Enablers Foundational work and Leadership Engagement around ALC Over 2016/17, the NSM LHIN secured outside resources to support the analysis of current state with regards to ALC. This evaluation took place over a year and included the data and feedback of hospitals, long-term care, home and community care, discharge planners, system navigators and community coordinators. This review provided the opportunity to investigate some of the root causes of the ALC issues in North Simcoe Muskoka and resulted in five key recommendations. As the recommendations from the ALC Strategy were informed by the community and endorsed by system leaders, continued engagement and leadership also becomes a key enabler for implementation of the recommendations. Sub-regional Planning Tables Engagement of multiple providers and sectors at the sub-regional level will facilitate the development of plans to improve flow and system navigation for patients and coordination and communication across providers. The integration of home and community care, primary care, and public health into local planning tables will increase the engagement and likelihood of success of new initiatives. Consistency of Client Record Systems: The relatively low number of disparate Health Information Systems and Electronic Medical Record (EMR) Systems and the high rate of EMR adoption in primary care across the LHIN, puts NSM in a favourable position to be early adopters and innovators of ehealth initiatives. This potential has been demonstrated in the past when NSM LHIN was selected to be the pilot for the provincial e-prescribing and Hospital Report Manager initiatives with very successful outcomes. NSM LHIN ehealth Advisory Committee The ehealth Advisory Committee acts as a central point of contact and collaborative planning around local digital health projects. The committee acts as a means for knowledge sharing, needs assessment, and gap identification and advises the NSM LHIN on matters related to information technology and information management. 44

107 Integrated Health Services Plan Strategic Priority: 3.0 Drive System Sustainability Description of the Priority This Strategic Priority reflects the NSM LHIN s imperative to promote system sustainability, including efficient use of system resources, return on investment, and accountability for results. The provincial health care system faces a significant challenge as historic levels of investment are not considered sustainable. Current Status Quality and Best Practice Implementation Quality of care can vary significantly between regions and across care settings. Variations in the delivery and utilization of health services can indicate potential opportunities to improve both patient care and value. Included under the Patients First Act are provisions for the development of a provincial Integrated Clinical Care Council, which will oversee the development of quality standards and performance measures to drive best practice implementation across the province. In developing these quality standards, the council has prioritized areas in which there are significant gaps between current and optimal practice, or where there is evidence of unnecessary variation. Current quality standards that have been introduced align with the mental health portfolio and include behavioural symptoms of dementia, major depression and schizophrenia. North Simcoe Muskoka s Regional Quality Advisory Council serves as a mechanism to ensure that clinicians in our region have an opportunity to provide input into the development of these standards and to support their local implementation. Accountability for Investments Health care expenditures currently account for approximately 42% of the provincial budget and without significant change are projected to represent 70% of spending within the next 12 years. This is reflected in considerable budgetary pressures for all health care providers across the province. Contributing to this challenge is the shift in demographics towards an increasing senior s population, which will result in higher costs to the system. Specifically, the cost of care for a senior is three times higher than that of the general population. 70 Ontarians are living longer and the baby boomers are now reaching an age where they will require more health care. 71 It is therefore necessary that resources are best utilized to ensure that NSM residents continue to receive appropriate care in the future. Both changing demographics and existing budgetary pressures reinforce the importance of the LHIN role in ensuring accountability for investments. Taken together, strong oversight, continued monitoring, and evidence-informed planning in all areas will ensure existing and new funding is best directed based on need, quality, and evidence of achieving intended outcomes. 70 Ministry of Health and Long-Term Care. Health system transformation: a year in review. Presented at Ontario Hospital Association Health Care Financial Management Conference; Ministry of Health and Long-Term Care. Health system funding reform update. Presented at Ontario Hospital Association Health Care Financial Management Conference;
108 Goal 3.1: Advance quality, best practice, and innovation across the local health care system. Consistency with Government Priorities The Excellent Care for All Act (ECFAA), came into effect in June 2010 and established a number of requirements for health care organizations. 72 ECFAA laid the foundation for evidence-based care and patient-centred funding, as well as broadening the mandate for the Ontario Health Quality Council (now Health Quality Ontario). The Auditor General s 2015 Annual Report called for LHINs and Health Quality Ontario (HQO) to work closely to support quality improvement across the province. 73 In 2015, HQO and the LHINs initiated partnerships to advance quality at the regional level through the establishment of Regional Quality Tables. The Regional Tables were intended to provide a mechanism to build local foundations for quality and improve alignment between regional and provincial strategic directions. The NSM LHIN established its Regional Quality Advisory Council in 2016, in partnership with HQO. This group provides a forum for advancing the foundations of clinical quality improvement in support of the NSM LHIN Integrated Health Service Plan. It also serves as an important mechanism for clinical leadership to achieve progress and momentum on quality in alignment with the work of the NSM LHIN Quality Improvement Network and the NSM LHIN Leadership Council. This table will be a valuable resource for the NSM LHIN, as it will provide a venue to discuss performance improvement, align efforts across sectors, and share best practices throughout the region. The Patients First Act includes provisions for the development of a provincial Integrated Clinical Care Council to oversee the development of consistent clinical standards to drive best practice implementation throughout the system. The Regional Quality Advisory Council is a means of ensuring that local clinicians have an opportunity to inform clinical standard development and to support local implementation work. Action Plans and Interventions Action Plans and Interventions Facilitate the local implementation of clinical quality standards leveraging resources and partnerships from HQO with an initial focus on the mental health cohort Work with the Regional Quality Advisory Council to develop a culture of quality throughout our LHIN and to provide oversight to the LHIN council structure on the development of actions in alignment with reducing readmissions Support existing LHIN councils and committees in aligning their scorecards and dashboards with the direction of the Regional Quality Advisory Council and the provincial quality framework Support data informed planning and decision-making by providing analysis and interpretation of regional and sub-regional level issues and trends Develop a regional quality improvement plan which each subregion will collaboratively monitor and measure Optimize physician EMR utilization and quality improvement efforts by supporting adoption of OntarioMD s EMR Dashboard. 2017/ / /20 Status % Status % Status % Not yet started 20 In progress 30 To be completed In progress 25 In progress 25 To be completed In progress 40 In progress 40 To be completed In progress 25 In progress 33 Not yet started To be completed To be completed In progress 35 To be completed Excellent Care for All Act, 2010, S.O. 2010, c Auditor General of Ontario. Annual report Office of the Auditor General of Ontario;
109 Measuring Success A number of the initiatives aligned with this goal are foundational or are enablers to the success of other projects and as such will be measured by level of completion. Metrics aligned with the implementation of clinical quality standards in mental health will be developed by the Improving & Driving Excellence across Sectors (IDEAS) cohort focused on this work. Indicators that will be monitored to measure progress toward this goal include: Readmissions within 30 days for selected HIG conditions (MLAA Target: 15.50%) Number of primary care providers implementing the EMR dashboard Risks and Mitigation Strategies Risks Data quality is critical to both planning and quality improvement. The LHIN is dependent on the accuracy of service provider data, which poses a risk in terms of measuring the impacts of change efforts or using evidence to inform planning. The physician political climate may pose a risk to the stability of the Regional Quality Advisory Council. The provincial clinical standards have been met with negativity by some clinicians. There may be resistance to the sharing of baseline data and quality initiatives by some health service providers. The development of an area of focus in alignment with the Regional Quality Advisory Committee may create tension from Councils that have historically set their own direction. This is a necessary direction, but may lead to Council membership turnover. Available data may not be fulsome at the sub-geographic level and trends in migration and resident movement patterns can be misleading. Predictive models are not always available or realistic. Mitigation Strategy Mitigate the risk by continuing to communicate the importance of data quality at the regional level. Facilitate local data quality committees and encourage service provider participation in ongoing training sessions or data blitzes delivered by the MOHLTC, the Ontario Hospital Association, and Canadian Institute for Health Information (CIHI). Engage providers at all levels to clearly communicate the correlation between data quality and effective regional planning and QI efforts. Continuing to focus on quality and striving for an improved system has maintained engagement at the Quality Advisory Council to date and is the LHIN s strategy going forward. Partner with HQO and leverage HQO resources to build partnerships and trust in advisory tables and committees. Re-engage and review Council Terms of Reference to ensure the existing Councils have appropriate membership. Accept the risk and work within the bounds of the information available, providing interpretive cautions when necessary Key Enablers NSM LHIN Clinical Planning Tables There are a number of planning tables, councils, and project steering committees that collaborate across organizations with regards to a specific topic or clinical discipline. Planning groups across the region include mental health and addictions, vascular, stroke, cardiac, emergency department, critical care, renal, and palliative as examples. Many of these groups have LHIN staff associated with them and linkages with these groups can be leveraged to identify gaps and opportunities with regards to improving quality and maximizing the use of available funding to meet the needs within the community. Regional Quality Advisory Council The NSM Regional Quality Advisory Council is an action-oriented, clinically-focused body, focused on regional quality challenges and initiatives, aligned with provincial quality priorities and structures. It is led by a regional Clinical Chair and includes regional clinical leads, sector leaders, and a Health Quality Ontario regional Quality Improvement Specialist. The Clinical Quality Chair for the NSM LHIN is a joint appointee of HQO and the LHIN, which supports a stronger alignment between the strategic directions of the region and those of the province. 47
110 Improving & Driving Excellence across Sectors (IDEAS) Cohort focused on Major Depression The Improving & Driving Excellence Across Sectors (IDEAS) program is an Ontario-wide initiative to support capacity building in quality improvement and change management across all sectors of the provincial health care system. IDEAS is delivered through a collaborative partnership among seven Ontario universities, Health Quality Ontario (HQO), the Institute for Clinical Evaluative Sciences, and the Institute of Health Policy, Management and Evaluation at the University of Toronto. The next cohort of the IDEAS Advanced Learning Program will target major depression, with participants focusing on the implementation of the Major Depression Quality Standards, released by HQO. The NSM LHIN will be supporting one or more local teams to engage in this work beginning in October
111 Goal 3.2: Ensure accountability for current investments and evaluate opportunities to improve capacity. Consistency with Government Priorities Transparency and accountability are essential elements of the Patients First Act. The LHIN has a role within this broader mandate to ensure that those who are providing LHIN-funded services account for the programs they are delivering and the patients they serve. The LHIN also has a system role, in partnership with stakeholders, providers and patients to plan services needed now and into the future. Protecting the system means controlling costs and targeting funding to services which improve patients outcomes in an effective and efficient way. Monitoring and reporting of existing investments is part of this equation. The LHIN monitors performance indicators for existing programs and also supports new programs in establishing evaluation criteria and metrics. As new programs are established they need to be monitored to ensure they meet expectations, any issues are noted early, and innovations are flagged for project spread. Newer programs to be the focus of work this year include the Nurse Practitioners in Long-Term Care Homes initiative, 74 mental health and additions programs in alignment with Open Minds, Healthy Minds: Ontario s Comprehensive Mental Health and Addictions Strategy, 75 diabetes and chronic disease reporting as aligned with the Ontario Diabetes Strategy 76. Initiatives currently under development still need to have indicators and deliverables identified so monitoring can take place in the future. Action Plans and Interventions Action Plans and Interventions Update current state assessment of mental health and addictions services across the NSM LHIN aligned with the Core Services outlined by Ontario s Mental Health and Addictions Leadership Advisory Council Continue to monitor existing supportive housing initiatives. Work with the Mental Health and Addictions Coordinating Council and sector stakeholders to assess opportunities to enhance access to supportive housing, in alignment with Ministry direction Develop a framework for performance monitoring and evaluation of the Specialized Geriatric Services Program, as elements of the program are developed In accordance with MOHLTC requirements, establish accountability indicators for the Nurse Practitioners in Long-Term Care Homes initiative and monitor quarterly performance Monitor the quarterly activity statistics for Adult and Pediatric Diabetes Education Programs as a means of informing regional and sub-regional planning Create a revised Enterprise Risk Management Policy and Framework. 2017/ / /20 Status % Status % Status % To be completed Not yet started In progress In progress 33 To be completed To be completed Not yet started To be completed In progress To be completed To be completed Ministry of Health and Long-Term Care. Nurse practitioners in long-term care homes. MOHLTC; Ministry of Health and Long-Term Care. Open minds, healthy minds. Ontario s comprehensive mental health and addictions strategy. Ministry of Health and Long-Term Care; Ministry of Health and Long-Term Care. Ontario diabetes strategy. MOHLTC;
112 Action Plans and Interventions Sponsor, oversee and manage nsmchip by clarifying deliverables and ensuring project management which enables successful implementation In collaboration with hospital sector partners, investigate hospital quarterly reporting; evaluate options to improve efficiencies and establish best practices to improve quality of data reported and optimize future year funding Monitor performance, apply new budgeting principles and share best practice through the Community Sector Advisory Group as a means toward increasing the percentage of HSPs achieving all four MSAA performance measures Develop a system-wide approach to capital planning across the region Develop a framework to be applied locally for hospitals renewing/upgrading their Hospital Information System (HIS) in alignment with the recommendations of the HIS Renewal Advisory Panel Streamline the system for submission and storage of data to support planning and oversight of LHIN investments. 2017/ / /20 Status % Status % Status % Not yet started To be completed To be completed To be completed Not yet started To be completed 50 To be completed To be completed Measuring Success A number of the initiatives aligned with this goal are foundational or include the development of performance metrics for other initiatives, and as such will be measured by level of completion. Indicators that will be measured to reflect progress toward this goal include: Number of clients interactions by Adult Diabetes Education Programs Number of clients interactions by Paediatric Diabetes Education Programs Number of signed nsmchip Master Services Agreements (Target: Increase over baseline of 17) Number of organizations fully/partially contributing data to nsmchip (Target: Increase over baseline of 6 partially contributing) Percentage of HSPs reporting a balanced budget (Target: 100%) Percentage of HSPs reporting portion of budget spent on admin is within LHIN specific target (Target: 100%) Percentage of HSPs meeting or exceeding 80% of functional centre level indicators for targeted service activity (Target: 100%) Percentage of HSPs meeting or exceeding 80% of functional centre level indicators for the number of individuals served (Target: 100%) Risks and Mitigation Strategies Risks Availability and accuracy of data is a risk to proper program oversight and monitoring. Outcome related data can also be subjective, difficult to quantify, and hard to collect. The quality of the local HIS renewal framework to be developed is at risk without the inclusion of all acute care partners. Local community engagement on this topic has also identified that community and primary care feedback on the framework is essential to ensure quality of the final product. 50 Mitigation Strategy This ongoing risk must be considered for evaluation initiatives across all programs. Reduce likelihood by leveraging the expertise of the subject matter experts in data analysis and performance to identify appropriate data sources. Mitigate the quality risk by embedding the project team who will develop the framework with LHIN support and oversight as part of the local ehealth Advisory Committee. Strong ties and communication with this committee will ensure that all interested stakeholders are involved.
