Bring your insurance card(s) and a picture identification card to your appointment.
|
|
|
- George Jefferson
- 5 years ago
- Views:
Transcription
1 Your appointment is on / / at :. Thank you for choosing Midwest Ear Specialists (a member of the BJC Medical Group) as your healthcare partner. We value communication, beginning with the new patient registration process; the information in this packet will help you prepare for your first visit to our office. Your packet contains directions to our office and general information about our office policies and procedures. Included below is a list of information you need to bring with you to the appointment. Bring your insurance card(s) and a picture identification card to your appointment. Bring a copy of your medication list to your appointment. You should request this from all treating physicians that you currently go to for health care. Bring payment for your copayment or coinsurance, as required by your insurance carrier. If you are not prepared to pay your copayment, you will need to reschedule your appointment. Please plan to arrive at the office at least 30 minutes prior to your scheduled appointment time. This will allow ample time to complete the registration process. You will be asked to read and sign the following notifications: Included in This Packet: Patient Information Form Patient Demographic Form Patient Medical History Form CHC/HIE Participation Form Authorization for Disclosure of Health Information At Your Visit: HIPAA Notice Financial Statement of Patient Responsibility Review of Systems Complete and bring the included forms. During your visit, we will ask you to describe your current symptoms. Again, we thank you for choosing our practice and we look forward to working with you to achieve your healthcare goals We encourage you to call the office if you have any questions about the information contained in this packet. Sincerely, The Doctors and Staff of Midwest Ear Specialists
2 OFFICE POLICIES & GENERAL PRACTICE INFORMATION Office Hours: Monday through Friday 8:30am - 4:15pm Appointments If you arrive more than 10 minutes late for your appointment, we may ask you to reschedule. 24-hour advance notice is required to cancel your appointment. Your doctor may ask you to find an alternate source of medical care if you repeatedly fail to keep your scheduled appointments. Medical Records When you need a copy of your current records, we must have a signed, HIPAA-compliant authorization. You can drop-off, mail, or fax the authorization form to us. We use a professional service to manage our medical records requests and, according to Missouri law, they may charge a fee for copying medical records. Please allow at least 14 days from the receipt of the signed authorization to receive your records. Medication Refills Rx We accept refill requests during regular office hours. We will fill refill requests or contact you about your request between the hours of 8:30am and 4:30pm. Please ask your pharmacy to fax your request to Please allow hours to process your request. After Hours Care If you have a non-life-threatening medical problem after office hours, you may contact one of our doctors through the exchange
3 Financial Expectations We have contracts with over 100 different insurance plans. As a result, it is your responsibility to know your insurance coverage for office visits, procedures, physicals, and labs. Accepted methods of payment are cash, check or credit card. Appointments Failure to arrive in time for your appointment may result in the need to reschedule your appointment. 24-hour advance notice is required to cancel your appointment. Patient who fail to show up or cancellations received less than 2 hours prior to a scheduled office appointment may be charged a fee of $25. Copays are due at the time of service or you may be asked to reschedule. Under-insured or No Health Insurance (1) Non-Procedural Office Visits: Pay a deposit of $50 prior to service. (2) Procedural Visits: Pay $75 prior to service. (3) Patients who are deemed self-pay according to the BJCMG s Self Pay Policy will receive a 25% discount off billed charges. This discount will be credited toward the remaining account balance but does not modify the amount of the above defined deposit. We will file claims for all services provided by our doctors with our contracted insurance plans, including Medicare under the Medicare plan guidelines. All non-covered, unpaid balances will remain the responsibility of the patient. Outstanding Account Balance If outstanding balance is greater than $250 you will need to contact the Central Business Office (CBO) to setup monthly payment arrangements ( ). BJC Medical Group offers several financial assistance plans. If you need additional information about financial assistance, please call the Central Business Office at (314) or (800) Cosmetic Services If requesting a medically unnecessary cosmetic service not covered by insurance, patient will pay 100% of estimated professional charges one week prior to scheduled appointment. Completion of Forms: (1) No Charge: FMLA forms for patient s own condition, Medication assistance forms, work excuse letters, health insurance and physical forms. (2) $25 Fee: FMLA forms for the patient s spouse/parent/caregiver, disability forms unless completed during patient visit, income protection forms, and all other forms not listed.
4
5 Patient Demographic Form Name: Date of Birth: / / How did you hear about us? Referral From a Friend Practice Website Other: In accordance with the American Recovery and Reinvestment Act of 2009, Midwest Ear Specialists is required to ask for the following information from our patients. Address: Cell Phone Number: - - Primary Dental Provider: Race (please select one): Language (please select one): Ethnicity (please select one): African American/Black Albanian Hispanic or Latino American Indian/Alaskan Native American Sign Language Not Hispanic or Latino Asian Arabic Unknown/Not Reported Caucasian/White Bosnian Hispanic/Latino Bulgarian Multiracial Central Khmer Not Provided Chinese Other Unknown English French German Haitian: Haitian Creole Hebrew Hindi Italian Japanese Korean Nepali Polish Portuguese Russian Somali Spanish; Castilian Swahili Thai Urdu Vietnamese
6 Date: / / Patient Name: Primary Care Doctor: Pharmacy Number: DOB: / / Referred by: List reason(s) for visit and duration of problem: Medical History Allergies to Medications: Current Medications: (Prescription and Over the Counter) 1. Dosage 2. Dosage 3. Dosage 4. Dosage 5. Dosage 6. Dosage Check any illness or condition you have had: Diabetes High Blood Pressure Heart Attack Heart Stents or Surgery Cancer: Emphysema/COPD Stroke/TIA Easy Bleeding Serious Reaction to Anesthesia Depression/Anxiety Allergies (seasonal/year round) Other: Past Surgical History Please list all prior surgeries with the approximate year in which the surgery took place: No past surgical history Surgery: Surgery: Surgery: Surgery: Year: Year: Year: Year: Social History What is your current marital status? Married Single Divorced Widowed Other Do you drink alcohol? Do you drink caffeine? Do you use tobacco? If quit, date quit: / / Yes Yes Yes No No No Formerly Formerly Formerly What is your current smoking status? Every day smoker Some day smoker Former smoker Never smoked Family History Please tell us about your family s medical history: No relevant family history Mother Age: Health Problems: Father Age: Health Problems: Brother / Sister (please circle) Age: Health Problems: Brother / Sister (please circle) Age: Health Problems:
7 Consent for Sharing of Information via Health Information Exchanges (HIE) ( HIE Consent ) General Consent I understand and agree that my health information may be stored in or exchanged through one or more electronic health information exchanges through which health care professionals and facilities and others involved in my care may view and obtain my information. I also understand and agree that, once my health information is exchanged in that way, it may be added into other treating providers medical records, and may be aggregated with the health information of others and used or disclosed to conduct data analysis, or for any other lawful purpose. Consent for Release of Sensitive Information I understand and agree that my health care providers may store or exchange through one or more health information exchanges health information related to any of the following: mental health or developmental disability treatment, alcohol or drug abuse treatment program services, HIV/AIDS testing or other communicable diseases, head trauma and brain injuries, genetic testing/counseling, sexual assault or artificial insemination (any or all of which are Sensitive Information. ). I specifically consent to the disclosure or receipt of such Sensitive Information for the purposes described above in the Consent for Sharing Information via Health Information Exchanges. I may have the right to inspect and copy any of my mental health or developmental disability information that will be shared. Duration of HIE Consent I understand that this HIE Consent applies to information generated prior to the date of this HIE Consent or during any subsequent time while this Consent is in effect. This HIE Consent is effective on the date of my signature (or the signature of my authorized representative below). The Consent for Release of Sensitive Information expires with respect to information about mental health and developmental disability services 25 years after the signature date on this HIE Consent. I may revoke this HIE Consent in writing, at any time; provided, however, that such revocation will not apply to any uses or sharing of my health information that occurred prior to the date the written revocation was received. Patient Signature Date Print Name of Patient Date of Birth If person other than patient has signed above, indicate relationship to patient: Name: Relationship to Patient:
8 Due to the federal privacy regulations, we cannot leave messages with protected health information on home answering machines or with family members without written permission. I give Midwest Ear Specialists permission to leave detailed messages: On my home answering machine / voic # On my work answering machine / voic # On my cell phone # With persons listed (name and relationship to patient) Signature Date I do not want any medical information released except to myself. Signature Date
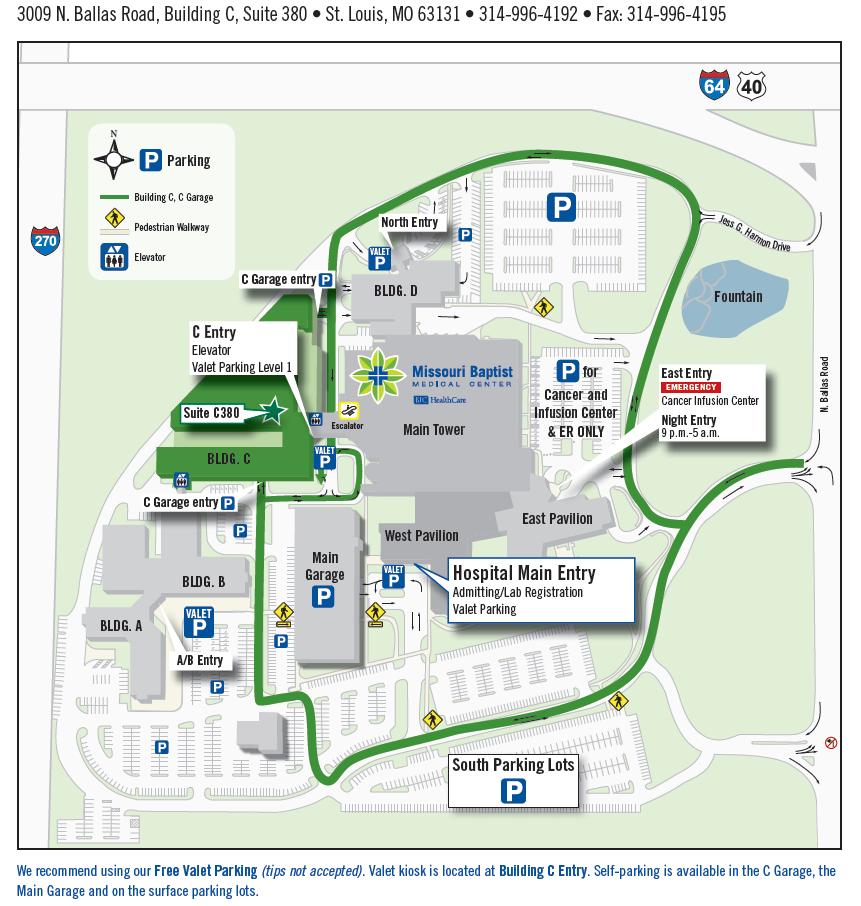
9 MISSOURI BAPTIST MEDICAL CENTER 3009 NORTH BALLAS ROAD, BUILDING C, SUITE 380 SAINT LOUIS, MO (314) FROM ILLINOIS (ALTERNATE ROUTE TO AVOID I-40[64]) DEPENDING ON YOUR STARTING POINT, TAKE I-255 (N OR S) TO I-270 AND THEN FOLLOW THE INSTRUCTIONS BELOW. FROM I-270 GET ON I-40 (64) EAST. GET OFF AT THE BALLAS ROAD EXIT. GO RIGHT AT THE LIGHT ONTO BALLAS ROAD. TURN RIGHT INTO MISSOURI BAPTIST MEDICAL CENTER. THEN TAKE OUR FIRST RIGHT AND FOLLOW SIGNS TO PROFESSIONAL BUILDING C. FROM I-40 (64) WESTBOUND (NOT COMING FROM I-270) GET OFF AT THE BALLAS ROAD EXIT AND GO LEFT. TURN RIGHT INTO MISSOURI BAPTIST MEDICAL CENTER. THEN YOU RE YOUR FIRST RIGHT AND FOLLOW SIGNS TO PROFESSIONAL BUILDING C. FROM I-40 (64) EASTBOUND. GET OFF AT THE BALLAS ROAD EXIT AND GO RIGHT. TURN RIGHT INTO THE MISSOURI BAPTIST MEDICAL CENTER. THEN TAKE YOUR FIRST RIGHT AND FOLLOW SIGNS TO PROFESSIONAL BUILDING C. BUILDING C OFFERS VALET PARKING OR THERE IS A PARKING GARAGE DIRECTLY UNDER BUILDING C.
10
Family Care Health Centers
 Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Thank you for choosing Oakland Medical Center as your Patient-Centered Medical Home
 Thank you for choosing Oakland Medical Center as your Patient-Centered Medical Home We ask that you complete the enclosed paperwork and bring it with you at the time of your appointment. We also ask that
Thank you for choosing Oakland Medical Center as your Patient-Centered Medical Home We ask that you complete the enclosed paperwork and bring it with you at the time of your appointment. We also ask that
Patient Registration Form
 908 South 10 th Street Office: 337.392.2330 Fax: 337.392.2580 West State Orthopedics and Sports Medicine Clinic, LLC Patient Registration Form Date: / / Patient Name: Birth Date: / / (last) (first) (mi)
908 South 10 th Street Office: 337.392.2330 Fax: 337.392.2580 West State Orthopedics and Sports Medicine Clinic, LLC Patient Registration Form Date: / / Patient Name: Birth Date: / / (last) (first) (mi)
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
NEW PATIENT PACKET. Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone. Address: Driver s License #:
 Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION CONSENT TO USE OR DISCLOSE MEDICAL INFORMATION
 Patient Name (PLEASE PRINT): Date of Birth: ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION The & Center of Southern Oregon, PC s Notice of Privacy Practices contains information about the uses and disclosures
Patient Name (PLEASE PRINT): Date of Birth: ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION The & Center of Southern Oregon, PC s Notice of Privacy Practices contains information about the uses and disclosures
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL
 Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
MAIN STREET MEDICAL NEW PATIENT QUESTIONNAIRE
 NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
Sage Medical Center New Patient Forms
 Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
PATIENT REGISTRATION FORM (ecw)
") PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
Patient Registration. City, State & Zip Code Date of Birth Age. Occupation: Family Physician: Married Single Other Spouse's Name
 *SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
*SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
NAME SS# ADDRESS CITY STATE ZIP. TELEPHONE (home) (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE
 (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE") REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
Patient Name:,, Address: Phones:,, Home Work Cell. Primary Physician: Emergency Contact: Phone#:
 Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
NEW PATIENT INFORMATION: ADULT
 NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology
 Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you
Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you
If you require films or CD, kindly give us 48 hour notice or make technologist aware at the time of your study.
