Plant the Seeds of Compliance with PEPPER. Prepared for: WiAHC June 8, Presented by: Caryn Adams, Manager
|
|
|
- Christiana Richard
- 5 years ago
- Views:
Transcription

1 Plant the Seeds of Compliance with PEPPER Prepared for: June 8, 2017 Presented by: Caryn Adams, Manager
2 Summary and Objectives Program for Evaluating Payment Electronic Report has been available to home health agencies since In the state of Wisconsin, less than 50% of HHAs have accessed their PEPPER reports. If government agencies are able to use this data, shouldn t we also? At the end of this session, the participants will be able to: Verbalize what PEPPER reports are Understand the data collected and reported in the PEPPER reports Effectively utilize PEPPER reports in your agency s compliance plan **Participants may bring their PEPPER reports to review if desired.

3 About the Presenter Caryn Adams, Health Care Manager Caryn is a senior consultant in Wipfli LLP s health care senior living practice. She has more than 25 years of experience in the health care industry. Her vast industry experience lends a deep understanding of the challenges faced by her clients. Caryn is dedicated to providing exceptional client service to assist longterm care, home care, hospice, and senior living providers in achieving their strategic goals.
4 Power Point Presentation

5 W i A H C J u n e 8, Objectives Verbalize what PEPPER reports are Understand the data collected and reported in the PEPPER reports Effectively utilize PEPPER reports in your agency s compliance plan 2 W h a t t h e h e c k i s P E P P E R a n y w a y? Pepper 1
6 PEPPER Program for Evaluating Payment Patterns Electronic Report 4 Summary Summarizes one agency s Medicare claims and compares it with data for the nation, MAC jurisdiction, and the state All providers Targets areas that are vulnerable to improper payments Overpayments and underpayments 5 Purpose Supports CMS s program integrity activities Provides education to providers 6 Pepper 2
7 Purpose Government Accountability Office (GAO) has designated Medicare as a program at high risk for fraud, waste, and abuse. Payments to HHAs have been identified as vulnerable to abuse. OIG has been encouraging providers to develop and implement a compliance program to protect its operations from fraud and abuse. 7 Target Data The Compare Targets Report displays statistics for target areas that have reportable data (11+ target count) in the most recent time period. Percentiles indicate how a home health agency's target area percent/rate compares to the target area percents/rates for all home health agencies in the respective comparison group. For example, if a home health agency's national percentile (see below) is 80.0, 80% of the home health agencies in the nation have a lower percent/rate value than that home health agency. (The home health agency's Medicare Administrative Contractor (MAC) jurisdiction percentile and the state percentile values (if displayed) should be interpreted in the same manner. Percentiles at or above the 80th percentile for any target area indicate that the home health agency may be at a higher risk for improper Medicare payments. The greater the percentile value, in particular the national and/or jurisdiction percentile, the greater the consideration that should be given to that target area. 8 Episode Episode = Claim Part A and Part B claims are eligible for inclusion 9 Pepper 3
8 Average Case Mix Numerator (N): Sum of case mix weight for all episodes paid to the HHA during the report period, excluding LUPAs and PEPs Denominator (D): Count of episodes paid to the HHA during the report period, excluding LUPAs and PEPs Reported as a rate, not a percent 10 Average Number of Episodes N: Count of episodes paid to the HHA D: Count of unique beneficiaries served by the HHA Reported as a rate, not a percent 11 Episodes With Five or Six Visits N: Count of episodes with five or six visits paid to the HHA D: Count of episodes paid to the HHA 12 Pepper 4
9 Non-LUPA Payments N: Count of episodes paid to the HHA that did not have a LUPA payment D: Count of episodes paid to the HHA 13 High Therapy Utilization Episodes N: Count of episodes with 20+ therapy visits paid to the HHA D: Count of episodes paid to the HHA 14 Outlier Payments N: Dollar amount of outlier payments for episodes paid to the HHA D: Dollar amount of total payments for episodes paid to the HHA 15 Pepper 5
10 Reports Organized in three 12 month time periods based on the fiscal year (FY) Summarizes statistics for three fiscal years Distributed in July 2017 Schedule is annually, on or about July 18, Compare An HHA is compared to other HHAs in three comparison groups: State, Medicare Administrative Contractor/Fiscal Intermediary jurisdiction, and nation. These comparisons enable a HHA to determine whether its results differ from other HHAs and whether it is at risk for improper Medicare payments (i.e., is an outlier ). 17 Uses PEPPER can be used to compare its claims data for areas of potential concern and to identify changes in billing practices 18 Pepper 6
11 PEPPER PEPPER determines outliers based on preset control limits. The upper control limit for all target areas is the national 80th percentile. Areas at risk for under coding also have a lower control limit, which is the national 20th percentile. PEPPER draws attention to any findings that are at or above the upper control limit (high outliers) or at the lower control limit (low outliers). 19 Do I Have to Use PEPPER? No Free data You don t have to compile it Why wouldn t you? 20 How to Use PEPPER As a tool for analyzing data, the PEPPER reports provide an opportunity for ongoing process improvement Guides questions to be asked for QAPI 21 Pepper 7
12 What Should I Do When I Get the Report? Do not panic High outlier does not prove anything, but it can prepare you if an audit occurs Determine, if possible, why you are an outlier - Audit a sample of claims - Review the documentation in the medical record - Review the claim: Was it coded and billed appropriately based on documentation in the medical record? Ensure following best practices even if you are not an outlier 22 Use the Resources on the PEPPER Website Share internally Guide auditing and monitoring Multiple facilities Compare and contrast Look for increases or decreases over time Identify root causes of increases or decreases Be proactive and preventive Avoid pay and chase 23 To Be Included: Claim facility type = 3 Include service of home health visits Services must have been provided during the report period Exclude nonpayment and interim claims Final action claim (all disputes and adjustments have been resolved) Medicare claim payment amount >0 Excludes HMO Excludes cancelled claims 24 Pepper 8
 Patient")
13 Also The numerator count needs to be 11 or more 25 Distributed annually in July PEPPER Resources Portal Click on PEPPER Distribution Follow the instructions on the portal Need six-digit CMS certification number (PTAN) Patient control number from a paid claim Need to be the CEO, administrator, president, or compliance officer 27 Pepper 9
14 P E P P E R R E V I E W What Should I Do With the Data? Review outliers Review accuracy of data Review systems and processes QAPI 29 Average Case Mix Risk of over-coding of clinical and functional status OASIS review Documentation to support OASIS education 30 Pepper 10
15 Average Number of Episodes Continuing to treat beyond medical necessity Review documentation Skilled documentation 31 Episodes With Five or Six Visits Using the minimum number of visits to avoid LUPA Review documentation Reasonable and necessary 32 Non-LUPA Payments Same as previous Review documentation Medical necessity Reasonable and necessary 33 Pepper 11
16 High Therapy Utilization Episodes Improper billing for therapy services Review documentation Reasonable and necessary Skilled 34 Outlier Payments Potential over-coding of clinical and functional status Review documentation OASIS review and education 35 Lets Look at a Report Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xl s 36 Pepper 12