113 Risks Integration of the Enterprise Risk Management program with existing CCAC risk management policies and approaches may increase the time required to implement and obtain approvals HSP performance is vulnerable to the inherent risks of any business. The following are examples of events that would reduce capacity to deliver service: inability to recruit or retain staff, legal action taken against HSP, inaccurate forecasting of expenses, changes in patient demand, and changes in revenue. Mitigation Strategy Reduce the likelihood of the risk by obtaining all the necessary CCAC risk management documents as early as possible for review. The LHIN is supporting HSPs to strengthen internal processes through new initiatives such as the selfassessment tool and Community Sector Advisory Group. Both items identify potential means of strengthen internal controls that help to mitigate risks. Key Enablers Mental Health and Addictions Project Team This group is made up of key leaders within the NSM LHIN who provide mental health and addictions services to clients. The Project Team provides a consistent forum for discussion and collaboration where the LHIN can engage with health service providers and leverage their collective clinical expertise and leadership. This expertise will be sought in the creation of a mental health and addiction current state inventory. Community Sector Advisory Group The Community Sector Advisory Group (CSAG) was implemented to create a forum for shared problem solving and collaborative innovation. This advisory group is comprised of senior leaders from across the NSM LHIN that represent all four community sectors- Community Care Access Centre, Community Mental Health and Addictions, Community Health Centres and Community Support Services. The group will support the development and implementation of NSM LHIN policy related to Multi-Sector Service Accountability Agreement financial targets, performance indicators and education. Provincial/Pan-LHIN Best Practices in Evaluation and Decision Making Pan LHIN and provincial resources provide a standardized foundation for evaluation, quality improvement and decision making. These include, as examples, the pan-lhin Decision Making Framework, the Health System Improvement Process (HSIP), the Joint Review Framework for capital planning, the LHIN Community Engagement Tool Kit, and the LHIN Physician Engagement Tool Kit. 51
114 Conclusion The North Simcoe Muskoka LHIN s Annual Business Plan (ABP) for 2017/18 presents the second year of operational planning to support delivery on the three strategic priorities articulated in the LHIN s Integrated Health Service Plan (IHSP). The 2017/18 ABP also reflects the expanded role of the LHIN subsequent to the passage of the Patients First Act, The three strategic priorities established in the LHIN s Integrated Health Service Plan are as follows: Improve Access to Appropriate Care Build Capacity and Enhance Coordination Drive System Sustainability The NSM LHIN s strategic priorities were developed in alignment with the direction of the Patients First Action Plan for Health Care and as such, these priorities continue to guide the LHIN s planning following the passing of the Act. To reflect the LHIN s enhanced role in the system, the NSM LHIN has revised the goals articulated in its IHSP to connect ongoing areas of focus with the new priority areas resulting from the Patients First Act. For each of the nine revised goals, the Annual Business Plan includes specific actions and associated indicators that will be measured to ensure LHIN accountability for results. The NSM LHIN and its Board of Directors have also committed to refreshing the LHIN s existing Mission, Vision, and Values to better reflect the role of the renewed LHIN. This work will take place in collaboration with local stakeholders and system partners to produce a collective vision for the transformation of the LHIN that reflects both provincial direction and local realities specific to North Simcoe Muskoka. Stakeholders participating in this process will include health service providers, the public, the LHIN s Patient Caregiver Family Advisory Panel, Indigenous and Métis partners, Francophone representatives, Public Health colleagues, and local municipalities. The implementation of the Patients First Act will be a multi-year journey and the LHIN s next several Annual Business Plans will reflect the work of this system transformation. The NSM LHIN and its Board of Directors will continue to leverage the collective expertise of its system partners and communities to move forward in delivering on our strategic priorities and the renewed vision for the system. It is in the spirit of collaboration that we embark on the transformative change through which NSM s health care system will evolve to achieve the vision of Patients First. 52
115 Appendix A: Integrated Communications Strategy Business Objectives The business objectives of the North Simcoe Muskoka Local Health Integration Network s (LHIN) 2017/18 Annual Business Plan support the strategic directions of the LHIN s IHSP , and the achievement of the health system transformation agenda as it is implemented by the province and across the LHIN: Improve Access to Appropriate Care Build Capacity and Enhance Coordination Drive System Sustainability These three strategic priorities will guide our communication activities with a primary focus on home and community care, fostering stronger relationships with primary care and public health, community based planning in our five sub-regions, expansion of digital health, seniors care, and capacity building. Health equity, quality, community engagement, collaboration and patient centred care will continue to be the lens for developing communication plans and tactics. Communications Objectives Build confidence among residents of the North Simcoe Muskoka LHIN, that: progress is being made to improve access to health services progress is being made to improve the patient experience the system is sustainable, being effectively managed, providing value for tax dollars the system is transparent. Increase health literacy to enable and support residents of the North Simcoe Muskoka LHIN to live healthy lives and manage their illness better. Support patients and caregivers by raising awareness of programs and services to improve their navigation of the system through outlets such as NSMhealthline.ca. Engage providers, stakeholders, and system leaders to become active participants in and ambassadors for transformation. Increase understanding amongst stakeholders and public about North Simcoe Muskoka LHIN programs, initiatives, and successes. Support the goals of the Annual Business Plan for 2017/18, Integrated Health Service Plan and build awareness of other North Simcoe Muskoka LHIN strategic directions and initiatives by identifying opportunities for alignment of communication planning and opportunities with health service providers and other system partners. Mitigate communication risks of negative publicity by proactive media monitoring and evaluation. Context The North Simcoe Muskoka LHIN has a critical role to play in advancing the Patients First: Action Plan for Health Care and the Patients First Act. The priorities of the North Simcoe Muskoka LHIN and the goals A-1
116 that cascade from them reflect alignment with both the strategic goals of Patients First and the priorities of the Ministry of Health and Long-Term Care. The priorities outlined in the ABP will support meaningful improvements in health system performance and integration. Subsequent communication materials will highlight system success and encourage further health system improvements, including: Improving access to the best possible care in the most appropriate setting to optimize health outcomes. Enabling patients to receive high quality, coordinated care across the care continuum while successfully navigating a complex health care system. Providing patients with the right information to make informed decisions about their health. Demonstrating system sustainability, including accountability for results, return on investment, access to services, and appropriate use of system resources to ensure the system is sustainable for generations to come. Delivering better coordinated and integrated home and community care and primary care. Creating a system that is built around the needs of the patient and the unique needs of our 5 sub-regions. The North Simcoe Muskoka LHIN s communications activities and products are well-positioned to align with priorities listed in the mandate letter to the Minister of Health and Long-Term Care, other provincial priorities and amongst the 13 other LHINs. Sub-region integration, primary care, home and community care, mental health and addictions, health equity and population health, patient and caregiver engagement, health system performance and reporting, digital health, capacity planning, will be the primary focus of communication initiatives for 2017/18. The activities which will be undertaken by the North Simcoe Muskoka LHIN over the coming year will ensure we continue to inform and educate the public and providers on the value of LHINs and the role they play in building a sustainable system, provide information for stakeholder and public engagement, and build confidence in the system. Target Audiences The North Simcoe Muskoka LHIN is accountable for communicating with a wide-variety of stakeholders. Depending on the nature of the communication initiative, the target audience for communication will include: Primary Audiences Patients/Family/Caregivers North Simcoe Muskoka LHIN Board and Staff North Simcoe Muskoka LHINs funded Health Service Providers Primary Care including Family Health Teams, Nurse Practitioner-Led Clinics, Community Health Centres and the Primary Care Network Physicians and Health Care Professionals Entité 4 Aboriginal Health Circle Public Diverse populations such as Francophone, Indigenous and Métis, seniors, and marginalized populations. Leadership Council Patient, Family, and Caregiver Advisory Council Secondary Audiences MPPs Ministry of Health and Long-Term Care Municipalities and representatives Media Other LHINs Other Ministries Health Care Associations including OHA, HSSO, OLTCA, etc. A-2
117 Key Messages The below key messages have been developed for 2017/18, however, it should be noted that as situations arise, further messages may be developed to address new projects or developing issues. Provincial Messages Related to Patients First The Patients First: Action Plan for Health Care is Ontario s plan to transform the health care system into one that puts the needs of patients at its centre. The Patients First: Action Plan for Health Care sets clear and ambitious goals for Ontario s health care system in order to put patients at the centre of our health care system by improving the health care experience: increasing access, connecting services, informing patients and protecting our health care system. We have made progress in all four priority areas, but we can do more to put patients first. By putting patients first in everything we do, we will provide faster access to the care patients need today and make the necessary investments to ensure our health system will be there for patients for generations to come. On December 7, 2016, Ontario passed the Patients First Act, 2016, an important step forward in the Patients First: Action Plan for Health Care. Once fully implemented, changes supported by the Patients First Act will make local health care more responsive to local needs: Patients will benefit from improved access to primary care, including a single number to call when they need health information or advice on where to find a new family doctor or nurse practitioner. Primary care providers, inter-professional health care teams, hospitals, public health units and home and community care providers will be better able to communicate and share information, to ensure a smoother patient experience and transitions. Our goal is that patients will only have to tell their story once. Administration of the health care system will be streamlined and reduced, with savings put back into improving patient care. The voices of patients and families in their own health care planning will be strengthened. There will be an increased focus on cultural sensitivity and the delivery of health care services to Indigenous peoples and French speaking people in Ontario. LHINs will ensure that any changes are seamless and that they simplify and improve patient experience. There will be no added bureaucracy and financial savings will go to patient care. Local LHIN Messages Health Equity Context 4.3% of North Simcoe Muskoka residents self-identify as Aboriginal which is the third highest proportion among the 14 LHINs 2.8% of North Simcoe Muskoka residents identify French as their mother tongue Key Messages The North Simcoe Muskoka LHIN continues to work with its partners to promote health equity and enable access to appropriate and culturally safe care. A-3
118 Primary Care Context Only 29.4% of adults in North Simcoe Muskoka report being able to see their doctor or nurse practitioner either the same or next day when ill. 61.1% of North Simcoe Muskoka patients report having difficulty accessing after-hours care without visiting an emergency department. Sub-Regions Context Sub-regions allow LHINs to better plan, integrate, and improve the performance of local health services. They also help the LHIN to identify and understand the diverse population needs be they cultural, linguistic, or other helping our health care system better respond to these needs. The North Simcoe Muskoka LHIN has 5 unique subregions: Barrie and Area Couchiching (Orillia and Area) Muskoka North Simcoe (Midland, Penetanguishene and Area) South Georgian Bay (Collingwood, Wasaga Beach and Area) Key Messages 96.5% of North Simcoe Muskoka patients report having access to a regular medical doctor. The North Simcoe Muskoka LHIN is committed to improving access to primary care. The North Simcoe Muskoka LHIN is fostering sub-region partnerships with primary care to improve access to care, including same day/next day appointments and after-hours care. Work is being done in partnership with primary and home and community care to plan care at a sub-region level. This will allow family doctors and nurse practitioners to better navigate services for their patients. Key Messages Sub-regions are not an added layer of bureaucracy. Sub-regions provide a local lens that will help the North Simcoe Muskoka LHIN better address patients' needs at the local level. Sub-regions will help to ensure that patients can access care that addresses their community s distinct needs, closer to home. Health Literacy Context In North Simcoe Muskoka, the rate of emergency visits for conditions that could be treated in alternative primary care setting consistently exceeds that of the province. Key Messages Work is being done to ensure that North Simcoe Muskoka residents know how to access care in the most appropriate setting. Public Health Context Under the Patients First Act, LHINs are required to promote health equity, reduce health disparities and recognize the social determinants of health, requiring a broader consideration of the health of the population. Key Messages The North Simcoe Muskoka LHIN has had a strong history of working collaboratively with the Simcoe Muskoka District Health Unit. We will continue to strengthen our relationship with public health to better understand and coordinate the population health needs in each of our unique communities. A-4
119 Additional Key Messages The North Simcoe Muskoka LHIN collaborates with health service providers and community partners, enabling them to play an active role in transforming the health system to provide quality care that meets the needs of residents today and into the future. The North Simcoe Muskoka LHIN is committed to building a more seamless and coordinated approach to patient care by working with our stakeholders to identifying current gaps in the health care system, and working together to develop solutions to close those gaps. The North Simcoe Muskoka LHIN is working together with health service providers, funded and non-funded, to provide care in the most appropriate setting. What does this mean for residents? It means getting the care they need, when they need it, in the most appropriate place, and by the most appropriate provider. The North Simcoe Muskoka LHIN is committed to ensuring accountability for current investments to improve capacity in the system, ensuring that our system is sustainable for generations to come. Tactics To help achieve the communications goals and objectives set out in this plan, the following activities are recommended: Communications Activity Internal LHIN Memos/Updates Frequency Responsibility Purpose As needed. Communications in collaboration with Executive Lead. Patient Information As needed. Communications in collaboration with program area. Communiques to Health Service Providers As needed, project/issue dependent. Executive and/or program leads to identify need, communications to support preparation and distribution. Seniors Report Annually. Communications and Seniors Lead. Physician Newsletter Quarterly. Physician Lead and Communications. Media Outreach As required. Communications and program lead. Good News Stories/LHINfo Minutes Monthly/ as required. Program leads and communications to identify communication opportunities and develop content. To ensure all North Simcoe Muskoka LHIN staff are aware of provincial and local developments, potential impacts on work, and key messages associated with priorities and milestones. To provide information on patient services, programs, policies, and procedures for activities related to home and community care. To ensure HSPs remain informed of project status and updates, and/or LHIN-wide or Provincial developments that may impact their clients or service delivery. To raise awareness of senior services in North Simcoe Muskoka LHIN, share information regarding system improvements, promote system success, share patient stories. To engage primary care leaders in North Simcoe Muskoka LHIN, keep informed of LHIN-wide and provincial priorities/projects, provide opportunities to get involved. To raise awareness and inform public audiences of significant achievements, developments, or changes, ministerial announcements. Support HSPs in disseminating important system-wide announcements. For both internal and external distribution, to be packaged in a variety of forms. Build confidence in the system, celebrate milestones and successes. A-5
120 Communications Activity Frequency Responsibility Purpose Community Reports As required. Program leads to identify opportunity for in-depth communication regarding a broader initiative. Conferences/ Speaking Opportunities Engagement with local government representatives Website Management and Updating French Language and Indigenous and Métis communication Board to Board Engagement As appropriate. Bi-annually/ as required. Ongoing. As required. As required. To be attended by relevant Program Lead/ Executive Lead/ CEO/ Board Chair. Key messages and presentations developed in collaboration with Communications. North Simcoe Muskoka LHIN CEO and Board Chair, supported by communications. Communications/ content to be developed by program lead. FLS/ FNMI Coordinator, with assistance from Communications. Collaboration with Entité 4 and Aboriginal Health Circle. North Simcoe Muskoka LHIN Board of Directors Opportunity to provide in-depth education and information about larger portfolios (i.e., HealthLinks, Seniors, Palliative Care). Provide public with information to make better choices regarding health care. Build confidence that work is being done to improve access to care in North Simcoe Muskoka. Opportunity for North Simcoe Muskoka LHIN staff to share best practices, achievements, and innovative health system solutions with public and partner organizations. Raise status and awareness of North Simcoe Muskoka LHIN. Keep local government representatives aware of goals, priorities, milestones, accomplishments. Provide data regarding access to health care, funding, and issues. Provide opportunities for engagement. Provide timely information regarding projects, initiatives, engagement opportunities, milestones, accomplishments, and accountability to public and stakeholders. To provide culturally appropriate information to specific stakeholder groups. Communication products will be created in collaboration with representatives from Entité 4 and the Aboriginal Health Circle to ensure appropriateness and completeness. Maintain open dialogue between North Simcoe Muskoka LHIN Board of Directors and HSP partner boards. Social Media Ongoing. Communications Provide timely information regarding projects, initiatives, engagement opportunities, milestones, accomplishments, and accountability to public and stakeholders. Promote engagement with online communities. Build relationships with partners by promoting and sharing other health system information. Strategic Approach To achieve our Communications Objectives, the following strategies will be used: Communication will be delivered in a variety of formats to accommodate our diverse audiences including our commitment to providing public communication in both official languages. Communication will be timely, clear, and transparent. Where applicable communications materials will include information to raise awareness of services to promote system navigation for patients and caregivers. The North Simcoe Muskoka LHIN s communication will be as proactive and forthcoming as possible. Materials and products will be coordinated with health service providers as appropriate. A-6
121 Communication will incorporate the vision, mission and values of the North Simcoe Muskoka LHIN and position us as a valued key player in the transformation of Ontario s health system. Evaluation Identifying and tracking critical communications success factors will enable the NSM LHIN to more effectively identify whether communication activities have been successful and develop additional strategies as may be appropriate. Critical success factors may include: Health service providers across the NSM LHIN are engaged early and frequently, and can see how their participation is impacting implementation. Online surveys will be utilized, in conjunction with face to face feedback opportunities, to establish a literacy baseline which will inform the focus for communications in future years. Through feedback mechanisms and ongoing assessment, the LHIN will monitor the effectiveness of communications vehicles and messages and adjust plans as needed to support the achievement of the Annual Business Plan s areas of focus. Performance measures to support the success factors listed above may include: Level of engagement by stakeholders, health service providers, persons with lived experience, and the public in response to LHIN community and stakeholder engagement efforts/activities/events. Comments received through the NSM public website. Comments received through engagement activity (feedback forms, interactive discussions). Feedback opportunities will be provided as needed (in person, via survey, or online) to evaluate understanding and effectiveness of communications vehicles/messages in conjunction with the Patient, Family, and Caregiver Advisory council and other community groups. Media monitor to evaluate the increase positive media coverage. Use Google analytics to monitor and measure website traffic and identify content that receives increased focus. Social media following, and level of social media engagement through shares, retweets, likes, and favourites. Work with health system partners to understand increased interest in programs and services following communications related to programs and services. A-7
122 Appendix B: Community Engagement Strategy Health care planning in North Simcoe Muskoka is centred on the needs and experiences of patients, residents, family members, and caregivers as key stakeholders. Community engagement continues to be a high priority as it relates to the planning and provision of high-quality, patient-centred care. Patientcentred care is a key pillar of the Patients First: Action Plan for Health Care with community engagement being a foundational element mandated by the Local Health System Integration Act: Meaningful involvement of stakeholders in the work of the LHIN and health service providers (at all levels), ranging from priority setting and planning to decision-making, implementation, review and evaluation. With the introduction and adoption in July 2016 of the revised Community Engagement Guidelines and Toolkit for all LHINs ( engaging with residents and stakeholders can now be customized to the specific needs and preferences of our communities and regions. There are a number of activities that occur on an ongoing basis in the North Simcoe Muskoka LHIN to ensure that health system planning is informed by residents, patients, health service providers, front line staff, and a broad range of community stakeholders. Notice of planned consultations, as well as any project or consultation-related reading materials are continuously posted on the NSM LHIN website. It is part of the LHIN s role to ensure health care planning is responsive to the needs of the community, residents, patients, health service providers, and other stakeholders. The planning tables, councils, and project steering committees across the region all bring with them a range of clinical and subject matter expertise that is leveraged to inform the creation of appropriate indicators, with which to measure system performance. Many of the LHIN planning tables include residents, patients, and/or caregivers who provide the voice of lived experience and represent a variety of different demographic or geographic areas. These participants are encouraged to share their stories and provide context to how the work of the committee has real potential implications for the members of the community. The NSM LHIN continually looks to increase participation and seek new ways of incorporating the patient voice into LHIN planning activities. The goals of community engagement in North Simcoe Muskoka are: To solidify the key role that patients, residents, health service providers, and other stakeholders play in identifying community needs, gaps, and successes and informing change across the local health care system; To be highly inclusive and equitable with a range of opportunities available for patients and stakeholders to provide their perspective; To identify gaps, needs, and successes that become a key form of evidence to drive planning and system improvement; To ensure stakeholders feel valued as contributors and see how their feedback and participation is impacting the design, quality, and sustainability of the health care system. As the health care system moves forward and continues to evolve, there will be ongoing opportunities for engaging stakeholders from the NSM community and beyond. Throughout the 2017/18 Annual Business Plan, community engagement activities through various committees and initiatives have been identified as key enablers of our work. As new areas of work are identified in the future, the NSM LHIN will B-1
123 continue to engage stakeholders in supporting home and community care, primary care transformation, and stronger collaboration with public health. The patient voice, the engagement of the community, and perspectives of health system partners are all be essential to success in these areas. Cross-Sector Community Engagement There are a number of community engagement events or initiatives that are ongoing in the NSM LHIN and do not represent one particular topic, sector, or clinical area. The following are a sampling of these broader community engagement initiatives, with additional engagements added as required for specific purposes. NSM LHIN Patient Caregiver Family Advisory Panel Established in March of 2015, the Patient Caregiver Family (PCF) Advisory Panel plays a crucial role in ensuring initiatives maintain a patient-centred focus and that the patient voice is heard and included in all levels of the planning, implementation and evaluation. Members of the Panel share their perspectives and vast experience with the local health care system to continue to improve services for all residents of our region. The panel also acts as a valuable resource for LHIN staff and partner organizations to work through current and future initiatives to ensure a patientcentred focus. Members provide input and feedback on the development of LHIN strategic priorities, and the inclusion of the patient and caregiver voice in LHIN communications. Panelists are now planning what the inclusion of the patient and caregiver voice will look like at the sub-regional level of NSM LHIN. Recruitment for membership is ongoing. NSM LHIN CEO Meetings with Patients, Caregivers, and Family Members In addition to being members of the NSM LHIN PCF Advisory Panel, the NSM LHIN CEO and Community Engagement Coordinator meet informally with people interested in sharing their stories, experiences and ideas regarding the health care system within North Simcoe Muskoka. Meetings occur regularly to ensure that the patient voice is heard directly by key LHIN decision makers and stories are shared with councils, committees and working groups to inform their ongoing work. Often, people the CEO meets with are invited to become directly involved with a council, committee or working group specific to the experiences of that individual patient or caregiver. NSM Care Connections Forum The annual Care Connections Forum is a large LHIN-wide event, in which approximately 300+ key stakeholders gather to strengthen relationships, share best practices, and transfer knowledge. In 2017, the NSM LHIN has partnered for the first time with the Aboriginal Health Circle to hold the NSM LHIN Care Connections and Aboriginal Health Forums on consecutive days (March 28 and 29, 2017). Experts from the Southcentral Foundation in Alaska have been invited to come and share their knowledge on the NUKA model of care. Their experience and expertise in transforming their local health care system to a more holistic, patient-centred model will be the theme running through both events. Community Surveys Community surveys are utilized frequently via the NSM LHIN website and Twitter to solicit feedback from residents, caregivers, health community partners and service providers. Surveys are provided in both French and English, and often include questions about the demographics of the participants, including self-identification to ensure the responses gained are reflective of a representative sample. Health System Funding Reform (HSFR) Local Partnership Group The province mandated the creation of a HSFR Local Partnership to assist with capacity planning and change management around Health System Funding Reform. The NSM LHIN s HSFR Local Partnership includes representation from hospitals, the CCAC, and long term care, and has been working collaboratively since January 2013 to implement Quality B-2
124 Based Procedures at the local level. The group informs the distribution of resources, shares best practices, and identifies models of care including care paths, policies and procedures to implement at an organizational level in order to meet provincial standards. The local partnership uses the results of the Quality Based Procedures Implementation Index to inform their work. Regional Quality Advisory Council The NSM LHIN partnered with Health Quality Ontario to establish a Regional Quality Advisory Council. This group will provide a forum to discuss quality improvement strategies across the LHIN and align these strategies with regional and provincial strategic directions. It is led by a regional clinical chair and is comprised of regional clinical leads, sector leaders, and a Health Quality Ontario regional quality improvement specialist. This table will be a valuable resource for the NSM LHIN, as it will provide a venue to discuss performance improvement, align efforts across sectors, develop standardized methods of care, and share best practices throughout the region. Service Accountability Agreement Information Sessions There are three Service Accountability Agreement Information Sessions that take place annually (as needed) across the LHIN; one for each sector including hospital, community, and long term care. They are conducted via webinar/teleconference and are attended predominantly by administrators, executive directors, and senior finance personnel. These sessions are a means of providing information and seeking feedback from health service providers on the inclusion of indicators, completion of schedules, and sign-backs for Service Accountability Agreements. This year, an advisory group was created to support the mandate for the community sectors under the MSAA. Simcoe County Local Immigration Partnership (SCLIP) Beginning in 2016/17, the LHIN French Language Services Coordinator, Aboriginal Health Liaison, and Equity Lead will be participating on the SCLIP with a lens on health equity. This partnership is led by the County of Simcoe and focused on the development of settlement strategies for newcomers to the region. As such, the LHIN Liaison will be building relationships, bringing opportunities forward with regards to building and improving health equity, and gathering feedback on behalf of the LHIN from this group. NSM LHIN Sub-Regional Engagement We will help guide the establishment of formal partnerships and collaborations between health care and community partners and local residents (patients and caregivers) in each of our 5 sub-regions to better meet the needs of specific client and patient populations in a geography to: Formally articulate and strengthen the continuum of care across HSPs and sectors for clients and patients with specific care conditions; Standardize approaches to care and service in focused sectors; Integrate programs and services to improve quality, access and outcomes; and, Build shared capacity in key back office functions that are necessary to support the efficient and effective delivery of care. Indigenous and Métis The LHIN funds a variety of services through six organizations, specifically serving individuals who identify as Indigenous or Métis, and also have many stakeholder partnerships across ministries and organizations that are not LHIN funded. Those who identify as Indigenous or Métis call attention to challenges they face in receiving equitable access to health services including funding issues, lack of sensitivity to their culture, and a lack of targeted programs that focus on their particular health needs. Engagement of the Indigenous and Métis communities helps to ensure that LHIN work continues to be informed by their needs and perspectives, and that traditional practices and the unique cultural needs of these populations are honoured and incorporated. The NSM LHIN makes concerted efforts to have individuals who identify B-3