 A Note to Our Patient: Your physician will be receiving a copy of your results via fax within two business days. Please contact your physician to go over your results and to obtain a copy of your report.
A Note to Our Patient: Your physician will be receiving a copy of your results via fax within two business days. Please contact your physician to go over your results and to obtain a copy of your report.
INSURANCE INFORMATION
 2014 575 Hill Country Dr. Ste 202 Kerrville, TX 78028 (830)258-6237 Office (830)315-1366 Fax Patient Name (last, first, MI) of Birth Social Security Number Mailing Address Home Telephone Work Telephone
2014 575 Hill Country Dr. Ste 202 Kerrville, TX 78028 (830)258-6237 Office (830)315-1366 Fax Patient Name (last, first, MI) of Birth Social Security Number Mailing Address Home Telephone Work Telephone
Patient Information Form
 Francisco J. Gomez, MD, FAHS, FAHA Tracy Posdzich, PMHNP-BC 110 Wolf Rd. Albany, NY 12205-1244 www.gomezneurology.com voice: 518-650-2090 fax: 888-698-2021 Patient Information Form Chief Complaint (reason
Francisco J. Gomez, MD, FAHS, FAHA Tracy Posdzich, PMHNP-BC 110 Wolf Rd. Albany, NY 12205-1244 www.gomezneurology.com voice: 518-650-2090 fax: 888-698-2021 Patient Information Form Chief Complaint (reason
Dear New Patient, Once again, we would like to thank you for choosing us as your primary health care provider. We look forward to working with you.
 307 West Central Street Wendy J. Parker, M.D. Natick, MA 01760 Deborah J. Riester, M.D. Telephone: 508-820-8383 Jo-Ann Suna,M.D. Fax: 508-820-0250 Hadia F. Tirmizi, M.D. Natalia Sedo, N.P. Christine Chang,
307 West Central Street Wendy J. Parker, M.D. Natick, MA 01760 Deborah J. Riester, M.D. Telephone: 508-820-8383 Jo-Ann Suna,M.D. Fax: 508-820-0250 Hadia F. Tirmizi, M.D. Natalia Sedo, N.P. Christine Chang,
Thank you, in advance, for being a partner in your care.
 477 Cooper Road, Suite 220 Westerville, OH 43081 614-818-0215 Your appointment with: Dr. David H. Brown Dr. Jed W. Henry Dr. Adam J. Clemens is scheduled for. Welcome to our practice. It is our desire
477 Cooper Road, Suite 220 Westerville, OH 43081 614-818-0215 Your appointment with: Dr. David H. Brown Dr. Jed W. Henry Dr. Adam J. Clemens is scheduled for. Welcome to our practice. It is our desire
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D KLONDIKE RD SW SUITE 205 CONYERS, GA TELEPHONE FAX
 PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c
 W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Welcome to the Southeastern Urology Associates meridianemr Patient Portal
 New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
Patient Registration Form
 Date: Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Patient Registration Form First Name Middle Last Name... Sex: M F Date of
Date: Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Patient Registration Form First Name Middle Last Name... Sex: M F Date of
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip
 PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Last Name First Middle. Mailing Address. City State Zip Phone. Date of Birth Age Soc. Sec# Cell. Employer Work Phone
 Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
Pediatric Patient History
 Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Social Security Number: Employment Status: Employed Unemployed Address: Student Retired
 Please complete all forms fully and to the best of your ability. If something does not apply to you please write N/A in the field. Patient Demographics: Name: Sex: Male Female Address: Apt: City: Marital
Please complete all forms fully and to the best of your ability. If something does not apply to you please write N/A in the field. Patient Demographics: Name: Sex: Male Female Address: Apt: City: Marital
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Patient Registration Form
 Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Date: Patient Registration Form First Name Middle Last Name... Sex: M F Preferred
Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Date: Patient Registration Form First Name Middle Last Name... Sex: M F Preferred
Lives (circle one): in assisted living with a relative alone
: in assisted living with a relative alone") Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
PATIENT'S NAME DATE OF BIRTH SOCIAL SECURITY # HOME PHONE # CELL PHONE # WORK PHONE #
 PATIENT INFORMATION PATIENT'S NAME DATE OF BIRTH SOCIAL SECURITY # STREET ADDRESS CITY, STATE, ZIP HOME PHONE # CELL PHONE # WORK PHONE # Emergency Contact & relationship: Phone #: Pharmacies local and
PATIENT INFORMATION PATIENT'S NAME DATE OF BIRTH SOCIAL SECURITY # STREET ADDRESS CITY, STATE, ZIP HOME PHONE # CELL PHONE # WORK PHONE # Emergency Contact & relationship: Phone #: Pharmacies local and
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Patient: Gender: Male Female. Mailing Address: Ethnicity: Not Hispanic or Latin Hispanic/Latin Home Phone #:
 5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
Emergency Contact Name: Relationship: Home #: ( ) Cell #: ( ) Alternate #: ( ) Pharmacy Information Pharmacy Name: Phone #: ( ) Location:
 Cell #: ( ) Alternate #: ( ) Pharmacy Information Pharmacy Name: Phone #: ( ) Location:") New Patient Office Information Last Name: First Name: Initial Date of Birth: SSN # Marital Status: Single Married Divorced Widowed Address: City: State: Zip: Gender: M Parent/ Legal Guardian if Patient
New Patient Office Information Last Name: First Name: Initial Date of Birth: SSN # Marital Status: Single Married Divorced Widowed Address: City: State: Zip: Gender: M Parent/ Legal Guardian if Patient
Re-Vita -Life. Sub-dermal Bio-identical Pellets
 Re-Vita -Life Sub-dermal Bio-identical Pellets Welcome and thank you for inquiring about Re-Vita-Life Bio-identical hormone replacement therapy. We have included a new patient information packet which
Re-Vita -Life Sub-dermal Bio-identical Pellets Welcome and thank you for inquiring about Re-Vita-Life Bio-identical hormone replacement therapy. We have included a new patient information packet which
Date: Name: Date of birth: Reason for today s visit: If yes, what are you allergic to and what type of reaction/symptoms did you have?
 Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
WILMINGTON HEALTH Patient Information
 WILMINGTON HEALTH Patient Information Account No. Doctor s No. PLEASE ANSWER ALL QUESTIONS PATIENT INFORMATION NAME: LAST BIRTHDATE SS# HOME PHONE CELL PHONE EMAIL ADDRESS FIRST MIDDLE SEX M F RACE White/Caucasian
WILMINGTON HEALTH Patient Information Account No. Doctor s No. PLEASE ANSWER ALL QUESTIONS PATIENT INFORMATION NAME: LAST BIRTHDATE SS# HOME PHONE CELL PHONE EMAIL ADDRESS FIRST MIDDLE SEX M F RACE White/Caucasian
Welcome to University Family Healthcare, PA.
 Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Date: Name: Date of birth: Reason for today s visit: If yes, what are you allergic to and what type of reaction/symptoms did you have?
 Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE Phone: Fax:
 Dear Parents/Guardians: School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE 19807 Phone: 651-2100 Fax: 651-2111 The Wilmington Charter/Cab Calloway
Dear Parents/Guardians: School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE 19807 Phone: 651-2100 Fax: 651-2111 The Wilmington Charter/Cab Calloway
PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD
 PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD General Consent for Treatment I have the legal right to consent to medical and surgical treatment because (a) I am the patient
PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD General Consent for Treatment I have the legal right to consent to medical and surgical treatment because (a) I am the patient
PATIENT NOTICE. If you are already taking any of the above medications, your provider may want to talk to you about alternative treatments.
 PATIENT NOTICE Our goal at is to provide quality medical care. Because of our concern for your health and well-being, there are certain types of medications we may not be able to prescribe to you. Examples
PATIENT NOTICE Our goal at is to provide quality medical care. Because of our concern for your health and well-being, there are certain types of medications we may not be able to prescribe to you. Examples
Neck & Spine Patient Demographic
 Neck & Spine Patient Demographic o New Patient o Return Patient o Update Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg.
Neck & Spine Patient Demographic o New Patient o Return Patient o Update Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg.
Welcome to the Office of Dr. Sam Van Kirk!
 Welcome to the Office of Dr. Sam Van Kirk! We understand that you have a choice in selecting your healthcare provider and we are pleased that you picked our practice. Our goal is to provide respectful,
Welcome to the Office of Dr. Sam Van Kirk! We understand that you have a choice in selecting your healthcare provider and we are pleased that you picked our practice. Our goal is to provide respectful,
The Home Doctor. Registration Checklist
 The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
Print Patient Name. Patient Signature
 . ASSIGNMENT OF BENEFITS Private insurance authorization for assignment of benefits and information release: I, the undersigned, authorize payment of medical benefits to Hill Country Pain for any services
. ASSIGNMENT OF BENEFITS Private insurance authorization for assignment of benefits and information release: I, the undersigned, authorize payment of medical benefits to Hill Country Pain for any services
Dear Kaniksu Patient,
 Dear Kaniksu Patient, Welcome to Kaniksu Health Services (KHS), a Community Health Center that provides quality and affordable medical, pediatric, dental, behavioral health and veteran care, regardless
Dear Kaniksu Patient, Welcome to Kaniksu Health Services (KHS), a Community Health Center that provides quality and affordable medical, pediatric, dental, behavioral health and veteran care, regardless
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Medications List. Allergies. Drug Name Dosage Directions Reason Taking
 Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Responsible Party (Guarantor) Info. Insurance Information
 Info. Insurance Information") Associates in Women s Health, P.C. 2801 YOUNGFIELD STREET, SUITE 200 GOLDEN, CO 80401 P: 303-940-1867 F: 303-940-1894 Please Circle Your Doctor: ELLIS GANTER PYTHON SCHOEN WESSELL, WHNP PATIENT INFORMATION
Associates in Women s Health, P.C. 2801 YOUNGFIELD STREET, SUITE 200 GOLDEN, CO 80401 P: 303-940-1867 F: 303-940-1894 Please Circle Your Doctor: ELLIS GANTER PYTHON SCHOEN WESSELL, WHNP PATIENT INFORMATION
LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W
 CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W") PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
REGISTRATION FORM (Minors)
") LEGAL NAME REGISTRATION FORM (Minors) Social Security#: Date of Birth: Sex: M or F Nickname: Religion: Church: Race (circle one): White Black-Asian AM Indian Alaska Native Native Hawaiian Pacific Islander-Unknown
LEGAL NAME REGISTRATION FORM (Minors) Social Security#: Date of Birth: Sex: M or F Nickname: Religion: Church: Race (circle one): White Black-Asian AM Indian Alaska Native Native Hawaiian Pacific Islander-Unknown
Adult Health History
 Adult Health History Name: DOB: Please list medications, including: vitamins, herbs, homeopathic remedies, and nonprescription medicines on the attached medication sheet. Medical History: High blood pressure
Adult Health History Name: DOB: Please list medications, including: vitamins, herbs, homeopathic remedies, and nonprescription medicines on the attached medication sheet. Medical History: High blood pressure
DENTON UROLOGY 2401 West Oak Street Ste. #102 Denton, Texas Phone: Fax:
 DETO UROLOG 2401 West Oak Street Ste. #102 Denton, Texas 76201 Phone: 940-387-2241 Fax: 940-380-1374 Acknowledgment of Review of otice of Privacy Practices I have reviewed this office s otice of Privacy
DETO UROLOG 2401 West Oak Street Ste. #102 Denton, Texas 76201 Phone: 940-387-2241 Fax: 940-380-1374 Acknowledgment of Review of otice of Privacy Practices I have reviewed this office s otice of Privacy
Lalita Matta, MD Estrela Chaves, NP, CDE
 PERSONAL INFORMATION Name of Patient: Maiden Name: Social Security No.: Date of Birth: Home Address: City: State: Zip: Home Phone: Mobile Phone: Work Phone: Email Address: Race/ Ethnicity: Marital Status:
PERSONAL INFORMATION Name of Patient: Maiden Name: Social Security No.: Date of Birth: Home Address: City: State: Zip: Home Phone: Mobile Phone: Work Phone: Email Address: Race/ Ethnicity: Marital Status:
HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed.
 Today date: HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed. Patient Full Name: Of Birth: Street: City: Zip Code:
Today date: HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed. Patient Full Name: Of Birth: Street: City: Zip Code:
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE Phone: Fax:
 School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
PATIENT INFORMATION Please Print
 PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
Fax: Do not mail the forms!
 Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
HEALTH HISTORY QUESTIONNAIRE
 Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
SPOUSE/GUARDIAN (If patient is married, give spouse information. If patient is a child, give parent information.)
") Please Fill Out Completely: St. Mary s Women s Center 1000 Cowles Clinic Way, Suite D-300 Greensboro, GA 30642 762-243-3860 phone 762-243-3879 fax Patient s Last Name First Name MI Social Security Number
Please Fill Out Completely: St. Mary s Women s Center 1000 Cowles Clinic Way, Suite D-300 Greensboro, GA 30642 762-243-3860 phone 762-243-3879 fax Patient s Last Name First Name MI Social Security Number
Amarillo Endoscopy Center Srinivas Pathapati, MD., PA 6833 Plum Creek Drive Amarillo, TX (806)
") Today s Date: / / PATIENT INFORMATION Patient s Last Name First Middle Mr. Miss Mrs. Ms. Marital Status (Circle one) Single / Mar / Div / Sep / Widow Legal Name (If applicable) Maiden Name Birth Date Age
Today s Date: / / PATIENT INFORMATION Patient s Last Name First Middle Mr. Miss Mrs. Ms. Marital Status (Circle one) Single / Mar / Div / Sep / Widow Legal Name (If applicable) Maiden Name Birth Date Age
Authorization to Disclose Protected Health Information (PHI)
") Authorization to Disclose Protected Health Information (PHI) Notice to Member: Completing this form will allow Health Net to share your health information with the person or group that you identify below.
Authorization to Disclose Protected Health Information (PHI) Notice to Member: Completing this form will allow Health Net to share your health information with the person or group that you identify below.
PATIENT INFORMATION When registering please provide proof of insurance and Picture ID Payment is expected at time of service.
