2011 Guidelines for Field Triage of Injured Patients
|
|
|
- Griselda McKinney
- 5 years ago
- Views:
Transcription
1 2011 Guidelines for Field Triage of Injured Patients
2 Slide 1 Welcome! Today, we are going to discuss the 2011 Guidelines for Field Triage of Injured Patients (2011 Guidelines). This presentation and the revised guidelines are designed to help you do your job as emergency medical services (EMS) providers by helping you to respond to severely injured patients more effectively.
3 Objectives Review the importance of accurate field triage Review the history of the American College of Surgeons Field Triage Decision Scheme Discuss changes in the 2011 Guidelines for Field Triage of Injured Patients Review CDC educational initiatives for the 2011 Guidelines for the Field Triage of Injured Patients
4 Slide 2 The goals for this presentation are to: review the importance of accurate field triage in trauma care; review the history of the American College of Surgeon s (ACS) Field Triage Decision Scheme; discuss the changes in the 2011 Guidelines for Field Triage of Injured Patients; and, finally, review the Centers for Disease Control and Prevention (CDC) s educational initiatives for the decision scheme.

5 Published: January 2012 Available for FREE at:
6 Slide 3 The decision scheme is based upon Guidelines for Field Triage of Injured Patients: Recommendations of the National Expert Panel on Field Triage, 2011 published in January 2012 in CDC s Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports.







7 10 Leading Causes of Death by Age Group, United States Source: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. Ten Leading Causes of Death,
8 Slide 4 Injury is the leading cause of death for Americans aged 144 years. So understandably, almost half of the 16.6 million transport calls per year that we the approximately 1 million EMS providers respond to are related to injury.
9 If you are severely injured, care at a Level I trauma center, rather than a nontrauma center, lowers your risk of death by 25%. Source: MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med Jan 26; 354(4):
10 Slide 5 CDC supported research shows that, if you are severely injured, care at a Level I trauma center, rather than a nontrauma center, lowers your risk of death by 25%. This statistic is important to remember because, as an EMS provider, you know that getting the right patient, to the right place, at the right time is critical. Not all injuries require care at a Level I trauma center. Transporting less severely injured patients to a lower level trauma center or nontrauma center can help ensure that resources at Level I trauma centers are available for those patients who need them most.

11 History of the Decision Scheme The American College of Surgeons-Committee on Trauma (ACS-COT) developed guidelines to designate trauma centers in Set standards for personnel, facilities, and processes necessary for the best care of injured persons Studies showed mortality reduction in regions with trauma centers
12 Slide 6 In 1976, the American College of Surgeons Committee on Trauma developed guidelines to authenticate trauma centers and set standards for personnel, facilities, and processes necessary for the best care of injured persons. Studies in the 1970s and early to mid 1980s showed a reduction in mortality in those regions with specialized trauma centers.

13 History of the Decision Scheme National consensus conference in 1987 resulted in first ACS field triage protocol, the Triage Decision Scheme The Decision Scheme serves as the basis for field triage of trauma patients in most EMS systems in the U.S.
14 Slide 7 These studies led to a national consensus conference in 1987 that resulted in the first ACS field triage protocol, known as the triage decision scheme for trauma patients. Since 1987, this decision scheme has served as the basis for field triage for trauma patients in most EMS systems in the United States.
, convened the National Expert Panel on Field Triage In 2011 the Panel reconvened to review and update the 2006")
15 History of the Decision Scheme The Decision Scheme has been revised five times (1990, 1993, 1999, 2006, 2011) In the Centers for Disease Control and Prevention (CDC), with support from the National Highway Traffic Safety Administration (NHTSA), convened the National Expert Panel on Field Triage In 2011 the Panel reconvened to review and update the 2006 Guidelines
16 Slide 8 Since its initial publication, the decision scheme has been revised five times: 1990, 1993, 1999, 2006, and We will discuss the 2011 decision scheme today. The 2011 decision scheme was developed when the National Expert Panel on Field Triage, which was initially formed to develop the 2006 Guidelines, reconvened to review the 2006 Guidelines in the context of recently published literature and experiences of states and local communities working to implement the Guidelines. The National Expert Panel on Field Triage comprises persons with expertise in acute injury care, including EMS providers and medical directors, state EMS directors, hospital administrators, emergency medicine physicians and nurses, adult and pediatric trauma surgeons, persons in the automotive industry, public health personnel, and representatives of federal agencies.

17 National Expert Panel on Field Triage Membership Members National leadership, expertise, and contributions in the realm of injury prevention and control EMS Providers and Medical Directors Emergency Medicine Physicians and Nurses Trauma Surgeons Public Health Federal Agencies Automotive Industry
18 Slide 9 This panel included professionals with a variety of backgrounds, including EMS, emergency medicine, trauma surgery, nursing, public health, research, and automotive engineering.