125 as Indigenous or Métis participate on all LHIN sub-region planning and engagement groups. Over the course of 2016/17 the number of groups with Indigenous and Métis representatives will be increased. The NSM LHIN and LHIN Aboriginal Lead will participate in the following engagements during 2017/18. Aboriginal Health Circle Meetings These meetings are led by Indigenous and Métis service providers in the community. They are attended by the LHIN, and are a valuable opportunity for the LHIN to learn more about the needs of the community, and communicate opportunities for Indigenous and Métis participation in regional initiatives. Aboriginal Health Forum The two-day Aboriginal Health Forum, held each spring, explores health issues across the life cycle, through a format of interactive workshops, key-note speakers, and community discussion. Participants gain a better understanding of the holistic perspective of health, wellness, and Mino'Bimaadziwin (meaning The Good Life ). The forum is attended by health care partners, the LHIN, and members of the community. It has strong attendance and increases the visibility of the Indigenous, Métis community in health care. Meetings with First Nation Band Councils In partnership with the Aboriginal Health Circle, LHIN leadership and the LHIN Aboriginal Lead have annual meetings with the leadership of the four First Nation s communities in North Simcoe Muskoka. These include the Beausoleil, Chippewas of Rama, Wahta Mohawk, and Moose Deer Point First Nations. The purpose of these engagements is to improve health equity and equity of outcomes for the Indigenous and Métis populations. Relationships are continually being built and strengthened to ensure that the Indigenous and Métis communities are engaged in health system improvement. Emerging issues can be identified, and feedback can be provided in terms of removing barriers in support of equitable access to care and equity of outcomes. These sessions also facilitate an improved LHIN understanding of existing regional, provincial, and federal health planning and service delivery within the Indigenous and Métis communities. The continued involvement and engagement of the NSM LHIN s Indigenous and Métis residents in system planning is crucial. French Language Services (FLS) There are currently eight health service providers that are identified and one that is designated to provide health care services in French throughout North Simcoe Muskoka. Community engagement efforts will be increased over the coming fiscal year to enable the completion of LHIN deliverables in a manner that is responsive to the needs of the community. A continued partnership with the French Language Health Planning Entity (Entité 4) is key in advancing the LHIN priority of meeting the needs of the Francophone community. The primary role of Entité 4 is to support the engagement of the Francophone population by soliciting feedback regarding health needs and priorities, health services available, and the potential identification of organizations for French language services. Feedback from the community can then be used as the foundation for informed, evidence-based, and patient-centred planning in each sub-region of NSM LHIN. NSM French Language Services Community of Practice (FLS COP) The FLS COP consists of all French language identified and designated health service providers in the region. Organizations that are not LHIN funded are also represented. This Community of Practice collaborates to share best practices, policies, resources, and lessons learned. In doing so, they enable the work of building and supporting French language services across the region. At the same time, the LHIN leverages the expertise of the B-4
126 group to overcome barriers and gaps which have been identified in an effort to assist in improving LHINwide service provision. Community Partners with Schools (COMPASS) Meetings These monthly meetings are attended by elementary and secondary school representatives and community mental health service providers. The goal is to enhance healthy child and youth development, and to reduce social, emotional, or behavioral barriers to learning. The LHIN French Language Services Coordinator is also linked to these groups as an ongoing opportunity to improve relationships between Francophone community organizations, school boards, and the LHIN. These partnerships support the development of French language services for Francophone youth with regards to mental health and addictions. Local Community Engagements The NSM LHIN continues to work closely with the French Language Health Planning (Entité 4) to maintain and enhance existing collaborative working relationships, and to continue to engage the Francophone community. Entité 4 plays a key role in addressing the needs of the Francophone community in the region. By partnering with and advising the LHIN on how best to overcome existing barriers, and improve access to and accessibility of French language services, Entité 4 continues to support the delivery of excellent care. Acute Care Stroke Steering Committee The NSM LHIN Integrated Stroke Plan will be implemented in three phases, the South, Central and North parts of NSM. The South Project has been in development all of since 2015/16 and is close to accepting its first patient by the end of 2016/17. The South Project has engaged physicians, allied professionals both inside and outside of the acute setting, and patients and their caregivers through a qualitative evaluation method. The tools used to engage the various stakeholders will be replicated through the development and implementation of phase two, the Central part of NSM, and phase three, the Northern part of NSM. NSM Local Critical Care Network The Local Critical Care Network meets regularly and is represented by the hospitals within NSM. Their role is to collaborate and support the implementation of the Ontario Critical Care Plan , with the key goal to provide standard and consistent critical care across the region. 77 Emergency Department (ED) Steering Committee The ED Steering Committee is a collaborative gathering of administrative and clinical leaders in emergency medicine. The committee enables sharing across health care providers of successful initiatives to improve emergency department flow and quality. As reforms in primary, home, and community care proceed, the emergency departments across the LHIN will be involved in planning proactively rather than simply responding to the impacts of the collective system. Community-Based Care Community Support Services (CSS) Collaborative The CSS Collaborative is comprised of leaders from across the community sector and is a key partnership for the LHIN to work through issues and create opportunities. The Collaborative also provides a forum for soliciting essential feedback on gaps and concerns. In order to complete the work, stakeholders come together regularly to better understand the 77 Critical Care Services Ontario. Ontario critical care plan CCSO; B-5
127 capacity of the system for central intake and the readiness of organizations to potentially implement an electronic solution. Palliative Care Planning Sessions and the NSM Regional Palliative Care Network (NSM RPCN) The NSM Regional Palliative Care Network Steering Committee was established in December, 2016 and includes key regional health care and community stakeholders and providers as well as patients/family members. The NSM RPCN is aligned with the Ontario Palliative Care Network (OPCN) and will be guiding hospice palliative care within NSM. The NSM RPCN will continue to work with regional providers, stakeholders and communities to support the development of a high-quality, coordinated hospice palliative care system. Community Sector Advisory Group The Community Sector Advisory Group (CSAG) was implemented to create a forum for shared problem solving and collaborative innovation. This advisory group is comprised of senior leaders from across the NSM LHIN that represent all four community sectors- Community Care Access Centre, Community Mental Health and Addictions, Community Health Centres and Community Support Services. The group will support the development and implementation of NSM LHIN policy related to Multi-Sector Service Accountability Agreement financial targets, performance indicators and education. Assisted Living Services for High Risk Seniors (ALS-HRS) Steering Committee ALS-HRS services within NSM are currently being evaluated through a framework developed with the support of the ALS-HRS Steering Committee. This evaluation will support the direction of planning for ALS-HRS in North Simcoe Muskoka. Muskoka and Area Health System Transformation (MAHST) Council As an implementation plan for a future model of health care for Muskoka and Area is developed, the NSM LHIN will continue to work in coordination with the local members of this group to support ongoing communications and community engagement activities and needs. Seniors Services Seniors Health Project Team The Seniors Health Project Team, as advisory to the LHIN and Specialized Geriatric Services Lead Agency, is accountable for regional system recommendations, ensuring that planning and implementation aligns with goals set out in relevant project charter(s). The team includes leaders from inside and outside the health system and partners with other planning groups such as the LHIN s Patient Caregiver Family Advisory Panel. The Seniors Health Project Team will support planning and community engagement associated with the Specialized Geriatric Services that have resources dedicated for these purposes. Long Term Care Sector Summits LHIN-led long term care sector summits will be conducted annually. These events will be held to ensure long term care is adequately represented in the planning and execution of ongoing work across the region. It is an opportunity for the LHIN to continue to build and strengthen relationships with long term care providers and their clients. Following these events, participants are encouraged to provide their feedback through an online survey. These summits have been well attended and the feedback has indicated that the commitment to this event is of value for both the LHIN and the participating long term care representatives. Primary Care LHIN Physician Lead, Clinical Planning and System Integration and NSM Primary Care Network The NSM LHIN Physician Lead, Clinical Planning and System Integration will support LHIN work in enabling access to timely and appropriate primary care. The Lead will continue to strengthen relationships, act as a B-6
128 champion and subject matter expert, and play a key role in the leadership of the NSM LHIN and the NSM Primary Care Network. The Primary Care Network is a collaborative group of local physician champions who work to move the system forward, identify potential issues, and educate and engage their peers to bring their perspective and contribute to new initiatives. Mental Health and Addiction Mental Health and Addictions Project Team The NSM LHIN benefits significantly from the inclusion of the Mental Health and Addictions Project Team within its decision making process and ongoing work. This group is made up of the key leaders within the NSM LHIN who provide or support mental health and addictions services. The LHIN works in coordination with the Project Team to enhance access to mental health and addictions services for residents through the development, planning, implementation, and evaluation of new and existing programs, services and initiatives. The Project Team provides a consistent forum for discussion and collaboration where the LHIN can engage with health service providers, leveraging their collective clinical expertise and leadership. Complex and Chronic Health Conditions Health Links Community of Practice The focus of the Health Links Community of Practice group is Health Link sustainability and standardization of practice and care. Areas of focus include reduction in the number of patients waiting for an alternate level of care (ALC), palliative care planning, data quality and consistency, Quality Improvement Plans, and a regional and sub-regional focus on activities to reduce 30 day readmissions. The group consists of Health Link leaders, care coordinators, and front line staff as required to inform specific initiatives or act as subject matter experts in project work. The Health Links Community of Practice is very focused on the outcomes of community and patient engagement in each Health Link, and utilizes patient satisfaction survey results and patient stories in every community of practice meeting to drive the work at a regional level. ehealth NSM LHIN ehealth Advisory Committee The committee is comprised of health service providers and leaders across multiple sectors. The purpose is to enable ehealth initiatives through the collective identification of gaps, needs, assets, and opportunities. Participants on the committee support the development and implementation of the LHIN ehealth Strategic Plan and act as subject matter experts regarding information technology, clinical workflow, and health administration. Members facilitate alignment between organizational and regional ehealth priorities, and champion the local implementation of projects initiated both regionally and provincially. The LHIN acts as a liaison to this group, and supports the facilitation of discussion and planning as needed in collaboration with the chairs. The LHIN shares the status of provincial and regional projects with the group, and brings back feedback from the committee to NSM LHIN, regional, and provincial tables. B-7
129 Appendix C: LHIN Operations Spending Plan LHIN Operations 2016/ / / /20 Sub-Category ($) Projected Actuals Allocation Planned Expenses Planned Expenses Salaries and Wages $2,320,330 $26,163,278 $26,163,278 $26,163,278 Total Salaries and Wages $2,320,330 $26,163,278 $26,163,278 $26,163,278 Employee Benefit HOOPP $233,386 $2,446,308 $2,446,308 $2,446,308 Other Benefits 277,797 4,081,983 4,081,983 4,081,983 Total Employee Benefits $511,183 $6,528,291 $6,528,291 $6,528,291 Transportation and Communication Staff Travel $37,584 $457,075 $457,075 $457,075 Governance Travel 25,286 28,000 28,000 28,000 Communications 35, , , ,116 Other Recruitment & Other 6,651 15,500 15,500 15,500 Total Transportation and Communication $104,616 $760,691 $760,691 $760,691 Services Accommodations $188,026 $1,286,805 $1,286,805 $1,286,805 Advertising 3, Banking 918 3,500 3,500 3,500 Community Engagement 139, , , ,415 Communications 0 5,000 5,000 5,000 Consulting Fees 217,928 55,767 55,767 55,767 Equipment Rentals 11, , , ,069 Governance Per Diems 115, , , ,000 Insurance 0 33,784 33,784 33,784 LSSO Shared Costs 318, Other Meeting Expenses 21,183 21,573 21,573 21,573 Other Governance Costs 19,036 24,000 24,000 24,000 Printing & Translation 13,577 41,205 41,205 41,205 Staff Development 88, , , ,250 Home Care Purchased Patient Services 0 69,665,884 69,665,884 69,665,884 Home Care Medical Supplies and Equipment 0 5,353,129 5,353,129 5,353,129 Total Services $1,138,434 $77,223,881 $77,223,881 $77,223,881 Supplies and Equipment Office Supplies and Equipment $13,823 $112,150 $112,150 $112,150 IT Equipment 63, , , ,322 Total Supplies and Equipment $77,092 $416,472 $416,472 $416,472 Total Planned Expenses (LHIN OPS) $4,151,655 $111,092,613 $111,092,613 $111,092,613 Annual Funding Target $4,151,655 $111,092,613 $111,092,613 $111,092,613 Variance Note: The Budget does not include funding and costs for other initiatives. C-1
130 Appendix D: LHIN Staffing Plan (Full-Time Equivalents) 2016/17 FTEs 2017/ / /20 Position Title as of Mar. 31/17 Forecast FTEs Forecast FTEs Forecast FTEs Chief Executive Officer Chief Operating Officer Vice-President of Clinical Vice-President of Home and Community Care Vice-President of Financial Health and Accountability Vice-President of System Transformation Vice-President of Quality and Performance Directors* Client Care Coordinators Team Assistants Nurse Practitioner Mental Health & Addictions Nurse Rapid Response Nurse Telehomecare Coordinator Information and Referral Managers* Application Specialist* Communications Community Engagement Contracts Advisor Executive Assistant Facilities Accounting* Administrative Assistant Analyst* Human Resources* Health Information Management Improvement Specialist Payroll Project Management* In-Service Education Total FTEs Note: * Funded in part through Initiatives. FTE numbers above do not include staffing for other initiatives. D-1
131 Briefing Note Title: Psychogeriatric Resource Consultants Integration by Funding Agenda Item: 3.9 Meeting Date: June 26, 2017 Item For: Information Submitted By: Ligaya Byrch Input/Direction Approved By: Neil Walker Decision Attachment(s): Yes (list below) No - Key Highlights from Committee: The Committee of the Whole discussed the various integration options available to the LHIN at this time. It was felt that since the two Health Service Providers already agree in principle to the context of the integration that the recommendation to integrate by funding be supported. Considerations for the Board: Majority of the Committee voted to support the proposed motion embedded below. Proposed Motion: That the NSM LHIN Board of Directors endorse the integration by funding of the Psychogeriatric Resource Consultant program that would result in the permanent transfer of all associated program resources, including $208,258 in LHIN funding, from Collingwood General and Marine Hospital Community Mental Health Service to Waypoint s regional Specialized Geriatric Services program effective October 1, Information as submitted to the Committee of the Whole on June 12, 2017: Issue/Context: In 2015 the NSM LHIN region completed a review of thirteen seniors health programs to understand opportunities related to the development of an integrated regional program for frail seniors. The report recommended the resources and responsibilities of the Psychogeriatric Resource Consultant (PRC) program at Collingwood General & Marine Hospital (CGMH) be integrated with the [now] NSM Specialized Geriatric Services (SGS) Program, led by Waypoint Centre for Mental Health Care. The purpose of this briefing note is: To secure LHIN Committee of the Whole support for integration by funding of Collingwood General & Marine Hospital s (CGMH) Psychogeriatric Resource Consultant (PRC) program with Waypoint Centre for Mental Health Care s NSM Specialized Geriatric Services (SGS) Program. Background: PRC History Ontario s Strategy for Alzheimer Disease & Related Dementias: The 1999 provincial Strategy for Alzheimer Disease and Related Dementias (ADRD) provided funding for 50 PRCs. Their role was to support health service providers in LTC and the community to work with people with ADRD, other complex mental health needs and associated behaviours. The PRCs had three primary roles: educator, consultant and networker/developer. In NSM, CGMH became the lead agency. Two PRCs were recruited in 2001.
