NHS Fife. Local Report ~ July Blood Transfusion
|
|
|
- Octavia Stanley
- 5 years ago
- Views:
Transcription

1 NHS Fife Local Report ~ July 2008 Blood Transfusion
2
3 kepcáñé içå~äoééçêíúgìäóommu _äçççqê~åëñìëáçå
4 içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók téü~îé~ëëéëëéçíüéééêñçêã~ååé~ëëéëëãéåíñìååíáçåñçêäáâéäóáãé~åíçåíüéëáñ Éèì~äáíóÖêçìéëÇÉÑáåÉÇÄó~ÖÉIÇáë~ÄáäáíóIÖÉåÇÉêIê~ÅÉIêÉäáÖáçåLÄÉäáÉÑ~åÇëÉñì~ä çêáéåí~íáçåkcçêíüáëéèì~äáíó~åççáîéêëáíóáãé~åí~ëëéëëãéåíiéäé~ëéëééçìêïéäëáíé EïïïKåÜëÜÉ~äíÜèì~äáíóKçêÖFKqÜÉÑìääêÉéçêíáåÉäÉÅíêçåáÅçêé~éÉêÑçêãáë~î~áä~ÄäÉçå êéèìéëíñêçãíüékepnfpbèì~äáíó~åçaáîéêëáíólññáåéêk «kepnì~äáíófãéêçîéãéåípåçíä~åçommu fp_knjuqqmqjqrvjv cáêëíéìääáëüéçgìäóommu vçìå~ååçéóçêêééêççìåéíüéáåñçêã~íáçåáåíüáëççåìãéåíñçêìëéïáíüáåkeppåçíä~åç ~åçñçêéçìå~íáçå~äéìêéçëéëkvçìãìëíåçíã~âé~éêçñáíìëáåöáåñçêã~íáçåáåíüáë ÇçÅìãÉåíK`çããÉêÅá~äçêÖ~åáë~íáçåëãìëíÖÉíçìêïêáííÉåéÉêãáëëáçåÄÉÑçêÉ êééêççìåáåöíüáëççåìãéåík fåñçêã~íáçååçåí~áåéçáåíüáëêééçêíü~ëäééåëìééäáéçäókepäç~êçëlkep çêö~åáë~íáçåëiçêí~âéåñêçãåìêêéåíkepäç~êçlkepçêö~åáë~íáçåëçìêåéëiìåäéëë çíüéêïáëéëí~íéçi~åçáëäéäáéîéçíçäéêéäá~ääéçåéìääáå~íáçåk ïïïkåüëüé~äíüèì~äáíókçêö
5 `çåíéåíë N péííáåöíüéëåéåé R O pìãã~êóçññáåçáåöë S P aéí~áäéçñáåçáåöë~ö~áåëííüéëí~åç~êçë NM ^éééåçáñnódäçëë~êóçñ~ääêéîá~íáçåë ^éééåçáñoóoéîáéïéêçåéëë ^éééåçáñpóaéí~áäëçñêéîáéïîáëáí PM PN PO içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu P
6 içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu Q
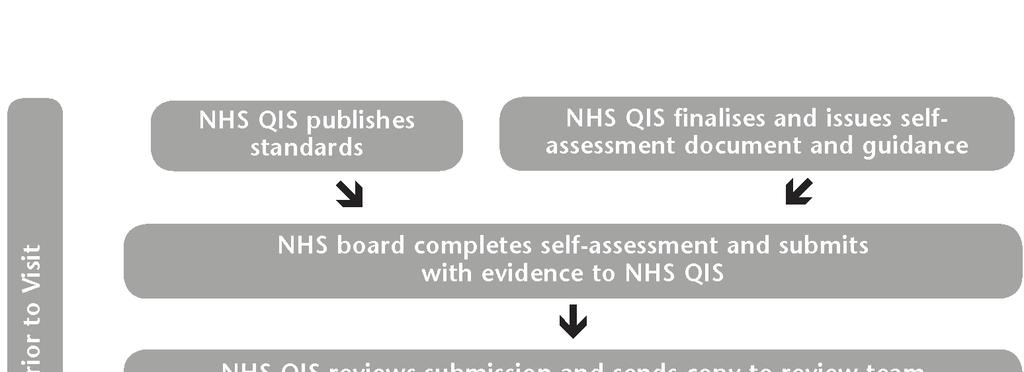
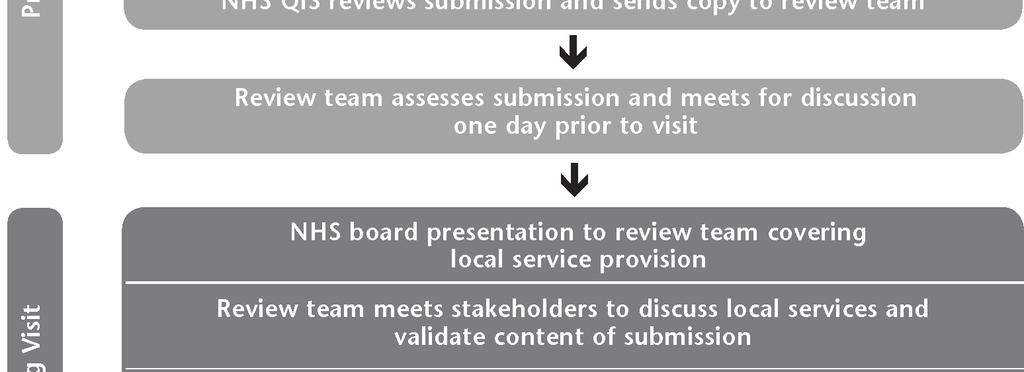
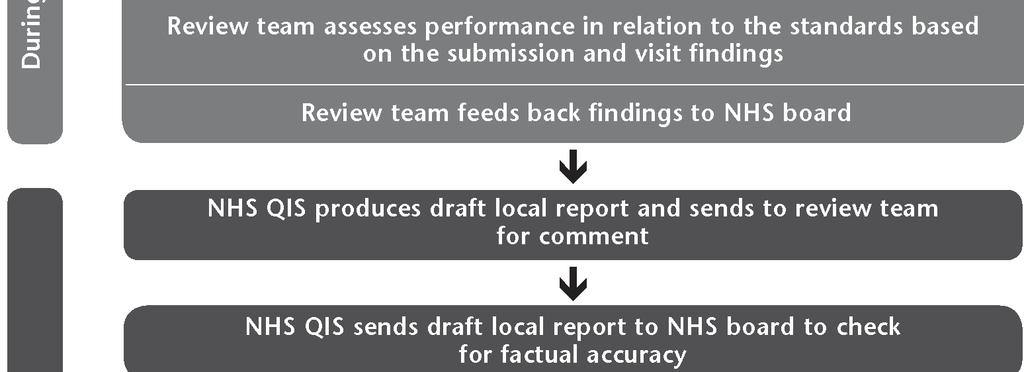
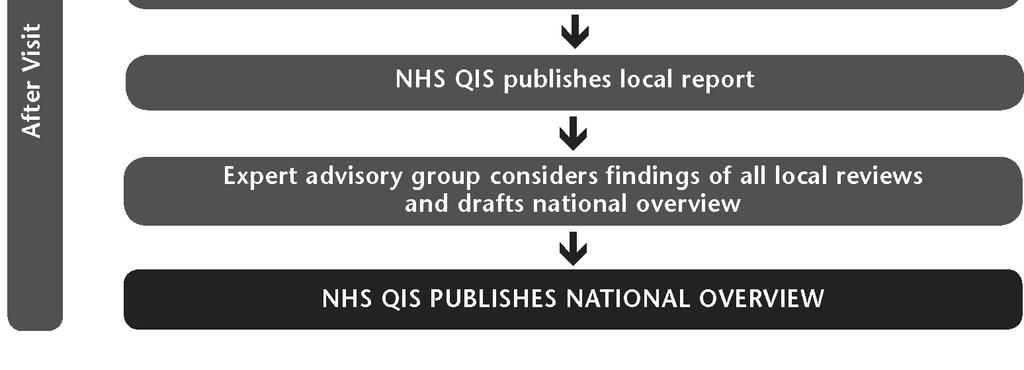
7 N péííáåöíüéëåéåé NHS Quality Improvement Scotland (NHS QIS) was set up by the Scottish Parliament in 2003 to take the lead in improving the quality of care and treatment delivered by NHSScotland. NHS QIS does this by setting standards and monitoring performance, and by providing NHSScotland with advice, guidance and support on effective clinical practice and service improvements. The Scottish National Blood Transfusion Service (SNBTS) is responsible for collecting, processing, storing and supplying all blood and blood components in Scotland and NHS boards are responsible for ordering and managing their supplies in a safe and effective manner. The Scottish Executive introduced a programme of work to improve and support transfusion practice in Scotland and, as a consequence, NHS QIS appointed a project group to develop clinical standards for blood transfusion practices. The project group developed four standards, covering: core principles; clinical management pre-transfusion; clinical management hospital transfusion laboratory; and clinical management blood and blood component collection, administration and monitoring. The Clinical Standards for Blood Transfusion were published in September These include details of the project group which set the standards and are available on request from NHS QIS or can be downloaded from the website ( About this report This report presents the findings from the peer review of NHS Fife s performance against the blood transfusion standards. The review process has three key phases: preparation prior to the visit; the visit; and the report production and publication following the visit. (See flow chart in Appendix 2 for further detail.) During the visit, each multidisciplinary review team assesses performance using the categories met, not met and not met (insufficient evidence), as detailed below. Met applies where the evidence demonstrates the standard and/or criterion is being attained. Not met applies where the evidence demonstrates the standard and/or criterion is not being attained. Not met (insufficient evidence) applies where no evidence is available for the review team, or where the evidence available is insufficient to allow an assessment to be made. A final category not applicable is used where a standard and/or criterion does not apply to the NHS board under review. Each review team is led by an experienced reviewer, who is responsible for guiding the team in their work and ensuring that team members are in agreement about the assessment reached. Membership of the review team visiting NHS Fife on 1 April 2008 can be found in Appendix 3. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu R
8 O pìãã~êóçññáåçáåöë OKN lîéêîáéïçñäçå~äëéêîáåééêçîáëáçå Fife is a relatively small region situated in east-central Scotland and has a population of around 358, The majority of the population live in urban areas, of which Dunfermline, Glenrothes and Kirkcaldy are the largest in the region. içå~äkepëóëíéã~åçëéêîáåéë Fife NHS Board is responsible for improving the health of the local population and for the delivery of the healthcare required. It provides strategic leadership and has responsibility for the efficient, effective and accountable performance of the NHS in Fife. At the time of the review visit, NHS Fife provided acute, primary and maternity services throughout the NHS board area. Transfusion procedures are carried out in nine areas within NHS Fife: Victoria Hospital, Kirkcaldy; Forth Park Maternity Hospital, Kirkcaldy, which covers the maternity and neonatal units for Fife; Queen Margaret Hospital, Dunfermline; Adamson Hospital, Cupar; Cameron Hospital, Leven; St Andrews Memorial Hospital; Glenrothes Hospital; Whiteman s Brae Hospital, Kirkcaldy; and Stratheden Hospital, Cupar. Further information about the local NHS system can be accessed via the website of NHS Fife ( NHS Fife s Victoria Hospital supplies blood and blood components to the primary care division across Fife. NHS Fife s blood bank laboratories are supplied with blood and blood components by Edinburgh & South East Scotland Blood Transfusion Service, based at the Royal Infirmary of Edinburgh. In the 12 months prior to the review visit, approximately 15,591 red cell units were transfused within NHS Fife. The NHSScotland Better Blood Transfusion Programme (BBTP) is supported by the transfusion practitioner who is assisted by the hospital transfusion team and link trainers. 1 General Register Office for Scotland. Mid-2006 Population Estimates Scotland: Population Estimates by Age and Sex and Administrative Area. First published on 26 April Revised 27 July Available from: içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu S
9 OKO pìãã~êóçññáåçáåöë~ö~áåëííüéëí~åç~êçë A summary of the findings from the review is presented in this section. A detailed description of performance against the standards/criteria is included in Section 3. `çêééêáååáéäéë NHS Fife has an established, active, hospital transfusion committee (HTC) that was formed in The HTC reports directly to the clinical governance steering group, whose chairman is also a member of the NHS Fife clinical governance committee. The HTC meet quarterly and includes membership from staff representatives from Queen Margaret Hospital, Victoria Hospital, and St Andrews Memorial Hospital. The review team encouraged the board to broaden its HTC membership by including representatives from paediatric services, other community hospitals and the SNBTS. NHS Fife provided good evidence of multidisciplinary audit being carried out throughout the NHS board area. Audits can be proposed by any members of staff in NHS Fife. The HTC agrees what blood transfusion audits will be carried out and will appoint a working group of various staff who carry out the audit feedback findings and recommendations to the HTC for sign off and action. NHS Fife uses several methods of communication when disseminating audit findings to staff and stakeholders. The review team noted in particular the SHARE newsletter as a good communication tool which is circulated to all staff and ward areas across NHS Fife. There is an established hospital transfusion team (HTT) that supports the HTC in promoting a training and education programme for staff involved in the hospital blood transfusion process. However, when the BBTP Level 1: Safe Transfusion Practice training programme was introduced, the board agreed that this would be led by the HTC, therefore, the HTT does not formally meet on a regular basis. The board recognised that a more active and formal approach was required for the HTT and, at the time of the review visit, staff reported that a schedule for future monthly HTT meetings was being developed. The transfusion practitioner provides updates to the HTC on BBTP progress. NHS Fife has a standard operating procedure (SOP) which describes the procedures for recording and investigating serious adverse blood reactions and events. There is a computerised risk management reporting system (DATIX) in operation across the NHS board area. The review team commended the board for its robust incident reporting framework. There are electronic blood stock management systems in place at Victoria Hospital and Queen Margaret Hospital, which provide an audit trail of all blood and blood component stock movement from the blood stock fridge to the return of the unit label to the laboratory. At the time of the review visit, Forth Park Maternity Hospital staff were using a paper system to monitor stock levels within its blood stock fridge, which is supplied by the blood bank laboratory at Victoria Hospital, however, staff reported that discussions were taking place to consider introducing the electronic tracking system to Forth Park Maternity Hospital. Electronic and paper copies of traceability documentation is maintained and securely stored for 30 years. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu T
10 Staff engaged in the blood transfusion process within NHS Fife are trained to establish and maintain patient identification at every stage of the blood transfusion process. However, at the time of the review visit, identification documentation did not include patient gender as part of the minimum data set at every stage of the blood transfusion process. The review team encouraged the board to develop a robust patient identification policy to address the issue of recording gender as part of the minimum data set at every stage of the blood transfusion process and to develop a risk-assessed form of identification. NHS Fife has adopted a red wristband system to alert staff to patients with special requirements, for example allergies or special circumstances. The wristband prompts staff to check the patient s medical records for further details. NHS Fife has also introduced a yellow wristband to alert staff to patients not wishing to receive a blood transfusion for religious reasons. `äáåáå~äã~å~öéãéåíóéêéjíê~åëñìëáçå NHS Fife staff reported that the blood and blood components clinical procedures manual outlines the procedure for staff to record discussions with patients on treatment options and alternatives to transfusion. While staff reported that discussions do take place, at the time of the review visit, there was no evidence available to confirm that detailed discussions with patients regarding transfusion are being documented. The introduction of a transfusion care pathway currently in development, will address this issue. A wide range of leaflets are available in all major transfusion areas. The transfusion practitioner is responsible for ensuring all clinical areas have sufficient stock of leaflets and are informed of any updates to patient leaflets. Patient information leaflets can be downloaded and printed from the NHS Fife intranet. In emergency situations, where pre-transfusion discussion is not possible, staff would endeavour to establish the identity of the patient through checking their personal belongings and making enquiries with accompanying relatives as to whether they have any treatment preferences. Findings from a small transfusion documentation audit carried out in January 2008 at Victoria Hospital showed full compliance with prescriptions being signed by qualified practitioners across the NHS board area. `äáåáå~äã~å~öéãéåíóüçëéáí~äíê~åëñìëáçåä~äçê~íçêó Both blood bank laboratories within NHS Fife are accredited by the Clinical Pathology Association (UK) Ltd (CPA) and are compliant with the Medicines and Healthcare products Regulatory Agency (MHRA). NHS Fife has a competency-based training assessment system in place at both laboratories and training records are maintained. All biomedical scientists (BMSs) are registered with the Health Professions Council. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu U
11 Both NHS Fife blood bank laboratories have stock management systems in place. Blood stocks are shared between Victoria Hospital and Queen Margaret Hospitals to minimise wastage rates. Units of O RhD negative blood are rotated regularly and expiry dates are tracked. Blood wastage rates are reported to the HTC. The review team commended the board for its robust traceability system. `äáåáå~äã~å~öéãéåíóääççç~åçääçççåçãéçåéåíåçääéåíáçåi ~Çãáåáëíê~íáçå~åÇãçåáíçêáåÖ There was evidence of theory and practical training being undertaken across the NHS board area. The BBTP is delivered by the transfusion practitioner, supported by the HTT and link trainers. The review team commended the board on the high number of senior medical staff who had undertaken training, and the introduction of BBTP Level 1 training as part of the senior medical staff s annual performance development assessment system. However, challenges had been identified in the low number of staff participating in training across all staff groups. At the time of the review visit, staff reported that an education and training plan had been developed to address the current training needs of staff employed within NHS Fife. Through audit, NHS Fife has identified challenges around recording the minimum data set requirements on blood transfusion documentation for patients. The review team encouraged the board to develop a robust positive patient identification policy to address this issue. NHS Fife s blood and blood components clinical procedures manual describes the monitoring process for patients receiving a blood transfusion. However, findings from a small audit found that timings of observations were not being adhered to and there was inconsistency on where results of these observations were recorded. Staff reported that discussions were taking place around introducing a transfusion care pathway which would address these issues. The review team commended NHS Fife for its robust incident reporting framework (DATIX) and procedures used to record and report near miss incidents and serious adverse blood reactions to Serious Hazards of Transfusion (SABRE) and Serious Hazards of Transfusion (SHOT). içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu V
12 P aéí~áäéçñáåçáåöë~ö~áåëííüéëí~åç~êçë pí~åç~êçn~w`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüéêé~êéëóëíéãëáåéä~åéëìééçêíáåöåäáåáå~äöçîéêå~ååéíçéåëìêéë~ñéiéññéåíáîé~åç ~ééêçéêá~íéääçççíê~åëñìëáçåk kepcáñé bëëéåíá~ä`êáíéêá~ N~KNW qüéêéáë~åéëí~ääáëüéçi~åíáîéiãìäíáçáëåáéäáå~êóüçëéáí~äíê~åëñìëáçååçããáííéé Eeq`FíÜ~íÜ~ëÇÉÑáåÉÇêÉëéçåëáÄáäáíáÉë~åÇ~ÅÅçìåí~ÄáäáíóíçíÜÉÅÜáÉÑ ÉñÉÅìíáîÉLkepÄç~êÇîá~íÜÉÅäáåáÅ~äÖçîÉêå~åÅÉëíêìÅíìêÉK pq^qrpwmet There is an established, active, multidisciplinary NHS Fife hospital transfusion committee (HTC) which was formed in The HTC committee meets quarterly, membership includes representatives from Victoria Hospital, Kirkcaldy; Queen Margaret Hospital, Dunfermline; and St Andrews Memorial Hospital. The review team noted that minutes submitted as evidence did not appear to include a representative from Scottish National Blood Transfusion Services (SNBTS). The board informed the review team that a representative from SNBTS had been invited to all HTC meetings. The review team encouraged the chair of the HTC to broaden membership of the group to include representatives from paediatric services, other community hospitals, and SNBTS to attend future HTC meetings. The HTC reports directly to the clinical governance steering group. The medical director for the operational division receives minutes from the HTC, he is a member of the NHS Fife clinical governance committee and chairman of the clinical governance steering group and is the main link with the HTC. The review team recommended the board update its organisation chart to define more clearly the reporting structure between the HTC, clinical governance and risk management groups. N~KOW qüéeq`ü~ëêçäéë~åçêéëéçåëáäáäáíáéë~ëçìíäáåéçáåjbienvvvfv~åç eaieommpfnvkqüéëéáååäìçéáåîçäîéãéåíáåãìäíájéêçñéëëáçå~ä~ìçáíiéçìå~íáçå ~åçíê~áåáåöiçéîéäçéãéåí~åçãççáñáå~íáçåçñöìáçéäáåéë~åçéêçíçåçäëi~åç áåîçäîéãéåíçñëí~âéüçäçéêëk pq^qrpwmet Staff reported that an audit programme was in place which included the Scottish hip revision study, which was ongoing at the time of the review visit; national GI bleeding audit; NHS Fife wristband audit; an ongoing renal registry national audit; maximum surgical blood ordering system (MSBOS) review; and audit of crossmatch and transfusion practice for elective caesarean sections. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NM
13 Audit activity is proposed by various members of staff. The HTC agrees a working group to lead the audit, outcomes from which are co-ordinated by the working group and proposals on ways forward are presented and discussed at the HTC. Following these discussions, appropriate actions are identified. The review team noted that several useful audits related to blood transfusion had been conducted and evidence of new practice implementation following outcomes from these audits was provided. For example an audit carried out in October 2004 to follow crossmatch and transfusion practice for elective caesarean sections at Forth Park Maternity Hospital, Kirkcaldy, revealed that women attending for planned caesarean sections were routinely having blood crossmatched in preparation for transfusion which indicated a diversion from agreed policy. As a result of the findings, a memo from the consultant obstetrician was circulated to appropriate staff members reiterating correct policy procedures. A re-audit of crossmatch and transfusion practice for elective caesarean sections at Forth Park Maternity Hospital carried out in March 2005, showed a significant improvement regarding adherence to policy, with crossmatches being performed only in appropriate circumstances. Audit data are disseminated widely to relevant staff groups and stakeholders using various methods of communication, for example the SHARE newsletter, presentations and training. Electronic and hard copies of audit reports are available from the clinical effectiveness group. NHS Fife aims to have all policies posted onto the intranet in the near future for staff to access. Changes to policies and protocols are undertaken by the NHS Fife policy group which disseminates the revised policies to relevant staff groups and stakeholders. All policies are ratified and disseminated in accordance with local guidance. The HTC is responsible for developing policies and protocols specific to blood transfusion. At the time of the review visit, the review team noted that a number of NHS Fife policies/procedures were overdue for review. Staff reported that a new policy template had been developed and was awaiting ratification by the policy group, which had resulted in the delay. Staff reported that all new policies are reviewed annually and advice from authors on the timings for reviewing existing policies would be sought. The review team encouraged the board to ensure that the ratification of the new policy template be carried out as a priority to ensure up-todate policies were available to all NHS Fife staff. The review team encouraged NHS Fife to generate a regular multidisciplinary audit programme and expand the participation of other specialties in audit. The role of the clinical effectiveness group in supporting audit work was noted as a strength for the board by the review team. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NN
14 N~KPW qüéeq`iáååçää~äçê~íáçåïáíüíüéåäáåáå~äöçîéêå~ååéåçããáííééiáãéäéãéåíë íüékeppåçíä~åç_éííéê_äçççqê~åëñìëáçåmêçöê~ããée qmfk pq^qrpwmet There is an established hospital transfusion team (HTT). Membership includes the transfusion practitioner, lead clinicians from Queen Margaret Hospital and Victoria Hospital and chief biomedical scientists (BMSs). A decision that the HTC leads the implementation of the Better Blood Transfusion Programme (BBTP) Level 1: Safe Transfusion Practice training programme was taken by the board on the introduction of BBTP. The transfusion practitioner attends HTC meetings and reports on all BBTP related work progress. Therefore, at present, the HTT group does not meet formally. The hospital transfusion practitioner, who undertakes staff training, meets weekly with individual HTT members to discuss and take forward any issues arising from HTC meetings. The HTT had identified the requirement to develop a more active group and plans are in progress to hold regular monthly HTT meetings. The review team encouraged the board to introduce a schedule for regular HTT monthly meetings. The transfusion practitioner is responsible for BBTP Level 1 training throughout NHS Fife with the support of link trainers, some of whom were noted to no longer be practising. The review team was informed that a review of link trainers is to be carried out to reduce the number to a more manageable group. N~KQW qüéeq`êéîáéïë~ääêééçêíëçñ~çîéêëééîéåíë~åçåé~êãáëëáååáçéåíëêéä~íáåöíç ÄäççÇíê~åëÑìëáçå~åÇIáåêÉëéçåëÉIáãéäÉãÉåíëÅÜ~åÖÉëáåéê~ÅíáÅÉïÜÉêÉ åéåéëë~êók pq^qrpwmet The NHS Fife incident management policy sets out a course of action which clearly details the procedures to be followed by staff to effectively record, investigate and manage adverse or near miss incidents across NHS Fife. All incidents are reported through a computerised risk management reporting system (DATIX). Staff complete a three part incident/near miss reporting form for all clinical and non-clinical incidents along with a traffic light grading matrix to determine the extent of the incident. Relevant coloured copies of the incident form are distributed in accordance with local policy. Red incidents are reported to NHS Fife risk management team for action, and changes in practice are implemented where appropriate. Lessons learned from incidents are shared with relevant staff and stakeholders via staff meetings, the SHARE newsletter and risk management conferences. The review team noted the NHS Fife s SHARE newsletter as particularly informative. Reports of serious adverse events or reactions and near miss incidents are also submitted to Serious Adverse Blood Reactions and Events (SABRE) and the Serious Hazards of Transfusion (SHOT) initiative. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NO
15 The transfusion practitioner reviews all adverse events and near miss incidents at regular intervals through a filtering facility available in DATIX, which highlights specific incidents related to blood transfusion. The transfusion practitioner attends monthly quality assurance laboratory meetings to discuss all adverse events and near miss incidents relating to blood transfusion. Information relating to adverse events or incidents are collated by the transfusion practitioner, the chief BMS and laboratory quality assurance officer s. The transfusion practitioner reports this information to the HTC (adverse events and near miss incidents is a standing item on the HTC agenda). içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NP
16 pí~åç~êçnäw`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüékepäç~êçü~ë~ëóëíéãáåéä~åéíçéåëìêéíü~íéîéêóìåáíçñääçççåçãéçåéåí êéåéáîéçáåíçíüéüçëéáí~äíê~åëñìëáçåä~äçê~íçêóå~åäéìåãáëí~â~ääóíê~åéçíçáíë êéåáéáéåíiçêíçáíëñáå~äñ~íéáñåçííê~åëñìëéçk kepcáñé bëëéåíá~ä`êáíéêáçå NÄKNW qüéêéáë~î~äáç~íéçëóëíéãíçéåëìêéíü~íéîáçéååéçñìåãáëí~â~ääéíê~åé~äáäáíóáë ÖÉåÉê~íÉÇIëíçêÉÇ~åÇ~ÅÅÉëëáÄäÉÑçêPMóÉ~êëK pq^qrpwmet NHS Fife has a standard operating procedure (SOP) to provide staff with guidance on blood transfusion traceability. The blood bank laboratories in Victoria Hospital and Queen Margaret Hospital use the bag and tag system which issues a traceability label from the pre-transfusion stage. The label is tracked throughout the journey of the blood unit until its return to the laboratory to confirm transfusion of the blood to the patient. The returned section of the traceability label is electronically scanned and the information securely stored both in paper and electronic form for the recommended period of 30 years. At present, Forth Park Maternity Hospital is using a paper-based system for monitoring stock levels within its blood fridge, however, the board are considering introducing the bag and tag system into Forth Park Maternity Hospital. The electronic (computerised) system used to store traceability information generates a daily report of unreturned traceability labels and follow-up action is taken by laboratory staff who contact the relevant wards to check the final fate of units within the timescales set out in the traceability flow chart. The review team commended NHS Fife for its comprehensive traceability flow chart which is displayed in all relevant ward areas. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NQ
17 pí~åç~êçnåw`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüéêéáë~êçäìëíëóëíéãáåéä~åéíçéëí~ääáëüé~íáéåíáçéåíáñáå~íáçåçéí~áäë~åçã~áåí~áå íüáë~íéîéêóëí~öéçñíüéåäáåáå~äíê~åëñìëáçåéêçåéëëk kepcáñé bëëéåíá~ä`êáíéêá~ NÅKNW qüéãáåáãìãáçéåíáñáå~íáçåç~í~ëéíeëìêå~ãéiñçêéå~ãéiëéñiç~íéçñäáêíü~åç ìåáèìéáçéåíáñáå~íáçååìãäéêiéö`çããìåáíóeé~äíüfåçéñx`efzfáëìëéç~íéîéêó ëí~öéçñíüéåäáåáå~äíê~åëñìëáçåéêçåéëëíçéçëáíáîéäóáçéåíáñóíüéé~íáéåík pq^qrpwnot met At the time of the review visit, the minimum data set in use across NHS Fife included four of the recommended five identifiers (surname, forename, date of birth and a unique identification number). A recent wristband audit carried out in August 2007 confirmed that gender was not routinely recorded as part of the minimum data set. The omission of gender at each stage of the clinical transfusion process means that the board has narrowly failed to meet this standard criterion. The findings from the wristband audit also showed that the Community Health Index (CHI) number was not always recorded on the wristband and, in these cases, the hospital number would be detailed. On occasions when patients were transferred from one hospital to another their wristband would contain several hospital numbers, which caused confusion for staff when recording minimum data set information. The board has identified this as an issue and staff reported that a decision to use the CHI number in future for positive patient identification recording had been agreed. One of the recommendations following the outcome of this audit is to develop an NHS Fife wide wristband/identification policy that will include specialist areas such as the special care nursery at Forth Park Maternity Hospital. The introduction of a board-wide positive patient identification policy will detail the use of the CHI number when recording the minimum data set for patients. All staff involved in the blood transfusion process are required to undertake BBTP Level 1 training which includes reference to ensuring positive patient identification. However, the board had identified challenges regarding low uptake of staff training in the blood transfusion process. Across NHS Fife, the transfusion practitioner has implemented statutory monthly face-to-face blood transfusion training sessions for nursing staff. Staff reported that the consultant haematologist had been instrumental in providing blood transfusion training for senior medical staff and training now features on their annual performance development assessment process. There are a large number of link trainers in place across NHS Fife, some of whom are no longer practicing. The transfusion practitioner reported that a review of link trainers would be carried out to reduce the number to a more manageable group. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NR
18 NÅKOW ^ääé~íáéåíëãìëíäéáçéåíáñá~ääé~í~ääíáãéëkfåé~íáéåíë~åçç~óé~íáéåíëãìëí ïé~ê~åáçéåíáñáå~íáçåïêáëíä~åçkfñíüéïêáëíä~åçäéåçãéëáå~ååéëëáääéñçê~åó êé~ëçåi~å~äíéêå~íáîéiêáëâj~ëëéëëéçñçêãçñáçéåíáñáå~íáçåáë~ççéíéçáããéçá~íéäók pq^qrpwnot met The NHS Fife blood and blood component clinical procedures manual states that patients receiving a blood transfusion must wear a wristband at all times. However, a wristband audit undertaken in August 2007 found a number of issues relating to positive patient identification and a small number of patients not wearing a wristband. Outcomes from this audit were discussed at the HTC and a working group was identified to lead investigations into resolving these issues which included information technology (IT) solutions for each of the three sites. At the time of the review visit, staff reported that they were nearing the end of their investigations and recommendations would be fed back to the next HTC meeting. There is no formal alternative risk-assessed form of identification if the wristband becomes inaccessible for any reason. The review team recommended that the board develop a robust positive patient identification system that includes a risk-assessed alternative to wristbands. NÅKPW qüéêéáë~ëóëíéãeéöçáëíáååíáîéïêáëíä~åçëfíç~äéêíèì~äáñáéçéê~åíáíáçåéêëíç é~íáéåíëïüçü~îéëééåáñáåíê~åëñìëáçåêéèìáêéãéåíëiáååäìçáåöíüéïáëüíçåçíäé íê~åëñìëéçk pq^qrpwmet NHS Fife has introduced a red wristband system to alert qualified practitioners to refer to patient s medical notes for information regarding allergy or special circumstances and requirements. The board also uses a yellow wristband to identify patients who do not wish to be transfused for religious reasons, although it was noted that patients have the right to refuse to wear this should they not wish to do so. NÅKQW cçêé~íáéåíëïüçëéáçéåíáíóå~ååçíäéåçåñáêãéçeéöìååçåëåáçìëé~íáéåíëçê é~íáéåíëïáíüåçããìåáå~íáçåçáññáåìäíáéëfi~ãáåáãìãçñöéåçéê~åççåéìåáèìé áçéåíáñáéêeéö~ååáçéåí~åçéãéêöéååóåìãäéêçê`efåìãäéêfáëéëëéåíá~äñçê éçëáíáîéé~íáéåíáçéåíáñáå~íáçåk pq^qrpwmet The NHS Fife major haemorrhage protocol includes guidance for staff on how to manage unidentified patients admitted to the accident and emergency (A&E) department. The procedure notes a patient would be allocated a typenex number and recorded as unnamed male or unnamed female until the patient s identity is confirmed. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NS
19 Guidelines are in place to assist staff when identifying patients with communication difficulties. Language Line 24-hour telephone translation services along with Fife community interpreting services are used across the NHS board area to support communication and establish positive patient identification details where appropriate. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NT
20 pí~åç~êçnçw`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüékepäç~êçü~ë~ëíê~íéöóñçêã~å~öéãéåíçñääçççëüçêí~öéëk kepcáñé bëëéåíá~ä`êáíéêáçå NÇKNW bãéêöéååóääçççã~å~öéãéåí~êê~åöéãéåíëeb_j^f~êééëí~ääáëüéç~ëçéñáåéç áåeaieommrfork pq^qrpwmet NHS Fife has an established emergency blood management arrangements (EBMA) group. The roles and responsibilities of individual staff members are clearly defined in its terms of reference. Following discussions at the HTC, an action plan for managing EBMA was drafted and signed off by the HTC. The NHS Fife laboratory EBMA document provides guidance on procedures for staff in times of blood shortages. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NU
21 pí~åç~êço~w`äáåáå~äj~å~öéãéåíómêéjqê~åëñìëáçå pí~åç~êçpí~íéãéåí qüéçéåáëáçåíçíê~åëñìëéáëã~çéñçääçïáåöåçåëáçéê~íáçåçñíüééçíéåíá~äêáëâë~åç ÄÉåÉÑáíëçÑI~åÇíÜÉ~äíÉêå~íáîÉëíçIíê~åëÑìëáçåKtÜÉêÉéçëëáÄäÉíÜáëáëÇáëÅìëëÉÇÄÉíïÉÉå íüéåäáåáåá~å~åçé~íáéåíeçêíüéáêäéö~äöì~êçá~åfáå~çî~ååéçñíê~åëñìëáçåk kepcáñé bëëéåíá~ä`êáíéêá~ O~KNW qüéé~íáéåíûëêéåçêçëåçåí~áåéîáçéååéíü~ííüéêé~ëçåñçêíê~åëñìëáçåçñääççççê ÄäççÇÅçãéçåÉåíëÜ~ëÄÉÉåÉñéä~áåÉÇ~åÇÇáëÅìëëÉÇïáíÜíÜÉé~íáÉåíKqÜáë áååäìçéëçáëåìëëáçåçñî~äáç~äíéêå~íáîéëíçíê~åëñìëáçå~åçíüéçéíáçåíçêéñìëék pq^qrpwnot met (insufficient evidence) Staff are made aware through educational material and the NHS Fife blood and blood components clinical procedures manual of the importance of ensuring that patients casenotes contain evidence that the reason for transfusion of blood and blood components has been discussed and includes valid alternatives to transfusion and the option to refuse. There is a patients/parents/guardian agreement form which includes a specific section to be ticked if blood transfusion is not to be undertaken. At the time of the review visit, staff assured the review team that discussions do take place, however, NHS Fife was unable to provide documented evidence to confirm compliance with this standard criterion. NHS Fife is addressing this issue through discussions regarding the development of a transfusion care pathway. O~KOW ié~ñäéíëéñéä~áåáåöíüéêáëâë~åçäéåéñáíëçñi~åç~äíéêå~íáîéëíçiíê~åëñìëáçå~êé êé~çáäó~î~áä~ääéñçêé~íáéåíëïüçã~óêéèìáêéíçäéiçêü~îéäééåíê~åëñìëéçk pq^qrpwmet NHS Fife reported that there is a high awareness of patient information leaflets among NHS Fife nursing staff. Information leaflets are available in all major blood transfusion areas. The transfusion practitioner distributes leaflets to all clinical areas. Ward staff are responsible for ensuring stock levels are monitored and supplies are requested from the transfusion practitioner. Leaflets are also available on the NHS Fife intranet. At the time of the review visit, the transfusion practitioner reported that NHS Fife plans to introduce a new style of leaflet currently under development by SNBTS, whereby transfusion information leaflets will contain a removable sticker which, once given to the patient, will be attached to the patient s notes as evidence they have received the leaflet. The review team noted that the introduction of the new leaflet would strengthen the already well-developed leaflet distribution process across NHS Fife. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu NV
22 O~KPW tüéêééêéjíê~åëñìëáçåçáëåìëëáçåáëåçíéçëëáääéeéöáå~åéãéêöéååófíüéêéáë~ ëóëíéãiåçãé~íáääéïáíüíüéé~íáéåíûëåäáåáå~äåééçëiíçáåîéëíáö~íé~åç~åíáå ~ÅÅçêÇ~åÅÉïáíÜíÜÉé~íáÉåíÛëíêÉ~íãÉåíéêÉÑÉêÉåÅÉëKqÜáëáåÅäìÇÉëÅçãéäá~åÅÉ ïáíü~å~çî~ååéçéåáëáçåççåìãéåík pq^qrpwmet In emergency situations, for example when an unconscious patient is admitted to the A&E department, staff ensure that measures are taken to try and establish the identity of a patient by checking their personal belongings and asking any accompanying relatives or friends to confirm their identity and whether they have any treatment preferences. The review team noted that NHS Fife has an operational policy non blood medical management Jehovah s Witness which states that a yellow wristband is offered to Jehovah s Witness patients as a means of alerting staff to ensure their religious beliefs are respected. The board encourages Jehovah s Witness patients to carry a signed advance directive and a copy of this is also placed in a prominent place in the medical notes. Board staff reported that NHS Fife s blood transfusion training and education materials have been adapted to include information for staff on the management of advance directives. The training material also highlights the importance of ensuring patients receive post-transfusion information in situations where a pre-transfusion discussion had not been possible. However, while the review team acknowledged the board s good practice of using yellow wristbands to alert staff to patient treatment preferences, it was further informed by board staff that in addition to yellow wristbands, a clear band with a yellow insert could also be used to identify patients of the Jehovah s Witness faith. The review team considered this practice to be potentially confusing for staff and would strongly recommend that staff follow the guidance as detailed in the board policy and use only one colour of yellow wristband. O~KQW tüéåéêéjíê~åëñìëáçåçáëåìëëáçåü~ëåçíí~âéåéä~åéiíüéêé~ëçåëñçêíê~åëñìëáçå EÄ~ëÉÇçåêáëâë~åÇÄÉåÉÑáíëF~êÉÇáëÅìëëÉÇïáíÜíÜÉé~íáÉåí~åÇïêáííÉå áåñçêã~íáçåçññéêéçêéíêçëééåíáîéäók pq^qrpwnot met (insufficient evidence) At the time of the review visit, staff reported that retrospective discussions following transfusion, and the recording of such discussions in patients notes, has been a challenge for the board. NHS Fife reported that with the introduction of a transfusion care pathway, currently under development, this will address the issue. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OM
23 pí~åç~êçoäw`äáåáå~äj~å~öéãéåíómêéjqê~åëñìëáçå pí~åç~êçpí~íéãéåí mçëáíáîéé~íáéåíáçéåíáñáå~íáçå~ííüéíáãéçñë~ãéäáåö~åçíüéìëéçñ~ãáåáãìã áçéåíáñáå~íáçåç~í~ëéíçåë~ãéäéë~åçêéèìéëíñçêãëáëéëëéåíá~äñçêéêéjíê~åëñìëáçåíéëíáåö ~åçääçççåçãéçåéåíêéèìéëíëk kepcáñé bëëéåíá~ä`êáíéêáçå OÄKNW _äçççë~ãéäéëñçêíê~åëñìëáçåéìêéçëéë~êéçäí~áåéç~åçä~äéääéçáå~ååçêç~ååé ïáíüäçå~äéêçíçåçäëiïüáåü~êéä~ëéççåå~íáçå~äöìáçéäáåéëk pq^qrpwnot met Blood samples are labelled in accordance with local protocols. However, these guidelines do not include gender as part of the minimum data set and, therefore, the review team agreed the board cannot meet this standard criterion. It was acknowledged that positive patient identification will be addressed in the new positive patient identification policy and the implementation of the proposed transfusion care pathway. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu ON
24 pí~åç~êçoåw`äáåáå~äj~å~öéãéåíómêéjqê~åëñìëáçå pí~åç~êçpí~íéãéåí _äççç~åçääçççåçãéçåéåíéêéëåêáäáåöáëíüéêéëéçåëáäáäáíóçñ~èì~äáñáéçéê~åíáíáçåéêk kepcáñé bëëéåíá~ä`êáíéêá~ OÅKNW ^ääéêéëåêáéíáçåëñçêääççç~åçääçççåçãéçåéåíë~êéëáöåéçäó~èì~äáñáéç éê~åíáíáçåéêk pq^qrpwmet The NHS Fife blood and blood components clinical procedures manual states that blood and blood components can be prescribed on a blood transfusion prescription form or an intravenous fluid prescription chart. Local policy also states all prescriptions must be signed by a medical officer. A small nursing transfusion documentation audit carried out in Victoria Hospital showed 100% compliance with this standard criterion. The review team encouraged the board to carry out a similar audit across its other sites. OÅKOW _äççç~åçääçççåçãéçåéåíéêéëåêáéíáçåëëééåáñówääçççåçãéçåéåííçäé ~ÇãáåáëíÉêÉÇXåìãÄÉêçÑìåáíëEãáääáäáíêÉëáåé~ÉÇá~íêáÅé~íáÉåíëFíçÄÉíê~åëÑìëÉÇX Çìê~íáçåçÑíê~åëÑìëáçåX~åóëéÉÅá~äêÉèìáêÉãÉåíëX~åÇ~åóëéÉÅá~äáåëíêìÅíáçåëK pq^qrpwnot met The review team acknowledged that the board had undertaken a small blood transfusion prescribing audit in January 2008 which confirmed that the blood and blood component prescriptions specified: the blood component to be administered; the number of units to be infused; the duration of transfusion; any special instructions; and special requirements. Blood components were noted to be prescribed on both the blood transfusion prescription form and the intravenous fluid prescription chart. However, staff reported that the board is considering using the intravenous fluid prescription chart solely for blood transfusion prescribing. While the review team recognised that the prescription forms used across NHS Fife did contain all essential prescribing requirements, the audit confirmed that not all prescriptions documented the duration of transfusion and, therefore, considered the board not to be fully compliant with this standard criterion. Results of the audit findings will be presented to the HTC for consideration and action. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OO
25 pí~åç~êçp~w`äáåáå~äj~å~öéãéåíóeçëéáí~äqê~åëñìëáçå i~äçê~íçêó pí~åç~êçpí~íéãéåí i~äçê~íçêóçééê~íáçåëåçãéäóïáíüåìêêéåíêéöìä~íçêóêéèìáêéãéåíëk kepcáñé bëëéåíá~ä`êáíéêá~ P~KNW ^ääíê~åëñìëáçåä~äçê~íçêáéëïáíüáåíüékepäç~êç~êé~ååêéçáíéçäó`äáåáå~ä m~íüçäçöó^ååêéçáí~íáçåerhfiíçe`m^fçêéèìáî~äéåí~åç~êéåçãéäá~åíïáíüíüé jéçáåáåéë~åçeé~äíüå~êééêççìåíëoéöìä~íçêó^öéååóejeo^fêéèìáêéãéåíëk pq^qrpwmet NHS Fife has two blood bank laboratories. Both hospital blood bank laboratories are accredited with Clinical Pathology Accreditation (UK) Ltd (CPA) and are also fully compliant with the Medicines and Healthcare products Regulatory Agency (MHRA) requirements. P~KOW `çãééíéååójä~ëéçíê~áåáåö~åç~ëëéëëãéåíëóëíéãë~êéáåéä~åé~åçíê~áåáåö êéåçêçë~êéã~áåí~áåéçk pq^qrpw Met Robust departmental training plans are in place for laboratory staff. All laboratory staff are registered with OrasGold TM online recording and assessment system. There are five computers which have been set up and are available to laboratory staff for online training. The laboratory manager, together with assistance from the quality assurance officer, is responsible for ensuring that all blood bank laboratory staff receive competencybased training and assessment in line with CPA requirements. Training records, which include competency levels, are documented and maintained by individual laboratory staff members. All qualified BMSs are registered with the Health Professions Council and are committed to continuing professional development that provides a range of learning activities which health professionals maintain and develop throughout their career to ensure that they retain their capacity to practise safely, effectively and legally within their evolving scope of practice. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OP
26 pí~åç~êçpäw`äáåáå~äj~å~öéãéåíóeçëéáí~äqê~åëñìëáçå i~äçê~íçêó pí~åç~êçpí~íéãéåí mêçåéçìêéë~êéáåéä~åéíççéíáãáëéääçççìëé~åçãáåáãáëéï~ëí~öék kepcáñé bëëéåíá~ä`êáíéêá~ PÄKNW mêçíçåçäëéåççêëéçäóíüéeq`~êéáåéä~åéiáååäìçáåöäìíåçíäáãáíéçíçwíüé ã~ñáãìãëìêöáå~äääççççêçéêáåöëåüéçìäéejp_lpfxã~ëëáîéääçççäçëëxã~àçê áååáçéåíëx~åçéãéêöéååóääçççã~å~öéãéåí~êê~åöéãéåíëk pq^qrpwmet Evidence submitted for the review visit detailed that the following protocols were in place: MSBOS; massive blood loss; major incidents; and EBMA. PÄKOW qüéêéáë~ëíçåâã~å~öéãéåíëóëíéãíçéäáãáå~íééñåéëëáåîéåíçêó~åçêéçìåé ï~ëíéiëìééçêíéçäó~åáåñçêã~íáçåíéåüåçäçöóefqfëóëíéãk pq^qrpwmet There are stock management systems in place at Victoria Hospital, Queen Margaret Hospital and Forth Park Maternity Hospital. Blood and blood component stocks are shared between both blood bank laboratories to help minimise wastage, and daily stock checks ensure the best use of blood and blood components. Protocols for the emergency issue of O RhD negative red cells are also in place and stocks of specialist blood, if unused, are rotated into normal stock for appropriate use. Throughout NHS Fife, stocks of O RhD negative blood are rotated regularly and expiry dates tracked. There is an IT system in place that supports blood stock management and provides a full audit trail of all blood stock electronically scanned onto the system. Wastage rates are discussed at HTC meetings. The review team commended NHS Fife for its robust traceability system and its traceability flow chart available in all relevant ward areas. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OQ
27 PÄKPW fååçää~äçê~íáçåïáíüåäáåáå~äëééåá~äíáéëiä~äçê~íçêóëí~ññé~êíáåáé~íéáå~ìçáíçñ íê~åëñìëáçåáëëìéëk pq^qrpwmet There was good evidence of NHS Fife s involvement in multidisciplinary local and national audit projects. Feedback on audit findings is provided to all appropriate staff groups using various methods of communication. Hospital blood bank laboratory staff assist the transfusion practitioner with clinical and self-audit activity. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OR
28 pí~åç~êçq~w`äáåáå~äj~å~öéãéåíó_äççç~åç_äççç `çãéçåéåí`çääéåíáçåi^çãáåáëíê~íáçå~åçjçåáíçêáåö pí~åç~êçpí~íéãéåí mçëáíáîéé~íáéåíáçéåíáñáå~íáçåáëééêñçêãéç~ö~áåëííüéääçççåçãéçåéåí~åç~åó ~ÅÅçãé~åóáåÖÇçÅìãÉåí~íáçå~íÉîÉêóëí~ÖÉçÑíÜÉÅäáåáÅ~äíê~åëÑìëáçåéêçÅÉëëK kepcáñé bëëéåíá~ä`êáíéêá~ Q~KNW låäóëí~ññïüçü~îéåçãéäéíéçíüé qmåçåíáåìáåöéçìå~íáçåéêçöê~ããéeçê Éèìáî~äÉåíF~ééêçéêá~íÉíçíÜÉáêêçäÉÅ~åé~êíáÅáé~íÉáåíÜÉÅäáåáÅ~äíê~åëÑìëáçå éêçåéëëk pq^qrpwnot met The review team was informed that all new staff receive appropriate BBTP Level 1 training for their role in the blood transfusion process as part of their induction. Staff are encouraged to complete blood transfusion training using the OrasGold TM online recording and assessment system, and the learn blood transfusion website ( which forms part of the theoretical competency assessment. Monthly elearning drop in sessions have been introduced by the transfusion practitioner for all staff. Newly appointed porters shadow existing porters until they are able to demonstrate competency in the collection and movement of blood. Face-to-face training sessions specific to the phlebotomist s role in the transfusion process are provided by the transfusion practitioner. BBTP Level 1 training is compulsory for all foundation year one (FY1) junior doctors as it is a requirement of the General Medical Council (GMC) registration. Staff reported that the consultant haematologist had been instrumental in blood transfusion training for senior medical staff. Figures to date show more than half of NHS Fife s consultants have completed face-to-face BBTP Level 1 training, the review team commended the board on its training figures for senior medical staff and the inclusion of blood transfusion training in senior medical staff s annual appraisal development system. However, significant challenges have been identified in the low number of staff participating in training across other staff groups. A training and education action plan has been developed to address these challenges. At present, there is no formal NHS Fife process to prohibit staff participating in the blood transfusion process if they are not trained. At the time of the review visit, staff reported that discussions for the introduction of a process which prevents untrained staff from participating in the transfusion process had taken place, and changes to the blood and blood components clinical procedure manual may be required when it is reviewed to reflect this process. NHS Fife is participating in the national BBTP pilot for the Trainers and Assessors Accreditation Programme (TAAP) and associated competency tools. NHS Fife plans içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OS
29 to implement competency assessment following the recommendations from the TAAP pilot. Q~KOW qüéãáåáãìãáçéåíáñáå~íáçåç~í~ëéíáëêéåçêçéççå~ääíê~åëñìëáçåççåìãéåí~íáçå EëÉÉëí~åÇ~êÇÅêáíÉêáçåNÅKNFK pq^qrpwnot met Board staff reported that a small nursing transfusion documentation audit carried out in January 2008 confirmed that gender was not being recorded as part of the minimum data set on all blood transfusion documentation. Discussions are in progress to develop a transfusion care pathway which will address this issue. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OT
30 pí~åç~êçqäw`äáåáå~äj~å~öéãéåíó_äççç~åç_äççç `çãéçåéåí`çääéåíáçåi^çãáåáëíê~íáçå~åçjçåáíçêáåö pí~åç~êçpí~íéãéåí m~íáéåíë~êéãçåáíçêéçñçê~åó~çîéêëééîéåíëçêêé~åíáçåëçìêáåö~åç~ñíéêíüé íê~åëñìëáçåéêçåéëë~ëåäáåáå~ääóáåçáå~íéçk kepcáñé bëëéåíá~ä`êáíéêá~ QÄKNW m~íáéåíë~êéãçåáíçêéç~ååçêçáåöíçüçëéáí~äíê~åëñìëáçåéçäáåó~åç~åóìåíçï~êç ÉîÉåíëEáåÅäìÇáåÖëìëéÉÅíÉÇ~ÇîÉêëÉêÉ~ÅíáçåëF~êÉáããÉÇá~íÉäóÅäáåáÅ~ääó ã~å~öéç~åçéêçãéíäóêééçêíéçíçíüéeqik pq^qrpwnot met Staff reported that patients receiving a blood transfusion have their pulse, temperature and blood pressure recorded prior to transfusion. The patient s temperature and pulse would be recorded 15 and then 30 minutes after the start of each unit of blood component, and thereafter, pulse, temperature and blood pressure would be recorded hourly until the end of the transfusion as detailed in local protocols. Any signs of transfusion reactions are reported immediately and managed in accordance with local guidelines. However, a small nursing transfusion documentation audit carried out in January 2008 concluded that there was a lack of consistency where observations were being recorded and the timings of the observations. NHS Fife is considering introducing a blood transfusion care pathway to address these issues. Recording patient observations will also be addressed at staff training sessions. The review team encouraged the board to progress with the introduction of a transfusion care pathway which would provide staff with an adequate documentation system for recording individual transfusion episodes, and also ensure that staff involved in the blood transfusion process receive appropriate training. QÄKOW péêáçìë~çîéêëééîéåíë~åçåé~êãáëëáååáçéåíë~êéêééçêíéççåíüéåäáåáå~ä áååáçéåíêééçêíáåöëóëíéãáå~ååçêç~ååéïáíüäçå~äéêçíçåçäëk pq^qrpwmet Adverse clinical events and near miss incidents are recorded on the DATIX adverse incident management system. The system ensures that appropriate follow-up action is taken using root cause analysis methodology. Investigations are carried out by laboratory staff, medical staff, nursing staff and the transfusion practitioner. Incidents are discussed at monthly haematology and blood transfusion quality assurance meetings and laboratory committee meetings, and information is fed back içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OU
31 to the HTC. The review team commended NHS Fife for its robust incident reporting framework. QÄKPW oééçêíëçñëéêáçìë~çîéêëééîéåíëçêêé~åíáçåë~åçåé~êãáëëáååáçéåíë~êé ëìäãáííéçíçpéêáçìë^çîéêëé_äçççoé~åíáçåë~åçbîéåíëep^_obf~åçíüépéêáçìë e~ò~êçëçñqê~åëñìëáçåepelqfáåáíá~íáîéäóíüéêéäéî~åíëí~ññk pq^qrpwmet There are designated individuals in both blood bank laboratories who are responsible for reporting serious adverse events or reactions and near miss incidents to SABRE and the SHOT initiative. içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu OV
32 içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu PM ^éééåçáñnódäçëë~êóçñ~ääêéîá~íáçåë ^ÄÄêÉîá~íáçå ^Cb ~ÅÅáÇÉåí~åÇÉãÉêÖÉåÅó qm _ÉííÉê_äççÇqê~åëÑìëáçåmêçÖê~ããÉ _`pe _êáíáëü`çããáííééñçêpí~åç~êçëáåe~éã~íçäçöó _jp ÄáçãÉÇáÅ~äëÅáÉåíáëí `ef `çããìåáíóeé~äíüfåçéñ `m^ `äáåáå~äm~íüçäçöó^ååêéçáí~íáçåerhfiíç b_j^ ÉãÉêÖÉåÅóÄäççÇã~å~ÖÉãÉåí~êê~åÖÉãÉåíë cvn ÑçìåÇ~íáçåóÉ~êçåÉ dj` déåéê~äjéçáå~ä`çìååáä eq` Üçëéáí~äíê~åëÑìëáçåÅçããáííÉÉ eqi Üçëéáí~äíê~åëÑìëáçåä~Äçê~íçêó eqq Üçëéáí~äíê~åëÑìëáçåíÉ~ã fq áåñçêã~íáçåíéåüåçäçöó jeo^ jéçáåáåéë~åçeé~äíüå~êééêççìåíëoéöìä~íçêó^öéååó jp_lp ã~ñáãìãëìêöáå~äääççççêçéêáåöëåüéçìäé kepnfp kepnì~äáíófãéêçîéãéåípåçíä~åç p^_ob péêáçìë^çîéêëé_äçççoé~åíáçåë~åçbîéåíë pelq péêáçìëe~ò~êçëçñqê~åëñìëáçå pk_qp påçííáëük~íáçå~ä_äçççqê~åëñìëáçåpéêîáåé plm ëí~åç~êççééê~íáåöéêçåéçìêé q^^m qê~áåéêë~åç^ëëéëëçêë^ååêéçáí~íáçåmêçöê~ããé
33 ^éééåçáñoóoéîáéïéêçåéëë içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu PN
NHS Grampian. Local Report ~ March Blood Transfusion
 NHS Grampian Local Report ~ March 2008 Blood Transfusion kepdê~ãéá~å içå~äoééçêíúj~êåüommu _äçççqê~åëñìëáçå içå~äoééçêíekepdê~ãéá~åfw_äçççqê~åëñìëáçåój~êåüommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
NHS Grampian Local Report ~ March 2008 Blood Transfusion kepdê~ãéá~å içå~äoééçêíúj~êåüommu _äçççqê~åëñìëáçå içå~äoééçêíekepdê~ãéá~åfw_äçççqê~åëñìëáçåój~êåüommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
NHS Forth Valley. Local Report ~ May Blood Transfusion
 NHS Forth Valley Local Report ~ May 2008 Blood Transfusion kepcçêíüs~ääéó içå~äoééçêíúj~óommu _äçççqê~åëñìëáçå içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
NHS Forth Valley Local Report ~ May 2008 Blood Transfusion kepcçêíüs~ääéó içå~äoééçêíúj~óommu _äçççqê~åëñìëáçå içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
Blood Transfusion Policy. Version Number: 6.1 Controlled Document Sponsor: Controlled Document Lead: On: December 2014.
 Blood Transfusion Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Clinical The policy describes the framework and principles required to deliver best transfusion
Blood Transfusion Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Clinical The policy describes the framework and principles required to deliver best transfusion
JOB DESCRIPTION. Specialist Practitioner of Transfusion for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:-
 JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
NHS Ayrshire & Arran. Local Report ~ July Healthcare Services for People with Learning Disabilities
 NHS Ayrshire & Arran Local Report ~ July 2009 Healthcare Services for People with Learning Disabilities kep^óêëüáêéc^êê~å içå~äoééçêíúgìäóommv eé~äíüå~êépéêîáåéëñçêméçéäé ïáíüié~êåáåöaáë~äáäáíáéë içå~äoééçêíekep^óêëüáêéc^êê~åfweé~äíüå~êépéêîáåéëñçêméçéäéïáíüié~êåáåöaáë~äáäáíáéëógìäóommv
NHS Ayrshire & Arran Local Report ~ July 2009 Healthcare Services for People with Learning Disabilities kep^óêëüáêéc^êê~å içå~äoééçêíúgìäóommv eé~äíüå~êépéêîáåéëñçêméçéäé ïáíüié~êåáåöaáë~äáäáíáéë içå~äoééçêíekep^óêëüáêéc^êê~åfweé~äíüå~êépéêîáåéëñçêméçéäéïáíüié~êåáåöaáë~äáäáíáéëógìäóommv
Trust Policy for Blood Transfusion
 Trust Policy for Blood Transfusion Approval and Authorisation Reviewed by Job Title Date Simon Middleton Chair of Hospital Transfusion Committee 03.09.2010 Rebecca Sampson Consultant Haematologist 01.09.2010
Trust Policy for Blood Transfusion Approval and Authorisation Reviewed by Job Title Date Simon Middleton Chair of Hospital Transfusion Committee 03.09.2010 Rebecca Sampson Consultant Haematologist 01.09.2010
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
REPORT OF BLOOD SAFETY REVIEW
 REPORT OF BLOOD SAFETY REVIEW 11 th February 2010 Table of Contents Acknowledgements 2 The Review Team 3 1 Context for Review 4-5 2 Background 6 3 HSS Circular MD 6/03: Better Blood Transfusion 7-8 4 National
REPORT OF BLOOD SAFETY REVIEW 11 th February 2010 Table of Contents Acknowledgements 2 The Review Team 3 1 Context for Review 4-5 2 Background 6 3 HSS Circular MD 6/03: Better Blood Transfusion 7-8 4 National
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
NHS Borders. Local Report ~ November Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services
 NHS Borders Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services NHS Borders Local Report ~ November 2009 Clinical Governance
NHS Borders Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services NHS Borders Local Report ~ November 2009 Clinical Governance
Clinical Standards ~ September Blood Transfusion
 Clinical Standards ~ September 2006 Blood Transfusion NHS Quality Improvement Scotland 2006 ISBN 1-84404-427-0 First published September 2006 You can copy or reproduce the information in this document
Clinical Standards ~ September 2006 Blood Transfusion NHS Quality Improvement Scotland 2006 ISBN 1-84404-427-0 First published September 2006 You can copy or reproduce the information in this document
Policy for the authorising of blood components by the Haematology Clinical Nurse Specialist V1.0
 Policy for the authorising of blood components by the Haematology Clinical Nurse Specialist V1.0 January 2016 Summary. This policy applies only to selected staff within the Haematology Department at the
Policy for the authorising of blood components by the Haematology Clinical Nurse Specialist V1.0 January 2016 Summary. This policy applies only to selected staff within the Haematology Department at the
Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear guidance on the use of irradiated blood products.
 Document Title: Document Purpose: Document Statement: Document Application: Responsible for Implementation: Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear
Document Title: Document Purpose: Document Statement: Document Application: Responsible for Implementation: Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear
Royal Wolverhampton Hospitals NHS Trust. Job Description Haematology
 Royal Wolverhampton Hospitals NHS Trust Job Description Haematology Job Title: Grade: A4C Band 3 (Point 7) Directorate: Pathology Department: Haematology Reports to: BMS staff and section senior Professionally
Royal Wolverhampton Hospitals NHS Trust Job Description Haematology Job Title: Grade: A4C Band 3 (Point 7) Directorate: Pathology Department: Haematology Reports to: BMS staff and section senior Professionally
Policy Summary. Policy Title: Policy and Procedure for Clinical Coding
 Policy Title: Policy and Procedure for Clinical Coding Reference and Version No: IG7 Version 6 Author and Job Title: Caroline Griffin Clinical Coding Manager Executive Lead - Chief Information and Technology
Policy Title: Policy and Procedure for Clinical Coding Reference and Version No: IG7 Version 6 Author and Job Title: Caroline Griffin Clinical Coding Manager Executive Lead - Chief Information and Technology
Intensive Psychiatric Care Units
 NHS Lothian Royal Edinburgh Hospital Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
NHS Lothian Royal Edinburgh Hospital Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Implementation Policy for NICE Guidelines
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Implementation Policy for NICE Guidelines Version No.: 5.3 Effective From: 08 May 2017 Expiry Date: 02 March 2019 Date Ratified: 23 February 2017
The Newcastle upon Tyne Hospitals NHS Foundation Trust Implementation Policy for NICE Guidelines Version No.: 5.3 Effective From: 08 May 2017 Expiry Date: 02 March 2019 Date Ratified: 23 February 2017
Diagnostic Testing Procedures in Urodynamics V3.0
 V3.0 09 01 18 Table of Contents Summary.... 1. Introduction... 3 1.1. Diagnostic testing information... 3 2. Purpose of this Policy/Procedure... 3 2.1. Approved Document Process... 3 3. Scope... 3 3.1.
V3.0 09 01 18 Table of Contents Summary.... 1. Introduction... 3 1.1. Diagnostic testing information... 3 2. Purpose of this Policy/Procedure... 3 2.1. Approved Document Process... 3 3. Scope... 3 3.1.
A Guide To Safe Blood Transfusion Practice
 A Guide To Safe Blood Transfusion Practice Introduction To Blood Transfusion Safety Marie Browett, Pavlina Sharp, Fiona Waller, Hafiz Qureshi, Malcolm Chambers (on behalf of the UHL Blood Transfusion Team)
A Guide To Safe Blood Transfusion Practice Introduction To Blood Transfusion Safety Marie Browett, Pavlina Sharp, Fiona Waller, Hafiz Qureshi, Malcolm Chambers (on behalf of the UHL Blood Transfusion Team)
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services
 Scottish Ambulance Service Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services Scottish Ambulance Service Local Report ~ November
Scottish Ambulance Service Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services Scottish Ambulance Service Local Report ~ November
Intensive Psychiatric Care Units
 NHS Tayside Carseview Centre, Dundee Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
NHS Tayside Carseview Centre, Dundee Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
Competency Framework for the Administration of all Blood Products
 Framework for the Administration of all Blood Products Ref No. Authors Others Consulted during preparation Date Created December 2006 Date reviewed March 2007 Date approved Implementation date April 2007
Framework for the Administration of all Blood Products Ref No. Authors Others Consulted during preparation Date Created December 2006 Date reviewed March 2007 Date approved Implementation date April 2007
Grampian University Hospitals NHS Trust. Local Report ~ February Older People in Acute Care
 Grampian University Hospitals NHS Trust Local Report ~ February 2004 Older People in Acute Care NHSScotland Board Areas 13 12 15 1 Argyll & Clyde 2 Ayrshire & Arran 3 Borders 9 7 4 Dumfries & Galloway
Grampian University Hospitals NHS Trust Local Report ~ February 2004 Older People in Acute Care NHSScotland Board Areas 13 12 15 1 Argyll & Clyde 2 Ayrshire & Arran 3 Borders 9 7 4 Dumfries & Galloway
Longer Term Impact of NHS QIS Peer Review Visits: Continuous Quality Improvement of Blood Transfusion Services in NHS Boards
 Longer Term Impact of NHS QIS Peer Review Visits: Continuous Quality Improvement of Blood Transfusion Services in NHS Boards Dr Steve Cross Human Reliability Dr Guro Huby University of Edinburgh Commissioned
Longer Term Impact of NHS QIS Peer Review Visits: Continuous Quality Improvement of Blood Transfusion Services in NHS Boards Dr Steve Cross Human Reliability Dr Guro Huby University of Edinburgh Commissioned
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Administration of Intrathecal Cytotoxic Chemotherapy in NHS Grampian
 Administration of Intrathecal Cytotoxic Chemotherapy in NHS Grampian Lead Author/Coordinator: Jeff Horn / Sarah Howlett Macmillan Haematology CNS/ Pharmacist Reviewer: Gavin Preston Consultant Haematologist
Administration of Intrathecal Cytotoxic Chemotherapy in NHS Grampian Lead Author/Coordinator: Jeff Horn / Sarah Howlett Macmillan Haematology CNS/ Pharmacist Reviewer: Gavin Preston Consultant Haematologist
Better Blood Transfusion & anti-d Immunoglobulin
 Better Blood Transfusion & anti-d Immunoglobulin - an analysis of adverse events reports from the Serious Hazards of Transfusion scheme Tony Davies - Transfusion Liaison Practitioner SHOT / NHSBT The Royal
Better Blood Transfusion & anti-d Immunoglobulin - an analysis of adverse events reports from the Serious Hazards of Transfusion scheme Tony Davies - Transfusion Liaison Practitioner SHOT / NHSBT The Royal
SUBJECT: CLINICAL GOVERNANCE
 Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Administration of blood components. Denise Watson Patient Blood Management Practitioner 11th January, 2016
 Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Policy for Patient Identification. Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead:
 CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
Patient Identification
 Patient Identification Reference No: Version: 5 Ratified by: P_CS_24 LCHS Trust Board Date ratified: 10 th April 2018 Name of originator/author: Name of approving committee/responsible individual: Date
Patient Identification Reference No: Version: 5 Ratified by: P_CS_24 LCHS Trust Board Date ratified: 10 th April 2018 Name of originator/author: Name of approving committee/responsible individual: Date
HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES:
 HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES: A Review of the arrangements in place across the Welsh National Health Service ACTION PLAN - UPDATED August 2010 RECOMMENDATION
HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES: A Review of the arrangements in place across the Welsh National Health Service ACTION PLAN - UPDATED August 2010 RECOMMENDATION
POLICY FOR THE TRANSFUSION OF BLOOD AND BLOOD COMPONENTS
 POLICY FOR THE TRANSFUSION OF BLOOD AND BLOOD COMPONENTS Document Author Written By: Transfusion Practitioner / Transfusion Laboratory Manager Authorised Authorised By: Chief Executive Date: July 2015
POLICY FOR THE TRANSFUSION OF BLOOD AND BLOOD COMPONENTS Document Author Written By: Transfusion Practitioner / Transfusion Laboratory Manager Authorised Authorised By: Chief Executive Date: July 2015
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE
 POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
NHSLA Risk Management Standards
 NHSLA Risk Management Standards 2012-13 for NHS Trusts providing Acute Services Brighton and Sussex University Hospitals NHS Trust Level 1 October 2012 Contents Executive Summary... 3 Assessment Outcome...
NHSLA Risk Management Standards 2012-13 for NHS Trusts providing Acute Services Brighton and Sussex University Hospitals NHS Trust Level 1 October 2012 Contents Executive Summary... 3 Assessment Outcome...
BLOOD STOCKS MANAGEMENT SCHEME. -- Inventory Practice Survey
 BLOOD STOCKS MANAGEMENT SCHEME -- Inventory Practice Survey 2002 -- Headline Summary Information extracted from the BSMS website is distributed and made available to a wide range of hospital personnel.
BLOOD STOCKS MANAGEMENT SCHEME -- Inventory Practice Survey 2002 -- Headline Summary Information extracted from the BSMS website is distributed and made available to a wide range of hospital personnel.
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Introduction and Development of New Clinical Interventional Procedures
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Introduction and Development of New Clinical Interventional Procedures Version No.: 2.1 Effective From: 27 November 2017 Expiry Date: 7 January 2019
The Newcastle upon Tyne Hospitals NHS Foundation Trust Introduction and Development of New Clinical Interventional Procedures Version No.: 2.1 Effective From: 27 November 2017 Expiry Date: 7 January 2019
NPSA Alert 03: Reducing the harm caused by oral Methotrexate. Implementation Progress Report July Learning and Sharing
 NPSA Alert 03: Reducing the harm caused by oral Methotrexate Implementation Progress Report July 2006 Learning and Sharing CONTENTS Page 1 Background 3 2 Findings 4 Appendix 1 Summary of responses 6 Appendix
NPSA Alert 03: Reducing the harm caused by oral Methotrexate Implementation Progress Report July 2006 Learning and Sharing CONTENTS Page 1 Background 3 2 Findings 4 Appendix 1 Summary of responses 6 Appendix
Non Medical Prescribing Policy
 Non Medical Prescribing Policy Author: Sponsor/Executive: Responsible committee: Ratified by: Consultation & Approval: (Committee/Groups which signed off the policy, including date) This document replaces:
Non Medical Prescribing Policy Author: Sponsor/Executive: Responsible committee: Ratified by: Consultation & Approval: (Committee/Groups which signed off the policy, including date) This document replaces:
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Systemic Anti-Cancer Therapy Delivery. June 2017 National External Review
 Systemic Anti-Cancer Therapy Delivery June 2017 National External Review Healthcare Improvement Scotland is committed to equality. We have assessed the review process for likely impact on equality protected
Systemic Anti-Cancer Therapy Delivery June 2017 National External Review Healthcare Improvement Scotland is committed to equality. We have assessed the review process for likely impact on equality protected
Job Description. TDL Laboratory Staff, Clients and Customers, Group Blood Transfusion Manager
 Job Description Job Title: Location: Reporting to: Accountable to: Liaises with: Senior Biomedical Scientist (Blood Transfusion) BMI London Independent Pathology Lead Group Laboratory Director Regional
Job Description Job Title: Location: Reporting to: Accountable to: Liaises with: Senior Biomedical Scientist (Blood Transfusion) BMI London Independent Pathology Lead Group Laboratory Director Regional
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
Unannounced Inspection Report. Aberdeen Maternity Hospital NHS Grampian. 9 October 2013
 Unannounced Inspection Report Aberdeen Maternity Hospital NHS Grampian 9 October 2013 The Healthcare Environment Inspectorate is a part of Healthcare Improvement Scotland Healthcare Improvement Scotland
Unannounced Inspection Report Aberdeen Maternity Hospital NHS Grampian 9 October 2013 The Healthcare Environment Inspectorate is a part of Healthcare Improvement Scotland Healthcare Improvement Scotland
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY
 DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
PROCEDURE FOR TAKING AND LABELLING A TRANSFUSION SAMPLE AND COMPLETING THE REQUEST FORM
 Mid-West Area Hospitals Page 1 of 5 Edition No.: 01 PROCEDURE FOR TAKING AND LABELLING A TRANSFUSION SAMPLE AND COMPLETING THE REQUEST FORM EDITION No 01 EFFECTIVE DATE 5 th February 2013 REVIEW INTERVAL
Mid-West Area Hospitals Page 1 of 5 Edition No.: 01 PROCEDURE FOR TAKING AND LABELLING A TRANSFUSION SAMPLE AND COMPLETING THE REQUEST FORM EDITION No 01 EFFECTIVE DATE 5 th February 2013 REVIEW INTERVAL
NHS Tayside. Local Report ~ May Out-of-Hours Emergency Dental Services
 NHS Tayside Local Report ~ May 2009 Out-of-Hours Emergency Dental Services NHS Tayside Local Report ~ May 2009 Out-of-Hours Emergency Dental Services NHS Quality Improvement Scotland (NHS QIS) is committed
NHS Tayside Local Report ~ May 2009 Out-of-Hours Emergency Dental Services NHS Tayside Local Report ~ May 2009 Out-of-Hours Emergency Dental Services NHS Quality Improvement Scotland (NHS QIS) is committed
Diagnostic Test Reporting & Acknowledgement Procedures. - Pathology & Clinical Imaging
 Diagnostic Test Reporting & Acknowledgement Procedures V2.0 November 2014 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5.
Diagnostic Test Reporting & Acknowledgement Procedures V2.0 November 2014 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5.
Management of Diagnostic Testing and Screening Procedures Policy
 Trust Policy Management of Diagnostic Testing and Screening Procedures Policy Purpose Date Version July 2012 2 The purpose of this policy is to ensure that all diagnostic and screening tests undertaken
Trust Policy Management of Diagnostic Testing and Screening Procedures Policy Purpose Date Version July 2012 2 The purpose of this policy is to ensure that all diagnostic and screening tests undertaken
Safety Reporting in Clinical Research Policy Final Version 4.0
 Safety Reporting in Clinical Research Policy Final Version 4.0 Category: Summary: Equality Assessment undertaken: Impact Policy The Medicines for Human Use (Clinical Trials) Regulations 2004 and subsequent
Safety Reporting in Clinical Research Policy Final Version 4.0 Category: Summary: Equality Assessment undertaken: Impact Policy The Medicines for Human Use (Clinical Trials) Regulations 2004 and subsequent
European network of paediatric research (EnprEMA)
") 17 February 2012 EMA/77450/2012 Human Medicines Development and Evaluation Recognition criteria for self assessment The European Medicines Agency is tasked with developing a European paediatric network
17 February 2012 EMA/77450/2012 Human Medicines Development and Evaluation Recognition criteria for self assessment The European Medicines Agency is tasked with developing a European paediatric network
GPs apply for inclusion in the NI PMPL and applications are reviewed against criteria specified in regulation.
 Policy for the Removal of Doctors from the NI Primary Medical Performers List (NIPMPL) where they have not provided primary medical services in the HSCB area in the Preceding 24 Months Context GPs cannot
Policy for the Removal of Doctors from the NI Primary Medical Performers List (NIPMPL) where they have not provided primary medical services in the HSCB area in the Preceding 24 Months Context GPs cannot
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Diagnostic Testing Procedures in Neurophysiology V1.0
 V1.0 10 September 2012 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the
V1.0 10 September 2012 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the
The Newcastle Upon Tyne Hospitals NHS Foundation Trust. Strategy for Non-Medical Prescribing
 The Newcastle Upon Tyne Hospitals NHS Foundation Trust Strategy for Non-Medical Prescribing Version No: 2.2 Effective From: 19 October 2016 Expiry Date: 19 October 2019 Date Ratified: 12 October 2016 Ratified
The Newcastle Upon Tyne Hospitals NHS Foundation Trust Strategy for Non-Medical Prescribing Version No: 2.2 Effective From: 19 October 2016 Expiry Date: 19 October 2019 Date Ratified: 12 October 2016 Ratified
NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report. Results for July Dec 2016
 NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report Results for July Dec 2016 March 2017 National Catering and Nutritional Services Specification: Half Yearly
NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report Results for July Dec 2016 March 2017 National Catering and Nutritional Services Specification: Half Yearly
Safe Blood Transfusion
 Safe Blood Transfusion Cardiff & Vale uhb & Welsh Blood Service Education Sub-group Objectives Complex pathway Overview ~ pre-transfusion blood sampling ~ collection from blood bank fridge ~ administration
Safe Blood Transfusion Cardiff & Vale uhb & Welsh Blood Service Education Sub-group Objectives Complex pathway Overview ~ pre-transfusion blood sampling ~ collection from blood bank fridge ~ administration
CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS
 CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS RATIONALE All Professionals/healthcare workers are personally accountable for their practice and, in the exercise of their professional accountability,
CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS RATIONALE All Professionals/healthcare workers are personally accountable for their practice and, in the exercise of their professional accountability,
Diagnostic Testing Procedures for Ophthalmic Science
 V4.0 01/08/17 Table of Contents 1. Introduction... 3 2. Purpose of this Policy... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the Managers... 3 5.3.
V4.0 01/08/17 Table of Contents 1. Introduction... 3 2. Purpose of this Policy... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 3 5.2. Role of the Managers... 3 5.3.
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
Title Controlled Storage of Blood and Blood Products Standard Operating Procedure
 Document Control Title Controlled Storage of Blood and Blood Products Standard Operating Procedure Author Transfusion Laboratory Manager Author s job title Transfusion Laboratory Manager Directorate Clinical
Document Control Title Controlled Storage of Blood and Blood Products Standard Operating Procedure Author Transfusion Laboratory Manager Author s job title Transfusion Laboratory Manager Directorate Clinical
MID CHESHIRE HOSPITALS NHS FOUNDATION TRUST WOMEN S AND CHILDREN S DIVISION JOB DESCRIPTION
 MID CHESHIRE HOSPITALS NHS FOUNDATION TRUST WOMEN S AND CHILDREN S DIVISION JOB DESCRIPTION Post: Responsible to: Accountable to: Base: LAS ST3+ Doctor (Fixed Term) in Obstetrics & Gynaecology (x 2.4 WTE)
MID CHESHIRE HOSPITALS NHS FOUNDATION TRUST WOMEN S AND CHILDREN S DIVISION JOB DESCRIPTION Post: Responsible to: Accountable to: Base: LAS ST3+ Doctor (Fixed Term) in Obstetrics & Gynaecology (x 2.4 WTE)
NHS Borders. Intensive Psychiatric Care Units
 NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Agenda Item: REPORT TO PUBLIC BOARD MEETING 31 May 2012
 Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
HYWEL DDA LOCAL HEALTH BOARD. Transfusion Policy. Completed Action: Addresses all aspects of transfusion with blood and blood components
 Policy Number: 278 Supersedes: Standards For Healthcare Services No/s Version No: 1 Date Of Review: Reviewer Name: Completed Action: Approved by: Date Approved: New Review Date: Brief Summary of Document:
Policy Number: 278 Supersedes: Standards For Healthcare Services No/s Version No: 1 Date Of Review: Reviewer Name: Completed Action: Approved by: Date Approved: New Review Date: Brief Summary of Document:
Blood / Blood Products Transfusion A Liquid Transplant
 Blood / Blood Products Transfusion A Liquid Transplant Caroline Holt Specialist Practitioner of Transfusion caroline.holt@tgh.nhs.uk Tel : 922 5484 Mob: 07759260044 The Transfusion Team Gillian Lewis Blood
Blood / Blood Products Transfusion A Liquid Transplant Caroline Holt Specialist Practitioner of Transfusion caroline.holt@tgh.nhs.uk Tel : 922 5484 Mob: 07759260044 The Transfusion Team Gillian Lewis Blood
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
LOCAL SUPERVISING AUTHORITY ANNUAL REPORT
 LOCAL SUPERVISING AUTHORITY ANNUAL REPORT 2006 Table of Contents 1.0 PURPOSE OF REPORT...1 2.0 ORGANISATION OF SUPERVISION OF MIDWIVES...1 2.1 Appointment of Supervisor of Midwives...1 2.2 Resignation/De-Selection
LOCAL SUPERVISING AUTHORITY ANNUAL REPORT 2006 Table of Contents 1.0 PURPOSE OF REPORT...1 2.0 ORGANISATION OF SUPERVISION OF MIDWIVES...1 2.1 Appointment of Supervisor of Midwives...1 2.2 Resignation/De-Selection
Changes in practice and organisation surrounding blood transfusion in NHS trusts in England
 See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
Promoting Effective Immunisation Practice
 4th Edition 2017 Contents Introduction 3 Who is the programme for? 3 Learning Outcomes 4 Notes for employers 4 Updating 5 Notes for students 6 What are the options for learning? 6 Brief overview of the
4th Edition 2017 Contents Introduction 3 Who is the programme for? 3 Learning Outcomes 4 Notes for employers 4 Updating 5 Notes for students 6 What are the options for learning? 6 Brief overview of the
CAUTION: Refer to the Document Library for the most recent version of this policy. Blood Transfusion Policy. Pathology Transfusion.
 Directorate Department Year Version Number Central Index Number Endorsing Committee Date Endorsed Approval Committee Date Approved Author Name and Job Title Key Words (for search purposes) Date Published
Directorate Department Year Version Number Central Index Number Endorsing Committee Date Endorsed Approval Committee Date Approved Author Name and Job Title Key Words (for search purposes) Date Published
Improving compliance with oral methotrexate guidelines. Action for the NHS
 Patient safety alert 13 Alert Immediate action Action Update Information request Ref: NPSA/2006/13 Improving compliance with oral methotrexate guidelines Oral methotrexate is a safe and effective medication
Patient safety alert 13 Alert Immediate action Action Update Information request Ref: NPSA/2006/13 Improving compliance with oral methotrexate guidelines Oral methotrexate is a safe and effective medication
UK TRANSFUSION LABORATORY COLLABORATIVE
 UK TRANSFUSION LABORATORY COLLABORATIVE 2017 survey indicates that staff shortages are not being addressed Authors: Hema Mistry, Rashmi Rook and Paula HB Bolton-Maggs No Disclosures Introduction UK transfusion
UK TRANSFUSION LABORATORY COLLABORATIVE 2017 survey indicates that staff shortages are not being addressed Authors: Hema Mistry, Rashmi Rook and Paula HB Bolton-Maggs No Disclosures Introduction UK transfusion
Plymouth Community Healthcare CIC. Observation Policy ( Mental Health Wards and Plymbridge ) Version 2.3
 Version 2.3") Plymouth Community Healthcare CIC Observation Policy ( Mental Health Wards and Plymbridge ) Version 2.3 Notice to staff using a paper copy of this guidance The policies and procedures page of Healthnet
Plymouth Community Healthcare CIC Observation Policy ( Mental Health Wards and Plymbridge ) Version 2.3 Notice to staff using a paper copy of this guidance The policies and procedures page of Healthnet
Quality Improvement Programme: Safe and Effective Transfusion in Scottish Hospitals The Role of the Transfusion Nurse Specialist (SAET Study)
") Quality Improvement Programme: Safe and Effective Transfusion in Scottish Hospitals The Role of the Transfusion Nurse Specialist (SAET Study) SUMMARY REPORT CEPS Project Number: 99/16 Grant-holder: Professor
Quality Improvement Programme: Safe and Effective Transfusion in Scottish Hospitals The Role of the Transfusion Nurse Specialist (SAET Study) SUMMARY REPORT CEPS Project Number: 99/16 Grant-holder: Professor
This controlled document shall not be copied in part or whole without the express permission of the author or the author s representative.
 This document is also available in large print and other formats and languages, upon request. Please call NHS Grampian Corporate Communications on (01224) 551116 or (01224) 552245. This controlled document
This document is also available in large print and other formats and languages, upon request. Please call NHS Grampian Corporate Communications on (01224) 551116 or (01224) 552245. This controlled document
HAEMOVIGILANCE. Ms. Emma O Riordan Haemovigilance, CNM2 (Acting) Ms. Bríd Doyle, MSc. FAMLS. Haemovigilance Co-ordinator, (Acting)
 Ms. Bríd Doyle, MSc. FAMLS. Haemovigilance Co-ordinator, (Acting)") HAEMOVIGILANCE a set of surveillance procedures covering the whole transfusion chain from the collection of blood and its components to the follow-up of its recipients, intended to collect and assess information
HAEMOVIGILANCE a set of surveillance procedures covering the whole transfusion chain from the collection of blood and its components to the follow-up of its recipients, intended to collect and assess information
NHS Lothian. Local Report ~ June Out-of-Hours Emergency Dental Services
 NHS Lothian Local Report ~ June 2009 Out-of-Hours Emergency Dental Services NHS Lothian Local Report ~ June 2009 Out-of-Hours Emergency Dental Services NHS Quality Improvement Scotland (NHS QIS) is committed
NHS Lothian Local Report ~ June 2009 Out-of-Hours Emergency Dental Services NHS Lothian Local Report ~ June 2009 Out-of-Hours Emergency Dental Services NHS Quality Improvement Scotland (NHS QIS) is committed
SOUTH CENTRAL NEONATAL NETWORK
 SOUTH CENTRAL NEONATAL NETWORK Audit of the current provision of education and training within the Neonatal South Central Network 1.0 Background The driving principles for the reform of the NHS education
SOUTH CENTRAL NEONATAL NETWORK Audit of the current provision of education and training within the Neonatal South Central Network 1.0 Background The driving principles for the reform of the NHS education
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
NHS SHETLAND CLINICAL GOVERNANCE STRATEGY
 NHS SHETLAND CLINICAL GOVERNANCE STRATEGY 2010-13 Clinical governance is the defining heart and inspiration of quality in the NHS Aidan Halligan 2006 Last version date: March 2007 Next Formal Review January
NHS SHETLAND CLINICAL GOVERNANCE STRATEGY 2010-13 Clinical governance is the defining heart and inspiration of quality in the NHS Aidan Halligan 2006 Last version date: March 2007 Next Formal Review January
Inspection Report. Royal Infirmary of Edinburgh. NHS Lothian 18 and 19 January February 2010
 Inspection Report Royal Infirmary of Edinburgh NHS Lothian 18 and 19 January 2010 2 February 2010 qüé=eé~äíüå~êé=båîáêçåãéåí=fåëééåíçê~íé=áë=~=é~êí=çñ=kep=nì~äáíó=fãéêçîéãéåí=påçíä~åç= The Healthcare Environment
Inspection Report Royal Infirmary of Edinburgh NHS Lothian 18 and 19 January 2010 2 February 2010 qüé=eé~äíüå~êé=båîáêçåãéåí=fåëééåíçê~íé=áë=~=é~êí=çñ=kep=nì~äáíó=fãéêçîéãéåí=påçíä~åç= The Healthcare Environment
Qualitative baseline evaluation of the GP Community Hub Fellowship pilot in NHS Fife and NHS Forth Valley Briefing paper
 Qualitative baseline evaluation of the GP Community Hub Fellowship pilot in NHS Fife and NHS Forth Valley Briefing paper This resource may also be made available on request in the following formats: 0131
Qualitative baseline evaluation of the GP Community Hub Fellowship pilot in NHS Fife and NHS Forth Valley Briefing paper This resource may also be made available on request in the following formats: 0131
ADVANCED NURSE PRACTITIONER STRATEGY
 ADVANCED NURSE PRACTITIONER STRATEGY 2016-2020 Lead Manager: Chair, GG&C Advanced Practice Group Responsible Director: Board Nurse Director Approved by: NMAHP Group Date approved Date for review: September
ADVANCED NURSE PRACTITIONER STRATEGY 2016-2020 Lead Manager: Chair, GG&C Advanced Practice Group Responsible Director: Board Nurse Director Approved by: NMAHP Group Date approved Date for review: September
2015 Survey of Patient Blood Management (PBM)
") 2015 Survey of Patient Blood Management (PBM) This is the second national Patient Blood Management (PBM) survey. In 2013 you were invited to participate in the first PBM survey which provided valuable
2015 Survey of Patient Blood Management (PBM) This is the second national Patient Blood Management (PBM) survey. In 2013 you were invited to participate in the first PBM survey which provided valuable
Intra-operative Cell Salvage. Competency Assessment Workbook. Trainee: Hospital: Trainer/Supervisor: Date Commenced: Date Completed:
 Intra-operative Cell Salvage Competency Assessment Workbook Trainee: Hospital: Trainer/Supervisor: Commenced: Completed: Contents Introduction 1-2 Record of Assessors 4 Confirmation of Required Pre-assessment
Intra-operative Cell Salvage Competency Assessment Workbook Trainee: Hospital: Trainer/Supervisor: Commenced: Completed: Contents Introduction 1-2 Record of Assessors 4 Confirmation of Required Pre-assessment
Blood Products Policy
 Blood Products Policy Originator: Corinne Revens, Ward Sister Jane Creed, Senior Registered Nurse Miranda Green, Registered Nurse Review date: August 2013 Revision date: August 2015 Approved by: Clinical
Blood Products Policy Originator: Corinne Revens, Ward Sister Jane Creed, Senior Registered Nurse Miranda Green, Registered Nurse Review date: August 2013 Revision date: August 2015 Approved by: Clinical
Apologies for absence were noted from Ms Claire Dobson, Dr I Gourley, Dr J Kennedy, Professor S McLean, Mr I Mohammed.
 CONFIRMED MINUTES OF THE MEETING OF THE FIFE DRUGS AND THERAPEUTICS COMMITTEE HELD AT 12.30PM ON WEDNESDAY 4 OCTOBER 2017 IN MEETING ROOM 2, WARD 6, VICTORIA HOSPITAL, KIRKCALDY. Present: Dr Frances Elliot
CONFIRMED MINUTES OF THE MEETING OF THE FIFE DRUGS AND THERAPEUTICS COMMITTEE HELD AT 12.30PM ON WEDNESDAY 4 OCTOBER 2017 IN MEETING ROOM 2, WARD 6, VICTORIA HOSPITAL, KIRKCALDY. Present: Dr Frances Elliot
Document Title Investigating Deaths (Mortality Review) Policy
 Policy") Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Quality Indicator Local Use of Data
 Quality Indicator Local Use of Data The clinical audit lead for each contributing site was contacted and asked to answer the following questions (in their own words) about the use of STAG data. In general,
Quality Indicator Local Use of Data The clinical audit lead for each contributing site was contacted and asked to answer the following questions (in their own words) about the use of STAG data. In general,
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Procedure for Monitoring of Delayed Transfers of Care
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Procedure for Monitoring of Delayed Transfers of Care Version No.: 2.2 Effective From: 17 March 2015 Expiry Date: 17 March 2018 Date Ratified: 25
The Newcastle upon Tyne Hospitals NHS Foundation Trust Procedure for Monitoring of Delayed Transfers of Care Version No.: 2.2 Effective From: 17 March 2015 Expiry Date: 17 March 2018 Date Ratified: 25
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Strong Potassium Solutions Safe Handling and Storage
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Strong Potassium Solutions Safe Handling and Storage Version : 5.3 Effective From: 19 January 2016 Expiry Date: 19 January 2019 Date Ratified: 14
The Newcastle upon Tyne Hospitals NHS Foundation Trust Strong Potassium Solutions Safe Handling and Storage Version : 5.3 Effective From: 19 January 2016 Expiry Date: 19 January 2019 Date Ratified: 14
Potential challenges when assessing organisational processes for assurance of clinical competence in labs with limited clinical staff resource
 Contents 1. Introduction... 1 2. Examples of Clinical Activity... 2 3. Automatic selection and reporting... 3 Appendix 1... 8 Appendix 2... 9 1. Introduction ISO 15189 is necessarily written such that
Contents 1. Introduction... 1 2. Examples of Clinical Activity... 2 3. Automatic selection and reporting... 3 Appendix 1... 8 Appendix 2... 9 1. Introduction ISO 15189 is necessarily written such that
PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH The aim of this report is to provide NHS Borders Board with a thematic review of:-
 Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
SystmOne COMMUNITY OPERATIONAL GUIDELINES
 SystmOne COMMUNITY OPERATIONAL GUIDELINES Guidelines IM&T 11 Date: August 2007 Document Management Title of document SystmOne Community Operational Guidelines Type of document Guidelines IM&T 11 Description
SystmOne COMMUNITY OPERATIONAL GUIDELINES Guidelines IM&T 11 Date: August 2007 Document Management Title of document SystmOne Community Operational Guidelines Type of document Guidelines IM&T 11 Description
Access to Health Records Procedure
 Access to Health Records Procedure Version: 1.0 Ratified by: Date ratified: 11/03/2015 Name of originator/author: Name of responsible individual: Information Governance Group Medical Records Manager, Jackie
Access to Health Records Procedure Version: 1.0 Ratified by: Date ratified: 11/03/2015 Name of originator/author: Name of responsible individual: Information Governance Group Medical Records Manager, Jackie