17 PEPPER 37 PEPPER Pepper 13

18 Pepper 14

19 Pepper 15

20 Pepper 16

 51")
21 49 Q API QAPI Compliance New CoPs More data collection and performance projects Goes into effect in 2018 (if you do not have a current QAPI) 51 Pepper 17
22 Element 1 Design and Scope Ongoing Comprehensive Facility self-assessment tool 52 Element 2 Governance and Leadership 53 Element 3 Feedback, Data Systems, and Monitoring 54 Pepper 18

23 Element 4 Performance Improvement Projects (PIP) 55 Element 5 Systematic Analysis and Systemic Action 56 Root Cause Analysis 57 Pepper 19
24 What Is Root Cause Analysis? Root cause analysis is a method that is used to address a problem or nonconformance in order to get to the root cause of the problem. It is used so we can correct or eliminate the cause and prevent the problem from recurring. Adapted from NASA Root Cause Analysis 58 Philosophy of Root Cause Analysis Each problem is an opportunity because it can tell a story about why and how it occurred It is critical that everyone take a personal and active role in improving quality The true problem must be understood before action is taken To do this well, you must be: Both focused and open-minded Both patient and quick Adapted from NASA Root Cause Analysis 59 What Is Root Cause? Root cause is the fundamental breakdown or failure of a process that, when resolved, prevents a recurrence of the problem Or, in other words: When you fix the root cause, the problem goes away and doesn t come back Root cause analysis is a systematic approach to get to the true root causes of our process problems Adapted from NASA Root Cause Analysis 60 Pepper 20

25 Types of Tools Used in Root Cause Analysis Brainstorming Fishbone diagram Flowchart Whys 61 Plan Do Check Act (PDCA) 62 PDCA PLAN Establish the objectives and processes necessary to deliver results in accordance with the expected target or goals. By establishing output expectations, the completeness and accuracy of the specification are also a part of the targeted improvement. When possible, start on a small scale to test possible effects. 63 Pepper 21
26 PDCA DO Implement the plan, execute the process, make the product. Collect data for charting and analysis in the following CHECK and ACT steps. 64 PDCA CHECK Study the actual results (measured and collected in DO above) and compare against the expected results (targets or goals from the PLAN ) to ascertain any differences. Look for deviation in implementation from the plan and also look for the appropriateness/completeness of the plan to enable the execution (i.e., Do ). Charting data can make it much easier to see trends over several PDCA cycles and in order to convert the collected data into information. Information is what you need for the next step ACT. 65 PDCA ACT Request corrective actions on significant differences between actual and planned results. Analyze the differences to determine their root causes. Determine where to apply changes that will include improvement of the process or product. When a passthrough these four steps does not result in the need to improve, the scope to which PDCA is applied may be refined to plan and improve with more detail in the next iteration of the cycle, or attention needs to be placed on a different stage of the process. 66 Pepper 22
27 Action Steps to QAPI Step 11 Step 11 Getting to the root of the problem Root cause analysis Focuses primarily on systems and processes, not individual performance Teach your staff the process 67 Header In seed time learn, in harvest teach, in winter enjoy. - William Blake 68 Cultivate your craft. Water it daily, pour some tender loving care into it, and watch it grow. Remember that a plant doesn t sprout immediately. Be patient, and know that in life you will reap what you sow. J.B. McG 69 Pepper 23
28 Questions? 70 Contact Information Caryn Adams RN, MSN, RAC-CT, DNS-CT, HCS-O, AHIMA- Approved ICD 10 CM/PCS Trainer Manager, Health Care Practice, Post-Acute Care Pepper 24
29 Attachment
 summarizes provider-specific data for Medicare")
30 Purpose of Home Health Agency Program for Evaluating Payment Patterns Electronic Report Visit PEPPERresources.org Data Report Through Q4CY15 Link to PEPPER Training , Provider D02271 The Program for Evaluating Payment Patterns Electronic Report (PEPPER) summarizes provider-specific data for Medicare services that may be at higher risk for improper Medicare payments. Please refer to the Home Health Agency PEPPER User's Guide at PEPPERresources.org for guidance using the report. If you need assistance, please contact TMF by visiting PEPPERresources.org and clicking on the Help/Contact Us tab. This is HHA PEPPER version Q4CY15 Jurisdiction: Demo Jurisdiction (DMSTR) PEPPER was developed by TMF Health Quality Institute under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the Department of Health and Human Services (HHS). Worksheet: Purpose File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
31 Definitions for Home Health Agency PEPPER Target Areas Home Health Target Area Avg Case Mix Home Health Target Area Definition N: sum of case mix weight for all episodes paid to the HHA during the report period, excluding LUPAs (identified by Part A NCH HHA LUPA code) and PEPs (identified as patient discharge status code equal to 06 ) D: count of episodes paid to the HHA during the report period, excluding LUPAs and PEPs Nbr Episodes N: count of episodes paid to the HHA during the report period D: count of unique beneficiaries served by the HHA during the report period 5 or 6 Visits N: count of episodes with 5 or 6 visits paid to the HHA during the report period D: count of episodes paid to the HHA during the report period NonLUPA N: count of episodes paid to the HHA that did not have a LUPA payment during the report period D: count of episodes paid to the HHA during the report period Hi Therapy Utiliz N: count of episodes with 20+ therapy visits paid to the HHA during the report period (first digit of HHRG equal to '5') D: count of episodes paid to the HHA during the report period Outlier N: sum of dollar amount of outlier payments (identified by the amount where Value Code equal to 17 ) for episodes paid to the HHA during the report period D: sum of dollar amount of total payments for episodes paid to the HHA during the report period
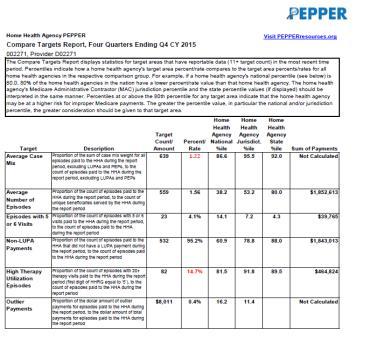
32 Home Health Agency PEPPER Visit PEPPERresources.org Compare Targets Report, Four Quarters Ending Q4 CY , Provider D02271 The Compare Targets Report displays statistics for target areas that have reportable data (11+ target count) in the most recent time period. Percentiles indicate how a home health agency's target area percent/rate compares to the target area percents/rates for all home health agencies in the respective comparison group. For example, if a home health agency's national percentile (see below) is 80.0, 80% of the home health agencies in the nation have a lower percent/rate value than that home health agency. The home health agency's Medicare Administrative Contractor (MAC) jurisdiction percentile and the state percentile values (if displayed) should be interpreted in the same manner. Percentiles at or above the 80th percentile for any target area indicate that the home health agency may be at a higher risk for improper Medicare payments. The greater the percentile value, in particular the national and/or jurisdiction percentile, the greater consideration should be given to that target area. Target Average Case Mix Description Proportion of the sum of case mix weight for all episodes paid to the HHA during the report period, excluding LUPAs and PEPs, to the count of episodes paid to the HHA during the report period, excluding LUPAs and PEPs Target Home Health Agency Home Health Agency Home