NEW PATIENT WELCOME LETTER
|
|
|
- Theodore Newton
- 5 years ago
- Views:
Transcription


.")
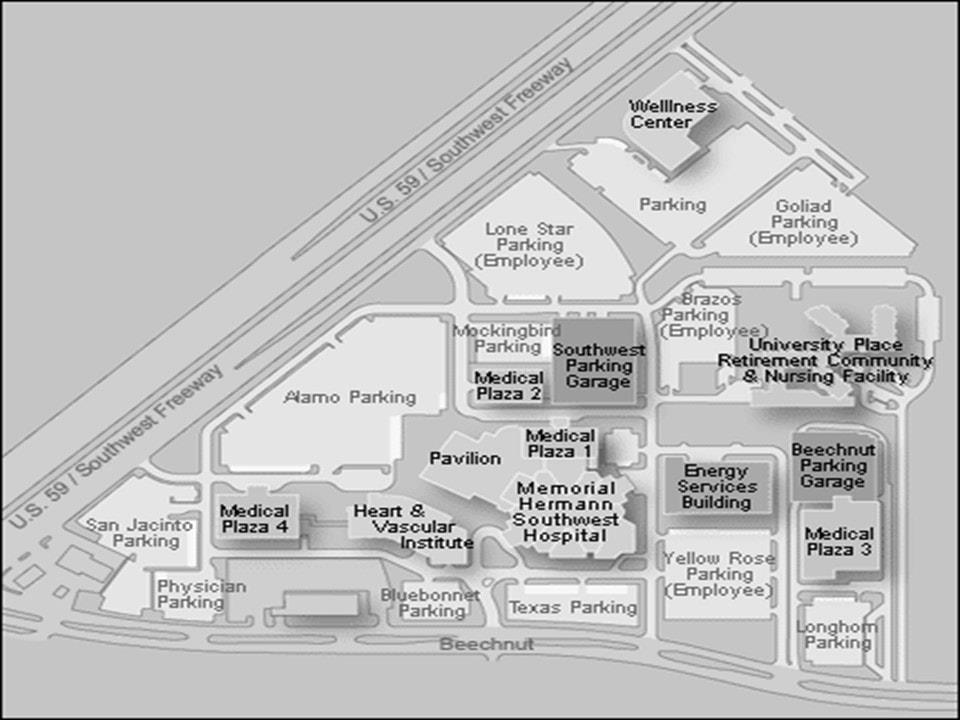
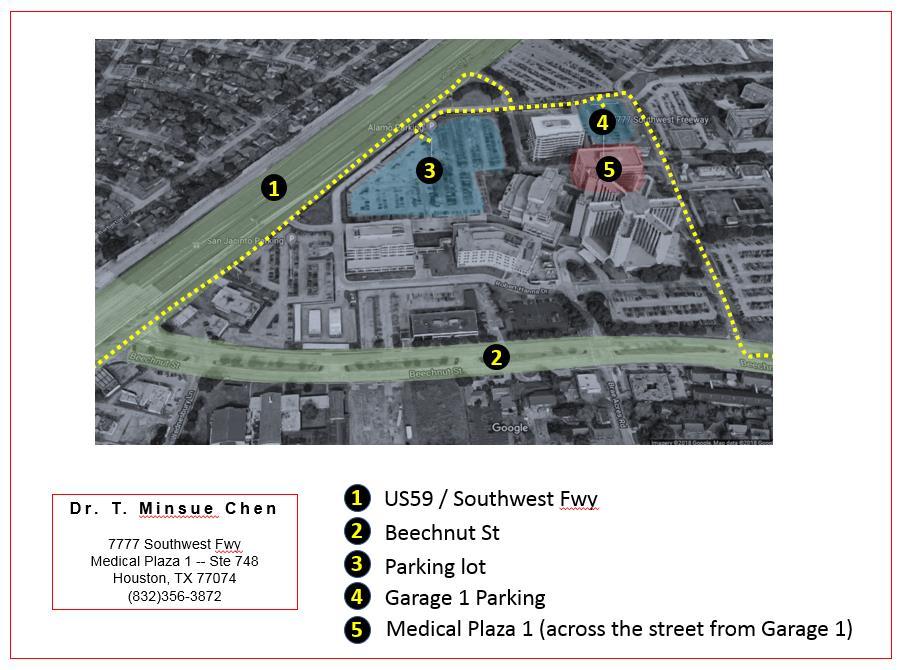
1 NEW PATIENT WELCOME LETTER We respect your time: In order for you (and the other patients on the schedule) to be seen with minimal wait, patient registration and paperwork must be completed BEFORE your appointment time. Therefore, plan to arrive at least 15 minutes before your scheduled appointment time. To expedite the process, NEW PATIENT forms can be printed and completed before your office visit. To prevent other delays, have your driver s license, insurance card, and payment ready when you check in. Tips on finding our office: Our address is: 7777 Southwest Fwy, Ste 748, Houston, TX Take the elevator to the seventh floor of Medical Plaza 1. CHEN SKIN AND CANCER SURGERY, P.A. is located adjacent to the Ladies Restroom. Parking: For easy access and your first visit to your office, we suggest you park in GARAGE ONE (covered parking garage attached to Medical Plaza SW Fwy). Medical Plaza SW Fwy is directly across from GARAGE ONE. Upon your arrival to CHEN SKIN AND CANCER SURGERY, P.A., sign-in and inquire about Parking Validation. Maps: Located at the Memorial Hermann Southwest Hospital campus, CHEN SKIN AND CANCER SURGERY, P.A. is directly adjacent to the hospital building. Directions to the medical campus are listed below: From US 59 N, travel South. Exit Gessner/ Beechnut and go left under 59 and another left on to US 59 N feeder road (or make a U-turn). Turn right at the 2nd driveway to the right onto the Southwest Hospital Campus. From Beltway 8, exit 59 North. Exit Gessner/ Beechnut. Continue on US 59 N feeder road, past Beechnut. Turn right at the 2nd driveway to the right onto the Southwest Hospital Campus. From IH 10 W, travel east to US 59, then South on 59. Exit Gessner/ Beechnut and go left under 59 and another left on to US 59 N feeder road (or make a U-turn). Turn right at the 2nd driveway to the right onto the Southwest Hospital Campus. From IH 10 E, travel west to US 59, then South on 59. Exit Gessner/ Beechnut and go left under 59 and another left on to US 59 N feeder road (or make a U-turn). Turn right at the 2nd driveway to the right onto the Southwest Hospital Campus. Bring the following to your appointment: 1) Your driver's license, insurance card, and credit card or debit card. The payment card will be put on file for no show and cancellation fee and any other charges assigned to your account, such as the balance determined by your insurer as your share of the expenses. You will always be notified before any charges are necessary for your account. You can pay either with a check or the payment card we have on file for you. Our office accepts Visa, MasterCard, and Discover (no American Express).
2
3 2) After printing the NEW PATIENT forms, please complete and bring the forms with you to your appointment. Before you arrive for your appointment, we can review our ice of Privacy Practices and ice of Services Agreement on our website ( 3) If you have a summary of your Health History, please bring it along. Specifically, Dr. Chen needs a list of your allergies, current medications, medical problems, and prior procedures. Additionally, if you have seen a doctor for your skin problem, it can sometimes be helpful to bring a copy of your medical records for Dr. Chen to review. What to expect from your appointment with us: Dr. Chen and her staff will review your Health History. This will be followed by examination of your skin concerns and discussion of treatment options, which may or may not include a procedure. Please remember that if you have medical insurance, you are responsible for your co-payment/coinsurance/deductible at the time of service. Additionally, office procedures may be performed on the same day only if the procedure has been pre-approved/pre-certified by your insurance company. Kindly contact your insurance company to see if pre-authorization is necessary. Contacting our office: Please do not hesitate to let us know if you have any questions. We are a small practice; therefore, if we do not answer the, it is because we are either caring for a patient who is in the office or on the with another patient. We have found that the fastest and most patient preferred method of communication is via TEXT messaging. Therefore, kindly send us a TEXT message to our office number (832) , and we will reply as soon as possible. Other methods to contact us include: 1) Send a HELLO from our website. 2) (info@drminsuechen.com). 3) Leave a detailed message on our voic (832) ) Send a Fax (888) All messages should be responded to by the end of the next business day. Please contact us again if you do not hear from us by the end of the next business day. Payment and collections policy: In order to keep this office open and staff paid, we need our patients to take financial responsibility for their accounts and pay their bills in a timely manner. Payment is due at the time of service, and any outstanding balance is to be paid in full before any additional services and/or items are provided by Chen Skin and Cancer Surgery, P.A. The cost of any date of service is not complete until the finished documentation of that visit is reviewed for accuracy and completion and you may be sent an additional statement. Some treatments require several visits to treat and each is billed separately. Cosmetic procedures are to be paid in full at the time of service and will not be billed to your insurance carrier. Chen Skin and Cancer Surgery, P.A. reserves the right to assign additional fees to your account in the following instances: compensation for extra administrative expenses incurred, any check returned for nonpayment, form completion fee, declined charge on credit card, and medical records fee. Our promise to you: Please review OUR PROMISE TO YOU webpage (SEE charges.html) regarding office policies and fee structure regarding: Timeliness; Payment Policies ($20 late fees; $50 returned check fee); Cancellation Policy ($150 to $500 fee depending on your reserved appointment type); Grounds for Termination of Patient-Physician Relationship; No Jerk Rule, and availability and fee schedule for Virtual Visits and Appointments outside of regular hours. See also our ice of Privacy Practices ( and ices of Service Agreement ( We look forward to caring for your skin health needs! Have a blessed day! Dr. Chen and staff
4 Date: THANK YOU FOR COMPLETING THESE IMPORTANT FORMS 1) Whom can we thank for referring you to our medical practice? 2) PATIENT DEMOGRAPHICS Patient Name (LEGAL): Last First Middle Nick Name: Age: Date of Birth: Gender (circle): M F : : Phone: Phone: Preferred Language (circle): English Spanish Other Status (circle): Minor Single Married Divorced Widowed Separated Domestic Partner Mailing Address: City: State: Zip: Social Security Number (required for some insurance): Employer Name: Phone: Address: City: State: Zip: Federal agencies require us to collect his following information regarding race and ethnic group: Race (circle): White Black American Indian Native Hawaiian/Pacific Islander Other PATIENT REFUSED Ethnic Group (circle): Hispanic or Latino Hispanic or Latino Other PATIENT REFUSED Advanced Directives: I, the patient, have an Advance Directive: YES NO If yes, please provide us with a copy. 3) WHO IS THE RESPONSIBLE PARTY OR GUARDIAN (if different from the patient)? Name: Date of Birth: Relationship to Patient: : : Mailing Address: City: State: Zip: Name of Employer: Phone: 4) WHICH IS YOUR PREFERRED PHARMACY? Preferred Pharmacy Name: Phone #: Nearest Major Intersection: City: Zip Code: 5) IN CASE OF EMERGENCY, PLEASE CONTACT: Emergency Contact: Phone: Mailing Address: City: State: Zip: Relationship to Patient: Mother s maiden name (for security use only) 6) Authorization for Treatment: I authorize the health care providers at Chen Skin and Cancer Surgery to perform medical and/or surgical procedures on me or the minor I am responsible for as she deems necessary for the treatment of skin conditions. X Signature of Patient / Responsible party / Guardian: Date:
5 Date: Name: Date of Birth: SKIN HISTORY When was your last SKIN SCREENING? What sunscreen do you use? What SPF? When is your PROCEDURE with Dr. Chen SCHEDULED? In your lifetime, how many SKIN CANCERS have you had? None In your lifetime, how many skin lesions have you had CUT OFF? None In your lifetime, how many times have you had MOHS SURGERY? None GENERAL HISTORY Occupation: Exercise / Activity: / week Pets: Smoking / Tobacco: packs/ day Hobbies: Alcohol: drinks/ day Upcoming activities (ie. social, travel, athletic, etc): MEDICAL / SURGICAL HISTORY Height: Weight: Allergies to medications: Medications: Vitamins / Supplements: Medical problems: Surgeries in the past: Family history of medical problems, cancer, etc: Your Health Care Team / Doctors: YOUR VISIT WITH US What is the reason for visit? Where is the problem located? How long has it been a problem? List the treatments so far: List the lab studies so far: Do you know anyone with a similar skin problem? What do you think is going on? What else do we need to know?
