Seeking Models for Sustaining Access to Health Care in Rural Communities
|
|
|
- Nathaniel Chase
- 5 years ago
- Views:
Transcription
1 Seeking Models for Sustaining Access to Health Care in Rural Communities Rural Hospital Conference of the Carolinas November 9, 2017 Andy Fosmire, M.S., VP for Rural Health Oklahoma Hospital Association
2
3 83 Hospital Closures Since 2010 In Oklahoma: Sayre Memorial Hospital Memorial Hospital & Physician Group (Frederick) Epic Medical Center (Eufaula) Pushmataha Hospital (Antlers) Bankruptcy Protection Atoka County Medical Center Bankruptcy Protection
4 83 Hospital Closures Since 2010 In North Carolina: Davie Medical Center-Mocksville Blowing Rock Hospital Vidant Pungo Hospital (Belhaven) Yadkin Valley Community Hospital (Yadkinville)
5
6 Oklahoma s Rural Hospital Financial Positions 65 truly rural hospitals in Oklahoma 53 have negative operating margins 37 have less than 14 days cash on hand 7 struggle to make payroll and payroll taxes Source: Eide Bailly 2017
7 Rural vs Urban Oklahoma Hospitals 2015

8
9 Death by a Thousand Cuts Sequestration cuts 2% for nine years Bad debt reimbursement cuts Documentation & coding cuts Readmission cuts Multiple therapy procedure cuts ESRD reimbursement cuts Super rural laboratory extender expired Outpatient hold harmless payments expired 508 reclassifications expired
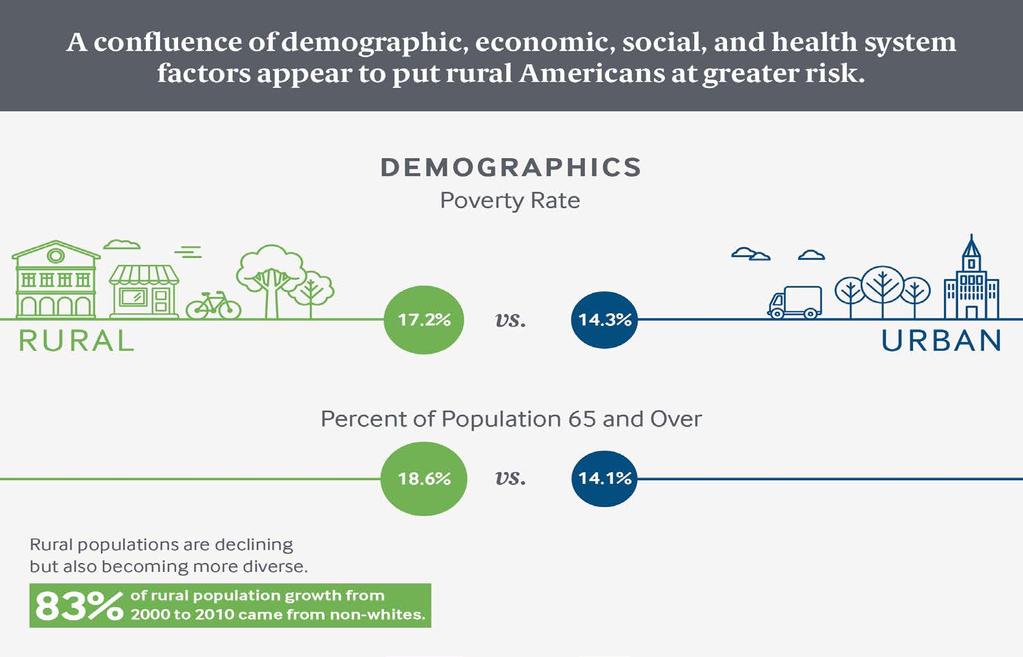
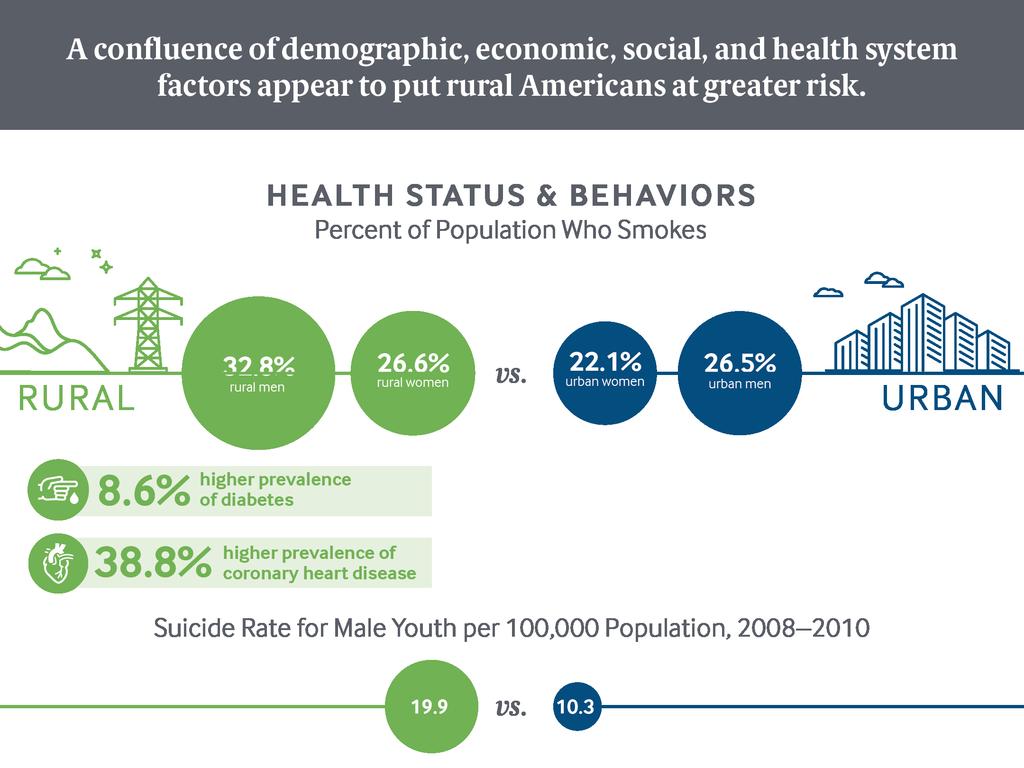
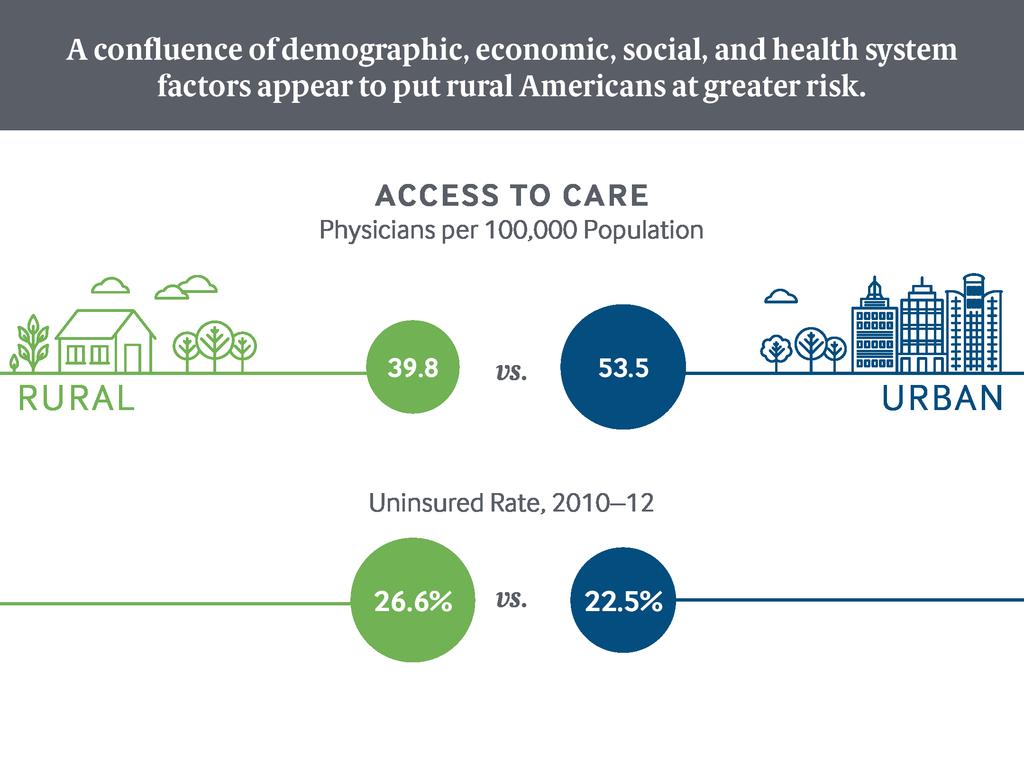
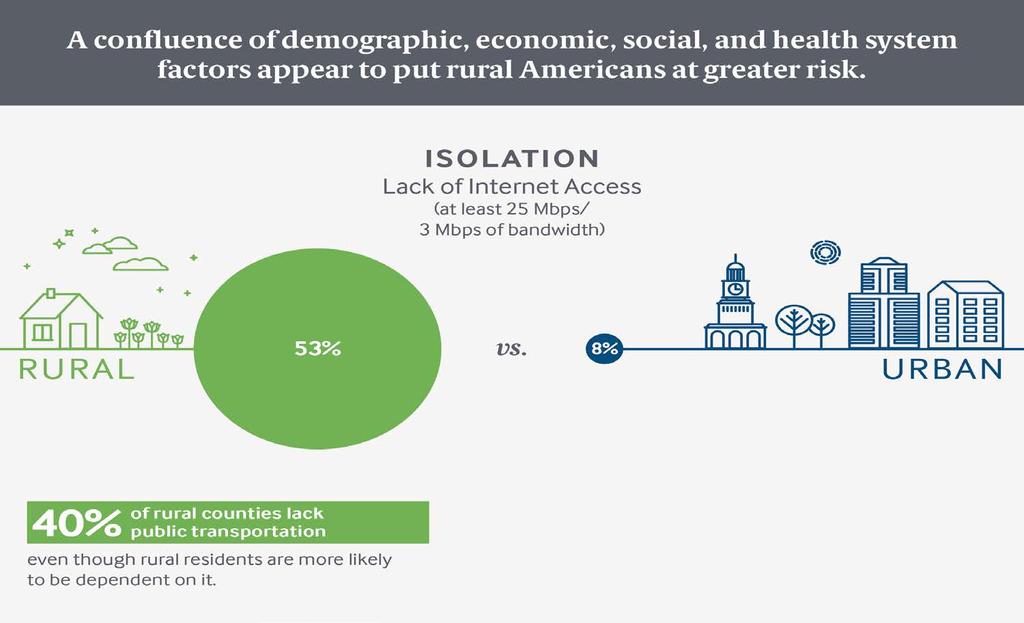
10 Rural/Urban Divide Rural folks tend to be poorer, sicker, and older that their urban counterparts Alan Morgan CEO, NRHA
11
12
13
14
15 Data: Hing, E, Hsiao, C. US Department of Health and Human Services. State Variability in Supply of Office-based Primary Care Providers: United States NCHS Data Brief, No. 151, May CDC s National Center for Health Statistics A. O Connor and G. Wellenius, Rural Urban Disparities in the Prevalence of Diabetes and Coronary Heart Disease, Public Health, Oct (10): M. Shan, Z. Jump, E. Lancet, Urban and Rural Disparities in Tobacco Use, National Conference on Health Statistics, August 8, 2012, C. A. Fontanella, D. L. Hiance-Steelesmith, and G. S. Phillips, Widening Rural Urban Disparities in Youth Suicides, United States, , JAMA Pediatrics, May (5): Source: M. Hostetter and S. Klein, In Focus: Reimagining Rural Health Care, Transforming Care: Reporting on Health System Improvement, The Commonwealth Fund, March 2017.

16 Searching for Solutions
17
18 Redefining Rural Health Summits: April 2015: Convened 12 state hospital associations to learn what steps they are taking to address rural hospitals in crisis. Discussed models/ideas states are investigating for sustaining future rural health services. Distributed a detailed summary report for states that were not in attendance. August 2015: Follow up meeting, 22 states, led to AHA Rural Affiliate group formation/monthly calls March 2016: First formal Rural Affiliate meeting
19 Purpose of the Summits: Convene other state hospital associations to identify common themes and discern elements for sustaining rural health services. Discuss models/ideas states are investigating for sustaining future rural health services. An opportunity for state associations to gain insight from others and guide their own efforts with rural communities. Identify forces impacting provision of rural healthcare. Develop guiding principals a common path forward.
20 Drivers Impacting Rural Communities: Money-Declining volumes, funding cuts, uncompensated care, regulations, workforce issues Continuity of care limited or no collaboration among rural providers collaborative disconnect Lifestyle issues: Rural hospitals act as default social services agencies, i.e. poor nutrition, poverty, and other uniquely rural factors Reform fatigue: Uncertain future, communities tired of continued effort to prop up their hospital Resistance to maintaining a medical presence in communities without a full service hospital
21 Redefining Rural Health Guiding Principals for Transformation: Patient first (community and population-based health) Enlightened governance and leadership Access to appropriate care Provide quality and value Collaborate among all providers (continuum of care) Leverage technology Adequate payment from state and federal sources
22 Structure for Rural Services New Provider Type, OR Amend Current Provider Type(s)? CAH (Critical Access Hospital) PPS (Prospective Payment System) RHC (Rural Health Clinic) FQHC (Federally Qualified Health Center) Ambulatory Surgery Centers FESC (Federal Extended Stay Clinic) Other? Combination of the two in a way that meets the Core needs
23 Amend Current Provider Type Rationale Limits entrants to only those currently in that particular type to move along a continuum at desired pace Creates flexibility based on need (documented through modified CHNA) Quicker legislative/regulatory path Administration open to New Provider type

24 We Are All Pushing the Same Rock
25 Kansas Hospital Association Summary KHA s Rural Health Visioning Technical Assistance Group (TAG) formed in 2012 and identified five areas of work: Establishing a case for change Identifying and reviewing best practices and emerging models Finding or developing models that could be an option Developing scenarios to assist members to structure leadership discussions about their role and future Providing resources for members to evaluate collaboration and affiliation
26 Minnesota Hospital Association Summary Critical Access Hospital Payment Reform Task Force member driven endeavor Analyzed HCRIS, operating margin profiles, admissions trends, case mix, and swing bed rates CAH Reform Model Concepts designed to: Be patient-centered, value driven home and community-based care Recognize provider-generated savings whether realized by Medicare or Medicaid Generate direct/indirect savings for CMS by improving quality and decreasing utilization Maintain access to emergency services
27 Illinois Hospital Association Summary IHA Transforming Illinois Health Care Task Force, Rural Health Subgroup 13 CAHS and 5 rural PPS hospitals formed in 2014 and convened to: Identify elements of new rural health care delivery models with government and finance mechanisms; and Develop pathways for members to transition to new models. Three subcommittees Model design Payment system Quality improvement
28 Washington State Hospital Association Summary WSHA and the Washington State Department of Health created the Washington Rural Health Access Preservation (WRHAP) to ensure continued access to essential health services in WA s most vulnerable communities using their CMS SIM grant. WRHAP has: Reviewed existing alternative rural healthcare models Frontier Extended Stay Clinic (FESC) Federal Community Health Integration Project (F- CHIP) Free standing ED (Georgia) Integrated interagency county/district/regional system
29 Washington State Hospital Association Summary continued Identified an initial list of essential services that need to be provided locally Described some potential payment models Fixed cost of the facility Prospective per member per month for primary care (including prevention) and possibly other services Extended stay payments Bundled payments for episodes of pre and postacute care


 The global budget")




 Rural Health")




30 Pennsylvania approach: Rural Global Budget Model is driven by a hospital-led transformation plan and enabled by a global budget (Project funded by a $25 million grant from CMMI) Fixed annual revenue (global budget) The global budget is fixed annually and paid out to hospitals monthly, providing a stable stream of revenue The objective of the global budget is to stabilize cash flow, allowing focus on investment and care quality The global budget is calculated based on historic data adjusted for transformation-related annual service changes Transformation support (Rural Health Redesign Center) Rural Health Redesign Center will provide tailored, end-to-end assistance at no cost to the hospital The objective of the RHRC is to minimize the burden of the transformation, allowing focus on successful implementation The RHRC will participate in all transformation phases: data collection, plan creation, implementation progress SOURCE: Pennsylvania Department of Health and Hospital Association of Pennsylvania 30
31 Oklahoma Hospital Association Summary Council on Rural Health Comprised of 15 rural CEOs from across the state and three ex-officio members. Provides a forum to address health care issues specific to rural communities across Oklahoma. Develop and address health policy and regulatory issues unique to rural settings. Advises the OHA board on ways to focus its resources to better assist rural hospitals in service to their communities.

32 Hey, This Direction
33 Hybrid of CAH and FQHC Oklahoma Options: Two Sub-models o Allows for acute inpatient, swing beds, outpatient services, cadre of required FQHC services (behavioral health, oral health, sliding fee scale) 24-Hr outpatient hospital o 24-hr emergency treatment, stabilization o Primary Care and Outpatient services o Short Term Observation o No inpatient beds (acute or swing) o Proposed edits to OSDH 667 Sub-Chapter 40
34 .
35 CMS Rural Solutions Summit: October 19, 2016 CMS gathered rural stakeholders in person at CMS headquarters to discuss ways to improve rural health access, support local innovations in care delivery, and serve as a CMS Rural Council listening session. Workgroups focused on: Essential healthcare services in rural communities Enhancing innovation in rural healthcare delivery Modernizing telemedicine
36 Outcome from the CMS Rural Solutions Summit Develop a proposal to CMS for a payment model demonstration project to pilot the Outpatient Hospital Model coordinating with: CMS/CMMI representatives Other state hospital assocations Federal Office of Rural Health policy American Hospital Association
37

38 Rural Hospital Initiative: Testing New Approaches to Payment & Delivery Presented and proposed by the hospital associations of Colorado*, Kansas, New Mexico and Oklahoma *Due to legislative changes in CO, they have withdrawn form active participation
39 Project Goals Promote collaboration at all levels of the project Federal, state, regional and local Develop and test: Health care access point in rural communities as an alternative to PPS hospital or CAH Predictable and flexible payment approach that incentivizes local health improvement, quality and efficiency Budget neutral or system savings while access is retained or improved
40 Tasks/Deliverables to Start Secure complete beneficiary Medicare data Identify and engage sites willing to participate Those testing new model Partner organization Discuss with and engage Medicaid and Third Party payers in collaboration Address and resolve key statutory and regulatory barriers at state and federal levels Path back to previous status if community chooses

41 Overview of the Model
42 Overview of Services Provided - CORE Primary health care including prenatal care Urgent & Emergency care Emergent and non-emergent transportation Observation Outpatient and ambulatory services Minor procedures Ancillary services to support primary care and basic diagnostic Care coordination, chronic disease management and other approaches to population health Active Telemedicine
43 Overview of Services Provided - OPTIONAL If unavailable locally, may be included in the payment model Rehabilitative services Subacute care Behavioral health Oral Health Services needed within a reasonable distance.* Must be consistent with community need and documented in data. *Distance will need to be determined with CMS input.
44 Services That Should Be Available Within Reasonable Distance Prenatal services, normal and/or emergency deliveries and subsequent newborn care Unique local and regional services Must be consistent with community need and documented in data If unavailable within a reasonable distance* may be included in the payment model *Distance will need to be determined with CMS
45 Payment Principles To preserve access and improve health, low volume facilities must be supported with a new approach to payment that is at least budget neutral Annual federal grants or support: Built into a fixed payment similar to MedPAC's approach Annual financial participation from the local community: To assist in supporting the continued access to services One time grant or transitional funding: To bridge challenges as CMS makes payment process changes to fund local costs of transition
46 Payment Principles (Cont.) An inclusive budget encompassing all services Incentivize clinical integration Allow flexible use of limited staff and resources to adjust to day-to-day changes in volume and service needs Ideally, all payers should participate in the demonstration to determine exactly how the model can balance the support of access and optimal health for a community as well as incentives for efficiency and high quality States in conversations with Medicaid agencies and third party payers as per discussions with CMS
47 Payment Methodology Blended Fixed and Encounter Payment LESS D E P E N D A B I L I T Y More $ Value Incentive $ Additional services $ Encounter Payments $ Grants $ Fixed Payment +/- 2% Risk/Reward of fixed payment Rural relevant quality, outcome and performance measures, aligned with scope of services provided by the model Phase in Report, Reward, Risk Traditional fee schedule reimbursement for non-core services Other revenue investment, grants, philanthropic contributions Third party payer payments for all non-governmental funded services if not included in demonstration Co-pays and deductibles collected in traditional manner Paid by all payers participating in demonstration For all core services Based on % of traditional fee schedule negotiated to account for fixed payments Federal Grant to ensure access to emergency services Local financial support at a minimum of 10% of Federal Grant Tied to Negotiated Base Budget for core services Multi-year agreement negotiated annually Paid monthly 1/12 th, no back-end reconciliation Includes all services and a capital allowance Operational incentive to be efficient and effective to meet budget
48 Incentives & Accountability Reporting, consistent with the nature of the facility, should document and assess* Local health improvement services, quality, local population served by core services, and operational efficiency measures and expense Measures should be consistent with the scope of services provided by the facility* Recognition should be given to identifying key measures and balancing accountability with burdensome processes Demonstration facilities would continue to submit encounter data To support the services provided To support the process of collecting co-pays and insurance To document and assess services provided, along with budget neutrality or savings Components of a value incentive are included to support the triple aim *Lessons can be learned from work to identify and test rural relevant measures from other sources
49 Test Site Eligibility Recommendations Any previous Medicare and Medicaid certified hospital located in a CMS designated rural area willing to meet the service, payment and accountability requirements, or May have been closed for up to 2-3 years Must be able to demonstrate community commitment (cash to the budget) Average acute census (TBD, likely > two) Partner Organizations Any PPS or CAH that provides Inpatient Acute services not sustainable in test site community Local and regional opportunities for collaboration and/or integration, such as primary care and EMS
50 Questions?
Reimbursement Models of the Future A Look at Proposed Models
 Experience the Eide Bailly Difference Reimbursement Models of the Future A Look at Proposed Models Ralph J. Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 Introduction CAH reimbursement
Experience the Eide Bailly Difference Reimbursement Models of the Future A Look at Proposed Models Ralph J. Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 Introduction CAH reimbursement
Rural Relevance in Oklahoma
 Rural Relevance in Oklahoma OHA Annual Conference 2017 November 1, 2017 Agenda Introductions The Rural Relevance Study Impact of Current and Proposed Health Policies on Rural Providers Oklahoma Rural Hospitals:
Rural Relevance in Oklahoma OHA Annual Conference 2017 November 1, 2017 Agenda Introductions The Rural Relevance Study Impact of Current and Proposed Health Policies on Rural Providers Oklahoma Rural Hospitals:
Appendix B: Formulae Used for Calculation of Hospital Performance Measures
 Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
The Essential Care, Everywhere study provides new insight into Washington s rural communities, and their 42 hospitals.