Health Agency Count/ Percent/ National Jurisdict. State Amount Rate %ile %ile %ile Sum of Payments Not Calculated Average Number of Episodes Episodes with 5 or 6 Visits Non-LUPA Payments Proportion of the count of episodes paid to the HHA during the report period, to the count of unique beneficiaries served by the HHA during the report period Proportion of the count of episodes with 5 or 6 visits paid to the HHA during the report period, to the count of episodes paid to the HHA during the report period Proportion of the count of episodes paid to the HHA that did not have a LUPA payment during the report period, to the count of episodes paid to the HHA during the report period $1,852, % $39, % $1,843,013 High Therapy Utilization Episodes Outlier Payments Proportion of the count of episodes with 20+ therapy visits paid to the HHA during the report period (first digit of HHRG equal to 5 ), to the count of episodes paid to the HHA during the report period Proportion of the dollar amount of outlier payments for episodes paid to the HHA during the report period, to the dollar amount of total payments for episodes paid to the HHA during the report period % $464,824 $8, % Not Calculated Note: State and/or jurisdiction %iles are not reported when there are fewer than 11 providers Worksheet: Compare with reportable data for the target area in the state and/or jurisdiction. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
33 Home Health Agency PEPPER , Provider D02271 Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify: Average Case Mix Visit PEPPERresources.org Link to Definitions Worksheet Increasing Target Rates over time resulting in greater risk of improper Medicare payments Your Target Rate (first row in the table below) is above the national 80th percentile Target Rate /1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Home Health Agency Natl: 80th %ile Juris: 80th %ile State: 80th %ile YOUR HOME HEATLH AGENCY 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Target Area Rate Target Count: (Numerator: sum of case mix weight for all episodes paid to the HHA during the report period, excluding LUPAs (identified by Part A NCH HHA LUPA code) and PEPs (identified as patient discharge status code equal to 06 ) Denominator Count (Denominator: count of episodes paid to the HHA during the report period, excluding LUPAs and PEPs) Denominator Average Length of Stay *Data not available when numerator count less than 11 Note: State and/or jurisdiction percentiles are zero if there are fewer than 11 providers with reportable data for the target area in the state and/or jurisdiction. COMPARATIVE DATA National 80th Percentile Jurisdiction 80th Percentile State 80th Percentile Note: HHRG case mix weights changed (decreased) in CY 2014 from CY 2013 SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE: This could indicate a risk of potential overcoding of beneficiaries' clinical and functional status. The HHA should determine whether beneficiaries' clinical and functional status as reported on the OASIS is supported and consistent with medical record documentation. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
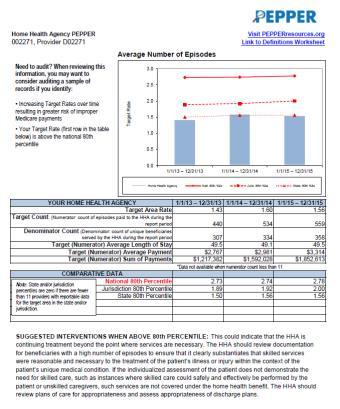
34 Home Health Agency PEPPER , Provider D02271 Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify: Average Number of Episodes Visit PEPPERresources.org Link to Definitions Worksheet Increasing Target Rates over time resulting in greater risk of improper Medicare payments Your Target Rate (first row in the table below) is above the national 80th percentile Target Rate /1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Home Health Agency Natl: 80th %ile Juris: 80th %ile State: 80th %ile YOUR HOME HEALTH AGENCY 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Target Area Rate Target Count: (Numerator: count of episodes paid to the HHA during the report period Denominator Count (Denominator: count of unique beneficiaries served by the HHA during the report period Target (Numerator) Average Length of Stay Target (Numerator) Average Payment $2,767 $2,981 $3,314 Target (Numerator) Sum of Payments $1,217,382 $1,592,028 $1,852,613 *Data not available when numerator count less than 11 Note: State and/or jurisdiction percentiles are zero if there are fewer than 11 providers with reportable data for the target area in the state and/or jurisdiction. COMPARATIVE DATA National 80th Percentile Jurisdiction 80th Percentile State 80th Percentile SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE: This could indicate that the HHA is continuing treatment beyond the point where services are necessary. The HHA should review documentation for beneficiaries with a high number of episodes to ensure that it clearly substantiates that skilled services were reasonable and necessary to the treatment of the patient s illness or injury within the context of the patient s unique medical condition. If the individualized assessment of the patient does not demonstrate the need for skilled care, such as instances where skilled care could safely and effectively be performed by the patient or unskilled caregivers, such services are not covered under the home health benefit. The HHA should review plans of care for appropriateness and assess appropriateness of discharge plans. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
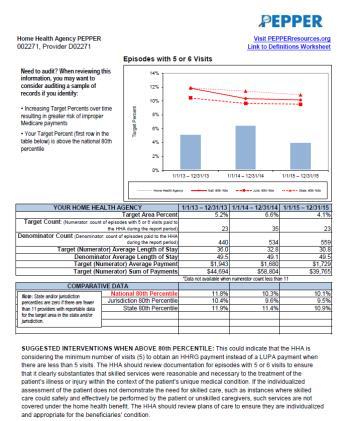
35 Home Health Agency PEPPER , Provider D02271 Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify: Increasing Target Percents over time resulting in greater risk of improper Medicare payments Your Target Percent (first row in the table below) is above the national 80th percentile Episodes with 5 or 6 Visits Target Percent 14% 12% 10% 8% 6% 4% 2% Visit PEPPERresources.org Link to Definitions Worksheet 0% 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Home Health Agency Natl: 80th %ile Juris: 80th %ile State: 80th %ile YOUR HOME HEALTH AGENCY 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Target Area Percent 5.2% 6.6% 4.1% Target Count: (Numerator: count of episodes with 5 or 6 visits paid to the HHA during the report period) Denominator Count (Denominator: count of episodes paid to the HHA during the report period) Target (Numerator) Average Length of Stay Denominator Average Length of Stay Target (Numerator) Average Payment $1,943 $1,680 $1,729 Target (Numerator) Sum of Payments $44,694 $58,804 $39,765 *Data not available when numerator count less than 11 Note: State and/or jurisdiction percentiles are zero if there are fewer than 11 providers with reportable data for the target area in the state and/or jurisdiction. COMPARATIVE DATA National 80th Percentile 11.8% 10.3% 10.1% Jurisdiction 80th Percentile 10.4% 9.6% 9.5% State 80th Percentile 11.9% 11.4% 10.9% SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE: This could indicate that the HHA is considering the minimum number of visits (5) to obtain an HHRG payment instead of a LUPA payment when there are less than 5 visits. The HHA should review documentation for episodes with 5 or 6 visits to ensure that it clearly substantiates that skilled services were reasonable and necessary to the treatment of the patient s illness or injury within the context of the patient s unique medical condition. If the individualized assessment of the patient does not demonstrate the need for skilled care, such as instances where skilled care could safely and effectively be performed by the patient or unskilled caregivers, such services are not covered under the home health benefit. The HHA should review plans of care to ensure they are individualized and appropriate for the beneficiaries condition. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