19 National Expert Panel on Field Triage The role of the Expert Panel is to: Periodically review the Decision Scheme Ensure criteria are consistent with existing evidence Ensure criteria are compatible with advances in technology Make necessary recommendations for revision
20 Slide 10 The National Expert Panel on Field Triage s role is to: periodically review the decision scheme, ensure that criteria are consistent with existing evidence, ensure that criteria are compatible with advances in technology, and make necessary recommendations for revision. Not an official advisory committee of CDC and does not have a fixed membership or an officially organized structure.
21 2011 Guidelines for Field Triage of Injured Patients
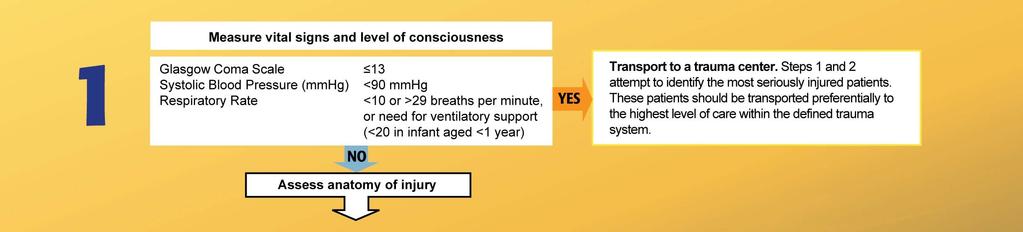
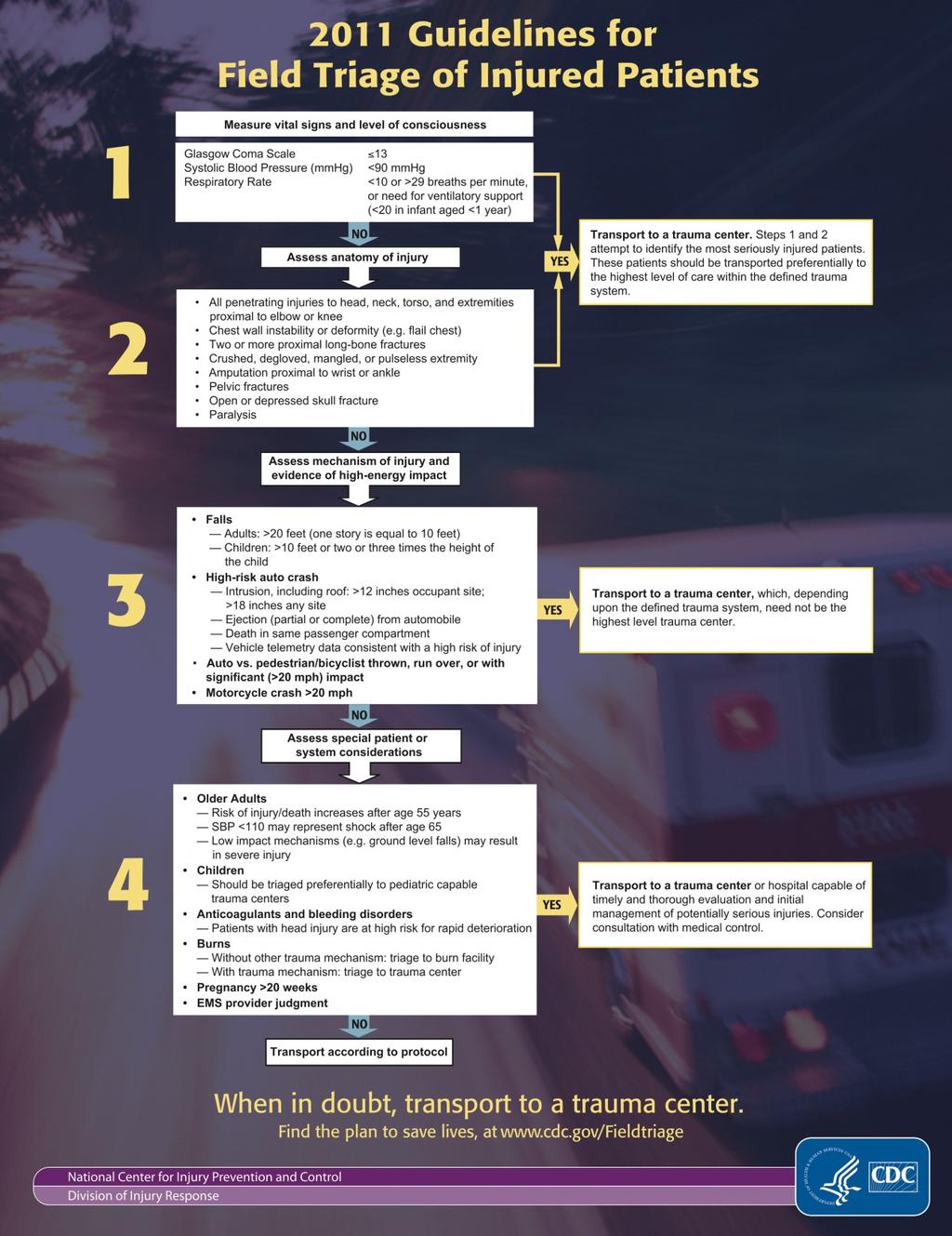
22 Slide 11 As I pointed out earlier, the decision scheme was developed to assist local medical directors and EMS providers with decisions about field triage and destination facility. It is the foundation for field triage protocols for trauma patients in most EMS systems across the United States. The decision scheme is divided into four steps: Step 1. Physiologic criteria, Step 2. Anatomic criteria, Step 3. Mechanism of injury criteria, and Step 4. Special patient or system considerations. After each step, the Guidelines includes two transition boxes. One box provides guidance on the appropriate destination for a patient that meets the criteria outlined in the preceding step. The other box moves the reader to the next step in the Guidelines if the patient does not meet the criteria in the preceding step. In essence, the Guidelines help you determine the gravity of the injury and the most appropriate destination facility for your patient, or it helps you move further through the decision scheme criteria.

23 Clarification and Explanation Purpose Utilization Guidelines name Literature and experience Future research
24 Slide 12 Purpose So what is the purpose of the Guidelines? They are intended to lay the foundation for developing local and regional field triage protocols, including areas with limited medical resources and/or geographic hurdles to transporting patients to trauma centers. The Guidelines were revised to facilitate more effective triage and better match trauma patients conditions with the medical resources best equipped to treat them. Utilization Purpose: Clearly states that this is not for mass casualty triage The Guidelines provided in this report are not intended for mass casualty or disaster triage; instead, they are designed for use with individual injured patients and provide guidance for EMS providers who care for and transport patients injured in U.S. communities daily through motorvehicle crashes, falls, penetrating injuries, and other injury mechanisms. The Guidelines cannot account for all EMS systems, every injury, or transportation. They must ultimately be based upon local data and analysis of systems. The Panel recognizes that these Guidelines cannot address the specific circumstances of each EMS system in the United States or all circumstances that might arise at the scene of injury or while the patient is being transported to a hospital or trauma center. The Guidelines discuss core elements of any well-managed field triage process; these guidelines should be adapted to fit the specific needs of local environments within the context of defined state, regional, or local trauma systems and in accord with an analysis of local data. In areas of uncertainty, or in those not addressed by the Guidelines, local EMS systems should rely on direction from local EMS medical directors, regulations, policies, and protocols. Guidelines name The Panel decided not to change or modify the name of the decision scheme because creating a new and different name would likely only add to or increase any confusion or misunderstanding that exists. The Panel recommended that the decision scheme be called either the field triage decision scheme or the guidelines for field triage of injured patients. The Panel also recommended that the Guidelines not be referred to as a national protocol because using the term protocol has an unintended proscriptive inference for the end-user that could restrict local adaptation required for optimal implementation. Literature and Experience Changes to the Guidelines are based upon literature review AND experience of states, regions, and communities working on field triage. Future Research More research on Field Triage is needed. Ensuring that the Guidelines are based on the best clinical evidence requires expanded surveillance, focused research using robust study designs, and consistent outcome measures.
25 Step 1: Physiologic Criteria Step 1: Physiologic Criteria
26 Slide 13 Now, let s take a look at the decision scheme step by step, starting with Step 1, Physiologic criteria.
 from <14 to GCS < 13.")
27 Step 1: 2011 Changes Modified Added Glasgow Coma Scale (GCS) from <14 to GCS < 13. Or need for Ventilatory Support
28 Slide 14 The criteria on the Glasgow Coma Scale (GCS) was changed from less than 14 to GCS less than or equal to 13. Experience with the 2006 Guidelines indicates that many readers interpreted this criterion as recommending that patients with a GCS of 14 or less should be taken to trauma centers. This was rewritten in an effort to reduce confusion. The need for Ventilatory Support was added to the respiratory rate criterion. After reviewing the literature, the Panel added or need for ventilatory support to the respiratory rate criterion, recognizing that adults and children requiring ventilatory support (including both bag-mask ventilation and intubation) represent a very high-risk group, whether or not they have a respiratory rate of <10 or >29 breaths per minute (<20 in infant aged <1 year).

29 Step 2: Anatomic Criteria
30 Slide 15 We now move to Step 2, Anatomic criteria.

31 Step 2: 2011 Changes Modified Crushed, degloved, mangled, or pulseless extremity Chest wall instability or deformity (e.g. flail chest) Penetrating injuries to head, neck, torso and extremities proximal to elbow or knee Amputation proximal to wrist or ankle
32 Slide 16 Pulseless was added to the criteria for crushed, degloved, or mangled extremity for the following reasons: vascular injuries of the extremity may lead to significant morbidity and mortality these injuries require a high level of specialized trauma care involving multiple medical specialties vascular injuries exist in the absence of a crushed, degloved, or mangled extremity. Flail chest was changed to chest wall instability or deformity (e.g., flail chest) for the following reasons: flail chest is rarely diagnosed by EMS providers the terminology chest wall instability or deformity more accurately describes what EMS providers are asked to identify in the field environment the broader terminology ensures that additional blunt trauma to the chest will be identified and transported to the appropriate facility. Penetrating injuries to head, neck, torso and extremities proximal to elbow or knee was modified. The wording of this criterion was modified from elbow and knee to elbow or knee to recognize that these types of injuries generally occur separately and that each can represent a severe injury. Amputation proximal to wrist or ankle was modified. It was changed from amputation proximal to wrist and ankle to amputation proximal to wrist or ankle recognizing that these types of injuries most commonly occur separately and that each can represent a severe injury.

33 Step 3: Mechanism of Injury Criteria
34 Slide 17 Moving on to Step 3, Mechanism of injury criteria.

35 Step 3: 2011 Changes Modified High-risk automobile crash
36 Slide 18 Including roof was added to the intrusion category for high-risk automobile crashes for the following reasons: the 2006 guidelines do not clearly convey that vertical roof intrusion carries the same implication for increased injury severity as horizontal intrusion into the vehicle occupant space current review of the literature confirms that intrusion, including vertical roof intrusion, is an important predictor of trauma center need.

37 Step 4: Special Considerations
38 Slide 19 We have reached Step 4, Special patient or system considerations.

39 Step 4: 2011 Changes Modified Older adults Anticoagulation and bleeding disorders
40 Slide 20 SBP <110 may represent shock after age 65 years and low impact mechanisms (e.g., ground level falls) may result in severe injury were added under Older Adults in Step 4 for the following reasons: undertriage of the older adult population is a substantial problem the evidence reviewed suggests that the physiologic parameters used in younger patients may not apply to older adults occult injury is likely to be greater among older adults low energy transfers (e.g., ground level falls) may result in serious injuries in this population there is a need to be more proactive in the field identification of serious injury among older adults. Patients with head injury are at high risk for rapid deterioration was added to anticoagulation and bleeding disorders. Anticoagulation use has been associated with an increased risk of intracranial hemorrhage following head injury. This criterion was modified to underscore the potential for anticoagulated patients who do not meet Step 1, Step 2, or Step 3 criteria, but have evidence of head injury, to undergo rapid deterioration.

41 Step 4: 2011 Changes Removed End-stage renal disease requiring dialysis Time sensitive extremity injury
42 Slide 21 End-stage renal disease requiring dialysis was removed because there is no research demonstrating the value of dialysis as a triage criterion for identifying patients with serious injury and that concerns regarding anticoagulation in this population are addressed under the anticoagulation and bleeding disorders criterion. Time sensitive extremity injury was removed because with the addition of pulseless to Step Two criteria, the panel thought this criterion was redundant.
43
44 Slide 22 The Decision Scheme layout was modified to make it easier to follow and use within any trauma system.

45 Decision Scheme Layout Modification Changed layout of the guidelines Modified specific language of the transition boxes
46 Slide 23 To improve the layout of the transition boxes, the Panel took two steps. First, because the transition boxes between Steps 1 and 2 communicate the exact same information, they were thought to be redundant, and were consolidated into one box. Second, all transition boxes were moved to the right side of the page for easier readability and determination of outputs for patients meeting different steps in the Guidelines. The Panel also modified the language within the boxes to ensure consistency between transitions in the Guidelines.
 Implementation guide for EMS leaders Large decision scheme")
47 Education Initiative CDC, in collaboration with partners and experts, has developed FREE educational tools: Morbidity and Mortality Weekly Reports (MMWR) Recommendations and Reports Guidelines for Field Triage of Injured Patients: Recommendations of the National Expert Panel on Field Triage (includes continuing education opportunity) Implementation guide for EMS leaders Large decision scheme poster- available in color and black & white (size: 17 x 22 inches) Small decision scheme poster - available in color and black & white (size: 8.5 x 11 inches) Badge (size: 2.5 x 3.5 inches) Pocket card (folded size: 2.5 x 6 inches) Implementation guide fact sheet Online course developed with the University of Michigan SmartPhone application
48 Slide 24 CDC and its partners have developed resources and tools to help educate EMS leaders and professionals learn about the decision scheme. These resources include: Morbidity and Mortality Weekly Reports (MMWR) Recommendations and Reports Guidelines for Field Triage of Injured Patients: Recommendations of the National Expert Panel on Field Triage (includes continuing education opportunity) Implementation guide for EMS leaders Large decision scheme posteravailable in color and black & white (size: 17 x 22 inches) Small decision scheme posteravailable in color and black & white (size: 8.5 x 11 inches) Badge (size: 2.5 x 3.5 inches) Pocket card (folded size: 2.5 x 6 inches) Implementation guide fact sheet Online course developed with the University of Michigan SmartPhone application

49 Endorsing Organizations (Partial Listing)
50 Slide 25 Thirty-seven organizations and agencies endorse the decision scheme with concurrence from the Federal Interagency Committee on Emergency Medical Services and the National Highway Traffic Safety Administration. They include: Air Medical Physician Association American Academy of Orthopedic Surgeons American Academy of Pediatrics American Association of Critical-Care Nurses American Association for Respiratory Care American Association for the Surgery of Trauma American Burn Association American College of Emergency Physicians American College of Osteopathic Surgeons American College of Surgeons American Public Health Association American Trauma Society Association of Air Medical Services Association of Critical Care Transport Association of Public-Safety Communications Officials Association of State and Territorial Health Officials Brain Trauma Foundation Commission on Accreditation of Medical Transport Systems Eastern Association for the Surgery of Trauma Emergency Nurses Association