 KENTUCKY FERTILITY, GYNECOLOGY AND OBSTETRICS PRIMARY HEALTH CARE 170 North Eagle Creek DR Suite 101 Lexington KY 40509 Phone 859-277-5736 Fax 859-276-2236 PATIENT INFORMATION When registering please provide
KENTUCKY FERTILITY, GYNECOLOGY AND OBSTETRICS PRIMARY HEALTH CARE 170 North Eagle Creek DR Suite 101 Lexington KY 40509 Phone 859-277-5736 Fax 859-276-2236 PATIENT INFORMATION When registering please provide
Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology
 Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you
Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you
Bay area Advanced Gastroenterology Care
 Authorization to Release Medical Information Date: Patient s Name: Patient s Address: Date of Birth: I hereby authorize you to transfer or make available all medical records or reports relating to my care
Authorization to Release Medical Information Date: Patient s Name: Patient s Address: Date of Birth: I hereby authorize you to transfer or make available all medical records or reports relating to my care
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease
 Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
To All Mission Ranch Primary Care Patients:
 To All Mission Ranch Primary Care Patients: At Mission Ranch Primary Care we strive to provide the best possible customer service. As a part of this, we ask that you fill out this paperwork and return
To All Mission Ranch Primary Care Patients: At Mission Ranch Primary Care we strive to provide the best possible customer service. As a part of this, we ask that you fill out this paperwork and return
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD
 Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
History Form. PAST SURGICAL HISTORY Surgeries/Hospitalizations Year Complications/Problems with anesthesia
 History Form Name: Date of Birth: Today's Date: Height: Weight: Date of Injury: Primary Care Physician: Address Who recommended this office? Address CHIEF COMPLAINT Why are you seeing the doctor today?
History Form Name: Date of Birth: Today's Date: Height: Weight: Date of Injury: Primary Care Physician: Address Who recommended this office? Address CHIEF COMPLAINT Why are you seeing the doctor today?
We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal.
 Appointment Date: Appointment Time: Dear Orion Member, We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal. Enclosed
Appointment Date: Appointment Time: Dear Orion Member, We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal. Enclosed
PATIENT REGISTRATION FORM
 Natalie A. Nealeigh, PA-C PATIENT REGISTRATION FORM PATIENT INFORMATION (PLEASE PRINT) Last Name: First Name: MI: Street Address: City: State: Zip: Home #: Cell #: Work #: DOB: Age: Sex (M/F): Marital
Natalie A. Nealeigh, PA-C PATIENT REGISTRATION FORM PATIENT INFORMATION (PLEASE PRINT) Last Name: First Name: MI: Street Address: City: State: Zip: Home #: Cell #: Work #: DOB: Age: Sex (M/F): Marital
DRUG / MEDICATION ALLERGIES: (include: Type/Reaction)
") NASSAU CHEST PHYSICIANS PC MEDICAL QUESTIONNAIRE 1 DATE: PATIENT NAME: DOB: DRUG / MEDICATION ALLERGIES: (include: Type/Reaction) 9/1/2014 PHARMACY NAME PHARMACY PHONE PHARMACY Street Address City State
NASSAU CHEST PHYSICIANS PC MEDICAL QUESTIONNAIRE 1 DATE: PATIENT NAME: DOB: DRUG / MEDICATION ALLERGIES: (include: Type/Reaction) 9/1/2014 PHARMACY NAME PHARMACY PHONE PHARMACY Street Address City State
714 Beacon Street, Newton Centre, MA,
 Nancy Cooper, MD Kari Emsbo, MD Yana Urman, MD 714 Beacon Street Newton Centre, MA 02459 617-332-1001 Phone 617-332-5154 Fax Dear Patient: On behalf of all of us at Beth Israel Deaconess HealthCare-Newton
Nancy Cooper, MD Kari Emsbo, MD Yana Urman, MD 714 Beacon Street Newton Centre, MA 02459 617-332-1001 Phone 617-332-5154 Fax Dear Patient: On behalf of all of us at Beth Israel Deaconess HealthCare-Newton
Over. 1. What is the primary reason that you are here? 2. What three aesthetic changes would you like to effect?
 New Patient Questionnaire Please help us help you by filling out the following information. It is our intention to make your consultation and surgical experience with us productive, enjoyable and goal
New Patient Questionnaire Please help us help you by filling out the following information. It is our intention to make your consultation and surgical experience with us productive, enjoyable and goal
Patient Name First Middle Last Address Street City State Zip Home Phone Work Phone Cell Phone. Date of Birth SS#
 PATIENT WILL NOT BE SEEN WITHOUT PHOTO ID Patient Information Kimberly Walpert, M.D. 1199 Prince Avenue Athens GA 30606 Ph 706-475-1870 Fax 706-475-1879 www.athensbrainandspine.com Patient Name First Middle
PATIENT WILL NOT BE SEEN WITHOUT PHOTO ID Patient Information Kimberly Walpert, M.D. 1199 Prince Avenue Athens GA 30606 Ph 706-475-1870 Fax 706-475-1879 www.athensbrainandspine.com Patient Name First Middle
Esthetician Services Registration Form
 Esthetician Services Registration Form PATIENT INFORMATION Name: Date of Birth: Address: Pharmacy: City, State, Zip: Phone #: Email Address: Medical Doctor: Home Phone: Phone #: Mobile Phone: Dermatologist:
Esthetician Services Registration Form PATIENT INFORMATION Name: Date of Birth: Address: Pharmacy: City, State, Zip: Phone #: Email Address: Medical Doctor: Home Phone: Phone #: Mobile Phone: Dermatologist:
CURE CARDIOVASCULAR CONSULTANTS
 NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
Planned Respite Referral Application
 Planned Respite Referral Application White Plains, NY 10605 (914) 948-4993 or (914) 564-3749 FAX: (914) 813-4364 Dear Applicant: Thank you for your interest in Planned Respite. Planned Respite is a short-term
Planned Respite Referral Application White Plains, NY 10605 (914) 948-4993 or (914) 564-3749 FAX: (914) 813-4364 Dear Applicant: Thank you for your interest in Planned Respite. Planned Respite is a short-term
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
Dear New Patient: Sincerely, The Scheduling Staff
 Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Medical History Form
 Medical History Form Patient Name of Birth Medical History Do you have or have you had any of the following? Condition Yes No Condition Yes No Condition Yes No ADHD Stroke Menopausal Syndrome Allergies
Medical History Form Patient Name of Birth Medical History Do you have or have you had any of the following? Condition Yes No Condition Yes No Condition Yes No ADHD Stroke Menopausal Syndrome Allergies
Date: Patient/Parent/Legal Guardian Signature CHCP Form #PCS104 (rev. 6/16 per UDS)
") : REGISTRATION FORM 1. Name (First and Last): M.I. of Birth: 2. Address: Apartment: City/State: Zip Code: Home Phone: Cell Phone: Work Phone: 3. E-mail address: Social Security: - - 4. *Gender Identity:
: REGISTRATION FORM 1. Name (First and Last): M.I. of Birth: 2. Address: Apartment: City/State: Zip Code: Home Phone: Cell Phone: Work Phone: 3. E-mail address: Social Security: - - 4. *Gender Identity:
ADMISSION FORM. Employment Status: Retired Unemployed Employed Full Time Employed Part Time
 Patient ID Number A. PATIENT INFORMATION: First Name & Middle Initial: Home Address: ADMISSION FORM Last Name: Apartment Number: City: State: Zip: Phone: Home Cell Second Phone: Work Cell Email Address:
Patient ID Number A. PATIENT INFORMATION: First Name & Middle Initial: Home Address: ADMISSION FORM Last Name: Apartment Number: City: State: Zip: Phone: Home Cell Second Phone: Work Cell Email Address:
MAIN STREET RADIOLOGY
 MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
CORAZON PANES SANCHEZ., M.D., L.L.C.
 PERRYVILLE, MD 21903 Rising sun, MD 21911 BALTIMORE, MD 21221 PATIENT REGISTRATION NAME: DOB: SEX: ( ) MALE ( ) FEMALE SOCIAL SECURITY #: - - ADDRESS: CITY/STATE: ZIP:_ TELEPHONE #: MOTHER S NAME: FATHER
PERRYVILLE, MD 21903 Rising sun, MD 21911 BALTIMORE, MD 21221 PATIENT REGISTRATION NAME: DOB: SEX: ( ) MALE ( ) FEMALE SOCIAL SECURITY #: - - ADDRESS: CITY/STATE: ZIP:_ TELEPHONE #: MOTHER S NAME: FATHER
PATIENT INFORMATION Indiana Plastic Surgery Center, PC
 PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
PATIENT HISTORY. Name Last First Middle/Maiden Name you Prefer. Address Street City State/Zip. Address
 PATIENT HISTORY GENERAL INFORMATION Name Last First Middle/Maiden Name you Prefer Address Street City State/Zip Home Phone ( ) - Cell Phone ( ) - E-Mail Address Age Sex Date of Birth / / Social Security#
PATIENT HISTORY GENERAL INFORMATION Name Last First Middle/Maiden Name you Prefer Address Street City State/Zip Home Phone ( ) - Cell Phone ( ) - E-Mail Address Age Sex Date of Birth / / Social Security#
MonaLisa Touch Patient Questionnaire & Health History
 MonaLisa Touch Patient Questionnaire & Health History Name: (Last) (First) (Middle) Date of Birth: Age: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address: May we
MonaLisa Touch Patient Questionnaire & Health History Name: (Last) (First) (Middle) Date of Birth: Age: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address: May we
Authorization, Fees, and Office Policy
 a Authorization, Fees, and Office Policy Authorization for Treatment I hereby authorize the staff of Compassionate Care Clinics of Pinellas to render medical services as deemed necessary. I also certify
a Authorization, Fees, and Office Policy Authorization for Treatment I hereby authorize the staff of Compassionate Care Clinics of Pinellas to render medical services as deemed necessary. I also certify
(Please Print) PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )
 PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )") (Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
(Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
The process has been designed to be user friendly and involves a few simple steps.
 HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to