36 Home Health Agency PEPPER , Provider D02271 Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify: Non-LUPA Payments 120% 100% Visit PEPPERresources.org Link to Definitions Worksheet Increasing Target Percents over time resulting in greater risk of improper Medicare payments Your Target Percent (first row in the table below) is above the national 80th percentile Target Percent 80% 60% 40% 20% 0% 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Home Health Agency Natl: 80th %ile Juris: 80th %ile State: 80th %ile YOUR HOME HEALTH AGENCY 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Target Area Percent 90.2% 92.7% 95.2% Target Count: (Numerator: count of episodes paid to the HHA that did not have a LUPA payment during the report period) Denominator Count (Denominator: count of episodes paid to the HHA during the report period) Target (Numerator) Average Length of Stay Denominator Average Length of Stay Target (Numerator) Average Payment $3,030 $3,188 $3,464 Target (Numerator) Sum of Payments $1,202,935 $1,578,228 $1,843,013 *Data not available when numerator count less than 11 Note: State and/or jurisdiction percentiles are zero if there are fewer than 11 providers with reportable data for the target area in the state and/or jurisdiction. COMPARATIVE DATA National 80th Percentile 97.6% 97.6% 97.5% Jurisdiction 80th Percentile 95.6% 95.9% 95.2% State 80th Percentile 91.3% 92.7% 93.5% SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE: This could indicate that the HHA is considering the minimum number of visits (5) to obtain an HHRG payment instead of a LUPA payment where there are less than 5 visits. The HHA should review documentation to ensure that it clearly substantiates that skilled services were reasonable and necessary to the treatment of the patient s illness or injury within the context of the patient s unique medical condition. If the individualized assessment of the patient does not demonstrate the need for skilled care, such as instances where skilled care could safely and effectively be performed by the patient or unskilled caregivers, such services are not covered under the home health benefit. The HHA should review plans of care to ensure they are individualized and appropriate for the beneficiaries condition. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
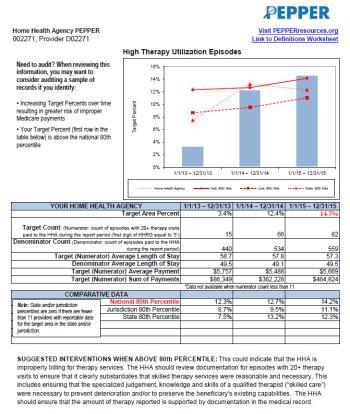
37 Home Health Agency PEPPER , Provider D02271 Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify: Increasing Target Percents over time resulting in greater risk of improper Medicare payments Your Target Percent (first row in the table below) is above the national 80th percentile High Therapy Utilization Episodes Target Percent 16% 14% 12% 10% 8% 6% 4% 2% Visit PEPPERresources.org Link to Definitions Worksheet 0% 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Home Health Agency Natl: 80th %ile Juris: 80th %ile State: 80th %ile YOUR HOME HEALTH AGENCY 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Target Area Percent 3.4% 12.4% 14.7% Target Count: (Numerator: count of episodes with 20+ therapy visits paid to the HHA during the report period (first digit of HHRG equal to '5') Denominator Count (Denominator: count of episodes paid to the HHA during the report period) Target (Numerator) Average Length of Stay Denominator Average Length of Stay Target (Numerator) Average Payment $5,757 $5,488 $5,669 Target (Numerator) Sum of Payments $86,349 $362,228 $464,824 *Data not available when numerator count less than 11 Note: State and/or jurisdiction percentiles are zero if there are fewer than 11 providers with reportable data for the target area in the state and/or jurisdiction. COMPARATIVE DATA National 80th Percentile 12.3% 12.7% 14.2% Jurisdiction 80th Percentile 8.7% 9.5% 11.1% State 80th Percentile 7.5% 13.2% 12.3% SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE: This could indicate that the HHA is improperly billing for therapy services. The HHA should review documentation for episodes with 20+ therapy visits to ensure that it clearly substantiates that skilled therapy services were reasonable and necessary. This includes ensuring that the specialized judgement, knowledge and skills of a qualified therapist ( skilled care ) were necessary to prevent deterioration and/or to preserve the beneficiary s existing capabilities. The HHA should ensure that the amount of therapy reported is supported by documentation in the medical record. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
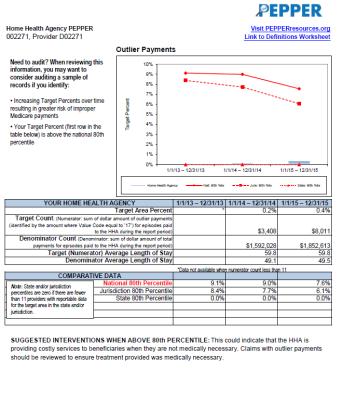
38 Home Health Agency PEPPER , Provider D02271 Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify: Increasing Target Percents over time resulting in greater risk of improper Medicare payments Your Target Percent (first row in the table below) is above the national 80th percentile Outlier Payments Target Percent 10% 9% 8% 7% 6% 5% 4% 3% 2% 1% Visit PEPPERresources.org Link to Definitions Worksheet 0% 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Home Health Agency Natl: 80th %ile Juris: 80th %ile State: 80th %ile YOUR HOME HEALTH AGENCY 1/1/13 12/31/13 1/1/14 12/31/14 1/1/15 12/31/15 Target Area Percent * 0.2% 0.4% Target Count: (Numerator: sum of dollar amount of outlier payments (identified by the amount where Value Code equal to 17 ) for episodes paid to the HHA during the report period) $3,408 $8,011 Denominator Count (Denominator: sum of dollar amount of total payments for episodes paid to the HHA during the report period) $1,592,028 $1,852,613 Target (Numerator) Average Length of Stay Denominator Average Length of Stay *Data not available when numerator count less than 11 Note: State and/or jurisdiction percentiles are zero if there are fewer than 11 providers with reportable data for the target area in the state and/or jurisdiction. COMPARATIVE DATA National 80th Percentile 9.1% 9.0% 7.6% Jurisdiction 80th Percentile 8.4% 7.7% 6.1% State 80th Percentile 0.0% 0.0% 0.0% SUGGESTED INTERVENTIONS WHEN ABOVE 80th PERCENTILE: This could indicate that the HHA is providing costly services to beneficiaries when they are not medically necessary. Claims with outlier payments should be reviewed to ensure treatment provided was medically necessary. File: Copy of _DMSTR_HHAPEPP_Q4CY15_Provider_D02271.xls
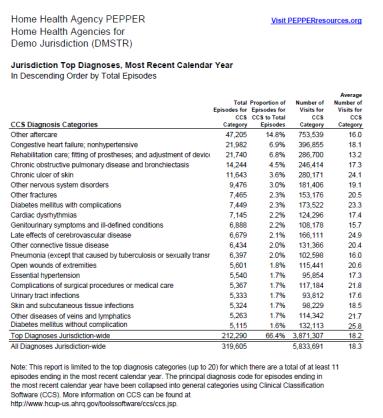
39 Home Health Agency PEPPER Top Diagnoses Provider D02271 Visit PEPPERresources.org Home Health Agency Top Diagnoses, Most Recent Calendar Year In Descending Order by Total Episodes CCS Diagnosis Categories Rehabilitation care; fitting of prostheses; and adjustment of device Other aftercare Congestive heart failure; nonhypertensive Chronic obstructive pulmonary disease and bronchiectasis Diabetes mellitus with complications Late effects of cerebrovascular disease Complications of surgical procedures or medical care Pneumonia (except that caused by tuberculosis or sexually transm Other nervous system disorders Other fractures Chronic ulcer of skin Diabetes mellitus without complication Delirium, dementia, and amnestic and other cognitive disorders Fracture of upper limb Acute myocardial infarction Cardiac dysrhythmias Total Episodes for CCS Category Proportion of Episodes for CCS to Total Episodes Number of Visits for CCS Category Average Number of Visits for CCS Category % % 1, % % % % % % % % % % % % % % Top Diagnoses % 7, All Diagnoses , Note: This report is limited to the top diagnosis categories (up to 20) for which there are a total of at least 11 episodes ending in the most recent calendar year. The principal diagnosis code for episodes ending in the most recent calendar year have been collapsed into general categories using Clinical Classification Software (CCS). More information on CCS can be found at