 Transforming the Delivery of Essential Care in Rural Communities Medical Design Forum AIA Seattle/AHP Medical Forum February 7, 2013 The Essential Care, Everywhere study provides new insight into Washington
Transforming the Delivery of Essential Care in Rural Communities Medical Design Forum AIA Seattle/AHP Medical Forum February 7, 2013 The Essential Care, Everywhere study provides new insight into Washington
May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics
 Hot Reimbursement Topics Rural Area Hospitals May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics RICHARD S. REID, MPA, FHFMA, CPA, Director,
Hot Reimbursement Topics Rural Area Hospitals May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics RICHARD S. REID, MPA, FHFMA, CPA, Director,
Rebalancing Health Care in the Heartland The Rural Imperative of Population Health Des Moines, IA
 Rebalancing Health Care in the Heartland The Rural Imperative of Population Health Des Moines, IA Brock Slabach, MPH, FACHE Sr. Vice-President National Rural Health Association Leawood, KS December 1,
Rebalancing Health Care in the Heartland The Rural Imperative of Population Health Des Moines, IA Brock Slabach, MPH, FACHE Sr. Vice-President National Rural Health Association Leawood, KS December 1,
Rural Health Disparities 5/22/2012. Rural is often defined by what it is not urban. May 3, The Rural Health Landscape
 5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
EXTENDED STAY PRIMARY CARE
 EXTENDED STAY PRIMARY CARE Working with Frontier Communities to Design Facilities that Work June 2000 Supported in part by the Federal Office of Rural Health Policy HRSA, DHHS Frontier Education Center
EXTENDED STAY PRIMARY CARE Working with Frontier Communities to Design Facilities that Work June 2000 Supported in part by the Federal Office of Rural Health Policy HRSA, DHHS Frontier Education Center
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Outcomes Measurement in Long-Term Care (LTC)
") ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
November 10, Alan Morgan Chief Executive Officer National Rural Health Association. New Approaches To Health Care Delivery
 November 10, 2016 Alan Morgan Chief Executive Officer National Rural Health Association New Approaches To Health Care Delivery Improving the health of millions who call rural America home. National Rural
November 10, 2016 Alan Morgan Chief Executive Officer National Rural Health Association New Approaches To Health Care Delivery Improving the health of millions who call rural America home. National Rural
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
Rural Health Clinics
 Rural Health Clinics * An Issue Paper of the National Rural Health Association originally issued in February 1997 This paper summarizes the history of the development and current status of Rural Health
Rural Health Clinics * An Issue Paper of the National Rural Health Association originally issued in February 1997 This paper summarizes the history of the development and current status of Rural Health
January 10, Glenn M. Hackbarth, J.D Hunnell Road Bend, OR Dear Mr. Hackbarth:
 Glenn M. Hackbarth, J.D. 64275 Hunnell Road Bend, OR 97701 Dear Mr. Hackbarth: The Medicare Payment Advisory Commission (MedPAC or the Commission) will vote next week on payment recommendations for fiscal
Glenn M. Hackbarth, J.D. 64275 Hunnell Road Bend, OR 97701 Dear Mr. Hackbarth: The Medicare Payment Advisory Commission (MedPAC or the Commission) will vote next week on payment recommendations for fiscal
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Global Budget Revenue. October 8, 2015
 Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Critical Access Hospitals and Cost-Based Reimbursement
 Critical Access Hospitals and Cost-Based Reimbursement Jared Heim, CPA, Partner jheim@eidebailly.com 563.557.6169 Agenda for Today Overview of Critical Access Hospitals Overview of Health Care Reform Behavioral
Critical Access Hospitals and Cost-Based Reimbursement Jared Heim, CPA, Partner jheim@eidebailly.com 563.557.6169 Agenda for Today Overview of Critical Access Hospitals Overview of Health Care Reform Behavioral
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
The Financial Effects of Wisconsin Critical Access Hospital Conversion
 The Financial Effects of Wisconsin Critical Access Hospital Conversion Richard Donkle, CPA Dale Gullickson, FHFMA Rural Wisconsin Health Cooperative For the Wisconsin Office of Rural Health Acknowledgements
The Financial Effects of Wisconsin Critical Access Hospital Conversion Richard Donkle, CPA Dale Gullickson, FHFMA Rural Wisconsin Health Cooperative For the Wisconsin Office of Rural Health Acknowledgements
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction
 Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
The Center for Medicare & Medicaid Innovations: Programs & Initiatives
 The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session. Comments of Christy Parque, MSW.
 New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session Comments of Christy Parque, MSW President and CEO November 29, 2017 The Coalition for Behavioral Health, Inc. (The Coalition)
New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session Comments of Christy Parque, MSW President and CEO November 29, 2017 The Coalition for Behavioral Health, Inc. (The Coalition)
Long term commitment to a new vision. Medical Director February 9, 2011
 ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
Navigating an Enhanced Rural Health Model for Maryland
 Executive Summary HEALTH MATTERS: Navigating an Enhanced Rural Health Model for Maryland LESSONS LEARNED FROM THE MID-SHORE COUNTIES To access the Report and Accompanied Technical Reports go to: go.umd.edu/ruralhealth
Executive Summary HEALTH MATTERS: Navigating an Enhanced Rural Health Model for Maryland LESSONS LEARNED FROM THE MID-SHORE COUNTIES To access the Report and Accompanied Technical Reports go to: go.umd.edu/ruralhealth
Medicaid MOA Update and Payment Reform Visioning Session
 Medicaid MOA Update and Payment Reform Visioning Session Where we are today, developing a vision for the future www.mpca.net The History PPS and Medicare cost-based reimbursement were created (2000) in
Medicaid MOA Update and Payment Reform Visioning Session Where we are today, developing a vision for the future www.mpca.net The History PPS and Medicare cost-based reimbursement were created (2000) in
Value-Based Reimbursements are Here: Are you Ready?
 Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Roadmap for Transforming America s Health Care System
 Roadmap for Transforming America s Health Care System America s health care system requires transformational change to provide all health care participants with broader access and choice, improved quality
Roadmap for Transforming America s Health Care System America s health care system requires transformational change to provide all health care participants with broader access and choice, improved quality
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Critical Access Hospital Quality
 Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
SNC BRIEF. Safety Net Clinics of Greater Kansas City EXECUTIVE SUMMARY CHALLENGES FACING SAFETY NET PROVIDERS TOP ISSUES:
 EXECUTIVE SUMMARY The Safety Net is a collection of health care providers and institutes that serve the uninsured and underinsured. Safety Net providers come in a variety of forms, including free health
EXECUTIVE SUMMARY The Safety Net is a collection of health care providers and institutes that serve the uninsured and underinsured. Safety Net providers come in a variety of forms, including free health
Background for Congressman Kevin Cramer s Health Care Reform Roundtable February 22, 2017 Consideration of Rural Health in Health Care Reform
 Background for Congressman Kevin Cramer s Health Care Reform Roundtable February 22, 2017 Consideration of Rural Health in Health Care Reform In rural health, health reform really means maintaining and
Background for Congressman Kevin Cramer s Health Care Reform Roundtable February 22, 2017 Consideration of Rural Health in Health Care Reform In rural health, health reform really means maintaining and
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
Trends in State Medicaid Programs: Emerging Models and Innovations
 Trends in State Medicaid Programs: Emerging Models and Innovations Speakers: Barbara Edwards, Principal, Steve Fitton, Principal, Tina Edlund, Managing Principal, Moderator: Annie Melia, Information Services
Trends in State Medicaid Programs: Emerging Models and Innovations Speakers: Barbara Edwards, Principal, Steve Fitton, Principal, Tina Edlund, Managing Principal, Moderator: Annie Melia, Information Services
VALUE BASED ORTHOPEDIC CARE
 VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
CLINICAL INTEGRATION DRIVERS, IMPACT, AND OPTIONS JOBY KOLSUN, D.O. MEDICAL DIRECTOR CLINICAL INTEGRATION LEE PHO
 CLINICAL INTEGRATION DRIVERS, IMPACT, AND OPTIONS JOBY KOLSUN, D.O. MEDICAL DIRECTOR CLINICAL INTEGRATION LEE PHO Disclaimers My current position I am not offering advice on clinical integration Items
CLINICAL INTEGRATION DRIVERS, IMPACT, AND OPTIONS JOBY KOLSUN, D.O. MEDICAL DIRECTOR CLINICAL INTEGRATION LEE PHO Disclaimers My current position I am not offering advice on clinical integration Items
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
Final Report No. 101 April Trends in Skilled Nursing Facility and Swing Bed Use in Rural Areas Following the Medicare Modernization Act of 2003
 Final Report No. 101 April 2011 Trends in Skilled Nursing Facility and Swing Bed Use in Rural Areas Following the Medicare Modernization Act of 2003 The North Carolina Rural Health Research & Policy Analysis
Final Report No. 101 April 2011 Trends in Skilled Nursing Facility and Swing Bed Use in Rural Areas Following the Medicare Modernization Act of 2003 The North Carolina Rural Health Research & Policy Analysis
Submission #1. Short Description: Medicare Payment to HOPDs, Section 603 of BiBA 2015
 Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Payment and Delivery System Reform in Vermont: 2016 and Beyond
 Payment and Delivery System Reform in Vermont: 2016 and Beyond Richard Slusky, Director of Reform Green Mountain Care Board Presentation to GMCB August 13, 2015 Transition Year 2016 1. Medicare Waiver
Payment and Delivery System Reform in Vermont: 2016 and Beyond Richard Slusky, Director of Reform Green Mountain Care Board Presentation to GMCB August 13, 2015 Transition Year 2016 1. Medicare Waiver
Medicaid 101: The Basics for Homeless Advocates
 Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Executive, Legislative & Regulatory 2017 AGENDA. unitypoint.org
 Executive, Legislative & Regulatory 2017 AGENDA unitypoint.org PRESIDENT S LETTER Dear Policy Makers and Community Stakeholders, 2017 presents many opportunities to meet needs, lower costs and continue
Executive, Legislative & Regulatory 2017 AGENDA unitypoint.org PRESIDENT S LETTER Dear Policy Makers and Community Stakeholders, 2017 presents many opportunities to meet needs, lower costs and continue
Decrease in Hospital Uncompensated Care in Michigan, 2015
 Decrease in Hospital Uncompensated Care in Michigan, 2015 July 2017 Introduction The Affordable Care Act (ACA) expanded access to health insurance coverage for Michigan residents in 2014 through the creation
Decrease in Hospital Uncompensated Care in Michigan, 2015 July 2017 Introduction The Affordable Care Act (ACA) expanded access to health insurance coverage for Michigan residents in 2014 through the creation
Executive, Legislative & Regulatory 2018 AGENDA. unitypoint.org/govaffairs
 Executive, Legislative & Regulatory 2018 AGENDA unitypoint.org/govaffairs Dear Policy Makers and Community Stakeholders, In the midst of tumultuous times, we bring you our 2018 State Legislative Agenda.
Executive, Legislative & Regulatory 2018 AGENDA unitypoint.org/govaffairs Dear Policy Makers and Community Stakeholders, In the midst of tumultuous times, we bring you our 2018 State Legislative Agenda.
The Accountable Care Organization Specific Objectives
 Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
Working Together for a Healthier Washington
 Working Together for a Healthier Washington Dorothy Teeter, HCA Director Nathan Johnson, HCA Chief Policy Officer All Alliance Meeting June 9, 2015 By 2019, we will have a Healthier Washington. Here s
Working Together for a Healthier Washington Dorothy Teeter, HCA Director Nathan Johnson, HCA Chief Policy Officer All Alliance Meeting June 9, 2015 By 2019, we will have a Healthier Washington. Here s
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Findings Brief. NC Rural Health Research Program
 Do Current Medicare Rural Hospital Payment Systems Align with Cost Determinants? Kristin Moss, MBA, MSPH; G. Mark Holmes, PhD; George H. Pink, PhD BACKGROUND The financial performance of small, rural hospitals
Do Current Medicare Rural Hospital Payment Systems Align with Cost Determinants? Kristin Moss, MBA, MSPH; G. Mark Holmes, PhD; George H. Pink, PhD BACKGROUND The financial performance of small, rural hospitals
Community Health Needs Assessment July 2015
 Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations
 Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations Executive Summary Rural networks across the nation have been working with rural providers to assist
Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations Executive Summary Rural networks across the nation have been working with rural providers to assist
Elizabeth Mitchell December 1, Transforming Healthcare in an Uncertain Environment
 Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Succeeding in Value-Based Care CareConnect Journey
 Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Testimony Robert E. O Connor, MD, MPH House Committee on Oversight and Government Reform June 22, 2007
 Testimony Robert E. O Connor, MD, MPH House Committee on Oversight and Government Reform June 22, 2007 Chairman Waxman, Ranking Member Davis, I would like to thank you for holding this hearing today on
Testimony Robert E. O Connor, MD, MPH House Committee on Oversight and Government Reform June 22, 2007 Chairman Waxman, Ranking Member Davis, I would like to thank you for holding this hearing today on
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together
 Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
MedPAC June 2013 Report to Congress: Medicare and the Health Care Delivery System
 MedPAC June 2013 Report to Congress: Medicare and the Health Care Delivery System STEPHANIE KENNAN, SENIOR VICE PRESIDENT 202.857.2922 skennan@mwcllc.com 2001 K Street N.W. Suite 400 Washington, DC 20006-1040
MedPAC June 2013 Report to Congress: Medicare and the Health Care Delivery System STEPHANIE KENNAN, SENIOR VICE PRESIDENT 202.857.2922 skennan@mwcllc.com 2001 K Street N.W. Suite 400 Washington, DC 20006-1040
Centers for Medicare and Medicaid CMS Updates. Christol Green, Anthem Inc.
 Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Presented to Midwestern Legislative Conference The Council of State Governments Milwaukee, Wisconsin July 17, 2016
 Presented to Midwestern Legislative Conference The Council of State Governments Milwaukee, Wisconsin July 17, 2016 Keith J. Mueller, PhD Director, RUPRI Center for Rural Health Policy Analysis Head, Department
Presented to Midwestern Legislative Conference The Council of State Governments Milwaukee, Wisconsin July 17, 2016 Keith J. Mueller, PhD Director, RUPRI Center for Rural Health Policy Analysis Head, Department
Lessons from the States: Oregon s APM Model
 Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Optimizing Operations through Data Collection and Dissemination. Raymond Belles, Jr. Managing Consultant
 Optimizing Operations through Data Collection and Dissemination Raymond Belles, Jr. Managing Consultant rbelles@bkd.com Learning Objectives Define the changing healthcare landscape Identify trends in home
Optimizing Operations through Data Collection and Dissemination Raymond Belles, Jr. Managing Consultant rbelles@bkd.com Learning Objectives Define the changing healthcare landscape Identify trends in home
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
The Financial Performance of Rural Hospitals and Implications for Elimination of the Critical Access Hospital Program
 The Financial Performance of Rural Hospitals and Implications for Elimination of the Critical Access Hospital Program George M. Holmes, George H. Pink, and Sarah A. Friedman University of North Carolina
The Financial Performance of Rural Hospitals and Implications for Elimination of the Critical Access Hospital Program George M. Holmes, George H. Pink, and Sarah A. Friedman University of North Carolina
Presented to the West Virginia Governance Forum May 2, 2014 Stonewall, West Virginia
 Keith J. Mueller, PhD Director, RUPRI Center for Rural Health Policy Analysis Head, Department of Health Management & Policy University of Iowa College of Public Health Keith-mueller@uiowa.edu Presented
Keith J. Mueller, PhD Director, RUPRI Center for Rural Health Policy Analysis Head, Department of Health Management & Policy University of Iowa College of Public Health Keith-mueller@uiowa.edu Presented
Chapter 9. Conclusions: Availability of Rural Health Services
 Chapter 9 Conclusions: Availability of Rural Health Services CONTENTS Page VIABILITY OF FACILITIES AND SERVICES.......................................... 211 FACILITY ADAPTATION TO CHANGES..........................................,.,.
Chapter 9 Conclusions: Availability of Rural Health Services CONTENTS Page VIABILITY OF FACILITIES AND SERVICES.......................................... 211 FACILITY ADAPTATION TO CHANGES..........................................,.,.
Bundled Payments. AMGA September 25, 2013 AGENDA. Who Are We. Our Business Challenge. Episode Process. Experience
 Bundled Payments AMGA September 25, 2013 Who Are We AGENDA Our Business Challenge Episode Process Experience 1 Cleveland Clinic is transforming Fee for service Fee for value 3 Fast Facts 41,200 employees
Bundled Payments AMGA September 25, 2013 Who Are We AGENDA Our Business Challenge Episode Process Experience 1 Cleveland Clinic is transforming Fee for service Fee for value 3 Fast Facts 41,200 employees
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Rural Essential Access Community Hospitals (REACH) For Rural America
 For Rural America") Rural Essential Access Community Hospitals (REACH) For Rural America Adopted, 3/29/01 This proposal was developed by individuals convened by the National Rural Health Association. This proposal is intended
Rural Essential Access Community Hospitals (REACH) For Rural America Adopted, 3/29/01 This proposal was developed by individuals convened by the National Rural Health Association. This proposal is intended
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
HEALTH PROFESSIONAL WORKFORCE
 HEALTH PROFESSIONAL WORKFORCE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care
HEALTH PROFESSIONAL WORKFORCE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Overview. Rural hospitals provide health care and critical care to 20 percent of Americans and are vital economic engines for their communities.
 Overview The delivery of health care in the United States is in flux, beset by unprecedented medical and fiscal challenges. Although rising health care costs and growing uncertainties affect every segment
Overview The delivery of health care in the United States is in flux, beset by unprecedented medical and fiscal challenges. Although rising health care costs and growing uncertainties affect every segment
HOT ISSUES FACING HOME HEALTH & HOSPICE AGENCIES. Luke James Chief Strategy Officer Encompass Home Health & Hospice
 HOT ISSUES FACING HOME HEALTH & HOSPICE AGENCIES Luke James Chief Strategy Officer Encompass Home Health & Hospice Hospice Challenges Past & Present Face-to-Face (F2F) Implementation Sequestration Cuts
HOT ISSUES FACING HOME HEALTH & HOSPICE AGENCIES Luke James Chief Strategy Officer Encompass Home Health & Hospice Hospice Challenges Past & Present Face-to-Face (F2F) Implementation Sequestration Cuts
Protecting Access to Medicare Act of 2014
 Protecting Access to Medicare Act of 2014 Protects Current Medicare Beneficiaries Doc Fix : Prevents the 24% cut in reimbursement to doctors who treat Medicare patients on April 1, 2014 and replaces it
Protecting Access to Medicare Act of 2014 Protects Current Medicare Beneficiaries Doc Fix : Prevents the 24% cut in reimbursement to doctors who treat Medicare patients on April 1, 2014 and replaces it
MEDICARE ENROLLMENT, HEALTH STATUS, SERVICE USE AND PAYMENT DATA FOR AMERICAN INDIANS & ALASKA NATIVES
 American Indian & Alaska Native Data Project of the Centers for Medicare and Medicaid Services Tribal Technical Advisory Group MEDICARE ENROLLMENT, HEALTH STATUS, SERVICE USE AND PAYMENT DATA FOR AMERICAN
American Indian & Alaska Native Data Project of the Centers for Medicare and Medicaid Services Tribal Technical Advisory Group MEDICARE ENROLLMENT, HEALTH STATUS, SERVICE USE AND PAYMENT DATA FOR AMERICAN
Rural Hospital Closures and Recent Financial Performance of Critical Access Hospitals in the Carolinas
 Rural Hospital Closures and Recent Financial Performance of Critical Access Hospitals in the Carolinas GH Pink and KL Reiter V Freeman, GM Holmes, A Howard, B Kaufman, J Perry, R Randolph, S Thomas, and
Rural Hospital Closures and Recent Financial Performance of Critical Access Hospitals in the Carolinas GH Pink and KL Reiter V Freeman, GM Holmes, A Howard, B Kaufman, J Perry, R Randolph, S Thomas, and
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
NYS Value Based Payments (VBP):
:") NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
Leveraging a CAH Health System Affiliation to Modernize Rural Health Care
 Leveraging a CAH Health System Affiliation to Modernize Rural Health Care Alisa Coleman President & CEO Ferrell Hospital Alan P. Richman President & CEO InnoVative Capital, LLC February 7, 2016 Jared Florence
Leveraging a CAH Health System Affiliation to Modernize Rural Health Care Alisa Coleman President & CEO Ferrell Hospital Alan P. Richman President & CEO InnoVative Capital, LLC February 7, 2016 Jared Florence
Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix
: The Doc Fix") April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population Health
 Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population Health B C Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population
Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population Health B C Executive Summary: Innovative Medicaid Payment Strategies for Upstream Prevention and Population
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
THE IMPACT OF BBA, BIPA and MEDICARE+CHOICE ON LTC (Why Medicare/Medicare Supplement is SHORT-TERM CARE)
") THE IMPACT OF BBA, BIPA and MEDICARE+CHOICE ON LTC (Why Medicare/Medicare Supplement is SHORT-TERM CARE) (For a complete description of Medicare, Medicare supplement and Medicare+Choice, see Appendix A
THE IMPACT OF BBA, BIPA and MEDICARE+CHOICE ON LTC (Why Medicare/Medicare Supplement is SHORT-TERM CARE) (For a complete description of Medicare, Medicare supplement and Medicare+Choice, see Appendix A
The Affordable Care Act
 The Affordable Care Act Medical City, Dallas, TX October 26, 2012 Presented by Cheryl West, MPH Director, Government Affairs, AARC Affordable Care Act (ACA) 2 What I m Not Going to Talk About 3 What I
The Affordable Care Act Medical City, Dallas, TX October 26, 2012 Presented by Cheryl West, MPH Director, Government Affairs, AARC Affordable Care Act (ACA) 2 What I m Not Going to Talk About 3 What I