6 Date: Name: Date of Birth: This often does not have anything to do with why you are here, but insurance requires that this paperwork be in your chart. Please circle those symptoms that apply to you at this time. If none of the symptoms apply to you, please check the area that says I have none of the above. REVIEW OF SYSTEMS (circle what you have now) Constitutional: Fever Weight loss Night sweats Fatigue Skin: Rashes Itching Hair change Nail change Eyes: Loss of vision Distorted vision Eye pain ENT: Loss of hearing Ringing Dizziness Nosebleeds Hoarseness Cardiovascular: Chest Pain Palpitations Swelling of legs Pulmonary: Cough Shortness of breath Wheezing Endocrine: Heat or cold intolerance Excessive thirst or hunger Gastrointestinal: Swallowing difficulty Heartburn Diarrhea Vomiting Genitourinary: Urinary frequency Blood in urine Urinary pain Musculoskeletal: Joint pain Muscle pain/ cramps Neurological: Headaches Numbness/tingling Weakness Blackouts Slurred speech Psychiatric: Anxiety Depression Mania Hematological: Easy bruising/ bleeding Anemia Immunological: Frequent infections Swollen lymph glands ( ) I have none of the above. ******* ALERTS: For your SAFETY, we review these alerts at EVERY visit. **************************** CHECK ALL THAT APPLY None of the issues below Problems with healing (ie. slow heal, thick scars, keloid scars) Cosmetic / Plastic surgery Pregnancy / Planning pregnancy Breast feeding Active Infection Frequent infection MRSA/ Staph infection Pacemaker / Defibrillator Blood thinners Bleeding problems PRE-procedure antibiotics recommended by your doctor Artificial heart valve VP shunt Artificial joint in past 2 years White coat syndrome Seizures Fainting / Passing out Allergy to Latex Allergy to Lidocaine Allergy to Adhesive Allergy to Topical Antibiotic Cancer in the past Radiation exposure (ie. acne, cancer, work-related) Organ transplant Diabetes (last HgbA1c ) Kidney problems (Cr ) Other NOTABLE ISSUES that the surgical team needs to be aware of? Hepatitis B / Hepatitis C HIV / AIDS Rapid heart with local numbing Problems with anesthesia
7 Name: Date of Birth: HOW AND WHO CAN WE CONTACT ABOUT YOUR CARE AND RESULTS? 1. I PREFER TO BE CONTACTED IN THIS ORDER: 1 st (first) preferred method to be 2 nd (second) preferred method to be 3 rd (third) preferred method to be 4 th (fourth) preferred method to be 5 th (fifth) preferred method to be 2. IF WE ARE UNABLE TO SPEAK WITH YOU, I WOULD LIKE THE OFFICE TO DO THE FOLLOWING: a) When calling my CELL PHONE (circle one): b) When sending a TEXT MESSAGE (circle one): c) When sending an message (circle one): d) When calling my HOME PHONE (circle one): e) When calling my WORK PHONE (circle one): f) I hereby give my consent that ANOTHER PERSON may be contacted about my health information in nonemergency situations. I understand that I MUST provide their names, relationship, & contact information below (circle one): *** with my Emergency Contact (if other, list below) ***Name: Relationship: Phone: : X Signature of Patient / Responsible party / Guardian: Date:
PLEASE FILL OUT FORM BELOW AND THEN FAX BACK TO: ADDITIONALLY, PLEASE BRING FORM WITH YOU ON THE DAY OF YOUR SCHEDULED APPOINTMENT.
 PLEASE FILL OUT FORM BELOW AND THEN FAX BACK TO: 516-354-8597 ADDITIONALLY, PLEASE BRING FORM WITH YOU ON THE DAY OF YOUR SCHEDULED APPOINTMENT. THANK YOU - 1 - NEW PATIENT MEDICAL INFORMATION Steven J.
PLEASE FILL OUT FORM BELOW AND THEN FAX BACK TO: 516-354-8597 ADDITIONALLY, PLEASE BRING FORM WITH YOU ON THE DAY OF YOUR SCHEDULED APPOINTMENT. THANK YOU - 1 - NEW PATIENT MEDICAL INFORMATION Steven J.
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION SHEET:
 PATIENT INFORMATION SHEET: LAST NAME: FIRST NAME/MI: ADDRESS: CITY: STATE: ZIP CODE: SOCIAL SECURITY #: HOME: CELL: WORK: SEX: M F BIRTHDATE: MARITAL STATUS: SINGLE MARRIED WIDOWED OTHER EMPLOYER NAME:
PATIENT INFORMATION SHEET: LAST NAME: FIRST NAME/MI: ADDRESS: CITY: STATE: ZIP CODE: SOCIAL SECURITY #: HOME: CELL: WORK: SEX: M F BIRTHDATE: MARITAL STATUS: SINGLE MARRIED WIDOWED OTHER EMPLOYER NAME:
Last Name First Middle. Mailing Address. City State Zip Phone. Date of Birth Age Soc. Sec# Cell. Employer Work Phone
 Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
Burton M. Sundin, M.D. / Reps B. Sundin, M.D. Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: address:
: Address: Zip, City, State: Home#: Work#: Cell#: address:") Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
PATIENT REGISTRATION FORM
 Natalie A. Nealeigh, PA-C PATIENT REGISTRATION FORM PATIENT INFORMATION (PLEASE PRINT) Last Name: First Name: MI: Street Address: City: State: Zip: Home #: Cell #: Work #: DOB: Age: Sex (M/F): Marital
Natalie A. Nealeigh, PA-C PATIENT REGISTRATION FORM PATIENT INFORMATION (PLEASE PRINT) Last Name: First Name: MI: Street Address: City: State: Zip: Home #: Cell #: Work #: DOB: Age: Sex (M/F): Marital
PATIENT INFORMATION. Patient s Name: Birthdate: ( ) F ( ) M LAST FIRST MI. ( ) Married ( ) Single ( ) Divorced ( ) Separated ( ) Widowed Occupation:
 F ( ) M LAST FIRST MI. ( ) Married ( ) Single ( ) Divorced ( ) Separated ( ) Widowed Occupation:") UPON COMPLETION OF PATIENT REGISTRATION PACKET, PLEASE BRING ALL FORMS TO YOUR APPOINTMENT. YOU MAY ALSO FAX COMPLETED FORMS TO THE OFFICE AT 910-575- 9103. THANK YOU. PATIENT INFORMATION Patient s Name:
UPON COMPLETION OF PATIENT REGISTRATION PACKET, PLEASE BRING ALL FORMS TO YOUR APPOINTMENT. YOU MAY ALSO FAX COMPLETED FORMS TO THE OFFICE AT 910-575- 9103. THANK YOU. PATIENT INFORMATION Patient s Name:
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
Patient Registration. City, State & Zip Code Date of Birth Age. Occupation: Family Physician: Married Single Other Spouse's Name
 *SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
*SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
PATIENT INFORMATION. Address: Sex: City: State: address: Cell Phone: Home Phone: Work Phone: address: Cell Phone:
 PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely)
") SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely) Name: Former/ Maiden Name: Date of Birth: Age: Today s Date: *Language: Race: Ethnicity: *Do
SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely) Name: Former/ Maiden Name: Date of Birth: Age: Today s Date: *Language: Race: Ethnicity: *Do
2200 Northern Boulevard, Suite 133 East Hills, NY Fax (516) Transitional Care
 Transitional Care") 2200 Northern Boulevard, Suite 133 East Hills, NY 11548 855-670-6077 Fax (516) 918-9039 Transitional Care Dear New Patient: We welcome you to our practice as a transitional patient. We will be managing
2200 Northern Boulevard, Suite 133 East Hills, NY 11548 855-670-6077 Fax (516) 918-9039 Transitional Care Dear New Patient: We welcome you to our practice as a transitional patient. We will be managing
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
DENTON UROLOGY 2401 West Oak Street Ste. #102 Denton, Texas Phone: Fax:
 DETO UROLOG 2401 West Oak Street Ste. #102 Denton, Texas 76201 Phone: 940-387-2241 Fax: 940-380-1374 Acknowledgment of Review of otice of Privacy Practices I have reviewed this office s otice of Privacy
DETO UROLOG 2401 West Oak Street Ste. #102 Denton, Texas 76201 Phone: 940-387-2241 Fax: 940-380-1374 Acknowledgment of Review of otice of Privacy Practices I have reviewed this office s otice of Privacy
Your annual preventive visit, or complete physical exam, is scheduled with. Dr. on at AM/PM.
 Dear: Your annual preventive visit, or complete physical exam, is scheduled with Dr. on at AM/PM. Please bring the following with you on the date of your appointment: A list of your current medication(s),
Dear: Your annual preventive visit, or complete physical exam, is scheduled with Dr. on at AM/PM. Please bring the following with you on the date of your appointment: A list of your current medication(s),
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Dear New Patient: Sincerely, The Scheduling Staff
 Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
Fax: Do not mail the forms!
 Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group
 DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
Welcome to the Southeastern Urology Associates meridianemr Patient Portal
 New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
Bellevue Neurology PATIENT DEMOGRAPHIC FORM
 PATIENT DEMOGRAPHIC FORM Name Today s date / / Last First M.I. Mailing Address Age Number, Street, Apartment Number City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Date of Birth / / SS # Marital
PATIENT DEMOGRAPHIC FORM Name Today s date / / Last First M.I. Mailing Address Age Number, Street, Apartment Number City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Date of Birth / / SS # Marital
James M. Wilson, M.D. - Medical Information to (fax to ) PATIENT INFORMATION Last name: First: D.O.
 PATIENT INFORMATION Last name: First: D.O.") James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
Patient: Gender: Male Female. Mailing Address: Ethnicity: Not Hispanic or Latin Hispanic/Latin Home Phone #:
 5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
To All Mission Ranch Primary Care Patients:
 To All Mission Ranch Primary Care Patients: At Mission Ranch Primary Care we strive to provide the best possible customer service. As a part of this, we ask that you fill out this paperwork and return
To All Mission Ranch Primary Care Patients: At Mission Ranch Primary Care we strive to provide the best possible customer service. As a part of this, we ask that you fill out this paperwork and return
FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty
 FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty Consent for Purposes of Treatment, Payment and Health Care Operations I consent to the use or disclosure of my protected health information by Florida
FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty Consent for Purposes of Treatment, Payment and Health Care Operations I consent to the use or disclosure of my protected health information by Florida
Virginia Heartburn & Hernia Institute
 Virginia Heartburn & Hernia Institute PATIENT INFORMATION FORM (Please make sure to print clearly and sign at the bottom of this page) Patient s Last Name: First: Middle Initial: Marital Status: Married
Virginia Heartburn & Hernia Institute PATIENT INFORMATION FORM (Please make sure to print clearly and sign at the bottom of this page) Patient s Last Name: First: Middle Initial: Marital Status: Married
DEMOGHRAPHICS INSURANCE INFORMATION
 DEMOGHRAPHICS Name: Date of Birth: / / AGE: Street Address: City: State: Zip: Home Phone #: ( ) Cellular Phone :( ) Social Security Number: E-mail: Marital Status: Single Married Divorced Widowed Employer:
DEMOGHRAPHICS Name: Date of Birth: / / AGE: Street Address: City: State: Zip: Home Phone #: ( ) Cellular Phone :( ) Social Security Number: E-mail: Marital Status: Single Married Divorced Widowed Employer:
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with?
 Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
Neck & Spine Patient Demographic
 Neck & Spine Patient Demographic o New Patient o Return Patient o Update Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg.
Neck & Spine Patient Demographic o New Patient o Return Patient o Update Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg.
PATIENT REGISTRATION
 PATIENT REGISTRATION Date: Patient Name Last First Middle Initial (Nickname) Home Address Street Apt# City State Zip ( ) Male ( ) Female Body part being evaluated Marital Status: ( ) Single ( ) Married
PATIENT REGISTRATION Date: Patient Name Last First Middle Initial (Nickname) Home Address Street Apt# City State Zip ( ) Male ( ) Female Body part being evaluated Marital Status: ( ) Single ( ) Married
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c
 W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
Patient Name First Middle Last Address Street City State Zip Home Phone Work Phone Cell Phone. Date of Birth SS#
 PATIENT WILL NOT BE SEEN WITHOUT PHOTO ID Patient Information Kimberly Walpert, M.D. 1199 Prince Avenue Athens GA 30606 Ph 706-475-1870 Fax 706-475-1879 www.athensbrainandspine.com Patient Name First Middle
PATIENT WILL NOT BE SEEN WITHOUT PHOTO ID Patient Information Kimberly Walpert, M.D. 1199 Prince Avenue Athens GA 30606 Ph 706-475-1870 Fax 706-475-1879 www.athensbrainandspine.com Patient Name First Middle
Would you like to follow us on: Twitter Facebook Physician's Signature
 PATIENT REGISTRATION INFORMATION TODAY S DATE: / / Last Name First Name MI Soc. Sec. # Date of Birth Sex Male Female Patient Address Apt. City, State, Zip Single Married Divorced Widow Home Phone Work
PATIENT REGISTRATION INFORMATION TODAY S DATE: / / Last Name First Name MI Soc. Sec. # Date of Birth Sex Male Female Patient Address Apt. City, State, Zip Single Married Divorced Widow Home Phone Work
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
NEW PATIENT INFORMATION Primary Care Physician
 Last Name NEW PATIENT INFORMATION Primary Care Physician Date: First Name MI Referring Provider Previous Name Date of Birth (mm/dd/yyyy) Address City Gender Male Female Marital Status Single Divorced Married
Last Name NEW PATIENT INFORMATION Primary Care Physician Date: First Name MI Referring Provider Previous Name Date of Birth (mm/dd/yyyy) Address City Gender Male Female Marital Status Single Divorced Married
Patient Name: Last First Middle
 Wilmington Ear Nose & Throat Associates, PA Patient Information Form Patient Name: Last First Middle Mailing Address: Street Address (if different from above): City: State: Zip Code: Social Security #:
Wilmington Ear Nose & Throat Associates, PA Patient Information Form Patient Name: Last First Middle Mailing Address: Street Address (if different from above): City: State: Zip Code: Social Security #:
If you wish to fill out the forms when you arrive, please arrive 20 minutes before your appointment.
 Dear patient, I would like to take a moment to personally welcome you to Conestoga Eye. At Conestoga Eye we see you, and we are excited that you will be visiting us soon. It is our mission to provide unparalleled
Dear patient, I would like to take a moment to personally welcome you to Conestoga Eye. At Conestoga Eye we see you, and we are excited that you will be visiting us soon. It is our mission to provide unparalleled
TODAYS DATE WHICH PHYSICIAN ARE YOU SEEING TODAY? NAME (LAST) (FIRST) (MI) ADDRESS CITY STATE ZIP DATE OF BIRTH
 (FIRST) (MI) ADDRESS CITY STATE ZIP DATE OF BIRTH") TODAYS DATE WHICH PHYSICIAN ARE YOU SEEING TODAY? NAME (LAST) (FIRST) (MI) ADDRESS CITY STATE ZIP HOME PHONE CELL PHONE WORK PHONE MALE FEMALE DATE OF BIRTH EMAIL SOCIAL SECURITY # DRIVERS LICENSE # DRIVERS
TODAYS DATE WHICH PHYSICIAN ARE YOU SEEING TODAY? NAME (LAST) (FIRST) (MI) ADDRESS CITY STATE ZIP HOME PHONE CELL PHONE WORK PHONE MALE FEMALE DATE OF BIRTH EMAIL SOCIAL SECURITY # DRIVERS LICENSE # DRIVERS
Age: Birthdate: Date of Last Physical exam:
 Name: : Age: Birthdate: of Last Physical exam: SYMPTOMS: Check symptoms you currently have OR have had within the past YEAR. General Fever Chills Weight loss Weight Gain Headache Depression Vertigo Ringing
Name: : Age: Birthdate: of Last Physical exam: SYMPTOMS: Check symptoms you currently have OR have had within the past YEAR. General Fever Chills Weight loss Weight Gain Headache Depression Vertigo Ringing
Workers' Compensation Demographic Form. Patient Information
 Workers Comp Patient Demographic Workers' Compensation Demographic Form Please Print Clearly Patient Information Date of Visit Account Number Workers' Compensation Coordinator Patient Name (Last, First,
Workers Comp Patient Demographic Workers' Compensation Demographic Form Please Print Clearly Patient Information Date of Visit Account Number Workers' Compensation Coordinator Patient Name (Last, First,
WELCOME TO USF HEALTH
 WELCOME TO USF HEALTH We appreciate you choosing USF Health for your healthcare needs. When you come to see a new healthcare provider, you may have questions about what to expect at your first visit. We
WELCOME TO USF HEALTH We appreciate you choosing USF Health for your healthcare needs. When you come to see a new healthcare provider, you may have questions about what to expect at your first visit. We
Thank you for choosing Southern WV Endocrinology. Enclosed you will find your new patient
 Welcome, Thank you for choosing Southern WV Endocrinology. Enclosed you will find your new patient paper work that must be completed and mailed back to us as soon as possible. Please bring your medication
Welcome, Thank you for choosing Southern WV Endocrinology. Enclosed you will find your new patient paper work that must be completed and mailed back to us as soon as possible. Please bring your medication
Patient Demographic Sheet
 Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD
 Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
Workers Compensation Demographic
 Workers Compensation Demographic Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg. Cell Phone o OK to Leave Msg. Email Do
Workers Compensation Demographic Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg. Cell Phone o OK to Leave Msg. Email Do
PATIENT REGISTRATION
 of Appointment: Referring Physician: Denton Watumull, M.D. Derek Rapp, M.D. Joshua Lemmon, M.D. Chase Derrick, M.D. Submit completed form to your patient coordinator s email, print out or email to: Bruce
of Appointment: Referring Physician: Denton Watumull, M.D. Derek Rapp, M.D. Joshua Lemmon, M.D. Chase Derrick, M.D. Submit completed form to your patient coordinator s email, print out or email to: Bruce
NAME MEDICAL HISTORY DATE Past Medical History: (Please circle all that apply): NONE Anxiety Coronary Artery Disease HIV/AIDS Seizures Arthritis Depre
: NONE Anxiety Coronary Artery Disease HIV/AIDS Seizures Arthritis Depre") GENERAL INFORMATION Patient Name Preferred Name of Birth / / Age Sex Height Weight Address Street City State Zip Home Phone Cell Phone Work Phone Social Security Number Email Emergency Contact: Name &
GENERAL INFORMATION Patient Name Preferred Name of Birth / / Age Sex Height Weight Address Street City State Zip Home Phone Cell Phone Work Phone Social Security Number Email Emergency Contact: Name &
Hello and Welcome! I truly look forward to working with you and your child on the journey towards optimal health. Warmly, Amanda H.
 Hello and Welcome! Attached you will find pediatric intake forms. Before your child s scheduled appointment, please fill out the forms as thoroughly as possible. I know your time is valuable and by bringing
Hello and Welcome! Attached you will find pediatric intake forms. Before your child s scheduled appointment, please fill out the forms as thoroughly as possible. I know your time is valuable and by bringing
Patient Name Age Date of Birth. Patient Address. City State Zip Code. Home Phone Cell Phone Work Phone
 Patient Registration Date Patient Information Patient Name Age Date of Birth Patient Address City State Zip Code Home Phone Cell Phone Work Phone Last 4 Digits of Your Social Security Number Email Marital
Patient Registration Date Patient Information Patient Name Age Date of Birth Patient Address City State Zip Code Home Phone Cell Phone Work Phone Last 4 Digits of Your Social Security Number Email Marital
Patient Communication Request
 Patient Communication Request Name: Date of Birth: Address: ZIP: Home Phone: Work Phone: Cell Phone: E-mail address: It is the policy of Capstone Family Practice to contact patients for any lab results.
Patient Communication Request Name: Date of Birth: Address: ZIP: Home Phone: Work Phone: Cell Phone: E-mail address: It is the policy of Capstone Family Practice to contact patients for any lab results.
May Family Chiropractic Health Information and Health History Patient Name: Gender: Male Female
 1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
Patient Information: Last Name First Name MI. Address Apt/Room # City Zip. Community name (if not at home) Martial Status: S M W D
 Martial Status: S M W D") HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
PLASTIC SURGERY ASSOCIATES OF LEHIGH VALLEY MEDICAL HISTORY QUESTIONNAIRE (MR: )
") PLASTIC SURGERY ASSOCIATES OF LEHIGH VALLEY MEDICAL HISTORY QUESTIONNAIRE DATE: (MR: ) Office Use Only PATIENT S NAME: (FIRST, MIDDLE INITIAL, LAST) DATE OF BIRTH AGE SOCIAL SECURITY # MALE/FEMALE ADDRESS
PLASTIC SURGERY ASSOCIATES OF LEHIGH VALLEY MEDICAL HISTORY QUESTIONNAIRE DATE: (MR: ) Office Use Only PATIENT S NAME: (FIRST, MIDDLE INITIAL, LAST) DATE OF BIRTH AGE SOCIAL SECURITY # MALE/FEMALE ADDRESS
SPOUSE/GUARDIAN (If patient is married, give spouse information. If patient is a child, give parent information.)
") Please Fill Out Completely: Infectious Disease Specialists of Athens 1500 Oglethorpe Ave, Suite 300B Athens, GA 30606 Phone: (706) 559-4405 Fax: (706) 559-4773 Patient s Last Name First Name MI Social
Please Fill Out Completely: Infectious Disease Specialists of Athens 1500 Oglethorpe Ave, Suite 300B Athens, GA 30606 Phone: (706) 559-4405 Fax: (706) 559-4773 Patient s Last Name First Name MI Social
Integrative Therapies 7E Oak Branch Drive Greensboro, NC
 Integrative Therapies 7E Oak Branch Drive Greensboro, NC 27407 www.integrativetherapies.net 336-294-0910 Hello! Welcome to Integrative Therapies and Integrative Pain Medicine, We are very happy that you
Integrative Therapies 7E Oak Branch Drive Greensboro, NC 27407 www.integrativetherapies.net 336-294-0910 Hello! Welcome to Integrative Therapies and Integrative Pain Medicine, We are very happy that you
Patient Name:,, Address: Phones:,, Home Work Cell. Primary Physician: Emergency Contact: Phone#:
 Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION CONSENT TO USE OR DISCLOSE MEDICAL INFORMATION
 Patient Name (PLEASE PRINT): Date of Birth: ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION The & Center of Southern Oregon, PC s Notice of Privacy Practices contains information about the uses and disclosures
Patient Name (PLEASE PRINT): Date of Birth: ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION The & Center of Southern Oregon, PC s Notice of Privacy Practices contains information about the uses and disclosures
NORTHSIDE PARK GASTROENTEROLOGY & ENDOSCOPY CENTER, PLLC
 NORTHSIDE PARK GASTROENTEROLOGY & ENDOSCOPY CENTER, PLLC PATIENT REGISTRATION Today s Date: / / Birthdate: / / S.S. # / / Patient Name: Age: Sex: Last First MI Address: City: State: Zip Code: Home Phone:
NORTHSIDE PARK GASTROENTEROLOGY & ENDOSCOPY CENTER, PLLC PATIENT REGISTRATION Today s Date: / / Birthdate: / / S.S. # / / Patient Name: Age: Sex: Last First MI Address: City: State: Zip Code: Home Phone:
New Patient Registration Form. Male Female
 New Patient Registration Form Today s Date Last Name Nickname Home Address DOB / / First Name Male Female City State Zip Code Email Medical Power of Attorney (if applicable) DOB / / Address City State
New Patient Registration Form Today s Date Last Name Nickname Home Address DOB / / First Name Male Female City State Zip Code Email Medical Power of Attorney (if applicable) DOB / / Address City State
Amarillo Bone & Joint Clinic. Welcome to Amarillo Bone & Joint Clinic,
 Welcome to Amarillo Bone & Joint Clinic, Our physician group is comprised of Drs. Keith Bjork, Brian Sims, Brad Veazey, T.M. Toby Risko, Joshua North, Brian Haseloff, Todd Bradshaw, and Lisa Longhofer,
Welcome to Amarillo Bone & Joint Clinic, Our physician group is comprised of Drs. Keith Bjork, Brian Sims, Brad Veazey, T.M. Toby Risko, Joshua North, Brian Haseloff, Todd Bradshaw, and Lisa Longhofer,
Patient Name: First Middle Last Address: City: State: Zip Code: Date of Birth: Social Security: Marital Status: S M D W
 Date: Sex: M or F Patient Name: First Middle Last Address: City: State: Zip Code: Date of Birth: Social Security: Marital Status: S M D W Home Phone: Work Phone: Cell Phone: Email Address: Employment Status:
Date: Sex: M or F Patient Name: First Middle Last Address: City: State: Zip Code: Date of Birth: Social Security: Marital Status: S M D W Home Phone: Work Phone: Cell Phone: Email Address: Employment Status:
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease
 Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
M or F Patient s Date of Birth Patient s Social Security Number Sex. Secondary Address: (if have, Northern) Street City State Zip Code
 Street City State Zip Code") PATIENT REGISTRATION PLEASE PRINT Today's Date: Referred by: Patient s Name: Last First M.I. M or F Patient s Date of Birth Patient s Social Security Number Sex Primary Address: Street Apt/Unit # City
PATIENT REGISTRATION PLEASE PRINT Today's Date: Referred by: Patient s Name: Last First M.I. M or F Patient s Date of Birth Patient s Social Security Number Sex Primary Address: Street Apt/Unit # City
Beaches Eye Center Patient Registration Form
 Beaches Eye Center Patient Registration Form How did you hear about us? Phonebook/Internet / TV /Newspaper Family / Friend / Insurance Plan / Hospital / Doctor Referral /By Whom? Your Primary Physician
Beaches Eye Center Patient Registration Form How did you hear about us? Phonebook/Internet / TV /Newspaper Family / Friend / Insurance Plan / Hospital / Doctor Referral /By Whom? Your Primary Physician
SYNERGY PLASTIC SURGERY
 Patient s Name Address First Middle Last Street & Apt # City State Zip Home Phone Cell Phone Other Phone Race Ethnicity Language Any restrictions for contacting you? No Yes E-mail Age Birthdate SS# Gender
Patient s Name Address First Middle Last Street & Apt # City State Zip Home Phone Cell Phone Other Phone Race Ethnicity Language Any restrictions for contacting you? No Yes E-mail Age Birthdate SS# Gender
New Patient Intake Questionnaire
 New Patient Intake Questionnaire NAME: DATE: / / BIRTHDATE: / / REFERRED BY: AGE: REASON FOR VISIT: LOCATION OF PAIN: BACK HIP BUTTOCK LEG FOOT RIGHT LEFT NECK ARM SHOULDER HAND RIGHT LEFT OTHER (DESCRIBE)
New Patient Intake Questionnaire NAME: DATE: / / BIRTHDATE: / / REFERRED BY: AGE: REASON FOR VISIT: LOCATION OF PAIN: BACK HIP BUTTOCK LEG FOOT RIGHT LEFT NECK ARM SHOULDER HAND RIGHT LEFT OTHER (DESCRIBE)
Patient Questionnaire
 Patient Questionnaire Name: Age: Date of Birth: / / Gender: M F Address: City: State: Zip: Telephone: Home: Work: Cell: E-mail: How did you hear about us? : In case of emergency, whom should we contact?
Patient Questionnaire Name: Age: Date of Birth: / / Gender: M F Address: City: State: Zip: Telephone: Home: Work: Cell: E-mail: How did you hear about us? : In case of emergency, whom should we contact?
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D KLONDIKE RD SW SUITE 205 CONYERS, GA TELEPHONE FAX
 PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
Name (First): (MI) (Last) Date: Address: City: State: Zip: Home Phone: Cell Phone: Driver s License #: Driver s License State: Occupation:
: (MI) (Last) Date: Address: City: State: Zip: Home Phone: Cell Phone: Driver s License #: Driver s License State: Occupation:") Board Certified & Fellowship Trained in Sports Medicine & Orthopaedic Arthroscopic Surgery 9980 Central Park Blvd North, Suite 222 Boca Raton, FL 33428 Please Print: Name (First): (MI) (Last) Date: Address:
Board Certified & Fellowship Trained in Sports Medicine & Orthopaedic Arthroscopic Surgery 9980 Central Park Blvd North, Suite 222 Boca Raton, FL 33428 Please Print: Name (First): (MI) (Last) Date: Address:
Allergies Drug Food Environmental. Previous Surgeries & Hospitalizations (Please list date, reason, and hospital)
") Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Prescription refills should be called in 24 hours before needing them. No refills will be made on weekends or holidays.
 TEXAS PULMONARY & CRITICAL CARE CONSULTANTS, P.A. Dr. Samer H. Fahoum Dr. R. Roger Gleason, III Dr. John W. Hollingsworth, II Dr. Obinna I. Okoye Dr. John T. Pender, Jr. 1201 Fairmount Avenue Fort Worth,
TEXAS PULMONARY & CRITICAL CARE CONSULTANTS, P.A. Dr. Samer H. Fahoum Dr. R. Roger Gleason, III Dr. John W. Hollingsworth, II Dr. Obinna I. Okoye Dr. John T. Pender, Jr. 1201 Fairmount Avenue Fort Worth,
Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD
 Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD PATIENT LAST NAME: FIRST NAME: MI: MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE: WORK PHONE: CELL PHONE: MARITAL STATUS: DATE OF BIRTH:
Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD PATIENT LAST NAME: FIRST NAME: MI: MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE: WORK PHONE: CELL PHONE: MARITAL STATUS: DATE OF BIRTH:
CURE CARDIOVASCULAR CONSULTANTS
 NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
Lubbock Sports Medicine Patient Registration
 Lubbock Sports Medicine Patient Registration PATIENT INFORMATION (Please Print) E-MAIL ADDRESS Check One: Male Female Patients Last Name First Name Middle Name Date of Birth Age Marital Status Social Security
Lubbock Sports Medicine Patient Registration PATIENT INFORMATION (Please Print) E-MAIL ADDRESS Check One: Male Female Patients Last Name First Name Middle Name Date of Birth Age Marital Status Social Security
MRN: (Office Use Only) Patient Information. Legal Name: (Last) Mr. Mrs. Ms. (First) (Middle)
 Patient Information. Legal Name: (Last) Mr. Mrs. Ms. (First) (Middle)") Patient Information MRN: (407) 260-2606 Fax (407) 260-6339 Date: Patient Information Legal Name: (Last) Mr. Mrs. Ms. (First) (Middle) Mailing Address: (Street) (City) (State) (ZIP) Phone: ( ) ( ) ( ) (Home)
Patient Information MRN: (407) 260-2606 Fax (407) 260-6339 Date: Patient Information Legal Name: (Last) Mr. Mrs. Ms. (First) (Middle) Mailing Address: (Street) (City) (State) (ZIP) Phone: ( ) ( ) ( ) (Home)
MICHELE S. GREEN, M.D.
 MICHELE S. GREEN, M.D. Name Last First Middle initial Address Number Street Apt# City, State Zip Home Cell Email Please Circle: Preferred Contact Number Home Cell Work Single Married Divorced Widowed Male
MICHELE S. GREEN, M.D. Name Last First Middle initial Address Number Street Apt# City, State Zip Home Cell Email Please Circle: Preferred Contact Number Home Cell Work Single Married Divorced Widowed Male
History Form. PAST SURGICAL HISTORY Surgeries/Hospitalizations Year Complications/Problems with anesthesia
 History Form Name: Date of Birth: Today's Date: Height: Weight: Date of Injury: Primary Care Physician: Address Who recommended this office? Address CHIEF COMPLAINT Why are you seeing the doctor today?
History Form Name: Date of Birth: Today's Date: Height: Weight: Date of Injury: Primary Care Physician: Address Who recommended this office? Address CHIEF COMPLAINT Why are you seeing the doctor today?
GRAHAM CHIROPRACTIC CENTER, INC. BRYAN GRAHAM, DC, CCSP
 New Patient Intake Form Patient Information Thank you for choosing our practice for your chiropractic needs. Please fill out this form as completely as possible. If you have any questions or concerns,
New Patient Intake Form Patient Information Thank you for choosing our practice for your chiropractic needs. Please fill out this form as completely as possible. If you have any questions or concerns,
PATIENT INFORMATION & CONDITION FORM
 PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
Medications List. Allergies. Drug Name Dosage Directions Reason Taking
 Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Tel: Fax:
 Laith Farjo, M.D. Providing state of the art orthopedic care in a friendly environment Your Appointment: Time: Please complete the enclosed forms in ink and bring them with you along with your photo ID
Laith Farjo, M.D. Providing state of the art orthopedic care in a friendly environment Your Appointment: Time: Please complete the enclosed forms in ink and bring them with you along with your photo ID
Statement of Financial Responsibility
 Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Sage Medical Center New Patient Forms
 Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
For Office Use Only: Physician Initials Nurse Initials Entered by. Patient Full Name Nickname used. Home Address City State Zip
 No Changes For Office Use Only: Physician Initials Nurse Initials Entered by Patient Information Today s Date Patient Full Name Nickname used _ Home Address City State Zip Social Security Number Date of
No Changes For Office Use Only: Physician Initials Nurse Initials Entered by Patient Information Today s Date Patient Full Name Nickname used _ Home Address City State Zip Social Security Number Date of
Patient Last Name: First: MI:
 California NeuroInstitute, Inc. Work Comp, Auto Accident or Personal Injury (All Information MUST be completed in order to bill your insurance company) Patient Last Name: First: MI: Date of Birth: Age:
California NeuroInstitute, Inc. Work Comp, Auto Accident or Personal Injury (All Information MUST be completed in order to bill your insurance company) Patient Last Name: First: MI: Date of Birth: Age:
New Patient Paperwork
 Your Vision Is Our Focus New Patient Paperwork Dear Patient, Please fill out all of the following pages, and bring them with you to your scheduled appointment time. If you have questions regarding your
Your Vision Is Our Focus New Patient Paperwork Dear Patient, Please fill out all of the following pages, and bring them with you to your scheduled appointment time. If you have questions regarding your
Your appointment is with:
 380 HOSPITAL DRIVE, SUITE 320 MACON, GA 31217 233 NORTH HOUSTON ROAD, SUITE 140F WARNER ROBINS, GA 31093 Office Phone: (478)742-5331 Office Fax: (478)750-1387 www.seurology.com W. Winston Wilfong, MD Lancing
380 HOSPITAL DRIVE, SUITE 320 MACON, GA 31217 233 NORTH HOUSTON ROAD, SUITE 140F WARNER ROBINS, GA 31093 Office Phone: (478)742-5331 Office Fax: (478)750-1387 www.seurology.com W. Winston Wilfong, MD Lancing
The Home Doctor. Registration Checklist
 The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
Last Name: First Name: Sex: Male Female. Birth Date: / / Age: Home Address: Home Phone #: Cell Phone #: Work Phone #:
 Today s Date: / / Last Name: First Name: Sex: Male Female Birth Date: / / Age: Email: Home Address: City: State: Zip Code: Home Phone #: Cell Phone #: Work Phone #: Which is the best number to reach you?
Today s Date: / / Last Name: First Name: Sex: Male Female Birth Date: / / Age: Email: Home Address: City: State: Zip Code: Home Phone #: Cell Phone #: Work Phone #: Which is the best number to reach you?
Seasons Women s Care Patient Registration Form
 Seasons Women s Care Patient Registration Form Name: of Birth: Address: City: St: Zip Home Phone: Cell: Best Number: Email: Race or Ethnicity: Marital Status: SS# Drivers Lic#: Employer: Work# Occupation:
Seasons Women s Care Patient Registration Form Name: of Birth: Address: City: St: Zip Home Phone: Cell: Best Number: Email: Race or Ethnicity: Marital Status: SS# Drivers Lic#: Employer: Work# Occupation: