( ) MANAGERS MANUAL. Community Monitoring of Health Services Under NRHM
|
|
|
- Dominick Hamilton
- 5 years ago
- Views:
Transcription



1 ( ) MANAGERS MANUAL Community Monitoring of Health Services Under NRHM
2 Managers Manual on Community based Monitoring of Health services under National Rural Health Mission Drawing from NRHM Framework of Implementation Prepared by Task force on Community Monitoring Of Advisory Group on Community Action Based on the Proposal sanctioned by Mission Directorate of NRHM, MoHFW, Government of India
3 Contents Editing Layout & Design Production Coordinator Abhijit Das, Sunita Singh & Ruth Vivek with support from Technical Advisory Group (TAG) & Advisory Group on Community Action (AGCA) Elisa Parija Runu Saxena, Rahul Sharma Moumita Ghosh Published December, 2008 Printed at Design Solutions ii
4 Preface The National Rural Health Mission (NRHM) was launched on the 12 April 2005, with the goal of improving the availability of and access to quality health care by people, especially for those residing in rural areas, the poor, women and children. To ensure that the services reach those for whom they are meant, the NRHM proposes an intensive accountability framework that includes community-based monitoring as one of its key strategies. The NRHM Framework for Implementation outlines the composition and broad roles of monitoring and planning committees at various levels. These outlines were to be subsequently elaborated for developing the process of community monitoring. The Advisory Group for Community Action (AGCA) is a standing committee within the NRHM, constituted to support and advise the MoHFW in implementation and review of the NRHM across the country. The AGCA took a lead in initiating discussions with the MoHFW to develop a detailed proposal on how Community Monitoring could be rolled out in a phased manner across the country. Through a process of discussions and deliberations, the AGCA developed a comprehensive proposal for decentralised Community Monitoring with the active partnership of the Department and civil society institutions. The proposal was then forwarded Union Ministry of Health and Family Welfare (MoHFW) for implementation on a national scale. The MoHFW has approved this first phase of the Community Monitoring proposal and has suggested the AGCA for a special Task Group for overseeing the implementation. The AGCA has established a Task Group for technical support and oversight in implementing the project and it is being chaired by Mr. A R Nanda of PFI, the convenor of AGCA. A Secretariat has also been established jointly by Population Foundation of India (PFI) and Centre for Health and Social Justice at New Delhi (CHSJ). This Manual is based on project proposal that has been approved for different stakeholders in the community. iii
5 Acknowledgements Ms S Jalaja, Ex-Mission Director, NRHM, MoHFW, Government of India. Mr G C Chaturvedi, Mission Director NRHM, MoHFW, Government of India. Mr Amarjeet Sinha, Joint Secretary, MoHFW, Government of India. Dr Tarun Seem, Director, NRHM, MoHFW, Government of India. Mr Ganga Kumar, Deputy Director, NRHM, MoHFW, Government of India. Mission Directors of Nine States; Mr S. K. Lohani, Mission Director, NRHM, Government of Odisha. Mr Madhukar Chwodhari, Mission Director, NRHM, Government of Maharashtra. Ms Darshaniya Ahluwalia Mission Director, NRHM, Government of Chhattisgarh. Dr J B Ekka, Mission Director, NRHM, Government of Assam. Dr Manohar Agnani, Mission Director, NRHM, Government of Madhya Pradesh. Ms Girija Vaidyanathan Mission Director, NRHM, Government of TamilNadu. Mr V. Srinivas Mission Director, NRHM, Government of Rajesthan. Dr Pradeep Kumar Singh Mission Director, NRHM, Government of Jharkhand. Mr Nilay Mitash Mission Director, NRHM, Government of Karnataka. All members of the Advisory Group on Community Action. All members of the Technical Advisory Group of AGCA. All members of State Mentoring Committee of concerned states. All State Nodal Organisations. All District and Block level NGOs. All Health Providers and Managers at District, Block, PHC and community level who were associated with the process. Members of the different Panchayati Raj Insititutions in the nine states. Members of the different level of Monitoring and Planning Committees in the nine states. Members of the Village Health and Sanitation Committees. And Citizens of India who were engaged in this process across the nine states. iv
6 Contents Preface Acknowledgements Glossary iii iv vi Section I Introduction to NRHM 3 Section II Community Monitoring in NRHM 7 Introduction to Community Monitoring 7 Objectives of Community Monitoring 7 Process of Community Monitoring 8 Section III First Phase of Community Monitoring 11 Scale of Implementation of the First Phase 12 Need for involving Civil Society Organisations/ NGOs in the First Phase 12 Role of Civil Society Organisations in the First Phase 14 Section IV Implementing the first phase of Community Monitoring 17 Preparatory Phase 17 District Level Implementation Phase 18 Section V Organisational responsibilities 25 National Level 25 State Level 26 District Level 28 Block Level & Below 28 Tables and Figures Table 1 Ambit & Scope of Community Monitoring at Different Levels 9 Table 2 Activities in the Preparatory Phase 18 Table 3 State Level Activities in the Preparatory Phase 18 Table 4 Criteria for NGO selection 22 Table 5 Format for NGO Selection 23 Table 6 Organisational Responsibilities at Different Levels 25 Figure 1 Geographical Spread 13 Figure 2 Organogram of Monitoring & Planning Committees 19 Figure 3 Process of Monitoring 21 Figure 4 Organogram 27 Annexures Annexure 1 NRHM Strategies 31 Annexure 2 Monitoring and Evaluation 32 Annexure 3 Community Monitoring Framework 33 Annexure 4 Composition, Roles and Responsibilities of Monitoring 35 Committees Annexure 5 Concrete Service Guarantees 42 Enclosed in CD-ROM - Managers' Manual, Training Manual, Monitoring Manual, format of Process Documentation and other related materials. v
7 Glossary AGCA AYUSH ASHA ANM AWW AIDS APL BPMC CHSJ CHC CBOs CSO CM CMO CMHO DOTS DHO DH DPMC FGD GoI GDP Advisory Group for Community Action Ayurveda Unani Siddha Homeopathy Accredited Social Health Activist Auxiliary Nurse Midwife Anganwadi Worker Acquired Inmmuno Deficiency Syndrome Above Poverty Line Block Planning and Monitoring Committee Centre for Health and Social Justice Community Health Centers Community Based Organisations Civil Society Organisations Community Monitoring Chief Medical Officer Chief Medical Health Officer Directly Observed Treatment, Short Course Chemotherapy District Health Officer District Hospital District Planning and Monitoring Committee Focus Group Discussion Government of India Gross Domestic Product MLA MLC NRHM NHP NHRC PFI PRIs PTA PHC PPMC RKS RTI SHG SHC SC ST STI TOT TAG VHSC VHC Minister of Legislative Assembly Minister of Legislative Council National Rural Health Mission National Health Programmes National Human Rights Commission Population Foundation of India Panchayati Raj Institutions Parent Teacher Association Primary Health Centre PHC Planning and Monitoring Committee Rogi Kalyan Samiti Reproductive Tract Infection Self Help Group Sub- Health Centre Scheduled Caste Scheduled Tribe Sexually Transmitted Infections Training of Trainers Technical Advisory Group Village Health and Sanitation Committee Village Health Committee HIV HO Human Immunodeficiency Virus Health Officer IPHS IMR Indian Public Health Standards Infant Mortality Rate MoHFW MDGs MTA MPW MMR MO Ministry of Health and Family Welfare Millennium Development Goals Mother Teacher Association Multi-Purpose Worker Maternal Mortality Rate Medical Officer

8
9
10 MANAGERS MANUAL COMMUNITY MONITORING SECTION-I Introduction to NRHM There is an increasing recognition that despite significant improvements in health parameters like life expectancy at birth of and the reduction of infant mortality, there are large parts of the country where people continue to have very poor access to health care services and their health status continues to be abysmal. A high proportion of the population continues to suffer from and die of preventable conditions like maternal deaths, malaria and tuberculosis. Persistent malnutrition and high levels of anaemia amongst children and women is widespread. Due to the poor status of public health systems people are also facing poverty and indebtedness from the costs incurred in seeking health care. Public spending on health in India, especially on preventive and promotive health is also very low in India. On the other hand, private and out of pocket, expenditure on health is very high, about three times higher than the public expenditure. Thus, there is an urgency to deal with multiple health related crisis that the rural poor in the country are faced with. There is also the need to transform the health system into an efficient, transparent and accountable system delivering affordable and quality services. The National Rural Health Mission has been conceptualised and is being implemented to bring about these fundamental changes in the way health GOALS Reduction in Infant Mortality Rate (IMR) and Maternal Mortality Ratio (MMR). Universal access to public health services such as Women's health, child health, water, sanitation & hygiene, immunization, and Nutrition. Prevention and control of communicable and non-communicable diseases, including locally endemic diseases. Access to integrated comprehensive primary healthcare. Population stabilization, gender and demographic balance. Revitalize local health traditions and mainstream AYUSH. Promotion of healthy life styles. 3
11 THE VISION OF THE MISSION To provide effective healthcare to rural population throughout the country with special focus on 18 states, which have weak public health indicators and/or weak infrastructure. 18 special focus states are Arunachal Pradesh, Assam, Bihar, Chattisgarh, Himachal Pradesh, Jharkhand, Jammu and Kashmir, Manipur, Mizoram, Meghalaya, Madhya Pradesh, Nagaland, Orissa, Rajasthan, Sikkim, Tripura, Uttaranchal and Uttar Pradesh. To raise public spending on health from 0.9% GDP to 2-3% of GDP, with improved arrangement for community financing and risk pooling. To undertake architectural correction of the health system to enable it to effectively handle increased allocations and promote policies that strengthen public health management and service delivery in the country. To revitalize local health traditions and mainstream AYUSH into the public health system. Effective integration of health concerns through decentralized management at district, with determinants of health like sanitation and hygiene, nutrition, safe drinking water, gender and social concerns. Address inter State and inter district disparities. Time bound goals and report publicly on progress. To improve access to rural people, especially poor women and children to equitable, affordable, accountable and effective primary health care. there is an urgency to deal with multiple health related crisis that the rural poor in the country are faced with care services are being delivered to the rural poor. The goal of the Mission is to improve the availability of and access to quality health care by people, especially for those residing in rural areas, the poor, women and children. The Mission seeks to provide universal access to equitable, affordable and quality health care which is accountable, at the same time responsive to the needs of the people, reduction of child and maternal deaths as well as population stabilisation, gender and demographic balance. In this process, the Mission would help achieve goals set under the National Health Policy and the Millennium Development Goals (MDGs). In order to achieve its goals and objectives the Mission seeks to forge effective partnerships between the Central, state and local governments. There are flexible mechanisms built into the Mission so that local needs and priorities can be identified and addressed and local initiatives promoted. Intersectoral convergence is also seen as a key strategy of the Mission for improving interventions in preventive and promotive health. The Panchayati Raj Institutions (PRIs) and the community have been given key roles in the management of primary health care programmes as well as infrastructure. Some of the key areas that have been identified for concerted action within the NRHM framework of action are as follows: Well functioning health facilities Quality and accountability in the delivery of health services. Taking care of the needs of the poor and vulnerable sections of the society and their empowerment. Prepare for health transition with appropriate health financing. Pro-people public private partnership. Convergence for effectiveness and efficiency. Responsive health system meeting people s health needs. The expected outcomes from the Mission are: Reduction of Infant Morality rate to 30/1000 live births by Reduction of Maternal Mortality to 100/100,000 live births by Reduction of Total Fertility Rate to 2.1 by Reduction of Malaria Mortality Rate by 50% up to 2010 and an additional 10% by Reduction of Kala Azar Mortality Rate by 100% by 2010 and sustaining elimination until Reduction of Filaria/Microfilaria Rate by 70% by 2010 by 80% by 2012 and elimination by
12 MANAGERS MANUAL COMMUNITY MONITORING Reduction of Dengue Mortality Rate by 50% by 2010 and sustaining at that level until Increasing Cataract operations to 46 lakh until Reducing Leprosy Prevalence Rate from 1.8 per 10,000 in 2005 to less that 1 per 10,000. Maintain 85% cure rate in the Tuberculosis DOTS series through the entire Mission Period and also sustain planned case detection rate. Upgrading all Community Health Centers (CHC) to Indian Public Health Standards (IPHS). Increase utilisation of First Referral Units through increased bed occupancy by referred cases from less than 20% to over 75%. Engaging 4,00,000 female Accredited Social Health Activists (ASHA). At the community level it is expected that: There will be increased awareness about preventive health including nutrition. There will be a trained worker available at the community level with a drug kit for common ailments. A monthly Health Day will be organised where services related to maternal and child health, for ex. immunisation, ante-natal check-ups and nutritional services will be available. Generic drugs for common ailments will be available at the sub centre and good hospital care will be assured through availability of doctors, drugs and quality services at PHC/CHC level. There will be improved facilities available for institutional deliveries and the Janani Suraksha Yojna will also provide opportunities for subsidised hospital care for those below the poverty line. Mobile medical units will ensure availability of services to remote underserved areas. There will be provision of safe drinking water and household toilets. To ensure that these outcomes are achieved, and quality and accountable health services which are responsive and take care of the needs of the poor and vulnerable sections of the society are attained community ownership and participation in management is seen as an important pre-requisite within NRHM. Thus, community monitoring is an important component for achieving these results. community ownership and participation in management is seen as an important pre-requisite within NRHM HOW TO TRIGGER COMMUNITY ACTION? Through household and health facility survey that involve Village Health Teams and discuss findings locally. Through Health Camps that bring a range of health services to the community and makes them aware of their entitlements. Through "Public Hearings" or Jan Sunawai oganized periodically where people share their experience of seeking health care. Such Jan Sunwais may be organized twice a year, or at least once a year at PHC, block and district levels. Through training and orientation of village Health Teams for community action. By building team of Community Workers like Aangan Wadi Sevika, ASHA, School Teacher, Mahila Samakhya worker, PTA/MTA' members, etc. By involving group like SHGs, Community based organizations, MTAs, PTAs, literacy volunteers, Containing Education Centre volunteers, etc. who have motivation for Community action. By making local level health functionaries visit households frequently. By making Block and District level Health Mission teams, including NGOs, organize a series of activities like health camps, public hearings, etc. 5
13
14 MANAGERS MANUAL COMMUNITY MONITORING SECTION-II Community Monitoring in NRHM Introduction to Community Monitoring The accountability framework proposed in the NRHM is a three-pronged process that includes internal monitoring, periodic surveys and studies and community based monitoring. Community monitoring is also seen as an important aspect of promoting community led action in the field of health. The provision for Monitoring and Planning Committees has been made at PHC, block, district and state levels. The adoption of a comprehensive framework for community-based monitoring and planning at various levels under NRHM, places people at the centre of the process of regularly assessing whether the health needs and rights of the community are being fulfilled. The community monitoring process involves a three way partnership between health care providers and managers (health system); the community, community based organisations and NGOs and the Panchayati Raj Institutions. The success of the community monitoring process will depend upon the ownership of the process by all three parties and a developmental spirit of fact-finding and learning lessons for improvement rather than fault finding. The objectives of community based monitoring are as follows: It will provide regular and systematic information about community needs, which will be used to guide the planning process appropriately. It will provide feedback according to the locally developed yardsticks, as well as on some key indicators. It will provide feedback on the status of fulfilment of entitlements, functioning of various levels of the public health 7
15 the provision for Monitoring and Planning Committees has been made at PHC, block, district and state levels system and service providers, identifying gaps, deficiencies in services and levels of community satisfaction, which can facilitate corrective action in a framework of accountability. It will enable the community and community-based organisations to become equal partners in the planning process. It would increase the community sense of involvement and participation to improve responsive functioning of the public health system. The community should emerge as active subjects rather than passive objects in the context of the public health system. It can also be used for validating the data collected by the ANM, Anganwadi worker and other functionaries of the public health system. Process of Community Monitoring The exercise of community monitoring involves drawing in, activating, motivating, and capacity building and allowing the community and its representatives e.g. Community Based Organisations (CBOs), people s movements, voluntary organisations and Panchayat representatives, to directly give feedback about the functioning of public health services, including giving inputs for improved planning of the same. The community and community-based organisations will monitor demand/need, coverage, access, quality, effectiveness, behaviour and presence of health care personnel at service points, possible denial of care and negligence. The monitoring process will include outreach services, public health facilities and the referral system. The key Institutions for Community Monitoring as laid out in the Framework of Implementation are: Village Health and Sanitation Committee (VHSC). The PHC Planning and Monitoring Committee. The Block Planning and Monitoring Committee. The District Planning and Monitoring Committee. The State Planning and Monitoring Committee. Guidelines regarding the composition, roles and powers of these committees have been laid out in detail in the Framework of Implementation and are reproduced in Annexure 4. The monitoring process will begin with a village report card being prepared by the Village Health and Sanitation Committee after consulting village records (ex. ASHA records or ANM records or the Village Health Register) and also by conducting interviews and meetings with potential beneficiaries (like women who are pregnant or have undergone childbirth in the recent past, or those with small children) to understand the community members experiences and problems faced, as well as assess the extent to which key services are being delivered effectively. The Monitoring Committee at each subsequent level would review and collate the reports coming from the committees dealing with units immediately below it. For example, Block Committee will receive and review the VHSC reports while the District Committee would receive and review the reports from all Block Committees. However, the monitoring committees would not only rely on reports, but would also make their own independent observations on selected key parameters. Each committee would appoint a small team drawn from among its civil society and PRI representatives who would visit on a quarterly/six-monthly basis, a small sample of units (say one facility or two villages) under their purview and directly review the conditions. This will enable the committee to not just rely on reports but to also have a first-hand assessment of conditions in their area. For example, the PHC committee representatives would visit two villages and conduct group discussions in each trimester selecting different villages by rotation. Similarly, the Block Committee representatives would visit one PHC by rotation in each trimester. The monitoring committees at 8
16 MANAGERS MANUAL COMMUNITY MONITORING PHC/Block/District levels will be responsible for making an assessment of the functioning of the major health care facility at their respective level (PHC/CHC/District Hospital). Sharing of the findings of monitoring committees will not only take place through the periodic report submitted to the next level of monitoring committee, but also through periodic public sharing. Monitoring committees at PHC, Block and District level will be involved in sixmonthly or annual Jan Samvads or public hearings at their respective levels, where committee members would share the results of their findings and also get direct feedback of the situation, including possible presentation of cases of denial of health care. Similarly, the State Planning and Monitoring Committee will conduct an annual public meeting open to all civil society representatives where the State Mission report and independent reports will be presented and various aspects of design and implementation of NRHM in the state, including state specific health schemes, would be reviewed and discussed enabling corrective action to be taken. A broad outline of the ambit and scope of community monitoring at different levels is given in the Table below Community Monitoring Committee Village Health and Sanitation Committee Table-1 Ambit & Scope of Community Monitoring at Different Level Periodicity of Monitoring Quarterly Activities to be undertaken a. Reviews Village Health register, Village health calendar. b. Reviews performance of ANM, MPW, ASHA. c. Reviews communities own experiences as beneficiaries of services. d. Sends brief three monthly report to PHC committee. PHC Monitoring and Planning Committee Block Monitoring and Planning Committee District Monitoring and Planning Committee State Monitoring and Planning Committee Quarterly Quarterly Quarterly Quarterly a. Reviews and collates reports from all VHSCs. b. An NGO / PRI sub team conducts FGDs in three sample. villages under PHC. c. Visit PHC, review records, discuss with RKS members. d. Send brief three monthly report to Block committee. a. Reviews and collates reports from all PHCs. b. NGO / PRI sub team visits at least one PHC of the block, conduct interviews with MO and make observations. c. Visit CHC and review records, discuss with RKS members. d. Send brief three monthly report to District committee. a. Reviews and collates reports from all Blocks. b. An NGO / PRI sub team visits at least one CHC of the District, conducts interviews with Incharge, meets Block committee members and RKS members, makes observations c. Visits District hospital and reviews records, discuss with RKS members. c. Send brief three monthly report to State committee. a. Reviews and collates reports from all Districts. b. An NGO / PRI sub team visits 3 to 5 Districts, conducts interviews with DHO and District Committee members, makes observations on DH. c. Sends six monthly report to NRHM / Union Health Ministry. 9
17
18 MANAGERS MANUAL COMMUNITY MONITORING SECTION-III First Phase of Community Monitoring The outlines of community monitoring process provided within the Framework of Implementation have been developed and elaborated upon by the Advisory Group on Community Action (AGCA). The first phase was seen as a learning phase because no similar community monitoring activity, either in the health sector or in other social sectors has been implemented on a countrywide scale before. Thus in the first phase the implementation was supervised at a national level by a specially constituted National Secretariat and Task Group constituted under the supervision of the Advisory Group. It was decided that the first phase would be of eleven months (March 07-Jan 08), which got extended till December 2008 and covered nine states. Some reasons because of which it was desirable to start with a learning phase, are as follows: Learning from experiences and mistakes on a smaller scale, then moving to a larger scale: This is probably the first time in the country that the official health system is institutionalising community monitoring of health services on a major scale. There is scope for many kinds of experiences and even deviation from objectives, so it is thought to be desirable to try out the process on a smaller scale and make corrections before moving to a statewide scale. The need to pool expertise and build an initial critical mass: The number of organisations with experience in rightsbased and accountability-oriented work related to the Health sector may not be very large in many states. Similarly, expertise and commitment related to this activity within Health departments may also be limited to begin with. It would be desirable for facilitating agencies both within and outside the Health department to come together, 11
19 no similar community monitoring activity, either in the health sector or in other social sectors has been implemented on a countrywide scale before share expertise, help launch pilots in a few areas, and analyse experiences, before going to scale at the state level. This would also strengthen ownership of the process within the Department. Starting directly with a widely generalized model would demand very extensive involvement of comparatively few facilitators from day one; they would have to immediately spread themselves thin not allowing much space for initial development of methodologies and building a critical mass. The process of developing community monitoring is a delicate process that needs to be handled carefully. Community mobilisation experiences in the Health sector show that the initial response of community representatives is often to assertively point out a whole range of problems, deficiencies, gaps and even alleged cases of denial of health care which may be quite difficult for the Health officials to digest and take in the right spirit which could even at times, lead to a virtual breakdown of dialogue. Maintaining the vitality and authenticity of the process, but not allowing complete polarisation, which would disrupt the dialogue and convergence process itself is a delicate task. Starting by launching the community monitoring process all over the state on a large scale may conceivably lead to potentially disruptive situations and even demotivation of Health functionaries which could be avoided by first working out the process in pilot areas and building appropriate checks and balances in the methodology before moving to generalisation. Scale of Implementation of the First Phase The first phase of the community monitoring component of NRHM was implemented in 36 selected districts of 9 states of the country. These are Assam Chhattisgarh Jharkhand Madhya Pradesh Maharashtra Orissa Rajasthan Tamil Nadu Karnataka In each of these states a number of districts were selected (between three and five depending upon the number of districts in the state) on the basis of regional diversity as well as the presence of a credible district level NGO/ Civil Society Organisation, which can facilitate the implementation. In each of these districts three blocks were chosen for the first phase, and from among these three blocks the operational area of three PHCs were selected. Five villages were selected for initiating community monitoring in each of the three PHC areas. The total numbers of districts, blocks, PHCs and villages is summarised below: For States with 15 to 29 districts: three pilot districts were selected. For States with 30 to 39 districts: four pilot districts were selected. For States with 40 and above districts: five pilot districts were selected. This will lead to a total of 36 districts spread across these nine states. In each district, three blocks were identified giving a total 108 blocks. In each of these blocks, three PHCs were identified giving a total 324 PHCs. In each PHC area, five revenue villages were identified giving a total 1620 villages. Need for involving Civil Society Organisations/ NGOs in the First Phase NGOs or Civil Society Organisations have been given crucial roles in the NRHM. It is envisaged that besides providing services in selected areas, they will not only be members in institutional arrangement at all levels, but will also act as resource organisations and provide support for evaluation, monitoring and social audit. These organisations had a crucial role to play in the first phase of community monitoring to ensure its success. Although state Health Departments would play an extremely important role in developing community monitoring activities, however the facilitation of community based monitoring was not left to state Health Departments. Some of the reasons for this are as follows: 12




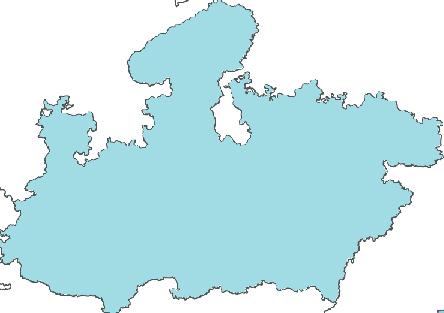
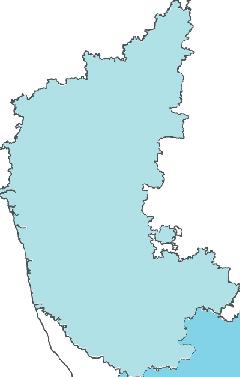

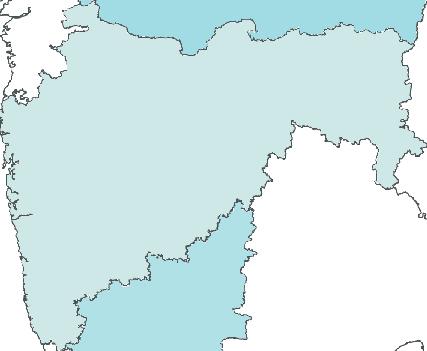

20 MANAGERS MANUAL COMMUNITY MONITORING Figure-1 Geographical Spread 13
21 facilitate change in the balance of power in the health sector, in favour of people It is largely the Health Department functionaries themselves who would be monitored; hence for the monitoring to be robustly independent, it is not sufficient to leave the entire task of developing the monitoring framework to the Health department alone. For effective community monitoring, capacity building of a whole set of actors like beneficiary representatives, CBOs, people s movements, voluntary organisations and Panchayat representatives - who will eventually do the monitoring - is imperative. Hence, involvement of networks, organisations and individuals with experience of community mobilisation and community based monitoring to facilitate involvement in the health system of this whole new set of actors is needed. To facilitate change in the balance of power in the health sector, in favour of people. The exercise of community monitoring carries meaning only if ordinary people and their spokespersons in form of both Panchayat representatives and CBOs, gain a degree of authority to identify gaps and correspondingly propose priorities and influence decision making regarding the health system. The kind of capacity required to develop a participatory community monitoring system is quite different from programme implementation and training usually conducted by the Health Department; hence involving voluntary sector agencies with some experience of accountability building and health rights work would be desirable to help facilitate this process. Role of Civil Society Organisations in the First Phase Civil Society Organisations i.e. Community Based Organisations (CBOs) and Non Governmental Organisations (NGOs) have three kinds of roles in the process of community based monitoring: Members of monitoring committees: Social organisations working in close, regular contact with communities on health related issues, especially from a rights-based perspective, would be able to present in various monitoring committees the community concerns, experiences and suggestions regarding improving public health system functioning. Resource groups for capacity building and facilitation: NGOs and CBOs will have the responsibility for overall facilitation of the initial process of committee formation and capacity building of community monitoring committee members about the process of community based monitoring. It includes the roles of members at different levels, including peripheral committees at PHC and village levels. Based on national model material, training modules and materials for orientation of community monitoring committee members would be adapted and published at state level and used for this capacity building process. All three types of members Panchayat representatives, civil society organisations and health system functionaries would benefit from such capacity building. Agencies helping to carry out independent collection of information: NGOs and CBOs would contribute to the collection of information relevant to the monitoring process at all levels from the village to state level. In these processes, an element of community mobilisation may be involved. Specific teams would dialogue with communities and would collect and process community-based information. These teams could be subgroups drawn from the larger monitoring committee at specific levels, but could also include some persons from beyond the monitoring committee. Formation of such teams should be encouraged especially at the PHC and block levels. Each team should include members from one or more facilitating NGOs and PRI members, and could also include representatives from among the health care providers. Such teams should undergo a short orientation exercise before they undertake the community monitoring exercise. 14

22
23
24 MANAGERS MANUAL COMMUNITY MONITORING SECTION-IV Implementing the first phase of Community Monitoring The first phase of the community monitoring process was implemented under the overall supervision of the specially constituted Task Group of the Advisory Group on Community Action. A National Secretariat was set up in Delhi through the collaboration of Population Foundation of India and Centre for Health and Social Justice. PREPARATORY PHASE The activities that were undertaken during the first phase and the persons responsible at each level are given in the table below. The preparatory phase lasted from March 2007 to June State Mentoring Group The State Mentoring Group was formed involving representatives of the state Health Department and state level health sector voluntary networks. Based on experience and demonstrated interest, the State Mission Director and the state designated AGCA members suggested names for this mentoring team. This team had definite responsibilities to develop community monitoring in the state during the first phase and beyond, which was clearly spelt out. This team had seven to eleven members, of which at least four to seven were civil society representatives. In addition, the designated national AGCA members were permanent invitees to the State Mentoring Team. State Nodal Organisation One of the state level NGOs with membership in the State Mentoring Team was selected to work as the state nodal NGO during the first phase. This state nodal NGO worked under the direction of the State Mentoring Team. 17
25 Table-2 Activities in the Preparatory Phase Activity Responsibility Support from Setting up Task Group. AGCA MoHFW, GOI Setting up National Secretariat. Contacting State Secretaries in the 9 states. Contacting Civil Society Organisations in the 9 states. Preparation of necessary Materials, Curricula and Modules. Meeting with state CSOs and identifying State Nodal organization. Meeting with State Health Secretary and NRHM Directorate and setting up State Community Monitoring Mentoring Group. AGCA- Task Group MoHFW, GOI Task Group National Secretariat AGCA- Task Group AGCA- Task Group Task Group National Secretariat National Secretariat Other state level activities that were carried out in the preparatory phase are as follows: A State Level Workshop was organised by the State Mentoring Team, State Nodal Organisation and State Health Mission involving all stakeholders (State Mission officials, District Health officials and PRI representatives from selected districts, NGO networks and civil society organisations from these districts) along with NRHM GoI representatives. The activities of the first phase were shared and the process finalised. Detailed timetable for district level meetings, formation and orientation of committees was worked out in this two-day state Activity Responsibility Support from Selection of districts and blocks for implementing the project. Selecting organizations which will be implementing activities at the district and block level. State level workshop to finalise the districts and modalities of district and block level activities. State level TOT. Table-3 State Level Activitie s in the Preparatory Phase Adapting and translating materials, curricula and modules for the state. State C M Mentoring Group. State C M Mentoring Group. State C M Mentoring Group. State C M Mentoring Group. State C M Mentoring Group. Task Group. National Secretariat. Task Group. National Secretariat. Task Group. National Secretariat. Task Group. National Secretariat. Task Group. National Secretariat. level workshop. A State level Training of Trainer s for the facilitating teams from all pilot districts was conducted. It was held primarily by voluntary sector facilitators in the first phase, since government officials may not have adequate experience in community monitoring activities. However state Health Department officials were present and involved in these workshops, enabling them to actively participate in further such trainings. Outcomes of the Preparatory Phase: National Secretariat was established. State Community Monitoring Mentoring Groups were established in all nine states. State Nodal Organisations were established in all nine states. State level workshops were organised in all states. State level TOT was organised in all states. Draft of materials, curriculum and modules were prepared. State level adaptation of the publications was begun. DISTRICT LEVEL IMPLEMENTATION PHASE Once the district and block level 18
26 MANAGERS MANUAL COMMUNITY MONITORING facilitating organisations were selected and traind, the key activities shifted to the district and block levels. The time allocated for these activities was July 2007 to December 2007 in the first phase. The activities at the district and block level proceeded in the following manner: Getting Ready for Community Monitoring District processes were facilitated by NGOs taking responsibility in the first phase districts along with the District Health officials and PRI representatives. A District Mentoring Team (including representatives of each of the three groups) to facilitate the community monitoring process was put in place, which facilitated the orientation activities in this and subsequent stages. In each district, one NGO was needed to take responsibility as the District Nodal NGO. This NGO was assisted by other civil society organisations that would take specific responsibility in various blocks. The process started with a District Level Workshop to share the concept, identify Figure- 2 Organogram of Monitoring & Planning Committees 19
27 the monitoring results were also shared at the village level, block and district level in the appropriate PRI fora blocks and PHCs, involving key District Health officials, PRI members and civil society organisations. Three blocks within the district were selected for pilot implementation. Block nodal civil society organisations took up the responsibility for specific blocks in coordination with the District Nodal NGO. There was need to conduct a block level training for at least a four member Block Community Monitoring Facilitation Team, including at least two NGO/ CBO members and half women. These Block Facilitation Team members were responsible for the subsequent committee formation and orientation processes. It was anticipated that these activities would be completed in the month of July Formation of Committees During the next four months (Aug Nov 2007), there was formation of committees at village, PHC and block levels in the selected blocks (in that order), along with organising primary orientation of their members. Formation of community monitoring committees started from village committees, PHC, block, and then district committees. A few members from VHCs were included in the PHC committee; similarly a few PHC committee members were included in the block committee. Therefore it was important to constitute the committees from village level upwards in such a sequential order. CBOs/NGOs and Panchayat representatives who had shown leading initiative in organising community monitoring activities at any level found representation in the next high-level committees. Adequate representation of women, dalits and adivasis was ensured in various committees. Following committee formation at the peripheral levels, the District Level Committee was also finalised and became functional by November In the first phase, at the state level, a provisional committee was formed by December This would be given final shape only after the next phase of Extended implementation is completed and at least half of the districts of the state have the Community Monitoring Committees in place, which could send representatives to the State Committee. Community Monitoring The community monitored need, coverage, access, quality, effectiveness, behaviour, presence of health care personnel at service points, possible denial of care and negligence. The monitoring process included outreach services, public health facilities and the referral system. The community monitoring exercises and collation of information was organised village wise, PHC wise, block-wise and district wise. In this way, these exercises aggregated information upwards. The monitoring results were also shared at the village level, block and district level in the appropriate PRI fora. Some of the frameworks on which community monitoring may be done, and which are included within the NRHM are as follows: Village Health Plan, District Health Plan. Entitlements under the Janani Suraksha Yojna. Roles and responsibilities of the ASHA. Indian Public Health Standards for different facilities like Sub Centre, PHC, CHC. Concrete Service Guarantees. Citizen s Charter and so on. Activities that was undertaken at the village level for community monitoring has already been outlined in Table 1- Section II, Page 9. PHC and block level community monitoring exercises included a public dialogue ( Jan Samvad ) or public hearing ( Jan Sunwai ) process by December Here individual testimonies and assessments by local CBOs/NGOs were presented. Individual testimonies were identified through the adverse outcome recording process. These public dialogues were moderated/facilitated by the District and Block Facilitation Groups in collaboration with Panchayat representatives and CBOs/NGOs working on the issue of health rights. The monitoring committee at each level 20
28 MANAGERS MANUAL COMMUNITY MONITORING Figure- 3 Process of Monitoring 21
29 monitoring committees did not only rely on reports, but also directly interacted in the field situation and got feedback reviewed and collated the summary reports from the committees dealing with units under it. This enabled it to make an assessment of the situation prevailing in all the units under its purview, and to make a report at its level. For example, the District Committee would receive and review the reports from all block committees. However monitoring committees did not only rely on reports, but also directly interacted in the field situation and got feedback. Firstly, each committee appointed a small sub-team drawn from its NGO and PRI representatives who visited on a regular basis, a small sample of units (say one facility or two villages) under their purview and directly reviewed the conditions. This enables the committee to not just rely on reports but to also have a first-hand assessment of conditions in their area. For example, the PHC committee representatives would visit two villages and conduct group discussions in each trimester, selecting different villages by rotation. Similarly, the Block Committee representatives would visit one PHC by rotation in each trimester. Secondly, monitoring committees at PHC, block and district level would be involved in six-monthly or annual Jan Samvads or Public hearings at their respective levels, where committee members would get direct feedback of the situation, including possible presentation of cases of denial of health care. Similarly, it is suggested that the State Health Mission could conduct an annual public meeting open to all civil society representatives Activity Profile A1- Income Generation A2 - Environment / Natural Resource Mgmt A3 - Education A4- Health Table-4 Criteria for NGO selection Community Mobilisation C1- Self Help Groups C2- Village Level Committees C3- Federations C4- Community Leadership training C5- Work with PRIs C6 Village based organisation and mobilisation on specific issues where the State Mission report and independent reports would be presented and various aspects of design and implementation of NRHM in the state, including state specific health schemes, would be reviewed and discussed enabling corrective action to be taken. Screening Civil Society Organisations for involvement in Community Monitoring In order to screen civil society organisations for their capacity to partner in community monitoring activities, and to participate in monitoring committees at various levels, a simple questionnaire was used. Such organisations may include CBOs (including Self-Help Groups and people s organisations) as well as NGOs working at the respective level, with documented activity in the area since at least three years. In addition to other questions about the organisation, the following issues will be included in the questionnaire. On the basis of their responses to their questionnaire, the following screening table will be used and any organisation having at least one entry in all the four aspects (with brief report of the activity carried out in that aspect) may be considered as having qualified. Any organisation with demonstrated experience of monitoring public services; organising public dialogues or public hearings should be given priority to participate in the community monitoring committees. Women s Empowerment Activities W1- Village level women s groups W2 Women s leadership development and training W3 Women and PRI WomeRights based Activities R1- Right to Healthcare R2- Right to Food R3- Right to Information R4- Right to Employment R5- Livelihood rights e.g. rights related to Forest, Land, Wages, Displacement etc. (specify) 22
30 MANAGERS MANUAL COMMUNITY MONITORING Table-5 Format for NGO Selection Name of CSO Activity Profile Community Mobilisation Activities Women s Empowerment Activities Rights based Activities A1 A2 A3 A4 C1 C2 C3 C4 C5 W1 W2 W3 W4 W5 W6 Key Considerations during Selection To ensure wide participation, diverse group of civil society networks and organisations involved in promotion of health rights and monitoring should be involved at various levels. The process of selecting civil society organisations to be involved in monitoring committees at all levels could be facilitated by the mentoring team of the respective level, with guidance from the mentoring team of the higher level. For example, the District Mentoring Team could suggest the names of civil society organisations to be involved in the District Monitoring Committee, with inputs from the State Mentoring Team as relevant. This should be a participatory process including various civil society networks and organisations. It should not be limited to NGOs, and should also definitely involve CBOs and people s organisations Civil society involvement in monitoring should not be focussed only on mother NGOs which are often deeply involved in implementation and who may not always be the most objective monitors of work which they themselves are involved in implementing. Particularly for the community monitoring process in NRHM, it is imperative that the idea is not confined to just leave it to mother NGOs. Rather, organisations with experience of rights based activities and accountability enforcing activities should be given adequate space and responsibility at all levels. Process Documentation and Review Since the first phase of the community monitoring process was a learning phase, it included process documentation and review as an important component. This included the following three distinct stages: Process Documentation To ensure uniformity of recording the activity, each activity of the project that has been mentioned above included a documentation procedure. These documents were filled in by the responsible agency at different levels and collated at the state level. The State Mentoring Team was responsible for analysing these documents and prepared a review report on the state implementation, reporting what interventions worked and why and suggesting changes. Evaluation of the State Level Intervention There was an independent evaluation of the different interventions and their impact on different stakeholders by a team of five experts. The evaluation included review of the documentation process, interviews with different stakeholders, including members of the community in a limited number of locations across each of the nine states. State Level Review Workshops The third component of the review process comprised of an end line workshop with those involved in implementing the first phase to review the process in each state. 23
31
32 MANAGERS MANUAL COMMUNITY MONITORING SECTION-V Organisational Responsibilities The entire range of activities during the first phase were needed to be supported by NRHM Mission Directorate from the Union Health Ministry level for rapidity of execution, given the compressed timeframe available. Responsibilities for handling funds and ensuring activities at various levels were allocated as follows: NATIONAL LEVEL At the national level, the Task Group of the Advisory Group on Community Action (AGCA) facilitated the entire process of community action in consultation with the Ministry of Health and Family Welfare. The Population Foundation of India is the Secretariat for the AGCA. AGCA-TAG (Sub-group of AGCA) Conceiving and planning the entire intervention. Periodic review. Support the relationship building with Table 6: Organisational Responsibilities at Different Levels Level National State District Block and below Responsibility Overall facilitation by AGCA (in consultation with NRHM officials). Financial responsibilities and coordination handled by AGCA Secretariat along with subgroup of AGCA. State Nodal NGO under guidance of State Mentoring Team (which would include State Mission Director). District nodal NGO under guidance of District Mentoring Team (which would include District Health Officer). Block nodal civil society organisation (in coordination with District Nodal NGO). 25
33 a National Secretariat was set up under the leadership of PFI along with Centre for Health and Social Justice at New Delhi the state government. Support the formation of State CM Mentoring Group. Identify State Level Nodal Organisation. Technical inputs. Generate training designs. Framing Community Monitoring Protocol. Jan Samvad protocols etc. Distil lessons learnt. National Secretariat on Community Action NRHM A National Secretariat was set up under the leadership of PFI along with Centre for Health and Social Justice at New Delhi. The Secretariat undertook special facilitation of the community monitoring process at the national level in consultation with the MoHFW and NRHM Mission. The National Secretariat functioned within the framework formulated by the AGCA for community based monitoring of programmes under NRHM. The National Secretariat had the following roles and responsibilities: Coordinating activities of the national preparatory phase, which includes developing tools, model curriculum, workshops, awareness materials and documentation formats for the programme. Assist the AGCA members and the state NRHM Directorates and NGO networks for the state preparatory stage. Facilitate process documentation and review of the pilot implementation phase in consultation with AGCA members. Develop a website on community based monitoring of processes and access to services under NRHM Manage the financial responsibility of the pilot programme Prepare progress reports, field visits and the national dissemination workshops of the programme at the national level Conduct quarterly review of AGCA for review of the pilot programme. Staffing: The National Secretariat was managed by two programme officers responsible for the overall programmatic and financial coordination of the programme. The officers reported to the Task Group of AGCA. STATE LEVEL At the state level, there was the State Community Monitoring Mentoring Group, State Resource Pool and the State Nodal Agency. State CM Mentoring Group Coordinate with the State Government. Prepare state level plan/design and budgets. Identify districts and blocks. Identify NGOs for district and block level. Review progress at the state level. Distil lessons learnt from the state level experiences. State Resource Pool Adaptation of manuals, protocols and materials for the state level situation. Translation of materials, manuals and protocols. Provide training and facilitation support for events trainings and workshops. State Nodal Agency Assist in implementing the decisions taken at the CM Mentoring Team. Arrange for technical and resource support to district/block level NGOs. Support the process of adaptation, translation and publication state level materials/manuals. Supervise community level documentation processes. Maintain documentation of state level processes. Provide progress, process and financial reports and documents to the National Secretariat on a regular basis. Financial support and disbursement to district level and block level processes. Maintain state level accounts. Supervise progress and support processes/activities at the district, block and community levels. 26
34 MANAGERS MANUAL COMMUNITY MONITORING Ministry of Health and Family Welfare (GoI)- NRHM Advisory Group on Community Action (AGCA) National Secretariat on Community Action- NRHM State Monitoring and Planning Committee State Mentoring Team State Nodal NGO (Out of the state mentoring team, one NGO Member will designated as State NodalNGO) District Mentoring Team (This team will include PRI representatives, district Health Officials and NGO representatives) District Nodal NGO The District level and Block level funds in the first phase in each state would be given to designated District nodal NGO to enable a fast startup and adequate flexibility in the process) District Monitoring and Planning Committee Block Nodal Civil Society Organizations (The District nodal NGO would collaborate with Block nodal civil society organisations for execution of activities in specific blocks) Block Community Monitoring Facilitation Team (Responsible for subsequent committee formation and orientation processes) Block Monitoring and Planning Committee PHC Monitoring and Planning Committee Village Health and Sanitation Committee Figure-4 Organogram 27
35 DISTRICT LEVEL At the district level, there is the District Community Monitoring Mentoring Group and the District Nodal Agency. District CM Mentoring Group Coordinate with the State and district level government. Prepare district level plan/design and budgets. Coordinate with blocks and provides technical support. Review progress at the district level and below. Distil lessons learnt from the district level and below experiences. Identify NGOs for district and block level for implementing the community monitoring programme. District Nodal Agency Assist in implementing decisions taken by mentoring group. Arrange for technical and resource support to district/ block level NGOs. Support process of adaptation, translation and publication state level materials/manuals. Supervise community level documentation processes. Coordinate with State Nodal Agency. Coordinate with district officials - Chief Medical Officer; Zilla Parishad, District Mentoring Team. Mobilisation and capacity building at district level. Collation of records and reports. Financial management. Mobilisation and capacity building at district and block level. Facilitate balance of power between stakeholders - liaison with different stakeholders. Declaring, dissemination - health entitlements within rights based approach. Reflect community/spokespersons of community concerns, experiences. Form committees at the village, PHC and block if such committees have not been formed. BLOCK LEVEL AND BELOW At the block level, there is a Block Nodal Agency in coordination with District Nodal NGO. The block level NGOs will appoint block facilitators for the execution of community monitoring. Block Nodal Agency Collaborate with District Nodal Agency for execution of activities in block. Mobilisation and capacity building at block level. Form committees at the village, PHC and block if such committees have not been formed. Coordinate with- Block Medical Officer; village Panchayat, Panchayat Samitis, District Mentoring Team. Supervise block facilitators for the execution of the Community Monitoring at block and village level. Community mobilisation at village level. Financial management at the block level. Encouraging participation of all stakeholders in community monitoring process. Conduct Jan Samvad at village, PHC and block level. Supervise community level documentation processes. Organise VHSC trainings. Handholding of VHSC members for community inquiry and preparation of report card 28
36

37
38 Annexures ANNEXURE 1: NRHM STRATEGIES (a) Core Strategies: Train and enhance capacity of Panchayati Raj Institutions (PRIs) to own, control and manage public health services. Promote access to improved healthcare at household level through the female health activist (ASHA). Health Plan for each village through Village Health Committee of the Panchayat. Strengthening sub centre through an untied fund to enable local planning and action and more Multi Purpose Workers (MPWs). Strengthening existing PHCs and CHCs, and provision of bedded CHC per lakh population for improved curative care to a normative standard (Indian Public Health Standards defining personnel, equipment and management standards). Preparation and Implementation of an inter-sectoral District Health Plan prepared by the District Health Mission, including drinking water, sanitation & hygiene and nutrition. Integrating vertical Health and Family Welfare programmes at national, state, block, and district levels. Technical support to National, State and District Health Missions, for public health management. Strengthening capacities for data collection, assessment and review for evidence based planning, monitoring and supervision. Formulation of transparent policies for deployment and career development of human resources for health. Developing capacities for preventive health care at all levels for promoting healthy life styles, reduction in consumption of tobacco and alcohol etc. Promoting non-profit sector particularly in under served areas. (b) Supplementary Strategies Regulation of private sector including the informal rural practitioners to ensure availability of quality service to citizens at reasonable cost. Promotion of Public Private Partnerships for achieving public health goals. Mainstreaming AYUSH -revitalising local health traditions. Reorienting medical education to support rural health issues including regulation of medical care and medical ethics. Effective and viable risk pooling and social health insurance to provide health security to the poor by ensuring accessible, affordable, accountable and good quality hospital care. 31
39 ANNEXURE 2: MONITORING AND EVALUATION Health MIS to be developed upto CHC level, and web-enabled for citizen scrutiny. Sub centres to report on performance to Panchayats, hospitals to Rogi Kalyan Samitis and District Health Mission to Zila Parishad. The District Health Mission to monitor compliance to Citizen s Charter at CHC level. Annual District Reports on People s Health (to be prepared by Govt/NGO collaboration). State and National Reports on People s Health to be tabled in Assemblies, Parliament. External evaluation/social audit through professional bodies/ngos. Mid-course reviews and appropriate correction. (From: NRHM Mission Document) Monitoring Outcomes of the Mission Right to health is recognised, as inalienable right of all citizens as brought out by the relevant rulings of the Supreme Court as well as the International Conventions to which India is a signatory. As rights convey entitlement to the citizens, these rights are to be incorporated in the monitoring framework of the Mission. Therefore, providing basic Health services to all the citizens as guaranteed entitlements would be attempted under the NRHHM. Preparation of household specific health cards that record information on: Record of births and deaths, record of illnesses and disease, record any expenditure on health care, food availability and water source, means of livelihood, age profile of family, record of age at marriage, sex ratio of children, available health facility and providers, food habits, alcohol and tobacco consumption, gender relations within family, etc, (by ASHA/AWW/Village Health Team). Preparation of habitation/village health register, on the basis of the household health cards (by the Village Health Team). Periodic health facility survey at SHC, PHC, CHC, district levels to see if service guarantees are being honoured (by district/block level Mission Teams/research and resource institutions). Formation of Health Monitoring and Planning Committees at PHC, block, district and State levels to ensure regular monitoring of activities at respective levels, along with facilitating relevant inputs for planning. Sharing of all data and discussion at habitation/village level to ensure full transparency. Display of agreed service guarantees at health facilities, details of human and financial resources available to the facility. Sample household and facility surveys (by external research organisations/ngos). Public reporting of household and health facility findings and its wider dissemination through public hearings and formal reporting. (From: NRHM Framework for Implementation) 32
40 ANNEXURE 3: COMMUNITY MONITORING FRAMEWORK We have discussed the overall monitoring framework in an earlier section (IV). The basic change that NRHM wishes to bring about in the monitoring framework is to involve local communities in planning and implementing programmes with a framework that allows them to assess progress against agreed benchmarks. While external institutions will also assess progress, they will do so on benchmarks that have been agreed with local communities and health institutions. The intention is to move towards a community based monitoring framework that allows continuous assessment of planning and implementation of NRHM. Besides the issues already mentioned earlier on the monitoring framework, the broad principles for community based monitoring are listed below: Given the overall objective that people should have complete access to rational, appropriate and effective health care, community based monitoring should preferably fulfil following objectives: It should provide regular and systematic information about community needs, which would guide related planning. It should provide feedback according to the locally developed yardsticks for monitoring as well as key indicators. This would essentially cover the status of entitlements, functioning of various levels of the public health system and service providers, identifying gaps, deficiencies and levels of community satisfaction, which can facilitate corrective action in a framework of accountability. It should enable the community and community-based organisations to become equal partners in the planning process. It would increase the community sense of involvement and participation to improve responsive functioning of the public health system. The community should emerge as active subjects rather than passive objects in the context of the public health system. It could be used for validating the data collected by the ANM, Anganwadi worker and other functionaries of the public health system. Ownership of Community Monitoring Process The Health Department functionaries need to be involved in the preparation and mobilisation phase of the initiative so as to enable ownership of the process and outcomes among the providers and users. PRIs, community based organisations and NGOs, along with Health Department functionaries should be involved in the preparation and mobilisation phase of the initiative so as to enable ownership of the process and outcomes among the providers and users. The government can enable such interactive processes through issuing relevant Government Orders, and by ensuring effective communication to all levels of public health functionaries. All the members of any committee that is formed (for example the Village Health Committee) must have their roles and responsibilities clearly defined and articulated. Power(s) and Capacity Building The committees that are formed at various levels must have concomitant authority i.e. they must have the power to initiate action. The capacities of the members of a village level committee have to be built continuously for them to be able to function effectively. This would require allocation of resources and capacity building inputs. This process must begin with full and ready access to information. The intent of the newly launched NRHM as mentioned in the core strategy is that it will promote community ownership and decentralised planning from village to district 33
41 level. This is supposed to be through participatory processes, by strengthening evidence based effective monitoring and evaluation. In order to actually do so it will be imperative that: The government should enable such interactive processes by issuing relevant Government Orders. One example of such orders is the one passed by the Government of Rajasthan for the formation of Convergence Committees at the district and PHC level. A similar example is the response of the Gujarat Government to the National Human Rights Commission, wherein coordination bodies at various levels of the Public Health System are proposed for operationalising a state level health services monitoring mechanism. All the members of any committee that is formed must have their roles and responsibilities clearly defined and articulated. Effective and quality monitoring requires institutional mechanisms at various levels beginning at the community and going upwards. Adequate investment (time and resources) must be made in capacity development at various levels. Analysis of the collected information must be undertaken at various levels so as to enable prompt action and corrections. The committees that are formed at various levels must have concomitant authority i.e. they must have the power to take action. The monitoring system must be directly linked to corrective decision making bodies at various levels. The information and issues emerging from monitoring must be communicated to the relevant official bodies responsible for taking action (from PHC to state level) so that monitoring results in prompt, effective and accountable remedial action. Overall Points to be Considered Effective community monitoring would change the status of community members from passive beneficiaries to active rights holders, enabling them to more effectively access health services. One must be realistic in setting indicators and planning activities. Communities need few and simple indicators for monitoring, and the time devoted by members, especially community representatives involved in various committees, must be utilised optimally. Community monitoring must be seen as an integral part of the Public Health System at all levels and for all activities, and not as a stand-alone process. Panchayati Raj Institutions are not synonymous with the community. For community ownership and effective monitoring, even if PRI representatives are involved, one still needs to involve user groups and beneficiaries, and to include CBOs. Involvement of the General Public by Means of Regular Public dialogue or Public hearing (Jan Samvad / Jan Sunwai) Most of the public participation in the monitoring process would be mediated by representatives of the community or community-linked organisations. However, to enable interested community members to be directly involved in exchange of information, and to improve transparency and accountability of the health care system, Public dialogues (Jan Samvad) or Public hearings ( Jan Sunwai ) would be need to organised at regular intervals (once or twice in a year, depending on the initiative of the local organisations) at PHC, block and district levels (see section IV page 21). What Should the Community Monitor? The community and community-based organisations should monitor demand/ need, coverage, access, quality, effectiveness, behaviour and presence of health care personnel at service points, possible denial of care and negligence. This should be monitored related to outreach services, public health facilities and the referral system. 34
42 ANNEXURE 4: COMPOSITION, ROLES AND RESPONSIBILITIES OF MONITORING COMMITTEES Village Health Committee This Committee would be formed at the level of the revenue village (more than one such villages may come under a single Gram Panchayat). Composition The Village Health Committee would consist of: Gram Panchayat members from the village. ASHA, Anganwadi Sevika, ANM. SHG leader, the PTA/MTA Secretary, village representative of any Community Based Organisation working in the village, user group representative. The chairperson would be the Panchayat member (preferably woman or SC/ST member) and the convener would be ASHA; where ASHA not in position it could be the Anganwadi Sevika of the village. Roles and Responsibilities Create public awareness about the essentials of health programmes, with focus on people s knowledge of entitlements to enable their involvement in the monitoring. Discuss and develop a Village Health Plan based on an assessment of the village situation and priorities identified by the village community. Analyse key issues and problems related to village level health and nutrition activities, give feedback on these to relevant functionaries and officials. Present an annual health report of the village in the Gram Sabha. Participatory Rapid Assessment to ascertain the major health problems and health related issues in the village Estimation of the annual expenditure incurred for management of all the morbidities may also be done. The mapping will also take into account the health resources and the unhealthy influences within village boundaries. Mapping will be done through participatory methods with involvement of all strata of people. The health mapping exercise shall provide quantitative and qualitative data to understand the health profile of the village. These would be village information (number of households caste, religion and income ranking, geographical distribution, access to drinking water sources, status of household and village sanitation, physical approach to village, nearest health facility for primary care, emergency obstetric care, and transport system) and the morbidity pattern. Maintain village health register and health information board/calendar The health register and board, put up at the most frequented section of the village will have information about mandated services, along with services actually rendered to all pregnant women, new born and infants, people suffering from chronic diseases etc. Similarly, dates of visit and activities expected to be performed during each visits by health functionaries may be displayed and monitored by means of a Village health calendar. These will be the most important document maintained by the village community about the exhibition of health status and health care services availability. This will also serve as the instrument for cross verification and validation of data. Ensure that the ANM and MPW visit the village on the fixed days and perform the stipulated activity; oversee the work of village health and nutrition functionaries like ANM, MPW and AWW. Obtain a bi-monthly health delivery report from health service providers during their visit to the village. Discuss the report submitted by ANM and MPW and take appropriate action. 35
43 Consider the problems of the community and the health and nutrition care providers and suggest mechanisms to solve it. Discuss every maternal death or neonatal death that occurs in their village, analyse it and suggest necessary action to prevent such deaths. Get these deaths registered in the Panchayat. Manage the village health fund. Power (s) of the Committee The convener will sign the attendance registers of the AWWs, Mid-Day Meal Sanchalak, MPWs, and ANMs. MPWs and ANMs will submit a bi-monthly village report to the committee along with the plan for next two months. Format and contents of the bi-monthly reports would be decided village health committee. The committee will receive funds of Rs.10, 000 per year. This fund may be used as per the discretion of the VHC. Yardsticks for Monitoring at Village Level Village Health Plan. NRHM indicators translated into Village health indicators. Tools for Monitoring at Village Level Village Health Register. Records of the ANM. Village health calendar. Infant and maternal death audit. Public dialogue (Jan Samvad). PHC Health Monitoring and Planning Committee The PHC Health Committee would function as the health monitoring and planning arm of the Panchayats coming under the PHC area. It is recommended that the PHC Committee have the following broad pattern of representation, including members from Panchayats, health care service providers and civil society: Composition 30% members should be representatives of Panchayat Institutions (Panchayat Samiti member from the PHC coverage area; two or more sarpanchs of which at least one is a woman). 20% members should be non-official representatives from the village health committees, coming from villages under the jurisdiction of the PHC, with annual rotation to enable representation from all the villages. 20% members should be representatives from NGOs/CBOs and people s organisations working on Community health and health rights in the area covered by the PHC. 30% members should be representatives of the health and nutrition care providers, including the Medical Officer Primary Health Centre and at least one ANM working in the PHC area. The chairperson of the PHC committee would be one of the Panchayat representatives, preferably a Panchayat Samiti member belonging to the PHC coverage area. The executive chairperson would be the Medical officer of the PHC. The secretary of the PHC committee would be one of the NGO/CBO representatives. 36
44 Roles and Responsibilities Consolidation of the village health plans and charting out the annual health action plan in order of priority. The plan should clearly lay down the goals for improvement in health services and key determinants. Presentation of the progress made at the village level, achievements, actions taken and difficulties faced followed by discussion on the progress of the achievements of the PHC, concerns and difficulties faced and support received to improve the access to health facilities in the area of that particular PHC. The discussion could include: Sharing of reports of Village Health Committees. Reports from ANM, MPW about the coverage of health facilities. Any efforts done at the village level to improve the access to health care services. Record and analysis of neonatal and maternal deaths. Any epidemic occurring in the area and preventive actions taken. Ensure that the Charter of citizens health rights is disseminated widely and displayed out side the PHC informing the people about the medicine facilities available at the PHC, timings of PHC and the facilities available free of cost. A suggestion box can be kept for the health care facility users to express their views about the facilities. These comments will be read at the coordination committee meeting to take necessary action. Monitor physical resources like, infrastructure, equipments, medicines, water connection etc at the PHC and inform the concerned government officials to improve it. Discuss and develop a PHC Health Plan based on an assessment of the situation and priorities identified by representatives of village health committees and community based organisations. Share information about any health awareness programme organised in the PHC s jurisdiction, its achievements, follow up actions, difficulties faced etc. Coordinate with local CBOs and NGOs to improve the health scenario of the PHC area. Review functioning of sub-centres operating under jurisdiction of the PHC and taking appropriate decisions to improve their functioning. Brief minutes of the meeting at the end of the meeting along with the action plan emphasising the actions to be taken by different committee members, which will be shared at the District Level Committee. The minutes will also serve as a reference point, while sharing the progress done between two committee meetings. Initiate appropriate action on instances of denial of right to health care reported or brought to the notice of the committee; initiate an enquiry if required and table report within two months in the committee. The report may become a part of the performance appraisal of the concerned staff member. The committee may recommend corrective measures to the next level (block/district). The decisions taken in the committee need to be forwarded to higher concerned officials and a copy to the corresponding health committee of that level who will be responsible to take necessary decision for action to be taken on the inquiry within a period of three months. Power(s) of the committee Contribute to annual performance appraisal of Medical officer/other functionaries at the PHC. Take collective decision about the utilisation of the special funds given to PHC (say Rs.25, 000) for the repairs, maintenance of equipments, health education etc and any other aspects, which will facilitate the improvement of access to health care services. The MO can utilise this fund after the discussion and approval from the committee. Yardsticks for Monitoring at PHC level Charter of Citizens Health Rights. IPHS or similar standards for PHC (this would include continuous availability of basic 37
45 outpatient services, indoor facility, delivery care, drugs, laboratory investigations and ambulance facilities). PHC Health Plan. Tools for Monitoring at PHC level Village health registers / calendars. PHC records. Discussions with and interviews of the PHC committee members. Public dialogue (Jan Samvad) or Public hearing (Jan Sunwai). Quarterly feedback from village Health Committees. Periodic assessment of the existing structural deficiencies. Block Health Monitoring and Planning Committee The committee constituted at the block level would be consistent with CHC. This committee would have members drawn from service providers, representatives of VHSCs and PPMCs, representative of panchayts. A local civil society organization will serve as its member secretary. The block CMO & HO will be the convener of this committee and it will be chaired by the Pradhan of Panchayat Samiti. Composition 30% members should be representatives of the Block Panchayat Samiti (Adhyaksha/ Adhyakshika of the Block Panchayat Samiti or members of the Block Panchayat samiti, with at least one woman). 20% members should be non-official representatives from the PHC health committees in the block, with annual rotation to enable representation from all PHCs over time. 20% members should be representatives from NGOs / CBOs and People s organizations working on community health and health rights in the block, and involved in facilitating monitoring of health services. 20% members should be officials such as the Block Medical Officer, the Block Development Officer, selected Medical Officers from PHCs of the block. 10% members should be representatives of the CHC level Rogi Kalyan Samiti. The chairperson of the Block committee would be one of the Block Panchayat Samiti representatives. The executive chairperson would be the Block medical officer. The secretary would be one of the NGO / CBO representatives. Roles and Responsibilities Consolidate PHC level health plans and charting out of the annual health action plan for the block. The plan should clearly lay down the goals for improvement in health services. Review progress made at the PHC levels, difficulties faced, actions taken and achievements made, followed by discussion on any further steps required to be taken for further improvement of health facilities in the block, including the CHC. Analyse records on neonatal and maternal deaths; and the status of other indicators, such as coverage for immunisation and other national programmes. Monitor physical resources like, infrastructure, equipments, medicine, water connection etc at the CHC; similar exercise for the manpower issues of the health facilities that come under the jurisdiction of the CHC. Coordinate with local CBOs and NGOs to improve the health services in the block. Review functioning of sub-centres and PHCs operating under jurisdiction of the CHC and taking appropriate decisions to improve their functioning. Initiate appropriate action on instances of denial of right to health care reported or brought to the notice of the committee; initiate an enquiry if required and table report 38
46 within two months in the Committee. The Committee may also recommend corrective measures to the district level. Power(s) of the committee Contribute to annual performance appraisal of Medical officer/other functionaries at the PHC and CHC. Take collective decision about the utilisation of the special funds given to CHC for the repairs, maintenance of equipments, health education etc and any other aspects, which will facilitate the improvement of access to health care services. The CMO can utilise this fund after the discussion and approval from the committee. Yardsticks for Monitoring at Block level IPHS or similar standards for CHC (this would include continuous availability of basic outpatient services, indoor facility, community outreach services, referral services, delivery and antenatal care, drugs, laboratory investigations and ambulance facilities). Charter of Citizens Health Rights for CHC. Block Health Plan. Tools for Monitoring at Block level PHC and CHC records. Discussions with and interviews of the CHC RKS members. Report of Public dialogue (Jan Samvad). Quarterly feedback from village and PHC Health Committees. Periodic assessment of the existing structural and functional deficiencies. District Health Monitoring and Planning Committee The committee constituted at the district level would contribute to the development of District Health Plan. This committee would have members drawn from service providers, representatives of VHSCs, PPMCs, BPMCs and representative of panchayts. The chairperson of the District Committee would be one of the Zilla Parishad representatives, preferably convenor or member of the Zilla Parishad Health committee. The executive chairperson would be the CMO/CMHO/DHO or officer of equivalent designation. The secretary of the PHC committee would be one of the NGO/CBO representatives. Composition 30% members should be representatives of the Zilla Parishad (esp. convenor and members of its Health Committee). 25% members should be district health officials, including the District Health Officer/Chief Medical Officer and Civil Surgeon or officials of parallel designation, along with representatives of the District Health Planning Team including management professionals. 15% members should be non-official representatives of block committees, with annual rotation to enable successive representation from all blocks. 20% members should be representatives from NGOs/CBOs and people s organisations working on Health rights and regularly involved in facilitating community based monitoring at other levels (PHC/block) in the district. 10% members should be representatives of Hospital Management Committees in the district. Roles and Responsibilities Discuss on the reports of the PHC health committees. Financial and solving blockages in flow of resources if any. Assess infrastructure, medicine and health personnel related information and 39
47 necessary steps required to correct the discrepancies. Review progress report of the PHCs emphasising the information on referrals utilisation of the services, quality of care etc. Contribute to development of the District Health Plan, based on an assessment of the situation and priorities for the district. This would be based on inputs from representatives of PHC health committees, community based organisations and NGOs. Ensure proper functioning of the Hospital Management Committees. Discuss on circulars, decisions or policy level changes done at the state level; deciding about their relevance for the district situation. Take into cognisance of the reported cases of the denial of health care and ensure proper redressal. Yardsticks for Monitoring at District Level Charters of Citizens Health Rights. District Action Plan. NRHM guidelines. Indian Public Health Standards. Tools for Monitoring at the District Level Report from the PHC Health committees. Report of the District Mission committee. Public Dialogue (Jan Samvad). State Health Monitoring and Planning Committee The committee constituted at the state level would contribute to the development of State Health Plan. This committee would have members drawn from service providers, representatives of VHSCs, PPMCs, BPMCs, DPMCs and representative of panchayts. The chairperson would be one of the elected members (MLAs). The executive chairperson would be the Secretary Health and Family Welfare. The secretary would be one of the NGO coalition representatives. Composition 30% of total members should be elected representatives, belonging to the State legislative body (MLAs/MLCs) or Convenors of Health committees of Zilla Parishads of selected districts (from different regions of the state) by rotation. 15% would be non-official members of district committees, by rotation from various districts belonging to different regions of the state. 20% members would be representatives from State health NGO coalitions working on Health rights, involved in facilitating community based monitoring. 25% members would belong to state Health Department. Secretary Health and Family Welfare, Commissioner Health, relevant officials from Directorate of Health Services (incl. NRHM Mission Director) along with technical experts from the State Health System Resource Centre / Planning cell. 10% members would be officials belonging to other related departments and programmes such as Women and Child Development, Water and Sanitation, Rural development. Roles and Responsibilities Discuss the programmatic and policy issues related to access to health care and to suggest necessary changes. Review and contribute to the development of the State Health Plan, including the plan for implementation of NRHM at the state level; the committee will suggest and review priorities and overall programmatic design of the State Health Plan. 40
48 Discuss Key issues arising from various district health committees, which cannot be resolved at that level (especially relating to budgetary allocations, recruitment policy, programmatic design etc) and initiate appropriate action initiated by the committee. Also discuss administrative and financial level queries, which need urgent attention. Institute a health rights redressal mechanism at all levels of the health system, which will take action within a time bound manner. Review summary report of the actions taken in response to the enquiry reports. Operationalise and assess the progress made in implementing the recommendations of the NHRC, to actualise the right to health care at the state level. Take proactive role to share any related information received from GOI and will also will share achievements at different levels. The copies of relevant documents will be shared. Power(s) of the committee Ensure that the different levels committees are properly constituted and they meet regularly and transact their mandates in letter and spirit Yardsticks for Monitoring at State Level NHRC recommendations and National Action Plan on Right to Health Care; responses of state Health Departments and actions to which the State Government has committed itself. NRHM state level plan and the State Health Mission guidelines. IPHS. Tools for Monitoring at State Level Reports of the district health committees. Periodic assessment reports by various taskforces/ state level committees about the progress made in formulating policies according to IPH Standards, NHRC recommendations and its implementation status etc. 41
49 ANNEXURE 5: CONCRETE SERVICE GUARANTEES Concrete Service Guarantees that NRHM will provide: Skilled attendance at all births. Emergency obstetric care. Basic neonatal care for new born. Full coverage of services related to childhood diseases/health conditions. Full coverage of services related to maternal diseases/health conditions. Full coverage of services related to low vision and blindness due to refractive errors and cataract. Full coverage for curative and restorative services related to leprosy. Full coverage of diagnostic and treatment services for tuberculosis. Full coverage of preventive, diagnostic and treatment services for vector borne diseases. Full coverage for minor injuries/illness (all problems manageable as part of standard outpatient care upto CHC level). Full coverage of services inpatient treatment of childhood diseases/health conditions. Full coverage of services inpatient treatment of maternal diseases/health conditions including safe abortion care (free for 50% user charges from APL). Full coverage of services for blindness, life style diseases, hypertension etc. Full coverage for providing secondary care services at sub-district and District Hospital. Full coverage for meeting unmet needs and spacing and permanent family planning services. Full coverage of diagnostic and treatment services for RI/STI and counselling for HIV AIDS services for adolescents. Health education and preventive health measures. 42
50 visitwww.nrhmcommunityaction.org
 Flat 3C, H Block, First Floor, Saket B-28, Qutab Institutional Area New Delhi - 110017 Tara Crescent, New Delhi - 110 016 Phone: + 91-11-40517478, 26511425, Fax: 26536041 Phone: +")
51 ( ) Published on behalf of Advisory Group on Community Action (AGCA) by National Secretariat on Community Action - NRHM Centre for Health and Social Justice (CHSJ) Population Foundation of India (PFI) Flat 3C, H Block, First Floor, Saket B-28, Qutab Institutional Area New Delhi Tara Crescent, New Delhi Phone: , , Fax: Phone: , Fax: chsj@chsj.org popfound@sify.com Website: Website:
National Rural Health Mission (NRHM) State Institute of Health & Family Welfare, Jaipur
 State Institute of Health & Family Welfare, Jaipur") National Rural Health Mission (NRHM) State Institute of Health & Family Welfare, Jaipur NRHM N Newer Initiatives. R Rural Poor Population H Holistic Holistic Health Package. M Monitoring mechanisms To
National Rural Health Mission (NRHM) State Institute of Health & Family Welfare, Jaipur NRHM N Newer Initiatives. R Rural Poor Population H Holistic Holistic Health Package. M Monitoring mechanisms To
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012
 Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Rural Health Care System in India
 Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
To evaluate the impact of NRHM interventions, by Agencies outside the Government, and make recommendations on:
 TOT OF ZONAL AGENCIES To evaluate the impact of NRHM interventions, by Agencies outside the Government, and make recommendations on: The institutional mechanisms and monitoring systems that have been put
TOT OF ZONAL AGENCIES To evaluate the impact of NRHM interventions, by Agencies outside the Government, and make recommendations on: The institutional mechanisms and monitoring systems that have been put
CHAPTER 30 HEALTH AND FAMILY WELFARE
 CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
A Report on the First Phase of Community Monitoring under NRHM
 Reviving Hopes Realising Rights A Report on the First Phase of Community Monitoring under NRHM Contents : Sunita Singh, Abhijit Das, Sona Sharma Editing : Elisa Parija Layout & Design : Kishor Production
Reviving Hopes Realising Rights A Report on the First Phase of Community Monitoring under NRHM Contents : Sunita Singh, Abhijit Das, Sona Sharma Editing : Elisa Parija Layout & Design : Kishor Production
Rural Health Care System in India. Rural Health Care System the structure and current scenario
 Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
NATIONAL RURAL HEALTH MISSION
 NATIONAL RURAL HEALTH MISSION Meeting people s health needs in rural areas Framework for Implementation 2005-2012 Ministry of Health and Family Welfare Government of India Nirman Bhawan New Delhi-110001
NATIONAL RURAL HEALTH MISSION Meeting people s health needs in rural areas Framework for Implementation 2005-2012 Ministry of Health and Family Welfare Government of India Nirman Bhawan New Delhi-110001
Rural Health Care System in India. Rural Health Care System the structure and current scenario
 Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA.
 UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
Evaluation Study on National Rural Health Mission (NRHM)
") Programme Evaluation Organisation Pla n n in g Com m s is io n Evaluation Study on National Rural Health Mission (NRHM) in Seven States Volume-I PEO Report No.217 Programme Evaluation Organisation Planning
Programme Evaluation Organisation Pla n n in g Com m s is io n Evaluation Study on National Rural Health Mission (NRHM) in Seven States Volume-I PEO Report No.217 Programme Evaluation Organisation Planning
Study Team. Bella Patel Uttekar Sandhya Barge Yashwant Deshpande Vasant Uttekar Jashoda Sharma Shweta Shahane
 Study Team Bella Patel Uttekar Sandhya Barge Yashwant Deshpande Vasant Uttekar Jashoda Sharma Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component of the National Rural Health Mission,
Study Team Bella Patel Uttekar Sandhya Barge Yashwant Deshpande Vasant Uttekar Jashoda Sharma Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component of the National Rural Health Mission,
A RAPID APPRAISAL OF FUNCTIONING OF ASHA UNDER NRHM IN UTTARAKHAND, INDIA
 May, 2012 A RAPID APPRAISAL OF FUNCTIONING OF ASHA UNDER NRHM IN UTTARAKHAND, INDIA By Hema Bhatt Management of Development Projects, EPFL CONTENT 1. ABSTRACT 2 2. INTRODUCTION..3 3. THE STATE OF PUBLIC
May, 2012 A RAPID APPRAISAL OF FUNCTIONING OF ASHA UNDER NRHM IN UTTARAKHAND, INDIA By Hema Bhatt Management of Development Projects, EPFL CONTENT 1. ABSTRACT 2 2. INTRODUCTION..3 3. THE STATE OF PUBLIC
Technical partner paper 7
 The Rockefeller Foundation Sponsored Initiative on the Role of the Private Sector in Health Systems in Developing Countries Technical partner paper 7 Andhra Pradesh Health Sector Reform A Narrative Case
The Rockefeller Foundation Sponsored Initiative on the Role of the Private Sector in Health Systems in Developing Countries Technical partner paper 7 Andhra Pradesh Health Sector Reform A Narrative Case
Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh
 Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh 1 CHAPTER Deepak Kumar,* Manisha* and Archana Dwivedi** INTRODUCTION Himachal Pradesh (HP) is one
Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh 1 CHAPTER Deepak Kumar,* Manisha* and Archana Dwivedi** INTRODUCTION Himachal Pradesh (HP) is one
Chapter II. Health Care System in India
 Chapter II Health Care System in India Chapter II HEALTHCARE SYSTEM IN INDIA 2.1- Introduction: Healthy citizens are the greatest assets any country can have Winston S. Churchill Health is a state subject
Chapter II Health Care System in India Chapter II HEALTHCARE SYSTEM IN INDIA 2.1- Introduction: Healthy citizens are the greatest assets any country can have Winston S. Churchill Health is a state subject
PRESENTATION ON UNIVERSAL HEALTH COVERAGE
 PRESENTATION ON UNIVERSAL HEALTH COVERAGE MEGHALAYA Date:09/01/2014 Introduction General Background Indicator Meghalaya India Demographic Profile* State Population Total (in lakhs) 29.64 12101. 02 State
PRESENTATION ON UNIVERSAL HEALTH COVERAGE MEGHALAYA Date:09/01/2014 Introduction General Background Indicator Meghalaya India Demographic Profile* State Population Total (in lakhs) 29.64 12101. 02 State
Health Reforms Initiatives in India A Brief Review. Abstract
 Health Reforms Initiatives in India A Brief Review By Ms. Savita Punjabi, Head, Dept. of Commerce, Badlapur (W) Abstract Globalisation has converted the world in a small town integrating its all activities
Health Reforms Initiatives in India A Brief Review By Ms. Savita Punjabi, Head, Dept. of Commerce, Badlapur (W) Abstract Globalisation has converted the world in a small town integrating its all activities
SCHEME OF GRANT-IN-AID FOR PROMOTION OF AYUSH INTERVENTION IN PUBLIC HEALTH INITIATIVES.
 SCHEME OF GRANT-IN-AID FOR PROMOTION OF AYUSH INTERVENTION IN PUBLIC HEALTH INITIATIVES. 1. Introduction There are approximately 7.00 lakh institutionally qualified AYUSH practitioners located in urban,
SCHEME OF GRANT-IN-AID FOR PROMOTION OF AYUSH INTERVENTION IN PUBLIC HEALTH INITIATIVES. 1. Introduction There are approximately 7.00 lakh institutionally qualified AYUSH practitioners located in urban,
Study Team. Bella Patel Uttekar Nayan Kumar Vasant Uttekar Jashoda Sharma Shweta Shahane
 Study Team Bella Patel Uttekar Nayan Kumar Vasant Uttekar Jashoda Sharma Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component of the National Rural Health Mission, launched in April
Study Team Bella Patel Uttekar Nayan Kumar Vasant Uttekar Jashoda Sharma Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component of the National Rural Health Mission, launched in April
GoI-UNDP Disaster Risk Management Programme. Project Management Board (PMB) GoI-UNDP Disaster Risk Management Programme [ ] Agenda Notes
![GoI-UNDP Disaster Risk Management Programme. Project Management Board (PMB) GoI-UNDP Disaster Risk Management Programme [ ] Agenda Notes](/thumbs/83/87290884.jpg "GoI-UNDP Disaster Risk Management Programme. Project Management Board (PMB) GoI-UNDP Disaster Risk Management Programme [ ] Agenda Notes") 3 rd Meeting of the Project Management Board (PMB) GoI-UNDP Disaster Risk Management Programme [2002-2007] Agenda Notes Part I 21 st December, 2004, New Delhi NDM Division, Ministry of Home Affairs, North
3 rd Meeting of the Project Management Board (PMB) GoI-UNDP Disaster Risk Management Programme [2002-2007] Agenda Notes Part I 21 st December, 2004, New Delhi NDM Division, Ministry of Home Affairs, North
Study Team. Bella Patel Uttekar Sandhya Barge Wajahat Khan Yashwant Deshpande Vasant Uttekar Jashoda Sharma Balaji Chakrawar Shweta Shahane
 Study Team Bella Patel Uttekar Sandhya Barge Wajahat Khan Yashwant Deshpande Vasant Uttekar Jashoda Sharma Balaji Chakrawar Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component
Study Team Bella Patel Uttekar Sandhya Barge Wajahat Khan Yashwant Deshpande Vasant Uttekar Jashoda Sharma Balaji Chakrawar Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component
0 MODEL DISTRICTS AS A ROADMAP FOR PUBLIC HEALTH SCALE UP IN INDIA
 MODEL DISTRICTS AS A ROADMAP FOR PUBLIC HEALTH SCALE UP IN INDIA Nirupam Bajpai, Megan Towle, and Jyothi Vynatheya Working Paper No. 4 July 2011 WORKING PAPERS SERIES Columbia Global Centers South Asia,
MODEL DISTRICTS AS A ROADMAP FOR PUBLIC HEALTH SCALE UP IN INDIA Nirupam Bajpai, Megan Towle, and Jyothi Vynatheya Working Paper No. 4 July 2011 WORKING PAPERS SERIES Columbia Global Centers South Asia,
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur
 State Institute of Health & Family Welfare, Jaipur") Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
DOI: /jemds/2014/1887 ORIGINAL ARTICLE
 EVALUATION OF ASHA PROGRAMME IN SELECTED BLOCK OF RAISEN DISTRICT OF MADHYA PRADESH UNDER THE NATIONAL RURAL HEALTH MISSION Bhagwan Waskel 1, Sanjay Dixit 2, Rama Singodia 3, D.K. Pal 4, Manju Toppo 5,
EVALUATION OF ASHA PROGRAMME IN SELECTED BLOCK OF RAISEN DISTRICT OF MADHYA PRADESH UNDER THE NATIONAL RURAL HEALTH MISSION Bhagwan Waskel 1, Sanjay Dixit 2, Rama Singodia 3, D.K. Pal 4, Manju Toppo 5,
Growth of Primary Health Care System in Kerala-A comparison with India
 Growth of Primary Health Care System in Kerala-A comparison with India Dr. Suby Elizabeth Oommen Assistant Professor Department of Economics, Christian College, Chengannur, Alappuzha, Kerala, INDIA, 689121
Growth of Primary Health Care System in Kerala-A comparison with India Dr. Suby Elizabeth Oommen Assistant Professor Department of Economics, Christian College, Chengannur, Alappuzha, Kerala, INDIA, 689121
Guidelines for Performance based Payment for ASHA under National Leprosy Eradication Programme
 Guidelines for Performance based Payment for ASHA under National Leprosy Eradication Programme Introduction: Under Health System, Multi-purpose Workers (MPW- Male & Female) at the sub- centre act as the
Guidelines for Performance based Payment for ASHA under National Leprosy Eradication Programme Introduction: Under Health System, Multi-purpose Workers (MPW- Male & Female) at the sub- centre act as the
Janani Suraksha Yojana ( JSY )
") Concurrent Assessment of Janani Suraksha Yojana ( JSY ) in Selected States Bihar, Madhya, Orissa, Rajasthan, Uttar United Nations Population Fund - India Concurrent Assessment of Janani Suraksha Yojana
Concurrent Assessment of Janani Suraksha Yojana ( JSY ) in Selected States Bihar, Madhya, Orissa, Rajasthan, Uttar United Nations Population Fund - India Concurrent Assessment of Janani Suraksha Yojana
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
INTERNATIONAL ASSOCIATION FOR NATIONAL YOUTH SERVICE
 Profile verified by: Mr. Vincent Senam Kuagbenu Executive Director of the Ghana National Service Scheme Date of Receipt: 12/04/2012 Country: Ghana INTRODUCTION: The Ghana National Service Scheme is a public
Profile verified by: Mr. Vincent Senam Kuagbenu Executive Director of the Ghana National Service Scheme Date of Receipt: 12/04/2012 Country: Ghana INTRODUCTION: The Ghana National Service Scheme is a public
Discussion Paper on Health Statistics
 Discussion Paper on Health Statistics National Statistical Commission (NSC), in its report for 2010-11, recommended the following data sets pertaining to health statistics, as the core statistics i) Health
Discussion Paper on Health Statistics National Statistical Commission (NSC), in its report for 2010-11, recommended the following data sets pertaining to health statistics, as the core statistics i) Health
Work-time analysis of ANM and ASHA: A Priority for Strengthening Health Systems
 Work-time analysis of ANM and ASHA: A Priority for Strengthening Health Systems Anu-Raga Mahalingashetty, Master of Public Health Candidate, Department of Population & Family Health, Global Health Track
Work-time analysis of ANM and ASHA: A Priority for Strengthening Health Systems Anu-Raga Mahalingashetty, Master of Public Health Candidate, Department of Population & Family Health, Global Health Track
ELECTION COMMISSION OF INDIA
 ELECTION COMMISSION OF INDIA Nirvachan Sadan, Ashoka Road, New Delhi 110001 No. 590/Training/Fund/2012 Dated 12th September, 2012 To, Subject: Madam / Sir, 1 The Chief Electoral Officers (All States /
ELECTION COMMISSION OF INDIA Nirvachan Sadan, Ashoka Road, New Delhi 110001 No. 590/Training/Fund/2012 Dated 12th September, 2012 To, Subject: Madam / Sir, 1 The Chief Electoral Officers (All States /
Request for Qualifications: Designing impact evaluations for Gram Varta and Nodal Anganwadi Centre initiatives under SWASTH, Bihar, India
 International Initiative for Impact evaluation Improving lives through impact evaluation Request for Qualifications: Designing impact evaluations for Gram Varta and Nodal Anganwadi Centre initiatives under
International Initiative for Impact evaluation Improving lives through impact evaluation Request for Qualifications: Designing impact evaluations for Gram Varta and Nodal Anganwadi Centre initiatives under
PART 1. RURAL HEALTH CARE SYSTEM IN INDIA
 PART 1. RURAL HEALTH CARE SYSTEM IN INDIA Rural Health Care System the structure and current scenario The primary health care infrastructure in rural areas has been developed as a three tier system and
PART 1. RURAL HEALTH CARE SYSTEM IN INDIA Rural Health Care System the structure and current scenario The primary health care infrastructure in rural areas has been developed as a three tier system and
Directory of Innovations Implemented in the Health Sector. December 2008
 First Draft, March 31, 2009 Directory of Innovations Implemented in the Health Sector December 2008 Supported by Department for International Development 1 !! "#!$ %%! & ' % % # # %(! ) * # % %# % +# ),
First Draft, March 31, 2009 Directory of Innovations Implemented in the Health Sector December 2008 Supported by Department for International Development 1 !! "#!$ %%! & ' % % # # %(! ) * # % %# % +# ),
National Health Policy 2015 Draft
 2015 National Health Policy 2015 Draft Placed in Public Domain for Comments, Suggestions, Feedback Ministry of Health & Family Welfare December, 2014 00 Table of Contents 1 Introduction 3 2 Situation Analysis
2015 National Health Policy 2015 Draft Placed in Public Domain for Comments, Suggestions, Feedback Ministry of Health & Family Welfare December, 2014 00 Table of Contents 1 Introduction 3 2 Situation Analysis
Application Form For JAPAN s Grant Assistance for Grassroots Projects (GGP)
") Application Form For JAPAN s Grant Assistance for Grassroots Projects (GGP) Attachment: Check List for Documents to be attached Embassy of Japan in India, The Consulate-General of Japan, Kolkata The Consulate-General
Application Form For JAPAN s Grant Assistance for Grassroots Projects (GGP) Attachment: Check List for Documents to be attached Embassy of Japan in India, The Consulate-General of Japan, Kolkata The Consulate-General
International Journal of Academic Research ISSN: : Vol.2, Issue-4(5), October-December, 2015 Impact Factor : 1.855
, October-December, 2015 Impact Factor : 1.855") Gopi M, Research Scholar, PG and Research department of Social Work, Sacred Heart College Tiruppattur,Vellore ( Dist ),Tamil Nadu. Dr. J Henry Rozario, Associate Professor Department of Social Work, Sacred
Gopi M, Research Scholar, PG and Research department of Social Work, Sacred Heart College Tiruppattur,Vellore ( Dist ),Tamil Nadu. Dr. J Henry Rozario, Associate Professor Department of Social Work, Sacred
AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE. CHF 7,993,000 2,240,000 beneficiaries. Programme no 01.29/99. The Context
 AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE CHF 7,993,000 2,240,000 beneficiaries Programme no 01.29/99 The Context Twenty years of conflict in Afghanistan have brought a constant deterioration
AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE CHF 7,993,000 2,240,000 beneficiaries Programme no 01.29/99 The Context Twenty years of conflict in Afghanistan have brought a constant deterioration
INTRODUCTION. 76 MCHIP End-of-Project Report. (accessed May 8, 2014).
.") Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor
 Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor Overview- What gets measured, gets done Operation ASHA -serving more than 54 Lakh people in
Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor Overview- What gets measured, gets done Operation ASHA -serving more than 54 Lakh people in
UHC. Moving toward. Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Annual Report. Strengthening Institutional Capacity for Nurses Training On HIV/AIDS in India (GFATM 7) (October September 10)
 (October September 10)") Annual Report Strengthening Institutional Capacity for Nurses Training On HIV/AIDS in India (GFATM 7) (October 2009- September 10) Annual Report 2009-10 1 Annual Report 2009-10 2 Contents Highlights 4
Annual Report Strengthening Institutional Capacity for Nurses Training On HIV/AIDS in India (GFATM 7) (October 2009- September 10) Annual Report 2009-10 1 Annual Report 2009-10 2 Contents Highlights 4
Request for Proposal
 Request for Proposal on Impact Assessment of ITC s Watershed Development Programmes implemented in partnership with NABARD in select districts of Andhra Pradesh Districts Guntur, Prakasam Deadline for
Request for Proposal on Impact Assessment of ITC s Watershed Development Programmes implemented in partnership with NABARD in select districts of Andhra Pradesh Districts Guntur, Prakasam Deadline for
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
Ministry of Panchayati Raj. Objective/Outcome Outlay Quantifiable Deliverables
 Statement of Outlays and Outcomes/Targets: Annual Plan 2005-06 (Rs. in crores) Sl.No. Name of the Scheme/ Programme 1. Training of elected representatives for implementing various developmental programmes
Statement of Outlays and Outcomes/Targets: Annual Plan 2005-06 (Rs. in crores) Sl.No. Name of the Scheme/ Programme 1. Training of elected representatives for implementing various developmental programmes
Environmental Impact Assessment
 Annual Report 2006-2007 Environmental Impact Assessment Introduction Keeping in view the tenets of Sustainable Development, it has been realized that all developmental efforts need to be harmonized with
Annual Report 2006-2007 Environmental Impact Assessment Introduction Keeping in view the tenets of Sustainable Development, it has been realized that all developmental efforts need to be harmonized with
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
ICDS in India: Policy, Design and Delivery Issues
 ICDS in India: Policy, Design and Delivery Issues Naresh C. Saxena and Nisha Srivastava Abstract India s excellent economic growth in the last two decades has made little impact on the nutrition levels
ICDS in India: Policy, Design and Delivery Issues Naresh C. Saxena and Nisha Srivastava Abstract India s excellent economic growth in the last two decades has made little impact on the nutrition levels
Scheme of Merit cum means based scholarship to students belonging to minority communities.
 Scheme of Merit cum means based scholarship to students belonging to minority communities. S. No. Objective : The objective of the Scheme is to provide financial assistance to the poor and meritorious
Scheme of Merit cum means based scholarship to students belonging to minority communities. S. No. Objective : The objective of the Scheme is to provide financial assistance to the poor and meritorious
Models of Supportive Supervision for IMNCI Implementation in Selected Districts of Bihar, Orissa and Rajasthan in India
 224 Indian Journal of Public Health Research & Development. January-March 2013, Vol. 4, No. 1 Models of Supportive Supervision for IMNCI Implementation in Selected Districts of Bihar, Orissa and Rajasthan
224 Indian Journal of Public Health Research & Development. January-March 2013, Vol. 4, No. 1 Models of Supportive Supervision for IMNCI Implementation in Selected Districts of Bihar, Orissa and Rajasthan
Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India
 Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India Suneeta Sharma, PhD MHA, Managing Director, Futures Group India Tanya Liberham, MA, Knowledge Management Officer,
Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India Suneeta Sharma, PhD MHA, Managing Director, Futures Group India Tanya Liberham, MA, Knowledge Management Officer,
Frontline Health Worker. Allied Health & Paramedics. Frontline Health Worker. Sector Health. Sub-Sector. Occupation
 Sector Health Sub-Sector Allied Health & Paramedics Occupation Frontline Health Worker Reference ID: HSS/ Q 8601, Version 1.0 NSQF level: 3 Frontline Health Worker Published by: All Rights Reserved, First
Sector Health Sub-Sector Allied Health & Paramedics Occupation Frontline Health Worker Reference ID: HSS/ Q 8601, Version 1.0 NSQF level: 3 Frontline Health Worker Published by: All Rights Reserved, First
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
Minister. Secretaries of State. Department of Planning and Health Information. Department of Human Resources Development
 KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
Medicine and surgery date back to the beginning of civilization. because diseases preceded humans on earth. Early medical treatment was
 History of Hospitals Medicine and surgery date back to the beginning of civilization because diseases preceded humans on earth. Early medical treatment was always identified with religious services and
History of Hospitals Medicine and surgery date back to the beginning of civilization because diseases preceded humans on earth. Early medical treatment was always identified with religious services and
National Rural Livelihoods Mission
 www.swaniti.in National Rural Livelihoods Mission (NRLM) A critical element in India s 12th Five Year Plan (2012-2017) is the generation of productive and gainful employment at scale. The aim is to absorb
www.swaniti.in National Rural Livelihoods Mission (NRLM) A critical element in India s 12th Five Year Plan (2012-2017) is the generation of productive and gainful employment at scale. The aim is to absorb
Joint Secretary (AYUSH)
") Integrating ti AYUSH in Health Research, Teaching and Practice Dr. D. D. Sharma Joint Secretary (AYUSH) 1 Preamble AYUSH: indigenous, time-tested, tested, cultural-friendly, socially acceptable, holds
Integrating ti AYUSH in Health Research, Teaching and Practice Dr. D. D. Sharma Joint Secretary (AYUSH) 1 Preamble AYUSH: indigenous, time-tested, tested, cultural-friendly, socially acceptable, holds
Workload and perceived constraints of Anganwadi workers
 Workload and perceived constraints of Anganwadi workers Damanpreet Kaur, Manjula Thakur, Amarjeet Singh, Sushma Kumari Saini Abstract : Integrated Child Development Service scheme is most important nutritional
Workload and perceived constraints of Anganwadi workers Damanpreet Kaur, Manjula Thakur, Amarjeet Singh, Sushma Kumari Saini Abstract : Integrated Child Development Service scheme is most important nutritional
TRAINING ON WATER, SANITATION, AND HYGIENE (WASH) TO THE FRONTLINE WORKERS (FLWS) IN A RURAL SET UP
 TO THE FRONTLINE WORKERS (FLWS) IN A RURAL SET UP") Management TRAINING ON WATER, SANITATION, AND HYGIENE (WASH) TO THE FRONTLINE WORKERS (FLWS) IN A RURAL SET UP Shyama Prasad Chattopadhyay *1 *1 MA(Economics), MBA, Assistant Professor, IIHMR University,
Management TRAINING ON WATER, SANITATION, AND HYGIENE (WASH) TO THE FRONTLINE WORKERS (FLWS) IN A RURAL SET UP Shyama Prasad Chattopadhyay *1 *1 MA(Economics), MBA, Assistant Professor, IIHMR University,
Guidelines for preparation of AWP&B for the year
 Guidelines for preparation of AWP&B for the year 2017-18 Annexure-I The guidelines for preparation of comprehensive Annual Work Plan & Budget for the year 2017-18 in the prescribed format are given below:-
Guidelines for preparation of AWP&B for the year 2017-18 Annexure-I The guidelines for preparation of comprehensive Annual Work Plan & Budget for the year 2017-18 in the prescribed format are given below:-
Integrated Child Development Services Scheme. Monitoring Visits. (Four Year s Time Interval Revisiting Exercise) 2008/ /12.
 2008/ /12.") Not to be Quoted Report No 34(1/2013-14) Integrated Child Development Services Scheme Monitoring Visits (Four Year s Time Interval Revisiting Exercise) 2008/09 2011/12 A Report Central Monitoring Unit
Not to be Quoted Report No 34(1/2013-14) Integrated Child Development Services Scheme Monitoring Visits (Four Year s Time Interval Revisiting Exercise) 2008/09 2011/12 A Report Central Monitoring Unit
Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala. Sunil Kumar
 End TB Strategy Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala Sunil Kumar The END TB strategy challenges the world to envision the End of the Tuberculosis pandemic and
End TB Strategy Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala Sunil Kumar The END TB strategy challenges the world to envision the End of the Tuberculosis pandemic and
MOTHER AND CHILD TRACKING SYSTEM (MCTS)
") MOTHER AND CHILD TRACKING SYSTEM (MCTS) 12/11/2013 Training Report Goa NATIONAL INSTITUTE OF HEALTH AND FAMILY WELFARE NEW DELHI MCTS Goa training Conducted by NIHFW (12 th - 13 th November, 2013) Introduction
MOTHER AND CHILD TRACKING SYSTEM (MCTS) 12/11/2013 Training Report Goa NATIONAL INSTITUTE OF HEALTH AND FAMILY WELFARE NEW DELHI MCTS Goa training Conducted by NIHFW (12 th - 13 th November, 2013) Introduction
India s mandate for Universal Health Coverage
 Chapter 4 Human Resources for Health Introduction: Effective, accountable and efficient Human Resources for Health for enabling Universal Health Coverage India s mandate for Universal Health Coverage (UHC)
Chapter 4 Human Resources for Health Introduction: Effective, accountable and efficient Human Resources for Health for enabling Universal Health Coverage India s mandate for Universal Health Coverage (UHC)
Improving Quality of Maternal and Newborn Health in India
 Improving Quality of Maternal and Newborn Health in India Fact Sheet: January 2017 Partners: Government of India (GoI), State Governments of Rajasthan, Maharashtra, Uttar Pradesh, Jharkhand, Andhra Pradesh
Improving Quality of Maternal and Newborn Health in India Fact Sheet: January 2017 Partners: Government of India (GoI), State Governments of Rajasthan, Maharashtra, Uttar Pradesh, Jharkhand, Andhra Pradesh
Safe Drinking Water and Sanitation for School Children Zimbabwe Final Report to the Isle of Man Overseas Aid Committee July 2011-April 2012
 Safe Drinking Water and Sanitation for School Children Zimbabwe Final Report to the Isle of Man Overseas Aid Committee July 2011-April 2012 Executive Summary The project was a community-based intervention
Safe Drinking Water and Sanitation for School Children Zimbabwe Final Report to the Isle of Man Overseas Aid Committee July 2011-April 2012 Executive Summary The project was a community-based intervention
Gramalaya Tiruchirappalli Annual Report for
 Gramalaya Tiruchirappalli Annual Report for 2007 2008 Gramalaya was established in 1987 with a group of committed youths in the field of rural development. Gramalaya got its legal entity by registering
Gramalaya Tiruchirappalli Annual Report for 2007 2008 Gramalaya was established in 1987 with a group of committed youths in the field of rural development. Gramalaya got its legal entity by registering
CORPORATE SOCIAL RESPONSIBILITY POLICY March, 2017 Version 1.2
 CORPORATE SOCIAL RESPONSIBILITY POLICY March, 2017 Version 1.2 Name of document Corporate Social Responsibility Policy Policy Version 1.2 Issued by CSR Committee Amendment date 22.03.2017 Effective Date
CORPORATE SOCIAL RESPONSIBILITY POLICY March, 2017 Version 1.2 Name of document Corporate Social Responsibility Policy Policy Version 1.2 Issued by CSR Committee Amendment date 22.03.2017 Effective Date
National Health Systems Resource Centre
 National Health Systems Resource Centre Technical Support Institution with National Rural Health Mission Ministry of Health & Family Welfare Government of India V ISION We are committed to facilitate the
National Health Systems Resource Centre Technical Support Institution with National Rural Health Mission Ministry of Health & Family Welfare Government of India V ISION We are committed to facilitate the
DISTRICT BASED NORMATIVE COSTING MODEL
 DISTRICT BASED NORMATIVE COSTING MODEL Oxford Policy Management, University Gadjah Mada and GTZ Team 17 th April 2009 Contents Contents... 1 1 Introduction... 2 2 Part A: Need and Demand... 3 2.1 Epidemiology
DISTRICT BASED NORMATIVE COSTING MODEL Oxford Policy Management, University Gadjah Mada and GTZ Team 17 th April 2009 Contents Contents... 1 1 Introduction... 2 2 Part A: Need and Demand... 3 2.1 Epidemiology
PRESENTATION ON UNIVERSAL HEALTH COVERAGE GOVERNMENT OF MEGHALAYA
 PRESENTATION ON UNIVERSAL HEALTH COVERAGE GOVERNMENT OF MEGHALAYA 1 1. Introduction General Background Indicator Meghalaya India Demographic Profile State Population Total (in lakhs) 29.64 12101. 02 State
PRESENTATION ON UNIVERSAL HEALTH COVERAGE GOVERNMENT OF MEGHALAYA 1 1. Introduction General Background Indicator Meghalaya India Demographic Profile State Population Total (in lakhs) 29.64 12101. 02 State
Strengthening primary healthcare in India: white paper on opportunities for partnership
 Strengthening primary healthcare in India: white paper on opportunities for partnership Mala Rao and David Mant explore how India and the UK can work together on education, professional development, affordable
Strengthening primary healthcare in India: white paper on opportunities for partnership Mala Rao and David Mant explore how India and the UK can work together on education, professional development, affordable
STATE HEALTH SOCIETY, PUNJAB
 STATE HEALTH SOCIETY, PUNJAB GUIDELINES FOR FAMILY HEALTH CAMPS National Rural Health Mission, Department of Health and Family Welfare, Punjab 1 INDEX Content Page No. Objectives and Framework of the camp
STATE HEALTH SOCIETY, PUNJAB GUIDELINES FOR FAMILY HEALTH CAMPS National Rural Health Mission, Department of Health and Family Welfare, Punjab 1 INDEX Content Page No. Objectives and Framework of the camp
Universal Health Coverage Manipur. Dr Suhel Akhtar, IAS Principal Secretary (Health & FW) Government of Manipur
 Government of Manipur") Universal Health Coverage Manipur Dr Suhel Akhtar, IAS Principal Secretary (Health & FW) Government of Manipur Overview Goal Essential factors for UHC State profile Health System Strengthening in the State
Universal Health Coverage Manipur Dr Suhel Akhtar, IAS Principal Secretary (Health & FW) Government of Manipur Overview Goal Essential factors for UHC State profile Health System Strengthening in the State
National Hygiene Education Policy Guideline
 ISLAMIC REPUBLIC OF AFGHANISTAN Ministry of Rural Rehabilitation & Development And Ministry of Public Health National Hygiene Education Policy Guideline Developed by: Hygiene Education Technical Working
ISLAMIC REPUBLIC OF AFGHANISTAN Ministry of Rural Rehabilitation & Development And Ministry of Public Health National Hygiene Education Policy Guideline Developed by: Hygiene Education Technical Working
REPUBLIC OF NAMIBIA MINISTRY OF HEALTH AND SOCIAL SERVICES
 REPUBLIC OF NAMIBIA MINISTRY OF HEALTH AND SOCIAL SERVICES Community-Based Health Care Policy (Including Roles) Draft 1/11/2007 ii MINISTRY OF HEALTH AND SOCIAL SERVICES Community Based Health Care Policy
REPUBLIC OF NAMIBIA MINISTRY OF HEALTH AND SOCIAL SERVICES Community-Based Health Care Policy (Including Roles) Draft 1/11/2007 ii MINISTRY OF HEALTH AND SOCIAL SERVICES Community Based Health Care Policy
Nutrition Moves. States create promising change in India
 Nutrition Moves States create promising change in India Acknowledgements The case studies presented in this publication are a testimony to the commitment by India s state governments to accelerate progress
Nutrition Moves States create promising change in India Acknowledgements The case studies presented in this publication are a testimony to the commitment by India s state governments to accelerate progress
SYNTHESIS REPORT OF HEALTH INFORMATION SYSTEMS IN INDIA
 SYNTHESIS REPORT OF HEALTH INFORMATION SYSTEMS IN INDIA May 2014 This publication was produced for review by the United States Agency for International Development and the Haryana National Rural Health
SYNTHESIS REPORT OF HEALTH INFORMATION SYSTEMS IN INDIA May 2014 This publication was produced for review by the United States Agency for International Development and the Haryana National Rural Health
SEA/HSD/305. The Regional Six-point Strategy for Health Systems Strengthening based on the Primary Health Care Approach
 SEA/HSD/305 The Regional Six-point Strategy for Health Systems Strengthening based on the Primary Health Care Approach World Health Organization 2007 This document is not a formal publication of the World
SEA/HSD/305 The Regional Six-point Strategy for Health Systems Strengthening based on the Primary Health Care Approach World Health Organization 2007 This document is not a formal publication of the World
HealthRise India Program Launch
 HealthRise India Program Launch MAMTA Health institute for Mother and Child Grantee & CAC Kick-Off Meetings November 19-20, 2015 New Delhi, India Outline About MAMTA HealthRise Objectives & Target Beneficiaries
HealthRise India Program Launch MAMTA Health institute for Mother and Child Grantee & CAC Kick-Off Meetings November 19-20, 2015 New Delhi, India Outline About MAMTA HealthRise Objectives & Target Beneficiaries
NOTE. Visit of Hon'ble Health Minister to Karnataka and Tamilnadu on 14/09/2008 to 17/09/2008.
 NOTE Subject:- Visit of Hon'ble Health Minister to Karnataka and Tamilnadu on 14/09/2008 to 17/09/2008. Hon'ble Health Minister, Prof. Laxmi Kanta Chawla accompanied by Sh.Satish Chandra, IAS, Secretary
NOTE Subject:- Visit of Hon'ble Health Minister to Karnataka and Tamilnadu on 14/09/2008 to 17/09/2008. Hon'ble Health Minister, Prof. Laxmi Kanta Chawla accompanied by Sh.Satish Chandra, IAS, Secretary
NEYVELI LIGNITE CORPROATION LIMITED
 NEYVELI LIGNITE CORPROATION LIMITED Corporate Social Responsibility Policy 1.0 Prelude : Neyveli Lignite Corporation (NLC), hereinafter referred as Company has been carrying out peripheral developmental
NEYVELI LIGNITE CORPROATION LIMITED Corporate Social Responsibility Policy 1.0 Prelude : Neyveli Lignite Corporation (NLC), hereinafter referred as Company has been carrying out peripheral developmental
Government Scholarship Scheme for Indian Muslim Students : Access and Impact
 Government Scholarship Scheme for Indian Muslim Students : Access and Impact Fahimuddin The Prime Minister s Point Programme for the welfare of minorities was announced in June, 006. It provided that a
Government Scholarship Scheme for Indian Muslim Students : Access and Impact Fahimuddin The Prime Minister s Point Programme for the welfare of minorities was announced in June, 006. It provided that a
OCIAL ACCOUNTABILITY SOUTH ASIA SUSTAINABLE DEVELOPMENT DEPARTMENT
 OCIAL ACCOUNTABILITY SOUTH ASIA SUSTAINABLE DEVELOPMENT DEPARTMENT Social Accountability Initiatives in South Asia Since 2005 a unique effort to initiate and mainstream Social Accountability (SAc) initiatives
OCIAL ACCOUNTABILITY SOUTH ASIA SUSTAINABLE DEVELOPMENT DEPARTMENT Social Accountability Initiatives in South Asia Since 2005 a unique effort to initiate and mainstream Social Accountability (SAc) initiatives
CHAPTER IV HEALTH SCENARIO IN ASSAM WITH SPECIAL REFERENCE TO CACHAR DISTRICT
 CHAPTER IV HEALTH SCENARIO IN ASSAM WITH SPECIAL REFERENCE TO CACHAR DISTRICT 4.1. Health Care System in India Health is a fundamental human right. It is the responsibility of the government to provide
CHAPTER IV HEALTH SCENARIO IN ASSAM WITH SPECIAL REFERENCE TO CACHAR DISTRICT 4.1. Health Care System in India Health is a fundamental human right. It is the responsibility of the government to provide
Minutes of Meeting Subject
 Minutes of Meeting Subject APPROVED: Generasi Impact Evaluation Proposal Host Joint Management Committee (JMC) Date August 04, 2015 Participants JMC, PSF Portfolio, PSF Cluster, PSF Generasi Agenda Confirmation
Minutes of Meeting Subject APPROVED: Generasi Impact Evaluation Proposal Host Joint Management Committee (JMC) Date August 04, 2015 Participants JMC, PSF Portfolio, PSF Cluster, PSF Generasi Agenda Confirmation
MOTHER AND CHILD TRACKING SYSTEM (MCTS)
") MOTHER AND CHILD TRACKING SYSTEM (MCTS) 10/26/2013 Training Report Leh Division NATIONAL INSTITUTE OF HEALTH AND FAMILY WELFARE NEW DELHI MCTS Leh training Conducted by NIHFW (24 th October- 25 nd October
MOTHER AND CHILD TRACKING SYSTEM (MCTS) 10/26/2013 Training Report Leh Division NATIONAL INSTITUTE OF HEALTH AND FAMILY WELFARE NEW DELHI MCTS Leh training Conducted by NIHFW (24 th October- 25 nd October
4 September 2011 PROVINCIAL GUIDELINES FOR THE IMPLEMENTATION OF THE THREE STREAMS OF PHC RE-ENGINEERING
 4 September 2011 PROVINCIAL GUIDELINES FOR THE IMPLEMENTATION OF THE THREE STREAMS OF PHC RE-ENGINEERING 1. Introduction 1.1. The National Health Council has mandated that in order to improve health outcomes
4 September 2011 PROVINCIAL GUIDELINES FOR THE IMPLEMENTATION OF THE THREE STREAMS OF PHC RE-ENGINEERING 1. Introduction 1.1. The National Health Council has mandated that in order to improve health outcomes
UPC. An Overview. The Urban Projects Concept. Financial support for improved access to water and sanitation
 WATER SERVICES TRUST FUND An Overview Financial support for improved access to water and sanitation WATER SERVICES TRUST FUND Water Ser vices Trust Fund [ Urban ] The booklet was prepared by the Water
WATER SERVICES TRUST FUND An Overview Financial support for improved access to water and sanitation WATER SERVICES TRUST FUND Water Ser vices Trust Fund [ Urban ] The booklet was prepared by the Water
SDC ICT4D STRATEGY WHERE WE ARE WHERE WE WANT TO BE HOW WE GET THERE A SUMMARY
 SDC ICT4D STRATEGY WHERE WE ARE WHERE WE WANT TO BE HOW WE GET THERE A SUMMARY 1 Introduction The 2005 Millennium Development Summit in New York showed that the Millennium Development Goals (MDGs) cannot
SDC ICT4D STRATEGY WHERE WE ARE WHERE WE WANT TO BE HOW WE GET THERE A SUMMARY 1 Introduction The 2005 Millennium Development Summit in New York showed that the Millennium Development Goals (MDGs) cannot
The Indian Institute of Culture Basavangudi, Bangalore RECENT DEVELOPMENTS IN MATERNITY AND CHILD WELFARE SERVICES IN INDIA
 The Indian Institute of Culture Basavangudi, Bangalore Transaction No. 27 RECENT DEVELOPMENTS IN MATERNITY AND CHILD WELFARE SERVICES IN INDIA By DR. SARYU BHATIA THE INDIAN INSTITUTE OF CULTURE 6, North
The Indian Institute of Culture Basavangudi, Bangalore Transaction No. 27 RECENT DEVELOPMENTS IN MATERNITY AND CHILD WELFARE SERVICES IN INDIA By DR. SARYU BHATIA THE INDIAN INSTITUTE OF CULTURE 6, North
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Review Article Human Resources for Health in India: An Overview K S. Nair Former Faculty, Department of Planning & Evaluation,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Review Article Human Resources for Health in India: An Overview K S. Nair Former Faculty, Department of Planning & Evaluation,
Part 1. Rural Health Care System in India 1. Table 1. State-Wise Area, Districts and Villages in India 28
 CONTENTS Page List of Abbreviations Highlights ii vii-x Part 1. Rural Health Care System in India 1 Part 2. Detailed Statistics Section I. Demographic Indicators Table 1. State-Wise Area, Districts and
CONTENTS Page List of Abbreviations Highlights ii vii-x Part 1. Rural Health Care System in India 1 Part 2. Detailed Statistics Section I. Demographic Indicators Table 1. State-Wise Area, Districts and
REVIEW ARTICLE Human Resource Requirement Under the Context of Universal Health Coverage (UHC) in Bangladesh: Current Situation and Future Challenges
 in Bangladesh: Current Situation and Future Challenges") REVIEW ARTICLE Human Resource Requirement Under the Context of Universal Health Coverage (UHC) in Bangladesh: Current Situation and Future Challenges *MHK Talukder 1, MM Rahman 2, M Nuruzzaman 3 1 Professor
REVIEW ARTICLE Human Resource Requirement Under the Context of Universal Health Coverage (UHC) in Bangladesh: Current Situation and Future Challenges *MHK Talukder 1, MM Rahman 2, M Nuruzzaman 3 1 Professor
Persons Affected with Leprosy Homes No. of PAL living in these homes
 DISTRICT PROFILE - KANPUR NAGAR (2008) Introduction was first carved out of erstwhile Kanpur in 1977. It was reunited with Kanpur Dehat in 1979, to separate again in 1981. is a commercial capital of Uttar
DISTRICT PROFILE - KANPUR NAGAR (2008) Introduction was first carved out of erstwhile Kanpur in 1977. It was reunited with Kanpur Dehat in 1979, to separate again in 1981. is a commercial capital of Uttar
P4P Case Studies. Paying for Performance: The Janani Suraksha Yojana Program in India
 Inside About the P4P Case Studies Series 2 Acronyms 2 Introduction 3 Background 4 JSY Program Design and Structure 7 Strengthening the JSY Program 15 Financing the JSY Program 17 Results 18 Key Challenges
Inside About the P4P Case Studies Series 2 Acronyms 2 Introduction 3 Background 4 JSY Program Design and Structure 7 Strengthening the JSY Program 15 Financing the JSY Program 17 Results 18 Key Challenges
Mission Antyodaya: Gram Samridhi evam Swachata Pakhwada (1-15 th October, 2017)
") Mission Antyodaya: Gram Samridhi evam Swachata Pakhwada (1-15 th October, 2017) An initiative of the Ministry of Rural Development, GoI along with with Ministries of Panchayati Raj, Drinking Water and
Mission Antyodaya: Gram Samridhi evam Swachata Pakhwada (1-15 th October, 2017) An initiative of the Ministry of Rural Development, GoI along with with Ministries of Panchayati Raj, Drinking Water and