Self-directed learning package
|
|
|
- Chester Anderson
- 5 years ago
- Views:
Transcription



1 Surgical Workbook Self-directed learning package To be read in conjunction with: HMO/Intern position description Surgical Unit orientation information NAME: Author: Dr Benjamin Scott July
2 Workbook Review End of Term Date: Comments: Completed Non-yet complete Term Supervisor Dr. Date Director of Clinical Training (or delegate) Dr. Date 2
3 Pre and Post Workbook Survey Many thanks for taking the time to complete the surgical workbook. I truly hope it helps you in approaching some of the common cases that you may see on the wards. A lot of work has gone into this project and it would be great to know if it is of any value to new surgical interns and residents. Could you please take the time to complete the first part of this survey prior to completing the work book and the second part once you have completed the relevant case. Each should take less than 2 minutes. Surgical education survey: First page to be done prior to completing the workbook If you were to encounter the following scenarios on the first day of your surgical rotation would you feel confident in managing; A patient presenting with cholecystitis Post-operative patient with a fever A patient presenting with appendicitis Strongly Agree Strongly Disagree Strongly Agree Strongly Disagree Strongly Agree Strongly Disagree A patient presenting with acute limb ischaemia Strongly Agree Strongly Disagree Assessing risk for Venous Thomboembolism and prevention strategies Strongly Agree Strongly Disagree Post-operative patient with hypotension Strongly Agree Strongly Disagree A patient presenting with a bowel obstruction Strongly Agree Strongly Disagree Assessment of fluid status and prescribing IV fluids Strongly Agree Strongly Disagree 3
4 Having done the workbook do you feel more confident managing the following clinical scenarios? A patient presenting with cholecystitis Post-operative patient with a fever A patient presenting with appendicitis Strongly Agree Strongly Disagree Strongly Agree Strongly Disagree Strongly Agree Strongly Disagree A patient presenting with acute limb ischaemia Strongly Agree Strongly Disagree Assessing risk for Venous Thomboembolism and prevention strategies Strongly Agree Strongly Disagree Post-operative patient with hypotension Strongly Agree Strongly Disagree A patient presenting with a bowel obstruction Strongly Agree Strongly Disagree Assessment of fluid status and prescribing IV fluids Strongly Agree Strongly Disagree Are there any other topics you would like to see included? Do you have any feed-back or improvements for the education resource? 4
, and to provide some more structure and real")
5 Self-directed workbook - Surgery This self-directed workbook as a guide for you to assess your knowledge and identify your learning needs by completing the workbook. It is not mandatory, but we would like to continue to use it as it assists with performance appraisals (which is essentially performance coaching), and to provide some more structure and real learning outcomes. The following diagram highlights the key objectives, with our aim to see more of does and shows how BHS Surgical Expected Learning Outcomes 1. To be able to manage patients with surgical presentations on the ward and referred by the Emergency Department. 2. Understand the management requirements for post-operative patients. Education The education series covers the following topics: 1. Abdominal Pain 2. Pyrexia Post op 3. Appendicitis 4. Ischaemia 5. Anticoagulation 6. Hypotension 7. Diabetes 8. Bowel Obstruction 9. Hypovolaemia The learning resources in this self-directed workbook cover these topics. The learner should complete the self-directed workbook to enhance their own understanding of their learning needs. Every section does not need to be completed. Use it to reinforce areas where your knowledge is strong, or to identify areas that need some work. In many cases this will mean on the job learning, rather than finding information in books. We suggest that completing this workbook in preparation for or duration of your surgical term is strongly advised. Formal educational activities occur throughout the week (Surgical terms) It is not possible for doctors to attend all sessions due to shift work, duration of rotations and leave etc. therefore we endeavor to publish for each topic the PowerPoint presentations and associated resources for people to read on the BHS education resource website: 5
6 Case 1: You have been asked to review Mrs. Robertson in the emergency department, a 38 year old female, who has presented with upper abdominal pain over the last 24 hours. She explains that it began in the epigastric region but moved to the right upper side about 8 hours ago. The pain is constant, 8/10 with no radiation. 1. What is your differential diagnosis for this patient (list 3) 2. What specific examination findings will you look for? From the end of the bed, Mrs. Robertson is obviously in pain and looks uncomfortable. She is not jaundiced. Blood pressure: 135/80 Heart Rate: 95 Respiratory Rate: 16 Temperature: 38.1 You examine her abdomen and find that she is tender in the RUQ and is murphy s sign positive. 3. What is murphy s sign and why does it cause pain? 4. What bedside tests or investigations will you order and why? 6



7 The following tests results are available: 5. What imaging will you request? 7

8 Radiology Report 6. Working with the diagnosis of cholecystitis, what will be your management for this patient (consider that the patient is in the emergency department currently, and the logistics that will be involved). a) Immediate management in ED b) Definitive Management 8
9 7. What are the common organisms that cause cholecystitis? 8. Mrs. Robertson is now ready for theatre. What approaches can be employed by the surgeon? 9. Mrs. Robertson has returned to the ward and her post-operative management needs to be commenced. a. Do we need to continue antibiotics? b. A nurse asks you if the patient can eat and drink? c. Is that patient at risk of a deep venous thrombosis (DVT)? How can these be prevented? d. What analgesia will you provide? e. What are the complications to look out for? f. When will you follow up this patient after discharge? g. Mrs Robertson works in a job that involves daily lifting of 15kg boxes. What advice will you give her regarding return to work. 9

10 Case 2 You are on the ward round and approach Mr. Thompson in bed 22a. He states that he is feeling a little bit off. You review the observation chart. 1. What are some potential origins for this temperature? Which is the most likely? 2. Currently the patient is looking well. You know that atelectasis commonly occurs during this time. Are there any preventative measures you can take for this? 10

11 You move to 22b and Mrs. Fung is looking unwell. She had abdominal surgery 8 days ago and as she lives alone in an isolated area, the team has decided to keep an eye on her until she improves. You review her observation chart. 3. What is the likely cause of this pattern of fever in a postoperative patient? 4. You examine the patient s abdomen and there is generalised tenderness. What actions will you take? 11

12 You move to 23a and Mr Gray is day 5 post hernia repair. He explains that the wound site feels sore. 5. What is the most likely cause of the fever in this case? What other pathologies can cause a fever during this time? 6. You take down the dressing (there is no excuse for not looking) and find a hot, erythematous (red) wound that has purulent discharge. What actions will you take? 12
13 Case 3 You have been asked to review Miss Stevenson, an 18 year old female has presented to the ED with abdominal pain. 1. What are the questions you will ask about abdominal pain? After a focused history you discover that the pain is in the right iliac fossa. The pain started 6 hours ago and was initially in the peri-umbilical area. Prior to this she has been experiencing nausea and anorexia for approximately 16 hours. The pain is exacerbated by coughing and was increased when driving over bumps on the car ride to the emergency department. 2. Based on the history, what is your differential diagnosis for this patient? 3. What specific signs will you be looking for on examination? 13
14 Examination findings Blood Pressure: 130/80 Heart Rate: 88 Respiratory Rate: 16 Temp: 38.1 From the end of the bed the patient appears uncomfortable. The peripheries are cool and the oral mucous membranes are dry. You find that the patient is tender at McBurney s point. Rebound tenderness is present. When palpating the left side of the abdomen, pain is experienced on the right side. Bowel sounds are present. You lay the patient on their left side and extend the right hip, which exacerbates the pain. 4. Where is McBurney s point? 5. What is Rosving s sign? 6. How do you elicit rebound tenderness? 7. What is the psoas sign? 8. What is your initial management for this patient? (Hint: consider analgesia, hydration, anti-infective and communication with appropriate staff) 14
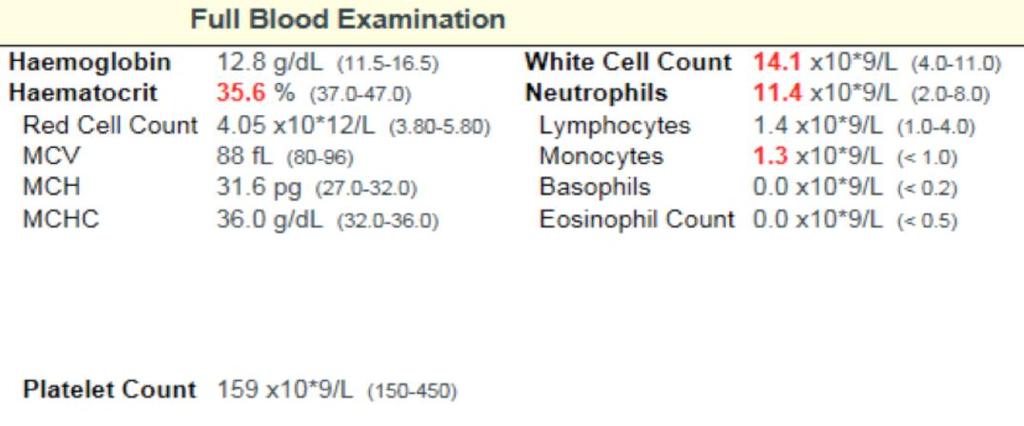
15 At this stage you are suspicious of acute appendicitis. 9. What blood tests will you order? Consider those that will also help to exclude other significant pathology. 15




16 The Pathology results are available for the following blood tests 16
17 10. Your next task is to contact the surgical registrar. Fill out the different sections of the ISBAR handover tool to cover what you will say in the conversation. ISBAR: Introduction, Situation, Background, Assessment, Recommendation/Request Introduction: Situation: Background: Assessment: Recommendation / Request: 11. Your surgical registrar explains that he is suspecting appendicitis. Is there any other imaging you should consider? What is the definitive management for acute appendicitis? The patient has been returned to the ward. 12. How will you manage this patient s pain? 13. Can she eat and drink? 17
 and these should not be")
18 14. Does she need prevention for venous thromboembolism? 15. What follow up will she need? 16. Do antibiotics need to be continued? A few days later the histopathology is returned. Note: It is an important lesson in this case that a patient may have appendicitis even in the absence of significantly abnormal blood tests (such as white cell count and CRP) and these should not be relied upon to confirm or refute the diagnosis of appendicitis. 18
19 Case 4 One of the local general practitioners has sent 55 year old, Mr. Johnson directly from their clinic to the emergency department. The letter from the GP reads acutely painful right lower limb, history of atrial fibrillation?limb ischaemia. The emergency department staff have contacted your registrar and asked you to see the patient. 1. What is critical limb ischaemia? What are the potential aetiologies of this condition? 2. What symptoms and risk factors will you specifically ask the patient about? After taking a focused history from the patient it is revealed that Mr. Johnson has had this pain in his leg for 2 hours. He describes it as an aching pain worsened by walking and elevation. You examine the patient and find that his right leg is paler than the left, cool to touch and has inconsistent sensory function on the dorsal aspect of the foot. Motor function is still in tact. Prior to this there has been no known history of peripheral vascular disease or intermittent claudication. The nurse hands you an ECG they obtained from the patient. 19

20 Patient: Mr. Johnson Age: 55 Gender: male ECG 20
21 3. What does the ECG show?. You hand this information over to your registrar and they tell you they are suspecting an acutely ischaemic limb 4. How are ischaemic limbs classified? 5. What are the other potential diagnoses? 6. How will you manage this patient both immediately and definitively? (cue: what management can you commence in the emergency department? Which team will need to be contacted for the definitive treatment?) 7. What services are available within the hospital to assist you in the management of this patient during the post operative period? 8. You are asked to review the patient post operatively and they are complaining of 10/10 pain in the right lower limb. What complication/s may have occurred? 21

22 Case 5 Mrs. Jenkins has just undergone a laparoscopic cholecystectomy and has returned to the ward. She is a 60-year-old woman who has a history of previous deep venous thrombosis. One of the junior nurses pages you and asks if you want anticoagulation for this patient. 1. What risk factors do you need to enquire about to assess the risk for a venous thromboembolism occurring? 2. What mechanical devices do we use to prevent VTE? 3. What pharmacological agents are available for prevention of VTE? 4. Chart an appropriate dose of enoxaparin. 22
23 Case 6 You are on the way to a clinical review for a patient with a low blood pressure. The patient is day 1 post hemi-colectomy. Vital Signs Heart Rate: 115 Blood Pressure: 98/80 Temperature: 36.9 Respiratory rate: 24 The patient is complaining of generalised abdominal pain that has been getting worse since the morning 1. What are the potential causes for hypotension in the post-operative patient? 2. How will you assess the patient to identify a cause? 3. What management will you initiate? 23
24 Your second patient for the day is also hypotensive but is 5 days following a cholecystectomy. The patient is short of breath and has convincing crackles in their left lower lobe. The patient is septic. 4. What is sepsis? What symptoms or signs will you look for? 5. What antibiotics would be used in this case? If you aren t sure you should review the surviving sepsis guidelines, which provide guidance on antibiotic choice in a wide range of clinical scenarios. 6. Who can be contacted if there are doubts about choice of antibiotics? 24
25 Case 7 Mr. Jones is a 55-year-old man who is having a hemi-colectomy in 2 days. The nursing staff want to know if you would like him to continue taking his regular medications. He is currently on Metformin 1g BD and Gliclazide 80mg Daily (dose). 1. What is your plan for these medications? Mrs. Ruffalo is a 61yo female, had a cholecystectomy 1 day ago and is expected to be in hospital for 2 more days. He has known type 2 diabetes. The nurse mentioned that the blood sugars have been somewhat erratic and unpredictable. You calculate the mean daily glucose is 17mmol/L. 2. How are you going to manage this patients blood sugars? You are attending morning ward round and are seeing Mr. Wong. He was brought into the Emergency Department last night and is to have an appendectomy. He is a Type 1 Diabetic and is normally on basal-bolus regimen of insulin. The patient is fasted and you have maintenance fluid running. Your student asks you if you will prescribe his normal insulin as they are concerned you will make the patient hypoglycaemic. 3. How will you respond to this statement? 25
26 Case 8 You have been asked by your registrar to see a 40 year old female in the Emergency department who has a suspected bowel obstruction. You attend the patient s bedside and a 2 day history of cramping abdominal pain with a recent onset of nausea and vomiting. There is a past history of hypertension, type 2 diabetes mellitus and a surgical history of an appendectomy 15 years ago and a cholecystectomy 5 years ago. 1. Is this likely to be a small bowel obstruction or a large bowel obstruction? 2. How do the presentations differ? 3. What are the causes of small bowel obstructions? 4. What are the causes of large bowel obstructions? 5. What imaging/investigations will you order for this patient? Activity Visit the website below to see excellent radiographic images of the different types of bowel obstruction. 26
27 6. How will you manage this patient? 7. While the patient is waiting for surgery you are called to the ward for a clinical review. The pain is now constant and the abdomen has generalized tenderness. The patient is guarding when you palpate. What do you think has happened? 27
28 Case 9 You have been asked to see Mrs. Lucas on the ward. She is currently nil orally and has a nasogastric tube inserted. The nurse in charge has asked you to prescribe some IV fluids as he thinks the patient is hypovolaemic. 1. What examination findings will you look for to confirm hypovolaemia? On examination you discover that Mrs. Lucas has cool peripheries, heart rate of 100 and a blood pressure of 125/80. You decide that this patient requires fluid resuscitation and routine maintenance. 2. If Mrs Lucas is 65kg and has no other comorbidities, what will you prescribe this patient? (use the flow chart on the next page if you need some guidance) These guidelines (quite short and well worth a read) break fluid prescription down to three components. 28

29 29
30 Surgery Skills and Procedures Checklist PGY 1 The PGY 1 Doctors in Training should work towards competency and be confident to perform the following procedures relevant to general surgery: Element Procedure/skill Observed Assisted Performed Minor surgical Wounds Tubes & drains Splinting Cannulation BLS Haemorrhage Control Emergency Assessment and Management Incision of drainage of sub cutaneous abscess Excision of skin lesions Closure of a superficial wound Surgical knots and simple suture insertion Removal of suture and staples Care of wound healing by secondary infection Debridement of superficial contaminated wound Removal of foreign body from eye, ear and nose Insertion of intercostal drain Placement of urethral catheter Placement of nasogastric tube Pleural/peritoneal tap Removal of wound drain Applying a plaster backslab splint Insertions of IV cannula Basic life support Superficial wound haemostasis Epistaxis Post-operative bleeding Acute abdomen Abdominal sepsis Septic shock GI Bleeding Referenced from the Royal Australasian College of Surgeons Essential Surgical Skills Please list any further skills and procedures experienced on Surgery rotation: include co-signature from supervisor Details of procedure/skill Observed Assisted Performed Comments/reflections from experiences listed in this section: 30
31 Skills and Procedures Checklist PGY 2+ By the end of PGY 2 Doctors in Training should be able to perform the above procedures and be working towards competency in these additional procedures relevant to surgery: Element Procedure/skill Observed Assisted Performed Insertion of IV cannula in children Paediatric Surgery Orthopaedic Surgery Vascular Surgery Pre-operative Postoperative care ALS Emergency Assessment and Management Maintenance of IV fluid management for children IV fluid resuscitation for children Advanced Paediatric Life Support Appropriate prescribing of analgesia for a child Recognises and initiated managements of orthopaedic emergencies Open fractures Compartment syndrome Cauda equine syndrome Acute bone and joint infections/sepsis Recognise and diagnoses common orthopaedic presentations Common fracture classification application Principles of closed reduction of simple fractures and dislocations Application of common upper and lower limb plaster casts Draping for upper and lower orthopaedic procedures Ordering equipment for uncomplicated primary hip and knee joint replacement surgery Supervised surgery for common upper and lower limb fractures Ankle fracture Neck of femur fracture Forearm fracture Reduction of colles wrist fracture Reduction of shoulder dislocation Assessment of acute limb ischaemia Investigation and management of patients with acute limb ischaemia Calculation of Ankle Brachial Index Care of angiographic puncture sites Appropriate assessments and investigations Post-operative care of common elective and trauma procedures Post-operative physiotherapy and rehabilitation after elective and trauma procedures Advanced life support Miscarriage Closed head Injury Compartment Syndrome Trauma Long Bone fractures Burns Tendon Injury Referenced from the Royal Australasian College of Surgeons Essential Surgical Skills 31
32 Please list any further skills and procedures experienced on Surgery rotation: include co-signature from supervisor Details of procedure/skill Observed Assisted Performed Comments/reflections from experiences listed in this section: 32
33 Mini-CEX Assessment 1 Introduction: A mini-cex exercise assessment (mini-cex) is a minute snapshot of doctor-patient interaction observed and assessed by a senior departmental doctor (Consultant or Registrar). Various skills to be assessed during a patient consultation include; medical interviewing, physical examination, communication, clinical judgement, professional qualities, counselling skills, organisation and efficiency. Instruction: During core rotations DiTs are expected to complete a minimum of 2 mini-cex assessments from the skills and procedure check list provided below. Department: Date: Clinical Problem: Assessment Criteria 1. Medical Interviewing 2. Physical examination skills Descriptors Elicits a history that is relevant, concise and accurate to patient s context and preferences Effectively uses appropriate questions Responds appropriately to verbal and non-verbal cues Performs a focused physical examination that is relevant and accurate Provides competent explanation to patient Sensitive to patient s comfort and modesty 3. Communication Develops rapport, trust and understanding with patient/family Accurately conveys relevant information and explanations to patients/family and other health professionals Develops a shared plan of care with patients/families and other health professionals 4. Clinical judgment 5. Professionalism/ Counselling skills 6. Organisation/ efficiency Demonstrates effective clinical problem solving and judgement to address patient problems Interprets available data and integrates information to generate differential diagnoses and management plans Exhibits honesty, integrity, compassion and respect Participates effectively and appropriately in an interprofessional healthcare team Appropriately manages conflicts of interest Aware of own limitations Effectively manages challenges such as obtaining informed consent, delivering bad news, addressing anger and misunderstanding Sets priorities and manages time efficiently Manages competing demands and stress Appropriately manages supervision, resources and staff. Overall Competent performance Not yet competent Assessor comments on candidate s strengths and areas for improvement. Results Competent Not yet competent Competent Not yet competent Competent Not yet competent Competent Not yet competent Competent Not yet competent Competent Not yet competent 33
34 Mini-CEX Assessment 2 Introduction: A mini-cex exercise assessment (mini-cex) is a minute snapshot of doctor-patient interaction observed and assessed by a senior departmental doctor (Consultant or Registrar). Various skills to be assessed during a patient consultation include; medical interviewing, physical examination, communication, clinical judgement, professional qualities, counselling skills, organisation and efficiency. Instruction: During core rotations DiTs are expected to complete a minimum of 2 mini-cex assessments from the skills and procedure check list provided below. Department: Date: Clinical Problem: Assessment Criteria 1. Medical Interviewing 2. Physical examination skills Descriptors Elicits a history that is relevant, concise and accurate to patient s context and preferences Effectively uses appropriate questions Responds appropriately to verbal and non-verbal cues Performs a focused physical examination that is relevant and accurate Provides competent explanation to patient Sensitive to patient s comfort and modesty 3. Communication Develops rapport, trust and understanding with patient/family Accurately conveys relevant information and explanations to patients/family and other health professionals Develops a shared plan of care with patients/families and other health professionals 4. Clinical judgment 5. Professionalism/ Counselling skills 6. Organisation/ efficiency Demonstrates effective clinical problem solving and judgement to address patient problems Interprets available data and integrates information to generate differential diagnoses and management plans Exhibits honesty, integrity, compassion and respect Participates effectively and appropriately in an interprofessional healthcare team Appropriately manages conflicts of interest Aware of own limitations Effectively manages challenges such as obtaining informed consent, delivering bad news, addressing anger and misunderstanding Sets priorities and manages time efficiently Manages competing demands and stress Appropriately manages supervision, resources and staff. Overall Competent performance Not yet competent Assessor comments on candidate s strengths and areas for improvement. Results Competent Not yet competent Competent Not yet competent Competent Not yet competent Competent Not yet competent Competent Not yet competent Competent Not yet competent 34
35 Case Based Presentation 1 Introduction: During core rotations DiTs are requested to record at least one case that provided a valuable learning opportunity. The purpose of this assessment is to assist staff, allowing them to reflect upon clinical practice and develop insight into recognising limitations. At the end of term rotation assessment, DiTs are encouraged to seek feedback on these journals. (De identify all cases -NO PATIENT ID PLEASE) Department: Case/Presentation Description: Overview of what has happened. Feelings: What were you thinking and/or feeling throughout? Evaluation: What was positive and/or negative about the experience? Analysis: What was the underlying cause/issue of the situation? Conclusion: What else could have been done? Action plan: If this case was presented again would you do anything differently? 35
36 Case Based Presentation 2 Introduction: During core rotations DiTs are requested to record at least one case that provided a valuable learning opportunity. The purpose of this assessment is to assist staff, allowing them to reflect upon clinical practice and develop insight into recognising limitations. At the end of term rotation assessment, DiTs are encouraged to seek feedback on these journals. (De identify all cases -NO PATIENT ID PLEASE) Department: Case/Presentation Description: Overview of what has happened. Feelings: What were you thinking and/or feeling throughout? Evaluation: What was positive and/or negative about the experience? Analysis: What was the underlying cause/issue of the situation? Conclusion: What else could have been done? Action plan: If this case was presented again would you do anything differently? 36
37 References: 1. Burns E. Atrial Fibrillation [Internet] [cited 2016 Jul 14]. Available from: The Medical Education team would like to acknowledge Dr. Ben Scott for his work in developing this resource for Doctors in training at Ballarat Health Services 37
Family Medicine Residency Surgery Rotation
 Family Medicine Residency Surgery Rotation Rotation Goal The overall goal for the educational experience provided in the areas of general surgery, trauma surgery, office orthopedic surgery and sports medicine,
Family Medicine Residency Surgery Rotation Rotation Goal The overall goal for the educational experience provided in the areas of general surgery, trauma surgery, office orthopedic surgery and sports medicine,
Laparoscopic Radical Nephrectomy
 Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Surgical Residency Curriculum
 Community Memorial Hospital Surgical Residency Curriculum Program Director: G. W. Iwasiuk MD FACS 2016 Educational Goals & Objectives Surgeons provide continuing care for patients with a myriad of surgical
Community Memorial Hospital Surgical Residency Curriculum Program Director: G. W. Iwasiuk MD FACS 2016 Educational Goals & Objectives Surgeons provide continuing care for patients with a myriad of surgical
SURGICAL ONCOLOGY MCVH
 SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
HOSPITAL MEDICAL OFFICER
 Position Title: Classification: Reports To: Department: Award / Enterprise Agreement: Hospital Medical Officer Hospital Medical Officer HM13 Director of Emergency Services Emergency In accordance with
Position Title: Classification: Reports To: Department: Award / Enterprise Agreement: Hospital Medical Officer Hospital Medical Officer HM13 Director of Emergency Services Emergency In accordance with
TRAUMA AND EMERGENCY SURGERY CORE OBJECTIVES: PGY 4
 TRAUMA AND EMERGENCY SURGERY CORE OBJECTIVES: PGY 4 GOALS Through rotation on the trauma and emergency surgery service, residents shall attain the following goals: I. Patient Care A. Trauma Resuscitations
TRAUMA AND EMERGENCY SURGERY CORE OBJECTIVES: PGY 4 GOALS Through rotation on the trauma and emergency surgery service, residents shall attain the following goals: I. Patient Care A. Trauma Resuscitations
Laparoscopic partial nephrectomy
 Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
SCOPE OF PRACTICE PGY 1-6
 PGY1 Complete history and physical on each patient admitted as assigned by the attending surgeon. Participate in daily ward rounds. Assist operating surgeons and senior residents in the operating room
PGY1 Complete history and physical on each patient admitted as assigned by the attending surgeon. Participate in daily ward rounds. Assist operating surgeons and senior residents in the operating room
Supervision of Residents/Chain of Command
 Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
A Total Colectomy is the surgical removal of the entire colon (last part of the intestine/gut). It does not involve the removal of the rectum.
. It does not involve the removal of the rectum.") Total Colectomy What is a Total Colectomy? A Total Colectomy is the surgical removal of the entire colon (last part of the intestine/gut). It does not involve the removal of the rectum. Before an ileostomy
Total Colectomy What is a Total Colectomy? A Total Colectomy is the surgical removal of the entire colon (last part of the intestine/gut). It does not involve the removal of the rectum. Before an ileostomy
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
You have been admitted with a hip fracture
 Hip fracture: Information for patients and relatives You have been admitted with a hip fracture This booklet has been designed by health professionals to provide you and your relatives with the information
Hip fracture: Information for patients and relatives You have been admitted with a hip fracture This booklet has been designed by health professionals to provide you and your relatives with the information
NEW JERSEY. Downloaded January 2011
 NEW JERSEY Downloaded January 2011 SUBCHAPTER 25. MANDATORY NURSE STAFFING 8:39 25.1 Mandatory policies and procedures for nurse staffing (a) There shall be a full time director of nursing or nursing administrator
NEW JERSEY Downloaded January 2011 SUBCHAPTER 25. MANDATORY NURSE STAFFING 8:39 25.1 Mandatory policies and procedures for nurse staffing (a) There shall be a full time director of nursing or nursing administrator
Trauma. Level 2. This resident can lead a to recognize common. This resident can. accurately diagnose. team that cares for traumatic conditions and
 Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
The School Of Nursing And Midwifery. CLINICAL SKILLS PASSPORT
 The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
Health Sciences Centre, Team C, Dr. M. Wells (Breast and Hernia) Medical Expert
 Medical Expert") Health Sciences Centre, Team C, Dr. M. Wells ( and ) Introduction The goal of this rotation is to afford senior residents the best possible opportunity to develop the foundational knowledge and skills
Health Sciences Centre, Team C, Dr. M. Wells ( and ) Introduction The goal of this rotation is to afford senior residents the best possible opportunity to develop the foundational knowledge and skills
Abdomino-perineal Resection/Excision of the Rectum
 Abdomino-perineal Resection/Excision of the Rectum What is an Abdomino-perineal Resection/Excision of Rectum? An Abdomino-perineal Resection/Excision of Rectum is the surgical removal of part of the large
Abdomino-perineal Resection/Excision of the Rectum What is an Abdomino-perineal Resection/Excision of Rectum? An Abdomino-perineal Resection/Excision of Rectum is the surgical removal of part of the large
The Gynaecology Ward, The Women s Centre. Minor Surgery. Your nursing care, recovery, and getting back to normal
 The Gynaecology Ward, The Women s Centre Minor Surgery Your nursing care, recovery, and getting back to normal Contents Admission 3 Medicines 3 Visiting Hours 3 Patientline 3 Preparation for your operation
The Gynaecology Ward, The Women s Centre Minor Surgery Your nursing care, recovery, and getting back to normal Contents Admission 3 Medicines 3 Visiting Hours 3 Patientline 3 Preparation for your operation
CONSENT FORM UROLOGICAL SURGERY
 CONSENT FORM for UROLOGICAL SURGERY (Designed in compliance with consent form 1) PATIENT AGREEMENT TO INVESTIGATION OR TREATMENT Patient Details or pre-printed label Patient s NHS Number or Hospital number
CONSENT FORM for UROLOGICAL SURGERY (Designed in compliance with consent form 1) PATIENT AGREEMENT TO INVESTIGATION OR TREATMENT Patient Details or pre-printed label Patient s NHS Number or Hospital number
8/19/2017. The OIG Report
 This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
RURAL & COMMUNITY SURGERY SMH, Gatineau, Joliette, Ormstown, Val D Or and Lakeshore Sites
 RURAL & COMMUNITY SURGERY SMH, Gatineau, Joliette, Ormstown, Val D Or and Lakeshore Sites Goals & Objectives Preamble The general objective of our rural and community surgery rotations is to provide the
RURAL & COMMUNITY SURGERY SMH, Gatineau, Joliette, Ormstown, Val D Or and Lakeshore Sites Goals & Objectives Preamble The general objective of our rural and community surgery rotations is to provide the
Pediatric Surgery Curriculum Clinical Base Year
 Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
PLASTIC AND HAND SURGERY CORE OBJECTIVES
 PLASTIC AND HAND SURGERY CORE OBJECTIVES Through rotation on the plastic and hand surgery service, residents shall attain the following goals: I. Patient Care A. Preoperative Care: Residents will evaluate
PLASTIC AND HAND SURGERY CORE OBJECTIVES Through rotation on the plastic and hand surgery service, residents shall attain the following goals: I. Patient Care A. Preoperative Care: Residents will evaluate
CONSENT FOR I & D PERIANAL ABSCESS
 Surgery > Immesive Scenario 8 CONSENT FOR I & D PERIANAL ABSCESS MODULE: GENERAL SURGERY TARGET: CT1 ST4 BACKGROUND: Junior surgical trainees are often expected to take consent for procedures in theatre
Surgery > Immesive Scenario 8 CONSENT FOR I & D PERIANAL ABSCESS MODULE: GENERAL SURGERY TARGET: CT1 ST4 BACKGROUND: Junior surgical trainees are often expected to take consent for procedures in theatre
OVERALL GOALS AND OBJECTIVES FOR EACH RESIDENT LEVEL 3 rd YEAR GENERAL SURGERY RESIDENT PATIENT CARE
 OVERALL GOALS AND OBJECTIVES FOR EACH RESIDENT LEVEL CRITERIA FOR ADVANCEMENT TO PGY-4 YEAR: Satisfactory completion of all rotations and fulfillment of all performance objectives listed above as judges
OVERALL GOALS AND OBJECTIVES FOR EACH RESIDENT LEVEL CRITERIA FOR ADVANCEMENT TO PGY-4 YEAR: Satisfactory completion of all rotations and fulfillment of all performance objectives listed above as judges
Hip fracture - DHS. Your broken hip joint - some information
 Page 1 Hip Fracture - DHS Your broken hip joint - some information These notes give a guide to your stay in hospital. They also give an idea about what it will be like afterwards. They do not cover everything.
Page 1 Hip Fracture - DHS Your broken hip joint - some information These notes give a guide to your stay in hospital. They also give an idea about what it will be like afterwards. They do not cover everything.
Cardio Oesophagectomy
 Cardio Oesophagectomy Information for patients Excellent Care with Compassion What is a Cardio - Oesophagectomy? It is the removal of the oesophagus (gullet) where the cancer is situated. Part of the stomach
Cardio Oesophagectomy Information for patients Excellent Care with Compassion What is a Cardio - Oesophagectomy? It is the removal of the oesophagus (gullet) where the cancer is situated. Part of the stomach
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVII. MANAGEMENT AND DELEGATION A. General Information: The judgments that you make in management and delegation situations have to be based on knowledge. You MUST know your content, and then you can move
XVII. MANAGEMENT AND DELEGATION A. General Information: The judgments that you make in management and delegation situations have to be based on knowledge. You MUST know your content, and then you can move
Bowel Surgery Hartmann s Procedure Your operation explained
 Bowel Surgery Hartmann s Procedure Your operation explained Introduction This information is for people considering having a Hartmann s Procedure operation. It explains what is involved and some possible
Bowel Surgery Hartmann s Procedure Your operation explained Introduction This information is for people considering having a Hartmann s Procedure operation. It explains what is involved and some possible
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
About Your Colectomy
 UW MEDICINE PATIENT EDUCATION About Your Colectomy How to prepare and what to expect This handout explains a colectomy operation, including how to prepare for surgery, what to expect afterward, recovering
UW MEDICINE PATIENT EDUCATION About Your Colectomy How to prepare and what to expect This handout explains a colectomy operation, including how to prepare for surgery, what to expect afterward, recovering
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Broad expectations of PRINT
 Congratulations on passing your finals! Now you ve got those out of the way, you can turn your attention to developing skills as interns rather than preparing for examinations. So, welcome to your PRINT
Congratulations on passing your finals! Now you ve got those out of the way, you can turn your attention to developing skills as interns rather than preparing for examinations. So, welcome to your PRINT
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
E-Learning Module M: Assessment Review
 E-Learning Module M: Assessment Review This Module requires the learner to have read Chapter 12 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised: August
E-Learning Module M: Assessment Review This Module requires the learner to have read Chapter 12 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised: August
PGY-1 Overall Goals & Objectives
 PGY-1 Overall Goals & Objectives PGY-1 residents are expected to accomplish and maintain the following objectives: Develop personal values and interpersonal skills appropriate for the surgical resident
PGY-1 Overall Goals & Objectives PGY-1 residents are expected to accomplish and maintain the following objectives: Develop personal values and interpersonal skills appropriate for the surgical resident
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
February 2009 [KU 1018] Sub. Code: 4717
![February 2009 [KU 1018] Sub. Code: 4717](/thumbs/79/78949052.jpg "February 2009 [KU 1018] Sub. Code: 4717") February 2009 [KU 1018] Sub. Code: 4717 Second Year Paper II MEDICAL SURGICAL NURSING - I Answer ALL questions. I. Essays: (2x15=30) 1. Mr.Mani 64 yrs old man is admitted with the diagnosis of Benign Prostatic
February 2009 [KU 1018] Sub. Code: 4717 Second Year Paper II MEDICAL SURGICAL NURSING - I Answer ALL questions. I. Essays: (2x15=30) 1. Mr.Mani 64 yrs old man is admitted with the diagnosis of Benign Prostatic
CERTIFICATE OF COMPLETION OF PAEDIATRIC LEVEL 1 COMPETENCY V1.0
 Applicants applying for ST4 posts in paediatrics may use this certificate to successful, satisfactory completion of Level 1 paediatric competences, as defined in the RCPCH Level 1 Paediatrics and Child
Applicants applying for ST4 posts in paediatrics may use this certificate to successful, satisfactory completion of Level 1 paediatric competences, as defined in the RCPCH Level 1 Paediatrics and Child
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
Patient Diary. Enhanced Recovery After Surgery (ERAS) Total Knee Replacement. Helping patients get better sooner after surgery.
 Total Knee Replacement. Helping patients get better sooner after surgery.") Contact numbers If you need any support or advice before or after surgery please do not hesitate to call us. Claire Ward enhanced recovery nurse (Monday Friday 8-4) 07816448518 Ward 12B 01494426398 How
Contact numbers If you need any support or advice before or after surgery please do not hesitate to call us. Claire Ward enhanced recovery nurse (Monday Friday 8-4) 07816448518 Ward 12B 01494426398 How
You will be having surgery to remove a the distal or tail part of your pancreas.
 Distal pancreatectomy You will be having surgery to remove a the distal or tail part of your pancreas. This handout will help you learn about the surgery, how to prepare for surgery and your care after
Distal pancreatectomy You will be having surgery to remove a the distal or tail part of your pancreas. This handout will help you learn about the surgery, how to prepare for surgery and your care after
Patient Information Varicose Vein Surgery Dr Marek Garbowski. Varicose Veins
 Contents: Welcome Varicose veins Our expectations Preadmission clinic The day of your operation In preparation of going home Discharge advice following varicose veins surgery Contacts Varicose Veins Welcome
Contents: Welcome Varicose veins Our expectations Preadmission clinic The day of your operation In preparation of going home Discharge advice following varicose veins surgery Contacts Varicose Veins Welcome
GENERAL SURGERY ROTATION SYLLABUS
 GENERAL SURGERY ROTATION SYLLABUS Level of Training PGY2, PGY3 Length of Rotation 4 weeks (required rotation) Contact Person: Donald A. Zorn, M.D. Phone: 431-5464 Beeper: 489-3601 Cell: 510-7133 Preceptor
GENERAL SURGERY ROTATION SYLLABUS Level of Training PGY2, PGY3 Length of Rotation 4 weeks (required rotation) Contact Person: Donald A. Zorn, M.D. Phone: 431-5464 Beeper: 489-3601 Cell: 510-7133 Preceptor
FOCUS CHARTING. The Focus Charting System is the accepted documentation system at Windsor Regional Hospital.
 FOCUS CHARTING The Focus Charting System is the accepted documentation system at Windsor Regional Hospital. Advantages of Focus Charting Flexible enough to adapt to any clinical practice setting and promotes
FOCUS CHARTING The Focus Charting System is the accepted documentation system at Windsor Regional Hospital. Advantages of Focus Charting Flexible enough to adapt to any clinical practice setting and promotes
Enhanced recovery after oesophagogastric surgery (EROS) Patient information and advice
 Patient information and advice") Enhanced recovery after oesophagogastric surgery (EROS) Patient information and advice Welcome to the enhanced recovery programme. The aim of the programme is to enable you to be well enough to go home
Enhanced recovery after oesophagogastric surgery (EROS) Patient information and advice Welcome to the enhanced recovery programme. The aim of the programme is to enable you to be well enough to go home
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition
 Nursing Competency Workbook 6th Edition") Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
West Middlesex Junior Doctors Handbook in Colorectal Surgery
 West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
Emergency Department Student Elective Goals and Objectives
 Emergency Department Student Elective Goals and Objectives Goals: During the Emergency Department (ED) rotation, the student will develop his/her knowledge and skills associated with the evaluation, treatment
Emergency Department Student Elective Goals and Objectives Goals: During the Emergency Department (ED) rotation, the student will develop his/her knowledge and skills associated with the evaluation, treatment
PRIVILEGE APPLICATION FORM - [Mercy Medical Center]
![PRIVILEGE APPLICATION FORM - [Mercy Medical Center]](/thumbs/85/91362180.jpg "PRIVILEGE APPLICATION FORM - [Mercy Medical Center]") Current Privilege Status Key Practitioner's Current Privilege status is signified in ( ) preceding each privilege. G = W = Withdrawn T = Temporary P = With Proctor A = Assist with C = With Consult E =
Current Privilege Status Key Practitioner's Current Privilege status is signified in ( ) preceding each privilege. G = W = Withdrawn T = Temporary P = With Proctor A = Assist with C = With Consult E =
Policy on Resident Supervision. University of South Florida College of Medicine General Surgery Residency Rev. July 2013
 Policy on Resident Supervision University of South Florida College of Medicine General Surgery Residency Rev. July 2013 Policy Definitions: 1. Resident: A medical school graduate who is enrolled in the
Policy on Resident Supervision University of South Florida College of Medicine General Surgery Residency Rev. July 2013 Policy Definitions: 1. Resident: A medical school graduate who is enrolled in the
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER. Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow
 SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
Liver Resection. Why do I need a liver resection? This procedure is done for many reasons. Talk to your doctor about why you are having this surgery.
 Liver Resection What is a liver resection? This is a surgical procedure where the surgeon removes part of the liver. It is done under general anesthetic which means you sleep during the procedure. Why
Liver Resection What is a liver resection? This is a surgical procedure where the surgeon removes part of the liver. It is done under general anesthetic which means you sleep during the procedure. Why
Shock - Hypovolaemia
 Shock - Hypovolaemia Research Staff: Participants should be asked to arrive dressed as they would for clinical placement. That is, in uniform, hair and jewellery appropriate, note pad, pen, watch, stethoscope,
Shock - Hypovolaemia Research Staff: Participants should be asked to arrive dressed as they would for clinical placement. That is, in uniform, hair and jewellery appropriate, note pad, pen, watch, stethoscope,
OPAT CELLULITIS PATHWAY
 OPAT CELLULITIS PATHWAY ANY exclusion criteria for OPAT Sepsis syndrome Active drug/alcohol abuse Active underlying orthopaedic condition Craniofacial cellulitis Failure to improve with > 48hrs IV Rx YES
OPAT CELLULITIS PATHWAY ANY exclusion criteria for OPAT Sepsis syndrome Active drug/alcohol abuse Active underlying orthopaedic condition Craniofacial cellulitis Failure to improve with > 48hrs IV Rx YES
Enhanced Recovery Programme for total hip and knee replacement Orthopaedic Department Patient Information Leaflet
 Enhanced Recovery Programme for total hip and knee replacement Orthopaedic Department Patient Information Leaflet What is the Enhanced Recovery Programme? This leaflet aims to give you information on what
Enhanced Recovery Programme for total hip and knee replacement Orthopaedic Department Patient Information Leaflet What is the Enhanced Recovery Programme? This leaflet aims to give you information on what
NURSE PRACTITIONER (NP) CLINICAL PRIVILEGES ORTHOPEDIC SURGERY
 CLINICAL PRIVILEGES ORTHOPEDIC SURGERY") Name: Page 1 Initial Appointment (initial privileges) Reappointment (renewal of privileges) All new applicants must meet the following requirements as approved by the governing body effective: / /. Applicant:
Name: Page 1 Initial Appointment (initial privileges) Reappointment (renewal of privileges) All new applicants must meet the following requirements as approved by the governing body effective: / /. Applicant:
Monitoring of the accomplishment of the stated objectives will be performed using the following methods:
 July 2011 ROTATION: PLASTIC SURGERY ROTATION DIRECTOR: Tim Miller, M.D. SITES: RRUMC; Greater Los Angeles VA Medical Center, Olive View UCLA Medical Center GOALS AND OBJECTIVES: 1. Obtain clinical experience
July 2011 ROTATION: PLASTIC SURGERY ROTATION DIRECTOR: Tim Miller, M.D. SITES: RRUMC; Greater Los Angeles VA Medical Center, Olive View UCLA Medical Center GOALS AND OBJECTIVES: 1. Obtain clinical experience
Colon Surgery Rapid Recovery Program
 Colon Surgery Rapid Recovery Program at Toronto Western Hospital Colon Esophagus Liver Stomach Colon Small Intestine Please visit the UHN Patient Education website for more health information: www.uhnpatienteducation.ca
Colon Surgery Rapid Recovery Program at Toronto Western Hospital Colon Esophagus Liver Stomach Colon Small Intestine Please visit the UHN Patient Education website for more health information: www.uhnpatienteducation.ca
C-GALL PATIENT INFORMATION LEAFLET
 C-GALL PATIENT INFORMATION LEAFLET The purpose of this study is to compare keyhole gall bladder surgery (laparoscopic cholecystectomy) with watchful waiting in people who suffer from pain due to gallstones
C-GALL PATIENT INFORMATION LEAFLET The purpose of this study is to compare keyhole gall bladder surgery (laparoscopic cholecystectomy) with watchful waiting in people who suffer from pain due to gallstones
Hysterectomy. What is a hysterectomy? How is this procedure done?
 Hysterectomy What is a hysterectomy? A hysterectomy is a surgery that removes your uterus (womb). The uterus is one of the organs of the female reproductive system. It is about the size of your closed
Hysterectomy What is a hysterectomy? A hysterectomy is a surgery that removes your uterus (womb). The uterus is one of the organs of the female reproductive system. It is about the size of your closed
Morton s neuroma. If you have any further questions, please speak to a doctor or nurse caring for you.
 Morton s neuroma This leaflet aims to answer your questions about having surgery for Morton s neuroma. It explains the benefits, risks and alternatives, as well as what you can expect when you come to
Morton s neuroma This leaflet aims to answer your questions about having surgery for Morton s neuroma. It explains the benefits, risks and alternatives, as well as what you can expect when you come to
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Thoracic Surgery Unit Information for Patients Having an Examination of the Lymph Glands Inside the Chest
 Thoracic Surgery Unit Information for Patients Having an Examination of the Lymph Glands Inside the Chest Cervical Mediastinoscopy (often simply Mediastinoscopy ) The following information has been prepared
Thoracic Surgery Unit Information for Patients Having an Examination of the Lymph Glands Inside the Chest Cervical Mediastinoscopy (often simply Mediastinoscopy ) The following information has been prepared
Primary Supervisors: Dr. Robert Atkinson (Office: ) Dr. Daniel Singer (Office: ) Dr. John Juliano Dr. Shim Ching (Plastic Surgery)
 Dr. Daniel Singer (Office: ) Dr. John Juliano Dr. Shim Ching (Plastic Surgery)") Hand Surgery Rotation At Queen s Medical Center, PGY-5 Description of Rotation The Hand Surgery rotations include a three-month rotation as a PGY-5 (Chief) resident. Residents on rotation participate in
Hand Surgery Rotation At Queen s Medical Center, PGY-5 Description of Rotation The Hand Surgery rotations include a three-month rotation as a PGY-5 (Chief) resident. Residents on rotation participate in
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Rotation Specific Learning Objectives CCFP-EM Residency Program. Plastic Surgery
 Rotation Specific Learning Objectives CCFP-EM Residency Program Plastic Surgery of the Rotation To utilize the relevant competencies contained within the CanMEDS-FM roles to effectively evaluate, diagnose
Rotation Specific Learning Objectives CCFP-EM Residency Program Plastic Surgery of the Rotation To utilize the relevant competencies contained within the CanMEDS-FM roles to effectively evaluate, diagnose
Course Outline and Assignments
 Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Inguinal hernia repair integrated care pathway (ICP)
") Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy
 Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy Overview of Scenario Simulated Patient Overview Target Audience (Part A): 2 nd year Speech Pathology students, 2 nd year Social Work students
Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy Overview of Scenario Simulated Patient Overview Target Audience (Part A): 2 nd year Speech Pathology students, 2 nd year Social Work students
Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet
 Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet Originator: Mr Raj Patel Date: May 2011 Version: 2 Date for Review: May 2014 DGOH Ref No: DGOH/PIL/00364
Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet Originator: Mr Raj Patel Date: May 2011 Version: 2 Date for Review: May 2014 DGOH Ref No: DGOH/PIL/00364
ANTERIOR RESECTION WHAT ARE THE BENEFITS OF HAVING AN ANTERIOR RESECTION?
 WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
Radical Prostatectomy Care Guide: A checklist of what to expect
 Radical Prostatectomy Care Guide: A checklist of what to expect Form: D-5473 How to prepare for your operation as an outpatient 1. Pre- Admission Visit Where to find us: Toronto General Hospital (TGH),
Radical Prostatectomy Care Guide: A checklist of what to expect Form: D-5473 How to prepare for your operation as an outpatient 1. Pre- Admission Visit Where to find us: Toronto General Hospital (TGH),
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
To ensure oversight of resident supervision and graded authority and responsibility, the following levels of supervision are recognized:
 Roles, Responsibilities and Patient Care Activities of Residents University of Washington Boise Internal Medicine and Saint Luke s Health Care System and Saint Alphonsus Health Care System Definitions
Roles, Responsibilities and Patient Care Activities of Residents University of Washington Boise Internal Medicine and Saint Luke s Health Care System and Saint Alphonsus Health Care System Definitions
River City AAPC. Jacksonville, FL
 1. A 15 year-old male arrives in the family practice physicians office complaining of severe low right side abdominal pain. Following the examination, the physician determines that patient has appendicitis
1. A 15 year-old male arrives in the family practice physicians office complaining of severe low right side abdominal pain. Following the examination, the physician determines that patient has appendicitis
EMERGENCY MEDICINE CLINICAL ROTATION COMPETENCY BASED CURRICULUM
 CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
Right Hemicolectomy. Patient information - General Surgery. Right Hemicolectomy
 Right Hemicolectomy General Surgery Right Hemicolectomy Patient information - General Surgery Introduction This booklet provides information about your operation. Please do not hesitate to ask any questions
Right Hemicolectomy General Surgery Right Hemicolectomy Patient information - General Surgery Introduction This booklet provides information about your operation. Please do not hesitate to ask any questions
Enhanced Recovery Programme for Nephrectomy (Kidney Removal)
") Enhanced Recovery Programme for Nephrectomy (Kidney Removal) This information leaflet will explain what will happen when you come to the hospital for your operation. The enhanced Recovery Programme is
Enhanced Recovery Programme for Nephrectomy (Kidney Removal) This information leaflet will explain what will happen when you come to the hospital for your operation. The enhanced Recovery Programme is
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SKILLED NURSING SERVICES
 DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
RIGHT HEMICOLECTOMY. Patient information Leaflet
 RIGHT HEMICOLECTOMY Patient information Leaflet April 2017 WHAT IS A RIGHT HEMICOLECTOMY? This is an operation that is designed to remove the right side of your large bowel. Part of the large bowel is
RIGHT HEMICOLECTOMY Patient information Leaflet April 2017 WHAT IS A RIGHT HEMICOLECTOMY? This is an operation that is designed to remove the right side of your large bowel. Part of the large bowel is
Mediastinal Venogram and Stent Insertion
 Mediastinal Venogram and Stent Insertion Radiology Department Patient information leaflet This leaflet tells you about the procedure known as a mediastinal venogram. It explains what is involved and the
Mediastinal Venogram and Stent Insertion Radiology Department Patient information leaflet This leaflet tells you about the procedure known as a mediastinal venogram. It explains what is involved and the
PRACTICAL SKILLS. Objective examination of the patient
 RACTICAL KILL tudent's data. These fields are completed by the student First and last name No of study book In the next tables, total of 76 practical skills are listed by topics that you should develop
RACTICAL KILL tudent's data. These fields are completed by the student First and last name No of study book In the next tables, total of 76 practical skills are listed by topics that you should develop
Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt
 Department of Neurosurgery Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt Information for patients Shunt surgery This leaflet explains what to expect when you are in hospital and during
Department of Neurosurgery Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt Information for patients Shunt surgery This leaflet explains what to expect when you are in hospital and during
NEONATAL-PERINATAL MEDICINE CLINICAL PRIVILEGES
 Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 8/5/2015. Applicant: Check off the Requested box for
Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 8/5/2015. Applicant: Check off the Requested box for
Whipple Procedure (Pancreaticoduodenectomy)
") Enhanced Recovery After Whipple Procedure (Pancreaticoduodenectomy) Your Path to Healing Your Pancreatic Surgical Oncology Team This expert team is an important part of the Pancreatic Surgery Program at
Enhanced Recovery After Whipple Procedure (Pancreaticoduodenectomy) Your Path to Healing Your Pancreatic Surgical Oncology Team This expert team is an important part of the Pancreatic Surgery Program at
Enhanced recovery after bowel surgery
 Patient information - Bowel Pre-operative Surgery Enhanced Assessment Recovery - WLE Enhanced recovery after bowel surgery Introduction This leaflet will explain what will happen when you come to the hospital
Patient information - Bowel Pre-operative Surgery Enhanced Assessment Recovery - WLE Enhanced recovery after bowel surgery Introduction This leaflet will explain what will happen when you come to the hospital
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
Scope of Practice for Student Nurses - Undergraduate & Entry to Professional Practice
 Scope of Practice for Student Nurses - Undergraduate & Entry to Professional Practice March 2017 2 nd edition The Royal Children's Hospital (RCH) Scope of Practice for Student Nurses. This scope of practice
Scope of Practice for Student Nurses - Undergraduate & Entry to Professional Practice March 2017 2 nd edition The Royal Children's Hospital (RCH) Scope of Practice for Student Nurses. This scope of practice
Having an open partial nephrectomy
 Having an open partial nephrectomy The aim of this information sheet is to help answer some of the questions you may have about having part of your kidney removed using conventional open surgery this is
Having an open partial nephrectomy The aim of this information sheet is to help answer some of the questions you may have about having part of your kidney removed using conventional open surgery this is
Urology Enhanced Recovery Programme: Laparoscopic/open simple/radical/partial/donor nephrectomy. Information For Patients
 Urology Enhanced Recovery Programme: Laparoscopic/open simple/radical/partial/donor nephrectomy Information For Patients 2 This information leaflet aims to help you understand the Enhanced Recovery Programme
Urology Enhanced Recovery Programme: Laparoscopic/open simple/radical/partial/donor nephrectomy Information For Patients 2 This information leaflet aims to help you understand the Enhanced Recovery Programme
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS
 Nursing Chapter 610-X-7 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS 610-X-7-.01 610-X-7-.02 610-X-7-.03 610-X-7-.04 610-X-7-.05
Nursing Chapter 610-X-7 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS 610-X-7-.01 610-X-7-.02 610-X-7-.03 610-X-7-.04 610-X-7-.05
Administration ~ Education and Training (919)
") The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
The Accreditation Council for Graduate Medical Education requires the educational program to provide a curriculum that must contain the following educational components to its Trainees; overall educational
Global Surgery Package for Professional Claims
 Manual: Policy Title: Reimbursement Policy Global Surgery Package for Professional Claims Section: Administrative Subsection: None Policy Number: RPM011 Date of Origin: 1/1/2000 Last Updated: 3/6/2017
Manual: Policy Title: Reimbursement Policy Global Surgery Package for Professional Claims Section: Administrative Subsection: None Policy Number: RPM011 Date of Origin: 1/1/2000 Last Updated: 3/6/2017
Your Hospital Stay After Fibular Free Flap Surgery
 Your Hospital Stay After Fibular Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your fibular free flap surgery. It includes where you will stay after
Your Hospital Stay After Fibular Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your fibular free flap surgery. It includes where you will stay after
Tenckhoff Catheter Insertion
 Tenckhoff Catheter Insertion Information for patients with chronic kidney disease (CKD) who have chosen to have peritoneal dialysis Renal Directorate Produced: May 2010 Review date: May 2012 This leaflet
Tenckhoff Catheter Insertion Information for patients with chronic kidney disease (CKD) who have chosen to have peritoneal dialysis Renal Directorate Produced: May 2010 Review date: May 2012 This leaflet
Percutaneous Transhepatic Biliary Drainage Interventional Radiology
 Percutaneous Transhepatic Biliary Drainage Interventional Radiology Your doctor has scheduled a percutaneous transhepatic biliary drainage to be done in the Interventional Radiology (IR) Department on
Percutaneous Transhepatic Biliary Drainage Interventional Radiology Your doctor has scheduled a percutaneous transhepatic biliary drainage to be done in the Interventional Radiology (IR) Department on