132 Over time, PRC roles evolved across the province with some regions eliminating PRCs and others changing the role and scope to support local needs. In NSM, PRC practice held to the original scope. Positions have been sustained because of the benefits from PRC leadership and capacity building. Since inception in 2001, the main focus of the NSM PRCs has been the LTC sector. NSM Initiatives: o Behaviour Intervention Response Team (BIRT) - In 2009/10, Waypoint received funding from the LHIN to establish BIRT. BIRT was intended to provide a wrap-around service to NSM LTC residents with significant cognitive impairment and severe/high risk behaviours. CGMH collaborated in developing the proposal and identified a service partnership whereby the PRCs would be an integral part of the service delivery model for BIRT. The service partnership vision was never realized. o Behaviour Support Ontario (BSO) - In 2011, the province launched BSO. The BSO Project was created to enhance services for those with behaviours associated with complex and challenging mental health, dementia or other neurological conditions wherever they live at home, in long-term care, or elsewhere. The NSM Behaviour Support System (BSS) Action Plan was developed by many partners including Waypoint and CGMH. The plan outlined the vision for NSM BSS resources and clinical services. Funding was received for an additional PRC in the region (total PRCs in NSM =3) for the intent to have one PRC lead each of the three LTC behaviour teams being developed. Currently, the PRCs work as partners alongside the LTC behaviour teams but never assumed the leadership role. NSM LHIN Direction Seniors Health Program Review - In 2015 the NSM LHIN region completed a review of thirteen targeted seniors health programs to better understand opportunities related to the development of an integrated regional program for frail seniors. The PRC program was reviewed. As an individual program, PRCs were identified as an important part of the NSM BSS team with some opportunities for change identified. Evaluators noted that PRCs did not benefit from corporate co-location with the Community Mental Health Service at CGMH and recommended the PRC resources and responsibilities be integrated within the mandate of a proposed IRSHP 1. It was further recommended that a single integrated Behaviour Support Team be developed inclusive of the PRCs. LHIN Action Plan: Based on the results of the Seniors Program Review, the NSM LHIN developed an Action Plan (July 2015) to establish an integrated regional Specialized Geriatric Services (SGS) Program. The plan included the development of a LHIN-wide basket of specialized geriatric services through redesign and integration, with early focus on individuals living with behaviours. NSM SGS Program: o Lead Agency - In late 2015, Waypoint was identified by the LHIN as the lead agency for the NSM SGS Program. As Lead Agency, Waypoint is accountable to the LHIN and LHIN Leadership Council for the NSM SGS Program. The NSM SGS Program was directed to establish an integrated regional Behaviour Support System as an early deliverable. o Clinical Design - In 2016, the NSM SGS Program completed the Clinical Design Report & Recommendations document. The document was endorsed by the NSM LHIN Seniors Health Project Team and the NSM Behaviour System Implementation Steering Committee and was circulated to LHIN Leadership Council. The document defines an ideal state for the clinical design of the program: Currently, services supporting older adults with cognitive impairment and responsive behaviours operate as distinct partners under the NSM BSS umbrella. In alignment with the recommendations of the Seniors Program Review (2015), the current behavior and geriatric psychiatry resources supporting this unique population will be redesigned and aligned under the [NSM SGS] clinical service to create an integrated regional system. 1 IRSHP was the concept proposed in this document that was re-named the NSM SGS Program by the LHIN. Page 2 of 5
133 Current State CGMH is funded to support three PRCs. This includes the original 2.0 FTE positions funded through the ADRD Strategy and the additional 1.0 FTE position funded via Waypoint through the provincial 2011 BSO initiative. The program receives $319,654 in funding, including $111,396 from Waypoint. The PRCs report under functional centre # (Health Prom/Educ & Dev Psycho-Geriatric) under the CGMH M-SAA. They have the following performance targets: Not Uniquely Identified Service Recipient Interactions 1200 Sessions 1200 Participant Attendances 4800 The PRCs did not achieve performance targets in and The main reason for variance was a PRC vacancy. The PRCs outperformed volume targets the previous 4 years. Analysis / Discussion In alignment with LHIN and NSM SGS Program directions, the SGS Program has been actively working with BSS partners over the last year to redesign the BSS team. As part of Phase 1 work, both County of Simcoe and Waypoint BSS resources have been redesigned: A BSS Manager role has been established. The Waypoint BIRT team has been disbanded and the resources redesigned to provide more specialized support within the BSS team for complex cases. The scope and role of LTC resources have been revised, including aligning a PSW with every NSM LTC beds to provide a more visible presence and just-in-time support to LTC providers for older adults with cognitive impairment and responsive behaviours. The BSS team have completed education in March 2017 that included certification in mental heath recovery as well as education in compassion fatigue and sexuality/intimacy in dementia. Additional education plans are being established to continue to build BSS team capacity. Standardized processes and tools are being established for use across the team. Phase 1 redesign took effect June 1, Phase 2 focuses on the redesign of remaining BSS team resources including the PRCs as well as community BSS resources aligned with the Alzheimer Society of Greater Simcoe County, Care Partners and Wendat. Integration by Funding To support Phase 2 BSS redesign, the LHIN is seeking approval from the Committee of the Whole / Board of Directors in June 2017 for integration by funding of the CGMH PRC program with Waypoint s regional SGS Program. Under LHSIA, Section 19 refers to Integration By Funding. This method of integration reflects a transfer, merge or amalgamation of services, operations, persons or entities. While the integration proposed by CGMH and Waypoint is within the LHIN CEO s Delegation of Authority, the nature of the Integration requires the approval of the LHIN Board of Directors. Benefits of Integration / Rationale Alignment with the MoHLTC s Alzheimer s Strategy and Provincial Behavioral Strategy, and NSM LHIN IHSP 2016_2019. Through integration the NSM region will move toward a single integrated regional BSS team. This will result in improved communication as well as a more standardized and collaborative approach to care across the region. PRCs have been building capacity in the LTC sector in NSM for 16 years. Through Phase 1 redesign, LTC BSS resources will increase their role in capacity building thereby creating an opportunity to explore the PRC capacitybuilding role in other sectors like acute care, primary care and the community sector (including the Retirement Home sector). Page 3 of 5
134 With 30 BSS resources in LTC and 7 BSS resources in the community it is important to explore BSS team redesign to build capacity in the community sector to promote aging in place and prevent premature admission to LTC. As identified during the Seniors Program Review, there is no benefit in corporate co-location of the PRC program with the Community Mental Health Service at CGMH. As a result of BSS redesign, including PRC integration, we anticipate better outcomes for older adults with cognitive impairment and responsive behaviours, their caregivers as well as health service providers. Through these changes it is anticipated (see Appendix A): Improved resident and caregiver outcomes (i.e. improved assessment and management of responsive behaviours, increased caregiver satisfaction). Enhanced system capacity (i.e. increased knowledge and skillsets of providers and caregivers). A more affordable, sustainable and accountable system (i.e. increased care of frail seniors and their caregivers in their home settings, reduced inappropriate use of hospital and LTC resources). Integration Terms & Conditions The CGMH and Waypoint senior teams have had lengthy discussion around this integration, with both teams supporting the integration. The following terms and conditions are proposed for this integration: Effective October 1, 2017 annual LHIN base funding for the PRC program in the amount of $208,258 be transferred permanently from the CGMH Community Mental Health Service to Waypoint s regional SGS Program. The agreement between Waypoint and CGMH for 1.0FTE PRC that results in the transfer of BSO funds in the amount of $111,396 will be terminated. To move toward the creation of a single integrated regional BSS team, leadership for the PRC staff will shift to the SGS Program effective July 4, An interim leadership plan will be put in place for the period July 4 September 30, 2017 to clarify organization accountabilities and responsibilities during the transition period from CGMH to Waypoint. Effective October 1, 2017 all 3 PRCs will become employees of Waypoint and the NSM SGS Program. No severance will be incurred as a result of this transfer. All wage adjustments resulting from the transfer of staff from CGMH to Waypoint will be addressed through current BSS team surpluses. It is anticipated that the annual cost of this transfer will be approximately $25,000. Current CGMH base funds used to address PRC program deficits will remain with CGMH. Key Risks & Mitigation Strategies Transition Cost The cost of transfer would be limited to the wage disparity that will result in the movement of staff from a non-unionized position at CGMH to a unionized position within Waypoint. The estimated annual cost of transfer is $25,000. Costs associated with program operations, currently paid through CGMH base funds will be absorbed through current BSS surpluses resulting in more appropriate alignment of provincial and LHIN funding. Through reduced travel, improved use of technology and other efficiencies we hope to offset some of this cost of transfer by reductions in program operating expenses. Role clarity As the role transfers and evolves, role clarity may become compromised. The SGS Program will engage with the PRCs and other key stakeholders in role evolution and leverage the SGS Program s communication strategy to promote role clarity. Retention There is always a risk that change will result in the loss of skilled and experienced clinicians. The SGS Program will promote open dialogue and work in partnership with the PRCs, HHR departments and organization leaders to support PRC transition. South Simcoe currently the PRCs support LTCHs in the South Simcoe region. This region is outside NSM LHIN boundaries and within the jurisdiction of the Central LHIN. The NSM SGS Program will work with the NSM LHIN and Central LHIN to define boundaries and role, given the integration of the PRCs within the NSM BSS team. Page 4 of 5
135 Services to South Simcoe will remain status quo until an appropriate plan of care is in place to support LTCH residents and their caregivers. Strategic Alignment IHSP Strategic Priority #2: Build Capacity and Enhance Coordination o 2.1 Establish infrastructure to improve care for seniors and older adults: Develop a strategy for an integrated regional seniors health program that builds on existing resources and infrastructure established through the Specialized Geriatrics Program. Develop and implement a plan for an integrated behavioural support system within the Specialized Geriatrics Services program IHSP Strategic Priority #3: Drive System Sustainability o 3.3 Enhance transparency in planning and directing future investments: Integrate services into a single funding envelope for the Specialized Geriatrics Services program to maximize efficiency and effectiveness Recommendation: It is recommended that the NSM LHIN Committee of the Whole / Board of Directors support an integration by funding of CGMH s PRC program with Waypoint s regional SGS Program under the Waypoint M-SAA. Proposed Motion: That the NSM LHIN Committee of the Whole recommend to the Board of Directors support for an integration by funding of the Psychogeriatric Resource Consultant program that would result in the permanent transfer of all associated program resources, including $208,258 in LHIN funding, from Collingwood General and Marine Hospital Community Mental Health Service to Waypoint s regional Specialized Geriatric Services program effective October 1, Page 5 of 5
136 Briefing Note Title: Broader Public Sector Accountability Act (BPSAA) Reporting Requirements Agenda Item: 3.10 Meeting Date: June 26, 2017 Item For: Information Submitted By: Jeff Kwan Input/Direction Approved By: Decision Attachment(s): Yes (list below) No - Key Highlights from Committee: The filing of the report is a requirement under the Broader Public Sector Accountability Act, 2010 (BPSAA) which helps protect the interests of taxpayers and increases accountability for those agencies covered under the Act. Considerations for the Board: The majority of the expenses outlined in the table are for travel, meals and accommodation and were claimed in accordance with the Management Board of Cabinet s Travel, Meal and Hospitality Expenses Directive which LHINs must follow. Proposed Motion (if required): That the NSM LHIN Board of Directors approve the 2016/17 Public Disclosure of Expenses report as outlined in Section 2. Information as submitted to the Committee of the Whole on June 12, 2017: Issue/Context: To seek NSM LHIN Committee of the Whole endorsement of the 2016/17 Public Disclosure of Expenses report required under the Broader Public Sector Accountability Act. Considerations: The Government of Ontario and various Broader Public Sector (BPS) organizations provide goods and services to Ontarians. Generally, the Broader Public Sector refers to the organizations that receive funding from the Government of Ontario. They are not, however, a part of the government itself. Examples of BPS organizations include LHINS, hospitals, universities, colleges, and school boards. The rules that govern accountability and transparency for the BPS are set out in legislation and in directives issued under legislation. The Broader Public Sector Accountability Act, 2010 (BPSAA) establishes requirements in the areas of compensation, expenses, perquisites, business documents and procurement, and is designed to improve accountability and transparency across the BPS. The Act prohibits designated BPS organizations from paying for a consultant lobbyist with public funds. It also contains specific requirements for hospitals and LHINs to report on the use of consultants and report publically on expense claim information. LHINs must report to the ministry on three topics: /17 Report on Use of Consultants: This report was approved at the May 29, 2017 LHIN Board of Directors meeting.
137 /17 Public Disclosure of Expenses LHINs are required to post expense information for designated persons. Designated persons is defined as the CEO and senior management team of the entity, the appointed members of the entity s board, as well as the top five expense claimants in a one-year period (should they not already be included in the aforementioned). The expenses for designated persons for fiscal year 2016/17 were as follows: Annual Expense Amounts for NSM LHIN Designated Persons for FY 2016/17 Name Title Total Expenses Jill Tettmann Chief Executive Officer $19, Robert Morton Board Chair $12, Neil Walker Chief Operating Officer $5, Tina Christman French Language Coordinator $5, Ligaya Byrch Senior Manager $4, Rebecca Van Iersel Physician Lead $3, Peter Preager Board Member $2, Larry Saunders Board Member $2, Barbara Dickson Board Member $1, Ellen Mary Mills Board Member $1, Ron Stevens Board Member $1, Ernest Vaillancourt Board Member $1, Leanne Vincent Corporate, Office Coordinator $ Tim Withey Board Member $ Andreas Ott Board Member $ Ewelina Chwilkowska Board Member $ Margaret Redmond Board Member $56.80 Total $63, LHIN Staff review expense claims to ensure adherence to the Travel, Meals, and Hospitality Directive: Identify any low cost items (Under $5): None Identify any items that exceed the maximum amount stipulated in the Travel, Meal and Hospitality Directive (eg: Dinner expense amount exceeding maximum stipulated in Directive): None Identify any travel outside the province: None Briefly identify contentious issues (eg: International travel that did not receive appropriate approval): None 3. Compliance Attestation LHINs are required to prepare quarterly attestations, made by its CEO, and approved by its board, attesting to: The completion and accuracy of reports required on the use of consultants Compliance with the prohibition on engaging lobbyist services using public funds Compliance with the applicable expense claim directives; Compliance with the applicable perquisites directives; and Compliance with the applicable procurement directives. In addition, although not a requirement under the BPSAA, the LHIN s CEO must attest to the following: That the LHIN has fulfilled its obligations under the Memorandum of Understanding; That the LHIN has fulfilled its obligations under the Ministry LHIN Accountability Agreement/Ministry LHIN Performance Agreement, in effect during the Reporting Period Page 2 of 3
138 This report was approved at the April 25, 2017 LHIN Board of Directors meeting. Proposed Motion: That the NSM LHIN Committee of the Whole recommend to the Board of Directors approval of the 2016/17 Public Disclosure of Expenses report as outlined in Section 2. Page 3 of 3
139 Briefing Note Title: North Simcoe Muskoka Community Care Access Centre Fiscal Audited Financial Statements Agenda Item: 7.1 Meeting Date: June 26, 2017 Item For: Information Submitted By: Tom Roberts Input/Direction Approved By: Jeff Kwan Decision Attachment(s): Yes (list below) No /17 NSM CCAC Audited Financial Statements Issue/Context: The North Simcoe Muskoka Community Care Access Centre (NSM CCAC) entered into an audit engagement with BDO Canada (BDO) for the fiscal year ending March 31, 2017; however, the audited financial statements for this engagement were not be ready for presentation by BDO prior to the dissolution of the NSM CCAC Board of Directors. As outlined in the Local Health System Integration Act (LHSIA) ss 34.5(7) the Chair and Chief Executive Officer (CEO) of the Local Health Integration Network (LHIN) have the requirement and authority to, make any filings or reports that a community care access corporation may make or that would have been required for the community care access corporation immediately before its dissolution. Background: Information was presented to the NSM LHIN Board of Directors on April 24, 2017, outlining the requirement for the Chair and CEO to complete all filings and reports for the legacy NSM CCAC. Similar to the process utilized for the NSM LHIN audited statements from fiscal , the Board of Directors is being provided with the opportunity to engage with the auditors (BDO). In addition to the requirement to produce audited financial statements, the legacy CCAC was also required to produce an audited Annual Reconciliation Report (ARR). The ARR is a reconciliation of all funding and expenses generated by CCAC, and is a process used by the Ministry of Health and Long-Term Care to verify if surplus funds are to be returned to the Minister of Finance. Considerations: The NSM LHIN Board is not obligated under LHSIA to do anything vis-à-vis the NSM CCAC audit. As such the Board may opt to: 1. Table a motion to approve the fiscal audited financial statements of the NSM CCAC; 2. Receive the audited financial statements as information only and ask questions of BDO; or 3. Defer all matters related to the NSM CCAC fiscal audit to the Chair and CEO. As LHSIA grants the Chair and CEO the legal authority and responsibility to make necessary filings and reports that the community care access corporation would have been required to complete, the LHIN Chair and CEO have protection under LHSIA s immunity provision in ss 35.1 against any claims for anything they do in good faith in exercising these duties under LHSIA. It is unclear if this provision would apply to the entire Board of Directors as LHSIA does not provide the legal authority to the Board to complete filings and reports for the NSM CCAC. As reporting to the governing body is a key component of appropriate good governance, the NSM CCAC audited financial statements for fiscal are being presented to the Board of Directors alongside the opportunity to ask questions of BDO.
140 Recommendation: To support the Board of Directors in exercising good governance, while adhering to the authorities granted in LHSIA, it is recommended that the NSM CCAC fiscal audited financial statements be provided to the Board of Directors as information only and that no Board motion be tabled. The Board Chair and CEO will make the necessary filings and reports with respect to the fiscal audit and ARR for the legacy NSM CCAC. Page 2 of 2
141
142
143

144 North Simcoe Muskoka Community Care Access Centre Final Report to the Board of Directors June 26, 2017
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/24/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/24/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
2017/2018. Annual Business Plan
 2017/2018 Annual Business Plan July 10, 2017 Table of Contents Introduction 3 Setting Context 4 Mandate and Strategic Directions... 4 Overview of Current and Forthcoming Programs and Activities... 5 Environmental
2017/2018 Annual Business Plan July 10, 2017 Table of Contents Introduction 3 Setting Context 4 Mandate and Strategic Directions... 4 Overview of Current and Forthcoming Programs and Activities... 5 Environmental
Accountability Framework and Organizational Requirements
 Ministry of Health and Long-Term Care Accountability Framework and Organizational Requirements Consultation Document Population and Public Health Division May 2017 Ministry of Health and Long-Term Care
Ministry of Health and Long-Term Care Accountability Framework and Organizational Requirements Consultation Document Population and Public Health Division May 2017 Ministry of Health and Long-Term Care
Community Health and Hospital Services Integration Planning Process DRAFT Integrated Service Delivery Model for Northumberland County December 2013
 Overview The Central East Local Health Integration Network is one of 14 Local Health Integration Networks (LHINs) established by the Government of Ontario in 2006. LHINs are community-based organizations
Overview The Central East Local Health Integration Network is one of 14 Local Health Integration Networks (LHINs) established by the Government of Ontario in 2006. LHINs are community-based organizations
OVERVIEW SCOPE & DEMONSTRATION OF IMPACT
 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
Enclosed please find a copy of the resolution and corresponding staff report and presentation.
 February 3, 2016 Tony Clement, MP Parry Sound-Muskoka 44A King William Street Huntsville, Ontario P1H 1G3 Dear Mr. Clement: Re: Proposal for a Contemporary Health System Please be advised that during the
February 3, 2016 Tony Clement, MP Parry Sound-Muskoka 44A King William Street Huntsville, Ontario P1H 1G3 Dear Mr. Clement: Re: Proposal for a Contemporary Health System Please be advised that during the
Service Accountability Agreements Update
 Service Accountability Agreements Update Central East Local Health Integration Network Board Meeting Date: December 21, 2016 Presented By: System Finance and Performance Management Overview Context Service
Service Accountability Agreements Update Central East Local Health Integration Network Board Meeting Date: December 21, 2016 Presented By: System Finance and Performance Management Overview Context Service
NORTH SIMCOE MUSKOKA LHIN CARE CONNECTIONS
 Committee Chair Carol Lambie NORTH SIMCOE MUSKOKA LHIN CARE CONNECTIONS Mental Health and Addictions Child and Adolescent Steering Committee March 27, 2015 9:00 11:30am System Coordinator Susan Lalonde
Committee Chair Carol Lambie NORTH SIMCOE MUSKOKA LHIN CARE CONNECTIONS Mental Health and Addictions Child and Adolescent Steering Committee March 27, 2015 9:00 11:30am System Coordinator Susan Lalonde
MINISTRY OF HEALTH AND LONG-TERM CARE
 THE ESTIMATES, 1 The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life for all Ontarians.
THE ESTIMATES, 1 The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life for all Ontarians.
The LHIN s role in creating integrated health service delivery systems
 PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
LHIN Quality Improvement Plans (QIPs) and Service Provider QIPs. Presentation to Service Provider Organizations April 2018
 and Service Provider QIPs. Presentation to Service Provider Organizations April 2018") LHIN Quality Improvement Plans (QIPs) and Service Provider QIPs Presentation to Service Provider Organizations April 2018 Purpose To provide an overview of: LHIN Quality Improvement Plan (QIP), and Service
LHIN Quality Improvement Plans (QIPs) and Service Provider QIPs Presentation to Service Provider Organizations April 2018 Purpose To provide an overview of: LHIN Quality Improvement Plan (QIP), and Service
Coordinated Care Planning
 Coordinated Care Planning What is a Coordinated Care Plan? A plan for your care that is created with you and your family (as per your direction) and involves all the members of your health care team. What
Coordinated Care Planning What is a Coordinated Care Plan? A plan for your care that is created with you and your family (as per your direction) and involves all the members of your health care team. What
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
COMMITTEE REPORTS TO THE BOARD
 Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
OVERVIEW. 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: Toll Free: Fax:
 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
Executive Compensation Policy and Framework BLUEWATER HEALTH
 Executive Compensation Policy and Framework BLUEWATER HEALTH 1. Background The Province of Ontario introduced The Broader Public Sector Accountability Act in 2010 (BPSAA), which introduced controls on
Executive Compensation Policy and Framework BLUEWATER HEALTH 1. Background The Province of Ontario introduced The Broader Public Sector Accountability Act in 2010 (BPSAA), which introduced controls on
Corporate Communication Plan. April 2011 March 2012
 Corporate Communication Plan April 2011 March 2012 Table of Contents Background 3 Our Roles and Responsibilities 3 Our Vision 3 Our Priorities 4 2010-2013 Integrated Health Service Plan Strategic Directions
Corporate Communication Plan April 2011 March 2012 Table of Contents Background 3 Our Roles and Responsibilities 3 Our Vision 3 Our Priorities 4 2010-2013 Integrated Health Service Plan Strategic Directions
Excellent Care for All Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP
: Progress Report for 2016/17 QIP") Excellent Care for All Quality Improvement Plans (QIP): Progress Report for QIP The Progress Report is a tool that will help organizations make linkages between change ide and improvement, and gain insight
Excellent Care for All Quality Improvement Plans (QIP): Progress Report for QIP The Progress Report is a tool that will help organizations make linkages between change ide and improvement, and gain insight
North Simcoe Muskoka Local Health Integration Network. Working Together to Achieve Better Health, Better Care, Better Value.
 North Simcoe Muskoka Local Health Integration Network Working Together to Achieve Better Health, Better Care, Better Value. Annual Business Plan 2010-2011 Table of Contents Annual Business Plan Context
North Simcoe Muskoka Local Health Integration Network Working Together to Achieve Better Health, Better Care, Better Value. Annual Business Plan 2010-2011 Table of Contents Annual Business Plan Context
Health Quality Ontario Business Plan
 Health Quality Ontario Business Plan 2017-20 October 2016 Table of Contents 1 Executive Summary...1 2 Mandate and Strategy...2 3 Environmental Scan...4 4 Programs and Activities...5 5 Risks... 18 6 Resources...
Health Quality Ontario Business Plan 2017-20 October 2016 Table of Contents 1 Executive Summary...1 2 Mandate and Strategy...2 3 Environmental Scan...4 4 Programs and Activities...5 5 Risks... 18 6 Resources...
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/26/2018 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/26/2018 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
The Patients First Act Backgrounder
 December 7, 2016 The Patients First Act, 2016 is part of the government s Patients First: Action Plan for Health Care to create a more patient-centered health care system in Ontario. Ontario s 14 Local
December 7, 2016 The Patients First Act, 2016 is part of the government s Patients First: Action Plan for Health Care to create a more patient-centered health care system in Ontario. Ontario s 14 Local
September Sub-Region Collaborative Meeting: Bramalea. September 13, 2018
 September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
Enabling Health Links with a Care Coordination Tool. February 2014
 Enabling Health Links with a Care Coordination Tool February 2014 Health Links highlighted the need for a care coordination tool Health Link business plans consistently highlight how technology could enable
Enabling Health Links with a Care Coordination Tool February 2014 Health Links highlighted the need for a care coordination tool Health Link business plans consistently highlight how technology could enable
How the Quality Improvement Plan and the Service Accountability Agreement Can Transform the Health Care System
 How the Quality Improvement Plan and the Service Accountability Agreement Can Transform the Health Care System Local Health Integration Network (LHIN) Health Quality Ontario (HQO) Quality Improvement Task
How the Quality Improvement Plan and the Service Accountability Agreement Can Transform the Health Care System Local Health Integration Network (LHIN) Health Quality Ontario (HQO) Quality Improvement Task
North Simcoe Muskoka LHIN
 Further NSM LHIN HEALTH SYSTEM IMPROVEMENT PROPOSAL FORM Instructions for Use: Download (save) the file to your hard-drive or network. Rename the file in the following manner: name of your organization_cfp_code.
Further NSM LHIN HEALTH SYSTEM IMPROVEMENT PROPOSAL FORM Instructions for Use: Download (save) the file to your hard-drive or network. Rename the file in the following manner: name of your organization_cfp_code.
MINISTRY OF HEALTH AND LONG-TERM CARE
 THE ESTIMATES, 2005-06 1 SUMMARY The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life
THE ESTIMATES, 2005-06 1 SUMMARY The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life
Changes to Managed Entry
 To: All Primary Care Physicians Published By: Primary Health Care Branch Date Issued: May 11, 2015 Corresponding Bulletin Reference #: 4654 Re: Supporting Areas of High Physician Need: Changes to Entry
To: All Primary Care Physicians Published By: Primary Health Care Branch Date Issued: May 11, 2015 Corresponding Bulletin Reference #: 4654 Re: Supporting Areas of High Physician Need: Changes to Entry
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 27/03/2019 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 27/03/2019 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Looking Back and Looking Forward. A Sneak Peek for the 2018/19 Home Care quality improvement plans (QIPs)
") Looking Back and Looking Forward A Sneak Peek for the 2018/19 Home Care quality improvement plans (QIPs) DANYAL MARTIN LAURIE DUNN NOVEMBER 20, 2017 Learning Objectives Share learnings from the 2017/18
Looking Back and Looking Forward A Sneak Peek for the 2018/19 Home Care quality improvement plans (QIPs) DANYAL MARTIN LAURIE DUNN NOVEMBER 20, 2017 Learning Objectives Share learnings from the 2017/18
MUSKOKA AND AREA HEALTH SYSTEM TRANSFORMATION COUNCIL TERMS OF REFERENCE
 MUSKOKA AND AREA HEALTH SYSTEM TRANSFORMATION COUNCIL TERMS OF REFERENCE Table of Contents Background... 1 Vision for our Future... 1 Purpose of Health System Transformation Council... 2 Accountability...
MUSKOKA AND AREA HEALTH SYSTEM TRANSFORMATION COUNCIL TERMS OF REFERENCE Table of Contents Background... 1 Vision for our Future... 1 Purpose of Health System Transformation Council... 2 Accountability...
Health System Transformation. Breakfast with the Chiefs June 6, 2013 Helen Angus Associate Deputy Minister, MOHLTC
 Health System Transformation Breakfast with the Chiefs June 6, 2013 Helen Angus Associate Deputy Minister, MOHLTC The Need for Change Historic levels of 6% investment are not sustainable The cost of care
Health System Transformation Breakfast with the Chiefs June 6, 2013 Helen Angus Associate Deputy Minister, MOHLTC The Need for Change Historic levels of 6% investment are not sustainable The cost of care
Agenda Item 9 Integration Strategy. Presentation to the Board of Directors
 Agenda Item 9 Integration Strategy Presentation to the Board of Directors What is Integration? Our integration lens reflects a continuum of approaches from Informal Relationships to Structured Collaboration
Agenda Item 9 Integration Strategy Presentation to the Board of Directors What is Integration? Our integration lens reflects a continuum of approaches from Informal Relationships to Structured Collaboration
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Telemedicine in Central East LHIN Opportunities to Strengthen the System. Central East LHIN Board February 2015
 Telemedicine in Central East LHIN Opportunities to Strengthen the System Central East LHIN Board February 2015 OTN and Telemedicine Enabled Organizations BACKGROUND 2 What is OTN Telemedicine? OTN is one
Telemedicine in Central East LHIN Opportunities to Strengthen the System Central East LHIN Board February 2015 OTN and Telemedicine Enabled Organizations BACKGROUND 2 What is OTN Telemedicine? OTN is one
Regional Complex Continuing Care Review: Final Report and Recommendations
 Regional Complex Continuing Care Review: Final Report and Recommendations Submitted to: North Simcoe Muskoka LHIN Leadership Council January 2010 Submitted by Sara Lankshear, RN PhD (c) Relevé Consulting
Regional Complex Continuing Care Review: Final Report and Recommendations Submitted to: North Simcoe Muskoka LHIN Leadership Council January 2010 Submitted by Sara Lankshear, RN PhD (c) Relevé Consulting
Ministère de la Santé et des Soins de longue durée Bureau du ministre
 Ministry of Health and Long-Term Care Office of the Minister 10 th Floor, Hepburn Block 80 Grosvenor Street Toronto ON M7A 2C4 Tel 416-327-4300 Fax 416-326-1571 www.ontario.ca/health May 1, 2017 Ministère
Ministry of Health and Long-Term Care Office of the Minister 10 th Floor, Hepburn Block 80 Grosvenor Street Toronto ON M7A 2C4 Tel 416-327-4300 Fax 416-326-1571 www.ontario.ca/health May 1, 2017 Ministère
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 12/23/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 12/23/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
COMMUNITY ACCOUNTABILITY PLANNING SUBMISSIONS (CAPS) & MULTI-SECTOR SERVICE ACCOUNTABILITY AGREEMENTS (MSAA) Educational Materials
 & MULTI-SECTOR SERVICE ACCOUNTABILITY AGREEMENTS (MSAA) Educational Materials") 2018-2019 COMMUNITY ACCOUNTABILITY PLANNING SUBMISSIONS (CAPS) & MULTI-SECTOR SERVICE ACCOUNTABILITY AGREEMENTS (MSAA) Educational Materials October 5, 2017 Contents A. MSAA Schedule Refresh Structure
2018-2019 COMMUNITY ACCOUNTABILITY PLANNING SUBMISSIONS (CAPS) & MULTI-SECTOR SERVICE ACCOUNTABILITY AGREEMENTS (MSAA) Educational Materials October 5, 2017 Contents A. MSAA Schedule Refresh Structure
North East Behavioural Supports Ontario Sustainability Plan
 North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 03/15/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 03/15/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Patient Care Groups: A new model of population based. primary health care. for Ontario
 : A new model of population based primary health care for Ontario A report on behalf of the Primary Health Care Expert Advisory Committee By David Price, Elizabeth Baker, Brian Golden and Rosemary Hannam
: A new model of population based primary health care for Ontario A report on behalf of the Primary Health Care Expert Advisory Committee By David Price, Elizabeth Baker, Brian Golden and Rosemary Hannam
Local Health Integration Network Authorities under the Local Health System Integration Act, 2006
 Purpose This document outlines principles that guide the potential use of the new Local Health Integration Network (LHIN) directive, investigatory and supervisory authorities ( statutory authorities )
Purpose This document outlines principles that guide the potential use of the new Local Health Integration Network (LHIN) directive, investigatory and supervisory authorities ( statutory authorities )
Annual Community Engagement Plan
 Annual Community Engagement Plan 2012-2013 Table of Contents Introduction 3 Background Overview 3 Our Role and Responsibilities 4 Erie St. Clair LHIN Vision 4 ESC LHIN Strategic Goals 4 Engagement Activities
Annual Community Engagement Plan 2012-2013 Table of Contents Introduction 3 Background Overview 3 Our Role and Responsibilities 4 Erie St. Clair LHIN Vision 4 ESC LHIN Strategic Goals 4 Engagement Activities
MSAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017
 is made as of the 1 st day of April, 2017") MSAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND THE SCHIZOPHRENIA
MSAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND THE SCHIZOPHRENIA
Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016
 Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016 Introduction The Ministry of Health and Long Term Care s (MOHLTC) Patients First: Action Plan for Health Care exemplifies
Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016 Introduction The Ministry of Health and Long Term Care s (MOHLTC) Patients First: Action Plan for Health Care exemplifies
MINISTRY OF HEALTH AND LONG-TERM CARE
 THE ESTIMATES, 2004-05 1 SUMMARY The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life
THE ESTIMATES, 2004-05 1 SUMMARY The Ministry provides for a health system that promotes wellness and improves health outcomes through accessible, integrated and quality services at every stage of life
Recommendations for Adoption: Diabetic Foot Ulcer. Recommendations to enable widespread adoption of this quality standard
 Recommendations for Adoption: Diabetic Foot Ulcer Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
Recommendations for Adoption: Diabetic Foot Ulcer Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
Sub-region Geography Data Analysis
 Region Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 128,573 Puslinch 7399 # Seniors (65+) 18,669 17,205 Puslinch 1,464 % Seniors (65+) 13.7% 13.4% Puslinch 19.8% %
Region Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 128,573 Puslinch 7399 # Seniors (65+) 18,669 17,205 Puslinch 1,464 % Seniors (65+) 13.7% 13.4% Puslinch 19.8% %
Sub-region Geography Data Analysis
 Guelph-Puslinch Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 Guelph 128,573 Puslinch 7399 # Seniors (65+) 18,669 Guelph 17,205 Puslinch 1,464 % Seniors (65+) 13.7%
Guelph-Puslinch Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 Guelph 128,573 Puslinch 7399 # Seniors (65+) 18,669 Guelph 17,205 Puslinch 1,464 % Seniors (65+) 13.7%
South West LHIN Primary Health Care Capacity Report Final Recommendations
 South West LHIN Primary Health Care Capacity Report Final Recommendations West Elgin Community Health Centre and the South West LHIN jointly sponsored a study called Understanding Health Inequities and
South West LHIN Primary Health Care Capacity Report Final Recommendations West Elgin Community Health Centre and the South West LHIN jointly sponsored a study called Understanding Health Inequities and
Strengthening Access, Performance and Accountability of Primary Health Care Implementation Framework Template Central East LHIN Response
 Strengthening Access, Performance and Accountability of Primary Health Care Implementation Framework Template Central East LHIN Response Advancing Integrated Systems of Care the Central East LHIN s Primary
Strengthening Access, Performance and Accountability of Primary Health Care Implementation Framework Template Central East LHIN Response Advancing Integrated Systems of Care the Central East LHIN s Primary
Community Engagement Plan
 Community Engagement Plan 2015/2016 1 Community Engagement C e n t r a l L H I N A n n u a l R e p o r t 2 0 1 5 / 2 0 1 6 Listening to the voices of our patients and caregivers, and continued engagement
Community Engagement Plan 2015/2016 1 Community Engagement C e n t r a l L H I N A n n u a l R e p o r t 2 0 1 5 / 2 0 1 6 Listening to the voices of our patients and caregivers, and continued engagement
ARH Strategic Plan:
 ARH Strategic Plan: 2017 2020 Table of Contents Section 1. Introduction 1.1 Why a Strategic Plan 1.2 Building on Previous Accomplishments 1.3 Where We Are Today 2. How We Developed Our New Plan: 2.1 Plan
ARH Strategic Plan: 2017 2020 Table of Contents Section 1. Introduction 1.1 Why a Strategic Plan 1.2 Building on Previous Accomplishments 1.3 Where We Are Today 2. How We Developed Our New Plan: 2.1 Plan
Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All
 Health Quality Branch Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All Ontario Long-Term Care Association Quality Forum June 12, 2013 Miin Alikhan Director,
Health Quality Branch Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All Ontario Long-Term Care Association Quality Forum June 12, 2013 Miin Alikhan Director,
Agenda Item Tab No. Time Presenter 1.0 MEETING CALLED TO ORDER 1:00 Mr. John Langs. 2.0 NOTICE/RECOGNITION OF A QUORUM 1 Mr.
 AGENDA BOARD OF DIRECTORS September 24, 2013 1:00pm- 3:00pm Central LHIN 60 Renfrew Drive, Markham ON Agenda Item Tab No. Time Presenter 1.0 MEETING CALLED TO ORDER 1:00 Mr. John Langs 2.0 NOTICE/RECOGNITION
AGENDA BOARD OF DIRECTORS September 24, 2013 1:00pm- 3:00pm Central LHIN 60 Renfrew Drive, Markham ON Agenda Item Tab No. Time Presenter 1.0 MEETING CALLED TO ORDER 1:00 Mr. John Langs 2.0 NOTICE/RECOGNITION
Annual Business Plan 2015/16. Central West Local Health Integration Network
 Annual Business Plan 2015/16 Central West Local Health Integration Network April 2015 Table of Contents A MESSAGE FROM THE BOARD CHAIR AND CEO... 2 OVERVIEW ABP 2015/2016... 3 SECTION 1 Context 1.1 LHIN
Annual Business Plan 2015/16 Central West Local Health Integration Network April 2015 Table of Contents A MESSAGE FROM THE BOARD CHAIR AND CEO... 2 OVERVIEW ABP 2015/2016... 3 SECTION 1 Context 1.1 LHIN
Shared Vision, Shared Outcomes: Building on the Foundation of Collaboration between Public Health and Comprehensive Primary Health Care in Ontario
 Shared Vision, Shared Outcomes: Building on the Foundation of Collaboration between Public Health and Comprehensive Primary Health Care in Ontario Submission from the Association of Ontario Health Centres
Shared Vision, Shared Outcomes: Building on the Foundation of Collaboration between Public Health and Comprehensive Primary Health Care in Ontario Submission from the Association of Ontario Health Centres
Mississauga Halton Local Health Integration Network
 Mississauga Halton Local Health tegration Network Annual Business Plan April 1, 2015 March 31, 2016 1 Mississauga Halton Local Health tegration Network Annual Business Plan 2015-16 Table of Contents 1.0
Mississauga Halton Local Health tegration Network Annual Business Plan April 1, 2015 March 31, 2016 1 Mississauga Halton Local Health tegration Network Annual Business Plan 2015-16 Table of Contents 1.0
Ontario Quality Standards Committee Draft Terms of Reference
 Ontario Quality Standards Committee Draft Terms of Reference 1. Introduction The Ontario Health Quality Council (Health Quality Ontario) officially commenced operation on April 1st, 2010. Created under
Ontario Quality Standards Committee Draft Terms of Reference 1. Introduction The Ontario Health Quality Council (Health Quality Ontario) officially commenced operation on April 1st, 2010. Created under
PO Box 1132 Station F Toronto, ON M4Y 2T8
 Doris Grinspun Chief Executive Officer Registered Nurses' Association of Ontario (RNAO) 158 Pearl Street, Toronto, Ontario M5H 1L3 Dear Doris: Thank you for giving the Green Party of Ontario the opportunity
Doris Grinspun Chief Executive Officer Registered Nurses' Association of Ontario (RNAO) 158 Pearl Street, Toronto, Ontario M5H 1L3 Dear Doris: Thank you for giving the Green Party of Ontario the opportunity
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017
 South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017 Overview of today s presentation Provide background on
South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017 Overview of today s presentation Provide background on
Multi-Sector Service Accountability Agreements (M-SAA)
") 2011-14 Multi-Sector Service Accountability Agreements (M-SAA) CE LHIN Board of Directors Meeting March 23 rd, 2011 The 2011-14 M-SAA Required under LHSIA and Ministry-LHIN Performance Agreement (MLPA),
2011-14 Multi-Sector Service Accountability Agreements (M-SAA) CE LHIN Board of Directors Meeting March 23 rd, 2011 The 2011-14 M-SAA Required under LHSIA and Ministry-LHIN Performance Agreement (MLPA),
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Workplace Violence Prevention indicator in hospital Quality Improvement Plans (QIPs)
") Workplace Violence Prevention indicator in hospital Quality Improvement Plans (QIPs) S U D H A K U T T Y, HQO, DIRECTOR, QUALITY IMPROVEMENT STRATEGIES & ADOPTION D A N Y A L MA R T I N, H Q O, MA N A
Workplace Violence Prevention indicator in hospital Quality Improvement Plans (QIPs) S U D H A K U T T Y, HQO, DIRECTOR, QUALITY IMPROVEMENT STRATEGIES & ADOPTION D A N Y A L MA R T I N, H Q O, MA N A
Health Links: Meeting the needs of Ontario s high needs users. Presentation to the Canadian Institute for Health Information January 27, 2016
 Health Links: Meeting the needs of Ontario s high needs users Presentation to the Canadian Institute for Health Information January 27, 2016 Agenda Items Health Links: Overview and successes to date Critical
Health Links: Meeting the needs of Ontario s high needs users Presentation to the Canadian Institute for Health Information January 27, 2016 Agenda Items Health Links: Overview and successes to date Critical
ehealth Report for Ed Clark November 10, 2016 My Background and Context:
 ehealth Report for Ed Clark November 10, 2016 My Background and Context: I worked for a number of years for OHIP at the Ministry of Health in Kingston. Several major project initiative involved converting
ehealth Report for Ed Clark November 10, 2016 My Background and Context: I worked for a number of years for OHIP at the Ministry of Health in Kingston. Several major project initiative involved converting
Sub-region Geography Data Analysis
 Kitchener-Waterloo-Wilmot-Wellesley-Woolwich (KW4) Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 391,521 Kitchener 231,482 Waterloo 104,165 Wilmot 20,240 Wellesley 11,216 Woolwich
Kitchener-Waterloo-Wilmot-Wellesley-Woolwich (KW4) Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 391,521 Kitchener 231,482 Waterloo 104,165 Wilmot 20,240 Wellesley 11,216 Woolwich
2014/15 Quality Improvement Plan (QIP) Narrative
 Narrative") 2014/15 Quality Improvement Plan (QIP) Narrative 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop a quality improvement plan.
2014/15 Quality Improvement Plan (QIP) Narrative 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop a quality improvement plan.
Management Report to the MH LHIN Board of Directors April/May, 2011
 700 Dorval Drive, Suite 500 Oakville, ON L6K 3V3 Tel: 905 337-7131 Fax: 905 337-8330 Toll Free: 1 866 371-5446 www.mississaugahaltonlhin.on.ca Management Report to the MH LHIN Board of Directors April/May,
700 Dorval Drive, Suite 500 Oakville, ON L6K 3V3 Tel: 905 337-7131 Fax: 905 337-8330 Toll Free: 1 866 371-5446 www.mississaugahaltonlhin.on.ca Management Report to the MH LHIN Board of Directors April/May,
MINUTES OF BOARD OF DIRECTORS MEETING. Burlington Art Centre 1333 Lakeshore Road, Burlington, ON
 MINUTES OF BOARD OF DIRECTORS MEETING Date: Wednesday, October 10, 2012 Location: Burlington Art Centre 1333 Lakeshore Road, Burlington, ON PRESENT: B. Alexander (Vice-Chair), V. Bayley, B. Brownlow, S.
MINUTES OF BOARD OF DIRECTORS MEETING Date: Wednesday, October 10, 2012 Location: Burlington Art Centre 1333 Lakeshore Road, Burlington, ON PRESENT: B. Alexander (Vice-Chair), V. Bayley, B. Brownlow, S.
Regional Hospice Palliative Care Model Action Plan
 ITEM 11.1 Regional Hospice Palliative Care Model Action Plan Central LHIN Board of Directors October 28, 2014 1 Agenda Background Declaration A Vision for Palliative Care in Ontario Central LHIN Approach
ITEM 11.1 Regional Hospice Palliative Care Model Action Plan Central LHIN Board of Directors October 28, 2014 1 Agenda Background Declaration A Vision for Palliative Care in Ontario Central LHIN Approach
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2014
 Narrative for Health Care Organizations in Ontario 3/30/2014") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
2017/18 Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") 2017/18 Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario March 31, 2017 This document is intended to provide health care organizations in Ontario with guidance as to how
2017/18 Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario March 31, 2017 This document is intended to provide health care organizations in Ontario with guidance as to how
Central East LHIN Strategic Aims
 Central East LHIN Strategic Aims Mental Health and Addictions Strategic Aim Update December 16, 2015 Presented By: Dr. Ian Dawe, Jai Mills and Marilee Suter Agenda Background and Overview Aim Metrics Update
Central East LHIN Strategic Aims Mental Health and Addictions Strategic Aim Update December 16, 2015 Presented By: Dr. Ian Dawe, Jai Mills and Marilee Suter Agenda Background and Overview Aim Metrics Update
Grand River Hospital Minutes Of A Public Meeting Of The Board Of Directors Held On September 27, 2016 In the Freeport Boardroom
 Present: G. Bellew D. Bennett J. Deganis D. Freeman D. Graham S. Hanmer P. Hendrikse H. Hoediono Staff: Bailey, T. Cheal, B. Karjaluoto, M. Grand River Hospital Minutes Of A Public Meeting Of The Board
Present: G. Bellew D. Bennett J. Deganis D. Freeman D. Graham S. Hanmer P. Hendrikse H. Hoediono Staff: Bailey, T. Cheal, B. Karjaluoto, M. Grand River Hospital Minutes Of A Public Meeting Of The Board
Program Design: Mental Health and Addiction Nurses in District School Board Program
 Program Design: Mental Health and Addiction Nurses in District School Board Program September 6, 2011 Table of Contents Program Design: Mental Health and Addiction Nurses in District School Boards Program
Program Design: Mental Health and Addiction Nurses in District School Board Program September 6, 2011 Table of Contents Program Design: Mental Health and Addiction Nurses in District School Boards Program
WATERLOO WELLINGTON LOCAL HEALTH INTEGRATION NETWORK
 WATERLOO WELLINGTON LOCAL HEALTH INTEGRATION NETWORK Finance and Audit Committee SUMMARY REPORT TO BOARD OF DIRECTORS DATE: April 24, 2012 From: D. Small, Chair of Finance and Audit Committee The Finance
WATERLOO WELLINGTON LOCAL HEALTH INTEGRATION NETWORK Finance and Audit Committee SUMMARY REPORT TO BOARD OF DIRECTORS DATE: April 24, 2012 From: D. Small, Chair of Finance and Audit Committee The Finance
Workplace Violence Prevention: A Provincial Approach to Improvement Presentation at OHA HealthAchieve
 Workplace Violence Prevention: A Provincial Approach to Improvement Presentation at OHA HealthAchieve SUDHA KUTTY NOVEMBER 6, 2017 1:30PM Agenda Provide an overview of the Quality Improvement Plan (QIP)
Workplace Violence Prevention: A Provincial Approach to Improvement Presentation at OHA HealthAchieve SUDHA KUTTY NOVEMBER 6, 2017 1:30PM Agenda Provide an overview of the Quality Improvement Plan (QIP)
Waterloo Wellington Community Care Access Centre. Community Needs Assessment
 Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Ministry of Health Patients as Partners Provincial Dialogue Report
 Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 2/22/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 2/22/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Where We Are Now. Three Key Areas for Investment
 Where We Are Now Everyone deserves the chance to live independently in their own home or community for as long as possible. For decades, Ontario s not-for-profit home and community support providers have
Where We Are Now Everyone deserves the chance to live independently in their own home or community for as long as possible. For decades, Ontario s not-for-profit home and community support providers have
Quality, Risk and Patient Safety Report Fiscal Year , Third Quarter Submitted to: Board of Directors March 3, 2017
 Quality, Risk and Patient Safety Report Fiscal Year 20, Third Quarter Submitted to: Board of Directors March 3, 2017 Analysis and Ideas for Improvement Contributed by Staff of the North East CCAC Date
Quality, Risk and Patient Safety Report Fiscal Year 20, Third Quarter Submitted to: Board of Directors March 3, 2017 Analysis and Ideas for Improvement Contributed by Staff of the North East CCAC Date
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard /10 Q3
 MLAA Performance Assessment Dashboard /10 Q3") MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
Executive Compensation Policy and Framework ALEXANDRA HOSPITAL INGERSOLL / TILLSONBURG DISTRICT MEMORIAL HOSPITAL
 Executive Compensation Policy and Framework ALEXANDRA HOSPITAL INGERSOLL / TILLSONBURG DISTRICT MEMORIAL HOSPITAL Front Page for Ministry Submission: Organization (Full Name): Last Name: Job Title: Address:
Executive Compensation Policy and Framework ALEXANDRA HOSPITAL INGERSOLL / TILLSONBURG DISTRICT MEMORIAL HOSPITAL Front Page for Ministry Submission: Organization (Full Name): Last Name: Job Title: Address:
Agenda Item 8.4 BRIEFING NOTE: Toronto Central Local Health Integration Network (LHIN)
") Agenda Item 8.4 BRIEFING NOTE: Toronto Central Local Health Integration Network (LHIN) SUBJECT: Voluntary Integration of the Assisted Living and Attendant Outreach Services from the Canadian Red Cross
Agenda Item 8.4 BRIEFING NOTE: Toronto Central Local Health Integration Network (LHIN) SUBJECT: Voluntary Integration of the Assisted Living and Attendant Outreach Services from the Canadian Red Cross
Central LHIN Community Governance Council Meeting. May 23 & 30, 2012
 Central LHIN Community Governance Council Meeting May 23 & 30, 2012 Agenda Wl Welcome and dit Introductions ti Central LHIN Overview Draft ftstrategic t Vision i and dprinciples i Community Sector Optimization
Central LHIN Community Governance Council Meeting May 23 & 30, 2012 Agenda Wl Welcome and dit Introductions ti Central LHIN Overview Draft ftstrategic t Vision i and dprinciples i Community Sector Optimization
Stronger Connections. Better Health. Primary Care Strategy Update
 Stronger Connections Better Health Primary Care Strategy Update Summer 2017 Get Involved: Connecting Primary Care through Networks Primary Care Providers have an important and unique perspective on the
Stronger Connections Better Health Primary Care Strategy Update Summer 2017 Get Involved: Connecting Primary Care through Networks Primary Care Providers have an important and unique perspective on the
PCFHC STRATEGIC PLAN
 PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
Recommendations for Adoption: Major Depression. Recommendations to enable widespread adoption of this quality standard
 Recommendations for Adoption: Major Depression Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
Recommendations for Adoption: Major Depression Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
January 18, Mike Horrobin Board Chair
 January 18, 2018 Dear Community Member, In 2014, the Government of Ontario began the process of developing public sector compensation frameworks to ensure a transparent and consistent approach to executive
January 18, 2018 Dear Community Member, In 2014, the Government of Ontario began the process of developing public sector compensation frameworks to ensure a transparent and consistent approach to executive
Toronto Central LHIN 2016/2017 QIP Snapshot Report. Health Quality Ontario The provincial advisor on the quality of health care in Ontario
 Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
What does the Patients First Act mean for Rural Communities?
 What does the Patients First Act mean for Rural Communities? Michael Barrett, CEO South West Local Health Integration Network (LHIN) ROMA Conference January 30, 017 Overview of Today s Presentation 1.
What does the Patients First Act mean for Rural Communities? Michael Barrett, CEO South West Local Health Integration Network (LHIN) ROMA Conference January 30, 017 Overview of Today s Presentation 1.
The Patient s Voice. Key findings from LHIN engagements with patients, families and caregivers. September 2015
 The Patient s Voice Key findings from LHIN engagements with patients, families and caregivers September 2015 Background The Integrated Health Service Plan is a strategic roadmap that enables LHINs to move
The Patient s Voice Key findings from LHIN engagements with patients, families and caregivers September 2015 Background The Integrated Health Service Plan is a strategic roadmap that enables LHINs to move
Health System Performance and Accountability Division MOHLTC. Transitional Care Program Framework
 Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Board of Directors Meeting Minutes
 Board of Directors Meeting Minutes DATE: Wednesday, June 26, 2013 TIME: 11:00 a.m. PLACE: 356 Oxford St. W., London CHAIR: RECORDER: MEMBERS: Linda Ballantyne, Board Secretary Cate Patchett, Corporate
Board of Directors Meeting Minutes DATE: Wednesday, June 26, 2013 TIME: 11:00 a.m. PLACE: 356 Oxford St. W., London CHAIR: RECORDER: MEMBERS: Linda Ballantyne, Board Secretary Cate Patchett, Corporate