40 Home Health Agency PEPPER Home Health Agencies for Demo Jurisdiction (DMSTR) Visit PEPPERresources.org Jurisdiction Top Diagnoses, Most Recent Calendar Year In Descending Order by Total Episodes Total Episodes for CCS Category Proportion of Episodes for CCS to Total Episodes Number of Visits for CCS Category Average Number of Visits for CCS Category CCS Diagnosis Categories Other aftercare 47, % 753, Congestive heart failure; nonhypertensive 21, % 396, Rehabilitation care; fitting of prostheses; and adjustment of device 21, % 286, Chronic obstructive pulmonary disease and bronchiectasis 14, % 246, Chronic ulcer of skin 11, % 280, Other nervous system disorders 9, % 181, Other fractures 7, % 153, Diabetes mellitus with complications 7, % 173, Cardiac dysrhythmias 7, % 124, Genitourinary symptoms and ill-defined conditions 6, % 108, Late effects of cerebrovascular disease 6, % 166, Other connective tissue disease 6, % 131, Pneumonia (except that caused by tuberculosis or sexually transm 6, % 102, Open wounds of extremities 5, % 115, Essential hypertension 5, % 95, Complications of surgical procedures or medical care 5, % 117, Urinary tract infections 5, % 93, Skin and subcutaneous tissue infections 5, % 98, Other diseases of veins and lymphatics 5, % 114, Diabetes mellitus without complication 5, % 132, Top Diagnoses Jurisdiction-wide 212, % 3,871, All Diagnoses Jurisdiction-wide 319,605 5,833, Note: This report is limited to the top diagnosis categories (up to 20) for which there are a total of at least 11 episodes ending in the most recent calendar year. The principal diagnosis code for episodes ending in the most recent calendar year have been collapsed into general categories using Clinical Classification Software (CCS). More information on CCS can be found at
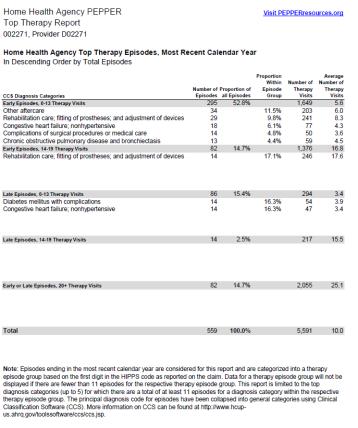
41 Home Health Agency PEPPER Top Therapy Report , Provider D02271 Visit PEPPERresources.org Home Health Agency Top Therapy Episodes, Most Recent Calendar Year In Descending Order by Total Episodes CCS Diagnosis Categories Early Episodes, 0-13 Therapy Visits Other aftercare Rehabilitation care; fitting of prostheses; and adjustment of devices Congestive heart failure; nonhypertensive Complications of surgical procedures or medical care Chronic obstructive pulmonary disease and bronchiectasis Early Episodes, Therapy Visits Rehabilitation care; fitting of prostheses; and adjustment of devices Number of Proportion of Episodes all Episodes Proportion Within Episode Group Number of Therapy Visits Average Number of Therapy Visits % 1, % % % % % % 1, % Late Episodes, 0-13 Therapy Visits Diabetes mellitus with complications Congestive heart failure; nonhypertensive % % % Late Episodes, Therapy Visits % Early or Late Episodes, 20+ Therapy Visits % 2, Total % 5, Note: Episodes ending in the most recent calendar year are considered for this report and are categorized into a therapy episode group based on the first digit in the HIPPS code as reported on the claim. Data for a therapy episode group will not be displayed if there are fewer than 11 episodes for the respective therapy episode group. This report is limited to the top diagnosis categories (up to 5) for which there are a total of at least 11 episodes for a diagnosis category within the respective therapy episode group. The principal diagnosis code for episodes have been collapsed into general categories using Clinical Classification Software (CCS). More information on CCS can be found at
42 Home Health Agency PEPPER Home Health Agencies for Demo Jurisdiction (DMSTR) Visit PEPPERresources.org Jurisdiction Top Therapy Episodes, Most Recent Calendar Year In Descending Order by Total Episodes CCS Diagnosis Categories Early Episodes, 0-13 Therapy Visits Other aftercare Rehabilitation care; fitting of prostheses; and adjustment of devices Congestive heart failure; nonhypertensive Chronic obstructive pulmonary disease and bronchiectasis Other nervous system disorders Early Episodes, Therapy Visits Other aftercare Rehabilitation care; fitting of prostheses; and adjustment of devices Other nervous system disorders Congestive heart failure; nonhypertensive Other fractures Late Episodes, 0-13 Therapy Visits Congestive heart failure; nonhypertensive Chronic ulcer of skin Genitourinary symptoms and ill-defined conditions Deficiency and other anemia Chronic obstructive pulmonary disease and bronchiectasis Late Episodes, Therapy Visits Rehabilitation care; fitting of prostheses; and adjustment of devices Congestive heart failure; nonhypertensive Other aftercare Other nervous system disorders Chronic ulcer of skin Early or Late Episodes, 20+ Therapy Visits Other aftercare Rehabilitation care; fitting of prostheses; and adjustment of devices Late effects of cerebrovascular disease Other nervous system disorders Congestive heart failure; nonhypertensive Total Number of Episodes Proportion of all Episodes Proportion Within Episode Group Number of Therapy Visits Average Number of Therapy Visits 202, % 900, , % 190, , % 115, , % 49, , % 35, , % 37, , % 418, , % 67, , % 53, , % 22, , % 20, , % 18, , % 159, , % 15, , % 7, , % 4, , % 3, , % 7, , % 85, % 10, % 6, % 4, % 4, % 3, , % 479, , % 51, , % 46, , % 44, , % 27, % 21, , % 2,042, Note: Episodes ending in the most recent calendar year are considered for this report and are categorized into a therapy episode group based on the first digit in the HIPPS code as reported on the claim. Data for a therapy episode group will not be displayed if there are fewer than 11 episodes for the respective therapy episode group. This report is limited to the top diagnosis categories (up to 5) for which there are a total of at least 11 episodes for a diagnosis category within the respective therapy episode group. The principal diagnosis code for episodes have been collapsed into general categories using Clinical Classification Software (CCS). More information on CCS can be found at
Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts
 PEPPER to Support Auditing and Monitoring Efforts") Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts July 30, 2015 Kimberly Hrehor 2 Agenda History and basics of PEPPER HHA PEPPER target areas Percents, rates and
Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts July 30, 2015 Kimberly Hrehor 2 Agenda History and basics of PEPPER HHA PEPPER target areas Percents, rates and
This educational presentation is provided by. The software that powers post-acute care. HOME HEALTH. HOSPICE. THERAPY.
 2 This educational presentation is provided by The software that powers post-acute care. HOME HEALTH. HOSPICE. THERAPY. PRIVATE DUTY We understand the challenges your business is facing. That s why Kinnser
2 This educational presentation is provided by The software that powers post-acute care. HOME HEALTH. HOSPICE. THERAPY. PRIVATE DUTY We understand the challenges your business is facing. That s why Kinnser
Surviving Targeted Probe & Educate
 Surviving Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe & Educate
Surviving Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe & Educate
Home Health Targeted Probe & Educate
 Home Health Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. WWW.TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe
Home Health Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. WWW.TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance
 PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1
 Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]
![August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]](/thumbs/83/88557772.jpg "August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]") Bridgepoint 1, Suite 300 5918 West Courtyard Drive, Austin TX 78730-5036 August 30, 2013 [Contact Name] SNF Name, 009168 [Address Line 1] [Address Line 2] [City], B8 [ZIP] RE: Program for Evaluating Payment
Bridgepoint 1, Suite 300 5918 West Courtyard Drive, Austin TX 78730-5036 August 30, 2013 [Contact Name] SNF Name, 009168 [Address Line 1] [Address Line 2] [City], B8 [ZIP] RE: Program for Evaluating Payment
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc.
 HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1
 PEPPER to Support Auditing and Monitoring Efforts: Session 1") Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Thank you for joining us!
 Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the Hospice Training and Resources section. A recording
Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the Hospice Training and Resources section. A recording
User s Guide Tenth Edition
 Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Tenth Edition Prepared by Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User
Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Tenth Edition Prepared by Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User
Thank you for joining us!
 Thank you for joining us! We will start at 1:00 p.m. CT. You will hear silence until the session begins. Audio Options: Recommended: Audio broadcast using your computer speakers (automatically join the
Thank you for joining us! We will start at 1:00 p.m. CT. You will hear silence until the session begins. Audio Options: Recommended: Audio broadcast using your computer speakers (automatically join the
Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report. User s Guide Sixth Edition. Prepared by
 Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report User s Guide Sixth Edition Prepared by Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report
Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report User s Guide Sixth Edition Prepared by Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report
Thank you for joining us!
 Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the SNF Training and Resources section. A recording of
Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the SNF Training and Resources section. A recording of
Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule
 Calendar Year (CY) 2013 Final Rule") Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
PEPPER and Data Analytics for Skilled Nursing Facilities, Hospices and Inpatient Rehabilitation Facilities. April 19, 2015 Kimberly Hrehor
 PEPPER and Data Analytics for Skilled Nursing Facilities, Hospices and Inpatient Rehabilitation Facilities April 19, 2015 Kimberly Hrehor Agenda What is PEPPER? Focus: Hospice PEPPER Focus: SNF PEPPER
PEPPER and Data Analytics for Skilled Nursing Facilities, Hospices and Inpatient Rehabilitation Facilities April 19, 2015 Kimberly Hrehor Agenda What is PEPPER? Focus: Hospice PEPPER Focus: SNF PEPPER
4/20/2015. NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals. Today s Objectives. Background
 NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
OASIS ITEM ITEM INTENT
 (M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
(M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
HHGM is Alive and Kicking: How Can You Prepare for What s Next?
 HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
Reading and Using the PEPPER Report
 Reading and Using the PEPPER Report PANAC Webinar September 25, 2014 Stephanie Kessler Partner, Senior Living Services Consulting Group Disclaimer The information contained herein is of a general nature
Reading and Using the PEPPER Report PANAC Webinar September 25, 2014 Stephanie Kessler Partner, Senior Living Services Consulting Group Disclaimer The information contained herein is of a general nature
Public Policy HCA Public Policy No
 Public Policy HCA Public Policy No.2-2014 TO: FROM: RE: HCA CHHA & LTHHCP PROVIDER MEMBERS PATRICK CONOLE, VICE PRESIDENT, FINANCE & MANAGEMENT UPDATES FROM NGS HOME HEALTH ADVISORY MEETING DATE: MARCH
Public Policy HCA Public Policy No.2-2014 TO: FROM: RE: HCA CHHA & LTHHCP PROVIDER MEMBERS PATRICK CONOLE, VICE PRESIDENT, FINANCE & MANAGEMENT UPDATES FROM NGS HOME HEALTH ADVISORY MEETING DATE: MARCH
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Develop a Taste for PEPPER: Interpreting
 Develop a Taste for PEPPER: Interpreting Your Organizational Results Cheryl Ericson, MS, RN Manager of Clinical Documentation Integrity, The Medical University of South Carolina (MUSC) Objectives Increase
Develop a Taste for PEPPER: Interpreting Your Organizational Results Cheryl Ericson, MS, RN Manager of Clinical Documentation Integrity, The Medical University of South Carolina (MUSC) Objectives Increase
What Did Your PEPPER Tell CMS?
 What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
Understanding the PEPPER
 Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC. Month Day Year / / Month Day Year
 / / UHHC. Month Day Year / / Month Day Year") Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
MDS Accuracy and Compliance: Where There s Smoke
 MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
OASIS Complete Webinar Series
 OASIS Complete Webinar Series Selecting Clinically Relevant and Fiscally Appropriate Diagnoses Presented By: Rhonda Marie Will, RN, BS, HCS-D, COS-C October 1, 2010 243 King Street, Suite 246 Northampton,
OASIS Complete Webinar Series Selecting Clinically Relevant and Fiscally Appropriate Diagnoses Presented By: Rhonda Marie Will, RN, BS, HCS-D, COS-C October 1, 2010 243 King Street, Suite 246 Northampton,
The following is a summary of each of the updates from the meeting.
 This week, National Government Services (NGS) conducted a home health advisory meeting in the Centers for Medicare and Medicaid Services (CMS ) Region V office in Chicago for the State Associations in
This week, National Government Services (NGS) conducted a home health advisory meeting in the Centers for Medicare and Medicaid Services (CMS ) Region V office in Chicago for the State Associations in
OASIS QUALITY IMPROVEMENT REPORTS
 6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
OASIS ITEM ITEM INTENT TIME POINTS ITEM(S) COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES
 COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES") (M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
(M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
Riding Herd on Fraud, Waste and Abuse
 Riding Herd on Fraud, Waste and Abuse Dan McCullough Judi McCabe Juanita Henry Kim Hrehor 1 Taking Stock: Surveying the Landscape of Fraud, Waste and Abuse 2 How Big is the Problem? The simple truth is
Riding Herd on Fraud, Waste and Abuse Dan McCullough Judi McCabe Juanita Henry Kim Hrehor 1 Taking Stock: Surveying the Landscape of Fraud, Waste and Abuse 2 How Big is the Problem? The simple truth is
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Key points. Home Care agency structures. Introduction to Physical Therapy in the Home Care Setting. Home care industry
 Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Essentials for Clinical Documentation Integrity 2017
 Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
Recovery Audit Contractors: AHA Perspective. Elizabeth Baskett, Policy, AHA February 23, 2012
 Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Medicare Home Health Prospective Payment System
 Medicare Home Health Prospective Payment System Payment Rule Brief Final Rule Program Year: CY 2013 Overview On November 8, 2012, the Centers for Medicare and Medicaid Services (CMS) officially released
Medicare Home Health Prospective Payment System Payment Rule Brief Final Rule Program Year: CY 2013 Overview On November 8, 2012, the Centers for Medicare and Medicaid Services (CMS) officially released
Today s educational presentation is provided by. The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE
 Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
Health Economics Program
 Health Economics Program Issue Brief 2006-02 February 2006 Health Conditions Associated With Minnesotans Hospital Use Health care spending by Minnesota residents accounts for approximately 12% of the state
Health Economics Program Issue Brief 2006-02 February 2006 Health Conditions Associated With Minnesotans Hospital Use Health care spending by Minnesota residents accounts for approximately 12% of the state
Therapy Documentation: What is Reasonable and Necessary?
