Patient and Provider Perspectives of Self-Management of Ulcers in SCI/D
|
|
|
- Gerard Haynes
- 5 years ago
- Views:
Transcription






1 OFFICE of RESEARCH & DEVELOPMENT Patient and Provider Perspectives of Self-Management of Ulcers in SCI/D Dawn Ehde, PhD 1 Marylou Guihan, PhD 2 August 28, 2013 VETERANS HEALTH ADMINISTRATION
2 Disclaimer This study was funded the Department of Veterans Affairs, Office of Research and Development, Health Services Research and Development Service (IIR ). The views expressed in this presentation are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the US government. VETERANS HEALTH ADMINISTRATION 1
3 Disclosure This study received Department of Veterans Affairs Funding and Staff Support. This continuing education activity is managed and accredited by Professional Education Services Group in cooperation with the Paralyzed Veterans of America. Neither PESG nor PVA nor any accrediting organization supports or endorses any product or service mentioned in this activity. PESG Staff and the Program Planning Committee have no financial interest to disclose. Commercial Support was not received for this activity. VETERANS HEALTH ADMINISTRATION 2
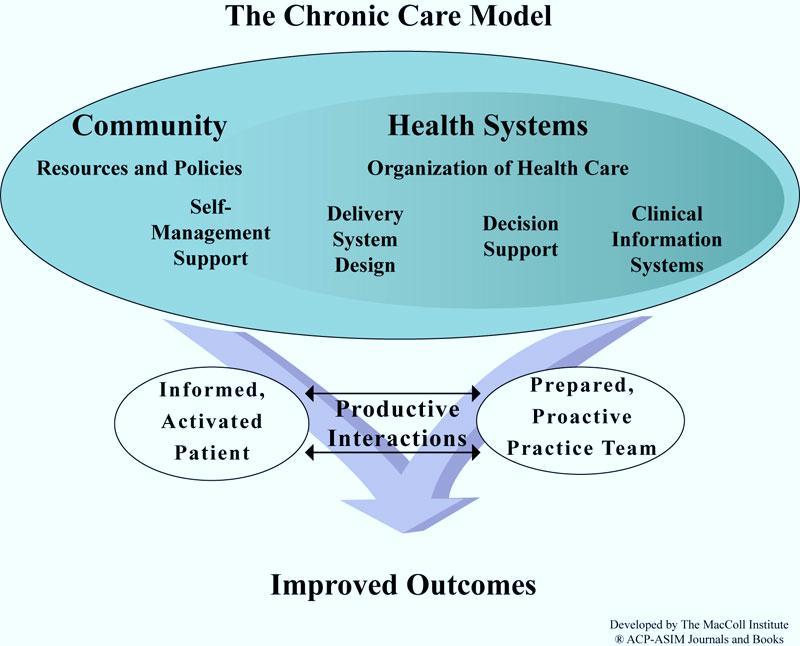
4 Overview Study Rationale Pressure ulcers (PrUs) as a chronic condition Chronic Care Model, which emphasizes selfmanagement Study of patient & providers perspectives on selfmanagement of PrUs Discussion of steps for integrating selfmanagement into the care of PrUs VETERANS HEALTH ADMINISTRATION 3
5 Why focus on PrUs in SCI? PrUs are the most common secondary complication after SCI. In FY 2012, there were 4,394 admissions for PrU treatment at VA SCI Centers. Only 1.3% of the PrUs treated in SCI units were hospitalacquired. Community-acquired pressure ulcers are the main reason for hospitalization of Veterans with SCI/D. Virtually all published literature on prevention is based on institutional settings, where the focus is provider behavior. VETERANS HEALTH ADMINISTRATION 4
6 PrU Prevalence and Recurrence Rates PrU prevalence rates in persons with SCI residing in the community range from 17-33%. High rates of recurrence (31% to 79%) also have been reported. Chen and colleagues found that although PrU risk was relatively stable during the first 10 years following SCI, there was a significant trend toward increased PrU prevalence years post-sci. The mean age of Veterans with SCI is 61 (sd=1.1)and the mean time since post-sci in Veterans with PrUs is 20 years. VETERANS HEALTH ADMINISTRATION 5
7 PrUs in SCI PrU etiology is multi-factorial, encompassing mechanical, metabolic, nutritional and environmental factors, all of which are influenced by a person's behavior. In a 2003 survey, VA SCI providers were nearly unanimous in their agreement that patients who comply with treatment recommendations can prevent PrUs. 1 Despite the strong opinions expressed by providers, the evidence supporting most SCI PrU CPG recommendations is based on expert consensus. VETERANS HEALTH ADMINISTRATION 6
8 PrU Risk Factors and Prevention Modifiable and non-modifiable risk factors (e.g., decreased mobility and lack of sensation, coupled with other physiologic changes), put everyone with SCI at lifelong risk for PrUs. PrU prevention typically focuses on patient education (e.g., pressure relief, skin hygiene, adequate nutrition, skin protective behaviors, avoiding substance use, proper equipment use and seeking timely medical attention). The role of motivation and self-efficacy in the self-management of other chronic conditions (e.g., diabetes) is seen as critical to long term outcomes. VETERANS HEALTH ADMINISTRATION 7
9 Pressure ulcers = chronic condition Why do we believe that PrUs in SCI should be re-conceptualized as a complex chronic condition? PrU prevention & management requires substantial and sustained changes in patient behavior & system support. VETERANS HEALTH ADMINISTRATION 8
10 Chronic vs. Acute Condition PrUs are a non-communicable condition characterized by: Duration Prognosis Pattern Sequelae VETERANS HEALTH ADMINISTRATION 9
11 Chronic Care Model (CCM) Why the Chronic Care Model? Because it has led to improved health care outcomes in other complex chronic health conditions, focusing on: Improving patient activation via education, improved motivation and self-management (SM) skill-building; Redesigning the healthcare system to provide more proactive patient support and productive patient-provider team interactions; Providing decision support to healthcare providers to maximize adherence to evidence-based guidelines; and Creating clinical information systems that provide timely data about patients and populations. VETERANS HEALTH ADMINISTRATION 10
12 11

13 Medical Versus Self-Management < 0.5% = Health care providers = Individual with pain VETERANS HEALTH ADMINISTRATION




14 What is Self-Management? what people do on a day to day basis to feel better and pursue the life they desire. Teresa Brady, PhD, Centers for Disease Control and Prevention, 2010 VETERANS HEALTH ADMINISTRATION 13
15 What is Self-Management? The tasks that the individual must do to live well with one or more chronic conditions. and skills Tasks include having the confidence to deal with: Medical management Role management Emotional management of their condition (IOM, 2004; Brady, 2011) VETERANS HEALTH ADMINISTRATION 14
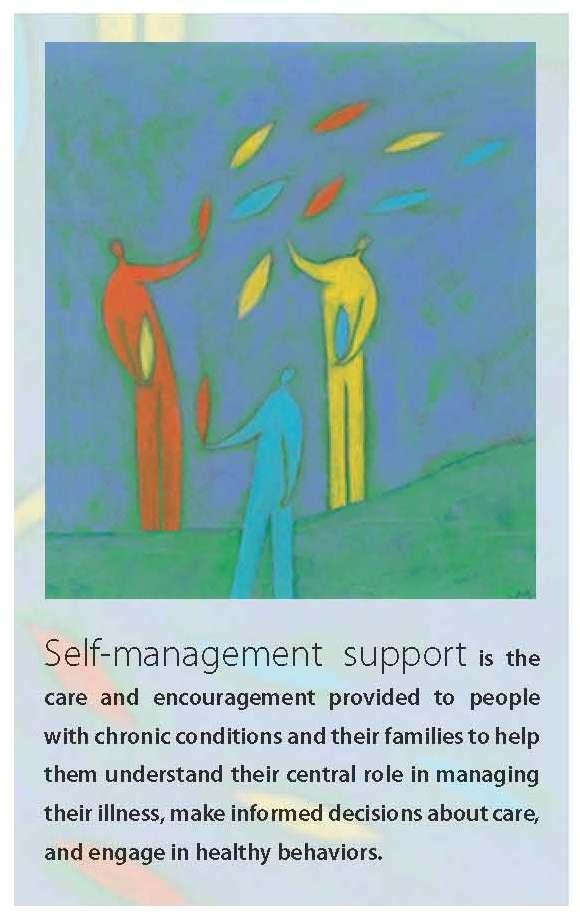
16 What is Self-Management Support? Self-management support may be viewed in two ways, as: A portfolio of techniques and tools that help patients choose healthy behaviors; and A fundamental transformation of the patient-caregiver relationship into a collaborative partnership. The purpose of self-management support is to aid and inspire patients to become informed about their conditions and take an active role in their treatment. 1 VETERANS HEALTH ADMINISTRATION 15
17 Self-Management Support Institute of Medicine: Systematic support is necessary to increase patients skills and confidence in managing their chronic conditions, including: Regular assessment of progress & problems Goal setting Problem-solving support Relapse prevention VETERANS HEALTH ADMINISTRATION 16
18 Reims Model to Promote High Leverage Changes to Improve SM at the System Level 1. Emphasizing the patient s central role 2. Assessing patient self-management knowledge, behaviors, confidence, and barriers 3. Providing effective behavior change interventions & ongoing support with peers or professionals 4. Using culturally competent, linguistically appropriate approaches in interactions and 5. Assuring collaborative care-planning and problem solving by the team. VETERANS HEALTH ADMINISTRATION 17

19 Gaps in Self-Management Support in SCI? Little is known about what people with SCI think about self-management. Little is known about what SCI care providers think about self-management support. VETERANS HEALTH ADMINISTRATION 18
20 Patient Viewpoint Patients vary in the roles and degree of control that they are willing or able to assume in self-management, including decisions about their own medical treatment. Many variables likely impact patients engagement in selfmanagement and health care, including: Health literacy and numeracy Sex, age, education, cultural differences Severity of illness Perception that they lack knowledge Perception that providers may not respect their preferences Lack of self-efficacy VETERANS HEALTH ADMINISTRATION 19
21 Patient Viewpoint One study found that even relatively affluent and welleducated patients felt compelled to conform to socially sanctioned roles and thus deferred to physicians during clinical consultations. Fear of being labeled as difficult prevented many patients from participating more fully in their own health care. VETERANS HEALTH ADMINISTRATION 20
22 Provider Viewpoint To effectively support SM, providers need to view patients as being the expert or central manager of their health care and decision-making. Shared decision making requires attitudes and skills that many providers may not possess or be familiar with. Partnering with a patient may require providers to counsel patients about lifestyle issues or attend to the patient s emotional distress. VETERANS HEALTH ADMINISTRATION 21
23 Provider Viewpoint Providers may also need to negotiate their own professional biases and emotions. Studies have shown that when faced with a patient they view as difficult, providers sometimes respond in problematic ways, (e.g., avoidance, anger, and stereotypes as a form of distancing). Incorporating tools for reflective self-awareness and strategies for how to address them into routine clinical practices may help providers to improve their skills. VETERANS HEALTH ADMINISTRATION 22
24 Provider Viewpoint Providers cannot assume that one size fits all in promoting shared decision making/self management, with everyone starting off with common meanings and application across different individuals or cultural groups. Providers need to be aware of cultural assumptions underlying the process and be sensitive to the needs and preferences of patients in diverse cultural groups. VETERANS HEALTH ADMINISTRATION 23
25 Current Study: Aims To examine how SCI healthcare providers and Veterans with SCI view pressure ulcer selfmanagement and self-management support VETERANS HEALTH ADMINISTRATION 24
26 Design Conducted concurrently with a large multi-site (4 VA SCI Centers) randomized controlled trial comparing 2 interventions for increasing skin protective behaviors. Primary Veteran inclusion criteria: Could not be participating in RCT; did not matter if 0 vs. 1+ PrUs. VETERANS HEALTH ADMINISTRATION 25
27 Methods, Participants Convenience sample participated in focus groups at each site n = 8 focus groups 1 for Veterans at each site 1 for providers at each site Veterans with SCI/D (n=35) SCI/D providers (n=39) VETERANS HEALTH ADMINISTRATION 26
28 Veteran Demographics Frequency Percent Gender Age Marital Status Employment Education Male Female Single Married Divorced Employed Unemployed Disabled/Retired < High School High School College/trade school Bachelors Degree Graduate Degree
29 Veteran Demographics Frequency Percent Level of Injury Service-Connected Status Number of previous /current PrUs Percent of Healthcare by VA Paraplegia Tetraplegia Yes <
30 Veteran Demographics Mean (S.D) Age at injury (years) 39.6 (15.2) Duration of SCI (years) 20.9 (12.4) 29
31 Provider Demographic characteristics N (%) Gender: Male 9 (23.1) Female 30 (76.9) Age: (15.4) (51.3) (33.3) Discipline: Physician 9 (23.1) Nurse Practitioner 2 (5.1) Nurse 8 (20.5) Therapist 15 (38.5) Other 5 (13.0) Trained in another area of specialization: Yes 15 (40.5) No 22 (59.5) 30
32 Provider Background N (%) Percent time spent in: Administration 31.1 (28.2) Direct Patient Care 75.3 (26) Other 30.2 (36.2) Patient care setting (s): Inpatient 60 (29.2) Outpatient 42 (30.9) Home Care 6 (8.4) Type of care provided: Initial rehabilitation 30.1 (26.1) Chronic SCI care 81.9 (80.4) 31
33 Provider background Mean (SD) Total years working in SCI: 11.9 (8.4) - VA SCI center 10.1 (7.7) - Model Systems facility 3 (4.5) - Non-Model Systems facility 3.7 (5.5) 32
34 Focus Groups Use focus group guides which consisted of openended questions, including asking them to: to define self management and skin management; to describe their skin management activities; to discuss barriers to and supports for skin management their views on patient-provider conversations about skin management. Also asked other questions/background info VETERANS HEALTH ADMINISTRATION 33
35 Procedures Conducted in by an experienced focus group facilitator Veteran groups: 90 minutes Provider groups: 60 minutes Veterans received a small honorarium; providers did not. VETERANS HEALTH ADMINISTRATION 34
36 Data Analysis Audio recordings transcribed verbatim Constant comparative techniques NVivo 8 used for analysis Reims conceptual framework was used to organize findings Sample quotes from Veterans and providers to illustrate findings VETERANS HEALTH ADMINISTRATION 35
37 Results: Veteran s Central Role in Skin Management Veterans recognized their responsibility in managing their own skin: That responsibility is yours and you have to take control of yourself. I have to take care of myself. And for self-advocacy: You know your body better than anybody else. And you have to know what to tell [your providers]. VETERANS HEALTH ADMINISTRATION 36
38 Veterans Central Role in Skin Management Veterans also recognized the need for help from others: You must pay attention to what your therapist tells you Listen to what they tell you and accept it If you don t listen to what they re saying [providers], [you re] the fool. You have to manage everyone around you, including yourself. VETERANS HEALTH ADMINISTRATION 37
39 Providers on Patients Role Providers also emphasized that Veterans have primary responsibility, although less emphatically: I know we re the train but [the Vet is] the engine. You got to run it and we will give you the help. VETERANS HEALTH ADMINISTRATION 38
40 Provider Role And with less optimism: [Some patients seem more] motivated by whatever else they need to do in their life than to feel empowered enough to go ahead and follow through with instructions [to properly care for SCI or skin problems]. VETERANS HEALTH ADMINISTRATION 39
41 Assessing SM Knowledge, Behaviors, Confidence, & Barriers Veterans reported possessing adequate knowledge about how to manage PrUs & engaging in many skinprotective behaviors: Basically just having a routine [is important] have a daily inspection, mornings & evenings. If you have a caretaker, they can see things you can t see & you can ask them to look. VETERANS HEALTH ADMINISTRATION 40
42 Barriers to SM identified by Veterans Personal factors: Depression or self-pity if you wallow in self-pity you begin to stop doing things that you should routinely do. External factors (most frequently reported): Lack of available CGs or CG time Lack of financial resources for CG time VETERANS HEALTH ADMINISTRATION 41
43 Barriers to SM identified by Providers Providers recognized the complexity of the lives of their patients with SCI & to some degree, how challenging SM can be even to the most motivated patients. But many comments focused on their perceptions of patient behavior & attitudes: The VA will care for me no matter what. no incentive to change [their] behavior. VETERANS HEALTH ADMINISTRATION 42
44 Provision of Behavior Change Interventions & Support: Veteran Perspectives Veterans were mixed on the adequacy of the support they get from providers & the system. They consistently stressed the impact & importance of non-medical interventions: especially peer modeling & groups as sources of knowledge, friendship, and emotional support that facilitated self-management. VETERANS HEALTH ADMINISTRATION 43
45 Peer Support: Examples I learned more from a couple guys that I was in rehab with that had been injured for quite a while, learned from then how to do things and how to take care of myself. Learning from other people, learning from your peers, learning from people who have been there is the biggest thing that you can accomplish. VETERANS HEALTH ADMINISTRATION 44
46 Provision of Behavior Change Interventions & Support: Provider Perspectives Some providers discussed using proactive methods to facilitate patient self-management, including a flexible approach to elicit behavior change: You have to negotiate with them Like, okay, what are you willing to do? I had this patient who [wanted to] sit for 12 hours, and I said, well 12 hours is a little too much. How much can you go down, what would be realistic for you? He said, well, 6; okay, we can start with 6. VETERANS HEALTH ADMINISTRATION 45
47 Provision of Behavior Change Interventions & Support: Provider Perspectives Providers also acknowledged the importance of social interventions in supporting change or selfmanagement: We have the peer partner program that pairs up a guy with a new injury with a guy who s been living successfully in the community for at least a year [Sometimes] that s a good way of kind of getting the education across. VETERANS HEALTH ADMINISTRATION 46
48 Use of Culturally Competent Approaches Veterans were mixed in their assessment of providers communication skills. Several providers described the need for multiple ways to approach and tailor information to individual patients. [I m always] trying to find a way, whatever connects with that patient [is important] because it s not going to be the same with every patient. How do you get them to remember and what influences them? VETERANS HEALTH ADMINISTRATION 47
49 Assure Collaborative Planning & Problem-Solving by Team Veterans acknowledged importance of healthcare team but did not discuss the importance or presence of an ongoing collaborative effort. Providers stressed importance of collaboration & communication among team members. But providers did not describe patients or caregivers as team members. VETERANS HEALTH ADMINISTRATION 48
50 Limitations Sample size May not be generalizable to civilians Findings need to be confirmed by further qualitative and quantitative research. Perspectives and roles of families and caregivers needs to be considered in future research. VETERANS HEALTH ADMINISTRATION 49
51 Discussion Some, but not all, of Reims recommended health care system changes for supporting patient selfmanagement were described by Veterans and providers. Veterans placed more emphasis on their own role (or that of peers) in facilitating self-management. Self-management support at the system level was not described in any detail. VETERANS HEALTH ADMINISTRATION 50
52 Discussion Like other areas of healthcare, self-management support likely occurs but may not be systematically integrated into the care environment. How much of this is due to terminology, a lack of understanding about SM support, insufficient SM support resources, or other factors is unknown. VETERANS HEALTH ADMINISTRATION 51
53 What Can We Do to Better integrate Self-Management Support into SCI Care? Battersby et al. (2010) recommendations Examples of self-management integration into SCI care VETERANS HEALTH ADMINISTRATION 52
54 Battersby et al. (2010) Evidence-Based Recommendations for Self-Management Support Integrating Self-Management Support into Clinical Practice Enhanced Visit Preparation Focused Visit Expand Options at Post-visit 1. Brief targeted assessment to guide SMS 2. Evidence-based information to guide shared decision making 3. Clinicians use a nonjudgmental approach 4. Collaborative priority and goal setting 5. Collaborative problem-solving 6. Diverse providers can offer SMS 7. Individual-, group-, telephone-, and selfinstruction formats can be employed 8. Enhance patient self-efficacy 9. Ensure active follow-up 10. Guideline-based case management for selected patients 11. Link patient to evidence-based communitybased self-management programs 12. Multifaceted interventions are more effective 53









55 Physician Psychologist Psychiatrist Feedback Decision support Care coordination Patient Care Manager Motivate adherence Monitor response to Tx Manualized therapy -CBT -Problem-solving -Physical activity Weekly case supervision Treatment adjustment Manage treat-to-target 54


56 High Impact Changes for Self- Management Before, During, and After the Visit Help patients understand their central role in managing their conditions and that the entire health care team is there to help. Before the Visit Ask patients to bring questions and concerns and health monitoring information. 55
57 During the Visit Collaboratively develop a visit agenda with the patient and family, handling as many concerns as possible, and plan return visits as appropriate. Engage the entire team in supporting patients, use warm handoff introductions, and explain team member roles to patients. Ask patient about their goals to improve their health and help them make action plans that build confidence in their ability to reach these goals. 56
58 During the Visit Prepare a written care plan or visit summary that includes goals and action plans to ensure patients and families know what to do when they leave the visit. Use group medical appointments, peer-led support groups, or patient education classes to provide opportunities for patients to share experiences and support. 57
59 After the Visit Organize follow-up support to help patients sustain healthy behaviors between visits. Extend care into the community by linking patients to community programs. 58
60 Build a Team Designate and train a lead coach for selfmanagement support, who will also support ongoing staff development of skills. Assign responsibility for self-management tasks to all team members. Identify team strategies to review patient charts, anticipate care needs, and enhance the flow of care. 59

61 60
62 Summary System-level changes are an area for further development & research in SCI PrU care. Future research should address questions of how to support self-management at the patient, caregiver, provider, & system level to improve PrU outcomes. The Chronic Care Model literature may serve as a useful model for such research and changes. VETERANS HEALTH ADMINISTRATION 61
Standards of Practice for Professional Ambulatory Care Nursing... 17
 Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Perceptions of Family Cancer Caregivers in Tanzania: A Qualitative Study. Allison Walker
 Perceptions of Family Cancer Caregivers in Tanzania: A Qualitative Study Allison Walker Motivation Upward trend in cancer cases in developing countries Lack of institutional facilities and specialists
Perceptions of Family Cancer Caregivers in Tanzania: A Qualitative Study Allison Walker Motivation Upward trend in cancer cases in developing countries Lack of institutional facilities and specialists
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Goal #1: Mastery of Clinical Knowledge with Integration of Basic Sciences
 Goal #1: Mastery of Clinical Knowledge with Integration of Basic Sciences Objective #1: To demonstrate comprehension of core basic science knowledge 1.1a) demonstrate knowledge of the basic principles
Goal #1: Mastery of Clinical Knowledge with Integration of Basic Sciences Objective #1: To demonstrate comprehension of core basic science knowledge 1.1a) demonstrate knowledge of the basic principles
CAPE/COP Educational Outcomes (approved 2016)
") CAPE/COP Educational Outcomes (approved 2016) Educational Outcomes Domain 1 Foundational Knowledge 1.1. Learner (Learner) - Develop, integrate, and apply knowledge from the foundational sciences (i.e.,
CAPE/COP Educational Outcomes (approved 2016) Educational Outcomes Domain 1 Foundational Knowledge 1.1. Learner (Learner) - Develop, integrate, and apply knowledge from the foundational sciences (i.e.,
Understanding Health Literacy Skills in Patients With Cardiovascular Disease and Diabetes Patrick Dunn, Ph.D. Vasileios Margaritis, Ph.D.
 Understanding Health Literacy Skills in Patients With Cardiovascular Disease and Diabetes Patrick Dunn, Ph.D. Vasileios Margaritis, Ph.D., & Cheryl Anderson, Ph.D. January 13, 2017 Prose Print Diabetes
Understanding Health Literacy Skills in Patients With Cardiovascular Disease and Diabetes Patrick Dunn, Ph.D. Vasileios Margaritis, Ph.D., & Cheryl Anderson, Ph.D. January 13, 2017 Prose Print Diabetes
Change is Good: You Go First
 Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
VHA Preventive Care Program. Clinician/Educator Programs
 Behavioral Medicine Careers in the VA Health Care System: Clinician/Educator Positions Michael Goldstein, MD, Associate Chief Consultant for Preventive Medicine Margaret (Peg) Dundon, PhD, National Program
Behavioral Medicine Careers in the VA Health Care System: Clinician/Educator Positions Michael Goldstein, MD, Associate Chief Consultant for Preventive Medicine Margaret (Peg) Dundon, PhD, National Program
Challenges and Innovations in Community Health Nursing
 Challenges and Innovations in Community Health Nursing Diana Lee Chair Professor of Nursing and Director The Nethersole School of Nursing The Chinese University of Hong Kong An outline The changing context
Challenges and Innovations in Community Health Nursing Diana Lee Chair Professor of Nursing and Director The Nethersole School of Nursing The Chinese University of Hong Kong An outline The changing context
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers
 Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Clinical Nurse Leader (CNL ) Certification Exam. Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012)
 Certification Exam. Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012)") Clinical Nurse Leader (CNL ) Certification Exam Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012) Subdomain Weight (%) Nursing Leadership Horizontal Leadership
Clinical Nurse Leader (CNL ) Certification Exam Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012) Subdomain Weight (%) Nursing Leadership Horizontal Leadership
When preparing for an ACE certification exam,
 Introduction to Coaching CHAPTER 1 APPENDIX B Exam Content Outline For the most up-todate version of the Exam Content Outline, please go to www.acefitness.org/ HealthCoachexamcontent and download a free
Introduction to Coaching CHAPTER 1 APPENDIX B Exam Content Outline For the most up-todate version of the Exam Content Outline, please go to www.acefitness.org/ HealthCoachexamcontent and download a free
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
SECTION 3. Behavioral Health Core Program Standards. Z. Health Home
 SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
Population Health: The Role of the DNP. Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare
 Population Health: The Role of the DNP Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare TOPICS in Population Health Definitions Hopkins Conceptual Model Interventions Relationship
Population Health: The Role of the DNP Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare TOPICS in Population Health Definitions Hopkins Conceptual Model Interventions Relationship
Stanford Self-Management Programs Effectiveness and Translation
 Stanford Self-Management Programs Effectiveness and Translation Kate Lorig, RN, DrPH Stanford Patient Education Center 1000 Welch Road, Suite 204 Palo Alto CA 94304 650-723-7935 self-management@stanford.edu
Stanford Self-Management Programs Effectiveness and Translation Kate Lorig, RN, DrPH Stanford Patient Education Center 1000 Welch Road, Suite 204 Palo Alto CA 94304 650-723-7935 self-management@stanford.edu
Enhancing Patient Care through Effective and Efficient Nursing Documentation
 Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Health Coaching: Filling a Gap In Primary Care
 Health Coaching: Filling a Gap In Primary Care Katie Ingle, DNP, FNP Cannon Falls, MN Introduction Katie Ingle, DNP-FNP Family nurse practitioner, working in family practice 2005 MSN graduate of AASU 2013
Health Coaching: Filling a Gap In Primary Care Katie Ingle, DNP, FNP Cannon Falls, MN Introduction Katie Ingle, DNP-FNP Family nurse practitioner, working in family practice 2005 MSN graduate of AASU 2013
Balbale et al. Implementation Science (2015) 10:130 DOI /s x Implementation Science
 10:130 DOI /s x Implementation Science") Balbale et al. Implementation Science (2015) 10:130 DOI 10.1186/s13012-015-0318-x Implementation Science RESEARCH Open Access Evaluating implementation of methicillinresistant Staphylococcus aureus (MRSA)
Balbale et al. Implementation Science (2015) 10:130 DOI 10.1186/s13012-015-0318-x Implementation Science RESEARCH Open Access Evaluating implementation of methicillinresistant Staphylococcus aureus (MRSA)
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa
 Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Impact of Implementing Designed Nursing Intervention Protocol on Clinical Outcome of Patient with Peptic Ulcer. Amal Mohamed Ahmad
 Impact of Implementing Designed Nursing Intervention Protocol on Clinical Outcome of Patient with Peptic Ulcer By Amal Mohamed Ahmad Assistant Professor, Medical-Surgical Nursing, Faculty of Nursing, Aswan
Impact of Implementing Designed Nursing Intervention Protocol on Clinical Outcome of Patient with Peptic Ulcer By Amal Mohamed Ahmad Assistant Professor, Medical-Surgical Nursing, Faculty of Nursing, Aswan
Being Prepared for Ongoing CPS Safety Management
 Being Prepared for Ongoing CPS Safety Management Introduction This month we start a series of safety intervention articles that will consider ongoing CPS safety management functions, roles, and responsibilities.
Being Prepared for Ongoing CPS Safety Management Introduction This month we start a series of safety intervention articles that will consider ongoing CPS safety management functions, roles, and responsibilities.
An Approach to Developing Social Work Practice Competencies in Mental Health Setting. Dr. Prashant Talwar UNIMAS
 An Approach to Developing Social Work Practice Competencies in Mental Health Setting. Dr. Prashant Talwar UNIMAS 1 Social Work O Social workers have been involved in the health care field since the turn
An Approach to Developing Social Work Practice Competencies in Mental Health Setting. Dr. Prashant Talwar UNIMAS 1 Social Work O Social workers have been involved in the health care field since the turn
DOCUMENT E FOR COMMENT
 DOCUMENT E FOR COMMENT TABLE 4. Alignment of Competencies, s and Curricular Recommendations Definitions Patient Represents patient, family, health care surrogate, community, and population. Direct Care
DOCUMENT E FOR COMMENT TABLE 4. Alignment of Competencies, s and Curricular Recommendations Definitions Patient Represents patient, family, health care surrogate, community, and population. Direct Care
Abstract Development:
 Abstract Development: How to write an abstract Fall 2017 Sara E. Dolan Looby, PhD, ANP-BC, FAAN Assistant Professor of Medicine, Harvard Medical School Neuroendocrine Unit/Program in Nutritional Metabolism
Abstract Development: How to write an abstract Fall 2017 Sara E. Dolan Looby, PhD, ANP-BC, FAAN Assistant Professor of Medicine, Harvard Medical School Neuroendocrine Unit/Program in Nutritional Metabolism
EVALUATING CAREGIVER PROGRAMS Andrew Scharlach, Ph.D. Nancy Giunta, M.A., M.S.W.
 EVALUATING CAREGIVER PROGRAMS Andrew Scharlach, Ph.D. Nancy Giunta, M.A., M.S.W. Paper Prepared for the Administration on Aging 2003 National Summit on Creating Caring Communities Overview of CASAS FCSP
EVALUATING CAREGIVER PROGRAMS Andrew Scharlach, Ph.D. Nancy Giunta, M.A., M.S.W. Paper Prepared for the Administration on Aging 2003 National Summit on Creating Caring Communities Overview of CASAS FCSP
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service
 WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
U.H. Maui College Allied Health Career Ladder Nursing Program
 U.H. Maui College Allied Health Career Ladder Nursing Program Progress toward level benchmarks is expected in each course of the curriculum. In their clinical practice students are expected to: 1. Provide
U.H. Maui College Allied Health Career Ladder Nursing Program Progress toward level benchmarks is expected in each course of the curriculum. In their clinical practice students are expected to: 1. Provide
WakeMed Rehab Spinal Cord Injury Scope of Service
 WakeMed Rehab Spinal Cord Injury Scope of Service The WakeMed Rehab Continuum provides an integrated, comprehensive delivery of rehabilitation services utilizing evidence-based practice directed toward
WakeMed Rehab Spinal Cord Injury Scope of Service The WakeMed Rehab Continuum provides an integrated, comprehensive delivery of rehabilitation services utilizing evidence-based practice directed toward
FIP STATEMENT OF POLICY Pharmacy: Gateway to Care
 Preamble Knowledge, prevention and management of disease has changed dramatically in recent decades. In addition to the responsibility of governments to provide the fundamental right of health, citizens
Preamble Knowledge, prevention and management of disease has changed dramatically in recent decades. In addition to the responsibility of governments to provide the fundamental right of health, citizens
Aurora Behavioral Health System
 Aurora Behavioral Health System Decades Program Overview Where healing starts and the road to recovery begins Aurora East 6350 S. Maple Ave. Tempe, AZ 85283 (The hospital is located on the NW corner of
Aurora Behavioral Health System Decades Program Overview Where healing starts and the road to recovery begins Aurora East 6350 S. Maple Ave. Tempe, AZ 85283 (The hospital is located on the NW corner of
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
Priorities and Interventions in SCI Rehabilitation: Incorporating the Patient s Voice Using PROMs. Vanessa Noonan, PhD PT
 Priorities and Interventions in SCI Rehabilitation: Incorporating the Patient s Voice Using PROMs Vanessa Noonan, PhD PT Needs and priorities of patients change throughout the SCI continuum. During the
Priorities and Interventions in SCI Rehabilitation: Incorporating the Patient s Voice Using PROMs Vanessa Noonan, PhD PT Needs and priorities of patients change throughout the SCI continuum. During the
Does The Chronic Care Model Work?
 Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Pursuing the Triple Aim: CareOregon
 Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Social and Behavioral Sciences (SBS)
") Social and Behavioral Sciences (SBS) 1 Social and Behavioral Sciences (SBS) Courses SBS 5001. Fundamentals of Public Health. 3 Credit Hours. This course encompasses historical and sociocultural approaches
Social and Behavioral Sciences (SBS) 1 Social and Behavioral Sciences (SBS) Courses SBS 5001. Fundamentals of Public Health. 3 Credit Hours. This course encompasses historical and sociocultural approaches
Reference materials are provided with the criteria and should be used to assist in the correct interpretation of the criteria.
 InterQual Level of Care Criteria Rehabilitation Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Rehabilitation Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
Effectively implementing multidisciplinary. population segments. A rapid review of existing evidence
 Effectively implementing multidisciplinary teams focused on population segments A rapid review of existing evidence October 2016 Francesca White, Daniel Heller, Cait Kielty-Adey Overview This review was
Effectively implementing multidisciplinary teams focused on population segments A rapid review of existing evidence October 2016 Francesca White, Daniel Heller, Cait Kielty-Adey Overview This review was
Military Wives Matter
 Military Wives Matter Military Wives Matter An Internet-based study of military wives mental health status and barriers to treatment Colleen Lewy PhD Celina Oliver PhD Bentson McFarland MD PhD Department
Military Wives Matter Military Wives Matter An Internet-based study of military wives mental health status and barriers to treatment Colleen Lewy PhD Celina Oliver PhD Bentson McFarland MD PhD Department
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Text-based Document. Developing Cultural Competence in Practicing Nurses: A Qualitative Inquiry. Edmonds, Michelle L.
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Strategies to Improve Medication Adherence It Can Be SIMPLE
 Strategies to Improve Medication Adherence It Can Be SIMPLE Shane Greene, Pharm.D. Director of Pharmacy Services Care N Care Insurance Company, Inc. Objectives Pharmacists: Identify predictors of medication
Strategies to Improve Medication Adherence It Can Be SIMPLE Shane Greene, Pharm.D. Director of Pharmacy Services Care N Care Insurance Company, Inc. Objectives Pharmacists: Identify predictors of medication
Convenient Care Clinic Nurse Practitioner Impact Analysis
 Convenient Care Clinic Nurse Practitioner Impact Analysis Debra R. Wallace DNP, FNP Ellen B. Daroszewski PhD, APRN Center for Health Engineering Research Let s start with a review of the healthcare environment
Convenient Care Clinic Nurse Practitioner Impact Analysis Debra R. Wallace DNP, FNP Ellen B. Daroszewski PhD, APRN Center for Health Engineering Research Let s start with a review of the healthcare environment
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Sandra V Heinsz, Ph.D. Informed Consent Services Agreement
 Welcome to my practice. This document (the Agreement) contains important information about my professional services and business policies. It also contains summary information about the Health Insurance
Welcome to my practice. This document (the Agreement) contains important information about my professional services and business policies. It also contains summary information about the Health Insurance
Allied Health Worker - Occupational Therapist
 Position Description January 2017 Position description Allied Health Worker - Occupational Therapist Section A: position details Position title: Employment Status: Classification and Salary: Location:
Position Description January 2017 Position description Allied Health Worker - Occupational Therapist Section A: position details Position title: Employment Status: Classification and Salary: Location:
Range of Variables Statements and Evidence Guide. December 2010
 Range of Variables Statements and Evidence Guide December 2010 Unit 1 Demonstrates knowledge sufficient to ensure safe practice. Each of the competency elements in this unit needs to be reflected in the
Range of Variables Statements and Evidence Guide December 2010 Unit 1 Demonstrates knowledge sufficient to ensure safe practice. Each of the competency elements in this unit needs to be reflected in the
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.
 MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.") CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Translating advanced practice nursing competence into clinical practice
 Translating advanced practice nursing competence into clinical practice Frances Kam Yuet WONG RN PhD School of Nursing The Hong Kong Polytechnic University Hong Kong Society for Nursing Education 25 th
Translating advanced practice nursing competence into clinical practice Frances Kam Yuet WONG RN PhD School of Nursing The Hong Kong Polytechnic University Hong Kong Society for Nursing Education 25 th
Pain Management Education for Nurses: Simulation vs. Traditional Lecture A Comparative Parallel-group Design Study
 Pain Management Education for Nurses: Simulation vs. Traditional Lecture A Comparative Parallel-group Design Study ASPMN Annual Conference September 16, 2017 Esther I. Bernhofer, PhD, RN-BC, CPE Nichole
Pain Management Education for Nurses: Simulation vs. Traditional Lecture A Comparative Parallel-group Design Study ASPMN Annual Conference September 16, 2017 Esther I. Bernhofer, PhD, RN-BC, CPE Nichole
Confronting the Challenges of Rare Disease:
 Confronting the Challenges of Rare Disease: SOLUTIONS ACROSS THE ENTIRE PRODUCT LIFE CYCLE The Orphan Drug Act of 1983 brought increased awareness to the need for new treatments for rare disease patients
Confronting the Challenges of Rare Disease: SOLUTIONS ACROSS THE ENTIRE PRODUCT LIFE CYCLE The Orphan Drug Act of 1983 brought increased awareness to the need for new treatments for rare disease patients
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION
 FOCUSED QUESTION") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION What is the effectiveness of a stress management program to address the occupational needs of caregivers for older adults? López, J., Crespo, M., & Zarit,
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION What is the effectiveness of a stress management program to address the occupational needs of caregivers for older adults? López, J., Crespo, M., & Zarit,
Arizona Living Well Institute
 HEALTH NET M A R C H 2 6, 2 0 1 5 J E N N A B U R K E, B S, C H E S I N T E R I M D I R E C T O R W W W. A Z L W I. O R G Agenda 1. 2. Learn of the background, structure and purpose of Healthy Living 3.
HEALTH NET M A R C H 2 6, 2 0 1 5 J E N N A B U R K E, B S, C H E S I N T E R I M D I R E C T O R W W W. A Z L W I. O R G Agenda 1. 2. Learn of the background, structure and purpose of Healthy Living 3.
Patient-Centered Case Management Assessment & Patient Interview Techniques
 Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
Healthcare 2015: Win-win or lose-lose?
 IBM Institute for Business Value Healthcare 2015: Win-win or lose-lose? A portrait and a path to successful transformation Presented at Disease Management Colloquium May 19, 2008 Jim Adams, IBM Center
IBM Institute for Business Value Healthcare 2015: Win-win or lose-lose? A portrait and a path to successful transformation Presented at Disease Management Colloquium May 19, 2008 Jim Adams, IBM Center
Effective Communication Between Elders and Providers
 Effective Communication Between Elders and Providers JOYCELYN DORSCHER MD ASSOCIATE DEAN FOR STUDENT AFFAIRS AND ADMISSIONS ASSOCIATE PROFESSOR, DEPARTMENT OF FAMILY MEDICINE UND SCHOOL OF MEDICINE AND
Effective Communication Between Elders and Providers JOYCELYN DORSCHER MD ASSOCIATE DEAN FOR STUDENT AFFAIRS AND ADMISSIONS ASSOCIATE PROFESSOR, DEPARTMENT OF FAMILY MEDICINE UND SCHOOL OF MEDICINE AND
Essential Skills and Abilities Requirements for Admission, Promotion, and Graduation in the Pharmacy Program
 Essential Skills and Abilities Requirements for Admission, Promotion, and Graduation in the Pharmacy Program INTRODUCTION The College of Pharmacy at the University of Manitoba is responsible to society
Essential Skills and Abilities Requirements for Admission, Promotion, and Graduation in the Pharmacy Program INTRODUCTION The College of Pharmacy at the University of Manitoba is responsible to society
Care Coordination is more than a Care Coordinator: Translating Research to Practice in Rural
 Care Coordination is more than a Care Coordinator: Translating Research to Practice in Rural Jennifer P. Lundblad, PhD, MBA Washington University PCOR Symposium April 5-6, 2016 Washington University 2016
Care Coordination is more than a Care Coordinator: Translating Research to Practice in Rural Jennifer P. Lundblad, PhD, MBA Washington University PCOR Symposium April 5-6, 2016 Washington University 2016
Qualitative Evidence for Practice: Why Not! Barbara Patterson, PhD, RN, ANEF Lehigh Valley Health Network Research Day 2016 October 28, 2016
 Qualitative Evidence for Practice: Why Not! Barbara Patterson, PhD, RN, ANEF Lehigh Valley Health Network Research Day 2016 October 28, 2016 OBJECTIVES At the completion of this presentation the learner
Qualitative Evidence for Practice: Why Not! Barbara Patterson, PhD, RN, ANEF Lehigh Valley Health Network Research Day 2016 October 28, 2016 OBJECTIVES At the completion of this presentation the learner
Describe the scientific method and illustrate how it informs the discovery and refinement of medical knowledge.
 1 Describe the scientific method and illustrate how it informs the discovery and refinement of medical knowledge. Apply core biomedical and social science knowledge to understand and manage human health
1 Describe the scientific method and illustrate how it informs the discovery and refinement of medical knowledge. Apply core biomedical and social science knowledge to understand and manage human health
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS) 1,2,3
 1,2,3") Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Hidden. Heroes. America s Military Caregivers. Rajeev Ramchand Terri Tanielian
 Hidden Heroes America s Military Caregivers Rajeev Ramchand Terri Tanielian Who is caring for disabled veterans? What resources are available to caregivers? Where are there gaps? 2 Methods and approach
Hidden Heroes America s Military Caregivers Rajeev Ramchand Terri Tanielian Who is caring for disabled veterans? What resources are available to caregivers? Where are there gaps? 2 Methods and approach
NURSING (MN) Nursing (MN) 1
 Nursing (MN) 1") Nursing (MN) 1 NURSING (MN) MN501: Advanced Nursing Roles This course explores skills and strategies essential to successful advanced nursing role implementation. Analysis of existing and emerging roles
Nursing (MN) 1 NURSING (MN) MN501: Advanced Nursing Roles This course explores skills and strategies essential to successful advanced nursing role implementation. Analysis of existing and emerging roles
Patient and Family Advisor Orientation Manual
 Patient and Family Advisor Orientation Manual Guide to Patient and Family Engagement Table of Contents About This Orientation Manual... 1 Section 1. Responsibilities and Expectations... 2 Section 2. Tips
Patient and Family Advisor Orientation Manual Guide to Patient and Family Engagement Table of Contents About This Orientation Manual... 1 Section 1. Responsibilities and Expectations... 2 Section 2. Tips
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
The FOCUS Program: Helping Cancer Patients and Family Their Caregivers. Laurel Northouse PhD, RN, FAAN Professor of Nursing University of Michigan
 The FOCUS Program: Helping Cancer Patients and Family Their Caregivers Laurel Northouse PhD, RN, FAAN Professor of Nursing University of Michigan Co-director, Socio-behavioral Program U of M Comprehensive
The FOCUS Program: Helping Cancer Patients and Family Their Caregivers Laurel Northouse PhD, RN, FAAN Professor of Nursing University of Michigan Co-director, Socio-behavioral Program U of M Comprehensive
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT
 A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
The Role of Occupational Therapy (OT) In Community-based Home Care Services
 In Community-based Home Care Services") The Role of Occupational Therapy (OT) In Community-based Home Care Services The Society of Occupational Therapists (SAOT) supports the 2008 statement of the Canadian Association of Occupational Therapists
The Role of Occupational Therapy (OT) In Community-based Home Care Services The Society of Occupational Therapists (SAOT) supports the 2008 statement of the Canadian Association of Occupational Therapists
Surgical Critical Care Sub I
 Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
This document applies to those who begin training on or after July 1, 2013.
 Objectives of Training in the Subspecialty of Occupational Medicine This document applies to those who begin training on or after July 1, 2013. DEFINITION 2013 VERSION 1.0 Occupational Medicine is that
Objectives of Training in the Subspecialty of Occupational Medicine This document applies to those who begin training on or after July 1, 2013. DEFINITION 2013 VERSION 1.0 Occupational Medicine is that
NATIONAL STANDARDS, ESSENTIAL ELEMENTS AND INTERPRETIVE GUIDANCE
 Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Obesity and corporate America: one Wisconsin employer s innovative approach
 Focus On... Obesity Obesity and corporate America: one Wisconsin employer s innovative approach Amy Helwig, MD, MS; Dennis Schultz, MD, MSPH; Len Quadracci, MD Introduction The United States has an obesity
Focus On... Obesity Obesity and corporate America: one Wisconsin employer s innovative approach Amy Helwig, MD, MS; Dennis Schultz, MD, MSPH; Len Quadracci, MD Introduction The United States has an obesity
Physicians Who Care for People with MS
 Physicians Who Care for People with MS Neurologists: Specialize in the diagnosis and treatment of conditions related to the nervous system including the brain, spinal cord, and nerves. Many neurologists
Physicians Who Care for People with MS Neurologists: Specialize in the diagnosis and treatment of conditions related to the nervous system including the brain, spinal cord, and nerves. Many neurologists
THE INTRAPARTUM NURSE S BELIEFS RELATED TO BIRTH PRACTICE
 THE INTRAPARTUM NURSE S BELIEFS RELATED TO BIRTH PRACTICE Ellise D. Adams PhD, CNM All Rights Reserved Contact author for permission to use The Intrapartum Nurse s Beliefs Related to Birth Practice (IPNBBP)
THE INTRAPARTUM NURSE S BELIEFS RELATED TO BIRTH PRACTICE Ellise D. Adams PhD, CNM All Rights Reserved Contact author for permission to use The Intrapartum Nurse s Beliefs Related to Birth Practice (IPNBBP)
Consumer Perception of Care Survey 2016 Executive Summary
 Maryland s Public Behavioral Health System Consumer Perception of Care Survey 2016 Executive Summary MARYLAND S PUBLIC BEHAVIORAL HEALTH SYSTEM 2016 CONSUMER PERCEPTION OF CARE SURVEY TABLE OF CONTENTS
Maryland s Public Behavioral Health System Consumer Perception of Care Survey 2016 Executive Summary MARYLAND S PUBLIC BEHAVIORAL HEALTH SYSTEM 2016 CONSUMER PERCEPTION OF CARE SURVEY TABLE OF CONTENTS
Chapter 2. At a glance. What is health coaching? How is health coaching defined?
 Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
Allied Health - Occupational Therapist
 Position Description December 2015 Position description Allied Health - Occupational Therapist Section A: position details Position title: Employment Status: Classification and Salary: Location: Hours:
Position Description December 2015 Position description Allied Health - Occupational Therapist Section A: position details Position title: Employment Status: Classification and Salary: Location: Hours:
Palliative Care Competencies for Occupational Therapists
 Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Nurse Link. Special Edition: Professional Practice Model. LUHS Nursing Professional Practice Model. Nursing Attributes
 Nurse Link V O L U M E 7, I S S U E 7 Special Edition: Professional Practice Model Author D E C E M B E R 2 0 1 3 A Professional Practice Model is the overarching conceptual framework for nurses, nursing
Nurse Link V O L U M E 7, I S S U E 7 Special Edition: Professional Practice Model Author D E C E M B E R 2 0 1 3 A Professional Practice Model is the overarching conceptual framework for nurses, nursing
Thank you for joining us today!
 Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Pay-for-Performance: Approaches of Professional Societies
 Pay-for-Performance: Approaches of Professional Societies CCCF 2011 Damon Scales MD PhD University of Toronto Disclosures 1.I currently hold a New Investigator Award from the Canadian Institutes for Health
Pay-for-Performance: Approaches of Professional Societies CCCF 2011 Damon Scales MD PhD University of Toronto Disclosures 1.I currently hold a New Investigator Award from the Canadian Institutes for Health
Critical Time Intervention (CTI) (State-Funded)
 (State-Funded)") Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
A pre- experimental study on the effect of Assertiveness training program among nursing students of a selected college of Nursing, Ajitgarh,
 2017; 3(5): 533-538 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2017; 3(5): 533-538 www.allresearchjournal.com Received: 25-03-2017 Accepted: 26-04-2017 Ritika Soni Rattan Group
2017; 3(5): 533-538 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2017; 3(5): 533-538 www.allresearchjournal.com Received: 25-03-2017 Accepted: 26-04-2017 Ritika Soni Rattan Group
Patient -Centered Comparative Effectiveness Research and Quality Improvement: Their Relationship in Transformative Research
 Patient -Centered Comparative Effectiveness Research and Quality Improvement: Their Relationship in Transformative Research Beth Kosiak, Ph.D. Program Officer Improving Healthcare Systems Program PCORI
Patient -Centered Comparative Effectiveness Research and Quality Improvement: Their Relationship in Transformative Research Beth Kosiak, Ph.D. Program Officer Improving Healthcare Systems Program PCORI
WPS Integrated Care Management Improving health, one member at a time
 WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
Inpatient Rehabilitation Program Information
 Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Using Innovation to Maximize Behavioral Health Accommodations. Regions Hospital Case Study
 Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
LICENSED CLINICAL SOCIAL WORKER-PATIENT SERVICES AGREEMENT
 LICENSED CLINICAL SOCIAL WORKER-PATIENT SERVICES AGREEMENT PLEASE KEEP THIS DOCUMENT FOR YOUR RECORDS Welcome to our practice. This document (the Agreement) contains important information about my professional
LICENSED CLINICAL SOCIAL WORKER-PATIENT SERVICES AGREEMENT PLEASE KEEP THIS DOCUMENT FOR YOUR RECORDS Welcome to our practice. This document (the Agreement) contains important information about my professional
MISSION, VISION AND GUIDING PRINCIPLES
 MISSION, VISION AND GUIDING PRINCIPLES MISSION STATEMENT: The mission of the University of Wisconsin-Madison Physician Assistant Program is to educate primary health care professionals committed to the
MISSION, VISION AND GUIDING PRINCIPLES MISSION STATEMENT: The mission of the University of Wisconsin-Madison Physician Assistant Program is to educate primary health care professionals committed to the