Panel Discussion: Home-Based Primary Care Led Population Management
|
|
|
- Blake Holt
- 5 years ago
- Views:
Transcription
1 Panel Discussion: Home-Based Primary Care Led Population Management Moderator: Steven Merhan, MD Panelists: Barbara Sutton, MSN APRN ACHPN Terri Hobbs Christopher Day, MPH MBA
2 Faculty Disclosures Day Kindred House Calls Employee and Stock Holder Hobbs no relevant disclosures Merhan US Medical Management - Employee Sutton no relevant disclosures
3 Objectives Use the information presented to help them improve their home-based care services. Describe how home-based primary care can assist with population management.
4 Population Health Steve Merhan, MD Chief Medical Officer US Medical Management

5 Population Health Management is a transformational approach to healthcare delivery that shifts the focus from caring for patients who self-select for care based on their own assessment of their condition to taking transcendent responsibility for the health status of a cohort or population of patients Steven Merahn, MD All Rights Reserved Not for publication or distribution without explicit permission of copyright holder


6 For population management, success is more than a full schedule and busy switchboard Patients who do NOT come in for care may be as important to consider as those in the waiting room.
7 What are the Goals for Population Management? To manage variables in order to deliver or add value, where value is the maximum benefit for least cost Value is audience specific: Patient Improved quality of care and quality of health Provider Revitalized professional identity and compensation Payer Efficiency and appropriate resource utilization

8 How Do We Operationalize the Triple Aim? Population Health Management is a clinical operating model for systemsbased practice that operationalizes the Triple Aim Accountable Care is a payment methodology that can be achieved using Population Health Management.

9 Implementing Population Health Management requires mastering a separate and distinct operating model from traditional care delivery, including a specialized infrastructure with its own functional requirements and an associated set of operating capabilities Steven Merahn, MD All Rights Reserved Not for publication or distribution without explicit permission of copyright holder
10 Three Interrelated Tiers Drive the Operation of Successful Systems Tier One MEET FUNCTIONAL REQUIREMENTS Tier Two MASTER OPERATING CAPABILITIES Tier Three OPTIMIZE INTERACTION DESIGN 2014 Steven Merahn, MD All Rights Reserved Not for publication or distribution without explicit permission of copyright holder
11 Example: Driving Tier One FUNCTIONAL REQUIREMENTS Power train Acceleration (fuel control and transmission) Deceleration (braking and transmission) Steering (directional management) Tier Two OPERATING CAPABILITIES Car: Use of the gas and brake pedals and steering wheel; gear shift/clutch Motorcycle: Use of the twist grip, hand and foot brake and foot gear shift Tier Three INTERACTION DESIGN Integrating the operational capabilities and following the rules of the road while driving with other vehicles 2014 Steven Merahn, MD All Rights Reserved Not for publication or distribution without explicit permission of copyright holder
12 Functional Requirements of a Population Management Infrastructure Clinical, Claims, PDD, Financial, Operational, Consumer Rules for Sorting & Categorizing Data System-Level Goals & Program Eligibility Inputs Communication & Activation Strategy Person-Level Goals, Shared Decision Making, & Coordination Resource Allocation & Standing Orders Programs & Services Data Analytics /Reporting Population Surveillance Segmentation & Targeting Outreach & Engagement Care Planning Clinical Strategy Resource Managed Care Delivery Care Coordination / Collaboration Generated Data The Functional Requirements of a Population Management Infrastructure: Systems Elements and Interaction Design 2014 Steven Merahn, MD All Rights Reserved All functional requirements must be fulfilled; however, different organizations may fulfill them differently with various configurations of programs, platforms, partners and personnel
13 How Is Value Really Created? Via the Essential Triad: Care Planning Continuity Collaboration
14 Population Health Management Requires Two-Level Care Plan Development PERSON-LEVEL GOALS SYSTEM-LEVEL GOALS Reduce patientspecific risk factors Improve or stabilize condition-specific health status Improve or stability quality of life Increase affinity and loyalty of patients and families Person- Level Goals System- Level Goals Reduce ED Utilization Reduce All-Cause Hospitalization Reduce SNF Utilization Reduce Readmission Rates Patient Satisfaction Scores ACO Measures IAH Measures HEDIS Measures 2014 Steven Merahn, MD All Rights Reserved Not for publication or distribution without explicit permission of copyright holder


15 While Quality Measures may be evidence-based, they are, on their own, insufficient to improve health status Improving health status or shifting patterns of resource utilization requires management of variables beyond QMs QMs Other EBP Other risks/conditions Patient engagement/satisfaction Life Life Life Life

16 Why Continuity Matters Right Brain Trumps Left Brain In Relationships Products and Services Primary Care Specialists Surgical Care Imaging Lab Tactical Performance Efficiency Consistency Availability Reliability Responsiveness Convenience Channels Medical Home Ambulatory inpatient Dignity Home care Authenticity Websites/App Integrity Empathy Sincerity Urgency Emotive Performance Affinity and Loyalty Are Built Through Experience
17 Continuity is critical because when providers and patients remain present in each others lives (even when they are absent from the daily schedule) the influence of the relationship extends beyond the immediate encounter.

18 Collaboration = Goal Achievement Collaboration is a mutually beneficial relationship between individuals or organizations who work toward common goals by sharing responsibility, authority and accountability for achieving results. 18

19 Home-based primary care is an extraordinary example of achievementoriented care delivery
20 Finally, lets not forget that improving the health status of individuals and populations fundamentally remains a human endeavor Thank You
21 Barbara Sutton, MSN APRN ACHPN Amita Healthcare
22 What is Population Health? Health care practitioners using similar treatment recommendations or guidelines for populations with a specific disease, injury or illness. Example: APRN & LCSW visits post hospitalization. Guidelines for each visit include medications, weights, diet. Visit frequency developed to maximize engagement and education.
23 Use of Best Practice Guidelines Elevate care management from art to science. Develop a unified approach to care management, bringing together patient data, provider data, and payer data. APRNs work closely with Heart Failure Clinic Ensure correct medications Exercise Weights and interventions
24 Engaging patients 99% of patient activity is not happening in the office, clinic or office: It happens at home! What is important to that patient? Their family?
25 Equity Patient subgroups can be defined by race or ethnicity, socioeconomic status, gender or geography. Eliminate inequalities deciding on treatment based on the overall health of the community, regardless of any one person s subgroup status.
26 Value for Employers Employers want employees to return to work sooner, and they want predictability in their total spending on healthcare. right care based on the evidence right time, right setting prompt access to care right price control the cost of care best life return to function and productivity best outcome patient satisfaction
27 Managing Costs Develop a continuum of partners Post discharge costs may exceed 50% of the total health care cost
28 Collaborating Develop relationships with Discharge planners, skilled nursing facilities, and home health agencies Reach out to develop community partnerships with senior services, housing agencies, transportation services, medication assistance programs.
29 Consider the broad determinants of health Health determinants include income and social status, social support networks, education, employment and working conditions, biology and genetic endowment, physical environment, personal health practices and coping skills, and health services.
30 Prevention Prevention - to prevent an event or to minimize its effect after it has occurred. Not every event is preventable, but every event does have a preventable component. Whenever possible, population-based practice emphasize primary prevention. Reduce hospital readmissions within 30 days
31 Collaborate Consolidate care management resources for high-risk patients. Care management works when the appropriate resources are brought together for these complex, high-cost patients.
32 References Williams, C A, & Highriter ME. Community health nursing: population focus and evaluation. Public Health Reviews. 1978, 7 (3-4): Turnock, B. Public Health: What It Is and How It Works. Gaithersburg, MD: Aspen Publishers, Inc., The Leading Lights Summit


33 Contract Negotiations Terri Hobbs, Executive Director

34
35 Population Current census over 1,450 homebound adults 500 patients from two payers = $700,000 in additional revenue Work force support $180, % enrolled in Med Advantage 35% are receiving additional stipends 15% of our patients on IAH (Medicare ffs) Over $1 million IAH shared savings Yr 1
36 Payers we approached Payer 1 Medicare/Medicaid Contractor FFS plus $100 stipend Nurse Practitioner 1 year Payer 2 Medicare Advantage plan FFS plus $150 stipend Palliative care contract Payer 3 Medicare Advantage plan PMPM cap no risk Payer 4 In negotiations
37 Provide Actual Data
38 Expenses vs Revenue Expenses Revenue 50% 26% 19% 4% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Expenses Fee for Service IAH Stipend MU Bonus
39 Key Points Get in front of the right person Prepare quality & patient outcome data Highlight the teams and functions Quality MU, PCPCH, PQRS & IAH Community partnerships and collaboration Polite persistence

40
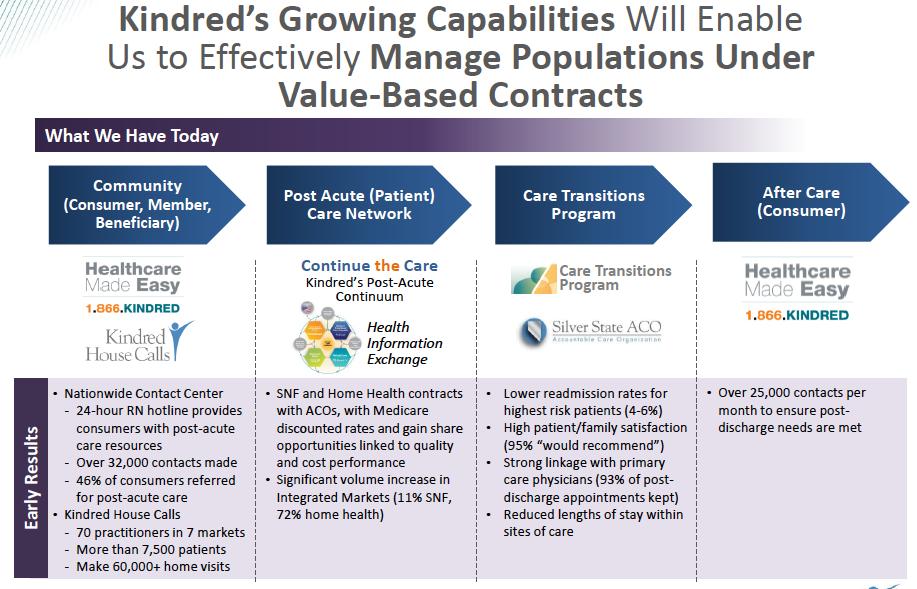
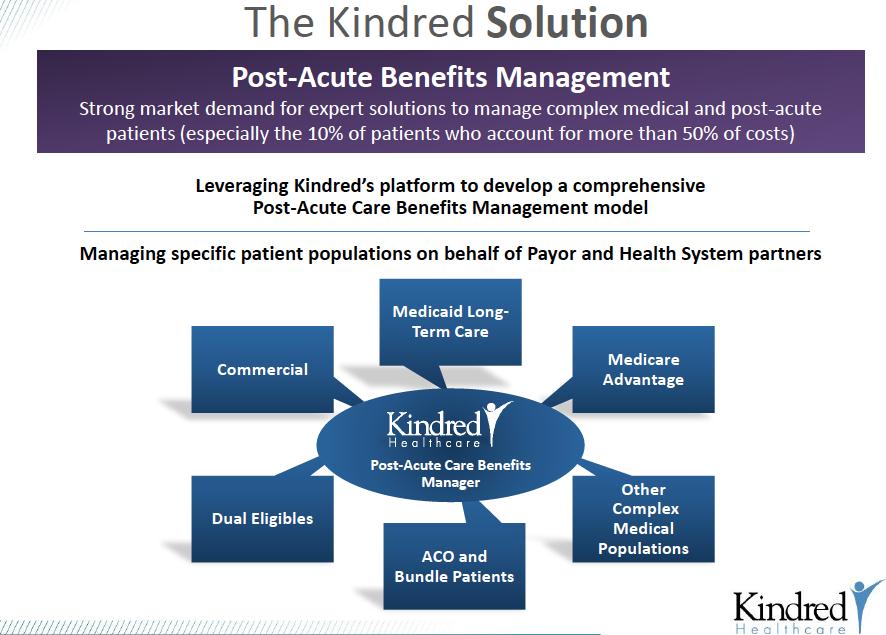
41 The Kindred Story Christopher Day, MPH MBA

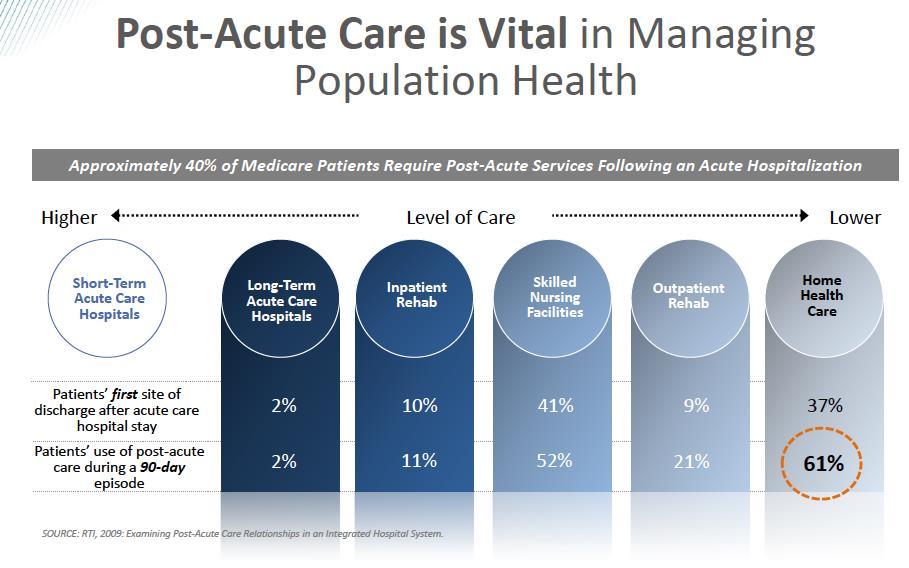
42 Concentration of Risk and $ in U.S. Healthcare


43 A Higher Number of Chronic Conditions Predicts Utilization and Spending Percentage of Medicare FFS Beneficiaries by Number of Inpatient Admissions and Number of Chronic Conditions Percentage of Hospital Readmissions Within 30 Days of Discharge by Number of Chronic Conditions and Age Per Capita Medicare Spending for Medicare FFS Beneficiaries by Number of Chronic Conditions Source: Chronic Conditions Among Medicare Beneficiaries, Chartbook: 2012

44 Exploding Number of Advanced Elderly with Functional Debility --> Growing Need for HBPC
45
46
47
48

49 Gap in Health Care Delivery System: Creating a Solution for Elderly High Utilizers Medicare Eligible Years Current System Chronic Disease 2-20 Years Gap In Care Delivery In Hospital Death or Hospice <6 months Tier 3A Patients Home- Based Primary Care Chronic Disease 2-20 Years Medicare Eligible Years In Hospital Death or Hospice <6 months Tier 3A Patients 49
50 The Case of Virginia Virginia is 85 years old, a typical Tier 3A patient with the following demographics: End Stage (Stage IV) Congestive Heart Failure (CHF) Other Chronic Diseases COPD Diabetes DJD CKD Mild Dementia A life expectancy of < 24 months Virginia lives in an independent senior apartment with ~2 hours private duty/day Her adult children all live in other states
51 Population Served: Snapshot Elderly, homelimited Mean Age 86 74% Female Average of 20 Diagnoses Average of 7 Chronic Conditions Estimated annual cost > $32,000 per patient


52 Home-Based Primary Care Led Care Management OUTCOMES Improved Quality and Patient Satisfaction Reducing Hospital Readmissions Lower Cost for an Episode of Care

53 Home-Based Primary Care Practice Standards Comprehensive Care Staff Structure and Teams Improve Patient Experience Access to In- Home Care Improve Health Cost effective care Medical and Psychosocial Issues Management
54 Operational Approach to HBPC Led Population Health Management Hospital Home or ALF/ILF Home Care Tier 3A HBPC Practitioner Care Coordinator SNF Analytics Remote Monitoring Electronic record Foundation of Care Management Hospice

55 Population Health Outcomes Measurement


56 Quality Dashboards Ability to monitor/manage the performance of each Care Team by analyzing reports available on the Community Analytics Portal
57 Conclusions: Advantages of Home-Based Primary Care Led Population Health Management Home-Based Primary Care + Post Acute + Care Management Programs can provide a fully Integrated, Comprehensive Care Solution for the Rapidly Growing Elderly in the U.S. Preferred Place of Service Care where it s needed and wanted the most Continuum Fit Aligns with the health care Continuum, especially home health, hospice and rehab Quality /Cost Outcomes High quality, low readmissions improved outcomes, longer home LOS at a lower total cost Vehicle for At- Risk Contracting Proven contract model with willing managed care partners Senior Community Innovation Model can provide a platform for best practices and future growth Care Management Hub Vehicle for population health and care redesign 57
58 Panel Discussion Go to: 2Shoesapp.com/AAHCM Click on the session you are in 2. Ask and vote on questions
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
Decreasing Medical. Costs. Are your members listening to you? PRESENTED BY: September 22, 2016
 Decreasing Medical Costs Are your members listening to you? PRESENTED BY: Aaron Crowell, Executive Vice President, MTM, Inc. Gary Jacobs, Executive Vice President, CareCentrix Dan Masciopinto, SVP of Product,
Decreasing Medical Costs Are your members listening to you? PRESENTED BY: Aaron Crowell, Executive Vice President, MTM, Inc. Gary Jacobs, Executive Vice President, CareCentrix Dan Masciopinto, SVP of Product,
Maryland s Integrated Care Network. Heading into Year Three
 Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Why Develop Some Local Management of Services for Frail Elderly Persons?
 12:30 1:30 PM Managing and Measuring 1 Why Develop Some Local Management of Services for Frail Elderly Persons? 1. Local entities could integrate social supports and health care 2. Local entities could
12:30 1:30 PM Managing and Measuring 1 Why Develop Some Local Management of Services for Frail Elderly Persons? 1. Local entities could integrate social supports and health care 2. Local entities could
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait
 Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Session #6: Population Health Must Haves Care Coordination
 Session #6: Population Health Must Haves Care Coordination Presenter: Robert Wieland, M.D. Arbor Lakes Saturday, Jan. 7, 2017 11:15 a.m. 12:15 p.m. Robert A. Wieland, M.D. Robert A. Wieland, M.D. (Bob)
Session #6: Population Health Must Haves Care Coordination Presenter: Robert Wieland, M.D. Arbor Lakes Saturday, Jan. 7, 2017 11:15 a.m. 12:15 p.m. Robert A. Wieland, M.D. Robert A. Wieland, M.D. (Bob)
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Beyond the Horizon: What s Next? Session PH6, March 5, 2018 Don Calcagno, President, Advocate Physician Partners
 Beyond the Horizon: What s Next? Session PH6, March 5, 2018 Don Calcagno, President, Advocate Physician Partners 1 Conflict of Interest Don Calcagno Has no real or apparent conflicts of interest to report.
Beyond the Horizon: What s Next? Session PH6, March 5, 2018 Don Calcagno, President, Advocate Physician Partners 1 Conflict of Interest Don Calcagno Has no real or apparent conflicts of interest to report.
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015
 Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Population Health. Collaborative Care. One interoperable platform. NextGen Care
 Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Rural and Independent Primary Care.
 Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
The greatest difficulty in the world is not for people to accept new ideas but to get them to forget their old ones.
 Dr. Marie S, Gustin Nursing Excellence Conference, 2012 The greatest difficulty in the world is not for people to accept new ideas but to get them to forget their old ones. John Maynard Keynes Chaos, Complexity,
Dr. Marie S, Gustin Nursing Excellence Conference, 2012 The greatest difficulty in the world is not for people to accept new ideas but to get them to forget their old ones. John Maynard Keynes Chaos, Complexity,
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Innovative Business Activities in Health Care with Commercial Partners
 Innovative Business Activities in Health Care with Commercial Partners Steve Witman, CPA, MBA Vice President of Business Development / Financial and Capital Planning LifeBridge Health March 4, 2014 Business
Innovative Business Activities in Health Care with Commercial Partners Steve Witman, CPA, MBA Vice President of Business Development / Financial and Capital Planning LifeBridge Health March 4, 2014 Business
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
Presentation Objectives
 At Home: Comprehensive Care of the Frail Elderly Ramiro Jervis, MD Asantewaa Poku, MPH Kristofer Smith, MD, MPP December 10, 2013 1 Presentation Objectives Develop, both culturally and operationally, an
At Home: Comprehensive Care of the Frail Elderly Ramiro Jervis, MD Asantewaa Poku, MPH Kristofer Smith, MD, MPP December 10, 2013 1 Presentation Objectives Develop, both culturally and operationally, an
Value Based Care: Trends for Boston Chicago Houston Los Angeles Miami San Francisco Washington, DC
 Value Based Care: Trends for 2018 Boston Chicago Houston Los Angeles Miami San Francisco Washington, DC Need head shot David Fairchild, MD Director BDC Advisors Dave Terry CEO & Co-Founder Archway Health
Value Based Care: Trends for 2018 Boston Chicago Houston Los Angeles Miami San Francisco Washington, DC Need head shot David Fairchild, MD Director BDC Advisors Dave Terry CEO & Co-Founder Archway Health
Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management
 Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management Christopher T. Olivia, MD, President Michael Renzi, DO, Chief Medical Officer March 18, 2014 2014, Continuum Health
Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management Christopher T. Olivia, MD, President Michael Renzi, DO, Chief Medical Officer March 18, 2014 2014, Continuum Health
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Health System Transformation. Discussion
 Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Accountable Care Organizations American Osteopathic Association Health Policy Day September 23, 2011
 Accountable Care Organizations American Osteopathic Association Health Policy Day September 23, 2011 Cary Sennett MD PhD Cary Sennett, MD, PhD Managing Director, Engelberg Center for Health Care Reform
Accountable Care Organizations American Osteopathic Association Health Policy Day September 23, 2011 Cary Sennett MD PhD Cary Sennett, MD, PhD Managing Director, Engelberg Center for Health Care Reform
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Payer Perspectives On Value-based Contracting
 Payer Perspectives On Value-based Contracting Miles Snowden, MD, MPH, CEBS Chief Medical Officer 1 A simple goal Making the health system work better for everyone 2 Optum serves 60,000,000+ individuals
Payer Perspectives On Value-based Contracting Miles Snowden, MD, MPH, CEBS Chief Medical Officer 1 A simple goal Making the health system work better for everyone 2 Optum serves 60,000,000+ individuals
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
The TeleHealth Model THE TELEHEALTH SOLUTION
 The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships
 MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships June 2014 avalerehealth.net Today s Panelists John Hackett - JHackett@extendicare.com o Vice President of Strategy & Development,
MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships June 2014 avalerehealth.net Today s Panelists John Hackett - JHackett@extendicare.com o Vice President of Strategy & Development,
OHA s Quality & Accountability Metrics: Measuring CCO Performance. State of Oregon Research Academy September 17, 2014
 OHA s Quality & Accountability Metrics: Measuring CCO Performance State of Oregon Research Academy September 17, 2014 Health System Transformation: Achieving the Triple Aim 2 Our Health System Transformation
OHA s Quality & Accountability Metrics: Measuring CCO Performance State of Oregon Research Academy September 17, 2014 Health System Transformation: Achieving the Triple Aim 2 Our Health System Transformation
A strategy for building a value-based care program
 3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Identifying and Treating Your High Risk Patient Population. Beth Hickerson Quality Improvement Advisor August 15, 2017
 Identifying and Treating Your High Risk Patient Population Beth Hickerson Quality Improvement Advisor August 15, 2017 HIGH RISK PATIENTS What and Why? What is a high-risk patient? High level of resource
Identifying and Treating Your High Risk Patient Population Beth Hickerson Quality Improvement Advisor August 15, 2017 HIGH RISK PATIENTS What and Why? What is a high-risk patient? High level of resource
Turning Big Data Into Better Care
 Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Transforming Physician Practices: Evolution of ACOs in California. National Association of ACOs - Washington, DC October 2015
 Transforming Physician Practices: Evolution of ACOs in California National Association of ACOs - Washington, DC October 2015 Integrated Healthcare Association Statewide multi-stakeholder leadership group
Transforming Physician Practices: Evolution of ACOs in California National Association of ACOs - Washington, DC October 2015 Integrated Healthcare Association Statewide multi-stakeholder leadership group
YOUR HEALTH INFORMATION EXCHANGE
 YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
Publication Development Guide Patent Risk Assessment & Stratification
 OVERVIEW ACLC s Mission: Accelerate the adoption of a range of accountable care delivery models throughout the country ACLC s Vision: Create a comprehensive list of competencies that a risk bearing entity
OVERVIEW ACLC s Mission: Accelerate the adoption of a range of accountable care delivery models throughout the country ACLC s Vision: Create a comprehensive list of competencies that a risk bearing entity
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Lessons from the States: Oregon s APM Model
 Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Medical Group and Hospital A Model for Clinical Integration
 Medical Group and Hospital A Model for Clinical Integration Richard Afable M.D., MPH President and CEO Hoag Memorial Hospital Presbyterian Alan Puzarne Chief Operating Officer Greater Newport Physicians
Medical Group and Hospital A Model for Clinical Integration Richard Afable M.D., MPH President and CEO Hoag Memorial Hospital Presbyterian Alan Puzarne Chief Operating Officer Greater Newport Physicians
Minnesota Perspective: Fairview Health Services. National Accountable Care Organization Congress October 25, 2010
 Minnesota Perspective: Fairview Health Services National Accountable Care Organization Congress October 25, 2010 Fairview Overview Not-for-profit organization established in 1906 Partner with the University
Minnesota Perspective: Fairview Health Services National Accountable Care Organization Congress October 25, 2010 Fairview Overview Not-for-profit organization established in 1906 Partner with the University
Using A Data Warehouse and Analytics to Drive Population Health Management
 Success Story Using A Data Warehouse and Analytics to Drive Population Health Management HEALTHCARE ORGANIZATION Large Medical Center TOP RESULTS Enabled pay-for-performance (P4P) incentive payment reporting
Success Story Using A Data Warehouse and Analytics to Drive Population Health Management HEALTHCARE ORGANIZATION Large Medical Center TOP RESULTS Enabled pay-for-performance (P4P) incentive payment reporting
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement
 to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement") Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
What s Next for CMS Innovation Center?
 What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
Succeeding with Accountable Care Organizations
 Succeeding with Accountable Care Organizations The Point B Webinar Series October 25, 2011 Today s Discussion Key ACO trends and emerging models Critical success factors for building an ACO Developing
Succeeding with Accountable Care Organizations The Point B Webinar Series October 25, 2011 Today s Discussion Key ACO trends and emerging models Critical success factors for building an ACO Developing
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Medicare Advantage in Practice: Enhanced Care Models for High Need Patients
 Medicare Advantage in Practice: Enhanced Care Models for High Need Patients Rebekah Dube, Pharm.D. VP, Health Plan Clinical Programs & Interim VP, Health Plan Products Who is Martin s Point Health Care?
Medicare Advantage in Practice: Enhanced Care Models for High Need Patients Rebekah Dube, Pharm.D. VP, Health Plan Clinical Programs & Interim VP, Health Plan Products Who is Martin s Point Health Care?
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Introduction Patient-Centered Outcomes Research Institute (PCORI)
") 2 Introduction The Patient-Centered Outcomes Research Institute (PCORI) is an independent, nonprofit health research organization authorized by the Patient Protection and Affordable Care Act of 2010. Its
2 Introduction The Patient-Centered Outcomes Research Institute (PCORI) is an independent, nonprofit health research organization authorized by the Patient Protection and Affordable Care Act of 2010. Its
Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim
 Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim Christopher T. Olivia, MD, President June 11, 2014, All Rights Reserved and CONTINUUM HEALTH
Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim Christopher T. Olivia, MD, President June 11, 2014, All Rights Reserved and CONTINUUM HEALTH
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Transforming Care for Older Adults AGE DIFFERENT. Jann Dorman, Alen Vartan, Faye Sahai, and Estee Neuwirth, Phd
 Transforming Care for Older Adults AGE DIFFERENT Jann Dorman, Alen Vartan, Faye Sahai, and Estee Neuwirth, Phd Minicourse 16 Annual IHI National Forum on Quality Improvement in Health Care Dec. 8, 2014
Transforming Care for Older Adults AGE DIFFERENT Jann Dorman, Alen Vartan, Faye Sahai, and Estee Neuwirth, Phd Minicourse 16 Annual IHI National Forum on Quality Improvement in Health Care Dec. 8, 2014