51 Endorsing Organizations (Partial Listing) With concurrence from the National Highway Traffic Safety Administration
52 Slide 26 Other organizations and agencies that endorse the decision scheme include: International Academies of Emergency Dispatch International Association of Emergency Medical Services Chiefs International Association of Fire Chiefs International Association of Flight and Critical Care Paramedics National Association of Emergency Medical Technicians National Association of EMS Educators National Association of EMS Physicians National Association of State EMS Officials National EMS Information System National EMS Management Association National Volunteer Fire Council Safe States Alliance Society for Academic Emergency Medicine Society for the Advancement of Violence and Injury Research Society of Emergency Medicine Physician Assistants Trauma Center Association of America Western Trauma Association Federal Interagency Committee on Emergency Medical Services (comprised of representatives from the U.S. Department of Health and Human Services, the U.S. Department of Transportation, the U.S. Department of Homeland Security, the U.S. Department of Defense, and the U.S. Federal Communications Commission). The National Highway Traffic Safety Administration concurs with these Guidelines.
53 References 1. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. Ten Leading Causes of Death, MacKenzie EJ, Rivara FP, Jurkovich GJ, Nahens AB, Frey KP, Egleston BL, Salkever DS, Scharfstein DO. A national evaluation of the effect of traumacenter care on mortality. N Engl J Med Jan 26; 354(4): Division of Injury Response, National Center for Injury Prevention and Control, CDC. Guidelines for field triage of injured patients: recommendations of the national expert panel on field triage, Atlanta, Georgia. MMWR Recomm Rep Jan 13;61(RR-1): Large Cost Savings Realized From The 2006 Field Triage Guideline: Reduction in Overtriage in U.S. Trauma Centers. Faul M, Wald MM, Sullivent EE, Sasser SM, Kapil V, Lerner EB, Hunt RC. Prehosp Emerg Care Oct 18. [Epub ahead of print]
54 Slide 27 Here are the references for this presentation. However, more than 85 references included in the MMWR article were used for revising the decision scheme.
55 Find the plan to save lives and money at:
56 Slide 28 I encourage you to visit CDC s Web site for more information about the decision scheme and to take advantage of the continuing education opportunity. You can also order or download the materials to use in your trauma system at no cost. The Web site is:
Field Triage Decision Scheme: The National Trauma Triage Protocol
 Field Triage Decision Scheme: The National Trauma Triage Protocol U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Injury Prevention and Control
Field Triage Decision Scheme: The National Trauma Triage Protocol U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Injury Prevention and Control
Emergency Medical Services Program
 County of Santa Cruz HEALTH SERVICES AGENCY 1080 EMELINE AVENUE, SANTA CRUZ, CA 95060 (831) 454-4120 FAX: (831) 454-4272 TDD: (831) 454-4123 EMERGENCY MEDICAL SERVICES PROGRAM Policy No. 7000 Reviewed
County of Santa Cruz HEALTH SERVICES AGENCY 1080 EMELINE AVENUE, SANTA CRUZ, CA 95060 (831) 454-4120 FAX: (831) 454-4272 TDD: (831) 454-4123 EMERGENCY MEDICAL SERVICES PROGRAM Policy No. 7000 Reviewed
POLICIES AND PROCEDURES
 POLICIES AND PROCEDURES POLICY: 553.25 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 5 I. AUTHORITY Division 2.5, California Health and Safety
POLICIES AND PROCEDURES POLICY: 553.25 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 5 I. AUTHORITY Division 2.5, California Health and Safety
Oakland County Medical Control Authority System Protocols Transportation Protocol Section Transportation Protocol.
 Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure A.
Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure A.
interventional cardiac facility (see Appendix 2). Notify receiving hospital, as soon as possible of impending arrival of the patient and give ETA.
. Notify receiving hospital, as soon as possible of impending arrival of the patient and give ETA.") Page 1 of 9 Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure
Page 1 of 9 Purpose: To define the decision-making process to be followed by EMS personnel in order to ensure patients are transported to a facility appropriate for their condition. I. Transportation Procedure
TITLE: Trauma Triage and Patient Destination EMS Policy No. 5210
 PURPOSE: The purpose of this policy is to establish triage criteria for trauma patients, identify appropriate receiving hospital destinations for trauma patients, and direct the actions of the prehospital,
PURPOSE: The purpose of this policy is to establish triage criteria for trauma patients, identify appropriate receiving hospital destinations for trauma patients, and direct the actions of the prehospital,
HOSPITALS TO ENTER PATIENTS INTO THE
 PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
The Trauma System. Prevention Pre-hospital care and transport Acute hospital care Rehab Research
 An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
FRAMEWORK AS APPROVED BY GTCNC 15 OCTOBER 2009 GEORGIA TRAUMA SYSTEM. Regional Trauma System Planning Framework
 FRAMEWORK AS APPROVED BY GTCNC 15 OCTOBER 2009 GEORGIA TRAUMA SYSTEM Regional Trauma System Planning Framework REV. 18 OCT 2009 FRAMEWORK AS APPROVED BY GTCNC 15 OCTOBER 2009 TABLE OF CONTENTS Acknowledgements...
FRAMEWORK AS APPROVED BY GTCNC 15 OCTOBER 2009 GEORGIA TRAUMA SYSTEM Regional Trauma System Planning Framework REV. 18 OCT 2009 FRAMEWORK AS APPROVED BY GTCNC 15 OCTOBER 2009 TABLE OF CONTENTS Acknowledgements...
Trauma Program Annual Report Red Deer Regional Hospital Central Zone
 Trauma Program Annual Report Red Deer Regional Hospital Central Zone April 1 2010 March 31 2011 Prepared by: Brenda Wiggins Central Zone Trauma Coordinator Kyla Hoogers Central Zone Trauma Data Analyst
Trauma Program Annual Report Red Deer Regional Hospital Central Zone April 1 2010 March 31 2011 Prepared by: Brenda Wiggins Central Zone Trauma Coordinator Kyla Hoogers Central Zone Trauma Data Analyst
Duke Regional Advisory Committee Meeting Minutes
 Duke Regional Advisory Committee Meeting Minutes Date: April 28, 2017 Time: 10:00 am- 1:00 pm Location: University Tower, 3100 Tower Blvd, Durham, NC 27707 Attendees:, Carolyn Foley, Sean Gibson, Nicole
Duke Regional Advisory Committee Meeting Minutes Date: April 28, 2017 Time: 10:00 am- 1:00 pm Location: University Tower, 3100 Tower Blvd, Durham, NC 27707 Attendees:, Carolyn Foley, Sean Gibson, Nicole
JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II
 July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
Modesto Junior College Course Outline of Record EMS 390
 Modesto Junior College Course Outline of Record EMS 390 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 390 Emergency Medical Technician 1 6 Units Limitations on Enrollment:
Modesto Junior College Course Outline of Record EMS 390 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 390 Emergency Medical Technician 1 6 Units Limitations on Enrollment:
Central Zone Trauma Program Annual Report
 2011-2012 Central Zone Trauma Program Annual Report Central Zone Trauma Program Red Deer Regional Hospital 2011-2012 Table of Contents Alberta Health Services Mission and Strategy... Page 4 Central Zone
2011-2012 Central Zone Trauma Program Annual Report Central Zone Trauma Program Red Deer Regional Hospital 2011-2012 Table of Contents Alberta Health Services Mission and Strategy... Page 4 Central Zone
Northwest Georgia - Region 1 EMS Regional Trauma Plan
 Northwest Georgia - Region 1 EMS Regional Trauma Plan "Building Excellence in a Page 1 of 203 Trauma System of Care through Collaboration" November 29, 2012 TABLE OF CONTENTS Executive Summary 2 Mission,
Northwest Georgia - Region 1 EMS Regional Trauma Plan "Building Excellence in a Page 1 of 203 Trauma System of Care through Collaboration" November 29, 2012 TABLE OF CONTENTS Executive Summary 2 Mission,
EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN
 EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN Approved by East Alabama Regional Trauma Advisory Council On 11.20.2008 EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN TABLE OF CONTENTS BACKGROUND 3 TRAUMA SYSTEM GOALS.
EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN Approved by East Alabama Regional Trauma Advisory Council On 11.20.2008 EAST ALABAMA REGIONAL TRAUMA SYSTEM PLAN TABLE OF CONTENTS BACKGROUND 3 TRAUMA SYSTEM GOALS.
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Trauma Service Area- B (BRAC) Regional Pediatric Plan
 Regional Pediatric Plan") Trauma Service Area - B (BRAC) Regional Pediatric Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, Texas 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran,
Trauma Service Area - B (BRAC) Regional Pediatric Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, Texas 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran,
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Modesto Junior College Course Outline of Record EMS 350
 Modesto Junior College Course Outline of Record EMS 350 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 350 First Responder with Healthcare Provider CPR 3 Units Formerly
Modesto Junior College Course Outline of Record EMS 350 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 350 First Responder with Healthcare Provider CPR 3 Units Formerly
Santa Cruz County EMS Agency Policy No. 7050
 TRAUMA PATIENT TRANSPORT AND HOSPITAL DESTINATION Authority for this policy is noted in Division 2.5, California Health and Safety Code, Sections 1797.222, 1798.162, 1798.163 California Code of Regulations
TRAUMA PATIENT TRANSPORT AND HOSPITAL DESTINATION Authority for this policy is noted in Division 2.5, California Health and Safety Code, Sections 1797.222, 1798.162, 1798.163 California Code of Regulations
Chapter 1. Learning Objectives. Learning Objectives 9/11/2012. Introduction to EMS Systems
 Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Deposited on: 06 May 2010
 Hornsby, J. and Quasim, T. and Dignon, N. and Puxty, A. (2010) Provision of trauma teams in Scotland: a national survey. Emergency Medical Journal, 27 (3). pp. 191-193. ISSN 1472-0205 http://eprints.gla.ac.uk/5279/
Hornsby, J. and Quasim, T. and Dignon, N. and Puxty, A. (2010) Provision of trauma teams in Scotland: a national survey. Emergency Medical Journal, 27 (3). pp. 191-193. ISSN 1472-0205 http://eprints.gla.ac.uk/5279/
AEC: INTERMEDIATE to PARAMEDIC BRIDGE PROGRAM STAFFORD TLC APRIL 18, 2016 through JANURARY 28, 2017
 AEC: INTERMEDIATE to PARAMEDIC BRIDGE PROGRAM TUESDAY/THURSDAY/FRIDAY @ STAFFORD TLC APRIL 18, 2016 through JANURARY 28, 2017 DAY/DATE/TIME CONTENT READING ASSIGNMENT Monday 04/18/16 04/19/16 04/21/16
AEC: INTERMEDIATE to PARAMEDIC BRIDGE PROGRAM TUESDAY/THURSDAY/FRIDAY @ STAFFORD TLC APRIL 18, 2016 through JANURARY 28, 2017 DAY/DATE/TIME CONTENT READING ASSIGNMENT Monday 04/18/16 04/19/16 04/21/16
Comparison: ITLS Provider and Trauma Nursing Core Course (TNCC)
") Overview International Trauma Life Support (ITLS) is a global organization dedicated to preventing death and disability from trauma through education and emergency care. ITLS educates emergency personnel
Overview International Trauma Life Support (ITLS) is a global organization dedicated to preventing death and disability from trauma through education and emergency care. ITLS educates emergency personnel
The development and features of the Spanish prehospital advanced triage method (META) for mass casualty incidents
 for mass casualty incidents") Arcos González et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:63 DOI 10.1186/s13049-016-0255-y COMMENTARY The development and features of the Spanish prehospital
Arcos González et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:63 DOI 10.1186/s13049-016-0255-y COMMENTARY The development and features of the Spanish prehospital
The following policy was adopted by the San Luis Obispo County EMS Agency and will become effective March 1, 2012 at 0800 hours.
 SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
Appendix 1 - Licensing and Audit Requirements for Emergency Department Services
 Appendix 1 - Licensing and Audit Requirements for Emergency Department Services Number Urgent Care Centres Emergency Department Emergency Department with Major Trauma Centre 1. Access 24/7 (This requirement
Appendix 1 - Licensing and Audit Requirements for Emergency Department Services Number Urgent Care Centres Emergency Department Emergency Department with Major Trauma Centre 1. Access 24/7 (This requirement
Developing a Trauma Center
 Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
WESTCHESTER REGIONAL
 WESTCHESTER REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL POLICY STATEMENT Supersedes/Updates: New Policy No. 11-02 Date: February 8, 2011 Re: EMS System Resource Utilization Pg(s): 5 INTRODUCTION The Westchester
WESTCHESTER REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL POLICY STATEMENT Supersedes/Updates: New Policy No. 11-02 Date: February 8, 2011 Re: EMS System Resource Utilization Pg(s): 5 INTRODUCTION The Westchester
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject References Emergency Medical Services Administrative Policies and Procedures Title
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject References Emergency Medical Services Administrative Policies and Procedures Title
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
Clinical Guideline Trauma Care: Accessing Trauma Services
 Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
Standards for Trauma Center Accreditation Pediatric Levels I & II. Effective Date: October 1, 2014
 2014-2015 Standards for Trauma Center Accreditation Pediatric Levels I & II ffective Date: October 1, 2014 PRFAC In 1985 Pennsylvania became the eighth state in the country to develop a trauma system through
2014-2015 Standards for Trauma Center Accreditation Pediatric Levels I & II ffective Date: October 1, 2014 PRFAC In 1985 Pennsylvania became the eighth state in the country to develop a trauma system through
South Central Region EMS & Trauma Care Council Patient Care Procedures
 South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
Alabama Trauma System Region One Plan
 Alabama Trauma System Region One Plan Published by Alabama Department of Public Health (ADPH)/Office of Emergency Medical Services (OEMS) Copyright 2013 ADPH/OEMS Original Release Date First Edition, V1.0/February
Alabama Trauma System Region One Plan Published by Alabama Department of Public Health (ADPH)/Office of Emergency Medical Services (OEMS) Copyright 2013 ADPH/OEMS Original Release Date First Edition, V1.0/February
Trauma Logistics: The things to know ED Charge RN
 The University East Bank Campus is verified by the American College of Surgeons as a Level II Trauma Center. We serve the metro and referring areas as a definitive care trauma center for our patients.
The University East Bank Campus is verified by the American College of Surgeons as a Level II Trauma Center. We serve the metro and referring areas as a definitive care trauma center for our patients.
Chapter 1, Part 2 EMS SYSTEMS EMS System A comprehensive network of personnel, equipment, and established to deliver aid and emergency medical care
 1 3 4 5 6 7 8 9 10 11 1 Chapter 1, Part EMS SYSTEMS EMS System A comprehensive network of personnel, equipment, and established to deliver aid and emergency medical care to the community. IN-HOSPITAL COMPONENTS
