BORN TO. 25 Years of India s Progress in Maternal and Child Health
|
|
|
- Lindsay May
- 5 years ago
- Views:
Transcription

1 BORN TO BE 25 Years of India s Progress in Maternal and Child Health 1

2 2

3 3
4 Born to BE Ministry of Health and Family Welfare, New Delhi, 2015 The contents of this publication may be reproduced for noncommercial use, provided the source is acknowledged. Requests for commercial reproduction should be directed to the Ministry of Health and Family Welfare, New Delhi. An attempt has been made through the Ministry of Health and Family Welfare to provide comprehensive, accurate and reliable information with no conflict of interest. Ministry of Health and Family Welfare Nirman Bhawan, New Delhi Website: Cover photo: Syed Altaf Ahmad/UNICEF India 4 Designed & Printed by: Rouge Communications
5 BORN TO BE 25 Years of India s Progress in Maternal and Child Health 1

6 2

7 An Eventful Journey 3
8 An Eventful Journey India is polio free. The progress in Millennium Development Goals 4 and 5 are reflected in a higher decline than the global average in under 5 mortality rate and maternal mortality ratio. Maternal and neonatal tetanus has been eliminated. The country has initiated a mission to ensure that every child is reached with life-saving vaccinations by There is a commitment to end preventable deaths of newborn children through the India Newborn Action Plan. Control, prevention and treatment of major preventable and treatable illnesses, such as acute respiratory tract infections and diarrheal diseases have proved effective. Institutional deliveries have increased to more than 79 per cent. 4
9 The progress India has witnessed over the last 25 years have resulted in reduction of deaths of children and mothers due to preventable causes. The Government of India s flagship programmes for maternal and child health along with initiatives of state governments are supported by bilateral and multilateral agencies, professional associations, academic institutions, civil society organisations and media. Today, the Indian health care network is among the largest and its tentacles reach almost every mother and child through a continuum of care approach across life stages. Quality services are being delivered at home: community and health facilities for newborn children, adolescents and pregnant mothers are available. With a large population of young people, the country is focused on nurturing a new generation that will grow healthy and realise its full potential. The journey has been an eventful one! India was the first country to have launched a Family Planning Programme in The maternal and child health programmes moved to a more focused and integrated approach through the Child Survival and Safe Motherhood programme in It covered all the districts of the country by The programme augmented activities under the oral rehydration therapy and acute respiratory infection programme for control of diarrhea and pneumonia in children. High coverage levels were achieved under the Universal Immunization Programme (UIP). The safe motherhood component focused on universal prophylaxis for control of anemia in pregnant women, provision of aseptic delivery kits, and strengthening of first referral units to deal with high risk and obstetric emergencies. After the International Conference Population and Development at Cairo in 1994, India was again the first to have converted its guidelines in to the Reproductive and Child Health (RCH) Programme in The immediate objectives were to address unmet needs of contraception, establish health care infrastructure and strengthen health personnel to achieve goals of reduction of infant mortality rate and maternal mortality ratio to less than 30/1,000 and less than 100/100,000 respectively. The design and learnings of RCH Phase I defined the contours of RCH II, that was launched in the new millenium. It saw a paradigm shift from one size fits all design to an approach where sub-national requirements, capacities and performances were considered. In addition, RCH Phase II moved from a stand alone and supply side approach to integrated approaches that stimulated demand for services. RCH Phase II also adopted the Integrated Management of Neonatal and Childhood Illnesses (IMNCI) strategy after adding the neonatal component which was missing in the original global strategy. This was done by adding components of care for a newborn in the first seven days of life. IMNCI focused on children less than five years old the age group that bears the highest burden of deaths from common childhood diseases such as sepsis, measles, malaria, diarrhoea, pneumonia and malnutrition. Although the major reason for developing the IMNCI strategy stemmed from the needs of curative care, the strategy also addressed social determinants for health such as nutrition and other important elements of disease prevention and health promotion. Prophylaxis with Vitamin A and iron and folic acid for preventing blindness and anemia in children, adolescents and pregnant women were also implemented. Under RCH II, the Universal Immunization Programme targeted six vaccine preventable diseases. For improving maternal health, schemes such as essential obstetric care, provision of emergency obstetric and neonatal care at first referral hospitals, safe abortion services and medical termination of pregnancy were put in place. The National Rural Health Mission (NRHM) launched in 2005 and eventually, subsumed by the National Health Mission (NHM) in 2013, heralded a period of remarkable increase in coverage and quality of health care for mothers and children. The mission empowered state governments through a special focus approach. The thrust was on establishing fully functional, community owned, decentralised health delivery mechanisms through evidence based planning and implementation. The importance of inter-sectoral convergence for maternal and child health at all levels was emphasised through concerted action on a wide range of health determinants such as water, sanitation, education, nutrition, social and gender equality. Integration within the health sector was expected to provide a focus on outcomes, measured against the Indian Public Health Standards for all health facilities. 5
10 A large part of successful delivery can be attributed to the vast and steadily growing numbers of community health workers, both volunteers and employees. An army of nearly one million community level workers Accredited Social Health Activists (ASHAs) are perhaps the most significant driver of maternal and child health care for a population of more than a billion. Increased efficiency in service delivery through effective programme monitoring and overall management, focus on improving health infrastructure and health care professionals have led India on a path that will ensure healthy mothers and survival and development of every child. Road ahead The Government of India s efforts over 25 years have borne fruit. Government health programmes are monitored, mid-course corrections are made, and new schemes within programmes are designed for greater effectiveness. It has been continually building on each of its disparate efforts to improve maternal and child care and linking each of them to the rest, resulting in a continuum of care for every mother and every child, and now, every adolescent. The Government of India affirms that health is a fundamental right. Inequity has reduced, the quality of service has improved, and community outreach has been outstanding. The Draft National Health Policy 2015 outlines further expansion of services, assures universal free delivery of comprehensive quality primary health care services as an entitlement for all aspects of reproductive, maternal, child and adolescent health. It intends to improve access to secondary and tertiary care services through strategic purchases from the private sector. Indian health care s continuum of care now reaches a widely spread and diverse population, across the stages of life from birth, childhood, adolescence and motherhood. A Strategic Approach to Reproductive, Maternal, Newborn, Child, and Adolescent Health (RMNCH+A) launched in 2013, seeks to reach underserved communities through its unique continuum of services, constant innovation and routine monitoring of interventions. The RMNCH+A strategy is guided by central tenets of equity, universal care, entitlement, and accountability. Mission Indradhanush targets immunization of all unimmunized children up to two years against seven vaccine preventable diseases. Rashtriya Kishor Swasthya Karyakram targets India s adolescent population consisting of about 253 million girls and boys between the ages of years. The national missions for Skill India, Digital India, Clean India (Swacch Bharat Abhiyan) and Beti Bachao, Beti Padao (Save Girls, Educate Girls) augur well to build a comprehensive approach that will enable INDIA to fulfill its promise to every mother and every child! 6

11 Born to Be is a compilation of photographs which depict how the Government of India, over 25 years, has designed health programmes to improve the way care is provided: from childhood to adolescence, to pregnant women, and infants, thereby, reducing maternal and child mortality. 7

12 Child Survival and Safe Motherhood On going programmes: Family Welfare 1997 Navjaat Shishu Suraksha Karyakram Universal Immunization Oral Rehydration Therapy Acute Respiratory Infection Programme Reproductive and Child Health, Phase I 2000 National Population Policy 2009 National Health Policy 2002 National Health Systems Resource Centre Reproductive and Child Health, Phase II National Rural Health Mission (NRHM) Integrated Management of Neonatal and Childhood Illnesses (IMNCI) Janani Suraksha Yojana First Accredited Social Health Activists (ASHA) deployed Rollout of Health Management Information System 8
 Rashtriya Bal Swasthya Karyakram (RBSK) 2013 National Vaccine Policy Janani Shishu Suraksha Karyakram Home Based Newborn Care")
13 Significant Moments National Deworming Day Elimination of maternal and neonatal tetanus Beti Bachao Beti Padhao Kayakalp Mother and Child Tracking System 2011 National Health Mission (NHM) Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) Rashtriya Bal Swasthya Karyakram (RBSK) 2013 National Vaccine Policy Janani Shishu Suraksha Karyakram Home Based Newborn Care Facility Based Newborn Care Facility Based Management of Children with Severe Acute Malnutrition India Newborn Action Plan 2014 Swachch Bharat Abhiyaan India declared polio free India Newborn Action Plan Rashtriya Kishor Swasthya Karyakram (RKSK) Intensified Diarrhoea Control Fortnight National Quality Assurance Framework for Health Facilities Mission Indradhanush 9

14 Promises to keep MDG 4 Child Mortality Rate


15 Child Mortality Rate in India declined by 61.1% compared to global decline of 48.9% 61.1% decline 48.9% decline India Global 11

16 Promises to keep MDG 5 Maternal Mortality Ratio

17 Maternal Mortality Ratio in India declined by 70.2% compared to global decline of 44.7% 70.2% decline 44.7% decline India Global

18 Hi five to success National Health Mission Proactive leadership Partnerships Programme management Innovations 14

19 15




20 36 Fostering Life 46 Saving Life 18 Nurturing New Life 70 Inspiring Life


21 A passage to pride 82 The Game Changers 108 A Vision for Every Mother Every Child

22 18


23 Nurturing New Life 19
24 Nurturing New Life Political leadership and support have accelerated progress in scaling up interventions that save newborn lives and gives every child the best possible start in life. The advent of newborn health programmes in India ensured that clinical policies and practices were well grounded in reliable research and are innovatively adapted to deliver results. 20
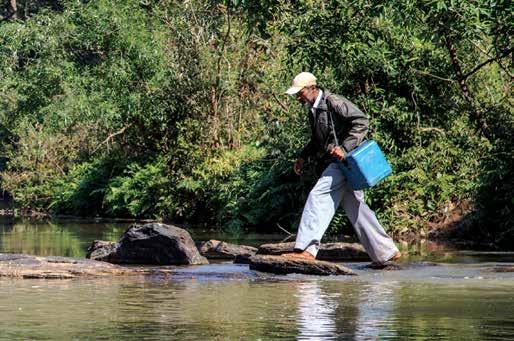
25 The results are out. Neonatal deaths have reduced by 46 per cent in the last 23 years. The momentum in decline was highest between 2008 and 2013 surpassing the global decline in the same period. India adapted the global Integrated Management of Childhood Illness by including Neonatal in its implementation plan for the country. Integrated Management of Neonatal and Childhood Illnesses was introduced at the community and facility level to implement standard case management of major causes of neonatal and childhood mortality and morbidity. Institutional delivery: Janani Suraksha Yojna, a conditional cash transfer scheme to promote institutional delivery; and Janani Shishu Suraksha Karyakaram (JSSK) aimed at reducing out of pocket expenses by making free health care (including transport, drugs, diagnostics) an entitlement and have contributed to the increase in institutional deliveries to more than 79 per cent. Facility based newborn care: Establishment of Newborn Care Corners (NBCCs) at all primary health care facilities; Newborn Stabilisation Units (NBSU) at the secondary level; and Special Newborn Care Units (SNCUs) at tertiary levels has led to multi-fold increase in availability and access to high-end facility based services for care of newborns. Investment in health infrastructure, equipment along with capacity building efforts for health staff through Navjat Shishu Suraksha Karyakram (NSSK) on basic newborn care and life saving skills of neonatal resuscitation has improved quality of facility based care. Home based newborn care: Mothers and newborns are especially vulnerable during the period immediately following delivery. Effective newborn care with a home based approach is extended by accredited social health activists for essential newborn support, postnatal care and early detection of illnesses. This is followed by referral and support to family for adoption of healthy practices. Home based newborn care (HBNC) surmounts the challenge of providing care for remote populations and saves more newborn lives each day. Incentives for ASHAs have been provided to support home based newborn care and has led to provision of quality services to every child and mother across the country. Policy led initiatives: Auxiliary Nurse Midwives are now authorised to administer: (1) a pre-referral dose of injectable gentamicin for suspected neonatal sepsis in infants and complete treatment for the full course under specific situations when referrals are not possible; and (2) a pre-referral dose of corticosteroids to women in preterm labour, improving the chances of survival of premature babies. Monitoring: An online real time reporting system with more than 250 parameters for special newborn care units is being extended to all states in India. Individual tracking and personal mobile based follow up to one year, through the mother and child tracking system, is being done along with death monitoring through child death reviews. Dedicated human resources and infrastructure for SNCUs with four doctors and staff nurses for a bedded units with an attractive remuneration package to retain talent is being adopted by state governments especially in high priority districts with vulnerable health parameters. Significant capital investment towards establishment of new maternal and child health wings and ambulances has been sanctioned in the public health system. These approaches are improving newborn health and ensuring that children survive and thrive to realise full potential. 21


26 22 Special newborn care units are equipped to manage complications that arise during delivery

27 Newborns should be sent home after the crucial first 48 hours of life, after mothers receive instructions on care and after postnatal visits are scheduled 23



28 24 Mothers are taught to keep babies warm, protect the baby at birth, keep the cord dry and look for danger signs

29 Mobile phones help frontline health workers interact with mothers 25

30 26 Community health workers identify and manage infections in children and maintain records



31 Health workers assess babies for signs of serious health problems; advise referral if necessary; and encourage timely vaccination according to national schedules 27

32 Currently 575 special new born care units in country with nearly half reporting online Nearly 700,000 neonates were admitted in special new born care units in , with around 10 per cent mortality during treatment Each bedded special new born care unit is staffed with 4 doctors and staff nurses 28 Newborn health facilities enable observation and provide immediate treatment

33 29


34 30 Staff posted at special newborn care units have skills to manage sick newborns and maintain records of every sick baby



35 31



36 32 Universal coverage of sick newborn care is envisioned through quality facilities and human resources in every district in the country

37 33

38 34 Special newborn care facilities at three levels have increased infant survival rates



39 An online monitoring system can analyse more than 250 parameters at click of a button Handwashing, the single most effective way to prevent the spread of infections 35

40 36

41 Fostering Life 37
42 Fostering Life The story of India s efforts in maternal and child health during the last two decades can be best witnessed in the transition that mothers have made from unassisted home delivery to delivery at a hospital or to birth at home assisted by a skilled birth attendant. 38
43 A child in India is well nourished and protected along with her mother right from conception. A generation of young Indians are now born in quality health care facilities indicating a healthy future for children. Extensive outreach campaigns and provision of quality services have led to mothers demanding services from health facilities and government schemes that support pregnancy care and child birth. They have learnt that immunization against tetanus, iron and folic acid prophylaxis as well as anemia management is available. They understand that nutrition and preparation for delivery is essential and at monthly village health and nutrition days, they also learn about antenatal care. After participating in mothers meetings and regular visits by a health worker, a mother knows how to prepare for birth, and then ensure the health of her newborn. There are village health, sanitation and nutrition committees across India promoting behaviour change and demand generation among mothers. The majority of mothers in India today avail support from Janani Suraksha Yojana and Janani Shishu Suraksha Karyakaram. Accredited social health activists help them understand benefits of institutional delivery and quite often play the role of a birth companion. Emergency obstetric care, 24-hour delivery services at primary health centres and safe abortion services are available to every mother to be. The public health system ensures that every mother receives a phone number for the vehicle that will take her to hospital, and receives a new delivery kit just in case she needs it. Mothers now know that safe delivery of healthy children is a reality. The five point strategy that made institutional delivery a reality in India is: Demand creation and financial protection: Janani Suraksha Yojana promotes institutional delivery through a conditional cash transfer. In response to the need for out of pocket expenses, the Janani Shishu Suraksha Karyakram was launched in 2011 to provide free and cashless services that covered care of the infant. These include normal delivery, C-sections and nutritional needs during their stay. Both mother and sick infants (up to one year) are given free drugs and consumables, diagnostics, blood, and transport facilities before and after delivery. Strengthening community processes: Accredited social health activists promote institutional delivery and facilitate organisation of monthly Village Health and Nutrition Days (VHNDs) thus ensuring that more than 75 per cent of mothers access antenatal services. In addition, they counsel pregnant women on birth preparedness, breastfeeding and complementary feeding, immunization, contraception, and prevention of reproductive tract/sexually transmitted infections. They are also navigators between the community and hospital. Emergency transport: Across India, several models of emergency transport systems have been developed to bring pregnant women to health facilities. More than 29 states and union territories in India have a state-wide emergency response and patient transport system. Three types of systems are most prevalent: a toll free number 108 at a centralised state level call centre which deploys state-of-art ambulances with a trained emergency medical technician and a professional management team. One third of its users are pregnant women. A more basic model involving variety of arrangements with local transport providers to render cashless travel service is also available. In some states, a toll free number 102 at district level call centres primarily allow transport to pregnant women through ambulances available in the public system. Ensuring service availability: The supply side for health services has been strengthened to meet increased demand by expanding the availability of RCH services. In order to cope with the demand, 24 X 7 Primary Health Centers and First Referral Units (FRUs) have been established. During the last few years there has been an eight-fold increase in 24x7 primary health centres and a five-fold increase in first referral units resulting in more women getting full antenatal care services. Skilled human resource: Medical officers (physicians) at public health facilities are being trained to provide specialist (gynecological and anesthetic) services during emergencies. 39

44 Many health facilities across the country have multi-skilled doctors who have been trained in emergency obstetric care and life saving anesthetic skills. So far, over 1,300 and 1,800 medical officers have been multi-skilled in emergency obstetric and anesthesia services. Ensuring service quality: Quality assurance through adoption of quality standards, establishment of standard treatment protocols, introduction of quality improvement programmes, provision of untied funds and maintenance grants to facilities to improve patient services have been the hallmark of recent efforts that India has made to ensure every child will be born in institutional care. Tracking each mother and child: The Government of India launched a nationwide web-based Health Management Information System to track service delivery. In 2010, a name based maternal and child tracking system for pregnant women, mothers and children, was introduced to ensure antenatal checks, postnatal care, immunization, etc. Better maternal health care saves lives of women and children in India, and with improved education, more mothers are aware of life-saving services that are available to them. The efforts are showing dividends in less mothers dying before and/or during delivery. 40 Providing appropriate antenatal care includes routine check-ups that help manage complications at the right time

45 Mobile technology enables community health workers to access current health information 41



46 42 Antenatal care begins with early registration, Iron and folic acid supplementation, nutrition counselling and birth preparedness

47 43

48 44 Free emergency transport and referral is available for pregnant mothers round the clock


49 Areas far away from hospitals benefit from ambulances that are equipped with an emergency delivery kit containing life saving equipment 45

50 46

51 Saving Life 47
52 Saving Life The period between conception and the first few years of a child s life is recognised as one of the greatest risk and greatest opportunity. India s progress in reducing maternal and neonatal mortality is supplemented by its remarkable efforts to deliver health beyond birth. 48
53 The major interventions in child health that helped children survive and thrive are: behaviours on early initiation and exclusive breastfeeding; age appropriate complementary feeding; adequate nutrition with Vitamin A and iron and folic acid supplementation; protection from vaccine preventable diseases by immunization; and integrated management of major illnesses - diarrhea, pneumonia and malaria. Over the past decades, several strategies have been developed on various aspects of child health and development. Starting with Growth Monitoring, Oral Rehydration Therapy, Breastfeeding and Immunization as vertical interventions in the eighties, the Child Survival and Safe Motherhood programme and Reproductive and Child Health Phase 1 programme ushered an integration of reproductive, maternal and child health interventions. The coverage of other important, proven, cost effective interventions such as provision of oral rehydration solution and zinc for diarrhea and antibiotics to treat pneumonia are now being stepped up. Exclusive breastfeeding for six months also protects children and is being actively promoted. In order to improve knowledge of health care providers, pre-service Integrated Management of Neonatal Childhood Illnesses training is being continued in over 100 medical and nursing colleges in India. Recognising the right of every child to survive, India s strategic approach to Reproductive, Maternal, Neonatal, Child and Adolescent Health (RMNCH+A) has adopted an equity-focused approach that targets disadvantaged and marginalised children to address disparities and also accelerate progress. The RMNCH+A strategy is based on provision of comprehensive care through the five pillars, or thematic areas, of reproductive, maternal, neonatal, child, and adolescent health, and is guided by central tenets of equity, universal care, entitlement, and accountability. This section illustrates the tenacious voyage undertaken during the last 25 years to deliver life saving vaccines that have helped save millions of lives of children in India. 49


54 50 Feeding practices, Vitamin A supplementation and treatment with oral rehydration solution are taught to mothers


55 51
56 Immunization: A cost-effective life saver Vaccination has a long and successful history in India. The journey from 1802 to make the country small pox free to the current efforts of ensuring that full immunization reaches all children has proven to be one of the most cost effective public health interventions for reduction of under five mortality rates. 52
57 Early days and the 70s : The birth of the expanded programme on immunization In 1802, India administered its first vaccine against small pox and finally achieved success as a small pox free nation in The long drawn battle against small pox had helped India set up systems, trained vaccinators, and acquire cold chain equipment and surveillance systems. This along with the WHO s Expanded Programme on Immunization launched in 1974 helped India to rapidly roll out the national immunization programme called Expanded Programme on Immunization (EPI) in 1978 with BCG, OPV, DPT and typhoid-paratyphoid vaccines. EPI targeted at least 80 per cent coverage in infancy. However, the vaccination was largely restricted to urban areas through major hospitals, hence the coverage remained low. 80s : Rebirth as Universal Immunization Programme The launch of Universal Immunization Programme (UIP) also led to inclusion of measles vaccine to the schedule. In 1986, focus on immunization was re-emphasised when it was added to the Prime Minister s 20 point programme. Immunization was given the status of one of the five National Technology Missions. 90s : Growth of the Universal Immunization Programme The World Summit for Children in 1990 emphasised increasing coverage with existing antigens and maternal and neonatal tetanus elimination. In the same year, India acted swiftly by universalising the geographical coverage of the UIP (from 31 districts) and targeting 100 per cent infants and pregnant women. In April 1991, maintenance of cold chains was handed over to states and union territories from UNICEF and commercial agencies : Maturing of the programme The National Technical Advisory Group on Immunization was formed in 2001 for informed decision making concerning introduction of new vaccines and strengthening the Universal Immunization Programme. In 2005, UIP became part of National Rural Health Mission in India. It also marked release of the first Multi-year ( ) strategic plan for UIP. In 2006, India conducted first immunization weeks for improving coverage with UIP antigens in poor performing districts. These strategic approaches led to improvement in full immunization coverage to 62.4 per cent in In 2007, national, state and district level Adverse Effects Following Immunization committees were constituted. By 2010 various guidelines and handbooks on UIP were released. In 2011, the National Vaccine Policy of India was released to develop a long term plan to strengthen the UIP. This policy addressed issues of vaccine security, management, regulation guidelines, vaccine research and development and product development. The year 2012 was observed as the Year of Intensification of Routine Immunization in India and led to intensive awareness and mobilisation campaigns. It is estimated that nearly 8.9 million children in the country do not receive all vaccines that are available under the UIP. However, this needs to be viewed in the context of 27 million children being born in India each year; further India has approximately 100 million children in the range of 1 to 5 years needing booster doses of vaccines and 30 million pregnant women who need tetanus toxoid vaccination every year. Mission Indradhanush was launched in 2014 to ensure total immunization using all available vaccines for all unimmunized children up to two years and pregnant women. 53


58 54 Pregnant mothers are vaccinated with tetanus toxoid, which also provides immunity to their children


59 Cold chains keep vaccines at prescribed temperatures The universal immunization programme has made significant contributions to reducing preventable child deaths 55



60 56 Ice packs and new syringes are crucial to ensure successful delivery of vaccines

61 Continued supervision of health workers takes place during immunization campaigns 57


62 58 Cold chain points were established across the country for storage of vaccines


63 Data on essential RMNCH+A services is maintained by health workers 59
64 Triumph over Polio and Neonatal Tetanus On 27th March 2014, India was officially declared polio free, by the World Health Organisation, having passed three years without any new case of wild poliovirus reported. The thirty three year long journey to achieving this global milestone in public health has been arduous. 60
65 Polio vaccination was initiated in India in 1978, under the Expanded Programme of Immunization (EPI). Yet by 1984, the programme had only provided 40 per cent of infants, the required three doses of oral polio vaccine (OPV). Vaccination continued under the Universal Immunization Programme from In 1988, the World Health Assembly passed a resolution for polio eradication by After the Global Polio Eradication Initiative in 1994 put polio elimination on the international development agenda, India launched the Pulse Polio Immunization Programme in 1995, aiming at 100 per cent coverage and eradication of wild poliovirus transmission. The strategy has continuously evolved over the two subsequent decades. The Pulse Polio Immunization Programme started as a boothbased activity, where children under age five, regardless of immunization status, were given OPV drops during mass immunization campaigns on designated days (known as National or Sub- National Immunization Days) as supplementation in routine immunization activities. By the late nineties, India increased its focus on polio and the polio drive moved from booth activity to house-tohouse campaigning. This was complemented by intense and focused interventions for high risk and migrant groups. Ultimately, three features of the programme have contributed to its success: a) Strong leadership and partnerships; b) A far-reaching social mobilisation campaign ; and c) Robust micro planning and analytics. Social mobilisation The Polio Social Mobilization Network recruited over 7,000 social mobilisers to conduct houseto-house counselling of parents, and other communication activities across high risk areas to persuade residents to accept vaccination. The campaign also engaged over 50,000 community influencers such as religious leaders, doctors, local medicine men and housewives as champions of the programme, to convince households refusing the vaccine to permit vaccination. Children were formed into groups (Bulawa Tolis) and involved as change agents. Polio classes were also conducted in schools. Robust planning, monitoring and supervision The polio programme made continuous use of data to identify, track, and eventually reach target groups that were typically missed; and micro plans were regularly adapted based on this evidence. Key strategies included tracking migrant/high risk groups; transit vaccination teams; grid plans and a focused approach to address underlying factors (poor water, sanitation, open-defecation, high incidence of diarrhea and low immunization rates). India validated for eliminating maternal and neonatal tetanus A significant public health milestone that India has recently achieved is its goal of eliminating maternal and neonatal tetanus. World Health Organisation (WHO), declared India free of maternal and neonatal tetanus on the 15th of May


66 62 Children were change agents to bring other children to vaccination booths Microplanning ensured two drops of life reached every child in India

67 Booths were set up at major railway stations and children were vaccinated in trains 63

68 64

69 Migrant population were immunized to make India polio free 65


70 66 Vaccinators visited every house in every city, town and village

71 The battle against Polio was won through social mobilisation of all sections of society 67


72 68 India s polio eradication programme is a model of excellence across the globe


73 69

74 70


75 Inspiring Life 71
76 Inspiring Life Adolescents aged years constitute about one-fifth of India s population. The transition stage of physical and psychological human development renders this particular group as important as it contributes towards the sustainable and inclusive growth of the nation. Therefore, ensuring their proper health and social development is imperative. 72
77 Poverty, education and societal and familial pressures impact the health of adolescents and to support this underserved group the Adolescent Reproductive and Sexual Health (ARSH) programme was launched under RCH II to delay age of marriage, reduce incidence of teenage pregnancies, maternal deaths, sexually transmitted diseases and HIV positive cases. Adolescent Reproductive and Sexual Health (ARSH) was identified as one of the four strategies (along with maternal health, child health, and family planning) to attain national goals of reduced maternal mortality ratio, infant mortality rate and total fertility rate. The impetus to consolidate the momentum of the existing efforts was developed under the Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) strategy. The strategy envisages an all inclusive continuum of care spanning all stages of the life cycle. Adolescence has emerged as a pivotal period linking one end (newborn and child) of continuum of care to the other (reproductive and maternal). The national adolescent health strategy was drafted and converted into Rashtriya Kishor Swasthya Karyakram (RKSK). The RKSK strategy is a more holistic, effective, and responsive approach. This programme moves from being largely curative, to one which emphasises communitybased health promotion and prevention, which in turn generates awareness and demand for facility based services. RKSK envisions that all adolescents in India are able to realise their full potential by making informed and responsible decisions related to their health and well-being. It focuses on six thematic areas of health: sexual and reproductive health, nutrition, injuries and violence (including gender based violence), non-communicable diseases, mental health and substance misuse. Interventions under RKSK include (i) the Weekly Iron Folic Supplementation (WIFS) programme aimed at reduction in anemia targeting 112 million adolescents (ii) a menstrual hygiene scheme for advocacy on hygienic menstrual practices and provision of subsidised sanitary napkins (iii) peer education programme as young people are more receptive to information communicated by their peers (iv) adolescent health days every quarter at the village level (v) adolescent friendly health clinics, of which over six thousand are functional and provide counselling and clinical services; and (vi) communication with special focus on SBCC. RKSK is being implemented across all states in a phased manner. Adolescent friendly health clinics are being strengthened with dedicated adolescent health counsellors at community health centres. The peer educator programme is a new community based intervention in the process of being rolled out. Every effort and each step forward in adolescent health is sweeping in its ambition as healthy adolescents bring great promise for India s future. 73


78 74 Adopting toilet use and eliminating open defecation for sustainable sanitation practices


79 Supplementing adolescents with iron and folic acid tablets that are distributed after the mid-day meal is served 75

80 76 A holistic programme has begun for adolescents

81 77


82 78 Adolescents health brought to the forefront


83 79

84 80

85 India is crucial to global health not just due to its population numbers and geographic size, but also because of the extraordinary progress it has made in health amongst other areas, which has taken millions out of poverty and is a source of inspiration for many nations Dr Margaret Chan WHO Director-General 81

86 82

87 The Game Changers During the journey of maternal and child health in India, gallant steps have secured attainment of a wellfunctioning health system. The following section illustrates health system strengthening efforts to bridge the gap in human resources for health and improve programme management and local governance for RMNCH+A service provision. 83
88 Putting People First Since the launch of the NRHM, challenges associated with the shortage of human resources for health were anticipated. Optimising the utilisation of existing manpower is a continuous process. States are incentivised to ensure rational deployment of human resources, with a focus on high-priority districts, high volume facilities in rural areas, and slum and low-income neighborhoods in urban areas. 84
89 Since the launch of NRHM, increased recognition of the challenges associated with the shortage of human resources for health has led to various steps to improve human resources practices. Broadly, these steps have followed three approaches: 1) optimising utilisation of existing manpower; 2) adding to the pool of service providers; and 3) building service providers capacities for improved workforce productivity and quality of services. Bridging the gap in human resources: The largest service provision platform in the country for RMNCH+A services is established with more than 160,000 skilled staff (specialists, medical officers, staff nurses, paramedical workers indicating over 74 per cent increase from the 2005 baseline. Adding to the pool of health specialists, a strategy of multi-skilling the existing medical officers (physicians) at public health facilities is bridging the shortfall of highly skilled specialist cadres. Medical officers (physicians) are trained to acquire skills of life saving services like emergency obstetric care and conduct cesareans during emergencies. Across the country, doctors trained in indigenous systems of medicine, such as ayurveda, yoga and naturopathy, unani, siddha and homeopathy (AYUSH), are being mainstreamed into the public health care system under the NHM. These doctors are co-located at public health facilities along with allopathic doctors in order to improve the availability of manpower in these facilities. About 5,000 AYUSH doctors are currently providing services under the NHM. To enhance the capacity of the nursing cadre, skill labs have been established at district hospitals, public nursing schools and colleges. A systematic curriculum is followed to improve existing knowledge and practice clinical skills, that preservice education at public nursing institutions provide. The existing training infrastructure is complemented by the establishment of skill labs. Nursing students practice clinical skills and develop competencies using simulation-based learning models. Pre-training and post-training assessments have shown significant improvements in knowledge and skills of students on key maternal and child health areas. 85


90 86 Skill labs provide practical training for health workers

91 Health practitioners at work 87


92 88 Standard curriculas for training in skill labs

93 Learning by doing: Skills lab provide opportunity to practice 89
94 ASHA Spreading Hope Originally designed for states and districts with low maternal and child health indicators, the Accredited Social Health Activists (ASHA) programme, has become a community level health workforce of nearly one million women, selected to represent and serve their communities. ASHAs now reach every village and ward, in almost every state and union territory of the country, in rural and urban areas. 90
95 Accredited Social Health Activists (ASHAs) play a key role in promoting institutional delivery including creation of awareness and quite often play the role of birth companion. In addition, they facilitate monthly Village Health and Nutrition Days leading to improvement in antenatal care services among pregnant women. The success of the ASHA ecosystem was made possible through high levels of political commitment. ASHAs are supportively supervised. Drugs and equipment kits are regularly replenished; performance based incentives and non-monetary benefits are designed to be motivating; and career opportunities, such as selection for auxiliary nursing midwife courses and support for higher education, are made available to them. The Government of India is doing all it can to nurture a system that effectively assures reach and delivery. The ASHA programme has also been integrated within health system reforms. From the original vision of a facilitator, an activist, and a provider of community level care, the ASHA is beginning to provide other functions that address the country s geographic, epidemiologic and demographic diversity. These include: support to village health committees with village demographic records creating awareness among communities on health and its determinants, village health planning, advocacy, utilisation of health services, counselling for birth preparedness, breastfeeding and complementary feeding, immunization, contraception, prevention of reproductive tract infections/sexually transmitted infections, accompanying pregnant women and children to health facilities for treatment and providing home based care to mothers and children. She is the village depot holder for ORS, IFA, OCP and condoms, and provides primary care for minor ailments such as diarrhea, fever and first aid. ASHAs have made immense contributions to the improved delivery of a range of maternal, newborn and child health and communicable disease programmes. They even exercise their agency and undertake several tasks that are not remunerated, but build and strengthen community trust and rapport. As unfinished agenda and newer challenges in maternal and child health emerge, the role of ASHAs will further evolve. In anticipation, certification of the ASHA through the National Open School System is proposed. It will provide an opportunity to assess and certify competencies and skills for a larger role in community based health care delivery. Another important aspect is the integration of ASHAs into the primary health care team. The health system finally recognises and acknowledges the strengths of community structures, where the ASHA is the fulcrum around community action and an integral part of the continuum of care for maternal and child health. 91

96 92 ASHAs reach out to more than a billion people to provide crucial maternal and child health related information and services

97 93


98 94 Diffusion of health care messages by ASHA

99 Speaking the language of transformation to healthy behaviours by putting mothers first 95


100 96 Door to door visits to provide home based care


101 Growth monitoring Capacity Building of ASHAs 97


102 98 Awareness campaigns, village health planning, mothers meetings and newborn care are all part of an ASHA s routine

103 99



104 100 ASHAs at work



105 101
106 Increasing efficiency The design and implementation of the National Rural Health Mission triggered increased fund flow for health service delivery. It became apparent that programme management would need to be strengthened at all levels in order to convert the increased flow of funds into improved health outcomes and delivery of results. 102
107 The strengthening of management capacities at national, state, district, facility and community levels was accomplished through six strategies: 1) creation of dedicated structures for management of the NRHM; 2) induction of programme management skills through contracted lateral infusion of professionals; 3) establishment of resource institutions for technical assistance; 4) decentralisation of planning; 5) introduction of flexible financing, and 6) strengthening monitoring and evaluation. The above led to a greater focus on outcomes, better utilisation of existing resources and more effective absorption of the increased allocation of funds to health. Decentralised management of the health system, community based and facility-level institutions have also been created. Village Health, Sanitation and Nutrition Committees (VHSNCs) take collective action on issues related to health and social determinants of health in the community, as well as leadership in village level health planning, implementation, monitoring and evaluation. There are VHSNCs working across India. At the facility level, Rogi Kalyan Samitis (hospital management societies) were established to manage functioning of health facilities and ensure quality of service throughout India. A system of allocation of flexible funds has been introduced under the NRHM to address local concerns at all levels of health facilities. Untied funds are also provided to the VHSNCs to promote financial devolution. As part of decentralised planning, district health action plans as well as village and block-level planning processes form the state programme implementation plan which is funded and monitored by the central government. Since 2008, a nationwide web-based Health Management Information System (HMIS) is functional to track service delivery. At present, all 36 states and union territories, including 676 districts and around 180,000 public health facilities, upload health-related data on a range of output and service delivery indicators on the HMIS each month. A maternal and child tracking system, a namebased tracking system for pregnant women, mothers and children, was introduced in 2010 to ensure necessary service delivery such as antenatal checks, postnatal care and immunization. All inputs taken together has gridded programme efficiency from inputs to outcomes for health. 103

108 104 Tracking every mother and child to universalise services



109 Daily reporting of campaigns, HMIS Portal and latest technology, linking the entire nation at one place 105


110 106 Decentralised management and governance structures help improve efficiency and also bring transparency and accountability

111 107

112 108


113 A Vision for Every Mother and Every child The focus of the National Health Mission is to expand the reach of services to the most vulnerable and marginalised groups within the country. As outlined in the draft National Health Policy 2015, the overarching vision is to achieve universal free delivery of comprehensive quality primary healthcare services as an entitlement for all aspects of reproductive, maternal, child and adolescent health and improved access to secondary and tertiary care services. This section, illustrates four recent initiatives that reaffirms the vision for maternal and child health in India and a commitment to accelerate results in the context of post 2015 agenda. 109

114 110


115 India Newborn Action Plan 111
116 India Newborn Action Plan Newborn health is a top national health priority. Standing firm on India s commitment in the 67th World Health Assembly, the India Newborn Action Plan (INAP) is another step towards India s commitment to the global agenda and affirms its priorities for newborns. INAP sets out the country s mandate with a vision, goals, strategic implementation packages and actions to end all preventable newborn deaths and still births. 112
117 The country observed a paradigm shift in its approach towards health care by adopting the Reproductive, Maternal, Newborn, Child Health and Adolescent Health Strategy (RMNCH+A). Newborn health occupies centre-stage in the overall strategy as all the inter linkages between various components have the greatest impact on the mortality and morbidity rates of a newborn. Building on the RMNCH+A approach, understanding the causes and challenges of newborn health, knowledge and tools are available to reduce the newborn deaths significantly. India puts greater focus on saving newborn lives through the India Newborn Action Plan. The Action Plan is an important step in contextualising and formalising the country s commitment in terms of improving health systems and health delivery platforms for accelerating efforts for improving newborn survival. Health outcomes of newborns are shaped by biological, social and economic factors along with the cultural environment. India s Newborn Action Plan is a response to the global Every Newborn Action Plan (ENAP) and outlines a targeted strategy for accelerating the reduction of preventable newborn deaths and stillbirths in India. The triumph over polio and neonatal tetanus has proved that it can reach even the most hard-to-reach and vulnerable children despite demographic, economic, and socio-cultural challenges. Neonatal deaths are the biggest contributor to child deaths. While the country has witnessed dramatic reduction in maternal and child mortality rates over the past two decades, the reduction of deaths of babies less than a month old has been much less as compared to deaths of all children under the age of 5. This is a major reason why the government has launched the India Newborn Action Plan. With a clear understanding that almost all of these deaths and subsequent disabilities are preventable, the plan is a concerted effort towards translating these commitments into meaningful change for newborns. The plan draws from the latest evidence on effective interventions, which will not only help in reducing the burden of stillbirths and neonatal mortality, but also maternal deaths. With clearly marked timelines for implementation, monitoring and evaluation, and scaling up of proposed interventions, the plan calls for all stakeholders to work towards improving newborn health in India with the dual goals of dramatically reducing newborn and stillborn death rates to a single digit by The plan is guided by the principles of integration, equity, gender, quality of care, convergence, accountability and partnerships. Its strength is built on its six pillars across the life stages. The six pillars include: preconception and antenatal care; care during labour and child birth; immediate newborn care; care of healthy newborns; care of small and sick newborns, and care beyond newborn survival. India has taken a vital step towards improving quality of life beyond survival for those newborns with birth defects/disabilities and for those who develop neurodevelopmental delay following sickness. For effective implementation, a systematic plan for monitoring and evaluation has been developed with a list of dashboard indicators. INAP is a guiding framework for states and districts to develop their own action plan with measurable indicators. 113


118 Nearly half of newborn deaths can be averted by ensuring safe delivery A safe delivery, a healthy infant and a secure childhood and adolescence leads to adults who contribute to society and the nation 114

119 Essential newborn care at all delivery points through functional newborn corners by trained personnel JSSK Healthy Newborn Sick Newborn All newborns delivered at home and health facility JSSK Sick newborn delivered at home or institution Facility-based newborn care at CHC & DH JSSK Setting up Newborn Stabilisation Units and Newborn Special Care Units Home-based newborn care Training ASHAs in HBNC Supportive supervision Referral systems JSSK JSSK (JANANI SHISHU SURAKSHA KARYAKRAM) 115 Continuum of care to the healthy and sick newborns



120 116 Regular home visits during the first 28 days and monitoring by health workers prevents and corrects complications during critical period of life

121 During home visits, the health worker can refer sick babies to specialised facilities for appropriate care 117

122 118


123 Mission Indradhanush 119
124 Mission Indradhanush Indradhanush refers to the rainbow. In December 2014, India launched Mission Indradhanush to expand immunization coverage to all children by year Representing the seven colours of the rainbow, the mission intends to immunize all children against seven vaccine preventable diseases namely diphtheria, pertussis, tetanus, childhood tuberculosis, polio, hepatitis B and measles. In addition to this, vaccines for Japanese Encephalitis (JE) and Haemophilus influenzae type B (Hib) are also provided in certain states. 120
125 The mission depicts the commitment to children by ensuring that immunization is accessible to every child and continues to remain the most effective intervention to protect children from life threatening conditions that are preventable. Mission Indradhanush reflects the seven colours of the rainbow and reaches the most unreached children with seven vaccines through special immunization drives. It is estimated that nearly 8.9 million children in the country do not receive all vaccines that are available under the universal immunization programme. Immunization coverage in India increased from 61 per cent to 65 per cent between , indicating only 1 per cent increase in coverage every year. To accelerate the process of immunization by covering 5 per cent and more children every year, a mission mode has been adopted to achieve the target of full coverage by Four special vaccination drives were held between April 2015 and July These drives will continue until 2020 with simultaneous immunization system strengthening efforts in high focus districts. Objectives: The government intends to cover 201 high focus districts in the first phase of year These districts have nearly 50 per cent of all unvaccinated or partially vaccinated children in India. Furthermore, another 297 districts will be targeted in the second phase of year Strategy of Mission Indradhanush: The outreach is planned through special vaccination campaigns. All vaccines are already available free of cost under the universal immunisation programme in India. Under this mission, the government plans to intensify its efforts and thus increase accessibility of these vaccines to all children in India. Special planning, capacity building and communication interventions brought both visibility and momentum to reaching hard to reach populations. Results achieved internally through excellent convergence with the government and partners also provided a model for future new vaccines introduction and immunization system strengthening. During the first four rounds of Mission Indradhanush, more than 900,000 sessions were held and about 20 million vaccines were administered to more than 9.6 million beneficiaries (7.5 million children and 2.1 million pregnant women). During these rounds about 2 million children were fully vaccinated thereby adding to the pool of fully immunized children in the country. Apart from increasing coverage, the mission has also increased its basket of services: more than 1.9 million doses of Vitamin A, more than 1.6 million ORS packets and about 5.7 million zinc tablets have been distributed during the sessions. Mission Indradhanush has also led to health systems strengthening through meticulous planning and preparation of robust microplans for frontline health workers, along with an accountability framework through task forces and rigorous monitoring structures. An extensive information, education and communication campaign, an integral part of the mission, created countrywide awareness regarding benefits of full immunization and social mobilisation at the community level. 121

126 122 Reaching the 201 high focus districts in the country in the first phase which have nearly 50 per cent of all unvaccinated or partially vaccinated children



127 123

128 124 Mobile transport to reach places where routine immunisation coverage is weak




129 Immunization sessions on the go 125


130 126 Mothers and caretakers prioritise their child s immunization


131 127

132 128

133 Beyond Survival 129
134 Beyond Survival Rashtriya Bal Swasthya Karyakram (RBSK) is an important initiative aimed at early identification and early interventions for children from birth to 18 years to cover 4 D s viz. Defects at birth, Deficiencies, Diseases, Development delays including disability. 130
135 Developmental delays are common in early childhood affecting at least 10 per cent of children. These delays, without timely intervention, may lead to permanent disabilities with regard to cognition, hearing and vision. There are also groups of diseases which are very common in children e.g., dental caries, otitis media, rheumatic heart disease and reactive airways diseases which can be cured if detected early. It is understood that early intervention and management can prevent these conditions from progressing into more severe and debilitating forms, thereby reducing hospitalisation and resulting in improved school attendance and access to opportunities for development. Rashtriya Bal Swasthya Karyakram was launched by the Government of India as a structured health screening and management programme for childhood health conditions. An operational guideline outlines the programme. Health screening of school going children is a continued intervention under the School Health Programme, and it is now being expanded to cover all children from birth to 18 years of age. RBSK enables screening and early intervention services for children with birth defects, diseases, deficiencies and developmental delays (including disabilities). The services aim to cover children of age 0-6 years in rural areas and urban slums, in addition to children enrolled in grades 1-12 in government and government aided schools. It is expected that these services will reach about 270 million children in a phased manner. The Child Health Screening and Early Intervention Services will also translate into economic benefits in the long run. Timely intervention would not only halt conditions that deteriorate but would also reduce the out-of-pocket expenditure of poor and marginalised populations in the country. Additionally, the Child Health Screening and Early Intervention Services will also provide countrywide epidemiological data on the 4 Ds (Defects at birth, Diseases, Deficiencies and Developmental Delays including Disabilities). Such data is expected to hold relevance for future planning of area specific services. The following mechanisms as per operational guidelines will be used to reach children for health screenings: i) Community based newborn screening at home through ASHAs for newborns till 6 weeks of age during home visitation; ii) anganwadi centre based screening by dedicated mobile health teams for children 6 weeks to 6 years; iii) government and government aided school based screening by dedicated mobile health teams for children 6 years to 18 years; and iv) facility based newborn screening at public health facilities, by existing health manpower. In addition to the community screening through mobile teams, an early intervention centre will be established at the district hospitals. The purpose of early intervention centres will be to provide referral support to children detected with health conditions during health screening in addition to establishing screening mechanisms for detection of hearing, visual and other developmental delays and birth defects. A multispecialty team consisting of a pediatrician, medical officer, dentist, physiotherapist, psychologist, staff nurses, paramedics, etc. will be engaged to provide services. Outreach screening will be done by dedicated Mobile health teams for 6 week to 6 year old children at anganwadi centres and for 6-18 year old children at schools. Child Health Screening and Early Intervention Services under RBSK envisage screening for 30 selected health condition, early detection and free management. States and union territories may also include diseases such as hypothyroidism, sickle cell anemia and beta thalassemia based on the epidemiological situation and availability of testing and specialised support facilities within state and union territories. Once the child is screened and referred from any of these points of identification, it would be ensured that the necessary treatment/intervention is delivered at zero cost to the family. 131


136 132 Children up to six years are screened at district early intervention centres for management of birth defects


137 133

138 134


139 Kayakalp: A commitment to quality 135
140 Kayakalp: A commitment to quality The constant endeavour of a public health care system is to establish quality benchmarks that are measured and monitored. One of the goals of the National Health Mission is to to improve the availability of and access to quality health care for people, especially for those residing in rural areas, the poor, women and children. 136
141 India s National Quality Assurance Programme (NQAP) seeks to establish comprehensive systems with adequate weightage for preventive and promotive components of care at public health facilities. The Indian Public Health Standards prescribe a set of uniform standards envisaged to improve the quality of health care delivery in the country. The guidelines laid down norms for physical infrastructure, services (essential and desirable), human resources, equipment, drugs and diagnostics at public health facilities. They address normative planning of health facilities. However, it was felt that processes were left out and there were no provisions for quality certification of facilities/services. A growing need for a separate quality assurance system for public sector facilities, which is evidence based, sustainable, affordable and addresses specific requirements of public sector facilities was highlighted in studies undertaken by the Ministry of Health and Family Welfare. In response to this need, the National Quality Assurance Programme was launched to extend the responsibility of public health facilities beyond providing curative services. National quality assurance standards have been developed with adequate weightage for preventive and promotive components of care. NQAP includes strengthening of a quality assurance institutional framework; explicit quality assurance standards for public health facilities; continual assessment; a health system driven approach; capacity building of the system; performance review through key performance indicators; certification; and incentivisation. Various states are in the process of implementing the quality assurance programme by reconstitution of State and District Quality Assurance Committees. The key process includes assessment of health facilities using NQAP tools, initiating actions for gap closure, implementation of standard operating procedures and reassessment. The National Quality Assurance Standards are organised around eight Areas of Concern : service provision; patient rights; inputs; support services; clinical services; infection control; quality management; outcome; explicit quality assurance standards for public health facilities. District hospitals have 70 quality standards, while community health centres and primary health centres have 65 and 50 quality standards respectively. Each quality standard has measurable elements which are used for assessing the degree of compliance. Further, each department in a health facility is assessed separately against quality standards. KAYAKALP, a commitment to the Clean India movement, was launched in 2015 to promote cleanliness and enhance the quality of public health facilities. The purpose of this initiative is to appreciate and recognise efforts in facilities to create a healthy environment. Cleanliness (Swachhta) guidelines for health facilities have been issued as a part of this initiative. The facilities have flexibility for phasing of quality assurance interventions. For example, quality certification of RMNCH+A services in a facility could be undertaken in the first year. Other areas could be covered in subsequent years. Incentivisation of states in adopting and sustaining NQAP standards are in-built in the quality assurance programme. More than 50 facilities have already been accredited under NQAP. In addition, the Government of India is committed to provide equitable and quality health care services in the country especially to reach the vulnerable and marginalised population. Adoption of quality standards, establishment of standard treatment protocols, introduction of a quality assurance system, scale-up of the Clinical Establishment Act, accreditation of private and public service providers, provision of untied funds and maintenance grants to facilities to improve patient services have been some recent efforts to ensure quality of care in public and private health facilities. The system of monitoring quality of services using a health systems framework of inputs, process and outcomes, including client perspectives is being instituted. National Guidelines for Clean Hospitals applicable to tertiary care hospitals, hospitals associated with medical colleges and super-specialty hospitals in India has taken shape in

142 138 Clean healthcare facilities lead to a clean India and a healthy India



143 139

144 140 The journey during the past 25 years to ensure that mothers and children in India are healthy has so far produced noteworthy results. There is greater resolve to accomplish unfinished tasks and deliver on the promises that every society makes to the health and well-being of its future generations. The Government of India has demonstrated leadership in global movements such as the Call to Action for Child Survival, Every Woman Every Child, A Promise Renewed, FP 2020 and other major forums, thus showing global solidarity to build on the progress made in maternal and child health indicators. Efforts for strengthening health systems, forging partnerships with stakeholders including the private sector and achieving synergy through convergence with other sectoral constituents to address all determinants of health will remain the crucial elements for future action. Aspirations of a country of one billion plus people demand transparent and accountable processes that show evidence of results. India s Health Mission is geared to embed innovative solutions that will keep its mothers and children healthy and happy.

145 141



























146 Credits Inside Cover WHO Page 2-3 UNICEF/2012/ Graham Crouch Page 7 MCH/WHO Page UNICEF/2014/ Syed Altaf Ahmad Page UNICEF/2014/ Syed Altaf Ahmad Page UNICEF/2014/ Syed Altaf Ahmad Page 18 Andy Hall/Save the Children Page 22 MCH/WHO Page 22 NHSRC Page 23 MCH/WHO Page 24 UNICEF/2006/Bartholo Page 24 NHSRC Page 24 Suzanne Lee/Save the Children Page 25 Prashant Panjiar/BMGF Page 26 UNICEF/2009/ Sondeep Shankar Page 27 USAID Page 27 Jhpiego Page 27 UNICEF/2009/ Sondeep Shankar Page 28 UNICEF Page 30 MCH/WHO Page 30 MCH/WHO Page 31 UNICEF/2015 Page 31 MCH/WHO 142 Page 31 MCH/WHO Page 32 Raj Yagnik/Save the Children Page 32 UNICEF/2012/Vishwan Page 32 MCH/WHO Page 33 MCH/WHO Page 34 UNICEF/2015



























147 Page 35 MCH/WHO Page 35 UNICEF/2011 Page 36 Parth Sanyal/Save the Children Page 40 Parth Sanyal/Save the Children Page 41 Sanchayta Singha Sarkar/NHM Page 42 UNICEF/2010/ Pirozzi Page 42 UNICEF/2014/Dhiraj Singh Page 42 UNICEF/2014/Dhiraj Singh Page 43 HLFPPT Page 44 Prashant Panjiar/BMGF Page 45 UNICEF/2008/Pietrasik Page 46 UNICEF/2015/ Syed Altaf Ahmad Page 50 UNICEF/2013/Romana Page 51 WHO Page 51 MCH/WHO Page 54 UNICEF/2003/Vitale Page 55 UNICEF/2012/Singh Page 55 MCH/WHO Page 56 UNICEF/2015 Page 56 Rachel Palmer/Save the Children Page 57 UNICEF/2014/Shome Basu Page 58 ITSU Page 58 MCH/WHO Page 59 Parth Sanyal/Save the Children Page 62 UNICEF/2010/Gurinder Osan Page 62 UNICEF/2012/Anindito Mukherjee Page 63 UNICEF/2006/Pietrasi Page 64 UNICEF/2015/ Sandeep Biswas Page 66 UNICEF/2015/ Sandeep Biswas Page 67 UNICEF/2013/Graham Crouch 143




























148 Page 68 UNICEF/2012/Graham Crouch Page 68 UNICEF/2012/Graham Crouch Page 69 UNICEF/2012/Graham Crouch Page 70 UNICEF/2014/Syed Altaf Ahmad Page 74 UNICEF/2012/Dhiraj Singh Page 74 Diwakar Mani/UNICEF Page 75 UNICEF/2014/Divakar Mani Page 76 UNICEF/2014/Divakar Mani Page 78 UNICEF/2013 Page 78 UNICEF/2012/Picasa Page 79 NHM Gujarat Page 82 UNICEF/2014/Syed Altaf Ahmad Page 86 NHSRC Page 87 HLFPPT Page 88 MCH/WHO Page 89 NHSRC Page 92 UNICEF/2014/Shome Basu Page 94 Ruhani Kaur/UNDP Page 95 UNICEF/2012/Vishwan Page 96 Ruhani Kaur/UNDP Page 97 MCH/WHO Page 97 Ryan Paul Lobo/BMGF Page 98 UNICEF/2008/Adam Ferguson Page 98 UNICEF/2014/Sumit Dayal 144 Page 98 Andy Hall/Save the Children Page 98 UNDP Page 99 Andy Hall/Save the Children Page 100 NHSRC Page 100 ITSU Page 100 NHSRC
























149 Page 101 Parth Sanyal/Save the Children Page 101 UNICEF/2014/Dhiraj Singh Page 101 Parth Sanyal/Save the Children Page 104 MCH/WHO Page 105 MCH/WHO Page 105 MCH/WHO Page 105 MCH/WHO Page 106 NHM Bihar Page 107 NHSRC Page 108 CJ Clarke/Save the Children Page 110 UNICEF/2012/Enrico Fabian Page 114 Jhpiego Page 115 MCH/WHO Page 116 Andy Hall/Save the Children Page 116 UNICEF/2009/Sondeep Shankar Page 116 Raj Yagnik/Save the Children Page 117 Bartholo/UNICEF Page 118 Pranab k aich/itsu Page 122 Claude Renault/ITSU Page 123 UNICEF/2015 Page 123 Claude Renault/ITSU Page 123 Claude Renault/ITSU Page 124 Pranab k aich/itsu Page 125 UNICEF/2015/Syed Altaf Ahmad Page 125 UNICEF/2015/Syed Altaf Ahmad Page 125 Claude Renault/ITSU Page 126 Claude Renault/ITSU Page 127 Pranab k aich/itsu Page 127 Priyaranjan/ITSU Page 128 MoHFW 145










150 Page 132 MoHFW Page 132 Rachel Palmer/Save the Children Page 133 MoHFW Page 133 MoHFW Page 133 MoHFW Page 134 NHSRC Page 138 WHO Page 139 NHSRC Page 139 MCH/WHO Page 139 MCH/WHO Page 141 UNICEF/2014/Singh 146

151 147
152 148
153 149

154 150
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012
 Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
INTRODUCTION. 76 MCHIP End-of-Project Report. (accessed May 8, 2014).
.") Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. Community IMCI. Community IMCI
 Implementation in the Western Pacific Region. Community IMCI. Community IMCI") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Saving Every Woman, Every Newborn and Every Child
 Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Nurturing children in body and mind
 Nurturing children in body and mind Dr Rachel Devi National Advisor for Family Health Ministry of Health and Medical Services, Fiji 11 th Pacific Health Ministers Meeting 15-17 April 2015 Yanuca Island,
Nurturing children in body and mind Dr Rachel Devi National Advisor for Family Health Ministry of Health and Medical Services, Fiji 11 th Pacific Health Ministers Meeting 15-17 April 2015 Yanuca Island,
Managing Programmes to Improve Child Health Overview. Department of Child and Adolescent Health and Development
 Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
CHAPTER 30 HEALTH AND FAMILY WELFARE
 CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
Frontline Health Worker. Allied Health & Paramedics. Frontline Health Worker. Sector Health. Sub-Sector. Occupation
 Sector Health Sub-Sector Allied Health & Paramedics Occupation Frontline Health Worker Reference ID: HSS/ Q 8601, Version 1.0 NSQF level: 3 Frontline Health Worker Published by: All Rights Reserved, First
Sector Health Sub-Sector Allied Health & Paramedics Occupation Frontline Health Worker Reference ID: HSS/ Q 8601, Version 1.0 NSQF level: 3 Frontline Health Worker Published by: All Rights Reserved, First
Egypt. MDG 4 and Beyond. Emad Ezzat, MD Head of PHC Sector. Ministry of Health & Population
 Egypt Ministry of Health & Population MDG 4 and Beyond Lessons Learnt Emad Ezzat, MD Head of PHC Sector EMRO high-level meeting, Dubai, Jan 2013 Trends of Under 5, Infant and Neonatal Mortality (1990 2008)
Egypt Ministry of Health & Population MDG 4 and Beyond Lessons Learnt Emad Ezzat, MD Head of PHC Sector EMRO high-level meeting, Dubai, Jan 2013 Trends of Under 5, Infant and Neonatal Mortality (1990 2008)
Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare
 An Evidence Brief for Policy Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare Executive Summary This policy brief was prepared by the Uganda
An Evidence Brief for Policy Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare Executive Summary This policy brief was prepared by the Uganda
Continuum of Care Services: A Holistic Approach to Using MOTECH Suite for Community Workers
 CASE STUDY Continuum of Care Services: A Holistic Approach to Using MOTECH Suite for Community Workers Providing coordinated care across the continuum of maternal and child health in Bihar, India PROJECT
CASE STUDY Continuum of Care Services: A Holistic Approach to Using MOTECH Suite for Community Workers Providing coordinated care across the continuum of maternal and child health in Bihar, India PROJECT
Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn
 Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn Dr. M L Jain Director State Institute of Healthand and Family Welfare, Rajasthan Jaipur SIHFW: an ISO 9001: 2008 certified
Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn Dr. M L Jain Director State Institute of Healthand and Family Welfare, Rajasthan Jaipur SIHFW: an ISO 9001: 2008 certified
Water, sanitation and hygiene in health care facilities in Asia and the Pacific
 Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
UHC. Moving toward. Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
CONCEPT NOTE Community Maternal and Child Health Project Relevance of the Action Final direct beneficiaries
 CONCEPT NOTE Project Title: Community Maternal and Child Health Project Location: Koh Kong, Kep and Kampot province, Cambodia Project Period: 24 months 1 Relevance of the Action 1.1 General analysis of
CONCEPT NOTE Project Title: Community Maternal and Child Health Project Location: Koh Kong, Kep and Kampot province, Cambodia Project Period: 24 months 1 Relevance of the Action 1.1 General analysis of
Situation Analysis Tool
 Situation Analysis Tool Developed by the Programme for Improving Mental Health CarE PRogramme for Improving Mental health care (PRIME) is a Research Programme Consortium (RPC) led by the Centre for Public
Situation Analysis Tool Developed by the Programme for Improving Mental Health CarE PRogramme for Improving Mental health care (PRIME) is a Research Programme Consortium (RPC) led by the Centre for Public
FINDING SOLUTIONS. for Women?s and Girls?Health and Education in Afghanistan
 FINDING SOLUTIONS for Women?s and Girls?Health and Education in Afghanistan 2016 A metaanalysis of 10 projects implemented by World Vision between 20072015 in Western Afghanistan 2 BACKGROUND Afghanistan
FINDING SOLUTIONS for Women?s and Girls?Health and Education in Afghanistan 2016 A metaanalysis of 10 projects implemented by World Vision between 20072015 in Western Afghanistan 2 BACKGROUND Afghanistan
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
Growth of Primary Health Care System in Kerala-A comparison with India
 Growth of Primary Health Care System in Kerala-A comparison with India Dr. Suby Elizabeth Oommen Assistant Professor Department of Economics, Christian College, Chengannur, Alappuzha, Kerala, INDIA, 689121
Growth of Primary Health Care System in Kerala-A comparison with India Dr. Suby Elizabeth Oommen Assistant Professor Department of Economics, Christian College, Chengannur, Alappuzha, Kerala, INDIA, 689121
IMCI and Health Systems Strengthening
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
The Syrian Arab Republic
 World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
STATUS OF MATERNAL, INFANT, AND YOUNG CHILD NUTRITION (MIYCN) IN MEDICAL COLLEGES & HOSPITALS
 IN MEDICAL COLLEGES & HOSPITALS") STATUS OF MATERNAL, INFANT, AND YOUNG CHILD NUTRITION (MIYCN) IN MEDICAL COLLEGES & HOSPITALS KEY FINDINGS BASELINE ASSESSMENT 2017 UTTAR PRADESH & BIHAR Image: Velocity Creative Introduction Despite a
STATUS OF MATERNAL, INFANT, AND YOUNG CHILD NUTRITION (MIYCN) IN MEDICAL COLLEGES & HOSPITALS KEY FINDINGS BASELINE ASSESSMENT 2017 UTTAR PRADESH & BIHAR Image: Velocity Creative Introduction Despite a
Eradicate Childhood Malnutrition, Madhya Pradesh, India
 Eradicate Childhood Malnutrition, Madhya Pradesh, India Date: May 6, 2017 I. Demographic Information 1. Districts and State: Barwani district in Madhya Pradesh, India 2. Organization: Real Medicine Foundation
Eradicate Childhood Malnutrition, Madhya Pradesh, India Date: May 6, 2017 I. Demographic Information 1. Districts and State: Barwani district in Madhya Pradesh, India 2. Organization: Real Medicine Foundation
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder
 Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
AREAS OF FOCUS POLICY STATEMENTS
 ENGLISH (EN) AREAS OF FOCUS POLICY STATEMENTS With respect to the areas of focus policy statements, The Rotary Foundation notes that 1. The goals of the Foundation are to increase efficiency in grant processing
ENGLISH (EN) AREAS OF FOCUS POLICY STATEMENTS With respect to the areas of focus policy statements, The Rotary Foundation notes that 1. The goals of the Foundation are to increase efficiency in grant processing
INDONESIA S COUNTRY REPORT
 The 4 th ASEAN & Japan High Level Officials Meeting on Caring Societies: Support to Vulnerable People in Welfare and Medical Services Collaboration of Social Welfare and Health Services, and Development
The 4 th ASEAN & Japan High Level Officials Meeting on Caring Societies: Support to Vulnerable People in Welfare and Medical Services Collaboration of Social Welfare and Health Services, and Development
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA.
 UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
Sources for Sick Child Care in India
 Sources for Sick Child Care in India Jessica Scranton The private sector is the dominant source of care in India. Understanding if and where sick children are taken for care is critical to improve case
Sources for Sick Child Care in India Jessica Scranton The private sector is the dominant source of care in India. Understanding if and where sick children are taken for care is critical to improve case
INTERNATIONAL ASSOCIATION FOR NATIONAL YOUTH SERVICE
 Profile verified by: Mr. Vincent Senam Kuagbenu Executive Director of the Ghana National Service Scheme Date of Receipt: 12/04/2012 Country: Ghana INTRODUCTION: The Ghana National Service Scheme is a public
Profile verified by: Mr. Vincent Senam Kuagbenu Executive Director of the Ghana National Service Scheme Date of Receipt: 12/04/2012 Country: Ghana INTRODUCTION: The Ghana National Service Scheme is a public
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005
 Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
8 November, RMNCAH Country Case-Studies: Summary of Findings from Six Countries
 8 November, 2012 RMNCAH Country Case-Studies: Summary of Findings from Six Countries Country Case-Studies: September October 2012 6 countries Bangladesh, India, Indonesia, Nepal, Papua New Guinea and Solomon
8 November, 2012 RMNCAH Country Case-Studies: Summary of Findings from Six Countries Country Case-Studies: September October 2012 6 countries Bangladesh, India, Indonesia, Nepal, Papua New Guinea and Solomon
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur
 State Institute of Health & Family Welfare, Jaipur") Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Indian Council of Medical Research
 Indian Council of Medical Research Call for Letters of Intent Grants Programme for Implementation Research on Maternal and Child Health Deadline: 31 May 2017 India has made significant progress in reducing
Indian Council of Medical Research Call for Letters of Intent Grants Programme for Implementation Research on Maternal and Child Health Deadline: 31 May 2017 India has made significant progress in reducing
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION
 COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION") UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
CONSOLIDATED RESULTS REPORT. Country: ANGOLA Programme Cycle: 2009 to
 CONSOLIDATED RESULTS REPORT Country: ANGOLA Programme Cycle: 2009 to 2014 1 1. Key Results modified or added 2. Key Progress Indicators 3. Description of Results Achieved PCR 1: Accelerated Child Survival
CONSOLIDATED RESULTS REPORT Country: ANGOLA Programme Cycle: 2009 to 2014 1 1. Key Results modified or added 2. Key Progress Indicators 3. Description of Results Achieved PCR 1: Accelerated Child Survival
International confederation of Midwives
 International confederation of Midwives Traditional Midwife The Palestinian Dayah 1 Midwifery Matters 2011 Issue 131 Page 17 2 In Education In Practice In Research In Profession New trends in midwifery
International confederation of Midwives Traditional Midwife The Palestinian Dayah 1 Midwifery Matters 2011 Issue 131 Page 17 2 In Education In Practice In Research In Profession New trends in midwifery
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW
 06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
National Health Strategy
 State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
Minister. Secretaries of State. Department of Planning and Health Information. Department of Human Resources Development
 KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
Amendments for Auxiliary Nurses and Midwives syllabus and regulation
 Amendments for Auxiliary Nurses and Midwives syllabus and regulation Duration of the course : The total duration of the course is 2 year (18 months + 6 months internship) First Year : i. Total weeks -
Amendments for Auxiliary Nurses and Midwives syllabus and regulation Duration of the course : The total duration of the course is 2 year (18 months + 6 months internship) First Year : i. Total weeks -
Sudan High priority 2b - The principal purpose of the project is to advance gender equality Gemta Birhanu,
 Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
IMCI at the Referral Level: Hospital IMCI
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
A Review on Health Systems in Transition in Myanmar
 A Review on Health Systems in Transition in Myanmar Resources and Services Dr. Nilar Tin Physical and human resources Physical Resources Capital stocks and investment no: of Infrastructure (as of 2013)
A Review on Health Systems in Transition in Myanmar Resources and Services Dr. Nilar Tin Physical and human resources Physical Resources Capital stocks and investment no: of Infrastructure (as of 2013)
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 TONGA Tonga is a lower-middle-income country in the Pacific Ocean with an estimated population of 102 371 (2005), of which 68% live on the main island Tongatapu and 32% are distributed on outer islands.
TONGA Tonga is a lower-middle-income country in the Pacific Ocean with an estimated population of 102 371 (2005), of which 68% live on the main island Tongatapu and 32% are distributed on outer islands.
MCH Programme in Vietnam Experiences for post Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam
 MCH Programme in Vietnam Experiences for post - 2015 Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam Current status: Under five mortality 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 58,0 45,8 26,8 24,4 24,1 22,5
MCH Programme in Vietnam Experiences for post - 2015 Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam Current status: Under five mortality 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 58,0 45,8 26,8 24,4 24,1 22,5
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health
 Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Development of Policy Conference Nay Pi Taw 15 th February
 Development of Policy Conference Nay Pi Taw 15 th February To outline some Country Examples of the Role of Community Volunteers in Health from the region To indicate success factors in improvements to
Development of Policy Conference Nay Pi Taw 15 th February To outline some Country Examples of the Role of Community Volunteers in Health from the region To indicate success factors in improvements to
AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE. CHF 7,993,000 2,240,000 beneficiaries. Programme no 01.29/99. The Context
 AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE CHF 7,993,000 2,240,000 beneficiaries Programme no 01.29/99 The Context Twenty years of conflict in Afghanistan have brought a constant deterioration
AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE CHF 7,993,000 2,240,000 beneficiaries Programme no 01.29/99 The Context Twenty years of conflict in Afghanistan have brought a constant deterioration
UNICEF WCARO October 2012
 UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
WORLD ALLIANCE FOR PATIENT SAFETY WHO GUIDELINES ON HAND HYGIENE IN HEALTH CARE (ADVANCED DRAFT): A SUMMARY CLEAN HANDS ARE SAFER HANDS
: A SUMMARY CLEAN HANDS ARE SAFER HANDS") WORLD ALLIANCE FOR PATIENT SAFETY WHO GUIDELINES ON HAND HYGIENE IN HEALTH CARE (ADVANCED DRAFT): A SUMMARY CLEAN HANDS ARE SAFER HANDS WHO Guidelines on Hand Hygiene in Health Care (Avanced Draft): A
WORLD ALLIANCE FOR PATIENT SAFETY WHO GUIDELINES ON HAND HYGIENE IN HEALTH CARE (ADVANCED DRAFT): A SUMMARY CLEAN HANDS ARE SAFER HANDS WHO Guidelines on Hand Hygiene in Health Care (Avanced Draft): A
HEALTH & NUTRITION Kenya Programme
 HEALTH & NUTRITION Kenya Programme 2016-2018 About Us Save the Children has been operational in Kenya since the 1950s, providing support to children through developmental and humanitarian relief programmes
HEALTH & NUTRITION Kenya Programme 2016-2018 About Us Save the Children has been operational in Kenya since the 1950s, providing support to children through developmental and humanitarian relief programmes
The USAID portfolio in Health, Population and Nutrition (HPN)
") The USAID portfolio in Health, Population and Nutrition (HPN) Goal: Promote and improve health and well-being of Malawians through investing in sustainable, high-impact health initiatives in line with
The USAID portfolio in Health, Population and Nutrition (HPN) Goal: Promote and improve health and well-being of Malawians through investing in sustainable, high-impact health initiatives in line with
FANTA III. Improving Pre-Service Nutrition Education and Training of Frontline Health Care Providers TECHNICAL BRIEF
 TECHNICAL BRIEF Food and Nutrition Technical Assistance III Project June 2018 Improving Pre-Service Nutrition Education and Training of Frontline Health Care Providers Introduction The purpose of this
TECHNICAL BRIEF Food and Nutrition Technical Assistance III Project June 2018 Improving Pre-Service Nutrition Education and Training of Frontline Health Care Providers Introduction The purpose of this
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. IMCI Monitoring and Evaluation
 Implementation in the Western Pacific Region. IMCI Monitoring and Evaluation") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI Monitoring and Evaluation 8 IMCI Monitoring and Evaluation Why is monitoring and evaluation of IMCI important?
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI Monitoring and Evaluation 8 IMCI Monitoring and Evaluation Why is monitoring and evaluation of IMCI important?
Incorporating the Right to Health into Health Workforce Plans
 Incorporating the Right to Health into Health Workforce Plans Key Considerations Health Workforce Advocacy Initiative November 2009 Using an easily accessible format, this document offers guidance to policymakers
Incorporating the Right to Health into Health Workforce Plans Key Considerations Health Workforce Advocacy Initiative November 2009 Using an easily accessible format, this document offers guidance to policymakers
Economic and Social Council
 United Nations E/CN.3/2015/20 Economic and Social Council Distr.: General 8 December 2014 Original: English Statistical Commission Forty-sixth session 3-6 March 2015 Item 4 (a) of the provisional agenda*
United Nations E/CN.3/2015/20 Economic and Social Council Distr.: General 8 December 2014 Original: English Statistical Commission Forty-sixth session 3-6 March 2015 Item 4 (a) of the provisional agenda*
Good practice in the field of Health Promotion and Primary Prevention
 Good practice in the field of Promotion and Primary Prevention Dr. Mohamed Bin Hamad Al Thani Med Cairo February 28 th March 1 st, 2017 - Cairo - Egypt 1 Definitions Promotion Optimal Life Style Change
Good practice in the field of Promotion and Primary Prevention Dr. Mohamed Bin Hamad Al Thani Med Cairo February 28 th March 1 st, 2017 - Cairo - Egypt 1 Definitions Promotion Optimal Life Style Change
Areas of Focus Statements of Purpose and Goals
 April 2012 Page 1 Exhibit A-13-d Areas of Focus Statements of Purpose and Goals With respect to the areas of focus policy statements, TRF notes that 1. The goals of Future Vision are to increase efficiency
April 2012 Page 1 Exhibit A-13-d Areas of Focus Statements of Purpose and Goals With respect to the areas of focus policy statements, TRF notes that 1. The goals of Future Vision are to increase efficiency
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 FAST FACTS THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL STATE OF THE WORLD S MIDWIFERY CHALLENGES The 73 countries
FAST FACTS THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL STATE OF THE WORLD S MIDWIFERY CHALLENGES The 73 countries
COUNTRY PROFILE: LIBERIA LIBERIA COMMUNITY HEALTH PROGRAMS JANUARY 2014
 COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
Grant Aid Projects/Standard Indicator Reference (Health)
") Examples of Setting Indicators for Each Development Strategic Objective Grant Aid Projects/Standard Indicator Reference (Health) Sector Development strategic objectives (*) Mid-term objectives Sub-targets
Examples of Setting Indicators for Each Development Strategic Objective Grant Aid Projects/Standard Indicator Reference (Health) Sector Development strategic objectives (*) Mid-term objectives Sub-targets
Standards for competence for registered midwives
 Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Child Survival among Urban Poor- Challenges and Approaches for Involving Pediatricians
 Child Survival among Urban Poor- Challenges and Approaches for Involving Pediatricians IAP Central Zone Workshop February 9th, 2006 Shreemaya Residency, Indore Dr. Siddharth Agarwal Urban Health Resource
Child Survival among Urban Poor- Challenges and Approaches for Involving Pediatricians IAP Central Zone Workshop February 9th, 2006 Shreemaya Residency, Indore Dr. Siddharth Agarwal Urban Health Resource
Provisional agenda (annotated)
") EXECUTIVE BOARD EB140/1 (annotated) 140th session 21 November 2016 Geneva, 23 January 1 February 2017 Provisional agenda (annotated) 1. Opening of the session 2. Adoption of the agenda 3. Report by the
EXECUTIVE BOARD EB140/1 (annotated) 140th session 21 November 2016 Geneva, 23 January 1 February 2017 Provisional agenda (annotated) 1. Opening of the session 2. Adoption of the agenda 3. Report by the
National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year
 National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year 2010-11 District :-Sriganganagar A RCH - TECHNICAL STRATEGIES & ACTIVITIES (RCH Flexible Pool) A.1 MATERNAL
National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year 2010-11 District :-Sriganganagar A RCH - TECHNICAL STRATEGIES & ACTIVITIES (RCH Flexible Pool) A.1 MATERNAL
Indian Healthcare System: Issues and Challenges
 Indian Healthcare System: Issues and Challenges Dr. Bimal Jaiswal1, Ms. Noor Us Saba1 1Department of Applied Economics, Faculty of Commerce, University of Lucknow, Lucknow, U.P. 2Visiting Faculty, Institute
Indian Healthcare System: Issues and Challenges Dr. Bimal Jaiswal1, Ms. Noor Us Saba1 1Department of Applied Economics, Faculty of Commerce, University of Lucknow, Lucknow, U.P. 2Visiting Faculty, Institute
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health
 Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
upscale: A digital health platform for effective health systems
 República de Moçambique Ministério da Saúde Direcção Nacional de Saúde Pública upscale: A digital health platform for effective health systems From 2009 to 2016, Malaria Consortium tested a number of interventions
República de Moçambique Ministério da Saúde Direcção Nacional de Saúde Pública upscale: A digital health platform for effective health systems From 2009 to 2016, Malaria Consortium tested a number of interventions
CITY COUNCIL OF KISUMU
 in collaboration with CITY COUNCIL OF KISUMU TRAINING OF COMMUNITY HEALTH WORKERS Increasing Access to Healthcare using a Community-based Approach MANYATTA B By Beldina Opiyo-Omolo 21 January - 4 February,
in collaboration with CITY COUNCIL OF KISUMU TRAINING OF COMMUNITY HEALTH WORKERS Increasing Access to Healthcare using a Community-based Approach MANYATTA B By Beldina Opiyo-Omolo 21 January - 4 February,
Uzbekistan: Woman and Child Health Development Project
 Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
Medical Care in Gujarat Current Scenario & Future
 Medical Care in Gujarat Current Scenario & Future Our Goals Reduce maternal and child mortality Address adverse sex ratio Provide state of the art health, medical services and medical education relevant
Medical Care in Gujarat Current Scenario & Future Our Goals Reduce maternal and child mortality Address adverse sex ratio Provide state of the art health, medical services and medical education relevant
Ethiopia Health MDG Support Program for Results
 Ethiopia Health MDG Support Program for Results Health outcome/output EDHS EDHS Change 2005 2011 Under 5 Mortality Rate 123 88 Decreased by 28% Infant Mortality Rate 77 59 Decreased by 23% Stunting in
Ethiopia Health MDG Support Program for Results Health outcome/output EDHS EDHS Change 2005 2011 Under 5 Mortality Rate 123 88 Decreased by 28% Infant Mortality Rate 77 59 Decreased by 23% Stunting in
South Sudan Country brief and funding request February 2015
 PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
Comprehensive Evaluation of the Community Health Program in Rwanda. Concern Worldwide. Theory of Change
 Comprehensive Evaluation of the Community Health Program in Rwanda Concern Worldwide Theory of Change Concern Worldwide 1. Program Theory of Change Impact Sexual and Reproductive Health Maternal health
Comprehensive Evaluation of the Community Health Program in Rwanda Concern Worldwide Theory of Change Concern Worldwide 1. Program Theory of Change Impact Sexual and Reproductive Health Maternal health
Position Title: Consultant to Assess the RWANDA Thousand Days in the Land of a Thousand Hills Communication Campaign. Level: Institutional contract
 Terms of Reference for a Special Service Agreement- Institutional Contract Position Title: Level: Location: Duration: Start Date: Consultant to Assess the RWANDA Thousand Days in the Land of a Thousand
Terms of Reference for a Special Service Agreement- Institutional Contract Position Title: Level: Location: Duration: Start Date: Consultant to Assess the RWANDA Thousand Days in the Land of a Thousand
GLOBAL GRANT MONITORING AND EVALUATION PLAN SUPPLEMENT
 ENGLISH (EN) GLOBAL GRANT MONITORING AND EVALUATION PLAN SUPPLEMENT Global grant sponsors for humanitarian projects and vocational training teams must incorporate monitoring and evaluation measures within
ENGLISH (EN) GLOBAL GRANT MONITORING AND EVALUATION PLAN SUPPLEMENT Global grant sponsors for humanitarian projects and vocational training teams must incorporate monitoring and evaluation measures within
Mauritania Red Crescent Programme Support Plan
 Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA
 COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
Global Health Workforce Crisis. Key messages
 Global Health Workforce Crisis Key messages - 2013 Despite the increased evidence that health workers are fundamental for ensuring equitable access to health services and achieving universal health coverage,
Global Health Workforce Crisis Key messages - 2013 Despite the increased evidence that health workers are fundamental for ensuring equitable access to health services and achieving universal health coverage,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES. Tajikistan
 CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
Primary objective: Gain a global perspective on child health by working in a resource- limited setting within a different cultural context.
 Global health elective competency- based objectives for pediatric residents (These objectives can be adapted by the resident s institution to pertain to a specific elective site) Primary objective: Gain
Global health elective competency- based objectives for pediatric residents (These objectives can be adapted by the resident s institution to pertain to a specific elective site) Primary objective: Gain
Digital Disruption meets Indian Healthcare-the role of IT in the transformation of the Indian healthcare system
 Digital Disruption meets Indian Healthcare-the role of IT in the transformation of the Indian healthcare system Introduction While the Indian healthcare system has made important progress over the last
Digital Disruption meets Indian Healthcare-the role of IT in the transformation of the Indian healthcare system Introduction While the Indian healthcare system has made important progress over the last
Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E
 Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E WHO-EM/RDO/002/E Shaping the future of health in the WHO Eastern Mediterranean Region:
Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E WHO-EM/RDO/002/E Shaping the future of health in the WHO Eastern Mediterranean Region:
APPENDIX TO TECHNICAL NOTE
 (Version dated 1 May 2015) APPENDIX TO TECHNICAL NOTE How WHO will report in 2017 to the United Nations General Assembly on the progress achieved in the implementation of commitments included in the 2011
(Version dated 1 May 2015) APPENDIX TO TECHNICAL NOTE How WHO will report in 2017 to the United Nations General Assembly on the progress achieved in the implementation of commitments included in the 2011
Integrated Management of Childhood Illness (IMCI)
") CHAPTER 5 III Integrated Management of Childhood Illness (IMCI) Tigest Ketsela, Phanuel Habimana, Jose Martines, Andrew Mbewe, Abimbola Williams, Jesca Nsungwa Sabiiti,Aboubacry Thiam, Indira Narayanan,
CHAPTER 5 III Integrated Management of Childhood Illness (IMCI) Tigest Ketsela, Phanuel Habimana, Jose Martines, Andrew Mbewe, Abimbola Williams, Jesca Nsungwa Sabiiti,Aboubacry Thiam, Indira Narayanan,
Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala. Sunil Kumar
 End TB Strategy Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala Sunil Kumar The END TB strategy challenges the world to envision the End of the Tuberculosis pandemic and
End TB Strategy Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala Sunil Kumar The END TB strategy challenges the world to envision the End of the Tuberculosis pandemic and
EMERGENCY CARE SYSTEMS
 OVERVIEW Emergency and Trauma Care Systems The DCP emergency components of essential packages WHO Emergency Care System Framework Emergency Care System Assessment Tool PREVENTION PREHOSPITAL & TRANSPORT
OVERVIEW Emergency and Trauma Care Systems The DCP emergency components of essential packages WHO Emergency Care System Framework Emergency Care System Assessment Tool PREVENTION PREHOSPITAL & TRANSPORT
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004
 UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
Biennial Collaborative Agreement
 Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Joint Secretary (AYUSH)
") Integrating ti AYUSH in Health Research, Teaching and Practice Dr. D. D. Sharma Joint Secretary (AYUSH) 1 Preamble AYUSH: indigenous, time-tested, tested, cultural-friendly, socially acceptable, holds
Integrating ti AYUSH in Health Research, Teaching and Practice Dr. D. D. Sharma Joint Secretary (AYUSH) 1 Preamble AYUSH: indigenous, time-tested, tested, cultural-friendly, socially acceptable, holds
Republic of South Sudan 2011
 Republic of South Sudan 2011 Appealing Agency Project Title Project Code Sector/Cluster Refugee project VOLUNTEER ORGANIZATION FOR THE INTERNATIONAL CO-OPERATION LA NOSTRA NOTRA FAMIGLIA) Strengthening
Republic of South Sudan 2011 Appealing Agency Project Title Project Code Sector/Cluster Refugee project VOLUNTEER ORGANIZATION FOR THE INTERNATIONAL CO-OPERATION LA NOSTRA NOTRA FAMIGLIA) Strengthening
Reproductive & Child Health. State Institute of Health & Family Welfare, Jaipur
 Reproductive & Child Health Program State Institute of Health & Family Welfare, Jaipur What is RCH.? Reproductive & Child Health program is a model developed through experiments in paradigm shifts, Clinic
Reproductive & Child Health Program State Institute of Health & Family Welfare, Jaipur What is RCH.? Reproductive & Child Health program is a model developed through experiments in paradigm shifts, Clinic