 Therapy Documentation: What is Reasonable and Necessary? Presented By: Cindy Krafft MS PT, COS-C Director of Rehabilitation Consulting Services President - Home Health Section APTA June 15, 2010 243 King
Therapy Documentation: What is Reasonable and Necessary? Presented By: Cindy Krafft MS PT, COS-C Director of Rehabilitation Consulting Services President - Home Health Section APTA June 15, 2010 243 King
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
THE PEPPER AND YOUR CDI PROGRAM. Kat McFarland, RN, MN, ACM Director Care Management Providence Regional Medical Center Everett 9/28/2018
 THE PEPPER AND YOUR CDI PROGRAM Kat McFarland, RN, MN, ACM Director Care Management Providence Regional Medical Center Everett 9/28/2018 https://pepperresources.org/training-resources/short-term-acute-care-hospitals/pepper-review
THE PEPPER AND YOUR CDI PROGRAM Kat McFarland, RN, MN, ACM Director Care Management Providence Regional Medical Center Everett 9/28/2018 https://pepperresources.org/training-resources/short-term-acute-care-hospitals/pepper-review
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals
 NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCS-D Exam Update. Tricia A. Twombly BSN RN HCS-D HCS-O COS-C CHCE AHIMA Approved ICD-10 CM Trainer Senior Director, DecisionHealth CEO, BMSC
 HCS-D Exam Update Lisa Selman-Holman JD, BSN, RN, HCS-D, HCS-O, COS-C AHIMA Approved ICD-10 CMPCS Trainer Owner, Selman-Holman and Associates Chair, BMSC Tricia A. Twombly BSN RN HCS-D HCS-O COS-C CHCE
HCS-D Exam Update Lisa Selman-Holman JD, BSN, RN, HCS-D, HCS-O, COS-C AHIMA Approved ICD-10 CMPCS Trainer Owner, Selman-Holman and Associates Chair, BMSC Tricia A. Twombly BSN RN HCS-D HCS-O COS-C CHCE
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Medicare Home Health Prospective Payment System Calendar Year 2015
 Proposed Rule Summary Medicare Home Health Prospective Payment System Calendar Year 2015 August 2014 1 P age TABLE OF CONTENTS Overview, Resources and Comment Submission... 1 Home Health Payment Rates...
Proposed Rule Summary Medicare Home Health Prospective Payment System Calendar Year 2015 August 2014 1 P age TABLE OF CONTENTS Overview, Resources and Comment Submission... 1 Home Health Payment Rates...
How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs. Program Objectives
 How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs 2015 NAHC Annual Meeting 106 October 28, 4:30 5:30 p.m. Nashville, Tennessee Kathleen Spooner, RN, CMC Kathleen A. Hessler,
How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs 2015 NAHC Annual Meeting 106 October 28, 4:30 5:30 p.m. Nashville, Tennessee Kathleen Spooner, RN, CMC Kathleen A. Hessler,
PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY. July 17, 2012
 PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY July 17, 2012 On July 6, 2012, the Centers for Medicare & Medicaid Services (CMS) made public a proposed
PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY July 17, 2012 On July 6, 2012, the Centers for Medicare & Medicaid Services (CMS) made public a proposed
Center for Clinical Standards and Quality/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
STATISTICAL BRIEF #9. Hospitalizations among Males, Highlights. Introduction. Findings. June 2006
 HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #9 Agency for Healthcare Research and Quality June 2006 Hospitalizations among Males, 2003 C. Allison Russo, M.P.H. and Anne Elixhauser, Ph.D.
HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #9 Agency for Healthcare Research and Quality June 2006 Hospitalizations among Males, 2003 C. Allison Russo, M.P.H. and Anne Elixhauser, Ph.D.
New in Current payment risks. Tips & strategies. Revenue Cycle: The Ca$h Connection. CPAs & ADVISORS
 Revenue Cycle: The Ca$h Connection CPAs & ADVISORS M. Aaron Little, CPA Managing Director Springfield, MO mlittle@bkd.com New in 2017 Current payment risks Tips & strategies 2 1 3 Payment rates SN HCPCS
Revenue Cycle: The Ca$h Connection CPAs & ADVISORS M. Aaron Little, CPA Managing Director Springfield, MO mlittle@bkd.com New in 2017 Current payment risks Tips & strategies 2 1 3 Payment rates SN HCPCS
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Compliance Objectives
 Eyeing Coding Compliance and CDI Compliance Programs What Compliance Officers Need to Know or Should Know By Diana Adams, RHIA (adamsrra@tx.rr.com) Compliance Objectives Discovering who are the healthcare
Eyeing Coding Compliance and CDI Compliance Programs What Compliance Officers Need to Know or Should Know By Diana Adams, RHIA (adamsrra@tx.rr.com) Compliance Objectives Discovering who are the healthcare
2017 FOCUSED ON DOCUMENTATION NECESSITIES & PRE-CLAIM REVIEW
 2017 FOCUSED ON DOCUMENTATION NECESSITIES & PRE-CLAIM REVIEW PRESENTED BY: MELINDA A. GABOURY, COS-C CHIEF EXECUTIVE OFFICER HEALTHCARE PROVIDER SOLUTIONS, INC. HEALTHCAREPROVIDERSOLUTIONS.COM ADDITIONAL
2017 FOCUSED ON DOCUMENTATION NECESSITIES & PRE-CLAIM REVIEW PRESENTED BY: MELINDA A. GABOURY, COS-C CHIEF EXECUTIVE OFFICER HEALTHCARE PROVIDER SOLUTIONS, INC. HEALTHCAREPROVIDERSOLUTIONS.COM ADDITIONAL
Home Care and Hospice: Payment and Reimbursement Update: AHLA Institute on Medicare and Medicaid Payment Issues
 Home Care and Hospice: Payment and Reimbursement Update: 2014 AHLA Institute on Medicare and Medicaid Payment Issues William A. Dombi Vice President for Law National Association for Home Care & Hospice
Home Care and Hospice: Payment and Reimbursement Update: 2014 AHLA Institute on Medicare and Medicaid Payment Issues William A. Dombi Vice President for Law National Association for Home Care & Hospice
Best Options for Responding to the Home Health PPS 2011 Cuts *revised handouts
 Best Options for Responding to the Home Health PPS 2011 Cuts *revised handouts Improve Your Revenues with OASIS and Coding Presented By: Rhonda Marie Will, RN, BS, HCS-D, COS-C Melanie R. Duerr, RN, MS,
Best Options for Responding to the Home Health PPS 2011 Cuts *revised handouts Improve Your Revenues with OASIS and Coding Presented By: Rhonda Marie Will, RN, BS, HCS-D, COS-C Melanie R. Duerr, RN, MS,
Specialized On-Demand Education for Home Care Staff
 Home Care Association of New Hampshire and RCTCLearn offer Specialized On-Demand Education for Home Care Staff Providing your agency s staff with high quality continuing professional education doesn t
Home Care Association of New Hampshire and RCTCLearn offer Specialized On-Demand Education for Home Care Staff Providing your agency s staff with high quality continuing professional education doesn t
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
ICD 10 CM State of Transition
 ICD 10 CM State of Transition Tricia A. Twombly, RN, BSN, HCS D, HCS C, COS C, CHCE, AHIMA ICD 10 Trainer, ICE Certified Credentialing Specialist, CEO Board of Medical Coding and Compliance, Senior Director
ICD 10 CM State of Transition Tricia A. Twombly, RN, BSN, HCS D, HCS C, COS C, CHCE, AHIMA ICD 10 Trainer, ICE Certified Credentialing Specialist, CEO Board of Medical Coding and Compliance, Senior Director
Is your Home Health Agency ready for the Final Rule to the Conditions of Participation?
 Is your Home Health Agency ready for the Final Rule to the Conditions of Participation? Medicare-certified home health agencies have almost doubled from 6,461 in 1990 to 12,268 in 2014 due to longer life
Is your Home Health Agency ready for the Final Rule to the Conditions of Participation? Medicare-certified home health agencies have almost doubled from 6,461 in 1990 to 12,268 in 2014 due to longer life
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Medicare Claims Processing Manual Chapter 10 - Home Health Agency Billing
 Medicare Claims Processing Manual Chapter 10 - Home Health Agency Billing Table of Contents (Rev. 2209 05-06-11) (Rev. 2249 07-01-11) Transmittals for Chapter 10 Crosswalk to Old Manual 10 - General Guidelines
Medicare Claims Processing Manual Chapter 10 - Home Health Agency Billing Table of Contents (Rev. 2209 05-06-11) (Rev. 2249 07-01-11) Transmittals for Chapter 10 Crosswalk to Old Manual 10 - General Guidelines
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
* HFMA staff and volunteers determined that this product has met specific criteria developed under. endorse or guaranty the use of this product.
 Latest Updates to the PEPPER: Utilizing New Report Data and Benchmarks to Support Your Compliance Efforts John Zelem, MD Senior Director, Audit, Compliance & Education Executive Health Resources * HFMA
Latest Updates to the PEPPER: Utilizing New Report Data and Benchmarks to Support Your Compliance Efforts John Zelem, MD Senior Director, Audit, Compliance & Education Executive Health Resources * HFMA
3/21/2018. Foundation Management Services, Inc All rights reserved. Unauthorized reproduction is strictly prohibited.
 Keys to Documentation Success in Home Health Coding DISCLAIMER This material is designed and provided to communicate information about compliance, ethics and coding in an educational format and manner.
Keys to Documentation Success in Home Health Coding DISCLAIMER This material is designed and provided to communicate information about compliance, ethics and coding in an educational format and manner.
2/18/2015. The Journey Begins. PEPPER and OSCAR/CASPER Reports. Objectives. Preparation for Change
 PEPPER and OSCAR/CASPER Reports Objectives Identify the purpose of the PEPPER and CASPER (OSCAR) reports Interpret the individual reports and identify the outlier data that places a facility at greater
PEPPER and OSCAR/CASPER Reports Objectives Identify the purpose of the PEPPER and CASPER (OSCAR) reports Interpret the individual reports and identify the outlier data that places a facility at greater
Effective Tools to Prevent and Manage Adverse Events
 Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
An Initial Review of the CY Medicare Home Health Rule. CY2018 Proposed Medicare Home Health Rate Rule and Much More
 An Initial Review of the CY 2018 2019 Medicare Home Health Rule Mary K. Carr William A. Dombi NAHC CY2018 Proposed Medicare Home Health Rate Rule and Much More Published July 25, 2017 https://www.cms.gov/medicare/medicare
An Initial Review of the CY 2018 2019 Medicare Home Health Rule Mary K. Carr William A. Dombi NAHC CY2018 Proposed Medicare Home Health Rate Rule and Much More Published July 25, 2017 https://www.cms.gov/medicare/medicare
06-01 FORM HCFA WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the
 06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Hospital Inpatient Quality Reporting (IQR) and Hospital Value-Based Purchasing (VBP) Programs Claims-Based Measures Hospital-Specific Report (HSR) Overview and Updates Questions and Answers Moderator Bethany
Hospital Inpatient Quality Reporting (IQR) and Hospital Value-Based Purchasing (VBP) Programs Claims-Based Measures Hospital-Specific Report (HSR) Overview and Updates Questions and Answers Moderator Bethany
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Polling Question #1. Denials and CDI: A Recovery Auditor s Perspective
 1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
Wound Care Reimbursement. Things Are A-Changing!
 Wound Care Reimbursement Things Are A-Changing! Kathleen D. Schaum, MS President Kathleen D. Schaum & Assoc., Inc. kathleendschaum@bellsouth.net 561-964-2470 Disclosure No relevant financial relationships
Wound Care Reimbursement Things Are A-Changing! Kathleen D. Schaum, MS President Kathleen D. Schaum & Assoc., Inc. kathleendschaum@bellsouth.net 561-964-2470 Disclosure No relevant financial relationships
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
RAC Targets, Bullseyes and Near Misses: What Your CDI Program Should Know
 RAC Targets, Bullseyes and Near Misses: What Your CDI Program Should Know Barbara Flynn, RHIA, CCS, Certified AHIMA ICD-10-CM/PCS Trainer, ICD10 Ambassador Vice President for Health Information Management
RAC Targets, Bullseyes and Near Misses: What Your CDI Program Should Know Barbara Flynn, RHIA, CCS, Certified AHIMA ICD-10-CM/PCS Trainer, ICD10 Ambassador Vice President for Health Information Management
SNF Compliance: What s at Stake?
 SNF Compliance: What s at Stake? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Elisa Bovee, MS OTR/L Vice President of Operations About Elisa Elisa
SNF Compliance: What s at Stake? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Elisa Bovee, MS OTR/L Vice President of Operations About Elisa Elisa
2017 Home Health PPS Rate Update
 2017 Home Health PPS Rate Update On November 3, 2016, CMS issued the Final Rule to update the Home Health Prospective Payment System (HH PPS) rates for Calendar Year (CY) 2017. In summary, this final rule:
2017 Home Health PPS Rate Update On November 3, 2016, CMS issued the Final Rule to update the Home Health Prospective Payment System (HH PPS) rates for Calendar Year (CY) 2017. In summary, this final rule:
Development of Updated Models of Non-Therapy Ancillary Costs
 Development of Updated Models of Non-Therapy Ancillary Costs Doug Wissoker A. Bowen Garrett A memo by staff from the Urban Institute for the Medicare Payment Advisory Commission Urban Institute MedPAC
Development of Updated Models of Non-Therapy Ancillary Costs Doug Wissoker A. Bowen Garrett A memo by staff from the Urban Institute for the Medicare Payment Advisory Commission Urban Institute MedPAC
(M1025) Case-Mix Diagnosis (Optional) OPTIONAL Complete only if a Z-code in Column 2 is reported in place of a resolved condition
 Case-Mix Diagnosis (Optional) OPTIONAL Complete only if a Z-code in Column 2 is reported in place of a resolved condition") HOME HEALTH 2017 PPS CALCULATION WORKSHEET PATIENT NAME: ID NUMBER: DATE: TYPE OF ASSESSMENT: Start of care Follow-up M0110 - EPISODE TIMING: Is the Medicare home health payment episode f which this assessment
HOME HEALTH 2017 PPS CALCULATION WORKSHEET PATIENT NAME: ID NUMBER: DATE: TYPE OF ASSESSMENT: Start of care Follow-up M0110 - EPISODE TIMING: Is the Medicare home health payment episode f which this assessment
National Provider Call: Hospital Value-Based Purchasing
 National Provider Call: Hospital Value-Based Purchasing Fiscal Year 2015 Overview for Beneficiaries, Providers, and Stakeholders Centers for Medicare & Medicaid Services 1 March 14, 2013 Medicare Learning
National Provider Call: Hospital Value-Based Purchasing Fiscal Year 2015 Overview for Beneficiaries, Providers, and Stakeholders Centers for Medicare & Medicaid Services 1 March 14, 2013 Medicare Learning
OASIS-C Home Health Outcome Measures
 OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
PPS Therapy. Medicare 2/28/ year Home Health clinician/contractor. 30 years Geriatric Rehab. Home Health consultant, author, speaker
 PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Regulatory Advisor Volume Eight
 Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health
 Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health Mary McGoldrick, MS, RN, CRNI Home Care and Hospice Consultant Saint Simons Island, GA Nothing to Disclose
Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health Mary McGoldrick, MS, RN, CRNI Home Care and Hospice Consultant Saint Simons Island, GA Nothing to Disclose
2017 HOME HEALTH PPS AND VALUE BASED PURCHASING UPDATE
 2017 HOME HEALTH PPS AND VALUE BASED PURCHASING UPDATE Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com FINAL 2017 PAYMENT RATES HOME HEALTH Outlier
2017 HOME HEALTH PPS AND VALUE BASED PURCHASING UPDATE Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. healthcareprovidersolutions.com FINAL 2017 PAYMENT RATES HOME HEALTH Outlier
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses