Welcome and Overview. Sepsis Mortality Reduction Boot Camp 3/20/2014
|
|
|
- Myron Dawson
- 5 years ago
- Views:
Transcription
1 Welcome and Overview Sepsis Mortality Reduction Boot Camp 3/20/2014
2 AHA Disclaimer Participation in this virtual event is by express written invitation of the AHA only. Unauthorized participants and/or any party that assists unauthorized participants may be subject to substantial criminal and civil penalties. If you have not been invited to take part in this call, please disconnect at this time. 2

3 AHA/HRET (HEN) Sepsis Mortality Reduction Boot Camp-Day 1 repeated Virtual Meeting Summary Disclosure & Accreditation Statement March 20, 2014 The planners and faculty of the AHA/HRET (HEN) Sepsis Mortality Reduction Boot Camp have indicated no relevant financial relationships to disclose in regard to the content of this activity with the following exception. Kathleen Vollman indicated she receives honorarium from Sage Products, Eloquest Healthcare & Hill-Rom. This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical education through the joint sponsorship of the American Board of Quality Assurance and Utilization Review Physicians, Inc. (ABQAURP) and Health Research & Education Trust (HRET). ABQAURP is accredited by the ACCME to provide continuing medical education for physicians. The American Board of Quality Assurance and Utilization Review Physicians, Inc. designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credits. Physicians should only claim credit commensurate with the extent of their participation in the activity.
4 AHA/HRET (HEN) Sepsis Mortality Reduction Boot Camp-Day 1 repeated Virtual Meeting Summary Disclosure & Accreditation Statement March 20, 2014 The American Board of Quality Assurance and Utilization Review Physicians, Inc. (ABQAURP) is an approved provider with the Florida Board of Nursing to provide continuing education for nurses. ABQAURP designates this activity for 3.75 Nursing Contact Hours through the Florida Board of Nursing, Provider # Congress St. New Port Richey, FL Toll Free Telephone
5 WebEx Introduction and Tutorial

6 WebEx Quick Reference Dial-in Info: Audio Button 1. Click on Audio Button 2. Pop up will open with: Dial-in number Your Access Code Your attendee ID # 6

7 WebEx Quick Reference Please use Chat to All Participants for questions For technology issues only, please Chat to Host Select Chat recipient Enter Text 7

8 To download the selected presentation, begin here. Downloading a given presentation to your electronic device
9 Select Save or Save As, then document.

10 Name file Choose.pdf format. Click Save

11 Develop an understanding of the impact of sepsis on hospital mortality Understand implementation of sepsis screening in the ED and the inpatient departments Learn how best to collect data and how to drive improvement Today s Objectives
12 Polling Question 1: Who is participating today?

13 Polling Question 2: Time Zone?

14 Polling Question 3: What size is your facility?
15 Impact of Sepsis Kathleen M Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Consultant ADVANCING NURSING LLC SEPSIS SOLUTIONS INTERNATIONAL Detroit MI 48168
16 Disclosures
17 Overview Significance of the problem Define the continuum Process for development of a hospital wide sepsis program: The Power of the Pyramid o Organizational support o Early Recognition Screening/triggers o Implementation/protocols o Measurement/CI
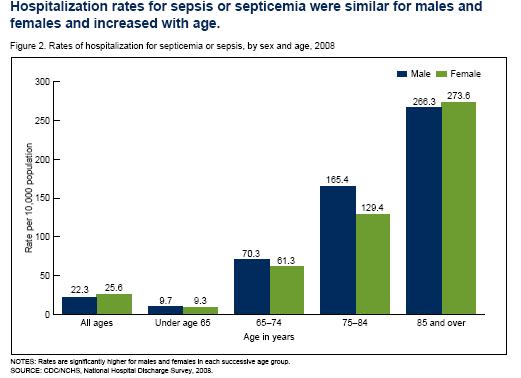
18 Severe Sepsis: A Significant Healthcare Challenge Hospitalizations have increased by 32% from *** Most costly reason for hospitalization in 2009** o 15.4 billion in aggregate hospital cost 1 out of 23 patients in hospital had septicemia** Rank in the top 4 most costly for all 4 payer groups*** Sixth most common inpatient diagnosis*** Major cause of morbidity and mortality worldwide o Leading cause of death in noncoronary ICU (US) 1 o 10th leading cause of death overall (US) 2 * In the US, more than 700 patients die of severe sepsis daily (1.6 million new cases per year)
19 Severe Sepsis: A Significant Healthcare Challenge * Based on data for septicemia Reflects hospital-wide cases of severe sepsis as defined by infection in the presence of organ dysfunction 1 Sands KE, et al. JAMA 1997;278: National Vital Statistics Reports Angus DC, et al. Crit Care Med 2001;29: **AHRQ Healthcare cost & Utilization Project October 2011 **AHRQ Healthcare cost & Utilization Project October 2011 *** Torio CM, Andrews RM (AHRQ). HCUP Statistical Brief #160. August 2013, AHRQ, Rockville, MD.
20 Severe Sepsis vs. Current Care Priorities U.S. Care Priorities # of Deaths Mortality Rate Incidence AMI (1) 900, ,000 25% Stroke (2) 700, ,500 23% Trauma (3) 2.9 million 42, % (Motor Vehicle) (injuries) Severe Sepsis (4) 751, ,000 29% Source: (1) Ryan TJ, et al. ACC/AHA Guidelines for management of patients with AMI. JACC. 1996; 28: (2) American Heart Association. Heart Disease and Stroke Statistics 2005 Update. Available at: (3) National Highway Traffic Safety Administration. Traffic Safety Facts 2003: A Compilation of Motor Vehicle Crash Data from the Fatality Analysis Reporting System and the General Estimates System. Available at (4) Angus DC et al. Crit Care Med 2001;29(7):
 for managing sepsis.")

21 A Sepsis Pilot Recognizes trouble before it starts Follows standard operating procedures (SOP) for managing sepsis. Does not take little things for granted. Understands the consequences: Immediate Long term Holds everyone accountable takes personal responsibility for outcomes.





22 Time Sensitive Diseases Changing the Paradigm of Practice AMI Stroke Trauma < 10% 8-25% < 5%
23 4-Tier Process for Severe Sepsis Program Implementation Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively SEPSIS SOLUTIONS INTERNATIONAL 2006
24 Tier I: Organizational Consensus and Support Milestones and Checklist 1. Define Sepsis Program Goal and aligned with organizational goals 2. Identify Executive sponsor 3. Collect Baseline Data essential step 4. Develop sepsis team(do we have all the right people here?) and schedule monthly(minimum) meeting for at least 6 months 5. Identify Sepsis Coordinator 6. Identify nursing and physician champions in ED and ICU and ensure champions attend team meeting 7. Begin to define action plan and timeline for program development and implementation 24

25 1. Define Sepsis Goal: Develop Project Team Charter
26 Economic Implications of an Evidence-based Sepsis Protocol: Can We Improve Outcomes and Lower Costs? Objective To determine financial impact of a sepsis protocol designed for use in the ED in a Academic, tertiary care hospital in US Design Analysis of results from recent prospective study comparing outcomes in patients with septic shock before and after initiation of sepsis protocol Adults (n=120) who sequentially presented to ED with septic shock, specifically o o o At least two systemic inflammatory response syndrome (SIRS) criteria Known or suspected infection (based on radiologic imaging and clinical suspicion) Shock requiring both fluid resuscitation and vasopressor administration ED = Emergency Department Shorr AF et al. Crit Care Med. 2007;35:
27 Summary of Results Post-protocol, savings of ~$6,000/patient observed Translated into total cost difference of $573,000 between the two groups Post-protocol, ICU costs reduced by ~35% (p=0.026) and ward costs fell by 30% (p=0.033) Protocol resulted in a reduction in overall hospital LOS of 5 days (p=0.023) Pre-protocol, 28-day mortality rate was 48.3% vs. 30.0% following protocol initiation (p=0.040) ICU, intensive care unit; LOS, length of stay Shorr AF et al. Crit Care Med. 2007;35:
28 Tier I: Organizational Consensus and Support Milestones and Checklist 1. Define Sepsis Program Goal and aligned with organizational goals 2. Identify Executive sponsor 3. Collect Baseline Data essential step 4. Develop sepsis team(do we have all the right people here?) and schedule monthly(minimum) meeting for at least 6 months 5. Identify Sepsis coordinator 6. Identify nursing and physician champions in ED and ICU and ensure champions attend team meeting 7. Begin to define action plan and timeline for program development and implementation 28
 on process aims, goals, targets, outcomes with the frontline team. o o Informative, not punitive.")
29 The Role of Executive Sponsorship 1. Sponsors are executive leaders explicitly tied to a process being improved. 2. Sr. executives round regularly (q week, q 2 weeks) on process aims, goals, targets, outcomes with the frontline team. o o Informative, not punitive. Accountable, not in trouble 3. Sponsors remove barriers to progress.

30 Role of Executive Sponsor Review project plans Review results from first team meeting Identify anticipated barriers that senior leader can help address Enlist support and help AND ASK for a sponsor to be assigned to the project
31 Baseline Data Collection Process: Defining Current State Pick time period for medical record query Sample size: minimum of 20 pts per ICU Query strategies: o ICD 9 codes: and o Patients in ICU on 1-2 antibiotics, vasopressor (review charts to see if meet criteria for severe sepsis with lactate > 4 or septic shock before including in outcome data or process data Select Data Collection Elements o Outcome: mortality, cost per case, LOS o Process 31
32 The Team Is KEY! Can Be Major Barrier If Not Functioning Well Must have nurse and physician champions from ED and ICU (need at least one physician at all meetings) Must be linked in the organization s quality or operational structure Are you linked? Must meet at least 1-2 times per month Team members must be well educated on the evidence and armed with tools and knowledge to change behavior at the bedside Does the team need more education? MUST have bedside nurses on team provide reality check and best knowledge of barriers Do you? 32
33 Tier I: Organizational Consensus and Support Milestones and Checklist Complete Team Charter Sepsis Goals aligned with organizational goals Identify sepsis coordinator/resource(s) for program Develop sepsis team(do we have all the right people here?) and schedule monthly(minimum) meeting for at least 6 months Identify nursing and physician champions in ED and ICU and ensure champions attend team meeting Collect Baseline Data essential step Begin to define action plan and timeline for program development and implementation
34 Sepsis Program Action Plan Item Responsibility Due Date Status 1. Assemble team 2. Identify executive sponsor 3. Educate team on evidence 4. Project Charter 5. Baseline data 34
35 Tier 1: Challenges and Barriers Scheduling meetings and consistent attendance Time Skipping key steps---charter, communication plan, align team/program within organization Baseline data 35
36 4-Tier Process for Severe Sepsis Program Implementation Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively SEPSIS SOLUTIONS INTERNATIONAL 2006
37 Screening for Sepsis and Performance Improvement 1. We recommend routine screening of potentially infected seriously ill patients for severe sepsis to increase the early identification of sepsis and allow implementation of early sepsis therapy (1C) 2. Performance improvement efforts in severe sepsis should be used to improve patient outcomes (UG) Dellinger RP, et al. Crit Care Med. 2013;
38 Severe Sepsis: Defining a Disease Continuum Infection Systemic Manifestations of infection Sepsis Severe Sepsis Adult Criteria A clinical response arising from a nonspecific insult, including 2 of the following: Temperature:> 38 C or < 36 C Heart Rate: > 90 beats/min Respiration: > 20/min WBC count: > 12,000/mm 3, or < 4,000/mm 3, or > 10% immature neutrophils Altered mental status BG >140 (non diabetic) SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest.1992;101: Systemic Manifestations of infection with a presumed or confirmed infectious process Sepsis with 1 sign of organ dysfunction, hypoperfusion or hypotension. Examples: Cardiovascular (refractory hypotension) Renal Respiratory Hepatic Hematologic Unexplained metabolic acidosis Shock
39 Signs & Symptoms of Sepsis Chills Alteration in LOC Tachypnea Unexplained metabolic acidosis Heart rate Altered blood pressure Platelets Bands Skin perfusion Urine output Skin mottling Poor capillary refill Hyperglycemia Purpura/petechia Levy M, et al. Crit Care Med 2003;31:
40 Definitions Sepsis: presence of infection (suspected or confirmed) with systemic manifestations of infection Severe Sepsis: Sepsis-induced tissue hypoperfusion or organ dysfunction Septic Shock: Hypotension that persists despite adequate fluid resuscitation
41 Why Do You Need to Have a Screening Process? TIME IS TISSUE!! o Similar to trauma, AMI, or stroke, the speed and appropriateness of therapy administered in the initial hours after severe sepsis develops are likely to influence outcomes. 1 To screen effectively, it must be part of the nurses daily routines i.e., part of admission and shift assessment Must define a process for what to do with the results of the screen If you don t screen you will miss patients that may have benefited from the interventions 1. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: Crit Care Med. 2008;36:
42 Screening for Severe Sepsis Yes Positive Screen for Severe Sepsis? No Surviving Sepsis Guidelines Monitor frequently whether on the ward or ICU Standard care
43 Tier II: Screening for Severe Sepsis Milestones and Checklist Develop screening process for ED, rapid response team and ICU (eventually housewide) Develop audit process to evaluate compliance and effectiveness Ensure screening process has clear next steps defined for nursing staff
44 Sepsis Program Action Plan Item Responsibility Due Date Status 1. Assemble team 2. Identify executive sponsor 3. Educate team on evidence 4. Project Charter 5. Baseline data 6. Define screening tool and process for ED, ICU, Floor, RRT 7. Define screening audit process 44
45 Tier III: Sepsis Bundle Implementation Milestones and Checklist Develop easy to use order sets (ED and ICU should be the same), organized by bundle Order sets approved by appropriate medical and nursing leadership/committees Identify resistance and barriers to bundle implementation and develop solutions o Ex: ability to get lactate quickly Identify equipment needs and make capital requests Develop triggers/processes to alert staff when time to move from first 3 hrs to shock bundle Define educational plan for all staff Develop implementation plan
46 Tier III: Develop and Implement the Education Plan o o o Content: (present to physicians, nurses and RTs) o Significance of problem o Sepsis continuum o Pathophysiology of severe sepsis o Prevention and management (share the evidence) o Case studies for staff to practice with bedside tools Methods: o Self learning modules o Classroom and/or small groups of staff on unit o Web-based: IE:ICU-USAPRO Ongoing: o build into orientation, o monthly for residents, o every 6 months for all staff, o one-on one during rounds
47 Implementation Hospital resources often focus on planning phase and then back off after implementation. The implementation phase is the most critical. Frequent rounds by project champion recommended on unit to support staff and answer questions. Defined resources for bedside nurse: o Project champion has pager to be available 24/7 initially o Clinical nurse champions identified on each ICU unit and ED to be resources to bedside staff (these staff should be members of the sepsis team/committee from the beginning)
48 TIER III: Develop Implementation Plan Identify who will oversee the implementation and the expectations of that person(sepsis nurse or program coordinator) Define ICU/ED resources for staff that they can call at any time for questions and assistance Create rounding schedule and process o Should begin as daily in the ICU and ED o Keep master list of all patients who go on the bundles (and those who should have but didn t if possible) o Do real time interventions to ensure patients get the evidence based practices o Define follow up process for review and evaluate missed opportunities
49 Sepsis Program Action Plan Item Responsibility Due Date Status 1. Assemble team 2. Identify executive sponsor 3. Educate team on evidence 4. Project Charter 5. Baseline data 6. Define screening tool and process for ED, ICU, Floor, RRT 7. Define screening audit process 8. Develop order sets/work through committees 9. Identify resistance and barriers to bundle implementation and develop solutions 10. Develop & implement an educational plan for all staff: 11. Develop an implementation plan 49

50 4-Tier Process for Severe Sepsis Program Implementation Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively SEPSIS SOLUTIONS INTERNATIONAL 2006
51 Tier IV: Measurement Milestones and Checklist Define outcome and process data elements that will be collected Develop and implement a data collection process Revise and update goals and action plan as needed Execute implementation plan
52 Data Collection Patient Log o o Define how will find all patients that receive the bundles Real time data collection is optimal then used as checklist to ensure patient receives all appropriate interventions Outcome o o o Process o Mortality (ICU and Hosp) Hosp LOS Cost per case (total and direct) SSC database o Data elements that measure process achievement of the 3 & 6 hour bundles & outcome measures of the 6hrs
53 Sepsis Program Action Plan Item Responsibility Due Date Status 1. Assemble team 2. Identify executive sponsor 3. Educate team on evidence 4. Project Charter 5. Baseline data 6. Define screening tool and process for ED, ICU, Floor, RRT 7. Define screening audit process 8. Develop order sets/work through committees 9. Identify resistance and barriers to bundle implementation and develop solutions 10. Develop & implement an educational plan for all staff: 11. Develop an implementation plan 12. Data measurement & feedback 53
54 Strategies for Keeping Sepsis Front and Center Align team with clinical and quality structures in organization Sepsis program/goals part of hospital quality plan Reporting progress and data quarterly to executive leadership Report to hospital board annually Standing agenda item on department meetings Communication plan---includes flyers, newsletters, postings in units etc. Code sepsis Real time data measurement and feedback 54
55 Seize the Opportunity The Power of The Pyramid Can Make a Difference in Implementing a Sepsis Program while Saving Lives & Money

56 Questions
57 Polling Question 3: Where is your team? Where is your organization on the sepsis climb? o Just started getting our team together o We have an order set o Almost to the top of the summit o Stuck on the mountain side and setting up camp o Moving along with a great team and we know where we are headed?
58 Optimizing Care for Patients with Severe Sepsis and Septic Shock Sean R. Townsend, MD VP Quality & Safety, California Pacific Med. Ctr. Clinical Assistant Professor University of California, San Francisco March 2014 This presenter has nothing to disclose.
59 Our Work Funded By:
60 Time Sensitive Interventions AMI Door to PCI o Focus on the timely return of blood flow to the affected areas of the heart. Stroke Time is Brain o The sooner that treatment begins, the better are one s chances of survival without disability. Trauma The Golden Hour o o Requires immediate response and medical care on the scene. Patients typically transferred to a qualified trauma center for care.
61 Mortality Increasing with Successive Organ Failures Mortality Rate # of Organ Dysfunctions 21.2% % % % 4 Source: Angus DC et al. Crit Care Med 2001;29(7):
62 Severe Sepsis vs. Current Care Priorities U.S. Care Priorities # of Deaths Mortality Rate Incidence AMI (1) 900, ,000 25% Stroke (2) 700, ,500 23% Trauma (3) 2.9 million 42, % (Motor Vehicle) (injuries) Severe Sepsis (4) 751, ,000 29% Source: (1) Ryan TJ, et al. ACC/AHA Guidelines for management of patients with AMI. JACC. 1996; 28: (2) American Heart Association. Heart Disease and Stroke Statistics 2005 Update. Available at: (3) National Highway Traffic Safety Administration. Traffic Safety Facts 2003: A Compilation of Motor Vehicle Crash Data from the Fatality Analysis Reporting System and the General Estimates System. Available at (4) Angus DC et al. Crit Care Med 2001;29(7):
63
64 National Hospital Discharge Database
65 Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012 R. Phillip Dellinger, Mitchell M. Levy, Andrew Rhodes, Djillali Annane, Herwig Gerlach, Steven M. Opal, Jonathan E. Sevransky, Charles L. Sprung, Ivor S. Douglas, Roman Jaeschke, Tiffany M. Osborn, Mark E. Nunnally, Sean R. Townsend, Konrad Reinhart, Ruth M. Kleinpell, Derek C. Angus, Clifford S. Deutschman, Flavia R. Machado,Gordon D. Rubenfeld, Steven A. Webb, Richard J. Beale, Jean-Louis Vincent, Rui Moreno, and the Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Crit Care Med 2013; 41: Intensive Care Medicine 2013;..
66 Screening for Sepsis and Performance Improvement 1. We recommend routine screening of potentially infected seriously ill patients for severe sepsis to increase the early identification of sepsis and allow implementation of early sepsis and allow implementation of early sepsis therapy (Grade 1C). 2. Performance improvement efforts in severe sepsis should be employed to improve patient outcomes (UG).
67 Initial Resuscitation 1. We recommend the protocolized, quantitative resuscitation of patients with sepsisinduced hypoperfusion (defined as hypotension persisting after initial fluid challenge or blood lactate concentration 4 mmol/l). This protocol should be initiated as soon as hypoperfusion is recognized and should not be delayed pending ICU admission. During the first 6 hrs of resuscitation, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as one part of a treatment protocol: Central venous pressure (CVP): 8 12mm Hg Mean arterial pressure (MAP) 65mm Hg Urine output 0.5mL.kg 1.hr 1 Superior vena cava oxygen saturation (ScvO2) or mixed venous oxygen saturation (SvO2) 70% or 65%, respectively. (Grade 1C)
68 Initial Resuscitation 2. We suggest targeting resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion (grade 2C).
69 Antibiotic therapy 1. We recommend that intravenous antimicrobial therapy be started as early as possible and within the first hour of recognition of septic shock (1B) and severe sepsis without septic shock (grade1c). Remark: Although the weight of evidence supports prompt administration of antibiotics following the recognition of severe sepsis and septic shock, the feasibility with which clinicians may achieve this ideal state has not been scientifically validated.
70 Antibiotic therapy 4. We suggest the use of low procalcitonin levels or similar biomarkers to assist the clinician in the discontinuation of empiric antibiotics in patients who appeared septic, but have no subsequent evidence of infection (grade 2C).
71 123
72 Surviving Sepsis Campaign: Data Analysis First analysis: 2 years 15,000 pts January 2005-December 2006 Current analysis: 4 years 28,150 pts January 2005-December 2008

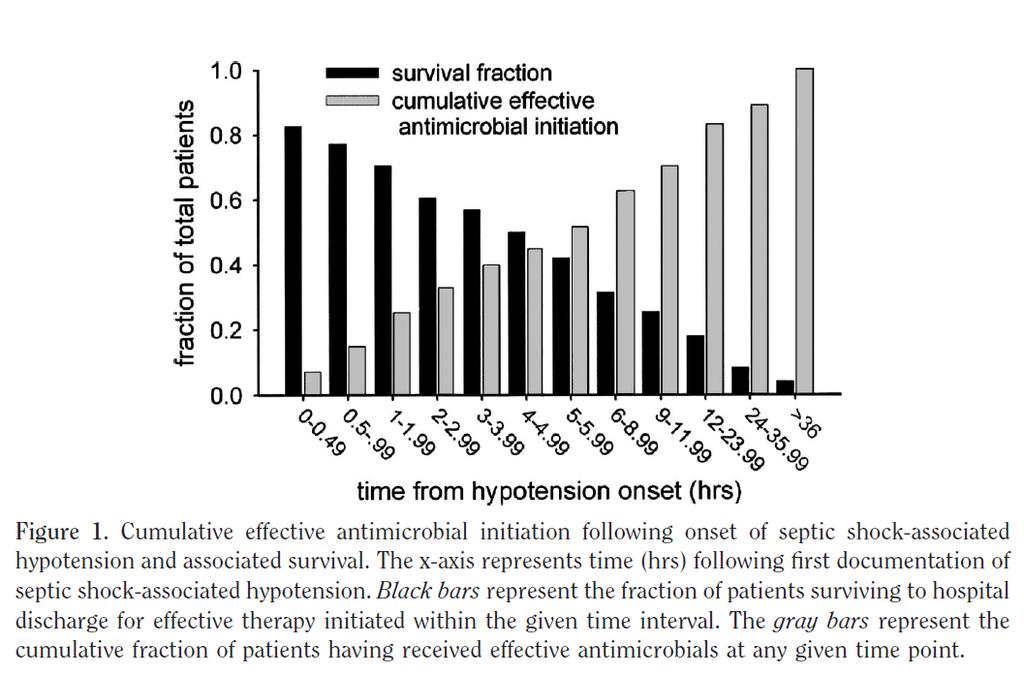
73 Hospital Mortality by Time to Antibiotics
74 Hospital Mortality by Time to Antibiotics
75 Source control 1. We recommend that a specific anatomical diagnosis of infection requiring consideration for emergent source control (e.g., necrotizing soft tissue infection, peritonitis, cholangitis, intestinal infarction) be sought and diagnosed or excluded as rapidly as possible, and intervention be undertaken for source control within the first 12 hr after the diagnosis is made, if feasible. (Grade 1C).
76 Fluid therapy 1. We recommend crystalloids be used in the initial fluid resuscitation of severe sepsis (Grade 1B). 2. We suggest the use of albumin in the fluid resuscitation of severe sepsis and septic shock when patients require substantial amounts of crystalloids (Grade 2C). Delaney AP, Dan A, McCaffrey J, et al: The role of albumin as a resuscitation fluid for patients with sepsis: A systematic review and meta-analysis. Crit Care Med 2011; 39: We recommend against the use of hydroxyethyl starches (HES) for fluid resuscitation of severe sepsis and septic shock (Grade 1B). (This recommendation is based on the results of the VISEP, CRYSTMAS, 6S and CHEST trials. The results of the recently completed CRYSTAL trial were not considered).
77 Fluid therapy 4. Initial fluid challenge in sepsis-induced tissue hypoperfusion (hypotension or elevated lactate) with suspicion of hypovolemia to be a minimum of 30ml/kg of crystalloids (a portion of this may be albumin equivalent). More rapid administration and greater amounts of fluid, may be needed in some patients (Grade 1C). 5. We recommend a fluid challenge technique be applied wherein fluid administration is continued as long as there is hemodynamic improvement either based on dynamic (e.g. change in pulse pressure, stroke volume variation) or static (e.g., arterial pressure, heart rate) variables (UG).
78 Vasopressors 1. We recommend that vasopressor therapy initially target a mean arterial pressure (MAP) of 65 mm Hg (grade 1C). 2. We recommend norepinephrine as the first choice vasopressor (Grade 1 B). 3. We suggest epinephrine (added to and potentially substituted for norepinephrine) when an additional agent is needed to maintain blood pressure (Grade 2B). 4. Vasopressin.03 units/min can be added to norepinephrine with the intent of raising MAP to target or decreasing or decreasing norepinephrine dosage (UG). 5. We suggest dopamine as an alternative vasopressor agent to norepinephrine in highly selected patients at very low risk of tachyarrhythmias and with relative or absolute bradycardia. (Grade 2C).
79 Vasopressors 1. Phenylephrine is not recommended in the treatment of septic shock except: Norepinephrine associated with serious arrhythmias Cardiac output is known to be high and blood pressure persistently low As salvage therapy when combined inotrope/vasopressor drugs and low dose vasopressin have failed to achieve MAP target (grade 1C).
80 Goals of Care and Communication of Prognosis 1. We recommend that goals of care and prognosis be discussed with patients and families (Grade 1B). 2. We recommend that these communications should be incorporated into treatment and endof-life care planning, utilizing palliative care principles where appropriate (Grade 1B). 3. We suggest that goals of care be addressed as early as feasible, but no later than within 72 hrs of ICU admission (Grade 2C).
81 NQF BUNDLE: Sepsis 0500 TO BE COMPLETED WITHIN 3 HOURS OF TIME OF PRESENTATION : 1. Measure lactate level 2. Obtain blood cultures prior to administration of antibiotics 3. Administer broad spectrum antibiotics 4. Administer 30ml/kg crystalloid for hypotension or lactate 4mmol/L time of presentation is defined as the time of triage in the Emergency Department or, if presenting from another care venue, from the earliest chart annotation consistent with all elements severe sepsis or septic shock ascertained through chart review.
82 NQF BUNDLE: Sepsis 0500 TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION: 5. Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation to maintain a mean arterial pressure (MAP) 65mmHg) 6. In the event of persistent arterial hypotension despite volume resuscitation (septic shock) or initial lactate 4 mmol/l (36mg/dl): - Measure central venous pressure (CVP)* - Measure central venous oxygen saturation (ScvO2)* 7. Remeasure lactate* * Targets for quantitative resuscitation included in the guidelines are CVP of 8 mm Hg, ScvO2 of 70% and lactate normalization
83 Change in Compliance Over Time Levy MM et al. CCM 38(2): , February 2010.
84 Change in Mortality Over Time Levy MM et al. CCM 38(2): , February 2010.
85 Mortality: Site Quarter Mortality over 4 year study period 36.7% to 27.5% ARR: 9.2% RRR: 25.0% P=0.005
86 Intermountain: SS & Shock
87 Intermountain: Shock Only
88 Questions?
89 Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky

90 59
91 About Us St. Claire Regional Medical Center is a 159-bed rural hospital centrally located between Lexington and Ashland, in Morehead, Kentucky. The emergency department has approximately 30,000 yearly visits, which accounts for for more than 70% of the admissions to the hospital. Nursing and physician leaders in the emergency department work closely together to advance the care of patients. 60
92 Case Study 62 year old male presenting from long-term care facility o paraplegic, bed-ridden o indwelling urinary catheter. Complaint: deteriorating mental status. Vital signs: blood pressure 80/50, heart rate 119, respiratory rate 23, temperature 98.5 C, spo 2 95% on 2 liters per minute via nasal cannula. Treatment is initiated. 61
93 Case Study (cont.) The patient remains in emergency department for several hours with limited IV fluids and a single antibiotic agent administered. The patient is admitted to the ICU and received a central line, arterial line, several boluses of IV fluids, additional antibiotics, and vasopressors. Why weren t these interventions initiated in the emergency department? 62
94 Discovering a Need Chart reviews of patients with primary diagnosis of sepsis for the months of January- March o 42 patients with primary diagnosis of sepsis. o 21 patients met SIRS criteria at triage o 13 of those 21 patients met SIRS criteria based on vital signs alone. o Only 3 of those 21 patients had the established sepsis order set initiated. 63
95 The Next Step Sepsis screening tool created and added into ED triage assessment. Performed on every adult patient upon arrival to emergency department. If patient meets the criteria, the Triage Sepsis order set is initiated by the nurse and the patient is flagged on the tracker.
96 Triage Sepsis Order Set CBC CMP Magnesium PTT, PT/INR Lactate Troponin BNP Blood culture x 2 Includes the following: UAMC CXR - portable EKG IV initiation and normal saline bolus Bedside telemetry, noninvasive blood pressure, and continuous pulse oximetry monitoring
97 Post-Intervention Data Screening initiated on January 15 th, positive screens from January 15 th,2013 through June 30 th, (48% of patients with positive screen) met criteria for diagnosis of sepsis. Main sources: o Sepsis of urinary origin. o Sepsis of pulmonary origin. 66
98 What s Next? Establishment of sepsis risk screening for inpatient units. Sepsis education for all nursing staff. Development of protocols to decrease the risk of developing sources of infection: o Criteria for indwelling catheter insertion to decreased incidence of catheter-associated urinary tract infections (CAUTIs). o Ventilator-associated pneumonia (VAP) prevention. 67
99 QUESTIONS? 68
100 Mortality Reduction Through Timely Identification of Sepsis on the Floors: the MOST Protocol Mary Ann Barnes-Daly RN BSN CCRN DC Regional Clinical Initiative Lead Sutter Health Sacramento, CA March 2014
101 About Us Sutter Amador Hospital Sutter Auburn Faith Hospital Sutter Davis Hospital Sutter Medical Center, Sacramento Sutter Roseville Medical Center Sutter Solano Medical Center Sacramento, California


102 About Our Project Pilot center in 2010 Regional in 2011 Sutter Amador Hospital Sutter Auburn Faith Hospital Sutter Davis Hospital Sutter Medical Center, Sacramento Sutter Roseville Medical Center Sutter Solano Medical Center Sacramento, California
103 Funding for the Project
104 Overview- Scope of project Continue quality improvement in ED and ICU Develop a process for identification of severe sepsis and early initiation of treatment for patients on the floors MOST units = o Medical o Oncology o Surgical o Telemetry
105 Why MOST? This cohort of patients is important because they tend to have a higher likelihood to die than patients who go from ED to ICU In other words patients who go directly from ED to ICU, although presumably sicker, survive more than patients who go from MOST to the ICU later. * *SSC data and our own showed the same trends

106 ICU admits from ED vs. transfer from inpatient units (severe sepsis and septic shock)
107 Mortality Rate Summary SRMC 2010 Patients Admitted to ICU from SRMC ED o Mortality rate = 21.4% Patients transferred to ICU from MOST* Units Mortality rate = 25.2% Conclusion: patients transferred from inpatient unit were 15% higher likelihood to die than patients admitted from ED to ICU directly *MOST= Medical Oncology Surgical Telemetry combined
108 Screening and Identification Strategies Step One: o Standardize the screening criteria-regional approach ISO = Infection SIRS - Organ Failure o Some screens lacked full list of SIRS criteria o Some screens lacked full list of organ failure criteria o Modifications such as replacing the P/F ratio with increasing O2 requirements to maintain SaO2 >90%
109 Screening and identification strategies continued Step Two: Educate and retrain including: o the pathophysiology of systemic inflammation and organ failure o how and when to screen o how to use the chain of command when challenges arise
110 Screening on the floors Step Three: o roll out screening with superusers/auditors/mentors Step Four: o Measure compliance with screening o Outcome metric for the grant
111 Now what? Your patient has a positive sepsis screen Process and resources for appropriate response to a new positive screen for severe sepsis Standardize the right response 24/7 Create hand-off specific for sepsis status Response for simple sepsis o Notify MD, ask for initial and serial lactates o Increase screening to twice per shift
112 Call RRT Response to screen positive for severe sepsis o RRT (ICU RN and RCP) arrives and interfaces with RN and validates screen o If incorrect-educate and coach RRT validates o If positive call SEPSIS ALERT o Initiate standing orders for ABG, Lab, Fluid bolus o Additional personnel include Lab tech, IVT, Nursing supervisor, Intensivist either live or on phone
113 Response to screen positive for severe sepsis If the patient is stable initiation of the 3 hour bundle can occur on MOST unit Most severe sepsis patients were quickly transferred to the ICU for resuscitation, observation and a quick turn-around (6-24 hours) No longer waiting for septic shock to occur Patient flow impact
114 Trend Line Shows Significant Reduction in Mortality for MOST Units

115 2011 Mortality Data ICU Patients combined severe sepsis and septic shock
116 Data Summary ED mortality reduction from 21.4% to 12.0% MOST units mortality reduction from 25.2% to 12.3% Overall ICU mortality reduction from 22.8% to 12.1%
117 Data Summary ED mortality now 12.0% MOST mortality now 12.3%
118 Overall improvements More patients going from ED directly to ICU ED mortality reduction Less patients transferred from MOST to ICU MOST mortality reduction Overall ICU severe sepsis and shock mortality reduction No impact on ICU bed availability

119


120 Thank you - barnesm4@sutterhealth.org
121 Got Lactate??? Karin Molander, MD Sepsis Physician Champion, Mills Peninsula Health Services Burlingame, CA

122 Mills Peninsula Health Services Mills-Peninsula Health Services o General medical and surgical hospital in Burlingame, CA, 393 licensed beds, includes: o SNF o Behavioral Health o Family Birth Center 44,738 ED visits ,819 admissions 3444 inpatient surgeries
123 MPHS Sepsis Mortality At Sutter hospitals severe sepsis and septic shock are the leading cause of death. Since 2006 we have been developing protocols on early recognition and rapid treatment of Severe Sepsis & Septic Shock. In 2007 MPHS Sepsis mortality was greater than 35%
124 PACE (Partners Advancing Clinical Excellence) Gordon and Betty Moore Foundation awarded Sutter a multi-million dollar grant to improve mortality in patients identified with Severe Sepsis (in addition to 5 other outcome measures) Involved 6 Sutter facilities RN and MD involvement Monthly call in meetings
125 Severe Sepsis/Septic Shock Diagnosis CBC Blood Cultures Source Cultures Lactate Radiographic studies Treatment Antibiotics within 1 hour of dx of Septic Shock Antibiotics within 3 hours of dx of Severe Sepsis Source control EGDT
126 Causes of Elevated Lactate Shock Post cardiac arrest Regional tissue ischemia DKA Thiamine deficiency Liver failure Malignancy Mitochondrial disease Drugs/toxins Alcohol, cocaine, CO, cyanide Pharmacologic agents metformin, epinephrine, linezolid, propofol Anaerobic muscle activity Seizure Heavy exercise
127 Lactate Elevated lactate associated with increased mortality if cause is due to hypoperfusion (Broder and Weil Science 1964; 143) Noted to be a predictor of mortality in ED patients presenting with suspected infection (Shapiro et al Ann Emerg Med 2005; 45)
128 RN Sepsis SIRS Protocol Allows ED triage RN to initiate work-up on patient presenting with suspected infection and positive SIRS screen. o CBC o Blood Cultures o Lactate o Saline lock
129 4Ts W Sugar Thought Tachypnea Tachycardia Temperature WBC Glucose > 120 (based on case study by Maureen D. Raynor)
130 Positive Sepsis Screen 2 of the following criteria and suspected infection: o T > 38 or < 36 o RR > 20 o HR > 90 o Confusion o WBC > 13 or < 4 or > 10% bands
131 Positive Sepsis Screen Other risk factors o Age > 60 o o o o Immunocompromised (recent chemo, steroids, HIV+) History of diabetes, liver disease, chronic renal disease Altered Mental Status Current use of antibiotics o Systolic BP < 100
132 Screening patients Developed badge cards for RN/MDs Nurse Protocols Best Practice Alert within EHR Mandatory Screen performed at triage and each shift Goal: develop automated BPA to prompt as laboratory and VS data entered into EHR
133 Best Practice Alert Prompt within Electronic Health Record Activated if Blood cultures are ordered Then prompts to order lactate, yes or no. Initially ran silently within EHR to verify low incidence of false alert Initially only activated in ED Now facility-wide
134 Lactate Audit 2/18/13 9/6/13 Utilize daily Epic workbench report to audit all lactates 2.0 for last 24 o in ED, critical care, med/surg. Chart review for MD identification of sepsis, severe sepsis, septic shock Total of pts with lactate # pts with lactate 2 and sepsis, severe sepsis or septic shock 441 # not septic 130 % sepsis 76.4 % not sepsis 23.6
 Normal WBC and Sepsis # pts with lactate 2 and sepsis 441 # pts with lactate 2,")
135 Lactate Audit 2/18/13 9/6/13 37% of patients with a lactate 2.0 and sepsis had a normal WBC (4 WBC 12) Normal WBC and Sepsis # pts with lactate 2 and sepsis 441 # pts with lactate 2, normal WBC and sepsis 168 % pts with sepsis and normal WBC 38.1
136 Septic Shock Jun Sept 2013 Severe Sepsis/Septic Shock Oct Jan 2014 First Lactate value > 6.0 Mortality numerator Mortality denominator mortality rate 13.0% 19.5% 18.1% 34.7% percent of total # pts 29.5% 39.5% 18.4% 12.6% First Lactate value Mortality numerator Mortality denominator mortality rate 13.7% 10.7% 14.5%
137 MPHS Mortality 45.0% MPHS Septic Shock and Severe Sepsis Mortality 40.0% 35.0% 30.0% 25.0% 20.0% 15.0% EHR Go Live Series1 10.0% 5.0% 0.0% ED RN SIRS Protocol Hospital-wide RN SIRS Protocol
138 MPHS Mortality reduction Individual feedback to RN/MD using Sepsis Bundle Compliance Audit Tool Monthly Sepsis Team meetings (RNs, MDs, pharmacists, Quality, ED scribes, Management, C suite) Daily Lactate audits POC lactate on RRT

139 MPHS Sepsis Team Members MPHS Sepsis Committee members accepting Patient Safety First award at November 2013 Beacon conference for reducing sepsis mortality by > 30% for > 6 months

140 Break Don t go far! We will begin again at the top of the hour!
141 Sepsis Mortality Reduction Journey Jonathan Kling, MBA, RN, CCRN Associate Chief Nursing Officer NCH Healthcare System Naples, Florida
142 Sepsis Mortality Reduction Journey The Highs and the Lows



143 About Us Non profit, multifacility Healthcare System in Naples, Fl. 715 total beds; 2 hospital system. Alliance of 650 physicians & medical facilities. throughout Collier County and SW Florida. Extensive inpatient and outpatient services. Member of the Mayo Clinic Network 37,284 admissions; 87,100 emergency room visits; 3,033 births; 416 open heart surgeries; 11,282 surgical procedures & 3,000employees. 2012, 2013 Most Wired. ANCC Pathways Designated, July
144 Goal: The Pre-Journey IHI Reducing Sepsis Mortality Collaborative October 09 to September 10 o Reduce sepsis mortality by 10% in ED to Critical Care admitted patients. o Bundle component compliance > 85%. Action: Created ED Sepsis Alert to ID potential sepsis patients sooner. 40% 35% 30% 25% 20% 15% 10% 5% 0% Sepsis Mortality Rate 34% 10% 24%
145 The Pre-Journey Thomson Reuter Sepsis Team September 10 August 11 Goal: Reduce Sepsis mortality by 10% within 6 months Action: Built additional sepsis PowerPlans for med/surg and critical care Results Mortality Index % 1.0 Q2-Q3'10 Q4'10-Q1'11 Top Decile
146 The Pre-Journey 35% 30% 25% 20% 15% 10% 5% 0% Mortality % August September 2011 Mortality = Patients with Primary MS-DRG of Sepsis who Died Total # of Patients with Primary MS-DRG of Sepsis
147 The Real Journey Begins Problem Identified Fall of 2011 Sepsis Mortality Rate of 32% Initial Goal: To reduce severe sepsis mortality rate of NCH inpatient population by 10% (from 32% to 22%) by 12/30/12 and maintain < 22%* mortality rate for 6 months. * CRG med 22.2 benchmark expected comparative for top deciles of large community hospital. 147
148 The SEPSIS Journey Select/Form Interdisciplinary Team o Physician Champion, Nurse Leaders, bedside RNs, IP, Pharmacy Employ Evidence-Based Practice (EBP) o Sepsis bundle, early identification & intervention, alert system Plan/Pilot Spread Implement/Monitor/Evaluate Sustain
149 The SEPSIS Journey Select/Form Team Employ EBP Plan/Pilot: ED and Critical Care (CC) o Raise awareness, SOS o Bundle compliance, sepsis alerts, PowerPlans, Spread: to non-cc, Hospitalists, NPs, PAs o Expand alerts to fire to RNs o RN escalation process/rapid response team Implement/Monitor/Evaluate Sustain
150 The SEPSIS Journey Select/Form Team Employ EBP Plan/Pilot Spread Implement/Monitor/Evaluate o Comprehensive raise awareness and education campaign o Sepsis Committee monthly review of stats, case studies, opportunity identification Sustain

151 The Journey 70% 60% Severe Sepsis Mortality July 2011 March % 40% 30% 20% 10% 0% Jul Aug Sep Oct Nov Dec Jan Feb Mar
152 The Journey: SOS S.O.S. = Suspect Onset of Sepsis 152
153 The Journey Badge Cards for Non-Critical Care, Critical Care and Emergency Department Personnel 153
154 The Journey: SOS Documented or Suspected Infection And 2 or more = SIRS/Systemic Inflammatory Response Syndrome Heart Rate>90 BPM Temperature <36 C(96.8 F) or >38.3 C (101 F) Respiratory Rate > 20 BPM White Blood Cell Count >12,000 And 1 or more s/s hypoperfusion and/or organ dysfunction: SBP <90 or MAP <70 or drop of 40 from baseline Lactate > 4 mmol/l (on ABG or LA) Worsening Hypoxemia Worsening altered mental status Decreased urine output (<30ml/hr x 4 hrs) Creatinine increase > 0.5 mg/dl above baseline INR > 1.5 or PTT > 80 Platelet count < 100,000 Bilirubin > 2mg/dL
155 The Journey: SOS If your patient presents with s/s of Severe Sepsis: Immediately notify the physician to obtain orders to initiate the Sepsis Critical Care Power Plan which includes: Obtain Serum Lactate (ABG or draw Lactic Acid stat) Obtain Blood Cultures (peripheral & IV access device prior to Abx) Administer IV Broad Spectrum Antibiotic(s) within 1 hour In the event of Hypoperfusion or Lactate > 4 mmol/l Administer IV Fluid Bolus (20 ml/kg/hr) Apply Vasopressors for hypotension not responding to initial Fluids (SBP>90 or MAP> 65 mmhg) Control Glucose Levels >70 but < 150 (begin IV insulin protocol prn) Central Line Placement Measure CVP goal 8-12 mmhg
156 The Journey 50% 45% 40% % Sepsis Mortality % % Expired 35% 30% 25% 20% 15% 10% 5% 32% 17% 31% 24% % 23% 17% 17% 16% 29% 13% 8% 14% 11% 19% 7% 24% 13% 33% 10% 21% 14% 0% 156
157 The Journey Continues 50% Sepsis Mortality % % 20% 10% 0%
158 Impact of Sepsis Improvements $3.7 m cost avoided. 172 lives saved Actual # Mortalities Projected # Mortalities
159 Sepsis Actual vs. Baseline 50% 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Actual Sepsis Mortality Rate Linear (Actual Sepsis Mortality Rate) Baseline / Proj Rate

160 The Journey Continues Select/Form Employ EBP Plan/Pilot Spread Implement/Monitor/Evaluate Sustain the Gain
161 Surviving Sepsis Campaign data collection to drive improvement Christa Schorr RN,MSN, FCCM Program Director of Critical Care Clinical Trials and Faculty for the Surviving Sepsis Campaign Cooper University Hospital, Camden, NJ
162 Past Present 6 & 24 hour bundle Previous Chart Review Database Version 3 162

163 Aggregate data 15,000 patients

164 Mortality results






165 New SSC database Enter new patient record; view/select records Built-in reports Export to local file and transmit to central site at SCCM 165

166 Inside the data collection tool
167 Monthly - Quarterly Reports
168 Data collection & feedback Adequate resources for data collection and analysis Consistency in data entry Clear understanding of sepsis and data elements Timely feedback Process to display aggregate results Instrument to provide individual clinician feedback

169 Where do we start? 169
170 6 Hour Sepsis Resuscitation Bundle Compliance Serum lactate within 6 Hrs 2005 Baseline Data Blood Culture before Antibiotics Antibiotic Compliance Fluids and Vasopressors for hypotension or elevated lactate CVP>=8mm Hg within 6 Hrs for shock or elevated lactate ScvO2>=70% or SvO2>=65% within 6 Hrs for shock or elevated lactate All applicable elements of the resuscitation bundle
171 Severe sepsis 6 hour resuscitation bundle compliance Nov-06 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07 Jul-07 Aug-07 Sep-07 Oct-07 Nov-07 Dec-07 Jan-08 Feb-08 Mar-08 Apr-08 Serum lactate within 6 Hrs Antibiotic Compliance 171
172 Time (hours) to antibiotic delivery Source of Infection Present Not Present p value Pneumonia* n= ± ± * UTI n= ± ± Abdomen* n= ± ± * Meningitis n= ± ± Skin n= ± ± Bone n= ± ± Wound n= ± ± Catheter n= ± ± Endocarditis n= ± ± Device n= ± ± Other n= ± ±
173 AUDIT & FEEDBACK
174 Dashboard reporting ICU Benchmarks per Surviving Sepsis Database BM 79% BM 78% Goal is 100% Goal is within 6 hr of present ation Goal is 100% 6 HR SEVERE SEPSIS RESUSCITATION BUNDLE Number of charts Serum lactate within 6 hr Median time to serum lactate measure Blood cultures collected before antibiotics 4 Q 10 1 Q 11 2 Q 11 3 Q 11 4 Q 11 1 Q 12 2 Q 12 3 Q 12 4 Q % 36/36 96% (48/50) 97% (37/38) 94% (29/31) (30/30) 100% (26/26) 100% 97% (30/29) 96% (25/26) 96% (23/24) 1 hr 1 hr 1 hr 1 hr 1hr 1hr 1 hr 1 hr 1hr 94% 34/36 90% (45/50) 87% (33/38) 87% (27/31) 97% (29/30) 88% (23/26) 90% (27/30) 96% (25/26) 83% (20/24) Data example reflects previous 6 & 24 bundles
175 Dashboard reporting ICU BM 68% Goal is 100% GOAL IS 3 hr for ED admits, or 1 hr for non- ED admits 6 HR SEVERE SEPSIS RESUSCITATION BUNDLE Antibiotic compliance Median time to antibiotic administration 4 Q 10 1 Q 11 2 Q 11 3 Q 11 4 Q 11 1 Q 12 2 Q 12 3 Q 12 69% 25/35 58% (29/50) 63% (24/38) 74% (23/31) 70% (21/30) 73% (19/26) 83% (25/30) 65% (17/26) 4 Q % (15/24) 2 hr 3 hr 3 hr 2 hr 2hr 2hr 2 hr 2 hr 2hr Data example reflects previous 6 & 24 bundles
176 Provider Report Card - example Chart review date Clinican team: nurse physician NP/PA resident fellow other name Date of service: Patient medical record # Indicator # Criteria to be completed with 3 hours of severe sepsis 1 Measure lactate Indicator compliance Elaspsed time to meet indicator NOTES: 2 Obtain blood culture prior to administration of antibiotics 3 Administer broad spectrum antibiotics 4 Administer 30 ml/kg crystalloid for hypotensionor lactate 4 mmol/l # applicable indicators # indicators met 3 hour bundle compliance Criteria to be completed within 6 hours of severe sepsis 5 Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) 65 mm Hg Team comments: In the event of persistent arterial hypotension despite volume resuscitation (septic shock) or initial lactate 4 mmol/l (36 mg/dl): 6 Measure central venous pressure (CVP) 7 Measure central venous oxygen saturation (Scvo2) 8 Remeasure lactate if initial lactate was elevated 9 Hospital Mortality (if known at time of report) # applicable indicators # indicators met 6 hour measured bundle compliance Achieve central venous pressure (CVP) 8 mm Hg Achieve central venous oxygen saturation (Scvo2) 70% Remeasure lactate if initial lactate was elevated 6 hour achieved bundle compliance


177 SSC-provider level feedback Clinical team Severe Sepsis Report Card Clinical team: nurse physician NP/PA resident fellow other name 3 hour bundle
178 Summary Importance of data collection Significance of drilling down to details Value of audit and feedback

179

180 Where do you start? Where will you look to improve?
181 Wrap Up Next Steps & CEU Instructions

182 Tune in tomorrow! Learn additional strategy and tools for sepsis mortality reduction SAME BAT TIME & CHANNEL
The Power of the Pyramid:
 The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Establishing an Emergency Department Sepsis Screen
 Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers
 Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care. Dial in # 855/ Reference conference ID#
 MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Current Status: Active PolicyStat ID: Guideline: Sepsis Identification And Management in Adults GUIDELINE: COPY
 Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
The Davies Award Is: The HIMSS Nicholas E. Davies Award of Excellence. Awarding IT. Improving Healthcare.
 The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Northwell Sepsis Collaborative Evidence Based Best Practice
 Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA. July 26 th, :00 a.m. 12:00 p.m. CDT
 AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
2014 Maryland Patient Safety Center s Call for Solutions
 Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
STARTER PACK: Webinar #1 SEPSIS
 STARTER PACK: Webinar #1 SEPSIS Welcome to the Sepsis Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps Gap
STARTER PACK: Webinar #1 SEPSIS Welcome to the Sepsis Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps Gap
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2
 Thursday, September 26 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2 John D Angelo, MD, FACEP Andy Odden, MD Diane Jacobsen,
Thursday, September 26 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2 John D Angelo, MD, FACEP Andy Odden, MD Diane Jacobsen,
Document Ratification Group Chairman s Action
 Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE. Early Recognition and Treatment of Severe Sepsis and Septic Shock
 SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
How Cookeville Regional Medical Center Set Up a Sepsis Program
 How Cookeville Regional Medical Center Set Up a Sepsis Program Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org SepsisSolutionsInternational
How Cookeville Regional Medical Center Set Up a Sepsis Program Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org SepsisSolutionsInternational
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation
 Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6
 Thursday, November 21, 2013 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6 Sean Townsend MD Terry Clemmer MD Diane Jacobsen MPH,
Thursday, November 21, 2013 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6 Sean Townsend MD Terry Clemmer MD Diane Jacobsen MPH,
Greater New York Hospital Association United Hospital Fund. STOP Sepsis Collaborative Toolkit. of Severe Sepsis in the Emergency Department
 Greater New York Hospital Association United Hospital Fund STOP Sepsis Collaborative Toolkit A Protocol-Based Approach to Early Identification and Treatment of Severe Sepsis in the Emergency Department
Greater New York Hospital Association United Hospital Fund STOP Sepsis Collaborative Toolkit A Protocol-Based Approach to Early Identification and Treatment of Severe Sepsis in the Emergency Department
Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum
 Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum Angela Craig APN, MS, CCNS Clinical Nurse Specialist Critical Care Cookeville Regional Medical Center Cookeville, TN acragi@crmchealth.org
Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum Angela Craig APN, MS, CCNS Clinical Nurse Specialist Critical Care Cookeville Regional Medical Center Cookeville, TN acragi@crmchealth.org
Goals today 6/14/2011. Disclosures, 2004-May Sepsis A Medical Emergency. Jim O Brien, MD, MSc So what is sepsis anyway?
 Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
The Value-Driven Laboratory. The new business model for expanded hematology parameters Immature Granulocytes (IG) Sysmex America White Paper
 Sysmex America White Paper") The Value-Driven Laboratory The new business model for expanded hematology parameters Immature Granulocytes (IG) Sysmex America White Paper 577 Aptakisic Road Lincolnshire, IL 60069 USA www.sysmex.com
The Value-Driven Laboratory The new business model for expanded hematology parameters Immature Granulocytes (IG) Sysmex America White Paper 577 Aptakisic Road Lincolnshire, IL 60069 USA www.sysmex.com
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Sepsis Mortality - A Four-Year Improvement Initiative
 Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Fundamental Critical Care Support (FCCS)
") Provided By: Fundamental Critical Care Support (FCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Needs Statement and Educational Gap: Early identification
Provided By: Fundamental Critical Care Support (FCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Needs Statement and Educational Gap: Early identification
Emergency. Best Critical Care Practices
 Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014
 Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Supplementary Appendix
 Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING
 SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS
 #9: EARLY DETECTION & TREATMENT OF SEPSIS") Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS Executive Summary Checklist Commitment from hospital governance and senior administrative leadership to support early
Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS Executive Summary Checklist Commitment from hospital governance and senior administrative leadership to support early
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Inpatient Quality Reporting Program
 The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Presentation Transcript Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead, Hospital
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Presentation Transcript Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead, Hospital
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
SEPSIS Management in Scotland
 SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
Stampede Sepsis: A Statewide Collaborative
 Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Learning Session 4: Required Infection Reporting for Minnesota CAH
 Learning Session 4: Required Infection Reporting for Minnesota CAH Presenters: Vicki Tang Olson Program Manager, Stratis Health Janet Lilleberg Quality Data Specialist, Stratis Health Marilyn Grafstrom,
Learning Session 4: Required Infection Reporting for Minnesota CAH Presenters: Vicki Tang Olson Program Manager, Stratis Health Janet Lilleberg Quality Data Specialist, Stratis Health Marilyn Grafstrom,
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Objectives 10/09/2015. Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935
 Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Preventing Sepsis Mortality
 Murray State's Digital Commons Scholars Week 2017 - Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Murray State's Digital Commons Scholars Week 2017 - Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Passage to Excellence Our Sepsis Journey
 Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
Use of TeleMedicine to Improve Clinical and Financial Outcomes
 Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Charting the Future: Implications and Insights for Informatics. Dana Alexander RN MSN MBA FHIMSS FAAN
 Charting the Future: Implications and Insights for Informatics Dana Alexander RN MSN MBA FHIMSS FAAN Conflict of Interest Disclosure Dana Alexander RN Has no real or apparent conflicts of interest to report.
Charting the Future: Implications and Insights for Informatics Dana Alexander RN MSN MBA FHIMSS FAAN Conflict of Interest Disclosure Dana Alexander RN Has no real or apparent conflicts of interest to report.
Kansas Heart and Stroke Collaborative
 Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Inpatient Quality Reporting Program
 The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Presentation Transcript Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Presentation Transcript Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Sepsis Kills: The challenges & solutions to reducing mortality
 Sepsis Kills: The challenges & solutions to reducing mortality Kevin Rooney, Ahmed Labib & Brent Foreman Who are we? Declaration of Conflict of Interest We have no financial conflict of interest in presenting
Sepsis Kills: The challenges & solutions to reducing mortality Kevin Rooney, Ahmed Labib & Brent Foreman Who are we? Declaration of Conflict of Interest We have no financial conflict of interest in presenting
Learning Objectives. Registration and Continental Breakfast 7:00 AM -7:30 AM
 Fundamental Critical Care Support Provided by USF Health Date: Program Number SF2014136B At CLS (Center for Advanced Medical Learning and Simulation) Tampa, Florida Day One Schedule Session Learning Format
Fundamental Critical Care Support Provided by USF Health Date: Program Number SF2014136B At CLS (Center for Advanced Medical Learning and Simulation) Tampa, Florida Day One Schedule Session Learning Format
COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL. Sepsis Treatment Order Sets Sepsis Treatment Order Sets
 Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
Southern California CSU DNP Consortium
 Southern California CSU DNP Consortium California State University, Fullerton California State University, Long Beach California State University, Los Angeles IMPLEMENTATION OF A SEPSIS PROTOCOL: A QUALITY
Southern California CSU DNP Consortium California State University, Fullerton California State University, Long Beach California State University, Los Angeles IMPLEMENTATION OF A SEPSIS PROTOCOL: A QUALITY
IHI Expedition. Today s Host 9/17/2014
 September 6, 204 Begins at 3:00 PM EST These presenters have nothing to disclose IHI Expedition Expedition: Appropriate Use of Blood Products Session 3: Transfusion Safety Program Infrastructure: Measures
September 6, 204 Begins at 3:00 PM EST These presenters have nothing to disclose IHI Expedition Expedition: Appropriate Use of Blood Products Session 3: Transfusion Safety Program Infrastructure: Measures
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
South Central HIINergy Partners
 South Central HIINergy Partners Six states partnering for quality and patient safety through the SEPSIS: Nursing and Front-Line Staff Empowerment for Early Identification and Prompt Treatment Welcome and
South Central HIINergy Partners Six states partnering for quality and patient safety through the SEPSIS: Nursing and Front-Line Staff Empowerment for Early Identification and Prompt Treatment Welcome and
ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative Funded by the Center for Medicare & Medicaid Innovation (CMMI)
 Network Sepsis Learning Collaborative Funded by the Center for Medicare & Medicaid Innovation (CMMI)") ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative 2016 Funded by the Center for Medicare & Medicaid Innovation (CMMI) Outline A Case Epidemiology of Sepsis Learn Baseline Protocolize
ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative 2016 Funded by the Center for Medicare & Medicaid Innovation (CMMI) Outline A Case Epidemiology of Sepsis Learn Baseline Protocolize
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
CDRL A006 Training Manual User's Guide for STAT! TM EMEDS ICU Serious Medical Game. Release v November 26, 2014
 CDRL A006 Training Manual User's Guide for STAT! TM EMEDS ICU Serious Medical Game Copyright 2014 Vcom3D, Inc. Release v1.0.0 - November 26, 2014 Sponsored by Air Force Research Laboratory (AFRL) Prepared
CDRL A006 Training Manual User's Guide for STAT! TM EMEDS ICU Serious Medical Game Copyright 2014 Vcom3D, Inc. Release v1.0.0 - November 26, 2014 Sponsored by Air Force Research Laboratory (AFRL) Prepared
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
Number of sepsis admissions to critical care and associated mortality, 1 April March 2013
 Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding