Welcome and Introductions. Peter Carpenter
|
|
|
- Valerie McGee
- 5 years ago
- Views:
Transcription
1 Welcome and Introductions Peter Carpenter
2 Acute presentation 14/03/18 Dr Hugh McIntyre

3 Acute Heart Failure Timeline
4 Acute Heart Failure Timeline Andrew Lansley speech to the BMA annual conference "just two weeks ago, I saw a programme which embodies everything I ve been talking about today - clinicians taking the initiative to improve their services, to improve quality of care, access to information and patient outcomes measuring their performance - not against national targets - but against their own standards, and working to improve the quality of the service they provide
5 Acute Heart Failure Timeline August 2010 Heart Failure EQ Programme 4 measures (LV function evaluation, ACEI or ARB for LVSD, Discharge Instructions, Adult Smoking Cessation) 100% Heart Failure Appropriate Care Score Composite Quality Score 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Jul-10 Sep-10 Nov-10 Jan-11 Mar-11 May-11 Jul-11 Sep-11 Nov-11 Jan-12 Mar-12 May-12 Jul-12 Sep-12 Nov-12 Jan-13 Mar-13 May-13 Jul-13 Sep-13 Nov-13 Jan-14 Mar-14 May-14 Jul-14 Sep-14 Nov-14 Jan-15
6 Acute Heart Failure Timeline March 2014 Collaborative Local Discontinuation of CQUIN Plateau in performance Measures? Utility - smoking NHFA specialist input, optimal meds and ward correlate with better outcome National context Acute HF CG 187 tariff 5 year planning: National audits Aligning EQR with NHFA Relevance
7 Acute Heart Failure Timeline April 2015 to date ACS & CQS since 2015 for KSS Trusts involved in the Heart Failure programme NHFA Aligned Tariff Outcomes Dashboard 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Apr-2015 May-2015 Jun-2015 Jul-2015 Aug-2015 Sep-2015 Oct-2015 Nov-2015 Dec-2015 Jan-2016 Feb-2016 Mar-2016 Apr-2016 May-2016 Jun-2016 Jul-2016 Aug-2016 Sep-2016 Oct-2016 Nov-2016 Dec-2016 Jan-2017 Feb-2017 Mar-2017 Apr-2017 May-2017 Jun-2017 Jul-2017 Aug-2017 Sep-2017 ACS CQS Linear (ACS) Linear (CQS)
8 Best Practice Tariff NHFA / HES data target is 70% Specialist Input target is 60% *Both must be achieved to obtain the BPT* Highlights 17/18 Q1 & Q2 6 of the 8 Trusts met the BPT criteria All met Specialist Input KPI 6 met data target 628k of a potential increased income of 816k achieved One Trust missed out on ~ 83k One Trust missed out on ~ 106k
9 Outcomes For information Not patient level (HES aggregate) One of the biggest achievements throughout the course of the programme is the reduction in the crude mortality rate. Across KSS there are 50,000+ patients with Heart Failure. As a rough estimate if all patients with HF were admitted, 1000 less would die in hospital in 2017 as opposed to ,640 patients with HF have benefitted from the NHFA care bundle measures since they were adopted in April 2015

10 Dashboard
11 Next? Data /Outcomes Tidy the NHFA / HES data gap STP (sustainability and Transformation Plans) CEC (Clinically Effective Commissioning) Atlas of Variation Right Care GIRFT (Getting it right first time)
12 But
13 PROMS results symptoms in the last 2 weeks Q1b) Difficulty walking 1 block on level ground responses: Q8b) Difficulty working or doing household chores responses: Severe 16% None 19% Much 32% None 27% Much 23% Slight 21% Moderate 20% Some 21% Q9) difficulty during daily physical activities? responses: Moderate 21% Lots / Cant 28% None 13% A bit 24% Some 35%
14 Tube Map
15 Thanks to you to Jen to Fats & Daniel to Justin
16 Refreshment break 11:30 12:00
17 Community heart failure dashboard update June 2017 December 2017 Dr Richard Blakey Atrial Fibrillation and Community Heart Failure Lead, Kent, Sussex & Surrey Academic Health Science Network
18 EQ / AHSN Timeline January 2010 snowy meeting The Hawth Crawley March 2010 appointed community HF lead April 2010 HF EQ into community June 2010 WSPCT LES?implemented Aug 2010 NICE CG108 Oct 2010 NTproBNP Jan 2011 Sir John Oldham Neighbourhood Care Teams Jan 2011 Changes to HF structure - Kent 4/ /50 community/acute HF nurse E.Sx 8/2011? BHF IV diuretic nurse Apr 2013 Change QOF coding from LVD to LVSD 11/2016 Sussex Community take over North of East Sussex 2017 Standardised EF cut off Surrey 2017 ESBT Cardiology pathway re-design
19
20 Community HF nurses Band 4 to 7 Area Surrey Kent East Sussex West Sussex? Brighton? 0 2
21 HF Nurses / GP HF registers (proven LVSD) EQ Baseline data Mean dose/max HF dose 2011 Heart Failure Nurses N = 350 GP registers n = 498* ACE/ARB 57.6% 48.7% Beta-blockers 42.4% 29.0% *12 GP surgeries

22 Summary 53% of patients seen within 2 weeks for the period April 2017 to December % on at least a 50% dose of ACE/ ARB 28% on at least a 50% dose of BB

23 ACE/ ARB Figures fairly static for April December 2017 (suggests that there isn t much improvement to be made having already come so far)
24 BB Similar story for BB as for ACE/ARB. Appears improvement has plateaued

25 The Goldilocks Dilemma Community Measures dose of ACE/ARB and BB Remove the measures? Change the measures? Or are they just right?

26 Atrial Fibrillation and anti-coagulant split Population with AF has increased to 39% for period April 2017 December 2017 Also, the %age on an anti-coagulant has also improved over the same period to 89% Warfarin remains the most popular choice followed by Rivaroxaban then Apixaban

27 AliveCor and Heart Failure AHSN has received 560 AliveCor devices to distribute across Primary, Community and Secondary care for AF identification Distribution to be prioritised to those users most likely to encounter un-diagnosed AF with high CHA2DS2-VASc score Users to report back newly identified AF Quick view of QRSD Algorithm being developed for QTc
28 East Sussex AliveCor Results to date 182 ECGs sent 126 new cases of AF reported 33 from Hastings practice 1; 16 new AF 26 from Hastings practice 2: 14 new AF If extrapolated across both CCGs would be >600 new cases detected Narrative from GPs didn t know I was supposed to tell you founds loads of AF use it all the time Any other way of finding out success of the use of AliveCor?
29 AliveCor cost effectiveness 126 new cases of AF detected and reported to me for 12, per new AF detected Cardiology 1 st OPA 16/17 = 166 x MFF For the two practices in Hastings: 17,000 population 5 devices ( 300) 30 new AF detected = 10 per case detected!

30 Long term conditions focusing on Chronic Kidney Disease CKD is the 4 th most common LTC amongst the KSS community HF population since this programme began in June 2015

31 Sick day rules Latest advice from Dr Ed Kingdon, AKI lead for AHSN Still no consensus on sick day rules or how to implement withdrawal and restarting HF medication
32 Referral Received to Assessment within 2 weeks trend since programme was updated in June 2015 The overall trend is a decline in the %age of patients seen within 2 weeks of initial referral However, in the current reporting period (April 2017 August 2017) there is a slight increase in the trend All of the points for the monthly referral to assessment %age falls somewhere between 50-80% which suggests that even though there are month to month changes they aren t dramatic enough to not be of normal variation



33 Where does Heart Failure feature for Primary care from April 2018?
34 NICE Proposed CCG Outcome Indicator Set Diagnosis, assessment and monitoring 1. Adults presenting to hospital with new suspected acute heart failure have a single measurement of natriuretic peptide 2. Adults admitted to hospital with new suspected acute heart failure and raised natriuretic peptide levels have a transthoracic Doppler 2D echocardiogram Organisation of care 3. Adults admitted to hospital with acute heart failure have input within 24 hours of admission from a dedicated specialist heart failure team 4. Adults with acute heart failure have a follow up clinical assessment by a member of the community or hospital based specialist heart failure team within 2 weeks of hospital discharge
35 Further Proposed Areas for HF Quality Assessment 6 monthly reviews Survey of primary care and pharmacy Local HF services Primary care involvement in HF management Review of medicines optimisation post hospital discharge Raising the priority of heart failure with STP decision makers
36 Sustainability & Transformation Partnership s (STPs) (Formerly Sustainability & Transformation Plan s) The NHS and local councils have formed partnerships in 44 areas covering all of England, to improve health and care. Each area has developed proposals built around the needs of the whole population in the area, not just those of individual organisations. There are 4 STPs that cover the Kent Surrey Sussex region. 1. Frimley Health and Care STP 2. Kent and Medway STP 3. Surrey Heartlands STP 4. Sussex and East Surrey STP STPs are a way for the NHS to develop its own, locally appropriate proposals to improve health and care for patients
37 CCG PREVALENCE NHS EASTBOURNE, HAILSHAM AND SEAFORD CCG 1.13 NHS HASTINGS AND ROTHER CCG 1.05 NHS COASTAL WEST SUSSEX CCG 0.88 NHS SWALE CCG 0.86 NHS THANET CCG 0.86 NHS MEDWAY CCG 0.75 NHS HIGH WEALD LEWES HAVENS CCG 0.73 NHS HORSHAM AND MID SUSSEX CCG 0.72 NHS SOUTH KENT COAST CCG 0.70 NHS CANTERBURY AND COASTAL CCG 0.66 NHS WEST KENT CCG 0.65 NHS EAST SURREY CCG 0.61 NHS ASHFORD CCG 0.60 NHS CRAWLEY CCG 0.58 NHS DARTFORD, GRAVESHAM AND SWANLEY CCG 0.58 NHS GUILDFORD AND WAVERLEY CCG 0.55 NHS NORTH WEST SURREY CCG 0.53 NHS BRIGHTON AND HOVE CCG 0.53 NHS SURREY DOWNS CCG 0.52 NHS SURREY HEATH CCG 0.51
38 CCG EXCEPTION NHS CRAWLEY CCG 5.88 NHS HORSHAM AND MID SUSSEX CCG 7.42 NHS CANTERBURY AND COASTAL CCG 7.49 NHS ASHFORD CCG 7.69 NHS GUILDFORD AND WAVERLEY CCG 7.97 NHS SURREY HEATH CCG 8.06 NHS EAST SURREY CCG 8.16 NHS NORTH WEST SURREY CCG 8.38 NHS BRIGHTON AND HOVE CCG 8.49 NHS HIGH WEALD LEWES HAVENS CCG 8.55 NHS EASTBOURNE, HAILSHAM AND SEAFORD CCG 8.93 NHS DARTFORD, GRAVESHAM AND SWANLEY CCG 9.15 NHS MEDWAY CCG 9.32 NHS SOUTH KENT COAST CCG 9.40 NHS SWALE CCG 9.50 NHS WEST KENT CCG NHS HASTINGS AND ROTHER CCG NHS THANET CCG NHS COASTAL WEST SUSSEX CCG NHS SURREY DOWNS CCG 11.44
39 CCG %LVSD ACE/BB NHS DARTFORD, GRAVESHAM AND SWANLEY CCG NHS NORTH WEST SURREY CCG NHS MEDWAY CCG NHS SWALE CCG NHS HASTINGS AND ROTHER CCG NHS CRAWLEY CCG NHS SURREY HEATH CCG NHS WEST KENT CCG NHS EAST SURREY CCG NHS SOUTH KENT COAST CCG NHS HORSHAM AND MID SUSSEX CCG NHS THANET CCG NHS CANTERBURY AND COASTAL CCG NHS GUILDFORD AND WAVERLEY CCG NHS ASHFORD CCG NHS BRIGHTON AND HOVE CCG NHS EASTBOURNE, HAILSHAM AND SEAFORD CCG NHS COASTAL WEST SUSSEX CCG NHS HIGH WEALD LEWES HAVENS CCG NHS SURREY DOWNS CCG 71.18
40 Kent, Sussex & Surrey HF and LVSD prevalence 2009/10 v 2016/17 HF 09/10 LVD 09/10 HF 16/17 LVSD 16/17 Register 29,677 14,461 43,589 10,882 Percentage (+40%) 0.23(-28%) % LVSD receiving ACE +BB Number treated for LVSD ACE + BB 42.1% 65.4% 6,093 7,120
41 Numbers LVSD treated ACE/BB PCT v CCG 2009/10 v 2016 v / /17 BRIGHTON AND HOVE PCT / CCG (-23.2%) ESDW / EHSCCG + HWLHCCG = 712 (+31%) HASTINGS AND ROTHER PCT / CCG (-19%) SURREY PCT / ES+SD+SH+NWS+G&W WEST SUSSEX PCT / CWS + C + H&MS = 1003 (-4.6%) (+6.6%) KENT (+29.1%) QOF CODING CHANGE 2013/14

42 Even the best of us need updating and refreshing with so much to know.


43 Red Flags 56 year old with suspected heart failure Little English Struggling with SOB Murmur - likely aortic stenosis Surgery been discussed in Bulgaria NTproBNP 8,334 ng/l BP 100/88 Ramipril started
 SOB and leg swelling Ramipril 10mg / Bisoprolol 10mg / Diltiazem 180mg XL OD NTproBNP 6,532ng/L Weight Pale.")
44 95 yr old Longstanding AF CKD3b with proteinuria? (but no ACR since at least 2010) SOB and leg swelling Ramipril 10mg / Bisoprolol 10mg / Diltiazem 180mg XL OD NTproBNP 6,532ng/L Weight Pale. 60Kg BP 100/60 heart rate 70 AF, few bilat basal creps Creatinine Clearance 19ml/min. No Hb since Plan: no echo, wean off ramipril 24 hr ECG

45
46 KSS AHSN ICHOM Heart Failure PROMS Pilot Frances Scott & Ishtar Al-Shammari Heart Failure Collaborative 14 March 2018

47 Ted 80 years old HF for 15 years Retired Allotment Reading Cooking
48 What is PROMS Patient Reported Outcome Measures? Used in clinical care (e.g. assessing health status and needs of patients and quality of life Format used usually by questionnaires
49 Why use PROMS with Heart Failure Patients? Help to monitor o patient progress o help professionals and patients discuss health issues with each other o and/or help to improve the quality of health services KSS AHSN worked with ICHOM using a standard set of PROMS questions adapted to use in KSS local setting





50 Outcome measurement drives value improvements for all stakeholders Key stakeholders Transparent, highquality outcomes data Patients will choose their provider based on expected outcomes and their share of the cost Clinicians will improve quality of care by comparing performance and learning from each other Hospitals will differentiate into areas where they deliver superior outcomes at competitive prices Value Payers will negotiate contracts based on results, not volume, and encourage innovation to achieve those results Life science will market their products on value, showing improved outcomes relative to costs
51 ICHOM was formed to catalyze the transformation to Value Based Health Care ICHOM History Our mission Founded in 2012 by thought leaders with the desire to use outcome measurement to unlock the potential of value-based health care. ICHOM is a nonprofit Independent 501(c)3 organization Idealistic and ambitious goals Global focus Engages diverse stakeholders Our mission Unlock the potential of value-based health care by defining global Standard Sets of outcome measures that matter most to patients across a wide range of medical conditions, and driving the adoption and reporting of these measures worldwide Value = Patient health outcomes achieved Cost of delivering those outcomes
52 ICHOM plays several roles along the journey that will enable value-based health care: our strategic agenda ICHOM defines internationally recognized Standard Sets of outcomes and related case-mix factors ICHOM will provide riskadjusted international benchmarks on outcomes by medical condition ICHOM will become a methodological partner with media to publish ratings based on ICHOM outcomes Define Standards Measure outcomes Benchmark on outcomes 1 Collaborate to improve value 1 Establish outcomes transparency Develop value-based payment models VBHC ICHOM facilitates adoption and implementation by sharing knowledge and supporting proof-of-concept ICHOM will enable cooperation to improve value by establishing value collaboratives ICHOM will engage payers and governments to realign financial incentives and promote transparency Core mission of ICHOM Enabler role Current focus 1. We are exploring the inclusion of resources data in benchmarks but the methodology is to be determined

53 ICHOM organizes Working Groups to define Standard Sets of outcomes we recommend all care providers track ICHOM facilitates a process with international physician and registry leaders, patient representatives and methodologists to develop a global Standard Set of outcomes that really matter to patients











54 We have completed 23 Standard Sets, covering >50% of the disease burden as defined by WHO Our current 23 Standard Sets commitments 1. Inflammatory arthritis 2. Oral health 3. Congenital upper limb anomalies 4. Paediatric facial palsy 5. Type II diabetes 6. Atrial fibrillation 7. Overall adult health 8. Diabetes In discussions to launch 1. Mental health package 2. Overall child health 3. Overall cancer 4. Pediatric epilepsy 5. Multiple sclerosis 6. COPD 7. Morbid obesity Numbers not representing prioritization/ likelihood



55 ICHOM is helping providers across the globe measure outcomes Direct capacity-building support Lighter-touch networked support Ad-hoc advisory support and workshops Coronary Artery Disease Implementation Community Partner with innovative providers to pilot outcomes measurement in their institutions and develop local capacity to scale Provide guidance and action items to global institutions implementing Standard Sets with a goal of benchmarking Kick-off implementation in more experienced organizations by introducing Standard Set content Currently supporting 43 organizations
56 ICHOM and KSS AHSN have completed the pilot phase of the project Key Tasks Preparation Diagnostic Roll Out Measurement Establish project team and governance structure Establish local clinician buy-in Assess and define scope of project Assess IT and informatics infrastructure within pilot sites Perform a gap analysis of what data is collected versus what isn t Determine and process map pilot implementation sites Secure additional IT/Information platforms to address data gaps Secure PROM licenses for Standard Set as required Deploy data capture solution Pilot data collection with part of dataset Assess Pilot period Refine Workflow and IT systems using PDSA cycles Scale up to implement full dataset Troubleshoot full dataset issues & quality assure data Begin to measure and analyze full dataset Change Management Copyright 2016 by the International Consortium for Health Outcomes Measurement. All rights reserved. 56
57 Outcomes measurement will lead to multiple benefits for private and public hospitals Identify and disseminate best practices Direct measurements and comparisons will enable identification and dissemination of best practices Benchmark sites/teams and drive continuous improvement Demonstrate superior outcomes Anchor reputation in facts Attract new patients in areas of excellence, also internationally Potential to charge a higher price for improved quality of care (depending on country/regulation) Enhance Management capabilities Take informed decisions for staff promotion and/or investments (based on outcomes achieved) Adapt delivery models to achieve similar outcomes at lower cost Be prepared for more transparency/new models Get prepared for value based payment models Quantify your performance and be ahead of the trend for more public transparency Demonstrate superior performance to obtain maximum reimbursement from value based payment models Starting outcomes measurement now will allow you to shape the global trend rather than merely respond

58 After a successful pilot, Aneurin Bevan University Health Board is scaling Standard Set implementation across the organization Background Aneurin Bevan University Health Board partners with ICHOM in 2015 to support translation of VBHC theory into practice Impact on Outcome 9 months into implementation, capture of demographic data reached 100% and Parkinson's PROMs reached 88% ICHOM Parkinson Standard Set Percent completion in ABUHB program Initial pilot: to implement one condition Parkinson s disease in one clinic Supported by an empowered and cross functional Steering Committee Board, IT, finance, clinical representation Dedicated project management team Fit-for-purpose IT solution Workflow revisions: patients complete PROMs in waiting area clinicians review data prior to consultation Post pilot, VBHC Team formed to provide central coordination of roll out of VBHC implementation across the organization Scaling implementation to four more condition lung cancer, heart failure, lower back pain, cataracts Organization-wide VBHC courses used to build awareness Falls Healthrelated quality of life Hospital admissions Ability to work Cognitive and psychiatric functioning Non-motor functioning Motor functioning Basic demographic information Patient-reported baseline information treatment variable information Clinicial-reported outcomes Patient-reported outcomes, non-motor Patient-reported outcomes, motor Patient-reported outcomes, PDQ Arora J, Lewis S, Cahill A. Implementing ICHOM s Standard Sets of Outcomes: Parkinson s Disease at Aneurin Bevan University Health Board in South Wales, UK. London, UK: International Consortium for Health Outcomes Measurement (ICHOM), March 2017 (available at
59 Sweden's best practice adoption in AMI has helped them achieve better outcomes and use of resources than UK Background Risk-adjusted data from national Swedish and UK quality registries compared Sweden Impact on Outcome 30-day mortality Standardized mortality rate 2 37% higher 30-day mortality in the UK compared to Sweden 7.6% % 1.37 Primary PCI 3 59% 22% UK β blocker at discharge 4 89% 78% Compared care and outcomes for all UK and Swedish AMI patients during Better uptake of evidence-based treatments in Sweden than the UK were shown to lead to lower AMI mortality rates Impact on Resources ALOS, AMI >40% shorter hospitalization time in Sweden 20-44% Sweden UK Year Source: Chung et al, Acute myocardial infarction: a comparison of short-term survival in national outcome registries in Sweden and the UK, The Lancet, Jan 23, OECD data
 Highlights 1.")

60 Brazil ANAHP Heart Failure Community Implementation ANAHP: National Association of Private Hospitals in Brazil 8 sites participate in the program (Sao Paulo, Porto Alegre, Belo Horizonte, Rio de Janeiro) Highlights 1. On site Project Manager coordinates the implementation between the 8 hospitals 2. Once the Implementation Community program is finished, each hospital will have the knowledge to move on to implementing the next Standard Sets 3. Implementation community support internal benchmarking between the participating sites, in the next phase sites plan to benchmark outcomes internationally
61 KSS Pilot.
 East Sussex Healthcare Trust West (Eastbourne) East Sussex Healthcare Trust, East (St")
62 Pilot Scope Initial pilot was for 9 months (Feb to Oct 2017) 4 Community HF Teams Kent Community Healthcare Trust, East (Whitstable) Kent Community Healthcare Trust, West (Sevenoaks) East Sussex Healthcare Trust West (Eastbourne) East Sussex Healthcare Trust, East (St Leonards)
63 Pilot - Aim To gather questionnaire data for a minimum of 50 patients per team (200 in total) To review this data comparing to Enhancing Quality outcomes data where the data was related. Shortness of Breath Odema/Swelling Questionnaire aimed to assess quality of care delivered to (All Cause) patients from the patient s perspective.
64 Results Total number of questionnaires given out is 500 Total number of questionnaires returned is 281 Estimated return rate 55% (skewed) Most robust sample - Kent Community Trust West - Return rate for 37%
65 Clinical Outcomes PROMS results What is it like living with Heart Failure? A serious, chronic condition that tends to gradually get worse over time. Eventually it can shorten patients life. Weight gain Shortness of Breath Coughing & Wheezing Swollen ankles, legs or abdomen Tiredness Need to urinate at night Dizziness Feeling frightened Depression Anxiety Rapid heart rate Loss of appetite
66 What did the patients report feeling 2 weeks post discharge and following first visit from HF Nurse? Physical All providers - Q1b) Walking 1 block on level ground responses: 0 = Extremely limited, 42, 15% 5 = Limited for other reasons or did not do the activity, 18, 6% 1 = Quite a bit limited, 47, 17% 4 = Not at all limited, 58, 21% 2 = Moderately limited, 55, 20% 3 = Slightly limited, 57, 21%
67 What did the patients say they felt having Heart Failure? Social All providers - Q6) Over the past 2 weeks, how much has your heart failure limited your enjoyment of life? responses: 0 = It has extremely limited my enjoyment of life, 40, 14% 4 = It has not limited my enjoyment of life at all, 65, 24% 1 = It has limited my enjoyment of life quite a bit, 62, 23% 3 = It has slightly limited my enjoyment of life, 57, 21% 2 = It has moderately limited my enjoyment of life, 51, 18%
68 What did the patients say they felt having Heart Failure? Social All providers - Q8a) Hobbies, recreational, activities responses: 0 = Severely limited, 53, 20% 5 = Does not apply or did not do for other reasons, 31, 11% 4 = Did not limit at all, 28, 10% 1 = Limited quite a bit, 59, 22% 3 = Slightly limited, 50, 18% 2 = Moderately limited, 51, 19%
69 What did the patients say they felt having Heart Failure? Psychological All providers - Q7) If you had to spend the rest of your life with your heart failure the way it is right now, how would you feel about this? responses: 0 = Not at all satisfied, 66, 24% 4 = Completely satisfied, 25, 9% 3 = Mostly satisfied, 62, 23% 1 = Mostly dissatisfied, 59, 21% 2 = Somewhat satisfied, 63, 23%
70 What did the patients say they felt having Heart Failure? Psychological 11a) Little interest or pleasure in doing things? responses: 3 = Nearly every day, 39, 14% 2 = More than half the days, 19, 7% 0 = Not at all, 130, 48% 1 = Several days, 84, 31%
71 What did the patients say they felt having Heart Failure? Psychological All providers - Q6) Over the past 2 weeks, how much has your heart failure limited your enjoyment of life? responses: 0 = It has extremely limited my enjoyment of life, 40, 14% 4 = It has not limited my enjoyment of life at all, 65, 24% 1 = It has limited my enjoyment of life quite a bit, 62, 23% 3 = It has slightly limited my enjoyment of life, 57, 21% 2 = It has moderately limited my enjoyment of life, 51, 18%
72 Do these results surprise you?
73 How does Heart Failure burden of symptoms compare to other long term conditions? Study comparing burden of symptoms of HF patients with advanced lung or pancreatic cancer Both conditions had similar scores but patients with more severe heart failure had a greater number of physical symptoms, higher depression scores and lower spiritual well-being than patients with advanced cancer. Bekelman, Rumsfeld, Havranek, Yamashita, Hutt, Gottlieb, Sydney and Kutner, Symptom Burden, Depression and Spiritual Well-Being: A Comparison of Heart Failure and Advanced Cancer patients - Journal of General Medicine (2009)
74 Challenges/Lessons Learnt Need clarity and understanding of all data items and processes Acknowledge HF teams are resourced differently and different roles complete multiple tasks which impact on the process of data collection Teams were at times overstretched to take on the additional requirement of the pilot having an impact on the data collection but did manage to upload data at a later date
75 Challenges/Lessons Learnt Questionnaires posted to patients deemed to be more successful Single point of co-ordination to record questionnaire sent and returned (Kent Community West team) Where possible integrate process with existing processes (ie. Posting care plan include PROMS questionnaire)
76 Next Steps Recommend to teams to utilise PROMS questionnaires as part of their quality audit Link into Quality programmes at Trusts Pilot teams to make recommendations to see if there are any opportunities to change and improve care Review pathway Review care plan to reflect Include PROMS results in MDT review Do patients need more psychological support? Work with ICHOM to benchmark results with other national and international pilots
77 Questions? Frances Scott Ishtar Al-Shammari kssahsn.net ichom.org
78 Lunch break 12:30 13:30
79 An introduction to the Health Service Engagement team

80 Ensure that everyone in the UK with CVD has access to high-quality, integrated health and social care services 81
81 Health Services Engagement Team Make the case for change at a health system level to improve evidence based CVD care eg working with RightCare, AHSNs, Public Health England Use BHF best practice portfolio and evidence based practice to challenge variation in care and identify sustainable solutions that respond to the challenges of the health system in quality, efficiency and effectiveness Act as a catalyst for change by convening senior decision makers and practitioners to identify challenges, opportunities and solutions to improve CVD care through communities of practice Educate and empower - signpost to training and resources for health professionals to optimise delivery of the best care to people living with or at risk of developing CVD (BHF Alliance)
82 Local success stories Learning from teams who have used the collaborative to make a change



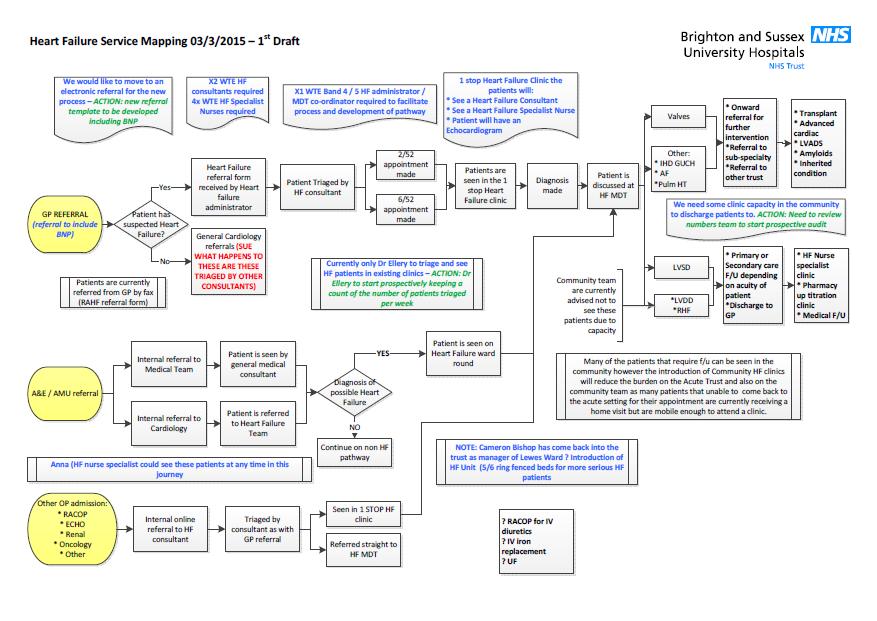
83 Celebrating Success: Using data to make improvements Sarah Young Nurse Consultant Cardiology On behalf of the BSUH team
84 The BSUH HF team - now 2 x HF Consultants Dr Ellery Dr Coombs 3.6 WTE HF nurses Nurse Consultant Cardiology Consultant pharmacist 0.6 WTE HF MDT co-ordinator Wider MDT cardiology and non cardiology teams, cardiac physiologists echo and pacing, palliative care, clinical psychologist, arrhythmia nurse specialists, cardiac rehab 5 non-medical prescribers Local protocols for non-prescribers
85 What we do Nursing team receive on average 100 referrals/mth Inpatients Online referrals HF ward rounds (nursing review in between) Tues and Thur RSCH average pts / round Mon and Thur PRH average 4-5 pts / round HF MDT Tues and Thur RSCH average 9 pts discussed on Tues, smaller number on Thursday Thur at PRH average 7 pts discussed
86 Outpatient referrals Education re HF and self management strategies Uptitration of HF meds Admissions avoidance Access to MDT re devices, specialist support 29 nurse-led clinic slots / week Outpatients Inpatients - early follow up after discharge Diuretics and renal function As above
87 Sacubitril valsartan since Aug 2016 AKI and heart failure Short stay patients ED NT pro-bnp RAHFC Acute cardiologist Ambulatory care
88 Other aspects of the service RAHFC on both sites timely echo Ferinject and recruiting for IRONMAN Ultrafiltration Devices CRTP/D Standard ICD information including deactivation Leadless pacemakers Subcutaneous ICD s Remote monitoring clinic / congestion alerts
89 Cardiology patients referred for advanced heart failure assessment Waiting list (two with LVAD) 4 Transplanted Referred 2 Removed 1
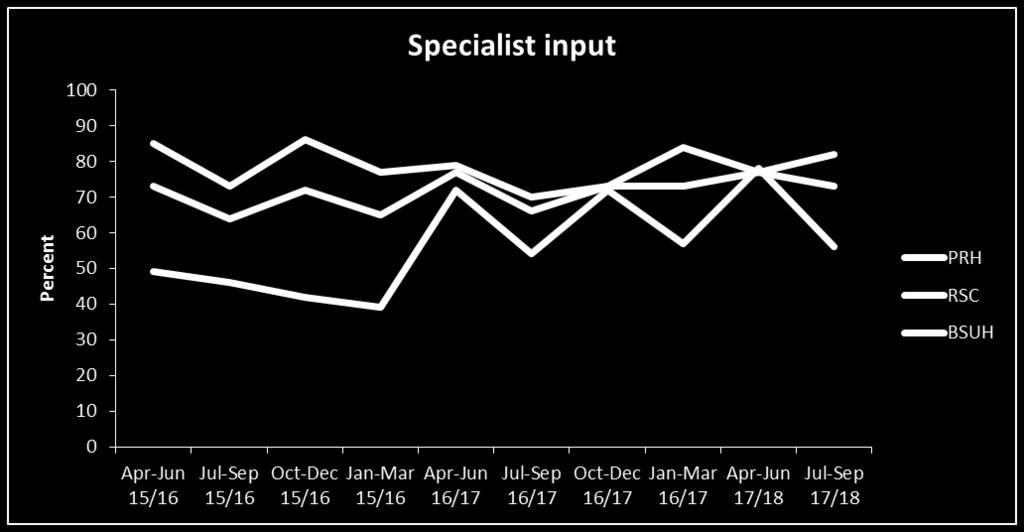
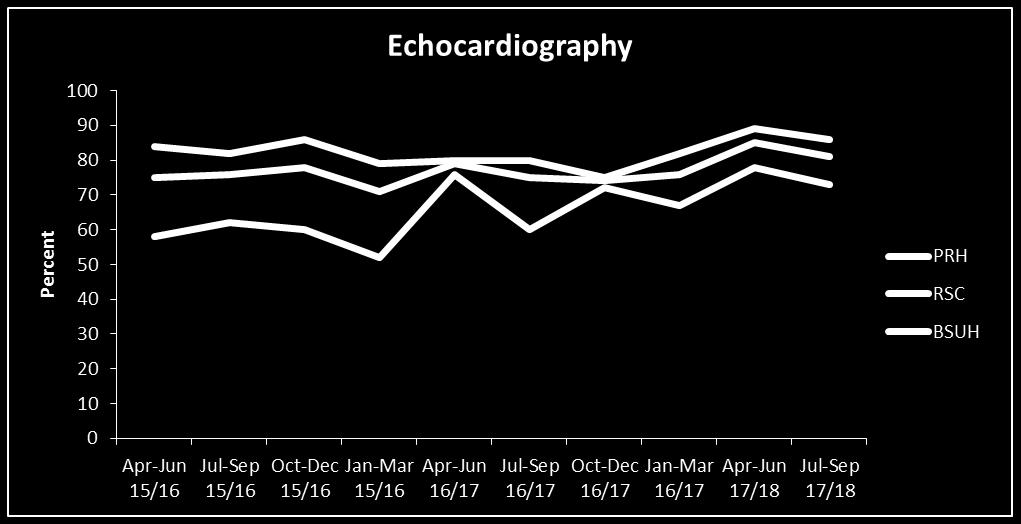
90 But not always like that. Inequity of care 15/16 Q1 EQ data RSCH PRH Specialist input 85% 49% Echocardiography 82% 58% Referral to HFNS (LVSD) 87% 50%
91 Addressing this inequity Took a long time. Started talking about this 5 years ago Tertiary centre, 2 hospitals Failed EQ targets (RSCH achieved, PRH not achieved) Trust asked questions EQR team support in the Trust for service redesign Pathway mapping March 2015 On line referral Additional manpower
92
93 Business case Cardiovascular directorate priority Business case started March 2015 Cost effective with devices, Best Practice Tariff, reduced hospital admissions Used EQ data to show inequity between RSCH and PRH sites
94 Difficulties No new money Chicken and the Egg Trust support / commissioner support Achieved Trust support (July- Sept) first secondary to commissioner support Local commissioners in Mid Sussex Education for primary care Admissions avoidance RAMU Specialist commissioners re devices NHS England
95 Business case signed off Jan 2016 Money available from April PA HF Consultant 1.0 WTE HFNS PRH 0.6 WTE MDT co-ordinator (admin) 1.0 WTE Cardiac physiologist (echo) 1.08 WTE Lab staff
96 What it means Access to Specialist care for all HF pts across the Trust Additional HF Consultant cover across both sites Additional 1 day in the lab for devices HFSN on site at PRH All HF admissions RAMU for admissions avoidance Onward referral to community HF nurses or FU in nurse-led HF clinic
97 Implementation at PRH HFNS 1.0 WTE HF admin co-ordinator 1 day / week Consultant HF ward round twice / week MDT with community HF team once / week Work with medical and nursing teams On line referral all cause HF Liaison with cardiac physiologists and prioritisation of echo s
98

99

100 PRH EQ data
101 National HF audit provisional RSCH April 16-March 17 (n=403) Echo 79% 69% ACE/ARB 93% 86% Beta Blocker 92% 83% MRA 76% 72% Specialist input 76% 65% HFNS referral (LVSD) 82% 79% PRH April 16-March 17 (n=204) Survival to discharge 357 (88%) 178 (87%)
102 More work to do 1.0 WTE - Cover for leave 0.25 WTE Band 6 HF nurse (1 yr secondment) Non LVSD patient follow up
103 Thank you to the PRH team!
104 Integrated Heart Failure Team Sarah Terry Specialist Heart Failure Nurse


105 Our population West Population approx. 184,290 and 23 GP Practices East Population approx. 183,000 and 33 GP Practices
106 The Integrated Heart Failure Team In 2004 three Community Heart Failure Specialist nurses were employed as part of the BHF project to recruit heart failure nurses across the country. The community nurses joined an existing acute heart failure specialist nurse. This formed an integrated heart failure team that crossed the secondary care and community boundary. Current team structure A mix of full/part time staff and includes: Acute Heart Failure Specialist Nurses Community Heart Failure Specialist Nurses Heart Failure And Device Specialist Nurses (West) 50/50 Acute/Community Heart Failure Specialist Nurses Heart Failure HCA s
107 Referrals and Caseload Average 108 referrals to the team each month. Referrals for all cause heart failure. Referrals can be made by: (to a generic central ) automated referral from the hospital system to the post face to face telephone. Average caseload varies between Systmone patient record system.
108 Key aspects of our roles Identify new admissions with known or potential heart failure. Ensure a confirmed diagnosis of heart failure by BNP testing and echo. All patients treated for heart failure with a confirmed diagnosis are discharged with a Transfer of Care document, follow up plan and appointment with a heart failure specialist nurse. Reducing hospital admissions and length of stay Medication titrations Education and Support End of Life care Education for staff Ongoing data collection and electronic patient record Weekly MDT and heart failure ward rounds Onward referrals e.g. Cardiac Rehabilitation, Breathlessness Clinic
109 The 6 month review project (East) Why did we make this change? As a team we discharge patients back to GP with open door access. In 2016 we identified that patients with reduced EF (<35%) that had been discharged to GP were a potential group of patients that we could review to revisit possible further medication titration and new indications for CRT. How did we do it? All patients with an EF<35% are added to a calendar for potential review in 6 months. Each month the patients names are reviewed to see if they have already or have pending a review with cardiology, GPwSI or other appropriate professional. If not the patient is invited to attend for review. If the patient has been seen by a relevant person they are added to the calendar in a further 6 months time, this is also the same for those who don t respond. The patients whom respond are asked to have an ECG (as appropriate) and a blood test. They are reviewed in clinic in the normal way.
110 Outcome Patients on the 6 monthly Calander RIP Invite letter sent Responded Required review Ongoing after 1st review Did not result in excessive demand on service Potential to reduce hospital admissions Patients have been identified that are now suitable for CRT We have been able to adjust medications and further titrate as per NICE guidelines
111 50/50 Role Why did we make this change? Improving patient support in the immediate post discharge period To reduce hospital readmissions and length of stay How did we do it? The nurse meets the patient in hospital and follows them up post discharge, up to 30 days. The patient is reviewed at home usually within a week of discharge and if not within 2 weeks. At 30 days the patient is either discharged to the GP (being added to the calendar for 6 monthly follow ups as indicated) or transferred to one of the community heart failure specialist nurse for further input.
112 50/50 Outcomes Patients are able to begin to build a relationship with the heart failure nurse prior to discharge Post discharge concerns/problems particularly those that are medication based are identified early The 30 day period allows for the nurses caseload to be lower and more fluid, enabling the flow of patients from hospital to be seen in a timely manner.


113 IV Diuresis in the community. Increased day case IV diuretics, as appropriate. Continued review of patients with a reduced EF (<35%) every 6 months. Support groups. Equitable access to support for heart failure patients who have CRT therapy.


114 For more information: Please contact Sarah Terry, Community Heart Specialist Nurse on or
115 Local plans for next steps Reflect on your team s next steps



116
117 EQ data Single site - Run chart. Median line is middle of data points Multiple sites Line graph. Line for each site and trust total. No median Tuesday, March 20,
118 Roundtable discussion Sit with your team/trust or bounce ideas with the person next to you. 45 minutes (including tea/coffee break) to discuss and plan for your next actions. Think about: What problems do you want to solve? What ideas do you have for doing this? Who else do you need to involve to make this happen? Create an action plan for who will do what and by when in order to get your change into practice Think about what you can do longer term, but also some small actions you can do next week or soon to help you get there.
119 Discussion Team name: What problems do we want to solve? What ideas do we have for doing this? Who else do we need to involve?
120 Action plan Team name: Action to be taken By when (in the next week, month, 3 months) By who


121 Feedback A brief 2 minute summary plan from each group. Remember to grab a tea/coffee.

122 The future working with the BHF
123 Award ceremony Celebrating the collaborative s success stories!
124 Summary and next steps
125 Thank you Helen O Kelly Health Service Engagement Lead (South East England) okellyh@bhf.org.uk Sian Martin Clinical Development Coordinator martins@bhf.org.uk
South East Coast Complex Cardiology Services
 South East Coast Complex Cardiology Services Dr Adam Jacques Clinical Director SEC CVD SCN June 4 th 2014 SEC Cardiovascular SCN Vision Cardiovascular Centres of Excellence Patients being diagnosed as
South East Coast Complex Cardiology Services Dr Adam Jacques Clinical Director SEC CVD SCN June 4 th 2014 SEC Cardiovascular SCN Vision Cardiovascular Centres of Excellence Patients being diagnosed as
Sussex Integrated Urgent Care Transformation Soft Market Testing Wednesday 26 th July 2017
 Sussex Integrated Urgent Care Transformation Soft Market Testing Wednesday 26 th July 2017 Welcome Agenda Welcome Purpose and programme for the day Sussex NHS 111Transformation The Context, Scope and Vision;
Sussex Integrated Urgent Care Transformation Soft Market Testing Wednesday 26 th July 2017 Welcome Agenda Welcome Purpose and programme for the day Sussex NHS 111Transformation The Context, Scope and Vision;
Models of community heart failure care pathways. Dr Jim Moore GP & GPSI Cardiology Cheltenham,GLOS
 Models of community heart failure care pathways Dr Jim Moore GP & GPSI Cardiology Cheltenham,GLOS Declaration of Conflict of Interests Dr Jim Moore GP and GPwSI in Cardiology, Cheltenham NICE Guideline
Models of community heart failure care pathways Dr Jim Moore GP & GPSI Cardiology Cheltenham,GLOS Declaration of Conflict of Interests Dr Jim Moore GP and GPwSI in Cardiology, Cheltenham NICE Guideline
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Local Needs Assessment Heart Failure and Cardiac Rehabilitation
 Local Needs Assessment Heart Failure and Cardiac Rehabilitation The Human Burden of Heart Failure Heart failure is a life-limiting condition that people can live with for a number of years and require
Local Needs Assessment Heart Failure and Cardiac Rehabilitation The Human Burden of Heart Failure Heart failure is a life-limiting condition that people can live with for a number of years and require
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Commissioning for Value insight pack
 Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure.
 Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure. Authors: Gareth Holyfield (Principal Pharmacist, Public Health Wales) Don Wilkes (Community Pharmacist,
Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure. Authors: Gareth Holyfield (Principal Pharmacist, Public Health Wales) Don Wilkes (Community Pharmacist,
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Tele Stroke ( Telemedicine in Practice)
") Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
National Clinical Audit & Patient Outcome Programme: An update
 National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
Urology Clinical Forum. 11 th March 2015
 Urology Clinical Forum 11 th March 2015 Welcome and Introductions Justin Vale, Chair of the LCA Urology Pathway Group Progress of the Urology Pathway Group Justin Vale, Chair of the LCA Urology Pathway
Urology Clinical Forum 11 th March 2015 Welcome and Introductions Justin Vale, Chair of the LCA Urology Pathway Group Progress of the Urology Pathway Group Justin Vale, Chair of the LCA Urology Pathway
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Outcomes benchmarking support packs: CCG level
 Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
In North Wales, four years ago, we had not seen the sudden increase in CKD referrals seen elsewhere in
 The development of the CKD nurse led service across North Wales BCUHB 2013 Background In North Wales, four years ago, we had not seen the sudden increase in CKD referrals seen elsewhere in the country.
The development of the CKD nurse led service across North Wales BCUHB 2013 Background In North Wales, four years ago, we had not seen the sudden increase in CKD referrals seen elsewhere in the country.
Improving Quality of Life of Long-Term Patient - From the Community Perspective
 Improving Quality of Life of Long-Term Patient - From the Community Perspective Dr Caz Sayer, Camden CCG Chair Working with the people of Camden to achieve the best health for all Context The Health and
Improving Quality of Life of Long-Term Patient - From the Community Perspective Dr Caz Sayer, Camden CCG Chair Working with the people of Camden to achieve the best health for all Context The Health and
PRIMARY CARE COMMISSIONING COMMITTEE
 PRIMARY CARE COMMISSIONING COMMITTEE 1. Date of Meeting: 2. Title of Report: Western Avenue Medical Centre Personal Medical Services (PMS) Reinvestment Report 3. Key Messages: The Personal Medical Services
PRIMARY CARE COMMISSIONING COMMITTEE 1. Date of Meeting: 2. Title of Report: Western Avenue Medical Centre Personal Medical Services (PMS) Reinvestment Report 3. Key Messages: The Personal Medical Services
Integrated respiratory action network for patients with COPD
 Integrated respiratory action network for patients with COPD In this Future Hospital Programme case study Dr Helen Ward describes how a team from The Royal Wolverhampton NHS Trust established a respiratory
Integrated respiratory action network for patients with COPD In this Future Hospital Programme case study Dr Helen Ward describes how a team from The Royal Wolverhampton NHS Trust established a respiratory
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Nurse Prescribing in Heart Failure (Integrated Service)
") Nurse Prescribing in Heart Failure (Integrated Service) Liz Killeen Community Heart Failure CNS & RNP. Galway PCCC. Introduction. Heart Failure affects more than 120,000 Irish people and is one of the
Nurse Prescribing in Heart Failure (Integrated Service) Liz Killeen Community Heart Failure CNS & RNP. Galway PCCC. Introduction. Heart Failure affects more than 120,000 Irish people and is one of the
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Preventing Heart Attacks and Strokes The Size of the Prize
 Preventing Heart Attacks and Strokes The Size of the Prize Dr Matt Kearney General Practitioner and National Clinical Director for CVD Prevention NHS England and Public Health England The NHS needs a radical
Preventing Heart Attacks and Strokes The Size of the Prize Dr Matt Kearney General Practitioner and National Clinical Director for CVD Prevention NHS England and Public Health England The NHS needs a radical
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
NHS Innovation Accelerator. Implementation Toolkit. mycopd
 NHS Innovation Accelerator Implementation Toolkit mycopd Introduction NHS England s Innovation and Technology Tariff (ITT) went live on 1 April 2017. This new Tariff was introduced to incentivise the adoption
NHS Innovation Accelerator Implementation Toolkit mycopd Introduction NHS England s Innovation and Technology Tariff (ITT) went live on 1 April 2017. This new Tariff was introduced to incentivise the adoption
Working in partnership to improve the identification and treatment of sepsis
 Identifying and Tackling Sepsis in Healthcare Tuesday 25 th April 2017 Working in partnership to improve the identification and treatment of sepsis Tracy Broom Associate Director Wessex Patient Safety
Identifying and Tackling Sepsis in Healthcare Tuesday 25 th April 2017 Working in partnership to improve the identification and treatment of sepsis Tracy Broom Associate Director Wessex Patient Safety
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Chrissie Bryant, Business Director Wales, GlaxoSmithKline - Chair of session. Date of Preparation 30/11/2012 UK/RESP/0115/12
 Bobby Bolt Divisional Director for Primary Care and Networks Dr Patrick Flood-Page - Project Lead Respiratory Consultant Dr Jackie Abbey, Project Lead GP Clinician Chrissie Bryant, Business Director Wales,
Bobby Bolt Divisional Director for Primary Care and Networks Dr Patrick Flood-Page - Project Lead Respiratory Consultant Dr Jackie Abbey, Project Lead GP Clinician Chrissie Bryant, Business Director Wales,
Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex
 in Wessex") Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex The case for change AKI is recognised as a major public health and patient safety concern nationally and
Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex The case for change AKI is recognised as a major public health and patient safety concern nationally and
NHS North Yorkshire and York
 CASE STUDY NHS North Yorkshire and York Managing long term conditions through redesigning the care pathways and integrating telehealth North Yorkshire and York The challenge Strategic plans NHS North Yorkshire
CASE STUDY NHS North Yorkshire and York Managing long term conditions through redesigning the care pathways and integrating telehealth North Yorkshire and York The challenge Strategic plans NHS North Yorkshire
Workflow. Optimisation. hereweare.org.uk. hereweare.org.uk
 Workflow Optimisation Dr. Paul Deffley & Jaivir Pall Clinical Lead & Commercial Lead About Here Not-for-profit social enterprise Membership organisation (our members are local GPs, Practice Managers, Practice
Workflow Optimisation Dr. Paul Deffley & Jaivir Pall Clinical Lead & Commercial Lead About Here Not-for-profit social enterprise Membership organisation (our members are local GPs, Practice Managers, Practice
Using Evidence to Support the Business Case the route to adoption
 Using Evidence to Support the Business Case the route to adoption Christopher P Price Department of Primary Care Health Sciences University of Oxford Technology Adoption in Healthcare innovation improving
Using Evidence to Support the Business Case the route to adoption Christopher P Price Department of Primary Care Health Sciences University of Oxford Technology Adoption in Healthcare innovation improving
Home administration of intravenous diuretics to heart failure patients:
 Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Monthly and Quarterly Activity Returns Statistics Consultation
 Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Northern Ireland COPD Audit
 Northern Ireland COPD Audit A regional audit of chronic obstructive pulmonary disease (COPD) care September 2017 www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care Contents
Northern Ireland COPD Audit A regional audit of chronic obstructive pulmonary disease (COPD) care September 2017 www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care Contents
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Value Based Healthcare
 Value Based Healthcare Dr Paul Buss Dr Sally Lewis Sir Muir Gray Speakers: Executive Medical Director/ Deputy CEO, Aneurin Bevan UHB Deputy Medical Director Aneurin Bevan UHB Chair, Health and Social Care
Value Based Healthcare Dr Paul Buss Dr Sally Lewis Sir Muir Gray Speakers: Executive Medical Director/ Deputy CEO, Aneurin Bevan UHB Deputy Medical Director Aneurin Bevan UHB Chair, Health and Social Care
Powys Teaching Health Board. Respiratory Delivery Plan
 Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Lorenzo for clinical outcomes transformation? Ben Bridgewater
 Lorenzo for clinical outcomes transformation? Ben Bridgewater Global Trends - Outcomes and Transformation: The Landscape The problems The obstacles The solutions Ageing population and consumerism Increasing
Lorenzo for clinical outcomes transformation? Ben Bridgewater Global Trends - Outcomes and Transformation: The Landscape The problems The obstacles The solutions Ageing population and consumerism Increasing
Service Transformation Report. Resource and Performance
 SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
Ambulatory emergency care Reimbursement under the national tariff
 HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
NON-EMERGENCY PATIENT TRANSPORT SERVICE
 South Central Ambulance Service NHS Foundation Trust NON-EMERGENCY PATIENT TRANSPORT SERVICE A reference guide for Healthcare Professionals - Sussex 2017 INTRODUCTION South Central Ambulance Service NHS
South Central Ambulance Service NHS Foundation Trust NON-EMERGENCY PATIENT TRANSPORT SERVICE A reference guide for Healthcare Professionals - Sussex 2017 INTRODUCTION South Central Ambulance Service NHS
NHS GRAMPIAN. Local Delivery Plan - Mental Health and Learning Disability Services
 NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
On behalf of COMMIT Team
 Dr Rashmi Sharma & Dr Achyut Guleri On behalf of COMMIT Team Quality Safety People Delivery Environment Cost Consultant Microbiologist Clinical Director- Laboratory Medicine, Blackpool Teaching Hospitals
Dr Rashmi Sharma & Dr Achyut Guleri On behalf of COMMIT Team Quality Safety People Delivery Environment Cost Consultant Microbiologist Clinical Director- Laboratory Medicine, Blackpool Teaching Hospitals
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Clinical Audit for Improvement: HQIP update
 Clinical Audit for Improvement: HQIP update Mirek Skrypak @MirekSkr Associate Director for Quality and Development National Clinical Audit and Patient Outcomes Programme Healthcare Quality Improvement
Clinical Audit for Improvement: HQIP update Mirek Skrypak @MirekSkr Associate Director for Quality and Development National Clinical Audit and Patient Outcomes Programme Healthcare Quality Improvement
Yorkshire & the Humber Acute Kidney Injury Patient Care Initiative (AKIPCI)
") Yorkshire & the Humber Acute Kidney Injury Patient Care Initiative (AKIPCI) Friday 17 th October 2014 1330-1700 Hatfeild Hall, Normanton Golf Club, Aberford Road, Wakefield, WF3 4JP Notes 1. Welcome, Introductions,
Yorkshire & the Humber Acute Kidney Injury Patient Care Initiative (AKIPCI) Friday 17 th October 2014 1330-1700 Hatfeild Hall, Normanton Golf Club, Aberford Road, Wakefield, WF3 4JP Notes 1. Welcome, Introductions,
Arrhythmia Care Coordinators An Update
 Arrhythmia Care Coordinators An Update Jayne Mudd Senior Arrhythmia Care Coordinator James Cook University Hospital Middlesbrough The Arrhythmia Care Coordinator Role first proposed within working groups
Arrhythmia Care Coordinators An Update Jayne Mudd Senior Arrhythmia Care Coordinator James Cook University Hospital Middlesbrough The Arrhythmia Care Coordinator Role first proposed within working groups
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance
 Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Delivering the QIPP programme: making existing services improve patient outcomes
 Delivering the QIPP programme: making existing services improve patient outcomes Produced by Glyn Davies MP, Chair All-Party Parliamentary Group on AF in association with the Atrial Fibrillation Association
Delivering the QIPP programme: making existing services improve patient outcomes Produced by Glyn Davies MP, Chair All-Party Parliamentary Group on AF in association with the Atrial Fibrillation Association
INNOVATION, HEALTH AND WEALTH A SCORECARD
 INNOVATION, HEALTH AND WEALTH A SCORECARD Page 2 CONTENTS 4 EXECUTIVE SUMMARY 6 INTRODUCTION 7 3 MILLION LIVES 9 INTRA-OPERATIVE FLUID MANAGEMENT/OESOPHAGEAL DOPPLER MONITORING 11 CHILD IN A CHAIR IN A
INNOVATION, HEALTH AND WEALTH A SCORECARD Page 2 CONTENTS 4 EXECUTIVE SUMMARY 6 INTRODUCTION 7 3 MILLION LIVES 9 INTRA-OPERATIVE FLUID MANAGEMENT/OESOPHAGEAL DOPPLER MONITORING 11 CHILD IN A CHAIR IN A
The prevention and self care workshop 16 th September Dr. Jenny Harries Regional Director PHE South Regional Office
 The prevention and self care workshop 16 th September 2016 Dr. Jenny Harries Regional Director PHE South Regional Office Jenny.harries@phe.gov.uk The health and wellbeing gap If the nation fails to get
The prevention and self care workshop 16 th September 2016 Dr. Jenny Harries Regional Director PHE South Regional Office Jenny.harries@phe.gov.uk The health and wellbeing gap If the nation fails to get
Nurse Led End of Life Care. Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough
 Nurse Led End of Life Care Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough SETTING THE SCENE Preferences for Place of Death 2014 Home 72% Hospice 10% Care
Nurse Led End of Life Care Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough SETTING THE SCENE Preferences for Place of Death 2014 Home 72% Hospice 10% Care
North West COPD Report Nov 2011
 North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
September Workforce pressures in the NHS
 September 2017 Workforce pressures in the NHS 2 Contents Foreword 3 Introduction and methodology 5 What professionals told us 6 The biggest workforce issues 7 The impact on professionals and people with
September 2017 Workforce pressures in the NHS 2 Contents Foreword 3 Introduction and methodology 5 What professionals told us 6 The biggest workforce issues 7 The impact on professionals and people with
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
West Midlands Strategic Clinical Network & Senate Improving the detection and management of Atrial Fibrillation in Primary Care
 West Midlands Strategic Clinical Network & Senate Improving the detection and management of Atrial Fibrillation in Primary Care Good Practice Guide Improving the detection and management of Atrial Fibrillation
West Midlands Strategic Clinical Network & Senate Improving the detection and management of Atrial Fibrillation in Primary Care Good Practice Guide Improving the detection and management of Atrial Fibrillation
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Commissioning effective anticoagulation services for the future: A resource pack for commissioners
 Commissioning effective anticoagulation services for the future: A resource pack for commissioners The development of this commissioning toolkit was supported by Bayer HealthCare. Bayer HealthCare paid
Commissioning effective anticoagulation services for the future: A resource pack for commissioners The development of this commissioning toolkit was supported by Bayer HealthCare. Bayer HealthCare paid
The pathway highlights a clear strategy for managing these patients which includes the following:
 James Cook University Hospital Streamlining the pathway for patients identified in surgical pre admission clinics (PAC) with previously undetected atrial fibrillation. Why was this project implemented?
James Cook University Hospital Streamlining the pathway for patients identified in surgical pre admission clinics (PAC) with previously undetected atrial fibrillation. Why was this project implemented?
EDS 2. Making sure that everyone counts Initial Self-Assessment
 EDS 2 Making sure that everyone counts Initial Self-Assessment Equality Delivery System for the NHS EDS2 Summary Report Implementation of the Equality Delivery System EDS2 is a requirement on both NHS
EDS 2 Making sure that everyone counts Initial Self-Assessment Equality Delivery System for the NHS EDS2 Summary Report Implementation of the Equality Delivery System EDS2 is a requirement on both NHS
Acute kidney injury Keeping kidneys healthy: The AKI programme board. Dr Richard Fluck, National Clinical Director (Renal) NHS England
 NHS England") Acute kidney injury Keeping kidneys healthy: The AKI programme board Dr Richard Fluck, National Clinical Director (Renal) NHS England NHS Outcomes Framework NHS Five Year Forward View A vision for the
Acute kidney injury Keeping kidneys healthy: The AKI programme board Dr Richard Fluck, National Clinical Director (Renal) NHS England NHS Outcomes Framework NHS Five Year Forward View A vision for the
COPD SERVICE RE-DESIGN
 COPD SERVICE RE-DESIGN Dr Mukesh Singh GP Principal & GPwSI Respiratory Medicine, Horse Fair Practice, Rugeley Clinical Lead LTC & Governing Body member Cannock Chase CCG COPD DRIVERS FOR RE-DESIGN DOH
COPD SERVICE RE-DESIGN Dr Mukesh Singh GP Principal & GPwSI Respiratory Medicine, Horse Fair Practice, Rugeley Clinical Lead LTC & Governing Body member Cannock Chase CCG COPD DRIVERS FOR RE-DESIGN DOH
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Acceleration for ACS. NSTEMI Event 09 November. Outputs from Table Discussions
 Acceleration for ACS NSTEMI Event 09 November Outputs from Table Discussions 1 1. What mechanism do we need to have to identify patients early (within 6 hours of admission to hospital)? Have identification
Acceleration for ACS NSTEMI Event 09 November Outputs from Table Discussions 1 1. What mechanism do we need to have to identify patients early (within 6 hours of admission to hospital)? Have identification
IAPT Service Review Norfolk and Waveney STP
 IAPT Service Review Norfolk and Waveney STP Intensive Support Team Mental Health 20 th April 2017 Context The Mental Health Intensive Support Team (IST) Part of the NHS Improvement A free resource to NHS
IAPT Service Review Norfolk and Waveney STP Intensive Support Team Mental Health 20 th April 2017 Context The Mental Health Intensive Support Team (IST) Part of the NHS Improvement A free resource to NHS
JOB DESCRIPTION. Consultant in Palliative Medicine GENERAL
 JOB DESCRIPTION JOB TITLE DEPARTMENT REPORTS TO ACCOUNTABLE TO Consultant in Palliative Medicine Medical Team Lead Consultant Director of Patient Care GENERAL ellenor is a specialist palliative care provider
JOB DESCRIPTION JOB TITLE DEPARTMENT REPORTS TO ACCOUNTABLE TO Consultant in Palliative Medicine Medical Team Lead Consultant Director of Patient Care GENERAL ellenor is a specialist palliative care provider
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
The new mental health access & waiting time standards
 The new mental health access & waiting time standards Dr Frank Burbach Consultant Clinical Psychologist Somerset Partnership NHS Foundation Trust frank.burbach@sompar.nhs.uk 1 NHS Presentation to [XXXX
The new mental health access & waiting time standards Dr Frank Burbach Consultant Clinical Psychologist Somerset Partnership NHS Foundation Trust frank.burbach@sompar.nhs.uk 1 NHS Presentation to [XXXX
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Reducing Elective Waits: Delivering 18 week pathways for patients. Programme Director NHS Elect Caroline Dove.
 Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Delivering the transformation of children and young people s mental health services
 Delivering the transformation of children and young people s mental health services Simon Medcalf Head of Mental Health, NHS England 4 October 2016 1 Context: Implementing the Five Year Forward View for
Delivering the transformation of children and young people s mental health services Simon Medcalf Head of Mental Health, NHS England 4 October 2016 1 Context: Implementing the Five Year Forward View for
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
NHS non-urgent Patient Transport Service (PTS) Engagement Report
 Engagement Report") NHS non-urgent Patient Transport Service (PTS) Engagement Report September 2015 Introduction The Sussex PTS is currently provided by the South East Coast Ambulance Service (SECAmb). Around 280,000 PTS
NHS non-urgent Patient Transport Service (PTS) Engagement Report September 2015 Introduction The Sussex PTS is currently provided by the South East Coast Ambulance Service (SECAmb). Around 280,000 PTS
To Dip or Not To Dip
 To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS
 THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
Dartford and Gravesham NHS Trust. Susan Acott Chief Executive
 Dartford and Gravesham NHS Trust Susan Acott Chief Executive A First in Kent Retired policeman Richard Oliver aged 59 was the first patient to be fitted with the EMBLEM, Subcutaneous Implantable Cardiac
Dartford and Gravesham NHS Trust Susan Acott Chief Executive A First in Kent Retired policeman Richard Oliver aged 59 was the first patient to be fitted with the EMBLEM, Subcutaneous Implantable Cardiac
Haringey and Islington
 Haringey and Islington Wellbeing Partnership Who we are Thoughts on system leadership and on leading within complex systems Observations from our experience Recognising where we are seeing and showing
Haringey and Islington Wellbeing Partnership Who we are Thoughts on system leadership and on leading within complex systems Observations from our experience Recognising where we are seeing and showing
COPD Management in the community
 COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services