1 3 4 5 6 7 8 9 10 11 1 Chapter 1, Part EMS SYSTEMS EMS System A comprehensive network of personnel, equipment, and established to deliver aid and emergency medical care to the community. IN-HOSPITAL COMPONENTS
San Diego County Trauma System
 Engineering Prevention Medical Treatment San Diego County Trauma System CIREN Center CIREN Program Report Commitment The San Diego CIREN center is committed to saving lives, and mitigating and preventing
Engineering Prevention Medical Treatment San Diego County Trauma System CIREN Center CIREN Program Report Commitment The San Diego CIREN center is committed to saving lives, and mitigating and preventing
Alabama Trauma System Region Three Plan
 Alabama Trauma System Region Three Plan Published by Alabama Department of Public Health/Office of Emergency Medical Services Copyright 2013 ADPH OEMS Original Release Date First Edition, V1.0/October
Alabama Trauma System Region Three Plan Published by Alabama Department of Public Health/Office of Emergency Medical Services Copyright 2013 ADPH OEMS Original Release Date First Edition, V1.0/October
Emergency Medical Services: More Than Just a Ride to the Hospital
 Emergency Medical Services: More Than Just a Ride to the Hospital Manish I. Shah, MD, MS Prehospital Domain Lead EMS for Children Innovation and Improvement Center Associate Professor Department of Pediatrics
Emergency Medical Services: More Than Just a Ride to the Hospital Manish I. Shah, MD, MS Prehospital Domain Lead EMS for Children Innovation and Improvement Center Associate Professor Department of Pediatrics
National EMS Scope of Practice Model Revision 2018
 1 2 3 4 5 6 National EMS Scope of Practice Model Revision 2018 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 THIS VERSION CONTAINS TWO PARTS: I. EMS LEVEL DESCRIPTIONS II. RAPID PROCESS FOR
1 2 3 4 5 6 National EMS Scope of Practice Model Revision 2018 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 THIS VERSION CONTAINS TWO PARTS: I. EMS LEVEL DESCRIPTIONS II. RAPID PROCESS FOR
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DESTINATION POLICY
 SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY I. PURPOSE DESTINATION POLICY Policy Reference No.: 5000 Supersedes: February 1, 2015 A. To identify the approved ambulance-transport destinations for the
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY I. PURPOSE DESTINATION POLICY Policy Reference No.: 5000 Supersedes: February 1, 2015 A. To identify the approved ambulance-transport destinations for the
Hospital Care and Trauma Management Nakhon Tipsunthonsak Witaya Chadbunchachai Trauma Center Khonkaen, Thailand
 Hospital Care and Trauma Management Nakhon Tipsunthonsak Witaya Chadbunchachai Trauma Center Khonkaen, Thailand Health protection and disease prevention Needs Assessment Disasters usually have an unforeseen,
Hospital Care and Trauma Management Nakhon Tipsunthonsak Witaya Chadbunchachai Trauma Center Khonkaen, Thailand Health protection and disease prevention Needs Assessment Disasters usually have an unforeseen,
Multi-Casualty Incidents and Triage
 Z03_CAMP7247_07_SE_A03.indd Page 1 8/23/11 9:22 PM user f-404 F-402 Multi-Casualty Incidents and Triage David Maatman, NREMT-P/IC Roy Alson, PhD, MD, FACEP Jere F. Baldwin, MD, FACEP, FAAFP John T. Stevens,
Z03_CAMP7247_07_SE_A03.indd Page 1 8/23/11 9:22 PM user f-404 F-402 Multi-Casualty Incidents and Triage David Maatman, NREMT-P/IC Roy Alson, PhD, MD, FACEP Jere F. Baldwin, MD, FACEP, FAAFP John T. Stevens,
San Joaquin County Emergency Medical Services Agency Policy and Procedure Manual
 Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221. I. Title Trauma team Activation Protocol/Roles & Responsibilities of the Trauma Team
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Level 3 Trauma Hospital Criteria
 Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Ambulance Provider Compliance Summary for EMERGENCY RESPONSE Compliance Criteria
 Ambulance Provider Compliance Summary for EMERGENCY RESPONSE Compliance Criteria Date: April 23, 2012 Source Information: Medicare Policy Purpose The United Mine Workers of America Health and Retirement
Ambulance Provider Compliance Summary for EMERGENCY RESPONSE Compliance Criteria Date: April 23, 2012 Source Information: Medicare Policy Purpose The United Mine Workers of America Health and Retirement
Incident title: Prison fire
 Incident title: Prison fire Reporter Incident location Dr. Patricio Cortés Picazo Director EMS SAMU Metropolitano Santiago de Chile 2010-2013 Emergency Medical Services SAMU Metropolitano Santiago de Chile
Incident title: Prison fire Reporter Incident location Dr. Patricio Cortés Picazo Director EMS SAMU Metropolitano Santiago de Chile 2010-2013 Emergency Medical Services SAMU Metropolitano Santiago de Chile
UPMC Trauma Care System
 A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC CONDUCT TRIAGE
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
EMS Subspecialty Certification Review Course. Learning Objectives
 EMS Subspecialty Certification Review Course Mass Gatherings: 4.3 Disaster Planning and Operations: 4.3.1 Human Resource Needs in Disaster Response 4.3.2 Care Teams 4.3.2.1 Physician Placement 4.3.2.2
EMS Subspecialty Certification Review Course Mass Gatherings: 4.3 Disaster Planning and Operations: 4.3.1 Human Resource Needs in Disaster Response 4.3.2 Care Teams 4.3.2.1 Physician Placement 4.3.2.2
COURSE DESCRIPTIONS. Emergency Health Sciences (EMSP)
") ` COURSE DESCRIPTIONS Emergency Health Sciences (EMSP) EMSP 4010. Emer Med Serv-Ambulance. 4 Credit Hours. Orientation to the San Antonio Fire Department Standard Medical Operating Procedures (SMOPs) and
` COURSE DESCRIPTIONS Emergency Health Sciences (EMSP) EMSP 4010. Emer Med Serv-Ambulance. 4 Credit Hours. Orientation to the San Antonio Fire Department Standard Medical Operating Procedures (SMOPs) and
Level 4 Trauma Hospital Criteria
 Level 4 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 4 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
San Joaquin County Emergency Medical Services Agency Policy and Procedure Manual
 Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2010-04 Bariatric Patient Transports 12/17/2010 2012-01 DNR and POLST
Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2010-04 Bariatric Patient Transports 12/17/2010 2012-01 DNR and POLST
EMS Subspecialty Certification Review Course. Learning Objectives. Scope of Practice
 EMS Subspecialty Certification Review Course 2.3.1 Scope of Practice Models 2.3.1.1 Military/federal government medical personnel 2.3.1.2 State vs. national scope of practice model 2.3.1.2.1 Levels of
EMS Subspecialty Certification Review Course 2.3.1 Scope of Practice Models 2.3.1.1 Military/federal government medical personnel 2.3.1.2 State vs. national scope of practice model 2.3.1.2.1 Levels of
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
among TEMS providers:
 The need for standardization among TEMS providers: Training, credentialing and roles By Scott Warner, MD, EMT Tactical teams which have integrated tactical medics and physicians into their law enforcement
The need for standardization among TEMS providers: Training, credentialing and roles By Scott Warner, MD, EMT Tactical teams which have integrated tactical medics and physicians into their law enforcement
Tactical & Hunter First Aid Workshop
 Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
Multiple Patient Management Plan
 2018 [NAME OF PLAN] Multiple Patient Management Plan Marin County Health & Human Services Emergency Medical Services Agency Supports the Marin County Operational Area Emergency Operations Plan and Medical
2018 [NAME OF PLAN] Multiple Patient Management Plan Marin County Health & Human Services Emergency Medical Services Agency Supports the Marin County Operational Area Emergency Operations Plan and Medical
San Joaquin County Emergency Medical Services Agency Policy and Procedure Manual
 Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
Policy Memorandum 2006-02 Clearing of Patients in Custody 4/27/2006 2009-01 Billing for services to non-transported patients 1/5/2009 2009-02 Emergency and Non-Emergency Patient Definitions 1/5/2009 2010-02
NWC EMSS EMT Class Fall Semester 2018 August 21 December 13 Tuesday / Thursday Six (6) Mandatory Saturdays. Date Subject Time & Instructor
 Mandatory Saturdays. Date Subject Time & Instructor") NWC EMSS EMT Class Fall Semester 2018 August 21 December 13 Tuesday / Thursday Six (6) Saturdays Date Subject Time & Instructor 08/14 EMS 110 Orientation Required pre class reading: Chapter 1 and Chapter
NWC EMSS EMT Class Fall Semester 2018 August 21 December 13 Tuesday / Thursday Six (6) Saturdays Date Subject Time & Instructor 08/14 EMS 110 Orientation Required pre class reading: Chapter 1 and Chapter
King Saud University. Updated Study Plan. Prince Sultan Bin Abdulaziz College for EMS. Bachelor of Science Program, Emergency Medical Services
 2013 King Saud University Prince Sultan Bin Abdulaziz College for EMS Bachelor of Science Program, Emergency Medical Services Updated Study Plan 1433 ه 1434- Prince Sultan Bin Abdulaziz College for EMS,
2013 King Saud University Prince Sultan Bin Abdulaziz College for EMS Bachelor of Science Program, Emergency Medical Services Updated Study Plan 1433 ه 1434- Prince Sultan Bin Abdulaziz College for EMS,
(K) Primary care specialty family/general practice, internal medicine, or pediatrics.
 Primary care specialty family/general practice, internal medicine, or pediatrics.") 19 CSR 30-40.303 Medical Director Required for All: Ambulance Services and Emergency Medical Response Agencies That Provide Advanced Life Support Services, Basic Life Support Services Utilizing Medications
19 CSR 30-40.303 Medical Director Required for All: Ambulance Services and Emergency Medical Response Agencies That Provide Advanced Life Support Services, Basic Life Support Services Utilizing Medications
EMT-B Course Syllabus. Instructor: Russell Cephus EMT. Instructor Contact Information: (570)
") EMT-B Course Syllabus Instructor: Russell Cephus EMT Instructor Contact Information: (570) 290-5718 diyinstructional@gmail.com Instructor Office Hours and Location: -, 9a to 5p by appointment only Course
EMT-B Course Syllabus Instructor: Russell Cephus EMT Instructor Contact Information: (570) 290-5718 diyinstructional@gmail.com Instructor Office Hours and Location: -, 9a to 5p by appointment only Course
EMT RECERT PROPOSAL (NCCP standards)
") EMT RECERT PROPOSAL (NCCP standards) The National Component requires 20 hours of the topic hours listed for recert: Modules I thru V. Module I TOPIC Airway and Neurotological Management Ventilation ETCO2
EMT RECERT PROPOSAL (NCCP standards) The National Component requires 20 hours of the topic hours listed for recert: Modules I thru V. Module I TOPIC Airway and Neurotological Management Ventilation ETCO2
PARAMEDIC STUDENT FIELD INTERNSHIP GUIDE
 Through field experience in the emergency ambulance, the paramedic student will develop a more comprehensive understanding of the pathophysiology of disease and trauma, rationale for treatments rendered,
Through field experience in the emergency ambulance, the paramedic student will develop a more comprehensive understanding of the pathophysiology of disease and trauma, rationale for treatments rendered,
This Annex describes the emergency medical service protocol to guide and coordinate actions during initial mass casualty medical response activities.
 A N N E X C : M A S S C A S U A L T Y E M S P R O T O C O L This Annex describes the emergency medical service protocol to guide and coordinate actions during initial mass casualty medical response activities.
A N N E X C : M A S S C A S U A L T Y E M S P R O T O C O L This Annex describes the emergency medical service protocol to guide and coordinate actions during initial mass casualty medical response activities.
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES BUREAU OF EMS, TRAUMA AND PREPAREDNESS EMS AND TRAUMA SERVICES SECTION STATEWIDE TRAUMA SYSTEM
 MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES BUREAU OF EMS, TRAUMA AND PREPAREDNESS EMS AND TRAUMA SERVICES SECTION STATEWIDE TRAUMA SYSTEM (By authority conferred on the department of health and human
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES BUREAU OF EMS, TRAUMA AND PREPAREDNESS EMS AND TRAUMA SERVICES SECTION STATEWIDE TRAUMA SYSTEM (By authority conferred on the department of health and human
Paramedic Course Syllabus. Instructor Contact Information: (504) ,
 ,") Paramedic Course Syllabus Instructor: Stephen Kershaw; NREMTP Anita M. Lindsay; MAED, BSHS, NREMTP Instructor Contact Information: (504) 496-7678, Email: alindsay@medexpress.net Instructor Office Hours
Paramedic Course Syllabus Instructor: Stephen Kershaw; NREMTP Anita M. Lindsay; MAED, BSHS, NREMTP Instructor Contact Information: (504) 496-7678, Email: alindsay@medexpress.net Instructor Office Hours
Regions Hospital Delineation of Privileges Critical Care
 Regions Hospital Delineation of Privileges Critical Care Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Regions Hospital Delineation of Privileges Critical Care Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Organization and Management for Hospitals and EMS Agencies
 Organization and Management for Hospitals and EMS Agencies For The Greater Kansas City Metropolitan Area A Community Plan for Diversion Approval Date: March 27, 2002 Implementation Date: May 1, 2002 Revised:
Organization and Management for Hospitals and EMS Agencies For The Greater Kansas City Metropolitan Area A Community Plan for Diversion Approval Date: March 27, 2002 Implementation Date: May 1, 2002 Revised:
NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT
 February 2015 NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT Improving patient outcomes from Out Of Hospital Cardiac Arrest David Hennelly AP MSc Jan 2015 THE ONE LIFE PROJECT IS BEING LED BY THE NATIONAL
February 2015 NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT Improving patient outcomes from Out Of Hospital Cardiac Arrest David Hennelly AP MSc Jan 2015 THE ONE LIFE PROJECT IS BEING LED BY THE NATIONAL
What is ICD10 and how will it affect me?
 What is ICD10 and how will it affect me? Vikki Lindemuth Blue Cross and Blue Shield of Kansas Statewide Specialty Provider Representative Nancy Ratzlaff Billing Director - LifeTeam Critical Care Ambulance
What is ICD10 and how will it affect me? Vikki Lindemuth Blue Cross and Blue Shield of Kansas Statewide Specialty Provider Representative Nancy Ratzlaff Billing Director - LifeTeam Critical Care Ambulance
PEDIATRIC TRAUMA CENTERS. Availability, Outcomes, and Federal Support Related to Pediatric Trauma Care. Report to Congressional Requesters
 United States Government Accountability Office Report to Congressional Requesters March 2017 PEDIATRIC TRAUMA CENTERS Availability, Outcomes, and Federal Support Related to Pediatric Trauma Care GAO-17-334
United States Government Accountability Office Report to Congressional Requesters March 2017 PEDIATRIC TRAUMA CENTERS Availability, Outcomes, and Federal Support Related to Pediatric Trauma Care GAO-17-334
BACKGROUND. Emergency Departments in Smaller Centres and Rural Communities
 EXPECTATIONS OF PHYSICIANS NOT CERTIFIED IN EMERGENCY MEDICINE INTENDING TO INCLUDE EMERGENCY MEDICINE AS PART OF THEIR RURAL PRACTICE CHANGING SCOPE OF PRACTICE PROCESS BACKGROUND The CPSO Ensuring Competence:
EXPECTATIONS OF PHYSICIANS NOT CERTIFIED IN EMERGENCY MEDICINE INTENDING TO INCLUDE EMERGENCY MEDICINE AS PART OF THEIR RURAL PRACTICE CHANGING SCOPE OF PRACTICE PROCESS BACKGROUND The CPSO Ensuring Competence:
Chapter 1. Emergency Medical Care Systems, Research, and Public Health. Copyright 2010 by Pearson Education, Inc. All rights reserved.
 Chapter 1 Emergency Medical Care Systems, Research, and Public Health Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 1 Emergency Medical Care Systems, Research, and Public Health Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Definitions. The following words and phrases shall have the following
 109-1-1. Definitions. The following words and phrases shall have the following meanings as used in this agency s regulations. (a) Administrator means the executive director of the emergency medical services
109-1-1. Definitions. The following words and phrases shall have the following meanings as used in this agency s regulations. (a) Administrator means the executive director of the emergency medical services
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy
 Policy") Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY RECEIVING HOSPITAL STANDARDS
 SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY I. PURPOSE RECEIVING HOSPITAL STANDARDS Policy Reference No.: 5010 Review Date: January 1, 2011 Supersedes: August 1, 2007 A. Establish minimum standards
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY I. PURPOSE RECEIVING HOSPITAL STANDARDS Policy Reference No.: 5010 Review Date: January 1, 2011 Supersedes: August 1, 2007 A. Establish minimum standards
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
National Trauma Data Standard DATA DICTIONARY Admissions
 National Trauma Data Standard DATA DICTIONARY 2012 Admissions July 2011 registry. 18 During 2004 through 2006, the ACSCOT Subcommittee on Trauma Registry Programs was Introduction Traumatic injury, both
National Trauma Data Standard DATA DICTIONARY 2012 Admissions July 2011 registry. 18 During 2004 through 2006, the ACSCOT Subcommittee on Trauma Registry Programs was Introduction Traumatic injury, both
Attachment B ORDINANCE NO. 14-
 ORDINANCE NO. 14- AN ORDINANCE OF THE COUNTY OF ORANGE, CALIFORNIA AMENDING SECTIONS 4-9-1 THROUGH 4-11-17 OF THE CODIFIED ORDINANCES OF THE COUNTY OF ORANGE REGARDING AMBULANCE SERVICE The Board of Supervisors
ORDINANCE NO. 14- AN ORDINANCE OF THE COUNTY OF ORANGE, CALIFORNIA AMENDING SECTIONS 4-9-1 THROUGH 4-11-17 OF THE CODIFIED ORDINANCES OF THE COUNTY OF ORANGE REGARDING AMBULANCE SERVICE The Board of Supervisors
Emergency Medical Technician (EMT)
") Emergency Medical Technician (EMT) When every second counts... when the situation is at its worst... when there s an accident or medical emergency that s when Emergency Medical Technicians (EMTs) are at
Emergency Medical Technician (EMT) When every second counts... when the situation is at its worst... when there s an accident or medical emergency that s when Emergency Medical Technicians (EMTs) are at
EMT Course Syllabus Spring 2017 (February - May)
") EMT Course Syllabus Spring 2017 (February - May) Instructor/Coordinator: Prescott Nadeau, AEMT / EMS I.C. Instructor/Coordinator Contact Information: Prescott Nadeau: (C) 802-999-5944 Email- pnadeau38@gmail.com
EMT Course Syllabus Spring 2017 (February - May) Instructor/Coordinator: Prescott Nadeau, AEMT / EMS I.C. Instructor/Coordinator Contact Information: Prescott Nadeau: (C) 802-999-5944 Email- pnadeau38@gmail.com
American Heart Association Classes CPR ACLS PALS Pediatric Advanced Life Support (PALS)
") ACE 4 EMS educators will be available to teach a course in your area during 2016. The dates are as follows: June 4 & 5, 2016 June 25 & 26, 2016 August 27 & 28, 2016 September 24 & 25, 2016 November 12
ACE 4 EMS educators will be available to teach a course in your area during 2016. The dates are as follows: June 4 & 5, 2016 June 25 & 26, 2016 August 27 & 28, 2016 September 24 & 25, 2016 November 12
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria)
") AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
Complexities & Progress in Graduate Medical Education
 Complexities & Progress in Graduate Medical Education NHPF Meeting on GME Atul Grover, M.D., Ph.D., FACP, FCCP Chief Public Policy Officer, AAMC September 6, 2013 Key Principles of Accountability Measures
Complexities & Progress in Graduate Medical Education NHPF Meeting on GME Atul Grover, M.D., Ph.D., FACP, FCCP Chief Public Policy Officer, AAMC September 6, 2013 Key Principles of Accountability Measures
Basic Standards for Residency Training in Orthopedic Surgery
 Basic Standards for Residency Training in Orthopedic Surgery American Osteopathic Association and American Osteopathic Academy of Orthopedics Approved/Effective July 1, 2012 TABLE OF CONTENTS Section I:
Basic Standards for Residency Training in Orthopedic Surgery American Osteopathic Association and American Osteopathic Academy of Orthopedics Approved/Effective July 1, 2012 TABLE OF CONTENTS Section I:
EMERGENCY MEDICAL SERVICES (EMS)
") Bismarck State College 2018-2019 Catalog 1 EMERGENCY MEDICAL SERVICES (EMS) EMS 110. Emergency Medical Technician Credits: 4 Prerequisite: Completion of a healthcare provider level CPR (BLS) Course. Corequisites:
Bismarck State College 2018-2019 Catalog 1 EMERGENCY MEDICAL SERVICES (EMS) EMS 110. Emergency Medical Technician Credits: 4 Prerequisite: Completion of a healthcare provider level CPR (BLS) Course. Corequisites:
The 2013 Boston Marathon Bombings
 The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
12/30/2011. Dan Spaite : PI NIH/NINDS 1R01NS A1. Ben Bobrow: PI NIH/NINDS 1R01NS A1
 Daniel Spaite, MD, FACEP Professor of Emergency Medicine Ben Bobrow, MD, FACEP Associate Professor of Emergency Medicine Dan Spaite : PI NIH/NINDS 1R01NS071049-01A1 Ben Bobrow: PI NIH/NINDS 1R01NS071049-01A1
Daniel Spaite, MD, FACEP Professor of Emergency Medicine Ben Bobrow, MD, FACEP Associate Professor of Emergency Medicine Dan Spaite : PI NIH/NINDS 1R01NS071049-01A1 Ben Bobrow: PI NIH/NINDS 1R01NS071049-01A1
Plane crash exercise Kuusamo
 Plane crash exercise Kuusamo Reporter Incident location Dr. Lasse Raatiniemi Role in incident: Treatment officer Co-authors Tommi pekanoja Role in incident: Observer, Field supervisor Pasi Lehto Role in
Plane crash exercise Kuusamo Reporter Incident location Dr. Lasse Raatiniemi Role in incident: Treatment officer Co-authors Tommi pekanoja Role in incident: Observer, Field supervisor Pasi Lehto Role in
9/10/2012. Chapter 62. Learning Objectives. Learning Objectives (Cont d) EMS Operations Command and Control
 EMS Operations Command and Control") Chapter 62 EMS Operations Command and Control 1 Learning Objectives Explain the need for an incident management system and an incident command system in managing EMS incidents Compare command procedures
Chapter 62 EMS Operations Command and Control 1 Learning Objectives Explain the need for an incident management system and an incident command system in managing EMS incidents Compare command procedures
Document Title: Trauma Patient Care in the Emergency Department : Pitfalls to Avoid
 Project: Ghana Emergency Medicine Collaborative Document Title: Trauma Patient Care in the Emergency Department : Pitfalls to Avoid Author(s): Jim Holliman, M.D., F.A.C.E.P. (Uniformed Services University
Project: Ghana Emergency Medicine Collaborative Document Title: Trauma Patient Care in the Emergency Department : Pitfalls to Avoid Author(s): Jim Holliman, M.D., F.A.C.E.P. (Uniformed Services University
UMBC Professional & Continuing Education Department of Emergency Health Services
 UMBC Professional & Continuing Education Department of Emergency Health Services PNCCT sm /NR Paramedic Refresher Requirements /Breakdown Comparison If you ARE an NCCP State, the following applies to you:
UMBC Professional & Continuing Education Department of Emergency Health Services PNCCT sm /NR Paramedic Refresher Requirements /Breakdown Comparison If you ARE an NCCP State, the following applies to you: