PEPPER and Data Analytics for Skilled Nursing Facilities, Hospices and Inpatient Rehabilitation Facilities. April 19, 2015 Kimberly Hrehor
|
|
|
- Edwina Sharp
- 5 years ago
- Views:
Transcription
1 PEPPER and Data Analytics for Skilled Nursing Facilities, Hospices and Inpatient Rehabilitation Facilities April 19, 2015 Kimberly Hrehor Agenda What is PEPPER? Focus: Hospice PEPPER Focus: SNF PEPPER Focus: IRF PEPPER Review strategies to mitigate audit risk Questions and Answers Target area listings for other providers 2 1
2 Providers are Under Focus: Office of Inspector General Work Plan Recovery Auditors Medicare Administrative Contractors 3 What is PEPPER? Patterns Electronic Report (PEPPER) summarizes Medicare claims data statistics for one provider in areas ( target areas ) that may be at risk for improper Medicare payments. PEPPER compares the provider s Medicare claims data statistics with aggregate Medicare data for all other providers in the nation, MAC jurisdiction and state. PEPPER cannot identify improper Medicare payments! 4 2
3 What is PEPPER? PEPPER was originally developed in 2003 for short term acute care PPS hospitals; it was made available through the Quality Improvement Organizations in support of efforts to identify and prevent improper Medicare payments through PEPPER is also available for long term (LT) acute care PPS hospitals, critical access hospitals (CAHs), inpatient psychiatric facilities (IPFs), inpatient rehabilitation facilities (IRFs), partial hospitalization programs (PHPs), hospices, skilled nursing facilities (SNFs) and in 2015 for home health agencies (HHAs). 5 Why are Providers Receiving PEPPER? CMS is tasked with protecting the Medicare Trust Fund from fraud, waste and abuse. The provision of PEPPER supports CMS program integrity activities. PEPPER is an educational tool that is intended to help providers assess their risk for improper Medicare payments. 6 3
4 PEPPER Summarizes Medicare Data Paid Medicare claims (no other payers) Medicare claim payment amount > $0 Exclude HMO (Medicare Advantage) claims Exclude canceled claims Medicare secondary payer claims included if Medicare payment > $0 7 PEPPER Data Organized in three 12 month time periods based on federal fiscal year (FY). FY 2012 FY 2013 FY 2014 Q4FY14 release contains statistics for discharges at the IRF that end between Oct. 1, 2011 through Sept. 30, 2014 (fiscal years 2012, 2013 and 2014). 8 4
5 Short term Acute Care Hospital PEPPER Data Summarized by federal fiscal year quarters according to the discharge date on the claim. Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Qx FYx Federal fiscal year begins Oct. 1 and ends Sept. 30. Q1 = October December Q2 = January March Q3 = April June Q4 = July September 9 Target Area Area identified as potentially at risk for improper payments. Focused on admission necessity or coding issues Constructed as a ratio: Numerator = discharges identified as potentially problematic (likely to be miscoded or admitted unnecessarily) Denominator = larger reference group that contains the numerator 10 5
6 Target Area Percents Target area percents are calculated by dividing the number of target discharges/episodes by the number of denominator discharges/episodes for each provider for each time period, then multiplying by 100. Example: Miscellaneous CMGs 11 Percent vs. Percentiles The target area percent measures the provider s billing patterns for each target area over time. Percentiles show how the provided compares to others in the nation, jurisdiction and state. Percentiles provide context

7 Context.. 63% 52% 49% 44% 43% 40% 33% 29% 24% 11% 80 th percentile 20 th percentile Where do you fall among the distribution? Does that make sense? Should you be concerned?

8 15 Comparisons in PEPPER PEPPER provides state, MAC jurisdiction and national comparisons. National Comparison MAC Jurisdiction Comparison State Comparison 16 8
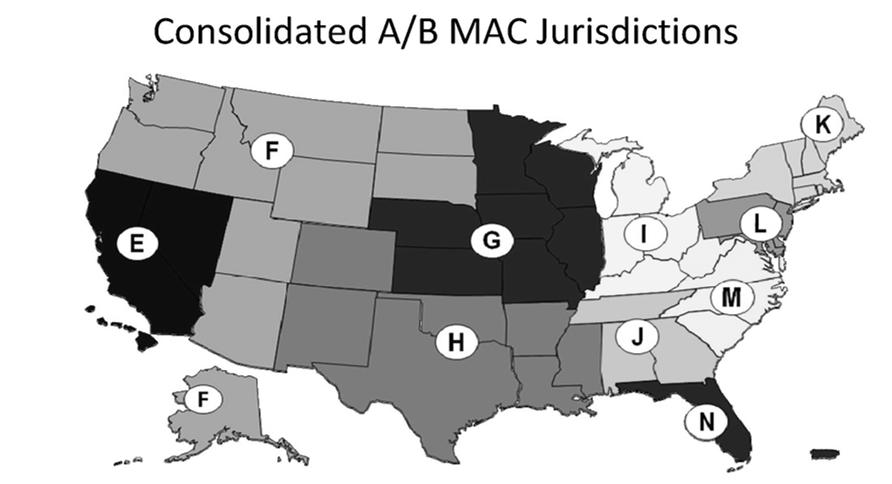
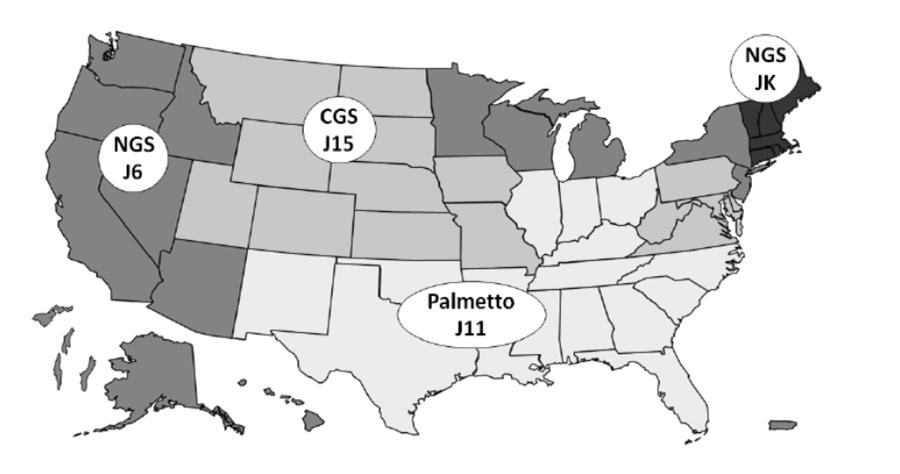
9 MAC Jurisdictions 17 Home Health/Hospice MACs 18 9
10 National level Data Reports 3/17/2015 National level Data National level data for the target areas (number of discharges for the numerator/denominator, average length of stay, total payments) is available at PEPPERresources.org on the Data page. The reports are updated following each release
11 How do I obtain my PEPPER? PEPPER is distributed in electronic format. PEPPER is no longer mailed to providers in hard copy format. PEPPER cannot be sent via STACH, CAH, IPF, Distinct Part Units (SNF, IRF, PHP) of Hospitals PEPPER is distributed via QualityNet to the hospital QualityNet Administrators and those with basic user accounts and the PEPPER recipient role. Available for 60 days from date TMF uploads the file. Providers can request we re upload the file (contact us through the Help Desk at PEPPERresources.org)

12 Pepper Resources website 3/17/2015 Hospices, LTCHs, Free standing SNFs, IRFs, PHPs PEPPER Resources Portal Visit PEPPERresources.org Click on the PEPPER Distribution Get Your PEPPER link Review instructions and access portal Each release will be available for approximately two years from the original release date


13 25 Who has Access to PEPPER? PEPPER is only available to the individual provider. PEPPER is not publicly available, cannot be released to consultants, etc. TMF does not send PEPPERs to MACs/Recovery Auditors, but does provide them with an Access database that contains the PEPPER statistics for providers in their jurisdiction/region
14 For assistance with PEPPER: Visit PEPPERresources.org for the PEPPER User s Guide and training materials. Submit request for assistance at PEPPERresources.org Help/Contact Us tab. 27 Strategies to Consider. Do Not Panic! Indication of high outlier does not necessarily mean that compliance issues exist. But: Determine Why You are an Outlier Sample claims using same inclusion criteria. Review documentation in medical record. Review claim; was it coded and billed appropriately based upon documentation in medical record? Ensure following best practices, even if not an outlier
15 Hospice PEPPER Target Areas Target Area Target Area Definition Live Discharges *revised as of the Q4FY13 release For discharges prior to July 1, 2012: N: count of beneficiary episodes discharged alive by the hospice (patient discharge status code not equal to 40, 41 or 42 with occurrence code "42" (date of termination of hospice benefit) Denominator (D): count of all beneficiary episodes discharged (by death or alive) by the hospice during the report period (obtained by considering all claims billed for a beneficiary by that hospice) 29 Hospice PEPPER Target Areas, 2 Target Area Target Area Definition Live Discharges *revised as of the Q4FY13 release For discharges beginning July 1, 2012: N: count of beneficiary episodes who were discharged alive by the hospice (patient discharge status code not equal to 40, 41 or 42, excluding: beneficiary transfers (patient discharge status code 50 or 51 ); beneficiary revocations (occurrence code 42 ); beneficiaries discharged for cause (condition code H2 ); beneficiaries who moved out of the service area (condition code 52 ) D: count of all beneficiary episodes discharged (by death or alive) by the hospice during the report period (obtained by considering all claims billed for a beneficiary by that hospice) 30 15
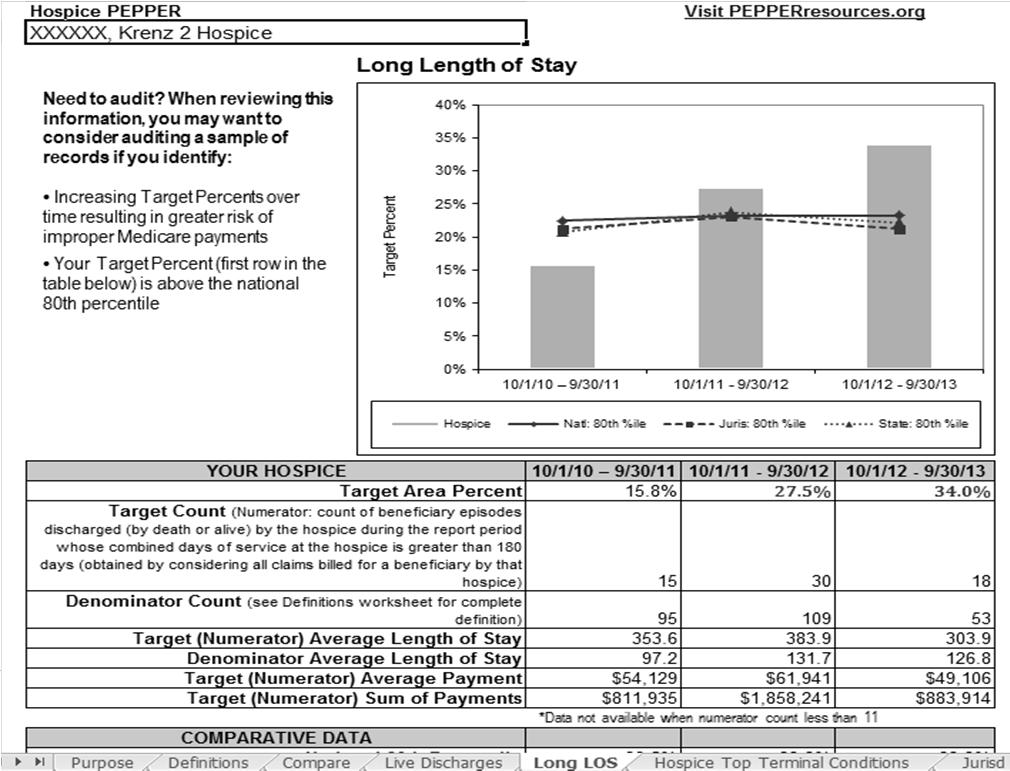
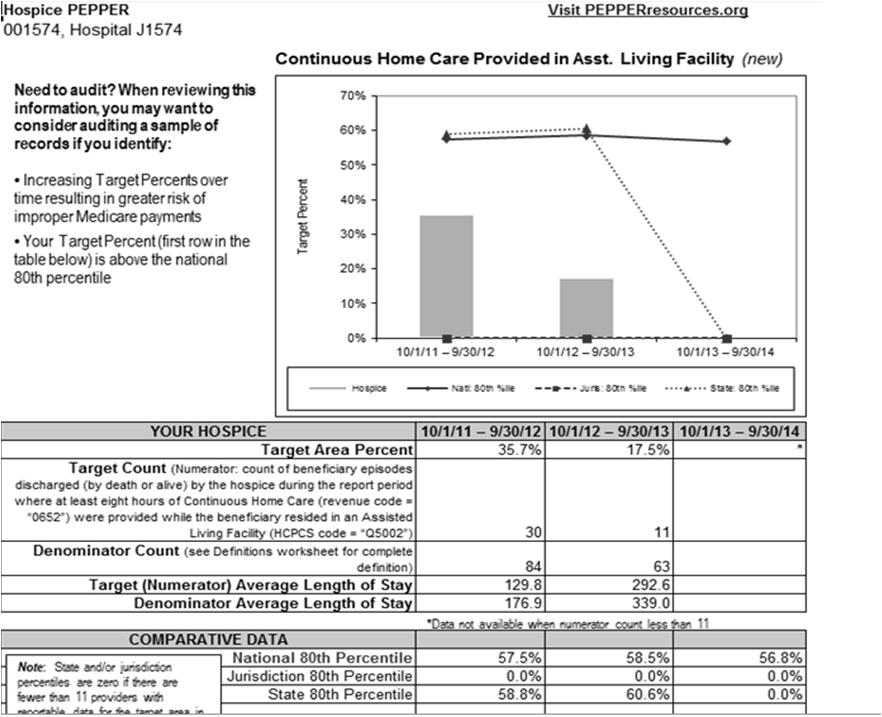
16 Hospice PEPPER Target Areas, 3 Target Area Long Length of Stay Target Area Definition N: count of beneficiary episodes discharged (by death or alive) by the hospice during the report period whose combined days of service at the hospice is greater than 180 days (obtained by considering all claims billed for a beneficiary by that hospice) D: count of all beneficiary episodes discharged (by death or alive) by the hospice during the report period 31 Hospice PEPPER Target Areas, 4 Target Area Target Area Definition Continuous Home Care Provided in an Assisted Living Facility *new as of the Q4FY14 release N: count of beneficiary episodes discharged (by death or alive) by the hospice during the report period where at least eight hours of Continuous Home Care (revenue code = 0652 ) were provided while the beneficiary resided in an Assisted Living Facility (HCPCS code = Q5002 ) D:count of all beneficiary episodes ending in the report period that indicate the beneficiary resided in an assisted living facility (HCPCS code = Q5002 ) for any portion of the episode 32 16
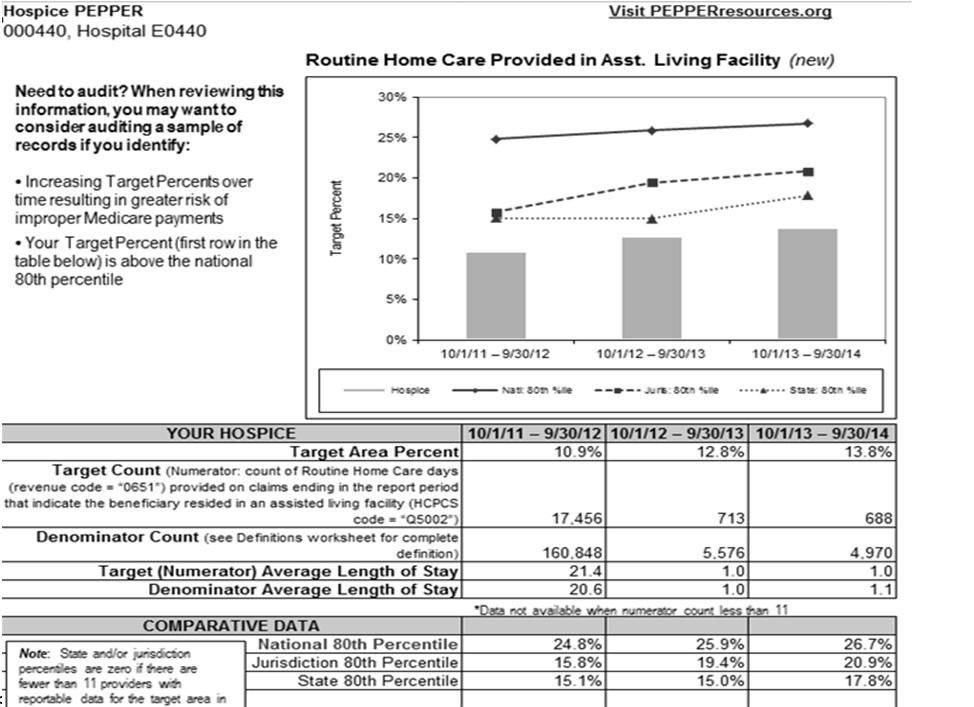
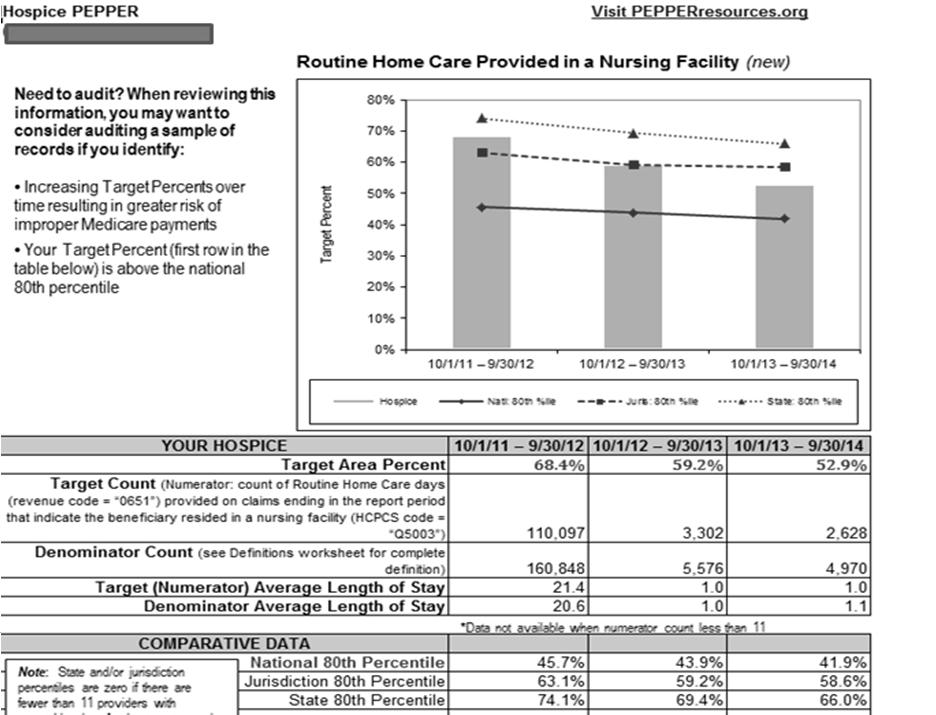
17 Hospice PEPPER Target Areas, 5 Target Area Target Area Definition Routine Home Care Provided in an Assisted Living Facility *new as of the Q4FY14 release N: count of Routine Home Care days (revenue code = 0651 ) provided on claims ending in the report period that indicate the beneficiary resided in an assisted living facility (HCPCS code = Q5002 ) D: count of all Routine Home Care days (revenue code = 0651 ) provided by the hospice on claims ending in the report period 33 Hospice PEPPER Target Areas, 6 Target Area Target Area Definition Routine Home Care Provided in a Nursing Facility *new as of the Q4FY14 release N: count of Routine Home Care days (revenue code = 0651 ) provided on claims ending in the report period that indicate the beneficiary resided in a nursing facility (HCPCS code = Q5003 ) D: count of all Routine Home Care days (revenue code = 0651 ) provided by the hospice on claims ending in the report period 34 17
18 Hospice PEPPER Target Areas, 7 Target Area Target Area Definition Routine Home Care Provided in a Skilled Nursing Facility *new as of the Q4FY14 release N: count of Routine Home Care days (revenue code = 0651 ) provided on claims ending in the report period that indicate the beneficiary resided in a skilled nursing facility (HCPCS code = Q5004 ) D: count of all Routine Home Care days (revenue code = 0651 ) provided by the hospice on claims ending in the report period 35 SNF PEPPER Target Areas Coding of ADL Target Area Therapy RUGs with High ADL Nontherapy RUGs with High ADL Change of Therapy Assessment Target Area Definition N: count of days billed with RUG equal to RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB D: count of days billed for all therapy RUGs N: count of days billed with RUG equal to SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, IB1 in RUG III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUG IV D: count of days billed for all nontherapy RUGs N: count of assessments with AI second digit D D: count of all assessments 36 18
19 SNF PEPPER Target Areas, 2 Therapy Target Area Ultrahigh Therapy RUGs Therapy RUGs 90+ Day Episodes of Care Target Area Definition N: count of days billed with RUG equal to RUX, RUL, RUC, RUB, RUA D: count of days billed for all therapy RUGs N: count of days billed for all therapy RUGs D: count of days billed for all therapy and nontherapy RUGs N: count of episodes of care at the SNF with LOS 90+ days D: count of all episodes of care at the SNF 37 IRF PEPPER Target Areas Target Area Miscellaneous CMGs CMGs at Risk for Unnecessary Admissions Target Area Definition N: count of discharges for Case Mix Groups (CMGs) 2001 (Miscellaneous M>49.15), 2002 (Miscellaneous M>38.75 and M<49.15), 2003 (Miscellaneous M>27.85 and M<38.75) or 2004 (Miscellaneous M<27.85) D: count of all discharges N: count of discharges with no tier group assignment for CMGs 0101 (Stroke M>51.05), 0501 (Non traumatic Spinal Cord Injury M>51.35), 0601 (Neurological M>47.75), 0801 (Replacement of Lower Extremity Joint M>49.55), 0802 (Replacement of Lower Extremity Joint M>37.05 and M<49.55), 0901 (Other Orthopedic M>44.75), 1401 (Cardiac M>48.85), or 1501 (Pulmonary M>49.25) D: count of all discharges 38 19
20 IRF PEPPER Target Areas, 2 Target Area Outlier Payments STACH Admissions following IRF Discharge Target Area Definition N: count of discharges with an outlier approved amount greater than $0 D: count of all discharges N: count of beneficiaries discharged from the IRF during the 12 month time period that were admitted to a short term acute care hospital within 30 days of discharge from the IRF; excluding beneficiaries that were transferred to a STACH, LTCH or IRF within one day of discharge as evidenced by a subsequent claim; excluding patient discharge status codes 07 (left against medical advice), 20 (expired) D: count of all discharges excluding beneficiaries that were transferred to a STACH, LTCH or IRF within one day of discharge as evidenced by a subsequent claim; and excluding patient discharge status codes 07, HHA PEPPER Target Areas Target Area Outlier Payments Average Number of Episodes Average Case Mix Target Area Definition N: dollar amount of outlier payments received by the HHA during the report period D: dollar amount of total payments received by the HHA during the report period N: count of episodes paid to the HHA during the report period D: count of beneficiaries served by the HHA during the report period N: sum of case mix weight for all episodes paid to the HHA during the report period, excluding LUPAs and PEPs D: count of episodes paid to the HHA during the report period, excluding LUPAs and PEPs 40 20
21 HHA PEPPER Target Areas, 2 Target Area Episodes with 5 or 6 Visits Non LUPA Payments High Therapy Utilization Episodes Target Area Definition N: count of episodes with 5 or 6 visits paid to the HHA during the report period D: count of episodes paid to the HHA during the report period N: count of episodes paid to the HHA that did not have a LUPA payment during the report period D: count of episodes paid to the HHA during the report period N: count of episodes with 20+ therapy visits paid to the HHA during the report period (first digit of HHRG equal to 5 ) D: count of episodes paid to the HHA during the report period 41 Short term Acute Care Hospital Target Areas Stroke Intracranial Hemorrhage Respiratory Infections Simple Pneumonia Septicemia Unrelated OR Procedures Medical DRGs with CC or MCC Surgical DRGs with CC or MCC Single CC or MCC Excisional Debridement Ventilator Support Transient Ischemic Attack Chronic Obstructive Pulmonary Disease PTCA with Stent Syncope Other Circulatory System Diagnoses Other Digestive System Diagnoses Medical Back Problems Spinal Fusion 3 day SNF qualifying Admissions 30 day Readmissions to Same Hospital or Elsewhere 30 day Readmissions to Same Hospital 2 DS Medical DRGs 2DS Surgical DRGs 1DS Medical DRGs 1DS Surgical DRGs Same day Stays Medical DRGs Same day Stays Surgical DRGs 42 21
22 Critical Access Hospital Target Areas Stroke Intracranial Hemorrhage Respiratory Infections Simple Pneumonia Septicemia Medical DRGs with CC or MCC Surgical DRGs with CC or MCC Single CC or MCC Chronic Obstructive Pulmonary Disease Syncope Medical Back Problems Swing Bed Transfers 3 day SNF qualifying Admissions 30 day Readmissions to Same Hospital or Elsewhere 30 day Readmissions to Same Hospital 2DS Heart Failure and Shock 2DS Cardiac Arrhythmia 2DS Esophagitis Gastroenteritis 2DS Nutritional & Metabolic Disorders 2DS Kidney & UTI 1DS Excluding Transfers 1DS Medical DRGs 43 IPF and LT Target Areas Inpatient Psychiatric Facility Target Areas: Outlier Payments 3 to 5 Day Readmissions 30 Day Readmissions Comorbidities Long term Acute Care Hospital Target Areas: Septicemia Excisional Debridement Short Stays Short Stays for Resp. Syst. Diagnoses Outlier Payments 30 Day Readmissions STACH Admissions following LT discharge 44 22
23 Partial Hospitalization Program Target Areas Days of Service with 4 Units Billed Group Therapy No Individual Psychotherapy 60+ Days of Service 30 day Readmissions 45 Questions? Help/Contact Us at PEPPERresources.org 46 23

24 Hospice PEPPER Reports and Your Compliance Program Kathryn Krenz Compliance Analyst Agenda Medicare Hospice Benefit Why PEPPER for Hospice? What is Hospice PEPPER? Hospice PEPPER target areas Case Study Auditing and Monitoring Considerations Questions 48 24
25 Medicare Hospice Benefit Overview Established in 1986 to provide palliative care and support to terminally ill patients and their families Is part of the Medicare Part A Hospital Benefit Paid on a per diem basis based on 4 levels of care Routine home care Respite care Short-term general inpatient care Continuous home care 49 Medicare Hospice Benefit Eligibility Patient must be eligible for Medicare Part A Patient must be certified terminally ill by two physicians with life expectancy of 6 months or less if the illness runs its usual course Patient must elect hospice Must be aware that care will be palliative vs. curative Must understand that election waives rights to other Medicare benefits 50 25
26 Medicare Hospice Benefit Covered Hospice Services Includes coverage of nursing medical social services physician services counseling short-term general inpatient care medical appliances and supplies aide and homemaker services PT, OT, ST other services related to the palliation of the terminal illness 51 Why PEPPER for Hospice? The Government Accountability Office has designated the Medicare hospice benefit as a high risk program for fraud and abuse Supports CMS program integrity efforts It is an educational tool to help providers assess risk Trends over time have generated concern Spending has increased by approximately $1 billion per year Diagnoses have changed from cancer to non-cancer Average length of stay has increased 52 26
27 What is Hospice PEPPER? Contains claims data statistics obtained from paid hospice Medicare claims for the most recent three federal fiscal years Oct 1 through September 30 Compares the provider s hospice data to other hospices in three comparison groups Nation Medicare Administrative Contractor jurisdiction State Identifies risk areas for improper Medicare payments based on preset upper control limit of the 80 th percentile 53 What is Hospice PEPPER? Claims included must meet criteria Must be a final action claim that was non-rejected and for which all adjustments and disputes have been resolved and payment made in an amount greater than zero Services must have been provided during the time period used to create the episode of service the beneficiary must have been discharged or did not return for care within 30 days for those claims to be included Excludes claims submitted to a Medicare Advantage plan Excludes cancelled claims Claims are collected for two years prior to each time period so that longer lengths of stay can be evaluated 54 27
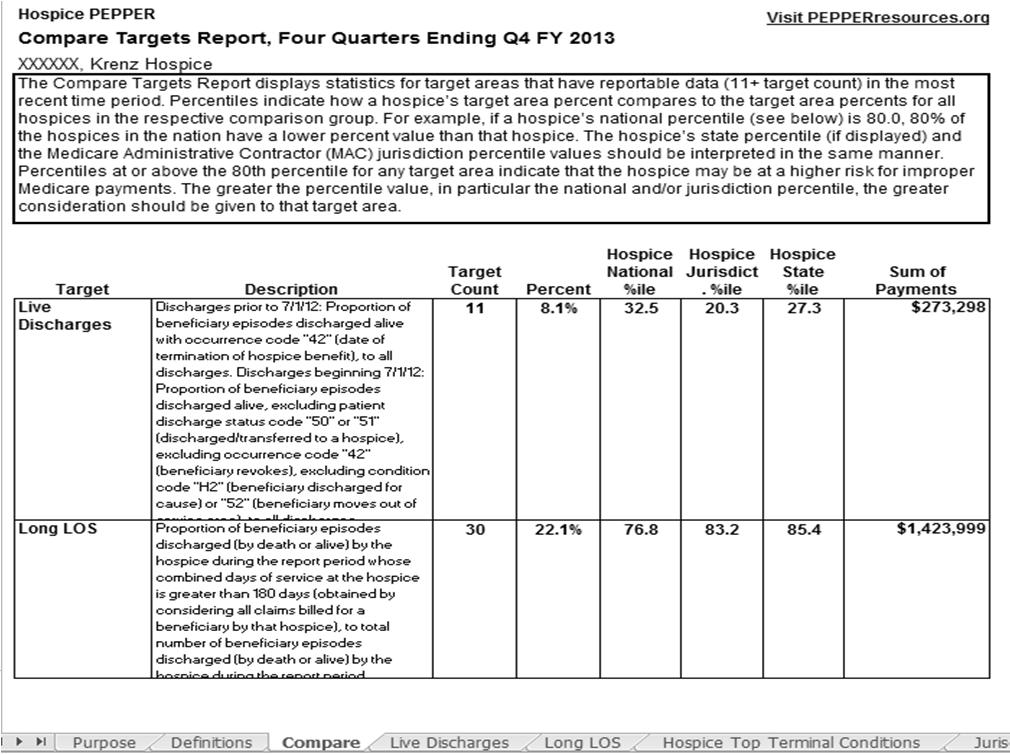
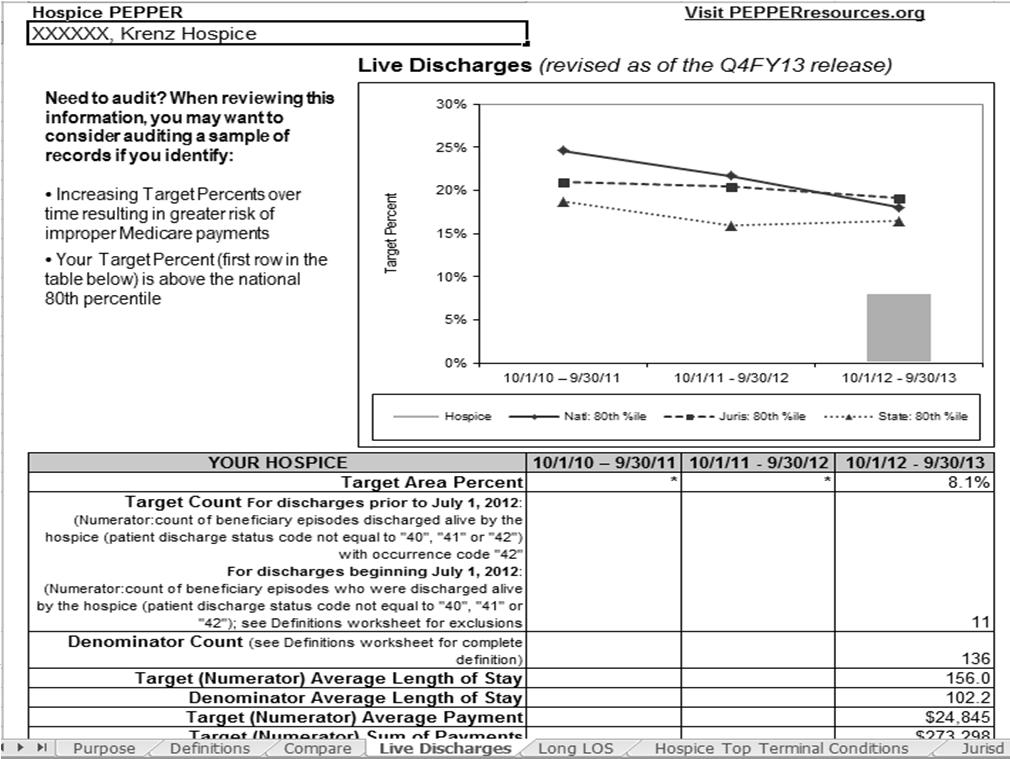
28 What is Hospice PEPPER? Has informational tabs in excel spreadsheet format Purpose tab gives hospice identifier and general report information Definitions tab explains how target area information for the hospice was generated Compare tab compares individual hospice data to nation, MAC jurisdiction and state hospices Target areas tabs (currently Live Discharges and Long LOS tabs) graphs out the agency related to nation, jurisdiction and state Hospice Top Terminal Conditions lists provider top diagnoses for time period of report (must be at least 11 decedents) Jurisdiction Top Terminal Conditions lists MAC top diagnoses for time period of report (must be at least 11 decedents) 55 PEPPER Hospice Target Areas Target Area Live Discharges (Live Discharges) Target Definition For discharges prior to July 1, 2012: Numerator (N): count of beneficiary episodes discharged alive by the hospice - patient discharge status code not equal to 40 (expired at home), 41 (expired in a medical facility) or 42 (expired place unknown)) with occurrence code "42" (date of termination of hospice benefit) Denominator (D): count of all beneficiary episodes discharged (by death or alive) by the hospice during the report period (obtained by considering all claims billed for a beneficiary by that hospice) For discharges beginning July 1, 2012: Numerator (N): count of beneficiary episodes who were discharged alive by the hospice - patient discharge status code not equal to 40 (expired at home), 41 (expired in a medical facility) or 42 (expired place unknown)), excluding: beneficiary transfers (patient discharge status code 50 or 51 ) beneficiary revocations (occurrence code 42 ) beneficiaries discharged for cause (condition code H2 ) beneficiaries who moved out of the service area (condition code 52 ) Denominator (D): count of all beneficiary episodes discharged (by death or alive) by the hospice during the report period (obtained by considering all claims billed for a beneficiary by that hospice) 56 28
29 PEPPER Hospice Target Areas-continued Target Area Long Length of Stay (Long LOS) Target Area Definition N: count of beneficiary episodes discharged (by death or alive) by the hospice during the report period whose combined days of service at the hospice is greater than 180 days (obtained by considering all claims billed for a beneficiary by that hospice) D: count of all beneficiary episodes discharged (by death or alive) by the hospice during the report period 57 PEPPER Hospice Target Areas-continued Target Area Continuous Home Care Provided in an Assisted Living Facility (CHC in ALF) *new as of the Q4FY14 release Target Area Definition N: count of beneficiary episodes discharged (by death or alive) by the hospice during the report period where at least eight hours of Continuous Home Care (revenue code = 0652 ) were provided while the beneficiary resided in an Assisted Living Facility (HCPCS code = Q5002 ) D: count of all beneficiary episodes ending in the report period that indicate the beneficiary resided in an assisted living facility (HCPCS code = Q5002 ) for any portion of the episode 58 29
30 PEPPER Hospice Target Areas-continued Target Area Routine Home Care Provided in an Assisted Living Facility (RHC in ALF) *new as of the Q4FY14 release Target Area Definition N: count of Routine Home Care days (revenue code = 0651 ) provided on claims ending in the report period that indicate the beneficiary resided in an assisted living facility (HCPCS code = Q5002 ) D: count of all Routine Home Care days (revenue code = 0651 ) provided by the hospice on claims ending in the report period 59 PEPPER Hospice Target Areas-continued Target Area Routine Home Care Provided in a Nursing Facility (RHC in NF) *new as of the Q4FY14 release Target Area Definition N: count of Routine Home Care days (revenue code = 0651 ) provided on claims ending in the report period that indicate the beneficiary resided in a nursing facility (HCPCS code = Q5003 ) D: count of all Routine Home Care days (revenue code = 0651 ) provided by the hospice on claims ending in the report period 60 30
31 PEPPER Hospice Target Areas-continued Target Area Routine Home Care Provided in a Skilled Nursing Facility (RHC in SNF) *new as of the Q4FY14 release Target Area Definition N: count of Routine Home Care days (revenue code = 0651 ) provided on claims ending in the report period that indicate the beneficiary resided in a skilled nursing facility (HCPCS code = Q5004 ) D: count of all Routine Home Care days (revenue code = 0651 ) provided by the hospice on claims ending in the report period 61 Why New Hospice Target Areas? RAC (Recovery Audit Contractor) Improvements Tasked with reviewing all provider types, including hospice First new contract awarded to Connolly for Region 5 on 12/30/ currently under post-award protest OIG reports on Medicare hospices July 2011 hospices that focus on NF residents January 2015 hospices have incentives to provide care in ALs 62 31
32 Case Study
33
34
35 69 35

36 Auditing and Monitoring Considerations Review the PEPPER for trends that point to risk for a single year and for changes over time Review hospice eligibility and admission criteria for your agency and change processes as needed Audit for accurate documentation and billing of discharge type Audit for accurate documentation of place of service Monitor for accurate hospice diagnosis coding Review for education needs for patients/families 72 36
37 Auditing and Monitoring Considerations continued Audit medical records Does documentation support terminal prognosis? Watch for cookie cutter or conflicting documentation, particularly in electronic medical records Monitor IDG notes for accuracy and completeness and agreement with the rest of the medical record Use audit findings to determine training needs 73 Auditing and Monitoring Considerations continued Monitor contractor sites for changes in LCDs/review focus/denial information Watch CMS Hospice Center for changes and areas that CMS is concerned about Review the OIG work plan yearly and any other pertinent OIG reports for areas to focus on in your audit/monitoring 74 37
38 Questions? Contact information: Kathryn Krenz, RN, BSN, CPC, CHC Compliance Analyst Brookdale Senior Living
39 PEPPER &Data Analytics: SNF Shawn Halcsik DPT, MEd, RAC CT, CPC, CHC Vice President of Compliance & Clinical Services Evergreen Rehabilitation Louisville, KY 2010 OIG Report OIG Report: $1.5 billion upcoded downcoded coverage correct 16.8 Therapy ADLs None 30.3 Specialty Care Oral/Nutrit 39
40 Continued Focus on SNFs 2015 OIG Work Plan The OIG will describe changes in SNF billing practices from FYs 2011 to 2013 RAC Review FY2013 SNF recoveries $1.8 million (6%) MAC Review MedPAC Report MDS Focused Surveys CMS Monitoring of RUGs 79 Therapy in the News Nursing Home Operator to Pay $48 Million to Resolve Allegations that Six California Facilities Billed for Unnecessary Therapy Extendicare Health Services Inc. Agrees to Pay $38 Million to Settle False Claims Act Allegations Relating to the Provision of Substandard Nursing Care and Medically Unnecessary Rehabilitation Therapy $3.8 million settlement shows nursing homes must oversee their therapy providers, feds say $1.3 million settlement marks second recent deal over SNF supervision of therapy providers 40
41 Mitigating Audit Risk 3 Ps Circle of Concern Train & Educate Continuous Audit Preparation Audit & Monitor Response Therapy Oversight Which Are You? 38 PEPPER No PEPPER 62 41



42 SNF PEPPER Target Areas SNF PEPPER Target Areas, cont. Therapy 42

43 High ADLs (11 16) If at/above 80 th percentile This could indicate a risk of potential overcoding of beneficiaries activities of daily living (ADL) status. The SNF should determine whether the amount of assistance beneficiaries need with ADL as reported on the MDS is supported and consistent with medical record documentation. Is the ADL score reported consistent with the intensity of therapy being provided If at/below 20 th percentile This could indicate a risk of potential undercoding of beneficiaries ADL status. The SNF should determine whether the amount of assistance beneficiaries need with ADL as reported on the MDS is supported and consistent with medical record documentation. Is the ADL score reported consistent with the intensity of therapy being provided 86 43
44
45 89 ADL Score Audit Tool 90 45
46 COT Considerations If at/above 80th percentile: SNF may be experiencing challenges with delivering services to the beneficiary Look at factors that lead to the need for the COT Communication between disciplines Missed therapy due to appointments, scheduling Scheduling conflicts Staffing Issues If at/below 20th percentile: Review process in facility for IDT review of minutes Process for Unscheduled Assessment Monitoring & Communication Length of Stay? 91 Target Therapy High ADL Description Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB, to days billed within episodes of care ending in the report period for all therapy RUGs SNF SNF Target National Jurisdict. SNF State Count Percent %ile %ile %ile 15, % Nontherapy High Proportion of days billed within episodes of care ending in the report period with RUG equal to SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, ADL IB1 in RUG III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUG IV, to days billed within episodes of care ending in the report period for all nontherapy RUGs % Change of Therapy Assessment Proportion of assessments with AI second digit equal to D within episodes of care ending in the report period, to all assessments within episodes of care ending in the report period % Ultrahigh Therapy RUGs Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RUL, RUC, RUB, RUA, to days billed within episodes of care ending in the report period for all therapy RUGs 32, % Therapy RUGs Proportion of days billed within episodes of care ending in the report period for therapy RUGs, to days billed within episodes of care ending in the report period for all therapy and nontherapy RUGs 34, % Day Proportion of episodes of care ending in the report period at the SNF with a length of stay of 90+ days, to all episodes of care ending in the Episodes of Care report period at the SNF %

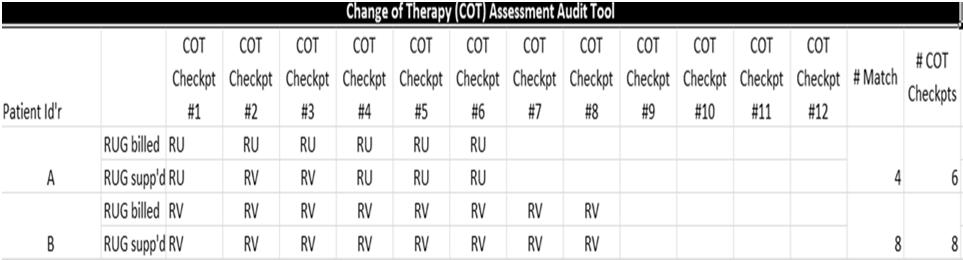
47 Change of Therapy (COT) Assessment Audit Tool 93 Change of Therapy (COT) Assessment Audit Tool 47
48 90+ Day Episode of Care If at/above 80th percentile: Could indicate that the SNF is continuing treatment beyond point where services are medically necessary If at/below 20th percentile: Review to assure that patients receive all necessary treatments prior to discharge = RISK MANAGEMENT 95 Target Therapy High ADL Description Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB, to days billed within episodes of care ending in the report period for all therapy RUGs SNF SNF Target National Jurisdict. SNF State Count Percent %ile %ile %ile 1, % Nontherapy High Proportion of days billed within episodes of care ending in the report period with RUG equal to SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, ADL IB1 in RUG III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUG IV, to days billed within episodes of care ending in the report period for all nontherapy RUGs % Change of Therapy Assessment Proportion of assessments with AI second digit equal to D within episodes of care ending in the report period, to all assessments within episodes of care ending in the report period % Ultrahigh Therapy RUGs Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RUL, RUC, RUB, RUA, to days billed within episodes of care ending in the report period for all therapy RUGs 2, % Therapy RUGs Proportion of days billed within episodes of care ending in the report period for therapy RUGs, to days billed within episodes of care ending in the report period for all therapy and nontherapy RUGs 4, % Day Proportion of episodes of care ending in the report period at the SNF with a length of stay of 90+ days, to all episodes of care ending in the Episodes of Care report period at the SNF %
49 Ultra High Therapy RUGs / Therapy RUGs If at/above 80th percentile Could indicate SNF is improperly billing for therapy services. Is clinical intensity appropriate based on patient need? If at/below 20th percentile Is clinical intensity appropriate based on patient need? Is staffing appropriate? 97 Target Therapy High ADL Description Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB, to days billed within episodes of care ending in the report period for all therapy RUGs SNF SNF Target National Jurisdict. SNF State Count Percent %ile %ile %ile 15, % Nontherapy High Proportion of days billed within episodes of care ending in the report period with RUG equal to SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, ADL IB1 in RUG III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUG IV, to days billed within episodes of care ending in the report period for all nontherapy RUGs % Change of Therapy Assessment Proportion of assessments with AI second digit equal to D within episodes of care ending in the report period, to all assessments within episodes of care ending in the report period % Ultrahigh Therapy RUGs Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RUL, RUC, RUB, RUA, to days billed within episodes of care ending in the report period for all therapy RUGs 32, % Therapy RUGs Proportion of days billed within episodes of care ending in the report period for therapy RUGs, to days billed within episodes of care ending in the report period for all therapy and nontherapy RUGs 34, % Day Proportion of episodes of care ending in the report period at the SNF with a length of stay of 90+ days, to all episodes of care ending in the Episodes of Care report period at the SNF %
50 Intensity & Duration Outlier Considerations Additional Data Length of Stay Community discharge % Functional Outcomes Section O Accuracy Scheduled Assessment ARD Communication Unscheduled Assessment Communication MDS Section O Verification RUG Level Setting Process How would therapists respond to question from investigator How amount/intensity of treatment is determined for their patient? LOS Determination Process How would facility staff respond to question from investigator related to pressure to keep on Part A Documentation Quality Intensity & Duration Outlier Considerations Documentation Review Technical Certifications Signed and dated timely and legible Technical Therapy Minute Recording Non MDS: evaluation Time, non skilled Modality Time MDS: Skilled Modality Minutes, Re eval Minutes, Set Up Minutes Co treat minutes Mode of Treatment Accuracy: Individual, Concurrent, Group Claim Triple Check RUGs match MDS Section O Verified ADL Score Supported Days match scheduled and unscheduled assessments completed 50
 nurse.")
51 Intensity & Duration Outlier Considerations Documentation Review Medical Necessity Nursing Medical Necessity & Daily Skill Nursing services are considered skilled when they are so inherently complex that they can be safely and effectively performed only by, or under the supervision of, a registered nurse or, when provided by regulation, a licensed practical (vocational) nurse. ADL score consistent with Therapy RUG Therapy Medical Necessity & Daily Skill Therapy services are considered skilled when they are so inherently complex that they can be safely and effectively performed only by, or under the supervision of, a qualified therapist. Therapy Plans of Care are individual, pt. centered, and match patient clinical presentation RUG Level (treatment intensity) and LOS (treatment duration) # disciplines d/c destination Level (severity) of decline from PLOF Diagnosis vs. Complexities/co morbidities Section O Audit Tool

52 Section O Audit Tool 103 Target Therapy High ADL Description Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB, to days billed within episodes of care ending in the report period for all therapy RUGs SNF SNF Target National Jurisdict. SNF State Count Percent %ile %ile %ile 1, % Nontherapy High Proportion of days billed within episodes of care ending in the report period with RUG equal to SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, ADL IB1 in RUG III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUG IV, to days billed within episodes of care ending in the report period for all nontherapy RUGs % Change of Therapy Assessment Proportion of assessments with AI second digit equal to D within episodes of care ending in the report period, to all assessments within episodes of care ending in the report period % Ultrahigh Therapy RUGs Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RUL, RUC, RUB, RUA, to days billed within episodes of care ending in the report period for all therapy RUGs 2, % Therapy RUGs Proportion of days billed within episodes of care ending in the report period for therapy RUGs, to days billed within episodes of care ending in the report period for all therapy and nontherapy RUGs 4, % Day Proportion of episodes of care ending in the report period at the SNF with a length of stay of 90+ days, to all episodes of care ending in the Episodes of Care report period at the SNF %
53 Target Therapy High ADL Description Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB, to days billed within episodes of care ending in the report period for all therapy RUGs SNF SNF Target National Jurisdict. SNF State Count Percent %ile %ile %ile 15, % Nontherapy High Proportion of days billed within episodes of care ending in the report period with RUG equal to SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, ADL IB1 in RUG III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUG IV, to days billed within episodes of care ending in the report period for all nontherapy RUGs % Change of Therapy Assessment Proportion of assessments with AI second digit equal to D within episodes of care ending in the report period, to all assessments within episodes of care ending in the report period % Ultrahigh Therapy RUGs Proportion of days billed within episodes of care ending in the report period with RUG equal to RUX, RUL, RUC, RUB, RUA, to days billed within episodes of care ending in the report period for all therapy RUGs 32, % Therapy RUGs Proportion of days billed within episodes of care ending in the report period for therapy RUGs, to days billed within episodes of care ending in the report period for all therapy and nontherapy RUGs 34, % Day Proportion of episodes of care ending in the report period at the SNF with a length of stay of 90+ days, to all episodes of care ending in the Episodes of Care report period at the SNF % Part A Data Monitoring You?? You?? You?? You?? You?? 49.1 State VA Nat'l You COT RU 90+ LOS Comm DC Source: PEPPER National Target Analysis; 53



54 Questions? Shawn Halcsik



55 COMPLIANCE OVERSIGHT External Oversight Corporate Internal Oversight Leadership Governing Body Internal Priority Structures Hospital Services 55
56 ADD SOME FLAVOR TO YOUR COMPLIANCE PROGRAM 1. Compliance Infrastructure- 2. Standards of Conduct 3. Education and Training 4. Process to Receive Reports of Non-Compliance 5. System to Respond to Allegations 6. Audits to Monitor Compliance 7. System to Investigate Problems 8. Program Effectiveness INPATIENT REHABILITATION FACILITY COMPLIANCE PRIORITIES OIG target Begin tracking adverse events in IRF s for Medicare beneficiaries in Condition of Participation- 42 CFR (a)(2)- requires hospitals to track adverse patient events. RAC target- Medical necessity of patients at time of admission and throughout the patient s stay. Operational Outcomes: Comorbidity capture 60% Compliance Reduction in non-community transfers- ACT, SNF Patient Outcomes Transition to community following IP stay. LOS management 56

57 MANAGING RISK ASSESS THE DATA An IRF s target area % is compared to other IRFs 5 in the State, MAC jurisdiction and Nation. If the IRF s target area percent is at/above the national 80 th percentile or at/below the national 20 th percentile, the IRF is identified as at risk for improper Medicare payments. Compare and target area reports: Red bold print- at or above the national 80 th percentile for the target area. 57
,")



58 EVALUATE RISK Determine how your facility compares to other IRFs If statistics are higher/lower than most other IRFs ( outlier ), ask why? Consider patient population and external factors Review documentation: does it support the CMG? If yes- note results of audit; reassess periodically; maintain documentation of audits If no- take necessary steps to address; reassess; continue to adjust if necessary. PEPPER AS A TOOL TO EVALUATE/MONITOR RISK Coding Length of Stay Mgt. Medical Necessity of Admissions Discharge Planning 58
59 IRF PEPPER TARGET AREAS Target Area Miscellaneou s CMGs CMGs at Risk for Unnecessary Admissions Target Area Definition N: count of discharges for Case-Mix Groups (CMGs) 2001 (Miscellaneous M>49.15), 2002 (Miscellaneous M>38.75 and M<49.15), 2003 (Miscellaneous M>27.85 and M<38.75) or 2004 (Miscellaneous M<27.85) D: count of all discharges N: count of discharges with no tier group assignment for CMGs 0101 (Stroke M>51.05), 0501 (Non-traumatic Spinal Cord Injury M>51.35), 0601 (Neurological M>47.75), 0801 (Replacement of Lower Extremity Joint M>49.55), 0802 (Replacement of Lower Extremity Joint M>37.05 and M<49.55), 0901 (Other Orthopedic M>44.75), 1401 (Cardiac M>48.85), or 1501 (Pulmonary M>49.25) D: count of all discharges IRF PEPPER TARGET AREAS Target Area Outlier Payments STACH Admissions following IRF Discharge Target Area Definition N: count of discharges with an outlier approved amount greater than $0 D: count of all discharges N: count of beneficiaries discharged from the IRF during the 12-month time period that were admitted to a shortterm acute care hospital within 30 days of discharge from the IRF; excluding beneficiaries that were transferred to a STACH, LTCH or IRF within one day of discharge as evidenced by a subsequent claim; excluding patient discharge status codes 07 (left against medical advice), 20 (expired) D: count of all discharges excluding beneficiaries that were transferred to a STACH, LTCH or IRF within one day of discharge as evidenced by a subsequent claim; and excluding patient discharge status codes 07, 20 59




60 IRF TARGET AREA- MISCELLANEOUS CMGS WHAT ARE THE RISKS? Is Coding to the most specific level possible? * % Compliance methodology. Does documentation clearly support why the patient needed an acute level of care in an intensive rehabilitation environment? Could the patient have been treated at a lower level of care? Was admission criteria met? 60


61 IRF TARGET AREA- CMG AT RISK FOR UNNECESSARY ADMISSIONS WHAT ARE THE RISKS? Are physicians and clinical screeners capturing all appropriate co-morbidities in their documentation? Are admit FIM scores accurately capturing the highest burden of care (lowest score) 61

")
62 IRF TARGET- OUTLIER PAYMENTS WHAT ARE THE RISKS? What causes the overpayment? Long length of stay Medical complexity of patient Cost to charge ratio (CCR) 62




63 IRF TARGET- STACH ADMISSIONS FOLLOWING IRF DISCHARGE WHAT ARE THE RISKS? Was patient not medically stable or prepared at time of discharge? Includes patients that were discharged to SNF and then return to acute Not easily tracked by an IRF. 63




64 OPPORTUNITIES Discharge Planning- was there family involvement? Additional needs? Were patient goals met? Patient follow-up after discharge Strategic Partnerships MANAGE THE RISK Build risk areas into performance improvement indicators Add targets to operational dashboards Internal Audits- Peer Audits Monitor targets in MEC and GB meetings so entire hospital/unit is monitoring on an ongoing basis. 64


65 65
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance
 PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
PEPPER for Home Health Agencies and Skilled Nursing Facilities: Practical Applications for Compliance April 19, 2016 Victor Kintz, Polaris Group and Kimberly Hrehor, TMF Agenda What is PEPPER? Focus: HHA
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1
 PEPPER to Support Auditing and Monitoring Efforts: Session 1") Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1
 Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
Thank you for joining us!
 Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the SNF Training and Resources section. A recording of
Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the SNF Training and Resources section. A recording of
Thank you for joining us!
 Thank you for joining us! We will start at 1:00 p.m. CT. You will hear silence until the session begins. Audio Options: Recommended: Audio broadcast using your computer speakers (automatically join the
Thank you for joining us! We will start at 1:00 p.m. CT. You will hear silence until the session begins. Audio Options: Recommended: Audio broadcast using your computer speakers (automatically join the
Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts
 PEPPER to Support Auditing and Monitoring Efforts") Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts July 30, 2015 Kimberly Hrehor 2 Agenda History and basics of PEPPER HHA PEPPER target areas Percents, rates and
Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts July 30, 2015 Kimberly Hrehor 2 Agenda History and basics of PEPPER HHA PEPPER target areas Percents, rates and
Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report. User s Guide Sixth Edition. Prepared by
 Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report User s Guide Sixth Edition Prepared by Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report
Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report User s Guide Sixth Edition Prepared by Skilled Nursing Facility Program for Evaluating Payment Patterns Electronic Report
August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]
![August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]](/thumbs/83/88557772.jpg "August 30, [Contact Name] SNF Name, [Address Line 1] [Address Line 2] [City], B8 [ZIP]") Bridgepoint 1, Suite 300 5918 West Courtyard Drive, Austin TX 78730-5036 August 30, 2013 [Contact Name] SNF Name, 009168 [Address Line 1] [Address Line 2] [City], B8 [ZIP] RE: Program for Evaluating Payment
Bridgepoint 1, Suite 300 5918 West Courtyard Drive, Austin TX 78730-5036 August 30, 2013 [Contact Name] SNF Name, 009168 [Address Line 1] [Address Line 2] [City], B8 [ZIP] RE: Program for Evaluating Payment
Reading and Using the PEPPER Report
 Reading and Using the PEPPER Report PANAC Webinar September 25, 2014 Stephanie Kessler Partner, Senior Living Services Consulting Group Disclaimer The information contained herein is of a general nature
Reading and Using the PEPPER Report PANAC Webinar September 25, 2014 Stephanie Kessler Partner, Senior Living Services Consulting Group Disclaimer The information contained herein is of a general nature
What Did Your PEPPER Tell CMS?
 What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
User s Guide Tenth Edition
 Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Tenth Edition Prepared by Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User
Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User s Guide Tenth Edition Prepared by Long-term Acute Care Program for Evaluating Payment Patterns Electronic Report User
THE PEPPER AND YOUR CDI PROGRAM. Kat McFarland, RN, MN, ACM Director Care Management Providence Regional Medical Center Everett 9/28/2018
 THE PEPPER AND YOUR CDI PROGRAM Kat McFarland, RN, MN, ACM Director Care Management Providence Regional Medical Center Everett 9/28/2018 https://pepperresources.org/training-resources/short-term-acute-care-hospitals/pepper-review
THE PEPPER AND YOUR CDI PROGRAM Kat McFarland, RN, MN, ACM Director Care Management Providence Regional Medical Center Everett 9/28/2018 https://pepperresources.org/training-resources/short-term-acute-care-hospitals/pepper-review
Thank you for joining us!
 Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the Hospice Training and Resources section. A recording
Thank you for joining us! We will start at 1 p.m. CT. You will hear silence until the session begins. Handout: Available at PEPPERresources.org in the Hospice Training and Resources section. A recording
Understanding the PEPPER
 Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Plant the Seeds of Compliance with PEPPER. Prepared for: WiAHC June 8, Presented by: Caryn Adams, Manager
 Plant the Seeds of Compliance with PEPPER Prepared for: June 8, 2017 Presented by: Caryn Adams, Manager Summary and Objectives Program for Evaluating Payment Electronic Report has been available to home
Plant the Seeds of Compliance with PEPPER Prepared for: June 8, 2017 Presented by: Caryn Adams, Manager Summary and Objectives Program for Evaluating Payment Electronic Report has been available to home
2/18/2015. The Journey Begins. PEPPER and OSCAR/CASPER Reports. Objectives. Preparation for Change
 PEPPER and OSCAR/CASPER Reports Objectives Identify the purpose of the PEPPER and CASPER (OSCAR) reports Interpret the individual reports and identify the outlier data that places a facility at greater
PEPPER and OSCAR/CASPER Reports Objectives Identify the purpose of the PEPPER and CASPER (OSCAR) reports Interpret the individual reports and identify the outlier data that places a facility at greater
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc.
 HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
Surviving Targeted Probe & Educate
 Surviving Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe & Educate
Surviving Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe & Educate
Home Health Targeted Probe & Educate
 Home Health Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. WWW.TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe
Home Health Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. WWW.TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Develop a Taste for PEPPER: Interpreting
 Develop a Taste for PEPPER: Interpreting Your Organizational Results Cheryl Ericson, MS, RN Manager of Clinical Documentation Integrity, The Medical University of South Carolina (MUSC) Objectives Increase
Develop a Taste for PEPPER: Interpreting Your Organizational Results Cheryl Ericson, MS, RN Manager of Clinical Documentation Integrity, The Medical University of South Carolina (MUSC) Objectives Increase
* HFMA staff and volunteers determined that this product has met specific criteria developed under. endorse or guaranty the use of this product.
 Latest Updates to the PEPPER: Utilizing New Report Data and Benchmarks to Support Your Compliance Efforts John Zelem, MD Senior Director, Audit, Compliance & Education Executive Health Resources * HFMA
Latest Updates to the PEPPER: Utilizing New Report Data and Benchmarks to Support Your Compliance Efforts John Zelem, MD Senior Director, Audit, Compliance & Education Executive Health Resources * HFMA
This educational presentation is provided by. The software that powers post-acute care. HOME HEALTH. HOSPICE. THERAPY.
 2 This educational presentation is provided by The software that powers post-acute care. HOME HEALTH. HOSPICE. THERAPY. PRIVATE DUTY We understand the challenges your business is facing. That s why Kinnser
2 This educational presentation is provided by The software that powers post-acute care. HOME HEALTH. HOSPICE. THERAPY. PRIVATE DUTY We understand the challenges your business is facing. That s why Kinnser
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1)
") CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
3/12/2012. DRG Validation, cont. New Challenges and Target Areas RACs. Update on RACs [Recovery Audit Contractors] & Other External Auditors
![3/12/2012. DRG Validation, cont. New Challenges and Target Areas RACs. Update on RACs [Recovery Audit Contractors] & Other External Auditors](/thumbs/82/85079861.jpg "3/12/2012. DRG Validation, cont. New Challenges and Target Areas RACs. Update on RACs [Recovery Audit Contractors] & Other External Auditors") Update on RACs [Recovery Audit Contractors] & Other External Auditors Presented by: Mary Legerski, RN, Esq., CHC, CPC, MBA, MPA New Challenges and Target Areas RACs CGI Targets as of 3/7/12 Inpatient claims
Update on RACs [Recovery Audit Contractors] & Other External Auditors Presented by: Mary Legerski, RN, Esq., CHC, CPC, MBA, MPA New Challenges and Target Areas RACs CGI Targets as of 3/7/12 Inpatient claims
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS)
") CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
3M Health Information Systems. A case study in coding compliance: Achieving accuracy and consistency
 3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
Patient-Driven Payment Model
 Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Using SNF Data to Manage Federal & State Audit Initiatives
 Using SNF Data to Manage Federal & State Audit Initiatives 2012 OIG & GAO Reports In 2009 OIG estimated that 47% of claims had misreported information on the MDS that caused significant errors in Billing
Using SNF Data to Manage Federal & State Audit Initiatives 2012 OIG & GAO Reports In 2009 OIG estimated that 47% of claims had misreported information on the MDS that caused significant errors in Billing
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
MDS Accuracy and Compliance: Where There s Smoke
 MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I ZIMMET HEALTHCARE 2018
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
The Shift is ON! Goodbye PPS, Hello RCS
 The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
OIG Work Plan Darci Friedman, Director of Regulatory Products Lynne Rinehimer, Sr. Healthcare Solutions Consultant
 OIG Work Plan 2014 Darci Friedman, Director of Regulatory Products Lynne Rinehimer, Sr. Healthcare Solutions Consultant Agenda Introduction to, and how to interpret, the OIG Work Plan Review of Hospital
OIG Work Plan 2014 Darci Friedman, Director of Regulatory Products Lynne Rinehimer, Sr. Healthcare Solutions Consultant Agenda Introduction to, and how to interpret, the OIG Work Plan Review of Hospital
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
4/20/2015. NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals. Today s Objectives. Background
 NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Riding Herd on Fraud, Waste and Abuse
 Riding Herd on Fraud, Waste and Abuse Dan McCullough Judi McCabe Juanita Henry Kim Hrehor 1 Taking Stock: Surveying the Landscape of Fraud, Waste and Abuse 2 How Big is the Problem? The simple truth is
Riding Herd on Fraud, Waste and Abuse Dan McCullough Judi McCabe Juanita Henry Kim Hrehor 1 Taking Stock: Surveying the Landscape of Fraud, Waste and Abuse 2 How Big is the Problem? The simple truth is
Transitioning to the New IRF-PAI
 Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
6/12/2017. The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group
 The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
SNF Compliance: What s at Stake?
 SNF Compliance: What s at Stake? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Elisa Bovee, MS OTR/L Vice President of Operations About Elisa Elisa
SNF Compliance: What s at Stake? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Elisa Bovee, MS OTR/L Vice President of Operations About Elisa Elisa
RAC Audits and Denials Management WHCA Fall Conference September 9, 2014
 JoLynn Munro, MS,OTR/L, Regional Vice President Infinity Rehab Carolyn Staples, CCC/SLP, Area Rehab Director Infinity Rehab RAC Audits and Denials Management WHCA Fall Conference September 9, 2014 Objectives
JoLynn Munro, MS,OTR/L, Regional Vice President Infinity Rehab Carolyn Staples, CCC/SLP, Area Rehab Director Infinity Rehab RAC Audits and Denials Management WHCA Fall Conference September 9, 2014 Objectives
Goodbye PPS: Hello RCS!
 Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #21 Compliance = Confidence! Tuesday, August 6 2:30 to 4:30 p.m. Diplomat 1 & 2 Upon completion of this presentation,
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #21 Compliance = Confidence! Tuesday, August 6 2:30 to 4:30 p.m. Diplomat 1 & 2 Upon completion of this presentation,
Payment Methodology. Acute Care Hospital - Inpatient Services
 Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Discharge to Community Measure
 The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
2013 OIG Work Plan. Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas
 2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015)
") 7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
06-01 FORM HCFA WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the
 06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Medicare Inpatient Psychiatric Facility Prospective Payment System
 Medicare Inpatient Psychiatric Facility Prospective Payment System Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview and Resources On April 24, 2015, the Centers for Medicare and Medicaid
Medicare Inpatient Psychiatric Facility Prospective Payment System Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview and Resources On April 24, 2015, the Centers for Medicare and Medicaid
MEDICARE INPATIENT PSYCHIATRIC FACILITY PROSPECTIVE PAYMENT SYSTEM
 MEDICARE INPATIENT PSYCHIATRIC FACILITY PROSPECTIVE PAYMENT SYSTEM PAYMENT RULE BRIEF PROPOSED RULE Program Year: FFY 2019 OVERVIEW AND RESOURCES The Centers for Medicare & Medicaid Services released the
MEDICARE INPATIENT PSYCHIATRIC FACILITY PROSPECTIVE PAYMENT SYSTEM PAYMENT RULE BRIEF PROPOSED RULE Program Year: FFY 2019 OVERVIEW AND RESOURCES The Centers for Medicare & Medicaid Services released the
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
routine services furnished by nursing facilities (other than NFs for individuals with intellectual Rev
 4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
The OIG Report: Audits are Here! About Kris. Harmony Healthcare International, Inc. Copyright 2013 All Rights Reserved 1. OIG Audits.
 The OIG Report: Audits are Here! Presented by: Kris Mastrangelo, President & CEO Harmony Healthcare International, (HHI) About Kris Kris Mastrangelo, OTR/L, LNHA, MBA Kris Mastrangelo, President and CEO,
The OIG Report: Audits are Here! Presented by: Kris Mastrangelo, President & CEO Harmony Healthcare International, (HHI) About Kris Kris Mastrangelo, OTR/L, LNHA, MBA Kris Mastrangelo, President and CEO,
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals
 NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Payment Rule Summary. Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013
 Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
Medicare Fee-For-Service (FFS) Hospital Readmissions: Q Q2 2014
 Hospital Readmissions: Q Q2 2014") Medicare Fee-For-Service (FFS) Hospital Readmissions: Q3 2013 Q2 2014 State of Florida Data Dictionary Provided on Page A Please contact Peggy Loesch via email at Peggy.Loesch@HCQIS.org or by phone at
Medicare Fee-For-Service (FFS) Hospital Readmissions: Q3 2013 Q2 2014 State of Florida Data Dictionary Provided on Page A Please contact Peggy Loesch via email at Peggy.Loesch@HCQIS.org or by phone at
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
General Inpatient Level of Care: Managing Risks
 General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
National Hospice and Palliative Care OrganizatioN. Facts AND Figures. Hospice Care in America. NHPCO Facts & Figures edition
 National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
Equalizing Medicare Payments for Select Patients in IRFs and SNFs
 Equalizing Medicare Payments for Select Patients in IRFs and SNFs Doug Wissoker Bowen Garrett A report by staff from the Urban Institute for the Medicare Payment Advisory Commission The Urban Institute
Equalizing Medicare Payments for Select Patients in IRFs and SNFs Doug Wissoker Bowen Garrett A report by staff from the Urban Institute for the Medicare Payment Advisory Commission The Urban Institute
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Reference Guide for Hospice Medicaid Services
 Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
OASIS ITEM ITEM INTENT TIME POINTS ITEM(S) COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES
 COMPLETED RESPONSE SPECIFIC INSTRUCTIONS DATA SOURCES / RESOURCES") (M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
(M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OT Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient s home
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.
 Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.") MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
05-11 FORM CMS (Cont.)
") 05-11 FORM CMS-2540-10 4100 4100. GENERAL The Paperwork Reduction Act (PRA) of 1995 requires that the private sector be informed as to why information is collected and what the information is used for
05-11 FORM CMS-2540-10 4100 4100. GENERAL The Paperwork Reduction Act (PRA) of 1995 requires that the private sector be informed as to why information is collected and what the information is used for
ENFORCEMENT, COMPLIANCE, & LONG TERM CARE: HOME HEALTH, HOSPICE, & NURSING HOMES
 ENFORCEMENT, COMPLIANCE, & LONG TERM CARE: HOME HEALTH, HOSPICE, & NURSING HOMES HEALTHCARE ENFORCEMENT COMPLIANCE INSTITUTE: OCTOBER 29, 2017 NICOLE MARTIN, DIRECTOR OF QUALITY & COMPLIANCE AT SAMARITAN
ENFORCEMENT, COMPLIANCE, & LONG TERM CARE: HOME HEALTH, HOSPICE, & NURSING HOMES HEALTHCARE ENFORCEMENT COMPLIANCE INSTITUTE: OCTOBER 29, 2017 NICOLE MARTIN, DIRECTOR OF QUALITY & COMPLIANCE AT SAMARITAN
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Hospice House Network Inpatient Conference
 Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
2014 AANAC 9_30_ AANA C AANA
 2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
HOMECARE AND HOSPICE REIMBURSEMENT
 Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN
 LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Recovery Audit Contractors: AHA Perspective. Elizabeth Baskett, Policy, AHA February 23, 2012
 Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Key points. Home Care agency structures. Introduction to Physical Therapy in the Home Care Setting. Home care industry
 Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
HHGM is Alive and Kicking: How Can You Prepare for What s Next?
 HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule
 CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Fiscal Year 2018 Hospital VBP Program, HAC Reduction Program and HRRP: Hospital Compare Data Update Questions and Answers Moderator Maria Gugliuzza, MBA Project Manager, Hospital Value-Based Purchasing
Fiscal Year 2018 Hospital VBP Program, HAC Reduction Program and HRRP: Hospital Compare Data Update Questions and Answers Moderator Maria Gugliuzza, MBA Project Manager, Hospital Value-Based Purchasing
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
on how to complete this line if you have a new program for which the period of years is less than Rev. 7
 4034 FORM CMS-2552-10 09-15 4034. WORKSHEET E-4 - DIRECT GRADUATE MEDICAL EDUCATION (GME) AND ESRD OUTPATIENT DIRECT MEDICAL EDUCATION COSTS Use this worksheet to calculate each program s payment (i.e.,
4034 FORM CMS-2552-10 09-15 4034. WORKSHEET E-4 - DIRECT GRADUATE MEDICAL EDUCATION (GME) AND ESRD OUTPATIENT DIRECT MEDICAL EDUCATION COSTS Use this worksheet to calculate each program s payment (i.e.,
Stakeholder input is gathered in several ways. Patients are given the opportunity to provide feedback, the SWOT analysis is based on information from
 Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Medicare Program Integrity Manual Chapter 6 - Intermediary MR Guidelines for Specific Services
 Medicare Program Integrity Manual Chapter 6 - Intermediary MR Guidelines for Specific Services Transmittals for Chapter 6 Table of Contents (Rev. 475, 07-19-13) 6.1 - Medical Review of Skilled Nursing
Medicare Program Integrity Manual Chapter 6 - Intermediary MR Guidelines for Specific Services Transmittals for Chapter 6 Table of Contents (Rev. 475, 07-19-13) 6.1 - Medical Review of Skilled Nursing
A1600 A1800: Most Recent Admission/Entry or Reentry into this Facility
 A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your